Predicting aneurysm enlargement in patients with persistent type II endoleaks
6
From the New England Society for Vascular Surgery Predicting aneurysm enlargement in patients with persistent type II endoleaks Carlos H. Timaran, MD, Takao Ohki, MD, PhD, Soo J. Rhee, MD, Frank J. Veith, MD, Nicholas J. Gargiulo III, MD, Hisako Toriumi, MD, Mahmood B. Malas, MD, William D. Suggs, MD, Reese A. Wain, MD, and Evan C. Lipsitz, MD, New York, NY Objective: The clinical significance of type II endoleaks is not well understood. Some evidence, however, indicates that some type II endoleaks might result in aneurysm enlargement and rupture. To identify factors that might contribute to aneurysm expansion, we analyzed the influence of several variables on aneurysm growth in patients with persistent type II endoleaks after endovascular aortic aneurysm repair (EVAR). Methods: In a series of 348 EVARs performed during a 10-year period, 32 patients (9.2%) developed type II endoleaks that persisted for more than 6 months. Variables analyzed included those defined by the reporting standards for EVAR (SVS/AAVS) as well as other endoleak characteristics. Univariate, receiver operating characteristic curve, and Cox regression analyses were used to determine the association between variables and aneurysm enlargement. Results: The median follow-up period was 26.5 months (range, 6-88 months). Thirteen patients (41%) had aneurysm enlargement by 5 mm or more (median increase in diameter, 10 mm), whereas 19 (59%) had stable or shrinking aneurysm diameter. Univariate and Cox regression analyses identified the maximum diameter of the endoleak cavity, ie, the size of the nidus as defined on contrast computed tomography scan, as a significant predictor for aneurysm enlargement (relative risk, 1.12; 95% confidence interval, 1.04-1.19; P .001). The median size of the nidus was 23 mm (range, 13-40 mm) in patients with aneurysm enlargement and 8 mm (range, 5-25 mm) in those without expansion (Mann-Whitney U test, P < .001). Moreover, receiver operating characteristic curve and Cox regression analyses showed that a maximum nidus diameter greater than 15 mm was particularly associated with an increased risk of aneurysm enlargement (relative risk, 11.1; 95% confidence interval, 1.4-85.8; P .02). Other risk factors including gender, smoking history, hypertension, need of anticoagulation, aneurysm diameter, type of endograft used, and number or type of collateral vessels were not significant predictors of aneurysm enlargement. Conclusions: In patients with persistent type II endoleaks after EVAR, the maximum diameter of the endoleak cavity or nidus is an important predictor of aneurysm growth and might indicate the need for more aggressive surveillance as well as earlier treatment. (J Vasc Surg 2004;39:1157-62.) The most frequent mechanism of failure after endovas- cular aortic aneurysm repair (EVAR) is the occurrence of an endoleak, ie, the persistence of blood flow in the aneurysm sac outside the endograft. 1,2 Type II endoleaks are attrib- uted to retrograde flow from patent lumbar arteries, infe- rior mesenteric artery, and other collateral aortic branch- es. 2-4 Although type II endoleaks are frequently evident in intraoperative angiograms after EVAR, the majority of these endoleaks resolve as a result of the reversal of antico- agulation and the subsequent thrombosis of the aneurysm sac and its side branches. 2 Persistent type II endoleaks develop in approximately 5% to 25% of the patients after EVAR. 1,2,5-9 The exact clinical significance of persistent type II endoleaks is not defined because these might be associated with aneurysm enlargement, stability, and shrinkage. 1,2,8,10 Therefore, the optimal method of diag- nosis and treatment of type II endoleaks is also controver- sial. 9 As more experience with the diagnosis and treatment of type II endoleaks has been reported, it is now well recognized that type II endoleaks are not always benign. For instance, recent studies have documented that type II endoleaks might produce systemic blood pressures within the aneurysm sac that might result in aneurysm enlarge- ment and rupture. 4,8,11-14 Because the risk of aneurysm rupture is related to the maximum diameter of the aneu- rysm, general agreement exists that persistent type II en- doleaks associated with aneurysm enlargement require ag- gressive management. However, it is still unknown which type II endoleaks will result in aneurysm expansion, thereby increasing the risk of rupture. This study was designed to assess the influence of several variables on aneurysm expansion in patients with persistent type II endoleaks after EVAR to define when a more aggressive approach of this type of endoleak is indi- cated. The most current recommended reporting standards were used to define the different variables. 15,16 METHODS Among 348 patients who underwent EVAR during a 10-year period (November 1992 to September 2002), 32 From the Division of Vascular Surgery, Department of Surgery, Montefiore Medical Center, Albert Einstein College of Medicine. Competition of interest: none. Presented at the Thirtieth Anniversary Meeting of the New England Society for Vascular Surgery, Newport, RI, Sep 19-21, 2003. Winning paper of the Darling Award of the New England Society for Vascular Surgery. Reprint requests: Takao Ohki, MD, Montefiore Medical Center, 111E 210th St, Bronx, NY 10467 (e-mail: [email protected]). 0741-5214/$30.00 Copyright © 2004 by The Society for Vascular Surgery. doi:10.1016/j.jvs.2003.12.033 1157
-
Upload
independent -
Category
Documents
-
view
0 -
download
0
Transcript of Predicting aneurysm enlargement in patients with persistent type II endoleaks

From the New England Society for Vascular Surgery
Predicting aneurysm enlargement in patients withpersistent type II endoleaksCarlos H. Timaran, MD, Takao Ohki, MD, PhD, Soo J. Rhee, MD, Frank J. Veith, MD, Nicholas J.Gargiulo III, MD, Hisako Toriumi, MD, Mahmood B. Malas, MD, William D. Suggs, MD, Reese A.Wain, MD, and Evan C. Lipsitz, MD, New York, NY
Objective: The clinical significance of type II endoleaks is not well understood. Some evidence, however, indicates thatsome type II endoleaks might result in aneurysm enlargement and rupture. To identify factors that might contribute toaneurysm expansion, we analyzed the influence of several variables on aneurysm growth in patients with persistent typeII endoleaks after endovascular aortic aneurysm repair (EVAR).Methods: In a series of 348 EVARs performed during a 10-year period, 32 patients (9.2%) developed type II endoleaks thatpersisted for more than 6 months. Variables analyzed included those defined by the reporting standards for EVAR(SVS/AAVS) as well as other endoleak characteristics. Univariate, receiver operating characteristic curve, and Coxregression analyses were used to determine the association between variables and aneurysm enlargement.Results: The median follow-up period was 26.5 months (range, 6-88 months). Thirteen patients (41%) had aneurysmenlargement by 5 mm or more (median increase in diameter, 10 mm), whereas 19 (59%) had stable or shrinking aneurysmdiameter. Univariate and Cox regression analyses identified the maximum diameter of the endoleak cavity, ie, the size ofthe nidus as defined on contrast computed tomography scan, as a significant predictor for aneurysm enlargement (relativerisk, 1.12; 95% confidence interval, 1.04-1.19; P � .001). The median size of the nidus was 23 mm (range, 13-40 mm)in patients with aneurysm enlargement and 8 mm (range, 5-25 mm) in those without expansion (Mann-Whitney U test,P < .001). Moreover, receiver operating characteristic curve and Cox regression analyses showed that a maximum nidusdiameter greater than 15 mm was particularly associated with an increased risk of aneurysm enlargement (relative risk,11.1; 95% confidence interval, 1.4-85.8; P � .02). Other risk factors including gender, smoking history, hypertension,need of anticoagulation, aneurysm diameter, type of endograft used, and number or type of collateral vessels were notsignificant predictors of aneurysm enlargement.Conclusions: In patients with persistent type II endoleaks after EVAR, the maximum diameter of the endoleak cavity ornidus is an important predictor of aneurysm growth and might indicate the need for more aggressive surveillance as wellas earlier treatment. (J Vasc Surg 2004;39:1157-62.)
The most frequent mechanism of failure after endovas-cular aortic aneurysm repair (EVAR) is the occurrence of anendoleak, ie, the persistence of blood flow in the aneurysmsac outside the endograft.1,2 Type II endoleaks are attrib-uted to retrograde flow from patent lumbar arteries, infe-rior mesenteric artery, and other collateral aortic branch-es.2-4 Although type II endoleaks are frequently evident inintraoperative angiograms after EVAR, the majority ofthese endoleaks resolve as a result of the reversal of antico-agulation and the subsequent thrombosis of the aneurysmsac and its side branches.2 Persistent type II endoleaksdevelop in approximately 5% to 25% of the patients afterEVAR.1,2,5-9 The exact clinical significance of persistenttype II endoleaks is not defined because these might beassociated with aneurysm enlargement, stability, and
From the Division of Vascular Surgery, Department of Surgery, MontefioreMedical Center, Albert Einstein College of Medicine.
Competition of interest: none.Presented at the Thirtieth Anniversary Meeting of the New England Society
for Vascular Surgery, Newport, RI, Sep 19-21, 2003. Winning paper ofthe Darling Award of the New England Society for Vascular Surgery.
Reprint requests: Takao Ohki, MD, Montefiore Medical Center, 111E210th St, Bronx, NY 10467 (e-mail: [email protected]).
0741-5214/$30.00Copyright © 2004 by The Society for Vascular Surgery.doi:10.1016/j.jvs.2003.12.033
shrinkage.1,2,8,10 Therefore, the optimal method of diag-nosis and treatment of type II endoleaks is also controver-sial.9 As more experience with the diagnosis and treatmentof type II endoleaks has been reported, it is now wellrecognized that type II endoleaks are not always benign.For instance, recent studies have documented that type IIendoleaks might produce systemic blood pressures withinthe aneurysm sac that might result in aneurysm enlarge-ment and rupture.4,8,11-14 Because the risk of aneurysmrupture is related to the maximum diameter of the aneu-rysm, general agreement exists that persistent type II en-doleaks associated with aneurysm enlargement require ag-gressive management. However, it is still unknown whichtype II endoleaks will result in aneurysm expansion, therebyincreasing the risk of rupture.
This study was designed to assess the influence ofseveral variables on aneurysm expansion in patients withpersistent type II endoleaks after EVAR to define when amore aggressive approach of this type of endoleak is indi-cated. The most current recommended reporting standardswere used to define the different variables.15,16
METHODS
Among 348 patients who underwent EVAR during a10-year period (November 1992 to September 2002), 32
1157

f the
JOURNAL OF VASCULAR SURGERYJune 20041158 Timaran et al
patients (9.2%) developed type II endoleaks that wereinitially observed at the first postoperative month or at anytime thereafter and persisted for more than 6 months.These 32 patients with persistent type II endoleaks wereincluded in a cohort study. Patients with type II endoleaksassociated with either type I or type III endoleaks at anytime were specifically excluded. Patient clinical and proce-dural characteristics and follow-up results of patients un-dergoing EVAR were prospectively collected. The medicalrecords, computed tomography (CT) scans, and angio-graphic studies of these patients were, however, furtherreviewed to define clinical characteristics, risk factors, mor-phologic features of endoleaks, and changes in aortic aneu-rysms according to the current reporting standards forEVAR prepared and revised by the Ad Hoc Committee forStandardized Reporting Practices in Vascular Surgery(SVS/AAVS).15,16 Patients with persistent type II en-doleaks underwent CT scans every 3 to 6 months, and nopatients were lost to follow-up. Axial thin-slice (1.5-3 mmthick) CT imaging and occasionally three-dimensional(3D) CT reconstruction models were obtained to confirmthe presence of an endoleak and to further define theetiology and the most likely classification of the leak. Se-quential changes in aneurysm size were determined withserial measurements of the maximum aneurysm diameterby using a standardized method previously described todecrease interobserver variability.17 Patients with persistenttype II endoleaks who had documented aneurysm enlarge-ment on follow-up CT scanning underwent diagnostic
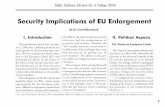
Fig 1. Maximum diameter measurements of the main enby using calipers or CT imaging analysis software with mnidus (2) measuring 9 mm. Although the endoleak chandiameter could be determined in all patients. B, Large enmore than one nidus was seen, the maximum diameter o
angiography to characterize the endoleak. Once a type IIendoleak was confirmed angiographically in patients withevidence of aneurysm expansion, additional treatment witheither transarterial or translumbar embolization was per-formed. The technique of these treatment modalities hasbeen described in detail before. Follow-up dynamic CTscans with 3-mm slice-thickness were obtained at 3, 6, and12 months and annually thereafter. Embolization was con-sidered to be technically successful when resolution of theendoleak was obtained with stabilization or shrinkage ofthe aneurysm sac.
All follow-up CT scans and angiograms of patients withpersistent type II endoleaks were reviewed to characterizethe endoleak channel in greater detail. Endoleak angiogra-phy and pressure measurements were available in patientswho underwent translumbar embolization. The number,origin, and outflow vessels feeding the endoleak were spec-ified as suggested by the current reporting standards.15 Thesize of the main endoleak cavity or nidus was recordedincluding the maximum diameter, short axis, and length ofthe endoleak cavity. Calipers or CT imaging analysis soft-ware with magnification and precise cursor placement wereused for diameter measurements obtained from CT scanimages (Fig 1).
Descriptive statistics for categorical variables are pre-sented as relative frequencies (percents). Univariate analy-ses of categorical variables were performed by using Fisherexact test (two-tailed P value) for group comparisons be-tween patients with type II endoleaks and evidence of
ak cavity or nidus (e) was obtained from CT scan imagescation and precise cursor placement. A, Small endoleakas sometimes irregular and complex, a maximum nidusk nidus measuring 23 mm in maximum diameter. Whenlargest nidus was selected.
doleagnifinel wdolea

JOURNAL OF VASCULAR SURGERYVolume 39, Number 6 Timaran et al 1159
aneurysm growth and those with stable or shrinking aneu-rysms. Morphologic changes in aneurysm dimension wereclassified according to the reporting standards for EVAR.16
Continuous variables were expressed as medians and rang-es; these were analyzed with the Mann-Whitney U test forunpaired comparisons. Kaplan-Meier survival estimateswere used to determine freedom from aneurysm ruptureand open conversion and patient survival. Cox regressionanalyses and receiver operating characteristics (ROC)curves were used to assess the influence of various riskfactors on aneurysm expansion. The relative risk (RR) and95% confidence intervals (95% CIs) for different variableswere estimated by Cox regression. Only univariate regres-sion analyses were performed because of the small numberof patients in the different subgroups. The risk factorsassessed included gender, smoking history, hypertension,need for chronic anticoagulation, initial aneurysm size,amount of wall calcification and sac thrombus, number andtype of branch vessels, size of the endoleak nidus, andendograft type. Findings were considered statistically sig-nificant if the resulting P value was less than .05. Forstatistical analyses, SPSS for Windows version 11.0 (SPSSInc, Chicago, Ill) and MedCalc statistical software version7.2.0.2 (MedCalc Software, Mariakerke, Belgium) wereused.
RESULTS
Study patients. Devices used for EVAR in patientswith persistent type II endoleaks included Zenith (n � 6;Cook, Bloomington, Ind), Excluder (n � 5; W. L. Gore &Associates, Flagstaff, Ariz), AneuRx (n � 5; MedtronicAVE, Santa Rosa, Calif), MEGS (n � 5; Montefiore Endo-vascular Graft System, New York, NY), Talent (n � 4;Medtronic AVE), Ancure (n � 3; Guidant, Menlo Park,Calif), Vanguard (n � 3; Boston Scientific Corp, Natick,Mass), and Quantum (n � 1; Cordis Endovascular, Miami,Fla). Thirteen patients (41%) with persistent type II en-doleaks after EVAR exhibited enlargement in aneurysmdiameter (by 5 mm or more), whereas 19 (59%) exhibitedno significant change in aneurysm dimension or shrinkage.The median increase in aneurysm diameter in patients withsignificant aneurysm enlargement was 10 mm (range, 5-32mm), which occurred at a mean of 9.7 � 6.4 months afterEVAR. Of the 19 patients without aneurysm enlargement,6 (19 %) exhibited significant reduction in sac diameter by5 mm or more (median reduction, 13 mm; range, 5-20mm).
There were no significant differences in clinical charac-teristics and comorbidities between patients with persistenttype II endoleaks and aneurysm enlargement and thosewith stable or shrinking aneurysms (Table I). The medianfollow-up period was similar, 31 months (range, 12-62months) for enlarging aneurysms and 25 months (range,6-88 months) for stable or shrinking aneurysms (P � .12).
Initial aneurysm morphology and EVAR proce-dures. Proximal neck diameter and length were not signif-icantly different between the two groups (Table II). Themedian maximum aneurysm diameter was the same in both
groups (6 cm; range, 5-9 cm in patients with aneurysmenlargement and 4.8-10 cm in patients with stable aneu-rysms). The amount of thrombus and wall calcification wasalso comparable (Table II). The number of aortic branchvessels and patency of the inferior mesenteric artery beforeEVAR were not significantly different between the groups.
There was no significant difference with regards to thetype of endograft used for EVAR between the two groups.However, stratified analysis revealed that aneurysm en-largement was more frequent in patients with persistenttype II endoleaks who had undergone procedures withTalent and Vanguard devices (RR, 3.1; 95% CI, 1.5-6.1;P � .01).
Postoperative morphologic changes and endoleakcharacteristics. Patency of the inferior mesenteric artery aswell as origin and outflow sources of the endoleak were notsignificantly different between the two groups (Table II).The median number of vessels feeding the endoleak was 3(range, 2-5) in the enlarging aneurysm group and 2 (range,1-4) in the stable/shrinking aneurysm group (P � .02).Despite this difference, Cox regression analysis failed toidentify the number of vessels feeding the endoleak as asignificant predictor of aneurysm enlargement (RR, 1.7;95% CI, 0.9-3.2; P � .07).
The maximum diameter of the nidus of the endoleakwas significantly larger in patients with aneurysm expansionthan in those with stable or shrinking aneurysms (P �.001). The median maximum nidus diameter in the enlarg-ing aneurysm group was 23 mm (range, 13-40 mm),whereas in patients with stable/shrinking aneurysms it was8 mm (range, 5-25 mm). Cox regression analysis revealedthat the maximum diameter of the nidus was a significantpredictor for aneurysm enlargement (RR, 1.12; 95% CI,1.04-1.19; P � .001). ROC curve analysis was used todetermine the optimal cutoff point for the maximum nidusdiameter to predict aneurysm enlargement (Fig 2). At acutoff value of 15 mm, the sensitivity of the maximumnidus diameter to predict aneurysm enlargement was 92.3%(95% CI, 63.9%-98.7%) with a specificity of 84.2% (95% CI,60.4%-96.4%). A maximum nidus diameter greater than 15
Table I. Clinical characteristics of patients with persitenttype II endoleaks: enlarging aneurysm group, and stable/shinking aneurysm group
Enlarginganeurysm
(%) (n � 13)
Stable/shrinkinganeurysm
(%) (n � 19) P
Median age (y) 79 77 .51Male sex 11 (85) 14 (71) .39Comorbidities
Hypertension 7 (54) 12 (63) .44Tobacco abuse 2 (11) 8 (42) .11Anticoagulation 4 (31) 5 (26) .54Coronary artery disease 10 (77) 10 (53) .15Diabetes mellitus 1 (8) 5 (26) .19Hyperlipidemia 5 (39) 10 (43) .34

JOURNAL OF VASCULAR SURGERYJune 20041160 Timaran et al
mm was also a significant predictor of aneurysm enlarge-ment by Cox regression analysis (RR, 11.1; 95% CI, 1.4-85.8; P � .02).
The median pressure in the nidus was the same in bothgroups (100 mm Hg; range, 60-130 mm Hg in patientswith aneurysm enlargement and 50-130 mm Hg in patientswith stable aneurysms; P � not significant). However, it isimportant to clarify that only 5 of 19 patients with stable/shrinking aneurysms underwent angiography and sac pres-sure measurements, whereas 12 of 13 patients with aneu-rysm enlargement had these additional investigations.
Clinical outcome. For all patients with persistent typeII endoleaks, freedom from aneurysm rupture rates at 1, 3,and 5 years was 100%, 92%, and 92%, whereas freedomfrom conversion to open aneurysm repair rates was 100%,84%, and 75%, respectively (Kaplan-Meier). Twelve pa-tients with persistent type II endoleaks and aneurysm en-largement underwent transarterial and/or translumbar em-bolization on average 12 months after EVAR. Four patientswithout significant aneurysm enlargement also underwentcoil embolization. The results of these procedures are de-scribed in detail elsewhere.2 Briefly, technical success fortranslumbar embolization was 71% (10 of 14), whereas fortransfemoral embolization it was 38% (3 of 8). All patientswith successful transarterial or translumbar embolization,ie, with resolution of the endoleak, had stabilization orshrinkage of the aneurysm sac.
Three patients had persistent type II endoleaks afterfailed translumbar and/or translumbar embolization. Oneof these patients collapsed and died suddenly without aprecise diagnosis. A presumed aneurysm rupture was notconfirmed because a postmortem examination was notperformed. The other two patients with persistent type IIendoleaks after failed translumbar embolization had nofurther aneurysm enlargement. One aneurysm rupture,retroperitoneal and intraperitoneal, occurred in a patientwith no previous treatment for his persistent type II en-doleak. After EVAR, his aneurysm diameter was 6 cm,whereas the maximum diameter of the endoleak nidus was
Table II. Distribution, characteristics, and procedural factgroup and stable/shrinking aneurysm group
E
Aneurysm diameter (cm) (median [range])Proximal neck diameter (mm) (median [range])Proximal neck length (mm) (median [range])Patent inferior mesenteric arteryPatent hypogastric arteriesAneurysm thrombus (median)Endograft configuration
BifurcatedAortouni-iliac
Endoleak channelNidus maximum diameter (mm) (median [range])Aortic branch vessels (number [range])
*Mann-Whitney U test.
16 mm. The aneurysm remained stable for approximately24 months, when significant enlargement occurred (26mm during a period of 3 months). An open procedurewithout explantation of the endograft for aneurysm rupturewas necessary. When the aneurysm was opened, backbleed-ing from four lumbar arteries was observed, confirming thediagnosis of a type II endoleak. The branches were over-sewn from within the sac. The patient had an uneventfulrecovery.
Overall, long-term survival was 95% at 1 year, 61% at 3years, and 41% at 5 years. Nine patients died during follow-up. No deaths were caused by confirmed aneurysm rupturein this series, although there was one death from a sus-pected aneurysm rupture, which could not be confirmedbecause a postmortem examination was not performed.
DISCUSSION
The results of our study indicate that the maximumdiameter of the endoleak cavity or nidus was a significantpredictor for aneurysm enlargement in patients with persis-tent type II endoleaks after EVAR. Because it is currentlyrecognized that type II endoleaks are not always benign,particularly when associated with aneurysm expansion, ourfindings provide an important guide for monitoring anddetermining the need for additional interventions in pa-tients with persistent type II endoleaks. Moreover, our dataalso support a selective approach toward patients with typeII endoleaks that persist after 6 months in the setting of ananeurysm sac that is neither enlarging nor shrinking. Thesestable aneurysms might be safely observed when the maxi-mum diameter of the endoleak nidus is smaller than 15 mmbecause the likelihood of subsequent aneurysm enlarge-ment is low, even though there is no spontaneous throm-bosis of the endoleak cavity. Conversely, a maximum en-doleak nidus diameter greater than 15 mm is associatedwith a greater than 10-fold increased risk of aneurysmexpansion, thereby justifying a more aggressive surveillancewith imaging studies obtained at shorter intervals andearlier interventions.
f 32 EVAR procedures comparing enalrging aneurysm
ing aneurysmn � 13)
Stable/shrinkinganeurysm (n � 19) P
(5–9) 6 (4.8–10.0) .83(18–26) 23 (19–29) .34(12–40) 20 (8–40) .2953.8% 57.9% .5969.2% 84.2% .2828.2% 24.1% .42
84.6% 78.9% .9915.4% 21.1% .99
(13–40) 8 (5–25) �.001*(2–5) 2 (1–4) .02*
ors o
nlarg(
62224
233

JOURNAL OF VASCULAR SURGERYVolume 39, Number 6 Timaran et al 1161
Several treatment options are available to treat patientswith persistent type II endoleaks. Both transarterial andtranslumbar embolizations with coils and other thrombo-genic materials are the most widely used methods of inter-vention.2,9,18,19 The size of the endoleak nidus has beenrecognized as an important factor to determine the ap-proach for embolization.2 In a previous study we reportedour experience with the treatment of type II endoleaks.2,*Translumbar embolization was safe and effective in themajority of patients and therefore was considered our treat-ment of choice, particularly for endoleaks with a large nidusand multiple feeding vessels. The size of the endoleak nidusis, therefore, not only an important predictor for technicalsuccess with the translumbar approach but also a significantrisk factor for aneurysm expansion and the need for trans-lumbar embolization.
Coil embolization with translumbar approach failed intwo patients whose endoleak channels remained patent.Interestingly, the aneurysm sac of both patients has re-mained stable since translumbar embolization was per-formed. The size of the endoleak channel decreased in sizesignificantly after coil embolization, with obliteration of thenidus as demonstrated by follow-up CT scans. This obser-vation further supports the premise of a direct relationshipbetween the size of the endoleak channel and the likelihoodof aneurysm expansion. Moreover, if the same observationis consistently observed in other patients, it would suggestthat the need for complete obliteration of the endoleakcavity by using translumbar embolization, although desir-able, might not be necessary to prevent further aneurysmenlargement.
Although the clinical significance of the maximumdiameter of the endoleak cavity or nidus as a significantpredictor for aneurysm enlargement after EVAR was sup-ported by the analysis of our data with ROC curve and Coxregression models, several limitations and concerns shouldbe considered with regard to our results and their potentialapplicability. First, all 6 patients with aneurysm shrinkageand 8 patients with stable aneurysms did not undergodiagnostic angiography as part of the evaluation of theirendoleaks, which is considered by some authors essentialfor the proper classification of all endoleaks.2,9 These pa-tients usually had evidence of aneurysm shrinkage andtherefore were not candidates for any intervention. How-ever, axial thin-slice CT images and 3D CT reconstructionswere sufficient to characterize their endoleaks further.These studies helped to identify the etiology of the en-doleak, excluding attachment site leaks and leaks derivedfrom endograft defects, ie, endoleaks type I and III, respec-tively. Because it is currently accepted that type II en-doleaks associated with a shrinking aneurysm do not re-quire treatment, the need for contrast angiography in thesepatients is no longer justified. Another limitation thatmight be attributed to the lack of angiographic studies in all
*Ohki T, Gargiulo NJ III, Kurvers H, Cynamon J, Lipsitz EC, Suggs WD,et al. The value and limitations of translumbar and transfemoral access inthe management of type II endoleaks after endovascular abdominal aorticaneurysm repair. Submitted for publication.
patients is that the number of vessels feeding the endoleakcould be overestimated in the enlarging aneurysm groupbecause of the greater sensitivity of angiography and CTcombined, because most patients in the stable/shrinkinggroup only underwent CT scans.
The maximum diameter of the main cavity of theendoleak or nidus was measured on images obtained withthin-cut (1 to 3 mm) spiral CT scanning with delayedimaging by using calipers or CT imaging analysis softwarewith magnification and precise cursor placement. Althoughthe endoleak channel was often complex and irregular, themaximum diameter of the main endoleak cavity or niduscould be determined in all patients, particularly those asso-ciated with aneurysm enlargement. Aneurysm sac volumeand volume of the endoleak channel were determined inonly seven patients in our study. Because changes in aneu-rysm size occur in three dimensions, ideally both sac max-imum diameter and volume should be considered to definechanges in aneurysm size.16 It is likely that patients withsignificant aneurysm sac volume expansion could have rel-atively minor diameter shifts of less than 5 mm and thuswere included in the stable/shrinking aneurysm group.However, aneurysm sac diameter is still the most widelyused parameter to measure changes in aneurysm size and to
Fig 2. ROC curve analysis is usually obtained to assess the accu-racy of a continuous test variable to detect a specific outcomethrough the graphic representation of the tradeoffs between sen-sitivity and specificity for every possible cutoff value. In the currentstudy, ROC curve analysis revealed that at a cutoff value of 15 mm,the sensitivity of maximum nidus diameter to detect aneurysmenlargement was 92.3% (95% CI, 63.9%-98.7%) with a specificityof 84.2% (95% CI, 60.4%-96.4%). Moreover, the proximity of theROC curve (bold line) to the left upper corner of the graphindicates that the maximum diameter of the nidus is an accuratepredictor of aneurysm enlargement; the opposite occurs when thecurve comes closer to the 45-degree diagonal of the ROC space(dotted line), which indicates that a test or predictor is less accurate.

JOURNAL OF VASCULAR SURGERYJune 20041162 Timaran et al
assess the risk of rupture.16,20-22 Other methods of moni-toring changes in aneurysm size, including total aneurysmsac volume, have not been validated, and their use mightnot be cost-effective. Moreover, the role of endoleak vol-ume has not been previously assessed; therefore its clinicalsignificance is unknown. The current reporting standardsfor EVAR do not consider endoleak volume as an impor-tant characteristic of the magnitude of endoleaks.16 There-fore, its clinical utility remains to be elucidated. Our opin-ion is that endoleak volume would be essential to predictthe risk of aneurysm enlargement in patients with persistentendoleaks after translumbar embolization. In this particularsituation it is difficult to determine the maximum diameterof the nidus because this is partially obliterated with coilsand other thrombogenic materials.
Finally, our study included a small number of patients,which prevented us from obtaining further stratified andmultivariate analyses that are necessary to confirm the in-dependence of any predictor of aneurysm enlargement.Moreover, only a limited number of variables were analyzedto prevent overinterpretation of our data. Univariate anal-yses with different methods, however, confirmed the statis-tically significant association between the maximum diam-eter of the nidus and aneurysm enlargement. Despite thesemethodologic limitations, our study represents one of thelargest series of patients with persistent type II endoleaksfrom a single institution. Of importance, our experienceincluded long-term follow-up, which might account for theinstances of aneurysm enlargement and rupture seen in ourseries.
In conclusion, our data suggest that the maximumdiameter of the endoleak channel is an important predictorof aneurysm enlargement in patients with persistent type IIendoleaks. A diameter of the endoleak nidus greater than15 mm is particularly significant because it is associatedwith a greater than 10-fold increased risk of aneurysmexpansion, thereby indicating the need for more aggressivesurveillance and possibly earlier intervention.
REFERENCES
1. Veith FJ, Baum RA, Ohki T, Amor M, Adiseshiah M, Blankensteijn JD,et al. Nature and significance of endoleaks and endotension: summary ofopinions expressed at an international conference. J Vasc Surg 2002;35:1029-35.
2. Rhee SJ, Ohki T, Veith FJ, Kurvers H. Current status of management oftype II endoleaks after endovascular repair of abdominal aortic aneu-rysms. Ann Vasc Surg 2003;17:335-44.
3. Gorich J, Rilinger N, Sokiranski R, Kramer S, Schutz A, Sunder-Plassmann L, et al. Embolization of type II endoleaks fed by the inferiormesenteric artery: using the superior mesenteric artery approach. JEndovasc Ther 2000;7:297-301.
4. Politz JK, Newman VS, Stewart MT. Late abdominal aortic aneurysmrupture after AneuRx repair: a report of three cases. J Vasc Surg2000;31:599-606.
5. White GH, May J, Waugh RC, Yu W. Type I and Type II endoleaks: amore useful classification for reporting results of endoluminal AAArepair. J Endovasc Surg 1998;5:189-91.
6. Harris PL, Vallabhaneni SR, Desgranges P, Becquemin JP, van Mar-rewijk C, Laheij RJ. Incidence and risk factors of late rupture, conver-sion, and death after endovascular repair of infrarenal aortic aneurysms:the EUROSTAR experience—European Collaborators on Stent/grafttechniques for aortic aneurysm repair. J Vasc Surg 2000;32:739-49.
7. Chuter TA, Faruqi RM, Sawhney R, Reilly LM, Kerlan RB, Canto CJ,et al. Endoleak after endovascular repair of abdominal aortic aneurysm.J Vasc Surg 2001;34:98-105.
8. van Marrewijk C, Buth J, Harris PL, Norgren L, Nevelsteen A, WyattMG. Significance of endoleaks after endovascular repair of abdominalaortic aneurysms: The EUROSTAR experience. J Vasc Surg 2002;35:461-73.
9. Baum RA, Carpenter JP, Golden MA, Velazquez OC, Clark TW,Stavropoulos SW, et al. Treatment of type 2 endoleaks after endovascu-lar repair of abdominal aortic aneurysms: comparison of transarterial andtranslumbar techniques. J Vasc Surg 2002;35:23-9.
10. Zarins CK, White RA, Hodgson KJ, Schwarten D, Fogarty TJ. En-doleak as a predictor of outcome after endovascular aneurysm repair:AneuRx multicenter clinical trial. J Vasc Surg 2000;32:90-107.
11. Baum RA, Carpenter JP, Cope C, Golden MA, Velazquez OC, NeschisDG, et al. Aneurysm sac pressure measurements after endovascularrepair of abdominal aortic aneurysms. J Vasc Surg 2001;33:32-41.
12. Hinchliffe RJ, Singh-Ranger R, Davidson IR, Hopkinson BR. Ruptureof an abdominal aortic aneurysm secondary to type II endoleak. Eur JVasc Endovasc Surg 2001;22:563-5.
13. Bade MA, Ohki T, Cynamon J, Veith FJ. Hypogastric artery aneurysmrupture after endovascular graft exclusion with shrinkage of the aneu-rysm: significance of endotension from a “virtual,” or thrombosed typeII endoleak. J Vasc Surg 2001;33:1271-4.
14. Bernhard VM, Mitchell RS, Matsumura JS, Brewster DC, Decker M,Lamparello P, et al. Ruptured abdominal aortic aneurysm after endo-vascular repair. J Vasc Surg 2002;35:1155-62.
15. Chaikof EL, Fillinger MF, Matsumura JS, Rutherford RB, White GH,Blankensteijn JD, et al. Identifying and grading factors that modify theoutcome of endovascular aortic aneurysm repair. J Vasc Surg 2002;35:1061-6.
16. Chaikof EL, Blankensteijn JD, Harris PL, White GH, Zarins CK,Bernhard VM, et al. Reporting standards for endovascular aortic aneu-rysm repair. J Vasc Surg 2002;35:1048-60.
17. Cayne NC, Veith FJ, Lipsitz EC, Ohki T, Mehta M, Gargiulo NJ III, etal. Variability of maximal aortic aneurysm diameter measurements onCT scan: significance and methods to minimize. J Vasc Surg. In press2004.
18. Solis MM, Ayerdi J, Babcock GA, Parra JR, McLafferty RB, GruneiroLA, et al. Mechanism of failure in the treatment of type II endoleak withpercutaneous coil embolization. J Vasc Surg 2002;36:485-91.
19. Kasirajan K, Matteson B, Marek JM, Langsfeld M. Technique andresults of transfemoral superselective coil embolization of type II lum-bar endoleak. J Vasc Surg 2003;38:61-6.
20. Cronenwett JL, Murphy TF, Zelenock GB, Whitehouse WM Jr, Lin-denauer SM, Graham LM, et al. Actuarial analysis of variables associatedwith rupture of small abdominal aortic aneurysms. Surgery 1985;98:472-83.
21. Brown PM, Pattenden R, Vernooy C, Zelt DT, Gutelius JR. Selectivemanagement of abdominal aortic aneurysms in a prospective measure-ment program. J Vasc Surg 1996;23:213-20.
22. Brown PM, Zelt DT, Sobolev B. The risk of rupture in untreatedaneurysms: the impact of size, gender, and expansion rate. J Vasc Surg2003;37:280-4.
Submitted Sep 18, 2003; accepted Dec 28, 2003.Available online Apr 2, 2003.