
Comparative Study of Deproteinized Bovine Bone Mineral and ...
9
The International Journal of Periodontics & Restorative Dentistry © 2021 BY QUINTESSENCE PUBLISHING CO, INC. PRINTING OF THIS DOCUMENT IS RESTRICTED TO PERSONAL USE ONLY. NO PART MAY BE REPRODUCED OR TRANSMITTED IN ANY FORM WITHOUT WRITTEN PERMISSION FROM THE PUBLISHER. © 2021 BY QUINTESSENCE PUBLISHING CO, INC. PRINTING OF THIS DOCUMENT IS RESTRICTED TO PERSONAL USE ONLY. NO PART MAY BE REPRODUCED OR TRANSMITTED IN ANY FORM WITHOUT WRITTEN PERMISSION FROM THE PUBLISHER.
-
Upload
khangminh22 -
Category
Documents
-
view
4 -
download
0
Transcript of Comparative Study of Deproteinized Bovine Bone Mineral and ...
The International Journal of Periodontics & Restorative Dentistry
© 2021 BY QUINTESSENCE PUBLISHING CO, INC. PRINTING OF THIS DOCUMENT IS RESTRICTED TO PERSONAL USE ONLY. NO PART MAY BE REPRODUCED OR TRANSMITTED IN ANY FORM WITHOUT WRITTEN PERMISSION FROM THE PUBLISHER. © 2021 BY QUINTESSENCE PUBLISHING CO, INC. PRINTING OF THIS DOCUMENT IS RESTRICTED TO PERSONAL USE ONLY. NO PART MAY BE REPRODUCED OR TRANSMITTED IN ANY FORM WITHOUT WRITTEN PERMISSION FROM THE PUBLISHER.

579
Volume 41, Number 4, 2021
Submitted September 4, 2019; accepted October 23, 2019. ©2021 by Quintessence Publishing Co Inc.
The aim of this histomorphometric study was to compare the outcome of sinus floor augmentation procedures using bovine bone mineral and a xenograft enriched with gelatin and a polymer. In 20 patients a single sinus floor elevation procedure with a lateral window approach was performed. In half of the patients, sinuses were grafted with a deproteinized bovine bone mineral—DBBM (control group)—while in the remaining 10, a xenograft enriched by polymer and gelatin—NBS (test group)—was applied. In the DBBM group, histomorphometric analysis revealed 23.14 ± 10.62% of lamellar bone, 19.43% ± 9.18% of woven bone, 23.35% ± 6.04% of osteoid, 17.16% ± 6.13% of biomaterial particles, and 16.93% ± 9.78% of medullary spaces. In the NBS group, histomorphometric analysis found 39.64% ± 12.02% of lamellar bone, 16.28% ± 7.75% of woven bone, 17.51% ± 4.87% of osteoid, 12.72% ± 5.36% of biomaterial particles, and 13.84% ± 6.53% of medullary spaces. Differences between groups for proportion of lamellar bone (P = .004) and osteoid (P = .0287) were statistically significant. Inflammatory infiltration was appreciated only in the NBS group. The enriched xenograft showed a statistically significant higher proportion of lamellar bone and osteoid; however, this was accompanied by an accentuated inflammatory infiltrate. Int J Periodontics Restorative Dent 2021;41:579–586. doi: 10.11607/prd.4630
Comparative Study of Deproteinized Bovine Bone Mineral and Bovine Bone Mineral Enriched with a Polymer and Gelatin in Maxillary Sinus Floor Elevation Procedures
1 Department of Biomedical, Surgical, and Dental Sciences, Università degli Studi di Milano, Milan, Italy; IRCCS Istituto Ortopedico Galeazzi, Milan, Italy.
2 Department of Periodontology & Dental Implantology, School of Dental Medicine, University of Tel Aviv, Tel Aviv-Yafo, Israel.
3 Department of Biomedical, Surgical, and Dental Sciences, Università degli Studi di Milano, Milan, Italy.
4 Department of Biomedical, Surgical, and Dental Sciences, Università degli Studi di Milano, Milan, Italy; IRCCS Istituto Ortopedico Galeazzi, Milan, Italy; Department of Oral Surgery, Institute of Dentistry, I. M. Sechenov First Moscow State Medical University, Moscow, Russia.
Correspondence to: Dr Stefano Corbella, Via R. Galeazzi 4, 20161, Milan, Italy. Email: [email protected]
Following tooth extraction, maxillary bone atrophy due to loss of function is usually seen together with micro-trauma during extraction.1 In the posterior maxilla, sinus pneumatiza-tion is also common.2
Implant-supported rehabilitation is a predictable treatment alternative to restore missing teeth. However, implant insertion requires adequate bone volume.3 Short dental implants may be considered a viable treat-ment option for cases with at least 4 to 5 mm of residual bone.4 Yet, in many cases, the available bone height under the sinus floor does not allow for implant placement, requir-ing bone augmentation procedures to overcome this limitation.5–7
Maxillary sinus floor elevation (MSFE) is intended to augment the bone volume in the latero- posterior maxillary areas.8,9 Depend-ing on the amount of residual bone and the desired outcome, either a transcrestal or a lateral opened ap-proach may be applied.10,11 Several systematic reviews in the literature have reported favorable outcomes in bone volume gain12,13 and implant survival rates11,14,15 after MSFE proce-dures, both in short- and long-term evaluations.
Among the grafting biomateri-als in MSFE procedures, autogenous bone has been considered the gold standard for years.15 Nonetheless, bone substitutes have been shown
Silvio Taschieri, MD, DDS1/Ofer Moses, DMD2 Claudia Dellavia, DDS3/Elena Canciani, PhD, MBiotech3
Carlos Nemcovsky, DMD2 Luca Francetti, MD, DDS1 Stefano Corbella, PhD, DDS4
© 2021 BY QUINTESSENCE PUBLISHING CO, INC. PRINTING OF THIS DOCUMENT IS RESTRICTED TO PERSONAL USE ONLY. NO PART MAY BE REPRODUCED OR TRANSMITTED IN ANY FORM WITHOUT WRITTEN PERMISSION FROM THE PUBLISHER. © 2021 BY QUINTESSENCE PUBLISHING CO, INC. PRINTING OF THIS DOCUMENT IS RESTRICTED TO PERSONAL USE ONLY. NO PART MAY BE REPRODUCED OR TRANSMITTED IN ANY FORM WITHOUT WRITTEN PERMISSION FROM THE PUBLISHER.

The International Journal of Periodontics & Restorative Dentistry
580
to be as effective as autogenous bone, even in extremely atrophic cases.3 Moreover, different materi-als could have different resorption times, thus optimizing the character-istics of the bone graft to the needs of the particular clinical case.16 Maxil-lary sinus floor augmentation by a lat-eral approach together with implant placement without applying any bio-material is feasible, as blood clot sta-bility could be sufficient to preserve a secluded space for obtaining bone regeneration.17,18 However, there are several anatomical situations in which this approach cannot be applied.19
Two systematic reviews evaluat-ed the histomorphometric results of new bone formation in MSFE proce-dures with different biomaterials,20,21 reporting no clear advantage of any graft. More recently, new bone sub-stitutes were proposed with a hybrid formulation, adding polymers or oth-er substances to xenografts in order to enhance the bone augmentation procedures.22 Such materials were hypothesized to enhance new bone formation by some authors reporting data on a small sample of subjects.23
The aim of the present com-parative prospective study was to evaluate whether one new bone substitute with adjunctive polymers could lead to higher new bone for-mation as compared to deprotein-ized bovine bone mineral (DBBM) when used in MSFE.
Materials and Methods
The study protocol was approved by the Scientific Board of the IRCCS Istituto Ortopedico Galeazzi in Mi-
lan, Italy, in 2018 and was included in one research project approved by the Italian Ministry of Health. All study phases were performed in accordance with the Declaration of Helsinki,24 and all patients signed an informed consent form before be-ginning the study.
This prospective, nonrandomized clinical study comprised 20 patients in which 20 MSFE procedures were per-formed (one procedure per patient).
Inclusion Criteria
Inclusion criteria were as follows: (1) American Association of Anes-thesiologists classification of ASA I or ASA II; (2) single or multiple eden-tulism in the latero-posterior area of the maxilla (premolars/molars); (3) < 5 mm of residual bone height; (4) no previous regenerative pro-cedures in the site of intervention; (5) nonsmokers, former smokers, and those smoking fewer than five cigarettes a day; and (6) no sinus pa-thology that could affect treatment outcome.
Allocation
Ten sinuses (control group) were grafted with DBBM while the other 10 (test group) were grafted with a xenograft enriched by polymer and gelatin (NBS).
Interventions
The same experienced surgeon (S.T.) performed all surgical interven-
tions. The DBBM (Bio-Oss, Geistlich) grain size was 0.25 to 1 mm. The NBS graft material was composed of bovine bone matrix and a poly-mer (L-lactic-co-e-caprolactone) in a gelatin scaffold with a grain size of 0.25 to 1 mm (SmartBone, Indust-rie Biomediche Insubri). Deciding the graft type for each patient was established by alternate allocating of subjects to the control group or the test group. All patients followed preoperative diagnostic CBCT scan-ning. The surgical intervention was performed following a standard procedure.
Briefly, after local anesthesia (with articaine 4% and adrenaline 1:100,000), a trapezoidal flap was elevated to access the sinus, which was identified by careful preopera-tive evaluation of the CBCT scans. Access was created by eroding the lateral bone wall with a round diamond bur mounted in a low-speed handpiece connected to physiodispenser (American Eagle Instruments), taking care to avoid injuring the sinus membrane. De-tachment of the membrane was carefully performed, and the cre-ated cavity was filled with the bio-material. After finalizing the sinus grafting, the access window was covered with a resorbable collagen membrane (GRAFT collagen mem-brane, Alpha-Bio Tec). The flap was repositioned and sutured with in-terrupted sutures (Ethilon, Ethicon, Johnson & Johnson). Patients were instructed to avoid any activity that would abruptly raise or lower pres-sure in the sinus cavity for 3 weeks after surgery, such as sneezing with their mouth closed, blowing their
© 2021 BY QUINTESSENCE PUBLISHING CO, INC. PRINTING OF THIS DOCUMENT IS RESTRICTED TO PERSONAL USE ONLY. NO PART MAY BE REPRODUCED OR TRANSMITTED IN ANY FORM WITHOUT WRITTEN PERMISSION FROM THE PUBLISHER. © 2021 BY QUINTESSENCE PUBLISHING CO, INC. PRINTING OF THIS DOCUMENT IS RESTRICTED TO PERSONAL USE ONLY. NO PART MAY BE REPRODUCED OR TRANSMITTED IN ANY FORM WITHOUT WRITTEN PERMISSION FROM THE PUBLISHER.

581
Volume 41, Number 4, 2021
nose, traveling on an airplane, suck-ing through a straw, diving, blowing balloons, or playing a wind instru-ment. Furthermore, patients were instructed to avoid vigorous mouth rinsing, hard and hot foods, strenu-ous exertion, smoking, and touch-ing the gums for at least 3 days after surgery. Patients were instructed to gently rinse with a 0.2% chlorhexi-dine digluconate solution twice a day for 10 days. All patients were prescribed nonsteroidal analgesics to be self-administered as needed. Antibiotic therapy with amoxicillin (1 g, twice a day for 6 days) was pre-scribed to all patients.
Six months after the MSFE, ra-diographic and clinical evaluations were performed, and implants were placed in the previously augmented areas. At this time, bone core sam-ples were retrieved with a 3.2-mm–diameter trephine bur in the direc-tion of implant site preparation.
Histologic Analysis
Retrieved tissue samples were fixed in 40% ethanol solution for 48 hours at 4ºC and then dehydrated with ethanol, propanol, and xylene for 48 hours. After dehydration, samples were infiltrated with a mixture of ethanol and acrylic resin in decreas-ing ratios (3 alcohol:1 resin, 1:1, 1:3, pure resin), and finally embedded in pure methyl-methacrylate resin (Technovit 7200 VLC, Kulzer). Using a mounted diamond blade, the vials containing the embedded samples were cut longitudinally in a coronal- apical direction and grinded to achieve 70-µm thickness. Two sec-
tions from each biopsy sample were mounted and then stained with tolu-idine blue on a hot plate. After dry-ing, each slide was analyzed under light microscope at different magnifi-cations (×2, ×4, ×10, ×20, and ×40). The highly mineralized matrices showed a brown color (biomaterial with high degree of mineralization), while the less-mineralized matrix showed a purple/dark blue color (os-teoid, woven bone, and polymer); in all sections, the connective tissue was stained light blue. Each sample was digitally recorded for histomor-phometric analysis (tissue fractions).25 The histomorphometry was per-formed on the overall image of the most representative section of each biopsy sample. ImageJ software (National Institutes of Health) was used for outcome measures.
Outcome Measures
The primary outcome was the new bone volume proportion (NBV). The secondary outcomes were: (1) bone substitute volume (BSV); (2) propor-tion of connective tissue volume (CTV) in the specimen; (3) occur-rence of complications; and (4) alve-olar bone height reduction (ABHR) available at the moment of implant placement, measured by compar-ing periapical radiographs immedi-ately after MSFE and before implant placement.
Statistical Analysis
Descriptive statistics provided mean and SDs for continuous variables.
Shapiro-Wilk test was applied to test normality of distributions of primary (NBV) and secondary (BSV and CTV) outcome variables. Differ-ences between groups for normally distributed variables were tested by means of Student t test. Statistical significance was established at P < .05.
Results
Demographic data are presented in Table 1. No surgical complications occurred. Results of the histomor-phometric analysis are presented in Table 2.
The qualitative evaluation of the sections included graft integration, the presence of osteoclast cells, and coating polymer degradation (Figs 1 and 2). In both groups, the grafted bone substitute appeared surrounded by newly formed bone, in close contact to the biomaterial, and was slightly mineralized (Figs 3 and 4).
In the DBBM group, multinucle-ated cells (probably osteoclasts) were clearly identified in close contact at the interface and between the new bone and the DBBM particles (Fig 5). In the NBS group, macrophages were detected both at the interface between bovine bone granules and newly formed bone but also in close contact with the graft (Fig 6).
In two samples in the NBS group, the polymer-coated mate-rial appeared to be surrounded by a dense layer, rich in cells (inflam-matory cells). In both groups, good vascularization of the newly formed tissues could be observed (Fig 7).
© 2021 BY QUINTESSENCE PUBLISHING CO, INC. PRINTING OF THIS DOCUMENT IS RESTRICTED TO PERSONAL USE ONLY. NO PART MAY BE REPRODUCED OR TRANSMITTED IN ANY FORM WITHOUT WRITTEN PERMISSION FROM THE PUBLISHER. © 2021 BY QUINTESSENCE PUBLISHING CO, INC. PRINTING OF THIS DOCUMENT IS RESTRICTED TO PERSONAL USE ONLY. NO PART MAY BE REPRODUCED OR TRANSMITTED IN ANY FORM WITHOUT WRITTEN PERMISSION FROM THE PUBLISHER.
The International Journal of Periodontics & Restorative Dentistry
582
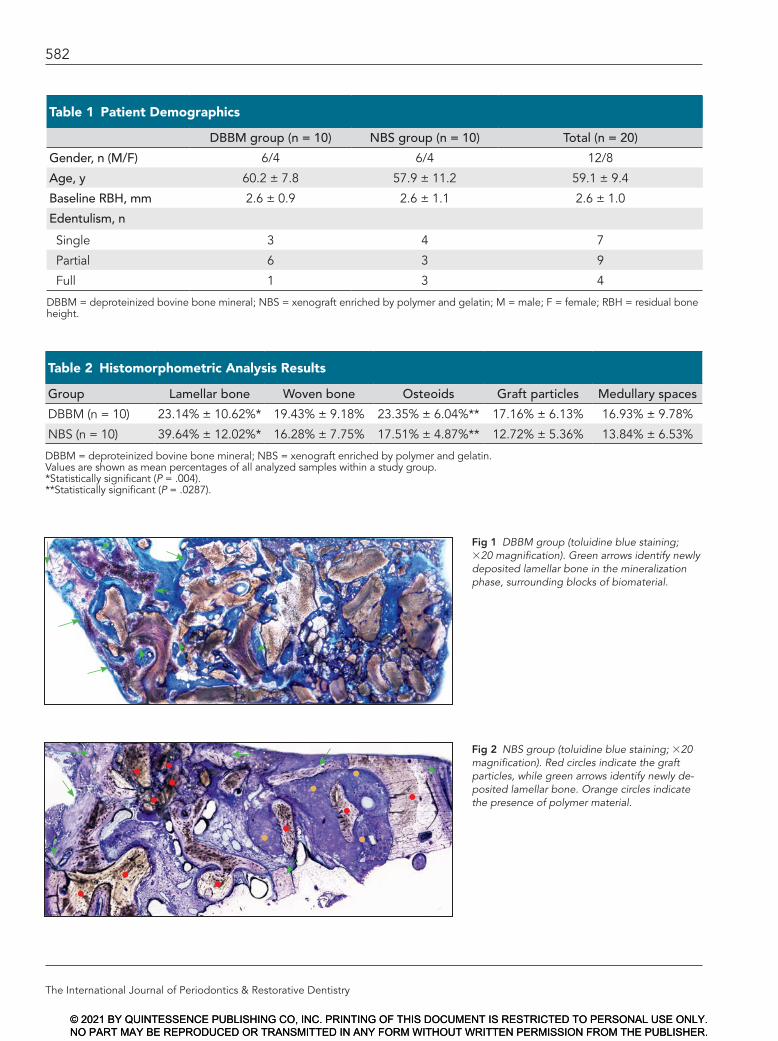
Table 2 Histomorphometric Analysis Results
Group Lamellar bone Woven bone Osteoids Graft particles Medullary spaces
DBBM (n = 10) 23.14% ± 10.62%* 19.43% ± 9.18% 23.35% ± 6.04%** 17.16% ± 6.13% 16.93% ± 9.78%
NBS (n = 10) 39.64% ± 12.02%* 16.28% ± 7.75% 17.51% ± 4.87%** 12.72% ± 5.36% 13.84% ± 6.53%
DBBM = deproteinized bovine bone mineral; NBS = xenograft enriched by polymer and gelatin.Values are shown as mean percentages of all analyzed samples within a study group. *Statistically significant (P = .004).**Statistically significant (P = .0287).
Table 1 Patient Demographics
DBBM group (n = 10) NBS group (n = 10) Total (n = 20)
Gender, n (M/F) 6/4 6/4 12/8
Age, y 60.2 ± 7.8 57.9 ± 11.2 59.1 ± 9.4
Baseline RBH, mm 2.6 ± 0.9 2.6 ± 1.1 2.6 ± 1.0
Edentulism, n
Single 3 4 7
Partial 6 3 9
Full 1 3 4
DBBM = deproteinized bovine bone mineral; NBS = xenograft enriched by polymer and gelatin; M = male; F = female; RBH = residual bone height.
Fig 1 DBBM group (toluidine blue staining; ×20 magnification). Green arrows identify newly deposited lamellar bone in the mineralization phase, surrounding blocks of biomaterial.
Fig 2 NBS group (toluidine blue staining; ×20 magnification). Red circles indicate the graft particles, while green arrows identify newly de-posited lamellar bone. Orange circles indicate the presence of polymer material.
© 2021 BY QUINTESSENCE PUBLISHING CO, INC. PRINTING OF THIS DOCUMENT IS RESTRICTED TO PERSONAL USE ONLY. NO PART MAY BE REPRODUCED OR TRANSMITTED IN ANY FORM WITHOUT WRITTEN PERMISSION FROM THE PUBLISHER. © 2021 BY QUINTESSENCE PUBLISHING CO, INC. PRINTING OF THIS DOCUMENT IS RESTRICTED TO PERSONAL USE ONLY. NO PART MAY BE REPRODUCED OR TRANSMITTED IN ANY FORM WITHOUT WRITTEN PERMISSION FROM THE PUBLISHER.
583
Volume 41, Number 4, 2021
In the DBBM group, the inflam-matory infiltrate was only a sporadic event where few inflammatory cells of small size were detected, pre-dominantly lymphocytes and granu-locytes. By contrast, infiltrates in the NBS group were observed in 2 of the 10 specimens.
Remodeling the graft after MSFE caused an ABHR of 2.7 ± 0.9 mm in the NBS group and 1.2 ± 0.5 mm in the DBBM group, which was statistically significant (P < .05).
Discussion
The present study revealed that the percentage of lamellar, mature bone was higher in the test group.
The main limitation of the study was its design, specifically the non-randomized allocation and sample
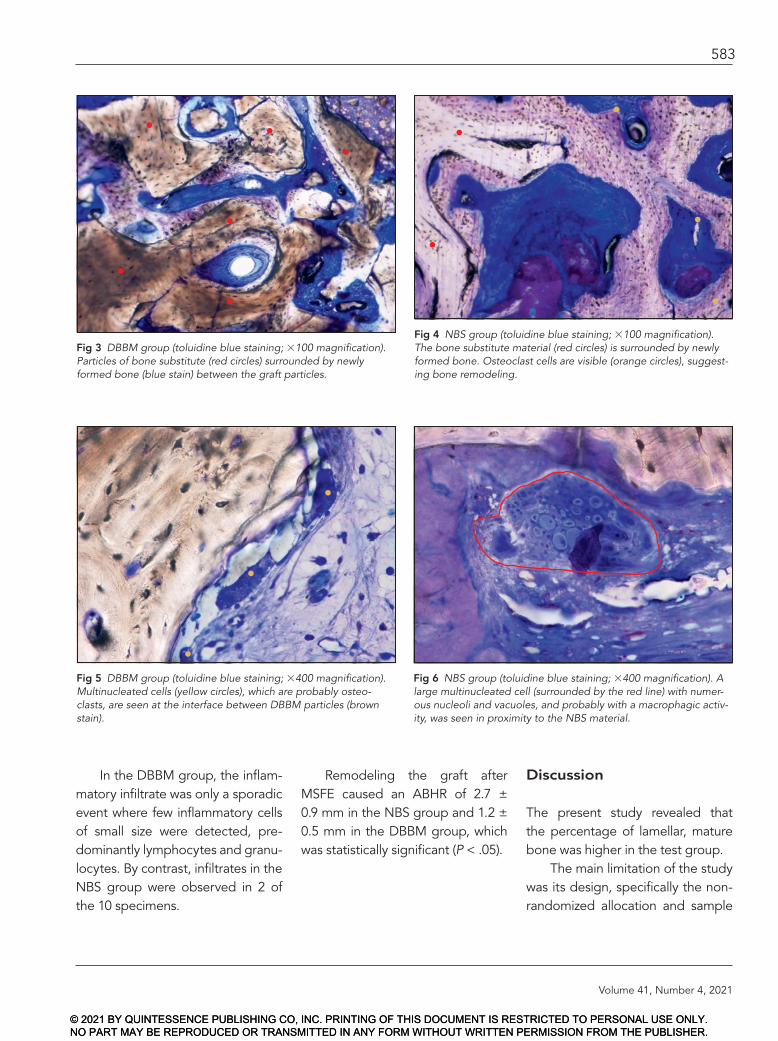
Fig 3 DBBM group (toluidine blue staining; ×100 magnification). Particles of bone substitute (red circles) surrounded by newly formed bone (blue stain) between the graft particles.
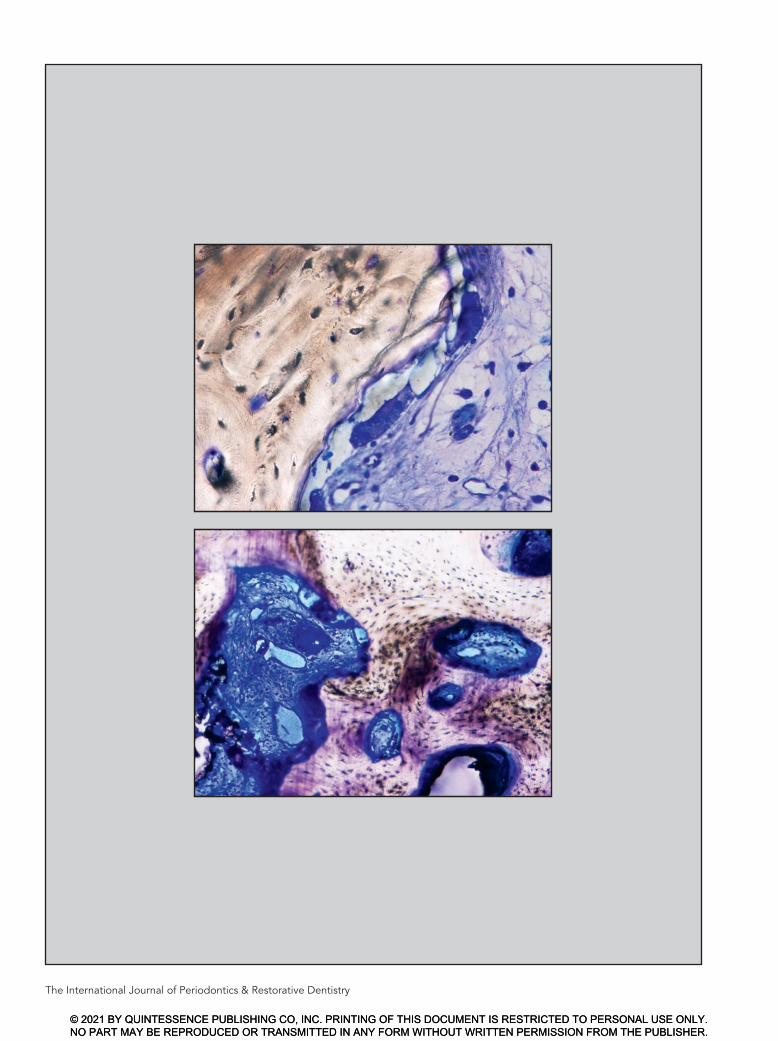
Fig 5 DBBM group (toluidine blue staining; ×400 magnification). Multinucleated cells (yellow circles), which are probably osteo-clasts, are seen at the interface between DBBM particles (brown stain).
Fig 6 NBS group (toluidine blue staining; ×400 magnification). A large multinucleated cell (surrounded by the red line) with numer-ous nucleoli and vacuoles, and probably with a macrophagic activ-ity, was seen in proximity to the NBS material.
Fig 4 NBS group (toluidine blue staining; ×100 magnification). The bone substitute material (red circles) is surrounded by newly formed bone. Osteoclast cells are visible (orange circles), suggest-ing bone remodeling.
© 2021 BY QUINTESSENCE PUBLISHING CO, INC. PRINTING OF THIS DOCUMENT IS RESTRICTED TO PERSONAL USE ONLY. NO PART MAY BE REPRODUCED OR TRANSMITTED IN ANY FORM WITHOUT WRITTEN PERMISSION FROM THE PUBLISHER. © 2021 BY QUINTESSENCE PUBLISHING CO, INC. PRINTING OF THIS DOCUMENT IS RESTRICTED TO PERSONAL USE ONLY. NO PART MAY BE REPRODUCED OR TRANSMITTED IN ANY FORM WITHOUT WRITTEN PERMISSION FROM THE PUBLISHER.

The International Journal of Periodontics & Restorative Dentistry
584
size. However, demographic char-acteristics of both groups were similar at baseline, both without any systemic disease or condition that might have affected the outcomes. With regard to sample size, even though a sample size calculation was not performed before the study began, the calculated power of the included sample (after collecting data) was 0.83, thus justifying the sample size. Finally, heterogeneity between the distribution of resto-ration type between groups was found. It was assumed that, despite such difference, the influence on histomorphometric outcomes could be negligible.
The aim of the study was to evaluate the histologic and histo-morphometric outcomes, not the clinical and radiographic extent of bone augmentation. As previously mentioned, no complications were recorded, and all implants were placed as planned.
A systematic review reported that, after 6 months of healing fol-lowing MSFE procedures with
DBBM, averages of 28.3% of mature bone and 27.8% of residual bio-material could be observed.20 The results of the present study were comparable to another systematic review that evaluated histomorpho-metric outcomes of different bioma-terials in MSFE procedures.21 The significant proportion of immature vital bone in close contact with the biomaterial particles and the mature bone indicated a high degree of in-tegration.
Whilst reports concerning the use of DBBM alone or in combina-tion with other bone substitutes are extensive, few studies have evalu-ated the biomaterial used in the NBS group (SmartBone) in oral and maxillofacial surgery.23,26–28 One study evaluated the outcomes of NBS used as grafting material in five cases with MSFE procedures.23 Contrary to the present findings, that study reported that a major-ity of the bone substitute material was not detectable 6 months after implantation.23 Moreover, the au-thors stated that the biomaterial
enhanced new bone formation, but this was not observed in the present study. Additionally, the present find-ings cannot confirm the reported histomorphometric results of other studies23 with 6-month follow-ups, maybe due to the larger sample size and the different methodology adopted in the present research. Other reports concerning the use of SmartBone biomaterial dealt with customized grafts in maxillofacial surgery for calvarial26 and zygomatic reconstructions.27 Although good outcomes were reported in those case reports, they cannot be gener-alized.
The present study found dif-ferences in the amount of lamellar bone and osteoids between the two groups; it can be hypothesized that such results are related to the different osteogenic properties be-tween NBS and DBBM. Because the osteoconductive properties of polymeric materials have not been clearly demonstrated,22 one can as-sume that this may have influenced the histomorphometric results.
Fig 7 Blood vessels (orange arrows) could be observed both (a) DBBM and (b) NBS groups (toluidine blue staining; ×100 magnification). Orange circles indicate sites where the polymer is in contact with the new bone matrix.
a b
© 2021 BY QUINTESSENCE PUBLISHING CO, INC. PRINTING OF THIS DOCUMENT IS RESTRICTED TO PERSONAL USE ONLY. NO PART MAY BE REPRODUCED OR TRANSMITTED IN ANY FORM WITHOUT WRITTEN PERMISSION FROM THE PUBLISHER. © 2021 BY QUINTESSENCE PUBLISHING CO, INC. PRINTING OF THIS DOCUMENT IS RESTRICTED TO PERSONAL USE ONLY. NO PART MAY BE REPRODUCED OR TRANSMITTED IN ANY FORM WITHOUT WRITTEN PERMISSION FROM THE PUBLISHER.

585
Volume 41, Number 4, 2021
Another important issue to be considered is the presence of an inflammatory infiltrate surrounding the polymer molecules, seen in two samples in the NBS group. Such findings should be further evalu-ated to elucidate the frequency of occurrence and whether it is part of the material’s integration/resorption process or related to a foreign-body reaction to the polymer.
Conclusions
Despite the limitations of the pres-ent study and although the propor-tion of lamellar bone was statisti-cally significantly higher in the NBS group than the DBBM group, it is still not clear which bone substi-tute performed better in the overall evaluation. The histomorphometric analysis showed that integration of the biomaterials was not complete 6 months after intervention and that residual polymer was found in the samples, sporadically associated with an inflammatory infiltrate.
Acknowledgments
The authors declare no conflicts of interest.
References
1. Araújo MG, Lindhe J. Ridge alterations following tooth extraction with and without flap elevation: An experimental study in the dog. Clin Oral Implants Res 2009;20:545–549.
2. Wagner W, Wiltfang J, Pistner H, et al. Bone formation with a biphasic calcium phosphate combined with fibrin sealant in maxillary sinus floor elevation for de-layed dental implant. Clin Oral Implants Res 2012;23:1112–1117.
3. Esposito M, Grusovin MG, Polyzos IP, Felice P, Worthington HV. Interventions for replacing missing teeth: Dental im-plants in fresh extraction sockets (imme-diate, immediate-delayed and delayed implants). The Cochrane Database Syst Rev 2010:CD005968.
4. Nielsen HB, Schou S, Isidor F, Christensen AE, Starch-Jensen T. Short implants (≤ 8 mm) compared to stan-dard length implants (> 8 mm) in con-junction with maxillary sinus floor aug-mentation: A systematic review and meta-analysis. Int J Oral Maxillofac Surg 2019;48:239–249.
5. Aghaloo TL, Misch C, Lin GH, Iacono VJ, Wang HL. Bone augmentation of the edentulous maxilla for implant place-ment: A systematic review. Int J Oral Maxillofac Implants 2016;31(suppl):s19–s30.
6. Chiapasco M, Casentini P, Zaniboni M. Bone augmentation procedures in im-plant dentistry. Int J Oral Maxillofac Im-plants 2009;24(suppl):237–259.
7. Friberg B. Bone augmentation for single tooth implants: A review of the litera-ture. Eur J Oral Implantol 2016;9(suppl 1):s123–s134.
8. Boyne PJ, James RA. Grafting of the maxillary sinus floor with autog-enous marrow and bone. J Oral Surg 1980;38:613–616.
9. Tatum H Jr. Maxillary and sinus implant reconstructions. Dent Clin North Am 1986;30:207–229.
10. Del Fabbro M, Corbella S, Weinstein T, Ceresoli V, Taschieri S. Implant survival rates after osteotome-mediated max-illary sinus augmentation: A system-atic review. Clin Implant Dent Relat Res 2012;14(suppl 1):e159–e168.
11. Tan WC, Lang NP, Zwahlen M, Pjetursson BE. A systematic review of the success of sinus floor elevation and survival of implants inserted in combination with sinus floor elevation. Part II: Transal-veolar technique. J Clin Periodontol 2008;35:241–254.
12. Temmerman A, Van Dessel J, Cortellini S, Jacobs R, Teughels W, Quirynen M. Volumetric changes of grafted volumes and the Schneiderian membrane after transcrestal and lateral sinus floor eleva-tion procedures: A clinical, pilot study. J Clin Periodontol 2017;44:660–671.
13. Younes F, Cosyn J, De Bruyckere T, Cleymaet R, Eghbali A. A 2-year pro-spective case series on volumetric changes, PROMs, and clinical outcomes following sinus floor elevation using de-proteinized bovine bone mineral as fill-ing material. Clin Implant Dent Relat Res 2019;21:301–309.
14. Corbella S, Taschieri S, Del Fabbro M. Long-term outcomes for the treatment of atrophic posterior maxilla: A system-atic review of literature. Clin Implant Dent Relat Res 2015;17:120–132
15. Nkenke E, Stelzle F. Clinical outcomes of sinus floor augmentation for implant placement using autogenous bone or bone substitutes: A systematic review. Clin Oral Implants Res 2009;20(suppl 4):124–133.
16. Bouler JM, Pilet P, Gauthier O, Verron E. Biphasic calcium phosphate ceram-ics for bone reconstruction: A review of biological response. Acta Biomater 2017;53:1–12.
17. Duan DH, Fu JH, Qi W, Du Y, Pan J, Wang HL. Graft-free maxillary si-nus floor elevation: A systematic re-view and meta-analysis. J Periodontol 2017;88:550–564.
18. Starch-Jensen T, Schou S. Maxillary si-nus membrane elevation with simulta-neous installation of implants without the use of a graft material: A systematic review. Implant Dent 2017;26:621–633.
19. Lundgren S, Cricchio G, Hallman M, Jungner M, Rasmusson L, Sennerby L. Sinus floor elevation procedures to en-able implant placement and integra-tion: Techniques, biological aspects and clinical outcomes. Periodontol 2000 2017;73:103–120.
20. Corbella S, Taschieri S, Weinstein R, Del Fabbro M. Histomorphometric out-comes after lateral sinus floor elevation procedure: A systematic review of the literature and meta-analysis. Clin Oral Implants Res 2016;27:1106–1122.
21. Danesh-Sani SA, Engebretson SP, Janal MN. Histomorphometric results of dif-ferent grafting materials and effect of healing time on bone maturation after sinus floor augmentation: A systematic review and meta-analysis. J Periodontal Res 2017;52:301–312.
22. Sanz M, Dahlin C, Apatzidou D, et al. Biomaterials and regenerative tech-nologies used in bone regeneration in the craniomaxillofacial region: Consen-sus report of group 2 of the 15th Euro-pean Workshop on Periodontology on Bone Regeneration. J Clin Periodontol 2019;46(suppl 21):82–91.
© 2021 BY QUINTESSENCE PUBLISHING CO, INC. PRINTING OF THIS DOCUMENT IS RESTRICTED TO PERSONAL USE ONLY. NO PART MAY BE REPRODUCED OR TRANSMITTED IN ANY FORM WITHOUT WRITTEN PERMISSION FROM THE PUBLISHER. © 2021 BY QUINTESSENCE PUBLISHING CO, INC. PRINTING OF THIS DOCUMENT IS RESTRICTED TO PERSONAL USE ONLY. NO PART MAY BE REPRODUCED OR TRANSMITTED IN ANY FORM WITHOUT WRITTEN PERMISSION FROM THE PUBLISHER.

The International Journal of Periodontics & Restorative Dentistry
586
23. D’Alessandro D, Perale G, Milazzo M, et al. Bovine bone matrix/poly(l-lactic-co-epsilon-caprolactone)/gelatin hy-brid scaffold (SmartBone) for maxillary sinus augmentation: A histologic study on bone regeneration. Int J Pharm 2017;523:534–544.
24. World Medical Association Declaration of Helsinki: Ethical principles for medi-cal research involving human subjects. JAMA 2000;284:3043–3045.
25. Maridati P, Dellavia C, Pellegrini G, Canciani E, Maragno A, Maiorana C. Histologic and radiographic compari-son of bone scraper and trephine bur for autologous bone harvesting in max-illary sinus augmentation. Int J Oral Maxillofac Implants 2015;30:1128–1136.
26. Facciuto E, Grottoli CF, Mattarocci M, et al. Three-dimensional craniofacial bone reconstruction with SmartBone on demand. J Craniofac Surg 2019;30:739–741.
27. Grecchi F, Perale G, Candotto V, Busato A, Pascali M, Carinci F. Reconstruction of the zygomatic bone with SmartBone: Case report. J Biol Regul Homeost Agents 2015;29:42–47.
28. Pertici G, Carinci F, Carusi G, et al. Composite polymer-coated mineral scaffolds for bone regeneration: From material characterization to human studies. J Biol Regul Homeost Agents 2015;29:136–148.
© 2021 BY QUINTESSENCE PUBLISHING CO, INC. PRINTING OF THIS DOCUMENT IS RESTRICTED TO PERSONAL USE ONLY. NO PART MAY BE REPRODUCED OR TRANSMITTED IN ANY FORM WITHOUT WRITTEN PERMISSION FROM THE PUBLISHER. © 2021 BY QUINTESSENCE PUBLISHING CO, INC. PRINTING OF THIS DOCUMENT IS RESTRICTED TO PERSONAL USE ONLY. NO PART MAY BE REPRODUCED OR TRANSMITTED IN ANY FORM WITHOUT WRITTEN PERMISSION FROM THE PUBLISHER.




















