Comercialización Petrolera
8
486 Cure of Interfascicular Reentrant Ventricular Tachycardia by Ablation of tbe Anterior Fascicle of tbe Left Bundle Brancb HARRY J.G.M. CRIJNS, M.D., JOEP L.R.M. SMEETS, M,D., LUZ MARIA RODRIGUEZ, M.D., ALBERT MEIJER, M.D,, and HEIN J.J. WELLENS, M,D. From the Department of Cardiology, University Hospital Maastricht, Maastricht, The Netherlands Ablation of Interfascicular Reentrant Tachycardia. Introduction: Fascicular reen- trant ventricular tachycardia (VT) using the anterior fascicle of the left bundle anterogradely is rare and may produce identical QRS morphology during sinus rhythm and VT. Catheter ablation of this type of VT has not been described in detail. Methods and Results: In a postinfaret patient with dilated left ventricle and recurrent VT (showing a QRS configuration of right bundle branch, left posterior fascicular block), endocar- dial recordings from the His-Purkinje system showed that VT was due to interfascicular reen- try. Induction of VT occurred after progressive retrograde conduction delay on increasing the prematurity of the extrastimulus. Anterograde conduction occurred exclusively over the left anterior fascicle, which caused identical QRS morphology during sinus rhythm and VT. Dur- ing VT, the left posterior fascicle was used retrogradely. The usual target for bundle branch reentry ablation, the right bundle, did not participate in the reentrant circuit. While perform- ing left ventricular endocardial mapping, VT was interrupted when positioning the caiheter on the left anterior fascicle, and "reversed" nonsustained bundle branch reentry occurred with anterograde conduction over the posterior fascicle and retrograde conduction over the anterior fascicle. Ablation of conduction in tbe anterior fascicle led to cure of the VT. Conclusion: Interfascicular reentrant VT witb right bundle branch block, right-axis QRS configuration can be cured by catheter ablation of anterior fascicle conduction. (J Cardiovasc Electrophysiol. Vol. 6. pp. 486-492, June 1995) interfascicular reentry, bundle branch reentry, ventricular tachycardia, catheter ablation, anterior fascicle Introduction Bundle branch reentry was suggested as a mech- anism for ventricular tachycardia (VT) more than 20 years ago.' Bundle branch reentrant VT occurs most frequently in the setting of structural heart disease, particularly in dilated he<uts.~' It tnay occur sporadically in patients in whom the only abnor- mality is conduction delay within the His-Purkinje Address (or correspondence: Harry J.G.M. Crijns. M.D.. Depiirl- mcnt of Cardiology. Thoraxcenier. University Hospital Gronin- gen. P.O. Box 30001. 9700 RB Groningen. The Netherlands. Fax: 31-50614391. Manuscript received 7 September 1994: Accepted for publication 17 April 1995. system.^ The conduction delay underlying reen- try tnay he functional, as has been described after the administration of a selective potassium channel blocker.^ The comtnon denominator for bundle branch reentry seems, thet^fore, to be slow His-Ptirkinje conduction. We describe a postinfaret patient with fitst-degree AV block, right bundle branch block (RBBB), and left posterior fascicu- lar block (LPFB) during sinus rhythm, presenting with interfascicular reentry, with VT morphology identical to tbat found during sinus rhythm. More than two decades ago, Spurrell et al.* showed that these tachycardias can be cured by surgical interruption of conduction in the left anterior fas- cicle. This report describes successful catheter abla- tion of VT by interruption of anterior fascicle con-
-
Upload
independent -
Category
Documents
-
view
0 -
download
0
Transcript of Comercialización Petrolera

486
Cure of Interfascicular Reentrant Ventricular Tachycardiaby Ablation of tbe Anterior Fascicle of tbe
Left Bundle Brancb
HARRY J.G.M. CRIJNS, M.D., JOEP L.R.M. SMEETS, M,D.,LUZ MARIA RODRIGUEZ, M.D., ALBERT MEIJER, M.D,, and
HEIN J.J. WELLENS, M,D.
From the Department of Cardiology, University Hospital Maastricht, Maastricht, The Netherlands
Ablation of Interfascicular Reentrant Tachycardia. Introduction: Fascicular reen-trant ventricular tachycardia (VT) using the anterior fascicle of the left bundle anterogradelyis rare and may produce identical QRS morphology during sinus rhythm and VT. Catheterablation of this type of VT has not been described in detail.
Methods and Results: In a postinfaret patient with dilated left ventricle and recurrent VT(showing a QRS configuration of right bundle branch, left posterior fascicular block), endocar-dial recordings from the His-Purkinje system showed that VT was due to interfascicular reen-try. Induction of VT occurred after progressive retrograde conduction delay on increasing theprematurity of the extrastimulus. Anterograde conduction occurred exclusively over the leftanterior fascicle, which caused identical QRS morphology during sinus rhythm and VT. Dur-ing VT, the left posterior fascicle was used retrogradely. The usual target for bundle branchreentry ablation, the right bundle, did not participate in the reentrant circuit. While perform-ing left ventricular endocardial mapping, VT was interrupted when positioning the caiheter onthe left anterior fascicle, and "reversed" nonsustained bundle branch reentry occurred withanterograde conduction over the posterior fascicle and retrograde conduction over the anteriorfascicle. Ablation of conduction in tbe anterior fascicle led to cure of the VT.
Conclusion: Interfascicular reentrant VT witb right bundle branch block, right-axis QRSconfiguration can be cured by catheter ablation of anterior fascicle conduction. (J CardiovascElectrophysiol. Vol. 6. pp. 486-492, June 1995)
interfascicular reentry, bundle branch reentry, ventricular tachycardia, catheter ablation, anteriorfascicle
Introduction
Bundle branch reentry was suggested as a mech-anism for ventricular tachycardia (VT) more than20 years ago.' Bundle branch reentrant VT occursmost frequently in the setting of structural heartdisease, particularly in dilated he<uts.~' It tnay occursporadically in patients in whom the only abnor-mality is conduction delay within the His-Purkinje
Address (or correspondence: Harry J.G.M. Crijns. M.D.. Depiirl-mcnt of Cardiology. Thoraxcenier. University Hospital Gronin-gen. P.O. Box 30001. 9700 RB Groningen. The Netherlands. Fax:31-50614391.
Manuscript received 7 September 1994: Accepted for publication17 April 1995.
system.^ The conduction delay underlying reen-try tnay he functional, as has been describedafter the administration of a selective potassiumchannel blocker.^ The comtnon denominator forbundle branch reentry seems, thet^fore, to be slowHis-Ptirkinje conduction. We describe a postinfaretpatient with fitst-degree AV block, right bundlebranch block (RBBB), and left posterior fascicu-lar block (LPFB) during sinus rhythm, presentingwith interfascicular reentry, with VT morphologyidentical to tbat found during sinus rhythm.More than two decades ago, Spurrell et al.* showedthat these tachycardias can be cured by surgicalinterruption of conduction in the left anterior fas-cicle. This report describes successful catheter abla-tion of VT by interruption of anterior fascicle con-

Crijns. et al. Ablation of Interfascicular Reentrant Tachycardia 487
duction. It also suggests that in VT with identical
QRS configuration as during sinus rhythm, the
QRS morphology is important in selecting an
appropriate ablation site-
Methods
Patient
A 72-year-oId male was admitted to our hos-pital with sustained VT. In 1977 he had sufferedan inferior wall myocardial infarct. Two years laterhe was resuscitated from ventricular fibrillationafter which he received long-term amiodarone. Thepatient had been well until 6 months before admis-sion, when unstable angina aiid heart failure neces-sitated coronary artery bypass grafting. Tbe pre-operative ECG showed an RBBB with right-axisdeviation due to LPFB. Amiodarone was stopped.Immediately postoperatively, transient completeAV block was observed for which an iutificial pace-maker was implanted. Three months before admis-sion, the patient had another episode of heart fail-ure. Left ventricular ejection fraction was 26% withglobal bypokinesia and moderate mitral incompe-tence. There were no tachycardias or iscbemia. Onthe day of admission, he had a sustained VT caus-ing palpitations and dyspnea. The tachycardia wastemiinated in-hospital by intravenous procainiunide.During admission the arrhythmia became inces-sant despite optim;il treatment tor heart failure, andeventually amiodiirone was reinstitutcd. However,tachycardias kept recurring, and, therefore, thepatient underwent an electrophysiologic study andVT ablation. Figure I shows the spontaneous onsetof VT from sinus rbytbm.
Electrophysiologic Study and Ablation Procedure
After positioning the high right atrium, His-bun-die, iind right ventricular apex catheters, a qu^ripo-lar ablation catheter (Polaris'" |Cordis Europa NV,Roden, The Netherlands]) was positioned to mapright bundle activation. Despite extensive mapping,a clear right bundle potential could not be recorded.Thereafter, the catheter was positioned in theoutflow tract of the lelt ventricle to record the His-bundle, common left bundle, and anterior fasciclepotentials. The posterior fascicle could not berecorded for technical reasons. Ablation was per-formed using a custom-available radiofrequencycurrent generator (HAT 200S"* IDr. Osypka,Wyhlen, Germany]).
Results
Figure 2 shows endocardial recordings from theHis bundle and left bundle during sinus rhythmand VT. Figure 3 shows a diagram of conductiontimes recorded from the His-Purkinje system dur-ing sinus rhytbm and VT. TTie diagram indicatesthat reentry occurred anterogradely over tbe ante-rior fascicle and retrogradely over the posterior fas-cicle (Fig. 2). The tachycardia frequently startedspontaneously during regular sinus rhytbm (Fig.1). It could also be initiated by single and doubleextrastimuli from the right ventricular apex. Dur-ing right ventricular extrastimulation. retrogradeHis-bundle activation was delayed progressivelywith increasing prematurity of the extrastimulus.With the basic drive interval S|S; set at 430 msec,the S|H| was 350 msec. S, was not followed byVH conduction. With progressive shortening of theS-,S, interval, the S,H, interval increa.sed from 350msec to a maximum of 440 msec at tbe onset ofthe tachycardia showing a cycle length of 390 msec(Fig. 4). At the onset of each tachycaidia, a His-bundle deflection with an HV interval of 70msec was recorded. Variations in the RR intervalduring tachycardia were preceded by HH intervalvariations while the HV interval remainedunchanged (Fig. 4). Similarly, the AF-AF intervaldetermined the subsequent VV interval.
It was decided to ablate the VT by interrupt-ing conduction in tbe anterior fascicle. Ablation ofposterior fascicle conduction was expected to beunsuccessful since it would not prevent reentryfrom the left ventricular myocardium into the leftanterior fascicle. In addition, selective ablation ofthe proximal left posterior fascicle wits deemed tootime-consuming in this patient. Before applyingradiofrequency current, the catheter was placedfirmly on the anterior fascicle wbile the patient wasin VT. This maneuver temiinated the tachycardiaby causing AF-V block. AF-V block was also seenduring subsequent sinus rhythm showing leftposterior fascicle conduction and an extremely longPR interval. In addition, "reversed" reentrant beatswere observed, anterogradely conducted over tbeposterior fascicle and retrogradely over the ante-rior fascicle (Fig. 5).
Before application of the radiofrequency cur-rent, anterior fascicle conduction resumed spon-taneously. Within 1.5 seconds after onset of theradiofrequency pulse, conduction over the anteriorfascicle disappeared, and anterograde left posteriorfascicle conduction with a long PR intervalemerged. After the ablation. VT could no longer
488 Journal of Cardiovascular Klectrophysiology Vol. 6. No. 6. Jutie 1995
941030
94584
400 msec
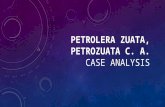
Figure 1. ECG following amiodarone treatment. To the right, onset of ventricular tachycardia (VT)frotn sinus rhythm. Dur-ing sinus rhythm, the PR interval measures 240 msec. The PR interval at the on.set of VT is decreased due to shortening of theRR interval caused by the first reentrant beat. Note identical QRS morphology during sinus rhythm and VT. P = P waves.
RA
100 msecFigure 2. Endocardial recordings from the left bundle (LB) and His bundle recorded across the tricuspid valve (HBE) duringsinus rhythm (panel A) and VT {panel B). Note 'he reversal of activation. The HV and LB-V inter\'als during .sinus rhvthm are100 and 85 msec, respectively, andduring VTc 'e 70and lOOmsec. respectively. RA — right atrium.

Crijns, et al. Ablation of Interfascicular Reentrant Tachycardia 489
SR VT
AO-108
TA-100
LB-100
AF-100
RB RBPF
Figure 3. Scheme showing conduction times in sinus rhythm (SR) and ventricular tachycardia (VT). Conduction in the His-Purkinje systetn is markedly delayed. During VT. the AF-V and LB-V intervals were identical (100 msec), ruling out antero-grade conduction over the common bundle. Consequently, the lefi posterior fascicle was the retrograde limb of the reentrantcircuit. AF = anterior fascicle: AO = measurement from the aortic root: HB = His bundle: LB = common left bundle; PF =posterior fascicle; RB = right bundle; TA = His-bundle potential recorded across the tricuspid annulus. Numbers indicateconduction times from the site shown to onset of ventricular activation {in msec).
•45*5
H
940925
Figure 4. Initiation of VT with double ventricular extrastimuli. Note the extremely long interval between the stimulus and ret-rograde His-bundle activation, consistent with an extreme conduction delay in the His-Purkinje system. The S,H, intervalmeasures 350 msec. After 5,. there is no VH conduction. With progressive shortening of the SSj interval from 380 to 240msec, the S^H, interval increased gradually from 350 to 440 msec. At the S,H, of 440 msec, VT started. Note the presence ofcomplete AV dissociation during ventricular pacing and ventricular tachycardia. The His bundle was recorded in the aorticroot. 5,5, = basic drive cycle length; 5; and S, ^ first and .second premature beats, respectively; S,H, = stimulus-to-H inter-val during the basic drive.

490 Journal of Cardiovascular Electrophysiology Vol. 6, No. 6. June 1995
94&86
941030 A100 msec
Figure 5. "Reversed" interfa.scicular reentry after catheter-induced anterograde block in the anterior fascicle. The sinus beatshows an extremely long PR interval (approximately 350 msec) and AF-V block. Considering the QRS configuration, antero-grade conduction occurs over the posterior fascicle. After anterograde conduction, there is retrograde penetration of theanterior fa.scicle and His bundle, followed by an anterograde reentry into the teft posterior fascicle. After the second reentrantbeat, retrograde penetration into the anterior fascicle fails and sinus rhythm resumes, again followed by retrograde anteriorpenetration. Note that the QRS morphology of sinus and VT beats are identical. H'andAF' = ret rogradely activated His andanterior fascicle potentials, respectively. Other abbreviations as in Figure 2.
be induced. During a 12-month foilow-up, therewere no spontaneous VT recurrences.
Discussion
This report describes cure of fascicular reentrantVT with RBBB, right-axis morphology by catheterablation of anterior fascicle conduction. The fea-sibility of surgical division of the anterior fasciclefor treatment of this type of VT has been reportedpreviously by Spurrell et al.* Left-sided catheterablation of bundle branch reentry was reported byBlanck et al. in two patients, and extensive elec-trophysiologic data were recently presented in onepatient.'
In contrast to fascicular reentry, the target sitefor ablation of bundle branch reentry VT usuallyis the right bundle branch.-'* The latter VTs fre-quently show a left bundle branch block (LBBB)morphology. However, with RBBB VT the rightbundle is mostly a bystander, i.e., the VT occurs
interfascicularly. This is supported by the recentreport by Mehdirad et al.^ demonstrating thatFurkinje reentry with a RBBB QRS morphologytends to occur within the left-sided His-Purkinjesystem. Therefore, ablation of the right bundle willappear futile in most cases of RBBB VTs usingone of the bundle branches or fascicles. In agree-ment with previous reports, the present case sup-ports the notion that bundle branch reentryshould be clearly distinguished from fascicularreentry when determining the target site for abla-tion.
The QRS moiphology of the VT was identicalto that In sinus rhythm. This may easily lead tomisdiagnosis of supraventricular tachycardia. Inthis patient, the 12-lead ECG showed AV disso-ciation, favoring a ventricular origin of the tachy-cardia. This report stresses the notion that in VTwith QRS morphology identical to that found insinus rhythm, bundle branch reentry or fascicularreentry should be entertained as a possible diag-

Crijns. et at. Ablation of Interfascicular Reentrant Tachycardia 49!
nosis. Similarity of the QRS morphology suggeststhat anterograde conduction occurs exclusively overone of the fascicles of the left bundle or over theright bundle.
Fascicular Reentry Versus BundleBranch Reentry
The present findings suggested intertascicuiarreentry rather than bundle branch reentry.^ VT.started invariably with the anterior fa.scicle poten-tial before the first VT beat, and the AF-AFinterval variations preceded the VV variations. VTinitiated frequently from normal sinus rhythm, i.e.,in the absence of premature beats. In addition,induction of the VT by premature stimuli was asso-ciated with a critical degree of retrograde His-Pur-kinje conduction delay (VH prolongation). Thesecriteria were, however, not helpful in differentiat-ing fascicular from bundle branch reentrant VTsince they apply for both types of reentry. In addi-tion, the His-bundle potential was not found tobe a bystander. In contrast, the following criteriastrongly supported fascicular reentry. First, theHVyj was considerably shorter than the HV j ,which virtually excluded bundle branch reentry.The HVvT being considerably shorter than the HV^in fa.scicular VT relates to the fact that the branch-ing point of the penetrating left bundle branch isthe starting point for activation of the various partsof the proximal conduction system (Fig. 3). Thispoint being relatively far from the His bundle causesrather early activation of the ventricle relative toretrograde His activation. It is, however, importantto keep in mind that the HVy, being shorter orlonger than the HV i during either bundle branchreentry or fascicular reentry depends on the bal-ance between anterograde and retrograde conduc-tion times during VT. Second, the H potentialfollowed rather than preceded the AF potential. Inbundle branch reentry, i.e., reentry using both bun-dle branches, the H ptitentiai would have precededthe AF potential.
Chien et al.'" advocated recording the rightbundle potentiiil in all Hi.s-Purkinje reentrant tachy-cardias, since in some cases the right bundle maybe a bystander rather than a prerequisite for sus-taining the arrhythoiia. The present case supportsthe contention that It is mandatory to record atleast the bundle branch or fascicle, which pro-vides the anterograde link during reentry. Thisbundle is, in fact, the final common pathway, andpermanent interruption of conduction in that finalcommon pathway may lead to cure of the VT.
Obviously, ablation of conduction in the retro-grade limb of the circuit leaves the possibility thatthe anterograde limb is activated from anotherretrograde pathway! On the other hand, ablationof the anterograde limb interrupts not only VTbut may also abolish normal AV conduction,thereby necessitating pacemaker implantation. Inaddition, it does not exclude the possibility ofanother tachycardia using the retrograde Hmbanterogradely.
Clinical Consequences
Bundle branch reentry or intedascicular reen-trant VT is not confined to patients with car-diomyopathy or aortic valvufar disease, but mayalso occur late after infarction in patients with adilated left ventricle, iUthough in postinfarct patientsone expects a myocardial .scar rather than the bun-dle branches to be the origin of VT. In addition,these types of reentry may be easily confused withaberrant conduction during supraventricular tachy-cardia, because of identical QRS morphology. Bothcircumstances favor misdiagnosis. and it may bept>stulated that in the postinfarct patient with uni-directional bundle branch block and a dilated ven-tricle, bundle branch or interfa.scicular reentry mayoccur more frequently than previously thought.Recognition of this type of VT is extremely impor-tant, since it can be cured relatively easily bycatheter ablation techniques."
The present findings stress that if VT ablationis considered, it is important to delineate at leastthe anterogTdde limb of the reentrant pathway. Abla-tion of conduction in that Hnal common pathwaywill lead to cure of the clinical VT. The QRS mor-phology of the VT gives the most important clueas to where to look for that final common path-way as a target for ablation. Bundle branch reen-try with LBBB and left-axis moiphology suggeststhe right bundle as the final pathway. Similarly, asin the present case. Interruption of conduction inthe left anterior fascicle is indicated in bundlebranch reentry with an RBBB, right-axis mor-phology. Finally, the left posterior fascicle can bean important target in the ablation of bundle branchreentrant VT showing an RBBB with left-axis devi-ation. Apart from these considerations, however,the optimal ablation site is also determined byaccessibility of the target site and the consequencesof ablation for AV conduction during sinus riiythm.
Acknowledgment: The authors thank Adri van den Dool for skill-fully preparing the figures.
492 Journal of Cardiovascular Electrophysiology Vol. 6. No. 6. June 1995
References1. Wellens HJJ, Schuilenburg RM, Durrer D: Eleclrical
stimulation of the heart in patients with ventriculartachycardia. Circulation 1972:46:216-226.
2. Blanck Z, Dhala A, Deshpande S. et al: Bundle branchreentrant ventricular tachycardia: Cumulative experi-ence in 48 patients. J Cardiovasc Electrophysioi1993;4:253-262.
3. Jo.sephson ME: Clinical Cardiac Electrophysiology:Techniques and Interpretations, 2nd ed. Lea &Febiger, Maivem. PA. 1993. pp. 469-475.
4. Blanck Z. Jazayeri M, Dhala A, et al: Bundle branchreentry: A mechanism of ventricular tachycardia in theabsence of myocardial or valvular dysfunction. J AmColl Cardiol 1993:22:1718-1722.
5. Crijns HJGM, Kingma JH. Gosselink ATM, et al:Comparison in the same patient of aberrant conductionand bundle branch reentry after dofetilide. a new selec-tive class III antiarrhythmic agent. PACE 1993;16:1006-1016.
6. Spurrell RAJ. Sowton E. Deuchar DC: Ventriculartachycardia in four patients evaluated by programmed
electrical stimulation of the heart and treated in twopatients by surgical division of anterior radiation of leftbundle-branch. BrHeartJ 1973:35:1014-1021.
7. Blanck Z. Deshpande S. Jazayeri MR. et al: Catheterablation of the left bundle branch for the treatment ofsustained bundle branch reentrant ventricular tachycar-dia. J Cardiovasc Electrophysiol 1995;6:40-43.
8. Caceres J, Jazayeri M, McKinnie J. et al: Sustainedbundle branch reentry as a mechanism of clinicaltachycardia. Circulation 1989;79:256-270.
9. Mehdirad AA. Keim S, Rist K. et al: Asymmetry ofretrograde conduction and reentry within the His-Pur-kinje system: A comparative analysis of left and rightventricular stimulation. J Am Coll Cardiol1994:24:177-184.
10. Chien WW. Scheinman MM. Cohen TJ, et al: Impor-tance of recording the right bundle branch deflection inthe diagnosis of His-Purkinje reentrant tachycardia.PACE 1992:15:1015-1024.
11. Miles WM: Bundle branch reentrant tachycardia: Achance to cure? J Cardiovasc Electrophysioll993;4:263-265.