CLINICAL NOTE Double Scalping Flap: A Versatile Technique in Scalp Reconstruction
8
Copyright @ 2009 Mutaz B. Habal, MD. Unauthorized reproduction of this article is prohibited. Double Scalping Flap: A Versatile Technique in Scalp Reconstruction Othon Papadopoulos, MD, PhD,*Þ Dimitrios Karypidis, MD,*þ Margarita Moustaki, MD,* Chrisostomos Chrisostomidis, MD,* Champsas Grigorios, MD,* Kostopoulos Epaminondas, MD,* and Marios Frangoulis, MD, PhD* Abstract: Scalp reconstruction is a challenging area in plastic surgery. The susceptibility of potentially exposed brain tissue is almost always a concern along with the provision of adequate soft tissue coverage in cases of full-thickness defects. The applied reconstructive strategy also affects efficiency in malignant disease treatment providing both local control of the disease and vigorous monitoring for recurrence or metastasis. The general condition of the patients presenting with malignant lesions of the scalp is often impaired because of old age or concomitant disease. Therefore, de- manding, long-lasting, or multistage procedures may often be un- desirable. The double scalping flap comprises a 1-stage procedure, which can be used in most full-thickness defects of the vertex of the scalp. Some of the primary advantages of the double scalping flap procedure are its versatility and arc of rotation, its minimal donor site morbidity, being relatively simple, and being a short technique. Disadvantages that may be considered are the loss of hair-bearing skin at the occipital region and the poor color and texture match between scalp skin and the split-thickness skin graft that is used on the donor site. We present 2 patients with exemplary case of neglected malignancy of the scalp and their successful treatment using the double scalping flap. Comparison and contrast of alter- native reconstructive procedures are also included to further in- vestigate scalp reconstruction. Key Words: Scalp, flap, double scalping flap, scalp reconstruction, sarcoma, squamous cell carcinoma (J Craniofac Surg 2009;20: 1484Y1491) D espite the fact that numerous techniques have been described for the management of scalp defects, scalp reconstruction remains a challenge for the plastic surgeon. Complexity in the reconstruction of such defects is primarily due to the surgical anatomy of the region that requires sophisticated procedures for aesthetic and functional restoration. Reconstruction mainly concerns defects after tumor resection, trauma, or congenital deformity. There are several techniques available in the reconstructive armamentarium, which should be tailored to meet the individual requirements of the patient, depending on the location, size, and depth of the defect. 1,2 The best replacement for scalp tissue is autologous scalp tissue. 2 Therefore, local flaps, with or without concurrent skin grafts, still remain the method of choice for the reconstruction of scalp defects, especially after tumor resection and when not amendable to primary closure. Most of these defects can be reconstructed using local tissue rearrangements that allow for coverage over the calvaria, restore the hair, and achieve good aesthetic results. 2 We report 2 patients who underwent resection of their neglected malignant tumor with immediate reconstruction of the subsequent large full- thickness defect using the 1-stage double scalping rotation advancement flap based on the superficial temporalis vessels bilaterally. This successful reconstruction of the scalp requires careful preoperative planning and intraoperative precision to achieve coverage of the calvaria while preserving vascularity. Avoiding disruption of the regional anatomy includes attention to native hair patterns and hair lines. Although local flaps are usually preferred, when local tissue rearrangements are inadequate for reconstruction, alternative techniques should be considered such as secondary intention healing for split-thickness defects, skin grafting, tissue expansion, and free tissue transfer. 1Y3 HISTORIC REVIEW The reconstruction of facial defects using flaps has been practiced since ancient times (circa 600 BC) when Sushruta of Varanasi-India 4 described in writings the use of a forehead flap, which is probably among the first applications of plastic surgery. These attempts, however, were not successful. The use of local flaps for facial reconstruction was described and well accepted during World War I, when surgeons faced the challenge of treating severe traumatic midface defects. 5 In 1942, during World War II, Converse 6 applied the 2-stage anterior scalping flap, originally for nasal reconstruction. It was a variation of the Bup and down[ flap of Gillies. 7 In the late 1970s, the scalping flap gained popularity and found applications in cheek, eyebrow, and orbital roof restoration successfully and later in nasopharynx, tonsils, and floor of the mouth reconstruction. 8,9 In 1964, Frezieres et al 10 presented the use of rotation flap for scalp defect reconstruction. In 1967, Orticochea 11Y13 described the 4-flap reconstruction technique, a more elaborate flap to achieve closure for larger defects of the occipital region of the scalp. A year later, he suggested the use of a 3-flap technique, providing enhanced CLINICAL NOTE 1484 The Journal of Craniofacial Surgery & Volume 20, Number 5, September 2009 From the *Plastic Surgery Department, BAndreas Syggros[ Hospital for Skin and Venereal Diseases; †2nd Department of Propedeutic Surgery, Faculty of Medicine, University of Athens, BLaiko[ General Hospital, Athens, Greece; and ‡Cardiff University Medical School, United Kingdom. Received January 16, 2009. Accepted for publication March 17, 2009. Address correspondence and reprint requests to Dimitrios Karypidis, MD, Plastic Surgery Department, BAndreas Syggros[ Hospital for Skin and Venereal Diseases, Cardiff University Medical School, United Kingdom; E-mail: [email protected] Copyright * 2009 by Mutaz B. Habal, MD ISSN: 1049-2275 DOI: 10.1097/SCS.0b013e3181b09ade
Transcript of CLINICAL NOTE Double Scalping Flap: A Versatile Technique in Scalp Reconstruction

Copyright @ 2009 Mutaz B. Habal, MD. Unauthorized reproduction of this article is prohibited.
Double Scalping Flap: A Versatile Techniquein Scalp Reconstruction
Othon Papadopoulos, MD, PhD,*Þ Dimitrios Karypidis, MD,*þ Margarita Moustaki, MD,*Chrisostomos Chrisostomidis, MD,* Champsas Grigorios, MD,* Kostopoulos Epaminondas, MD,*
and Marios Frangoulis, MD, PhD*
Abstract: Scalp reconstruction is a challenging area in plasticsurgery. The susceptibility of potentially exposed brain tissue isalmost always a concern along with the provision of adequate softtissue coverage in cases of full-thickness defects. The appliedreconstructive strategy also affects efficiency in malignant diseasetreatment providing both local control of the disease and vigorousmonitoring for recurrence or metastasis. The general condition ofthe patients presenting with malignant lesions of the scalp is oftenimpaired because of old age or concomitant disease. Therefore, de-manding, long-lasting, or multistage procedures may often be un-desirable. The double scalping flap comprises a 1-stage procedure,which can be used in most full-thickness defects of the vertex of thescalp. Some of the primary advantages of the double scalping flapprocedure are its versatility and arc of rotation, its minimal donorsite morbidity, being relatively simple, and being a short technique.Disadvantages that may be considered are the loss of hair-bearingskin at the occipital region and the poor color and texture matchbetween scalp skin and the split-thickness skin graft that is usedon the donor site. We present 2 patients with exemplary case ofneglected malignancy of the scalp and their successful treatmentusing the double scalping flap. Comparison and contrast of alter-native reconstructive procedures are also included to further in-vestigate scalp reconstruction.
Key Words: Scalp, flap, double scalping flap, scalp reconstruction,sarcoma, squamous cell carcinoma
(J Craniofac Surg 2009;20: 1484Y1491)
Despite the fact that numerous techniques have been described forthe management of scalp defects, scalp reconstruction remains a
challenge for the plastic surgeon. Complexity in the reconstructionof such defects is primarily due to the surgical anatomy of the regionthat requires sophisticated procedures for aesthetic and functionalrestoration. Reconstruction mainly concerns defects after tumorresection, trauma, or congenital deformity. There are severaltechniques available in the reconstructive armamentarium, whichshould be tailored to meet the individual requirements of the patient,depending on the location, size, and depth of the defect.1,2
The best replacement for scalp tissue is autologous scalptissue.2 Therefore, local flaps, with or without concurrent skin grafts,still remain the method of choice for the reconstruction of scalpdefects, especially after tumor resection and when not amendable toprimary closure. Most of these defects can be reconstructed usinglocal tissue rearrangements that allow for coverage over the calvaria,restore the hair, and achieve good aesthetic results.2 We report2 patients who underwent resection of their neglected malignanttumor with immediate reconstruction of the subsequent large full-thickness defect using the 1-stage double scalping rotationadvancement flap based on the superficial temporalis vesselsbilaterally. This successful reconstruction of the scalp requirescareful preoperative planning and intraoperative precision to achievecoverage of the calvaria while preserving vascularity. Avoidingdisruption of the regional anatomy includes attention to native hairpatterns and hair lines. Although local flaps are usually preferred,when local tissue rearrangements are inadequate for reconstruction,alternative techniques should be considered such as secondaryintention healing for split-thickness defects, skin grafting, tissueexpansion, and free tissue transfer.1Y3
HISTORIC REVIEWThe reconstruction of facial defects using flaps has been
practiced since ancient times (circa 600 BC) when Sushruta ofVaranasi-India4 described in writings the use of a forehead flap,which is probably among the first applications of plastic surgery.These attempts, however, were not successful. The use of local flapsfor facial reconstruction was described and well accepted duringWorld War I, when surgeons faced the challenge of treating severetraumatic midface defects.5 In 1942, duringWorld War II, Converse6
applied the 2-stage anterior scalping flap, originally for nasalreconstruction. It was a variation of the Bup and down[ flap ofGillies.7 In the late 1970s, the scalping flap gained popularity andfound applications in cheek, eyebrow, and orbital roof restorationsuccessfully and later in nasopharynx, tonsils, and floor of the mouthreconstruction.8,9
In 1964, Frezieres et al10 presented the use of rotation flap forscalp defect reconstruction. In 1967, Orticochea11Y13 described the4-flap reconstruction technique, a more elaborate flap to achieveclosure for larger defects of the occipital region of the scalp. A yearlater, he suggested the use of a 3-flap technique, providing enhanced
CLINICAL NOTE
1484 The Journal of Craniofacial Surgery & Volume 20, Number 5, September 2009
From the *Plastic Surgery Department, BAndreas Syggros[Hospital for Skinand Venereal Diseases; †2nd Department of Propedeutic Surgery, Faculty ofMedicine, University of Athens, BLaiko[ General Hospital, Athens, Greece;and ‡Cardiff University Medical School, United Kingdom.Received January 16, 2009.Accepted for publication March 17, 2009.Address correspondence and reprint requests to Dimitrios Karypidis, MD,
Plastic Surgery Department, BAndreas Syggros[ Hospital for Skin andVenereal Diseases, Cardiff University Medical School, United Kingdom;E-mail: [email protected]
Copyright * 2009 by Mutaz B. Habal, MDISSN: 1049-2275DOI: 10.1097/SCS.0b013e3181b09ade

Copyright @ 2009 Mutaz B. Habal, MD. Unauthorized reproduction of this article is prohibited.
flap vascularity over the 4-flap technique and less postoperativecomplications. Juri et al14 published in 1975 the use of parieto-occipital flaps in the surgical treatment of alopecia.
In 1977, Arena15 first recommended the posterior neck skinas a tissue supply, similar to facial skin, which led to the descriptionof a 2-stage posterior scalping flap. As an extension of theretroauricular-temporal flap introduced by Washio16 in 1969, thisflap fulfills many of the objectives of the anterior scalping flap,without the defect of a forehead scar, owing to its effortlesslycamouflaged donor site in the nape of the neck. Although this flapwas introduced more than 20 years ago, there is a paucity of reports
regarding its use. In 2000, Mandell et al17 published their experiencein the use of the posterior scalping flap, reporting that this flap couldbe a viable reconstructive technique capable of providing functionaland cosmetic restoration of the midface.
Vecchione and Griffith18 reported in 1978 their treatment ofscalp defects by using multiple flaps in a pinwheel design. In 1979,Runne et al19 described a double-flap method in the frontal andtemporal areas to cover larger defects resulting from several surgicalprocedures. In the same year, Becker20 first described a rhomboid-to-W technique for excision of some skin lesions and closure. Sincethen, other applications of this type of flap have been reported21Y23
FIGURE 1. Surgical technique design during the preoperative stage: the location of the defect is shown in mid-gray and thearea of the flaps bilaterally in light gray and dark gray are shown in anterior, profile, top, and back views. Reference points (A-F)assist in understanding the rotation and themobilization of the flap. Note the exact outline of the flaps (black solid line) and that oftumor excision margin (gray line). In surgical planning, the maximum sagittal diameter of the defect (B-C distance) must be equalor smaller than the sagittal length of both flaps (D-C distance). The coronal diameter of the defect must not be longer than thesum of the posterior widths of the flaps (D-E distance + D-E distance). In the profile, the vascular supply of the right flap is shown.FB indicates frontal branch of the superficial temporal artery; OA, occipital artery; PAA, posterior auricular artery; PB, parietalbranch of the superficial temporal artery; STA, superficial temporal artery; STSG, split-thickness skin graft.
FIGURE 2. Surgical technique design during the postoperative stage: the new position of the flaps after their mobilization. Thedefect is covered. The change of the position of the reference points shows the rotation of the flaps. Point C is moved forward andsutured medially to point B (anterior border point of the defect). Points D and E are similarly moved anteriorly. Note the newposition of the supplying artery and the dog ears at the frontotemporal region owing to the folding of the flaps bilaterally.Secondary arteries such as the occipital and the posterior auricular arteries are ligated.
The Journal of Craniofacial Surgery & Volume 20, Number 5, September 2009 Double Scalping Flap
* 2009 Mutaz B. Habal, MD 1485

Copyright @ 2009 Mutaz B. Habal, MD. Unauthorized reproduction of this article is prohibited.
in localized scalp lesions until 1990 when Stough and Stough24
presented the triple rhomboid flap as a method for reducing vertexalopecia and for defect reconstruction.
In 1980, Sawhney25 described the use of transposition flapsfor the reconstruction of inextensible skin such as the scalp.However, transposition flaps such as Limberg and bilobed flapscontinued to have fewer applications in scalp than in foreheadreconstruction.2 In 1988, Ahieja26 provided a geometric consider-ation in the classic transposition and rotation flap.
In the early 1990s, Spinelli et al27 reported the applicability ofanterior scalping flap for reconstruction of upper cranial and cranialbase defects, including the soft tissue coverage of the anterior uppercranium, skull base, and nasal unit resulting from resection ofvarious malignancies. Their next reports in 1998 (Spinelli et al5) and2008 (Patel and Spinelli28) only confirmed their belief that scalpingflap maintains a definite role in soft tissue coverage of upper cranialand cranial base defects and offers an acceptable aesthetic andfunctional outcome.27Y29
In 1999, Davis30 reported the VY scalp flap as a particularlywell-suited flap for the reconstruction of the temporal sideburn. Theredirected hair follicles match the missing hair-bearing pattern,whereas the resulting donor scar is well concealed behind thesuperior helix of the ear.
In 2000, Iida et al31 described the use of a simply designedbilobed flap for the reconstruction of parietal scalp defects. In 2001,De Haro et al32 reported the use of a bipedicled fronto-occipital flapfor the postoncologic defects of the lateral scalp.
SURGICAL TECHNIQUESurgical excision of the lesion is designed according to the
diagnosis so as to ensure tumor-free margin. The defect in whichtumor extirpation will result is accurately measured by outlining theexcision margins. A sagittal incision is performed from the posteriorborder of the defect (point C, Fig. 1) to the lower point of the scalpdesign (point D, Fig. 1). A second incision is then made in thepostauricular region (A-E distance, Fig. 1) parallel to the previous
one, and the 2 incisions are linked with another one, parallel tothe superior nuchal line (E-D distance, Fig. 1). The postauricularincision should not be carried any further anteriorly (point A, Fig. 1)than the superior attachment of the helix to avoid transection of thesuperficial temporal artery. The flaps are then raised after dissectionof the skin and subcutaneous down to galea aponeurotica and at thelevel of the loose areolar connective tissue layer of the scalp. Whenthe perforating occipital and posterior auricular vessels are en-countered, they are divided and ligated (Fig. 2). The rotation of bothflaps is performed so as to cover the soft tissue defect of the scalp,and they are sutured along the anterior excisional margin (B-Bdistance, Fig. 1). Both flaps are also sutured along their midsagittalpart (D-C distance, Fig. 2). The lateral dog ears due to the anteriorfolding of the flaps bilaterally serve by providing drainage outletduring the immediate postoperative period. Revision of the area cantake place 3 weeks after the operation.
PATIENT 1A 70-year-old woman presented with neglected squamous
cell carcinoma of the scalp (T4 N0 M0). Meticulous preoperativeevaluation took place. A computed tomographic scan of the craniumshowed bone and dura involvement. In collaboration with theneurosurgeon, a wide excision of the tumor including the underlyingcranial border and dura was performed. Mersilene mesh (Ethicon,Somerville, NJ) was used for dura repair, and methyl methacrylate
FIGURE 3. Neglected squamous cell carcinoma in a70-year-old woman (patient 1), occupying the vertex andthe top aspect of the scalp.
FIGURE 4. Computed tomographic scan reveals full-thicknesslesion involving the bone and the superficial layer of thedura mater. Superior sagittal sinus was not involved.
FIGURE 5. Side view and design of the right flap in patient 1.
Papadopoulos et al The Journal of Craniofacial Surgery & Volume 20, Number 5, September 2009
1486 * 2009 Mutaz B. Habal, MD

Copyright @ 2009 Mutaz B. Habal, MD. Unauthorized reproduction of this article is prohibited.
was applied to repair the bone defect. Two scalping flaps based onthe superficial temporal vessels were used to repair the soft tissuedefect, and a split-thickness skin graft was used to cover the donorsites bilaterally. The procedure lasted 3.5 hours. Metastasis in theparotid gland was noted 7 months after the operation. Superficialparotidectomy and supraomohyoid neck dissection were performed.Presently, 2 years after the operation, the patient is free of recurrenceor metastasis (Figs. 3Y11).
PATIENT 2An 85-year-old man presents with soft tissue sarcoma of the
scalp. Wide excision of the tumor and ostectomy of the involvedcranium and of the underlying dura were performed. Methylmethacrylate was used for bone replacement, and a double scalpingflap was used for soft tissue repair. Operative time was 4 hours.Local control of the tumor was achieved 2 years after the operation(Figs. 12Y20).
DISCUSSIONThere are many options for repairing large scalp defects.
Methodical analysis of the defect is of paramount importance in theselection of the surgical method to be used. There are a number offactors concerning the defect, which are important when making thatchoice, such as size, location, structures exposed, aesthetic subunits,contour, and the environment of the wound (e.g., surgical scars or
previously irradiated tissue).2 Analysis of the wound also takes placein the context of the particular patient. Thus, a thorough knowledgeof the patient’s surgical and medical history is necessary forestablishing an intelligent reconstructive strategy. In addition, theetiology of the surgical wound to be restored (e.g., after tumorextirpation or traumatic), the mechanism of injury or associatedtrauma, the age, and the general condition of the patient greatlyaffect the prognosis.1
Restoring the hair of the scalp is desired in the repair of scalpdefects. This is an important reason why the use of local flaps isconsidered more advantageous in our center than the use of tissueexpansion techniques. If this is not possible, we proceed with the useof regional or distant flaps using microsurgical techniques.3,33Y35
FIGURE 8. Postoperative view of patient 1. The finalposition and suturing of the 2 scalp flaps is shown. Note thecoronal and midsagittal suture lines. Also note the bilateraldog ears over the frontal-temporal areas owing to thekinking of the flap.
FIGURE 9. Postoperative back view of patient 1. The donorsite of the flap covered with split-thickness skin graft is alsoshown.FIGURE 7. Side view and design of the left flap in patient 1.
FIGURE 6. Top view in patient 1. The excision margin isoutlined around the lesion.
The Journal of Craniofacial Surgery & Volume 20, Number 5, September 2009 Double Scalping Flap
* 2009 Mutaz B. Habal, MD 1487
Copyright @ 2009 Mutaz B. Habal, MD. Unauthorized reproduction of this article is prohibited.
Although primary closure is feasible in some cases, in most patientsundergoing oncologic resection, scalp defects after the procedure arenot amendable either to primary closure or to skin grafting.Moreover, in such patients, reconstruction can be even moreconvoluted down to a history of radiation therapy, presence ofcerebrospinal fluid leak, infected alloplastic material, or devitalizedbone after craniotomy.33
Although primary closure is the simplest method of recon-struction, it can be rarely applied in practice after major oncologicresection.33 Healing on secondary intention is also an alternative forrepairing scalp defects. Nevertheless, the applicability of this optionis limited in cases of large defects with pericranium deficit.3
Moderately sized scalp defects could be ideally restored withadjacent scalp tissue. This is one reason why the scalping flapmaintains a noteworthy role in soft tissue coverage of upper cranialand cranial base defects. For larger defects, combinations of localflaps, such as the double scalping flap, may be used to recruitsufficient amount of tissue into the defect.3,36
When designed carefully, local flaps can provide a durableand well-vascularized skin, with appropriate color and texture forthe coverage of compromised wound (e.g., radiated, infected). Inboth of our patients, we used the double scalping flap as the solereconstructive procedure, which resulted in sufficient defectcoverage and restoration of the scalp contiguousness, with softtissue of acceptable cosmetic and functional properties. The pro-cedure was easily performed within the same operative field, welltolerated by the patient, and with a short average hospitalizationtime. No major complications and no morbidity of the free skindonor site were observed during the follow-up period.
Compared with double scalping flap, the use of other localflaps, such as the temporalis flap,28 may be limited owing to the
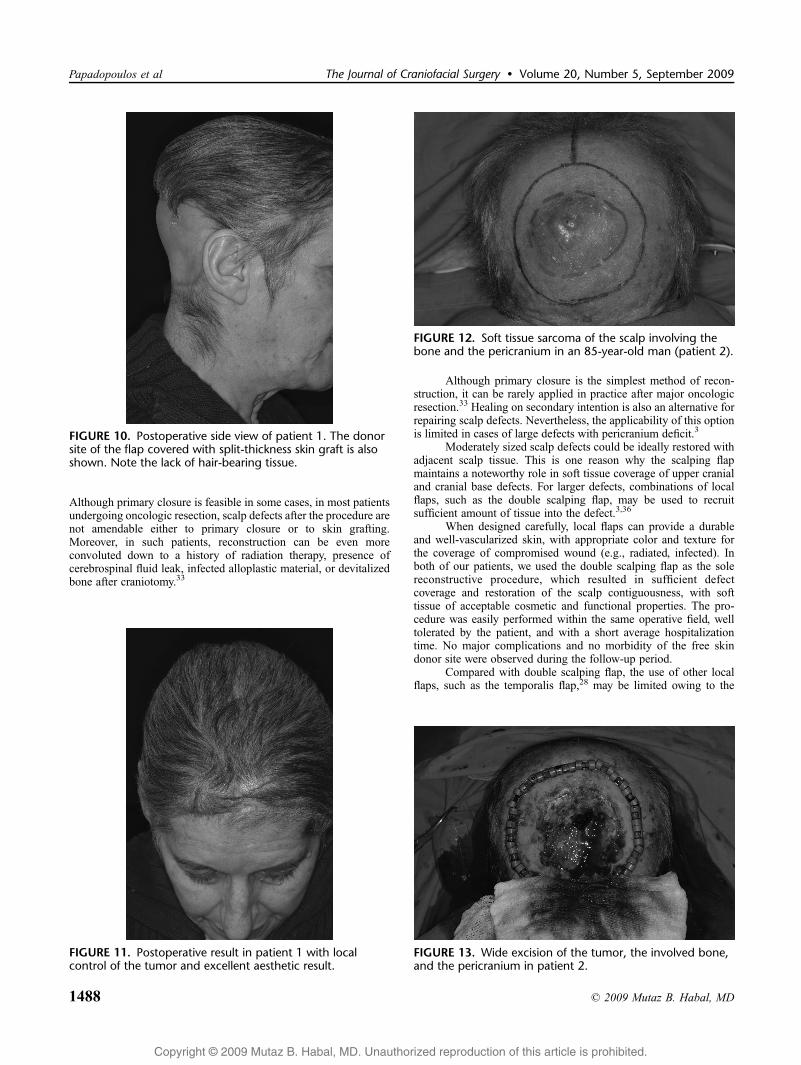
FIGURE 12. Soft tissue sarcoma of the scalp involving thebone and the pericranium in an 85-year-old man (patient 2).
FIGURE 13. Wide excision of the tumor, the involved bone,and the pericranium in patient 2.
FIGURE 11. Postoperative result in patient 1 with localcontrol of the tumor and excellent aesthetic result.
FIGURE 10. Postoperative side view of patient 1. The donorsite of the flap covered with split-thickness skin graft is alsoshown. Note the lack of hair-bearing tissue.
Papadopoulos et al The Journal of Craniofacial Surgery & Volume 20, Number 5, September 2009
1488 * 2009 Mutaz B. Habal, MD

Copyright @ 2009 Mutaz B. Habal, MD. Unauthorized reproduction of this article is prohibited.
smaller arc of rotation and size, the considerable donor site defect,and the limited ability to support a skin island.
Split-thickness skin grafts, or less commonly full-thickness skingrafts, can be usedmainly in hairless patients to reconstructmoderatelysized defects but are more reliable when sufficient grafting bed isavailable (i.e., periosteum or subcutaneous tissues) to be placed ontowell-vascularized tissue.33,35 In addition, careful hemostasis of thereceptor bed is important because the formation of hematomas wouldcompromise graft success. Alternatively, skin grafts are commonlyused to cover donor sites in scalp reconstruction with local flaps, aftercovering the exposed calvarium with a pedicled local fascial flap orpericranial tissue or after removing the outer cortex of the calvarium.3
The aesthetic outcome of skin grafting in scalp reconstructionis inferior when compared with the results achieved by local flapsbecause skin grafting usually results in hypopigmented anddepressed areas compared with the adjacent scalp. Alopecia isalso a disadvantage when using skin grafts.3,37 Conversely, properlydesigned local flaps could easily restore the correct orientation andalignment of hair follicles in the area to be reconstructed in caseswhere flaps are indicated. Avoiding transection of hair folliclestypically prevents alopecia along the resulting scar. Furthermore,scars could be easily hidden away because skin incisions are placedwithin hair-bearing regions, improving the cosmetic result.
In skull-exposing defects and dural repairs in the absence ofpericranium, and if grafting is the only option, perforations in theexternal cortical layer of the skull lead to the formation ofgranulation tissue, which fills the concavity of the scalp wound.Although this may be a time-consuming 2-stage procedure, itusually improves the prognosis of subsequent skin grafting and scalpwound contour. It has been reported that time to produce granulationtissue may be shortened using negative atmospheric pressure.2
Vacuum-assisted closure (VAC; Kinetic Concepts, San Antonio,TX) is a technology used in patients with inauspicious wounds andin those who have no local and regional options and are notcandidates for free flap closure. It is also suggested that the VACdevice may effectively remove wound fluid, decrease the bacterialcounts in wounds, significantly increase the vascularity, and stabilizeskin grafts because it conforms to the wound.38,39 When comparedwith the usual 2-stage approach to skin grafting the exposed skull,this method spares the patient a longer hospital stay and a secondoperative procedure, and it results in major cost savings.
However, at present, the VAC system remains an alternativein cases where flap coverage may not be an option owing to thelimited local tissue availability or to the general condition of thepatient, which may not allow long periods under anesthesia.38 Inaddition, in some patients, temporary healing and wound cover maybe desirable to allow for a more desirable reconstructive procedure
FIGURE 16. Intraoperative view of patient 2. The finalsuturing of both flaps bilaterally. Both suture lines and thelateral dog ears are also shown.
FIGURE 15. Intraoperative view of patient 2. The mobilizedflaps are rotated and positioned so as to adequately coverthe defect. FIGURE 17. The resected tumor, bone, and pericranium.
FIGURE 14. Meticulous hemostasis is of paramountimportance. The use of Surgicel (Johnson & Johnson Medical,Arlington, TX) assisted hemostasis.
The Journal of Craniofacial Surgery & Volume 20, Number 5, September 2009 Double Scalping Flap
* 2009 Mutaz B. Habal, MD 1489

Copyright @ 2009 Mutaz B. Habal, MD. Unauthorized reproduction of this article is prohibited.
such as tissue expansion at a later date when the patient recoversfrom potential concurrent injuries.
Tissue expansion is typically not an option for immediatereconstruction of oncologic scalp defects. However, it has beenproved useful for secondary revisions. Despite the reported rate ofcomplications and the need for serial procedures, it offers goodaesthetic results.33,40 Still, the aesthetic appearance of tissue-expanded scalp is compromised compared with a double scalpingflap reconstruction owing to the reduced density of hair follicles thattissue expansion results in.3 However, tissue expansion cansometimes be used in conjunction with scalping flaps as a second-stage procedure to restore the hair in the donor site of the flaps.
Regional pedicled musculocutaneous flaps41,47 from thetrunk such as the pectoralis major musculocutaneous flap,36,42,43
the trapezius,3,36,42,44,48 and the latissimus dorsi3,36,42,45 muscleflaps are also options for scalp repair, especially when the defect siteis located in the posterior scalp or occipital region, providing goodblood supply and viable tissue. Another common indication includesscalp reconstruction in patients with recurrent skin cancer, in whichprior radiation therapy or scarring due to previous surgery mayreduce the reliability of local flaps. However, the subclavicularlocation of their vascular attachments can compromise perfusion tothe flap because adequate reach often requires stretching of the flapand significant tension on the tissue.28,37,46 In addition, the use of thelatissimus dorsi and trapezius flaps may require intraoperativerepositioning of the patient to use the flap as well as supplementaryrevision procedures because of the increased bulk.
Free tissue transfer is another option for patients with poorquality and/or amount of local tissues. Consequently, scalp defectsthat are too large or too compound to reconstruct using local flapsare frequently repaired using free flaps that allow complete scalprestoration after tumor extirpation in a single stage. Despite thepostoperative atrophy of the free muscle, tissue bulk may also be aproblem after free muscle transfer, requiring follow-up revisions. Inpatients with oncologic defect, bulky free flaps may also make thedetection of cancer recurrence more difficult. Furthermore, there isoften a poor match for scalp skin regarding skin color and texture aswell as the alopecia in the area of reconstruction (with the exceptionof hair-bearing temporoparietal free flaps).3,28 In addition, free flapsexpose the patients to a more complex surgical procedure that maynot be desirable in patients with impaired general condition.
Therefore, the double scalping flap comprises a time-savingand relatively simple procedure without major complications anddemanding postoperative care compared with free tissue transfer.Although the selection of a method mainly relies on accurateindications and surgical planning regarding each individual patient,in our view, the double scalping flap is an excellent example of scalpreconstruction adequate to offer a less complex and well-toleratedoperation resulting in a very satisfactory functional and aestheticoutcome.
FIGURE 19. Postoperative result in patient 2: top view. Localcontrol of the tumor.
FIGURE 20. Posterior view of the postoperative result inpatient 2. Good aesthetic result despite the localized loss ofhair-bearing skin.
FIGURE 18. Intraoperative view of patient 2. Soft tissuesarcoma has been excised along with the bone and thepericranium. Bone deficit is covered with methyl methacrylate.The flaps have been meticulously dissected and mobilizedbilaterally.
Papadopoulos et al The Journal of Craniofacial Surgery & Volume 20, Number 5, September 2009
1490 * 2009 Mutaz B. Habal, MD

Copyright @ 2009 Mutaz B. Habal, MD. Unauthorized reproduction of this article is prohibited.
REFERENCES1. Leedy J, Janis J, Rohrich R. Reconstruction of acquired scalp defects: an
algorithmic approach. Plast Reconstr Surg 2005;116:54eY72e2. Temple C, Ross D. Scalp and forehead reconstruction. Clin Plast Surg
2005;32:377Y3903. Blackwell K, Rawnsley J. Aesthetic considerations in scalp
reconstruction. Facial Plast Surg 2000;24:11Y214. Singhal GD, Patterson TJS. Synopsis of Ayurveda. New York: Oxford
University Press, 19935. Spinelli HM, Bahtijarevic ZMD, Rinker B. Reconstruction of upper and
cranial base defects utilizing the scalping flap. Plast Reconstr Surg1998;101:930Y936
6. Converse JM. Reconstruction of the nose by the scalping flap technique.Surg Clin North Am 1959;39:335Y365
7. Gillies HD. Experiences with tubed pedicle flaps. Surg Gynecol Obstet1959;39:335Y365
8. Converse JM. Clinical applications of the scalping flap in reconstructionof the nose. Plast Reconstr Surg 1969;43:247Y259
9. Converse JM, McCarthy JG. The scalping forehead flap revisited.Clin Plast Surg 1981;8:413Y434
10. Frezieres H, Fave A, Burel P. Rotation flap of the scalp. Bull MensSoc Med Mil Fr 1964;58:204Y207
11. Orticochea M. Four flap scalp reconstruction technique. Br J Plast Surg1967;20:159Y171
12. Orticochea M. Use of the 4-flap technique for reconstruction of theforehead and parietal regions. Ann Chir Plast 1969;14:153Y158
13. Orticochea M. New three-flap reconstruction technique. Br J Plast Surg1971;24:184Y188
14. Juri J, Juri C, Arufe HN. Use of rotation scalp flaps for treatment ofoccipital baldness. Plast Reconstr Surg 1978;61:23Y26
15. Arena S. The posterior scalping flap. Laryngoscope 1977;87:98Y10416. Washio H. Retroauricular temporal flap. Keisei Geka 1968;11:285Y29017. Mandell DL, Genden EM, Biller HF, et al. Posterior scalping flap
revisited. Arch Otolaryngol Head Neck Surg 2000;126:303Y30718. Vecchione TR, Griffith L. Closure of scalp defects by using multiple
flaps in a pinwheel design. Plast Reconstr Surg 1978;62:74Y7719. Runne U, Bloch PH, Tritsch H. Double flap method in the frontal and
temporal area to cover larger defects left by surgery. Z Hautkr 1979;54:444Y448
20. Becker H. The rhomboid-to-W technique for excision of some skinlesions and closure. Plast Reconstr Surg 1979;64:444Y447
21. Izaguirre H, Navarro C. Rhomboid-to-BW[ technique for excision andclosure of facial skin lesions. J Maxillofac Surg 1983;11:207Y210
22. Lober CW, Mendelsohn HE, Fenske NA. Rhomboid transposition flaps.Aesthetic Plast Surg 1985;9:121Y124
23. Lister G. Local flaps to the hand. Hand Clin 1985;1:621Y64024. Stough DB, Stough DB. Triple rhomboid flap for crown alopecia
correction. J Dermatol Surg Oncol 1990;16:543Y548.25. Sawhney CP. Transposition flaps of inextensible skin such as the scalp.
Br J Plast Surg 1980;33:119Y12126. Ahieja RB. Geometric considerations in the design of rotation flaps
in the scalp and forehead region. Plast Reconstr Surg 1988;81:900Y906
27. Spinelli HM, Persing JA, Walser B. Reconstruction of the cranial base.Clin Plast Surg 1995;22:555Y561
28. Patel MP, Spinelli HM. The scalping flap for reconstruction of uppercranial and cranial base defects. Plast Reconstr Surg 2004;114:186Y189
29. Spinelli HM, Irizarry D, McCarthy JG, et al. An analysis of extraduraldead space after fronto-orbital surgery. Am J Otolaryngol 1999;20:287Y293
30. Davis WH. Sideburn reconstruction with an arterial V-Y hair-bearingscalp flap after the excision of basal cell carcinoma. Plast Reconstr Surg2000;106:94Y97
31. Iida N, Ohsumi N, Tonegawa M, et al. Reconstruction of scalp defectsusing simple designed bilobed flap. Aesthetic Plast Surg 2000;24:137Y140
32. De Haro F, Giraldo F. Bipedicled fronto-occipital flap for reconstructionof postoncologic defects of the lateral scalp. Plast Reconstr Surg2001;107:506Y510
33. Mehrara BJ, Disa JJ, Pusic A. Scalp reconstruction. J Surg Oncol2006;94:504Y508
34. Menick FJ. Facial reconstruction with local and distant tissue: theinterface of aesthetic and reconstructive surgery. Plast Reconstr Surg1998;102:1424Y1433
35. Garcı́a del Campo JA, Garcı́a de Marcos JA, del Castillo Pardo de VeraJL, et al. Local flap reconstruction of large scalp defects. Med OralPatol Oral Cir Bucal 2008;13:E666YE670
36. Frodel JL Jr, Ahlstrom K. Reconstruction of complex scalp defects:the Bbanana peel[ revisited. Arch Facial Plast Surg 2004;6:54Y60
37. Hurvitz KA, Kobayashi M, Evans GR. Current options in head and neckreconstruction. Plast Reconstr Surg 2006;118:122eY133e
38. Molnar JA, DeFranzo AJ, Marks MW. Single-stage approach to skingrafting the exposed skull. Plast Reconstr Surg 2000;105:174
39. Schintler MV, Prandl EC, Wittguber G, et al. The impact of theVAC-treatment for locally advanced malignancy of the scalp.Zentralbl Chir 2004;129(suppl 1):S41YS46
40. Nazerani S, Motamedi MH. Reconstruction of hair-bearing areas ofthe head and face in patients with burns. Eplasty 2008;8:e41
41. Langstein HN, Chang DW, Robb GL. Coverage of skull base defects.Clin Plast Surg 2001;28:375Y387
42. Tellio?lu AT, Cimen K, A0ar HI, et al. Scalp reconstruction with islandhair-bearing flaps. Plast Reconstr Surg 2005;115:1366Y1371
43. Resto VA, McKenna MJ, Deschler DG. Pectoralis major flap incomposite lateral skull base defect reconstruction. Arch OtolaryngolHead Neck Surg 2007;133:490Y494
44. Darzi MA, Iqbal S, Chowdri NA, et al. Trapezius myocutaneousflap for reconstruction of a large scalp defect following theexcision of postburn scar carcinoma (Marjolin’s ulcer). Burns1992;18:429Y431
45. Har-El G, Bhaya M, Sundaram K. Latissimus dorsi myocutaneousflap for secondary head and neck reconstruction. Am J Otolaryngol1999;20:287Y293
46. Friedman M, Grybauskas V, Skolnik E, et al. Parietal occipital napeof neck flap. A myocutaneous flap for selected head and neckreconstruction. Arch Otolaryngol Head Neck Surg1986;112:309Y315
47. Newman MI, Hanasono MM, Disa JJ, et al. Scalp reconstruction:a 15-year experience. Ann Plast Surg 2004;52:501Y506
48. Ozbek MR, Kutlu N. Vertical trapezius myocutaneous flap forcovering wide scalp defects. Handchir Mikrochir Plast Chir 1990;22:326Y329
The Journal of Craniofacial Surgery & Volume 20, Number 5, September 2009 Double Scalping Flap
* 2009 Mutaz B. Habal, MD 1491