
The effect of fontanel on scalp EEG potentials in the neonate
8
The effect of fontanel on scalp EEG potentials in the neonate P. Gargiulo a,b , P. Belfiore c , E.A. Friðgeirsson d , S. Vanhatalo e,⇑ , C. Ramon a,f a Institute of Biomedical and Neural Engineering, Reykjavik University, Iceland b Department of Science, Landspitali University Hospital, Reykjavik, Iceland c Department of Biomedical, Electronic and Telecommunication Engineering, University Federico II of Naples, Italy d Department of Development CE and IT, Landspitali University Hospital, Reykjavik, Iceland e Department of Children’s Clinical Neurophysiology, HUS Medical Imaging Center and Children’s Hospital, Helsinki University Central Hospital and University of Helsinki, Helsinki, Finland f Department of Electrical Engineering, University of Washington, Seattle, WA 98195, USA article info Article history: Accepted 4 December 2014 Available online xxxx Keywords: Neonatal EEG High density EEG Source localization Head model highlights Fontanels in the neonatal skull form spatial discontinuity in the head models. EEG simulation of the whole cortex activity discloses no distortion by fontanels. The relative effect of fontanels on scalp EEG potentials is negligible. abstract Objective: To define how fontanels affect scalp EEG potentials in neonates. Method: Realistic finite element method head models were generated with and without fontanels. The electrical activity of the whole cortex was simulated using distributed 54,620 concurrently active cortical dipoles with a uniform random distribution of current densities (0–40 lA/cm 2 ). The overall effects of fontanels on scalp potentials were calculated from finite element forward solution in the vicinity the fon- tanel region by relative difference measure (RDM ⁄ ) and magnification factor (MAG), and the skull conduc- tivity was systematically varied from 0.003 to 0.3 S/m. Results: The neonatal scalp EEG topographies are comparable in models with and without fontanels, with highest amplitudes directly above the anterior fontanel. Quantitatively, comparison of these models elic- its negligible differences (RDM ⁄ 2% and MAG 1.0). However, fontanel contribution to scalp potential was shown to increase sharply with decreases in skull conductivity. Conclusions: These results suggest that fontanels may affect neonatal scalp EEG much less than tradition- ally assumed, and the effect is strongly dependent on skull conductivity. Significance: Most neonatal EEG studies can be adequately performed without assuming distortions by fontanels. Ó 2014 International Federation of Clinical Neurophysiology. Published by Elsevier Ireland Ltd. All rights reserved. 1. Introduction Rapid advancement of early developmental neuroscience has significantly increased the interest in functional brain assessment, which is commonly studied with neonatal/infant EEG. Several recent studies have illustrated that signal gain in neonatal/infant EEG is limited by the number of recording electrodes (Grieve et al., 2004; Odabaee et al., 2013, 2014). Better spatial resolution is possible by using higher density EEG (hdEEG) systems, which are now commercially available for the laboratory (Fifer et al., 2006; Grieve et al., 2003; Odabaee et al., 2013; Roche-Labarbe et al., 2008) and have even been employed in intensive care units (Stjerna et al., 2012; Vanhatalo et al., 2008; Welch et al., 2013). Increasing the number of recording electrodes leads to clear experimental benefits, including the possibility for genuine source localization of neonatal/infant EEG (Beauchemin et al., 2011; Despotovic et al., 2013; Roche-Labarbe et al., 2008). However, this method for improved source localization is only possible if the EEG data qualities at each site is ubiquitous. Dense electrode arrays have been associated with an increase risk of signal distortion http://dx.doi.org/10.1016/j.clinph.2014.12.002 1388-2457/Ó 2014 International Federation of Clinical Neurophysiology. Published by Elsevier Ireland Ltd. All rights reserved. ⇑ Corresponding author at: Department of Clinical Neurophysiology, Children’s Hospital, Helsinki University Hospital, P.O. Box 280, 00029 HUS, Finland. E-mail address: sampsa.vanhatalo@helsinki.fi (S. Vanhatalo). Clinical Neurophysiology xxx (2014) xxx–xxx Contents lists available at ScienceDirect Clinical Neurophysiology journal homepage: www.elsevier.com/locate/clinph Please cite this article in press as: Gargiulo P et al. The effect of fontanel on scalp EEG potentials in the neonate. Clin Neurophysiol (2014), http://dx.doi.org/ 10.1016/j.clinph.2014.12.002
-
Upload
independent -
Category
Documents
-
view
4 -
download
0
Transcript of The effect of fontanel on scalp EEG potentials in the neonate

Clinical Neurophysiology xxx (2014) xxx–xxx
Contents lists available at ScienceDirect
Clinical Neurophysiology
journal homepage: www.elsevier .com/locate /c l inph
The effect of fontanel on scalp EEG potentials in the neonate
http://dx.doi.org/10.1016/j.clinph.2014.12.0021388-2457/� 2014 International Federation of Clinical Neurophysiology. Published by Elsevier Ireland Ltd. All rights reserved.
⇑ Corresponding author at: Department of Clinical Neurophysiology, Children’sHospital, Helsinki University Hospital, P.O. Box 280, 00029 HUS, Finland.
E-mail address: [email protected] (S. Vanhatalo).
Please cite this article in press as: Gargiulo P et al. The effect of fontanel on scalp EEG potentials in the neonate. Clin Neurophysiol (2014), http://dx.d10.1016/j.clinph.2014.12.002
P. Gargiulo a,b, P. Belfiore c, E.A. Friðgeirsson d, S. Vanhatalo e,⇑, C. Ramon a,f
a Institute of Biomedical and Neural Engineering, Reykjavik University, Icelandb Department of Science, Landspitali University Hospital, Reykjavik, Icelandc Department of Biomedical, Electronic and Telecommunication Engineering, University Federico II of Naples, Italyd Department of Development CE and IT, Landspitali University Hospital, Reykjavik, Icelande Department of Children’s Clinical Neurophysiology, HUS Medical Imaging Center and Children’s Hospital, Helsinki University Central Hospital and University of Helsinki, Helsinki,Finlandf Department of Electrical Engineering, University of Washington, Seattle, WA 98195, USA
a r t i c l e i n f o h i g h l i g h t s
Article history:Accepted 4 December 2014Available online xxxx
Keywords:Neonatal EEGHigh density EEGSource localizationHead model
� Fontanels in the neonatal skull form spatial discontinuity in the head models.� EEG simulation of the whole cortex activity discloses no distortion by fontanels.� The relative effect of fontanels on scalp EEG potentials is negligible.
a b s t r a c t
Objective: To define how fontanels affect scalp EEG potentials in neonates.Method: Realistic finite element method head models were generated with and without fontanels. Theelectrical activity of the whole cortex was simulated using distributed 54,620 concurrently active corticaldipoles with a uniform random distribution of current densities (0–40 lA/cm2). The overall effects offontanels on scalp potentials were calculated from finite element forward solution in the vicinity the fon-tanel region by relative difference measure (RDM⁄) and magnification factor (MAG), and the skull conduc-tivity was systematically varied from 0.003 to 0.3 S/m.Results: The neonatal scalp EEG topographies are comparable in models with and without fontanels, withhighest amplitudes directly above the anterior fontanel. Quantitatively, comparison of these models elic-its negligible differences (RDM⁄ �2% and MAG �1.0). However, fontanel contribution to scalp potentialwas shown to increase sharply with decreases in skull conductivity.Conclusions: These results suggest that fontanels may affect neonatal scalp EEG much less than tradition-ally assumed, and the effect is strongly dependent on skull conductivity.Significance: Most neonatal EEG studies can be adequately performed without assuming distortions byfontanels.� 2014 International Federation of Clinical Neurophysiology. Published by Elsevier Ireland Ltd. All rights
reserved.
1. Introduction
Rapid advancement of early developmental neuroscience hassignificantly increased the interest in functional brain assessment,which is commonly studied with neonatal/infant EEG. Severalrecent studies have illustrated that signal gain in neonatal/infantEEG is limited by the number of recording electrodes (Grieveet al., 2004; Odabaee et al., 2013, 2014). Better spatial resolution
is possible by using higher density EEG (hdEEG) systems, whichare now commercially available for the laboratory (Fifer et al.,2006; Grieve et al., 2003; Odabaee et al., 2013; Roche-Labarbeet al., 2008) and have even been employed in intensive care units(Stjerna et al., 2012; Vanhatalo et al., 2008; Welch et al., 2013).
Increasing the number of recording electrodes leads to clearexperimental benefits, including the possibility for genuine sourcelocalization of neonatal/infant EEG (Beauchemin et al., 2011;Despotovic et al., 2013; Roche-Labarbe et al., 2008). However, thismethod for improved source localization is only possible if the EEGdata qualities at each site is ubiquitous. Dense electrode arrayshave been associated with an increase risk of signal distortion
oi.org/

Fig. 1. Workflow of the study.
2 P. Gargiulo et al. / Clinical Neurophysiology xxx (2014) xxx–xxx
caused by electrode bridges. A key challenge in obtaining adequatesource localization is in solving the forward problem with realistichead models that include all macroscopic details of an infant’shead. The most significant feature of a newborn-specific headmodel is the inclusion of fontanels, or the soft membranous gapsbetween the incompletely formed cranial bones that allow for cra-nial growth from early expansion of brain. In infant cranial skulldevelopment, the brain grows quicker than the rate of local ossifi-cation, resulting in the formation of four relatively wide gaps priorto eventual cranial suture development: the anterior, posterior,sphenoidal, and anterolateral fontanels (Cornette et al., 2002).Based on the vast literature on adult EEG source localization, allof these openings in the skull layer should lead to severe spatialdistortions in the scalp EEG (Heasman et al., 2002; Li et al., 2007).
Our recent work showed that the neonatal skull likely has anelectrical conductivity level close to those of other soft tissues,which is orders of magnitude higher than the conductivity of adultcranial bones (Odabaee et al., 2014; see also Despotovic et al.,2013). This would indirectly suggest that infant fontanels mayhave less significance than what is expected from correspondingskull openings in adults; however, the effect of fontanels has notbeen directly tested in realistic conditions. The implications fromcharacterizing fontanel effects on infant EEG are twofold. First, thisinvestigation would directly affect the design of realistic sourcelocalization methods required to advance signal gain from neona-tal EEG. Second, knowing the EEG sensitivity to fontanels would becrucial for the comparative assessment of EEG and magnetoen-cephalography (MEG), which are currently assessed using headmodels without realistic conduction properties (Lew et al., 2013).
From this motivation, our present work set out to analyze theeffects of fontanels on infant scalp EEG potentials in realistic con-ditions where scalp EEG is produced by the widespread corticalactivity. We used realistic head models both with and without fon-tanels and including all cranial tissue compartments. This studyaimed to elucidate whether the scalp potential topography is dis-torted around fontanel region and whether the relative quantita-tive effects from fontanels may be affected by different levels ofconductivity in the fontanel region.
2. Material and methods
A schematic outlining the methods utilized in our study isshown in Fig. 1. Two sets of finite element (FEM) head models, bothincluding models with and without fontanels, were generated tosimulate scalp EEG. Two head models were utilized to assesswhether changes in skull conductivity during infant developmentwould change the fontanel effects. These scalp potential distribu-tions were compared between head models, and we likewiseassessed the effects of fontanel conductivity. The analytic protocolswere the same for both head models.
2.1. Subject and head model generation
MRI images taken from a two week old healthy male born at theterm age (110 axial MR slices, image matrix = 256 � 256 � 110,slice resolution 256 � 256, pixel size = 0.938 mm, field ofview = 240.00 mm and slice thickness = 1 mm). MRI images weresegmented using the commercial medical image processing plat-form MIMICS 16 from Materialise (MIMICS, 2013; available at:http://www.materialise.com), and the results were qualitativelyconfirmed for consistency. We segmented the following tissuestructures (Ramon et al., 2006): white and gray matter, cerebellum,CSF, skull, dura layer, skin, eyes, and crystalline lens. Since some ofthese structures were not separable with clearly distinguishedintensity thresholds, we used special segmentation techniques
Please cite this article in press as: Gargiulo P et al. The effect of fontanel on scalp10.1016/j.clinph.2014.12.002
such as morphological, Boolean, and manual editing tools to isolatethem from the surroundings as described previously (Gargiuloet al., 2008, 2011). The skull diameter was 9.38 cm and the averagethickness of the skull layer was 2.8 mm. The segmentations areshown in axial and coronal planes as well as in 3D in Fig. 2.
2.2. Tissue conductivities
Tissue conductivities were adopted from previous literature(Ramon et al., 2006) and are summarized in Table 1. However, itshould be noted that the conductivity of the dura layer is not wellknown. We assumed a midrange value of 0.06 S/m from the range0.02–0.1 S/m described in literature. For simplicity, we usedisotropic tissue conductivities, although it is known that, in adults,white matter and the skull are anisotropic (Güllmar et al., 2010).Including anisotropy could improve model accuracy, but requiresdiffusion tensor imaging to extract the anisotropic tissue conduc-tivities (Marin et al., 1998). Moreover, the dimensions in the babyhead structures (e.g. skull thickness) are already at the limit of MRIvoxel resolution, which limits the inclusion of anisotropy in ormodels.
For the skull conductivity, we adopted values that have beenrecently proposed in the theoretical and empirical papers on neo-natal EEG, which suggest an order of magnitude higher conductiv-ity in neonates than in adults (Roche-Labarbe et al., 2008; Songet al., 2013). For the analyses of scalp potential topography,fontanel conductivity was taken as the cerebrospinal fluid(CSF = 1.54 S/m) conductivity since fontanels are essentially wetsubcutaneous tissue without major resistive layers and using CSFconductivity allows for a maximal contrast between head modelswith and without fontanels. We also combined conductivities forsoft and hard bone, which can simply be defined as skull conduc-tivity (Song et al., 2013). Infant scalp potentials were simulatedusing two different skull conductivity values: one to represent highskull conductivities in newborns (0.2 S/m; Odabaee et al., 2014)
EEG potentials in the neonate. Clin Neurophysiol (2014), http://dx.doi.org/

Fig. 2. Head model generation. (A) MRI image segmented into 10 tissue compartments: soft tissue (cyan), soft bone (light green), hard bone (dark cyan), gray matter (violet),white matter (blue), CSF (orange), cerebellum (yellow), eyes (gray), fontanels (red) and fat (green). (B) 3Dmodel of the infant skull showing fontanel positions in red (front andtop views). (C) The source vectors within a segmented slice of the brain. The normal vectors (blue) between white matter (green) and gray matter (orange). Inset gives adetailed in small area. (D) Example of adaptive FEM meshing. The picture shows an adaptive FEM grid and the details of the grid in the vicinity of the cortical sources. The FEMsoftware automatically adjusts the grid resolution in each iteration to achieve the desired L2-norm while keeping the computational errors to a minimum level. Note that theelement size varies and depends on distance to the source. For instance, elements in cerebellum are bigger than the elements close to the gray–white matter boundaries. (Forinterpretation of the references to colour in this figure legend, the reader is referred to the web version of this article.)
Table 1Mean conductivities for the segmented tissues in adults.
Tissue Conductivities (S/m)
Brain white matter 0.143Brain gray matter 0.333Spinal cord and cerebellum 0.15385Cerebrospinal fluid 1.54Hard bone 0.00625Soft bone 0.04Blood 0.625Muscle 0.1Fat 0.04Scalp 0.435Soft tissue 0.2Air (internal moist) 0.005
P. Gargiulo et al. / Clinical Neurophysiology xxx (2014) xxx–xxx 3
and the other assumed to represent the moderate skull conductiv-ity of older infants (0.05 S/m).
2.3. Generation of the source space
This study was aimed to simulate the natural, spontaneousbrain activity that always produces complex global EEG patternsas opposed to the more simple EEG topographies produced byclassical dipolar sources (e.g. Lew et al., 2013). To this end, wesimulated realistic spatial mixing of cortical activity by assumingthat dipolar sources are located in the cortex with uniform randomdistribution of dipolar intensities.
To define surface nodes, we used the isosurface algorithm inMatlab (MATLAB version 7.10.0. Natick, Massachusetts: The Math-Works Inc., 2010) on a binary image matrix from the boundary
Please cite this article in press as: Gargiulo P et al. The effect of fontanel on scalp10.1016/j.clinph.2014.12.002
between white and gray matters. This program likewise allowedfor the computation of normal vectors using the central finitedifference approximation to the numerical gradient at nodeswithin the binary matrix. Therefore, for each surface node f(x, y,z), the three gradient components may be found by (1):
@f@x¼ f xþ hx
2
� �� f x� hx
2
� �
@f@y¼ f yþ hy
2
� �� f y� hy
2
� �
@f@z¼ f zþ hz
2
� �� f z� hz
2
� �ð1Þ
where hx, hy and hz are the separations between the adjacent pointsin the x, y, and z directions, respectively.
In this method of computation, surface nodes are fixed whilethe gradient components are perpendicular to the surface andtherefore considered normal vector components. The normal vec-tor distribution within a segmented slice of the brain is shown inFig. 2C.
The next step was to create a distribution of normally-orienteddipolar sources in the cortical layer. Source spaces consisting ofapproximately 8 � 106 dipolar sources, were created using a previ-ously described method (Song et al., 2013) that computes voltagesat the nodes surrounding the dipole. This has been shown to beaccurate when the distance to a computed electric field issignificantly larger than the dipole spacing (Song et al., 2013). Inour case, source spacing was approximately 1.0 mm, and thedistance to scalp was up to few cm from the sources. The selectedcurrent density of each dipole was chosen to be from J = 0 to40 lA/cm2 with a uniform random distribution. The maximumvalue of 40 lA/cm2 was computed based on the cortical voxel.
EEG potentials in the neonate. Clin Neurophysiol (2014), http://dx.doi.org/

4 P. Gargiulo et al. / Clinical Neurophysiology xxx (2014) xxx–xxx
For each normal vector, the current density of the normal vectorcomponents was calculated with:
Jx ¼ j � @f@x
Jy ¼ j � @f@y
Jz ¼ j � @f@z
ð2Þ
The origin of the normal vector was fixed at a reference voltage,and the voltages at the neighboring nodes were calculated usingthe equation DV ¼ I � R where the resistance along an edge in thevoxel is found from the resistivity of gray matter (300 Xcm). Thiswas repeated for all normal vectors, superimposing the vectorswhen a node was influenced by more than one dipole.
2.4. Scalp EEG simulation
Using an adaptive FEM solver, potentials and flux distributionsin the whole head model were computed for a given dipole inten-sity distribution. We used an adaptive FEM solver software, Galer-wint, developed at the University of Washington (Schimpf et al.,1996). The allowable element size varied from 1 to 32 voxels,and an exact match of elements to segment boundaries wasenforced. The solver used the Joint Conjugate Gradient method tocompute fluxes in the whole model. The electrical activity in eachcortical voxel was represented by a dipolar source, which repre-sented an averaged sum of volume currents of all neurons in onehypercolumn. Here, our assumption was that a cortical voxel couldbe treated as a hypercolumn. In general, a hypercolumn has about80 � 103 to 100 � 103 neurons (Horton and Adams, 2005).
Fig. 2D shows an adaptive FEM grid and the details of this gridin the vicinity of the cortical sources. The FEM software automati-cally adjusts the grid resolution in each iteration to achieve the
Table 2The run parameters for one of the simulation.
Run parameters Fontanels Non-fontanel
#Dipoles 54,620 54,620#Elements 815,830 815,627#Nodes 916,267 916,233
Fig. 3. Comparison of scalp potential topographies in newborn (A and B) and infant (C andm) including (left) and without (right) fontanels shows very similar overall pattern. (B)models with vs. without fontanel. The figures show a minor difference that is strictly lim0.05 S/m) including (left) and without (right) fontanels shows very similar overall pattermodels with and without fontanel. The figures show a minor difference that is strictly l
Please cite this article in press as: Gargiulo P et al. The effect of fontanel on scalp10.1016/j.clinph.2014.12.002
desired L2-norm while keeping the computational errors to a min-imum level.
A total of ten runs were made with different uniform randomdistributions of dipolar intensities. The dipoles in the voxels wereoriented normal to the local normal surface of the white and graymatter boundary with the orientation of the local normal vectorpointing from white to gray matter. For each dipole, the intensitywas set to 0–40 lA/cm2 (dipole moment 0.4 nA m) with a randomuniform distribution, and all dipoles were set to be active simulta-neously. The number of dipoles and the simulation parameters areshown in Table 2.
2.5. Analyses comparing head models
In order to evaluate the effect of fontanels on scalp potentials, wecompared two head models: one that had fontanel conductivity setto the conductivity of CSF (1.54 S/m), and the other that had fonta-nels replaced with infant bone tissue as previously defined (new-born and infant models). The latter is hereafter referred to as the‘‘non-fontanel model’’. Firstly, we inspected the topographic distri-butions of scalp potentials to see whether gross differences can beobserved according to presence of fontanels. Secondly, we analyzedthe topographic differences between models by subtracting scalppotential distributions (fontanel minus non-fontanel). Thirdly, wequantified the regional effects of fontanels on the scalp potentialsusing the relative difference measure (RDM⁄) and magnification fac-tor (MAG) on a fixed, 3100 mm2 region of interest on the scalp thatsurrounds the fontanel areas (which had a total surface of35,000 mm2). This choice of region was obviously arbitrary, but itsurrounded the region where our subtraction images showed thedifference (Fig 3), and it also roughly corresponded to the areawhere distortion of EEG potentials by fontanels is commonlyexpected to occur. While the numerical results do obviously co-varywith the choice of region, we assumed a limited region to allow for abetter estimation of fontanel effects than using global measures ofMAG and RDM⁄. The RDM⁄ is computed as follows (Schimpf et al.,2002; Malmivuo and Plonsey, 1995; Ramon et al., 2014):
RDM� ¼
ffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiXN
n¼1
VFiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiPNi¼1ðV
Fi Þ2q � VNiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiPN
i¼1ðVNi Þ2
q0B@
1CA
2vuuuut ð3Þ
D) head models. (A) Comparison of newborn head models (skull conductivity 0.2 S/Three views of the scalp potential topography from subtraction of newborn headited to the fontanel area. (C) Comparison of infant head models (skull conductivity
n. (D) Three views of the scalp potential topography from subtraction of infant headimited to the fontanel area.
EEG potentials in the neonate. Clin Neurophysiol (2014), http://dx.doi.org/
P. Gargiulo et al. / Clinical Neurophysiology xxx (2014) xxx–xxx 5
where the summation is over all sampling points (the total numberof spatial sampling points at scalp are N = 31,942. VF indicates thepotentials computed from the fontanel model, and VN indicatespotentials computed from the non-fontanel model.
The MAG is calculated as follows:
MAG ¼
ffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiPNi¼1ðV
Fi Þ2PNi¼1ðV
Ni Þ2
vuut ð4Þ
As evidenced by these equations, if the two models are same,the RDM⁄ will be zero and MAG will be unity.
Lastly, we varied the fontanel conductivity levels to assess thesensitivity of RDM⁄ and/or MAG to scalp conductivity in head mod-els with neonatal or infant dimensions.
2.6. Interaction between fontanel effects and skull conductivity
Theoretically, it is possible that a higher skull conductivity inneonates could be responsible for the lack of fontanel-relatedEEG distortion seen in adults (Heasman et al., 2002; Li et al.,2007). Hence, we examined the relative fontanel-related distor-tions when skull conductivities were varied from the lowest sug-gested levels in adults (0.003 S/m) to the highest suggested levelsin neonates (0.3 S/m).
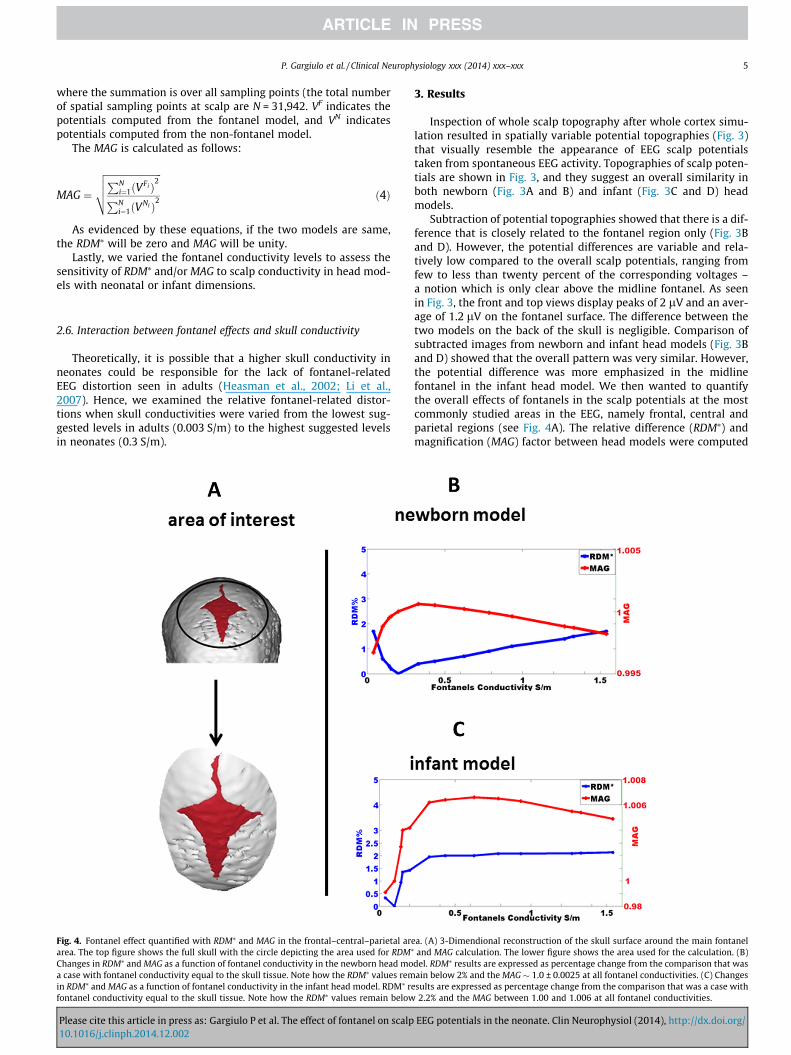
Fig. 4. Fontanel effect quantified with RDM⁄ and MAG in the frontal–central–parietal ararea. The top figure shows the full skull with the circle depicting the area used for RDM⁄
Changes in RDM⁄ and MAG as a function of fontanel conductivity in the newborn head moa case with fontanel conductivity equal to the skull tissue. Note how the RDM⁄ values remin RDM⁄ and MAG as a function of fontanel conductivity in the infant head model. RDM⁄ refontanel conductivity equal to the skull tissue. Note how the RDM⁄ values remain below
Please cite this article in press as: Gargiulo P et al. The effect of fontanel on scalp10.1016/j.clinph.2014.12.002
3. Results
Inspection of whole scalp topography after whole cortex simu-lation resulted in spatially variable potential topographies (Fig. 3)that visually resemble the appearance of EEG scalp potentialstaken from spontaneous EEG activity. Topographies of scalp poten-tials are shown in Fig. 3, and they suggest an overall similarity inboth newborn (Fig. 3A and B) and infant (Fig. 3C and D) headmodels.
Subtraction of potential topographies showed that there is a dif-ference that is closely related to the fontanel region only (Fig. 3Band D). However, the potential differences are variable and rela-tively low compared to the overall scalp potentials, ranging fromfew to less than twenty percent of the corresponding voltages –a notion which is only clear above the midline fontanel. As seenin Fig. 3, the front and top views display peaks of 2 lV and an aver-age of 1.2 lV on the fontanel surface. The difference between thetwo models on the back of the skull is negligible. Comparison ofsubtracted images from newborn and infant head models (Fig. 3Band D) showed that the overall pattern was very similar. However,the potential difference was more emphasized in the midlinefontanel in the infant head model. We then wanted to quantifythe overall effects of fontanels in the scalp potentials at the mostcommonly studied areas in the EEG, namely frontal, central andparietal regions (see Fig. 4A). The relative difference (RDM⁄) andmagnification (MAG) factor between head models were computed
ea. (A) 3-Dimendional reconstruction of the skull surface around the main fontaneland MAG calculation. The lower figure shows the area used for the calculation. (B)
del. RDM⁄ results are expressed as percentage change from the comparison that wasain below 2% and the MAG � 1.0 ± 0.0025 at all fontanel conductivities. (C) Changessults are expressed as percentage change from the comparison that was a case with2.2% and the MAG between 1.00 and 1.006 at all fontanel conductivities.
EEG potentials in the neonate. Clin Neurophysiol (2014), http://dx.doi.org/
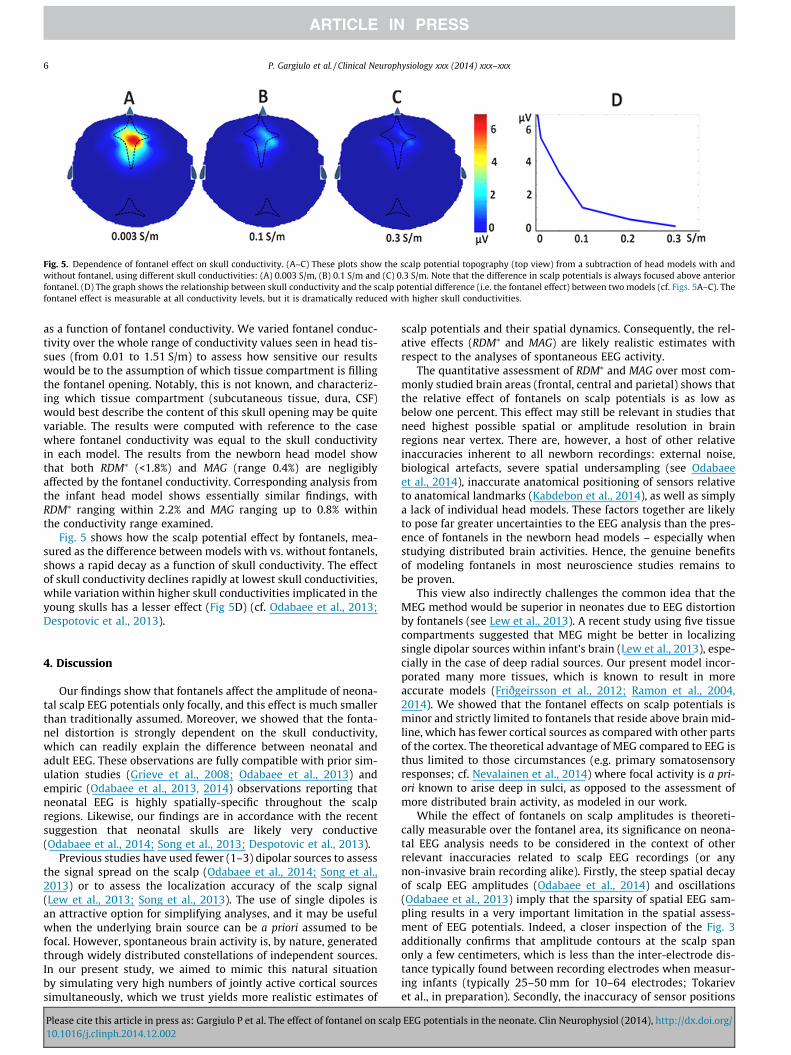
Fig. 5. Dependence of fontanel effect on skull conductivity. (A–C) These plots show the scalp potential topography (top view) from a subtraction of head models with andwithout fontanel, using different skull conductivities: (A) 0.003 S/m, (B) 0.1 S/m and (C) 0.3 S/m. Note that the difference in scalp potentials is always focused above anteriorfontanel. (D) The graph shows the relationship between skull conductivity and the scalp potential difference (i.e. the fontanel effect) between two models (cf. Figs. 5A–C). Thefontanel effect is measurable at all conductivity levels, but it is dramatically reduced with higher skull conductivities.
6 P. Gargiulo et al. / Clinical Neurophysiology xxx (2014) xxx–xxx
as a function of fontanel conductivity. We varied fontanel conduc-tivity over the whole range of conductivity values seen in head tis-sues (from 0.01 to 1.51 S/m) to assess how sensitive our resultswould be to the assumption of which tissue compartment is fillingthe fontanel opening. Notably, this is not known, and characteriz-ing which tissue compartment (subcutaneous tissue, dura, CSF)would best describe the content of this skull opening may be quitevariable. The results were computed with reference to the casewhere fontanel conductivity was equal to the skull conductivityin each model. The results from the newborn head model showthat both RDM⁄ (<1.8%) and MAG (range 0.4%) are negligiblyaffected by the fontanel conductivity. Corresponding analysis fromthe infant head model shows essentially similar findings, withRDM⁄ ranging within 2.2% and MAG ranging up to 0.8% withinthe conductivity range examined.
Fig. 5 shows how the scalp potential effect by fontanels, mea-sured as the difference between models with vs. without fontanels,shows a rapid decay as a function of skull conductivity. The effectof skull conductivity declines rapidly at lowest skull conductivities,while variation within higher skull conductivities implicated in theyoung skulls has a lesser effect (Fig 5D) (cf. Odabaee et al., 2013;Despotovic et al., 2013).
4. Discussion
Our findings show that fontanels affect the amplitude of neona-tal scalp EEG potentials only focally, and this effect is much smallerthan traditionally assumed. Moreover, we showed that the fonta-nel distortion is strongly dependent on the skull conductivity,which can readily explain the difference between neonatal andadult EEG. These observations are fully compatible with prior sim-ulation studies (Grieve et al., 2008; Odabaee et al., 2013) andempiric (Odabaee et al., 2013, 2014) observations reporting thatneonatal EEG is highly spatially-specific throughout the scalpregions. Likewise, our findings are in accordance with the recentsuggestion that neonatal skulls are likely very conductive(Odabaee et al., 2014; Song et al., 2013; Despotovic et al., 2013).
Previous studies have used fewer (1–3) dipolar sources to assessthe signal spread on the scalp (Odabaee et al., 2014; Song et al.,2013) or to assess the localization accuracy of the scalp signal(Lew et al., 2013; Song et al., 2013). The use of single dipoles isan attractive option for simplifying analyses, and it may be usefulwhen the underlying brain source can be a priori assumed to befocal. However, spontaneous brain activity is, by nature, generatedthrough widely distributed constellations of independent sources.In our present study, we aimed to mimic this natural situationby simulating very high numbers of jointly active cortical sourcessimultaneously, which we trust yields more realistic estimates of
Please cite this article in press as: Gargiulo P et al. The effect of fontanel on scalp10.1016/j.clinph.2014.12.002
scalp potentials and their spatial dynamics. Consequently, the rel-ative effects (RDM⁄ and MAG) are likely realistic estimates withrespect to the analyses of spontaneous EEG activity.
The quantitative assessment of RDM⁄ and MAG over most com-monly studied brain areas (frontal, central and parietal) shows thatthe relative effect of fontanels on scalp potentials is as low asbelow one percent. This effect may still be relevant in studies thatneed highest possible spatial or amplitude resolution in brainregions near vertex. There are, however, a host of other relativeinaccuracies inherent to all newborn recordings: external noise,biological artefacts, severe spatial undersampling (see Odabaeeet al., 2014), inaccurate anatomical positioning of sensors relativeto anatomical landmarks (Kabdebon et al., 2014), as well as simplya lack of individual head models. These factors together are likelyto pose far greater uncertainties to the EEG analysis than the pres-ence of fontanels in the newborn head models – especially whenstudying distributed brain activities. Hence, the genuine benefitsof modeling fontanels in most neuroscience studies remains tobe proven.
This view also indirectly challenges the common idea that theMEG method would be superior in neonates due to EEG distortionby fontanels (see Lew et al., 2013). A recent study using five tissuecompartments suggested that MEG might be better in localizingsingle dipolar sources within infant’s brain (Lew et al., 2013), espe-cially in the case of deep radial sources. Our present model incor-porated many more tissues, which is known to result in moreaccurate models (Friðgeirsson et al., 2012; Ramon et al., 2004,2014). We showed that the fontanel effects on scalp potentials isminor and strictly limited to fontanels that reside above brain mid-line, which has fewer cortical sources as compared with other partsof the cortex. The theoretical advantage of MEG compared to EEG isthus limited to those circumstances (e.g. primary somatosensoryresponses; cf. Nevalainen et al., 2014) where focal activity is a pri-ori known to arise deep in sulci, as opposed to the assessment ofmore distributed brain activity, as modeled in our work.
While the effect of fontanels on scalp amplitudes is theoreti-cally measurable over the fontanel area, its significance on neona-tal EEG analysis needs to be considered in the context of otherrelevant inaccuracies related to scalp EEG recordings (or anynon-invasive brain recording alike). Firstly, the steep spatial decayof scalp EEG amplitudes (Odabaee et al., 2014) and oscillations(Odabaee et al., 2013) imply that the sparsity of spatial EEG sam-pling results in a very important limitation in the spatial assess-ment of EEG potentials. Indeed, a closer inspection of the Fig. 3additionally confirms that amplitude contours at the scalp spanonly a few centimeters, which is less than the inter-electrode dis-tance typically found between recording electrodes when measur-ing infants (typically 25–50 mm for 10–64 electrodes; Tokarievet al., in preparation). Secondly, the inaccuracy of sensor positions
EEG potentials in the neonate. Clin Neurophysiol (2014), http://dx.doi.org/

P. Gargiulo et al. / Clinical Neurophysiology xxx (2014) xxx–xxx 7
relative to cortical areas is known to be in the order of 10–20 mm(Hellström et al., 1963; Kabdebon et al., 2014), which, togetherwith spatial amplitude decays (Odabaee et al., 2014), presents biasthat is stronger than direct fontanel effects – even above the fonta-nel. Thirdly, the technical and biological noise needs to be consid-ered, as it is always present in the recording session and mayreadily exceed the fontanel effects.
The assumption that neonatal EEG is distorted by the presenceof fontanels arose from ignoring the geometry and particulardevelopmental histology in the neonatal skull tissue. The skullthickness in neonates (2–3 mm; cf. Despotovic et al., 2013) com-pared to adults (3–6 mm) makes the relative contribution of skulltissue small in the first place, and the presumably high conductionin the neonatal skull layer (Odabaee et al., 2014) makes the con-ductive pathways relatively similar in and around the fontanelareas. The high conduction of neonatal skull bone is readilyexplained by its key properties: it is non-ossified at birth, andthe histological structure remains trabecular for a longer time(Ernst et al., 2011; Silau, 1995), hence providing tissue pathwayswith high electric conductivity until the skull becomes fully ossi-fied later in life.
Neonatal EEG source localization has recently gained consider-able interest when the recording methods have allowed for betterspatial EEG collection (Fifer et al., 2006; Grieve et al., 2008; Roche-Labarbe et al., 2008; Welch et al., 2013; Vanhatalo et al., 2008;Despotovic et al., 2013), while the theoretical studies have pro-vided better understanding for improved source localization meth-ods (Song et al., 2013; Odabaee et al., 2013, 2014). Our study didnot assess source localization directly; however, the absence ofmajor effects of fontanels in the forward solutions suggests thatadequate source localization (within the constraints of the record-ing configuration) may be feasible. This idea has a significant impli-cation: it allows the use of boundary element methods (BEM)models that are widely available in user-friendly analysis pack-ages, while FEM required for models with fontanel have been avail-able in selected and more demanding academic analysisenvironments only.
The immediate impacts of our findings to clinical practice maybe more limited than their impacts to more advanced academicwork. Currently, most clinical centers are still recording infantswith only 8–10 electrodes (cf. Andre et al., 2010), and the conven-tional visual waveform assessment is rough enough to ignore pos-sible amplitude variations of this magnitude. However, increasingnumbers of advanced medical centers are performing EEG record-ings with EEG caps or other electrode nets (see above), whichresults in more spatial data being collected at and near fontanelareas. It is thereby becoming increasingly important to acknowl-edge that the scalp EEG in neonates is spatially accurate and it isnot meaningfully confounded by fontanels. Based on recent studiesand known cranial histology, it may be assumed that the presentfindings can be qualitatively comparable in preterm babies as well.Finally, many clinicians are now using Laplacian derivations avail-able in more advanced EEG review softwares. Our present resultssupport the use of spherical splined amplitude interpolations forcommon implementation in these EEG softwares.
Acknowledgments
S.V. was supported by the Academy of Finland, as well as by theEuropean Community’s Seventh Framework Programme, EuropeanCommunity (FP7-PEOPLE-2009-IOF, grant agreement no. 254235,as well as FP7-HEALTH-2009-4-2-1, grant agreement no. 241479,The NEMO Project).
Conflict of interest: Nothing to declare.
Please cite this article in press as: Gargiulo P et al. The effect of fontanel on scalp10.1016/j.clinph.2014.12.002
References
André M, Lamblin MD, d’Allest AM, Curzi-Dascalova L, Moussalli-Salefranque F, SNguyen The T, et al. Electroencephalography in premature and full-term infants.Developmental features and glossary. Neurophysiol Clin 2010;40:59–124.
Beauchemin M, González-Frankenberger B, Tremblay J, Vannasing P, Martínez-Montes E, Belin P, et al. Mother and stranger: an electrophysiological study ofvoice processing in newborns. Cereb Cortex 2011;21:1705–11.
Cornette LG, Tanner SF, Ramenghi LA, Miall LS, Childs AM, Arthur RJ, et al. Magneticresonance imaging of the infant brain: anatomical characteristics and clinicalsignificance of punctate lesions. Arch Dis Child Fetal Neonatal Ed2002;86:F171–7.
Despotovic I, Cherian PJ, Vos M, Hallez H, Deburchgraeve W, Govaert P, et al.Relationship of EEG sources of neonatal seizures to acute perinatal brain lesionsseen on MRI: a pilot study. Hum Brain Mapp 2013;34:2402–17.
Ernst LM, Ruchelli ED, Huff DS. Color atlas of fetal and neonatal histology. 1sted. London: Springer; 2011.
Fifer WP, Grieve PG, Grose-Fifer J, Isler JR, Byrd D. High-densityelectroencephalogram monitoring in the neonate. Clin Perinatol 2006;33:679–91.
Friðgeirsson EA, Gargiulo P, Ramon C, Haueisen J. 3D segmented model of head formodelling electrical activity of brain. Eur J Transl Myol 2012;22:57–60.
Gargiulo P, Vatnsdal B, Ingvarsson P, Knutsdottir S, Gudmundsdottir V, Yngvason S,Helgason T. Restoration of muscle volume and shape induced by electricalstimulation of denervated degenerated muscles: qualitative and quantitativemeasurement of changes in rectus femoris using computer tomography andimage segmentation. Artif Organs 2008;32:609–13.
Gargiulo P, Helgason T, Reynisson PJ, Helgason B, Kern H, Mayr W, et al. Monitoringof muscle and bone recovery in spinal cord injury patients treated withelectrical stimulation using three-dimensional imaging and segmentationtechniques: methodological assessment. Artif Organs 2011;35:275–81.
Grieve PG, Emerson RG, Fifer WP, Isler JR, Stark RI. Spatial correlation of the infantand adult electroencephalogram. Clin Neurophysiol 2003;114:1594–608.
Grieve PG, Emerson RG, Isler JR, Stark RI. Quantitative analysis of spatial samplingerror in the infant and adult electroencephalogram. NeuroImage2004;21:1260–74.
Grieve PG, Isler JR, Izraelit A, Peterson BS, Fifer WP, Myers MM, Stark RI. EEGfunctional connectivity in term age extremely low birth weight infants. ClinNeurophys 2008;119:2712–20.
Güllmar D, Haueisen J, Reichenbach JR. Influence of anisotropic electricalconductivity in white matter tissue on the EEG/MEG forward and inversesolution. A high-resolution whole head simulation study. NeuroImage2010;51:145–63.
Heasman BC, Valentín A, Alarcón G, Seoane JJG, Binnie CD, Guy CN. A hole in theskull distorts substantially the distribution of extracranial electrical fields in anin vitro model. J Clin Neurophys 2002;19:163–71.
Hellström B, Karlsson B, Müssbichler H. Electrode placement in EEG of infants andits anatomical relationship studied radiographically. Electroenceph ClinNeurophysiol 1963;15:115–7.
Horton CJ, Adams DL. The cortical column: a structure without a function. PhilosTrans R Soc Lond B Biol Sci 2005;360:837–62.
Kabdebon C, Leroy F, Simmonet H, Perrot M, Dubois J, Dehaene-Lambertz G.Anatomical correlations of the international 10–20 sensor placement system ininfants. NeuroImage 2014;99:342–56.
Lew S, Sliva DD, Choe MS, Grant PE, Okada Y, Wolters CH, Hämäläinen MS. Effects ofsutures and fontanels on MEG and EEG source analysis in a realistic infant headmodel. NeuroImage 2013;76:282–93.
Li J, Wang K, Zhu S, He B. Effects of holes on EEG forward solutions using a realisticgeometry head model. J Neural Eng 2007;4:197.
Malmivuo J, Plonsey R. Bioelectromagnetism: principles and applications ofbioelectric and biomagnetic fields. 1st ed. Oxford: Oxford University Press;.
Marin G, Guerin C, Baillet S, Garnero L, Meunier G. Influence of skull anisotropy forthe forward and inverse problem in EEG: simulation studies using FEM onrealistic head models. Hum Brain Mapp 1998;6:250–69.
Nevalainen P, Lauronen L, Pihko E. Development of human somatosensory corticalfunctions–what have we learned from magnetoencephalography: a review.Front Hum Neurosci 2014;8:158.
Odabaee M, Tokariev A, Layeghy S, Mesbah M, Colditz PB, Ramon C, Vanhatalo S.Neonatal EEG at scalp is focal and implies high skull conductivity in realisticneonatal head models. NeuroImage 2014;96:73–80.
Odabaee M, Freeman WJ, Colditz PB, Ramon C, Vanhatalo S. Spatial patterning of theneonatal EEG suggests a need for a high number of electrodes. NeuroImage2013;68:229–35.
Ramon C, Schimpf P, Haueisen J, Holmes M, Ishimaru A. Role of soft bone, CSF andgray matter in EEG simulations. Brain Topogr 2004;16:245–8.
Ramon C, Schimpf PH, Haueisen J. Influence of head models on EEG simulations andinverse source localizations. Biomed Eng Online 2006;5:10.
Ramon C, Gargiulo P, Friðgeirsson EA, Haueisen J. Changes in scalp potentials andspatial smoothing effects of inclusion of dura layer inhuman head models forEEG simulations. Front Neuroeng 2014;7:32.
Roche-Labarbe N, Aarabi A, Kongolo G, Gondry-Jouet C, Dümpelmann M, Grebe R,Wallois F. High-resolution electroencephalography and source localization inneonates. Hum Brain Mapp 2008;29:167–76.
EEG potentials in the neonate. Clin Neurophysiol (2014), http://dx.doi.org/

8 P. Gargiulo et al. / Clinical Neurophysiology xxx (2014) xxx–xxx
Schimpf PH, Haynor DR, Kim Y. Object-free adaptive meshing in highlyheterogeneous 3-D domains. Int J Biomed Comp 1996;40:209–25.
Schimpf PH, Ramon C, Haueisen J. Dipole models for the EEG and MEG. IEEE TransBiomed Eng 2002;49:409–18.
Silau AM. Normal prenatal development of the human parietal bone andinterparietal suture. J Cran Gen Dev Biol 1995;15:81–6.
Song J, Morgan K, Turovets S, Li K. Anatomically accurate head models and theirderivatives for dense array EEG source localization. Funct Neurol Rehabil Ergon2013;3:275–93.
Please cite this article in press as: Gargiulo P et al. The effect of fontanel on scalp10.1016/j.clinph.2014.12.002
Stjerna S, Voipio J, Metsäranta M, Kaila K, Vanhatalo S. Preterm EEG: a multimodalneurophysiological protocol. J Vis Exp 2012;60:e3774.
Vanhatalo S, Metsäranta M, Andersson S. High-fidelity recording of brain activity inthe extremely preterm babies: feasibility study in the incubator. ClinNeurophysiol 2008;119:439–45.
Welch MG, Myers MM, Grieve PG, Isler JR, Fifer WP, Sahni R, et al.Electroencephalographic activity of preterm infants is increased by FamilyNurture Intervention: a randomized controlled trial in the NICU. ClinNeurophysiol 2013;125:675–84.
EEG potentials in the neonate. Clin Neurophysiol (2014), http://dx.doi.org/




















