Idiopathic" mental retardation and new chromosomal abnormalities

ARTICLE IN PRESS+Model
J Pediatr (Rio J) 2014xxx(xx)xxx---xxx
wwwjpedcombr
ORIGINAL ARTICLE
Chromosomal microarrays testing in children withdevelopmental disabilities and congenital anomalies
Guillermo Lay-Sonablowast Karena Espinozaa Cecilia Viala Juan C RiveraaMariacutea L Guzmaacutenab Gabriela M Repettoab
a Center for Human Genetics Facultad de Medicina Cliacutenica Alemana Universidad del Desarrollo Santiago Chileb Hospital Padre Hurtado Santiago Chile
Received 20 March 2014 accepted 9 July 2014
KEYWORDSMicroarraysCongenitalanomaliesDevelopmentaldisabilitiesCopy numbervariantsDiagnosis
AbstractObjectives Clinical use of microarray-based techniques for the analysis of many developmen-tal disorders has emerged during the last decade Thus chromosomal microarray has beenpositioned as a first-tier test This study reports the first experience in a Chilean cohortMethods Chilean patients with developmental disabilities and congenital anomalies were stud-ied with a high-density microarray (CytoScanTM HD Array Affymetrix Inc Santa Clara CAUSA) Patients had previous cytogenetic studies with either a normal result or a poorly charac-terized anomalyResults This study tested 40 patients selected by two or more criteria including major con-genital anomalies facial dysmorphism developmental delay and intellectual disability Copynumber variants (CNVs) were found in 725 of patients while a pathogenic CNV was found in25 of patients and a CNV of uncertain clinical significance was found in 25 of patientsConclusion Chromosomal microarray analysis is a useful and powerful tool for diagnosis of
developmental diseases by allowing accurate diagnosis improving the diagnosis rate anddiscovering new etiologies The higher cost is a limitation for widespread use in this settingcopy 2014 Sociedade Brasileira de Pediatria Published by Elsevier Editora Ltda All rights reserved
Please cite this article as Lay-Son G Espinoza K Vial C Rivera JC Guzmaacuten ML Repetto GM Chromosomal microarrays testing in childrenwith developmental disabilities and congenital anomalies J Pediatr (Rio J) 2014 httpdxdoiorg101016jjped201407003
lowast Corresponding authorE-mail glaysonuddcl (G Lay-Son)
httpdxdoiorg101016jjped2014070030021-7557copy 2014 Sociedade Brasileira de Pediatria Published by Elsevier Editora Ltda All rights reserved
JPED-218 No of Pages 6
ARTICLE IN PRESS+Model
2 Lay-Son G et al
PALAVRAS-CHAVEMicroarraysAnomaliascongecircnitasAtraso dedesenvolvimentoVariante do nuacutemerode coacutepiaDiagnoacutestico
Anaacutelise cromossocircmica por microarray em criancas com deficiecircncias dedesenvolvimento e anomalias congecircnitas
ResumoObjetivo O uso cliacutenico de teacutecnicas baseadas em microarrays para a anaacutelise de transtornos dedesenvolvimento tem surgido durante a uacuteltima deacutecada Assim o microarray cromossocircmico temsido posicionado como um teste de primeiro niacutevel cliacutenico Relatamos a primeira experiecircncia emuma coorte chilenaMeacutetodos Pacientes chilenos com atraso de desenvolvimento e anomalias congecircnitas foramestudados com um microarray de alta densidade (CytoScanTM HD Array Affymetrix Inc SantaClara CA EUA) Pacientes tiveram estudos citogeneacuteticos anteriores ou um resultado normalou de uma anomalia natildeo bem caracterizadaResultados Foram analisados 40 pacientes selecionados por dois ou mais criteacuterios incluindoanomalias congecircnitas maiores dismorfismo facial atraso de desenvolvimento e deficiecircncia int-electual Uma variante do nuacutemero de coacutepia (CNV) foi encontrada em 725 dos pacientesenquanto que uma CNV patogecircnica foi encontrada em 25 dos pacientes e uma CNV de signifi-cado cliacutenico incerto foi encontrada em 25 dos pacientesConclusotildees A anaacutelise cromossocircmica microarray eacute uma ferramenta uacutetil e poderosa emtranstornos de desenvolvimento permitindo um diagnoacutestico preciso melhorando a taxa dediagnoacutestico e descobrindo novas etiologias O custo mais elevado eacute uma limitacatildeo para um usodifundido em nossa realidadecopy 2014 Sociedade Brasileira de Pediatria Publicado por Elsevier Editora Ltda Todos os direitosreservados
I
Mlara
tomipds
isnktocntinos(htI
sctvf
acybteo
it
M
P
Fpa
t(ocause for the disorder
ntroduction
ajor congenital anomalies affect two to three of every 100ive newborns and are a leading cause of infant mortalitynd disability12 Although most are isolated and multifacto-ial in origin patients with multiple abnormalities requiren assessment to identify an underlying genetic cause
In recent years the etiological study of developmen-al disorders has been enriched with the clinical usef microarray-based techniques In developed countriesolecular karyotyping or chromosomal microarray (CMA)
s considered the first-line technique for the analysis ofatients with multiple congenital anomalies nonsyndromicevelopmental delayintellectual disability and autismpectrum disorders3---7
In contrast in developing nations such as Latin Amer-can countries detection of chromosomal anomalies istill performed mainly by conventional cytogenetic tech-iques GTG (G-bands by trypsin using Giemsa) bandingaryotyping in lymphocytes has been mainly used to iden-ify chromosomal abnormalities with a resolution equalr greater than 5-10 megabases (5-10 Mb)8---11 Fluores-ent in situ hybridization (FISH) is available for a limitedumber of diseases caused by chromosomal microdele-ionsmicroduplications and has a resolution of 2-5 Mbn metaphase and between 50-150 Kb in interphaseuclei8911---13 Other molecular techniques have been devel-ped to look for small microdeletionsmicroduplicationsuch as multiplex ligation-dependent probe amplificationMLPA)14 In contrast to these conventional techniques CMA
as a higher resolution which reaches up to 50 Kb a tenimes higher resolution than conventional karyotyping1315
t seeks genetic imbalances (gains or losses of chromosomalhs
egments) across the genome and has allowed the identifi-ation of new syndromes that are not readily detected byhe methods described above16---18 The discovery of normalariation as copy number variations (CNVs) poses a challengeor the clinical interpretation15
Whilst diagnostic studies for individuals with congenitalnomalies or intellectual disability based on conventionalytogenetics have a diagnostic yield close to 3 CMA has aield of around 15 to 20 over five timesgreater than G-anded karyotype6 justifying its use as a first line diagnosticest for patients with an unknown clinical diagnosis It isstimated that CMA alone is capable of detecting over 99f all karyotype abnormalities5
This report presents the authorsrsquo pioneering experiencen the use of CMA in a cohort of Chilean patients with mul-iple congenital anomalies without etiological diagnosis
ethods
atients
orty patients were selected from the Genetic Clinics at Hos-ital Padre Hurtado (Santiago Chile) between May of 2012nd November of 2012
This study included patients who had at least two ofhe following clinical features major congenital anomaliesMCAs) facial dysmorphism (FD) developmental delay (DD)r intellectual disability (ID) All patients lacked a definite
Of all patients 36 had a normal karyotype two patientsad an uncharacterized small additional marker chromo-ome (sSMC) one had a derivative chromosome one had an
ARTICLE IN PRESS+Model
Chromosomal microarrays in children 3
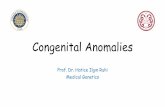
Figure 1 Summary of clinical features and genetic imbalances found in this cohortation
s(aihKCcubanOPHpC
R
CMA chromosomal microarray FISH fluorescent in situ hybridizsSMC supernumerary small marker chromosome
inherited Robertsonian translocation and one patient hadmonosomy X but with unusual additional features
The local ethics committee approved this study and writ-ten informed consent was obtained from all patients andorparentsguardians
Sample Processing
Genomic DNA was purified from peripheral blood mono-nuclear cells with AxyPrep Blood Genomic DNA Miniprep Kit(Axygen Biosciences Union City CA USA) following manu-facturerrsquos instructions Genomic DNA of each patient washybridized with the CytoScanTM HD Array (Affymetrix IncSanta Clara CA USA) according to manufacturerrsquos instruc-tions This is a custom high-density comparative genomichybridization array with almost 27 million of geneticmarkers includes 700000 single nucleotide polymorphism(SNP) markers and over 19 oligonucleotide non-polymorphicprobes for CNV detection
Data Analysis
Array data were analyzed using the Affymetrixreg Chromo-some Analysis Software Suite (ChAS) v122 (AffymetrixInc Santa Clara CA USA) based on the reference genome
Or4h
NA not applicable by age NOR nucleolar organizer region
equence of the UCSC Genome Browser hg19 Feb 2009GRCh37hg19) The authors analyzed CNVs over 400 Kbs recommended6 With this higher-resolution platformt was possible to evaluate smaller CNVs but no patientad clinically relevant abnormalities between 100 and 400b so this limit was kept for purposes of this reportNVs over 400 Kb were categorized by clinical signifi-ance as CNV of clear clinical relevance (group 1) CNV ofnclear relevance or uncertain significance (group 2) orenign or polymorphic CNV (group 3) using the publiclyvailable databases ISCA (International Standard Cytoge-omic Array)19 DGV (Database of Genomic Variants)2021
MIM (Online Mendelian Inheritance in Man)22 DECI-HER(Database of Chromosomal Imbalance and Phenotype inumans Using Ensembl Resources)2324 and ECARUCA (Euro-ean Cytogeneticists Association Register of Unbalancedhromosome Aberrations)25
esults
f the 40 patients analyzed 16 (41) were female Agesanged from 1 month to 25 years with a median age of2 years As selected the vast majority of the patientsave multiple anomalies including structural and functional
ARTICLE IN+Model
4
Group 1 Group 2 Group 3
29 patients
40 patients
12 CNVs9L3G
1 CNVs0L1G
42 CNVs2L40G
55 CNVs11L44G
0 CNVs
A
B
10 patients 1 patient
11 patients
25 patients
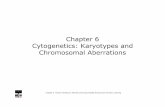
Figure 2 Characterization of CNVs larger than 400 Kb inChilean cohortA among 40 patients CNVs were not found in 11 individuals Inthe remaining 29 patients 55 CNVs were found (11 losses and 44gains) B each patient may have CNV of more than one group ata time CNVs were categorized by clinical significance as CNV ofclear clinical relevance (group 1) CNV of uncertain significance(C
dF
C
FpOs2s
t
bpti3
D
Iitph
sai
lo
tdstsg
C
TovIc
(
spds
D
TCecoipdd
ahddaTorhsstf
lomapc
group 2) or benign or polymorphic CNV (group 3)NVs copy number variants G gains L losses
evelopmental disorders Clinical details are summarized inig 1
NV characterization (Fig 2)
ifty-five CNVs over 400 Kb were observed in 29 of 40atients (725) ranging between 0 and 4 CNVs per patientf the total 11 were losses and 44 were gains (Fig 2A) Theize of chromosomal imbalances ranged from 4209 Kb to52 Mb The latter corresponded to one patient with anSMC detected by karyotype
These 55 CNVs were classified into three groups based onheir clinical interpretation
According to the classification adopted (Fig 2B) 218elonged to group 1 (clear clinical relevance related to thehenotype) 18 to group 2 (unclear relevance) and 764o group 3 (benign or polymorphic) Losses were predom-nant in group 1 while gains were predominant in group
iagnostic yield
n Group 1 two patients had two terminal chromosomembalances each probably derived from unbalanced crypticranslocations Seven patients had a microdeletion and oneatient had a mosaic partial trisomy 20 (one of the patientsad an sSMC) More details are summarized in Fig 1
In Group 2 only one patient had a variant of uncertainignificance (VOUS)26 This patient had a 2 Mb triplicationt 9p23 [arr 9p23(9323653-11359708)x3] but with thenformation available in the databases and in biomedical
aof1
PRESSLay-Son G et al
iterature a definitive pathogenic effect could not be ruledut or assigned
The authors failed to find true genetic imbalances inhe second patient with an sSMC and the patient with aerivative chromosome 16 In the patient with the Robert-onian translocation no genomic imbalance that explainedhe phenotype was found Finally in the patient with mono-omy X the deletion of one X was confirmed but additionalenomic imbalances were not found (fig 1)
linical interpretation
his study found a pathogenic CNV that was not previouslybserved by (n = 9) or not well characterized (n = 1) by con-entional karyotype in ten of 40 patients of group 1 (250)n addition a known cytogenetic anomaly in one patient wasorroborated (monosomy X)
If only the patients with normal karyotype are considered35 patients) the diagnosis rate increased to 285
Additionally this study found a CNV of uncertain clinicalignificance or VOUS (group 2) in one additional patient Thisatient is waiting for additional testing and follow up toefine the clinical relevance of this finding It is planned totudy both parents with FISH andor MLPA
iscussion
his is the first report of the CMA testing in a cohort ofhilean patients with developmental disabilities consid-ring that there are few studies of the clinical use ofhromosomal microarrays in Latin America as experiencesf individual cases are the norm Within South Amer-ca a similar experience was reported with a group ofatients from Brazil2728 Those authors analyzed 95 syn-romic patients with normal karyotypes and reported aiagnostic yield of 1728
The present study detected over 25 pathogenic alter-tions in this cohort which is in the upper range thatas been reported in the literature In patients with syn-romic and nonsyndromic developmental delayintellectualisability with normal karyotypeFISH meta-analysis shows
diagnostic yield of 78-138 ranging from 5 to 50529
his is largely explained by heterogeneity in the designf studies especially in patient selection previous testingealized and array platforms used In the present case theigh rate of diagnosis can be explained by the fact that thetudied cohort was relatively small had the bias of veryelected patients many of whom have remained for longime without diagnosis and finally used a high-density plat-orm
Over time different online public databases have col-ected phenotypic and genomic information of thousandsf anonymous patients which allow elucidating the vastajority of CNVs as benign or polymorphic without further
nalysis In fact the majority of this studyrsquos findings wereolymorphic CNVs (copy number polymorphisms [CNPs])orroborated in those cytogenomic databases and from the
uthorsrsquo own cohort data Recurrent CNVs over 400 Kb werebserved in half of these patients mainly involving theollowing chromosomal loci 10q1122 14q3222 16p1127q2131 Yq11223 and Yq1123 Only one case that had
IN+Model
dolcupr
taaoadnoo
F
GA
C
T
A
TBtCt
R
ARTICLEChromosomal microarrays in children
a VOUS required further analysis to determine possiblepathogenicity This patient was one year and 11 monthswith DD language delay hearing deficit inguinal herniaand short stature He had a 46XY karyotype and the arrayshowed a 2 Mb gain in chromosome 9p23 including par-tial triplication of one gene PTPRD The protein Ptprd isa receptor-type protein-tyrosine phosphatase is expressedin certain regions of the brain such as the hippocampus andcould have a role in learning and memory30 and the synapticorganization31 No phenotype has been assigned to the fulltriplication of this gene
Although CMA is a very robust and reliable techniqueit has limitations it is unable to detect balanced genomicabnormalities such as inversions reciprocal and Robert-sonian translocations Depending on the platform usedlow-level mosaicism and some polyploidies cannot bedetected When CMA technique is used as the first line ofstudy it has been described that this situation can occur in078 of cases5 Finally CMA does not give information onposition of the rearrangement FISH is often used as comple-mentary method to identify possible rearrangements withimplications for genetic counseling732
In the present cohort it was found that three patientswith previously known cytogenetic abnormalities resultedin a normal molecular karyotype As expected the patientwho is carrier for a Robertsonian translocation had a nor-malbalanced aCGH result In the case of one of the twopatients with sSMC the coverage of the array the genomicsequences involved and the size sSMC may explain whythat genetic material were undetected by this method19
Thus this small bisatellited chromosome likely correspondsto highly repetitive sequences typical of acrocentric chro-mosomes not included in the array that was demonstratedby nucleolus organizer region (NOR) banding In the patientwith a derivative chromosome 16 with an abnormal band-ing pattern and morphology (more metacentric than usual)a pericentric inversion is the most plausible explanation
Thus karyotype remains more suitable to evaluatepotential carriers of chromosomal rearrangements coupleswith recurrent miscarriage or patients with a distinctiveaneuploidy phenotype However FISH is more suitable if aspecific microdeletion syndrome is highly suspected7
Chromosome microarrays are a highly accurate robustand high-throughput method This study used a combinedoligonucleotide-based array plus SNP array which has manyadvantages where the SNP array significantly improvesthe accuracy and sensitivity of the CNV detection andmosaicism also allowing the detection of copy-neutralvariants33 In the case of the chip used in this report(Cytoscan HD Affymetrix) the platform chemistry andits algorithms analyze the oligonucleotide and SNP probesindependently and thus each CNV can be detected andconfirmed at the same time without requiring any furtherconfirmation3233 In this case instead of a confirmation ofthe array finding FISH analysis allows for determination ofthe type of rearrangement32
A limitation for widespread use of molecular karyotypeis the high cost of the test In Chile CMA is approximately
four to seven times more expensive than a karyotype andorFISH and is currently not covered by health insurance How-ever to reach an early diagnosis in selected patients withmultiple congenital anomalies andor global developmental
PRESS5
elay it can avoid unnecessary testing (the lsquolsquodiagnosticdysseyrsquorsquo) and allow focusing on specific issues which in theong term can be cost-effective34---38 It may be expected thatosts will decrease over time enabling its more widespreadse Finally it should be mentioned that there are otherlatforms that have lower resolution but at a relativelyeduced cost
Recognizing its limitations there is growing evidence ofhe clinical impact of this technology In many patients
definitive diagnosis can impact not only on informationnd counseling for their family environment39 but alson active surveillance in search of possible complicationsmong other types of medical interventions3738 The presentata show the usefulness of CMA allowing improved diag-ostic capability with remarkable precision and optimizationf the management and supervision of health in this groupf patients with special needs
unding
rant support from Child Health Foundation in Birminghamlabama
onflicts of interest
he authors declare to have no conflicts of interest
cknowledgments
he authors are grateful to the Child Health Foundation inirmingham Alabama for their grant support for this worko the participating patients and families and to Dr Silviaastillo and cytogeneticist Ana Mariacutea Fuentes for review ofhe conventional karyotype results
eferences
1 Christianson A Howson M Modell B March of Dimes globalreport on birth defects The hidden toll of dying and disabledchildren White Plains NY March of Dimes Birth Defects Foun-dation 2006
2 Kumar P Burton BK Dysmorphology In Kumar P Burton BKeditors Congenital malformations evidence-based evaluationand management New York McGraw-Hill Prof MedTech 2007p 3---11
3 Rauch A Hoyer J Guth S Zweier C Kraus C Becker C et alDiagnostic yield of various genetic approaches in patients withunexplained developmental delay or mental retardation Am JMed Genet A 20061402063---74
4 Vermeesch JR Fiegler H de Leeuw N Szuhai K Schoumans JCiccone R et al Guidelines for molecular karyotyping in consti-tutional genetic diagnosis Eur J Hum Genet 2007151105---14
5 Hochstenbach R van Binsbergen E Engelen J Nieuwint APolstra A Poddighe P et al Array analysis and karyotyp-ing workflow consequences based on a retrospective studyof 36325 patients with idiopathic developmental delay in theNetherlands Eur J Med Genet 200952161---9
6 Miller DT Adam MP Aradhya S Biesecker LG Brothman AR
Carter NP et al Consensus statement chromosomal microarrayis a first-tier clinical diagnostic test for individuals with devel-opmental disabilities or congenital anomalies Am J Hum Genet201086749---64
IN+Model
6
1
1
1
1
1
1
1
1
1
1
2
2
2
2
2
2
2
2
2
2
3
3
3
3
3
3
3
3
3Hoppman N et al Chromosomal microarray impacts clinical
ARTICLE
7 Manning M Hudgins L Professional Practice and GuidelinesCommittee Array-based technology and recommendations forutilization in medical genetics practice for detection of chro-mosomal abnormalities Genet Med 201012742---5
8 Shaffer LG Ledbetter DH Lupski JR Molecular cytogeneticsof contiguous gene syndromes mechanisms and consequencesof gene dosage imbalance In Scriver CR Beaudet AL Sly WSValle D Childs B Kinzler KW et al editors The metabolic andmolecular basis of inherited disease New York McGraw Hill2001 p 1291---324
9 Trask BJ Human cytogenetics 46 chromosomes 46 years andcounting Nat Rev Genet 20023769---78
0 Salman M Jhanwar SC Ostrer H Will the new cytogeneticsreplace the old cytogenetics Clin Genet 200466265---75
1 Smeets DF Historical prospective of human cytogenetics frommicroscope to microarray Clin Biochem 200437439---46
2 Turleau C Vekemans M New developments in cytogenetics MedSci (Paris) 200521940---6
3 Edelmann L Hirschhorn K Clinical utility of array CGH for thedetection of chromosomal imbalances associated with mentalretardation and multiple congenital anomalies Ann N Y AcadSci 20091151157---66
4 Jehee FS Takamori JT Medeiros PF Pordeus AC Latini FRBertola DR et al Using a combination of MLPA kits to detectchromosomal imbalances in patients with multiple congenitalanomalies and mental retardation is a valuable choice for devel-oping countries Eur J Med Genet 201154e425---32
5 Lee C Iafrate AJ Brothman AR Copy number variations andclinical cytogenetic diagnosis of constitutional disorders NatGenet 200739S48---54
6 Shaffer LG Bejjani BA Torchia B Kirkpatrick S Coppinger JBallif BC The identification of microdeletion syndromes andother chromosome abnormalities cytogenetic methods of thepast new technologies for the future Am J Med Genet C SeminMed Genet 2007145C335---45
7 Schluth-Bolard C Till M Edery P Sanlaville D New chromosomalsyndromes Pathol Biol (Paris) 200856380---7
8 Slavotinek AM Novel microdeletion syndromes detected bychromosome microarrays Hum Genet 20081241---17
9 International Collaboration for Clinical Genomics (ICCG)International Standard Cytogenomic Array (ISCA) ConsortiumDatabase Search [cited 4 March 2014] Available fromhttpwwwiccgorg
0 MacDonald JR Ziman R Yuen RK Feuk L Scherer SW TheDatabase of Genomic Variants a curated collection of struc-tural variation in the human genome Nucleic Acids Res201442D986---92
1 Database of Genomic Variants (DGV) [cited 4 March 2014]Available from httpdgvtcagcadgvapphome
2 Online Mendelian Inheritance in Man OMIMreg McKusick-Nathans Institute of Genetic Medicine Johns Hopkins University(Baltimore MD) [cited 10 March 2014] Available fromhttpomimorg
3 Firth HV Richards SM Bevan AP Clayton S Corpas M Rajan Det al DECIPHER Database of Chromosomal Imbalance and Phe-notype in Humans Using Ensembl Resources Am J Hum Genet
200984524---33
4 Database of Chromosomal Imbalance and Phenotype in Humansusing Ensembl Resources (DECIPHER) [cited 10 March 2014]Available from httpsdeciphersangeracuk
3
PRESSLay-Son G et al
5 European Cytogeneticists Association Register of UnbalancedChromosome Aberrations (ECARUCA) [cited 10 March 2014]Available from httpumcecaruca01externumcnnl8080ecarucaecarucajsp
6 de Leeuw N Dijkhuizen T Hehir-Kwa JY Carter NP FeukL Firth HV et al Diagnostic interpretation of array datausing public databases and internet sources Hum Mutat2012
7 Rosenberg C Knijnenburg J Bakker E Vianna-Morgante AMSloos W Otto PA et al Array-CGH detection of micro rearrange-ments in mentally retarded individuals clinical significance ofimbalances present both in affected children and normal par-ents J Med Genet 200643180---6
8 Krepischi-Santos AC Vianna-Morgante AM Jehee FS Passos-Bueno MR Knijnenburg J Szuhai K et al Whole-genomearray-CGH screening in undiagnosed syndromic patients oldsyndromes revisited and new alterations Cytogenet GenomeRes 2006115254---61
9 Michelson DJ Shevell MI Sherr EH Moeschler JB Gropman ALAshwal S Evidence report Genetic and metabolic testing onchildren with global developmental delay report of the QualityStandards Subcommittee of the American Academy of Neurol-ogy and the Practice Committee of the Child Neurology SocietyNeurology 2011771629---35
0 Uetani N Kato K Ogura H Mizuno K Kawano K MikoshibaK et al Impaired learning with enhanced hippocampallong-term potentiation in PTPdelta-deficient mice EMBO J2000192775---85
1 Takahashi H Craig AM Protein tyrosine phosphatases PTPPTP and LAR presynaptic hubs for synapse organizationTrends Neurosci 201336522---34
2 Bui TH Vetro A Zuffardi O Shaffer LG Current controversiesin prenatal diagnosis 3 is conventional chromosome analysisnecessary in the post-array CGH era Prenat Diagn 201131235---43
3 Mason-Suares H Kim W Grimmett L Williams ES Horner VLKunig D et al Density matters comparison of array platformsfor detection of copy-number variation and copy-neutral abnor-malities Genet Med 201315706---12
4 Wordsworth S Buchanan J Regan R Davison V Smith KDyer S et al Diagnosing idiopathic learning disability acost-effectiveness analysis of microarray technology in theNational Health Service of the United Kingdom Genomic Med2007135---45
5 Newman WG Hamilton S Ayres J Sanghera N Smith A GauntL et al Array comparative genomic hybridization for diagno-sis of developmental delay an exploratory cost-consequencesanalysis Clin Genet 200771254---9
6 Trakadis Y Shevell M Microarray as a first genetic test in globaldevelopmental delay a cost-effectiveness analysis Dev MedChild Neurol 201153994---9
7 Coulter ME Miller DT Harris DJ Hawley P Picker J RobertsAE et al Chromosomal microarray testing influences medicalmanagement Genet Med 201113770---6
8 Riggs E Wain K Riethmaier D Smith-Packard B Faucett W
management Clin Genet 20139 Pina-Neto JM Genetic counseling J Pediatr (Rio J)
200884S20---6

ARTICLE IN PRESS+Model
2 Lay-Son G et al
PALAVRAS-CHAVEMicroarraysAnomaliascongecircnitasAtraso dedesenvolvimentoVariante do nuacutemerode coacutepiaDiagnoacutestico
Anaacutelise cromossocircmica por microarray em criancas com deficiecircncias dedesenvolvimento e anomalias congecircnitas
ResumoObjetivo O uso cliacutenico de teacutecnicas baseadas em microarrays para a anaacutelise de transtornos dedesenvolvimento tem surgido durante a uacuteltima deacutecada Assim o microarray cromossocircmico temsido posicionado como um teste de primeiro niacutevel cliacutenico Relatamos a primeira experiecircncia emuma coorte chilenaMeacutetodos Pacientes chilenos com atraso de desenvolvimento e anomalias congecircnitas foramestudados com um microarray de alta densidade (CytoScanTM HD Array Affymetrix Inc SantaClara CA EUA) Pacientes tiveram estudos citogeneacuteticos anteriores ou um resultado normalou de uma anomalia natildeo bem caracterizadaResultados Foram analisados 40 pacientes selecionados por dois ou mais criteacuterios incluindoanomalias congecircnitas maiores dismorfismo facial atraso de desenvolvimento e deficiecircncia int-electual Uma variante do nuacutemero de coacutepia (CNV) foi encontrada em 725 dos pacientesenquanto que uma CNV patogecircnica foi encontrada em 25 dos pacientes e uma CNV de signifi-cado cliacutenico incerto foi encontrada em 25 dos pacientesConclusotildees A anaacutelise cromossocircmica microarray eacute uma ferramenta uacutetil e poderosa emtranstornos de desenvolvimento permitindo um diagnoacutestico preciso melhorando a taxa dediagnoacutestico e descobrindo novas etiologias O custo mais elevado eacute uma limitacatildeo para um usodifundido em nossa realidadecopy 2014 Sociedade Brasileira de Pediatria Publicado por Elsevier Editora Ltda Todos os direitosreservados
I
Mlara
tomipds
isnktocntinos(htI
sctvf
acybteo
it
M
P
Fpa
t(ocause for the disorder
ntroduction
ajor congenital anomalies affect two to three of every 100ive newborns and are a leading cause of infant mortalitynd disability12 Although most are isolated and multifacto-ial in origin patients with multiple abnormalities requiren assessment to identify an underlying genetic cause
In recent years the etiological study of developmen-al disorders has been enriched with the clinical usef microarray-based techniques In developed countriesolecular karyotyping or chromosomal microarray (CMA)
s considered the first-line technique for the analysis ofatients with multiple congenital anomalies nonsyndromicevelopmental delayintellectual disability and autismpectrum disorders3---7
In contrast in developing nations such as Latin Amer-can countries detection of chromosomal anomalies istill performed mainly by conventional cytogenetic tech-iques GTG (G-bands by trypsin using Giemsa) bandingaryotyping in lymphocytes has been mainly used to iden-ify chromosomal abnormalities with a resolution equalr greater than 5-10 megabases (5-10 Mb)8---11 Fluores-ent in situ hybridization (FISH) is available for a limitedumber of diseases caused by chromosomal microdele-ionsmicroduplications and has a resolution of 2-5 Mbn metaphase and between 50-150 Kb in interphaseuclei8911---13 Other molecular techniques have been devel-ped to look for small microdeletionsmicroduplicationsuch as multiplex ligation-dependent probe amplificationMLPA)14 In contrast to these conventional techniques CMA
as a higher resolution which reaches up to 50 Kb a tenimes higher resolution than conventional karyotyping1315
t seeks genetic imbalances (gains or losses of chromosomalhs
egments) across the genome and has allowed the identifi-ation of new syndromes that are not readily detected byhe methods described above16---18 The discovery of normalariation as copy number variations (CNVs) poses a challengeor the clinical interpretation15
Whilst diagnostic studies for individuals with congenitalnomalies or intellectual disability based on conventionalytogenetics have a diagnostic yield close to 3 CMA has aield of around 15 to 20 over five timesgreater than G-anded karyotype6 justifying its use as a first line diagnosticest for patients with an unknown clinical diagnosis It isstimated that CMA alone is capable of detecting over 99f all karyotype abnormalities5
This report presents the authorsrsquo pioneering experiencen the use of CMA in a cohort of Chilean patients with mul-iple congenital anomalies without etiological diagnosis
ethods
atients
orty patients were selected from the Genetic Clinics at Hos-ital Padre Hurtado (Santiago Chile) between May of 2012nd November of 2012
This study included patients who had at least two ofhe following clinical features major congenital anomaliesMCAs) facial dysmorphism (FD) developmental delay (DD)r intellectual disability (ID) All patients lacked a definite
Of all patients 36 had a normal karyotype two patientsad an uncharacterized small additional marker chromo-ome (sSMC) one had a derivative chromosome one had an
ARTICLE IN PRESS+Model
Chromosomal microarrays in children 3
Figure 1 Summary of clinical features and genetic imbalances found in this cohortation
s(aihKCcubanOPHpC
R
CMA chromosomal microarray FISH fluorescent in situ hybridizsSMC supernumerary small marker chromosome
inherited Robertsonian translocation and one patient hadmonosomy X but with unusual additional features
The local ethics committee approved this study and writ-ten informed consent was obtained from all patients andorparentsguardians
Sample Processing
Genomic DNA was purified from peripheral blood mono-nuclear cells with AxyPrep Blood Genomic DNA Miniprep Kit(Axygen Biosciences Union City CA USA) following manu-facturerrsquos instructions Genomic DNA of each patient washybridized with the CytoScanTM HD Array (Affymetrix IncSanta Clara CA USA) according to manufacturerrsquos instruc-tions This is a custom high-density comparative genomichybridization array with almost 27 million of geneticmarkers includes 700000 single nucleotide polymorphism(SNP) markers and over 19 oligonucleotide non-polymorphicprobes for CNV detection
Data Analysis
Array data were analyzed using the Affymetrixreg Chromo-some Analysis Software Suite (ChAS) v122 (AffymetrixInc Santa Clara CA USA) based on the reference genome
Or4h
NA not applicable by age NOR nucleolar organizer region
equence of the UCSC Genome Browser hg19 Feb 2009GRCh37hg19) The authors analyzed CNVs over 400 Kbs recommended6 With this higher-resolution platformt was possible to evaluate smaller CNVs but no patientad clinically relevant abnormalities between 100 and 400b so this limit was kept for purposes of this reportNVs over 400 Kb were categorized by clinical signifi-ance as CNV of clear clinical relevance (group 1) CNV ofnclear relevance or uncertain significance (group 2) orenign or polymorphic CNV (group 3) using the publiclyvailable databases ISCA (International Standard Cytoge-omic Array)19 DGV (Database of Genomic Variants)2021
MIM (Online Mendelian Inheritance in Man)22 DECI-HER(Database of Chromosomal Imbalance and Phenotype inumans Using Ensembl Resources)2324 and ECARUCA (Euro-ean Cytogeneticists Association Register of Unbalancedhromosome Aberrations)25
esults
f the 40 patients analyzed 16 (41) were female Agesanged from 1 month to 25 years with a median age of2 years As selected the vast majority of the patientsave multiple anomalies including structural and functional
ARTICLE IN+Model
4
Group 1 Group 2 Group 3
29 patients
40 patients
12 CNVs9L3G
1 CNVs0L1G
42 CNVs2L40G
55 CNVs11L44G
0 CNVs
A
B
10 patients 1 patient
11 patients
25 patients
Figure 2 Characterization of CNVs larger than 400 Kb inChilean cohortA among 40 patients CNVs were not found in 11 individuals Inthe remaining 29 patients 55 CNVs were found (11 losses and 44gains) B each patient may have CNV of more than one group ata time CNVs were categorized by clinical significance as CNV ofclear clinical relevance (group 1) CNV of uncertain significance(C
dF
C
FpOs2s
t
bpti3
D
Iitph
sai
lo
tdstsg
C
TovIc
(
spds
D
TCecoipdd
ahddaTorhsstf
lomapc
group 2) or benign or polymorphic CNV (group 3)NVs copy number variants G gains L losses
evelopmental disorders Clinical details are summarized inig 1
NV characterization (Fig 2)
ifty-five CNVs over 400 Kb were observed in 29 of 40atients (725) ranging between 0 and 4 CNVs per patientf the total 11 were losses and 44 were gains (Fig 2A) Theize of chromosomal imbalances ranged from 4209 Kb to52 Mb The latter corresponded to one patient with anSMC detected by karyotype
These 55 CNVs were classified into three groups based onheir clinical interpretation
According to the classification adopted (Fig 2B) 218elonged to group 1 (clear clinical relevance related to thehenotype) 18 to group 2 (unclear relevance) and 764o group 3 (benign or polymorphic) Losses were predom-nant in group 1 while gains were predominant in group
iagnostic yield
n Group 1 two patients had two terminal chromosomembalances each probably derived from unbalanced crypticranslocations Seven patients had a microdeletion and oneatient had a mosaic partial trisomy 20 (one of the patientsad an sSMC) More details are summarized in Fig 1
In Group 2 only one patient had a variant of uncertainignificance (VOUS)26 This patient had a 2 Mb triplicationt 9p23 [arr 9p23(9323653-11359708)x3] but with thenformation available in the databases and in biomedical
aof1
PRESSLay-Son G et al
iterature a definitive pathogenic effect could not be ruledut or assigned
The authors failed to find true genetic imbalances inhe second patient with an sSMC and the patient with aerivative chromosome 16 In the patient with the Robert-onian translocation no genomic imbalance that explainedhe phenotype was found Finally in the patient with mono-omy X the deletion of one X was confirmed but additionalenomic imbalances were not found (fig 1)
linical interpretation
his study found a pathogenic CNV that was not previouslybserved by (n = 9) or not well characterized (n = 1) by con-entional karyotype in ten of 40 patients of group 1 (250)n addition a known cytogenetic anomaly in one patient wasorroborated (monosomy X)
If only the patients with normal karyotype are considered35 patients) the diagnosis rate increased to 285
Additionally this study found a CNV of uncertain clinicalignificance or VOUS (group 2) in one additional patient Thisatient is waiting for additional testing and follow up toefine the clinical relevance of this finding It is planned totudy both parents with FISH andor MLPA
iscussion
his is the first report of the CMA testing in a cohort ofhilean patients with developmental disabilities consid-ring that there are few studies of the clinical use ofhromosomal microarrays in Latin America as experiencesf individual cases are the norm Within South Amer-ca a similar experience was reported with a group ofatients from Brazil2728 Those authors analyzed 95 syn-romic patients with normal karyotypes and reported aiagnostic yield of 1728
The present study detected over 25 pathogenic alter-tions in this cohort which is in the upper range thatas been reported in the literature In patients with syn-romic and nonsyndromic developmental delayintellectualisability with normal karyotypeFISH meta-analysis shows
diagnostic yield of 78-138 ranging from 5 to 50529
his is largely explained by heterogeneity in the designf studies especially in patient selection previous testingealized and array platforms used In the present case theigh rate of diagnosis can be explained by the fact that thetudied cohort was relatively small had the bias of veryelected patients many of whom have remained for longime without diagnosis and finally used a high-density plat-orm
Over time different online public databases have col-ected phenotypic and genomic information of thousandsf anonymous patients which allow elucidating the vastajority of CNVs as benign or polymorphic without further
nalysis In fact the majority of this studyrsquos findings wereolymorphic CNVs (copy number polymorphisms [CNPs])orroborated in those cytogenomic databases and from the
uthorsrsquo own cohort data Recurrent CNVs over 400 Kb werebserved in half of these patients mainly involving theollowing chromosomal loci 10q1122 14q3222 16p1127q2131 Yq11223 and Yq1123 Only one case that had
IN+Model
dolcupr
taaoadnoo
F
GA
C
T
A
TBtCt
R
ARTICLEChromosomal microarrays in children
a VOUS required further analysis to determine possiblepathogenicity This patient was one year and 11 monthswith DD language delay hearing deficit inguinal herniaand short stature He had a 46XY karyotype and the arrayshowed a 2 Mb gain in chromosome 9p23 including par-tial triplication of one gene PTPRD The protein Ptprd isa receptor-type protein-tyrosine phosphatase is expressedin certain regions of the brain such as the hippocampus andcould have a role in learning and memory30 and the synapticorganization31 No phenotype has been assigned to the fulltriplication of this gene
Although CMA is a very robust and reliable techniqueit has limitations it is unable to detect balanced genomicabnormalities such as inversions reciprocal and Robert-sonian translocations Depending on the platform usedlow-level mosaicism and some polyploidies cannot bedetected When CMA technique is used as the first line ofstudy it has been described that this situation can occur in078 of cases5 Finally CMA does not give information onposition of the rearrangement FISH is often used as comple-mentary method to identify possible rearrangements withimplications for genetic counseling732
In the present cohort it was found that three patientswith previously known cytogenetic abnormalities resultedin a normal molecular karyotype As expected the patientwho is carrier for a Robertsonian translocation had a nor-malbalanced aCGH result In the case of one of the twopatients with sSMC the coverage of the array the genomicsequences involved and the size sSMC may explain whythat genetic material were undetected by this method19
Thus this small bisatellited chromosome likely correspondsto highly repetitive sequences typical of acrocentric chro-mosomes not included in the array that was demonstratedby nucleolus organizer region (NOR) banding In the patientwith a derivative chromosome 16 with an abnormal band-ing pattern and morphology (more metacentric than usual)a pericentric inversion is the most plausible explanation
Thus karyotype remains more suitable to evaluatepotential carriers of chromosomal rearrangements coupleswith recurrent miscarriage or patients with a distinctiveaneuploidy phenotype However FISH is more suitable if aspecific microdeletion syndrome is highly suspected7
Chromosome microarrays are a highly accurate robustand high-throughput method This study used a combinedoligonucleotide-based array plus SNP array which has manyadvantages where the SNP array significantly improvesthe accuracy and sensitivity of the CNV detection andmosaicism also allowing the detection of copy-neutralvariants33 In the case of the chip used in this report(Cytoscan HD Affymetrix) the platform chemistry andits algorithms analyze the oligonucleotide and SNP probesindependently and thus each CNV can be detected andconfirmed at the same time without requiring any furtherconfirmation3233 In this case instead of a confirmation ofthe array finding FISH analysis allows for determination ofthe type of rearrangement32
A limitation for widespread use of molecular karyotypeis the high cost of the test In Chile CMA is approximately
four to seven times more expensive than a karyotype andorFISH and is currently not covered by health insurance How-ever to reach an early diagnosis in selected patients withmultiple congenital anomalies andor global developmental
PRESS5
elay it can avoid unnecessary testing (the lsquolsquodiagnosticdysseyrsquorsquo) and allow focusing on specific issues which in theong term can be cost-effective34---38 It may be expected thatosts will decrease over time enabling its more widespreadse Finally it should be mentioned that there are otherlatforms that have lower resolution but at a relativelyeduced cost
Recognizing its limitations there is growing evidence ofhe clinical impact of this technology In many patients
definitive diagnosis can impact not only on informationnd counseling for their family environment39 but alson active surveillance in search of possible complicationsmong other types of medical interventions3738 The presentata show the usefulness of CMA allowing improved diag-ostic capability with remarkable precision and optimizationf the management and supervision of health in this groupf patients with special needs
unding
rant support from Child Health Foundation in Birminghamlabama
onflicts of interest
he authors declare to have no conflicts of interest
cknowledgments
he authors are grateful to the Child Health Foundation inirmingham Alabama for their grant support for this worko the participating patients and families and to Dr Silviaastillo and cytogeneticist Ana Mariacutea Fuentes for review ofhe conventional karyotype results
eferences
1 Christianson A Howson M Modell B March of Dimes globalreport on birth defects The hidden toll of dying and disabledchildren White Plains NY March of Dimes Birth Defects Foun-dation 2006
2 Kumar P Burton BK Dysmorphology In Kumar P Burton BKeditors Congenital malformations evidence-based evaluationand management New York McGraw-Hill Prof MedTech 2007p 3---11
3 Rauch A Hoyer J Guth S Zweier C Kraus C Becker C et alDiagnostic yield of various genetic approaches in patients withunexplained developmental delay or mental retardation Am JMed Genet A 20061402063---74
4 Vermeesch JR Fiegler H de Leeuw N Szuhai K Schoumans JCiccone R et al Guidelines for molecular karyotyping in consti-tutional genetic diagnosis Eur J Hum Genet 2007151105---14
5 Hochstenbach R van Binsbergen E Engelen J Nieuwint APolstra A Poddighe P et al Array analysis and karyotyp-ing workflow consequences based on a retrospective studyof 36325 patients with idiopathic developmental delay in theNetherlands Eur J Med Genet 200952161---9
6 Miller DT Adam MP Aradhya S Biesecker LG Brothman AR
Carter NP et al Consensus statement chromosomal microarrayis a first-tier clinical diagnostic test for individuals with devel-opmental disabilities or congenital anomalies Am J Hum Genet201086749---64
IN+Model
6
1
1
1
1
1
1
1
1
1
1
2
2
2
2
2
2
2
2
2
2
3
3
3
3
3
3
3
3
3Hoppman N et al Chromosomal microarray impacts clinical
ARTICLE
7 Manning M Hudgins L Professional Practice and GuidelinesCommittee Array-based technology and recommendations forutilization in medical genetics practice for detection of chro-mosomal abnormalities Genet Med 201012742---5
8 Shaffer LG Ledbetter DH Lupski JR Molecular cytogeneticsof contiguous gene syndromes mechanisms and consequencesof gene dosage imbalance In Scriver CR Beaudet AL Sly WSValle D Childs B Kinzler KW et al editors The metabolic andmolecular basis of inherited disease New York McGraw Hill2001 p 1291---324
9 Trask BJ Human cytogenetics 46 chromosomes 46 years andcounting Nat Rev Genet 20023769---78
0 Salman M Jhanwar SC Ostrer H Will the new cytogeneticsreplace the old cytogenetics Clin Genet 200466265---75
1 Smeets DF Historical prospective of human cytogenetics frommicroscope to microarray Clin Biochem 200437439---46
2 Turleau C Vekemans M New developments in cytogenetics MedSci (Paris) 200521940---6
3 Edelmann L Hirschhorn K Clinical utility of array CGH for thedetection of chromosomal imbalances associated with mentalretardation and multiple congenital anomalies Ann N Y AcadSci 20091151157---66
4 Jehee FS Takamori JT Medeiros PF Pordeus AC Latini FRBertola DR et al Using a combination of MLPA kits to detectchromosomal imbalances in patients with multiple congenitalanomalies and mental retardation is a valuable choice for devel-oping countries Eur J Med Genet 201154e425---32
5 Lee C Iafrate AJ Brothman AR Copy number variations andclinical cytogenetic diagnosis of constitutional disorders NatGenet 200739S48---54
6 Shaffer LG Bejjani BA Torchia B Kirkpatrick S Coppinger JBallif BC The identification of microdeletion syndromes andother chromosome abnormalities cytogenetic methods of thepast new technologies for the future Am J Med Genet C SeminMed Genet 2007145C335---45
7 Schluth-Bolard C Till M Edery P Sanlaville D New chromosomalsyndromes Pathol Biol (Paris) 200856380---7
8 Slavotinek AM Novel microdeletion syndromes detected bychromosome microarrays Hum Genet 20081241---17
9 International Collaboration for Clinical Genomics (ICCG)International Standard Cytogenomic Array (ISCA) ConsortiumDatabase Search [cited 4 March 2014] Available fromhttpwwwiccgorg
0 MacDonald JR Ziman R Yuen RK Feuk L Scherer SW TheDatabase of Genomic Variants a curated collection of struc-tural variation in the human genome Nucleic Acids Res201442D986---92
1 Database of Genomic Variants (DGV) [cited 4 March 2014]Available from httpdgvtcagcadgvapphome
2 Online Mendelian Inheritance in Man OMIMreg McKusick-Nathans Institute of Genetic Medicine Johns Hopkins University(Baltimore MD) [cited 10 March 2014] Available fromhttpomimorg
3 Firth HV Richards SM Bevan AP Clayton S Corpas M Rajan Det al DECIPHER Database of Chromosomal Imbalance and Phe-notype in Humans Using Ensembl Resources Am J Hum Genet
200984524---33
4 Database of Chromosomal Imbalance and Phenotype in Humansusing Ensembl Resources (DECIPHER) [cited 10 March 2014]Available from httpsdeciphersangeracuk
3
PRESSLay-Son G et al
5 European Cytogeneticists Association Register of UnbalancedChromosome Aberrations (ECARUCA) [cited 10 March 2014]Available from httpumcecaruca01externumcnnl8080ecarucaecarucajsp
6 de Leeuw N Dijkhuizen T Hehir-Kwa JY Carter NP FeukL Firth HV et al Diagnostic interpretation of array datausing public databases and internet sources Hum Mutat2012
7 Rosenberg C Knijnenburg J Bakker E Vianna-Morgante AMSloos W Otto PA et al Array-CGH detection of micro rearrange-ments in mentally retarded individuals clinical significance ofimbalances present both in affected children and normal par-ents J Med Genet 200643180---6
8 Krepischi-Santos AC Vianna-Morgante AM Jehee FS Passos-Bueno MR Knijnenburg J Szuhai K et al Whole-genomearray-CGH screening in undiagnosed syndromic patients oldsyndromes revisited and new alterations Cytogenet GenomeRes 2006115254---61
9 Michelson DJ Shevell MI Sherr EH Moeschler JB Gropman ALAshwal S Evidence report Genetic and metabolic testing onchildren with global developmental delay report of the QualityStandards Subcommittee of the American Academy of Neurol-ogy and the Practice Committee of the Child Neurology SocietyNeurology 2011771629---35
0 Uetani N Kato K Ogura H Mizuno K Kawano K MikoshibaK et al Impaired learning with enhanced hippocampallong-term potentiation in PTPdelta-deficient mice EMBO J2000192775---85
1 Takahashi H Craig AM Protein tyrosine phosphatases PTPPTP and LAR presynaptic hubs for synapse organizationTrends Neurosci 201336522---34
2 Bui TH Vetro A Zuffardi O Shaffer LG Current controversiesin prenatal diagnosis 3 is conventional chromosome analysisnecessary in the post-array CGH era Prenat Diagn 201131235---43
3 Mason-Suares H Kim W Grimmett L Williams ES Horner VLKunig D et al Density matters comparison of array platformsfor detection of copy-number variation and copy-neutral abnor-malities Genet Med 201315706---12
4 Wordsworth S Buchanan J Regan R Davison V Smith KDyer S et al Diagnosing idiopathic learning disability acost-effectiveness analysis of microarray technology in theNational Health Service of the United Kingdom Genomic Med2007135---45
5 Newman WG Hamilton S Ayres J Sanghera N Smith A GauntL et al Array comparative genomic hybridization for diagno-sis of developmental delay an exploratory cost-consequencesanalysis Clin Genet 200771254---9
6 Trakadis Y Shevell M Microarray as a first genetic test in globaldevelopmental delay a cost-effectiveness analysis Dev MedChild Neurol 201153994---9
7 Coulter ME Miller DT Harris DJ Hawley P Picker J RobertsAE et al Chromosomal microarray testing influences medicalmanagement Genet Med 201113770---6
8 Riggs E Wain K Riethmaier D Smith-Packard B Faucett W
management Clin Genet 20139 Pina-Neto JM Genetic counseling J Pediatr (Rio J)
200884S20---6

ARTICLE IN PRESS+Model
Chromosomal microarrays in children 3
Figure 1 Summary of clinical features and genetic imbalances found in this cohortation
s(aihKCcubanOPHpC
R
CMA chromosomal microarray FISH fluorescent in situ hybridizsSMC supernumerary small marker chromosome
inherited Robertsonian translocation and one patient hadmonosomy X but with unusual additional features
The local ethics committee approved this study and writ-ten informed consent was obtained from all patients andorparentsguardians
Sample Processing
Genomic DNA was purified from peripheral blood mono-nuclear cells with AxyPrep Blood Genomic DNA Miniprep Kit(Axygen Biosciences Union City CA USA) following manu-facturerrsquos instructions Genomic DNA of each patient washybridized with the CytoScanTM HD Array (Affymetrix IncSanta Clara CA USA) according to manufacturerrsquos instruc-tions This is a custom high-density comparative genomichybridization array with almost 27 million of geneticmarkers includes 700000 single nucleotide polymorphism(SNP) markers and over 19 oligonucleotide non-polymorphicprobes for CNV detection
Data Analysis
Array data were analyzed using the Affymetrixreg Chromo-some Analysis Software Suite (ChAS) v122 (AffymetrixInc Santa Clara CA USA) based on the reference genome
Or4h
NA not applicable by age NOR nucleolar organizer region
equence of the UCSC Genome Browser hg19 Feb 2009GRCh37hg19) The authors analyzed CNVs over 400 Kbs recommended6 With this higher-resolution platformt was possible to evaluate smaller CNVs but no patientad clinically relevant abnormalities between 100 and 400b so this limit was kept for purposes of this reportNVs over 400 Kb were categorized by clinical signifi-ance as CNV of clear clinical relevance (group 1) CNV ofnclear relevance or uncertain significance (group 2) orenign or polymorphic CNV (group 3) using the publiclyvailable databases ISCA (International Standard Cytoge-omic Array)19 DGV (Database of Genomic Variants)2021
MIM (Online Mendelian Inheritance in Man)22 DECI-HER(Database of Chromosomal Imbalance and Phenotype inumans Using Ensembl Resources)2324 and ECARUCA (Euro-ean Cytogeneticists Association Register of Unbalancedhromosome Aberrations)25
esults
f the 40 patients analyzed 16 (41) were female Agesanged from 1 month to 25 years with a median age of2 years As selected the vast majority of the patientsave multiple anomalies including structural and functional
ARTICLE IN+Model
4
Group 1 Group 2 Group 3
29 patients
40 patients
12 CNVs9L3G
1 CNVs0L1G
42 CNVs2L40G
55 CNVs11L44G
0 CNVs
A
B
10 patients 1 patient
11 patients
25 patients
Figure 2 Characterization of CNVs larger than 400 Kb inChilean cohortA among 40 patients CNVs were not found in 11 individuals Inthe remaining 29 patients 55 CNVs were found (11 losses and 44gains) B each patient may have CNV of more than one group ata time CNVs were categorized by clinical significance as CNV ofclear clinical relevance (group 1) CNV of uncertain significance(C
dF
C
FpOs2s
t
bpti3
D
Iitph
sai
lo
tdstsg
C
TovIc
(
spds
D
TCecoipdd
ahddaTorhsstf
lomapc
group 2) or benign or polymorphic CNV (group 3)NVs copy number variants G gains L losses
evelopmental disorders Clinical details are summarized inig 1
NV characterization (Fig 2)
ifty-five CNVs over 400 Kb were observed in 29 of 40atients (725) ranging between 0 and 4 CNVs per patientf the total 11 were losses and 44 were gains (Fig 2A) Theize of chromosomal imbalances ranged from 4209 Kb to52 Mb The latter corresponded to one patient with anSMC detected by karyotype
These 55 CNVs were classified into three groups based onheir clinical interpretation
According to the classification adopted (Fig 2B) 218elonged to group 1 (clear clinical relevance related to thehenotype) 18 to group 2 (unclear relevance) and 764o group 3 (benign or polymorphic) Losses were predom-nant in group 1 while gains were predominant in group
iagnostic yield
n Group 1 two patients had two terminal chromosomembalances each probably derived from unbalanced crypticranslocations Seven patients had a microdeletion and oneatient had a mosaic partial trisomy 20 (one of the patientsad an sSMC) More details are summarized in Fig 1
In Group 2 only one patient had a variant of uncertainignificance (VOUS)26 This patient had a 2 Mb triplicationt 9p23 [arr 9p23(9323653-11359708)x3] but with thenformation available in the databases and in biomedical
aof1
PRESSLay-Son G et al
iterature a definitive pathogenic effect could not be ruledut or assigned
The authors failed to find true genetic imbalances inhe second patient with an sSMC and the patient with aerivative chromosome 16 In the patient with the Robert-onian translocation no genomic imbalance that explainedhe phenotype was found Finally in the patient with mono-omy X the deletion of one X was confirmed but additionalenomic imbalances were not found (fig 1)
linical interpretation
his study found a pathogenic CNV that was not previouslybserved by (n = 9) or not well characterized (n = 1) by con-entional karyotype in ten of 40 patients of group 1 (250)n addition a known cytogenetic anomaly in one patient wasorroborated (monosomy X)
If only the patients with normal karyotype are considered35 patients) the diagnosis rate increased to 285
Additionally this study found a CNV of uncertain clinicalignificance or VOUS (group 2) in one additional patient Thisatient is waiting for additional testing and follow up toefine the clinical relevance of this finding It is planned totudy both parents with FISH andor MLPA
iscussion
his is the first report of the CMA testing in a cohort ofhilean patients with developmental disabilities consid-ring that there are few studies of the clinical use ofhromosomal microarrays in Latin America as experiencesf individual cases are the norm Within South Amer-ca a similar experience was reported with a group ofatients from Brazil2728 Those authors analyzed 95 syn-romic patients with normal karyotypes and reported aiagnostic yield of 1728
The present study detected over 25 pathogenic alter-tions in this cohort which is in the upper range thatas been reported in the literature In patients with syn-romic and nonsyndromic developmental delayintellectualisability with normal karyotypeFISH meta-analysis shows
diagnostic yield of 78-138 ranging from 5 to 50529
his is largely explained by heterogeneity in the designf studies especially in patient selection previous testingealized and array platforms used In the present case theigh rate of diagnosis can be explained by the fact that thetudied cohort was relatively small had the bias of veryelected patients many of whom have remained for longime without diagnosis and finally used a high-density plat-orm
Over time different online public databases have col-ected phenotypic and genomic information of thousandsf anonymous patients which allow elucidating the vastajority of CNVs as benign or polymorphic without further
nalysis In fact the majority of this studyrsquos findings wereolymorphic CNVs (copy number polymorphisms [CNPs])orroborated in those cytogenomic databases and from the
uthorsrsquo own cohort data Recurrent CNVs over 400 Kb werebserved in half of these patients mainly involving theollowing chromosomal loci 10q1122 14q3222 16p1127q2131 Yq11223 and Yq1123 Only one case that had
IN+Model
dolcupr
taaoadnoo
F
GA
C
T
A
TBtCt
R
ARTICLEChromosomal microarrays in children
a VOUS required further analysis to determine possiblepathogenicity This patient was one year and 11 monthswith DD language delay hearing deficit inguinal herniaand short stature He had a 46XY karyotype and the arrayshowed a 2 Mb gain in chromosome 9p23 including par-tial triplication of one gene PTPRD The protein Ptprd isa receptor-type protein-tyrosine phosphatase is expressedin certain regions of the brain such as the hippocampus andcould have a role in learning and memory30 and the synapticorganization31 No phenotype has been assigned to the fulltriplication of this gene
Although CMA is a very robust and reliable techniqueit has limitations it is unable to detect balanced genomicabnormalities such as inversions reciprocal and Robert-sonian translocations Depending on the platform usedlow-level mosaicism and some polyploidies cannot bedetected When CMA technique is used as the first line ofstudy it has been described that this situation can occur in078 of cases5 Finally CMA does not give information onposition of the rearrangement FISH is often used as comple-mentary method to identify possible rearrangements withimplications for genetic counseling732
In the present cohort it was found that three patientswith previously known cytogenetic abnormalities resultedin a normal molecular karyotype As expected the patientwho is carrier for a Robertsonian translocation had a nor-malbalanced aCGH result In the case of one of the twopatients with sSMC the coverage of the array the genomicsequences involved and the size sSMC may explain whythat genetic material were undetected by this method19
Thus this small bisatellited chromosome likely correspondsto highly repetitive sequences typical of acrocentric chro-mosomes not included in the array that was demonstratedby nucleolus organizer region (NOR) banding In the patientwith a derivative chromosome 16 with an abnormal band-ing pattern and morphology (more metacentric than usual)a pericentric inversion is the most plausible explanation
Thus karyotype remains more suitable to evaluatepotential carriers of chromosomal rearrangements coupleswith recurrent miscarriage or patients with a distinctiveaneuploidy phenotype However FISH is more suitable if aspecific microdeletion syndrome is highly suspected7
Chromosome microarrays are a highly accurate robustand high-throughput method This study used a combinedoligonucleotide-based array plus SNP array which has manyadvantages where the SNP array significantly improvesthe accuracy and sensitivity of the CNV detection andmosaicism also allowing the detection of copy-neutralvariants33 In the case of the chip used in this report(Cytoscan HD Affymetrix) the platform chemistry andits algorithms analyze the oligonucleotide and SNP probesindependently and thus each CNV can be detected andconfirmed at the same time without requiring any furtherconfirmation3233 In this case instead of a confirmation ofthe array finding FISH analysis allows for determination ofthe type of rearrangement32
A limitation for widespread use of molecular karyotypeis the high cost of the test In Chile CMA is approximately
four to seven times more expensive than a karyotype andorFISH and is currently not covered by health insurance How-ever to reach an early diagnosis in selected patients withmultiple congenital anomalies andor global developmental
PRESS5
elay it can avoid unnecessary testing (the lsquolsquodiagnosticdysseyrsquorsquo) and allow focusing on specific issues which in theong term can be cost-effective34---38 It may be expected thatosts will decrease over time enabling its more widespreadse Finally it should be mentioned that there are otherlatforms that have lower resolution but at a relativelyeduced cost
Recognizing its limitations there is growing evidence ofhe clinical impact of this technology In many patients
definitive diagnosis can impact not only on informationnd counseling for their family environment39 but alson active surveillance in search of possible complicationsmong other types of medical interventions3738 The presentata show the usefulness of CMA allowing improved diag-ostic capability with remarkable precision and optimizationf the management and supervision of health in this groupf patients with special needs
unding
rant support from Child Health Foundation in Birminghamlabama
onflicts of interest
he authors declare to have no conflicts of interest
cknowledgments
he authors are grateful to the Child Health Foundation inirmingham Alabama for their grant support for this worko the participating patients and families and to Dr Silviaastillo and cytogeneticist Ana Mariacutea Fuentes for review ofhe conventional karyotype results
eferences
1 Christianson A Howson M Modell B March of Dimes globalreport on birth defects The hidden toll of dying and disabledchildren White Plains NY March of Dimes Birth Defects Foun-dation 2006
2 Kumar P Burton BK Dysmorphology In Kumar P Burton BKeditors Congenital malformations evidence-based evaluationand management New York McGraw-Hill Prof MedTech 2007p 3---11
3 Rauch A Hoyer J Guth S Zweier C Kraus C Becker C et alDiagnostic yield of various genetic approaches in patients withunexplained developmental delay or mental retardation Am JMed Genet A 20061402063---74
4 Vermeesch JR Fiegler H de Leeuw N Szuhai K Schoumans JCiccone R et al Guidelines for molecular karyotyping in consti-tutional genetic diagnosis Eur J Hum Genet 2007151105---14
5 Hochstenbach R van Binsbergen E Engelen J Nieuwint APolstra A Poddighe P et al Array analysis and karyotyp-ing workflow consequences based on a retrospective studyof 36325 patients with idiopathic developmental delay in theNetherlands Eur J Med Genet 200952161---9
6 Miller DT Adam MP Aradhya S Biesecker LG Brothman AR
Carter NP et al Consensus statement chromosomal microarrayis a first-tier clinical diagnostic test for individuals with devel-opmental disabilities or congenital anomalies Am J Hum Genet201086749---64
IN+Model
6
1
1
1
1
1
1
1
1
1
1
2
2
2
2
2
2
2
2
2
2
3
3
3
3
3
3
3
3
3Hoppman N et al Chromosomal microarray impacts clinical
ARTICLE
7 Manning M Hudgins L Professional Practice and GuidelinesCommittee Array-based technology and recommendations forutilization in medical genetics practice for detection of chro-mosomal abnormalities Genet Med 201012742---5
8 Shaffer LG Ledbetter DH Lupski JR Molecular cytogeneticsof contiguous gene syndromes mechanisms and consequencesof gene dosage imbalance In Scriver CR Beaudet AL Sly WSValle D Childs B Kinzler KW et al editors The metabolic andmolecular basis of inherited disease New York McGraw Hill2001 p 1291---324
9 Trask BJ Human cytogenetics 46 chromosomes 46 years andcounting Nat Rev Genet 20023769---78
0 Salman M Jhanwar SC Ostrer H Will the new cytogeneticsreplace the old cytogenetics Clin Genet 200466265---75
1 Smeets DF Historical prospective of human cytogenetics frommicroscope to microarray Clin Biochem 200437439---46
2 Turleau C Vekemans M New developments in cytogenetics MedSci (Paris) 200521940---6
3 Edelmann L Hirschhorn K Clinical utility of array CGH for thedetection of chromosomal imbalances associated with mentalretardation and multiple congenital anomalies Ann N Y AcadSci 20091151157---66
4 Jehee FS Takamori JT Medeiros PF Pordeus AC Latini FRBertola DR et al Using a combination of MLPA kits to detectchromosomal imbalances in patients with multiple congenitalanomalies and mental retardation is a valuable choice for devel-oping countries Eur J Med Genet 201154e425---32
5 Lee C Iafrate AJ Brothman AR Copy number variations andclinical cytogenetic diagnosis of constitutional disorders NatGenet 200739S48---54
6 Shaffer LG Bejjani BA Torchia B Kirkpatrick S Coppinger JBallif BC The identification of microdeletion syndromes andother chromosome abnormalities cytogenetic methods of thepast new technologies for the future Am J Med Genet C SeminMed Genet 2007145C335---45
7 Schluth-Bolard C Till M Edery P Sanlaville D New chromosomalsyndromes Pathol Biol (Paris) 200856380---7
8 Slavotinek AM Novel microdeletion syndromes detected bychromosome microarrays Hum Genet 20081241---17
9 International Collaboration for Clinical Genomics (ICCG)International Standard Cytogenomic Array (ISCA) ConsortiumDatabase Search [cited 4 March 2014] Available fromhttpwwwiccgorg
0 MacDonald JR Ziman R Yuen RK Feuk L Scherer SW TheDatabase of Genomic Variants a curated collection of struc-tural variation in the human genome Nucleic Acids Res201442D986---92
1 Database of Genomic Variants (DGV) [cited 4 March 2014]Available from httpdgvtcagcadgvapphome
2 Online Mendelian Inheritance in Man OMIMreg McKusick-Nathans Institute of Genetic Medicine Johns Hopkins University(Baltimore MD) [cited 10 March 2014] Available fromhttpomimorg
3 Firth HV Richards SM Bevan AP Clayton S Corpas M Rajan Det al DECIPHER Database of Chromosomal Imbalance and Phe-notype in Humans Using Ensembl Resources Am J Hum Genet
200984524---33
4 Database of Chromosomal Imbalance and Phenotype in Humansusing Ensembl Resources (DECIPHER) [cited 10 March 2014]Available from httpsdeciphersangeracuk
3
PRESSLay-Son G et al
5 European Cytogeneticists Association Register of UnbalancedChromosome Aberrations (ECARUCA) [cited 10 March 2014]Available from httpumcecaruca01externumcnnl8080ecarucaecarucajsp
6 de Leeuw N Dijkhuizen T Hehir-Kwa JY Carter NP FeukL Firth HV et al Diagnostic interpretation of array datausing public databases and internet sources Hum Mutat2012
7 Rosenberg C Knijnenburg J Bakker E Vianna-Morgante AMSloos W Otto PA et al Array-CGH detection of micro rearrange-ments in mentally retarded individuals clinical significance ofimbalances present both in affected children and normal par-ents J Med Genet 200643180---6
8 Krepischi-Santos AC Vianna-Morgante AM Jehee FS Passos-Bueno MR Knijnenburg J Szuhai K et al Whole-genomearray-CGH screening in undiagnosed syndromic patients oldsyndromes revisited and new alterations Cytogenet GenomeRes 2006115254---61
9 Michelson DJ Shevell MI Sherr EH Moeschler JB Gropman ALAshwal S Evidence report Genetic and metabolic testing onchildren with global developmental delay report of the QualityStandards Subcommittee of the American Academy of Neurol-ogy and the Practice Committee of the Child Neurology SocietyNeurology 2011771629---35
0 Uetani N Kato K Ogura H Mizuno K Kawano K MikoshibaK et al Impaired learning with enhanced hippocampallong-term potentiation in PTPdelta-deficient mice EMBO J2000192775---85
1 Takahashi H Craig AM Protein tyrosine phosphatases PTPPTP and LAR presynaptic hubs for synapse organizationTrends Neurosci 201336522---34
2 Bui TH Vetro A Zuffardi O Shaffer LG Current controversiesin prenatal diagnosis 3 is conventional chromosome analysisnecessary in the post-array CGH era Prenat Diagn 201131235---43
3 Mason-Suares H Kim W Grimmett L Williams ES Horner VLKunig D et al Density matters comparison of array platformsfor detection of copy-number variation and copy-neutral abnor-malities Genet Med 201315706---12
4 Wordsworth S Buchanan J Regan R Davison V Smith KDyer S et al Diagnosing idiopathic learning disability acost-effectiveness analysis of microarray technology in theNational Health Service of the United Kingdom Genomic Med2007135---45
5 Newman WG Hamilton S Ayres J Sanghera N Smith A GauntL et al Array comparative genomic hybridization for diagno-sis of developmental delay an exploratory cost-consequencesanalysis Clin Genet 200771254---9
6 Trakadis Y Shevell M Microarray as a first genetic test in globaldevelopmental delay a cost-effectiveness analysis Dev MedChild Neurol 201153994---9
7 Coulter ME Miller DT Harris DJ Hawley P Picker J RobertsAE et al Chromosomal microarray testing influences medicalmanagement Genet Med 201113770---6
8 Riggs E Wain K Riethmaier D Smith-Packard B Faucett W
management Clin Genet 20139 Pina-Neto JM Genetic counseling J Pediatr (Rio J)
200884S20---6

ARTICLE IN+Model
4
Group 1 Group 2 Group 3
29 patients
40 patients
12 CNVs9L3G
1 CNVs0L1G
42 CNVs2L40G
55 CNVs11L44G
0 CNVs
A
B
10 patients 1 patient
11 patients
25 patients
Figure 2 Characterization of CNVs larger than 400 Kb inChilean cohortA among 40 patients CNVs were not found in 11 individuals Inthe remaining 29 patients 55 CNVs were found (11 losses and 44gains) B each patient may have CNV of more than one group ata time CNVs were categorized by clinical significance as CNV ofclear clinical relevance (group 1) CNV of uncertain significance(C
dF
C
FpOs2s
t
bpti3
D
Iitph
sai
lo
tdstsg
C
TovIc
(
spds
D
TCecoipdd
ahddaTorhsstf
lomapc
group 2) or benign or polymorphic CNV (group 3)NVs copy number variants G gains L losses
evelopmental disorders Clinical details are summarized inig 1
NV characterization (Fig 2)
ifty-five CNVs over 400 Kb were observed in 29 of 40atients (725) ranging between 0 and 4 CNVs per patientf the total 11 were losses and 44 were gains (Fig 2A) Theize of chromosomal imbalances ranged from 4209 Kb to52 Mb The latter corresponded to one patient with anSMC detected by karyotype
These 55 CNVs were classified into three groups based onheir clinical interpretation
According to the classification adopted (Fig 2B) 218elonged to group 1 (clear clinical relevance related to thehenotype) 18 to group 2 (unclear relevance) and 764o group 3 (benign or polymorphic) Losses were predom-nant in group 1 while gains were predominant in group
iagnostic yield
n Group 1 two patients had two terminal chromosomembalances each probably derived from unbalanced crypticranslocations Seven patients had a microdeletion and oneatient had a mosaic partial trisomy 20 (one of the patientsad an sSMC) More details are summarized in Fig 1
In Group 2 only one patient had a variant of uncertainignificance (VOUS)26 This patient had a 2 Mb triplicationt 9p23 [arr 9p23(9323653-11359708)x3] but with thenformation available in the databases and in biomedical
aof1
PRESSLay-Son G et al
iterature a definitive pathogenic effect could not be ruledut or assigned
The authors failed to find true genetic imbalances inhe second patient with an sSMC and the patient with aerivative chromosome 16 In the patient with the Robert-onian translocation no genomic imbalance that explainedhe phenotype was found Finally in the patient with mono-omy X the deletion of one X was confirmed but additionalenomic imbalances were not found (fig 1)
linical interpretation
his study found a pathogenic CNV that was not previouslybserved by (n = 9) or not well characterized (n = 1) by con-entional karyotype in ten of 40 patients of group 1 (250)n addition a known cytogenetic anomaly in one patient wasorroborated (monosomy X)
If only the patients with normal karyotype are considered35 patients) the diagnosis rate increased to 285
Additionally this study found a CNV of uncertain clinicalignificance or VOUS (group 2) in one additional patient Thisatient is waiting for additional testing and follow up toefine the clinical relevance of this finding It is planned totudy both parents with FISH andor MLPA
iscussion
his is the first report of the CMA testing in a cohort ofhilean patients with developmental disabilities consid-ring that there are few studies of the clinical use ofhromosomal microarrays in Latin America as experiencesf individual cases are the norm Within South Amer-ca a similar experience was reported with a group ofatients from Brazil2728 Those authors analyzed 95 syn-romic patients with normal karyotypes and reported aiagnostic yield of 1728
The present study detected over 25 pathogenic alter-tions in this cohort which is in the upper range thatas been reported in the literature In patients with syn-romic and nonsyndromic developmental delayintellectualisability with normal karyotypeFISH meta-analysis shows
diagnostic yield of 78-138 ranging from 5 to 50529
his is largely explained by heterogeneity in the designf studies especially in patient selection previous testingealized and array platforms used In the present case theigh rate of diagnosis can be explained by the fact that thetudied cohort was relatively small had the bias of veryelected patients many of whom have remained for longime without diagnosis and finally used a high-density plat-orm
Over time different online public databases have col-ected phenotypic and genomic information of thousandsf anonymous patients which allow elucidating the vastajority of CNVs as benign or polymorphic without further
nalysis In fact the majority of this studyrsquos findings wereolymorphic CNVs (copy number polymorphisms [CNPs])orroborated in those cytogenomic databases and from the
uthorsrsquo own cohort data Recurrent CNVs over 400 Kb werebserved in half of these patients mainly involving theollowing chromosomal loci 10q1122 14q3222 16p1127q2131 Yq11223 and Yq1123 Only one case that had
IN+Model
dolcupr
taaoadnoo
F
GA
C
T
A
TBtCt
R
ARTICLEChromosomal microarrays in children
a VOUS required further analysis to determine possiblepathogenicity This patient was one year and 11 monthswith DD language delay hearing deficit inguinal herniaand short stature He had a 46XY karyotype and the arrayshowed a 2 Mb gain in chromosome 9p23 including par-tial triplication of one gene PTPRD The protein Ptprd isa receptor-type protein-tyrosine phosphatase is expressedin certain regions of the brain such as the hippocampus andcould have a role in learning and memory30 and the synapticorganization31 No phenotype has been assigned to the fulltriplication of this gene
Although CMA is a very robust and reliable techniqueit has limitations it is unable to detect balanced genomicabnormalities such as inversions reciprocal and Robert-sonian translocations Depending on the platform usedlow-level mosaicism and some polyploidies cannot bedetected When CMA technique is used as the first line ofstudy it has been described that this situation can occur in078 of cases5 Finally CMA does not give information onposition of the rearrangement FISH is often used as comple-mentary method to identify possible rearrangements withimplications for genetic counseling732
In the present cohort it was found that three patientswith previously known cytogenetic abnormalities resultedin a normal molecular karyotype As expected the patientwho is carrier for a Robertsonian translocation had a nor-malbalanced aCGH result In the case of one of the twopatients with sSMC the coverage of the array the genomicsequences involved and the size sSMC may explain whythat genetic material were undetected by this method19
Thus this small bisatellited chromosome likely correspondsto highly repetitive sequences typical of acrocentric chro-mosomes not included in the array that was demonstratedby nucleolus organizer region (NOR) banding In the patientwith a derivative chromosome 16 with an abnormal band-ing pattern and morphology (more metacentric than usual)a pericentric inversion is the most plausible explanation
Thus karyotype remains more suitable to evaluatepotential carriers of chromosomal rearrangements coupleswith recurrent miscarriage or patients with a distinctiveaneuploidy phenotype However FISH is more suitable if aspecific microdeletion syndrome is highly suspected7
Chromosome microarrays are a highly accurate robustand high-throughput method This study used a combinedoligonucleotide-based array plus SNP array which has manyadvantages where the SNP array significantly improvesthe accuracy and sensitivity of the CNV detection andmosaicism also allowing the detection of copy-neutralvariants33 In the case of the chip used in this report(Cytoscan HD Affymetrix) the platform chemistry andits algorithms analyze the oligonucleotide and SNP probesindependently and thus each CNV can be detected andconfirmed at the same time without requiring any furtherconfirmation3233 In this case instead of a confirmation ofthe array finding FISH analysis allows for determination ofthe type of rearrangement32
A limitation for widespread use of molecular karyotypeis the high cost of the test In Chile CMA is approximately
four to seven times more expensive than a karyotype andorFISH and is currently not covered by health insurance How-ever to reach an early diagnosis in selected patients withmultiple congenital anomalies andor global developmental
PRESS5
elay it can avoid unnecessary testing (the lsquolsquodiagnosticdysseyrsquorsquo) and allow focusing on specific issues which in theong term can be cost-effective34---38 It may be expected thatosts will decrease over time enabling its more widespreadse Finally it should be mentioned that there are otherlatforms that have lower resolution but at a relativelyeduced cost
Recognizing its limitations there is growing evidence ofhe clinical impact of this technology In many patients
definitive diagnosis can impact not only on informationnd counseling for their family environment39 but alson active surveillance in search of possible complicationsmong other types of medical interventions3738 The presentata show the usefulness of CMA allowing improved diag-ostic capability with remarkable precision and optimizationf the management and supervision of health in this groupf patients with special needs
unding
rant support from Child Health Foundation in Birminghamlabama
onflicts of interest
he authors declare to have no conflicts of interest
cknowledgments
he authors are grateful to the Child Health Foundation inirmingham Alabama for their grant support for this worko the participating patients and families and to Dr Silviaastillo and cytogeneticist Ana Mariacutea Fuentes for review ofhe conventional karyotype results
eferences
1 Christianson A Howson M Modell B March of Dimes globalreport on birth defects The hidden toll of dying and disabledchildren White Plains NY March of Dimes Birth Defects Foun-dation 2006
2 Kumar P Burton BK Dysmorphology In Kumar P Burton BKeditors Congenital malformations evidence-based evaluationand management New York McGraw-Hill Prof MedTech 2007p 3---11
3 Rauch A Hoyer J Guth S Zweier C Kraus C Becker C et alDiagnostic yield of various genetic approaches in patients withunexplained developmental delay or mental retardation Am JMed Genet A 20061402063---74
4 Vermeesch JR Fiegler H de Leeuw N Szuhai K Schoumans JCiccone R et al Guidelines for molecular karyotyping in consti-tutional genetic diagnosis Eur J Hum Genet 2007151105---14
5 Hochstenbach R van Binsbergen E Engelen J Nieuwint APolstra A Poddighe P et al Array analysis and karyotyp-ing workflow consequences based on a retrospective studyof 36325 patients with idiopathic developmental delay in theNetherlands Eur J Med Genet 200952161---9
6 Miller DT Adam MP Aradhya S Biesecker LG Brothman AR
Carter NP et al Consensus statement chromosomal microarrayis a first-tier clinical diagnostic test for individuals with devel-opmental disabilities or congenital anomalies Am J Hum Genet201086749---64
IN+Model
6
1
1
1
1
1
1
1
1
1
1
2
2
2
2
2
2
2
2
2
2
3
3
3
3
3
3
3
3
3Hoppman N et al Chromosomal microarray impacts clinical
ARTICLE
7 Manning M Hudgins L Professional Practice and GuidelinesCommittee Array-based technology and recommendations forutilization in medical genetics practice for detection of chro-mosomal abnormalities Genet Med 201012742---5
8 Shaffer LG Ledbetter DH Lupski JR Molecular cytogeneticsof contiguous gene syndromes mechanisms and consequencesof gene dosage imbalance In Scriver CR Beaudet AL Sly WSValle D Childs B Kinzler KW et al editors The metabolic andmolecular basis of inherited disease New York McGraw Hill2001 p 1291---324
9 Trask BJ Human cytogenetics 46 chromosomes 46 years andcounting Nat Rev Genet 20023769---78
0 Salman M Jhanwar SC Ostrer H Will the new cytogeneticsreplace the old cytogenetics Clin Genet 200466265---75
1 Smeets DF Historical prospective of human cytogenetics frommicroscope to microarray Clin Biochem 200437439---46
2 Turleau C Vekemans M New developments in cytogenetics MedSci (Paris) 200521940---6
3 Edelmann L Hirschhorn K Clinical utility of array CGH for thedetection of chromosomal imbalances associated with mentalretardation and multiple congenital anomalies Ann N Y AcadSci 20091151157---66
4 Jehee FS Takamori JT Medeiros PF Pordeus AC Latini FRBertola DR et al Using a combination of MLPA kits to detectchromosomal imbalances in patients with multiple congenitalanomalies and mental retardation is a valuable choice for devel-oping countries Eur J Med Genet 201154e425---32
5 Lee C Iafrate AJ Brothman AR Copy number variations andclinical cytogenetic diagnosis of constitutional disorders NatGenet 200739S48---54
6 Shaffer LG Bejjani BA Torchia B Kirkpatrick S Coppinger JBallif BC The identification of microdeletion syndromes andother chromosome abnormalities cytogenetic methods of thepast new technologies for the future Am J Med Genet C SeminMed Genet 2007145C335---45
7 Schluth-Bolard C Till M Edery P Sanlaville D New chromosomalsyndromes Pathol Biol (Paris) 200856380---7
8 Slavotinek AM Novel microdeletion syndromes detected bychromosome microarrays Hum Genet 20081241---17
9 International Collaboration for Clinical Genomics (ICCG)International Standard Cytogenomic Array (ISCA) ConsortiumDatabase Search [cited 4 March 2014] Available fromhttpwwwiccgorg
0 MacDonald JR Ziman R Yuen RK Feuk L Scherer SW TheDatabase of Genomic Variants a curated collection of struc-tural variation in the human genome Nucleic Acids Res201442D986---92
1 Database of Genomic Variants (DGV) [cited 4 March 2014]Available from httpdgvtcagcadgvapphome
2 Online Mendelian Inheritance in Man OMIMreg McKusick-Nathans Institute of Genetic Medicine Johns Hopkins University(Baltimore MD) [cited 10 March 2014] Available fromhttpomimorg
3 Firth HV Richards SM Bevan AP Clayton S Corpas M Rajan Det al DECIPHER Database of Chromosomal Imbalance and Phe-notype in Humans Using Ensembl Resources Am J Hum Genet
200984524---33
4 Database of Chromosomal Imbalance and Phenotype in Humansusing Ensembl Resources (DECIPHER) [cited 10 March 2014]Available from httpsdeciphersangeracuk
3
PRESSLay-Son G et al
5 European Cytogeneticists Association Register of UnbalancedChromosome Aberrations (ECARUCA) [cited 10 March 2014]Available from httpumcecaruca01externumcnnl8080ecarucaecarucajsp
6 de Leeuw N Dijkhuizen T Hehir-Kwa JY Carter NP FeukL Firth HV et al Diagnostic interpretation of array datausing public databases and internet sources Hum Mutat2012
7 Rosenberg C Knijnenburg J Bakker E Vianna-Morgante AMSloos W Otto PA et al Array-CGH detection of micro rearrange-ments in mentally retarded individuals clinical significance ofimbalances present both in affected children and normal par-ents J Med Genet 200643180---6
8 Krepischi-Santos AC Vianna-Morgante AM Jehee FS Passos-Bueno MR Knijnenburg J Szuhai K et al Whole-genomearray-CGH screening in undiagnosed syndromic patients oldsyndromes revisited and new alterations Cytogenet GenomeRes 2006115254---61
9 Michelson DJ Shevell MI Sherr EH Moeschler JB Gropman ALAshwal S Evidence report Genetic and metabolic testing onchildren with global developmental delay report of the QualityStandards Subcommittee of the American Academy of Neurol-ogy and the Practice Committee of the Child Neurology SocietyNeurology 2011771629---35
0 Uetani N Kato K Ogura H Mizuno K Kawano K MikoshibaK et al Impaired learning with enhanced hippocampallong-term potentiation in PTPdelta-deficient mice EMBO J2000192775---85
1 Takahashi H Craig AM Protein tyrosine phosphatases PTPPTP and LAR presynaptic hubs for synapse organizationTrends Neurosci 201336522---34
2 Bui TH Vetro A Zuffardi O Shaffer LG Current controversiesin prenatal diagnosis 3 is conventional chromosome analysisnecessary in the post-array CGH era Prenat Diagn 201131235---43
3 Mason-Suares H Kim W Grimmett L Williams ES Horner VLKunig D et al Density matters comparison of array platformsfor detection of copy-number variation and copy-neutral abnor-malities Genet Med 201315706---12
4 Wordsworth S Buchanan J Regan R Davison V Smith KDyer S et al Diagnosing idiopathic learning disability acost-effectiveness analysis of microarray technology in theNational Health Service of the United Kingdom Genomic Med2007135---45
5 Newman WG Hamilton S Ayres J Sanghera N Smith A GauntL et al Array comparative genomic hybridization for diagno-sis of developmental delay an exploratory cost-consequencesanalysis Clin Genet 200771254---9
6 Trakadis Y Shevell M Microarray as a first genetic test in globaldevelopmental delay a cost-effectiveness analysis Dev MedChild Neurol 201153994---9
7 Coulter ME Miller DT Harris DJ Hawley P Picker J RobertsAE et al Chromosomal microarray testing influences medicalmanagement Genet Med 201113770---6
8 Riggs E Wain K Riethmaier D Smith-Packard B Faucett W
management Clin Genet 20139 Pina-Neto JM Genetic counseling J Pediatr (Rio J)
200884S20---6

IN+Model
dolcupr
taaoadnoo
F
GA
C
T
A
TBtCt
R
ARTICLEChromosomal microarrays in children
a VOUS required further analysis to determine possiblepathogenicity This patient was one year and 11 monthswith DD language delay hearing deficit inguinal herniaand short stature He had a 46XY karyotype and the arrayshowed a 2 Mb gain in chromosome 9p23 including par-tial triplication of one gene PTPRD The protein Ptprd isa receptor-type protein-tyrosine phosphatase is expressedin certain regions of the brain such as the hippocampus andcould have a role in learning and memory30 and the synapticorganization31 No phenotype has been assigned to the fulltriplication of this gene
Although CMA is a very robust and reliable techniqueit has limitations it is unable to detect balanced genomicabnormalities such as inversions reciprocal and Robert-sonian translocations Depending on the platform usedlow-level mosaicism and some polyploidies cannot bedetected When CMA technique is used as the first line ofstudy it has been described that this situation can occur in078 of cases5 Finally CMA does not give information onposition of the rearrangement FISH is often used as comple-mentary method to identify possible rearrangements withimplications for genetic counseling732
In the present cohort it was found that three patientswith previously known cytogenetic abnormalities resultedin a normal molecular karyotype As expected the patientwho is carrier for a Robertsonian translocation had a nor-malbalanced aCGH result In the case of one of the twopatients with sSMC the coverage of the array the genomicsequences involved and the size sSMC may explain whythat genetic material were undetected by this method19
Thus this small bisatellited chromosome likely correspondsto highly repetitive sequences typical of acrocentric chro-mosomes not included in the array that was demonstratedby nucleolus organizer region (NOR) banding In the patientwith a derivative chromosome 16 with an abnormal band-ing pattern and morphology (more metacentric than usual)a pericentric inversion is the most plausible explanation
Thus karyotype remains more suitable to evaluatepotential carriers of chromosomal rearrangements coupleswith recurrent miscarriage or patients with a distinctiveaneuploidy phenotype However FISH is more suitable if aspecific microdeletion syndrome is highly suspected7
Chromosome microarrays are a highly accurate robustand high-throughput method This study used a combinedoligonucleotide-based array plus SNP array which has manyadvantages where the SNP array significantly improvesthe accuracy and sensitivity of the CNV detection andmosaicism also allowing the detection of copy-neutralvariants33 In the case of the chip used in this report(Cytoscan HD Affymetrix) the platform chemistry andits algorithms analyze the oligonucleotide and SNP probesindependently and thus each CNV can be detected andconfirmed at the same time without requiring any furtherconfirmation3233 In this case instead of a confirmation ofthe array finding FISH analysis allows for determination ofthe type of rearrangement32
A limitation for widespread use of molecular karyotypeis the high cost of the test In Chile CMA is approximately
four to seven times more expensive than a karyotype andorFISH and is currently not covered by health insurance How-ever to reach an early diagnosis in selected patients withmultiple congenital anomalies andor global developmental
PRESS5
elay it can avoid unnecessary testing (the lsquolsquodiagnosticdysseyrsquorsquo) and allow focusing on specific issues which in theong term can be cost-effective34---38 It may be expected thatosts will decrease over time enabling its more widespreadse Finally it should be mentioned that there are otherlatforms that have lower resolution but at a relativelyeduced cost
Recognizing its limitations there is growing evidence ofhe clinical impact of this technology In many patients
definitive diagnosis can impact not only on informationnd counseling for their family environment39 but alson active surveillance in search of possible complicationsmong other types of medical interventions3738 The presentata show the usefulness of CMA allowing improved diag-ostic capability with remarkable precision and optimizationf the management and supervision of health in this groupf patients with special needs
unding
rant support from Child Health Foundation in Birminghamlabama
onflicts of interest
he authors declare to have no conflicts of interest
cknowledgments
he authors are grateful to the Child Health Foundation inirmingham Alabama for their grant support for this worko the participating patients and families and to Dr Silviaastillo and cytogeneticist Ana Mariacutea Fuentes for review ofhe conventional karyotype results
eferences
1 Christianson A Howson M Modell B March of Dimes globalreport on birth defects The hidden toll of dying and disabledchildren White Plains NY March of Dimes Birth Defects Foun-dation 2006
2 Kumar P Burton BK Dysmorphology In Kumar P Burton BKeditors Congenital malformations evidence-based evaluationand management New York McGraw-Hill Prof MedTech 2007p 3---11
3 Rauch A Hoyer J Guth S Zweier C Kraus C Becker C et alDiagnostic yield of various genetic approaches in patients withunexplained developmental delay or mental retardation Am JMed Genet A 20061402063---74
4 Vermeesch JR Fiegler H de Leeuw N Szuhai K Schoumans JCiccone R et al Guidelines for molecular karyotyping in consti-tutional genetic diagnosis Eur J Hum Genet 2007151105---14
5 Hochstenbach R van Binsbergen E Engelen J Nieuwint APolstra A Poddighe P et al Array analysis and karyotyp-ing workflow consequences based on a retrospective studyof 36325 patients with idiopathic developmental delay in theNetherlands Eur J Med Genet 200952161---9
6 Miller DT Adam MP Aradhya S Biesecker LG Brothman AR
Carter NP et al Consensus statement chromosomal microarrayis a first-tier clinical diagnostic test for individuals with devel-opmental disabilities or congenital anomalies Am J Hum Genet201086749---64
IN+Model
6
1
1
1
1
1
1
1
1
1
1
2
2
2
2
2
2
2
2
2
2
3
3
3
3
3
3
3
3
3Hoppman N et al Chromosomal microarray impacts clinical
ARTICLE
7 Manning M Hudgins L Professional Practice and GuidelinesCommittee Array-based technology and recommendations forutilization in medical genetics practice for detection of chro-mosomal abnormalities Genet Med 201012742---5
8 Shaffer LG Ledbetter DH Lupski JR Molecular cytogeneticsof contiguous gene syndromes mechanisms and consequencesof gene dosage imbalance In Scriver CR Beaudet AL Sly WSValle D Childs B Kinzler KW et al editors The metabolic andmolecular basis of inherited disease New York McGraw Hill2001 p 1291---324
9 Trask BJ Human cytogenetics 46 chromosomes 46 years andcounting Nat Rev Genet 20023769---78
0 Salman M Jhanwar SC Ostrer H Will the new cytogeneticsreplace the old cytogenetics Clin Genet 200466265---75
1 Smeets DF Historical prospective of human cytogenetics frommicroscope to microarray Clin Biochem 200437439---46
2 Turleau C Vekemans M New developments in cytogenetics MedSci (Paris) 200521940---6
3 Edelmann L Hirschhorn K Clinical utility of array CGH for thedetection of chromosomal imbalances associated with mentalretardation and multiple congenital anomalies Ann N Y AcadSci 20091151157---66
4 Jehee FS Takamori JT Medeiros PF Pordeus AC Latini FRBertola DR et al Using a combination of MLPA kits to detectchromosomal imbalances in patients with multiple congenitalanomalies and mental retardation is a valuable choice for devel-oping countries Eur J Med Genet 201154e425---32
5 Lee C Iafrate AJ Brothman AR Copy number variations andclinical cytogenetic diagnosis of constitutional disorders NatGenet 200739S48---54
6 Shaffer LG Bejjani BA Torchia B Kirkpatrick S Coppinger JBallif BC The identification of microdeletion syndromes andother chromosome abnormalities cytogenetic methods of thepast new technologies for the future Am J Med Genet C SeminMed Genet 2007145C335---45
7 Schluth-Bolard C Till M Edery P Sanlaville D New chromosomalsyndromes Pathol Biol (Paris) 200856380---7
8 Slavotinek AM Novel microdeletion syndromes detected bychromosome microarrays Hum Genet 20081241---17
9 International Collaboration for Clinical Genomics (ICCG)International Standard Cytogenomic Array (ISCA) ConsortiumDatabase Search [cited 4 March 2014] Available fromhttpwwwiccgorg
0 MacDonald JR Ziman R Yuen RK Feuk L Scherer SW TheDatabase of Genomic Variants a curated collection of struc-tural variation in the human genome Nucleic Acids Res201442D986---92
1 Database of Genomic Variants (DGV) [cited 4 March 2014]Available from httpdgvtcagcadgvapphome
2 Online Mendelian Inheritance in Man OMIMreg McKusick-Nathans Institute of Genetic Medicine Johns Hopkins University(Baltimore MD) [cited 10 March 2014] Available fromhttpomimorg
3 Firth HV Richards SM Bevan AP Clayton S Corpas M Rajan Det al DECIPHER Database of Chromosomal Imbalance and Phe-notype in Humans Using Ensembl Resources Am J Hum Genet
200984524---33
4 Database of Chromosomal Imbalance and Phenotype in Humansusing Ensembl Resources (DECIPHER) [cited 10 March 2014]Available from httpsdeciphersangeracuk
3
PRESSLay-Son G et al
5 European Cytogeneticists Association Register of UnbalancedChromosome Aberrations (ECARUCA) [cited 10 March 2014]Available from httpumcecaruca01externumcnnl8080ecarucaecarucajsp
6 de Leeuw N Dijkhuizen T Hehir-Kwa JY Carter NP FeukL Firth HV et al Diagnostic interpretation of array datausing public databases and internet sources Hum Mutat2012
7 Rosenberg C Knijnenburg J Bakker E Vianna-Morgante AMSloos W Otto PA et al Array-CGH detection of micro rearrange-ments in mentally retarded individuals clinical significance ofimbalances present both in affected children and normal par-ents J Med Genet 200643180---6
8 Krepischi-Santos AC Vianna-Morgante AM Jehee FS Passos-Bueno MR Knijnenburg J Szuhai K et al Whole-genomearray-CGH screening in undiagnosed syndromic patients oldsyndromes revisited and new alterations Cytogenet GenomeRes 2006115254---61
9 Michelson DJ Shevell MI Sherr EH Moeschler JB Gropman ALAshwal S Evidence report Genetic and metabolic testing onchildren with global developmental delay report of the QualityStandards Subcommittee of the American Academy of Neurol-ogy and the Practice Committee of the Child Neurology SocietyNeurology 2011771629---35
0 Uetani N Kato K Ogura H Mizuno K Kawano K MikoshibaK et al Impaired learning with enhanced hippocampallong-term potentiation in PTPdelta-deficient mice EMBO J2000192775---85
1 Takahashi H Craig AM Protein tyrosine phosphatases PTPPTP and LAR presynaptic hubs for synapse organizationTrends Neurosci 201336522---34
2 Bui TH Vetro A Zuffardi O Shaffer LG Current controversiesin prenatal diagnosis 3 is conventional chromosome analysisnecessary in the post-array CGH era Prenat Diagn 201131235---43
3 Mason-Suares H Kim W Grimmett L Williams ES Horner VLKunig D et al Density matters comparison of array platformsfor detection of copy-number variation and copy-neutral abnor-malities Genet Med 201315706---12
4 Wordsworth S Buchanan J Regan R Davison V Smith KDyer S et al Diagnosing idiopathic learning disability acost-effectiveness analysis of microarray technology in theNational Health Service of the United Kingdom Genomic Med2007135---45
5 Newman WG Hamilton S Ayres J Sanghera N Smith A GauntL et al Array comparative genomic hybridization for diagno-sis of developmental delay an exploratory cost-consequencesanalysis Clin Genet 200771254---9
6 Trakadis Y Shevell M Microarray as a first genetic test in globaldevelopmental delay a cost-effectiveness analysis Dev MedChild Neurol 201153994---9
7 Coulter ME Miller DT Harris DJ Hawley P Picker J RobertsAE et al Chromosomal microarray testing influences medicalmanagement Genet Med 201113770---6
8 Riggs E Wain K Riethmaier D Smith-Packard B Faucett W
management Clin Genet 20139 Pina-Neto JM Genetic counseling J Pediatr (Rio J)
200884S20---6

IN+Model
6
1
1
1
1
1
1
1
1
1
1
2
2
2
2
2
2
2
2
2
2
3
3
3
3
3
3
3
3
3Hoppman N et al Chromosomal microarray impacts clinical
ARTICLE
7 Manning M Hudgins L Professional Practice and GuidelinesCommittee Array-based technology and recommendations forutilization in medical genetics practice for detection of chro-mosomal abnormalities Genet Med 201012742---5
8 Shaffer LG Ledbetter DH Lupski JR Molecular cytogeneticsof contiguous gene syndromes mechanisms and consequencesof gene dosage imbalance In Scriver CR Beaudet AL Sly WSValle D Childs B Kinzler KW et al editors The metabolic andmolecular basis of inherited disease New York McGraw Hill2001 p 1291---324
9 Trask BJ Human cytogenetics 46 chromosomes 46 years andcounting Nat Rev Genet 20023769---78
0 Salman M Jhanwar SC Ostrer H Will the new cytogeneticsreplace the old cytogenetics Clin Genet 200466265---75
1 Smeets DF Historical prospective of human cytogenetics frommicroscope to microarray Clin Biochem 200437439---46
2 Turleau C Vekemans M New developments in cytogenetics MedSci (Paris) 200521940---6
3 Edelmann L Hirschhorn K Clinical utility of array CGH for thedetection of chromosomal imbalances associated with mentalretardation and multiple congenital anomalies Ann N Y AcadSci 20091151157---66
4 Jehee FS Takamori JT Medeiros PF Pordeus AC Latini FRBertola DR et al Using a combination of MLPA kits to detectchromosomal imbalances in patients with multiple congenitalanomalies and mental retardation is a valuable choice for devel-oping countries Eur J Med Genet 201154e425---32
5 Lee C Iafrate AJ Brothman AR Copy number variations andclinical cytogenetic diagnosis of constitutional disorders NatGenet 200739S48---54
6 Shaffer LG Bejjani BA Torchia B Kirkpatrick S Coppinger JBallif BC The identification of microdeletion syndromes andother chromosome abnormalities cytogenetic methods of thepast new technologies for the future Am J Med Genet C SeminMed Genet 2007145C335---45
7 Schluth-Bolard C Till M Edery P Sanlaville D New chromosomalsyndromes Pathol Biol (Paris) 200856380---7
8 Slavotinek AM Novel microdeletion syndromes detected bychromosome microarrays Hum Genet 20081241---17
9 International Collaboration for Clinical Genomics (ICCG)International Standard Cytogenomic Array (ISCA) ConsortiumDatabase Search [cited 4 March 2014] Available fromhttpwwwiccgorg
0 MacDonald JR Ziman R Yuen RK Feuk L Scherer SW TheDatabase of Genomic Variants a curated collection of struc-tural variation in the human genome Nucleic Acids Res201442D986---92
1 Database of Genomic Variants (DGV) [cited 4 March 2014]Available from httpdgvtcagcadgvapphome
2 Online Mendelian Inheritance in Man OMIMreg McKusick-Nathans Institute of Genetic Medicine Johns Hopkins University(Baltimore MD) [cited 10 March 2014] Available fromhttpomimorg
3 Firth HV Richards SM Bevan AP Clayton S Corpas M Rajan Det al DECIPHER Database of Chromosomal Imbalance and Phe-notype in Humans Using Ensembl Resources Am J Hum Genet
200984524---33
4 Database of Chromosomal Imbalance and Phenotype in Humansusing Ensembl Resources (DECIPHER) [cited 10 March 2014]Available from httpsdeciphersangeracuk
3
PRESSLay-Son G et al
5 European Cytogeneticists Association Register of UnbalancedChromosome Aberrations (ECARUCA) [cited 10 March 2014]Available from httpumcecaruca01externumcnnl8080ecarucaecarucajsp
6 de Leeuw N Dijkhuizen T Hehir-Kwa JY Carter NP FeukL Firth HV et al Diagnostic interpretation of array datausing public databases and internet sources Hum Mutat2012
7 Rosenberg C Knijnenburg J Bakker E Vianna-Morgante AMSloos W Otto PA et al Array-CGH detection of micro rearrange-ments in mentally retarded individuals clinical significance ofimbalances present both in affected children and normal par-ents J Med Genet 200643180---6
8 Krepischi-Santos AC Vianna-Morgante AM Jehee FS Passos-Bueno MR Knijnenburg J Szuhai K et al Whole-genomearray-CGH screening in undiagnosed syndromic patients oldsyndromes revisited and new alterations Cytogenet GenomeRes 2006115254---61
9 Michelson DJ Shevell MI Sherr EH Moeschler JB Gropman ALAshwal S Evidence report Genetic and metabolic testing onchildren with global developmental delay report of the QualityStandards Subcommittee of the American Academy of Neurol-ogy and the Practice Committee of the Child Neurology SocietyNeurology 2011771629---35
0 Uetani N Kato K Ogura H Mizuno K Kawano K MikoshibaK et al Impaired learning with enhanced hippocampallong-term potentiation in PTPdelta-deficient mice EMBO J2000192775---85
1 Takahashi H Craig AM Protein tyrosine phosphatases PTPPTP and LAR presynaptic hubs for synapse organizationTrends Neurosci 201336522---34
2 Bui TH Vetro A Zuffardi O Shaffer LG Current controversiesin prenatal diagnosis 3 is conventional chromosome analysisnecessary in the post-array CGH era Prenat Diagn 201131235---43
3 Mason-Suares H Kim W Grimmett L Williams ES Horner VLKunig D et al Density matters comparison of array platformsfor detection of copy-number variation and copy-neutral abnor-malities Genet Med 201315706---12
4 Wordsworth S Buchanan J Regan R Davison V Smith KDyer S et al Diagnosing idiopathic learning disability acost-effectiveness analysis of microarray technology in theNational Health Service of the United Kingdom Genomic Med2007135---45
5 Newman WG Hamilton S Ayres J Sanghera N Smith A GauntL et al Array comparative genomic hybridization for diagno-sis of developmental delay an exploratory cost-consequencesanalysis Clin Genet 200771254---9
6 Trakadis Y Shevell M Microarray as a first genetic test in globaldevelopmental delay a cost-effectiveness analysis Dev MedChild Neurol 201153994---9
7 Coulter ME Miller DT Harris DJ Hawley P Picker J RobertsAE et al Chromosomal microarray testing influences medicalmanagement Genet Med 201113770---6
8 Riggs E Wain K Riethmaier D Smith-Packard B Faucett W
management Clin Genet 20139 Pina-Neto JM Genetic counseling J Pediatr (Rio J)
200884S20---6
Copyright © 2022 FDOKUMEN