
Can remittances compensate for manpower outflows : The case of Philippine physicians
17
Transcript of Can remittances compensate for manpower outflows : The case of Philippine physicians
Filipino-born rather than U.S. nationals. 2 That is, the U.S. stock of Philippine physicians was over 75 percent of the Philippine stock in active practice3 It can be drp,ued that some Filipino physicians *Nere only in the U.S. temporarily, but several studies of foreign medical graduates1 (Fans) suggest that the large majority of such individuals intend to stay permanently.”
There is no mystery about the individual doctor’s motivation for migration. Available estimates of relative doctor incomes in ahe U.S. versus the Philippines indicate that the private return to migration for a nzwly- trained doctor is extremely high? But this high private r&urn in no sensT guarantees a positive social return to the Philippines fr3m doctor migration. Indeed, a stegative social return might at first blush be cxmted. Given that developing nations generally face capital scarcity, the use 0 trahn doctors who the.n leave would seem a low-yield use of issue is the following: why did the Philippine government allow :,hc use of scare capital for expansion of medical education when so m&any doctors then chose 10 leave? While pohtical and sociological explanations abound, are then? also explanations providing an economic rationale? In particular, remi.ttances from Filipinc doctors practicing overseas might be sizeable enough to compensate for losses associated with emigration. That is, it may ‘pay’ to train doctors for export. Tlhis paper presents an analytical framework which permits us to evaluate this proposition.
“The 13,380 figure is from World Health Organization (1978, p. 38). The 10,410 figure is from American Medical Association statistics as reported in Mejia et al. (1980, p. 5). The assertion that very few Philippine-trained doctors are U.S. born is supported by three pieces of evidence. first, ?dejia et al. report that of all Philippine FM& who entered the U.S. between 1966 and 1968, 80 percent were Philippine citizens, 1 percent were naturalized citizens of the U.S., less thqn 0.5 pet-cent were citizens by birth of the U.S., 3 perent were citizens of other CoutWz-s, and fd pmxnt were unidentified by citizenship (table 1.7, p. 14). Second, AMA data reported by
ejia et al. show that of 57,217 FMCs in the U.S. in 1970, 5,972 (around JO perent) were U.S. born. Out of the 5,972 U.S. born FMGs, 5,662 received their medical training in 13 countries: 12 countries in Europe pius Mexicc. The other 318 U.S. born FMGs representeli Iess i/&an I pmeenr
qf rhe FA4Gs frum the remafrtirg FMG-supplyirrg mmtries (table 1.8, p. 16). Third, a study by S:evens et al. (1978) drew 2~ sa*:lple of FN& serving as hospital house stafi iI; the U.S. in 197% ?t. Out of 732 FMGs, only 36 were U.S. bo*.n and 6 were naturalized U.S. citizens.
30f course, there were more than 13,480 individuals trained as physici ns residing in thu SOW of ihose trained as physicians da not lind it wrrrth
‘Stevens et al. found that 75 percen! of a sample of F Gs working us h .NJS~ stafT in 1973- 74 ~~~~en{~ed to stay in the C1.S. This may understate thz true percentage, since. those on temporary \ isas have incentives to misstate intentions. Haug and Stevens found that, of d cohort of I:MGs I~re III 1963, over 80 percent were still here in 1971. Neither stutly is ~~~~~~~~d LO ~hl~ipp~t~~ EVlGS.
rovide indications tilat the return to physician training sn the Phil aken into account. First, if it pru unteci value of physician training is
Four comments are in order. First, the argument that it ~nay ‘pay’ to tra*,ij
n made to the authors several times by indivfdu; Is teCXXlt press articles iniicat%I, t
d’ This paper was partly provoked s that ‘it pays’ cculd be correct.
h there is no s ific mechanism re voluntary, d depend ori
can question the reliability of such and explore under what conditions they
worth stressin that, CGk there exists no E Philippine pkq-sician remittances,
ignoble increments to family income. [Ministry of tht: Budget ( 1379)]
n U.S. dollars for selected occupations In 1979 were: pharmacist $1256. A remittance age U.S. doctor income in 19%
would rqresent a signikant increment to family income.’ Third, one possible counter to the argument that training doctxs is a
‘bad’ investment (in the absence of remittances) might be the following: ‘P‘s d investment if mi rating doctors pay the full cost of their training.’
Our framework allows us to evaluate this argument. A fourth comment is a non-exhaustive list of competing explanations for
ration flow. First, expansion of medical training facilities may reflect
The su,ggestion that remittance. may compensate: for doctor out-mtgration has ken madt: to the authors several timcs. One q-kit pubhshed st*~tsment appears m congrewonai testlmoAq by Dr. Robert V&s:
‘Indeed it is stated that the third largest cash crop of the Philippines is its foreign medical ~~d~~t~ m tans of the amount sf money they send home when employed in this count ia II is try that this has n our finding in terms of inter views with Philippine ph~~~~~~~* in te ms of rhci ing iunds hiJrnt . 1 he average salary in government service for 8 Filipino p qkcian is tS.S. 8 month. 1 ou can readily see that it wuld be very
~~h~~~~ ian warkrt this owntry, mm at a salary much MOW that which CCMAM by rni ny ~rneric~~n ~hy~~ci~~~~ to nci that much money ho
4 R. Go ftljbrb et ai., Remittatmjlflows, migration
political pr~sure from elites, who wish to provide their children with a mobile form of human capital. This makes special sense for families faced with a political situation which could change suddenly and drastically.* Second, a large portion of the -medical training cap&t universities, and governmental political ability to control un mix” may be limited. Thild, the government may perceive a the doctor/population ratio in the Philippines, implying sup training. Combining such support with political or econontk constraints preventing legal knitation of physician emigration would account for lack of gorfernment limits on medical training? We do not explicitly analyze the% alternative explanations in detail. Instead, we focus on ‘remittttnoes as compensation’, presenting iin analytical framework which aIfows this explanation to be evaluated.
To evaluate the ‘remittances as compensation explanation, two quite distinct public policy <uestiuns are relevant. One involves the broad ‘regime choice’: suppose a government interested in maximizing Philippine social welfare were in charge of the economy, a-ad had a choice between two mutually exclusive regjmev. In regime I, doctors were trained, bu outmigration was prohibited. In regime II, doctors also were trained, but each doctor had the option of migrating or lnot migrating. Which regime would the government choose? This question addresses the broad issue of whether a policy alEowipg mi;yation of tsaineid doctors has a positive net
ayoff to the domestic economy. The second issue has a very different focus. G&n that migration is ff~~~~?~~,
is the number of doctors trained as chosen by the private sector lower, gher, or the same as the tevel that would maximize social welfare? This cund question is relevant under two quite different scenarios. In the first
scenario the social-welfare maximizing government chooses the mi the second question then becomes important for optimal ent of the preferred regime. In the second scenario, the
ave chosen the migration regime, but is ‘stuck’ s. Here, the second question can be thou ht of as an e second best’ issue,
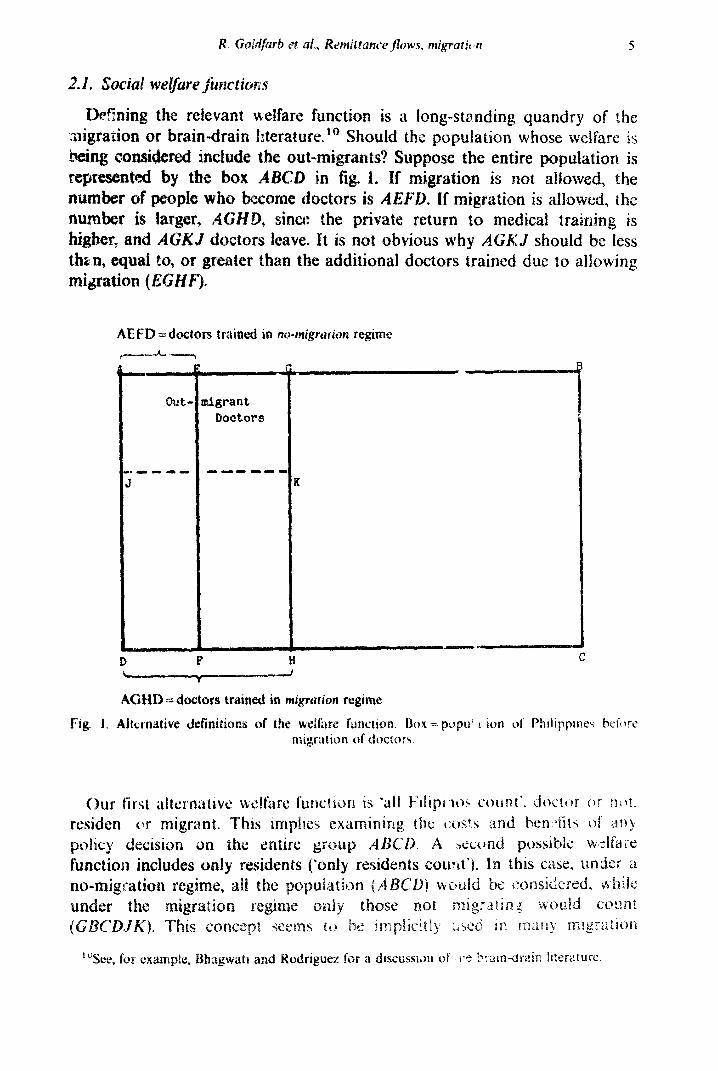
t welfare functlion is a Iong-stmding quandry o whose wei
the entire ~~u~at~~~ is ix3 is not alluwed, the ~g~at~~n is a~~~~~d~ the to medical traiaing is
GKJ shmld be Iess cd due to aflowing
Eligrant Doctors
6
studies. In estimating benefits of migration, these analyses frequently net out foregone consumption of out-migrants.’ 1
A third possible function is the opposite of the first and excludes all potential doctors: ‘only non-doctors count’. Thus, one would look only at the group GBCH. This alternative stems from a difficulty with the second welfare concept. Using ‘only resident? count’ a comparison of the mi and the non-migration regin e would mean comparing the w~lfar~ different populations, ABGD ilnd GBCDJK. Therefore, it may the approptiate fixed popul;ition base is GBCH, excludin doctors under any possible re@ne.
Each alternative welfare function has its strengths and weaknesses. Below we focus on ‘only residents Izount”, but will indicate how using the other al terna tires aBect results.
3. The regime chaire ptstioltll
We first address the question, which regime should be chosen, using t;he ‘only residents count’ welfare function. Consider the ‘social’ cost--benefit analysis associated with training one more doctor if no doctor, once trained, csuld emigrate. The stream of social benefits BN (where the subscript N denotes the non-migration case) from such training could be indicat
where S is years of medical training required of a medical student, T is the expected length of the physician’s working life after training, YD1 is the doctor’s earnings in the Philippines in year i, YOi is the earnin would have achieved in year i if he had not become a doctor, 6 is a term representing any social externality provided by the doctor’s service the relevant social discount rate. Except for the s correction, this fo of social benefits assumes that earnings represent soei productivity.
The social costs C associated with trainin one more doctor are
’ (&+yOi) C=K+~------- i=l (l+rqi ’
eq. (2) still holds, but ey. ( ?), the
nefits to the Philippines of trh-hg one
in the Philippines v ill be in octsr’s U.S. eamin s in year i, Cb is the
nsity to consvmc. and ~r~~ffj~~~~~~ ae term hY& is meant ?t~ captu~
tlon r~~~~~re~~cnt~ b~ca*rse ihe doctor is nc~ longer +I
t hc that R is z O~WUW _v rtznCItuatv.q; t hi ate that remit tanoes shoukl be calculated
ign exchange* The first tt’r of H, is R, t the dc_xtot is in the Phih ines in year i.
exogenous to P ppine decision makers igration from Philippines. and there
~XCSS demand fer these limited immigration ~~~rt~~itj~~.‘~
How can these: equations k used to analyze ‘regime choice‘, the choice t~ct~n a policy of training hxtors and allcjwing export versus a policy of
d~tors and not all-rwing export‘? ‘t”ote th:kt ~1, the number of trained under a ‘migrAtic)n allowed’ policy, i% :ikelv to be difftxnt
from n, the number of doctors trained under a ‘no-mi;r stion police The net M . knefits (from one cohort of students) of a policy alloumg migration is
w :rere B&q indicates that B, has bm~ redefined lo substitute ma product for Yni and YGs. EVHI if YDi (and analogously YOr) ~XJU~S rn~rgin~~l product for small changes in the stock of doctors, it will not (summedjl marginal product for large changes in the stock of dact
would umierstate C MPbi because YDi would equal the m the mth doctor, which would, because of d~~i~is~~~ ma be lower than the marginal product of the (m_i)th doctor.
SimilaxIy, the net benefits of a no-migration policy is
Thus, allowing migration is the preferred policy if (4) >(5), To make further progress, one must specify how m and n are det k consider two possibilities. In the first, the number of training slots is
controlled by the government which chooses m under a migration regime and pt under a no-migration regime to maximize net social benefits. The second possibility is that the number of slots in medical schools is determined by the demand of (qualified) students. In this second case, a larger number of slots can be expected if migration is allowed, since the possibility of migration raises the expected private return to medical trainin That is, under this alternative, m > II.
3.1. F&t nltlernatke: rn and PI selected to mmcimize net social bmefits
Here, the government controls the number of slots and chooses m and n to maximize net social benefits. Thus, we must compare the net social yields of allowing migration (assuming m is chosen optimally) with not glowing migration (assuming n is chosen optimally).
Selecting m optimaliy requires maximizing eq. (4) with res Selecting n optimally requires similar maximization of eq. (5). requires selecting yt so that for the rzth trainee, Bh = C,
s I ~~
iC1 +E)- Yoi _I_-
i=S+l (1 +r)i -=”
Number of
Doctors trained
3.2. Second altemative: Number of trainees --Determined by student demand
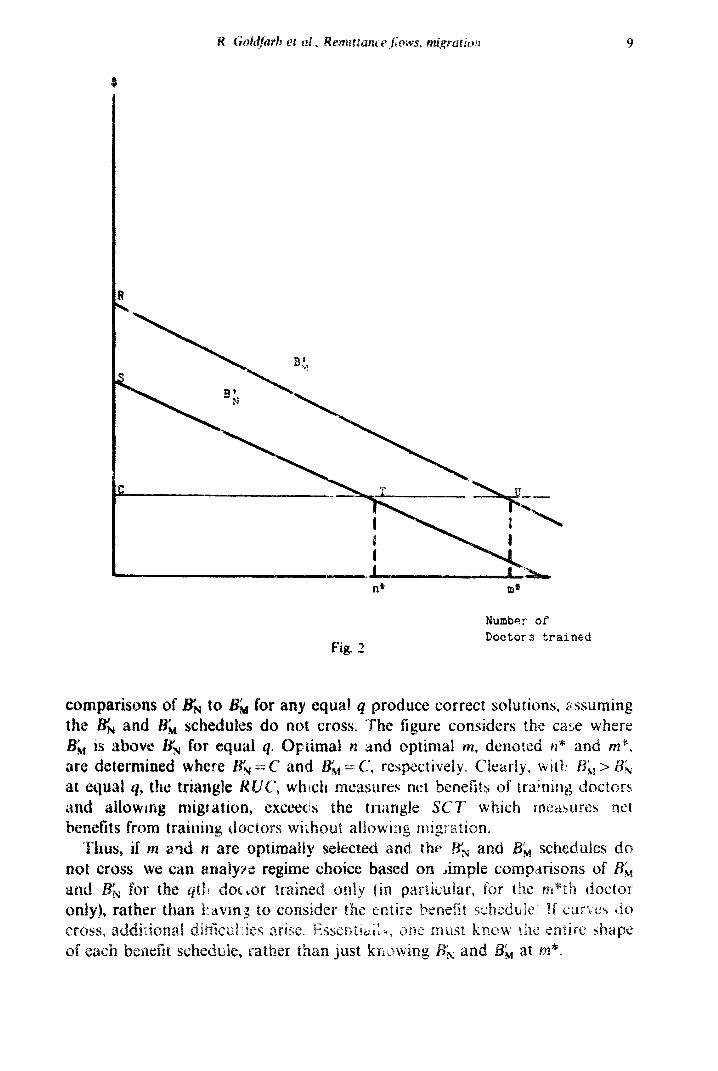
klere, more slots result if migration is allowc:d, since the possibility of migra.iio:\ raises the expected private return to medical trail& under this &emative. &era1 subcases can be considered. Suppose one schedule ilie(j: everywhere above the other, and C is constant and SLT, for the mth doctor traixd. It r;an be shown (a demonstration is available from the al&x-s) that for & ~rs;lJ for equal 4, a migration policy dominates a no- migration policy. On the other hand, if EN> B;, for equal 9, the outcome is ambiguous, and depends on the shapes of the entire benefit schedules. Suppose insltead th;rt one sch cdule lies everywhere above the other, asld (‘ is constant bur. greater than BM for the mth doctor. Then all results depend on the entire benefit schedules. All kinds of additional complications arise if the scheduIes cross. Thus, for this second alternative, one must know the enlire shape of each benefit schedule, and wh< ther Cs EM at actual m. This additional complication about the relatlonsLhip between C and BM did not arise when the government chose n and nz optimally because choosing m optimally implied C = i-rl, at m*.
3.3. Can empirical tjlesk’ be put on t~~ese analytical ‘bones’?
Consider the first alternative above, in which the government chooses the number of training slots optimally. In that world, if betlqfit schedules do nat m~s, we could choose between regimes by comparing & to BE, at &@. This simple comparison is attractive because obl.aining believable evidence on the entire B& and Bh schedules seems improbable. On the other hand, estimation of SE,, and B;, at I-II* is conceivable. Sb at m* is the benefit the last doctor traine:d under current rules (allowing migration) would provide to the Philippines [that is, eq. (3) for the m*th doctor]. Data on current doctor incomes in the U.S. and Philip actual migration propensities, remittance ratios, and so forth woul w estimation of (3) for the nr*th doctor. Sk at m* [that is, cc+ (1) for the mth doctor] could be estimated Lsing tile same data.
Four important warnings about the limitations of such a calculation are in or&~-. First, we sySpert that private demand, not government aptimizin PM? .c ~~~~~~~, we know that th\z benefit curves may well cross. Both of these limitations suggest that simple comparisons of BE, and RN at actual PII may
e in~on~~u~ive~ The third ~in~~ta~ion is subtler. We are trying to estimate SrN data from the ‘migration allowed’ regime. But & refer regime , tind (since there might be important differences
regime@ editnates of BN based an the migration regime may be biased. Fourth, our timatjon procedure provides an estimate of L& at (1 -p)m*
rather than nt*! That is, by usi data generated by a regime where nl* drop are trai te, WE are looking at values of YDi ~do~~st~~ doctor i~~~~~s) d~t~~in~ by ‘only’ (1 -p)m* hew trainees. This
scrhedufe at (1 -p)m*, not m*! Thus, if the our estin~ate of RN at ~2* overstates &.
pucks we ignore a11 these difficuJties and and &M at m*. First, subtract S;, om BM at m*
(3) minus (1 )I. Simplifying terms gives the following condition for
That i% the lifetime income of a doctor in the U.S. (c Y”,i) times the remittance percenta R plus Iifetime consumption savings from migration (GbGi) - each term appropriately discounted and weighted by the probability (p,) of being in the U.S. - must exceed the lifetime income plus externalities of a doctor in the Philippines 7, YDi( 1 + E), ako appropriately discounted and weighted.
If /?i is constant over i, eq. (7) can be rearranged
S+T
c y / S+T
us
i c t&i) i.zS+l(l+r)‘/
__- i=S+*(i +r)’
,1-t&--hZ
R ’
as follows:
where 2=x YDi, which must be less than 1. Eq. (8) implies that migration is d only it U.S. doctor income exceeds Philippine doctor income by a larger percentage than ( 1 -t E -- bZ)/R. l6
Results analogous to eq. (81 can be derived for the other two social welfare functions discussed above. In the ‘only nor-doctors count” case, the ne N version
. (8) has (I -o- E---b)/W on the right-hand side, instead of ( 1 +c -MM. arance of Z, the new version is more favorable to migration
atively, in the ‘all Filipinos count’ case, the eW versxon of IS) b’) on the right~hand side. The h’ indicates z ~rr(;_“tf~on Tar
different tax systems in the two cou erivation:j of thi5s results a~ available from the authors.
We can for illustrative purposes use values from the existing (
e a0 co I^ f es-e
12 R. Gordfarb et al., Remittance Jews, migrcttion
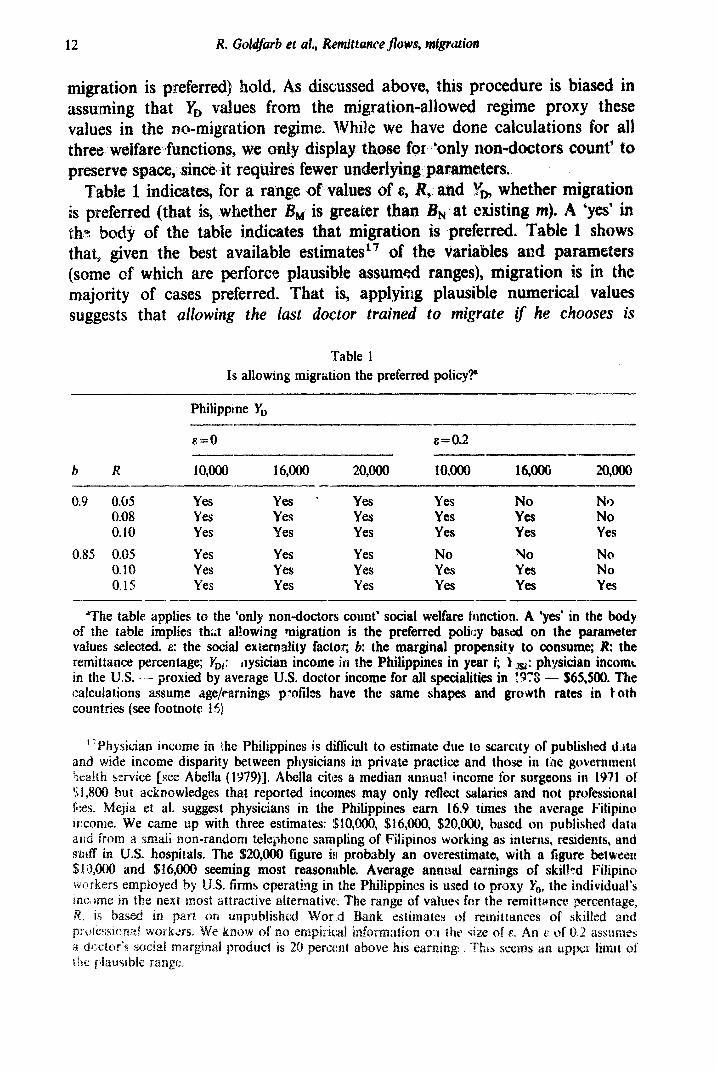
migration is preferred) hold, As dkussed above, this procedure is biased in assuming that YD values from the migration-allowed regime proxy these values in the no-migration regime. While we have done calculations for all thres welfare functions, we only display those for ‘only non-doctors count” to preserve space, since it requires fewer underlying parameters.
Table II indicates, for a range of values of 8, R, and whether migr~t~on is preferred (that i3, whether 18, is greater than BN at existing m). A ‘yes’ in eh(? body of the table indicates that migration is preferred. Table 1 shows that, given the best available estimates *7 of the variables and parameters (some of which are perforce plausible assum ranges), migration is in the majority of cases preferred. That is, applying plausible numerical valu suggests that atlowing the lust doctor trained to migrate zf he chooses is
Table 1
Is allowing migration the preferred policy?”
Philippine YD
E.=O &=0.2
b R 10,000 16,000 20,000 10,000 16,000 Qm --
0.9 0.05 Yes Yes ; Yes Yes NO N9 0.08 Yes Yes Yes Yes YeS No 0.10 Yes Yes Yes YeS Yes Yes
0.85 0.05 Yes Yes Yes No YO No 0.10 Yes Yes Yes Yes Yes No 0.15 YEi Yes Yes YeS Yes Yes
_---- _-
“The table applies to the ‘only nondoctors count’ social welfare famction. A ‘yes’ in the body of the table implies tha;t allowing migration is the preferred polity based on the parameter values selected. E: the social externality factor; b: the marginal propensity to consume; I?: the remittance percentage; rDi: ilysician income in the Philippines in year i; ‘t +Jsl: physician incomt in the U.S. - - proxied by average U.S. doctor income for all specialities in ITS -- !$65,!80. The calculations assume age/earnings profiles have the same shapes and growth rates in t oth countries (see footnote 15)
’ ‘Physician income in ihe Philippines is difficult to estimate due to scarcslty of publish~ d.jta and wide income disparity between physicians in private practice and those in tk g~v~rnrn~n~
13
precedes ~~~ the P~~l~pp~ne~’ peint of ukw) YU fix-bidding m@ation. This
f the large disparity between YUS and Yn.
set forth above, the following ‘regime iven that the Philippines already has a
e.+ the i~forrn~ti~~ in tab:: 1 provides ~~~~1~~~~~ no an” regime. Even t ough the data iases associakd with currently
gains from ‘closing the borders”. Sin the borders’ wou involve administrative costs
dcd rn the current analysis, the
t‘ welfare I‘unctio give results
ents count’ welfa function, on the other hand, . Three comments abut this ‘rever a major source oi’
u&s are biased againct a migration regkme; a ‘true’ at resu:ts do change
of examining the nsitivity of results to welfare function assumptions. Third, even with the
reversal, we still do not have strong evidence against a migration regime.
4. Private versus ial optimality of training under a migration regime
A second issue is raised by the ‘remittances as compensation’ argument. Suppsse a ‘migration-allowed’ me has already been chosen, either because it is economically optimal or to political constraints. Suppose further that, under this regime, the num P of doctors trained is determined
or demand. The fotlo issue arises: is the number of her, or the same as tie level that would maximize national
this issue, one must compare the private indiGdu;al’~ decision with what t ~~~i~~-wel~~r~ maximizing governmeN
al. The privrrtc i ividu~~ views it as dcsir i-k tc\ obtairl
period as pi, rather thafl 0 or 1; The right-band side is the discjounted earniags in his alternative (non-doctoring) occupatf Dn. By using pretax incomes in eq. (9), we assume that tihe individual views taxes as prices for government servicrt:s received; that is, he acts as if*he is subject to a perfmt ben&t tax.’ This assumption ‘avoids additional algebraic compl
Haw does the private decision compare to the quilibri welfare maximizing government would desire? count” sociaf welfare function, the government taking place so long as the following condition trainee:
S+T piRY,,i+(i -pi)Yni(i +E)+pibY& c i=S+l (i +rfi
Using the ‘anly r~side~i~ would like to s trainisl holds for each prospective
where CG is the total (private plus public) cost of training a doctor, is the remittance percentage out of pretax: income, and & is also pretax, The first term on the left indicates that, from the social-welfare maximizing government’s point of view, benefits of training a doctor include his remittances and saved consumpiion if he leaves, and bBs income plus externalities if he stays. If the optimal number is trained from the government’s point of view, the 2 is replaced by an equal sign in (10) for the marginal trainee.
Since the right-hand side of (9) is identical to the right-hand side of (lo), private decisions wial lead to the socially optimal number of doctors trained if
‘+’ PiRY”,i*t(l-pi)YDi(l +&)+PibY*i c c (1 fr)” -- ‘G i=S+l
S+T Pi KSi +I1 -pi)YDi = c 1- --__
(1 i-r)’ c
i--S+1 Pr’
The equality in eq. (1 ‘I-; states that the net social benefit of the M trainee is equal to the net. private benefit.
ere are at least two useful ways to analyze eq. (11). irst, solve for the
“Treating taxes as pure costs involves multiplying I’,, by (1 -“- tu,J and Yni and Y& by (1 r,l, where t, and t, are the releva;lt CJ.S. and Philippine tax rates. If taxes are entered in this way, then even in the absence uf m@gration and externalitks (c), it CStn easily be shown that, ta
al decisions by the private stvtor, private costs (ic,,) must be below full CQSIS (C,) private in~~du~ oniy ~~~l~t~
* (1 -- IJ of cos;is. It atiscs the tlm su~si 0 avoi 3:
15
irate derisions KI produce a social ost of training (C,)
reduction externality tim externality prs-
vate gains, YUq( ii - R),
te that K turns private
t on she cfairn t~~~t the P~~~~~~~~~~S should
trainees pay full costs. Eq. ( 12) shows this erpreted as the right-
nd ar,d third terms ample if E=O and
QY*, = Y&( I- R). Eq. ( 12) hig~~jig~ts the idea that, if externalities a:e present, s that pricing embody corrections [or these externalities. It to note that, given plausible vatuel for parameters (such as
in table l), students might have to be charged amounts well above actual training costs in w=der to achieve optimali:y. Using the values in
unts in five figures are not hard to generate. ond way to look at eq. ( 11) is to ask: ‘if schools charse fw ” costs (so
C, = C,,), will tc’o many or too few doctors be trained? Private &cisions lead to too many doctors if
Ults foI~o~ frOm ( 13). First, suppose pi is constant. Then if c: =. 0, sector trains tot ~~~~~y doctors if
prrPfr?es jhave the sarnc shape in each country,
This p;s*pcr addresses two questions about Philipp& physician out- migration: is it economically preferable to allow migration or t‘o rtxtrict it; and if migration is allowed, do private market decisiotlzs result in a socially optimaI vohm~e of training? Lack of data plus uncertainty about the approprjate welfare function precludes reaching unequivocal c~n~~usi~ns. Never&hdess, available empirical evidence does not favor restrictin migratior;~. We have alslo shown that, even if medical schools char costs, the private market may train too many doctors.
Using information from a ‘.migration’ regime, approximate estimates can be made of physician incomes in the Philippines and the U.S., consumption
ropenslt~es, and “guesstimates” of externaiities and remittances. These are used to &c: does a migration regime return greater social &x&its than a no- ~~at~c’~~ regime? The numbers suggest the answer may weli be
uncier alternative rq$mes. Moreov

the brain drain,
w: An eco~lomic kssues and policks
in the U.S. in 1963 and in 1971:
1 graduates (Heath,
rnes 19-m ~~~~~Q~ City). and frmge benefit survey -
Pakistan, World Bank stti working paper DO.
Stevens, ~~~~~~y~ Louis Goodman and Stephen ,Wick, 1978, The alien doctors (Wiley, ‘New Y Orb;).
World Health 0 1978, World hea th statistics, Vo. 111 (Geneva).




















