
HMOs and Managed Care: Implications for Rural Physician Manpower Planning
15
Weiner 3 73 HMOs and Managed Care: Implications for Rural Physician Manpower Planning“ Jonathan P. Weiner ABSTRACT American health care is changing dramatically. Health maintenance organizations (HMOs) and other managed care plans are central to this change. Today, the majority of Americans living in metropolitan areas receive their care from these types of plans. The goal of this article is two-fold. First, it will discuss the potential implications of HMOs and managed care for physician needs and supply in rural regions. Second, it will deriveinsight intoalternativeapproaches for meeting rural health manpower needs by analyzing H M O staffing patterns. As HMOs and other managed care plans expand, rural physicians, their practices, and their patients will almost certainly be affected. A s described in this paper, most of these effects are likely to be positive. The staffing patterns used by HMOs provide an interesting point of comparison for those responsible for rural health manpower planning and resourcedevelopment. HMOs appear to meet the needs of their enrollees with significantly fewer providers than areavailable nationally or suggested by the federal standards. Moreover, HMOs makegreater useof nonphysician providers such as nurse practitionersand physician assistants. The American health care system of 1990bears little resemblance to that of even 10 years ago. Major features of this “new medical marketplace” include: payer’s aggressive application of utilization review protocols to contain costs, vertical integration of provider organizations, limitations on consumer’s choice to select providers, and alternative financing mecha- nisms such as capitation and prospective payment (Stoline & Weiner, 1988). These dramatic changes all come together within the health maintenance organization (HMO). Today, the majority of Americans belong to HMOs or other related managed care plans. In addition to the various types of HMOs, managed care is usually considered to encompass preferred provider organizations (PPOs)and indemnity plans that manage their program outlays via inten- sive utilization review controls, such as prehospital certification or ”gatekeepers” (Gabel, Jajich-Toth,DeLissovoy, Rice, & Cohen, 1988). Many believe that the growth of HMOs and managed care has been fostered by the increasing supply of physicians: during the last 20 years, there has been almost a two-fold increase in the number of practicing * For further information, contact Jonathan P. Weiner, PhD, Associate Professor, School of Hygiene and Public Health, Johns Hopkins University, Hampton House, Room 605,624 N. Broadway, Baltimore, MD 21205. The Journal of Rural Health Volume 7, Number 4-Supplemental 1991
-
Upload
johnshopkins -
Category
Documents
-
view
1 -
download
0
Transcript of HMOs and Managed Care: Implications for Rural Physician Manpower Planning

Weiner 3 73
HMOs and Managed Care: Implications for Rural Physician Manpower Planning“
Jonathan P . Weiner
ABSTRACT American health care is changing dramatically. Health maintenance organizations ( H M O s ) and other managed care plans are central to this change. Today, the majority of Americans living in metropolitan areas receive their care from these types of plans. The goal of this article is two-fold. First, it will discuss the potential implications of HMOs and managed care for physician needs and supply in rural regions. Second, it will deriveinsight intoalternativeapproaches for meeting rural health manpower needs by analyzing H M O staffing patterns.
As HMOs and other managed care plans expand, rural physicians, their practices, and their patients will almost certainly be affected. A s described in this paper, most of these effects are likely t o be positive.
The staffing patterns used by H M O s provide an interesting point of comparison for those responsible for rural health manpower planning and resourcedevelopment. H M O s appear to meet the needs of their enrollees with significantly fewer providers than areavailable nationally or suggested by the federal standards. Moreover, HMOs makegreater useof nonphysician providers such as nurse practitioner sand physician assistants.
The American health care system of 1990 bears little resemblance to that of even 10 years ago. Major features of this “new medical marketplace” include: payer’s aggressive application of utilization review protocols to contain costs, vertical integration of provider organizations, limitations on consumer’s choice to select providers, and alternative financing mecha- nisms such as capitation and prospective payment (Stoline & Weiner, 1988). These dramatic changes all come together within the health maintenance organization (HMO).
Today, the majority of Americans belong to HMOs or other related managed care plans. In addition to the various types of HMOs, managed care is usually considered to encompass preferred provider organizations (PPOs) and indemnity plans that manage their program outlays via inten- sive utilization review controls, such as prehospital certification or ”gatekeepers” (Gabel, Jajich-Toth, DeLissovoy, Rice, & Cohen, 1988).
Many believe that the growth of HMOs and managed care has been fostered by the increasing supply of physicians: during the last 20 years, there has been almost a two-fold increase in the number of practicing
* For further information, contact Jonathan P. Weiner, PhD, Associate Professor, School of Hygiene and Public Health, Johns Hopkins University, Hampton House, Room 605,624 N. Broadway, Baltimore, MD 21205.
The Journal of Rural Health Volume 7, Number 4-Supplemental 1991

3 74 The journal of Rural Health
physicians. In this era of abundance, providers have been far more likely to play by the payer’s rules. It is estimated that more than one half of all U.S. physicians now participate in at least one HMO or PPO and virtually all come under the scrutiny of the utilization review agents of at least one managed indemnity insurance plan. The scenarios just described are more apt for some parts of our nation than others. We have (at least) two parallel sets of delivery systems: the systems found in the urban centers and their suburban rings; and those of the nonmetropolitan small cities and towns and rural frontiers. While rural health care systems are intertwined with those of urban areas, to a significant degree they also function as indepen- dent, geographically contained microsystems. The dynamics and problems within these subsystems are unique. One of these special problems is the shortage of health care providers.
This paper has two primary goals. First, to discuss the potential implica- tions of HMOs and managed care for future physician needs and supply in rural regions. That is, as HMOs and related health plans expand within urban America and diffuse into rural locales, what impact will this have on the adequacy of the physician stock in nonmetropolitan areas? Will this trend improve or exacerbate current problems?
The second goal of this paper is to offer insight into alternative ap- proaches for meeting rural health manpower needs by using the HMO as a self-contained laboratory. That is, can we learn anything by assessing the staffing approaches that established HMOs have chosen to serve their enrolled populations? This discussion should be relevant for those con- cerned with physician supply adequacy for all populations, not just where HMOs and other managed care health plans are operating.
The Managed Care Decade: A Summary
In 1980,95 percent of insured Americans were enrolled in conventional indemnity-style health plans. By 1990, these types of arrangements consti- tuted the minority-managed care predominated. Less than 25 percent of families with employment-linked plans had indemnity health insurance policies (e.g., traditional Blue Cross/Blue Shield). And, with government programs included, the proportion of Americans with conventional insur- ance was estimated to have fallen below 45 percent.
The health maintenance organization was the arrangement of choice for about 5 percent of Americans in 1980. At that time, 80 percent of the ”prepaid” enrollees received care from staff or group model HMOs in which the physicians practiced in organized clinic-like settings. The re- mainder were enrolled in “open-panel” independent practice association (IPA) model HMOs which were made up largely of solo and small-group practitioners who wished to compete with the larger ”closed-panel” plans (Interstudy, 1989).

Weiner 3 75
Many believe that the old-line HMOs provided the paradigms for the managed care movement, but that the spark for the explosive growth came from elsewhere-employers and government. As the financiers of the enterprise, these parties adopted proactive cost-containment mechanisms in an attempt to manage rather than simply expend resources.
Today, there are more than 1,500 distinct managed care entities in the United States. They include not only established prepaid group practice model HMOs and IPAs, but also newer plans that have been variably labelled: preferred provider organizations, case manager plans, managed indemnity plans, health insuring organizations, triple option plans, exclu- sive provide organizations, point-of-service plans, and open-ended HMOs (Stoline & Weiner, 1988; Gabel, et al., 1988).
Managed Care in Rural America
HMOs focus on populations, unlike other U.S. providers, they serve a predefined group of patients and are paid on the basis of this “denomina- tor.’’ Therefore, the more numerous the population, the greater the reim- bursement. Moreover, all types of managed care plans, like most business ventures, target themselves at large consumer markets. In rural areas, large populations are not easy to come by; accordingly, these areas have not supported many managed care plans and their penetration rate is far lower than in urban locales. Where managed care plans are available to consumers in nonmetropolitan areas, there are rarely more than one or two plans in a typical rural market. It is not uncommon to find more than a dozen managed care plans in a typical urban area.
Although not major providers, HMOs and rural areas are not strangers to one another. Some have cited an early prepaid group practice, started by a farmers’ cooperative in Oklahoma, as America’s first HMO (Christianson, Shadle, Hunter, Hartwell, & McGee, 1986, Christianson, 1989). It has been estimated that of the 600 or more HMOs operating today, more than 100 do business in nonurban areas. Although exact statistics are not available, only a small subset of these plans limit their markets only to rural areas. It can be roughly estimated that somewhere between 5 and 10 percent of rural residents belong to an HMO. This is about one half the rate of urban residents.
It is even more difficult to estimate the proportion of rural residents enrolled in all types of managed care plans, but based on an assumption of one half the national market penetration rate, an estimate in the 15 to 30 percent range seems reasonable.
There are several nonmetropolitan locations (e.g., Marshfield, WI) with large established group practices that sponsor HMOs. Increasingly, state medical societies and other statewide organizations (e.g., Blue Cross) are sponsoring IPA-model HMOs, open to physicians throughout the state.

376 The \ournal of Rural Health
Other types of managed care plans, such as PPOs, are also beginning to spread, particularly to serve statewide employers, Medicaid recipients, or consumers enrolled in statewide health insurance plans.
A national health insurance program is once again being debated. Many of the schemes that have been proposed, prominently feature HMOs and managed care approaches (Enthoven, 1989). Also, Medicare and Medicaid have an ongoing interest in promoting managed care (also known as "coordinated" care) programs for their beneficiaries (Health Care Financ- ing Administration, 1986). These developments within the public sector could dramatically increase the importance of managed care for the entire country, including rural areas.
Possible Effects of Managed Care on Rural Physician Supply
It is difficult to predict the precise effects of HMOs and managed care on the supply of providers in rural areas. There are, however, a number of direct effects that might be expected as HMOs continue redefining their markets to include urban fringe areas and nonmetropolitan cities and towns. Furthermore, even if HMOs and managed care are not widely adopted in rural locales, most agree they will continue their expansion in metropolitan areas. This could also have a variety of indirect effects on rural physician supply. One major indirect effect relates to the competitive impact of HMOs on those doctors not actively participating in such plans.
Intrinsic to the HMO concept is that patients must limit their choice of provider only to a subset of participating physicians. The ratio of physicians to enrolled patients within HMOs is significantly lower than the overall doctor-to-population ratios in most urban geographic areas. Therefore, it has been suggested that this phenomenon will further exacerbate the "oversupply" situation that many believe now exists in the non-HMO community (Tarlov, 1988). That is, as HMOs grow, those physicians not involved in such plans will find themselves with a decreasing base of potential patients. This could lead some physicians to seek practice options were there is less competition. This might increase the likelihood that providers will gravitate toward nonurban locales where there are fewer competing HMOs and private practitioners.
Capitation payment mechanisms are common among HMOs and this scheme is very appealing to primary care doctors. It assures a predictable revenue, is more certain than collecting fee-for-service payment from patients, and involves less red tape than most third-party fee-for-service payers now require. As capitation mechanisms spread, the ability of pri- mary care doctors to make a go of rural practices might increase, as long as their patient base is adequate.
Another interesting advantage of capitation-based payments is that

Weiner 3 77
many HMOs have developed payment rates that are uniform across the state. This has the benefit of circumventing the urban/rural payment differential that now is ingrained within the usual-customary-reasonable based fee schedules used by most fee-for-service payers. If the trend toward statewide HMOs continues, this could have the effect of making rural practice more attractive.
It should also be acknowledged that HMOs whose markets are limited to rural areas have had some difficulty setting viable capitation rates because payers, such as Medicare, have insisted on using historical usual- customary-reasonable payments as the basis of the capitation formula. Under such a circumstance, capitation payment schemes would not offer this special incentive to rural physicians.
HMOs, by design, are legally responsible for identifying providers of care. Unlike conventional insurance companies, state Medicaid programs, and Medicare, HMOs (and PPOs to a degree) are obliged to provide, or arrange for the provision of, services to their beneficiaries. If a plan enrolls patients in a rural area, it takes on the responsibility of assuring that an adequate number of providers are reasonably accessible. Given the limited success that the public sector has had in this regard, it will be interesting to see whether the private sector can achieve this goal.
HMOs, PPOs, and other managed care entities prefer to negotiate with pre-existing organized networks of providers, such as group practices, hospital chains, or medical societies. In this manner, one contract can give them a single provider that can service an entire geographic area. The other, less appealing alternative, is for the plan to negotiate distinct contracts with numerous providers. This factor may increase the pressure on rural physi- cians to join (or start) collectives. One scenario might find rural providers forming networks on a regional, cross-country basis, to increase their leverage with and appeal to managed care plans. The supply of rural providers might increase as administrative, financial, and social support systems found within these collectives improve the rural practice environ- ment.
HMOs have historically made efficient use of nonphysician primary care providers such as nurse practitioners and physician assistants (Weiner, Steinwachs, & Williamson, 1986). In the past, these so-called physician "extenders" or "substitutes" have been introduced into rural areas with some success, but it is possible that the HMO framework may provide a vehicle for attracting more of these providers.
While it is likely that HMOs and managed care will help increase the available health manpower in at least some rural areas, they will probably never prosper in small isolated towns or in frontier areas because of the lack of an adequate population base. Moreover, without government subsidy, they cannot be expected to address the very significant problem of the uninsured. Like other private or public sector insurance programs, man- aged care plans do not serve those who do not meet eligibility criteria.

3 78 The Iournal of Ritral Health
Aside from any changes that HMOs may introduce into the rural health care environment, they also offer insight into a variety of physician man- power planning issues.
HMO Staffing: Lessons for Rural Manpower Planning Background
HMOs represent unique laboratories for manpower modeling research.
They are self-contained systems of care where the patient base (denominator) is fixed. Almost all (about 95%) of their enrollees’ care is delivered within the ”closed” organization. They are one of few ”insurance” arrangements with first-dollar coverage for services that include preventive care. Once enrolled, HMO members face few financial access barriers. These traits are not found within most other insurance plans. They represent privately run, efficient systems of care with strong incentives to reach the best balance between cost containment and quality. Many have excellent computerized information systems that offer the data items required to construct manpower models.
Even before they were common, HMOs’ staffing patterns were used by manpower planners as a benchmark for assessing physician adequacy within a given geographic region (Mason, 1972; Office of Technology Assessment, 1980). It was assumed that if the physician-to-population ratio in a particular geographic location was similar to that found within a large HMO, then the area probably was being served by a reasonably adequate supply of physicians. Given that HMOs are generally considered to provide comprehensive, high-quality care, there is a degree of logic to this approach. In addition to the direct use of HMO staffing patterns as requirement standards, other manpower planning methodologies, such as demand and need-based modes, have also relied on data derived from HMOs (Schwartz, Sloan, & Mendelson, 1988).
Although HMOs have been important to manpower modeling, several concerns have been raised regarding the validity of HMO-based method- ologies.
There is some evidence that HMOs serve younger, less poor and possibly healthier patients than found in the U.S. population at large. Therefore, without adjustment, HMO patients’ use patterns might underestimate the true need of a representative cross section of Americans. Clinical practices in HMOs are different from those found in the fee-for-service sector. For example, patients receive more ambula-
HMOs have several characteristics that lend themselves to this activity. 1.
2.
3.
4.
1.
2.

Weiner 3 79
tory care, less surgery and less hospital care. Therefore, when one adopts HMO staffing as an ideal, indirectly, these standards of practice are also adopted. It is not always reasonable to assume that the organizational efficiency attained by HMOs can be replicated throughout the non- HMO sector. For example, less sparsely populated areas cannot be expected to serve their populations using large clinic-like group practice settings. Also, the productivity levels of physicians in some HMOs has been shown to be somewhat higher than that of the average U.S. physician (though not the average rural physician).
The technical and philosophical controversies surrounding health man- power adequacy are many, but in the final analysis, most agree that no one planning approach offers an incontrovertible gold standard (Weiner, 1989). With this in mind, the thesis of this paper is that the staffing patterns at established, successful HMOs can offer at least one point of reference useful in assessing whether a population is served adequately.
The remainder of this section compares and contrasts the staffing pat- terns of 10 large HMO sites (as documented by two recent studies) to the actual U.S. physician supply and the ”ideal” needs-based requirement standards adopted by the Graduate Medical Education National Advisory Committee (GMENAC).
3.
Physician-to-Population Ratios
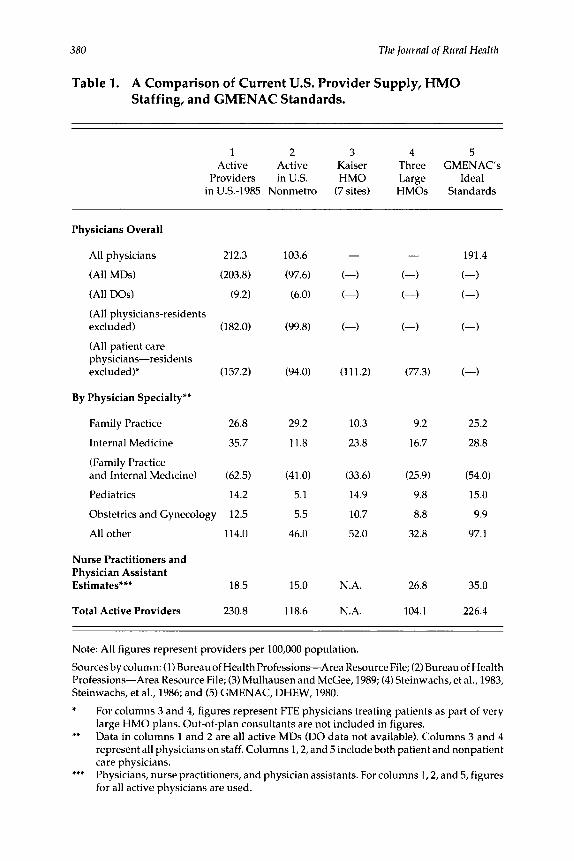
Table 1 presents a comparison of HMO, US., and GMENAC provider- to-population ratios. On an overall basis, and for specific specialty catego- ries (including nonphysician providers, i.e., nurse practitioners and physi- cian assistants), each of the five columns of this table presents the number of providers (per 100,000 population) as derived from five different sources: (1) the actual overall US. supply for Dec. 31,1985; (2) the actual 1985 supply in nonmetropolitan areas of the country; (3) the average staffing ratio across seven regions of the country’s largest HMO-Kaiser Permanente; (4) the average staffing ratios at three large (non-Kaiser) HMOs; and (5) the requirement (i.e., “need”) standards suggested for the U.S. 1990 population by the landmark GMENAC study.
Table 1 suggests that the overall 1985 US. physician supply exceeded GMENAC’s ideal standards. That is, the figure of 212.3 active physicians per population is higher that the suggested ideal rate of 191.4 per 100,000. For virtually all specialities presented on the table, the national rates are similar to, or higher than, GMENAC’s.
The rural physician-to-population ratios for 1985 were far lower than the U.S. overall average (Kindig & Movassaghi, 1989; DeFriese & Ricketts, 1989). The active number of physicians in nonmetropolitan areas is less than
380 The Iournal of Rural Health
Table 1. A Comparison of Current U.S. Provider Supply, HMO Staffing, and GMENAC Standards.
1 2 3 4 5 Active Active Kaiser Three GMENAC's
Providers inU.S. HMO Large Ideal in US-1985 Nonmetro (7 sites) HMOs Standards
Physicians Overall
All physicians 212.3
(All MDs) (203.8)
(All DOs) (9.2)
(All physicians-residents excluded) (182.0)
(All patient care physicians-residents excluded)* (157.2)
103.6
(97.6)
(6.0)
(99.8)
(94.0) (111.2) (77.3)
By Physician Specialty**
Family Practice 26.8
Internal Medicine 35.7
(Family Practice and Internal Medicine) (62.5)
Pediatrics 14.2
Obstetrics and Gynecology 12.5
All other 114.0
29.2
11.8
10.3
23.8
9.2
16.7
25.2
28.8
(41 .O)
5.1
5.5
46.0
(33.6)
14.9
10.7
52.0
(25.9)
9.8
8.8
32.8
(54.0)
15.0
9.9
97.1
Nurse Practitioners and Physician Assistant Estimates*** 18.5 15.0
118.6
N.A.
N.A.
26.8
104.1
35.0
226.4 Total Active Providers 230.8
Note: All figures represent providers per 100,000 population.
Sources by column: (1) Bureau of Health Professions-Area Resource File; (2) Bureau of Health Professions-Area Resource File; (3) Mulhausen and McGee, 1989; (4) Steinwachs, et al., 1983, Steinwachs, et al., 1986; and (5) GMENAC, DHEW, 1980. * For columns 3 and 4, figures represent FTE physicians treating patients as part of very
large HMO plans. Out-of-plan consultants are not included in figures. ** Data in columns 1 and 2 are all active MDs (DO data not available). Columns 3 and 4
represent all physicians on staff. Columns 1,2, and 5 include both patient and nonpatient care physicians. Physicians, nurse practitioners, and physician assistants. For columns 1,2, and 5, figures for all active physicians are used.
***

Weiner 381
one half that of the national average, although when only patient care physicians who are posttraining are considered, the rural rate is about 60 percent of the national average. Note that at the specialty-specific level, only the rural supply of family practitioners is higher than GMENAC’s standard, but when taken in conjunction with general internists, there are still fewer ”adult medicine” physicians (i.e., family practitioners plus internists) avail- able than the standard suggests are needed.
GMENAC never intended that all rural regions have physician supplies meeting the national ideals. For one thing, the ideal rates include managers, residents, research, and tertiary care subspecialists. In general, GMENAC’s ”geographic panel” considered the minimum requirement for nonurban health services catchment areas to be approximately 50 percent of the stated national ideals (Department of Health and Human Services, 1980).
Columns three and four of Table 1 present the staffing ratios at two sets of HMOs. Each set of figures represents the panel of providers serving the members enrolled at very large HMO plans. It can be estimated that the HMOs’ providers deliver somewhere between 90 percent and 95 percent of the all medical care received by the plans’ enrollees, and these figures should be considered accordingly. (A small percentage of ”in-plan” subspecialty care is delivered by nonpanel physicians on a fee-for-service basis. A similar percentage is believed to be obtained by enrollees indepen- dently from “out-of-plan” providers.)
Column three represents the average staffing levels across seven major regions of the Kaiser-Permanente HMO for 1983. A total of 4.2 million persons are served by these closed multispecialty group physician panels. The providers at these sites serve only Kaiser enrollees on a capitation basis-they see no other patients. The figures in column four were derived (in 1981) from three large (more than 100,000 members) HMOs: the Harvard Community Health Plan, Boston, MA; the MedCenters Health Plan, Minne- apolis, MN; and the Maxicare Health Plan, Los Angeles, CA. The Harvard plan is a staff model HMO, theother two aregroup/networkmodels, where fee-for-service patients are also treated by the groups serving the HMO enrollees (Mulhasuen & McGee, 1989; Steinwachs et al., 1986, Steinwachs, Shapiro, Weiner, 1983).
The two sets of HMO staffing rates are reasonably similar to one another, although the Kaiser plans appear to have somewhat higher physician staffing levels than do the other three HMOs. The staffing levels at the HMOs are significantly lower than the national (overall) rates, as well as the GMENAC ideal standards.
As identified previously, there is some concern that adopting HMO staffing levels as ideals might lead to an underestimation of the ”true need” within a general population. When considering them as requirement stan- dards outside HMOs, an upward adjustment of all HMO-based staffing levels to compensate for those factors identified earlier is suggested. De-

382 The journal of Rural Heulth
pending on the age of the population of interest, adjustments in the 10 to 25 percent range appear warranted (i.e., up to 25% more physicians will be required than are available in the HMOs). Even with such adjustments, the HMO staff levels are well below the current overall U.S. supply and the standards suggested by GMENAC.
Of special relevance is a comparison of the HMO rates to the current (i.e., 1985) supply in nonmetropolitan US. areas (i.e., column 2 of Table 1). Note that the rural rate of 94.0 nontrainee patient care physicians (which is probably the most appropriate figure to compare to the HMOs) is higher than the non-Kaiser HMO rate of 77.3, but slightly lower than the Kaiser plan rate of 11 1.2. It is also interesting to note that for adult medicine and ”all other” specialties, the rural rates appear comparable or higher. The pediat- ric and obstetric/gynecology rates are lower in the rural areas. It is not clear whether this reflects the younger nature of HMO populations; the greater use of family practitioners in rural areas-who may be substituting for these specialities; or an indication of a possible inadequacy in nonmetropolitan areas.
A comparison of the nonphysician provider supply rates across the columns of Table 1 leads to some interesting findings. But first, some methodologic notes. The nonphysician provider rates for the nonmetropolitan areas were not available, a rate of 15.0 per 100,000 was assumed. This figure is slightly, but not dramatically, lower than the overall national rate of 18.5. Unfortunately, the nonphysician provider rates for the Kaiser plans were also not available. No rates were assumed, but many Kaiser sites are known to make significant use of nonphysician providers. It should also be noted that the ideal rates adopted by GMENAC were based on the assumption of an available supply of 70,000 nonphysician providers in 1990. (This assumption has, in retrospect, proven to be too high.) Originally, GMENAC suggested that an even greater supply of nonphysician providers would be ideal (Weiner et al., 1986).
Based on the use of nurse practitioners and physician assistants at the three non-Kaiser HMOs, it appears that HMOs make significantly greater use of nonphysician providers than is the case nationally, although even these rates are, on average lower than what GMENAC suggested as ideal. Among the three plans averaged together in column 4 of Table 1, there was a tremendous degree of variability in the reliance on nonphysician provid- ers. (This cross-plan variability was far higher than that observed for physicians.) The nonphysician provider rates varied from a high of 67.2 per 100,000 at the Harvard plan to a low of 4.4 at Maxicare. This suggests that the level of delegation to nonphysician providers could go well beyond even the rate suggested by GMENAC.
To better compare and contrast this and other differences between the staffing patterns at the three non-Kaiser plans and GMENAC’s suggested ideals, a series of ”sensitivity” analyses are presented.

Weiner 383
Why the HMOs’ Staffing Differs from GMENAC’s Standards
My colleagues and I completed a study under federal contract in which we replicated the GMENAC needs-based requirement model, parameter by parameter, using empirical data from three HMOs. (The three non- Kaiser HMOs) (Steinwachs et al., 1983, Steinwachs, et al., 1986; Weiner, et al., 1987). In general, the original GMENAC models were based on norma- tive (nonempirical) input from expert panels. Using the HMO data, we were able to empirically derive the individual pieces of GMENAC’s model, which included: incidence of disease; visits made per episode (or year) of illness; the distribution of visits to primary care generalists versus special- ists; the proportion of visits that were delegated to nurse practitioners, and physician assistants (i.e., nonphysician providers); and the productivity of providers (i.e., patient visits per year). The results of our study for the “child health specialty (pediatrics and family practitioners) and the ”adult health” specialty (internists and family practitioners) are discussed below.
As might be expected from the staffing patterns presented earlier on Table 1, when the HMO-derived data are used to recalculate GMENAC’s physician requirement model, significantly fewer providers than originally recommended by GMENAC would be “needed.” With adjustments for out- of-plan use, socioeconomic and age differences, we calculated that the HMO-based standards for child care was about 78 percent of GMENAC’s. For adult care, the HMO-based ideal was 50 percent of what GMENAC suggested (Steinwachs, et al., 1986).
Because we reconstituted GMENAC’s model piece by piece, we were able to perform a sensitivity analysis that suggested how each individual HMO-derived parameter would affect the final result of the requirement model. In other words, we were able to assess how GMENAC’s ideal standards would change, if only one of the HMOs characteristics was adopted while the others were not (i.e., GMENAC’s normative assump- tions were retained).
Table 2 presents the results of these sensitivity analyses or the two major primary care specialties. On this table, all original GMENAC model param- eters, except the one noted, is used to recalculate the requirement model. For each variable, the results are presented separately for each of the three HMOs and on an average basis. The numbers are expressed in terms of the percentage of the original GMENAC requirement. For example, figures higher than 100 percent indicate that the HMO-derived model would lead to a higher standard than GMENAC, whereas figures less than 100 percent, indicated a lower requirement standard.
Table 2 suggests that for the first three sets of variables-incidence, visits per episode, and proportion of care given by generalists-adapting the empirical, HMO-derived parameters would lead to a lower physician requirement than GMENAC’s. These results suggest that original GMENAC

384 The journal of Rural Health
Table 2. Sensitivity of GMENAC's Model for Primary Care Physician Requirement to the Actual Practice Characteristics at Three HMOs.*
Variable/HMO*' Child Health Care Adult Health Care
Percent of GMENAC**'
Disease IncidencelPrevalence Maxicare MedCenters Harvard 67 Average 66
Visits Per Patient Per Year Maxicare MedCenters Harvard 93 Average 90
49 82 88 82
91 85 58 59
Percent of Visits to Generalists**** Maxicare 84 MedCenters 87 Harvard 95 79 Average 89 70
Delegation Rate to Nonphysician Providers**** Maxicare 137 MedCenters 125 Harvard 104 73 Average 122 111
Productivity Maxicare MedCenters Harvard 140 Average 121
97 125
121 -
82 76
62 56
80 51
126 133
103 138
Source: Steinwachs, et al., 1983; Steinwachs, et al., 1986.
*
**
*** ****
All of GMENAC's normative variables are used in the model projection except for the identified variable, which is estimated from the HMO data base. MedCenters denotes MedCenters Health Plan; Harvard denotes Harvard Community Health Plan. Projected requirements are shown as a percentage of GMENAC's original projections. Generalists refer to internists, family practitioners, and pediatricians. Nonphysician providers include practitioners and physician assistants.

Weiner 385
panels were probably liberal in their estimates of how frequently people would have need for medical care. It also suggests that HMOs make more use of nongeneralists than GMENAC assumed would be the case.
For the last two variables on Table 2-delegation to nonphysician providers and productivity-the results, in general, indicate that if actual HMO practices were adopted as norms, more physicians than suggested by GMENAC would be needed. (One exception is the delegation result at the Harvard Health Plan, where there was a very high nonphysician provider delegation rate.) These findings suggest that HMOs neither delegate visits to nonphysician providers at the rate GMENAC assumed, nor are their physicians as productive in terms of patients seen per year. One possible explanation for the decreased physician productivity is that because of higher than (United States) average delegation to nonphysician providers, the mix of patients retained by the doctors may be more intensive than average, thereby requiring a longer time per visit.
The issue of productivity is an interesting one. In general, group prac- tices, which form the basis of our sample HMOs, have relatively high productivity rates, but at the three study plans, only one plan (Maxicare) approached GMENAC’s suggested annual ambulatory productivity rate of about 5,500 for pediatricians and family practitioners, and 3,700 for inter- nists. This is a very important factor in assessing the adequacy of a supply in a given area; and one that practitioner controls to a significant degree.
Summary
If HMOs and other managed care plans continue to flourish and expand their market shares into nonmetropolitan regions, then rural physicians, their practices and patients, will almost certainly be affected. While it is difficult to forecast these effects with any certainty, their general nature can be anticipated. These trends are summarized following, as are their ex- pected impacts on the health personnel available to rural residents.
As HMOs place additional competitive pressures on physicians practicing, or wishing to practice, in urban areas, it is possible that there may be increased openness to setting up practice in rural locations. As managed care further emphasizes nonhospital care, the demand for outpatient and preventive services is likely to increase among rural HMO enrollees. This may increase the need for primary care providers. (As an aside, this trend may add further financial pressures on rural hospitals not already offering comprehensive outpatient services.) As HMOs spread into rural areas, capitation payment arrangement will become more evident. This could have the effect of strengthen- ing the financial viability of primary care practices.
1.
2.
3.

386 The Iournal of Rural Heulfh
4. As managed care plans become more common in rural areas, it is possible that the responsibility for ensuring adequate access to providers will be accepted by the insuring corporation. This con- cern, will of course only be limited to enrollees of the plan. The critical needs of uninsured patients will not be addressed without government subsidy to the managed care plans. It is possible that more nurse practitioners and physician assistants will enter practice in rural regions as HMOs provide an efficient framework for their employment. It is likely that networks of providers will increase in rural regions to allow for more efficient contracting with managed care plans. By serving to strengthen the organizational infrastructure of practices in rural regions, these networks could have implications for all residents, including those not enrolled in the plans. The effects of HMOs and other managed care plans on rural areas will probably be most pronounced in “rural” locales bordering metropolitan regions and in nonmetropolitan cities and large towns. Because of the very small, widely dispersed, population base found in other rural regions, managed care plans will be difficult to establish there.
In additon to the potential effects of HMOs on physicians’ practices, the staffing patterns of these organizations provide an interesting point of comparison for those responsible for rural health manpower planning and resource development programs. Some of the points that are evident from an assessment of the staffing at 10 large HMOs are as follows.
The HMOs meet the needs of their enrollees with significantly fewer providers than are available nationally, or suggested by GMENAC. Although there are differences in the types of patients served and the environmental contexts, this suggests that the extent of the perceived physician ”shortage” in rural areas may not be as large as some believe. From the staffing at the HMOs, further evidence is offered for the potential of nurse practitioners and physician assistants to meet the health care needs of a defined population. An analysis of the sensitivity of the original normative GMENAC model to the actual practices at three large HMOs suggests that GMENAC’s estimates of medical need may have been liberally high; delegation of nurse practitioners and physician assistants were unrealistically high, largely because of unavailability of this type of provider; and physician productivity was unrealistically high, suggesting that more providers may be needed to deliver the same level of care.
The health care system is changing rapidly and the HMO and managed care movements are inseparable from this phenomenon. These new mecha-
5.
6.
7.
1 .
2.
3.

Weiner 387
nisms for health care organization and financing are likely to have a very significant impact on the way in which the health care needs of rural Americans will be met.
REFERENCES
Christianson, J.B., Shadle, M., Hunter, S., Hartwell, S., & McGee, J. (1986, Spring). The new
Christianson, J.B. (1989). Alternative delivery systems in rural areas. Health Services Research,
DeFries, G.H., & Ricketts, T. (1989). Primary health care in rural areas: An agenda for research. Health Sewices Research, 23 (6), 931-974.
Department of Health and Human Services. (1980). Report of the Graduate Medical Education National Advisory Committee (GMENAC), Vols. 2-7. (DHHS publication nos. HRA 81-651 through HRA 81-657). Hyattsville, MD: Health Resources Administration.
Enthoven, A S . (1989). A consumer choice health plan for the 1990s. New England journal of Medicine, 320,94-101.
Gabel, J., Jajich-Toth, C., DeLissovoy, G., Rice, T., & Cohen, H. (1988, Summer). The changing world of group health insurance. Health Affairs, 48-67.
Health Care Financing Administration. (1986, Annual Supplement). Competition in a chang- ing health care environment. Health Care Financing Review.
InterStudy. (1989). Quarterly report of H M O growth and enrollment. Excelsior, MN: Author. Kindig, D.A., & Movassaghi, H. (1989, Summer). Physician supply in small rural counties.
Mason, R. (1972). Manpower needs by specialty.)ournalofthe American Medical Association, 216,
Mulhausen, R., & McGee, J. (1989). Physician need: An alternative projection from a study of large prepaid group practices. Iournal of the American Medical Association, 216,1930.
Office of Technology Assessment. (1980). Forecasts of physician supply and requirement, 2980. (GPO publication no. 052-003-00746-1). Washington, DC: Government Printing Office.
Schwartz, W., Sloan, F.A., & Mendelson, D.N. (1988). Why there will be little or no physician surplus between now and the year 2000. New England journal of Medicine, 318,892-897.
Steinwachs, D., Shapiro, S., Weiner, J. (1983). A n application of the GMENAC physician require- ment model to empirical data derived from three HMOs. Baltimore, MD: Johns Hopkins University Health Services Research and Development Center.
Steinwachs, D., Weiner, J., Shapiro, S., Batalden, P. Cotlin, K., & Wasserman, F. (1986). A comparison of the requirements for primary care physicians in HMOs with projections made by the GMENAC. New England journal of Medicine, 314,217-222.
Stoline, A,, & Weiner, J. (1988). The new medical marketplace: A physician's guide to the health care revolution. Baltimore, MD: The Johns Hopkins University Press.
Tarlov, R. (1986). HMO growth and physicians: The third compartment. Health Affairs, 5,23- 35.
Weiner, J.P., Steinwachs, D.M., & Williamson, J. (1986). Nurse practitioner and physician assistant practice in three HMOs: Implications for future US. health manpower needs. American Iaurnal of Public Health, 76,507-511.
Weiner, J.P., Steinwachs, D.M., Shapiro, S., Coltin, K.L., Ershott, J., & OConnor, J.P. (1987). Assessing a methodology for physician requirement forecasting: Replication of GMENAC's needs-based model for the pediatric specialty. Medical Care, 25,426-436.
Weiner, J.P. (1989, Winter). Forecasting physician supply: Recent developments. Health Affairs,
environment for rural HMOs. Health Affairs, 105-121.
23 (6), 849-890.
Health Afiairs, 64-76.
1621 -1626.
173-179.




















