
Benign hereditary chorea: Clinical and neuroimaging features in an Italian family
18
Brief Reports Characteristic Head Drops and Axial Extension in Advanced Chorea-Acanthocytosis Susanne A. Schneider, MD, PhD, 1,2 Anthony E. Lang, MD, 3 Elena Moro, MD, 3 Benedikt Bader, MD, 4 Adrian Danek, MD, 4 and Kailash P. Bhatia MD 1 * 1 Sobell Department of Motor Neuroscience and Movement Disorders, UCL, Institute of Neurology, Queen Square, London, United Kingdom; 2 Schilling-Section of Neurogenetics, Department of Neurology, University of Lu ¨ beck, Lu ¨ beck, Germany; 3 Morton and Gloria Shulman Movement Disorders Centre, Toronto Western Hospital, University of Toronto, UHN, Toronto, Ontario, Canada; 4 Neurologische Klinik und Poliklinik, Ludwig-Maximilians- Universita ¨t Mu ¨ nchen, Munich, Germany Video Abstract: Chorea-acanthocytosis is a rare autosomal reces- sive neurodegenerative disorder with a complex clinical presentation comprising of a mixed movement disorder (mostly chorea and dystonia), seizures, neuropathy and myopathy, autonomic features as well as dementia and psychiatric features. Because the differential diagnosis is wide, clinical clues and red flags are important. We report here our observation of characteristic neck and trunk flexion and extension spasms in four cases with advanced chorea-acanthocytosis. Ó 2010 Movement Disorder Society Key words: chorea-acanthocytosis; acanthocytes; neuroa- canthocytosis; head drops; trunk flexion; trunk extension; orobulbar features INTRODUCTION Chorea-acanthocytosis is a rare autosomal recessive adult-onset neurodegenerative disorder due to VPS13A gene mutations, encoding chorein. 1,2 Clinical manifestations consist of a mixed movement disorder, seizures, neuropathy, myopathy, autonomic features, dementia, and psychiatric features. 3 The dif- ferential diagnosis is wide. Acanthocytes are not always detected by the screening test of the peripheral blood smear. Hence, clinical clues and red flags are an important aid for clinicians. In evaluating patients with chorea-acanthocytosis in our tertiary referral centers, we have observed typical flexions of neck (presenting as head drops) and trunk as a charac- teristic feature in advanced chorea-acanthocytosis which in our view have not been explicitly described before. We feel that these features may be a pathognomic clinical sign for chorea-acanthocystosis and a useful clue toward the diagnosis, particularly if self-mutilatory mouth move- ments or feeding-related tongue dystonia are also present. We illustrate our observations by videos including a series of videos over time for Case 1 showing that head drops become prominent late in the disease course. All patients gave written informed consent. A summary of the demo- graphic and clinical details are shown in Table 1. Case 1 This 40-year-old patient developed slowly progres- sive frontal lobe dysfunction from age 32, followed by chorea and slurred speech from age 34. He developed falls at age 36. At age 38, he developed difficulty eat- ing with tongue biting. On examination then he had generalized chorea, intermittent mild head drops, gait ataxia, and severe bruxism (Video Segment 1). At age 39, he presented with his first generalized tonic-clonic seizure and developed autonomic dysfunction with pro- gressive loss of bladder control. On last follow-up, aged 40, memory function was relatively preserved. He was depressed; however, aggression, self-injurious behaviour, or psychosis were absent. Saccades were hypometric. He had orobulbar involvement with marked dysarthria, slow tongue movements, and swallowing difficulties. Because of severe bruxism culminating in tongue biting and damage of his teeth, he wore a gum shield. He had *Correspondence to: Kailash P. Bhatia, Sobell Department of Motor Neuroscience and Movement Disorders, The National Hospital for Neurology and Neurosurgery, UCL, Institute of Neurology, Lon- don WC1N 3 BG, United Kingdom. E-mail: [email protected] Potential conflict of interest: Nothing to report. Received 29 October 2009; Revised 9 December 2009; Accepted 25 January 2010 Published online 11 June 2010 in Wiley InterScience (www. interscience.wiley.com). DOI: 10.1002/mds.23052 1487 Movement Disorders Vol. 25, No. 10, 2010, pp. 1487–1504 Ó 2010 Movement Disorder Society
-
Upload
independent -
Category
Documents
-
view
2 -
download
0
Transcript of Benign hereditary chorea: Clinical and neuroimaging features in an Italian family

Brief Reports
Characteristic Head Drops andAxial Extension in Advanced
Chorea-Acanthocytosis
Susanne A. Schneider, MD, PhD,1,2
Anthony E. Lang, MD,3 Elena Moro, MD,3
Benedikt Bader, MD,4 Adrian Danek, MD,4
and Kailash P. Bhatia MD1*
1Sobell Department of Motor Neuroscience and MovementDisorders, UCL, Institute of Neurology, Queen Square,
London, United Kingdom; 2Schilling-Section ofNeurogenetics, Department of Neurology, University ofLubeck, Lubeck, Germany; 3Morton and Gloria ShulmanMovement Disorders Centre, Toronto Western Hospital,University of Toronto, UHN, Toronto, Ontario, Canada;
4Neurologische Klinik und Poliklinik, Ludwig-Maximilians-Universitat Munchen, Munich, Germany
Video
Abstract: Chorea-acanthocytosis is a rare autosomal reces-sive neurodegenerative disorder with a complex clinicalpresentation comprising of a mixed movement disorder(mostly chorea and dystonia), seizures, neuropathy andmyopathy, autonomic features as well as dementia andpsychiatric features. Because the differential diagnosisis wide, clinical clues and red flags are important.We report here our observation of characteristic neckand trunk flexion and extension spasms in four caseswith advanced chorea-acanthocytosis. � 2010 MovementDisorder Society
Key words: chorea-acanthocytosis; acanthocytes; neuroa-canthocytosis; head drops; trunk flexion; trunk extension;orobulbar features
INTRODUCTION
Chorea-acanthocytosis is a rare autosomal recessive
adult-onset neurodegenerative disorder due to VPS13Agene mutations, encoding chorein.1,2
Clinical manifestations consist of a mixed movement
disorder, seizures, neuropathy, myopathy, autonomic
features, dementia, and psychiatric features.3 The dif-
ferential diagnosis is wide. Acanthocytes are not
always detected by the screening test of the peripheral
blood smear. Hence, clinical clues and red flags are an
important aid for clinicians.
In evaluating patients with chorea-acanthocytosis in our
tertiary referral centers, we have observed typical flexions
of neck (presenting as head drops) and trunk as a charac-
teristic feature in advanced chorea-acanthocytosis which
in our view have not been explicitly described before. We
feel that these features may be a pathognomic clinical
sign for chorea-acanthocystosis and a useful clue toward
the diagnosis, particularly if self-mutilatory mouth move-
ments or feeding-related tongue dystonia are also present.
We illustrate our observations by videos including a series
of videos over time for Case 1 showing that head drops
become prominent late in the disease course. All patients
gave written informed consent. A summary of the demo-
graphic and clinical details are shown in Table 1.
Case 1
This 40-year-old patient developed slowly progres-
sive frontal lobe dysfunction from age 32, followed by
chorea and slurred speech from age 34. He developed
falls at age 36. At age 38, he developed difficulty eat-
ing with tongue biting. On examination then he had
generalized chorea, intermittent mild head drops, gait
ataxia, and severe bruxism (Video Segment 1). At age
39, he presented with his first generalized tonic-clonic
seizure and developed autonomic dysfunction with pro-
gressive loss of bladder control.
On last follow-up, aged 40, memory function was
relatively preserved. He was depressed; however,
aggression, self-injurious behaviour, or psychosis were
absent. Saccades were hypometric. He had orobulbar
involvement with marked dysarthria, slow tongue
movements, and swallowing difficulties. Because
of severe bruxism culminating in tongue biting and
damage of his teeth, he wore a gum shield. He had
*Correspondence to: Kailash P. Bhatia, Sobell Department ofMotor Neuroscience and Movement Disorders, The National Hospitalfor Neurology and Neurosurgery, UCL, Institute of Neurology, Lon-don WC1N 3 BG, United Kingdom. E-mail: [email protected]
Potential conflict of interest: Nothing to report.Received 29 October 2009; Revised 9 December 2009; Accepted
25 January 2010Published online 11 June 2010 in Wiley InterScience (www.
interscience.wiley.com). DOI: 10.1002/mds.23052
1487
Movement DisordersVol. 25, No. 10, 2010, pp. 1487–1504� 2010 Movement Disorder Society

generalized chorea and his head drops had become
more severe resulting in head and face injuries (Video
Segment 2). His gait was very unstable and lurching.
Investigations demonstrated presence of 5% acantho-
cytes. The protein assay4 revealed absent chorein. Cre-
atine kinase (CK) was raised to 224 at age 39 and to
429 on last follow-up, at age 40 (normal <150). Cop-
per studies were normal. Genetic testing was negative
for Huntington’s disease, DRPLA, SCA17, and juncto-philin-3 (HDL2). VPS13A testing was not performed.
Electrophysiological studies suggested mild myopathy
and mild chronic sensory motor axonal neuropathy.
Tetrabenazine worsened his depression and had to be
withdrawn. He continues to receive botulinum toxin
injections in the masseter muscles to alleviate the brux-
ism, antidepressants, benzodiazepines and, for seizure
control, valproate. In view of loss of bladder control, a
catheter had to be inserted.
There was no family history of neurological disease.
His sister was asymptomatic. She had normal (how-
ever, at the lower limit of the normal range) levels of
chorein in the protein assay.4
Case 2
This woman from an extended French-Canadian kin-
dred with VPS13A mutations5,6 presented at age 43
with a 6-year history of generalized abnormal move-
ments. Her parents were first cousins. One sister and
two cousins, also the products of a consanguineous
marriage, were similarly affected. Examination at age
43 demonstrated moderate generalized chorea with
dystonia of the trunk and legs, mild action hand
tremor, and absent lower limb deep tendon reflexes.
Mild ‘‘tic-like’’ behavior was noted including humming
and mild swearing. At age 45, her trunk and knees
began to ‘‘give-way’’. While sitting unsupported her
trunk would occasionally extend forwards or back-
wards involuntarily (Video Segment 2).
Peripheral smear demonstrated 10% acanthocytes.
CK levels were 3212. CT scans demonstrated caudate
atrophy. Fluorodeoxyglucose positron emission tomog-
raphy revealed absence of FDG uptake in the caudate-
putamen area. Neuropsychological assessment showed
only mild reduction in verbal fluency and procedural
learning. She failed trials of multiple medications.
Case 3
This 32-year-old man, one of the affected cousins of
Patient 2, was seen for consideration of bilateral globus
pallidus internus (GPi) deep brain stimulation (DBS)
surgery.
At age 22, he noted clumsiness in his hands and
dysarthria. He developed involuntary movements of his
tongue and jaw, with severe biting of his cheeks and
tongue. He also developed facial tics, anterocollis, and
opisthotonus. He fell while walking, due to imbalance
and involuntary leg movements. When kneeling, there
were involuntary backward trunk movements. His older
brother was in a nursing due to the same disease and
had exactly the same backward movements. His dys-
phagia and dysarthria progressively worsened. He had
feeding dystonia needing to lie down to drink liquids
and to push the food inside his mouth with his fingers
or a fork. Genetic analysis at age 24 revealed he was
compound heterozygous for the French Canadian foun-
der mutation EX70_EX73del5 and a splice site
(c.424211G>T) VPS13A gene mutation.
On exam, speech was dystonic and severely slurred.
There was severe drooling. He had what were inter-
preted as tics involving blinks and shoulder shrugs. He
had occasional simple vocalizations (‘‘hmm’’ sounds).
He also had compulsive nose picking and skin scratch-
ing to the point of bleeding and wore gloves to prevent
him from this behavior. His head was held mostly
flexed. He demonstrated prominent backwards trunk
movements, which occasionally caused him to knock
his head quite hard on the wall behind him and he
wore a soft helmet as a protection (Video Segment 3).
Hand movements were slow, but tone was normal.
A variety of medications provided only partial relief.
Botulinum toxin injections of the masseters and ptery-
goid muscles markedly reduced cheek and tongue bit-
ing. Bilateral GPi DBS surgery was performed at age
31 with clinical improvement.
Case 4
This 36-year-old male patient is taken from the
archival video database of Professor David Marsden’s
and was previously reported by Hardie et al. as Case
18.7 There was a 3-year history of progressive speech
impairment, dysphagia, intermittent muscle spasms
affecting the left-sided limbs, and difficulty walking
with occasional falls. On examination, there were a
fine slow tongue tremor at rest and action tongue dys-
tonia and facial dystonia when speaking. His speech
was dysarthric. He spontaneously made intermittent
loud sucking and blowing noises and his head dropped
intermittently (Video Segment 4). Optic fundi and eye
movements were normal. Limb tone and power were
normal, but rapid finger movements were mildly
impaired in the left hand. There was leg dystonia when
walking. Tendon reflexes were all reduced. Plantar
1488 S.A. SCHNEIDER ET AL.
Movement Disorders, Vol. 25, No. 10, 2010

responses were flexor. About 5% acanthocytes was
present in peripheral blood. CK was elevated at 692.
Mutation analysis revealed a VPS13A mutation in exon
57.8
DISCUSSION
Movements in chorea-acanthocytosis are often com-
plex. Chorea, dystonia with prominent orofacial
involvement, tics and parkinsonism have all been
described.
We noted the occurrence of sudden and striking
movements of the trunk and head, sometimes resem-
bling sudden loss of tone as seen in negative myoclo-
nus. In more severe Cases (#2 and 3), the trunk move-
ments were profound causing drops from the waist
downward so that the head would go into the lap. In
less severe presentations, there were characteristic head
drops with ballistic flexion of the neck as seen in two
of our Patients (#1 and 4).
Case 3 had axial drops but also equally sudden and
striking extensor movements. Thus, in addition to sud-
den loss of tone resulting in the head to drop, exten-
sion movements are equally possible. Interestingly, we
noted intrafamilial homogeneity of the movement.
Patient 3 and his similarly affected brother showed
exactly the same backward movements. Overall, these
axial movements appeared to be a distinctive feature
which may be a clue towards the diagnosis.
As a consequence, one of our patients (Case 1) had
various injuries at the back of his head and the fore-
head. This was initially misinterpreted as self-injurious
behaviour which may also occur in chorea-acanthocy-
tosis.9 However, psychiatric assessment revealed no
suggestion to support voluntary self-injurious tenden-
cies in our case.
The type of myoclonus-like movements we describe
here may also be seen in myoclonic disorders, for
example Unverricht-Lundborg disease.10 However, in
the latter, myoclonus is generalized, whereas in our
patients it predominantly affected the trunk or neck.
Also, the overall phenomenology in chorea-acanthocy-
tosis is much more complex.
The differential diagnosis of a mixed movement dis-
order with both myoclonic jerks and dystonia also
includes myoclonus dystonia (DYT11). However, the
onset of myoclonus dystonia is usually very early in
life with ‘‘lightening jerks’’ in contrast to neuroacan-
thocytosis where onset is in adulthood. In addition,
none of our patients had a beneficial response to
TABLE 1. Demographic and main clinical characteristics of Cases 1–4
Case 1 Case 2 Case 3 Case 4
Age at onset 32 37 22 33Age at last follow-up 40 47 32 36Age when video was taken 38 and 40 47 32 36Previously reported as No previous reports Dobson-Stone et al.,
2005 Cases 4–7Dobson-Stone et al.,
2005 Case 4–3Hardie et al., 1991,
Case 18;Dobson-Stone et al.,2002 Case 32
Family history Negative Positive Cousin of Case 2 n.k.Onset symptom Frontal lobe dysfunction
(32); chorea (34)Nervous breakdown
(34) and chorea (37)Clumsiness, dysarthria Speech impairment,
muscle spasms,gait difficulty
Predominant movement disorder Chorea Chorea, leg dystonia,action tremor, tic-likevocalizations
Dystonia, motorand vocal tics, neckand and gait problems
Tongue dystonia,tongue tremor,leg dystonia
Onset of axial flexion/extensor spasms
38 45 24 n.k. precisely
Description of axial flexion/extensor spasms
Head drops Trunk flexion forwardto 90 degrees
Head and trunk flexionand extension
Head drops
Onset of oromandibular features 38 n/a 23 33Cognitive function Relatively well
preservedRelatively well
preservedReduced judgement ability n.k.
Psychiatric features Depression Nervous breakdown Poor judgement n.k.Self-injurious behaviour Absent Absent Present AbsentEffective Treatment Btx for head drops None Btx for cheek biting;
Bilateral GPi DBS;n.k.
Numbers in brackets refer to the age when this symptom or sign was first noted.n.k., not known; n/a, not applicable; Btx, botulinum toxin injections; GPi DBS, globus pallidus internus deep brain stimulation surgery.
1489AXIAL JERKS IN CHOREA-ACANTHOCYTOSIS
Movement Disorders, Vol. 25, No. 10, 2010

alcohol which is a characteristic feature DYT11 dysto-
nia. Furthermore, inheritance in the latter is autosomal
dominant in contrast to chorea-acanthocytosis where
inheritance is recessive.
The differential diagnosis of sudden head move-
ments furthermore includes tic disorders. Although two
of our patients exhibited tic-like features like vocaliza-
tions (Cases 2 and 3) and motor tics (Case 3), Patients
1 and 4 had no tics and denied any inner urge to
move. Also, tics can usually be suppressed, but Cases
2 and 3 had no control over their axial movements.
Finally, there is phenotypic overlap with stereotypic
‘‘head banging’’ as seen in mentally disabled children11
for example those with Down syndrome, autism, or
following amphetamine poisoning.12
The classification of the movements we observed is
not straight forward. As discussed earlier, there are simi-
larities to myoclonus and tics; however, they could also
represent a choreic movement especially as the direction
included both flexion and extension. The movements
could also be dystonic, in view of the prominent opis-
thotonus with dystonic arching present in Case 3. Inter-
estingly and perhaps related, a pattern of trunk flexion
(‘‘feet-clasping posture’’) is a characteristic feature in the
R6/2 Huntington’s disease mouse model.13
Treatment responses ranged from very good to
unsatisfactory. In one Patient (#1), the head move-
ments could be alleviated by botulinum toxin injec-
tions. Patient 2 failed trials of multiple medications. In
Patient 3, bilateral GPi DBS markedly improved swal-
lowing, axial dropping, and extensor movements.
We encourage physicians to look for these clinical
signs, the spectrum of which ranges from mild to
severe, and if present to screen for acanthocytes.14 A
technically much simpler and more sensitive laboratory
parameter in chorea-acanthocytosis, however, is deter-
mination of CK which generally is elevated.15 Protein
assays4 or genetic testing1,2 can confirm the diagnosis.
Legends to the Video
Segment 1. Patient with chorea-acanthocytosis. The
first part of the clip, shows the patient aged 38. While
sitting there is generalized chorea with intermittent
head drops (resembling a sudden loss of tone). The
patient is also asked to shortly take the toothbrush out
of his mouth which he uses to protect his teeth from
clenching. After having done this, there is severe brux-
ism. The second part of the clip shows the patient at
age 40 when walking. His forward head drops have
become more severe. His gait is very unstable and
with intermittent loss of tone in the legs.
Segment 2. The patient (shown at age 47) with cho-
rea-acanthocytosis has generalized chorea. When sitting,
she demonstrates involuntary sudden forward flexions of
the trunk.
Segment 3. This patient with genetically proven
chorea-acanthocytosis (compound heterozygous:
EX70_EX73del and c.424211G>T VPS13A muta-
tions) was recorded prior to GPi DBS surgery at age
32. When walking there is involuntary loss of tone in
the legs and also sudden head drops. The postural sta-
bility is markedly impaired.
Segment 4. The patient aged 36 years with chorea-
acanthocytosis makes loud sucking and blowing noises.
Towards the end of the clip, there are intermittent
involuntary forward head drops.
Acknowledgments: This research was supported by anintramural research grant by the University of Lubeck, Ger-many (SAS). BB and AD are funded partially by the Advo-cacy for Neuroacanthocytosis Patients (London, UK). Weacknowledge The Advocacy for Neuroacanthocytosis Patientsat www.naadvocacy.org, and Ginger and Glenn Irvine forsupporting to offer the chorein protein test free of charge.
Financial Disclosures: SAS: Sources of support: NovartisFoundation for Therapeutic Medicine. University of Lubeck,Germany (Employment). AEL: Advisor: Biovail, Boerhinger-Ingelheim, Cephalon, Ceregene, Eisai, Medtronic, LundbeckA/S, NeuroMolecular, Novartis, Solvay, Taro, Teva; Grants:Canadian Institutes of Health Research, Dystonia MedicalResearch Foundation, Michael J. Fox Foundation, NationalParkinson Foundation, Ontario Problem Gambling ResearchCentre, Parkinson’s Disease Foundation, Taro; Speaker orother support: GSK, UCB. EM: Honoraria for lecturing fromMedtronic. BB: BB is supported by the Advocacy for Neuroa-canthocytosis Patients; by the Bayerische Forschungsallianz;and by the Bundesministerium fur Bildung und Forschung.AD: Grants from Bayerische Forschungsstiftung and Bayeri-sche Forschungsallianz, Munchner Universitatsgesellschaft,Deutsch-Franzosische Hochschulstiftung, and the Advocacy forNeuroacanthocytosis Patients. Honoraria as speaker fromMerz, Pfizer, and Neuro-Update. KB: Advisor/honoraria/finan-cial support to speak/attend meetings from GSK, Boehringer-Ingelheim, Ipsen, Merz, and Orion pharma companies. Grantsby the Dystonia Society UK and the Halley Stuart Trust.
Author Roles: Conception (KB), Organization (SAS,AEL, EM, KB), Execution (SAS, AEL), Chorein Westernblot (BB), Manuscript Writing of the first draft (SAS, AEL),and review and critique (KB, EM, BB, AD).
REFERENCES
1. Rampoldi L, Danek A, Monaco AP. Clinical features and molec-ular bases of neuroacanthocytosis J Mol Med 2002;80:475–491.
2. Ueno S, Maruki Y, Nakamura M, et al. The gene encoding anewly discovered protein, chorein, is mutated in chorea-acantho-cytosis Nat Genet 2001;28:121–122.
3. Schneider SA, Walker RH, Bhatia KP. The Huntington’s disease-like syndromes: what to consider in patients with a negative
1490 S.A. SCHNEIDER ET AL.
Movement Disorders, Vol. 25, No. 10, 2010

Huntington’s disease gene test Nat Clin Pract Neurol 2007;3:517–525.
4. Dobson-Stone C, Velayos-Baeza A, Filippone LA, et al. Choreindetection for the diagnosis of chorea-acanthocytosis Ann Neurol2004;56:299–302.
5. Dobson-Stone C, Velayos-Baeza A, Jansen A, et al. Identificationof a VPS13A founder mutation in French Canadian families withchorea-acanthocytosis Neurogenetics 2005;6:151–158.
6. Al-Asmi A, Jansen AC, Badhwar A, et al. Familial temporallobe epilepsy as a presenting feature of choreoacanthocytosisEpilepsia 2005;46:1256–1263.
7. Hardie RJ, Pullon HW, Harding AE, et al. Neuroacanthocytosis.A clinical, haematological and pathological study of 19 casesBrain 1991;114:13–49.
8. Dobson-Stone C, Danek A, Rampoldi L, et al. Mutational spec-trum of the CHAC gene in patients with chorea-acanthocytosisEur J Hum Genet 2002;10:773–781.
9. Walker RH, Liu Q, Ichiba M, et al. Self-mutilation in chorea-acanthocytosis: manifestation of movement disorder or psychopa-thology? Mov Disord 2006;21:2268–2269.
10. Chew NK, Mir P, Edwards MJ, et al. The natural history ofUnverricht-Lundborg disease: a report of eight genetically provencases Mov Disord 2008;23:107–113.
11. Shoumitro DEB. Self-injurious behaviour as part of genetic syn-dromes BR J PSYCH 1998;172:385–388.
12. Espelin DE, Done AK. Amphetamine poisoning: effect-iveness of chlorpromazine N Engl J Med 1968;278:1361–1365.
13. Mangiarini L, Sathasivam K, Seller M, et al. Exon 1 of the HDgene with an expanded CAG repeat is sufficient to cause a pro-gressive neurological phenotype in transgenic mice Cell 1996;87:493–506.
14. Storch A, Kornhass M, Schwarz J. Testing for acanthocytosis aprospective reader-blinded study in movement disorder patientsJ Neurol 2005;252:84–90.
15. Walker RH, Jung HH, Dobson-Stone C, et al. Neurologic phe-notypes associated with acanthocytosis Neurology 2007;68:92–98.
Benign Hereditary Chorea:Clinical and NeuroimagingFeatures in an Italian Family
Elena Salvatore, MD, PhD,1 Luigi Di Maio, MD, PhD,1
Alessandro Filla, MD,1 Alfonso M. Ferrara, MD,2
Carlo Rinaldi, MD,1 Francesco Sacca, MD,1
Silvio Peluso, MD,1 Paolo E. Macchia, MD, PhD,2
Sabina Pappata, MD,3 and Giuseppe De Michele, MD1*
1Department of Neurological Sciences, Federico IIUniversity, Naples, Italy; 2Department of Endocrinology andMolecular and Clinical Oncology, Federico II University,Naples, Italy; 3Biostructure and Bioimaging Institute, CNR,
Naples, Italy
Video
Abstract: Benign hereditary chorea is an autosomal domi-nant disorder characterized by early onset nonprogressivechorea, caused by mutations of the thyroid transcriptionfactor-1 (TITF-1) gene. Clinical heterogeneity has beenreported and thyroid and respiratory abnormalities maybe present. We describe 3 patients of an Italian familycarrying the S145X mutation in the TITF-1 gene withmild motor delay, childhood onset dyskinesias, and subtlecognitive impairment. A child in the third generation pre-sented with congenital hypothyroidism and neonatal respi-ratory distress. Imaging studies in 2 patients showed mildventricular enlargement and empty sella at magnetic reso-nance imaging and hypometabolism of basal ganglia andcortex at 18-Fluoro-2-deoxy-glucose positron emissiontomography. � 2010 Movement Disorder Society
Key words: benign hereditary chorea; thyroid transcrip-tion factor-1; congenital hypothyroidism; MRI; FDG-PET
Benign hereditary chorea (BHC) is an autosomal
dominant disorder characterized by childhood onset
chorea with little or no progression into adult life.
Mental deterioration does not occur, but slightly lower
I.Q. scores have been reported. Mutations in the thy-roid transcription factor-1 (TITF-1) gene on chromo-
Additional Supporting Information may be found in the onlineversion of this article.
Elena Salvatore and Luigi Di Maio contributed equally to thestudy, and both should be considered as first authors.
*Correspondence to: Dr. Giuseppe De Michele, Dipartimento diScienze Neurologiche, Universita degli Studi di Napoli Federico II,Via Pansini 5, I-80131, Napoli, Italy. E-mail: [email protected]
Potential conflict of interest: Nothing to report.Received 23 September 2009; Revised 28 December 2009;
Accepted 28 January 2010Published online 11 June 2010 in Wiley InterScience (www.
interscience.wiley.com). DOI: 10.1002/mds.23065
1491BENIGN HEREDITARY CHOREA IN AN ITALIAN FAMILY
Movement Disorders, Vol. 25, No. 10, 2010

some 14q have been identified as causative in several
families, most of them recently reviewed.1,2 A second
locus (8q21) for BHC has been recently mapped in
two Japanese families with adult onset chorea.3
The TITF-1 gene is a homeodomain-containing tran-
scription factor essential for the organogenesis of lung,
thyroid, and basal ganglia.4 Thus, it is not surprising
that the clinical spectrum in families carrying TITF-1mutations includes thyroid and lung disorders, such as
congenital hypothyroidism and respiratory distress. The
putative mechanism of disease results from gene hap-
loinsufficiency and reduced protein product.
We previously described molecular and functional
data of the novel TITF-1 S145X mutation in an Italian
pedigree.5 Here, we report in detail the clinical features
and the neuroimaging data of the family.
CASE REPORTS
This three-generation family shows three affected
individuals, one for each generation, all carrying a pre-
viously unreported mutation of the TITF-1 gene. The
genetic defect and the molecular mechanisms have
been described in the previous article.5 The index
patient was Patient 1, who had been referred for exclu-
sion of Huntington’s disease (HD). The information
that her father (Pt. 2) had abnormal movements and
that her son (Pt. 3) had congenital hypothyroidism led
to the clinical suspicion of BHC and to the molecular
analysis of the TITF-1 gene.
Patient 1, 26 years old, began walking at the age of
18 months, but she was clumsy and fell repeatedly.
Her gait much improved around puberty. Mild general-
ized choreic movements appeared at the age of 7 years
and remained stable thereafter. No mental or behav-
ioral abnormalities were present, she did not encounter
difficulties at school, and she was graduated at a Hotel
school. During puerperium, when she was 19 years
old, her chorea worsened and she presented with a
postpartum psychosis, characterized by depression and
aggressiveness toward the newborn and successfully
treated with risperidone and lamotrigine.
At the age of 23 years she was admitted to our hos-
pital. Neurological examination showed generalized
choreic movements (video) and was otherwise normal.
Neuropsychological evaluation demonstrated long term
verbal memory deficit and low-normal score at Raven
Matrices test.
Molecular analysis of HD gene and laboratory test-
ing were normal, a part from elevation of thyroid-stim-
ulating hormone.5 Thyroid hormone replacement was
started. Brain magnetic resonance imaging (MRI)
revealed ventricular dilatation, more marked in the
posterior part of lateral ventricles (Fig. 1a–c) and par-
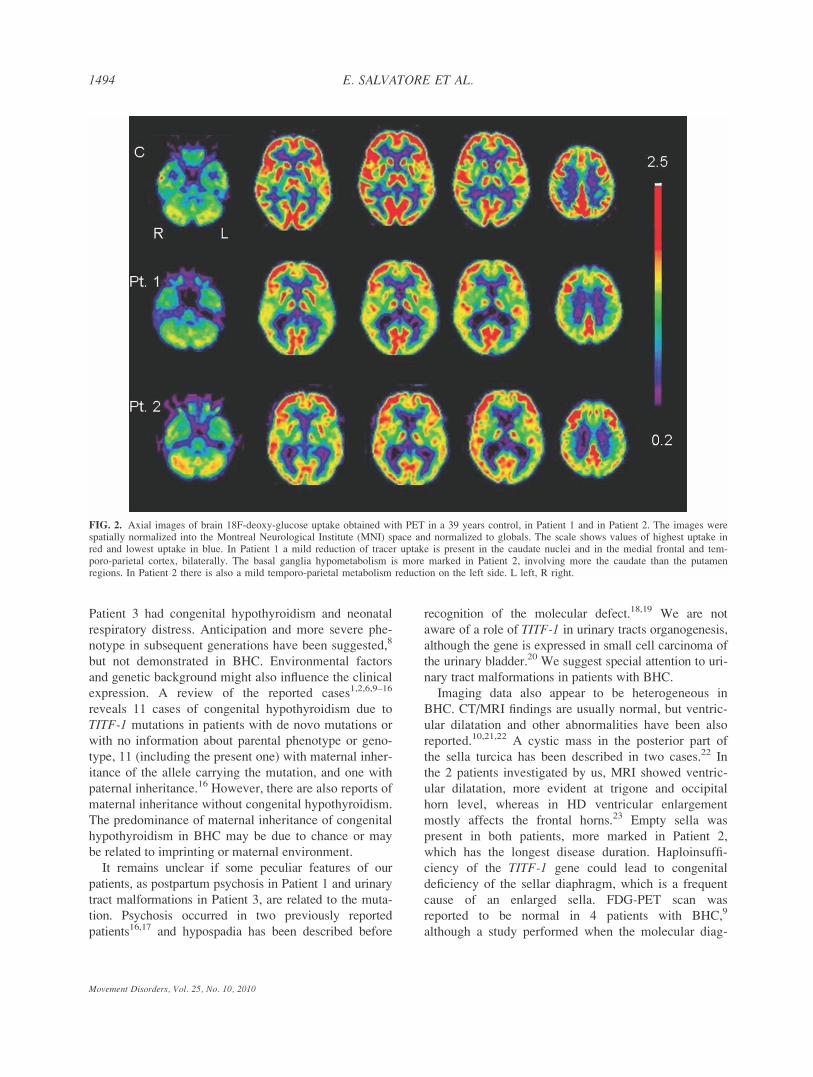
tial empty sella (Fig. 1d). Brain 18-Fluoro-2-Deoxy-
Glucose Positron Emission Tomography (FDG-PET)
showed slight relative hypometabolism of the caudate
nuclei and of the medial frontal and temporo-parietal
cortices (Fig. 2). The patient was treated with tetrabe-
nazine up to 75 mg daily, with mild improvement. At
the age of 26 years she withdrew the therapy abruptly
and presented marked worsening of chorea, irritability,
emotional lability, poor sleep, inappropriate dress, and
behavior. She was admitted to our hospital again,
treated with quetiapine, 75 mg/daily, and discharged
improved after a week.
Patient 2, the proband’s father, 56 years old, had
meningitis at the age of 6 months. Subsequent motor
development was delayed with walking starting at the
age of 5 years and normal language skills. His school
performances were poor. Since childhood, slight, spo-
radic, hyperkinesias were present, which mainly
involved the abdomen and had been stable over time.
He did not report improvement by alcohol. He worked
as a school-caretaker and had a normal social life. At
examination jerky abdominal movements were evident;
mild and rare choreic movements were present in other
body regions (video). Neuropsychological evaluation
showed short term verbal and spatial memory deficit,
slight attentional deficit, and constructive apraxia.
Thyroid hormone screening showed primary hypo-
thyroidism with increased TSH and mildly reduced
FT3. Brain MRI evidenced slight, asymmetrical ven-
tricular dilatation, more marked in the right side and in
the posterior part of lateral ventricles (Fig. 1e–g), and
complete empty sella (Fig. 1h). FDG-PET demon-
strated relative hypometabolism of basal ganglia, more
prominent in the caudate nuclei, and a slight relative
hypometabolism of the left temporo-parieto-occipital
cortex (Fig. 2). Tetrabenazine, up to 50 mg daily, was
prescribed, but the drug was withdrawn for insomnia
and nervousness.
Patient 3, the 5 years old proband’s son, born at term
by cesarean delivery because of transverse position,
received continuous positive airway pressure therapy
for neonatal respiratory distress. The infant presented
with multiple congenital anomalies: severe bilateral
vesicoureteral reflux with pyelectasis and megabladder,
patent foramen ovale, and congenital hypothyroidism
for which thyroid replacement treatment was started.
Psychomotor development was delayed: sitting at
10 months, walking at 26 months, first words at 26
months, at present only few words in vocabulary and
lack of sphincter control. His I.Q. was 76 at the age of
Movement Disorders, Vol. 25, No. 10, 2010
1492 E. SALVATORE ET AL.

4 years. He is a pleasant boy, has no behavioral prob-
lem and developed normal social relationships. At the
age of 4 years he developed slight, generalized choreic
movements (video).
Molecular analysis: Direct sequencing of the TITF-1gene showed, in all the 3 patients, the new heterozy-
gous mutation C609A in exon 2, resulting in a substi-
tution of serine at codon 145 for a stop codon
(S145X). The mutation predicted a truncated protein of
about 14.5 kDa that lacks the entire homeodomain and
the carboxy-terminus portion.5
DISCUSSION
BHC shows heterogeneity of the clinical presentation
within and among the families. In the present family
the neurologic presentation, characterized by mild
motor delay, early-onset dyskinesias, and slightly lower
intelligence, was quite similar in the 3 patients,
although the abnormal movements are somewhat differ-
ent among individuals. Although chorea is the move-
ment disorder characteristic of BHC, dystonia, myo-
clonic jerks, and ataxia have been also described.6 The
distinction among chorea, myoclonus, and jerky dysto-
nia may be difficult. The diagnosis of chorea, which is
characterized by a random flow of rapid, unpredictable
abnormal movements,7 better applies to Patients. 1 and
3, whereas the sudden, more predictable and repetitive
abdominal jerks in Patient 2 seem to be more consistent
with myoclonus. As described in other patients with
BHC,6 dyskinesias, contrary to myoclonus-dystonia,
were not worsened by action nor improved by alcohol.
Concerning extra-neurologic features subclinical
hypothyroidism was present in Patients 1 and 2, whereas
FIG. 1. Axial T2-weighted (Pt. 1 a–c; Pt. 2 e–g) and sagittal T1-weighted (Pt. 1 d; Pt. 2 h) MR images. Dilatation of supratentorial ventricularsystem is evident in both patients. Enlargement of the third ventricle is also evident in Patient 2. In both patients there is evidence of empty sella,partial in Patient 1, complete and prominent in Patient 2.
1493BENIGN HEREDITARY CHOREA IN AN ITALIAN FAMILY
Movement Disorders, Vol. 25, No. 10, 2010
Patient 3 had congenital hypothyroidism and neonatal
respiratory distress. Anticipation and more severe phe-
notype in subsequent generations have been suggested,8
but not demonstrated in BHC. Environmental factors
and genetic background might also influence the clinical
expression. A review of the reported cases1,2,6,9–16
reveals 11 cases of congenital hypothyroidism due to
TITF-1 mutations in patients with de novo mutations or
with no information about parental phenotype or geno-
type, 11 (including the present one) with maternal inher-
itance of the allele carrying the mutation, and one with
paternal inheritance.16 However, there are also reports of
maternal inheritance without congenital hypothyroidism.
The predominance of maternal inheritance of congenital
hypothyroidism in BHC may be due to chance or may
be related to imprinting or maternal environment.
It remains unclear if some peculiar features of our
patients, as postpartum psychosis in Patient 1 and urinary
tract malformations in Patient 3, are related to the muta-
tion. Psychosis occurred in two previously reported
patients16,17 and hypospadia has been described before
recognition of the molecular defect.18,19 We are not
aware of a role of TITF-1 in urinary tracts organogenesis,
although the gene is expressed in small cell carcinoma of
the urinary bladder.20 We suggest special attention to uri-
nary tract malformations in patients with BHC.
Imaging data also appear to be heterogeneous in
BHC. CT/MRI findings are usually normal, but ventric-
ular dilatation and other abnormalities have been also
reported.10,21,22 A cystic mass in the posterior part of
the sella turcica has been described in two cases.22 In
the 2 patients investigated by us, MRI showed ventric-
ular dilatation, more evident at trigone and occipital
horn level, whereas in HD ventricular enlargement
mostly affects the frontal horns.23 Empty sella was
present in both patients, more marked in Patient 2,
which has the longest disease duration. Haploinsuffi-
ciency of the TITF-1 gene could lead to congenital
deficiency of the sellar diaphragm, which is a frequent
cause of an enlarged sella. FDG-PET scan was
reported to be normal in 4 patients with BHC,9
although a study performed when the molecular diag-
FIG. 2. Axial images of brain 18F-deoxy-glucose uptake obtained with PET in a 39 years control, in Patient 1 and in Patient 2. The images werespatially normalized into the Montreal Neurological Institute (MNI) space and normalized to globals. The scale shows values of highest uptake inred and lowest uptake in blue. In Patient 1 a mild reduction of tracer uptake is present in the caudate nuclei and in the medial frontal and tem-poro-parietal cortex, bilaterally. The basal ganglia hypometabolism is more marked in Patient 2, involving more the caudate than the putamenregions. In Patient 2 there is also a mild temporo-parietal metabolism reduction on the left side. L left, R right.
1494 E. SALVATORE ET AL.
Movement Disorders, Vol. 25, No. 10, 2010

nosis was not available showed caudate hypometabo-
lism.24 More recently reduction of technetium 99 m
ethyl cysteinate dimer uptake has been demonstrated in
the basal ganglia of two children studied by SPECT.25
Using FDG-PET we showed cortex and basal ganglia
hypometabolism in both Patient 1 and Patient 2. These
findings are consistent with the significant reduction of
striatal and neocortical interneurons demonstrated by
immunohistochemical staining in BHC26 and with the
patients’ choreic syndrome and mild cognitive impair-
ment. The pattern of metabolic changes is similar, but
less severe than that found in HD,23 consistently with
the milder, non progressive BHC phenotype.
Legends to the Videos
Segment 1. Patient 1 examination shows general-
ized, moderate to marked, choreic movements involv-
ing the face, the neck, the trunk, the limbs, both proxi-
mally and distally. Finger-to-nose and walking do not
worsen the abnormal movements. Mild unsteadiness is
also evident.
Segment 2. Slightly staggering gait and mild limb
choreic movements, not worsened by action, in Patient
2. Brisk abdominal wall contractions are evident.
Segment 3. In Patient 3 mild choreic movements
involved the trunk and the four limbs, both proximally
and distally, not worsened by action. Brisk myoclonic-
like movements are also evident. Tottering was prob-
ably too marked for his age.
Acknowledgments: Financial Disclosures: Elena Salva-tore, Luigi Di Maio, Alfonso M. Ferrara, Carlo Rinaldi, Fran-cesco Sacca, Silvio Peluso, Paolo E. Macchia, and SabinaPappata: report no disclosures. Alessandro Filla: funded byresearch grants and serves as study coordinator of a projectfunded by the EUROSCA association. Giuseppe De Michele:receives research support from the EURO-HD Network.
Author Roles: Salvatore E.—Organization and executionof research project, writing of the first draft of the manu-script. Di Maio L.—Organization and execution of researchproject, writing of the first draft of the manuscript. Filla A.—Review and critique of manuscript. Ferrara AM.—Executionof research project. Rinaldi C.—Execution of research projectand writing of the first draft of the manuscript. Sacca F.—Execution of research project. Peluso S.—Execution ofresearch project. Macchia PE.—Organization of research pro-ject. Pappata S.—Execution of research project and reviewand critique of manuscript. De Michele G.—Conception ofresearch project and review and critique of manuscript.
REFERENCES
1. Kleiner-Fisman G, Lang AE. Benign hereditary chorea revisited:a journey to understanding. Mov Disord 2007;22:2297–2305.
2. Carre A, Szinnai G, Castanet M, et al. Five new TTF1/NKX2.1mutations in brain-lung-thyroid syndrome: rescue by PAX8 syn-ergism in one case. Hum Mol Genet 2009;18:2266–2276.
3. Shimohata T, Hara K, Sanpei K, et al. Novel locus for benignhereditary chorea with adult onset maps to chromosome 8q21.3q23.3. Brain 2007;130:2302–2309.
4. Breedveld GJ, van Dongen JW, Danesino C, et al. Mutations inTITF-1 are associated with benign hereditary chorea. Hum MolGenet 2002;11:971–979.
5. Ferrara AM, De Michele G, Salvatore E, et al. A novel NKX2.1mutation in a family with hypothyroidism and benign hereditarychorea. Thyroid 2008;18:1005–1009.
6. Asmus F, Devlin A, Munz M, Zimprich A, Gasser T, ChinneryPF. Clinical differentiation of genetically proven benign heredi-tary chorea and myoclonus-dystonia. Mov Disord 2007;22:2104–2119.
7. Schrag A, Quinn NP, Bhatia KP, Marsden CD. Benign hereditarychorea–entity or syndrome? Mov Disord 2000;15:280–288.
8. Breedveld GJ, Percy AK, MacDonald ME, et al. Clinical andgenetic heterogeneity in benign hereditary chorea. Neurology2002;59:579–584.
9. Kleiner-Fisman G, Rogaeva E, Halliday W, et al. Benign heredi-tary chorea: clinical, genetic, and pathological findings. AnnNeurol 2003;54:244–247.
10. do Carmo Costa M, Costa C, Silva AP, et al. Nonsense mutationin TITF1 in a Portuguese family with benign hereditary chorea.Neurogenetics 2005;6:209–215.
11. Asmus F, Horber V, Pohlenz J, et al. A novel TITF-1 mutationcauses benign hereditary chorea with response to levodopa. Neu-rology 2005;64:1952–1954.
12. Devos D, Vuillaume I, de Becdelievre A, et al. New syndromicform of benign hereditary chorea is associated with a deletion ofTITF-1 and PAX-9 contiguous genes. Mov Disord 2006;21:2237–2240.
13. Moya CM, Perez de Nanclares G, Castano L, et al. Functionalstudy of a novel single deletion in the TITF1/NKX2.1 homeoboxgene that produces congenital hypothyroidism and benign choreabut not pulmonary distress. J Clin Endocrinol Metab 2006;91:1832–1841.
14. Provenzano C, Veneziano L, Appleton R, Frontali M, CivitarealeD. Functional characterization of a novel mutation in TITF-1 ina patient with benign hereditary chorea. J Neurol Sci 2008;264:56–62.
15. Maquet E, Costagliola S, Parma J, et al. Lethal respiratory failureand mild primary hypothyroidism in a term girl with a de novoheterozygous mutation in the TITF1/NKX2.1 gene. J Clin Endo-crinol Metab 2009;94:197–203.
16. Glik A, Vuillaume I, Devos D, Inzelberg R. Psychosis, short stat-ure in benign hereditary chorea: a novel thyroid transcription fac-tor-1 mutation. Mov Disord 2008;23:1744–1747.
17. de Vries BB, Arts WF, Breedveld GJ, Hoogeboom JJ, NiermeijerMF, Heutink P. Benign hereditary chorea of early onset maps tochromosome 14q. Am J Hum Genet 2000;66:136–142.
18. Chun RW, Daly RF, Mansheim BJ, Jr, Wolcott GJ. Benign fami-lial chorea with onset in childhood. JAMA 1973;225:1603–1607.
19. Burns J, Neuhauser G, Tomasi L. Benign hereditary non-progres-sive chorea of early onset. Clinical genetics of the syndrome andreport of a new family. Neuropadiatrie 1976;7:431–438.
20. Jones TD, Kernek KM, Yang XJ, et al. Thyroid transcription fac-tor 1 expression in small cell carcinoma of the urinary bladder:an immunohistochemical profile of 44 cases. Hum Pathol 2005;36:718–723.
21. Iwatani N, Mabe H, Devriendt K, Kodama M, Miike T. Deletionof NKX2.1 gene encoding thyroid transcription factor-1 in twosiblings with hypothyroidism and respiratory failure. J Pediatr2000;137:272–276.
22. Krude H, Schutz B, Biebermann H, et al. Choreoathetosis, hypo-thyroidism, and pulmonary alterations due to human NKX2–1haploinsufficiency. J Clin Invest 2002;109:475–480.
1495BENIGN HEREDITARY CHOREA IN AN ITALIAN FAMILY
Movement Disorders, Vol. 25, No. 10, 2010

23. Montoya A, Price BH, Menear M, Lepage M. Brain imaging andcognitive dysfunctions in Huntington’s disease. J Psychiatry Neu-rosci 2006;31:21–29.
24. Suchowersky O, Hayden MR, Martin WR, Stoessl AJ, Hilde-brand AM, Pate BD. Cerebral metabolism of glucose in benignhereditary chorea. Mov Disord 1986;1:33–44.
25. Mahajnah M, Inbar D, Steinmetz A, Heutink P, Breedveld GJ,Straussberg R. Benign hereditary chorea: clinical, neuroimaging,and genetic findings. J Child Neurol 2007;22:1231–1234.
26. Kleiner-Fisman G, Calingasan NY, Putt M, Chen J, Beal MF,Lang AE. Alterations of striatal neurons in benign hereditarychorea. Mov Disord 2005;20:1353–1357.
Long-Term Effect of UnilateralPallidotomy on Levodopa-Induced
Dyskinesia
Galit Kleiner-Fisman, MD, FRCPC,1,2*Andres Lozano, MD, PhD, FRCPS,3
Elena Moro, MD, PhD,1 Yu-Yan Poon, RN,1
and Anthony E. Lang, MD, FRCPC1
1Morton and Gloria Shulman Movement Disorders Center,Toronto Western Hospital, University of Toronto,
Toronto, Ontario, Canada; 2Baycrest Geriatric Hospital,University of Toronto, Toronto, Ontario,
Canada; 3Department of Neurosurgery, TorontoWestern Hospital, University of Toronto, Toronto,
Ontario, Canada
Abstract: Unilateral pallidotomy has been effectively usedto treat parkinsonism and reduce levodopa induced dyski-nesia (LID). We sought to determine the long-term effectsof pallidotomy on LID in 10 patients who had initialbenefit from pallidotomy but went on to require DBS sur-gery for symptom progression. The Dyskinesia RatingScale (DRS) was used to rate and quantify LID in ablinded fashion. Though sample size was small, there wasa trend towards a reduction in LID lasting up to 12 yearssuggesting that posteroventral pallidotomy may providesustained benefit in reducing LID. � 2010 MovementDisorder Society
Key words: Parkinson’s disease; pallidotomy; dyskinesia
In the era before DBS, as well as currently, in many
countries around the world, unilateral postero-ventral
pallidotomy as a treatment for Parkinson’s disease
(PD) has been the surgical alternative of choice. Pallid-
otomy ameliorates parkinsonism and is particularly
effective in reducing levodopa-induced dyskinesia
(LID) most prominently in the contralateral hemibody.1
Despite initial control of disabling symptoms, parkin-
sonism generally worsens several years following pal-
lidotomy and many patients have subsequently under-
gone STN DBS when their symptoms again became re-
sistant to medical regimens.2–4
No long-term follow-up studies have blindly eval-
uated the persistent effects of unilateral pallidotomy on
LID. It has been our personal experience that the anti-
dyskinetic effects may be evident many years after the
original surgery and Hariz reported that these effects
could last up to 13.5 years.5
We sought to determine the long-term effect of pal-
lidotomy on dyskinesia in a selected sample of patients
who had previously undergone pallidotomy and were
undergoing preoperative evaluation for STN DBS due
to symptom progression. Given the extensive preopera-
tive assessment for DBS, ON/OFF evaluations were
available for review in these patients. We evaluated ef-
ficacy of pallidotomy on dyskinesia by comparing con-
tralateral and ipsilateral dyskinesia at the STN-DBS
preoperative evaluation. We postulated that there
would be a difference between sides due to lasting
effects of pallidal lesioning with less severe dyskinesia
contralateral to the previous surgery.
PATIENTS AND METHODS
Patient Population
Ten patients (8 male) with PD and prior pallidotomy
on average 7.3 years (range 2–12 years) earlier were
evaluated for consideration of STN DBS. All patients
were felt to have obtained an initial good response to
pallidotomy with respect to parkinsonism and particu-
larly LID. Not all patients had received pallidotomy at
our center; pre and postoperative LID scores were
available in 6 of the 10. Before DBS patients were
evaluated under the protocol of the Core Assessment
Program for Intracerebral Transplantation6 (CAPSIT)
before STN DBS surgery. Dyskinesia was assessed
using the Dyskinesia Rating Scale (DRS) (maximum
score for unilateral limbs 5 8). The dosage of anti-par-
kinsonian medication required by the patient was
recorded; levodopa equivalent doses (LED) were calcu-
lated in a manner described elsewhere.7 Evaluations
*Correspondence to: Dr. Galit Kleiner-Fisman, Morton and GloriaShulman Movement Disorders Center, Toronto Western Hospital,University of Toronto, 399 Bathurst Street, McL-7, Toronto, Ontario,M5T 2S8 Canada. E-mail: [email protected]
Potential conflict of interest: None reported.Received 4 March 2009; Revised 27 May 2009; Accepted 8
October 2009Published online 21 June 2010 in Wiley InterScience (www.
interscience.wiley.com). DOI: 10.1002/mds.23155
1496 G. KLEINER-FISMAN ET AL.
Movement Disorders, Vol. 25, No. 10, 2010

were made while the anti-parkinsonian medication was
in effect (medication-on period) and following overnight
withdrawal from medication (medication-off period).
These assessments were video-taped and a blinded-rater
(blinded to patient, side of previous pallidotomy, and
medication state) quantified and identified the type of
dyskinesia utilizing the DRS.
Statistical Analysis
Effectiveness of initial pallidotomy on dyskinesia
was assessed comparing pre and postoperative DRS
scores using the Wilcoxon sign-rank test. Pairwise
comparisons were made between the limbs ipsilateral
and contralateral to prior pallidotomy for ‘‘ON’’ dyski-
nesia and ‘‘OFF’’ dystonia using a paired t-test.
RESULTS
All patients had undergone pallidotomy contralateral
to their most severely affected side (parkinsonism and
LID). The available data demonstrated that at 12
months following pallidotomy patients had a significant
reduction in dyskinesia: ipsilateral dyskinesia (mean
reduction 1.25 points; minimum change 0 points, maxi-
mum change 2.5 points, P 5 0.04), contralateral dyski-
nesia (mean reduction 2 points; minimum change 1
point, maximum change 3.5 points, P 5 0.03), and
axial dyskinesia (mean reduction 1.75 points; minimum
change 0 points, maximum change 2 points P 5 0.05).
Mean age at pallidotomy was 51.5 6 5.9 with disease
duration before pallidotomy of 9.5 6 2 years. Mean
LED at the time of pallidotomy was 754.3 6 450 mg
and at time of STN DBS was 1287.8 6 419.2 mg.
The results of blinded assessment of dyskinesia
before STN DBS are displayed in Table 1. There was
a small difference in LID between sides with a trend
toward less LID in the contralateral versus the ipsilat-
eral limbs (P 5 0.09). In 5 of 8 patients, who demon-
strated on-period LID, these were more severe (mark-
edly in 3) on the side ipsilateral to the previous pal-
lidotomy. There was no difference in OFF dystonia
found between limbs.
DISCUSSION
Pallidotomy has a prolonged effect on contralateral
dyskinesia with previous studies having reported bene-
fit lasting up to 13.5 years even when akinesia and
other PD symptoms had returned.5 Other studies have
also reported sustained benefit from unilateral pallidot-
omy on contralateral dyskinesia.1,8,9 None of these
studies evaluated LID in a blinded fashion. In this
study, only patients who were undergoing subsequent
DBS were included due to availability of data, and
therefore, this may be a biased cohort of patients with
suboptimal outcomes given the need for further inter-
vention. There are other patients who underwent pallid-
otomy at our Center who have had sustained long-term
improvement of LID (as evidenced by on-period clini-
cal assessments demonstrating minimal or no dyskine-
sia contralateral to their previous surgery); however,
video-taped CAPSIT evaluations of these patients
were not available for blinded review. Our evaluated
patients were all felt to have had an initial good
effect on LID from pallidotomy; however, progression
of parkinsonian symptoms necessitated consideration
of DBS.
Although sample size in our case series was too
small to achieve statistical significance, there was a
trend toward significance lasting up to 12 years fol-
lowing the original surgery, consistent with previous
reports of sustained benefit. This finding again sug-
gests that postero-ventral pallidotomy remains a rea-
sonable alternative therapy for disabling LID, espe-
cially in patients for whom DBS surgery is not a ther-
apeutic option.
Financial Disclosures: GKF: honoraria from Santhera,Teva Pharmaceuticals. AL: consultant for Medtronic, ElyLilly, Cergene, and St. Jude. YYP: Nothing to disclose. EM:consultant to and honoraria from Medtronic. AEL: advisor,Allon Therapeutics, Biovail, Boehringer-Ingelheim, Cepha-lon, Ceregene, Eisai, Medtronic, Lundbeck A/S, Neuromolec-ular, Novartis, Merck Serono, Solvay, Taro, Teva; grantsfrom Canadian Institutes of Health Research, Dystonia Medi-cal Research Foundation, Michael J. Fox Foundation,
TABLE 1. Dyskinesia characteristics
Yrs sincepallidotomy
DRSipsilateral(ON)
DRScontralateral
(ON)
OFFdystonia
(ipsilateral)
OFFdystonia
(contralateral)
1. 12 4 0 2 02. 5 4 2 0 03. 4 4 5 0 14. 10 4 5 0 05. 9 0 1 2 06. 2 0 0 0 17. 9 2 0 0 08. 7 6 1 0 09. 7 0 0 0 010. 8 7 0 0 0Mean 7.3 3.1 1.4
DRS, dyskinesia rating scale.
Movement Disorders, Vol. 25, No. 10, 2010
1497LONG-TERM EFFECT OF UNILATERAL PALLIDOTOMY ON LID

National Parkinson Foundation, Ontario Problem GamblingResearch Centre, Parkinson’s Disease Foundation, Taro;speaker fees or other support from GSK, UCB.
REFERENCES
1. Fine J, Duff J, Chen R, et al. Long-term follow-up of unilateralpallidotomy in advanced Parkinson’s disease. N Engl J Med2000;342:1708–1714.
2. Kleiner-Fisman G, Fisman DN, Zamir O, et al. Subthalamic nu-cleus deep brain stimulation for Parkinson’s disease after success-ful pallidotomy: clinical and electrophysiological observations.Mov Disord 2004;19:1209–1214.
3. Ondo WG, Silay Y, Almaguer M, Jankovic J. Subthalamic deepbrain stimulation in patients with a previous pallidotomy. MovDisord 2006;21:1252–1254.
4. Mogilner AY, Sterio D, Rezai AR, Zonenshayn M, Kelly PJ,Beric A. Subthalamic nucleus stimulation in patients with a priorpallidotomy. J Neurosurg 2002;96:660–665.
5. Hariz MI, Bergenheim AT. A 10-year follow-up review ofpatients who underwent Leksell’s posteroventral pallidotomy forParkinson disease. J Neurosurg 2001;94:552–558.
6. Langston JW, Widner H, Goetz CG, et al. Core assessment pro-gram for intracerebral transplantations (CAPIT). Mov Disord 1992;7:2–13.
7. Hobson DE, Lang AE, Martin WR, Razmy A, Rivest J, FlemingJ. Excessive daytime sleepiness and sudden-onset sleep in Parkin-son disease: a survey by the Canadian Movement DisordersGroup. JAMA 2002;287:455–463.
8. Strutt AM, Lai EC, Jankovic J, et al. Five-year follow-up of uni-lateral posteroventral pallidotomy in Parkinson’s disease. SurgNeurol 2008.
9. Vitek JL, Bakay RA, Freeman A, et al. Randomized trial of pal-lidotomy versus medical therapy for Parkinson’s disease. AnnNeurol 2003;53:558–569.
Increased Reaction Time PredictsVisual Learning Deficits in
Parkinson’s Disease
Lucio Marinelli, MD, PhD,1* Bernardo Perfetti, PhD,2
Clara Moisello, PhD,2 Alessandro Di Rocco, MD,3
David Eidelberg, MD,4 Giovanni Abbruzzese, MD,1
and Maria Felice Ghilardi, MD2*1Department of Neurosciences, Ophthalmology and Genetics,University of Genova, Italy; 2Department of Physiology andPharmacology, CUNY Medical School, New York, New York,USA; 3Department of Neurology, NYU, New York, New York,USA; 4Center for Neurosciences, The Feinstein Institute forMedical Research, North Shore-Long Island Jewish Health
System, Manhasset, New York, USA
Abstract: To determine whether the process involved inmovement preparation of patients in the early stages of Par-kinson’s disease (PD) shares attentional resources with vis-ual learning, we tested 23 patients with PD and 13 healthycontrols with two different tasks. The first was a motor taskwhere subjects were required to move as soon as possible torandomly presented targets by minimizing reaction time.The second was a visual learning task where targets werepresented in a preset order and subjects were asked to learnthe sequence order by attending to the display without mov-ing. Patients with PD showed higher reaction and movementtimes, while visual learning was reduced compared with con-trols. For patients with PD, reaction times, but not move-ment times, displayed an inverse significant correlation withthe scores of visual learning. We conclude that visual declar-ative learning and movement preparation might share simi-lar attentional and working memory resources. � 2010Movement Disorder Society
Key words: Parkinson’s disease; executive function;attention; motor control
Motor slowness in Parkinson’s disease (PD) is a gen-
eral term that encompasses: akinesia, a poverty of move-
ment production and delay in movement initiation; bra-
dykinesia, a reduction in movement speed; and hypoki-
nesia, a reduction in movement size.1 In experimental
motor tasks, akinesia is reflected by increased reaction
times, a finding often reported in patients with PD.1
*Correspondence to: L. Marinelli, Department of Neurosciences,Ophthalmology and Genetics, via De Toni 5, University of Genova,16132 Genova, Italy. E-mail: [email protected] or M.F. Ghilardi,Department of Pharmacology and Physiology, Harris Hall 202, 138thstreet and Convent Avenue, City University of New York MedicalSchool, New York, New York 10031. E-mail: [email protected]
Potential conflict of interest: Nothing to report.Received 11 August 2009; Revised 19 January 2010; Accepted 16
March 2010Published online 21 June 2010 in Wiley InterScience (www.
interscience.wiley.com). DOI: 10.1002/mds.23156
1498 L. MARINELLI ET AL.
Movement Disorders, Vol. 25, No. 10, 2010

During the few hundred milliseconds between stimu-
lus presentation and movement onset, many processes
take place, including attentional and stimulus processing,
decision making, and movement programming. Some of
these processes and resources are also engaged during
visuospatial learning that occurs without movement.2 In
fact, activation of frontoparietal areas, the likely neural
substrate of these processes, occurs during many tasks,
independent of the modality and of the learning load.3,4
It is now well known that PD impairs not only
motor functions but also attentional and learning proc-
esses.5 However, the connection between the two defi-
cits has not been explored.
Here, we hypothesize that if movement preparation
shares neural resources with visual spatial learning, in
patients with PD, abnormalities in reaction time and
impairment of sequence learning that requires no
movement should be correlated.
PATIENTS AND METHODS
Twenty-three patients with idiopathic PD (17 men
and 6 women; mean age 6 SE: 60.0 6 6.8 years)
in early stages of the disease (Hoehn and Yahr stages
I–II) and 13 age-matched healthy controls (6 men and
7 women; 56.5 6 2.7 years) participated in the study.
All subjects were right-handed, underwent a clinical
interview to determine that he or she did not meet the
DSM-III-R criteria for depression or dementia, scored
more than 27 at Mini-Mental State Examination, and
had a normal brain MRI.
Mean UPDRS score (part 3) of patients with PD was
8.8 (1.8, SE). The most involved side was the right in 10
patients and the left in the remaining 13 patients.
At the time of testing, all patients were in stable con-
ditions. Thirteen patients were drug-naive; 4 had been
treated with deprenyl alone, 4 with levodopa (L-dopa)/
carbidopa, and 2 with a combination of dopamine ago-
nists and L-dopa/carbidopa. However, all patients were
drug-free for at least 12 hours before testing. Written
informed consent was obtained from all participants
under a protocol approved by the institutional review
board of the participating institutions.
Detailed features of the tasks have been previously
reported.6,7 Briefly, in both tasks, one of eight targets
appeared on a screen with a common starting point, in
synchrony with a tone at 1-second intervals. Each trial
block lasted for 90 seconds.
The two tasks, which were presented in a random-
ized order, were:
1. Motor task: targets were presented in a pseudorandom
and unpredictable order. Movements were performed
on a digitizing tablet with the right dominant hand.
Instructions were to reach each target as soon as possi-
ble, minimizing reaction time but avoiding target
anticipation. Target distance was 1.8 cm.
2. Visual learning task: subjects were instructed to learn the
order of a repeating sequence of eight targets that was
presented in the 90-second block. At the end of the block,
verbal reports about the sequence order were collected.6,7
For each movement we computed: reaction time,
movement duration, peak velocity, hand-path length,
and spatial error.6,7
At the end of the visual block, declarative scored
were computed from 0 (unawareness of a sequence) to
8 (complete correct sequence).6,7
Factorial analysis of variance was performed to
compare patients with PD and healthy controls’ values.
Linear regression analyses were also performed to
determine correlations between kinematic and other
variables. Level of significance was P < 0.05.
RESULTS
There was no difference between the performance indi-
ces of treated and drug-naıve patients and between right
and left hemiparkinsonian patients. Therefore, patients’
data were combined and compared with those of controls.
Data are summarized in Figure 1. On average, reac-
tion times were prolonged in patients with PD when
FIG. 1. Kinematic and learning indices. Mean 6 SE of kinematicand learning indices (* see text for statistics).
1499REACTION TIME PREDICTS VISUAL LEARNING IN PD
Movement Disorders, Vol. 25, No. 10, 2010

compared with controls [F(1,34)5 5.6, P 5 0.02]. Simi-
larly, in patients with PD, movement durations were sig-
nificantly longer [F(1,34) 5 8.0, P 5 0.008] and peak of
velocity reduced [F(1,34) 5 6.9, P 5 0.01]. Spatial ac-
curacy, expressed by spatial error, was similar in the two
groups [F(1,34) 5 1.9, P 5 0.2]; however, hand-path
lengths were reduced in patients with PD when com-
pared with controls [F(1,34) 5 9.0, P 5 0.005].
The declarative scores reflecting visual learning
were significantly lower in patients compared with
controls [F(1,34) 5 13.2, P 5 0.0009], indicating
impairment in visuospatial learning.
We then ascertained whether declarative scores in
the visual task were associated to kinematic measure-
ments. In patients with PD, declarative scores were
negatively correlated with reaction times: the higher
the reaction time, the lower the declarative score (r 520.66, P 5 0.0006). No significant correlations were
found between declarative scores versus movement
times (r 5 20.23, P 5 0.3), peak velocity (r 5 0.05,
P 5 0.8), or hand-path length (r 5 20.20, P 5 0.4).
In addition, there were no correlations between
UPDRS (part 3) scores and either reaction times (r 50.06, P 5 0.8), movement times (r 5 0.12, P 5 0.7),
hand-path length (r50.21, P 5 0.5), or declarative
scores (r 5 20.13, P 5 0.7). In patients with
PD, there was no significant correlation between reac-
tion times and movement duration or peak velocity
(r 5 0.29, P 5 0.2). As expected, movement time and
peak velocity values were instead highly correlated
(r 5 20.87, P < 0.0001).
Finally, in healthy controls we did not find any cor-
relation between learning scores with either reaction
time (r 5 0.39, P 5 0.2) or movement time (r 50.004, P 5 1.0).
DISCUSSION
This study shows that, in agreement with previous
work, in patients with early stage PD increased reac-
tion times and impaired visual sequence learning are
significantly correlated: patients with higher reaction
times are also more impaired in sequence learning,
suggesting that movement preparation shares resources
with learning of visuospatial sequences.
Increased reaction time in patients with PD is con-
sidered the experimental hallmark of akinesia.1 Our
motor task also captured other characteristic features of
PD: hypokinesia, with reduced hand-path length and
bradikinesia,1 with significant increases in movement
time and reductions of peak velocity. Interestingly, the
clinical motor UPDRS scores did not correlate with
any of the kinematic measures. This lack of correspon-
dence is likely due to the fact that motor UPDRS
scores reflect global motor impairment, as this scale
embraces multiple motor aspects. Interestingly, in our
PD population, reaction and movement time did not
correlate, adding evidence that their respective neural
mechanisms may not overlap.
As previously shown,5,6 our patients with PD display
abnormal visual sequence learning, a learning that is
declarative and explicit in nature, requires no motor
involvement but loads working memory and attention
buffers, possibly like movement preparation. Patients
with PD also show alteration in visuospatial and cen-
tral executive abilities.8 It has been suggested that all
these deficits stem from malfunction of the frontoparie-
tal network.9 In fact, this network is engaged in many
and various facets of cognitive control, as it might be
responsible for the active representation of attended
and goal-relevant stimuli, and thus for promoting
adequate domain-dependent information processing.2 In
fact, even the simple shift between attended stimuli
leads to an update of this network.10
The exclusive correlation of declarative scores with
reaction times, but not with other kinematic parame-
ters, suggests that, first, the neural resources for move-
ment preparation and those for visuospatial learning
partly overlap and, second, PD significantly hampers
such resources. Moreover, these data suggest that
motor and cognitive functions are not completely inde-
pendent processes but share similar resources, implying
that some motor and nonmotor parkinsonian signs
might have common neural bases. Such results are im-
portant in designing novel rehabilitative approaches to
improve specific aspects of motor performance and the
quality of life of patients.
Acknowledgments: This study was supported by NationalParkinson Foundation, McDonnell Foundation (MFG), andNIH grant R01NS054864 (MFG).
Financial Disclosures: Giovanni Abbruzzese: AdvisoryBoard: Novartis and Lundbeck; Honoraria: Boehringer.
Author Roles: L. Marinelli: research project organizationand execution, writing the first draft of the manuscript. B.Perfetti: statistical analysis design and execution, manuscriptcritique. C. Moisello: statistical analysis design and execu-tion, manuscript critique. A. Di Rocco: statistical analysisreview and critique, manuscript review and critique. D.Eidelberg: research project conception, statistical analysisreview and critique, manuscript review and critique. G.Abbruzzese: statistical analysis review and critique, manu-script review and critique. M.F. Ghilardi: research projectconception, statistical analysis review and critique, manu-script review and critique.
Movement Disorders, Vol. 25, No. 10, 2010
1500 L. MARINELLI ET AL.

REFERENCES
1. Berardelli A, Rothwell JC, Thompson PD, Hallett M. Pathophysi-ology of bradykinesia in Parkinson’s disease. Brain 2001;124:2131–2146.
2. Miller EK, Cohen JD. An integrative theory of prefrontal cortexfunction. Ann Rev Neurosci 2001;24:167–202.
3. Funahashi S. Prefrontal cortex and working memory processes.Neuroscience 2006;139:251–261.
4. Rounis E, Stephan KE, Lee L, et al. Acute changes in frontopari-etal activity after repetitive transcranial magnetic stimulation overthe dorsolateral prefrontal cortex in a cued reaction time task. JNeurosci 2006;26:9629–9638.
5. Doyon J. Motor sequence learning and movement disorders. CurrOpin Neurol 2008;21:478–483.
6. Ghilardi M, Eidelberg D, Silvestri G, Ghez C. The differentialeffect of PD and normal aging on early explicit sequence learn-ing. Neurology 2003;60:1313–1319.
7. Ghilardi MF, Silvestri G, Feigin A, et al. Implicit and explicitaspects of sequence learning in pre-symptomatic Huntington’sdisease. Parkinsonism Relat Disord 2008;14:457–464.
8. Kemps E, Szmalec A, Vandierendonck A, Crevits L. Visuo-spa-tial processing in Parkinson’s disease: evidence for diminishedvisuo-spatial sketch pad and central executive resources. Parkin-sonism Relat Disord 2005;11:181–186.
9. Nakamura T, Ghilardi MF, Mentis M, et al. Functional networksin motor sequence learning: abnormal topographies in Parkin-son’s disease. Hum Brain Mapp 2001;12:42–60.
10. Hon N, Epstein RA, Owen AM, Duncan J. Frontoparietal activitywith minimal decision and control. J Neurosci 2006;26:9805–9809.
Psychogenic Paralysis andRecovery After Motor Cortex
Transcranial Magnetic Stimulation
Nathalie Chastan, MD, PhD*and Dominique Parain, MD, PhD
Department of Neurophysiology, Rouen University Hospital,Rouen, France
Abstract: Psychogenic paralysis presents a real treatmentchallenge. Despite psychotherapy, physiotherapy, antide-pressants, acupuncture, or hypnosis, the outcome is notalways satisfactory with persistent symptoms after long-term follow-up. We conducted a retrospective study toassess clinical features and to propose an alternativetreatment based on repetitive transcranial magneticstimulation (rTMS). Seventy patients (44 F/26 M, meanage: 24.7 6 16.6 years) experienced paraparesis (57%),monoparesis (37%), tetraparesis (3%), or hemiparesis(3%). A precipitating event was observed in 42 patients,primarily as a psychosocial event or a physical injury.An average of 30 stimuli over the motor cortex contra-lateral to the corresponding paralysis was delivered atlow frequency with a circular coil. The rTMS waseffective in 89% of cases, with a significantly betteroutcome for acute rather than chronic symptoms. Inconclusion, motor cortex rTMS seem to be very effec-tive in patients with psychogenic paralysis and could beconsidered a useful therapeutic option. � 2010 Move-ment Disorder Society
Key words: conversion disorder; motor paralysis; trans-cranial magnetic stimulation; motor cortex
Psychogenic disorders imply that the patient has no
voluntary control over the production of symptoms,
with no known organic syndrome to explain the symp-
toms. Psychogenic disorders are frequently related to
the motor system,1 as psychogenic paralysis,2–6 and
present a real treatment challenge.
The initial aim of this study was to evaluate clinical
features of patients with psychogenic paralysis. We
performed a retrospective study of 70 adults and chil-
dren. The second aim was to assess a promising new
*Correspondence to: Dr. Nathalie Chastan, CHU de Rouen—Hopi-tal Charles Nicolle, Service de Neurophysiologie, 1 rue de Germont,76031 Rouen Cedex, France. E-mail: [email protected]
Potential conflict of interest: The authors confirm that there was noconflict of interest. The authors have no financial disclosures or addi-tional information to disclose.
Received 11 November 2009; Revised 28 January 2010; Accepted23 March 2010
Published online 21 June 2010 in Wiley InterScience (www.
interscience.wiley.com). DOI: 10.1002/mds.23187
1501PSYCHOGENIC PARALYSIS AND RTMS
Movement Disorders, Vol. 25, No. 10, 2010

treatment based on repetitive transcranial magnetic
stimulation (rTMS), which is known to modulate corti-
cal excitability, for patients with psychogenic paralysis
characterized by a decreased activation of the primary
motor cortex.7 Motor-evoked potentials have been sug-
gested to be useful in the diagnosis of psychogenic pa-
ralysis, as they are normal.8–10 As some patients,
before the onset of this study, had recovered immedi-
ately after several magnetic stimulations used for diag-
nostic motor-evoked potentials, we decided to apply
rTMS to these patients.
PATIENTS AND METHODS
Patients
We retrospectively reviewed the medical records of
70 patients with psychogenic paralysis who received
therapeutic rTMS between April 1999 and November
2008 in the Neurophysiology Department of the
Rouen University Hospital. The rTMS was used for
routine diagnostic purposes for each patient. The
study was approved by the local Ethics Committee.
The nature, onset, duration of the symptoms, and
precipitating events were recorded. We defined symp-
toms as acute or subacute symptoms, <30-day or
>30-day duration at the moment of the rTMS admin-
istration, respectively.
The diagnosis was explained to each individual
patient, particularly regarding the nature of
‘‘functional’’ paralysis, i.e., a nervous system dysfunc-
tion without lesion. TMS was introduced principally as
a diagnostic test and sometimes as a treatment that
could possibly alleviate their symptoms. We tried to
avoid suggestion in most cases. We spent 15 minutes
explaining and performing the rTMS session.
Methods
An average of 30 stimuli delivered at low frequency
(the device allowed stimulation every 4–5 seconds)
and maximal intensity of 2.5 Tesla were attempted
with a circular coil (P/N 9784-00) during 2 to 3
minutes. Another session of 30 stimuli was sometimes
delivered a few minutes later in cases of incomplete
improvement. The rTMS was applied to the motor cor-
tex opposite from the corresponding paralysis or on
both sides for bilateral paralysis. The rTMS efficacy
was classified in two groups: effective (total recovery
or dramatic improvement) or ineffective (mild
improvement or failure). Patient follow-up was per-
formed in most cases by the general practitioner, pedi-
atrician, or neurologist.
Statistical Analysis
To assess the influence of certain characteristics on
outcome, the comparison of rTMS efficacy between
different situations (men versus women, etc.) was
measured using the Fisher’s exact test. The accepted
significance level was P < 0.05.
RESULTS
Seventy patients (44 women and 26 men) were
referred by different units: the Department of Pediatrics
(n 5 28), Neurology (n 5 19), Neurosurgery (n 5 11),
Orthopedics (n 5 7), Rheumatology (n 5 3), and Emer-
gency (n 5 2). They were aged 24.7 6 16.6 years (mean
6 SD; minimum–maximum: 8–79 years). The majority
of patients (41 patients, i.e., 59%) were adolescents
(Fig. 1).
All patients experienced an abrupt onset or rapidly
progressive onset of the paralysis. At least one precipi-
tating event was observed in 42 of 48 patients for whom
information was available: a physically traumatic event
(n 5 12, in the affected limbs [n 5 5] or in a diffuse
way [n 5 7], with a minor injury for six patients); a psy-
chosocial precipitating event (n 5 21, death of a relative
[n 5 2], family conflict [n 5 11], work conflict [n 5 3],
and academic problems [n 5 4]); cephalalgia (n 5 8);
malaise (n 5 8); an unusual physical effort (n 5 3); and
an infection (n 5 2).
The symptoms were a paraparesis (n 5 40, 57%),
monoparesis (n 5 26, 37%), tetraparesis (n 5 2, 3%),
and hemiparesis (n 5 2, 3%). Paraparesis affected sig-
nificantly more children than adults (P 5 0.0003) and
monoparesis more adults than children (P 5 0.01).
The motor symptoms were isolated (n 5 24, 34%)
or were associated with sensory symptoms (n 5 27,
39%), with pain (n 5 11, 16%), or with both sensory
FIG. 1. Age distribution of patients with a psychogenic paralysis.The number of patients in different age groups in units of 10 years.
1502 N. CHASTAN AND D. PARAIN
Movement Disorders, Vol. 25, No. 10, 2010

symptoms and pain (n 5 8, 11%). The symptoms me-
dian duration at the time of the consultation was 5
days (minimum–maximum: 1–1080, Fig. 2). The symp-
toms were acute in 55 patients (median duration: 4
days) and subacute (even chronic) in 15 patients (me-
dian duration: 240 days).
The patients’ medical history revealed the following:
a comorbid psychiatric disorder (n 5 28, anxiety
and depressive disorders [n 5 21], eating disorders
[n 5 3], and posttraumatic stress disorders [n 5 4]);
physical injury history different from the precipitating
event (n 5 15, in the same area of the current paraly-
sis [n 5 13] or in a diffuse way [n 5 2]); ‘‘back trou-
ble’’ (n 5 10, sciatica, spinal injury, or surgery); a per-
sonal neurologic pathology (n 5 8 with 6 migraine);
or a familial neurologic pathology (n 5 4).
The rTMS was effective in 62 patients (89%), with a
total recovery in 53 patients (immediately after rTMS
[n 5 43], quasi-immediately [within a few minutes or
hours, n 5 8], and a few days later [n 5 2]) or a dra-
matic improvement in nine patients. The rTMS was inef-
fective in eight patients (11%), with a mild improvement
(n 5 5) or a failure (n 5 3). It was significantly more
effective for acute symptoms than subacute symptoms
(P 5 0.009). No significant difference of rTMS outcome
was observed between children and adults, men and
women, symptoms characteristics, concerning the pre-
cipitating events, or patients’ medical history.
The symptoms recurred in eight patients, always with
the same paralysis, with a single recurrence of paralysis
(n 5 5) after a 160-day average delay and multiple
recurrences (n 5 3) after a 150-day average delay. The
rTMS was applied again in six of the eight patients with
recurrence and was effective for all patients.
DISCUSSION
Description of a Population with Psychogenic
Paralysis
Although many studies have described adults with
psychogenic paralysis,2–4,6,11,12 data are most limited
in children.13 As previously reported,2,6,11,13 the major-
ity of patients were women. Paraparesis appeared twice
as less in the literature probably because of the adult
population.3,11 Only two patients (two adults) experi-
enced a hemiparesis, whereas this symptom occurred
between 32% and 47% in the previously described
adult population,3,4,11 probably because of our predom-
inant pediatric population. As previously described, tet-
raparesis was a rare symptom.4,11
At least one precipitating event was observed in 42
patients, mainly a psychosocial precipitating event
(work or familial conflict)11 or a physical injury,14
although of a trivial nature that could be sufficient to
produce psychogenic symptoms.13
As previously described,11 medical history revealed
the importance of psychiatric comorbidity and organic
disease (physical injury in the paralyzed limb and pre-
vious back problems) as risk factors for psychogenic
paralysis.
Efficiency of Repetitive TMS on Psychogenic
Paralysis
Limited evidence exists regarding the optimal choice
of treatment in psychogenic disorders. In some patients
with mild symptoms, explanation and reassurance with
encouragement may be sufficient. In patients with
more resistant symptoms, a combination of psychother-
apy and physiotherapy may be helpful. Cognitive-be-
havioral therapy,15 antidepressants,16 hypnosis,17,18 and
acupuncture19 can also be effective. Despite all these
treatments, outcome is not satisfactory in all patients;
37% to 83% of patients continue to experience symp-
toms 2 to 16 years after diagnosis.2,3,6,12
In our study, rTMS applied over the motor cortex is
associated with a very good outcome in 89%. As previ-
ously described,2,3,13 the factor significantly associated
with a favorable outcome was acute onset of symptoms,
but not the age13 or the sex.12 In contrast to previous
studies, we did not find a significant good outcome for
patients with a comorbid psychiatric disorder.3 Despite
an improvement in paralysis, a psychologic follow-up is
sometimes required in certain patients.
Three studies have reported a therapeutic benefit
from diagnostic20 and rTMS21,22 in patients with psy-
chogenic paralysis. Four patients were treated with 15-
FIG. 2. Symptoms duration of patients with a psychogenic paralysisat the time of consultation. The number of patients in different symp-tom duration groups (d).
Movement Disorders, Vol. 25, No. 10, 2010
1503PSYCHOGENIC PARALYSIS AND RTMS

Hz rTMS sessions of motor cortex for 5 to 12 weeks,22
with variable benefits (one total recovery, two marked
improvement, and one failure). We have previously
reported a spectacular recovery immediately after only
one session of low frequency rTMS (50 stimuli) over
the motor cortex in a psychogenic aphonia.21
Why has rTMS proved so effective? First, the possi-
bility of a placebo effect cannot be ruled out because
of symptom variability in psychogenic paralysis and
the possible symptoms attenuation or disappearance
with suggestion and persuasion. Nevertheless, 89% of
rTMS efficacy is impressive and seemed be specific to
rTMS, without the same efficacy for other therapies
usually used.2,3,6,12 Second, rTMS delivered over the
motor cortex produces a muscular activation, allowing
the patient to become aware of the movement possibil-
ity that could help in their management. Third, we sug-
gest that rTMS may have the ability to restore an
appropriate cerebral connectivity by activating a sup-
pressed motor cortex. Functional magnetic resonance
imaging studies have demonstrated a decreased activa-
tion of primary motor7 and an increased activation of
prefrontal regions,23 suggesting an active inhibition
from prefrontal areas to primary motor areas.23–25
CONCLUSION
Our results suggest that motor cortex rTMS could be
an effective treatment in patients with psychogenic pa-
ralysis, although further randomized controlled trial
versus placebo is necessary. Nevertheless, the physio-
pathologic and rTMS efficacy mechanisms of psycho-
genic disorders remain unknown.
Acknowledgments: We thank Richard Medeiros, RouenUniversity Hospital Medical Editor, for editing the manuscript.
Financial Disclosures: Nathalie Chastan and DominiqueParain: stock ownership in medically related fields.
Author Roles: Nathalie Chastan: research project (concep-tion, organization, and execution); statistical analysis (design,execution, review, and critique); manuscript (writing of the firstdraft, review, and critique). Dominique Parain: research project(conception, organization, and execution); statistical analysis(review and critique); manuscript (review and critique).
REFERENCES
1. Lempert T, Dieterich M, Huppert D, Brandt T. Psychogenic dis-orders in neurology: frequency and clinical spectrum. Acta Neu-rol Scand 1990;82:335–340.
2. Couprie W, Wijdicks EF, Rooijmans HG, van Gijn J. Outcomein conversion disorder: a follow up study. J Neurol NeurosurgPsychiatry 1995;58:750–752.
3. Crimlisk HL, Bhatia K, Cope H, David A, Marsden CD, Ron MA.Slater revisited: 6 year follow up study of patients with medicallyunexplained motor symptoms. BMJ 1998;316:582–586.
4. Heruti RJ, Reznik J, Adunski A, Levy A, Weingarden H, Ohry A.Conversion motor paralysis disorder: analysis of 34 consecutivereferrals. Spinal Cord 2002;40:335–340.
5. Letonoff EJ, Williams TR, Sidhu KS. Hysterical paralysis: a reportof three cases and a review of the literature. Spine 2002; 27:E441–E445.
6. Stone J, Sharpe M, Rothwell PM, Warlow CP. The 12 year progno-sis of unilateral functional weakness and sensory disturbance. JNeurol Neurosurg Psychiatry 2003;74:591–596.
7. Burgmer M, Konrad C, Jansen A, et al. Abnormal brain activationduring movement observation in patients with conversion paralysis.Neuroimage 2006;29:1336–1343.
8. Cantello R, Boccagni C, Comi C, Civardi C, Monaco F. Diagnosisof psychogenic paralysis: the role of motor evoked potentials. JNeurol 2001;248:889–897.
9. Foong J, Ridding M, Cope H, Marsden CD, Ron MA. Corticospinalfunction in conversion disorder. J Neuropsychiatry Clin Neurosci1997;9:302–303.
10. Pillai JJ, Markind S, Streletz LJ, Field HL, Herbison G. Motorevoked potentials in psychogenic paralysis. Neurology 1992;42:935–936.
11. Binzer M, Andersen PM, Kullgren G. Clinical characteristics ofpatients with motor disability due to conversion disorder: a prospectivecontrol group study. J Neurol Neurosurg Psychiatry 1997;63:83–88.
12. Binzer M, Kullgren G. Motor conversion disorder. A prospective2- to 5-year follow-up study. Psychosomatics 1998;39:519–527.
13. Schwingenschuh P, Pont-Sunyer C, Surtees R, Edwards MJ, BhatiaKP. Psychogenic movement disorders in children: a report of 15cases and a review of the literature. Mov Disord 2008; 23:1882–1888.
14. Stone J, Carson A, Aditya H, et al. The role of physical injury inmotor and sensory conversion symptoms: a systematic and narra-tive review. J Psychosom Res 2009;66:383–390.
15. Kroenke K, Swindle R. Cognitive-behavioral therapy for somatiza-tion and symptom syndromes: a critical review of controlled clini-cal trials. Psychother Psychosom 2000;69:205–215.
16. O’Malley PG, Jackson JL, Santoro J, Tomkins G, Balden E,Kroenke K. Antidepressant therapy for unexplained symptoms andsymptom syndromes. J Fam Pract 1999;48:980–990.
17. Moene FC, Spinhoven P, Hoogduin KA, van Dyck R. A rando-mised controlled clinical trial on the additional effect of hypnosisin a comprehensive treatment programme for in-patients with con-version disorder of the motor type. Psychother Psychosom2002;71:66–76.
18. Moene FC, Spinhoven P, Hoogduin KA, van Dyck R. A random-ized controlled clinical trial of a hypnosis-based treatment forpatients with conversion disorder, motor type. Int J Clin Exp Hypn2003;51:29–50.
19. Zhang ZY, Yuan YM, Yan BW, Tian YQ, Wang W, Fan LM. Anobservation of 1316 cases of hysterical paralysis treated by acu-puncture. J Tradit Chin Med 1987;7:113–115.
20. Jellinek DA, Bradford R, Bailey I, Symon L. The role of motorevoked potentials in the management of hysterical paraplegia: casereport. Paraplegia 1992;30:300–302.
21. Chastan N, Parain D, Verin E, Weber J, Faure MA, Marie JP. Psycho-genic aphonia: spectacular recovery after motor cortex transcranialmagnetic stimulation. J Neurol Neurosurg Psychiatry 2009;80:94.
22. Schonfeldt-Lecuona C, Connemann BJ, Viviani R, Spitzer M, Her-wig U. Transcranial magnetic stimulation in motor conversion dis-order: a short case series. J Clin Neurophysiol 2006; 23:472–475.
23. Marshall JC, Halligan PW, Fink GR, Wade DT, Frackowiak RS.The functional anatomy of a hysterical paralysis. Cognition1997;64:B1–B8.
24. Geraldes R, Coelho M, Rosa MM, Severino L, Castro J, de Car-valho M. Abnormal transcranial magnetic stimulation in a patientwith presumed psychogenic paralysis. J Neurol Neurosurg Psychia-try 2008;79:1412–1413.
25. Hurwitz TA, Prichard JW. Conversion disorder and fMRI. Neurol-ogy 2006;67:1914–1915.
1504 N. CHASTAN AND D. PARAIN
Movement Disorders, Vol. 25, No. 10, 2010




















