
The immunological monitoring of alloreactive responses in liver transplant recipients: A review
Upload
independentCategory
view
1download
0
© 2014 Informa UK, Ltd. This provisional PDF corresponds to the article as it appeared upon acceptance. Fully formatted PDF and full text (HTML) versions will be made available soon.
DISCLAIMER: The ideas and opinions expressed in the journal’s Just Accepted articles do not necessarily reflect those of Informa Healthcare (the Publisher), the Editors or the journal. The Publisher does not assume any responsibility for any injury and/or damage to persons or property arising from or related to any use of the material contained in these articles. The reader is advised to check the appropriate medical literature and the product information currently provided by the manufacturer of each drug to be administered to verify the dosages, the method and duration of administration, and contraindications. It is the responsibility of the treating physician or other health care professional, relying on his or her independent experience and knowledge of the patient, to determine drug dosages and the best treatment for the patient. Just Accepted articles have undergone full scientific review but none of the additional editorial preparation, such as copyediting, typesetting, and proofreading, as have articles published in the traditional manner. There may, therefore, be errors in Just Accepted articles that will be corrected in the final print and final online version of the article. Any use of the Just Accepted articles is subject to the express understanding that the papers have not yet gone through the full quality control process prior to publication.
Just Accepted by Leukemia & Lymphoma
Allogeneic hematopoietic stem cell transplantation for hematological malignancies from mismatched 9/10 HLA unrelated donors: Comparison with transplantations from 10/10 unrelated donors and HLA identical siblingsMauricette Michallet, Mohamad Sobh, Caroline Serrier, Stéphane Morisset, Hélène Labussière, Sophie Ducastelle, Fiorenza Barraco, Lila Gilis, Xavier Thomas, Franck E Nicolini
Doi: 10.3109/10428194.2014.944518
ABSTRACT
We retrospectively studied the outcome of 213 consecutive patients who received allo-HSCT for hematological malignancies, 121 (57%) from HLA identical siblings, 63 (29%) from 10/10 HLA identical unrelated donors and 29 (14%) from 9/10 HLA mismatched unrelated donors between 2006 and 2011 in our institution. Engraftment was significantly lower in the 9/10 HLA group (90%) than in the 10/10 HLA group (95%) than in the siblings group (99%), (p=0.03). The median OS was 10 months (5-21), 18 months (11-NR) and 60 months (31-NR) respectively with a 2-years probability of 19% (8-44), 43% (31-59) and 63% (54-74) respectively. TRM was significantly higher in the 9/10 HLA group with 1 year cumulative incidence of 45% (35-55), compared to 33% (27-39) in the unrelated 10/10 HLA group and 12% (9-15) in the siblings group (p<0.001). Disease status at transplantation less than first CR/chronic phase was associated with worse OS [HR=3 (1.4-6), p=0.003].
Leu
k L
ymph
oma
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
INSE
RM
on
07/2
9/14
For
pers
onal
use
onl
y.

JUST
ACC
EPTE
D
1
Allogeneic hematopoietic stem cell transplantation for
hematological malignancies from mismatched 9/10 HLA
unrelated donors: Comparison with transplantations from 10/10
unrelated donors and HLA identical siblings
Mauricette Michallet, Mohamad Sobh, Caroline Serrier, Stéphane Morisset, Hélène
Labussière, Sophie Ducastelle, Fiorenza Barraco, Lila Gilis, Xavier Thomas, Franck E
Nicolini
Blood and Marrow Transplant Unit, Department of Hematology, Centre Hospitalier Lyon
Sud, Pierre Benite, France.
Correspondence: Mauricette Michallet, MD, PhD, Blood and Marrow Transplant Unit, Department of Hematology, Centre Hospitalier Lyon Sud, University of Lyon, Lyon, France, Pavillon Marcel Berard bâtiment 1G, 165 Chemin du Grand Revoyet, 69495 Pierre Bénite CEDEX France. Tel: +33 4 78 86 22 33. Fax: +33 4 72 66 64 40. E-mail: [email protected]
Short title: Allo-HSCT from 9/10 HLA unrelated donors
ABSTRACT
We retrospectively studied the outcome of 213 consecutive patients who received allo-HSCT for hematological malignancies, 121 (57%) from HLA identical siblings, 63 (29%) from 10/10 HLA identical unrelated donors and 29 (14%) from 9/10 HLA mismatched unrelated donors between 2006 and 2011 in our institution. Engraftment was significantly lower in the 9/10 HLA group (90%) than in the 10/10 HLA group (95%) than in the siblings group (99%), (p=0.03). The median OS was 10 months (5-21), 18 months (11-NR) and 60 months (31-NR) respectively with a 2-years probability of 19% (8-44), 43% (31-59) and 63% (54-74) respectively. TRM was significantly higher in the 9/10 HLA group with 1 year cumulative incidence of 45% (35-55), compared to 33% (27-39) in the unrelated 10/10 HLA group and 12% (9-15) in the siblings group (p<0.001). Disease status at transplantation less than first CR/chronic phase was associated with worse OS [HR=3 (1.4-6), p=0.003].
Key words: unrelated donors, 9/10 HLA, 10/10 HLA, identical siblings
Leu
k L
ymph
oma
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
INSE
RM
on
07/2
9/14
For
pers
onal
use
onl
y.

JUST
ACC
EPTE
D
2
INTRODUCTION
Allogeneic hematopoietic stem cell transplantation (allo-HSCT)
represents the only potential treatment strategy to cure wide types of
hematological malignancies aiming to eradicate the malignant clone
using the immunological conflict inherent to donor hematopoietic stem
cells installation in the recipient. The potential benefits of allogeneic
hematopoietic cell transplantation accrue from the ability to use
myeloablative chemoradiotherapy and the immune-mediated reaction
of donor lymphocytes directly against residual disease cells in the
recipient (i.e. the graft versus leukemia reaction). Myeloablative
conditioning regimens are limited to younger patients and to those in
good medical condition [1]. Reduced intensity conditioning (RIC)
regimens were developed with the aim to decrease transplantation-
related-mortality (TRM) in elderly patients, in heavily pretreated
patients or in those with medical comorbidities precluding the use of
standard conditioning regimens [2-4]. However, one risk of RIC
regimens is graft failure because of the low intensity of the
conditioning and the higher risk of disease relapse. The different
possible cell sources, either bone marrow, peripheral blood or cord
blood and the better knowledge of HLA typing has led to the
development of new transplantation techniques and modalities which
have improved patient survival and transplantation outcomes. Best
outcomes were obtained when the donor was an HLA-identical sibling
[5-7]. A patient has 30% of chance to find a HLA-identical sibling
donor while the rest of patients should find an alternative unrelated
donor through the Bone Marrow Donor Worldwide (BMDW registry)
Leu
k L
ymph
oma
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
INSE
RM
on
07/2
9/14
For
pers
onal
use
onl
y.

JUST
ACC
EPTE
D
3
[8]. The use of 10/10 HLA matched unrelated transplants has been
used as a main alternative and with its unavailability, when available,
a 9/10 HLA mismatched unrelated transplant has been used. The
outcome of this last mismatched transplant is not very clear and its
use according to patient and disease conditions has not been well
defined yet. Previous studies have shown that matching for all alleles
of the HLA-A, -B, -C, and -DRB1 loci was associated with the highest
survival rates in transplantation with unrelated donors (URD) [9-12].
Recently, the National Marrow Donor Program (NMDP) and the
Center for International Blood and Marrow Transplant Research
(CIBMTR) published guidelines defining the minimal requirements for
appropriate HLA typing resolution and matching criteria for URD, they
recommended whenever possible, donors who are high-resolution
matched at HLA-A, -B, -C, and -DRB1, and when such a donor is not
available, a single-locus mismatched donor (HLA-A, -B, -C, or -DRB1)
can be used with acceptable risks of transplant related mortality
(TRM) [13,14]. We aimed in this study to evaluate the outcome of allo-
HSCT in patients with hematological malignancies with either 9/10
HLA mismatched unrelated donors, 10/10 HLA identical unrelated
donors or HLA identical siblings; and to define which category of
patients can benefit the most of each strategy.
MATERIAL AND METHODS
We have retrospectively studied the outcome of 213 consecutive
patients who received allo-HSCT for different hematological
malignancies, 121 (57%) from HLA identical siblings, 63 (29%) from
10/10 HLA identical unrelated donors and 29 (14%) from 9/10 HLA
Leu
k L
ymph
oma
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
INSE
RM
on
07/2
9/14
For
pers
onal
use
onl
y.
JUST
ACC
EPTE
D
4
mismatched unrelated donors between 2006 and 2011 at our bone
marrow transplantation center. There were 124 (58%) males and 89
(42%) females with a median age of 44 years (range: 18-66), 52%
had myeloid malignancy, and 48% had lymphoid malignancy. At time
of transplantation, 34% of patients were in first complete remission
(CR1) or first chronic phase (CP1), 19% were in CR2 or CP2 and 47%
were in less than CR. The median time between diagnosis and allo-
HSCT was 13.5 months (range: 2-219). As conditioning regimen, 53%
received a myelo-ablative conditioning and 47% a reduced intensity
one, while the HSC source was bone marrow in 55% of cases and
peripheral blood stem cells in 45% of cases. For sex-matching, in
22% of patients, it was a female donor to a male recipient and in 23%
of patients it was a male donor to a female recipient. Major ABO
incompatibility was present in 23% of cases and minor incompatibility
in 16%. All HLA typings were performed at high resolution levels,
thus, in the 9/10 HLA mismatched group, 12 of 29 patients (41, 4%)
had the mismatch at HLA-A locus, 7 patients (24,1%) at the HLA-B, 7
(24,1%) at the HLA-C and 3 (10,4%) at the HLA-DQ. The different
characteristics according to the 3 HLA groups are detailed in Table 1.
ENDPOINTS
Neutrophil recovery was defined by an absolute neutrophil count of at
least 500 cells/mm3 for three consecutive days. GVHD was reported
and graded according to published criteria [15]. Chronic GVHD was
diagnosed according to standard criteria on patients who survived at
least 90 days after transplantation [16]. Transplantation-related
mortality (TRM) was defined as death from any cause other than
Leu
k L
ymph
oma
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
INSE
RM
on
07/2
9/14
For
pers
onal
use
onl
y.

JUST
ACC
EPTE
D
5
relapse occurring after transplantation. Relapse was defined on basis
of morphologic evidence of hematopoietic disease in bone marrow or
other sites. Overall survival (OS) was defined as the time from
transplantation to any cause of death and progression-free survival
(PFS) was defined as survival from transplantation to disease
progression or death.
STATISTICAL ANALYSIS
Categorical variables related to patients, disease and transplantation
procedure were analyzed using chi-square statistic and continuous
variables with Mann-Whitney test. Cumulative incidence curves in
competing-risks settings were used to estimate incidence over time for
neutrophil recovery, acute and chronic GVHD, TRM and relapse. Fine
and Gray models [17] were used to estimate pre-transplant variables
and the competing risks regression for the multivariate analysis. OS
and PFS were estimated by the Kaplan-Meier method with log-rank
test for univariate analysis [18]. Cox proportional-hazards regression
models were used to assess the influence of pre-transplant variables
on OS and PFS [19]. The multivariate analysis on OS, PFS and TRM
was made after stratification on diagnosis studying the following
variables: pre-transplant disease status, age of the recipient, sex
matching, HLA group, ABO matching, CMV matching, HSC source
(bone marrow or peripheral blood) and conditioning regimen.
Statistical analysis was performed with R statistical software (version
2.9.2).
Leu
k L
ymph
oma
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
INSE
RM
on
07/2
9/14
For
pers
onal
use
onl
y.

JUST
ACC
EPTE
D
6
RESULTS Engraftment and chimerism results
After HSCT, the cumulative incidence of engraftment was significantly
lower in the 9/10 HLA group (90%) than in the 10/10 HLA group (95%)
than in the sibling group (99%), (p=0.03). The cumulative incidence of
complete donor chimerism among evaluable patients, defined as
having at least 95% of donor cells, was at 3 months after allo-HSCT,
90% in the 9/10 HLA group, 91% in the 10/10 HLA group and 93% in
the siblings group.
Graft versus host disease
The cumulative incidence of acute GVHD≥2 at 3 months was 32%
(23-41), 20% (15-26) and 27% (23-32) for HLA 9/10 group, unrelated
HLA 10/10 and siblings groups respectively [(p=not significant (NS)]
(Figure 1). The cumulative incidence of limited GVHD at one year was
14% (11-18), 11% (7-15) and 4% (0-8), and for the extensive GVHD,
it was 21% (13-30), 9% (5-13) and 17% (14-21) for the 3 groups
respectively (global, p= NS).
Overall survival, relapse incidence and transplant related
mortality
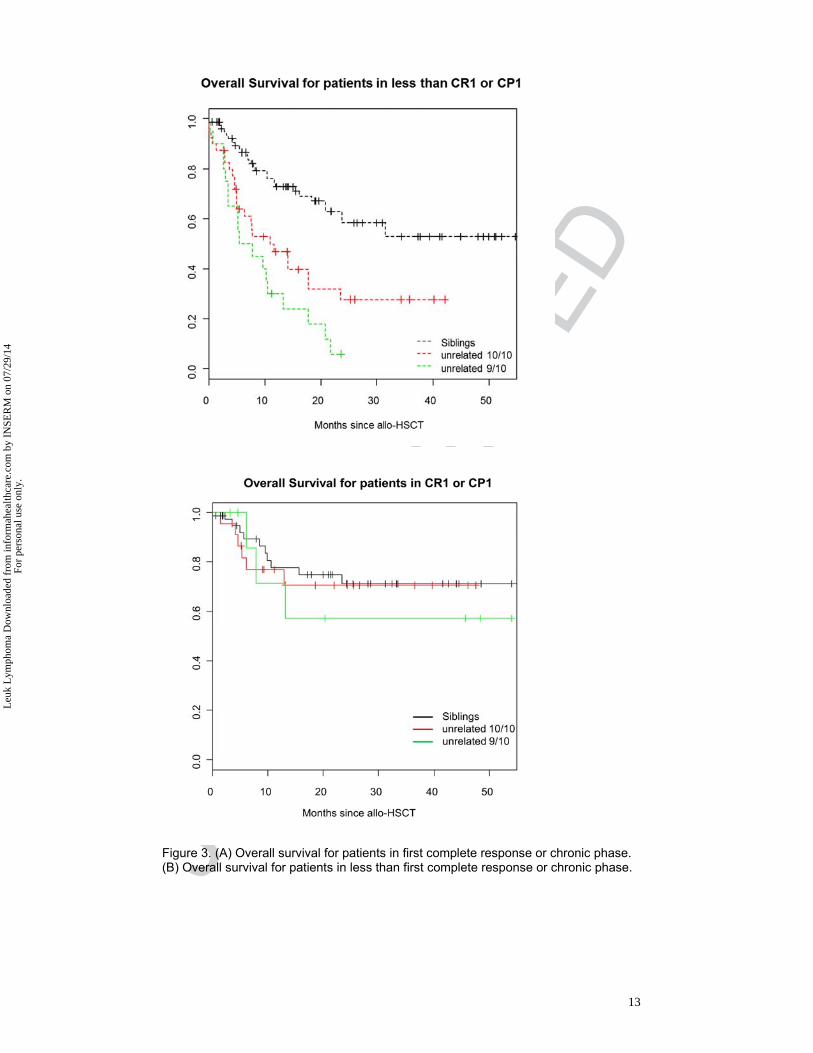
After a median follow-up of 8 months (0-54) in the 9/10 HLA group, 10
months (0-60) in the 10/10 HLA group and 18 months in the siblings
group, the median overall survival (OS) was 10 months (5-21), 18
months (11-NR) and 60 months (31-NR) respectively with a 2-years
probability of 19% (8-44), 43% (31-59) and 63% (54-74) respectively
(Figure 2). Interestingly, when we stratified the patients on disease
status pre-transplantation, all patients from unrelated groups
Leu
k L
ymph
oma
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
INSE
RM
on
07/2
9/14
For
pers
onal
use
onl
y.

JUST
ACC
EPTE
D
7
(matched or mismatched) in CR1/CP1 showed similar results to HLA
identical siblings group in terms of OS (Figure 3A, B). There was a
higher but not significant relapse incidence at one year in the 9/10
HLA group (26%, 95% CI: 17-35) compared to the unrelated 10/10
HLA group (15%, 95% CI: 9-20) and identical siblings group (17%,
95%CI: 14-20) (Figure 4). The transplant related mortality (TRM) was
significantly higher in the 9/10 HLA group with a cumulative incidence
at 1 year of 45% (35-55), compared to 33% (27-39) in the unrelated
10/10 HLA group and 12% (9-15) in the identical siblings group
(p<0.001) (Figure 5). No statistical difference was observed according
to infection related death between the different groups.
Multivariate analysis
In multivariate analysis, OS was negatively affected by unrelated
donors [9/10 HLA mismatched unrelated group: HR=5 (95% CI: 2.7-
10), p=0.0001; 10/10 HLA matched unrelated group: HR=2 (95% CI:
1.2-4), p=0.01], female donors to male patients [HR=2 (95% CI: 1.4-
4), p=0.03] and disease status <CR1 or <chronic phase (CP)1 [HR=3
(95% CI: 1.4-6), p=0.003]; while the TRM was negatively affected by
unrelated donors [9/10 HLA mismatched unrelated group: HR=9 (95%
CI: 4-20), p<0.001; 10/10 HLA matched unrelated group: HR=4 (95%
CI: 1.2-10), p=0.03], female donors to male patients [HR=3 (95% CI:
1.2-7), p=0.01] and ABO minor incompatibility [HR=2.5 (95% CI: 1.2-
5), p=0.01]. The funnel plot showing the adjusted TRM according to all
covariates and comparing to the global population death rate, shows
that the 9/10 HLA group has the worse TRM independently of any
other factor.
Leu
k L
ymph
oma
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
INSE
RM
on
07/2
9/14
For
pers
onal
use
onl
y.

JUST
ACC
EPTE
D
8
DISCUSSION
We showed that allo-HSCT from 9/10 HLA mismatched unrelated
donors have a significantly worse OS than those from 10/10 HLA
matched unrelated donors and from HLA identical siblings, this was
mainly due to an increased TRM. Patients in this group also showed a
significantly lower engraftment rate compared to other groups while
acute and chronic GVHD incidences were not statistically different.
Kröger et al. showed similar results in terms of GVHD incidence, OS,
TRM, and relapse between patients receiving allo-HSCT from fully
matched unrelated donors, having one mismatch (9/10) or more (6-
8/10). This study showed the interest of pre-transplant anti-
thymoglobulin use in the HSCT settings [20], where only unrelated
10/10 and 9/10 have received ATG during the conditioning regimen.
Recently, Saber et al. found that 8/8 matched HSCT recipients had a
similar survival rate compared with HLA identical siblings recipients
while 7/8 matched HSCT recipients had higher early mortality than
matched siblings HCT; this study included only patients with acute
myeloid leukemia [21]. With the emergence of cord blood use as HSC
source, recent studies have compared their outcomes to outcomes
from HLA mismatched donors with the unavailability of matched
related or unrelated donors; results seem similar but still uncertainties
about the type of mismatched locus, the retrospective nature of these
studies and the heterogeneous patients and the different HSCT
settings limits their validation [22,23]. When stratified on disease
status pre-transplantation, patients in our study in first CR or CP and
receiving transplants from 9/10 HLA mismatched donors showed
Leu
k L
ymph
oma
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
INSE
RM
on
07/2
9/14
For
pers
onal
use
onl
y.

JUST
ACC
EPTE
D
9
comparable outcomes to other groups suggesting the more weight the
disease status has, when compared to HLA matching. It is important
to note that the effect of a single-allele mismatch may vary with the
underlying diagnosis. In a study on 948 donor-recipient pairs at the
Fred Hutchinson Cancer Research Center, it was found that a single-
allele mismatch conferred a higher risk of death, but only for low risk
patients, defined as those with chronic myeloid leukemia (CML) within
2 years of diagnosis [24]. In contrast, a single allele mismatch had no
effect on survival among higher risk patients, such as those with more
advanced CML, acute leukemia, or myelodysplastic syndromes.
Similar outcomes are reported in a recent report from an Italian group
[25]. When only a single HLA mismatch was present, the mortality risk
was higher than among 10/10 matched unrelated pairs in patients
transplanted with acute leukemia in the first CR, but not in patients
with advanced diseases. These results suggest that the potential
benefit of HLA matching was offset by the negative impact of
advanced disease. Concerning the type of mismatch, the results from
different studies are very discordant; ones confirmed that mismatches
at HLA-B or -C level were better tolerated than those at HLA-A or -
DRB1 level, whereas others suggested worse survival for HLA-C but
not HLA-A mismatches [11,26]. On the other hand, the effect of
isolated mismatches in the low expression loci HLA-DRB3, -DRB4, -
DRB5, -DQ, and -DP in transplant outcome has been difficult to prove
and their effect may be demonstrable only in combination with
mismatches in other loci [9,10]. Although, in our study, the
mismatched group contained only 29 patients distributed among the
Leu
k L
ymph
oma
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
INSE
RM
on
07/2
9/14
For
pers
onal
use
onl
y.

JUST
ACC
EPTE
D
10
different loci which makes difficult to do a sub-analysis and does not
allow us to draw any conclusions on this point.
Finally, the debate on the donor choice with the absence of HLA
matched donor is still ongoing. We showed that patients with 9/10
HLA matched donors experience higher TRM rates, not for CR
patients. Results from other studies show controversial results
concerning the involvement of the type of HLA locus and especially
with heterogeneous patients, disease and transplantation
characteristics. Cord blood source has been used in this settings with
satisfying outcomes, we stress out the need of prospective
randomized studies evaluating the different unrelated sources with
more homogeneous populations and transplantation settings.
Potential conflict of interest: None
REFERENCES
1. Sorror ML, Giralt S, Sandmaier BM, et al. . Hematopoietic cell transplantation specific comorbidity index as an outcome predictor for patients with acute myeloid leukemia in first remission: combined FHCRC and MDACC experiences. Blood 2007;110:4606-4613.
2. Storb R. Can reduced-intensity allogeneic transplantation cure older adults with AML? Best Pract Res Clin Haematol 2007;20:85-90.
3. Champlin R, Khouri I, Komblau S, Molidrem J, Giralt S. Reinventing bone marrow transplantation. Nonmyeloablative preparative regimens and induction of graft-vs-malignancy effect. Oncology (Williston Park) 1999;13:621-628; discussion 631, 635-628, 641.
4. Aoudjhane M, Labopin M, Gorin NC, et al. . Comparative outcome of reduced intensity and myeloablative conditioning regimen in HLA identical sibling allogeneic haematopoietic stem cell transplantation for patients older than 50 years of age with acute myeloblastic leukaemia: a retrospective survey from the Acute Leukemia Working Party (ALWP) of the European group for Blood and Marrow Transplantation (EBMT). Leukemia 2005;19:2304-2312.
5. Beatty PG, Clift RA, Mickelson EM, et al. . Marrow transplantation from related donors other than HLA-identical siblings. N Engl J Med 1985;313:765-771.
6. Saber W, Opie S, Rizzo JD, Zhang MJ, Horowitz MM, Schriber J. Outcomes after matched unrelated donor versus identical sibling hematopoietic cell transplantation in adults with acute myelogenous leukemia. Blood 2013;119:3908-3916.
7. Arora M, Weisdorf DJ, Spellman SR, et al. . HLA-identical sibling compared with 8/8 matched and mismatched unrelated donor bone marrow transplant for chronic phase chronic myeloid leukemia. J Clin Oncol 2009;27:1644-1652.
8. Tiercy JM, Nicoloso G, Passweg J, et al. . The probability of identifying a 10/10 HLA allele-matched unrelated donor is highly predictable. Bone Marrow Transplant 2007;40:515-522.
Leu
k L
ymph
oma
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
INSE
RM
on
07/2
9/14
For
pers
onal
use
onl
y.

JUST
ACC
EPTE
D
11
9. Flomenberg N, Baxter-Lowe LA, Confer D, et al. . Impact of HLA class I and class II high-resolution matching on outcomes of unrelated donor bone marrow transplantation: HLA-C mismatching is associated with a strong adverse effect on transplantation outcome. Blood 2004;104:1923-1930.
10. Lee SJ, Klein J, Haagenson M, et al. . High-resolution donor-recipient HLA matching contributes to the success of unrelated donor marrow transplantation. Blood 2007;110:4576-4583.
11. Woolfrey A, Klein JP, Haagenson M, et al. . HLA-C antigen mismatch is associated with worse outcome in unrelated donor peripheral blood stem cell transplantation. Biol Blood Marrow Transplant 2011;17:885-892.
12. Horan J, Wang T, Haagenson M, et al. . Evaluation of HLA matching in unrelated hematopoietic stem cell transplantation for nonmalignant disorders. Blood 2012;120:2918-2924.
13. Spellman SR, Eapen M, Logan BR, et al. . A perspective on the selection of unrelated donors and cord blood units for transplantation. Blood 2012;120:259-265.
14. Bray RA, Hurley CK, Kamani NR, et al. . National marrow donor program HLA matching guidelines for unrelated adult donor hematopoietic cell transplants. Biol Blood Marrow Transplant 2008;14:45-53.
15. Glucksberg H, Storb R, Fefer A, et al. . Clinical manifestations of graft-versus-host disease in human recipients of marrow from HL-A-matched sibling donors. Transplantation 1974;18:295-304.
16. Shulman HM, Sullivan KM, Weiden PL, et al. . Chronic graft-versus-host syndrome in man. A long-term clinicopathologic study of 20 Seattle patients. Am J Med 1980;69:204-217.
17. Fine J, Gray R. A Proportional Hazards Model for the Subdistribution of a Competing Risk. Journal of the American Statistical Association 1999;94:496-509.
18. Kaplan E, Meier P. Non parametric estimationfrominomplete observations. J Am Stat Assoc 1958;53:457.
19. Cox D. Regression models and life tables. J Royal Stat Soc B 1972;34:187-220. 20. Kroger N, Zabelina T, Binder T, et al. . HLA-mismatched unrelated donors as an
alternative graft source for allogeneic stem cell transplantation after antithymocyte globulin-containing conditioning regimen. Biol Blood Marrow Transplant 2009;15:454-462.
21. Saber W, Opie S, Rizzo JD, Zhang MJ, Horowitz MM, Schriber J. Outcomes after matched unrelated donor versus identical sibling hematopoietic cell transplantation in adults with acute myelogenous leukemia. Blood 2012;119:3908-3916.
22. Kanda J, Ichinohe T, Kato S, et al. . Unrelated cord blood transplantation vs related transplantation with HLA 1-antigen mismatch in the graft-versus-host direction. Leukemia 2012;27:286-294.
23. Malard F, Furst S, Loirat M, et al. . Effect of graft source on mismatched unrelated donor hemopoietic stem cell transplantation after reduced intensity conditioning. Leukemia 2013.
24. Petersdorf EW, Anasetti C, Martin PJ, et al. . Limits of HLA mismatching in unrelated hematopoietic cell transplantation. Blood 2004;104:2976-2980.
25. Crocchiolo R, Ciceri F, Fleischhauer K, et al. . HLA matching affects clinical outcome of adult patients undergoing haematopoietic SCT from unrelated donors: a study from the Gruppo Italiano Trapianto di Midollo Osseo and Italian Bone Marrow Donor Registry. Bone Marrow Transplant 2009;44:571-577.
26. Petersdorf EW, Gooley T, Malkki M, Horowitz M. Clinical significance of donor-recipient HLA matching on survival after myeloablative hematopoietic cell transplantation from unrelated donors. Tissue Antigens 2007;69 Suppl 1:25-30.
Leu
k L
ymph
oma
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
INSE
RM
on
07/2
9/14
For
pers
onal
use
onl
y.

JUST
ACC
EPTE
D
12
Figures Legends:
Figure 1. Cumulative incidence of acute GVHD grade ≥ II according to different HLA groups.
Figure 2. Overall survival according to different HLA groups.
Leu
k L
ymph
oma
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
INSE
RM
on
07/2
9/14
For
pers
onal
use
onl
y.
JUST
ACC
EPTE
D
13
Figure 3. (A) Overall survival for patients in first complete response or chronic phase. (B) Overall survival for patients in less than first complete response or chronic phase.
Leu
k L
ymph
oma
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
INSE
RM
on
07/2
9/14
For
pers
onal
use
onl
y.

JUST
ACC
EPTE
D
14
Figure 4. Cumulative incidence of relapse according to different HLA groups.
Figure 5. Cumulative incidence of transplant related mortality according to different HLA groups.
Leu
k L
ymph
oma
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
INSE
RM
on
07/2
9/14
For
pers
onal
use
onl
y.

JUST
ACC
EPTE
D
15
Table 1. patients characteristics
HLA identical siblings group
N=121 10/10 HLA unrelated
group N=63 9/10 HLA unrelated
group N=29 p-valuePATIENTS DESCRIPTION
Gender Male 69 (62%) 37 (59%) 18 (62%) NS Female 52 (38%) 26 (41%) 11 (38% NS Age Median, years 45 (18-66) 44 (20-64) 38 (19-61) NS Disease Myeloid leukemia 71 (59%) 23 (37%) 16 (55%) NS
AML / MDS 54 / 7 15 / 0 13 / 2 CML / MPS 3 / 7 2 / 6 1 / 0
Lymphoid leukemia 50 (41%) 40 (63%) 13 (45%) NS ALL / MM 18 / 13 20 / 15 7 / 2
Lymphoma / CLL 14 / 5 5 / 0 4 / 0 Disease status NS
CR1/CP1 40 (33%) 23 (37%) 9 (31%) CR2/CP2 26 (21%) 7 (11%) 7 (24%)
<CR2/CP2 55 (45%) 33 (52%) 13 (45%) Conditioning NS
Full-intensity 64 (53%) 32 (51%) 16 (55%) Reduced-intensity 57 (47%) 31 (49%) 13 (45%)
Cell source PBSC 55 (45%) 28 (44%) 13 (45%)
BM 66 (55%) 35 (56%) 16 (55%) Sex-mismatching 0,03
Fd-Mr 30 (25%) 9 (14%) 8 (28%) Md-Fr 22 (18%) 19 (30%) 9 (31%)
CMV-mismatching 0,07D- R+ 25 (21%) 13 (21%) 8 (28%) D+ R- 16 (13%) 14 (22%) 6 (21%)
ABO-mactching major 22 (18%) 21 (33%) 6 (21%) <0,0001minor 7 (9%) 20 (32%) 8 (28%)
Interval diag-HSCT 16 months (2-219) 14 months (4-136) 9 months (4-87) NS Median FU 18 months (0-60) 10 months (0-48) 8 months (0-54)
Leu
k L
ymph
oma
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
INSE
RM
on
07/2
9/14
For
pers
onal
use
onl
y.
Copyright © 2022 FDOKUMEN




















