
Induction immunotherapy in pediatric heart transplant recipients: a multicenter study
Interventions to improve medication adherence in adult kidneytransplant recipients: a systematic review
Jac Kee Low1, Allison Williams1, Elizabeth Manias2, Kimberley Crawford1
1 Faculty of Medicine, Nursing and Health Sciences, Monash University, Victoria, Australia2 Faculty of Medicine, Dentistry and Health Sciences, The University ofMelbourne, Victoria, Australia
AbstractBackground. Research has documented the negative consequences ofmedication non-adherence amongst kidney transplant recipients,and yet little is known about an effective strategy that iswidely implemented against non-adherence. This systematic reviewaimed to examine the effectiveness of interventions that havebeen implemented to improve medication adherence in adult kidneytransplant patients.Methods. A total of eight electronic databases: Medline, PubMed,CINAHL, Web of Science, Embase, ScienceDirect, Scopus andPsycINFO were searched from inception to November 2013. Onlyprimary intervention studies, which reported measurement of adultpatients’ adherence to immunosuppressive medications after kidneytransplantation, were included. The quality of all studies wasassessed using the CONSORT checklist for randomized studies andthe TREND checklist for non-randomized studies.Results. The search identified twelve relevant interventionstudies that were conducted in Belgium, Switzerland, the UnitedKingdom, and the United States of America. Recruited participantswere predominantly male and aged on average from 42.4 to 52.1years. In general, effective interventions were implemented for3, 6 and 12 months. Medication adherence rates were greatlyenhanced when educational-behavioural interventions were led byhealthcare professionals whereas one-off feedback from a nurseand financial assistance programs offered little improvement. Adose administration aid when used in conjunction with a self-monitoring device was proven to improve patients’ adherence aswell. In comparison, although regimen simplification increased

overall adherence by eliminating the burden of the evening doseon patients, the number of patients who had a drug-holiday (atleast 1-day interval without a dose) was higher in a once-dailyregimen than a twice-daily regimen. Quality of studies rangedfrom 16.0% to 80.5%, as appraised using the CONSORT and TRENDchecklists.Conclusion. Findings of this review suggest a combination ofeducational and behavioural interventions delivered by healthcareprofessionals, in addition to emotional support, is effective inenhancing medication adherence. Simple personal reminders, whencoupled with real-time feedback through a self-monitoring device,also enhance patient adherence.
Keywords: adults; intervention; kidney transplantation; medicationadherence; systematic review

Introduction
With the incidence of end-stage kidney disease projected toincrease dramatically, the demand for kidney transplants willalso rise [1]. Kidney transplantation is the preferred treatmentfor end-stage kidney disease, because it increases patient’squality-adjusted-life years 5-fold [2] and is more economicalwhen compared to dialysis [3]. However, kidney transplantationinvolves the inherent risk of graft rejection where therecipient’s immune system does not accept the transplant. Notonly does rejection elevate the risk of kidney loss; it incurscostly hospitalizations, laboratory tests, and anti-rejectiontreatments, which are associated with poor patient outcomes [4].To minimize the risk of rejection, recipients are routinelytested for signs of rejection and are placed on life-longregimens of immunosuppressive medication. Not takingimmunosuppressive medications as prescribed (defined as takingmedications <95.1% of days) is associated with a 60% increasedrisk of kidney transplant failure and graft loss [5]. It istherefore evident that immunosuppressive medications arenecessary in kidney transplantation, but are only effective iftaken as prescribed.
Adherence can be defined as the extent to which peoplefollow the instructions they are given for prescribed treatments[6]. Medication adherence is greatly influenced by the patient’sperspectives, medication properties, ease of access to thehealthcare system [7] and medication regimen [8]. Given thatmedication adherence in kidney transplantation is critical to thesuccess of the graft [5], it is surprising that up to 67% ofpeople who have kidney transplants do not take theirimmunosuppressive medications as prescribed [9]. There isundoubtedly a compelling need for interventions to improvemedication adherence. Ultimately, better medication adherenceresults in improved general wellbeing for the transplant patientand reduced healthcare costs.
Many studies have been conducted to explore the causalrelationships between medication non-adherence andimmunosuppressant properties as well as patients’ perspectives.However, little is known about intervention programs that can
improve medication adherent behaviour amongst kidney transplantrecipients. In 2009, De Blesser [10] systematically examinedtwelve intervention studies that have been conducted to improvemedication adherence rates in solid organ transplant patients.Five reports focused on adult kidney transplant recipients [10]and only two of these studies successfully incorporatedmultidimensional interventions that were effective, whichinvolved a combination of a counselling and education program oftransplant [11] or medication [12]. Since then, many refinementsand developments have occurred to help keep patients engaged intheir medication treatment. Innovative health technologies andpolicies, which were not widely available or thoroughlyresearched in the early 2000s, have since proven to be effectivein enhancing patient’s medication adherence in chronic illnessmanagement [13, 14], even in resource-limited settings such asthe Nyanza Province [15].
Accordingly, a systematic review of all intervention studiesaimed at improving immunosuppressant therapy adherence in adultpatients who have received a live (i.e. elective surgery) ordeceased (i.e. cadaveric) transplanted kidney was undertaken.This systematic review sought to consolidate and synthesizeinformation contained in published studies on the effectivenessof interventions to promote medication adherence in kidneytransplantation.

Materials and methods
The Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA statement) was used as a guideline to ensureclarity and quality of the systematic review [16].
Literature search
A total of 8 electronic databases: Medline, PubMed, CINAHL, Webof Science, Embase, ScienceDirect, Scopus and PsycINFO weresearched for articles published from inception to November 2013.An initial trial search using Medline and Embase databasesrevealed no studies. This search was then followed by preliminarysearches of the National Library of Medicine and Elsevier, withreference to the literature previously identified by De Blesser[10], to determine highly relevant topical terms. This was toensure that the searches were as thorough as possible and searchterms were consistent. The term “intervention” was found to beneither a popular Medical Subject Headings nor a widely usedEmtree thesaurus term to categorize studies that investigated theefficacy of interventions to improve medication adherence inkidney transplant recipients. To ensure rigour, “intervention”was used in combination with “kidney transplantation”, which alsorevealed no relevant studies. Therefore, “intervention” wasomitted except if it was shown in the word index generator ofother electronic databases.
For most searches, the key term “kidney transplant” was usedin conjunction with either “medication adherence” or “patientcompliance” and combined with “immunosuppressive agents” toretrieve all relevant primary research studies (Appendix 1).Although the terms “adherence” and “compliance” are distinct inmeaning in the health care lexicon as proposed by World HealthOrganization [17], “patient adherence” and “patient compliance”in this context were inter-changeable and both referred to theextent to which consumers follow the instructions they are givenfor prescribed treatments [6].
Selection criteria
Inclusion criteria for this review were primary research studiesthat were written in English and those that described specific
interventions aiming to improve adherence to prescribedmedications, where participants were aged 18 years and above,and medication adherence was reported as an outcome measure.
Full-text articles written in a language other than Englishwere excluded. Case reports, conference abstracts that lackeddetails on the method and all published non-primary researcharticles (précis, letters to the editor, reviews and bookchapters) were not included in this review. In the absence of anabstract, the full text was sourced. Intervention studies thatdid not address medication adherence as an outcome were alsodeemed ineligible.
Additionally, reference lists of retrieved studies andreviews on the topic were checked for relevant articles notidentified by the previous search strategies. After removing allduplicates, all authors screened study titles and abstracts anddiscarded those that did not fit the inclusion criteria. Full-text papers were sourced on retrieved references that lacked anabstract or contained an abstract with insufficient details.Studies that appeared to include relevant data or informationwere retrieved and full-text versions were examined for inclusioneligibility. Two reviewers (J.K.L & K.C.) independently assessedthe articles for possible inclusion. Differences in assessmentwere resolved with discussion until the reviewers came to aconsensus.
Data extraction and quality ratings
Data extracted from selected articles included year ofpublication, country, study design, patient group, indexmedications (Table 1), duration, control, standard or usual care,interventions as well as measurement of medication adherence(Table 2). The quality of intervention studies in this reviewwere critically appraised using standardized evaluation tools,the 25-item Consolidated Standards of Reporting Trials (CONSORT)checklist for all randomized controlled trials studies (RCT) [18]and the 22-item Transparent Reporting of Evaluations withNonrandomized Designs (TREND) checklist for other study designs[19]. Both checklists are proposed to evaluate the critical

factors that should be present in a quality report, which canprovide the most reliable evidence on the efficacy of health careinterventions [18, 19]. In order to compare the quality ofretrieved studies that were assessed with different evaluationtools, a percentage was calculated of the obtained score dividedby the total number of the potential score and multiplied by 100for each study.
Attempts were made to contact corresponding authors toobtain details not found in the full text. Corresponding authorswere given two weeks to respond and any field that was left blankprovides evidence of a vain attempt.
Results
The initial search yielded 1742 citations, of which 1739 werefound through electronic databases and three citations throughreferences [11, 20, 21]. A total of 772 citations wereduplicates. Three highly relevant citations were excluded becausefull-texts were either not published [11] or published in alanguage other than English [21, 22]. After close examination,twelve studies that met the inclusion criteria were included forthis literature review (Figure 1). Of these, two studies did notexplicitly state the age group of individuals that was recruited.Both studies were included because corresponding author was notsuccessfully contacted and terms indicative of a non-adultpatient group (e.g. children, paediatric, adolescent, parents,less than 18 years old) were not used in the article [23, 24]. Assuch, kidney transplant group participants for both studies areclassified as “all patients” in Table 1.
Study characteristics and quality
As summarized in Table 1, the final sample consisted of tworetrospective cohort studies [25, 26], two studies with no pairedcomparison data [27, 28] and eight randomized controlled trials[12, 20, 23, 24, 29-32], of which two were pilot studies [31,32]. Of all twelve studies, only two studies had multiple datacollection sites. In one study, which was conducted inSwitzerland, two hospital sites were used [32] and in one studyconducted in Belgium, six clinical sites were used [30] whereasthe remainder were carried out in the United Kingdom (n = 2) [24]and the United States of America (n = 8) [12, 20, 23, 25, 27-29,31]. Of all studies, only three studies pre-determined the samplesize needed to obtain sufficient power to support findings oninterventional efficacy [29, 30, 32] and the number of patientsallotted to the control or intervention group ranged from 5 to519. Without the numerical values of three studies [23, 24, 30],participants aged on average from 42.4 to 52.1 years. Overall,more male participants were recruited except for studiesconducted by Russell [31] and Kuypers [30]; however, two studiesdid not report the male to female ratio [20, 23, 24]. Regardless
of the dosage frequency, all studies included a measurement ofadherence to immunosuppressive medications.
A quality assessment was performed individually for eachstudy using the CONSORT or TREND statements. Papers assessedusing the TREND checklist [25-28] achieved an average score of59.7%, and the quality ranged from 38.7% to 74.5%. Two out offour non-RCT studies appraised using the TREND checklist onlyexamined the adherence rate of one group of patients [26-28]. Forthese studies, intervention involved was relatively simple andeasy to execute because all patients were provided with freeimmunosuppressive agents [27, 28]. Therefore, the followingitems: group assignment, delivery method and statistical methodsto compare group differences, were non-applicable and weretherefore excluded when assessing these non-RCT studies [27, 28].The quality of randomized controlled trials ranged 16.0% [24] to80.5% [29] with an average score of 52.7%. Most of the includedRCT studies lacked transparency when detailing the steps taken toensure that group assignment was randomized. Additionally, studyparticipants, coordinators and investigators of most studies werenot blinded to group assignment.
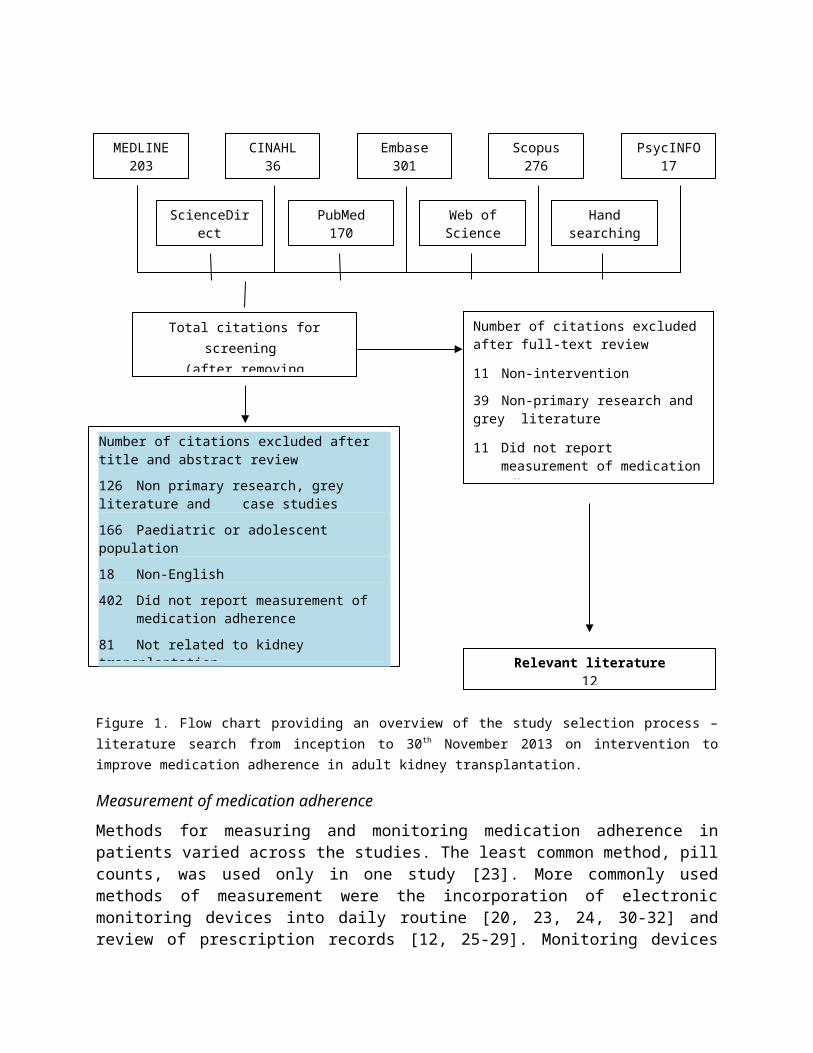
Figure 1. Flow chart providing an overview of the study selection process –literature search from inception to 30th November 2013 on intervention toimprove medication adherence in adult kidney transplantation.
Measurement of medication adherence
Methods for measuring and monitoring medication adherence inpatients varied across the studies. The least common method, pillcounts, was used only in one study [23]. More commonly usedmethods of measurement were the incorporation of electronicmonitoring devices into daily routine [20, 23, 24, 30-32] andreview of prescription records [12, 25-29]. Monitoring devices
Web ofScience
MEDLINE203
CINAHL36
Embase301
Scopus276
ScienceDirect
PubMed170
Handsearching
PsycINFO17
Total citations forscreening
(after removing
Number of citations excluded after title and abstract review 126 Non primary research, grey literature and case studies166 Paediatric or adolescent population 18 Non-English402 Did not report measurement of
medication adherence81 Not related to kidney transplantation Relevant literature
12
Number of citations excludedafter full-text review
11 Non-intervention
39 Non-primary research and grey literature
11 Did not report measurement of medicationadherence

used in the studies included a pill bottle with a specialized lid[23, 24, 31, 32], the 28-compartment MedMinderTM medication tray[20]; and the pocket-sized Helping HandTM for blister packs [30].Researchers used pill bottles [23, 24, 31, 32] and Helping HandTM
[30] to electronically monitor patient’s adherence to a singleimmunosuppressive medication. In comparison, the MedMinderTM traywas large enough to accommodate both immunosuppressive and non-immunosuppressive medications, and thus appropriate to monitorpatient’s adherence to all medications [20]. All these devicesare equipped with a microchip that registers the date and time ofcap or tray opening; and re-insertion of the blister pack.
Using missed doses to represent non-adherence, an arbitrarythreshold value of 80% [12, 27, 28] was applied to adherencemeasured with prescription refill records whereas adherence ratesof 85% [20, 31] and 98% [32] were applied when measuring withelectronic devices. Patients with an adherence rate less thanthese cut-off points were categorized as non-adherent inrespective studies [12, 20, 27, 28, 31, 32]. On the other hand,the operational definition of non-adherence was different in therandomized controlled trials conducted by Hardstaff [23, 24],where both incidences of missed and extra doses of medicationswere considered as non-adherence. Further details regardingadherence rate calculations are summarized in Table 2.
To confirm adherence, some studies included routinelaboratory tests comprising of immunosuppressive serumconcentrations [12, 27, 28]. In contrast, other studies involvedassessment of the economic outcomes and health care utilizationof patients [26, 29] as well as patients’ adherence to other non-immunosuppressive medications by measuring patients’ restingblood pressure [17]. When compared to adherent patients, a higherproportion of non-adherent patients displayed less-than-satisfactory serum concentrations of the index medication [12,27], they also had higher all-cause hospitalization [29] and wereless successful in controlling the key parameter of theircomorbid condition such as blood pressure [20]. All studiesincluded were not designed and powered to detect graft rejectionor graft loss as a long term outcome of medication non-adherence.Interventions and outcomes
Interventions that targeted behavioural, financial andaffective (feelings, emotions and perspectives) changes wereimplemented for different lengths of time (Table 2). Except forthe trials conducted by Hardstaff [23, 24], which only included aone-off feedback from a registered nurse, all programs wereimplemented for at least three months [12, 20, 23, 25-32]. Inaddition to an implementation period, a handful of studies alsoincluded an extended monitoring period, which comprised ofbaseline monitoring [20, 30, 31], follow-up [29] and acombination of both [32]. Only one study, which was led by Kupers[30], included baseline adherent behaviour of all patients in thefinal analysis. In comparison, studies led by McGillicudy [20],Russell [31] and De Geest [32] used a baseline monitoring periodas a screening phase to identify non-adherent individuals. Forthese three studies, only patients with a medication adherencescores of less than 85% [20, 31] and 98% [32] were eligible forrandomization into either the control or intervention group.
The method of intervention delivery by either a nurse or apharmacist differed across the studies. For instance, in onestudy, patients received feedback about their medicationadherence as documented by an electronic monitoring device [24]whereas other studies involved adoption of interviews [31, 32],personal counselling [12, 25] and semi-structured discussions[29]. Other types of interventions included in the retrievedstudies were the provision of immunosuppressant therapy free ofcharge [27, 28], regimen simplification of tacrolimus [30],patient-tailored medication-intake reminders [20]; and educationmaterials about transplant medications [25].
Five out of the twelve interventions included in this reviewfound a significant improvement in patient’s score of medicationadherence [12, 20, 25, 29, 31]. One of the shortest and effectiveintervention was implemented for three months in hypertensivekidney transplant patients [20]. These patients were equippedwith an electronic, 28-compartment medication tray, personalreminder system) and were also taught to self-monitor theirresting blood pressure [20]. Combined together, the patientsreceived real-time feedback about their own performance,resulting in significant improvements in medication adherence andthus, blood pressure [20]. The remaining four studies implemented

effective multidimensional interventions, which included acombination of behavioural modification with educationalmaterials [12, 25] and involvement of patients’ significantothers [29, 31]. All interventions were carried out by either anurse or a pharmacist and patients were attended individually[12, 25, 29, 31]. To modify patients’ behaviour, instructionabout the time to take medications were given specifically (e.g.8.00am and 8.00pm instead of twice-daily), medicine-taking timewas scheduled to coincide with regular routine [12, 31] andpersonalized reminders of their regular prescription refill weregiven [25]. Some studies included a verbal or written contractbetween the patient and the researcher [29, 31] to foster thedevelopment of the patient’s self-efficacy. To avoid confusionand to help ensure patients realize that immunosuppressantmedications were necessary to keep their grafts functioning, somestudies incorporated medication education. Patients were educatedabout the purpose of their immunosuppressant medication [25],benefits of adherence [12] and consequences of non-adherence[29]. When possible, significant others were encouraged to play arole in preparing, reminding and filling the patient’sprescription, to motivate them to stay engaged with theirmedication regimen and take their medications as prescribed [29,31]. Adherence-enhancing intervention for these four studies wereimplemented for 6 [31] and 12 months [12, 25, 29], respectively.A pilot study conducted by De Geest [32], which was the first totest the efficacy of an educational-behavioural intervention innon-adherent adult kidney transplant patients, had a relativelysmall sample size (intervention group, n = 4). There appeared tobe a trend that the intervention benefitted the patients duringthe implementation but lacked statistical significance [32].
In contrast, interventions involving one-off feedback from anurse [24] and financial assistance programs [27, 28] did not successfully improve patient’s medication adherence. In two studies conducted by Chisholm [27, 28], the efficacy of reduced medication-related costs on patients’ adherence was greatly hindered by the lack of paired-comparison data. However, these studies provided insight into the development of suboptimal adherence and showed that medication costs alone was not a determining factor of non-adherence [27, 28]. This was proven by

the drop in percentage of patients who remained adherent from 95%at five months to less than 50% at the twelfth month post-transplant point [27, 28]. Besides the one-off feedback and financial assistance programs, a simplified regimen of tacrolimuswas found to benefit patients immediately after the intervention, as demonstrated by the difference in adherence rateof patients before (twice-daily: 82.2%) and after (once-daily: 88.2%) the implementation [30]. However, this initial impact did not last long [30]. A higher proportion of patients in the once-daily dosing regimen was found to have at least a one-day interval without a dose per month when compared to the twice-daily group (62% vs. 40%) [30].
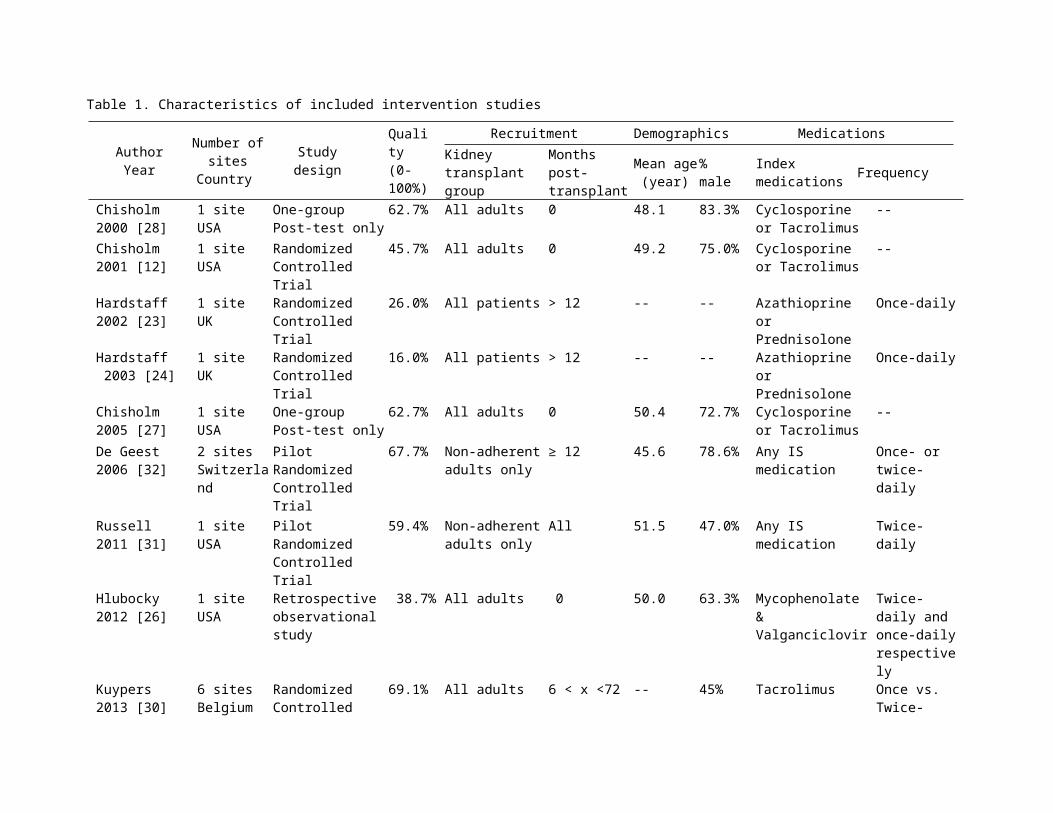
Table 1. Characteristics of included intervention studies
AuthorYear
Number ofsites
Country
Studydesign
Quality(0-100%)
Recruitment Demographics MedicationsKidney transplant group
Monthspost-transplant
Mean age (year)
% male
Index medications Frequency
Chisholm2000 [28]
1 siteUSA
One-group Post-test only
62.7% All adults 0 48.1 83.3% Cyclosporine or Tacrolimus
--
Chisholm2001 [12]
1 siteUSA
Randomized Controlled Trial
45.7% All adults 0 49.2 75.0% Cyclosporine or Tacrolimus
--
Hardstaff2002 [23]
1 siteUK
Randomized Controlled Trial
26.0% All patients > 12 -- -- Azathioprine orPrednisolone
Once-daily
Hardstaff 2003 [24]
1 siteUK
Randomized Controlled Trial
16.0% All patients > 12 -- -- Azathioprine orPrednisolone
Once-daily
Chisholm2005 [27]
1 siteUSA
One-group Post-test only
62.7% All adults 0 50.4 72.7% Cyclosporine or Tacrolimus
--
De Geest2006 [32]
2 sitesSwitzerland
Pilot Randomized Controlled Trial
67.7% Non-adherentadults only
≥ 12 45.6 78.6% Any IS medication
Once- or twice-daily
Russell2011 [31]
1 siteUSA
Pilot Randomized Controlled Trial
59.4% Non-adherentadults only
All 51.5 47.0% Any IS medication
Twice-daily
Hlubocky2012 [26]
1 siteUSA
Retrospective observational study
38.7% All adults 0 50.0 63.3% Mycophenolate & Valganciclovir
Twice-daily and once-dailyrespectively
Kuypers2013 [30]
6 sitesBelgium
Randomized Controlled
69.1% All adults 6 < x <72 -- 45% Tacrolimus Once vs. Twice-
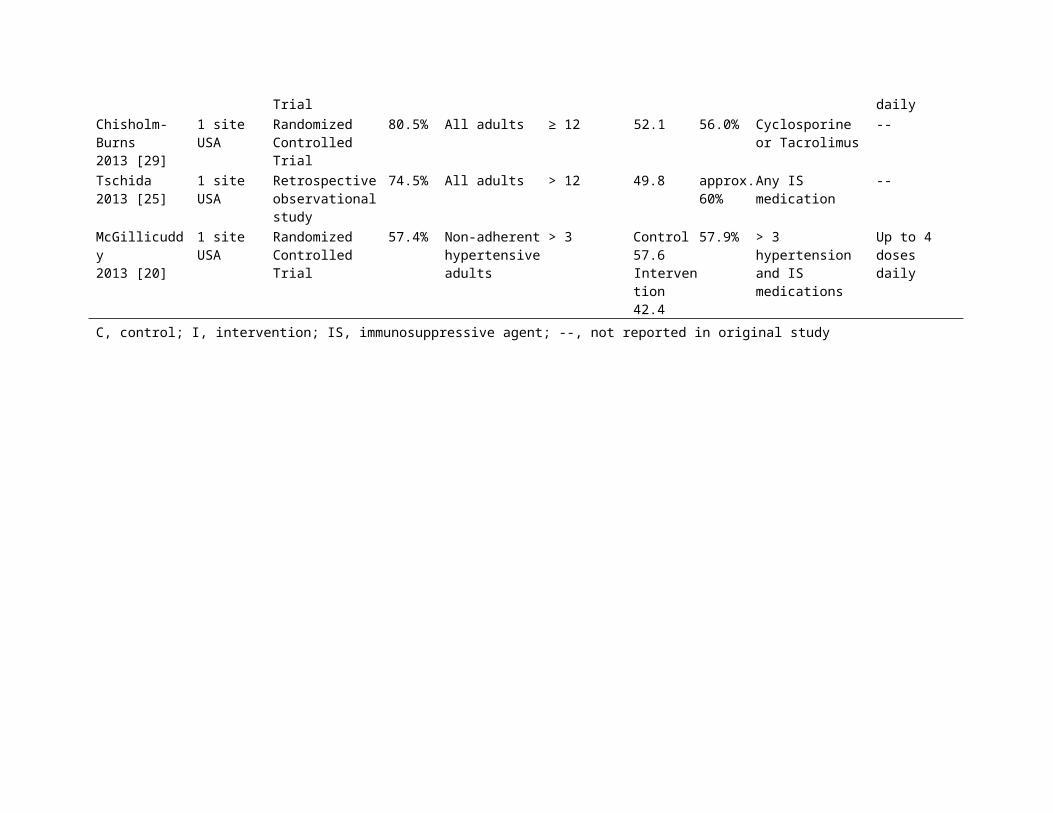
Trial dailyChisholm-Burns2013 [29]
1 siteUSA
Randomized Controlled Trial
80.5% All adults ≥ 12 52.1 56.0% Cyclosporine or Tacrolimus
--
Tschida2013 [25]
1 siteUSA
Retrospective observational study
74.5% All adults > 12 49.8 approx.60%
Any IS medication
--
McGillicuddy2013 [20]
1 siteUSA
Randomized Controlled Trial
57.4% Non-adherenthypertensiveadults
> 3 Control 57.6Intervention 42.4
57.9% > 3 hypertension and IS medications
Up to 4 doses daily
C, control; I, intervention; IS, immunosuppressive agent; --, not reported in original study

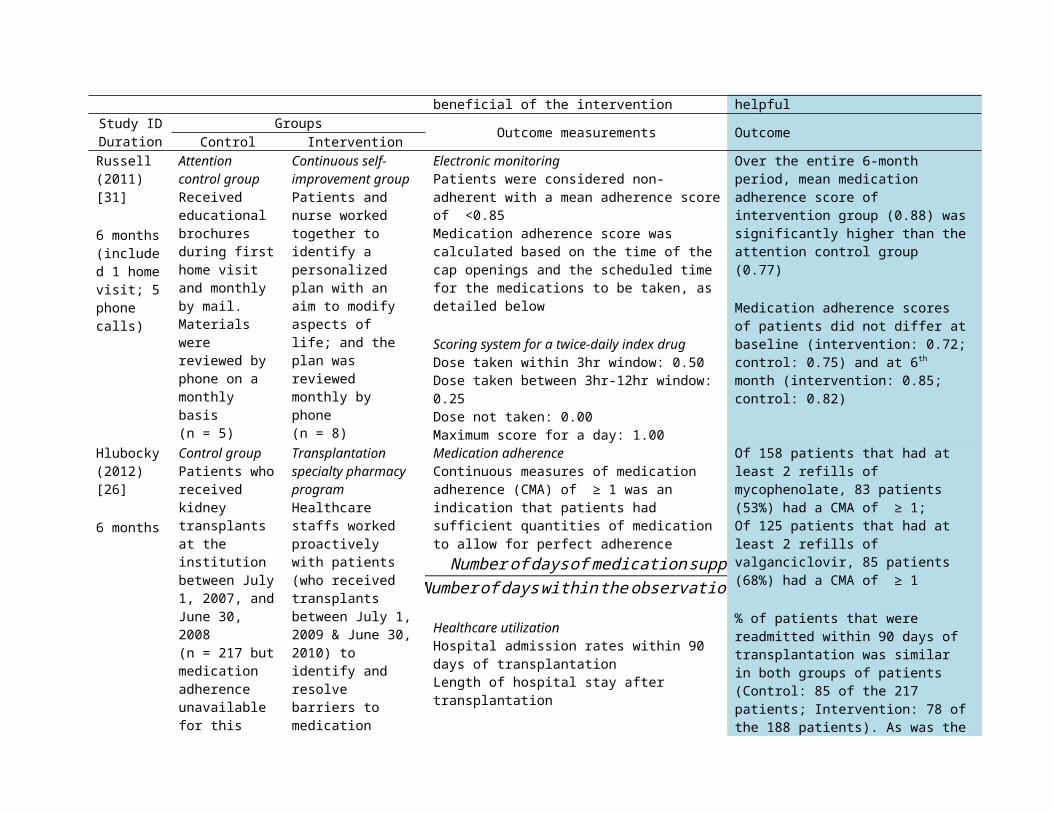
Table 2. Interventions and outcomes of retrieved intervention studies
Study IDDuration
Groups Outcome measurements OutcomeControl InterventionChisholm(2000)[28]
12 months(Free medications)
No control group
All participants received free immunosuppres-sants(N = 18)
(a) Pharmacy refill records<80% consumption of dose was considered non-compliant
Compliance rate (%) =Numberofimmunosuppressantdosesfilled
Numberofdosesprescribed x100
(b) On-target serum concentrations of immunosuppressantCyclosporine: ≥ 250 ng/mLTacrolimus: ≥ 8 ng/mL
Percentage of patients that remained compliant each monthdecreased over timeAt 5 months: about 95% of the patients;At 7 months: 75% of the patients;At 12 months: only 48% of thepatients remained compliant
Percentage of patients with sub-target immunosuppressant concentrations was significantly higher in non-compliant group (48%) than compliant group (14%)
Chisholm(2001)[12]
12 months
Received usual routine careand had no contact withpharmacist(n = 12)
Clinical pharmacist-led intervention Monthly medication counselling, with the use ofcompliance enhancement principles(n = 12)
(a) Pharmacy refill records<80% consumption of dose was considered non-compliant
Compliance rate (%) =Numberofimmunosuppressantdosesfilled
Numberofdosesprescribed x100
(b) On-target serum concentrations of immunosuppressantCyclosporine: 250-400 ng/mLTacrolimus: 8-15 ng/mL
Mean compliance rate for intervention group (96%) was significantly higher than control group (82%);Percentage of patients that remained compliant every month for 12 months was significantly higher in intervention group (75%) thancontrol group (33%);Percentage of patients with “on target” serum concentrations in intervention group was significantly higher than

control group (64% vs. 48%)Hardstaff(2002)[23]
3 months
Plain top bottlesPatients were interviewed by a nurse about their compliance during theirregular clinic visits and the remaining tablets werecounted(n = 25)
Smart top bottlesPatients were monitored electronically and had bring their bottle tothe regular outpatient appointment; nointerview with nurse practitioner(n = 75)
Electronic monitoring or a combination of pill counts and interviewsFor group with plain tops, compliance was calculated as the total number of missed doses of medications
For group with smart top bottles, compliance was calculated as the total number of missed or extra openings of the bottle
Compliance rate calculation formula was not provided
54% of the patients in plain bottle group and 39% of the patients in smart top bottle group were 100% compliant throughout the study
Of 67 patients in the smart top bottle group, 7% of them missed consecutive doses and 31% of them took extra doses
Study IDDuration
Groups Outcome measurements OutcomeControl InterventionHardstaff(2003)[24]
12 months(Monitoring only)
Received no feedback(n = 25)
One-off feedback from a nurse on their compliance at the clinic appointment(n = 23)
Electronic monitoringCompliance was calculated as a % of missed or extra doses of medications
The number of days prior to feedbackwas counted and the compliance in that time period was compared to exactly the same number of days after feedback
Compliance rate calculation formula was not provided
Overall, 83% of patients missed ≥ 1 dose; 54% of themtook extra doses; 23%of them missed consecutive doses and only 6% took medications accurately in the12 months of the study
Of the 23 patients in intervention group, 26% subsequently improved and 39%worsened;Of the 25 patients in controlgroup, 20% subsequently improved and 40% worsened

Chisholm(2005)[27]
12 months(Free medications)
No control group
All participants received free immunosuppres-santstacrolimus vs. cyclosporine(N = 33)
(a) Pharmacy refill records<80% consumption of dose was considered non-adherentMonthly adherence rate (%) =
1−Daysbetweenrefills−TotaldayssupplyDaysbetweenrefills
x100
(b) On-target serum concentrations of immunosuppressantCyclosporine: ≥ 250 ng/mLTacrolimus: ≥ 8 ng/mL
A higher percentage of patients that received tacrolimus (63%) remained compliant when compared with those taking cyclosporine (33%);At 12 months post-transplant,only 14 patients (i.e. 42% ofthe patients) remained adherent
Percentage of patients with sub-target serum concentrations was higher in non-adherent (75%) patients than adherent patients (24%);
De Geest(2006)[32]
9 months(3-monthenhancedusual care /intervention; 6-monthfollow up)
Enhanced usual care groupReceived usual care and treatingphysicians were allowedto interveneif patient was found tobe non-adherent(n = 12)
Behavioural - educational interventionsElectronic Monitoring feedback in addition to a patient-tailored plan drafted at first home visit between the nurse and patient; the plane was reviewed by 3 follow-up phoneinterviews(n = 6)
Electronic Monitoring<98% consumption of dose was considered non-adherent(a) Taking adherence =Numberofcapopeningsrecorded
Numberofdosesprescribedx100
(b) Drug holidays was defined as no intake for >36 h for a twice daily dosing regimen OR >60 h for a once daily dosing regimen
(c) Timing adherence was also measured
Qualitative assessment of interventionIntervention group was asked an open-ended question about the
Absolute values of adherence rates (calculated by taking adherence), drug holidays andtiming adherence were not reported. Instead, chance of non-adherence was calculated.No statistical significance was found throughout the study.In both groups of patients, non-adherence rate during thefirst 3 months was reported to decrease significantly andchance of non-adherence increased gradually during the follow-up period
Patients felt that electronicmonitoring feedback was most
beneficial of the intervention helpfulStudy IDDuration
Groups Outcome measurements OutcomeControl InterventionRussell(2011)[31]
6 months(included 1 homevisit; 5phone calls)
Attention control groupReceived educational brochures during firsthome visit and monthly by mail. Materials were reviewed by phone on a monthly basis(n = 5)
Continuous self-improvement groupPatients and nurse worked together to identify a personalized plan with an aim to modify aspects of life; and the plan was reviewed monthly by phone(n = 8)
Electronic monitoringPatients were considered non-adherent with a mean adherence scoreof <0.85Medication adherence score was calculated based on the time of the cap openings and the scheduled time for the medications to be taken, as detailed below
Scoring system for a twice-daily index drugDose taken within 3hr window: 0.50Dose taken between 3hr-12hr window: 0.25Dose not taken: 0.00Maximum score for a day: 1.00
Over the entire 6-month period, mean medication adherence score of intervention group (0.88) wassignificantly higher than theattention control group (0.77)
Medication adherence scores of patients did not differ atbaseline (intervention: 0.72;control: 0.75) and at 6th month (intervention: 0.85; control: 0.82)
Hlubocky(2012)[26]
6 months
Control groupPatients whoreceived kidney transplantsat the institution between July1, 2007, andJune 30, 2008(n = 217 butmedication adherence unavailable for this
Transplantation specialty pharmacy programHealthcare staffs worked proactively with patients (who received transplants between July 1,2009 & June 30,2010) to identify and resolve barriers to medication
Medication adherenceContinuous measures of medication adherence (CMA) of ≥ 1 was an indication that patients had sufficient quantities of medication to allow for perfect adherence
¿ Numberofdaysof medicationsuppliedNumberofdayswithintheobservationperiod
Healthcare utilizationHospital admission rates within 90 days of transplantationLength of hospital stay after transplantation
Of 158 patients that had at least 2 refills of mycophenolate, 83 patients (53%) had a CMA of ≥ 1;Of 125 patients that had at least 2 refills of valganciclovir, 85 patients (68%) had a CMA of ≥ 1
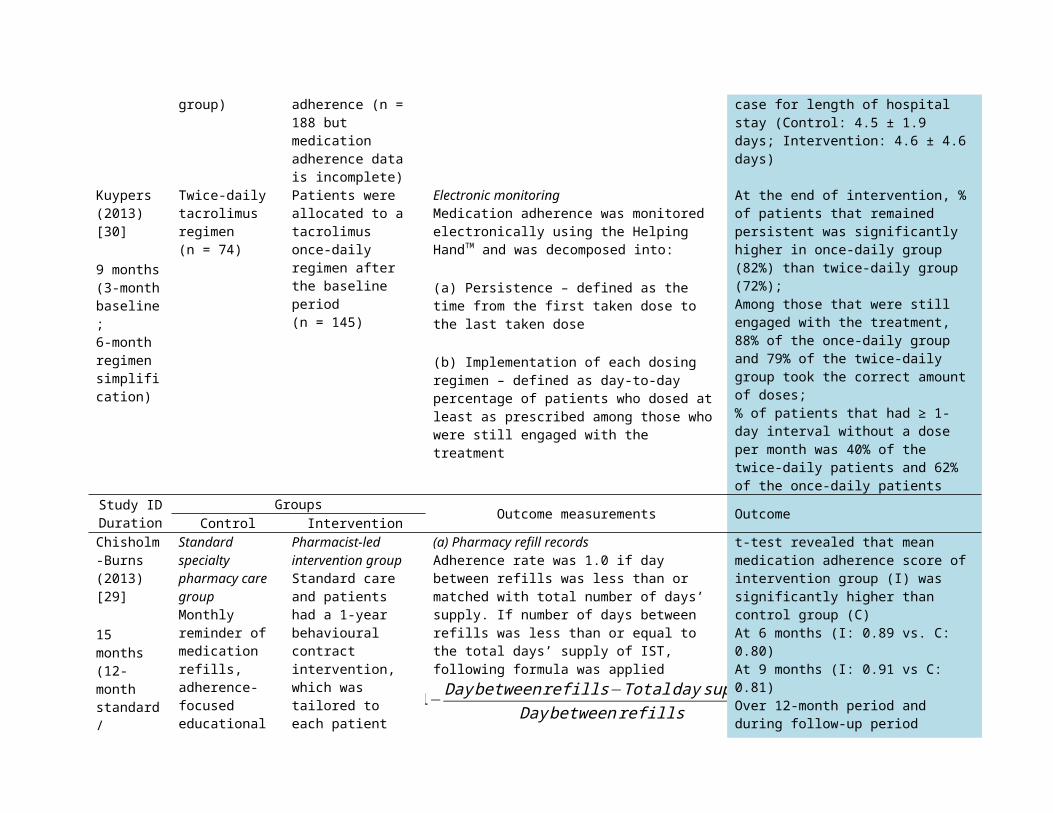
% of patients that were readmitted within 90 days of transplantation was similar in both groups of patients (Control: 85 of the 217 patients; Intervention: 78 ofthe 188 patients). As was the
group) adherence (n = 188 but medication adherence data is incomplete)
case for length of hospital stay (Control: 4.5 ± 1.9 days; Intervention: 4.6 ± 4.6days)
Kuypers(2013)[30]
9 months(3-monthbaseline;6-month regimen simplification)
Twice-daily tacrolimus regimen(n = 74)
Patients were allocated to a tacrolimus once-daily regimen after the baseline period(n = 145)
Electronic monitoringMedication adherence was monitored electronically using the Helping HandTM and was decomposed into:
(a) Persistence – defined as the time from the first taken dose to the last taken dose
(b) Implementation of each dosing regimen – defined as day-to-day percentage of patients who dosed at least as prescribed among those who were still engaged with the treatment
At the end of intervention, %of patients that remained persistent was significantly higher in once-daily group (82%) than twice-daily group (72%);Among those that were still engaged with the treatment, 88% of the once-daily group and 79% of the twice-daily group took the correct amountof doses;% of patients that had ≥ 1-day interval without a dose per month was 40% of the twice-daily patients and 62% of the once-daily patients
Study IDDuration
Groups Outcome measurements OutcomeControl InterventionChisholm-Burns(2013)[29]
15 months(12-month standard/
Standard specialty pharmacy care groupMonthly reminder of medication refills, adherence-focusededucational
Pharmacist-led intervention groupStandard care and patients had a 1-year behavioural contract intervention, which was tailored to each patient
(a) Pharmacy refill recordsAdherence rate was 1.0 if day between refills was less than or matched with total number of days’ supply. If number of days between refills was less than or equal to the total days’ supply of IST, following formula was applied
1−Daybetweenrefills−Totaldaysupply
Daybetweenrefills
t-test revealed that mean medication adherence score ofintervention group (I) was significantly higher thancontrol group (C)At 6 months (I: 0.89 vs. C: 0.80)At 9 months (I: 0.91 vs C: 0.81)Over 12-month period and during follow-up period
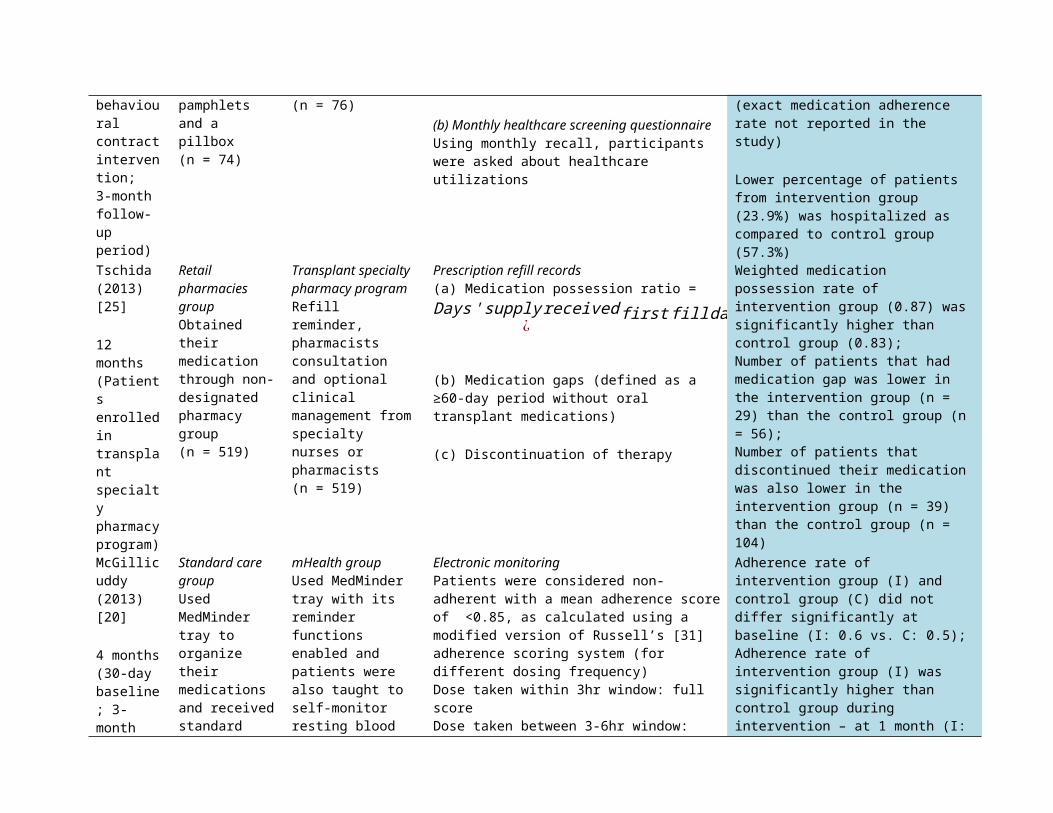
behavioural contractintervention;3-month follow-up period)
pamphlets and a pillbox(n = 74)
(n = 76)(b) Monthly healthcare screening questionnaireUsing monthly recall, participants were asked about healthcare utilizations
(exact medication adherence rate not reported in the study)
Lower percentage of patients from intervention group (23.9%) was hospitalized as compared to control group (57.3%)
Tschida(2013)[25]
12 months(Patients enrolledin transplant specialty pharmacyprogram)
Retail pharmacies groupObtained their medication through non-designated pharmacy group(n = 519)
Transplant specialty pharmacy programRefill reminder, pharmacists consultation and optional clinical management fromspecialty nurses or pharmacists(n = 519)
Prescription refill records(a) Medication possession ratio =Days'supplyreceived
¿firstfilldate¿¿endof reviewperiod¿ ¿
Numberofdays¿
firstfilldate¿¿endofreviewperiod¿¿
(b) Medication gaps (defined as a ≥60-day period without oral transplant medications)
(c) Discontinuation of therapy
Weighted medication possession rate of intervention group (0.87) wassignificantly higher than control group (0.83);Number of patients that had medication gap was lower in the intervention group (n = 29) than the control group (n= 56);Number of patients that discontinued their medicationwas also lower in the intervention group (n = 39) than the control group (n = 104)
McGillicuddy(2013)[20]
4 months(30-day baseline; 3-month
Standard care groupUsed MedMinder tray to organize their medications and receivedstandard
mHealth group Used MedMinder tray with its reminder functions enabled and patients were also taught to self-monitor resting blood
Electronic monitoringPatients were considered non-adherent with a mean adherence scoreof <0.85, as calculated using a modified version of Russell’s [31] adherence scoring system (for different dosing frequency)Dose taken within 3hr window: full scoreDose taken between 3-6hr window:
Adherence rate of intervention group (I) and control group (C) did not differ significantly at baseline (I: 0.6 vs. C: 0.5);Adherence rate of intervention group (I) was significantly higher than control group during intervention – at 1 month (I:
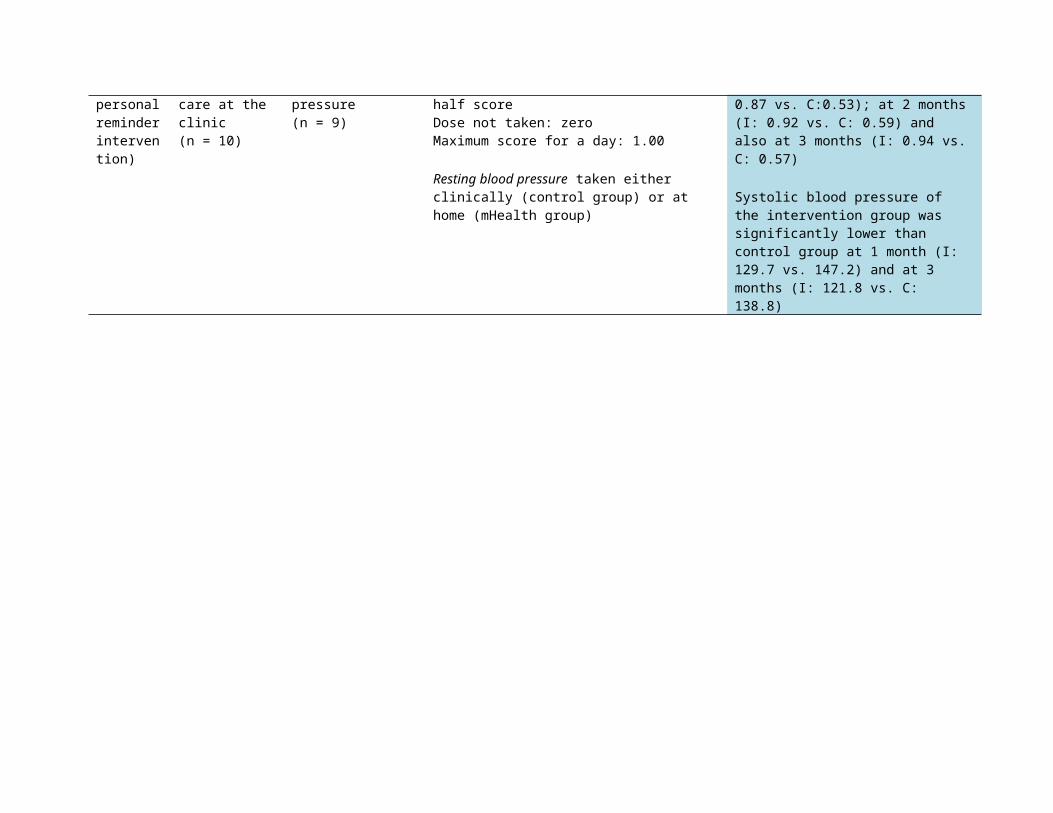
personalreminderintervention)
care at the clinic(n = 10)
pressure(n = 9)
half scoreDose not taken: zeroMaximum score for a day: 1.00
Resting blood pressure taken either clinically (control group) or at home (mHealth group)
0.87 vs. C:0.53); at 2 months(I: 0.92 vs. C: 0.59) and also at 3 months (I: 0.94 vs.C: 0.57)
Systolic blood pressure of the intervention group was significantly lower than control group at 1 month (I: 129.7 vs. 147.2) and at 3 months (I: 121.8 vs. C: 138.8)
Discussion
Methodological considerations
The search strategy adopted in this systematic review wassufficiently broad enough to capture most studies of interest asdemonstrated by the low number of studies found through retrievedreferences (n = 3). Surprisingly, out of the 970 retrievedcitations, 17% was related to biomedical characteristics such asdrug development, assay and effect; 10% measured patients’beliefs and expectations; whereas only 1% was dedicated toimproving medication adherence. This review revealed thatsuboptimal adherence to medication regimens is a well-recognizedbut poorly managed problem. It is evident that limitedintervention research exists in the kidney transplant literatureand more research needs to be undertaken before an effectivestrategy can be incorporated into current usual care services.
There are many different methods to assess adherence tomedications, either directly or indirectly, but no one singlemethod is without its limitations and is unequivocally superioracross all scenarios. In most of the included studies,measurement of medication adherence relied heavily on a singlemethod. Without a secondary confirmation measurement, it wasimpossible to suggest that patients were taking their medicationsafter they refilled their prescription [25, 26], or removed themedications from either the blister pack [30] or bottle [23, 24,31, 32] . However, the sensitivity and accuracy of adherencemeasurements could be greatly enhanced if electronic monitoringdevices and/or prescription refill records are coupled with oneof the following methods: measurement of the serum level ofmedication or metabolite (e.g. tacrolimus or cyclosporine);evaluation of graft function (e.g. serum creatinine); monitoringof comorbid conditions; self-report (e.g. Morisky scale) andpatient diaries; and medication-taking questionnaires using alikert scale.
The choice of measurement of adherence is very important. Asreported by Hardstaff, the percentage of patients who were 100%adherent was higher in the “plain bottle” group than theelectronically monitored group [23]. Even though both methods ofsurveillance included the involvement of a nurse practitioner at

the end of the trial, the control group (plain bottle) satthrough an interview with a nurse to conduct a pill-count;whereas for the patients in the electronic monitoring group,bottles were returned without any further contact with the nurse[23]. Data collected under such circumstances were highlyunreliable because patients could easily manipulate the number ofpills with an intention to appear more adherent in the presenceof an authority figure and such action is impossible to track.This claim is supported by a randomized controlled trialundertaken by Hardstaff et al. [24], in which a group of adultkidney transplant patients were monitored electronically. Theone-off contact that the patients had with the nurse practitionerdid not have an impact on the patients’ medication-takingbehaviour. In line with this finding, Russell and colleagues [31]reported that the consistent difference between control andintervention groups during the first five months of themonitoring period diminished at the end of the intervention. Thiscould be due to the cessation of surveillance at completion ofthe study, which increased patients’ awareness of being studiedand was not a true effect of long-term change in behaviour [31].For future intervention studies that involve frequent contactbetween patients and healthcare professionals, it is extremelyimportant to use a robust method of adherence measurement thatcontinues after study completion to estimate true behaviouralchange.
The implementation period of the intervention warrants moreattention as more than 50% of adult kidney transplant patientswho were receiving their immunosuppressive medications free ofcharge became non-adherent at the twelfth month post-transplantation point [27, 28]. Beneficiary effects ofbehavioural and/or educational interventions may be maximized ifthe interventions are implemented during the early post-transplantation period (first six months) before any patientattempts to deviate from the prescribed regimen. Moreover,implementation of an intervention for as short as three monthsgreatly assisted kidney transplant recipients to adhere to theirmedication [20] but for behavioural-educational interventions, a

longer implementation period will definitely benefit patients inthe long term [32]. It is therefore evident that the involvementof patients as active agents, for more than three months duringthe early post-transplantation period, will greatly motivatethem. Patients will eventually learn to self-regulate theirmedication adherent behaviour and care for their graft.
Quality of studies and future researchTo date, only a handful of intervention studies with an aim toimprove medication adherence among kidney transplant recipientshave been completed. Due to the limited number of relevantpublications, all studies that met the broad inclusion criteriawere included in this review despite the weak quality of studiesas demonstrated by the low average quality score of 56.5%.Published articles that lacked details [23, 24] and three studiesthat did not have any data for comparison purposes [26-28] wereincluded in this review. In addition, steps taken to ensureconcealment of group allocation were not detailed in moststudies. Preliminary findings of pilot studies were not confirmedby any follow-up study [31, 32] and only two of twelve studiesincluded had multiple data collection sites [30, 32]. Therefore,the designs of most studies included were relatively weak andalthough findings were valuable, intervention involved cannot bebroadly applied or generalized.
Furthermore, medication adherence is a continuum, shapedthrough a complex interplay of influential factors at theindividual and interpersonal level. Factors such as gender, age[36], ease of access to the healthcare system [7] and ethnicity[37] were reported to play a role in the health outcomes ofpatients. However, most studies failed to include a cleardescription of patient demographics, healthcare settings, usualcare provided and most importantly, content of interventionsperformed. This situation makes it very difficult for futureinvestigators to adopt, reproduce and refine the strategyexamined in past research. As such, attention to detail inreporting research is important for meaningful analysis of thefindings and also for future research. Results of this currentreview also point towards extending the monitoring period
whenever possible, to include a baseline monitoring period and afollow-up period, to better assess the impact of theintervention.
Limitations of the reviewMost corresponding authors were not able to be contacted to
follow up on details in their studies. Moreover, a question thatfrequently arises in systematic reviews is the potentialselection bias produced by the key terms used to generate thelist of references. To address this issue, preliminary searchesof the National Library of Medicine and Elsevier, with referenceto the literature previously identified by De Blesser [10], weredone to determine highly relevant topical terms. Anotherlimitation is that this review only included articles publishedin English but there may be articles published in otherlanguages, which can provide significant insight into theefficacy of intervention.
ConclusionAlthough not explicitly specified in some studies, elements ofsocial cognitive theory, self-determination theory andmotivational interviewing were embedded in some of theinterventions. All these conceptual models share a similarunderlying idea, which is that behavioural modification can onlybe realized and become permanent if an individual takes on anactive role, to constantly self-regulate behaviour through self-observation (monitoring own behaviour, its determinants, and itseffects) and reflection (evaluates own behaviour in relation topersonal standards and environmental circumstance) [33-35]. Formost studies, patients were encouraged to actively participate inmaking decisions through various forms, such as the management oftheir therapy [12, 31], self-monitoring of blood pressure [20]and contact with healthcare professionals if they had anyconcerns about their medication regimen [12, 25]. The six-monthcontinuous self-improvement intervention, which was implementedby Russell [31] and colleagues, effectively enhanced medicationadherence scores throughout the study. Similarly, Chisholm-Burns[29] successfully demonstrated that the patients continuously
benefitted from the behavioural contracting intervention even at3 months after its completion [29]. Both interventions deliveredby Russell [31] and Chisholm-Burns [29] assisted patients toidentify both barriers to medication adherence and strategies forovercoming these barriers. Other than a patient-tailoredstrategy, interventions led by a pharmacist with an emphasis onmedication counselling were found to be effective in improvingpatients’ adherence as well [12, 25]. Additionally, a simpleself-regulatory approach, with the incorporation of a doseadministration aid in conjunction with a self-monitoring device,was proven to be effective [20]. Self-monitoring increasespatients’ awareness about their non-adherent behaviour and alsoallows healthcare professionals to monitor patients’ performance.If a patient is detected to be having difficulty in following themedication regimen, early behavioural and educationalinterventions can be implemented to support optimal behaviour.
One major setback of most of these effective patient-tailored interventions is the involvement of a pharmacist or anurse, which is hard to be adopted in current healthcaresettings. It is time-consuming and costly to implement.Nevertheless, this workforce cost may be off-set by the reductionof health care costs as a result of medication non-adherence[13]. Additionally, future adherence-enhancing interventionscould be done with a focus on a supportive, cost-effective andmultidimensional intervention delivered by non-nursing personnelthat are not responsible for the daily care of the patient.Kidney transplant recipients should also be encouraged to beinvolved actively in the design of an intervention, to increasemedication adherence.
Acknowledgement. This work was supported by the National Health andMedical Research Council (NHMRC) Partnerships for Better Healthgrant (APP1056717)
Conflict of interest statement. None declared.
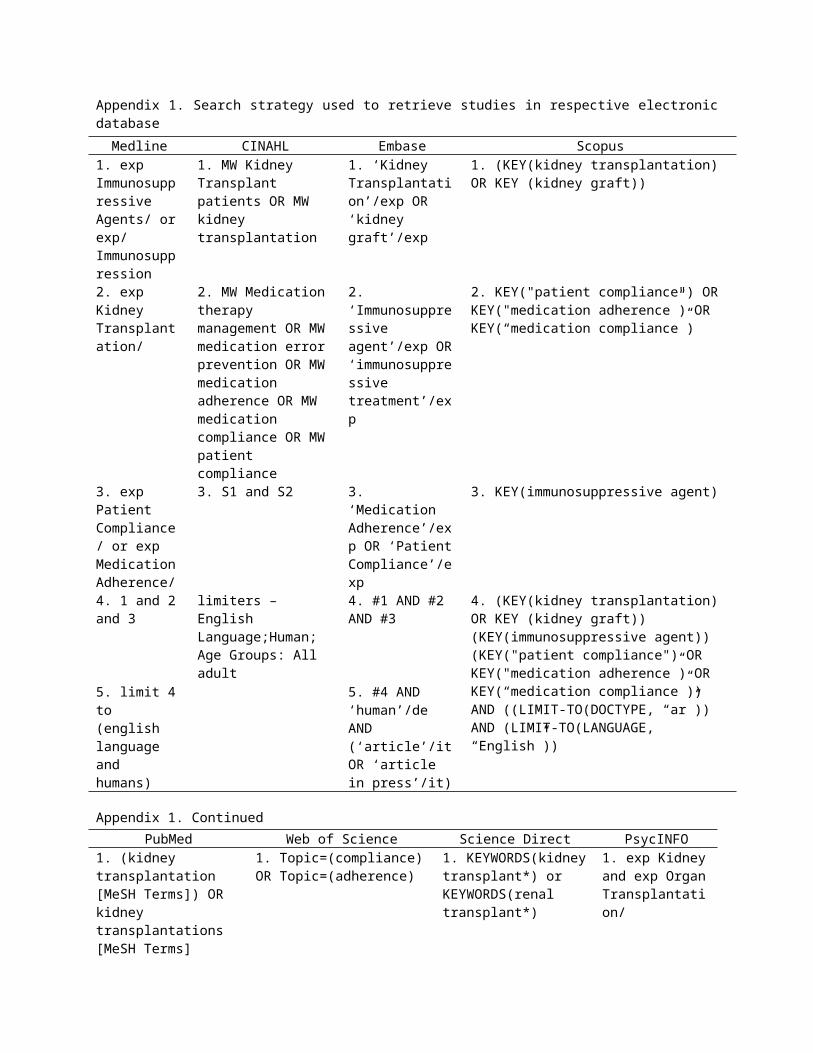
Appendix 1. Search strategy used to retrieve studies in respective electronicdatabaseMedline CINAHL Embase Scopus
1. exp Immunosuppressive Agents/ orexp/ Immunosuppression
1. MW Kidney Transplant patients OR MW kidney transplantation
1. ‘Kidney Transplantation’/exp OR ‘kidney graft’/exp
1. (KEY(kidney transplantation) OR KEY (kidney graft))
2. exp Kidney Transplantation/
2. MW Medication therapy management OR MW medication error prevention OR MW medication adherence OR MW medication compliance OR MW patient compliance
2. ‘Immunosuppressive agent’/exp OR‘immunosuppressive treatment’/exp
2. KEY("patient compliance") OR KEY("medication adherence”) OR KEY(“medication compliance”)
3. exp Patient Compliance/ or exp MedicationAdherence/
3. S1 and S2 3. ‘Medication Adherence’/exp OR ‘PatientCompliance’/exp
3. KEY(immunosuppressive agent)
4. 1 and 2and 3
limiters – English Language;Human; Age Groups: All adult
4. #1 AND #2 AND #3
4. (KEY(kidney transplantation) OR KEY (kidney graft)) (KEY(immunosuppressive agent)) (KEY("patient compliance") OR KEY("medication adherence”) OR KEY(“medication compliance”))AND ((LIMIT-TO(DOCTYPE, “ar”)) AND (LIMIT-TO(LANGUAGE, “English”))
5. limit 4to (english language and humans)
5. #4 AND ‘human’/de AND (‘article’/itOR ‘article in press’/it)
Appendix 1. ContinuedPubMed Web of Science Science Direct PsycINFO
1. (kidney transplantation [MeSH Terms]) OR kidney transplantations [MeSH Terms]
1. Topic=(compliance)OR Topic=(adherence)
1. KEYWORDS(kidneytransplant*) or KEYWORDS(renal transplant*)
1. exp Kidneyand exp OrganTransplantation/

2. (medication adherence [MeSH Terms]) OR medication compliance [MeSH terms]) OR patientcompliance [MeSH terms]
2. Topic=(medication)OR Topic(=immunosuppressive) OR Topic=(immunosuppressant)
2. (FULL-TEXT(medication adherence) or FULL-text(medication compliance)) OR FULL-TEXT (patientcompliance)
2. exp Drug Therapy/ or exp Health Behavior/ or exp TreatmentCompliance/
3. ((agents, immunosuppressive [MeSH terms]) OR immunosuppressants[MeSH terms]) OR immunosuppressive agents [MeSH terms]
3. Topic=(“kidney transplant”) OR Topic=(“kidney transplantation”) OR Topic=(“renal transplant”) OR Topic=(“renal transplantation”)
3.( KEYWORDS(kidney transplant*) or KEYWORDS(renal transplant*)) AND ((FULL-TEXT(medication adherence) or FULL-text(medication compliance)) OR FULL-TEXT (patientcompliance))
3. 1 and 2
4. (1 and 2 and 3)Filters: Humans; English; Adults
4. #3 AND #2 AND #1Refined by: Document Types=(ARTICLE) AND Languages=(ENGLISH) AND Database=(WOS)
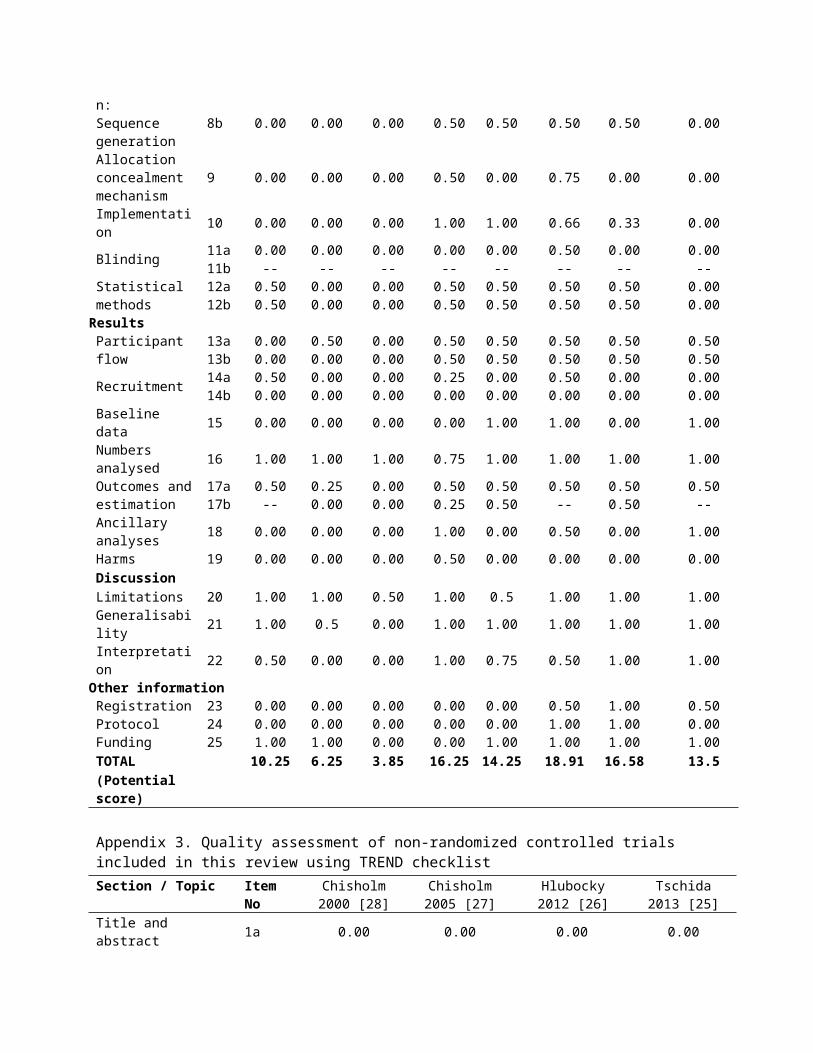
Appendix 2. Quality assessment of Randomized Controlled Trials included in this review using CONSORT checklist
Section / Topic
ItemNo
Chisholm2001[12]
Hardstaff2002[23]
Hardstaff2003[24]
De Geest2006[32]
Russell2011[31]
Chisholm-Burns2013[29]
Kuypers(2013)[30]
McGillicuddy2013 [20]
Title and abstract1a 0.00 0.00 0.00 0.50 0.5 0.5 0.50 0.501b 0.50 0.00 0.00 0.50 0.5 0.5 0.50 0.50
IntroductionBackground and objective
2a 0.50 0.25 0.50 0.50 0.5 0.5 0.50 0.50
2b 0.50 0.00 0.00 0.50 0.5 0.5 0.50 0.50Methods
Trial design 3a 0.25 0.00 0.50 0.50 0.25 0.50 0.50 0.253b 0.00 0.00 0.50 0.00 0.00 0.00 0.00 0.00
Participants 4a 0.50 0.25 0.10 0.50 0.50 0.50 0.50 0.504b 0.50 0.25 0.25 0.50 0.25 0.50 0.25 0.25
Interventions 5 1.00 0.75 0.00 1.00 1.00 1.00 1.00 1.00
Outcomes 6a 0.50 0.50 0.50 0.50 0.50 0.50 0.50 0.506b 0.00 0.00 0.00 0.00 0.00 0.00 0.00 0.00
Sample size 7a 0.00 0.00 0.00 0.50 0.00 0.50 0.50 0.007b -- -- -- -- -- -- -- --
Randomisatio 8a 0.00 0.00 0.00 0.50 0.00 0.50 0.50 0.00
n:Sequence generation
8b 0.00 0.00 0.00 0.50 0.50 0.50 0.50 0.00
Allocation concealment mechanism
9 0.00 0.00 0.00 0.50 0.00 0.75 0.00 0.00
Implementation 10 0.00 0.00 0.00 1.00 1.00 0.66 0.33 0.00
Blinding 11a 0.00 0.00 0.00 0.00 0.00 0.50 0.00 0.0011b -- -- -- -- -- -- -- --
Statistical methods
12a 0.50 0.00 0.00 0.50 0.50 0.50 0.50 0.0012b 0.50 0.00 0.00 0.50 0.50 0.50 0.50 0.00
ResultsParticipant flow
13a 0.00 0.50 0.00 0.50 0.50 0.50 0.50 0.5013b 0.00 0.00 0.00 0.50 0.50 0.50 0.50 0.50
Recruitment 14a 0.50 0.00 0.00 0.25 0.00 0.50 0.00 0.0014b 0.00 0.00 0.00 0.00 0.00 0.00 0.00 0.00
Baseline data 15 0.00 0.00 0.00 0.00 1.00 1.00 0.00 1.00
Numbers analysed 16 1.00 1.00 1.00 0.75 1.00 1.00 1.00 1.00
Outcomes andestimation
17a 0.50 0.25 0.00 0.50 0.50 0.50 0.50 0.5017b -- 0.00 0.00 0.25 0.50 -- 0.50 --
Ancillary analyses 18 0.00 0.00 0.00 1.00 0.00 0.50 0.00 1.00
Harms 19 0.00 0.00 0.00 0.50 0.00 0.00 0.00 0.00DiscussionLimitations 20 1.00 1.00 0.50 1.00 0.5 1.00 1.00 1.00Generalisability 21 1.00 0.5 0.00 1.00 1.00 1.00 1.00 1.00
Interpretation 22 0.50 0.00 0.00 1.00 0.75 0.50 1.00 1.00
Other informationRegistration 23 0.00 0.00 0.00 0.00 0.00 0.50 1.00 0.50Protocol 24 0.00 0.00 0.00 0.00 0.00 1.00 1.00 0.00Funding 25 1.00 1.00 0.00 0.00 1.00 1.00 1.00 1.00TOTAL 10.25 6.25 3.85 16.25 14.25 18.91 16.58 13.5(Potential score)
Appendix 3. Quality assessment of non-randomized controlled trials included in this review using TREND checklistSection / Topic Item
NoChisholm2000 [28]
Chisholm2005 [27]
Hlubocky2012 [26]
Tschida2013 [25]
Title and abstract 1a 0.00 0.00 0.00 0.00
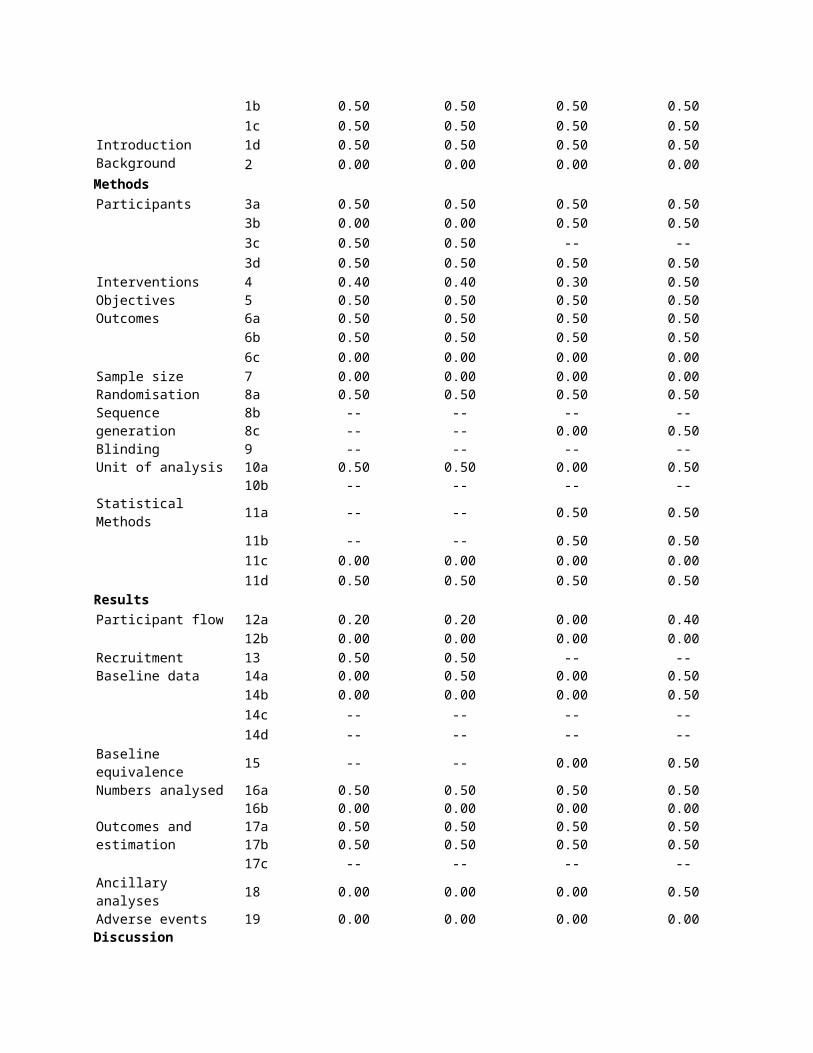
1b 0.50 0.50 0.50 0.501c 0.50 0.50 0.50 0.50
Introduction 1d 0.50 0.50 0.50 0.50Background 2 0.00 0.00 0.00 0.00MethodsParticipants 3a 0.50 0.50 0.50 0.50
3b 0.00 0.00 0.50 0.503c 0.50 0.50 -- --3d 0.50 0.50 0.50 0.50
Interventions 4 0.40 0.40 0.30 0.50Objectives 5 0.50 0.50 0.50 0.50Outcomes 6a 0.50 0.50 0.50 0.50
6b 0.50 0.50 0.50 0.506c 0.00 0.00 0.00 0.00
Sample size 7 0.00 0.00 0.00 0.00RandomisationSequence generation
8a 0.50 0.50 0.50 0.508b -- -- -- --8c -- -- 0.00 0.50
Blinding 9 -- -- -- --Unit of analysis 10a 0.50 0.50 0.00 0.50
10b -- -- -- --Statistical Methods 11a -- -- 0.50 0.50
11b -- -- 0.50 0.5011c 0.00 0.00 0.00 0.0011d 0.50 0.50 0.50 0.50
ResultsParticipant flow 12a 0.20 0.20 0.00 0.40
12b 0.00 0.00 0.00 0.00Recruitment 13 0.50 0.50 -- --Baseline data 14a 0.00 0.50 0.00 0.50
14b 0.00 0.00 0.00 0.5014c -- -- -- --14d -- -- -- --
Baseline equivalence 15 -- -- 0.00 0.50
Numbers analysed 16a 0.50 0.50 0.50 0.5016b 0.00 0.00 0.00 0.00
Outcomes and estimation
17a 0.50 0.50 0.50 0.5017b 0.50 0.50 0.50 0.5017c -- -- -- --
Ancillary analyses 18 0.00 0.00 0.00 0.50
Adverse events 19 0.00 0.00 0.00 0.00Discussion

Interpretation 20a 0.50 0.50 0.25 0.5020b 0.00 0.00 0.00 0.0020c 0.50 0.50 0.00 0.5020d 0.50 0.50 0.00 0.50
Generalisability 21 0.00 0.00 0.00 0.50Overall evidence 22 0.50 0.50 0.00 0.50TOTAL 11.10 11.10 7.55 14.90
1. AIHW. Projections of the incidence of treated end-stagekidney disease in Australia, 2010-2020. Australian Instituteof Health and Welfare, Canberra: 2011.
2. Howard K, Salkeld G, White S et al. The cost-effectiveness ofincreasing kidney transplantation and home-based dialysis.Nephrology (Carlton), 2009; 1: 123-32.
3. Cass A, Chadban S, Gallagher M et al. The Economic impact ofend stage kidney disease in Australia: Projections to 2020.Kidney Health Australia: 2006.
4. Morrissey PE, Flynn ML, Lin S. Medication noncompliance andits implications in transplant recipients. Drugs, 2007; 10:1463-81.
5. Pinsky BW, Takemoto SK, Lentine KL et al. Transplant outcomesand economic costs associated with patient noncompliance toimmunosuppression. Am J Transplant, 2009; 11: 2597-606.
6. Haynes RB, Ackloo E, Sahota N, McDonald HP, Yao X.Interventions for enhancing medication adherence. CochraneDatabase Syst Rev, 2008; 2:
7. Tong A, Howell M, Wong G et al. The perspectives of kidneytransplant recipients on medicine taking: a systematicreview of qualitative studies. Nephrol Dial Transplant,2011; 1: 344-54.
8. Hardinger KL, Hutcherson T, Preston D, Murillo D. Influenceof pill burden and drug cost on renal function aftertransplantation. Pharmacotherapy, 2012; 5: 427-432.
9. Denhaerynck K, Dobbels F, Cleemput I et al. Prevalence,consequences, and determinants of nonadherence in adultrenal transplant patients: a literature review. Transplantinternational : official journal of the European Society forOrgan Transplantation, 2005; 10: 1121-33.
10. De Bleser L, Matteson M, Dobbels F, Russell C, De Geest S.Interventions to improve medication-adherence after

transplantation: a systematic review. Transplantinternational : official journal of the European Society forOrgan Transplantation, 2009; 8: 780-97.
11. Dejean N, Rontaing L, Lapeyre-Mestre M, Roge B, Durand D.Educational program to reduce noncompliance after renaltransplantation. in 41st Congress Abstract (European RenalAssociation and the European Dialysis and TransplantationAssociation). 2004. Lisbon (Portugal)
12. Chisholm MA, Mulloy LL, Jagadeesan M, DiPiro JT. Impact ofclinical pharmacy services on renal transplant patients'compliance with immunosuppressive medications. ClinTransplant, 2001; 5: 330-6.
13. Cutler DM, Everett W. Thinking outside the pillbox--medication adherence as a priority for health care reform. NEngl J Med, 2010; 17: 1553-5.
14. Patel S, Jacobus-Kantor L, Marshall L et al. Mobilizing yourmedications: an automated medication reminder applicationfor mobile phones and hypertension medication adherence in ahigh-risk urban population. J Diabetes Sci Technol, 2013;3: 630-9.
15. Pop-Eleches C, Thirumurthy H, Habyarimana JP et al. Mobilephone technologies improve adherence to antiretroviraltreatment in a resource-limited setting: a randomizedcontrolled trial of text message reminders. AIDS, 2011; 6:825-34.
16. Moher D, Liberati A, Tetzlaff J, Altman DG, Group P.Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. BMJ, 2009: b2535.
17. Sabaté E. Adherence to long-term therapies. Evidence foraction. World Health Organization, Switzerland: 2003.
18. Schulz KF, Altman DG, Moher D, Group C. CONSORT 2010statement: updated guidelines for reporting parallel grouprandomized trials. Ann Intern Med, 2010; 11: 726-32.
19. Treasure E. The TREND statement. Evidence-based dentistry,2004; 4: 88-91.
20. McGillicuddy JW, Gregoski MJ, Weiland AK et al. Mobile HealthMedication Adherence and Blood Pressure Control in RenalTransplant Recipients: A Proof-of-Concept RandomizedControlled Trial. JMIR Res Protoc, 2013; 2: e32.
21. Zhang J-l, Tang X. Influence of post-discharge continuousnursing intervention on psychological quality and compliancewith immunosuppressants treatment in patients with renaltransplantation. Chinese Journal of Practical Nursing, 2013;27:
22. Huang Y, Yu X. Effect of healthy education on improving thedrug compliance of patients after renal transplantation.Journal of Clinical Rehabilitative Tissue EngineeringResearch, 2007; 43: 8773-8775.
23. Hardstaff R, Green K, Talbot D. Noncompliance postrenaltransplantation: measuring the extent of the problem usingelectronic surveillance and nurse practitioner interviews.Transplant Proc, 2002; 5: 1608.
24. Hardstaff R, Green K, Talbot D. Measurement of complianceposttransplantation--the results of a 12-month study usingelectronic monitoring. Transplant Proc, 2003; 2: 796-7.
25. Tschida S, Aslam S, Khan TT et al. Managing specialtymedication services through a specialty pharmacy program:the case of oral renal transplant immunosuppressantmedications. J Manag Care Pharm, 2013; 1: 26-41.
26. Hlubocky JM, Stuckey LJ, Schuman AD, Stevenson JG.Evaluation of a transplantation specialty pharmacy program.Am J Health Syst Pharm, 2012; 4: 340-7.
27. Chisholm MA, Mulloy LL, DiPiro JT. Comparing renaltransplant patients' adherence to free cyclosporine and freetacrolimus immunosuppressant therapy. Clin Transplant, 2005;1: 77-82.
28. Chisholm MA, Vollenweider LJ, Mulloy LL et al. Renaltransplant patient compliance with free immunosuppressivemedications. Transplantation, 2000; 8: 1240-4.
29. Chisholm-Burns MA, Spivey CA, Graff Zivin J et al. Improvingoutcomes of renal transplant recipients with behavioraladherence contracts: a randomized controlled trial. Am JTransplant, 2013; 9: 2364-73.
30. Kuypers DR, Peeters PC, Sennesael JJ et al. Improved adherenceto tacrolimus once-daily formulation in renal recipients: arandomized controlled trial using electronic monitoring.Transplantation, 2013; 2: 333-40.

31. Russell C, Conn V, Ashbaugh C et al. Taking immunosuppressivemedications effectively (TIMELink): a pilot randomizedcontrolled trial in adult kidney transplant recipients. ClinTransplant, 2011; 6: 864-70.
32. De Geest S, Schafer-Keller P, Denhaerynck K et al. Supportingmedication adherence in renal transplantation (SMART): apilot RCT to improve adherence to immunosuppressiveregimens. Clin Transplant, 2006; 3: 359-68.
33. Bandura A. Self-efficacy: toward a unifying theory ofbehavioral change. Psychol Rev, 1977; 2: 191-215.
34. Miller WR, Rollnick S. Meeting in the middle: motivationalinterviewing and self-determination theory. Int J Behav NutrPhys Act, 2012: 25.
35. Ryan RM, Deci EL. Self-determination theory and thefacilitation of intrinsic motivation, social development,and well-being. Am Psychol, 2000; 1: 68-78.
36. Denhaerynck K, Steiger J, Bock A et al. Prevalence and riskfactors of non-adherence with immunosuppressive medicationin kidney transplant patients. Am J Transplant, 2007; 1:108-16.
37. Weng FL, Israni AK, Joffe MM et al. Race and electronicallymeasured adherence to immunosuppressive medications afterdeceased donor renal transplantation. J Am Soc Nephrol,2005; 6: 1839-48.
Copyright © 2022 FDOKUMEN




















