Organ procurement: Spanish transplant procurement management
11
Invited Review Organ procurement: Spanish transplant procurement management Martı ´ Manyalich 1,2,3,4 , Carlos A Mestres 5 , Chloe ¨ Balleste ´ 2,4 , Gloria Pa ´ez 3,4 , Ricard Valero 2,3,4,6 and Marı ´a Paula Go ´ mez 4 Abstract Transplantation is an accepted therapeutic option to save or improve the quality of life when organ failure occurs or tissue replacements are needed. However, the lack of organs is the major limitation. The deceased organ procurement organization and professionals provide the solution to this international problem. In this review, we identify the elements involved in the organ procurement management process to analyze the possibility of implementation of deceased organ procurement for a transplantation program. While the donation rates are subject to several negative factors including religious, economic, cultural, and legal issues, the existence of well-trained professionals may considerably increase them. Professional training in organ donation along with the establishment of a solid organizational system has been identified as the crucial factor in developing efficient organ donation and transplantation programs. Keywords organ transplantation, Spain, staff development, tissue and organ procurement Introduction The increase in the world’s population is the main factor to be considered by healthcare programs in the near future. In 2008, the population was estimated to be 6,500 million, and it is expected to rise to 9,000 million by 2050, an increase of 50% in only 50 years. 1 The group with a higher quality of life is growing, thus worldwide life expectancy has risen to the current 64.3 years. 1 Society is changing, and social and health- care needs will consequently be affected in the coming years. The patterns of disease differ depending on the age range of the population studied. With a mean age of 60 years, consideration of chronic diseases generat- ing a higher demand on healthcare systems will be man- datory. Transplantation of organs and tissues will have to increase in availability according to the new needs of society. The main difference between transplantation and other medical therapies is that a donor program has to be simultaneously implemented in a given coun- try, because ‘‘without donors there are no organs, and without organs there are no transplants’’. Principles of organ transplantation Some principles are mandatory. Organ transplantation must be accepted as a successful and definitive therapy for endstage organ failure by healthcare professionals directly related to transplantation and also by political, business, and religious leaders. It is essential that the government and healthcare authorities support this belief to give credibility to transplant and donation pro- fessionals. Transplantation must be considered a finan- cially effective and efficient therapy. Dedication of financial resources to transplantation has to be accepted as an added value to the medical system. Organ procurement must be recognized as an essential Asian Cardiovascular & Thoracic Annals 19(3/4) 268–278 ß The Author(s) 2011 Reprints and permissions: sagepub.co.uk/journalsPermissions.nav DOI: 10.1177/0218492311411590 aan.sagepub.com 1 Transplant Coordination Service, Hospital Clinic, University of Barcelona. 2 Department of Surgery and Surgical Specialties, School of Medicine, University of Barcelona. 3 Transplant Procurement Management, Barcelona Scientific Park, University of Barcelona. 4 Donation and Transplantation Institute, Barcelona Scientific Park, University of Barcelona. 5 Department of Cardiovascular Surgery, Hospital Clinic, University of Barcelona. 6 Department of Anesthesiology, Hospital Clinic, University of Barcelona, Barcelona, Spain. Corresponding author: Martı ´Manyalich, Assessor on Transplantation, Medical Director, Hospital Clinic, University of Barcelona, Villarroel 170, 08036 Barcelona, Spain Email: [email protected] at PENNSYLVANIA STATE UNIV on September 12, 2016 aan.sagepub.com Downloaded from
-
Upload
khangminh22 -
Category
Documents
-
view
2 -
download
0
Transcript of Organ procurement: Spanish transplant procurement management

Invited Review
Organ procurement: Spanish transplantprocurement management
Martı Manyalich1,2,3,4, Carlos A Mestres5, Chloe Balleste2,4,Gloria Paez3,4, Ricard Valero2,3,4,6 and Marıa Paula Gomez4
Abstract
Transplantation is an accepted therapeutic option to save or improve the quality of life when organ failure occurs or
tissue replacements are needed. However, the lack of organs is the major limitation. The deceased organ procurement
organization and professionals provide the solution to this international problem. In this review, we identify the elements
involved in the organ procurement management process to analyze the possibility of implementation of deceased organ
procurement for a transplantation program. While the donation rates are subject to several negative factors including
religious, economic, cultural, and legal issues, the existence of well-trained professionals may considerably increase them.
Professional training in organ donation along with the establishment of a solid organizational system has been identified
as the crucial factor in developing efficient organ donation and transplantation programs.
Keywords
organ transplantation, Spain, staff development, tissue and organ procurement
Introduction
The increase in the world’s population is the mainfactor to be considered by healthcare programs in thenear future. In 2008, the population was estimated to be6,500 million, and it is expected to rise to 9,000 millionby 2050, an increase of 50% in only 50 years.1 Thegroup with a higher quality of life is growing, thusworldwide life expectancy has risen to the current64.3 years.1 Society is changing, and social and health-care needs will consequently be affected in the comingyears. The patterns of disease differ depending on theage range of the population studied. With a mean ageof 60 years, consideration of chronic diseases generat-ing a higher demand on healthcare systems will be man-datory. Transplantation of organs and tissues will haveto increase in availability according to the new needs ofsociety. The main difference between transplantationand other medical therapies is that a donor programhas to be simultaneously implemented in a given coun-try, because ‘‘without donors there are no organs, andwithout organs there are no transplants’’.
Principles of organ transplantation
Some principles are mandatory. Organ transplantationmust be accepted as a successful and definitive therapy
for endstage organ failure by healthcare professionalsdirectly related to transplantation and also by political,business, and religious leaders. It is essential that thegovernment and healthcare authorities support thisbelief to give credibility to transplant and donation pro-fessionals. Transplantation must be considered a finan-cially effective and efficient therapy. Dedication offinancial resources to transplantation has to beaccepted as an added value to the medical system.Organ procurement must be recognized as an essential
Asian Cardiovascular & Thoracic Annals
19(3/4) 268–278
� The Author(s) 2011
Reprints and permissions:
sagepub.co.uk/journalsPermissions.nav
DOI: 10.1177/0218492311411590
aan.sagepub.com
1Transplant Coordination Service, Hospital Clinic, University of
Barcelona.2Department of Surgery and Surgical Specialties, School of Medicine,
University of Barcelona.3Transplant Procurement Management, Barcelona Scientific Park,
University of Barcelona.4Donation and Transplantation Institute, Barcelona Scientific Park,
University of Barcelona.5Department of Cardiovascular Surgery, Hospital Clinic, University of
Barcelona.6Department of Anesthesiology, Hospital Clinic, University of Barcelona,
Barcelona, Spain.
Corresponding author:
Martı Manyalich, Assessor on Transplantation, Medical Director, Hospital
Clinic, University of Barcelona, Villarroel 170, 08036 Barcelona, Spain
Email: [email protected]
at PENNSYLVANIA STATE UNIV on September 12, 2016aan.sagepub.comDownloaded from

component of the transplantation process. Investmentmust be allocated at a level equivalent to the act oftransplantation. The mainstay of success in a transplantprogram is maintaining the highest level of trust indonation. Integrity, honesty, and professionalism aremandatory to convey openness, sincerity, and transpar-ency in all policies, practices, and behavior of thehealthcare organization in charge of the donation andtransplantation programs.
Transplant Coordination
The first transplant coordination team in Spain wascreated in 1985 at the Hospital Clinic of theUniversity of Barcelona.2 Transplant coordination sub-sequently became a specific institutional departmentrequired for the development and growth of the insti-tution’s organ, tissue, and cell transplant programs.This model was introduced in other centers, regions,and countries.3 It was found that implementation oftransplant coordination departments with transplantprocurement management (TPM) specialists increasedthe activity of transplant programs, increasing thedonations for more wait-listed patients.4
Donors and Donations
Two types of donor can generate organs and tissues:deceased and living. Legal and ethical implicationsdiffer depending on the type of donation.5,6 A compar-ison of how a given country has developed and orga-nized a donation system shows clear differencesbetween continents regarding the distribution patternof deceased and living donors.7–9 As shown inFigure 1, European donations are predominantlybased on deceased donors, and Asian countries basi-cally focus on living donation. The USA has a mixedprogram; the rates of living and deceased donors aresimilar. There is consensus that the most importantproblem in transplantation is the scarcity of donors,and consequently, a shortage of organs for thenumber of potential recipients.5 All efforts in donationare focused on increasing the donation rate of eachcountry.8
The implications of the 2 types of donation are dif-ferent. Deceased donation is the only one allowingimportant structural changes in the global donationrates. Deceased donation is stable, transparent, lessaggressive, and better accepted by society. The struc-ture required to make possible a deceased donationmodel is complex and expensive, but where it is created,it permits a regulated and trusted donation and trans-plantation program. Furthermore, this structuredsystem facilitates the development of a living donation
program. This is due to the medical organization, thealready trained healthcare professionals, and an edu-cated population. Currently, most European countriesfocus on deceased donation and promote living dona-tion under a highly regulated and structured frameworkto avoid organ shortage.10 The key, under internationalagreement, is to create a strong deceased donation pro-gram. When this structure has been demonstrated to beefficient and trustworthy, a living donor program canbe developed.11
The essential step in donation and transplantation isto detect donors so as to obtain organs. The 2 types ofdonor include deceased donors, which can be after car-diac death or after brain death, and living donors(Figure 2). The most common multiorgan donors aredeceased after brain death. Brain death occurs when theintracranial pressure is higher than the blood pressure;then, there is no blood flow to the brain (Figure 3).12
The diagnosis of brain death has to be carried out veryaccurately following specific clinical examinations, andconfirmed by instrument tests (Table 1).13 There arealso deceased donors after cardiac death.14 Diagnosisof death is performed according to cardiorespiratorycriteria (irreversible cardiac arrest). Organs are affectedby a period of warm ischemia. These donors can bedivided into 2 main groups: uncontrolled deceasedafter cardiac death (Maastricht categories I-II), whenunexpected cardiac arrest occurs, or controlleddeceased after cardiac death (Maastricht categoriesIII-IV), also known as awaiting cardiac arrest.Considering donors deceased after cardiac death,fewer organs (mainly kidneys and livers) can be consid-ered for transplantation compared to those deceasedafter brain death. In the case of living donors, usuallyonly kidneys and liver are considered. Ethically, thereare more questions, and the balance of risks to benefitsis not as clear as with cadaveric donors.15 Furthermore,the protection of the donor has to be assured by thehealthcare system.10
Essential Elements in Developing aTransplant Procurement ManagementModel
To perform a global analysis of the implemention of anorgan and tissue donation and transplantation systemin a region or country, it is necessary to take intoaccount each of the essential elements, known as thestars of TPM (Figure 4).16 Society and social attitudesare the foundations of the system. Not taking societyinto consideration would make the creation of a posi-tive attitude towards donation impossible. Unlikeother medical practices, transplantation activity doesnot depend only on technical, surgical, and
Manyalich et al. 269
at PENNSYLVANIA STATE UNIV on September 12, 2016aan.sagepub.comDownloaded from

pharmacological aspects, but also on the altruistic andfree donation of members of society. Therefore, organtransplantation requires both skilled medical expertiseand high levels of trust, support, and participation fromthe general public. Without the willingness of membersof society to donate, transplantation cannot beconsidered.
Society’s attitude towards donation is directlyrelated to the economic development and welfare ofthe population, the percentage of gross national prod-uct invested in health, and the type of healthcare systemsupported by the government. Furthermore, history,religion and cultural relationships with the concept ofdeath are factors influencing society’s positive attitude,and consequently, the rates of organ and tissue dona-tion. Society also closes the cycle by evaluating theentire process. The population should be aware of thequality of life of transplant patients, the results of trans-plant programs, and the graft and patient survivalrates. Without this feedback, society could hardlybuild an opinion about the process.
Education
Initially, a key factor in the success of donation andtransplantation processes is the motivation, trust, andpositive attitude of healthcare professionals includingphysicians, nurses, and paramedics working in hospi-tals with potential donors. This positive attitude is pos-sible thanks to the education of these professionals.17
The process of obtaining organs and tissues entails aseries of procedures and skills that are fundamental toraise the number and quality of transplants.Professionals involved in transplant coordinationrequire solid and comprehensive training, essential tointegrate donation and transplantation processes in theclinical field.
Education does not have to be focused only onhealthcare professionals directly related to donationand transplantation. It is essential that the wholehealthcare body receives clear scientific informationand learns the skills for diagnosis of brain death, thephysiology and treatment of the organs of a deadpatient, and the legal and ethical aspects of donation.
0.0%
20.0%
40.0%
60.0%
80.0%
100.0%
120.0%
Bangla
desh
Libya
Japa
nIra
n
Turke
y
Mex
ico
Cypru
s
NewZea
l
Roman
iaBra
zil
Austra
lia
Venez
uela
Canad
a
Norway
Israe
l
Malt
a
Greec
e
Argen
tina
Qatar
Belgium
Portu
gal
Hunga
ry
Czech
Rep
Franc
eSpa
in
Urugu
ay
Estonia
Cuba
Bolivia
Living Donation
Deceased
Living Donation versus Deceased Donors
Figure 1. International donation rates: figures comparing living donation and deceased donation.
270 Asian Cardiovascular & Thoracic Annals 19(3/4)
at PENNSYLVANIA STATE UNIV on September 12, 2016aan.sagepub.comDownloaded from

Priority given to the education of healthcare profes-sionals will facilitate the entire donation and transplan-tation process because they can teach the general publicand other allied professionals.18
On a second level, the next step should be to educatethe general population. Public educational programsshould take into account the fact that their maingoals are to give information about the essentials ofthe process in an easy and clear manner and toanswer basic questions such as who can donate, whatcan be donated, when and where somebody can becomea donor, and for which diseases organ and tissue
transplantation is indicated. Such programs shouldalso explain that organ and tissue transplantation is anecessary and accepted part of medical care. The tar-gets of an educational program should be the key mem-bers of society, especially young people.18 Adults can bereached either directly or through their children.University students are a target to consider as theywill become the future professionals.
Mass media have an enormous impact on the pop-ulation, but the cost of campaigning is usually very highand the cost-effectiveness is low. It is most important totransmit positive news about donation and inform
0% 10% 20% 30% 40% 50% 60% 70% 80% 90% 100%
BangladeshGeorgia
LibyaTrin
JapanDominic
IranTunisiaTurkey
UkraineMexico
BulgariaCyprus
Saudi ArabNew Zeal
NetherlandRomania
Hong KongBrazil
SwitzerlanAustraliaMalaysia
VenezuelaDenmark
CanadaUK
NorwaySweden
IsraelUSA
MaltaRussia
GreeceGermanyArgentina
AustraQatar
Slovak RepBelgium
ItalyPortugal
PuertoHungary
ColombiaCzech RepLithuania
FranceCroatia
SpainFinland
UruguayPolandEstoniaIreland
CubaLatvia
BoliviaSlovenia
Living Donation
Deceased Donation
Figure 1. Continued.
Manyalich et al. 271
at PENNSYLVANIA STATE UNIV on September 12, 2016aan.sagepub.comDownloaded from

society about transplantation success. Meetings andpublic campaigns to explain the essentials of donation,using different groups such as social or cultural associ-ations, opinion or religious groups, are highly recom-mended. All efforts invested in education should aim atobtaining a long-lasting impact on society.
Healthcare System
Depending on the type of healthcare system, the TPMwill be conceived differently. Society’s opinion aboutthis system has an essential impact on the attitudetowards donation. One of the keys to the success ofthe Spanish system of donation of organs and tissuesis the trust of the Spanish population in its universalhealthcare system. Because everybody has the samechance of receiving a transplant, the act of donationis easily accepted.19,20 The establishment of a donationand transplantation program entails a new goal for
healthcare professionals. When a patient is declaredbrain dead or presents with cardiorespiratoty arrest,the hospital’s new goal consists of generating organs,tissues, and cells to save or improve the quality of life ofothers.21,22
National Economy
Population welfare is directly related to the economy ofa country or region. Stable economic support to start atransplant program is essential because it representshigh human, material, and financial costs. Resourcemanagement is one of the responsibilities of the TPM.All resources necessary to generate a donor, organ, andtissue, determine the cost that should be known andnegotiated. The TPM must know which resources areneeded for the mission and how to get them. Therefore,planning and negotiation are absolutely requiredskills.23–25
ALIVE D.B.D. CARDIAC-ARREST EXITUS
D.C.D.
TISSUES
ORGANS AND TISSUES
KIDNEYS+
LIVERS +
TISSUES
Deceased donors Livingdonors
Figure 2. Types of donor. D.B.D.= deceased after brain death, D.C.D.= deceased after cardiac death.
Figure 3. Diagnostic imaging of brain death. (A) Angiography. (B) Scintigraphy.
272 Asian Cardiovascular & Thoracic Annals 19(3/4)
at PENNSYLVANIA STATE UNIV on September 12, 2016aan.sagepub.comDownloaded from

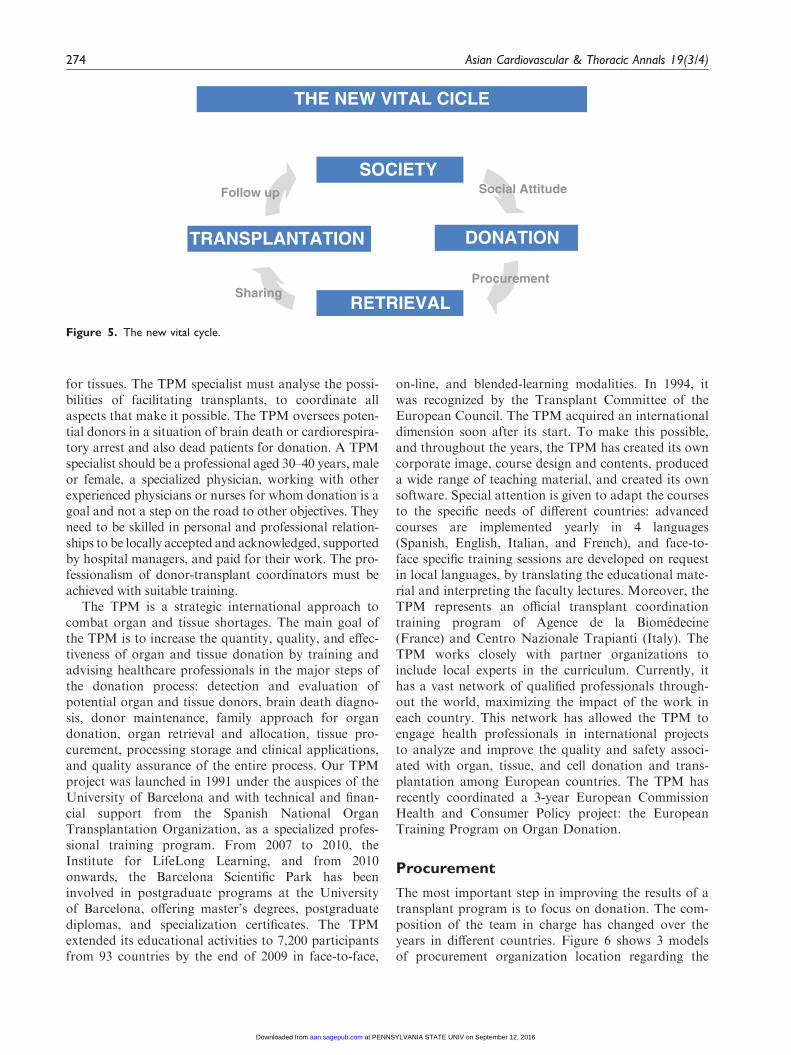
New Vital Cycle
Transplantation is possible thanks to a new vital cycleenabling a society that donates and has transplant coor-dination to benefit from the process (Figure 5). Society,thanks to a positive attitude that depends on cultural,religious, economic, and educational factors, donates
according to an altruistic process. Donation is the pro-cess that converts society’s will into the procurement oforgans, tissues, and cells. The TPM is in charge of thisprocess.26,27 Consequently, it is possible thanks todonor detection, the people responsible for this process,authorized centers, regulatory provisions, trained organand tissue retrieval teams, and the organizational workperformed by TPM departments. The organ sharingand allocation system must be organized to ensure themost ethical and fairest procedures, making the best useof the available organs, and increasing patients’ trans-plantation possibilities.11 The process involves waitinglist management systems and distribution criteria basedon consensus. Once the organ has been allocated, trans-plants can be performed, and the recipients monitoredin authorized centers. These centers organize thefollow-up of recipients and living donors. Resourcesand procedures to promote good graft survival aswell as measures to treat complications are mandatory.The creation of national and international registries iscritical to normalize the activity developed in the coun-try.8 Registries offer the opportunity to promote resultsand experiences among professionals, institutions, andsociety. The positive attitude of society will be empow-ered through well-planned mass media campaigning.
Transplant Procurement Management
The success of a transplant program lies in profession-alizing donation and sharing responsibilities.28,29
Within this framework, TPM staff are responsible fordonations, transplant teams for transplant programs,and medical specialists and tissue bank professionals
SOCIAL ATTITUDE
EDUCATIONPublic Health Professionals
HEALTH SYSTEM
NATIONAL ECONOMY
NEW LIFE CYCLE
TPM : Transplant Procurement Management
PROCUREMENT OPO, centres, others
SHARINGTransplant Office, ABM, ET,
ONT, SKT, others...
TRANSPLANTFollow-up, inmunosupression
PAYMENTProfessionals, transplant centre
QUALITY Safety, quality control, efficacy
RESEARCH AND DEVELOPMENT
Figure 4. The stars of transplant procurement management.
Table 1. Protocol of clinical examinations and instrument tests
for diagnosis of brain death
Type of Assessment
Clinical examination
Pupils in medium or dilated position
Absence of photomotor reflex
Absence of ocular movements
Absence of spontaneous blinking
Absence of corneal reflex
Absence of facial movements
Absence of spontaneous muscle movements
Absence of oculovestibular reflexes
Absence of oculocephalic reflexes
Absence of nausea reflex
Absence of cough reflex
Absence of response to atropine
Absence of spontaneous breathing
Spinal motor responses can exist
Instrument test
Electroencephalogram
Multimodality evoked potentials
Transcranial Doppler sonography
Cerebral arteriography
Radionuclide scanning
Others
Manyalich et al. 273
at PENNSYLVANIA STATE UNIV on September 12, 2016aan.sagepub.comDownloaded from
for tissues. The TPM specialist must analyse the possi-bilities of facilitating transplants, to coordinate allaspects that make it possible. The TPM oversees poten-tial donors in a situation of brain death or cardiorespira-tory arrest and also dead patients for donation. A TPMspecialist should be a professional aged 30–40 years, maleor female, a specialized physician, working with otherexperienced physicians or nurses for whom donation is agoal and not a step on the road to other objectives. Theyneed to be skilled in personal and professional relation-ships to be locally accepted and acknowledged, supportedby hospital managers, and paid for their work. The pro-fessionalism of donor-transplant coordinators must beachieved with suitable training.
The TPM is a strategic international approach tocombat organ and tissue shortages. The main goal ofthe TPM is to increase the quantity, quality, and effec-tiveness of organ and tissue donation by training andadvising healthcare professionals in the major steps ofthe donation process: detection and evaluation ofpotential organ and tissue donors, brain death diagno-sis, donor maintenance, family approach for organdonation, organ retrieval and allocation, tissue pro-curement, processing storage and clinical applications,and quality assurance of the entire process. Our TPMproject was launched in 1991 under the auspices of theUniversity of Barcelona and with technical and finan-cial support from the Spanish National OrganTransplantation Organization, as a specialized profes-sional training program. From 2007 to 2010, theInstitute for LifeLong Learning, and from 2010onwards, the Barcelona Scientific Park has beeninvolved in postgraduate programs at the Universityof Barcelona, offering master’s degrees, postgraduatediplomas, and specialization certificates. The TPMextended its educational activities to 7,200 participantsfrom 93 countries by the end of 2009 in face-to-face,
on-line, and blended-learning modalities. In 1994, itwas recognized by the Transplant Committee of theEuropean Council. The TPM acquired an internationaldimension soon after its start. To make this possible,and throughout the years, the TPM has created its owncorporate image, course design and contents, produceda wide range of teaching material, and created its ownsoftware. Special attention is given to adapt the coursesto the specific needs of different countries: advancedcourses are implemented yearly in 4 languages(Spanish, English, Italian, and French), and face-to-face specific training sessions are developed on requestin local languages, by translating the educational mate-rial and interpreting the faculty lectures. Moreover, theTPM represents an official transplant coordinationtraining program of Agence de la Biomedecine(France) and Centro Nazionale Trapianti (Italy). TheTPM works closely with partner organizations toinclude local experts in the curriculum. Currently, ithas a vast network of qualified professionals through-out the world, maximizing the impact of the work ineach country. This network has allowed the TPM toengage health professionals in international projectsto analyze and improve the quality and safety associ-ated with organ, tissue, and cell donation and trans-plantation among European countries. The TPM hasrecently coordinated a 3-year European CommissionHealth and Consumer Policy project: the EuropeanTraining Program on Organ Donation.
Procurement
The most important step in improving the results of atransplant program is to focus on donation. The com-position of the team in charge has changed over theyears in different countries. Figure 6 shows 3 modelsof procurement organization location regarding the
THE NEW VITAL CICLE
SOCIETY
DONATIONTRANSPLANTATION
RETRIEVAL
Social Attitude
ProcurementSharing
Follow up
Figure 5. The new vital cycle.
274 Asian Cardiovascular & Thoracic Annals 19(3/4)
at PENNSYLVANIA STATE UNIV on September 12, 2016aan.sagepub.comDownloaded from

hospital. The pioneer model is the one in which hospitaltransplant teams are in charge of procurement manage-ment in addition to their normal activity of transplan-tation. Ethical aspects can also be discussed. It is themost commonly used model at the beginning of theimplementation of a TPM organization. In othermodels, the procurement organization depends onexternal organizations (in another building far fromthe hospital) as is the case with American organ pro-curement organizations, where some of the personnelmust be assigned to the promotion of donor detection.This model fits vast geographic areas because it allowsthe control of more than one center, but it has to besupported by strong campaigns to make sure braindead patients are reported as potential donors, avoid-ing donor loss.
The system known as the Spanish model considersthat the TPM specialist is in charge of the donation oforgans and tissues and acts as a particular service of thehospital.4 Because such specialists work for and providea service to everyone, they must be staff members andhierarchically under the responsibility of the medicaldirector so as to maintain their independence withinthe hospital. Experience has shown that there is no per-fect model, and each country has to adapt the procure-ment organization to its own reality, taking intoaccount the healthcare system, the hospitals, and theextension of the concerned areas.11
Sharing
Distribution and exchange of organs must be well orga-nized in order to allocate them as ethically and legallyas possible, facilitating a policy of exchanges, maximis-ing the procured organ’s benefit and the transplantrecipient’s chances. An organ allocation system impliesmore management standards in waiting list coordina-tion and more consensus-based distribution criteria.
Each transplant system has to define who is responsiblefor donor detection and transplantation. This task usu-ally lies within the hospital. The national or regionalorganization has to organize and manage the transplantnetwork, collaborating with donation promotion andeducation. As an example, in Spain, the NationalOrgan Transplantation Organization arranges the pro-cess between donors and recipients based on criteriaestablished by healthcare professionals. The SpanishNational Organ Transplantation Organization isresponsible for editing consensus documents, partici-pating in international quality meetings, and promotingpolicies aimed at benefiting transplantation through anational discussion forum (interregional council).Organ donation and distribution is the responsibilityof the health administration, which should be obligedto provide the necessary resources and guarantee thefairness, transparency, and safety of the entire system.
Transplantation
Transplantation must be lead by experts and well-trained transplant teams, with human, material, andfinancial resources dedicated to transplantation. Thetransplantation has to be carried out and the recipientfollowed up in these specialist centers, with experience,resources, and authorisation, demonstrating good graftsurvival rates. Patients have to be monitored in a well-organised fashion, immunosuppressive drugs must beavailable, and the team must be able to treatcomplications.
Payment
Providing adequate financial resources is critical toensure the normal functioning of donation and trans-plantation organization. A solid budget must begranted to pay for staff, equipment, administrative
LATIPSOHLATIPSOH HOSPITAL
Tx. Teams Tx.Teams
Tx. Teams
ORGANIZATION
TPM
TransplantProcurementManagement
National Independent Organizations
Transplant Teams
Figure 6. Models of procurement organizations. TPM = transplant procurement management, Tx = transplantation.
Manyalich et al. 275
at PENNSYLVANIA STATE UNIV on September 12, 2016aan.sagepub.comDownloaded from

facilities, and the educational activities of the program.Financial costs for donor recovery and associatedtesting should also be considered for payment. TheTPM payment system should be mixed, with a fixedpart for a day’s work, equivalent to other specialistsof the center, and a variable part according to activity.Depending on the department capacity to generatedonors, the TPM contract should be considered afull-time job.16
Quality
The TPM should always strive to establish all necessarymechanisms to ensure quality in all steps of the dona-tion and transplantation process. To this end, the TPMshould establish appropriate standard operating proce-dures, develop a registry of all activity performed, keepa complete clinical donor record including all requireddocuments and legal procedures, and follow-up alldonor viability studies and laboratory results thatcould affect the quality of the organ and/or tissue trans-planted. Furthermore, it is advisable to implementsome of the internationally recognized quality controlsystems for each process, and in the future, secureaccreditation for transplant coordination units andthe TPM through national and international officiallyapproved societies, organizations, or universities, toachieve better performance and quality. The donationand transplantation process is lengthy and complex; itrequires continuous assessment to detect where, when,and why donors are lost, and attempt to define the bestpossible solutions. It is necessary to identify the areas inwhich efforts should be directed. Improvement is thesingle objective of this assessment process.
It is of great interest to participate in national andinternational registries for the purpose of comparingresults and experiences, such as quality control of theprograms.8,10 The record of these values ensures thetraceability and transparency of the activity. A registryhas, therefore, become a mandatory requirement forthe TPM in a hospital at regional, national, and inter-national levels. There are various registries according tothe factors to be analyzed. The hospital registry allowsthe control of each donation and transplantation casewithin the hospital area; it is a compulsory part of theorgan and tissue procurement coordination. Thenational registry normalizes the activity developed inthe country by promoting its evaluation and thedesign of new strategies to improve the results. Theinternational registry is a consultation tool allowingcomparison of the activity in different countries.There are several active international registries compil-ing donation and transplantation activity according todifferent variables.1,7 All registries offer the opportunity
to promote their results and experiences of donationand transplantation activity.
Finally, quality must be assured from the outset ofimplementation of the donation and transplantationsystem in a country or region. Initial advice and furtheranalysis of the results are mandatory to ensure ade-quate development of the process. Several institutions,such as the Donation and Transplantation Institute(www.dtifoundation.org), have been effective in givingsupport to developing programs.
Research and Development
The aim of the research and development of a TPMspecialist is to increase the quality and number oforgans and tissues for transplantation. Donor detectionsystem improvement is another field to analyse anddevelop, including measurement of donation potential-ity, control of the efficiency of the process, and theusage rate of generated organs. Donor maintenance,brain death diagnosis, organ perfusion, non-beatingheart donation, ischemia-reperfusion, and transplantpreconditioning are important study topics. Workingon the use of expanded-criteria donors opens new pos-sibilities for donation, including the use of organs fromC virus antibody-positive donors, elderly hepaticdonors, hepatic and cardiac domino donors for tissues,double renal transplants, partial hepatic transplantsfrom living donors, combined transplants from differ-ent organs, and adult-pediatric transplants. Moreover,human tissues are also of interest for study. There arestudies on cell viability, sterilization, bioengineering,and cryobiology. The TPM can also participate in gen-erating tissues and cells for research, such as pancreaticislets, hepatocyte islets for implants or a hepatic biore-actor, olfactory ganglia, vascular tissue for culture, andcardiac tissue for functionalism among others.
Conclusions
Organ and tissue donation and transplantation repre-sents a social good that must be protected and pro-moted, from the administration to the healthprofessionals. Society must be deeply involved. Thereare several elements that can influence attitudestowards organ donation. Legislation, financial support,specialized training for health professionals, and cul-tural acceptance of the process are key issues in thesuccess of an organ procurement program.19,20 Thefirst step is education of the health professionals whowill spread their positive attitude and knowledge oforgan donation to the population.17,18 Secondly, it isconvenient to start with a deceased donor system as it iseasier to ensure transparency and establish a larger andstronger structure. After efficient implementation of a
276 Asian Cardiovascular & Thoracic Annals 19(3/4)
at PENNSYLVANIA STATE UNIV on September 12, 2016aan.sagepub.comDownloaded from

deceased donor organization (after brain death andafter cardiac death), the extension to living donationwill be easier. Living donation has to be a secondoption after brain death and cardiac death, becauseliving donors restrict procurement to fewer organs perdonor and require more organization than deceaseddonation.10 It is essential to be well trained and advisedbefore implementing any system, to make sure that theprocess will be clear, transparent, and fair, in order toguarantee quality.
Funding
This research received no specific grant from any fundingagency in the public, commercial, or not-for-profit sectors.
Conflict of interest statement
No author has conflict of interest to disclose with regards thissubmission.
References
1. World Health Organization. (WHO) Data and Statistics.
Available at: http://www.who.int/research/en.2. Beltran JJ, Fornaguera J, Manalich M, Sentıs J, Planella
VL and Nalda MA. Removal of organs from patients
attended in an emergency resuscitation unit. Rev Esp
Anestesiol Reanim 1985; 32: 234–235.
3. Espinel E, Deulofeu R, Sabater R, Manalich M,
Domingo P and Rue M. The capacity for organ genera-
tion of hospitals in Catalonia, Spain: a multicenter study.
Transplant Proc 1989; 21: 1419–1421.4. Manyalich M, Cabrer C, Sanchez-Ibanez J, Valero J and
Umbert B. The Spanish model: keys to procurement:
Transplant Procurement Management (TPM).
In: Phillips GO (ed.) Advances in Tissue Banking. World
Scientific. 1997, pp.35–40.5. The Declaration of Istanbul on Organ Trafficking and
Transplant Tourism. Available at: http://www.
declarationofistanbul.org.6. World Health Assembly Resolution 57.18. Human organ
and tissue transplantation. 22 May 2004. Available at:
http://www.who.int/gb/ebwha/pdf_files/WHA57/
A57_R18-en.pdf.7. International Registry of Organ Donation and
Transplantation. Available at: www.tpm.org.8. Manalich M, Paez G, Valero R and Manyalich M.
IRODaT: the International Online Registry for Organ
Donation and Transplantation 2007. Transplant Proc
2009; 41: 2030–2034.9. Transplantation Committee of the Council of Europe.
International figures on organ donation and transplanta-
tion activities 1993-1997. Organs and Tissues 1998; (1):
5–11.10. Manyalich M, Ricart A, Martınez I, Balleste C, Paredes
D, Vilardell J, et al. EULID project: European living
donation and public health. Transplant Proc 2009; 41:
2021–2024.
11. Manyalich M. Organization of organ donation and role
of coordinators. Transplant Procurement Management.
Saudi J Kidney Dis Transplant 1999; 10: 175–82.12. Domınguez-Roldan JM, Murillo-Cabezas F, Munoz-
Sanchez A, Santamarıa-Mifsut JL and Villen-Nieto J.
Changes in the Doppler waveform of intracranial arteries
in patients with brain-death status. Transplant Proc 1995;
27: 2391–2392.13. Guidelines for the determination of death. Report of the
medical consultants on the diagnosis of death to the
President’s Commission for the Study of Ethical
Problems in Medicine and Biomedical and Behavioral
Research. JAMA 1981; 246: 2184–2186.
14. Valero R, Cabrer C, Oppenheimer F, Trias E, Sanchez-
Ibanez J, De Cabo FM, et al. Normothermic recircula-
tion reduces primary graft dysfunction of kidneys
obtained from non-heart-beating donors. Transpl Int
2000; 13: 303–310.15. The Ethics Committee of the Transplantation Society.
The consensus statement of the Amsterdam Forum on
the Care of the Live Kidney Donor. Transplantation
2004; 78: 491–492.16. Manyalich M, Valero R and Paez G. Transplant
Coordination Manual, TPM—Fundacio IL3—
Universitat de Barcelona, Barcelona (Espana), 2007.
ISBN: 978-84-612-0565-3.17. Paez G, Valero R and Manyalich M. Training of health
care students and professionals: a pivotal element in the
process of optimal organ donation awareness and profes-
sionalization. Transplant Proc 2009; 41: 2025–2029.
18. Manyalich M, Paredes D, Balleste C and Menjıvar A.
The PIERDUB project: International Project on
Education and Research in Donation at University of
Barcelona: training university students about donation
and transplantation. Transplant Proc 2010; 42: 117–120.19. Ley 30/1979, de 27 de octubre, por la cual se dictan las
disposiciones sobre la extraccion y el trasplante de orga-
nos (BOE num. 266, de 06.11.1979).
20. Real decreto 2070/1999, de 30 de diciembre, por el cual se
regulan las actividades de obtencion y utilizacion clınica
de organos humanos y la coordinacion territorial en
materia de donacion y trasplante de organos y tejidos
(BOE num. 3, de 04.01.2000).21. Ghirardini A, Nanni-Costa A, Venturi S, Ridolfi L,
Petrini F, Taddei S, et al. Efficiency of organ procure-
ment and transplantation programs. Transpl Int 2000;
13(Suppl 1): S267–S271.
22. Ghirardini A, Costa AN, Venturi S, Ridolfi L, Petrini F,
Taddei S, et al. Evaluation of the efficiency of organ pro-
curement and transplantation program. Transplant Proc
2000; 32: 100–103.
23. Manyalich M, Cabrer C, Felipe C, Miranda B and
Matesanz R. Coordinator training. In: Matesanz R,
Miranda B (eds) Organ donation for transplantation: the
Spanish model. Aula Medica: 1996, pp.67–79.
24. Manyalich M. TPM: modello organizzativo di
coordinamento dei Trapianti per il reperimento del
donatori en Manuale del Corso Nazionale per
coordinatori alla donazione e prelievo di organi.
Manyalich et al. 277
at PENNSYLVANIA STATE UNIV on September 12, 2016aan.sagepub.comDownloaded from

Bolonia (Italia): Editrice Compositori s.r.l. 2004. ISBN:88-7794-467–6.
25. Manyalich M. Trasplante de organos y tejidos ‘‘Medicina
Interna. Farreras-Rozman’’. Madrid: Ediciones Harcourt,2000, p.53.
26. Manyalich M, Cabrer C, Valero R, Paredes D,Navarro A, Trias E, et al. Transplant Procurement
Management: a specialization. Les Cahiers du ForumEuropeen. Forum Europeen des Managers de Sante,2003. ISBN: 2-9521163-0-X.
27. Paredes D, Valero R, Navarro A, et al. Transplant pro-curement manager (TPM): uno strumento formativo per
aumentare le donazione. Manuale del corso nazionale percoordinatori alla donazione e prelievo di organi. Bologna:Editrice Composition 2000, p.5.
28. Manyalich M, Cabrer CA, Garcia-Fages LC, Valero R,Salvador L and Sanchez J. Training the transplant pro-curement management (TPM) coordinator. In: TouraineJL (ed.) Organ Shortage: The Solutions. Dordrecht:
Kluwer Academic Publishers, 1995, pp.191–195.29. Paredes D, Valero R, Navarro A, Miranda B, Viedma
MA, Cabrer C, et al. Transplant Procurement
Management: a training tool to increase donation.Transplant Proc 1999; 31: 2610–2611.
278 Asian Cardiovascular & Thoracic Annals 19(3/4)
at PENNSYLVANIA STATE UNIV on September 12, 2016aan.sagepub.comDownloaded from