
All-Epiphyseal Anterior Cruciate Ligament Reconstruction in Skeletally Immature Patients: A Surgical...
7
All-Epiphyseal Anterior Cruciate Ligament Reconstruction in Skeletally Immature Patients: A Surgical Technique Using a Split Tibial Tunnel Marios G. Lykissas, M.D., Ph.D., Senthil T. Nathan, M.D., and Eric J. Wall, M.D. Abstract: Many techniques have been described for anterior cruciate ligament (ACL) reconstruction in skeletally immature patients, including extra-articular, complete or partial transphyseal, and physeal-sparing techniques. An all-epiphyseal technique places the tendon and its tunnels and fixation all within the child’s epiphysis, leaving the growth plates untouched. We describe an all-epiphyseal quadruple-hamstring ACL reconstruction using a split tibial tunnel. The split tibial tunnels drop the tunnel size down to 4.5 to 5.5 mm from 7 to 8 mm because only half the total graft diameter passes through each of the split tunnels. This increases the safety margin for keeping the tunnel within the tibial epiphysis, in addition to avoiding damage into the growth plate. The bone bridge between the 2 tunnels serves as a solid low-profile fixation post. Femoral graft fixation is achieved with an interference screw, which allows precise tensioning and low-profile fixation entirely within the femoral tunnel. By placing the graft at the native ACL’s anatomic attachment points without spanning or violating the growth plates at any step of the procedure, an all-epiphyseal ACL reconstruction with a split tibial tunnel theoretically minimizes the risk of growth disturbance in an ACL-deficient child. T he natural history of nonoperative treatment of an- terior cruciate ligament (ACL) tears in skeletally immature patients who return to sports is very poor. These children have recurrent instability episodes, poor satisfaction with sports performance, subsequent menis- cal tears, and early degenerative changes. Many tech- niques have been described for ACL reconstruction in skeletally immature patients, including extra-articular, complete or partial transphyseal, and physeal-sparing techniques, such as the transepiphyseal technique. 1-3 Extra-articular techniques are nonanatomic and do not restore isometry, whereas transphyseal techniques vio- late and can tether the growth plate and may cause leg length discrepancies or angular deformities. In the tran- sepiphyseal technique, as described by Anderson, 3 ana- tomic ACL reconstruction is performed by drilling the femoral and tibial tunnels within the epiphysis, avoiding disruption of the growth plate. However, the tibial graft is fixed to the metaphysis, which can potentially cause growth disturbance through a “tether effect.” We describe a modification of the Anderson technique for all-epiphyseal ACL reconstruction in an ACL- deficient child: an all-epiphyseal quadruple-hamstring ACL reconstruction using a split tibial tunnel (Fig 1). The graft, the bone tunnels, and graft fixation are placed entirely within the epiphysis. An all-epiphyseal tech- nique should minimize the risk of growth disturbance by avoiding drilling or tethering the growth plate. It should also minimize the risk of subsequent cartilage damage from recurrent knee instability by its anatomic graft placement. The split tibial tunnels drop the tunnel size down to 4.5 to 5.5 mm from 7 to 8 mm because only half the total graft diameter passes through each of the split From the Division of Orthopaedic Surgery, Cincinnati Chil- dren’s Hospital Medical Center, Cincinnati, Ohio, U.S.A. The authors report that they have no conflicts of interest in the authorship and publication of this article. Received March 29, 2012; accepted May 23, 2012. Address correspondence to Eric J. Wall, M.D., Division of Orthopaedic Surgery, Cincinnati Children’s Hospital Medical Center, 3333 Burnet Ave, MLC 2017, Cincinnati, OH 45229, U.S.A. E-mail: [email protected] © 2012 by the Arthroscopy Association of North America 2212-6287/12202/$36.00 http://dx.doi.org/10.1016/j.eats.2012.05.005 e133 Arthroscopy Techniques, Vol 1, No 1 (September), 2012: pp e133-e139
-
Upload
independent -
Category
Documents
-
view
0 -
download
0
Transcript of All-Epiphyseal Anterior Cruciate Ligament Reconstruction in Skeletally Immature Patients: A Surgical...

d
a
OCU
All-Epiphyseal Anterior Cruciate Ligament Reconstruction inSkeletally Immature Patients: A Surgical Technique Using a
Split Tibial Tunnel
Marios G. Lykissas, M.D., Ph.D., Senthil T. Nathan, M.D., and Eric J. Wall, M.D.
Abstract: Many techniques have been described for anterior cruciate ligament (ACL) reconstructionin skeletally immature patients, including extra-articular, complete or partial transphyseal, andphyseal-sparing techniques. An all-epiphyseal technique places the tendon and its tunnels andfixation all within the child’s epiphysis, leaving the growth plates untouched. We describe anall-epiphyseal quadruple-hamstring ACL reconstruction using a split tibial tunnel. The split tibialtunnels drop the tunnel size down to 4.5 to 5.5 mm from 7 to 8 mm because only half the total graftdiameter passes through each of the split tunnels. This increases the safety margin for keeping thetunnel within the tibial epiphysis, in addition to avoiding damage into the growth plate. The bonebridge between the 2 tunnels serves as a solid low-profile fixation post. Femoral graft fixation isachieved with an interference screw, which allows precise tensioning and low-profile fixation entirelywithin the femoral tunnel. By placing the graft at the native ACL’s anatomic attachment pointswithout spanning or violating the growth plates at any step of the procedure, an all-epiphyseal ACLreconstruction with a split tibial tunnel theoretically minimizes the risk of growth disturbance in anACL-deficient child.
The natural history of nonoperative treatment of an-terior cruciate ligament (ACL) tears in skeletally
immature patients who return to sports is very poor.These children have recurrent instability episodes, poorsatisfaction with sports performance, subsequent menis-cal tears, and early degenerative changes. Many tech-niques have been described for ACL reconstruction inskeletally immature patients, including extra-articular,complete or partial transphyseal, and physeal-sparingtechniques, such as the transepiphyseal technique.1-3
Extra-articular techniques are nonanatomic and do not
From the Division of Orthopaedic Surgery, Cincinnati Chil-ren’s Hospital Medical Center, Cincinnati, Ohio, U.S.A.The authors report that they have no conflicts of interest in the
uthorship and publication of this article.Received March 29, 2012; accepted May 23, 2012.Address correspondence to Eric J. Wall, M.D., Division ofrthopaedic Surgery, Cincinnati Children’s Hospital Medicalenter, 3333 Burnet Ave, MLC 2017, Cincinnati, OH 45229,.S.A. E-mail: [email protected]© 2012 by the Arthroscopy Association of North America2212-6287/12202/$36.00
http://dx.doi.org/10.1016/j.eats.2012.05.005Arthroscopy Techniques, Vol 1, No 1 (S
restore isometry, whereas transphyseal techniques vio-late and can tether the growth plate and may cause leglength discrepancies or angular deformities. In the tran-sepiphyseal technique, as described by Anderson,3 ana-tomic ACL reconstruction is performed by drilling thefemoral and tibial tunnels within the epiphysis, avoidingdisruption of the growth plate. However, the tibial graftis fixed to the metaphysis, which can potentially causegrowth disturbance through a “tether effect.”
We describe a modification of the Anderson techniquefor all-epiphyseal ACL reconstruction in an ACL-deficient child: an all-epiphyseal quadruple-hamstringACL reconstruction using a split tibial tunnel (Fig 1).The graft, the bone tunnels, and graft fixation are placedentirely within the epiphysis. An all-epiphyseal tech-nique should minimize the risk of growth disturbance byavoiding drilling or tethering the growth plate. It shouldalso minimize the risk of subsequent cartilage damagefrom recurrent knee instability by its anatomic graftplacement. The split tibial tunnels drop the tunnel sizedown to 4.5 to 5.5 mm from 7 to 8 mm because only half
the total graft diameter passes through each of the splite133eptember), 2012: pp e133-e139

ined. (Cas the
e134 M. G. LYKISSAS ET AL.
tunnels. This increases the safety margin for keeping thetunnel within the tibial epiphysis, in addition to avoidingdamage into the growth plate. The bone bridge betweenthe 2 tunnels serves a solid low-profile fixation post.
Surgical Technique
Joint Preparation
The patient is positioned supine on a fluoroscopy-compatible operating room table with the table footextended. A non-circumferential leg holder is ele-vated under the thigh so that the hip is flexed about25° to facilitate lateral cross-table fluoroscopy ofthe knee. If the surgeon is certain that the ACL isruptured, surgery begins with a 4-cm vertical inci-sion made over the proximal medial tibia about 2cm medial to the tibial tubercle. The skin incisionstarts just below the joint line to facilitate drillingof the tibial epiphyseal tunnels and is extendeddistally to allow harvest of the gracilis and semi-tendinosus tendons in standard fashion. The sur-geon should not try to gain extra tendon length bystripping the periosteum as hamstrings originate offthe proximal tibia because this may stimulate me-dial overgrowth (proximal tibia vara).
A diagnostic arthroscopy is performed first throughstandard portals with chondral or meniscal surgery asindicated. The remnants of the ACL are removed, anda minimal (2- to 4-mm) notchplasty is performed toallow adequate visualization of the anatomic ACLfootprint on the femur.
The muscle is removed by use of a metal ruler, andNo. 2 FiberLoop sutures (Arthrex, Naples, FL) are
FIGURE 1. Modified all-epiphyseal ACL reconstruction. (A) A fefemoral and proximal tibial epiphysis, respectively. (B) A biocomptunnel. A 1-cm bone bridge between the 2 tibial tunnels is maintacorrect position of the femoral tunnel in the lateral plane, as well
used to sew the 2 tendons together at their proximal
and distal ends with a whipstitch. To create a double-strand graft with similar diameters at both ends, thethick proximal end of the gracilis is sewn to the thindistal end of the semitendinosus and vice versa. Thecentral 12 cm of the doubled graft is left free of sutureso that the intra-articular portion will be pure tendonwithout suture (Fig 2). The doubled tendons are foldedover, and Vicryl suture (Ethicon, Somerville, NJ) islooped around the center of the forelimb. The diame-ters of the quadrupled graft and each of the doubledends are measured by use of the appropriate tendonsizers from the Biotenodesis set (Arthrex). The diam-eter of the quadrupled graft typically ranges from 6 to8 mm and will be fixed in the single femoral tunnel.The doubled-end diameter measures 4 to 5.5 mm, andeach side of the doubled graft will reside in its ownseparate tunnel. The tendons are then placed under 10lb of tension on the back table with the use of the
unnel and a split tibial tunnel are placed entirely within the distalterference screw (Matryx) is used to fix the graft into the femoral) Lateral illustration of the all-epiphyseal technique showing the
looped end of the graft around the anteromedial tibial epiphysis.
FIGURE 2. Graft preparation in all-epiphyseal ACL reconstructionwith split tibial tunnel. The proximal end of the gracilis is sewn tothe thin distal end of the semitendinosus with a whipstitch and viceversa by use of No. 2 FiberLoop sutures. The central 12 cm of thedoubled graft is left free of suture. The doubled tendons are foldedover, and Vicryl suture is looped around the midpoint of the graft.The tendons are then placed under 10 lb of tension for 20 minutes
moral tosite in
on the back table with the use of the GraftMaster device.

awtTo
e135ALL-EPIPHYSEAL ACL RECONSTRUCTION IN CHILDREN
GraftMaster device (Acufex Smith & Nephew, An-dover, MA).
Tunnel Preparation
The femoral tunnel is approached first. The arthro-scope is moved from the anterolateral portal to theanteromedial portal. The Arthrex femoral RetroDrillguide is inserted through the anterolateral portal, anda 2.4-mm K-wire is placed percutaneously through thelateral femoral condyle from outside in (Video 1). The2.4-mm guide pin is directed into the notch underanteroposterior fluoroscopy, staying parallel and justdistal to the femoral growth plate. A small stab inci-sion on the lateral thigh facilitates insertion of theguidewire to bone. With the C-arm in the lateralposition, the guidewire should enter the lateral femo-ral condyle at a point that is one-fourth of the distancefrom posterior to anterior along the Blumensaat lineand one-fourth of the distance down from the Blumen-saat line. The guidewire is visualized arthroscopicallyentering into the intercondylar notch at a point corre-sponding to the center of the anatomic footprint of theACL on the femur. The femoral tunnel is reamed afterthe tibial tunnel guide pins are placed.
The tibial tunnel is prepared after repositioning ofthe C-arm into the cross-table lateral position so thatthe extension of the proximal tibial physis into thetibial tubercle can be visualized. A first guidewire isinserted into the anteromedial tibial epiphysis justmedial to the patellar tendon. The guidewire is drilledfreehand or with a tibial guide into the epiphysis under
FIGURE 3. Tibial tunnel preparation in all-epiphyseal ACL recons9-year-old boy with a complete midsubstance ACL tear. The firsthile the probe is used for triangulation. (B) Arthroscopic view of
ip of the probe is placed at the desired exit point of the guidewire.he tip of the guidewire is visualized arthroscopically while enter
f the free edge of the lateral meniscus.fluoroscopic guidance and directed to the medial as-pect of the tibial ACL footprint at the level of the freeedge of the anterior horn of the lateral meniscus (Fig3). In the freehand technique, the guidewire is visual-ized arthroscopically while entering the joint. To ac-curately aim the guidewire, triangulation is used byplacing the tip of an arthroscopic probe at the desiredexit point. A second guidewire is placed about 1.5 cmmore medially and directed so that it converges in thejoint with the first guidewire (Fig 4). Similarly, thesecond guidewire should be drilled entirely withinthe epiphysis and should not cross the physis. Careshould be taken to ensure that a 1-cm bone bridgebetween the 2 tunnels remains after reaming. Theaccurate position of both guidewires is confirmed flu-oroscopically.
The medial guidewire is pulled back but left in theepiphysis while an appropriately size drill is used toream over the lateral tibial tunnel to match the size ofa doubled end of the graft, generally 4.5 to 5.5 mm(Fig 5). The medial guidewire is then advanced intothe joint, and an appropriately size drill is used toream over the medial tibial tunnel. If there is a differ-ence in the diameters of the limbs of the graft, thesmallest drill should be used for reaming the medialtibial tunnel because the margin for error is reducedcompared with the lateral tibial tunnel that resides inthe edge of the tibial tubercle expansion of the epiph-ysis. The tibial guidewires are then removed, and thesoft tissue around the outer entrance of the tibialtunnels is shaved so that it will not fold inward and
n with split tibial tunnel. (A) Lateral radiograph of the left knee ofuidewire is drilled into the epiphysis under fluoroscopic guidance
me knee through the anterolateral portal. One should note that thethroscopic view of the same knee through the anterolateral portal.knee joint at the medial aspect of the ACL footprint at the level
tructiotibial gthe sa(C) Aring the

e136 M. G. LYKISSAS ET AL.
impede graft passage. The skin is incised around thefemoral guidewire to accommodate the reamer fromoutside in. An appropriately size drill is used to reamthe femoral tunnel over the guidewire, usually 7 to 8mm in diameter (Fig 6).
Graft Retrieval
A looped 22-gauge wire is placed from outsidein through the femoral tunnel and retrieved with an
FIGURE 5. Tibial tunnel preparation in all-epiphyseal ACL recon-struction with split tibial tunnel: lateral radiograph of the left kneeof a 9-year-old boy with a complete midsubstance ACL tear. Tibialtunnel drilling begins with the lateral tibial tunnel after the medial
guidewire has been pulled back.arthroscopic grasper or probe through 1 of the tibialtunnels. A second looped 22-gauge wire is placedthrough the femoral tunnel and retrieved in a similarmanner through the other tibial tunnel. Sutures from 1end of the graft are placed through the looped portionof the first wire (emerging from the medial tunnel) andretrieved from the lateral femoral condyle. Suturesfrom the other end of the graft are placed through thelooped portion of the second wire (emerging from thelateral tunnel) and retrieved from the lateral femoralcondyle in a similar manner. The individual doubledgraft limbs are held upside-down and are advancedindependently through the tibial tunnels to the intra-articular end of the femoral tunnel (Fig 7). Then, thegraft limbs are pulled up through the femoral tunnelsimultaneously by use of the back side of an angledcurette to guide the graft into the femoral tunnel. Afteradvancement of the graft, the suture loop that hadbeen placed at the halfway point of the graft duringpreparation should overlie the center of the tibial bonebridge.
Graft Fixation
The knee is fully extended while tension is appliedto the graft to rule out impingement on the intercon-dylar notch arthroscopically. The knee is then cycled,and tension of approximately 15 lb is applied to thetendons proximally. A biocomposite interferencescrew (Matryx; ConMed Linvatec, Largo, FL) thatmatches the size of the bone tunnel “line to line” isplaced in the femoral tunnel for graft fixation whilethe knee is positioned in approximately 30° of flex-
FIGURE 4. Tibial tunnel prep-aration in all-epiphyseal ACLreconstruction with split tibialtunnel: lateral radiograph (A)and arthroscopic view throughthe anterolateral portal (B) ofthe left knee of a 9-year-oldboy with a complete midsub-stance ACL tear. It should benoted that the second tibialguidewire is placed in a con-vergent way to the first tibialpin.
ion. Wound closure then proceeds in a standard
datspctmptdtfs
cgsst
tmpdserasrti
ndtaSweppii
w9ainccpt
e137ALL-EPIPHYSEAL ACL RECONSTRUCTION IN CHILDREN
fashion, and the extremity is immobilized in a bracebefore the patient leaves the operative suite.
DISCUSSION
The great variety of ACL reconstruction proce-ures described for restoration of knee stabilityfter ACL intrasubstance tears in skeletally imma-ure patients reflects the fact that there is no con-ensus on how to treat ACL injuries in this patientopulation. In an adult-style transphyseal ACL re-onstruction, graft tunnels and fixation devices ex-end into the distal femoral and proximal tibialetaphysis. In children with wide-open growth
lates, a solidly fixed and tensioned graft may po-entially cause a tether effect and resultant growthisturbance without forming a bone bridge acrosshe growth plate.4 To avoid tether or bone barormation, multiple partial or complete physeal-paring techniques have been proposed.1-3
Theoretically, physeal-sparing procedures do notause growth disturbances by minimizing the risk ofrowth plate injury. In the over-the-top “physeal-paring” reconstruction described by Kocher et al.,1 atrip of iliotibial band that is left attached to the Gerdy
FIGURE 6. Femoral tunnel preparation in all-epiphyseal ACLreconstruction with split tibial tunnel: lateral radiograph of the leftknee of a 9-year-old boy with a complete midsubstance ACL tearafter drilling of the femoral tunnel.
ubercle is passed around the over-the-top position on s
he femur, through the notch, and under the transverseeniscal ligament and is fixed to the anterior tibial
eriosteum distal to the physis. In a recent adult ca-averic biomechanical study, iliotibial band recon-truction was found to be advantageous over trans-piphyseal and transphyseal techniques in terms ofestoration of normal anteroposterior tibial translationnd rotatory stability.4 However, this technique re-ulted in an overconstrained knee with respect tootation at higher flexion angles. It is also a nonana-omic ACL replacement and, thus, does not providesometry.
In the transepiphyseal ACL reconstruction tech-ique of Anderson,3 the femoral and tibial tunnels arerilled entirely within the epiphysis, avoiding pene-ration of the growth plate. The doubled hamstringutograft is looped over an EndoButton (Acufexmith & Nephew) and washer on the femoral side,hereas the tibial graft is tunneled through the tibial
piphysis and then spans the proximal tibial growthlate and is fixed to the tibial metaphysis with a screwost in the metaphysis. Advantages of the techniquenclude no growth plate drilling and the restoration ofsometry by placing the graft in an anatomic location
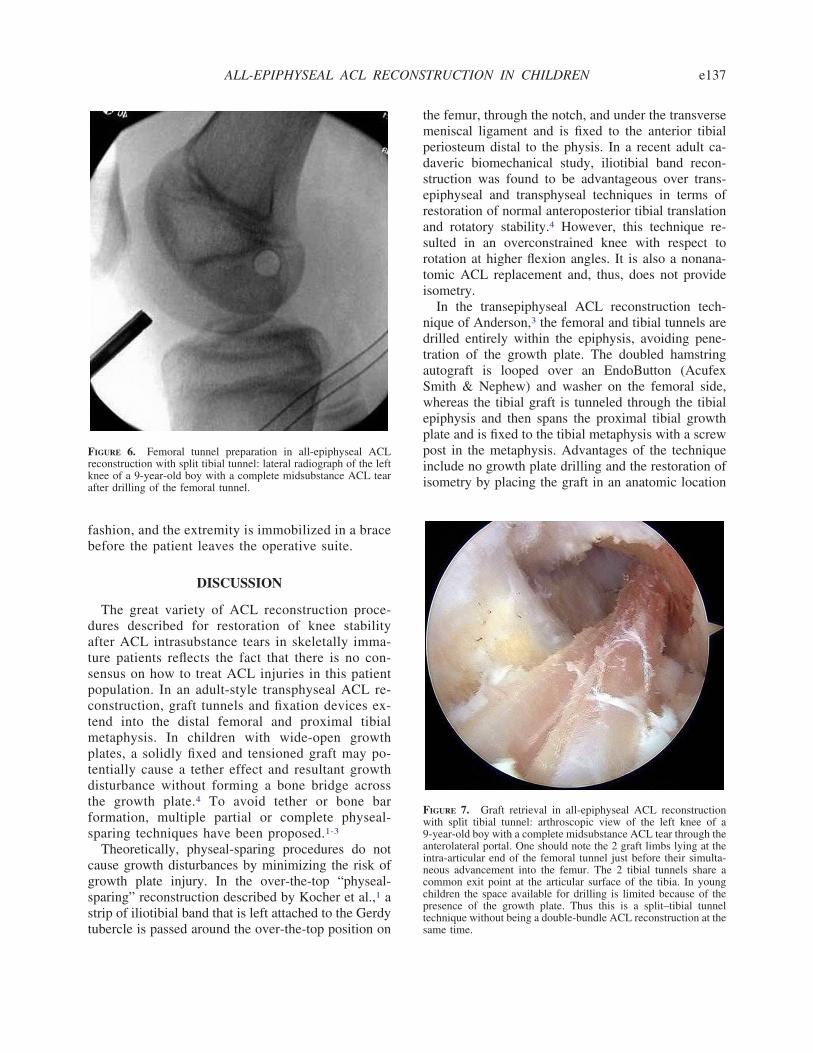
FIGURE 7. Graft retrieval in all-epiphyseal ACL reconstructionith split tibial tunnel: arthroscopic view of the left knee of a-year-old boy with a complete midsubstance ACL tear through thenterolateral portal. One should note the 2 graft limbs lying at thentra-articular end of the femoral tunnel just before their simulta-eous advancement into the femur. The 2 tibial tunnels share aommon exit point at the articular surface of the tibia. In younghildren the space available for drilling is limited because of theresence of the growth plate. Thus this is a split–tibial tunnelechnique without being a double-bundle ACL reconstruction at the
ame time.
rmftt
f
A
e138 M. G. LYKISSAS ET AL.
on both the tibia and the femur (Table 1). The onlydisadvantage of the technique is the tibial fixation ofthe graft that spans the growth plate, which can po-tentially result in a tether effect, especially in childrenwith significant growth remaining. It is also difficult todrill a 7- to 8-mm single tunnel in the small tibialepiphysis of children aged younger than 10 years.
In the surgical technique we describe, the graft, thebone tunnels, and both tibial fixation and femoralfixation are placed entirely within the epiphysis. It is apure all-epiphyseal ACL reconstruction and re-createsthe native epiphyseal-to-epiphyseal ACL anatomy ofthe child. The intra-articular portion reproduces theanatomic attachments of the ACL, which is the bestway to restore rotational and anteroposterior stabilityof the knee. It also allows for immediate weight bear-ing, no restriction of motion, and aggressive knee
TABLE 1. Advantages, Risks/Limitations, Tips, andTibi
Advantages Risks/Limitations
voids drilling through the growthplate
Growth plate injuryfrom inadequate tibitunnel drilling
Avoids tethering the growth plate Limb overgrowth duestimulation of thephyses(hypervascularity duto drilling nearphyses)
Minimizes the risk of permanentgrowth arrest
Surgery through theperiosteum near thetibial physis may alsstimulate growth
Restores the isometry by anatomicgraft placement
Minimizes the risk of cartilagedamage from recurrent kneeinstability
The decreased diameter of the tibialtunnels increases the safetymargin for keeping the tunnelswithin the tibial epiphysis
The bone bridge between the 2tibial tunnels serves as a solidlow-profile fixation post
rehabilitation. A split tibial tunnel with an intervening1-cm cortical bone bridge ensures secure low-profiletibial graft fixation while reducing the tunnel size,which increases the margin of safety between thegrowth plate and the joint when one is drilling the thintibial epiphysis. Femoral graft fixation is achievedwith an interference screw, which allows precise ten-sioning and low-profile fixation entirely within thefemoral tunnel.3
Although the described technique minimizes theisk of growth disturbance, damage to the growth plateay still occur during drilling of the epiphysis on the
emur or the tibia. Our technique with split tibialunnels increases the margin of safety by decreasinghe tunnel diameter.
The described technique is a promising alternativeor ACL reconstruction in skeletal immature patients
s of All-Epiphyseal ACL Reconstruction Using Splitnel
Tips Pearls
Start the skin incision forgraft harvesting justbelow the joint line tofacilitate drilling of thetibial epiphysealtunnels
Do not try to gain extratendon length by strippingthe periosteum because thismay stimulate medialovergrowth of the proximaltibia
Perform a minimalnotchplasty to allowadequate visualizationof the anatomic ACLfootprint on the femur
Sew the thick proximal endof the gracilis to the thindistal end of thesemitendinosus and viceversa
During graft retrieval,pull the graft limbsthrough the femoraltunnel simultaneously
Avoid sutures at the central12 cm of the doubled graft
Fix the graft in 30° offlexion
Do not ream the femoraltunnel until the tibialtunnels are placed
If there is a difference in thediameter of the limbs ofthe graft, the smallest drillshould be used for reamingthe medial tibial tunnel
Ensure that a 1-cm bonebridge will remain betweenthe 2 tunnels after reaming
After advancing the graft, thesuture loop that had beenplaced at the center of thegraft during preparationshould overlie the center of
Pearlal Tun
al
to
e
o
the tibial bone bridge

2
3
4
e139ALL-EPIPHYSEAL ACL RECONSTRUCTION IN CHILDREN
with significant growth remaining (Table 2). By plac-ing the graft at the native ACL’s anatomic attachment
TABLE 2. Indications and Contraindications of All-Epiphyseal ACL Reconstruction Using Split Tibial Tunnel
Indications Contraindications
Boys with a midsubstanceACL tear and a boneage �14.5 yr who wishto return to cuttingsports
Children who strictly avoid cuttingsports and do not have recurrentknee instability episodes
Girls with a midsubstanceACL tear and a boneage �13 yr who wishto return to cuttingsports
Skeletally immature athletes withbone ages �14.5 yr for boysand �13 yr for girls
points without spanning or drilling the growth plates
at any step of the procedure, all-epiphyseal ACL re-construction with a split tibial tunnel theoreticallyminimizes the risk of growth disturbance in an ACL-deficient child.
REFERENCES
1. Kocher MS, Garg S, Micheli LJ. Physeal sparing reconstructionof the anterior cruciate ligament in skeletally immature prepu-bescent children and adolescents. J Bone Joint Surg Am 2005;87:2371-2379.
. Guzzanti V, Falciglia F, Stanitski CL. Physeal-sparing intraar-ticular anterior cruciate ligament reconstruction in preadoles-cents. Am J Sports Med 2003;31:949-953.
. Anderson AF. Transepiphyseal replacement of the anterior cru-ciate ligament in skeletally immature patients. A preliminaryreport. J Bone Joint Surg Am 2003;85:1255-1263.
. Kennedy A, Coughlin DG, Metzger MF, et al. Biomechanical
evaluation of pediatric anterior cruciate ligament reconstructiontechniques. Am J Sports Med 2011;39:964-971.



















