Anterior cruciate ligament reconstruction and joint dynamics during stair climbing
11
After online publication, subscribers (personal/institutional) to this journal will have access to the complete article via the DOI using the URL: If you would like to know when your article has been published online, take advantage of our free alert service. For registration and further information, go to: . Due to the electronic nature of the procedure, the manuscript and the original figures will only be returned to you on special request. When you return your corrections, please inform us, if you would like to have these documents returned. Dear Author Here are the proofs of your article. • You can submit your corrections online, via e-mail or by fax. • For online submission please insert your corrections in the online correction form. Always indicate the line number to which the correction refers. • You can also insert your corrections in the proof PDF and email the annotated PDF. • For fax submission, please ensure that your corrections are clearly legible. Use a fine black pen and write the correction in the margin, not too close to the edge of the page. • Remember to note the journal title, article number, and your name when sending your response via e-mail or fax. • Check the metadata sheet to make sure that the header information, especially author names and the corresponding affiliations are correctly shown. • Check the questions that may have arisen during copy editing and insert your answers/corrections. • Check that the text is complete and that all figures, tables and their legends are included. Also check the accuracy of special characters, equations, and electronic supplementary material if applicable. If necessary refer to the Edited manuscript. • The publication of inaccurate data such as dosages and units can have serious consequences. Please take particular care that all such details are correct. • Please do not make changes that involve only matters of style. We have generally introduced forms that follow the journal’s style. • Substantial changes in content, e.g., new results, corrected values, title and authorship are not allowed without the approval of the responsible editor. In such a case, please contact the Editorial Office and return his/her consent together with the proof. • If we do not receive your corrections within 48 hours, we will send you a reminder. • Your article will be published Online First approximately one week after receipt of your corrected proofs. This is the official first publication citable with the DOI. Further changes are, therefore, not possible. • The printed version will follow in a forthcoming issue. Please note http://www.link.springer.com http://dx.doi.org/10.1007/s00264-014-2513-9
-
Upload
eeeeeeeeeeeeeeeeee -
Category
Documents
-
view
0 -
download
0
Transcript of Anterior cruciate ligament reconstruction and joint dynamics during stair climbing
After online publication, subscribers (personal/institutional) to this journal will haveaccess to the complete article via the DOI using the URL:
If you would like to know when your article has been published online, take advantageof our free alert service. For registration and further information, go to:
.
Due to the electronic nature of the procedure, the manuscript and the original figureswill only be returned to you on special request. When you return your corrections,please inform us, if you would like to have these documents returned.
Dear Author
Here are the proofs of your article.
• You can submit your corrections online, via e-mail or by fax.
• For online submission please insert your corrections in the online correction form.
Always indicate the line number to which the correction refers.
• You can also insert your corrections in the proof PDF and email the annotated PDF.
• For fax submission, please ensure that your corrections are clearly legible. Use a fine
black pen and write the correction in the margin, not too close to the edge of the page.
• Remember to note the journal title, article number, and your name when sending your
response via e-mail or fax.
• Check the metadata sheet to make sure that the header information, especially author
names and the corresponding affiliations are correctly shown.
• Check the questions that may have arisen during copy editing and insert your
answers/corrections.
• Check that the text is complete and that all figures, tables and their legends are included.
Also check the accuracy of special characters, equations, and electronic supplementary
material if applicable. If necessary refer to the Edited manuscript.
• The publication of inaccurate data such as dosages and units can have serious
consequences. Please take particular care that all such details are correct.
• Please do not make changes that involve only matters of style. We have generally
introduced forms that follow the journal’s style.
• Substantial changes in content, e.g., new results, corrected values, title and authorship are
not allowed without the approval of the responsible editor. In such a case, please contact
the Editorial Office and return his/her consent together with the proof.
• If we do not receive your corrections within 48 hours, we will send you a reminder.
• Your article will be published Online First approximately one week after receipt of your
corrected proofs. This is the official first publication citable with the DOI. Further
changes are, therefore, not possible.
• The printed version will follow in a forthcoming issue.
Please note
http://www.link.springer.com
http://dx.doi.org/10.1007/s00264-014-2513-9
AUTHOR'S PROOF!
Metadata of the article that will be visualized in OnlineFirst
1 Article Title Anterior cruciate ligament reconstruction and return to sport
activ ity: postural control as the key to success
2 Article Sub- Title
3 Article Copyright -Year
SICOT aisbl 2014(This will be the copyright line in the final PDF)
4 Journal Name International Orthopaedics
5
Corresponding
Author
Family Name Maffulli
6 Particle
7 Given Name Nicola
8 Suffix
9 Organization University of Salerno
10 Division Department of Musculoskeletal Disorders, Facultyof Medicine and Surgery
11 Address Baronissi 84081, Salerno, Italy
12 Organization Mile End Hospital
13 Division Centre for Sports and Exercise Medicine, Bartsand The London School of Medicine andDentistry
14 Address 275 Bancroft Road, London E1 4DG, UK
15 e-mail n.maffull [email protected]
16
Author
Family Name Papalia
17 Particle
18 Given Name Rocco
19 Suffix
20 Organization Campus Bio-Medico University of Rome
21 Division Department of Orthopaedic and Trauma Surgery
22 Address Via Alvaro del Porti l lo 200, Rome, Italy
23 e-mail
24
Author
Family Name Franceschi
25 Particle
26 Given Name Francesco
27 Suffix
28 Organization Campus Bio-Medico University of Rome

AUTHOR'S PROOF!
29 Division Department of Orthopaedic and Trauma Surgery
30 Address Via Alvaro del Porti l lo 200, Rome, Italy
31 e-mail
32
Author
Family Name Tecame
33 Particle
34 Given Name Andrea
35 Suffix
36 Organization Campus Bio-Medico University of Rome
37 Division Department of Orthopaedic and Trauma Surgery
38 Address Via Alvaro del Porti l lo 200, Rome, Italy
39 e-mail
40
Author
Family Name D’Adamio
41 Particle
42 Given Name Stefano
43 Suffix
44 Organization Campus Bio-Medico University of Rome
45 Division Department of Orthopaedic and Trauma Surgery
46 Address Via Alvaro del Porti l lo 200, Rome, Italy
47 e-mail
48
Author
Family Name Denaro
49 Particle
50 Given Name Vincenzo
51 Suffix
52 Organization Campus Bio-Medico University of Rome
53 Division Department of Orthopaedic and Trauma Surgery
54 Address Via Alvaro del Porti l lo 200, Rome, Italy
55 e-mail
56
Schedule
Received 3 August 2014
57 Revised
58 Accepted 14 August 2014
59 Abstract
60 Keywordsseparated by ' - '
ACL - Reconstruction - Semitendinosus and gracil is - Patellartendon - Rehabilitation - KAM
61 Foot noteinformation

AUTHOR'S PROOF!
UNCORRECTEDPROOF
1
23 ORIGINAL PAPER
4 Anterior cruciate ligament reconstruction and return to sport5 activity: postural control as the key to success
7 Rocco Papalia & Francesco Franceschi & Andrea Tecame &
8 Stefano D’Adamio & Nicola Maffulli & Vincenzo Denaro9
10
11 Received: 3 August 2014 /Accepted: 14 August 201412 # SICOT aisbl 2014
13 Abstract14 Purpose The risk for re-tear following anterior cruciate liga-15 ment (ACL) reconstruction is influenced by several hormonal,16 neuromuscular, biomechanical and anatomic factors. One of17 the most important negative prognostic factors that markedly18 increase the risk for ACL re-tear is the presence of high knee-19 abduction moment (KAM), which can be measured immedi-20 ately by landing on both feet after a vertical jump. We evalu-21 ated the effect in postoperative values for KAM according to22 the type of graft used for ACL reconstruction (hamstring vs23 patellar tendon) and a specific rehabilitation protocol focusing24 on recovery of muscular strength, proprioception and joint25 stabilisation.26 Methods From November 2010 to September 2012, we en-27 rolled 40 female recreational athletes with clinical and imag-28 ing evidence of ACL tear and randomised them in two groups.29 One group of patients underwent reconstruction with a30 hamstring-tendon graft and the second with a patellar-tendon31 graft. A custom rehabilitation programme focusing on propri-32 oception was adopted. Clinical outcomes [International Knee33 Documentation Committee (IKDC) and Lysholm scores] and34 performance in functional test for stability (single-leg hop,
35timed hop, crossover triple hop, KAM test) were assessed36preoperatively at 3 and 6 months postoperatively.37Results All patients showed statistically significant clinical38improvements postoperatively when compared with preoper-39ative values (P<0.0001). No significant intergroup difference40was observed in all clinical scores and functional tests, with41the exception of the value registered for the KAM test42(P<0.0001).43Conclusions ACL reconstruction using patellar-tendon graft44followed by rehabilitation centred on strength, proprioception45and stability restoration can produce satisfactory values for46KAM within the physiological range. The surgical strategies47should be adapted to the patient on the basis of a multidisci-48plinary approach.
49Keywords ACL . Reconstruction . Semitendinosus and50gracilis . Patellar tendon . Rehabilitation . KAM
51Introduction
52Biomechanical, neuromuscular, psychological, hormonal and53anatomical factors all impact on the risk of developing anterior54cruciate ligament (ACL) tears [1–5]. In particular, epidemio-55logical data show that women are particularly at risk for re-tear56following ACL reconstruction [6, 7]. Biomechanical studies57focusing on the knee-abduction moment (KAM), an index of58knee stability, report that the higher the KAM value, the59greater the risk of ACL re-tear [7–9]. Several factors influence60KAM values; the most important are knee valgus moment,61range of motion (ROM) in knee flexion, body mass, tibial62length and quadriceps:flexor muscle ratio [8]. In women,63KAM values are physiologically higher than in men [10],64possibly (at least partially) explaining the higher incidence65of re-tear in women. If using autologous semitendinosus and66gracilis tendons as the graft for ACL reconstruction, the
R. Papalia : F. Franceschi :A. Tecame : S. D’Adamio :V. DenaroDepartment of Orthopaedic and Trauma Surgery, CampusBio-Medico University of Rome, Via Alvaro del Portillo 200, Rome,Italy
N. Maffulli (*)Department of Musculoskeletal Disorders, Faculty of Medicine andSurgery, University of Salerno, 84081 Baronissi, Salerno, Italye-mail: [email protected]
N. MaffulliCentre for Sports and Exercise Medicine, Barts and The LondonSchool of Medicine and Dentistry, Mile End Hospital, 275 BancroftRoad, London E1 4DG, UK
International Orthopaedics (SICOT)DOI 10.1007/s00264-014-2513-9
JrnlID 264_ArtID 2513_Proof# 1 - 03/09/2014

AUTHOR'S PROOF!
UNCORRECTEDPROOF
67 harvest can alter the ratio of strength between knee extensor68 and flexor muscles, resulting in even higher postoperative69 KAM values in these patients [11].70 The definitive aim of the study was to compare the KAM71 values assesses in different patients to evaluate the possible72 different effects of the two surgical approaches (reconstruction73 using semitendinosus and gracilis vs patellar tendon) on knee74 stability restoration. Along with this primary intention, we75 attempted to verify the hypothesis of no difference in func-76 tional score [International Knee Documentation Committee77 (IKDC) and Lysholm score) in patient undergoing ACL re-78 construction using either semitendinosus and gracilis or patel-79 lar tendon as graft choice in a population of female recrea-80 tional athletes. We also aimedd to verify whether a rehabilita-81 tion protocol based on recovery of knee proprioception and82 postural control can improve postoperative KAM values com-83 pared with a historical control group in which a standard84 rehabilitation protocol was followed after surgery.
85 Materials and methods
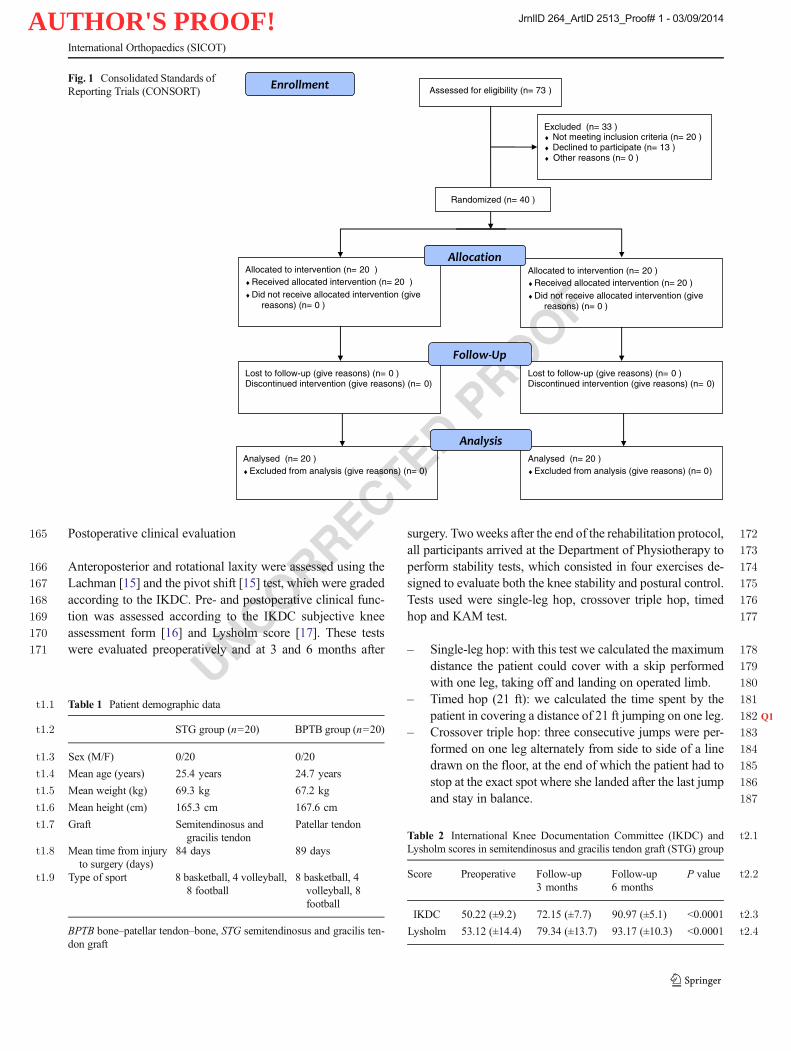
86 Patients studied were recreational female athletes with a87 symptomatic, complete ACL tear detected on clinical (pos-88 itive Lachman and pivot shift tests [12]) and imaging:89 lateral and anteroposterior (AP) weight-bearing radio-90 graphs to detect fractures, osteoarthritis grading and var-91 us–valgus malalignment assessment; MRI to evaluate le-92 sions to the ACL, cartilage, menisci and other knee93 ligaments.94 Patients were all scheduled to undergo ACL reconstruc-95 tion using a semitendinosus and gracilis or patellar tendon96 graft, followed by a standardised postoperative rehabilita-97 tion programme for 24 weeks. Patients requiring concom-98 itant surgical management of meniscal lesions were also99 included in the study. Exclusion criteria were history of100 previous surgery on either knee, detection of cartilage101 lesions or osteoarthritic changes (joint-space narrowing102 >50 % in any compartment), multiligamentous involve-103 ment [posterior cruciate ligament (PCL), lateral collateral104 ligament (LCL), medial collateral ligament (MCL), pos-105 terolateral corner], concomitant ipsilateral leg fracture and106 cardiovascular disease.107 A total of 73 consecutive female recreational athletes op-108 erated at out institution between 2010 and 2012 met our109 inclusion criteria. However, 13 patients did not want to par-110 ticipate in the study, five had a grade III or IV chondral lesion,111 seven had multiligamentous injury and eight had positive112 history of surgery to the same knee; these patients were113 excluded. Ultimately, 40 patients were considered eligible114 for the study. The Consolidated Standards of Reporting Trials115 (CONSORT) flowchart [13] for this trial is presented in Fig. 1.116 Patients were then randomised into two groups using a
117computerised combination generator operaded by an investi-118gator with no clinical involvement in the trial (SD). The first119group consisted of patients who underwent ACL reconstruc-120tion using semitendinosus and gracilis tendon grafts (STG121group); the second group consisted of patients undergoing122ACL reconstruction using the middle third of the patellar123tendon for reconstruction [bone–patellar tendon–bone124(BPTB) group].125All patients played either football (N=16), volleyball (N=1268) or basketball (N=16). Although they all participated in127sports before the accident, significant differences were found128given the different types of training, intensity and physical129load between required for the different sports. Mean follow-up130was 12 months; mean interval of time from injury to surgery131was 84 days [standard deviation (SD)±20, 95 % confidence132interval (CI) 64–104] for the STG group and 89 days (SD±27,13395%CI 72–100) for the BPTB group. Prior to data collection,134each athlete read and signed an informed consent to partici-135pate in the study, which was approved by our Institution ethics136committee. The study was conducted at the Department of137Orthopaedic and Trauma Surgery of the Campus Bio-Medico138University Hospital in Rome.
139Operative findings and surgical technique
140All patients were operated by two experienced orthopaedic141surgeons (RP and FF) who performed routine ACL recon-142structions using the transtibial technique [11, 14]. At diagnos-143tic arthroscopy, all 40 patients were confirmed to have com-144plete ACL tears. In the STG group, six underwent partial145meniscectomies (three medial and three lateral) and three146medial meniscus repair for a red–red zone tear. In the BPTB147group, six patients underwent partial meniscectomies (three148medial and three lateral) and two a meniscal repair: one for a149red–red zone and one for a white–red zone tear. In the BPTB150group, fixation was accomplished using metal interference151screws (Arthrex, Naples, FL, USA); in the STG group, fem-152oral fixation was accomplished using the TightRope® system153(Arthrex). In the tibia, the graft was fixed using absorbable154screw (Arthrex).
155Rehabilitation protocol
156All recruited patients followed a standard rehabilitation pro-157gramme for a period of 24 weeks that consisted of five phases158focusing on different recovery objectives: ROM (1–2 weeks),159force (3–4 weeks), proprioception and stability (5–11 weeks),160run (9–14 weeks), power (15–24 weeks). Particular attention161was paid to the third stage—fifth to 11th week—during which162patients trained proprioception and postural stability. No pa-163tient withdrew from the study, and all attended at least 85% of164the rehabilitation sessions.
International Orthopaedics (SICOT)
JrnlID 264_ArtID 2513_Proof# 1 - 03/09/2014
AUTHOR'S PROOF!
UNCORRECTEDPROOF
165 Postoperative clinical evaluation
166 Anteroposterior and rotational laxity were assessed using the167 Lachman [15] and the pivot shift [15] test, which were graded168 according to the IKDC. Pre- and postoperative clinical func-169 tion was assessed according to the IKDC subjective knee170 assessment form [16] and Lysholm score [17]. These tests171 were evaluated preoperatively and at 3 and 6 months after
172surgery. Twoweeks after the end of the rehabilitation protocol,173all participants arrived at the Department of Physiotherapy to174perform stability tests, which consisted in four exercises de-175signed to evaluate both the knee stability and postural control.176Tests used were single-leg hop, crossover triple hop, timed177hop and KAM test.
178– Single-leg hop: with this test we calculated the maximum179distance the patient could cover with a skip performed180with one leg, taking off and landing on operated limb.181– Timed hop (21 ft): we calculated the time spent by the182patient in covering a distance of 21 ft jumping on one leg. Q1
183– Crossover triple hop: three consecutive jumps were per-184formed on one leg alternately from side to side of a line185drawn on the floor, at the end of which the patient had to186stop at the exact spot where she landed after the last jump187and stay in balance.
Assessed for eligibility (n= 73 )
Excluded (n= 33 )Not meeting inclusion criteria (n= 20 )Declined to participate (n= 13 )Other reasons (n= 0 )
Analysed (n= 20 )Excluded from analysis (give reasons) (n= 0)
Lost to follow-up (give reasons) (n= 0 )Discontinued intervention (give reasons) (n= 0)
Allocated to intervention (n= 20 )Received allocated intervention (n= 20 )Did not receive allocated intervention (give
reasons) (n= 0 )
Lost to follow-up (give reasons) (n= 0 )Discontinued intervention (give reasons) (n= 0)
Allocated to intervention (n= 20 )Received allocated intervention (n= 20 )Did not receive allocated intervention (give
reasons) (n= 0 )
Analysed (n= 20 )Excluded from analysis (give reasons) (n= 0)
Randomized (n= 40 )
Fig. 1 Consolidated Standards ofReporting Trials (CONSORT)
t1:1 Table 1 Patient demographic data
t1:2 STG group (n=20) BPTB group (n=20)
t1:3 Sex (M/F) 0/20 0/20
t1:4 Mean age (years) 25.4 years 24.7 years
t1:5 Mean weight (kg) 69.3 kg 67.2 kg
t1:6 Mean height (cm) 165.3 cm 167.6 cm
t1:7 Graft Semitendinosus andgracilis tendon
Patellar tendon
t1:8 Mean time from injuryto surgery (days)
84 days 89 days
t1:9 Type of sport 8 basketball, 4 volleyball,8 football
8 basketball, 4volleyball, 8football
BPTB bone–patellar tendon–bone, STG semitendinosus and gracilis ten-don graft
t2:1Table 2 International Knee Documentation Committee (IKDC) andLysholm scores in semitendinosus and gracilis tendon graft (STG) group
t2:2Score Preoperative Follow-up3 months
Follow-up6 months
P value
t2:3IKDC 50.22 (±9.2) 72.15 (±7.7) 90.97 (±5.1) <0.0001
t2:4Lysholm 53.12 (±14.4) 79.34 (±13.7) 93.17 (±10.3) <0.0001
International Orthopaedics (SICOT)
JrnlID 264_ArtID 2513_Proof# 1 - 03/09/2014
AUTHOR'S PROOF!
UNCORRECTEDPROOF
188 – KAM test: Patients were asked to jump from a box 30 cm189 high and, once they had touched the ground, to maintain190 the position of equilibrium. The exercise was repeated191 twice, and in the third repetition, two jumps as high as192 possible were performed after landing. This exercise pri-193 marily evaluated KAM and valgus attitude upon landing,194 an element that is particularly significant in predicting the195 risk of re-tear of the ACL. Upon landing, the patients’196 ability to absorb the shock with their gluteus without197 subsequent knee failure was also evaluated. To supervise198 proper execution of this exercise, the instructor directed199 each patient to land with the weight equally divided200 between both lower limbs. This test was conducted under201 the supervision of two observers: a trained orthopaedic202 surgeon described the task and supervised the patient203 during the entire exercise to guarantee correct execution204 while preventing injuries. The other observer recorded205 the task using a series of HD video recorders located206 precisely in front and at both sides of the individual at a207 distance of 5 m from the landing surface. This individual208 measured knee angles in the coronal and sagittal planes209 by tracing the axes of interest using computer software on210 single frames. Knee abduction angles were the primary211 points of interest of these measurements, being a reliable212 indicator of KAM borne by the knee.
213 Statistical analysis
214 Descriptive statistics were calculated. Clinical improvement215 over time was assessed using analysis of variance (ANOVA)216 with repeated-measures analysis in clinical and functional217 scores. A P value of <0.05 was considered to be statistically218 significant. Statistical analysis was carried out using the
219Statistical Package for the Social Sciences (SPSS) software220version 20.0 (SPSS Inc., Chicago, IL, USA).221We performed a priori power analysis to estimate the222sample size: we took into account a large anticipated effect223size (Cohen’s d value) of 0.9, setting statistical significance (P224value) at 0.05 to reach a desired statistical power of ∼0.80,225obtaining a minimum required sample size per group of 20226patients to achieve this level of significance for our227comparison.228
229Results
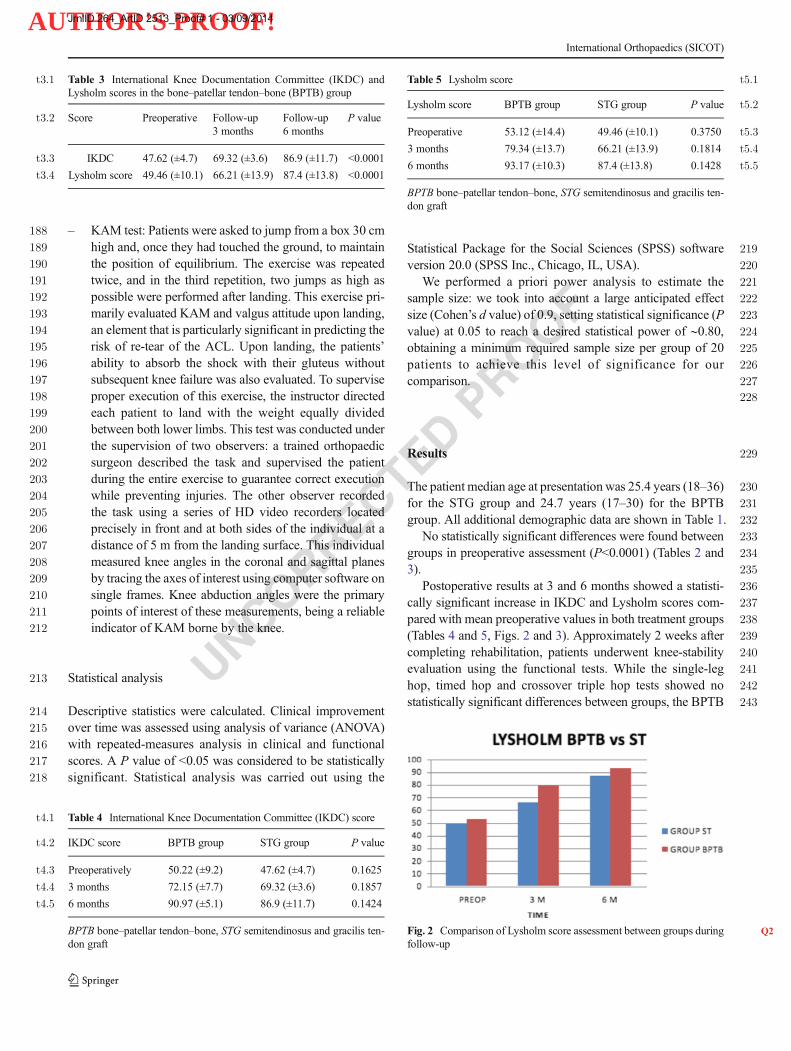
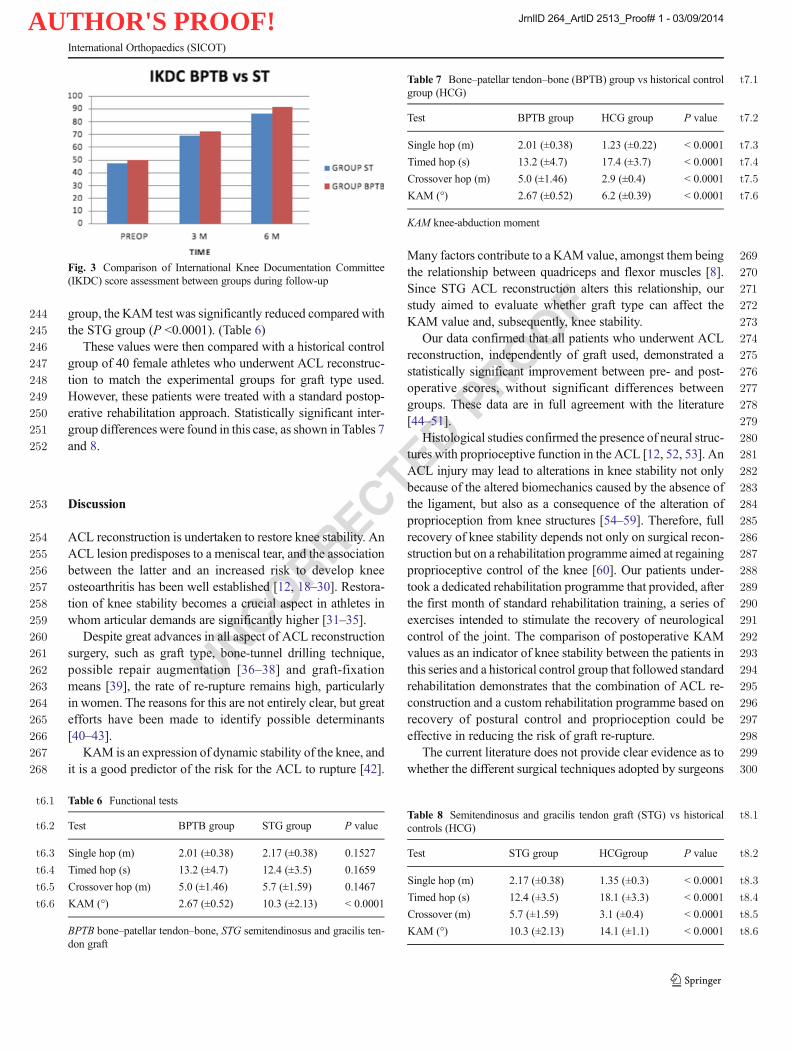
230The patient median age at presentation was 25.4 years (18–36)231for the STG group and 24.7 years (17–30) for the BPTB232group. All additional demographic data are shown in Table 1.233No statistically significant differences were found between234groups in preoperative assessment (P<0.0001) (Tables 2 and2353).236Postoperative results at 3 and 6 months showed a statisti-237cally significant increase in IKDC and Lysholm scores com-238pared with mean preoperative values in both treatment groups239(Tables 4 and 5, Figs. 2 and 3). Approximately 2 weeks after240completing rehabilitation, patients underwent knee-stability241evaluation using the functional tests. While the single-leg242hop, timed hop and crossover triple hop tests showed no243statistically significant differences between groups, the BPTB
t3:1 Table 3 International Knee Documentation Committee (IKDC) andLysholm scores in the bone–patellar tendon–bone (BPTB) group
t3:2 Score Preoperative Follow-up3 months
Follow-up6 months
P value
t3:3 IKDC 47.62 (±4.7) 69.32 (±3.6) 86.9 (±11.7) <0.0001
t3:4 Lysholm score 49.46 (±10.1) 66.21 (±13.9) 87.4 (±13.8) <0.0001
t4:1 Table 4 International Knee Documentation Committee (IKDC) score
t4:2 IKDC score BPTB group STG group P value
t4:3 Preoperatively 50.22 (±9.2) 47.62 (±4.7) 0.1625
t4:4 3 months 72.15 (±7.7) 69.32 (±3.6) 0.1857
t4:5 6 months 90.97 (±5.1) 86.9 (±11.7) 0.1424
BPTB bone–patellar tendon–bone, STG semitendinosus and gracilis ten-don graft
t5:1Table 5 Lysholm score
t5:2Lysholm score BPTB group STG group P value
t5:3Preoperative 53.12 (±14.4) 49.46 (±10.1) 0.3750
t5:43 months 79.34 (±13.7) 66.21 (±13.9) 0.1814
t5:56 months 93.17 (±10.3) 87.4 (±13.8) 0.1428
BPTB bone–patellar tendon–bone, STG semitendinosus and gracilis ten-don graft
Fig. 2 Q2Comparison of Lysholm score assessment between groups duringfollow-up
International Orthopaedics (SICOT)
JrnlID 264_ArtID 2513_Proof# 1 - 03/09/2014
AUTHOR'S PROOF!
UNCORRECTEDPROOF244 group, the KAM test was significantly reduced compared with
245 the STG group (P <0.0001). (Table 6)246 These values were then compared with a historical control247 group of 40 female athletes who underwent ACL reconstruc-248 tion to match the experimental groups for graft type used.249 However, these patients were treated with a standard postop-250 erative rehabilitation approach. Statistically significant inter-251 group differenceswere found in this case, as shown in Tables 7252 and 8.
253 Discussion
254 ACL reconstruction is undertaken to restore knee stability. An255 ACL lesion predisposes to a meniscal tear, and the association256 between the latter and an increased risk to develop knee257 osteoarthritis has been well established [12, 18–30]. Restora-258 tion of knee stability becomes a crucial aspect in athletes in259 whom articular demands are significantly higher [31–35].260 Despite great advances in all aspect of ACL reconstruction261 surgery, such as graft type, bone-tunnel drilling technique,262 possible repair augmentation [36–38] and graft-fixation263 means [39], the rate of re-rupture remains high, particularly264 in women. The reasons for this are not entirely clear, but great265 efforts have been made to identify possible determinants266 [40–43].267 KAM is an expression of dynamic stability of the knee, and268 it is a good predictor of the risk for the ACL to rupture [42].
269Many factors contribute to a KAM value, amongst them being270the relationship between quadriceps and flexor muscles [8].271Since STG ACL reconstruction alters this relationship, our272study aimed to evaluate whether graft type can affect the273KAM value and, subsequently, knee stability.274Our data confirmed that all patients who underwent ACL275reconstruction, independently of graft used, demonstrated a276statistically significant improvement between pre- and post-277operative scores, without significant differences between278groups. These data are in full agreement with the literature279[44–51].280Histological studies confirmed the presence of neural struc-281tures with proprioceptive function in the ACL [12, 52, 53]. An282ACL injury may lead to alterations in knee stability not only283because of the altered biomechanics caused by the absence of284the ligament, but also as a consequence of the alteration of285proprioception from knee structures [54–59]. Therefore, full286recovery of knee stability depends not only on surgical recon-287struction but on a rehabilitation programme aimed at regaining288proprioceptive control of the knee [60]. Our patients under-289took a dedicated rehabilitation programme that provided, after290the first month of standard rehabilitation training, a series of291exercises intended to stimulate the recovery of neurological292control of the joint. The comparison of postoperative KAM293values as an indicator of knee stability between the patients in294this series and a historical control group that followed standard295rehabilitation demonstrates that the combination of ACL re-296construction and a custom rehabilitation programme based on297recovery of postural control and proprioception could be298effective in reducing the risk of graft re-rupture.299The current literature does not provide clear evidence as to300whether the different surgical techniques adopted by surgeons
Fig. 3 Comparison of International Knee Documentation Committee(IKDC) score assessment between groups during follow-up
t6:1 Table 6 Functional tests
t6:2 Test BPTB group STG group P value
t6:3 Single hop (m) 2.01 (±0.38) 2.17 (±0.38) 0.1527
t6:4 Timed hop (s) 13.2 (±4.7) 12.4 (±3.5) 0.1659
t6:5 Crossover hop (m) 5.0 (±1.46) 5.7 (±1.59) 0.1467
t6:6 KAM (°) 2.67 (±0.52) 10.3 (±2.13) < 0.0001
BPTB bone–patellar tendon–bone, STG semitendinosus and gracilis ten-don graft
t7:1Table 7 Bone–patellar tendon–bone (BPTB) group vs historical controlgroup (HCG)
t7:2Test BPTB group HCG group P value
t7:3Single hop (m) 2.01 (±0.38) 1.23 (±0.22) < 0.0001
t7:4Timed hop (s) 13.2 (±4.7) 17.4 (±3.7) < 0.0001
t7:5Crossover hop (m) 5.0 (±1.46) 2.9 (±0.4) < 0.0001
t7:6KAM (°) 2.67 (±0.52) 6.2 (±0.39) < 0.0001
KAM knee-abduction moment
t8:1Table 8 Semitendinosus and gracilis tendon graft (STG) vs historicalcontrols (HCG)
t8:2Test STG group HCGgroup P value
t8:3Single hop (m) 2.17 (±0.38) 1.35 (±0.3) < 0.0001
t8:4Timed hop (s) 12.4 (±3.5) 18.1 (±3.3) < 0.0001
t8:5Crossover (m) 5.7 (±1.59) 3.1 (±0.4) < 0.0001
t8:6KAM (°) 10.3 (±2.13) 14.1 (±1.1) < 0.0001
International Orthopaedics (SICOT)
JrnlID 264_ArtID 2513_Proof# 1 - 03/09/2014

AUTHOR'S PROOF!
UNCORRECTEDPROOF
301 for ACL reconstruction exert any other effect on postoperative302 KAM. Investigating this point was the main objective of our303 study. Results showed that KAM assessment through a func-304 tional test exhibited statistically significant differences be-305 tween patients in whom the ACL was reconstructed using306 hamstring tendons compared with those in whom the patellar307 tendon was used. The latter showed lower KAM values,308 which are related to a lower risk of re-tear after surgery. From309 this observation, it is possible to hypothesise that surgical310 technique may have a primary role in attaining maximum311 knee stability following the intervention in female athletes,312 confirming previous suggestions of some authors, who dem-313 onstrated significantly greater postoperative laxity in recon-314 structed knees of female patients when using hamstring versus315 patellar tendons [61]. KAM is influenced by the relationship316 between quadriceps and flexor muscles of the lower limb.317 Using the BPTB graft does not alter this relationship, in318 contrast to using STG [62], and KAM may benefit from this319 approach. However, it is difficult to ascertain whether the320 greatest benefit regarding knee stability using this technique321 is due not only to alteration of muscle ratio or from other322 biomechanical and constitutional factors.323 Strengths of this study are its prospective randomised324 design, the presence of two experienced orthopaedic surgeons,325 the presence of an independent operator for data collection326 and the use of standardised integrated tools to evaluate knee327 stability and, in particular, KAM. The design is pragmatic and328 compliant with CONSORT [13] criteria. Limitations are the329 relatively short follow-up and the small cohort.330 Both a surgical and rehabilitation approach focusing on331 KAM conservation following ACL reconstruction in female332 athletes can improve stability of the operated knee, thus re-333 ducing the risk of postoperative re-ruptures. Results suggest334 considering the use of the patellar tendon as a graft combined335 with a dedicated rehabilitation protocol mostly focusing on336 recovery of postural control, proprioception and stability in337 female athletes with ACL deficiency.
338339 Conflict of interest None.
340 References341
342 1. Hewett TE, Lindenfeld TN, Riccobene JV, Noyes FR (1999) The343 effect of neuromuscular training on the incidence of knee injury in344 female athletes. A prospective study. Am J Sports Med 27(6):699–345 706346 2. Hewett TE, Myer GD, Ford KR (2006) Anterior cruciate ligament347 injuries in female athletes: part 1, mechanisms and risk factors. Am J348 Sports Med 34(2):299–311. doi:10.1177/0363546505284183349 3. Hewett TE, Ford KR, Myer GD (2006) Anterior cruciate ligament350 injuries in female athletes: Part 2, a meta-analysis of neuromuscular351 interventions aimed at injury prevention. Am J Sports Med 34(3):352 490–498. doi:10.1177/0363546505282619
3534. Wojtys EM, Huston LJ, Lindenfeld TN, Hewett TE, Greenfield354ML (1998) Association between the menstrual cycle and anterior355cruciate ligament injuries in female athletes. Am J Sports Med35626(5):614–6193575. Ciuffreda P, Lelario M, Milillo P, Vinci R, Coppolino F, Stoppino L,358Genovese E, Macarini L (2013) Mechanism of traumatic knee inju-359ries and MRI findings. Musculoskelet Surg 97(2):127–1353606. Lyman S, Koulouvaris P, Sherman S, Do H, Mandl LA, Marx RG361(2009) Epidemiology of anterior cruciate ligament reconstruction:362trends, readmissions, and subsequent knee surgery. J Bone Joint Surg363Am 91(10):2321–2328. doi:10.2106/JBJS.H.005393647. Hewett TE, Myer GD, Ford KR (2005) Reducing knee and365anterior cruciate ligament injuries among female athletes: a sys-366tematic review of neuromuscular training interventions. J Knee367Surg 18(1):82–883688. Myer GD, Ford KR, Khoury J, Hewett TE (2011) Three-dimensional369motion analysis validation of a clinic-based nomogram designed to370identify high ACL injury risk in female athletes. Phys Sportsmed37139(1):19–28. doi:10.3810/psm.2011.02.18583729. Paterno MV, Schmitt LC, Ford KR, Rauh MJ, Myer GD, Huang B,373Hewett TE (2010) Biomechanical measures during landing and pos-374tural stability predict second anterior cruciate ligament injury after375anterior cruciate ligament reconstruction and return to sport. Am J376Sports Med 38(10):1968–1978. doi:10.1177/036354651037605337710. Webster KE, Feller JA (2012) The knee adduction moment in ham-378string and patellar tendon anterior cruciate ligament reconstructed379knees. Knee Surg Sports Traumatol Arthrosc: Off J ESSKA 20(11):3802214–2219. doi:10.1007/s00167-011-1835-z38111. Pinczewski LA, Deehan DJ, Salmon LJ, Russell VJ, Clingeleffer A382(2002) A five-year comparison of patellar tendon versus four-strand383hamstring tendon autograft for arthroscopic reconstruction of the384anterior cruciate ligament. Am J Sports Med 30(4):523–53638512. Papalia R, Franceschi F, Zampogna B, TecameA,Maffulli N, Denaro386V (2014) Surgical management of partial tears of the anterior cruciate387ligament. Knee Surg Sports Traumatol Arthrosc : Off J ESSKA38822(1):154–165. doi:10.1007/s00167-012-2339-138913. Schulz KF, Altman DG, Moher D, Group C (2010) CONSORT 2010390statement: updated guidelines for reporting parallel group391randomised trials. BMJ 340:c332. doi:10.1136/bmj.c33239214. Franceschi F, Papalia R, Rizzello G, Del Buono A, Maffulli N,393Denaro V (2013) Anteromedial portal versus transtibial drilling tech-394niques in anterior cruciate ligament reconstruction: any clinical rele-395vance? A retrospective comparative study. Arthroscopy: J Arthrosc396Relat Surg : Off Publ Arthroscopy Assoc N Am Int Arthroscopy397Assoc 29(8):1330–1337. doi:10.1016/j.arthro.2013.05.02039815. Prins M (2006) The Lachman test is the most sensitive and the pivot399shift the most specific test for the diagnosis of ACL rupture. Aust J400Physiother 52(1):6640116. Hefti F, Muller W, Jakob RP, Staubli HU (1993) Evaluation of knee402ligament injuries with the IKDC form. Knee Surg Sports Traumatol403Arthrosc : Off J ESSKA 1(3–4):226–23440417. Briggs KK, Lysholm J, Tegner Y, Rodkey WG, Kocher MS,405Steadman JR (2009) The reliability, validity, and responsiveness of406the Lysholm score and Tegner activity scale for anterior cruciate407ligament injuries of the knee: 25 years later. Am J Sports Med40837(5):890–897. doi:10.1177/036354650833014340918. Barrios JA, Higginson JS, Royer TD, Davis IS (2009) Static and410dynamic correlates of the knee adduction moment in healthy knees411ranging from normal to varus-aligned. Clin Biomech 24(10):850–412854. doi:10.1016/j.clinbiomech.2009.07.01641319. Barber FA, Click SD (1997) Meniscus repair rehabilitation with414concurrent anterior cruciate reconstruction. Arthroscopy: J Arthrosc415Relat Surg : Off Publ Arthroscopy Assoc of N Am Int Arthroscopy416Assoc 13(4):433–43741720. Clatworthy M, Amendola A (1999) The anterior cruciate ligament418and arthritis. Clin Sports Med 18(1):173–198, vii
International Orthopaedics (SICOT)
JrnlID 264_ArtID 2513_Proof# 1 - 03/09/2014
AUTHOR'S PROOF!
UNCORRECTEDPROOF
419 21. Maffulli N, Osti L (2013) ACL stability, function, and arthritis: what420 have we been missing? Orthopedics 36(2):90–92. doi:10.3928/421 01477447-20130122-02422 22. Hara K, Niga S, Ikeda H, Cho S, Muneta T (2008) Isolated423 anterior cruciate ligament reconstruction in patients with chronic424 anterior cruciate ligament insufficiency combined with grade II425 valgus laxity. Am J Sports Med 36(2):333–339. doi:10.1177/426 0363546507307501427 23. Jacobsen K (1977) Osteoarthrosis following insufficiency of the428 cruciate ligaments in man. A clinical study. Acta Orthop Scand429 48(5):520–526430 24. van der Hart CP, van den Bekerom MP, Patt TW (2008) The occur-431 rence of osteoarthritis at a minimum of ten years after reconstruction432 of the anterior cruciate ligament. J Orthop Surg Res 3:24433 25. Cebesoy O (2006) What are the risk factors in the development of434 osteoarthritis following ACL reconstruction? Int Orthop 30(5):431–435 431436 26. Krishnan SR, Randle R (2009) ACL reconstruction with unicondylar437 replacement in knee with functional instability and osteoarthritis. J438 Orthop Surg Res 4:43439 27. Madhusudhan T, Kumar T, Bastawrous S, Sinha A (2008) Clinical440 examination, MRI and arthroscopy and meniscal and ligamentous441 knee Injuries – a prospective study. J Orthop Surg Res 3:19442 28. Papalia R, Zampogna B, Torre G, Lanotte A, Vasta S, Albo E,443 Tecame A, Denaro V (2014) Sarcopenia and its relationship with444 osteoarthritis: risk factor or direct consequence? Musculoskeletal445 surgery:1–6446 29. Maffulli N, Binfield PM, King JB (2003) Articular cartilage lesions447 in the symptomatic anterior cruciate ligament-deficient knee.448 Arthroscopy:J Arthrosc Relat Surg 19(7):685–690449 30. Osti L, Papalia R, Del Buono A, Leonardi F, Denaro V, Maffulli N450 (2011) Surgery for ACL deficiency in patients over 50. Knee Surg451 Sports Traumatol Arthrosc 19(3):412–417452 31. Osti L, Papalia R, Del Buono A, Leonardi F, Denaro V, Maffulli N453 (2011) Surgery for ACL deficiency in patients over 50. Knee Surg454 Sports Traumatol Arthrosc : Off J ESSKA 19(3):412–417. doi:10.455 1007/s00167-010-1242-x456 32. Feller J, Webster KE (2013) Return to sport following anterior457 cruciate ligament reconstruction. Int Orthop 37(2):285–290458 33. Chaves SF, Marques NP, Silva RL, Rebouças NS, de Freitas LM, de459 Paula Lima PO, de Oliveira RR (2012) Neuromuscular efficiency of460 the vastus medialis obliquus and postural balance in professional461 soccer athletes after anterior cruciate ligament reconstruction. MLTJ462 2(2):121463 34. Joseph C, Pathak SS, Aravinda M, Rajan D (2008) Is ACL recon-464 struction only for athletes? Int Orthop 32(1):57–61465 35. Li R,Maffulli N, Hsu YC, ChanKM (1996) Isokinetic strength of the466 quadriceps and hamstrings and functional ability of anterior cruciate467 deficient knees in recreational athletes. Br J Sports Med 30(2):161–468 164469 36. Yuan T, Zhang C-Q, Wang JH (2013) Augmenting tendon and470 ligament repair with platelet-rich plasma (PRP). MLTJ 3(3):139471 37. Kanazawa T, Soejima T, Noguchi K, Tabuchi K, Noyama M,472 Nakamura K, Shiba N Tendon-to-bone healing using autologous473 bone marrow-derived mesenchymal stem cells in ACL reconstruc-474 tion without a tibial bone tunnel-A histological study. Muscle,475 Ligaments and Tendons Journal 4 (2):201–206476 38. Filomeno P, Dayan V, Touriño C (2012) Stem cell research and477 clinical development in tendon repair. MLTJ 2(3):204478 39. Chambat P, Guier C, Sonnery-Cottet B, Fayard J-M, Thaunat M479 (2013) The evolution of ACL reconstruction over the last fifty years.480 Int Orthop 37(2):181–186481 40. Samuelsson K, Andersson D, AhldenM, Fu FH, Musahl V, Karlsson482 J (2013) Trends in surgeon preferences on anterior cruciate ligament483 reconstructive techniques. Clin Sports Med 32(1):111–126. doi:10.484 1016/j.csm.2012.08.011
48541. Salmon L, Russell V, Musgrove T, Pinczewski L, Refshauge K (2005)486Incidence and risk factors for graft rupture and contralateral rupture487after anterior cruciate ligament reconstruction. Arthroscopy: J Arthrosc488Relat Surg : Off Publ Arthroscopy Assoc of N Am Int Arthroscopy489Assoc 21(8):948–957. doi:10.1016/j.arthro.2005.04.11049042. Myer GD, Ford KR, Khoury J, Succop P, Hewett TE (2010)491Development and validation of a clinic-based prediction tool to492identify female athletes at high risk for anterior cruciate ligament493injury. Am J Sports Med 38(10):2025–2033. doi:10.1177/494036354651037093349543. Lui P, Zhang P, Chan K, Qin L (2010) Biology and augmentation of496tendon-bone insertion repair. J Orthop Surg Res 5(1):1–1449744. Aglietti P, Buzzi R, D’Andria S, Zaccherotti G (1992) Arthroscopic498anterior cruciate ligament reconstruction with patellar tendon.499Arthroscopy: J Arthrosc Relat Surg : Off Publ Arthroscopy Assoc500of N Am Int Arthroscopy Assoc 8(4):510–51650145. Aglietti P, Zaccherotti G, Menchetti PP, De Biase P (1995) A com-502parison of clinical and radiological parameters with two arthroscopic503techniques for anterior cruciate ligament reconstruction. Knee Surg504Sports Traumatol Arthrosc : Off J ESSKA 3(1):2–850546. Aglietti P, Buzzi R, Giron F, Simeone AJ, Zaccherotti G (1997)506Arthroscopic-assisted anterior cruciate ligament reconstruction with507the central third patellar tendon. A 5-8-year follow-up. Knee Surg508Sports Traumatol Arthrosc : Off J ESSKA 5(3):138–14450947. Aglietti P, Buzzi R, Menchetti PM, Giron F (1996) Arthroscopically510assisted semitendinosus and gracilis tendon graft in reconstruction for511acute anterior cruciate ligament injuries in athletes. Am J Sports Med51224(6):726–73151348. Freedman KB, D’Amato MJ, Nedeff DD, Kaz A, Bach BR Jr (2003)514Arthroscopic anterior cruciate ligament reconstruction: a515metaanalysis comparing patellar tendon and hamstring tendon auto-516grafts. Am J Sports Med 31(1):2–1151749. Meighan AA, Keating JF, Will E (2003) Outcome after reconstruc-518tion of the anterior cruciate ligament in athletic patients. A compar-519ison of early versus delayed surgery. J Bone Joint Surg Br Vol 85(4):520521–52452150. Mohammadi F, Salavati M, Akhbari B, Mazaheri M, Mohsen Mir S,522Etemadi Y (2013) Comparison of functional outcome measures after523ACL reconstruction in competitive soccer players: a randomized trial. J524Bone Joint Surg Am 95(14):1271–1277. doi:10.2106/JBJS.L.0072452551. Streich NA, Zimmermann D, Bode G, Schmitt H (2011)526Reconstructive versus non-reconstructive treatment of anterior cru-527ciate ligament insufficiency. A retrospective matched-pair long-term528follow-up. Int Orthop 35(4):607–61352952. Katayama M, Higuchi H, Kimura M, Kobayashi A, Hatayama K,530Terauchi M, Takagishi K (2004) Proprioception and performance531after anterior cruciate ligament rupture. Int Orthop 28(5):278–28153253. Haus J, Halata Z (1990) Innervation of the anterior cruciate ligament.533Int Orthop 14(3):293–29653454. Fonseca ST, Ocarino JM, Silva PL, Guimaraes RB, Oliveira MC,535Lage CA (2005) Proprioception in individuals with ACL-deficient536knee and good muscular and functional performance. Res Sports537Med 13(1):47–61. doi:10.1080/1543862059092209553855. Jensen TO, Fischer-Rasmussen T, Kjaer M, Magnusson SP (2002)539Proprioception in poor- and well-functioning anterior cruciate liga-540ment deficient patients. J Rehabil Med : Off J UEMS (EBPRM)54134(3):141–14954256. Schultz RA, Miller DC, Kerr CS, Michel i L (1984)543Mechanoreceptors in human cruciate ligaments. A histological544study. J Bone Joint Surg Am 66(7):1072–107654557. Woo SL-Y, Wu C, Dede O, Vercillo F, Noorani S (2006)546Biomechanics and anterior cruciate ligament reconstruction. J547Orthop Surg Res 1 (2)54858. Dhillon MS, Bali K, Prabhakar S (2012) Differences among mech-549anoreceptors in healthy and injured anterior cruciate ligaments and550their clinical importance. MLTJ 2(1):38
International Orthopaedics (SICOT)
JrnlID 264_ArtID 2513_Proof# 1 - 03/09/2014
AUTHOR'S PROOF!
UNCORRECTEDPROOF
551 59. Papalia R, Franceschi F, Vasta S, DiMartinoA,Maffulli N, Denaro V552 (2012) Sparing the anterior cruciate ligament remnant: is it worth the553 hassle? Br Med Bull 104(1):91–111554 60. Mohammadi F, Salavati M, Akhbari B, Mazaheri M, Khorrami M,555 Negahban H (2012) Static and dynamic postural control in compet-556 itive athletes after anterior cruciate ligament reconstruction and con-557 trols. Knee Surg Sports Traumatol Arthrosc : Off J ESSKA 20(8):558 1603–1610. doi:10.1007/s00167-011-1806-4
55961. Gobbi A, Domzalski M, Pascual J (2004) Comparison of anterior560cruciate ligament reconstruction in male and female athletes using the561patellar tendon and hamstring autografts. Knee Surg Sports562Traumatol Arthrosc: Off J ESSKA 12(6):534–539. doi:10.1007/563s00167-003-0486-056462. Barenius B, Webster WK, McClelland J, Feller J (2013) Hamstring565tendon anterior cruciate ligament reconstruction: does gracilis tendon566harvest matter? Int Orthop 37(2):207–212
567
International Orthopaedics (SICOT)
JrnlID 264_ArtID 2513_Proof# 1 - 03/09/2014