
Anterior and Posterior Cruciate Ligaments at Different Patient Ages: MR Imaging Findings
10
Anterior and Posterior Cruciate Ligaments at Different Patient Ages: MR Imaging Findings 1 Hee Kyung Kim, MD Tal Laor, MD Norah J. Shire, PhD, MPH Judy A. Bean, PhD Bernard J. Dardzinski, PhD Purpose: To retrospectively compile normative data on the anterior cruciate ligament (ACL) and the posterior cruciate liga- ment (PCL) in children and young adults. Materials and Methods: This HIPAA-compliant study was approved by the institu- tional review board. The requirement for informed patient consent was waived. Knee MR imaging examinations (n 324) were performed in 168 female and 156 male patients (age range, 1–20 years) at 1.5 and 3.0 T, and the image findings were retrospectively evaluated by two blinded radiologists separately. One radiologist reviewed all im- ages twice at two sessions, and the other reviewed a random subset of half the images during one session. Dis- cordant assessments were resolved by consensus. The sagittal and coronal ACL-tibial angles, Blumensaat line– ACL angle, angle of inclination of the intercondylar roof, ACL-tibial insertion site, and PCL angle and horizontal component–to–vertical component ratio were measured. The associations between these values and patient age, patient sex, and physeal patency were assessed. Linear and fractional polynomial regression models were used to evaluate the relationships between measurements. Results: ACL-tibial angles became significantly larger (P .001) with increasing age during skeletal growth and approached adult values after physeal fusion. The Blumensaat line– ACL angle was constant after age 2 years. The inclination of intercondylar roof angle became significantly smaller (P .001) with increasing age. The ACL-tibial insertion site was constant at the junction of the anterior and middle thirds of the tibial anteroposterior diameter and was not age dependent. The PCL angle became significantly larger (P .001) with advancing age and in children who had fused as opposed to open physes. The horizontal compo- nent–to–vertical component PCL ratio became signifi- cantly smaller with advancing age (P .001). Conclusion: During growth, angulation of the ACL is age dependent. The angle and morphologic changes of the PCL are age dependent throughout skeletal maturation. RSNA, 2008 1 From the Department of Radiology and Imaging Re- search Center (H.K.K., T.L., B.J.D.) and Center for Epide- miology and Biostatistics (J.A.B.), Cincinnati Children’s Hospital Medical Center, 3333 Burnet Ave, Cincinnati, OH 45229-3039; and Division of Epidemiology and Biostatis- tics, University of Cincinnati, Division of Digestive Dis- eases, Cincinnati, Ohio (N.J.S.). Received June 22, 2007; revision requested August 27; revision received October 29; accepted January 8, 2008; final version accepted January 16. Address correspondence to T.L. (e-mail: [email protected] ). RSNA, 2008 ORIGINAL RESEARCH PEDIATRIC IMAGING 826 Radiology: Volume 247: Number 3—June 2008 Note: This copy is for your personal non-commercial use only. To order presentation-ready copies for distribution to your colleagues or clients, contact us at www.rsna.org/rsnarights.
-
Upload
independent -
Category
Documents
-
view
0 -
download
0
Transcript of Anterior and Posterior Cruciate Ligaments at Different Patient Ages: MR Imaging Findings

Anterior and Posterior CruciateLigaments at Different PatientAges: MR Imaging Findings1
Hee Kyung Kim, MDTal Laor, MDNorah J. Shire, PhD, MPHJudy A. Bean, PhDBernard J. Dardzinski, PhD
Purpose: To retrospectively compile normative data on the anteriorcruciate ligament (ACL) and the posterior cruciate liga-ment (PCL) in children and young adults.
Materials andMethods:
This HIPAA-compliant study was approved by the institu-tional review board. The requirement for informed patientconsent was waived. Knee MR imaging examinations (n �324) were performed in 168 female and 156 male patients(age range, 1–20 years) at 1.5 and 3.0 T, and the imagefindings were retrospectively evaluated by two blindedradiologists separately. One radiologist reviewed all im-ages twice at two sessions, and the other reviewed arandom subset of half the images during one session. Dis-cordant assessments were resolved by consensus. Thesagittal and coronal ACL-tibial angles, Blumensaat line–ACL angle, angle of inclination of the intercondylar roof,ACL-tibial insertion site, and PCL angle and horizontalcomponent–to–vertical component ratio were measured.The associations between these values and patient age,patient sex, and physeal patency were assessed. Linearand fractional polynomial regression models were used toevaluate the relationships between measurements.
Results: ACL-tibial angles became significantly larger (P � .001)with increasing age during skeletal growth and approachedadult values after physeal fusion. The Blumensaat line–ACL angle was constant after age 2 years. The inclinationof intercondylar roof angle became significantly smaller(P � .001) with increasing age. The ACL-tibial insertionsite was constant at the junction of the anterior and middlethirds of the tibial anteroposterior diameter and was notage dependent. The PCL angle became significantly larger(P � .001) with advancing age and in children who hadfused as opposed to open physes. The horizontal compo-nent–to–vertical component PCL ratio became signifi-cantly smaller with advancing age (P � .001).
Conclusion: During growth, angulation of the ACL is age dependent.The angle and morphologic changes of the PCL are agedependent throughout skeletal maturation.
� RSNA, 2008
1 From the Department of Radiology and Imaging Re-search Center (H.K.K., T.L., B.J.D.) and Center for Epide-miology and Biostatistics (J.A.B.), Cincinnati Children’sHospital Medical Center, 3333 Burnet Ave, Cincinnati, OH45229-3039; and Division of Epidemiology and Biostatis-tics, University of Cincinnati, Division of Digestive Dis-eases, Cincinnati, Ohio (N.J.S.). Received June 22, 2007;revision requested August 27; revision received October29; accepted January 8, 2008; final version acceptedJanuary 16. Address correspondence to T.L. (e-mail:[email protected] ).
� RSNA, 2008
ORIG
INAL
RESE
ARCH
�PE
DIAT
RIC
IMAG
ING
826 Radiology: Volume 247: Number 3—June 2008
Note: This copy is for your personal non-commercial use only. To order presentation-ready copies for distribution to your colleagues or clients, contact us at www.rsna.org/rsnarights.

Magnetic resonance (MR) imag-ing findings of normal anteriorcruciate ligament (ACL) and
posterior cruciate ligament (PCL) align-ment and morphology in the knees ofadults are well documented (1,2). Be-cause the immature skeleton undergoescontinuous growth and remodeling (3),the anatomic relationships between lig-aments and bone that are well de-scribed in adults (4,5) may be differentin children. This difference may affectthe reliability of using alterations in thenormal anatomy described in adults,such as buckling of the PCL as a second-ary sign of ACL disruption (6), to evalu-ate the knees of children.
Study findings suggest that ACL in-jury is now more frequently recognizedin children and adolescents (3,7–10).Several study investigators have advo-cated early ACL reconstruction in se-lected patients for prevention of addi-tional injury and to allow early return tosports activities (7–10). Successful ACLreconstruction requires correct ana-tomic placement and angulation of a lig-ament graft with respect to the tibia andfemur to avoid impingement and jointmovement limitation (11,12). With theincrease in reparative surgeries per-formed in younger children, similar an-atomic data on the knees of younger
patients are necessary. Although therehave been reports of normal anatomy ofthe proximal tibia and tibial attachmentsites of the ACL in children (13), to ourknowledge, normative data on the MRimaging appearances of the ACL and thePCL in children have not been com-piled. Thus, the purpose of our studywas to retrospectively compile norma-tive data on the ACL and the PCL inchildren and young adults.
Materials and Methods
Our Health Insurance Portability and Ac-countability Act–compliant study was ap-proved by the institutional review boardof Cincinnati Children’s Hospital Medi-cal Center. The requirement for informedpatient consent was waived.
MR Imaging ExaminationsData from picture archiving and com-munication systems computer recordsof all patients who underwent kneeMR imaging examinations betweenJanuary 2000 and August 2006 (n �2519) were extracted. Patients weregrouped in 1-year age intervals. Our goalwas to retrospectively evaluate the find-ings of up to 25 examinations for eachage group, when available. A patient’sdata were included in our study if theMR imaging examination was per-formed at our hospital and included, atminimum, a sagittal and coronal inter-mediate- or T2-weighted (conventionalor fast spin-echo) MR imaging series ora fast inversion-recovery MR imagingseries that adequately depicted the
ACL and the PCL. These sequencesenabled differentiation between thecruciate ligaments and nonossifiedepiphyseal cartilage. Patients were ex-cluded if their imaging report includeda diagnosis (where applicable) or his-tory of partial or complete disruptionof the ACL and/or PCL, previous re-parative surgery, distal femoral orproximal tibial fractures, congenitalstructural anomalies, developmentaldelay, non–weight-bearing states, orsyndromes. Because the normal mor-phologies of the ACL and PCL changewith knee hyperextension or flexion(14,15), the MR images that depicteda femoral-tibial angle larger than 5° ofhyperextension or larger than 15° offlexion were also excluded.
The findings of a total of 324 kneeMR examinations performed in 313children and young adults were in-cluded. Three patients underwent twoimaging examinations performed 5,14, and 27 months apart. The 324 ex-aminations were performed in 168knees of female patients and in 156knees of male patients. The patients’ages ranged from 1 to 20 years (Table1). In eight patients (three childrenaged 1 to �2 years and one patienteach aged 2 to �3 years, 4 to �5years, 7 to �8 years, 10 to �11 years,and 11 to �12 years), both knees wereimaged on the same day. In four ofthese children, the knees were imagedtogether, and in four of them, theknees were imaged separately. For ev-
Published online10.1148/radiol.2473071097
Radiology 2008; 247:826–835
Abbreviations:ACL � anterior cruciate ligamentPCL � posterior cruciate ligament
Author contributions:Guarantors of integrity of entire study, H.K.K., T.L., B.J.D.;study concepts/study design or data acquisition or dataanalysis/interpretation, all authors; manuscript drafting ormanuscript revision for important intellectual content, allauthors; manuscript final version approval, all authors;literature research, H.K.K., T.L., B.J.D.; clinical studies, allauthors; statistical analysis, all authors; and manuscriptediting, all authors
Authors stated no financial relationship to disclose.
Advances in Knowledge
� The angle between the anteriorcruciate ligament (ACL) and thetibia as seen on sagittal and coro-nal MR images is significantlysmaller in younger children thanin older children.
� The angle of the posterior cruci-ate ligament (PCL) in youngerchildren, as seen on sagittal MRimages, is significantly smallerthan that in older children.
� The morphology of the PCLchanges during normal skeletalgrowth, with the horizontal com-ponent–to–vertical componentratio becoming relatively smaller.
� The attachment site of the ACLrelative to the proximal tibia re-mains stable throughout all agesof childhood development.
Implications for Patient Care
� Since ACL repair is now beingperformed in younger children,recognition of the normal devel-opmental changes of the cruciateligaments may be important forsuccessful ACL graft placement.
� Use of the described PCL mor-phology in adults as a secondarysign of ACL injury in children mayrequire further study, because theangle and configuration of thenormal PCL change with skeletalgrowth.
PEDIATRIC IMAGING: MR of Anterior and Posterior Cruciate Ligaments Kim et al
Radiology: Volume 247: Number 3—June 2008 827

ery patient in whom the data on bothknees were included in our study, thevalues were sufficiently different andwere measured during different ses-sions approximately 1 week apart tominimize intrapatient correlationbias.
In all patients, imaging was per-formed by using a 1.5-T (Signa Hori-zon LX Echospeed, Excite HD Echo-speed, or Signa LX Echospeed Plus,GE Medical Systems, Milwaukee, Wis[137 patients]; Symphony or Magne-tom Espree, Siemens Medical Solu-tions, Erlangen, Germany [151 pa-tients]) or 3.0-T (Magnetom Trio; Sie-mens Medical Solutions [36 patients])imaging system. The knee was posi-tioned at full or nearly full extension.All examinations included, at mini-mum, the following sequences per-formed at 1.5 T: sagittal and coronalintermediate- or T2-weighted fastspin-echo or turbo spin-echo se-quences (2500–4500/17–34 [repeti-tion time msec/echo time msec]and/or 2500 – 4500/68 –102 [effec-tive], echo train length of six to eight,two signals acquired), conventional
spin-echo intermediate- and T2-weighted sequences (2000 –3000/12–15 and 2000–3000/64–80, onesignal acquired), or a fast inversion-recovery sequence (3500–4500/34/155 [repetition time msec/echo timemsec/inversion time msec], echo train
length of six to eight, two signals ac-quired). The following parameterswere used for 3.0-T MR imaging:3000/8–18 and/or 3000–3500/56–64,a turbo factor of five to seven, and onesignal acquired. For all sequences, thesection thickness was 3–5 mm with an
Figure 1
Figure 1: Sagittal ACL-tibial angle. (a) Turbo spin-echo intermediate-weighted sagittal MR image (3000/8.8) of left knee of 3-year-old girl. The plane of the tibial plateau is demarcated (dotted line) on a lateral image.(b) On sagittal midline MR image obtained with the same sequence in same patient, the plane of the tibial pla-teau is superimposed, forming an angle with the most anterior margin of the ACL. In this girl, the angle is38.5°. (c) Turbo spin-echo intermediate-weighted sagittal MR image (2000/16) of right knee of 19-year-oldboy. The plane of the tibial plateau is demarcated (dotted line) on a lateral image. (d) On sagittal midline MRimage obtained with the same sequence in same patient, the plane of the tibial plateau is superimposed, form-ing an angle with the most anterior margin of the ACL. In this boy, the angle is 53.9°.
Table 1
Knee Examinations Performed in1-year-Interval Patient Age Groups
Age Interval (y)No. of Knee MR Examinations(n � 324)
1 to �2 102 to �3 143 to �4 84 to �5 145 to �6 156 to �7 197 to �8 178 to �9 189 to �10 15
10 to �11 2411 to �12 2512 to �13 2313 to �14 1514 to �15 2015 to �16 1916 to �17 1617 to �18 1318 to �19 1619 to �20 1220 to �21 11
PEDIATRIC IMAGING: MR of Anterior and Posterior Cruciate Ligaments Kim et al
828 Radiology: Volume 247: Number 3—June 2008
intersection gap of 0.5–1.5 mm and amatrix of (256–512) � (192–256) wasused, depending on the patient’s size.Sagittal and coronal sequences wereprescribed from an axial sequence.
All knees were imaged by using atransmit-receive or receive-only ex-tremity coil, torso or cardiac phased-array coil, neonatal body coil, orquadrature head coil. The choice of
coil was based on the size of the pa-tient, the desired field of view, and theneed for unilateral versus bilateralknee imaging. When necessary, thepatient was sedated according to radi-ology department guidelines.
MR Imaging Analysis of Physeal PatencyPatients were assigned (H.K.K., withmusculoskeletal training and 5 years ex-
perience) to an open physes group orclosed or closing physes group. Patientswere considered to be skeletally imma-ture or to have open physes when thesignal intensity of the cartilage was seenin its entirety across both the distal fem-oral physis and the proximal tibial phy-sis. Patients were considered to haveclosed or closing physes when the phy-seal cartilage signal intensity was dis-continuous or absent across the physes.
All numeric measurements wereperformed by one author (H.K.K.).This author validated all physeal groupassignments and measurements a sec-ond time. If the two measurementswere different, the average value wasused. A second author (T.L., pediatricmusculoskeletal radiologist with 15years experience) independently vali-dated a random subset of half the mea-surements and the determination ofphyseal patency. All discordant assess-ments between authors were resolvedby means of consensus measurement.During the image readings and measure-ments, the radiologists were blinded to thepatients’ sex and age.
The following data were thengrouped according to 1-year age inter-val, patient sex, and whether the physesabout the knee were open or closed. Foreach examination, the following valueswere measured by using clinical picturearchiving and communication systemssoftware (Centricity Enterprise PACS;GE Medical Systems).
MR Measurements of ACLSagittal ACL-tibial angle.—This anglewas created between a line parallelingthe midlateral tibial plateau (Fig 1, a,c) and a line demarcating the anterior-most margin of the ACL, drawn on themidline image best depicting the ACL(Fig 1b, 1d). Measurement of this an-gle is the technique used by Gentili etal (6).
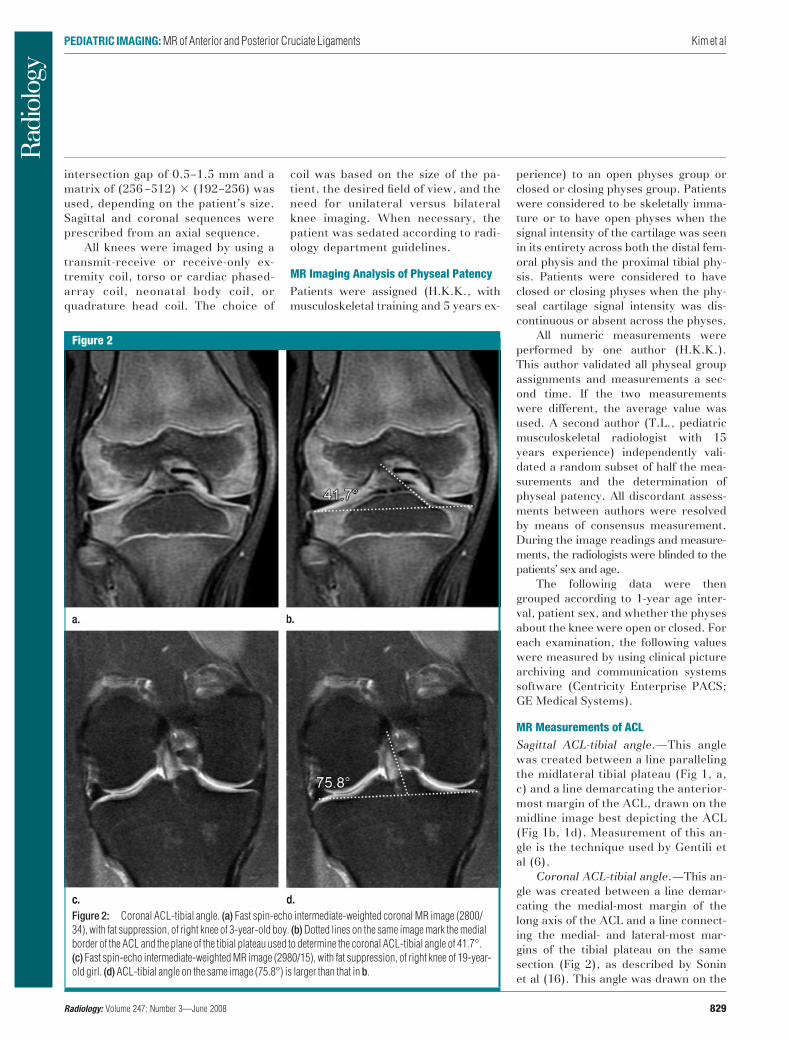
Coronal ACL-tibial angle.—This an-gle was created between a line demar-cating the medial-most margin of thelong axis of the ACL and a line connect-ing the medial- and lateral-most mar-gins of the tibial plateau on the samesection (Fig 2), as described by Soninet al (16). This angle was drawn on the
Figure 2
Figure 2: Coronal ACL-tibial angle. (a) Fast spin-echo intermediate-weighted coronal MR image (2800/34), with fat suppression, of right knee of 3-year-old boy. (b) Dotted lines on the same image mark the medialborder of the ACL and the plane of the tibial plateau used to determine the coronal ACL-tibial angle of 41.7°.(c) Fast spin-echo intermediate-weighted MR image (2980/15), with fat suppression, of right knee of 19-year-old girl. (d) ACL-tibial angle on the same image (75.8°) is larger than that in b.
PEDIATRIC IMAGING: MR of Anterior and Posterior Cruciate Ligaments Kim et al
Radiology: Volume 247: Number 3—June 2008 829

midcoronal image best depicting theACL.
Blumensaat line–ACL angle.—This angle was created between a linedrawn along the edge of the intercon-dylar roof (ie, Blumensaat line) andthe anterior-most margin of the ACLon the sagittal view best depicting thisligament (Fig 3).
Angle of inclination of the intercon-dylar roof.—This angle was created be-tween a line drawn along the edge of theintercondylar roof and the long axis ofthe femur (13) (Fig 3) on a midline sag-ittal image.
ACL-tibial insertion site.—On thesagittal image that best depicted theACL, the distance from the anterior-most tibial border (at the level of theproximal physis) to the anterior edge ofthe ACL was measured and dividedby the longest tibial anteroposterior dis-tance measured on the same image, atthe level of the proximal tibial physis(Fig 4). This is the method used by Sheaet al (13).
MR Measurements of PCLPCL angle.—This angle was created be-tween a line connecting the origin site ofthe PCL on the femur to a point placedat the point of directional change of thePCL and a line drawn from the samepoint to the distal-most point of PCLinsertion on the tibia, as described byGentili et al (6) (Fig 5). A single imagebest depicting the PCL was used for thismeasurement.
PCL horizontal component–to–ver-tical component ratio.—On the sameimage used to measure the PCL angle,we measured the ratio of the length ofthe horizontal component of the PCLfrom the origin site to the site of direc-tional change, divided by the verticallength from this same site to the distal-most PCL attachment site on the poste-rior tibia (Fig 6).
Statistical AnalysesData normality was assessed by usingthe Shapiro-Wilk test. Nonnormal datawere transformed when an appropriatetransformation was possible; then nor-mality was reassessed. Between-groupanalyses of patient sex– and physeal
patency–based differences were con-ducted by using the rank sum test or theStudent t test. Nonparametric analyses(eg, rank sum test) were used when noappropriate transformation was possi-ble. Linear and fractional polynomial re-gression models were used to assess re-lationships between outcome variables(sagittal and coronal ACL-tibial angles,Blumensaat line–ACL angle, inclinationof intercondylar roof angle, ACL-tibialinsertion site, PCL angle, and PCL hori-zontal component–to–vertical compo-nent ratio) and predictor variables (pa-tient sex, patient age, and physeal pa-tency). Analysis results were stratifiedby sex, with regression functions fittedto the data for each sex. The goodnessof fit for each model was assessed byusing likelihood-ratio �2 statistics andadjusted coefficients of determinationfor multivariate analysis (R2). Becauseinterpretation of fractional polynomialregression functions is not always intui-tive, we graphically represented thosedata with the best-fitting models. Changeswith age are reported with linearity as-
sumed, although changes over time maynot progress in a linear fashion. All anal-yses were conducted by using software(Stata, version 8.2; Stata, College Sta-tion, Tex), and two-tailed P values lessthan or equal to .05 were considered toindicate statistical significance in allcases.
Results
Open physes were identified at 237 ex-aminations, while closed physes wereidentified at 87 examinations. Measure-ments and statistical significance ana-lyzed according to physeal patency andpatient sex are listed in Table 2.
ACL MeasurementsSagittal ACL-tibial angle.—This anglewas significantly larger as a function ofpatient age (P � .001) and sex (P � .039)in the fractional polynomial regressionmodel. The mean measurement was55.5° � 6.7 (standard deviation) for allfemale patients versus 53.9° � 5.8 for all
Figure 3
Figure 3: Blumensaat line–ACL angle andinclination of the intercondylar roof angle depictedon turbo spin-echo intermediate-weighted sagittalMR image (2000/16) of right knee of 19-year-oldboy. Dotted line along edge of the intercondylarroof (Blumensaat line) and dotted line along mostanterior border of the ACL form a 9.9° angle. Anglebetween the longitudinal femoral axis and theintercondylar roof is 44.7°.
Figure 4
Figure 4: ACL-tibial insertion site depicted onturbo spin-echo intermediate-weighted sagittalMR image (2000/16) of right knee of 14-year-oldboy. Distance between the anterior-most portion ofthe insertion of the ACL and the anterior aspect ofthe tibia (as determined at level of physis) (shortdotted line) divided by the anteroposterior dis-tance at the level of the proximal tibial physis (longdotted line) yields an insertion site of the ACL at33% of the anteroposterior tibial diameter.
PEDIATRIC IMAGING: MR of Anterior and Posterior Cruciate Ligaments Kim et al
830 Radiology: Volume 247: Number 3—June 2008

male patients. After controlling data forsex in a linear model, data showed thatthe angle became larger by a mean of0.71° � 0.05 with each additional yearof age. In our patient cohort, the valuescontinued to increase with increasingage in all groups, with a significant dif-ference in angle between all patientswith open physes (53.2° � 6.2) and allpatients with closed physes (58.8° �4.9) (P � .001) (Figs 1, 7). However,when we stratified the data according toopen versus closed physes and madeadjustments for sex, age was shown tobe a significant predictor of sagittalACL-tibial angle if the physes were openbut not if they were closed.
Coronal ACL-tibial angle.—Thisangle changed significantly with age inthe fractional polynomial regressionmodel (P � .001): It became a mean1.3° � 0.08 larger with each addi-tional year of age after we controlleddata for sex (Figs 2, 8). The difference inangle between the sexes was also signifi-cant: The mean angle measurement was62.9° � 10.0 for all female patientsversus 60.7° � 9.8 for all male patients(P � .04). The difference in meancoronal ACL-tibial angle between allthe patients with open physes (59.2° �9.4) and all those with closed physes(69.1° � 7.4) also was significant (P �.001). Again, after adjustments for sex,age was no longer a significant predictorof coronal ACL-tibial angle when thephyses were closed.
Blumensaat line–ACL angle.—Whenthe data of patients younger than 2years were excluded, there was no sig-nificant effect of age, sex, or physealpatency on measurement of the Blu-mensaat line–ACL angle. When datafrom the youngest patients were in-cluded, this angle became larger in acurvilinear manner as a function ofage.
Angle of inclination of the intercondy-lar roof.—A fractional polynomial modelwas fit to the angle between the longitu-dinal femoral axis and the anterior mar-gin of the intercondylar roof (Blumen-saat line). This angle became signifi-cantly smaller, by a mean of 0.42° �0.05, with each additional year of age(P � .001) after we controlled the data
Figure 5
Figure 5: PCL angle. (a) On turbo spin-echo intermediate-weighted sagittal MR image (3000/8.8) in3-year-old girl, PCL angle is measured (dotted lines) between a line from the femoral origin site to the site ofangular change and a line from this same site to the distal-most insertion site on the posterior tibia. The angleis 106.3°. The origin site is at the distal-most aspect of the intercondylar roof at the level of the joint surface.(b) Turbo spin-echo intermediate-weighted sagittal MR image (2000/16) in 19-year-old girl shows PCL angleof 122.8°. The origin of the PCL is now slightly more proximal on the intercondylar roof, a few millimetersabove the joint surface.
Figure 6
Figure 6: PCL horizontal component–to–vertical component ratio. (a) Turbo spin-echo intermediate-weighted sagittal MR image (3000/8.8) in 3-year-old girl. Dividing the horizontal component length of thePCL by the vertical component length resulted in a ratio of 0.88. The knee is enlarged to approximate the sizeof the knee in b. (b) Fast spin-echo intermediate-weighted sagittal MR image (2000/16) in 19-year-old girlshows a horizontal component–to–vertical component ratio of 0.48. Note the larger posterior tibial protrusioncompared with that in a.
PEDIATRIC IMAGING: MR of Anterior and Posterior Cruciate Ligaments Kim et al
Radiology: Volume 247: Number 3—June 2008 831

for sex, and it differed significantly ac-cording to sex (mean angle, 44.4° � 5.1for all female patients vs 46.5° � 5.3 forall male patients; P � .001). There wasa significant difference (P � .001) in thisangle between all the patients with openphyses (46.5° � 4.8) and all those withclosed physes (42.3° � 5.3).
ACL-tibial insertion site.—The lo-cation of the insertion of the anteriorborder of the ACL with respect to thetibial plateau did not change signifi-cantly according to age, sex, or phy-seal patency. The mean insertion sitepercentage (of the anteroposteriortibial diameter) for both the open phy-ses group and the closed physes groupwas 31% � 4 (P � .59).
PCL MeasurementsPCL angle.—This angle as measured onsagittal MR images was best describedwith a curvilinear model and was largerby a mean of 0.68° � 0.09 with eachadditional year of age (P � .001). ThePCL angle also differed according tophyseal patency, with mean values of113.9° � 8.1 in the open physes groupand 121.9° � 8.7 in the closed physesgroup (P � .001). The difference in PCLangle between all the female patientsand all the male patients was not signif-icant (Figs 5, 9).
PCL horizontal component–to–ver-tical component ratio.—This ratio di-minished linearly and significantly, by amean of 0.02 � 0.01, with each addi-
tional year of age (P � .001), but it wasunaffected by patient sex. There was arelatively shorter horizontal componentand a longer vertical component withincreasing age. There was a significantdifference in mean horizontal compo-nent–to–vertical component ratio be-tween the open physes group (0.67 �0.12) and the closed physes group(0.56 � 0.18) (P � .001) (Fig 6).
Discussion
In our study, we identified on both sag-ittal and coronal MR images a signifi-cantly larger angle that the ACL formswith the tibial plateau with advancingage; measurements of this angle ap-
Table 2
Measurements and Statistical Significance Based on Physeal Patency and Patient Sex
MeasurementOpen Physes Closed Physes Physes
Male Patients Female Patients P Value Male Patients Female Patients P Value Open Closed P Value
Sagittal ACL-tibial angle(degrees) 52.9 � 0.52 53.5 � 0.62 .47 57.9 � 0.72 59.3 � 0.71 .19 53.2 � 6.2 58.8 � 4.9 �.001*
53.1 53.3 58.2 59.2 53.1 58.938.9–65.4 39.2–66.9 50.5–64.8 43.5–71.2 36.1–74.8 43.5–71.2
Coronal ACL-tibial angle(degrees) 59.0 � 9.3 59.4 � 9.5 .72 67.9 � 8.5 69.6 � 6.8 .30 59.2 � 9.4 69.1 � 7.4 �.001*
59.2 59.4 65.7 69.9 59.2 69.534.4–78.9 38.9–85.0 55.1–84.4 52.5–83.5 34.4–85 52.5–84.4
Blumensaat line–ACL angle(degrees) 7.5 � 5.1 7.5 � 4.8 .78† 8.6 � 5.8 7.4 � 4.3 .55† 7.5 � 5.0 7.8 � 4.8 .52†
6.8 7.2 7.7 7.8 6.9 7.80.0–30.2 0.23–27.8 0.15–22.8 0.34–16.8 0.1–30.2 0.2–22.8
Inclination of intercondylarroof angle (degrees) 42.1 � 4.9 45.7 � 4.7 .005† 43.3 � 6.13 41.8 � 4.8 .10† 46.5 � 4.8 42.3 � 5.3 �.001*†
47.5 46.0 44.2 41.2 46.9 43.525.3–57.6 34.4–58.1 24.4–52.2 32.4–51.5 25.3–58.1 24.4–52.2
ACL-tibial insertion site(%)‡ 31 � 4 31 � 5 .34 30 � 4 31 � 3 .58 31 � 4 31 � 4 .59
31 31 30 30 31 3019–39 21–41 18–39 21–40 19–41 18–40
PCL angle (degrees) 114.0 � 8.2 113.7 � 8.1 .67† 122.0 � 8.4 121.9 � 8.9 .91† 113.9 � 8.1 121.9 � 8.7 �.001†
113.0 112.9 121.7 122.4 112.9 122.494.0–133.5 95.9–139.0 108.4–138.8 101.6–139.4 94.0–139.0 101.6–139.4
PCL horizontal-to-verticalcomponent ratio 0.67 � 0.13 0.68 � 0.12 .66† 0.55 � 0.07 0.56 � 0.10 .53 0.67 � 0.12 0.56 � 0.18 �.001†
0.65 0.65 0.57 0.57 0.7 0.60.34–0.99 0.42–0.97 0.42–0.75 0.32–0.75 0.3–1.0 0.4–0.8
Note.—With exception of P values, value on first line is mean measurement � standard deviation, value on second line is median, and value on third line is range.
* Sex-adjusted P value in regression model.† P value determined with rank sum testing.‡ Values cited as percentages of the anteroposterior tibial diameter.
PEDIATRIC IMAGING: MR of Anterior and Posterior Cruciate Ligaments Kim et al
832 Radiology: Volume 247: Number 3—June 2008

proach adult values with skeletal matu-rity. Gentili et al (6) described a normalsagittal ACL-tibial angle of 55.6° inadults, with a cutoff angle smaller than45° being suggestive of an ACL tearwith 91% sensitivity and 97% specific-ity. The mean sagittal ACL-tibial anglein the knees of the youngest patients(aged 1 year, n � 10) in our study was46.4° � 4.9 versus a mean angle of60.4° � 3.1 in the knees of the oldestpatients (aged 20 years, n � 11). Thenormal sagittal ACL-tibial angle in theyoungest patients was similar to the cut-off angle used to suggest ACL tears inadults. On the coronal images, the meanACL-tibial angle was 49.3° � 6.8 in theyoungest patients and 71.1° � 5.9 in theoldest patients. Sonin et al (16) calcu-lated a normal mean coronal ACL-tibialangle of 76° in adults. The differencesbetween the angles measured in the pa-tients in our study and those describedin adults may be representative of nor-mal growth.
We suggest that the larger ACL-tib-ial angle with advancing age in bothplanes is induced by an alteration in themorphology of the growing knee. Ourstudy findings show that as a child ma-tures, there is an increase in steepnessof the intercondylar roof on sagittal im-ages that reaches significance. Thistranslates to a greater height of the in-tercondylar notch on coronal images.Because the ACL originates from theposterior part of the medial surface ofthe lateral femoral condyle (4), as thisarea elongates, it may “pull up” the ACLorigin site.
The ACL-tibial insertion site re-mains proportionally stable relative tothe anteroposterior diameter of the tib-ial plateau in children and adults (13).We found the insertion site to be lo-cated at a mean of 31% of the tibialdiameter across the age ranges assessedin our study, similar to a published valueof 28% in children aged 12–14 years(13). In addition, the Blumensaat line–ACL angle remained constant withgrowth after age 2 years. This was ex-pected, because the smaller inclinationof intercondylar roof angle comple-ments the larger ACL-tibial sagittal an-gle, and, thus, the relationship between
Figure 7
Figure 7: Sagittal ACL-tibial angle as a function of patient age and sex. Polynomial regression curves, withcorresponding 95% confidence intervals (shaded), show that the angle became larger by a mean of 0.71° �0.05 with each additional year of age. Age was a significant predictor of the sagittal ACL-tibial angle when thephyses were open but not when they were closed. The data obtained between the sexes were significantly dif-ferent (P � .039).
Figure 8
Figure 8: Coronal ACL-tibial angle as a function of patient age and sex. Polynomial regression curves,with corresponding 95% confidence intervals (shaded), show that the angle became larger by a mean of1.3° � 0.08 with each additional year of age. Age was a significant predictor of the coronal ACL-tibial anglewhen the physes were open but not when they were closed. The data obtained between sexes were significantlydifferent (P � .04).
PEDIATRIC IMAGING: MR of Anterior and Posterior Cruciate Ligaments Kim et al
Radiology: Volume 247: Number 3—June 2008 833

the distal femoral intercondylar roofand the ACL remains constant. In thegroups with the youngest patients, therewere a small number of imaging studiesavailable for inclusion, and this possiblyaccounted for the variation in the Blu-mensaat line–ACL angle at ages youngerthan 2 years. The significant differencein sagittal and coronal ACL-tibial anglesbetween the sexes likely reflected thedifference in growth rates betweenmale and female individuals (17).
We suggest that the measurementchanges with growth of the PCL mayreflect the relationship between the PCLand the morphology of the distal femur.The origin of the PCL on sagittal imagesof the knees of very young subjects ap-pears to lie at the inferior-most aspectof the distal femoral epiphysis, along thearticular surface. Our study results indi-cate that the angle of inclination of theintercondylar roof was smaller in theolder patients, resulting in a steeperroof. We postulate that because the or-igin of the PCL is on the lateral surfaceof the medial femoral condyle in theintercondylar notch (4), the steeperroof at older ages might result in amore proximal translation of the ori-gin, which is slightly cranial to the ar-ticular surface in older children. Thisrelative upward migration of the ori-gin site may be reflected in an increasein the PCL angle. The mean PCL anglein adults with an intact ACL is 123°(6), but it is substantially smaller(106°) in patients with an acutely tornACL. However, in our younger patientpopulation, the mean normal PCL an-gle was 113.9°, which is smaller thanthis angle in adults. This finding sug-gests that using a decrease in the PCLangle on the basis of values deter-mined in adults as a secondary sign ofACL injury in the skeletally immaturepatient may not always be useful.
In addition to undergoing a gradualincrease in the sagittal angle, the PCLalso undergoes a configurational changewith age. Early in life, the horizontalcomponent of the PCL is just slightlyshorter than the vertical component.However, the horizontal component–to–vertical component ratio becomessignificantly smaller with advancing age
because of a relative lengthening of thevertical component. The tibial insertionsite in the more skeletally mature kneeis at a prominent tibial protrusion pos-teriorly (4). Change in the shape of theposterior tibia may be responsible forthe relative lengthening of the verticalcomponent of the PCL in older children.Further study of the morphologic changesin the knee bones of pediatric subjectswith age might be helpful to better un-derstand the changes in the cruciate lig-aments that we have observed.
The changes in the cruciate liga-ments seen as children grow may haveclinical importance because youngerchildren are undergoing knee surgerymore frequently. Although reconstruc-tive treatment of ACL injuries in skele-tally immature children is associatedwith a risk of physeal injury and subse-quent growth disturbance, use of non-surgical therapy can result in instabilityand meniscal and chondral injuries (7).ACL reconstruction is now advocated inselected patients for prevention of addi-tional injury (7–10,18). When surgeryis performed in younger patients, recog-
nition of the immature skeletal anatomymay be important for successful ACLgraft placement. To avoid graft laxityand loss of flexion in adults, an anglesmaller than 75° in the coronal plane isoptimal (19). To our knowledge, the op-timal angle for graft placement in chil-dren is not known.
One limitation of our study was itsretrospective design. In addition, thecases included were from a cross-sec-tional group and were not followed up ina longitudinal fashion. Because the ex-aminations were performed for variousindications, the imaging sequences andparameters used were not identical. Weattempted to exclude knees that werepositioned with exaggerated degrees offlexion or extension, but a dedicatedknee holder was not used. We could notcontrol for minor degrees of variation insection angulation. In addition, half themeasurements were validated by oneauthor only. Limited data for the youngerchildren were available because fewerexaminations had been performed insubjects in this age group. We used bi-lateral knee data in a small subset of
Figure 9
Figure 9: PCL angle as a function of patient age and sex. Polynomial regression curves, with correspond-ing 95% confidence intervals (shaded), show the angle became larger by a mean of 0.68° � 0.09 with eachadditional year of age. Age was a significant predictor of the PCL angle. The PCL angle also differed signifi-cantly between the open and closed physes groups. Data obtained between the sexes were not significantlydifferent.
PEDIATRIC IMAGING: MR of Anterior and Posterior Cruciate Ligaments Kim et al
834 Radiology: Volume 247: Number 3—June 2008

cases, although measurements in thetwo knees were different. Althoughprior literature on adult findings de-scribes an optimal graft location relativeto the location of the posterior portionof the ACL footprint on the tibia toavoid graft impingement (20), we choseto measure the anterior-most margin onthe sagittal images and the medial-mostmargin on the coronal images. Thesemargins were identified most consis-tently and reliably in the children.
Further study is needed to deter-mine if changes in the length and vol-ume of the ACL occur with growth, be-cause this additional information mayprove useful when planning surgical re-pair. We did not directly assess thechange in the width of the intercondylarnotch of the distal femur, which possiblyhas an important role in cruciate liga-ment injury in children, or the change inthe contour of the proximal tibia.
In summary, we found that duringgrowth, there are significant angularand morphologic changes involving theACL and the PCL. These changes mayreflect normal developmental alter-ations in the osseous structures aboutthe knee, such as steepening of the in-tercondylar roof. Once there is no po-tential for further growth in the knee,the appearance and position of the cru-ciate ligaments approach those de-scribed in adults and do not change sig-nificantly with age. The findings of ourstudy may help to further elucidate thecomplex anatomy of the knee in chil-dren. Additional study is needed to de-termine whether the same parametersdescribed as secondary signs of ACL in-jury described in the literature on adultsare applicable to children.
References1. Moore SL. Imaging the anterior cruciate lig-
ament. Orthop Clin North Am 2002;33:663–674.
2. Sonin AH, Fitzgerald SW, Hoff FL, FriedmanH, Bresler ME. MR imaging of the posteriorcruciate ligament: normal, abnormal, andassociated injury patterns. RadioGraphics1995;15:551–561.
3. Odgen JA. Injury to the immature skeleton.In: Odgen JA, ed. Skeletal injury in the child.3rd ed. New York, NY: Springer-Verlag,2000; 48.
4. Girgis FG, Marshall JL, Monajem A. Thecruciate ligaments of the knee joint: anatom-ical, functional and experimental analysis.Clin Orthop Relat Res 1975;106:216–231.
5. Staubli HU, Rauschning W. Tibial attach-ment area of the anterior cruciate ligamentin the extended knee position: anatomy andcryosections in vitro complemented by mag-netic resonance arthrography in vivo. KneeSurg Sports Traumatol Arthrosc 1994;2:138–146.
6. Gentili A, Seeger LL, Yao L, Do HM. Ante-rior cruciate ligament tear: indirect signs atMR imaging. Radiology 1994;193:835–840.
7. Shea KG, Apel PJ, Pfeiffer RP. Anterior cru-ciate ligament injury in paediatric and ado-lescent patients: a review of basic scienceand clinical research. Sports Med 2003;33:455–471.
8. Micheli LJ, Metzl JD, Di Canzio J,Zurakowski D. Anterior cruciate ligamentreconstructive surgery in adolescent soc-cer and basketball players. Clin J SportMed 1999;9:138–141.
9. Lo IK, Bell DM, Fowler PJ. Anterior cruciateligament injuries in the skeletally immaturepatient. Instr Course Lect 1998;47:351–359.
10. Fehnel DJ, Johnson R. Anterior cruciate in-juries in the skeletally immature athlete: areview of treatment outcomes. Sports Med2000;29:51–63.
11. Shea KG, Apel PJ, Pfeiffer RP, Traughber
PD. The anatomy of the proximal tibia inpediatric and adolescent patients: implica-tions for ACL reconstruction and preventionof physeal arrest. Knee Surg Sports Trauma-tol Arthrosc 2007;15:320–327.
12. Kocher MS, Hovis WD, Curtin MJ, HawkinsRJ. Anterior cruciate ligament reconstruc-tion in skeletally immature knees: an ana-tomic study. Am J Orthop 2005;34:285–290.
13. Shea KG, Apel PJ, Pfeiffer RP, ShowalterLD, Traughber PD. The tibial attachment ofthe anterior cruciate ligament in childrenand adolescents: analysis of magnetic reso-nance imaging. Knee Surg Sports TraumatolArthrosc 2002;10:102–108.
14. Nakanishi K, Horibe S, Shiozaki Y, et al. MRIof normal anterior cruciate ligament (ACL)and reconstructed ACL: comparison of whenthe knee is extended with when the knee isflexed. Eur Radiol 1997;7:1020–1024.
15. Grover JS, Bassett LW, Gross ML, Seeger LL,Finerman GA. Posterior cruciate ligament: MRimaging. Radiology 1990;174:527–530.
16. Sonin AH, Hsieh P, Dunfee W, Traina S. MRimaging assessment of the normal ACL anglein the coronal plane. Presented at the 28thannual meeting of the Society for SkeletalRadiology, Orlando, Fla, March 13–16,2005.
17. Hensinger RN. Lower extremity. In: HensingerRN, ed. Standards in pediatric orthopedics: ta-bles, charts, and graphs illustrating growth. NewYork, NY: Raven, 1986; 238–243.
18. Hawkins CA, Rosen JE. ACL injuries in theskeletally immature patient. Bull Hosp Jt Dis2000;59:227–231.
19. Howell SM, Gittins ME, Gottlieb JE, TrainaSM, Zoellner TM. The relationship betweenthe angle of the tibial tunnel in the coronalplane and loss of flexion and anterior laxityafter anterior cruciate ligament reconstruc-tion. Am J Sports Med 2001;29:567–574.
20. Howell SM, Clark JA, Farley TE. A rationalefor predicting anterior cruciate graft im-pingement by the intercondylar roof: a mag-netic resonance imaging study. Am J SportsMed 1991;19:276–282.
PEDIATRIC IMAGING: MR of Anterior and Posterior Cruciate Ligaments Kim et al
Radiology: Volume 247: Number 3—June 2008 835












![[Posterior cortical atrophy]](https://static.fdokumen.com/doc/165x107/6331b9d14e01430403005392/posterior-cortical-atrophy.jpg)







