Biomechanical robustness of a new proximal epiphyseal hip replacement to patient variability and...
11
Please cite this article in press as: Martelli S, et al. Biomechanical robustness of a new proximal epiphyseal hip replacement to patient variability and surgical uncertainties: A FE study. Med Eng Phys (2011), doi:10.1016/j.medengphy.2011.07.006 ARTICLE IN PRESS G Model JJBE-1923; No. of Pages 11 Medical Engineering & Physics xxx (2011) xxx–xxx Contents lists available at ScienceDirect Medical Engineering & Physics jou rnal h omepa g e: www.elsevier.com/locate/medengphy Biomechanical robustness of a new proximal epiphyseal hip replacement to patient variability and surgical uncertainties: A FE study S. Martelli a,∗ , F. Taddei a , E. Schileo a , L. Cristofolini a,b , Neil Rushton c , M. Viceconti a a Laboratorio di Tecnologia Medica, Istituto Ortopedico Rizzoli, Bologna, Italy b Facoltà di Ingegneria, Università degli Studi di Bologna, Bologna, Italy c The Orthopaedic Research Unit, University of Cambridge, UK a r t i c l e i n f o Article history: Received 29 December 2010 Received in revised form 8 June 2011 Accepted 11 July 2011 Keywords: Hip prosthesis Biomechanics Finite element model Failure risk sensitivity Numerical pre-clinical validation Epiphyseal hip replacement robustness Femoral head resurfacing a b s t r a c t The biomechanical behaviour of current hip epiphyseal replacements is notably sensitive to the typi- cal variability of conditions following a standard surgery. The aim of the present study was to assess the biomechanical robustness to the variability of post-operative conditions of an innovative proxi- mal epiphyseal replacement (PER) hip device featuring a short, curved and cemented stem. The risk of femoral neck fractures, prosthesis fractures and aseptic loosening were assessed through a validated finite element procedure following a systematic approach. Risk changes due to anatomical variations were assessed mimicking extreme conditions in terms of femoral size and level of osteoporosis. Fail- ure risks associated with surgical uncertainties were assessed mimicking extreme conditions in terms of uncertainties on the prosthesis position/alignment, cement–bone interdigitation depth, and friction between the prosthesis and the hosting cavity. The femoral neck strength increased after implantation from 9% to 49% and was most sensitive to changes of the anatomo-physiological variables. The risk of stem fractures was low in all studied configurations. The risk of stem loosening was low and most sen- sitive to surgical uncertainties. In conclusion, the new device can be considered an effective alternative to current epiphyseal replacements. Care is recommended in a proper seating of the prosthesis in the femur. © 2011 IPEM. Published by Elsevier Ltd. All rights reserved. Abbreviations: BL, biomechanical length of the femur; BW, body weight; FE, finite element; PER, proximal epiphyseal replacement (new device tested in this study); THR, total hip replacement; CT, computed tomography; RMSE, root mean square error; OP, osteoporosis; Sz, size; I, interdigitation depth; Pr, proximalisation; Lt, lateralisation; O, orientation; Fr, friction coefficient; R FRACT , risk of femoral neck fractures; FRR, fracture risk ratio (variation after implantation of the risk of neck fracture); RSTEM, risk for stem fracture; RLOOS, risk for aseptic loosening of the pros- thesis (due to concurrent factors); RCEM, risk for cement fracture; R BONEDAM , risk for cancellous bone damage; RFIBR, risk for adverse peri-prosthetic tissue fibrotic dif- ferentiation; RFRETT, risk for excessive fretting wear of the cement; RBRES, risk for long time excessive bone resorption of the peri-prosthetic bone; EPTO1, princi- pal tensile bone strain; EPTO3, principal compressive bone strain; S, strain energy density per unit of mass in bone; Sref, homeostatic value of the strain energy den- sity per unit of mass; S1, principal tensile stem stress; Se, fatigue endurance limit; Mp, micromovement of the prosthesis in its hosting cavity; MT1, prosthesis–cement micromovement threshold below which no excessive fretting wear is expected; MT2, prosthesis–bone micromovement threshold below which an effective bone in-growth is expected. ∗ Corresponding author at: Laboratorio di Tecnologia Medica - Istituto Ortopedico Rizzoli, Via di Barbiano 1/10, 40136 Bologna, Italy, Tel.: +39 051 636 6864; fax: +39 051 636 6863. E-mail address: [email protected] (S. Martelli). 1. Introduction Contemporary hip epiphyseal replacements are promising a number of advantages in the field of total hip replacements (THR) including increased bone preservation, reduced alteration of the hip anatomy and biomechanics, better proprioception and negligi- ble risk for recurrent dislocations [1–3]. These expected advantages and the encouraging early clinical outcomes [3–5] are driving an increasing use of hip epiphyseal replacements in clinical con- texts [6,7]. However, the clinical experience gathered over the past decade showed that individual factors and the intrinsic variabil- ity of the surgical procedure are possible sources of biomechanical concerns [3,7–12]. Among hip epiphyseal devices, investigations into resurfacing failures found that a combination of poor cementing techniques, improper implant seating and femoral neck notching had caused fractures [8,9,12]. Specifically, Shimmin and Back [9] determined varus placement to be detrimental. Furthermore, it has been found that bone quality is related to femoral neck fracture [3,10]. Cement fixation has also been associated to the failure of retrieved implants [8]. Some numerical studies [13,14] have highlighted a strong vari- ability of the risk of biomechanical failure through different bone anatomies, while others [7,11] suggested that the implant design 1350-4533/$ – see front matter © 2011 IPEM. Published by Elsevier Ltd. All rights reserved. doi:10.1016/j.medengphy.2011.07.006
Transcript of Biomechanical robustness of a new proximal epiphyseal hip replacement to patient variability and...

G
J
Bp
Sa
b
c
a
ARRA
KHBFFNEF
fissLfftcflpdsMmMi
Rf
1d
ARTICLE IN PRESS Model
JBE-1923; No. of Pages 11
Medical Engineering & Physics xxx (2011) xxx– xxx
Contents lists available at ScienceDirect
Medical Engineering & Physics
jou rna l h omepa g e: www.elsev ier .com/ locate /medengphy
iomechanical robustness of a new proximal epiphyseal hip replacement toatient variability and surgical uncertainties: A FE study
. Martelli a,∗, F. Taddeia, E. Schileoa, L. Cristofolinia,b, Neil Rushtonc, M. Viceconti a
Laboratorio di Tecnologia Medica, Istituto Ortopedico Rizzoli, Bologna, ItalyFacoltà di Ingegneria, Università degli Studi di Bologna, Bologna, ItalyThe Orthopaedic Research Unit, University of Cambridge, UK
r t i c l e i n f o
rticle history:eceived 29 December 2010eceived in revised form 8 June 2011ccepted 11 July 2011
eywords:ip prosthesisiomechanicsinite element modelailure risk sensitivity
a b s t r a c t
The biomechanical behaviour of current hip epiphyseal replacements is notably sensitive to the typi-cal variability of conditions following a standard surgery. The aim of the present study was to assessthe biomechanical robustness to the variability of post-operative conditions of an innovative proxi-mal epiphyseal replacement (PER) hip device featuring a short, curved and cemented stem. The riskof femoral neck fractures, prosthesis fractures and aseptic loosening were assessed through a validatedfinite element procedure following a systematic approach. Risk changes due to anatomical variationswere assessed mimicking extreme conditions in terms of femoral size and level of osteoporosis. Fail-ure risks associated with surgical uncertainties were assessed mimicking extreme conditions in termsof uncertainties on the prosthesis position/alignment, cement–bone interdigitation depth, and friction
umerical pre-clinical validationpiphyseal hip replacement robustnessemoral head resurfacing
between the prosthesis and the hosting cavity. The femoral neck strength increased after implantationfrom 9% to 49% and was most sensitive to changes of the anatomo-physiological variables. The risk ofstem fractures was low in all studied configurations. The risk of stem loosening was low and most sen-sitive to surgical uncertainties. In conclusion, the new device can be considered an effective alternativeto current epiphyseal replacements. Care is recommended in a proper seating of the prosthesis in thefemur.
Please cite this article in press as: Martelli S, et al. Biomechanical robustnesand surgical uncertainties: A FE study. Med Eng Phys (2011), doi:10.1016/j
Abbreviations: BL, biomechanical length of the femur; BW, body weight; FE,nite element; PER, proximal epiphyseal replacement (new device tested in thistudy); THR, total hip replacement; CT, computed tomography; RMSE, root meanquare error; OP, osteoporosis; Sz, size; I, interdigitation depth; Pr, proximalisation;t, lateralisation; O, orientation; Fr, friction coefficient; RFRACT, risk of femoral neckractures; FRR, fracture risk ratio (variation after implantation of the risk of neckracture); RSTEM, risk for stem fracture; RLOOS, risk for aseptic loosening of the pros-hesis (due to concurrent factors); RCEM, risk for cement fracture; RBONEDAM, risk forancellous bone damage; RFIBR, risk for adverse peri-prosthetic tissue fibrotic dif-erentiation; RFRETT, risk for excessive fretting wear of the cement; RBRES, risk forong time excessive bone resorption of the peri-prosthetic bone; EPTO1, princi-al tensile bone strain; EPTO3, principal compressive bone strain; S, strain energyensity per unit of mass in bone; Sref, homeostatic value of the strain energy den-ity per unit of mass; S1, principal tensile stem stress; Se, fatigue endurance limit;p, micromovement of the prosthesis in its hosting cavity; MT1, prosthesis–cementicromovement threshold below which no excessive fretting wear is expected;T2, prosthesis–bone micromovement threshold below which an effective bone
n-growth is expected.∗ Corresponding author at: Laboratorio di Tecnologia Medica - Istituto Ortopedicoizzoli, Via di Barbiano 1/10, 40136 Bologna, Italy, Tel.: +39 051 636 6864;
ax: +39 051 636 6863.E-mail address: [email protected] (S. Martelli).
350-4533/$ – see front matter © 2011 IPEM. Published by Elsevier Ltd. All rights reserveoi:10.1016/j.medengphy.2011.07.006
© 2011 IPEM. Published by Elsevier Ltd. All rights reserved.
1. Introduction
Contemporary hip epiphyseal replacements are promising anumber of advantages in the field of total hip replacements (THR)including increased bone preservation, reduced alteration of thehip anatomy and biomechanics, better proprioception and negligi-ble risk for recurrent dislocations [1–3]. These expected advantagesand the encouraging early clinical outcomes [3–5] are drivingan increasing use of hip epiphyseal replacements in clinical con-texts [6,7]. However, the clinical experience gathered over the pastdecade showed that individual factors and the intrinsic variabil-ity of the surgical procedure are possible sources of biomechanicalconcerns [3,7–12].
Among hip epiphyseal devices, investigations into resurfacingfailures found that a combination of poor cementing techniques,improper implant seating and femoral neck notching had causedfractures [8,9,12]. Specifically, Shimmin and Back [9] determinedvarus placement to be detrimental. Furthermore, it has been foundthat bone quality is related to femoral neck fracture [3,10]. Cement
s of a new proximal epiphyseal hip replacement to patient variability.medengphy.2011.07.006
fixation has also been associated to the failure of retrieved implants[8]. Some numerical studies [13,14] have highlighted a strong vari-ability of the risk of biomechanical failure through different boneanatomies, while others [7,11] suggested that the implant design
d.

ING Model
J
2 eering
auditeScTfcfmdainwdPmgndtlr[i
iidct
otodoiso
2
iilivobwaae
2
fy
ARTICLEJBE-1923; No. of Pages 11
S. Martelli et al. / Medical Engin
nd the relative surgical procedure play a fundamental role in fail-re. Statistical investigation into the less diffused short-stemmedevices (Proxima, DePuy Inc., Warsaw, USA) showed a relevant
nfluence of different bone anatomies and surgical outcomes onhe implant mechanics [15]. More recently, an innovative proximalpiphyseal replacement (PER, Stryker Orthopaedics, Hérouville-aint-Clair, France) has been proposed [16–18]. The PER deviceonsists of a modular head and a short, curved and cemented stem.he implant design involves the removal of a large fraction of theemoral head to minimise, in this region, the risk of necrosis as aonsequence of blood supply loss [19]. The short curved stem trans-er a consistent fraction of the articular load from the head to the
edial cortical shell in the calcar region [18]. The geometry of theevice was finalised following an original numerical–experimentalpproach to optimise the loading transfer mechanism between themplant and the reamed bone [18]. The results showed a nearlyatural bone mechanics in PER implants. The same conclusionas confirmed through the experimental comparison between PERevices and the most successful resurfacing devices. In fact, onER implants, superficial bone strains more closely matched thoseeasured on intact femurs [16]. Furthermore destructive tests sug-
ested that PER implants better preserve the natural risk of femoraleck fracture [17]. These differences are likely a consequence of aifferent mechanism in transferring the acetabular load betweenhe two devices. In fact, on resurfaced femurs, the majority of theoad is intended to be transferred through the metallic shell to theeamed femoral head, leaving the stem the duty of alignment only20]. This mechanism has been recently hypothesised to play a rolen short-term neck fractures [20] of resurfaced femurs.
However, despite the promising results obtained for PERmplants, little is known about the effect of the typical variabil-ty of a standard surgery and of the bone structure on the risk ofifferent biomechanical failure scenarios. Indeed, the only numeri-al study was conducted on a single implant [18], while pre-clinicalests were conducted on a small set of cadaveric implants [17].
The aim of this study was to assess the robustness of the riskf potential biomechanical failure scenarios (i.e. femoral neck frac-ures, prosthesis fracture and aseptic loosening of the prosthesis)f the PER device to the typical variability of conditions due toifferent patient and surgical factors (i.e. femoral size, level ofsteoporosis, surgical misalignment of the device, bone–cementnterdigitation depth). The study was conducted using a risk analy-is for hip epiphyseal replacements recently proposed [21], a designf experiment approach and a validated FE procedure.
. Materials and methods
A recently published risk analysis procedure was [18,21] usedn this study to address a number of possible failure scenarios,ncluding femoral neck fractures, prosthesis fractures and asepticoosening. The risk values for an average sized femur implanted indeal conditions from a previous study were chosen as referencealues [18]. Seven variables were explored to investigate changesn the risk of biomechanical failure throughout the range of possi-le anatomo-physiological and surgical conditions. Two FE modelsere generated for each variable by setting its extreme values, one
t a time, not accounting for factor interactions. Models were gener-ted following a validated procedure [22,23]. Risk indicators werextracted and compared to identify the most influencing variables.
.1. Selection of the CT dataset
Please cite this article in press as: Martelli S, et al. Biomechanical robustnesand surgical uncertainties: A FE study. Med Eng Phys (2011), doi:10.1016/j
The study was based on a CT scan of an average sized humanemur (biomechanical length 417 mm) from a male donor (age 51ears, weight 75 kg, height 175 cm) for which a detailed descrip-
PRESS & Physics xxx (2011) xxx– xxx
tion is given in an earlier publication [24]. In summary, the femurdid not show abnormalities or defects to a radiographic inspection.The CT scan was obtained through an axial scan protocol (scannermodel: HiSpeed, General Electric Co., USA) using typical physicalsettings for clinical examinations (tube current: 180 mA, 120 kVP).The slice thickness was 1 mm and the spacing was 2 mm in the prox-imal region (from the top of the femoral head down to the lessertrochanter) and 4 mm in the rest of the femur. The pixel spacingwas 0.46 mm.
2.2. Definition of the investigated variables
The investigated variables were: femoral size (Sz), cement inter-digitation depth (I), friction (Fr) at the prosthesis interface, surgicaluncertainties including planar prosthesis misplacements (Pr and Lt)and misrotations (O) and osteoporosis level (T-score). Each variableis below discussed separately.
2.2.1. Femoral size (Sz)To represent the largest variations in size two additional femur
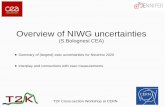
CT scans where chosen. Selection was based on the IOR (IstitutoOrtopedico Rizzoli, Bologna, Italy) database containing over thanthousand CT scans from patients who received a THR. Datasets wereordered according to femur biomechanical length. The two femursthat showed the smallest and the largest biomechanical lengthwere selected to represent a small and a large size femur (Table 1).The ideal prosthesis position and size was virtually defined foreach anatomy by an experienced surgeon (Fig. 1) in a surgery pre-planning environment (Hip-Op©, B3C, Italy).
2.2.2. Interdigitation depth (I)The maximum cement–bone interdigitation depth (4 mm) in the
bone layer encircling the stem was estimated from the exposedfracture of seven cadaveric femurs implanted with a PER deviceduring a separate study [17]. The interdigitated bone was mod-elled as a uniform layer for which the constant interdigitation depthvariable (I) was assumed to range between 0 and 4 mm [25]. In thislayer, the mechanical properties of the resulting mixture betweenbone, cement and other materials that cannot carry loads (e.g. mar-row, fat or physiological fluids) are dependent on an extremelycomplex interdigitation process. This process induces an averageincrease of the stiffness of the elastic support of the prosthesis [26].This stiffness increase was simulated, as a first approximation, byassigning the elastic properties of the cement (E = 2700 MPa) to theinterdigitated bone layer in those regions where the bone elasticmodulus was lower than that of the cement.
2.2.3. Friction (Fr)No perfect bond can be expected in the immediate post-
operative period at both the cement–prosthesis and thebone–prosthesis interface [27], thus the friction coefficientwas varied between 0.0 and 0.6 to include extreme frictionconditions [28].
2.2.4. Surgery uncertaintiesAn experienced surgeon carried out seven virtual implanta-
tions of the device using a surgical planning software (HipOp©,B3C, Italy) [29]. The reference implant position was assumed theideal position defined in [18]. On a frontal projection, six dif-ferent device positions were defined consistently with extremeconditions for a normal surgery (Fig. 2). Each new position of thedevice was defined using a planar coordinate system with the
s of a new proximal epiphyseal hip replacement to patient variability.medengphy.2011.07.006
origin in the centre of the prosthesis cup in the ideal position.The vertical axis was assumed parallel to the femoral diaph-ysis while the horizontal axis was assumed pointing laterallywhile lying on the vertical symmetry plane of the femoral neck.

ARTICLE IN PRESSG Model
JJBE-1923; No. of Pages 11
S. Martelli et al. / Medical Engineering & Physics xxx (2011) xxx– xxx 3
Table 1In the first column the femoral size. In the following columns the subjects’ details. In sequence, the subject age (years), the sex, the femoral side, the body-weight (kg), thepatient body mass index (BMI) and the biomechanical length (mm) that was used to define the size variable.
Size Subject age (years) Sex Side Subject body-weight (kg) Body mass index (BMI) Biomechanical length (mm)
Small 53 Female Right 58 24.8 370Medium 51 Male Right 75 24.8 417Large 66 Male Right 88 24.4 480
F On thi
Tmpdavevw
Fsa
ig. 1. On the left the three geometrical models extracted from the CT volumes.
mplanted in the ideal position in the CT volume of the averaged sized femur.
hree variables were defined to describe each specific misplace-ent/misalignment: (1) proximal-distal displacement assuming
ositive misplacements pointing proximally (Pr), (2) medio-lateralisplacement (Lt) assuming positive misplacements pointing later-lly and (3) rotations (O) assuming positive misalignment pointingarus. The highest misplacement possible was assumed 3 mm in
Please cite this article in press as: Martelli S, et al. Biomechanical robustnesand surgical uncertainties: A FE study. Med Eng Phys (2011), doi:10.1016/j
ach direction and the highest misalignment were assumed 10◦ inarus and −2◦ in valgus, that was the maximum rotation possibleithout reaming of the medial cortex.
ig. 2. The variables proximal-distal (Pr), medio-lateral (Lt) and rotations (O) arehown superimposed to PER implant and their positive and negative direction islso indicated by + and − signs.
e right a screenshot of the surgical planning software where the PER device was
2.2.5. Osteoporosis (T-score)The modelling strategy was based on the established defini-
tion of osteoporosis in terms of T-score [30]. The T-score value ofthe average sized femur was extracted from the CT data following[31]. The osteoporosis process was assumed to resorb cancel-lous bone twice as quickly as the cortical bone [32], accordingto the hypothesis of bone resorption depending on available freesurface and in vivo observed patterns [33,34]. The surface sepa-rating the cortical from the trabecular bone volume was visuallyidentified in a software environment (LHPBuilder, SCS, Italy). Theaverage Hounsfield units among the CT voxels crossing the cortical-trabecular separating surface was estimated and the correspondingbone ash density was calculated using a published relationship [35].In the finite-element model this value (0.5 g/cm3) was used to sep-arate cortical from trabecular elements. The intermediate T-scorevalue from [18] was −3.42. Two scaling factors, one for the corticaland one for the trabecular regions, were used to scale separatelythe ash density associated to each mesh element. Two additionalmodels were generated representing a non-osteoporotic (non-OPmodel) and a highly (highly OP model) osteoporotic femur. Thenon-OP level was that of the mean population of young adults(T-score = 0) while the highly OP level was assigned T-score = −5(Table 2). The map of the bone elastic modulus was re-calculatedfor both femur models using the aforementioned published rela-tionship [35].
2.3. The FE modelling procedure
s of a new proximal epiphyseal hip replacement to patient variability.medengphy.2011.07.006
The FE modelling procedure for which a more detailed descrip-tion can be found in [24,36], is here only briefly summarised. Thebone anatomy was extracted from the CT data [37]. An experiencedsurgeon carried out the virtual implantation of the prosthesis. The

ARTICLE IN PRESSG Model
JJBE-1923; No. of Pages 11
4 S. Martelli et al. / Medical Engineering & Physics xxx (2011) xxx– xxx
Table 2The variables and their ranges considered in the present study. The average implant condition was defined by average values of all the investigated variables (column “Mid”).The variables (column “Factor”) were assumed to vary between their lower values (column “Low”) and their maximum values (column “High”). In the “Unit” column, theunit used to present the variable values.
Factor Description Unit Low Mid High
Sz Femoral size Small Medium LargeI Cement interdigitation depth mm 0 2 4Pr Stem proximal misplacement mm −3 0 3Lt Stem lateral misplacement mm −3 0 3O Stream mis-orientation deg −2 0 10
core
iup[ivsafctdth5Tc2titcapm
a
FpsTr
T-score Osteoporosis level T-sFr Friction coefficient
ntact and the implanted bone volume were meshed (10-nodednstructured tetrahedral mesh) and the inhomogeneous materialroperties were extracted from CT data (Bonemat V3, B3C, Italy)38,39] (Fig. 3) following a procedure described in [24,36]. In themplanted model, the cement mantle was assigned E = 2700 MPa,
= 0.3 (Simplex P, Stryker Orthopaedics, USA) [40] and the prosthe-is was assigned the material properties of cobalt–chrome (CoCr)lloy (E = 210 GPa, v = 0.3). The bone–cement interface was assumedully bonded. Either the prosthesis–bone or the prosthesis–cementontact surfaces were assumed to be in frictional unilateral contact,he friction coefficient variable was defined between extreme con-itions according to the study design (see Section 2.2 for details). Inhe present study only model verification was performed using postoc indicators [41]; the 90th percentile of the error distribution was% for the prosthesis, 8% for the cement, and 12% for the femur.he contact penetration was used as convergence indicator of theontact problem; the contact penetration was always lower than
�m. The average model was taken from an earlier study [18] andhe same procedure was repeated to explore the range of possiblemplant conditions by setting the extreme values of each inves-igated variable (Table 2). To allow an element-by-element result
Please cite this article in press as: Martelli S, et al. Biomechanical robustnesand surgical uncertainties: A FE study. Med Eng Phys (2011), doi:10.1016/j
omparison for each implanted model, an intact model was gener-ted using the implanted bone model as an intact sub-model. Therocess resulted in 28 FE models (14 intact and 14 implanted femurodels).
ig. 3. The FE model of the implanted femur superimposed to the CT dataset. On the lrosthesis–cement complex in wireframe (top) and the FE model (bottom) showing the mections (Sez. A and Sez. B) show the inner implanted epiphysis superimposed to the rahe inner trabecular bone and external femoral cortex are presented by using different coeferred to the web version of the article.)
−5 −3.42 00 0.3 0.6
2.4. Definition and analysis of the risk of failure
The risk analysis was published in a previous study [18,21]. Insummary, the three investigated scenarios of failure were: femoralneck fractures (a), fractures of the prosthetic component (b) andaseptic loosening (c). For each of them, the list of investigated fail-ure modes were:
) The ratio between the peak of the principal tensile strain pre-dicted in the cortical bone (EPTO1impl) and the tensile strainthreshold (EPTO1T) for fracture [23] was used as an indicatorof the risk of femoral neck fracture (RFRACT):
RFRACT = EPTO1impl
EPTO1T× 100;
An additional indicator was defined to address changes of thebone fracture load at the femoral neck after implantation. Thefracture risk ratio (FRR) was defined as:
FRR = EPTO1impl − EPTO1int × 100;
s of a new proximal epiphyseal hip replacement to patient variability.medengphy.2011.07.006
EPTO1int
where EPTO1int is the peak of the principal tensile strain pre-dicted in the cortical bone by the intact femur model.
eft two projections of the radiographic volume with the planned position of theap of the elasticity modulus distribution derived from CT values. On the right two
diographic volume. The colour maps show the distribution of material properties.lour scales. (For interpretation of the references to colour in this text, the reader is

ING Model
J
eering
b
c
i
ii
i
Ffip
ARTICLEJBE-1923; No. of Pages 11
S. Martelli et al. / Medical Engin
) An indicator of the risk of prosthesis fracture (RSTEM) wasassessed verifying that peak VonMises stress (SQV) did notinduce in the prosthesis any permanent damage. The endurancelimit (SQVT = 200 MPa) was assumed the lowest threshold of thecobalt–chrome alloys currently used for implant manufacturing[42].
RSTEM = SQVSQVT
× 100;
) The risk for aseptic loosening of the implant was computedconsidering concurrent failure modes (i.e. cement fracture,fibrotic tissue differentiation, fretting wear of the cement,peri-prosthetic bone damage and excessive resorption of theperi-prosthetic bone) [43]. The loosened area was computed asthe union of the loosened areas caused by each failure mode.The overall indicator for aseptic loosening (RLOOS) was definedas the ratio between the loosened area and the total area of theprosthesis interface. The failure modes were studied as follows:
i. The ratio between the predicted maximum principal tensilestress (S1) and the endurance limit (Se = 11.3 MPa) for acrylicbone cement (Simplex P, Stryker Orthopaedics, USA) [40] was
Please cite this article in press as: Martelli S, et al. Biomechanical robustnesand surgical uncertainties: A FE study. Med Eng Phys (2011), doi:10.1016/j
used as the indicator of the risk for cement fracture (RCEM):
RCEM = S1Se
× 100
ig. 4. The maps for all the investigated failure risks (risk of femoral neck fracture RF
brotic tissue differentiation at the bone–prosthesis interface RFIBR (c), cement fracture Reri-prosthetic bone RBRES (f)) estimated for the ideal surgery condition.
PRESS & Physics xxx (2011) xxx– xxx 5
i. The ratio between the predicted relative micromovement (MP)at the cement–prosthesis interface (Fig. 4e) and the thresholdMT1 = 50 �m was used as the indicator of the risk fretting wear ofthe cement (RFRETT). This threshold represent the stick–slip limitat the cement–prosthesis interface below which no fretting wearis expected [44,45]:
RFRETT = MP
MT1× 100
i. The ratio between the predicted relative micromovement (MP)at the bone–prosthesis interface (Fig. 4c) and the threshold(MT2 = 150 �m) above which a fibrotic tissue differentiation pre-vails (150 �m) [46,47] was used as the indicator of the riskfor adverse fibrotic differentiation (RFIBR) of the peri-prostheticbone:
RFIBR = MP
MT2× 100
v. The risk for peri-prosthetic bone damage (RBONEDAM) was com-puted as the highest risk between the risk indicator of boneoverload in compressive and tensile conditions. RBONEDAM in
s of a new proximal epiphyseal hip replacement to patient variability.medengphy.2011.07.006
compressive conditions was the ratio between the highest prin-cipal compressive bone strain (EPTO3) predicted by the modeland its safe threshold (EPTO3T = −1.04%) [48]. RBONEDAM in tensileconditions was the ratio between the highest principal tensile
RACT (a), risk of aseptic loosening for peri-prosthetic bone damage RBONEDAM (b),CEM (d), fretting wear of the cement RFRETT (e) and adverse bone resorption of the

ING Model
J
6 eering
v
R
2
t[TfFttlstowv
3
wdcb
Fs
ARTICLEJBE-1923; No. of Pages 11
S. Martelli et al. / Medical Engin
bone strain (EPTO1) predicted by the model and its safe threshold(EPTO1T = 0.73%) [48].
RBONEDAM = max(
EPTO1EPTO1T
; − EPTO3EPTO3T
)× 100
. Changes (S − Sref) of the strain energy density per unit of mass(S) with respect to its homeostatic value (Sref) can be consideredas the mechanical signal driving bone remodelling. However,a certain level of abnormality of the signal must be exceededbefore the bone respond. This level s defines the boundaries ofthe so-called dead zone within which no bone remodelling isexpected [49]; s was assigned 0.75, a level that was found toproduce realistic predictions for hip implants [50]. Assumingthe possibility for the bone resorption and apposition processto initiate for RBRES < −100% and RBRES > +100%, respectively, thecorresponding risk value was computed as follows:
BRES =(
S − Sref
Sref
)· 100
s, s = 0.75;
.5. Selection of the most critical loading scenario
The loads applied to the proximal femur mimicked the execu-ion of selected activities of daily living from a large public database43,51]. The FE model was fully constrained in the condylar region.he loads applied to the proximal femur were selected for eachailure scenario. The risk for femoral neck fractures (RFRACT andRR) was studied mimicking a single leg stance loading conditionhat was found to replicate clinically relevant spontaneous frac-ures [52]. The risk for prosthesis fracture (RSTEM) and for asepticoosening (RLOOS) were studied mimicking the peak load duringtair-climbing, a severe activity of daily living that produces some ofhe largest hip reaction loads [43]. The only exception was the riskf adverse bone resorption of the peri-prosthetic bone (RBRES) thatas investigated mimicking the peak load during level-walking, a
ery frequent activity of daily living.
. Results
For the average model, i.e. when all the investigated variables
Please cite this article in press as: Martelli S, et al. Biomechanical robustnesand surgical uncertainties: A FE study. Med Eng Phys (2011), doi:10.1016/j
ere set to intermediate values mimicking an ideal surgery con-ition, the results were taken from [18] and here reported forompleteness (Fig. 4). For this implant condition, the highest risk ofiomechanical failure was the risk for cement fracture (RCEM = 58%).
ig. 5. The interaction plots between the fracture risk ratio FRR computed for the bone
trength of the neck with implant would be lower than that left intact in all cases (FRR < 0
PRESS & Physics xxx (2011) xxx– xxx
Among all other investigated scenarios lower values of the high-est risk were found only for the large size femur and the deeplyinterdigitated scenarios (53% and the 50%, respectively). Failure wasnot predicted for any of the studied conditions but for the extremelyvalgus implant, for which fracture of the cement was predictedin a very localised region close to the distal tip. In the followingthe results obtained for each scenario are discussed separately. Foreach risk, results are presented as (1) maximum and minimumpredicted risk levels and (2) variables producing the highest riskchanges.
3.1. Femoral neck fracture
In all cases, the implantation of the prosthesis produced adecrease of the risk of femoral neck fracture. This decrease wasminimum for the smallest femur size (FRR = −9%) and maximumfor the 3 mm lateral displaced stem (FRR = −49%). Size and OP levelinduced FRR variations above 20% while all the other parametersinduced lower changes (Fig. 5).
The cortical bone tensile strain was highly sensitive to the dif-ferent implant configurations; RFRACT ranged from 15% of the smallsize to 52% of the severely osteoporotic femur. Variations of the OPlevel induced the highest RFRACT changes (31%) while variations ofall the other parameters induced RFRACT changes below 20% (Fig. 6).
3.2. Prosthesis fracture
The peak Von Mises stress in the prosthesis was highly sensi-tive to the different implant configurations; RSTEM was predictedto range from 32% to 69%. Variations of the OP level and the stemorientation induced RSTEM changes of 30% while variations of all theother parameters induced smaller changes (Fig. 7).
3.3. Aseptic loosening
None of the investigated risks (RCEM, RFRETT, RFIBR, RBONEDAM)exceeded the safe threshold in any of the investigated scenariosapart from the risk for cement fatigue fractures (Figs. 8 and 9).In the case of a valgus stem (O = −2◦) the cement stress exceededthe endurance limit in a very localised region of the distal cementwhere RCEM reached 111%, leading to failure of a very small portionof the total area of interface (RLOOS = 0.15%). Each failure mode is
s of a new proximal epiphyseal hip replacement to patient variability.medengphy.2011.07.006
separately discussed in the following:
i. RCEM varied from RCEM = 46% reached for the non-osteoporoticand the 10◦ varus stem to RCEM = 111% of the 2◦ valgus stem.
at the femoral neck and the investigated variables (Sz, I, Fr, O, Pr, Lt, T-score). The). Low, centre and high are parameter values from Table 2.

ARTICLE IN PRESSG Model
JJBE-1923; No. of Pages 11
S. Martelli et al. / Medical Engineering & Physics xxx (2011) xxx– xxx 7
Fig. 6. The interaction plots (left) between RFRACT computed for the bone at the femoral neck and the investigated variables (Sz, I, Fr, O, Pr, Lt, T-score) and the histograms(right) show the changes of RFRACT due to the variations of each investigated variable within the studied range. For none of the investigated cases femoral neck fracture waspredicted (RFRACT < 100%). Low, centre and high are parameter values from Table 2.
F (RSTEM
t d varia param
i
ii
iv
v
ig. 7. On the right the interactions plot between the predicted risk of stem fracturehe histograms show the changes of RSTEM due to the variations of each investigateccumulation is predicted in the prosthesis (RSTEM < 100%). Low, centre and high are
Variations of O and Lt induced RCEM changes of 65% and 41%,respectively, while variations of all the other parameters inducedRCEM changes below 28%.
i. RFRETT varied from 24% of the 10◦ varus stem to 74% of the 3 mmlaterally displaced stem. Variations of Lt induced RFRETT changesof 40% while variations of all the other parameters induced RFRETTchanges below 26%.
i. RFIBR was always lower than 23% obtained with the zero-frictionmodel. RFIBR changes induced by variation of all parameters wereall below 12%.
. RBONEDAM varied from 22% of the small size femur to 90% of the3 mm lateral stem. Variations of Lt and T-score induced RBONEDAMchanges of 52% and 64%, respectively, while all the other param-eter induced change below 34%.
. The map of the risk of bone resorption (RBRES) showed a verysmall bone region (<2.3% of the femoral epiphysis) exceedingthe activation threshold of the bone resorption process in most
Please cite this article in press as: Martelli S, et al. Biomechanical robustnesand surgical uncertainties: A FE study. Med Eng Phys (2011), doi:10.1016/j
of the studied configurations. Only the large size and the severelyosteoporotic models showed higher risks; in these cases thevolume at risk for resorption was 8.9% and 24% of the femurepiphyseal volume, respectively (Fig. 10).
) and the investigated influencing variables (Sz, I, Fr, O, Pr, Lt, T-score). On the right,able within the studied range. For none of the investigated cases no cyclic damage
eter values from Table 2.
4. Discussion
The risk of biomechanical failure of the most common epiphy-seal replacements has been found to be significantly sensitive to thedifferent post-operative conditions depending on individual factorsand on the variability of the surgical procedure [12,53]. The aimof the present study was to assess the biomechanical robustnessof the innovative PER device to individual factors and to surgicaluncertainties.
The implant was found stable in all the investigated condi-tions. Considering the surgical uncertainties only, the lowest risk ofbiomechanical failure was found for the implant in the ideal posi-tion. This suggests that the ideal position planned by the surgeonis nearly ideal also from a biomechanical standpoint.
Individual and surgical factors affected the biomechanical risk offailure in different ways. The femoral neck strength increased afterimplantation in all studied conditions, from 9% of the small size
s of a new proximal epiphyseal hip replacement to patient variability.medengphy.2011.07.006
femur to 49% increase of the laterally displaced stem. The risk ofstem fracture was low in all cases. The overall risk for aseptic loos-ening throughout the prosthesis interface was low for each studiedcondition but high-risk values where found in very small regions

ARTICLE IN PRESSG Model
JJBE-1923; No. of Pages 11
8 S. Martelli et al. / Medical Engineering & Physics xxx (2011) xxx– xxx
Fig. 8. Plots of the interactions between the predicted risk for the investigated failure modes (RCEM, RBONEDAM, RFIBR, RFRETT) potentially concurring in aseptic loosening of theprosthesis and the investigated variables of influence (Sz, I, Fr, O, Pr, Lt, T-score). The occurrence of each failure mode is predicted when the corresponding computed riske ter val
oaeeIpv(cstib
tef(ofcIar
ml
xceed the threshold 100% (horizontal solid line). Low, centre and high are parame
f the prosthesis interface, suggesting loosening as the most prob-ble failure scenario for PER implants. The risk of cement fracturesxceeded the safe threshold in a very localised region (0.15% of thentire prosthesis interface) when the stem was placed in valgus.n this condition the stem tip was very close to the medial cortexroducing a stiff linkage yielding high cement stresses. High-riskalues were also found for the risk of peri-prosthetic bone damageRBONEDAM < 90%) when the stem was laterally displaced. Long-timeoncerns for stem mobilisation were found to occur more likely oneverely osteoporotic femurs (T-score = −5). Indeed, results showhat a larger portion of peri-prosthetic bone experiences large load-ng alterations after surgery as the bone weakens due to adverseone resorption.
The implant biomechanics of PER implants showed impor-ant differences from what observed for the most largely diffusedpiphyseal replacements (i.e. resurfacing devices). The risk ofemoral neck fractures was lower than that of the intact femur−49% < FRR < −9%), whereas in resurfacing devices the post-perative increase of bone strains has been associated with earlyemoral neck fractures [11]. This is likely due to a more physiologi-al mechanism in transferring the acetabular load of PER implants.n fact, post-surgical alterations of both the superficial bone strainsnd the fracture load were found smaller in PER implant than in
Please cite this article in press as: Martelli S, et al. Biomechanical robustnesand surgical uncertainties: A FE study. Med Eng Phys (2011), doi:10.1016/j
esurfaced femurs [16,17].The range of predicted risk of fractures (minimum RFRACT = 15%;
aximum RFRACT = 52%, difference = 37%) was consistent with ear-ier experimental studies (fracture load = 11.4 ± 34% times body
ues from Table 2.
weight [17]). This range is also consistent with the range of princi-pal bone strains found in 16 resurfaced femurs [13,14]. The fractureload of PER implants was highly sensitive to surgical uncertainties(−49% < FRR < −21%) accordingly, again, to what found for resur-faced femurs [11,14]. However, while varus stems induced a riskdecrease in PER implants the same varus rotation induced a riskincrease in resurfaced femurs [11]. In fact, rotating the curved PERstem in varus, the articular load is transferred through stiffer link-age with a considerably more dense bone close to the medial cortex.This change increases the bone compressive strains in the strongmedial cortex while it decreases the bone tensile strains in the thincortex of the lateral neck. For resurfaced femurs, on the contrary,an increase of bone strains in the lateral neck was shown as thedevice was rotated in varus [14]. The risk of aseptic loosening waslow accordingly to what found for resurfaced femurs [21] high-lighting two most likely failure modes: cement fatigue fracturesand peri-prosthetic bone overload. The risk of cement fractureswas highly sensitive to surgical errors (46% < RCEM < 111%), in accor-dance with what found on resurfaced femurs [11,13,14] althoughwith a different dependency. While valgus orientations reduced byapproximately two-third the cement stresses in resurfaced femurs[11,14], cement stresses did benefit of varus and laterally displacedstems in the PER implant.
s of a new proximal epiphyseal hip replacement to patient variability.medengphy.2011.07.006
The risk for peri-prosthetic bone damage RBONEDAM variedbetween 25% and 89%, reaching the highest level for the severelyosteoporotic bone. Although damage at the peri-prosthetic bonewas never predicted, this high value make the peri-prosthetic bone

ARTICLE IN PRESSG Model
JJBE-1923; No. of Pages 11
S. Martelli et al. / Medical Engineering & Physics xxx (2011) xxx– xxx 9
F ning (w
dw[
sr
Frasf
ig. 9. The histograms show the changes of the computed risk concurring in looseithin the studied range.
amage one of the most probable scenarios. Similar conclusionsere drawn for resurfaced femurs from radiological observations
Please cite this article in press as: Martelli S, et al. Biomechanical robustnesand surgical uncertainties: A FE study. Med Eng Phys (2011), doi:10.1016/j
54].An effective PER implants stability over time was predicted con-
istently with contemporary epiphyseal replacements. The highestisk for excessive bone resorption (24% of the epiphyseal bone)
ig. 10. Histogram reporting the volume fraction of the epiphyseal bone region atisk for activation of the bone remodelling process (RBRES). The bone volume fractiont risk for excessive bone resorption did never exceed the 2.3% of the reamed epiphy-eal bone apart from the large size model (RBRES = 8.9%) and the severely osteoporoticemur (RBRES = 24%).
RCEM, RFRETT, RFIBR and RBONEDAM) due to the variations of each investigated variable
was found for the severely osteoporotic (T-score = −5) femur. Com-paring different solutions, it can be noted that a larger portionof trabecular bone experiences large loading differences as thebone weaken. Particularly, the peri-prostetic trabecular bone expe-riences the highest resorption speed [32] and alterations of theimplant mechanics. However, such a high OP level is normally con-sidered a strong contra-indication for epiphyseal replacements [3].
The present study has some limitations. The first limitation is therelatively small number of variables used. On one hand, additionalparameters (e.g. femoral neck length, head diameter and antev-ersion angle, out of plane prosthesis misplacements, erroneousselection of the prosthesis size, press-fit level and probably others)might have allowed a better description of the entire range of pos-sible implant conditions, but requiring a much larger effort. Moreresearch towards a completely parametric model would make itefficiently feasible. In the author’s opinion, however, the large rangeof anatomies here used (biomechanical length range: 370–480 mm,neck length range: 32–44 mm, head diameter range: 21–52 mmand anteversion angle range: 9–14◦) and the extreme prosthesispositions here investigated can provide meaningful first informa-tion on the risk of biomechanical failure in a broad range of clinicalconditions.
Furthermore, not all variables were defined symmetrically withrespect to the implant assumed ideal (i.e. the stem mis-orientationlevels were −2◦; 0◦; 10◦ and the osteoporosis T-score levels were−5; −3.42; 0). This inevitably distorts the information on the riskssensitivity to the investigated variables. However, the aim of thisstudy was to assess the robustness of the implant biomechanics to
s of a new proximal epiphyseal hip replacement to patient variability.medengphy.2011.07.006
extreme post-surgical conditions.The models were verified but not validated for practical reasons.
However, confidence about the models result could be gatheredfrom earlier findings based on the same procedure here adopted

ING Model
J
1 eering
[milbm
biicisiet
ctfcsbtrb
iars
ih([teamPaboinea
rrbbiir
pti
A
O
[
[
[
[
[
[
[
[
[
[
[
[
[
[
ARTICLEJBE-1923; No. of Pages 11
0 S. Martelli et al. / Medical Engin
21,24,36]. Comparing predictions with experimental measure-ents on cadaveric bones, the accuracy was approximately 10%
n predicting the superficial bone strains [36,55] and the fractureoad [23]. On a resurfaced femur, the error in predictions of theone-implant micromotions was below 20 �m [24] and, the sameodel allowed good predictions of relevant clinical outcomes [21].The study design neglected the factor interactions while a com-
ination of detrimental factors has been hypothesised to play a rolen failure of similar hip epiphyseal implants [7,13,14]. But again,n the authors’ opinion the large differences between the studiedonfigurations can provide meaningful information while factornteractions could be more easily investigated designing exten-ive statistical studies. To this purpose the knowledge of the mostmportant factors provided in this study may help in the design offficient statistical simulations while keeping the large computa-ional time required [15] still reasonable.
The head remnant was assumed to consist of native bone inontact with the prosthesis surface (Fig. 4c). However, it is likelyhat during insertion of the prosthesis some cement can expandrom the stem region under the prosthesis dome, creating a thinement layer at the prosthesis interface. Although this should notignificantly alter the implant mechanics [11], the failure mode toe checked this case might change from fibrotic tissue differen-iation to fretting wear of the cement. However, given the smallelative micromovements predicted (<30 �m), a good implant sta-ility should be expected in all cases.
Although the simulated loads mimic important everyday activ-ties, additional motion tasks should be investigated since eachctivity type might induce specific skeletal loads. In fact clinicallyelevant femoral neck fractures were obtained on relatively largeeries of cadaveric femurs using a specific loading scenario [7].
The last study limitation concerns the definition of the stud-ed failure modes. Other failure modes, not included in this study,ave been hypothesised to play a role in failure of similar devicesi.e. neck narrowing [4,54,56] and peri-prosthetic bone necrosis57]). However, follow-up studies found femoral neck narrowingo be not clinically relevant [4,54,56] and the PER implants arexpected to be moderately prone to avascular necrosis [16]. Inddition, it cannot completely be excluded that unexpected failureodes might appear in the clinics due to the differences between
ER and resurfacing prosthesis [58]. However, the choice to use risk analysis based on the resurfacing devices seems reasonableecause (a) a strict geometric similarity, (b) the complete absencef clinical information for the PER devices, and (c) the large clin-cal experience on the resurfacing devices. Nevertheless this doesot guarantee that other unexpected scenarios might become rel-vant during future clinical trials. Should this happen, the presentnalysis can be extended accordingly.
The relevant risk for short-term femoral neck fractures ofesurfaced femurs [9] is constraining the current clinical practiceestricting clinical indications to younger patients with sufficientone stock [3] and recommending moderate activity during reha-ilitation [20]. Present results suggest that less strict clinical
ndication might be used for PER implants and might also providemportant information in designing the surgical procedure so as toeduce the risk of post-operative failures.
In conclusion the innovative PER device could be considered aotential alternative to current resurfacing devices although addi-ional statistical studies should be considered to account for factornteractions.
Please cite this article in press as: Martelli S, et al. Biomechanical robustnesand surgical uncertainties: A FE study. Med Eng Phys (2011), doi:10.1016/j
cknowledgments
This work was partially financially supported by Strykerrthopaedics - Benoist Girard (Hérouville Saint Clair, France). The
[
PRESS & Physics xxx (2011) xxx– xxx
authors would also acknowledge Carolin Ohman for the valuablediscussion.
Conflict of interest statement
To cover the costs of this study, Istituto Ortopedico Rizzolireceived funds from Stryker Orthopaedics - Benoist Girard (Hérou-ville Saint Clair, France). Two of the Authors personally receivedfunds from Stryker Orthopaedics - Benoist Girard for tasks con-tracted in relation to the present study. This manuscript wasindependently written by the Authors, with no direct involvementof Stryker in the analysis or interpretation of the results, nor inmanuscript preparation.
References
[1] Grigoris P, Roberts P, Panousis K, Jin Z. Hip resurfacing arthroplasty: the evolu-tion of contemporary designs. Proc Inst Mech Eng [H] 2006;220:95–105.
[2] McMinn D, Daniel J. History and modern concepts in surface replacement. ProcInst Mech Eng [H] 2006;220:239–51.
[3] Mont MA, Ragland PS, Etienne G, Seyler TM, Schmalzried TP. Hip resurfacingarthroplasty. J Am Acad Orthop Surg 2006;14:454–63.
[4] Back DL, Dalziel R, Young D, Shimmin A. Early results of primary Birminghamhip resurfacings. An independent prospective study of the first 230 hips. J BoneJoint Surg Br 2005;87:324–9.
[5] Itayem R, Arndt A, Nistor L, McMinn D, Lundberg A. Stability of the Birming-ham hip resurfacing arthroplasty at two years. A radiostereophotogrammetricanalysis study. J Bone Joint Surg Br 2005;87:158–62.
[6] Buergi ML, Walter WL. Hip resurfacing arthroplasty: the Australian experience.J Arthroplasty 2007;22:61–5.
[7] Ong KL, Manley MT, Kurtz SM. Have contemporary hip resurfacing designsreached maturity? A review. J Bone Joint Surg Am 2008;90:81–8.
[8] Morlock MM, Bishop N, Zustin J, Hahn M, Ruther W, Amling M. Modes of implantfailure after hip resurfacing: morphological and wear analysis of 267 retrievalspecimens. J Bone Joint Surg Am 2008;90:89–95.
[9] Shimmin AJ, Back D. Femoral neck fractures following Birmingham hip resur-facing: a national review of 50 cases. J Bone Joint Surg Br 2005;87:463–4.
10] Amstutz HC, Campbell PA, Le Duff MJ. Fracture of the neck of the femur aftersurface arthroplasty of the hip. J Bone Joint Surg Am 2004;8:1874–7, 6-A.
11] Long JP, Bartel DL. Surgical variables affect the mechanics of a hip resurfacingsystem. Clin Orthop Relat Res 2006;453:115–22.
12] Marker DR, Seyler TM, Jinnah RH, Delanois RE, Ulrich SD, Mont MA. Femoralneck fractures after metal-on-metal total hip resurfacing: a prospective cohortstudy. J Arthroplasty 2007;22:66–71.
13] Radcliffe IA, Taylor M. Investigation into the affect of cementing techniqueson load transfer in the resurfaced femoral head: a multi-femur finite elementanalysis. Clin Biomech (Bristol, Avon) 2007;22:422–30.
14] Radcliffe IA, Taylor M. Investigation into the effect of varus–valgus orientationon load transfer in the resurfaced femoral head: a multi-femur finite elementanalysis. Clin Biomech (Bristol, Avon) 2007;22:780–6.
15] Dopico-González C, New AM, Browne M. Probabilistic finite element analysis ofthe uncemented hip replacement—effect of femur characteristics and implantdesign geometry. J Biomech 2010;43:512–20.
16] Cristofolini L, Juszczyk M, Taddei F, Field RE, Rushton N, Viceconti M. Stressshielding and stress concentration of contemporary epiphyseal hip prostheses.Proc Inst Mech Eng [H] 2009;223:27–44.
17] Cristofolini L, Juszczyk M, Taddei F, Field RE, Rushton N, Viceconti M. Assess-ment of femoral neck fracture risk for a novel proximal epiphyseal hipprosthesis. Clin Biomech (Bristol Avon) 2011;26:585–91.
18] Martelli S, Taddei F, Cristofolini L, Schileo E, Field RE, Rushton N, et al. A newhip epiphyseal prosthesis: design revision driven by a validated numericalprocedure. Med Eng Phys 2011, in press.
19] Steffen RT, Smith SR, Urban JP, McLardy-Smith P, Beard DJ, Gill HS, et al. Theeffect of hip resurfacing on oxygen concentration in the femoral head. J BoneJoint Surg Br 2005;87:1468–74.
20] Long JP, Santner TJ, Bartel DL. Hip resurfacing increases bone strains associatedwith short-term femoral neck fracture. J Orthop Res 2009;27:1319–25.
21] Martelli S, Taddei F, Cristofolini L, Gill HS, Viceconti M. Extensive riskanalysis of mechanical failure for epiphyseal prosthesis: a combinednumerical–experimental approach. Proc Inst Mech Eng [H] 2010.
22] Schileo E, Dall’ara E, Taddei F, Malandrino A, Schotkamp T, Baleani M, et al. Anaccurate estimation of bone density improves the accuracy of subject-specificfinite element models. J Biomech 2008;41:2483–91.
23] Schileo E, Taddei F, Cristofolini L, Viceconti M. Subject-specific finite elementmodels implementing a maximum principal strain criterion are able to estimate
s of a new proximal epiphyseal hip replacement to patient variability.medengphy.2011.07.006
failure risk and fracture location on human femurs tested in vitro. J Biomech2008;41:356–67.
24] Taddei F, Martelli S, Gill HS, Cristofolini L, Viceconti M. Finite element model-ing of resurfacing hip prosthesis: estimation of accuracy through experimentalvalidation. J Biomech Eng 2010;132:021002–21011.

ING Model
J
eering
[
[
[
[
[
[[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
ARTICLEJBE-1923; No. of Pages 11
S. Martelli et al. / Medical Engin
25] Morlock M, Bishop N, Rüther W, Delling G, Hahn M. Biomechanical, morpholog-ical, and histological analysis of early failures in hip resurfacing arthroplasty.Proc Inst Mech Eng [H] 2006;220:333–44.
26] Waanders D, Janssen D, Mann KA, Verdonschot N. The mechanical effects ofdifferent levels of cement penetration at the cement–bone interface. J Biomech2010;43:1167–75.
27] Little JP, Taddei F, Viceconti M, Murray DW, Gill HS. Changes in femurstress after hip resurfacing arthroplasty: response to physiological loads. ClinBiomech (Bristol, Avon) 2007;22:440–8.
28] Nuno N, Groppetti R, Senin N. Static coefficient of friction between stain-less steel and PMMA used in cemented hip and knee implants. Clin Biomech2006;20:20.
29] Lattanzi R, Viceconti M, Zannoni C, Quadrani P, Toni A. Hip-Op: an innova-tive software to plan total hip replacement surgery. Med Inform Internet Med2002;27:71–83.
30] AJM 1991. Osteoporosis Consensus Development Conference. 1991.31] Kroger H, Lunt M, Reeve J, Dequeker J, Adams JE, Birkenhager JC, et al. Bone
density reduction in various measurement sites in men and women with osteo-porotic fractures of spine and hip: the European quantitation of osteoporosisstudy. Calcif Tissue Int 1999;64:191–9.
32] Polikeit A, Nolte LP, Ferguson SJ. Simulated influence of osteoporosis and discdegeneration on the load transfer in a lumbar functional spinal unit. J Biomech2004;37:1061–9.
33] Rouhi G, Epstein M, Sudak L, Herzog W. Free surface density and microdam-age in the bone remodeling equation: theoretical considerations. Int J Eng Sci2006;44:456–69.
34] Horikoshi T, Endo N, Uchiyama T, Tanizawa T, Takahashi HE. Peripheral quanti-tative computed tomography of the femoral neck in 60 Japanese women. CalcifTissue Int 1999;65:447–53.
35] Morgan EF, Bayraktar HH, Keaveny TM. Trabecular bone modulus–density rela-tionships depend on anatomic site. J Biomech 2003;36:897–904.
36] Taddei F, Cristofolini L, Martelli S, Gill HS, Viceconti M. Subject-specific finiteelement models of long bones: an in vitro evaluation of the overall accuracy. JBiomech 2006;39:2457–67.
37] Testi D, Zannoni C, Cappello A, Viceconti M. Border-tracing algorithmimplementation for the femoral geometry reconstruction. Comput MethodsPrograms Biomed 2001;65:175–82.
38] Taddei F, Pancanti A, Viceconti M. An improved method for the automatic map-ping of computed tomography numbers onto finite element models. Med EngPhys 2004;26:61–9.
39] Taddei F, Schileo E, Helgason B, Cristofolini L, Viceconti M. The material map-ping strategy influences the accuracy of CT-based finite element models of
Please cite this article in press as: Martelli S, et al. Biomechanical robustnesand surgical uncertainties: A FE study. Med Eng Phys (2011), doi:10.1016/j
bones: an evaluation against experimental measurements. Med Eng Phys2007;29:973–9.
40] Lewis G. Fatigue testing and performance of acrylic bone–cement materi-als: state-of-the-art review. J Biomed Mater Res B: Appl Biomater 2003;66B:457–86.
[
[
PRESS & Physics xxx (2011) xxx– xxx 11
41] Zienkiewicz OC, Zhu JZ. A simple error estimator and adaptive procedure forpractical engineering analysis. Int J Numer Methods Eng 1987;24:337–57.
42] Black J, Hastings G. Handbook of biomaterial properties. 1st ed. Chapman &Hall; 1998.
43] Bergmann G, Deuretzbacher G, Heller M, Graichen F, Rohlmann A, Strauss J,et al. Hip contact forces and gait patterns from routine activities. J Biomech2001;34:859–71.
44] Verdonschot N, Huiskes R. Surface roughness of debonded straight-taperedstems in cemented THA reduces subsidence but not cement damage. Biomate-rials 1998;19:1773–9.
45] Zhou ZR, Pellerin V, Vincent L. Fretting—wear of aluminium and titanium alloys.In: Coulon PA, editor. Titanium & aluminium. I.I.T.T. International; 1989. p.145–53.
46] Kienapfel H, Sprey C, Wilke A, Griss P. Implant fixation by bone ingrowth. JArthoplasty 1999;14:355–68.
47] Cehreli M, Sahin S, Akca K. Role of mechanical environment and implant designon bone tissue differentiation: current knowledge and future contexts. J Dent2004;32:123–32.
48] Bayraktar HH, Keaveny TM. Mechanisms of uniformity of yield strains for tra-becular bone. J Biomech 2004;37:1671–8.
49] Huiskes R, Weinans H, van Rietbergen B. The relationship between stress shield-ing and bone resorption around total hip stems and the effects of flexiblematerials. Clin Orthop Relat Res 1992;12:4–34.
50] Kuiper JH, Huiskes R. The predictive value of stress shielding for quantifi-cation of adaptive bone resorption around hip replacements. J Biomech Eng1997;119:228–31.
51] Heller MO, Bergmann G, Kassi JP, Claes L, Haas NP, Duda GN. Determinationof muscle loading at the hip joint for use in pre-clinical testing. J Biomech2005;38:1155–63.
52] Cristofolini L, Juszczyk M, Martelli S, Taddei F, Viceconti M. In vitro repli-cation of spontaneous fractures of the proximal human femur. J Biomech2007;40:2837–45.
53] Corten K, MacDonald S. Hip resurfacing data from national joint registries: whatdo they tell us? What do they not tell us? Clin Orthop 2010;468:351–7.
54] Steffen RT, Pandit HP, Palan J, Beard DJ, Gundle R, McLardy-Smith P, et al. Thefive-year results of the Birmingham Hip Resurfacing arthroplasty: an indepen-dent series. J Bone Joint Surg Br 2008;9:436–41, 0-B.
55] Schileo E, Taddei F, Malandrino A, Cristofolini L, Viceconti M. Subject-specificfinite element models can accurately predict strain levels in long bones. JBiomech 2007;40:2982–9.
56] Clarke IC, Donaldson T, Bowsher JG, Nasser S, Takahashi T. Current concepts ofmetal-on-metal hip resurfacing. Orthop Clin North Am 2005;36:143–62, viii.
s of a new proximal epiphyseal hip replacement to patient variability.medengphy.2011.07.006
57] Masella RS, Meister M. Current concepts in the biology of orthodontic toothmovement. Am J Orthod Dentofacial Orthop 2006;129:458–68.
58] Viceconti M, Affatato S, Baleani M, Bordini B, Cristofolini L, Taddei F. Pre-clinicalvalidation of joint prostheses: a systematic approach. J Mech Behav BiomedMater 2009;2:120–7.