
biomechanical characterization and simulation of the
247
BIOMECHANICAL CHARACTERIZATION AND SIMULATION OF THE TRICUSPID VALVE A Dissertation Presented to The Graduate Faculty of The University of Akron In Partial Fulfillment Of the Requirements for the Degree Doctor of Philosophy Keyvan Amini Khoiy December 2018
-
Upload
khangminh22 -
Category
Documents
-
view
2 -
download
0
Transcript of biomechanical characterization and simulation of the

BIOMECHANICAL CHARACTERIZATION AND SIMULATION OF THE
TRICUSPID VALVE
A Dissertation
Presented to
The Graduate Faculty of The University of Akron
In Partial Fulfillment
Of the Requirements for the Degree
Doctor of Philosophy
Keyvan Amini Khoiy
December 2018

ii
BIOMECHANICAL CHARACTERIZATION AND SIMULATION OF THE
TRICUSPID VALVE
Keyvan Amini Khoiy
Dissertation
Approved: Accepted:
Advisor
Dr. Rouzbeh Amini
Department Chair
Dr. Rebecca K. Willits
Committee Member
Dr. Brian L. Davis
Dean of the College
Dr. Craig Menzemer
Committee Member
Dr. Ge Zhang
Dean of the Graduate School
Dr. Chand K. Midha
Committee Member
Dr. Francis Loth
Date
Committee Member
Dr. Rolando J.J. Ramirez
iii
ABSTRACT
The tricuspid valve, which is located on the right side of the heart, prevents blood
backflow from the right ventricle to the right atrium. Regurgitation in this valve occurs
when its leaflets do not close normally. Tricuspid valve regurgitation is one of the most
common tricuspid valve dysfunctions, often requiring valve repair or replacement. The
long-term success rate of the repair surgeries has not been promising; in many cases,
reoperations are required within a few years after the first surgery. A limiting factor in
understanding the etiology of tricuspid valve repair failure is our lack of knowledge
regarding tricuspid valve biomechanics. In particular, tricuspid valve mechanical behavior
has not been accurately studied. In addition, there is no precise analytical and/or
computerized model to predict the mechanical responses of the valve under normal and
pathological conditions. In the current study, we have used biaxial tensile testing, small
angle light scattering, ex-vivo passive heart beating simulation, and sonomicrometry
techniques to quantify the mechanical characteristics, microstructure, dynamic
deformations, and geometric parameters of the tricuspid valve. We aimed to develop a
more accurate computerized model of the tricuspid valve for simulation purposes. Our
studies are important both for understanding the normal valvular function as well as for
development/improvement of surgical procedures and medical devices.

iv
DEDICATION
To my mother for her loving support and inspiration

v
ACKNOWLEDGEMENTS
I would like to express my sincere appreciation to my supervisor Dr. Rouzbeh
Amini, who consistently and enthusiastically conveyed a spirit of adventure regarding
research, as well as excitement for making progress in all aspects of life. Without his
guidance and persistence, the completion of this work would not have been possible.
I would like to thank my committee members, Dr. Brian L. Davis, Dr. Ge Zhang,
Dr. Francis Loth, and Dr. Rolando J. J. Ramirez, who have demonstrated to me that an
appreciation for global concerns should always outpace all our substantial goals.
I also thank Thomas Decker, Dipankar Biswas, and Anthony Black, whose help
added to the quality and flow of this work, as well as Sheila Pearson, whose grammatical
advice has aided in improving the quality of my publications.
I would also like to thank my roommates, Evan Stern and Gigi Jumbert, as well as
Sharon Stern and Robin Henry. They were in fact my family in the U.S., caring about me
and protecting me so that I would not feel lonely while I was away from my family, who
are living thousands of miles away.
My family are the most important people to me in the pursuit of this study, and
always. I would like to thank them all, specifically my mother, whose love, patience,
diligence, and perseverance has at all times been my inspiration—even though we have not
been able to meet in person for the last four years.

vi
TABLE OF CONTENTS
Page
LIST OF TABELS ............................................................................................................. xi
LIST OF FIGURES ......................................................................................................... xiv
CHAPTERS
I. INTRODUCTION ............................................................................................................1
1.1 Anatomy and Function of the Heart .......................................................... 1
1.2 Tricuspid Valve Anatomy ......................................................................... 2
1.3 Tricuspid Valve Microstructure ................................................................ 5
1.4 Tricuspid Valve Pathophysiology ............................................................. 7
1.5 Tricuspid Valve Mechanical Behavior ...................................................... 9
1.6 Material Models ........................................................................................ 9
1.7 Computerized Simulation ........................................................................ 11
1.8 Open Questions ....................................................................................... 15
II. BIAXIAL MECHANICAL RESPONSE OF THE TRICUSPID VALVE
LEAFLETS ........................................................................................................................19
2.1 Summary ................................................................................................. 19
2.2 Introduction ............................................................................................. 19
2.3 Materials and Methods ............................................................................ 21
2.3.1 Biaxial Tensile Testing Equipment ................................................... 21
2.3.2 Specimen Preparation ........................................................................ 22
2.3.3 Biaxial Tensile Testing Protocols ..................................................... 23

vii
2.3.4 Strain and Stress Calculation ............................................................. 25
2.4 Results ..................................................................................................... 27
2.5 Discussion ............................................................................................... 34
III. QUANTIFICATION OF MATERIAL CONSTANTS FOR A
PHENOMENOLOGICAL CONSTITUTIVE MODEL OF THE TRICUSPID
VALVE LEAFLETS .........................................................................................................36
3.1 Summary ................................................................................................. 36
3.2 Introduction ............................................................................................. 37
3.3 Materials and Methods ............................................................................ 38
3.3.1 Planar Biaxial Tensile Strains and Stresses ....................................... 38
3.3.2 Constitutive Modeling ....................................................................... 39
3.3.3 Average Models ................................................................................ 40
3.4 Results ..................................................................................................... 46
3.4.1 Stress Response Functions ................................................................ 46
3.4.2 Constitutive Modeling Results .......................................................... 47
3.4.3 Average Modeling Results ................................................................ 51
3.5 Discussion ............................................................................................... 59
3.5.1 Constitutive Model ............................................................................ 59
3.5.2 Average Models ................................................................................ 64
3.5.3 Limitations ........................................................................................ 66
3.6 Conclusion ............................................................................................... 67
IV. DYNAMIC DEFORMATIONS AND SURFACE STRAINS OF THE
TRICUSPID VALVE LEAFLETS ....................................................................................68
4.1 Summary ................................................................................................. 68
4.2 Introduction ............................................................................................. 69

viii
4.3 Methods ................................................................................................... 71
4.3.1 Ex-vivo Heart Apparatus ................................................................... 71
4.3.2 Sample Preparation ........................................................................... 75
4.3.3 Strain Calculation .............................................................................. 76
4.3.4 Pressures Data Analysis .................................................................... 77
4.4 Results ..................................................................................................... 78
4.4.1 Pressure ............................................................................................. 78
4.4.2 Deformation ...................................................................................... 79
4.5 Discussion ............................................................................................... 84
V. DYNAMIC DEFORMATIONS OF THE TRICUSPID VALVE ANNULUS,
INTACT AND AFTER CHORDAE RUPTURE ..............................................................90
5.1 Summary ................................................................................................. 90
5.2 Introduction ............................................................................................. 91
5.3 Materials and Methods ............................................................................ 93
5.3.1 Ex-vivo Heart Apparatus ................................................................... 93
5.3.2 Sample Preparation ........................................................................... 94
5.3.3 Data Analysis .................................................................................... 96
5.3.4 Statistical Analysis ............................................................................ 98
5.4 Results ..................................................................................................... 99
5.4.1 Pressure ............................................................................................. 99
5.4.2 Annulus Area, Circumference, and Radius Values ......................... 100
5.4.3 Annulus Dilation Due to the Chordae Rupture ............................... 104
5.4.4 Changes in Annulus Geometry Throughout the Cardiac Cycle ...... 105
5.4.5 Annulus Curve ................................................................................. 109

ix
5.5 Discussion ............................................................................................. 109
VI. EFFECTS OF CHORDAE RUPTURE ON THE SURFACE STRAINS OF THE
TRICUSPID VALVE LEAFLETS ..................................................................................115
6.1 Summary ............................................................................................... 115
6.2 Introduction ........................................................................................... 116
6.3 Materials and Methods .......................................................................... 118
6.3.1 Ex-vivo Heart Apparatus ................................................................. 118
6.3.2 Sample Preparation ......................................................................... 119
6.3.3 Data Acquisition .............................................................................. 119
6.3.4 Pressure Data Analysis .................................................................... 120
6.3.5 Deformation Data Processing and Analysis .................................... 121
6.3.6 Average Model ................................................................................ 121
6.3.7 Statistical Analysis .......................................................................... 122
6.4 Results ................................................................................................... 122
6.4.1 Average Model ................................................................................ 122
6.4.2 Pressures .......................................................................................... 123
6.4.3 Leaflet Deformation and Strain Spatial Distribution ...................... 125
6.4.4 Temporal Distribution of the Strains ............................................... 129
6.5 Discussion ............................................................................................. 130
6.6 Conclusion ............................................................................................. 133
VII. FINITE ELEMENT MODELING AND SIMULATION OF THE TRICUSPID
VALVE ............................................................................................................................135
7.1 Introduction ........................................................................................... 135
7.2 Materials and Methods .......................................................................... 136
x
7.2.1 Modeling the Geometry of the Tricuspid Valve ............................. 136
7.2.2 Finite Element Model of the Tricuspid Valve ................................. 141
7.3 Results ................................................................................................... 144
7.4 Discussion ............................................................................................. 146
VIII. CONCLUSIONS AND FUTURE WORK .............................................................150
8.1 Conclusions ........................................................................................... 150
8.2 Future Work .......................................................................................... 157
BIBLIOGRAPHY ............................................................................................................159
APPENDICES .................................................................................................................182
APPENDIX A. THE DEVELOPED AVERAGE STRESS–STRAIN RESPONSES
FOR THE POSTERIOR AND SEPTAL LEAFLETS (Supplementary Materials to
Chapter III).......................................................................................................................183
APPENDIX B. QUANTIFICATION OF THE SURFACE STRAINS USING FOUR-
DIMENSIONAL SPATIOTEMPORAL COORDINATES OF SURFACE
MARKERS ......................................................................................................................190
B.1 Strain Calculation .................................................................................. 190
B.2 Nomenclature ........................................................................................ 193
APPENDIX C. QUANTIFICATION OF THE MATERIAL CONSTANTS FOR A
PHENOMENOLOGICAL CONSTITUTIVE MODEL OF SMALL BOWEL
MESENTERY (Applications of the Method Developed in Chapters II and III) .............196
C.1 Summary ............................................................................................... 196
C.2 Introduction ........................................................................................... 197
C.3 Material and Methods............................................................................ 198
C.3.1 Biaxial Tensile Testing Equipment ................................................. 198
C.3.2 Specimen Preparation ...................................................................... 199
C.3.3 Planar Biaxial Tensile Testing ........................................................ 200
xi
C.3.4 Strain and Stress Calculation ........................................................... 202
C.3.5 Constitutive Modeling ..................................................................... 203
C.3.6 Average Model Development ......................................................... 205
C.4 Results ................................................................................................... 207
C.4.1 Dimensional Measurements ............................................................ 207
C.4.2 Biaxial Mechanical Responses ........................................................ 207
C.4.3 Response Function Interpretation .................................................... 212
C.4.4 Constitutive Modeling ..................................................................... 213
C.4.5 Average Modeling ........................................................................... 216
C.5 Discussion ............................................................................................. 218

xii
LIST OF TABELS
Table Page
1.1 A list of the material models that have been widely used in the literature to model
the mechanical properties of soft tissue ..................................................................... 11
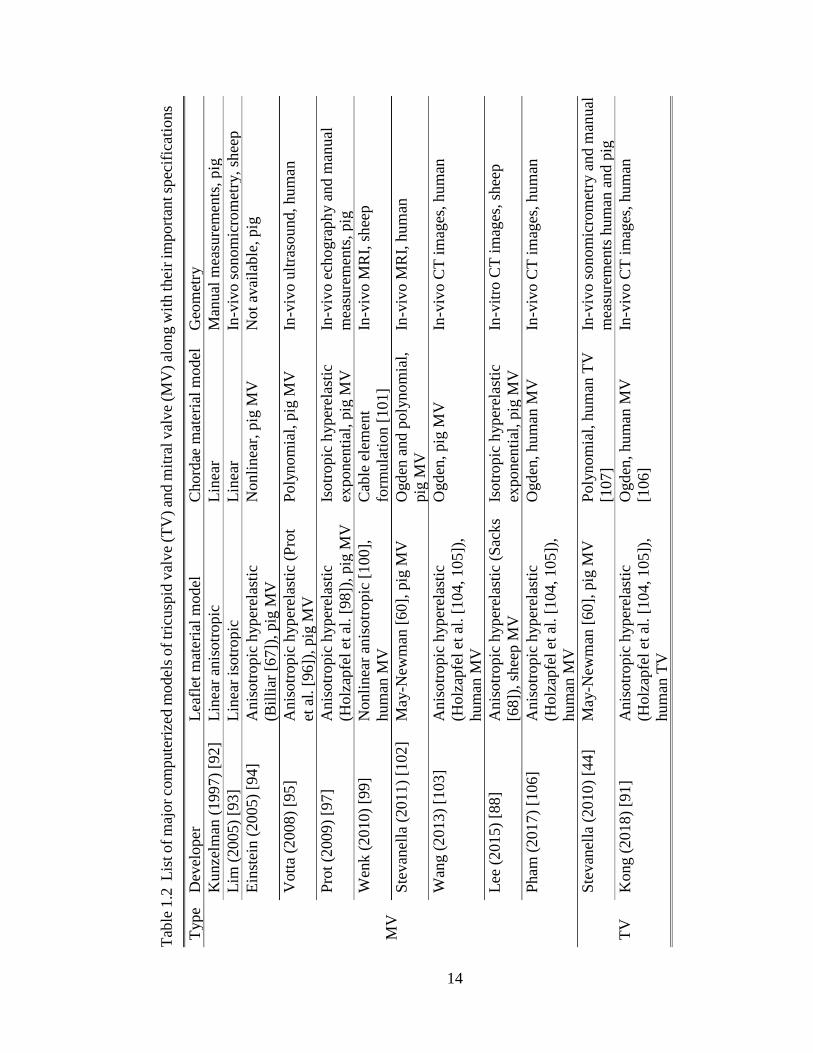
1.2 List of major computerized models of tricuspid valve (TV) and mitral valve (MV)
along with their important specifications .................................................................. 14
1.3 The abbreviations used in this document are listed in this table alphabetically. ....... 18
2.1 Biaxial loadings protocols applied for each specimen ............................................... 24
2.2 Measured thicknesses for the leaflets of all the hearts used during the experiment .. 28
2.3 The average maximum rigid body rotation ωmax, the average maximum shear
angle θmax, and the average of the ratio of the maximum Cauchy shear stress to
the maximum Cauchy normal stress r presented for each loading protocol and
leaflet type (for each protocol and leaflet type the data is averaged over all hearts
and presented in the form of average ± standard error). ............................................ 33
3.1 The maximum membrane tension of each tension-controlled loading protocol for
circumferential c and radial r directions. The tension ratios were kept constant
during the experiments: Tc: Tr = 1: 1, 1: 0.75, 0.75: 1, 1: 0.5, 0.5: 1 ........................ 38
3.2 Material constants along with the R2 of the fit and anisotropy index AI calculated
for individual specimens by fitting the experimental data into the proposed
constitutive model ..................................................................................................... 50
3.3 Material constants for the tension-based average model data (AVG) as well as the
average data minus one standard error (AVG – SE) and average data plus one
standard error (AVG + SE). The corresponding R2 value of the fit and the
anisotropy index AI are also presented. ..................................................................... 55
3.4 Material constants for the first Piola–Kirchhoff-stress–based average model data
(AVG) as well as the average data minus one standard error (AVG – SE) and
average data plus one standard error (AVG + SE). The corresponding R2 value
of the fit and the anisotropy index AI are also presented. ......................................... 55

xiii
3.5 Material constants for the Cauchy-stress–based average model data. The
corresponding R2 value of the fit and the anisotropy index AI are also presented
in the table. ................................................................................................................ 55
5.1 Calculated area at minimum and maximum right ventricular pressure (RVP) for
intact and post chordae rupture (PCR) conditions. The values are presented for all
eight hearts used in the experiments along with the average (AVG) and standard
deviation (STD). Comparing the average values showed an increase in the area
post chordae rupture. ............................................................................................... 101
5.2 Calculated circumference at minimum and maximum right ventricular pressure
(RVP) for intact and post chordae rupture (PCR) conditions. The values are
presented for all eight hearts used in the experiments along with the average
(AVG) and standard deviation (STD). Comparing the average values showed an
increase in the circumference post chordae rupture. ............................................... 103
5.3 Calculated radius using the triangulation method (R) along with the radii
calculated from the area (RA) and circumference (RC), using the assumption of
flat annuli, at minimum and maximum right ventricular pressure (RVP) for intact
and post chordae rupture (PCR) conditions. The values are presented for all eight
experimental hearts along with the average (AVG) and standard deviation (STD).
Comparison between R, RA, and RC showed that the three different methods of
calculating the radius produced the same results. ................................................... 103
5.4 Geometric dilation in area, circumference, and radius of the heart annuli due to
chordae rupture at maximum right ventricular pressure (RVP) calculated using
Equation (5.1) along with the average (AVG) and standard deviation (STD) for
each quantity. ........................................................................................................... 105
5.5 Dilation in the length of annulus anterior segment (AAS), annulus posterior
segment (APS), and annulus septal segment (ASS) due to the chordae rupture at
maximum right ventricular pressure (RVP) calculated using Equation (5.1) along
with the average (AVG) and standard deviation (STD) for each quantity. The
largest dilation occurred at the AAS. ...................................................................... 105
5.6 Average geometric changes at maximum right ventricular pressure (RVP) for
intact and post chordae rupture (PCR) conditions calculated using Equation (5.2).
The last column shows the percentage of the change in geometric parameters with
intact-to-PCR dilation included in calculations. The geometrical parameters at
minimum RVP were selected as the reference to calculate the changes. ................ 108
7.1 The measured perimeter (Prmtr), anterior segment length (ASL), posterior
segment length (PSL), septal segment length (SSL), anterior leaflet height (ALH),
posterior leaflet height (PLH), septal leaflet height (SLH), anteroposterior
commissure height (ACH), posteroseptal commissure height (PCH), and
anteroseptal commissure height (SCH) for three different porcine heart valves.
xiv
The table also includes the normalized values for each valve, the normalized
average (Nrmlzd AVG), and the scaled average values. The scaled average
(AVG) values were used in the modeling of the valve geometry. .......................... 138
7.2 Average (AVG) number of first- and second-order chordae counted based on the
dissected porcine TVs and used in the geometry modeling. ................................... 138
8.1 Parameters of a Fung-type model for human heart valves [42] ................................152
C.1 Five different loading protocols used in the tangential (Tang) and radial directions
during the experiments to evaluate the mechanical response of different regions
of porcine mesentery. .............................................................................................. 202
C.2 Measured thicknesses for the individual specimens of the distal avascular, distal
vascular, and root regions of the porcine mesentery. .............................................. 208
C.3 The average maximum rigid body rotation wmax, the average maximum shear
angle θmax, and the average ratio of the maximum Cauchy shear stress to the
maximum Cauchy normal stress r presented for each loading protocol and
mesentery region (for each protocol and mesentery region the data are averaged
over all samples (n=8) and presented in the form of average ± standard error). ..... 211
C.4 Material parameters computed for individual samples by fitting the experimental
data to the proposed constitutive model along with the fitting R-squared values
(R2) and the anisotropy index (AI). ......................................................................... 214
C.5 Material parameters computed by fitting the averaged stress–strain data to the
proposed constitutive model along with the fitting R-squared (R2) and the
anisotropy index (AI). .............................................................................................. 220

xv
LIST OF FIGURES
Figure Page
1.1 The heart structure and parts. (Image adopted from Cook et al. [2]) ........................... 2
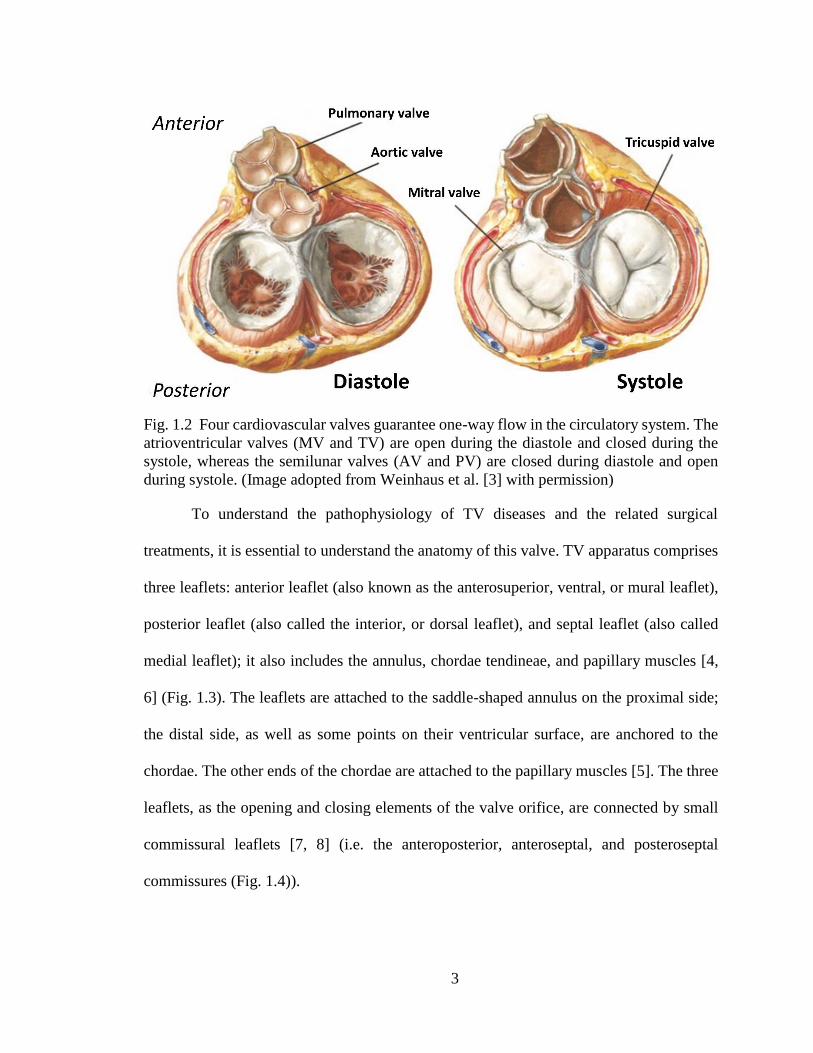
1.2 Four cardiovascular valves guarantee one-way flow in the circulatory system. The
atrioventricular valves (MV and TV) are open during the diastole and closed
during the systole, whereas the semilunar valves (AV and PV) are closed during
diastole and open during systole. (Image adopted from Weinhaus et al. [3]) ............. 3
1.3 TV apparatus comprises of anterior leaflet, posterior leaflet, septal leaflet, annulus,
chordae tendineae, and papillary muscles. (Image adopted from Weinhaus et al.
[3] and Chan [5].) ........................................................................................................ 4
1.4 Illustration of the tricuspid valve leaflets, their connection to each other, and their
attachment to the chordae. (Image adapted from Carpentier et al. [8].) ...................... 5
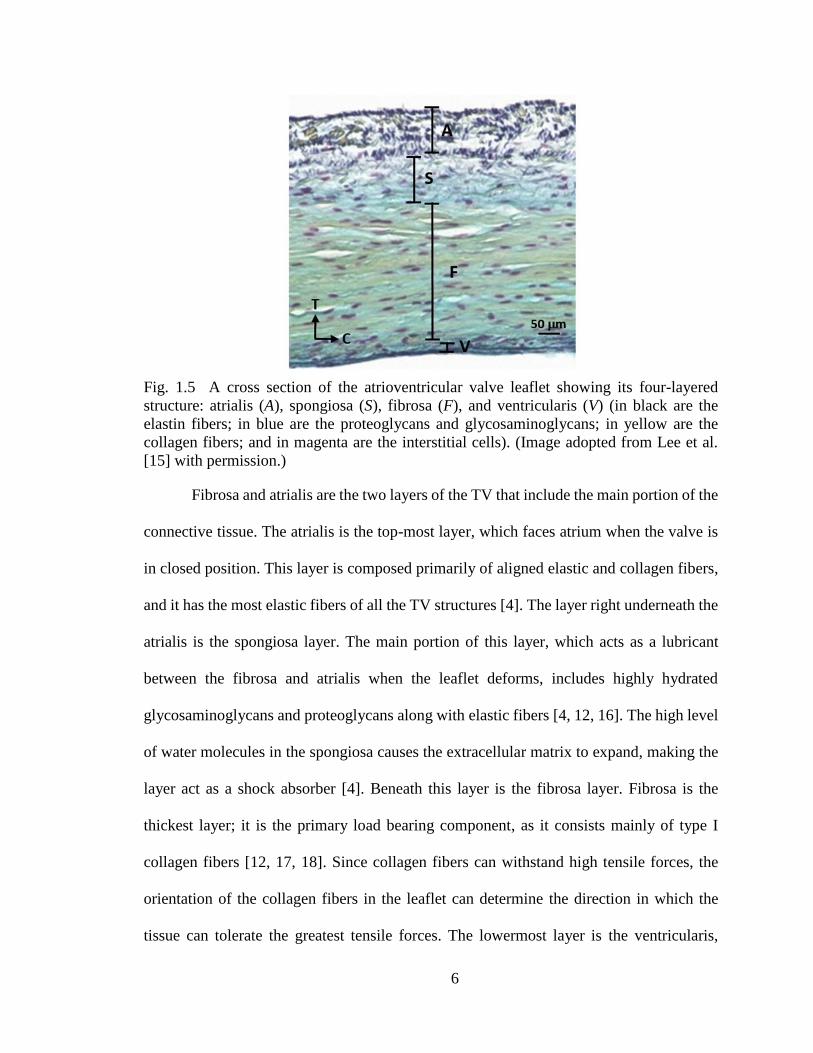
1.5 A cross section of the atrioventricular valve leaflet showing its four-layered
structure: atrialis (A), spongiosa (S), fibrosa (F), and ventricularis (V) (in black
are the elastin fibers; in blue are the proteoglycans and glycosaminoglycans; in
yellow are the collagen fibers; and in magenta are the interstitial cells). (Image
adopted from Lee et al. [15].) ...................................................................................... 6
2.1 Custom-made biaxial tensile testing equipment ........................................................ 22
2.2 a) Specially designed phantom to facilitate the attachment of the leaflets to the
biaxial tensile testing equipment. b) Specimen attached to the equipment using
fishhooks and suture lines. ........................................................................................ 24
2.3 The three leaflets of the tricuspid valve and the position and shape of the
specimens. ................................................................................................................. 27
2.4 The average membrane tension versus stretch ratio for the loading protocols a)
number 1 (equibiaxial), b) number 2, c) number 3, d) number 4, and e) number 5
for the anterior leaflet. The circumferential (Circ) and radial directions are in solid
red and dash-dotted blue, respectively. The bars are standard errors. The green
dashed line shows the maximum physiological tension level (Max Physio), while
the tension level goes up to 100 N/m in case of hypertension. ................................ 30

xvi
2.5 The average membrane tension versus stretch ratio for the loading protocols a)
number 1 (equibiaxial), b) number 2, c) number 3, d) number 4, and e) number 5
for the posterior leaflet. The circumferential (Circ) and radial directions are in
solid red and dash-dotted blue, respectively. The bars are standard errors. The
green dashed line shows the maximum physiological tension level (Max Physio),
while the tension level goes up to 100 N/m in case of hypertension. ...................... 31
2.6 The average membrane tension versus stretch ratio for the loading protocols a)
number 1 (equibiaxial), b) number 2, c) number 3, d) number 4, and e) number 5
for the septal leaflet. The circumferential (Circ) and radial directions are in solid
red and dash-dotted blue, respectively. The bars are standard errors. The green
dashed line shows the maximum physiological tension level (Max Physio), while
the tension level goes up to 100 N/m in case of hypertension. ................................. 32
3.1 Comparison between the accuracy of linear interpolation and exponential fit to
estimate the original data for averaging. ................................................................... 43
3.2 The constant stress contours produced using the response functions of Equation
(2.2) plotted over the strain field for typical leaflets: (a,b) anterior, (c,d) posterior,
and (e,f) septal leaflets. .............................................................................................. 47
3.3 The result of the five-protocol fit along with the experimentally measured
circumferential (Circ) and radial data for typical leaflets: (a) anterior, (b)
posterior, and (c) septal. The numbers represent the protocol numbers listed in
Table 3.1. ................................................................................................................... 49
3.4 The average stress–strain responses developed based on identical tension states
from loading protocols (a) number 1 (equibiaxial), (b) number 2, (c) number 3,
(d) number 4, and (e) number 5 of Table 3.1 for the anterior leaflet. The vertical
axis is the second Piola–Kirchhoff stress, and the horizontal axis is the Green
strain. These data were used to calculate the average material constants presented
in Table 3.3. ............................................................................................................... 52
3.5 The average stress–strain responses developed based on identical first Piola–Kirchhoff stress states from loading protocols (a) number 1 (equibiaxial), (b)
number 2, (c) number 3, (d) number 4, and (e) number 5 of Table 3.1 for the
anterior leaflet. The vertical axis is the second Piola–Kirchhoff stress, and the
horizontal axis is the Green strain. These data were used to calculate the average
material constants presented in Table 3.4.................................................................. 53
3.6 The average stress–strain responses developed based on identical Cauchy stress
states from loading protocols (a) number 1 (equibiaxial), (b) number 2, (c) number
3, (d) number 4, and (e) number 5 of Table 3.1 for the anterior leaflet. The vertical
axis is the second Piola–Kirchhoff stress, and the horizontal axis is the Green
strain. These data were used to calculate the average material constants presented
in Table 3.5. ............................................................................................................... 54

xvii
3.7 The five stress-controlled protocols used to reconstruct the tissue responses based
on the developed average models. The horizontal axis is the circumferential
second Piola–Kirchhoff stress, and the vertical axis is the radial second Piola–
Kirchhoff stress. ........................................................................................................ 56
3.8 Tissue response of the anterior leaflet to five stress-controlled loading protocols
(Fig. 3.7) reconstructed using the material constants of the arithmetic average (A-
B) from Table 3.2, the tension-based average model (T-B) from Table 3.3, the
first Piola–Kirchhoff-stress–based average model (P-B) from Table 3.4, and the
Cauchy-stress–based average model (C-B) from Table 3.5. The vertical axis is the
second Piola–Kirchhoff stress, and the horizontal axis is the Green strain. The
subscripts cc and rr denote the circumferential and radial directions, respectively.
................................................................................................................................... 57
3.9 Tissue response of the posterior leaflet to five stress-controlled loading protocols
(Fig. 3.7) reconstructed using the material constants of the arithmetic average (A-
B) from Table 3.2, the tension based average model (T-B) from Table 3.3, the
first Piola–Kirchhoff-stress–based average model (P-B) from Table 3.4, and the
Cauchy-stress–based average model (C-B) from Table 3.5. The vertical axis is the
second Piola–Kirchhoff stress, and the horizontal axis is the Green strain. The
subscripts cc and rr denote the circumferential and radial directions, respectively.
................................................................................................................................... 58
3.10 Tissue response of the septal leaflet to five stress-controlled loading protocols
(Fig. 3.7) reconstructed using the material constants of the arithmetic average (A-
B) from Table 3.2, the tension based average model (T-B) from Table 3.3, the
first Piola–Kirchhoff-stress–based average model (P-B) from Table 3.4, and the
Cauchy-stress–based average model (C-B) from Table 3.5. The vertical axis is the
second Piola–Kirchhoff stress, and the horizontal axis is the Green strain. The
subscripts cc and rr denote the circumferential and radial directions, respectively.
................................................................................................................................... 59
3.11 Small-angle light-scattering (SALS) scan of the midsection of a typical tricuspid
valve anterior leaflet. Each arrow shows the main direction of the extracellular
matrix fibers over a 250 μm × 250 μm region. The color map shows the degree
of alignment. The warmest color, corresponding to 1, indicates a network in which
all fibers are in the same direction; the coolest color, corresponding to 0, indicates
a network in which the probability of a fiber existing in any directions is the same.
................................................................................................................................... 62
3.12 Constant strain energy contours plotted over the Green strain field for the (a)
anterior, (b) posterior, and (c) septal leaflets of a typical tricuspid valve. ................ 63
3.13 The strain energy contours plotted over the strain field for posterior leaflet of the
specimen listed as Sample 3 in Table 3.2. The contours are nonconvex, violating
the integrity of the developed constitutive model for this specific leaflet. ............... 64

xviii
4.1 a) Schematic of the ex-vivo beating heart apparatus and b) a picture of the actual
apparatus. ................................................................................................................... 71
4.2 The T-shaped pipefitting connected to the right atrium through a straight barbed
hose fitting (1). The Luer Lok assembly was connected to the other side of the t-
shaped pipe fitting to support the pressure sensor. The other straight barbed hose
fitting (2) connected the right ventricle to the pump. Crystal wires came out
through the inferior vena cava. The umbilical clamp was used to prevent leakage
from the inferior vena cava. ....................................................................................... 74
4.3 Umbilical clamps, cable ties, and worm-drive clamps were used for sealing. .......... 74
4.4 The arrangement of the sonocrystals over the surface of the septal leaflet. The red
lines show the triangular element used for strain calculation. The radial direction
was defined by a vector connecting crystal 4 to crystal 7. ........................................ 76
4.5 Right heart pressure during the cardiac cycle averaged over all of the hearts. The
bars are standard errors (n=8). The vertical lines show the opening and closure of
the pulmonary valve (PV) and tricuspid valve (TV): TV closed at 0.2 s and opened
at 0.54 s; the pulmonary valve opened at 0.29 s and closed at 0.44 s. ...................... 79
4.6 Average peak areal, maximum principal (Max Princ), circumferential (Circ), and
radial strains at the leaflet midpoint measured with respect to reference 1 (Ref1,
minimum RAP) and reference 2 (Ref2, end diastole). The error bars are standard
error (n=8). ................................................................................................................ 81
4.7 The temporal strain variations during the cardiac cycle. (a) The areal, (b)
maximum principal, (c) circumferential, and (d) radial strains at the leaflet
midpoint averaged over all of the hearts. The shaded area shows the standard error
(n=8). Vertical lines show the time points for TV closing, PV opening, maximum
RVP, PV closing and TV opening respectively from left to right............................. 82
4.8 The areal, maximum principal, circumferential, and radial strains at maximum
RVP. The strains are averaged over all the hearts (n=8) and are presented on a
typical septal leaflet. Minimum RAP is used as the reference for strain calculation.
The arrows are showing the direction of the strains at the center of each triangular
surface........................................................................................................................ 83
4.9 Distribution of the maximum principal strain over the leaflet during the septal
entire cardiac cycle. Maximum principal strain is averaged over all of the hearts
(n=8) and showed over a typical septal leaflet during the cardiac cycle. .................. 84
5.1 Eight sonocrystals (2 mm in diameter) sutured around the valve annulus (a) before
the experiment and (b) after the experiment. The pulmonary side of the heart has
been cut open for better visualization of the positions of the crystals....................... 95

xix
5.2 Method used to calculate the area, circumference, and radius of the annulus. A
lower resolution of the original triangulation is presented for illustrative purposes.
................................................................................................................................... 97
5.3 Average right ventricular pressure (RVP), pulmonary artery pressure (PAP), and
right atrial pressure (RAP) measured for the intact and post chordae rupture (PCR)
cases. ........................................................................................................................ 100
5.4 Comparison of the average values of (a) the area, (b) circumference, and (c) radius
between the intact and post chordae rupture (PCR) conditions at minimum and
maximum right ventricular pressure (RVP). The Wilcoxon signed rank test p-
values for area, circumference, and radius were 0.01 at maximum RVP and 0.04
at minimum RAP. The asterisks (*) show significant differences (p < 0.05,
Wilcoxon signed rank test). Error bars show the standard errors. ........................... 102
5.5 Comparison of the dilation (due to the chordae rupture) between annulus anterior
segment (AAS), annulus posterior segment (APS), and annulus septal segment
(ASS) at maximum right ventricular pressure (RVP). The Wilcoxon signed rank
test p-values were 0.55, 0.38, and 0.74 between the AAS and APS, the AAS and
ASS, and the APS and ASS, respectively. No significant differences were
observed (p > 0.05, Wilcoxon signed rank test). Error bars show the standard
errors. ....................................................................................................................... 104
5.6 Changes in (a) area, (c) circumference, and (e) radius as well as the absolute values
of (b) area, (d) circumference, and (f) radius throughout the cardiac cycle
averaged over all the annuli for intact and post chordae rupture (PCR) conditions.
The shaded regions show the standard errors. The temporal position of the
maximum right ventricular pressure (RVP) as well as the opening and closure of
the tricuspid and pulmonary valves for the intact case are shown in the graphs as
a better illustration of the deformations that occur throughout the cardiac cycle. .. 107
5.7 Comparison of the change in the length of the annulus anterior segment (AAS),
annulus posterior segment (APS), and annulus septal segment (ASS) in intact and
post chordae rupture (PCR) conditions at maximum right ventricular pressure
(RVP). The PCR values include the dilation as well. For a comparison of the
change in length between the intact and PCR conditions, the Wilcoxon signed
rank test was used; p-values were 0.02 for AAS and ASS and 0.38 for APS. The
p-values were 0.03, 0.02, and 0.84 for the comparison of the change in length for
the intact case between the AAS and APS, the AAS and ASS, and the APS and
ASS, respectively. The asterisks (*) indicate significant differences (p < 0.05,
Wilcoxon signed rank test). Error bars show the standard errors. ........................... 108
6.1 TV septal leaflet and annulus average geometry at reference frame (minimum
RAP) for normal (blue) and PCR (red) conditions. ................................................. 123

xx
6.2 Average hemodynamic pressures during the cardiac cycle for intact conditions.
The shaded areas show the standard error. .............................................................. 124
6.3 Average hemodynamic pressures during the cardiac cycle for post chordae rupture
(PCR) conditions. The shaded areas show the standard error. ................................ 125
6.4 Spatial distribution of areal, maximum principal (Max Princ), circumferential
(Circ), and radial strains demonstrated over the developed average septal leaflet
geometry at maximum right ventricular pressure (RVP) before (top row) and after
(bottom row) chordae rupture. ................................................................................. 127
6.5 Comparison of the average (over all the hearts) of maximum of the strain’s spatial
average signal (strain is averaged over the leaflet surface throughout the cardiac
cycle). Error bars show the standard error. .............................................................. 128
6.6 Comparison of the maximum of maximum principal strain between intact and post
chordae rupture (PCR) cases for Crystal 1 and Crystal 2, shown in Fig. 6.1. ......... 128
6.7 Calculated average TV septal leaflet maximum principal strain, plotted at different
timepoints to show the deformation of the leaflet throughout the cardiac cycle for
both intact (top row) and post chordae rupture (bottom row) conditions. The color
map shows the distribution of the maximum principle strain. ................................ 129
6.8 Temporal distribution of the spatial average of the strains throughout the cardiac
cycle for intact and post chordae rupture (PCR) conditions averaged for all hearts.
The shaded area shows the standard error. .............................................................. 130
7.1 The important dimensions of the tricuspid valve, which include anterior segment
length (ASL), posterior segment length (PSL), septal segment length (SSL),
anterior leaflet height (ALH), posterior leaflet height (PLH), septal leaflet height
(SLH), anteroposterior commissure height (ACH), posteroseptal commissure
height (PCH), and anteroseptal commissure height (SCH), as measured from
dissected porcine heart valve apparatus. ................................................................. 137
7.2 Reconstructed wireframe used for modeling the tricuspid valve geometry. Refer
to Table 7.1 for abbreviations and dimensions. ....................................................... 140
7.3 The reconstructed TV apparatus geometry used in the finite element analysis. ...... 140
7.4 Finite element mesh for the reconstructed TV geometry......................................... 144
7.5 Maximum in-plane principal strain distribution illustrated over the anterior (A),
posterior (P), and septal (S) valve leaflets at different points in time during the
valve closure simulation. ......................................................................................... 145

xxi
7.6 Distribution of maximum in-plane principal strain over the septal leaflet at
maximum right ventricular pressure. ....................................................................... 146
7.7 Maximum in-plane principal stress distribution illustrated over the anterior (A),
posterior (P), and septal (S) valve leaflets at different points in time during the
valve closure simulation. ......................................................................................... 147
7.8 Comparison of effects of changes in the annulus boundary conditions on the strain
distribution and deformations of the septal leaflet. The top plot shows the result
of the simulation with the moving annulus boundary conditions (as the simulation
of the intact case), and the bottom plot shows the result of the simulation with the
fixed annulus boundary conditions (as the simulation of rigid ring annuloplasty). .148
A.1 The average stress–strain responses developed based on identical tension states
from loading protocols (a) number 1 (equibiaxial), (b) number 2, (c) number 3,
(d) number 4, and (e) number 5 of Table 3.1 (of the main manuscript) for the
posterior leaflet. The vertical axis is the second Piola–Kirchhoff stress, and the
horizontal axis is the Green strain. These data were used to calculate the average
material constants presented in Table 3.3................................................................ 184
A.2 The average stress–strain responses developed based on identical first Piola–
Kirchhoff stress states from loading protocols (a) number 1 (equibiaxial), (b)
number 2, (c) number 3, (d) number 4, and (e) number 5 of Table 3.1 (of the main
manuscript) for the posterior leaflet. The vertical axis is the second Piola–
Kirchhoff stress, and the horizontal axis is the Green strain. These data were used
to calculate the average material constants presented in Table 3.4. ........................ 185
A.3 The average stress–strain responses developed based on identical Cauchy stress
states from loading protocols (a) number 1 (equibiaxial), (b) number 2, (c) number
3, (d) number 4, and (e) number 5 of Table 3.1 (of the main manuscript) for the
posterior leaflet. The vertical axis is the second Piola–Kirchhoff stress, and the
horizontal axis is the Green strain. These data were used to calculate the average
material constants presented in Table 3.5................................................................ 186
A.4 The average stress–strain responses developed based on identical tension states
from loading protocols (a) number 1 (equibiaxial), (b) number 2, (c) number 3,
(d) number 4, and (e) number 5 of Table 3.1 (of the main manuscript) for the
septal leaflet. The vertical axis is the second Piola–Kirchhoff stress and the
horizontal axis is the Green strain. These data were used to calculate the average
material constants presented in Table 3.3................................................................ 187
A.5 The average stress–strain responses developed based on identical first Piola–
Kirchhoff stress states from loading protocols (a) number 1 (equibiaxial), (b)
number 2, (c) number 3, (d) number 4, and (e) number 5 of Table 3.1 (of the main
manuscript) for the septal leaflet. The vertical axis is the second Piola–Kirchhoff

xxii
stress, and the horizontal axis is the Green strain. These data were used to
calculate the average material constants presented in Table 3.4. ............................ 188
A.6 The average stress–strain responses developed based on identical Cauchy stress
states from loading protocols (a) number 1 (equibiaxial), (b) number 2, (c) number
3, (d) number 4, and (e) number 5 of Table 3.1 (of the main manuscript) for the
septal leaflet. The vertical axis is the second Piola–Kirchhoff stress, and the
horizontal axis is the Green strain. These data were used to calculate the average
material constants presented in Table 3.5.................................................................189
C.1 The specimens were excised from (A) the distal avascular region, (B) the distal
vascular region, and (C) the root region of the porcine mesenteries. ...................... 200
C.2 (a) Suture lines are connected to the specimen using fishhooks. (b) Specimen
attached to the specifically-designed carriages of the equipment using suture-
lines.......................................................................................................................... 201
C.3 The average membrane tension versus stretch ratio for the equibiaxial loading
protocol for (a) the distal avascular, (b) the distal vascular, and (c) the root regions
of the porcine mesenteries (n=8, the bars are standard errors). ............................... 210
C.4 The mean stretch values at 40 N ⁄ m measured at three different regions of the
mesentery shown in Fig. C.1 for radial and tangential (Tang) directions. Bars are
the standard error (n=8). .......................................................................................... 210
C.5 The constant stress contours for (a) and (b) the distal avascular, (c) and (d) the
distal vascular, and (e) and (f) the root regions of a typical porcine mesentery
specimens. ............................................................................................................... 212
C.6 The experimentally measured data and the result of the five-protocol fitting for
(a) the distal avascular, (b) the distal vascular, and (c) the root regions of a typical
porcine mesentery specimen. The numbers are associated with the protocol
numbers in Table C.1. ............................................................................................. 215
C.7 Average second Piola–Kirchhoff stress versus Green strain in tangential (Tang)
and radial directions for loading protocols (a) number 1 (equibiaxial), (b) number
2, (c) number 3, (d) number 4, and (e) number 5 of Table C.1 for the distal
avascular region. ...................................................................................................... 216
C.8 Average second Piola–Kirchhoff stress versus Green strain in tangential (Tang)
and radial directions for loading protocols (a) number 1 (equibiaxial), (b) number
2, (c) number 3, (d) number 4, and (e) number 5 of Table C.1 for the distal
vascular region......................................................................................................... 217

xxiii
C.9 Average second Piola–Kirchhoff stress versus Green strain in tangential (Tang)
and radial directions for loading protocols (a) number 1 (equibiaxial), (b) number
2, (c) number 3, (d) number 4, and (e) number 5 of Table C.1 for the root region. 217
C.10 Constant energy contours plotted over the strain field for typical samples of (a)
the distal avascular, (b) the distal vascular, and (c) the root regions of the porcine
mesentery. ................................................................................................................ 222
C.11 The mechanical responses observed for the root region of the porcine mesentery
did not always follow the same trend. For example, tissue was (a) stiffer in
tangential direction, or (b) had similar stiffness in both directions, noticeably
different from other typical cases in this region (Fig. C.6c). The numbers are
associated with the protocol numbers in Table C.1. ................................................ 223

1
CHAPTER 1I
INTRODUCTION
1.1 Anatomy and Function of the Heart
The heart, one of the most vital organs of the body, is a combination of two separate
pumps that are attached to one another. The right side pumps blood through the pulmonary
circulation in order to transfer oxygen to blood in the lungs. Conversely, the left side pumps
blood into the systemic circulation to provide the organs and tissues of the body with
necessary oxygen and nutrients. Each side of the heart incorporates an atrium and a
ventricle [1] (Fig. 1.1).
A recurrent contraction in the heart muscles provides the force to pump the blood,
and four one-way valves (including two atrioventricular and two semilunar valves) guide
the blood in the appropriate direction in the circulation process (Fig. 1.2). During systole,
the atrioventricular valves—the mitral valve (MV) on the right and the tricuspid valve (TV)
in the left) force—close the valve orifice to prevent blood from the ventricles from back
into the atria. Analogically during diastole, the semilunar valves close to prevent the blood
from flowing back from the aorta (aortic valve (AV)) and pulmonary arteries (pulmonary
valve (PV)). Opening and closure of these four valves are passive procedures (i.e. a
backward pressure gradient closes the valves, and a forward pressure gradient causes them
to open) [1].

2
Fig. 1.1 The heart structure and parts. (Image adopted from Cook et al. [2] with permission)
Each of these valve apparatuses consists of several parts that, in combination with
the other parts of the heart, create a powerful blood pump that can beat an average of more
than three billion times during a human lifetime. In the current study, we are focusing on
the TV; therefore, in the following sections of this chapter, we discuss this apparatus in
more detail.
1.2 Tricuspid Valve Anatomy
The TV, as one of the two atrioventricular valves, is a composite of several
structures located in the right heart between the right atrium and right ventricle, and it has
a roughly triangular orifice. The structures of the TV work together in order to open during
diastole and close during systole to maintain a one-way flow of blood and to prevent blood
backflow from the right ventricle to the right atrium during the systole [4, 5].
3
Fig. 1.2 Four cardiovascular valves guarantee one-way flow in the circulatory system. The
atrioventricular valves (MV and TV) are open during the diastole and closed during the
systole, whereas the semilunar valves (AV and PV) are closed during diastole and open
during systole. (Image adopted from Weinhaus et al. [3] with permission)
To understand the pathophysiology of TV diseases and the related surgical
treatments, it is essential to understand the anatomy of this valve. TV apparatus comprises
three leaflets: anterior leaflet (also known as the anterosuperior, ventral, or mural leaflet),
posterior leaflet (also called the interior, or dorsal leaflet), and septal leaflet (also called
medial leaflet); it also includes the annulus, chordae tendineae, and papillary muscles [4,
6] (Fig. 1.3). The leaflets are attached to the saddle-shaped annulus on the proximal side;
the distal side, as well as some points on their ventricular surface, are anchored to the
chordae. The other ends of the chordae are attached to the papillary muscles [5]. The three
leaflets, as the opening and closing elements of the valve orifice, are connected by small
commissural leaflets [7, 8] (i.e. the anteroposterior, anteroseptal, and posteroseptal
commissures (Fig. 1.4)).

4
Fig. 1.3 TV apparatus comprises of anterior leaflet, posterior leaflet, septal leaflet, annulus,
chordae tendineae, and papillary muscles. (Image adopted from Weinhaus et al. [3] and
Chan [5] with permission.)
Perfect closure relies on the precise coaptation of the three leaflets, which implies
a perfect fit between the surface area and shape of the leaflets and the annulus [9]. The
chordae tendineae, along with the papillary muscles, construct a suspension system for the
leaflets to sit on. This suspension system prevents excessive upward displacement of the
leaflets during the systole and eases the opening of the valve orifice during the diastole.
Papillary muscles, which have contractile properties and are attached to the ventricular wall
at the proximal side, are normally categorized in three groups (anterior, posterior, and
septal, as mentioned previously). The chordae tendineae, which are the intermediate parts
between the papillary muscles and the leaflets, are fibrous cords that possess elastic
properties. Based on their attachment to the leaflet, three types of chordae tendineae can
be distinguished: basal chordae (attached to the base of the leaflets), intermediary or
second-order chordae (attached to the belly of the leaflet at the ventricular side), and
marginal chordae or first-order (attached to the free edge of the leaflets) [8-10]. The
majority of the chordae tendineae branch before inserting into the leaflet. In this

5
dissertation, we use the abovementioned convention for chordae tendineae categorization;
however, other methods of categorization with different approaches also exist [8, 9].
Fig. 1.4 Illustration of the tricuspid valve leaflets, their connection to each other, and their
attachment to the chordae. (Image adapted from Carpetier et al. [8])
The TV apparatus—along with the right atrium, right ventricle, and blood flow—
are interconnected components of the same hemodynamic system, and TV function is
heavily influenced by the operation of all other components [8].
1.3 Tricuspid Valve Microstructure
Different parts of the TV apparatus have different structural components based on
their complex functions. TV leaflets contain interstitial fibroblasts and connective tissue
fibers [11], including collagen and elastin, within an extracellular matrix [4]. They have a
four-layer structure in cross section including atrialis, spongiosa, fibrosa, and ventricularis,
covered by a layer of endothelial cells [4, 12-15] (Fig. 1.5).
6
Fig. 1.5 A cross section of the atrioventricular valve leaflet showing its four-layered
structure: atrialis (A), spongiosa (S), fibrosa (F), and ventricularis (V) (in black are the
elastin fibers; in blue are the proteoglycans and glycosaminoglycans; in yellow are the
collagen fibers; and in magenta are the interstitial cells). (Image adopted from Lee et al.
[15] with permission.)
Fibrosa and atrialis are the two layers of the TV that include the main portion of the
connective tissue. The atrialis is the top-most layer, which faces atrium when the valve is
in closed position. This layer is composed primarily of aligned elastic and collagen fibers,
and it has the most elastic fibers of all the TV structures [4]. The layer right underneath the
atrialis is the spongiosa layer. The main portion of this layer, which acts as a lubricant
between the fibrosa and atrialis when the leaflet deforms, includes highly hydrated
glycosaminoglycans and proteoglycans along with elastic fibers [4, 12, 16]. The high level
of water molecules in the spongiosa causes the extracellular matrix to expand, making the
layer act as a shock absorber [4]. Beneath this layer is the fibrosa layer. Fibrosa is the
thickest layer; it is the primary load bearing component, as it consists mainly of type I
collagen fibers [12, 17, 18]. Since collagen fibers can withstand high tensile forces, the
orientation of the collagen fibers in the leaflet can determine the direction in which the
tissue can tolerate the greatest tensile forces. The lowermost layer is the ventricularis,

7
which consist of sheets of endothelial cells that overlay the elastic and collagen fibers [4].
The thickness of these layers will vary according to their proximity to the annulus.
Proximal to the annulus, the fibrosa is thick and gradually becomes thinner towards the
distal side of the leaflets, vanishing about two-thirds of the way through. In contrast,
spongiosa and atrialis are relatively thin at the proximity of the annulus and increasingly
thicken distally to become the main components at the free edges of the leaflets [4]. The
TV annulus has a fibrous structure, which gradually transitions from the collagen-rich area
at the leaflet’s side to the elastin-rich area towards the myocardium wall [12, 18]. The
chordae tendineae are composed of collagen fibers parallel to the chordae long axis [18];
they provide the necessary strength for the chordae to carry tensile loads when the valve is
pressurized.
1.4 Tricuspid Valve Pathophysiology
Etiologically, TV regurgitation can be divided into two types, functional
regurgitation and organic regurgitation. Functional TV regurgitation (FTR), also known as
secondary TV regurgitation, is the primary reason for TV malfunction. It is the type of
regurgitation that develops after a disturbance in the coordination of the valve elements
without any organic valvular or myocardial lesion [4, 8]. This dysfunction, which could be
reversible, is considered to be functional, as the morphology of the leaflets is normal [5,
19]. MV diseases, right ventricular dysfunction, and pulmonary hypertension diseases are
the main reasons for development of FTR [8]. For example, approximately one half of the
patients suffering from MV regurgitation have at least moderate FTR [20, 21]. In addition,
more than 30% of the patients with MV stenosis have developed moderate to severe FTR
[22, 23].

8
On the other hand, organic TV regurgitation is primarily due to either the
involvement of the TV in certain diseases or a diseased myocardium. No matter what the
etiology of the disease is, it can cause lesions that affect different components including
the annulus (dilatation, abscess), leaflets (excess leaflet tissue, thickening, vegetation,
abscess, perforation, tear), commissures (fusion, thickening), chordae (rupture, elongation,
thickening, shortening, fusion), papillary muscles (rupture, elongation), and/or ventricle
(infarction, fibrosis, dilatation) [8]. Three different types of TV regurgitation have been
defined based on leaflet motion [8]: type I (normal leaflet motion), type II (excessive leaflet
motion or leaflet prolapse), and type III (restricted leaflet motion, including restricted
leaflet opening and restricted leaflet closure). Severe restriction to the leaflet motion as a
result of commissural fusion, leaflet thickening, chordae fusion, and calcification causes a
reduction in blood flow from the atrium to the ventricle; this condition is categorized as
TV stenosis [4, 8].
As one of the most common TV dysfunctions, TV regurgitation often requires TV
repair or replacement [24, 25]. From 1999 to 2008, approximately 150,000 patients
underwent TV repair surgeries [24] in the United States. Overall, TV repair has better
outcomes when compared to TV replacement with prosthetic devices [8, 26, 27]. However,
according to the Society of Thoracic Surgery Database, in terms of morbidity and mortality,
TV surgery is still the most high-risk valve operation [28]. The frequency of TV repair
procedures has been increasing recently, as many investigators are now in favor of more
aggressive surgical approaches to FTR in the absence of any organic TV lesions [24, 29-
31]. Roughly 1.6 million people in the United States suffer secondary TV regurgitation,
raising the number of potential candidates for TV repair [32-34].

9
1.5 Tricuspid Valve Mechanical Behavior
The success level of TV surgeries is highly tied to our knowledge of TV mechanical
properties as, similar to the other cardiovascular valves, TV function is linked to the valve’s
biomechanical behavior and complex geometry. The mechanical behavior of any material,
in turn, is tied to its microstructure. As discussed above, the microstructure of TV
components is extremely complex, complicating the overall mechanical behavior of the
valve. Given the in-situ loading conditions of the desired valve leaflets during the operation
of the heart, biaxial tensile tests have been used to provide precise and realistic data on the
mechanical response of the heart valve leaflets. Many studies have addressed the
mechanical behaviors of soft tissue including the MV and AV [35-42]. May-Newman et
al. studied the biaxial mechanical behavior of the porcine MV [35], and Billiar et al. probed
the biaxial responses of the natural and glutaraldehyde-treated AV cups [36]. Grashow et
al. studied creep and strain relaxation as well as the effect of strain rate on the mechanical
behavior of the anterior leaflet of the MV [37, 38]. Sacks et al. explored the surface strains
of the MV anterior leaflet [39]. However, TV mechanical behavior has been understudied
in comparison to the behavior of other heart valves, and it has not yet been accurately
characterized, leaving it to become known as “the forgotten valve” [43]. For example, the
only available computational model of the TV [44] has been constructed based on a grossly
simplified geometry using the homogenous mechanical properties of the MV.
1.6 Material Models
Mechanical response modeling is an essential step in the accurate quantification of
normal biomechanical behavior of the native valve tissue during the cardiac cycle. Material
models are necessary for a better understanding of the mechanical behavior of the tissue

10
and are designed to model the mechanical responses under a generalized form of loading
in a computerized simulations. For this purpose, researchers develop equations, namely
constitutive models, that can approximate the response of the desired material (i.e. the
strains) to the environmental stimuli (i.e. forces). These models can be derived as the
empirical relationship between the stimuli and the response, which are known as
phenomenological models, or they can be derived based on basic principles and
microstructure of the desired material, which are known as structural models. Several
different phenomenological and structural models have been proposed to represent the
mechanical behavior of different materials [45-49] based on their inherent microstructure
and composition. For example, the Mooney–Rivlin model (developed initially by Mooney
[45] and modified by Rivlin et al. [46]) and the Ogden model (proposed by Ogden [47])
were developed to represent the mechanical behavior of isotropic rubber materials.
Soft tissue materials (including heart valve tissue) are often considered
incompressible. Because of their oriented fibrous structure, they are known to exhibit
anisotropic responses. They express highly nonlinear stress–strain response and undergo
large strains and rotations [12, 50]. All these characteristics induce complexity in their
mechanical behavior and make their accurate modeling highly challenging. Researchers
have proposed different models to represent the mechanical responses of soft tissues,
including heart valves [15, 42, 50-73]. Different variations of a Fung-type model, originally
proposed by Fung [52], have been widely used in modeling mechanical behavior of soft
tissues including skin [53], pericardium [54, 55], abdominal aorta [56], urinary bladder
[57], small intestine [58], coronary artery [59], and heart valves [42]. May-Newman and
Yin proposed a specific phenomenological constitutive model with three material constants
11
to represent the mechanical behavior of the MV [60]. Choi et al. introduced a
phenomenological constitutive model to address orthotropic mechanical properties of the
pericardium [61-63], which was later used by other researchers to model the mechanical
responses of the abdominal aorta [64, 65]. In addition to the phenomenological constitutive
models, structural models have also been widely used to capture the mechanical responses
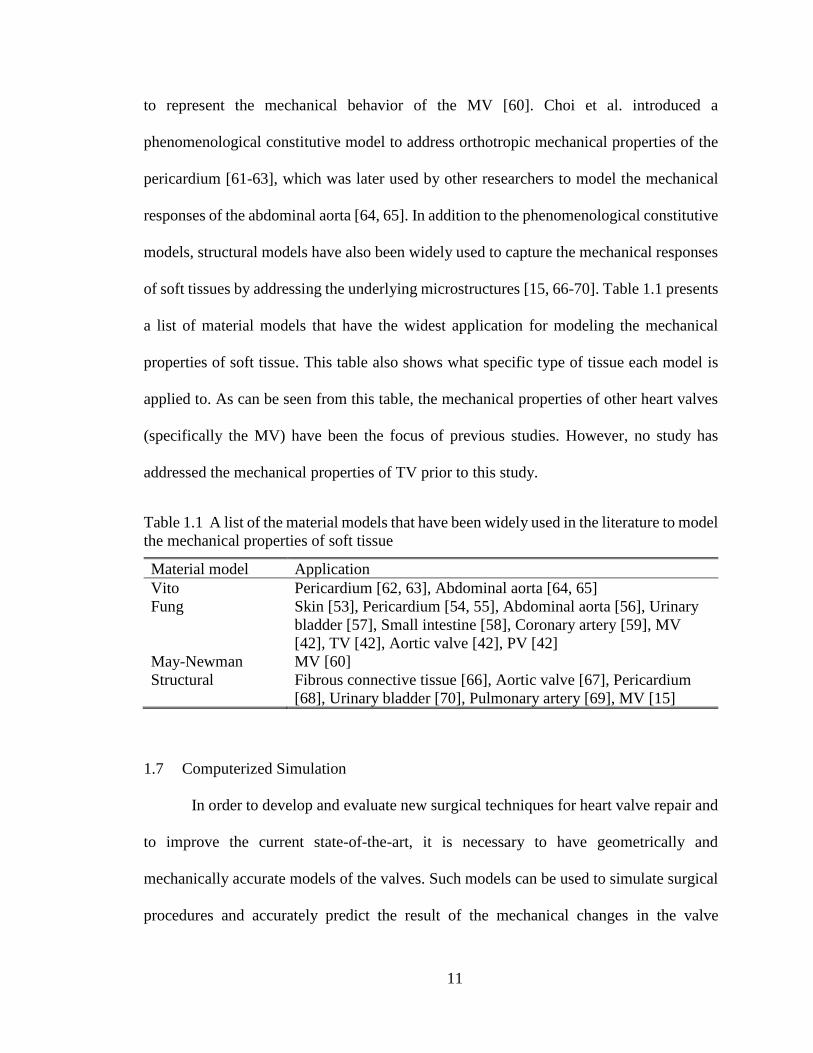
of soft tissues by addressing the underlying microstructures [15, 66-70]. Table 1.1 presents
a list of material models that have the widest application for modeling the mechanical
properties of soft tissue. This table also shows what specific type of tissue each model is
applied to. As can be seen from this table, the mechanical properties of other heart valves
(specifically the MV) have been the focus of previous studies. However, no study has
addressed the mechanical properties of TV prior to this study.
Table 1.1 A list of the material models that have been widely used in the literature to model
the mechanical properties of soft tissue
Material model Application
Vito Pericardium [62, 63], Abdominal aorta [64, 65]
Fung Skin [53], Pericardium [54, 55], Abdominal aorta [56], Urinary
bladder [57], Small intestine [58], Coronary artery [59], MV
[42], TV [42], Aortic valve [42], PV [42]
May-Newman MV [60]
Structural Fibrous connective tissue [66], Aortic valve [67], Pericardium
[68], Urinary bladder [70], Pulmonary artery [69], MV [15]
1.7 Computerized Simulation
In order to develop and evaluate new surgical techniques for heart valve repair and
to improve the current state-of-the-art, it is necessary to have geometrically and
mechanically accurate models of the valves. Such models can be used to simulate surgical
procedures and accurately predict the result of the mechanical changes in the valve

12
apparatus or the boundary conditions. In addition, these models contribute to the
development of new prosthetic valves that are designed to mimic native valve behaviors.
To develop such models accurately and to validate them, one should consider the following
factors:
Appropriate mechanical properties. A computerized model needs to reflect the
realistic mechanical response of the original tissue under a generalized loading condition.
Obtaining such properties can be accomplished by accurately measuring the mechanical
properties of the tissue and using appropriate material models [74, 75].
Accurate geometry and underlying microstructure. Manual measurements or 2D
and 3D imaging can be used to reconstruct the geometry of the TV. Small angle light
scattering (SALS) techniques [76-79] can be used to extract the microstructure of the leaflet
tissues and the distribution of the fiber orientations.
Loading and boundary conditions. In case of the heart valve, loading can be
accomplished by incorporating the transvalvular pressures or the blood flow into the
simulation. In this case, boundary conditions might be the deformation of the annulus and
papillary muscles throughout the cardiac cycle. Sonomicrometry [80-83] or other
techniques [84] can be used to track and record these boundary conditions.
Experimental measurements for validation purposes. A reliable method to evaluate
the accuracy of the developed computerized model is to experimentally measure the
deformations in a specific case and compare them with the results of the computerized
simulation. Sonomicrometry techniques [26, 85], videofluoroscopy [30], or camera
tracking systems [39] can be used to capture the heart valve deformations and extract the

13
mechanical strains [86, 87] while the heart is beating. These strains can be compared to the
simulation results to validate the model.
Such a geometrically and mechanically accurate model, once it has been
experimentally validated, can be used to simulate the heart valve lesions and surgical
procedures as well as evaluate the effects of mechanical alterations on the valve apparatus
and/or develop new prosthetic valves. Lee et al. have recently published a detailed article
regarding such a model that they have developed for the MV [88, 89]. In this study, high-
resolution micro-CT images of MV were used to reconstruct an accurate geometry. The
microstructure of the tissues was characterized using SALS, and the material model
proposed by Fan et al. [90] was used to represent the mechanical behavior of the MV
leaflets. However, by the start of the study described in this dissertation, no accurate
computerized model of TV was available in the literature. The only available model at that
time was established based on a grossly simplified geometry, and a material model for the
MV was used to represent the mechanical properties [44]. Another model later was
proposed by Kong et al. in 2018 [91], was based on a more accurately developed geometry
obtained from CT images, and TV mechanical properties were used to represent the
mechanical responses. However, no data were presented to verify the validity of this model.
Consequently, it was necessary to develop a more accurate and verifiable finite element
(FE) model of the TV to be used in computerized simulations in order to study TV behavior
under different circumstances and environmental changes, including simulation of valvular
lesions and treatments. Table 1.2 summarizes the major computerized models for the MV
and the only two available computerized models for the TV, along with their important
specifications (including the material models).
14
Tab
le 1
.2 L
ist of
maj
or
com
pute
rize
d m
odel
s of
tric
usp
id v
alve
(TV
) an
d m
itra
l val
ve
(MV
) al
on
g w
ith thei
r im
port
ant sp
ecif
icat
ions
Type
Dev
eloper
L
eafl
et m
ater
ial
model
C
hord
ae m
ater
ial
model
G
eom
etry
MV
Kunze
lman
(1997)
[92]
Lin
ear
anis
otr
opic
L
inea
r M
anual
mea
sure
men
ts, p
ig
Lim
(2005)
[93]
Lin
ear
isotr
opic
L
inea
r In
-viv
o s
onom
icro
met
ry,
shee
p
Ein
stei
n (
2005)
[94]
Anis
otr
opic
hyp
erel
asti
c
(Bil
liar
[67])
, pig
MV
Nonli
nea
r, p
ig M
V
Not
avai
lable
, pig
Vott
a (2
008)
[95]
Anis
otr
opic
hyp
erel
asti
c (P
rot
et a
l. [
96])
, pig
MV
Poly
nom
ial,
pig
MV
In
-viv
o u
ltra
sound, hum
an
Pro
t (2
009)
[97]
Anis
otr
opic
hyp
erel
asti
c
(Holz
apfe
l et
al.
[98])
, pig
MV
Isotr
opic
hyper
elas
tic
exponen
tial
, pig
MV
In-v
ivo e
cho
gra
ph
y a
nd m
anual
mea
sure
men
ts, pig
Wen
k (
2010)
[99]
Nonli
nea
r an
isotr
opic
[1
00],
hum
an M
V
Cab
le e
lem
ent
form
ula
tion [
101]
In-v
ivo M
RI,
sh
eep
Ste
van
ella
(2011)
[102]
May
-New
man
[60],
pig
MV
O
gd
en a
nd p
oly
nom
ial,
pig
MV
In-v
ivo M
RI,
hum
an
Wan
g (
2013)
[103]
Anis
otr
opic
hyp
erel
asti
c
(Holz
apfe
l et
al.
[104, 105])
,
hum
an M
V
Ogd
en,
pig
MV
In
-viv
o C
T i
mag
es, h
um
an
Lee
(2015)
[88]
Anis
otr
opic
hyp
erel
asti
c (S
acks
[68])
, sh
eep M
V
Isotr
opic
hyper
elas
tic
exponen
tial
, pig
MV
In-v
itro
CT
im
ages
, sh
eep
Pham
(2017)
[106]
Anis
otr
opic
hyp
erel
asti
c
(Holz
apfe
l et
al.
[104, 105])
,
hum
an M
V
Ogd
en, hum
an M
V
In-v
ivo C
T i
mag
es, hum
an
TV
Ste
van
ella
(2010)
[44]
May
-New
man
[60],
pig
MV
P
oly
nom
ial,
hum
an T
V
[107]
In-v
ivo s
onom
icro
met
ry a
nd m
anual
mea
sure
men
ts h
um
an a
nd p
ig
Kong (
2018)
[91]
Anis
otr
opic
hyp
erel
asti
c
(Holz
apfe
l et
al.
[104, 105])
,
hum
an T
V
Ogd
en,
hum
an M
V
[106]
In-v
ivo
CT
im
ages
, h
um
an

15
1.8 Open Questions
The TV is the most understudied of the four cardiac valves, leaving it to be known
as “the forgotten valve” [43]. While many studies have been conducted to examine the
mechanical characteristics of the MV and AV [35-39], the biaxial mechanical responses of
the TV have not yet been accurately quantified.
Moreover, a large group of researchers has studied the biomechanical behavior and
dynamic deformations of the MV [12, 26, 30, 39, 82, 85, 108, 109], the atrioventricular
valve analogous to the TV on the left side of the heart. In addition, a few studies focus on
TV geometry and annulus deformation [80, 81, 83, 84, 110]. While these studies are
extremely important, they provide no information about the dynamic mechanical strains of
TV leaflets. In terms of experimental techniques, the previous valvular studies can be
categorized into two main groups: in-vivo studies [26, 30, 80-82, 85, 108-110] and in-vitro
studies [39, 111, 112]. In-vivo ovine and porcine studies are frequently used as models
prior to clinical studies [26, 82, 85]. Such studies, however, require surgical operating
rooms and animal care facilities, which are often costly and should be used only prior to
clinical approaches. In-vitro studies, while less costly, were previously conducted only on
excised valves [39, 112]. In these studies, the excised valves are generally mounted on a
prosthetic rigid annulus and subjected to pulsatile pressure in a flow simulator. The
outcome of such studies is limited, since it has been shown that the cardiac valve annulus
is dynamically deforming during the cardiac cycle [82]; thus, valve annulus restriction
could significantly alter the leaflet strains [26]. Recently, an ex-vivo apparatus using the
entire porcine heart (instead of using isolated valves) has been developed to image valve
motion and to study hemodynamics in the left chambers of the heart [113]. Nevertheless,

16
the author did not find any study on the dynamic mechanical strains of the TV in the
literature.
Finally, a few researchers have published studies on accurate development of
computerized models for the MV [88] and AV [114, 115]. However, despite the importance
of computational simulations for the TV, no verified model for the TV is currently
available. The only available computational model at the start of the current study was
developed by Stevanella et al. [44] based on grossly simplified assumptions. In their model,
the geometry was constructed based on the dimensions manually measured from the
excised valves and sonomicrometry data that was available in the literature. Moreover,
without access to accurate TV data, the mechanical responses were estimated using data
available for the MV with the assumption of uniform mechanical properties over all
leaflets.
As such, the following questions are still open:
• Unlike other heart valves (MV and AV), the mechanical properties of TV have not yet
been accurately measured. Do all leaflets of TV have similar mechanical responses and
are these responses the same as the other valves? If yes, to what extent are they are
similar? If no, how will each TV leaflet respond to mechanical loading? Is it possible
to develop a constitutive material model to represent the mechanical properties of TV
leaflets? Which material model can best represent the mechanical properties of TV
leaflets? Is the microstructure of the TV leaflets similar to that of other heart valve
leaflets? The answer to these questions can be found in chapters II and III of the current
document.

17
• The pathophysiology of TV regurgitation is closely related to the dynamic
deformations of the valve annulus and leaflet coaptation [116]. Any alteration in
mechanical environment of the valve (i.e. chordae rupture) can cause long-term valve
regeneration. To understand the mechanism behind these long-term changes, it is
necessary to study normal TV deformations and probe the immediate effects of changes
in the mechanical environment of the valve. Moreover, valve deformations and strain
distributions on the leaflets can be used as boundary conditions as well as validation
data for computerized models. What is the normal deformation on TV leaflets and
annulus during the cardiac cycle? What is the distribution of the strains on the surface
of the TV leaflets and how does it change throughout the cardiac cycle? How do the
valve deficiencies affect the strain distribution and deformation of TV leaflets and TV
annulus? These questions are addressed in detail in chapters IV, V, and VI.
• The only available computerized model for the TV uses poor geometry and the
mechanical properties of another heart valve. Does geometry improvement and
application of realistic TV mechanical properties provide us with a computerized model
that can accurately simulate TV behavior? The answer to this question is provided in
chapter VII.
In the remaining chapters of this document, answers to these questions will be
provided, and a final chapter is dedicated to conclusions and possible future work. All
experiments and measurements in this study are conducted on the porcine heart. The pigs
were female or castrated males ranging from 6 to 8 months in age and weighing around
200 𝑙𝑏𝑠.

18
Table 1.3 The abbreviations used in this document are listed in this table alphabetically.
Abbreviation Full expression
ACH Anteroposterior Commissure Height
ALH Anterior Leaflet Height
ASL Anterior Segment Length
AV Aortic Valve
AVG Average
CTR Chordae Tendinea Rupture
FE Finite Element
FTR Functional Tricuspid Regurgitation
MV Mitral Valve
PAP Pulmonary Artery Pressure
PBS Phosphate Buffered Saline
PCH Posteroseptal Commissure Height
PCR Post Chordae Rupture
PLH Posterior Leaflet Height
PSL Posterior Segment Length
PV Pulmonary Valve
RAP Right Atrial Pressure
RVP Right Ventricular Pressure
SCH Anteroseptal Commissure Height
SE Standard Error
SLH Septal Leaflet Height
SSL Septal Segment Length
STD Standard Deviation
TV Tricuspid Valve

19
CHAPTER 2II
BIAXIAL MECHANICAL RESPONSE OF THE TRICUSPID VALVE LEAFLETS
(The content of this chapter was published in JBME (Aug 2016) as “On the Biaxial
Mechanical Response of Porcine Tricuspid Valve Leaflets” [117].)
2.1 Summary
Located on the right side of the heart, TV prevents blood backflow from the right
ventricle to the right atrium. Similar to other cardiac valves, quantification of TV biaxial
mechanical properties is essential in developing accurate computational models. In the
current study, for the first time, biaxial stress-strain behavior of porcine TV was measured
ex vivo under different loading protocols using biaxial tensile testing equipment. The
results showed a highly nonlinear response including a compliant region followed by a
rapid transition to a stiff region for all of TV leaflets in both the circumferential and radial
directions. Based on the data analysis, all the three leaflets were found to be anisotropic,
and they were stiffer in the circumferential direction in comparison to the radial direction.
It was also concluded that the posterior leaflet was the most anisotropic leaflet.
2.2 Introduction
TV, which is located between the right atrium and the right ventricle of the heart,
prevents blood backflow from the ventricle to the atrium during ventricular systole [1].
Absent the normal closure of TV leaflets, blood flow may regurgitate back into the right
atrium during systole, a condition that may require valvular repair surgery. From 1999 to

20
2008, approximately 30,000 patients have undergone TV repair surgeries [24]. Overall,
TV repair has better outcomes when compared to TV replacement with prosthetic devices
[25, 118, 119]. However, according to the Society of Thoracic Surgery Database, in terms
of morbidity and mortality, TV surgery is still the most high-risk valve operation [120].
The frequency of TV repair procedures has been increasing recently, as many investigators
are now in favor of more aggressive surgical approaches to functional tricuspid
regurgitation (FTR), also known as secondary TV regurgitation, in the absence of any
organic lesions of TV [20, 21, 121, 122]. Although FTR could be caused by diseases
specific to the right side of the heart (e.g. pulmonary hypertension or right atrial tumors),
it frequently develops in the presence of left-sided heart diseases and in particular coexists
with MV lesions. For example, approximately one half of the patients suffering from MV
regurgitation have at least moderate FTR [123, 124]. In addition, more than 30% of
patients with MV stenosis have developed moderate to severe FTR [125, 126]. Roughly
1.6 million people in the United States suffer secondary TV regurgitation, raising the
number of potential candidates for TV repair [32-34].
In order to develop new surgical techniques for TV leaflet repair and to improve
the current state-of-the-art, it is necessary to understand the biomechanical properties of
native TV tissues. Given the in-situ loading conditions of TV leaflets during the operation
of the heart, a biaxial tensile test could provide precise and realistic data on the mechanical
response of the valve leaflets. While many studies have been conducted to examine the
mechanical characteristics of MV and AV[35-39], the biaxial mechanical responses of TV
have not yet been accurately quantified, leaving TV to become known as “the forgotten
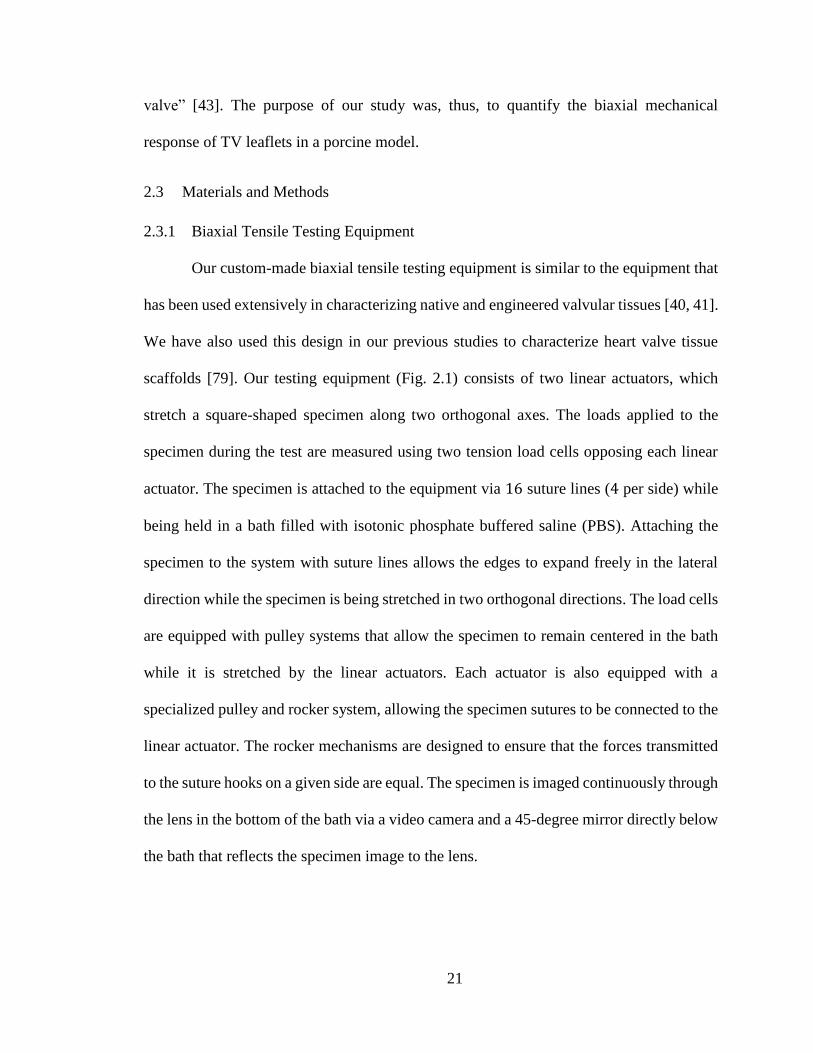
21
valve” [43]. The purpose of our study was, thus, to quantify the biaxial mechanical
response of TV leaflets in a porcine model.
2.3 Materials and Methods
2.3.1 Biaxial Tensile Testing Equipment
Our custom-made biaxial tensile testing equipment is similar to the equipment that
has been used extensively in characterizing native and engineered valvular tissues [40, 41].
We have also used this design in our previous studies to characterize heart valve tissue
scaffolds [79]. Our testing equipment (Fig. 2.1) consists of two linear actuators, which
stretch a square-shaped specimen along two orthogonal axes. The loads applied to the
specimen during the test are measured using two tension load cells opposing each linear
actuator. The specimen is attached to the equipment via 16 suture lines (4 per side) while
being held in a bath filled with isotonic phosphate buffered saline (PBS). Attaching the
specimen to the system with suture lines allows the edges to expand freely in the lateral
direction while the specimen is being stretched in two orthogonal directions. The load cells
are equipped with pulley systems that allow the specimen to remain centered in the bath
while it is stretched by the linear actuators. Each actuator is also equipped with a
specialized pulley and rocker system, allowing the specimen sutures to be connected to the
linear actuator. The rocker mechanisms are designed to ensure that the forces transmitted
to the suture hooks on a given side are equal. The specimen is imaged continuously through
the lens in the bottom of the bath via a video camera and a 45-degree mirror directly below
the bath that reflects the specimen image to the lens.
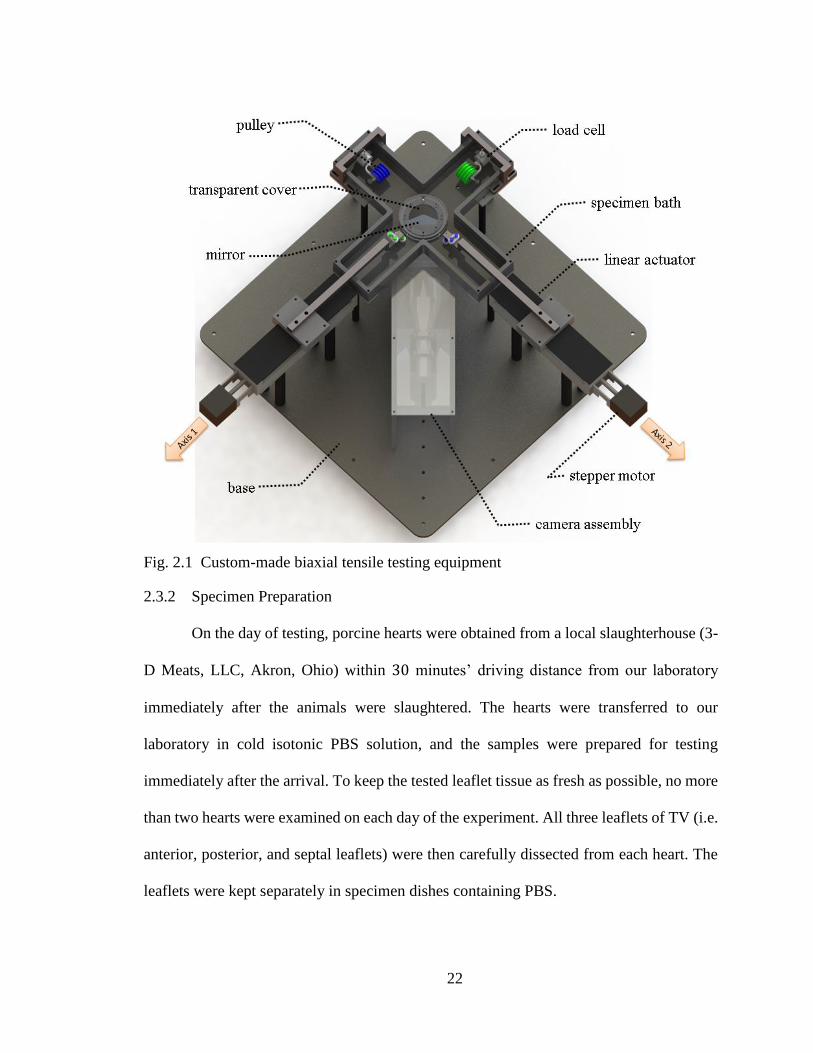
22
Fig. 2.1 Custom-made biaxial tensile testing equipment
2.3.2 Specimen Preparation
On the day of testing, porcine hearts were obtained from a local slaughterhouse (3-
D Meats, LLC, Akron, Ohio) within 30 minutes’ driving distance from our laboratory
immediately after the animals were slaughtered. The hearts were transferred to our
laboratory in cold isotonic PBS solution, and the samples were prepared for testing
immediately after the arrival. To keep the tested leaflet tissue as fresh as possible, no more
than two hearts were examined on each day of the experiment. All three leaflets of TV (i.e.
anterior, posterior, and septal leaflets) were then carefully dissected from each heart. The
leaflets were kept separately in specimen dishes containing PBS.

23
Removing a square-shaped specimen from the leaflet and attaching it to the biaxial
tensile testing equipment was facilitated by a specially designed phantom (Fig. 2.2a). Not
only did the phantom make it much easier and faster to attach the specimen to the system,
it also decreased the probability of damaging the tissue during the preparation process. The
leaflets were carefully positioned between the two halves of the phantom, trimmed using
surgical scissors, and attached to the fishhooks-suture-line setup through the grooves in the
phantom. The grooves facilitated the uniform attachment of the fishhooks, which was
necessary to obtain a uniform strain field. They were designed in 1 𝑚𝑚 distance from each
other on all the edges. These suture lines were then used to mount the specimen on the
testing equipment. The phantom was designed in such a way that it did not put any pressure
on the leaflet and was clamped to the leaflet edges only. Thus, any chance of damage due
to specimen preparation was minimized.
In total, ten sets of TV leaflets were tested, with each set coming from the same
heart. We performed all of the tests within 2 to 6 hours postmortem to eliminate erroneous
results that might be obtained from testing leaflets that had been frozen and thawed. The
dimensions of the trimmed specimens were 11 𝑚𝑚 by 11 𝑚𝑚 and the fishhooks were
attached on the sides of a 7.6 𝑚𝑚 by 7.6 𝑚𝑚 square (center to center). Four small glass
beads (0.5 𝑚𝑚 in diameter) were attached to the specimen in a 2 by 2 array (3 𝑚𝑚 apart
in each direction) as fiducial markers for quantification of the in-plane deformation.
2.3.3 Biaxial Tensile Testing Protocols
Specimens were mounted to the biaxial tensile testing equipment in the specimen
bath containing isotonic PBS at room temperature (Fig. 2.2b) with the circumferential
direction (i.e. commissure-to-commissure direction) aligned with one stretching direction

24
(axis 1 in Fig. 2.1) and the radial direction aligned with the other direction (axis 2 in Fig.
2.1). Before collecting the data, the samples were preconditioned using ten cycles of
equibiaxial loading. Each leaflet then experienced seven different loading protocols
starting with equibiaxial loading, which loaded it up to a maximum of 100 𝑁/𝑚 on each
axis. The other four loading types were non-equibiaxial as shown in the Table 2.1. In all
cases, a tare load of 0.5 𝑔 was first applied [36]. Each loading-unloading cycle took
20 seconds to complete.
Fig. 2.2 a) Specially designed phantom to facilitate the attachment of the leaflets to the
biaxial tensile testing equipment. b) Specimen attached to the equipment using fishhooks
and suture lines.
Table 2.1 Biaxial loadings protocols applied for each specimen
Maximum membrane tension (𝑁/𝑚)
Loading protocol no. Circumferential axis Radial axis
1 100 100
2 100 80
3 80 100
4 100 50
5 50 100

25
2.3.4 Strain and Stress Calculation
The in-plane positions of the fiducial markers were obtained using the camera
setup. Homogeneity of the strain field primarily depends on how uniform and regular the
suture lines are connected around the specimen and how close the connection points are
from the adjacent edges [74, 75]. The aforementioned phantom used to attach the fishhooks
guaranteed the uniform connection of the suture lines to the specimen. Since in our biaxial
testing equipment, four connections (i.e. the fish hooks) are applied on each side of the
specimen, uniform strain field was expected at the region covering 35% of the central area
of the specimen [75]. The fiducial markers were attached on the central area of the
specimen in a 3 𝑚𝑚 by 3 𝑚𝑚 square format. Since total area of the specimen was a
7.6 𝑚𝑚 by 7.6 𝑚𝑚 square (i.e. the area between the fishhooks), fiducial markers were
positioned within the 35% uniform strain field. The positional data were used to calculate
in-plane deformation gradient tensor F using methods explained previously [86, 127]. The
Green strain tensor was then calculated using the following equation:
E =
1
2(C − I) (2.1)
where I is the identity tensor and C, the right Cauchy-Green deformation tensor,
was defined by
C = FTF (2.2)
The thickness of each specimen was measured in six different locations using a dial
micrometer with an accuracy of 25 microns, and the average was calculated. As the square-

26
shaped specimens were cut from the central region of each leaflet, as shown in Fig. 2.3, the
thickness value was not measured beyond this square area.
To calculate the first Piola-Kirchhoff stress tensor P, each axis force was divided
by the cross-sectional area of the specimen normal to that axis. Such cross-sectional area
was calculated as the product of the distance between the fishhooks, which are connected
on two opposite sides of the specimen, and the measured thickness of the specimen. The
normal stresses P11 and P22 were then calculated. Since the specimens were thin enough
and only under planar loads and with the assumption of no shear forces applied [50], all
other components of first Piola-Kirchhoff stress tensor were considered to be zero. The
second Piola-Kirchhoff stress tensor S was then calculated:
S = F−1P (2.3)
The rigid body rotation angles ω were also calculated to determine how much of
the deformation was due to the rigid body rotation during the tests:
ω = tan−1(
𝑅21
𝑅11) (2.4)
where rotation matrix R was given by
R = FU−1 (2.5)
and U was the right stretch tensor:
C = U2 (2.6)

27
Fig. 2.3 The three leaflets of the tricuspid valve and the position and shape of the
specimens.
The tethered mounting configurations, used in the current study, allows for free
lateral displacements which provides more homogeneous stress field based on the applied
boundary loads [74]. As mentioned before, the elements of the first Piola-Kirchhoff stress
tensor are determined based on the assumption that there is no shear stress.
The shear angle θ, a measure of shear deformation, was also calculated using the
following equation:
θ = cos−1(
𝐶12
𝐶11𝐶22) (2.7)
2.4 Results
The thickness values for all of the tested specimens (including average and standard
deviation by leaflet type) are listed in Table 2.2. The Student’s t-test analysis revealed that
there was no significant difference between the thicknesses of the anterior and posterior

28
leaflets (𝑝 = 0.27). The septal leaflet, however, was significantly thicker than the anterior
and posterior leaflets (𝑝 < 10−4 for both cases). Another notable outcome was that the
septal leaflets had the smallest overall standard deviation in measured thickness values.
Table 2.2 Measured thicknesses for the leaflets of all the hearts used during the experiment
Leaflet Thickness (𝜇𝑚)
Heart No Anterior Posterior Septal
1 241 377 440
2 318 271 508
3 406 453 478
4 258 288 411
5 368 406 521
6 300 269 528
7 262 330 587
8 246 386 478
9 432 330 483
10 300 347 479
AVG 313 346 491
STD 68 61 49
The tension-stretch behavior of the specimens for all protocols listed in Table 2.1
was recorded. Fig. 2.4 demonstrates the average membrane tension versus stretch ratio of
the anterior leaflet for each loading protocol (averaged over all of the 10 specimens).
Figures 2.5 and 2.6 show the same graphs for posterior and septal leaflets, respectively.
The bars in these figures are the standard errors. The standard error was from 0.00 to 0.02
for circumferential direction and for radial direction it was from 0.00 to 0.04 for all three
types of leaflets and all the protocols. As shown in Figs. 2.4–2.6 the largest difference
between mechanical responses in the circumferential direction and the radial direction for
the equibiaxial loading was observed for the posterior leaflet, indicating that the posterior
leaflet presented more anisotropic responses than the other two leaflets.

29
The average values of the maximum rigid body rotation angles 𝜔𝑚𝑎𝑥 for each
leaflet type and loading protocol are presented in Table 2.3. In this table, the largest value
of rigid body rotation was less than 3 degrees indicating that the rigid body rotation was
negligible in the current experiment.
The average maximum shear angles θmax for each leaflet type and loading protocol
are also presented in Table 2.3. The largest maximum shear angle (4.2 ± 0.9 degrees) was
calculated for protocol number 5, in which the leaflet experienced one of the two most
anisotropic loading conditions. The shear angles calculated for the other protocols were
around 3 degrees. Table 2.3 also displays the average ratio of the maximum Cauchy shear
stresses to the maximum Cauchy normal stresses r measured for each leaflet type under
different loading protocols. The average maximum shear stress is in the range of 3.5% to
7.2% of the maximum normal stress.

30
Fig. 2.4 The average membrane tension versus stretch ratio for the loading protocols a)
number 1 (equibiaxial), b) number 2, c) number 3, d) number 4, and e) number 5 for the
anterior leaflet. The circumferential (Circ) and radial directions are in solid red and dash-
dotted blue, respectively. The bars are standard errors. The green dashed line shows the
maximum physiological tension level (Max Physio), while the tension level goes up to
100 𝑁/𝑚 in case of hypertension.

31
Fig. 2.5 The average membrane tension versus stretch ratio for the loading protocols a)
number 1 (equibiaxial), b) number 2, c) number 3, d) number 4, and e) number 5 for the
posterior leaflet. The circumferential (Circ) and radial directions are in solid red and dash-
dotted blue, respectively. The bars are standard errors. The green dashed line shows the
maximum physiological tension level (Max Physio), while the tension level goes up to
100 𝑁/𝑚 in case of hypertension.
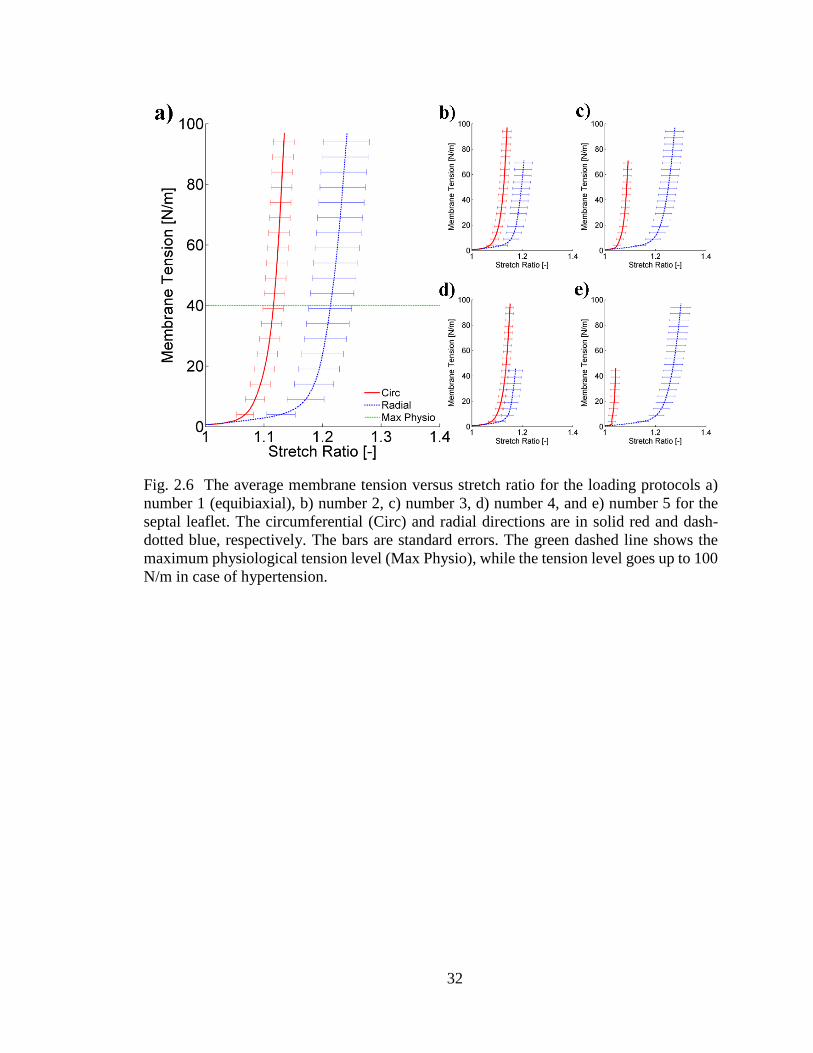
32
Fig. 2.6 The average membrane tension versus stretch ratio for the loading protocols a)
number 1 (equibiaxial), b) number 2, c) number 3, d) number 4, and e) number 5 for the
septal leaflet. The circumferential (Circ) and radial directions are in solid red and dash-
dotted blue, respectively. The bars are standard errors. The green dashed line shows the
maximum physiological tension level (Max Physio), while the tension level goes up to 100
N/m in case of hypertension.

33
Tab
le 2
.3 T
he
aver
age
max
imum
rig
id b
od
y r
ota
tion 𝜔
𝑚𝑎
𝑥, th
e av
erag
e m
axim
um
sh
ear
angle
𝜃𝑚
𝑎𝑥, an
d t
he
aver
age
of
the
rati
o o
f
the
max
imum
Cau
chy s
hea
r st
ress
to
the
max
imum
Cau
chy n
orm
al s
tres
s 𝑟
pre
sente
d f
or
each
lo
adin
g p
roto
col
and l
eafl
et t
yp
e (f
or
each
pro
toco
l an
d l
eafl
et t
ype
the
dat
a is
aver
aged
over
all
hea
rts
and p
rese
nte
d i
n t
he
form
of
aver
age
± s
tandar
d e
rror)
.
Load
ing
Pro
toco
l N
o.
Ante
rior
Lea
flet
Post
erio
r L
eafl
et
S
epta
l L
eafl
et
𝜔𝑚
𝑎𝑥
(deg
ree)
𝜃 𝑚𝑎
𝑥
(deg
ree)
r
(%)
𝜔
𝑚𝑎
𝑥
(deg
ree)
𝜃 𝑚𝑎
𝑥
(deg
ree)
r
(%)
𝜔
𝑚𝑎
𝑥
(deg
ree)
𝜃 𝑚𝑎
𝑥
(deg
ree)
r
(%)
1
2.5
3±
0.4
9
3.4
3±
0.8
1
7.2
1±
1.6
9
1.7
9±
0.4
4
2.8
8±
0.7
3
5.5
9±
1.4
3
1.2
3±
0.2
9
3.4
9±
0.6
4
5.8
0±
0.8
4
2
2.3
8±
0.4
5
3.1
9±
0.8
3
7.2
1±
1.8
9
1.6
5±
0.4
8
2.7
5±
0.7
0
5.7
2±
1.6
9
1.4
7±
0.2
6
3.4
6±
0.6
4
5.4
2±
0.9
0
3
2.5
7±
0.4
9
3.5
0±
0.8
1
5.4
7±
1.1
3
1.8
0±
0.4
6
2.9
6±
0.7
6
4.6
8±
1.0
6
1.2
6±
0.2
2
3.1
4±
0.6
6
4.8
1±
0.7
3
4
2.2
7±
0.4
0
3.1
3±
0.9
2
6.5
6±
1.7
5
1.7
0±
0.4
7
2.6
9±
0.7
1
4.5
8±
1.5
2
1.8
8±
0.3
7
3.2
3±
0.5
8
4.3
4±
0.8
9
5
2.8
7±
0.5
4
4.2
0±
0.9
0
4.3
7±
0.6
8
2.0
2±
0.4
9
3.3
0±
0.8
5
3.5
1±
0.7
1
1.6
0±
0.2
1
3.4
3±
0.7
5
3.8
6±
0.7
0

34
2.5 Discussion
In this study, we quantified the biaxial mechanical response of the porcine TV
leaflets. The outcomes of our study are useful for quantification of the mechanical
properties of TV leaflets and for developing FE models because such models rely on the
accurate quantification of the tissue mechanical properties [44].
The peak load values used in biaxial stretching were selected based on the
estimation of maximum stresses on the leaflets both for normal physiological right
ventricular pressure (RVP) and for the case of pulmonary hypertension. The reported
maximum RVP is approximately 30 𝑚𝑚 𝐻𝑔 for a normal heart [128], while during
pulmonary hypertension it can reach as high as 80 𝑚𝑚 𝐻𝑔 [129, 130]. Based on different
anatomical measurements we approximated the mean radius of curvature of TV to be
around 2 𝑐𝑚 [131, 132]. Using these numbers along with the law of Laplace, one can
estimate the maximum tension on TV leaflets to be approximately 40 𝑁/𝑚 and 100 𝑁/𝑚
under normal physiological conditions and in the case of pulmonary hypertension,
respectively. In Figs. 2.4a, 2.5a, and 2.6a the maximum physiological level of loading is
determined with the horizontal green dashed line. Therefore, the presented tension-
deformation data can be referred to both for physiological levels and for hypertensive levels
of loading.
The overall trends of the tension–stretch graph showed a highly nonlinear behavior,
as the leaflets were more compliant at the beginning of the loading (i.e. over the toe region)
and then they rapidly became stiff (i.e. transition to the lockout region) both in the radial
and in the circumferential directions. The latter behavior was not observed in the few
mechanical tests conducted on TV previously due to the small level of strains used in such

35
experiments [133]. In all of the specimens tested, the leaflets were stiffer in the
circumferential direction than the radial direction, a phenomenon observed in other cardiac
valves as well [35-39]. As there was no significant difference between the thicknesses of
the anterior and posterior leaflets, even without using any specific material model, one can
conclude from the tension–stretch data that these two leaflets had the same stiffness in the
circumferential direction. The anterior leaflet, however, was much stiffer than the posterior
one in the radial direction, as the anterior leaflet deforms much less under the same loading
conditions. The septal leaflet was more compliant than the other two leaflets in the
circumferential direction, as it showed nearly the same deformation under the same loading
conditions while being significantly thicker (as discussed previously). For the radial
direction, the septal leaflet deformed slightly more in comparison to the anterior leaflet,
and it also was thicker. Therefore, it can also be concluded that the septal leaflet is more
compliant in the radial direction than the anterior leaflet.
36
CHAPTER 3III
QUANTIFICATION OF MATERIAL CONSTANTS FOR A PHENOMENOLOGICAL
CONSTITUTIVE MODEL OF THE TRICUSPID VALVE LEAFLETS
(The content of this chapter was published in JBME (May 2018) as “Quantification of
Material Constants for a Phenomenological Constitutive Model of Porcine Tricuspid
Valve Leaflets for Simulation Applications” [134].)
3.1 Summary
TV is a one-way valve on the pulmonary side of the heart, which prevents backflow
of blood during ventricular contractions. Development of computational models of TV is
important both in understanding the normal valvular function and in the
development/improvement of surgical procedures and medical devices. A key step in the
development of such models is quantification of the mechanical properties of TV leaflets.
In this study, after examining previously measured five-loading-protocol biaxial stress–
strain response of porcine TVs, a phenomenological constitutive framework was chosen to
represent this response. The material constants were quantified for all three leaflets, which
were shown to be highly anisotropic with average anisotropy indices of less than 0.5 (an
anisotropy index value of 1 indicates a perfectly isotropic response, whereas a smaller
value of the anisotropy index indicates an anisotropic response). To obtain mean values of
material constants, stress–strain responses of the leaflet samples were averaged and then
fitted to the constitutive model (average 𝑅𝟐 over 0.9). Since the sample thicknesses were
37
not hugely different, averaging the data using the same tension levels and stress levels
produced similar average material constants for each leaflet.
3.2 Introduction
TV, a one-way valve that opens and closes in response to changes in ventricular
pressure [135], prevents the backflow of blood from the right ventricle to the right atrium
during ventricular systole [1]. The main malfunctions of TV, namely valvular regurgitation
and stenosis, may require surgical interventions such as total valve replacement or valvular
repair [136, 137]. In the United States, approximately 150,000 patients undergo TV
surgeries annually [24, 25, 138]. While TV repair surgeries have better outcomes when
compared to total TV replacement procedures [32-34], the outcomes of TV repair surgeries
are still not completely satisfying, and TV surgery remains one of the most high-risk valve
procedures [120]. To improve existing surgical techniques and develop more successful
valve repair procedures, accurate quantification of the biomechanical properties of native
TV tissues is essential. Such data are necessary both in the development of tissue-
equivalent biomaterials [79] and as input parameters for generating computational models
of healthy and diseased TVs [44, 89, 139]. Despite the need for data on the mechanical
behavior of this valve, TV has been understudied in comparison to the other valves of the
heart [35, 37-39, 42, 43, 67].
Considering the native loading environment of the cardiac valves, we have
previously used biaxial tensile testing to evaluate the stress–strain response of porcine TV
leaflets [117]. In the current study, we utilized a phenomenological constitutive model to
quantify the anisotropic and nonlinear material properties of the porcine TV leaflets. Since
material properties of porcine TV leaflets were not available, previous FE models relied on

38
material properties derived from the mitral and AVs [44], which are expected to be
different from those of TV. In this study, we aimed to provide material constants that can
be used in the development of TV FE models to mimic its deformation in vivo [81] and ex
vivo [140].
3.3 Materials and Methods
3.3.1 Planar Biaxial Tensile Strains and Stresses
The planar biaxial tensile testing procedure and the strain and stress calculations
are presented in detail in our previous publication [117]. Briefly, a total of 30
(11 𝑚𝑚 × 11 𝑚𝑚) square-shaped samples (i.e., one sample per each TV leaflet of ten
porcine hearts) were freshly excised and mounted on the biaxial tensile testing equipment
[40, 41, 79, 117] with the circumferential and radial directions of the leaflets aligned with
stretching axes of the equipment. Five different tension-controlled loading protocols with
a constant tension ratio of 𝑇𝑐: 𝑇𝑟 = 1: 1, 1: 0.75, 0.75: 1, 1: 0.5, 0.5: 1 were then performed
on each specimen with a maximum tension of 100 𝑁/𝑚 as shown in Table 3.1. The strains
and stresses were subsequently calculated from tension–deformation data. More
information about the stress–strain responses are provided in our previous publication
[117].
Table 3.1 The maximum membrane tension of each tension-controlled loading protocol
for circumferential 𝑐 and radial 𝑟 directions. The tension ratios were kept constant during
the experiments: 𝑇𝑐: 𝑇𝑟 = 1: 1, 1: 0.75, 0.75: 1, 1: 0.5, 0.5: 1
Loading protocol no. 𝑇𝑐,𝑚𝑎𝑥 (𝑁 𝑚⁄ ) 𝑇𝑟,𝑚𝑎𝑥 (𝑁 𝑚⁄ )
1 100 100
2 100 75
3 75 100
4 100 50
5 50 100

39
3.3.2 Constitutive Modeling
Similar to the tissue in other cardiac valves, TV leaflet tissue was assumed to be
incompressible, homogenous, and hyperelastic, undergoing finite deformations within the
small specimen region [60]. Hence, following the concept of pseudoelasticity [141], its
mechanical response was expressed using a strain energy function 𝑊 and the components
of the second Piola–Kirchhoff stress tensor 𝑆𝑖𝑗 were evaluated:
𝑆𝑖𝑗 =
𝜕𝑊
𝜕𝐸𝑖𝑗 (3.1)
where 𝐸𝑖𝑗 were the components of the Green strain tensor and 𝑖 and 𝑗 were dummy indices.
To examine the pseudoelastic response of TV leaflets and choose a suitable form
for the strain energy function, all the stress–strain data were independently fitted to the
following response functions for each directional component [56, 142].
𝑆𝑐𝑐 = 𝑐0 (𝑐1𝐸𝑐𝑐 + 𝑐3𝐸𝑟𝑟 + 𝑐4𝐸𝑐𝑐𝐸𝑟𝑟 +1
2𝑐5𝐸𝑟𝑟
2 + 𝑐6𝐸𝑐𝑐𝐸𝑟𝑟2
+ 2𝑐7𝐸𝑐𝑐3 ) 𝑒𝑄
𝑆𝑟𝑟 = 𝑐0 (𝑐2𝐸𝑟𝑟 + 𝑐3𝐸𝑐𝑐 + 𝑐5𝐸𝑐𝑐𝐸𝑟𝑟 +1
2𝑐4𝐸𝑐𝑐
2 + 𝑐6𝐸𝑐𝑐2 𝐸𝑟𝑟
+ 2𝑐8𝐸𝑟𝑟3 ) 𝑒𝑄
(3.2)
where 𝑐𝑐 and 𝑟𝑟 denote the circumferential and radial directions, respectively, and
𝑄 = (𝑐1𝐸𝑐𝑐2 + 𝑐2𝐸𝑟𝑟
2 + 2𝑐3𝐸𝑐𝑐𝐸𝑟𝑟 + 𝑐4𝐸𝑐𝑐2 𝐸𝑟𝑟 + 𝑐5𝐸𝑟𝑟
2 𝐸𝑐𝑐
+ 𝑐6𝐸𝑐𝑐2 𝐸𝑟𝑟
2 + 𝑐7𝐸𝑐𝑐4 + 𝑐8𝐸𝑟𝑟
4 )
(3.3)

40
It is worth noting that the above equations do not describe a constitutive model.
They are merely a set of response functions that were utilized to interpolate the stress
components over the entire strain field.
Specific forms of the resulting stress surfaces were carefully examined, and an
anisotropic Fung-type strain energy function was subsequently chosen [53, 142]. As shear
stresses were negligible [117], the strain energy function 𝑊 was expressed as:
𝑊 = 𝑐
2(𝑒𝑎1𝐸𝑐𝑐
2 +𝑎2𝐸𝑟𝑟2 +2𝑎3𝐸𝑐𝑐𝐸𝑟𝑟 − 1) (3.4)
where 𝑐 and 𝑎𝑖 were the material constants and 𝐸𝑐𝑐 and 𝐸𝑟𝑟 were the components of the
Green strain tensor in the circumferential and radial directions, respectively. To calculate
the material constants, the measured biaxial stress–strain data for each specimen were fitted
to this model using a custom MATLAB code (MathWorks, Natick, MA) and the Trust-
Region-Reflective algorithm [143]. An anisotropy index 𝐴𝐼 was also calculated [58]:
𝐴𝐼 = 𝑚𝑖𝑛 (
𝑎1 + 𝑎3
𝑎2 + 𝑎3,𝑎2 + 𝑎3
𝑎1 + 𝑎3) (3.5)
3.3.3 Average Models
An important outcome of accurate constitutive modeling of soft tissues is the
application of the resultant material constants in generating computational simulations of
tissue deformation. One approach in performing such simulations is to use sets of
specimen-specific material constants. However, introducing a set of material constants to
represent the generic (average) tissue mechanical behavior could be also beneficial. In such
a case, one could perform parametric studies to identify how each parameter (both material
and geometric parameters) influence the simulation outcomes [144-147].

41
For linear elastic materials, the moduli of elasticity can be calculated by evaluating
the individual specimen-specific moduli of elasticity and then finding the average moduli
by calculating the arithmetic mean. In our study, however, a simple arithmetic mean of the
constitutive model material constants cannot accurately characterize the cumulative
behavior of the tissue due to the nonlinearity of the mechanical behavior and the resultant
choice of a nonlinear constitutive model. As described by other investigators [58, 64], one
way to resolve this issue is to first generate an average curve for each protocol by
calculating the arithmetic mean of experimentally measured strain values for all specimens.
Next, we can fit these average curves into the proposed model to calculate the generic
material constants. Averaging the strains is only appropriate over similar stress (or tension)
states. Our biaxial testing device was set up in such way that the shear components of the
stress tensors were considered to be negligible. As such, in our experiment, a similar stress
(or tension) state simply means that the normal stress (or tension) at each direction must be
equal among all samples being used in the averaging of the strains. Consistent with the
approach of other investigators [58, 64], we used tension control protocols in our
experiments. In the following sections, the procedures for calculating the average values
for similar tension states and similar stress states are described.
Average model development using tension. As our experiments were conducted
using tension-controlled protocol, having a similar tension state was guaranteed for similar
protocols of different samples. In our experiment, duration of the deformation was identical
for each specimen, and the strain data were collected at a similar time interval in all cases.
Although we had a high frequency for collecting the data, strain data were not necessarily
available for each specific tension value. As such, a procedure to approximate the strain
42
data at any specific tension value was necessary. Prior to our study, other investigators had
employed exponential functions to fit each tension–strain curve independently [58, 64] and
used that expression to interpolate the data. The exponential fit, however, cannot efficiently
predict the tension–strain response in cases where the Poisson’s effect induces a drift in the
tension–strain curves. In such cases, discrete mathematical functions are simply unable to
accurately fit the data since (due to the Poisson’s effect) more than one tension value may
exist for a single strain value. To overcome this hurdle in our study, we calculate the strains
at desired tension values by linearly interpolating the original data. As we had performed
our experiments with a relatively high frequency of data collection, we were able to capture
the Poisson’s effect in our estimated values of strains at each specified tension value. In
addition, more accurate estimations of strains—particularly at the lower strain regions—
were obtained in comparison to the exponential fits. The advantages of using the linear
interpolation over the exponential fit in this application is illustrated in Fig. 3.1. As shown
in this picture, the linear interpolation follows the original data accurately while the
exponential fit extremely deviates.
The specified tension values for each protocol were chosen as the average tension
𝑇𝑎𝑣𝑔,𝑖𝑖. For each protocol, the approximated strain values were averaged over the samples
to compute the average strain 𝐸𝑎𝑣𝑔,𝑖𝑖. The subscript 𝑖𝑖 refers to the circumferential 𝑐𝑐 and
radial 𝑟𝑟 directions.

43
Fig. 3.1 Comparison between the accuracy of linear interpolation and exponential fit to
estimate the original data for averaging.
Next, the following equation was used to estimate the normal components of the
average first Piola–Kirchhoff stress tensor 𝑃𝑎𝑣𝑔,𝑖𝑖 [58].
𝑃𝑎𝑣𝑔,𝑖𝑖 =
𝑇𝑎𝑣𝑔,𝑖𝑖
𝑛∑
1
ℎ𝑖
𝑛
𝑖=1
(3.6)
where ℎ𝑖 are the individual leaflet thicknesses and 𝑛 is number of specimens. The diagonal
components of the average deformation gradient tensor 𝐹𝑎𝑣𝑔,𝑖𝑖 were approximated using
the following equation, with the assumption of negligible shear deformations:
𝐹𝑎𝑣𝑔,𝑖𝑖 = √2𝐸𝑎𝑣𝑔,𝑖𝑖 + 1 (3.7)
The normal components of the average first Piola–Kirchhoff stress tensor 𝑃𝑎𝑣𝑔,𝑖𝑖
and deformation gradient tensor 𝐹𝑎𝑣𝑔,𝑖𝑖 were used to assemble their corresponding tensor

44
with the assumption of zero off-diagonal components. These tensors were then used to
calculate the average second Piola–Kirchhoff stress tensor:
𝑺𝑎𝑣𝑔 = 𝑷𝑎𝑣𝑔. 𝑭𝑎𝑣𝑔−𝑇 (3.8)
Finally, to calculate the average material constants, the 𝑺𝑎𝑣𝑔 − 𝑬𝑎𝑣𝑔 data were
fitted into the proposed constitutive model.
Average model development using the first Piola–Kirchhoff stress. The response of
valvular tissues to tension depends on the thickness of the leaflet specimens. As the
thickness of leaflets varies from one specimen to another, in theory, the average model
developed based on the equal tension values could be erroneous. Although this error might
seem to be trivial, in practice, due to the small variations of the thicknesses and
experimental convenience, biaxial testing of the valves has been generally conducted in a
tension-controlled manner [36, 38, 58, 59, 148]. To evaluate the potential errors in using
equal-tension values in the averaging process, we performed a second averaging procedure,
this time based on the first Piola–Kirchhoff stress values. Since for each protocol the ratio
of the tension in the radial direction over the tension in the circumferential direction was
kept constant, after calculating the first Piola–Kirchhoff stresses (by dividing tension over
the individual leaflet thicknesses), we were able to obtain the similar stress states necessary
for the averaging process. While the stress ratios were constant for all specimens for each
protocol, dividing the tensions by the specimen thicknesses resulted in different maximum
values of first Piola–Kirchhoff stresses. As such, it was necessary to truncate the data to
the point where there existed experimental data for all samples. This process led to the loss
of data at the high-tension values for some specimens.

45
Averaging was accomplished by linearly interpolating the first Piola–Kirchhoff
stresses and averaging the strains similar to the method explained above. In particular, for
each protocol, the first Piola–Kirchhoff stress components 𝑃𝑎𝑣𝑔,𝑖𝑖 were directly specified
from the experimental data with the necessary linear interpolation. For each specified stress
value, the strains were averaged over all the samples to obtain the components of average
Green strains 𝐸𝑎𝑣𝑔,𝑖𝑖. As before, the subscript 𝑖𝑖 indicates the circumferential 𝑐𝑐 or radial 𝑟𝑟
direction. Subsequently, Equation (3.7) was used to approximate the average deformation
gradient tensor diagonal components 𝐹𝑎𝑣𝑔,𝑖𝑖. Finally, the average second Piola–Kirchhoff
stress tensor 𝑺𝑎𝑣𝑔 was calculated using Equation (3.8).
Average model development using the predefined constitutive model and Cauchy
stress. As the Cauchy stress is the true stress borne by the tissue during the loading process,
it is probably the best candidate upon which the averaging procedure should be built. Since
the experiments were conducted in a tension-controlled manner, similar Cauchy stress
states were not directly available. Therefore, similar stress states were reconstructed by
choosing (sampling) a set of five-protocol Cauchy stress loadings and evaluating their
corresponding strains using the material constants obtained from the specimen-specific
constitutive modeling. Here, the desired data needed for averaging method based on
Cauchy stress were chosen a priori. Consequently, we used these chosen values as the
components of average Cauchy stress 𝜎𝑎𝑣𝑔,𝑖𝑖 and averaged the calculated strains over all
samples to compute the components of average Green strain 𝐸𝑎𝑣𝑔,𝑖𝑖 for each protocol.
Then, using Equation (3.7), we calculated the components of the deformation gradient
tensor 𝐹𝑎𝑣𝑔,𝑖𝑖. Finally, with the assumption of negligible shear stress and deformation, we
46
assembled the Cauchy stress tensor and deformation gradient tensor and used them to
calculate the average second Piola–Kirchhoff stress tensor:
𝑺𝑎𝑣𝑔 = 𝐽. 𝑭𝑎𝑣𝑔−1 . 𝝈𝑎𝑣𝑔. 𝑭𝑎𝑣𝑔
−𝑇 (3.9)
where 𝐽 is the determinant of 𝑭 which is equal to 1, as the valvular tissue was considered
to be incompressible.
3.4 Results
Detailed explanation of the biaxial mechanical responses of TV leaflets and the
tension–deformation data are presented in our previous publication [117]. Briefly, all three
leaflets responded in an anisotropic manner. Similar to tissues in other cardiac valves, TV
leaflets were more compliant at lower strain values but became stiffer when the strain
increased.
3.4.1 Stress Response Functions
The stress–strain data were fitted to the response functions described in Equation
(3.2) independently for each directional component. The 𝑅𝟐 (mean ± standard deviation)
for these fitted curves were 0.92 ± .06, 0.93 ± .09, and 0.93 ± .07 for the anterior,
posterior, and septal leaflets, respectively. The resulting fitting parameters were used to
plot the constant stress contours over the strain field. As shown in Fig. 3.2, for typical (i.e.,
randomly selected) anterior, posterior, and septal leaflets, the contours were asymmetric
around the 𝐸𝑐𝑐 = 𝐸𝑟𝑟 line for nearly all samples. In a perfectly isotropic material, the
response should be symmetric with respect to this line. Therefore, it was further confirmed
that the mechanical responses were anisotropic for all three leaflets as had been visually
inferred in our previous investigations [117]. The rapid increase in the stress values versus

47
the strains, along with the assumption of negligibility of shear stresses and the anisotropic
nature of the responses observed here, justified the choice of our Fung-type
phenomenological model [53] as well as the specific strain energy function 𝑊 defined in
Equation (3.4).
Fig. 3.2 The constant stress contours produced using the response functions of Equation
(2.2) plotted over the strain field for typical leaflets: (a,b) anterior, (c,d) posterior, and (e,f)
septal leaflets.
3.4.2 Constitutive Modeling Results
All five protocols of the biaxial stress–strain (second Piola–Kirchhoff stress versus
Green strain) data were simultaneously fitted to the Fung-type constitutive model of
Equation (3.4). As shown in Fig. 3.3 for typical anterior, posterior, and septal leaflets, the
results showed a reasonably accurate fit with the average 𝑅𝟐 (mean ± standard deviation)
of 0.92 ± 0.05, 0.89 ± 0.10, and 0.89 ± 0.10 for the anterior, posterior, and septal

48
leaflets, respectively. The material constants resulting from the specimen-specific fitting
method are shown in Table 3.2. The 𝑅2 as well as the anisotropy index 𝐴𝐼 are also presented
in Table 3.2 for each fit. An anisotropy index value of 1 indicates a perfectly isotropic
response, whereas a smaller value of 𝐴𝐼 indicates an anisotropic response [58]. As shown
in Table 3.2, the anisotropy index ranged from 0.22 to 1.00, from 0.09 to 0.58, and from
0.21 to 1.00, for the anterior, posterior, and septal leaflets, respectively.

49
Fig. 3.3 The result of the five-protocol fit along with the experimentally measured
circumferential (Circ) and radial data for typical leaflets: (a) anterior, (b) posterior, and (c)
septal. The numbers represent the protocol numbers listed in Table 3.1.
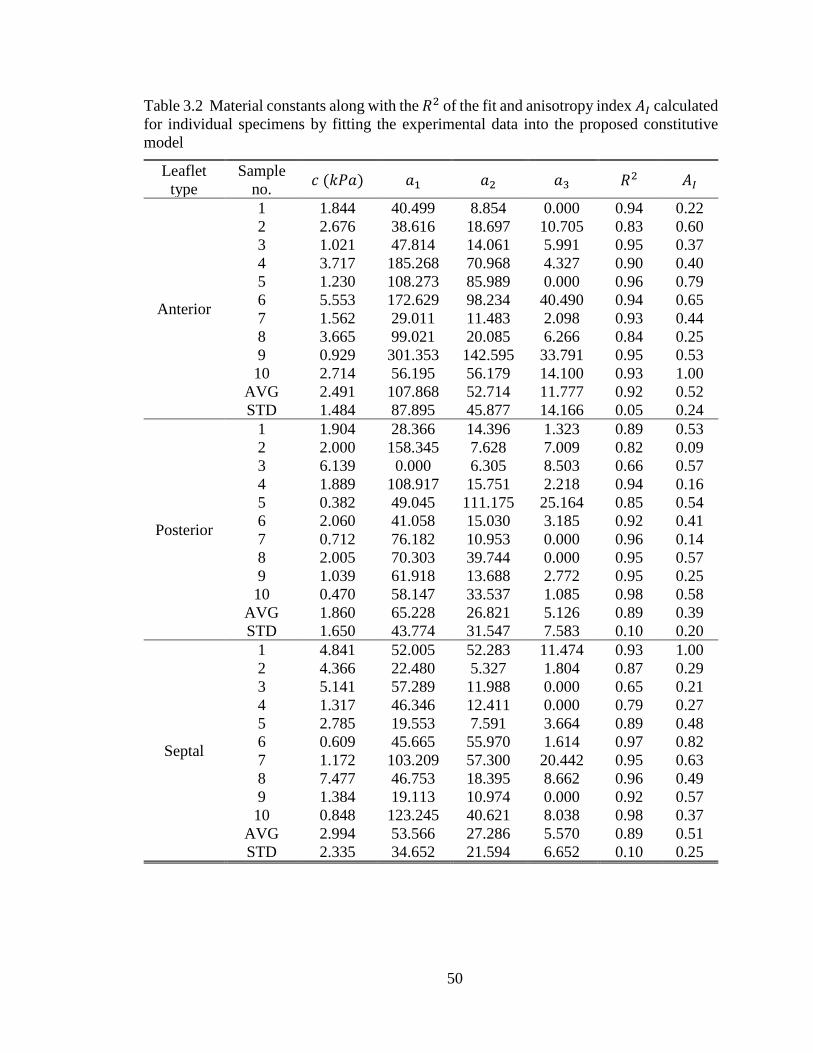
50
Table 3.2 Material constants along with the 𝑅2 of the fit and anisotropy index 𝐴𝐼 calculated
for individual specimens by fitting the experimental data into the proposed constitutive
model
Leaflet
type
Sample
no. 𝑐 (𝑘𝑃𝑎) 𝑎1 𝑎2 𝑎3 𝑅2 𝐴𝐼
Anterior
1 1.844 40.499 8.854 0.000 0.94 0.22
2 2.676 38.616 18.697 10.705 0.83 0.60
3 1.021 47.814 14.061 5.991 0.95 0.37
4 3.717 185.268 70.968 4.327 0.90 0.40
5 1.230 108.273 85.989 0.000 0.96 0.79
6 5.553 172.629 98.234 40.490 0.94 0.65
7 1.562 29.011 11.483 2.098 0.93 0.44
8 3.665 99.021 20.085 6.266 0.84 0.25
9 0.929 301.353 142.595 33.791 0.95 0.53
10 2.714 56.195 56.179 14.100 0.93 1.00
AVG 2.491 107.868 52.714 11.777 0.92 0.52
STD 1.484 87.895 45.877 14.166 0.05 0.24
Posterior
1 1.904 28.366 14.396 1.323 0.89 0.53
2 2.000 158.345 7.628 7.009 0.82 0.09
3 6.139 0.000 6.305 8.503 0.66 0.57
4 1.889 108.917 15.751 2.218 0.94 0.16
5 0.382 49.045 111.175 25.164 0.85 0.54
6 2.060 41.058 15.030 3.185 0.92 0.41
7 0.712 76.182 10.953 0.000 0.96 0.14
8 2.005 70.303 39.744 0.000 0.95 0.57
9 1.039 61.918 13.688 2.772 0.95 0.25
10 0.470 58.147 33.537 1.085 0.98 0.58
AVG 1.860 65.228 26.821 5.126 0.89 0.39
STD 1.650 43.774 31.547 7.583 0.10 0.20
Septal
1 4.841 52.005 52.283 11.474 0.93 1.00
2 4.366 22.480 5.327 1.804 0.87 0.29
3 5.141 57.289 11.988 0.000 0.65 0.21
4 1.317 46.346 12.411 0.000 0.79 0.27
5 2.785 19.553 7.591 3.664 0.89 0.48
6 0.609 45.665 55.970 1.614 0.97 0.82
7 1.172 103.209 57.300 20.442 0.95 0.63
8 7.477 46.753 18.395 8.662 0.96 0.49
9 1.384 19.113 10.974 0.000 0.92 0.57
10 0.848 123.245 40.621 8.038 0.98 0.37
AVG 2.994 53.566 27.286 5.570 0.89 0.51
STD 2.335 34.652 21.594 6.652 0.10 0.25

51
3.4.3 Average Modeling Results
The average stress–strain (second Piola–Kirchhoff stress versus Green strain)
responses developed for the anterior leaflet based on identical tension states are shown in
Fig. 3.4. This figure shows that the same ratio of tension in the radial and circumferential
directions (listed in Table 3.1) does not exist for the second Piola–Kirchhoff stresses. For
example, the tension-controlled equibiaxial protocol does not produce an equibiaxial
second Piola–Kirchhoff stress state. Figures 3.5 and 3.6 show similar graphs for the
average stress–strain responses developed based on identical first Piola–Kirchhoff stress
states and identical Cauchy stress states for the anterior leaflet. Similar graphs for the
posterior and septal leaflets are provided in APPENDIX A.
For each set of average response curves, the proposed phenomenological
constitutive model was also utilized to develop the average material model and calculate
the average material constants for each leaflet type. Table 3.3 shows the material constants
computed for the average response curves developed based on identical tensions along with
the 𝑅2 of the fit and the anisotropy index 𝐴𝐼. The data fitted the model with 𝑅2 of 0.85,
0.95, and 0.94 for anterior, posterior, and septal leaflets, respectively. Tables 3.4 and 3.5
show the same quantities obtained after fitting the average response curves developed
based on identical first Piola–Kirchhoff stresses and Cauchy stresses into the proposed
constitutive model. As expected, the values for the material constants are different from
the arithmetic average of the constants calculated for the individual specimens, as listed in
Table 3.2.

52
Fig. 3.4 The average stress–strain responses developed based on identical tension states
from loading protocols (a) number 1 (equibiaxial), (b) number 2, (c) number 3, (d) number
4, and (e) number 5 of Table 3.1 for the anterior leaflet. The vertical axis is the second
Piola–Kirchhoff stress, and the horizontal axis is the Green strain. These data were used to
calculate the average material constants presented in Table 3.3.

53
Fig. 3.5 The average stress–strain responses developed based on identical first Piola–Kirchhoff stress states from loading protocols (a) number 1 (equibiaxial), (b) number 2, (c)
number 3, (d) number 4, and (e) number 5 of Table 3.1 for the anterior leaflet. The vertical
axis is the second Piola–Kirchhoff stress, and the horizontal axis is the Green strain. These
data were used to calculate the average material constants presented in Table 3.4.

54
Fig. 3.6 The average stress–strain responses developed based on identical Cauchy stress
states from loading protocols (a) number 1 (equibiaxial), (b) number 2, (c) number 3, (d)
number 4, and (e) number 5 of Table 3.1 for the anterior leaflet. The vertical axis is the
second Piola–Kirchhoff stress, and the horizontal axis is the Green strain. These data were
used to calculate the average material constants presented in Table 3.5.

55
Table 3.3 Material constants for the tension-based average model data (AVG) as well as
the average data minus one standard error (AVG – SE) and average data plus one standard
error (AVG + SE). The corresponding 𝑅2 value of the fit and the anisotropy index 𝐴𝐼 are
also presented.
Leaflet type Data type 𝑐 (𝑘𝑃𝑎) 𝑎1 𝑎2 𝑎3 𝑅2 𝐴𝐼
Anterior
AVG - SE 4.137 74.935 31.156 8.438 0.86 0.47
AVG 3.702 60.171 23.129 5.098 0.85 0.43
AVG + SE 3.439 49.372 17.875 3.201 0.85 0.40
Posterior
AVG - SE 0.933 80.526 24.339 4.368 0.95 0.34
AVG 0.946 63.831 18.940 3.279 0.95 0.33
AVG + SE 0.980 51.610 15.099 2.557 0.97 0.33
Septal
AVG - SE 1.980 55.638 23.449 7.281 0.95 0.49
AVG 2.135 45.504 17.610 3.335 0.94 0.43
AVG + SE 2.498 36.945 13.462 1.141 0.91 0.38
Table 3.4 Material constants for the first Piola–Kirchhoff-stress–based average model data
(AVG) as well as the average data minus one standard error (AVG – SE) and average data
plus one standard error (AVG + SE). The corresponding 𝑅2 value of the fit and the
anisotropy index 𝐴𝐼 are also presented.
Leaflet type Data type 𝑐 (𝑘𝑃𝑎) 𝑎1 𝑎2 𝑎3 𝑅2 𝐴𝐼
Anterior
AVG - SE 3.257 78.060 33.025 8.946 0.88 0.48
AVG 2.943 62.608 24.443 5.395 0.87 0.44
AVG + SE 2.758 51.329 18.847 3.379 0.87 0.41
Posterior
AVG - SE 0.780 85.602 25.542 4.152 0.95 0.33
AVG 0.802 67.054 19.926 3.207 0.95 0.33
AVG + SE 0.842 53.680 15.911 2.567 0.96 0.33
Septal
AVG - SE 1.712 57.094 24.531 7.916 0.96 0.50
AVG 1.876 46.460 18.253 3.646 0.94 0.44
AVG + SE 2.234 37.476 13.842 1.296 0.91 0.39
Table 3.5 Material constants for the Cauchy-stress–based average model data. The
corresponding 𝑅2 value of the fit and the anisotropy index 𝐴𝐼 are also presented in the
table.
Leaflet type 𝑐 (𝑘𝑃𝑎) 𝑎1 𝑎2 𝑎3 𝑅2 𝐴𝐼
Anterior 1.961 70.589 27.856 6.473 1.00 0.45
Posterior 1.248 57.783 17.877 1.795 1.00 0.33
Septal 2.321 40.420 16.784 2.954 1.00 0.46
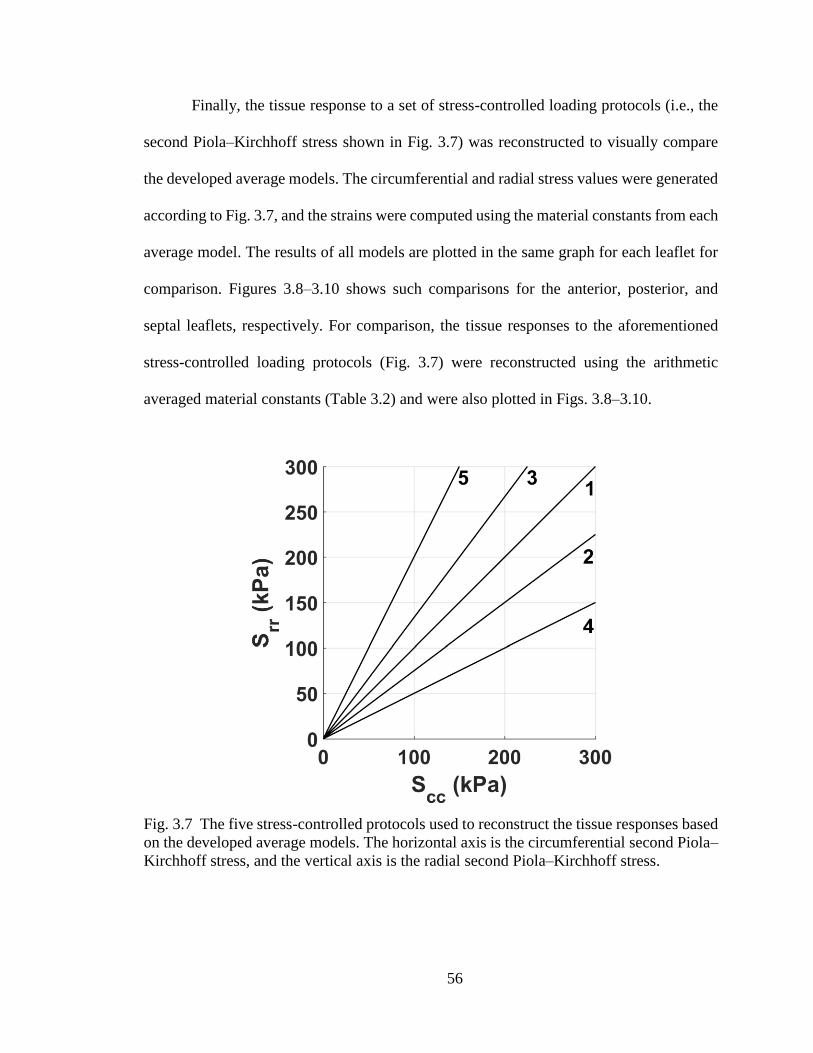
56
Finally, the tissue response to a set of stress-controlled loading protocols (i.e., the
second Piola–Kirchhoff stress shown in Fig. 3.7) was reconstructed to visually compare
the developed average models. The circumferential and radial stress values were generated
according to Fig. 3.7, and the strains were computed using the material constants from each
average model. The results of all models are plotted in the same graph for each leaflet for
comparison. Figures 3.8–3.10 shows such comparisons for the anterior, posterior, and
septal leaflets, respectively. For comparison, the tissue responses to the aforementioned
stress-controlled loading protocols (Fig. 3.7) were reconstructed using the arithmetic
averaged material constants (Table 3.2) and were also plotted in Figs. 3.8–3.10.
Fig. 3.7 The five stress-controlled protocols used to reconstruct the tissue responses based
on the developed average models. The horizontal axis is the circumferential second Piola–
Kirchhoff stress, and the vertical axis is the radial second Piola–Kirchhoff stress.

57
Fig. 3.8 Tissue response of the anterior leaflet to five stress-controlled loading protocols
(Fig. 3.7) reconstructed using the material constants of the arithmetic average (A-B) from
Table 3.2, the tension-based average model (T-B) from Table 3.3, the first Piola–Kirchhoff-stress–based average model (P-B) from Table 3.4, and the Cauchy-stress–based average
model (C-B) from Table 3.5. The vertical axis is the second Piola–Kirchhoff stress, and
the horizontal axis is the Green strain. The subscripts 𝑐𝑐 and 𝑟𝑟 denote the circumferential
and radial directions, respectively.

58
Fig. 3.9 Tissue response of the posterior leaflet to five stress-controlled loading protocols
(Fig. 3.7) reconstructed using the material constants of the arithmetic average (A-B) from
Table 3.2, the tension based average model (T-B) from Table 3.3, the first Piola–Kirchhoff-stress–based average model (P-B) from Table 3.4, and the Cauchy-stress–based average
model (C-B) from Table 3.5. The vertical axis is the second Piola–Kirchhoff stress, and
the horizontal axis is the Green strain. The subscripts 𝑐𝑐 and 𝑟𝑟 denote the circumferential
and radial directions, respectively.

59
Fig. 3.10 Tissue response of the septal leaflet to five stress-controlled loading protocols
(Fig. 3.7) reconstructed using the material constants of the arithmetic average (A-B) from
Table 3.2, the tension based average model (T-B) from Table 3.3, the first Piola–Kirchhoff-stress–based average model (P-B) from Table 3.4, and the Cauchy-stress–based average
model (C-B) from Table 3.5. The vertical axis is the second Piola–Kirchhoff stress, and
the horizontal axis is the Green strain. The subscripts 𝑐𝑐 and 𝑟𝑟 denote the circumferential
and radial directions, respectively.
3.5 Discussion
3.5.1 Constitutive Model
The constant stress contour plots (Fig. 3.2) led us to choose a Fung-type strain
energy function as our phenomenological constitutive framework. As listed in Table 3.2,
the selected constitutive model fitted the data reasonably well for all samples. The only
exception was a posterior leaflet, listed as heart number 3 in Table 3.2. For this specific
sample, the constant 𝑎1 vanished when fitting was performed with positive-constant
constraints (𝑅2 = 0.66) [149]. Even without enforcement of positive-constant constraints,
the value of 𝑎1 did not change, and the quality of fitting did not improve (𝑅2 = 0.66). In
addition, an 𝑎1 of zero is physically impossible, as it implies that there exists no direct

60
relation between deformation and the stress state in the circumferential direction. As such,
the data for this posterior leaflet, listed as Sample 3 in Table 3.2, were eliminated in the
average models. For a small number of other samples, the constant 𝑎3 vanished when the
positive constant constraints were imposed (Table 3.2). Such results indicated that in these
specific samples, the product of strains in both directions did not influence the calculated
stress values.
To evaluate how effective the model was in predicting the response of the tissue,
we first fitted protocols 1, 2, 4, and 5 (listed in Table 3.1) to the proposed constitutive
model. We then used the parameters obtained from the model to predict the response of the
model to protocol 3 (listed in Table 3.1). The 𝑅2 values for the fitting process were 0.915,
0.893, and 0.886 for the anterior, posterior, and septal leaflets, respectively. The 𝑅2 values
for the comparison between the model prediction and experimentally measured data (i.e.,
protocol 3) were 0.936, 0.875, and 0.907 for the anterior, posterior, and septal leaflets,
respectively. The 𝑅2 values for the prediction of the experimental data were all close to
1.0. Such proximity to 1.0 indicated that parameters obtained from fitting a large portion
of the strain energy space to the constitutive model were reliable for predicting the regions
of the strain energy space not included in the parameter fitting process. After the ability of
the model to predict the tissue response was confirmed, all five-protocol were used in the
fitting process as described in the method section.
The average anisotropy indices were 0.52, 0.39, and 0.51 for anterior, posterior,
and septal leaflets, respectively (Table 3.2). The anisotropy indices were much smaller than
1, confirming that, similar to other cardiac valves, TV leaflet tissue response was
anisotropic [38, 42, 60, 67, 148]. As shown in Fig. 3.11, quantitative analysis of tissue

61
microstructure using small angle light scattering [77, 86, 150-152] confirmed that the main
direction of the extracellular matrix fibers was along the circumferential direction, and TV
leaflets were thus expected to be anisotropic. The porcine leaflets were qualitatively similar
to human tissues, as all three leaflets were stiffer in the circumferential direction in
comparison to the radial direction for both species [42]. The average anisotropy index of
the posterior leaflet was slightly smaller than the other two leaflets; however, the difference
was not significant (𝑝 ≈ 0.1 for both comparisons, Student t-test).
In FE analysis, using a convex strain energy function in the material model is
crucial for the stability of the numerical methods [153]. Hence, supplementary inspections
were performed to validate the integrity of the developed phenomenological constitutive
models by plotting the constant strain energy contours over the strain field using the
calculated material constants. As illustrated in Fig. 3.12, the strain energy contours for
typical TV leaflets were convex in all cases, which further confirmed the reliability of the
developed individual models. The only exception, as initially suspected, was the posterior
leaflet of the sample listed as Sample 3 in Table 3.2. In this specific case, the strain energy
was nonconvex (Fig. 3.13). As such, in future development of FE models of TV, using the
material constants of this specific sample is not recommended. Using similar methods, we
observed that the strain energy functions for the average models were all convex.
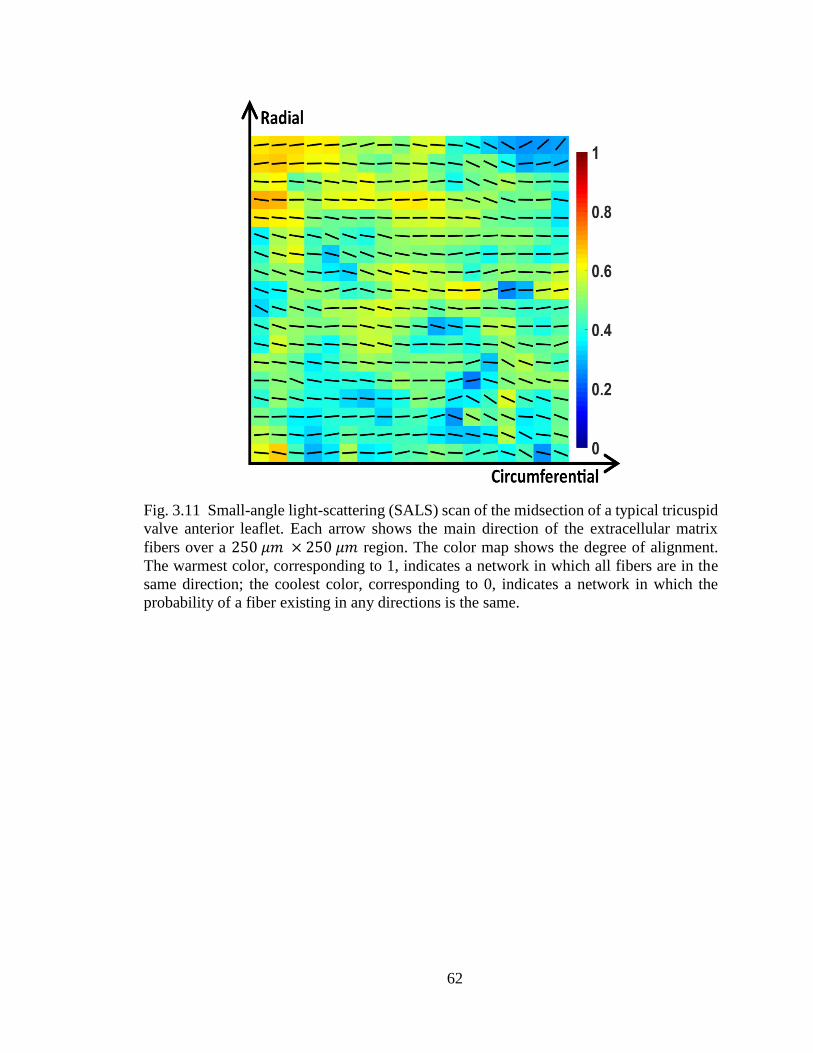
62
Fig. 3.11 Small-angle light-scattering (SALS) scan of the midsection of a typical tricuspid
valve anterior leaflet. Each arrow shows the main direction of the extracellular matrix
fibers over a 250 𝜇𝑚 × 250 𝜇𝑚 region. The color map shows the degree of alignment.
The warmest color, corresponding to 1, indicates a network in which all fibers are in the
same direction; the coolest color, corresponding to 0, indicates a network in which the
probability of a fiber existing in any directions is the same.

63
Fig. 3.12 Constant strain energy contours plotted over the Green strain field for the (a)
anterior, (b) posterior, and (c) septal leaflets of a typical tricuspid valve.
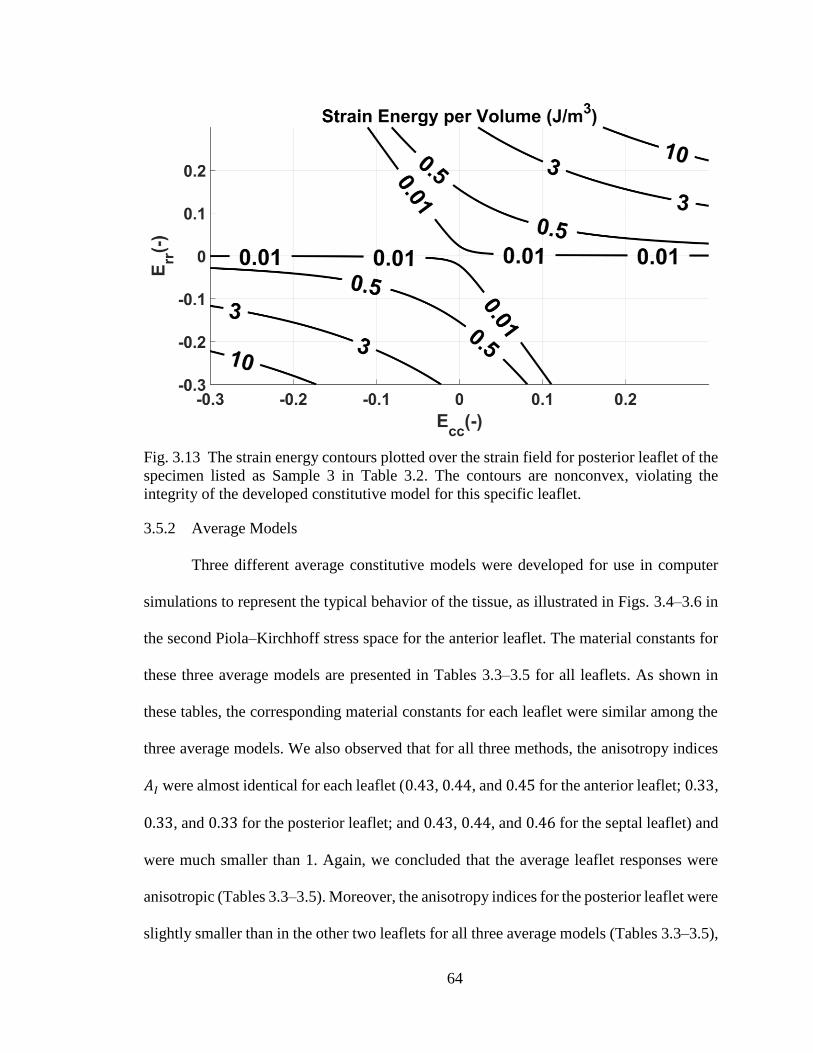
64
Fig. 3.13 The strain energy contours plotted over the strain field for posterior leaflet of the
specimen listed as Sample 3 in Table 3.2. The contours are nonconvex, violating the
integrity of the developed constitutive model for this specific leaflet.
3.5.2 Average Models
Three different average constitutive models were developed for use in computer
simulations to represent the typical behavior of the tissue, as illustrated in Figs. 3.4–3.6 in
the second Piola–Kirchhoff stress space for the anterior leaflet. The material constants for
these three average models are presented in Tables 3.3–3.5 for all leaflets. As shown in
these tables, the corresponding material constants for each leaflet were similar among the
three average models. We also observed that for all three methods, the anisotropy indices
𝐴𝐼 were almost identical for each leaflet (0.43, 0.44, and 0.45 for the anterior leaflet; 0.33,
0.33, and 0.33 for the posterior leaflet; and 0.43, 0.44, and 0.46 for the septal leaflet) and
were much smaller than 1. Again, we concluded that the average leaflet responses were
anisotropic (Tables 3.3–3.5). Moreover, the anisotropy indices for the posterior leaflet were
slightly smaller than in the other two leaflets for all three average models (Tables 3.3–3.5),

65
as were the arithmetic averages (Table 3.2). As shown in Figs. 3.8–3.10, the responses for
the three developed average models were highly similar. One reason for the similarity
could be the small variations in thickness of the different specimens for each leaflet. Had
the tissue thicknesses varied dramatically among the samples, one would have expected
that the average values obtained from the same tension states (thickness-dependent) to be
different from those obtained from same states of first Piola–Kirckhoff stress (thickness-
independent). Our analysis confirmed the fidelity of the tension-controlled biaxial testing
loading protocols and the subsequent averaging procedure in the tension space [36, 38, 58,
59, 148] when there are only small variations in the thickness of the specimens. It is,
however, more reasonable to avoid potential error in future investigations by performing
stress-controlled tests, especially when the tissue thickness varies significantly between the
specimens.
Figures 3.8–3.10 also show the arithmetically averaged material constant
responses. Based on these figures, while the responses of the three models for averaging
the experimental data (i.e., tension-based, first-Piola-Kirchhoff-stess–based, and Cauchy-
stress–based approaches), were notably similar, the responses generated from
arithmetically averaging the material constants were different, especially in the radial
direction. Such differences and similarities can be further investigated by comparing the
material constants for average models from Tables 3.3 and 3.4 with the arithmetic average
of the material constants of the individual fits from Table 3.2. For example, As shown in
these tables for septal leaflet, 𝑐 ranged from 1.876 to 2.321 𝑘𝑃𝑎, 𝑎1 ranged from 40.420
to 46.460, 𝑎2 ranged from 16.784 to 18.253, and 𝑎3 ranged from 2.954 to 3.646 for the
average models, wheras the arithmetically averaged values 𝑐, 𝑎1, 𝑎2, and 𝑎3 for the same

66
leaflet were 2.994 𝑘𝑃𝑎, 53.566, 27.286, and 5.570, respectively. The arithmetically
averaged material constants are all outside of the range of average model material
constants, consistent with our conclusion regarding Figs. 3.8–3.10.
Since stress is a tensor, the large difference between the values, even if it is only in
the radial direction, indicates a completely altered state of stress. This observation further
exemplifies that the arithmetically averaged values of the individual material constants may
not represent the generic tissue responses accurately.
3.5.3 Limitations
While phenomenological constitutive models are powerful in predicting the
responses of the tissue, they do not provide much insight about the mechanical environment
at the underlying extracellular matrix/cellular levels. In other words, model parameters
cannot be quantitatively related to structural components of the tissue, such as extracellular
matrix protein volume fractions or extracellular matrix morphology. Such information is
of particular interest in the field of mechanobiology, for which constitutive frameworks
that include structural components of the tissue are more relevant [66-70]. Another
limitation pertains to the use of porcine tissues. Although many of the conclusions of this
study (e.g. the choice of the averaging method) seemed to be independent of the species,
caution should always be taken when drawing conclusions for human subjects based on
animal studies. Another limitation is that all of the experiments in were conducted at room
temperature, and the response of the tissue might be different at body temperature. Finally,
previous studies have shown that in vivo residual strains are present in ovine MV leaflets,
and they relax after dissection [26]. If such a phenomenon does exist for TV, any change
67
in the deformation should be taken into consideration in the development of future
computational models.
3.6 Conclusion
We used results from biaxial mechanical testing and obtained material constants
for a Fung-type phenomenological model to predict the mechanical response of the porcine
TV leaflet. Similar to other cardiac valves, we observed that TV leaflets were highly
anisotropic. We also conducted a series of studies to identify the most appropriate method
for finding representative material parameters for TV leaflets. Since the thicknesses did not
differ significantly in our sample groups, we found that both tension-based and stress-based
averaging methods provided acceptable outcomes. However, to prevent potential errors
when sample thickness varies more considerably, it is recommended to employ the stress-
based averaging method.

68
CHAPTER 4IV
DYNAMIC DEFORMATIONS AND SURFACE STRAINS OF THE TRICUSPID
VALVE LEAFLETS
(The content of this chapter was published in JBME (Oct 2016) as “Surface Strains of
Porcine Tricuspid Valve Septal Leaflets Measured in Ex Vivo Beating Hearts” [140].)
4.1 Summary
Quantification of TV leaflets mechanical strain is important in order to understand
valve pathophysiology and to develop effective treatment strategies. Many of the
traditional methods used to dynamically open and close the cardiac valves in vitro via flow
simulators require valve dissection. Recent studies, however, have shown that restriction
of the atrioventricular valve annuli could significantly change their in-vivo deformation.
For the first time, the porcine valve leaflets deformation was measured in a passive ex-vivo
beating heart without isolating and remounting the valve annuli. In particular, the right
ventricular apexes of porcine hearts (n = 8) were connected to a pulse-duplicator pump that
maintained a pulsatile flow from and to a reservoir connected to the right atrium and the
pulmonary arteries. This pump provided an RVP waveform that closely matched
physiological values. The pressure environment caused the tricuspid and PVs to open/close
similar to that in vivo. At the mid-section of the valve leaflets, the peak areal strain was 9.8
± 2.0% (mean ± standard error). The peak strain was 5.6 ± 1.1% and 4.3 ± 1.0% in the
circumferential and radial directions, respectively. Although the right ventricle was beating
passively, the leaflet peak areal strains closely matched the values measured in other

69
atrioventricular valves (i.e., MV) in vivo. This technique can be used to measure leaflet
strains with and without the presence of valve lesions to help develop/evaluate treatment
strategies to restore normal valve deformation.
4.2 Introduction
As a one-way valve, TV guides the blood from the right atrium to the right ventricle
during the atrial systole and prevents its backflow during the ventricular systole [1]. During
the process of valve closure, its leaflets undergo complicated dynamic deformation and
loadings. Quantification of such dynamic deformations is important because the
development of treatment strategies for TV dysfunctions relies on a comprehensive
understanding of its normal biomechanical environment. Among TV dysfunctions, TV
regurgitation is one of the most common ones, which in most cases requires TV repair or
total valve replacement [24, 25]. The pathophysiology of TV regurgitation is closely
related to the dynamic deformation of the valve annulus and leaflet coaptation [116].
Accurate quantification of normal biomechanical behavior of TV leaflets during the cardiac
cycle is essential for the development and evaluation of efficient repair strategies and/or
prosthetic valves that aim to mimic native valves.
A large group of researchers have studied the biomechanical behavior and dynamic
deformations of MV [12, 26, 30, 39, 82, 85, 108, 109], the atrioventricular valve analogous
to TV on the left heart. There are also a few studies that focus on TV geometry and annulus
deformation [80, 81, 110]. While these studies are extremely important, they provide no
information about the dynamic mechanical strains of TV leaflets. In terms of experimental
techniques, the previous valvular studies can be categorized into two main groups: in-vivo
studies [26, 30, 80-82, 85, 108-110] and in-vitro studies [39, 111, 112]. In-vivo ovine and

70
porcine studies are frequently used as excellent models prior to clinical studies [26, 82, 85].
Such studies, however, require surgical operating rooms and animal care facilities, which
are often costly and should be used only prior to clinical approaches. In-vitro studies, while
less costly, were previously only conducted on excised valves [39, 111]. In these studies,
the excised valves are generally mounted on a prosthetic rigid annulus and subjected to
pulsatile pressure in a flow simulator. The outcome of such studies is limited since it has
been shown that the cardiac valve annulus is dynamically deforming during the cardiac
cycle [82] and, thus, valve annulus restriction could significantly alter the leafletstrains
[26].
Recently, an ex-vivo approach using the entire porcine heart (instead of using
isolated valves) has been developed to image valve motion and to study hemodynamics in
the left chambers of the heart [113]. In the presented study, we have used a modified ex-
vivo apparatus to open and close cardiac valves in the right side of the heart passively. In
particular, for the first time, we have been able to visualize the dynamic deformations of
TV and measure the mechanical strains on the septal leaflet. Our method has enabled us to
study the intact TVs without mounting them on a rigid annulus. Since porcine tissues are
available within a few minutes after the animals are slaughtered at a local slaughterhouse,
no surgical rooms and animal facilities were required for our experiments.
In the present study, we measured the deformation of porcine TV septal leaflets
using small positional markers while the heart was passively beating in our ex-vivo
apparatus. The measured deformation data were then used to quantify the in-plane ex-vivo
mechanical strains of TV septal leaflet.

71
Fig. 4.1 a) Schematic of the ex-vivo beating heart apparatus and b) a picture of the actual
apparatus.
4.3 Methods
4.3.1 Ex-vivo Heart Apparatus
A schematic of the ex-vivo apparatus and the circulation loop and an image of the
setup are shown in Fig. 4.1. The outlet of a reservoir was connected to the superior vena
cava, and the pulmonary artery was connected to the inlet of the reservoir. A positive

72
displacement pump (SuperPump AR Series, Vivitro Labs Inc., BC, Canada) was connected
to the apex of the right ventricle after an incision was carefully made at this location (as
described in more detail below). This pump is widely used for valve testing [154-158].
The pump setup included a controller unit, which enabled us to control the waveform, the
stroke volume, and the frequency of the beating. The continuous pulsatile flow in the right
side of the heart was initiated as follows:
• When the pump piston moved back (towards the left direction in Fig. 4.1a), it
pulled the fluid from the reservoir into the heart; thus, TV opened and the PV
closed.
• When the pump piston moved forward (towards the right direction in Fig. 4.1b),
due to an increase in the RVP, TV closed; after sufficient pressure had built up,
the PV opened, guiding the fluid back to the reservoir through the pulmonary
artery and the connected tubes.
Flow rate was measured using a transonic flowmeter (T108, Transonic Systems
Inc., Ithaca, NY) at the inflow tube proximal to the heart. Catheter type pressure probes
(SPR-524 and PCU-2000, ADInstruments, Colorado Springs, CO) were used to record
transient right atrial pressure (RAP), RVP, and pulmonary artery pressure (PAP). To
control the back-pressure over the PV, a mechanical valve was placed in the circuit after
the pulmonary artery.
Aluminum profiles (80/20 Inc., Columbia City, IN & Flexaframe™, Fisher
Scientific™, Waltham, MA) and rods were used as the framework for the ex-vivo
apparatus (Fig. 4.1b). All other parts, including a 15 liter reservoir, were assembled over

73
this framework. The reservoir was connected to the superior vena cava using flexible tubes.
To connect the right ventricle to the pump, a hole was created at the right apex using
scalpels and scissors where a straight barbed hose fitting was inserted. The hole was made
with extreme caution to avoid any damage to the papillary muscles and chordae tendineae
such to minimize the effect on valve function. The pulmonary artery was connected back
to the reservoir to complete the hydraulic circuit. To measure the pressure as close to the
right ventricle as possible without disturbing the circulation, a T-shaped pipe-fitting was
placed just after of the straight barbed hose fitting connected to the right ventricle. A
modified Luer Lok connector with a long tail was used to provide a safe passage for the
pressure probe through the T-shaped pipe fitting as it was inserted into the ventricular
chamber (Fig. 4.2). To allow one to visualize the leaflet motion, a backup seal followed by
a dome valve was assembled inside the T-shaped pipe fitting before the Luer Lok assembly.
As such, at any point during the experiment, we were able to remove the Luer Lok assembly
and insert an endoscopic camera without causing any leaks. The same assembly was used
to connect the pressure transducer to the superior vena cava and pulmonary artery as well.
The inferior vena cava and other critical vessels were sealed using umbilical clamps to
prevent leaks (Fig. 4.3). Cable ties or worm-drive clamps were used at the other
connections to prevent leaks. Flexible ¾-inch PVC tubes were used for all the tubing, and
the connections and fittings were selected accordingly.

74
Fig. 4.2 The T-shaped pipefitting connected to the right atrium through a straight barbed
hose fitting (1). The Luer Lok assembly was connected to the other side of the t-shaped
pipe fitting to support the pressure sensor. The other straight barbed hose fitting (2)
connected the right ventricle to the pump. Crystal wires came out through the inferior vena
cava. The umbilical clamp was used to prevent leakage from the inferior vena cava.
Fig. 4.3 Umbilical clamps, cable ties, and worm-drive clamps were used for sealing.

75
4.3.2 Sample Preparation
Fresh porcine hearts were obtained from a local slaughterhouse (3-D Meats, Dalton,
OH) and were transported to our laboratory (in approximately 30 minutes) while
submerged in isotonic PBS and covered with ice immediately after the animals were
slaughtered. The hearts were flushed using PBS to remove blood clots. In order to measure
positional data, a total of 16 sonocrystals (Sonometrics Co., ON, Canada) were sutured to
the valve annulus, septal leaflets, and myocardium (Fig. 4.4). To prevent any damage to
the hearts, the sonocrystal wires were passed into the ventricle through the inferior vena
cava and the suturing process was conducted via the superior vena cava. As shown in Fig.
4.4, two crystals (1 𝑚𝑚) were sutured close to the edge, three (1 𝑚𝑚) at the midsection
and three (2 𝑚𝑚) close to the annulus on the septal leaflet. Five more crystals (2 𝑚𝑚) were
sutured around the annulus. In addition, three crystals (3 𝑚𝑚) were connected outside of
the heart close to the apex in order to define the reference frame for positional
measurements. All crystal wires were passed through the inferior vena cava. PBS with PH
of 7.4 was used as the circulation fluid to help prevent the myocardium, especially the
endocardium, from degenerating rapidly. During preparation and data collection, samples
were submerged in PBS and/or PBS was sprayed on the surfaces exposed to the air to
prevent drying. The sonocrystals were connected to the sonomicrometer device (TRX
Series 16, Sonometrics Co., ON, Canada) to acquire the positional data. The pressure and
flow signals were sent to the sonomicrometer as well as a data acquisition card (6036E,
National Instruments, Austin, TX) directly connected to the computer. The pump controller
provided a standard 70 bpm waveform which was used in the experiment. This waveform
complied with the requirements of the International Standard Organization (ISO 5840) and

76
US Food and Drug Administration guidelines for heart valve testing [159]. After
stabilization of the flow rate and periodic pressure signals, the sonomicrometer
potentiometers were adjusted to maximize signal-to-noise ratio. Finally, an endoscopic
camera (SSVR-710 Snakescope) was inserted into the heart to visualize the leaflet motion
and ensure that the leaflets were coapting properly. The data acquisition was then initiated
with a rate of 100 Hz (according to ISO 5840 requirements) and for a period of 20 seconds
(2000 data points). Eight hearts were tested using the aforementioned procedure.
Fig. 4.4 The arrangement of the sonocrystals over the surface of the septal leaflet. The red
lines show the triangular element used for strain calculation. The radial direction was
defined by a vector connecting crystal 4 to crystal 7.
4.3.3 Strain Calculation
SonoSOFT (Sonometrics Co., ON, Canada) software was used to modify the
recorded displacement and pressure signals. SonoXYZ (Sonometrics Co., ON, Canada)
software was used to calculate the positional coordinates of the crystals during each cardiac
cycle with respect to a defined coordinate system. These positional data were used to

77
calculate the strain tensor based on a previously used method [26, 86, 87]. The triangulation
was done manually according to pattern shown in Fig. 4.4. Since only eight crystals were
sutured on the septal leaflet (the remaining eight crystals were sutured on the annulus and
outside of the heart, as stated previously), their positioning was the same for all eight hearts
and no automated triangulation was necessary.
After calculating the crystal positional data from the recorded raw data, the
positional data were averaged over the 22 recorded beats for all crystals in each heart. The
average positional data were then used to calculate the strains and stretches using the
method explained in APPENDIX B.
4.3.4 Pressures Data Analysis
The sonomicrometer data acquisition system was used to obtain both pressure and
displacement signals. No synchronization process was necessary as the data were already
synchronized for each node and heart. During all of the experiments, the signals of RAP,
RVP, and PAP were monitored and recorded. Before using such data, however, a few
pressure corrections were conducted in the signals from each heart. The first correction
was made to adjust the zero level. In particular, in each heart, there was a height difference
between the free surface of the fluid in the reservoir and the right atrium. To remove the
hydrostatic pressure magnitude in the measurement, the height was measured for each heart
and the equivalent hydrostatic pressure was subtracted from the pressure signals. As a
result, the minimum of the RVP and RAP shifted to a level close to zero. In addition, as
the hearts were assembled vertically, there was a height difference between the bottom of
the ventricle and the pulmonary artery where the pressure sensors were positioned to
measure RVP and PAP, respectively. This height difference was also measured for each

78
heart, and the equivalent hydrostatic pressure was subtracted from the PAP. Although these
heights and their equivalent hydrostatic pressures were small, this correction process was
necessary to obtain a consistent and comparable cardiac pressure graph for all experiments.
In all eight experiments, the recorded pressures and positional data were averaged over all
the 22 recorded beats.
4.4 Results
4.4.1 Pressure
As shown in Fig. 4.5, although the porcine hearts were passively beating, the
recorded pressure compared well with in-vivo human cardiac pressures [160]. The small
standard errors show that despite the variability among the porcine samples, the pressures
for each heart do not deviate much from the average value for the eight hearts. The
measured RVP ranged from values close to zero up to approximately 30 𝑚𝑚 𝐻𝑔, similar
to the reported porcine values (2 to 33 𝑚𝑚 𝐻𝑔 [161-164]). The measured PAP ranged
from approximately 6 to 30 𝑚𝑚 𝐻𝑔. The RAP remained relatively close to zero during
diastole. We were not able to find reliable PAP and RAP values for porcine hearts in the
literature but the measured values for these two signals (Fig. 4.5) were comparable to those
of human [160]. The RVP average signal also shows a small drop right at the beginning of
the diastole. A closer examination of the RVP signal in Fig. 4.5 shows that TV closes at
approximately 0.2 𝑠, where the RVP intersects with the RAP; the PV opens at 0.29 𝑠,
where the RVP meets the PAP; the PV closes approximately at 0.44 𝑠, where the RVP
separates from the PAP; and finally TV opens approximately at 0.54 𝑠, where the RVP
crosses the RAP once more. The average flow rate for all the hearts was 2.63 ±
0.13 𝑙/𝑚𝑖𝑛.
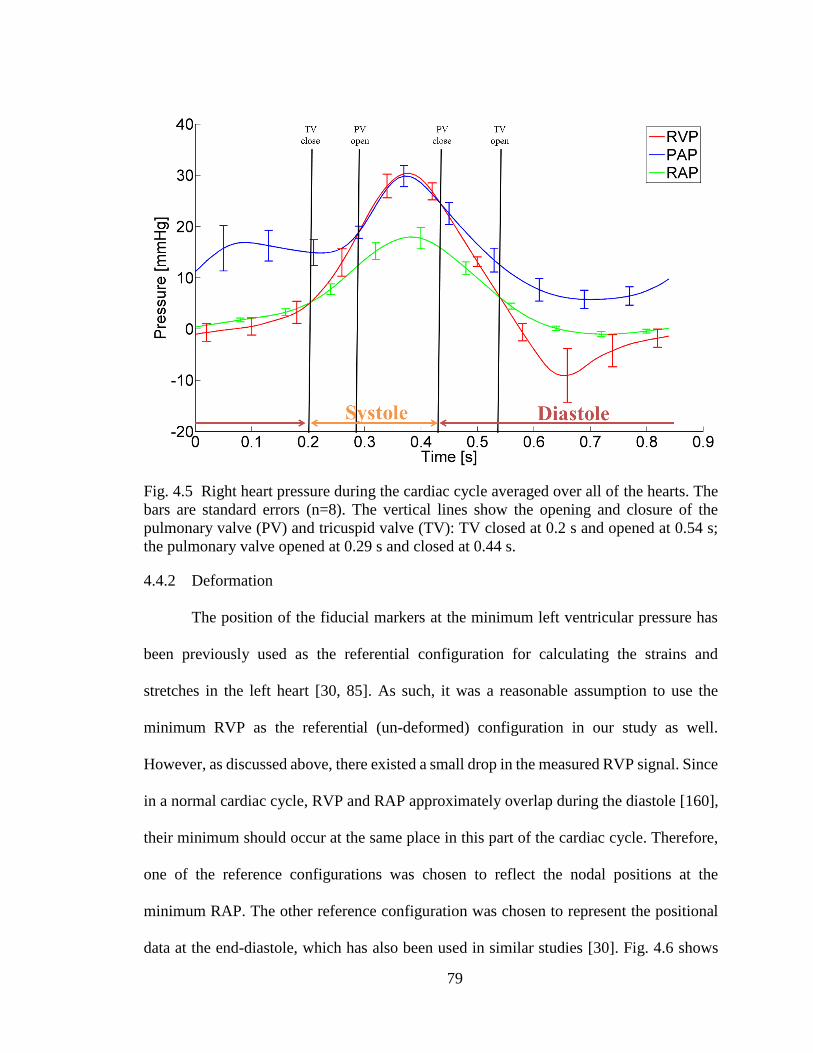
79
Fig. 4.5 Right heart pressure during the cardiac cycle averaged over all of the hearts. The
bars are standard errors (n=8). The vertical lines show the opening and closure of the
pulmonary valve (PV) and tricuspid valve (TV): TV closed at 0.2 s and opened at 0.54 s;
the pulmonary valve opened at 0.29 s and closed at 0.44 s.
4.4.2 Deformation
The position of the fiducial markers at the minimum left ventricular pressure has
been previously used as the referential configuration for calculating the strains and
stretches in the left heart [30, 85]. As such, it was a reasonable assumption to use the
minimum RVP as the referential (un-deformed) configuration in our study as well.
However, as discussed above, there existed a small drop in the measured RVP signal. Since
in a normal cardiac cycle, RVP and RAP approximately overlap during the diastole [160],
their minimum should occur at the same place in this part of the cardiac cycle. Therefore,
one of the reference configurations was chosen to reflect the nodal positions at the
minimum RAP. The other reference configuration was chosen to represent the positional
data at the end-diastole, which has also been used in similar studies [30]. Fig. 4.6 shows

80
the calculated peak areal strain, maximum principal strain, circumferential strain and radial
strain at the center point of the leaflet (point number 4) averaged for all eight hearts using
the two aforementioned references. Fig. 4.6 also shows the strain standard errors for the
eight hearts. There was no significant difference between the strains measured using two
different reference configurations (𝑝 > 0.14 in all cases, paired Student t-test). The same
observation has been reported for MV anterior leaflet [30]. As shown in Fig. 4.6, the peak
areal strain (9.8%) and the peak maximum principal strain (11.2%) were significantly
different (𝑝 < 0.008 in all cases, paired Student t-test) from the peak circumferential strain
(5.6%) and the peak radial strain (4.3%). However, there was no significant difference
(𝑝 ≈ 0.24, paired Student t-test) between the peak circumferential and the peak radial
strains (the numbers quantified using minimum RAP as the un-deformed reference (Ref1
in Fig. 4.6)).
Figure 4.7 shows the temporal strain variations over a cardiac cycle. The strain
values were averaged at the leaflet midpoint for the eight hearts at each time point. The
leaflets experienced positive strain for the majority of the times points during the cardiac
cycle. Comparing the strain graphs with the pressure graph shows that immediately after
TV closed (𝑡 = 0.2 𝑠), all the quantified strains rose rapidly and reached their peaks
values at the maximum RVP (𝑡 ≈ 0.4 𝑠). The strains subsequently dropped, reaching their
minimum values at 𝑡 ≈ 0.65 𝑠, with the exception of the radial strain, which reached the
minimum value at 𝑡 ≈ 0.5 𝑠. Overall, the strain values were extremely small during
diastole and increased during systole. Note that the peak of the means (Fig. 4.6) is always
less than (or ideally equal to) the mean of the peaks (Fig. 4.7) since the maximum values
of the signals for each heart do not necessarily happen exactly at the same time.

81
Fig. 4.6 Average peak areal, maximum principal (Max Princ), circumferential (Circ), and
radial strains at the leaflet midpoint measured with respect to reference 1 (Ref1, minimum
RAP) and reference 2 (Ref2, end diastole). The error bars are standard error (n=8).
Figure 4.8 shows the spatial distribution of the strains over the leaflet at the
maximum RVP. At this pressure level, the strains were averaged over all eight hearts. The
averaged data are illustrated for a typical septal leaflet. As shown in Fig. 4.8, the maximum
principal strain is distributed uniformly over the leaflet at maximum RVP, while the areal
strain is not as uniform. There is much heterogeneity in the spatial distribution of the
circumferential strain and radial strain over the septal leaflet. While higher values for
circumferential strain were observed toward the posterior of the leaflet, the radial strains
reached higher values in areas near the anterior.
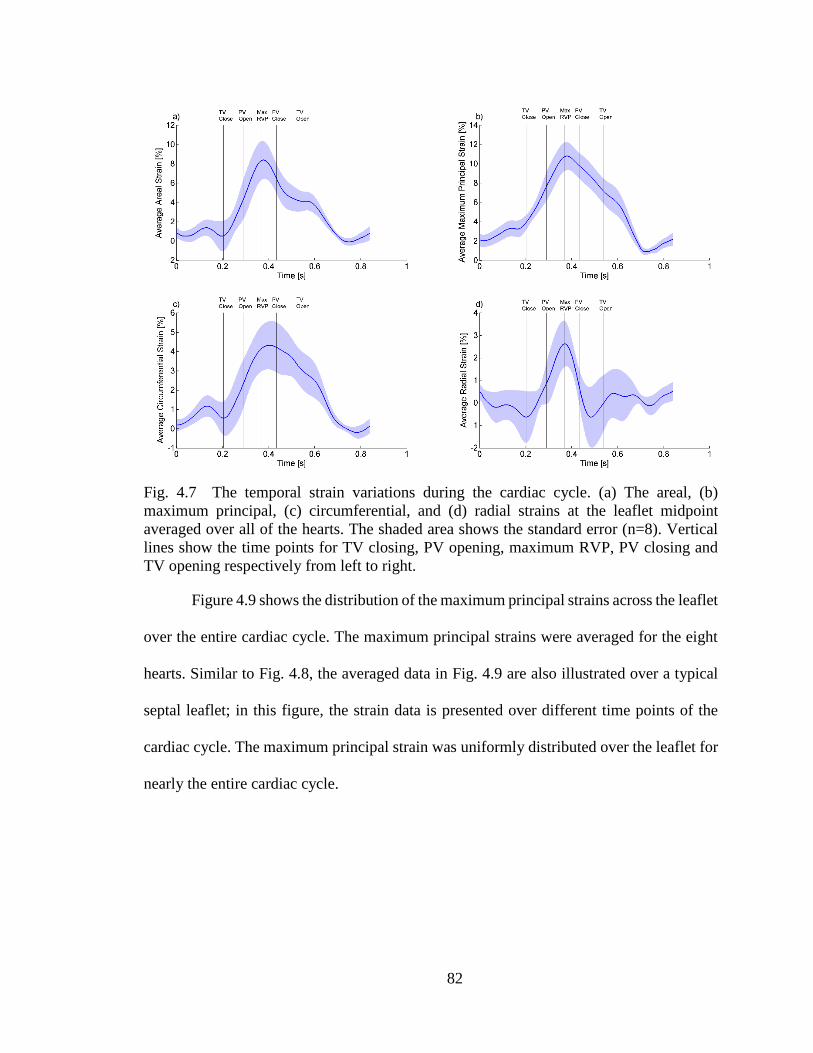
82
Fig. 4.7 The temporal strain variations during the cardiac cycle. (a) The areal, (b)
maximum principal, (c) circumferential, and (d) radial strains at the leaflet midpoint
averaged over all of the hearts. The shaded area shows the standard error (n=8). Vertical
lines show the time points for TV closing, PV opening, maximum RVP, PV closing and
TV opening respectively from left to right.
Figure 4.9 shows the distribution of the maximum principal strains across the leaflet
over the entire cardiac cycle. The maximum principal strains were averaged for the eight
hearts. Similar to Fig. 4.8, the averaged data in Fig. 4.9 are also illustrated over a typical
septal leaflet; in this figure, the strain data is presented over different time points of the
cardiac cycle. The maximum principal strain was uniformly distributed over the leaflet for
nearly the entire cardiac cycle.
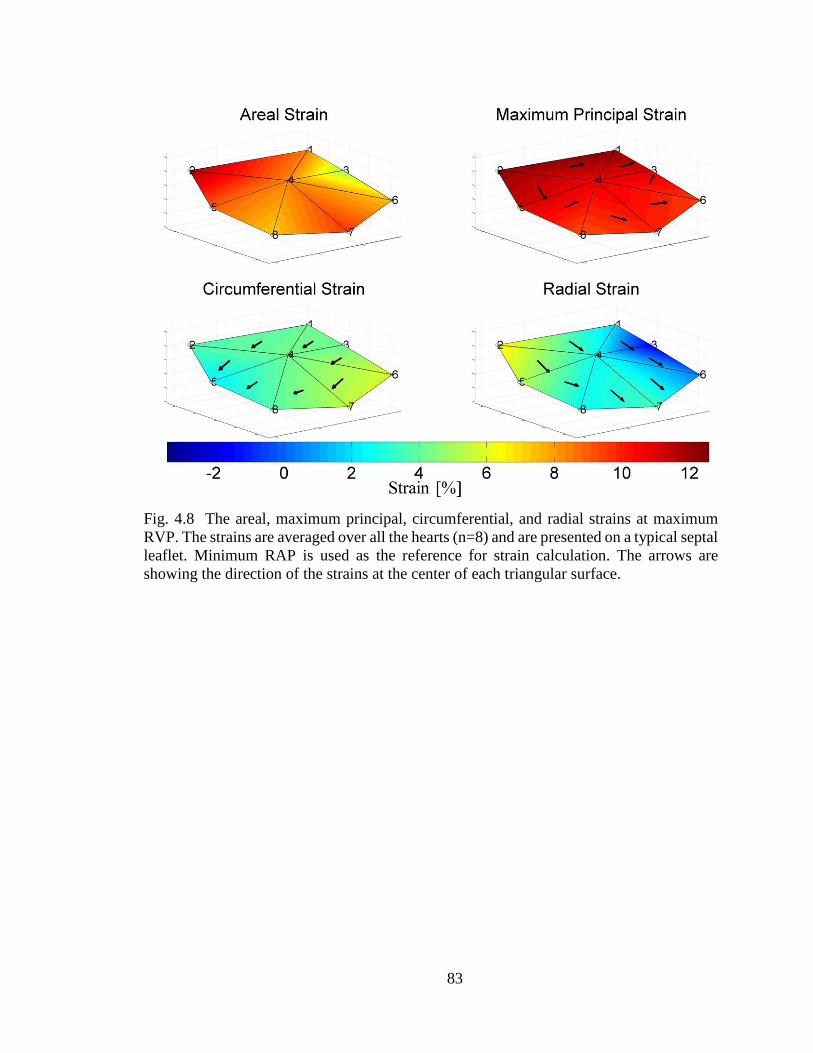
83
Fig. 4.8 The areal, maximum principal, circumferential, and radial strains at maximum
RVP. The strains are averaged over all the hearts (n=8) and are presented on a typical septal
leaflet. Minimum RAP is used as the reference for strain calculation. The arrows are
showing the direction of the strains at the center of each triangular surface.

84
Fig. 4.9 Distribution of the maximum principal strain over the leaflet during the septal
entire cardiac cycle. Maximum principal strain is averaged over all of the hearts (n=8) and
showed over a typical septal leaflet during the cardiac cycle.
4.5 Discussion
Our novel ex-vivo beating heart apparatus was able to produce repeatable data with
high temporal resolution. Using our passive beating heart, we were able to reproduce
ventricular pressure waves that matched the physiological values of an active heart [160].
Porcine hearts are excellent models for valve studies and pressure values at the pulmonary
side are similar in human and porcine hearts. In particular, human RVP ranges
approximately from zero to 30 𝑚𝑚 𝐻𝑔 [128, 160] and porcine RVP ranges roughly from
zero up to around 33 𝑚𝑚 𝐻𝑔 [161-164]. Such a similarity also exists in the system side
of the heart [1, 165].
To our best knowledge, the in-vivo strains in porcine TV leaflets have not yet been
quantified. Thus, it is not possible to compare our deformation results with in-vivo TV
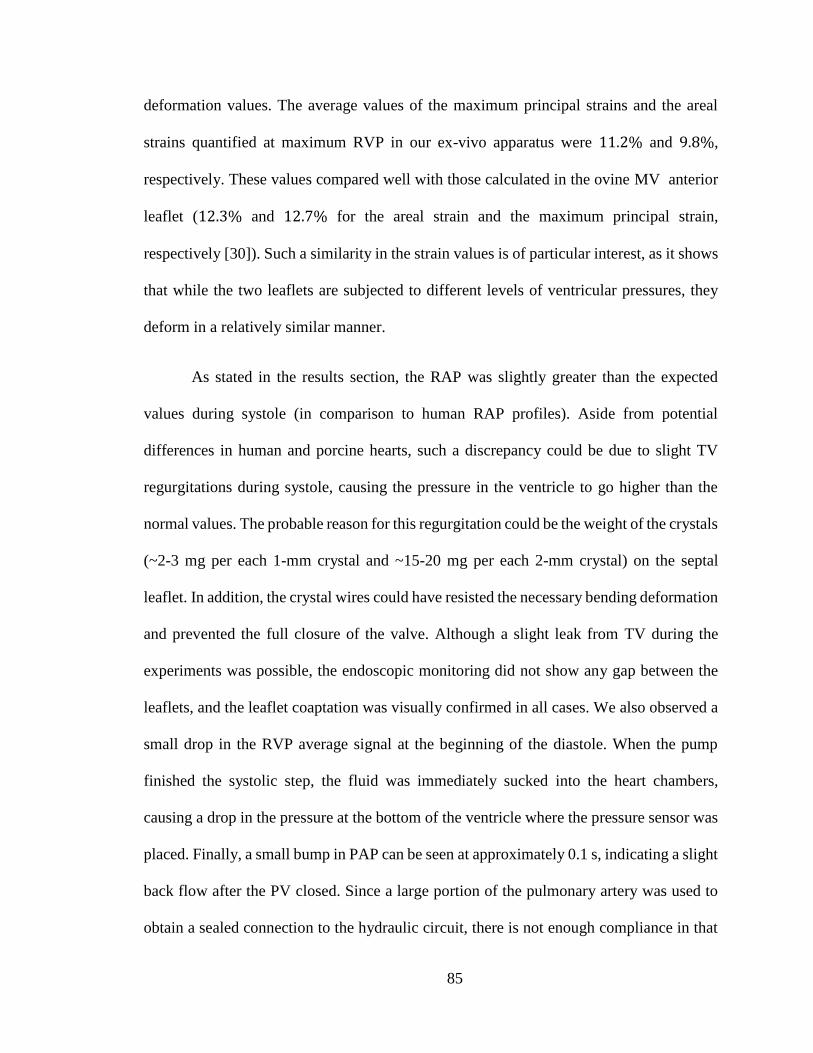
85
deformation values. The average values of the maximum principal strains and the areal
strains quantified at maximum RVP in our ex-vivo apparatus were 11.2% and 9.8%,
respectively. These values compared well with those calculated in the ovine MV anterior
leaflet (12.3% and 12.7% for the areal strain and the maximum principal strain,
respectively [30]). Such a similarity in the strain values is of particular interest, as it shows
that while the two leaflets are subjected to different levels of ventricular pressures, they
deform in a relatively similar manner.
As stated in the results section, the RAP was slightly greater than the expected
values during systole (in comparison to human RAP profiles). Aside from potential
differences in human and porcine hearts, such a discrepancy could be due to slight TV
regurgitations during systole, causing the pressure in the ventricle to go higher than the
normal values. The probable reason for this regurgitation could be the weight of the crystals
(~2-3 mg per each 1-mm crystal and ~15-20 mg per each 2-mm crystal) on the septal
leaflet. In addition, the crystal wires could have resisted the necessary bending deformation
and prevented the full closure of the valve. Although a slight leak from TV during the
experiments was possible, the endoscopic monitoring did not show any gap between the
leaflets, and the leaflet coaptation was visually confirmed in all cases. We also observed a
small drop in the RVP average signal at the beginning of the diastole. When the pump
finished the systolic step, the fluid was immediately sucked into the heart chambers,
causing a drop in the pressure at the bottom of the ventricle where the pressure sensor was
placed. Finally, a small bump in PAP can be seen at approximately 0.1 s, indicating a slight
back flow after the PV closed. Since a large portion of the pulmonary artery was used to
obtain a sealed connection to the hydraulic circuit, there is not enough compliance in that

86
area to dampen the changes in the pressure. A well-tuned compliance chamber might be
useful for eliminating this inertial effect in the PAP signal. Although, more realistic
pressure waveforms can be obtained using a compliance chamber with specific
adjustments, we chose a less complicated approach that will be more easily reproduced by
other researchers.
Unlike MV leaflets, in which significant differences exist between the maximum
strain in the circumferential and radial directions [26, 30, 111], no significant difference
existed between circumferential and radial strains in TV septal leaflet at the maximum
RVP. A potential explanation is that TV septal leaflet has a more isotropic extracellular
matrix microstructural architecture in comparison to MV anterior and posterior leaflets.
The anisotropic nature of MV anterior leaflet has been demonstrated previously [35].
Biaxial mechanical testing and measurement of tissue microstructural architecture (e.g. via
small angle light scattering could identify the degree of anisotropy in TV septal leaflets.
Due to the fact that the number of channels available for sonomicrometry crystals was
limited to 16, we were not able to measure the deformation of TV anterior and posterior
leaflets to make such a comparison among the ex-vivo strain values. Further research is
required to quantify strain values in TV anterior and posterior leaflets in the future [117,
166].
There are many advantages in using porcine hearts in our experiment, as fresh
tissues can be obtained and the biomechanical behavior of the valves is less affected by the
activity of degenerative enzymes in the extracellular matrix. In addition, in comparison to
human cadaverous tissues, younger porcine samples with less variability are available [35].
However, one should always be cautious in drawing conclusions regarding human tissue
87
responses based solely on animal studies [167]. The advantage of our ex-vivo apparatus is
that, if necessary, human cadaverous tissues can be used in conducting similar experiments
without any additional complications.
Sonomicrometry crystals may affect the measured deformations in different ways.
The process of attaching the crystals to the leaflet may cause some localized and permanent
changes to the leaflet structural properties. Although these changes were not measurable in
our setup, much caution was used to prevent damage to the tissue during the suturing
process. In is noteworthy that these changes were presumably restricted to the immediate
vicinity of the crystal. As per potential of error due to buoyancy and/or inertia, the piezo
crystals had same density as that of water or tissue. In addition, the crystals were extremely
small compared to the size of their surrounding tissues. Therefore, their interference with
natural leaflet motion was minimal. Crystals, of course, were connected the
sonomicrometer instrument via wires. One may consider the tethering effects of these
connecting wires as a potential source for leaflet motion restriction. The crystals were
connected to sonomicrometer using 38 gauge copper wires, which were flexible. In order
for the crystal wires to alter the natural motion of the leaflets in any way, the wires should
have been tethered close to the leaflet surface, with little or no out-of-plane slack. As such,
we made sure that the wires had enough slack to prevent physically restraining the natural
motion of the leaflets. Despite its few limitations, sonomicrometry have been used
extensively in the valve studies [26, 81, 82, 167-170].
A major limitation of our experiment is the passive nature of the beating heart. The
contraction of papillary muscles and the activation of ventricular and atrial muscles
potentially change the loading condition on the leaflet annulus and chordae tendineae.

88
Although the ex-vivo passive beating heart is not identical to the in-vivo active hearts,
unlike the in-vitro studies of the excised cardiac valves [39, 111, 112], TV annulus is not
restricted in the ex-vivo apparatus. In-vivo studies of TV motion have shown that TV
annulus size dynamically changes during the normal cardiac cycle [81]. The ex-vivo
beating heart at least maintains the passive component of such deformation in TV annulus.
In short, even though the ex-vivo beating heart experiment is not identical to the in-vivo
heart, it is more realistic than the isolated valve experiments when it comes to the valve
annulus deformation.
There exists a major advantage in using a passive beating heart in the verification
of combined valve and ventricle computational models [171]. In particular, because the
cardiac muscles are not active and the ventricular pressure is the only load applied to the
cardiac tissues, one could use the ex-vivo beating heart to validate combined valve and
ventricle models absent the active stress components of the cardiac tissues. In addition to
detailed pressure and strain measurements, the entire heart can be imaged and segmented
following the experiment to provide a subject-specific computational model.
Although our study was conducted using PBS, there is no limitation in using other
non-clear fluids in our apparatus, as our strain measurement does not rely on visual access
to the valves. Such a capability is of great importance because recent studies have shown
that the flow properties (particularly the transition to turbulence) could be significantly
different in blood in comparison to optically clear viscosity-matched blood substitutes
[172]. Since the transition to turbulence could happen in the proximity of the cardiac
valves, measurements of valve deformation using blood should be conducted in the future.
89
In summary, we developed an experimental setup to measure the dynamic
deformation of the porcine TV septal leaflets. We observed that the leaflet strain values are
similar to those measured in-vivo in leaflets of the other atrioventricular valve (i.e. MV).
In future studies, our experimental model can be used to evaluate mechanical strains on
different TV leaflets. In addition, our experimental setup can be beneficial in studying
primary valve lesions such as chordae rupture, secondary valve lesions such as pulmonary
hypertension, and valve repair procedures such as ring annuloplasty and/or leaflet
resection.
90
CHAPTER 5V
DYNAMIC DEFORMATIONS OF THE TRICUSPID VALVE ANNULUS, INTACT
AND AFTER CHORDAE RUPTURE
(The content of this chapter was published in PLOSE ONE (Nov 2018) as “Dilation of
Tricuspid Valve Annulus Immediately After Rupture of Chordae Tendineae in Ex-vivo
Porcine Hearts” [173].)
5.1 Summary
Chordae rupture is one of the main lesions observed in traumatic heart events that
might lead to severe TV regurgitation. TV regurgitation following chordae rupture is often
well tolerated with few or no symptoms for most patients. However, early repair of TV is
of great importance, as it might prevent further exacerbation of the regurgitation due to
remodeling responses. To understand how TV regurgitation develops following this acute
event, we investigated the changes on TV geometry, mechanics, and function of ex-vivo
porcine hearts following chordae rupture.
Sonomicrometry techniques were employed in an ex-vivo heart apparatus to
identify how the annulus geometry alters throughout the cardiac cycle after chordae
rupture, leading to the development of TV regurgitation.
We observed that TV annulus significantly dilated (~9% in area) immediately after
chordae rupture. The annulus area and circumference ranged from 11.4 ± 2.8 to 13.3 ±
2.9 cm2 and from 12.5 ± 1.5 to 13.5 ± 1.3 cm, respectively, during the cardiac cycle for
91
the intact heart. After chordae rupture, the annulus area and circumference were larger and
ranged from 12.3 ± 3.0 to 14.4 ± 2.9 cm2 and from 13.0 ± 1.5 to 14.0 ± 1.2 cm,
respectively.
In our ex-vivo study, we showed for the first time that TV annulus dilates
immediately after chordae rupture. Consequently, secondary TV regurgitation may be
developed because of such changes in the annulus geometry. In addition, TV leaflet and
the right ventricle myocardium are subjected to a different mechanical environment,
potentially causing further negative remodeling responses and exacerbating the detrimental
outcomes of chordae rupture.
5.2 Introduction
TV guides the blood from the right atrium to the right ventricle and prevents
backflow during ventricular contraction. The leaflets and annulus of TV undergo
complicated dynamic deformations during normal cardiac cycles [80, 81]. Any disturbance
in the normal deformation of the valve leaflets and/or annulus could lead to valvular
regurgitation [174, 175] and changes in the valve’s mechanical response [134, 142]. In
most cases, TV regurgitation—whether it is caused by primary valvular lesions (e.g., due
to congenital malformations [176], trauma [177, 178] or degenerative diseases such as
Marfan syndrome [179, 180]) or takes place as a result of other cardiovascular diseases
(e.g. secondary to pulmonary hypertension [181])—will require surgical intervention
[182].
While TV regurgitation is most often caused by chronic diseases, acute cases could
occur following traumatic events such as vehicular accidents [183, 184]. In the majority of

92
trauma-related cases, chordae rupture is the main lesion present [185]. Many accident
victims also suffer from other injuries such as lacerations, fractures, and closed head
injuries [151]. With these more severe concurrent injuries present immediately after
trauma, the acute TV regurgitation can be easily overlooked when making a diagnosis.
Although advances in diagnostic procedures such as echocardiography have improved in
recent years [186], isolated TV regurgitation is often well tolerated, and most patients
experience few or no symptoms in the weeks and months following the trauma [187, 188].
In fact, the average time from the trauma to the initial diagnosis of TV regurgitation is three
years [189] (with the time to diagnosis ranging from within 15 days of the trauma to as
long as 25 years later). However, early repair of the regurgitative TV following chordae
rupture is of critical importance. Among many benefits, early repair may prevent further
detrimental complications such as thickening and fibrosis of TV leaflets and/or changes in
the sinus rhythm due to right atrial dilation [189].
Previous studies have shown that acute biomechanical changes in cardiac valves
could induce remodeling responses that may negatively affect the valve structure,
mechanical properties, and function [117, 134, 190]. Considering the importance of such
acute events, in this study we aimed to identify how TV regurgitation develops
immediately following chordae rupture. Since normal TV function relies on precise and
complex interactions among the various components (i.e. annulus, leaflets, chordae), it is
expected that chordae rupture disturbs the normal deformation of the valve annulus and
leads to insufficient leaflet coaptation. It has been previously shown that valve
insufficiency can lead to ventricular and annulus dilation due to remodeling responses.
However, based on the assumption that intact chordae tendineae mechanically

93
support/anchor the normal TV annulus, for the first time in this ex-vivo study we have
shown that immediately following chordae rupture, TV annulus dilates in porcine hearts.
5.3 Materials and Methods
5.3.1 Ex-vivo Heart Apparatus
We have previously developed an ex-vivo passive beating heart apparatus to mimic
TV deformation without the need to dissect the valve and remount the annulus [140]. The
schematic of this apparatus is shown in Fig. 4.1a. In short, a positive displacement pump
(SuperPump AR Series, Vivitro Labs, Inc., Victoria, BC, Canada) was utilized to induce
passive beating in porcine hearts through pressure differences (without actively engaging
the muscle tissue). The pump, heart, and a fluid reservoir filled with isotonic PBS were
connected together using tubes and tube fittings to build a closed hydraulic circuit, in which
the pump could circulate the fluid from the reservoir into the heart and back to the reservoir.
Backward movement of the pump piston (towards the left in Fig. 4.1a) causes TV to open
and pulls the PBS from the right atrium (which is connected to the reservoir) into the right
ventricle. Forward movement of the pump piston (towards the right in Fig. 4.1a) causes
TV to close and the PV to open by increasing the pressure inside the ventricle, pushing the
PBS back into the reservoir through the pulmonary artery. As such, the pump is able to
circulate the PBS throughout the system and generate movement and deformation of TV
leaflets and annulus. A transonic flowmeter (T108, Transonic Systems, Inc., Ithaca, NY)
was used to monitor the flow rate, and three catheter-type pressure probes (SPR-524 probes
with a PCU-2000 controller, ADInstruments, Colorado Springs, CO) were used to monitor
RAP, RVP, and PAP. Based on the requirements of the heart valve testing procedures
established by the International Standard Organization (ISO 5840) and U.S. Food and Drug

94
Administration guidelines, a standard waveform of the pump with frequency of 70 𝑏𝑝𝑚
was used during the experiment. The other parameters of the pump controller were set to
ensure that the hydrodynamic pressure of the flow would closely match those of a heart
under normal physiological conditions.
5.3.2 Sample Preparation
Fresh porcine hearts were obtained from a local slaughterhouse (3-D Meats, Dalton,
OH) and were transferred to the laboratory in bags filled with PBS that were covered with
ice. Upon arrival at the lab, the hearts then were flushed out using PBS at room temperature
and checked to ensure that no blood clots were stuck inside the chambers or in the area
around TV apparatus. In order to measure annulus deformation, a total of eight sonocrystals
(Sonometrics Co., London, ON, Canada), 2 𝑚𝑚 in diameter, were carefully sutured around
the valve annulus (Fig. 5.1). The suturing process was conducted through the superior vena
cava, and the crystal wires were passed through the inferior vena cava to prevent any
damage to the heart. To form a reference frame for calculating the positional data, three
more sonocrystals, 3 𝑚𝑚 in diameter, were attached to the outside of the myocardium
close to the apex. A sonomicrometer (TRX Series 16, Somometrics Co., London, ON,
Canada) was used to collect data from the sonocrystals. The pressure and flow signals were
also collected via the sonomicrometer input channels to record all data in a synchronized
manner. After setup of the system but prior to recording any data, an endoscopic camera
(Snakescope SSVR-710) was sent into the right atrium through the superior vena cava to
verify the accurate functionality of the valve apparatus. The positional data of the
sonocrystals were recorded using a sampling rate of 100 𝐻𝑧 for a period of 20 seconds
during each experiment. After recording the data for the intact TV in each experiment, the
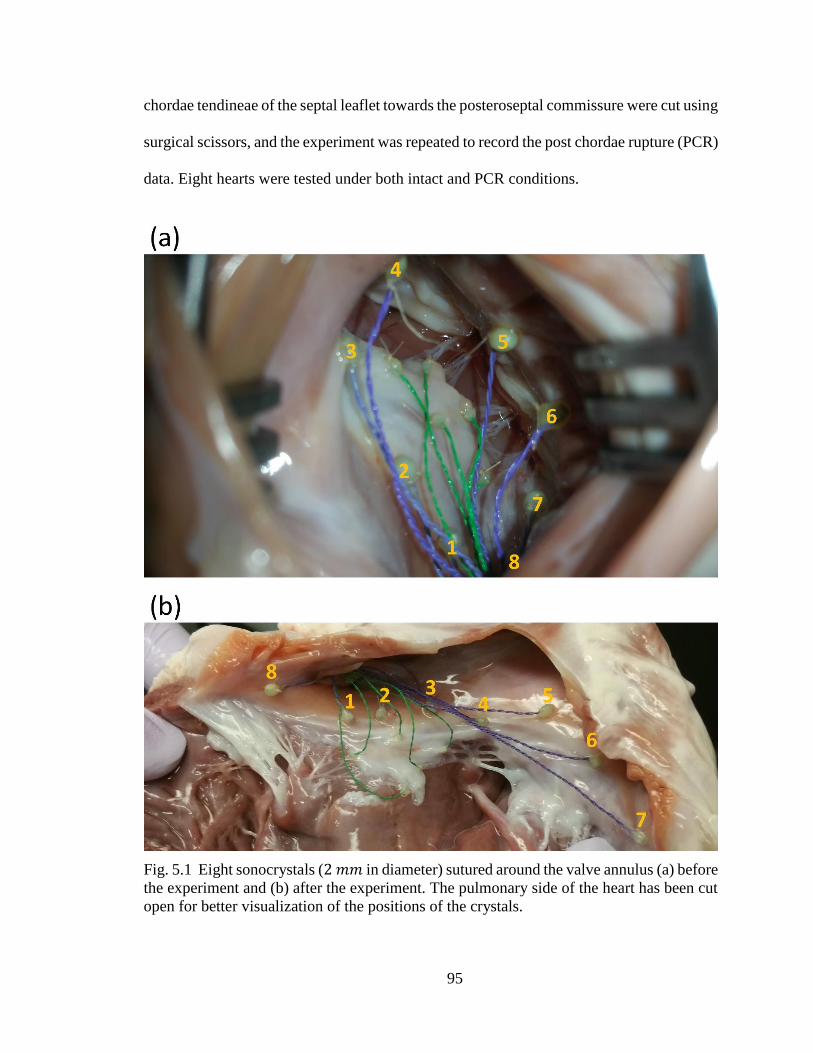
95
chordae tendineae of the septal leaflet towards the posteroseptal commissure were cut using
surgical scissors, and the experiment was repeated to record the post chordae rupture (PCR)
data. Eight hearts were tested under both intact and PCR conditions.
Fig. 5.1 Eight sonocrystals (2 𝑚𝑚 in diameter) sutured around the valve annulus (a) before
the experiment and (b) after the experiment. The pulmonary side of the heart has been cut
open for better visualization of the positions of the crystals.

96
5.3.3 Data Analysis
In order to calculate the area and circumference of the annulus at each moment
during the cardiac cycle, a cubic spline was fitted to the positional data [82, 83] of the
crystals around the annulus (Fig. 5.2). The length of the spline was calculated and
considered as the circumference of the annulus at each moment [83]. The area of the
annulus was approximated as follows:
1- The average of the three-dimensional position vectors collected by the
sonocrystals was calculated as the center of the annulus.
2- A triangulated virtual surface was built by connecting 10,000 equally-spaced
points on the spline representing the annulus to the calculated central point.
3- The sum of the surface areas of all the constructed triangles was calculated as
an approximation for the area of the annulus.
The approximation procedure is illustrated in Fig. 5.2 using a lower resolution of
the points on a typical annulus for better illustrative purposes (24 points for illustrative
purposes in Fig. 5.2; the resolution used in the calculation was 10,001 points). The average
of the measured distance between each point on the spline and the central point was
calculated as the average radius of the annulus. The calculated area and circumference were
also used to calculate the radius for comparison purposes by assuming that the annulus is
a circle on a flat plane.
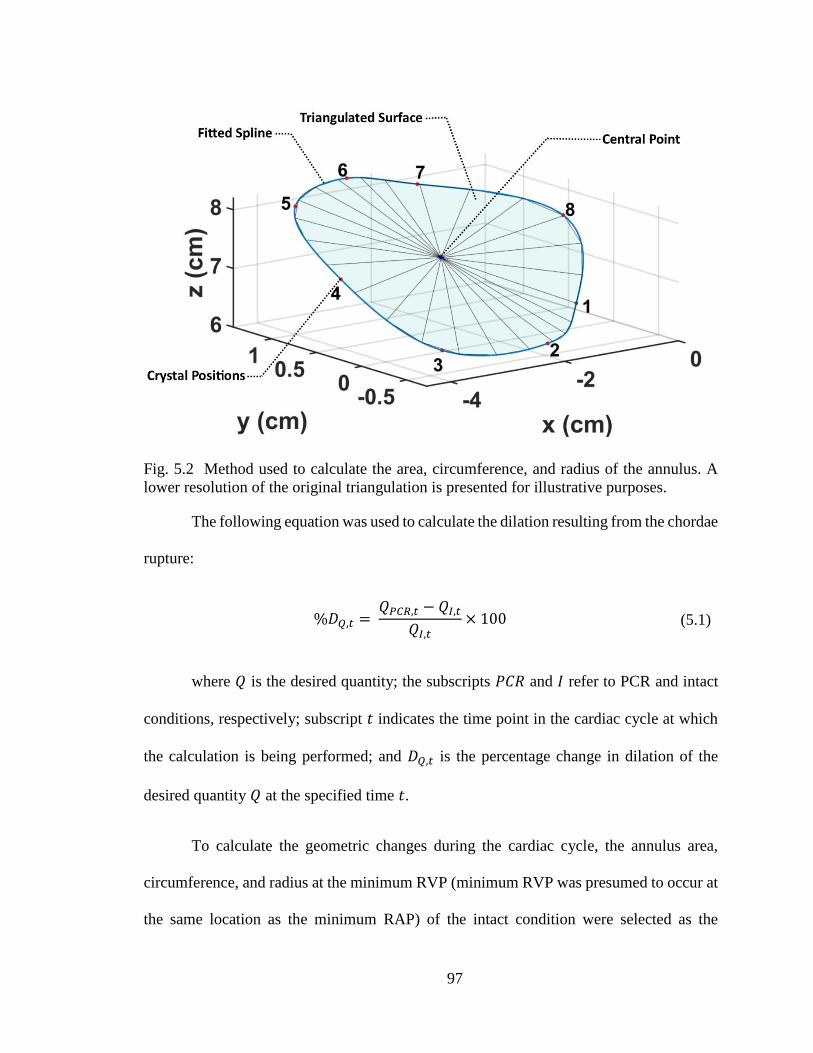
97
Fig. 5.2 Method used to calculate the area, circumference, and radius of the annulus. A
lower resolution of the original triangulation is presented for illustrative purposes.
The following equation was used to calculate the dilation resulting from the chordae
rupture:
%𝐷𝑄,𝑡 =
𝑄𝑃𝐶𝑅,𝑡 − 𝑄𝐼,𝑡
𝑄𝐼,𝑡× 100 (5.1)
where 𝑄 is the desired quantity; the subscripts 𝑃𝐶𝑅 and 𝐼 refer to PCR and intact
conditions, respectively; subscript 𝑡 indicates the time point in the cardiac cycle at which
the calculation is being performed; and 𝐷𝑄,𝑡 is the percentage change in dilation of the
desired quantity 𝑄 at the specified time 𝑡.
To calculate the geometric changes during the cardiac cycle, the annulus area,
circumference, and radius at the minimum RVP (minimum RVP was presumed to occur at
the same location as the minimum RAP) of the intact condition were selected as the

98
reference area (𝐴0), reference circumference (𝐶0), and reference radius (𝑅0), respectively.
Next, using Equation (5.2), we calculated the changes in area, circumference, and radius
for the annulus under both intact and PCR conditions.
%𝐶𝑄 =
𝑄𝑡 − 𝑄0
𝑄0× 100 (5.2)
where 𝑄𝑡 is the desired quantity at the current time, 𝑄0 is the initial (reference)
value of this quantity, and 𝐶𝑄 shows the percentage change. For comparison purposes, we
also calculated the approximate changes in annulus anterior segment (AAS), annulus
posterior segment (APS), and annulus septal segment (ASS) using the position of the
markers attached to each segment.
Finally, we developed an average annulus curve from the measured 3D data to
evaluate its shape. As the data was recorded independently for each TV annulus based on
its own reference frame and coordinate system, registration of marker positional data from
different annuli was necessary to match the corresponding marker positions with a
minimum error for averaging. Therefore, using singular value decomposition, the
measured positional data for all TV annuli were transformed to closely register the
corresponding marker points, and the resulting data points were averaged to develop an
average annulus curve similar to the ones developed in previous studies [83].
5.3.4 Statistical Analysis
All data presented in this paper are reported in the form of mean ± standard
deviation. Although much intervariability was observed among the measured values of
different subjects (more details in this regard can be found in the Results section), the

99
standard deviation due to measurement errors for 22 consecutive cardiac cycles was ~0.1%
of the mean value of the measured quantity. Nevertheless, to minimize the intervariability
due to measurement errors for each sample, the measured data of all 22 consecutive cardiac
cycles were averaged at the corresponding time points in the cardiac cycle and were used
for analysis. The Wilcoxon signed rank test was used for all statistical analysis, where any
result with 𝑝 < 0.05 is considered to be statistically significant.
5.4 Results
5.4.1 Pressure
The average recorded RVP, PAP, and RAP are shown in Fig. 5.3 for the intact and
PCR cases. As illustrated in this figure, the average measured pressures in this ex-vivo
setup closely match the in-vivo ones [160]. The range of pressure values for the intact case
were approximately from 0 to 30 𝑚𝑚 𝐻𝑔 and from 6 to 30 𝑚𝑚 𝐻𝑔 for RVP and PAP,
respectively. However, the pressures for RVP and PAP after chordae rupture ranged from
0 to 25 𝑚𝑚 𝐻𝑔 and from 5 to 24 𝑚𝑚 𝐻𝑔, respectively. The range for the RVP closely
matched the range reported for the porcine RVP in the literature [161-164]. We were not
able to find reported PAP or RAP values for porcine hearts; however, the recorded pressure
values closely matched those measured in human hearts [160].

100
Fig. 5.3 Average right ventricular pressure (RVP), pulmonary artery pressure (PAP), and
right atrial pressure (RAP) measured for the intact and post chordae rupture (PCR) cases.
5.4.2 Annulus Area, Circumference, and Radius Values
The results obtained for the area, circumference, and radius at the minimum and
maximum RVP for intact and PCR ex-vivo porcine hearts are listed in Tables 5.1–5.3.
Throughout the cardiac cycle, in intact hearts, the mean area, circumference, and radius of
the annulus ranged from 11.4 ± 2.8 to 13.3 ± 2.9 𝑐𝑚2, from 12.5 ± 1.5 to 13.5 ± 1.3 𝑐𝑚,
and from 1.9 ± 0.2 to 2.0 ± 0.2 𝑐𝑚, respectively. After chordae rupture, the mean area,
circumference, and radius of the annulus ranged from 12.3 ± 3.0 to 14.4 ± 2.9 𝑐𝑚2, from
13.0 ± 1.5 to 14.0 ± 1.2 𝑐𝑚, and from 1.9 ± 0.2 to 2.1 ± 0.2 𝑐𝑚, respectively. The
numbers provided here are the average of the minimum and maximum values of the
quantities, while Tables 5.1–5.3 list the values at minimum and maximum RVP; thus, there
might be a slight difference between the averages and standard deviations provided here
and those presented in Tables 5.1–5.3. Significant increases in the annulus area,
circumference, and radius were observed following chordae rupture (Fig. 5.4; 𝑝 = 0.01

101
for values measured at maximum RVP and 𝑝 = 0.04 for values measured at minimum
RAP, according to the Wilcoxon signed rank test). A segment-specific statistical analysis
revealed that the APS did not vary significantly after chordae rupture (𝑝 = 0.38 for values
measured at maximum RVP and 𝑝 = 0.64 for those measured at minimum RAP,
according to the Wilcoxon signed rank test), while the AAS and ASS increased
significantly (𝑝 = 0.02 for AAS values measured at maximum RVP, 𝑝 = 0.04 for AAS
values measured at minimum RAP, and 𝑝 = 0.02 for ASS values measured both at
maximum RVP and at minimum RAP, according to the Wilcoxon signed rank test). Table
5.3 also lists the radii estimated from the calculated areas and circumferences (𝑅𝐴 and 𝑅𝐶)
when the annulus was considered as a flat circle. These estimated radii values, especially
those calculated from the areas, were quite similar to those calculated using the previously
explained method.
Table 5.1 Calculated area at minimum and maximum right ventricular pressure (RVP) for
intact and post chordae rupture (PCR) conditions. The values are presented for all eight
hearts used in the experiments along with the average (AVG) and standard deviation
(STD). Comparing the average values showed an increase in the area post chordae rupture.
Area (𝑐𝑚2)
At minimum RVP At maximum RVP
Heart no. Intact PCR Intact PCR
1 12.7 12.7 13.7 14.0
2 8.8 8.7 11.5 12.1
3 8.8 9.9 10.9 12.2
4 13.8 13.9 15.3 15.5
5 8.0 9.4 9.8 11.5
6 16.2 17.7 19.1 20.2
7 11.6 14.7 12.8 15.5
8 11.5 12.0 13.0 13.6
AVG 11.4 12.4 13.3 14.3
STD 2.8 3.0 2.9 2.8

102
Fig. 5.4 Comparison of the average values of (a) the area, (b) circumference, and (c) radius
between the intact and post chordae rupture (PCR) conditions at minimum and maximum
right ventricular pressure (RVP). The Wilcoxon signed rank test p-values for area,
circumference, and radius were 0.01 at maximum RVP and 0.04 at minimum RAP. The
asterisks (*) show significant differences (𝑝 < 0.05, Wilcoxon signed rank test). Error bars
show the standard errors.

103
Table 5.2 Calculated circumference at minimum and maximum right ventricular pressure
(RVP) for intact and post chordae rupture (PCR) conditions. The values are presented for
all eight hearts used in the experiments along with the average (AVG) and standard
deviation (STD). Comparing the average values showed an increase in the circumference
post chordae rupture.
Circumference (𝑐𝑚)
At minimum RVP At maximum RVP
Heart no. Intact PCR Intact PCR
1 13.2 13.2 13.7 13.8
2 11.0 11.0 12.5 12.9
3 10.9 11.7 12.2 12.9
4 13.7 13.8 14.4 14.5
5 10.9 11.8 11.9 12.9
6 14.9 15.5 16.0 16.4
7 12.9 14.2 13.4 14.6
8 12.8 13.0 13.4 13.8
AVG 12.5 13.0 13.4 14.0
STD 1.5 1.5 1.3 1.2
Table 5.3 Calculated radius using the triangulation method (𝑅) along with the radii
calculated from the area (𝑅𝐴) and circumference (𝑅𝐶), using the assumption of flat annuli,
at minimum and maximum right ventricular pressure (RVP) for intact and post chordae
rupture (PCR) conditions. The values are presented for all eight experimental hearts along
with the average (AVG) and standard deviation (STD). Comparison between 𝑅, 𝑅𝐴, and
𝑅𝐶 showed that the three different methods of calculating the radius produced the same
results.
Radius (𝑐𝑚) At minimum RVP At maximum RVP
Heart Intact PCR Intact PCR no. 𝑅 𝑅𝐴 𝑅𝐶 𝑅 𝑅𝐴 𝑅𝐶 𝑅 𝑅𝐴 𝑅𝐶 𝑅 𝑅𝐴 𝑅𝐶
1 2.0 2.0 2.1 2.0 2.0 2.1 2.1 2.1 2.2 2.1 2.1 2.2
2 1.7 1.7 1.8 1.6 1.7 1.8 1.9 1.9 2.0 1.9 2.0 2.1
3 1.7 1.7 1.7 1.8 1.8 1.9 1.9 1.9 1.9 2.0 2.0 2.1
4 2.1 2.1 2.2 2.1 2.1 2.2 2.2 2.2 2.3 2.2 2.2 2.3
5 1.6 1.6 1.7 1.7 1.7 1.9 1.7 1.8 1.9 1.9 1.9 2.1
6 2.3 2.3 2.4 2.4 2.4 2.5 2.4 2.5 2.5 2.5 2.5 2.6
7 2.0 1.9 2.1 2.2 2.2 2.3 2.0 2.0 2.1 2.2 2.2 2.3
8 1.9 1.9 2.0 1.9 2.0 2.1 2.0 2.0 2.1 2.1 2.1 2.2
AVG 1.9 1.9 2.0 2.0 2.0 2.1 2.0 2.1 2.1 2.1 2.1 2.2
STD 0.2 0.2 0.3 0.3 0.2 0.2 0.2 0.2 0.2 0.2 0.2 0.2

104
5.4.3 Annulus Dilation Due to the Chordae Rupture
Table 5.4 shows the increase in area, circumference, and radius of the annuli (i.e.,
a measure of annuli dilation) due to the chordae rupture averaged over all ex-vivo porcine
hearts at maximum RVP. The area of the annuli dilated an average of 8.8% at maximum
RVP. The dilation at this point for both the circumference and the radius was approximately
4% on average. The segment-specific dilations were also calculated and are presented in
Table 5.5 for the AAS, APS, and ASS of the annuli. The largest average dilation in the
circumference of the annuli (6.3%) occurred at the AAS, whereas the lowest average
dilation (2.4%) occurred at the APS. Fig. 5.5 shows a comparison among the average
dilations (at maximum RVP) of three annulus segments. Statistical analyses showed that
there was no significant difference between the dilations in the different segments of the
annuli (Fig. 5.5).
Fig. 5.5 Comparison of the dilation (due to the chordae rupture) between annulus anterior
segment (AAS), annulus posterior segment (APS), and annulus septal segment (ASS) at
maximum right ventricular pressure (RVP). The Wilcoxon signed rank test p-values were
0.55, 0.38, and 0.74 between the AAS and APS, the AAS and ASS, and the APS and ASS,
respectively. No significant differences were observed (𝑝 > 0.05, Wilcoxon signed rank
test). Error bars show the standard errors.

105
Table 5.4 Geometric dilation in area, circumference, and radius of the heart annuli due to
chordae rupture at maximum right ventricular pressure (RVP) calculated using Equation
(5.1) along with the average (AVG) and standard deviation (STD) for each quantity.
Dilation at maximum RVP (%)
Heart no. Area Circumference Radius
1 2.4 1.0 1.1
2 5.2 3.2 2.5
3 11.9 6.4 5.1
4 1.0 0.4 0.9
5 17.1 8.1 8.3
6 5.9 2.6 3.3
7 20.8 8.6 9.3
8 5.9 2.5 2.9
AVG 8.8 4.1 4.2
STD 7.1 3.2 3.2
Table 5.5 Dilation in the length of annulus anterior segment (AAS), annulus posterior
segment (APS), and annulus septal segment (ASS) due to the chordae rupture at maximum
right ventricular pressure (RVP) calculated using Equation (5.1) along with the average
(AVG) and standard deviation (STD) for each quantity. The largest dilation occurred at the
AAS.
Dilation at Maximum RVP (%)
Heart No. AAS APS ASS
1 -1.2 2.3 1.9
2 7.6 -1.8 3.8
3 19.1 -5.2 -0.3
4 0.7 -1.4 5.6
5 10.2 7.6 4.5
6 2.8 1.4 3.8
7 9.2 12.8 2.3
8 1.8 3.5 2.4
AVG 6.3 2.4 3.0
STD 6.6 5.7 1.8
5.4.4 Changes in Annulus Geometry Throughout the Cardiac Cycle
The changes in metrics of each annulus throughout the cardiac cycle were
calculated using Equation (5.2), and the resulting values were averaged over all eight
annuli, as shown in Fig. 5.6. Table 5.6 also shows the average changes (calculated using

106
Equation (5.2)) at maximum RVP for normal and PCR ex-vivo porcine hearts. From the
minimum to the maximum RVP, the annulus area increased by 17 and 18% in intact and
PCR hearts, respectively. However, when accounting for the annulus dilation following
chordae rupture, the maximum change in area was found to exceed 27%. In other words,
the same PCR annuli showed more dilation if the changes were always referenced to the
corresponding intact hearts. The maximum changes in circumference and radius (in both
intact and PCR conditions) ranged roughly from 7.5% to 8.5%. Again, accounting for
chordae rupture–induced annulus dilation, approximately 12% maximum circumferential
and radial changes were calculated. The maximum change in segment-specific
circumferences during the cardiac cycle are also shown in Table 5.6. From this table, it can
be noticed that the AAS of the annulus circumference experienced a larger average change
during the cardiac cycle when compared with APS and ASS. Figure 5.7 shows the change
in the length of three segments of the annulus at maximum RVP for both intact and PCR
conditions. For the intact hearts, the changes in the length of the AAS during the cardiac
cycle were significantly higher than those for the other two segments (𝑝 = 0.03 for the
comparison between AAS and APS, 𝑝 = 0.02 for the comparison between AAS and ASS,
and 𝑝 = 0.84 for the comparison between APS and ASS, according to the Wilcoxon signed
rank test). There was, however, no significant difference between changes in the lengths of
different segments after chordae rupture (The smallest p-value was 0.08, according to the
Wilcoxon signed rank test for each comparison).

107
Fig. 5.6 Changes in (a) area, (c) circumference, and (e) radius as well as the absolute values
of (b) area, (d) circumference, and (f) radius throughout the cardiac cycle averaged over all
the annuli for intact and post chordae rupture (PCR) conditions. The shaded regions show
the standard errors. The temporal position of the maximum right ventricular pressure
(RVP) as well as the opening and closure of the tricuspid and pulmonary valves for the
intact case are shown in the graphs as a better illustration of the deformations that occur
throughout the cardiac cycle.

108
Fig. 5.7 Comparison of the change in the length of the annulus anterior segment (AAS),
annulus posterior segment (APS), and annulus septal segment (ASS) in intact and post
chordae rupture (PCR) conditions at maximum right ventricular pressure (RVP). The PCR
values include the dilation as well. For a comparison of the change in length between the
intact and PCR conditions, the Wilcoxon signed rank test was used; p-values were 0.02 for
AAS and ASS and 0.38 for APS. The p-values were 0.03, 0.02, and 0.84 for the
comparison of the change in length for the intact case between the AAS and APS, the AAS
and ASS, and the APS and ASS, respectively. The asterisks (*) indicate significant
differences (𝑝 < 0.05, Wilcoxon signed rank test). Error bars show the standard errors.
Table 5.6 Average geometric changes at maximum right ventricular pressure (RVP) for
intact and post chordae rupture (PCR) conditions calculated using Equation (5.2). The last
column shows the percentage of the change in geometric parameters with intact-to-PCR
dilation included in calculations. The geometrical parameters at minimum RVP were
selected as the reference to calculate the changes.
Geometrical Change at Maximum RVP (%)
Quantity Intact PCR PCR with dilation
Areal 17.2 18.1 27.6
Circumferential 7.4 7.9 11.9
Radial 8.0 8.6 12.6
Change in AAS 9.0 9.6 16.1
Change in APS 6.3 6.9 8.8
Change in ASS 6.1 6.7 9.3

109
5.4.5 Annulus Curve
The resulting average TV annulus has the shape of a nonplanar saddle curve. The
maximum points of this curve were on the AAS and APS close to the anteroseptal and
posteroseptal commissures, respectively. One of the minimum points, on the other hand,
was approximately placed at the middle of the ASS, and the other was on the AAS close
to the anteroposterior commissure. These observations are consistent with those reported
for the in-vivo TV annulus in an ovine model [80].
5.5 Discussion
The positional data obtained from the sonocrystals sutured around the ex-vivo
porcine heart annulus were used to analyze the annulus deformation during the cardiac
cycle. The effects of the chordae rupture were also investigated on this deformation by
cutting one of the septal chordae proximal to the posterior commissure. The analyses
showed that if we consider the annulus as a flat circle and use the calculated area and
circumference to estimate the radius, the estimated values are comparable to the values for
the radius that were calculated directly from the annulus geometry.
Throughout the cardiac cycle, the geometry of the annulus alters considerably such
that from the minimum RVP to the maximum RVP, the area roughly experiences a 20%
increase, and the circumference extends approximately 8%. Our analysis showed that these
deformations do not occur uniformly along the annulus. For example, the AAS experiences
the largest deformation (about 9% on average). In most TV repair procedures, a prosthetic
annuloplasty ring is used to decrease the annulus size and improve the valve hemodynamics
[8]. Considering the dynamic deformation of TV annulus observed in our study, further

110
research is needed to identify how the valve deformation changes following ring
annuloplasty [26].
Due to the inherent differences between the in-vivo and the ex-vivo cases, the
results reported in this study might not exactly match the in-vivo outcomes. The absence
of muscular contraction (including those of the myocardium and papillary muscles) and
the lack of the interaction between the right and left ventricles in the ex-vivo experiments
might affect the results in comparison to those of the in-vivo cases. As such, much caution
should be taken in interpretation of our results. For example, it has been reported in in-vivo
studies that the annulus dimensions decrease during the systole [81, 83]; for the ex-vivo
case, however, they increase during the systole. In actively beating hearts, the contraction
of the heart muscles decreases the annulus as well. In contrast, in passively beating hearts,
no active contraction is present, and the increased ventricular pressure causes the annulus
to expand during the systole. In particular, unlike our ex-vivo results, Rausch and
colleagues recently observed 7.17 ± 1.93 𝑐𝑚2 as the minima of the annular area during
systole in in-vivo ovine hearts, which was significantly smaller than the annular area during
diastole (i.e., 8.65 ± 1.98 𝑐𝑚2) in the same hearts [83]. A similar trend was also observed
for the measured perimeters in this in-vivo model (i.e., 10.2 ± 1.28 𝑐𝑚 systolic value as
compared to a significantly smaller diastolic value of 11.2 ± 1.27 𝑐𝑚 ). It is worth noting
that quantitative comparison of the in-vivo active beating heart measurements [83] with
our ex-vivo passive beating heart measurements should be conducted with caution due to
the inherent differences in ovine versus porcine models.
In addition, in many different types of soft tissues, even in those that are not as
mechanically active as cardiac muscles, the mechanical properties are different in the ex-

111
vivo setups as compared to those measured in the native in-vivo environment [191]. Such
differences have been attributed to the lack of perfusion and metabolic activities in the ex-
vivo environments. As such, potential differences in the mechanical responses of the
tissues in the in-vivo versus ex-vivo setups should also be considered in the interpretation
of our results. Nevertheless, during the diastole, when the right ventricle is expected to be
at its least active state, the measured ex-vivo area and circumference values (11.4 ±
2.8 𝑐𝑚2 and 12.5 ± 1.5 𝑐𝑚, respectively) closely matched those of the in-vivo
measurements (8.65 ± 1.97 𝑐𝑚2 and 11.1 ± 1.27 𝑐𝑚, respectively) [83]. It should be
noted that since plane projection of the three-dimensional geometry was used to calculate
the area in the aforementioned in-vivo study, the area calculated in our study was slightly
larger, as was expected. Furthermore, Fawzy et al. [81] reported that most changes in
circumference occur in the anterior segment of the annulus in the in-vivo hearts, which is
consistent with the findings of our study (Fig. 5.7).
In atrioventricular valves, the structures of the chordae tendineae and papillary
muscles anchor the valve leaflets and prevent them from billowing into the atrium during
ventricular contraction [8]. As such, one would expect that regurgitation might occur when
such constraints are removed from the leaflet(s) following chordae rupture. However, it is
not just the billowing effects that are prevented by the parachute-like structure of the
chordae tendineae and the papillary muscles. Our experiments showed that there exists a
mechanical interdependency among TV chordae tendineae, leaflets, and annulus. We
observed that immediately after chordae rupture, the dynamic deformation of TV annulus
changed extensively, with a significant increase in the annulus area, circumference and
radius. Annulus dilation, whether it develops over time or occurs acutely (as in the case of

112
trauma-induced chordae rupture), is expected to change the coaptation of the valve leaflets
and induce regurgitation [182]. Our measurements showed that, on average, the flow into
the right atrium decreased by 26% immediately after the septal chordae tendineae close to
the posteroseptal commissure was cut. Moreover, the maximum RVP dropped from 30 mm
Hg to 25 mm Hg, which is a 17% decrease. A similar decrease was observed in the PAP.
These changes show how chordae rupture can alter the hemodynamics of the heart.
Recent ex-vivo studies have shown that TV annulus and leaflets are under tension
[140, 192]. An increase in the annulus area following chordae rupture may change the
annulus tension and alter the homeostatic mechanical environment to which the leaflets
and the myocardium surrounding the annulus are subjected. The homeostatic mechanical
environment is extremely important for the normal function of TV and its surrounding
tissues and can alter its normal mechanical properties [134, 140]. In all types of cardiac
valves, valve interstitial cells reside within the leaflet tissue [193-197]. The valve
interstitial cells, by means of protein synthesis and enzymatic degradation, maintain the
structural integrity of the leaflet tissue. In all types of soft tissues, collagen type I, which is
the main load-bearing protein of the extracellular matrix, scales with tissue stiffness [198].
The in-vivo valve interstitial cells respond to changes in mechanical loading and alter the
tissue stiffness via collagen synthesis or degradation. For example, in murine TVs,
increasing the mechanical load to which the leaflets are subjected led to increased mRNA
amounts of both collagen type I and III as well as to higher collagen turnover [199].
Conversely, in an ovine model, MV collagen content was decreased when the ventricular
pressure (and consequently the mechanical loading on the leaflets) decreased [190].
113
It is worth noting that cells are not the only components that are sensitive to changes
in mechanical loading [86]. While large mechanical strains could increase the rate of
extracellular matrix catabolism in cardiac valves [200], studies have shown that the
extracellular matrix collagen is more stable and degrades more slowly under homeostatic
mechanical strain [78, 201, 202]. Considering such an important influence of the tissue
mechanical milieu on short-term as well as long-term valve responses, it is essential to not
ignore dilation in the annulus following chordae rupture. Surely, further in-vivo animal
studies are necessary to better examine the long-term effects of chordae rupture on TV
function and structure. It is, however, expected that, in addition to the immediate effects of
annulus dilation in generating secondary tricuspid regurgitation, in the long term, changes
in the mechanical environment of TV leaflet and right ventricle myocardium could cause
further negative remodeling responses and exacerbate the detrimental outcomes of chordae
rupture.
In summary, we employed an ex-vivo heart setup and measured the deformation of
porcine TV annuli during simulated cardiac cycles. Regurgitation was induced by cutting
the chordae tendineae of the septal leaflets. For the first time, we observed that TV annulus
dilates immediately after the rupture of the chordae tendineae. Although TV may be
initially asymptomatic, instantaneous annulus dilation following chordae rupture could
lead to exacerbation of TV regurgitation and potentially to mechanically-induced
remodeling responses in TV leaflets, the remaining intact chordae tendineae, the papillary
muscles, and/or the ventricular myocardium. More careful examinations and early surgical
interventions might be necessary to prevent mid-term/long-term negative effects of

114
mechanically-induced remodeling in asymptomatic TVs following the rupture of the
chordae tendineae.
115
CHAPTER 6VI
EFFECTS OF CHORDAE RUPTURE ON THE SURFACE STRAINS OF THE
TRICUSPID VALVE LEAFLETS
(The content of this chapter will be published as a journal paper entitled “Effects of
Chordae Rupture on the Strains of Tricuspid Valve Septal Leaflet: An Ex-vivo Study on
Porcine Hearts”.)
6.1 Summary
Between 2000 and 2012, roughly 40,000 cases of chordae tendinea rupture (CTR)
were reported in the US by the National Inpatient Sample. This lesion is often overlooked,
especially when it comes to CTR of TV. To date, abnormal TV mechanical response in the
presence of CTR is still poorly understood. While recent studies have shown that
significant alteration of in-vivo valve deformation could happen when the conditions in the
atrioventricular valve annuli change, many traditional methods for examining cardiac valve
deformations require dissection of the valve. In the current work, however, porcine valve
leaflet deformation was studied in an intact heart in an ex-vivo setup using sonomicrometry
techniques, and the effects of CTR were examined by severing the septal chordae adjacent
to the posteroseptal commissure.
Following chordae rupture, the maximum RVP dropped from 31 𝑚𝑚 𝐻𝑔 to
25 𝑚𝑚 𝐻𝑔, and the flow rate decreased by 26%, showing that regurgitation occurred
immediately after chordae rupture. The chordae rupture significantly altered the

116
distribution of the strains over the septal leaflet surface. For example, a maximum increase
from 14.64 ± 2.96 to 18.15 ± 3.44 in maximum principal strain was observed after
chordae rupture at the distal edge of the septal leaflet with the p-vale of 0.013.
In this ex-vivo study, we were able to observe the primary regurgitation and record
the immediate decrease in the pressure and flowrate as well as the instantaneous alteration
in the distribution of the strains over the septal leaflet right after CTR. These changes in
the strain distribution shows that, PCR, the tricuspid apparatus and the myocardium could
become exposed to new mechanical loading, potentially resulting in further remodeling
responses and aggravating the negative effects of this lesion.
6.2 Introduction
TV regurgitation arises from a lack of leaflet coaptation that may result from
complications stemming from a few pathologies of the left side of the heart. Chief among
the left side heart diseases is MV regurgitation. TV regurgitation (i.e., non-functional)
poses a greater long-term risk to the patient, since it is well tolerated and the patient may
seem to be asymptomatic [185, 189, 203-205]. Increased morbidity and mortality arises
when the condition is undetected, as right ventricular dysfunction and atrial fibrillation are
likely to lead to chronic heart failure [185]. In many cases involving severe blunt chest
trauma (such as automobile accidents), studies in the literature and various case reports
point to CTR as a likely outcome [189, 204, 206, 207]. In the aforementioned cases, the
rapid compression of the right ventricle induces regurgitation of the atrioventricular valve;
this will result in fatal damage to the heart or, at a minimum, a ruptured chordae tendineae
[208]. In addition to being induced by chest trauma, CTR has also been reported as an
unforeseen outcome of medical procedures such as right heart catherization, where

117
penetrating chest trauma can induce structural disruption of TV structure. Finally, various
cardiovascular pathologies may also play a role in weakening the chordae structure, as can
occur in degenerative valve diseases (myxomatous valve diseases) such as Marfan
syndrome, which can lead to chordae elongation and ultimately to rupture and valvular
insufficiency [209].
Although no definite figure is known for how many cases of CTR in TV have been
documented, its prevalence is likely to be higher than the numbers indicated in the reported
statistics [186, 187]. Between 1999 and 2008, a total of 28,726 operations involving TV
were performed [24], with CTR cited as the most common cause for TV regurgitation (with
one study placing the incidence at 55% of patients). The number of reported cases is likely
to be underestimated for two main reasons [185, 189]. First, as the aforementioned TV
surgery study was limited to participants over the age of 30, it does not account for cases
in younger adults or children. Second, TV regurgitation, whether a result of CTR or not, is
often overlooked during diagnosis [187]. While TV regurgitation can be properly
diagnosed via transthoracic echocardiography and transesophageal echocardiography, it is
usually concurrent with the diagnosis of another condition [203, 210]. The fact that most
individuals with TV regurgitation have been misdiagnosed, were only diagnosed while
physicians were searching for a different indication, or have simply gone undiagnosed
should be cause for alarm [185, 189, 203, 205].
Current techniques to address CTR include reconstruction or replacement. Both of
these options involve the use of chordae implants and may even resort to chordae
transposition, which may not be ideal due to the natural and brittle structure of TV [185].
Because of the risks of undetected and untreated TV regurgitation, coupled with the delay
118
in treatment due to the long time between onset and diagnosis (up to 11 years in some
cases) [177, 211], a proper understanding of CTR is key to developing an approach to either
repair or replace the affected chordae. The abundant insights into CTR and its implications
for the left side of the heart overshadows the detrimental effects on TV apparatus and the
heart as a whole. In this study, we document the behavior of TV septal leaflet mechanics
before and after simulating CTR. Our objective is to examine the changes is the
hemodynamics of TV and alteration of the leaflet strains PCR in an effort to provide
quantitative and comprehensive data that will prove invaluable in determining the best
procedure to address this condition.
6.3 Materials and Methods
6.3.1 Ex-vivo Heart Apparatus
In a previously developed ex-vivo passive beating heart apparatus (Fig. 4.1a), a
positive displacement pump (SuperPump AR Series, Vivitro Labs, Inc., Victoria, BC,
Canada) was utilized to beat porcine hearts passively by circulating PBS into the hearts
[140]. The resulting transvalvular pressure from this circulation forces TV to open and
close, imitating the native deformations of intact TV leaflets. The apparatus was developed
in a way that allowed the monitoring and recording of RAP, RVP, PAP, and the mean flow
rate throughout the cardiac cycle. Based on the International Standard Organization (ISO
5840) and U.S. Food and Drug Administration regulations for heart valve testing, the
pump’s standard 70 𝑏𝑝𝑚 waveform was used, and other pump parameters were set to keep
the hydrodynamic pressures in TVs in the test setup consistent with those in a native valve
during the cardiac cycle. More details about this setup can be found in our previous
publication [140].

119
6.3.2 Sample Preparation
Fresh porcine hearts were transferred to the lab from a local slaughterhouse (3-D
meats, Dalton, OH) in bags filled with PBS that were covered in ice. The right chambers
of the hearts were flushed out with PBS and checked carefully with an endoscopic camera
(an SSVR-710 Snakescope) to ensure that no blood clots were present inside the chambers
or around the valves. Eight sonocrystals (Somometrics Co., London, ON, Canada), 1 or
2 mm in diameter, were then sutured over the septal leaflet in a predefined arrangement
(Fig. 4.4). To eliminate any cutting and patching of the heart chambers, suturing was
performed through the superior vena cava, and the sonocrystal wires were passed through
the inferior vena cava. Umbilical clamps were used to prevent any leakage from the inferior
vena cava and the coronary vein. The heart was then connected to the ex-vivo beating heart
apparatus through the superior vena cava, pulmonary artery, and an incision made at the
bottom of the right apex, as explained in our previous publication [140]. To make a
reference frame for the positional data of the sonocrystals, three 3-mm-diameter
sonocrystals were attached to the outside of the myocardium around the apex.
6.3.3 Data Acquisition
A sonomicrometer (TRX Series 16, Somometrics Co., London, ON, Canada) was
utilized to trigger the sonocrystals and record their signals. The sonomicrometer
communicated with a computer through a USB port using SonoLabDS3 software
(Somometrics Co., London, ON, Canada). To make the data synchronization easier, the
pressure sensors were also connected to analog input channels of the sonomicrometer.
After running the pump, an endoscopic camera (SSVR-710 Snakescope) was sent into the
right atrium — through a probe embedded into the superior vena cava connector [140] —

120
to visually assess the coaptation of the valve leaflets during the beating of the heart. An
oscilloscope (MSO2014B, Tektronix, Beaverton, OR) was used to visualize the signals and
adjust the sensitivity of the sonocrystals to reduce the signal-to-noise ratio. After adjusting
the necessary parameters, the sonocrystal and pressure signals were recorded with a
frequency of 100 Hz for 20 seconds using SonoLabDS3 software. The mean flow rate was
also read from the flowmeter and recorded in each experiment. To model CTR, the chordae
tendineae of the septal leaflet in the proximity of the posteroseptal commissure was cut
using surgical scissors. The experiment was repeated, and the data were recorded for
another 20 seconds with a frequency of 100 Hz. In total, eight successful experiments were
conducted.
6.3.4 Pressure Data Analysis
The hemodynamic pressures (RAP, RVP, and PAP) were recorded during the
cardiac cycle for all experiments for the intact and PCR conditions. As the relative
transvalvular pressures drive the deformation of the valve and the flow, the effects of
hydrostatic pressures on the pressure signals due to the elevation differences between the
pressure probes and the free surface of the liquid (see Fig. 4.1a) were negated by shifting
the average pressure signals. As such, the average RAP and RVP were shifted in such a
way that they are close to zero during the diastole (if a shift was necessary). The PAP was
also adjusted slightly to match these shifts. This process can be interpreted as deducting
the pressure equivalent of the vertical distance between the free surface of the reservoir
fluid and the right atrium, which shifted the diastole portion of the RVP and RAP close to
zero, and the shift in the PAP to compensate for the vertical distance between the bottom
of the right ventricle (where the RVP sensor was located) and entrance of the pulmonary

121
artery (where the PAP sensor was located). As pressure levels are relatively low in the right
side of the heart, the adjustments for these equivalent hydrostatic pressures were necessary
to obtain more consistent pressure curves.
6.3.5 Deformation Data Processing and Analysis
The distance between each pair of sonocrystals was recorded throughout the
experiment. The recorded signals were processed using SonoVIEW software (Sonometrics
Co.) to remove the noise and determine unusable signals (signals with too much noise or
drift). Utilizing SonoXYZ software (Sonometrics Co.), the modified signals were then used
to reconstruct the absolute positional coordinates for each sonocrystal with respect to a
defined coordinate system throughout the entire cardiac cycle. These positional data, which
represent the deformation of the septal leaflet surface during the cardiac cycle, were used
to calculate the strains for both intact and PCR conditions [26, 86, 87, 140]. More
information regarding the triangulation and strain calculation can be found in our previous
publication [140].
6.3.6 Average Model
The measured deformations for all samples were used to develop an average
geometry and deformation model. This average model can provide more insight regarding
the geometry of septal leaflet as well as its deformation throughout the cardiac cycle. As
the recorded data for each sample were in their own reference frame, it was necessary to
represent the data for all the samples in a unique coordinate system for averaging. As such,
the singular value decomposition method [212, 213] was used to transform all the data into
one coordinate system and register the corresponding markers on top of each other with a
minimum cumulative error. The transformed data were then averaged over all samples in

122
a frame-by-frame manner to generate the average geometry and deformation along the
cardiac cycle [83]. This average model was generated for both intact and PCR cases.
6.3.7 Statistical Analysis
The displacement and pressure signals were recorded for 20 seconds, which is
equivalent to approximately 23 cardiac cycles. The standard deviation of the comparison
of these consecutive cardiac cycles was ~0.1% of the mean value of the measured quantity.
Therefore, the signals did not show any significant intervariability among different cardiac
cycles. However, to further reduce noise in the signals, the recorded displacement and
pressure signals were averaged over all cardiac cycles. These average signals were used
for subsequent calculations and analysis. Student’s t-test was used for all statistical
analyses conducted in this study, where any result with 𝑝 < 0.05 was considered to be
statistically significant. Data are presented in the form of mean ± standard deviation,
wherever necessary.
6.4 Results
6.4.1 Average Model
An average model was generated using the measured positional data for all eight
hearts. Figure 6.1 shows this average geometry at the reference frame (minimum RAP) for
normal hearts and PCR cases. This figure shows the position of the markers around the
annulus and across the septal leaflet for both intact and PCR cases simultaneously. Crystals
are numbered in this figure to facilitate tracking of their positions from the intact condition
to the PCR case. In this plot, it can be noticed that Crystal 6 is close to the posteroseptal
commissure and Crystal 8 is near the anteroseptal commissure. To generate the average
model, such a geometry was developed for each frame throughout the cardiac cycle.

123
Fig. 6.1 TV septal leaflet and annulus average geometry at reference frame (minimum
RAP) for normal (blue) and PCR (red) conditions.
6.4.2 Pressures
Figure 6.2 illustrates the average pressure signals for the intact case. This graph
shows that while the experiments were conducted in an ex-vivo setup, the pressure signals
were comparable with those of in-vivo hearts [160]. The RVP, which were mostly close to
zero during the diastole, showed a rise to 31 mm Hg in the peak area of systole. As shown
in Fig. 6.2, a slight drop was observed in the RVP right after the start of the diastole phase.
The PAP ranged approximately from 6 to 31 mm Hg. While the RAP remained close to
zero during diastole, it had a peak of 17 mm Hg during the systole, which does not occur
in a normal human RAP signal. The range of the RVP closely matched those reported for
porcine hearts [161-164]. While we were not able to find reliable PAP and RAP values
reported for porcine hearts in the literature, these signals (Fig. 6.2) closely matched those

124
of human hearts [160]. The standard errors, shown in the shaded areas in Fig. 6.2, were
small—indicating that the pressures measured for different hearts did not deviate much
from the calculated average, despite the variability of the porcine hearts used in the
experiments. A small minimum was observed in the RVP signal right before it plateaued
during diastole after dropping from its peak during systole (Fig. 6.2). As shown in Fig. 6.2,
a closer inspection of the pressure signals showed that RVP and RAP separate at 0.19 s
and come back together at 0.56 s, which indicates TV closure and opening, respectively,
at these time points. Moreover, the signal for the RVP crosses the signal for the PAP at
0.29 s and 0.44 s, indicating the PV opening and closure, respectively, at these points.
Fig. 6.2 Average hemodynamic pressures during the cardiac cycle for intact conditions.
The shaded areas show the standard error.
In Fig. 6.3, pressure signals are presented for the PCR condition. After chordae
rupture, the RVP ranges from close to zero to 25 mm Hg, and the PAP ranges
approximately from 5 to 24 mm Hg. The pressure signals for RVP and PAP intersect first

125
at 0.31 s (when the PV opens), and again at 0.49 s (when the PV closes again). The
pressure signals for RAP, on the other hand, range from close to zero to more than
18 mm Hg.
Fig. 6.3 Average hemodynamic pressures during the cardiac cycle for post chordae rupture
(PCR) conditions. The shaded areas show the standard error.
6.4.3 Leaflet Deformation and Strain Spatial Distribution
The position of the fiducial markers (sonocrystals) were utilized to calculate the
strains over the septal leaflet of TV for both normal and PCR cases. More details regarding
these calculations can be found in our previous publication [140]. To illustrate the spatial
distribution of the strains, the developed average geometry of the septal leaf was used.
Figure 6.4 compares the spatial distribution of areal, maximum principal, circumferential,
and radial strains obtained over the developed average septal leaflet geometry at maximum
RVP before and after chordae rupture. The strains showed in this figure are averaged over
all eight hearts. The bold black edge that connects Crystals 6, 7, and 8 is the annulus side
126
of the leaflet (for a better understanding of the leaflet directions, please refer to Fig. 6.1).
This figure (Fig. 6.4) showed that the spatial distribution of the strains was largely altered
following the chordae rupture. While the strains are more uniformly distributed over the
leaflet surface when the leaflet is intact, they vary widely throughout the leaflet surface
after chordae rupture. From this figure, it can be noticed that the concentration of the strains
moves towards the edge where the chordae has been severed (i.e., toward Crystal 1).
Averaging the strains over the leaflet (spatial average), we obtain a single strain
signal (for each of the areal, maximum principal, circumferential, and radial strains)
throughout the cardiac cycle for each heart. Figure 6.5 presents a comparison of the
maximum of these strain signals averaged over all eight hearts (the error bars show the
standard errors) for different types of strains. Except for the circumferential strain, all
average strains showed an increase after chordae rupture. The maximum principal strain in
this figure increased from 11.19 ± 1.51 for the intact case to 11.95 ± 1.95 for the PCR
case, and the p-value for comparison between these two cases was 0.292. Figure 6.6
presents a comparison of the maximum principal strain averaged over all hearts along with
the standard errors for intact and PCR cases for the sonocrystals located on the distal edge
of the leaflet (Sonocrystals 1 and 2, as shown in Fig. 6.1). An increase from 14.64 ± 2.96
to 18.15 ± 3.44 and 13.15 ± 2.00 to 15.18 ± 2.30 in maximum principal strain was
observed after chordae rupture at the position of Crystals 1 and 2, respectively. The p-value
for this comparison was 0.013 for Crystal 1 and 0.166 for Crystal 2. To see how the heart
deforms throughout the cardiac cycle, the averaged septal leaflet geometry was plotted at
different time points, as illustrated in Fig. 6.7. This figure shows the leaflet deformation
for both intact and PCR cases for comparison purposes. The colormaps in this figure show

127
the distribution of the maximum principal strain over the septal leaflet at different time
points in the cardiac cycle. The change in the valve deformations and the deviation of the
strain distribution was notable following the chordae rupture (Fig. 6.7).
Fig. 6.4 Spatial distribution of areal, maximum principal (Max Princ), circumferential
(Circ), and radial strains demonstrated over the developed average septal leaflet geometry
at maximum right ventricular pressure (RVP) before (top row) and after (bottom row)
chordae rupture.

128
Fig. 6.5 Comparison of the average (over all the hearts) of maximum of the strain’s spatial
average signal (strain is averaged over the leaflet surface throughout the cardiac cycle).
Error bars show the standard error.
Fig. 6.6 Comparison of the maximum of maximum principal strain between intact and post
chordae rupture (PCR) cases for Crystal 1 and Crystal 2, shown in Fig. 6.1.

129
Fig. 6.7 Calculated average TV septal leaflet maximum principal strain, plotted at different
timepoints to show the deformation of the leaflet throughout the cardiac cycle for both
intact (top row) and post chordae rupture (bottom row) conditions. The color map shows
the distribution of the maximum principle strain.
6.4.4 Temporal Distribution of the Strains
To track the changes in the strains throughout the cardiac cycle and compare their
temporal distribution, the spatial average of the strains was calculated at each time point.
This averaging provided a single strain curve for each type of strain, showing the changes
over time for each heart. These signals were averaged for all eight hearts, and the resulting
curves for areal, maximum principal, circumferential, and radial strains before and after
chordae rupture were plotted (Fig. 6.8). Opening and closure of the valves shown in this
graph are based on the intact conditions. These plots showed that, while the spatial
distribution of the strains was significantly altered following chordae rupture (see Fig. 6.4),
the strains, on average, did not change significantly throughout the cardiac cycle and
followed relatively the same shape. Specifically, the spatial average of the maximum

130
principal strain maintained the same shape throughout the cardiac cycle after the chordae
was severed. Based on Fig. 6.8, the rapid growth in strain can be observed immediately
after closure of TV (at 0.2 s). Comparison of the plots in this figure with the pressure plots
in Figs. 6.2 and 6.3 show that the maximum strains occurred at nearly the same time as the
RVP reached its peak (at around 0.4 s). After this peak, the strains rapidly dropped towards
the end of the systole. During the diastole, the strains mostly remained close to zero.
Fig. 6.8 Temporal distribution of the spatial average of the strains throughout the cardiac
cycle for intact and post chordae rupture (PCR) conditions averaged for all hearts. The
shaded area shows the standard error.
6.5 Discussion
Chordae rupture was found to significantly alter TV leaflet strain distribution and
annulus geometry during the cardiac cycle. As such, annulus dilation is an indicator of the
development of TV regurgitation. In addition, alteration in mechanical strains immediately
following CTR may result in remodeling responses that could further influence TV
function/malfunction.

131
Chordae rupture changed the normal geometry of the annulus and septal leaflet
considerably. In addition to the dilation of the annulus, severe alteration occurred after
chordae rupture in the portion of the septal leaflet adjacent to the ruptured chordae (Crystals
1, 2, 3, and 4, as shown in Fig. 6.1). The trajectory of this alteration throughout the cardiac
cycle generates a waveform movement in this area of the septal leaflet in the PCR case that
is not present in the intact leaflet.
Our ex-vivo beating heart apparatus was able to reproduce ventricular pressure
waveforms that closely match those of an active heart [160]. As the hemodynamic
parameters of the pulmonary side are similar in human and porcine hearts, studying porcine
TV deformations can provide significant information regarding the deformations of TV in
a human heart. For example, human and porcine RVP ranges are very close: the RVP
ranges roughly from zero to 30 mm Hg for the human heart and from zero to 33 mm Hg
for the porcine heart [128, 160-164].
The chordae rupture prevented proper coaptation of TV. As such, when the pump
pushed the liquid back into the ventricle during the systole phase, a portion of the liquid
regurgitated back into the right atrium through TV, preventing it from coaptating properly.
Therefore, the average flow rate reduced by approximately 26% after chordae rupture. This
regurgitation following the chordae rupture prevented the pressure from rising to the peak
in the intact condition, and an approximate drop of 6 𝑚𝑚 𝐻𝑔 in the maximum RVP was
observed (Figs. 6.2 and 6.3).
As shown in Fig. 6.2, RAP rises slightly above the normal human pressure profile
during the systole, which may be due to a slight regurgitation during this phase. While the

132
coaptation of the leaflet was verified visually during each experiment, the weight of the
sonocrystals and the resistance of the attached wires to bending could have prevented the
leaflets from closing tightly [140]. The pressure increases after chordae rupture (Fig. 6.3)
confirms that additional regurgitation is occurring due to the chordae rupture.
Closer examination of Figs. 6.2 and 6.3 shows that PV opening was slightly delayed
after chordae rupture. This can be explained by considering the fact that due to the
regurgitation (and reduced flow rate), it takes more time for the pressure to rise high enough
to open the PV. Moreover, the PV closes with a notable delay after chordae rupture in
comparison to the intact case. To explain this delay, we should consider the fact that due
to the regurgitation, the pressure levels during the systole dropped. Thus, during the systole,
the pulmonary artery is subjected to lower pressures, which indicates that this compliant
artery expands less than normal. As a result, when the pressures pass their peak during the
systole, the pulmonary artery pushes against the fluid with a lower force and causes a delay
in the closure of the PV.
The positional data of the sonocrystals sutured to TV septal leaflet of the ex-vivo
beating heart were used to analyze deformations and calculate the strains throughout the
cardiac cycle [140]. By cutting the septal chordae adjacent to the posteroseptal
commissure, it was possible to investigate the effects of chordae rupture on the
deformations and strains. In previous studies, the strains and stretches were calculated
based on the position of the fiducial markers at the minimum left/right ventricular pressure
[30, 85]. However, as a small drop was observed in the measured RVP in the current
study—which creates an artificial global minimum in this RVP signal—the positions of
the sonocrystals at the minimum RAP were chosen as the reference configuration. This
133
was a reasonable choice, since the minimum RVP and RAP show some overlap under
normal conditions [140, 160].
Figure 6.80 shows the spatial average strain signals, which are also averaged over
all the hearts, while Fig. 6.5 shows the average of the maximums of the spatial average
strain signals. It should be noted from these figures that the peak of the means (the peak of
each signal in Fig. 6.8) is always less than (or ideally equal to) the mean of the peaks (the
corresponding value in Fig. 6.5).
The average values for the maximum principal strains and areal strains measured
in this experiment were 11.2% and 9.8%, respectively, before chordae rupture and 12.0%
and 10.0%, respectively, after chordae rupture. While the in-vivo strains in porcine TV
leaflets have not yet been reported in the literature, the values obtained in this study are
comparable to those reported for the anterior leaflet of an ovine MV [30].
6.6 Conclusion
A uniquely developed ex-vivo apparatus to facilitate passive beating of a porcine
heart (Fig. 4.1a) and sonomicrometry techniques were used to examine the effects of CTR
on the deformation of TV septal leaflet [140]. Experiments were conducted on eight intact
porcine hearts as well as on the same hearts after the septal chordae tendineae were severed
at a location adjacent to the posteroseptal commissure. The chordae rupture resulted in
immediate dilation of TV annulus following a drop of 19% in the maximum RVP (Figs.
6.2 and 6.3) and an increase of 26% in the average flow rate. Changes in the pressure levels
and the flowrate revealed the presence of regurgitation immediately following chordae
rupture. The deformation of the leaflet was observed to change right after chordae rupture

134
(Fig. 6.1), and the analysis of the surface strains over the septal leaflet revealed a significant
alteration of the strain distributions over the leaflet surface throughout the cardiac cycle
(Figs. 6.4 and 6.7). Long-term remodeling responses are expected to occur due to changes
in the mechanical environment of the valve apparatus that might alter the normal behavior
of the valve. Finally, we emphasize the limitations inherent in using an ex-vivo setup in
this study. Any application of the results from this study must take the ex-vivo nature of
the results into account.
135
CHAPTER 7VII
FINITE ELEMENT MODELING AND SIMULATION OF THE TRICUSPID VALVE
7.1 Introduction
In order to develop new surgical techniques for TV repair and improve the available
strategies, it is necessary to have an accurate FE model for the TV. Such a model can be
used to simulate surgical procedures and predict the outcomes before the surgery is
performed, helping the surgeon to preplan the procedure so as to maximize the quality of
the result. This model could also be used in the development of new prosthetic heart valves
that can more accurately mimic the behavior of a native valve. Such a development will
facilitate in-silico examination of valve repair techniques and will aid in predicting
alterations in the biomechanical behavior of TV following such surgeries.
To date, the MV has been more widely studied, and a larger number of well-
developed FE models have been proposed to simulate its behavior [10, 42, 88, 89, 92, 214-
219]. In contrast, comparatively few researchers have studied TV [9, 42, 107, 220], and
only one very elementary model had been published [44] before this study due to the lack
of accurate geometrical and mechanical information for this valve. Later, a more accurate
FE model of TV was developed [91]; however, insufficient information was provided for
its outcome to be validated.
In our previous studies (described in chapters II and III, [117, 134]), a material
model was developed to represent the mechanical behavior of the TV in response to
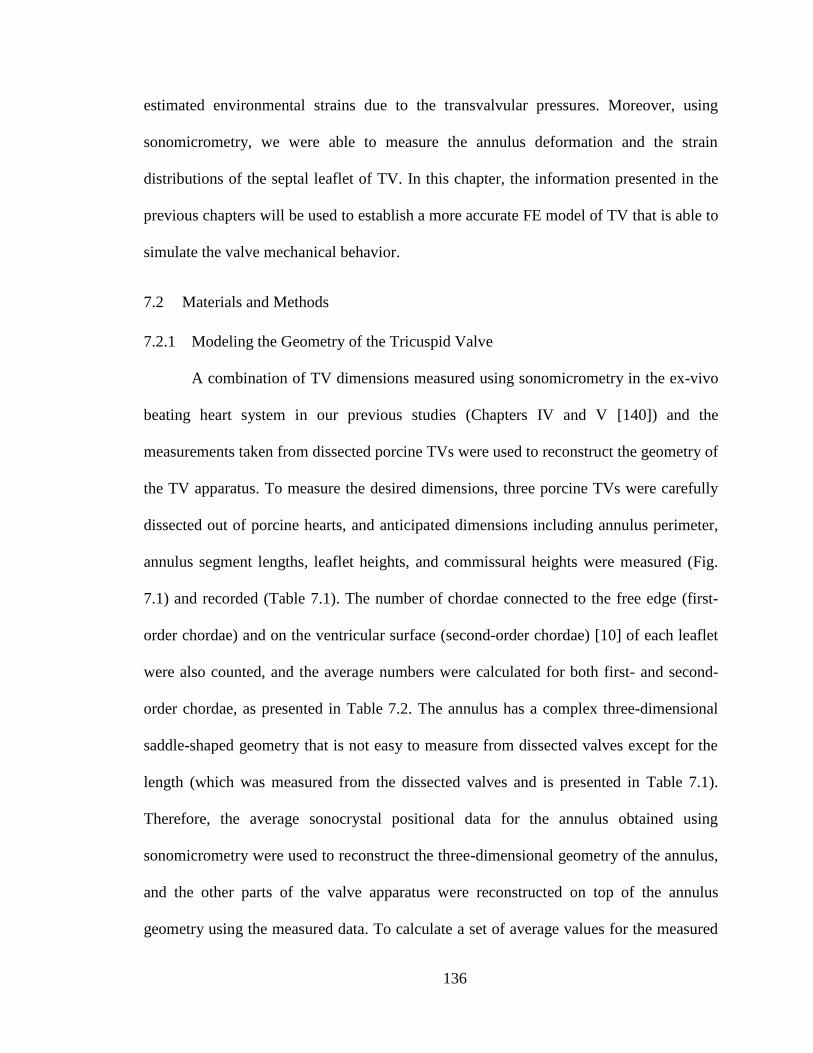
136
estimated environmental strains due to the transvalvular pressures. Moreover, using
sonomicrometry, we were able to measure the annulus deformation and the strain
distributions of the septal leaflet of TV. In this chapter, the information presented in the
previous chapters will be used to establish a more accurate FE model of TV that is able to
simulate the valve mechanical behavior.
7.2 Materials and Methods
7.2.1 Modeling the Geometry of the Tricuspid Valve
A combination of TV dimensions measured using sonomicrometry in the ex-vivo
beating heart system in our previous studies (Chapters IV and V [140]) and the
measurements taken from dissected porcine TVs were used to reconstruct the geometry of
the TV apparatus. To measure the desired dimensions, three porcine TVs were carefully
dissected out of porcine hearts, and anticipated dimensions including annulus perimeter,
annulus segment lengths, leaflet heights, and commissural heights were measured (Fig.
7.1) and recorded (Table 7.1). The number of chordae connected to the free edge (first-
order chordae) and on the ventricular surface (second-order chordae) [10] of each leaflet
were also counted, and the average numbers were calculated for both first- and second-
order chordae, as presented in Table 7.2. The annulus has a complex three-dimensional
saddle-shaped geometry that is not easy to measure from dissected valves except for the
length (which was measured from the dissected valves and is presented in Table 7.1).
Therefore, the average sonocrystal positional data for the annulus obtained using
sonomicrometry were used to reconstruct the three-dimensional geometry of the annulus,
and the other parts of the valve apparatus were reconstructed on top of the annulus
geometry using the measured data. To calculate a set of average values for the measured
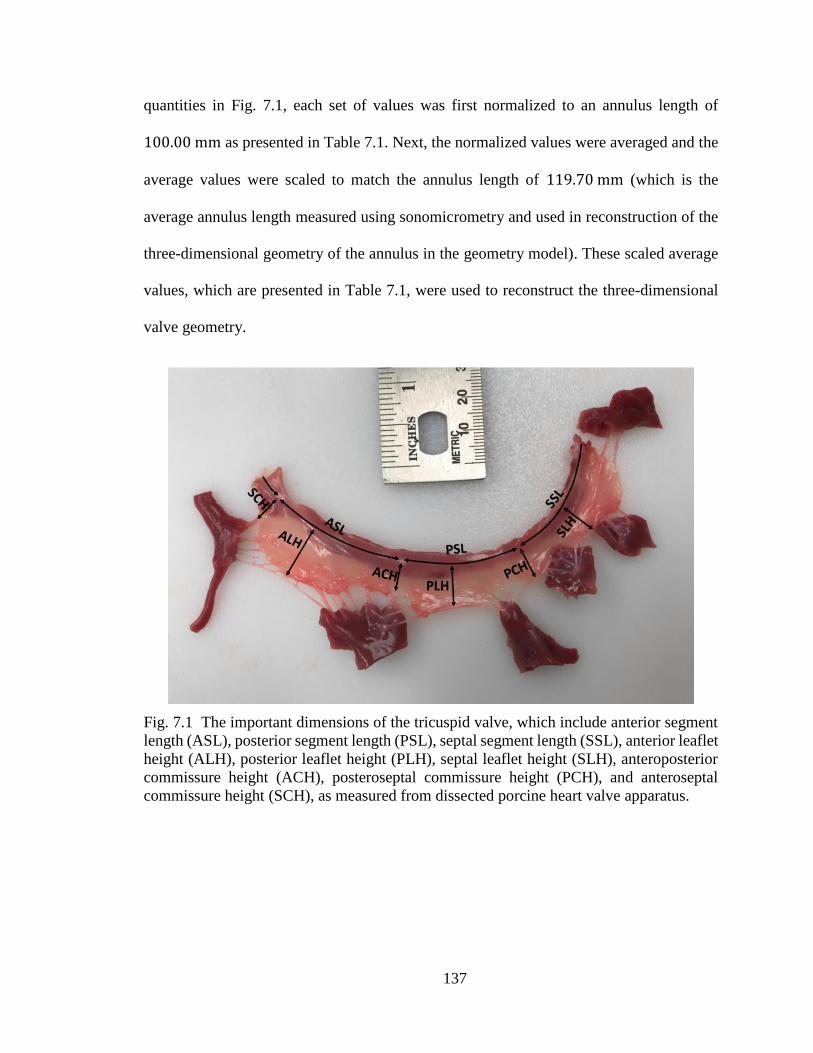
137
quantities in Fig. 7.1, each set of values was first normalized to an annulus length of
100.00 mm as presented in Table 7.1. Next, the normalized values were averaged and the
average values were scaled to match the annulus length of 119.70 mm (which is the
average annulus length measured using sonomicrometry and used in reconstruction of the
three-dimensional geometry of the annulus in the geometry model). These scaled average
values, which are presented in Table 7.1, were used to reconstruct the three-dimensional
valve geometry.
Fig. 7.1 The important dimensions of the tricuspid valve, which include anterior segment
length (ASL), posterior segment length (PSL), septal segment length (SSL), anterior leaflet
height (ALH), posterior leaflet height (PLH), septal leaflet height (SLH), anteroposterior
commissure height (ACH), posteroseptal commissure height (PCH), and anteroseptal
commissure height (SCH), as measured from dissected porcine heart valve apparatus.
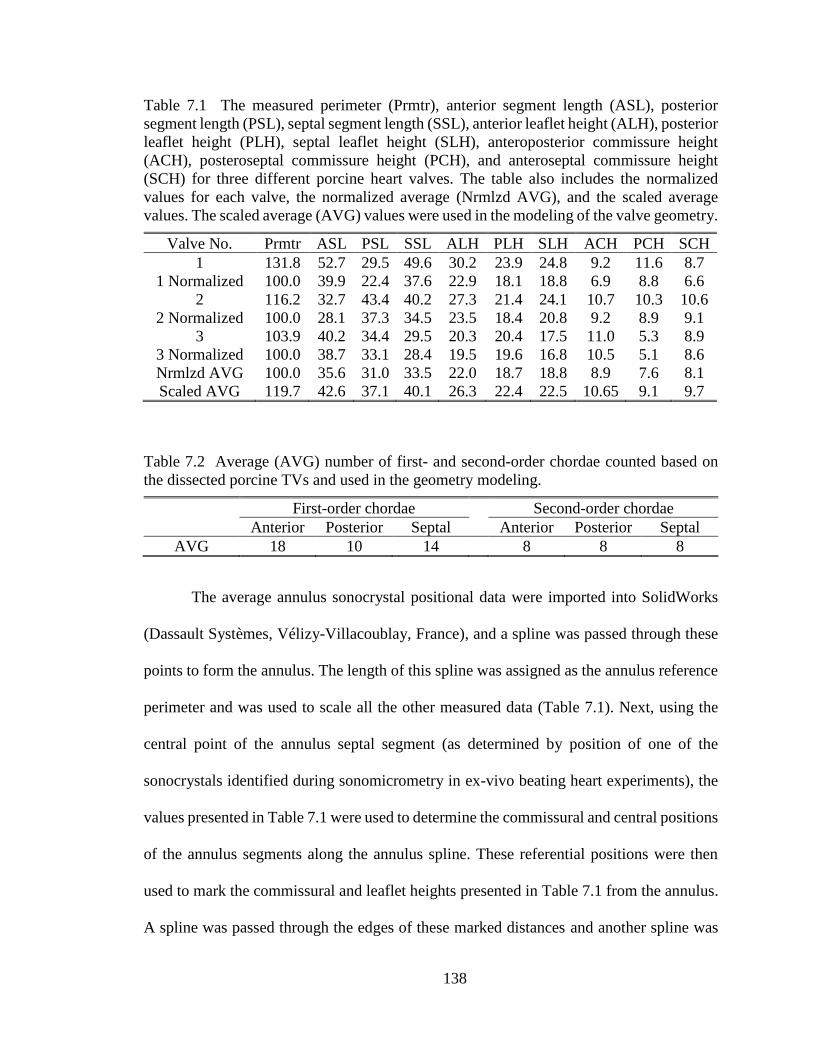
138
Table 7.1 The measured perimeter (Prmtr), anterior segment length (ASL), posterior
segment length (PSL), septal segment length (SSL), anterior leaflet height (ALH), posterior
leaflet height (PLH), septal leaflet height (SLH), anteroposterior commissure height
(ACH), posteroseptal commissure height (PCH), and anteroseptal commissure height
(SCH) for three different porcine heart valves. The table also includes the normalized
values for each valve, the normalized average (Nrmlzd AVG), and the scaled average
values. The scaled average (AVG) values were used in the modeling of the valve geometry.
Valve No. Prmtr ASL PSL SSL ALH PLH SLH ACH PCH SCH
1 131.8 52.7 29.5 49.6 30.2 23.9 24.8 9.2 11.6 8.7
1 Normalized 100.0 39.9 22.4 37.6 22.9 18.1 18.8 6.9 8.8 6.6
2 116.2 32.7 43.4 40.2 27.3 21.4 24.1 10.7 10.3 10.6
2 Normalized 100.0 28.1 37.3 34.5 23.5 18.4 20.8 9.2 8.9 9.1
3 103.9 40.2 34.4 29.5 20.3 20.4 17.5 11.0 5.3 8.9
3 Normalized 100.0 38.7 33.1 28.4 19.5 19.6 16.8 10.5 5.1 8.6
Nrmlzd AVG 100.0 35.6 31.0 33.5 22.0 18.7 18.8 8.9 7.6 8.1
Scaled AVG 119.7 42.6 37.1 40.1 26.3 22.4 22.5 10.65 9.1 9.7
Table 7.2 Average (AVG) number of first- and second-order chordae counted based on
the dissected porcine TVs and used in the geometry modeling.
First-order chordae Second-order chordae
Anterior Posterior Septal Anterior Posterior Septal
AVG 18 10 14 8 8 8
The average annulus sonocrystal positional data were imported into SolidWorks
(Dassault Systèmes, Vélizy-Villacoublay, France), and a spline was passed through these
points to form the annulus. The length of this spline was assigned as the annulus reference
perimeter and was used to scale all the other measured data (Table 7.1). Next, using the
central point of the annulus septal segment (as determined by position of one of the
sonocrystals identified during sonomicrometry in ex-vivo beating heart experiments), the
values presented in Table 7.1 were used to determine the commissural and central positions
of the annulus segments along the annulus spline. These referential positions were then
used to mark the commissural and leaflet heights presented in Table 7.1 from the annulus.
A spline was passed through the edges of these marked distances and another spline was

139
passed through points halfway between the lines that connected the marked points to the
annulus spline (Fig. 7.2). The Surface Loft feature in SolidWorks was used to pass a surface
through all three splines. The TV was assumed to have three papillary muscles
(anteroposterior, anteroseptal, and posteroseptal papillary muscles), each considered as a
single point in which all the chordae of that area merge. The position of these points (e.g.,
the tips of the assumed papillary muscles) were considered to be right under the
commissures at almost the same elevation as the lowest position of the valve leaflets, based
on the observations made for porcine heart TVs. First- and second-order chordae were
modeled in the geometry. First-order chordae (chordae on the edge) were assumed to be
distributed uniformly along the edge for each leaflet. Second-order chordae (chordae
entering to the back of the leaflet) were assumed to be uniformly distributed on the surface
of each leaflet and positioned at a distance about one-third of the total leaflet length from
the leaflet distal (free) edges. The number of chordae used in the model are based on the
chordae counted (presented in Table 7.2). The final developed geometry of the TV
apparatus used in the FE analysis is shown in Fig. 7.3.

140
Fig. 7.2 Reconstructed wireframe used for modeling the tricuspid valve geometry. Refer
to Table 7.1 for abbreviations and dimensions.
Fig. 7.3 The reconstructed TV apparatus geometry used in the finite element analysis.
141
7.2.2 Finite Element Model of the Tricuspid Valve
The developed TV apparatus geometry was imported into Abaqus (Dassault
Systèmes, Vélizy-Villacoublay, France) for FE modeling. For importation into Abaqus, the
leaflet geometry was saved in “.x_b” file format and the chordae geometries were saved as
“.step” files. All files were imported into Abaqus to create a Part. To create a base to apply
the annulus deformation boundary conditions, in the Part module, the position of the
annulus markers was marked on the annulus in the part containing the leaflets. The
Partition Edge: Enter Parameter command in Abaqus was then used, and the normalized
relative distances of the marker positions from SolidWorks were applied. In the Part
module, a local coordinate system was established on the center surface of each leaflet in
the part containing the leaflets in order to show the circumferential and radial directions
for each leaflet. This was accomplished using the Abaqus command Datum CSYS: 3 Points,
and the coordinates of the point were transferred from the coordinate system built in
SolidWorks. As previously mentioned, the leaflets’ mechanical response are anisotropic;
therefore, these coordinate systems were necessary to define the material orientation for
the Fung-type material model that was assigned to the leaflets by using the Assign Material
Orientation command in the Property module. To prevent stress concentration on the
annulus while applying the annulus deformation boundary conditions throughout the
cardiac cycle, stringers on the annulus were defined by using the Create Stringer command
in the Property module. In this way, the deformation of the sonocrystal positional points
could be uniformly transferred to all points around the annulus without stress
concentration. The same procedure was utilized to reduce the stress concentration on the
insertion points of the chordae tendineae into the leaflet edges and commissural areas.

142
Although the Fung-type material model developed in chapter III [134] was initially
intended to be used in the model, due to the computational limitations, it was not used in
the final simulations. Instead, a linear elastic model with parameters obtained from the
literature [93] was used. Based on this linear elastic model, the modulus of elasticity for all
TV leaflets was considered to be equal to 0.4 𝑀𝑃𝑎. Considering the fact that the leaflets in
the TV are more fragile than those in the MV, this value is half of the elasticity modulus
reported in the literature for linearly simulated MV leaflets [93]. Moreover, a Poisson’s
ratio of 0.45 was assumed based on values obtained from the literature [93]. Chordae
tendineae mechanical response was modeled using an isotropic hyperelastic Ogden
material model developed for the chordae tendineae of the MV [91, 92, 106]. The same
properties were defined for the stringer on the edge of the leaflets. The stringers on the
annulus, however, were defined to be stronger so that the deformation boundary condition
could adequately and uniformly transfer to all points on the annulus through the movement
of sonocrystal positional points throughout the cardiac cycle. The homogenous shell type
section was used for the anterior leaflet with a thickness of 0.313 mm, and the
corresponding hyperplastic material developed in the previous chapters was assigned to
this section. Similarly, sections were defined for the posterior and septal leaflets as having
a thickness of 0.346 mm and 0.491 mm, respectively, and the corresponding material
properties were assigned to each. Although different average cross-sectional areas have
been reported for the TV chordae tendineae [9, 44, 107], all chordae were assumed to be
unbranched with an initial cross-sectional area of 0.171 mm2 [44, 107], and a general truss
section was defined to represent them. As we did not consider free lengths for the chordae,
their cross-sectional areas were later adjusted during the simulation to ensure coaptation of

143
the leaflets. The same type of section was defined for the edge stringer. To assign beam
sections to the annulus and commissural stringers, circular profiles were defined with radii
of 2 mm and 0.75 mm, respectively. Next, a beam type section was defined by assigning
the corresponding profiles and materials for each stringer. The defined sections were
assigned to the corresponding entities in the parts.
A structured technique was implemented to mesh the leaflets using standard linear
quadratic-shape shell elements with an approximate global size of 0.5 mm (Fig. 7.4). The
chordae were meshed using standard linear truss elements with an approximate global size
of 7 mm (Fig. 7.4). In the Assembly module, the necessary instances were imported into
the assembly using the Create Instance command. In the Step module, a Dynamic Explicit
step was defined to simulate the valve closure period after loading. The closing time was
chosen to be 0.38 second, which is when the average RVP reached its maximum in the ex-
vivo experiments [140].
In the Interaction module in Abaqus, an interaction property was defined to
represent the tangential and normal behavior of the leaflet surfaces in the TV model. The
friction coefficient was chosen to be 0.2 [221, 222], and the contact was defined as hard.
Next, a General Contact was created in the initial step and the above interaction property
was assigned to it. This contact was propagated to the dynamic step. Tie constraints were
used to attach each chorda to the edge or surface of the leaflets. The normalized amplitudes
for the average relative transvalvular pressure and the average positional change for all
sonocrystals on the annulus were imported into the Abaqus model as amplitudes using the
Create Amplitude command. The maximum relative transvalvular pressure (i.e.
~ 14 mm 𝐻𝑔) was uniformly placed on the outer surface of all three leaflets, and the

144
corresponding amplitudes were assigned to it, simulating the smooth pressure change
throughout the valve closure. The papillary muscles were fixed in the initial step and
propagated to the dynamic step. All sonocrystal positions on the annulus were fixed in the
initial step. In the dynamic step, these positions were moved to their corresponding
positions at the maximum RVP (as measured in the ex-vivo experiments), and the
corresponding amplitudes were assigned to simulate the smooth movement at these
points—and thus the deformation of the annulus—throughout the cardiac cycle.
Fig. 7.4 Finite element mesh for the reconstructed TV geometry.
7.3 Results
The developed model was used to simulate closure of TV. In Fig. 7.5, the
deformation of the valve during the closure simulation is illustrated at different time points.
This figure showed that the developed model is able to simulate the valve closure. The
color map in Fig. 7.5 shows the maximum in-plane principal strain distribution. The

145
maximum principal strain was under 25% for most locations based on this figure, and the
strains appeared to be uniform at the belly areas over the surface of the leaflets. The
distribution of the maximum in-plane principal strains on the septal leaflet surface is shown
separately in Fig. 7.6. As can be noticed from this figure, the strains in the belly area range
from approximately 8 to 15%. If we compare this data with the strain values measured for
the same region (belly area) in the ex-vivo experiments shown in Fig. 4.8 (the values of
maximum principal strain in Fig. 4.8 at the belly area range from approximately 9 to 13%.),
we notice a close match between the measured values and the results of this simulation,
further verifying the result of the simulation and the accuracy of the developed model.
Fig. 7.5 Maximum in-plane principal strain distribution illustrated over the anterior (A),
posterior (P), and septal (S) valve leaflets at different points in time during the valve closure
simulation.

146
Fig. 7.6 Distribution of maximum in-plane principal strain over the septal leaflet at
maximum right ventricular pressure.
Figure 7.7 shows the spatial distribution of the maximum in-plane principal stress
at different time points throughout the closure simulation. This stress reached values as
high as 120 kPa. The distribution of the stresses shows that the anterior leaflet experiences
the highest stress, while the septal leaflet experiences the lowest stress. Moreover, a slight
stress concentration can be seen around the area of the annulus. However, there is no
significant stress concentration at the connection points of the chordae on the leaflet
surfaces or at the edges of the leaflets.
7.4 Discussion
By running the FE simulation and applying the transvalvular pressure signal (which
is a function of time), the leaflets began to move toward each other, and coaptation
happened gradually (Fig. 7.5). The progressive change in the shape of the annulus shows
that the improvised annulus stringer perfectly transfers the movement of the sonocrystal
positional data to all the nodes around the annulus, implementing the expected boundary
conditions of the annulus (Fig. 7.5). In Fig. 7.6, the distribution of the maximum in-plane

147
principal strain illustrated over the septal leaflet showed that the levels of maximum in-
plane principal strains at the central area of this leaflet are around 12%, which closely
matches the values measured in the ex-vivo beating heart experiment [140], where the
average of maximum principal strain was roughly 11% (Fig. 4.8).
The level of stresses in the FE model (Fig. 7.7) are comparable to the estimated
values for normal physiological stress levels on the leaflet surfaces [117] from the biaxial
experiments (the values ranged roughly from 80 kPa for the septal leaflet to 130 kPa for
the anterior leaflet). The slight stress concentration observed around the annulus in this
figure might result from imposing the boundary conditions through the annulus stringer.
On the other hand, the stringers improvised into the edges of the leaflets prevented the
strain concentration from occurring at these areas by more uniformly transferring the load
from the chordae to the leaflets and vice versa.
Fig. 7.7 Maximum in-plane principal stress distribution illustrated over the anterior (A),
posterior (P), and septal (S) valve leaflets at different points in time during the valve closure
simulation.

148
Fig. 7.8 Comparison of effects of changes in the annulus boundary conditions on the strain
distribution and deformations of the septal leaflet. The top plot shows the result of the
simulation with the moving annulus boundary conditions (as the simulation of the intact
case), and the bottom plot shows the result of the simulation with the fixed annulus
boundary conditions (as the simulation of rigid ring annuloplasty).
Finally, to show how the results of this study can be used in real applications, we
simulated the ring annuloplasty using the developed FE model to see how valvular
treatments can alter the normal dynamic deformations of the TV. If we assume that the
annulus loses its ability to move as a result of rigid ring annuloplasty, we modeled the ring
annuloplasty by fixing the annulus. In Fig. 7.8, we have compared the strain distribution
and deformations of the septal leaflet from the simulation with a fixed annulus and the
simulation with moving annulus boundary conditions. As shown in this figure, there was a
slight increase in the range of the strains in the belly area. However, in the areas close to
the commissures, the strain distributions and the leaflet deformations were notably altered.
This alteration in the strain distribution and leaflet deformation shows how changing the

149
normal biomechanical environment of TV as a result of valvular treatments can affect the
valve, leading to potential tissue regeneration and long-term valvular failure.

150
CHAPTER 8VIII
CONCLUSIONS AND FUTURE WORK
8.1 Conclusions
Using custom-designed biaxial tensile testing equipment, we measured the biaxial
mechanical responses of the porcine TV leaflets under loading conditions that were
estimated based on physiological pressure levels and approximations of TV structure
geometries [128-132]. The overall trend of the measured tension–stretch data showed a
highly nonlinear behavior both in the radial and in the circumferential directions, as the
leaflets were more compliant at lower strains (i.e. over the toe region) following by a rapid
transition to a stiffer response (i.e. transition to the lockout region). The latter behavior was
not observed in the few mechanical tests conducted on the TV previously due to the small
level of strains used in such experiments [133]. TV leaflets were stiffer in the
circumferential direction, indicating an anisotropic response, a phenomenon that is also
observed in other cardiac valves [35-39]. The largest difference between mechanical
responses in the circumferential direction and the radial direction for the equibiaxial
loading was observed for the posterior leaflet, signifying a more anisotropic response in
this leaflet as compared to the other two leaflets. While no significant difference was
observed between the thicknesses of the anterior and posterior leaflets (𝑝 = 0.27,
Student’s t-test), the septal leaflet was significantly thicker than both of the other leaflets.
The anterior and posterior leaflets had the same stiffness in the circumferential direction,
151
but the anterior leaflet was much stiffer in the radial direction. The septal leaflet was more
compliant than the other two leaflets in the circumferential direction.
Next, we used the experimentally measured mechanical response data from our
biaxial mechanical testing to develop a material model to represent the mechanical
responses of TV leaflets in a general loading condition. The initial analysis of these data
led us to choose a Fung-type strain energy function as the phenomenological constitutive
framework, which was further justified by the high quality of the fitted models to the data.
The calculated anisotropy indices (i.e. 0.52, 0.39, and 0.51 for the anterior, posterior, and
septal leaflets, respectively) revealed that, similar to other cardiac valves [38, 42, 60, 67,
148], TV leaflets were highly anisotropic, further confirming our previous observation.
Quantitative analysis of tissue microstructure using small angle light scattering [77, 86,
150-152] confirmed that the main direction of the extracellular matrix fibers was along the
circumferential direction, and TV leaflets were thus expected to be anisotropic. In terms of
anisotropy, the porcine leaflets were qualitatively similar to human tissues: for both
species, all three leaflets were stiffer in the circumferential direction in comparison to the
radial direction [42].
To develop a set of representative material constants to be used in FE analysis,
average constitutive models were developed considering the nonlinear responses of the
native tissues. Our analysis on the three presented averaging approaches (i.e., tension-
based, first-Piola-Kirchhoff-stress–based, and Cauchy-stress–based approaches)
confirmed the fidelity of the tension-controlled biaxial testing loading protocols and the
subsequent averaging procedure in the tension space [36, 38, 58, 59, 148] when only small
variations in the thickness of the specimens exist. It is, however, more reasonable to avoid

152
potential errors by performing stress-controlled tests, especially when the tissue thickness
varies significantly between the specimens. While the responses of the three average
models were notably similar, the responses generated from arithmetical averaging of the
material constants were completely different. This observation further exemplifies that the
arithmetically averaged values of the individual material constants of a nonlinear model
may not represent the generic tissue responses accurately. Statistical comparison of the
mechanical responses and the material model developed here for the TV using responses
and material models available in the literature for other heart valves is not possible due to
differences in the models that have been used in each case as well as the limited amount of
available data. However, the parameters presented in Table 8.1 are parameters calculated
for human heart valves that are available in the literature [42] for a seven-parameter Fung-
type model, allowing a simple one-to-one comparison to be made.
Table 8.1 Parameters of a Fung-type model for human heart valves [42]
Valve C (𝑘𝑃𝑎) 𝑎1 𝑎2 𝑎3 𝑎4 𝑎5 𝑎6
MV 0.369 188.75 91.80 -2.143 100 -11.37 -12.51
AV 0.132 186.43 74.45 59.84 100 -6.78 -14.49
PV 0.587 43.68 20.66 6.49 10 0.16 -1.38
TV 0.684 59.42 29.05 1.25 10 1.66 -0.29
Additional inspections were also performed to validate the integrity of the
developed phenomenological constitutive models by examining the convexity of their
strain energy functions, as this convexity is crucial for the stability of the numerical
methods in computerized simulations [153].
Next, we developed an experimental setup to measure the dynamic deformation of
the porcine TV complex. Our novel ex-vivo passive beating heart apparatus was able to

153
produce repeatable data with high temporal resolution. Using our passive beating heart
system, we were able to reproduce ventricular pressure waves that matched the
physiological values of an actively beating heart [160]. Due to their excellent similarities
to the human heart in terms of pressure values on the pulmonary side, porcine hearts were
used in this simulation. In particular, human RVP ranges approximately from zero to
30 𝑚𝑚 𝐻𝑔 [128, 160], and porcine RVP ranges roughly from zero up to 33 𝑚𝑚 𝐻𝑔 [161-
164]. Such a similarity also exists in the systemic side of the heart [1, 165]. Using this
simulation apparatus and sonomicrometry techniques [26, 80-83, 85-87], we were able to
visualize the deformations and the strains of the valve septal leaflet and annulus.
The average values of the maximum principal strains and the areal strains
quantified at maximum RVP on the surface of the septal leaflet were 11.2% and 9.8%,
respectively. These values compared well with those calculated for the ovine MV anterior
leaflet (12.3% and 12.7% for the areal strain and the maximum principal strain,
respectively [30]). Such a similarity in the strain values is of particular interest, as it shows
that while the two leaflets are subjected to different levels of ventricular pressure, they
deform in a relatively similar manner. We noticed that the maximum principal strain is
distributed uniformly over the leaflet for nearly the entire cardiac cycle, while the areal
strain is not as uniform. There is much heterogeneity in the spatial distribution of the
circumferential strain and radial strain over the septal leaflet. While higher values for
circumferential strain were observed toward the posterior side of the leaflet, the radial
strains reached higher values in areas near the anterior side. However, unlike MV leaflets,
in which significant differences exist between the maximum strain in the circumferential
and radial directions [26, 30, 111], no significant difference was observed between

154
circumferential and radial strains in the septal leaflet of the TV at the maximum RVP. A
possible explanation for this finding is that the septal leaflet of the TV has a more isotropic
extracellular matrix microstructural architecture in comparison to the anterior and posterior
leaflets of the MV [35].
Positional data obtained from the sonocrystals sutured around the ex-vivo porcine
heart annulus were used to develop an average annulus model and analyze the annulus
shape and deformation throughout the cardiac cycle. The effects of chordae rupture were
also investigated on these deformations and strain distributions by cutting one of the septal
chordae proximal to the posteroseptal commissure. We observed that the geometry of the
annulus is considerably altered during the cardiac cycle such that, from the minimum RVP
to the maximum RVP, the area experiences a roughly 20% increase, and the circumference
extends approximately 8%. Our analysis showed that these deformations do not occur
uniformly along the annulus. For example, the annulus anterior segment (AAS)
experiences the largest deformation (about 9% on average).
Our experiments showed that there exists a mechanical interdependency among the
chordae tendineae, leaflets, and annulus of the TV. We observed that immediately after
chordae rupture, the dynamic deformation of the TV annulus changed extensively, with a
significant increase in the annulus area, circumference and radius. Annulus dilation is
expected to change the coaptation of the valve leaflets and induce regurgitation [182]. Our
measurements showed that the flow into the right atrium decreased by 26% and RVP
dropped by 17%, altering the hemodynamics of the heart immediately after the septal
chordae tendineae was cut. Moreover, the deformation and the strain distribution of the

155
septal leaflet significantly changed throughout the cardiac cycle following the rupture of
the chordae.
Although the TV may be initially asymptomatic, instantaneous annulus dilation and
changes in the leaflets strain distribution following chordae rupture could lead to
exacerbation of TV regurgitation and potentially to mechanically-induced remodeling
responses in the TV leaflets, the remaining intact chordae tendineae, the papillary muscles,
and/or the ventricular myocardium. Hence, careful examination and early surgical
intervention might be necessary to prevent mid-term/long-term negative effects of
mechanically-induced remodeling in asymptomatic TVs following the rupture of the
chordae tendineae.
Finally, a basic model of TV was developed in Abaqus using mechanical properties
of the native TV, microstructure, accurate annulus boundary conditions, and the 3D surface
geometry of TV. This model was used to simulate the closure of the TV during the cardiac
cycle. The distribution of stresses showed that the anterior and septal leaflets experience
the highest and the lowest stresses, respectively. To validate the model, the distribution of
the maximum in-plane principal strain over the septal leaflet from the model was compared
to the corresponding distribution that was measured in experiments using the ex-vivo setup
and sonomicrometry [140]. This comparison revealed that the level of the maximum in-
plane principal strain at the belly area of this leaflet (where we measured strains
experimentally [140]) is around 15%, closely matching the values measured in the ex-vivo
beating heart experiment [140], which were roughly 12% maximum principal strain.
Moreover, the maximum in-plane principal stress in the simulation results reached values
as high as 133.6 𝑘𝑃𝑎 on TV leaflet surfaces. This was comparable to the estimated values

156
of normal physiological stress levels on the leaflet surfaces [117] for the biaxial
experiments (where the values ranged from roughly 80 𝑘𝑃𝑎 for the septal leaflet to
130 𝑘𝑃𝑎 for the anterior leaflet), further validating our developed model.
In summary, in this doctoral research, we obtained important new knowledge of
TV biomechanics including the strain-stress responses, leaflets microstructure, geometry
and dynamic deformations of the annulus, and dynamic deformations and stress
distributions of the septal leaflet throughout the cardiac cycle. In addition, we developed a
computerized model of the TV for simulation applications. Development of such an
accurate and verified model will facilitate in-silico examination of different valve repair
surgeries and provide insight into the possible changes in the biomechanical environment
of the TV following such procedures. With further modifications, verifications, and
validations, our model has the potential to shed light on appropriate modifications for TV
surgical procedures in order for their outcomes to most efficiently mimic the native valve
biomechanics.
Once more, it should be noted that all experiments in the current study were
performed on porcine hearts and porcine valvular tissues. There are many advantages in
using porcine hearts, as fresh tissues can be obtained so the biomechanical behavior of the
valves is less affected by the activity of degenerative enzymes in the extracellular matrix.
In addition, in comparison to human cadaverous tissues, younger porcine samples with less
variability are available [35]. Nevertheless, one should always be cautious in drawing
conclusions regarding human tissue responses based solely on animal studies [167].

157
8.2 Future Work
The findings of the current work can be used as the basis for several other
interesting studies. For example:
Similar to its application in the simulation of chordae rupture, the developed ex-
vivo beating heart apparatus can be used for simulation of the other valvular lesions, such
as valve perforation. Moreover, this apparatus can be used for simulation of valvular
treatments. For example, in most TV repair procedures, a prosthetic annuloplasty ring is
used to decrease the annulus size and improve the valve hemodynamics [8]. Considering
the dynamic deformation of the TV annulus observed in our study, further research can be
accomplished under similar procedures to identify how the valve deformation changes
following ring annuloplasty [26].
Due to the limited number of sonomicrometry crystal channels (16 channels)
employed in this study, we were not able to measure deformation of the anterior and
posterior leaflets of the TV. Further research can be established to quantify strain values in
the anterior and posterior leaflets and compare the results with those for the septal leaflet.
Although our study was conducted using PBS, there is no reason why non-clear
fluids cannot be used in our ex-vivo apparatus, as our strain measurements do not rely on
visual access to the markers. Such a capability is of great importance, because recent
studies have shown that the flow properties (particularly the transition to turbulence) could
be significantly different in blood in comparison to optically clear, viscosity-matched blood
substitutes [172]. Since the transition to turbulence could occur in proximity to the cardiac
valves, measurements of valve deformation using blood can be performed in the future.

158
In addition, the computerized model developed in this study can be improved to
provide more realistic outcomes. For example, while phenomenological constitutive
models are powerful in predicting the responses of the tissue, they do not provide much
insight about the mechanical environment at the underlying extracellular matrix/cellular
levels. In other words, model parameters cannot be quantitatively related to structural
components of the tissue, such as extracellular matrix protein volume fractions or
extracellular matrix morphology. Such information is of particular interest in the field of
mechanobiology, for which constitutive frameworks that include structural components of
the tissue are more relevant [66-70]. Using the experimentally measured mechanical
responses and the mapped microstructure of TV leaflets in the current study, further work
is necessary to develop such structural models that incorporate the microstructure of the
leaflets in the mechanical response.
Moreover, after adequate degrees of verification, the developed computerized
model can also be used in the simulation of valvular lesions and their treatments.
Finally, the data provided in the current work pertain to the use of porcine tissues.
Although many of the conclusions of this study seem to be independent of the species,
further studies can be done on the human heart for better understanding and comparison.
As such, the methods established in the current study can be applied in the same manner
on human cadaveric hearts, as this may provide more accurate insight into the mechanical
behavior of the native human TV and lead to development of more reliable computerized
models.

159
BIBLIOGRAPHY
[1] Hall, J. E., 2015, Guyton and Hall textbook of medical physiology e-Book, Elsevier
Health Sciences.
[2] Cook, M. S., and Weinhaus, A. J., 2015, "Anatomy of the Thoracic Wall,
Pulmonary Cavities, and Mediastinum," Handbook of Cardiac Anatomy,
Physiology, and Devices, P. A. Iaizzo, ed., Springer International Publishing,
Cham, pp. 35-60.
[3] Weinhaus, A. J., and Roberts, K. P., 2005, "Anatomy of the Human Heart,"
Handbook of Cardiac Anatomy, Physiology, and Devices, P. A. Iaizzo, ed.,
Humana Press, Totowa, NJ, pp. 51-79.
[4] Soliman, O. I., Folkert, J., and Cate, T., 2018, Practical Manual of Tricuspid Valve
Diseases, Springer.
[5] Chan, K. M. J., "Functional Mitral and Tricuspid Regurgitation."
[6] Hinton, R. B., and Yutzey, K. E., 2011, "Heart valve structure and function in
development and disease," Annual review of physiology, 73, pp. 29-46.
[7] Joudinaud, T. M., Flecher, E. M., and Duran, C., 2006, "Functional terminology for
the tricuspid valve," The Journal of heart valve disease, 15(3), pp. 382-388.
[8] Carpentier, A., Adams, D. H., and Filsoufi, F., 2011, Carpentier's Reconstructive
Valve Surgery E-Book, Elsevier Health Sciences.
[9] Silver, M. D., Lam, J. H., Ranganathan, N., and Wigle, E. D., 1971, "Morphology
of the human tricuspid valve," Circulation, 43(3), pp. 333-348.
[10] Gunnal, S., Wabale, R., and Farooqui, M., 2015, "Morphological study of chordae
tendinae in human cadaveric hearts," Heart views: the official journal of the Gulf
Heart Association, 16(1), p. 1.
[11] Ushiki, T., 2002, "Collagen fibers, reticular fibers and elastic fibers. A
comprehensive understanding from a morphological viewpoint," Archives of
histology and cytology, 65(2), pp. 109-126.
[12] Sacks, M. S., Merryman, W. D., and Schmidt, D. E., 2009, "On the biomechanics
of heart valve function," Journal of Biomechanics, 42(12), pp. 1804-1824.

160
[13] Schoen, F., 1997, "Aortic valve structure-function correlations: role of elastic fibers
no longer a stretch of the imagination," The Journal of heart valve disease, 6(1), p.
1.
[14] Thubrikar, M., 2018, The aortic valve, Routledge.
[15] Lee, C.-H., Zhang, W., Liao, J., Carruthers, C. A., Sacks, J. I., and Sacks, M. S.,
2015, "On the presence of affine fibril and fiber kinematics in the mitral valve
anterior leaflet," Biophysical journal, 108(8), pp. 2074-2087.
[16] Simionescu, D., Lovekamp, J., and Vyavahare, N., 2003, "Degeneration of
bioprosthetic heart valve cusp and wall tissues is initiated during tissue preparation:
an ultrastructural study," The Journal of heart valve disease, 12(2), pp. 226-234.
[17] Vesely, I., 1997, "The role of elastin in aortic valve mechanics," Journal of
biomechanics, 31(2), pp. 115-123.
[18] Misfeld, M., and Sievers, H.-H., 2007, "Heart valve macro-and microstructure,"
Philosophical Transactions of the Royal Society of London B: Biological Sciences,
362(1484), pp. 1421-1436.
[19] Spinner, E. M., Lerakis, S., Higginson, J., Pernetz, M., Howell, S., Veledar, E., and
Yoganathan, A. P., 2012, "Correlates of tricuspid regurgitation as determined by
3D echocardiography: pulmonary arterial pressure, ventricle geometry, annular
dilatation, and papillary muscle displacement," Circulation: Cardiovascular
Imaging, 5(1), pp. 43-50.
[20] Dreyfus, G. D., Corbi, P. J., Chan, K. M. J., and Bahrami, T., 2005, "Secondary
tricuspid regurgitation or dilatation: which should be the criteria for surgical
repair?," The Annals of Thoracic Surgery, 79(1), pp. 127-132.
[21] Lee, J.-W., Song, J.-M., Park, J. P., Lee, J. W., Kang, D.-H., and Song, J.-K., 2010,
"Long-term prognosis of isolated significant tricuspid regurgitation," Circulation
Journal, 74(2), pp. 375-380.
[22] Fung, Y. C., and Liu, S. Q., 1989, "Change of residual strains in arteries due to
hypertrophy caused by aortic constriction," Circulation research, 65(5), pp. 1340-
1349.
[23] Fung, Y. C., 1991, "What are the residual stresses doing in our blood vessels?,"
Annals of Biomedical Engineering, 19(3), pp. 237-249.
[24] Vassileva, C. M., Shabosky, J., Boley, T., Markwell, S., and Hazelrigg, S., 2012,
"Tricuspid valve surgery: the past 10 years from the Nationwide Inpatient Sample
(NIS) database," The Journal of thoracic and cardiovascular surgery, 143(5), pp.
1043-1049.

161
[25] Guenther, T., Noebauer, C., Mazzitelli, D., Busch, R., Tassani-Prell, P., and Lange,
R., 2008, "Tricuspid valve surgery: a thirty-year assessment of early and late
outcome," European journal of cardio-thoracic surgery : official journal of the
European Association for Cardio-thoracic Surgery, 34(2), pp. 402-409; discussion
409.
[26] Amini, R., Eckert, C. E., Koomalsingh, K., McGarvey, J., Minakawa, M., Gorman,
J. H., Gorman, R. C., and Sacks, M. S., 2012, "On the in vivo deformation of the
mitral valve anterior leaflet: effects of annular geometry and referential
configuration," Annals of Biomedical Engineering, 40(7), pp. 1455-1467.
[27] Chikwe, J., Itagaki, S., Anyanwu, A., and Adams, D. H., 2015, "Impact of
concomitant tricuspid annuloplasty on tricuspid regurgitation, right ventricular
function, and pulmonary artery hypertension after repair of mitral valve prolapse,"
Journal of the American College of Cardiology, 65(18), pp. 1931-1938.
[28] Mahmood, F., Gorman, J. H., Subramaniam, B., Gorman, R. C., Panzica, P. J.,
Hagberg, R. C., Lerner, A. B., Hess, P. E., Maslow, A., and Khabbaz, K. R., 2010,
"Changes in mitral valve annular geometry after repair: saddle-shaped versus flat
annuloplasty rings," The Annals of Thoracic Surgery, 90(4), pp. 1212-1220.
[29] Mahmood, F., Subramaniam, B., Gorman, J. H., Levine, R. M., Gorman, R. C.,
Maslow, A., Panzica, P. J., Hagberg, R. M., Karthik, S., and Khabbaz, K. R., 2009,
"Three-dimensional echocardiographic assessment of changes in mitral valve
geometry after valve repair," The Annals of Thoracic Surgery, 88(6), pp. 1838-
1844.
[30] Rausch, M. K., Bothe, W., Kvitting, J.-P. E., Göktepe, S., Miller, D. C., and Kuhl,
E., 2011, "In vivo dynamic strains of the ovine anterior mitral valve leaflet," Journal
of Biomechanics, 44(6), pp. 1149-1157.
[31] Bothe, W., Kvitting, J.-P. E., Swanson, J. C., Hartnett, S., Ingels, N. B., and Miller,
D. C., 2010, "Effects of different annuloplasty rings on anterior mitral leaflet
dimensions," The Journal of thoracic and cardiovascular surgery, 139(5), pp. 1114-
1122.
[32] Singh, J. P., Evans, J. C., Levy, D., Larson, M. G., Freed, L. A., Fuller, D. L.,
Lehman, B., and Benjamin, E. J., 1999, "Prevalence and clinical determinants of
mitral, tricuspid, and aortic regurgitation (the Framingham Heart Study)," The
American Journal of Cardiology, 83(6), pp. 897-902.
[33] Stuge, O., and Liddicoat, J., 2006, "Emerging opportunities for cardiac surgeons
within structural heart disease," The Journal of thoracic and cardiovascular surgery,
132(6), pp. 1258-1261.

162
[34] Taramasso, M., Vanermen, H., Maisano, F., Guidotti, A., La Canna, G., and Alfieri,
O., 2012, "The growing clinical importance of secondary tricuspid regurgitation,"
Journal of the American College of Cardiology, 59(8), pp. 703-710.
[35] May-Newman, K., and Yin, F. C., 1995, "Biaxial mechanical behavior of excised
porcine mitral valve leaflets," The American Journal of Physiology, 269(4 Pt 2),
pp. H1319-1327.
[36] Billiar, K. L., and Sacks, M. S., 2000, "Biaxial mechanical properties of the natural
and glutaraldehyde treated aortic valve cusp—part I: experimental results," Journal
of Biomechanical Engineering, 122(1), pp. 23-30.
[37] Grashow, J. S., Yoganathan, A. P., and Sacks, M. S., 2006, "Biaixal stress–stretch
behavior of the mitral valve anterior leaflet at physiologic strain rates," Annals of
Biomedical Engineering, 34(2), pp. 315-325.
[38] Grashow, J. S., Sacks, M. S., Liao, J., and Yoganathan, A. P., 2006, "Planar biaxial
creep and stress relaxation of the mitral valve anterior leaflet," Annals of
Biomedical Engineering, 34(10), pp. 1509-1518.
[39] Sacks, M. S., He, Z., Baijens, L., Wanant, S., Shah, P., Sugimoto, H., and
Yoganathan, A. P., 2002, "Surface strains in the anterior leaflet of the functioning
mitral valve," Annals of Biomedical Engineering, 30(10), pp. 1281-1290.
[40] Boronyak, S. M., and Merryman, W. D., 2012, "Development of a simultaneous
cryo-anchoring and radiofrequency ablation catheter for percutaneous treatment of
mitral valve prolapse," Annals of Biomedical Engineering, 40(9), pp. 1971-1981.
[41] Price, S. L., Norwood, C. G., Williams, J. L., McElderry, H. T., and Merryman, W.
D., 2010, "Radiofrequency ablation directionally alters geometry and
biomechanical compliance of mitral valve leaflets: refinement of a novel
percutaneous treatment strategy," Cardiovascular Engineering and Technology,
1(3), pp. 194-201.
[42] Pham, T., Sulejmani, F., Shin, E., Wang, D., and Sun, W., 2017, "Quantification
and comparison of the mechanical properties of four human cardiac valves," Acta
Biomaterialia, 54, pp. 345-355.
[43] McCarthy, P. M., and Sales, V. L., 2010, "Evolving indications for tricuspid valve
surgery," Current treatment options in cardiovascular medicine, 12(6), pp. 587-597.
[44] Stevanella, M., Votta, E., Lemma, M., Antona, C., and Redaelli, A., 2010, "Finite
element modelling of the tricuspid valve: a preliminary study," Medical
engineering & physics, 32(10), pp. 1213-1223.

163
[45] Mooney, M., 1940, "A theory of large elastic deformation," Journal of applied
physics, 11(9), pp. 582-592.
[46] Rivlin, R., and Saunders, D., 1997, "Large elastic deformations of isotropic
materials," Collected papers of RS Rivlin, Springer, pp. 157-194.
[47] Ogden, R. W., 1972, "Large deformation isotropic elasticity–on the correlation of
theory and experiment for incompressible rubberlike solids," Proc. R. Soc. Lond.
A, 326(1567), pp. 565-584.
[48] Ogden, R. W., 1997, Non-linear elastic deformations, Courier Corporation.
[49] Shahzad, M., Kamran, A., Siddiqui, M. Z., and Farhan, M., 2015, "Mechanical
characterization and FE modelling of a hyperelastic material," Materials Research,
18(5), pp. 918-924.
[50] Sacks, M. S., 2000, "Biaxial mechanical evaluation of planar biological materials,"
Journal of elasticity and the physical science of solids, 61(1-3), pp. 199-246.
[51] Sacks, M. S., and Sun, W., 2003, "Multiaxial mechanical behavior of biological
materials," Annual review of biomedical engineering, 5(1), pp. 251-284.
[52] Fung, Y.-C. B., 1973, "Biorheology of soft tissues," Biorheology, 10(2), pp. 139-
155.
[53] Tong, P., and Fung, Y.-C., 1976, "The stress-strain relationship for the skin,"
Journal of Biomechanics, 9(10), pp. 649-657.
[54] Sacks, M. S., 1999, "A Method for Planar Biaxial Mechanical Testing That
Includes In-Plane Shear," Journal of Biomechanical Engineering, 121(5), pp. 551-
555.
[55] Sun, W., Sacks, M. S., Sellaro, T. L., Slaughter, W. S., and Scott, M. J., 2003,
"Biaxial mechanical response of bioprosthetic heart valve biomaterials to high in-
plane shear," Journal of Biomechanical Engineering, 125(3), pp. 372-380.
[56] Vande Geest, J. P., Sacks, M. S., and Vorp, D. A., 2004, "Age dependency of the
biaxial biomechanical behavior of human abdominal aorta," Journal of
Biomechanical Engineering, 126(6), pp. 815-822.
[57] Gilbert, T. W., Wognum, S., Joyce, E. M., Freytes, D. O., Sacks, M. S., and
Badylak, S. F., 2008, "Collagen fiber alignment and biaxial mechanical behavior
of porcine urinary bladder derived extracellular matrix," Biomaterials, 29(36), pp.
4775-4782.

164
[58] Bellini, C., Glass, P., Sitti, M., and Di Martino, E. S., 2011, "Biaxial mechanical
modeling of the small intestine," Journal of the mechanical behavior of biomedical
materials, 4(8), pp. 1727-1740.
[59] Keyes, J. T., Lockwood, D. R., Utzinger, U., Montilla, L. G., Witte, R. S., and
Vande Geest, J. P., 2013, "Comparisons of Planar and Tubular Biaxial Tensile
Testing Protocols of the Same Porcine Coronary Arteries," Annals of Biomedical
Engineering, 41(7), pp. 1579-1591.
[60] May-Newman, K., and Yin, F. C. P., 1998, "A constitutive law for mitral valve
tissue," Journal of Biomechanical Engineering, 120(1), pp. 38-47.
[61] Choi, H., 1990, "Mechanical properties of canine pericardium."
[62] Choi, H. S., and Vito, R. P., 1990, "Two-Dimensional Stress-Strain Relationship
for Canine Pericardium," Journal of Biomechanical Engineering, 112(2), pp. 153-
159.
[63] Sacks, M. S., and Chuong, C. J., 1998, "Orthotropic Mechanical Properties of
Chemically Treated Bovine Pericardium," Annals of Biomedical Engineering,
26(5), pp. 892-902.
[64] Vande Geest, J. P., Sacks, M. S., and Vorp, D. A., 2006, "The effects of aneurysm
on the biaxial mechanical behavior of human abdominal aorta," Journal of
Biomechanics, 39(7), pp. 1324-1334.
[65] O’Leary, S. A., Healey, D. A., Kavanagh, E. G., Walsh, M. T., McGloughlin, T.
M., and Doyle, B. J., 2014, "The Biaxial Biomechanical Behavior of Abdominal
Aortic Aneurysm Tissue," Annals of Biomedical Engineering, 42(12), pp. 2440-
2450.
[66] Lanir, Y., 1983, "Constitutive equations for fibrous connective tissues," Journal of
Biomechanics, 16(1), pp. 1-12.
[67] Billiar, K. L., and Sacks, M. S., 2000, "Biaxial mechanical properties of the native
and glutaraldehyde-treated aortic valve cusp: part II—a structural constitutive
model," Journal of Biomechanical Engineering, 122(4), pp. 327-335.
[68] Sacks, M. S., 2003, "Incorporation of experimentally-derived fiber orientation into
a structural constitutive model for planar collagenous tissues," Journal of
Biomechanical Engineering, 125(2), pp. 280-287.
[69] Fata, B., Zhang, W., Amini, R., and Sacks, M. S., 2014, "Insights into regional
adaptations in the growing pulmonary artery using a meso-scale structural model:
effects of ascending aorta impingement," Journal of Biomechanical Engineering,
136(2), p. 021009.
165
[70] Wognum, S., Schmidt, D. E., and Sacks, M. S., 2009, "On the mechanical role of
de novo synthesized elastin in the urinary bladder wall," Journal of biomechanical
engineering, 131(10), p. 101018.
[71] Lanir, Y., 1979, "A structural theory for the homogeneous biaxial stress-strain
relationships in flat collagenous tissues," Journal of Biomechanics, 12(6), pp. 423-
436.
[72] Lanir, Y., and Fung, Y. C., 1974, "Two-dimensional mechanical properties of
rabbit skin—II. Experimental results," Journal of Biomechanics, 7(2), pp. 171-182.
[73] Lanir, Y., and Fung, Y. C., 1974, "Two-dimensional mechanical properties of
rabbit skin—I. Experimental system," Journal of Biomechanics, 7(1), pp. 29-34.
[74] Zhang, W., Feng, Y., Lee, C.-H., Billiar, K. L., and Sacks, M. S., 2015, "A
generalized method for the analysis of planar biaxial mechanical data using tethered
testing configurations," Journal of Biomechanical Engineering, 137(6), p. 064501.
[75] Eilaghi, A., Flanagan, J. G., Brodland, G. W., and Ethier, C. R., 2009, "Strain
uniformity in biaxial specimens is highly sensitive to attachment details," Journal
of Biomechanical Engineering, 131(9), p. 091003.
[76] Cochran, R., Kunzelman, K., Chuong, C., Sacks, M., and Eberhart, R., 1991,
"Nondestructive analysis of mitral valve collagen fiber orientation," ASAIO
transactions, 37(3), pp. M447-448.
[77] Sacks, M. S., Smith, D. B., and Hiester, E. D., 1997, "A small angle light scattering
device for planar connective tissue microstructural analysis," Annals of Biomedical
Engineering, 25(4), pp. 678-689.
[78] Robitaille, M. C., Zareian, R., DiMarzio, C. A., Wan, K.-T., and Ruberti, J. W.,
2011, "Small-angle light scattering to detect strain-directed collagen degradation in
native tissue," Interface Focus, 1(5), pp. 767-776.
[79] Hobson, C. M., Amoroso, N. J., Amini, R., Ungchusri, E., Hong, Y., D'Amore, A.,
Sacks, M. S., and Wagner, W. R., 2015, "Fabrication of elastomeric scaffolds with
curvilinear fibrous structures for heart valve leaflet engineering," Journal of
Biomedical Materials Research Part A, 103(9), pp. 3101-3106.
[80] Hiro, M. E., Jouan, J., Pagel, M. R., Lansac, E., Lim, K. H., Lim, H.-S., and Duran,
C. M. G., 2004, "Sonometric study of the normal tricuspid valve annulus in sheep,"
Journal of Heart Valve Disease, 13(3), pp. 452-460.
[81] Fawzy, H., Fukamachi, K., Mazer, C. D., Harrington, A., Latter, D., Bonneau, D.,
and Errett, L., 2011, "Complete mapping of the tricuspid valve apparatus using

166
three-dimensional sonomicrometry," The Journal of thoracic and cardiovascular
surgery, 141(4), pp. 1037-1043.
[82] Eckert, C. E., Zubiate, B., Vergnat, M., Gorman Iii, J. H., Gorman, R. C., and Sacks,
M. S., 2009, "In vivo dynamic deformation of the mitral valve annulus," Annals of
Biomedical Engineering, 37(9), pp. 1757-1771.
[83] Rausch, M. K., Malinowski, M., Wilton, P., Khaghani, A., and Timek, T. A., 2017,
"Engineering Analysis of Tricuspid Annular Dynamics in the Beating Ovine
Heart," Annals of Biomedical Engineering.
[84] Tsakiris, A. G., Mair, D. D., Seki, S., Titus, J. L., and Wood, E. H., 1975, "Motion
of the tricuspid valve annulus in anesthetized intact dogs," Circulation research,
36(1), pp. 43-48.
[85] Sacks, M. S., Enomoto, Y., Graybill, J. R., Merryman, W. D., Zeeshan, A.,
Yoganathan, A. P., Levy, R. J., Gorman, R. C., and Gorman, J. H., 2006, "In-vivo
dynamic deformation of the mitral valve anterior leaflet," The Annals of Thoracic
Surgery, 82(4), pp. 1369-1377.
[86] Amini, R., Voycheck, C. A., and Debski, R. E., 2014, "A Method for Predicting
Collagen Fiber Realignment in Non-Planar Tissue Surfaces as Applied to
Glenohumeral Capsule During Clinically Relevant Deformation," Journal of
Biomechanical Engineering, 136(3), p. 031003.
[87] Filas, B. A., Knutsen, A. K., Bayly, P. V., and Taber, L. A., 2008, "A new method
for measuring deformation of folding surfaces during morphogenesis," Journal of
Biomechanical Engineering, 130(6), p. 061010.
[88] Lee, C.-H., Rabbah, J.-P., Yoganathan, A. P., Gorman, R. C., Gorman Iii, J. H., and
Sacks, M. S., 2015, "On the effects of leaflet microstructure and constitutive model
on the closing behavior of the mitral valve," Biomechanics and modeling in
mechanobiology, 14(6), pp. 1281-1302.
[89] Lee, C.-H., Oomen, P. J., Rabbah, J. P., Yoganathan, A., Gorman, R. C., Gorman,
J. H., Amini, R., and Sacks, M. S., 2013, "A high-fidelity and micro-anatomically
accurate 3D finite element model for simulations of functional mitral valve,"
International Conference on Functional Imaging and Modeling of the Heart,
Springer, pp. 416-424.
[90] Fan, R., and Sacks, M. S., 2014, "Simulation of planar soft tissues using a structural
constitutive model: finite element implementation and validation," Journal of
biomechanics, 47(9), pp. 2043-2054.
[91] Kong, F., Pham, T., Martin, C., McKay, R., Primiano, C., Hashim, S., Kodali, S.,
and Sun, W., 2018, "Finite Element Analysis of Tricuspid Valve Deformation from

167
Multi-slice Computed Tomography Images," Annals of biomedical engineering,
pp. 1-16.
[92] Kunzelman, K., Reimink, M., and Cochran, R., 1997, "Annular dilatation increases
stress in the mitral valve and delays coaptation: a finite element computer model,"
Cardiovascular Surgery, 5(4), pp. 427-434.
[93] Lim, K. H., Yeo, J. H., and Duran, C., 2005, "Three-dimensional asymmetrical
modeling of the mitral valve: a finite element study with dynamic boundaries," J
Heart Valve Dis, 14(3), pp. 386-392.
[94] Einstein, D. R., Kunzelman, K. S., Reinhall, P. G., Nicosia, M. A., and Cochran, R.
P., 2005, "Non-linear fluid-coupled computational model of the mitral valve," J.
Heart Valve Dis, 14(3), pp. 376-385.
[95] Votta, E., Caiani, E., Veronesi, F., Soncini, M., Montevecchi, F. M., and Redaelli,
A., 2008, "Mitral valve finite-element modelling from ultrasound data: a pilot study
for a new approach to understand mitral function and clinical scenarios,"
Philosophical Transactions of the Royal Society of London A: Mathematical,
Physical and Engineering Sciences, 366(1879), pp. 3411-3434.
[96] Prot, V., Skallerud, B., and Holzapfel, G., 2007, "Transversely isotropic membrane
shells with application to mitral valve mechanics. Constitutive modelling and finite
element implementation," International journal for numerical methods in
engineering, 71(8), pp. 987-1008.
[97] Prot, V., Haaverstad, R., and Skallerud, B., 2009, "Finite element analysis of the
mitral apparatus: annulus shape effect and chordal force distribution,"
Biomechanics and modeling in mechanobiology, 8(1), pp. 43-55.
[98] Holzapfel, G. A., Sommer, G., Gasser, C. T., and Regitnig, P., 2005,
"Determination of layer-specific mechanical properties of human coronary arteries
with nonatherosclerotic intimal thickening and related constitutive modeling,"
American Journal of Physiology-Heart and Circulatory Physiology, 289(5), pp.
H2048-H2058.
[99] Wenk, J. F., Zhang, Z., Cheng, G., Malhotra, D., Acevedo-Bolton, G., Burger, M.,
Suzuki, T., Saloner, D. A., Wallace, A. W., and Guccione, J. M., 2010, "First finite
element model of the left ventricle with mitral valve: insights into ischemic mitral
regurgitation," The Annals of thoracic surgery, 89(5), pp. 1546-1553.
[100] Quapp, K., and Weiss, J., 1998, "Material characterization of human medial
collateral ligament," Journal of biomechanical engineering, 120(6), pp. 757-763.
[101] Hallquist, J. O., 2006, "LS-DYNA theory manual," Livermore software
Technology corporation, 3, pp. 25-31.

168
[102] Stevanella, M., Maffessanti, F., Conti, C. A., Votta, E., Arnoldi, A., Lombardi, M.,
Parodi, O., Caiani, E. G., and Redaelli, A., 2011, "Mitral valve patient-specific
finite element modeling from cardiac MRI: application to an annuloplasty
procedure," Cardiovascular Engineering and Technology, 2(2), pp. 66-76.
[103] Wang, Q., and Sun, W., 2013, "Finite element modeling of mitral valve dynamic
deformation using patient-specific multi-slices computed tomography scans,"
Annals of biomedical engineering, 41(1), pp. 142-153.
[104] Gasser, T. C., Ogden, R. W., and Holzapfel, G. A., 2006, "Hyperelastic modelling
of arterial layers with distributed collagen fibre orientations," Journal of the royal
society interface, 3(6), pp. 15-35.
[105] Holzapfel, G. A., Gasser, T. C., and Ogden, R. W., 2000, "A new constitutive
framework for arterial wall mechanics and a comparative study of material
models," Journal of elasticity and the physical science of solids, 61(1-3), pp. 1-48.
[106] Pham, T., Kong, F., Martin, C., Wang, Q., Primiano, C., McKay, R., Elefteriades,
J., and Sun, W., 2017, "Finite element analysis of patient-specific mitral valve with
mitral regurgitation," Cardiovascular engineering and technology, 8(1), pp. 3-16.
[107] Lim, K. O., 1980, "Mechanical properties and ultrastructure of normal human
tricuspid valve chordae tendineae," The Japanese journal of physiology, 30(3), pp.
455-464.
[108] Krishnamurthy, G., Itoh, A., Bothe, W., Swanson, J. C., Kuhl, E., Karlsson, M.,
Miller, D. C., and Ingels, N. B., 2009, "Stress–strain behavior of mitral valve
leaflets in the beating ovine heart," Journal of Biomechanics, 42(12), pp. 1909-
1916.
[109] Krishnamurthy, G., Itoh, A., Swanson, J. C., Bothe, W., Karlsson, M., Kuhl, E.,
Miller, D. C., and Ingels, N. B., 2009, "Regional stiffening of the mitral valve
anterior leaflet in the beating ovine heart," Journal of Biomechanics, 42(16), pp.
2697-2701.
[110] Jouan, J., Pagel, M. R., Hiro, M. E., Lim, K. H., Lansac, E., and Duran, C. M. G.,
2007, "Further information from a sonometric study of the normal tricuspid valve
annulus in sheep: geometric changes during the cardiac cycle," Journal of Heart
Valve Disease, 16(5), p. 511.
[111] He, Z., Ritchie, J., Grashow, J. S., Sacks, M. S., and Yoganathan, A. P., 2005, "In
vitro dynamic strain behavior of the mitral valve posterior leaflet," Journal of
Biomechanical Engineering, 127(3), pp. 504-511.

169
[112] He, Z., Sacks, M. S., Baijens, L., Wanant, S., Shah, P., and Yoganathan, A. P.,
2003, "Effects of papillary muscle position on in-vitro dynamic strain on the
porcine mitral valve," The Journal of heart valve disease, 12(4), pp. 488-494.
[113] Leopaldi, A. M., Vismara, R., Lemma, M., Valerio, L., Cervo, M., Mangini, A.,
Contino, M., Redaelli, A., Antona, C., and Fiore, G. B., 2012, "In vitro
hemodynamics and valve imaging in passive beating hearts," Journal of
Biomechanics, 45(7), pp. 1133-1139.
[114] Jermihov, P. N., Jia, L., Sacks, M. S., Gorman, R. C., Gorman, J. H., and Chandran,
K. B., 2011, "Effect of geometry on the leaflet stresses in simulated models of
congenital bicuspid aortic valves," Cardiovascular engineering and technology,
2(1), pp. 48-56.
[115] Weinberg, E. J., and Mofrad, M. R. K., 2008, "A multiscale computational
comparison of the bicuspid and tricuspid aortic valves in relation to calcific aortic
stenosis," Journal of biomechanics, 41(16), pp. 3482-3487.
[116] Come, P. C., and Riley, M. F., 1985, "Tricuspid anular dilatation and failure of
tricuspid leaflet coaptation in tricuspid regurgitation," The American Journal of
Cardiology, 55(5), pp. 599-601.
[117] Amini Khoiy, K., and Amini, R., 2016, "On the Biaxial Mechanical Response of
Porcine Tricuspid Valve Leaflets," Journal of Biomechanical Engineering, 138(10),
p. 104504.
[118] Navia, J. L., Brozzi, N. A., Klein, A. L., Ling, L. F., Kittayarak, C., Nowicki, E. R.,
Batizy, L. H., Zhong, J., and Blackstone, E. H., 2012, "Moderate tricuspid
regurgitation with left-sided degenerative heart valve disease: to repair or not to
repair?," The Annals of thoracic surgery, 93(1), pp. 59-69.
[119] Singh, S. K., Tang, G. H., Maganti, M. D., Armstrong, S., Williams, W. G., David,
T. E., and Borger, M. A., 2006, "Midterm outcomes of tricuspid valve repair versus
replacement for organic tricuspid disease," The Annals of thoracic surgery, 82(5),
pp. 1735-1741.
[120] Rankin, J. S., Hammill, B. G., Ferguson, T. B., Glower, D. D., O’Brien, S. M.,
DeLong, E. R., Peterson, E. D., and Edwards, F. H., 2006, "Determinants of
operative mortality in valvular heart surgery," The Journal of thoracic and
cardiovascular surgery, 131(3), pp. 547-557.
[121] Desai, R. R., Abello, L. M. V., Klein, A. L., Marwick, T. H., Krasuski, R. A., Ye,
Y., Nowicki, E. R., Rajeswaran, J., Blackstone, E. H., and Pettersson, G. B., 2013,
"Tricuspid regurgitation and right ventricular function after mitral valve surgery
with or without concomitant tricuspid valve procedure," The Journal of thoracic
and cardiovascular surgery, 146(5), pp. 1126-1132. e1110.
170
[122] Chan, V., Burwash, I. G., Lam, B.-K., Auyeung, T., Tran, A., Mesana, T. G., and
Ruel, M., 2009, "Clinical and echocardiographic impact of functional tricuspid
regurgitation repair at the time of mitral valve replacement," The Annals of
Thoracic Surgery, 88(4), pp. 1209-1215.
[123] Cohen, S., Sell, J., McIntosh, C., and Clark, R., 1987, "Tricuspid regurgitation in
patients with acquired, chronic, pure mitral regurgitation. I. Prevalence, diagnosis,
and comparison of preoperative clinical and hemodynamic features in patients with
and without tricuspid regurgitation," The Journal of thoracic and cardiovascular
surgery, 94(4), pp. 481-487.
[124] Koelling, T. M., Aaronson, K. D., Cody, R. J., Bach, D. S., and Armstrong, W. F.,
2002, "Prognostic significance of mitral regurgitation and tricuspid regurgitation in
patients with left ventricular systolic dysfunction," American heart journal, 144(3),
pp. 524-529.
[125] Sagie, A., Freitas, N., Chen, M. H., Marshall, J. E., Weyman, A. E., and Levine, R.
A., 1997, "Echocardiographic assessment of mitral stenosis and its associated
valvular lesions in 205 patients and lack of association with mitral valve prolapse,"
Journal of the American Society of Echocardiography, 10(2), pp. 141-148.
[126] Boyaci, A., Gokce, V., Topaloglu, S., Korkmaz, S., and Goksel, S., 2007, "Outcome
of significant functional tricuspid regurgitation late after mitral valve replacement
for predominant rheumatic mitral stenosis," Angiology, 58(3), pp. 336-342.
[127] Lake, S. P., and Barocas, V. H., 2011, "Mechanical and structural contribution of
non-fibrillar matrix in uniaxial tension: a collagen-agarose co-gel model," Annals
of Biomedical Engineering, 39(7), pp. 1891-1903.
[128] Redington, A. N., Gray, H. H., Hodson, M. E., Rigby, M. L., and Oldershaw, P. J.,
1988, "Characterisation of the normal right ventricular pressure-volume relation by
biplane angiography and simultaneous micromanometer pressure measurements,"
British heart journal, 59(1), pp. 23-30.
[129] Naeije, R., Brimioulle, S., and Dewachter, L., 2014, "Biomechanics of the right
ventricle in health and disease (2013 Grover Conference series)," Pulmonary
circulation, 4(3), pp. 395-406.
[130] Redington, A. N., Rigby, M. L., Shinebourne, E. A., and Oldershaw, P. J., 1990,
"Changes in the pressure-volume relation of the right ventricle when its loading
conditions are modified," British heart journal, 63(1), pp. 45-49.
[131] Anwar, A. M., Geleijnse, M. L., Soliman, O., II, McGhie, J. S., Frowijn, R., Nemes,
A., van den Bosch, A. E., Galema, T. W., and Folkert, J., 2007, "Assessment of
normal tricuspid valve anatomy in adults by real-time three-dimensional
171
echocardiography," The international journal of cardiovascular imaging, 23(6), pp.
717-724.
[132] Tei, C., Pilgrim, J. P., Shah, P. M., Ormiston, J. A., and Wong, M., 1982, "The
tricuspid valve annulus: study of size and motion in normal subjects and in patients
with tricuspid regurgitation," Circulation, 66(3), pp. 665-671.
[133] Heyden, S., Nagler, A., Bertoglio, C., Biehler, J., Gee, M. W., Wall, W. A., and
Ortiz, M., 2015, "Material modeling of cardiac valve tissue: Experiments,
constitutive analysis and numerical investigation," Journal of Biomechanics.
[134] Amini Khoiy, K., Pant, A. D., and Amini, R., 2018, "Quantification of Material
Constants for a Phenomenological Constitutive Model of Porcine Tricuspid Valve
Leaflets for Simulation Applications," Journal of Biomechanical Engineering,
140(9), pp. 094503-094503-094511.
[135] Cooper, T., Napolitano, L. M., Fitzgerald, M. J. T., Moore, K. E., Daggett, W. M.,
Willman, V. L., Sonnenblick, E. H., and Hanlon, C. R., 1966, "Structural basis of
cardiac valvar function," Archives of Surgery, 93(5), pp. 767-771.
[136] Lauten, A., Doenst, T., Hamadanchi, A., Franz, M., and Figulla, H. R., 2014,
"Percutaneous bicaval valve implantation for transcatheter treatment of tricuspid
regurgitation: clinical observations and 12-month follow-up,"
Circulation.Cardiovascular interventions, 7(2), pp. 268-272.
[137] Rodés-Cabau, J., Hahn, R. T., Latib, A., Laule, M., Lauten, A., Maisano, F.,
Schofer, J., Campelo-Parada, F., Puri, R., and Vahanian, A., 2016, "Transcatheter
therapies for treating tricuspid regurgitation," Journal of the American College of
Cardiology, 67(15), pp. 1829-1845.
[138] Kilic, A., Saha-Chaudhuri, P., Rankin, J. S., and Conte, J. V., 2013, "Trends and
outcomes of tricuspid valve surgery in North America: an analysis of more than
50,000 patients from the Society of Thoracic Surgeons database," The Annals of
thoracic surgery, 96(5), pp. 1546-1552.
[139] Lee, C.-H., Amini, R., Sakamoto, Y., Carruthers, C. A., Aggarwal, A., Gorman, R.
C., Gorman III, J. H., and Sacks, M. S., 2015, "Mitral valves: a computational
framework," Multiscale Modeling in Biomechanics and Mechanobiology,
Springer, London, UK, pp. 223-255.
[140] Amini Khoiy, K., Biswas, D., Decker, T. N., Asgarian, K. T., Loth, F., and Amini,
R., 2016, "Surface Strains of Porcine Tricuspid Valve Septal Leaflets Measured in
Ex Vivo Beating Hearts," Journal of Biomechanical Engineering, 138(11), p.
111006.

172
[141] Fung, Y.-c., 2013, Biomechanics: mechanical properties of living tissues, Springer
Science & Business Media, New York.
[142] Amini Khoiy, K., Abdulhai, S., Glenn, I. C., Ponsky, T. A., and Amini, R., 2018,
"Anisotropic and nonlinear biaxial mechanical response of porcine small bowel
mesentery," Journal of the mechanical behavior of biomedical materials, 78, pp.
154-163.
[143] Conn, A. R., Gould, N. I., and Toint, P. L., 2000, Trust region methods, SIAM,
Philadelphia, PA.
[144] Voorhees, A., Jan, N.-J., and Sigal, I., 2017, "Effects of collagen microstructure
and material properties on the deformation of the neural tissues of the lamina
cribrosa," Acta Biomaterialia(58), pp. 278-290.
[145] Voorhees, A., Grimm, J., Bilonick, R., Kagemann, L., Ishikawa, H., Schuman, J.,
Wollstein, G., and Sigal, I., 2016, "What is a typical optic nerve head?,"
Experimental eye research, 149, pp. 40-47.
[146] Gsellman, L., and Amini, R., 2016, "Patients With Intravitreal Gas Bubbles at Risk
of High Intraocular Pressure Without Exceeding Elevation of Surgery: Theoretical
AnalysisVitrectomy, High IOP, and No High Altitude Travel," Investigative
Ophthalmology & Visual Science, 57(7), pp. 3340-3347.
[147] Amini, R., Barocas, V. H., Kavehpour, H. P., and Hubschman, J. P., 2011,
"Computational simulation of altitude change-induced intraocular pressure
alteration in patients with intravitreal gas bubbles," Retina, 31(8), pp. 1656-1663.
[148] Stella, J. A., Liao, J., and Sacks, M. S., 2007, "Time-dependent biaxial mechanical
behavior of the aortic heart valve leaflet," Journal of biomechanics, 40(14), pp.
3169-3177.
[149] Humphrey, J. D., 1999, "An evaluation of pseudoelastic descriptors used in arterial
mechanics," TRANSACTIONS-AMERICAN SOCIETY OF MECHANICAL
ENGINEERS JOURNAL OF BIOMECHANICAL ENGINEERING, 121, pp. 259-
262.
[150] Girard, M. J., Dahlmann-Noor, A., Rayapureddi, S., Bechara, J. A., Bertin, B. M.,
Jones, H., Albon, J., Khaw, P. T., and Ethier, C. R., 2011, "Quantitative mapping
of scleral fiber orientation in normal rat eyes," Investigative ophthalmology &
visual science, 52(13), pp. 9684-9693.
[151] Haskett, D., Johnson, G., Zhou, A., Utzinger, U., and Geest, J. V., 2010,
"Microstructural and biomechanical alterations of the human aorta as a function of
age and location," Biomechanics and modeling in mechanobiology, 9(6), pp. 725-
736.

173
[152] Pant, A. D., Thomas, V. S., Black, A. L., Verba, T., Lesicko, J. G., and Amini, R.,
2018, "Pressure-induced microstructural changes in porcine tricuspid valve
leaflets," Acta Biomaterialia, 67, pp. 248-258.
[153] Federico, S., Grillo, A., Giaquinta, G., and Herzog, W., 2008, "Convex Fung-type
potentials for biological tissues," Meccanica, 43(3), pp. 279-288.
[154] Chaudhury, R. A., Atlasman, V., Pathangey, G., Pracht, N., Adrian, R. J., and
Frakes, D. H., 2016, "A High Performance Pulsatile Pump for Aortic Flow
Experiments in 3-Dimensional Models," Cardiovascular Engineering and
Technology, pp. 1-11.
[155] Evin, M., Guivier‐Curien, C., Pibarot, P., Kadem, L., and Rieu, R., 2016, "Are the
Current Doppler Echocardiography Criteria Able to Discriminate Mitral Bileaflet
Mechanical Heart Valve Malfunction? An In Vitro Study," Artificial Organs.
[156] Trawiński, Z., Wójcik, J., Nowicki, A., Olszewski, R., Balcerzak, A., Frankowska,
E., Zegadło, A., and Rydzyński, P., 2015, "Strain examinations of the left ventricle
phantom by ultrasound and multislices computed tomography imaging,"
Biocybernetics and Biomedical Engineering, 35(4), pp. 255-263.
[157] Rahmani, B., Tzamtzis, S., Ghanbari, H., Burriesci, G., and Seifalian, A. M., 2012,
"Manufacturing and hydrodynamic assessment of a novel aortic valve made of a
new nanocomposite polymer," Journal of Biomechanics, 45(7), pp. 1205-1211.
[158] Cygan, S., Werys, K., Błaszczyk, Ł., Kubik, T., and Kałużyński, K., 2014, "Left
ventricle phantom and experimental setup for MRI and echocardiography–
Preliminary results of data acquisitions," Biocybernetics and Biomedical
Engineering, 34(1), pp. 19-24.
[159] Nolan, S. P., 1994, "The International Standard Cardiovascular implants--Cardiac
Valve Prostheses (ISO 5840:1989) and the FDA Draft Replacement Heart Valve
Guidance (Version 4.0)," The Journal of heart valve disease, 3(4), pp. 347-349.
[160] Mohrman, D. E., and Heller, L. J., 2002, "Cardiovascular physiology."
[161] Greyson, C., Xu, Y., Cohen, J., and Schwartz, G. G., 1997, "Right ventricular
dysfunction persists following brief right ventricular pressure overload,"
Cardiovascular research, 34(2), pp. 281-288.
[162] Greyson, C., Xu, Y., Lu, L., and Schwartz, G. G., 2000, "Right ventricular pressure
and dilation during pressure overload determine dysfunction after pressure
overload," American journal of physiology.Heart and circulatory physiology,
278(5), pp. H1414-1420.

174
[163] Schmitto, J. D., Doerge, H., Post, H., Coulibaly, M., Sellin, C., Popov, A. F.,
Sossalla, S., and Schoendube, F. A., 2009, "Progressive right ventricular failure is
not explained by myocardial ischemia in a pig model of right ventricular pressure
overload," European journal of cardio-thoracic surgery : official journal of the
European Association for Cardio-thoracic Surgery, 35(2), pp. 229-234.
[164] Solomon, S. B., and Glantz, S. A., 1999, "Regional ischemia increases sensitivity
of left ventricular relaxation to volume in pigs," The American Journal of
Physiology, 276(6 Pt 2), pp. H1994-2005.
[165] Hannon, J. P., Bossone, C. A., and Wade, C. E., 1990, "Normal physiological
values for conscious pigs used in biomedical research," Laboratory animal science,
40(3), pp. 293-298.
[166] Billiar, K. L., and Sacks, M. S., 1997, "A method to quantify the fiber kinematics
of planar tissues under biaxial stretch," Journal of Biomechanics, 30(7), pp. 753-
756.
[167] Martin, C., and Sun, W., 2012, "Biomechanical characterization of aortic valve
tissue in humans and common animal models," Journal of Biomedical Materials
Research Part A, 100(6), pp. 1591-1599.
[168] Gorman III, J. H., Jackson, B. M., Enomoto, Y., and Gorman, R. C., 2004, "The
effect of regional ischemia on mitral valve annular saddle shape," The Annals of
thoracic surgery, 77(2), pp. 544-548.
[169] Gorman, J. H., Gorman, R. C., Jackson, B. M., Enomoto, Y., John-Sutton, M. G.
S., and Edmunds, L. H., 2003, "Annuloplasty ring selection for chronic ischemic
mitral regurgitation: lessons from the ovine model," The Annals of Thoracic
Surgery, 76(5), pp. 1556-1563.
[170] Gorman III, J. H., Gupta, K. B., Streicher, J. T., Gorman, R. C., Jackson, B. M.,
Ratcliffe, M. B., Bogen, D. K., and Edmunds Jr, L. H., 1996, "Dynamic three-
dimensional imaging of the mitral valve and left ventricle by rapid sonomicrometry
array localization," The Journal of thoracic and cardiovascular surgery, 112(3), pp.
712-724.
[171] Ge, L., Morrel, W. G., Ward, A., Mishra, R., Zhang, Z., Guccione, J. M., Grossi,
E. A., and Ratcliffe, M. B., 2014, "Measurement of mitral leaflet and annular
geometry and stress after repair of posterior leaflet prolapse: virtual repair using a
patient-specific finite element simulation," The Annals of Thoracic Surgery, 97(5),
pp. 1496-1503.
[172] Biswas, D., Casey, D., Crowder, D., Steinman, D. A., Yun, H. Y., and Loth, F.,
2016, "Characterization of Transition to Turbulence for Blood in a Straight Pipe
under Steady Flow Conditions," Journal of Biomechanical Engineering.

175
[173] Khoiy, K. A., Asgarian, K. T., Loth, F., and Amini, R., 2018, "Dilation of tricuspid
valve annulus immediately after rupture of chordae tendineae in ex-vivo porcine
hearts," PloS one, 13(11), p. e0206744.
[174] Waller, B. F., Moriarty, A. T., Eble, J. N., Davey, D. M., Hawley, D. A., and Pless,
J. E., 1986, "Etiology of pure tricuspid regurgitation based on anular circumference
and leaflet area: Analysis of 45 necropsy patients with clinical and morphologic
evidence of pure tricuspid regurgitation," Journal of the American College of
Cardiology, 7(5), pp. 1063-1074.
[175] Carpentier, A., 1983, "Cardiac valve surgery-the "French correction"," J Thorac
Cardiovasc Surg, 86, pp. 323-337.
[176] Jost, C. H. A., Connolly, H. M., Dearani, J. A., Edwards, W. D., and Danielson, G.
K., 2007, "Ebstein’s anomaly," Circulation, 115(2), pp. 277-285.
[177] Brandenburg, R. O., McGoon, D. C., Campeau, L., and Giuliani, E. R., 1966,
"Traumatic rupture of the chordae tendineae of the tricuspid valve: successful repair
twenty-four years later," The American journal of cardiology, 18(6), pp. 911-915.
[178] Naja, I., Pomar, J., Barriuso, C., Mestres, C., and Mulet, J., 1991, "Traumatic
tricuspid regurgitation," The Journal of cardiovascular surgery, 33(2), pp. 256-258.
[179] Shankar, K. R., Hultgren, M. K., Lauer, R. M., and Diehl, A. M., 1967, "Lethal
tricuspid and mitral regurgitation in Marfan's syndrome∗," The American Journal
of Cardiology, 20(1), pp. 122-128.
[180] Phornphutkul, C., Rosenthal, A., and Nadas, A. S., 1973, "Cardiac Manifestations
of Marfan Syndrome in Infancy and Childhood," Circulation, 47(3), p. 587.
[181] Berger, M., Haimowitz, A., Van Tosh, A., Berdoff, R. L., and Goldberg, E., 1985,
"Quantitative assessment of pulmonary hypertension in patients with tricuspid
regurgitation using continuous wave Doppler ultrasound," Journal of the American
College of Cardiology, 6(2), pp. 359-365.
[182] Rogers, J. H., and Bolling, S. F., 2009, "The tricuspid valve," Circulation, 119(20),
pp. 2718-2725.
[183] Noera, G., Sanguinetti, M., Pensa, P., Biagi, B., Cremonesi, A., Lodi, R., Lessana,
A., and Carbone, C., 1991, "Tricuspid valve incompetence caused by
nonpenetrating thoracic trauma," The Annals of thoracic surgery, 51(2), pp. 320-
322.
[184] Dontigny, L., Baillot, R., Panneton, J., Page, P., and Cossette, R., 1992, "Surgical
repair of traumatic tricuspid insufficiency: report of three cases," Journal of Trauma
and Acute Care Surgery, 33(2), pp. 266-269.

176
[185] Maisano, F., Lorusso, R., Sandrelli, L., Torracca, L., Coletti, G., La, G. C., and
Alfieri, O., 1996, "Valve repair for traumatic tricuspid regurgitation," European
journal of cardio-thoracic surgery: official journal of the European Association for
Cardio-thoracic Surgery, 10(10), pp. 867-873.
[186] Vayre, F., Richard, P., and Ollivier, J., 1996, "Traumatic tricuspid insufficiency,"
Archives des maladies du coeur et des vaisseaux, 89(4), pp. 459-463.
[187] Gayet, C., Pierre, B., Delahaye, J.-P., Champsaur, G., Andre-Fouet, X., and Rueff,
P., 1987, "Traumatic tricuspid insufficiency: an underdiagnosed disease," Chest,
92(3), pp. 429-432.
[188] Croxson, M. S., O'Brien, K. P., and Lowe, J. B., 1971, "Traumatic tricuspid
regurgitation. Long-term survival," British heart journal, 33(5), p. 750.
[189] Ma, W.-G., Luo, G.-H., Sun, H.-S., Xu, J.-P., Hu, S.-S., and Zhu, X.-D., 2010,
"Surgical treatment of traumatic tricuspid insufficiency: experience in 13 cases,"
The Annals of thoracic surgery, 90(6), pp. 1934-1938.
[190] Stephens, E. H., Nguyen, T. C., Itoh, A., Ingels, N. B., Miller, D. C., and Grande-
Allen, K. J., 2008, "The effects of mitral regurgitation alone are sufficient for leaflet
remodeling," Circulation, 118(14 suppl 1), pp. S243-S249.
[191] Guertler, C. A., Okamoto, R. J., Schmidt, J. L., Badachhape, A. A., Johnson, C. L.,
and Bayly, P. V., 2018, "Mechanical properties of porcine brain tissue in vivo and
ex vivo estimated by MR elastography," Journal of Biomechanics, 69, pp. 10-18.
[192] Basu, A., and He, Z., 2016, "Annulus Tension on the Tricuspid Valve: An In-Vitro
Study," Cardiovascular Engineering and Technology, 7(3), pp. 270-279.
[193] Filip, D. A., Radu, A., and Simionescu, M., 1986, "Interstitial cells of the heart
valves possess characteristics similar to smooth muscle cells," Circulation research,
59(3), pp. 310-320.
[194] Messier, R. H., Bass, B. L., Aly, H. M., Jones, J. L., Domkowski, P. W., Wallace,
R. B., and Hopkins, R. A., 1994, "Dual structural and functional phenotypes of the
porcine aortic valve interstitial population: characteristics of the leaflet
myofibroblast," Journal of Surgical Research, 57(1), pp. 1-21.
[195] Mulholland, D. L., and Gotlieb, A. I., 1996, "Cell biology of valvular interstitial
cells," The Canadian journal of cardiology, 12(3), pp. 231-236.
[196] Taylor, P. M., Batten, P., Brand, N. J., Thomas, P. S., and Yacoub, M. H., 2003,
"The cardiac valve interstitial cell," The international journal of biochemistry &
cell biology, 35(2), pp. 113-118.

177
[197] Bairati, A., and DeBiasi, S., 1981, "Presence of a smooth muscle system in aortic
valve leaflets," Anatomy and embryology, 161(3), pp. 329-340.
[198] Swift, J., Ivanovska, I. L., Buxboim, A., Harada, T., Dingal, P. D. P., Pinter, J.,
Pajerowski, J. D., Spinler, K. R., Shin, J.-W., and Tewari, M., 2013, "Nuclear
lamin-A scales with tissue stiffness and enhances matrix-directed differentiation,"
Science, 341(6149), p. 1240104.
[199] Willems, I., Havenith, M. G., Smits, J., and Daemen, M., 1994, "Structural
alterations in heart valves during left ventricular pressure overload in the rat,"
Laboratory investigation; a journal of technical methods and pathology, 71(1), pp.
127-133.
[200] Huang, S., and Huang, H.-Y. S., 2015, "Biaxial stress relaxation of semilunar heart
valve leaflets during simulated collagen catabolism: Effects of collagenase
concentration and equibiaxial strain state," Proceedings of the Institution of
Mechanical Engineers, Part H: Journal of Engineering in Medicine, 229(10), pp.
721-731.
[201] Zareian, R., Church, K. P., Saeidi, N., Flynn, B. P., Beale, J. W., and Ruberti, J.
W., 2010, "Probing collagen/enzyme mechanochemistry in native tissue with
dynamic, enzyme-induced creep," Langmuir, 26(12), pp. 9917-9926.
[202] Flynn, B. P., Bhole, A. P., Saeidi, N., Liles, M., DiMarzio, C. A., and Ruberti, J.
W., 2010, "Mechanical strain stabilizes reconstituted collagen fibrils against
enzymatic degradation by mammalian collagenase matrix metalloproteinase 8
(MMP-8)," PLoS One, 5(8), p. e12337.
[203] Lancellotti, P., Moura, L., Pierard, L. A., Agricola, E., Popescu, B. A., Tribouilloy,
C., Hagendorff, A., Monin, J.-L., Badano, L., Zamorano, J. L., on behalf of the
European Association of, E., Document, R., Sicari, R., Vahanian, A., and Roelandt,
J. R. T. C., 2010, "European Association of Echocardiography recommendations
for the assessment of valvular regurgitation. Part 2: mitral and tricuspid
regurgitation (native valve disease)," European Journal of Echocardiography,
11(4), pp. 307-332.
[204] Lin, S.-J., Chen, C.-W., Chou, C.-J., Liu, K.-T., Su, H.-M., Lin, T.-H., Voon, W.-
C., Lai, W.-T., and Sheu, S.-H., 2006, "Traumatic Tricuspid Insufficiency with
Chordae Tendinae Rupture: A Case Report and Literature Review," The Kaohsiung
Journal of Medical Sciences, 22(12), pp. 626-629.
[205] Yun Yong, J., Jonghwan, M., Sang Hyun, L., Yeo Jin, K., Hyoeun, A., and and
Sung Yong, P., 2016, "Undiagnosed Traumatic Tricuspid Regurgitation Identified
by Intraoperative Transesophageal Echocardiography," J Acute Care Surg, 6(2), pp.
68-70.

178
[206] DOUNIS, G., MATSAKAS, E., POULARAS, J., PAPAKONSTANTINOU, K.,
KALOGEROMITROS, A., and KARABINIS, A., 2002, "Traumatic tricuspid
insufficiency: a case report with a review of the literature," European Journal of
Emergency Medicine, 9(3), pp. 258-261.
[207] Schuster, I., Graf, S., Klaar, U., Seitelberger, R., Mundigler, G., and Binder, T.,
2008, "Heterogeneity of traumatic injury of the tricuspid valve: A report of four
cases," Wiener klinische Wochenschrift, 120(15), pp. 499-503.
[208] 1992, "Blunt chest injuries in 1696 patients," European Journal of Cardio-Thoracic
Surgery, 6(6), pp. 284-287.
[209] Emine, B. S., Murat, A., Mehmet, B., Mustafa, K., and Gokturk, I., 2008, "Flail
mitral and tricuspid valves due to myxomatous disease," European Journal of
Echocardiography, 9(2), pp. 304-305.
[210] Reddy, V. K., Nanda, S., Bandarupalli, N., Pothineni, K. R., and Nanda, N. C.,
2008, "Traumatic Tricuspid Papillary Muscle and Chordae Rupture: Emerging
Role of Three‐Dimensional Echocardiography," Echocardiography, 25(6), pp. 653-
657.
[211] Richard, P., Vayre, F., Sabouret, P., Gandjbakhch, I., and Ollivier, J. P., 1997,
"Outcome of traumatic tricuspid insufficiency, treated surgically. Apropos of 9
cases," Archives des maladies du coeur et des vaisseaux, 90(4), pp. 451-456.
[212] Golub, G. H., and Reinsch, C., 1970, "Singular value decomposition and least
squares solutions," Numerische mathematik, 14(5), pp. 403-420.
[213] De Lathauwer, L., De Moor, B., and Vandewalle, J., 2000, "A multilinear singular
value decomposition," SIAM journal on Matrix Analysis and Applications, 21(4),
pp. 1253-1278.
[214] Kunzelman, K., and Cochran, R., 1990, "Mechanical properties of basal and
marginal mitral valve chordae tendineae," ASAIO transactions, 36(3), pp. M405-
408.
[215] Zuo, K., Pham, T., Li, K., Martin, C., He, Z., and Sun, W., 2016, "Characterization
of biomechanical properties of aged human and ovine mitral valve chordae
tendineae," Journal of the mechanical behavior of biomedical materials, 62, pp.
607-618.
[216] Liao, J., and Vesely, I., 2003, "A structural basis for the size-related mechanical
properties of mitral valve chordae tendineae," Journal of biomechanics, 36(8), pp.
1125-1133.

179
[217] Stevanella, M., Krishnamurthy, G., Votta, E., Swanson, J. C., Redaelli, A., and
Ingels, N. B., 2011, "Mitral leaflet modeling: Importance of in vivo shape and
material properties," Journal of Biomechanics, 44(12), pp. 2229-2235.
[218] Barber, J. E., Kasper, F. K., Ratliff, N. B., Cosgrove, D. M., Griffin, B. P., and
Vesely, I., 2001, "Mechanical properties of myxomatous mitral valves," The
Journal of thoracic and cardiovascular surgery, 122(5), pp. 955-962.
[219] Ritchie, J., Jimenez, J., He, Z., Sacks, M. S., and Yoganathan, A. P., 2006, "The
material properties of the native porcine mitral valve chordae tendineae: an in vitro
investigation," Journal of biomechanics, 39(6), pp. 1129-1135.
[220] Lim, K. O., Boughner, D. R., and Perkins, D. G., 1983, "Ultrastructure and
mechanical properties of chordae tendineae from a myxomatous tricuspid valve,"
Japanese heart journal, 24(4), pp. 539-548.
[221] Rashid, B., Destrade, M., and Gilchrist, M. D., 2012, "Determination of friction
coefficient in unconfined compression of brain tissue," journal of the mechanical
behavior of biomedical materials, 14, pp. 163-171.
[222] Jin, Z., and Dowson, D., 2013, "Bio-friction," Friction, 1(2), pp. 100-113.
[223] Torres, A. M., and Ziegler, M. M., 1993, "Malrotation of the intestine," World
journal of surgery, 17(3), pp. 326-331.
[224] Strouse, P. J., 2004, "Disorders of intestinal rotation and fixation (“malrotation”),"
Pediatric Radiology, 34(11), pp. 837-851.
[225] Pracros, J. P., Sann, L., Genin, G., Tran-Minh, V. A., de Finfe, C. H. M., Foray, P.,
and Louis, D., 1992, "Ultrasound diagnosis of midgut volvulus: the “whirlpool”
sign," Pediatric radiology, 22(1), pp. 18-20.
[226] Applegate, K. E., Goske, M. J., Pierce, G., and Murphy, D., 1999, "Situs Revisited:
Imaging of the Heterotaxy Syndrome," RadioGraphics, 19(4), pp. 837-852.
[227] Malek, M. M., and Burd, R. S., 2005, "Surgical treatment of malrotation after
infancy: a population-based study," Journal of Pediatric Surgery, 40(1), pp. 285-
289.
[228] El-Gohary, Y., Alagtal, M., and Gillick, J., 2010, "Long-term complications
following operative intervention for intestinal malrotation: a 10-year review,"
Pediatric Surgery International, 26(2), pp. 203-206.
[229] Murphy, F. L., and Sparnon, A. L., 2006, "Long-term complications following
intestinal malrotation and the Ladd’s procedure: a 15 year review," Pediatric
Surgery International, 22(4), pp. 326-329.
180
[230] McVay, M. R., Kokoska, E. R., Jackson, R. J., and Smith, S. D., 2007, "The
changing spectrum of intestinal malrotation: diagnosis and management," The
American Journal of Surgery, 194(6), pp. 712-719.
[231] Graziano, K., Islam, S., Dasgupta, R., Lopez, M. E., Austin, M., Chen, L. E.,
Goldin, A., Downard, C. D., Renaud, E., and Abdullah, F., 2015, "Asymptomatic
malrotation: Diagnosis and surgical management," Journal of Pediatric Surgery,
50(10), pp. 1783-1790.
[232] Fung, Y., 1967, "Elasticity of soft tissues in simple elongation," American Journal
of Physiology--Legacy Content, 213(6), pp. 1532-1544.
[233] Savin, T., Shyer, A. E., and Mahadevan, L., 2012, "A method for tensile tests of
biological tissues at the mesoscale," Journal of Applied Physics, 111(7), p. 074704.
[234] D'Amore, A., Yoshizumi, T., Luketich, S. K., Wolf, M. T., Gu, X., Cammarata, M.,
Hoff, R., Badylak, S. F., and Wagner, W. R., 2016, "Bi-layered polyurethane –
Extracellular matrix cardiac patch improves ischemic ventricular wall remodeling
in a rat model," Biomaterials, 107, pp. 1-14.
[235] Kahan, L. G., Guertler, C., Blatnik, J. A., and Lake, S. P., 2017, "Validation of
Single C-Arm Fluoroscopic Technique for Measuring In Vivo Abdominal Wall
Deformation," Journal of Biomechanical Engineering, 139(8), pp. 084502-084502-
084507.
[236] Sigal, I. A., Flanagan, J. G., and Ethier, C. R., 2005, "Factors Influencing Optic
Nerve Head Biomechanics," Investigative Ophthalmology & Visual Science,
46(11), pp. 4189-4199.
[237] Humphrey, J. D., Vawter, D. L., and Vito, R. P., 1987, "Quantification of strains in
biaxially tested soft tissues," Journal of Biomechanics, 20(1), pp. 59-65.
[238] Parekh, A., Cigan, A. D., Wognum, S., Heise, R. L., Chancellor, M. B., and Sacks,
M. S., 2010, "Ex vivo deformations of the urinary bladder wall during whole
bladder filling: Contributions of extracellular matrix and smooth muscle," Journal
of Biomechanics, 43(9), pp. 1708-1716.
[239] Natali, A. N., Carniel, E. L., and Gregersen, H., 2009, "Biomechanical behaviour
of oesophageal tissues: Material and structural configuration, experimental data and
constitutive analysis," Medical Engineering & Physics, 31(9), pp. 1056-1062.
[240] Feola, A., Moalli, P., Alperin, M., Duerr, R., Gandley, R. E., and Abramowitch, S.,
2011, "Impact of Pregnancy and Vaginal Delivery on the Passive and Active
Mechanics of the Rat Vagina," Annals of Biomedical Engineering, 39(1), pp. 549-
558.

181
[241] Miller, E., and Ullrey, D., 1987, "The pig as a model for human nutrition," Annual
review of nutrition, 7(1), pp. 361-382.

182
APPENDICES

183
APPENDIX A
THE DEVELOPED AVERAGE STRESS–STRAIN RESPONSES FOR THE
POSTERIOR AND SEPTAL LEAFLETS (SUPPLEMENTARY MATERIALS TO
CHAPTER III)
The graphs showing the average stress–strain responses developed for the posterior
(Figs. A.1–A.3) and septal (Figs. A.4–A.6) leaflets based on identical tension states (Figs.
A.1 and A.4), identical first Piola–Kirchhoff stress states (Figs. A.2 and A.5), and identical
Cauchy stress states (Figs. A.3 and A.6) are presented here.
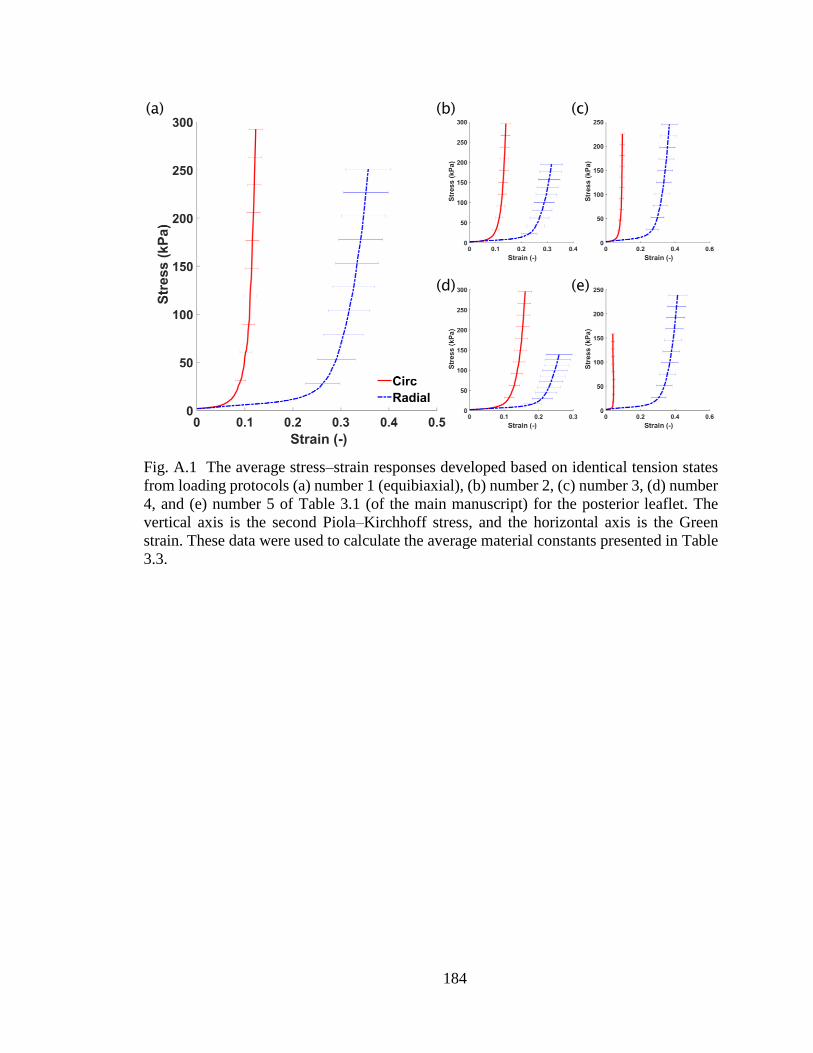
184
Fig. A.1 The average stress–strain responses developed based on identical tension states
from loading protocols (a) number 1 (equibiaxial), (b) number 2, (c) number 3, (d) number
4, and (e) number 5 of Table 3.1 (of the main manuscript) for the posterior leaflet. The
vertical axis is the second Piola–Kirchhoff stress, and the horizontal axis is the Green
strain. These data were used to calculate the average material constants presented in Table
3.3.

185
Fig. A.2 The average stress–strain responses developed based on identical first Piola–
Kirchhoff stress states from loading protocols (a) number 1 (equibiaxial), (b) number 2, (c)
number 3, (d) number 4, and (e) number 5 of Table 3.1 (of the main manuscript) for the
posterior leaflet. The vertical axis is the second Piola–Kirchhoff stress, and the horizontal
axis is the Green strain. These data were used to calculate the average material constants
presented in Table 3.4.

186
Fig. A.3 The average stress–strain responses developed based on identical Cauchy stress
states from loading protocols (a) number 1 (equibiaxial), (b) number 2, (c) number 3, (d)
number 4, and (e) number 5 of Table 3.1 (of the main manuscript) for the posterior leaflet.
The vertical axis is the second Piola–Kirchhoff stress, and the horizontal axis is the Green
strain. These data were used to calculate the average material constants presented in Table
3.5.

187
Fig. A.4 The average stress–strain responses developed based on identical tension states
from loading protocols (a) number 1 (equibiaxial), (b) number 2, (c) number 3, (d) number
4, and (e) number 5 of Table 3.1 (of the main manuscript) for the septal leaflet. The vertical
axis is the second Piola–Kirchhoff stress and the horizontal axis is the Green strain. These
data were used to calculate the average material constants presented in Table 3.3.

188
Fig. A.5 The average stress–strain responses developed based on identical first Piola–
Kirchhoff stress states from loading protocols (a) number 1 (equibiaxial), (b) number 2, (c)
number 3, (d) number 4, and (e) number 5 of Table 3.1 (of the main manuscript) for the
septal leaflet. The vertical axis is the second Piola–Kirchhoff stress, and the horizontal axis
is the Green strain. These data were used to calculate the average material constants
presented in Table 3.4.

189
Fig. A.6 The average stress–strain responses developed based on identical Cauchy stress
states from loading protocols (a) number 1 (equibiaxial), (b) number 2, (c) number 3, (d)
number 4, and (e) number 5 of Table 3.1 (of the main manuscript) for the septal leaflet.
The vertical axis is the second Piola–Kirchhoff stress, and the horizontal axis is the Green
strain. These data were used to calculate the average material constants presented in Table
3.5.

190
APPENDIX B
QUANTIFICATION OF THE SURFACE STRAINS USING FOUR-DIMENSIONAL
SPATIOTEMPORAL COORDINATES OF SURFACE MARKERS
The technique presented here measures the surface strains based on the general
nonlinear membrane theory of shells. This method can be used to calculate the deformation
gradient, strains, and other kinematic quantities using spatiotemporal coordinates from any
type of deformation [87].
B.1 Strain Calculation
The initial and current positions of the crystals, which will be referred to as nodes
from this point forward, are represented by �̂� and �̂�, respectively. The position vector of
each point on the surface of each triangular element is defined by the bilinear interpolation
of the nodal elements of the triangle:
𝑷 = ∑ 𝜔𝑖(𝜉, 𝜂)�̂�𝑖3𝑖=1 (B.1)
𝒑 = ∑ 𝜔𝑖(𝜉, 𝜂)�̂�𝑖3𝑖=1 (B.2)
where 𝜔𝑖(𝜉, 𝜂) are the bilinear basis functions and 𝜉 (∈ [0 1]) and 𝜂 (∈ [0 1]) are the
computational domain coordinates.
During the deformation, 𝑋𝑖 represented the reference (material) coordinates and 𝑥𝑖
represented the current (spatial) coordinates. The deformed coordinate was defined as a
function of the reference coordinate 𝑥𝑖 = 𝑥𝑖(𝑋𝑖), where 𝑖 = 1, 2, and 3; assuming that

191
𝑋3 = 𝑋3(𝑋1, 𝑋2), 𝑥𝑖 was rewritten as 𝑥𝑖 = 𝑥𝑖(𝑋1, 𝑋2) [87]. Therefore, the position vector
of a point at the reference configuration and that of the current configuration is written as:
𝑷 = 𝑋𝛼𝒆𝛼 + 𝑋3(𝑋1, 𝑋2)𝒆3 (B.3)
𝒑 = 𝑥𝛼(𝑋1, 𝑋2)𝒆𝛼 + 𝑥3(𝑋1, 𝑋2)𝒆3 (B.4)
where 𝛼 take values of 1 and 2 and the summation convention on repeated indices is
implied; and where 𝒆𝑖 represents an orthogonal coordinate system. The covariant base
vectors in un-deformed and deformed configurations are:
𝑮𝛼 = 𝑷,𝛼 = 𝒆𝛼 + 𝑋3,𝛼𝒆3 (B.5)
𝒈𝛼 = 𝒑,𝛼 = 𝑥𝛽,𝛼𝒆𝛽 + 𝑥3
,𝛼𝒆3 (B.6)
where 𝛼 and 𝛽 take values of 1 and 2 and the summation convention on repeated indices
is implied; and where ,𝛼 denotes derivative with respect to 𝑋𝛼 (𝜕 𝜕𝑋𝛼⁄ ). The third
covariant base vectors 𝑮3 and 𝒈3 were calculated as described previously [86]:
𝑮3 =𝑮1×𝑮2
‖𝑮1×𝑮2‖ (B.7)
𝒈3 =𝒈1×𝒈2
‖𝒈1×𝒈2‖ (B.8)
The components of the un-deformed metric tensors 𝐺𝑖𝑗 and the deformed metric
tensor 𝑔𝑖𝑗 were calculated using the covariant base vectors in the referential and current
configurations. The elements of the metric tensors are:
𝐺𝑖𝑗 = 𝑮𝑖 . 𝑮𝑗 (B.9)

192
𝑔𝑖𝑗 = 𝒈𝑖. 𝒈𝑗 (B.10)
Consistent with other valve studies, we chose the Eulerian strain as the main
measure of deformation in our calculation [30, 85]. The components of Eulerian strain were
calculated using
𝑒𝑖𝑗 = 𝑔𝑖𝑗−𝐺𝑖𝑗
2 (B.11)
where the Eulerian strain tensor is 𝐞 = 𝑒𝑖𝑗𝒈𝑖𝒈𝑗 and the contravariant base vectors in the
deformed configuration are defined by:
𝒈1 =𝒈2×𝒈3
√𝑔 (B.12)
𝒈2 =𝒈3×𝒈1
√𝑔 (B.13)
𝒈3 =𝒈1×𝒈2
√𝑔 (B.14)
where
√𝑔 = 𝒈1. (𝒈2 × 𝒈3) (B.15)
The maximum strain 𝑒𝑚𝑎𝑥 and its direction 𝑽𝑚𝑎𝑥 were calculated by solving the
eigenvalue problem for the Eulerian strain tensor. As shown in Fig. 4.4, the vector from
Crystal 4 to Crystal 7 was chosen as the global radial direction. To calculate the radial and
circumferential directions for each triangular element, the normal vector to the element was
calculated using the cross product of two side vectors of the element. The cross product of
the normal vector with the global radial direction vector provided the circumferential
direction vector 𝑽𝑐𝑖𝑟 in the triangular element plane; the cross product of the normal vector

193
with the local circumferential direction vector provided the local radial direction vector
𝑽𝑟𝑎𝑑 in the triangular element plan. The circumferential and radial strains were then
calculated:
𝑒𝑐𝑖𝑟 = 𝑽𝑐𝑖𝑟 . 𝐞. 𝑽𝑐𝑖𝑟 (B.16)
𝑒𝑟𝑎𝑑 = 𝑽𝑟𝑎𝑑 . 𝐞. 𝑽𝑟𝑎𝑑 (B.17)
where 𝑒𝑐𝑖𝑟 and 𝑒𝑟𝑎𝑑 were circumferential and radial strains, respectively.
Finally, using the Eulerian strain definition, the areal strain was calculated as
𝑒𝑎𝑟𝑒𝑎𝑙 = 1 − 1
𝜆𝑎𝑟𝑒𝑎𝑙 (B.18)
where 𝜆𝑎𝑟𝑒𝑎𝑙, the areal change, was given by
𝜆𝑎𝑟𝑒𝑎𝑙 = √𝑑𝑒𝑡(𝑔𝑖𝑗)
𝑑𝑒𝑡(𝐺𝑖𝑗) (B.19)
B.2 Nomenclature
𝐞 = Eulerian strain tensor
𝑒𝑎𝑟𝑒𝑎𝑙 = Areal change
𝑒𝑐𝑖𝑟 = Circumferential strain
𝒆𝑖 = Orthogonal unit vectors
𝑒𝑖𝑗 = Components of the Eulerian strain tensor
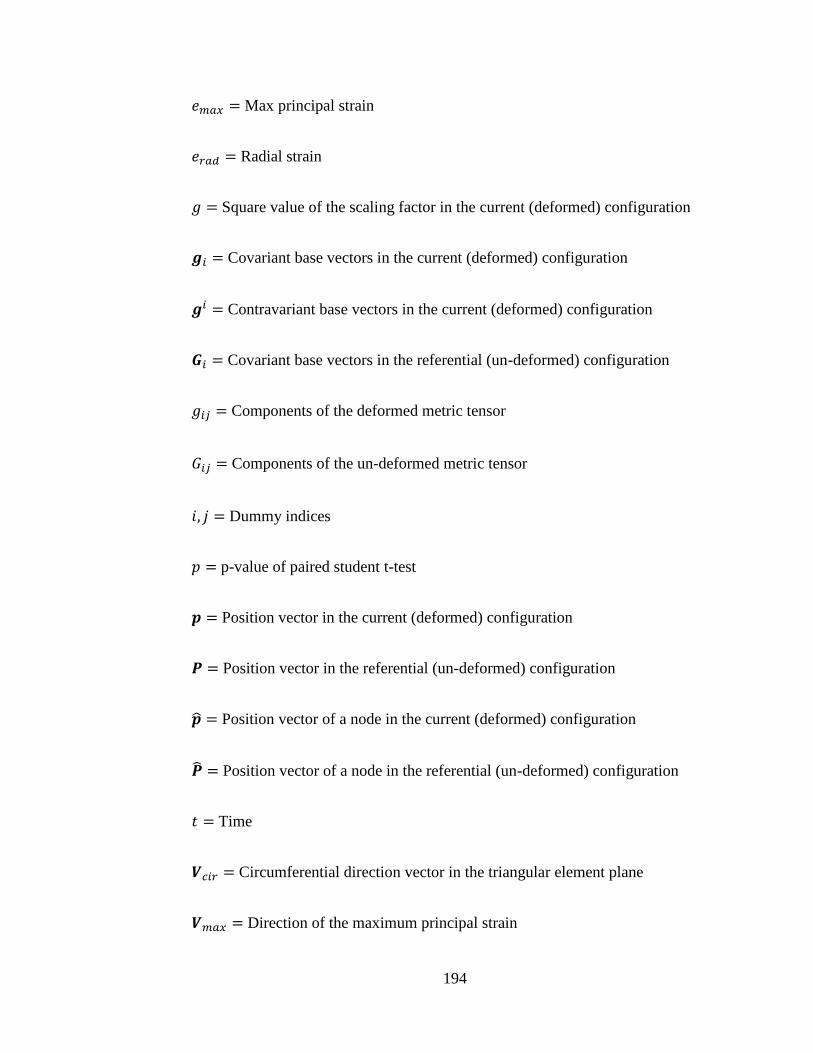
194
𝑒𝑚𝑎𝑥 = Max principal strain
𝑒𝑟𝑎𝑑 = Radial strain
𝑔 = Square value of the scaling factor in the current (deformed) configuration
𝒈𝑖 = Covariant base vectors in the current (deformed) configuration
𝒈𝑖 = Contravariant base vectors in the current (deformed) configuration
𝑮𝑖 = Covariant base vectors in the referential (un-deformed) configuration
𝑔𝑖𝑗 = Components of the deformed metric tensor
𝐺𝑖𝑗 = Components of the un-deformed metric tensor
𝑖, 𝑗 = Dummy indices
𝑝 = p-value of paired student t-test
𝒑 = Position vector in the current (deformed) configuration
𝑷 = Position vector in the referential (un-deformed) configuration
�̂� = Position vector of a node in the current (deformed) configuration
�̂� = Position vector of a node in the referential (un-deformed) configuration
𝑡 = Time
𝑽𝑐𝑖𝑟 = Circumferential direction vector in the triangular element plane
𝑽𝑚𝑎𝑥 = Direction of the maximum principal strain
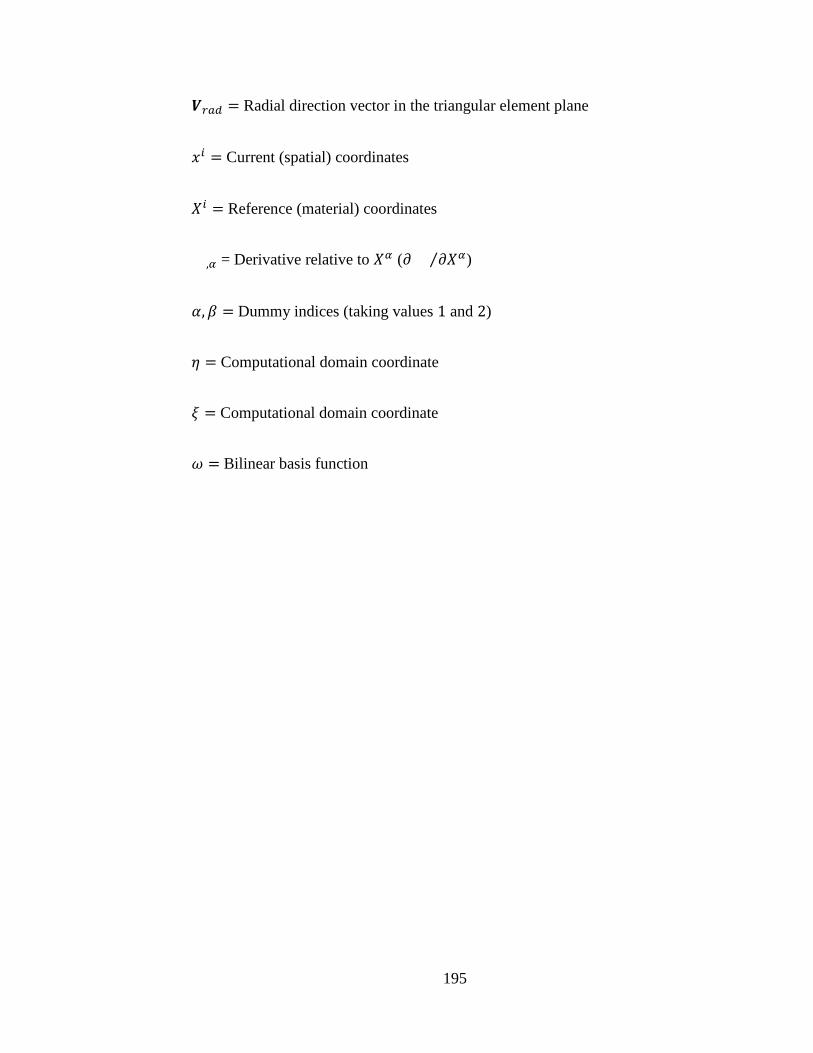
195
𝑽𝑟𝑎𝑑 = Radial direction vector in the triangular element plane
𝑥𝑖 = Current (spatial) coordinates
𝑋𝑖 = Reference (material) coordinates
,𝛼 = Derivative relative to 𝑋𝛼 (𝜕 𝜕𝑋𝛼⁄ )
𝛼, 𝛽 = Dummy indices (taking values 1 and 2)
𝜂 = Computational domain coordinate
𝜉 = Computational domain coordinate
𝜔 = Bilinear basis function
196
APPENDIX C
QUANTIFICATION OF THE MATERIAL CONSTANTS FOR A
PHENOMENOLOGICAL CONSTITUTIVE MODEL OF SMALL BOWEL
MESENTERY (APPLICATIONS OF THE METHOD DEVELOPED IN CHAPTERS II
AND III)
(The content of this chapter was published in JMBBM (Nov 2017) as “Anisotropic and
Nonlinear Biaxial Mechanical Responses of Porcine Small Bowel Mesentery” [142].)
C.1 Summary
Intestinal malrotation places pediatric patients at the risk of midgut volvulus, a
complication that can lead to ischemic bowel, short gut syndrome, and even death. Even
though the treatments for symptomatic patients of this complication are clear, it is still a
challenge to identify asymptomatic patients who are at a higher risk of midgut volvulus
and decide on a suitable course of treatment. Development of an accurate computerized
model of this intestinal abnormality could help in gaining a better understanding of its
integral behavior. To aid in developing such a model, in the current study, we have
characterized the biaxial mechanical properties of the porcine small bowl mesentery. First,
the tissue stress–strain response was determined using a biaxial tensile testing equipment.
The stress–strain data were then fitted into a Fung-type phenomenological constitutive
model to quantify the tissue material parameters. The stress–strain responses were highly
nonlinear showing more compliance at the lower strains following by a rapid transition into
a stiffer response at higher strains. The tissue was anisotropic and showed more stiffness

197
in the radial direction. The data fitted the Fung-type constitutive model with an average R-
squared value of 0.93. An averaging scheme was used to produce a set of material
parameters which can represent the generic mechanical behavior of the tissue in the
models.
C.2 Introduction
Intestinal malrotation, which occurs approximately in 1 out of 500 live births, is a
congenital disorder that is characterized by incomplete rotation and fixation of the
gastrointestinal tract to the abdominal wall during fetal development [223]. This
developmental arrest may occur during any of the phases of midgut development, resulting
in a wide spectrum of abnormalities, characterized by a narrowed mesenteric base [224].
This narrowed base predisposes a patient to midgut volvulus and possible subsequent
ischemic bowel disease, short gut syndrome and death. Midgut volvulus is one of the most
critical abdominal emergencies in the pediatric population. It is characterized by torsion of
small bowel and mesentery that could lead to blockage of mesenteric blood vessels and
ischemia of the small bowel. Midgut volvulus may lead to intestinal necrosis within a few
hours; thus, it requires immediate surgical intervention [225].
Increased imaging of patients has resulted in more incidental findings of
malrotation during workup for other anomalies [226]. While it is clear how to manage
symptomatic patients with malrotation, managing the treatment of asymptomatic patients
is more difficult because it is not known which patients are at a higher risk of midgut
volvulus. Because of this uncertainty coupled with the high morbidity and mortality
associated with volvulus, it is recommended by some to perform preventative operations
(i.e. a Ladd’s procedure) on all malrotation patients [227]. Others argue that the potential

198
long-term complications after a Ladd’s procedure, specifically future hospitalizations for
small bowel obstructions in 8.7 to 24% of patients, do not outweigh the relatively low risk
of midgut volvulus, and so recommend observation for asymptomatic patients [228-231].
This lack of consensus in the management of incidentally found intestinal
malrotation is likely due to the lack of quality data to support appropriate
recommendations, specifically, the lack of understanding of what degree of malrotation
results in increased propensity to torsion. Development of computational models of the
native and malrotated small bowel is useful to better understand the pathophysiology of
midgut volvulus. Using such models, one could examine how much mechanical torque is
required to deform tissues at different levels of malrotation and how such values compare
with normal cases. An important step in developing such models is the characterization of
the mechanical properties of the small bowel mesentery, which as a member of
gastrointestinal tract, plays an important role in this syndrome. Without accurate
mechanical properties for the small bowl mesentery, it is not possible to develop accurate
three-dimensional FE models of native and malrotated geometries. Previously, the
mechanical response of the mesentery has been quantified using uniaxial extension [232,
233]. In the current study, we used a biaxial mechanical testing equipment to quantify the
biaxial stress–strain response of the small bowel mesentery tissue. We further used a
phenomenological constitutive model to specify tissue material properties.
C.3 Material and Methods
C.3.1 Biaxial Tensile Testing Equipment
In this study, custom-made biaxial tensile testing equipment [40, 41, 117, 234] was
used to stretch specimens in two orthogonal directions under controlled loading. More

199
details about this testing equipment is provided in our previous publication [117]. Briefly,
a load cell measured the force applied in each direction independently. To quantify the
deformation, an optical deformation measurement system was used to track small fiducial
markers attached on the sample surface during the course of the experiment.
C.3.2 Specimen Preparation
On the day of the experiment, porcine mesenteries were obtained from a local
slaughterhouse (Duma Meats Inc., Mogadore, Ohio) within 20 minutes driving distance
from the laboratory. The pigs were about 6 months old and they weighed in approximately
300 𝑙𝑏 when slaughtered. Immediately after the animals were slaughtered, the mesenteries
were placed inside plastic bags filled with isotonic PBS and were covered with ice in a
cooling box for transport. Upon arrival at the lab, the proximal jejunum of the mesentery
was removed and 11 by 11 𝑚𝑚 square-shaped specimens were excised from three
different regions (distal avascular, distal vascular, and root) of the mesentery as shown in
Fig. C.1. The specimens were cut in such a way that the edges were aligned in the radial
and tangential directions of the mesentery. Using a dial micrometer (Anytime Inc., Los
Angeles, CA), the thicknesses were measured in six different locations on each specimen
and the result were averaged. All experiments were conducted at room temperature. Four
small glass beads (< 0.5 𝑚𝑚 in diameter) were glued on the surface of each specimen in
a 2 by 2 array format as the fiducial markers for optical deformation tracking.

200
Fig. C.1 The specimens were excised from (A) the distal avascular region, (B) the distal
vascular region, and (C) the root region of the porcine mesenteries.
C.3.3 Planar Biaxial Tensile Testing
The details of the experimental procedure are similar to those in our previous study
on TV leaflets [117]. In short, before attaching the specimen, the equipment bath was filled
with isotonic PBS at room temperature. Using suture-lines and small fishhooks (O. Mustad
& Son A.S., Gjörvik, Norway), the specimens were attached to the stretching carriages in
such a way that the radial direction was aligned with one axis and the tangential direction
with the other (Fig. C.2). This special technique for connecting samples to the stretching
components and the specific design of the carriages allow free lateral deformation of the
specimen and uniform and shear-free loading, which guarantees the uniform deformation
[117].
Each specimen experienced tension-controlled loading protocols with five different
tension ratios (𝑇𝑡: 𝑇𝑟 = 1: 1, 1: 0.75, 0.75: 1, 1: 0.5, 0.5: 1 with 𝑇𝑡 being the tangential
tension and 𝑇𝑟 being the radial tension). Table C.1 lists the loading protocols for each
specific region of the mesentery. Nine cycles of preconditioning were performed for each

201
loading protocol and data from the tenth cycle were utilized in the analysis. While a
minimum tare load of 0.5 𝑔 was applied for each case, the maximum tensions of 50, 100,
and 130 𝑁/𝑚 were selected for the distal avascular region, the distal vascular region, and
the root region of mesentery, respectively, as the strength of the tissue was not the same at
different regions. These maximum loads were selected experimentally based on the tissue
strength in order to prevent plastic deformation. Our data showed that the mechanical
response of the tissue samples did not change during the experiment with the chosen
maximum tension for each specific region. Each cycle lasted 10 seconds for the loading
step and 10 seconds for the unloading step. Therefore, the loading was quasi-static with
average strain rates of 3.2% and 2.5% per second for tangential and radial directions,
respectively.
Fig. C.2 (a) Suture lines are connected to the specimen using fishhooks. (b) Specimen
attached to the specifically-designed carriages of the equipment using suture-lines.
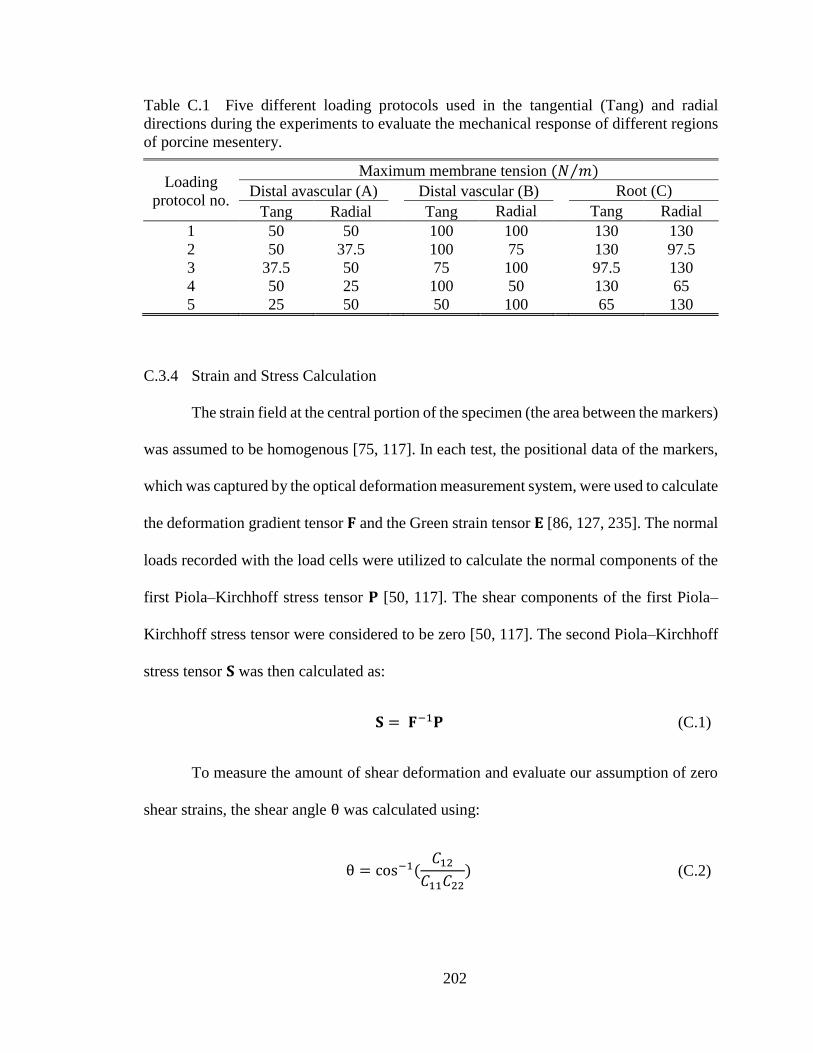
202
Table C.1 Five different loading protocols used in the tangential (Tang) and radial
directions during the experiments to evaluate the mechanical response of different regions
of porcine mesentery.
Loading
protocol no.
Maximum membrane tension (𝑁 𝑚⁄ )
Distal avascular (A) Distal vascular (B) Root (C)
Tang Radial Tang Radial Tang Radial
1 50 50 100 100 130 130
2 50 37.5 100 75 130 97.5
3 37.5 50 75 100 97.5 130
4 50 25 100 50 130 65
5 25 50 50 100 65 130
C.3.4 Strain and Stress Calculation
The strain field at the central portion of the specimen (the area between the markers)
was assumed to be homogenous [75, 117]. In each test, the positional data of the markers,
which was captured by the optical deformation measurement system, were used to calculate
the deformation gradient tensor 𝐅 and the Green strain tensor 𝐄 [86, 127, 235]. The normal
loads recorded with the load cells were utilized to calculate the normal components of the
first Piola–Kirchhoff stress tensor 𝐏 [50, 117]. The shear components of the first Piola–
Kirchhoff stress tensor were considered to be zero [50, 117]. The second Piola–Kirchhoff
stress tensor 𝐒 was then calculated as:
𝐒 = 𝐅−1𝐏 (C.1)
To measure the amount of shear deformation and evaluate our assumption of zero
shear strains, the shear angle θ was calculated using:
θ = cos−1(
𝐶12
𝐶11𝐶22) (C.2)

203
where 𝐶𝑖𝑗 were the components of the right Cauchy–Green deformation tensor 𝐂 defined
by
𝐂 = 𝐅T𝐅 (C.3)
The rigid body rotation angle ω was also calculated [117]:
ω = tan−1(
𝑅21
𝑅11) (C.4)
where rotation matrix 𝐑 was given by
𝐑 = 𝐅𝐔−1 (C.5)
and 𝐔 was the right stretch tensor:
𝐂 = 𝐔2 (C.6)
C.3.5 Constitutive Modeling
At each region, mesentery tissue was assumed to be incompressible, homogenous,
and hyperelastic undergoing finite deformations similar to other soft tissues [42, 53, 57-60,
62, 63, 65]. As such, we assumed that the mesentery tissue samples followed the concept
of pseudoelasticity [141]. The components of the second Piola–Kirchhoff stress tensor
were then evaluated using a strain energy function 𝑊:
𝑆𝑖𝑗 =
𝜕𝑊
𝜕𝐸𝑖𝑗 (C.7)
To determine an appropriate type of the strain energy function, the method
described by Vande Geest et al. [56] were utilized and the stress–strain behavior of the

204
tissue were carefully examined. Based on the Vande Geest et al. method, the stress–strain
data were independently fitted into the following response functions for each direction in
such a way that each normal component of the second Piola–Kirchhoff stress had its own
unique parameters:
𝑆𝑡𝑡 = 𝑐0 (𝑐1𝐸𝑡𝑡 + 𝑐3𝐸𝑟𝑟 + 𝑐4𝐸𝑡𝑡𝐸𝑟𝑟 +1
2𝑐5𝐸𝑟𝑟
2 + 𝑐6𝐸𝑡𝑡𝐸𝑟𝑟2
+ 2𝑐7𝐸𝑡𝑡3 ) 𝑒𝑄
𝑆𝑟𝑟 = 𝑐0 (𝑐2𝐸𝑟𝑟 + 𝑐3𝐸𝑡𝑡 + 𝑐5𝐸𝑡𝑡𝐸𝑟𝑟 +1
2𝑐4𝐸𝑡𝑡
2 + 𝑐6𝐸𝑡𝑡2 𝐸𝑟𝑟
+ 2𝑐8𝐸𝑟𝑟3 ) 𝑒𝑄
(C.8)
where 𝑡𝑡 and 𝑟𝑟 denoted tangential and radial directions, respectively, 𝐸𝑡𝑡 and 𝐸𝑟𝑟 were
the components of the Green strain tensor, and
𝑄 = (𝑐1𝐸𝑡𝑡2 + 𝑐2𝐸𝑟𝑟
2 + 2𝑐3𝐸𝑡𝑡𝐸𝑟𝑟 + 𝑐4𝐸𝑡𝑡2 𝐸𝑟𝑟 + 𝑐5𝐸𝑟𝑟
2 𝐸𝑡𝑡
+ 𝑐6𝐸𝑡𝑡2 𝐸𝑟𝑟
2 + 𝑐7𝐸𝑡𝑡4 + 𝑐8𝐸𝑟𝑟
4 )
(C.9)
It is important to note that the above equations did not represent a constitutive
model but they denoted a set of response functions, which were fitted to the data for each
direction independently allowing us to interpolate the stress components over the strain
field. After careful examination of the result of the fitting outcomes (the details are
explained in section 0
Response Function Interpretation), a Fung-type strain energy function 𝑊 [53] was
chosen to model the mechanical behavior of the mesentery:

205
𝑊 = 𝑐
2(𝑒𝑎1𝐸𝑡𝑡
2 +𝑎2𝐸𝑟𝑟2 +2𝑎3𝐸𝑡𝑡𝐸𝑟𝑟 − 1) (C.10)
where 𝑐 and 𝑎𝑖 were the material parameters and 𝐸𝑡𝑡 and 𝐸𝑟𝑟 were the component
of the Green strain tensor in the tangential and radial directions, respectively. The
experimental data for each specimen were fitted to this model to calculate the material
parameters in each case. To obtain a measure of the anisotropy of the responses, the
anisotropy index 𝐴𝐼 was also calculated for each set of material parameters. The anisotropy
index was calculated as described previously by Bellini et al. [58]:
𝐴𝐼 = 𝑚𝑖𝑛 (
𝑎1 + 𝑎3
𝑎2 + 𝑎3,𝑎2 + 𝑎3
𝑎1 + 𝑎3) (C.11)
C.3.6 Average Model Development
An ultimate goal of soft tissue mechanical characterization is to implement such
mechanical properties in computational models to be developed for simulation of the tissue
deformation. Certainly, one could apply each set of the specimen-specific constitutive
model parameters in subject-specific computational models or, alternatively, conduct
parametric studies to examine a range of mechanical properties [146, 236]. Yet, in many
cases, it is useful to produce a set of parameters representing the generic (average) tissue
mechanical behavior. In the case of linear elastic materials, one could evaluate the elastic
modulus for each specimen and then take the arithmetic mean of all values to obtain a
single average elastic modulus. However, in the presence of nonlinearity in the constitutive
model (similar to the model used in this study), a simple arithmetic average of the model
parameters cannot represent the overall behavior of the tissue. One way to overcome this
problem is to fit the constitutive model to the averaged experimental stress–strain curve
[58, 64]. In the current study, we first averaged the experimental strain values for each

206
protocol over all of the specimens. Clearly, we were only allowed to average the strains
over the same stress (loading) states. In such a case, the corresponding normal components
of stress in each direction had to be equal for all samples used in the averaging process (the
off-diagonal shear components of the stress tensor were supposed to be zero). Since the
biaxial tests were conducted in a tension-controlled manner, the same tension states were
available from similar protocols for all samples. However, it did not necessarily guarantee
that for every specific tension state in each sample, the identical values are available in
other samples. To solve this issue, other investigators [58, 64] had fitted the tension–strain
data into an exponential function for each test and evaluated the strains at the specific
tension values. The problem with using an exponential function is that it does not represent
the Poisson’s effect accurately. Since our data were dense enough, we were able to use an
interpolation method to estimate the tension value at any desired tension state. The
resulting data were then used to calculate the average tensions 𝑇𝑎𝑣𝑔,𝑖 and the average strains
𝐸𝑎𝑣𝑔,𝑖𝑖 were calculated by averaging the strains between all samples (𝑛 = 8) for each
protocol. The subscript 𝑖𝑖 refers to tangential 𝑡𝑡 and radial 𝑟𝑟 directions.
The components of the average first Piola–Kirchhoff stress tensor 𝑃𝑎𝑣𝑔,𝑖𝑖 were then
estimated as suggested by Bellini et al. [58]:
𝑃𝑎𝑣𝑔,𝑖𝑖 =
𝑇𝑎𝑣𝑔,𝑖
𝑛∑
1
ℎ𝑘
𝑛
𝑘=1
(C.12)
where ℎ𝑘 was the 𝑘th sample thickness. With the assumption of negligible shear
deformations, the diagonal components of the average deformation gradient tensor 𝐹𝑎𝑣𝑔,𝑖𝑖
were calculated:

207
𝐹𝑎𝑣𝑔,𝑖𝑖 = √2𝐸𝑎𝑣𝑔,𝑖𝑖 + 1 (C.13)
Finally, the average first Piola–Kirchhoff stress tensor and the average deformation
gradient tensor were used to calculate the average second Piola–Kirchhoff stress tensor:
𝑺𝑎𝑣𝑔 = 𝑷𝑎𝑣𝑔. 𝑭𝑎𝑣𝑔−𝑇 (C.14)
To develop the average constitutive model for each region of the mesentery,
𝑺𝑎𝑣𝑔 − 𝑬𝑎𝑣𝑔 data were fitted to the proposed strain energy function as described above
and the corresponding material parameters were evaluated.
C.4 Results
C.4.1 Dimensional Measurements
In total, twenty-four specimens in eight sets (𝑛 = 8 for each region) were tested.
Each set included one specimen from each region (distal avascular, distal vascular, and
root) of the same animal. All tests were performed within 2 to 6 hours postmortem to
eliminate probable erroneous results associated with the freezing and thawing of the
tissues. The measured thicknesses were 604 ± 279 𝜇𝑚 (mean ± standard deviation) for
the distal avascular, 1195 ± 531 𝜇𝑚 for the distal vascular, and 2162 ± 357 𝜇𝑚 for the
root region of the mesentery. Table C.2 shows the measured thicknesses for all the
specimens and for each region. The Student’s t-test analysis revealed that the thicknesses
were significantly different in all three regions (𝑝 < 0.015 for all comparisons).
C.4.2 Biaxial Mechanical Responses
Figure C.3 shows the average membrane tension versus the stretch ratio in different
regions of the porcine mesentery for the equibiaxial protocol. The maximum standard
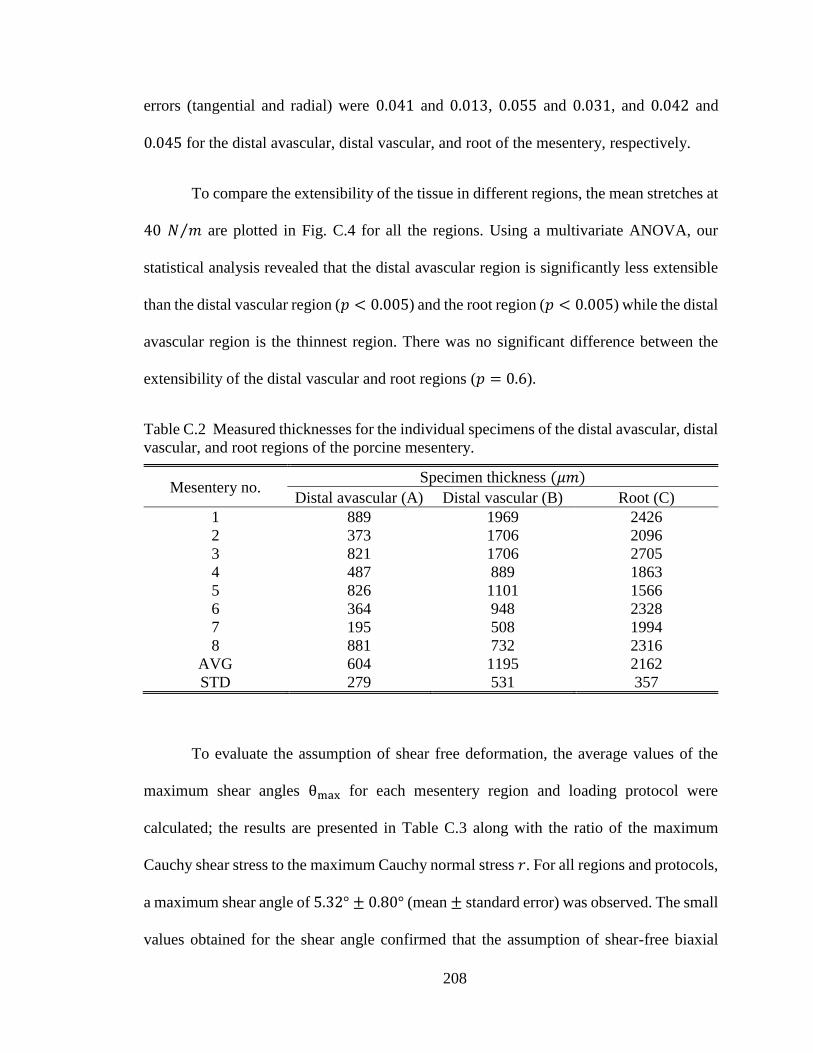
208
errors (tangential and radial) were 0.041 and 0.013, 0.055 and 0.031, and 0.042 and
0.045 for the distal avascular, distal vascular, and root of the mesentery, respectively.
To compare the extensibility of the tissue in different regions, the mean stretches at
40 𝑁 𝑚⁄ are plotted in Fig. C.4 for all the regions. Using a multivariate ANOVA, our
statistical analysis revealed that the distal avascular region is significantly less extensible
than the distal vascular region (𝑝 < 0.005) and the root region (𝑝 < 0.005) while the distal
avascular region is the thinnest region. There was no significant difference between the
extensibility of the distal vascular and root regions (𝑝 = 0.6).
Table C.2 Measured thicknesses for the individual specimens of the distal avascular, distal
vascular, and root regions of the porcine mesentery.
Mesentery no. Specimen thickness (𝜇𝑚)
Distal avascular (A) Distal vascular (B) Root (C)
1 889 1969 2426
2 373 1706 2096
3 821 1706 2705
4 487 889 1863
5 826 1101 1566
6 364 948 2328
7 195 508 1994
8 881 732 2316
AVG 604 1195 2162
STD 279 531 357
To evaluate the assumption of shear free deformation, the average values of the
maximum shear angles θmax for each mesentery region and loading protocol were
calculated; the results are presented in Table C.3 along with the ratio of the maximum
Cauchy shear stress to the maximum Cauchy normal stress 𝑟. For all regions and protocols,
a maximum shear angle of 5.32° ± 0.80° (mean ± standard error) was observed. The small
values obtained for the shear angle confirmed that the assumption of shear-free biaxial

209
loading was reasonable. Moreover, the average maximum values of 𝑟 were 2.7%, 4.4%,
and 10.3% for distal avascular, distal vascular, and root region, respectively. These small
values of 𝑟 (particularly for distal avascular and distal vascular regions) further show the
Cauchy shear stresses in comparison to the Cauchy normal stresses were negligible.
Moreover, the average maximum values of 𝑟 were 2.7%, 4.4%, and 10.3% for distal
avascular, distal vascular, and root region, respectively. These small values of 𝑟
(particularly for distal avascular and distal vascular regions) further show the Cauchy shear
stresses in comparison to the Cauchy normal stresses were negligible.
Table C.3 also represents the maximum rigid body rotation angles 𝜔𝑚𝑎𝑥. The
largest value of rigid body rotation was approximately 3 degrees, indicating minimal rigid
body rotation happened during the experiments.

210
Fig. C.3 The average membrane tension versus stretch ratio for the equibiaxial loading
protocol for (a) the distal avascular, (b) the distal vascular, and (c) the root regions of the
porcine mesenteries (n=8, the bars are standard errors).
Fig. C.4 The mean stretch values at 40 𝑁 ⁄ 𝑚 measured at three different regions of the
mesentery shown in Fig. C.1 for radial and tangential (Tang) directions. Bars are the
standard error (n=8).

211
Tab
le C
.3
The
aver
age
max
imum
rig
id b
od
y r
ota
tion 𝑤
𝑚𝑎
𝑥,
the
aver
age
max
imum
shea
r an
gle
𝜃𝑚
𝑎𝑥,
and t
he
aver
age
rati
o o
f th
e
max
imum
Cau
chy s
hea
r st
ress
to t
he
max
imum
Cau
chy n
orm
al s
tres
s 𝑟
pre
sente
d f
or
each
load
ing p
roto
col
and m
esen
tery
reg
ion
(for
each
pro
toco
l an
d m
esen
tery
reg
ion the
dat
a ar
e av
erag
ed o
ver
all
sam
ple
s (n
=8
) an
d p
rese
nte
d in the
form
of
aver
age
± s
tandar
d
erro
r).
Lo
adin
g
pro
toco
l no.
Dis
tal
avas
cula
r (A
)
Dis
tal
vas
cula
r (B
)
Root
(C)
𝜔𝑚
𝑎𝑥
(°)
𝜃 𝑚
𝑎𝑥
(°)
𝑟
(%)
𝜔
𝑚𝑎
𝑥 (
°)
𝜃𝑚
𝑎𝑥
(°)
r
(%)
𝜔
𝑚𝑎
𝑥 (
°)
𝜃 𝑚𝑎
𝑥 (
°)
r (%
)
1
1.0
±0.2
1.3
±0.2
2.7
±0.6
1.1
±0.2
3.1
±0.7
4.4
±1.1
3.1
±0.6
4.1
±0.7
10.3
±1.7
2
1.1
±0.3
1.4
±0.2
2.6
±0.5
1.1
±0.2
2.9
±0.6
4.0
±0.9
3.1
±0.6
4.6
±0.7
9.3
±1.6
3
1.0
±0.2
1.2
±0.2
2.4
±0.5
1.0
±0.2
3.1
±0.7
3.7
±0.8
3.0
±0.4
4.2
±0.7
10.1
±1.7
4
1.4
±0.3
1.6
±0.2
2.3
±0.4
1.2
±0.2
2.9
±0.7
3.7
±0.8
3.2
±0.8
5.3
±0.8
7.4
±1.2
5
1.2
±0.2
1.3
±0.3
2.1
±0.4
1.2
±0.2
3.2
±0.6
3.6
±0.5
2.9
±0.2
4.2
±0.7
8.7
±1.6

212
C.4.3 Response Function Interpretation
The measured biaxial stress–strain data fitted the response functions of Equation
(C.8) relatively well, with an R-squared value of 0.95 ± 0.05 (mean ± standard deviation).
To facilitate the selection of the strain energy function, graphs of constant stresses were
plotted over the strain field (versus 𝐸𝑡𝑡 and 𝐸𝑟𝑟). For an ideal isotropic material, the
constant stress contours are expected to be symmetric with respect to 𝐸𝑡𝑡 = 𝐸𝑟𝑟 line. As
shown in Fig. C.5 for typical specimens, the stress contours were asymmetric for all three
regions, indicating an anisotropic mechanical response. Moreover, the stress increased in
an exponential manner when strains increased. Such a specific form of the stress surfaces
and the negligibility of the shear stresses was the basis for the selection of an anisotropic
Fung-type [53] strain energy function 𝑊 in Equation (C.10).
Fig. C.5 The constant stress contours for (a) and (b) the distal avascular, (c) and (d) the
distal vascular, and (e) and (f) the root regions of a typical porcine mesentery specimens.

213
C.4.4 Constitutive Modeling
The data from all five biaxial protocols were simultaneously fit to the Fung-type
constitutive model represented by Equations (C.7) and (C.10). The result showed an
acceptable fit with the average R-squared values of 0.96, 0.94, and 0.89 for the distal
avascular, the distal vascular, and the root regions of the mesentery, respectively. Table
C.4 lists the material parameters calculated for each specimen as well as its corresponding
R-squared value for the fitted function. The calculated values for the anisotropy index are
also presented in Table C.4. An anisotropy index equal to 1 represented a perfectly
isotropic material while the smaller values of this index indicated the more anisotropic
response. Fig. C.6 shows the experimental biaxial data as well as the results for the five-
protocol fit for typical specimens from different regions of the mesentery.

214
Table C.4 Material parameters computed for individual samples by fitting the experimental
data to the proposed constitutive model along with the fitting R-squared values (𝑅2) and
the anisotropy index (𝐴𝐼).
Region Sample
no. 𝑐 (𝑘𝑃𝑎) 𝑎1 𝑎2 𝑎3 𝑅2 𝐴𝐼
Distal
avascular
(A)
1 3.857 53.954 72.196 8.801 0.955 0.775
2 11.702 46.903 54.974 22.641 0.986 0.896
3 0.827 75.819 361.473 0.000 0.952 0.210
4 2.654 5.207 39.053 1.814 0.919 0.172
5 1.918 15.547 67.351 6.228 0.957 0.296
6 1.273 39.360 43.100 0.000 0.983 0.913
7 11.974 42.318 37.526 15.170 0.946 0.917
8 2.415 69.101 49.698 20.429 0.975 0.783
AVG 4.578 43.526 90.671 9.385 0.959 0.620
STD 4.573 24.163 110.145 9.063 0.022 0.333
Distal
vascular
(B)
1 0.178 6.695 5.879 3.802 0.926 0.922
2 0.737 25.789 13.146 4.895 0.915 0.588
3 0.712 5.719 27.726 0.917 0.872 0.232
4 0.401 6.287 12.832 3.210 0.956 0.592
5 0.455 2.449 6.107 1.590 0.973 0.525
6 0.555 12.805 15.030 0.000 0.977 0.852
7 2.781 21.028 33.547 2.531 0.966 0.653
8 1.866 17.669 9.374 0.000 0.899 0.531
AVG 0.960 12.305 15.455 2.118 0.936 0.612
STD 0.894 8.410 10.045 1.797 0.038 0.212
Root
(C)
1 1.037 3.584 10.333 0.656 0.953 0.386
2 0.871 49.595 14.884 5.502 0.895 0.370
3 0.559 11.107 3.413 0.528 0.930 0.339
4 0.271 4.877 10.045 2.951 0.963 0.602
5 19.196 1.730 2.500 0.973 0.785 0.778
6 1.133 6.078 4.227 2.399 0.851 0.782
7 0.916 11.839 4.778 2.592 0.787 0.511
8 0.247 9.624 24.819 3.037 0.929 0.455
AVG 3.029 12.304 9.375 2.330 0.877 0.528
STD 6.541 15.497 7.566 1.644 0.071 0.177
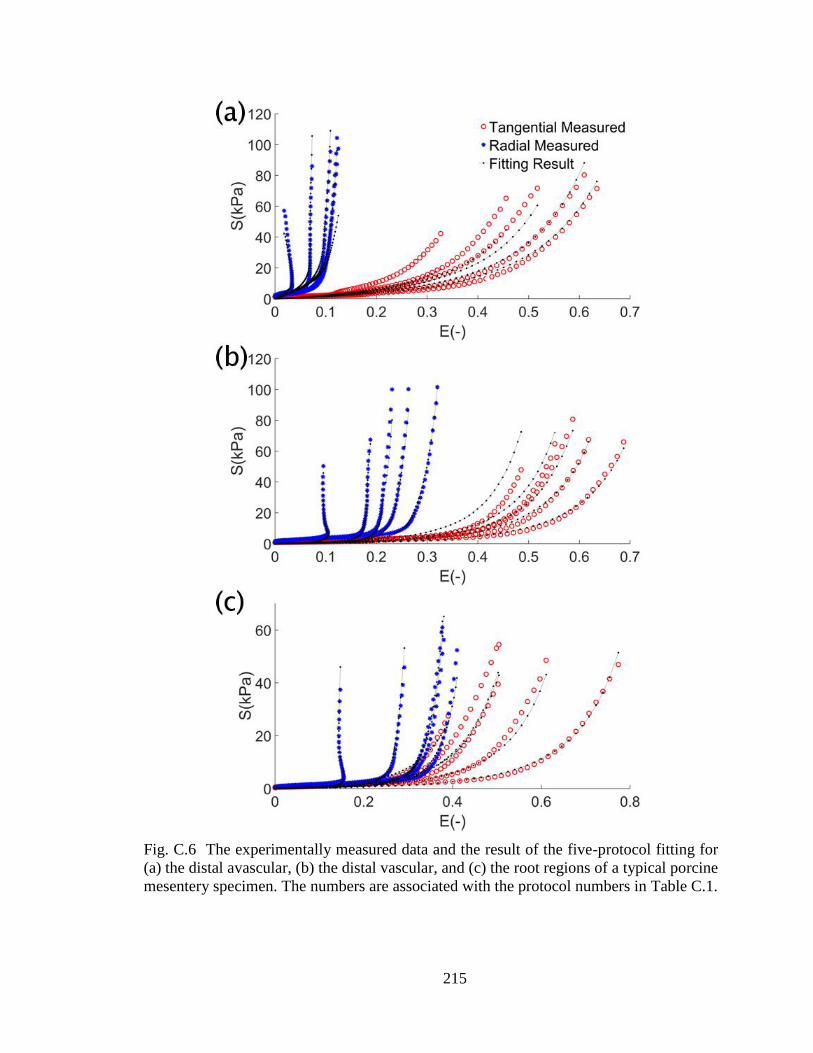
215
Fig. C.6 The experimentally measured data and the result of the five-protocol fitting for
(a) the distal avascular, (b) the distal vascular, and (c) the root regions of a typical porcine
mesentery specimen. The numbers are associated with the protocol numbers in Table C.1.

216
C.4.5 Average Modeling
The developed average stress–strain (second Piola–Kirchhoff stress versus Green
strain) responses are shown in Fig. C.7 for the distal avascular region for all five protocols.
Figures C.8 and C.9 show the same graphs for the distal vascular and root regions of the
mesentery, respectively. The same form of strain energy function was used to develop the
average material model. The averaged data fit the model with R-squared values of 0.97,
0.98, and 0.77 for the distal avascular, distal vascular, and root regions, respectively. The
calculated average material parameters are listed in Table C.5. As expected, these values
are different from the arithmetic average of the parameters calculated for each specimen
(listed in Table C.4). For comparison, Table C.5 also presents the anisotropy index 𝐴𝐼
calculated for the average models using Equation (C.11).
Fig. C.7 Average second Piola–Kirchhoff stress versus Green strain in tangential (Tang)
and radial directions for loading protocols (a) number 1 (equibiaxial), (b) number 2, (c)
number 3, (d) number 4, and (e) number 5 of Table C.1 for the distal avascular region.
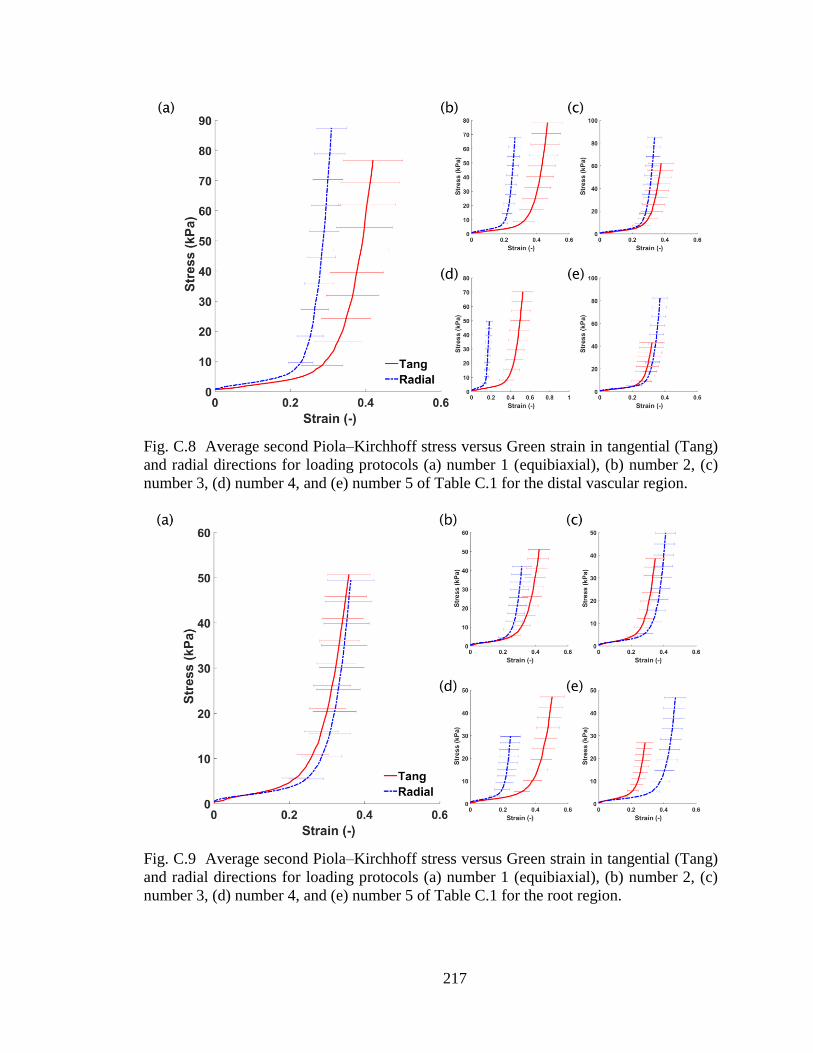
217
Fig. C.8 Average second Piola–Kirchhoff stress versus Green strain in tangential (Tang)
and radial directions for loading protocols (a) number 1 (equibiaxial), (b) number 2, (c)
number 3, (d) number 4, and (e) number 5 of Table C.1 for the distal vascular region.
Fig. C.9 Average second Piola–Kirchhoff stress versus Green strain in tangential (Tang)
and radial directions for loading protocols (a) number 1 (equibiaxial), (b) number 2, (c)
number 3, (d) number 4, and (e) number 5 of Table C.1 for the root region.

218
C.5 Discussion
Although uniaxial extension can be an acceptable method in mechanical
characterization of tissues under in-situ one-dimensional loading, it has been deemed
insufficient for characterization of the mechanical responses of soft tissues experiencing
multiaxial loading in their native environment [237]. As biological soft tissues are
generally considered incompressible [42, 53, 57-60, 62, 63, 65], planar biaxial testing
provides a two-dimensional stress-state, allowing full characterization of the mechanical
properties of the tissues [50].
The thickness of the tissue varied significantly among the three regions (𝑝 < 0.02
for all comparisons). The thickest region, i.e. the root region, was found to be
approximately 3.5 times thicker than the distal avascular region, which was the thinnest.
These substantial differences among the thicknesses led to the use of different maximum
tensions for each region.
The mesentery tissue showed a highly nonlinear behavior in all three regions with
low stiffness at small strains and dramatically higher stiffness at larger strains, which was
a typical behavior for a soft tissue [69, 238-240]. Both in the avascular region and in the
vascular region of the distal mesentery, the deformation was larger in the tangential
direction in comparison to that of the radial direction indicating an anisotropic tissue
behavior (Fig. C.3). In the root region, however, no notable differences were observed
between the stretch values in the tangential and radial directions.
219
The distal avascular region was significantly less extensible in comparison to the
other two regions (Fig. C.4). Since this region was significantly thinner than the distal
vascular and the root regions (Table C.2), it was by far the stiffest region.
Table C.3 also presents the ratio of the maximum Cauchy shear stress to the
maximum Cauchy normal stress 𝑟 for each loading protocol and each region. These ratios
showed relatively the same increase for all protocols from regions A through C. As we
have increased the maximum tension from region A to C (according to Table C.1), the
increase in 𝑟 indicated a direct relation between the maximum tension applied on the tissue
and the percentage of the shear stress generated during the test.
The mechanical responses of the porcine mesentery in three different regions shown
in Fig. C.1 were modeled using a constitutive model based on the Fung-type strain energy
function. The Fung-type constitutive model was selected based on the form of the response
functions fitted to the stress–strain data (Fig. C.5). Based on the fitting R-squared values
(Table C.4), the selected constitutive model was able to capture the experimental data well.
For a strain energy function of this type to be physically realistic, it should be shown that
all the material parameters must be positive [149]. When these limits were imposed, a
number of the 𝑎3 parameters from the distal avascular and distal vascular regions
approached zero (Table C.4). However, with the smallest R-squared value of 0.90, neither
of them resulted in an unacceptable fit.
Additional investigations were conducted to validate the integrity of the developed
constitutive models for use in FE analysis by further inspecting the resulted strain energy
functions. The convexity of the strain energy function is essential for stability of the

220
material model in FE analysis [153]. Hence, the evaluated material parameters for the
proposed constitutive model were used to plot the constant strain energy contours over the
strain field in each case. Investigation of these plots showed that all the estimated material
parameters resulted in convex potentials, as shown in Fig. C.10 for typical specimens of
all three regions of the mesentery, further improving the integrity of the developed model.
An average model was developed that can be used in computer simulations to
predict the average mechanical behavior of the tissue. Figures C.7–C.9 show the averaged
stress-stain data calculated for three regions of the mesentery; the material parameters
computed by fitting these average responses to the proposed constitutive model are listed
in Table C.5. The fitting R-squared value for the distal avascular region was 0.97 and for
the distal vascular regions was 0.98, showing a reliable fit for these data. As expected, the
material parameters computed for average model were different from the arithmetic
averages of the material parameters of individual specimens listed in Table C.4. The
anisotropy index 𝐴𝐼 obtained from the average model (Table C.5) for the distal avascular
and distal vascular regions (0.502 and 0.702, respectively) indicated anisotropic behavior
of the tissue at these two regions, which was consistent with the plots in Figs. C.3, C.7, and
C.8 and also with the averaged 𝐴𝐼 presented in Table C.4 (0.620 and 0.612, respectively).
Table C.5 Material parameters computed by fitting the averaged stress–strain data to the
proposed constitutive model along with the fitting R-squared (𝑅2) and the anisotropy index
(𝐴𝐼).
Region 𝑐 (𝑘𝑃𝑎) 𝑎1 𝑎2 𝑎3 𝑅2 𝐴𝐼
Distal avascular (A) 2.808 29.870 65.742 6.287 0.972 0.502
Distal vascular (B) 0.381 9.741 14.811 2.175 0.975 0.702
Root (C) 1.521 5.528 5.447 2.204 0.765 0.990
221
Midgut volvulus is a critical condition that primarily occurs in pediatric patients.
Considering the ethical issues involved in the use of human donor tissues, especially
pediatric tissues, we chose a large animal (i.e. porcine) model for our mechanical testing.
In addition, there are advantages in using the porcine model, as samples with lower
variability are readily available. Pigs mature much faster than humans; a three-year old pig
is considered to be fully mature [241]. Nevertheless, one should be aware of the limitations
of animal models in drawing conclusions regarding human tissue response.
For the root region, however, the 𝐴𝐼 of 0.990 indicated an isotropic response for
the average model. Although this conclusion was consistent with the plots in Figs. C.3 and
C.9, it was not consistent with the mean 𝐴𝐼 presented in Table C.4 (0.528) for the root
region. Further investigation of the 𝐴𝐼s in Table C.4 for individual specimens from the root
region revealed that most showed highly anisotropic responses. Plotting the stress–strain
data for the individual specimens in the root region showed that the mechanical responses
did not follow any determined pattern between the specimens. In other words, if a stiffer
direction existed, it could have switched from tangential to radial direction in any
specimen. As shown in Fig. C.6c, in a typical sample from the root region, the radial
direction was noticeably stiffer than the tangential direction. In other samples, also excised
from the root region, the tangential direction was the stiffer one (e.g. Fig. C.11a). There
also existed representative cases (e.g. Fig. C.11b), in which the tissue responded in a more
isotropic manner. One reason for such an inconsistency could be that, at the root region,
the definition of the radial and tangential directions is less meaningful and the tissue
constituent fibers could be in any direction, aligned or not aligned.

222
Fig. C.10 Constant energy contours plotted over the strain field for typical samples of (a)
the distal avascular, (b) the distal vascular, and (c) the root regions of the porcine
mesentery.

223
Fig. C.11 The mechanical responses observed for the root region of the porcine mesentery
did not always follow the same trend. For example, tissue was (a) stiffer in tangential
direction, or (b) had similar stiffness in both directions, noticeably different from other
typical cases in this region (Fig. C.6c). The numbers are associated with the protocol
numbers in Table C.1.

224
Based on our analysis using the response functions, we chose an appropriate form
of a phenomenological Fung-type constitutive model. Predicting tissue responses using
only a few parameters is extremely advantageous, as increasing the number of model
parameters can adversely affect the uniqueness of the fitted values. The phenomenological
models, however, are inherently limited as they provide little or no insight into the micro-
scale mechanical environment. For investigations that require knowledge of extracellular
and/or cellular-level biomechanical responses of the tissues, the use of more complex
structurally-based models is more appropriate [69].
As previously mentioned, development of a computerized model to better
understand the pathophysiology of midgut volvulus is essential. To bring us one step closer
to this goal, in the current study, the biaxial mechanical properties of the small bowel
mesentery, a tissue with major influence in the deformation of small bowel during midgut
volvulus, was characterized. The parameters quantified in this study can be employed in
FE models to simulate the mechanical behavior of the mesentery in different geometries.




















