
Aberrant epigenetic patterns in the etiology of gastrointestinal cancers
10
Introduction Gastrointestinal (GI) cancers account for about 20% of all cancers worldwide. In the global inci- dence of cancer, gastric cancer is the second, colorectal cancer is the third, and esophageal can- cer is the sixth most common tumor (Chan et al. 2006). In neoplasms, including GI cancers, epigenetic changes play a key role in the process of tumorigenesis (Baylin and Bestor 2002; Baylin and Ohm 2006). Epigenetics in the broad sense may be defined as the study of phenomena that modify gene ex- pression without changing the underlying DNA sequence. More specifically, epigenetics is the study of collective interaction of multiple mecha- nisms in establishing states of chromatin structure, histone modification, transcriptional activity, and DNA methylation. Evidence accumulated in re- cent years clearly demonstrates that epigenetic ab- normalities are important factors in the etiology of virtually all human cancer types (Laird 2005; Goldberg et al. 2007). DNA methylation is the most widely studied epigenetic abnormality in tumorigenesis. It refers to methylation of cytosine at CpG dinucleotides. CpG dinucleotides are not randomly distributed throughout the human genome. CpG-rich regions, known as CpG islands, are usually unmethylated in normal cells (with the exception of imprinted genes and several genes located on chromosome X) and are typically found associated with 5’ promoter end and first exon of numerous genes (Plass 2002). It is estimated that there are about 29 000 CpG islands within the human genome. Approximately 50–60% of all genes contain CpG islands. Alter- ations of cytosine methylation are prevalent in hu- man sporadic cancers (Costello and Plass 2001). Methylation defects include genome hypo- methylation (resulting in epigenetic activation of oncogenes and retroelements) and localized aber- rant hypermethylation of CpG islands, resulting in transcriptional repression of many important J Appl Genet 49(1), 2008, pp. 1–10 Invited Editorial Aberrant epigenetic patterns in the etiology of gastrointestinal cancers Pawe³ Karpiñski 1 , Maria M. S¹siadek 1 , Nikolaus Blin 2 1 Department of Genetics, Wroclaw Medical University, Poland 2 Division of Molecular Genetics, Institute of Human Genetics, University of Tuebingen, Germany Abstract. A body of evidence accumulated over the past decade suggests that epigenetic mechanisms play an es- sential role in maintaining important cellular functions. Changes in epigenetic patterns (mainly DNA hyper- and hypomethylation and, more recently, histone modifications) may contribute to the development of cancer. Aber- rant epigenetic events expand thorough tumor progression from the earliest to latest stages, therefore they can serve as convenient markers for detection and prognosis of cancer. The potential reversibility of epigenetic states in the tumor cell is an attractive target for cancer therapy. Much of our current knowledge on epigenetic alterna- tions in cancer comes from studies on gastrointestinal malignancies, mainly on colorectal cancer, which currently serves as a model for epigenetic tumorigenesis. This review summarizes the current knowledge of epigenetic changes in gastrointestinal cancers and how this relates directly to disease progression and prognosis. Keywords: CpG island methylator phenotype, DNA methylation, gastrointestinal cancer epigenetics, long-range epigenetic silencing. Received: November 28, 2007. Accepted: December 7, 2007. Correspondence: P. Karpiñski, Department of Genetics, Wroclaw Medical University, Marcinkowskiego 1, 50–368 Wroc³aw, Poland; e-mail: [email protected]
-
Upload
independent -
Category
Documents
-
view
0 -
download
0
Transcript of Aberrant epigenetic patterns in the etiology of gastrointestinal cancers
Introduction
Gastrointestinal (GI) cancers account for about20% of all cancers worldwide. In the global inci-dence of cancer, gastric cancer is the second,colorectal cancer is the third, and esophageal can-cer is the sixth most common tumor (Chan et al.2006). In neoplasms, including GI cancers,epigenetic changes play a key role in the processof tumorigenesis (Baylin and Bestor 2002; Baylinand Ohm 2006).
Epigenetics in the broad sense may be defined
as the study of phenomena that modify gene ex-
pression without changing the underlying DNA
sequence. More specifically, epigenetics is the
study of collective interaction of multiple mecha-
nisms in establishing states of chromatin structure,
histone modification, transcriptional activity, and
DNA methylation. Evidence accumulated in re-
cent years clearly demonstrates that epigenetic ab-
normalities are important factors in the etiology of
virtually all human cancer types (Laird 2005;
Goldberg et al. 2007).DNA methylation is the most widely studied
epigenetic abnormality in tumorigenesis. It refersto methylation of cytosine at CpG dinucleotides.CpG dinucleotides are not randomly distributedthroughout the human genome. CpG-rich regions,known as CpG islands, are usually unmethylated innormal cells (with the exception of imprinted genesand several genes located on chromosome X) andare typically found associated with 5’ promoter endand first exon of numerous genes (Plass 2002). It isestimated that there are about 29 000 CpG islandswithin the human genome. Approximately50–60% of all genes contain CpG islands. Alter-ations of cytosine methylation are prevalent in hu-man sporadic cancers (Costello and Plass 2001).Methylation defects include genome hypo-methylation (resulting in epigenetic activation ofoncogenes and retroelements) and localized aber-rant hypermethylation of CpG islands, resulting intranscriptional repression of many important
J Appl Genet 49(1), 2008, pp. 1–10
Invited Editorial
Aberrant epigenetic patterns in the etiology of gastrointestinal
cancers
Pawe³ Karpiñski1, Maria M. S¹siadek1, Nikolaus Blin2
1Department of Genetics, Wroclaw Medical University, Poland2Division of Molecular Genetics, Institute of Human Genetics, University of Tuebingen, Germany
Abstract. A body of evidence accumulated over the past decade suggests that epigenetic mechanisms play an es-
sential role in maintaining important cellular functions. Changes in epigenetic patterns (mainly DNA hyper- and
hypomethylation and, more recently, histone modifications) may contribute to the development of cancer. Aber-
rant epigenetic events expand thorough tumor progression from the earliest to latest stages, therefore they can
serve as convenient markers for detection and prognosis of cancer. The potential reversibility of epigenetic states
in the tumor cell is an attractive target for cancer therapy. Much of our current knowledge on epigenetic alterna-
tions in cancer comes from studies on gastrointestinal malignancies, mainly on colorectal cancer, which currently
serves as a model for epigenetic tumorigenesis. This review summarizes the current knowledge of epigenetic
changes in gastrointestinal cancers and how this relates directly to disease progression and prognosis.
Keywords: CpG island methylator phenotype, DNA methylation, gastrointestinal cancer epigenetics, long-range
epigenetic silencing.
Received: November 28, 2007. Accepted: December 7, 2007.
Correspondence: P. Karpiñski, Department of Genetics, Wroclaw Medical University, Marcinkowskiego 1, 50–368 Wroc³aw,
Poland; e-mail: [email protected]
genes (Ting et al. 2006). Promoter hyper-methylation patterns in human cancer show strongspecificity with respect to the tissue of origin, andcan be found early in tumorigenesis. Tumor sup-pressor genes that undergo aberrant methylation inmultiple tumor types may virtually belong to allcellular pathways, thus aberrant promoterhypermethylation has relevant consequences forcarcinogenesis. Moreover, the methylation statusof an individual gene promoter may be used for as-sessing the prediction, general prognosis, and re-sponse to therapy, underlying the importance ofstudies on specific patterns of promoterhypermethylation in tumors (Esteller 2005).
In GI cancers, epigenetic analysis has revealed
a number of genes and pathways inactivated by
methylation-associated silencing (Esteller et al.
2001a; Kang et al. 2003). This review focuses on
our current knowledge of aberrant methylation of
CpG islands in GI cancers, with special emphasis
on similarities and differences of promoter
hypermethylation of tumor suppressor genes with
respect to the tissue of origin. We also emphasize
recent advances in promoter hypermethylation
profiling in regard to prediction and general prog-
nosis in GI cancers.
Gastric cancer (GC)
GC is the second most common cancer in the
world and a main cause of cancer-related mortal-
ity. According to Laurén (1965), GC can be di-
vided into 2 types: intestinal (well-differentiated)
and diffuse (undifferentiated, more aggressive).
These types differ in etiology, pathogenesis and
behavior (Stadtländer and Waterbor 1999;
Meireles et al. 2004).Gastric carcinogenesis is a multi-step process
involving genetic and epigenetic alterations of tu-mor-related genes involving proto-oncogenes(RAB32), tumor suppressor genes (APC,RASSF1A), cell-cycle regulator genes (p16,COX-2), tissue-invasion-related genes (CDH1,TIMP-3, DAPK, THBS1), metabolic enzymes(GSTP1), and DNA repair genes (hMLH1,MGMT). Previous studies have demonstrated thatin GC, several genes are silenced by promoterhypermethylation and the number of genesaberrantly methylated in GC is growing rapidly(Table 1). In addition, promoter hypermethylationappears to be associated with certain types andstages of GC. As reported by Oue et al. (2003),
hypermethylation of CDH1 and RAR-� genes wasfound more frequently in diffuse than in intesti-
nal-type GC. Such tendencies were also describedby other authors for p16 and CDH1 genes (Tamuraet al. 2000; Oue et al. 2002). Recently a compre-hensive survey of specific methylation patterns indiffuse and intestinal-type GC cell lines revealed10 novel genes that were more frequentlyhypermethylated in diffuse GC (Yamashita et al.2005). In addition to this specific profile, in tumorcells already the lesion steps leading from chronicgastritis thorough intestinal metaplasia and gastricadenoma to GC, display specific methylation pat-terns in 12 marker genes (Kang et al. 2003). Sur-prisingly, methylation frequency of APC, CDH1and MGMT genes were equal in each step, ques-tioning the role of their methylation in gastriccarcinogenesis. Nevertheless, some other markers(e.g. hMLH1, COX-2 and p16) showed an increas-ing tendency of methylation along multistep pro-gression. Gene methylation also appeared to followa chronological order, defining methylation ofAPC, CDH1 and MGMT as early events, andhMLH1, RASF1A and GSTP1 as late events in gas-tric carcinogenesis (Kang et al. 2003).
Two distinct molecular pathways have been
identified in gastric carcinogenesis, which are also
characteristic of colorectal cancer: microsatellite
instability (MSI) and CpG island methylator phe-
notype (CIMP). Mutations in mismatch repair
(MMR) genes hMLH1 and hMSH2 have been
rarely observed in GCs, but MSI has been found in
15–39% of sporadic GCs. Leung et al. (1999) have
shown that this MMR deficiency is a direct conse-
quence of aberrant methylation of the hMLH1 pro-
moter in GCs. Because GCs with a high frequency
of MSI are associated with specific clinico-
pathological characteristics (e.g. intestinal-type
differentiation, less lymph node metastasis, and
better survival rate), this finding additionally un-
derlines the importance of aberrant methylation in
gastric carcinogenesis (Toyota et al. 1999a).
In 1999, Toyota et al. described a CpG island
methylator phenotype (CIMP) as a distinct subset
of GCs, characterized by concordant methylation
of multiple genes and associated with p16 and
hMLH1 hypermethylation and MSI (Toyota et al.
1999a). Several other studies confirmed the exis-
tence of this trait in GC (Kang et al. 2003; Oue
et al. 2003; Chang et al. 2006). CIMP in GC has
also been associated with better survival in GC
generally and in intestinal-type GC (Oue et al.
2003; An et al. 2005). Nevertheless, the primary
cause of methylation machinery defect responsi-
ble for CIMP in GCs remains unknown.
It is becoming increasingly apparent that infec-
tious agents, such as Helicobacter pylori and Ep-
2 P. Karpiñski et al.

stein-Barr virus (EBV), may be involved in
aberrant methylation in GC. Infection with
H. pylori can lead to gastric inflammation and is
known as a major cause of chronic gastritis. Be-
cause in the stomach the presence of methylation
at several genes was found in chronic gastritis, it is
possible that gene methylation in GC could be
a result of chronic inflammation caused by
H. pylori infection, but this hypothesis should be
addressed carefully (Kang et al. 2001, 2003; Chan
et al. 2003).
EBV is an oncogenic virus that is known to in-
duce cellular transformation and is implied in sev-
eral human cancers (Burkit’s lymphoma,
nasopharyngeal cancer, and Hodgkin disease).
EBV has also been shown to alter the expression
of human DNA methyltransferases (Tsai et al.
2002). Although EBV incidence in GC is modest
(ca 5–25%), it has been shown that EBV posi-
tively correlates with higher frequencies of meth-
ylated genes and with CIMP (Kang et al. 2002;
Chang et al. 2006). Although the direct role of
EBV in the etiology of CIMP in GC is unknown,
these data suggest that aberrant methylation might
be an important mechanism of EBV-related gas-
tric carcinogenesis.
Colorectal cancer (CRC)
CRC is the second to fourth most common cancer
in the world. Epigenetic changes play a key role in
its initiation and progression, and studies of CRC
are notably leading the way to understanding
cancer epigenetics. One of the reasons why CRC
provides a useful model of epigenetic alternations
in tumorigenesis is the wide accessibility of vari-
ous stages of CRC development, from aberrant
crypt foci to advanced carcinoma (Wong et al.
2007).
Histologic and genetic observations have
shown that most CRCs develop through multistep
carcinogenesis, known as adenoma to carcinoma
sequence proposed by Fearon and Vogelstein
(1990). According to their model, CRCs develop
from normal epithelium, through aberrant crypt
foci (that contain hyperplastic cells), benign pre-
cursor lesions (adenomas or serrated polyps), to
advanced stages of adenoma, and finally carci-
noma. Studies over the past 15 years showed that
specific genetic and, notably, epigenetic changes
are accumulated during this sequential tumor de-
velopment (Baylin and Ohm 2006; Young et al.
2007).
DNA methylation is a common epigenetic
event in CRC and coincides with a growing list of
promoter regions of many functionally important
genes (Table 2). Not surprisingly, aberrant
methylation in CRC shares a lot of similarities
with GC according to affected genes (e.g. hMLH1,
APC, p16). In CRCs as in GCs, specific profiles of
aberrant methylation in multistep carcinogenesis
were observed (Takahashi et al. 2006). On the ba-
sis of methylation analysis of 12 markers, Lee
et al. (2004) demonstrated a stepwise increase in
DNA methylation, from normal colon tissue to
Aberrant epigenetic patterns in GI cancers 3
Table 1. Frequency of promoter methylation in various genes in gastric carcinoma
Gene Gene function Frequency (%) References
APC signal transduction 17–80 Kang et al. 2003; Esteller et al. 2001a; Kim et al. 2005
RASSF1A cell cycle regulation ~6 Esteller et al. 2001a
p16 cell cycle regulation 25–40 Kang et al. 2003; Esteller et al. 2001a; Oue et al. 2003,Chang et al. 2006
COX-2 cell cycle regulation, apoptosis ~46 Kang et al. 2003
CDH1 cell signaling 50–80 Esteller et al. 2001a; Oue et al. 2003
TIMP-3 matrix remodeling, tissue invasion 10–65 Kang et al. 2001, 2003; Chang et al. 2006
DAPK apoptosis 30–60 Kang et al. 2001, 2003; Chang et al. 2006
THBS1 angiogenesis 50–60 Kang et al. 2001, 2003
GSTP1 xenobiotic metabolism 0–40 Kang et al. 2001, 2003; Esteller et al. 2001a; Chang et al.2006
MGMT DNA repair 16–26 Kang et al. 2003; Esteller et al. 2001a; Oue et al. 2003;Chang et al. 2006
hMLH1 DNA mismatch repair 16–30 Kang et al. 2001, 2003; Esteller et al. 2001a; Oue et al.2003; Chang et al. 2006
carcinoma. Recent studies also suggest differ-
ences in methylation profile within benign precur-
sor lesions of CRC, indicating that serrated polyps
are more prone to aberrant methylation than
adenomas (Jass 2007; Young et al. 2007).
Epigenetic and genetic similarities between
the etiology of CRC and GC are also underlined by
the presence of 2 distinct molecular pathways that
are also characteristic of GC: microsatellite insta-
bility (MSI) and CpG island methylator phenotype
(CIMP) (Samowitz et al. 2005; Weisenberger
et al. 2006). It has to be emphasized that these
2 pathways were originally described for CRC and
afterwards for GC (Aaltonen et al. 1993; Toyota
et al. 1999b). The MSI pathway was recognized
because of its correlation with hereditary non-
polyposis colon cancer (HNPCC); a few years
later, hMLH1 promoter hypermethylation, fol-
lowed by hMLH1 transcriptional silencing, was
directly correlated with the development of the
15% of sporadic CRCs that also displayed MSI.
MSI-CRCs are poorly differentiated and show
proximal location (Esteller et al. 1998). Paradoxi-
cally, despite poor differentiation, they carry a
more favorable prognosis than microsatellite-sta-
ble (MSS) cancers (Popat et al. 2005). In 1999,
Toyota et al. proposed that a subset of sporadic
CRCs display a promoter CpG island methylator
phenotype (CIMP), which manifests itself as an
exceptionally high frequency of methylation of
discrete CpG islands (Toyota et al. 1999b). Al-
though the existence of CIMP has not been de-
tected in CRCs associated with the CpG island
methylation of a number of genes across the ge-
nome by some investigators (Yamashita et al.
2003; Anacleto et al. 2005), subsequent popula-
tion-based studies have confirmed the presence of
a subset (Samowitz et al. 2005; Ogino et al.
2006a). In 2006, Weisenberger et al., studying
a large carefully selected marker panel in a cohort
of sporadic CRCs, definitively confirmed the exis-
tence of CIMP. Importantly, those authors found
that MSI was fully explained by CIMP-associated
hMLH1 methylation (Weisenberger et al. 2006).
In accordance with this finding, sporadic
colorectal tumors displaying CIMP show many
features typical of MSI tumors, such as proximal
location, a higher frequency in females, high
grade, mucinous histology, and the BRAF V600E
mutation (Ogino et al. 2006b). However, approxi-
mately half of CIMP-positive CRCs are
microsatellite-stable, which underscores the bio-
logical uniqueness of CIMP-positive CRCs
(Weisenberger et al. 2006).
As in GCs, the primary cause for the defect of
the methylation machinery leading to CIMP in
CRC remains mysterious, although 2 hypotheses
are still a matter of debate: genetic and environ-
mental. To date no specific genetic event that
aberrantly changes the mechanisms responsible
for spreading or blocking of DNA methylation
have been described (Issa 2004; Issa et al. 2005).
Nevertheless, recent studies have brought some
evidence for environmentally-related CIMP etiol-
4 P. Karpiñski et al.
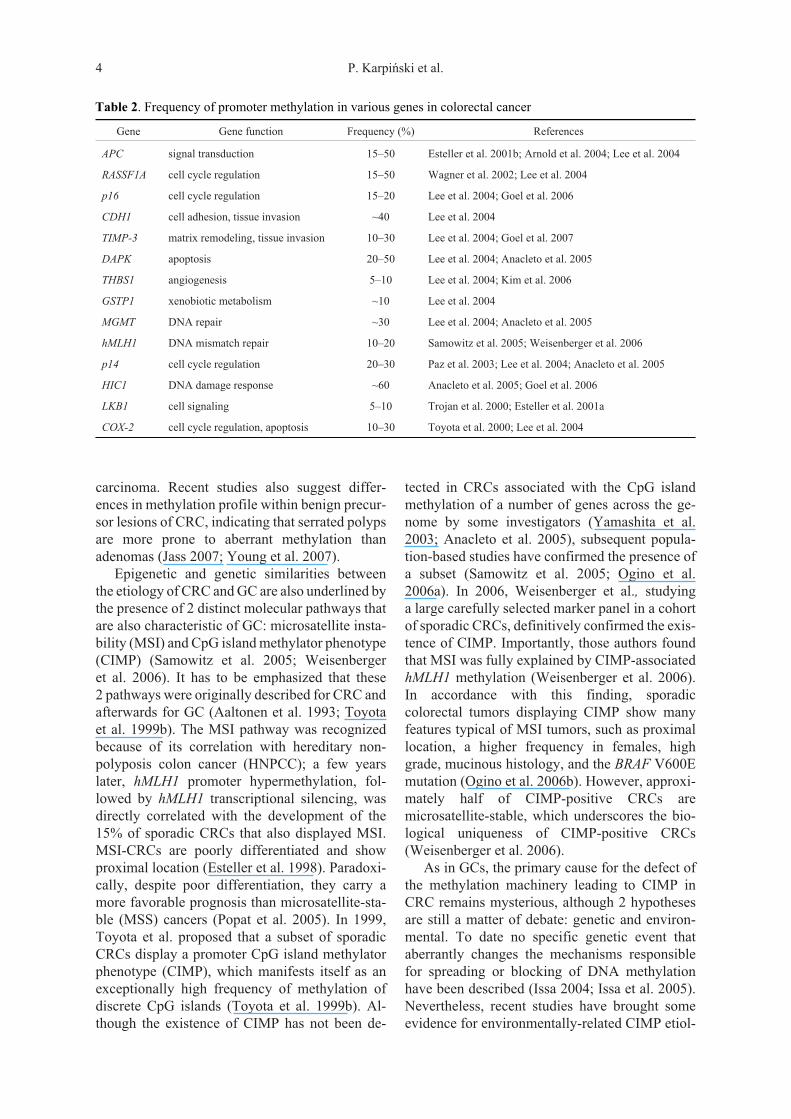
Table 2. Frequency of promoter methylation in various genes in colorectal cancer
Gene Gene function Frequency (%) References
APC signal transduction 15–50 Esteller et al. 2001b; Arnold et al. 2004; Lee et al. 2004
RASSF1A cell cycle regulation 15–50 Wagner et al. 2002; Lee et al. 2004
p16 cell cycle regulation 15–20 Lee et al. 2004; Goel et al. 2006
CDH1 cell adhesion, tissue invasion ~40 Lee et al. 2004
TIMP-3 matrix remodeling, tissue invasion 10–30 Lee et al. 2004; Goel et al. 2007
DAPK apoptosis 20–50 Lee et al. 2004; Anacleto et al. 2005
THBS1 angiogenesis 5–10 Lee et al. 2004; Kim et al. 2006
GSTP1 xenobiotic metabolism ~10 Lee et al. 2004
MGMT DNA repair ~30 Lee et al. 2004; Anacleto et al. 2005
hMLH1 DNA mismatch repair 10–20 Samowitz et al. 2005; Weisenberger et al. 2006
p14 cell cycle regulation 20–30 Paz et al. 2003; Lee et al. 2004; Anacleto et al. 2005
HIC1 DNA damage response ~60 Anacleto et al. 2005; Goel et al. 2006
LKB1 cell signaling 5–10 Trojan et al. 2000; Esteller et al. 2001a
COX-2 cell cycle regulation, apoptosis 10–30 Toyota et al. 2000; Lee et al. 2004

ogy. Curtin et al. (2007) studied the relationships
between dietary factors and single-nucleotide
polymorphisms in methyl-group metabolizing
genes as well as CIMP. Those authors hypothe-
sized that polymorphisms involved in provision of
methyl groups, potentially modified by a diet,
would be associated with CIMP. Their research
team found a few weak associations specific for
CIMP tumors and noted a possible influence of
MTHFR 1298A/C polymorphism together with
low folate and high alcohol intake (Curtin et al.
2007). In contrast, Samowitz et al. (2006) ob-
served in a large group a significant relationship
between heavy smoking and CIMP. While the pre-
cise mechanism between smoking and CIMP re-
mains currently unclear, studies on aberrant
methylation of several genes in lung cancer pa-
tients demonstrated a significantly higher fre-
quency of promoter methylation among smokers
(Liu et al. 2006). As in the GCs, there is mounting
evidence that infectious agents influence aberrant
methylation in CRCs. In fact, a recent paper by
Goel et al. (2006) describes an association be-
tween JC virus T-antigen expression and aberrant
methylation of multiple tumor-suppressor genes
in sporadic CRC. Oncogenic viruses, like JC virus,
frequently exploit different epigenetic mecha-
nisms to avoid host immune response or to take
over complete control of cellular gene expression,
e.g. by interaction of their specific proteins with
host DNA methyltransferases. Considering this,
the finding of Goel et al. (2006) raises the possibil-
ity that JC virus may play a mechanistic role in the
etiology of CIMP or at least in aberrant DNA
methylation in CRC (Flanagan 2007).
For many years, DNA methylation followed by
transcriptional silencing of genes was considered
as an event that is restricted to discrete CpG is-
lands. This view has been recently challenged by
Frigola et al. (2006), who demonstrated that
epigenetic silencing is not solely a focal event in
CRCs, but encompasses a large 4-Mb domain of
chromosomal region 2q14. This phenomenon was
termed long-range epigenetic silencing (LRES).
Those authors found that LRES at 2q14 was asso-
ciated with DNA methylation in 3 enriched CpG
island clusters. Interestingly, DNA methylation in
each of these clusters was associated with suppres-
sion of flanking genes despite the fact that these
genes themselves remained unmethylated. Fur-
thermore, this suppression was caused by
methylation of histone H3 at Lys9 (H3-K9), inde-
pendent of DNA methylation. Those data suggest
that the extent and spread of DNA hyper-
methylation may influence the long-range sup-
pression of neighboring genes by modifications in
histone code, followed by chromatin remodeling
(Frigola et al. 2006; Clark 2007). A very recent pa-
per by Hitchins et al. (2007) describes LRES
where a whole region located in 3p22, spanning
1.1Mb, was transcriptionally suppressed in
MSI-sporadic CRCs that displayed hMLH1 pro-
moter hypermethylation. Importantly, those au-
thors observed the same relation between DNA
methylation, histone modifications and
transcriptional silencing as Frigola et al. (2006).
Curiously, hMLH1 methylation-associated MSI
generally does not occur among sporadic CRCs
outside the context of CIMP, indicating that LRES
across 3p22 might be specific to CIMP CRCs
(Weisenberger et al. 2006; Hitchins et al. 2007).
It is also noteworthy that both examples of LRES
are associated with transcriptional silencing of
genes that are known to play an important role in
carcinogenesis, e.g. hMLH1, EN1 (Wnt signaling
pathway), GLI2 (sonic hedgehog signaling path-
way), DLEC1 (tumor suppressor), and CTDSPL
(tumor suppressor) (Frigola et al. 2006; Hitchins
et al. 2007). These observations have been con-
firmed by our studies of a larger group of sporadic
CRCs, indicating a strong association between
CIMP and LRES (unpublished). All these results
together suggest an interrelationship between
MSI, CIMP and LRES in the etiology of CRC, but
the chronology of key events still remains to be
elucidated.
Esophageal cancer (EC)
EC is a less frequent malignancy, as compared to
CRC or GC, but its incidence has increased rapidly
in the Western World (Tabernero et al. 2005).
There are 2 main subtypes of EC: esophageal
squamous cell carcinoma (ESCC) and esophageal
adenocarcinoma (EAC) (McManus et al. 2004).
As in the case of GC and CRC, EAC arises from
a multistep process that includes the transition
from normal squamous epithelium through colum-
nar, metaplastic epithelium (e.g. Barret’s esopha-
gus), to subsequent dysplastic lesions that give rise
to invasive adenocarcinoma (Jankowski et al.
1999; Fitzgerald 2006). In contrast, the molecular
progression of ESCC is much less characterized
(Guo et al. 2006).
Similarly to GI cancers described above, DNA
methylation is a common epigenetic event in EC,
but ECs have not been as extensively studied in
Aberrant epigenetic patterns in GI cancers 5
this context (Eads et al. 2001). As it has been re-
ported for other GI cancers, DNA methylation is a
common silencing event in both types of EC and
concerns a wide variety of important genes (Ta-
ble 3). Like in GC and CRC, aberrant methylation
accumulates gradually to the histologic changes
during esophageal carcinogenesis (Eads et al.
2001; Guo et al. 2006; Ishii et al. 2007). The earli-
est stages of EAC involve, for example, aberrant
methylation of MGMT and TIMP3, whereas
hypermethylation of APC, hMLH1 and p16 could
be observed in more advanced histological stages.
Similarly as in EAC, aberrant methylation of
MGMT is observed early in ESCC, but
hypermethylation of APC, hMLH1 and p16 could
be observed in less advanced stages (Eads et al.
2001; Guo et al. 2006). This finding supports the
utility of methylation markers in characterizing
both esophageal malignancies. Interestingly, a pa-
per by Brock et al. (2003) suggests that frequent
hypermethylation of multiple genes is a predictor
of poor prognosis in EAC.
In contrast to GC and CRC, microsatellite in-
stability is less frequently observed in EC, and
hMLH1/MSH2 expression appears to be at normal
levels (Kulke et al. 2001; McManus et al. 2004).
As in GCs, MSI in EC is directly associated with
aberrant hypermethylation of the hMLH1 gene,
underlining the importance of aberrant
methylation in esophageal carcinogenesis (Kulke
et al. 2001; Guo et al. 2006). Interestingly, hMLH1
methylation-associated MSI is a more frequent
and pronounced event in ESCC than in EAC
(Kulke et al. 2001; Matsumoto et al. 2007).
To date, the supporting evidence of CpG island
methylator phenotype in EC has not been found,
although the data published by Eads et al. (2001)
and Brock et al. (2003) suggest that this trait in fact
may be present in ECs. It is likely that the use of
unbiased approach and a carefully selected marker
panel on a cohort of ECs, as Weisenberger et al.
(2006) did on CRCs, will finally and undoubtedly
confirm the existence of CIMP in ECs.
As in the case of CIMP, no data confirming the
long-range epigenetic silencing (LRES) in EC
have been published to date. However, the finding
of frequent and concordant hypermethylation of
three HLA class I genes located on 6p21.3 and
subsequent loss of their expression in ESCC sug-
gests the existence of LRES, at least in this sub-
type of EC (Nie et al. 2001; Clark 2007).
Hypomethylation in GI cancers
Tumor cells from almost every human malignancy
undergo dramatic global hypomethylation that
contributes to all the stages thorough the multistep
carcinogenesis. Hypomethylation appears to trig-
ger several mechanisms that are related to neoplas-
tic progression. Extensive demethylation in
centromeric regions may play a role in aneuploidy,
whereas demethylation within the body of a num-
ber of a genes may induce oncogene activation,
loss of imprinting, and retrotransposon reactiva-
tion (Esteller 2005).
In contrast to aberrant CpG island methylation,
much less is known about the impact of the ge-
nome-wide hypomethylation on GI carcinogenesis.
Hypomethylation is known to occur early during
gastric carcinogenesis, and it is associated with ab-
errant activation of expression of Maspin
(a proto-oncogene that regulates cell adhesion, mo-
tility, apoptosis, and angiogenesis), synuclein or
SNCG (stimulating cancer cells), cyclin D2 (im-
plied in cell cycle regulation), and finally the
6 P. Karpiñski et al.
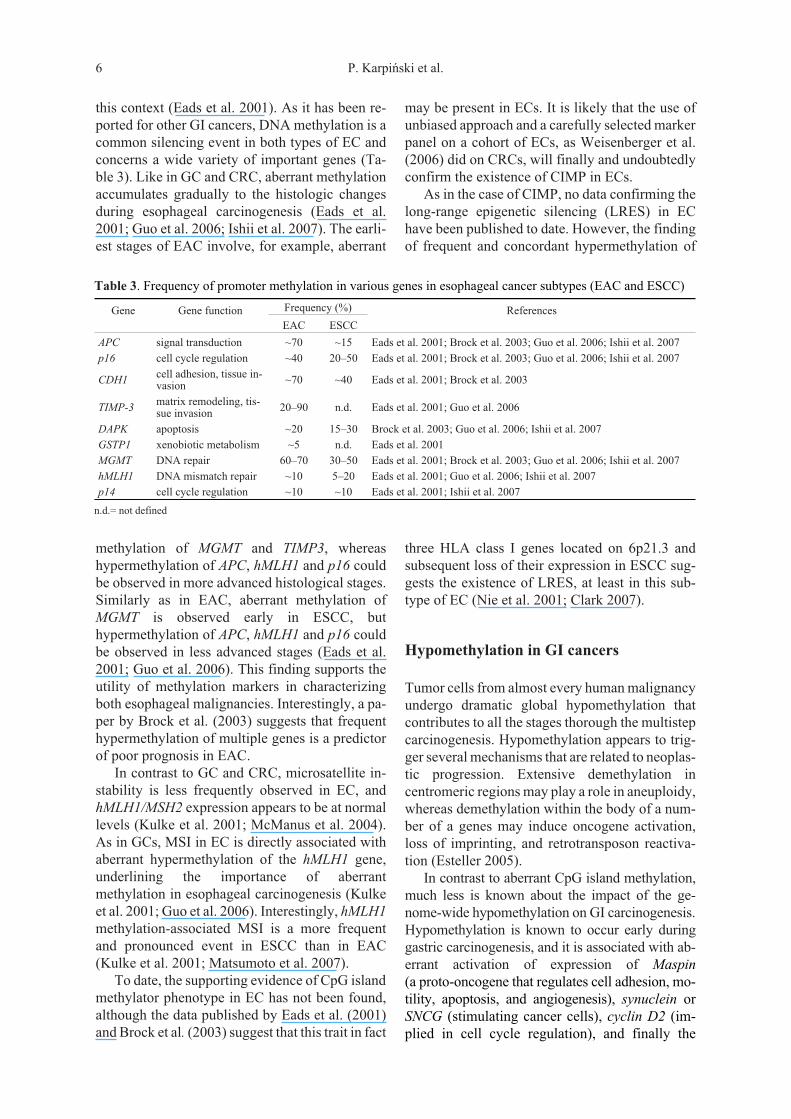
Table 3. Frequency of promoter methylation in various genes in esophageal cancer subtypes (EAC and ESCC)
Gene Gene function Frequency (%) References
EAC ESCC
APC signal transduction ~70 ~15 Eads et al. 2001; Brock et al. 2003; Guo et al. 2006; Ishii et al. 2007
p16 cell cycle regulation ~40 20–50 Eads et al. 2001; Brock et al. 2003; Guo et al. 2006; Ishii et al. 2007
CDH1cell adhesion, tissue in-vasion
~70 ~40 Eads et al. 2001; Brock et al. 2003
TIMP-3matrix remodeling, tis-sue invasion
20–90 n.d. Eads et al. 2001; Guo et al. 2006
DAPK apoptosis ~20 15–30 Brock et al. 2003; Guo et al. 2006; Ishii et al. 2007
GSTP1 xenobiotic metabolism ~5 n.d. Eads et al. 2001
MGMT DNA repair 60–70 30–50 Eads et al. 2001; Brock et al. 2003; Guo et al. 2006; Ishii et al. 2007
hMLH1 DNA mismatch repair ~10 5–20 Eads et al. 2001; Guo et al. 2006; Ishii et al. 2007
p14 cell cycle regulation ~10 ~10 Eads et al. 2001; Ishii et al. 2007
n.d.= not defined

proto-oncogene R-RAS (Cravo et al. 1996;
Akiyama et al. 2003; Oshimo et al. 2003;
Yanagawa et al. 2004; Nishigaki et al. 2005).
DNA hypomethylation is a common and also early
trait of colorectal cancer. In CRCs, hypo-
methylation is associated with a loss of imprinting
of H19 and IGF2 (insulin-like growth factor-II)
genes and activation of L1 retrotransposon that
may subsequently, by its aberrant integration,
cause disruption of the APC gene (Miki et al.
1992; Cui et al. 2002; Suter et al. 2004). Finally,
hypomethylation has been directly linked with
chromosomal instability in CRC (Rodriguez et al.
2006). The interrelations between DNA hypo-
methylation and hypermethylation in GI
tumorigenesis are still not well understood. Some
papers (e.g. Frigola et al. 2005) describe independ-
ent correlations for DNA hypomethylation and
hypermethylation in CRCs, whereas some others
(e.g. Suzuki et al. 2006) show that both DNA
methylation alternations are positively correlated
in CRCs and GCs. Regardless of these controver-
sies, the cited reports found positive associations
between hypomethylation and both a decreased
survival and a worse prognosis, either for CRC
or GC.
Summary
Although the molecular mechanisms responsible
for aberrant DNA methylation during
carcinogenesis are still not well characterized, the
implications of DNA hypomethylation and
hypermethylation in the etiology of GI
tumorigenesis have become quite clear. As de-
scribed in this review, the aberrant DNA
methylation patterns, apart from their functional
significance, can be exploited for the classification
of cancers arising in the same tissue with regard to
histologic subtype, stage and prognosis. A large
variety of techniques are now available to deter-
mine DNA methylation of the genome, allowing
the detection of malignant cells with remarkable
sensitivity and specificity, as e.g. shown for detec-
tion of DNA methylation in stools of CRC patients
or for aberrant methylation of p16 in serum of GC
patients (Kanyama et al. 2003; Laird 2003;
Belshaw et al. 2004). Similarly, APC methylation
in plasma was found to be a useful biomarker in
detection and prognosis of the patients with esoph-
ageal adenocarcinoma (Kawakami et al. 2000).
More importantly, the potential reversibility of
epigenetic changes offers promising targets for
cancer therapy. Indeed, DNA methyltransferases
and histone deacetylases have been among the ma-
jor epigenetic targets in cancer therapy to date
(Laird 2005).
In the last decade, research on epigenetic
changes in GI cancers brought a better understand-
ing of the mechanisms that underlie their etiology
and molecular pathways that lead to neoplastic
transformation. This was mostly apparent in the
case of colorectal cancer, where novel phenom-
ena, such as CIMP and LRES, have lately been
characterized (Frigola et al. 2006; Weisenberger
et al. 2006; Hitchins et al. 2007). Hopefully, these
recent findings should lead to development of
novel epigenetic drugs and effective anticancer
therapies.
Acknowledgements. The epigenetic cancer research
in the Department of Genetics (Wroclaw Medical
University) is supported by the State Committee for
Scientific Research, Polish Ministry for Scientific
Research and Information Technology (grant
no. 1423/P01/2007/32), 2007–2010.
REFERENCES
Aaltonen LA, Peltomaki P, Leach FS, Sistonen P,Pylkkanen L, Mecklin JP, et al. 1993. Clues to thepathogenesis of familial colorectal cancer. Science260: 812–816.
Akiyama Y, Maesawa C, Ogasawara S, Terashima M,Masuda T, 2003. Cell-type-specific repression ofthe Maspin gene is disrupted frequently bydemethylation at the promoter region in gastric in-testinal metaplasia and cancer cells. Am J Pathol163: 1911–1919.
An C, Choi I, Yao JC, Worah S, Xie K, Mansfield PF,et al. 2005. Prognostic significance of CpG islandmethylator phenotype and microsatellite instabilityingastriccarcinoma.ClinCancerRes11:656–663.
Anacleto C, Leopoldino AM, Rossi B, Soares FA,Lopes A, Rocha JC, et al. 2005. Colorectal cancer“methylator phenotype”: fact or artifact? Neopla-sia 7: 331–335.
Arnold CN, Goel A, Niedzwiecki D, Dowell JM,Wasserman L, Compton C, et al. 2004. APC pro-moter hypermethylation contributes to the loss ofAPCexpressionincolorectalcancerswithallelic losson 5q. Cancer Biol Ther 3: 960–964.
Baylin SB, Bestor TH, 2002. Altered methylation pat-terns in cancer cell genomes: cause or consequence?Cancer Cell 1: 299–305.
Baylin SB, Ohm JE, 2006. Epigenetic gene silencing incancer – a mechanism for early oncogenic pathwayaddiction? Nat Rev Cancer 6: 107–116.
Belshaw NJ, Giles O, Elliott GO, Williams EA,David M, Bradburn DM, et al. 2004. Use of DNAfrom human stools to detect aberrant CpG islandmethylation of genes implicated in colorectal can-
Aberrant epigenetic patterns in GI cancers 7

cer. Cancer Epidemiol Biomarkers Prev 13:1495–1501.
Brock MV, Gou M, Akiyama Y, Ar AM, Wu TT,Montgomery E, et al. 2003. Prognostic importanceof promoter hypermethylation of multiple genes inesophageal adenocarcinoma. Clin Cancer Res 9:2912–2919.
Chan AOO, Lam SK, Wong BCY, Kwong YL, 2003.Gene methylation in non-neoplastic mucosa of gas-tric cancer: age or Helicobacter pylori related?Am J Pathol 163: 370–373.
Chan AOO, Rashid A, 2006. CpG island methylation inprecursors of gastrointestinal malignancies.CurrMol Med 6: 401–408.
Chang MS, Uozaki H, Chong JM, Ushiku T,Sakuma K, Ishikawa S, et al. 2006. CpG islandmethylation status in gastric carcinoma with andwithout infection of Epstein-Barr virus. Clin CancerRes 12: 2995–3002.
Costello JF, Plass C, 2001. Methylation matters. J MedGenet 38: 285–303.
Clark JS, 2007. Action at a distance: epigenetic silencingof large chromosomal regions in carcinogenesis.Hum Mol Genet 16: R88–R95.
Cravo M, Pinto R, Fidalgo P, Chaves P, Glória L,Nobre-Leit�o C, et al. 1996. Global DNA hypo-methylation occurs in the early stages of intesti-nal-type gastric carcinoma. Gut 39: 434–438.
Cui H, Onyango P, Brandenburg S, Wu Y, Hsieh CL,Feinberg AP, 2002. Loss of imprinting in colorectalcancer linked to hypomethylation of H19 and IGF2.Cancer Res 62: 6442–6446.
Curtin K, Slattery ML, Ulrich CM, Bigler J, Levin TR,et al. 2007. Genetic polymorphisms in one-carbonmetabolism: associations with CpG islandmethylator phenotype (CIMP) in colon cancer andthe modifying effects of diet. Carcinogenesis 28:1672–1679.
Eads CA, Lord RV, Wickramasinghe K, Long TI,Kurumboor SK, Bernstein L, et al. 2001. Epigeneticpatterns in the progression of esophagealadenocarcinoma. Cancer Res 61: 3410–3418.
Esteller M, Levine R, Baylin SB, Ellenson LH,Herman JG, 1998. MLH1 promoter hyper-methylation is associated with the microsatellite in-stability phenotype in sporadic endometrial carci-nomas. Oncogene 17: 2413–2417.
Esteller M, Corn PG, Baylin SB, Herman JG, 2001a.
A gene hypermethylation profile of human cancer.
Cancer Res 61: 3225–3229.
Esteller M, Fraga MF, Guo M, Garcia-Foncillas J,Hedenfalk I, Godwin AK, et al. 2001b. DNAmethylation patterns in hereditary human cancersmimic sporadic tumorigenesis. Hum Mol Genet 10:3001–3007.
Esteller M, 2005. Aberrant DNA methylation as a can-cer-inducing mechanism. Annu Rev PharmacolToxicol 45: 629-56.
Fearon ER, Vogelstein B, 1990. A genetic model forcolorectal tumorigenesis. Cell 61: 759–767.
Flanagan JM, 2007. Host epigenetic modifications byoncogenic viruses. Br J Cancer 96: 183–188.
Fitzgerald RC, 2006. Molecular basis of Barrett’s oe-sophagus and oesophageal adenocarcinoma. Gut55: 1810–1820.
FrigolaJ,SoléX,PazMF,MorenoV,EstellerM,CapellàG, et al. 2005. Differential DNA hypermethylationandhypomethylationsignatures incolorectal cancer.Hum Mol Genet 14: 319–326.
Frigola J, Song J, Stirzaker C, Hinshelwood RA,Peinado MA, Clark SJ, 2006. Epigenetic remodel-ing in colorectal cancer results in coordinate genesuppression across an entire chromosome band. NatGenet 38: 540–549.
Goldberg AD, Allis CD, Bernstein E, 2007. Epigenetics:a landscape takes shape. Cell 128: 635–638.
Goel A, Li MS, Nagasaka T, Shin SK, Fuerst F,Ricciardiello L, et al. 2006. Association of JC virusT-antigen expression with the methylator pheno-type in sporadic colorectal cancers. Gastro-enterology 130: 1950–1961.
Goel A, Nagasaka T, Arnold CN, Inoue T, Hamilton C,Niedzwiecki D, et al. 2007. The CpG islandmethylator phenotype and chromosomal instabilityare inversely correlated in sporadic colorectal can-cer. Gastroenterology 132: 127–138.
Guo M, Ren J, House MG, Qi Y, Brock MV,Herman JG, 2006. Accumulation of promotermethylation suggests epigenetic progression insquamous cell carcinoma of the esophagus. ClinCancer Res 12: 4515–4522.
Hitchins MP, Lin VA, Buckle A, Cheong K, Halani N,Ku S, et al. 2007. Epigenetic inactivation of a clus-ter of genes flanking MLH1 in microsatellite- unsta-ble colorectal cancer. Cancer Res 67: 9107–9116.
Ishii T, Murakami J, Notohara K, Cullings HM,Sasamoto H, Kambara T, et al. 2007. Oesophagealsquamous cell carcinoma may develop within abackground of accumulating DNA methylation innormal and dysplastic mucosa. Gut 56: 13–19.
Issa JP, 2004. CpG island methylator phenotype in can-cer. Nat Rev Cancer 4: 988–993.
Issa JP, Shen L, Toyota M, 2005. CIMP, at last.Gastroenterology 129: 1121–1124.
Jankowski JA, Wright NA, Meltzer SJ,Triadafilopoulos G, Geboes K, Casson AG, et al.1999. Molecular evolution of the metaplasia-dysplasia-adenocarcinoma sequence in the esopha-gus. Am J Pathol 154: 965–973.
Jass JR, 2007. Classification of colorectal cancer basedon correlation of clinical, morphological and mo-lecular features. Histopathology 50: 113–130.
Kang GH, Shim YH, Jung HY, Kim WH, Ro JY,Rhyu MG, 2001. CpG island methylation inpremalignant stages of gastric carcinoma. CancerRes 6: 2847–2851.
Kang GH, Kim WH, Hye Won, Lee HW, Kim JC,Rhyu MG, Ro JY, 2002. Epstein-Barr vi-rus-positive gastric carcinoma demonstrates fre-quent aberrant methylation of multiple genes andconstitutes CpG island methylator pheno-
8 P. Karpiñski et al.
type-positive gastric carcinoma. Am J Pathol 160:787–794.
Kang GH, Lee S, Kim JS, Jung HY, 2003. Profile of ab-errant CpG island methylation along multistep gas-tric carcinogenesis. Lab Invest 83: 519–526.
Kim CH, Roh SA, Yu CS, Yook JH, Oh ST, Kim BS,et al. 2005. Aberrant CpG island methylation inearly-onset sporadic gastric carcinoma. J of CancRes and Clin Oncol 131: 733–740.
Kim YH, Petko Z, Dzieciatkowski S, Lin L, Ghiassi M,Stain S, et al. 2006. CpG island methylation ofgenes accumulates during the adenoma progressionstep of the multistep pathogenesis of colorectal can-cer. Genes Chromosomes Cancer 45: 781–789.
Kanyama Y, Hibi K, Nakayama H, Kodera Y, Ito K,Akiyama S, et al. 2003. Detection of p16 promoterhypermethylation in serum of gastric cancer pa-tients. Cancer Sci 94: 418–420.
Kawakami K, Brabender J, Lord RV, Groshen S, Green-wald BD, Krasna MJ, et al. 2000. HypermethylatedAPC DNA in plasma and prognosis of patients withesophageal adenocarcinoma. J Natl Cancer Inst 92:1805–1811.
Kulke MH, Thakore KS, Thomas G, Wang H, Loda M,Eng C, et al. 2001. Microsatellite instability andhMLH1/hMSH2 expression in Barrett esopha-gus-associated adenocarcinoma. Cancer 91:1451–1457.
Laird PW, 2003. The power and the promise of DNAmethylation markers. Nat Rev Cancer 3: 253-266.
Laird PW, 2005. Cancer epigenetics. Hum Mol Genet14: R65–R76.
Laurén R, 1965. The two histological main types of gas-tric carcinoma: diffuse and so-called intestinal-typecarcinoma: an attempt at a histoclinical classifica-tion. Acta Phatol Microbiol Scand 64: 31–49.
Lee S, Hwang KS, Lee HJ, Kim JS, Kang GH, 2004.Aberrant CpG island hypermethylation of multiplegenes in colorectal neoplasia. Lab Invest 84:884–893.
Leung SY, Yuen ST, Chung LP, Chu KM, Chan AS,HoJC,1999.hMLH1Promotermethylationand lackofhMLH1expression insporadicgastriccarcinomaswith high-frequency microsatellite instability. Can-cer Res 59: 159–164.
Liu Y, Lan Q, Siegfried JM, Luketich JD, Keohavong P,2006. Aberrant promoter methylation of p16 andMGMT genes in lung tumors from smokingand never-smoking lung cancer patients. Neopla-sia 8: 46–51.
Matsumoto Y, Nagasaka T, Kambara T, Hoshizima N,Murakami J, Sasamoto H, et al. 2007. Microsatelliteinstability and clinicopathological features inesophageal squamous cell cancer. Oncol Rep18:1123–1127.
McManus DT, Olaru A, Meltzer SJ, 2004. Biomarkersof esophageal adenocarcinoma and Barrett’s esoph-agus. Cancer Res 64: 1561–1569.
Meireles SI, Cristo EB, Carvalho AF, Hirata R,Pelosof A, Gomes LI, et al. 2004. Molecular classifi-ers for gastric cancer and nonmalignant diseases ofthe gastric mucosa. Cancer Res 64: 1255–1265.
Miki Y, Nishisho I, Horii A, Miyoshi Y, Utsunomiya J,Kinzler KW, et al. 1992. Disruption of the APCgene by a retrotransposal insertion of L1 sequencein a colon cancer. Cancer Res 52: 643–645.
Nie Y, Yang G, Song Y, Zhao X, So C, Liao J, et al.2001. DNA hypermethylation is a mechanism forloss of expression of the HLA class I genes in hu-man esophageal squamous cell carcinomas.Carcinogenesis 22: 1615–1623.
Nishigaki M, Aoyagi K, Danjoh I, Fukaya M,Yanagihara K, Sakamoto H, et al. 2005. Discoveryof aberrant expression of R-RAS by cancer-linkedDNA hypomethylation in gastric cancer usingmicroarrays. Cancer Res 65: 2115–2124.
Ogino S, Cantor M, Kawasaki T, Brahmandam M,Kirkner GJ, Weisenberger DJ, et al. 2006a. CpG is-land methylator phenotype (CIMP) of colorectalcancer is best characterised by quantitative DNAmethylation analysis and prospective cohort stud-ies. Gut 55: 1000–1006.
Ogino S, Odze RD, Kawasaki T, Brahmandam M,Kirkner GJ, Laird PW, et al. 2006b. Correlation ofpathologic features with CpG island methylator phe-notype (CIMP) by quantitative DNA methylationanalysis in colorectal carcinoma. Am J Surg Pathol30: 1175–1183.
Oshimo Y, Nakayama H, Ito R, Kitadai Y, Yoshida K,Chayama K, Yasui W, 2003. Promoter methylationof cyclin D2 gene in gastric carcinoma. Int J Oncol23: 1663–1670.
Oue N, Motoshita J, Yokozaki H, Hayashi K, Tahara E,Taniyama K, et al. 2002. Distinct promoterhypermethylation of p16INK4a, CDH1, andRAR-beta in intestinal, diffuse-adherent, and dif-fuse-scattered type gastric carcinomas. J Pathol 198:55–59.
Oue N, Oshimo Y, Nakayama H, Ito R, Yoshida K,Matsusaki K, et al. 2003. DNA methylation of multi-ple genes in gastric carcinoma: Association withhistological type and CpG island methylator pheno-type. Canc Sci 94: 901–905.
Paz MF, Fraga MF, Avila S, Guo M, Pollan M,HermanJG,EstellerM,2003.AsystematicprofileofDNA methylation in human cancer cell lines. CancerRes 63: 1114–1121.
Plass C, 2002. Cancer epigenomics. Hum Mol Genet 11:2479–2488.
Popat S, Hubner R , Houlston RS, 2005. Systematic re-view of microsatellite instability and colorectal can-cer prognosis. J Clin Oncol 23: 609–618.
Rodriguez J, Frigola J, Vendrell E, Risques RA,Fraga MF, Morales C, et al. 2006. Chromosomal in-stability correlates with genome-wide DNAdemethylation in human primary colorectal cancers.Cancer Res 66: 8462–9468.
Samowitz WS, Albertsen H, Herrick J, Levin TR, Swee-ney S, Murtaugh MA, et al. 2005. Evaluation ofa large, population-based sample supports a CpG is-land methylator phenotype in colon cancer.Gastroenterology 129: 837–845.
Samowitz WS, Albertsen H, Sweeney C, Herrick J,Bette J, Caan BJ, et al. 2006. Association of smoking,CpG island methylator phenotype, and V600E
Aberrant epigenetic patterns in GI cancers 9
BRAF mutations in colon cancer. J Natl CancerInst 98: 1731–1738.
Stadtländer CT, Waterbor J, 1999. Molecular epidemi-ology, pathogenesis and prevention of gastric can-cer. Carcinogenesis. 20: 2195–2208.
Suter CM, Martin DI, Ward RL, 2004. Hypomethylationof L1 retrotransposons in colorectal cancer and adja-centnormaltissue.IntJColorectalDis19: 95–101.
Suzuki K, Suzuki I, Leodolter A, Alonso S, Horiuchi S,Yamashita K, et al. 2006. Global DNA demethylationin gastrointestinal cancer is age-dependent and pre-cedes genomic damage. Cancer Cell 9: 199–207.
Takahashi T, Shigematsu H, Shivapurkar N, Reddy J,Zheng Y, Feng Z, et al. 2006. Aberrant promotermethylation of multiple genes during multisteppathogenesis of colorectal cancers. Int J Cancer118: 924–931.
Tamura G, Yin J, Wang S, Fleisher AS, Zou T, Abra-ham JM, et al. 2000. E-cadherin gene promoterhypermethylation in primary human gastric carci-nomas. J Natl Cancer Inst 5: 569–573.
Tabernero J, Macarulla T, Ramos FJ, Baselga J, 2005.Novel targeted therapies in the treatment of gastricand esophageal cancer. Ann Onc 16: 1740–1748.
Ting AH, McGarvey KM, Baylin S, 2006. The cancerepigenom – components and functional correlates.Genes & Dev 20: 3215–3231.
Toyota M, Ahuja N, Suzuki H, Itoh F, Ohe-Toyota M,Imai K, et al. 1999a. Aberrant methylation in gastriccancer associated with the CpG island methylatorphenotype. Cancer Res 59: 5438–5442.
Toyota M, Ahuja N, Ohe-Toyota M, Herman JG,Baylin SB, Issa JP, 1999b. CpG island methylatorphenotype in colorectal cancer. Proc Natl AcadSci 96: 8681–8686.
Toyota M, Shen L, Ohe-Toyota M, Hamilton SR,.Sinicrope FA, Issa JP, 2000. Aberrant methylationof the cyclooxygenase 2 CpG island in colorectaltumors. Cancer Res 60: 4044–4048.
Trojan J, Brieger A, Raedle J, Esteller M, Zeuzem S,2000. 5’-CpG island methylation of the LKB1/STK11 promoter and allelic loss at chromosome19p13.3 in sporadic colorectal cancer. Gut 47:272–276.
Tsai CN, Tsai CL, Tse KP, Chang HY, Chang YS, 2002.The Epstein-Barr virus oncogene product, latentmembrane protein 1, induces the downregulation ofE-cadherin gene expression via activation of DNAmethyltransferases. Proc Natl Acad Sci 99:10084–10089.
Wagner KJ, Cooper WN, Grundy RG, Caldwell G,Jones C, Wadey RB, et al. 2002. Frequent RASSF1Atumour suppressor gene promoter methylation inWilms’ tumour and colorectal cancer. Oncogene 21:7277–7282.
Weisenberger DJ, Siegmund KD, Campan M, Young J,Long TI, Faasse MA, et al. 2006. CpG islandmethylator phenotype underlies sporadicmicrosatellite instability and is tightly associatedwith BRAF mutation in colorectal cancer. NatGenet 38: 787–793.
Wong JL, Hawkins NJ, Ward RL, 2007. Colorectalcancer: a model for epigenetic tumorigenesis. Gut56: 140–148.
Yamashita K, Dai T, Dai Y, Yamamoto F, Perucho M,2003. Genetics supersedes epigenetics in colon can-cer phenotype. Cancer Cell 4: 121–131.
Yamashita K, Lui Park HL, Sook Kim MS, Osada M,Tokumaru Y, Inoue H, et al. 2005. PGP9.5methylation in diffuse-type gastric cancer. CancerRes 65: 4963–4968.
Yanagawa N, Tamura G, Honda T, Endoh M,Nishizuka S, Motoyama T, 2004. Demethylation ofthe Synuclein-gamma Gene CpG island in primarygastric cancers and gastric cancer cell lines. ClinCancer Res 10: 2447–2451.
Young J, Jenkins M, Parry S, Young B, Nancarrow D,English D, et al. 2007. Serrated pathway colorectalcancer in the population: genetic consideration.Gut 56: 1453–1459.
10 P. Karpiñski et al.




















