



































A Practical Study of Malaria - Forgotten Books
509
-
Upload
khangminh22 -
Category
Documents
-
view
2 -
download
0
Transcript of A Practical Study of Malaria - Forgotten Books



PREFACE
WHILE there is a number o f good books on malaria,I be
lieve there is a place for a work written by one engaged entirely
in private practice largely in country districts , in the home of the“
severer forms of the disease.
I n the endeavor to make the work as practical as possible “
especial attention has been devoted to that mystic paramalarial.syndrome
, hemoglobinuric fever, and to the d iagnosis and “
treat
ment of malaria. Prophylaxis has been considered in the lightofRbss ’ epoch—mak ing d iscovery .
The'
p arthenogenetic cycle of the parasite , Whose significancewas first recognized by “
S zchaudinn ,and which affords the on ly
rational exp lanation of”latency and relapse , is described for the
first time , perhaps , in our language.
While I have not hesitated to draw from the literature for the“illustration of practical points, due cred it is given in the reference
portion . I am especially indebted to the works of Ew ing, D ock,
Barker, M archiafava a nd Bignami , and Kelsch and K iener forpathologic data.
I am grateful tomy Wife for copying the manuscrip t and for
assistance in “
reading the p-
r-Oof, to M r. W. C .
“
Seckler for the
photographic work , and to the'
w. B . Saunders ‘
Co. for cou’
rtes -ies
throughout the Publication of the book .
W.
’ H. D .
M ARI AN'
NA,ARK ANSAS , O ctober, 1909.

CHAPTER I I
D issemination of M alaria by M osquitoes
T -
jh'
e Malaria- bearing M osquitoes
Classification of the M osquitoes of North and M iddle AmericaThe Parasites of M al-aria
PathogenesisEtiology of Perni-cions Malaria
CHAPTER iv
Chronic Malaria
S ompilistat ion'
s and S equel'
ae,
Diagnosis of‘
Perni‘
ciou'
s Mai-aria

14 cofimNrs
CHARTERfor th e D estruction of M osquitoes
Toward the D estn iction of Parasites
to Prevent the Access of M osquitoes
of
CHAPTER IX
TREATMENT


A PRACTICAL
CHAPTER. 1
A CERTAIN dusky tropical queen was wont to say that she
d id not'
fear the'
invasion of the White man ,for she had two
mighty gene rals , The Fever and The Forest .Malaria has been one o f civ i lizat ion ’
3 greatest foe-s both int ime of war and in peace . Where shot and she l l have . s laintheir thousands , malaria has . slain its tens of thousandsM alaria I S the Chieftain of the army of d isease . EvenNapo
leon acknow ledged its suprema'
cy When he Wrote his min istero f war on the occas ion of the d isastrous Englishexped it ion : We are rejo iced to see that the English themselves are in the morasses of Zealand. L et them be kept onlyin check , and the bad air and f evers pecul iar to the climate w ills oon destroy the ir army . I t 13 said that the French crowed
over the expedit ion ‘ ‘
w ith the fOrce of reason, the bitternessof sarcasm , and the playfulness of How accuratelyNapo leon ’
s pred ict ion Was verified is wel l known .
I n the tropics the man Who works the soi l digs his Qwn
grave. Gigant ic commercial enterprises have been undertakenand then abandoned onaccount
—o i the havocWrought by thisscourge . O nly recently has it been r ecogniz ed that the m-
edicalman must precede and prepare the way
- for the eng ineer and
the laborer.
But Warring and canal;digging are not the on ly stages uponthe malarial tragedy is ? enacted . Withinthe fam ily , at2 17
18 THE STUD Y or MALARI A
home , the d isease appears in a“
varied succession .of forms ,
rap idly fatal , or s low ly sapping the v itality ,influencing the
birth-.rateg longevity , and even the intelligence and moral ity
of entire countries .
I n highly malarial reg ions , as the mortal ity increases thenatal ity d imin ishes on account Of abort ions and steri l ity ,
Pre
mature-
seni lity is frequent and advanced age is not so com
monly attained .
M alaria, leav ing its subjects anemic and neurotic, is respon
sible for inertia, loss of w ill power, intemperance , and generalmental and moral degradation. Jones , who - maintains thatmalaria was a potent factor in the decl ine o f Greece and Rome ,
concludes that “
malaria made the Greek weak and inefficient ;it turned. the sturdy Roman into a bloodthirsty brute.
”.Mon
falcon attributes abort ion , in fant ici'
de , un iversal l ibert in ism ,
drunkenness , want of relig ion , gross superst ition , assassinat ion ,
and other crimes to the d irect influence o f malaria.
M alaria costs the South incalculable wealth. Besides lossthroug h unti lled acres , d imin ished earning capacity ,
loss of
t ime , and death, it produces in its v ict ims a d isincl inat ion forwork whose influence cannot be estimated in money . A con
servative computat ion of the loss to the S outhern S tates
through malaria is fifty millions o f dollars annually.
The importance to the world at large of the subj ect of
malaria is ev idenced by the fact that two of the seven Nobelprizes in med icine wh ich have been awarded have been grantedfor d iscoveries“ in malaria—to Ross in 1902 , and to L averan
in 1907.
The history o f malaria may be traced to the age o f fable .
The story o f Hercules and the Hydra is a fami liar one . Thismonster dwelt in the morasses in the ne ighborhood o f the Lakeof L erna, where Hercules was d ispatched to destroy him. As
each of the n ine heads was struck off two new ones appeared .
With the aid of his faithful servant , I olaus , who burned eachwound caused by the removed head , the beast was final ly con
quered . Even be fore the birth of Christ t h is myth was con
strued to typi fy the reclamation of swamp lands , un inhabitable '
on account of the prevalence of malaria. Antipater wrote ,

INTROD UCTI ON
‘
Hercules , the greatest subduer of the foggy atmosphere int imes past , was placed among the ”gods for hav ing destroyedthe Hydra ; in other words, for hav ing reclaimed the marshy
desert. The s lay ing by Apollo of the Python which. arose
from the fert ile ground after - the recess ion of the flood is. s imilarly interpreted.
M ore than one thousand years be fore . the birth of Christmalarial d isease is mention-cd in the O rphic poems , and the
tert ian and quartan types are alluded to . I n the I liad of .
Homer-
and in the Wasps o'
f Aris tophanes al lus ions are made
to a fever which was probably malarial . Palud ism was probably introduced “ into
-
Greece fromEgypt. Accord ing to Groffthe word AAT , which is found among the inscriptions o f thetemple of D enderah, re ferred to a d isease , doubtless malan a,
which recurred every year at the same season .
”
Hippocrates d iv ided malarial fevers into cont inuous . and .
intermittent , which he subd ivided into quot id ian, tertlan , and
quartan . He recognized the et iolog ic influence of season , rains ,and stagnant water, and the dangers of malignancy , dropsy ,
and affect ions of the spleen . P lato descr ibes splen ic en largement , and other early Greek wi iters undoubtedly refer to
malaria.
Re ferences by Roman . writersl
to malaria are not numerous ,
the earliest be ing that o f Plautus , who “
d ied 184 B . c . Cato
speaks of black bile and swollen spleen , and C icero , Varro ,Celsus , ”
L ivy , and others show unm istakable ev idence .of a
know ledge of the d isease,Pass ing over the
“
deve lopment during the midd le ages”
of the
know ledge o f malaria, the names of M orton,L ancis i , Syden
ham, and Torti appear.M orton , gave accurate clin ic des.c
_
r1ptio-
ns of the pern icious and s imple intermittent fevers , and attributed them to
miasmat ic effl'
uv ia. He was an ardent advocate of cinchona,whose value was at that period being hot ly contested .
Sydenham ,172 3, accurately descrIbed the malarial fevers .
The interm ittent fevers. be div ided into spring and . autumn
fevers .
I
He justly concluded that the interm ittent and con
'
tinu‘
ous forms o i malaria were due to the same cause.
'
S y_den
20 THE STUD Y OF MALARI A
ham ably de fended cinchona, and, after cl in ic experimentsWithits
-
use , formulated use ful rules for its admin istrat ion .
L ancis i , 1717, stated the et iolog ic relat ionship betweenmarshy reg ions and malaria, and was the first to seek for a
microscop ic organ ism as the cause o f the d isease.
Tort i , 1753, w rote an exhaust ive treat ise upon the variousforms o f malaria. His class ificat ion of the pern icious forms
has become class ical . Numerous quotat ions from Torti’streat ise are to be found even in recent works upon malaria.
Varro , 1 18 - 29 B . c .,exp ressed the opin ion that malarial
fever was caused by an imals so minute that they could not be
seen by the naked eye , and wh ich enter the body w ith the air
through the nose and mouth. S imilar opinions were held byColumella, Palladius , and Vitruv ius . Rasor1 I S quoted as say
ing,“
For many years I have held the opin ion that the intermittent fevers are produced by paras ites , which renew the
paroxysm by the act o f the ir reproduct ion , wh ich occurs more
or less rapid ly accord ing to the variety o f the ir species .
”L e
D iberder, 1869 , maintained that the fever was due to the
presence in the bloodl
of an imalswhich preyed upon the blood ,and that the paroxysms depended upon reproduct ive acts
'
be
tween which apyrexia occurred.
M itchel , 1849 , claimed to have found in the sputa of malarial subjects fungous spores in great numbers , which he believed to have been insp ired w ith marsh air and to have causedthe d isease .
S alisbury , 1866, announced the d iscovery in the urine and
sweat of malarial pat ients of a species of alga, palmella,com
mon on the marshy reg ions along the O hio and M iss iss ippiRivers which he alleged to be the causat ive element.
Untll the true paras ite o f malaria was d iscovered the mostw idely accepted paras it ic theory w as that proposed in 1879
by Klebs and Tommasi Crudel i . These invest igators foundconstantly present in the mud of the Roman marshes a shortbaci llus . They were able to cultivate it upon fish gelatine , andwhen injected into rabbits produced a fever s imilar to malaria.
They named it the bacillus malaria.
The malarial paras ites were undoubtedly seen and described


THE STUD Y OF MALARIA
il several years later ;'
now it has - been confirmed the worldr. Among Americans who first corroborated L averan
’
s
vs may be ment ioned S ternberg , Councilman and Abbott ,er , James , D ock , Thayer and Hew etson, Barker, WoldertWelch .he d iscoveries of Golg i in 1885 were of great importance1 re ference to the l ife history oft he paras ite . He was ableollow tert ian and quartan paras ites throughout the endogencycle of deve lopment , and showed that a close relat ionshipIted between certain phases of parasit icgrowth and certain(es of the paroxysm. O ther I talian invest igators provedsame for the estivo—autumnal paras ites .
1 vague suspicion that malaria andmosquitoes were in some
fin ite way Connected has been entertained in certain coun
s for a long period . A defin ite mosquito theory , however ,born in America. While re ference is somet imes made toaper on the
“
M osquital O rig in of M alarial D isease ,” s up
d to have been published by D r. John Craw ford i n the
timore O bserver, 1807, no such article has been . found ,
the re ference is probably erroneous .
n 1848 D r. Jos iah Nott , 2 of M obile , published a paper upon
ow fever,in which he maintained the d isseminat ion of that
:ase by insects , and suggested that malaria was spread by“
mosquito of the low lands .
”
.
‘
he most complete theory was proposed by K ing3 in 1883.
“
v iew s are supported by n ineteen arguments , most of whichincontestable at the present day .
“
hat mosquitoes are agents in the spread of malaria was
anced by Koch in 1884 , by L averan in 1884 , by Fliigge in
1 , by M anson in 1894, and by BignamI m 1896.
lndertak ing the work at M anson’
s suggest ion , and afteraral years ( 1895 - 1898 ) of to il and d iscouragement , Ross
ved conclus ive ly that certain species of mosquitoes are con
1cd in the dissemination of malaria. The debt owed him
mankind was acknowledged by the g i ft of a Nobel prize ;own feel ings over the d iscovery are expressed in these l ines ,ch he wrote
F ig. 2 .—M ajor Ronald Ross , the “
d iscoverer of the role of the mosquito .


INTROD UCTI ON 2
This day relenI
t
I
ing GodHath placed w ithin my hand
A wondrous thing , and GodBe praised. At his command
S eeking His secret . deeds ,With tears and toiling breath,
I find thy cunning seeds,
O h million murdering death.
I know this little thingA
_
my riad men w ill save ;O h ,
death,where is thy sting ,
Thy victory , oh grave ?”
A d iscovery , secondary in importance only those.
L averan and of Ross, was made by M acCallum in 1898 , wh
demonstrated that the flage lla represent male sexual elements
analogous to spermatozoa.
HI STORY or HEMOGLOI
B'
INURI C FEVER
I t is probably un ique in historical pathology that a comple:of symptoms so striking as hemog lobinuric fever should hav‘
such an obscure h istory . As this obscurity is int imately asso
ciatedWith the etiology and symptomatology of the conditio z
an investigation of some o f the factors in its history I s no
w ithout interest . A fter a short statement Of the h istory 0
hemog lobinuric fever we w ill briefly cons ider how far it ha
been influenced by ( 1 ) its con fusion w ith bilious remitten
fever and yellow fever, ( 2 ) the introduct ion O f cinchona bar]and its alkalo ids into the treatment o f malaria, and (3) th
advent of Europeans into endem ic reg ions .
I n the years fr om 1850 to 1853 blackwater fever Was described by L ebeau,
D aul le, and L eroy de M ericourt , phys icianof the French navy , who Observed it in '
M adagascar , and espe
cially on the I sland of No ssi . Bé, off the northwest coast 0
the former island. They named the cond it ion "cleric pe-m ielou
fever. I n 186 1 cases Observed in the'
Antilles , Guiana, anc
Senegal were described by . Dutroul'
eau as hematum’
c‘
, blliou
fever.
I
I n the early s ixt iesI
Barthelemy - Benoit also describehematum
’
cbilious fever, and in 1874 appeared the monograpl
O i Berenger- Ferand on melamm'
c bilious, fever. This write

24 THE STUD Y DE - MALARI A
states that the d isease has ex isted inH
Goree s ince 1845 , and inS t; L ouis , in S enegal , accord ing to the h osp ital records - of thatc1ty , at least s ince 182 0 ,
shortly after the settling of the Euro
peans there . The first twenty - three settlers at Gabun , in.
1843,
were attacked w ith blackwater fever and almost all o f them
d ied . A great increase in frequency has occurred S ince 1850
Crosse“ believes his own case , in 1888, to be the first on
record in the Niger Territories , though he states that thed isease was said by O ld coasters to have ex isted in the Niger.D elta since 1882 . F . F lehn 5 does not bel ieve the d isease to
be O f recent introduct ion into West A frica, but attributes its
comparat ive ly late recognition'
to two facts—first,that the
suscept ible populat ion , who formerly l ived as traders 011 ah
chored hulks , began to take up the ir abode on the shore ;second, that the d isease was formerly con founded w ith yel lowfever. I t has been known in S enegambia s ince and in
the D utch East I nd ies s ince the Atj eh War, 1874 Cal
mette saw a number of cases in Gabun in 1886 - 87, and Fluit
in S an Juan del S ur , has seen numerous cases s ince 1850 .
The: cond it ion was n ot described in I nd ia unti l 1855, - and
S ambon9 regards this as conclus ive o f its recent introduction ,
as“
it'
would be absurd to think that it could have escaped the
attention of such men as Annesley , Chevers , Carter , M artin ,
Fayrer, M orehead , and M aclean had they .met w ith it .D r. Elliotson ,
10 in 1832 , mentioned a case of ague aecom
panied by a d ischarge of bloody urine during t'
l1eI
cold stage .
Todd ,” in 1849 , asserted that“
a state
I
of general cachex ia,such as O ften occurs in scurvy , may bring on hematuria, or
such as results from an aguish state brought on by the malariao f marshy d istrict s .
”
I n the Un ited S tates hemog lobinuric fever was first described by D r. J . C . Cummings , “ o f M onroe
,L ouI S I ana, in
1859 . He reported 6 cases,and refers to numerous cases
during the prev ious season . Faget12treated the d isease as
early as 1859 ,_
and states that cases w ith hematuria and
hematemes is had frequently been seen in New O rleans and
been mistaken for yellow fever. I nasmuch as Faget consid
ered hematemesis a common symptom of hemog lobinuric fever ,
INTRODUCTI ON 25
it“
is possible that he himsel f con founded the two d iseases insome instances. I n 1867
'
D r. T . C . O sborn ,
13of Greensboro
Ala. , observed I O cases ,_ 5 of wh ich ended fatally , some w ith
anuria Iand uremia. All“
the pat ients had been repeated ly at
tacked w ith malaria. A few months later his son , D r. J . D .
O sborn ,
14read a
’
paper before the Greensboro'
M ed ical S ociety ,
from wh ich it is ev ident that the disease was becom ing more
prevalent , and that the country people were regard ing it as
yellow fever. D r. H. C . Gl1ent,1 5 -o i Port Sul livan ,Texas , in
1866 reported hemog lobinuric fever endem ic in parts of Texas .
I n M arch,1869 , D r. R. F . M ichel , of M ontgomery , Ala. , read
a paper before the M ed ical Association of the S tate of A labama
in which he spoke of the d isease as“
a malignant malarialfever, follow ing repeated attacks O f interm ittent , characterizedby intense nausea and vom it ing , v ery rap id and Complete j aund iced cond it ion O i the surface as w e ll as most o f the internalorgans o f the body, an impacted gall - bladder , and hemorrhagesfrom the kidneys . These phenomena presented themselves inan almos t un interrupted l ink, attended by remiss ions and exac
erbations. I t is a fever peculiar to the Un ited S tates. He
recorded the morbid anatomy . ih , one o f his fatal cases . I n
Arkansas hemog lobinuric fever -was first recorded“
by D r. E.
R. D uval l , of Fort Smith, in a paper“
read be fore the S tate
S ociety in 1871 . He,bel ieved the case he recorded to be the
first to occur in the S tate. This paper is said to be a modelof accurate cl inic Observat ion . I n 1880 D r; G . B . M alone , inM onroe County , A I kansas reported I 55 cas es met inhis prae
t ice. The affect ion was first reported in Georg ia by D r. W.
A . Greene , of Americus , in 1872 , and in North Carol ina byD r. Norcom
,of Edenton ,
in 1874. Norcom asse ts that the
d isease did not , as Some claimed , make its first appearance a
few years ago, but that it had long been recogn ized . D r.
M cD aniel,10
of Camden ,A labama, described hemoglobinuric
fever in 1874 , and says , I n calling up my own remimscences ,
I am sure that I have occas ionally ever s ince my boyhood seen
isolated cases of what was cons idered intense bilious fever w iththe surfaces and under t issues stained deeply yellow and w iththe urine deep red. They were nearly all fatal , and w ere

26 THE STUD Y OF M
I
ALARI A
called in older phrase bilious '
congeStive , and in more recent
“
pern icious bilious .
”I have also, but more rarely , known
groups of 31m ilar cases associated,say 3 or 4 cases occurring
on the‘
same premises or in the same fam ily , about the same
t ime. All such cases , in add it ion - to the deep so—called bil iousco lor and the red urine , had jact itat ion ,
suspirous breathing ,
inordinate thirst , and vom iting of various shaded and t intedso - called bilious matters . By d il igent ly inquiring I have ascer
tained that very many O ld phys icians , some of whom havenow ret ired from pract ice , are sat isfied that theyhave observeds imi lar cases , sometimes s ingly and somet imes in groups.
_
The late - lamented D r. A . G. M abry , in a report O f a . case
of intermitt ing icterode hematuric fever made to this associat ion in 1870 , says ,
“
I t‘ is a mistake to suppose that this is a
new form of d isease. M ore than tw enty- five years ago I
treated ,in the v icin ity of S elma, cases of intermitt ing fever
present ing In a marked degree all the symptoms characterist icof these cases at the present day .
”
- The acrimon ious dispute of the earl iest writers on the sub;
j ect of What constituted the coloring matter of the urine isparal lelled only by that occurring later concern ing quin ine inthe treatment . Wh ile D aul le and B -e
'
reng er—Féraud stoutly
maintained that the dark color was due to the presence of bilein the urine , D utrouleau, Pellarin ,
Barthelemy - Benoit , Anto
niades , and Corre ascribed it to blood . I t is remarkable thatnone of the first American w riters attributed the color of
the urine to bile , but cons idered it due to blood . Corre ( 188 1 )and Karamitsas ( 1882 ) proved that the process was a hemo
globinuria instead o f a hematuria.
The cred it of first d irect ing attent ion to the et iolog ic relat ion between quin ine and hemog lobinuric fever is generallycred ited to Tomasell i , who published his first observat ions in1874 , but this is an error. At a
“
meet ing of the Greek M edicalS ociety , November 6 , I 858 Veretas
l '5reported that the majo i
ity of phys icians pract ising in the marshy reg ions of Greecehad not iced hematuria follow ing the admin istrat ion of quin ine .
He adds ,“Among these observers my father has a place , hav
ing attent ively Observed this action of the medicament not

28 THE STUDY OF MALARI A
m ittent fever , s ince formerly bile and malaria w ere pract icallysynonymous .
I t has been mentioned that the first re l iable records o f the
ex istence of hemog lobinuric fever were , accord ing to Be’
renger
Ferand, those of the hospital of S t. L ouis in S enegal , whereit is shown to have ex isted as early as 1820. I t is a singularcoincidence that this city afforded , in 1778 , the first epidem icof yellow fever occurring in Africa.
1 8L ater Plehn
5
gave as
one of his reasonsI
foI
r be l iev ing that hemog lobinuric fever wasnot a new d isease in West A frica,
that it had formerly beenm istaken for ye llow fever. Bes ides S enegal , two of the otherreg ions where hemog lobinuric fev er was first seen , the West
I ndies and Guiana, were yel low - fever foci. I nI
the Un itedS tates we have the early statement of D r. J. D . O sborne thatthe cond it ion was then regarded as yellow fever.
The s imi larity of the symptoms and the relat ive immun ityof the black race to both d iseases render the m istake s omewhatexcusable. As recently as 1897
‘ Below448 maintained the ident ity of yel low fever and blackwater fever.
2 . Cinchona bark was introduced into Europe in 1640 by
the Countess del Cinchon , w i fe o f the v ice - regent of Peru,in
whose honor it has rece ived its name. The efficacy o f the barkin malaria was first known to the I nd ians in the reg ion of
L oxa,in the southern port ion of Ecuador. The Correg idor
of L oxa, hearing of the severe i llness o f the countess w ithtert ian fever at L ima,
in 1638 , adv ised her physician , de Vega,
to g ive the bark a trial , wh ich effected a prompt cure , and inthose days was regarded as nothing short of miraculous .
When the ‘
countess returned to Spain she took a supply Of thebark w ith her. Here it seems first to have been employedchiefly by the Jesuits , who introduced it into Rome in 1649 .
I t was then known as countess’
powder, or Jesuits ’ powder.
I ts use was antagon ized by other relig ious denominat ions and
by the med ical pro fession . Bark was imported into Eng landin 1671 by S ir Robert Talbot , an Engl ish quack , who kept theremedy a secret and sold it for one hundred louis d ’
or per
pound . L ouis XI V , who was attacked w ith a rebell ious and
severe intermittent in the year 1679 , was cured by Talbot w ith
I NTROD UCTI ON 29
a concentrated v inous t incture of the bark , “
purchased and
made public the secret remedy , for wh ich he paid and
a l i fe annuity of £2000.
I n I nd ia the remedy was employed by Bogue20 as early as
1657. I n these t imes in S pan ish - America, where the bark wasind igenous , extraord inary methods w ere employed to preventthe nature of the drug becom ing recogn ized. But during the
eighteenth century cinchona bark was almost universal lyknown . L ind is said to have employed in L ower S enegal ,during 1765 , over 140 pounds of the bark. I n .1714 Ramazzin i“ wrote that should a fever pat ient die it was cons idered a
crime not to have employed cinchona. I n fact , so w idespreadwas the
I
use of large - doses of bark that CalmeneroCasat i D aval Ramaz z ini and others
w rote vehemently against the abuse of the drug .
Pel let ier and Caventou, in 1820 ,succeeded in isolat ing
quin ine from the bark .The inst itut ion of cinchona plantations in Java in 1854 and
in Cey lon in 1859 caused a drop in the price of quin ine , whichhad formerly sold for its actual we ight in gold , to‘
one - twenti
eth the orig inal price.
M archiafava and Bignami seek to explain the seeming lateappearance of hemog lobinuric fever by the use of quininebecoming prevalent at the t ime when the d isease was firstdescribed. I t is probable that this factor has caused an increasein certain localit ies , but a comparison of the history of the
d isease w ith that of the drug show s no very intimate chronolog ic relat ions. Further, blackwater fever i s on the decrease
in some reg ions Where the use of quinine is becoming moregeneral . This is reported to be the case in German East A fricaby M e ixner,” in Cameroon by Ziemann ,
23 in Togo by A .
Plehn ,
24and
' by K ohlbrugge" in '
the M alay A rchipe lago. The
large number of cases occurring w ithout the prev ious use of
quinine should also be cons idered .
3. A cons ideration of the importance , in the history of
hemoglobinuric fever, of the immigration of Europeans intoreg ions where the condition is endemic involves the historyof the tropics and subtropics. Th is factor is man i festly an

30 THE STUD Y OF MALARI A
essential in countries where the nat ives are nearly immune , asin parts of A frica. Historic events , which were p robablypotent in the development of blackwater fever, were the discovery Of America, the Portuguese d iscover ies and settlementson the coast o f A frica, the A frican s lave trade and the laterefforts to abolish the same, the advent to A frica of miss ionaries and explorers , especially in the early part of the n ineteenth century , and the operations of the East Ind ia Company .
The access ion of Europeans was influent ial_
in the historyof hemog lobinuric fever in several ways—by the increase of
suscept ible populat ion , by the importat ion of quin ine , and by
the advent of physicians competent to recogn ize and to describethe d isease
CHAPTER I I
North America —I n the Un ited S tates it is chiefly the
southeasternI
portion inwhich malaria ismost prevalent . A longthe Atlantic coast, south of New Y ork and especial ly the lowlands of M aryland and
.
o f Virgin ia, and in the Carol inasGeorg ia, and Florida the
I
disease occurs frequently . Along theGul f coast and up the M iss issipp i River and its tributariesmalaria is Widely prevalent. The port ions of the S tates
‘ ly ingalong theAppalachian Range are almos t exempt , but the . dis
ease'
appears as the M ississ ippi River and the Atlant ic’
coast
upon e ither s ide are approached . West o f the'
M iss issipp'i ,Arkansas , L ouis iana, and Texas present the most numerous
foci of malaria. I n port ions o f Pennsylvania and -New. York
autoch thonous cases are not in frequently Observed. 111 the
more‘
southern New Eng land S tates malaria is still encountered ,and in some places . is even increasmg I n frequency , I n the
neighborhood o f the Great L akes m’
alaria'
is very rare , except
ing , poss ibly , that o f lL ake Erie and of L ake M ich igan . I n
the Central S tates malaria has almost or quite d isappeared ,
except in certain low river valleys . A long the Pacific coast
the d isease is not So frequent as along the At lant ic. I n Wash
ington it occurs in the Puget S ound Bas in and the Co lumbiaRiver, Chehalis , and the Yakima valleys . I n O regon malariais found in the Columbia, Williamette , Rogue , and the Um
'
a
t ill'a val leys , and in Cal iforn ia in the S acramento S an Joaquin ,
Tulare , Kern , and S anta ClaraI
_
valleys . I n certain parts O f
New M ex ico malaria is occas ionally met w ith.Canada is free from pa lud ism except along the northern
shore of Lake O ntario .
I n Mex ico severe forms of malaria occur, particularly inthe low coast reg ions.
32 THE STUD Y OF MALARI A
M alaria abounds in Central America along theAtlant ic coastand to a less extent upon the Pacific s ide.
S outh Amer ica.-
.The eastern coast Of S outh America is
more intensely infested w ith malaria than is the western coast.
Venezuela ( in the val leys ) , Guiana, and the greater port ion of
Brazil are highly malarial . Port ions of Paraguay and of
Bo liv ia afford a great many cases , while the d isease is muchless prevalent in Uruguay and almost absent from theArgen
a
t ine Republic. O n the Pacific border the deep valleys o f Peru
and o f Ecuador are malar ial centers .
_
The ent ire is land o f Cuba I S malarial to a greater or lessextent , as is also Jamaica. O f the L esser Ant illes , S t. . V in
cent , Ant igua, and Barbadoes are relatively exempt .“
M alar iais said to be almost unknown in the Bermudas.
Europe—Great Britain ,
once infested , is now free fromendem ic malaria. I n G ermany the d isease occurs in frequentlyin the Rhine and D anube valleys and near the mouths of riversalong the coast. M alaria is met in
“
Hol land , chiefly upon the
island of Zeeland and in North and S outh HOlland. The
valley of the D anube , in Austria,affords a cons iderable num
ber Of cases . Thereare few reg ions in Hungary in which thed isease does not occur, but it is especial ly along the western
hal f o f the southern border that it is prevalent . Themarshesalong the west coast and in the south o f France g ive rise toa number o f cases o f malaria. I n Sp ain and Portugal malariaoccurs in the coast reg ions and in the larger river valleys. The
d isease is pract ically unknown in Norway , but is occas ionallyreported from Sw eden , as wel l as from certain of the islandso f D enmark . I n Russia it is in the southern port ion , particu
larly along the coasts and along the valleys of the rivers flowing southward , that malaria is encountered . Cases
'
are occa
sionally observed in the southwest of Sw itzerland . The por
t ions of Bulgaria most highly malarial are the D anube valley ,
the coast reg ion , and the southern part. A lmost the whole of
I taly is sorely afflicted w ith malaria, as are also S ici ly and
S ard in ia. Greece is the most severely scourged country of
Europe . I t is said that in the plains “O f Thessaly , Phthiotis ,

GEOGRAPHI C D I S TRI BUTI ON 33
ACarnania, Boeot ia, Elis ,’
M essen ia,Argos , and L aconia hard ly
a'
I
S ingle inhabitant escapes'
the d isease .
“
As ia n—As ia M inor, Arabia, and Pers ia present foci o f malaria, , both in the coast ne ighborhoods and in the interior lowlands. I n the swampy reg ions o f A fghanistan and Beloot iS
tan‘
I
malaria is'
common and Severe. I n I nd ia -
port ions of the
northwest prov inces and of the Bengal and Bombay Pres idencies are intensely malarial . The foothills of the Himalayas,the Duars , and Te rai are famous malarial seats. Both the
coast regiI
Ons and the interior h ighlands of Cey lon are endem icterritory . Burmah , S iam, the M alay Pen insula, and French
.I ndo - Ch ina are malarial in port ions of the ir extent , and parts
o f Chinaare intensely in fested . M alaria is found in Japan ,
Formosa, and the Philippines , and port ions o f the East I ndies
are among'
the most highly malarial reg ions of the w orld.
A fr ica—On the w est coast the territory ,between the
S enegal and the Congo Rivers , is headquarters for malaria o f
malignant type. Approaching S outh A fr ica the d isease d iminishes in frequency and in severity . On the east the reg ion
fromD elagoa Bay to Eritrea i s malarial . I n the interior o f
Central A frica,I
excepting the high e levat ions , malaria is w idespread . M alaria abounds in M adagascar except ing upon t henortheast coast and
I
the mountainous interior. Reunion and
M aurit ius are also malarial . I n Egy pt it is chiefly the reg ionoverflow ed by the Nile in which the d isease is most prevalent .M alaria abounds about the coasts and marsh-
es o f A lgeria.
I n Australiamalaria occurs from Cape York to Brisbane ,on the east coast , d im inishing toward the south. New Zealandis apparently free frOm r
malaria, and the S andw ich I slands andmost of the other Pacific islands are remarkably exempt .
The relat ive frequency of the forms‘
of malarial in fectionvaries greatly . I t may be stated as a general propos it ion that
the quartan is the rarest form,the tertian
I
is the form prevailing in temperate reg ions , and the est ivo - autumnal in Warm and
hot cl imates. There are reg ions , however, in which the quartanpredominates , as in certain portions o f I taly and of I nd ia;in other local it ies it is the on ly form O f malaria present , as
upon the island M erite , of the Bismarck Archipelago .
I

34 THE STUD Y OF .MALARIA ‘
The .following table ShowS the re lat ive frequency of the
types of malaria in variOus regions
Tertian . QuarLocality . Authority. tan .
Texas M oore 23 0
Georgia Curry26
34 0
Camp Wi‘koff Ew ing 74 0
New O rleans Charity Hospital Records 373 1
Baltimore Thayer and Hewetson”
. 338 5Panama Kendal
3°22 0
S t. Lucia Gray and Low 12 2
Panama Gorgas32
8I taly Koch
33
32 5I taly 202 15Greece Cardamatis and D ia
‘
messis 87 3Bulgaria M ollow
“
99 I 0
I taly I talian S tatisticsBritish M alaya Wright
“
78 56
British M alaya Watson"8
19 4Philippines Craig
”98 8
I ndia Hope"0
2 17 933Cyprus Williamson I 2 8East I ndie Koch
‘ z
57Philippines Chamberlain 55 3I ndia Rogers
“
71I ndia Buchanan
“
56 12
A ssam Bentley“
134 46Japan Tsuz uk i47
12
naTogo Ziemann“
I 7German East Africa . M e ixner
“
5 I
German East Africa Grothusen‘ 0
5 7S enegal Thiroux and cl
’
Anfreville”°
7 44German East A frica . Kudick e
M
3 2
German East Africa . Exner52
1 1 4German East Africa . O llwig
52
7 0
German East Africa . S chOrnich z I 2
I n fect ions w ith morethanone form of the parasite are not
uncommon. O f these a combination of the tert ian and the
est ivo- autumnal is the most frequent , the tert ian w ith the quartan be ing rare , and the three forms together very rare.
GEOGRAPHI C D I STRI BUTI ON OF HEMOGLOB INURI C FEVER
I n North Amer ica hemog lobinuric fever is found in the
S outhern S tates , especial ly parts of Texas , L ouis iana, Arkansas , M ississipp i , Tennessee , A labama, Georg ia, F lorida, NorthCarolina , S outh Carol ina , and Virg in ia. I t is prevalent inCentra l America, part icularly in Honduras , Nicaragua, and
Costa Rica. I t is found in the Greater Ant illes , but appears
to be rare in Hayt i . I n the L esser Anti lles it is more common

36 THE STUD YI
or MALAR I A
Thus it is seen t hat , while the “
peculiar geographic d istribut ion of hemog lobinuria is embraced by that of malaria,
it is
not coextenswe w ith the latter. And herethe relat ion ceases.
While all localit ies in which blackwater feverI
eXI StS endemi
cally are highly malarial , there are very extens ive reg ions inwhich the severest forms of trop ical malaria are rampant
where hemog lobinuric fever i s unknown .
I t has been attempted to'
explain the d istribut ion by say ingthat the frequency of hemog lobinuria in a g iven locality is In
d irect rat io to the endem ic index of that lOcalityI—that is, the
percentage of nat ive- born children whose b lood harbors malarial parasiteS—but this explanation also presents d ifficult ies,as the d isease is not present in all local it ies whose endemicindex is high.We llman
5'6 maintains a close relat ionship between the geo
graphical d istribut ion - of M y z omyia fuaes la in Angola and
that o f blackwater fever. D an ie ls 5 7 bel ieves that i f the d iseaseis due to one or all o f several variet ies -
of mosquitoesWhich hement ions , IV .
‘
funes t-as must be one of those impl icated. F .
Plehn5 8 suggested a poss ible relat ion betweenthe geographicrange of hemog lobinuric fever and that of certain mosquitoes.I n certain local it ie s the d isease seems to be on the increase .
Crosse“says that it is increas ing in certain parts . of West
A frica. M anson5 9
re fers to the belief ’
o f competent observersthat it is yearly
'
becoming more common in A frica. Johnson”and F . Plehn
6 1assert that it is undoubted ly becoming
I
more
prevalent 011 the w est coast of A frica,and A . Plehn
6 2 bel ievesthat it is increas ing in frequency in New Guinea. The inhabi
tants of the reg ion o f Jalpaiguri , in I nd ia are recently saidto be alarmed at its increase in that sect ion.
On the other hand , there are places'
in which it is becomingless frequent . The med ical report from German East A fricafor t
I
he'
year 1903- 04 Show s a decrease from the preceding
year. The Ireport from D uala show s a steady annual decreasefrom 190 1 to 1904 inclusive .
49I
K. ohlbru-
gge7
I
declares that itis becoming rarer . in the M alayArchipelago . A . Plehn
,
“after
mention ing the decrease in certain sect ions of West Africa,
prophesied that in hal f a century this scourge of tropical A frica

GEOGRAPHI C D I STRI BUTI ON 37
would become i f not a hi storic remin iscence , at least an insignificant rarity . I t is probably becoming less frequent in some
O f '
the S outhern S tatesEpidemics of hemoglobinuric fever have been described .
M aster’
man“stat-es that in 1893 there was
'
a regular epidemico f malaria in and around Jaffa, and among the fatal casesWere a g i eat many of hemog lobinuria. S ays Plehn ,
“1 “
Not
in frequently the d isease appears in ep idemic form“
, as was
the case several years ago in Goree , Quittah , and Bonny ”
S ambon9 ment ions S everal epidem ics , as follows .
“
Thed iseasebroke out among the laborers employed in making the canalthrough the I sthmus o f Corinth ;it attacked the Chinese laborers on the Congo Railway ; and in 1885 , accord ing to D r.
Wenyon , of Fatshan , China,it ravaged , l ike a plague, the
Chinese army on the Tonquin border of Kwangs i . I n colleet ive dwell ings—such as barracks , hOSpitals , schools—it may
attack several persons at the same t ime. I n 1885 it broke out
in a prison in Castiades ,‘ S ard inia, at tacking 24 out of 800
conv icts .
”
CHAPTER I I I
.E
I
T I O LOGY
D EPEND II
NG as it does for its ex istence upon the l i fe historiesof three species o f an imals , malaria is of rather complexet iology . While w ithin the blood of man the parasite is notsubj ect tog reat variations
I
o f env ironment , no matter what the
season or the lat itude , nevertl1eless exposure to cold , wet
or heat , d ietary or other excesses , w i ll have the effect o f awakening latent malaria.
But it is the influence o f externalI factors upon the l i fe his
tory of the mosquito . that determ ine -
s the greatest variat ions inthe prevalence o f malaria accord ing to Climate , season , tem
perature , rain fal l , alt itude , etc.
Climate—I t may be said , as. a general rule, that the frequeney and v irulence o f malaria increase as w e approach theequator. The condit ions of warmth and moisture are more
prop it ious for the development Of parasites w ithin the bod iesof mosquitoes in trop ic than I n co lder Climates ; this is espe
cially true of the est ivo - autumnal form o f the malarial paras ite.
Exposure to the heat o f the trop ical sun pred isposes to the
cerebral forms of pernicious malaria, and undue exposure to
the sun’
s rays i s o fttimes sufficient to st imulate sporulat ionof the paras ites of latent malaria.
With respect to latitude Hirsch . reached the follow ing con
clusions as to the northern boundary o fmalaria in the northern
hemisphere. The l ine starts from 5 5°
N. on the western s ideo f North America, s inks to 45
°
on its eastern S ide, r ises to63
°
or 64°
on the western s ide of the o ld world ( Sweden and
F inland ) , and runs across Northern Asia in about the lat itudeof 5
L ong be fore the d iscovery of the rOle of the mo squito inmalaria it was known that the disease was not endemic “
unlessthe summer temperature maintained a certain average. Dur
ing the middle of the last century D rake” assumed that an
38
ETI OLOGY 39
average summer tempe1ature of s ixty degrees is necessai y to
the ex istence of malaria, and that it w i ll not prevail as an
epidemicw here the average tempe1ature falls below s ixty - five
also,that the fever w ill occur in Winter at all places wh ere that
season has a mean temperature of Sixty degrees or upward .
Hirsch maintained that the summer isobar of 59°
- oo.8°
F .
marks the limit of the occurrence of malarial fever, and thatthose reg ions where the mean summer temperature does not
reach that height are exempt from the d isease. Curiouslyenough, it “
has been recently repeatedly demonstrated that thisis the lowest temperature at which the paras ite w ill developin the body of the mosquito.
S eason .—VVhile relapses may occur at any season , and in
certain trop ic reg ions fresh infect ions may occur during any
period of the year, in all temperate and most tropic reg ionsthere are seasons during which the d isease is especially prevalent . This is common ly known as the malarial s eason
,and
varies accord ing to lat itude , temperature , rainfal l , so il , etc.
The season of primary attacks depends ent irely upon the
l i fe history o f the malaria- bearing mosquitoes . This season
usually beg ins a few w eeks after the first brood of anophel inesappears , which i s at the height of - summer
,and cont inues, in
temperate cl imates ,'
unti l after the nights b ecome cool . I n
each ind iv idual locality the beg inn ing of the season is rather
definite , the d isease recurring at a certam period each yearw ith more or less exact itude. I n most of the reg ions of the
S outhern S tates the malarial season beg ins in the earlier hal fof July . I n the lat itude of Balt imore the most notable increasein cases beg ins during August. The malarial season in Cal iformia is fromA ugust to O ctober.
The follow ing seasonal d istribut ion of malaria in Panama
is compiled from the“
Reports of the D epartment of S an itat ion of the I sthmian Canal Comm ission , and is the aggregate
of the three years , 1906- 1908 :
January JulyFebruary August
M arch S eptemberApril O ctober
NovemberJune D ecember

40 THE STUD Y OF MALARI A
I n I taly a large number of cases from various sources
are d istributed as fol low s :
‘
JanuaryFebruaryAdarch
April
M ayJuneI n Guiana the season o f greatest prevalence is said to be
from O ctober to D ecember 1nclusive ;in S t. Lucia, W. I ,from
January to M arch ; in Germany , from'
the end of July to the
m idd le of S eptember ;Holland , from the midd le of M ay to
m iddle of“
S eptember ; F rance , from“ July to November ;Bulgaria, M ay to O ctober I taly , from i
'
the end o f June to November ;Greece , from M ay to . November ; in Tonkin ,
from Apri lto November ; Calcutta, from O ctober to D ecember;Cyprus ,
Fig.- D iagram showing relation between rainfall and malaria (Plehn) .
M alaria morbidity .
Rainfall.~
Rainy days .
from July to O ctober ; S ingapore , April to July ; German.
New Guinea, from November to June ;Northern A frica, fromthe middle of June to November ;and in German East A frica,from Apri l to July .
Where both tert ian and est ivo - autumnal malaria are endem icthe malarial season is usually ushered in by cases of the for
mer, the estivo - autumnal variety appearing at the height of
ETI OLOGY 41
the season . The pern1c10us forms o f malaria occur with greatest frequence at the he ight of est ivo - autumnal prevalence . I n
I taly quartan malaria beg ins late in the summer and continueslate in the fall. I n America. this variety is too in frequent tojust i fy any defin ite conclus ions . M ixed and mult iple infect ions occur more frequently late in the season than early .
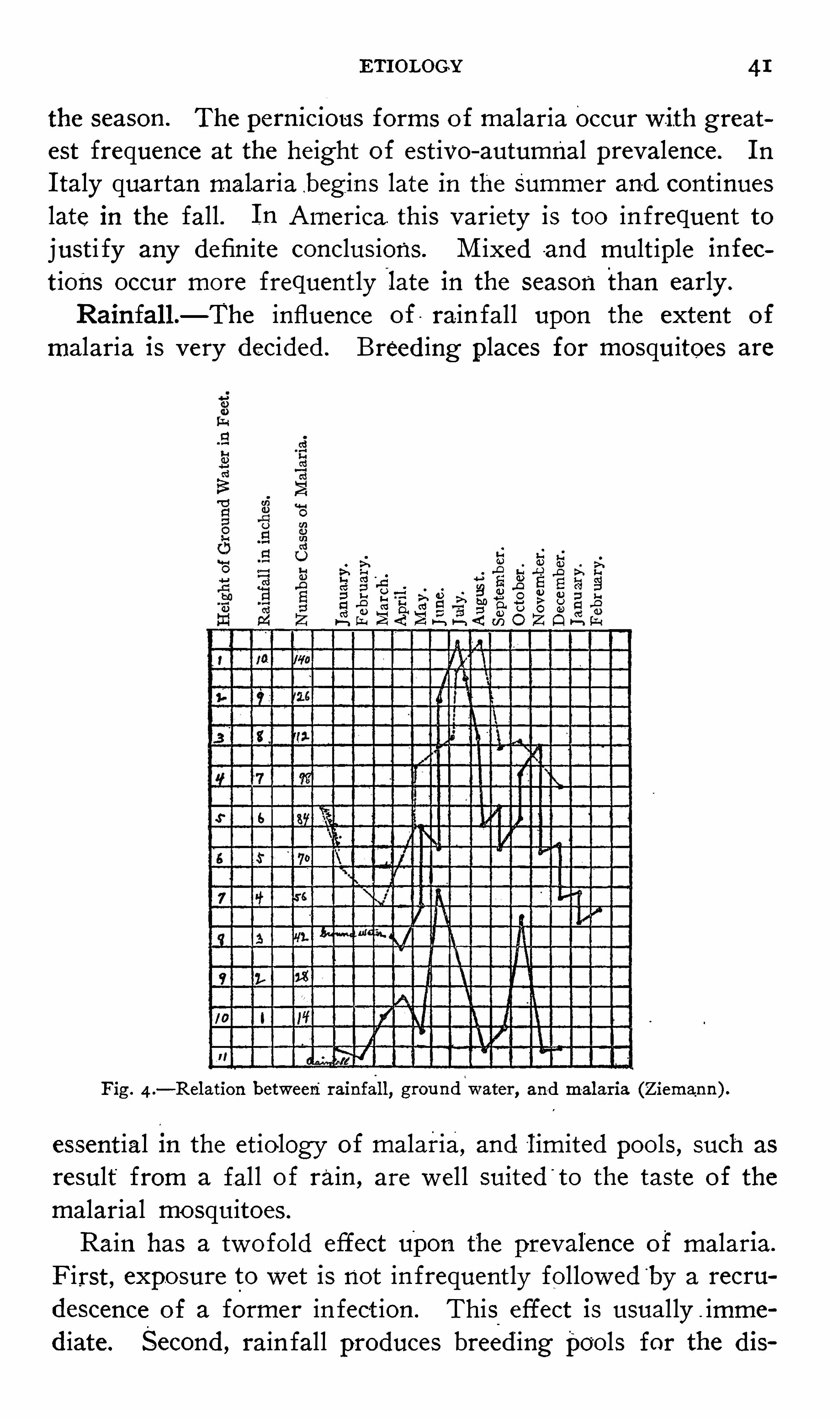
Rainfall.—The influence of rain fal l upon the extent of
malaria is very decided . Breed ing places for mosquitoes are
23>\ H
. Q ui dW
.0 rd :a u gm k o
a fi ak a a b m a
fl > ° a fld o b
Fig . 4 .—Relation between rainfall
, groundwater, and malaria (Ziemann ) .
essent ial in the etio logy of malaria, and lim ited pools , such as
result from a fal l of rain , are wel l suited '
to the taste of the
malarial mo squitoes .
Rain has a twofold effect upon the prevalence of malar1a.
F irst , exposure to wet is not in frequently followed“
by a recru
descence of a former in fect ion . This effect is usual ly imme
d iate. S econd , rain fall produces breed ing pools for the dis

THE STUDY or MALARIAnators
“
of malaria. The“
effect of fresh breeding) t shown immed iately . Allowmg tw enty days i
tic stages of the mosquito , ten days for the-mosquit
re paras ite , and a l ike period for the incubat ive si
.i t would be , obv ious ly , several w eeks be fore an i1
talaria could be expected from such a source.
exempl ified in the trop1es , where so_
much depend’all. Here the height of the malaria curve is a
rd the end of the rainy season or shortly'
after .
heavy rainfall in the spring and early summer he
zhe reputat ion of be ing favorable to the spread of n
h i le rainfall is essent ial to the deve lopment of n
cessive it may have the oppos ite effect by scouring)oo1s and d estroy ing the contamed ova and young
tuito. M oderate rains at short intervals are more 1) f breed ingpools than heavy downpours at long inie
,
"
the number of rainy days , as w ell as the actual 1shes
,is a factor in the et iology of malaria.
very low countries rainy years may be healthyis said tobethe case in the Netherlands .
6 6
W and a high atmospheric moisture w ere formerlyw ith being factors in the cause of malaria. .Ti
tless on account of the w ell - recogn ized dangering malaria between sunset and sunrise . O ther 11dex o f ground
- mo isture it is d oubt ful whetheric mo isture bears any relat ion to primary infectior
ria.
li1.—The chem ical compos it ion of the so i l has ar.
the re ign of malaria only so far as the relat ionto the retent ion of water is concernédfi M ore (5
the phys ical con format ion than upon the geolog i‘istics of the so il . As a _rule , clay soils retain mr than the sandy , though there are exceptions.
ms are less apt to harbor breed ing pools because 0
1age, but pools upon a rock- bed are very persistentmust be of such a character as to retain surfacez iently long for the aquat ic stages of mosquito lifi)leted . .
44 THE STUD Y OF MALARI A
abounds in Swamps , from wh ich ev en t he san i
are not entire ly free . This cont inues to be
t ill we reach the flanks of the Cumberland Meast and those of the O zark Hills to the w est .
theM iss issippi to themouth of the M issouri wfloods leav ing small lakes , ponds , swamps, and
in the “
aggregate are o f great extent. and but I
or dried up before the next inundat ion . Nc
seen , the whole of this reg ion is infested w ithbeyond any other portion of the val ley .
-
“
I n North A labama, Tennessee , and K entutalmost unknown , except along the few r ivers v
bottom lands, most of wh ich , moreover,an
inundat ion . The r1vers , how ever, are s inuous ,Sluggish and pondy , and it is in the ir v icinautumnal fever prevails . I n the S tates of I I
and O hio the rivers general ly flow through w ico f wh ich are l iable to be overflowed . Smal l laswamps are also frequent in certain port ions 1
and it is precise ly these local it ies which are mo
the east of all the S tates ment ioned , as we c.
tains , the sur face '
water is nolonger found mstreams generally have a
-
rapid current , dov
rocky channels , and here autumnal fever ne z
or when -
present is confined to thevalley of s
stream. Everywhere w est of the S tates of Ark:
and I owa s ur face water is scarce, the decl iv iwhich stretches from the Rocky M ountains fav iwhi le the subjacent sand almost absorbs ev t
rivers . Thus , as we advance into that "
dese i
the same t ime to the l imits of the surface wa
umnal fever. I n the North there is no defl
whole country is essent ially lacustrine , and 1
lat itude the fever prevails .» Thus the shores o
and L ake Erie , w ith those o f the southern extn
and M ichigan , are in fested ,and suffer far mo
lands which surround them . But beyond thesshores of the two latter. lakes iand on those of

ETI OLOGY 45
the"
fever, as we have seen ,1s never epidemic, although water
is abundant ;and st ill further North , where small lakes and
their connect ing streams ex ist in countless numbers , the d iseaseI S unknown , show ing that , while water 1s essent ial to the production o f this fever, other causes must coope rate to g ive it
power.
”
Canals , dams,stock , and other
'
ponds , .railroad and levéeborrow pits and other co llect ions o f water, part icularly whenstagnant , o ften breed anophel ine larvae, hence favoring the
development of palud ism.
I t is generally believed that salt marshes are never malarious , and that anopheles larvae cannot develop in s eawater.
This is , however, not strict ly true . D eV ogel6 8has recently
shown that'
anopheles larvae may develop in sea—w ater evapo
rated to hal f its in it ial volume , and a number of other observers h ave found larvae in salt water. But marshes of1-
.pure
sea- water are not nearly so nox ious as those of brackish w ater,
a m ixture of salt and fresh water, wh ich are famous anopheles
breeders. I t appears that in some instances where salt water
I S 1n1m1cal to the development of the aquat ic stages of mos
quitoes they may gradually become accustomed to the env ironment.
Alt itude—M alaria is essential ly a d isease of the low lands ,high altitude being relat ively exempt. This is part ially ac
counted for by the better drainage of e levated alt itudes and
fewer pools in wh ich malarial mosquitoes may breed . The
lower temperature of high altitudes is also a factor in maintain ing a low malarial morbidity in these reg ions .
I t is known t‘
hat'
anopheline mosquitoes do not .fly to great
he ights . Hence sleeping in an upper story or in a bui ld ings ituated high above the ground g ives a measure of protect ionfrom malaria. Laborers employed in highly malarial sect ions ,and who s leep in the
'
surrounding hills , even of moderate alt itude , o
'ften rema in entirely free from in fect ion .
A few hundred feet in altitude may "
show a more markedd ifference in the prevalence of malaria than as many m i lesin lat itude.
The general'
rule that malaria is a d isease of low coun tries
THE STUD Y or MALARI A
le excepti 'ons . This is especially true in the tropics .
he d isease may be encountered at v ery high alt itudes .
be said that the alt itude at wh ich malaria may occur
1 inverse rat io to latitude.
ria has been found on L ake Nyssa at an alt itude o i
etres at Co lico ,metres ;in the Himalaya M oun
metres ;in the Andes , at metres ;at Blanfeet ;German East A frica, at metres ; at
11 Central A frica , at he ights of over . feet ; andof
’
the high -llying valleys of Syria, at altitudes of
etres.
of the cases in high alt itudes reported .as malaria mayakes in d iagnos is ; other cases may be malaria con
.n the low lands. Thus Tosari , at an e levat ion of
had been cited as a place where malaria prevai led w ithpresence of mosquitoes , and this was used -
“
as an argu
gainst the mosquito theory . Koch, 6 9 invest igat ingin 1899 , examined the blood of e ighty - two children ;was the paras ite of malaria detected. The only case
ria found was in a man who , twelve days before the1g of his i llness , had spent the night in a highly malae upon the coast.
malaria is endemic in certain places of high alt iiuch are Eritrea,
in alt itudes of metres ;Upper
at metres ;parts of Madagascar, at metres ;
Reun ion I sland , metres ; in Java, atand in the Phil ipp ines it is said that , while certainire almost free from malar ia, the hills in the v icin ityriously in fected.
70 Wright ,3 8 in Brit ish M alaya, found'
S larvae in pools at an elevat ion of feet ..quakes and volcamc erupt ions have been follow ed by
levelopment of malaria. Examples are _
cited of Rome
in Reggio in 1783, and Palermo in 1828 . R emarkances have occurred in Peru also. The most recent
on is that of Amboina,in the East I ndies , which had
55 been remarkably free from malaria. I n that yearearthquake occurred , and s ince then the malaria has1 both in extent and intensity.
18
ETI OLOGY 47
Such results can be explained on ly by an increase of stagnantwater fol low ing these
'
violent d isturbances , probably throughthe interrupt ion of the flow of ground
- water.
I nundat ions .—S ince very early t imes overflows have been
recogn ized as a prol ific cause of epidemics of malaria. Tacitus ,Suetonious , L ivy , D ionys ius , Cass io , and S trabo ment ion such
results from inundat ions of the Tiber. This stream experi
enced an overflow in 1695 , which was described by L ancis i .The water covered a broad area of country, fill ing d itches ,sewers , and canals . The fol lowing June, July , and August
w ere extremely hot . An epidem ic of malignant malarial feverensued and , spread ing far and w ide , occas ioned a great mor—f‘tality .
_
I n g iv ing a descript ion of a trip up the Tigris River, L indg ives the
“
follow ing account of a curious strategem-
z“
Here
we were in formed that the Arabs had broken down the -banksof the river near B assora, w ith a design to cover w ith water
the deserts in its neighborhood . This , it seems, is the usualmethod of revenge taken by the Arabs for any injury donethem by the Turks in Bassora,
and it was represented to us
as an act of the most shocking .barbarity ,s ince a general con
suming s ickness would undoubted ly be the consequence. Th iswas the case fifteen years be fore , when the Arabs , by demol
ishing . the banks of this river, laid the env irons of Bassoraunder water. The stagnat ing and putrid water in the adjacentcountry and the great quant ity of dead and corrupted fish at
that t ime ly ing upon the shore polluted the whole atmosphere
and produced a putrid and mortal fever. O f this fever between and o f the inhabitants d ied ;at the same
t ime not above two or three of the Europeans who w ere set
tled there escaped w ith life.
”
Ep idemics of malaria follow ing _ overflow s of - the Ni le ,Ganges , I ndus , Euphrates , Niger , S enegal , Volga,
D anube ,S aone , Rhone , L oire , M ississ ipp i , and other rivers have beendescribed .
The immediate effect ofa n inundat ion is to check the devel0pment of malaria. This is a result o f a destruct ive effect ofthe flood upon the breed ing pools
'
of mosquitoes. h is only

48 THE STUDY “
or MALAR I A
after the waters h ave subs ided and poo ls and marshes are
left that the epidemic deve lops .
“
T rees and V egetat ion .—I t was formerly bel ieved that ,
while decay ing vegetat ion was the caus e of malaria, l iv ingplant li fe greatly retarded its development . Whole vo lumeshave been devoted to this subj ect . I t w as supposed that vege
tation filtered themiasm from the air. I t w as argued that i fair v itiated by respiration "
be confined in a bottle containinga liv ingp lant and exposed - to the rays of the sun , the carbonicacid gas w il l be absorbed and the ai
‘
r
‘
restored to its orig inalcond it ion , plant l i fe consum ing carbon d iox ide and exhal ingoxygen . S o firm was this be l ie f that in the days of ancientRome trees w ere protected
'
by law,I t is needless to say .
_that the protect ive power of l iv ing
plants was as much o verest imated as the faculty 0f decay ingvegetation tg w
cause malaria. Their pow er o f absorbing moisture from the
"
soil“
i1sr more than outw e ighed by the shade theyafford the ground .
Whi le the clearing of land of trees and vegetation may be
followed by an outbreak o f malaria, this may be due to the
overturning of the so i l , which usually goes hand in hand w ithopen ing land , and to the hardships attending such labor. The
ultimate effect of clearing trees from the land is to d im inishmalaria by perm itt ing the sun to dry the so il .I f trees have any protect ive v irtue whatever it is probably
through afford ing shelter and food for mosquitoes . The cul
ture of eucalyptus trees is now “known to have no prophy lact iceffect upon malaria.
Weeds and other vegetation gr0W111g 111 the water favorthe development of mosquito larvae by protect ing the surfaceof the water from ag itation by the wind .
V egetable decompos it ion bears no relation to the et iologyof malaria other than as an index to heat and moisture .
Wind .—'
The w ind was formerly held responsible for transm itt ing malaria long d istances. I t was bel ieved that the malaria of Ed inburgh was imported by the w inds from Hol land ,
and that I taly'
became malarious through the agency of the
A frican S il‘ OCCO .
‘
The land breezes, especial ly i f they blew

ETI OLOGY 49
over marshy areas , were regarded as more h ighly nox iousthan the sea breezes.
As a matter of fact , the wind has l ittle or no power to
transm it malaria for d istances 0f any consequence. Whileit is theoret ically possible for in fected mosquitoes to be borneby the w ind , in real ity these insects , especially the anopheles ,being weak fliers , seek Shelter while a breeze is blow ing .
The immun ity from mosquito bites afforded by the I nd ianpunkah , or a common fan ,
is ev idence of this .
Furthermore , the d isturbing effect of the w ind upon the
surface of the water interferes w ith ov ipos it ion o f the adultsand w ith respirat ion of larva and pupae.
Exposure to cold w inds may have the effect of arousinglatent malaria. An incident related by Watson
72 is a Strikingi llustrat ion . Thirty ladies and gentlemen had sai led to . the
mouth of the Tiber on an excurs ion of pleasure. Suddenlythe breeze shi fted to the south and began to blow over a
marshy tract of land s ituated to w indward of them. Twentyn ine of the thirty were immed iately after attacked w ith tertianague.
The o ccurrence of malaria upon shipboard has been -citedas
'
an argument that malaria is an air- borne d isease . Bilgewater in the holds of vessels has also been accred ited w ithproducing malaria at sea. The dangers o f malaria from car
goes-
of sugar and fruits were recogn ized by old writers .
M alaria occurring upon ships -
'
may _
be accounted for in sev
eral ways. These cases may be man i festat ions of .malariacontracted upon shore. Even cases
‘
occurring long after em
barking may be explos ions of latent malaria. I f vessels anchortoo c lose inshore in malarial reg ions in fected mosquitoes may
easi ly gain access to the crew—a hal f mile from shore is
probably a safe d istance. I t has been proven that mosquitoesmay be carried for cons iderable periods in the holds and sleeping apartments o f ships .
Commercial vessels are more apt to carry mosquitoes thanare warships , through load ing and un load ing o f cargoes.
There are many places where , notw ithstanding apparentlyfavorable topographic and meteorolog ic cond itions , malaria is

50 THE STUDY OF MALARI A
ent irely absent. This is due to the absence of e ither malariabearing mosquitoes , or'
malarial paras1tes , or of both. Amonga number - of such places may be ment ioned the city of Rome
and other port ions of I taly ,M ade ira, port ions of Cameroon,
Chole I s land , Comoro I s land , Rodrique z I s land , the S ey
chelles I s lands , port ions Of I nd ia and of Borneo , the F renchI slands , Ponape , S aipan , S amoa, .New Caledon ia,
Tahit i , Barbadoes , and port ions of Brazil and of the Argent ine Republic;The majority of such local it ies are islands and in the southernhemisphere.
Race - I mmun ity .—Certain protozoan d iseases among lower
animals con fer immun ity . I n the Texas fever of cattle an
attack, i f recovered from , is followed by immunity . Thereare said to be breeds of cattle natural ly immune to the d isease.
I n the large game an imals of A frica one in fect ion w ith trypcmosoma brucei confers immun ity . Koch found that birdsthat had been in fected w ith proteosoma gras
'
m'
i could,not be re
in fected.
F rom analogy it might there fore be expected that immun ityto malaria might ex ist w ith some ind iv iduals or races. Thisis true , however, in on ly a l imited sense.
While the various races of mankind vary somewhat in sus
ceptibility to malaria none can be said to possess absolute “
immun ity .
Caucas ians res id ing ln non -malarial countries are , whenexposed , most l iable to contract malaria. Negroes bred inhighly malarial reg ions are , as long as they remain upon the
native: so il , least suscept ible to paludal infect ion .
Immunity w ithin the race increases general ly as we go to
ward the equator. Thus the negroes of the S outhern S tatesd isplay less immunity than the negroes of t he West I ndies or
o f tropic A frica. L ikew ise it may be said that immun ity ismuch more marked in countries w ith a high than in thosew ith a low , endemic index.
The immun ity of the negro race has been variously est imated , some observers maintaining that they are absolutelyproo f against malarial invas ion , while others hold that theyareas suscept ible as the whites. _ The truth l ies between these

52 THE STUD Y or MALA’
RIA
A ccord ing to Hirsch , 18 there d ied of malarial fevers perthousand of population in Cey lon
Negroes
IndiansM alay sS ingaleseEnglish
D uring the C iv i l War both the morbid ity and mortal ityfrom malaria in the negro race were greater than in the Whiterace. However, the negro soldiers are said to have . beenmore exposed to malaria than the whites , haVing been aggre
gated in malarial local ities.
76
With the better hyg ien ic surround ings and more l im itedexposure of the wh ites the negroes would probably be attackedless o ften than they are. Whether the color, thickness , or
other qual it ies of the skin o f this race have anything to do
w ith the ir re lative immun ity is not known .
The Chinese are said to be v ery suscept ible to malarialin fection. The Arabians and the S iamese are almost as fre
quent ly and as gravely attacked as the Europeans."
Laveranlstates that it is difficult to est imate exact ly the
relat ive frequence o fmalarial fevers in the Europeans and in
the A lgerians , s ince the latter o ften escape observat ion , but
he bel ieves the nat ives have a degree of res istance and of
tolerance not possessed by the Europeans .
The d isease is said to be relat ively rare in the nat ives of
M adagascar. Adult F i lipinos are more frequent ly attackedthan the A frican negroes . The Abyssimans are o ften in
fected . The M alays , Javanese , and Tami ls are much lesssuscept ible than the Caucas ians .
At S tephan sort Koch42 f0und various races in fected in the
follow ing proportions :Number of Per Number infectedsons Examined . with M alaria.
2 1 12
240 63209264 29
734 157
Immun ity from malaria is probably an acquired immunity “
in the great majority of instances , though the contrary op inion

ETI OLOGY 53
is held by some competent authorit ies upon the subject. The
reasons for believ ing that this immunity'
is acquired by re"
p eated in fect ion , especially in childhood , and by-"
prolongedres idence in a malarial reg ion , a sort of accl imat ization , are
that immunity is much more prevalent in adults than in ch ildren ; that immun ity is often d imin ished by a change of res i
dence, or may be ent irely lost by a temporary res idence in a
non - malarial climate ;and that immun ity in an indiv idual may
ex ist toward one form of malaria and not toward others.
That immunity is much more man i fest in adults than in
children is ev ident from the considerat ion of the endemicindex of amalarial reg ion , part icularly of countries where thelatter - is high. D uring the . first years of l ife many l
individuals
examined Show ev idence of malarial in fect ion, older childrenin a less proport ion , and adults ev ince a relat ive immun ity .
This would hard ly be the case i f the immun ity were racialand congen ital.The effect of a change of res idence upon malarial immun ity
is a wel l- known fact. Plehn says that the S oudan negroes ,
relat ively immune at home , are often afflicted with malariawhen going as sold iers to other parts of the continent. iSmith"states that , while the nat ive negroes of S ierra L eone are ln
frequently at tacked , and on ly w ith m i ld degrees of malaria,
in the‘West I nd ies reg iment of negroes stat ioned in S ierra
L eone the fev er is of a very severe and o ften fatal character.
I nd iv iduals once immune to malaria may become suscept ibleon return ing . home from a temporary residence in a
‘
malariafree country . Plehn
i "
ment ions three Cameroon negroes who ,
shortly after return ing from a several years ’ sojourn in Europe , were attacked w ith severe remittent fever.
Repeated in fection and consequent immunity . to one formof malaria does not usually protect the ind iv idual from the
other forms . Koch78 found certain islands among the Bis -r
marck Archipelago where quartan fever ,
alone was endemic.
L aborers from these islands s ickened readi ly w ith tert ian and
est ivo- autumnal malaria in S tephensort . Elt ing79 has shownthat persons who could not be art ificially inoculated w ith a
certain variety of the paras ite could be w ith another
54 THE STUD Y or MALARI A
I n the-
South there is little d ifference betw een the races as
regards suscept ibil ity to the various forms of malarial in fe ct ion—te rtian , quartan , and est ivo - autumnal . Cl inically , however, pern icious cases , cachex ia and hemog lobinur ic fever, arerarer in the negro .
“
I nstances of cachexia followed by immun ity have been oh
served,’
especially by the I talian school . I n these cases , afterrecess ion -
of the spleen and l iver, and restoration of the bloodelements , a stable immun ity resulted . Subjects of ex ist ingcachex ia, even though free from cl in ic ev idences of acute
malaria for years , can hard ly be regarded as immune.
Rarely are persons encountered in highly malarial local itieswho have never been attacked w ith malaria. Such persons aresupposed to possess congenital immunity . Cell i80 obtained precise histories of four persons l iv ing in the Pont ine M arsheswho were absolutely immune , hav ing never had malaria,though they took no prophy lact ic precaut ions ;the ir color wasgood , and the ir l ivers and spleens normal. I n persons claiming never to have had malaria al lowances must be made forthe poss ibil ity of unrecogn i zed attacks , especially in early childhood , which might g ive rise to an acquired immun ity .
I n conclus ion , the res istance off the black race .to malariais due to repeated attacks in early childhood , and not to any
great extent to hered ity . While in a'
sense natural select ionis a factor, it is largely an ind iv idual struggle , the se lect ionof the fittest occurring in in fancy , and but l ittle be ing derivedfrom progen itors .
S ex.—As a general rule, females are less o ften attacked
w ith malaria than males , though in'
childhood the proportionis about even.
That women are less frequently in fected is not due to a
higher degree of resistance , but to the fact that they are lesso ften exposed and are more temperate in the ir habits.
‘
I t is
probable that i f they were equally exposed w ith males theyWould be even more o ften in fected than the latter, on account
of the greater del icacy of the skin and the manner of dress.
I n certain local it ies women are not less frequent ly attackedthan men . I n Panama there is said to be very l ittle , if . any ,
ETIOLOGY 55
d ifference - between the sexes in this respect.30 I n the D utch
East I nd ies European women are more suscept ible thanmen.
”
D avidson6 6
says that from 1871-
75 the death rate of"
sold iers ’w ives in I nd ia was 4 .2o v
per thousand , as compared w ithfor the men ;and that
.
in Bombay, 1885 - 86 , the female deathrate
“
was that of males, 7.
The followmg are some figures Show ing the sex d istribut ionm a few local ities
0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0
O O O O O O O O O O O O O O O O O O O O O O O O O O O O O O O O O
O O O O O O O O O O O O O O O O O O O O O O O O O O O O O O O O O O O O O
0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0
0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0
o o o o o o o o o c o o o o o o o o o o o o o o o o o o o o o o o o o o o
O O O O O O O O O O O O O O O O O O O O O O O O O O O O O O O O O O O
0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0
o o o o o o o o o o o o o o o o o o o o o o o o o o o o o o o o o o
I n an inst itut ion in A labama S imms and Warw ick8 5 foundamong deaf mutes per cent . o f the males and 6 per cent .
of the females in fected ;among blind , 6 per cent . of the malesand 3 per cent. of the females .
Pregnant women are probably less o ften infected because ,on account of the ir cond it ion ,
they are less o ften exposed ;
When exposed they are very susceptible. The puerperium pre
disposes to malaria.
Age .—Ch ildren are more frequently and more severely af
flicted w ith malaria than adults._This 1s probably due to the ir
more delicate skin ,the ir manner of dress , sounder and more
prolonged s leep , and inability to defend themselves againstmosquito bites. The fact that cases of malaria in childrenmore o ften escape correct diagnos is may account somewhatfor the greater frequency , especially of relapses .
The subjoined figures Show the d istribution of malariaaccord ing to age
Age 0 - 10 10 - 20 ao -
3o 30-
4o 40 -
50 50- 60 60 - 70 70
- 80 80 - 90
Thayer and Hew et
son29
18 146 204 130 65 36 11 3Rogers 2 13 10 3Cardamatis 729 499 398 230 144 100 55 15Conti
82245 E _
83 61.
Total 994 804 695 424“
272 15 6 66 18
56 THE STUDY or MALARI A
O f malarial subj ects observed by D e Brun86 at Beirutwere chi ldren and under e ight years of age.
O f 1 ,784 cases recorded by Hope ,4° ”
862 were in childrenunder fifteen and 92 2 in persons o f fifteen or over.
M alaria causes a greater number of deaths in children thanamong adults . S trachan87 tabulates deaths from malaria,
of which occurred in children under one year of age ,
275 from one to five years of age , 157 from five to‘
twenty ,
and 5 17 fr0m twenty to seventy- five years of age .
The follow ing figures Show the percentage mortality of
malaria, accord ing to age , compiled from the table of S avas68
in Greece0 -
5 Years . 20 -
40 Years .
54
Endem ic I ndex.—The percentage of children in fected m a
g iven local ity I S the index to the prevalence of malaria in thatreg ion (Fig . As Ross88 expresses it,
“ There is probably
Fig. 6 .- Spleen rate in British Central Africa (after D aniels) .
only one really accurate method “
by which w e can determinethe degree of malaria in a g iven locality ,
and that is by ascer
tain ing the average time in whichI
a newcomer becomes in
fected. The shorter this period the greater, ev idently , the


58 THE STUDY or MALARI A
Under one
From one to‘
two years
From two to three yearsFrom three to four years
F rom four to five y earsFrom five to s ix years
F rom six to seven years
From seven to eight y earsFrom eight to nine yearsF rom nine to ten years
Ten years and over
Craig reports the endemic index about Campas follows
From one to five y earsFrom five to ten years
From ten to fifteen y ears
I n calculat ing the endemic index a sufficient ly lof persons should be examined in order to elir.
I t has been estimated that i f fifty persons be exarr
blood of twenty- five found to contain paras ites ,
of error be ing 20 per cent. , the index would n<
cent , but between 30 and 70 per cent . Furthern
high index . ind icates widespread malaria , an in
must not be construed to ind icate an ent ire ab.
d isease , s ince experience has shown that it may
the index , estimatedI
in this manner, is zero.
I n comparing the ind ices ofI
two local it ies the fibe taken at correspond ing seasons , s ince the inde:locality varies according to season. Thus Roge1in the tea gardens of Assam that the endemic it.80 per cent . in O ctober, but Was only 30 per cent.
place early in April . L averan1States that , while
index of a certain port ion of Java was per 0
ary , it fell to 32 per_
cent . in M ay .
The, prevalence of splenic enlargement has be
to calculate the extent of palud ism , this meth (much less t ime than the examination of the blo
unhealthy v illages of Borneo , Nieuwenhuis86 four.
enlarged in 80 per cent . of the children examined.
found the Spleen index at F inschhafen to be 84 p

ETI OLOGY 59
examinat ion of the school chi ldren held at M arathon in O cto
ber, 1906 , Showed that en largement of the sp leen was to be
found in every pup i l.9 3The spleen rate and the
I
endemic index , est imated by a microS cop ic examinat ion of the blood
,do not usually correspond
even approx imately. I n Algeria the S ergents86 found the
spleen rate in childrenfrom one to five years old to be 63.58
per cent , while the paras ite rate was only per cent.
S tephen-s and Christ0phersg4 have prepared the fol low ing table
to i llustrate the relat ion between the Spleen rate and the
paras ite rate
Locality. Spleen Rate . Endemic Index.
CalcuttaJalpaiguriBustee
S chool children
Babu children
M ainaguriI
Rungamutty 1.
S am S ingKurseong IKurseong I IThese invest igators draw the follow ing conclus ions1 . A high endemic index may ex ist w ithout any appreciable
spleen rate (A frica) .
2 . A high spleen rate may ex ist inadults w ithout a corre
sponding parasite infect ion .
3. I n I nd ia (Bengal ) among children a high Spleen rate is
a fair ind icat ion of the parasite :infection .
4. The spleen rate , u nl ike the paras ite rate , increases up
to a certain age lim it and may be cons iderable when the paras ite rate is nil.
The writer does not be l ieve that the spleen rate would disclose the true endemic index o i reg ions in the S outhern S tates.
L ength of Res idence .—I n highly malarial reg ions , espe
cially in the trop ics , newcomers areusually in fected during thefirst year. C raig70 says that of the hundreds of cases of
malaria occurring in our sold iers in Cuba almost 95 per cent.
gave a history of being there from two to six weeks beforethe onset of the d isease , and that one month was the periodmost common ly g iven .
60 THE STUDY or MALARI A
I n the S outhern S tates the period before in fection variesgreat ly accord ing to circumstances.
I
Newcomers who l ive inhyg ienic surround ings , and who observe ord inary precaut ions ,may go for years w ithout developing
I
the d isease. O n the other
hand , persons coming S outh who take no precautions , and
who expose themse lves carelessly , are liable to be attackedearly . Thus , it is said that when the Beaumont oil fields w ere
Opened up peopleI
flocked there from nearly every sect ion of
the country , and nearly every newcomer was struck down
w ith in a few weeks w ith malarial fever in some form.
Res idence , even prolonged , in a malarial local ity does not
con fer absolute immun ity to malaria.
Change of Residence—The effect of a change of res idenceupon the immunity in the negro race has been re ferred to.
I t is a common observat ion that mov ing to another local itybrings the malaria out of the system. This“
malaria is
usual ly latent—always so,of course , i f the new res idence is
in a non- malarial reg ion. I t is not uncommon for persons
who have never had recogn izable paroxysms to suffer an out
break upon leav ing the endemic reg ion.
O ccupation .—This is a factor - in the etiology of malaria
in two respects : first , by reason of certain occupat ions expos ingthe person to the bites of mosquitoes ; second , by reason of
the exposure and exert ion attend ingcertain occupat ions awakening latent
I
malaria.
Rural avocat ions more commonly expose to malaria than
urban .
‘
O ccupat ions which necess itate res idence at h ighlymalarious spots are especial ly dangerous , as wel l as those thatrequire be ing out of doors at n ight .O verturn ing the soil , as in garden ing , farming , d itch ing ,
rai lroad , levée , and canal construct ion , pred isposes to malaria]in fect ion .
I
F ishermen , sold iers , n ight - watchmen, eng ineers ,
and timber - workers are o ften exposed.
Rice culture , requiring as it does the retent ion of water
from the surface of the ground ,is not
'
an unalloyed boon as
an innovat ion into many of our S outhern S tates . The dangers
to the community from the grow th o f rice w ere recogn izedmany decades ago near S avannah and Charleston . M alaria


ETI OLOGY 61
I S said to have almost d isappeared from the reg ions of Parmaand Vincenza when rice culture was d iscontinued .
S ocial C ondit ion . Civ i liz ation.- Formerly malaria at
tacked all classes. M any'
noted persons were frequentfy in
fected , and James I and Cromwel l d ied of the d isease . M oats
and lakes near castles and country estates were doubt less toblame .
Now malaria is chiefly a d isease of . the poor and ignorantclasses. The man in the w el l - constructed and properlyscreened res idence is much less l iable to become in fected thanthe one in the loosely bui lt and unprotected hut. The occupa
t ions and food of the poorer classes are a lso factors in the
greater prevalence among them.
Persons l iv ing in cities and towns are much less apt to be
exposed to in fect ion than those in v illages and in the country .
M any towns. and cit ies in the heart of malarial areas are relatively free from the d isease. Suburbs are more highly malarions than the more dense populated sect ions , for the reason
that the mosquito has more opportun ity to breed 1n the former.
O ther Factors .—There are certain factors of the utmost
importance in the et iology of malaria, and be fore the truthwas known were looked upon as caus ing the disease.
I
Theseare overwork , fat igue , exposure to sun , ram , and co ld , excessesin Bacchus and in Venus , psychic emotions , loss of sleep , traumatism, surg ical intervent ion , 0vereating ,
'
hunger , thirst , d igest iv e d isorders , menstruat ion, parturit ion,
intercurrent affec~
t ions , and the administ rat ion of certain med icaments .
Watermelons , muscad ines , cucumbers , and other art icleshave yet the reputat ion in . p arts of the S outh ‘
of caus ing chills .
The admin istrat ion of tubercul in and of potass ium iod ideare said to be followed not in frequently by outbursts of
malaria.
I t is obv ious that the influence of these factors is upon latentmalaria, or the parthenogenetic cycle of the parasite ’
s l i fe history .
I nsufficient and improper food both low ers the res istanceto new in fect ions and kind les latent malaria into activ ity.
62 THE STUD Y or MALARI A
The effect of deficient nourishment upon malar ia mortal ityis well i llustrated by the follow ing table , compi led by Rouxfrom statist ics in I nd ia, where rice is the staple food of the
lower classes :D eaths from M alaria .
0 0 0 0 0 0 0 000 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0
0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0
0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0
0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0
O O O O O O O O O O O O O O O O O O O O O O O O O O O O O
While the major port ion of many older works on malariawas devoted to the réle of drinking water in the contag ion of
malaria, it is now known that it_
is of m inor importance.
Cell i67 had several healthy ind iv iduals , in the S an S piritoHospital of Rome , to drink for a number of days water
obtained from the Pont ine marshes and from stagnant pools .
The results were uni formly negat ive .
Zeri6 7 conducted three series of experiments w ith waterfrom malarious local it ies: 1 . He had nine ind iv iduals drinkfrom 1% to 3
' l itres of water dai ly from five to twenty days ,
each person consuming from 10 to 60 l itres of the water. 2 . I n
s ixteen indiv iduals the mucous membranes of the resp iratorytract were Sprayed w ith marsh water“
by means of a com
pressed- air atom izer.
_
3. I n five persons Water from malarialplaces was injected into the rectum. The results of all theseexperiments w ere negat ive .
I t has been maintained that water in which mosquitoes harboring paras ites have ‘
d ied is capable of producing malar1a.
This is based upon the s ingle expe riment of Ros s , who had
an I nd ian nat ive drink a small quant ity of water in whichthere were dead mosquitoes which h ad fed upon malarialblood. Eleven days later the nat ive developed fever whichterminated spontaneously after three days w ithout relapsing .
I n the blood were found ring forms of the est ivo - autumnalparasite. This experiment was repeated , but the result couldnot be confirmed ,
so must be regarded as co - incidental .. I n regard to the immun ity to malaria enjoyed by opium
eaters , ,
Russell9 5 states that the observat ions of several sur
64 THE STUDY or MALARI A
s ion;of malaria necessary a to cons ider are : 1 , congen ital ;art ificial moculation , and 3, inoculat ion
“
through the bitescertain species of mosquitoes .
Congen ital M alaria—I t was formerly bel ieved that malaWas not in frequently trans ferred from mother to fet
D ucheckg‘? published a case , in 1858 , of a child whose mot]
suffered from malarial paroxysms during pregnancy .
’
l
chi ld dy ing three hours after birth , at autopsy the l iver a
Spleen w ere found to be enlarged , and the “
Spleen and . blc
of the portal vein contained cons iderable pigment.
Two cases are reported by Felkin .
9 7 I n the first case
diagnos is was based upon intrauterine quivering of the fet
en larged spleen at birth , and fever later ,I
the date of whichnot recorded. I n the second case the mother had never l.
malaria, hav ing never been outs ide of Ed inburgh , butin fect ion is attributed to the father, who had contracted ma
ria in A frica several years prev iously and , as Felkin believ
had transmitted the d isease to no less than three in fants .
Watson72cites the case of a woman who was suffering w
tert ian ague. On alternate days when She m issed the par(ysms she could feel the child shiver w ith chills. Bark v
prescribed and the paroxysms of the fetus were first intrupted , then those of the mother.
However, of numerous cases recorded by a score or m«
of early writers, all are Open to two object ions : F irst ,d iagnos is was not certainly established ; second ly , postnain fect ion .was not excluded .
I
M archiafava and Bignami ment ion four cases in wh
the blood of the fetuses of malarial mothers was ent irnegat iveThayer records a case of a negress who had had mala
at least five months and whose blood contained three groiof the quartan paras ites when she g ave birth. duringparoxysm,to a child whose blood , upon repeated examinati
i
was found free from paras ites and p igment . Wh ile both pas ites “
and pigment were found upon the maternal s ide of
placenta,none was found upon the “fetal s ide .
S ereni , 8 6 who examined the blood of four in fants born

ETI OLOGY 65
malarialmothers , w as unable to find ev idences of malaria inany case .
Ziemann ,
48 l ikew ise, in four cases of new - born children of
malarial in fected mothers , had un iformly negat ive results .
The writer has upon several occas ions obtained blood fromin fants , immed iately after birth , whose mothers harboredmalarial paras ites, and in no case have parasites been detected .
S im i lar results have been obtained by B ast ianel li , 22 Caccin i ,Borne ,“ 90 S ch00 , 9 ° F . Plehn ,
5Terburgh,
79 A . Plehn ,
9 9Wellman ,
and others .
Pe z opoulos and CardamatisLOO based the follow ing conclu
s ions uponI
six cases , five ful l - term labors and one abort ion ,
which they stud ied .
1 . I n the blood of the six mothers there were paras ites ,more or less
I
abundant .
2 . Inthe blood of the new - born and of the aborted foetus ,examined a few hours after expuls ion , there were no parasites .
3. I n the blood of the l iver and spleen , as
I
well as in sect ionso f these .organs of the . two fetuses which were examinedpostmortem , no paras ites were found .
4 . I n the blood . taken from the maternal surface of the
placenta: o f the five new - born children there w ere parasites 1n
abundance,while in the blood taken from the fetal surface
there were'
no parasites , or at most a v ery few .
5 . I n blood taken from the umbilical cord no paras ites were
found.
6 . I n the blood of theI
placenta of the aborted fetus no
paras ites could be detected .
Bein and K ohlstocki01
are said to have found malarial paras ites in the blood of a four- months - old child born somet imeafter the arrival of them other in a reg ion free from malaria.
Winslow l'
02records a case which he believes to be congen ital ,
though the paras ites were not detected unt i l the child was
eleven weeks old.
A case of malarial fever in in fancy thought to be maternalin orig in is reported by Peters .
1°3The examination of the
blood o n the second and third days after birth was negat ive ,though parasites were found onthe fifty - first day.
5

66 THE STUD Y or MALARI A
M offatt -
104observed a case Supposed to be congen ital malaria,
though the paras ites were not detected be fore the seventhWeek.Bouz1an , in A lgeria, detected parasites in the blood of an
in fant only twelve days old.
Hitte106 collected from the literature 2 1 cases of malariacons idered congen ital . I n 13 of these the blood was not
examined ; in 1 parasites were detected four months afterbirth;and in 5 cases paras ites were found from several weeksto two months after birth. The remain ing 2 cases were ob
servedI
by Hitte personal ly , who claims to have found paras itesin the blood obtained from the umbilical cords. The mothers
of both children w ere suffering ._
with malaria.
Paras ites were found by S imms and Warw ick in the bloodof three babies between three and seven days old ;the mothershad prev ious ly had malarial paroxysms.
Holt107 ment ions a case' in which he states there seems l itt le
doubt that the d isease was contracted in ntero. The motherhad been suffering w ith tertian intermittent . Eighteen hoursafter birth the child show ed ev idences of a malarial paroxysm.
The next day malarial organ isms were found in the blood.
Economous1i08 reports 6 cases w ith almost conclus ive ev i
dence of congen ital origin . I n each of these cases the blood,examined from e ight ,
to forty - e ight hours after birth , contained malarial paras ites . Themothers had , prev ious todcl ivery , suffered w ith malaria.
Bel109 ment ions a female pat ient Who d ied of p ernicious .
malaria. The paras ite was found in the blood , pericard ium,
men inges , and spleen , as wel l as in a seven - months fetus.
As may be in ferred , properly proven cases of congen italmalaria are rare. This reluctance of the paras ites to
_pass
through the placenta - is in keep ing w ith their avers ion to leavethe blood—vessels . I t has been pointed out that no paras itesare found in the hemorrhages and perivascular exudates in
cases of pern icious malaria, though they may ex ist in hordesw ithin the vessels “ Congen ital malaria is probably to be ex
plained in the majority of cases through placental les ionspermitting d irect ming ling of maternal and fetal blood durmgparturit ion.

ETI OLOGY 67
I noculation .—Even before the parasite of malaria was dis
covered Gerhardt"10 succeeded , employ ing the blood of malarial subj ects , in inoculat ing healthy persons w ith malaria.
S ince then many s imilar experiments have been performed .
Tert ian malaria has been transmitted by inoculat ion by Bein ,
Bacelli, Antolisei and Ange lin i,M annaberg , Elting , and others ;quartan by Guald i and Antolisei, D i M attei , Calandruccio ,
Bacelli, and Ce lli and S antori ;est ivo—autumnal by Guald i andAntolisei, D i
'
M attei, Cell i and S antori , Bastianell i and Bignami , and Elting .
The . inject ion o f blood contain ing on ly crescents gave nega
tive results inI
the experiments of Thayer, Bastiane lli , Bignami , and Elting. D i M atte i and Calandruccio , however,observed an irregular form of fever t o follow such an inj ect ion. ,This can be explained only by parthenogenesis.
The inject ion of blood contain ing~
a-
certain Species of para
s ites is followed by fever characterist ic of that species , and
these paras ites are to be found in the blood of the person
inoculated.
There are on ly two experiments which , at first s ight , seemto contradict this specificity of the d ifferent paras ites . Thesewere performed by Guald i and Antolisei. Blood fromtwo
pat ients suffering with quartan malariaI
was inoculated intotwo healthy persons . I n one case the in ject ion was followedin ten days by irregular fever and est i—vo—autumnal paras iteswere detected
_
in the blood. I n the other case after twelvedays
I
an irregular feverbegan and est ivo—autumnal and a few
quartan paras ites w ere f ound in the blood . I t was later discovered that the pat ients from whom the blood was takenhad recently suffered w ith quot id ian , tert ian , quartan , and
irregular fever, hence it is ev ident that a_ pure culture of
quartan paras ites was not obtained . These same observ ers , insubsequent experiments , found that the inject ion of one speciesof paras ite was followed by the characteristic fever and the
appearance of the same species of paras‘ ites in the blood of
the person inoculated .
There are those who cannot be success fully inoculated w ithone species of parasite but can w ith another. .I t has b een

68 THE STUDY OF MAI
LARI A
shown also that one speciesof paras ite o ften d isappearthe blood upon inoculat ion w ith a d ifferent species .
”
D i
found that the inoculation w ith estivo- autumnal paras itpat ient already in fected w ith quartan malaria caused a
pearance of the quartan and a development o f the
autumnal paras ites , and that the inoculat ion w ith qparasites of a pat ient already in fected w ith estivo- au
caused a d isappearance of the latter and a deve lopmthe quartan paras ites.
The degree of development of the parasites apparen
no effect upon the result , s ince the d isease develops as
after the inj ect ion of blood contain ing adult organ iafter that containing young parasites . I t is immateri
whether the blood be in j ected intravenously or subcutan
A very _
smal l amount of blood , even less than one d
o ften sufficient for inoculat ion .
The inj ect ion of defibrinated blood , of centrifugalim
puscles , and of blood d i luted w ith an equal quant ityt i lled water and inoculated immediately have g iven I
results. The inj ect ion of d issolved dried blood , and
d i luted w ith an equal quant ity of d ist illed water a nd z
to stand an hour, have proven negat ive.
Jeffriesm
reports the case of a New York surgeon wnever had malaria supposed to have "
contracted the dis
pricking his finger several t imes during an operat ionwoman in fected w ith malaria.
I
S ixteen days after the
t ion the surgeon had the first chill and had severalquently . The blood contained I
many est ivo- autumna
s ites.
D ochmann86
attempted to inoculate malaria fromman by means of the serum from a herpet ic vesicle.
he claims to have succeeded , the results of his expe:
have never been confirmed .
Efforts to inoculate the lower an imals w ith humanhave been fruit less. Such a ttempts have b een mad
horses , mules , dogs , monkeys , rabbits , mice, guinc
hedge - hogs , bats , wolves,
cats , pigeons , “
doves , n
screech - ow ls , turtles , frogs , '
and l izards .
ETIoLOGY 69
D I SSEMI
INA’
I'
I ON or MALARIA BY MOSQUI TOES
The d iscovery by Ross of the réle o f the mosquito in the
d isseminat ion of malaria is the most startl ing achievement of
modern med ical science .
M osquitoes ‘
do not cause malaria ; they carry it from in
fected to healthy persons . The paras ites , sucked w ith bloodfrom a malarial indiv idual, undergo a cycle of development
w ith in the body of the mosquito, and are then inoculated intohealthy persons. M an is merely the intermediate host of theparasite , the mosquito is the definit ive host , and it has beensaid that man g ives malaria to the mosquito, and not the
mosquito to man.
Not all species of mosquitoes can serve'
as hosts for themalarial paras ite. I t is on ly certain members “
of the sub
family Anophelinw that have" been found to act in this capacity . O f this subfam ily the follow ing have been determined ,
w ith more or less certainty , to be malaria carriers z'
Anopheles annnlipes .
Anopheles bifurcatns .
Anopheles cohacsns .
Anopheles crucians .
Anopheles foranti.Anopheles flnoialis .
Anopheles forni osaz nsis .
Anopheles ni acnlipennis .
Anopheles martini .
Anopheles punctipennis .
Anopheles pm sati.I
Anopheles vagns .
Anopheles vincenti.
Cellia albipes .
Cellia argyrotarsns .
Cellia pharoensis .
M yeomyia Chris tophersi.
M yz omyia culicifacies .
M yaomyia fnnes ta.
M yz oni yia Hisp'
aniola.
M yz omyia L is toni.
M yaomyia Ludlowii.
M yz omyia Luiz ii.
M yz omyia picla
M yz omyia Rossa .
M y'
aomyia a khadi.
M yz orhynchns barbiros tris .
M yz orhynchns Cous tani.
M yz orhynchns paludis .
M yaorhynchns sinensis .
M yaorhynchns Z iemanni .
Nyssorhynchns fnliginosns .
Nyssorhynchns J amesii.
Nyssorhynchns macnlatns .
Nyssorhynchns maculipalpis .
Nyss orhynchns S tephensii.
Nyssorhynchns Theobaldi.
Pynetophorns Chandoyei.
Pyretophorus cos talis .
Pyretophom s j eypnrensis .
Pyretophorns superpictus .
70 THE STUDY OF MALARI A
Not all of the se mosquitoes serve equal]the malarial paras ites . M yz omyia Rossii i“
rier of malaria, while the Chm’
s tophers z'
is 2
r ier.As yet very l itt le is known of the re]
species of mosquitoes and species of malariz
tophom s cos talis is known to transmit teiestivo - autumnal malaria, while M yz orhyncltertian and quartan , but not est ivo - autumn
'
I t is possible that some mosquitoes acq'
mun ity to malaria which may account for
as malar ia disseminators . There are cert:
in spite o f members of a malaria-b earing s
and the immigrat ion of infected persons ,
spread , though temperature and other cor.
ently favorable .
The food o f mosquitoes has much to dobility to in fect ion . Experiments have sho
maculipennis fed upon fruits and sweets
fected from feed ing upon malar ial blood , 1
water for several days be fore and after flblood they are almost alway s in fected .
O ne feed ing upon blood contain ing parasisuffice to infect the mosquito. D aniels “ 2
subject , examined fifty- seven mosquitoes vs
or o ftener at intervals of two days .
Nineteen fed only once , and five had z ygotes
Thirteen fed tw ice, and six had z ygotes
S ixteen fed three times, and ten‘
had z ygotes
Nine fed four times, and six had z ygotes .
O f these 57 anopheles 27,or per cen
The “
effect of ferti lizat ion upon the powe
transm it malaria is not defin itely settled , bsome that ferti l ized females are the mos
72 THE STUDY or MALARI A
theory. That malaria is more eas ily contracted at n ightunderstood from the feeding habits of the malarial mosquitoes.
That all measures d irected toward the prevent ion of mosquitobites are followed by a commensurate reduct ion of the preva
lence of malar ia is one of the strongest arguments . The
analogy w ith filiariasis , Texas fever , hematozoan in fect ion of
birds , and s imi lar d iseases strengthens the theory . Numerous
and accurate experiments have absolutely proven the d issemi
nat ion of malaria by certain mosquitoes . O ne of the earl iestof these was that of D r. Patrick M anson . M osquitoes fed on
tert ian malarial blood in Rome under the superv is ion of Bas
tianelli were sent in suitable cages to L ondon . There theywere permitted to bite D r. Thurburn M anson and M r. GeorgeWarren ,
ne ither of whom had ever been prev iously exposed
to malaria. I n due t ime both developed malaria, and tertianparas ites w ere found in the blood at this t ime and later duringseveral relapses.
The sexual cycle of the paras ite w ithin the mosquito hasbeen followed many t imes.
An object ion that has been frequent ly urged against themosquito theory” is that there are numerous localit ies inwhich mosquitoes abound and from which malaria is ent irelyabsent ; indeed ,
mosquitoes are said to be we l l n igh intolerablein port ions of the arct ic reg ions . . I t must be remembered ,however, that on ly a
”
certain subfam ily of mosquitoes can
serve as hosts for the parasite . Furthermore , the surround ingtemperature must be suitable for the sexual development of
the paras ites w ithin the defin it ive host . But it cannot be den iedthat there are areas , even in the m idst of a malarial country ,
in wh ich anophe lines are present, the temperature is favorable ,and other cond it ions apparently suitable
,but autochthonous
malaria does not appear. Among such local ities reported may
be ment ioned S ingapore , Penan ‘
g , M alacca, S oekaboemie , and
port ions of Brazil , of I taly , and of L ow er Egy pt. This hasnot as yet been sat is factorily explained , but may be due to an
acquired immunity on the part of the mosquito , or to the
influence of the ir food on the development of the paras ite.
I t was formerly maintained that there were highly malarial

ETI OLOGY 73
reg ions in which there were no mosquitoe s , and a number of
such places have been reported . But in each case whereinvestigated by a competent observer anophe l ine mosquitoeshave,been found where malaria is endem ic. Koch6
9 ment ionsthat at Tosari , e levated metres , while there was some
malar1a, there w ere no anopheles. The malaria occurred ,
however, in those who w ere employed in the ne ighboring lowlands and not in the children who remained inthe town .
The habits of the anopheline mosquitoes are such that theymay be easi ly overlooked except by an expert . Retiring to
dark recesses during the day , bit ing only at night , and not
s inging a great deal , their presence may not be fe lt , especiallyby persons .in whom the bites do “
not.
cause much irritation .
I t may there fore be stated confident ly that there is no
endemic malaria w ithout mosquitoes .
The misproport ion between the number of infected anophe
lines and the number of cases o f malaria has been cited to
overthrow the mosquito doctrine . I n A lg iers S ergent9 ° found4 per cent . of the anopheles and 100 per cent . of the childrenin fected . A. Plehn
79 found in one of the most malarial local i;t ies , Cameroon , among 860 anopheles only per cent . in
fected. S tephens and ChristOphers113 be l ieve that about
i
5 per
cent . of all the anopheles of tropic Africa are in fected. At
Aro they found the sporo z oit rate in anopheles caught in nat ivehuts to be 50 per cent .
I t should be borne in mind that one infected anophe linemosquito is capable of in fect ing a number of persons . A lsothe sporo z oit rate varies accord ing to season and accord ingto the kind of mosquito, .s ince it has been shown that some
species are better malaria carriers than others .
The fact that malaria is decreasing in , or has d isappearedfrom, reg ions formerly highly malarial , but in which malariabearing mosquitoes are yet found ,
“
is another argument whichhas been proposed against the re lat ion of the mosquito to
malaria. With re ference to Great Britain,Nuttall , Cobbett
and S trangeways- Pigg
mconcluded that '
I . The d isappearance o f ague from Great“ Britain does not
depend upon the ext inction of mosquitoes capable of harbor ingthe paras ites of malaria.
74 THE STUD Y OF MALARI A
2 .
_
‘
T hree species of anopheles (A . macnlipennls , A . bifur
calns , A . nigm'
pes ) are to be found in .Great Britain in all
d istricts w hich were formerly malarious , but also in placesconcern ing which there is no record of the former prevalenceof ague .
3. The anophe les to - day are most numerous in low - ly ingland contain ing many d itches , ponds , and s lowly - flow ing water ,
suitable for the ir habitat , and corresponding to the d istrictsWhere ague was formerly prevalent .4 . S ince the disappearance of ague does not
' depend upon
the ext inct ion of anophe les , it is probably due to several causesoperat ing together :(a ) A reduct ion in the number
,
_
of these insects consequentupon drainage of the land ; this be ing in accord w ith all the
older authors , who attributed the d isappearance of ague large lyto this cause .
(17) Reduct ion of the populat ion in in fected d istricts as the
result of emigrat ion about the t ime when ague d isappearedfrom Eng land . This would naturally reduce the number of
in fected ind iv iduals and thus lessen the chance of the anophelesbecom ing in fected.
( C ) I t is poss ible that the use Of quin ine“
has reduced the
chances of in fect ing the anophe les through check ing the development of the paras ites in the blood o f subjects affected w ithague .
F inally , it has been maintained that persons who have never
had malaria have contracted it in un inhabited w i ldernesseswhere , obv ious ly , only un in fected anophel ineswould be found ,
s ince man is the only intermed iate“ host of the parasite.
To this it may be answered that no such instance has beenso accurately reported as to prove conclus ive ly that in fect ionhas ever occurred
“
under these circumstances .
THE M ALARIA—BEARING MosomTO Es
The genus Anopheles was established in 18 18 by JohannM eigen. The bestowal of the name appears prescient , sinceanopheles s ign ifies tz onblesome or hurtful.O f the fifty
'
or more species'
and subspecies of anophel ines

ETI OLOGY 75
now known seven occur in the Un ited S tates :A . macnh'
pennls ,
A . pnnelipennz'
s,A . crucians , A . fz anclscanns , A. barbem
’
, C .
argyrotai'sns
,and C . alblpes
B reed ing P laces—Thed ifferent species of anophelines varya great deal in the choice of a breed ing place . Furthermore,w ith each species there maybe said
-
to be places of'
cho ice and
places of necessity .
Contrary to the usual custom of culex , the anopheles usual lyselects water more or less pure in which to depos it her ova.
Ground water appearing at the surface is especially suitable.
Pools of at least some degree of permanence are pre ferredto those which m ight dry
'
before the aquat ic stage of the
insect is completed. Natural accumulat ions of water more
o ften contain anopheles larvae than do artificial collect ions .
Poo ls , ponds , swamps , inlets of lakes , and of small , slow lyfiow ing streams , d itches along roads ide‘
s, canals , borrow pitsalong rai lroads and levées , and rice fields are common breeding
. places . Water contained in the tracks o f a n imals may
harbor larvae.
When water is scarce,as during the dry season , anophe line
larvae may be found in tubs , barrels , boats , buckets , bottles ,cisterns , mollusc and cocoanut shells ; in w ater retained bythe leaves and stalks of tropic plants , or even within Vases in
dwellings , though these locat ions are to be regarded as placesof necess ity and not of
’
choice.
While , as said , clean water is u sually chosen by these mos
quitoes , at least one species , M . Rossn'
,is known to breed in
very foul pools . Another species , M . L is toni, is said to breedin sw i ftly - flowing streams , which is contrary to the usual habitof this subfamily .
I n regard to salt water as a med ium for anophel ine larvaemany opin ions are he ld . I t seems
“
that the species indigenousto the United S tates do not breed in salt water, and th is wasthe experience of Celli and other I talian invest igators . How
ever, Centann i and O rta11 5 found anopheles larvae in water
containing per I,ooo of sod ium chloride . F icalbi and
othersl“15 found them in water containing 40 to 50 grams of
sod ium chloride per l itre . I n Alg iers and the D utch I ndies
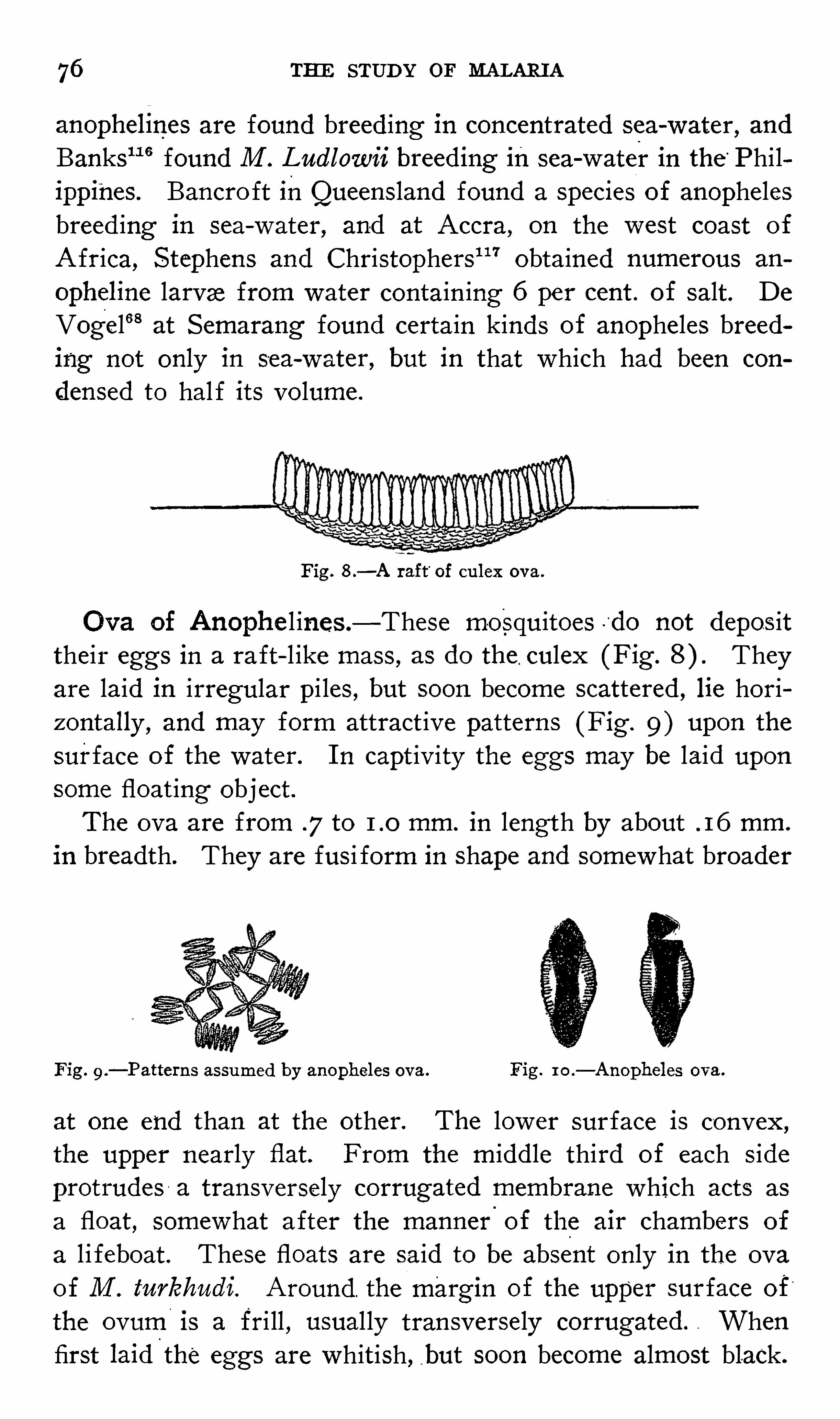
76 THE STUD Y or MALARI A
anophellnes are found breed ing in concentrated sea- water, and
Banks11 6 found M . Ludlowii breed1ng in sea- waterin the “
Philippines. Bancro ft inQueens land found a species of anophelesbreed ing in sea- water, and at Accra, on the west coast of
A frica, S tephens and Christophers1 17 obtained numerous an
0pheline larvae from water contain ing 6 per cent . of salt . D e
Vog'
el68 at S emarang found certain kinds of anopheles breeding not only in sea- water, but in that which had been con
densed to hal f its volume .
Fig. 8 .—A raft
“
of culex ova.
O va of Anophe l ines .—These mosquitoes -
'
do not depos ittheir eggs in a raft- l ike mass , as do the culex (F ig. Theyare laid in irregular pi les , but soon become scattered , lie horiz ontally , and may form attract ive patterns (F ig . 9 ) upon the
surface of the water. I n capt iv ity the eggs may be laid upon
some float ing obj ect .The ova are from .7 to mm. in length by about . 16 mm .
in breadth. They are fusi form in shape and somewhat broader
F ig . 9 .—Patte1ns assumed by anopheles ova. Fig. 1 0 .
—Anopheles ova.
at one end than at the other. The lower surface is convex ,
the upper nearly flat. From the middle third of each s ideprotrudes a transversely corrugated membrane which acts as
a float , somewhat after the manner
'
of the air chambers of
a l i feboat . These floats are said to be absent only in the ova
of M . tnrkhndl. Around . the marg in of the upper surface of“
the ovumis a fri ll , usual ly transversely corrugated . Whenfirst laid
'
the eggs are whitish , but soon become almost black.

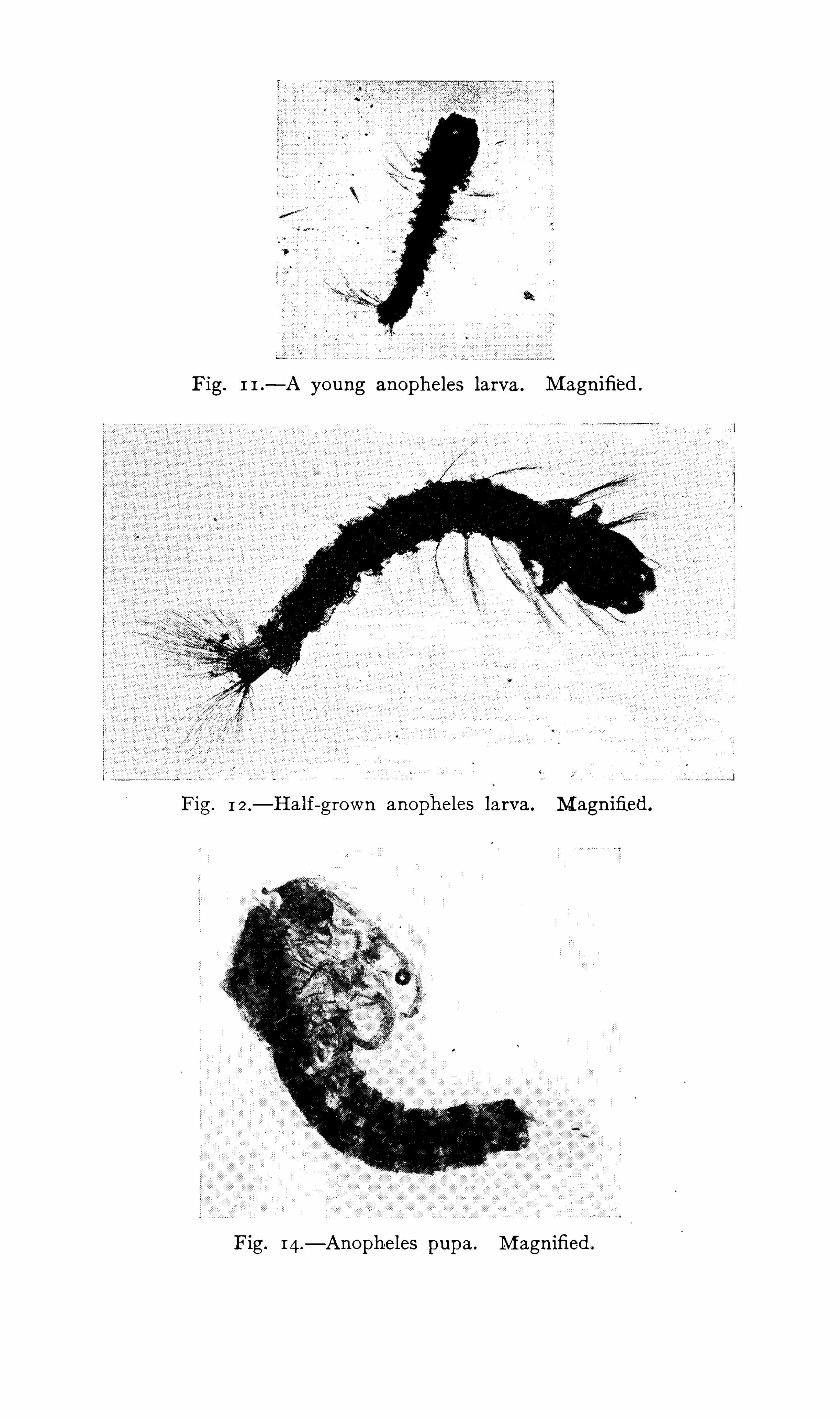
Fig. 1 1 .—A young anopheles larva . M agnified .
Fig. 1 2 .—Half—grown anopheles larva. M agnified .
Fig. 14.—Anoph-eles pupa . M agnified .
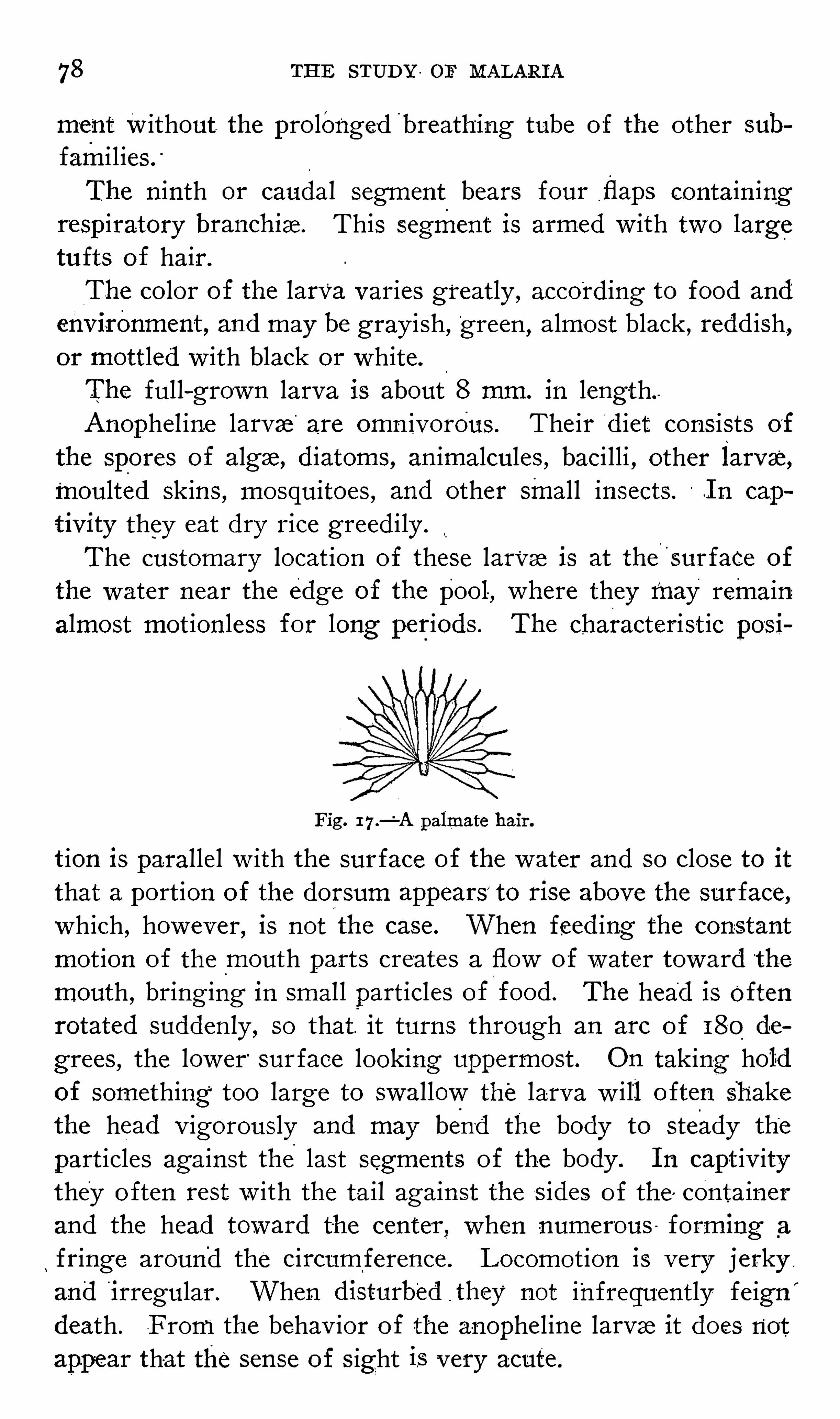
78 THE STUDY or MALARIA
ment Without. the pro longe -d'
breathing tube of the other sub
fami l ies .
“
The n inth or caudal segment bears four,flaps contain ing
resp iratory branchlae. This segment is armed w ith two largetufts of hair.
The color of the larva varies greatly , accord ing to food and
env1ronment , and may be gray ish ,”
green ,almost black , redd ish,
or mottled w ith black or whiteThe full - grown larva is about 8 mm. in length.Anophel ine larvae are omn ivorous . The ir d iet? consists of
the spores of algae, d iatoms, an imalcules , baci lli , other larvae,moulted skins
,mosquitoes , and other smal l insects . .I n cap
tivity they eat dry rice greed i ly .
The customary locat ion of these larvae is at thel
'
surfaCe of
the water near the edge of the pool, where they may remain:
almost mot ion less for long periods . The characterist ic pos i
Fig. 17.—'
A palmate hair.
t ion is parallel w ith the surface of the water and so close to itthat a portion of the dorsum appears to rise above the surface ,which , however, is not the case. When feed ing the constant
mot ion of the mouth parts creates a flow of water toward“
the
mouth , bring ing in smal l particles of food . The head is oftenrotated sudden ly , so that . it turns through an arc of 180 de
grees , the lower “
sur face looking uppermost . O n taking holdof something too large to swallow the larva w i ll o ften shakethe head v igorously and may bend the body to steady the
part icles against the.
last segments of the body . I n capt iv itythey o ften rest w ith the tail against the s ides of the , containerand the head toward the center , when numerous forming _
a
fringe around the circum ference . L ocomot ion is very j erky .
and i rregular . When disturb'
ed they not infrequently fe ign”
death . F rom the behav ior of the anopheline larvae it does notappear that the sense of s ight is very acute .

Fig. 1 5 .—Head of anopheles . M agnified .
Fig. 16 .—T ail of anophe les larva . M agnified .

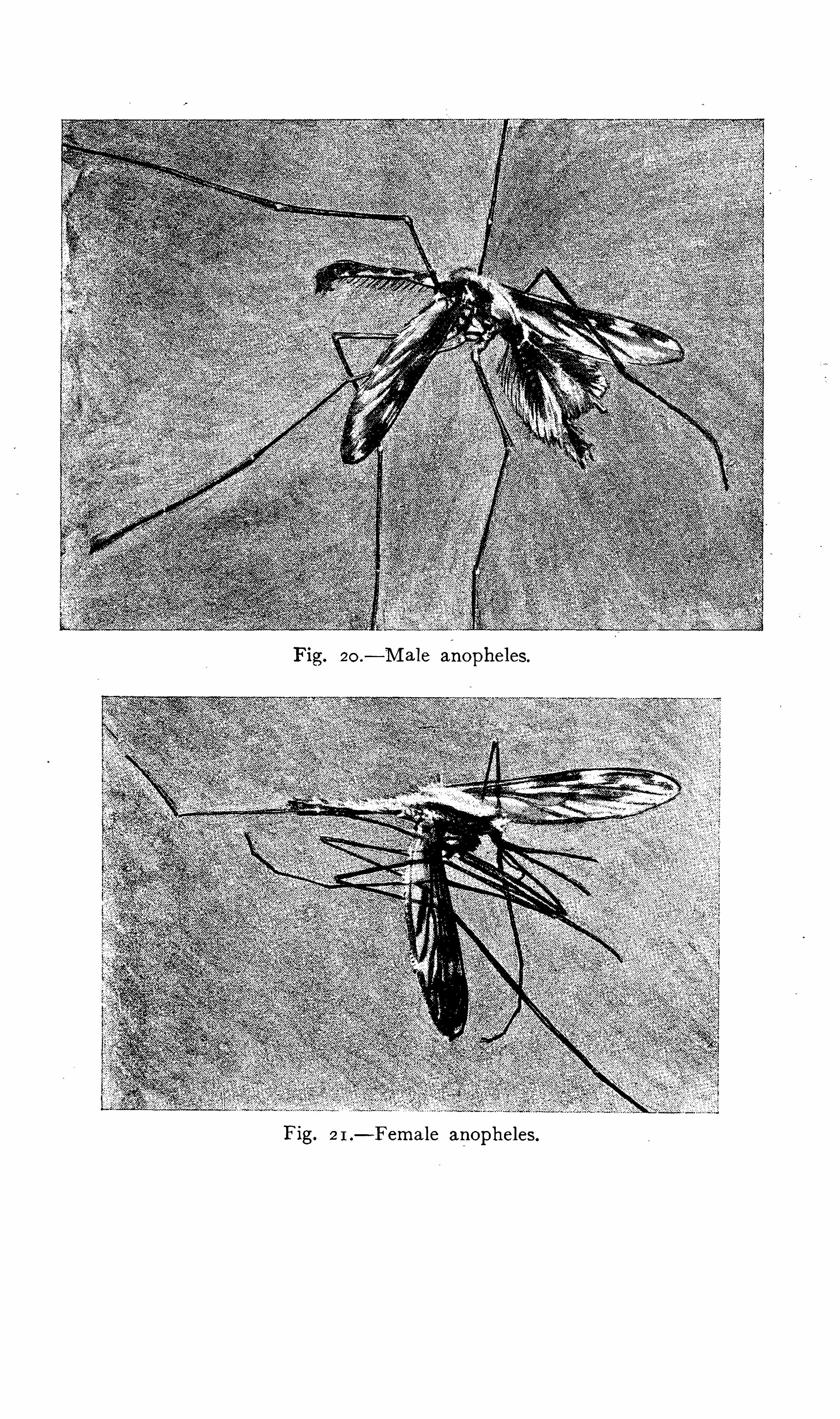


ETI OLOGY 79
Culex larvae have been thawed “
out of ice in which theywere imbedded and have proceeded to develop into inse‘
cts , but
so far as the writer is aware this has not been done w ithanopheles. The latter have , how ever , been found in water
Fig. 18 .—Adult culex larva.
under a frozen surface . They may ex1st for a few hours to a
few days upon mo ist mud.
The du'
rat ion of the larval stage varies accord ing to tem
perature , food , and poss ibly other cond itions . The l imits may
be placed at from ten to twentya six days . I n warm
Fig. 1 9 .- Resting positions of larvae a, Culex ; b, anopheles .
mates when suitable food is abundant the durat ion is ord inarilytwe lve“
or fourteen days . I n cooler climates and seasons the
durat ion is longer.
Anopheles and culex larvae may be d ifferent iated by the follow ing gross “
characteristics
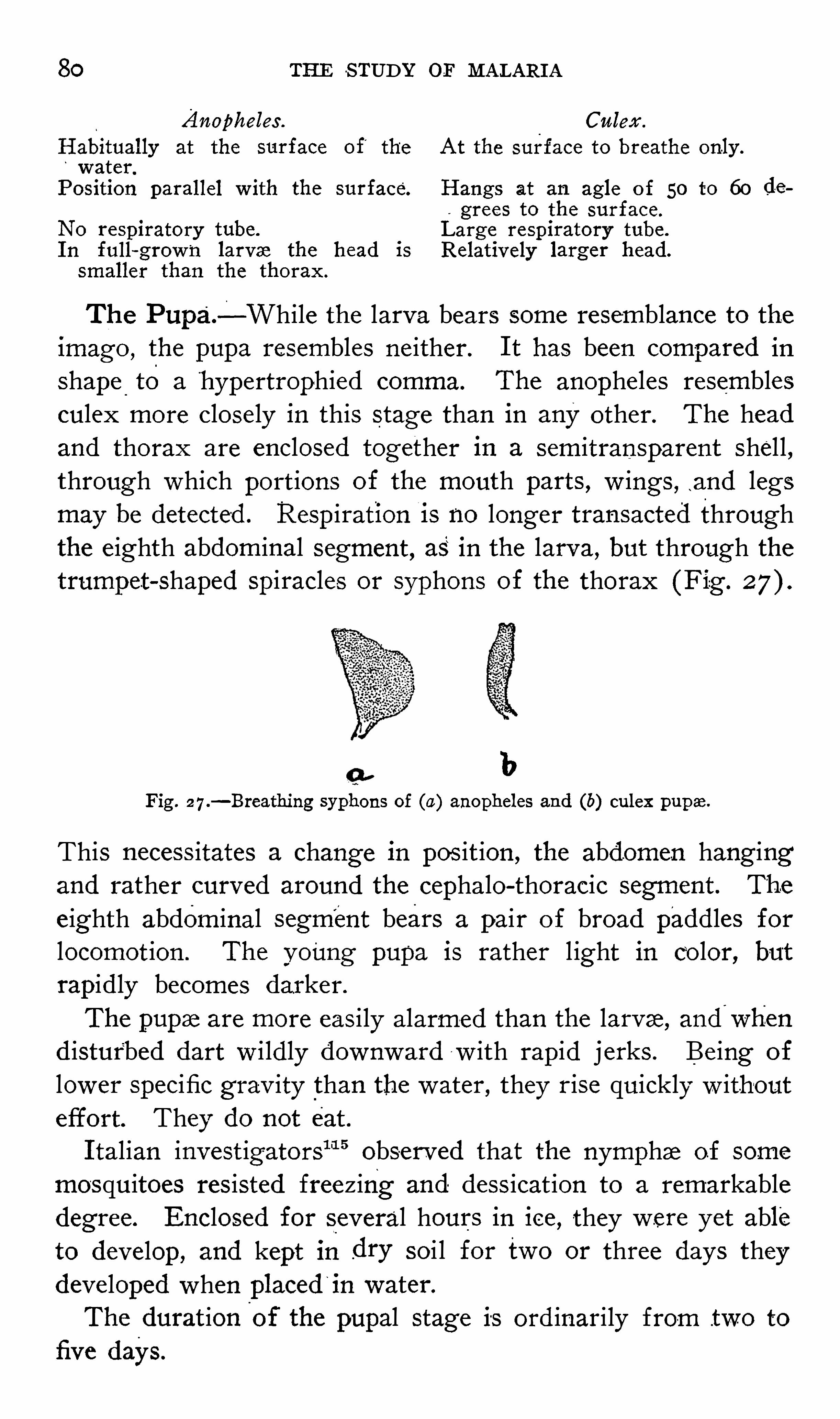
80 THE S TUDY or MALARI A
Anopheles . Culex .
Habitually at the surface of'
the At the surface to breathe only .
water.
Position parallel w ith the surface. Hangs at an agle o f 50 to 60 de
grees to the surface.
No respiratory tube. Large respiratory tube .
I n full- grown larvae the head is Relatively larger head.
smaller than the thorax .
The Pupa.—While the larva bears some resemblance to the
imago , the pupa resembles ne ither. I t has been compared in
shape to a hypertrophied comma. The anopheles resemblesculex more closely in this stage than in any other. The headand thorax are enclosed together in a semitransparent shel l ,through which port ions of the mouth parts , w ings , .and legsmay be detected . Respiration i s no longer transacted throughthe e ighth abdominal segment , as in the larva, but through thetrumpet
- shaped spiracles or syphons of the thorax (Fig .
bFig. 2 7.—Breathing syphons of (a) anopheles and (b) culex pupae.
This necess itates a change in pos it ion , the abdomen hang ingand rather curved around the cephalo- thoracic segment . The
e ighth abdominal segment bears a pair o f broad paddles forlocomot ion . The young pupa is rather l ight in color, butrapid ly becomes darker.
The pupae are more eas ily alarmed than the larvae, and'
wh'
en
d isturbed dart w i ldly downward w ith rapid j erks . Be ing of
lower specific grav ity than the water , they rise quickly w ithouteffort. They do not eat .
I talian invest igators“ 15 obse rved that the nymphae of some
mosquitoes res isted freezing and dess icat ion to a remarkabledegree. Enclosed for several hours in ice , they were yet ableto develop , and kept in dry soi l for two or three days theydeve loped when placed
‘
in water.
The durat ioni
of the pupal stage is ord inarily from .two to
five days.

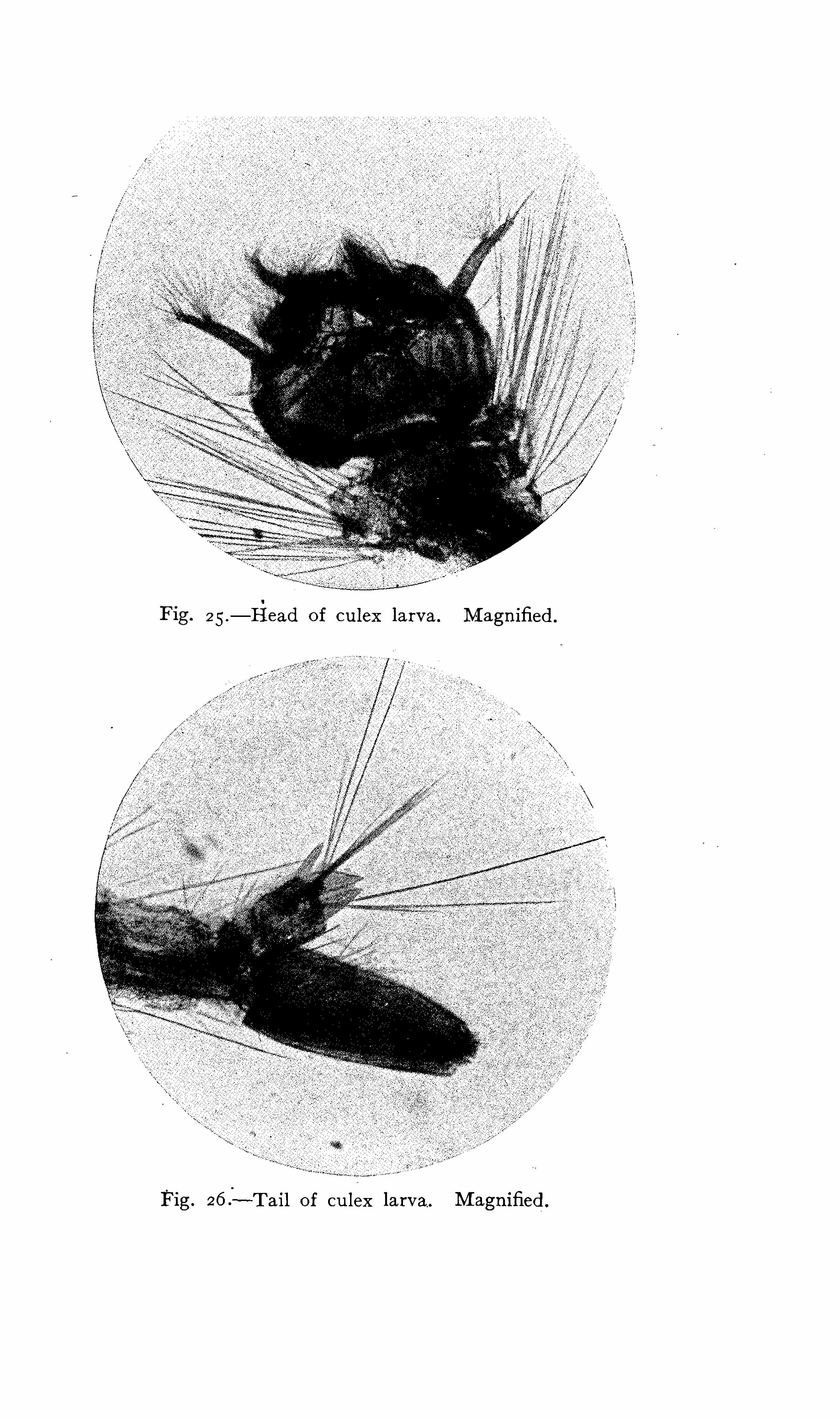
2 5 .—F1ead of culex larva. M agnified .
Fig.- ~T ail of culex larva. M agnified .




Fig. 30 .—Young stegomyia larva. M agnified .
Fig. 31 .—G rown stegomyia larva. M agnified .
Fig. 32 .—S tegomyia pupaf M agnified .




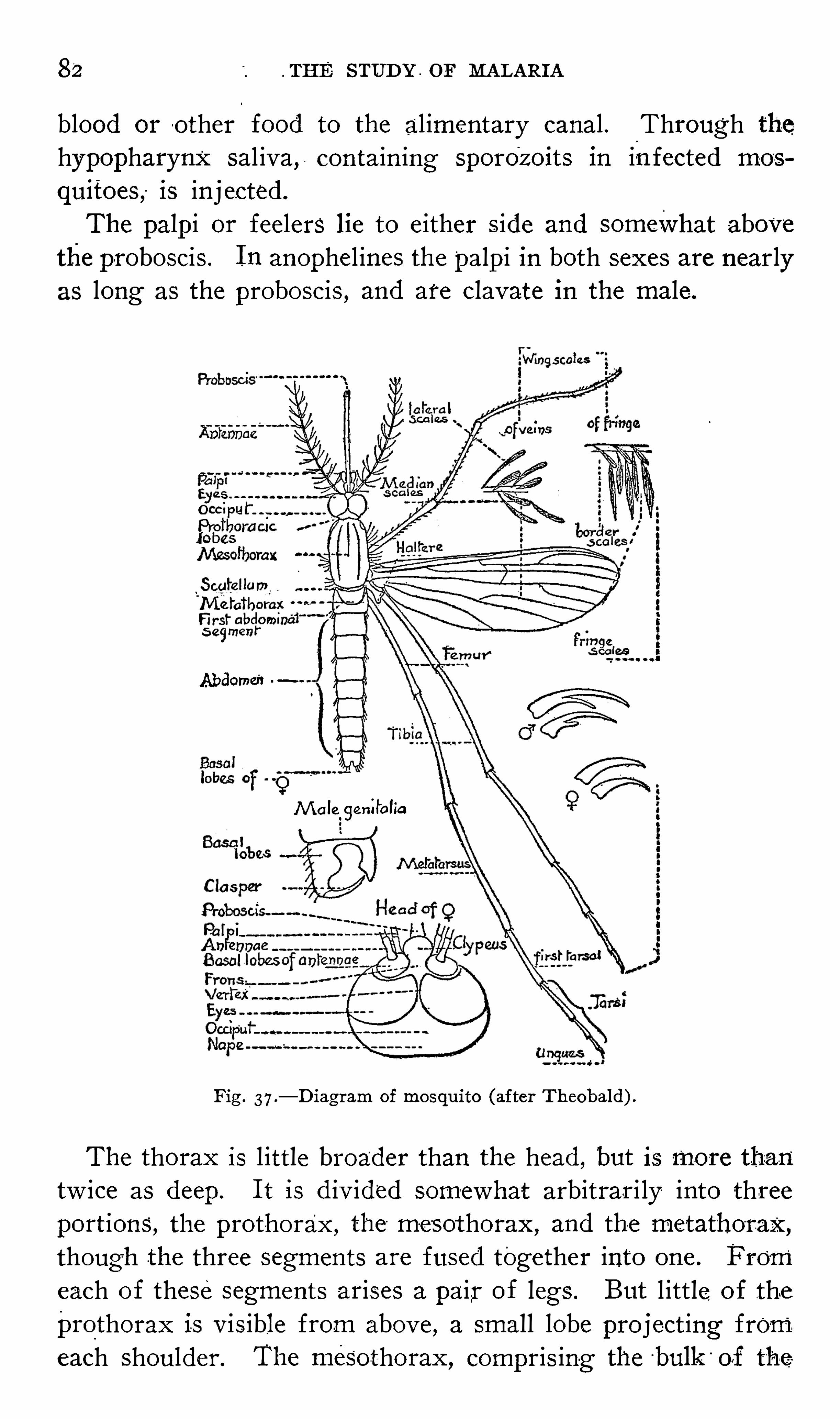
82 . THE STUD Y . or MALARI A
blood or o ther food to the al imentary canal . Through thehypopharynx sal iva, contain ing sporo
‘
z oits in infected mos
quitoes, is inj ected.
The palpi or feelers lie to e ither s ide and somevVhat abovethe proboscis . I n anophel ines the palp i in both sexes are nearlylong the proboscis , and are clavate in the male .
Abdomen
M aleogenilolia
Fig . 37.—D iagram of mosquito (after Theobald) .
The thorax is l ittle broader than the head , but is more than
tw ice as deep . I t is d iv ided somewhat arbitrar i ly into threeport ions, the prothorax , the mesothorax
, and the metathorax,
though the three segments are fused together into one . From
each of these segments arises a pair of legs . But l ittle of the
prothorax is v isible from abov e,a small lobe project ing from.
each shoulder. The mesothorax , compris ing the‘bulk
'
off the
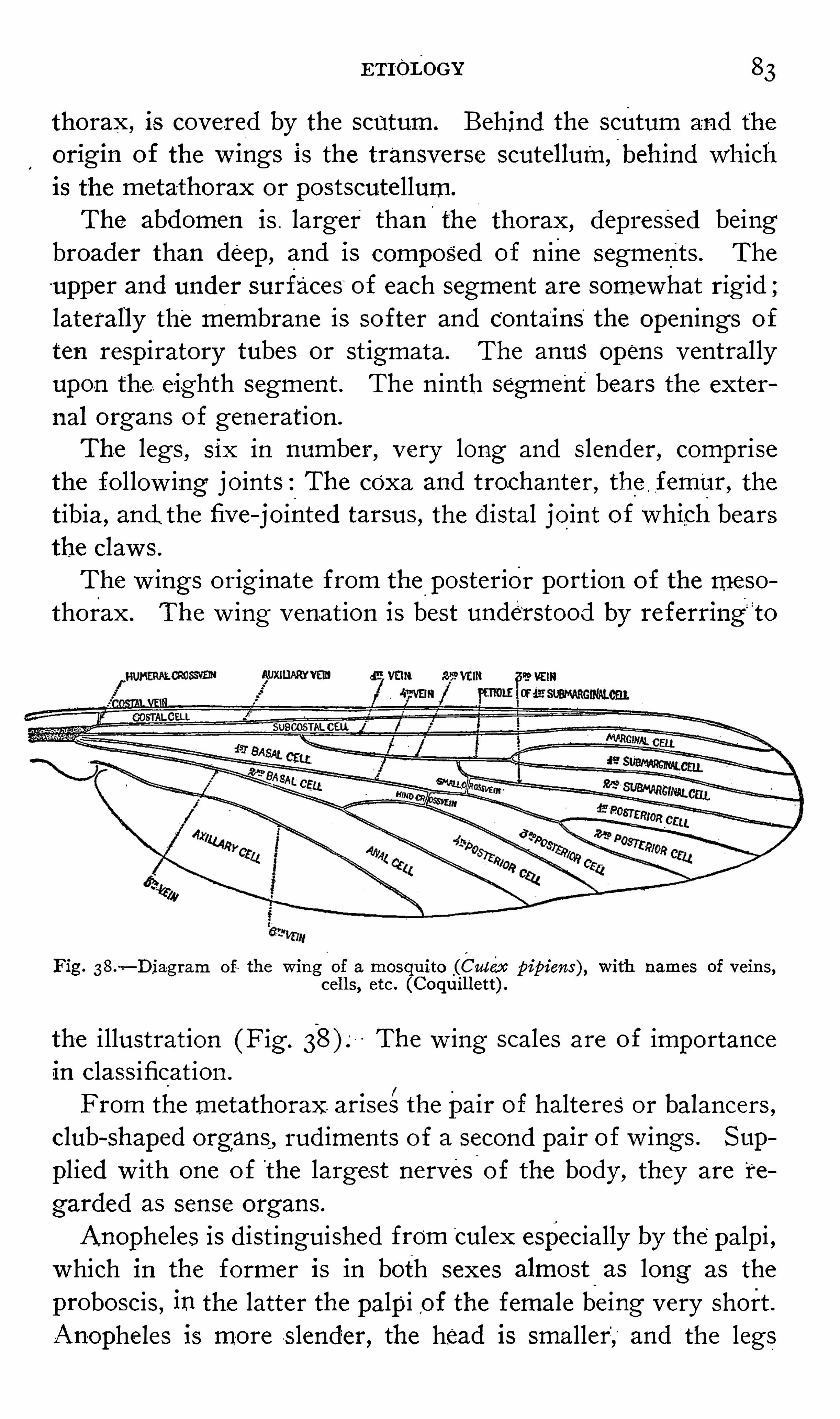
ETI-oDOGY 83
thorax ,is covered by the scutum . Behind the scutum and the
or1g1n of the wmgs is the transverse scutellum,
i
behind whichis the meta-thorax or postscutellum.
The abdomen is . larger than the thorax , depressed beingbroader than deep, and is composed of n ine segment s . The
upper and under surfaces of each segment are somewhat rig id ;laterally the membrane is softer and contains the open ings of
ten respiratory tubes or st igmata. The anus opens ventrallyupon the e ighth segment . The n inth segment bears the exter
nal organs o f generat ionThe legs , six in number
,very long and slender, comprise
the fo l low ing joints : The coxa and trochanter , the flfem
’
ur, the
t ibia, and the five - jointed tarsus , the d istal joint of which bearsthe claw s .
The w ings orig inate from the posterior port ion of the meso
thorax . The w ing venat ion is best understood by referring‘
t o
89 VEIK
Fig .—D iagram of the m ug of a mosquito (Culex pipiens) , with names of veins,
cells , etc . (Coquillett) .
the i llustrat ion (Fig . The w ing scales are of importancein class ificat ionFrom the metathorax. ar1se"the pair of halteres or balancers ,
club - shaped organs, rud iments o f a second pa1r of w ings . Sup
pl ied w ith one o f the large-st nervesi
o f the body , they are t e
garded as sense organs .
Anopheles is d ist inguished from"
culex especially by the palpi ,which in the former is in both sexes almost as long as the
proboscis , in the latter the palpi ,of the female be ing very short .
Anopheles 15 more S lender, the head is smaller; and the legs
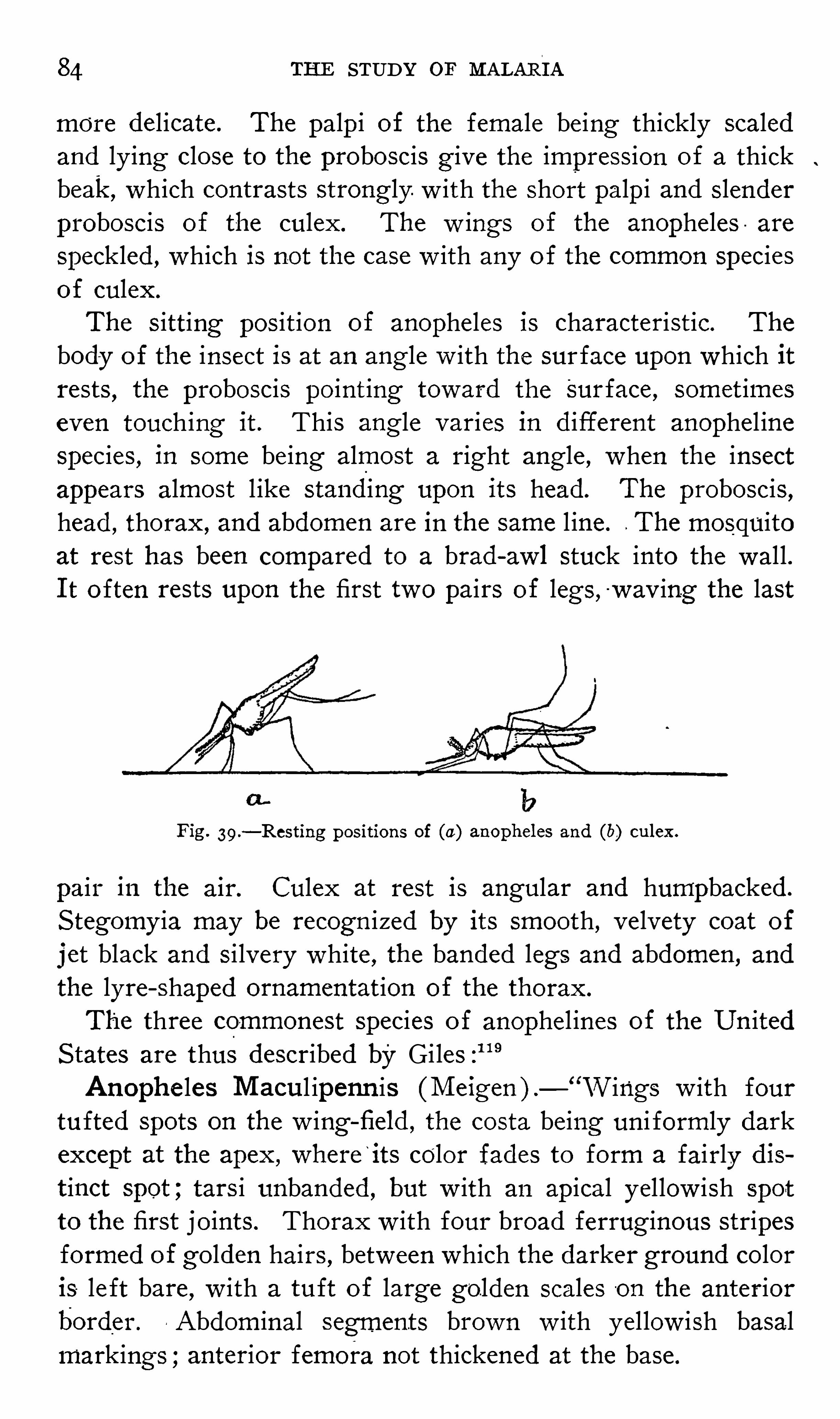
84 THE STUDY OF MALARTA
more delicate. The palp i of the female be ing thickly scaledand ly ing close to the proboscis g ive the impress ion of a thickbeak, which contrasts strongly w ith the short palpi and slenderproboscis of the culex. The w ings of the anopheles are
speckled , which is not the case w ith any of the common speciesof culex.
The s itting pos it ion of anopheles is characteristic. The
body o f the insect is at an ang le w ith the surface upon which itrests
,the proboscis point ing toward the Surface , somet imes
even touching it . This angle varies in d ifferent anophel inespecies , in some being almost a right angle , when the insectappears almost l ike stand ing upon its head. The proboscis ,head , thorax , and abdomen are in the same l ine. The mosquitoat rest has been compared to a brad - awl stuck into the wal l .I t o ften rests upon the first two pairs of legs , w av ing the last
Fig . 39 .—Resting positions of (a) anopheles and (b) culex.
pair in the air. Culex at rest is angular and humpbacked.
S tegomy ia may be recogn ized by its smooth , v elvety coat of
j et black and s i lvery white , the banded legs and abdomen , and
the lyre - shaped ornamentat ion of the thorax.
The three commonest species of anophel ines of the Un itedS tates are thus described by GilesAnophe les M acul ipenn is (M eigen ) . Wings w ith four
tufted spots on the w ing - field , the costa being un i formly darkexcept at the apex , where
‘
its color fades to form a fairly dist inct Spot ; tars i unbanded , but w ith an ap ical yel low ish spot
to the first jo ints . Thorax w ith four broad ferrug inous stripesformed of golden hairs , between which the darker ground coloris le ft bare
,w ith a tuft of large golden scales on the anterior
border .. Abdom inal segments brown w ith yel low ish basal
markings ;anterior femora not thickened at the base.

86 THE STUDY O F MALARI A
to be a triangular swelling at the base o f the abdominal segments . I t may be d ist inguished from An. em eto
-
ns by the costa
of the latter being uni form ly dark. and by its hav ing two insteadOf three dark Spots on the s ixth long itud inal ve in. The midd lespot extends much further across the w ing than in the S inensisgroup , and the tars i are unbanded . L eng th 5 t o 7 mm .
Anophe les Cruc ians —“Wings w ith white spots
here and there on the- brown ve ins , uni form along the costa ;
tars i unbanded , dusky brown ;ad men un i formly brown w ithgrey hairs . Thorax red - brown w ith linear markings .
“
D escription fromWied . ,A . Z . I . , p . 12
‘Tawny ;the thoraxw ith three deeper—t inted l ines ;the abdomen covered w ith greyhairs ;the w ings w ith dusky spots and costa. L ength 272 l ines
“
Coquillett , in his recent synopt ic table of North AmericanCnllclo
’w, states that
‘
the scales “
of the last veins are white ,marked w ith three black spots ;palpi marked w ith white at the
bases o f the last f our jo ints , ’ and w ithout any spot on the
costa, as seen in A . pnnetipennls .
“
Pro fessor Nuttal l sent M r. Theobald two females fromAmerica in spirit , which , although much damaged , show the
two features ment ioned by Coquillett very clearly , read i ly distinguishing the species - from the C . pnnetipennls of S ay .
”
The fol low ing key to the mosquitoes of North and M idd leAmerica is that
“
of M r. Coquillett ,12°
o f the D epartment of
Agriculture , by w hose kind permiss ion it is here reproduced'
A. CLAS S IFI CAT I ON O F THE M O SQUITO ES O F NO RTH AND M I DDLE
AM ER I CA
TABLE OF THE S UBFAM I'
LI ES
A . S cutellum convex behind, never distinctly three - lobed ; poste rior end ofthe thorax bare ; small cross—v einusually situated considerably be forethe root o f the third v ein and con
nected w ith it by a stump o f a vein
claw s of the“
female simple .
B . Proboscis straight or almost so ; back of the head devoid ofbroad appres sed scales , but w ith manynarrow outstanding ones ;body never
w ith metalescent scales ; first sub~
marginal ce ll longer than its petiole ;~
claw s simple in both sexes.
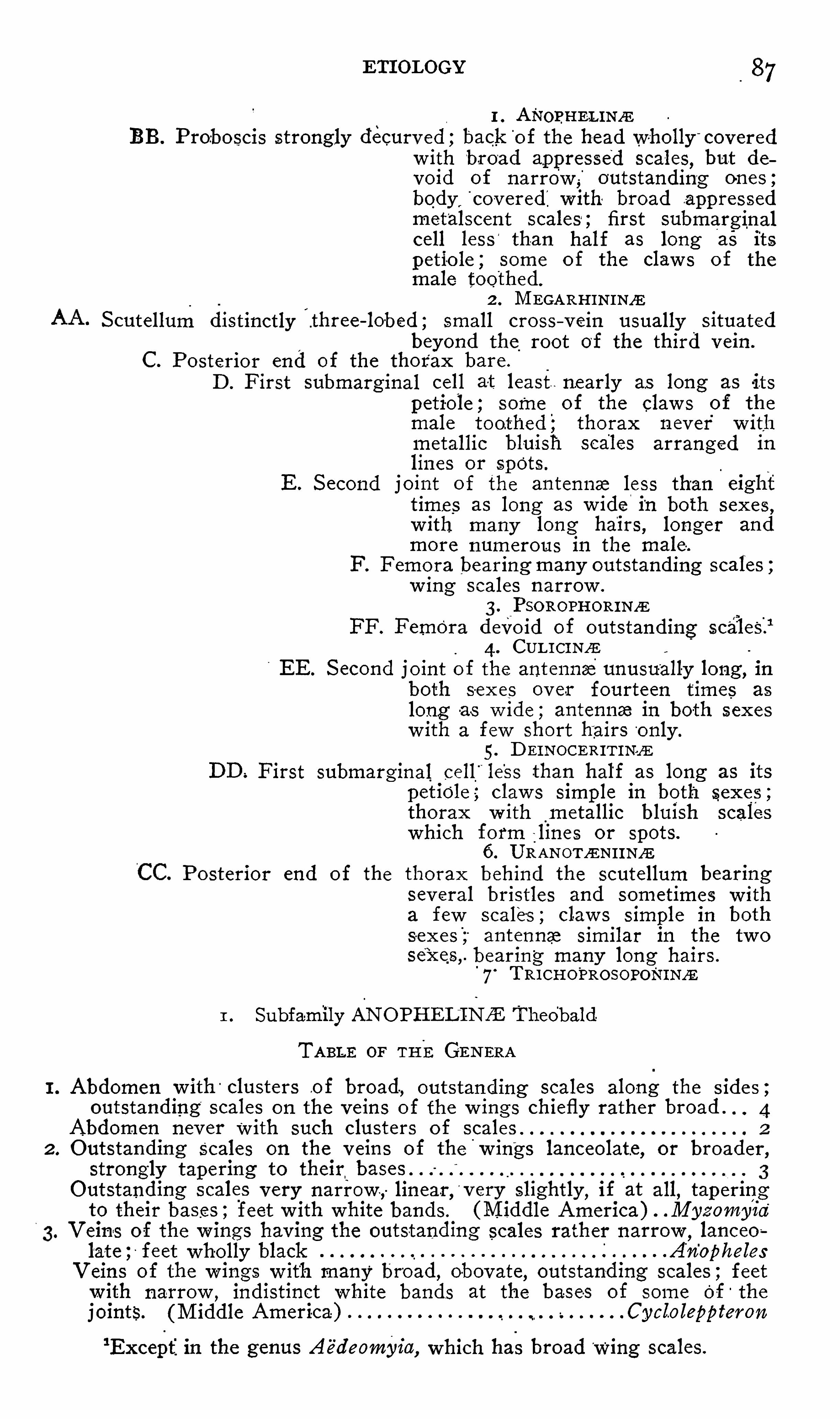
ETI OLOGY 87
1 . ANOPHEu Nz EBB. Proboscis strongly decurv ed ;back o f the head wholly covered
w ith broad appressed scales, but de
void of narrow,
outstanding ones ;body cov ered w ith broad appressedmetalscent scales ; first submarginalcell less
‘
than half as long as its
petio le , some o f the claw s o f themale toothed.
J
2 . M EGARHINI NfE
S cutellum distinctly three - lobed ; small cross v ein usually situatedbeyond the root of the third vein .
C. Posterior end of the thorax bare .
D . First submarg inal cell at least nearly as long as its
petiole ; some of the claw s of themale toothed ; thorax n ev er
'
w ithmetallic bluish scales arranged inlines or spots .
E. S econd joint of the an tennae less than eighttime s as long as w ide in both sexes ,
w ith many long hairs , longer andmore numerous in the male .
F. F emora bearing many outstanding scales ;w ing scales narrow .
3. PSOROPHORINZE
FF . Femora devoid of outstanding scales.
4. CUc e E
EE. S econd j oint o f the antennae unusually long , 1nboth sex es ov er fourteen times as
long as w ide ; antennae in both sexes
w ith a few short hjairs o nly .
5 . D EI NOCERI T INJ E
DD . First submarg inal cell less than half as long as its
petiole , claw s simple in both sexes ;thorax w ith m etallic bluish scales
which form lines or spots.
6. URANOTAEZNI I NfE
Posterior end of the thorax behind the scutellum bearingsev eral bristles and sometimes w ith
a few scales ; claw s simple in bothsexes ; antennae similar in the tw o
bearing many long hairs .
“
7. TRI CHO'
PRO SOPONINZE
1 . Subfamily ANO PHEL tN/a Theobald
TABLE OF THEGENERA
I . Abdomen w ith'
clusters .of broad , outstanding scales along the side s ;outstanding scales on the veins of the w ings chiefly rather broad . 4
Abdomen nev er with such clusters o f scal . .es
2 . Outstanding scales on the v eins of the w ings lanceolat. ,e or broader ,
strongly tapering to their
Outstanding scales very narrow ,linear
,v ery slightly , if at all
,tapering
to their bases ; feet w ith white bands. (M iddle America) . M y z omy z a
V ein s of the w ings having the outstanding scales rather narrow,lanceo
late ; feet wholly black AnophelesV eins of the w ings w ith many broad , obovate, outstanding scales ; feet
w ith narrow ,indistinct white bands at the base-s of some of the
joints. (M iddle America) . Cycloleppteron
‘Except
'
in the genus Aé’
deomy z’
a,which has broad wing scales.

88 THE STUDY or MALARI A
4. Upper side of thorax and scutellum bearing many appressed lanceolatescales ; outstanding scales on the
,
veins of the w ings rather narrow ,
lanceolate. (Florida and southward ) CelliaUpper side of thorax and scutellum w ith hairs only ;many rather broad ,obovate
'
outstanding scales on the v eins o f the w ings . (M iddleAmerica) Noto'
trieha n . gen.
G enus M YZOM Y I A Blanchard
( S ynonym : Grassia Theobald )
Wings black—scaled and w ith several white - scaled patches ; feet black ,banded w ith white ; thorax gray and w ith four black stripes . (West
I ndies ) lntz il Theob.
G enus ANO PHELES M eigem
(a ) TABLE OR THE S PECI ES
1. Wings marked w ith spots of dark or light - colored scales 2
Wings unspotted ; length of the head and body about 3 mm.
barberi Coq.
2 . F ront margin of the w ings w ith a patch of whitish S cales at a pointabout three - fourths of the way frombase to apex of the w ing . 5
F ront margin of the w ings wholly black - scaled 3
3. S ixth, or last , vein of the w ings wholly black - scaled 4S ixth vein white - scaled and w ith three patches of black scales.
crucians Wied.
4. Hind tibia yellow ish - white - scaled on the apical fourth ; first vein'
of
the w ings w ith a patch of yellow scales before its middle and another
on the apex. ( Central America)Hind tibia narrow ly yellow ish
- white scaled at the extreme apex only ,first and other veins w ith black s cales only macnlipennis M eig.
5 . S cales of the last vein of the w ings white , those at its apex black ;third v ein white—scaled and w ith two patches of black scales 6
S cales of the last vein white, those at each end black ; third vein black
scaled , the extreme apex white - scaled . punctipennis S ay .
6. Fourth vein of the w ings black - scaled , the apices of the forks and
usually also a patch at the cross veins white - scaled.
franciscanns M cC .
Fourth vein white—scaled,the fork s ( except their apices ) and on either
side of the cross veins black - scaled . .ps endopnnctipenn z’
s Theob.
( b) L I ST OF THE S PECI ES AND S YNONY M S
barberi Coq. maculipennis M eig .
crucians Wied. annulimanus van der Wulp .
1
eiseni Coq. blfnrcatns M eigen ( 1804 ; not of
francisc'
anus M cCrack en . L inné ,quadriinocnlatns S ay .
pseudOpunctipennis Theob.
punctipenn is S ay .
hyemalis F itch.
( c) UNRECOGNI ZED S PECI ESblfnreatus Linné , nigripes S ta ger , and walheri Theobald. These species
are said to have unspotted w ings , like barberi , but are larger, have yellow
scales on the thorax ,etc.
pictns -Loew . Thl-S speci es , descrlbed from As1a M inor, was also re
corded from North America by its author, but he ev idently mistook some
1At my request D r. C. Ritsema C z compared Specimens of ynacnlipennzls
w ith the type of. annnlimanns in the L eyden M useum, and informed me
that they ,are identical.
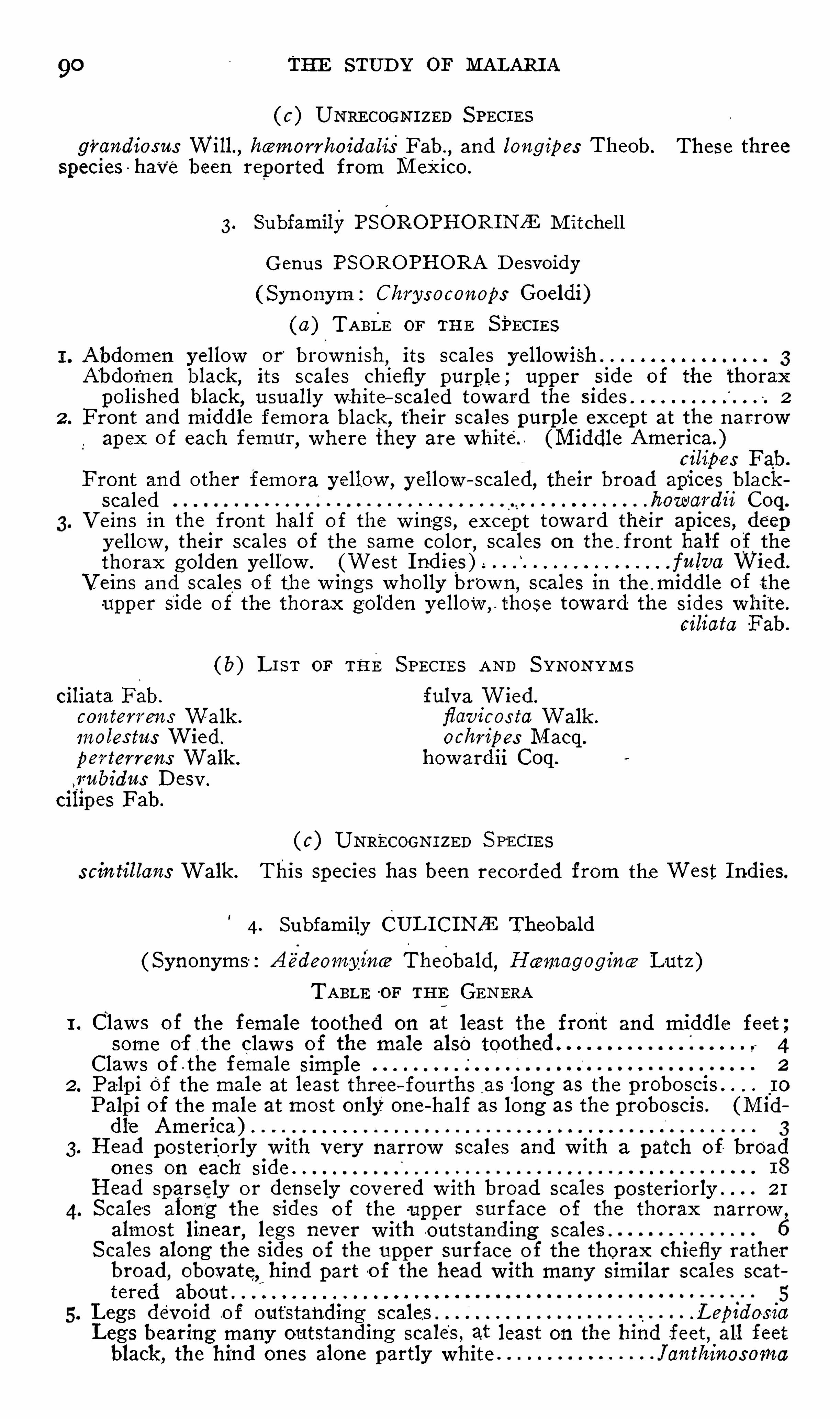
90 THE STUD Y OF MALAR I A
( c) UNRECOGNI ZED S PEC I ESgrandiosns Will , he morrhoidalis Fab.
,and long ipes Theob. These three
Species have been reported from M exico.
3. Subfamily PSOROPHORINZE M itchell
G enus PSO RO PHORA D esvoidy
( S yn onym : Chrysoconops Goeldi)
( o ) TABLE or THE SPECI ES
Abdomen yellow or bi ownish,its scales y ellow ish
A‘
bdor‘
nen black , its scales chiefly purple ; upper side o f the thorax
polished black , usually white—scaled toward the sides 2
2 . Front and middle femora black , their scales purple except at the narrow
ap ex of each femur,where they are white. (M iddle America.
cilipes Fab.
F ront and other femora y ellow , yellow scaled, their broad apices black
scaled hon-1111d11 Coq.
V e ins in the fron t half o f the w in-
gs , except toward their apices , deepy ellow ,
their scales of the same color,scales on the front half of the
thorax golden yellow . (West I nd ies ) . fnlva Wied.
V eins and scales o f the w ings wholly brow n, scales In the .middle of the
upper side o f the thorax golden yellow ,those toward the sides white .
ez hata Fab.
( b) L I S T or THE S PECI ES AND S YNONY M S
ciliata Fab. fulva Wied.
con tew'
ens Walk . flavicos ta Walk .
1noles t11s Wied. ochm'
pes M acq.
perterrens Walk . howardii Coq.
,1fnbidns D esv .
cilipes Fab.
( c) UNRECOGNI ZED S PECI ESscln tillans Walk . This species has been recorded from the West I ndies.
4. Subfamily CUL I C INZE Theobald
( Synonyms : Ae
'
deomy inm Theobald, Haemogogince Lut z )
TABLE -OF THE GENERA
I . Claw s of the female toothed on at least the front and middle feet ;some of the claw s of the male also toothed 4
Claw s of the female simple 2
2. Palp i of the male at least thre e fourths as long as the I o
Palpi of the male at most only one - half as long as the proboscis. (Middl
'
e America) .
3. Head posteriorly w ith very narrow scales and w ith a patch of broad
on es on each side
Head sparsely or densely cov ered w ith broad scales posteriorly ” 2 I
S cales along the sides of the upper surface o f the thorax narrow ,
almost lin ,ear legs never w ith outstanding scales .
S cales along the sides of the upper surface o
o
f the thorax chiefly rather
broad , obovate, hind part o f the head w ith many similar scales scat
tered aboutLegs devoid of outstanding scales .L epz dos-1a
L egs bearing many outstanding scales , at least on the hind feet , all feetblack ,
the hind ones alone partly white Janth1noso1na

ETI OLOGY
part of the head densely covered with broad , appressed s
l
ept sometimes a narrow stripe in the“
part of the head sparsely covered w ith narrow,almost 1
iles and w ith a patch of broad ones on each side .
eus bearing several scales or hairs,scutellum w ith broad s
S tegous bare
, scutellum w ith narrow scales only . (M iddle Ame1
V emf
veins having the outstanding scales narrow , lanceolate ,ghtly
.
tap ering to the base .
g veins hav ing many v ery broad outstanding scales whichongly to their bases ; sev eral of the scales are hollow ed o
:ir ap ices L epido;i of the male less than one fourth as long as the proboscis ”
i of the male about as long as the proboscis O chlei’o1 densely cov ered behind w ith broad , _
appressed scales, excr
rrow strip e in the middle,or else the thorax has six line
very scales
1 bearing narrow ,almost linear appressed scale s behind and
patch of broad ones on each side ; thorax never w ith line
very scales:tanding scales on the veins behind the first one narrow an
arly a uniform w idth .
:tanding scales on at least the apical half of the w ings broad ,lerably narrow ed at their bases
white at each end of some o f the joints or else wholly lwhich case the abdomen 1s wholly black
~ scaled,or else it has c
nds of light colored scales ”
white at the bases only of Some of the j oints, or else w
l ,in which case the abdomen I S black scaled and w ith the :
rners o f some of the segments white scaled . .Gmbha of the w ings not spotted .
a black - scaled and w ith three large spots o f pale yellow 5 1
fi ddle America)rax w ith two distinct bare stripes near the middle of the 1
le ; hind cross—vein at least its own length from the smallin C112fax w ithout bare stripes .
es of the w ings collected into spots ; hind cross—v ein muchin its length from the small cross vein Theol
s of the w ings uniformly distributed .
i cross - vein much less than its own length from the smal
éc
In 11
l cros s—vein situated at . least nearly its own length .from the
) ss - vein
.1half of the w ings hav ing the outstanding scales of the veins
w and almost linear ; proboscis wholly black . M elonoc
Ll half of the w ings having many broad, outstanding scales 0
ms
g v eins hav ing the outstanding scales narrow,almost linear . .
g v eins hav ing the outstanding scales rather broad , oblance <
lpi of the male almost one -
,half those of the female less than
th,as long as the proboscis T1
°
no
i in both sexes about one - third as long as the proboscis . M 161
i in both sexes -less than one - fifth as long as the proboscis .
I sos tomy ia n
outstanding scales on the veins of the w ings only mode
sad,over tw ice as long as broad , their apices rounded ; pro]
(1 feet usually w ith light - colored bands Coqn1lle
outstanding scales chiefly unusually broad, their apices fl[ low ed out
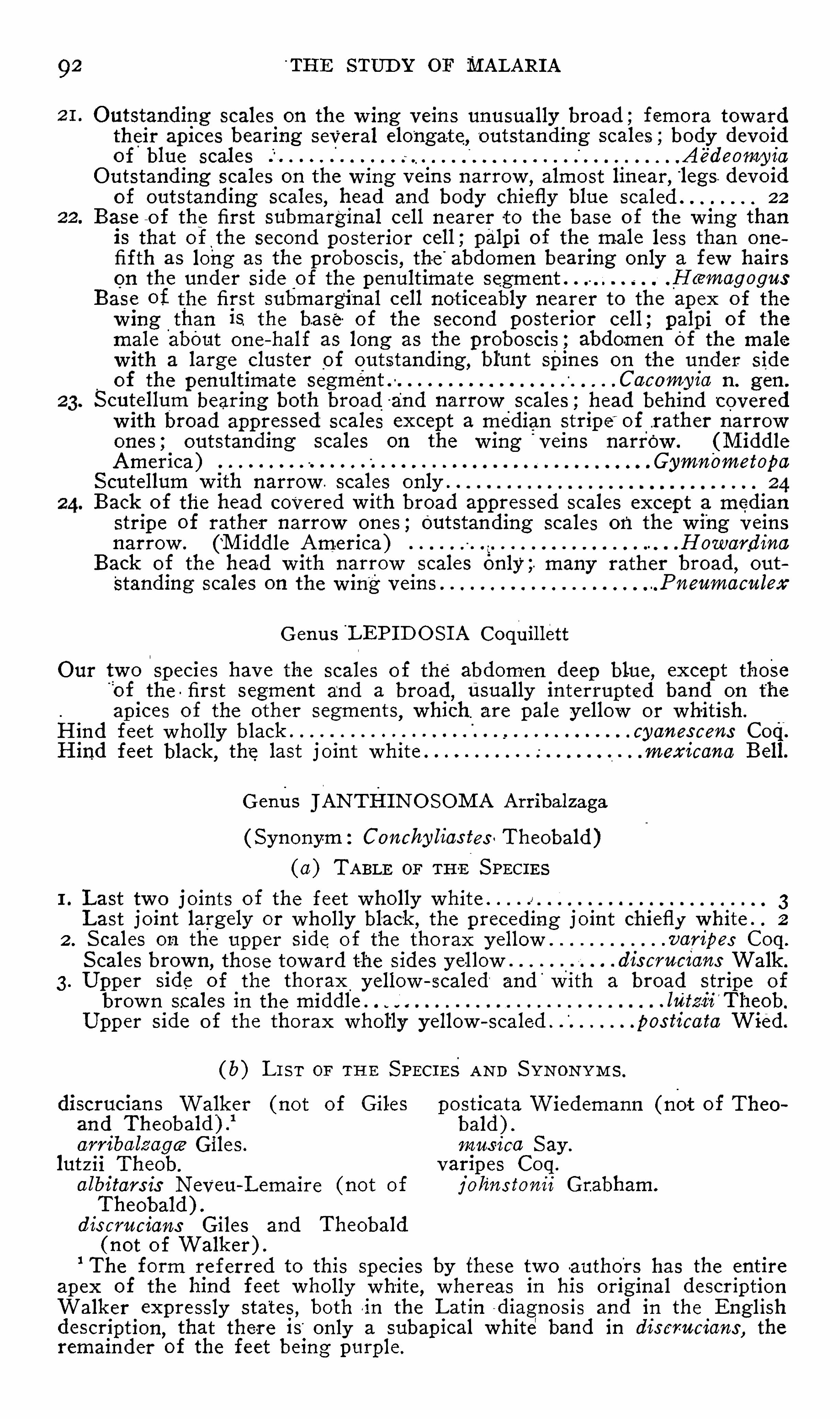
92 T HE STUD Y or MALARI A
Outstanding scales on the w ing veins unusually broad ; femora towardtheir ap i ces bearing several elongate, outstanding scales ;body devoidof blue scales A
°
e°
deo1ny1°
a
O utstanding scales on the w ing veins narrow,almost linear
, legs devoidof outstanding scales
,head and body chiefly blue scaled 22
Base of the first submarginal cell nearer to the base of the w ing thanis that of the second posterior cell , palpi of the male less than onefifth as long as the proboscis , the abdomen bearing only a few hairson the under side o f the penultimate segment . H (emogogns
Base of the first submarginal cell noticeably nearerto the apex of thew ing than is the ba se of the second posterior cell; palpi of themale about on e—half as long as the proboscis ; abdom en
pot the male
w ith a large cluster of outstanding , blunt Spines on the under side
of the penultimate segment Caeomyio n. gen.
S cutellumpbearing both broad and narrow scales ; head behind covered
w ith broad appressed scales except a median strip e of .rather narrow
ones ; outstanding scales on the w ing veins narrow . (M iddleAmerica) Gymnometopa
S cutellum w ith narrow . scales only .
Back of the head Covered w ith broad appressed scales except a medianstripe of rather narrow ones ; Outstanding scales on the w ing v einsnarrow . (M iddle America) Howardina
Back of the head w ith narrow scales only ; many rather broad,out
Standing scales on the w ing veins Pneumaenlex
G enus L EP I D O S I A Coquillett
Our two species have the scales of the abdomen deep blue , except those’
of the first s egment and a broad,Usually interrupted band on the
ap ices of the other segmen ts,which are pale y ellow or whitish.
Hind feet w holly black cyanes cens Coq.
Hind feet black , the last j oint white . mexicano Bell.
G enus JANTHINO SOM A Arribalz aga
( S ynonym : Conchy lias tes Theobald )
(a) TABLE or TH -E S PECI ES
1. Last two j oints of the feet wholly white . . 3Last joint largely or wholly black ,
the preceding j oint chiefly white . 2
2 . S cales on the upper side o f the thorax y ellow .varipes Coq.
S cales brown,those toward the sides y ellow . dis crucians Walk .
3. Upper side o f the thorax y ellow scaled and wi th a broad s tripe
brow n scales I n the middle . l11'
tz 1°
1 Theob.
Upp er s ide of the thorax wholly y ellow- scaled . pos ticata Wied.
( b) L I S T or THE S PEC I ES AND S YNONY M S .
discrucians Walk er (not of Giles posticataWiedemann (not o f Theoand Theobald ) .
1
bald ) .orrlbolz agw Giles . mus i c-a S ay .
lut z ii Theob. varipes Coq.
albltars is NeVeu—L emaire (not of j oh‘
ns z‘
onn°
Grabham.
Theobald ) .dis crucians Giles and Theobald
( not o f Walk er ) .
1The form referred to this species by these two authors has the entire
ap ex of the hind feet wholly white , whereas in his original descriptionWalker expressly states , both in the Latin diagnosis and in the Englishdescription,
that there i s only a subapical whiter
band in discrucians , theremainder of the feet being purple.
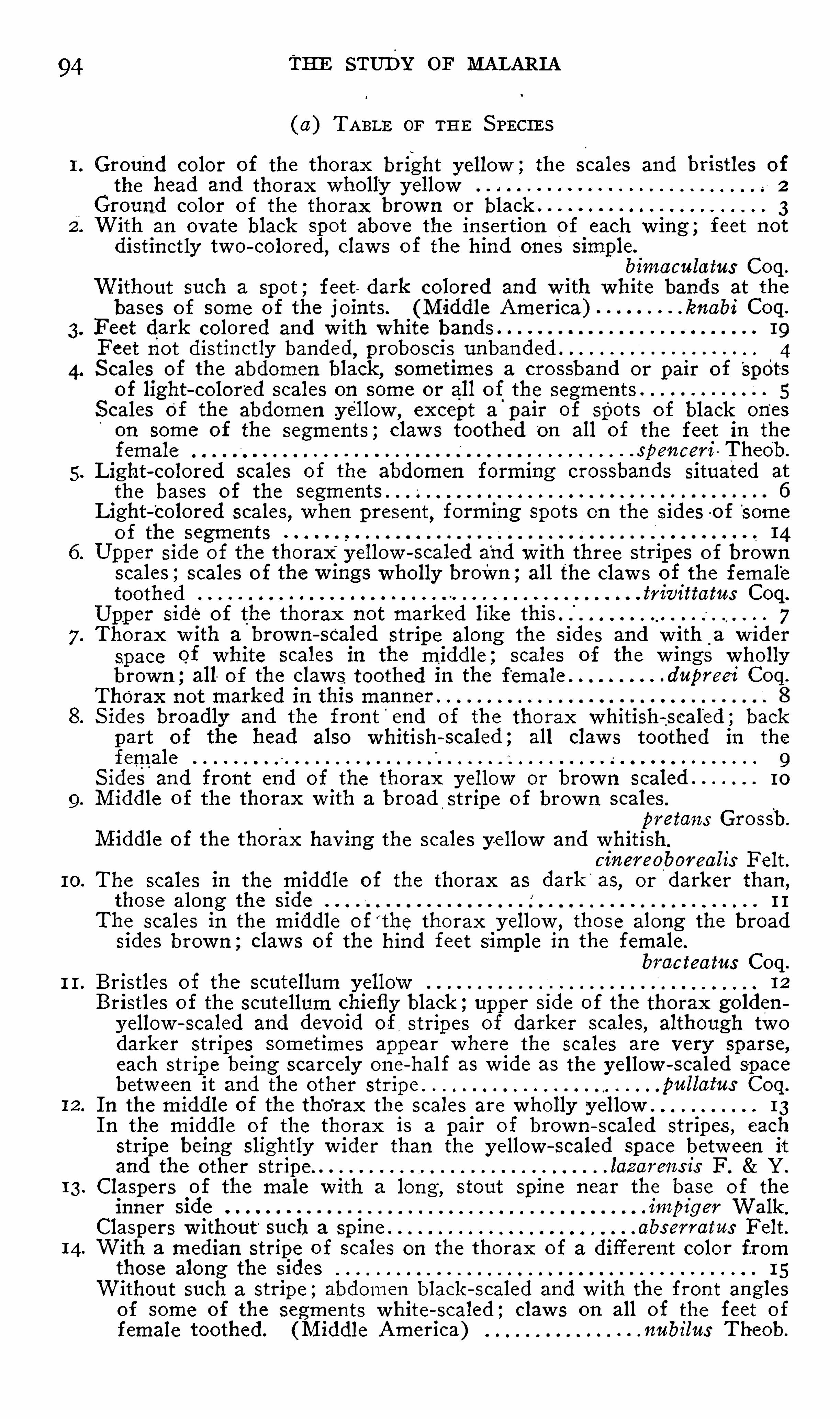
94
I O .
I I .
12 .
I 3.
14.
THE STUDY or MALAR I A
( 11) TABLE or THE S PECIES
Ground color of the thorax bright yellow ; the Scales and bristles ofthe head and thorax wholly y ellow 2
Ground color of the thorax brown o r black 3With an ovate black spot abov e the insertion of each w ing ; feet not
distinctly two colored , claw s of the hind ones simple.
bimaculatns Coq.
Without such a spot ; feet dark colored and w ith white bands at the
bases of some of the j oints. (M iddle America) . lanab1°
Coq.
Feet dark colored and w ith white bands
F eet not distinctly banded, p roboscis unbanded . . 4S cales of the abdomen black , sometimes a crosSband or pair of Spot-
s
of light color‘
ed scales on some or all of_
the segments .
S calesgof the abdomen .yellow ,
except a pai r of spots of black ones
on some of the segments ; claw s toothed on all of the feet in the
female spencerl TheOb.
L ight colored scales o f the abdomen forming crossbands situated at
the bases of the
Light - Colored scales , when present, forming spots on the sides o f Some
o f the segments
Upper side of the thorax y ellow scaled and w ith three stripes of brown
scales ; scales of the wings wholly broWn ;all the claw s of the female
toothed trivittatns Coq.
Upper side of the thorax not mark ed like this . 7Thorax w ith a brown sealed stripe along the s ides and w ith
_
a w ider
space of white scales in the middle ; scales of the w ings whollybrown ;all of the claw s toothed in the female . .d11p1
’ee1
°
Coq.
Thorax not mark ed in this manner
S ides broadly and the front end of the thorax whitish—scaled ; backpart of the head also whitish scaled ; all claw s toothed in the
female 9S ides and front end of the thorax y ellowor brown scaled 10
M iddle o f the thorax w ith a broad_
stripe o f brown scales .
pretans Grossb.
M iddle o f the thorax hav ing the scales y ellow and whitishclnereoborealis Felt .
The scales in the middle of the thorax as dark'
as,or darker than ,
those along the side 11
The scales in the middle o ff
the thorax y ellow , those along the broadsides brow n ; claw s of the hind feet S imple in the female.
bracteatns Coq.
Bristles o f the scutellum y ellow 12
Bristles of the scutellum chiefly black ;upper side of the thorax golden
y ellow - scaled and devoid of stripes of darker scales,although tw o
dark er strip es sometimes appear where the scales are very sparse,each stripe being scarcely one half as w ide as the yellow scaled space
betw een i t and the other stripe ” pnllatns Coq.
I n the m iddle o f the thorax the scales are w holly yellow 13I n the middle of the thorax i s a pair of brown scaled stripes , each
stripe being slightly w ider than the y ellow—scaled space betw een it
and the other stripe. . loz orens is F . Y .
Claspers of the male w ith a long , stout Spine near the base o f theinner side . 1
'
n1p1'
g er Walk .
Claspers w ithout such a sp ine abs ew atus F elt .With a median stripe of scales on the thorax o f a different color fr omthose along the sides 15Without such a strip e ; abdomen black - scaled and w ith the front angles
of some of the segments white - scaled ; claw s on all of the feet o f
female toothed. (M iddle America) Theob.

ETI OLOGY 95
15. S cales in themiddle of the thorax , at‘ least on its anterior half
, white,the remainder brown ; claw s on all of the feet of the female
toothedS cales in the middle of the thorax black
,the
“
remainder yellow or
whitish 1816. S tripe of wh ite scales in the middle of the thorax extending entirely
across the latter
S tripe of white scales confined to the anterior tw o thirds o f the
thorax confirmatns Arrib.
17. White scaled stripe of the thorax much narrow er than the brown
scaled portion on each side of it s erratus Theob.
White scaled stripe w ider than the brown - scaled portion on each
side of it dnpeeei Coq.
18. Upper surface of the thorax white - scaled toward the sides ; claw s on
the hind feet of the female simple triSenlatns S ay .
Upper surface o f the thorax golden yellow scaled toward the sides ;claw s on the hind feet o f the female toothed amnfer Coq.
19 . Proboscis blackish and w ith a white band near the middle ; whitebands o f the feet confined to the bases of the j oints , excep t on
nhind f eet,the last j oint of which is sometimes wholly white
Proboscis blackish, not distinctly banded near the middle . 22
20. Abdomen black—scaled,each segment w ith a basal
,band and median
longitudinal strip e o f yellow ish scales, and w ith a white - scaled spot
in the middle o f each side 2 1
Abdomen“
black scaled , each segment w ith a band at the base and a
Spot in the middle of each side white scaled,w ing seales wholly
black tceniorhynchns Wied.
2 1. Wing scales mixed black and yellow ish ; light colored scales o f the
legs y ellow ,usually a whitish band in the
b
middle of the first jointof
3
the feet . . sol1'
c1'
tans Walk .
Wing scales wholly black ; light colored scales o f . the legs pure w hite,first joint o f the feet nev er w ith a light colored band In the middle .
n11tchellce D yar .
22 . Joints of the feet hav ing the white band'
s situated at both ends o f
some of them,las t j oint o f the hind feet white 23Joints of the feet hav ing the white bands situated at the bases only
of some of them,last j oint of the hind feet black except sometimes
its extreme base 2823. Black scales mix ed w ith white ones on the w ings ; abdomen whitish
or y ellow scaled and w ith a pair of black scaled spots on some ofthe segments
Black scales only on the w ings , abdomen black scaled,some times w ith
a band of w hite scales at the bases o f the segments 25S tripe of scales in
_
the middle of the thorax deep golden brown, cover
ing more than one fifth of the w idth of thegthorax
,its borders
w ell defined. ( S alt water species ) latim'
ttatns C oq.
S tripe pale brown , covering less than one n inth of the w idth of thethorax
,its borders not strongly mark ed
,usually a narrow stripe o f
brown scales on each side of it separated by y ellow ish white scales .
(Fresh water species ) . cnrriel Coq.
2 5. Upper side of the thorax light yellow scaled and w ith a broad stripeof black scales
°
In the middle ;palp i wholly black - scaled in both sexes ;abdomen black scaled and w ith a band o f white scales at the base ofeach segment otropolpns Coq.
Upper side of the thorax not marked as abov e ; palpi w ith whitishsca
l
les at the ap ices in the female and w ith bands of them in thema e
26. S egments of the abdomen w ith distinct whitish bands at their bases ;scales of the upper side of the thorax brown and light yellow ish.
varipalpns Coq.
S egments of the abdomen never w ith distinct whitish bands ; scales ofthe upper side of the thorax wholly yellow 27
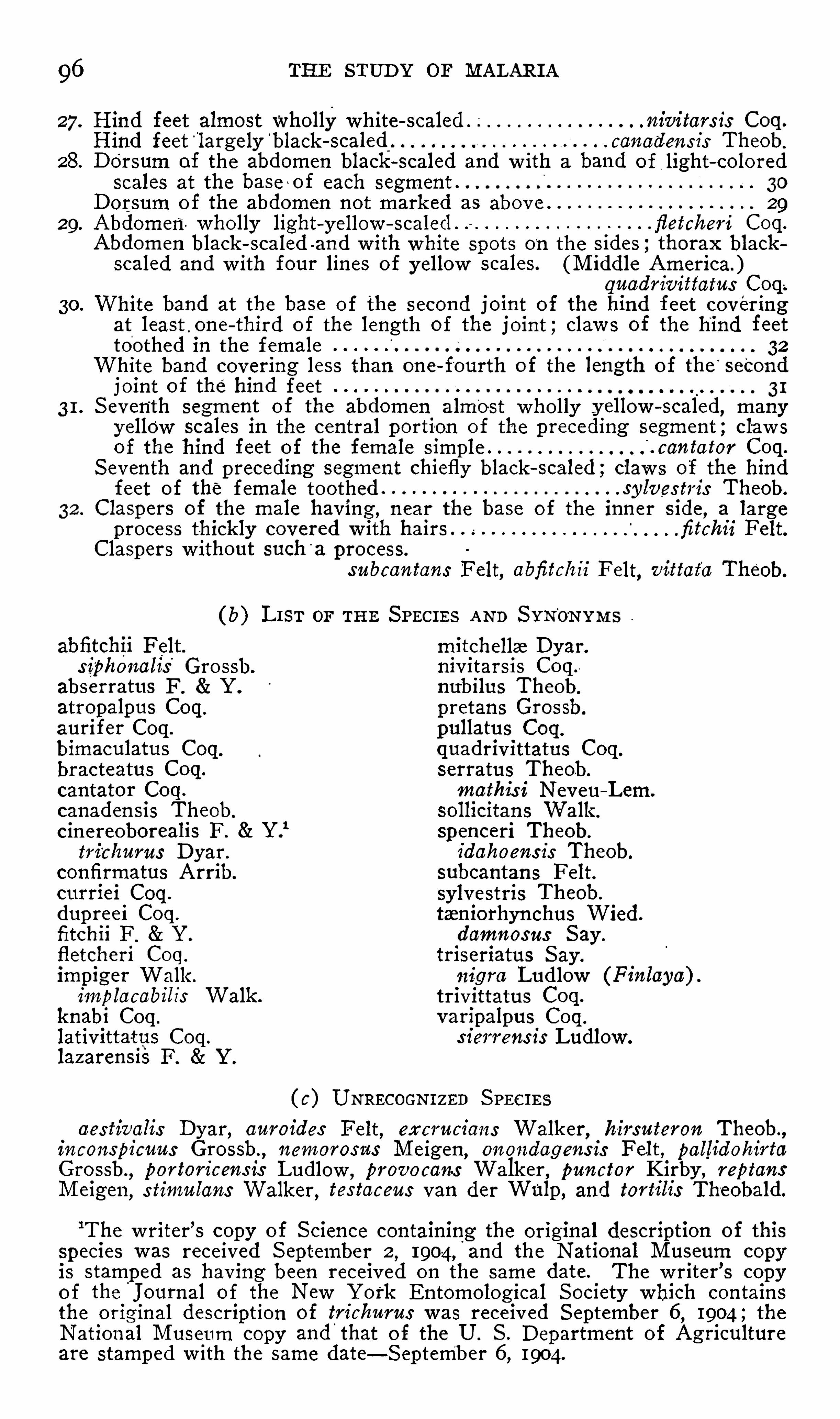
96 THE STUD Y or MALARI A
Hind feet almost wholly white - scaled ; nivitars is Coq.
Hind feet“
largely b lack - scaled canadens is Theob.
28. D o'
rsum of the abdomen black - scaled and w ith a band of_1ight - colored
scales at the base of each segment .
D orsum of the abdomen not mark ed as abov e . 2929. Abdomen wholly light—y ellow - scaled . fletcheri Coq.
Abdomen black - scaled -and w ith white spots on the sides ; thorax blackscaled and w ith four lines of y ellow scales. (M iddle America.)
qnodriw’
ttatns Coq.
30. White band at the base o f the second joint of the hind feet coveringat least . one - third of the length of the joint ; claw s of the hind feettoothed in the female 32
White band covering less than one - fourth o f the length of the‘
secondj oint of the hind feet31. S eventh segment of the abdomen almost wholly y ellow - scaled
,many
yellow scales in the central portion of the preceding segment ; claw s
of the hind feet of the female simple'
. can tator Coq.
S eventh and p receding segment chiefly black - scaled ; claw s of the hindfeet of the female toothed . sylves tm
'
s Theob.
Claspers of the male having ,near the base of the inner side , a large
process thickly covered w ith hairs . fitehz'
i Felt.Claspers w ithout such
'
a process.
subcantans Felt, abfiteh z z F elt, wittafo Theob.
( b) L I S T or THE SPECI ES AND S YN'
o-
NYM S
abfitchii Felt. mitchella D yar.siphonalis
’
Grossh. niv itarsis Coq.
abserratus F . Y . nubilus Theob.
atropalpus Coq. pretans Grossb.
aurifer Coq. pullatus Coq.
bimaculatus Coq quadriv ittatus Coq.
bracteatus Coq. serratus Theob.
cantator Coq. mathis i Neveu—Lem.
canaden sis Theob. sollicitans Walk .
cinereoborealis F . Y .
1spenceri Theob.
trichnrns D yar. idahoens is Theob.
confirmatus Arrib. subcantans Felt.
curriei Coq. sylvestris Theob.
dupreei Coq. ta niorhynchus Wied.
fitchii F . Y . domnosns S ayfletcheri Coq. triseriatus S ay .
impiger Walk . 111-gm Ludlow (Finlaya) .
implacabilis Walk . trivittatus Coq.
knabi Coq. varipalpus Coq.
lativittatus Coq. s ierrens is Ludlow .
laz arensiS F . Y .
( c) UNRECOGNI ZED S PECI ESaes tivah
'
s D yar, anroides Felt , excrucians Walker,hirsnteron Theob.,
inconspicnns Grossb., nen1oros 1-
1s M eigem, onondagens is Felt , pallidohirta
Grossb., por torieensis Ludlow , prooocans Walk er
, pnnctor K irby , reptans
M eigen ,s timulans Walker
,tes tacens van der Wulp , and tort1
°
11°
s Theobald.
1The w riter
’
s copy o f S cience containing the original description of this
species was received S eptember 2,1904,
'
and the National M useum copyis stamped as hav ing been received on the same date . The w riter
’
s copyo f the
'
Journal of the New York Entomological S ociety which contains
the original description of triehnm s was receiv ed S eptember 6, 1904 ; the
National M useum copy and'
that of the U. S . D epartment of Agriculture
are stamped w ith the same date—S eptemb er 6, 1904.
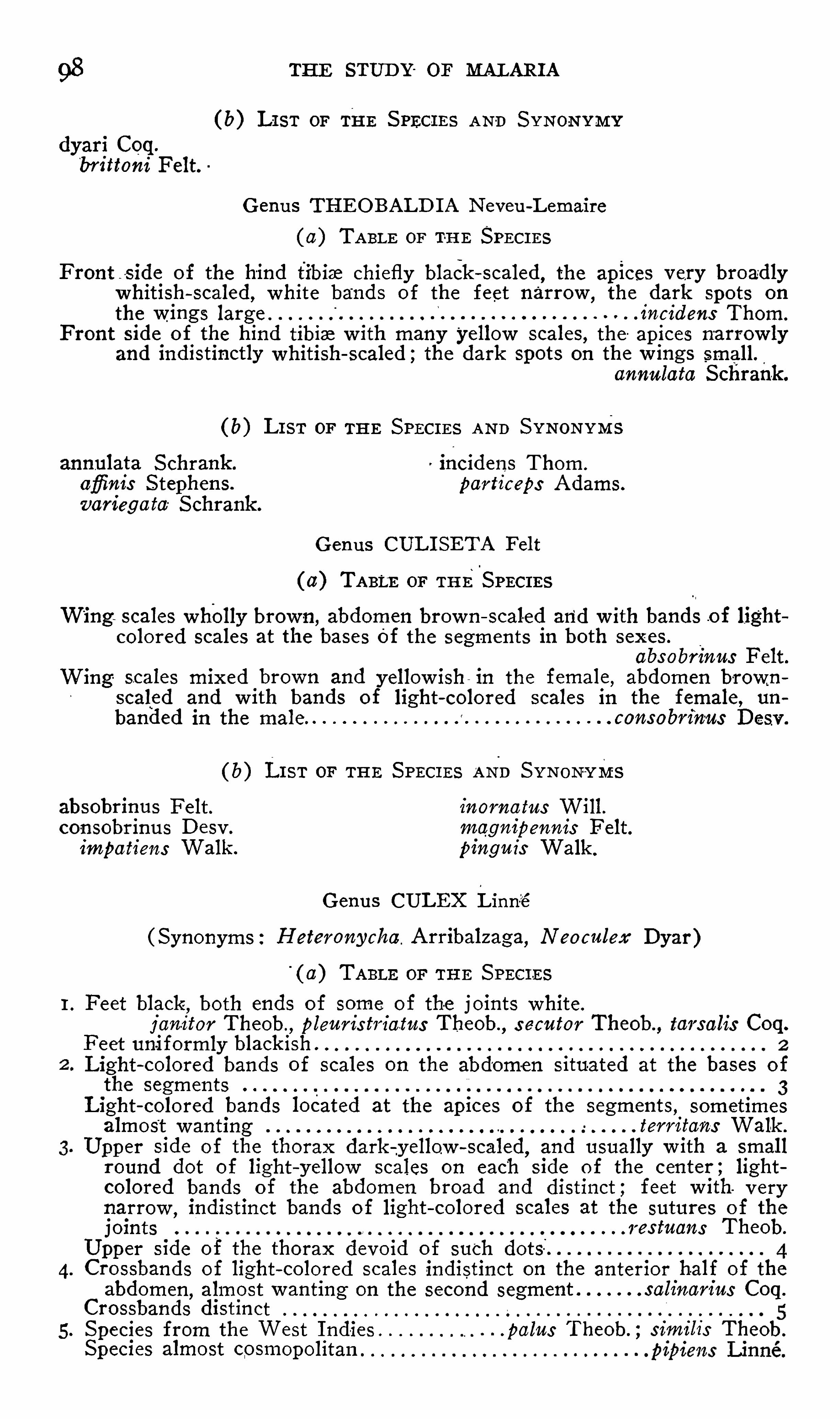
98 THE STUD Y or MALARI A
(b) L I ST or THE S PECI ES AND S YNONYM Y
dyari Coq.
brittoni Felt.
G enus THEO BALD I A Neveu - L emaire
( 11) TABLE or T-HE SPECI ES
F ront s ide of the hind tibia chiefly black scaled,the apices very broadly
whitish scaled , white bands of the feet narrow,the dark spots on
the wings large 1°
nc1°
dens Thom.
Front side of the hind tibia w ith many yellow scales, the apices narrow lyand indistinctly whitish scaled ; the
ydark spots on the w ings small.
annulata S chrank.
( b) L I ST or THE S PECI ES AND S YNONYMS
annulata S chrank .' incidens Thorn .
afl’inis S tephens. particeps Adams.
variegata S chrank .
G enus CUL I SETA Felt
( 11) TABLE or THES PECI ES
Wing scales wholly brown , abdomen brown scaled and w ith bands .of lightcolored scales at the bases of the segments in both sexes .
abs obrinus Felt .Wing scales mixed brown and y ellow ish in the female
,abdomen brown
scaled and w ith bands of light colored scales in the female , umbanded in the male consobmnus D esv .
( b) L I S T or THE S PECI ES AND S YNON-YMS
absobrinus Felt. inornatus Will.consobrinus D esv . mognlpennls F elt.impatiens Walk . pinguis Walk .
G enus CULEX Linn-e
( S ynonyms : Heteronycha. Arribalz aga, Neoculex Dyar)'
( a) TABLE or THE S PECI ES
1. Feet black,both ends of some of the j oints white.
j anitor Theob., pleuris triatus Theob., s ecutor Theob., tarsalis Coq.
F eet uniformly black ish .
Light - colored bands of scales on the abdomen situated at the bases ofthe segments
L ight colored bands located at the apices of the segments , sometimesalmost wanting lew itans Walk .
Upper side of the thorax dark y ellow - scaled,and usually w ith a small
round dot of light -
y ellow scales on each side of the cen ter , lightcolored bands of the abdomen broad and distinct ; feet w ith verynarrow
,indistinct bands o f light colored scales at the sutures of the
joints 1 es tuous Theob.
Upper side of the thorax devoid of such
4. Crossbands of light colored scales indistinct on the anterior half of theabdomen
, almost wanting on the second segment salinam'
us Coq.
Crossbands distinct
5 . S pecies from the West I ndies “ .palus Theob. ; s1°
1n 1°
l1°
s Theob.
Species almost cosmopolitan

ETI OLOGY 99
( b) L I ST or THE S PEC I ES A ND S YNONYM S
janitor Theob. salinarius Coq.
palus Theob nigm'
tulus auct. (North Americanp ipiens Linne. references ) .bos ciz D esv . secutor Theob.
cubensis Bigot. similis Theob.
fatigons auct .”L
(North'
American tarsalis Coq.
references ) .afiinis Adams ( not of S tephens ) .ferruginosus Wied. (Anopheles . leelloggu
°
Theob.
pung ens Wied. peus Speiser.
quinquefas ciotus S ay . w illis toni Giles.
pleuristriatus Theob. territan s Walk .
restuans Theob. apieolis _Adams.
( c) UNRECOGNI ZED S PECI ESflam
'
pes M acquart , biocellatus Theobald, inflletus Theob., microsquamosusTheob.
, nigripalpus Theob.,and s axatilis
“Grossbeck .
(C. penafieh° Williston has never been described.)
G enus M ELANO CONI ON Theobald
1. Hind and other feet wholly black 2
Hind feet white scaled on the broad base of the fourth joint , abdomen
black—scaled, a row of violet scaled spots along the S ides . (M iddleAmerica) 11ch1
°
1°
Coq.
2 . .Thorax on the anterior half golden y ellow scaled and w ith a pair of
black scaled spots , the posterior half black scaled and w ith two stripesof y ellow scales (M iddle America) ” splsslpes Theob.
Thorax wholly golden brown scaled 33. Abdomen w ith bands of y ellow ish scales at the bases of the segments.
(M iddle America) humilis Theob.
Abdomen unbanded
4. Front angles of the segments o f the abdomen yellow ish - scaled.
atratus Theob.
Front angles and whole of the abdominal segments black°
- scaled.
lndecom bilis Theob., melanurus Coq.
G enus T INO ‘
LESTES Coquillett
Feet unicolorous black ; scales of the upper side of the body black andw ith light colored ones in the front angles o f some of the segmentsof the abdomen . lotisquama Coq.
G enus M I CRAED ES Coquillett
Proboscis and feet unicolorous black ; scales of the abdomen purple blackand w ith light colored ones in the front angles of Some of thesegments bisulcatus Coq.
G enus I SO STOM Y IA Coquillett
Proboscis , feet , and abdomen wholly black scaled perturbons Will.(A
'
édes nigricorpus Theobald may
y
also belong to this genus. )
1I n response to my request , M ajor A Alcock , superintendent of the
natural history section of the I ndian M useum at Calcutta, I ndia, sent meSpecimens of this species in all the stages . The larvae have been examinedby Dr. H. G. Dyar and M r. F . Knab, who report having discovered differemees betw een them and the corresponding stage of the North Americanspecimens of pipiens .

100 THE STUD Y OF MALARI A
G enus CO QUI LLE‘
TT I D I A D yar
( 11) TABLE OF THE S PECI ES
I . S cales of the w ings mixed black and light colored , those of the costa
not forming distinct spots ; scales of the feet black and w ith white
ones at the bases o f some of the j ointsS cales of the w ings w holly black . (M iddle America) .
2 . Abdomen black scaled and w ith a white band at the base of each segment ; hind tibia w ith a broad light colored band before the apex .
perturbons Walk .
Abdomen golden yellow scaled and w ith several black scales on the firstthree segments ; hind tibia devoid of a distinct light colored band.
(M iddle America) .flaveolus Coq .
3. Feet black—scaled and w ith white bands at the sutures of some of thejoints , femora w ith a whitish_
spot or band at a_point near .three
fourths of their lengthF eet wholly black except at the base of the first joint , femora devoidof a distinct white mark near three fourths of their length ; abdomenblack - scaled and w ith a white band or median spot at the base of eachof the last four segments and a white spot in the front angles of
each segment :palliatus Coq .
4. S cales on the upper s ide of the abdomen black and w ith spots of wh iteones along the sides
S cales on the abdomen whollyblack ,on the thorax wholly brown .
arribaleagce Theob.
5 . White spots on the S ides of the abdomen situated in the frOnt angles
of the segments ; scales in the middle of the thorax y ellow ,those
toward the sides chiefly black nigm'
cans Coq.
White spots on the sides of the abdomen situated near the middle of
the segments ; scales of the thorax brown and w ith several lines oflight yellow ones . . .fas ciolatus Arrib.
(b) UNRECOGNI ZED SPECI ES
niger Giles , described from Antigua, West I ndies.richordi Ficalbi, a European species reported from Canada by Theobald.
( c) S PECI ES WRONGLY REFERRED To TH I S GENU S
antique Giles and confinis Arribalz aga belong to Grabhomio; fulvusWiedemann belongs to Psorophom ; sierrens is Ludlow belongs to O chlero
G enus TZENI ORRHYNCHUS Arribalz aga
(Synonyms M ansonia, Panoplz'
tes Theobald)
( 11) TABLE or THE S PECI ES
Third joint of the feet black scaled , the base narrowly white- scaled,scales
of the tibia not forming distinct spots or bands titillons Walk .
Third joint of the hind feet wholly white scaled , black and yellow ish scalesof the tibia collected into distinct bands and spots fascipes Coq.
(b) L I ST or THE S PECI ES AND S YNONYM Y
fascipes Coq. titillans Walk .
taniorhynchus Arrib. (not ofWiedemann) .
G enus AED EOM Y I A Theobald
Proboscis w ith a white ring near the middle ; joints of the feet white at
at their bases ; scales of the w ings brown, yellow ,and white.
sqnamlpennis Arrib.
102 THE STUD Y OF MALARIA
6 . Subfamily URANO TZENI INZE L ahille
G enus URANOTAENI A Arribalz aga
( a) TABLE or THE SPECI ES
I . Thorax w ith a median line of bluish scales ; feet wholly black 2
Thorax w ithout a median line ;hind feet white on at least the last two
joints and broad apex of the third . 32 . Bluish median line o f the thorax prolonged
'
to the scutellum.
sapphirina O . S .
Bluish line obliterated be fore reaching the scutellum. .socialis Theob.
3. S cutellum w ith blue scales ; a patch of blue scales on the thorax a con~
siderable distance in front o f the scutellum ; feet white at the sutures
of many of the joints. (M iddle America) geometrica Theob.
S cutellum without blue scales ; no patch of blue scales on the thoraxin front of it ; feet wholly black except the last two joints and apex
of the third in the hind ones . .lowli Theob.
( b) UNRECOGNI ZED S PECI ESapiealis Theobald and pulcherrima Arribalz aga. Both of these have been
reported from the West I ndies.
7. subfamily‘
TRI CHOPRO SO PoNINz E Theobald
(Synonyms Hyloconopz'
nce L utz , D endromyinae Lut z , S abettz'
nce Blanchard )
TABLE or THE GENERA
1. M ale palpi at least one half as long as the proboscis ; clypeus hairy .
(M iddle America) TrichoprosoponM ale palpi less than one - fourth as long as the probiscis ; clypeus bare" 2
2 . V eins of the w ings having the outstanding scales narrow and nearlylinear ; hind cross v ein situated at least its own length before the
small cross - vein ; legs never fringed w ith scales Wy eomyiaV ein
ghav ing many rather broad
c°
outstanding scales. (M iddle Amer
I ca 3Hind cross - vein S lightly before, opposite, or ,beyond the small cross
vein,each foot bearing two claw s “ 7
Hind cross—vein at least tw ice its own length before the small cross
vein ; legs never fringed w ith scales 4With two claw s on each hind foot ; no scales on. the posterior end ofthe thorax below the scutellum 5With only one claw on each hind foot
°
In both sexes ; posterior end o fthe thorax below the scutellum bearing several broad scales in addition to the bristles 6
5 . Proboscis Shorter than the body ;thickened before itsProboscis longer than the body , not thickened toward i ts apex.
Phoniomy ia. M ale proboscis strongly curved
°
In the outer half and w ith a cluster ofscales at each end of the curved portion L imatus
Legs not fringed S abethoz'
desLegs fringed
°
In places w ith outstanding scales°
I n both sexes . . .S abethes
G enus TR I CHO PRO SOPON Theobald
( S ynonym : J oblot1°
a Blanchard )
Feet wholly blackF eet black
,
ythe last four joints o f the middle feet and the last two of the
hind ones white 111°
w°
pes Theob.
ETI OLOGY
G enus WYEOM YIA”
Th‘
e'
obald
Proboscis and upper side of the abdomen wholly black - sc .aled
gray i Theob., per t1'
11a11s Coq.
G enus D ENDROM Y IA Theobald
Abdomen wholly black scaled on the upper side ; humeri black scaled ; firstjoint o f the hind feet Shorter than their Theob.
G enus PHONI OM Y'
IA Theobald
( 11) TABLE OF THE SPECI ES
Abdomen black - scaled,the front angles of the segments white - scaled.
l'011g1'
rois‘
tris Theob.
(b) L I ST OF THE SPECI ES AND SYNONYMY
longirostris Theob.trinidadens z
’
s Theob
G enus L IMATUS Theobald
( S ynonym: S imondella Laveran )
Thorax golden -
y ellow scaled , a median, Y - shaped spot , w ith the prong snearest the head
,and a large spot above each Wing v iolet - blue
Scaled durhami1 Theob.
G enus SABETHO I DES Theobald
Abdomen black -
wscaled the under side and front angles of the segmentswhitish scaled
,the white scaled front angles
g
prolonged so as . to
form a crossband Which is interrupted except somet imes on the lastthree segments . .confusas Theob.
Abdomen black scaled,the under side whitish scaled , and encroaching on
the sides of the dorsum,the border of the two colors strongly undu
lating undosus Coq.
G enus SABETHES D esvoidy
( 11) TABLE OF THE S PECI ES
1. Front and hind legs not fringedF ront and other legs fringed in places w ith outstanding scales ;middlelegs white scaled before and beyond the fringed portion , the broadapices of the hind feet chiefly White scaled 10119 111133 Fab.
2 . L egs black sc,
aled the apical part of the fringe on the middle legs white .
nitidus Theob.
L egs wholly black- sealed l-ocuples D esv .
(6) L I S T O F THE SPECI ES AND SYNONYMY
l-ocuples D esv . longipes _Fab.
remipes Wied. nitidus Theob.
The hatching of the first brood of anophe l ines bears an int imate relat ion to the seasonal occurrences of malaria. The
seasonal v ariat ions of d ifferent species are probably dependentupon the presence or absence of breed ing pools suitable to
part icular species . Temperature also exerts an influence , thehibernat ing females of some species leav ing “
w inter quarters

104 THE STUD Y OF MALARI A
earl ier than Others , and hibernat ing larvae mature at d iffetemperatures.
While the anophel ines are mosquitoes o f low alt itudes,1
may be found at cons iderable elevat ions . Thus I n the 1
they are found at an altitude of metres ; in the
penines at metres ; in Java at metres ; at Ha
at metres ; in Africa at metres , and in the lplateaus of M ex ico at metres .
”15
I t is the rule among mosquitoes that only the femalesblood suckers , hence it is this sex alone that is concerne <
the propagat ion of malaria. The female insects suck not 1the blood of man , but of other mammals , birds , occas ionof Co ld - blooded an imals
,and even other insects . Blooc
necessary for both the procreat ion of (mosquitoes and the dé0pment of the sexual cycle of the malarial organ ism. Wboth Sexes have the blood - sucking apparatus , the punctur
port ion of the proboscis - of the male is much w eaker than 1of the female.
There are a fewexcept ions to the rule that males - do
bite. Whi le males do not in frequently l ight upon the skinprobe around w ith the proboscis , they usual ly fly away w ithpartaking of blood .
°
But the male S tegomyia fasciata has I:known to bite. D octor S t i les”14 is said to have been bittena male C 1131110111115 , and the male of
“
Culex elegans is1
by S ambonL21
to be quite as bloodthirsty as the f emale.
habitual d iet ofmale mosquitoes , however, is vegetarian . Tare very fond of fruits , as bananas , dates , pears , apples , mel<
and of the nectar of flow ers , w ine , and beer. I n captiv ity nquitoes may be kept alive for some days upon a d iet me ]
o f sweetened water.
Anophel ine mosquitoes rarely suck blood except dur ingn ight . A fter feed ing they usually retire to remote and d
corners or to breed ing places to ov iposit . Persons may
bitten during s leep w ithout be ing d isturbed , since these inS 1are not noisy and the ir bite is not part icularly pain ful . D ur
the day their reserved habits make them d ifficult of detectiThey w ill ord inari ly feed in a few hours after hate-hingcaptiv ity , however, it may be d ifficult to induce them to f

106 THE STUD Y - OF MALARI A
mum l imit of fl ight . They are poorer flyers than most otherspecies . For this reason they are less o ften borne
_
by the WindSince they seek shelter when a breeze arises.While the w indnot soflgenerally
“
a vehiele for the d isseminat ion '
o fmosquitoesas commonly bel ieved , certain species , especially of salt waterbreeders , are borne by the w ind for several mi les .
_
“
The greater
prevalence o f mosquitoes in dwell ings after a w ind may often
be duetothe ir ret iring th ither for protect ion . Mosquitoes may
be carried in wagons loaded w ith straw , hay , or fruit , and
upon railroad cars . M any local it ies formerly f ree from the
pests date the ir afflict ion w ith mosquitoes from the introduct iono f rai lroads. Vesse ls may not only transport the insects forgreat d istances , but may even afford breed ing places .
The pre ference of anophel ines for certain colors has beendemonstrated by Nuttall .123. Boxes lined w ith cloth of d ifferent colors were placed where the mosquitoes w ere plent i ful ,and on seventeen days the number on each box was counted ,
w ith the follow ing resultColor of box.
Navy blueD ark red
Brown,
“
reddish
S carletS late grayD ark green ( olive )V ioletLeaf green
Pearl grayPale green
0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0
o o o o o o o o o o o o o o o o o o o o o o o o o o o o o o o o o o o o o o o o
Galli - Valerio and D e Jongh124
counted I 19 anophelines rest
ing upon dark colors and 33 upon bright colors , and 349 culexupon dark colors and 120 upon bright .M osquitoes are fond of the odorof leather and are usually
plent iful upon harness hang ing in stables . They are said topre fer the odor of the negro to that of the white man.
Number of Anopheles malculipmnis coun ted
in each box during seventeen days.
108
go
81
49
31
241817I 1
9
4
32
2
I

ETI OLOGY
Anophelines , l ike other male factors , pre fer darkness rat
than l ight , and seek the sequestered nooks during the day .
A meal of blood is a prerequis ite to fert i lizat ion . Fem;
confined w ith males,
. then isolated and fed , do not depferti le eggs , but must be fed first. A s ing le fertiliz atiorsuflicient for several batches of eggs. These are usuallypos ited between dusk and dawn . S t il l water is necessary ,
S i
the female may be drowned i f the surface I S ag itated.
female sits upon the water or upon the edge of floating leaor debris . The ova of anophe lines are depos it-ed
°
.upon
water in clumps , but soon separate and lie hori z ontal ly .
batch of ova usually numbers from 100 to 150 . Pressa
has calculated , on a bas is of 150 ova for each female , hatch50 per cent. females , that a s ing le female in one Season 1:
duces about five billion mosquitoes .
Parthenogenesis has occasionally been observed in”
mosc
toes. K ellogg“ 4reared a female mosquito from the p l
which almost immed iately depos ited eggs ; she had . not bferti lized. L arvae deve loped from the ova and nearly reac?
ful l growth be fore dy ing . Un fert il ized ’ female S tegom
fasciata and Culex pipiem have “
also been known to'
dept
ova , which , however, were not fertile.
I t is imposs ible to determine the length of l ife of mosquit
in nature , though even in capt iv ity they have been keptweeks. Anophel ines have been kept
.
al ive five days
out food or water , and for about two months fed 11]
bananas. .The males are not so long l ived as the fema
M itchell126 has kept S tegomyia fasciata S ixty - one days. I
w ell known that mosquitoes surv ive long droughts , as w ellh ibernate.
S tephens and Christophers say there is ev idence thatova can surv ive for some months in moist earth and expo
to frost . E yselll ‘27
and -
'
GallieV alerio and D e Jonghm
st
that the ova of most species of mosquitoes of the northtemperate and frig id zones may hibernate.
M osquitoes hibernate in the larval stage also. Smitl
found , in New Jersey , larvae of C11lex pungens in ice contai1in pitcher plants , and bel ieves that larval hibernat ion must
108 THE STUD Y OF MALARI A
extremely common. M itchell” 6 found anopheles larvae in
tanks and barrels in the Botan ical Gardens of Washington ,
D . C . , during w inter, and Woldert l'28 found these larvae in
D ecember at Ty ler, Texas .
M itchell126 be l ieves it probable that mosquitoes do not bibernate in the pupal stage , though Galli - Valerio and D e Jongh
m
maintain the opposite op1n10n.
I t is chiefly in the w inged stage that mosquitoes hibernate.
I n the late fal l the males die , the fecundated females seekingshe lter in dwell ings , cellars , stable , barns , cisterns , hol low trees ,
or under bridges . Annett and Duttonm thus describe the
hibernation of Anopheles maculipennis in Eng land :I . The att itude is pecul iar, the insect ly ing quite flat upon
the surface w ith its legs spread out.‘
I n this pos it ionthe undersurface of the thorax touches , or nearly touches , the wal l.2 . O nly females are found , and these are always fert ili z ed ,
and have the spermatheca filled .w ith spermatozoa.
The insects are d ifficult to arouse and very s lugg ish inany movements they make .
34. They do not . feed un less the temperature is raised . I f
kept at a low temperature (prov ided the air is mo ist ) theyremain for weeks w ithout feeding .
5 . I f aroused by- rais ing the temperature they feed read ily
and the ovaries rap idly deve lop. Eggs -
are laid , and in mostcases the female d ies after their deposit ion .
S tudy of M osquitoes—To obtain adult mosquitoes theymay be either captured or bred from larvae. M osquitoes are
best captured by placing very care ful ly the mouth of a test
tube orbottle over the insects while rest ing. They are killedpre ferably by the cyanide bottle , by chloro form, or by tobaccosmoke. The cyan ide bottle is prepared .by placing inthe bottom of a w ide- mouthed bottle a number of small pieces of
potass ium cyanide and covering w ith liquid plaster of Paris .
When the plaster has hardened the bottle is ready foruse , andshould then be kept t ightly corked , as the fumes are poisonous .
M osquitoes should not be k i lled immed iately after hatching ,
as the exoskeleton is then so ft and marked shrivell ing occurs .
A net should not'
be used for capturing adult mosquitoes , for
1 10 THE STUD Y OF MALARIA
layer of sand in the bottom, and covered w ith gauze held inplace by means of a rubber band . The larvae in each j arshould benear the same s ize , otherw ise the larger w il l d evourthe smal ler ones , and they should n ot be too numerous . A
few grains of dry rice should be drop-
ped in for food..
Adults also should be kept in such jars,which “
should,how
ever, contain on ly a small quant ity of water, upon whichshould float a thin sheet of cork, and each j ar should containa s lant ing strip upon which the insects may rest . A benthairpin makes a good hook upon which to suspend a p iece of
fruit from the edge of the j ar.
I n order to in fect mosquitoes w ith malaria they must , of
course , be fed upon blood containing paras ites . They may
be fed by hold ing . the moistened s forearm against the gauzecovering
'
of'
the j ar o r“
they may be placed in cages covered
Fig. 42 .—S tomach of infected mosquito.
w ith w ire nett ing, one end of wh ich has an opening protectedby a s leeve through which the arm may be introduced . The
mosquitoes should be fed in twenty- fOur to forty—eight hours
after hatching and thereafter every day for several days .
I n invest igat ing the mosquito cycle of the p aras ite of malaria the sexual forms must be sought for in the m idgut or
stomach , and the sporo z oits in the sal ivary g lands.
I n the d issect ion of the m idgut proceed as fo llow s
D o not d issect the mosquito unt il the blood from the lastfeed ing is d igested , wh ich may be ascertained by the disap
pearance of the dark color on the low er surface of the abdomen .
Kill the mosquito by means o f cyan ide fumes , chloro form ,
ether, or tobacco smoke .
Pull off the w ings and legs and remove the scales w ith a
small camel ’s—hair brush.


112 THE STUD Y OF MALARI A
THE PARAS I TES OF MALARIA
Zoolog ical Re lat ions—The paras ites of malariabelong tothe an imal kingdom , to the d iv is ion o f protozoa, to the classo f sporozoa ,
‘
and to the order o f hemos‘
poridi ‘a. The hemo
cytozoa are not pecul iar to man , but are found in other classeso f vertebrates , and are d istributed by ManSOn5 9 into threegenera, as fol lows
HAEMOCYTOZOA
I . G ENUS H1EM AMCEBA
Names.
subtertiana.
tertiana.
quartana.
relicta (Proteosoma)
D anielew sk i (Halteridium )Kochi.melaniphera.
M etchnikovi.
2 . GENUS .PI RO PLASM A
Bovines ; transmitted by the cattle
(Boo'
philus bov is ) .D ogs.
S heep .
I I orse .
M an .
3. GENUS HzEM OGR-
EGARI NA
H. ranarum (D repanidium ) ; F rog (Rana esculenta) .H. splendens . Frog (Rana esculenta) .H. magna. Frog (Rana esculenta) .H. lacertarum. Liz ard (Lacerta mu-
ralis )
About tw enty additional but less readily pro-
cured species.
There are three sharply defined species of parasite -s
ria, the parasite of tert ian malaria, the paras ite o f quartan
malaria, and the parasite o f est ivo - autumnal malaria. The
latter i s d iv ided by mos t observers into three , or at least two ,
varieties , the tert ian and the quot id ian , of wh ich latter'
variety
a pigmented form and an unpigmented form are described.
The w riter’s opin ion is that there are two variet ies of the
est ivo - autumnal paras ite , the tertian and the quot id ian , and
that the pigmented and the unpigmented quot id ians are merelyforms of one variety .
HOs is .
The malaria parasites ofman , the sexual
phase being evolved in“
mosquitoes ofthe genus Anopheles
Birds ; sexual phase . in mosquitoes ofthe genus Culex.
Birds .
S everal species of monkeys .
Bat (M iniopterus S hre‘
ibersu ) .Trionyx indicus.

E'
I fI QLOGY 1 13
A number of ~stud.ents. of mal Laveran
“
at their
head, maintaining the unity of the malarial parasites , holdthat the several “ species are on ly forms of one species “
whichupon which
Fig. 45 .—D iag-ram illustrating the cycles. of the parasite.
their theory is based are so unsound in the l ight of our present“knowledge that it I s unnecessary to review them.
B'
iol-01gfy .x- e The l i fe history of the parasites of mala-
ria is
somewhat .eomplica-ted
,inasmuch as man, the mosquito, and
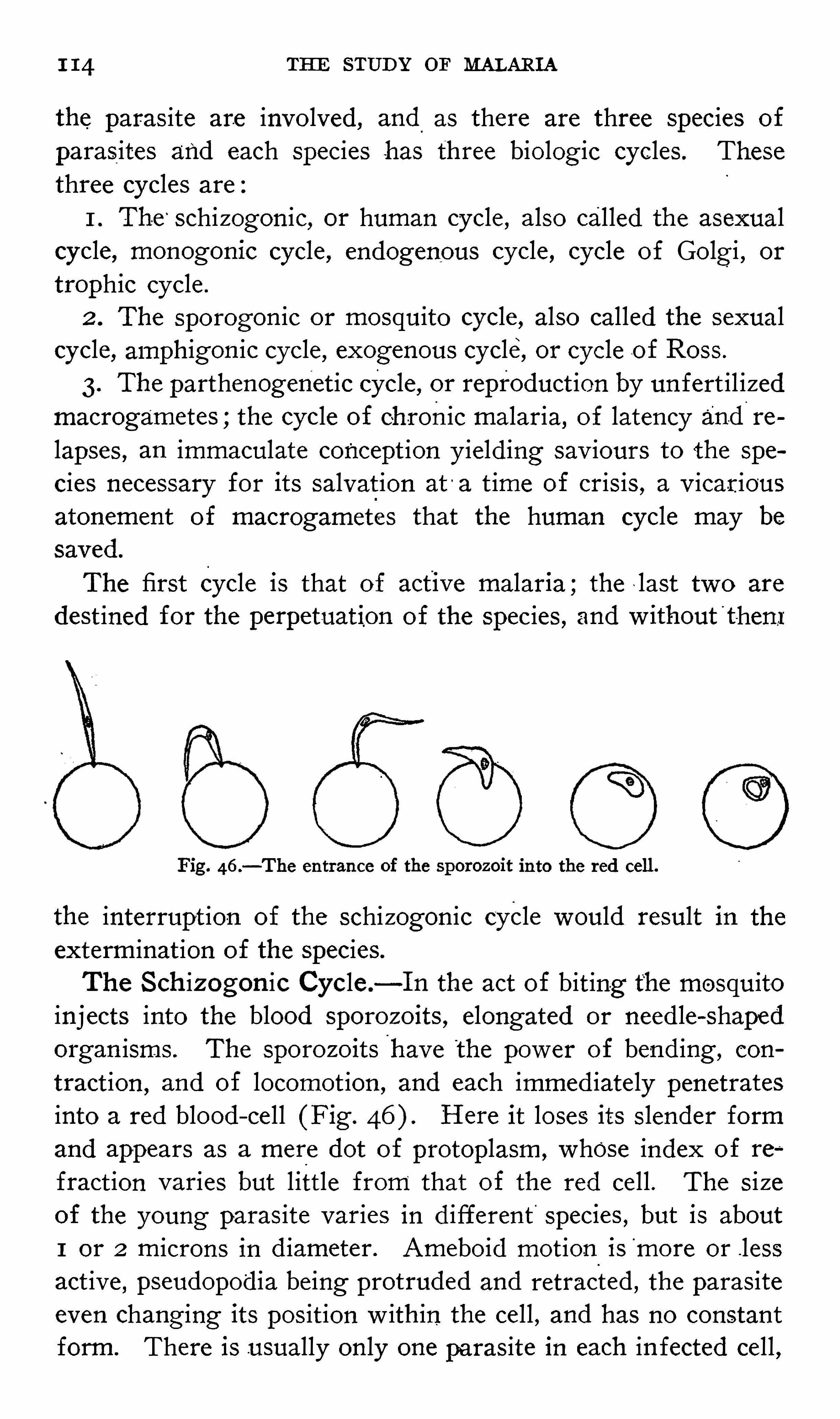
1 14 THE STUD Y OF MALARI A
the paras ite are invo lved , and.
as there are three species of
parasites and each species has three biolog ic cycles . Thesethree cycles are
1 . The‘
schizogonic, or human cycle , also called the asexualcycle, monogonie cycle , endogenous cycle , cycle of Golgi , or
trophic cycle .
2 . The sporogon ic or mosquito cycle , also called the sexualcycle, amphigon ic cycle , exogenous cycle, or cycle o f Ross .
3. The parthenogenet ic cycle , or reproduct ion by un fert il izedmacrogametes ;the cycle of chronic malaria, of latency and re
lapses , an immaculate concept ion y ield ing sav iours to the spe
cies necessary for its salvat ion at'
a t ime of crisis , a v icariousatonement of macrogametes that the human cycle may be
saved .
The first Cycle is that of active malar1a ; the last two are
destined for the perpetuation of the species , and w ithout'
t -hent
Fig. 46 .—The entrance of the sporoz oit into the red cell.
the interrupt ion of the schizogonic cycle would result in the
exterminat ion of the species.
The S ch i z ogon ic Cycle—I n the act of biting the mosquitoinjects into the blood sporo z oits , elongated or needle - Shapedorgan isms . The sporo z oits have the power of bend ing , con
tract ion,and of locomot ion , and each immed iately penetrates
into a red blood—ce ll (Fig . Here it loses its S lender formand appears as a mere dot of protoplasm , whose index o f re
fract ion varies but l ittle from that of the red cell . The s izeof the young parasite varies in d ifferent species , but is about1 or 2 microns in d iameter. Ameboid motion ismore or .lessact ive
, pseudopodia be ing protruded and retracted , the parasiteeven chang ing its pos it ion w ith in the cell , and has no constant
form. There is usually only one paras ite in each in fected cell ,
1 16 THE STUD Y or MALARIA
parasites are about one - fifth the s i z e of the red blood corpus
cles a nd unp1gmented. They are difficult-
to distinguish'
f-
rom
the young paras ites of t he other spec1es . .They are act ive lyameboid, protrud ing and retracting short pseudopod ia w ithrap id ity ;Y - shapes , T
- Shapes , and crosses are common f01ms .
The index of refract ion of the paras I tes I S low ,so that the ir
contours are not clearly d ist inguished from the substance ofthe'
red blood—cells . As the parasite increases in s ize pigment
gradually appears . The°
pigment of the tert ian paras ite is .
_
-fine,
rod—shaped , rather l ight in color, and z inactive mot ion. This
mot ion of the p igment has been compared to the bubbling of
boil ing water and to the swarming of insects . The infectedredeell becomes and pale.
‘
°
The half-
grown
parasite fil ls about hal f or two- thirds of the red blood cor
puscle . At th is stage the paras ite assumes fantast ic and bizarreShapes . The - adult paras ite is more or less Spher ical , as largeas or larger than a normal red cell , and occup ies three - fourthsor
'
four—fifths of the swo llen infected cel l , the marg in of wh ichmay be d ifficult
'
to see on account of its pale color. The pig
ment tends to become more abundant about the periphery .
When sporulation'
is imminent the paras ite and . its p igment
becomes less act ive or motion less , the p igment g athers in
clumps at the center , and rad ial striat ions appear from the
periphery toward the center. Usually the’
sporulating tert ianparas ite is not so
,
symmetrical as the correspond ing stage of
the quartan , resembling , rather, a bunch of grapes or a mul
berry . L ess o ften there are two concentric row s o f spores .
The spores are smal l and oval and vary in numberfrom twelveor fourteen to twenty
—six , o ftenest'
s ixteen , and more o ften an
even than an uneven number. S porulat ion takes place espe
cially°
I n the circulat ion of certain v iscera,but sporulat ing ter
t ian paras ites are much more frequent ly encountered in the
peripheral circulat ion than in'
the case of est ivo - autu’
mnal inteet ions.
The parasites develop w ith remarkable un i formity ,nearly
all appearing to be of the same age . Even in in fect ions w ithtwo groups of tert ian paras ites , which is very common ,
it is
unusual to find a paras ite which does not belong to one brood .





1 18 THE STUD Y or MALARI A
M 1°
c1foga111etocy tes. M acrogametes.
Plasma hyaline. Plasma granular.Pigment abundant, in thick . rods , Pigment in . fine rods and granules,brownish y ellow. brownish black .
Not larger than a red blood - cell. Larger than a red cell.Chromatin profuse. Chromatin less abundant .Little ameboid motion. M ore or less ameboid motion.
Nucleus toward center. Nucleus toward periphery .
I n stained films the early stage o f the tert ian paras ite isseen as a ring “ O ften the ring is not of the same thicknessthroughout its circum ference , but is composed o f a thin seg
ment , and a thicker segment , the chromatin ,
°
being upon the
thin segment. Usually the chromat in dot is immed iate ly w ithinthering , but may lie outs ide , and is surrounded by a pale zone .
The achromat ic zone may be regarded as the nucleus and the
chromat in as the nucleolus . As the paras ite dev elops one arc
becomes much thickened , g iv ing the appearance o f the S ignetring. The forms of the hal f - grown parasite are varied and
peculiar. P igment appears first and most abundantly in the
peripheral region , and does not invade the clear zone . The
red cell is enlarged and does not stain deeply.
A pecul iarst ippl ing o f the infected red cells is shown in films contammg
tert ian paras ites and stained w ith the Romanowsky stain or
one of its mod ifications . When the paras ite fil ls one - third of
the cel l a number of fine , red—stained points , S chiiffner ’
s dots ,
appear, which increase in s ize but not in number as the paras itegrows. I n the process of sporulat ion the chromat in becomessubd iv ided and surrounded by a .clear zone and encircled bythe blue cytoplasm, const itut ing the spore.
Th e Quartan Paras ite (Haz 111a111ceba malaria,H . quartame,
Plas1110d-111111 malaria),L averania 111alarice ) .
—The duration of
the schizogon ic cycle of the quartan paras I te I s seventy—two
hours . The young forms of the paras ite appear as small ,hyal ine , unp igmented b its o f protoplasm. They are h ighlyrefract ive and the contour is much more sharply defined thanthe tertian paras ite . Ameboid mot ion is slugg ish and the
organ ism may be watched some t ime unt i l motion is detected .
Pigment appears w ith in tw enty- four hours . I t is . in larger
quant it ies than in the tert ian paras ite , in coarser grains or rods ,and dark brown . or black in color. The pigment is accumu

ETI OLOGY 1 19
lated around the marg in, and its motionis very s low . I n the
half -
grown paras ites the peculiar forms observed in the tert ianorgan isms are
'
not seen, and ameboid movements become more
s lugg ish or cease altogether. red blood - ce ll in fested w iththe quartan paras ite does not enlarge and decolorize as in
tert ian infections , but , i f there is any dev iat ion from normal ,becomes smaller and darker, perhaps greenish and brassy . The
adult paras ites are almost as large as the red cells . Prior tosporulation the pigment collects toward the center, o ften in
'
a rad ial arrangement. S porulat ion proceeds after themanner
of t he tert ian paras ite, but is slower. The Sporulat ing forms
are beautifully symmetrical , and are typical rosettes. The
spores are round or oval , relat ively large and S ix to twelve innumber , o ftenest
_
e ight . Sporulat ing quartan paras ites ,a re
much more common ly observed in the peripheralblood thanare the correspond ing forms of the other species.
Quartan gametes are but rarely encountered . The '
fnacro
gametes are spherical in shape , and as long as they remainintracorpuscular are smaller than tert ian gametes, but are
equally.as large when
.
they . become extra'
corpuscular. Ex
flagellated mic-rogametocytes have been observed ; they are
somewhat smaller than the tertianforms, but no less active .
The stain ing react ions of the quartan paras ite are 31mi larto those of the tert ian. The young form is a ring and so
clos ely resembles the tert ian that it cannot be dist inguished w ithcertainty . After twelve to twenty
- four hours the paras ite becomes d isc or band shapedu The latter forms are character
istic. The parasite extends across the center of the in festedcel l as a more or leSs broad band, often rather quadrilateral ,the p igment be ing arranged more pro fusely along the marg inof the band. The chromatin body of the quartan species stainsless intensely and Spl it-
s earlier than in the tert ian. The adultusually fills the corpuscle , which may be no longer apparent .
The sexes of the gametes are d ifferent iated by the same characters as in the tert ian.
The Est ivo - autumnal Paras ite (Hcemamaeba pm cox,
Flaw /1003111111 prcecox,Hcemamceba immaculata, L averania p12
coir, Haemomenas prwcox,Plasmodium immaculatum Hema

120 THE STUD Y OF MALARI A
mceba parva, H2 111111020011falciform,Plasmodium faleipamm )
—The young forms of the est ivo - autumnal paras ites are s im i larto those o f the other species , but are smaller, be ing from one
fifth to one - s ixth the s ize of the in fested corpuscle . Ameboidmot ion is rather act ive , stars , c rosses , and irregular shapesoccurring in succes s ion. At rest the paras ites . appear annularor d iscoid . M ore than one paras ite in a s ing le cell is relatively
-
more common than in tertian and quartan in fect ions.
Advanced stages of development are rare ly seen in peripheralblood .
°
The in fested red cells oftenbecome shrive lled, cre
nated , darker, and of a The adult paras ites donot attain the s ize of the red blood corpuscles . S porulat ionproceeds in
i
a manner s imilar to t hat of the~
s imple tert ian .
parasite . The spores'
number fromfive to twenty- five or even .
thirty . Sporulat ion is not so un i form as in the other infect ions ; sporulat ing forms may be associated w ith
'
young or
hal f—grown paras ites .
'
Estivo - autumnal . gametes occur in the formof crescents ,
and o f fusi form, ovoid , and spherical bod ies . The crescent is
characterist ic, being found in this form of malaria alone. Theyare cy l indrical , tapering s l ightly at each extrem ity , and
s l ightly curved upon themselves. They are longer than the
d iameter of the red cell and about a t hird as broad as long.The changes from crescent to ovoid and round bod ies may
be easily observed under the m icroscope. The gametes appear
only after the in fect ion has pers isted for about a week. The
crescent may lie w ithin the cell or may have the appearance
of the red cell be ing attached to the concave s ide ; in seme
instance-s there is no ev idence le ft of the in fested blood - cell .The cel l may be stretched across the concav ity of the crescent ,
and is usually almost deco lorized . The crescents have g ivenev idence of a double outl ine . They possess no ameboid move
ment , and the pigment in the form of rods or granules ismot ionless . Before exflagellation the crescent assumes the
spherical form, smal ler than the tert ian , and s im i lar to the
quartan.
The staining reactions of the estivo - autumnal schizonts are
s imilar to those of the tert ian and quartan . The young para

D ESCRI PT I ON O F F LATES I V AND V 1
The drawings were made with the assistan of th e camera lucida from Specimens of freshblood . AWinck e l microscope , obj ect lve 14 (oil immersion ) , ocular 4, was used . Figures 4 , I 3, 23,24, and 42 of Plate I V were d rawn from fresh blood , w ith out th e camera 1u01da.
PLATE I V
THE PARASI TE O F TERTI AN FEV ER.
1.- Normal red corpuscle .
2, 3, 4.—Young h yaline forms . I n 4, a corpuscle con tains th ree d i st inct parasites .
5 , 21.—Beginn i ng of igmentation . Th e paras1te was observed to form a true ring by th e con
fluence of two p seudopo ia . D uring observation th e body burst from th e corpuscle ,w h ich became
decolori z ed and d isappeared from v iew . Th e parasite became , almost immed iately , d eformed andmotionless , as sh own in Fig . 21.
6, 7, 8.—Partly d evelop ed p igm ented forms .
9 ,
—Full-
grown body .
10—14.—S egmen ting bod ies .
15 .—Form simulat ing a segmenting body . Th e significance of th ese forms , several of wh ich
have been observed , was not clear to D rs . Th ay er and Hewetson , wh o h ad never met with s imilarbod ies in stained specimens so as to be able to stud y th e structure of th e ind ividual - segments .
16, 17.-Precocious se entation .
18, 19, 20.—Large swo len and fragmenting extracellular bod ies .
22.—Flagellate body .
23, 24.—Vacuoli z ation .
THE PARAS I TE OF QUAETAN FEVER.
25 .—Normal red corpuscle.—Young hyaline form .
27—34.—Gradual d evelopmen t of th e intracorpuscular bod ies ,
35 .—Full -
grown body . Th e substan ce of th e red corpuscle is no more via ble in th e freshspecimen .
36- 39.—S egment ing bod ies .—Large swollen extracellular form .
41.—F lagellate body .
42.—Vacuoli z ation .
PLATE V
THE PARAS I TE OF JEs'r rvo—AUTUM NAL FEV ER.
1, 2.—Small refractive ring
- lik e bod ies .
3—6.—Larger d isk - lik e and ameboid forms.
7.—Ring - lik e bod y with a few p igment -
granules in a brassy , sh runk en corpuscle .
8, 9 , 10, 12.—S imilar pi mented bod ies .
11.—Ameboid body w it pi ment .
13.—Body with a central c ump of pigment in a corpuscle ,
“
sh ow ing a retraction of th e h emo
globin- containing substance about th e parasite .
14—20.—Larger bod ies w ith cen tral pigment clumps or block s .
21- 24.—Segment ing bod ies from th e spleen . F igs . 21—23 represent one bod y wh ere th e en tire
process o f segmentat ion was observed . Th e segments , eigh teen in number,were accurately
counted before separation; as in Fig . 23. Th e sudden separation of th e'
segments , occurring asth ough some retain ing membrane were ruptured , was observed .
25—33.- Cr
‘
escents and ovoid bod ies . Figs . 30 and 31 represent one body , wh ich was seen to
extrude slow ly , and later to w ith d raw , two round ed protrusions.
34, 35 .—Round .bod ies .
36. Gemmation ,
”fragmentation .
37.—Vacuoli z ation of a crescent .
38- 40.—Flagellation . Th e figures represent one organ ism . Th e blood was tak en from th e car
at p .m . ; at th e body was as represented in Fig . At th e flagella appeared ; attwo of th e flagella h ad already brok en away from th e moth er bod y .
41—45 .—Phagocytosis . Traced w ith th e cam era lucida .
"Th ese illustrations are reproduced by permission from th e art icle by D rs . Thayer and Hewetson in The J ohns Hopkins Hosp ital Reports , vol . v ., 1895 .
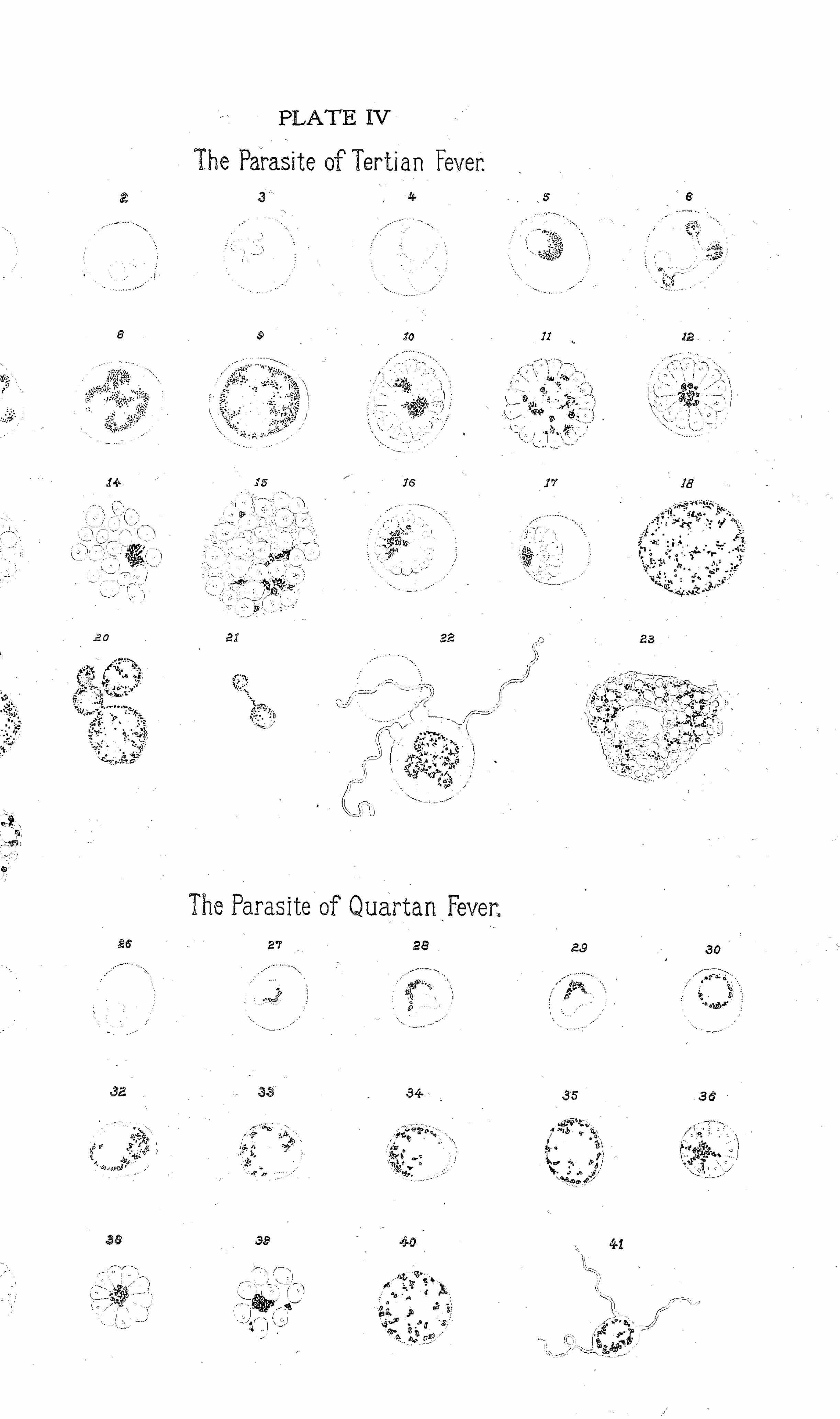


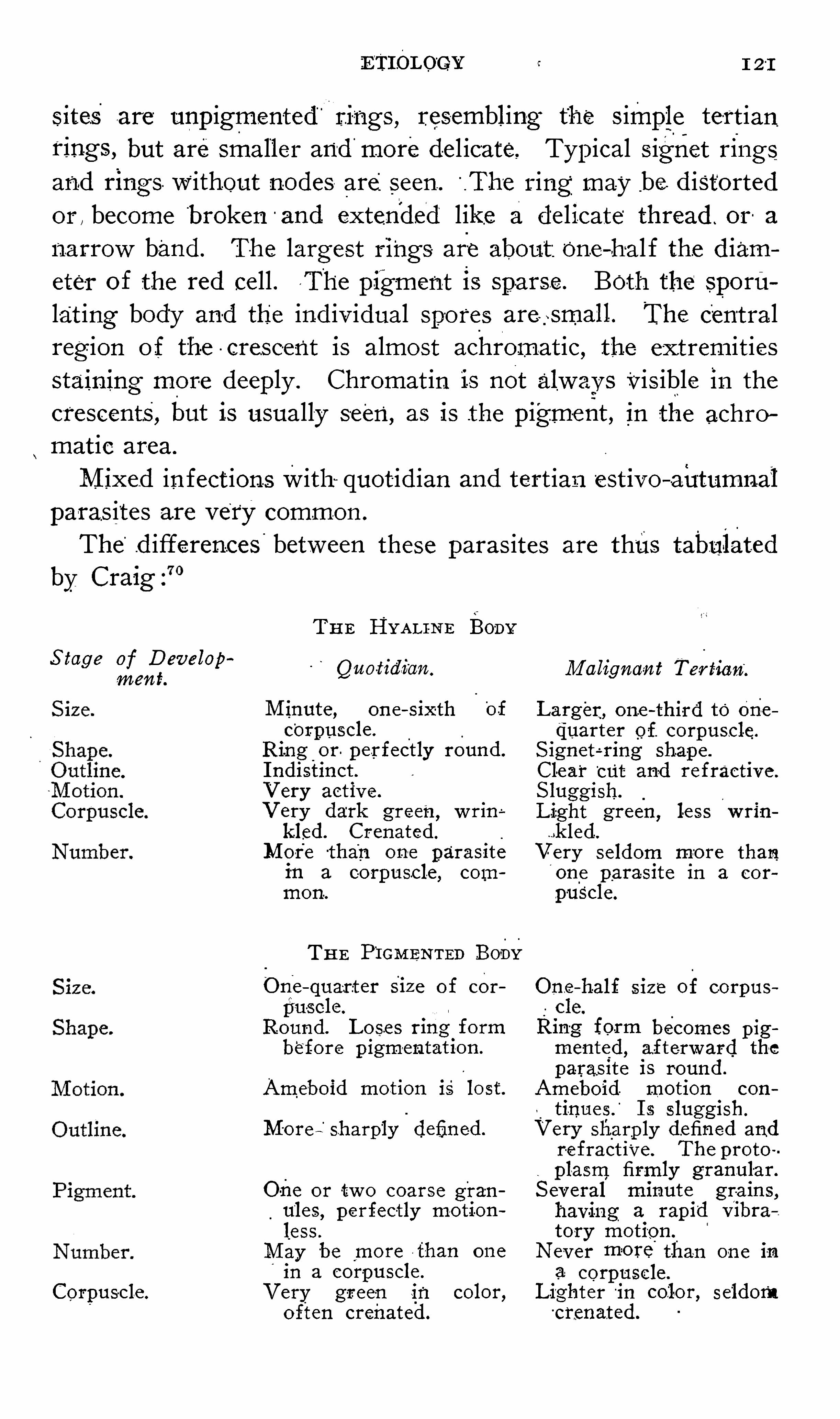
ETIOLOGY c 1 21
sites are unpigmented “
rings , resembling the s imple tert ianrings , but are smaller and more del icate, Typical s ignet ringsand rings. without nodes are
_
seen .
“
.The ring may _be d istorted
or , become broken -
and extended like a del icate thread . or a
narrow band . The largest rings are about:One—ha l f the d iameter of the red cell . T he pig -ment is sparse . Both the spornlat ing body and the ind iv idual spo res are gsmall. The centralregion o f the - crescent is almost achromat ic, the extrem itiesstaining more deeply . Chromat in is not alway s Vis ible in the
crescents, but is usually seen, as is the pigment , _
in the achro
matic area.
M ixed infect ions with quot id ian and tertian est ivo—autumnal
paras ites are very common .
The“
d ifferences between these paras ites are thus tabulatedby Craig
THE HYAL I -NE Fony
S tage of D evelopment Quo-tidian .
M inute , one—sixth'
of
corpuscle .
Ring or . perfectly round .
I ndistinct .
V ery activ e .
V ery dark green,w rin
kled. Crenated.
M ore than one parasite
in a corpuscle , common.
THE F I GM E-NTED Bony
O ne—quart er siz e of cor
pu-scle.
Round . Lose s ring formbefore p igmentat ion .
Ameboid motion is lost .
M ore" sharply defined .
One or tw o coarse gran
u‘
les, perfectly motion
less .
M ay ber
more than one
in a corpuscle .
Corpuscle . V ery green in color,often crenated.
M aligna-n t Ter tian;
Larger, one—third to Onequarter of. corpuscle.
S ignet é ring shape .
Clear“
cut and refractive .
S luggish.
L ight green ,less w rin
..k led.
V ery seldom mo re than'
one parasite in a cor
.pus'
cle.
One - half siz e of corpus
Rin-
g form becomes pigmented , afterward the
parasite is round .
Ameboid. motion con
tinnes.
‘
I s sluggish.
V ery sharp ly defined andrefract ive. The proto
plasm firmly granular.
S everal minute gra ins,having a rap id V ibr
tory motion.Never more than one in
a corpuscle .
Lighter'ih color, seldom
c remated.
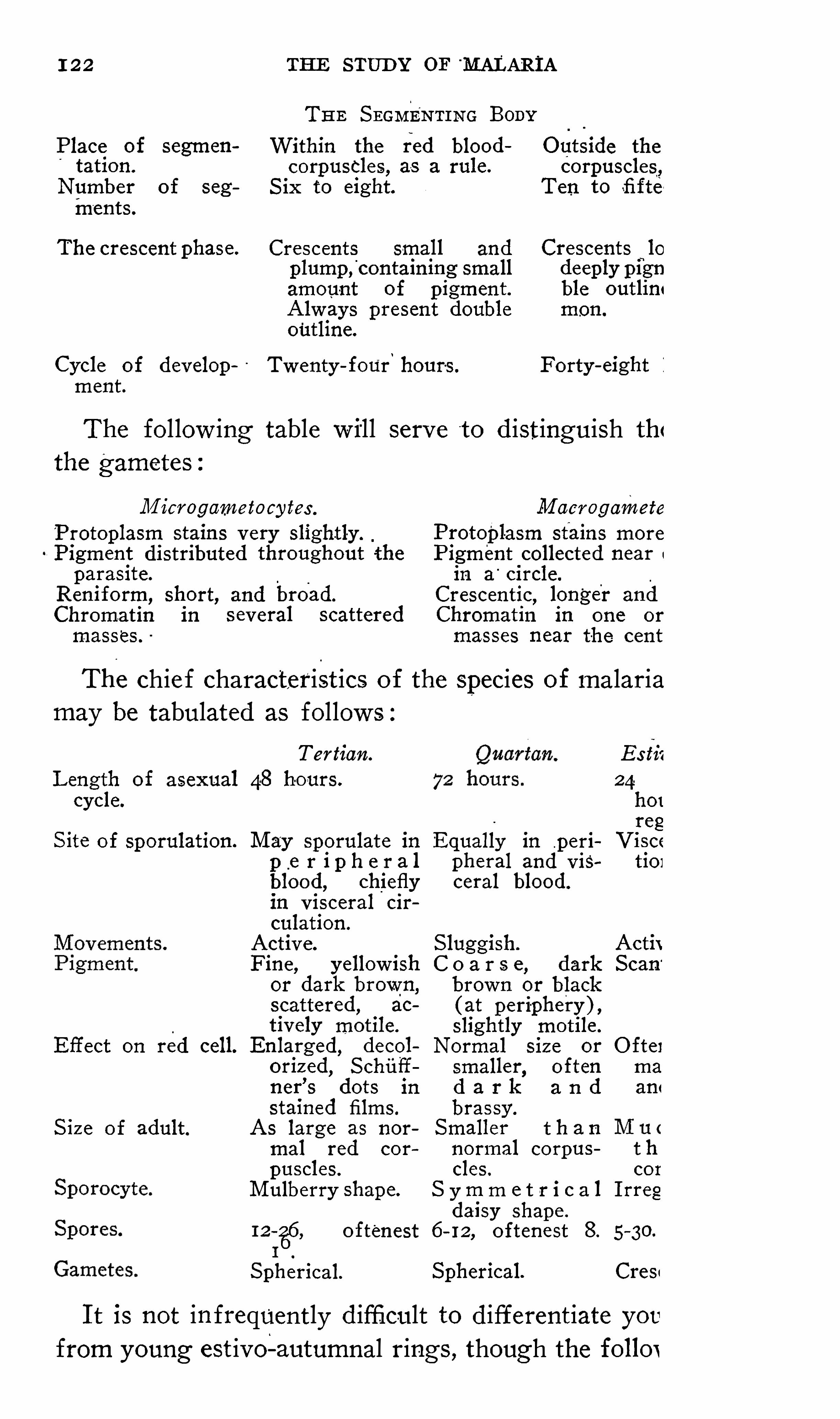
1 22 THE STUD Y OF M ALARIATHE S EGMENTI NG BODY
Place of segmen Within the red blood O utside the
tation. corpuscles, as a rule. corpuscles.,Number of seg S ix to eight Ten to sfifte
ments.
The crescent phase. Crescents small and Crescentsfi
lo
plump ,contain ing small deeply pignamount of pigment. ble outlini
Always present double mon.
outline.
Cycle of develop Twenty - four hours. Forty - eight i
ment.
The fol low ing table will serve t o d istinguish th<the gametes
M icrogametocy tes . M acrogamete
Protoplasm stains very slightly ._
Protopl-asm stains more
Pigment distributed throughout the Pigment collected near
parasite. in a circle.
Reniform, short, and broad. Crescentic,longer and
Chromatin in s everal scattered Chromatin in one or
masses . masses near the cent
The chie f characterist ics of the species of malariamay be tabulated as follows :
Tertian. Es t
-
ii
L ength of asexual 48 hours. 24cycle. hor
regS ite of sporulation. M ay sporulate in Equally in peri V isce
p e r i p h e r a l pheral and V is tion
blood , chiefly ceral blood.
in v isceral cir
culation.
Active. S luggish. Actit
Fine, yellow ish C o a r s e , dark S can'
or dark brown, brown or black
scattered,
ac ( at periphery ) ,tively motile. slightly motile .
Effect on red cell. Enlarged, decol Normal siz e or O ftei
oriz ed,S chiii
’
f smaller,
often ma
ner’
s dots in d a r k a n d am
stained films. brassy .
S iz e o f adult. As large as nor Smaller t h a n
mal red cor normal corpus t h
puscles. cles . cor
M ulberry shape. S y m m e t r i c a 1 I rregdaisy shape .
12 - 2
6
6, oftenest 6 - 12,
oftenest 8. 5 - 30.
I
S pherical. Spherical. Cres
I t is not infrequently d ifficult to differentiate youfrom young est ivo- autumnal rings , though the follox

124 THE STUD Y or MALARI A
the res idual body oft he sporoblast unt il the oocyst bursts , whenthe sporo z oits escape into the body cav ity . F inally , throughthe lacunar c irculat ion , they arrive - at the salivary g lands ,where they congregate in hordes , The sporo z oits numberfrom a
’
few hundreds to ten thousand or more,l
each'
measures
about 14 microns in length , about eight t imes as long as broad ,be ing Very s lender, tapering at both ”
ends ,“
and endow ed with
serpent ine movements . Fro‘
m the sal ivary g lands the sporo
z oits are inj ected by the mosquito , in the _act of prey ing uponits v ict ims , Where each sporo z oit soo‘
n enters a red ce ll and goesthrough the schizogon ic cycle . The durat ion of the mosquito'
cycle varies frome ight to s ixteen Or more days , depend ingmainly upon the temperature , but poss ibly also upon other
'factors' .The three species of paras ites are closely s im il iar in
i
their
stages of exogenous development. The d iffer ences betweenthe tert ian and the
.
est ivo - autumnal organisms are that in the
former the zygote is round or oval instead of pyriform or
ovo id , the protoplasm is less re fract ive , the character istic pig '
ment mai ntains , the sporoblasts are larger and less numerous ,
the sporo z oits are less dense and more regularly'
arranged,
often rad ially w ithin the sporoblast , and black sporeshave not
been found .
The quartan paras ite is the most d ifficult to develop w ithinthe mosquito .
The Parthenogenet ic Cyc le .—Parthenogenes is ,
“
or v irg inbirth
,is reproduct ion by un fert i lized fem-
ales .
This phenomenon,known also as the
“
alternat ion of genera
t ions ,” has been most care ful ly studied.
in p lant l ice , the
Aphidw. The eggs , which are laid in the - fal l and have hibernated
,hatch in the spring into females , hav ing the pow er of
g iv ing birth , w ithout fert i lizat ion, to v iv iparous young ,
"
whichinherit the faculty of parthenogenesis , and procreate in thismanner unt i l the advent of cold w eather or the f ai lure of
nourishment when males and ov iparous females are'
brought
forth . F rom these latter, after copulat ion , ova are produced ,
and the cycle reco-mmences .
Parthenogenetic reproduct ion is known to occur in a number
ETI OLOGY
Pf species , as hemoproteus , certain rotifera, j -e lly - fis]
ntomostracea, acarina, and certain insects , the s i lk - rr'
.
[uitoes, gall fl ies , ants , bees , wasps , chironomus , etc.
This l i fe cycle o f the parasite of malaria i s the moc
ec0gniz ed and least known o f its cycles. S ince the .
if the paras ite the gametes have been regarded
.llied w ith the - chron ic malaria and re lapses. Gol;
tated it a s his belief that the crescent was the p:
evers recurring at long intervals .
Canal is,131 in 1889 , described and pictured spheri<
lerived from crescents in the act of sporulation.
Xntolisei and Angelinil ‘”
confirmed the observation o
, ewkow icz l ‘32reported , in 1897, that he had S een 3;
rescents some o f which contained as many as thirtyGrass i133 expressed the Op in ion in 190 1 that the pa
nalaria underwent a parthenogenet ic cycle of dei
vhereby the species was perpetuated after the dea'
chiz onts.
He cited a number of arguments in support of ti
.nd re ferred to a s imilar process in other protozoaPrichosphcem
'
um,and Volvox
I t was S chaud inn134 who ,in 1902 , first observed
ectly interpreted parthenogenesis o‘
f tert ian macn
The ca se in which this was observed was that of Fravho , duringthe spring and summer ofseveral precedlad suffered occas ional paroxysms . O n Apri l 2 9 ar
wo severe paroxysms occurred .
“
At the height of
in M ay 1 the blood was examined and tertian '
paras in abundance bes ides schizonts , male and femalevere numerous , showmg that it w as
_
a typical re lapse.
day the blood was examined regularly and found tertian gametes in greater or less numbers .
'
O n M
lOOH, the blood examinat ion showed no markedrom the usual find ings , except that the parasites w «
vhat more plent i ful . I n every preparat ion were I O - 2
:ametes and occas ional microgametocytes . The ter
vas normal . O n the morning of M ay 26 a remarkal
ion of the macrogametes , w ith noteworthy nuclear

126 THE STUD Y or MALARI A
described below ,were detected . The blood was examined
every two hours , and the temperature was taken w ith the follow ing results
A . M . Gentigrade ,
At and at 2 P . M . parthenogenet ic forms were mostabundant. I n the even ing , bes ides unchanged sexual organisms, very y0ung endog lobular sch izonts were found.On M ay 27 the blood was examined tw ice at 7 A . M . Only
young endog lobular schizonts were found , the temperature
at 8 P . M . only'
scanty , hal f- grown schizonts were found ,
and the temperature was 37.
On M ay 28'
the typ ical attack (depend ing on asexual S -
porue
lation ) occurred , w ith the followm-
g temperature course
Cent-igrade.
0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0
0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 00
0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0
The result of the blood examinat ion was as usual in suchattacks .
The next morning most of the young paras ites were foundto be gametes . Thus a true
‘
alternation of generations . I t
should be observed that , while the sporulat ion of the unfer
tiliz ed macrogametes or parthenogametes ( i f it is permissibleto coin a much- needed term ) caused a slight rise of tempera
ture , it did not compare to the he ight reached during schizogonic sporulation. I t is indeed highly probable that sporulat ion '
of a small number of parthenogametes might occur w ith
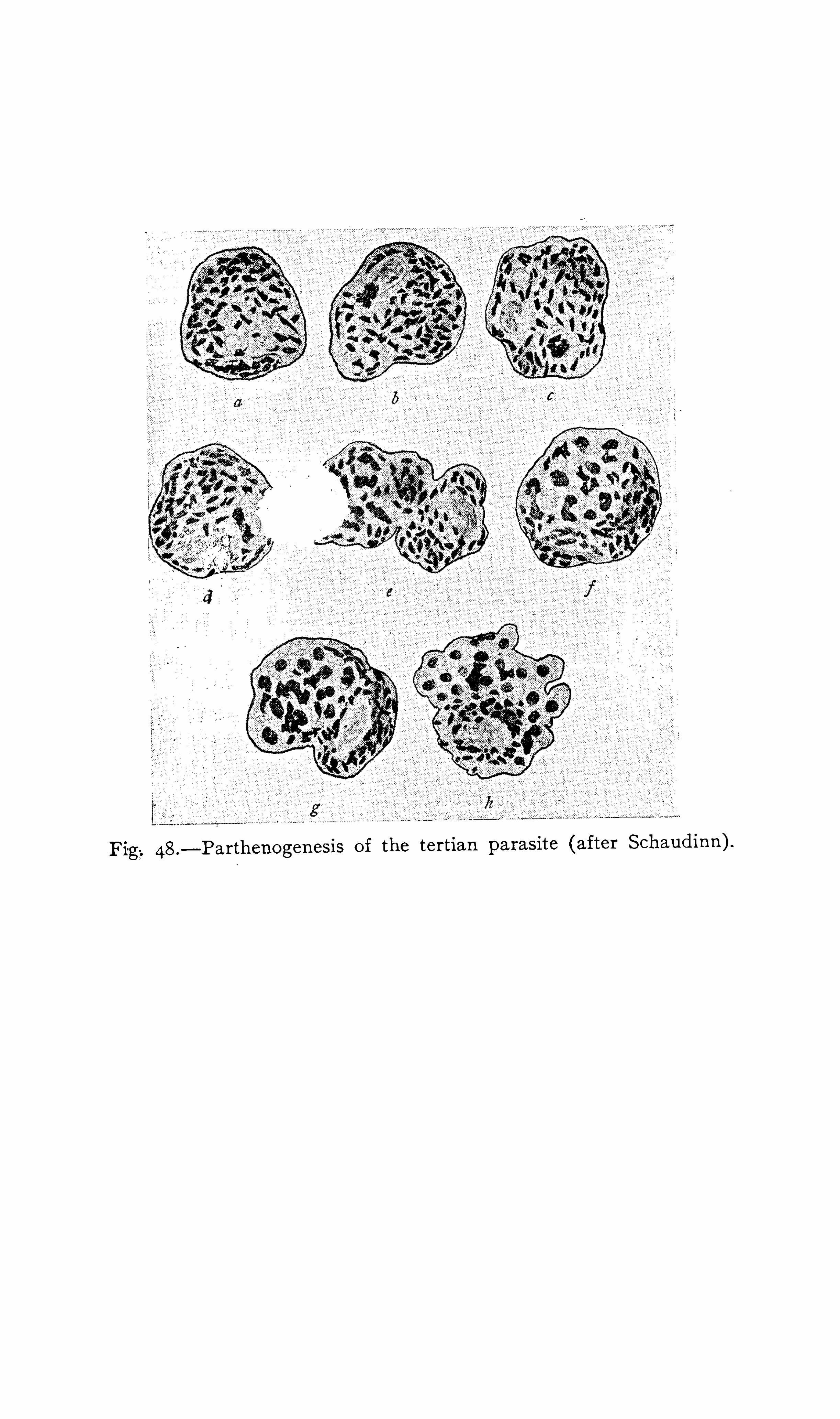
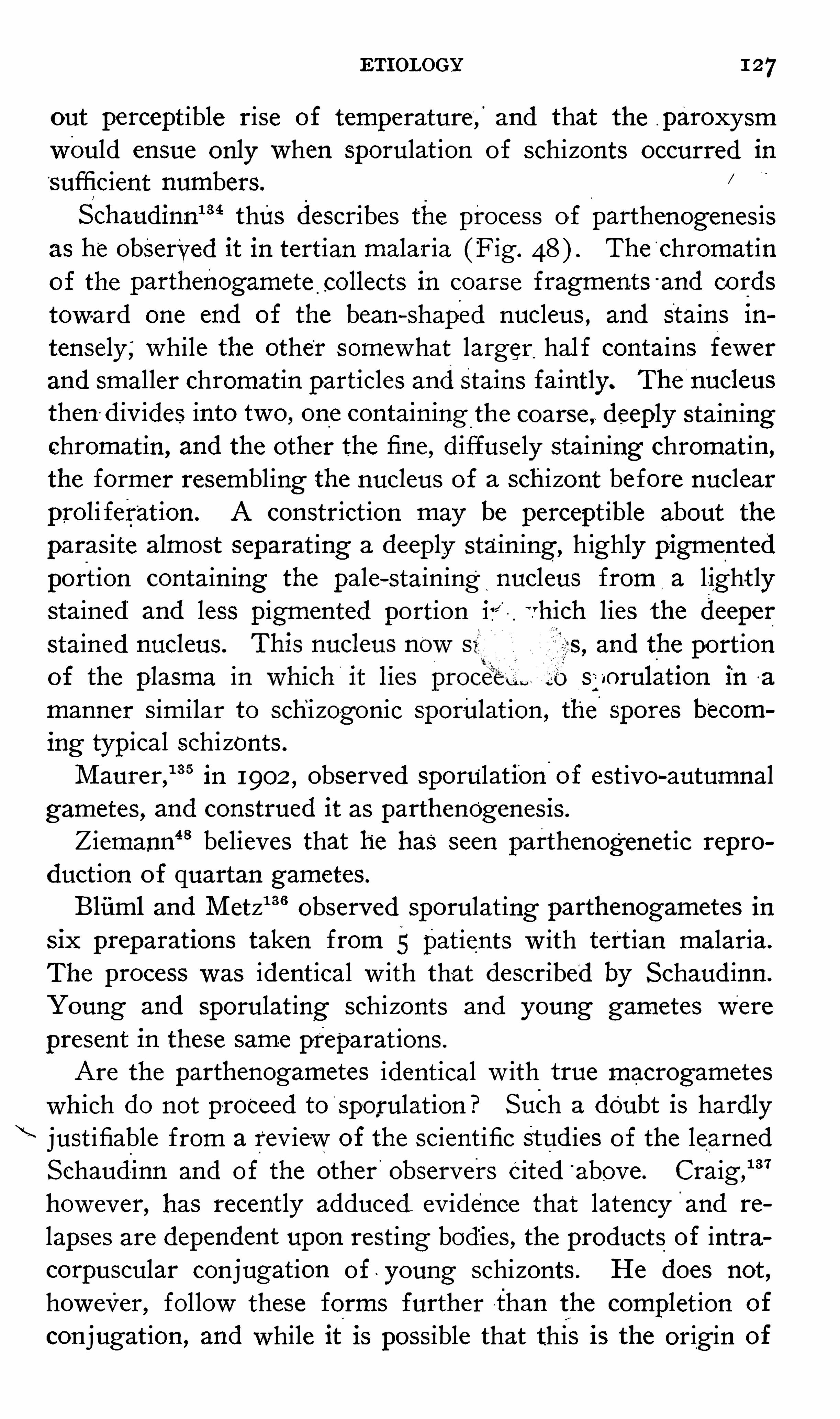
ETI OLOGY 1 27
out percept ible rise of temperature, and that the p aroxysmwould ensue only when sporulat ion of schizonts occurred in
sufficient numbers.S chaudinnm thus describes the process of parthenogenes is
as he observed it in tert ian malaria (Fig. The chromat ino f the parthenogamete collects in coarse fragments -
and co rds
toward one end of the bean—shaped nucleus , and stains intensely;while the other somewhat larger hal f contains fewerand smaller chromat in particles and stains faintly. The
‘
nucleus
then d iv ides into two , one contain ing -
the coarse , deeply stain ingchromat in , and the other the fine , d iffusely staining chromat in ,
the former resembling the nucleus of a sch izont before nuclearproli ferat ion . A constrict ion may be percept ible about theparasite almost separat ing a deeply stain ing,
highly pigmented
port ion containing the pale- stain ing nucleus from a l ight lystained and less pigmented portion ir V hich l ies the deeperstained nucleus. 5 , and the portionof the plasma i sworulation in a
manner s imilar to sch izogonic sporulat ion , the spores becom
ing typical schizonts.M aurer ,
135 in 1902 , observed sporulation-
of est ivo- autumnalgametes , and construed it as parthenOgenesis .
Ziemann‘18 believes that he has seen parthenogenet ic repro
duct ion of quartan gametes .
Bliiml and M etz136 observed sporulat ing parthenogametes in
six preparations taken from 5 patients w ith tert ian malaria.
The process was ident ical w ith that described by S chaud inn.
Young and sporulat ing schizonts and young gametes Werepresent in these same preparat ions .
Are the parthenogametes identical w ith true macrogametes
wh ich do not proceed to S porulation ? Such a doubt is hardlyjust ifiable from a rev iew of the scient ific Stud ies of the learnedS chaud inn and of the other observers c ited above . Craig ,
"37
however, has recently adduced ev idence that latency and re
lapses are dependent upon rest ing bod ies , the products of intracorpuscular conjugation of young schizonts . He does not ,
however, follow these forms further than the complet ion of
conjugation , and while it is possible that this is the orig in of
1 28 THE STUD Y OF MALAR IA
the parthenogametes , there is as yet no pos it ive ev idence thatthe latter are not true macrogametes.
I nasmuch as d ifferent terms are employed by various authorsto describe the morphology of the malarial parasite , to the
great con fus ion of the student , the w riter has prepared a brie fg lossary o f these terms . The defin it ions must not be takenin the w ide zoolog ic sense , but on ly as appl ied by the maj ority
of w riters to the paras ite o f malariaAmplz lgony . S ee S porogony .
Amphiont. S ee Zygote.
Androspore. S ee M icrogamete.
An theridium. S ee M icrogametocyte.
Asexual Cy cle, the schiz ogonic or
human cycle of parasitic repro
duction .
Blas t. S ee S poro z oit.Blas tophore. S ee Sporoblast.
Copula. S ee Zygote.
C1',
es cent one form of the estivoautumnal gamete.
D efinitive S poroblas t S ee Zygote.
Endog enous Cycle. S ee S chiz ogony.
Enhemospore. S ee M ero z oite.
Exog enous Cycle. S ee S porogony .
Exo tospore S ee S poro z oit .F lagella, microgametes .
Game te,sexual
c,
form of the parasite .
Gametoblas t. S ee S poro z oit .Gametocy te, cell giv ing origin to
gametes.
Gametospore. S ee Zygote .
Germinal Rod. S ee S poro z oit.Gymnospore, a schiz ogonic spore or
mero z oit.Gynospore. S ee M acrogamete .
Haemosporldia, the suborder o f p ro
to z oa to which the malarial para
site belongs .
Human Cycle, the schiz ogonic or
endogenous cycle.
M acrogamete, a female gamete .
M acrogametocy te, a female gameto
cy te.
M acrospore. S ee M acrogamete .
M eroz oite,a spore the product of
schiz ogony ; also applied to the
sporo z oit after it has entered thered cell.
M icrogame te,a male gamete , flagel
lum, spermato z oan .
M icrogame tocy te, a male gameto
cy te .
M icrospove. S ee M icrogametocvte.
M onogony . S ee S chiz ogony .
M onon t. S ee S chiz ont.M osquito Cycle, the sexual or sporo
gonic cycle .
Nomospore. S ee M ero z oit .Ondeterospore . S ee S chiz ont.Oocys t, an ency sted z ygote .
Ookinete. S ee Zygote.
Ovoid, one form o f the estivoautumnal gamete.
Par thenogamete ( new word ) , an
unfertiliz ed sporulating macrogamete.
Parthenog -cnes is, V irg ina] reproduc
tion.
Polymitus , an exflagellated micro
gametocy te.
Reproductive Cycle, the sporogon icor mosquito cycle.
S chiz ont,the asexual form of the
parasite .
S chiz ogony , the asexual,human or
endogenous cycle of development.
S exual Cycle, the sporogonic, mos
quito or exogenous cycle.
S perm- mothercell. S ee M icrogame
tocy te.
S pore - cys t. S ee O ocyst.S pore - mothercell. S ee S poroblast.S poroblas t, spherical or polygonalbodies contained in the oocyst ,
g iving orig in to the sporo z oits.S porocy te, a Sporulating schiz ont.5 1701agony , the sexual cycle of dev eIOpment .
S poron t. S ee O ocy st.S [901oz oa the class of proto z oa to
which the malarial parasi te be
longs .
SP0704 01t a spore the product o f
Sporogony .
S y z yg z'
es , the products o f conj ugating parasites .
Trophic Cy cle, the asexual cycle.
Trophoz oit, a young intracellular
parasite of asexual origin ; a“ mero z oit which has entered the
red cell.
V ermicule. S ee Zygote .
Z ob’
id . S ee S poro z oit .Zygote, a fertiliz ed macrogamete.
Zygotoblas t. S ee S poro z oit.Z ygotomere. S ee S poroblast.

130'
THE STUD Y OF MALAR I A
uponthe entrance into fresh red “
ce lls of the young generat ionof paras ites. This , how ever
,is shown to be erroneous by the
fact that a properly timed and adequate dose o f quin ine g ivenbefore the chill is expected does not prevent the access thoughit does destroy the young paras ites , prevent ing the ir invas iono f the ce lls .
The true explanat ion of t he orig in : of the paroxysm is
through the agency of a tox in l iberated by the sporulat ive act .
The ex istence o f a tox in , the product of the'
malarial paras ite ,
0b
a
0
Fig.49 .—The relation etween the stages of the parasite and the paroxysm;
is almost un iversally assumed by students of malaria.
“
The
grounds for this assumpt ion may be recounted as fol low s
1 . An analogy w ith other infect ious d iseases .
2 . Immun ity ;this immun ity is not absolute , but that a relat ive immun ity to malaria ex ists there is no room for doubt .3. The format ion of an antitox in F0rd
’
s14 0
experiments
be ing conclusive as to the ex istence of such .
4 . D egenerat ive changes in the kidneys , l iver, spleen , and
other organs not otherw ise explainable.
5 . Blood changes , as anemia out of proportion ,to the num
ETI OLOGY 13,1
ber of parasites , and brassy degeneration , st ippl ing , and po lychromatophilia of the red cells .
6 . I ncreased toxicity of the urine and sweat .
71The ex istence of coma in malaria w ithout paras ites or
pigment in the brain.
8. The fever and its relat ion to paras it ic sporulation .
‘
9 . Experimental proo f . The negat ive results of Guald i ,M ontesano ,
79 M annaberg , and Cel li80 are devoid of we ightagainst the conv incing experiments o f Rosenau, Parker, Francis and Beyerf
i zwho demonstrated the ex istence in malarial
blood o f a poison capable of reproducing the symptoms of
the d isease when injected into the veins of other men . The
details of their experiment with tert ian malaria are reproduced
as fo llows“
Andre z M endez (Case LXVI ) , 39 years old ; born in LaLuz , Estado de Guanajuato ;never had fever in his nat ive place.
I n 1878 ,had yellow fever in S an Antonio ,
Estado de
Guanajuato , w ith which he says he was s ick about one month .He came to Vera Cruz three years ago, and has had feversfive or s ix t imes s ince. Present i llness dates from aboutNovember 3, but states that he had been troubled w ith m ildattacks of fever for a month , which he describes as comingon alternate days , - but not sufficiently severe to keep him fromhis work.
“
The fever wh ich in it iated his present s ickness began w ith asevere chill and was followed by
“ fever and sweat , and was
associated w ith some nausea and vomit ing . He states that
these paroxysms w ere repeated daily unt il his admiss ion to
S an S ebast ian Hospital ,’
November 6 , 1903.
“ Blood examinat ion showed that he had a heavy in fectionw ith tertian parasites , and he was immed iately transferred to
the laboratory of Working Party No . 2,Y ellow F ever I nst i
tute.
“
The man was physically robust , but -c-V ery anemic, mucousmembranes part icularly pale , skin cold and damp.
“
At about noon on this date (November 6 ) the patient was
sei zed w ith a chill .“
By hal f an hour later , the rigor was very marked ;he
132 THE STUD Y OF MALARI A
lay in bed w ith a blanket drawn over his head , and was'
shak
ing v iolent ly ; he‘
could'
not hold a thermometer in his mouthand the pulse was taken w ith d ifficulty . D uring this t ime thetemperature was rap id ly ris ing, it be ing now 39 1
°
C.
“
At blood'
was drawn from one of the superficial v einsat the bend of the e lbow . O n account
“
of the rigor there wassome d ifficulty in introducing the
“
need le. The blood flowed
freely ; 12 5 cc. w ere quickly drawn . I t was pe rmitted . to flow
into a porcelain d ish and immed iatelyd-efibrinated by whippingw ith steri lized forks . Clott ing took place very i quickly , so
that the fibrin was readi ly and quickly separated from the fluid .
“ Judg ing from the S ize of the clot and color, the fibrin hadenmeshed a number ‘
of corpuscles . The defibrinated fluidshowed no further tendency to clot , and on m icroscopicalexamination looked l ike fresh blood containing a normal number of corpuscles .
“
To 2 5 cc. of defibrinated blood was added 2 5 cc. of phys iolog ical salt solut ion ,
and this d iluted blood was filtered throughthe same Berkefield filter in the same manner
'
as was done
w ith the blood of F ilomena M artinez. This filter when testedlater, M arch 1 , 1904, held back S taphylococcus [) yogenesaureus .
“ Nine cc. of the filtrate w ere injected into the right bas i licve in o f L ouis Peredo as soon as this amount could be obtained.
This inj ect ion took place at I .4O'
P . M . I t only took aboutforty minutes to defibrinate and filter the blood , which, process
was done as rapid ly as possible .
“
S tained smears o f the filtrate showed no morpholog ic ele
ments . The filtrate had a distinct red color.
“
As a control,Jose O j eira, at 2 P . M ., was g iven an inject ion
into his le ft bas il ic vein of 4 cc. of,
the unfiltered mixture. As
the blood was d iluted w ith equal parts of salt solut ion ,he ,
therefore,rece ived 2 cc. of M endez ’s blood .
“
The unfiltered m ixture of defibrinated blood and salt solut ion , upon microsc0pic examinat ion shortly after O j eira re
ceived his inject ion , show ed amebo id tert ian organisms w ithdancing pigment .
“
A fter draw ing the blood from -M endez he cont inued to have

134 THE S TUD Y or MALARI A
For further detai ls of themanner in which the blood serum
was obtained and the filtrat ion performed , see the aboverecords of F ilomena M artinez.
“
Peredo was carefully watched from the h our he was in
j ected , but he remained in good health , and no dev iat ion fromthe normal was detected .
“
His temperature was taken every four hours during the
n ight and day , both be fore and fo llow ing the inj ect ion , as
w ill be seen by the temperature charts No symptoms developed .
“
His blood was examined'
daily for plasmod ium, but none
was found .. The result of th is inject ion must, there fore , be
considered negat ive.
“
Ten days later he was again injected w ith filtered -malaria lblood under d ifferent circumstances and w ith pos
‘ it ive results.
“
At P . M .,November 6 ,
he was g iven an intravenousinject ion of the
—
blood of Andres M endez, passed through the
same Berkefield filter as be fore. M endez was suffer ing w ithtert ian in fect ion ; his blood “
was drawn during hischill and be fore the height . of the paroxysm, as
'
w ill be seen
by reference to the temperature chart .5
“ Thinking that al low ing the blood to clot four or five hoursin the ice chest in order to obtain a clear serum for filtrat ionm ight be too severe a tax upon the V ital ity of the malarialparasite , w e th is t ime defibrinated the blood as quickly as
poss ible , d iluted it as before w ith an equal volume of physiolog ic salt so lut ion , and filtered it through the same Berkefield filter in the same manner as was done w ith blood of
F ilomena M art inez.“
As soon as 9 cc . o f the filtrate could be obtained it was in
j ected into the basi lic ve in of the right arm of L ouis Peredo.
This inj ect ion took place at 1540 P . M .
“
About thirty—five minutes after receiv ing the injection hebegan hav ing chi lly sensat ions and headaches , and presentlywent to bed , covering h imsel f w ith his blanket 5 P .
F ive minutes later he was hav ing a v iolent chill , his teeth chattering so that we could “
not trust the thermometer in his mouth .The rigor of the entire .body was so marked that there was

ETiorooY 135
d ifficulty in taking the rad ial pulse . . The face was pale , and
at this t ime he vomited most o f the d inner he had eaten a
short t ime before receiv ing the inject ion“
The pat ient complained of headache , which he local ized at
the forehead and occiput ; says he felt cold and had pains in
the k nees . At this t ime the skin was dry . The chill lastedsomewhat over half an hour.
“At 3 P . M . the patient had trans ient chilly creeps
“
; very
s light rigor.
“
At P . M . he said he felt ‘
warm ins ide , ’ and all sense
of ch ill iness had d isappeared ;st il l his headache .
“At P . M . he complained of marked pain in his legs .
At P . M . he vomited the remainder of his dinner._
I t w il l be seen from the temperature chart .that during thistime his temperature was rapidly ris ing , and reached its
“
h ighest po int C. ) at 4 P . just two hours and twenty
minutes after rece iv ing the inject ion .
“
The pains inthe knees and back cont inued and nausea and
vomiting now - became a d istress ing feature 01 the paroxysms
for the pat ient .“
The fever gradually subsided , and reached normal atA . M. the next morn ing .
“
As the fever'
subsided the skin became mo ist , the nausea
and pains gradual ly d isappeared , so that by 6 P . M thepat ientwas quiet a nd d0zing . The ent ire paroxysm , there fore , ao
cord ing to the temperature record , lasted about e ight hours ,although the pat ient - was sleeping quietly five hours afterreceiv ing the injection.
“
I t is interest ing to note that th is man (Pedro ) had w hatseemed to be a typical malarial paroxysm,
beg inn ing w ith a
d ist inct rigor associated w ith a rise of temperature and fol
lowed by S light sweat ing . I t is o f particular interest to note
that his paroxysm,so far as symptoms were concerned , was
very much l ike the paroxysm from which Andres M endezsuffered , especially the nausea
“
and vomit ing .
“
Pedro was kept under very close scrutiny unt il November24 , eighteen days fol low ing the inject ion , during which t imehe rema ined ent irely normal and no plasmod ium appeared in
136 THE S TUDY or MALARIA
his peripheral blood , which was frequent ly examined , as fol
lows“
November °
6 P . M .,8 P . M . No malaria.
November 7—4 .3o A . M .
,A . M .,
P . M ., 5 P . M
11 P .
'
M . No malaria.
November 8 -
7A. M .,1 P . M .
,6 P . M .
, P M . No malaria.
November 9—7.30 -A . P . M . No malaria.
Nov ember 10—2 A . M .,
P . M .,8 P . M .,
“
five minutes each.No malaria.
November 1 1—4 , 7, I O'
A.M .,
1
2 , 6 , 1 1 P . M .,five minutes
each. No malaria.
November 12—1 .30 , 5 A .-M., fiveminutes each.
“
No malaria.
November 13—7 A . M . , P
'
. M .,five - minutes each . No
malaria.
November 14—8 A . M .
,8 P. M .,
five m inutes each. Nomalaria.
November 15—8 A . M .
,P . M .
,five m inutes each . No
malaria.
November 16—7 A . M .,
P . M .,five m inutes each . N
'
o
malaria.
November 17—8 A .M.
,8 P . M .
,five minutes each. No malaria.
“ Jose O j eira (Case XXI I I ) , a volunteer from Jalapa,18
years old ; he had never lived on the coast , and says that henever had fever of any kind . O n
"
exam inat ion in Jalapa,
August 1 1,he was f ound to be physical ly sound , of robust
physique ; urine showed no albumin, and blood examinationfor malaria was negat ive }
“
He was taken to Vera Cruz August 13 and immed iatelytrans ferred to a mosquito—proo f room in the laboratory , wherehe was kept under close observat ion .
“
O n August 28 , at 9 .30 A . M . , he was bitten by four mosqui
toes , two of which had bitten Antonio L eal (Case XXXV ) ,a yellow - fever pat ient , fift een days seventeen hours prev iously ,
and the other two had bitten the same case fourteen days
twenty- three hours prev ious ly .
“
The man was kept under close observation in a mosquitoproo f room , but show ed no react ion . . T here was no rise of
temperature , nor did he present any untoward symptoms.
“
O n O ctober 27, 7 P . he received intravenously 20 cc. of

138 THE STUDY OF MALARI A
I t w i ll be no'
ticed'
that 2 cc. of this blood caused but a
s light react ion in the case of O j eira , while cc. caused a
more marked react ion , w ith a rise o f temperature to 38 7°
C .
in the case of Peredo , ind icat ing in a very defin ite manner thatthe severity of
'
the symptoms were d irect ly due to the quant ityof poison introduced f O j eira did not have a chill or other
man i festations of a malarial paroxysm other than a rise of
temperature and nausea. He vomited gastric mucus severalt imes.
“
O n November I O , the fourth day follow ing the injection ,
O j eira had a typical malarial paroxysm , w ith tert ian paras itesin his peripheral blood . He suffered w ith a double in fect ion ,
hav ing a chill every day , as w i l l be not iced by re ference to
the temperature chart.“The character of the paras ites in his blood and the cl in ical
course o f the"
d isease resembled in all respects those of Mende z ,
fromwhom the blood was taken . Both cases were ent irelycontro l led by quin ine.
The paras ites of tert ian and quartan in fect ions developuni formly , one generat ion at a t ime
, hence typical paroxysmsare the rule. S ometimes , it is true , sporulat ing forms are met
w ith - betweenthe accesses , but a certain dose of tox inis necessary to excite a fit . The estivo—autumnal paras ites , o n the
other hand , do not sporulate so un i formly , hence the poison isl iberated in broken doses and typical paroxysms are more fre
quently lacking and the fever more cont inuous or . irregular.
I f sporulation occurred more nearly s imultaneously ,as in the
tert ian and quartan forms of malaria, it is probable that thesudden d ischarge o f the more highly poisonous est ivo—autumnaltox in would be more often attended w ith serious consequences .
The un i form sporulat ion o f the tertian and quartan parasitesmay be l ikened to a body of sold iers firing by vol leys , wh ilethat o f the estivo - autumnal paras ites is s imilar to sold iersfiring at w il l .The change of type of malarial attacks has been used as
an arg ument for the un ity of the malarial paras ites. I t is
w ell known , how ever, that such occurrences are best explainedby a number o f different spec
‘
ies . Quot idian malarial parox
ETI OLOGY 139
ysms dueto two generat ions o f tertianorgan isms may become
tertian 1n character by the“
destruct ion of one generat ion .
Quot idi’an paroxysms due to a triple quartan in fect ion may
become quartan or double quartan by the death of two genera
t ions or o f a s ing le “
generat ion of paras ites. O n the contrary,
tert ian and quartan accesses may become quot id ian by the
development into act iv ity of one or two addit ional generat ions .
I t is remarkable in mult iple infect ions by d ifferent generat ions of the same species of paras1te that they almost always
sporulate on d ifferent days and very o ften about the same
t ime each day .
'Thus it ,is v ery rare in double tert ian in fections that two paroxysms should occur w ith in one day f ollowedby a fever—free day . Th is is probably best explained by t hemode o f infect ion . I t is known that the malarial mosquitoesfeed almost so lely at n ight and usually on ly once during the
n ight . I f a subj ect is inoculated by the mosquito on two suc
cessive n ights it is obv ious that the paras ite would becomemature w ith an interval of about tw enty
- four hours betw een
the generat ions . I f inoculat ion should occur upon three or
more success ive nights it is probable that the th ird and succeed
ing generat ions would sporulate , after incubat ion ,s imul
taneously w ith the first and second . The interval between
mult iple quartan in fect ions may be explained s imi larly .
L atency and relapses w ere formerly explained upon the
theory that so long as the paras ites remained below a certainlevel o f asexual reproduct ion the d isease was latent , and whenthe. paras ites exceeded in number th is level a relapse occurred.
S ims has est imated the greatest number of adult paras iteswhich the body can endure w ithout symptoms as about two »
bill ions. I t is probable that brief periods o f latency may be
thus explained , especially in persons possess ing a relat ive immun ity , but it is ev ident that this 15 not a common mode , par
ticularly of relapses at long intervals , s ince the asexual cycleis known to w ear out spontaneously after certain periods.
These relapses at long intervals can be explained by parthenogenes is alone . A fter the schizonts have perished , while the
micr0gametocytes do not pers ist long , the macrogametes re
main for indefin ite periods . They may sporulate more or less
140 THE STUD Y OF MALARI A
regularly , causing paroxysms at intervals of about a week “
, or
multiples thereo f , or may lie dormant unt i l aroused into repro
ductive act iv ity by exposure or d ietary or other excesses. I t
is highly probable that the parthenogenetic cycle of reproduc
t ion is conducted almost altogether in the v isceral Circulat ion ,
part icularly in the spleen . As ev idence o f this may be citedthe outbreaks of malaria follow ing cold douching , electricalst imulat ion , and trauma of the splen ic reg ion .
The anem ia o f malaria depends upon three,
factors : . 1 , the
mechan ical destruct ion of cel ls by the paras ites ; 2 , the e ffectof tox ins , and, 3, the act iv ity of the blood - making organs .
L iberated hemog lobin is tranSfor-med by the l iver int-o
“ bilepigment. When the hemog lobin is
"l iberated too fast for thel iver to ut i lize , h emog lobinemia results , and hemosiderin is
precipitated from the blood. The increased activ ity of the
l iver results in polycholia and icterus . I t is probable that jaund1ee is due also when the l iver capacity is overtaxed to hemo
globinemia. When hemog lobinem ia exceeds a certain l imit thehemog lobin is excreted by the kidneys , result ing in hemo
globinuria.
Splenic enlargement'
is effected through hyperemia, depos it ion of detritus of destroyed erythrocytes , accumulat ion of
paras ites , and hyperplasia of the pulp.
S pontaneous cure is probably due to the natural weaken ingof the reproduct ive powers of the paras ite , a phenomenon
occurring in strains throughout the vegetable and an imal kingdoms , and poss ibly also to the influence of an antitox in.
Phagocytosis plays , in the opinion of the writer, a much lessprominent role than is usual ly attributed to it . I t is probablethat this function is exercised mainly after the parasites havelost v ital -ity from other causes .
ETI OLOGY OF PERNI CI OUS MALARI A
Pern icious malaria is that form of malaria so acute that ,independently of compl icat ions , l i fe I S endangered in a few
hours or a few days . This grav ity maybe due to the intens ification of ord inary malarial symptoms or to the advent
I
o f
unusual ones. I t should be clearly understood that pern icious
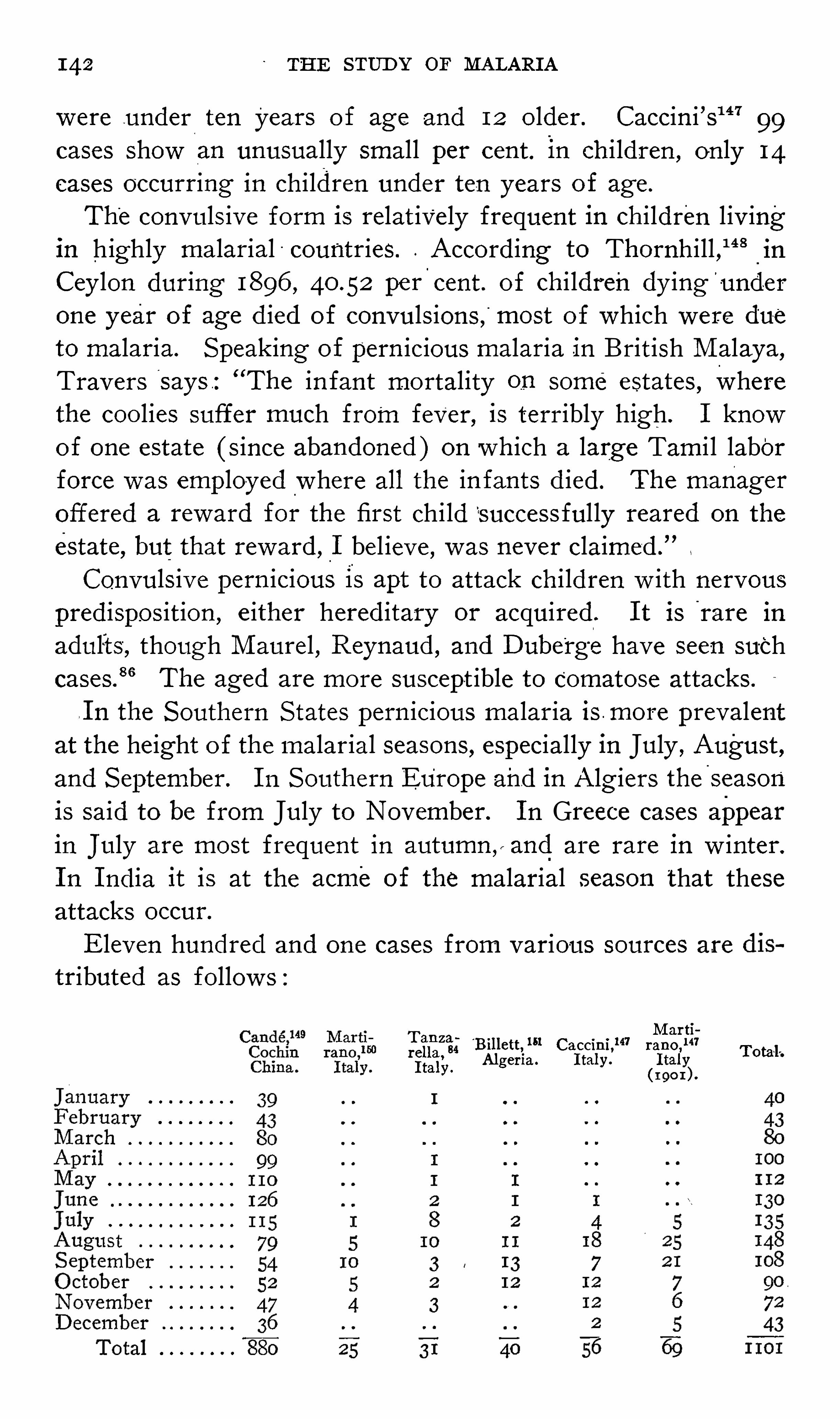
142 THE STUD Y OF MALARI A
were under ten years o f age and 12 o lder. Caccini ’s147 99cases show an unusually small per cent. in ch i ldren
, on ly 14
cases occurring in children under ten years o f age.
The convuls ive form is relat ively frequent in children l iv ingin highly malarial countries. Accord ing to Thornhill , “ 8
in
Cey lon during 1896 , 40 .52 pe r cent . of chi ldren dy ing underone year of age d ied of convuls ions , most of which were dueto malaria. S peaking of pern icious malaria in Brit ish M alaya,Travers says : “
The in fant mortality on some estates , wherethe coo lies suffer much from fever, is terribly high. I knowof one estate ( s ince abandoned ) on wh ich a large Tami l laborforce was employed where all the infants d ied. The manager
offered a reward for the first child success ful ly reared on the
estate , but that reward ,_
I bel ieve , was never claimed .
”
Convuls ive pern icious is apt to attack chi ldren w ith nervouspredispos ition , e ither hered itary or acquired . I t is rare in
adults , though M aurel , Reynaud , and D ube'
rge have seen suchcases
? 6The aged are more suscept ible to Comatose attacks.
.I n the S outhern S tates pern icious malaria is more prevalentat the height o f the malarial seasons , especially in July , August ,and S eptember. I n S outhern Europe and in Alg iers the
'
season
is said to be from July to November. I n Greece cases appearin j uly are most frequent in autumn y and are rare 1n w inter.
I n I nd ia it is at the acme of the malarial season that theseattacks occur.
Eleven hundred and one cases from various sources are
tributed as follow s :M arti
T an z a 151 141 14134 Billett , Caccini, rano, Tota-lrella, Algeria. I taly . I talyI taly .
( I 90 I )
I
0 0 0 0 0 0 0 0
0 0 0 0 0 0 0 0 0 0 0 0
0 0 0 0 0 0 0 0 0 0 0 0 0
O O O O O O O O O O O O O
0 0 0 0 0 0 0 0 0 0
O O O O O O O0 0 0 0 0 0 0 0 0
0 0 0 0 0 0 0 0

ETI OLOGY 143
The influence of inundat ions on the et iology o f perniciousfever 1s well recognized. In 182 6 j ohnson
16w rote .
“ There 15
no unmixed good 1n th is w orld, _The inundat ions of the Ni leand t he Ganges , while f they scatter ferti lity over
'
the val ley of
Egypt and the plains of B engal, sow with a l iberal hand at the
same t ime the seeds of dread ful d iseases . This is in all probability true o f the M iss iss ippi and other large rivers of
'
0ur
country . I n 1854 Frerichs recorded an epidemic of pern iciousmalaria fol lowing an overflow o f the O der where there had
previously been only m i ld cases o f malaria.
The length of res idence in a malarial reg1on 1s probablynot an important factor in '
t he et iology of the affect lon; Wh ileS ims“ . and others believe that it occurs main ly in the earlyperiod of res idence , most of M aurel
’
s75
cases were in persons
who had been in the colony a long t ime . Plehn5 ment ions the
case o f a young phys ician who d ied of pernicious malaria s1x
days after arrival at Banana.
. M aure l7 5 states that outbreaks of pernicious malar1a mayoccur several years after return to France from the tropics,and w ithout new in fect ion . D uring and shortly after the war
w ith Spain numerous cases which were in fected ln Cuba and
the Ph ilipp ines w ere treated in American hospitals . Rees1 5 3
records the case of a man who had spent only five days m an
endemic reg ion a nd developed comatose malaria w ith fatalterminat ion in a few weeks after his return to L ondon . S atter
lee ,15 4 Hall 1 5 5 Neer, 1 5 6 and others have observed s imilar cases
inAmerica. I n the maj ority o f such cases the outbreak occursw ithin a few weeks afte r leav ing the endemic area.
O ccupations Which subject not on ly to malarial infect ion ,
but to hardships and exposure , especia lly to the sun , pred isposeto p ern icious attacks . M anson
".
39cites the case
-
of_
Hong Kong ,
formerly healthy enough ,but
‘
when barracks and houses w ere
being built and roads laid out the soldiers died by the hundred
of pernicious fevers . Homem“ ?7 asserts that these cases occur
in Rio de . Janeiro , particularly‘
when the sewerage , _-
'
gas , and
water compan ies are makingdeep and extens ive excavations inthe more central streets of - the city . Early - in the last century ,
when themarsh of Chartreuse , near Bordeaux, was drained ,

THE STUD Y OF MALARI A
an epidemic of severe malaria prevai led , and in 1805
people were stricken , of whom d ied in five months .
A s it is especially'
in the laboring and poorer classes thatprimary in fect ions do not rece iv e adequate treatment , it islargely in this class that pern icious '
attacks - are'
found .
Pern icious attacks may be first attacks or they may occur
in cachectics , but it is chiefly between thes e extremes that most
attacks orig inate , namely ,in those hav ing had prev ious attacks
o f malaria , but who are not saturated to the degree of cachexia.
L averan ,
1M archiafava and B ignami , 22 and S ambon 9 hav e
never seen pernicious attacks w ithout prev ious malaria.
Ruge ,15 8 however
,states that such cases are not uncommon in
I nd ia and both the east and west coasts o f A frica. Col inandAntoniades have observed l ike cases.
11 5 9 Wurtz and Thiroux16 0
say _
_that the typho id form is most often a fever o ffi rst inva
s ion. Roux161 knows o f numerous - examples of pern icious
fet/fer as the first man ifestat ion -
of malaria. M annaberg111‘
asserts that it may attack those who have never be fore sufferedfrom malaria, as wel l as those who have undergone repeated
attacks . Homemm says that in many cases the perniciousparoxysm is preceded by s imple ones ; in others the pat ient isattacked while 1n perfect health . I t 15 the comatose form thatis most frequently Seen in those who . have not prev iously beenattacked w ith malaria. Crespin ’
s111
experience is that the at
tacks are exceptional 1n chronic malarials . Smart76
records it
that during the C iv i l War pern icious attacks occurred not onlyin persons
‘
who were for the first t ime exposed to a highlymalarial atmosphere , but also among t hose who had sufferedmore or less from the malarial influence be fore the superven
t ion o f the congest ive se izure . I n 50 cases observed by Cardamat is and D iamessis
3 5on ly one developed as a primary attack
M ost of the alg id and comatose cases of M aure l were in sub
j ects of chron ic malaria. Thayer9 8 and Craig70 say that it is
customary for malarial paroxysms to precede . S chel long”agrees w ith M artin that pern1c10us fever“
attacks -
persons al
ready rendered anemic from malaria;While it is probably true that in the majority
‘
of instancestypical paroxysms precede pern icious attacks , it is of the utmost
146 THE STUD Y or MALARI A
due'
to the in fect ion w ith the tropical parasites , it cannot nowbe maintained that tert ian and quartan infect ions are not occa
sionally accompan ied by pern iciousness . Craig161 says that anyof the malarial paras ites may cause pernicious in fect ions , leading to death. Crespin16 5 in forms us that it is not rare to find
on exam inat ion tert ian and quartan paras ites in these cases .
Billet1 5 1 found the large tertian in 6 of 40 cases of typho idpern icious . Ziem'
ann9 6
observed a case of pern icious malariadue to the ben ign tertian . Thiroux
sz6 found this paras ite in
a case of convuls ive pern1c10us m a mulatto in fant. Ew ing ,
27
in 64 cases of the cerebral type of pern icious , found the largetert ian paras ite alone in 5 . F rench16 6 reports
'
a case of coma
tose malaria in a man, aged twenty- one , Whose blood harboredthe tertian parasite. Hunt16 7 observed a case of common tertiancomplicated by alarming hemateme5 1s m a boy aged eleven.
M cElroy16 8had a case of comatose pern icious due to tert ian
infect ion in a negro male , aged thirty. Ficucci1'6 9
records a
case w ith a pern icious meningo- cerebellar syndrome due‘
to
tert ian paras ites; Fenner170
g ives the history of a case of the
comatose type in an adult ; the blood exam inat ions showed
crescents and large tert ian forms.
Craig16 4 makes the assert ion that quartan infections are
more apt to become pern icious than tert ian. The writer, however , agrees w ith D av idson ,
6 6who says that pernicious symp
toms occur more rarely in connect ion w ith the quartan infect ions than w ith s imple tertian . The reasons for this are probably the relat ive rarity of
“ quartan fever and the more even
d istribut ion o f paras ites throughout the circulation , there be ings light tendency to form accumulat ions .
I t is not yet known w ith certainty which variety of the
est ivo - autumnal paras ite g ives rise most frequently‘
to pern iciousness . M archiafava and Bignami16 2 and M annaberg
111
hold that the tert ian estivo - autumnal infect ions are the most
dangerous , only a few cases show ing the quot id ian . Craig ,
70
how ever,found the quotid ian paras ite most o ften in cases in
fected in Cuba and in the Philippines; This was also the expe
rience ofWright"18 in Brit ish M alaya, who found the pigmented

ETI OLOGY 147
quot id ian paras ite most frequently associated w ith the cerebraland gastro
- intestinal types of'
pernicious malaria.
The part played by the crescents in the pathogenesis of pernicious paroxysms is worthy of brie f cons iderat ion . M archiafava and Bignami , 22 Celli ,” M annaberg ,
”11 A . Plehn ,
171
Koch,
” 2M anson ,
5 9 Thayer, 9 8 and others be lieve that this formof the organ ism is non -
pyrogen ic. Ew ing ,
” 0how ever
"
, holds ,w ith L averan ,
that it is by no means certain that the format ionand
'
development of the crescents are entire ly innocuous to thepatient . Ew ing , doubtless in part , ' bases this opin ion on the
find ing of crescents alone in 33 of 64 cases of cerebral pernicious .
27 Whether the blood examined in these cases was per
ipheral or v isceral is not stated, but as only three were fatalit may fairly be assumed that in most instances at least it was.
peripheral . That the crescent ic form of the paras ite has “
an
intimate relation to - the production of the pernicious fevers 1s
improbable , for the follow ing reasons : F irst , crescents alonemay be found in the peripheral blood , and intense local izat ionof active forms be present in the brain or other v iscera. The
number o f paras ites in the superficial circulat ion is not a reliableguide to the sev erity o f the attack. O f Ew ing ’
s 64 cerebralcases no paras ites w ere ident ified in I I
,and,
in many o f his
33 cases_
in which crescents alone were found the .search was
success ful only after '
one and two hours. S econd , crescents
are rarely ,.if ever, present in the parasitic local izations and
thrombi frequent ly observed in pern1c10us cases.
O f the pathogenet ic factors which excite pern iciousness thefol low ing are to be regarded as the most important and ap
prox imately of relat ively equal 1mportance1 . An excess ive number of parasites.2 . L ocal izat ions of parasites .
3. Tox ins .
4. I nd iv idual predisposit ion and external eti010gic influences.Number of Paras ites .
—Golgi’
s law , that the number of
parasites determines the severity of the attack , has been generally accepted. Cases inWhich the paras ites are in very great
numbers in the peripheral blood are usually accompanied bycoma.
148 THE STUD Y or MALARI A
We have no means o f est imat ing even app-r0x1mately the
total number o f malarial paras ites in the body of a malarialpatient , as the d istribut ion o f the former varies w ithin the
w idest l imits . They may be numerous in the peripheral andv isceral circulation general ly ;they may be scanty or absent inthe peripheral circulat ion and numerous in most of the v iscera ;or they may ex ist in moderate numbers or be absent except incertain areas
“
where they may be intens ive ly local ized . Thatthe paras ites are abundant , either absolutely
'
in the body as a
whole or relat ively in certain areas , probably holds good ina great majority o f the cases , though , “
as Cell i80 states ,'
we
cannot always attribute pern iciousness to the large numberof paras it ic forms . M arch iafavaand Bignami” call attent ionto certain grave cases of comatose , convuls ive
,delirious or
m ixed pern icious , in which from beg inn ing to e nd and even
at autopsy v ery few paras ites are found . M annaberg1411
says :“
From the general impress ion wh ich I have obtained natural lyfrom the per ipheral blood , the number in mal ignant fevers isperhaps larger, yet the d ifference scarcely s eems
-
so decided as
to make th is factor alone responsible for the pern iciousness .
As appl ied to the number of paras ites in the peripheral blood ,
Gol-gi’
s rule is applicable on ly in a very g eneral sense. Bacelli173
says that fatal cases of malaria occur in wh ich there cannot
be found any known form o f the paras ite .
Ziemann‘18
states that the number of paras ites in the per
iphe ral blood is not always in d irect relat ion to the severityo f the attack . Crespin 1“1 1 acknow ledges that he had d ifficultyin find ing the paras ites , which w ere always scanty in thesecases . He g ives the detai ls of a case in which there w ere
neither paras ites nor p igment in the peripheral blood , but they
w ere numerous in the vessels of certain v iscera. This w riterquotes Nocht as say ing :
“
I n'
pernicious attacks the hematozoaare not found in the peripheral blood , but on ly in the v iscera.
”
M oore25
says :“
I have o ften seen cases where the symptoms
in no w ise seemed commensurate'
w ith the number o f paras itesobserved in the specimen of blood .
”Accord ing to Kendall ,”
there may be on ly a few paras ites in the peripheral circulat ion ,
or‘ it may be ev en imposs ible to find them. M annaberg
141states
I 50 THE STUD Y OF MALARI A
Local i z at ions of Paras ites .—Accumulat ions of paras ites in
the brain were first described by P laner and by F re
richs ( 1861 ) those in the l iver by Guarn ieri M ore
recently the m inute observations‘
of M archiafava and Bignami ,D ock , Barker and Ew ing have taught us that pernicious malaria ,
in many of its varied mani festat ions , is dependent on
these localizat ions in one or more of a mult ipl icity of local ities .
L ocalizat ions in the brain have been found - associated w ith a
w ide variety o f cerebral symptoms ; inthe mucosa of the ali
mentary tract , the gastro- intestinal symptoms , and typ ical alg id
attacks ; in t he heart, w ith cardiac symptoms ; in the medulla,
w ith bulbar. paralys is ; in the ret ina , w ith a
’
rnblyopia ; in the
pancreas , w ith hemorrhag ic pancreatitis , '
etc. I n proportion tothe amount o f damage sustained by the kidneys in malariathere is less tendency for parasites in pern icious attacks to accu
mulate in these organs"
than ln any othe r of the body . The
most care fully stud ied case o f this cond it ion is that of Ew ing .
177
These localizations cons ist , in the main , of parasite—in fectedred blood—cel ls . T here may be , how ever, pigmented leucocytesand free paras ites and pigment . The paras ites in each particu
lar case may be of the same or 0f d ifferent stages of development . The pigmented and sporulat ing forms are probablyo ftenest seen , but the earlier phases are frequently observed .
I t would seem reasonable that the crescents , on account of the irs ize , would frequently form an important e lement in these accumulations of parasites , but such does not appear to be the case.
The cause of the parasit ic concentrat ions is problemat ical .I t cannot be due to the s ize , we ight or loss of elast icity of the
in fected cells , for, as M annaberg1 ‘11
states , the benign'
parasite
would'
be more apt to form thrombi i f this w ere the cause .
Ke lsch and Kiener178 and others have observed endothel ialswell ings in the smal l cerebral vessels , w ith consequent constrict ion of cal ibre
, but whether this is a cause or an effect cannot
be said . Vasomotor disturbances and phagocytos is have alsobeen invoked in explanat ion . The most probable theory is thato f M annaberg ,
111who attributes the cond ition to a sort of
agglutinat ion or adhes iveness that holds the erythrocytes tothe vessel walls.

ETI OLOGY 151
The symptoms present in cases in which , on post- mortem
examination , local izat ions ofparas ites are demonstrated are not
always referableto these aggregat ions alone , since changes arefrequently observed wh ich are secondary to paras it ic thrbosis , and may outwe igh the latter 1n pathogen ic i .mportance
The most conspicuous of these changes are perivasculardat ion ,
hemorrhage and . necr05 1s . The hemorrhages are usu
ally punctate , but Blanc179 and Ziemann report large ce rebralclots .
This propens ity of the paras ites in pern icious fever to con
gregate undoubted ly explains the course of“
many cases , but
by no means all. Fatal cases of comatose malaria have beenobserved w ith no paras ites at all in the brain . Ford
18°reports
a case w ith serious pulmonary symptoms in which the ‘
parasites
were no more numerous in the lung than in the general “
circu
lat ion.
“
The severity of the renal lesion, w ith the absence of
paras ites in the renal vessels , also requires ment ion .
” 18 1
I t 15 not known whether paras it ic thrombi may ex istWithoutproducing symptoms“ Frerichs, 9 ‘1 who frequently observedthrombotic occlusions of the cerebral vessels , insisted that toomuch stress should not be laid onthem on account of the richcollateral circulat ion . He likew ise affirmed that he had more
than once seen marked ly pigmented bra1ns w ithout cerebralsymptoms during l i fe .
'
Based on a case in which the pat ient was suddenly attackedw ith trans ient coma three t imes in five days , Ew ing 18 1 believesthat the embol ic processes are factors 1n some instances .
This 1s the most probable explanat ion of thes-e cases .
T ox ins—Theev idence of the ex istence of a tox in in malariahas been detailed above .
I ndiv idual Pred ispos it ion and External'
Etiolog ic I nfluences—“We ought , then ,
in case s of pernicious fever , to seekin the cond it ions of the ground, wh0se qual ity is so different ,and
‘
not in the quant ity of the seed , the reason which shall explain to us the grav ity o f the disease .
” 15 7
The qual ity of the soil , in the sense so aptly employed byHomem, as a factor in the -
pathogenes is of pern icious malariahas probably not rece ived the attention it deserves . This influ

152 THE STUD Y OF MALARI A
ence , in many instances , doubtless not on ly induces the attack ,but determines lts type. O rgans or systems en feebled by ante
cedent ailments are apt to play the t it le role inthe pern icioustragedy . Thus alg id and cho leraic attacks may be
- associatedw ith a history of intest inal catarrh ;the comatose and deliriouscases , w ith a history of abuse of alcohol ; the convuls ive w ithep ilepsy, etc. I t is not improbable that some cases of dysenteric,card ialg ic, syncopal , tetan ic, catalept ic, paralyt ic, pneumon ic,pleurit ic
'
, gastralg ic , and other forms d escribed by the olderw riters may be s im ilarly explained. M ercier182 goes so far as
to say that all pern icious attacks are merely visceral complicat ions .
M alarial subj ects who are much ‘
exposed to the heat of the
sun are l iable to be stricken w ith pernicious fever, especially of
the cerebral type. This danger is enhanced i f to the solar heatare added fatigue , deficient or improper food , or other hardships. Certain psychic states have causat ive s ign ificance.
Hertz183 states that he has seen the local izat ion of pern icioussymptoms determined by injuries of the skull through a fal lor a blow .
I n add it ion to the four principal factors enumerated , con
gest ion of v iscera and parasitic obstruct ion of the hepat ic capillaries have been regarded as important. I t is probable that theyhave l ittle influence.
A feeble phagocyt ic act iv ity was cons idered by Golg i aspred ispos ing to pern icious attacks . I n the present state o f our
know ledge "
it is imposs ible to define the relat ion of this funct ion to perniciousness .
A considerat ion of the relat ive frequency w ith w hich theseveral factors are concerned in the pathogenes is of the variousforms of pern icious malaria w i l l necessarily be brie f . I n the
comatose variety any of the four ch ie f agents may take part ;id iosyncrasy and external influences may unite w ith any of the“
other factors ; an extraord inary number o f paras ites in the
general circulat ion , w ithout accumulations in the brain ,is pro
ductive o f coma probably because of the toxin . Ew ing18 1 saysthat the majority of cases of comatose malaria coming to
autopsy do not show a mass ing of paras ites in the brain. He

154 THE . STUD Y OF MALARI A
rate , phenacet in , arsen iuretted hydrogen , methy lene b lue,phosphorus , oxalic acid , certain i lluminat ing gases, he lve lla escu
lenta, and snake venom. Hemog lobinuria is a common symptom of Texas fever in catt le, and is seen occas ionally in sheep,dogs , goats , horses , and mules , follow ing in fect ion w ith hemato z oa resembling the malarial paras ite.
Race .—Hemoglobinuric fever is chiefly a d isease o f the
wh ite race. The negro is not absolutely immune , though not afew observers of w ide experience have not seen cases in thisrace . Th is relat ive immunity canbe explained only by naturalselection. I t varies markedly in d ifferent tribes , and membersof an insuscept ible tribe may be attacked on mov ing to a blackwater fever focus. F . Plehn
5refers to anextens ive outbreak
that '
occurred among the Cameroon negroes , especially thosewho came from the interior to the coast. According to D rye
pondt ,8 6the negroes recruited for the Congo Free
'
S tate“
in
1890 to 1892 paid a large tribute to this malady. D eGreny8
saw 2 0 cases in negroes imported from the Brit ish Ant i lles forrailroad con struct ion work on the lower Congo . I n the med icalreport from Germa
’
n'
East A frica for the official year, 1903-
4 ,
there were l isted 8 cases in negroes. Corre ,8D onny ,
8the
younger M oncorvo ,
8 Hanley ,
18 ‘1A . Plehn ,
9 9 Rudolph Plehn ,
185
Wittrock ,1 9 Brunn ,
‘1 9Curry ,
186Ey les ,1°1 D oering ,
187 Reynolds ,Easn1on ,
1°1' W' icke , Gaertner,9 0
Quartey~Papafio,
1°1'O
’
Sulli
van - Beare , Vieth , 90 Goltman and Krauss , 189 M cElroy ,19°
Be' renger - Ferand ,
19 11 Ziemann ,
"36F isch , O llwig ,
5 1Greisert
5 1
L ew is , 192 Francez , 193 M inor , 19 1 M cKay ,Tyson , Gorgas ,
and Wendland ‘1 9 have seen cases in negroes . The writer hasseen two cases in mulattoes and two in black negroes. Chineseimported into blackwater fever reg ions are almost as suscepti
ble as whites. M anson5 9
says that many of the Chinese laborers 011 the Congo rai lway d ied o f hemoglobinuric fever. Im
ported I nd ians are affected,but , accord ing to D an iels , 197 are
only about one - fourth as susceptible as Europeans . As may
be in ferred from one of the names ,“
fiévre jaune cles creoles ,creoles are not in frequently attacked . M asterman
6 1reports
that it is common among the Jews of Palest ine . RothsChuh8
saw cases ln m1xed breeds and pure I nd ians in Nicaragua.
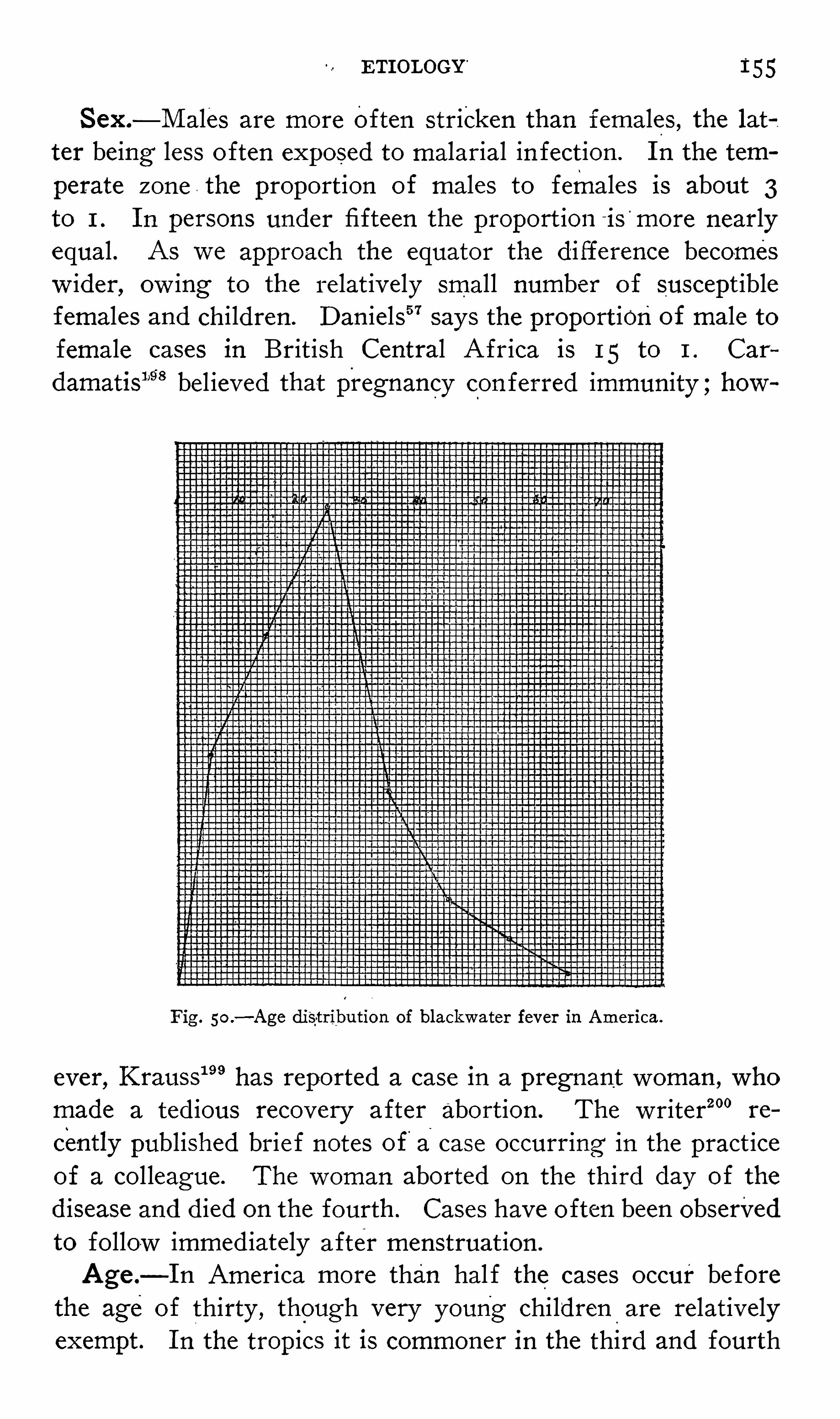
ETI OLOGY“
1“
55
S ex.—M ales are more often stricken than females , the lat
ter being less o ften exposed to malarial in fect ion . I n the tem
perate zone . the proportion of males to females is about 3to 1 . I n persons under fifteen the proport ion ~is
'
more nearlyequal . As we approach the equator the d ifference becomesw ider, ow ing to the relat ively small number of suscept iblefemales and children . D an iels 5 7 says the proport ionof male tofemale cases in Brit ish Central A frica is 15 to 1 . Car
damatis1’9
'
8 bel ieved that pregnancy con ferred immunity ;how
Fig . 50 .—Age distribution of blackwater fever in America.
ever, K rauss11’9has reported a case in a pregnant woman , who
made a ted ious recovery after abort ion . The writer200 re
cently published brie f notes of'
acase occurring in the pract iceof a col league. The woman aborted on the th ird dav of the
d isease and died on the fourth . Cases have o ften been observedto fo llow immed iately after menstruat ion .
Age .—I n America more than hal f the cases occur be fore
the age of thirty , though very young children are relativelyexempt . I n the tropics it is commoner in the third and fourth

156 THE STUD Y or MALARIA
decades of li fe because .most of the suscepti ble populat1on 15
w ithin these ages . D an ie ls 5 7 saw a case in a hal f - caste aboutfive years old ;Wendland ,1 9 V an der S cheer, and K aramit
sas1 5
observed cases in children of four ;L ipari202 mentions 2
cases in children o f three ;M asterman6 1
1 in a g irl of two , and
O etkerf‘:21 in a two—year- old ch i ld ;F isch203 saw cases in ch il
dren of fourteen months and two and one - hal f years ,”
and
M cElroyz.
011 at tw e lve months .
S eason—I n the trop ics , l ike malaria, it is perenn ial , occurring w ithout marked seasonal prevalence , though probably com
moner in the trans it ion period from the'
moist to the dry season.
I n the temperate zone it appears at the height of, or immedi
ately fo llow ing, the malarial season , the second hal f of theyear show ing by far the greater number o f cases , especiallyAugust , S eptember, and O ctober. A few cases are seen in the
first six '
months . I n Greece it is during the months of November and D ecember that the maj ority of cases occur.
Fam i ly Pred isposition . bel ieved in a wel lmarked fami ly tendency ,
hav ing observed cases in several mem
bers of the same fami ly. D an iels 5 7 re fers to three fam il ies inwhich he not iced this pred ispos it ion. Three such fami l ies are
known to the w riter. Cardamatis206
relates the case of a fam ilyof seven , ofWh ich the father, mother, and one daughter w ere
w ithin a few days attacked and d ied w ith blackwater fever.
The others,remov ing to
'
Athens , w ere all subsequently at
tacked , but fortunately recovered . Nine years later a daughterhad the fever again and recovered. S utherland16 8 speaks of a
fami ly of which all the children , six in number , d ied w ithhemog lobinuric fever,
'
I d iosyncrasy .—An id iosyncrasy in suscept ible ind iv iduals
has long been assumed and by many pass ively accepted as the
sole explanat ion of the mysteries o f pathogenesis . Foustanos207
holds that idiosyncrasy is e ither congen ital or acquired , as the
result of debil ity or bod ily changes due to syphilis , malaria,
etc. There I S not sufficient ev idence to show that hered ityplays an important part in Whatever is meant by this vague
term.
Prev ious A ttack s of Hemog lob inur ia .—Who has had

158 THE STUD Y or MALARI A
which this is specified is that ofHoward , twenty- three years
in Central A frica, though in 5 of M cElroy’
s214
cases the length0f residence was longer than twenty :
years .
A lt itude .—Hemog lobinuric fever is o ften considered a
d isease of the low lands , though cases are common ly observedat heights of feet . The results of D an iels ’ 5 7 observat ionson the influence of altitude may be stated as fol lowsThe greater number of recorded cases have occurred in the
highlands at or about feet above the sea lev el . Thereare two reasons .for this :F irst, the number of res idents inthese highlands is much greater than in the other d istricts.
This correct ion alone reverses the figures ;. secondly , many of
these cases were v is it ing the highlands on account of health orfor other reasons . O thers were pass ing through the highlandswhen invalided home . S ome had recent ly v is ited the '
lowlands.
A true correct ion that would attribute each case to thed istrictin which the d isease was acquired is imposs ible , but taking an
arbitrary period o f a fortn ight as represent ing a not improbablelatent period we should find that the place of res idence a fortn ight or more prev ious to Onset would g ive a very different distriet d istribut ion to that g iven by cons idering the place of onset .Corrected for proport ional numbers of suscept ible -
persons in
each d istrict and for place o f res idence two weeks prev ious toonset
, the d istribut ion per 10 of populat ion is as follows :in the h ighlands , at the lake level (L ake Nyassa, altitudeabout feet ) , and in the lower shire reg ions. Accord
ing to L averan ,
1it was necessary , on account of the frequency
of blackwater fever, to abandon certain posts in Congo'
estab
lished a t heights of 500 to 700 meters.
Change of res idence is a not uncommon cause for an out
break, especially if the d ifference in alt itude or climate is de
cided. I n A frica not on ly those com ing from the mountainsto the low lands , but also those mov ing from the insalubriousl ittoral to the re freshing high—ly ing d istricts are pred isposed .
This change seems to be independent o f the hardships of travel .After L eav ing Endem ic Reg ion .
—Such cases have beenobserved in Eng land by Bassett - Smith ,
217 Hughes ,218Sylivan ,
8
Crosse ,‘1M anson ,
“ 9D an ie ls , 6 7 and Parker ;220 in I reland by

ETI OLOGY 1 59
M owbray ; in Germany by S chlayer, 222 A . Plehn ,
”‘
K le ine,Koch221 and F . Plehn ;
211'
in F rance by Burot and L egrand ,
L e D antec,226 Kelsch and Kiener, 178 Rouv ier, 227 Vincent , 8 Bo is
son ,
86Troussaint
86 and L averan ;1 in Belg ium by D ryepondt
and V ancanpenhout228
and Bertrand ; and in Balt imore by
Brem.
21 5M any of these cases were not mere r elapses ; indeed ,
in the majority in'
which the number of prev ious attacks wasspecifically stated they were first attacks . The onset may occur
from a few days to five months or1 more after leav ing the
endemic area. I nclement weather and fat igue seem to be
factors in some of these cases . The mortality is low .
Occupat ion which requires res idence in a malaria l local ityand which necess itates overturn ing Of the soil , as garden ing ,
farming , d itching , railroad const ruction , etc , is largely pre
d lsposing . Not a few cases occur among t imber workers .
The d isease prevai led extens ively among those engaged 1n the
construct ion of the canal of Corinth. M anson5 9tel ls us that
many of the Ch inese laborers on the Congo railroad d ied of“
hemog lobinuric fever, and D eGreny 8 foundmany cases in bothnegroes and whites in the railroad work on the lower Congo .
Crosse209
says that it is s ign ificant that his first three gardenersd ied of blackwater fever, and that for some cons iderable t ime
cases occurred only near the plantat ions , and as the plantat ionsbecame more numerous the d isease spread to the other stat ionsin the territories .
O ccas ional“
Causes—O i these , exposure to cold and damp
ness is probably the most efficacious , show ing somewhat analogous to paroxysmal hemog lobinuria. O verexert ion precedessome cases . The influence of alcoho l has probably been over
est imated. Trauma has a slight et iolog ic importance . ThusM ould230 ment ions a caSe developing after a sprained ankle ;Plehn
61one in which a man was wounded in a bush fight and
bled considerably . Crosse‘” 9and Plehn
5saw cases immed iately
fol low ing confinement . Psychic states , as anger, grie f , and
fear, exposure to sun ,fat igue , excess ive venery ,
syph i l is , andthe mercury cure have been ment ioned as occas ional causes.
Cardamatis86 lays stress on the association w ith rheumat ic
d iathesis, 12 of his 30 cases be ing rheumat ic. A lexander

160 THE STUD Y or MALARI A
Haig -
231 believes there is an int imate relation , most probablycausat ive , betw een an excess of uric acid in the blood and
hemoglobinuric fever. He makes the un founded statement
that the ord inary acid sulphate of quin ine is about one - fifth
xanthin , which is phy siolog ically and patholog ically equivalentto uric acid , and here in , he bel ieves , l ies its supposed power to
producehemog lobinuria. Johnson60 'holds that a meat d iet pred isposes to blackwater fever.
Prev ious M a laria—I t may be said w ith almost absolutecertainty that prev ious in fect ion w ith malaria is essent ial . I n
fact , a majority of care ful observers make the unqualifiedassert ion. The extreme rarity of cases in Which preced ingmalarial in fect ion I S den ied almost forces us to the conclus ionthat it may have been ov erlooked , as m ight occur in latent ormasked in fection . I t is
,however, not imposs ible that hemo
globinuria may exceptional ly accompany the first outbursts ofmalaria, as in cases o f F . Plehn ,
5Goltman and Krauss , 1139 and
Brem.
“ 5 I n all of the cases of Tomasell i and Koch , the most
ardent advocates of the quin ine"
theory , there was a history of
antecedent malaria. Tomasell i2°5 states in ital icized words thatthe two condit ions w hich favor the hemolyt ic act ion of quin ineare : 1 , M alarial in fect ion
,chron ic or somet imes recent ; 2 , a
special id iosyncrasy o ften hereditary .
Cardamatis206
cites several w riters who have seen cases w ithout preced ing malaria, and V an der S cheer2°1 is said to haveseen such a case .
Pathogenes is—There are three chie f theories as to the
nature of hemog lobinuric fever : 1 , that it is malaria ; 2 , thatit is quin ine poison ing ;3, that it is a d isease sui generis .
I . Against the malarial nature of hemog lobinuric fever may
be urged the follow ing object ions :1 . The paras ites are o ften absent ;when present they are not
numerically proportionate to the severity of the attack , and
usually d isappear as the d isease progresses ; sporulat ion doesnot correspond in t ime w ith the Symptoms ; hemoglobinuriamay be associated w ith d ifferent forms of the malaria paras ite .
2 . I n malaria very numerous parasites may be present w ithout producing hemog lobinuria.
162 THE STUD Y or MALARI A
As'
stated in the first obj ect ion , the paras ites when presenttend to d isappear as the d isease progresses . The follow ingfigures show the d ifference in results of examinat ion at d ifferent periods . The great frequency w ith which they are foundtheday before the attack should be notedS tephens and Christophers
D ay before attack parasites present in 95 per cent. of cases.
D ay of attack parasites p resent in 70 per cent. 0f cases.
D ay after attack parasites present in 20 per cent . o f cases.
M annabergl
D ay before attack parasites p resent in per cent. of cases.
D ay of attack parasites p resent in 63 per cent . o f'
cases.
D ay after attack parasites present in per Cent . o f cases.
The reasons for the rapid d isappearance of the organ ismsare , first , that o ften quinine has
"been - taken before the “
exam inat ion ; second ly , that in “
the terrific hemolys is the weaker cells ,includ ing those contain ing paras it es , are usually the first tosuccumb.The hemoglobinuria occurring in Texas fever of cattle 1s
cited w ith some show of reason as an argument forthe purelymalarial orig in of blackwater fever. There are essent ial differences , however, in the occurrences of blackwater
'
in malar1aand Texas fever. F irst
,malaria is fo llowed by blackwater in
a very smal l percentage o f cases , malaria be ing . common , hem
globinuric fever much rarer ; in Texas fever blackwater is a
common symptom , occurring in nearly all severe cases . S econd ,
in blackwater fever in man the number of paras ites show s no
proportion whatever to the severity of thed isease. I n Texasfever
,on the other hand , as is show n by Sm ith and Kil
bourne , 218 the number of paras ites is in d irect relat ion to .the
severity of the process and increases as a fatal term inat ionapproaches . I n human malaria the paras ites may ex ist in very
large numbers . w ithout the development of hemog lobinuria ;th is is not the case in Texas fever. Bonome found in the
icterohemog lobinuria o f sheep the same r elat ion betw een the
number and behav ior of the hematozoa and the intens ity and
progress of the attack as obtains w ith Texas fever.
The form of parasite found in blackwater fever is , in the
g reat majority o f instances , the est ivo - autumnal . O nly excep
ETI OLOGY
.
163
tionally is hemog lobinuria combined w ith in fect ions With theben ig n organisms. The tert ian paras ite has been observed incases of Ziemann, Panse ,
7 9O rme ,
249Pecori , 6 9 Carducci , 6 9 V an
der Horst , Hughes ,218 Koch23 ‘1
( 5 caseS) , A Plehn (3cases ) , O llw ig ,
4 9 M cElroy ,
211Goltman and Krauss , Brem ,
“ 5
Herrick25 1 and Curl2 5 1 3 cases ) . The quartan paras ite hasoccurred in cases of V incen z if16 Grocco ,
9 6 Klei'ne,223'
K’
ujd icke ,5 1
and O tto.
5 1"Thiroux
8.
6and L averan
11are said to have found
the large form of paras ite , but whether tert ian or quartan isnot stated. T he fact that parasites other thanest ivo - autumnalhave been found is no argument agalnst the malarial natureof blackwater fever, s ince cases o f pern icious malaria in whichly the
~ large tert ian paras ites were found have been,
reported
by French,16 6Ew ing18 1 (2 and others .
Some writers believe that in add it ion to the mechan ical destruction -
o f the red cells by the parasites the latter g ive ,off
tox ins wh ich have hemolytic pow ers . The facts , however,
that intense hemolys is may occur w ith very few paras ites-
in
the blood;and that the paras ites when present do not bear a
d irect relat ion to '
the severity o f the'
disease , but rapidly diminish as the d isease progresses , speak strong ly against the= role
of. a paras itic tox in in blackwater fever.
The number o f cases in which the paras ite_
is found i f theexam inat ion is made early const itutes conclus ive ev idence of
an int imate relat ionsh ip to malaria. This , however, is not all.
The test imony furn ished by the"
paras ites is corroborated bythe two subs id iary ev idences of
‘
malaria - z first , pigmented“lenko
cytes ; second ly ,mononuclear leukocytos is . Given ,
therefore ,
the presence of the parasites in the first hours of attack , andthe almost constant find ing of p igmented leukocytes and
mononuclear leukocytos is , it is imposs ible to deny that malariap lays an important role 111 its product ion.
The pecul iarity of the geographic d istr ibut ion o f hemo
globinuric fever is no argument again '
st its malarial nature.
While it does not occur in all,even h ighly ,
malarial countries ,it is not met except in markedly miasmat ic reg ions . Ne itherdoes the
"
d istribut ion of quartan.
fever or some forms o
’
f‘
perni
cions fever coincide w ith that of malaria in general . Nor is
164 THE STUD Y OF MALARI A
the s l ight d ifference of seasonal prevalence of any we ight .The d ifferent forms ofmalaria have d ifferent seasons of prevalence , as “
Spring tert ian ,
”and est ivo- autumnal .
Favorable , therefore , to malaria l character are1.Geographic d istribut ion .
2 . L ength of res idence in endemic reg ion .
,3. Prev ious attacks .of malar1a.
4. M alarial prophy lax is 1S prophy lact ic of blackwater fever.
5 . Blood find ings : parasites , pigmented leukocytes , mono
nuclear leukocytos is .
The fact that hemog lobinuric fever does not respond to
quin ine is one of the strongest-
ev idences that it is n ot an attackof malaria (per se ) .The w riter ’
s op1n1on of the r e lat ion of malaria _to blackwaterfever is that the former is essent ially and solely the predisposing cause , and that in some cases it may also act as the excitingcause.
I I . Tomasell i first published his observations as to the et iologic relation between quinine and blackwater fever in 1 874.
M ore recent ly Koch has d irected attention toward it. The
w idespread controversy that followed the publicat ion of.
Koch ’sv iews was bitter in the extreme ;the matter was even aired inthe L ondon lay press. The misunde rstand ing was probablydue to two causes ;first , ignorance of Koch ’s utterance at firsthand ;second ly , the somewhat non - committal manner in whichhe expresses his
”idea of the relat ion to malaria.
'
While he. is
very emphat ic that blackwater fever is not an attack "
of
malaria;he is not clear as to the pred ispos ing role of the latter.
He does not even assert that quin ine is the exciting cause in all
cases , but admits that , although he saw no cases of blackwaterfever in which quin ine could be excluded , he could not go so
far as to maintain that every case of blackwater fever isquinine poison ing .
172 There I S no doubt but that this acridd ispute was product ive of d ire results , inasmuch as it broughtthe specific into d iscred it not only w ith the laity, but w ithmany o f the pro fess ion. Even yet it is necessary in some placeson account of a fear of hemog lobinuria to d isguise quininebefore it can be g iven.
166 THE STUD Y or MALARI A
Hopkins , Carg i ll , 26 1 M ould , Hoffm'
ann , D an iels 5 7 Ran
k in “
sCardamatis
206
(32 cases ) , Y o
5
fé,8 6M offatt , 2 5 3 S chlayer , 22
Curry,1 8 6 M cElroy ,
264D 11Bose ,
25 5 “
Hearseyf5 5 Ziemann ,
8
Ere Bignami , 231 D oering18 5 and S hropshire25 7 ( 15 per centof his cases ) . The w riter has seen 4 cases where quin ine coul (be excluded from the et iology.Hemoglobinuric fever occurring on ly in malarial subject
and quin ine be ing specific for n1alaria ,_
it is but a most natura
sequence of events that a large number of the cases of hemo
globinuric fever have developed after the administrat ion 0
quinine. The bare fact that blackwater fever o ften fol lowquin ine is weak ev idence for quinine et iology in the face 0
the numerous cases in wh ich prev ious quinine could be abSo
lutely excluded .
When , how ever, attacks can be produced repeatedly at w il
by a dose of quin ine the question assumes a very d ifferen '
aspect . Such cases are those of M urri ,26 8 Hoffman ,Koch, 17
M anson ,
“ 3 Ketchen ,
238 H0pkins ,26 0 Bertrand , 229 A . Plehnf
'
O llw ig ,
‘1 9 M arsden ,
26 9D an iels , 5 7 Kleine ,"225 Tomasell i , V in
cen z i, and Grocco .
As Stated above , there 15 no relation between the amount 0 :
quin ine and the intens ity o f the attack. Ketchen238 precipitated an attack , expe11mentally , w ith 1% grains. This patienstated that one - e ighteenth of a gram had prev iously produce <blackwater. Karamitsas ,
8 5Chomatianos ,
5 5Pampoukis ,
8 5 Kanell i Koch , Kle ine ,225 S h1opshi1e , 26 ‘
M oscato ,
8 6 A . Plehn ,
2
Boxer,” 0and others report outbreaks el icited by less than - one
hal f gram . Panse25 2 bel ieves that the usual dose preced ing ar
outbreak to_
be from one—tenth to 1 gram. Ton1aselli2°5 has
observed attacks to fol low the adm in istrat ion of doses as smalas from one - tw ent1eth to one - tenth gram, and Koch” 1
report:
a case after one - tenth gram had'
been admin istered . Kudicke5
and M archiafava and Bignami22 state the min imum quant it)as one—twentieth gram ,
L averan1and Ziemann
15. as 1 centi
gram , and Ruge1 5 5
as 1 mil ligram.
Ton1aselli2°5 examined various preparat ions of quin ine t(
ascertain whether thetoxic effect was dependent upon adulterat ion , and concluded that such was not the case , but that the

ETI OLOGY 167
sxic propert ies were inherent to qu1n1ne itsel f and to all the
e parations contain ing quinine .
The t ime interven ing between the administrat ion of quin ine1d the onset o f hemog lobinur ia 1s almost un i formly fixed byarious observers at from one to ,
six hours . .With six hours
them ax imum interval , the cases really due to quin ine wouldWind le cons iderably .
I t - is believed by some w riters that quin ine hypoderm1cally
) es not produce blackwater, even in persons suscept ible whenlministered orally . T his , how ever; is not the case. Toma
:111205has shown that subcutaneous inj ections of qu1n1ne are
“
)llowed more promptly by hemog lobinuria than is the orallministration . K ohlbrugge
7thinks that only the
”
inorgamc
.lts of qu1n1ne are “
tox ic, and states that the tannate , even in
largest doses g iven to s uscept ible persons , fails to:
fcause
moglob-inuria. M cK ay
449has
'
recently attempted to showa t hemolys is follow ing the admin istrat ion o f the sulphatequin ine is due to the sulphate and not to the quin ine. This
eW,how-
ever, is not- Supported -by clin ic experience . Furthers
ore , the results of experiments upon which M cKay based
s conclus ion could not be v erified by Christophers and Benty. I t is probable that neither the mode of
'
administration
) r the preparat ion used , i f absorbed , g ives any d ifference insults .
The role of quin ine in hemoglobinuric fever is probably.ghly complex . I t w i ll be
"
shown that it is of value as a
o phylactic when sys temat ically employed ; i f not thus used ,
1d malarial in fection be perm itted to occur , it may ,in some
:rsons thus pred isposed , act as the excit ing cause . I n the
tack itsel f it - is poss ibly o f value 111 destroying'
the paras iteshen these are present , or it may act harm ful ly in“
aiding‘
hemo
Even after a care ful study it is not easy to define precise lye respect ive potency of malaria and quin ine as et iolog ic facrs. To quote S hropsh ire -
7 5 7 “
To establish the cause of any
sease w e must apply the agent to the subj ect , .and have , as
1iform result, the But if there are two agents sus
:cted as causat ive which appl ied together produce the d isease ,

168 THE STUD Y or MALARI A
but applied separately to the Same ind iv idual , the one produce
it , the other never,we can attribute on ly to the one a causative
p lace , and to the other an accidental presence . Such is the
case before us. M alaria taken as‘
the cause and appl ied w ithout quin ine to an individual of such tendency , hemog lobinuriaresults in 15 per cent . of the case s be fore us . Quin ine hasprobably been appl ied to all the cases before us
'Without thepresence of malaria and no hemog lobinuria resulting . Whichproduces it
Favoring malaria as against quin1ne we have1 . Antecedent malaria essent ial .2 . Relat ive immun ity o f the negro. Racial immun ity to
d isease w ell known ; racial suscept ibil ity to drugs rare or um
known.
3. O ccurs o ften w ithout th e admin istrat ion of quinine .
We may safely conclude that the pred ispos ing cause is ai
ways malaria ;the excit ing causes are fresh malarial invas1on ,
quinine or other med icaments , exposure , exertion ,mental
states; etc.
I I I . The most enthusi ast ic champion of the v iew that blackwater fev er is ne ither malaria nor quinine po ison ing , but a
d isease sui generis , is S ambon .
121 M anson272 formerly advo
cated this theory . The two reasons for his bel ie f are a s im ilarity to paroxysmal hemog lobinuria and an analogy w ithTexas fever. S talkarrtf
’5 9 Rho ,
273 Vincent , 8 and others be
l ieve that_
it is a d istinct d isease . While the s imilarity to
paroxysmal hemog lobinuria cannot be den ied , the relat ion —toTexas fever, as we have seen , is far from close , and the ev idence that it is a d isease sui generis is inadequate. Yersin
27 ‘1
found baci l li in the casts and epithel ium in the urine of 2
pat ients , and bel ieved that he had d iscovered the cause o f the
d isease. Breaudat ,275
how ever , show ed that these Were the
bacillus Coli communis .
Collet276 has recently , w ithout grounds , how ever , suggested
that there may be a causal relat ion between the bacillus M ega
them'
um and blackwater fever.
The theory that green beans and the ir blossoms were
the cause o f many cases . o f hemog lobinuric fever seems

I 70 THE S TUD Y OF MALARI A
tox ic to rabbits.I njected i nto the animals intravenously indoses of 5 cc. it quickly kills the animals, caus ing infra vitam
a solut ion of red cells . Such a hemolytic serum then acts the
same as a bacterial poison . For example , to keep to'
our i llustration , rabbits are inj ected first w ith very smal l doses of thisspecific hemolyt ic serum . The dose
“
is gradual ly increasedunt il it is found that .the an imal tolerates amounts that -wouldbe absolutely fatal to animals not so treated . I f some o f the
serum of this an imal is now abstracted and added to the
specific hemolyt ic serum it is found that the power of the
latter w il l be inhibited. This show s that an ant ihemolys inhas been formed .
”
These statements re fer to the employment of heterologousserum ; that is , the serum of. d ifferent species
'
o i an imals .
I solys is , due to the employment of blood of the'
same spe cies ,is exempl ified in cases fol low ing the transfusion 0f bloodfrom man to man. Examples of autolys is , due to the bloodof the ind iv idual , are cases that have occurred after resorptionof extravasated blood ,
as the rupture of ectopic pregnancy .
Based on these facts , which have been amply demonstrated ,
Bignam i22 states his theory as fol low s
1 . An alteration in the p lasma which is effected , l ittle byl ittle , as a consequence o f a specific change in the red bloodcorpuscles through which a certain number of them come to
.behave , in respect to the organ ism, l ike the corpuscles in the
blood of another species of an imal . 2 . The format ion in
consequence o f this change of a substance in the plasma whichis capable , under certain cond it ions , of becom1ng hemolytic.
The w riter278 some t ime'
ago mod ified and elaborated Bignami ’s hypothes is , and expressed it for the first t ime in the
terms of Ehrl ich ’
s s ide—chain theory .
For the better understanding of the w riter’s hypothesis thepathogenes is may be d iv ided into the fol low ing stages : 1 ,
erythrorrhexis ;2 ,hepatic st imulat ion and product ion of ambo
ceptors ; 3, act ion of complement ; 4 ,hemolys is “
and hemo
globinuria, or the format ion of an antihemolys in.
1 . This primary blood destruct ion is due d irectly to the
malarial paras ite , chiefly through the act of sporulation , poss i
ETI OLOGY“
171
bly also by the production of a tox in. The hemog lobin thusl iberated is carried to the liver, where it is elaborated into bilep igment. We have seen that this erythrorrhex1s 1s 1nsufficient
to account for hemoglobinuri
2 . O n reaching the l iver.
the h emoglobin is acted upon by
certain of the molecules or atom groups Of the liver- ce lls ,wh ich have an affin ity for it . When all o f the atom groups
have been “
combined w ith by the hemog lobin , which happensWhen th is funct ion of the l iver has been frequent ly or recentlyexerted
,or when the amount of l iberated hemog lobin is veryliver is st imulated to the product ion of more such
atom groups. Th is stimulat ion is responded to by an over
production of atom groups , some of wh ich gain access to thegeneral circulation . Translated into the terms o f Ehrl ich ’s’
theory ,it may be said that certain -
r eceptors of the l iver cel ls"hav e the p roperty of trans forming free hemog lobin into
“ bilepigment ;when these receptors are exhausted the deficiency ismet by overproduction. When the cells become overfilled some
“
of these s ide - chains are cast off into the general circulat ion.
"
Here the receptor becomes an amboceptor. The pathology of
the l iver in this cond it ion fully supports the v iew of'
over
stimulat ion. .Karyokines is and other changes .in '
the l ivercel ls suggest that it responds to this st imulat ion. I n the pres
ent state of our' know ledge we cannot determ ine the chemic
nature o f the immune body,
3. Hav ing gained access to the general circulation , the
amboceptor meets the complement which ‘ is present in normalserum , and the complete hemolys in is formed .
4. The reaction of amboceptor w ith complement , if not
antagonized by an ant ihemolysin ,causes
_
a hemolys is , wh ich i fsufficiently extens ive results in hemoglobinuria. I t is highlyprobable that when the product ion of the hemolys in
'
does not
proceed w ith too great rapid ity there is formed , parm’
prism ,
an antihemolysin , which may exactly balance the hemolys inw ithout destroy ing it. This is probably the symbiosis re ferredto by Krauss.
199 S o long as the equil ibrium betw een hemo
lys in'
and antihemolysin - is maintained 110 hemolys is occurs ,
but let this equilibrium be greatly d isturbed by fresh malarial

172 THE STUD Y OF MALARI A
invas ion, quinine, exposure , fat igue or other, and probablyunknown , factors , hemolys is occurs and hemog lobinuria em
sues . Under'
this exact equi librium the subject may be saidto possess id iosyncrasy , and is in a condition very s imilar tothat of paroxysmal hemog lobinuria. Casagrandi
82has ré
cently found in malarial blood a hemolys in the presence of
which is masked by an ant ihemolys in .
I t is possible that a s l ight and temporary loss of equil ibriummay result in a l imited hemolys is producing hemog lobinemia,
but not hemoglob1nur1a. I n this way may be explained some
cases of anemia, cachex ia,and post
- malarial secondary fever,in which the paras ites i f present , are not in proport ion to theresults.
I t is believed that th is hypothes is explains the occurrence
of hemoglobinuric fever during and after malarial in fect ion ,
w ith or w ithout the adm in istrat ion of quin ine ;it explains whythe malarial attack may precede by months the appearance of
blackwater ;why exposure , exertion , etc., may el icit an attack ;why the hemo lysis does not always coincide in t ime With thesporulation of the paras ites in . the cases in which the latterare present ;it accounts in a measure for the complex relat ionw ith quin ine and explains obscure anemia, quinine fever, postmalarial secondary fever, and post
- hemog lobinuric fever.
L astly , it coincides w ith the prevalent ideas of trop ic phys iciansof an int imate relation between hemog lobinuric fever and“ biliousness.
”
Christophers and Bent ley, const ituting a committee ap
pointed by the Government of I nd ia to conduct an inquiryregard ing the nature of blackwater fever, have recently pub“
lished an extens ive monograph contain ing a record o f theirexperiments and the conclus ions which they reached as a re
sult of these experiments . They exclude paras it ic, osmot ic,and chemic actions as causes of hemolys is , and show that thehemolys in is probably derived from auto - immuni zation againstthe organ ism ’
s own red cells , an autolysin , confirming thusfar Bignami
’
s and the w riter’s theory. These experiments ,
w hich are the most complete and conv incing that have beenconducted in connect ion w ith hemog lobinuric fever, are too
CHAPTER I V
PATHOLOGIC ANATOMY
ACUTE MALARIA
THE pathognomonic anatomic feature of malaria is intravascular melanin , which is a product of hemog lobin converted
through the biolog ic agency of the;malarial paras ites . M elanin occurs in '
the t issues also , but here there is some doubtas to its orig in. I t is brownish black in in fine
grains , coarse part icles , or in lumps ;does not y ield the reac
t ion for iron , and is insoluble in acids , but is readi ly dissolvedby
fammonium sulphide . T his should not be con fused With
hemos iderin , wh ich"
is a chemic derivat ive of the hemog lobinof broken—down red blood - cells ;is yellow ish in color ;respondsto the react ion for I ron ;is insoluble in acids , alkal ies , alcohol ,and water, and ex ists especially extravascularly . I t is regarded
as a result of prolonged hemog lobinemia follow ing severe or
chron ic in fect ions .
The general plan of d istribution of melan in may be thusstated : I n the blood current it may ex ist free or , more com
monly ,is contained w ithin the phagocytes and the red cells
in fected w ith pigmented parasites , and is more abundant inthe capil laries than in the larger vesse ls . I n the
'
viscera it iso ftenest seen in the spleen , bone—marrow , brain , and l iver,especial ly in the endothel ial cells , but in the spleen "
and -bonemarrow it ex ists also outs ide the vessels and e ither betweenor w ithin the cells proper to these t issues .
The d istribut ion of the parasites varies according to the
type of the attack ; it has been shown that the latter dependslargely upon the local izat ions of the paras ites . They are usu
ally abundant in the splen ic blood irresp ect ive of the formassumed by the attack. I t occasionally happens that deathsupervenes , notw ithstand ing a progress ive d iminution of the
174



176 THE STUDY OF MALARIA
is o ften d istended w ith a quant ity ~ of dark, inspissated bile.
M icroscopically paras ites are not so abundant as in the spleen.
P igment is found in the vessels , especially in the blood capil
laries . Here are found also altered paras ites , melani ferousleukocytes , and large endothel ial cells contain ing coarse grainsof pigment. The macrophages are sometimes of an
“
enormous
s ize . The p igmented endothel ial cel ls are swol len and the
cap illaries are not infrequent ly ent irely obstructed w ith pigmented cellular e lements . The hepatic cells do not
'
containmelan in , but are frequently charged w ith hemosiderin , and
may show evidences of cloudy swel ling , atrophy , or necrosis .
Karyokines is is occas ionally noted Areas of focal necros ishave been described .
The k idneys on gross inspection show few changes ; theymay be s l ightly enlarged
-
and hyperemic. M icroscopic exami
nat ion show s a marked p1gment’
ation of the .M alpighian cor
puscles , together w ith degenerated—
tubular epithel ium. Whilethe epithel ium o f the tubules may be healthy , it o ften showscloudy swel ling and necros is. I n the straight tubules theremay be casts of various sorts . M elan in is found in the g lome
rul i , less o ften in the tubules . The cells may contain hemos iderin granules . Paras ites are rare in the g lomerular ves
se ls , but may be found in the‘ intertubular cap i llaries.
Ew ing ’
s177
case w ith massing of the paras ites in the renalcapil laries has been mentioned . A true g lomerul it is has beenfound in cases o f the alg id type.
I n cerebral cases the only variation from the normal _con
d it ion of"
the s tomach and bow e ls may be a sl ight pigmeu
tation . I n fatal cases of the alg id and choleraic forms thegastro
—intest inal tract may contain a bloody fluid and the
mucous membrane may be swol len , hyperemic, pigmented ,
necrot ic, or ulcerated. The foll icles and Peyer’
s patches maybe hypertrophied and prominent . M icroscopical ly there is
V iv id inject ion , parasit ic and pigmentary thrombos1s of the
capi llaries , hemorrhag ic points , and necros is . The peritoneumis usually normal .M acroscopical ly the lungs may show nothing abnormal save ,
probably , sl ight results of hypostas is , which in some cases may
PATHOLOGIC ANATOMY 177“
be cadaveric lesions. O ccasional ly there are hemorrhag icareas . M icroscopically neither. pigment nor p aras ites are so
ev ident as in certain of the other organs. The capillaries are
congested , sometimes thrombosed, and contain infected ery
throcytes , phagocytes ,'
which o ften show signs of degenera
t ion , and macrophages . The cap i llary epithel ium may’
b e sWollen , but is on ly occas ionally pigmented . The pleurae show
nothing abnormal.The h eart muscle is ordinari ly pale and flabby, but the
muscular fibers do not usually afford degenerat ive The
capillaries may contain paras ites in greater or less number, andthe endothel ium may be swollen. Cases in which the paras itesare very numerous in the card iac capi llaries, such as that of
Ew ing ,
” 1are very rare.
I n cerebral cases the men inges . Of the brain are deeplyhyperem ic, and excess of serum is found in the - meshes of
the pia, in the ventricles , and at the base of the brain . The‘
cerebral substance is c ommonly darkly pigmented and con .
gested , and may s how hemorrhages, usually punct i form, occa
sionally larger. The hemorrhages occur
.
o ftener . in the cere
brum, but may be present in the cerebellum. I n the abdominalform the brain may show but few patholog ic changes. M icros copically in the cerebral cases the capi llaries are seen to be
filled , even to occlus ion , w ith p igment, paras ites, and phago
cytes , the latter in the same or in d ifferent stages of schizogony ; gametes are seldom found. I n some instances nearlyevery red cel l contains one or more paras ites . Local izat ion -
of
parasites are founa t only in the cerebrum, but'
also in the
cerebellum and medulla. .The capillary endothel ium may be
swollen , pigmented , and undergo ing fatty degeneration. S ec
ondary changes , such as perivascular exudat ion ,hemorrhages,
and necros is , are not uncommon results of thrombosis. D e
g enerat ive changes in the gangl ion cel ls have been detected.
The bone -marrow is of a'
dark color approaching “
that of
thespleen , and somet imes d iffluent. M icroscopic examinationreveals hyperemia, the capillaries being engorged w ith pigmented parasites and g iant cel ls cl ing ing to the vessel walls.The paras ites ex ist as free spores , schizonts , which are fre
12
178 THE STUDY OF MALARIA
quently sporulat ing , and gametes in large numbers . Extra
vascular paras ites and free p igment are also found.
CHRONI C MALARIA
The spleen is always enl-arged .
'
The form is usually preserved. I ts average we ight is from 700 to 800 grams , _ though
it may attain four or five t imes this weight . I n cons istenceit is usually firmer than normal. The capsule is thickened ,especially at the convex ity . Upon the surface ’
are scattered
indurated whitish plaques of fibrous , occasionally calcareous ,cons istence, ev idences of perisplenitis. Adhesions to the
d iaphragm or“
other parts are not in frequent. Subcapsularin farcts are occas ional ly encountered. I n sect ion the paren
chymais usual ly found firm, on ly rarely is it of d imin ishedconsistence. The color varies from that of muscular t issue tos late . color. The thickened trabeculae, l ike white bands , are
very ev ident. The M alpighian'
follicles are somet imes con
spicuOus , sometimes ind istinct. I n old cases there is an over
grow th of connect ive t issue , part icularly near the capsule . His
tologically the chie f changes found are trabecular hyperplas iaand venous d i latation. The process somet imes resembles a
hypertrophic cirrhosis. The fibrOus trabeculae are hypertro
phied and there is formation of new connect ive t issue . The
venules are notably d i lated , the wal ls th ickened , and the bloodrich in pigmented leukocytes and macrophages . The depos itionof pigm ent . 13 in general s imilar to that in
.acute malaria.
There is at t imes l itt le change in the lympho id t issue formingthe arterial sheaths and M alpighian
-
bodies , but this may be
hyperplast ic. Necros is of the spleen pulp is observed ,sur
rounded by ev idences of regeneration. These regenerat iveprocesses consist chiefly of increased vascularizat ion , format ion of connect ive- t issue network enclosing g iant cells , and
hyperplas ia of lymphoid t issue beg inn ing in the M alpighianbod ies .
The liver is not so constantly en larged as is the spleen and
never attains so excessive a degree of hypertrophy . I t may
weigh from 2 to 4 kilograms . I n rare instances it is atrophic.
The consistence is firm , occas ionally somewhat doughy . The

PATHOLOGI C ANATOMY 179
capsule is tense and may be thickened. There may be present“
whit ish bands or patches , the results '
of perihepat it is . The
color varies - from redd ish to almost black. The cut surfaceis usually found to be congested and may drip w ith blood. The
color is more or less '
dark red . There may'
SOmetimes be de
tected on gross inspection an increase of connect ive t issue.
M icroscopically the hepatic cells are seen'
to be hypertroph iedand hyperplastic, show ing ev idences of cloudy swelling and
necrosis , or atrophied as a consequence of vascular d ilatat ion.
I n certain areas there may be a complete d isappearance of
hepatic cel ls , which are replaced by connect ive t issue , Kupffer’sce lls, or beg inn ing format ion o f new hepat ic ce lls . T he nucle iare frequently mult iple , and when s ing le may be much largerthan normal and contain one or two nucleol i. The hepat iccells may be charged w ith hemos iderin . P igment
'
is containedin the endothel ial and Kupffer ’s cells, especially
'
in congested
areas and in the periphery of the lobule. There is sometimes
d iffuse overgrowth of connect ive t issue . The blood capi llariesare usually d i lated and congested w ith blood r ich in pigmented
leukocytes ; the circulation is Common ly s lugg ish ._
The bilecapillaries are ordinarily unaltered . The perivascular lymphchannels may be d i lated. Amy loid degenerat ion beg inningapparently at the periphery of the lobules is not rare.
The kidneys are usually increased involume and in weight .The contracted kidney has been described in connection w ithmalaria, but there ”
is some doubt as to the et iolog ic relat ionsh ip. The surface
‘
of the kidney is smooth , the color is darkred , and the consistence is slightly increased. Upon sect ionthe cortical substance is redd ish gray . The pyramids are
markedly hyperemic, the red t int being most decided at the
border of the pyramidal substance. Upon microsc0pic ex
aminat ion the convolut ed tubules and ascending limb of
Henle ’s loop are found d ilated . The ep ithel ium is swollen ,
charged w ith hemosiderin , and may be undergoing degeneration . I n the collect ing tubules the epithel ium is
, as a rule, on lyslight ly altered. These tubules rarely contain granular or
hyal ine casts or desquamated‘
epithelium . Bowman’
s capsulepresents changes s imilar to those of the convoluted tubules .

180 THE STUDY OE MALARI A
The renal arterioles are congested and the capillaries are d ilatedand gorged w ith blood rich in leukocytes , more marked in thepyramidal than in the cort ical substance . M elanemia is notso decided in the kidney even
'
when pro fuse in'
the spleen and
l iver. There is generally l ittle change in the connective t issue .
Here“
and there is a sl ight th icken ing .Of - the' intertubular con
nective t issue . The blood—vessels, the glomerul i , and the wallsof the renal tubules may undergo amy loid degenerat ion . Thisis more d iffuse in the kidneys in chronicmalaria than in the
other org ans.
The al imentary tract may show ev idence of amyloid degenerat ion in
'
the stomach or bowel and dysenteric les ions “
in
the colon .
I n the lungs may be pigmentation and anemia, _
and in the
pleural cav ity an effus ion.
The heart is re laxed and o ften d ilated and somet imes show sevidence o f degeneration o f the musculature.
The bone -marrow is of firmer cons istence, and more deeplycolored“
than normal , especial ly toward the ends of the longbones . There is usually a decrease of fat and a proli ferat iono f marrow cel ls
,together w ith large cel ls , some undergo ing
karyokines is , lympho id cel ls , and nucleated red cel ls . The
vesse l walls are thickened. I n some instances there is atrophyof the bone - marrow .
The el iminat ion of the p igment probably consumes threeor four months after the cessat ion of in fect ion , though thisvaries w ith the act ivity o f the
“
e l iminat ive processes .
HEMOGLOBINURI C FEVER
The patholog ic findings .vary in proport ion to the prox1m1ty
and intens ity of the malarial attack. Inaddit ion to the changescharacteristic of malaria there ; are found , in blackwater feversubj ects
,the results of hemog lobinemia and polycholia chiefly
in the kidneys and l iver. O ccas ionally post mOrtems do not
reveal malarial ev idences , as in two cases reported by Curry ,
186
but this is very except ional . The body is usually deeply jaund iced . There may
"
or may not }be edema. The muscular sys
tem is O ften icteric.

PAT-HOLOGI C ANATOMY 1 81
The sp leen - is enlarged , often enormously so,.and congested .
The surface color varies from grayish to redd ish brown , almost
black. The capsule is thickened and usually strips '
eas i ly , but
may be adherent . The con-sistence'
of the organ is often so
d imin ished that it appears l ike a pulpy sac. The trabeculaeare thickened and fibrous ;the pulp is decided ly increased . The
M alpighian corpuscles are usually hypertrophied , somet imes
g iv ing the appearance of sa'
go spleen ; P igment is usuallyabundant. I t is contained w ithin the cells or ly ing between
them. The cells of the M alpigh ian bodies show the greatest
quant ity and largest masses . The large mononuclear cells and .
g iant cells are pigmented. The leukocytes ly ing external tothe walls of the small ve ins may show more p igment . than thosescattered here and there throughout the pulp . The color of
thep igment varies from yellow to almost black, and may con
s ist of hemos iderin or melanin; The walls Of the smallervessels are thickened , and the lumen may be obliterated . The
s inuses may be obliterated w ith pigmented and other cells .
The endothel ial cells ”
may be prol i ferating ,and o ften contain
granules of pigment . Parasites and pigmented leukocytes may
be present in the spleen when not d iscoverable in the generalcirculat ion . There may be round ce ll infiltrat ion around the
trabeculae.
The l iv er is enlarged , congested , and surcharged w ith bile.
I t varies in color from a decided yellow to a dark brown . The
capsule is slightly adherent. The surface is usually - smooth ,
but there may be subcapsular nodules from the“
s ize of a pin
head to that of a pea, which On section exude a th ick , cheesymatter. There is abrindant pigmentat ion , o ften rod - shaped ,
especially of the endothel ial cells , macrophages , and leukocytes .
The course of the capi llaries may ,
be well marked by the pigment contained in the -endothelial cells and that between the
wal l and the adjacent liver cells . Both the yellow and blackp igments are found , the former especially ,
in the l iver cells.
P igmentat ion is o ften more pronounced in the center of the
lobule. Thrombi ofp igmented cells in the capillaries and sub
lobular - ve ins occur , w ith cloudy swe lling and fatty degenerat ion of l iver cel ls . These retrogressive processes are in the
182 THE STUDY OF MALARI A
form of islands . The biliary inject ion , more intense in the
center of the hepatic lobule , may extend to the smal lestbranches. Regenerat ive efforts on the part of the l iver cellsare very much more common than - in pernicious malaria (M ar
chiafava and Bignami ) . =
K aryokinetic barrels and'
manasters
predom inate.
~This ' is interpreted .
_
by Bastianel l i as ev idenceof hyperfunct ion of the l iver. M archiafava and Bast iane ll iboth agree in bel iev ing that this multipl ication of the hepaticcells is an attempt On the part of the l iver to meet the in
creased demands for work 1n e l iminat ing the detritus of hemo
g lobin (Thayer) . The gall - bladder is usually d istended w ithbile .
The k idneys are general ly congested , we igh more , and are
softer than normal . The capsule is loosely attached . O n
Sect ion the cortex is o ften yellow ish ;the pyramids may present
brown ish streaks , more intense toward the apices. I n the
cortex may be found wedge- shaped hemorrhages w ith basestoward the capsule and apices po inting toward the medulla.
The medullary pyramids may Show minute hemorrhages. Theg lomerul i o ften escape undamaged ; there is rarely any p1g
mentat ion of the ce lls w ithin Bowman’
s capsule ;there maybecloudy swell ing , and s light epithelial desquamat ion . The
epithel ia of the convoluted tubules usually Show cloudy swelling , fatty degenerat ion , or coagulat ion necros is . There may be
pigmentat ion o f the epithe lial cells . The lumina are o ftenplugged w ith hemog lobin casts hold ing the epithel ia in place.
The changes in the straight tubules are S imi lar , but casts are
more numerous . The epithelium of Henle ’
s loops is betterpreserved , but the lumen is usually choked w ith casts of hemoglobin and epithel ial detritus from the convoluted tubules.
Biliary pigment also occurs here. Karyokinesis is sometimes
seen in the epithelium of Henle ’s loops and of‘
the convolutedtubules .
The s tomach and intestines may’
be negative. The serous
coat may be pale , the mucous membrane congested and bilestained , especial ly near the open ing Of the common bile—duct .There may be isolated hemorrhages , excoriations , and pigmeutation . The pancreas is normal .

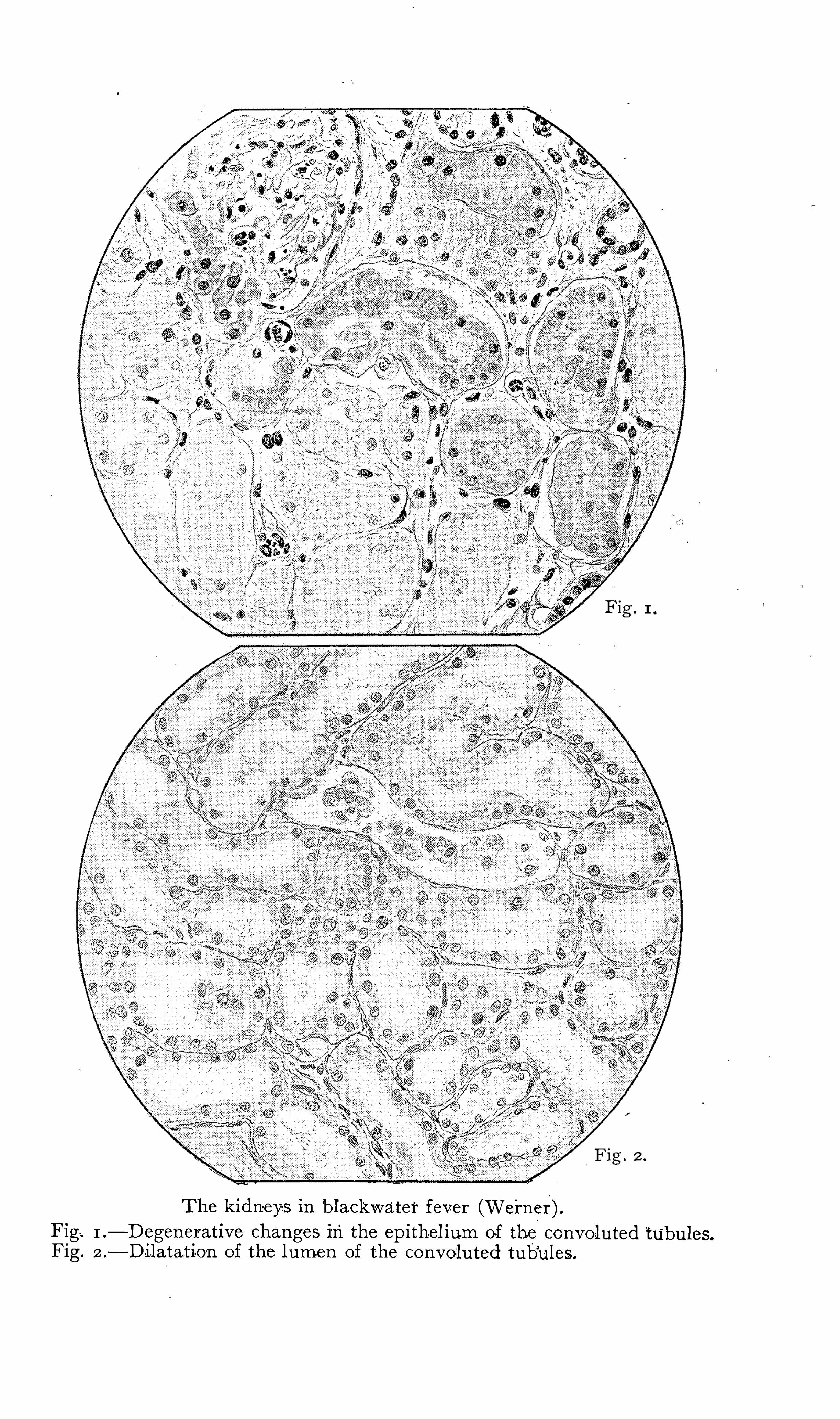


PATHOLOG I C ANATOMY 183
The pleura may Show punctate hemorrhages and the“
cav itymay contain a quant ity of serous fluid. The surface of the
lungs may Show S laty Specks and striae. The cut surface isvery pale , and exudes avery smal l amount of very pale , frothy ,serous fluid. There may be an ashy d iscolorat ion in the course
of the vessels, hypostat ic congest ion,and edema.
The pericardium may contain from a few drams to severalounces of a clear or sanguineous fluid,and may present hemor
rhages vary1ng 1n s1z e from that of a millet seed to that of acent . The heart is pale and o ften flabby . The muscularfibers are eas ily separable ; the walls may be very thin; The
le ft ventricle is usually strongly contracted, the right collapsed.
Auricles and ventricles may contain coagula or thrombi.M icroscopically the fibers stain wel l and show striations perfectly ; there are some areas of S light pigmentat ion and some
of connect ive - t issue prol i ferat ion ; the nerve trunks 1n the
transverse sect ion show marked degenerat ion ; empty nerve
sheaths are seen , and some connective- t issue proli ferat ion 1nto
fun iculus (Goltman and K rau'
ss ) .
The brain is usually pale and unpigmented ; the latter ven
tricles may contain an excess of fluid. The convex-ity of the
pia may show s l ight cloudiness ln-
the course of the vessels.
The puncta vasculosa may “
be scarcely v is ible. The bonemarrow shows the usual changes of malaria. M elan in , hemos iderin , and pro li ferat ing normoblasts may be found .

CHAPTER V
THE S implest and most lOgic class ificat ion of the malarialfevers is, accord ing to the form Of the several paras ites caus1ng them, into tertian, quartan , and
‘
est ivo autumnal . The en
deavor to affil ia te the ' tertian and quartan paras ites w ith theintermittent fevers and the est1vo - autu
'
mnal w ith the remittent
is fruitless , for a remittent temperature 15 by no means a
characterist ic o f est ivo—autumnal in fect ions. Neither is the
d1v15 1on 1nto quot idian , tert ian , and quartan'
consistent"
Quoti
d ian paroxysms may
.
be due to . e'
st ivo - autumnal infect ion,
double tert ian or triple quartan . Tert ian paroxysms may be
produced by estiV -O - autumnal paras ites or by s imple tertian .
The three forms of malar1a w i ll-
be stud ied in_the ir acute and
chron ic courses , larvated or masked forms , w ith the “
compl icas
t ions and sequelae.
ACUTE MALARI A
I ncubat ion—The period of incubat ion varies'
w ithin very
w ide l imits . I t may be stated as a general propos it ion that theincubat ion period is longest in quartan in fect ions and Shortest
in the est ivo- autumnal . The average period is , for quartan ,
twelve to e ighteen days ; tertian , six to fourteen days , and
est ivo—autumnal , two to ten days . M uch'
longer periods , run
n ing into several months,have been rel iably recorded. These
must be regarded as cases of chron ic malaria where the latentstage precedes the act ive , and are analogous to those cases o f
syphi l is in.which the secondary
i
mani festat ions occur"
'
w ithout
recogn ized primary les ion , and are to be explained sat is factori lyon ly by parthenogenes is.
General D escr ipt ion o f a M alar ial Paro -xysm .
‘—The formsof acute malaria have so many points in common that it is
conven ient to describe first the typic malarial paroxysm.
184
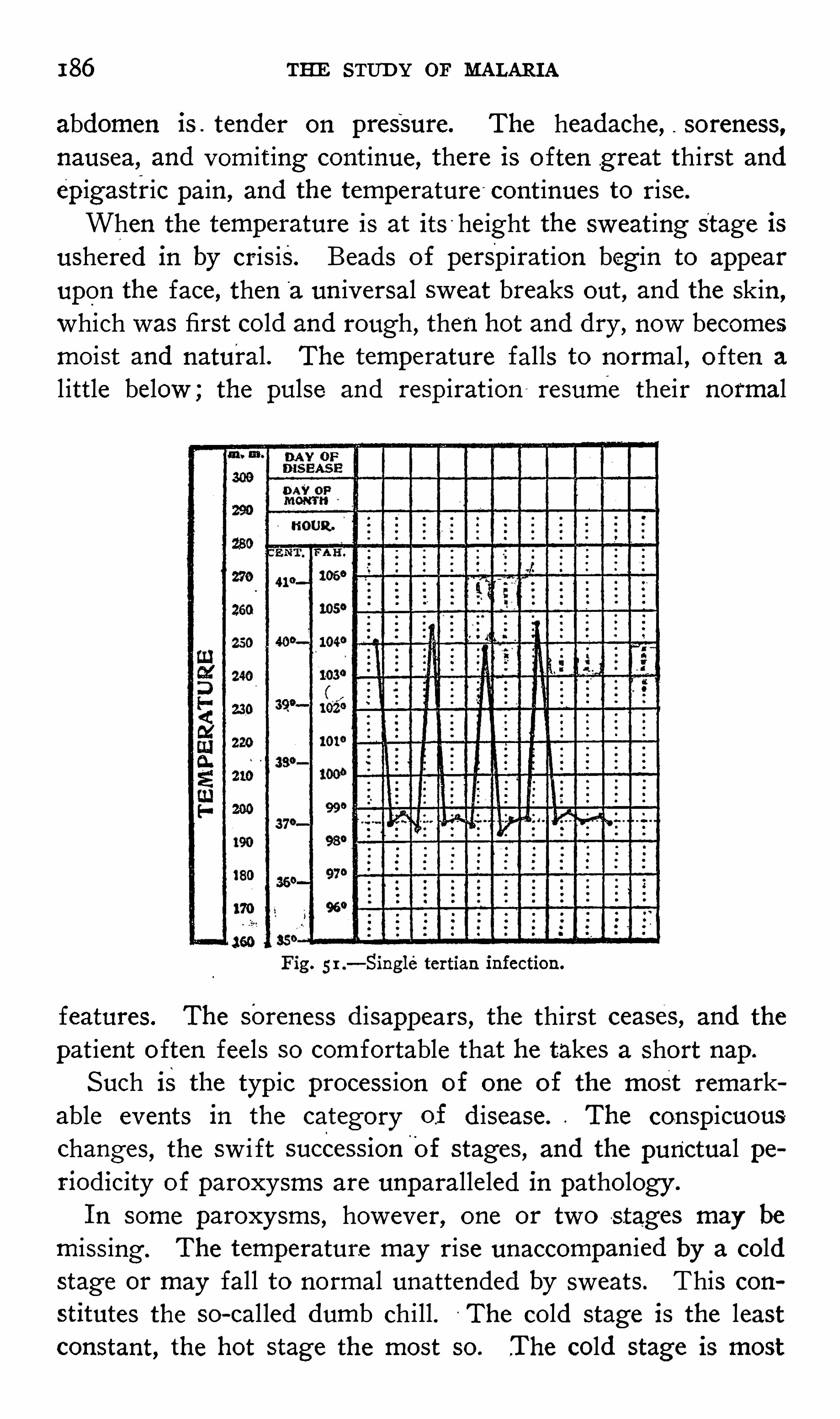
186 THE STUD Y OF MALARIA
abdomen is . tender on pressure. The headache , soreness,
nausea, and vomit ing cont inue, there is o ften g reat thirst andepigastric pain , and the temperature continues to rise.
When the temperature is at its - height the sweat ing Stage isushered in by cris is. Beads of perspirat ion beg in to appear
upon the face , then“
a un iversal sweat breaks out , and the skin ,
which was first cold and rough , then hot and dry , now becomesmoist and natural. The temperature falls to normal , o ften a
l ittle below ; the pulse and respirat ion resume their normal
Fig. 5 1 .—Single tertian infection.
features. The Soreness d isappears , the thirst ceases, and the
pat ient o ften feels so comfortable that he takes a short nap.
Such is the typic process ion of one of the most remarkable events in the category of d isease. The conspicuouschanges , the sw i ft succession
'
Of stages , and the punctual periodicity of paroxysms are unparalleled in pathology .
I n some paroxysms , however, one or two s tages may be
miss ing . The temperature may rise unaccompanied by a coldstage or may fall to normal unattended by sweats. This con
stitutes the so - cal led dumb chill. ~The cold stage is the leastconstant, the hot stage the most so.
_The cold stage is most
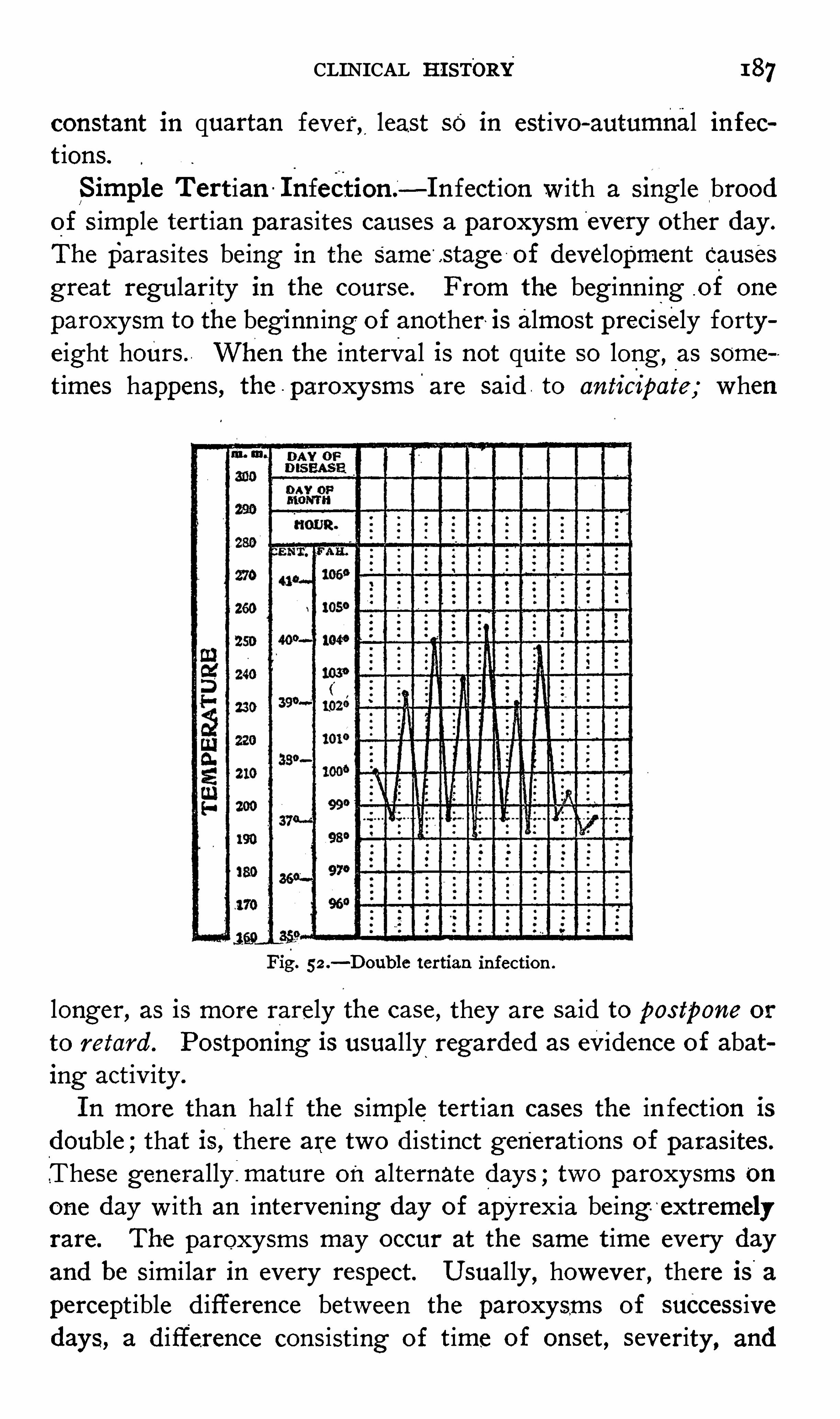
CLINICAL HI STORY 187
constant in quartan fever, least so in estivo - autumnal infect ions.
S imple T ert ian I nfect ion .—I nfect ion w ith a S ingle brood
of s imple tert ian paras ites causes a paroxysm every other day .
The paras ites being I n the Same .stage of development causesgreat regularity in the course . From the beginn ing .of one
paroxysm to the beginn ing o f another is almost precisely fortyeight hours . When the interval is not quite so long ,
as some
times happens , the - paroxysms'
are said . to anticipate; when
Fig. 5 2 .—D oub1e tertian infection .
longer, as is more rarely the case , they are said to pos tpone or
to retard . Postpomng 1s usually regarded as evidence of abating activ ity .
I n more than hal f the S imple tert ian cases the in fect ion isdouble ;that is, there are two d ist inct generat ions of paras ites.
.These generally:mature on alternate days ; two paroxysms onone day w ith an intervening day of apyrex ia being- e xtremelyrare. The paroxysms may occur at the same t ime every day
and be s imi lar in every respect. Usually ,however, there is a
percept ible d ifference between the paroxysms of successivedays, a d ifference consist ing of t ime of onset , severity , and

188 THE STUD Y OF MALARIArelat ive length of the stages of the paroxysms. I t very rarelyhappens that the paroxysms are so lengthen-ed
, and one so
ant icipates that its .onset occurs during the latter stage of the
preced ing paroxysm. They are sty led subintmnt attacks.
A change of type fromquot idian to tertian paroxysms, or
vice versd, is commonly observed . The change from quot id ianto tert ian may be Spontaneous or the result of incomplete
-
'
med icat ion or improvement in hyg ien ic condit ions , one group of
parasites perish ing . A change from tert ian to quotidian may
Fig. 53.—S ingle quartan infection .
occur w ithout apparent cause or fo llow ing ind iscretions of
various sorts.
The onset is probably more common during .the morn ing ,
but this '
is ne ither constant nor of d iagnost ic d ign ity . The
invas ion is almost always w ith .a chil l . The temperature risessudden ly and falls l ikew ise. Commonly there are no grave
symptoms , but a mi ld d e lirium is not rare . The temperatureusual ly goes as high as 103
°
to 105°
F . The average durat ionof the paroxysm is from eight to twelve hours.
D uring apyrex ia the pat ient may feel perfectly wel l excepts light weakness , headache , or vertigo. He is usual ly able to

190 THE STUD Y OF MALARI A
those of the typic paroxysm and are w el l'
marked. The Coldst age is not only more constant than in the other forms , but ismore intense and usually of longer durat ion. The three stages
are‘
sharply contrasted. P ern icious symptoms are very rarelyobserved in connect ion w ith quartan in fections. This may be
accounted for by the more equal d istribution through the cirenlation of the paras ites which Show no tendency to congregate ,
and by the longer apyrex ia] periods , between t he paroxysms.The average duration of the paroxysm is e ight or ten hours.
Fig . 5 5 .—T riple quartan infection .
obstinate dispos ition of quartan fever to r ecur beena matter of common know ledge for centuries , and is st il l apopular idea. This may doubtless be accounted for at this day '
by the probability that , ow ing to the greater interval betweenthe accesses , the specific is not properly taken. M ost phys iciansw i l l agree that quartan fever is just '
as amenable to appropriatetherapy as the other acute forms. As in tertian fever, analmost complete feeling Of w ell be ing may be experienced between paroxysms , the pat ient usually being able to attend to
business.Estivo - autumnal . I nfection—The chief feature of infec
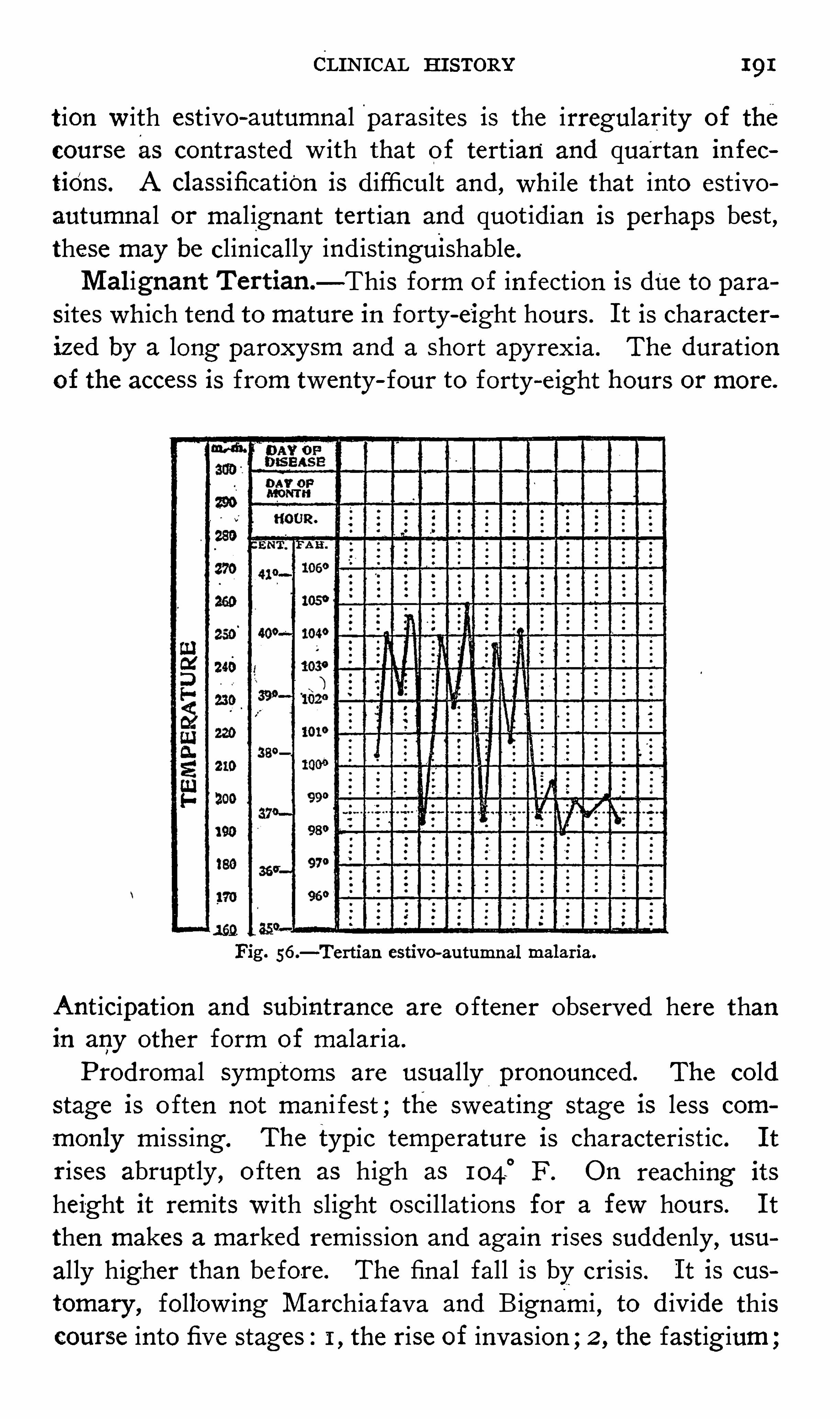
CLINICAL HI STORY 191
t ion w ith est ivo - autumnal paras ites is the irregularity of the
course as contrasted w ith that of tert ian and quartan infec
tiOnS . A classificatiOn is d ifficult and , wh i le that into est ivoautumnal or mal ignant tert ian and quot idian is perhaps best ,these may be clin ically ind ist inguishable.
M alignant T ertian—This form of in fect ion is due to paras ites wh ich tend to mature in forty - eight hours . I t is characteriz ed by a long paroxysm and a Short apy rex ia. The durat ionof the access is from twenty
- four to forty—e ight hours or more.
Fig. 56.—Tertian estivo- autumnal malaria.
Anticipation and subintrance are o ftener observed here thanin any other form of malaria.
Prodromal symptoms are usually pronounced. The coldstage is o ften not man i fest ; the sweat ing stage is less com
monly m iss ing . The typic temperature is characterist ic. I t
rises abruptly , o ften as high as 1040
F . O n reaching its
height it remits w ith slight oscil lat ions for a few hours . I t
then makes a marked remiss ion and again rises suddenly , usually higher than before. The final fall is by crisis. I t is cus
tomary , follow ing M archiafava and Bignami , to d iv ide thiscourse into five stages : I , the rise of invasion ;2 , the fastig ium

192 THE STUD Y OF "MALARI A
3, the pseudocrisis ;4 , the precritical rise ; 5 , the cris is. ThisCurve is simulated on ly by S imple tert ian fever w ith subintrantattacks , which is uncommon. Unfortunately this typicsequence is far from constant ;
'
the mod ificat ions are very
numerous and are too irregular to analyze.
The symptoms of the hot stage are more. pronounced than inthe in fect ions prev iously described . The headache and backache are worse , the general depression 15 .more pro found , stuporand del irium may appear, and pern icious symptoms may arise.
Dur1ug the Short interval the pat ient does not regain his ease
Fig. 5 7.—Quotidian estivo - au
’
tumnal malaria.
as in the s imple intermittent fevers , but the aching and pros
tration cont inue , and he may be unaware that the fever hasle ft.Quotidian .
—The quot idian estivo - autumnal fever.
is more
regular in its Course than the tert ian , especially at first , thoughthere is nothing -
characteristic in the temperature Curve , whichmay closely resemble a double tertian or a triple quartan.
Later it is apt to lose some of its regularity by anticipat ionor by lengthening of the paroxysms , whose average durat ionis from six to ten hours. The chill is rather more constant
194 THE STUD Y OE MALARI A
rather lower during the fever- free interval than in the others .
The typic run of tert ian est ivo - autumnal has been g iven as
follows : I , the stage o f in it ial ascent ;2 ,the fastig ium, during
which the temperaturemay Show fluctuat ions of a hal f degreeto a degree ; 3, the pseudocrisis ; 4, the precrit ical or finalascent ;and , 5 , the crisis .
Cont inued temperature in malaria is not as common as usu
al ly regarded ;remittent fever was formal ly thought to be therule in the summer- autumn malarial fevers. The causes of
this error are three ;firSt , in tert ian estivo- autumnal infect ionsthe apyretic interval is short , secondly , this interval o ftenoccurs during the n ight or early morn ing hours ; thirdly , the
patient , guided by the discomfort which Continues during the
interval usual ly den ies that he has been free ‘ from ' fever.
Nevertheless , a cont inued temperature is occas ionally noted
in malaria, especially in tertian est ivo - autumnal in fect ions . I t
may'
be regularly rem ittent or may be irregular. The following are the Chie f causes of a cont inued malar ial temperature
1 . Prolongat ion of the paroxysms.
2 . Ant icipat ion of the paroxysms .
3. I n fect ion w ith more than one brood of the same speciesof paras ite .
4 . I n fect ion w ith more than one Species .
5 . Compl icat ions.
S o - called Spontaneous recovery may occur in either form of
malaria.
.
AS a rule , the recovery is on ly temporary'
and is
merely“
the trans ition from the act ive to the latent stage , re
lapses usually occurring sooner Or later. Favorable hyg ien iccond it ions encourage spontaneous cure .
The durat ion of untreated acute malaria is too indefin iteto permit of exact statements . While s imple tertian may
terminate after a few paroxysms , an est ivo - autumnal fevermay continue three Or four w eeks i f it does not in the mean
t ime become pern icious.
A postmalarial secondary fever, or spodogenous fever, isoccas ional ly observed after the in fect ion , particularly est ivoautumnal , has lasted for some t ime . I t pers ists for days or
w eeks uninfluenced by quinine . The blood examinat ion is

CLINICAL HI STORY 195
negative for paras ites . Resorpt ion of débris , tox ins , and v is
ceral les ions have been O ffered'l'
as explanations of this process ,but
/
none of these are ent irely sat isfactory .
Circulatory S ystem.—The '
Blood .—The blood , being the
habitat of the paras ites , furn ishing the ir pabulum, contain ingthe ir tox in , bes ides carry ing one of the host ’s mechan ism of
de fense against the ir depredat ions , Show s important changes.
The volume of the blood as a whole is somewhat d imin ished.
The specific g ravity is Only sl ightly lowered , and usually onlyin recent infect ions, the destruct ion of the sol id e lements be ingnearly compensated by the excret ion of fluids .
i The '
density ,
at first lowered , approaches normal as the in fect ion pers ists .
The experiments that have been performed w ith re ference tothe ton icity of the blood in
i
malaria u have uni formly shown
that this is increased .
The parasites of malaria have a very unequal d istribut ion ,
some be ing almost constant ly found in the superficial circulat ion throughout the ir asexual cycle , others on ly during the
early stages of the ir development,modestly ret iring to the
recesses .of the v iscera for procreat ion . -The organisms '
are
somet imes scanty in the-
peripheral blood, occ’
asronally ent irelyabsent.The tertian parasite , more abundant in the deep circulat ion ,
may be observed in the peripheral'
circulat ion throughout thecourse of the asexual cycle , except ing the Sporulat ing forms ,wh ich are only except ionally seen . The. gametes are not in
frequently detected .
The quartan paras ite ismost evenly d istributed ,being about
equally common in the v isceral and superficial blood . Fur
thermore , all stages of the asexual development , includ ingthe Sporulating forms , may be followed in blood obtainedfrom the peripheral circulation. Quartan gametes are rarelyseen.
.The estivo- autumnal parasites are seen in on ly the earliestphases. I n some local it ies the gametes .are very commonly
'
ob
served after the in fect ion has pers isted a week or more ; in
others , even where severe in fect ions of long standing are en
countered, they are more rarely noted.
196 THE STUD Y OF MALARI A
P igment is most frequent ly contained w ithin the large mononuclear, less often the polymorphonuclear , leukocytes , but may
ex ist free in the blood Current .‘
I t is of a dark redd ish - brownor black co lor, and occurs as granules , rodl
'
ets, or irregular
c lumps .
O ne o f the best - known facts in the study of malaria- is the
rapid and w idespread destruct ion of the red blood - cells .
“
A
certain number of erythrocytes perish w ith e ach paras it icsporulation l ike sold iers after a vol ley from the enemy . I t is
not uncommon for a fourth - to a hal f mil lion red cells percmm . to be destroyed during each o f the first “
two or threeparoxysms , and this may progress unt il the count is cons iderably less than one -mi ll ion per cmm. A S a rule , in uncompli
cated benign malaria t his erythrorrhexis is greater'
during the
early paroxysms, dimin ish ing w ith each success ive paroxysm,
the cells apparently requiring some sort of immun ity . I t is
l ikew ise usual for the marked early destruct ion to be rapidlyCompensated , or
“
nearly S O , by the act iv ity of the blood - formingorgans . L ater it is more d ifficult for these organs to rep laceeven the smaller number o f destroyed ce lls . Hence the anemia
is common ly in proport ion to the severity and durat ion of the .
attack. Rest itut ion o f the red cells is more rapid and certainw ith tert ian and quartan than w ith est ivo - autumnal in fect ions.Race , age , and const itut ion are also factors in the rap id ity of
reconstruct ion.
There are certain changes that occur in the in fected cel lswhich
°
should be ment ioned. The cells contain ing the S impletertian parasites are swo l len and somewhat decolorized . Those '
contain ing the quartan paras ites a re shrunken and somewhatdarker in co lor. The ce lls
-
harboring est ivo - autumnal organisms have the appearance of old gold or of brass , and become
Somewhat smaller. A curious appearance of some infectedcells is what has been termed st ippl ing , This may be seen in
both s imple tert ian and est ivo—autumnal in fect ions , but presents”
features more or less characteristic in each . I n simple tert ianthe dots are fi ne and abundant . I n est ivo - autumnal they are
coarse , irregular , maybe cleft - l ike, and few in number—from
two to six. The fine st ippl ing o f tert ian in fect ion is also

198 THE S TUD Y OF MALARI A
phers have recorded that there is nO'
increase of“
the largemononuclears during pyrexia, but that the increase is pronOunced in the
“
apyretic interval , or Immed iately fol low ing therise of temperature , i f only one such occurs. They also noted
that in certain cases this change was extraord inari ly marked ,the large mononuclears during the interval even exceed ing innumber the polymorphonuclears. They observed further thatin some cases the mononuCI -ear increase was to be detected even
during the fever stage , but in these cases I t was sti ll furtherev ident during the interval . Rogers
44concludes that the mono
nuclear increase is decidedly more marked and frequent'
in
ben ign than in malignant tei tians. He accounts for this bythe shorter apyret ic interval of the latter. Krauss28 1 believesthat it is not so much the absolute 1nc1ease of the large» mono
nuclear e lements -
as the relat ive increase over the smal l lymphocytes ,Which is
'
characterist ic of malaria. Ziemann48 states thatin the beg inn ing O f the access there is o ften a transient polymOrphonuclear leukocytos is , which recedes during the acme of
the fev er s imultaneous w ith a relat ive increase of the largemononuclears , wh ichmay reach I 5 per cent . or more.
Eos inophilia, in the writer ’
s experience , denotes Compl icat ions , ord inari ly intest inal he lminthias is.
Billings 16 cases showed the follow ing average
Per cent .
Small mononuclears
Large mononuclearsPolymorphonuclears
Krauss ’28 1 204 cases
SmallLarge lymphocy tesPolymorphonuclearsEosinophiles
Rogers44 found that the large mononuclear leukocytes num
bered0 8 per cent . in
8 - 12 per cent. in12 - 15 p er cent . " in15 - 20 per cent . in
O ver 20 per cent .
CLINI CAL HI STORY 199
The leukocytes occasional ly undergo degenerative changes ,among which are fatty degenerat ion and vacuol izat ion o f the
protoplasm and fragmentat ion and chromatolysis of the
nucleus .
The blood platelet-s are somewhat increased in malaria, espe
cially during the interval follow ing a severe attack.The care ful ly conducted experiments Of. Capograss i84 tend
to show that , while malarial blood possesses agglutinat iveproperties , it is o f no d iagnost ic importance.
Celli , Carducci , and Casagrandi,147 investigat ing together,
were unable to determ ine defin itely the existence of an hemo
lys in , but concluded that such a body probably ex isted. Later
Casagrandi was able to veri fy the presence of an hemolys inin malarial blood, and concluded that it was masked by an
ant ibody . D e Blas i82 found in a watery solut ion o f centrifu
gated red cells antihemolyt ic action in 15 cases out of 19 . The
4 negat ive cases were in chronic malarias who had beenunder the influence of quinine a long t ime . This hemolyt icact ion isnot specific for malaria, occurring in meas les , typhus ,erysipelas , and scarlat ina, but not _
in healthy persons .
At the height of the fever the pulse may“
reach 130 or
more. D uring the' interval it usually becomes almost quite
normal in tert ian and quartan in fections. I n est ivo- au'
tumnalfever it depends upon the severity of the attack and the res istance of the pat ient . O ccasionally the rapid ity of the pulse doesnot Show the usual relat ion to the height of the temperature ,but may be below 100 , w ith high fever. This is somet imes
observed during the attack, but is rather more common duringconvalescence. D uring the
“
cold stage o f the paroxysm the
blood pressure rises decidedly , falling during the second stage ,
to become normal in the sweat ing stage. This is fairly con
stant , v ariations being due not to a d ifference of paras ites ,but to ind iv idual cond itions . An anemic murmur may be heardover the heart. A sense of precordial oppress ion or acute painare common complaints .
Respiratory O rgans .—Respiration is usually accelerated in
proportion to the temperature . C ough is a frequent symptom.
I n children a frequently repeated superficial hacking cough is

200 THE STUD Y'
OF MALARI A
O ften an indication of nausea. Bronchial catarrh is not intrequently observed , a ccompan ied by sibilant rides on auscultat ion. Ep istax is may occur and is occasionally alarming ly profuse.
Gas tro—intes tinal O rgans—While the paroxysm is on , the
appet ite is usually completely lost . I n tert ian and quartanmalaria th is may be regained during the interval , but in est ivoautumnal anorex ia general ly pers ists throughout apyrexia; Thepatient ord inari ly complains of a bitter taste in the mouth and
fulness , d iscomfort , or pain in the epigastric reg ion . The
tongue is large , flabby ,thickly coated , usually anem ic, and
show ing the prints of the teeth along the edges . Nausea is
nearly a constant symptom, and retching’
and Vom it ing are dis
tressing . The vom itus con5 1sts of matters ingested ,
°
bile , or
sl imy mucus . The boWels are constipated ,regular, or
'
loose , . in
the order of frequency named ; choleraic or dysenteric discharges occas ionally appear. M ore or less enlargement o f theSp leen is a Usual occurrence , together w ith pain and tenderness
in the le ft hypochondrium. I n primary acute in fect ions theenlargement may not be prominent ; in later in fections the
Spleen is o ften palpable beyond the costa] marg in . The spleenis rarely much enlarged in the negro. Enlargement of the l iveris much less constant and less marked than Splen ic hypertrophy .
There usually ex ists tenderness 1n the epigastric and righthypochondriac reg ions .
Genito—i z rinary O rgans .—Urine.
—As a general rule , “
the
urine emitted during a cold stage is paler in Color and that of
the stage of fever highly colored , but ind iv idual circumstances
may produce numerous except ions to this rule .
“
I n certaincases of est ivo- autumnal fever the urine may be very highlycolored and contain a heavy depos it . I n these Cases the urinecontains biliary coloring matters and an excess of urobilin .
The d iazo react ion sometimes obtains. The ind ican is fre
quently increased . Intert ian and quartan cases the quantityof the urine is somewhat augmented , in est ivo - autumnal d iminished . Polyuria of tert ian and quartan malaria and that occurring somet imes in est ivo - autumnal occurs under two cond it ions ,the po lyuria of the paroxysm and that of convalescence or post
202 THE STUD Y OF MALARIA
the denominator indicating the number of cases'
of'
malaria,the
'
numerator the number in which albuminwas found
CoSta79
F .
M archoux
BOrne9°
Thay er and Hew etson
S olon86
S choo90
Thayer2
Anders
Atkin son
ChamberlainF reri chs
6 1
Cook285
“
M arch iafava and Bignami say that albuminuria‘
is. rare in
the ir experience , though Ke lsch and K iener178 hold the oppos iteV iew , and Craig70 states. that it occurs in a - majority of the
severe cases .
An increased , tox icity of the urine has been found in largeper cent. of cases o f malaria, greatest during l
apyrex1a and usu
ally " intens i fy ing With each success ive paroxysm._
Brousse’i 6
arrived at the fo llow ing conclus ions : I . The urotox ic coefficient ,calculated by means of the formula of Bouchard , -
'
the,average
coefficient being .464, r ises during the attack , and the phy s io~logic
v
effects observed are those usual ly noted after the inj eCt ion of urine ;dyspnea , ,
mios is , fall'
of temperature , exophthal
mia,bes ides convuls ions . 2 . Th is tox icity is d imin ished during
the period of convalescence from the intermittent fevers very
much below’
that of the urine during the access , and , furthermore , more feeble than that o f normal urine.
Nervoas S ys tem .—Heada
'
che is one of the most invariablesymptoms of malaria. Backache and somat ic soreness are
severe . S omet imes hyperesthes ia is seen . V ertigo is the rule ,especially when the pat ient is upright . Neuralg ia, facial orintercostal , i s a not in frequent symptom . S tupor and deliriumare present in
'
grave cases , part icularly in children .
S kin—D uring the first stage of. the paroxysm the skin isblanched and cold , during the second stage hot , dry , and per
haps turg id , during the third bathed with sw eat, becoming
natural toward apyrexia. I cterus is not a pronounced symptom
CLINI CAL HI STORY 203
in acute cases except in'
certain pern icious forms . With theposs ible except ion o f pneumon ia herpes is seen more frequentlyin
,malaria than in any other d isease. I ts commonest s ites are
the l ips and -
nose, but it may appear elsewhere. I t is not nearlyso . common in the n egro as in the white. Urticaria and
erythema are sometimes observed.
PERNI C I OUS M ALAR IA
M alaria threatens or destroys l i fe through its inherent dangers , acutely expressed, through the sequelae o f chron ic man ifestations
,or through compl icat ions in any stage. Pern icious
malaria is that form of malaria, extremely acute , which , independent ly of compl icat ions , endangers l i fe in a few hours or
a few days . This grav ity may be due to the intensificat ion of
ord inary malarial symptoms or to the advent of unusual ones.
I t should be clearly understood that pernicious fever is not a
patholog ic ent ity , but is a form of malaria from the s implemodes of which it somet imes d iffers only in degree . I ts patho
genesis is int imately associated w ith the life history of the
malarial'
parasite , much more so than is hemoglobinuric fever.I ntermed iate forms may be encountered which may be d ifficultto place , as cases w ith s l ight somnolence , abundant sweats , orcold sur face.
Though the pern icious forms of malaria w ere alluded to
by Hippocrates and by Ce lsus , they did not rece ive any de
tailed cons iderat ion unt il 1743, when Tort i described them.
This pyretolog ist d iv ided the pern icious fevers into solitariw,
those characterized by the continuity or acuteness of the ord inary symptoms , and the comitatce, in which one grave symptompredominated . The comitatce he subd iv ided into the colliquat ive , includ ing the choleraic, dysenteric, atrabil ia
'
ry , cardialg ic,and d iaphoret ic, and the coagulat ive , includ ing the syncopal ,alg id , and letharg ic forms .
A l ibert , in 1804 , d ist inguished twenty variet ies of perniciousmalaria.
Rotix , follow ing Jaccoud ’
s class ificat ion , looks on all as
originating in the vasomotor and sympathet ic systems or in
the cerebrospinal system.

204 THE STUDY OF MALARI A
Ke lsch and Kiener adopt Tort i ’s system -w ith sl ight modifica
t ions .
M archiafava and Bignami arrange the -
pern icious forms , ao
cord ing to the course of“
temperature , into tert ian , quot id ian ,
subcontinuous , and larval .M anson groups them roughly into cerebral—includ ing the
hyperpy rex ial , comatose , . convuls iv e,and - paret ic forms—and
alg id , includ ing the syncopal , choleriform, ,dysenteric, and
hemog lobinuric forms.
D antec class ifies the variet ies anatomically accord ing to the
organs which bear the brunt o f the attack , namely : ( 1 ) Thebrain , (2 ) the medulla, (3) the spinal cord, (4) the heart , ( 5 )the - lungs , and (6 ) the d igestive tube.
Homem d escribes fifteen definite forms,bes ides several un
defined variet ies.
Cardamatis d istinguishes seventeen variet ies .
M ore than thirty S O - cal led variet ies of pern icious malariahave been described . A partial
'
list of these includes the apo
plectic, atax ic, Comatose , sudoral or diaphoretic, del irious ,eclamptic
'
or convulsive , tetan ic, typho id , amaurotic, aphas ic,ardent , _
exanthematous , hemipleg ic, hydrophobic neuralg ic,cerebromen ingeal, card ialg ic, dyspenic or asthmat ic, pneumo
nic, pleurit ic, syncopal , hemoptoic, alg id, choleraic , dysenteric,gastric or gastralg ic, hemorrhag ic, bilious or hepat ic, lymphat ic,rheumat ic , and nephritic forms .
This multipl icity is due to two causes : first , the fanci ful andunnecessary subd iv ision of typ ic forms ; second , the mistakingof compl ications for true pernicious attacks .
Any class ificat ion is not absolute ly essential , and all are more
or less arbitrary . Nevertheless , for convenience , all forms of
true pern icious malaria may be easily and log ical ly arranged
into cerebrospinal , ( 2 ) thoracic, and 3) abdominal forms .
Cerebrospinal F orms .—The representat ive type of cerebro
spinal pernicious malaria is the comatose variety ,which is , as
w el l , the most frequent of all variet ies .
Comatose malaria may make its appearance as the first manifestation of malaria or
,more commonly , after the lapse of
one or more paroxysms , typ ic Or irregular. Vio lent head

206 THE STUD Y OF MALARI A
unequal and “
may _
or may not react to light . S trabis'
mus is an
occas ional symptom. The face is congested in'
indiv iduals re
cently attacked or pall id in o lder sufferers . The skin is at
first hot and dry , perhaps S l ightly jaund iced ; later it may be
bathed w ith sweat . Petechim are occas ionally Seen . Trismusmay be
-
present , but the extremities are usually completely re
laxed , though sensat ion and motion are o ften not ent irely abolished , as somet imes ev idenced by res istence ' —to hypodermicmed icat ion . Cases man i festing muscular rig id ity and toniccontractures have been reported by S chellong
g2and by
Brown .
28 6 Hyperesthes ia and muscular tremOrSa re not in fre
quently present . The reflexes may be increased or d im in ished .
There may be tw itching of the muscles of the face , usuallyconfined to one s ide . L oud calls may not el icit respon
'
se , and
shaking'
only groans and unintelligible utterances . The coma
may be.
intermittent , runn ing parallel w ith the temperature .
The fever in most cases varies from 10 1°
to 103°
F . , but
may be subnormal or hyperpyrex ial . The pulse is at firstfu11 and bounding , later smal l
,rapid , and feeble. D i lat ion
of the right S ide of the heart may ex ist and an anem ic murmur may Somet imes be heard . The respirat ion may
-
be quiet ,s low or rapid , or blow ing and stertorous , w ith Cheyne - S tokescharacterist ics late in the course . Edema o f the lungs is an
occas ional late occurrence . Nausea and vomit ing are seen
early in the attack , i f they are present at all. The mouthand tongue are dry , the latter deeply coated. Herpes and
sordes are sometimes noted . Hiccough is an occas ional symptom. The tongue when protruded may be drawn to one s ide.
I n cases of recent in fect ion the Spleen may be on ly sl ight ly or
not at all enlarged ; in other cases it may be greatly en larged,constitut ing a valuable d iagnostic S ign.
The l iver may be tender, but is usually not much enlarged.
The evacuat ions of bowels and bladder may be involuntary or
there may be retent ion of urine. The bowels are o ften con
stipated .
,
I n favorable cases the coma gradually fades , consciousnessslow ly dawns , the temperature d rops to or below normal , thepulse regains its normal characterist ics , and, save the phys ical.
CL INI CAL HI STORY
ness and a degree of mental hebetude, all is well v1iatient.
unfavorable cases the coma becomes absolute, the pines rapid , thready , and irregular, the breathing 1S stert
1nd of Cheyne S tokes type , tracheal ratt l ing appears ,becomes cyanot ic, and death ensues from convulsions. collapse.
1e durat ion of an attack is from a few hours to a f
rt z183
Speaks Of cases of apparent death arising in;e of comatose attacks . He describes these cases as i
Inder this form of pernicious interm ittent must also(1 those cases O f apparent death which may last frian hour to four hours . Persons subject to such attairemain ent irely conscious , seeing and hearing
'
everythi
occurs or is said around them, but unable to move or
a sound ;or they may be ent irely unconscious, respiratited , pulse and heart beat not to be recogn ized, and. cv
’
.1arpest irritants applied to the body call ing forth no S ig
fe unt il , at the beg inn ing .Of the sweat ing Stage,i
t
.1t comes to him-sel f and the varioUS organs again 51011
fest the ir act iv ity . Trousseau reports the case of a 111
had had fainting . fits on two occas ions in Alg iers , andsequent attack fel l into this cond it ion of S imulated dea'
.s not unt i l he had been carried into the post -
.mortem ro<
:vidences of l i fe were observed about him, whereuponr
eturned to his bed and recovered under quinine tre.
lapses may occurafter the apparently favorable deferv~of the symptoms . Laveran1 saw three success ive attac
sold ier. Colin86 reports several examples of pernicic
:s assailing the same subject repeated ly at intervals1 to twenty days . M ayer states that in a third of 1
another attack supervened in eight or ten days . M c
:hree are very rare , but Homem records the case 01
5studentWho died'
after hav ing S ix pern ic ious paroxysrilong ' been maintained that the third attack is fatal.

208 THE STUD Y OF MALARIA
usually holds trUe that the success ive paroxysms increas e inseverity and danger to the patient. I n the interval the pat ientmay
’
be apathet ic ormay complain of headache . The relapsemay appear in the form of a d ifferent type of pern iciousparoxysm , as algid or -choleraic , but such cases are very rare .
A S intimated , the apoplect ic form of pern icious malaria ismerely a fulminant variety of comatose malaria. I n these rare
cases the onset is equally a s sudden as in'
cerebral hemorrhage ,whence. the name . L averan
,
1Cardamatis
28 7and Crespin
mare
incl ined to doubt the ex istence “
of th is variety , but cases have
been reported by M orris , 2 88 D av idson ,
6 6M aurel , 7 5 and others .
Ew ing ’s case is remarkable .
' “
The patient , wh ile S itt ing up in
bed smok ing , three t imes in five'
d‘
ays sudden ly became .uncon
scious , his p ipe fell to the floor, and he remai-ned stuporous
for three or four hours. At the end Of that period he wouldwake up ,
at once pick'
up his p ipe , and resume smoking.
”
"Symptoms orig inating from the cerebe llum are present
rare instances. SuCh are s low ,monotonous Speech , drow s iness ,
severe depression , and incoOrdination of vo luntary movements .
M archiafava and -Bignami” describe as follow s the interesting bulbar Symptoms which Occas ionally pr esent themse lves“When a physician unexpected ly encounters this d isease he iseas ily incl ined at the . first g lance to .
. think that the case is one
of a pat ient w ith bulbar paralys is who has become in fectedw ith malaria, but this suspi cion d isappears after a care ful exam inat ion and after see ing the gradual resolut ion o f the symptoms . The Chief symptoms -are :D ifficulty in art iculat ion , whichmay even reach anarthria ; a weak and nasal voice ; inferiorfacialparalys is , o ften o f one S ide on ly ;a half—open month fromwhich droo ls the sal iva ; a pendent lower lip ; a dry and On lyS lightly movable tongue ;d ifficult or abol ished deg lut it ion . I f
the attack tends to a fatal issue we have the added -
symptoms
o f sopor , a thready interm ittent pulse , labored and stertorous
breathing , and clammy Sweat . When , how ever , the result isfavorable the pat ient . recovers
" from the more severe symptom
as soon as the fever falls ;the bulbar symptoms usual ly pers istfor some days t although in mi lder form ,
and then graduallyd isappear , the dysphag ia going first , then the dysarthria
'
and
2 10 Tm STUD Y OF MALARI A
typ ic case. The most prominent symptoms are usually trismus and
'
op isthotonos ; emprosthotonos and pleurosthotonos
are but rarely Observed .
O ccas ionally amauros is arises in the course o f a comatose
attack. I t may .be trans ient or, in rare instances , permanent .I n the only case occurring under my observat ion v is ion beganto improve at the end of the attack, but was not fully restored
unt i l after several weeks . Accord ing to Poncet ,” 1
the -
per
s istence of amblyopia in these cases is due"
to opt ic neuritis ,peripap illary edema, extravasat
'ion of leukocytes , plugg ing o f
ret inal and choroidal vessels by paras ites or p igmented lenkocytes , and consequent mult iple hemorrhages:
_
A rare form of pernicious malaria, the atax ic, has beendescribed, part icularly by Angellini and Tort i .“ .The principal symptoms are scanning Speech , dysarthria, w eakness of
low er l imbs , vert igo , Unsteady gait w ith'
a d ispos it ion to fal lforward , muscular tremors , and exaggerated reflexes . M a
'
urel75records 22 cases , but it appears that some of these cases at
least do not belong to the atax ic type .
“
M anson”thus describes the so- cal led ardent
,
fever : I n the
course o f what seemed to be an ord inary malarial attack , thebody temperature , instead of stopping at 104
°
or 105°
F . ,
may cont inue to rise,and , pass ing 1 07
°
F . , rapidly mount to
1 10°
or even to 1 12°
F . The pat ient , after a brie f - stage of
w ild , man iacal , or perhaps muttering del irium, becomes rapidlyunconscious , then comatose , and d ies w ithin a few hours or
perhaps w ithin an hour after the onset of the pern icious Symptoms . Both the cases of . this type observed by Homem1 5 7
ended fatally .
Typhoid pern icious has been most care fully studied by Billet.
1 5 1 I n these cases the cl in ic p icture is almost ident ical w iththat presented in typhoid fever. The temperature is period ically intermittent or, as is more common ,
remittent , and usu
ally ranges from 10 1°
to 103°
'F . , but may reach 106°
F .
There are headache , backache , rap id pulse , torp id digest ivetract , sordes ,
'
splenomegaly , apathy ,and stupor. There may
be diarrhea or const ipat ion ,and bilious vomit ing occurs in
some cases. The abdomen is usually tympan it ic and there
n.

CL INI CAL H I STORY
may exist tenderness and gurgling in"
the right i liac fossa.
Epistax i s I S frequent . I ncoherent speech, del irium, and incon
tinence o f urine-
and feces are-
s ymptoms o f severe cases . All
of Billet ’s 40 cases Showed the presence of malarial paras itesand a
“ large mononuclear leukocytos is , and an absence of rose
spotsand the Widal react ion . Theaverage durat ion was fouror five days .
Thoracic F orms .—The immun ity of the organs of the Chest
to,
lOCaliz ations o f the malarial paras ites and to the effects .of
their tox ins i s remarkable . I ndeed , the thoracic forms are
much rarer than . the'
i‘ecords would import , for the O lder
w riters especially w ere prOne to attribute any complicat ion thatm ight present itsel f to the e ffect of the mysterious malarialpo ison .
Ew ing 1 79 has m inutely reco -
rded a case in which the autopsy
Showed an enormous number o f paras ites in the cap illaries o f
the heart muscle . The symptoms re ferable to the heart Werefeeble pulse , 124 to the minute , and very feeble heart Soundson - auscultat ion . The p atient was comatose .
-
' Benvenut i179 hasreported a case in which the capi llaries o f the myocard ium ,
brain,and kidney were filled w ith in fected red cells . The prin
cipal symptoms w ere coma and dyspnea.
Formerly cases o f pneumon ic pern icious malaria were more
frequently report ed than at present , S ince more exact methods
o f observat ion have come into use it i s certain that many of
thes e cases w ere compl icat ing lobar pneumon ias . That themalarial paras ite is
'
unable to Cause true inflammat ion of lungtissue is now w idely recogn ized , and w as maintained byCol in ,
233 J ’
accoud,289 'ROux ,
16 1and M arch iafava and Bignam i .
Nevertheless , grav e symptoms re ferable to the lung , and more
or less resembling pneumon ia,may arise in malarial in fect ions .
L averan ,
1who doubts the ex istence o f
'
a pneumon ic pern icious ,admits that in certain pat ients attacked w ith interm ittent
"
fever
there may be observed , w ith each attack, pulmonary conges
t ion , accompanied w ith subcrepitant rales , wh ich may lead toa belief in the ex istence of a pneumon ic intermittent . Bacelli
proved the ex istence of a group of cases nearly resemblingpneumon ia in symptomatology . The Characterist ic cough ,
2 1 2 THE STUD Y OF MALARIAdyspnea, and pain in the side are present. There may bemoderate dulness and coarse , sonorous, and s ibilant ralesheard
‘
over the port ion of the lung involved. O ther w ritersdescribe intermittent lung symptoms and s igns met in cases
of pern icious malaria. L e D antec226
records the fol low ingcase , occurring in the person of his friend , D r. Grosset , Who ,
after several paroxysms of intermittent , was taken in the
course of an attack of fever w ith dyspneaf Percuss ion showedincomplete dulness throughout the entire extent o f the chest .
Auscultat ion revealed crepitant rales . The face and fingernai ls were cyanosed , the intelligence was unimpaired ,
'
but the
peripheral sens ibi l ity had almost d isappeared . The chest wascovered w ith cupp ing-
g lasses , and several hypodermic inj ections of quin ine were g iven. This alarm ing cond it ion lastedalmost twenty
- fourhours , when , at the moment a fatal issuewas expected , the sens ibil ity returned and every trace of pul
monary congest ion d isappeared as i f_
by mag ic. Cases pre
sent ing profuse hemorrhages from the lungs and nose havebeen . recorded but rarely .
The pathogenes is o f this cond it ion is not known , as therehave been insufficient post mortems . F rom analogy w ith findings in other forms of pern icious malaria these cases must be
attributed to accumulat ions of paras ites in the pulmonary capil
laries . Gries inger290 early compared the fill ing up of the lungthat takes place in these cases to the enlargement of the
Spleen .
Abdominal Forms—The representat ive type of abdominalpernicious malaria is the alg id . The reasons for class ing thistype as an abdominal form have been briefly stated when con
sidering the pathogenes is of the d ifferent varieties. The pic
ture presented is that of abdominal shock“; it is periton ismminus the periton it is .
Tort i believed that the alg id attack was merely the intensification of the cold stage of a malarial paroxysm. But thereare essent ial d ifferences. F irst , the alg id attack almost alwaysoccurs during the febrile period and does not correspond in
t ime to the first . stage . S econdly , in the cold stage of the ord inary paroxysm the pat ient experiences a sensation o f chill iness ;
2 14 THE STUD Y OF MALARI A
I n favorable cases the character of the circulat ion and respirat ion
_
improves , the body warmth is gradually restored , the
patient ceases to complain , and convalescence is impeded onlyby the
'
extreme weakness .
“ When,in add it ion to the symptoms of alg id ity already de
tailed , there ex ist symptoms s imulat ing true cholera,there is
the variety o i alg id malaria usual ly spoken of as choleraicpernicious. The onset is w ith pro fuse d iarrhea and vomiting .
The stools are thin and watery and o ften rice—water- like .
There_
may likew ise be shown the muscular cramps of the
lower l imbs frequent in cho lera.The temperature is usuallye levated and pains in the abdomen and preco
’
rdia and smgultus
may be experienced The urine isusual ly scanty and may. be
come suppressed.
The condit ion of algor w ith which drenching'
d iap-horesis
occurs“
const itutes the so- called sudoral or d iaphoretic formof pern icious fever. These sweats , which are so profuse thatnot only the clothing of the pat ient , but also the bedclothes aresaturated , usual ly supervene toward the close of a paroxysm.
The celebrated Torti , who was “himsel f the v ictim o f such anattack , says that he was just congratulat ing himsel f uponescaping the fever when the abundant sweats occurred to con
v ince him that his cond it ion was crit ical .I n the course of an alg id access s yncope occasionally occurs
when any exert ion , even the sl ightest , is attempted or whenthe pat ient ’s head is l i fted from the pi llow . This dangeroussymptom
”
usually comes quite unexpectedly , and i f the pat ientsurv1ves the first onset a subsequent one may rapidly provefatal .The gastralg ic or card ialgic type is characterized by excru
ciating pain in the abdomen,especially the epigastric region ,
or m .the precord ia. The pain is o ften so intense that the
patient doubles up and rolls in agony upon the bed. The
abdomen is tender and vomit ing is a common symptom. Theremay be hematemesis , sometimes pro fuse . D iarrhea and singultus are occas ional symptoms .
Whi le the ex istence of dysenteric pern icious malaria hasbeen den ied by Col in29 1 and more recently by Kanellis and Car
CL INI CAL HI STORY
damatis ,292the frequent occurrence of severe dysenteric
toms,due solely to malarial in fection , has been definitelj
onstrated by Craig .
293The attack may follow other"
for
abdom inal pern icious ‘
or may come on sudden ly . The
frequent act ions of bloody mucus , v iolent tenesmus , c
pains in theabdomen, e levation of temperature , and som
emaciat ion. A lg id symptoms are not common . Occasi
abundant hemorrhages from the bowels occur. The)
prove'
rap idly fatal , especial ly if “
the pat ient is alreadyedly anemic.
I cterus and bilious vomit ing are not rare in malarai
a rule, these are not gra'
ve s ymptoms, but there are ca
which the ir pers istence and intensity form a complex of
toms described as bil ious pern icious malaria.
“
The“
fe
usually high , nausea constant , icterus marked , and voi
of bile d istressing . Bile is present in‘
the urine , o ften int ities , and somet imes albumin . Epistax is and hemat l
have been noted . The epigastrium is often pain ful and stus may add to the d iscomfort _of the patient . Toward t]
of the severe cases there are apathy and carphology , a1scene usually closes w ith del irium and coma.
Waton290
observed a case w ith symptoms resemblingof periton itis. LaVeran" re fers to several s imi lar cases .
101294
treated 3 Cases 111 wh ich the clin ic picture was id iw ith that of acute periton it is . O ne case which he diagnoperforat ion due to typhoid ulcerat ion was operated upon .
operat ion proved a
'
mistaken d iagnos is. The blood was
ined ,malarial
_paras1tes found , and the pat ient rec<
promptly after the“
subcutaneous inject ion o f xyz gra:
quin ine.
Wol f ,2 9 5 Chamberlain , and Craig report cases pres
symptoms which would lead to a d iagnos is of appen <
Ford180
records 5 such cases , one of which was operated
and the append ix found to be healthy .
Ross and D an iels29 8 performed an autopsy on a mar
was not supposed to have d ied ofmalaria, and found a h
rhagic pancreatitis w ith extens ive massing of paras itespancreas. Parasites were also very numerous in the
2 16 THE STUD Y or MALARI A
laries o f the stomach and intestines , and these organs showed
extens ive necros is .
The ur1ne 1s usual ly highly colored . The amount varies
inversely w ith the quant ity of sweat , bow el movement , and
vom ited matter, the specific grav ity varies inverse ly w ith the
amount . Early in the attack albumin may be absent , thoughlater ' it .is often present in large quant it ies , . together w ithnumerous tube casts .
The blood in various forms of p ern icious malaria show s ,besides paras itic find ings p rev ious ly ment ioned , a pronounced
reduct ion of red ce lls , averag ing a hal f to one million per
paroxysm. Polychromatophi l ia of red cells may be observed .
Contrary tothe case of s imple malar1a, there is usually a pro
nounced leukocytos is . There may be as many as per
cm. Thayergsobserved a case o f the alg id type in which there
were. in number. The d ifferent ial . form'
ula usual inmalaria, the relat ive increase o f large mononuclear e lements
,
is maintained . Accord ing to Billet , 15 1 the average of thesecells is 10- 15 per cent . in 9 of _his 40 cases it varied ' from 2 0 - 2 5
per cent . , and in I case they ex isted in the proportion of 30 per
cent . Great numbers of these cel ls were p igmented .
HEM O GLO B INURI C FEV ER
Hemog lobinuric fever is known by many names , some of
which are mere localisms . Among them ore general synonyms
are : malarial hematuria,hemog lobinuric fever , swamp fever,
blackwater fever,bilious hematuric fever , melanur ic fever, etc.
A fter a severe chill the temperature rises rapidly and a
copious d ischarge o f red , almost black, ur1ne I S v01ded . The
pat ient complains of headache and pain in the loins and epigas
trium , and is afflicted w ith nausea and v io lent bilious vomit ing .
Thirst is torturing and insat iable because of the gastric disturbance . There may be more or less tympan ites . The l iverand spleen , especially the latter , may be . en larged and tender.
I n a few hours icterus beg ins and the pat ient soonbecomes as
yellow as a pumpkin. He is very restless and has an anx iousexpression . I f the attack is mild the durat ion may not be
2 18 THE STUD Y or MALARIA
the - cases the onset is w ith a rigor, usually intense and pro
tracted . S omet imes , as in ordinary malaria,the first stage is
obsci1re or wanting , and the attack begins w ith fever and
vomit ing . O ccas ionally the passage o f black water precedesthe other symptoms , as i n one of my cases
, where the pat ienthad had a mild rigor the day be fore , but felt well - enough toride out on horseback in search of his cow . While five mi lesfrom home he was dumbfounded at pass ing an abundance of
almost black urine . He immediately set out to consult me, andhad ridden six miles when he
“
was prevailed upon . to return
home. D eath from '
exhaustion occurred on the fourth day .
Rare ly the onset is characterized by v iolent pain in the abdomen . The intens ity of the onset is no guide to the severityo f the attack.There are four symptoms which are present in nearly all
cases . These are : fever , hemog lobinuria, icterus , and vomit
There is nothing characterist ic in the temperature . I ts usualrange is from 10 1
°
to 105°
F . Hyperpyrex ia is unusual ,though very high temperatures have been recorded . ThusM arsden
269noted a case in which the temperature reached
109°
F . Cases in which the temperature is normal or sub
normal throughout are not unknown ; for example , 2 reported
by Baldw in S eal .25 8 Ne ither'
o i these pat ients had taken any
quinine . As a rule , in mild cases the temperature reaches thefast ig ium Short ly after onset , from which point it drops progressively to or a l ittle below normal . I n other
'
cases it is '
intermittent , remittent , or irregular, and may resemble the
curve of sept ic fever. When rigors occur during the course ,
they are accompan ied by a rise of temperature . Periodicity isnot a consp icuous feature nor is the characteristic curve of
M archiafava and Bignam i seen . The average durat ion of the
fever is from a few hours to several days. I t usually out laststhe hemog lobinuria, but not in all cases. The height of the
temperature in hemog lobinuric fever is possessed of little or
no prognost ic import.A rare occurrence is the obst inate tenacity or subsequent rise
of the fever after hemog lobinuria has subsided. The durat ion


220 THE STUD Y OF MALARI A
press ion , and Kudicke'
observed 2 fatal cases in Which anuriapers isted thirteen days .
The color , o ften described as port w ine , varies from a
light claret to that of black coffee . The latter color obtainswhen the urine of a severe attack is examined in a thick layerby reflected light . I n a test—tube by transm itted l ight it ap
pears of a lighter co lor. The froth varies from yellow to red
d ish a greenish color is said to be due to the presence of bile.
The coloring matter is more o ften in the form of methema
g lobin , though oxyhemaglobin is found . I t is pr'
obably not
present in a true so lut ion , S ince 1t 15 more abundant in the
sed iment of a centri fugali z ed urine than in the Supernatantfluid , and d isappears from the latter first w ith improvement .The hemog lobinuriamay be interm ittent or cont inuous . S te
phens and Christ0phers1 18
observed that blackwater urine made
alkaline w ith potash and then boiled produced a purple color ,giv ing the bands of hemochromogen , Show ing that the urineitsel f contained reducing bodies . A . Plehn ment ions that on
boil ing the urine and al low ing it to stand for - some t ime a
bright purple color appears . O n stand ing an abundant d irtybrown ish sed iment is depos ited , the amount vary ingw ith theconcentrat ion of the fluid . The urine stains l inen a d irty red .
The - react ion is generally slightly acid , but may be neutral oralkaline . The Specific grav ity varies inversely w ith the quant ity . Albiimin is always present. I t 1s common ly in excess
of the hemoglobin and pers ists for a longer period , though thecurves run more or less parallel . S erum album in , albumose ,
globul in , and nucleo—albumin are found. Plehn5
g ives the
l im its o f_
quant ity as - 2 grams per liter , est imated accordingto Esbach ’s method . The w riter has very frequently observedtw ice as much as his max imum l imit , and in I of his cases the
amount was 14 grams with the Esbach instrument . S ome
urines ,on being boi led become almost completely sol id ified .
Bile is , as a rule , absent ; it is never present in proportion to
the polychol ia. I t was not found by the Plehns5 or._ by D an iels5 7in any of their cases . Urobilin is common. S tephens and
Christ0phers118
assert that it occasionally appears before the
attack , but more constantly after the oxyhemoglobin has dis


s somewhat larger than otherw ise ,'
and . that the excret
:xtended over a longer period of t ime in a regularly ir.ng and decreas ing curve wh ich is uninfluenced by the
globin content
.
of the urine . This 1ncreased excreti
luin ine in the urine inhemog lobinuric fever would lead.nference that the organ ism is not capable , as it usually) rotecting itself from the poisonous alkaloid by Splitti1
.n olecule . M archoux29 9 claims that hemog lobinuricI rine has no hemo lyt ic act ion on the red blood - cells of r.
) ersons .
O n microscop ic examinat ion the field appears littere <
1 brown ish amorphous detritus , the _products of brokenred blood corpuscles . Whole red blood—cells are not get
found and rarely in considerable numbers . Casts are
:lant , especially the granular ; also hyal ine and epit
These casts are somet imes almost covered w ith the gr:
pigment . Renal and vesical ep ithel ium are commor.
mucus and crystals of hemato id in ‘
may‘ be found . L euc
'
tyros in are rare . Wi lliams,
301 M ackey302 and Brem215
described d ifferent pecul iar bod ies found in the urine .
nature and S ign ificance of these bod ies are unknown .
There are often present ves ical tenesmus and pain ov
bladder. Retent ion of urine , burn ing in the urethra, ar
derness over the kidneys are not uncommon symptoms.
urine may be voided drop by drop.
A fter a few hours jaundice beg ins to appear and ,em
the mi ldest cases , deve lops rapidly unt i l the skin and
are of a pronounced saffron yellow . I t usually outlas
fever a few days . I tching of the skin is not common . l
[ S relat ively in frequent and petech iae are rare. The ocen
of the latter is said to imply a grave prognos is . Ede
anasarca may be encountered , especially in cases whereis unusual involvement of the kidneys . Sw eats may o
'
cct
222 THE STUD Y OF MALARI A
the decl ine o f the fever or w ith collapse . The skindry . S ometimes the perspirat ion is charged w ith bileBanks210 ment ions a pecul iar odor emanat ing“ from bl.fever pat ients . He claims that it enables one , toget
the express ion , to make a d iagnos is be fore the urineined . S o far as the '
w riter know s , he has not beenrated
“
, though in suppress ion cases a uremic odor ma“
ceptible.
Vomit ing is usually one of the earl iest symptoms
quently the most d istressing . A fter the stomach convo ided the vom it cons ists of a yel low ish or green bilesionally it is a grass
-
green or peculiar bluish -green , c
be very'
dark , almost black,somewhat resembling t
vom it of yel low fever. The vomiting'
is independertaking of food , and is “
probably more“
or less of centr:I n very mi ld cases v omit ing may be very 1ns1gn1
‘
:
absent . Nausea is usually in proport ion to the vomit i 'bowe ls may be const ipated or there may be a bil iousO ccas ionally the deject ions are thin and w atery ,
o f a
brown co lor,and may close ly resemble the urine.
This is thought to be due to the extravasation of l
binuric serum into the intest ine , and is usually S
cases on ly . D ysenteric symptoms are in frequent .rhage from stomach or bowel . is rare . M eteorism i
in frequent symptom . There may be severe colicy pai
abdomen . Pain is usual ly present in thes ep'igastric 1
over the l iver and spleen . These are usually tender, to ften g reat ly en larged , the l iver less so . The appet
but mi ld cases is completely lost . Thirst is intense ar
be allev iated for the vomit ing . The tongue is an t
heav ily coated . S ordes o f the teeth and l ips are o fteextreme cases. The sal iva may stain the l inen a t
yellow. The pulse is rapid , out o f proportion to theture , at first full and bound ing ,
later small and com
A hemic murmur , systol ic in t ime,is somet imes heard
precord ia , not transm itted Respirat ion is accelerate<is o ften sense of Oppress ion in the chest . D yspnea
prominent symptom , due to anemia or to edema o f t

224 THE STUD Y OF MALARI A
Christophers and Bentley h ave made interesting observationson the phagocytos is of red blood corpuscles in the spleen o f a
case of blackwater fever. I n a d ifferential count of
Spleen cells per cent . were large macrophages containingred cel ls and per cent . were small mononuclear cells con
tain ing red blood - cel ls . I n both kinds of ce lls were seen bloodcorpuscles show ing no ev ident alterations , corpuscles more or
less decolorized , and clear vacuoles about the s ize of red bloodcel ls . The closest scrutlny of the engulfed cells “failed to revealthe presence of paras iteso r other ev idence of parasitic invasion .
This extensive phagocytos is of apparently normal Ce lls is of
interest from the standpointI
o f pathogenesis. The plateletsare numerous and of large s i ze. The alkal in ity of the
“blood iso ften d iminished . I n spite of the d estruction of r ed cel ls thespecific grav ity remaIns relat ively high . This is . no doubt dueto the quant ity of material in solut ion in the serum.
“
D uringconvalescence the specific grav1ty falls. S tephens and Christophers
5 7
g ive the follow ing as the result o f their observat ion on
ton icity : “
I n blackwater there is occas ionally a remarkably lowtonicity r in other cases it has the normal value or somewhatraised value , as in malaria. The low or normal value in blackwater may be due , as we have prev iously suggested , to the factthat the weak corpuscles—those o f h igh tonicity—are de
stroyed , or it may be due to the fact that the tonicity of . the
corpuscles as a whole is changed after the l iberat ion of hemo
g lobin.
”The presence of malarial paras ites has been dealt
w ith .Blackwater fever is not a very pain ful affection , but the
vomit ing and th irst make the pat ient intensely w retched . Be
s ides the abdominal pains there are headache and aching of the
back and l imbs . He is usually terrified at the appearance of
the urine . His express ion is one of anx iety and apprehens ion ,
and a fear of death o ften se I Zes him . He is restless and irritable. I n chi ldren especially there is frequent toss ing of the
head from s ide to S ide . L ater there is prostration ,
’ intenselanguor, perhaps somno lence. Form icat ion and numbness inthe fingers and toes are occasional complaints . D elirium whenpresent is usually quiet . When suppress ion ensues the symp
CLINI CAL HI STORY
may be . typic of those in uremia, but this is not
t;delirium “
may be of the low , muttering variety ; co5 are o ften missing,“ and the m ind may be cleartly before death ,
'
when coma supervenes . T here m;
luntary discharge of urine and feces.
‘
rie causes of death are three : S uppress ion o f urine. exand card iac paralys is . Suppress ion is the comm
e. This sometimes takes place when the ur1ne is'
cle
alreadyclear. Uremic symptoms do not result fromsion in blackwater
‘ fev er as frequently as in other c
Th is is probably due to two caus es . F irst , eliminugh vomiting and purg ing is free ;second ly , metabolinished as the result o f deficient oxygenat ion . Exhat
sually the result of the tremendous destruction '
of btogether with inability of the hema
’
topo iet ic orgaz
the deficiency , or to pyrex ia. O ccas ionally hiccough.e in exhaust ion . The patient may die early w ith symt
lOCk or may l inger several days in a typhoid state . Ca
ly sis is usually due to thrombosis of the heart. P
rds this as. a common cause o f death . Goltmann
1ss18 9hav e Shown that in some cases of death from syr
exists a marked card iac nerve degenerat ion and e
.ders .
would mani festly be of great practical importance i)toms o f an impend ing attack o f hemog lobinuria 1
ec0gniz ed . This is possible , i f at all, only in a
ral way . Plehn says that an onset is to be f<
1 the pat ient has'
lived some six months in a blacks7
area and has had malaria at short intervals, wher.
ria has been treated improperly w ith insufficient quge , when he looks downcast , and perhaps show s a
us of the sclera and skin. This might , however , foreapse o f ordinary malaria. S omet imes , he further S
‘
occurs a certain depressed cond ition ,
~
a characte'
al apathy w ith phys ical restlessness , phenomena whic
to describe , but have often been encountered by one
een many cases develop.
I
Also the_ presence of albumi '
1d cause susp icion , as this tends to be'
absent in S i
2 26 THE STUD Y OF MALARI A“
tropic fever, even w ith a temperature of 4 1°
C . Koch des
ignates as“ blackwater fever c and idates those in whom a
few hours after taking quin ine the temperature mounts to
38°
C . or more,the urine becomes decided ly darker , and the
next morning amild icterus is ev ident. Ziemann‘i 8has fre
quently observed in blackwater fever cand idates the fol low ingblood changes , which, however, are not constant
1 . The more frequent appearance of decided basophile and
polychromatophile d egenerat ion of the . red ce lls.
2 . The rapid solut ion of the '
red -
cells in a salt Sol-ution ,in
which normal cells do not d issolve.
3. A decided d iminut ion of the coagulability of the blood.
This writer also regards urobilinuria as a valuable prognost icS ign.
Relapses are not in frequent and several may occur , o ftenbe fal ling the patient when he is thought to be do ing we .ll I t
may be d ifficult to d istinguish relapses from recurrences .
Convalescence may very properly be regarded as the d iv idingl ine , those occurring during convalescence be ing cons idered as
relapses and those later as recurrences . Plehn bel ieves thatrecurrences are rare un less provoked by quin ine. O f e ighteenrecurrences recorded by V edy
m One occurred after less thanthree months , fourteen from three to -six months , two from S ix
to twelve months , and one longer. I t is remarkable that n inerecurrences happened just three months fro-m the date of the
last attack . The w riter ’
s experience has been that in personshav ing more than one attack the attacks are more o ften separated by intervals of a year or more .
Complications and S equoia—These are singularly few in .
variety . Nephrit is in some degree is an almost constant com
pl ication , and may cause death from suppre ss ion during the
attack. I t may heal in a remarkably Short t ime . As a sequelait is not in frequent and may pers ist for days or w eeks , caus ings low and incomplete convalescence or death . The changes in
the kidney may be attributed to the irritating effect of hemoglobinuric urine and to the pyrex ia.
I n 16 cases .the w riter has been able to make examinat ionso f urine at periods varying ‘
from a few days to fourteen years
228 THE STUD Y or MALARIA
CHRONI C MALARI A
There I S a great deal of confus ion as to what is compre
hended by chronic malaria. M uch of this chaos is due to
includ ing the manifestations of malarial cachexia w ith those
o f chron ic malaria, between which , however , there are essen
t ial d ifferences . Chromc malar ia impl ies a supply of v italres istance equal to the demand ;malarial cachexia denotes an
exhaustion o f this supply . Chron ic malaria I s an antagon isticequi librium between pal asite and host ;cachex ia, a 1uptuI e of
equi l ibrium. Chron ic malaria is a confl ict , cachex ia a con
quest . The relation betwe en chron ic malaria and cachex ia hasbeen 'fitly compared to that existing betwe en a - compensated
heart lesion and broken compensation . Chronic malaria is an
active form o f malaria, cachexia is a sequel . Cachex ia beinga sequel , usual ly of chronic malaria, it may be d ifficult to say
where "
the influence of the latter ends“
and the former beg ins .
Onthe other hand , it is frequently d ifficult or impossible to
d ifferent iate between a relapse in chron ic malaria and a re
ihfection.
For conven ience of study , chron ic malaria may be div idedinto a latent or pass ive stage and an act ive “
stage , or Stage of
re lapse.
I t is more frequently observed in r
'
children . I t has alreadybeen shown that the frequency w ith which children nat ive tothe S oi l are in fected constitutes the true end emic index o f a
local ity .
Ch i on I C mala11a may be“due to one infection , but occurr ing
chiefly in reg ions whe1e repeated I einfection is poss ible , it ishighly p l obable that 1einfection I s an important factor.
An analysis by the w riter of a la1ge number o f cases Show sthe follow ing results :Quartan and tert ian in fect ions are mo I e
prone to relapse than estivoautumnal . The percentage of
1elapses to total number of cases of qua1tan , tertian , and-
est ivoautumnal is , respect ively , 65 , 55 , and 45 . The pert inacity of
quartan may be regarded as a conservative effort o f nature toperpetuate the Species. I t is , indeed , remarkable how this formo f the parasite “
is conserved in certain places where it is so very
rare . However , the greater tendency to relapse Shown by the

Parthenogenes is is the bridge across the gap cause
rupt ion of the schizogon ic cycle .
The most frequent course is for chronic malarione or more acute attacks. I n some instances, hclatent stage may precede the act ive . Thus it is not
rare to me et cases w ith ev idences of chron ic mal
have no history o f act ive mani festations.
The latent stage o f chronic malaria resembles I ]spects a period of incubation ; in fact , the case
w ith unduly long stages of incubation are doubtle
but latent stages of the chronic d isease . Duringstage paras ites may or may not be found in the
blood.
Symptoms during the latent stage may be altoget
in wh ich case latency is absolute , or there may be p
tain Symptoms , subject ively ins ignificant , constitutilatency . These symptoms are ordinarily S im i lar tdromata of acute malaria : malaise , loss o f appetite ,the back and legs , d igest ive d isorders , etc.
, tog t
anemia and enlarged Spleen. L atent malaria is thevery numerous in fect ions , and is o f the utmost i
from the v iewpo int of prophy lax is .
The duration o f latency is exceed ing ly variable.
occur at short-er or“
at longer intervals.
Relapses at Short intervals h ave been recogniz ec
t ime of Hippocrates. L ater the septenary periods 1
for a tendency to Show relapses , . and this idea is S
prevalent among the laity . This shorter intervalcorresponds more -or less closely to the sexual cyparas ite and to the period of incubation . I t isalso ll
230 THE S TUD Y“
OF MALARI A
w ith the law “
o f Tre i lle3°4 and w ith the Stud ies of Cohenupon the period of freedom from paroxysms follow ing a S ing leinject ion of quinine. The duration wof this period is from five
to twenty- one days , o ftenest from five to ten . Relapses at
shorter intervals occas ionally exhibit a striking period icity .
Relapses at longer intervals occur at from one to twe lvemonths, exceptionally longer. Very long periods o f freedomhave been recorded , even up to s ixty years .
306Undoubted ly
many o f these are errors , due e ither to mistaken d iagnos is or
to the occurrence in the interval of unrecogn ized or' masked
paroxysms . How ever, periods as long as three years havebeen re l iably . recorded .
4 8
I t be ing clin ically imposs ible to dist inguish between a re lapseand a re in fect ion , the writer has adopted Celli’s80 rule , it be ingequally adapted to the seasonal prevalence of malaria in thiscountry . This authority regards as a relapse every case o f
fever I ’Vh'lCh repeats itsel f in the same ind iv idual during the
ep idemic year of malaria , from July of one year to the end
Of the follow ing June. I t is true that this may include some
cases of re in fect ion ,but it is unquestionably ,
the most pract icalguide and el iminates a max imum of error.
S econdary et iolog ic influences play a much more prominentrOle in re lapses than in primary in fect ions . O f these the most
important are change of res idence , fat igue , abuse of alcohol ,exposure , and gastro
- intest inal d isturbances . All are fami liarw ith the frequence w ith which a change of reS 1dence
“ bringsthe malaria out .
” These influences are much commoner factorsin the relaps es at long intervals than in those at Shorter intervals .
I t is ord inari ly the relapse that brings the chronic malarialto the phys ician. The relapse may cons ist of one or more
typic malarial paroxysms or
'
they may be atypic . Very - o ftenthe first stage of the paroxysm is wanting. They may exhibitquot id ian , tert ian , or quartan period icity , or may be altogetherirregular. The pat ient usually rhas an anemic t int and may ,
in
advanced cases , be jaund iced . O ccas ionally the complex ionmay be earthy , a t other t imes bronzed . The skin is dry and
o ften scaly . The eyes may be deep set ;they often bear a hag
232 THE STUD Y OF MALARI A
not a rare cond ition 1n chron ic malaria, and ep istaxis is some
t imes profuse.
D igest ive d isorders are v ery common and marked meteorismmay ex ist . The cond it ion o f the bOw els 15 not constant , d iarrhea somet imes alternat ing w ith const ipat ion . D ysentericmanifestat lons are frequent .The
.
spleen may be of normal proport ions in m ild cases , but
is usual ly enlarged ,somet imes enormous ly so , pass ing the
med ian line of the abdomen and the i l iac crest .“
I t may ormaynot be tender or painful ;in the former.
_
case the pa1n 1S usuallyof a pul ling nature and re ferred to the le ft Shoulder. I f perisplen it is With adhes ions does not o ccur the Spleen may be
movable or float ing .
“
O ften the Spleen en larges during the
act ive stage to recede slol dur1ng latency . The liver is oftenS l ightly en larged and tender.
Headache , nervousness , rest lessness , v ert igo ,insomnia, and ,
Severe cases , impaired memory , are observed . The urine iso ften album inous .
M ask ed M alar ia—M asked or larvate malaria, l ike pern icionsmalaria, needs complete overhaul ing . Nearly every dis
ease in the '
category has been confounded/
With malaria and
classed as larvate . This heterogeneous group has been ex
panded to embrace d iseases unrelated in any way to malaria,d iseases complicat ing malaria ,
and symptoms and sequela of
malaria. The frequency of masked malaria varies inverselyw ith the care employed in d iagnosis . M asked malaria is merelyatyp ic malaria. The symptoms be ing o f little value in diagnosis, this must be made by the anamnes is , the microscopic ex
aminat ion of the blood , and by the therapeut ic test . Nervous ,
gastro- intest inal
,and cutaneous d isorders are those most fre
quently recorded as masked . M ost o f these are to be consid
ered under Compl icat ions and S equelm.
COMPLI CATIONS AND SEQUELZ’E
Circalatory S ys tem .—M alaria is very frequently complicated
by heart d isorders . I n the negro population of the S outh ,in.
whom syph ilis , abuse o f alcohol and tobacco , pneumonia, and
other etiolog ic'
factors are ve ry prevalent , lesions of the Cir

CLINI CAL HI STORY 233
rstem, part icularly valvular les ions of the heart , oftengrav ity of severe.malarial infect ions . These are toed almost invariably as complicat ions and not as
Circulatory les ions , the d irect result of malarial inremarkably rare . M any such cases were repo rted
d iscovery of the parasite , but are for this reason
valueless .
found card iac hypertrophy in 6 of 6 1 , and Kelsch” 8 in 34 of 80 autops ies on malarial subjects . I t 18 ,
)y no means certain that malaria was respons ible fo r‘
ophy in these cases.
y the commonest card iac Sequel of malaria is myoSlight ev idences of degeneration of the heart musclemes found after death in cases which presented no
during l i fe . Triantaphyllides31 1
Observed 2 6=
cases
:oms of~myocarditis in cases of malar1a ;theselieves due solely to malaria. The cases of So—called>rais follow ing malaria are probably cases o f myo
) ilatation may fol low myocard it is . L ocalizat ions o f
1 the blood—vessels of the heart have been ment ioneddering pern icious malaria.
pectoris I S occasionally observed in connect ion w ithit may ex ist as a complicat ion or as the card ialgic'
n icious malaria.
ras formerly w ritten about malarial endocarditis ,d endarterit is . These occur but rarely and on ly as
ms . Ulcerat ive endocard itis has occasionally beenfter pneumon ia compl icat ing malaria. I t Should beind that the“
temperature o f sept ic endocard it is may.
0 that of malaria; Pericard it is and aort ic aneurisml compl icat ions . Phlebit is and thrombosis have been
234 THE STUD Y or M ALARI A
to malaria, especially during t mseasonable w eather. Bronchit isis a common compl ication , during a portion of the malarial“
season occurring w ith marked frequency . I t is observedo ftener in the negro than in the white race . S ubacute or
chron ic bronchit is is usually in chron ic malaria and cachex ia.
Ziemann reports the case of a healthy young man who , dur
ing an attack of est ivo—autumnal malar ia , was afflicted . w ithinterm ittent spasm o f the laryngeal muscles . The spasms
co incided w ith the malarial paroxysms, parasites were foundin the blood , and both the
'
malaria and the laryngeal troubley ie lded promptly to quin ine .
A pecul iar cond it ion of the pulmonary ap ices has been described . I t cons ists of a rap id and a trans ient congest ion of
the apex o f one or both lungs , aris ing_
and d isappearing w iththe paroxysm. The cough is dry and pain ful , the expectorationis scanty , occas ionally bloody , and there may be bronchialbreathing and increased vocal fremitus . The w riter has hadno experience w ith this compl ication.
Pneumon ia was long considered a man i festat ion or a sequelo f malaria , but it is now known that they are ent irely d ist inctd iseases .
Either lobular or lobar pneumon ia may compl icate malaria,
the latter more frequently than theformer. L obar pneumon iasomet imes occurs w ith acute malaria, but much more com
monly w ith chron ic malaria and cachex ia. I t is probably themost frequent mode of ex it of the cachect ic, in whom the
pneumonia o ften assumes the low form and is especially l iableto compl icat ions , as delayed resolut ion , gangrene , abscess , andpyothorax . Pneumon ia compl icat ing malaria is apt to be
atyp ic, though the pneumon ic symptoms usually predominate .
Both lungs are more apt to be affected , pro fuse hemoptosis
occasionally occurs , and malarial paras ites may be found inthe expectorated blood. F ibroid pneumonia somet imes com
pl icates malarial cachex ia. The prognos is in malaria compl icated w ith pneumon ia is grave.
P leurisy 18 not a common compl ication of palud ism. I t has
been maintained312 that the enlarged spleen , especially i f perisplenit is ex ists , pred isposes to inflammation of the left pleura ,
236 THE STUD Y OF MALARI A
paludism. O f these by far the most common is the Ascarislu
’
mbricoides . Uncinariasis is not an in frequent compl icat ionin
“
some sect ions . The writer has observed an infect ion w ithHymenolepis maria associated w ith malaria. I t is not improbable that intest inal he lminthiasis aggravates the anemia and
the gastro—intest inal and nervous symptoms . I n examining
the blood'
f or the malarial paras ite the presence of eos inophiliacalls for an exam inat ion of the feces .
C irrhosis of the l iver, the d irect result o f malarial in fect ion ,
described as relat ively frequent in certain_pO I
‘
t fl S'
O f the
tropics , appears to be rare in th is sect ion . Hypertrophichepatit is may result from prolonged infect ion . Ascites occa
sionally develops , particularly in chron ic malaria and cachex ia.
The Blood and S pleen—L eukemia fol low s malaria on lyrarely , probably nev er as
_
a true sequela. I n 124 cases of leukemia M oS ler
79determined that on ly 8 or 10 bore any etiologic
relation to malaria._
M archiafaval
and Bignami22 observed a
case Of splenomedul lary' leukem ia in an adult male , aged
twenty—e ight. The symptoms Were enormous enlargement of
the Spleen and l iver, d iarrhea, and grave anem ia. The case
had been diagnosed malarial cachex ia. Bast ianell i6 7 Observed a
S imi lar case . Ziemann48
treated a case in the ten -
year- old
daughter o f a Duala chie f ; the g irl had suffered repeated at
tacks oi malaria, and pigmented leukocytes were found in theblood . S akorraphos
79des cribed I O cases of leukemia in per
sons who had formerly l ived ln malarial local it ies . However ,
the blood examination showed no parasites nor was there any
elevat ion of the temperature Brown79saw a case of lymphatic
leukem ia fol low malaria. The w riter has had no experiencefavoring an et iolog ic relat ion between leukemia and malaria}The relation -
o i splen ic anem ia (Bant i ’s disease ) to malariais not clear. Two o f Hemmeter
’
s314
cases follow ed‘
malaria,
and of 15 which O sler316 observed malaria preceded 5 . Cohen
and Rosenberger-31 5
observed a case“
of chronic malarial infect ion w ith Spleen and blood lesions closely resembling those of
Banti ’s d isease . I njections o f quin ine and urea w ere used w ithgood results . S plen ic anemia may come into consideration in
d ifferent ial d iagnos is .
CLINI CAL HI STORY 237
M alarial Cachexia.—I h. this cond it ion the paras ites have
obtained und isputed possess ion of the host. The defens iveforces have been completely conquered , the blood - making or
gans can no‘
longer meet the demands made upon - them,and
tox ins , unopposed , work changes, often irreparable, in important organs . Cachexia has been classified as dry or humid ,accord ing to the absence or presence of anasarca, and as acute
or chron ic. Acute cachex ia is characterized by a rapid onset
and development of symptoms , and usually, follow s acute malaria , occas ionally after on ly one or two attacks . These cases
are infrequent. Chronic cachex ia,the usual form,
is a sequela .
o f chron ic malaria.
M alarial cachex ia is found where the severe forms of' mala
ria are endemic. I t may be stated as a general rule that thefrequency of cachexia among the wh ite race is an index to theprevalence of grave in fect ions . I t ismuch more common in
the white race than in the negro . Wh ile .negro ch ildrenare
not in frequent ly the subj ects o f malarial cachex ia,it is much
rarer in the adult negro . O f adults , males are more common lycachect ic than females ;among children the proportlon 1S abouteven . The cond it ion rare ly develops in persons o f. the betterclass , but is seen in those liv ing under improper hyg ien ic con
d itions and who neglect the treatment o f acute malaria.
Caseso f cachex ia developing w ithout preced ing malaria havebeen reported , but are subj ect to quest ion . The malaria may
have been unrecogn ized , as might happen w ith latent or maskedinfect ions . I n reg ions where kala—azar is endem ic it is on lyrecently that th is d isease has been different iated from malarialcachex ia. I nfect ions With the est ivo—autumnal parasite-
s are
fol lowed by cachexia much -more frequently than tert ian and
quartan in fect ions.
The cachect ic usually presents aS ingular appearance . The
emaciated limbs are in“
marked contrast to the big belly , and
the features are aged beyond the years . The most pronounced
phenomena are the anemia and the_
enlarged'
spleen . The red
blood - cells may be reduced to seven or e ight hundred thousandper c.mm. The leukocytes are generally normal in numberor a l ittle below . Numerous different ial counts have shown a

238 THE STUD Y OF MALARI A
relat iv e increase of the large mononuclear elements . The red
Cel ls '
may Show basophile degeneration, polychromatoph il ia,poiki locytos is , and nuclei , but none of these changes are by
any means constant . Accord ing to my experience paras itesare rarely found in the peripheral blood. The spleen often
extends to the umbilicus and to the crest of the i lium, some;
t imes beyond. I t is usually hard and“
the anterior border presents a Sharp edge . Pain and tenderness on
“
pressure are not
always felt. O ccas ionally a bruit 'is . to be“
detected over the
Splen ic area.
The pulse is small , compress ible , and may be irregular. Pal
pitation o f the heart and hemorrhages , especially ep istax is ,may occur. An anem ic murmur “
over the precord ia is often
heard .. M yocard it is and d ilatat ion are not in frequent . The
breath is Short, somet imes amount ing to actual dyspnea. A
cough is common and s igns of bronchit is may be el icited . Pul
monary edema - is a late symptom.
The temperature may be normal or subnormal for longperiods , though even ing rises are o ften observed . .Typ ic paroxysms are not frequent. Fever o ften follow s imprudences.
Whether the fever o f cachex ia is due d irectly to parasit ic activity or to organ ic changes is not defin ite ly known. The appet iteis generally poor and the d igest ion tardy . Epigastric pain,
nausea,and vomit ing may be complained of. The tongue and
oral mucous membrane are pale.
'
D iarrhea'
and dysentery fre
quent ly occur. M eteorism is common . The l iver is usual lysomewhat enlarged at first ; later it may become atrophic.
Ascites is not a rare man i festat ion . When fever ex ists theurine is ord inari ly scanty and highly colored . D elayed development of the gen itals is common in the young and d iminished
'
sexual pow er is n ot rare in the adult . I nd ifference , intellectual torpor, somnolence , headache , and vertigo are observedin cachectics . Resistance to cold is lessened and rheumat icpains are experienced . The Skin is pal lid , dry ,
and rough ,and
may exhibit sores or purpuric spots . Anasarca may supervene .
Pneumon ia, dysentery ,hemog lobinuric fever, and nephritis
are common complicat ions of cachex ia, and amyloid degenerat ion , especially of the kidneys , an occas ional sequela. Peri

CLINI CAL HI STORY
splen it is occas ionally occurs and may be the cause of S 6
pain ,- especially if adhes ions take place. A heavy spleen
cause relaxat ion of its supports and become“ float ing” or
dering .
”This cond it ion is seen more often in multipa
females . By pressure on neighboring organs a wandc
Spleen may cause pain , d igest ive d isorders , or ~even intesocclus ion . The ped icle may become tw isted , as occurred
fatal case of M archiafava and Bignami? 2Rupture of the spleen is an infrequent compl icat ion of n
rial cachex ia. I t is very rarely associated w ith acute mal
though a case has been recorded by Palmer“ 7 in which rui
occurredWithin seven days of the onset of the fever.
writer observed a case in a subject of cachex ia who h;large, hard Spleen . Recovery followed , notw ithstand ingtens ive hemorrhage . I n some countries , especially in I 1
rupture o f the Spleen has assumed med icolegal importAccord ing to Brault, 3 18 it is popularly known in Kharkovthe malarial spleen is very friable , and that combatants engin fist fights strive to strike the reg ion of the spleen , w iti.result that 5 per cent . of the official autops ies Show rupt
of this organ . The rupture may be Spontaneous or the n
of blows and falls . O f'
19 cases - of rupture of the mal;
spleen co llected by M esserer3 19
15 were Spontaneous and
4 the result of trauma.However, 35 cases stud ied by Russwere due to trauma, and no cases of spontaneous rupture I
noted. A large , so ft spleen is'
much more l iable to rupture
1 hard one,and fatal hemorrhage is more apt to occur in
former case. A ful l stomach pred isposes to Splen ic rupt
especially of the concave -
s ide. The capsule is usually ruptt
)ut when thickened , as may result from prev ious perispler.t may escape untorn. The capsule was not ruptured in
1 of Russell ’s9 5 35 cases . The'
laceration occurs w ith a'
qual frequency on the Concave and convex s ides of the Sp]Fears of the inner aspect may occur w ithout marks of '
v iol:
) f e ither the skin or the convex surface o f the spleen . A li
;harp blow tends to injure the convex surface ;a fal l or cr'
.ng blow , the concave s ide . The symptoms of rupture of
pleen cons ist of v iolent pain in the splenic reg ion referre
240 THE STUD Y OF MALARI A
the le ft shoulder,together w ith ev idences o f shock and hemor
rhage . The mortal ity of cases not treated w ith Splenectomyis exceeding ly high. D eath may o ccur in from a few hoursto five days .
Abscess of the spleen is a rarer complicat ion of malaria even
than rupture . The Writer i s able to co llect from the literaturement ion of not more than 50 cases . The common pyogen iccocci and the bacillus coli commun is are the bacteria usuallypresent in splenic abscesses . The symptoms
—are somet imes as
vague as those of abscess o f the l iver. There may be pain inthe left hypochondrium , especially i f the abscess is superficialand the peritoneum “
is invo lved . The pain is o ften re ferred tothe le ft Shoulder. Pain may ,
however,be ent irely want ing .
The temperature is usually e levated , though in I are instancesmay be normal or subnormal. I t is usual ly intermittent and
associated w ith ch i lls and sweats . Emaciat ion may be extreme ,
notw ithstand ing the appet ite is somet imes voracious . Abscesso f the spleen may be con fused w ith uncompl icated malaria, and
renal , gast1ic , or pancreat ic d isease . The presence of leuko
cytos is and the therapeut ic test are valuable d iagnost ic points .
S ignore ll i ’s spleen point may be a useful guide . This is a
pain ful area correspond ing to the fifth intercostal Space near
the left n ipple . The examinat ion of the urine may mislead .
I n a case o f splen ic abscess observed by Goltman320
the urinecontained albumin, casts , pus cells, renal cells , and some red
blood—ce lls . Aspirat ion is attended w ith“
some danger, but may
be done as a last resort , especially i f the pat ient is prepared foroperation . The abscess may rupture externally into the pleuralcav ity or lung of the left s ide , or into the stomach , intest ine , orperitoneal cav ity . Without operat ion the prognos is is very
grave ; w ith t imely incis ion and drainage a cons iderable percent . recover.
I n farcts and gangrene of the spleen are noted among the
rare complicat ions of the spleen in malarial cachex ia.
Genito—i irinary O rgans . Nepli ritis .—The frequency of ne
phritis recorded as a sequela of malaria varies greatly w ithlocality , type of fever , and w ith the ' idea o f what const itutesnephrit is . Thus , while Ford
l s"observed acute nephritis in
242 THE STUD Y OF MALARI A
cl imate, or other factors .
“
Dupreym '
has recently describedthree cases o f Impotence follow ing est ivo - autumnal fever.
M etrorrhag ia and , more o ften , menorrhag ia and amenorrheaare not in frequently seen w ith malaria. S terility has beencharged to palud ism.
I t was formerly bel ieved that pregnancy con ferred a degree
of immunity against mal-aria. This is now known not to be
true. I f the pregnant woman is attacked less o ften w ithmalaria it is because she is less often e xposed to in fection and
not on account of any immun ity which pregnancy con fers uponher.
A l ist of cases is appended to g ive an idea'
of the frequencyw ith which abort ion and premattI re . labor occur as the resultof malaria complicat ing pregnancy . The first c olumn of. fig
ures record s the number of cases I n w hich the complicat ionappeared ; the second column Show s the number of abortionsand premature labors wh ich occurred
Pascali
Weatherly , I n I ndia . .
Weatherly , in EnglandWeatherly , in A fricaWeatherly , in Florida
Hospital, Rome
Lwow’" 3
Goth324
Bonfils
Williams
This percentage is at least tw ice as large as that resultingfrom my experience .
The w riter is incl ined to the“belief that the negro 1s much '
less liable to suffer abort ion or premature del ivery than is thewhite . This is in keeping w ith the well—known relat ive immun ity of the negro to some o f the effects o f malaria. M er
cierl s zhas observed an unusually large number.of abort ions in
Creole women in fected[
w ith malaria. I t is .Well known thatthis race is markedly suscept ible to the s everer forms o f
malaria.
Cases accompanied by continued high temperature , retching ,
and vomit ing , and which are more res istent to treatment , are
CL INI CAL HI STORY
those in which abortion most frequently occurs.
follows that abort ion is more often due to est ivofever than to tertian and quartan ,
and to mult iplethan to S ing le.
The danger of abortion and premature del iveryin proport ion as the pregnancy is advanced . Thus Oi19 cases expuls ion of the uterine contents occurred
the fourth month , once in the fifth month , three tins ixth month , five t imes in the seventh month , and r
in the eighth month .The factors in the interruption of pregnancy are
fever, retching , vomiting , anemia, and tox ins . I t -i
improbable that in some cases paras it ic localiz atiO '
uterine vessels excite pains or cause placental sthough for this theory there is as yet no patholog ic prI f the malarial in fect ion cities not terminate the I
the labor at full term is apt to be S low , especially the f.Children born at full term o f malarial mothers are
smaller and l ighter than normal , and the mortality is 1L abor o ften rekind les latent malaria
,which , in
perium,is not in frequently atypic, the first or third
the paroxysm or complete intermission of the ter
Sometimes lacking. S ubinvolut ion , postpartum her
and suppression ofmilk may occur w ith puerperal mNervous S ys tem .
—I t is o ften impossible to 1
whether nervous man i festat ions in malaria are com
or sequelae. I t is certain that many cases reported
malaria are purely complicat ions. This is the case 1
t' iple neuritis , o f wh ich numerous cases have been as
malaria. I n by far the majority of cases the exi
malaria was not established by blood examination ;it is not certain that the neuritis. was due to malaria.
Glogner,327
r
in the East I ndies , described 6 cases of
ritis occurring during and after malarial disease. I
the parasites were found in the blood. The chie fwere d iffuse pains in the lower l imbs, formication , t.
of the nerves and muscles , and motor weakness , whilereflexes were sometimes intact , somet imes abolished .
244 THE STUD Y OF MALARIA
tric excitability of the nerves and muscles was d iminished,while sens ibil ity was retained . Edema of the legs was present
in some o f the cases .
Price328 records a case in a g irl , e ight years old , who fol
low ing malarial in fect ion , had mult iple neurit is which lastede ighteen mOnthS . Her symptom
-S were pain , paresthes ia, handtremor, w eakness of .the extremities , w ith characterist ic footdrOp . Estivo4autumnal paras ites w ere detected on blood ex
amination ,and quin ine effected a cure.
“
Ziemann"‘ 8
observed a Case o fperipheral neuritis in '
a young
German merchant who had been in Cameroon four months .
Two 'days be fore his entrance into the hospital he Was takenw ith “ high fever w ithout a preceding cold stage. S imultaneously he noted almost complete paralys is o f both legs , espe
cially of the right . Neither the bladder no r
“ bow el funct ionsw ere affected , nor
'
was there marked sensory disturbance .
The temperature did'
not exceed 103.5°
F . The peripheralblood showed an enormous number of est ivo - autumnal parasites . While the -
paralysis of the left leg pers isted Only a fewdays during convalescence
,that of the right leg was slow in
d imin ishing , notw ithstand ing massage and’
electric. treatment
for several w eeks , so that at the end of four months the pat ientwas sti l l compe lled to walk w ith the aid of a stick .I t is not in frequently d ifficult to d ifferentiate between poly
neurit is and myel itis .
L averan1“
descri bes a case o f parapleg ia which he Observed inConstant ine . The patient had had several attacks of malariaand underwent a re lapse after adm iss ion to the hosp ital , duringwhich the paras ite was found on microscopic examination .
The paralys is of the lower l imbs was not accompanied by any
alterat ion o f sens ibil ity nor of nutrition , and micturition and
de fecation were normal . Unfortunately for an exact d iagnosisthe patient had had syphilis also. M ercury and potass iumiod ide were prescribed w ithout appreciable result. Quininecaused a d isappearance of the paras ites , but had
'
no effect on
the paralys is .
A fatal case show ing parapleg ia was treated by Ziemann .
The patient was a strong negro man . Bladder paralys is , re
246 THE STUD Y or MALARI A
The Sclerotic les ions are said not to have resembled those dueto syphilis , and the symptoms are bel ieved tohave been dueto the paras it ic thromboses of the
“
capillarles and not to the
scleros is .
Hem ip leg ia, parapleg ia, and various monopleg ias , e ither w ithor . w ithout aphasia or sensory d isturbances , are not infre
quent ly associated w ith malar1a.
Cerebellar syndromes“
are rarely observed in malaria, Theycons ist of general weakness , rig id ity ,
and pain in the back ofthe neck, intense headache;atax ic gait w ith a tendency to fal lbackward and to the left , tremors , incoord inat ion of move
ment“
, dysarthria, nystagmus , and vomit ing . The tert ian paras ite is usually present in these cases.
Bulbar symptoms are occasmnally encountered . Such are
hypoglossal and facial paralys is , atax ia of arm,dy
'
sarthria or
anarthria, and staggering gait. These symptoms are usual lyobst inate.
Various psychoses occur in connect ion w ith malaria, e itherduring or follow ing acute or chron ic malaria. The commonest
of the se d isorders are weakened memory , melanchol ia, man ia,and delus ional insanity . Suicidal and erotic tendencies may
be observed. Below are brie f notes on 4 cases under the care
of Ziemann333 in Cameroon
I . A merchant , thirty - six years of age , slender , pale , w itha history o f neurasthen ia but not
'
of alcohol ism, l iv ing in a very
unhealthy local ity , but us ing no prophylact ic quin ine , hav inghad several moderate and light attacks of est ivo - autumnalfev er
, was suddenly seized w ith - a-
v iolent paroxysm . D uringthe seizure he had strong delus ions of persecut ion. He se izedhis gun in order to shoot down the ne ighbors whomhe thoughtpursuing him. Energet ic quin ine therapy was followed bycomplete cure excepting that the idea that the neighbors hadpersecuted him during the n ight of his i llness pers isted.
2 . A strong young merchant,w ith no hered itary taint nor
alcohol ic history , not hav ing employed quinine pro'
phy lactical ly ,
had an attack of est ivo - autumnal malaria. D uring'
the access
he d ist inctly heard the voices o f his father and other relat ivesin Europe , and conversed With them upon his prospects in

CLINI CAL HI STORY 247
omplete cure fo llowed the admin istrat ion of
the fixed idea that his relat ives had v is ited him.ess and that he was more quiet , pecul iar, and
He was returned home on the failure of his
merchant had been in Cameroon two years en
’ditions for the purpose o f obtain ing rubber.
xpeditions he did not u'
s'
e quinine as a prophy1 he suffered repeated malarial attacks . O n a
7 merchant he was-
suddenly taken w ith a paroxllCh he d ist inctly saw an arm extended
“ from the
L'
revolver aimed at him. S e ized w ith terror, he'
om be ing murdered. Quin ine cured the fever,
)n of the arm and the revo lver as to that parrsisted .
young merchant of healthy fami ly and w ithoutDholism or nervous d isorder was se ized three°ival in Cameroon w ith a severe est ivo - autumnal 'ring the attack he labored under the delusionfues , who in real ity nursed him attent ively ,
had
him. After energetic treatment w ith quininee .was effected except ing the persistence of the
ersecution by his colleagues.
not a rare phenomenon during palud ism. I t is
Sult of anem ia in pred isposed persons. As it
ther of a multitude Of forms , its chie f signifithe v iewpoint of diagnosis.
asthen ia is probably due d irectly to malaria inand preex isting neurasthen ia“
is o ften aggra
ial infect ion. The usual symptoms are restless:ss , insomn ia, and annoy lng d ist inctness of the
etiring .
tr‘ iv bel ieved that intercurrent malaria exercised

THE STUD Y OF MALARIA
The Eye—I nject ion of the conj unctiva'
is not infrequentlyassociated w ith neuralg ia of the fifth nerve . True interm ittent conjunctiv it is occurs but rarely i f at all. Both interstitial and dendrit ic keratit is are occas ionally ;
observed w ithmalaria, though it is doubt ful whether either form can be
attributed to malaria. The same prob-ably holds true for
ves icular“ kerat it is or the so- called cOrneal herpes. I n pernicious se i zures w ith coma- v ig i l the eyes are more or less ex
posed todamage .
I rit is ex ists as a compl ication“
of malaria in rare instances .
Choroid it is occasionally occurs in connect ion w ith ret in it is .
O ptic neuritis is observed chiefly in cachectics..
"
I n the maj orityof case s it proceeds to atrophy .
Ret inal hemorrhages ar'
e o ftenest minute and located farforward , hence they may be eas i ly overlooked. O ccas ionally ,
how ever,they are peripapillary or macular and o f large S ize .
I n the latter case the prognosis ismore serious. Persistent orperiod ic amaurosiswithout ev ident ret inal changes is somet imes
se en. The w riter has seen one case of hem ianop ia fol low ingpern icious malaria of the comatose form which terminated incomplete restorat ion of V I S I On . Rarer opt ic mani festat ionsoccurring in conjunct ion w ith malaria are hemorrhage and
infiltrat ion into the v itreous humor.
The Ear .—O talg ia,
labyrinthine vert igo , ot it is med ia, and
les ions of the internal ear and auditory nerve have been de
scribed as occurring w ith malaria, but in no case has the bloodbeen examined .
The Senses o f taste.
and sme ll are said to be'
d iminished or
abol ished in rare cases of malaria.
The S kin—The frequency w ith wh ich herpes occurs in
malaria has already been ment ioned. Next to herpes , urt icariais the most frequent cutaneous les ion associated w ith malaria.
I t may occas ionally resemble the eruption of measles . The pos
sibility o f the erupt ion being caused by quinine should be re
membered . Erythema is not an uncommon erupt ion w ithmalaria , and may simulate the eruption of scarlat ina. Pruritusmay be present . Erythema nodosum has occas ionally beenobserved . Petechiz e and large purpuric spots are not rare in
2 50 THE S TUD Y OF MALARI A
immun ity toward itsel f should immun ize against or antagon izeother d iseases , and such is the result of experience .
Typhoid Fa wn—The compl ication of typho id fever w ithmalaria is not very rare . A search o f the l iterature revealsrecords of 2 I 5 cases in which the presence of malarial parasitesand the typho id bacill i or
'
the Widal react ion . conclusivelyproved the associat ion .
Typho id fever is more frequently compl icated w ith tertianthan w ith est ivo - autumnal malaria. Craig337
'
has reported the
on ly Case o f s imultaneous typhoid fever and quartan malariaof which the w riter ‘
has any know ledge.
Usually the malarial symptoms arise and - the parasi tes are
detected during convalescence from the typho id fever, thoughthey may be present during the course o f the latter. Whenthe onset o f the malaria precedes that of the typho id fever themalarial parasites o ften d isappear from the peripheral circulation upon the advent of the typho id fever, somet imes re
appearing and producing symptoms during the convalescence.from typhoid. This is analagous to the result of inoculat inga g iven variety of malarial parasites into a malarial pat ientharboring a d ifferent form, the o lder in fect ion usually sur
rendering to‘
the fresh . M alaria occurring at the height of
typhoid fever may or may not mod i fy the course of the
latter. The mortal ity o f the compl icat ion of these two feversis higher than that of uncompl icated typhoid.
The term“
typhomalarial fever, i f used at all,should be
restricted to those cases .in which exact methods o f d iagnos isprove it applicable . Howev er, the combinat ion o f typhoid and
malarial fevers is no more ent it led , e ither by v irtue of int imacy
or frequency , to a hyphenated appellat ion than is tuberculosisor gonorrhea in associat ion w ith malaria. I t w as formerlybel ieved that a mysterious fus ion o f both d iseases produced a
hybrid patholog ic ent ity . I t is now defin itely known that thisis not the case. Such a d iagnos is is ord inari ly a compromisebased 011 a lack of frankness to acknow ledge inabil ity to d iagnose certain cases o f fever in the earl iest stages , and is not onlyloose and unscient ific, but is , in many instances , actually harmful, as it o ften leads to the - abuse of purgat ives and quin ine.

complicat ion . Ziemann , W’ ittrock, 4 9 and Marchiafava and
Bignam i22 observed I case each, and Hemmeter
314 ment ionsrecords of 198 urinalyses in cases
‘
of malaria gathered fromvarious hospitals , only 2 of which ind icated d iabetes mell itus.
The writer recalls the case o f a d iabetic , passing more than 5per cent . of sugar, who was attacked w ith est ivo - autumnalmalaria. The latter ran an unevent ful course '
and s eemed to
have “
no effect on the sugar excretion . The patient d ied Several months later of bronchitisPolyuria in malarial subjects has already been ment ioned .
Tuberculosis—Tu the S outh , where tuberculos is is very
prevalent in the negro race , the negro death rate from tuberculosis rang ing from 100 to 150 per cent . h igher than in the
“
white race , tuberculos is and malaria not infrequently concur,
especially inthe colored race . M alarial cachex ia pred isposesto tuberculosis on ly in a S l ight measure , i f at all. T he negro ,
who 15 less o ften the subject of cachex iathan the white , more
o ften Show s the combinat ion of malaria and tuberculos is. The
malaria may prove rapidly fatal, . both d iseases may be um
mod ified in the ir progress , or the tuberculos is may assume a
more rapid course. The old idea that the two d iseases are
antagonist ic is d isproved not on ly by their not uncommon
occurrence in the same indiv idual , but Kelsch and Kiener178have even found , in Several autops ies , ev idence of both diseases in the same organs , as the l iver and spleen .
I nfluen z a. be lieves that there ex ists a decidedantagon ism between malaria and influen z a. S imms and War
w ick , 8 5 however, mention s imultaneous epidemics of malariaand influenza in Alabama, when ,
“
of those .in fected w ith malaria, 60 per cent . were brought down w ith this d isease , and itwas much more severe than in those who were not in fected .
Cam en—Based on the suppos ition t hat cancer is not so frequent in tropic latitudes , and on the report of K rz owit z , in
252 THE STUD Y OF MALARI A
1 776,of a case of cancer of the breast heal ing after an attacko f doiible tert ian malaria,L Offler'33 8
assumed an'
antagonismbetw een
—the two d iseases , and proposed , as a therapeut ic measure ,
the inoculat ion w ith malar ia o f cancerous patients . A few
experiments and“
numerous reports of cancer among tropicpeople and malarial subj ects have Shown the absolute uselessness of suCh a proced .ure O n the other hand
,it is bel ieved
that malaria o f long stand ing pred isposes to cancer of the liver.
Smalipox is an infrequent complicat ion Of malar1a. L a:
veran1observed several such cases in Constant ine . Th e mala
rial paras ites usually d isappeared/
from the blood w ith theonset o f the smallpox where the onset o f the latter Succeededthat of the former. T he mortality of these cases was . umusu
al ly high. Py-em ic foci and hemorrhages“
w ere O bserved .
S yphilis is .a common compl icat ion '
of palud ism. Under
these C ircums tances syph i l is is more rapid in its course and is
rebel lious to treatment in proportion to the chron icity of the
malarial infect ion . I n malarial cachectics ant isyphilit ic treatment is sometimes all but impotent . Syphilit i 'c buboes are
more apt to supp-"i rate and'
become-
ug ly indolent ulcers. M alarial invas ion may arouse latent syph il is .
Vincent1 5 9 is of the opin i on that the colon baci llus o ften as
sumes pathogenic importance in malarial infect ions,and he
terms the result “
coli—malarial fever.
”The patients are pro
foundly malarial ; they present a fever of c ont inued type and
typho id phenomena,subdel irium , coma, d iarrhea,
etc . At
autopsy there are no intestinal les ions save a few psorenteric
plagues; S ome Show extens ive foci of necros1s 1n the Spleenor small miliary abscesses ; others suppurat ing points in t hekidneys . S ideros is is found in the s pleen and l iver.Bacteriolog ic examinat ion show s a general ized in fect ion w ith the bacillus col i commumis . The eccentric and iconoclast ic fL -
e-
grain2'5 '5
bel ieves that the rOle o f the colon baci llus in exotic pathology isimmense .
I n the present state of our know ledge it is imposs ible to determine the part played by the colon
'
bacillus 1n the fevers of
warm countries. I n .Subtropic and tropic climates , w ith an
exuberant flora ,it is theoretically not imposs ible that the colon
254 THE STUD Y or MALARI A
stage , while not at all rare in the negro , is more frequentlylacking than in the accesses in the whitef Herpes 1S re lat ivelyrarer
'
in the black. Uncontrollable vomit ing is not nearly so
frequent in the colored race as in the white. M arked Splen icen largement is much less common in the negro , palpable spleensin the adult negro being in frequent. The extremely low hemog lobinpercentages, which are not rare in chron ic malaria and
cachex ia o f '
white persons , are far less frequently observed inthe negro . As prev ious ly stated, cachex ia is decidedly moreprevalent in the wh ite race. M alarial paras ites are altogetherabsent from the peripheral blood of negroes in a larger percent . of cases than they are wanting in white pat ients . Whenpresent they are more frequently Scanty . O n the other hand ,the negro may harbor large numbers of parasites w ithoutman i fest ing any symptoms . Pulmonary compl icat ions , bronchitis, pneumon ia, and tuberculos is are more frequent in the
negro . Nephrit is is another compl icat ion of which this istrue. Hysteria and other neuroses are probably more common
in the Colored f emale . The abuse of snuff, which is under
mining the nervous stability of the majority of adult negro
females in the S outh , may help to account for this . Thereis less tendency to abort during pregnancy compl icated w ithmalaria in the colored female than in the white . Spontaneous
cure after only one or two paroxysms is a common terminat ion of malaria in the negro . Every phys ician pract is ingamong th is race is fam il iar w ith the frequency w ith whichthe ir attacks of malaria end after a round
”of -purgative
'
and
a pot ion o f“
tea”of some sort . The grave forms . of malaria
occurring less o ften , the mortal ity is consequently“ lower in
the negro race.
The Surgical Aspect of M alar ia.—Trauma may aggravate
act ive malaria or arouse it from latency . O n the other hand ,
malarial in fection reacts upon w ounds. S lightw ounds , suchas that caused by the extract ion of a tooth , may in cachectics
g ive rise to excessive hemorrhage. F ractures healmore slowlyin malarial subjects . The w riter has more than once observedsuppurat ion , ulcerat ion , and sloughing in the wounds , asept ically treated , of malarial persons , especially sawmi ll employes
C LI NI CAL HI STORY 255
and t imbermen . I f surg ical measures are Contemplated in
patients w ith a history Of recent malar1a the blood shouldbe examined care ful ly for ev idences of malar1a, which, i fpresent, might figure ln the result.With re ference to the surg ical relat ions of malaria the follow ing conclus ions are just ifiable
I . I n subjects of act ive malaria, wounds are apt to aggravate
the malaria.
2 . I n s ubj e'
cts o f latent malaria, trauma is apt to excite thelatter into activ ity .
3. Chrome malaria and cachexia may compl icate wounds
by increas ing the tendency to hemorrhage, suppurat ion ,
s loughing , indolence , or even gangrene.
4. The mere presence of parasites in the blood Without producing symptoms (absolute latency) is no bar to Operation , as
the Specific treatment may be pursued w ith the surg ical “5 . I n badly debilitated subjects of chronic malaria, and of
cachex ia only operat ions of necess ity Should be undertaken ,
’
and then quin ine. and t-
onics Should form part of the after
treatment.
CHAPTER V I
DIAGNO S IS
M ALARI A is the scapegoat of tropic pathology and quin inethe high priest.Too often is the mocking equat ion o f L egrain ,
F ever 2 M alaria: Quim'
h e ,
employed to solve the d iag nost ic problems of the fevers of
warm climates
There are three sources from which in format ion may be
drawn to make a d iagnos is o f malaria; first,from the symp
toms ; second , from the examinat ion of the blood ; and third ,
from the effect of quin ine upon the symptoms.
I . O f the cl in ical history the most important feature to becons idered is period icity . Tertian and quartanperiod icity are
pathognomon ic of malar1a. S omet imes the statements of
patients cannot be '
relied on w ith respect to the course o f theirailments, and tertian and quartan period icity must be abso
lutely determined to be of d iagnostic value. By this is not
meant that the d isease must be observed by the phys ician un
treated until such period icity is established , but that value of
this symptom is I n proportion to the rel iability of the source
from which the history is de rived . Unfortunately this periodicity is
i
o f l ittle value in est ivo - autumnal in fect ions , in whichthe importance and d ifficulty of d iagnos is are greater.
Quot id ian period icity is not only worthless , but actuallymislead ing in the d iagnos is .of malaria I t is especially in
septic cond it ions that m istakes are o ftenest made , where not
infrequently is the rhythmic quot id ian succession o f chill ,fever, and sweat mistaken for the metric march of malaria.
A noted clinician has sa id that he has rarely seen
'
a case of
abscess of the l iver that had not been drenched w ith quin ine ,
and his exper1ence is not un ique in this respect . M alaria is256
258 THE STUD Y OF MALARI A
of malaria has certain ly been overrated . I n reg ions wherethere is little malaria, the endemic index being low ,
it is probably a point of some worth. O n the other hand , in malarialregions of high - index endemicus it is worth much less. I t is
almost valueless in malaria occurring in negroe‘
s,
'
as it is infre
quently sufficiently enlarged to be palpable , and un less palpableis of
'
no d iagnost ic value . Phys icians in malarial reg ions are
all“familiar w ith the frequency w ith . which the enlarged spleen
of the subject o f chronic malaria or cachex ia complicates otherdiseases . I f the phys ician is sufficiently fam iliar
'
w ith thepatient to know that the “
Splen ic en largement i s acute , it be
comes a matter of some importance , but the statement of the
pat ient as to the former cond it ion Of the organ , even when the
latter is .immense , is not always to be relied uponHerpes when present is an aid to d iagnos is . T heo -only dis
ease in which it occurs w ith anyth ing like the frequency itdoes in malaria is pneumon ia.
2 . The m1croscopic exam ination of the blood for the d iagnos is of malaria determines the presence or
“
absence of para
s ites , pigment , and leukocytos is , and the numeric relat ion of
the leukocytes .
Before attempting the d iagnosis of malaria by the microscopic examinat ion of the blood the beg inner must become
thoroughly famil iar w ith the appearance of normal blood and
w ith the techn ic of examinat ion , and he Should not.rely too
much upon the result o f an examinat ion unti l he has 'had con
siderable experience w ithmalar ial blood .
While L averan made his d iscovery w ith a one - s ixth- inchlens , only a one - twel fth - inch oil immersion lens , w ith appro
priate condenser and d iaphragm , Should be employed , and themechan ic stage greatly facil itates the work. Thin s lides and
cover-
g lasses should be used.
While stained films of. the blood have a w ider field of use
fulness to the general pract itioner than preparat ions of the
unstained blood , he Should become famil iar w ith the technico f each .
When about to obtain blood to be examined , fresh and
unstained , several s l ides and cover-
g lasses , hav ing been washed


F ig. 67.—Mak
_ing the puncture .
Fig. 68 .—O btaining the blood .
F ig. 69 .—O btaining the blood betw een Slide and cover—glass.

260 THE STUD Y or MALARI A“
a manner that one edge of‘
the cover-
g lass co incides exactlyw ith the edge of the s l ide near its middle: He ld rather firmlyin this pos it ion by the thumb and forefinger, the Coapted
edges are appl ied to the blood - drop when the blood spreads
evenly betw een the s lide and cover-
g lass (Fig . Whenthe blood has almost reached the oppo s ite edge o f. the cover
g lass”
enough blood .has been obtained . Two cov er-
g lassesmay be used instead o f a s lide and cover -
g lass , and when ready
to be examined one of the cover-
g lasses cemented at the corner
or edge to a s l ide by meanso f Canada balsam .
The advantages of'
dried films over fresh preparations of
blood are several. Cleanl iness of the part-
_from wh ich the
blood is taken and the s ize o f the i
drop are not so important .This advantage is appreciated by the pract it ioner who o ften
has to make the preparat ion in the remote corner of an illl ighted cabin . The s lides may be laid as ide and examined at
leisure , weeks or even months later. The d ifferent ial leukocytecount can be made on the same slide .
I t is not necessary that the reg ion from which the blood istaken should be per fectly clean
,but i f perspiration is present
this should be w iped off. The ear is held and the puncture
made as described for wet films. The S lide , held in the righthand , is rested against the thumb and forefinger hold ing the
lobe of the ear, and gradual ly low ered unt i l it rece ives the dropof blood near one end .
The smear may be made by e ither one of three useful methods . The s implest is to hold the S l ide in the left hand and w iththe right lay the Shaft o f the need le across the drop of blood(F ig . A fter wait ing a few moments
,for the blood to
spread out betw een the need le and the S lide,the needle is
evenly and gradually drawn to the oppos ite end of the sl ide .
D ry ing the film by rapidly Wav ing it in the air preserves the
form of the red cells .
I nstead o f the need le the end o f another S lide may be appl iedto the drop of blood (Fig. 71 ) so that the two S lides meet at
an angle o f about 45 degrees ; after w aiting for the blood tospread along the edge of the s l id e , the upper s lide is then
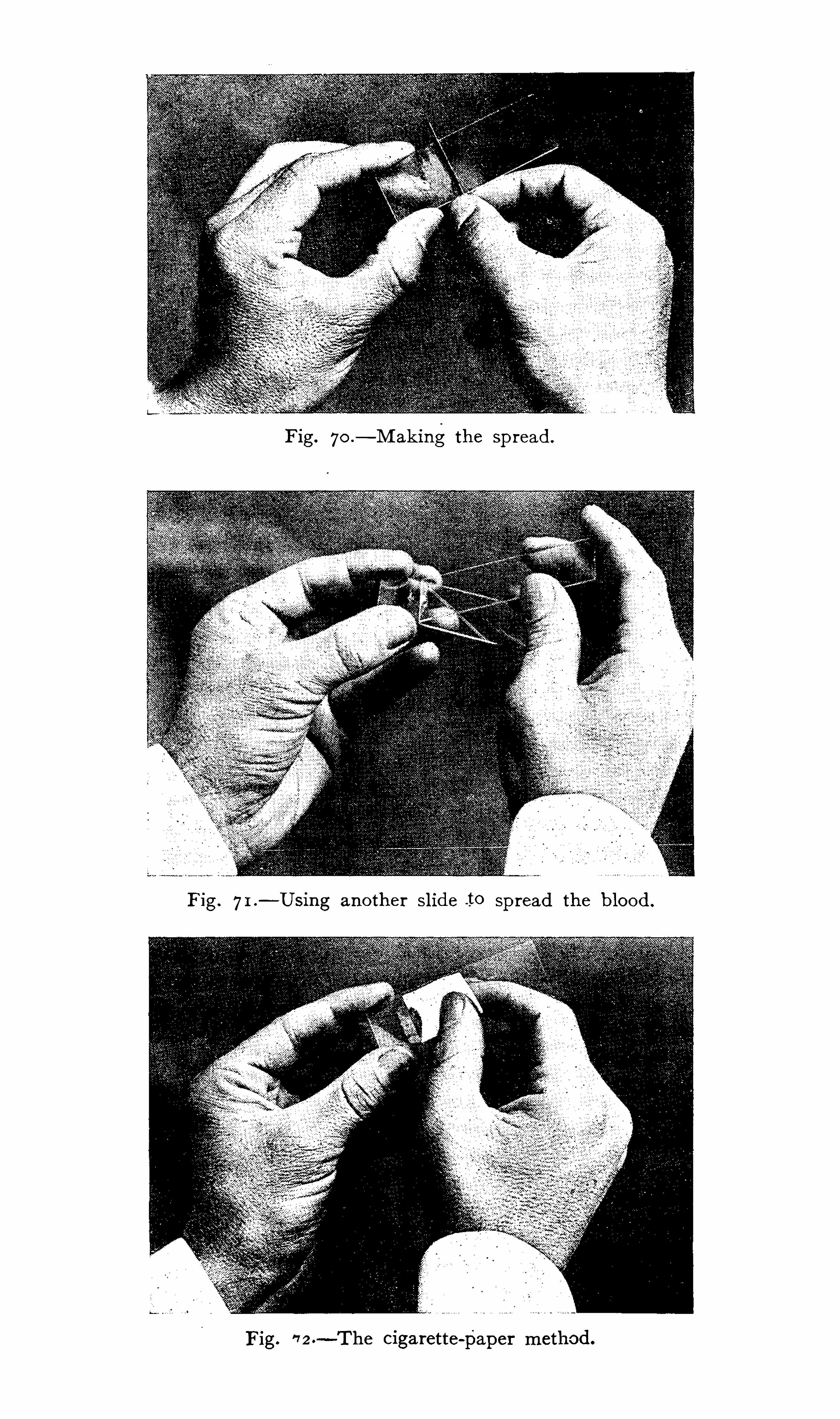
Fig. 7o .—M ak ing the sp read .
F ig. 7I .—Using another Slide .to Spread the blood .
Fig.'7 2 .
- The cigarette - paper method .

262 THE STUD Y or MALARIA
though the inethylene - blue solut ion may be filtered before mixing w ith the eos in i f desired . The mixture is poured into a
watch -
g lass and the films floated blood S ide down upon its
surface for two or three hours .~ They are then washed in
water, dried , and mounted.
Ew ing 13° -describes Nocht ’s mod ification of“
Romanowsky ’
s
method as fol lows'
I . To I ounce o f polychrome methylene—blue (Grubler ) add5 drops of 3 per cent . solut ion of acet ic acid (U. S . P . 33 per
cent .
2 . M ake a saturated ( 1 per cent . ) water solut ion of“
methylene—blue , pre ferably Ehrl ich ’s rect . (Grubler ) , or Koch ’s , dissolv ing the dye by gent le heat . This solution improves withage , and should be at least one week old .
3. M ake a I per cent . solut ion I n water of (Grubler’
s ) aqueous eos in .
The:
mixture is prepared as followsTo 10 cc. of watera dd 4 drops of the eos in solut ion , 6 drops
of neutral ized p o lychrome blue , _
and 2 drops of 1 per cent .
methy lene - blue , m ix ing w el l. The Specimens fixed in alcoholor by heat are immersed for two hours , specimen s ide down ,
and w i ll not overstain in twenty- four hours . The dens ity of
the blue stain may be varied to suit ind iv idual pre ferences . The
above proport ions need not be rig idly followed , but the polychrome solut ion Should be accurately neutralized.
L eishman’
s solution combines the fix ing and stain ing proper
t ies into one solution ,the whole process requiring on ly a few
minutes. I ts manufacture i s , however , rather ted ious . Two
solutions are necessary . The first consists of Grubler’
s
methy lene—blue , 1 part ; sod ium carbonate , 0;5 part ; d ist illedwater, 100 parts . This solution
'
is rendered polychrome by
heat ing to 65°
C . for twelve hours , then expos ing to room tem
perature for a week or ten days . The other is a 1 : 1000
watery so lut ion of Grubler’
s eos in . Equal parts ,of these solut ions are mixed and allowed to stand for S ix to twelve hours ,st irring occas ional ly . The m1xture is then filtered and the
filtrate thoroughly washed w ith disti lled water and dried . The
dried filtrate is the stain , and gram is d issolved in 100 cc.
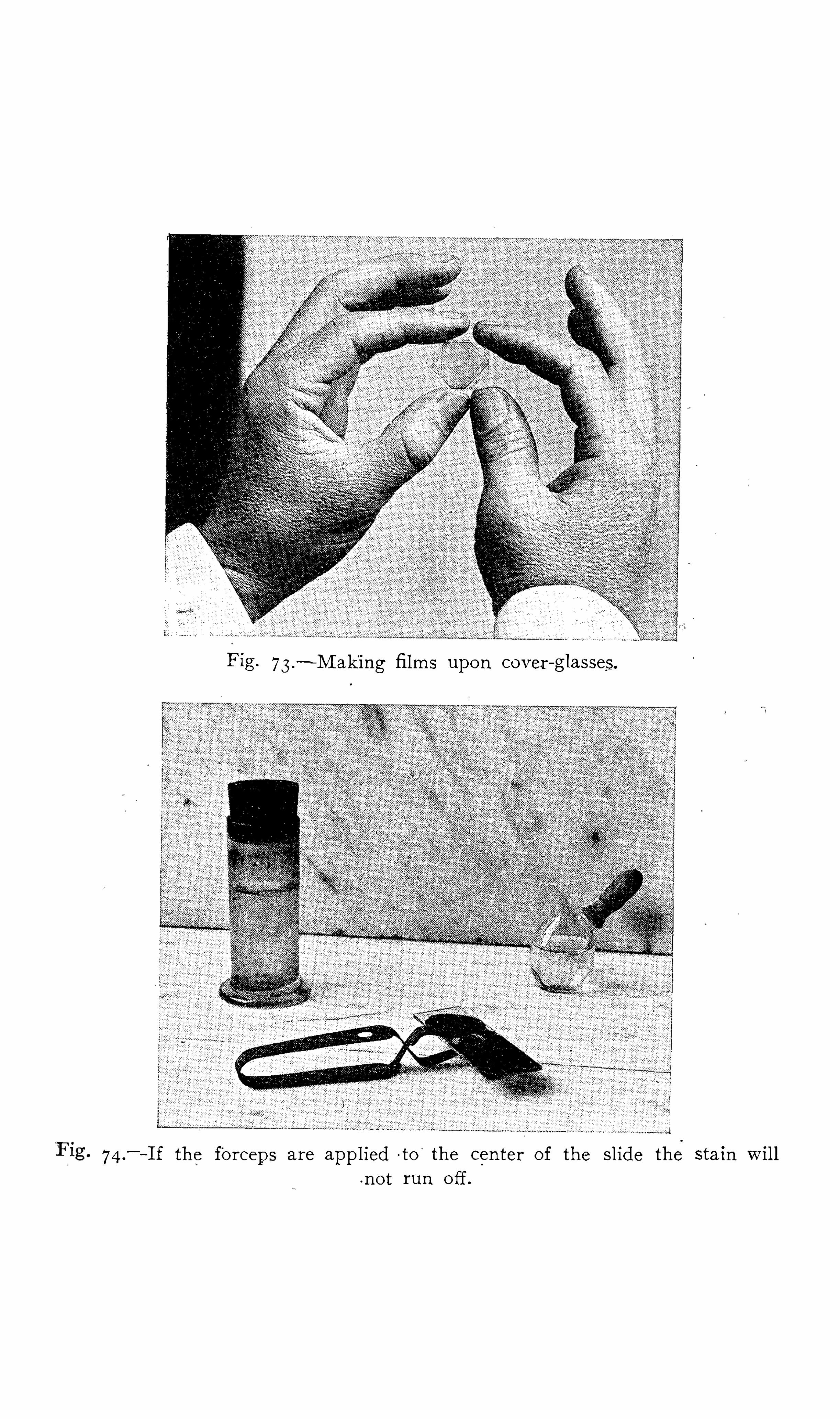
Fig. 73.—M aking films upon cover -
glasses.
74 .—I f the forceps are applied
- to‘
the center of the Slide the stain will.no t
“
run off.


264 THE STUD Y or MALARI A
The mixture is . next to be steamed in an ord inary steam
steri li z er at . 100°
C . for one hour, count ing the time after‘
steam is up.
’
The heat ing should not be done in a pressure
steri l izer, or in a water - bath , or in any other way than as
stated . Th is steam ing o f the alkal ine solut ion of methy leneblue effects certain changes in the methy lene - blue whereby a
polychromatic property ls g iven to it , so that the compound
w ith eos in , which is later to. be formed w ith it , has the property not only of d ifferentially stain ing the chromat in -of the
malarial paras ite , but also of d ifferent iat ing and bring ing out
more Sharply the nuclei and granules of the white blood cor
puScles.
“When the steaming is completed the mixture is removed
from the steri lizer and allow ed to cool, the flask being placed
in cold water i f des ired. When it is cold , w ithout filtering ,
pour it into a large d ish or flask -
and add to it , st irring or Shaking meanwhile , a sufficient quant ity of a I : 1000 solut ion of
eosin (Grubler, yellow ish , soluble in water ) unti l the mixture ,los ing its blue color
,becomes purple in color and ai scum w ith
yel low ish metal lic - lustre forms on the surface , whi le on closeinspect ion a finely granular black precipitate appears in suspen
s ion . This w i ll require about 500 cc. of the eos in solut ion for100 cc. of the alkal ine methy lene - blue solut ion . These are
quant it ies which are conven ient and suitable to employ .
“
The precip itate is co llected on a filter and , w ithout wa shing ,
is al lowed to dry thereon. When thoroughly dry d issolve “
thisprecip itate in pure methy l - alcohol in the proport ion of
_
0 .5 gm.
to 100 cc. of alcohol . This a lcoho l ic solut ion is the stain ingfluid. I t is not necessary to filter it . I t w il l keep indefinitely ,as w ill also the dry precipitate . Precaut ions should be takento keep the alcohol from evaporating ,
for thus the solut ionmay become too saturated and precipitates may form on the
blood film in the process of stain ing . I f the staining fl uiddeposits such precipitates it should be filtered and a small quant ity of methy l - alcohol added to it .
The films of blood , which should be spread thinly , are al
lowed to dry in the air. When dry , as much of the stainingfluid is poured upon the film as the cover-
glass w ill readily
D I AGNOS I S 265
hold w ithout draining off. Allow the stain ing fluid to remainin contact
“
w ith the film,
for one minute . This chiefly serves
the purposeof fixing the blood corpuscles. The cover -
glassis most conven iently manipulated by means of cover -
glassforceps .
“
Next add to the staining fluid on the cover -
glass d ist illedwater, drop by drop , unt il a del icate . scum w ith iridescent
metallic lustre forms on the surface. The amount of water
required w il l vary w ith the amount of staining fluid o n the
preparat ion , but , .in a general way, it may be said - that S ix or
eight drops w ill be required i f a seven - eighth- inch squarecover-
g lass is “
used. The amount of water added must nOt besufficient t o make the fluid transparent.
“
The stain ing fluid , thus d iluted , is allowed to r emainon the“
preparat ion for two or three minutes , during wh ich t ime the
real staining of the preparat ion takes place , and i s then washedin water.
“
The blood film w ill now be seen to have a blue or purple
color, and i f examined w ith the microscope the red blood coi
puscles w i ll be seen to be stained blue.
“
The next step is to develop the d ifferent ial staining of the
various elements in the preparat ion . This is done by washingthe preparat ion in water—pre ferably d ist illed water—unt i lthe better spread port ions of the film appear yellow ish or red
d ish ln color. S ome‘
tap waters may spo i l the staining . I f
des ired, the process of d ifferent iat ion may be read i ly observedby placing the cover-
g lass film s ide uppermost on a s l ide , covering it w ith “
water , and examining it w ith the microscope undera low magni fy ing power.
I,
The red blood corpuscles , which ,as be fore stated ,
at first have a blue color, w ill become greenish ,
then yel low ish , and finally orange or pinkish in color,depend
ing upon the depth of the orig inal stain ing , wh ich varies w iththe length of t ime that the diluted stain ing fluid has been al
low ed to act and w ith the degree of its d ilut ion.
“
The d ifferent iat ion by washing in water seems to be ess en
tially“
a process of decolorizat ion by which some of the blueconst ituent of the dye is removed ,
for the water that drains offf rom the preparation has a blue color . This differentiation or
266 THE STUD Y OF MALARI A
decolorizat ion proceeds S low ly , and may require one or more
minutes , “
depend ing upon the‘ intens ity of the staining and
upon thetint sought to be obtained in the red corpuscles .
“I t is apparent from the above that w ith a l ittle experience
w ith the method the color of the red corpuscles may be made
e ither Orange or p ink , as the operator des ires . When the de
s ired color is obtained in'
the red corpuscles the preparat ion isthen quickly dried between layers of filter paper and mounted
in balsam . I t is important to stop the decolorizat ion by dry ingthe preparat ion as soon as the des ired t int in the red corpusclesis obtained ,
for it may be carried too far.
“
D ried Stains on the upper surface of the cover-
g lass may
be easi ly removed w ith ord inary alcohol .“
I n the l ight of the forego ing explanations the fo llow ingsummary of the method of staining blood films w i ll be intelligible :
1 . M ake films of the blood , spread thinly , and al low themto dry in the air.
“
2 . Cover the preparat ion w ith the stain ing fluid for o ne
minute.
“
3. Add to the stain ing fluid on the preparat ion sufficientwater, drop by drop , unt i l a del icate iridescent , metal lic scum
forms on the surface . A llow this -mixture to remain on the
preparation for two or three minutes .
“
4 . Wash in water, preferably in d istil led water, until thefilm has a pinkish t int in its thinner or better- spread port ionsand the red corpuscles acquire a yel low or p ink color.
5 . D ry between filter paper and mount in'
balsam.
The preparat ions retain the ir colors as long as any prepara
t ion stained w ith an il ine dyes .
“
Unstained blood films may be kept for some w eeks w ithoutimpairment of their stain ing propert ies . F i lms months old
w i ll probably not g ive good results.
The red cells are orange or pink in color. Polychromato
philia and punctate basophilia or granular degeneration are wel lbrought out. The nucleated red cel ls have deep- blue nucleiand the cytoplasm is usually of a bluish t int.
The lymphocytes have dark purpl ish - blue nuclei and rob

268 THE STUD Y or MALARIA
With than those upon cover-
g lasses . The cedar oil is dropped
directly'
upon the stained film.
The examinat ion should be protracted for thirty minutesbe fore be ing pronounced negat ive . While para-
sites , i f present ,are usual ly found w ithin five or ten m inutes , it is not uncom
mon to detect the first organ isms after a search of twenty tothirty minutes .
Cedar oil may be removed from the film by w iping gent lywith a so ft cloth mo istened w ith xy lol .The
“
thick film process”is occa5 1onarlly useful where the
parasites are very scanty .
.
The blood is smeared upon the
s lide in a much thicker layer than for other methods . A fterdry ing , a l ittle. d ist illed water is added and al lowed to remainfifteen minutes , which causes the d issolut-ion o f the hemoglobin.
A fter "
dry ing again the film is stained by one of the usualmethods . While the outl ines of the red cel ls are st i l l v is ible ,the cel ls are transparent and parasites may be detected , thoughly ing under several cells . The advantage of this method isthat a much larger volume of blood may be examined in a
sh6rter Space of t ime than is the case w ith the thin film.
F lagella are much more eas ily demonstrated in the gametes
of the est ivo- autumnal than of the tert ian and quartanparas ites. The crescent becomes oval and then spheric be foreexflagellation is observed . To e ncourage this process the
method o f S tephens and Christ0phers”is most pract ical . A
number of rather thick drops of blood are placed upon a serieso f S l ides . The s l ides are then inverted , w ith the hang ing dropsover holes cut in blotting paper, mo istened w ith water, and
spread on a pane of g lass. A series of mo ist chambers is thusmade. A s l ide is removed at intervals of five minutes , theblood spread in the usual manner and stained . Exflagellation
is also observed in preparat ions of fresh blood . The w arm
stage , breathing upon the specimen , and the add it ion of a l ittlewater are recommended to .hasten the process .
S ources‘
of Error.—I n the examinat ion of blood for mala
rial paras ites there are several objects which may m islead . Pit
falls are probably more common in fresh blood than in stainedfilms .
DIAGNO S I S 269
Vacuoles and retractions of hemog lobin inred cel ls of freshpreparat ions are delusive and not in frequent ly
'mistaken for
the y oung hyaline forms, of the parasite . They are most commonin the center of the cell , wh i le paras ites are found in any
port ion. Vacuo les are highly refract ive , hav ing we ll - defined ,
clear- cut edges ;the margins of the parasites are dim and fadegradual ly into
'
the substance of the red cel ls . The vacuolesmay Show slight c hanges of form, but do not possess true
ameboid motion .nor pigment. While the'
vacuoles are per
fectly clear, the parasites Show a s light opalescence. I n stainedspecimens areas Which do not take the stain may dece ive .
These areas may be of circular fo rm in the center of the Cell ,or of ring form surround ing the center, ormay be oval , horseShoe shaped , crucial or 1rregular. When present they are apt
tob e abundant in some port ions of the film and ent irely absente lsewhere.
Crenat ions of red cells may present a hyaline appearance
somewhat resembling an amebo id paras ite . Their nature may
be determined by chang ing the focus .
Bent or buckled corpuscles occas ionally resemble crescents.
The absence of pigment and the S ize of corpuscle Should , however, enable a d ist inction. O verlapping of the corpuscles may
produce a ring Or crescent appearance which dece ives the beg inner.
The object in stained Spreads wh ich proves most deceiv ingto the
'
inexperienced is probably the blood platelet. These cor
puscles may lie upon or‘
w ith‘
in the red cell-s , in the center,
near the periphery , or only part ially enclosed by them . Theyare from one - seventh to one - half the size o f a red blood - cell ,and are round , oval , or elongated in Shape. They are o ftenof mulberrry Shape and “
ret icular structure , and , w ith the
Romanowsky class Of stains , approach'
more nearly“
purple or
l i lac than the characterist ic - blue of the paras ites . The marg inis surrounded by a pale or unstained area resembling a halo.
There is , of course , an absence of“
pigment and chromatin .
O ccurring in groups , as it frequently does , it has not rarelybeen mistaken for a Sporulat ing body , and isolated for a free
270 THE STUD Y OF MALARI A
spore. Bod ies resembling free spores should , however , be
d isregarded for d iagnost ic purposes.
- The nucle i o f nucleated red corpuscles may be mistaken forparas ites , but this should rarely occur if the morphology and
stain ing react ions o f. both bod ies is borne in mind.
Cabot“ 2and others have found in the ' blood of .pat ients
afflicted w ith pern icious anemia, leukem ia, and lead poison ingring - shaped bod ies occurring w ithin the red cells and not unlikemalarial paras ites . Their orig in or S ign ificance is not known ,
but they are thought to represent nuclear remains .
Pigmented leukocytes .have been m istaken for paras ites , butthe amebo id mot ion o f the former ln fresh Specimens and the
stain ing react ions in dried fi lms should prevent confus ion .
Hemokon ia, or blood - dust , may be con fused w ith free spores.
They are small , highly re fract ive , micrococcus - l ike bod ies averag ing one - hal f micron in diameter and possessed of very ani
mated motion. As stated , free Spores Should not be sought for
d iagnos is , and bod ies resembling them should be ignored .
.Extraneous d irt , leukocyte granulations , and stain precipi
tates must be care fully d ist inguished from pigment .
The amateur in examinat ions of malarial blood is apt to become decided ly d iscouraged , even when he has sat isfactor ilymastered the techn ic in the laboratory.
3
M ost students gain theimpress ion that all that is necessary to find the parasites is tolocate a malarial subject w ith any
i form of the d isease and
obtain the necessary blood at any stage of paras it ic development , to stain it properly , and to inspect it under a high - pow er
lens . Usually this is what he has been taught by text - booksand by teachers , and when he fai ls to detect the characterist icorgan isms in undoubted cases of malaria he is d isgusted. The
results of such teach ing throw d iscred it upon a d iscovery whosepract ical importance is unsurpassed in modern med icine.
To est imate the value of a report on the result of m icroscopic examinat ion of the blood for malarial paras ites it isalways des irable to know something of the experience of the
examiner. I n add ition to competence and proper techn ic thereare several factors which influence the result of the examination for parasites. The most important of these are : (a) the

272 THE STUD Y OF MALARI A
I f not found at the first examinat ion , as frequently occurs ,
subsequent searches are usually success ful . O n the contrary ,
in chron ic malaria the paras ites are far from constant dur1ng
the Stage o f latency , and pro longed search may fai l to revealthem during the relapse . Paras ites are often absent from the
peripheral blood of malarial cachectics . I n the paramalarial
syndrome , hemog lobinuric fever , the paras ites , i f present be foreonset , afterward d isappear in the majority o f cases .
(d ) The behav ior of the d ifferent kinds of paras ite in the irvarious stages has been re ferred to. AS a rule, the quartanparasite is most certain ly found on first examination ,
the est ivoautumnal least so , on account of its habit of resort ing to the
deep circulat ion when approaching maturity . I t is very unfor
tunate for rap id diagnos1s that the est ivo—autumnal paras itesare less read ily detected than those of the ben ign in fect ions ,but , fortunately , .are usually easi ly found in pern icious Cases ofestivofautumnal in fect ion .
( e ) That malarial parasites are found less frequent ly and
in smaller numbers in the superficial circulat ion of negroes w ithmalaria ' the w riter is conv inced , though .the d ifference is sl ight .This opinion is confirmed in part by the observat ions of K iilz ,247who found malarial parasites much less frequently in his negromalarial pat ients than in white .
(f) A long the Northern borders o fmalarial distribut ion theparasites are probably more read ily detected. This may be
accounted for partial ly by the greater re lat ive frequency of
S imple tertian in fect ions . Whether the more northern negro
shows the same scanty distribution o f parasites in the peripheralblood as man i fested by his southern brother the w riter has nomeans of determin ing . I t is surprising w ith what frequencycrescents are found in higher latitudes
'
in the blood of pat ientsmov ing from h ighly malarial local it ies where crescents are not
so frequent ly observed . Whether this is a conservat ive measure
related to the relat ive rarity .of anophe line mosquitoes cannot
be stated pos it ively , but it is known that the l i fe histories of
an imals are , in some instances , pecul iarly interdependent , especially in the case o f paras ite and host .
(g ) Why it is that in certain unquestionable cases of malaria

D I AGNOS I S 273
which have rece ived no quin ine and in'
which every cond it ionseems favorable to finding the paras ites prolonged and repeated
examinat ion shows none is. not known , but such cases are sometimes encountered.
As before said , where the specific can be w ithheld and re
peated examinat ions made—by a competent m icroscop ist i f notfound at the first exam inat ion , the paras ite may be found in
almost 100 per cent . of cases of mal-aria. The quest ion , whichis o f the utmost practical importance to the phys ician, arises :I n what proport ion of cases is the parasite to be found at a
s ing le examinat ion ? O n this depends in great measure the
pract ical value - of L averan’
s d iscovery , for in not a few case s
in general pract ice for reasons of conven ience the examinat ioncannot be repeated , in others in which the d iagnos is seems
more or less clear urgent symptoms are demand ingthe Specific.
The two factors which more than the others influence the resultare whether or not the patient has rece ived quinine s
and the
phaseof paras it ic development attained when the blood 15 w ithdrawn for the examinat ion . Ne ither of these factors is alwaysw ithin the control of the phys ician who desires to make a d iagnos is upon examinat ion o f the blood taken when the pat ientfirst comes under his observation . S ince a very large proportionOf the malaria o f the land is treated by country doctors , the
practical value of a d iagnostic test is largely in proport ion as
it is appl icable by them.
With reference to the number of cases inwhich the paras itecan be found at the first examinat ion the w riter w il l state hisexperience. Froma record kept of the number of malarialcases which had taken quinine in some form be fore comingunder observat ion it “
was learned that this reached somethingover 50 per cent . of the total number of cases treated. The
d iagnos is in these cases was obv iously based upon the cl in icalhistory and the therapeut ic test , S ince the search for parasitesin the blood of persons hav ing rece ived quinineis so discouragéing that this has not been done in rout ine work , but on ly inSpecial cases . A llow ing for errors in d iagnosis might reducethis number to 50 per cent . A Specimen of blood was alwaystaken from malarial pat ients who had not recently rece ived
18
274 THE STUDY or MALARI A
quinine when they . came under observat ion for the first t ime ,irrespect ive o f the stage of the access. The blood from frankcases on ly has beenincluded , no cases of atyp ic or latent malaria or of cachexia figuring in the result . Parasites were foundin approximately two- thirds of the cases and the examinat ionwas negative in about o ne - third . No d ifference as to clin iccourse , severity , or the efficacy of quin ine could be detectedbetween the cases inwhich paras ites were found and those in
which none'
were observed . From this experience may be in
ferred that in local it ies in which hal f of the malarial subj ectstake quinine in some formbe fore consult ing a phys ician the
paras ite can be detected at a s ing le examinat ion o f the periphe
ral blood taken at random w ith respect to the stage of parasit icgrow th in approx imately one - third :
of the cases only . The
prevalence o f se l f- med ication w ith quin ine products d ependslargely upon local cus tom and upon the energy of the patent
medicine industry .
The experience of the w riter being somewhat at variancew ith the convent ional text—book teaching , he feels it incumbentupon
“
him to cite the experience of others in this matter of the
most v ital interest.Craig70 says , “
O ften i f the blood be '
examined but .once none
at all w i ll be found .
”
Fornario3 43
observes that the parasites are missed w ith ex
treme frequency, and S o lian i , 147 in an analys is of 6 12 cases
under his Care , says that in many cases the first examinat ionwas negat ive .
. M cElroy“ 4
says , I have been struck w ith the frequency Withwhich I ' have been unable t o find parasites in cases where Iam strongly impressed w ith the malarial nature from the
cl in ical history .
”
Plehn345
states that'
the paras ites are frequently lacking inthe malaria of nat ives , or at least they are not found in the
peripheral blood , where the temperature curve . is typic and
pigmented leukocytes ind icate malaria.
The experience of Ew ing27 at Camp Wikoff is interest ing .
I n the 605 cases of malaria the plasmodia were found in the
blood in 335 cases , While in 270 cases the d iagnos is was based
276 THE STUD Y OF MALARIA
respons ible for the symptoms which instigate the blood ex
amination ?I n local ities where a cons iderable per cent . o f the inhabitants
carry-malarial germs in the ir blood '
without show ing malarialsymptoms it is mani festly poss ible that paras ites m ight befound in the blood o f such inhabitants during the course of
other ailments. And such is actually the case in certain reg ionsw ith a very high endemic index , to such an extent , indeed; thatthe w idely exper1enced Albert Plehn ,
9 9 in Cameroon , declaredthat the presence or absence of malarial parasites in the bloodof theWest A frican coast negro is of no diganostic value .
I n cases of coma in which malarial paras ites are detected
and'
which g ive a history o f exposure to v io lent heat or o f the
abuse of alcohol , it is not in frequently d ifficult to determine the'
part played by the parasite . I n cases of coma accompan ied bymalarial paras ites in the blood and albumin and
'
caSts in the
urine the d iagnos is may be obscure . Fever .occurrlng duringthe puerperium in subj ects of former malaria w ill make the
thought ful phys ician uneasy for a Short while at least , even i fparasites are found on blood examinat ion .
These are main ly problems,however, wh ich are involved in
other fields of d iagnosis and serve to impress the fact that compl icat ions must be excluded or , i f found , weighed . Whilethese cont ingencies should not be lost S ight o f, in the immense
majority of cases in this country active forms of the malarialparas ite detected in the blood are respons ible for the symptoms
which bring the pat ient under the care of the physician or
which prompt the phys icianto make the examinat ion .
I t w ill be noted that the ‘
word active is emphas ized . What ,then ,
is the value to be attached to the d iscovery “
of gametes
alone ?Formerly it was believed that the sole funct ion o f these peen
l iar bod ies was the perpetuat ion o f the species through themosquito cycle. Under this l imited v iew the detect ion of
gametes alone was on a diagnostic par With anemia and splenomegaly , sequelae of malaria, and not necessarily proo f of ex isting malaria
, even latent . S ince it has become known , however,that under certain not well understood conditions the macro
D I AGNO S I S 277
gametes can immediately , by the process of parthenogenes is ,g ive rise to pyrogenic paras ites without undergomg the mos
quito cycle , our v iew s must be mod ified , and these forms must
be regarded clinical ly as the'
paras ites of latent malaria. Relat ive to active - malaria, they may be looked upon as ev idenceso f past and potential , but not necessarily . of present , act ivemalaria.
I n regard to the number of paras ites in a g iven film of bloodthe fol low ing class ificat ion appl ies to estivo - autumnal infections :
Abundant when there is an average of two or more paras itesto each field of the microscope ;they are detected immed iate ly .
M oderately numerous when present in on ly one of severalfields ; found after a few minutes ’ search.S canty when only a ifew paras ites are detected in the ent ire
film, as commonly prepared , aften ten to thirty minutes " Search .
While there are many cases o f est ivo - autumnal in fect ion inwhich the paras ites are scanty , large numbers of est ivoautumnal parasites are occasionally -
observed in the peripheralblood , especially of
‘
pernicious cases . As many as 75 per cent .
of the-
red ce lls have been found in fested in several cases re
ported , and Rogers“ ment ions -
a rapid ly fatal case in '
which
the blood show ed‘
more paras ites than erythrocytes .
What is the diagnostic ‘
value of a negat ive resultThe w riter can by no means agree w ith those who maintain
that such a result pos it ively excludes a d iagnos is of malaria.
The failure to find parasiteS in the blood of a s ing le film takenw ithout reference to the period of the paroxysm , while of somevalue
,is not conclus ive, and i f the pat ient has recently received
quin ine is abso lutely w orthless . O n the other hand ,i f the blood
o f a pat ient who has not‘
recently taken quin ine be examinedrepeatedly by a competent person w ith the result that no paras ites are found , it is very strong ev idence against malaria.
The d iagnostic value , then , of a negat ive find ing depends uponthe presence or absence of the Cond it ions wh ich have beenenumerated , the chie f o f which is -the administration of quin ine .
When the examination of the peripheral blood is negativepuncture of the Spleen has been adv ised
,as the parasites in all

278 THE STUD Y or -MALARI A
stages are eas ily detected in theblood of this organ. This procedure , however , . is attended w ith some degree o f danger, especially of hemorrhage , and Should be resorted to on ly in cases
where an immed iate d iagnos is is imperat ive . I t has been est imated that the mortal ity of asp iration o f the spleen is 1% per
cent .1 5 8 M any fatalit ies have resulted in I ndia '
recently fromthis method of obtain ing blood for the study of the L eishmann
D onovan parasites .
4 4 When decided upon the follow ing ”
pre
caut ions should be observed : An asp-irating sy ringe or even
an ord inary hypodermic syringe may be employed . A flex ibleconnect ion between need le and nipple , such as comes With theregular ant itox in syringe , is valuable to prevent lacerat ion of
the capsule of the spleen in the event o f sudden respiratorymovements . Both the syringe and the S ite of inject ion Shouldbe rendered steri le . Cutaneous sensat ion may be deadened w ithcocaine or w ith ethy l chloride . The pat ient Should be instructed to hold the breath on deep insp irat ion , and the spleenshould be steadied against the ribs and d iaphragm. The need leS hould be inserted deeply and when the syringe is half filledShould be partially withdrawn ,
then filled , to obtain the bloodfrom two points . The operat ion Should be performed quickly ,
that'
the patient may not have to breathe during the process ,
as the danger of lacerat ion is thereby increased . A fterward
the cutaneous puncture Should be sealed w ith col lod ion , the
patient kept at rest in the recumbent pos it ion for twenty - fourhours , and cold appl icat ions placed over the reg ion of the
spleen . A dose o f calcium chloride adm in istered half an hourbefore the procedure might lessen the tendency to hemorrhage .
Upon'
failure to d iscover paras ites in the blood there are two
other blood s igns which must be considered . These are the
presence of pigment and a relat ive increase in the large mononuclear leukocytes . These s igns are termed subs id iary evi
dences Of malaria,because , being secondary in diagnost ic
portance to the paras ites , they are general ly'
called upon on lyin the absence of the latter.
M elanin is pathognomon ic of malaria, and its presence is
not cont ingent upon the stage of development o f the paras iteso r upon the prev ious admin istrat ion of quin ine. Theoret ically ,

280 THE STUD Y or MALARI A
smear it w i l l make quite a d ifference , particularly in the relat ionof the small lymphocytes to the large mononuclears , and
this relat ion is s ign ificant. I t is an interesting experimentto make and compare d ifferential leukocyte counts at both thebeg inn ing and the end of the spread . For accuracy at least500 cells Should be counted , though 2 50 g ive a fairly correct
estimate .
Perhaps the chie f difficulty in the procedure is the almost
arbitrary .d ist inct ion between the smal l mononuclear and the
large mononuclear leukocytes .
_
An invest igat ion of the l iterature upon the subj ect conv inces that the definit ions of the largemononuclear leukocyte are essent ially d ifferent . Furt ,hermore
S ince the chie f d ifference , s ize , is one of degree on ly , it is
obv ious that there is much room for error in the applicationo f any one of these defin it ions and that it requires a good dealo f experience to become skil ful in the employment of thisd iagnost ic measure.
When there is ev idence of leukoeytosis the d ifferential countalone must not be relied upon , S ince an absolute increase may
exist .under these circumstances when the d ifferent ial countw i ll show only a small per
“
cent . Here the absolute count must
be made also.
I n d ifferent iat ing malaria from typhoid fever the d ifferent ialcount is o f value on ly in the first two weeks of a fever, S inceafter that t ime the relat ive proportions of the leukocytes are
S imi lar in the two d iseases .
Notw ithstand ing its d ifficult ies , the d ifferent ial leukocytecount madeby an experienced examiner may render importantaid in the d iagnos is of malaria where the paras ite cannot be
detected , and a mononuclear leukocytosis reaching I 5 per cent .
must be regarded as strong ev idence o f malaria.
Bes ides the presence of pigment and a large mononuclearincrease there is another po int ascertained by microscopic ex
am ination of the blood , this is the presence or absence of
leukocytosis. Between malaria and typho id fever this po inthas no d ifferent ial value , and it w il l be remembered that a
leukocytos is is frequent in pern icious malaria. I t is , however,in sept ic cond it ions which somet imes so closely resemble mala
D I AGNOS I S 281
ria in which a marked leukocytosis may serve to excludemalaria.
3. The Therapeut ic T est. —The d iagnostic value of the
therapeut ic test has” been known s ince the days of Tort i ,
though neither its value nor its l imitat ions are yet widely realiz ed . O n the one hand, there are theoret ic and
'
ultrascien -tific
writers , apparent ly valuing a microscopic d iagnosis more highlythan human l i fe , who advocate w ithhold ing the Specific indefinitely unti l the parasite may be found . O n the Other hand ,there are phys icians who cont inue the admin istration of quin inein heroic doses for days , or even weeks , in fevers which donot Show the sl ightest suscept ibility .
Here d iagnos is and treatment meet Very closely , the former
encroaching somewhat upon the field o f the latter , the diagnostic test o ften becoming a therapeutic and l i fe s- aving measure .
The therapeut ic test is of especial value in cases which havealready had insufficient quinine , thereby caus ing only the dis
appearance of the parasites from ' the superficial circulat ion and
d istortion of the fever curve. I n these cases it has at lea-st as
much - stand ing in clin ical med icine as ant isyphil it ics in obscurecases thought to be syphilis or antitoxin in cases of susp iciousang ina in which a bacteriolog ic examinat ion is impossible .
When properly appl ied it can hard ly be product ive of,
harm.
A fever which res ists quin ine is not a malarial fever. .I n
order to test the res istance of a fever to quinine the drug mustbe cont inued for asufficient length of t ime and in proper doses
at suitable intervals , and , what is most important , it must beabsorbed .
The max imum period of“
resistance of malaria to quinine isord inari ly stated as four days . As far as the w riter ’s observat ions go , they tend to Show that in many cases the fever is
broken by the end of thirty - six hours , in at least hal f the cases
in forty - eight hours , and in three -fourths the Cases in S ixtyhours . I t is highly probable that in cases of malaria pers ist ing“longer than four days the Specific is not being absorbed . A
case is recalled in which . the fever cont inued notw ithstand ingthe admin istration in capsules of 24 grains of a soluble salt ofquinine during the twenty
- four hours for nearly S ix days .

282 THE STUD Y or.MALARI A
Paras ites hav ing beenfound before‘
the quininewas begun , the
drugWas then g iven ln solut ion, when the fever responded during the
_
seventh day . There had been no . evidences of cin
chOnism unti l the solut ion was employed . C inchon ism, how
ever, is not a guide in the employment of the therapeut ic test ;the specific is d irected toward the paras ites and not toward
the patient , and pat ients man i fest various degrees of sens itiveness toward quin ineOw ing to thecond it ions under which the therapeut ic test is
usually employed it is better to use moderate doses at regularintervals during both day and n ight . Three or 4 grains every
three hours are sufficient . Pills and tablets of quin ine shouldnever be rel ied upon ;the result may be not on ly misleading butdangerous . Capsules , if fresh, are usually
’
satisfactory ;a few
pin punctures in each end aids solut ion . Where the fever pers ists and there is reason to bel ieve that the medicine ' is not be ingabsorbed it should be g ivenin solut ion or even intramuscularly.I n c onnect ion w ith the therapeutic test the law of Treillei‘04
is interest-ing .
“
I t may be stated as fo llow s :”
I n malarial fever quinine g iven in a s ing le -
proper dose at
the beg inn ing of a paroxysm'
does not 1nfluence that paroxysm ,
but always suppresses the follow ing for a min imum period of
five days .
“
D es ignat ing the day upon which quin ine is administered as 1
, the min imum durat ion of apyrexia as 5 , and the
day of recurrence'
as I, the formula may be graphically repre
sented as 1 -
5- 1 . I n the case of quot idian and quartan fevers
the durat ion o f apyrex ia is o ften a mult iple of 5 . The formulais
, then, I- m5
- 1 . Treille regards as a proper dose : for quartanfever, 2 5
;
cent igrams ;for quot id ian , 2 .5'
grams , and for tertian ,
2 grams .
The writer cannot vouch for the detai ls of these propos it ions ,but the general principle has ample support. I n thorough accord are the recently recorded and accurate observat ions of
Cohenf”05who ascertained that a S ing le subcutaneous injection
of 15 grains of quin ine and urea, g iven pre ferably during theparoxysm or shortly after, produced an apyretic period of
approximately S ix and a hal f days or approx imately thirteendays .

284 THE STUD Y or .MALARA
D IFFERENTIAL D I AGNOS I S
The d ifferent ial d iagnos is between the malarial in fectionscan best be madeWith the m icroscope . I n on ly one type of
infection , the quartan , e ither s ingle Or double , can the d ifferential d iagnos is be made cl inically w ith certainty .
The d ifferent iation of chron ic malaria from cachex ia is
somet imes very d ifficult , the re lation being one of d isease ent ityand sequel , and the d ifference . somet imes one of degree on ly.
The d iagnos is of latent '
malaria must be based solely upOn
the detect ion of paras ites in the blood .
’
Basophile granulat ionof the red cells and urobilinuria cannot be rel ied upon as ev i
dences of latent malaria.
Abscess of the L iven—S eptic .
eonditions are very o ftend iagnosed as malaria ;this is especially true of hepat ic abscess .
There are two classes of cas es o f abscess of the l iver that may
be d ifficult at first examination to“
d istinguish from”
malaria ;first , where the local symptoms are absent or '
not wel l defined ;second , where there is enlargement of both liver and Spleen and
a history of both dysentery and malaria. The fact that thesepatients have usually
.
been drenched unsystemat ically w ithquin ine may compl icate the d iagnos is . I n typ ic cases of hepat icabscess there is usually a history of dysentery , and amebae may
be present in the feces . There is usually a dragg ing pain inthe l iver, somet imes re ferred to the right shoulder , increase of
l iver dulness , and tenderness on pressure . The spleen is not
necessari ly en larged . The'
temperature does not o ften riseh igh , and there is apt to be pro fuse perspirat ion , especiallyduring r sleep. O n microscopic examinat ion o f the blood thereis usually a leukocytos is to be found , though this is want ingin a few cases , and its absence should not be taken to excludeabscess . There are neither parasites , p igment , nor a relat iveincrease of the large mononuclear leukocytes. Exploratoryasp irat ion is
'
valuable in some cases . Jaund ice is a veryvar iablesymptom and may bemislead ing .
I nfect iv e endocard it is may present period ic paroxysms of
ch ill , fever, and sw eat . The phys ical examinat ion o f the heartand the m icroscopic examinat ion of the blood should establishthe d iagnos is .
D I AGNOS I S 285
Puerperal S ept icemia.—Women who h ave had malaria
during pregnancy are prone to Suffer relapses during'
the puer
perium. I n this cond it ion malaria 18 not in frequently atyp ic :the first or third stages o f the paroxysm are somet imes lackingand complete intermiss ion of temperature is o ften wanting .
The follow ing may serve to d ifferentiate typic cases of malariaand puerperal sepsis :
M alaria.
Onset from a few hours to tw entyone day s after labor.
O ften a history of malaria.
T emperature curve more or less
typ ic.
S ymptoms decline w ith temperature .
No local symptoms.Blood examinat ion positive.
Therapeutic test positive .
The so - called urethral fever may be accompanied by paroxysms somewhat resembling those o f malaria. The writer hasrecently seen a case in which the introduction of a steel soundevery other day was accompan ied for a Short t ime by corre
sponding paroxysms not due to malaria. The d ifferent iat ionfrom malaria Should present no d ifficulties.
Perinephrit ic abscess , pyelit is , cho lecystit is , and other septic
processes may be associated w ith fever which bears a more or
less close resemblance to that of malaria. LOCal symptoms , the
blood exam inat ion,and the therapeut ic test
'
rarely leave the
d iagnos is in “
doubt but a short while .
Typho id Fever.—S ince L averan ’
s d iscovery and s ince theknow ledge of the prompt efficacy of quin ine in malaria and the
value o f theWidal react ion have become thoroughly establishedmistakes in the d iagnos is of typho id fever and malaria shouldbe relat ively in frequent . This is un fortunately not the case .
Witness the lesson of the S pan ish—Amer ican 'War : O f
cases of typho id fever-
occurring in the American army ,
or'
per cent . , were correctly d iagnosed by reg imental orhospital surgeons . M ost of the remainder w ere called malaria ;ten thousand mistakes in one season , and the board of inves
tigation concludes that in recogn izing about hal f the cases of
Puerperal S epticemia.
Rare after the fifth day .
M alarial h istory usually absent.I rregular.
No relation betw een symptoms andtemperature.
L ocal symptoms present.
Negative .
Negative .
286 THE STUD Y or MALARIA
typho id fever the army Surgeon probably did better than the
average phys ician throughout the country _does in his private
pract ice.
I n proportion to the reliance placed upon symptomatology inthe d ifferent iat ion of typho id and malarial fevers so frequentlyw il l mistakes occur. Chills , cont inued fever, bronchit is , en
larged spleen , S light tenderness and gurg l ing in the right i liacfossa, tympan ites , d iarrhea , the D iazo react ion
,del irium, and
the typho id State may occur w ith e ither d isease . Herpes is
strong ly. ind icat ive of malaria and rose spots of typho id fever,but these Spots are more frequently absent than present in thetypho id fever of warm countries .
A correct d iagnos is must rest upon the results of the exami
nat ion of the blood and“
the therapeut ic test .The number, e ither abso lute or relat ive ,
_
‘
of the leukocytesis not as valuable in this connect ion as elsewhere , and i f thecase . is seen early the d iagnos is may be made '
before the Widalreact ion is appl icable , but this latter test is eminent ly use ful inmany cases .
“ ’
Proper prophy lact ic precautions Should be -
observed fromthe start in cases
'
of doubtful d iagnos is.
Tuberculos is is somet imes S imilar in its course to malaria.
I t is especially so in the early stage when the local-
s igns and
symptoms are i ll - defined or absent and the bacillus cannot be
detected , and in the stage of secondary infect ion when sept icsymptoms supervene. M iliary tuberculos is has not in frequent lybeen mistaken for malaria. For the d iagnos is between tuberculosis and malaria the m icroscopic examinat ion o f the bloodand Sputum , the phys ical exam ination ,
and therapeut ic test areusually ample .
I nfluen z a has sometimes been con fused w ith malaria. I f
the epidemic occurrence , d ifferent seasonal prevalence , catarrhaland other symptoms are insufficient upon which to"
make a
d iagnos is , the absence o f characteristic blood find ings are gen
erally conclus ive.
Y e l low fev er in some cases so close ly resembles the so - calledbilious remittent fever that in reg ions where both d iseases occurthe d ifferential d iagnos is by cl in ical history alone is impossible.

288 THE STUD Y OF MALARIA
of pernicious attacks found in c oma to be taken to the policestation Instead O f the hospital and the true cond it ion not
“
sus
pected unt il the pat ient-
S fai l to “
Sober up” in due t ime , whenit is usually too late for treatment t o avail .Negat ive examinations of the -
peripheral blood in desperatecases justify risking the dangers of splen ic puncture .
I n cases show ing the presence of p aras ites compl icationsmust be rig id ly excluded . I n some cases th1S ls attended w ithd ifficulties .
J
I n Comatose malaria, bes ides the ev idence obtained by an
examinat ion of the blood , a history of - exposure to of attacksof malaria, the general appearance and age o f. the pat ient , theabsence o f atheroma, the early e levat ion of temperature , and
perhaps the enlargement “
of the Spleen and S l ight ' jaund iceshould exclude cerebral hemorrhage. The d ifferent iat ion of
malarial coma from sunstroke is . often hard ; in fact , the - two
not'
infrequently-
co which case it may be imposs ibleto apport ion the et iolog ic Share Of each in the cl in ic picture .
Cardamatis287
states that in this type of pern icious malariac
‘
oma is the dom inat ing symptom , while in sunstroke are Ob
served coma, convuls ions , d e lirium, and h yperpyrexia. Uremic
coma may S imulate that due tomalaria. Un fortunately , the
urinalys is throws no . l ight on the“
d iagnosis , as in both‘ cond it ions we may find albumin and casts: The blood examinat ion ,
the temperature , and the'
an'
amnesis serve to make the d iagnosis.
For the d ifferent iat ion -oi alcoho l ic from malarial coma the
blood examinat ion is essent ial . The h istory may be _
of Value ,but the odor of the breathmay be mislead ing . To d iscriminatebetween-malarial coma and d iabetic coma the presence of the
paras ites , on one hand, and of g lycosuria, on the other,'
are
sufficient . I n d ifferent iat ing between the various comas w ithre ference tomalari-a two po ints should be remembered : F irst ,that comatose malaria may occur in persons w ith the odor of
alcohol on the breath , and , secondly , that coma: from causes
other than malaria may attack malarial cachectics . To d istinguish epi lepsy , opium . po ison ing , tetanus , and mening it is frompernicious malaria should rarely present d ifficulties i f the bloodis examined . The follow ing table of d ifferent features of

D I AGNO S I S 289
amblyopia due to quinine and tomalaria is borrowed from
M anson5 9
Quinine A'
mbl‘
yopia. M alarial Amblyopia.
History .—Quinine tak en in large History .
—Quinine may have beendoses
,not less than 30 grain s. tak en
,but not necessarily in large
d oses
O nset—S udden,
“
accompan ied by O nset —Not usually sudden, but it
deafness ; both eyes . are affected . may be so if hemorrhage has Occurred in the macular region.
There '
I S no deafness , and both
eye s are no t neces sar ily: affected .
Pupils .“ Widely dilated , and while Pup ils—React to light .
105 3 o f vision cont inues they do
not r eact to light .
V ision .—Comp letely lost for a time. V ision.
—Never completely lost.0phthalmo
l
scop ic Appearances .—A Ophthalmoscopic Appearances.
white haz e over fundus ; cherry There i s Optic neuritis ; Op tic disk
red spot at macula ; Optic disk is of characteristic gray ish red
pale ; retinal v essels markedly color , retinal hemorrhages_
and
constricted. sometimes v itreous Opacities.
Terminationg—Usually - S ome per Termination .—S ome cases recover
mane'
nt defect in the field “
of completely ; in others greaterO
or,
v ision or in_color vision. Cen less permanent defect of Vision
tral v ision recovers first ; optic remains .
disk is“
unusually white, and reti
nal vessels small.Treatment—S top quinine . Amyl Treatment .
'
- Give quinine:
nitrite has been recommended to
induce dilation of . retinal vessels.
A lg id attacks “
somet imes resemble perforat ion , o-r typho id, or
gastric ulcers , or rupture of the S pleen . The m icroscope and
the local symptoms should render the d iagnos is certain . The
cases resembling append icit is and periton it is have beentioned ; here, again , the microscopicexam ination o f the bloodmay save l ives . I n countries in whic-h
'
ch'
olera is endem ic thed iagnos is beween this d isease and the choleraic type of pern1
cious malaria was formerly d ifficult or imposs ible . Laveran ’
s
d iscovery has removed this d ifficulty and - rendered poss ible a
d iagnos is Of the utmost-
importance . The find ing of the hema
to z oa d ifferentiates the hemorrhag ic , bilious , and typhoid typesfrom typhoid and yellow fevers .
D I AGNOS I S OF HEMOGLOBINURIC FEVER
This is usually made and , as a rule , correct ly be fore the
phys ician arrives . The history o f malaria ,the fever , vomit ing ,
jaund ice , and black water are pathognomonic. Though theparas ites are so frequentlymissed , on examination of the blood
290 THE STUD Y OF MALARIA
there 15 usually a mononuclear leukocytos is, and p1gmented
leukocytes -may be found .
The d iagnos is from paroxysmal hemog lobinuria might prevent d ifficult ies . I n this rare cond ition the attacks usually follow chilling o f. some port ion of the body ,
.and the attack isusually of Short duration and seldom fatal. I n hemoglobinu
fever there 1S g iven a h istory of several years o f res idence in an
endemic reg ion , repeated a ttacks of malaria, w ith o ften the
presence of paras ites , p igmented leukocytes , and a mononuclearleukocytos is in the blood.
The cond it ions which have been most frequently confoundedw ith hemoglobinuric fever are yellow fever and bilious rem ittent fever.
local it ies where yellow fever and blackwater fever prevai ltheir d ifferent iat ion is not easy . The fo llow ing are the ch ie fpo ints of d ifference
Hemog lobinur ic F ever. Yellow F ever.
Endemic. Ep idemic.
O ne attack predisposes . O ne attack confers immunity .
Occurs usually after several years Attack s also new comersO f residence .
M alarial history alw ay s given. M ay be no history of malaria.
Prodromata common. Uncommon.
I cterus inten se,
“
early , alway s pres I cterus usually slight , begins on
ent. third or fourth day may be ab
sent .
Conjunctiva jaundiced. Usually congested at first.Hemoglobinuria. Albuminuria or hematuria.
Blood may Show malarial parasites, Absent .
p igmented leukocytes , and mono
nuclear leukocy tos is .
Bilious v om i ting . V omit clear or black .
Hemorrhages uncommon . Relatively common .
S pleen usually much enlarged. Enlargement S light .I ncreasing pulse. Pulse retards w ith stationary or
creasing temperature ( Faget’
s
S ign ) .
Albuminuria from beginning . Usually appears from second t o
fourth day .
A ratherstriking co incidence is the relat ive immunity o f the
negro to both d iseases .
Certain cases of bilious rem ittent fever present points of
striking S imilarity . This is w ell i llustrated by the follow ingcase wh ich was represented to me by the messenger and by
the fam ily on my arrival as one of“ hematuria”

CHAPTER V I I'
S pontaneous Recovery .
’—I t is a fami liar fact that malaria,
after the manner of other infectious infrequentlyundergoes what is termed Spontaneous cure . Phys icians inma larial reg ions O ften see pat ients whose paroxysms, typic andw ith characterist ic period icity, have ceased w ithout med icat ionor after nothing but a purgat ive dose .
I t' is doubt ful , however, whether this cessat ion may w ith pro
priety be termed a cure. I n the majority o f instances relapsesfo llow at Shorter or longer intervals . I t is better, therefore ,for pract ical purposes to c ons ider th is but a transit ion fromact ive malaria to latency . The greater frequency w ith whichgametes are found after the so - called Spontaneous recovery
just ifies this assumption .
S pontaneous cure occurs more frequently in tert1an and
quartan infect ions. This statement appl ies merely to the temporary cessat ion o f paroxysms and not to the tendency to re
lapse .
I t is more frequently Observed in the negro than in the whiterace , permanent cures Occurring not rare ly in the former race
in theabsence Of all med icat ion.
S ex may exert a slight influence upon the tendency to spon
taneous recovery , the female , on account of less severe exposureto deleterious influences , probably man i fest ing a greater dis
posit ion .
"
The d iscontinuance of paroxysms may be sudden or more
o ften gradual , the accesses becoming less severe or the intervallonger, or in in fect ions w ith more than one generat ion of para
s ites one may be sudden ly destroyed , the others later.
Prognos is—Th is“
is influenced to some extent by local ity .
I t is mani fest that in regions where only the tert ian and quartan292
‘
PROGNOS I S 293
infections are prevalent the mortality is le ss than where severe
estivo - autumnal fevers are w idespread . There is , furthermore ,
quite ad ifference in the mortality rate in countries where theestivo - autumnal in fect ions are
“
equally d istributed.
Race as a factor in the mortal ity of malaria has already beendealt w ith .A majority O f deaths from malaria occur in children. There
is no doubt but that many chi ldren die of malaria Which hasnot been d iagnosed in t ime. Inthe yOungp ern I CIouS symptoms ,
especially cerebral , are prone to supervene , or the attack may
be fol lowed by extreme anemia and drops ies . M alaria is l ikew ise much more serious in advanced age than in the interme
d iate ages .
O ccupat ion and social cond it ions play a part 1n prognosis .
Excess ive toi l and exposure may render pern icious attacksotherw ise ben ign, and t imely treatment , usually resorted to by
the better classes , enhances the chance of recovery .
1
The outlook is probably more favorable in attacks occurringw ithout the malarial season than w ithin .
M an ifestly the cond ition of the pat ient w ith re ference to theresults of prev ious d isease is of importance . Anem ia
,alcohol
ism, dysentery , and other cond it ions not fully recovered f rom
contribute grav ity to the prospect .The type of malarial in fect ion is of the greatest importance .
I n the tert ian and quartan types it is only very rare ly that
serious symptoms result . I t is n ot yet certainly known in
which variety of est ivo - autumnal in fect ion the prognos is ismost grave . Whi le March iafava and Bignami162 and M anna
berg 141 hold that the«
tert ian estivo - autumnal ' in fections are
most often attended w ith danger, Craig70 and Wright8 8 maintain the oppos ite v iew.
Postponement and ant icipat ion of the paroxysms were for
merly regarded as“favorable .and unfavorable , respect ively .
However , ow ing to the irregularity of the estivo - autumnalfevers , these can be said strictly to be properties O f tert ianand quartan in fect ions only , and are consequently of l ittle prognost ic import. Violent headache, somnolence , s igh ing respirat ion , S light mental aberrat ion , de fect ive art iculation and v is ion ,
THE STUD Y OF MALARI A
urface , and rapid ,feeble purse are some of the symp
forebode ev i l.prognost ic value of the microscopic exam inatio.
ood is l im ited . While , as a general rule , the severitttack is in proportion to the number of paras ites , 1
metimeS scanty“
in the peripheral circulat ion even in g
Sporulat ing and advanced stages of estivo - autu'
tes are rarely s een'
in the superficial blood excel
nely severe cases .
aney346
regards a reduction of leukocytes to or b
as of grave prognost ic value . The w riter is unabthis from his experience , s ince in his cases of pern i1ia there has ex isted a leukocytos is .
ni le in tertian and quartan infect ions a paroxysm m2
:ted approx imately from the results of blood examinaI n attempt w ith est ivo - autumnal malar1a may prov e1g . An impend ing paroxysm dependent on mature 1n the v isceral circulat ion cannot be foretold .
ercurrent d iseases complicating malaria aggravate
LO S IS . This is especiallv the case in chron ic malariaxia
, w ith which pneumon ia, dysentery , and other dis1
frequently fatal associat ions.
e grav ity o f pregnancy as a compl icat ion of malari:Onsidered .
nephrit is o f malarial orig in the prospect is , as a
I f, however, the pat ient is repeated ly subj ecte‘
ia or other harmful influences the prognos is is not p
e prognos is of the nervous sequelae is ord inari ly fThe various paralyses and mental symptoms are granS itory , but may occas ional ly become pers istent . B
toms are usual ly slow to d isappear.
e course of chron ic cachex ia may be extended for y
cachex ia runs a more rap id course . I n mild ca:
e of climate and ton ictreatment do a great deal fOI t ; advanced cases rarely recover. D eath may 1
exhaust ion , but is more commonly due to perni' ia and to compl icat ions , o f wh ich the most frequer.

296 THE STUDY OEM ALARI A
Anemia fromprev ious attacks o f malaria or other causes ,
alcoholism ,
-
or organ ic d isease of important v iscera -
add to the
grav ity of the case . The cerebral types are less serious in theyoung and vigorous , very fatal in the aged . A S a rule , patientsseen early and treated skilfully and energet ically have a betterchance for li fe , butmany cases en
'
d f atally in Spiteof the be stand most time ly treatment .
Thenumber of paras ites - in the peripheral c'
irculation" '
is not
always a re liable guide as '
to the severity -or_ progress o f the
attack . With apparent amel iorat ion ‘
o f the symptoms the
phys ician Should be circumspect in his prognos is and—
bear inm ind the possibil ity of further paroxysms .
I n .
'
the writer’
s op in ion ,the alg id type is
'
the'
most lethal ,the _ typhoid and the dysenteric least so , though th is is not
exactly in accord w ith 'Colin ,
29 1who arranges the
“
types accord
ing to the“follow ing descend ing scale Of grav ity:
'
S yncOpal,
algid , card ialg ic, de lirious , comatose , icteric , choleraic. S chellong 9 2 regards the comatose as the most dangerous and L e
Dantec,26
. the delirious and alg id.
Parryi’ 5 7
states that average mortalityof pern icious malariais I out of every 8 cases ;Wharton35 8 est imates it as 1 of every
12 or 15 ; Haspel8 6
and Borius,“ 9
one - third ; Pampouki sf;62 1 .4
- 2 5 4 per cent . L e .D a11tec,226
220 - 50 per cent ., and C res
pin ,
1442 0 -
70 per cent . The alg id type'
is said by Pampoukis8 6 tobe fatal in 5 5 .5 per cent . of cases . Cardamatis
287states that
the comatose variety is “
fatal in 20—40 per cent .,Bergeand
35 9
bel ieves the mortal ity of this type to be 50 per cent .
The fol low ing list o f cases of pe rn icious malaria,comp1led from the l iterature , Shows a mortality of per
cent . The first column of figures Show s the number o f cases ,
the second the .number Of fatalities :Number of Number ofCases . D eaths .
Laveran1
104Bailly
3°°886
NeppleAntonini and M onardM aillot
86
Grall25 6
Burot and L egrand2
Smart”
T ravers
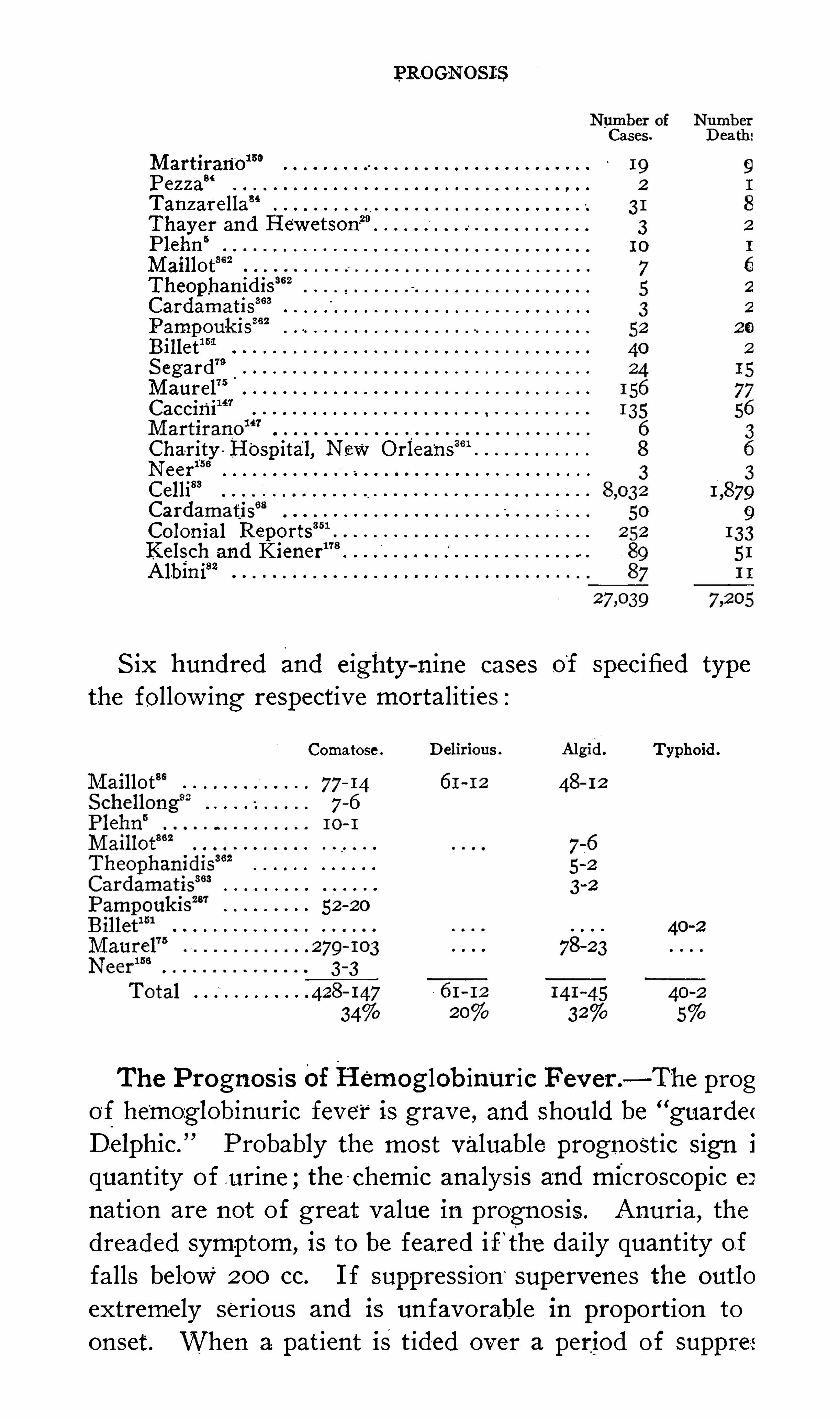
_PROGNOS I ZS
Cases
M artirano
Pe z z a“
Tan z a-rella
Thayer and I'
I ew etson29
Plehn“
M aillot
TheophamdisCardamatis
363
362Pampouk isBillet
”1
S egard79
M aurel75
Caccini
Charity H'
ospital, New O rleansNeer15 8
Celli83
CardamatisColon ial Reports
Kelsch and KienerAlbini82
S ix hundred and e ighty - n ine cases of Specified type
the follow ing respect ive mortalit ies :
Comatose . Typhoid .
0 0 0 0 0 0
0 0 0 0 0 0 0 0 0
0 0 0 0 0 0 0 0 0 0 0 0 0 0
The Prognos is OfHemog lobinuric F ev er .—The prog
of he'
mozglobinuric fever is grave , and should be “
guarde <
D -elphic.
”Probably the most valuable prognost ic S ign i
quant ity of u rine ;the -
chemic analys is and microscopic e:
nation are not of great value in prognos is . Anuria,the
dreaded Symptom,is to be feared if- ‘the daily quantity o f
falls below 200 cc. I f suppress ion supervenes the outlo
extremely serious and is un favorable in proport ion to
onset . When a pat ient is t id'
ed over a period of suppres

298 THE STUD Y OF MALARI A
as occas1onally happens , he usually d ies during convalescenceof exhaust ion ,
subsequent nephrit is , or embol ism.
Excess ive and uncontrollable vomiting is a bad omen, ex
h austing the sufferer and inter fering with nutrit ion and medi
cat ion . D iarrhea is probably in many cases , w ith suppress ionor a tendency thereto , a l i fe - saving measure , and may be par
tially respons ible for the relative rarity o f uremic symptoms
under these circumstances . S ingultus is present in a majo r ityo f fatal cases , and when obstinate is always un favorable . Re
mittent or intermittent temperature is usual ly favorable . S om
nolence , w ith d iminishing “
amount of urine ;coma, especially of
early onset , petech iae, ep istax is or other hemorrhage , and algorforebode ev i l.Thrombus formation in the heart Or large vessels may cause
sudden death when the pat ient is thought to be progress ingfavorably . Plehn
5 believes that loud heart murmurs accom
panied w ith weak , irregular pulse denote heart thrombus. Thiscond it ion is almost certainly fatal , usual ly in five to e ight days .
The larger the share partaken i by quinine in the et iology O f
the ind iv idual case the better the prognos is, prov ided the case
is not further aggravated by quin ine.
Cases occurring in v ictims of malarial cachex ia or of com
pl icat ions are usually more serious.
.The mortal ity varies unaccountably from year to year , some
seasons ev incing a series of mi ld cases , others an appallingmortality . I n a certain parish of L ouis iana in 1867 many
cases are said to have occurred , of which not less than '
95 per
cent. d ied 3“ F isch , 19 1 who placed the mortal ity on the GoldCoast at 20 per cent. , states that unt i l two or three decadesprev iously nearly all who w ere attacked d ied. O n the other
hand , Banks210 makes the well - n igh incred ible statement thathe treated over 100 cases in the Congo S tate w ithout a death.Pampoukis
9 6
g ives the mortality of blackwater fever as
per cent . Crosse ,420 per cent . Kanellis ,
8 67
per cent .
Berenger- Féraud ,
9 6
per cent . ; Barthelemy - BenOit ,9 6
2 5
per cent . Bertrand ,
2292 5 per cent . Carré,
1 9 127 per cent . Cas
san ,
9 8
per cent. M ichel , 36 8 33 to 50 per cent . S chellong,
19 1
42 per cent . Reynolds ? “ 50 per cent . ;S cott ,36 7 60 per cent .
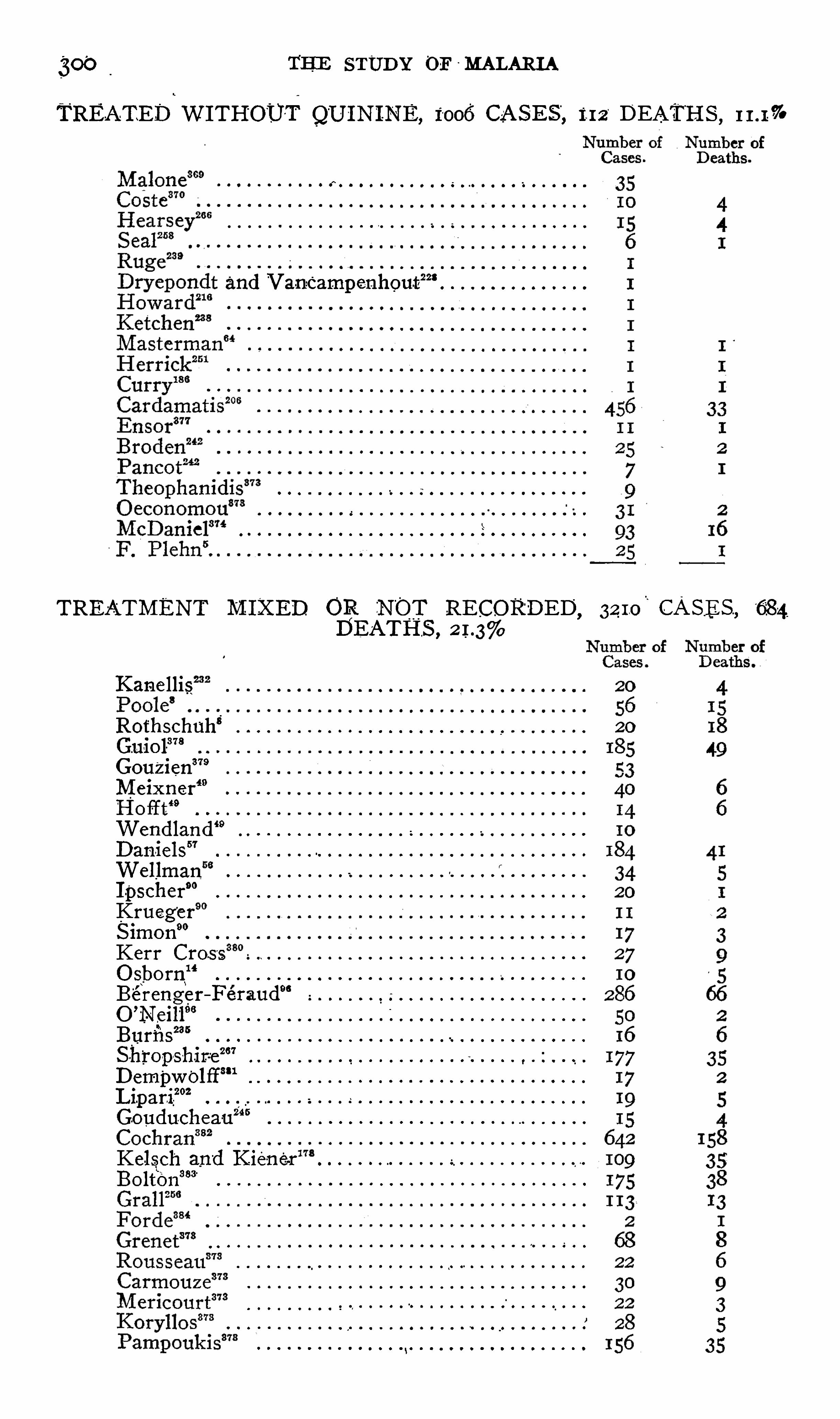
THE STUD Y OF - MALARI A
TREATED WI THOUTQUININE, 1006 CASES“
,m DEATHS ,
o o o o o - o o o o o o o n o -o o o o o 'o o 0 0 0 0 0 0 0 0 0 0 0 0 0 0
228and V anc
‘
ampe—nhout
- l 0 0 0 0 0 0 O O O O O O O O O O O O O O O O O O O O
lo o o o o o o o o o o o o o o o o o o o o o o o o o o o o o o o o
0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0
TREATMENT M IXED OR NOT RECORDED ,GASES ,
DEATHS ,
Kanellis
Rothschuh‘
20
Guiol378
Gou‘
z ien379
M eixner‘9
Ho it t‘9
Wendland49
D aniels”
Wellmanf
I pscher”
Krueger
S imon90
Kerr Cros sO sborn
“
Berenger—Feraud“
O’
Neill96
Burfi sm
S -h'
ropshir-ez a7
D empwolff‘“1
’
202LipariGouduchea-u
z “ s
Kelsch and K ie-ne-rL:
Bolton383
o o o o o o o oo
o o o o o o o o o o o o ooo oo o o o o o o o o o o o o
0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0
0 0 0 0 0 0 0 0 0 o oo
o o o o ooo o o o o o o o o o o o o o o
oo o o
o o o o o o o o o o o o oo o o o o o o o o o o o o o o
oo o o o o o o o o

C'
ases.
Cardamatis”
373Parathy ris
ut383
ThompStOn-e
German Protector ate Repor-ts
Plehn5 asserts that mortality‘
is highest 11]
but the follow ing table o f Daniels” does not bear himO f 136 first attacks . .31 or p er cent; w ere
Of as third or fourth attacks.'2 or per cent. w ere

CHAPTER VI I I
THE immortal d iscovery Of Ross is to the prophylax1s of
malariaWhat that O f L averan I s to the d iagnos is, and , althoughrecent , has already been instrumental in sav ing untold ,
suffering ,
“ incalculable economic loss , and thousands of human lives.
I t has been explained how the paras ite is abstracted by cer
tain Species of mosquitoes w ith the blood of in fected ind ividuals , undergoes essential changes I n the body of the mos
quito ,and is then inoculated into healthy persons. _
I t is, therefore , ev ident that if this cycle be broken at any po int in fect ioncannot occur, and that i f. it '
wer'
e un iversal ly interrupted duringa sufficiently long period o f. t ime the d isease would be '
annihi
lated . Hence prophylactic measures may be d irected againstthe destruct ion of the malarial paras ites w ithin the body of
man , the destruct ion of the mosquitoes wh ich are capable of
transmitt ing the paras ites , and the prevent ion o f mosquitoesgain ing access to man . The paras ite may be opposed e ither inman or in the mosquito . The mosquito may be
'
combatede ither in its aquat ic or in . its aerial s tage . Prophy lax is may
be conducted by a commun ity or by an ind iv idual , may be
public or private , O ffens ive or de fens ive .
A S is w el l known , malaria is now almost or ent irely absentfrom reg ions in which it was formerly very prevalent ,
~and in
other places is rapid ly d imin ish ing . I n the reg ions in -mind thechange was I ndependent o f des igned efforts for the erad icat iono f the d isease ;in fact , it occurred in most instances before thed iscovery of e ither the malarial paras ite or of the rOle of the
mosquito in the d issemination of the d isease , and‘
was an um
expected result Of the progress O i civ il izat ion . This uncon
scious prophy lax is was probably the product of several factors ,which may be classed as agricultural , therapeut ic, and hyg ienic.
302

304 THE S TUD Y OF M ALAR I A
were probably destroyed by fish. I t was ev ident that mosquitoreduct ion was to be the '
ch ie f end , though old cases of malariarece ived v igorous treatment. M arshes were . filled w ith sand
and the irrigation channels were deepened or treated w ith oil.
This pre liminary work was conducted w ith a brigade of on lyfour men , though
'
many others were employed later for theextens ive permanent work. From 1885 unti l 1902 inclusivethe number o f cases ofmalaria at I smailia had averaged nearly1800 annual ly. I n 1903 there occurred 2 14 cases ; in 1904 ,
90 ,and in 1905 on ly 37. I t is said that it is
’
now poss ible tosleep w ith comfort in the place Without nets . The cost of the
campaign is estimated at an in itial expend iture o f francs ,and an annual outlay of francs per head o f populat ion .
The results of the campaign conducted by Travers andWat
son at Klang and Port Swettenham ,in the F ederated M alay
S tates , are hard ly less-
striking . Klang had inhabitantsin 190 1 . Port Sw ettenham ,
five miles away ,‘
had a populat ionof about
-
700 . The population o f the d istrict surround ing thetwo towns was “
about"
'
I n the latter part'
of 190 1
malaria was so extens ive ly prevalent that probably not more
than three houses in Klan'
g escaped in fect ion , and Port Sw et
tenham was be ing ,abandoned by the workmen . The,
antimala
rial campaign , which was confined to the towns of Klang and
Port Swettenham,began in 1902 . Swamps were filled , a con
tour drain established to intercept incoming water from sur
round ing springs , and forest and mangrove trees Were fel led .
After the epidemic had begun to subs ide screens were furn ishedmany of the houses and quin ine was d istributed . The cost o f
the operat lons to the end of 1905 consisted of a primary
expense of and an annual expense of £4 10 .
The fo llow ing table Shows the mortal ity from malar1a w ithinthe towns as compared w ith that of the unprotected d istrict
1902 1903 1904
Towns 59 46 48
D istrict 227 230 286
The most brill iant results in the prophy lax is of malaria were
those obtained by Gorgas in Panama,one of the most insalu
brious reg ions upon the face of the earth , hav ing been called



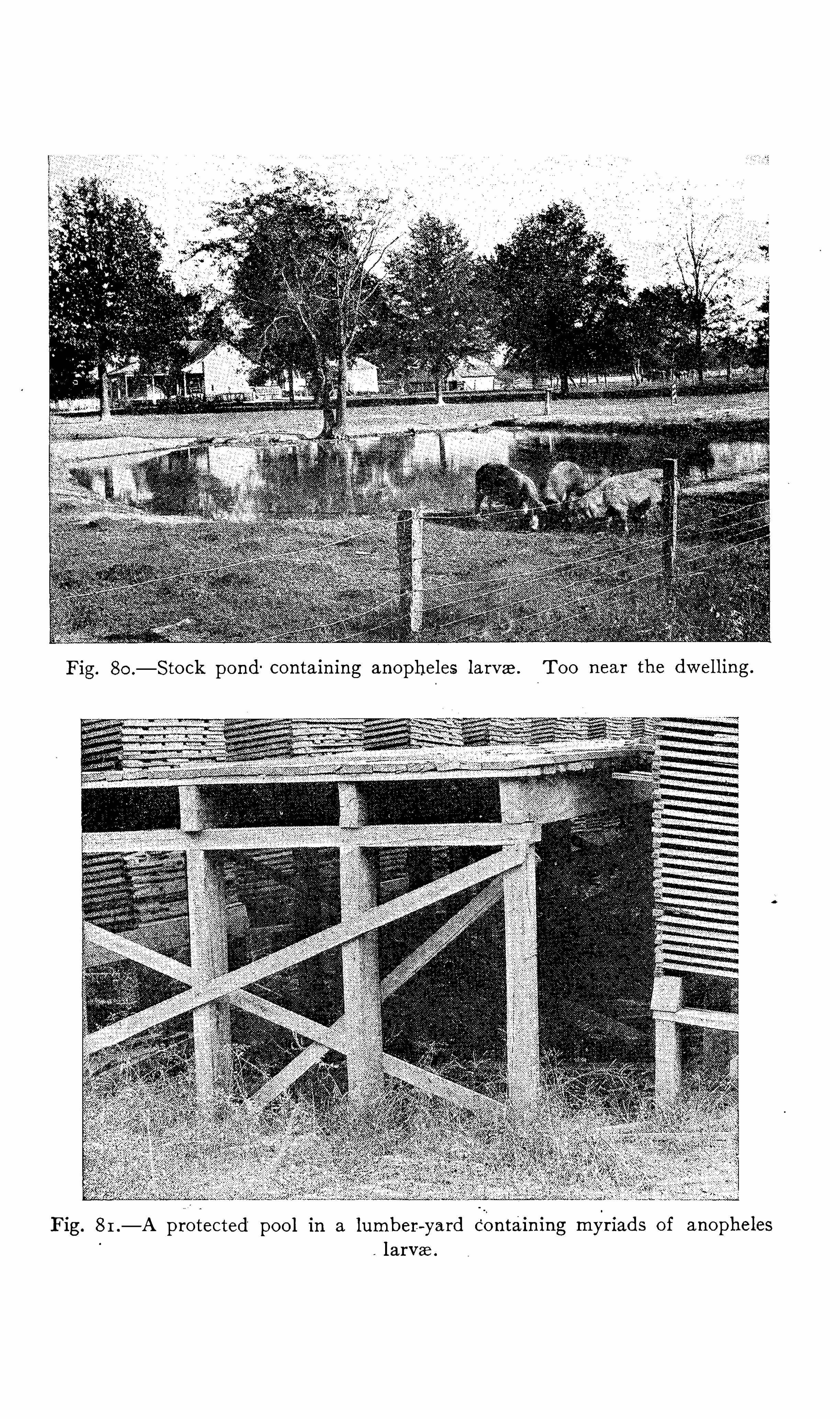


PROPHYLAXI S 305
during French occupat ion the F renchman’
s Grace . I t is a
common report that in the- rai lroad between Panama and Co lonev ery cross—tie '
represents'
the corpse of a laborer.
'
The canal zone I S fifty m i les in length ,.
With Panama and
Colon at e ach end. The average number of employes 15 40,000 .
The efforts cons isted in the destruct ion Of breed ing places onlyw ithin 2 00 yards Of the camps and v i llages , no attempts be ingmade to deal w ith those farther O ff. All the houses w ere
screened and“
the people w ere urged to use mosquito bars .
Quin ine was furn ished them and they w ei e adv ised to take 3grains dai ly . The abol ition of the breed ing pools w as rega1ded
most important measure . Ow ing to the heavy rainfal l andthe luxuriant vegetation the d itches filled rap
-id ly w ith grass ,and it
:
was found much cheaper to concrete them . Subso il’ ingby means o f the t ile drain covered w ith rock and soil
.
was used
wherever poss ible .
The result is that the death rate has been low ered unti l itdoes not exceed that o f New Y ork C ity .
I . MEASURES DIRECTED F OR THE DESTRUCTI ON OF
MOSQUITOES
D es truct ion of breed ing pools for the anophe les‘
is an effi
cient prevent ive measure . I t is chiefly through the erad icationof breeding places that S O - c alled uncons cious prophylax is hasaccomplished its results . This method has received the ch ie fconsiderat ion in the greatest ant imalarial campaigns . I t is
more permanent and possesses the further. advantage in manyinstances o f be ing cheaper 1n the end .
I t I s ne ither necessaI y nor in every case adv isable to remove
the surface water fromthe whole of a malarial country , but
on ly 111 the reg ion of habitations 0 1_
where anopheles are knownto breed . I n the Panama campaign the area of destruct ionextended only 2 00 yai dS from camps and habitations . ThisShould probably be the m in imum rad ius , though w ork at a
much g I eater d istance I S On ly a useless expense .
I n the"
area to be protected the land should be cleared '
of
weeds, undergrow th , _
bushes, and unnecessary trees to pro
mote . evaporation and prevent the . format ion of p udd les .

306 THE S TUD Y OF MALARI A
Grocery cans , broken'
bottles , ”buckets and Old tinware whichmight retain water should best beburied . Water- barrels
, tanks ,cisterns , and w ells should be empt ied , filled , or screened . Gut
ters Should be maintained ln such a cond it ion that water cannot
accumulate .0
'
The stock pond , so common in the v icin ity o f habitat ions insome Sections , is a menace to both man and beast and Shouldnot be tolerated.
The care of streams and large bod ies of water is ord inarilyS imple , s ince these rarely threaten san itat ion as anophelesbreeders . Within the protected area the banks should be
cleared of dense weeds and bushes,eddies
p prevented where
possible , and pools along the edges drained into - the channel .I n the case Of streams that
—get very low after the rainy
season,leav ing a chain Of pools along the river-
.bed , these poolsShould be drained into each other and an attempt made to
reestablish a flow and'
to permit of scouring and the“
access of
fish fromthe larger poo ls . Where the poo ls are smal l muchwater canbe gotten rid o f by the use of brooms.
I n the case of large bod ies of Water subj ect to overflow the
problem is more d ifficult. The primary effect o f the Submerg
ing of land , while the water is high , is to d iminish malaria.
The secondary effect , after the'
I
waters have receded ,is to
cause a marked increase . A remarkable example which illustrates this occurred in Holland in 1748 . The D utch al low edthe land , for defens ive purposes , to become overflowed. Peace
being concluded during the middle of the summer, the inundat ion was caused to subs ide , whereupon a serious outbreak o fmalaria occurred . The ep idemic was not success ful ly com
bated unti l the land was again submerged and kept SO untilthe advent of
'
w inter. The effect . upon malaria of inundationsis almost yearly observed in the val leys of the Ni le, of the
M iss issippi , and of other large streams. L eve'
es; dykes , and
other engineering means of large d imens ions are the onlyremed ies ; these being expens ive are rarely employed merelyfor san itary purposes.
M arshes and swamps when too extensive to be filled may
be effect ively drained . The drai ns should be narrow , of suffi

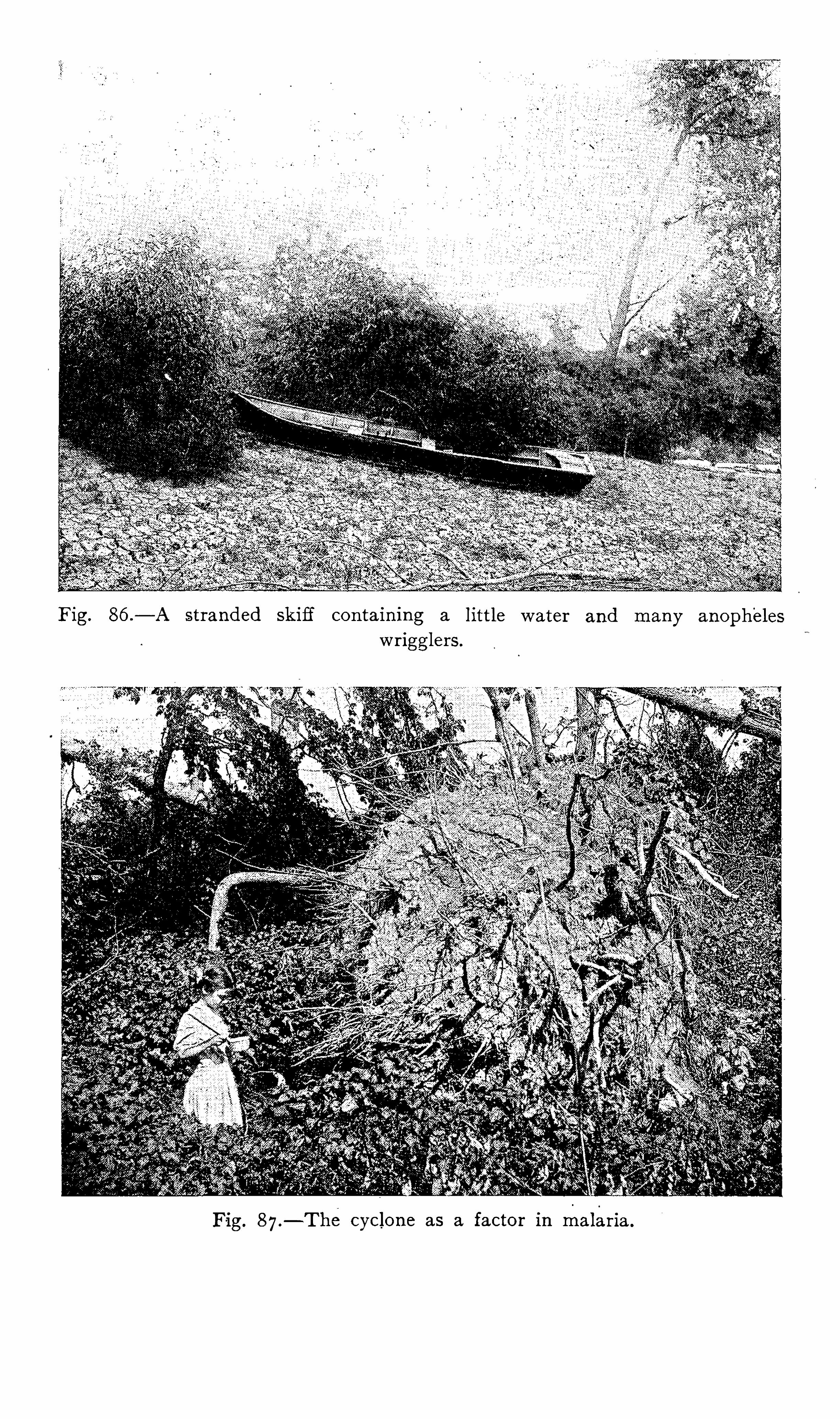






PROPHYLAXI S 307
cient depth and fall to drain effect ively , and may be paral lel ,crow foot fashion or otherw ise , as best suited to local cond it ions . I f concreted they _
_
require less after- treatment and may“
be cheaper in the end . I f not concreted they should be irequently inspected to prevent cavmg , depos it ,
'
O r fill ing w ithvegetation . Tile - drains are usually very efficient .L arge swamps in the v icin ity O f streams
- have been rendered
unfit as breed ing places by d irect ing the course of the stream
through them. The water is thus g iven a current , and if the
stream contains much mud in suspens ion the bed o f the marshis gradually filled .
F resh—water ponds close to the sea have been success fullytreated by filling w ith salt water. I t I S said that a large freshwater lake back O f the hotels at Virgin ia Beach wh ich b rednumerous
‘
mosquitoes was filled w ith salt water by means of
machinery w ith a sat isfactory result . Water strong ln salt isnot attract ive for ‘
breeding purposes , though brackish water
may harbor numerous larva .
The rendering innocuous o f borrow p its along railroad l ines(Fig . 9 1 ) is d ifficult . I t is much eas ier to prevent the stagna
t ion of water during the construction of the road than it is
to remedy the defect after comple t ion . F illing and dramage
are the best correct ives . I t should be the duty o f s ome one
to see that the construct ion of railroads,canals , a nd s imi lar
enterprises does not render a country more unsan itary .
The dest ruct ion of smaller pools and puddles is usual lyS imple and goes far toward prophy lax is , S ince it is in such
p laces that anophel ine mosquitoes breed by pre ference. F i llingis by far the mo st permanent , hence the cheapest and most
desirable method by wh ich to deal w ith these collect ions of
water. Poo ls in d itches along the S ides of roads (Fig .
wheel ruts , hoo fprints o f stock in so ft -
ground , water remaining in natural inequal it ies in the ground
-
and in e xcavat ionsfor various p urposes should be assiduously attended . The
work should be conducted by one'
who is famil iar w ith therud imentary principles of
”
drainage . The organ izat ion for thispurpose of
“
mosquito brigades” was first Suggested and put
into pract ice by RO S S , whose adv ice “
is as follows : “
Attack

308 THE STUD Y OE M ALARI A
first those col lect ions of water the obliteration of which w illremove the - largest number Of mosquitoes for the least amount
of money . Thus it is quite use less to drain stagnant water
S imply because it is stagnant water. The supermtendent Shouldfirst assure h imse l f that - it does actually contain larvae, and ,
better , that it constantlycontains them. AS already ment ioned ,
some pools are too large , others are too small , and others are
subj ect to scouring , and , though these cond it ions o ften changeat certain seasons , when ,
for instance , large pools dry up , yet
some pools appear to be habitually unsuited to the larva I t
is use less .to Spend much money over these. Again , it is not
adv isable to.
“
attack w ithout d iscrim inat ion even the poo ls wh ichdo contain larva . Some contain many more larvae than others
do ;and , in my experience , while larva do occur in Some con
siderable bod ies of water , such as marshes or ponds , they are
generally much more'
numerous in small pools . Now , it is
ev ident ly bad economy to Spend large sums ov er draining largebod ies O f water when smal l pudd les , eas i ly dealt w ith , reallycause more m ischie f. The superintendent must suppose noth
ing—he must never suppose because a marsh ex ists in a neigh
borhood that it is the only or the pr1ncipal cause o f malaria.
He must study . the point by care ful search for anopheles
larva ;and may O ften find that a "
smal l , unobserv ed pool in thestreet is more dangerous than a marsh a mile away .
The number and nature of the breed ing pools depend S O
much upon the configurat ion of the ground , the character of
the S o il , and the amount o f the rain fal l that it is imposs ible tog ive very minute d irect ions regard ing the method of deal ingw ith them. The superintendent must be guided by his own
judgment,remembering on ly the max im, which applies to most
kinds o f work , “
The S implest measures first .”The he ight o f the ground water is very int imately associated
w ith the prevalence of malaria, S ince the quantity '
o f surface
water depends largely upon the height of the ground water, andthe latter , when appearing upon the
”
surface , is a favoritebreed ing s ite for malarial mosquitoes . Hence , measures
d irected tow ard the lowering of the ground water are of the
highest efficacy in the prophy lax is of malaria. This is ev i

PROPHYLAX I Sdenced by the results O f the t i ling of land and
t ion o f drainage districts'
for the reclamation o f
S uch procedures often render unnecessary the e.
labor or money for the removal of breed ing poo lslarVal steps .
Ground water is lowered by various metho
prim it ive of - which is d itching .
“These d itchesor are part ly filled w ith gravel or stone , then w itf
ung lazed t ile drain is v ery effect iv e ; perforatecbeen employed also.
I n certain reg ions where the hardpan o'
r imperis respons ible for a high -
ground water excellen1
been obtained by boring through this, thereby
water = to escape into the permeable earth beneatlthe SO - called absorbing w ells .
I t is well known that rice culture increases thereg ion to a great extent (Fig . 93 I n some 01
countries the crop is a necess ity , but in reg ions 1
dependent upon the crop the cult ivat ion of rice rr
upon as an ev i l . I n fact , some governments have
certain restrict ions around the industry or ha
proh ibited it .S ince the t ime of P liny it
'
has been -
theither
render a locality more salubrious by filter ingexhalat ions . The eucalyptus globulus has attainereputat ion in this respect , probably from a bel ie f 1mo isture from “
the so i l and renders it drier. I
ments in I taly have,however, shown that this
effect in decreasing malaria,and that it even aff.
lent shelter for anopheles mosquitoes .
Sunflowers and castor—oil plants , which are
beneficial in the prophy lax is of malaria, are
’
prob
such v irtue .
There are circumstances“
under which it isdestroy the breed ing pools . Here the use of pet i
cated . This O il is also use ful in antimalariala temporary measure in part of the work whmeans are be ing employed elsewhere.

310"
THE'
STUD Y OF M ALAR I A
While the valueo f petro leum as a larv icide was known early1n the n ineteenth century , to Howard be longs the cred it of. its
pract ical applicat ion .
A11 oil Should be chosen wh ich Spreads rapid ly and evapo
rates S low ly . The refined i llum inat ing O il evaporates read i ly ,hence is too expens iv e for work on a large scale. The most
suitable is the fue l oil or blast - furnace oil. The oil, form inga film upon
'
the ent ire surface of the water ,'
chokes the air
tubes o f the larvae, Which come to the surface to breathe .
The pupae exp ire even earlier thanthe larva ,s ince they require
more ai r. Furthermore,not a few adult femalemosquitoes in
the act o f ov ipos it ion are thereby destroyed .
The poo l Should be cleared , as far .as possible , from Weedsand alga which interfere w ith the“
Spread of the oil. The“
oil
should be poured from a watering pot , Sprayed by means ofa
force pump ,or painted over the surface w ith saturated cloths
t ied to the ends of st icks . An automat ic o iler may be' imp
v ised . by p lacing _
a barre l o f oil a few feet above the Water tog ive the O il the necessary Spread , and having a perforat ion inthe bottom of the barre l to drop about tw enty t imes to the
m1nute .
The quant ity o f O ilWhich has been found amply sufficientis I
.
ounce for each'
1 5 square feet o f surface . I t has -been est imated that a barrel o f o il cost ing on ly a few do llars is suffi
cient to cover square feet of surface .
Evaporat ion , rains , and . w inds prevent permanent -
results , sothat .the o iling must be repeated . I ntervals of two or threew eeks are the proper average, and certain days o f themonthShould be systemat ical ly chosen . I t is best to beg in the o i lingin the spring to prev ent the first generat ions .
Nearly ev ery ant isept ic. and pOison has been employed forthe destruct ion of mosquito larva . The an i l ine derivat ivesare valuable , especially that known as L arvicide, which .destroys
also fish and other forms of l i fe wh ich may be luseful in kill inglarva . The same object ion appl ies to Phinotas Oil, a cresolcombinat ion
, and saprol, which are effect ive larvicides . Forrnalin , corros ive sublimate ,
“
carbolic. acid, and.
lysol are '
too s lowin the ir effects upon larva . to be of pract ical value . Perman
312 THE STUD Y OF MAL -ARIA
the former, exercised a“
very unfavorable influence upon the
development Of mosquito larva .
The c ult ivat ion of the .water pest (anac‘
haris alsina-s trum ) ,which S O thickly covers the surface o f the water as to prevent
the larva and pupae from gain ing access to the air, has been
recommended as a prophy lact ic measure . I t'
is >said that in
certain local ities the d isappearance of malaria co incides chronos
log ica lly w ith the appearance of the - water pest .
The natural enemies“
of adult mosquitoes are few and prae-J
t ically insign ificant . D ragon- fl ies,n ight—hawks , whip—poor
w i lls , swallow s, bats , and certain -
species of lizards destroy a
number afid some are killed by paras it ic m ites and a smal lsuctorial fly .
An ideal p'
rophy lax i s destroys"
the breed ing pools or the
aquatic stages of mos-
quitoes , but remed ies against the adult
insects are somet imes neces sary . For this purpos e . a great
variety of substances has been tried . O ne o f the most primit iveof measures is the smoldering fire of ch ips , rags , and feathers ,to be seen . in summer tw i l ight to the w indward of nearly every
negro cabiThe most pract ical means are the fumes of burn ing sulphur
and of pyrethrum powder. The room to be fumigated Shouldbe made as nearly airt ight as poss ible .
O f sulphur , from 2 to 5 pounds Should be used for every
cubic feet of space . I ts deleterious effect upon metalsand de licate fabrics l imits its use somewhat . Sulphur d iox idefumes have been found to be an exce llent insect icide .
'
Rose
nau39 3
says“
of it :.
“ Very d iluted atmospheres of the gas“
w i llquickly kill mosquitoes . I t is as efficacious for th is purposewhen dry as when m01st , whereas the dry gas has pract ically no
pow er ag ainst bacteria. Contrary to formaldehyde , it has surpris ing pow ers of penetrat ing through clothing and fabrics ,kill ing the mosquitoes even when hidden under four layerso f tow el ing , in one hour ’s t ime
, and in very d iluted proportions .
This substance , which has been so long d isparaged as a disin
fectant because it fai ls to kill Spores , must now be consideredas hold ing first rank in d is in fect ion against ye llow fever ,malaria, filariasis , and other 1nsect—borne diseases .
”
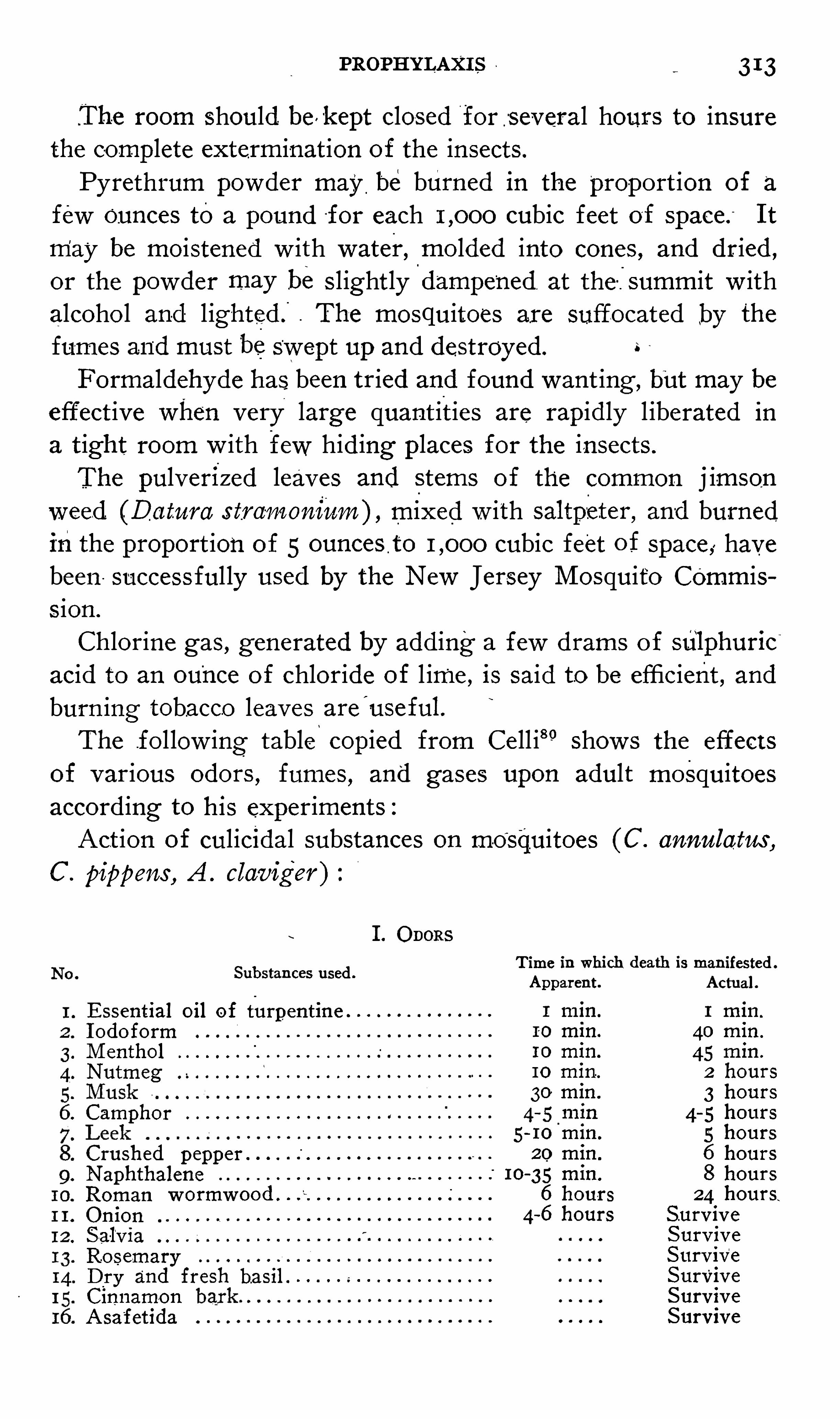
PROPHYLAXI S 313
.The room should bevkept closed for -
several hours to insurethe complete extermination of the insects.
Pyrethrum powder may be burned in the proport ion of a
few Ounces toa pound for each cubic feet of space.
“
I t
may be moistened w ith water, molded into cones , and dried ,
or the powder may be s lightly“
dampened . at the -fsummit w ithalcoho l and l ightedQ . The mosquitoes are suffocated by the
fumes and must beSwept up and destroyed.
Formaldehyde has. been tried and found want ing , but may be
effect ive when very large quant ities are rapidly l iberated ina t ight room w ith few hid ing places for the insects .
The pulverized leaves and S tems of the common j imson
weed (Da tum s tra-moniam) , mixed w ith saltpzeter , and burnedinthe proport ion of 5 ounces t o cubic feet of space , havebeen success ful ly used by the New Jersey M osquito Commiss ion .
Chlorine gas , generated by add ing a few drams o f sulphur1c
acid to an ounce of chloride of l ime , is said to be efficient , andburn ing tobacco leaves are
'
useful.
The fol low ing table copied from Ce ll i8° Shows the effectsof various odors , fumes
,and gases upon adult mosquitoes
accord ing to his experiments :
Act ion of culicidal substances on mosquitoes (C . annulatus ,
C . pippens , A . claviger )
I . O DORS
Substances used .
Essential oil of turpentineI odoformM enthol
Nutmeg
Camphor
Crushed pepper
NaphthaleneRoman
OnionS -al
‘
v ia
RosemaryD ry and fresh ba sil .
I CinnamonA sa
'
fetida
Time in which death is manifested .
Apparent.
1 min.
10 min.
I O min.
10 min.
30 min .
4- 5 min
5 - 10'
min.
20 min .
10-
35 min.
6 hours
4—6 hours
Actual
1 min.
40 min .
45 min .
2 hours
3 hours
4- 5 hours
5 hours
6 hours
8 hours24 hours.
SurviveS urv ive
Surv iveSurviveS urvive
Survive
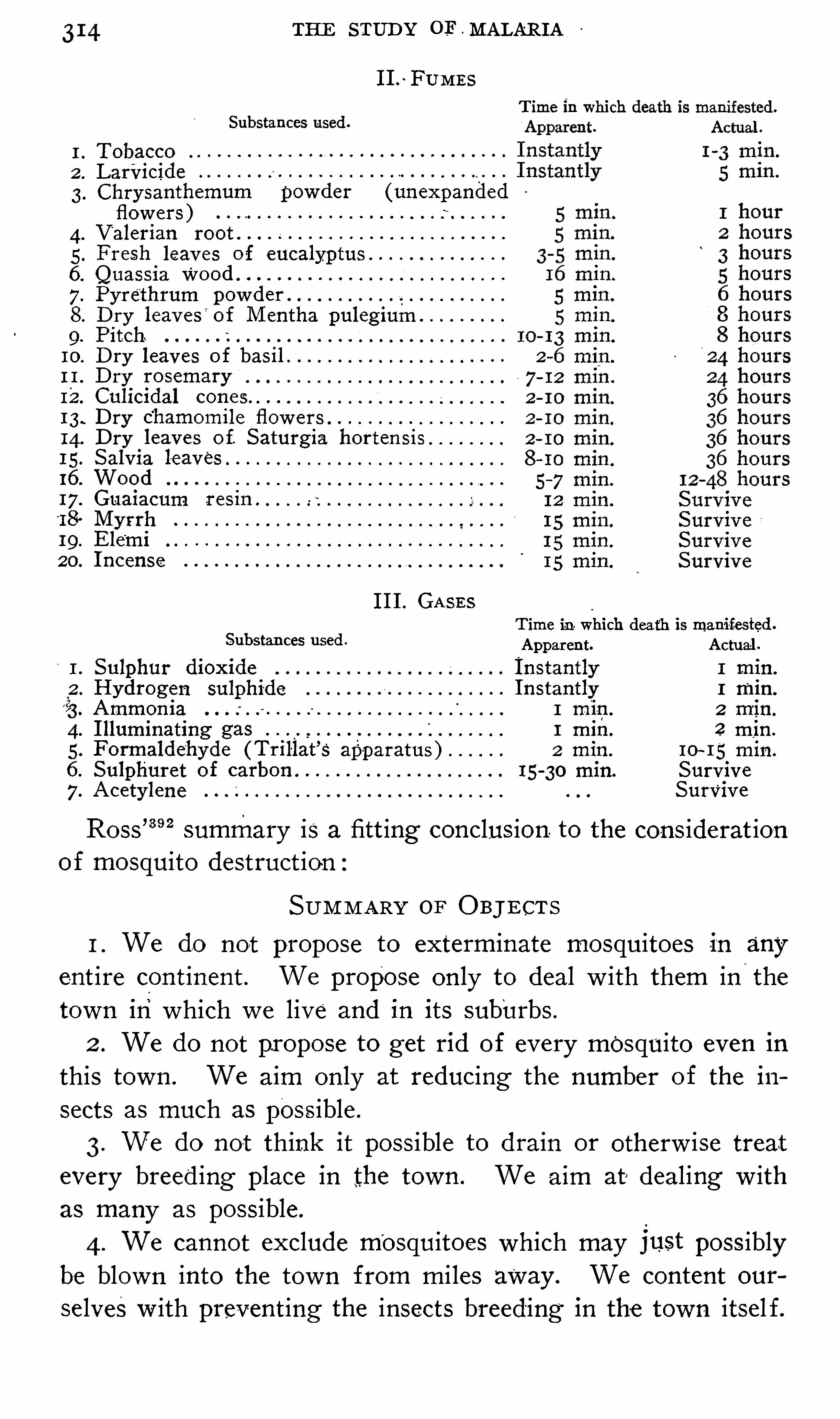
THE STUD Y OF - MALARI A
I I .~FUM ES
T ime in whichSubstances used .
TobaccoLarvicideChry santhemum powder (unexpandedflowers )V alerian root .
Fresh leaves of eucalyptus
Quassia WoodPyrethrum pow der .
D ry leaves of M entha pulegium. Pitch
10. D ry leaves of basil .
11. D ry rosemaryI 2. Culicidal cones .
13. D ry chamomile flow ers
14. D ry leaves o f. S aturgia horten sis15 . S alvia leaves
G
an
ge
s
wa
s
16. Wood17. Guaiacum res in .
“
18. M yrrh19 . Ele
‘
mi20. I ncense
I I I . GASES
T ime in which death 15 mani fested .
Substances used . Apparent. Actual.
I . Sulphur dioxide I nstantly 1 min.
2 . Hydrogen sulphide I nstantly 1 min.
3 . Ammonia 1 min . 2 min.
4. I lluminating gas 1 min . 2 min .
5 . Formaldehyde (Trillat’
s apparatus ) 2 min . I O~ I S m in .
6. Sulphuret of carbon 15 -
30 min. S urv ive
7. Acetylene S urvive
Ross’39 2
summary is a fitt ing conclus ion. to the cons iderat ionof mosquito destruct ion
SUM M ARY OF O BJ ECT S
I . We do not propose to exterminate mosquitoes in anyent ire cont inent . We propose on ly to deal w ith them in
‘
thetown inwhich w e live and in its suburbs .
2 . We do not propose to get rid of every mosquito even in
this town . We aim on ly at reducing the number of the i11
S ects as much as poss ible .
3. We do not think it poss ible to drain or otherw ise treatevery breed ing place in the town . We aim at» dealing w ithas many as possible .
4 . We cannot exclude mosquitoes which may just poss iblybe blown into the town from mi les away . We content our
selves w ith preventing the insects breeding in the town itsel f.
316 THE STUD Y OF MALARI A
danger to the community . The second mode consist s of the
administration , to persons not necessarily in fected , o f a drug
which destroys the para s ite soon after the latter is introducedinto the body , before the incubat ive stage is completed .
Cases of latent and atypic malaria (Fig . 94 ) are of greater
importance to prophy lax is , being sources of greaterdanger to
commun it ies than are typic acute cases } The durat ion of the
acute attack is Short , the pat ient is apt to be placed under relatively favorable cond it ions and to rece ive quin ine ; he doesnot wander and d isseminate the d isease
,and his blood may
contain but few sexual forms of the paras ite. O n the otherhand , the Subj ect of latent malaria may harbor paras ites formonths , and , the cond ition being unrecogn ized
-
or ignored, hedoes not take quin ine
,and is a fountain of in fect ion in d iverse
places and for prolonged periods .
Koch has maintained‘
that the prompt and permanent cure
of all acute cases of malar1a and the Systemat ic search for , andappropriate treatment Of, all latent cases in a reg ion w ill resultin the exterminat ionof the d isease from such a local ity . Thisi
’
S theoret ically poss ible , but could be pract ised on ly in smallcommun it ies under
'
perfect control. Nevertheless , it is cer
tainly the duty of phys icians to endeavor to effect rad ical curesof the cases which come under the ir observat ion , a duty owed
not on ly to the pat ient , but to the public, and such efforts w i llgo far toward the erad icat ion Of the d isease .
Quin ine Prophy laxis—Theoret ical ly the adm in istrat ion of
quinine to healthy ind iv iduals for the prevention of malaria isnot an ideal method of prophy lax is , for, strict ly Speaking, itdoes not prevent in fect ion , but destroys the paras ites in the
incubative stage after inoculation into the human body . But
no one method sat isfies all cond it ions each has its advantagesand its limitations ,
'
and frequently two or more methods mustbe employed S imultaneously.
Quin ine prophy lax is is ind icated in proportion to the diffi
culty of pursuing more permanent methods; I t is valuablewhere screens and bars are not available , as in camp ing ,
marching , traveling , or where the occupatiop takes one out at
night . When res idents of non - malarial countries go into mala


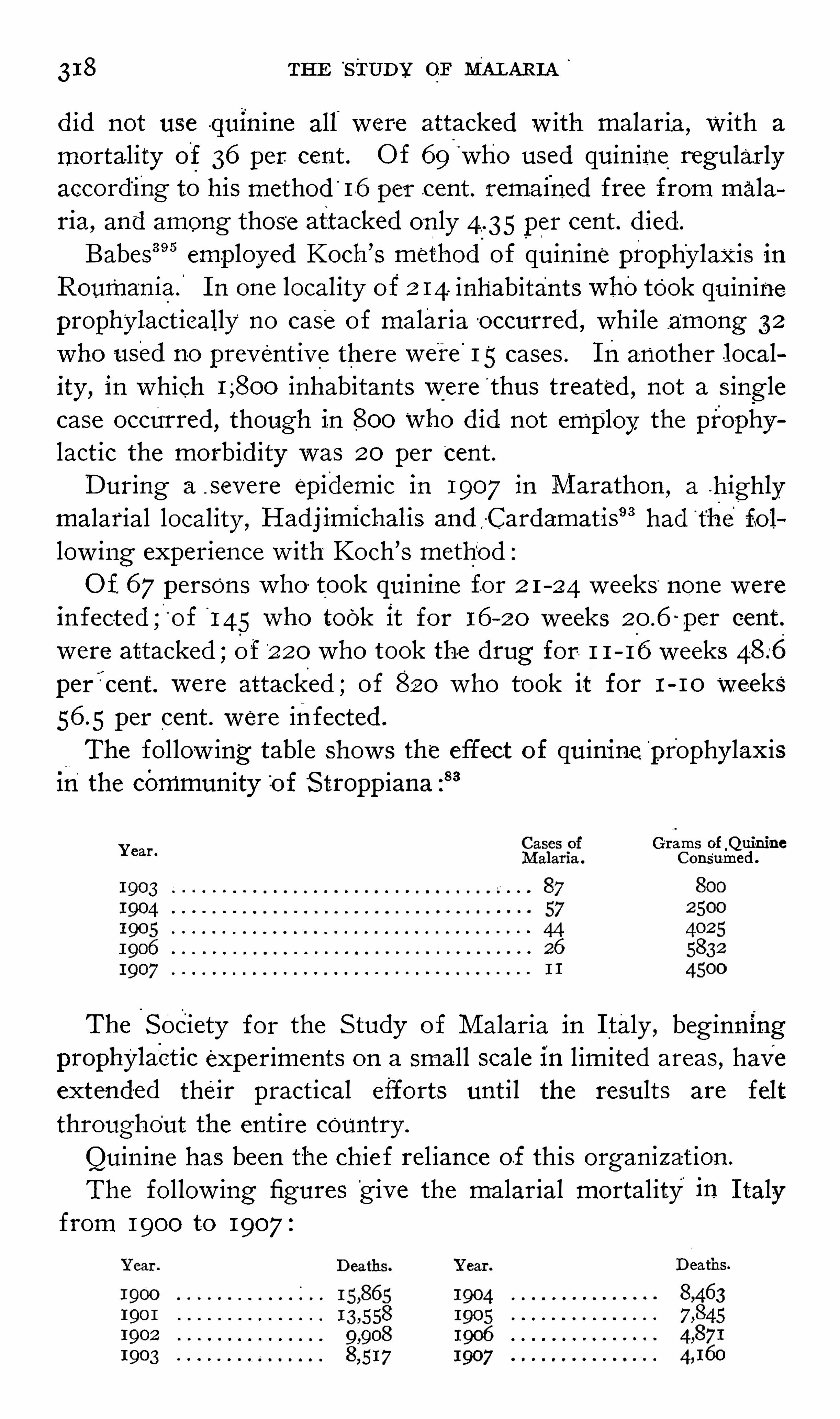
318 THE S TUD Y OF MALARI A
did not use quinine all were attacked w ith malaria, with a
mortality of 36 per cent . O f 69"
who used quin ine regular lyaccording to his method '
16 per cent . remained free from malaria, and among those attacked on ly 4.35 per cent . d ied .
Babes39 5 employed Koch ’
s method.
of quin ine prophylaxis inRoumaniaf I n one local ity of 2 14. inhabitants whotook quin ineprophylact ically no case o f malaria o ccurred , wh i le among 32
who used no prevent ive there were I'
5 cases . Inanother locality , in which inhabitants were '
thus treated not a S inglecase occurred , though in 800 who did not employ the prophylact ic the morbid ity was 20 per cent .
D uring a _ S evere epidemic in 1907 in M arathon,a .highly
malarial local ity , Hadj imichalis and -Cardamatis9 3had
“
the fo llow ing experience w ith Koch ’s method :
O f 67 persons who took quin ine for 2 1 - 24 w eeks none w ere
1nfec- ;ted O f 145 who took it for 16 20 weeks per cent .
were attacked ;o f 2 20 who took the drug for 1 1 16 weeksper cent. were attacked ; of 820 who took it for 1 - 10 weeks
per cent . were infected .
The fol low ing table Show s the effect of quinine '
pr'
ophy lax isIn the community of “
S troppiana :83
Grams of_QuimaoYear .
Consumed .
The'
Society for the S tudy of M alaria in I taly beg inningprOphylaet1c experiments on a small scale in l imited areas , haveextend-
ed their pract ical efforts unt i l the results are feltthroughout the ent ire country .
Quin ine has been the chie f rel iance of this organ1z ation .
The fol low ing figures'
g ive the malarial mortal ity in I talyfrom 1900 to 1907
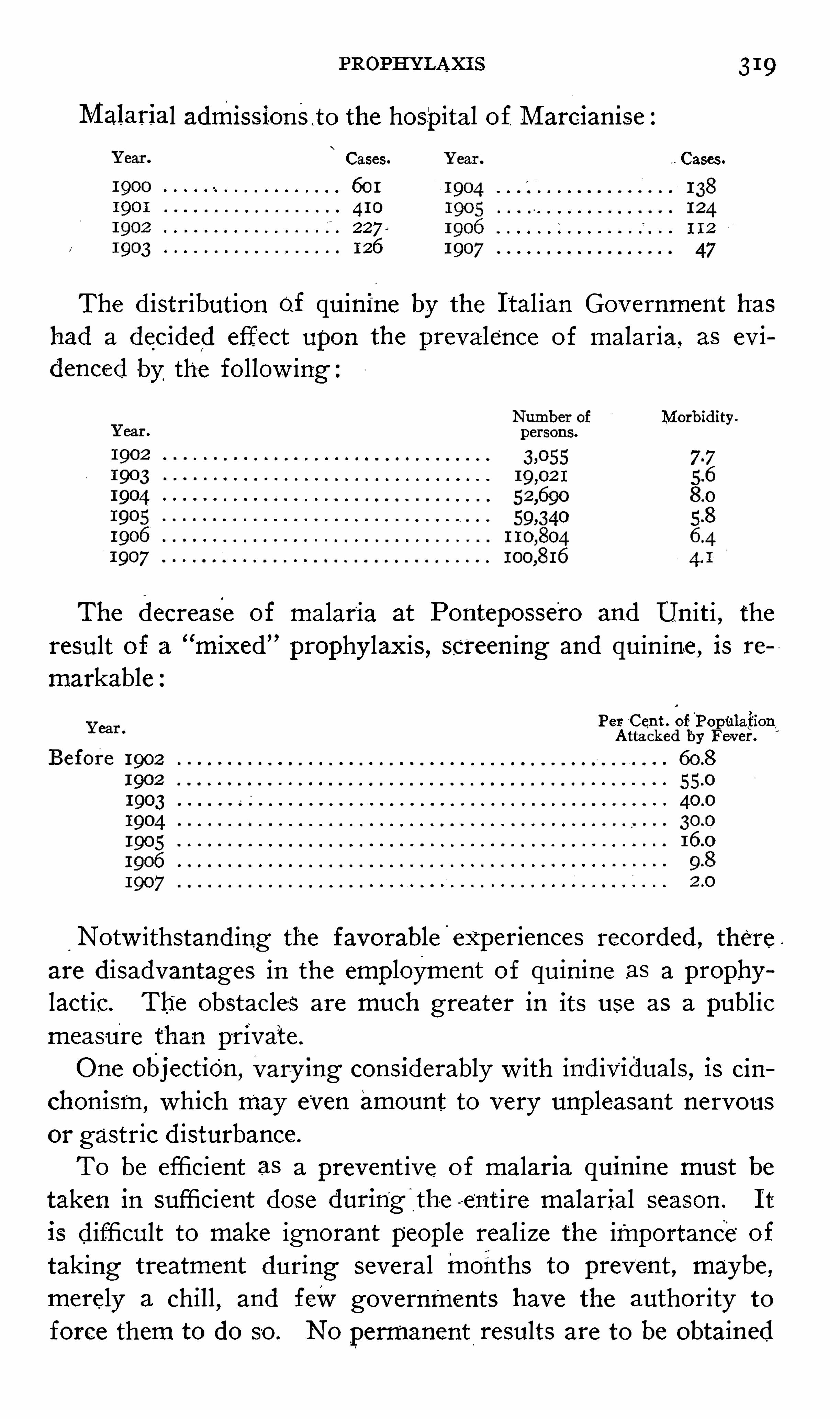
PROPHYLAXI S 319
Malarial admissionsto the hospital of. M arciamse
Cases. Cases.
The d istribution of quinine by the I tal ian Gov ernment has
had a decided effect upon the prevalence of malaria, as ev i
denced by the follow ingMorbidity .
The decrease of malaria at Pontepossero and Unit i , theresult o f a “
mixed” prophylaxis , Screening and quinine , is re
markablePer C ent . ofPopula
tion
,
Attacked by Fever.
Notw ithstand ing the favorable'
experiences recorded , there
are d isadvantages in the employment of quin ine as a prophy
lact ic. Th‘
e obstacles are much greater in its use as a publicmeasure than private .
O ne obj ecti0n ,vary ing considerably w ith ind ividuals , is cin
chonism, which may even amount to very unpleasant nervousor gastric disturbance.
To be efficient as a prevent ive o f malar1a quinine must betaken in sufficient dose during
'
the -ent ire malarial season . I t
is difficult to make ignorant people real ize the importance“
of
taking treatment during several months to prevent , maybe ,merely a chill
,and few governments have the authority to
force them to do so . No permanent,
results are to be obtained
320 THE STUD Y OF MALARI A
in this way unless all take the drug throughout the malarialseason and all cases o f malaria are
‘
radically cured.
The”
expense of public prophy laxis w ith quin ine on a largescale is enormous ; in
.
fact , in some instances p'
rohibitory .
M oney spent for quin ine to be g iven in inadequate doses at
irregular intervals is wasted .
The size of the dose and the interval at wh ich the prophylact ic is administered
‘
are of the utmost importance ._Very
vary ing quant it ies hav e been employed at d ifferent intervals ,but the established methods have about settled down to thosedescribed below :
The method canom z ed by Koch “
con5 1sts in g iv ing 1 gram of
quinine every s ixth and sev enth day , seventh and eighth , e ighthand n inth , or n inth and tenth day, accord ing to the danger of
infection . This man i fest ly leaves several intervening days inwhich there “
is no quin ine in the circulation. I n local ities , therefore, in which est ivo - autumnal malaria is prevalent , the shorterinterval of admin istrat ion should be pre ferred on account -o f
the Shorter period of incubation of. this form of malaria.
This method has proved very v aluable in many hands .
Ziemann48 describes his method of“
universal prophylax isas follow s :
1 . O ne gram o f qu1n1ne I S g iven every four days, three daysinterven ing . The drug is g iv en in solut ion w ith 5 drops of
hydrochloric acid . I f cinchonism is marked , I gram of potas
S ium bromide i s g iven .
2 . I f 1 gram of quinine is not wel l borne , 1 gram of euqui
n ine is ‘
g iven .
3. I f t his produces too decided cinchon ism, yo, gram of
quin ine is g iv en as abov e .
4 . I f V2 gram o f quin ine cannot be taken , V2 gram o f euqui
n ine is admin istered .
The drug is g iven early in the morn ing or one and a hal f totwo hours after a meal . The rule is to g ive a dose on the firstof each month and thereafter on each day of the monthd iv is ible by four.
By this method it is bel ieved that quin ine is constantly inthe blood current , and that this result is accompl ished w ith a
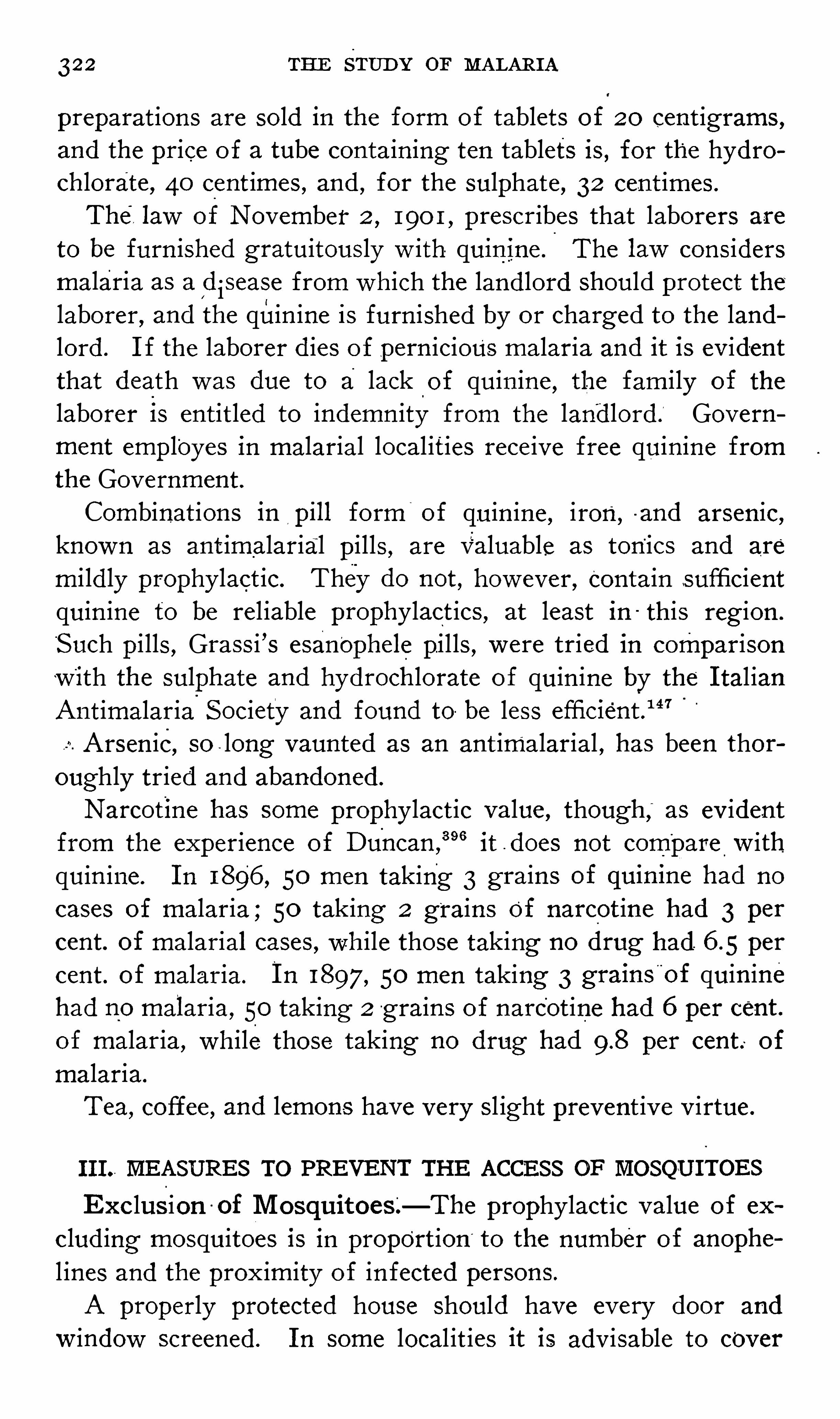
322 THE STUD Y or M ALARI A
preparations are sold in the form of tablets o f 20 cent igrams ,
and the price o f a tube containing ten tablets is , for the hydrochlorate , 40 cent imes , and , for the sulphate , 32 cent imes .
The, law of November 2, 190 1 , prescribes that laborers are
to be furn ished gratuitously w ith quin ine.
The law cons idersmalaria as a
[
d isease from which the landlord should protect thelaborer , and the quin ine is furn ished by or charged to the landlord . I f the laborer d ies o f pern icious malaria and it is ev identthat death was due to a lack
“
of quin ine , the fam ily of the
laborer is entitled to indemn ity from the land lord. Government employes in malarial local ities rece ive free quinine fromthe Government .
Combinations in pill form"
of quin ine , iron, a nd arsen ic,known as ant imalarial pills , are valuable as ton
'ics and are
m i ld ly prophy lact ic. They do not , how ever , Contain sufficientquin ine to be rel iable prophy lact ics , at least in this reg ion .
“
S uch pi lls , Grass i ’s esan'
ophele pil ls , w ere tried in comparisonw ith the sulphate and hydroch lorate o f quin ine by the I tal ianAntimalaria
'
S ociety and found to be less efficient .1 47
Arsen ic, so long vaunted as an ant imalarial , has been thoroughly tried and abandoned.
Narcotine has some prophy lact ic value , though ,
“
as ev identfrom the experience of Duncan ,
39 6 it d oes not compare w ithquin ine . I n 1896 , 50 men taking 3 grains of qu1n1ne had no
cases of malaria ; 50 taking 2 grains of narcot ine had 3 percent. of malaria] cases , wh ile those taking no drug had per
cent. of malaria. I n 1897, 50 men taking 3 grains"
of quin inehad no malaria, 50 taking 2 g rains of narcot ine had 6 per cent .of malaria, while those taking no drug had per cent. of
malaria.
Tea,coffee , and lemons have very s l ight prevent ive v irtue.
I I I .. MEASURES TO PREVENT THE ACCESS OF MOSQUI TOES
Exc lus ion -
of M osquitoesL—The prophy lact ic value of ex
clud ing mosquitoes i s in proport ion ‘
to the number of anophe
l ines and the prox imity of in fected persons.
A properly protected house Should have every door and
Window screened . I n some local it ies it is adv isable to cover
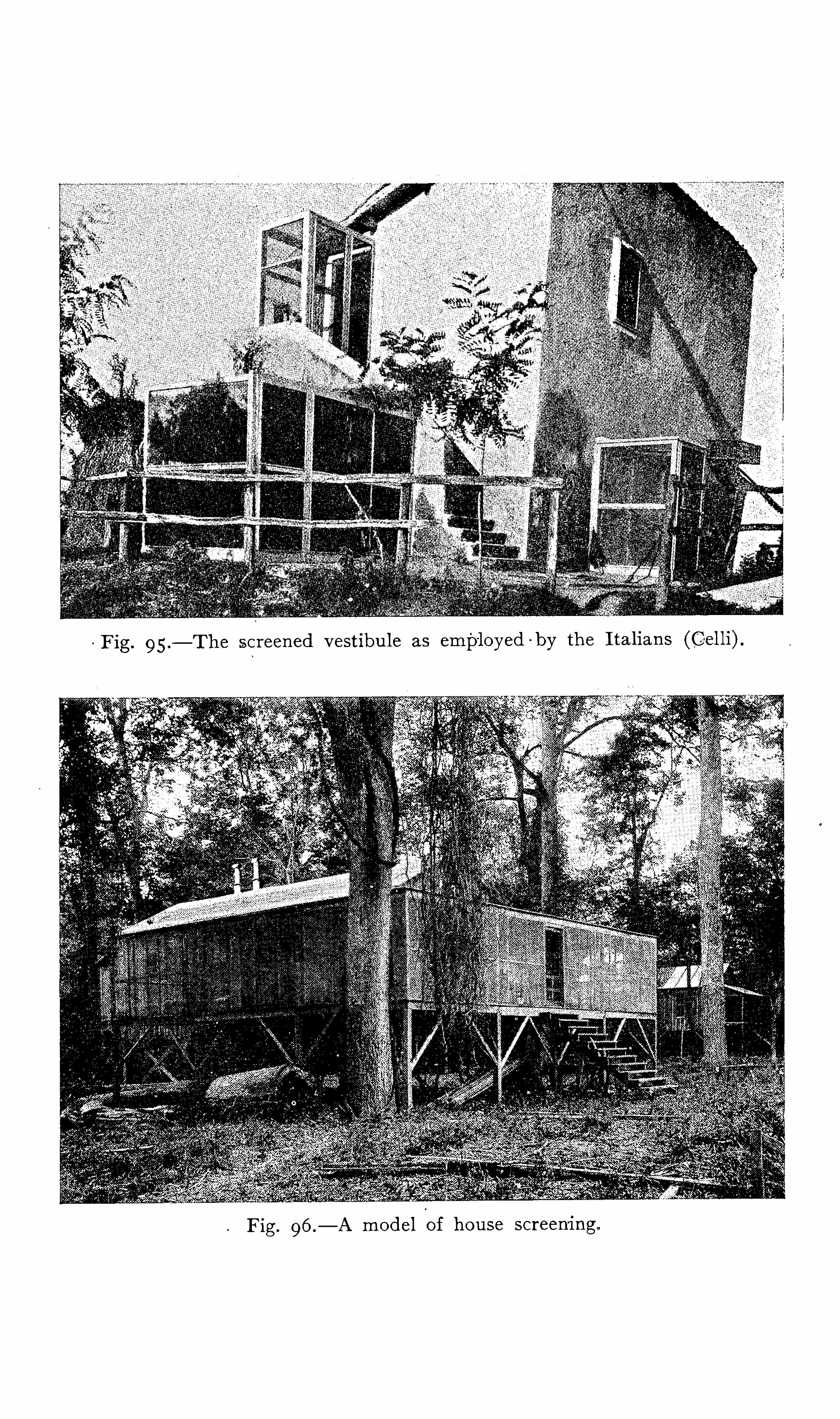



PR‘
OPHYLAXI S 323
even the chimneys w ith Wire nett ing . D oors Should be provided w ith ‘
spri-
ngs to necess itate closure. Where mosquitoesare plent i ful , and;
a door is much used, a double door , w ith aninterven ing vest ibule , after the"
manner of the I tal ians (Fig .
is to be pre ferred . A screened porch permits of S itt ingin the air in the evening when ‘
it would be dangerous to do so
otherw ise.
The select ion of the gauze for screens is of the h ighestimportance. The mesh of the w ire nett ing often used , No. 12 ,
is too large , permitt ing smal l mosquitoes to pass (Figs . 98
and None Should be used w ith fewer meshes than 18
to the inch . I n the abSence o f w ire gauze , cotton mosquitonetting
'
may be'
employed , but , be ing frai l , soon becomes torn
and useless.
Persons whose ocupations keep them out at night in highlymalarial places, as watchmen and others , Should be protectedw ith ve ils and w ith leather g loves hav ing gauntlets .
The mosquito bar is ind ispensable in malarial countries . Be
s ides be ing very effect ive when properly adjusted , it is the
most inexpens ive o f all prophylactic methods.
“
S tephens and Christ0phers1 13
rel ied personally almost en
tirely upon the protect ion afforded by the mosquito bar. Theysay :
“
The net Should be square (not a bel l n et ) Should not
have a S ing le , even m inute , hole ;should hang outside the poles ,i f these are used ; should be tucked under the mattress , and
should not trai l on the ground . A p iece o f close ly “
wovenmaterial , fastened on all round at the level of the - body , is a neces
sary add it ion in order to protect the l imbs during S leep frombites through the net . When not in use the ends of the net
Should be tw isted up Somewhat and then thrown over the top .
We always arranged our nets ourselves,never trust ing to ser
vants , and ,further, tobe doubly certain , we always carefully
Searched the interior w ith '
a candle be fore go ing to S leep. To
these minute precaut ions solely we attribute our absolute freedom from malaria. Employed w ithout care and attent ion a
mosquito net is of l ittle protect ion in such malarious places as
most up- country A frican stat ions .
”
The Public Health and M arine Hospital Serv ice issues the

324 THE STUD Y or MALARI A
follow ing instruct ions in regard to screening against mosquitoes :397
1 . The nett ing used Should have meshes fine enough to
prevent the passage of mosquitoes (at least 18- 20 to the inch ) .
2 . I t is important to screen the w indow s and doors of the
house . I t is doubly important to screen the beds of feverpat ients .
3. M osquitoes can bite through the mosquito nets when any
part o f the body is in contact w ith the nett ing .
4. Frequent exam inat ions Should be made to see that there
are no torn places in the nett ing or that no mosquitoes havefound a lodg ing ins ide.
5 . The netting should be well tucked in to keep mosquitoesfrom entering .
Fig. roo .—British experimental hut near O stia (M anson) .
6 . I f mosquitoes are found w ith in the nett ing they shouldbe killed ins ide , and not merely driven or Shaken out .
The results obtained from mechanical prophy lax is have beenv ery sat is factory . The celebrated experiment
'
of S ambon and
L ow”9 8 is striking . Under the auspices of the Eng l ish Co lonial
O ffice and the L ondon S chool of Tr0pic M ed icine these scien
tists Spent the ent ire malarial season of 1900 near O st ia, in one
o f the most malarial parts of the Roman Campagna. The hut
in which they l ived was constructed in L ondon for the purpose ,and was thoroughly screened . They drank the same water and
worked in the marsh w ith the nat ives. They took no quin ine ,and , in fact , observed no prophy lact ic precautions except ing to
326 THE STUD Y or MALARI A
consider the screen ing'
of all the houses , both on acconi
the expense and because o f t he poor construct ion of mar
them ,
“
permitt ing mosquitoes to enter through crev icesother open ings . The fact that screens offer a S l ight hind ito the free circulat ion of air in hot
'
countries is of l ittle mo
in the face of the benefits derived from the ir use , and
must be considered as one of the most effect ive mean
private prophylax is.
O f local applications to drive away mosquitoes many
stances have been tried , part icularly the essential o i ls , of vthe o ils of citronella,
eucalyptus -
and lavender are probabl ‘most efficacious. Petro leum , in fus ion of quass ia, naphth z
powdered sulphur, camphor, garl ic, the o i ls o f cloves ,pennyroyal ,
'
chrysanthemum ,and an ise have been empl
w ith vary ing degrees of Success .
The follow ing preparat ions are highly recommended
Cedar o il 1 ounce ,
O il of citronella 2 ounces ;
Sp irits of camphor 2 ounces—“
M .
S ig. :Apply a few drops to a cloth and hang upon the bed.
”
5322121011’ as 1 ounce ;
O il of lavender 1 dram.—M .
S ig : Apply to the Sk in .
Quinine—glycerine 1 1000
S ig . : Apply to the sk in.
Ether ,Alcohol
Aq . colomensis,
01. eucalyptusTr. py rethrum -
,M .
S ig . : D ilute w ith four or five parts of water and apply to
the sk in .
“
For the local rel ie f of mosquito bites , touching w ith vof ammon ia or w ith g lycerin are efficient .I n I nd ia the punk-a is employed to keep the air in motion
for this reason is found to be of serv ice in driv ing away
quitoes . The e lectric fan has this effect also, but for obi
reasons Should not be employed for this purpose during 5
The value of smoke against mosquitoes is wel l knthough it is not always ent irely effect ive . The writer recaloccason while on an island off the Gul f coast of Florida w

‘
PROPHYLAXI S 327
smoke was of no avai l against the terrific onslaught o f bloodthirsty mosquitoes , and it became necessary to bury himsel f upto the neck in the sand and to cover the head with a coat .
I so lat ion of the malar ial pat ient I S as truly ind icated -as in
ye llow fever , both "
d iseases be ing conveyed in the same manner.
M osquitoes must become infected be fore they can in fect man ;
breaking the v icious circle at th is po int would ext irpate mala-4
ria. I so lat ion is demanded not on ly for the good o f the com
mun ity , but t o prevent re in fection o f the pat ient , who Shouldbe confined under a w ell—adjusted bar unt il a rad ical (ture iseffected . I t is not to be expected , however, that asmuch canbe accompl ished from the iso lat ion o f malaria as from isola~
t ion of yellow fever. M any cases of ~ malaria ent irely escape
med ical treatment,and a malarial subject may be a source o f
in fect ion for a year or more , wh ile yellow fever is infect iousfor only a few days .
'
S ince it has become ev ident that so great a propd rtio-
n of
the inhabitants , especially the children of trop ic countries ,harbor malarial paras ites in the
“blood , segregat ion of the
Whites from the nat ives has been proposed and in some in.
stances pract ised w ith success . While the question is of some
import in this country , the negro quarters in most,
of our
towns are fairly we ll defined from those o f the Wh ite . Upon
the premises the householder Should see that his servants’
quarters are
-
as thoroughly screened as his own. I n the choiceo f c amp s ites nat ive houses should be avoided beyond the
l imit o f fl ight o f mosquitoes , i f possible.
Great good is be ing accompl ished in the prophy laxis of
tuberculos is by educat ion ,keeping the main facts in the et iology
and prevent ion constant ly before the eyes of the people . S o
much cannot be expected for malaria on account of the igno
rance and carelessness of the class and race of people most
scourged ,but undoubtedly some good may accrue from this
method . The Europeans , at home and in their co lonies , haveobtained some results in the prophy lax is of malaria by teaching the people the elements of the cause and prevention o f
the d isease .
L ectures , illustrated by st'
ereopt icon v iew s , are held publicly.
328 THE STUD Y or MALARI A
Publications in s imple language , _
in the form of circulars and
tracts , and even appropriately i llustrated postcards_
are scat
tered broadcast . The I talian S ociety for the S tudy of M alariahas d istributed about two m ill ions ,of these circulars . The
principles of prophy lax is are insti lled into the minds of the
schoo l chi ldren , and made attract ive and impressed by means
of i llustrated charts . The lay press has been used to advan
tage . With such means the format ion of an ant imalarialleague can do much fora commun ity . A l ittle can be aecom
plished by educat ion , and this l ittle should not be neg lected .
S choo ls and departments of tr0pic med icine have done a
great deal to d isseminate a know ledge o f this very importantsubj ect , and evenmore stress should be laid upon t h is important branch of med ical science .
3
To“
be thorough , malar ial prophylax is should be handledby the Government . D estruction o f the breed ing places of
the mosquitoes, which is by far the most radical method , is ,in many instances , too expens ive to be done
'
by ind iv iduals .
The format ion of drainage d istricts, the expenses of which arepaid by those benefited ,
is an effective plan , and so enhances
the value of r eal estate , from both agricultural and - san itarystandpoints , that there should be no oppos ition . The w riteris conv inced that these d istricts , which are being formed in
various parts of the S outh , are decreas ing the malaria in a
decided degree . I t is highly probable that malaria w ill beexterminated as a natural consequence o f the drainage of the
soi l be fore the Government or the people are educated to
the point of taking prophylactic steps. Governments wil lspend m illions o f money in the erad icat ion o f malaria fromfore ign laborers in orderto further g igant ic commercial enterprises , but make no prophy lact ic efforts against the malariaunderm in ing the v itality and destroy ing the l iv es of cit izens .
I nd iv iduals who Should know better permit anophe les mosqui
toes to breed at their doors and to"
have access to their houses ,and allow the ir malaria to go untreated .
The I nternat ional Congress of Hyg iene at its Brusselsmeeting , S eptember, recommended to all Governments
the'
adoption o f the fol low ing measures :14“
330 THE STUD Y or MALAR I A
drip - cans at their heads . The oil cans are raised three feetabove the water to g ive a w ide Spread to each drop , and are
arranged to drop about 20 drops to the minute . The oil used
is a rather heavy dark grade , which - costs the department$4.34
a barrel . About barrels of. oil were used w ithin the lastyear.
“
All streams are kept free from algae and are kept w ithinrestricted banks as far as possible ;this is done by blow ing out
the rap ids or falls to produce a uni form flow , and the edges
are filled in by hand .
“
All swamps, pools , or even temporary col lect ions of water
are o iled at . least weekly , and in the rainy season o ftener ;this applies
_
to the smal lest collection of water, even animaltracks , ruts from wagon wheels , and crab holes . I t entails a
great amount o f work, Which is done by colored labor under
cont inual superv is ion.
“
All receptacles hold ing water must be screened or o iled.
Water barrels are screened by covering w ith a board w ith a
small , screened open ing in the center for the inflow . Belowthis board are two Screened holes for the overflow , and the
water is drawn from a faucet at the bottom . Buckets and
pails in daily use in a household are not permitted to stand
filled more than twenty- four hours . All tin cans , bottles , etc. ,
must be buried . No gutters are al lowed on houses. There isa dai ly inspect ion of all water receptacles , and weekly the
inspector at the head of the stat ion must make a personalinspection and report any receptacle found containing mosquitolarvae. The second offense , after a warning , means the arrest
and fine of the househo lder.
All old machinery , which is foun d in great quant ity all over
the zone canal , le ft from the French occupat ion ,
“
is drainedby punching holes in any part that w i ll hold water or
,where
this is not poss ible , such places are filled w ith d irt.“
Even patent car couplings on the trains in use must be
inspected and o i led , as they are often found to contain mos
quito larvae.
“When any house or camp is found to contain any numberof mosquitoes it is fumigated w ith sulphur by the dry method.
PROPHYLAXI S ‘
All cracks or openings . are pasted over w ith paper ; enoughpots , each contain ing 5 pounds of sulphur , are pla ted at intervals on the floors to make about 1 pot for each cubic '
feet of space . A fter fumigat ion the house is le ft closed fromthree to f0ur hours.
“
All barracks , whether for black or white laborers , bachelorquarters , married quarters , offices , churches , lodge - rooms
, and
other rooms used for S leep ing ,l iv ing , or eat ing quarters are
screened..
The S an itary D epartment is respons ible for all re
pairs of this screen ing , and employs a large force of carpentersfor this
“
purpose .
“
The phys icians in each d istrict make a weekly - report o n
the number o f cases o f malaria in the d ifferent camps ; thesereports are tabulated in the central office of the S an itary D e
partment and compared w ith the prev ious records , and i f anincrease of even a fract ion of 1 per cent . is Shown for any
local ity the local inspector is telephoned and ordered to locatethe point of in fect ion and erad icate the breed ing places . Long
cont inued stat ist ics show how n icely this system work-s .
'
I f
any more serious increase occurs a Special mosquito inspectoris sent out from the central office to locate the trouble andreport on the best measures to be taken.
“
The d ifficulties of this work are . numerous. The constant
increase of population requires new s ites for camps to be
made in the unimproved , brush - covered country ; the ever
chang ing cond it ions due to the canal work are“
a cont inuedsource of trouble ; the progress of each steam—Shovel or of
each of the extens ive dumps produces new problems to be
so lved in the way of drainage , and, above all, the recurringdeluges of the rainy season cause ris ing creeks and rivers and
overflow of low lands so irregular as to be impossible to foresee.
“
The‘
S anitary D epartment has , as ide from its office force ,about thirty san itary inspectors and employs between .
and laborers . The total cost of the S an itary I nspector ’sD epartment is between . three and four hundred thousand dollars .
”
I t Should be the duty of the authorities of every malarial
332 THE STUD Y OF MALARI A
country to remove the duty from quin ine and to maintain a
high standard of purity and a“
low price .
3
I n m i litary pract ice permanent quarters should be properlyScreened , and all breed ing pools w ithin the radius of danger
S hould be destroyed . Temporary quarters Should be chosenw ith:reference to the breed ing of mosquitoes , and the forceShould ,
_
if necessary , be subj ected to Koch ’
s quinine pro
phy lax is . S hips should not anchor too'
near the shore o f
malarial local it ies .
Private prophy lax is,cons ists of measures having reference
to the person and to the premises . Personal prophy laxis issynonymous w ith proper hyg iene . Suitable food , water , and
clothing are essent ial. Regular hours must be kept , and'
con'
st_
ipation , chilling of the body ,and excesses o f all kinds must
be avoided . Prophy lact ic quin ine is not constantly necessary
for res idents i f the prem ises are in proper cond ition, but is
suitable f or strangers and under cond itions where mosquitoescannot be excluded . Person s S leeping upstairs are less l iableto in fect ion than
l
those upon the first floor.
Poo ls are to be filled , drained ,or o i led , and vessels emptied .
I t has been suggested that a tub o f water be kept on the placeto tempt mosquitoes to breed , and that this be empt ied every
few days . S tock ponds Should be '
drained , o i led , or stockedw ith fish . The houses Should be thorough ly screened , and
where these are not effect ive , or i f infection occurs , bars mustbe employed .
'
PROPHYLAXI S OF HEMOGLOBINURI C FEVER
A . Plehn has Shown that hemog lobinuric fever is preventable to a greater degree even than malaria. I n 1897
-
99 among
the officers of Cameroon who used no prophy lact ic there oc
curred in 578 months o f res idence 287 cases of malar ia and
31 of blackwater fever , or 1'
malaria case for every two
months and 1 of blackwater fever for each months. Ten
per cent . o f the blackwater cases terminated fatally . D uringthe same period among those who used prophy lax is there were
in 446'
months of res idence 90 cases of malaria and 6 of hemo
globinuric fev er , or 1 case of malaria for each five months
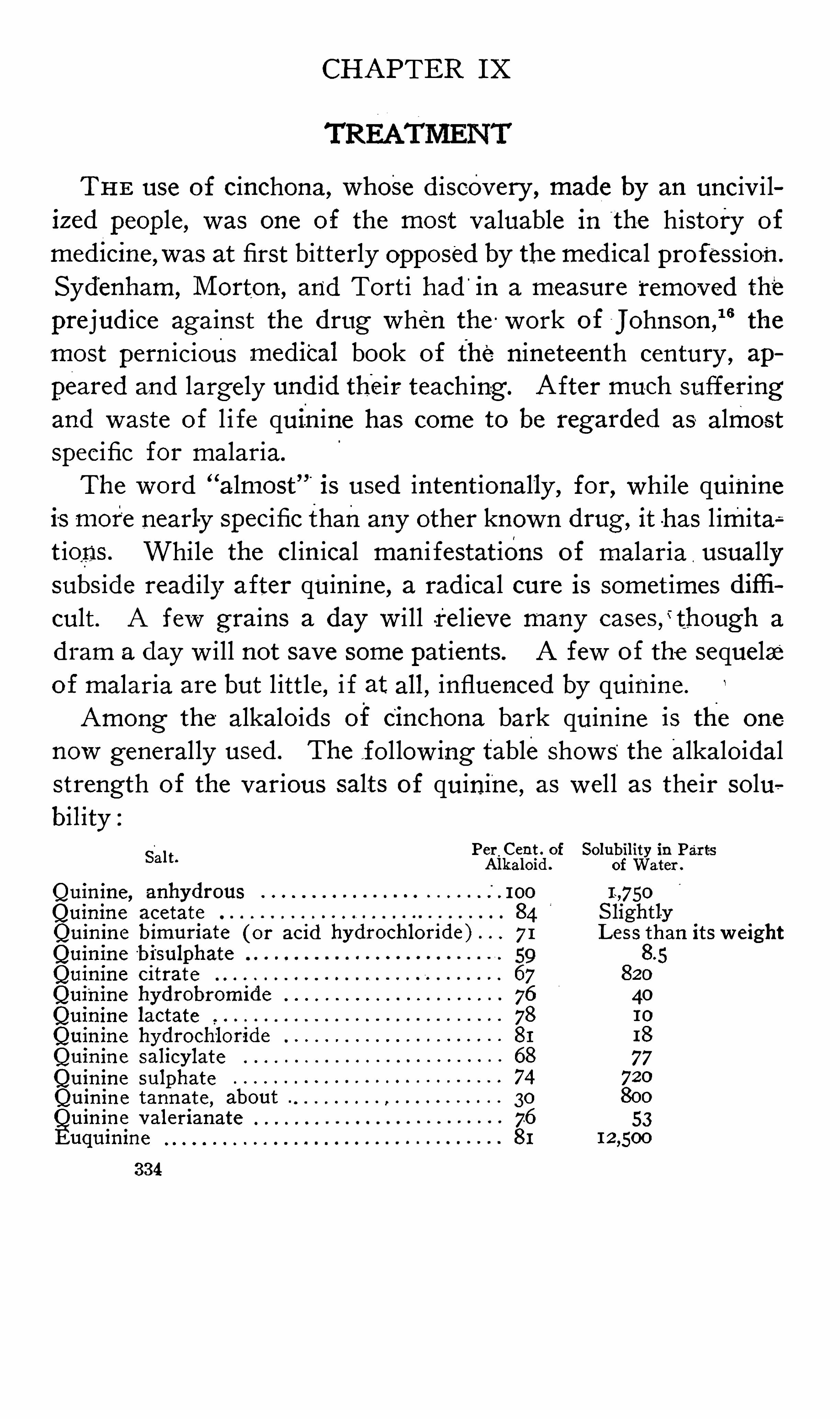
CHAPTER IX
THE use of cinchona, whose d iscovery , made by an unciv i liz ed people , was one of the most valuable in the history of
med icme,was at first bitterly opposed by the med ical profess ion.
Syd'
enham, M orton , and Tort i had ”
in a measure“
removed the
prejud ice against the drug when the work of J ohnson ,
16the
most pern icious mediCal book of the nineteenth century , ap
peared and largely und id their teaching. After much sufferingand waste o f l i fe quinine has come to be regarded as almostspecific for malaria.
The word“
almost '
is used intent ionally , for , Wh ile quinineis more nearly specific thanany other known drug , it has l imita;
t ions . While the cl in ical man i festat ions of malaria,usual ly
subs ide readily after quin ine , a rad ical cure is somet imes diffi
cult . A few grains a day w i ll rel ieve many cas a
dram a day w ill not save some pat ients. A few of the sequelae‘
of malaria are but l ittle , i f at all, influenced by quinine.
Among the alkaloids of cinchona bark quin ine is the one
now general ly used . The fol low ing table shows“
the alkaloidalstrength of the various salts of quinine , as wel l as the ir solubility :
Salt. Per_Cent . of
Alkaloid .
Quinine , anhydrous . 100
Quinine acetate 84Quin ine bimuriate ( or acid 71
Quinine'bi
'
sulphate
Quinine citrate 67
Quinine hydrobromide 76
Quinine lactate 78
Quinine hydrochloride 81
Quinine Salicylate 68
Quinine sulphate 74
Quinine tannate , about 30
Quinine valerianate 76
Euquinine 81
334
Solubility in PartsofWater .
I ~,7SO
S lightlyL ess than its w eight
820
40
I o
18
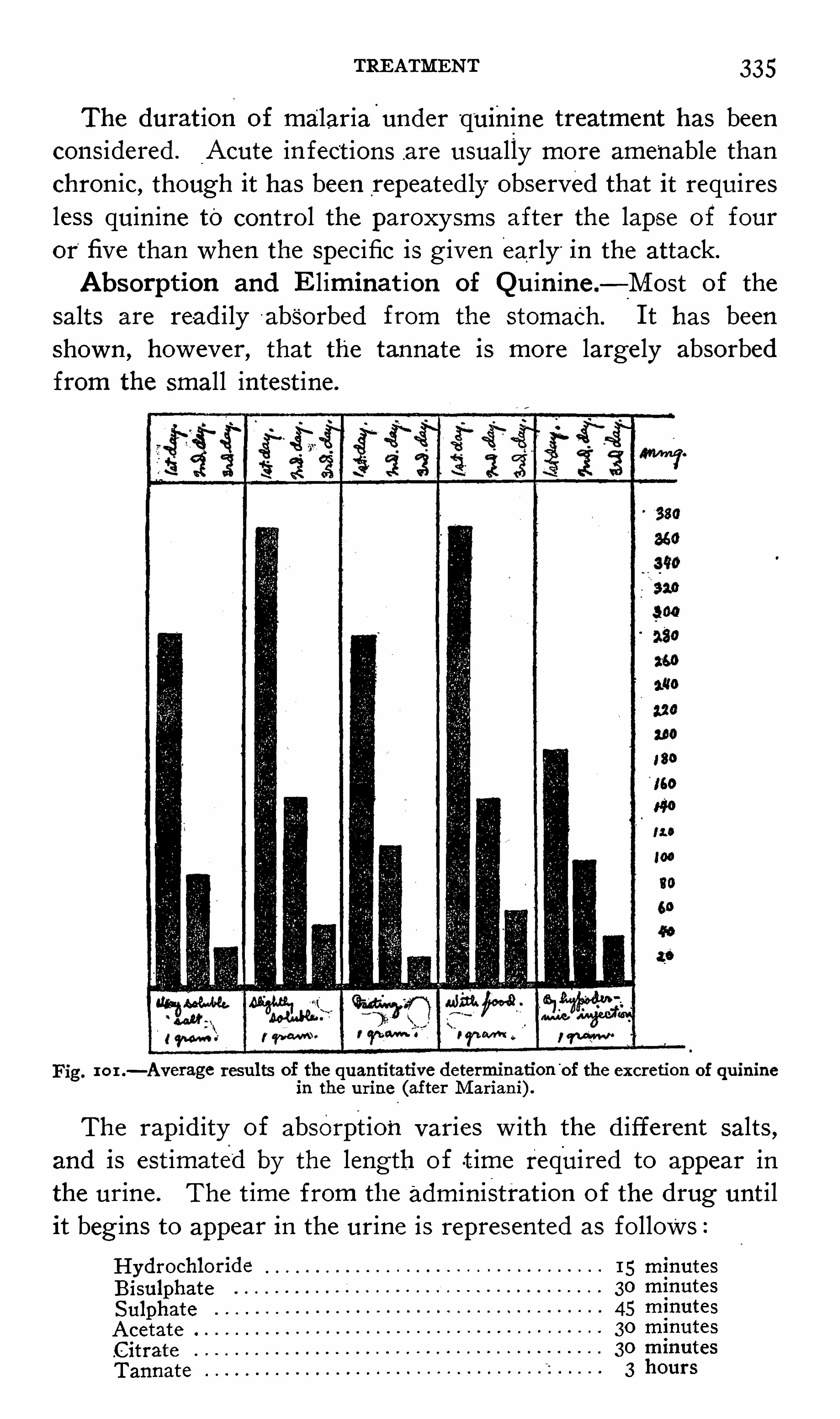
TREATMENT 335
The durat ion of malaria-
under“quinine treatment has been
cons idered . Acute in fect ions are usually more amenable thanchron ic, though it has been repeated ly observed that it requiresless quin ine to contro l the paroxysms after the lapse of four
or’
five than when the Specific is g iven early “
in the attack.Absorption and Eliminat ion of Qu in ine .
—M ost of the
salts are read ily '
absorbed from the stomach .'
I t has beenShown , however, that the tannate is more large ly absorbedfrom the small intest ine.
ran—Average results of the quantitative determination“
of the excretion of quinine
in the urine (after M ariani) .
The rap id ity of absorption varies w ith the d ifferent salts ,and is est imated by the length of t ime required to appear in
the urine . The t ime from the administrat ion of the drug unt ilit beg ins to appear in the urine is represented as follows °
Hydrochloride 15 minutes
Bisulphate 30 minutes
Sulphate 45 minutes
Acetate 30 minutes
.Citrate 30 minutes
Tannate 3 hours
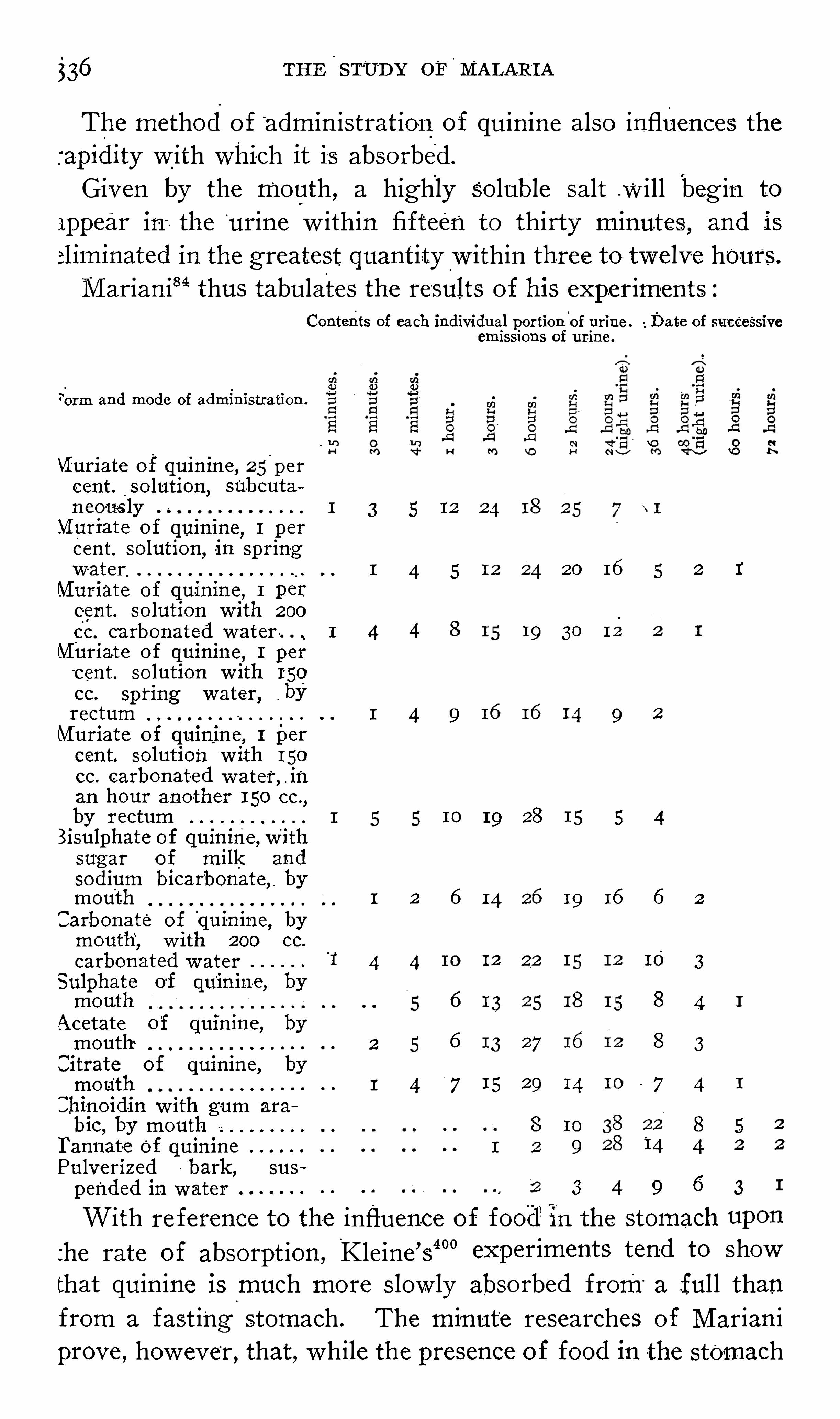
$36 THE S TUD Y OF MALARI A
The method o f admin istrat ion of quin ine also influences the'
apidity w ith whi-eh it is absorbed .
Given by the mouth , a highly soluble salt .will beg in to
ippear ia the'
urine w ithin fifteen to thirty minutes , and is
>liminated in the greatest quantity w ithin three to twe lve h0urs.
M arian i84 thus tabulates the results of his experiments :
Contents of each individual portion of urine . Date of successiveeni i S S ions of urine .
7orm and mode of administration
Vfuriate o f quinine, 25'
per
cent . solution,Subcuta
n eo-usly 1 3 5 12 24
.VI uriate of quinine, 1 p er
cent. solution ,in sp ring
water 1 4 5 20 16 5 2 1
Muriate of quinine , 1 percent . solution w ith 200
cc. carbonated water . . 1_4 4 8 19 30 12
Muriate of quinine , 1 perc ent . solution w ith 150
cc. Spring water, ,
byrectum 1 4 9 9 2
Muriate of quinine, 1 percent. solution w ith 150
cc. carbonated w ater,in
an hour another 150 cc,
by rectum 19 28 5 4Bisulphate of quinine ,Withsugar of milk and
sodium bicarbonate, bymouth 1 2 6 14 19 16 6 2
Carbonate of quinine, bymouth , with 200 cc.
carbonated w ater'
1'
4 4 12 22 10 3
Sulphate of quinin-e, bymouth 6 18 15 8 4
Acetate of quinine , bymouth 2 5 6 27 8 3
Citrate of quinine , bymouth 1 4
"
7 15 29 14 7 4
Chi-noid-in w ith gum ara
bic,by mouth 8 10 8 5
I‘
annat-e of quinine 1 2 9“
14 4
Pulveriz ed bark , sus
pended in water 3 9 6 3
With re ference to the influence of food"in the stomach
the rate of absorpt ion , Kleine ’
s40°
experiments tend to Showthat quin ine is much more S low ly absorbed from“
a full thanfrom a fast ing stomach . The minute researches of M arian iprove , however
,that , while the presence of food in the stomach

338"
THE S TUDY or MALARI A
TABLE I
One gram daily o f Quinine hydrochloride in water, at a S ingle dose, bymouth.
‘
No . Patient.
2 . 3. 4 . 5 . 6 .
Total quantity of urine excreted in per cent .
F irst day 18.5S econd dayThird dayFourth d-ayF ifth dayS ixth dayS ev enth day 2 .9Eighth dayNinth dayTenth day
Av erage
Total average, per cent .
Remarks.—I n patient No
‘
. 4 the feces were examined,1n which only a
trace of quinine could be detected w ith the thalleo -
quinine reaction .
TABLE I I
One . gram daily of quinine hydrochloride in wafers,
.2 grami
'
every two
hours.
No. Patient .
Total quantity of urine excreted in per cent.
First dayS econd day .
Third dayFourth dayFifth day 29 2 32 8S ixth dayS eventh day 29 10
Eighth dayNinth dayT enth day
Average
Total av erage , 27.8 p er cent .
RemarkS.—I n patient No. 8 the urine of second , third , and fourth daysw ere thrown out by mistak e. I n patient No . 3 the feces w ere examinedonly traces of quinine could be detected by the thalleo -
quinine reaction.
“
While it is a w idely prevalent bel ie f that the soluble saltsof quinine are much more rapidly and completely absorbedfrom the stomach than are the insoluble preparat ions , experiments show that such is not the case .
M arian i84 records his results as follow s
Administered on an
emp ty stomach .
Per cent .
Easily soluble quinine salt
Hardly soluble quinine salt

“
TREATMENT 339
Giemsa and S chaumann3°° observed that the average per
centage excreted w ithin the first twenty- four h ours after ad
m inistrat ion o f a soluble salt of quin ine was per cent.
whi le w ith an insoluble .Salt it was per and they
conclude that the salts of quin ine , hardly soluble in water , areat leas t as energet ically absorbed from the d igest ive tract as
the Soluble ones.
'
The results of clinical experience w ith .euquinine and the
tan -nate of quin ine ful ly support such a conclus ion .
Briquet and Quevenne‘101 formerly maintained,
that the ab
sorpt ion and excret ion of quin ine proceeded one - S ixth more
rapidly in f emales than in males . This conclus ion , as yet un
confirmed ,Should be determ ined on ly after a long series of
experiments.
Employed hypodermically the rapidity and thoroughness of
absorpt ion depends upon the . solubility of the salt and the con e
centrat ion of the solut ion . The latter is of the utmost t importance
,S ince , no matter how soluble the salt , i f given in strong
solution it w il l not be absorbed .
I n order to determine the effect upon - human blood andserum of quin ine injections , _
Giemsa and S chaumann“? added
to 1 cc. of l ight red human serum 1 cc. of solut ions of differentstrengths of vari0us salts of quin ine . Their results were as
follows °
Contepts
S trength -oiequiva ent Behavior of the mixture .
P ti n . to anh drousrepara oSO IUUOD
quiz ,“ Immed iately . After twenty - four hours .
(per cent ) .
Cloudiness.
M arked preCip itation.
Hydrochloride 1 35 M arked cloudi
ness.
Rimur iate
Bimuriate w ith urea
BisulphateHydrochloride
Bimuriate
Bimuriate With urea
Precipitation .
M ore decided
p r e cipitation ,
gray coloredI ncreased pre
cipitation,co
agulation.
Clear coagulum,Cloudy gray co
gray colored. agulum.
Clear coagulur-
n,Cloudy gray co
gray colored. agulum.
Cloudiness. Precipitation.
M arked cloudi Precipitation.
ness.
Cloudiness. Precipitation.
Cloudiness. Precipitation.
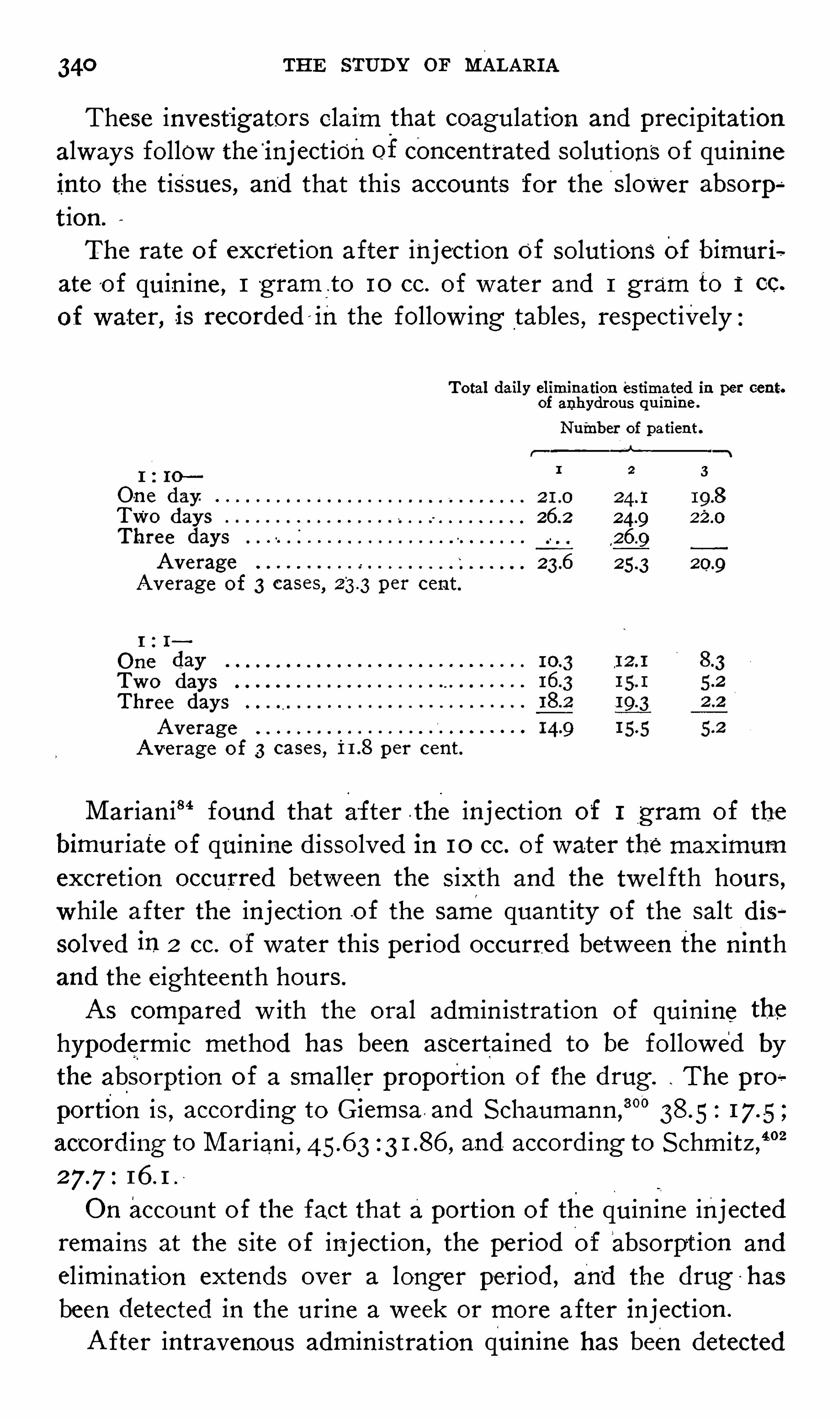
340 THE STUD Y or MALARI A
These invest igators claim that coagulation and precipitat ionalways follow the
'
inj eet ionof concentrated solut ions of quin ineinto the t issues , and that this accounts for the S lower absorp
a
t ion.
The rate of excret ion after inject ion of so lut ions of bimuriaate o f quin ine , 1 -
gram _
.to 10 cc. of water and 1 gram to 1 cc.
water, is recorded—ih the follow ing tables , respect ive ly
Total daily elimination estimated in per cent.of anhydrous quinine .
Number of patient .
On e day.
TWO days 26 2Three days 22
Average 23.6
Average of 3 cases,23.3per cent.
1 1
O ne dayTwo daysThree days
Average
Average of 3 cases , per cent.
M arian i8 4 found that after .the inject ion of 1 g ram of the
bimuriate of quin ine d isso lved in 10 cc. of water the max imumexcretion occurred between the s ixth and the twel fth hours ,while after the inject ion .of the same quant ity of the salt dissolved in 2 cc. o f water th is period occurred between the ninthand the e ighteenth hours .
AS compared w ith the oral adm in istrat ion of quinine the
hypodermic method has been ascertained to be followed bythe absorpt ion o f a smaller proport ion o f the drug . The pro
portion is , accord ing to Giemsa and S chaumann ,
“ 0
accord ing to M arian i , and accord ing to S chmitz ,4°02
O n account of the fact that aport ion of the quin ine inj ectedremains at the S ite o f in ject ion
,the period of absorpt ion and
el iminat ion extends over a longer period , and the drug has
been detected in the urine a week or more after inject ion .
A fter intravenous admin istrat ion quinine has been detected

342 THE STUD Y or MALARI A
next forty - e ight hours . Given just before segmentat ion and
repeated at intervals of three hours , the drug acts upon the
p lasmod ia not only whi le free in the plasma, but also upon
every stage o f the ir human l i fe cycle , and it is thus possibleto study the morpholog ic changes produced by quin ine in every
stage of the ir deve lopment.“
The young‘
ring
'
forms’
stain very intensely after the ad
m in istrat ion o f quinine , thep rotoplasm stain ing a much darkerblue than normal , while the chromat in stains a dark crimson .
Bes ides the increase in the intens ity o f the stain, the on ly Othermorpholog ic change observed is the loss of the unstained area,
which , in normal specimens , always surrounds the chromat in.
“
I n tertian plasmodia a litt le further advanced in developnt the stain ing reactions are the Same as in the
‘
ring forms , ’but the increased motility o f the paras ites is shown in the great ,
number and the‘bizarre ’
arrangement o f the“
pseudopodia.
Fragmentat ion is observed even be fore the format ion of pig
ment , some of the plasmod ia at this stage being broken up
into deeply stained port ions , the chromat in ly ing in one of
these port ions or free near the periphery of the erythrocyte .
“
A fter the format ion of pigment , and especially after theplasmod ia are from one—hal f to three - quarters grown , the ev i
dence of fragmentat ion and of extrus ion of the chromat infrom the paras ite become more marked. M any of the erythrocy tes contained port ions of deeply stained protoplasm , the chro
matin o f the plasmod ium ly ing free at some port ion of the
red cel l. The latter is often S ituated at the extreme peripheryor part ly outs ide of the erythrocyte .
“
At this stage numerous extracel lular plasmod ia are seen ,
e ither undergoing fragmentat ion or hydrop ic degenerat ion.
M any of the fragments are entirely devo id of pigment , staining a un i form deep blue throughout , while some may be almostfilled w ith pigment granules. “
The unstained area
“
about thechromatin is always absent , nor is there any ind icat ion of an
increase in the amount of chromat in which is so not iceablein the normal plasmod ia at this stage .
“While at this stagemany fragmented plasmod ia are usuallyobserved , in some instances no ev idence of - tli is process is
TREATMENT
The protoplasm stains a uni form dark blue , the pigmcollected, as a rule
,about “
the periphery , while the ch
.1 stains intensely and'
may be S ituated at any port ion)rganism, but usually near the periphery . There is.ined area surround ing the chromat in.
.1 many instances the chromat in is S ituated at the extre
hery of the plasmod ium or may lie partly or wholly c
of it w ithin the erythrocyte , thus prov ing that quin,S ses the power of caus ing extrus ion of the chroma .
rendering the plasmod ium sterile .
‘
ogether w ith the absence o f the vesicular port ion of
us , as Shown by the loss o f the unstained area surrou:
de chromatin , there is but se ldom, even in thoseorganis
.1 are not undergo ing fragmentat ion , any ev idence o f
e of the chromat in, and never any ev idence of its .d iv is i
Vhen the tert ian plasmod ium is nearly full grown "quino ften causes fragmentation ,
many of the fragme'
nta
i isms be ing free from chromat in,but the characteris
"e from the normal at this stage of grow th consists1Ct that , although the chromatin may be present and st
intensely ,it has increased but l itt le or not at all in amor
l iv is ion is either absent or imper fect , on ly two or th
masses be ing present , which lie close together near
hery of the organism . I n tertian plasmodia which heen influenced by quin ine and have reached this stage
0pment , the chromat in . has always increased largelynt and div ided
‘
into several smal l clumps , which are sc
throughout the organ ism. The morphology o f the pl
a at this period of their growth ind icates clearly t
ne preven ts an increase in the amount of the chromai
:ither hinders d iv is ion orstops it altogether.
.t th is stage the protoplasm of the organ ism stains dee ]he p igment is collected about the periphery in blocksileS , or d istributed throughout the protoplasm in the fo
granules 0r small clumps .
he unstained area about the chromat in is always abstplasmod ia which sporulate after being exposed to
i
'
o f the quinine throughout the ir ent ire cycle of devel
THE STUD Y OF M ALARI A
ment present very'
marked morpho log ic ev idences of"
the injurions effect of the drug . While Sporulat ion may not be ent irelyprevented , the majority of the spores are devo id of chromat inand are undoubtedly steri le . The segments are also decreasedin number and may be d istorted in Shape , while in the seg
ments which Show the presence of chromat in the latter is in theform of irregular masses , very d istinct from the usual formas seen in normal plasmod ia. Very o ften Sporulat ing bod iesare observed in wh ich on ly two or three of the segments pos
sess chromat in ; in such'
segments the protoplasm stains a deep
blue and there is no unstained area surround ing the chromat in .
“
Associated w ith the chromat in contain ing segments are
from - six to'
eight , or perhaps more,deeply stained segments
contain ing no chromat in .
“
I n the_segmenting
'
plasmodia the p igment , instead of be ingcol lected in a dense , compact mass , as is the rule in the normaltert1an plasmodia,
is reduced inamount and scattered in smallclumps or . granules betw een the segments.
“
F rom the morpholog ic changes described it is ev ident thatquin ine , admin istered in div ided doses , exercises a markedly
injurious effect upon every stage in the human life'
cycle of
the tertian plasmod ium, either caus ing t he death o f'
the organ
ism at some period of its development or prevent ing normalSporulat ion by restrain ing the d iv is ion of the chromat in priorto segmentat ion . The death of the organ ism i s ev idenced byfragmentat ion or the extrus ion of the chromatin , while the
effect up0n Sporulat ion is . Shown by the l im ited d ivis ion of
the chromat in and the large number of segments which are
devoid o f this essential port ion o f the nucleus .
“
I f quin ine is admin istered in one large dose , wh ich is not
repeated , at any"
stage of the deve lopment of the tert ian plasmodium prior to segmentat ion , the changes produced are the
same in kind as those already described , but a comparat ive lylarge number escape entirely or are but little injured .
’
“When quin ine is administered just prior to segmentation itdoes not , as has been maintained by numerous author ities ,prevent segmentat ion ,
'
nor do the stained preparat ions Showany d istinct morpholog ic changes in the segment ing bod ies .

346 THE STUD Y or MALARI A
ring in the tert ian and quartan plasmod ia, cons isting in frmentat ion ,
loss of the unstained area surround ing the ch:
matin , and extrus ion of the“
chromatin .
”
I t is wel l known that the sexual forms o f the malarial pa;S ites are very res istant to quin ine , pers ist ing in the bloodweeks and months desp ite the . l iberal use of quin ine .
While young and hal f- grown tert ian and quartan game
are sometimes destroyed by quin ine , those of the estii
autumnal . variety are exceed ing ly d ifficult to kill . I n fact ,has been maintained that the administrat ion o f quin inepat ients harboring on ly the asexual forms favors thedevelcment of crescents .
S chaud inn134 in fected anopheles mosquitoes w ith tertigametes from the blood of his servant g irl , who had be
taking a'
gram of quin ine three t imes weekly for a month.Guald i and“
M artirano15 0 arrived at the followmg conclusic
w ith respect to the effect'
of quin ine upon crescents
1 . Quinine admin istered in a s ing le dose of grams or
to grams for many consecut ive days is .not ablecause the disappearance of crescents from the blood.
2 . Quin ine in doses sufficient to destroy amebo id forms
the parasite not only do not destroy the crescents ,"
but do i
inh ibit the ir deve lopment w ithin the ‘
body of the mosquito .
3. Quin ine does not appreciably Shorten the period duriwh ich crescents remain in the blood after the cessat ion of fev
the period which represents the contag ious term of the disea
M acrogametes are more res istant to the effects of quimithan are the microgametocytes . This may poss ibly be duethe thieker protoplasmic body of the former, and explains 1difficulty of interrupt ing the parthenogenet ic cycle , the cy
of chronic or latent malaria.
Binz observed that in fusoria were st imulated to increas
movement by quin ine. The Same has been noted w ith tparasites of malaria.
According to M annaberg, a Short t ime after the adminfrat ion of quinine med ium- s ized t ert ian paras ites are o ft
observed in very act ive , even convuls ive , movement ,_
frt
which it appears that the paras ites are at first irritated
TREATMENT
increased movement . Bacelli131 observed the same in
tan paras ites .
“
Cohen305 believes this act ion o f quin ine to be use ful innosis . He States that in cases of doubt ful diagnos is thet ion of a quantity of the drug not sufficient to insure a dc
freedom period w ill frequently cause the appearance iperipheral blood of organ isms recognizable . as normal orforms of the hemameba of malaria, and this has beenObs
so- frequent ly and in so many d iverse c ond itions thatincl ined to look upon its absence after, say ,
hal f a dozent ions , vary ing from three day s to a w eek apart and in
increas ing from to 1 gram, as v irtually exclud ing min fect ion. He is of the Op in ion that in Such cases the orgis rest ing in some larval form , probably in the Spleen or
,
marrow , and. that its appearance peripherally is part offens ive , reproduct ive react ionto the paratoxic effect of qu
.That small doses of quin ine are able to arouse latent mis , in the writer ’
s Op in ion , unquest ionable. This can or
explained sat isfactorily by assuming that quin ine st imthe parthenogametes into a compensatory reproduct ion .
The relat ion of the t ime when the quin ine is admin i
to the temperature curve and the behavior of the '
p‘
arasit t
been care ful ly stud ied by M archiafava and Bignami ,22 tisults of whose observat ions may be summarized as
lows :1 . I f the quin ine is admin istered during the cris is
attack and cont inued during the apyrex ia, wh ich follow s
majority o f cases , the next expected attack is . inhibit
there is mere ly a slight elevat ion of temperature , w ith a
sense of d iscomfort . I n a smaller number of cases , evenstrong doses of quin ine are g iven during the cris is an
period of apyrexia, the attack is not prevented , but is (it
and abort ive.
2 . I f quin ine in the usual dose is admin istered w ith.six hours preceding the expected attack it may have no
ence at all upon the temperature of the succeeding paro.
I n other cases there - is not iced a sl ight“
delay in the a

348'
THE STUD Y OF MALARIA
this case the temperature curve is the typ ic one of an est ivaltertian . Subsequent attacks as a rule , do not occur .
I f the remedy is adm in istered at the onset o f the attackin the majority of cases the attack w il l come on in the usualway ,
and may even be grave and prolonged ;very o ften , how
ever , there are some mod ificat ions in the curv e. A subsequentattack does hot usual ly occur, although there may be frequentiri egular e levat ions of temperature .
4. When the quin ine is g iven during the febrile attack be
g inn ing short ly after the . onset and cont inuing throughout thecourse of the fever in a series of cases the characterist ic. curve
o f the - tert ian is not appreciably mod ified , while in another
series there are various modificat ions . I n a whole series of
cases when the quin ine has been g iven in large amount duringthe attack , there are apt to be no subsequent attacks, or on the
fo llow ing day or days there are . on ly S light e levat ions of tem
perature.
5 . I f“ quin ine is -
g iven near the t ime of the cris is when the
blood contains on ly young non -
p igmented paras ites , and i fits administrat ion is cont inued for about twelve hours , theparas ites cont inue to be seen in the peripheral blood for
nearly twenty- four hours , together w ith pigmented lenko
cytes .
6 . I f quin ine is g iven in the last hours preced ing the attack ,when the on ly bod ies found in the blood are the pigmented
adult parasites , or these predominate , then the paras ites goon to the ir development up to fiss ion , but the new generat ion ,
as a rule , does not present itsel f in the follow ing attack. I n
other cases , while we do not see the generat ion of young para
S ites , w e have bod ies belong ing to the crescent group ;it‘
would
appear that in this case the paras ites , instead of .
going on to
sporulation , take the other '
road wh ich leads to the format ion of
crescent forms.
7. When the remedy is g iven at the beg inn ing o f the attack ,
at the t ime when in the blood we find fiss ion forms , or thosethat have already become d iv ided , the act ion of the remedy
is subsequently recogn ized by the fact that the ameba of the
new generat ionbecome extremely scarce , and i f the quin ine'
be

350 THE STUD Y OF MALARI A
same effect had several t imes formerly resulted from smal ldoses of quinine .
The other case was that of a woman w ith a mitral regurgitant
_
murmur,Who stated that every t ime in her l i fe that quin inehad been
-
g iven her She thought she would die o f suffocat ion .
Three grains of euquinine in powder were g iven her, and in
a short t ime she was prostrated , suffering w ith severe dyspnea
and fear of death . These symptoms lasted about an hour.
Gudden405 . observed in several pat ients as a result of 5
1 gram
of quin ine , headache , nausea, vomit ing , a sense of burningheat ,a ch il l , and elevat ion of temperature to F .
, and pulse toThe urine contained no albumin .
Plehn““06
records a case of a woman who , a few m inutes aftertaking V2 g ram of quin ine , was
,seized w ith itch ing o f the
Sk in,an erythematous rash upon the neck and breast , a ch ill ,
and rise o f fever to 102°
F . After the intramuscular in jectionof 1 gram of quin ine the temperature became 104
?
F .
'
The
urine was normal and the elevat ion o f temperature lasted on lya few hours .
Trousseau and Pidoux report the case of a pat ient Whotook at one dose 3 ,grams of quin ine for the cure o f asthma,
wh ich recurred every day at a certain hour. Four hours laterhe experienced ringing in the ears , d izziness , and terrific vom iting . S even hours after taking the drug he was blind and deaf ,del irious , and unable to walk on account of vert igo . He was
vomit ing constant ly . These symptoms ceded Spontaneouslyd uring the m idd le o f the night .Gren ier“07 cites the example of a g irl of fifteen years who
took a moderate dose of quin ine for an attack of fever. A
Short time later She had nausea,vert igo , deafness , v isual dis
turbances , sw ell ing of the face , dyspnea , profound p rostration ,
general urt icaria, edema of the hands and feet , and vomiting .
These symptoms d isappeared in the course of six hours , butreturned each t ime even a small dose of quin ine was g iven ,
even though unrecogn ized .
L arge doses of quin ine_
may even prov e fatal . L averan1
Speaks of two sold iers , intend ing to take sulphate of soda as
a purgat ive , took by mistake 12 grams each of quinine. I n
TREATMENT
11 hour they were taken w ith cramping in the st
.ng , facial pallor, dilatat ion of the pup ils , superfictn
, chi ll iness ;pulse Small , irregular, somet imes ins
tendency to syncope . One of the patients recoveidied in collapse .
reports the"
case of a pat ient who tooksulphate of quin ine . Tox ic symptoms appeared
tinutes these were retching and vomit ing , uncO i
‘ low and labored respirat ion , a barely perceptiblelsions , affect ing chiefly the lower extrem ities. D e:
soon .
nerons other cases of quin ine poison ing could bt
ymptoms most f requently recorded are headacf
muscular weakness, staggering gait , dyspnea, 0
tss , amauros is , psych ic d isturbance , cutaneous - err
rhages , and fever.
er caused by quin ine was recogn ized as early 3
thnemann . He says :“
For experiment’
s sake,
tins of cinchona bark tw ice daily for a few cons
my feet and hands became cold ,fo llow ed by a fee
e, pa lp itat ion of the heart , pulse hard and rapid,apprehens ion , then a beating headache , flushingthirst , and all the usual Symptoms of intermitten i
Symptoms lasted two to three hours each t ime
1 after each dose I stopped the bark and
y .
nerons cases have s ince been observed . F . Plehr
number of cases , bel ieves that , wh ile it appear
in tropic than in temperate cl imates , it may Occur iave never suffered w ith malaria, and occurs oft t
iidents than in newcomers . The fever may be pi
hi ll , is accompan ied w ith other ev idences of cinelsomet imes associated w ith the cutaneous manifes
n ine “
.
the report o f a case in th is country , With an inteo f the l iterature and a bibliography , the reade i
to the article of Goodman.
409 This writer bel ie

352 THE STUD Y OF MALARI A
explanat ion of this untoward effect of quin ine to be 1
chemic changes in the blood act on the heat - dissipat
ratus in persons who - have,or hav e had ,malaria.
The cond it ion is as yet too obscure to warrant an
s ions . A care ful Study of the blood might reveal tgenes is . S ome cases probably bear an analogy to t
t iori produced by quin ine in certain “
persons Wh (
des ignates “ blackwater- fever candidates .
”
Quinine in large d oses . is undoubted ly somewhat c
to the heart , as exempl ified in some o f the cases re
may cause syncope , or even co llapse and death. I n f
the heart is said to be arrested in d iastole.
Quin ine may cause temporary psychic d isturbancesan ity and del irium. The latter occurs either innoisy form , w ith loquacity and ag itat ion , or in a qt
w ith stupor and depression .
The chie f d igest ive d isorders re ferable to quin ine ai
vomiting , anorex ia, and gastric and intest inal catarrhand intest inal hemorrhages have been attributed t <
of the drug , as w ell as hemorrhages from the“
mou
nose , lungs , "
Skin, and conjunct iva.
The cutaneous erupt ions ofq uin ine orig in may be
small'
doses . They are most apt to follow theT
admi
o f the Sulphate . The w riter has seen persons in“
i
sulphate had always produced annoy ing urticaria ,
bimuriate w ith no untoward effect . The pruritussome of these erupt ions is somet imes agonizing , th
declaring that the remedy is worse than the diSease.
I t is said that laborers in the manufacture of qui i
experience pruritus of the hands and forearms , foredness and a l icheno id .erupt ion , somet imes w ith S ithe face and gen itals.
Urt icaria is , in the experience o f the writer, the
quent of these man i festat ions . I t may be genera.
local,and is somet imes attended w ith edema of the
hands . The w riter has seen only one such case inrace .
Erythema,scarlat inal or morbill i form in appearanc
354 THE STUD Y O F MALARI A
preex ist ing uterine contract ions , it is extremely doubtfulwhether it in it iates labor pains except in a very l imited numberof cases . The writer has several t imes seen pat ients threatenedw ith
-
m iscarriage whose pains w ere promptly quieted by the
immed iate adm inistrat ion of quin ine , and he bel ieves that abort ion in these cases is o ftener due to too l ittle quin ine than to
too much . Pregnant women may take quin ine prophy lact icallyfor long periods , and i f they keep free from malaria they Show
no tendency to abort.The effect of quin ine upon the eye is somet imes a matter
of much concern . Total blindness may result , but fortunatelythis severe degree does not last long , though _
S ome constrict ionof the v isual field may pers ist permanently . Quin ine amblyopia is usual ly accompan ied by other tox ic effects
,being due
ord inarily to large doses of the drug cont inued for severaldays . The cond it ion is usual ly bilateral and a ttended w ithphotophobia, d ilated pup ils , d im in ished pupi l lary react ion
,color
blindness , concentric restrict ion of the v isual field ,
‘
ret inalanem ia, w ith vascular constrict ion and atrophy o f the opticnerve . D eS chw einit z found quinine and urea more tox ic w ithre ference to the eye than any other preparation he employed .
The prognos is is usually good , normal v is ion be ing ent irelyregained in the majority of cases
,but the cond it ion may per
s ist for months . The d ifferent iat ion of th is cond it ion frommalarial amauros is has been cons idered .
Tinn itus and a degree of deafness are common results of
quinine . The deafness may be temporarily complete. Con
gestion of the malleolus , w ith opacity and retract ion of the
drum ,
’
are the common cond itions present .The act ion of quin ine on the Spleen is doubt ful . While
Catan i , 410 Rochfontaine , 4 10 Herrlich ,409 and Piorry86 maintain
that it causes a contract ion , even of the healthy organ , the irresults could not be confirmed by Valleix and Briquet .
8 6
The behav ior of the leukocytes under the influence of quin ineis d isputed . Vincent and Bast ianell i8 6 observed that the ad
m inistrat ion of quin ine caused an increase in the number of
mononuclear leukocytes . Billet86 noted that w ithin three to fivehours after admin istrat ion there occurred a d iminut ion of the

to veri ty th ese observat ions
M archiafava and Bignam i observed a rem
ment in the phagocyte phenomena after the
of the salts of quinine , but bel ieved that it wincrease in the phagocyte energy brought abc
but to the greater quant ity of necrotic forr.
pigment, which is d iffused in the blood in cor.
d irect act ion of the remedy 011 the paras ites ,remov ing the dead forms which render the ble
that these w riters could say w ith certainty w e
of quin ine do not hinder the phagocyte a‘
ctiv i
blood corpuscles , nor is their mobility mod ified .
D isselhorst and others233
proved by experim
that the mot il ity and the phagocyte funct ion 0
is un impaired by quinine . M annaberg404
phagocytes in the internal organs have the irweakened than st imulated by quin ine .
Coutt a—indications to the Us e of Quinine .
ment o f the patient that he is unable - to takeconstitute no bar to the use of the Specific. Tl.
invariable sequence of very severe Skin man ifperhaps lead the phys ician to employ one of th
quin ine .
Card iac depression and dyspnea are a decidet ion to the adm in istrat ion of the drug .
The treatment o fmalaria complicating pregtially the same as under other cond it ions . A
more fancied than real , o f the oxytocic propertw idely prevalent , but of the d ilemma , malarialatter is certainly the shorter horn . The pregn
far less risk of abortion w ith . rational quininew ithout . M alaria during pregnancy is notori
and , while the attack Should be treated w ith thnecessary to effect a prompt cure , systemat ic

356 THE STUD Y OF MALARI A
quin ine prophy lax is is necessary to prevent recurrences . I f
laborpains have begun opiumShould be administered w ith thequin ine .
Thehistory of hemoglobinuric.
fever is no contra- ind icat ionto the use of quin ine. Whi le the admin istrat ion of the drug is
somet imes the occasion o f an outbreak of blackwater fever, thelatter is generally due to too l ittle quin ine rather than to too
much . Nor is it adv isable to restrict the s ize of the dose
unnecessari ly through fear of an attack , S ince it has been Shownthat the amount of quin ine is of little importance in the eti
ology , very smal l quant it ies being as prone to occasion the
attack as moderate amounts .
Choice of Preparat ion .—This is influenced by the age of
the patient , the mode of admin istrat ion , the severity of the
attack, and
'
other factors.
The sulphate , on account“
o f its cheapness and”
ease w ithwhich it is obtained , isWidely employed . The w riter , however ,now rarely employs it , and then only in suspens ion in syrup of
yerba santa for children . I t“
is probable that it g ives rise to
fnore gastro- intestinal and nervous d isturbances than any other
salt of quin ine,and it is
'
these mani festations produced , as a
rule , by this salt . which cause"
so many persons to say to the
phys ician that they cannot take quin ine .
The bisulphate , the hydrobromide Or bromide , and the hydrochloride are use ful preparat ions , be ing easi ly d issolved and
read i ly absorbed .
The bimuriate , or acid hydrochloride , or bihydrochlorate is
the most valuable salt o f quin ine . I ts great so lubility adapts it
for solution to be g iven by mouth , by ’
rectum, intramuscularly ,
or intravenously .
Euquinine, or quin ine ethy l carbonate , has beenthoroughlytried and has g iven satisfactory results in the writer ’s hands.
Being pract ical ly tasteless , it is eas i ly admin istered,e ither in
powder or'
suspended in a
'
neutral syrup ,to children. An acid
w ith the drug or immed iately fol low ing develops a bitter taste .
The Object ions to the preparat ion are its expense and the fact
that it is patented .
The tannate of quin ine , on account o f its small proport ion of
358 THE STUD Y OF MALARI A
by the M oa th—I n s imple cases of malaria, administration of
quinine by t he mouth is thei
rule by other methods the excep
t ion . I t is probable t hat n inety - n ine - one - hundredths o f the
quin ine consumed is g iven by the Oral route .
There are those , not object ing to the taste of quin ine , whow ill take it in the powdered form ; in fact , it is a common
method among the S outhern negroes to l ick it from the palmof the hand . The taste is , however , so repulsive to most persons that , w ith the except ion of the tannate and euquinine ,
it
must be g iven in some other form.
The same object ion appl ies to g iv ing the drug in’
solution ,
though this is unquestionably the most rel iable form in whichto g ive it by the mouth , but for obv ious reasons it cannot be
so - extens ively employed in this manner in private practice .
The solut ion is more ' quickly and completely absorbed . The
bimuriate and the bisulphate are the salts most suitable forsolut ion , but i f ne ither of these is at hand the sulphate may be
employed by add ing a drop of d ilute hydrochloric or sulphuricacid for each grain of the quin ine.
The most efficient veh icle for d isguis ing the taste of the
sulphate of quinine is the syrup
'
of yerba santa. Two grains
of quin ine tothe dram.
of the syrup is the suitable proport ion .
S yrup of choco late , fluidextract of l icorice , g inger, coffee ,
mi lk , honey , ol ive oil, and other med ia have been recommended,
but are far from sat is factory . Acid fruit juices and syrups
usual ly enhance the bitter taste .
Where prejud ice again st quinine makes it necessary to disguise the appearance of the drug ,
this may be accompl ishedeffect ively by add ing a small quantity of charcoal , _
turmeric,or methy lene—blue to the bimuriate , bisulphate , or other salt .P ills and tablets are conven ient to administer and not un
pleasant to take . but cannot be rel ied upon . The coat ing o ftenbecomes so hard as to make solut ion d ifficult or imposs ible .
The Writer has several t imes seen quinine g iven in . this formpass from the bO
‘Wel wholly unaffected. P ills and tabletsshould not be g iven when capsules can be obtained . Capsules ,when fresh
,are easily d issolved . I f there is any doubt as
to the ir qual ity they may be punctured several t imes in each

TREATMENT 359
end w ith a pin, or maybe followed by a few drops .of a dilutem ineral acid.
I n t he absence .o f capsule s quin1ne has been rolled in a l ittleball w ith cigarette paper. Absorpt ion is extremely s low and
uncertain ,and this method should not be resort-ed to.
The tannate of quin ine has been compounded with the chocolateconfection fora dministratior
i
to chi ldren , and in this form,
if re liably made 1s read ily taken , and-
in sufficient dose isefficient .
i
HypodeMmc M ethod .—Quinine was used hypodermically at
least as early as 1863, when BourdOn289 employed the sulphate
d issolved 111 water w ith tartaric acid . The same year M oore“
.
1
recommended the use . of 30 gG rains of the sulphate of qui
d issolved in /2 ounce of Water by means of 8 or I O drops
of d i lute sulphuric acid , from I to I /2 drams of this solut ion to be used at a dose. Bad results were common.
Arnould ,
“ 2in 1867, reported in 95 cases thus injected 2
indurated nodes , 4 eschars,and 1 5 abscesses. I n 1888 Rem
mann and Villeje introduced for hypodermic use the bi
muriate in the followmg formula, which “
is sti ll widelyployed °
Qumme bimuriateD ist i lled w ater to I O cc.
Kobner recommends
Quinine hydrochlorateGlycerine ,D istilled water
Grimmaux
Quinine hydrochlorico - sulphate
Aqua dest .
Klein 96
Quinine hydrobromate
S ulphuric ether
Alcohol
T riulz is‘6
added ant ipyrine to promote solut ion and d imin ish
Quinine m-uriate .
Anti‘
pyrine
Aqua
360 THE STUD Y OF MALARI A
Vincent and Burot :9 6Quinine muriateAnalgesm
GaglioQuinine hydrochlorateUrethan e 3 gm . ;
Aqua .
The add it ion .o f cocaine has been recommended alsoto'
lessen
the pain .
The'
mos‘
t suitable salt of quinine for inj ection is unques
tionably the bimuriate . The tablets of bimuriate of quinineand urea are convement and insure accurate dosage . The 3
grain tablets contain approx imately 2% grams of the quin inesalt .The advantages of giv ing quin ine by the n eed lein pernicious
malaria are obv iously . be ing able to admin ister it to pat ientsunableto swal lowor to retain it
, and the certainty and promptness of absorpt ion . Nevertheless , these great benefits are somewhat d iscounted by the bad results which somet imes appear.
Formerly tetanus was to be feared. Bartholow4 13 ment ion-
s
several such cases reported from New O rleans and -
2 occurr1ng
in'
one reg iment of the Brit ish I nd ian Army .
"Vincent , “ in a
late report , recalls the . numerous cases fol low ing,
the sub
cutaneous use of quin ine . M cCampbell41 5
speaks of a fatalcase o f tetanus shortly .follow ing a hypoderm ic inject ion of
the_
hydrochlorate o f quin ine , though the“
experiments of th iswriter fail t o corroborate those of Vincent to the effect thatthe injection of quin ine favors the development o f the tetanus
bacillusf'
I n the late F rench campaigninM adagascar 6 cases
o f tetanus subsequent to hypodermic-
s of qu1n1ne came under
observat ion . But there are other consequences which, whi lenot so deadly , are more commonly met . Nodules , necros is ,s loughing ,
and abscess formation are re ferred to .
'
Plehnm
and Bliimchen416have frequently seen necro -ses.
“
and -
abscessesresult from hypodermics of quin ine. Thayer9 8 says there isalways d anger of subsequent abscess or necros1s. L averan1
states that injections made into the Skin often g ive .rise to
THE STUD Y O F MALARI A
much of this as needed may be injected in one or severals-
ns .
solut ions should not be inj ected hypodermically , but
luscularly , s ince in the latter locat ion the in ject ion is
certainly absorbed , is less apt to cause indurat ion and
s , and is less pain ful . I n some cases of perniciousa the superficial circulat ion is v ery poor, absorpt ion cor
Ldingly inadequate , and necros is almos t inev itable.i f the
e is not deeply 1n j ected . I n a case of alg id malaria inactice where the quin ine was g iven hypodermically theEinject ion began to turn blue w ithin ten minutes and
most black w ithin two hours.
in itial dose should ord inarily be 15 grains . A fterward5 to I O grams should be inj ect ed every six or e ight hours1g as the symptoms demand it . F or children under
ears the first dose may be I VZ grains for each year of
The statement of Homem,
1 5 7that in the admin istrat ion
nine in pern iciousmalaria it is best rather to sin by prod
than by parsimony , is open to quest ion . While therew drugs so potent as quin ine hav ing so few tox ic effects ,:sults do somet imes follow excess ive doses. S chellong9 2fl that large doses added to the insult to the nervous
1 and had a depress ing effect on the heart. As Plehn5
:ses it , there is a un iversal tendency to attribute all bad
mena to the d isease and all favorable ones to the remedy.
ver, after us ing in 5 cases 5 to 6 grams in d iv ided doses ,ed at short intervals during the height of fever, this,te observer noted cons iderable depress ion of the heart ,i s system , and general cond it ion of the pat ients.
at of the cont inental w riters recommend the Pravaz or
syringes , w ith plat in - irid ium need les , but the ord inaryxin syringe , as used by Sutherland168 for this purpose ,rs as well. A so ft - rubber tubing connect ion between theand the n ipple of the syringe is advantageous , as it may
It the breaking of a needle in a strugg l ing pat ient . O ne
se syringes , a small steril izing pan , and alcohol lamp docupy much space , and ,
be ing almost ind ispensable in theseshould be easily access ible during the malarial season to
best location for injection is in the g luteal reg ion wel lthe ischial tuberos it ies , though the interscapular reg ion11 chosen'
techni’
c_
of intramuscular inject ions of quin ine may be
lariz ed in these precaut ion s : Have the solut ion freshlythorough , d ilute , and steri le ; render the syringe and
jeet ion s ite aseptic ;insert the needle into muscular t issue ,.V 01d breaking the needle.
ravenous M ethode—I n 1890 Bacelli422 introduced the in
i ous adm in istration of quin ine in the treatment of pern imalaria, claiming thereby to have reduced the mortal ityI 7 to 6 per cent . The followmg formula was
‘ii sed :
Quin ine hy drochlorateS odium chloride
D istilled water
e arm is bound above'
the elbow in order to d istend theof the forearm, into one of wh ich the need le is intro1 in the d irect ion of the blood current , and the solut ionted very s low ly after remov ing the constriction . The
:ure should be covered w ith a steri le dress ing . The solushould be warm and
”
sterile , and care should be takenno air is injected . I f swelling occurs at s ite o f the inj ec'
.t is ev ident - that the vein has not been entered . I t is said .
I gramof quinine thus inj ected produces a solut ion in thel of I w hich - is the strengt h deemed necessary by
to destroy protozoa. Rogers44thinkswel l of this method ,
[as abandoned in favor of _ it the subcutaneous route. How
it probably has no advantages over the intramuscularnistration. M oreover, it is not in frequently almost imposto locate the veins, . especially in young negroes.
upodermoclysiS .—Quin ine d issolved in normal salt solution
1 by hypodermoclys is has been recommended by Grrall25 6
364 THE STUD Y OF MALARI A
and others . F rom I O to 30 grains of the bimuriate are dis
so lved in a pint of normal salt solut ion , and as much as des iredis injected into the loose Subcutaneous t issue. I t is extolledespecially by Glatard86 in the treatment o f children sufferingw ith pern icious malaria. This method is probably not adapted
to the treatment of alg id malaria on account of the deficientsuperficial circulat ion . Besides , the necessary apparatus is fre
quently want ingGut ierrez423 had success w ith inject ions of quin ine directlyinto the spleen , but such a dangerous procedure is ent irelyunjust ifiable . F leury ,
424act ing upon the theory that the nearer
the spleen the quin ine is injected the better the result , injecteddeeply into the structures below the ribs in themidax i llary l ineupon the le ft s ide . His results
'
doinot appear to have exce lled
those follow ing inj ect ions in other s ites .
j oussetm
treated pern icious malaria w ith “inj ect ions of
quinine into the trachea by insert ing the needle immed iatelybelow the crico id cart i lage and inject ing a I O per cent. solutiondrop by drop.
Le D antec226
suggests that in cases o f tetanic pern iciousmalaria the subarachno id inject ions of quin ine , after the
method of Jaboulay , might prove efficacious. S o far. as known ,
this method has not been tried in this cond ition.
Rectal Adminis tration—This method , though uncertain ,is
of value where quin ine cannot be retained by the stomach , andthere are obj ect ions to the intramuscular inject ion , especiallyin ch ildren . I t may also be used as an adjuvant: to the int-
ra
muscular '
or intravenous inject ion in pern icious cases . A
soluble “
salt should be used , pre ferably the bimuriate ._
The
water should be about the temperature of the body , and shouldnot exceed a few ounces in quant ity. Two or three times as
much quin ine should be g iven by the rectum as by the mouth ,and the injection should be made high into the bowel . Ten
or 15 drops of t incture of opium should be added to prevent
tenesmus and aid retention. Ant ipyrine has been recommended
by some , but should be used w ith care where there is depression . A cleansing inject ion should be g iven first i f the patientis conscious .
366 THE STUD Y or MALARI A
paroxysm i s not prevented ;in fact , it may be ent irely unmodi
fied but such a dose , properly t imed , usual ly secures apyrex iasubsequently for several d ays ;I n
‘
double“
tert ian infect ions a s ing le dose g iven in th is way
may change the quot id ian paroxysms into tert ian , and if re
peated , in multiple tert ian and quartan in fect ions , const itutesa sort o f fract ional steri l ization of the blood .
Themethod Of Sydenham , the English method, consists of
a s ing le dose , averag ing 15 grains , g iven in the sweat ing stage
or the d ecline o f the paroxysm. This dose“
usually preventssucceed ing paroxysms i
‘
f One should occur it is usually abort ive.
This method requires less know ledge of the exact nature of
the in fect ion and of the stage of development than the formermethod , hence it may be more effect ively appl ied by the busypract it ioner. What experience the w riter has had w ith it hasbeen sat isfactory .
“
The third method , that of smal l doses at frequent intervals ,has numerous advantages over the one - dose methods .
1 . Quin ine g iven in this way is better borne by the d igest iveand nervous systems.
2 . The loss of one dose-
by vom it ing or fai lure of absorpt ionis not of so much importance .
3. The method is adapted to tert ian , quartan , or est ivoautumnal in fect ions ; this is important , for somet imes thesecannot be d ifferent iated cl in ically .
4. I t is adapted especial ly to estivo—autumnal in fect ionsw here sporulat ion is not so nearly synchronous .
5 . The t ime of admin istrat ion is not dependent on parasiticfind ings or defin ite stages , both of which may be obscure wherethe pat ient has prev ious ly taken quinine .
6. An experience in many hundreds o f cases has proved its
value .
The writer g ives quin ine in this way almost exclusively .
The average dose is a grain an hour, given usually 2 grainsevery. two hours , 3 grains every three hours or 4
'
grains everyfour hours day and n ight . I t is especial ly 1mportant that the
drug be g iven during the night , s ince thus only may the
TREATMENT
od be charged during the day , when sporulaicurs.
I t is not necessary to defer or d iscont inue the usaccount o f fever, as is bel ieved by,
some . M on
ore years ago M ai llot showed that to w ithhold tis reason Was not on ly use less, but dangerous .
C inchon ism is no guide to the“quant ity to be g iv
e patient toward which the quin ine is d irected ,b
es .
The specific Should not be d iscont inued as soon
rature is normal , but should be kept up for z
ys longer in the quant ity employed during the fewter about 15 grains on two success ive days of
ould be g iven for at least two or three months
lapse , even though the pat ient leave the mala1few davs
’
treatment w ith quin ine no more cu
1an does a few w eeks’
rubbing w ith mercury cur
Hyg ien ic and S ymptomat ic T reatment—RéLnt in the treatment of malaria not on ly during:t ive symptoms
,but during convalescence; E
)unteract the benefits o f
tses y ield after confinement to'
bed Which hasted quin ine . A relapse may be provoked by
'
:sumpt ion of duty . Rest is especially importanttent of est ivo - autumnal infect ions.
Butterm i lk is one of the most acceptable and ea
rticles o f d iet . Sweet milk , meat broths , ve
‘uit juices w ith egg -albumen , Soft - boi led eggs ,
sually allowable Q'
Where there is much gast) od had better be w ithheld temporarily .
The room and bed should be screened ; in
in othermembers o f the household be sat is fact“
he room should be thorough ly vent ilated an
rotected from draughts .
I t is customary to beg in the med ical treatment
alomel is the drug most eas i ly administeredhe drug need not exceed 5 or 6 grains , and shou
v a sal ine . The quin ine should not be delayed
368 THE STUD Y O F MALARI A
of the purgat ive . As has been said , cases orig inally v iolentalmost invariably die whi le preparing for the quin ine,and thoseof moderate severity become worse under the preparc
'
t tion.
” 6 6
Calomel has been frightfully abused in most malarial countries . I t was formerly the un iversal pract ice to g ive the drugunt i l the gums w ere “
touched”and the teeth irreparably dam
aged . I t was more the abuse o f calomel than of any otherdrug that led O l iver Wendell Holmes
“25to declare
'
that , ex
cepting a few drugs , .
“
ir the whole materia medica,as now
used, could be sunk to the bottom Of the sea it would be all
the better for mankind—and all the worse for the fishes .
”
D uring the cold stage blankets , hot drinks , and the externalappl icat ion of heat are ind icated . Atrop ine hypodermical ly isuse ful , and morphine -is indicated in some cases.
I n the hot stage , i f the temperature runs high , cold appl icat ions to the head , tep id spong ing , and cold rectal - inject ionsmay be used . The coal—tar ant ipyret ics are not o ften ind icated .
Cold drinks may be g iven.
For the headache cold applicat ions , code ine , and acet’
anilid ,or chloral and bromide of soda are use ful , and , i f the paindemands it , morphine need not be w ithheld . I f nervousness
is marked the monobromated camphor should be adm inisteredw ith the qu1n1ne 1n capsules , or the bromide o f soda, in solut ion , w ith each do se of the specific.
For vomit ing ,i f intense and not relieved by the applicat ion
of a mustard plaster to the epigastrium ,morph ine should be
employed subcutaneously .
Chron icM alaria.- I n - the treatment o f chronic malaria .two
parasitie cycles have to be combated , t he schizogon ic and the
parthenogenet ic. The treatment of the asexual cycle of para
s itie evolut ion in chron ic malaria is that of acute malaria.
The tendency to relapse at multiples of approx imate ly seven
days has long been recogn ized , these periods be ing known as
the s eptenary periods . I t is now known that these re lapsesdepend upon the sporulation of the parthenogametes
, a cycled ifficult to interrupt except during the stage o f free spores .
After success ively meeting the act ive symptoms by quin ine ,administered as above outl ined , the prevent ion of a relapse is

370 THE STUD Y - O F MALARI A
amauros is as a tox ic result of atoxy l should be' borne in
m ind.
I ron is nearly . always indicated ;the organ ic preparat ions of
iron and manganese are usually well borne by the stomach .
The pi l l of Blaud ’
s mass,2%
“
grains atoxyl , one - third grain ,
may be tried , or the class ic ant imalarial pil l of iron ,quin ine ,
arsen ic, and strychn ine.
”I nject ions of med icaments d irect ly into the Spleen ,
-
as_
somea
t imes adv ised , are unjust ifiable .
Counter - irritat ion over the splen ic area may aid in'
the rea
duction o f the en larged spleen .
“
The best agent is the , o intment
of the red iod ide of mercury . A piece the s ize-
of a pea or
larger should be thoroughly rubbed in , the Splenic reg ion be ingbared to the sun
’
s rays or to the heat of a fire . This shouldbe repeated dai ly unt il the skin becomes so irritated as to
make frict ion painful , When it should be d iscontinued , to be
resumed again when the cond it ion '
of the skin w i ll perm it .I odine , turpentine , mustard , firing w ith the actual “ cautery ,
and other counter- irritants have been recommended .
Hydrotherapeut ics and electricity have not g iven generalsat is fact ion . The ir use - is somet imes followed by an act iveoutburst of malaria.
While the x—rays have a destruct ive effect upon certainprotozoa , they do not appear to have such act ion upon the
parasites of malaria w ith in the circulat ion . D emarchifz f‘ as
a result o f his experiments , is conv inced that,wh ile these rays
are use less against the in fect ion itsel f , they appear to havea beneficial effect upon the enlarged Spleen when the paras iteshav e d isappeared spontaneous ly or as the result of med icat ion .
Splenectomy may be performed in very anemic pat ients w ithlarge , pain ful spleens , especial ly i f freely movable , in whom a
change of cl imate is imposs ible and therapeut ic measures havefai led. The writer had the opportunity of treating an obsti
nate case .of est ivo - autumnal malaria in an adult female whohad had , sev eral years prev iously , the spleen removed
“
on ac
count of malarial cachex ia. Hemog lobin percentage was onlys l ightly affected by the attack , and convalescence was rapid .
Brachio"27 has recent ly suggested a un ique method o f treat

TREATMENT 371
ment of splenomegaly . He had observed that in patients w ithsplen ic enlargements who suffered suppurative compl icat ions ,as mastoidit is , empyema, cancrum oris , etc., the spleen rap idlyd imin ished in s ize. At the same t ime a leukocytos is was pro
duced where these cells had prev iously been d im inished , and
to this phenomenon he attributed the improvement. I n order
to produce leukocytos is this w riter inj ected subcutaneous ly5 min ims of turpent ine in the splen ic reg ion ,
which resultedin abscess format ion and a consequent increase in the numberOf leukocytes; Nearly 2 0 cases were treated in th is manner
w ith the most encourag lng .results . Wh i le 1n - cases‘
w ith verylarge spleens it was necessary to repeat the 1n j ection ,
in onlyI case was the third inj ection required.
T reatment of M alaria in Ch ildren .—Inthe treatment of
malaria ln. children it is the pract ice of the wr iterto admimster
the quin1ne at short intervals every two or three hours .
While children bear quin ine in’
relat ively larger doses thanadults , the s ize o f the dose should be regulated by the severityof the attack and the age of the pat ient . I n average cases
children from one- half t o two years of age may be g ivenfrom V2 to I grain o f quin1ne every three hours , from three
to five years from 1 to 2 grains , and from six to ten years
from 2 to 2% grams . The sequant it ies may be increased insevere attacks .
“
The drug is ord inarily g iven by the mouth. Where capsulescannot be used , recourse must be had to a tasteless preparat ionor to a d isguising vehicle . Euquinine and the tannate o f
quin ine are the best ' of. the tasteless preparat ions . The former
st be“
g iven “
in sl ightly larger doses , the latter _
up to doublethe doses indicated a bove . The most efficient l iquid for disguis ing the taste Of the sulphate of quin ine is the “
syrup of
yerba santa, at least 1 dram of which should be given for
each 2 grains o f the quin ines I n cases w ith pern icious symp
toms the drug should , of course , be 1n j ected intramuscularly .
Rectal admin istrat ion of a Solut ion or suppos itory may be
employed to supplement other modes. The buttocks shouldbe pressed together for hal f an hour after insertion to
.
aid
retent ion .

372' THE STUD Y O F MALARI A
Calome l, mercury w ith chalk , and castor oil are efficient
purgatives in the treatment of malaria in children .
T t e -
atrnent of —When‘
malaria is eomplicated w ith other d iseases each should rece ive appropriate treatment . Themalaria should be promptly treated as under ord inary
“
c ircumstances. O n ly a few complications need specialconsiderat ion .
For“
rupture of the spleen immed iate laparotomy should beper formed . With early operat ion over hal f recover, w ithoutoperat ion the mortal ity i s nearly 100 per cent .Abscess of the sp leen is a surg ical condit ion. The cho1ce
of’
Operat ion betw een Splenectomy and splenotomy must bebased upon ind iv idual cond it ions . Two cases reported by
Be ll428 and by Groltmani 29
recovered ;after operat ion .
I n the treatment of quin ine amauros is the quin1ne__
must , Of
course , be d iscont inued . Nitrite of amy l and n itrog lycerine ,w ith ton ics , are recommended .
.S ‘ubst itutes for Quin ine.—I n the treatment of malar1a
there is no other drug that can compare in efficacy to “
the saltsof quin ine ;nevertheless , in rare instances , it becomes n ecessary
on account o f id iosyncrasy to resort to the use o f other reme
d ial agents.
4
O f the new er preparat ions of quin ine, euquinine , saloquinine ,aristochin
,etc.
, while purported to ..be free from the'
tox icpropert ies of the official salts , the w rite -r has seen I case in
which euquinine caused d istress ing d yspnea,and another case
in which this preparat ion caused v iolent urt icaria. Euqui
n ine is probably the most valuable of these preparat ions .
The alkalo ids o f cinchona, other than quin ine , are now but
rarely employed , and op in ions vary w idely as to the ir merits .
C inchon id ine is probably the most use ful o f these alkalo ids .
I t must be g iven in dos es about tw ice as large as of quinine.
These alkalo ids , especially cinchon ine and quin id ine are more
tox ic than quin ine , producing nervous and gastric d isorderand , in tox ic doses , convuls ions .
I n order to determine the value of these alkaloids in the
treatment of malaria the Eng l ish Government , in I nd ia,in
1866 , appointed a commiss ion to investigate the subject .16 1
374 THE STUD Y OF MALARI A
days . Ruge has given as much as 15 grains daily for fourweeks w ithout bad results . I t is best g iven incapsules . Kunst9 °1nj ected subcutaneously
'
5 cc. of a 5 per cent. solut ion ;in some
cases he gave even as much as 1 gram in th is manner. I n the
latter cases the pat ients became green ish - blue all over, the
injection s ite remained pain ful for ten days and became par
tially gangrenous .
I t is believed by some observers that methy lene - blue hasmore decided curat ive effect upon chron ic than upon acute
malaria. I t is probably most effect ive in tert ian and quartanin fect ions than in est ivo - autumnal . I t is thought . that
fmethyl
ene—blue affects especially the plasma of the paras ites , and is
consequently most effect ive in the stage where this cel l element
abounds . The drug causes a d iminut ion of amebo id mot ionofthe paras ites and a splitt lng of the plasma substance into sev
eral -
spheric masses .
Untoward symptoms caused by the admin istration ofmethy lene - blue are headache
, nausea, vom1ting , d iarrhea, strangury ,
and album inuria. These effects are less apt to supervene whena
’
p ure art icle is g iven . D e Blasif$2 is of the opin ion that it
causes contract ions “
of the“
pregnant uterus . The add it ion Of2 or 3 grains of powdered nutmeg lessens the tendency to
strangury . The pat ient should always be forewarned of the
blue color imparted to the urine and feces .
Thayer433 reached the follow ing conclus ions after us ingmethy lene—blue in a few cases
1 . M ethy lene - blue has a defin ite act ion against malarialfever, accompl ishing its end by destroy ing the specific organ
ism ;but'
it is materially less efficacious than quinine , fail ing toaccompl ish its purpose in many cases where quin ine acts sat isfactorily .
2 . The act ion appears to be rapid , the chills d isappearing or
the temperature , in the remittent cases , fall ing to normal during the first four or five days ;but later, however, s if a sufficientnumber of organ isms have resisted the drug ,
- they appear to
develop again d irectly under its influence , causing a return of
the symptoms .
TREATMENT 375
ethy lene - blue seems to have no advantages over quin ineNould warrant its further use .
re and who treated 10 cases of malaria w ith.ns daily of methy lene - blue
, g ive the follow ing as their
ions :ethy lene - blue w ill destroy malarial paras ites in many
)ut is less certain than quin ine .
[ethy lene - blue is probably most valuable in chron ic cases ,no advantage over quin inehe effects o f methy lene - blue are ordinarily more un
.t than quin ine .
is useful 1n cases that cannot take quin ine on account
e idiosyncrasy toward it. I ts use in cases of pregnancy.termined .
is probably valuable in treat ing hematuric and hemotric fevers on account of its d iuretic act ion ; th is has as
be determined. We have had no chance to test its use
1 cases .
Ve believe that quin ine “
is quicker and more certain , and
rely upon it rather than upon methy lene - blue.
:r its introduct ion in 1842 by Boud in arsenic enjoyed ,'
ecently , cons iderable reputat ion in the treatment of
1. The old schoo l of phys icians claimed results but[ ferior to those w ith quin ine. M ore recent observat ions.hat i f this agent has any value in the treatment of
t it is in the chronic form. Whether its good effectsre chiefly upon the -
anemia and as a general ton ic or
r it has some act ion upon the parthenogenet ic cycle istermined . Fow ler’s solut ionand the arsenous acid are
parations usually employed . The dose at the beg inn ingbe smal l and gradually increased . Upon the appearance
iness of the eyelids , col icky pains in the abdomen , and
3a the dose should be “
dim inished or its use temporari ly:inued . The arsenous acid may we l l be combined w ithjuinine , and strychnine in the treatment of chronic1.
recent preparations of arsen ic, arrhenal or d isod icarsenate , and sodium cacodylate have been vaunted as

376 THE STUD Y or MALARI A
ant imalarials by Gaut ier and others . They are rich in arsen ic,but less tox ic. Both preparat ions have been used in cases
where'
abort1on threatened ,and good results have been claimed .
They are usually g1ven hypoderm ically in doses o f from to
I %, grains d ai ly .
The benefits derived from atoxyl in the treatment of trypanoa
somiaSis led to an invest igat ion of its merits in malaria.
Chem ical ly , atoxy l i s sod ium aminOphenyl arsenate , contain ingabout 2 5 per cent . o f arsen ic and soluble , at 20
°
C . ,in
parts“
of water. The usual dose is . from "
one—third to I
grain , g iven every day or every other day , usually hypodermical ly.
Grosch43 5 cured w ith atoxy l a case ofmalaria that obst inatelyres isted quin1ne for a long period .
'
Fusco had sat is factory re
sults in 3 cases . Koch,ln report ing his experience with atoxy l
in thetreatment of Sleep ing s ickness , states that m cases‘
thatwere complicated w ith malaria
, usually of the estivo autumnal
variety ,the malar ial paras ites d im in ished markedly , but w ere
not so decidedly influenced by the drug as w ere the trypano
somes .
S latineano and Gal‘
esesco , employ ing large doses of atoxy lin 15 cases of malaria
,had 10 cures and 5 fai lures:‘ The fai l -4
ures w ere experienced most ly w ith double in fect ion'
s . Georgopulos , after its use in 14 cases , reported that the paroxysms
ceased , the spleen d im in ished in size , the paras ites d isappearedfrom the blood , and the general cond it ion of the pat ient im~
proved . I n 6 cases treated by Gonder and D apas the pat ientsimproved during the treatment
,in 2 cases the splen ic en large
ment d iminished cons iderably , but in on ly I case did the para
s ites d isappear ent irely . The res istance of the gametes , espe
cially the macrogametes , to the drug was noteworthy.
436 Vas
sal437
claims good results , especial ly in malarial cachex ia, by
the use o f atoxy l w ith the quinine.
While the experience of the w riter w ith atoxy l has beenlimited ,
he bel ieves that it is a valuable adjuvant to quin ine inthe cases where the latter is insufficient , particularly in cases
o f cachexia and extreme anemia. I ts good effect in these cases
may be due to the increased amount of arsen ic which may be
378 THE STUD Y OF MALARI A
A large number of other substances have been recommended
as substitutes for qu1n1ne .
"
The chie f o f these are phenocoll,eucalyptus, salicin
,salicylic acid
,s odium hyposulphite, etc.
The ir-
ant imalarial value , i f , indeed , they possess any , is so
s l ight as to render a detailed cons iderat ion not worth thewhi le .
The serum treatment of malaria has not yet reached the
stage of pract ical ut i lity . I ndeed,the experiments of Ford14°
alone have resulted in the isolation of an ant itox in . I n h is
first series of 9 cases of ben ign tert ian malaria 7 were cured ,
I was temporari ly benefited, while in the other the result was
negat ive. I n his second series of 2 0 cases of ben ign tert ian17w ere cured , while 3 were apparently quite uninfluenced.
Crit z mann8 6had several cachectic pat ients eat three t imes
daily 50 grams of chopped beef spleen m ixed With the yolkof an egg and 10 grams of bone - marrow . Burot and L e
grand225
used the same treatment in numerous cases o f cachexiain the hospital of Roche fort . I n the course of about fifteendays th e patient acquired a d isgust for the repast. While thepreparat ion had no effect upon the fever , it seemed to act as
a reconst ituent .M ore recently Carpenter“39 claims remarkable success in the
treatment of malaria w ith powdered splen ic extract'
in the dose
of 5 grains every two to four hours , preferably in capsules .
He says :“
Inmore than six years’
cont inuous experience and
in the treatment of hundreds of cases of malarial infect ionso f all types , both s imple and compl icated by all sorts o f cond it ions not a s ing le case has been met w ith which did not yie ldto th1s remedy .
” He further states that it is equally as rel iablea remedy as quin ine.
The Treatment of Pernicious M alaria—There are cer
tain cases apparently on the borderl ine between benign malariaand pern icious malaria of the cerebral type which may cause
hes itat ion as to the mode of administrat ion . I n these cases ,
usually in children , the pat ients , though stupefied , or even semi :comatose , can be aroused and made to swallow and usuallyretain the med icine . I n such cases , i f .the pat ient can be
watched , the quin ine may be g iven in solut ion by the mouth .
w i tn orai ad m in i st rat ion o r t h e S uluU UH wu c i-
e 1L c a n u
lowed , and even the rectum may be employed also.
As prev iously stated , qu in ine for intramuscular itshould be in d ilute solut ion ;1 5 grains to 2% drams o
is a suitable proport ion . The g luteal reg ion , above thetuberos it ies, is the best s ite for inject ion . I n pernicior
about 15 grains is the quant ity to be used at first inSubsequent doses may be from 5 to 10 grains in j ecte i
S ix to eight hours as needed . The techn ic of such in '
has already been g iven .
Inst as ant isyphil it ics may cause the gumma to meltbut are powerless to restore the t issue it has destro '
quin ine has its limitat ions in the therapeut ics of malashould be borne in mind that in its relat ion to the p:
quin ine is a toxin , _but not an ant itox in . I t is possil
where the paras ites are accumulated to the extent of
bosis the quin ine in solut ion in the blood d oes not reac
in tox ic quant it ies , and where perivascular exudat ion,
rhage, and necros is have resulted from these thrombi tl.hilation of the paras ites avai ls nothing . This i s corro
'
.
by those cases end ing fatally , notw ithstanding a rapidpearance of the paras ites , and in which post morter.
secondary changes are found . All that can be expe
quin ine is to destroy the paras ites , and this it may
accomplish from not be ing absorbed or not being prethe blood in sufficient quant ities or at the t ime when ths ites are most suscept ible to its act ion , or on account of
bot ic occlusions it '
may not gain access to the paras itesthe symptoms. Quin ine is probably a true specific icases of pern icious malariaOnly in which , in the abs
irreparable changes due to tox ins or to thrombi , thedestruct ion of the paras ites would be attended by an
s imultaneous cessat ion of symptoms .
O ther than the specific treatment there“
are importantomatic indicat ions to be met .
380 THE STUD Y OE MALARI A
I n cases w ith high temperature and hot dry skin cool ingbaths Should be used . FOr heart depress ion strychn ine or
d ig italis are useful .I n
"
the cerebral types the ice - bag to the head is called forand an act ive cathart ic should be-
g iven i f poss ible. Where thiscannot be swal lowed , a drop of croton oil on the back of thetongue m ay be tried .
'I f delirium is marked , a solut ion of
chloral and the bromides should beg iven by the rectum. Wherethere are convuls ions , chloral and bromides by the rectum,
morph ine hypodermically ,or even inhalat ions of chloroform
may be necessary . Bell'
employed lumbar puncture in a_
case
of malarial coma to relieve the increase in the cerebrospinalfluid - which usually ex ists in these cases , but the result wasd isappo int ing .
In alg id attacks for. the rel ie f of cold surface-
”
ands dyspnea,
especially i f choleraic symptoms are present, nothing‘
is so suitable as a combination of morphine and atropine . The heartusually . requires stimulat ion by strychnine and d ig italis; Hypodermics of ether may be necessary . I f dysenteric symptoms
ar ise they should - be treated w ith op ium and bismuth , togetherw ith sal ine irrigat ions .
I f compl icat ions appear they should rece ive ‘
appropriatetreatment .
D uring convalescence a t on ic of a rsen ic, strychnine , iron ,
and quinine is usually ind icated . I n cases where it is feas ible ,a change of c limate should be ordered unt i l recovery is thoroughly established .
T reatment of Hemog lobinuric Fever.—The d iscuss ionof
the treatment of hemog lobinuric fever has probably been productive o f more harsh and prejud iced controvers ies than hasany other quest ion in therapeut ics . The bone of contentionis quin ine .
I t is unnecessary to rev iew the history of the d iscuss ionsor to rehearse the arguments for or against the etiolog ic r elat ion of quinine to blackwater fever. No valid conclus ion can
be reached except through“
results of'
a larg e series of cases
treated w ith and w ithout quin ine . T he collect ion recorded
under Prognos is shows a mortal ity of 2 per cent. in cases

382 THE STUD Y OF MALARI A
2 . I f parasites are not found in the blood quinine should not
be g iven.
3.
'
I f quin ine .
‘
has already been g iven before the hemoglo
binuria has appeared and no paras ites are found , its use shouldbe suspended ;but i f paras ites pers ist it should be cont inued .
Thayer98 states his rules , mod ified from Bastianell i, thus
I . I f the a ttack occ’
urs spontaneous ly w ith a malarial paroxysm, the blood show ing the presence of paras ites , quin ineshould be freely admin istered hypodermically or intravenously .
2 . I f the paras ites have d isappeared , e ither as a result of“
the paroxysm itsel f or of doses of quin ine already g iven , it
may be as we ll to abstain ,at least for a t ime , fromthe admin
istration of the drug . I t cannot ame liorate the further course
of the paroxysm , and the poss ibil ity , if it has been alreadyg iven , that the symptoms may be in part due to quinine may
be thought of.3. I f an attack arise in the middle of an ord inary malarialin fect ion ,
after taking quin ine , it - is best to abstain ,_
for a t ime ,at any rate , from the further use of the drug . That “
which hasbeen g iven may _ have been enough to contro l the affection.
4 . I f,however, in an attack coming on after quin ine , the par;
as ites cont inue to deve lop ,quin ine should be again adminis
tered , despite theSl ight poss ibil ity of its injurious action . The
dangers from the further dev elopment of the paras ites are
probably the greater.
5 . I n pos tmalarial hemog lobinuria quin ine is , of course , useless .
The follow ing rules o f V edy are pract ical :I . I f l iv ing parasites (not merely ev idence Of their former
ex istence , pigment ) are detected tw enty- four hourS ‘
after the
beg inn ing of the attack 80 centigrams of a salt of quin inemay be in jected subcutaneously .
2 . I f the paras ites are not v is ible do not admin iste r quin ine .
3. I f in doubt , that is to say ,if the m icro-scopic examination
o f the blood cannot be made , do not g ive quin ine.
I t may be seen that the authorit ies quoted lay great stress
on the presence o f the paras ite as a guide to the adm in istrat ionof quin ine. The w riter
,how ev er , cannot agree w ith those who
TREATMENT 383
ho ld that quinine should be exh ibited in every case where themicroscopic examinat ion show s the presence of parasites . I t
has been shown conclus ively that paras ites are present in a
very large proport ion of cases examined early . I t has alsobeen shown that in . an equal ly large number of cases the para
s ites d isappear spontaneously . I n these cases quin ine is , tosay the least , superfluous.
I n the w riter ’s Op in ion , the only conditions in which quinine
is indicated a re : firs t, where the paras ites show no tendency
to disappear after forty - eight hours from ons et; second, in
the infrequent cases of intermitten t hemoglobinuriawhere the
outbreak corresponds with parasitic sporulation.
I f it is decided to g ive quin ine it should be injected , in diliitesolution , into the muscles as d irected for the treatment of
pern icious malaria. Given by the mouth it upsets-
t he stomachand may not be absorbed .
Even in cases of mi ldest onset the pat ient should be '
confined
to bed from the start , and should be kept quiet e ither bysuas ion or by sedat ives . Sudden death on sl ight exertion some
t imes occurs . The pat ient should not be transported fromone
place to another ; the Plehn brothers o bserved anuria as“
a
frequent consequence of moving pat ients from place to place.
Chilling of the body , especial lywhen the temperature is low ,
should be care fully avoided. When vomiting is not a prominen t feature
'
liquid nourishment may be g iven freely ; buttermilk and albumen water are the most suitable. Sw eet milk iso ften e jected as a th ick curd ,
molded ropy by the esophagus
in the act o f vom it-ing . Animal broths , barley and oatmealwater
,lemonade , and orange juice
'
are allowable. Rectal ali
mentat ion is unsat is factory .
There is no specific. M ethylene- blue has proved d isappoint
ing . Bes ides being a renal irritant , it masks the color of the
urine , a most serious objection. S al icy l ic acid probably hasno effect further than to upset the stomach and increase thed iscomfort . With the false idea that a hemorrhage has to bechecked , gall ic and tannic acids , ergot , and s imilar drugs are
frequently g iven ;these cannot po ssibly be of any benefit . Car
bolic acid and other renal irritants should not be used.

384 THE STUD Y OF MALARI A
The bow els should be '
moved early and o ften , and calomelpossesses advantages over other purgat ives ; it is more
s
easilyretained ,
is'
a bland d iuret ic, and is the best of intest inal ant iseptics . Too large doses are usually adv ised ; 3 to 5 grainsare , as a rule , sufficient , repeated pro re nata.
Quennec’
s440
chloroform treatment has been success ful insome hands . The orig inator claims for the method threepo ints _
of valueI . Controls vomit ing .
2. I ncreases output of urine.
3. D im in ishes albuminuria.
'He treated more than 50 cases w ith no mortality. The fol
low ing is his formula : Chloro form, 6 grams ;gum arabic, 8grams ; sweetened water
,2 50 grams . This amount is used
dai ly , a sip taken every ten m inutes . I n add it ion , Quennec
used quin ine , 1 gram'
daily subcutaneous ly , and sulphate of
soda and senna by rectum. The excess ive admin istrat ion of
chloro form m ight be harm ful , as it is a card iac depressant ,renal irritant , and lowers the blood pressure .
Cardamatis206
gives ether in every case of hemog lobinuricfever. I n ordinary cases he prescribes a teaspoonful in sweet
ened water every three hours , and increases the d ose i f theurine d iminishes in quant ity . I n cases of suppression he g ivesas much as a teaspoon ful every hour, at the same t ime inject ,
ing hypodermically I cc. every two or three hours . He maintains that by this means the pulse “
is strengthened ,
“
.precord ialanxiety , dyspnea, and vom it ing are rel ieved , and a pro fused iures is is provoked .
The w riter has had no experience w ith ether in the treatment
o f blackwater fever,but would cons ider it too irritat ing to the
kidneys for general use .
Hearsey26 6
used w ith good results a mod ificat ion of S tern
berg’
s yellow—fever treatment. The orig inal S ternberg . for
mula is : sod ium bicarbonate , I 50 grains ;mercury perchloride ,one - third grain ;water, 2 pints . S ig . : ounces every hour.
Hearsey g ives sodium bicarbonate , I O grains ;l iquor hydrargyriperchloridi, 30 minims every two to three hours .
A method of treatment recent ly introduced and extrava
386 THE STUDY OF MALARI A
V omit ing , i f not intense , is often benefited by a mustard
p laster on the epigastrium . The fly- blister formerly used
should'
be abandoned. D raughts of hot water Or carbonatedwater sometimes ass ist in re l iev ing this troublesome symptom.
Cracked ice may be tried.
“
M orphine hypodermically shouldbe g iven unhes itat ing ly when other measures fai l . Any ev ileffects are more
-
than outwe ighed by its enabling the stomachto retain l iquids .
An important measure toward the prevent ion a nd re lie f ofnausea and vomit ing is to maintain t he recumbent pos it ion.
M ed icine, water, and nourishment should be taken througha drinking tube or the ord inary inval id ’
s cup , and the ,bed‘
;
pan or urinal should be used When evacuat ing the bowels or
bladder.
I t is imperat ive to allay the rest lessness o ften present in thesecaSes . For this purpose chloral and brom ide of soda byrectum,
“morphine hypodermical ly , or sulphonal or smal l doses.o f chloro form by mouth are use ful .Probably the most important ind icat ion in the treatment is
the prevent ion of suppression . M edicinal diuretics usual ly doharm. O ne , turpent ine, w idely used in some sections
,sh ould
be condemned in the strongest terms . I t is one of the most
v iolent renal irr itants,and in some persons smal l doses may
cause suppress ion or hematuria. Water is the best d iuret ic ,and as much Should be g iv en by mouth as w ill be retained.
L ew is } 92 of North Caro l ina, was the first t '
o
'
recommend theuse Of normal salt solut ion by hypodermoclys is and by the
rectum in the treatment of hemog lobinuric fever , though L averan
ilattributes the priority to Gouz ien . The latter recom
mends the dai ly inject ion of 100 to 300 grams of a n ine- tenthsper cent . solut ion , in conjunct ion w ith the rectal inj ect ion of
200 grams,four to six t imes in twenty
- four hOurs . The use
of salt solut ion is the very best-
means of combat ing and treat
ing anuria. I t is probably better to use a hyperton ic solut ion .
I n mild casesWhere the urine is free the rectal u se is usuallysufficient , but in cases where suppress ion threatens or i s immi
nent the solut ion should be used subcutaneously or intravenously and in larger quantit ies and o ftener than adv ised by

U U U L I M L L Q .L VL L l u b u u l -I L V J l l . 1 J L G L L U L L U V v ; b l l b .l . b Sl - V L J . V J . L L L M Ex a u n
may be tried.
Werner,4“ in 1902 , suggested nephrotomy for anuria. S
an operat ion has been recorded in on ly three instances . 2
mann48 ment ions a case in a young female pat ient in wh
suppress ion had ex isted two days . The capsule of the ri
kidney was Split and peeled off to the hi lum and nephrotc
performed through the convex ity of the organ . The operat
was we ll borne , and subsequently 200 cc. of cloudy , albuminurine was voided from the bladder. D uring the followdays complete suppress ion recurred , and the pat ient d ied .
I n Kruger’s“ 5case decorticat ion of . one kidney was (1
five days after the onset of anuria, and , although the secret
of ur ine was pro fusely reestablished , the patient d ied of r
gress1ve weakness.K iilz
M 6reports a case in a
s man during his second att z
Three and a hal f days after the onset of anuria nephrotcupon one kidney was performed through S imon
’
s incisiVomiting , which was formerly uncontro llable , ceased i
'
mi
diately . Three hours after the operat ion 30 cc. of blood wvo ided from the bladder. I n e ight hours the dress ing 1
saturated w ith bloody icteric urine , which necess itated cha
ing the dress ing every three hours . Twenty - four hours at
the operat ion the pat ient d ied. Though a m icroscopic examit ion of the kidney c ould not be made , upon gross inspectthe nephrotomiz ed kidney appeared much more nearly nori
than the other.
S upportive measures“
are essent ial . A lcohol in all its fo i
is inadm iss ible . S tryc‘
hn ine is use ful , and should be '
g i
hypodermically When circumstances perm it D ig ital isproved serv iceable in the ‘
w riter’
s hands . D oering18 7had g s
effects from strophanthus . The aromatic spirits o f amme
and hypodermic inject ions of ether have been recommenc
Trans fusion of blood has been used, it is said , w ith excel]results. The elder Plehn” says that he had four attacks .
which K ohlstock treated him w ith inhalations of Oxygen ,
that nothing else did him so much good . Un fortunately ,1
method of t reatment is not o ften possible in private practice
388 THE STUD Y O F M ALARI A
The after- treatment should have a care for the d iet , whichshould be non- nitrogenous and cons ist largely of l iquids at
first. '
A ton ic of'
organic iron is ind icated , and d igest ive disorders
'
when present should receive appropriate treatment .
A quest ion of pract ical importance is , how soon after '
the
attack to beg in the“
admin istration of quin ine. A dose g iventoo early might possibly ,
- in'
some persons , precipitate hemolys1s. O n the other hand , delay may perm it an outbreak of
malaria accompanied by hemog lobinuria.
_
Upon the ground
that most o f the sens itive cel ls have succumbed during the at
tack and that the new ly formed'
cel ls are probably more sus
ceptible than those that have -w ithstood the attack, the w riteris of the op inion that quin ine should be begun , c are fully at
first , a short t ime after the attack4 has subsided and be foreblood regenerat ion is fairly established . O ne grain o f quininethree t imes daily , increased gradually every other ‘
day , is a
safe procedure. I f the temperature rises or the ur1ne becomesd ist inctly darker no further attempt to increase the dose shouldbe made.
a-I n the present state of our know ledge it is probably Utopianto d iscuss the treatment of hemog lobinuric fever by antihemo
lyt ic sera, but such has recently been success fully accompl ishedby Widal and Rostaine447 in paroxysmal hemoglobinuria.
REFERENCES
1. Laveran : Traité da Paludisme,Paris
, 1907.
2 . New O rleans M ed . and S urg . Jour.,iv , 563, 1848.
3. King : Popular S cience M onthly , S ept , 1883.
4. Crosse : Blackwater Fev er,London
,1899 .
5 . Plehn : D ie Kamerun K iiste, .Berlin ,1898.
6. M ense : Arch. fiir S chiffs . u. T rop . Hyg ,iii
, 4.
7. Kohlbrugge : Arch. fiir S chiffs. u. Trop . Hyg .,iii
, 2 .
8. Cited by M ense
9 . S ambon : The Practitioner,M arch ,
1901.
10. Cited by S ternberg11 . Cummings : N. O . M ed . New s and Hosp . Gaz .
, vi, 811.
12 . Faget : N. 0 . M ed . Jour.,O ct .
,.1868.
13. O sborne : I bid,1868, 644.
I 4. O sborne : I bid.,xxii
,61.
15 . Ghent : Richmond and Louisville M ed. Jour., v ,271.
Cited by Cardamatis17. Johnson : I nfluence of Trop ical Climates , etc.
,New York , 1826.
'
18. Cleghorn : D iseases of- M inorca, London ,1762 .
0
19 . Hirsch : Handbook of Geog. and Hist. Pathology ,London
,1883, vol. 1.
Cited by Rogers2 1 . Rama z z ini : Sur l
’
Abus du Quinquina, Paris Repr int , 1905 .
101.
102 .
103.
104.
105 .
106.
107.
108.
109.
11 1.
1 12 .
1 13.
1 14.
1 15 .
116.
117.
118.
1 19 .
120.
12 1.
122 .
123.
124.
125 .
126.
127.
128.
129.
130.
131 .
132 .
133134I 3S136.
I 37138 .
THE STUD Y OF MALARI A
Celli : La Malaria . S econdo le Nuove Ricerche, Rome .
Erni : A rch. fi'
i r S chiffs .
‘
u. Tr0p . Hyg ,Jun e
,1899 .
A tti della . S ocieta per gli S tudi della M alaria,Rome
, 1906.I bz d 1908.
119105 1904.Jour. Am. M ed.
'
Assoc , 5 1, 9 16.
Cited by L averan ( I ) .
S trachan : Brit . M ed. Jour.,M arch
Ross : Brit. M ed . Jour ., S ept . 14, 1901.
Panse : Arch. fur S'
chiffs. u. T rop . Hyg .,1902 , No. 12 .
Cited by RugeCraig . Yale M ed . Jour.,
June,1907.
S chellong : D ie M alariakrankheiten ,Be rlin
,1890.
Hadj imichalis and Cardamatis,Ann . T r0p . M ed. and Par.,
ii,
Report to the M alarial Committee,6th S eries
,London
,1902 .
Russell : M alaria and I njuries o f the Spleen , Calcutta, 1880.
Cited by M annabergF elkin : Edinb. M ed . Jour.
, June, 1889.
Thayer ; L ectures on the M alarial Fevers,New York
,1901.
A Plehn“
: D ie M alaria der . Afrikan ischen Negerbevolkerung, Jena,1902 .
Pe z opoulos and Cardamatis : Arch. de Med. des Enfants , ] an4 1907.
Cited by M anson
Winslow : Boston M ed. and Surg . Jour ., M ay 27, 1897.
Peters : Johns Hopk ins Hosp . Eu-ll.,June
,1902 .
M offatt : Brit . M ed. Jour.,M ay 4, 1907.
Cited by CrespinHitte : These de M ontpell
-ier,1902 .
'
Holt : D iseases of I n fancy and Childhood, New York,1908.
Eco- :nomous Bull. de la S oc. d’
Obstet ., x , 70, 1907.Bell : Jo-ar. Am . M ed. Assoc , 5 1 , 1993.
Cited by Thay er and Hew etsonJeffries : M ed . Record, 57, 654.
D aniels : Brit. M ed. Jour., Jan. 26
,1901.
S tephens and Christ0phers : Thomp . Yates Lab. Rep ., v i.
Cited by How ard
Cited by Galli V allerio et de JonghBank s : The Philipp ine Journal of S cience , D ec ,
1907.
Cited by Austin ,The Practitioner, M arch ,
1901.
S tephens and Christ0phers : Practical S tudy of M alaria,London, 1904.
Giles The Gnats or M osquitoes , London ,1902 .
Coqui
6
llett : Class. of the M osq. of North and M iddle America, Wash:,190
S ambon : Brit. M ed. Jour.,S ept 24, 1908.
Howard“
: M osquitoes , New York,1902 .
Nuttall : Brit. M ed. Jour .,S ept . 14, 1901 .
Galli V allerio et de Jongh : M anuel pour la Lutte , etc.,Paris, 1906.
Pressat : L e Paludisme et les M oustiques , Paris, 1 905 .
M itchell : M osquito L ife ,1907.
Ey esell : Arch . fiir S chiff s . u. T rop ,Hyg .,
xi,6.
Woldert : Jour. Am . M ed . Assoc, 50,
1249 .
Cited by S tephens and ChristophersEw ing : Jour. Exp . M ed.,
M arch 25 , 1901 .
Cited by M annabergCited by EwingCited by S chaudinn ( 134)S chaudinn : Albeiten aus den Kaiser] . Ges . Amt.
,-19 , 2 .
M aurer : Centralbl. fur Parasit., etc.,Nov . 5, 1902 .
Bliiml and M et z : Arch fiir S chiffs . und Trop . Hyg .,xii
'
,249.
Craig : I nternational Clinics , 17th S eries, iii.Cited by Craig

REFERENCES 391
139. Cited by Thayer140. Ford : Jour. Am. M ed. Assoc , 48, 133 ;M ed. Record, 66, 1001.
141. M annaberg : M alarial D iseases,Phila.
,1905.
Rosenau et al. . Exp . S tud . in Yellow Fever and M alaria, Wash ,
1905 .
143. Koch : D eut . M ed . Woch. , M ay 3, 1900.
144. Crespin : Précis du Paludisme,Paris
, 1905 .
145 . Bell : The Lancet,Aug . 24, 1900.
146. S antos : L’
I nfluence de l’
Impaludisme,e tc. Rio de Janeiro , 1888.
147. Atti della S ocieta p er gli S tudi della M alaria,Rome
,1902 .
1 48. Thornhill : I ndian M ed . Ga z .,M arch
,1898.
149. Cited by Burot et L egrand
150. Atti della S ocieta per gli S tudi della M alaria,Rome
, _ 1901.
15 1. Billet . Revue de M edicine, D ec,1902 .
152 . S ims : Jour. Trop . M ed. J an . 190 -2 .
153. Rees : Brit. M ed.
p
Jour.,F eb. 1900.
154. S atterlee : New York M ed . J0ur ., April 11, 1908.
155 . Hall : D enver M ed. Times,April 1908.
156. Neer : Jour. Am. M ed. A ssoc, 50 ,
1890157. Homem : Pernicious F ever, D etroit
,1904.
158. Ruge : Einfiihrung in das S tudium der M alariakrankheiten, Jena,159 . Cited by L e D antec
160. Wurt z and Thiroux : D iag . et S ém. des M alad . T r0p .,Paris , 1905.
161. Roux : M aladies des Pays Chauds, Paris , 1886 .
162 . M a
ghiafava and Bignami : Summer and Autumn, M al. Fever, London ,
I 4163. V an der S cheer : V irchow
’
s Archiv .,139 , 1.
164. Craig . O sler’
s M odern M edicine,Phila.
,1907, vol. i.
165 . Crespin : La Caducée , M ay166. French : New York M ed . Jour .
,M ay 23, 1896.
167. Hunt : New York Post
168. Cited by S utherland . M emphis M ed. M onthly , July , 1905 .
169. Ficucci : Rev . in M ed. Record , 71 , 870.
170. F enner : N. O . M ed. and S urg . Jour.,D ec , 1903.
171. A . Plehn : B'
eitr. z ur k ennt . der Trop . M alaria, Berlin ,1896.
172 . Koch : Arbeiten aus den Kaiser] . Gesundh. Amt ,
173. Cited by Rho . La M alaria, Turin,1896.
174. Bark er : S tudy of S ome Fatal Cases of M alaria, Baltimore , 1895 .
175 . Zeri : I l Policlinico ,April, 1904.
Bloomberg and Cofiin : Am M ed , Nov . 25 , 1905 .
177. Ew ing : Am. Jour. M ed. S c1., O ct ., 190
178. K elsch and Kiener : M aladies des Pays Chauds, Paris, 1889 .
179. Cited by Ew ing180. Ford : M ed. Record, April 5 , 1902 .
181. Ew ing Jour. Exp . M ed. , Feb. 5 , 1902 .
182 . M ercier : Le Paludisme Observé sous les Tropiques , Paris , 1905.183. Hert z . Ziemssen
’
s Cyclopedia, New York,1875 , vol. i i .
184. Hanley : Jour. T rop . M ed,1899 , p . 85 .
Cited by F . Flehn
186. Curry : Jour. Am. M ed. Assoc ,.38, 1130.
187. D oerring : D eut . M ed. Woch.,Nov . 14, 1895 .
190. Personal Communication “
191. Cited by F . Plehri
192 . L ew is .
y.N C . M ed Jour.
,M arch 5 , 1899 .
193. F rance z : N. 0 . M ed and Surg. Jour., July , 1902 .
M inos : M ed. New s , Nov . 24, 1883.
195. M cK ay Am. F ract. and New s , June196. Ty son : M e .d New s , M ay
197. D aniels : Laboratory S tudies in Tropical M edicine ,
392 THE STUD Y OF MALARI A
198 Cardamatis : La Grece M édicale, April, 1900.
199 . Krauss : M emphis M ed. M onthly ,'
April, 1902 .
200. D eaderick : -M emphis M ed . M onthly , Aug , 1907.201 M ense : Arch. fiir S chiffs. u. Trop . Hyg .,
June,1899.
202 . L ipari : I l M orgagni,203 Cited by S cheube
204. Cited‘
by Burns
205206.
Tomaselli,
: La I ntossicaz ione Chinica, etc., Catani, 1897.
Cardamat is : La F iévre B i lieuse Hémoglobinurique , Paris, 1902.
207. Foustanos : La Grece M édicale, April, 1900.
2082092 10
F . Plehn : Arch. fiir S chiffs. 11. Tw p . Hyg., iii, 6.Crosse : Brit . M ed. Jour., O ct . 8, 1898.
Bank s : Jour. Trop . M ed., D ec. 15 , 1900.
2 11. F . Plehn : Tropenhygiene, Jena, 1906.
2 12 .
2 13.
2 14.
2 15.2 16.2 17.
2 18.
220.
22 1.
222 .
223.
224.
225 .
226.
227.
228.
229 .
230.
231.
232 .
233.
234.
235 .236.
237.
238.
239.
240.
241.
242 .
243.
244 .
245 .
246.
248.
249.
250.
25 1.
252 .
253.
254.
255 .
256.
BUI
é
Ot and L egrand : M aladies da S oldat aux Pay s Chauds , Paris,1 97.
Védy : La F ievre Bilieuse Hémoglobinurique ,‘
etc.,Brussels
,1907.
M cElroy : M emphis'
M ed . M onthly , M ay and June, 1905 .Brem : Jour. Am. M ed. Assoc ,
D ec. 8- 15 , 1906.
Howard : Jour. T rop . M ed., M arch 1,1907.
Bassett - Smith : Jour. Trop. M ed., 1907, x ,69 .
Hughes : Jour. Trop . M ed.,June
,
M anson : Brit. M ed . Jour.,M ay 16, 1903.
Park er : Brit.'
M ed. Jour.,S ept . 9 , 1899.
M owbray : The Lancet, Aug . 26, 1905 .S chlayer : D eut . M ed . Woch.
, July 10,1902Kleine‘
: Brit . M ed. Jour., S ept. 14, 1901.Koch Jour. Trop . M ed.,July 15, 1899 .
Burot et Legrand : Thérapeutique du Paludisme,Paris
,1897.
Le D antec : Path010gie Exotique, Paris, 1905.
Cited by Kelsch and KienerD ryepondt and V ancampenhout : Jour de Med. de Bruxelles , 1899 , 9.
B ertrand : Ann . S oc. M ed .- Chi. d
’
Anvers, Nov . and D ec,1899.
M ould : Brit. M ed. Jour.,S ept . 9 , 1899.
Haig : The Lancet,-Ap ril 2 , 1898.
Cited by M en se : Archiv. fiir .S chiffs . u. Trop . Hyg .,iii
,2 .
Cited by M archiafava and BignamiCited by A . F lehnBurns : Jour. Am. M ed . A ssoc
,Nov . 17, 10
,1900.
Crosse : The Lancet , Jan. 6 , 1900.
Thin : Brit. M ed. Jour .,S ept . 1, 1900.Ketchen : Brit . M ed . Jour., Nov . 10
,
Ruge : D eut . M ed . Woch.,July 10
,1902 .
Woldert : New York M ed. Jour., Feb. 23, 1895 .
Hartsock : New York M ed . Jour .,S ept . 13, 1902 .
Broden : T rav . du Lab. M ed. (165 Leopoldv ille , Brussels, 1906.
Cited by' Cardamatis
Cardamatis : Progres M edical,1902 , Nos . 37
-
40.
V irchow’s Jahresbericht
,bd.
,1,1907.
Grattan : Jour. Royal A rmy M ed . Corps , 1907, ix , 3, p . 237.Kulz : Arch. fur S chiffs. u. Trop . Hyg .,xii,
“
242 .
Smith and Kilbourne,T exas or S outhern Cattle Fever, Washington,
1893.
O rme : Jour. Trop . M ed., Feb. 1 , 1908.
Cited by CrosseCited by BremCited by V edyCited by Koch : Arch . fur S chifi
'
s. u. Trop . Hyg., June , 1899.
Ellenbeck - Hilden,Beobachtungen uber M alaria,
Berlin ,1905 .
L egrain : I ntrod . a l’
Etude des Fievres des Pays Chauds , Paris , 1899.
Grall : Pathologie Exotique , Paris, 1900.
394 THE STUD Y or MALARI A
318. Brault : M aladies des Pay s Chauds , Paris , 1900.
319 . M esserer z'
These de Paris , 1886.
320. Goltman : M emphis M ed . M onthly ,'
-Nov ., 1905.
32 1 M oore : Am. M ed .,D ec. 28
,1901 .
322 . Duprey : Jour. Trop . M ed., S ept. 16, 1907.
323. Cited by Behrmann : Berlin Klin . Woch.,Aug. 24, 1885 .
324. Goth : Zeitschr. fiir Geb. u. Gynak .,v ii
, 1 , 1881.325 . Bonfils : Paludisme et Puerperalité, Paris , 1885 .
326. Williams : A Text - book of Obstetrics, New York
,1903.
327.
'
Glogner V irchow’
s Archiv .,1895 , 140, p . 481.
328. Price : Am . M ed.,June 3, 1905 .
329 . D aCosta : I nternational Clinics,S eries 1891, iii.
330. Fornaca : I l Policlinico,1907,
331. Torti : Riforma M ed .,1891 ,
'
xii.
332 . S piller : Am.Jour. M ed . S ci.,D ec
, .1900.
333. Ziemann : A rch . fiir S chiffs . u. Trop . Hyg .,xii
, 501.
334. Winfield : New York M ed. Jour. ,Aug .
335 . Bastianelli and Bignami : Bull. (1. S oc. Lancis , Rome,1890, 1x ,
336. D eaderick : S outhern M ed . Jour., O ct.,1908.
337. Anders : Phila. Hosp . Reports , iv ,1895 .
338. Loffler : D eut . M ed. Woch .,1901, No . 42 .
339. V alenti : I l Policlinico,x iv , 48,
340. L ioubenet z ky : S emaine,M ed.
,1908, 18.
M allory and Wright Pathological T echnique, Phila.,1904.
342. Cabot : Am. M ed .,D ec. 20, 1902 ; Bost. M ed. and Surg. Jour. M arch
24, 1904.
343. Fornario : D eut'
. M ed. Woch., Jan. 2 2 , 1903.
344 . M cElroy : M emphis M ed . M onthly ,Nov .,
1902 .
345 . A . Plehn :Weiteres iiber M alaria,etc.
,Jena
,1901.
346. D elaney : Brit. M ed. Jour.,M arch 28
,1903.
347. V incent : Ann . de l’
I nstitut . Pasteur,D ec. 25 , 1897.
Ross : The Lancet, Nov . 17, 1906.
Ross : The Lancet , S ept . 28 , 1907.
350. Hagen :A rch.,
fiir S‘
chifi‘ s u. T r0p . Hyg .,iv , iii.
35 1. Jour. Tr0p . M ed .,vol. x i.
352 . Haw : Jour. T rop. M ed., O ct. 16
,1899 .
353. Lav eran : Bull. de l’
Acad. de M éd .,lxix
, 32 .
354. Gorgas : Jour. Am . M ed. Assoc , 46, 1417.
355 . Annual Reports , .U . S . P. H. and M . H. S ., 1905 - 07.
356. M ediz inal Berichte iiber die D eutsch, S chut z geb.,1903- 06.
357. Parry : Am. Jour. M ed. S ci., v ii, 339.
359. Cited by Cardamatis
360._
Cited by Wood : Practical M edicine,Phila.
,1847.
361. Charity Hosp . Repo rts , New O rleans,1906- 07.
362 . Cited by Cardamatis
363. Cardamatis : Bull. de la S oc. de Méd. de Gand.,Nov ., 1900.
364. Cited by Cardamatis
365 . Cardamatis : Bull. de la S oc. de M'
éd. de Gand., O ct., 1900.
366. Jenk ins : Trans . Ark . M ed. S oc , 1904, 203.
367. Cited by S ambon
368. M ichel : N. O . Jour. of M ed.,1869.
369. M alone : T rans. A rk . M ed. S oc , 1880, v , 74.
370. Coste : Rev . in La Presse M ed.,S ept. 12 , 1906.
371. S teggall : M ed . Record ,372 . Austin : Brit. M ed. Jour.,
Feb. 10, 1900.
373. Cited by Cardamatis , F . B . : Hemoglobinurique , S yra, 1901.
374. M cD aniel : M ed . New s , Nov . 24. 1883.
375 . Henric : Arch. de M ed . Nav .,M ay ,
1898.
376. K ohlstock : D eut . M ed Woch., Nov . 14, 1895 .
377. Ensor : Arch. fiir S chiffs. u. Trop. Hyg.,108.
378. Cited by F . Plehn
REFERENCES 395
379 . Cited by Hopk insCited by Prentice : Brit. M ed; 24, 1898.
381. D empw olfi’
: A rch. fiir S chifi'
s . u. Trop . Hyg.,June, 1899.
382 . Cited by Hare : Ther. Ga z .,July 15 , 1892 .
383. Cited by L ew isForde : Jo‘
ur. T rop . M ed,F eb . 1
,1908.
Cardamatis : F ievre Bilieuse Hémoglobinurique, S yra, 1901.386. Prout : Brit. M ed. Nov . 9 , 1907.
387. Jaco‘
bs : New York M ed. Jour., O ct . 12,1907.
388. D eCruz : I ndian M ed .
D eBlasi : Gaz et’._
degli O Sp ed ., April 26, 1903.
390. O rme : Jou-
r. Tr0p . M ed .,x i, 38.
39 1. Thompstone : Jour._
Trop . M ed,xi
, 14.
392 . Ross : M osquito Brigades , New York, 1902 .
Rosenau : D is infection Against M osquitoes , etc., Washington, 1901.
394. Cited by Smart
395 . Babes : M iinch. M ed. Woch .,Ap ril 4, 1905 .
396. D uncan : Brit. M ed . Jour ., S ept. 1 , 1900.
Annual Report U. S .
'
P . H. and M . H. S ., Washington , 1906.
398. S ambon and Low : Brit . M ed . Jour., D ec . 8,1900.
399 . Busck : Jour. Trop . M ed .,xi
,252 .Kleine : Zeitschr. fur Hyg . I nfek ., 38, 1907.
401. Cited by Giemsa and S chaumann
402 . S chmit z : Arch. fiir Exp. Path. 11. Pharm.,1907.
403. Craig : Am. M ed.,April and M ay , 1906.
404.
'
M annaberg : D ie M alaria Parasiten , V ienna, 1893.
405 . Gudden : Arch. fiir S chiffs . u. T rop.
‘
Hyg .,1905 , 500.
406. A . Plehn : A rch. fiir S chiffs . u. T rop . Hyg .,ii, 4.
407. Grenier : I ndian M ed . Gaz .,Feb.,
1898.
Quill : Rev . in M ed . New s , D ec 5 , 1903.
409. Goodman : M ed. Record , 70, 865 .
410. Cited by Tomaselli
41 1. M oore : The Lancet,1863, 660.
412 . Cited by M auv ie z : L e Paludisme a D iego - S uare z , Paris, 1905 .
413. Bartholow : M ateria M edica, New York
,1894.
414. Cited‘
by M ccampbell
415 . M cCampbell : Jour. Am. M ed. Assoc ,
416. Bliimchen : D eut. M ed . Woch.,1901 , No . 17.
417. M anson : L ectures on T rop ical D iseases , Chicago , 1905 .
418. Cited by M cElroy
419 . Gros : Bull. de la S oc. de M ed. de Gand , O ct., 1900.
S hoemaker : M ed . Record, O ct. 29 , 1904.
Cited by V ande‘
rhoof : Jour. :Am. M ed . Assoc , 48, 1333.
Bacelli : Gaz . degli. O Sped .,Feb.
,1890 ;Riform. M ed:, 1890, 6.
423. Guiterre z : Rev. in Jour. Am . M ed. Assoc , Nov . 1902 .
424. F leury : Jour.Ami M ed. Assoc, Dec. 24, 1904.
425 . Holmes : Medical Essay s , Boston,1895 .
426. D emarchi : Policlinico,1906, xiii, 6.
427. Brachio : I ndian M ed . Ga z .,M arch
,1908.
428. Bell z'
The M ilitary Surgeon , August , 1907.
429 . Goltman : M emphis M ed. M onthly ,Nov, ,
1905 .
430. Guttman and Ehrlich : Berlin Klin . Woch.,1891, 39.
431. Wood : M ed . New s , M arch 4, 1905 .
432 . D e Blasi : Gaz . degli O spedali, M arch
433. Thayer : Bull. Johns Hopk ins Hosp .,M ay , 1892.
434. M oore and'
Allison : M ed . New s, D ec. 6, 1902.
435 . Grosch : M ed. Klinik .,1907, 20 .
436. Wiener : Klin . Woch.,June 4, 1908.
437. V assal : Le Caduccée, ninth year, 9.
438. Duncan : Jour. Trop . M ed , O ct. 16, 1899 .
Carpenter : M ed. Record , 70, 165 .

'
THE STUD Y OF MALARI A
Quennec :Arch. fur S chiffs. u. Trop . Hyg.,iii
,2.
V incent : Compt. Rend . S oc. Biol., D ec. 15 , 1905.Polli : Brit. M ed:Jour., Nov. 16, 1867.
O’
Sullivan - Beare : The Lancet,F eb. 1
,1902.
Werner : D eut. M ed. Woch.,1902 , 42 .
Cited by Werner : D ie Nieren beim S chwarz wasserfieber,1907.
K iilz : Arch. fur S chifi'
s. u. T rop . Hyg.,x i
, 508.
Cited by . Ed. Jour. Am. M ed. Assoc ,June 24, 1905.
Below : Berl. Klin. Woch., Nov . 15 , 1897.M cKay : G lasgow M ed; Jour., M arch, 1908.

398 INDEXChronic malaria, 2 28 D uration of larval stage, 79
treatment , 368 D ysenteric form ,2 14
Cinchona, history, 28
Circulatory system, complications, 232
symptoms ,
“
195
C iviliz ation ,6 1
Classification of mosquitoes, 86
of parasites, 11 2
of pernicious'
malariao 203
Clearing of land, 48
Climate , 38
Clinical history, 184
Colon bacillus, 25 2
Colors and mosquitoes, 106
Comatose malaria, 204
Complications, 232of hemoglobinuric fever , 226
treatment , 372
Congenital immunity, 54“
malaria, 64
Contra—indications to quinine , 355Convulsive form, 209
Coquillettidia , 100
Crescents, 231
pyrogenic properties , 147
Ctilex, 98
Culicella, 97
Culicinae, 87, 90
Culiseta , 98
Cu-ltivation experiments, 1 29
Cycles of the parasites , 1 14Cycloleppteron , 89
D EINOCER'
I TES , 10 1
D einoceritina , 87, 10 1
D endromyia, 103D estruction
_
oi mosquitoes, 305of parasites , 315
D iabetes, complication , 25 1
D iagnosis , 256
differential, 284
of hemoglobinuric fever, 289
of pernicious malaria, 287
D iaphoretic form, 2 14
D ifferential diagnosis, 284
D isappearance of malaria, 73D issection of mosquitoes, 1 10
D issemination by mosquitoes, 69D osage of quinine , 365
D rinking-water, 62
EAR complications, 248
Earthquakes, 46
Eclamptic form, 209
Education and prophylaxis, 327Eggs of mosquitoes , 76 , 107Elimination of quinine , 335
Endemic index, 56Endocarditis , diagnosis , 284
Endogenous cycle , 1 14
Epidemics, 63'
oi hemoglobinuric fever, 37
Error, sources of, 268
Estivo- autumnall
in-
fection , symptoms,190
parasites, 1 19
differentiation , 12 1
Etiology , 38of hemoglobinuric fever, 153of pernicious malafia, 140
Europeans and hemoglobinuric fever, 29
Examination of blood , 258
Exclusion of mosquitoes, 322
Exflagellation , 1 17
Exogenous cycle, 1 23
Exposure , 60
to wind , 49
External etiologic influences, 15 1
Eye complications, 248
FAM I LY predisposition and . hemoglo
binuria, 156
Feeding of mosquitoes,'
70, 1 10 7
Females,susceptibility of, 54
Fertiliz ation of mosquitoes, 70 , 107
Fish and prophylaxis, 31 1
Flagella,'
1 17, 268
Flight of mosquitoes, 105
Food in etiology, 6 1
of mosquitoes, 70 , 104
GAMETES , differentiation, 1 17, 122
estivo - autumnal, 120
quartan , 1 19
tertian , 1 17
Gastralgic form,2 14
Gastro - intestinal organs, complications,
235
IND EX 399
G astro - intestinal organs, symptoms, 200 History of malaria, 18
G enito - urinary organs, complications, Howardina, 10 1
240 Human cycle , - 1 14
symptoms, 200 Hydrophobic form, 209
Geographic distribution , 31 Hygienic treatment , 365of hemoglobinuric fever, 34 Hypod
-
erm-ic method , 359G lossary of terms, 1 28
G rabhamia, 97G round water, 43, 308
Gymnometopa, 101
HAB I TS of mosquitoes, 104
Hamamoeba immacu‘
lata, 1 19
malaria , 1 18
pra cox, 1 19
quartana , 1 18
tertiana , 1 15
vivax, 1 15
Hamato z oén falciform, 120
Hamocyto z oa, 1 1 2
Hamogogus, 10 1
Hamomenas pra cox, 1 19
Hayem’s method , 259
Heart, pathology, 177, 180 , 183Hematuria. See
'
Hemoglobinurz'
c fever .
Hemiplegia, 209Hemoglobinuric fever, complications,
226 JANTHI NO SOMA, 92
diagnosis, 289
etiology, 153 K EY to mosquitoes, 86'
geographic distribution, 34 K idneys, pathology, 176, 179 , 182
history, 23 K illing mosquitoes, 108
pathogenesis, 160
pathology, 180
prognosis, 297
prophylaxis, 332
quinine and ,
sequela , 226
symptoms, 2 16
treatment , 380
Hemolysin , 199
Hemosiderin , 174
Hibemation of larva , 107
mosquitoes, 108
ova, 1-o7
parasites, 71
pupa , 108
History of cinchona, 28
of hemoglobinuric fever,“
23
I D I OSYNCRASY , 1 56
I mago of mosquitoes, 81
Immunity, 50‘
congenital, 54
I ncubation , 184
I ndex endemicus, 56
I ndividual predisposition , 15 1
I nfection ,modes of
,63
I nfluen z a, complication , 25 1
diagnosis, 286
I nheritance of parasites by mosquitoes,
I noculation , 67
I nsecticides, 31 2
I ntestines, pathology, 176, 182
I ntravenous method , 363
I ntroduction , 17
I nundations , 47, 143
I solation of patients , 327
I sostomyia, 99
LARVAE, differentiation , 79hibernation , 107
Larval stage , duration , 79Latent malaria, 228
pathogenesis , 139
Laverania malaria , 1 18'
pra cox, 1 19
L eishman’s stain, 262
L ength of fl ight of mosquitoes, 105of life of mosquitoes , 107
of residence , 59 , 143, 157
L epidoplatys , 93L epidosia, 9 2
L eukemia, d iagnosis, 287L eukocytes, 197, 2 23, 279L ife of mosquitoes, length , 107




z~ S A UN D E R S
’
B O O K S O JV
K e e 11’
J‘ S urgery
AN UNABRI DUED TREAT I S E FORTHE S URGEON AND
THE GENERAL PRACT I T IONER
S urgery I TS PRI NC I PLES AND PRACT I CE. Written by 66 eminespecialis ts. Edited by WW. KEEN
,M .D .,
HON. EN
AND ED I N Emeritus Professor of the Piinciples of S urgery and
Clinical S urgery at the Jefferson M edical Co llege . Five octavos of I O
pages each,containing 2 500 text - illustrations and 50 co lored p late
Per vo lume : Cloth,
net ; Half M orocco,
net .
iN F IVE VOLUMES—2500 TEXTLCUT’
S AND 50 COLORED RLATES
THE F I FTH AND LAS T V O LUM E Now R EADY
THE EM INENT CONTRIBUTORS
Robert'
Abbe , M .D . D . N. Eisendrath,M .D .
J. G . Adami, M .D . Wm. L . Estes, M .D .
E. Wyllys Andrews, M .D . J. M . T . Finney, M .D .
G Q E. Arms trong , M .D . John M . Fisher, M .D .
A. D . Bevan , M .D . John A . Ford y ce , M .D .
Warren S . Bickham , M .D : Chas. H. Fraz ie r, M_
.D
John F. Binnie , M .D . L eonard Freeman, M .D .
P. Brook e Bland , M .D . Frederick H . Gerrish , M iD .
G eorge E. Brewer , M .D . John H Gibbon M D
J. Bland S utton, F .R.C .S . G eorg Gottstein , M . D .
A . T . Cabot, M .D . Hobart A . Hai e , M . D .
Hampton L . Carson , Esq. L udv ig Hek'
toen ,M .D .
EfA . Codman ,M .D . O rville Horwitz , M .D .
\Vm. B . Coley , M .D . Allen B . K an-
avel, M .D .
W. M . L . Coplin, M .D . Albert K ocher,M .D .
George W. Crile , M .
_
D .
”
K arl Gustav .L e -nnan-der M .D
Harvey Cushing, M .D . Bransford L ewis, M .D .
J. Chalmers D aCosta , M .D . R. W. Lovett , M .D .
John C . M .D . Edward M artin , M .D .
E. B . D ench ,M .D . Rudolph M atas
,M .D .
F . X. D ercum ,M .D . Chas. A . M ayo , M .D .
G . E. deS chw einit z , M . D . Wm . J . M ayo , M .D .
D avid L . Ed sall, M . D . M aj . Walter D . M cCaw , M .D .
E. E. M ontgomery , M .D .
B . G . A . .M oynihan , F .R. .C S
J . G . M umford, M .D .
John C .
-
M unro, M .D .
John B . MUrphy, M .D.E. H. Nichols , M .D .
A . J. O ch sner, M .D .
Surg. Re illy,U;S .
Edmund Owen,F .R.CS .
Jos . Ransohoff,M .D . , F .R.C
Surg .- Gen.
_
P. M . Rixey,U.S .N
John B . Roberts, M .D .
A . W. M ayo Robson , F .R.C .
W. L . Rodman, M .D .
Eugene A .
Harmon Smith , M .D .
Wm . G . Spiller, M .D .
Weller V an Hook , M .D .
J. P. VVarbasse , M .D .
F . Cf VVood , M .D .
G eorge Woolsey , M .D .
Hugh H. Young, M .D .
Fredrik Zachrisson , M .D.

S URGER Y AND ANA TOM Y 3
Kelly and Noble’
s
Gy neco logy
an?) Abdominal S urgery
Gy necology and Abdom ina l S urgery . f Edited by HOWARD A .
K EL LY,M . D . ,
Professor of Gyneco logy in Joh nsHopkinsUniversity ;
and CHARLES P.NOBLE,M . D .
,Clinical
'
Profe ssor of Gyneco logy in theWoman ’sM edical College , P hiladelphia. Two imperial octav o vo lumes
of 9 50 pages each, containing 880 original illustrations some in co lors .
Per vo lume : Cloth,
net ; Half M orocco,
net .
BOTH VO LUM ES NOW READY
WI TH 880 I LLUS TRAT I ONS BY HERMANN BECKER AND MAXBRODEL
I n v iew of the intimate association of“
gynecology With abdominal surgery
“
the
editors have combined these two important subj ects in on e work . For this reason
the work w ill be doubly valuable,for not Only the gynecologist and general prac
titioner will find it an exhaustiv e treatise, but th e surgeon also will find here the
latest technic of the various abdominal operation s . I t possesses a number of
valuable features not to be found in any oth er publication cov ering th e same fields .
I t conta ins a. chapter upon the bacteriology and one upon the pathology of gyne
cology ,dealingfully with the scientific basis of gynecology . I n no other work
can this information , prepared by specialists , be found as separate chapters .
There is a large Chapter devoted en tirely to medical gy necology , written esp ecially
for the physician engaged in gen eral practice . Heretofore the general p racti
tioner was compelled to search th rough an ent-ire work in order to obtain the in
formation desired . A bdom z'
mz l surg ery proper , as distinct from gynecology ,is

o t t o n’
s
D islocations an? o int Fracture s
D is locat ion s an d J o in t Fractures . B y FRED ERI C JAY COTTON,M . D .
,
A ssociate Professor O f Clinical S urgery at Tuft’
s M edical S chool,Boston .
O ctavo volume“
O f 600 pages , w ith 850 original illus trations .
PREPARING—ORIG INAL ,I LLUSTRAT I ONS
D r . Cotton’
s clinical and teach ing experience in this field has '
e specially fittedhim to write a practical w ork on this subj ect . He has w ritten a book clear and
definite in style ,systematic in pre sen tation , and accurate
'
in statement . The
illustrations possess t he feature Of show ing j ust th ose poin ts the author w ishes to
emphasi z e . T his is made possible because th e author is h im self the artist,by
far the greater maj ority Of the illustrations being the work of his Own hand .
They are str1k 1n crly artistic as w ell as unusually practical.
Kemp on“
Gastro
intestinal D iseasesD iagnos is and Treatm ent of ( i-as t ro = intes t ina l D isea ses . By ROB
ERT CO LE -M AN KEM P,M . D .
,Profes sor Of Gas tro - intes tinal D iseases at
the New Y ork S choo l O f C linical M edicm'
e . O ctavo of 750 pages , w ith
2 50 original illustrations .
PREPARING—f—ELABORATELY I LLUS TRATED
Of the many w ork s on gastro i- nte stinal d iseases , this is perhaps the only one
in Wh ich the n eed s of th e general p ractit ioner are giv en pre—emi-
n ent emphasis .
I t I S the practition er who first meets w ith these case s ,and it is h e Upon whom the
burden O f d iagnosis . rests . After th e diagnosis is e stablish ed , the practitioner, if
properly equipped ,could frequently treat th e case him self instead Of transferring
it to a spe cialist . Th is w ork I S intended to equip th e p i actitioner w ith this end
v iew . A s v isceral“
d isplacements hav e assum ed such an importan t po sition , the1r
symptom s,d iagnosis , and treatm en t , notably by m echan ical m e thods , are Specially
described . Typhoid fev e r is also included because of its localm anifestation s . A
chapter is dev oted to d iv erticulitis , now a subje ct of much importance . The illu.s
tration s ,
'
-all original,’
represent photograph s Of actual cases.

B i e r s
Hyp e r em i c T r eatm en tBy w in x M EYER. M . D . , and Prof. v . scnmmom
B ier’
s Hy perem ic Treatment in S urgery , M edicine,and the S pecial
ties : A M anual .O f its Practical App licatio n. By WI L LY M EYER,M . D .
,
Professor O f S urge ry at the New Y ork Post—Graduate M edical S choo land Hospital and .PRO F . D R. V I CTOR S CHM I EDEN,
A ss istant to Prof.
Bier,Unive rsity of Berlin ,
Germany . O ctavo O f 280 pages , withoriginal il lustrations . C loth , net.
JUST READY—THE NEW (2d ) ED I T I ON—FOR THE PRACT IT I ONER
For the prae z‘z'
l z‘
oner th is work has a particular value , because it give s special
attention to the hyperemic treatment of those Cond ition s w ith which he comes in
daily“
contact . Ye t the needs of the surg eon and the sp ecialist hav e not, by any
means , been neglected . The work is not a translation , but an entirely original
book ,by D r . Willy M eyer , who has practised the treatment for the past fifteen
years , and Prof. S chmiede n ,Professor Bier
’
s assistant at Berlin Univ ersity . . I n
the first part the three methods of inducing hyperemia are described ; in the second ,
are tak en'
up the details of application .
New York S tate Journal of M edicine
We commend this work_
to all those who are in terested in the treatmen t of infec tions
e ither acute or chronic ,for it is the only authoritative treatise we have in the English language .
C ampbe ll’
s S urgical Anatomy
A Text = Book of S urgica l Anatomy . By WI LL I AM FRANC I S CAM P
BELL,M . D .
,Professor of Anatomy ,
L ong I s land Co llege Hospital.O ctavo O f 675 pages , w ith 319 original illustrations . Cloth, net ;
Half M orocco,
net .
WITH 319 PRACT I CAL I LLUS TRAT I ONS
The first aim in the preparation of this original work was to emphasiz e the
practical. I t is in the fullest sense an applied anatomy—ah anatomy that w ill beof inestimable value to th e surgeon because only those facts are discussed a nd
only those structure s and regions emphasiz ed that hav e a peculiar interest to him .
D r. Campbell has treated h is subj ect in a v ery systematic way . The magnificentOriginal illustrations w ill be found extremely practical.
Boston M edical and S urgical Journal“
T he author has an exce llen t command of his sub jec t , and treats it w ith the freedom andthe conviction of the experienced anatomist . He is also an admirable clinician .
S cu d d er -
’
s
Tr ea tm ent o f F r a c tu resWITH NO TE S O N D I S L O C A T I O NS
The Treatment of Fractures : w ith Notes on a few Common
Dil cations . By CHARLES-L . S CUD D ER
,M .D .
,S urgeon to the M assa
:hus etts General Hospital , Boston . O ctavo O f 6 28 pages ,with 854
) riginal illustrations . Po lished Buckram ,net ; Half Morocco
,
net .
THE NEW (oth ) ED IT ION. REV I S ED‘
AND ENLARGED
OVER 26.-
500 COPIES
The fact that this work ha s attained a sixth edition indicates its practical
value . I n.
this edition D r. S cudder has made numerous additions throughout
the text , and has added many new illustration s , greatly enhancing the value of
the work . The articles on D islocations ,illustrated
'
in that practical mannerwh ich has . made D r. S cudder
’
s work so useful, w ill be found extremely val
uable .
Joseph D . Bryant , M .D P rofessor of t/z e Pr inciples and Practice of Surgery, Un ivezl
’
su‘yana
’'B ellez /ue Hosp ifal M edical College.
As a p ractical d emonstration O f the top ic it is excellent , and as an example of bookmakingit is h ighly commendable .
Bickham’
s O p erative ery
A Text = Book of Operat iv e S urge ry . ByWARREN S TONE B I CK HAM,
M . D .,
O f New O rleans.
'
O ctavo of I aOO'
pages ,. w ith 854
original illustrations. Cloth , net ; Half M orocco,
net.
‘
THE NEW (3d ) ED IT I ON
This absolutely newwork completely cov ers the surgical anatomy and opera
tiv e technic involv ed in the operations'
of general surgery . The practicability of
the work is particularly emphasi z ed in the 854 magn ificent illustrations which forma useful and strik ing feature .
Boston Medical and S urgical Journal“The book is a valuable con tribution to . the literatui'e O f Operative su-rgery . I t represents
a vast amount of careful work and technical knowledge on the part of the'
author. For the sur
geon in active practice or the instructor O f surgery , it is an unusually good review O f the subj ect .
'
M oy nih an’
s
Abdominal“
ration s
Abdom inal Operat ions . By B . G. A . M OYNI HAN,M . S . (L OND ),
F S enior Assistant S urgeon ,L eeds Gen
-
eral I nfirmary ,England.
O ctavo ,beautifully illustrated . C loth
,net ;HalfM orocco
,net.
THE NEw (2d) EDITI ON
Two LARGE EDm ONs 1N ONE YEAR
I t has been said of M r. M oynihan that in describing details of Operations he
is at his best . The appearance Of th is ,his latest w ork , therefore ,
w ill be w idely
welcomed by the medical profession , giv ing ,as it does
, in most clear and exact
language, not only the actual 7noclus op erand i of th e various abdominal operations ,
but also the preliminary technic of preparation and . steriliz ation . Complications
and sequelae and after - treatment are“
presented in the same clear , clean—cut manner
asthe operations themselves . The beautiful illustrationsh av e been especially drawn .
Edward Martin. M . D .
Pr ofessor of Clin ical S urg ery , Un iv ers ity of Pennsy lv an ia
I t is a w onderfully good _
book . He has achiev ed comp le te success in illustrating , both
by words and p ictures , the be st te chn ic Of the abdom inal operations now commonly p erformed .
M oyn ihan on Gall - stones
Ga ll= s tones and Their S urg ica l Treatm ent . By B . G. A . M OYNI
HAN,M . S . S enior A ssis tant S urgeon ,
L eeds GeneralI nfirmary ,
England . O ctavo O f 458 pages , fully illustrated . Cloth ,net ; Half M orocco
,net .
THE NEW (2d ) ED ITI ON
M r. M oynihan , in rev ising his book,has made many additions to the text , so
as to include th e most recent advance s . Especial atten tion has been given to a
detailed description of the early symptoms in cholelithiasis , enabling a diagnosis
to be'
made in the s tage in wh ich surgical treatment can be m ost "
safely adopted .
Ev ery phrase of gall- stone d isease is dealt w ith ,
and is - illustrated by a large
number of clin ical records . Th e account Of the Operativ e treatment of all the
form s an d complication s of gall- stone disease i s full and accurate . A number of
the illustrations are in color .
British M edical Journal
He exp resses h is views with admirable clearness , and he supports them by a large num
ber of clinical example s , w hich w ill be much p riz ed by those who know the difli cult problems
and tas k s which gall- stone surgery not .infrequently p resents .
l o SAUND ERS ’
B ooKs'
oN
Eisendrath’
s
S urgical D iagno sisA Text = Book of S urg ica l D iagnos is . By D ANI EL N. EI SENDRAT
M .D .,Professor o f S urgery in the Co llege Of Phy sicians and S urgeon
Chicago . O ctavo O f_800 pages , With 500 entire ly new and origin
text - illustrations and some co lored p lates . C loth,
net ; Ha
M orocco,
net .
JUS T I S S UED—THE NEW (2d ). ED I T ION
Of first importance in every surgical condition- is a correct diagnosI S , for up
this depends the treatment to be pursued and the two—diagnos is and treatment
constitute the most practical part of practical surgery . D r. Eisendrath tak es
each disease and injury amenable to surgical treatment; and sets forth the'
mea
of correct diagnosis in a systema tic and comprehensive Way . D efinite directiOas to
'
methods of examination are presented clearly and concisely , prov iding fall contingencies that
'
migh t arise in any g1v en case . Each illustration in
cates precisely how to diagnose the condition considered .
S urgery , Gynecology , and O bste trics
The book is onewhich is well adap ted to the uses O f th e p ractising surgeon who des iinformation concise ly and accurately given . No thing O f d iagnostic importance is omitte
ye t the ah thor does no t run in to end less de tail.
isendrath’
s linical AnatomyA Text = Book of Clin ical Anatomy . By
'
D ANI EI . N. EI S ENDRAT
A .B .,M .D ., Professor O f S urgery in the College Of Phy sicians a
S urgeons , Chicago . O ctavo Of 535 pages , illustrated . Cloth, $5 .
net ; Half M orocco,
THE NEw (2d ) ED ITIoN
This new anatomy discusses the subj ect from ‘
the clinical standpoint . A p
tion of each chapter is dev oted to the examination of the liv ing through palpati
and mark ing Of surface outline s of landmark s,v essels , nerve s , thoracic a
abdominal v isce ra . The illustrations are from new and original draw ings a
photograph s . Th is ed ition has be en carefully revised .
M edical Re cord , New York
A sp ecial recommendation for th e figures is that they are mo stly original and w
mad e for the purpose in v iew . T he se ct ions O f j oints and trunks are those of formalin i
cadav ers and are unimp eachable in accuracy .
In tern a tion a l
ext -B o ok Of u e ryS ECOND EDITION. THORovcuLYREV I SED AND ENLARGED
The In ternat ional Text = Book'
of Surgery . I n two vo lumes ._
By
American and British authors . Edited by J. COLL I NS WARREN,M .D .,
(Hon ), Professor O f S urgery ,Harvard M ed ical
S choo l,andA . PEARCE GOULD ,
M .S,F .R .C.S
,of London,England .
V ol. I . General and Operativ e S urg ery . Royal octavo , 975 pages ,
46 1 illustrations , 9 full - page colored plates—V ol. I I : Special or
Regional. S urg ery . Royal octavo , 1 122 pages , 499 illus tratiOns , _
and
8 full - page Colored plates .
Per vo lume : Cloth, net ;
'
Half M orocco,
net.
American TEXT - BO OK or S urgeryFOURTH ED IT IoN, RECENTLY I S S UED—OVER 43.1i00 CO PI ES
AmericanText = Book of S urgery . Edited by w w . K EEN,
_
LL .D . HON. F .R .C .S . ENG . AND ED IN .,and J . WI LL I AM WHI TE
,M . D .
,
PH .D . Octavo,
1363 pages , 5 5 1 text cuts and 39 colored and half- tone
plates . Cloth , net ; _Half M orocco , net .
Robson an?) Cammidgeon th e Pancreas
The Pancrea s : . it s S urgery and Pathology . By A . W. M AYO RO B~
S ON,F . R . C . S .
, Of Lond on ,England and P . J . CAM M I D GE
,F . R . C . S .
,of
London ,England . O ctavo Of 546pages , illustrated . Cloth
,net Half
M orocco , $6 .5 0 net .
I LLUS TRATED
This new work ,upon on e Of the most w idely :d iscussed subj ects of the times ,
represents th e original inv e stigation s of th ese eminent authorities . There are
special chap ters on Ch emical Pathology and D iabetes .
Boston M ed ical and S urgical Journal
For the general p ractition er and surge on it is the most valuable volume on the subj ect of
surgical d isease s of the pancreas wh ich has been published I n English up to this time .

I - 2
Gould’
s O p eration s on th e
I n t est in e s an d S tomach
The Techn ic of Operat ions upon the lntest ines and S tomach .
A LFRED H. GOULD ,M . D .
,of Boston .
'
L arge octavo,w ith 190 origin
illustrations , some in co lors . Cloth,
net ; Half M orocco ,
WITH 190 ORI G INAL I LLUS TRATI ONS
D r. Gould’
s new work is the result of e xhaustive experimentation , the tech
of the operations described being simplified as far as possible by experiments
animals , thus leading to the developmen t of many new features . The text is p
posely concise , the technic being presented very clearly by the numerous practi
illustrations , all made from actual Operations
i
done e ith er upon the animal . or t
human being . As the success of gastro—intest-inal surgery depends upon an acc
ate knowledge-o f the elementary step s , a thorough account Of . repair is include
New York , S tate Journal o f M edicine
The illustration s are so good that on e scarce ly need s the text to elucidate the steps
the operations described . The _work repre sents the b est surgical knowledge and skill.
DaCosta’
s M odern S urgerM odern S urgery
—GENERAL AND O PERAT I VE. By JOHN CHALMED ACO STA ,
M . D .,Profes sor Of S urgery and of Clinical S urgery in t
Jeffe rson M edical College , Philadelphia. O ctavo Of'
1283 pages , wi
872 illustrations . Cloth,
net ; Half M orocco,
net.
THE NEW (sth ) ED ITI ON
For this new fifth edition the w ork has been entirely rewritten and reset . C
hundred and fifty new illustrations have been added and theWork has beenlarged by the addition of tw o hundred pages . To k eep the book of a siz e to ban
conv enien tly , a thinner but high-
grade paper has been used . D aCosta’
s Surg
in this edition will more than maintain the reputation . already won .
Boston M edical and S urgical J our-nal
We commend the book , as we have prev iously commend ed it,to surge ons and to stude
as the most satisfactory one - volume contemporaneous treastise on surgery published in 1
coun try .
"

14 SA UND ERS'
B O OK S'
ON
Ha y n e s’
A n a tom y
A M anual of Anatomy . By I e No S . HAYNES,M .D .
,Professor of Pra
tical Anatomy ,Corne ll Univers ity Me d ical Co llege . O ctavo
,680 pages
w ith 42 d iagrams and 134 full-
page half- tone s . C lo th
,na
Th is book is the w ork of a p ract ical ins tructor—one w ho k now s by expe rience the requirments O f the av erag e stud ent , and I S able to meet these requirements in a v e ry satisfactorway .
” Th e M ed i cal R ecor d , New York .
Just Re adAm e r ic a n P o c k e t D ic tio n a ry S ixth Edifio
The American Pock et M ed ical Dict ionary . Ed ited by W. A . NEWM AD O RLAND
,A .M .
,M .D .
,As s is tant O bs te trician
,Hosp ital O f the University
Pennsylvania , e tc . 598 page s . Full leather,lim
‘
p ,w ith gold edges ,
ne t ;w ith pate nt thumb ind ex ,n e t.
I am’
struck at once w ith adm irat ion at the compac t s iz e and attractiv e exterior}I can recom
mend_
1t to our s tud ents w 1thout rese rv e .
”—JAM E SW. HOL LAND , M .D .. P rof essor of M edica
Ch emi s try and Tox i cology , a t the yqfl'
er son M ed ica l colleg e ,
Barton and We lls’
M edical The saurus
A Th esaurus of M ed icalWord s and Ph ras e s . By WI LFRED M . BARTO i
M . D . ,Assistant to Profe ssor Of M ateria Medica and Therapeutics , and Le (
turer on Pharmacy , G eorgetown Un iv ersity , Wash ington , D .
'
C . andWALTE
A . WEL L S , M . D . ,D emon strator of Laryngology , Georgetown Un iv ersity
Washington , D . C . 12mo of 534“
page s . Flexible leather , net ; w it
thumb index ,$3.00 n et .
S toney’
s S urgical Te chnic The New éi’
f’
éfifigBact eriology and S urg ical Techn ic for Nurses . By EM I LY A . M . STONES
Superintendent at the Carney Hospital, S outh Rev ised b
FREDERI C R . GR I F F I TH ,M . D . , Surgeon , of New York . 121110, 300 page
illustrated . 11
These subj ects are treated most accurately and up to d ate , w ithout the sup erfluous read in
wh ich is so often employed . Nurses w ill find th is book of the g reates t value.
”
Tr a in ed Nur se an d Hosp ita l Rev iew .
G r a n t on F a c e , M ou th . a n d J aw s
A Text = Book of the S urg ical Principles and S urg ical Dis eases of th
Face , M outh , and J aw s . For D ental S tudents . By H. HO RACE GRAN
A .M .,M .D Profe ssor O f S urge ry and O f C linical S urge ry , Hosp ital C o lleg
of M ed icine . O ctavo O f 231 pages ,w ith 68 illus trations . C lo th
,ne
language of the book is S im-
p le and clear. We recommend the work to those
whom it is in te nd ed .
”—P lz iladolp lu '
a M ed ical j ournal .
S URGE] ? Y AND ANA TOM E.
“
1 5
American I llustrated D ictionary The New
The American lllust rated M ed ica l Dict iona ry . With tables
of Arteries,M uscles
,Nerves , V eins, e tc . ;
'
of Bacilli,Bacteria, e tc . 3
Eponymic Tables of D iseases , O perations, S tains, Tests , etc . By W. A .
NEWM AN D ORLAND,M .D . Large octavo
, 876 pages . Flexible leather,
net ;with thumb index,
net .
Howard A. Ke lly , M .D P rof essor of Gy necology , j ohns Hophirz s Univers ily ,B altimore.
“D r. D orland
'
s d ictionary is adm irable . I t is so well gotten up and of such con
ven ient s iz e . NO errors have been found in my use of it .
G olebiew sk i and Bai ley’
s Accident Disease s'
At la s and Epitome of D iseases Caused by Accident s . By D R.
ED . G O LEB I EWSK I,ofBerlin . Edited ,
w ith add itions,by PEARCE BAI LEY
M .D . Consulting Neurologist to S t . Luke’s Hospital, .New York City.
With 71 colored figurés l
on 40 plates , 143 text - cuts,and 5 49 pages of
text . Cloth,
net . [ h S a zmo’ers
’ Hand - A tlas S eries .
He lferich and Bloodg‘
ood on Fracture s
At las and Ep itome of Traum at ic Fractures and D is locat ions
By PROF . DR . H . HELFERI CH, of G reifswald , Prussia . Ed ited,with ad
ditions,
. by JO SEPH C . BLOOD GO OD ,M . D . , Associate in Surgery , Johns
Hopkins University , Baltimore . 2 1 6 colored figures on 64 lithographicplates , 1 90 text
- cuts,and 353pages of text .
-Cloth ,net . [ 72 S emi
o’ers
’
A tlas S eries .
S ultan and C oley on Abdominal Hernia-s
At las and Epitome of Abdom ina l He rn ias . By PR. D r. G . SUL
I AN, of Gottingen . Edi ted
,w ith additions
,by WM . B . COLEY ,
M .
Clinical Lecturer and I nstructor in Surgery, Columbia University, New
York . 1 19 illustrations , 36 in colors,and 2 77 pages of text . Cloth ,
net . [ 72 S aw z o’ers
’
fl orid - A tlas S eries .
S e condWarren’
s S urgical Pathology . Edifion
S urg ica l Pathology . and Th e rapeut ics . By J . COLLINS WARREN,
M .D ., (HON ) , Professor of Surgery, Harvard M ed ical
S chool. O ctavo ,873 pages ; 136 illustrations , 33 in colors . C loth
,
net ; HalfM orocco,
net .
S e condZuckerkandl and D aC o sta
’
s surgery Ed i-tion
At la s and Ep itome of Ope rat iv e S urge ry . By D R . 0 . ZUCKER
KAND L, _
of V ienna. Ed ited , w ith add itions, by J . CHALM ERs DACO STA ,
M . D .,Professor of Surgery and C lin ical Surgery , Jefferson M edical Col
lege , Phila . 40 colored plates, 2 78 text—cuts , and 4 10 pages of text .
Cloth , net . [ 72 S o zmders’
A tlas S eries .
16 S URGERY AND ANA TOM Y
M oo r e’
s O r th op e d ic S u rge ryA M anual of Orthoped ic S urgery . By JAM ES E. M O ORE , M .D . , Professor
ofCliniCal Surgery , Univ ersity ofM innesota, College of M edicine and Surgery.
O ctavo of 356 pages , handsomely illustrated . C loth , $2 . 50 net .
The book is eminently p ract ical. I t is a safe guid e in the und e rs tand ing and treatment oforthop edi c cases . S hould be owned by every surgeon and practitione r.
”-Ami als of S urg ery .
Fow ler’
s O perating Room New (2d ) Edition
The O perat ing Room and t he Pat ient . By RUsSEL L S . FOWL ER , M . D . ,
Surgeon to the German Hospital, Brooklyn , New York . O ctavo of 284
pages , illustrated . Cloth , net.
D r. Fowle r has written h is book for surge ons ,nurses assisting at an Operation, internes ,
and all o the rs who se duties bring them in to the operating room . I t con tains explicitd ire ctions fo r the p reparation of material
, ins trumen ts needed, , p osition of pa tient , e tc . ,
all beautifully illustrated .
Na n c r e d e ’
s P r in c ip les of S u rge ry New (2d ) EditionLecture s on the Principles of S urgery . By CHAS . B . NANCREDE, M .D . ,
LL .D . , Professor of S urgery and of Clinical S urgery , University of M ichigan ,
Ann Arbor . O ctavo , 407‘
page s , illustrated . Cloth , net .
“ We can strong ly recommend th is book to all stud ents and those w howould see some th ingOf th e sc ientific foundat ion upon wh ich the art of surgery is built .
—Quar ter ly M ed ical j ou rna l ,S h efi ie ld ,
Eng land .
rNa n c r e d e 5 E s s e n t i a ls o f A n a tom y .S e v enth Edition
Es sent ials Of Anatomy , including the Anatomy of the V iscera . By CHAS .
B . NANCRED '
E, M .D . , Professor of S urgery and of Clinical S urgery , University
of M ichigan , Ann Arbor. Crown octavo , 388 pages ; 180 cuts . With an
Appendix containing
'
over 60 illustrations of the osteology of the body. Based
on Gray’
s A nalomry . Cloth ,net. [ h S armo’ers
’
Qaeslioh _
Comp eh a’s.
T he ques tions have been w isely selected , and the answ ers accurately and concisely g iven .
d ical M ag a z ine .
M a rt in’
s E s s e n tia ls o f S u rge ry .
S e v eggggeg
ifi on
Es s ent ials of S urgery . Containing also V enereal D iseases , Surgical Land
mark s, M inor and Operative Surgery ,
and‘
a complete description ,with illus
trations, of the Handk erchief and Roller Bandages . By EDWARD MARTI N,
A .M . , M .D . ,Professor of Clinical Surgery , University of Pennsylvania , etc.
Crown octavo , 338 pages , illustrated . With an Appendix on An tiseptic S ur
gery , etc . Cloth ,net. [ 72 S aunders
’
Queslioh Comfiena’s.
Writ ten to ass is t the s tud ent , it w ill be of undoubted v alue to the p rac tit ioner , con tain ing as itd oes the essence of surg ical work .
”—B os ton M ed ical and S urg ica l j ourna l.
M a r tin’
s E s s e n tia ls o f M in o r S u rge ry , B an d
agin g. a n d V e n e r e a l D is e a s e s .S emgfiifig
is e d
Es s ent ials of .M inor S urgery , Bandaging , and Venereal D is eas es . By
EDWARD M ART I N, A .M . , M .D . Professor of Clinical S urgery , University of
Pennsylvania , etc . Crown octavo , 166 pages , w ith _78 illustrations .
Cloth ,net . [ 71 S auiiders
’
Qa es z‘ioh Compena’s.
The be st cond ensat ion of the subj ects of w h ich it treats yet placed before the p rofession .
fi e M ed ica l N ew s , P h ilade lphia .