
511.full.pdf - Cjasn
10
Article A Systematic Review and Jurisdictional Scan of the Evidence Characterizing and Evaluating Assisted Peritoneal Dialysis Models Mark Hofmeister, 1,2 Scott Klarenbach, 3 Lesley Soril, 1,2 Nairne Scott-Douglas, 4 and Fiona Clement 1,2 Abstract Background and objectives Compared with hemodialysis, home peritoneal dialysis alleviates the burden of travel, facilitates independence, and is less costly. Physical, cognitive, or psychosocial factors may preclude peritoneal dialysis in otherwise eligible patients. Assisted peritoneal dialysis, where trained personnel assist with home peritoneal dialysis, may be an option, but the optimal model is unknown. The objective of this work is to characterize existing assisted peritoneal dialysis models and synthesize clinical outcomes. Design, setting, participants, & measurements A systematic review of MEDLINE, Cochrane Central Register of Controlled Trails, Cochrane Database of Systematic Reviews, Embase, PsycINFO, and CINAHL was conducted (search dates: January 1995–September 2018). A focused gray literature search was also completed, limited to developed nations. Included studies focused on home-based assisted peritoneal dialysis; studies with the assist provided exclusively by unpaid family caregivers were excluded. All outcomes were narratively synthesized; quantitative outcomes were graphically depicted. Results We included 34 studies, totaling 46,597 patients, with assisted peritoneal dialysis programs identified in 20 jurisdictions. Two categories emerged for models of assisted peritoneal dialysis on the basis of type of assistance: health care and non–health care professional assistance. Reported outcomes were heterogeneous, ranging from patient-level outcomes of survival, to resource use and transfer to hemodialysis;however, the comparative effect of assisted peritoneal dialysis was unclear. In two qualitative studies examining the patient experience, the maintenance of independence was identified as an important theme. Conclusions Reported outcomes and quality were heterogeneous, and relative efficacy of assisted peritoneal dialysis could not be determined from included studies. Although the patient voice was under-represented, suggestions to improve assisted peritoneal dialysis included using a person-centered model of care, ensuring continuity of nurses providing the peritoneal dialysis assist, and measures to support patient independence. Although attractive elements of assisted peritoneal dialysis are identified, further evidence is needed to connect assisted peritoneal dialysis outcomes with programmatic features and their associated funding models. CJASN 15: 511–520, 2020. doi: https://doi.org/10.2215/CJN.11951019 Introduction The number of patients on KRT exceeds 2 million worldwide, and in many countries, the need for these services greatly outweighs provision (1). In- center hemodialysis (HD) is the most common type of dialysis therapy initiated for patients with ESKD in developed nations (1). Peritoneal dialysis (PD) achieves similar clinical outcomes to in-center HD in eligible patients (2), however, the selection of dialysis modality can depend on many factors be- yond clinical effectiveness. As a home-based therapy, PD alleviates the significant burden and fatigue of travel to and from the hospital or dialysis unit for patients (3). From a health care system perspective, providing HD is often more costly than PD, because of added human and/or infrastructural resource requirements (3,4). In many settings, efforts are being made to increase the proportion of patients receiving PD, at least in part owing to the reduced cost relative to HD (1–3). Some patients eligible for PD may face barriers to use of this dialysis modality, such as physical, cognitive, or psychosocial factors preventing in-home performance of PD. If these barriers cannot be overcome, these patients are likely to receive in-center HD. The pro- vision of formal external assistance may increase the utilization of PD among eligible patients (4). Assisted PD is the provision of assistance for the PD procedure by individuals in the patient’s home, and may be offered to individuals unable to perform PD (4). The type of assistance offered can vary in terms of breadth and frequency of assistance and may evolve over time with patient needs (4). As dialysis pro- grams struggle with increasing demand, resource 1 Department of Community Health Sciences, University of Calgary, Calgary, Alberta, Canada; 2 Health Technology Assessment Unit, O’Brien Institute for Public Health, University of Calgary, Calgary, Alberta, Canada; 3 Department of Medicine, University of Alberta, Edmonton, Alberta, Canada; and 4 Department of Medicine, University of Calgary, Calgary, Alberta, Canada Correspondence: Dr. Fiona Clement, Community Health Sciences, University of Calgary Cumming School of Medicine, Teaching Research and Wellness Building, 3D14, 3280 Hospital Drive NW, Calgary, AB T2N 4N1, Canada. Email: [email protected] www.cjasn.org Vol 15 April, 2020 Copyright © 2020 by the American Society of Nephrology 511
-
Upload
khangminh22 -
Category
Documents
-
view
0 -
download
0
Transcript of 511.full.pdf - Cjasn

Article
A Systematic Review and Jurisdictional Scan of theEvidence Characterizing and Evaluating AssistedPeritoneal Dialysis Models
Mark Hofmeister,1,2 Scott Klarenbach,3 Lesley Soril,1,2 Nairne Scott-Douglas,4 and Fiona Clement1,2
AbstractBackground andobjectivesComparedwith hemodialysis, homeperitoneal dialysis alleviates theburdenof travel,facilitates independence, and is less costly. Physical, cognitive, or psychosocial factors may preclude peritonealdialysis in otherwise eligible patients. Assisted peritoneal dialysis, where trained personnel assist with homeperitoneal dialysis, may be an option, but the optimal model is unknown. The objective of this work is tocharacterize existing assisted peritoneal dialysis models and synthesize clinical outcomes.
Design, setting, participants, & measurements A systematic review of MEDLINE, Cochrane Central Register ofControlled Trails, Cochrane Database of Systematic Reviews, Embase, PsycINFO, and CINAHL was conducted(search dates: January 1995–September 2018). A focused gray literature search was also completed, limited todeveloped nations. Included studies focused on home-based assisted peritoneal dialysis; studies with the assistprovided exclusively by unpaid family caregivers were excluded. All outcomes were narratively synthesized;quantitative outcomes were graphically depicted.
ResultsWe included 34 studies, totaling 46,597 patients, with assisted peritoneal dialysis programs identified in20 jurisdictions.Twocategories emerged formodelsofassistedperitonealdialysison thebasisof typeofassistance:health care and non–health care professional assistance. Reported outcomes were heterogeneous, ranging frompatient-leveloutcomesof survival, to resourceuseandtransfer tohemodialysis;however, thecomparativeeffectofassisted peritoneal dialysis was unclear. In two qualitative studies examining the patient experience, themaintenance of independence was identified as an important theme.
Conclusions Reported outcomes and quality were heterogeneous, and relative efficacy of assisted peritonealdialysis could not be determined from included studies. Although the patient voice was under-represented,suggestions to improve assisted peritoneal dialysis included using a person-centered model of care, ensuringcontinuity of nurses providing the peritoneal dialysis assist, and measures to support patient independence.Although attractive elements of assisted peritoneal dialysis are identified, further evidence is needed to connectassisted peritoneal dialysis outcomes with programmatic features and their associated funding models.
CJASN 15: 511–520, 2020. doi: https://doi.org/10.2215/CJN.11951019
IntroductionThe number of patients on KRT exceeds 2 millionworldwide, and in many countries, the need forthese services greatly outweighs provision (1). In-center hemodialysis (HD) is the most common typeof dialysis therapy initiated for patients with ESKDin developed nations (1). Peritoneal dialysis (PD)achieves similar clinical outcomes to in-center HDin eligible patients (2), however, the selection ofdialysis modality can depend on many factors be-yond clinical effectiveness. As a home-based therapy,PD alleviates the significant burden and fatigue oftravel to and from the hospital or dialysis unit forpatients (3). From a health care system perspective,providing HD is often more costly than PD, becauseof added human and/or infrastructural resourcerequirements (3,4).
In many settings, efforts are being made to increasethe proportion of patients receiving PD, at least in partowing to the reduced cost relative to HD (1–3). Somepatients eligible for PD may face barriers to use ofthis dialysis modality, such as physical, cognitive, orpsychosocial factors preventing in-home performanceof PD. If these barriers cannot be overcome, thesepatients are likely to receive in-center HD. The pro-vision of formal external assistance may increase theutilization of PD among eligible patients (4).Assisted PD is the provision of assistance for the PD
procedure by individuals in the patient’s home, andmay be offered to individuals unable to perform PD(4). The type of assistance offered can vary in terms ofbreadth and frequency of assistance and may evolveover time with patient needs (4). As dialysis pro-grams struggle with increasing demand, resource
1Department ofCommunity HealthSciences, University ofCalgary, Calgary,Alberta, Canada;2Health TechnologyAssessment Unit,O’Brien Institute forPublic Health,University of Calgary,Calgary, Alberta,Canada; 3Departmentof Medicine,University of Alberta,Edmonton, Alberta,Canada; and4Department ofMedicine, Universityof Calgary, Calgary,Alberta, Canada
Correspondence:Dr. Fiona Clement,Community HealthSciences, University ofCalgary CummingSchool of Medicine,Teaching Researchand WellnessBuilding, 3D14, 3280Hospital Drive NW,Calgary, AB T2N 4N1,Canada. Email:[email protected]
www.cjasn.org Vol 15 April, 2020 Copyright © 2020 by the American Society of Nephrology 511

constraints, and evolving patient needs and preferences,assisted PD is an option to complement existing dialy-sis provision. However, there is no comprehensive syn-thesis of clinical outcomes, complications, and risks ofassisted PD. The objective of this work is to systemati-cally characterize existing assisted PD models and syn-thesize outcomes.
Materials and MethodsA systematic review was conducted, guided by Joanna
Briggs Institute methodology (5) and Preferred ReportingItems for Systematic Reviews and Meta-Analyses reportingstandards (6). To capture the literature characterizing assistedPD models internationally, the gray literature was searchedextensively.
Search StrategyMEDLINE, Cochrane Central Register of Controlled
Trails, Cochrane Database of Systematic Reviews, Embase,PsycINFO, and CINAHL were searched from January 1995to September 26, 2018. The search strategy was developedin consultation with an expert medical librarian. Searchterms combined controlled language and text words for PDwith words for assistance (full MEDLINE search strategy inSupplemental Appendix 1). The date limit was applied toidentify only modern implementations of assisted PD. Animalstudies, infant or child studies, comments, editorials, letters,and review articles were excluded.Gray literature searches were guided by the “Grey
Matters” tool (7). Websites of relevant organizations(e.g., kidney care organizations) were also searched (Sup-plemental Appendix 2). On the basis of a previous healthtechnology assessment of dialysis modalities, a targetedscan of international jurisdictions was completed, focusingon: Canada, Australia, the United Kingdom (UK), theUnited States (Medicare and Medicaid programs), France,Belgium, Denmark, Spain, Switzerland, Germany, TheNetherlands, Italy, and Brazil (8).
Study SelectionTitles and abstracts, and full texts were screened in-
dependently in duplicate. Abstracts included by eitherreviewer proceeded to full-text review. At full-text screen-ing, disagreement was resolved through discussion. Re-cords were included if the following criteria were met:reported original data in a peer-reviewed publication;designed as a randomized, controlled trial, quasi-experimentalor implementation study, observational cohort study, survey,qualitative description (e.g., interviews, focus groups), or casestudy of implementation experiences; focused on home-based assisted PD (as identified by the study); publishedin English or French; and reported outcomes relatedto evaluation, characterization, patient eligibility, andimplementation/delivery considerations of assisted PDmodels, or any patient-reported outcomes related topreferences, experience, barriers, and facilitators. Pub-lished conference abstracts were considered as full textsfor inclusion. Records with only a title available wereexcluded. Dialysis modalities other than assisted PD, orassisted PD provided outside the home, or exclusivelyprovided by unpaid family caregivers, were excluded.
Data from included published studies were extractedindependently in duplicate using standardized dataextraction forms. The following data were extracted: pub-lication date, study design, jurisdiction or country, incep-tion date of assisted PD program, type of PD technology(automated PD or continuous ambulatory PD), targetedand/or eligible patients, type of individual providing theassistance (e.g., registered nurse, nurse assistant or healthcare aid, home assistant), scope of PD assistance, frequencyof assistance, description of training, implementation re-quirements, comparator groups (if relevant), follow-up, andmain study outcomes (with any summary measure). Giventhe variety of definitions for the type of professional pro-viding assistance, we applied the below definitions:
c Registered nurses: self-regulated health care professionalsthat work autonomously and in collaboration to achieveoptimal levels of health, at all stages of life, and in situationsof health, illness, injury, anddisability (9). Registerednursesdeliver direct health care services, coordinate care, andsupport clients to manage their own health (9).
c Licensed practical nurses: self-regulated health care pro-fessionals that work independently or in collaborationwithother members of a health care team to assess, plan, im-plement, and evaluate care for patients (9).
c Health care aides: unregulated health care workers thatprovide daily living support to clients, through assistance infeeding, mobility, exercise, bathing, grooming, dressing,toileting, and personal hygiene activities (10).
Because of variation in reporting in gray literature, limiteddata were extracted: name of jurisdiction/country, patientpopulation, type and scope of assistance, program details,and implementation considerations.
Statistical AnalysesIncluded studies were synthesized by type of assisted
PD. All outcomes were narratively synthesized; quantita-tive outcomes in studies with a comparator were graphicallydepicted. Study quality was assessed with the Methodo-logical Index for Non-Randomized Studies tool, the Crit-ical Appraisal Skills Program Qualitative Checklist, or theConsensus Health Economic Criteria (11–13).
ResultsIncluded Published and Gray LiteratureA total of 1982 unique citations were identified (Figure 1).
Of these, 78 proceeded to full-text review. One publicationwas identified through gray literature (14,15); gray liter-ature documents were also identified for two programsdocumented in published literature (16–18). Assisted PDprograms were identified in 20 unique jurisdictions, with15 follow-up evaluations of those models (Table 1) (19–33).The final data set included 34 studies and a total of 46,597patients (Supplemental Appendix 3).Included studies were cohort studies (n524), cross-
sectional survey studies (n54), quasi-experimental designs(n53, pilot implementation trials), and one descriptive caseexample of an assisted PD experience. The two remainingstudies used qualitative study designs. Detailed character-istics of included studies are in Supplemental Appendix 3.
512 CJASN

Identified Models of Assisted PDAssisted PD programs were identified in 20 unique
jurisdictions, with two categories for models of assisted PDon the basis of the type of assistant or individual providingthe assistance emerging: the health care professional assis-tance model and the non–health care professional assis-tance model (Table 1). Among included studies, qualitywas heterogeneous (Supplemental Appendix 4). Norandomized, controlled trials were identified, and vari-ation in jurisdictions for assisted PD was present.
Scope of Assistance for PDWithin the health care professional assistance model,
three types of individuals providing assistance were com-monly described: a registered nurse (18–31,34–41), a li-censed practical nurse (14,15), and a nurse assistant/healthcare aide (16,32,33,42–44) (Table 1).In general, there is a coreset of procedural assistance that can be provided by allPD assistants in the characterized models (dark blue box,Figure 2) (45). Home assistants, with the support of patient’sfamily, are trained to provide the most basic assistance withthe operation of the PD machine, including machine set-upand dismantling, machine connections, PD bag exchange,and ordering and disposal of PD supplies (46–52). Homeassistants can also provide social support and assistancewith activities of daily living (45).Additional support for more complex medical care of
patients receiving assisted PD is permitted in health care
professional assistance models (14,22,34–39,42–44,53).Nurse assistants or health care aides offer support withmedication assistance to patients receiving assisted PD(42–44), and documentation of status (e.g., BP monitoring,monitoring weight) for the PD nurse and/or nephrologycare team overseeing the assisted PD program (light bluebox, Figure 2) (10,54). Assisted PD provided by an licensedpractical nurse (14,15) increases the scope of assistance toinclude medication administration and wound care, althoughhealth care aides may also perform the latter (green box,Figure 2) (55,56). The broadest scope of assistance wasdocumented with the registered nurse models of assistedPD (red box, Figure 2) (22,34–39,53). In addition to theaforementioned, assistance by registered nurse includescare for infections and/or mechanical complications, de-tailed clinical assessments, and patient education (57,58).The main difference between licensed practical nurse andregistered nurse support is the registered nurse’s ability tocare for more serious adverse events (57,58).
Health Care Professional Assistance ModelsUse of registered nurses for assisted PD was identified
in six European countries, including France (19–21,23–25,30,31,36), Belgium (22), Denmark (28,35), Germany(37), Sweden (53), and Switzerland (22), as well as specificregions in Spain (Canary Islands) (22), Australia (Westernregion) (34), the United States (Stony Brook, NY) (38), andCanada (Toronto, Ontario) (18,26,27,29,39–41). The number
Incl
ud
edE
ligib
ility
Scr
een
ing
Iden
tifi
cati
on
Additional records identified throughother sources
(n = 11)
Records after duplicates removed(n = 1982)
Records screened(n = 1982)
Records excluded(n = 1904)
Full-text articles assessedfor eligibility
(n = 78)
Records identified through databasesearching (n = 2793)
MEDLINE = 1021EMBASE = 1209CINAHL =407Central Register of controlled trials = 82Cochrane Database of Systematic Reviews = 43PsycINFO = 31
Included in synthesis(n = 34)
Seminal characterization and/or evaluationof assisted PD program: n=19
Follow-up characterization and/orevaluation of assisted PD program: n=15
Full-text articles excluded(n = 44)
No full-text or abstract: n=12Not English or French: n=5Incorrect intervention: n=13Not on primary objective: n=3Not original data: n=10Incorrect study design: n=1
Figure 1. | Flowchart of included published and gray literature assisted peritoneal dialysis (PD) models. Thirty-four studies were included.
CJASN 15: 511–520, April, 2020 Characterizing and Evaluating Assisted Peritoneal Dialysis Models, Hofmeister et al. 513

Table 1. Overview of assisted PD models identified from the published and gray literature
Assisted PDModel Type of Assistant Frequency of Assistance Jurisdiction Targeted or Eligible Patients with ESKD Assisted PD Model Features
Health careprofessionalassistance
Registered nurse 1–4 visits per day Australia(Western) (34)
c Patients with a working PD catheter, willingness toconsent, reasonable house condition, and a phone
c Assistance provided for automated PD
Shorterdurationofvisit (,1hr) with increasingfrequency of visits
c Patient, family, or other individual providingassistance (e.g., paid home assistant) required toperform connections and disconnections, importantin case of alarms or emergency
c Survey of current patients onPDorHDwas conducted in one center todetermine potential uptake of assisted PD
c Assistanceprovided topatients requiring immediatedialysis awaitingself-care training (i.e., short term), for existing patients ondialysiswhowould otherwise be hospitalized, and respite care from family-assisted PD
c Coordinated through existing ‘Home Link’ nursing services in onehospital
c A“onevisitperday”policywasestablished for theprogrambecauseoffunding restrictions
Belgium (22) NR c Assistance provided for automated PD and continuousambulatory PD
c Transportation and (re)training are not considered in scope of paidassistance
Denmark (28,35) c Frail, mainly elderly, patients characterized by loss ofphysical independence
c Assistance provided for automated PD
c Sole inclusion criterion was physical dependency onanother individual or caregiver to set up and possiblyconnect and disconnect PD machine
c Coordinated (training and support) provided by dedicated PD nursesin outpatient clinic
France (19–21,23–25,30,31,36)
c Adult patients who were unable to perform their PDexchanges alone
c Assistance provided for automated PD and continuousambulatory PD
c Evaluation of a patient’s ability to perform PDexchanges was on the basis of subjective assessmentby physician and PD nurses
c Established network of privately paid nurses across the country,trained and available to assist with at-home PD
c Publicly paid PD nurses (in hospital) perform home visits, conducttraining, and coordinate assistance of private nurses
c Private nurses tend to be located near the patient’s homec Supplementary assistance provided by family members whenavailable
Germany (37) NR c Assistance provided for automated PD and continuousambulatory PD
New York, USA(38)
c Elderly and disabled patients with multiple medicaland social problems
c Assistance provided for automated PD and continuousambulatory PD
c Longer-termand short-term (owing to acutedeteriorationofpatient orpartner resulting in inability to perform PD) assistance offered
c Coordinated with a nursing agency to identify and train nursesOntario, Canada(18,26,27,29,39–41)
c Patients with at least one medical or social conditionthat could be a barrier to PD
c Assistance provided for automated PD and continuousambulatory PD
c For Toronto program (Sunnybrook Health SciencesCentre): patients required to live in area of home caresupport; and patients, family, or other individual hadto be able to perform disconnection from cycler in theevent of an emergency (i.e., a fire in the home)
c Assistance available for both long-stay and short-stay, includingrespite, patients on assisted PD
c Partnered with community-based nursing agency that trained nursesc Multidisciplinary patient assessment by physician, nurse, and socialworker
c Dedicated case manager or program coordinator for regionalprograms
cAssistedPDprovided through twodeliverymodels: localhealth integrationnetworkswith other home care services, and hospital regional nephrologyprograms as part of integrated dialysis care models
Spain (22) NR c Assistance provided for automated PD and continuousambulatory PD
c Programonly available (and reimbursed) in the autonomous region ofthe Canary Islands
Sweden (53) NR c Assistance provided for automated PD and continuousambulatory PD
c Supplementary assistance from family providedwhen necessary (e.g.,initiating fluid exchange if nurse was late)
Switzerland (22) NR c Nurses employed through organization (Spitex) that is decentralizedat the level of cantons and communities
Licensed practicalnurse
2 visits per day Manitoba,Canada (14,15)
c Patients with suitable abdomen wanting PD, butunable to manage physical and/or mental tasksassociated with procedure
c Program only available in one urban area (Winnipeg)c Respite care also available for patients (or their caregivers) who arerecovering from other issues
514
CJASN
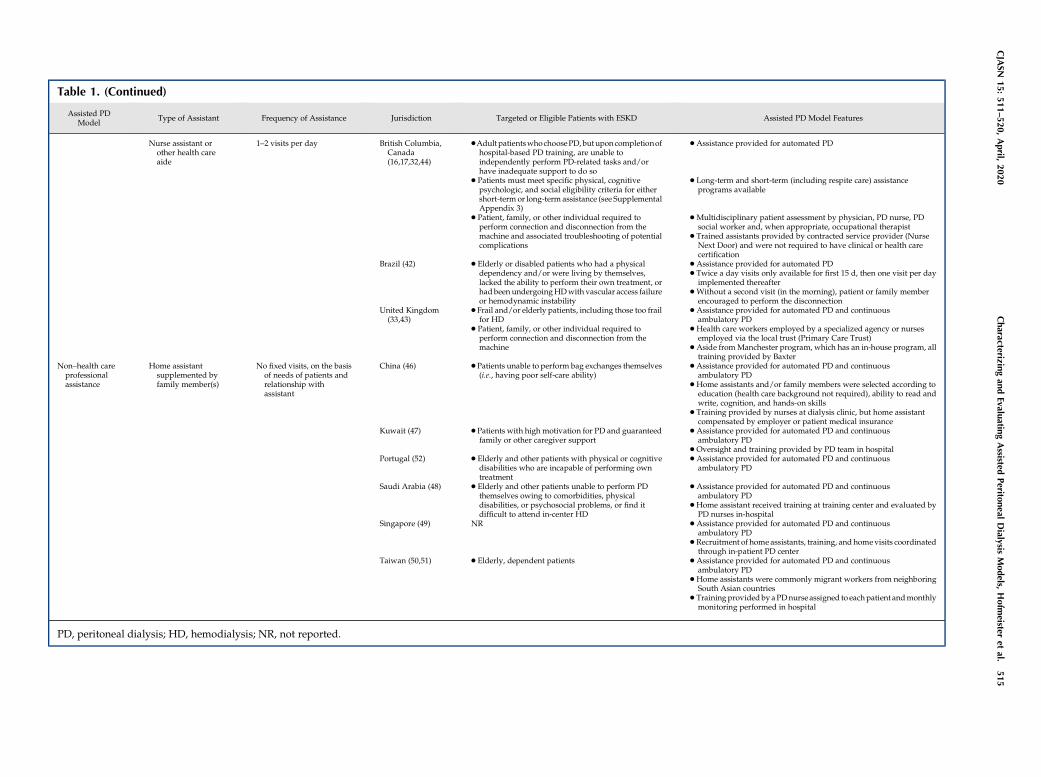
Table 1. (Continued)
Assisted PDModel Type of Assistant Frequency of Assistance Jurisdiction Targeted or Eligible Patients with ESKD Assisted PD Model Features
Nurse assistant orother health careaide
1–2 visits per day British Columbia,Canada(16,17,32,44)
cAdult patientswhochoosePD,butuponcompletionofhospital-based PD training, are unable toindependently perform PD-related tasks and/orhave inadequate support to do so
c Assistance provided for automated PD
c Patients must meet specific physical, cognitivepsychologic, and social eligibility criteria for eithershort-term or long-term assistance (see SupplementalAppendix 3)
c Long-term and short-term (including respite care) assistanceprograms available
c Patient, family, or other individual required toperform connection and disconnection from themachine and associated troubleshooting of potentialcomplications
c Multidisciplinary patient assessment by physician, PD nurse, PDsocial worker and, when appropriate, occupational therapist
c Trained assistants provided by contracted service provider (NurseNext Door) and were not required to have clinical or health carecertification
Brazil (42) c Elderly or disabled patients who had a physicaldependency and/or were living by themselves,lacked the ability to perform their own treatment, orhad been undergoingHDwith vascular access failureor hemodynamic instability
c Assistance provided for automated PDc Twice a day visits only available for first 15 d, then one visit per dayimplemented thereafter
c Without a second visit (in the morning), patient or family memberencouraged to perform the disconnection
United Kingdom(33,43)
c Frail and/or elderly patients, including those too frailfor HD
c Assistance provided for automated PD and continuousambulatory PD
c Patient, family, or other individual required toperform connection and disconnection from themachine
c Health care workers employed by a specialized agency or nursesemployed via the local trust (Primary Care Trust)
c Aside fromManchester program, which has an in-house program, alltraining provided by Baxter
Non–health careprofessionalassistance
Home assistantsupplemented byfamily member(s)
No fixed visits, on the basisof needs of patients andrelationship withassistant
China (46) c Patients unable to perform bag exchanges themselves(i.e., having poor self-care ability)
c Assistance provided for automated PD and continuousambulatory PD
c Home assistants and/or family members were selected according toeducation (health care background not required), ability to read andwrite, cognition, and hands-on skills
c Training provided by nurses at dialysis clinic, but home assistantcompensated by employer or patient medical insurance
Kuwait (47) c Patients with high motivation for PD and guaranteedfamily or other caregiver support
c Assistance provided for automated PD and continuousambulatory PD
c Oversight and training provided by PD team in hospitalPortugal (52) c Elderly and other patients with physical or cognitive
disabilities who are incapable of performing owntreatment
c Assistance provided for automated PD and continuousambulatory PD
Saudi Arabia (48) c Elderly and other patients unable to perform PDthemselves owing to comorbidities, physicaldisabilities, or psychosocial problems, or find itdifficult to attend in-center HD
c Assistance provided for automated PD and continuousambulatory PD
cHome assistant received training at training center and evaluated byPD nurses in-hospital
Singapore (49) NR c Assistance provided for automated PD and continuousambulatory PD
c Recruitment of home assistants, training, and homevisits coordinatedthrough in-patient PD center
Taiwan (50,51) c Elderly, dependent patients c Assistance provided for automated PD and continuousambulatory PD
c Home assistants were commonly migrant workers from neighboringSouth Asian countries
c Training provided byaPDnurse assigned to eachpatient andmonthlymonitoring performed in hospital
PD, peritoneal dialysis; HD, hemodialysis; NR, not reported.
CJASN
15:511–5
20,April,
2020
Characteriz
ingan
dEvalu
atingAssisted
Perito
neal
Dialysis
Models,
Hofm
eisteret
al.515

of visits made by registered nurses to assist patients receivingPD at home varied across jurisdictions and ranged from oneto four times a day, with visit duration inversely related tonumber of visits. All jurisdictions described assistance forthe automated PD procedure, whereas assistance for bothautomated PD and continuous ambulatory PDwas describedin seven jurisdictions (22,36–39,53). Use of registered nurseassistance for long-term patients on assisted PD wascommonly described. However, short-term assisted PDand respite care was also documented in three jurisdic-tions (34,38,39).Use of licensed practical nurses was documented only in
Winnipeg, Canada (14,15). In this model, licensed practicalnurses visited the patient home up to twice per day andprovided both short-term (including respite) and long-termassistance for PD (14,15).Lastly, assisted PD provided by nurse assistants or
health care aides was identified in Brazil (42), the UnitedKingdom (England and Northern Ireland) (33,43), and oneCanadian province (British Columbia [BC]) (16,17,32,44).Generally, nurse assistants or health care aides visitedpatients’ homes once or twice daily to provide PD assistance.In Brazil, twice-daily visits occurred within the first 15 daysafter a patient begins automated assisted PD and once a daythereafter. All jurisdictions encouraged additional assistancefrom family member(s) for the PD procedure. In both theUnited Kingdom and BC models, nurse assistants or healthcare aides were employed by contract agencies or serviceproviders for both automated PD and continuous
ambulatory PD (16,17,32,33,43,44). Further, both long-termand short-term (including respite) assisted PD was docu-mented in only the BC assisted PD model (16,17,32,44).
Non–Health Care Professional Assistance ModelsIn this assisted PD model, assistance is provided by a
home assistant, such as a domestic worker who is not alicensed health care professional, with no prior training inhealth care. This model was identified in six jurisdictions:China (46), Kuwait (47), Saudi Arabia (48), Singapore (49),Taiwan (50,51), and Portugal (52). Typically, home assis-tants received assisted PD training through in-hospitalprograms or dialysis clinics (46–51). In all jurisdictions,patients’ family members or informal caregivers also pro-vide supplemental assistance for PD, and so undergo thesame assisted PD training as home assistants. Given thiscoordinated support, there are no fixed number of visitsdescribed for this assisted PD model. Assistance for boththe automated PD and continuous ambulatory PD proce-dures were also provided (46–52).
Patient EligibilityThe most common requirement or characteristic de-
scribed for patients to receive assisted PD is the inabilityto autonomously perform the PD procedure in their homebecause of either physical, cognitive, and/or psychoso-cial barriers (14,35,36,39,42,44,46,48,52). Across the includedassisted PD models, patients were often frail and
Appendix
• Machine set-up and dismantling• Connecting and disconnecting patient to machine• PD bag exchange and disposal, and supply ordering• Patient personal assistance (e.g., bathing, dressing, eating) and social support
• Document & report patient status (e.g., blood pressure, weight)• Medication assistance
• Medication administration• Wound care†
• Clinical assessment (e.g., blood pressure, fluid assessment, nutrition)*• Information support and patient education*• Care for infectious (e.g., exit site infection) or mechanical complications
Home Assistant,supplemented byFamily Member(s)
Nurse Assistant orHealthcare Aide
Licensed Practical Nurse
Registered Nurse
† May be performed by nurse assistant or healthcare aide with training 60,61
* May be performed by licensed practical nurse 62,63
Figure 2. | Scope of peritoneal dialysis (PD) assistance by type of assistant. With increased professional regulation and qualifications, moreadvanced clinical care tasks may be completed.
516 CJASN
elderly individuals, or adults with physical disability(14,34–36,38,39,42–44,46,48,51,52).In certain jurisdictions, particularly with the health care
professional assistance models, additional eligibility crite-ria are described. For instance, in Australia (34), Ontario(39), BC (17,44), and the United Kingdom (43), the patientor a family member must be able to perform the connec-tions and disconnections to the PD machine to be eligiblefor assisted PD. This enables the registered nurse or thenurse assistant to visit once per day to the patient’s home,and is described as insurance against emergencies ormachine malfunctions that may occur outside of theassisted PD visit (34,39,44). The BC assisted PD programalso has distinct eligibility criteria on the basis of definedphysical, cognitive, psychologic, and social factors: healthstatus prevents dismantling/setting up the cycler; dexterity/strength/vision deficits limit the ability of the client tocomplete necessary tasks; cognitive function or learning deficits(such as memory, problem solving, or decision making) affectthe client’s ability to safely complete necessary tasks; confidenceto perform necessary tasks independently is absent; and absentor intermittent availability of support person(s) after identifi-cation that such support to manage PD is needed (59).
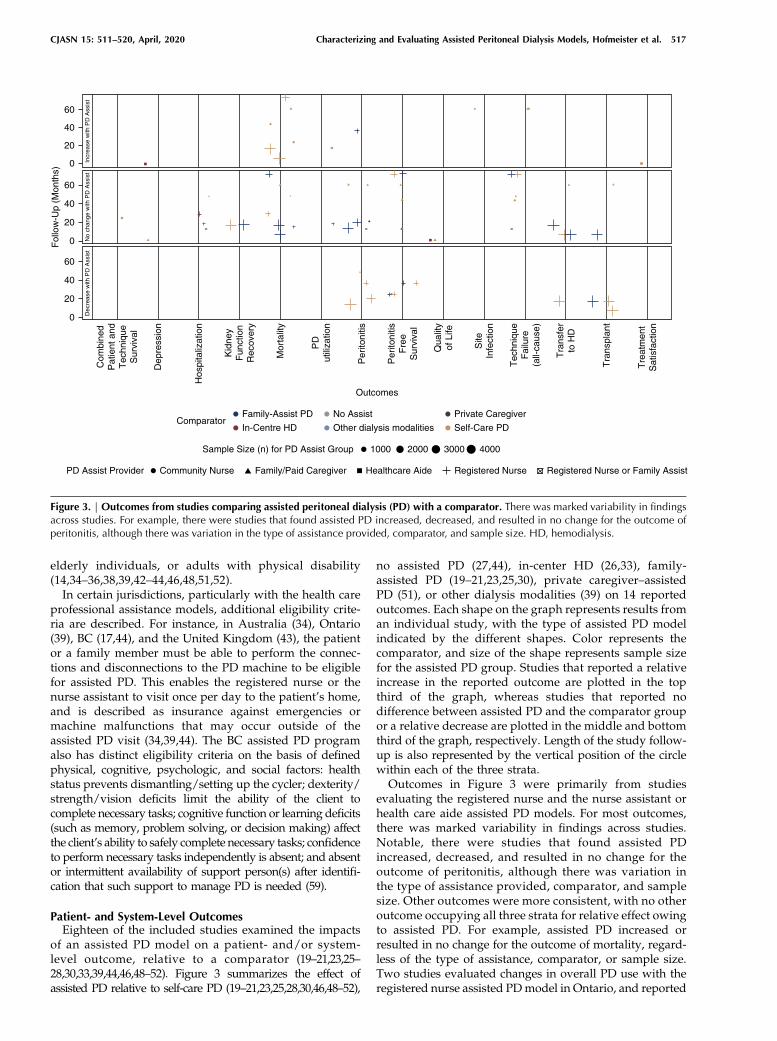
Patient- and System-Level OutcomesEighteen of the included studies examined the impacts
of an assisted PD model on a patient- and/or system-level outcome, relative to a comparator (19–21,23,25–28,30,33,39,44,46,48–52). Figure 3 summarizes the effect ofassisted PD relative to self-care PD (19–21,23,25,28,30,46,48–52),
no assisted PD (27,44), in-center HD (26,33), family-assisted PD (19–21,23,25,30), private caregiver–assistedPD (51), or other dialysis modalities (39) on 14 reportedoutcomes. Each shape on the graph represents results froman individual study, with the type of assisted PD modelindicated by the different shapes. Color represents thecomparator, and size of the shape represents sample sizefor the assisted PD group. Studies that reported a relativeincrease in the reported outcome are plotted in the topthird of the graph, whereas studies that reported nodifference between assisted PD and the comparator groupor a relative decrease are plotted in the middle and bottomthird of the graph, respectively. Length of the study follow-up is also represented by the vertical position of the circlewithin each of the three strata.Outcomes in Figure 3 were primarily from studies
evaluating the registered nurse and the nurse assistant orhealth care aide assisted PD models. For most outcomes,there was marked variability in findings across studies.Notable, there were studies that found assisted PDincreased, decreased, and resulted in no change for theoutcome of peritonitis, although there was variation inthe type of assistance provided, comparator, and samplesize. Other outcomes were more consistent, with no otheroutcome occupying all three strata for relative effect owingto assisted PD. For example, assisted PD increased orresulted in no change for the outcome of mortality, regard-less of the type of assistance, comparator, or sample size.Two studies evaluated changes in overall PD use with theregistered nurse assisted PDmodel in Ontario, and reported
Fol
low
-Up
(Mon
ths)
Incr
ease
with
PD
Ass
ist
No
chan
ge w
ith P
D A
ssis
tD
ecre
ase
with
PD
Ass
ist
60
40
20
60
40
20
0
60
40
20
0
0
Tra
nspl
ant
Com
bine
dP
atie
nt a
ndT
echn
ique
Sur
viva
l
Dep
ress
ion
Kid
ney
Fun
ctio
nR
ecov
ery
Mor
talit
y
PD
utili
zatio
n
Per
itoni
tis
Per
itoni
tisF
ree
Sur
viva
l
Qua
lity
of L
ife
Site
Infe
ctio
n
Tec
hniq
ueF
ailu
re(a
ll-ca
use)
Tra
nsfe
rto
HD
Tre
atm
ent
Sat
isfa
ctio
n
Outcomes
Sample Size (n) for PD Assist Group 1000 2000 3000 4000
ComparatorNo Assist Private CaregiverFamily-Assist PD
In-Centre HD Other dialysis modalities Self-Care PD
PD Assist Provider Community Nurse Healthcare Aide Registered Nurse Registered Nurse or Family AssistFamily/Paid Caregiver
Hos
pita
lizat
ion
Figure 3. | Outcomes from studies comparing assisted peritoneal dialysis (PD) with a comparator. There was marked variability in findingsacross studies. For example, there were studies that found assisted PD increased, decreased, and resulted in no change for the outcome ofperitonitis, although there was variation in the type of assistance provided, comparator, and sample size. HD, hemodialysis.
CJASN 15: 511–520, April, 2020 Characterizing and Evaluating Assisted Peritoneal Dialysis Models, Hofmeister et al. 517

an increase (27) relative to no assist, or no difference relativeto other dialysis modalities (39). The effect of the licensedpractical nurse assisted PD model was not evaluated in anyof the included studies.
Patient ExperienceTwo included studies evaluated the experience of patients
receiving assisted PD (32,53). Petersson and Lennerling(53) applied a hermeneutic phenomenological approach toexplore experiences of persons living with assisted PD inSweden. Bevilacqua et al. (32) used semistructured interviewsto identify potential values, enablers, barriers, and sugges-tions to improve an assisted PD program in BC. Broadly,patients valued the ability to maintain independence, thefeeling of support, and the relief from burden associated withself-care PD. The phenomenon of living with assisted PDwascharacterized in four main themes: facing new demands,managing daily life, partnerships in care, and experiencinga meaningful life (53). Suggestions to improve assisted PDincluded using a person-centered model of care, ensuringcontinuity of nurses providing the PD assist, and providingmeasures to support patient independence (e.g., education,telephone support) (32,53).
DiscussionThis review identified assisted PD models in 20 jurisdic-
tions in Europe, Asia, South America, Australia, Canada, andthe United States. Two categories of assisted PD modelsemerged: assistance from health care professionals and assis-tance from non–health care professionals. The most estab-lished and commonly implemented model was registerednurse assisted PD. Licensed practical nurse and nurse assistantor health care aide models are documented in more recentliterature from Canada and the United Kingdom.Most assisted PD models were delivered in large urban
centers, where there is likely a high prevalence of eligiblepatients in a circumscribed geographic area. For eligiblepatients living in rural/remote settings, the same physical,cognitive, or psychosocial barriers preventing the autonomousconduct of PD likely also contribute to difficulties accessing in-center HD. The provision of assisted PD to these patientswill require efforts to overcome barriers such as increasedtravel distance, difficulties recruiting care assistants, andlack of choice of care assistants (60). In general, differen-tiation of the level of assistance required by patients inincluded studies was not well described. And regardless ofsetting, there were no discernible trends in outcomes bytype of assistance provided.Although clinical outcomes with assisted PD were
evaluated, heterogeneous quality, reporting, and resultsdo not allow conclusions to be made. Further, despite itbeing likely that availability of assisted PD increases PDutilization, this was rarely evaluated. Available data makesit challenging to assess to what extent provision of assistedPD increased the proportion of patients on assisted PD, andcorrelation of PD utilization with programmatic features.This outcome is expected to depend on jurisdiction specificfeatures also, such as the funding model.Giuliani et al. (4) cautions that although assisted PD may
be an alternative for dependent patients that would other-wise receive in-center HD, many factors besides clinical
indications may influence the distribution of dialysis modal-ities. Themes associated with assisted PD of facing newdemands, managing daily life, partnerships in care, andexperiencing a meaningful life complement findings thatpatients receiving assisted PD value the maintenance ofindependence, the feeling of support, and relief fromburden associated with self-care (32,53). The success ofassisted PD programs is likely influenced by the ability tomeet these needs, although they are rarely used as metricsfor evaluation. This review supports findings by Giulianiet al. (4) that assisted PD should be intended to expandmodality choices and enhance patient centricity.In a review of PD first or favored policies, Liu et al. (61)
suggests that an important component of PD first policiesis the objective evaluation of patient outcomes afterimplementation. Although many objective outcomes arefrequently measured, it is unclear if patients do worse, thesame, or better with assisted PD than the appropriatecomparator. Further, the effect of assisted PD on PD utili-zation rates is rarely reported. Our recommendation is morefocused than that of Liu et al. (61): if the goal of PD-favoringprograms, such as assisted PD, is to increase PD utilization,this outcome should be explicitly reported in evaluations ofassisted PD.Although searches of published and gray literature were
extensive, this systematic review was limited to evidencein either English or French. Pooled analysis of reportedoutcome measures was not feasible because of heteroge-neity in comparators and point estimates/measures ofassociation. In commonly reported outcomes (e.g., transferto HD, peritonitis, mortality, etc.), there was markedvariability reported for all model types. No protocol forthis systematic review was registered. And on the EquatorNetwork website, there was no suitable tool for the qualityassessment of the study by Dratwa (22,62). Although theConsensus on Health Economic Criteria was used, manyitems were not relevant to this study.Many studies were identified characterizing and evaluat-
ing assisted PD; however, the evidence was limited. Relativeeffectiveness could not be determined from available studies.No randomized, controlled trials were identified, whichlimits validity of reported outcomes, and the patientvoice was under-represented. Further evidence is neededto connect assisted PD outcomes with programmaticfeatures and their associated funding models.
Acknowledgments
Because this work is a secondary analysis of already publishedwork, ethics approval is not required.
DisclosuresDr. Klarenbach reports a proportion of his salary is paid for by Al-
bertaHealth Services in his role as Co-Scientific Director of theKidneyHealth Strategic Clinical Network. Dr. Clement, Mr. Hofmeister,Dr. Scott-Douglas, and Dr. Soril have nothing to disclose.
FundingThis report was supported by a financial contribution from Al-
berta Health through the Alberta Health Evidence Review Process,the Alberta model for health technology assessment and policyanalysis.Theviewsexpressedhereindonotnecessarily represent theofficial policy of Alberta Health.
518 CJASN

Supplemental MaterialThis article contains the followingsupplementalmaterial online at
http://cjasn.asnjournals.org/lookup/suppl/doi:10.2215/CJN.11951019/-/DCSupplemental.Supplemental Appendix 1. MEDLINE search strategy.Supplemental Appendix 2. Search strategy of gray literature.Supplemental Appendix 3. Characteristics of included studies
from the published literature.Supplemental Appendix 4. Quality assessment.
References1. Mendelssohn DC, Wish JB: Dialysis delivery in Canada and
the United States: A view from the trenches. Am J Kidney Dis 54:954–964, 2009
2. Yeates K, Zhu N, Vonesh E, Trpeski L, Blake P, Fenton S: Hemo-dialysis and peritoneal dialysis are associated with similaroutcomes for end-stage renal disease treatment in Canada.Nephrol Dial Transplant 27: 3568–3575, 2012
3. Mehrotra R, Devuyst O,Davies SJ, JohnsonDW: The current stateof peritoneal dialysis. J Am Soc Nephrol 27: 3238–3252, 2016
4. GiulianiA,KaropadiAN,Prieto-VelascoM,Manani SM,CrepaldiC, Ronco C: Worldwide experiences with assisted peritonealdialysis. Perit Dial Int 37: 503–508, 2017
5. Aromataris E, Munn Z, editor: Joanna Briggs Institute Reviewer’sManual, North Adelaide, Australia, The Joanna Briggs Institute,2017
6. Moher D, Liberati A, Tetzlaff J, Altman DG; PRISMA Group:Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. BMJ 339: b2535, 2009
7. Canadian Agency for Drugs and Technologies in Health: GreyMatters: A practical tool for searching health-related greyliterature, 2019. Available at: https://www.cadth.ca/resources/finding-evidence/grey-matters. Accessed September 1, 2018
8. Sinclair A, Cimon K, Loncar M, Sood M, Komenda P, Severn M,Klarenbach S, SoH, Tsoi B,QuinnR, Pauly R, TonelliM,Manns B,Rader T, Moulton K, Moulton K, Helis E, Crain J, Pullman D:Dialysis Modalities for the Treatment of End-Stage Kidney Dis-ease: A Health Technology Assessment, Ottawa, ON, CanadianAgency for Drugs and Technologies in Health, 2017
9. Canadian Institute for Health Information: Licensed practicalnurses, 2019. Available at: https://www.cihi.ca/en/registered-nursesnurse-practitioners. Accessed September 1, 2019
10. Alberta Health Services: Health care aide, 2019. Available at:https://www.albertahealthservices.ca/careers/Page11729.aspx.Accessed September 1, 2019
11. Slim K, Nini E, Forestier D, Kwiatkowski F, Panis Y, Chipponi J:Methodological index for non-randomized studies (minors):Development and validation of a new instrument. ANZ J Surg73: 712–716, 2003
12. Critical Appraisal Skills Programme: CASP qualitative checklist,2018. Available at: https://casp-uk.net/wp-content/uploads/2018/03/CASP-Qualitative-Checklist-2018_fillable_form.pdf.Accessed September 1, 2018
13. Evers S,GoossensM,deVetH, vanTulderM,AmentA:Criteria listfor assessment of methodological quality of economic evalua-tions: Consensus on Health Economic Criteria. Int J TechnolAssess Health Care 21: 240–245, 2005
14. Manitoba Renal Program: PD community care program, 2019.Available at: http://www.kidneyhealth.ca/wp/pd-community-care-program/. Accessed September 10, 2019
15. Manitoba Renal Program: Home dialysis: Information aboutperitoneal dialysis and home hemodialysis, 2016. Available at:http://www.kidneyhealth.ca/wp/wp-content/uploads/patients/HomeDialysisHandbook_web.pdf. Accessed September 1,2019
16. BevilacquaM,Hill P, Turnbull L, Er L,ChiuH: Evaluationof thePDassist pilot project: Outcomes at 12months. BCRenal: An agencyof the provincial health services authority. 2015
17. BritishColumbiaRenalAgency:Best practices:Peritonealdialysisprograms, 2018. Available at: http://www.bcrenalagency.ca/resource-gallery/Documents/Best%20Practices-Peritoneal%20Dialysis%20Programs.pdf. Accessed September 1, 2019
18. Ontario Renal Network: 2018/19 Chronic Kidney DiseaseFundingGuide:Hospital and Community Funding, Toronto,ON,Ontario Renal Network, 2018
19. Bechade C, Guittet L, Evans D, Verger C, Ryckelynck JP,LobbedezT: Early failure inpatients startingperitoneal dialysis:Acompeting risks approach. Nephrol Dial Transplant 29: 2127–2135, 2014
20. BenabedA,BechadeC,FicheuxM,VergerC,LobbedezT:Effectofassistance on peritonitis risk in diabetic patients treated by peri-toneal dialysis: Report from the French Language PeritonealDialysis Registry. Nephrol Dial Transplant 31: 656–662, 2016
21. Castrale C, EvansD, Verger C, Fabre E, AguileraD, Ryckelynck JP,LobbedezT:Peritonealdialysis inelderlypatients:Report fromtheFrench Peritoneal Dialysis Registry (RDPLF). Nephrol DialTransplant 25: 255–262, 2010
22. Dratwa M: Costs of home assistance for peritoneal dialysis: Re-sults of a European survey. Kidney Int Suppl 73: S72–S75, 2008
23. Duquennoy S, Bechade C, Verger C, Ficheux M, Ryckelynck JP,Lobbedez T: Is peritonitis risk increased in elderly patients onperitoneal dialysis? Report from the french language peritonealdialysis registry (rdplf). Perit Dial Int 36: 291–296, 2016
24. Guillouet S, Lobbedez T, Lanot A, Verger C, Ficheux M, BechadeC: Factors associated with nurse assistance among peritonealdialysis patients: A cohort study from the French LanguagePeritoneal Dialysis Registry. Nephrol Dial Transplant 33:1446–1452, 2018
25. Lobbedez T, Verger C, Ryckelynck JP, Fabre E, Evans D: Is assistedperitoneal dialysis associated with technique survival whencompeting events are considered? Clin J Am Soc Nephrol 7:612–618, 2012
26. OliverMJ,Al-JaishiAA,DixonSN,Perl J, JainAK, LavoieSD,NashDM, Paterson JM, Lok CE, Quinn RR: Hospitalization rates forpatients on assisted peritoneal dialysis compared with in-centerhemodialysis. Clin J Am Soc Nephrol 11: 1606–1614, 2016
27. Oliver MJ, Garg AX, Blake PG, Johnson JF, Verrelli M, ZachariasJM, Pandeya S,Quinn RR: Impact of contraindications, barriers toself-care and support on incident peritoneal dialysis utilization.Nephrol Dial Transplant 25: 2737–2744, 2010
28. Povlsen JV, Ivarsen P: Assisted peritoneal dialysis: Also for the latereferred elderly patient. Perit Dial Int 28: 461–467, 2008
29. Sunder S, TaskapanH, Jojoa J, KrishnanM, KhandelwalM, Izatt S,Chu M, Subramanian P, Chinthalapalli H, Lobbedez T, Jassal SV,Bargman JM, Oreopoulos DG: Chronic peritoneal dialysis in thetenth decade of life. Int Urol Nephrol 36: 605–609, 2004
30. Verger C, Duman M, Durand PY, Veniez G, Fabre E, RyckelynckJP: Influence of autonomy and type of home assistance on theprevention of peritonitis in assisted automated peritoneal dialysispatients. An analysis of data from the French Language PeritonealDialysis Registry.Nephrol Dial Transplant 22: 1218–1223, 2007
31. Verger C, Ryckelynck JP, Duman M, Veniez G, Lobbedez T,Boulanger E, Moranne O: French peritoneal dialysis registry(RDPLF): Outline and main results. Kidney Int Suppl (103):S12–S20, 2006
32. Bevilacqua MU, Chiu HH, Saunders S, Turnbull L, Taylor PA,Singh RS, Salyers V: The value of patient and provider reportedexperiences in evaluating home-based assisted peritoneal di-alysis. Eur J Pers Cent Healthc 5: 404–412, 2017
33. Iyasere OU, Brown EA, Johansson L, Huson L, Smee J, MaxwellAP, Farrington K, Davenport A: Quality of life and physicalfunction in older patients on dialysis: A comparison of assistedperitoneal dialysis with hemodialysis. Clin J Am Soc Nephrol 11:423–430, 2016
34. Fortnum D, Chakera A, Hawkins N, Vandepeer G: With a littlehelp from my friends: Developing an assisted automated peri-tonealdialysisprograminWesternAustralia.RenalSocAustralas J13: 83–89, 2017
35. Povlsen JV, Ivarsen P: Assisted automated peritoneal dialysis(AAPD) for the functionally dependent and elderly patient. PeritDial Int 25[Suppl 3]: S60–S63, 2005
36. LobbedezT,MoldovanR,LecameM,Hurault deLignyB, ElHagganW, Ryckelynck JP: Assisted peritoneal dialysis. Experience in aFrench renal department. Perit Dial Int 26: 671–676, 2006
37. Pommer W, Wagner S, Muller D, Thumfart J: Attitudes of ne-phrologists towards assisted home dialysis in Germany. ClinKidney J 11: 400–405, 2018
CJASN 15: 511–520, April, 2020 Characterizing and Evaluating Assisted Peritoneal Dialysis Models, Hofmeister et al. 519

38. Wadhwa NK, Suh H, Cabralda T, Sokol E, Sokunbi D, Solomon M:Peritoneal dialysiswith trained home nurses in elderly and disabledend-stage renal disease patients. Adv Perit Dial 9: 130–133, 1993
39. OliverMJ,Quinn RR, Richardson EP, Kiss AJ, LampingDL,MannsBJ:Homecare assistance and theutilizationof peritoneal dialysis.Kidney Int 71: 673–678, 2007
40. Murray MA, Twolan C, Owens G, Ferguson C, Benard M, Verch-Whittington J: Evaluation of a newmodel of care to support homeperitoneal dialysis patients: The nephrology integrated caredemonstration project.CanadianAssocNephrolNurses Tech 22:17, 2012
41. Brunier G, Gray B, Coulis N, Savage J, Manuel A, McConnell H,Mildon B, Sherlock AM: The use of community nurses for homeperitoneal dialysis: Is it cost-effective? Perit Dial Int 16[Suppl 1]:S479–S482, 1996
42. FrancoMRG,FernandesN,RibeiroCA,QureshiAR,Divino-FilhoJC, da Gloria Lima M: A Brazilian experience in assisted auto-mated peritoneal dialysis: A reliable and effective home careapproach. Perit Dial Int 33: 252–258, 2013
43. Brown N, Vardhan A: Developing an assisted automated peri-toneal dialysis (aAPD) service-a single-centre experience. NDTPlus 4[Suppl 3]: iii16–iii18, 2011
44. BevilacquaMU, Turnbull L, Saunders S, Er L, ChiuH,Hill P, SinghRS, Levin A, Copland MA, Jamal A, Brumby C, Dunne O, TaylorPA: Evaluation of a 12-month pilot of long-term and temporaryassisted peritoneal dialysis. Perit Dial Int 37: 307–313, 2017
45. Alberta Health Services: Keeping you well and independent:Home care, 2017. Available at: https://www.albertahealthservices.ca/assets/info/seniors/if-sen-home-care-brochure.pdf. AccessedSeptember 1, 2019
46. Xu R, Zhuo M, Yang Z, Dong J: Experiences with assisted peri-toneal dialysis in China. Perit Dial Int 32: 94–101, 2012
47. Al-Hilali N, Nampoory MRN, Ninan TV, Ali JH, Gawish A, JohnyKV: Viability of home peritoneal dialysis: Experience with 100patients from an Arab population. Perit Dial Int 23[Suppl 2]:S165–S169, 2003
48. AlWakeel JS, Al GhonaimMA, Aldohayan A, Usama S, Al ObailiS, Tarakji AR, Alkhowaiter M: Appraising the outcome andcomplications of peritoneal dialysis patients in self-care perito-neal dialysis and assisted peritoneal dialysis: A 5-year review of asingle Saudi center. Saudi J Kidney Dis Transpl 29: 71–80, 2018
49. Griva K, Goh CS, Kang WCA, Yu ZL, Chan MC, Wu SY,Krishnasamy T, Foo M: Quality of life and emotional distress inpatients andburden in caregivers:Acomparisonbetweenassistedperitoneal dialysis and self-care peritoneal dialysis.Qual Life Res25: 373–384, 2016
50. ChengCH,ShuKH,ChuangYW,HuangST,ChouMC,ChangHR:Clinical outcome of elderly peritoneal dialysis patients with as-sisted care in a single medical centre: A 25 year experience.Nephrology (Carlton) 18: 468–473, 2013
51. HsiehCY, Fang JT, YangCW, Lai PC,Hu SA, ChenYM, YuCC, TianYC, Chien CC, Hung CC: The impact of type of assistance on
characteristics of peritonitis in elderly peritoneal dialysis patients.Int Urol Nephrol 42: 1117–1124, 2010
52. Querido S, Branco PQ, Costa E, Pereira S, Gaspar MA, Barata JD:Results in assisted peritoneal dialysis: A ten-year experience. Int JNephrol 2015: 712539, 2015
53. Petersson I, Lennerling A: Experiences of living with assistedperitoneal dialysis - a qualitative study.PeritDial Int37: 605–612,2017
54. Alberta Health Services: Health care aide role in medicationassistance:Acompanion to theAlbertaprovincial continuingcaremedication assistance program (MAP) manual, 2016.Available at: https://www.albertahealthservices.ca/assets/info/seniors/if-sen-companion-to-map-hca-role-in-med-assist.pdf.Accessed September 1, 2019
55. Alberta Health Services: Licensed practical nurse, 2019. Avail-able at: https://www.albertahealthservices.ca/careers/page11730.aspx. Accessed September 1, 2019
56. College of Licensed Practical Nurses of Alberta: LPN scope ofpracticeexplained innewfact sheetandvideo,2013.Availableat:https://www.clpna.com/2013/07/fact-sheet-scope-of-practice-for-lpns-in-alberta/. Accessed September 1, 2019
57. College andAssociation of RegisteredNurses ofAlberta: Entry-to-Practice competencies for the registered nurses profession, 2013.Available at: http://www.nurses.ab.ca/content/dam/carna/pdfs/DocumentList/Standards/RN_En-tryPracticeCompetencies_May2013.pdf. Accessed September 1,2019
58. College and Association of Registered Nurses of Alberta: Scopeof practices for registered nurses, 2011. Available at: http://www.nurses.ab.ca/content/dam/carna/pdfs/DocumentList/Standards/RN_ScopeOfPractice_May2011.pdf. AccessedSeptember 1, 2019
59. PeritonealDialysis Assist: Information for PDprograms and nursenext door. 2017. Available at: http://www.bcrenalagency.ca/about/news-stories/news-releases/province-wide-support-pro-gram-helps-pd-patients-maintain-care-at-home. AccessedMarch 1, 2019
60. McCann S, RyanAA,McKennaH: The challenges associatedwithproviding community care for peoplewith complexneeds in ruralareas: A qualitative investigation. Health Soc Care Community13: 462–469, 2005
61. Liu FX,GaoX, IngleseG,ChuengsamanP, Pecoits-FilhoR, YuA:Aglobal overviewof the impact of peritoneal dialysis first or favoredpolicies: An opinion. Perit Dial Int 35: 406–420, 2015
62. UK EQUATOR Centre. EQUATORNetwork: Search for reportingguidelines: UK EQUATOR Centre. Available at: https://www.e-quator-network.org/. Accessed March, 1 2020
Received: October 7, 2019 Accepted: February 20, 2020
Published online ahead of print. Publication date available atwww.cjasn.org.
520 CJASN
http://www.nurses.ab.ca/content/dam/carna/pdfs/DocumentList/Standards/RN_ScopeOfPractice_May2011.pdf
http://www.nurses.ab.ca/content/dam/carna/pdfs/DocumentList/Standards/RN_ScopeOfPractice_May2011.pdf




















