
3-D shape analysis of palatal surface in patients with unilateral complete cleft lip and palate
8
3-D shape analysis of palatal surface in patients with unilateral complete cleft lip and palate Hana Rusková a , Sárka Bejdová a , Miroslav Peterka b , Václav Krají cek a, c , Jana Velemínská a, * a Department of Anthropology and Human Genetics (Head: Assoc. Prof. Vladimír Sládek, M.Sc., Ph.D.), Faculty of Science, Charles University in Prague, Vini cná 7, 128 43 Prague 2, Czech Republic b Institute of Experimental Medicine Academy of Sciences CR (Head: Prof. Eva Syková, M.D., D.Sc.), Prague, Czech Republic c Department of Software and Computer Science Education (Head: Assoc. Prof. Dr. Pavel Töpfer, Ph.D.), Faculty of Mathematics and Physics, Charles University in Prague, Prague, Czech Republic article info Article history: Paper received 21 December 2012 Accepted 17 July 2013 Keywords: Unilateral cleft of lip and palate Palatal shape Surface scanning 3-D geometric morphometrics Dense correspondence analysis abstract Facial development of patients with unilateral complete cleft lip and palate (UCLP) is associated with many problems including deformity of the palate. The aim of this study was to evaluate palatal morphology and variability in patients with UCLP compared with Czech norms using methods of geo- metric morphometrics. The study was based on virtual dental cast analysis of 29 UCLP patients and 29 control individuals at the age of 15 years. The variability of palatal shape in UCLP patients was greater than that in nonclefted palates. Only 24% of clefted palates fell within the variability of controls. The palatal form of UCLP patients (range from 11.8 to 17.2 years) was not correlated with age. Compared with control palates, palates of UCLP patients were narrower, more anteriorly than pos- teriorly. Apart from the praemaxilla region, they were also shallower, and the difference increased posteriorly. The UCLP palate was characterised by the asymmetry of its vault. The maximum height of the palatal vault was anterior on the clefted side, whereas it was posterior on the nonclefted side. The slope of the UCLP palate was more inclined compared with the control group. The praemaxilla was therefore situated more inferiorly. Ó 2013 European Association for Cranio-Maxillo-Facial Surgery. Published by Elsevier Ltd. All rights reserved. 1. Introduction Orofacial clefts in newborns are some of the most common facial deformities; their causes are multifactorial. They are gener- ated by hypoplasia of facial prominences and palatal shelves and growth retardation of the mandible in human (O’Rahilly and Müller, 1992), as well as by experimental models (Jelínek and Peterka, 1977; Peterka and Jelínek, 1983). The incidence of the orofacial clefts is about 1e 7 per 1000 liveborn babies. The children with orofacial clefts need multidis- ciplinary care from birth to adulthood (e.g. Dürwald and Dannhauer, 2007; Vlastos et al., 2009). The presence of malfor- mation has a long-lasting adverse outcomes for health and social integration. The communication of the cleft patients is affected because of their problems with speech and hearing. The later timing of hard palate closure significantly affects speech develop- ment (e.g. Krey et al., 2009; Mossey et al., 2009). Unilateral complete cleft lip and palate (UCLP), the subject of our study, is the most frequent type of orofacial malformation. For these individuals, growth disturbance of the maxilla and the large number of orthodontic anomalies is typical (Jelínek et al., 1983). In order to choose the correct surgical technique and the timing of the surgery and start of orthodontic treatment, it is essential to know the growth potential of the patient’s jaws (Peterka and P enkava, 1975). For individuals with UCLP, decreased growth of the maxilla anteriorly is typical. In addition to reduced palatal growth, poste- riorotation of the mandible often develops. Significant deteriora- tion in intermaxillary relationships occurs mainly during puberty in relation to the eruption of permanent teeth. Limited pubertal ac- celeration with significant growth of the mandible is typical in UCLP individuals ( Smahel and Brejcha, 1983). Increase in alveolar arch is important for the correct placement of teeth, which is also limited in this case. Hypoplasia of the upper jaw can also lead to * Corresponding author. Tel.: þ420 221 951 612; fax: þ420 221 951 619. E-mail address: [email protected] (J. Velemínská). Contents lists available at ScienceDirect Journal of Cranio-Maxillo-Facial Surgery journal homepage: www.jcmfs.com 1010-5182/$ e see front matter Ó 2013 European Association for Cranio-Maxillo-Facial Surgery. Published by Elsevier Ltd. All rights reserved. http://dx.doi.org/10.1016/j.jcms.2013.07.011 Journal of Cranio-Maxillo-Facial Surgery xxx (2013) 1e8 Please cite this article in press as: Rusková H, et al., 3-D shape analysis of palatal surface in patients with unilateral complete cleft lip and palate, Journal of Cranio-Maxillo-Facial Surgery (2013), http://dx.doi.org/10.1016/j.jcms.2013.07.011
Transcript of 3-D shape analysis of palatal surface in patients with unilateral complete cleft lip and palate

lable at ScienceDirect
Journal of Cranio-Maxillo-Facial Surgery xxx (2013) 1e8
Contents lists avai
Journal of Cranio-Maxillo-Facial Surgery
journal homepage: www.jcmfs.com
3-D shape analysis of palatal surface in patients with unilateralcomplete cleft lip and palate
Hana Rusková a, �Sárka Bejdová a, Miroslav Peterka b, Václav Krají�cek a,c, Jana Velemínská a,*
aDepartment of Anthropology and Human Genetics (Head: Assoc. Prof. Vladimír Sládek, M.Sc., Ph.D.), Faculty of Science, Charles University in Prague,Vini�cná 7, 128 43 Prague 2, Czech Republicb Institute of Experimental Medicine Academy of Sciences CR (Head: Prof. Eva Syková, M.D., D.Sc.), Prague, Czech RepubliccDepartment of Software and Computer Science Education (Head: Assoc. Prof. Dr. Pavel Töpfer, Ph.D.), Faculty of Mathematics and Physics, CharlesUniversity in Prague, Prague, Czech Republic
a r t i c l e i n f o
Article history:Paper received 21 December 2012Accepted 17 July 2013
Keywords:Unilateral cleft of lip and palatePalatal shapeSurface scanning3-D geometric morphometricsDense correspondence analysis
* Corresponding author. Tel.: þ420 221 951 612; faE-mail address: [email protected] (J. Velemí
1010-5182/$ e see front matter � 2013 European Asshttp://dx.doi.org/10.1016/j.jcms.2013.07.011
Please cite this article in press as: Rusková HJournal of Cranio-Maxillo-Facial Surgery (20
a b s t r a c t
Facial development of patients with unilateral complete cleft lip and palate (UCLP) is associated withmany problems including deformity of the palate. The aim of this study was to evaluate palatalmorphology and variability in patients with UCLP compared with Czech norms using methods of geo-metric morphometrics. The study was based on virtual dental cast analysis of 29 UCLP patients and 29control individuals at the age of 15 years.
The variability of palatal shape in UCLP patients was greater than that in nonclefted palates. Only 24%of clefted palates fell within the variability of controls. The palatal form of UCLP patients (range from 11.8to 17.2 years) was not correlated with age.
Compared with control palates, palates of UCLP patients were narrower, more anteriorly than pos-teriorly. Apart from the praemaxilla region, they were also shallower, and the difference increasedposteriorly. The UCLP palate was characterised by the asymmetry of its vault. The maximum height of thepalatal vault was anterior on the clefted side, whereas it was posterior on the nonclefted side. The slopeof the UCLP palate was more inclined compared with the control group. The praemaxilla was thereforesituated more inferiorly.
� 2013 European Association for Cranio-Maxillo-Facial Surgery. Published by Elsevier Ltd. All rightsreserved.
1. Introduction
Orofacial clefts in newborns are some of the most commonfacial deformities; their causes are multifactorial. They are gener-ated by hypoplasia of facial prominences and palatal shelves andgrowth retardation of the mandible in human (O’Rahilly andMüller, 1992), as well as by experimental models (Jelínek andPeterka, 1977; Peterka and Jelínek, 1983).
The incidence of the orofacial clefts is about 1e7 per 1000liveborn babies. The children with orofacial clefts need multidis-ciplinary care from birth to adulthood (e.g. Dürwald andDannhauer, 2007; Vlastos et al., 2009). The presence of malfor-mation has a long-lasting adverse outcomes for health and socialintegration. The communication of the cleft patients is affectedbecause of their problems with speech and hearing. The later
x: þ420 221 951 619.nská).
ociation for Cranio-Maxillo-Facial
, et al., 3-D shape analysis of p13), http://dx.doi.org/10.1016
timing of hard palate closure significantly affects speech develop-ment (e.g. Krey et al., 2009; Mossey et al., 2009).
Unilateral complete cleft lip and palate (UCLP), the subject of ourstudy, is themost frequent type of orofacial malformation. For theseindividuals, growth disturbance of the maxilla and the largenumber of orthodontic anomalies is typical (Jelínek et al., 1983). Inorder to choose the correct surgical technique and the timing of thesurgery and start of orthodontic treatment, it is essential to knowthe growth potential of the patient’s jaws (Peterka and P�enkava,1975).
For individuals with UCLP, decreased growth of the maxillaanteriorly is typical. In addition to reduced palatal growth, poste-riorotation of the mandible often develops. Significant deteriora-tion in intermaxillary relationships occursmainly during puberty inrelation to the eruption of permanent teeth. Limited pubertal ac-celeration with significant growth of the mandible is typical inUCLP individuals (�Smahel and Brejcha, 1983). Increase in alveolararch is important for the correct placement of teeth, which is alsolimited in this case. Hypoplasia of the upper jaw can also lead to
Surgery. Published by Elsevier Ltd. All rights reserved.
alatal surface in patients with unilateral complete cleft lip and palate,/j.jcms.2013.07.011

H. Rusková et al. / Journal of Cranio-Maxillo-Facial Surgery xxx (2013) 1e82
anterior crossbite and to palatal or vestibular eruption of teeth(Peterka et al., 1980).
Later development of the upper jaw is the result of suturalgrowth, bone remodelling, growth of the alveolar ridges anderuption of the teeth (Enlow and Hans, 1996). In early postnataldevelopment, round arch forms change into oval arch forms(Sillman, 1964; Kramer et al., 1992). The dental arch of 3-year-oldchildren with UCLP or bilateral cleft lip and palate (BCLP) beforesurgery is wider than the unaffected dental arch. This is caused byunconnected segments of the alveolar arch (Jelínek et al., 1983).Indeed, measurements are significantly larger in unoperated adultswith BCLP than in controls because of the unmerged parts of thepalate (Diah et al., 2007). The antero-posterior dimension of thealveolar arch in UCLP, BCLP and cleft palate patients is shorter(Jelínek et al., 1983). An important feature of UCLP individuals isthat their palate surface is smaller than in healthy subjects(Huddart et al., 1978; Lo et al., 2003), which suggests that there is anintrinsic tissue deficiency in the palate/maxilla before palatoplasty(Lo et al., 2003). After lip surgery, the dental arch narrows (Huanget al., 2002).
A rapid reduction of palatal width was found after palatoplasty,which patients undergo from 3 to 6 years of age. Also, diminishedpalatal length has been described during all the evaluated periodsfrom 3 to 18 years (Peterka et al., 1980). According to Schliephakeet al. (2006), asymmetry (cleft side vs. noncleft side) of the ante-rior part of the palate in UCLP patients is greater than that of themolar area, and it increases with age. In another study, UCLP pa-tients in at 15 years were characterised by a certain asymmetrycompared with the control group palates (�Smahel et al., 2004).
The palate as a whole was shallower than in controls(Kilpeläinen et al., 1996; �Smahel et al., 2004). All maxillary dentalarch dimensions in UCLP patients at ages 3e12were smaller than incontrols, except for intermolar width at age 12 (Athanasiou et al.,1988). The width between permanent first molars in 12-year-oldUCLP patients was close to that of controls (Peterka et al., 1980). Atage 15, dental arch width was narrower across all palatal surfaces.Arch length was assessed only between the first molars, and therewas no reduction compared with controls (�Smahel et al., 2004).
To evaluate the shape of the palate in the above-mentionedstudies, traditional morphometry was used. These studies oftensuffer from magnification errors, with consequent loss of infor-mation from the third dimension (Bugaighis et al., 2010).
Previous research of �Smahel et al. (2004) was based on evalu-ation of more than 200 dimensions, but it did not evaluate palatalshape variability or detailed praemaxilla description. From amethodological point of view, our study was built on the researchof Bejdová et al. (2012), wherein the shape of the palate wasevaluated in BCLP patients. Shape analysis, including the densecorrespondence algorithm (DCA; Hutton et al., 2001), principalcomponent analysis (PCA) and finite element scaling analysis(FESA), made it possible to evaluate the surface of the palate as awhole, its average changes and its interindividual variability.
The aim of this study was to use geometric morphometric toolsto evaluate the variability and average differences of palatal shapein patients with UCLP compared with those in healthy Czechchildren.
2. Material and methods
2.1. Patients and control group
We analysed two groups consisting of 58 plaster casts of themaxillary alveolar arch and palate.
The UCLP sample consisted of 29 plaster casts of Czech boys. Thecasts were made as a part of the treatment record. Eighteen clefts
Please cite this article in press as: Rusková H, et al., 3-D shape analysis of pJournal of Cranio-Maxillo-Facial Surgery (2013), http://dx.doi.org/10.1016
were left sides and 11 clefts were of the right. Average age of thepatients was 14.8 years (range from 11.8 to 17.2). All surgery wasperformed at the Clinic of Plastic Surgery in Prague from1975 to 1980by the same method. Lip surgery was performed according to Ten-nison, with primary periosteoplasty at an average age of 8.5 months(range, 5e17 months). Palatoplasty by pushback with two flaps andpharyngealflap surgerywas performed onpatients at average age 4.9years (range from 3.0 to 5.9). After surgery, the patients underwentlong-term orthodontic treatment (Kuderová et al., 1996). �Smahelet al. (2004) have evaluated the treatment in detail. In our study,only UCLP patients without a bony bridge were included. Otherconditions were absence of imperfections in the dental cast surfaceand at least partial eruption of both permanent second molars.
The control group consisted of plaster casts of 29 healthy boys ofCzech origin. The average age was 14.7 years (range from 14.1 to15.7). The casts had been taken in the 1970s in schools in the city ofBrno. Conditions for inclusion in the study were at least partialeruption of both permanent second molars and absence of ortho-dontic anomalies (rotation, tooth position in the alveolar arch,crowding). Only individuals with an ideal occlusion were involved.
2.2. Methods
The maxillary plaster casts were digitised using laser scannerRoland LPX-250 (Roland DG, Hamamatsu, Japan) with a lateralresolution of 200 mm. The casts were scanned perpendicular to theocclusal plane using Dr. Picza 3 software (Roland DG), and the rawscanned data were processed using Pixform reverse engineeringsoftware (Roland DG). This software was used to revise the rawscans by removing the teeth from the models before analysis,because only the shape of the palate was evaluated (Fig. 1). It is wellknown that majority of the UCLP is localized on the left side. Oursample of UCLP patients comprised both left- and right-sided clefts.In order to have homogenized cleft side for further 3D shapeanalysis, the scans of right-sided clefts were flipped horizontallyand evaluated as left-sided clefts.
The models were processed using the software MorphoStudio3.02 and geometric morphometrics. DCA was used to convert themodels to the same number of triangular faces (Hutton et al., 2001).In the first step, a set of four hand-placed landmarks was situatedon each evaluated palatal surface. The first landmark was placedbetween the central incisors at the incisive papilla. The second andthird landmarks were situated on the most medial cervical marginsof the second premolars. The fourth landmark was placed in themiddle of a line connecting the first molars at the most medialcervical margins between the mesiodistal and distopalatal cusps(more details in Bejdová et al., 2012).
The next step was the Procrustes superimposition (Zelditchet al., 2004), which was used to find the average landmarkconfiguration of all four landmarks. After that, the models weretransformed by thin-plate spline interpolation so that their land-mark configurations fitted the average landmark configuration. Allpoints or vertices of the polygon mesh can be further considered aslandmarks and as the initial data for multivariate analysis.
Shape variability of clefted and nonclefted palates was analysedusing principal component analysis (PCA). This method was suit-able for studying individual variability as well as for comparingbetween groups of patients and controls, for which PCA score plotsare suitable. Using the software mentioned above, we were able toreconstruct the palatal shape of any individual in the sample oralong the axis of any principal component score. This methodologyhas frequently been used to evaluate facial variability (e.g., Singhet al., 2007; Weinberg et al., 2009).
As the age range in our UCLP sample was wide (from 11.8 to 17.2years), linear regression was used to describe the relation between
alatal surface in patients with unilateral complete cleft lip and palate,/j.jcms.2013.07.011
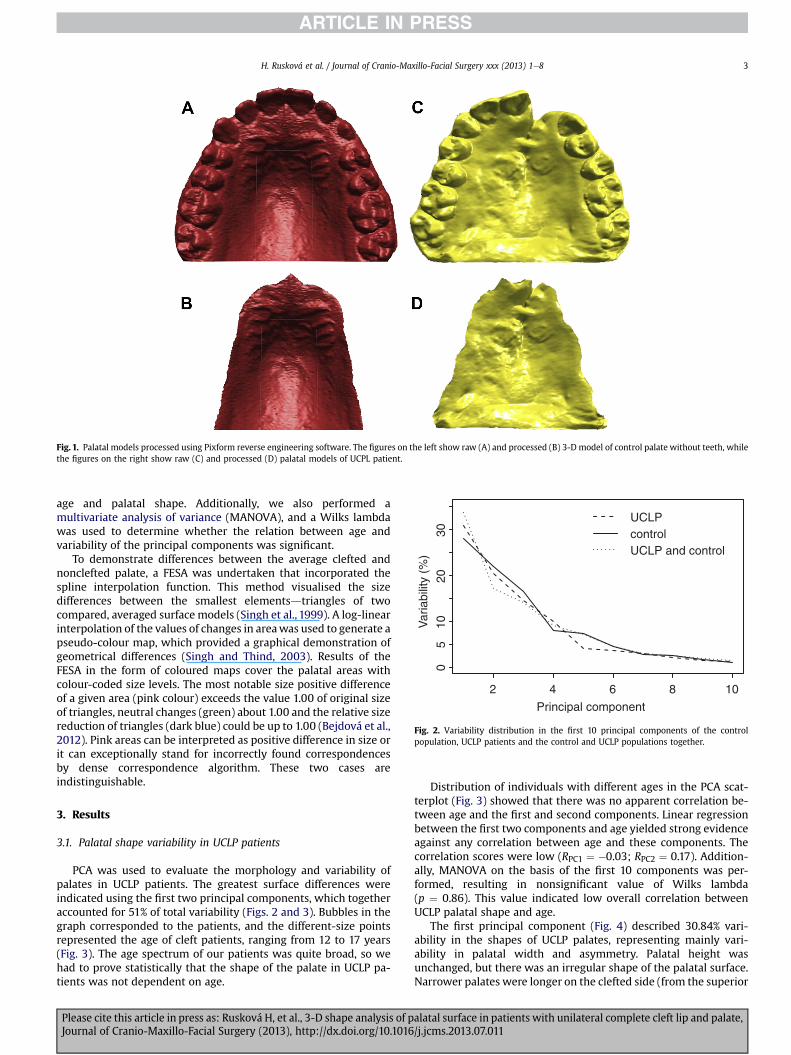
Fig. 2. Variability distribution in the first 10 principal components of the controlpopulation, UCLP patients and the control and UCLP populations together.
Fig. 1. Palatal models processed using Pixform reverse engineering software. The figures on the left show raw (A) and processed (B) 3-D model of control palate without teeth, whilethe figures on the right show raw (C) and processed (D) palatal models of UCPL patient.
H. Rusková et al. / Journal of Cranio-Maxillo-Facial Surgery xxx (2013) 1e8 3
age and palatal shape. Additionally, we also performed amultivariate analysis of variance (MANOVA), and a Wilks lambdawas used to determine whether the relation between age andvariability of the principal components was significant.
To demonstrate differences between the average clefted andnonclefted palate, a FESA was undertaken that incorporated thespline interpolation function. This method visualised the sizedifferences between the smallest elementsdtriangles of twocompared, averaged surface models (Singh et al., 1999). A log-linearinterpolation of the values of changes in areawas used to generate apseudo-colour map, which provided a graphical demonstration ofgeometrical differences (Singh and Thind, 2003). Results of theFESA in the form of coloured maps cover the palatal areas withcolour-coded size levels. The most notable size positive differenceof a given area (pink colour) exceeds the value 1.00 of original sizeof triangles, neutral changes (green) about 1.00 and the relative sizereduction of triangles (dark blue) could be up to 1.00 (Bejdová et al.,2012). Pink areas can be interpreted as positive difference in size orit can exceptionally stand for incorrectly found correspondencesby dense correspondence algorithm. These two cases areindistinguishable.
3. Results
3.1. Palatal shape variability in UCLP patients
PCA was used to evaluate the morphology and variability ofpalates in UCLP patients. The greatest surface differences wereindicated using the first two principal components, which togetheraccounted for 51% of total variability (Figs. 2 and 3). Bubbles in thegraph corresponded to the patients, and the different-size pointsrepresented the age of cleft patients, ranging from 12 to 17 years(Fig. 3). The age spectrum of our patients was quite broad, so wehad to prove statistically that the shape of the palate in UCLP pa-tients was not dependent on age.
Please cite this article in press as: Rusková H, et al., 3-D shape analysis of pJournal of Cranio-Maxillo-Facial Surgery (2013), http://dx.doi.org/10.1016
Distribution of individuals with different ages in the PCA scat-terplot (Fig. 3) showed that there was no apparent correlation be-tween age and the first and second components. Linear regressionbetween the first two components and age yielded strong evidenceagainst any correlation between age and these components. Thecorrelation scores were low (RPC1 ¼ �0.03; RPC2 ¼ 0.17). Addition-ally, MANOVA on the basis of the first 10 components was per-formed, resulting in nonsignificant value of Wilks lambda(p ¼ 0.86). This value indicated low overall correlation betweenUCLP palatal shape and age.
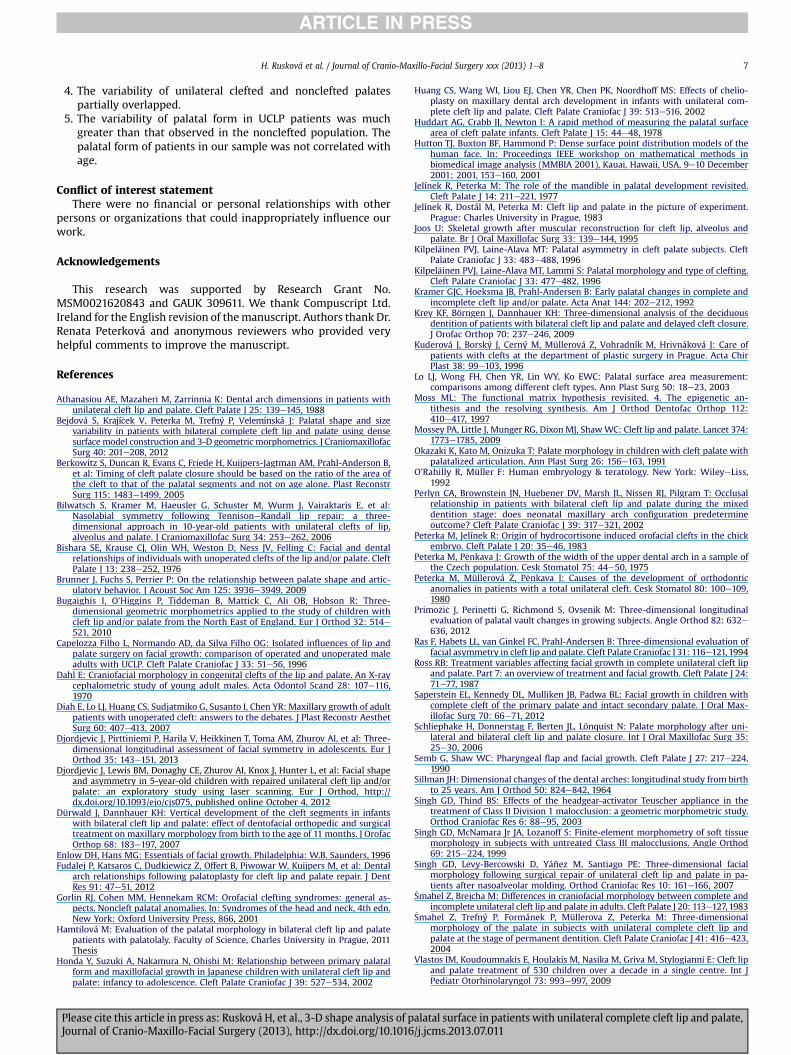
The first principal component (Fig. 4) described 30.84% vari-ability in the shapes of UCLP palates, representing mainly vari-ability in palatal width and asymmetry. Palatal height wasunchanged, but there was an irregular shape of the palatal surface.Narrower palates were longer on the clefted side (from the superior
alatal surface in patients with unilateral complete cleft lip and palate,/j.jcms.2013.07.011
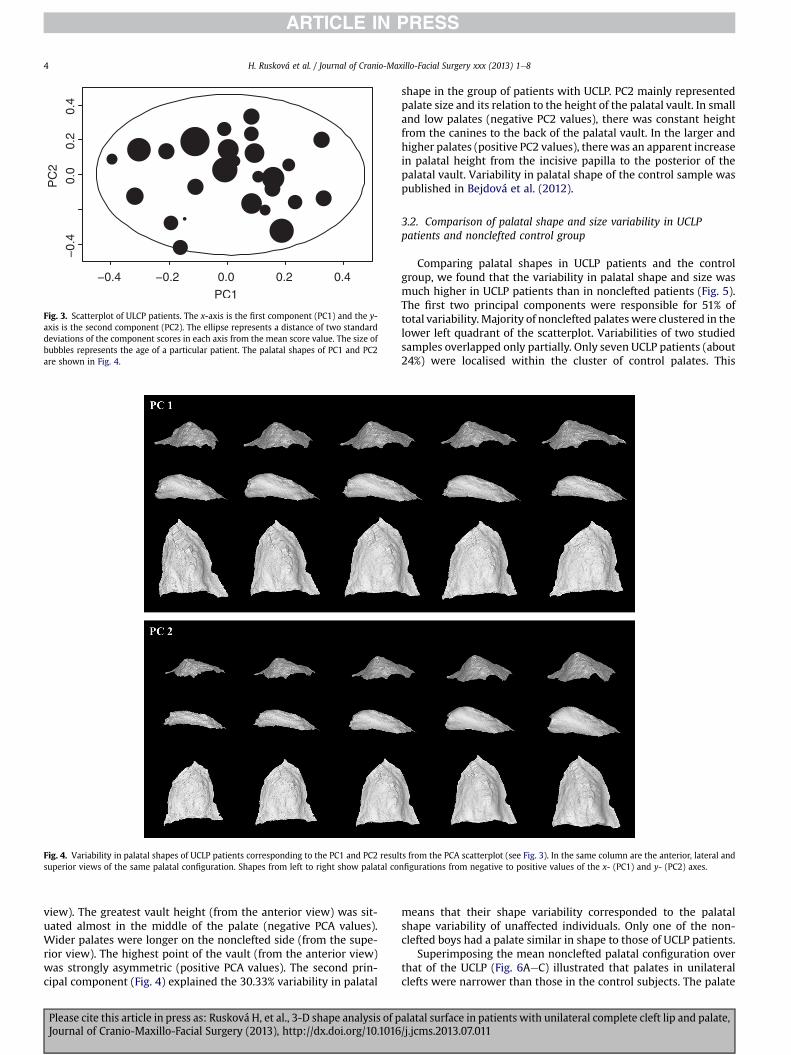
Fig. 3. Scatterplot of ULCP patients. The x-axis is the first component (PC1) and the y-axis is the second component (PC2). The ellipse represents a distance of two standarddeviations of the component scores in each axis from the mean score value. The size ofbubbles represents the age of a particular patient. The palatal shapes of PC1 and PC2are shown in Fig. 4.
Fig. 4. Variability in palatal shapes of UCLP patients corresponding to the PC1 and PC2 results from the PCA scatterplot (see Fig. 3). In the same column are the anterior, lateral andsuperior views of the same palatal configuration. Shapes from left to right show palatal configurations from negative to positive values of the x- (PC1) and y- (PC2) axes.
H. Rusková et al. / Journal of Cranio-Maxillo-Facial Surgery xxx (2013) 1e84
view). The greatest vault height (from the anterior view) was sit-uated almost in the middle of the palate (negative PCA values).Wider palates were longer on the nonclefted side (from the supe-rior view). The highest point of the vault (from the anterior view)was strongly asymmetric (positive PCA values). The second prin-cipal component (Fig. 4) explained the 30.33% variability in palatal
Please cite this article in press as: Rusková H, et al., 3-D shape analysis of pJournal of Cranio-Maxillo-Facial Surgery (2013), http://dx.doi.org/10.1016
shape in the group of patients with UCLP. PC2 mainly representedpalate size and its relation to the height of the palatal vault. In smalland low palates (negative PC2 values), there was constant heightfrom the canines to the back of the palatal vault. In the larger andhigher palates (positive PC2 values), therewas an apparent increasein palatal height from the incisive papilla to the posterior of thepalatal vault. Variability in palatal shape of the control sample waspublished in Bejdová et al. (2012).
3.2. Comparison of palatal shape and size variability in UCLPpatients and nonclefted control group
Comparing palatal shapes in UCLP patients and the controlgroup, we found that the variability in palatal shape and size wasmuch higher in UCLP patients than in nonclefted patients (Fig. 5).The first two principal components were responsible for 51% oftotal variability. Majority of nonclefted palates were clustered in thelower left quadrant of the scatterplot. Variabilities of two studiedsamples overlapped only partially. Only seven UCLP patients (about24%) were localised within the cluster of control palates. This
means that their shape variability corresponded to the palatalshape variability of unaffected individuals. Only one of the non-clefted boys had a palate similar in shape to those of UCLP patients.
Superimposing the mean nonclefted palatal configuration overthat of the UCLP (Fig. 6AeC) illustrated that palates in unilateralclefts were narrower than those in the control subjects. The palate
alatal surface in patients with unilateral complete cleft lip and palate,/j.jcms.2013.07.011

Fig. 5. PCA scatterplot of control population and ULCP patients together. The x-axis isthe first component (PC1) and the y-axis is the second component (PC2). The ellipserepresents a distance of two standard deviations of the component scores in each axisfrom the nonclefted mean score. The size of bubbles represents the age of an individualpatient.
Fig. 6. Mean palatal shape comparison. Figures on the left (A, B, C) compare the mean control palatal configuration with the clefted palatal configuration from anterior (A), lateral(B) and superior views (C). The mean nonclefted palatal shape is grey, and it is overlapped by the mean clefted palatal shape, which is green. Figures on the right (D, E, F) show thesize differences mapped into the mean affected configuration (anterior, lateral and superior views). Blue and turquoise areas are locations that illustrate the size reductions of thepalatal surface of UCLP patients compared with control. Red and pink areas illustrate the greatest positive size difference of the palatal surface.
H. Rusková et al. / Journal of Cranio-Maxillo-Facial Surgery xxx (2013) 1e8 5
was narrower throughout its whole extent, more anteriorly thanposteriorly. The height of the vault of control palates was ratherconstant in their posterior half. The height of the vault of the cleftedpalates was less, reaching maximum more posteriorly than incontrol palates, and then decreased again to the posterior palatalboundary (Fig. 6B). The palate as a whole was less vaulted than incontrols (Fig. 6A); the only exception was the anterior part on theclefted side where the palate was more vaulted than in controls.The palate was considerably asymmetrical. Noteworthy was the
Please cite this article in press as: Rusková H, et al., 3-D shape analysis of pJournal of Cranio-Maxillo-Facial Surgery (2013), http://dx.doi.org/10.1016
finding that the point on the incisive papilla lays more inferiorly inUCLP patients than in controls.
The results of FESA are shown in Fig. 6DeF. The coloured mapcovering the palatal surface informs about size differences betweenthe average left-side clefted palate and nonclefted palate. Thegreatest positive size differences (pink), which exceed 1.0 in cleftedpalates, were situated at scars and in the posterior region of palate(Fig. 6F). In these locations, the biggest size differences were foundbetween the UCLP palates and controls. The prevailing light-bluecolour illustrates the maximum size reductions in the clefted pal-ate surface compared with the average control palate. Distributionof the blue colour was uniform, with a slight predominance on theclefted side. The anterior pink area (on the clefted side) corre-sponds to themaximum height of the anterior palatal vault in UCLP.The red area in the third quarter of the posterior palatal vaultcorresponds to the highest point of its region (Fig. 6D, F). In otherwords, these results graphically illustrate the asymmetrical shapeof the average, unilateral, left-side clefted palate. This asymmetrychanges from clefted to nonclefted side throughout the palate isclearly visible in Fig. 4.
4. Discussion
In general, cleft palate may develop because of hypoplasticgrowth of the palatal segments, failure of the palate to elevateabove the tongue, excessively wide head and other reasons.
The aetiology of abnormal palatal morphology in orofacial cleftsmay thus be multifactorial (Ross, 1987). It is possible to distinguishintrinsic developmental deficiencies (Dahl, 1970; Yoshida et al.,1992; Lo et al., 2003; Ye et al., 2012), iatrogenic factors
alatal surface in patients with unilateral complete cleft lip and palate,/j.jcms.2013.07.011

H. Rusková et al. / Journal of Cranio-Maxillo-Facial Surgery xxx (2013) 1e86
introduced by treatment (Bishara et al., 1976; Fudalej et al., 2012)and functional distortions affecting the position and growth of bothnormal and pathological parts (Joos, 1995; Moss, 1997; Gorlin et al.,2001). In the literature, many differences in opinion regarding therelative importance of each factor exist (Capelozza Filho et al., 1996;Bugaighis et al., 2010; Xu et al., 2012). The question whether hy-poplasia is the cause or the effect of other factors (Lo et al., 2003)might be answered by analysing operated and nonoperated pa-tients with orofacial clefts. Such an analysis was made by Ye et al.(2012), who were inclined to believe that an intrinsic tissue defi-ciency in the palate/maxilla of unilateral, complete cleft lip andpalate patients exists.
As we investigated palatal shape in 11.8e17.2-year-old boys, wefound that the influence of intrinsic and iatrogenic factors was notpossible to distinguish. Palatoplasty was supposed to have a crucialinfluence (Von den Hoff et al., 2006; Saperstein et al., 2012; Xuet al., 2012), but the results of Berkowitz et al. (2005) confirmedthat delaying cleft surgery until 5 years of age and older does notnecessarily maximise palatal growth and that more than one goodtype of palatal surgery is suitable (Fudalej et al., 2012). Surgery bypushback with two flaps and pharyngeal flap was performed inpatients of our sample. The palatal shape of these UCLP patientswas different in terms of both average value and variabilitycompared with controls.
The UCLP patients included in the present study had undergonepalatoplasty with pharyngeal flap surgery. Ross (1987) has reportedthat the palatoplasty disturbs the antero-posterior growth andposition of the upper jaw. The influence of the pharyngeal flapsurgery has been investigated by Semb and Shaw (1990). Theseauthors have compared the skeletal pattern between the childrenwith cleft lip and palate with and without a pharyngeal flap. Post-operative measures failed to identify any important differences ingrowth after pharyngeal flap, suggesting that the superiorly basedpharyngeal flap brings no systematic risk of interference withsubsequent facial growth (Semb and Shaw, 1990).
A rapid reduction of palatal width was found after palatoplasty,which patients undergo from 3 to 6 years of age (Peterka et al.,1980). Width reduction between the canines appears at age 5(but significant values were only from 12 to 19 years), whereasreduction between second molars was not found (Peterka et al.,1980; Athanasiou et al., 1988). Shorter arch length from the inci-sive papilla to the maxillary tuberosity throughout the evaluatedperiod has been described (Peterka et al., 1980). Our results were inaccordance with these studies, although different geometricmorphometric methodology was used.
Using 3-D measurements, Okazaki et al. (1991), Kilpeläinen andLaine-Alava (1996) and Bugaighis et al. (2010) found that, afterpalatoplasty, the palate is shallower, narrower, shorter and moreasymmetrical than controls. These facts were supported by ouraverage results, too. The palate as a whole was lower than in con-trols (Kilpeläinen and Laine-Alava, 1996; �Smahel et al., 2004), andthe highest point of the palate was situatedmore posteriorly in cleftsubjects compared with controls (Kilpeläinen et al., 1996), which isalso in agreement with our results.
The palatal surface area was significantly more reduced in theUCLP group than in the noncleft control group (Berkowitz et al.,2005; Ye et al., 2012). Palatal surface area appears to be more reli-able than palatal volume in assessing growth modification (Primo�zi�cet al., 2012). As a consequence of surface decrease, less space for thetongue in UCLP patients influences the quality of speech (Okazakiet al., 1991; Brunner et al., 2009; Hamtilová, 2011). The relevanceof hard palate morphology to the development of speech should beconfirmed by further research (Schliephake et al., 2006).
Studies evaluating the palate after palatoplasty in patients withcomplete cleft lip and palate have dealt with its asymmetry. The
Please cite this article in press as: Rusková H, et al., 3-D shape analysis of pJournal of Cranio-Maxillo-Facial Surgery (2013), http://dx.doi.org/10.1016
average UCLP palate of our samplewas characterised by asymmetryof the palatal vault, which was apparent especially using the FESAmethod. Colour-coded maps provide insight into the amount andlocalization of facial asymmetry and a solid basis for diagnostic andtherapeutic purposes (Djordjevic et al., 2012). Themaximumheightof the anterior palatal vault was on the clefted side, whereas in theposterior part, it was on the nonclefted side, which is in accordancewith �Smahel et al. (2004). In the Schliephake et al. (2006) study,asymmetry of the anterior portion of the palate in UCLP patientswas greater compared with the molar area. This fact is also inagreement with our results. With age, this asymmetry wasincreased (Schliephake et al., 2006). Evaluation of facial asymmetryin the nasolabial region was found in many studies (e.g., Ras et al.,1994; Bilwatsch et al., 2006; Djordjevic et al., 2013), but it repre-sented only a small part of the variance among the control and cleftgroups (Bugaighis et al., 2010).
Using DCA, we computed average surface models and obtainednew information about the slope and position of the praemaxilla.Superimposing the mean nonclefted palatal configuration on thatof the clefted palate showed that the front of the UCLP palate(praemaxilla) was inferior to the mean control palate. This meansthat the incisive papilla lay most inferiorly on the plane of the UCLPpalate and that the slope of this plane was more inclined than thatof the control group. The same trend was also observed in BCLPpatients (Bejdová et al., 2012).
Using interactive MorphoStudio software, evaluation of vari-ability of the palatal surface was possible. As the age range of UCLPpatients in our sample was broad (11.8e17.2 years), we have toexclude the fact that the form of the palate was influenced by age.No significant correlation between age and palatal formwas found,which is in accordance with the results of our previous study(Bejdová et al., 2012).
The variability in UCLP patients was much higher compared withthe more homogenous control group. Our results are comparablewith the study of Bejdová et al. (2012), which exhibited the sametrend. This result was also in accordancewith the results of the Singhet al. (2007) and Bugaighis et al. (2010) studies. In these, a largervariability in the shape of the face in UCLP patients was observed.
Although our surgical method was always the same, the shapeof the palate became altered in different ways. One explanation forthis could be that the growth potential was under individual ge-netic control and subsequent orthodontic treatment was differentin each patient (�Smahel and Brejcha, 1983; Honda et al., 2002;Perlyn et al., 2002). According to our results, smaller palates wereshallower (lower growth potential) and larger palates were higherin the posterior part of their vault. More apparent vault asymmetrywas noted in wider palates (patients with greater palatal growth).
Palatal variability of UCLP and nonclefted groups partiallyoverlapped. The palatal morphology of only seven patients wascomparable with standards. One individual from the control grouphad a palate shaped like a clefted palate.
5. Conclusions
1. The average UCLP palate in 15-year-old boys was shallower,narrower, shorter and more asymmetrical compared withcontrols.
2. The maximum height of the anterior palatal vault was on theclefted side, whereas that of the posterior part was on thenonclefted side.
3. Superimposition of the average clefted and control palatalconfiguration showed that the slope of the UCLP palate wasmore inclined compared with that of the control group. Thepraemaxilla of UCLP subjects was therefore situated moreinferiorly.
alatal surface in patients with unilateral complete cleft lip and palate,/j.jcms.2013.07.011
H. Rusková et al. / Journal of Cranio-Maxillo-Facial Surgery xxx (2013) 1e8 7
4. The variability of unilateral clefted and nonclefted palatespartially overlapped.
5. The variability of palatal form in UCLP patients was muchgreater than that observed in the nonclefted population. Thepalatal form of patients in our sample was not correlated withage.
Conflict of interest statementThere were no financial or personal relationships with other
persons or organizations that could inappropriately influence ourwork.
Acknowledgements
This research was supported by Research Grant No.MSM0021620843 and GAUK 309611. We thank Compuscript Ltd.Ireland for the English revision of themanuscript. Authors thank Dr.Renata Peterková and anonymous reviewers who provided veryhelpful comments to improve the manuscript.
References
Athanasiou AE, Mazaheri M, Zarrinnia K: Dental arch dimensions in patients withunilateral cleft lip and palate. Cleft Palate J 25: 139e145, 1988
Bejdová �S, Krají�cek V, Peterka M, Trefný P, Velemínská J: Palatal shape and sizevariability in patients with bilateral complete cleft lip and palate using densesurface model construction and 3-D geometric morphometrics. J CraniomaxillofacSurg 40: 201e208, 2012
Berkowitz S, Duncan R, Evans C, Friede H, Kuijpers-Jagtman AM, Prahl-Anderson B,et al: Timing of cleft palate closure should be based on the ratio of the area ofthe cleft to that of the palatal segments and not on age alone. Plast ReconstrSurg 115: 1483e1499, 2005
Bilwatsch S, Kramer M, Haeusler G, Schuster M, Wurm J, Vairaktaris E, et al:Nasolabial symmetry following TennisoneRandall lip repair: a three-dimensional approach in 10-year-old patients with unilateral clefts of lip,alveolus and palate. J Craniomaxillofac Surg 34: 253e262, 2006
Bishara SE, Krause CJ, Olin WH, Weston D, Ness JV, Felling C: Facial and dentalrelationships of individuals with unoperated clefts of the lip and/or palate. CleftPalate J 13: 238e252, 1976
Brunner J, Fuchs S, Perrier P: On the relationship between palate shape and artic-ulatory behavior. J Acoust Soc Am 125: 3936e3949, 2009
Bugaighis I, O’Higgins P, Tiddeman B, Mattick C, Ali OB, Hobson R: Three-dimensional geometric morphometrics applied to the study of children withcleft lip and/or palate from the North East of England. Eur J Orthod 32: 514e521, 2010
Capelozza Filho L, Normando AD, da Silva Filho OG: Isolated influences of lip andpalate surgery on facial growth: comparison of operated and unoperated maleadults with UCLP. Cleft Palate Craniofac J 33: 51e56, 1996
Dahl E: Craniofacial morphology in congenital clefts of the lip and palate. An X-raycephalometric study of young adult males. Acta Odontol Scand 28: 107e116,1970
Diah E, Lo LJ, Huang CS, Sudjatmiko G, Susanto I, Chen YR: Maxillary growth of adultpatients with unoperated cleft: answers to the debates. J Plast Reconstr AesthetSurg 60: 407e413, 2007
Djordjevic J, Pirttiniemi P, Harila V, Heikkinen T, Toma AM, Zhurov AI, et al: Three-dimensional longitudinal assessment of facial symmetry in adolescents. Eur JOrthod 35: 143e151, 2013
Djordjevic J, Lewis BM, Donaghy CE, Zhurov AI, Knox J, Hunter L, et al: Facial shapeand asymmetry in 5-year-old children with repaired unilateral cleft lip and/orpalate: an exploratory study using laser scanning. Eur J Orthod, http://dx.doi.org/10.1093/ejo/cjs075, published online October 4, 2012
Dürwald J, Dannhauer KH: Vertical development of the cleft segments in infantswith bilateral cleft lip and palate: effect of dentofacial orthopedic and surgicaltreatment on maxillary morphology from birth to the age of 11 months. J OrofacOrthop 68: 183e197, 2007
Enlow DH, Hans MG: Essentials of facial growth. Philadelphia: W.B. Saunders, 1996Fudalej P, Katsaros C, Dudkiewicz Z, Offert B, Piwowar W, Kuijpers M, et al: Dental
arch relationships following palatoplasty for cleft lip and palate repair. J DentRes 91: 47e51, 2012
Gorlin RJ, Cohen MM, Hennekam RCM: Orofacial clefting syndromes: general as-pects. Noncleft palatal anomalies. In: Syndromes of the head and neck, 4th edn.New York: Oxford University Press, 866, 2001
Hamtilová M: Evaluation of the palatal morphology in bilateral cleft lip and palatepatients with palatolaly. Faculty of Science, Charles University in Prague, 2011Thesis
Honda Y, Suzuki A, Nakamura N, Ohishi M: Relationship between primary palatalform and maxillofacial growth in Japanese children with unilateral cleft lip andpalate: infancy to adolescence. Cleft Palate Craniofac J 39: 527e534, 2002
Please cite this article in press as: Rusková H, et al., 3-D shape analysis of pJournal of Cranio-Maxillo-Facial Surgery (2013), http://dx.doi.org/10.1016
Huang CS, Wang WI, Liou EJ, Chen YR, Chen PK, Noordhoff MS: Effects of chelio-plasty on maxillary dental arch development in infants with unilateral com-plete cleft lip and palate. Cleft Palate Craniofac J 39: 513e516, 2002
Huddart AG, Crabb JJ, Newton I: A rapid method of measuring the palatal surfacearea of cleft palate infants. Cleft Palate J 15: 44e48, 1978
Hutton TJ, Buxton BF, Hammond P: Dense surface point distribution models of thehuman face. In: Proceedings IEEE workshop on mathematical methods inbiomedical image analysis (MMBIA 2001), Kauai, Hawaii, USA, 9e10 December2001; 2001, 153e160, 2001
Jelínek R, Peterka M: The role of the mandible in palatal development revisited.Cleft Palate J 14: 211e221, 1977
Jelínek R, Dostál M, Peterka M: Cleft lip and palate in the picture of experiment.Prague: Charles University in Prague, 1983
Joos U: Skeletal growth after muscular reconstruction for cleft lip, alveolus andpalate. Br J Oral Maxillofac Surg 33: 139e144, 1995
Kilpeläinen PVJ, Laine-Alava MT: Palatal asymmetry in cleft palate subjects. CleftPalate Craniofac J 33: 483e488, 1996
Kilpeläinen PVJ, Laine-Alava MT, Lammi S: Palatal morphology and type of clefting.Cleft Palate Craniofac J 33: 477e482, 1996
Kramer GJC, Hoeksma JB, Prahl-Andersen B: Early palatal changes in complete andincomplete cleft lip and/or palate. Acta Anat 144: 202e212, 1992
Krey KF, Börngen J, Dannhauer KH: Three-dimensional analysis of the deciduousdentition of patients with bilateral cleft lip and palate and delayed cleft closure.J Orofac Orthop 70: 237e246, 2009
Kuderová J, Borský J, Cerný M, Müllerová Z, Vohradník M, Hrivnáková J: Care ofpatients with clefts at the department of plastic surgery in Prague. Acta ChirPlast 38: 99e103, 1996
Lo LJ, Wong FH, Chen YR, Lin WY, Ko EWC: Palatal surface area measurement:comparisons among different cleft types. Ann Plast Surg 50: 18e23, 2003
Moss ML: The functional matrix hypothesis revisited. 4. The epigenetic an-tithesis and the resolving synthesis. Am J Orthod Dentofac Orthop 112:410e417, 1997
Mossey PA, Little J, Munger RG, Dixon MJ, ShawWC: Cleft lip and palate. Lancet 374:1773e1785, 2009
Okazaki K, Kato M, Onizuka T: Palate morphology in children with cleft palate withpalatalized articulation. Ann Plast Surg 26: 156e163, 1991
O’Rahilly R, Müller F: Human embryology & teratology. New York: WileyeLiss,1992
Perlyn CA, Brownstein JN, Huebener DV, Marsh JL, Nissen RJ, Pilgram T: Occlusalrelationship in patients with bilateral cleft lip and palate during the mixeddentition stage: does neonatal maxillary arch configuration predetermineoutcome? Cleft Palate Craniofac J 39: 317e321, 2002
Peterka M, Jelínek R: Origin of hydrocortisone induced orofacial clefts in the chickembryo. Cleft Palate J 20: 35e46, 1983
Peterka M, P�enkava J: Growth of the width of the upper dental arch in a sample ofthe Czech population. Cesk Stomatol 75: 44e50, 1975
Peterka M, Müllerová �Z, P�enkava J: Causes of the development of orthodonticanomalies in patients with a total unilateral cleft. Cesk Stomatol 80: 100e109,1980
Primo�zi�c J, Perinetti G, Richmond S, Ovsenik M: Three-dimensional longitudinalevaluation of palatal vault changes in growing subjects. Angle Orthod 82: 632e636, 2012
Ras F, Habets LL, van Ginkel FC, Prahl-Andersen B: Three-dimensional evaluation offacial asymmetry in cleft lip and palate. Cleft Palate Craniofac J 31: 116e121,1994
Ross RB: Treatment variables affecting facial growth in complete unilateral cleft lipand palate. Part 7: an overview of treatment and facial growth. Cleft Palate J 24:71e77, 1987
Saperstein EL, Kennedy DL, Mulliken JB, Padwa BL: Facial growth in children withcomplete cleft of the primary palate and intact secondary palate. J Oral Max-illofac Surg 70: 66e71, 2012
Schliephake H, Donnerstag F, Berten JL, Lönquist N: Palate morphology after uni-lateral and bilateral cleft lip and palate closure. Int J Oral Maxillofac Surg 35:25e30, 2006
Semb G, Shaw WC: Pharyngeal flap and facial growth. Cleft Palate J 27: 217e224,1990
Sillman JH: Dimensional changes of the dental arches: longitudinal study from birthto 25 years. Am J Orthod 50: 824e842, 1964
Singh GD, Thind BS: Effects of the headgear-activator Teuscher appliance in thetreatment of Class II Division 1 malocclusion: a geometric morphometric study.Orthod Craniofac Res 6: 88e95, 2003
Singh GD, McNamara Jr JA, Lozanoff S: Finite-element morphometry of soft tissuemorphology in subjects with untreated Class III malocclusions. Angle Orthod69: 215e224, 1999
Singh GD, Levy-Bercowski D, Yáñez M, Santiago PE: Three-dimensional facialmorphology following surgical repair of unilateral cleft lip and palate in pa-tients after nasoalveolar molding. Orthod Craniofac Res 10: 161e166, 2007
�Smahel Z, Brejcha M: Differences in craniofacial morphology between complete andincomplete unilateral cleft lip and palate in adults. Cleft Palate J 20: 113e127,1983
�Smahel Z, Trefný P, Formánek P, Müllerova Z, Peterka M: Three-dimensionalmorphology of the palate in subjects with unilateral complete cleft lip andpalate at the stage of permanent dentition. Cleft Palate Craniofac J 41: 416e423,2004
Vlastos IM, Koudoumnakis E, Houlakis M, Nasika M, Griva M, Stylogianni E: Cleft lipand palate treatment of 530 children over a decade in a single centre. Int JPediatr Otorhinolaryngol 73: 993e997, 2009
alatal surface in patients with unilateral complete cleft lip and palate,/j.jcms.2013.07.011
H. Rusková et al. / Journal of Cranio-Maxillo-Facial Surgery xxx (2013) 1e88
Von den Hoff J, Maltha JC, Kuijpers-Jagtman AM: Palatal wound healing: the effectsof scarring on growth. In: Berkowitz S (ed.), Cleft lip and palate. Diagnosis andmanagement, 2nd edn. Springer Verlag, 301e313, 2006
Weinberg SM, Naidoo SD, Bardi KM, Brandon CA, Neiswanger K, Resick JM, et al:Face shape of unaffected parents with cleft affected offspring: combining threedimensional surface imaging and geometric morphometrics. Orthod CraniofacRes 12: 271e281, 2009
Xu X, Zheng Q, Lu D, Huang N, Li J, Li S, et al: Timing of palate repair affectinggrowth in complete unilateral cleft lip and palate. J Craniomaxillofac Surg 40:358e362, 2012
Please cite this article in press as: Rusková H, et al., 3-D shape analysis of pJournal of Cranio-Maxillo-Facial Surgery (2013), http://dx.doi.org/10.1016
Ye B, Ruan C, Hu J, Yang Y, Thomas J, Zhang G: A comparative study on the mea-surements of palatal shelf area and gradient for adult patients with unoperatedcleft palate. Cleft Palate Craniofac J 49: 561e565, 2012
Yoshida H, Nakamura A, Michi K, Wang GM, Liu K, Qiu WL: Cephalometric analysisof maxillofacial morphology in unoperated cleft palate patients. Cleft PalateCraniofac J 29: 419e424, 1992
Zelditch ML, Swiderski DL, Sheets DH, Fink WL: Superimposition methods. In:Zelditch ML (ed.), Geometric morphometrics for biologists: a primer. New York:Elsevier Academic Press, 105e128, 2004
alatal surface in patients with unilateral complete cleft lip and palate,/j.jcms.2013.07.011










![4* • Pharingeal grooves/cleft : 4 • [Pharyngeal membrane]](https://static.fdokumen.com/doc/165x107/6334ea00b9085e0bf5093ec7/4-pharingeal-groovescleft-4-pharyngeal-membrane.jpg)









