
Repair of congenital sternal cleft in infants and adolescents
6
1998;66:1151-1154 Ann Thorac Surg Hélio Minamoto, Eduardo de Campos Werebe and Fabio B. Jatene José Ribas M. de Campos, Luiz T.B. Filomeno, Angelo Fernandez, Raul Lopes Ruiz, Repair of congenital sternal cleft in infants and adolescents http://ats.ctsnetjournals.org/cgi/content/full/66/4/1151 on the World Wide Web at: The online version of this article, along with updated information and services, is located Print ISSN: 0003-4975; eISSN: 1552-6259. Southern Thoracic Surgical Association. Copyright © 1998 by The Society of Thoracic Surgeons. is the official journal of The Society of Thoracic Surgeons and the The Annals of Thoracic Surgery by on June 8, 2013 ats.ctsnetjournals.org Downloaded from
-
Upload
independent -
Category
Documents
-
view
5 -
download
0
Transcript of Repair of congenital sternal cleft in infants and adolescents

1998;66:1151-1154 Ann Thorac SurgHélio Minamoto, Eduardo de Campos Werebe and Fabio B. Jatene
José Ribas M. de Campos, Luiz T.B. Filomeno, Angelo Fernandez, Raul Lopes Ruiz, Repair of congenital sternal cleft in infants and adolescents
http://ats.ctsnetjournals.org/cgi/content/full/66/4/1151on the World Wide Web at:
The online version of this article, along with updated information and services, is located
Print ISSN: 0003-4975; eISSN: 1552-6259. Southern Thoracic Surgical Association. Copyright © 1998 by The Society of Thoracic Surgeons.
is the official journal of The Society of Thoracic Surgeons and theThe Annals of Thoracic Surgery
by on June 8, 2013 ats.ctsnetjournals.orgDownloaded from

Repair of Congenital Sternal Cleft in Infants andAdolescentsJose Ribas M. de Campos, MD, Luiz T. B. Filomeno, MD, Angelo Fernandez, MD,Raul Lopes Ruiz, MD, Helio Minamoto, MD, Eduardo de Campos Werebe, MD, andFabio B. Jatene, MDThoracic Division, Hospital das Clınicas, University of Sao Paulo Medical Center, Sao Paulo, Brazil
Background. Clinical and surgical aspects of sternalcleft repair are presented. Primary repair in the neonatalperiod is the best management for this rare condition, butnone of the patients in this report were referred to usduring that period. Autologous repair is suitable forolder patients because it avoids problems related to theimplant of prosthetic materials.
Methods. This article reviews 8 cases of sternal cleft notassociated with ectopia cordis in patients presentingbetween October 1979 and November 1997. Surgicalrepair consisted of three sliding chondrotomies, threeposterior sternal wall repairs, one combination with theRavitch technique for pectus excavatum repair, and oneposterior sternal wall repair associated with total repairof Cantrell’s pentalogy.
Results. All patients who submitted to surgical correc-tion had good aesthetic and structural results. The post-operative period was uneventful except that a subcuta-neous fluid collection developed in 1 patient. The meanhospital stay was 5.8 days. The patients were followed upfrom 4 months to 18 years.
Conclusions. Whether dealing with older children oryoung adults, the technique of reconstructing a newsternum with a posterior periosteal flap from sternal barsand chondral grafts is a simple, quick, inexpensive, andeffective option.
(Ann Thorac Surg 1998;66:1151–4)© 1998 by The Society of Thoracic Surgeons
Since the 1850s, fascination with cleft of the manu-brium has been evident because the heart and great
vessels visibly beat under the skin. This produces analternate protrusion and retraction movement upon res-piration, specifically during coughing or the Valsalvamaneuver. In this challenging anomaly, the underlyingmediastinal structures (heart and great vessels) mayeasily be injured by external trauma. In addition, it is anunpleasant cosmetic deformity and quite alarming to theyoung patient’s family.
Congenital sternal cleft is rare, and hence it is usuallyreported as an isolated case presentation. The first sur-gical correction was reported by Lannelongue in 1888, ascited by Ravitch [1], but the first successful repair waspublished by Burton in 1947 [2]. It is postulated that thesternum has a common origin with the pectoral muscu-lature, which develops from lateral plate mesoderm, andthat isolated sternal clefts arise from a failure in eitherdevelopment or fusion of the mesenchymal elements asshould normally occur by the eighth week of fetal life [3].
At one time this anomaly was erroneously known as“sternal agenesia,” a complete misnomer because thetwo sternal bars exist in these patients but they areunfused. Little is known about its incidence and patho-genesis. No familial, teratogenic, or nutritional factorshave been implicated. As mentioned, most cases are
sporadic [4] and there is only one report of 2 cases in thesame family [5]. Experimentally, Ramirez-Solis and col-leagues [6] in 1993 reported that disruption of the Hoxb-4gene in the mouse led to alterations in their paraxialmesoderm and that one of the animals presented a totalsternal cleft.
This report describes our experience with sternal cleftrepair in 8 patients, stressing the different surgical tech-niques required for each case and presenting anotheroption for selected patients.
Patients and Methods
Between May 1979 and September 1997, 8 patients (6 girlsand women and 2 boys), ages ranging from 1.5 to 19 years(mean, 7.2 years), were treated. Five were asymptomaticand underwent the operation for cosmetic reasons aswell as to shield the unprotected mediastinal structures.Although asymptomatic, the defect in an 11-year-old boywas associated with pectus excavatum. In anotherasymptomatic patient, the defect corresponded toCantrell’s pentalogy. The eighth patient presented withcongenital muscular subaortic stenosis; both cardiac andsternal defects were corrected at the same operation. Thepeculiar midline scar was present in 5 patients (Table 1).
The defect was corrected in 3 patients by slidingchondrotomies [7]. In 3 older patients the same techniquewas also attempted, but the sternal bars did not meet. Wethen decided to create a posterior sternal wall (PSW) with
Accepted for publication April 23, 1998.
Address reprint requests to Dr de Campos, Rua Almirante Soares Dutran. 520, Sao Paulo 05654.000, Brazil (e-mail: [email protected]).
© 1998 by The Society of Thoracic Surgeons 0003-4975/98/$19.00Published by Elsevier Science Inc PII S0003-4975(98)00596-7
by on June 8, 2013 ats.ctsnetjournals.orgDownloaded from
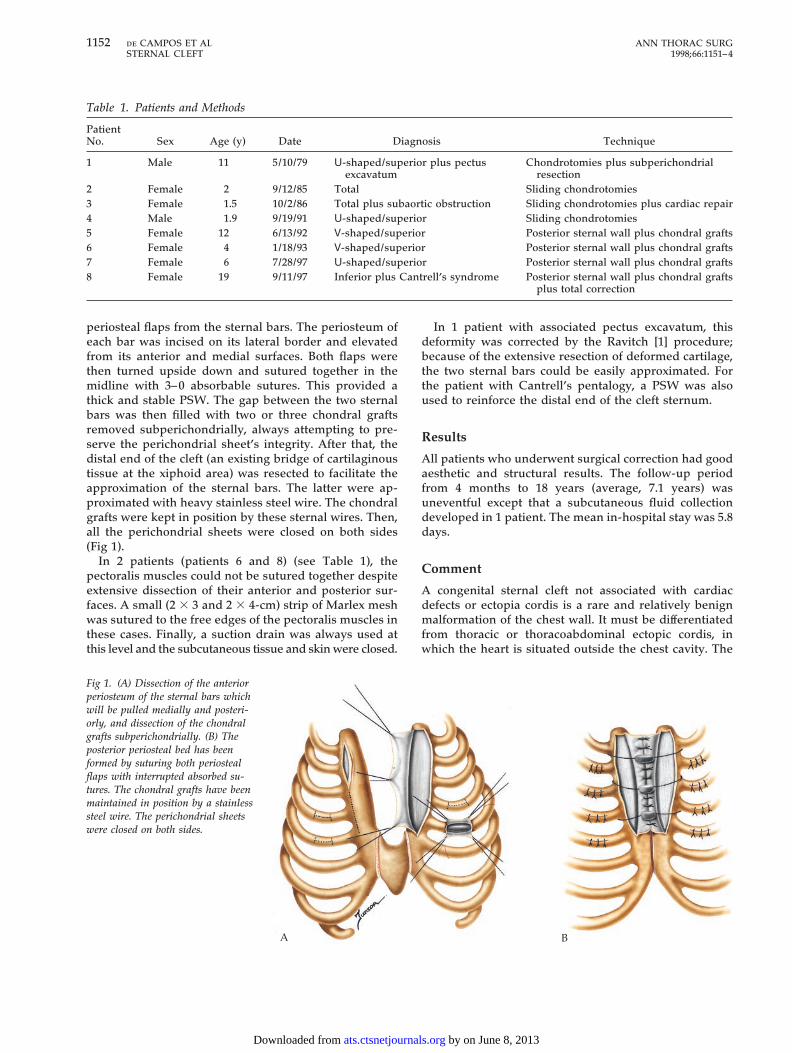
periosteal flaps from the sternal bars. The periosteum ofeach bar was incised on its lateral border and elevatedfrom its anterior and medial surfaces. Both flaps werethen turned upside down and sutured together in themidline with 3–0 absorbable sutures. This provided athick and stable PSW. The gap between the two sternalbars was then filled with two or three chondral graftsremoved subperichondrially, always attempting to pre-serve the perichondrial sheet’s integrity. After that, thedistal end of the cleft (an existing bridge of cartilaginoustissue at the xiphoid area) was resected to facilitate theapproximation of the sternal bars. The latter were ap-proximated with heavy stainless steel wire. The chondralgrafts were kept in position by these sternal wires. Then,all the perichondrial sheets were closed on both sides(Fig 1).
In 2 patients (patients 6 and 8) (see Table 1), thepectoralis muscles could not be sutured together despiteextensive dissection of their anterior and posterior sur-faces. A small (2 3 3 and 2 3 4-cm) strip of Marlex meshwas sutured to the free edges of the pectoralis muscles inthese cases. Finally, a suction drain was always used atthis level and the subcutaneous tissue and skin were closed.
In 1 patient with associated pectus excavatum, thisdeformity was corrected by the Ravitch [1] procedure;because of the extensive resection of deformed cartilage,the two sternal bars could be easily approximated. Forthe patient with Cantrell’s pentalogy, a PSW was alsoused to reinforce the distal end of the cleft sternum.
Results
All patients who underwent surgical correction had goodaesthetic and structural results. The follow-up periodfrom 4 months to 18 years (average, 7.1 years) wasuneventful except that a subcutaneous fluid collectiondeveloped in 1 patient. The mean in-hospital stay was 5.8days.
Comment
A congenital sternal cleft not associated with cardiacdefects or ectopia cordis is a rare and relatively benignmalformation of the chest wall. It must be differentiatedfrom thoracic or thoracoabdominal ectopic cordis, inwhich the heart is situated outside the chest cavity. The
A B
Fig 1. (A) Dissection of the anteriorperiosteum of the sternal bars whichwill be pulled medially and posteri-orly, and dissection of the chondralgrafts subperichondrially. (B) Theposterior periosteal bed has beenformed by suturing both periostealflaps with interrupted absorbed su-tures. The chondral grafts have beenmaintained in position by a stainlesssteel wire. The perichondrial sheetswere closed on both sides.
Table 1. Patients and Methods
PatientNo. Sex Age (y) Date Diagnosis Technique
1 Male 11 5/10/79 U-shaped/superior plus pectusexcavatum
Chondrotomies plus subperichondrialresection
2 Female 2 9/12/85 Total Sliding chondrotomies3 Female 1.5 10/2/86 Total plus subaortic obstruction Sliding chondrotomies plus cardiac repair4 Male 1.9 9/19/91 U-shaped/superior Sliding chondrotomies5 Female 12 6/13/92 V-shaped/superior Posterior sternal wall plus chondral grafts6 Female 4 1/18/93 V-shaped/superior Posterior sternal wall plus chondral grafts7 Female 6 7/28/97 U-shaped/superior Posterior sternal wall plus chondral grafts8 Female 19 9/11/97 Inferior plus Cantrell’s syndrome Posterior sternal wall plus chondral grafts
plus total correction
1152 de CAMPOS ET AL ANN THORAC SURGSTERNAL CLEFT 1998;66:1151–4
by on June 8, 2013 ats.ctsnetjournals.orgDownloaded from

latter two conditions are associated with a high mortalityrate because complex or uncorrectable cardiac anomaliesare also present.
Congenital sternal cleft can be classified as complete orincomplete [8]. A complete cleft is the rarest form andfewer than 10 cases have been reported in the medicalliterature [3, 5]. Incomplete clefts are subdivided intosuperior or inferior ones. The latter may occur as anisolated entity, although it is usually associated withother developmental defects of the anterior chest wallsuch as ectopia cordis, or a combination of defectsinvolving the abdominal wall, sternum, diaphragm, peri-cardium, and heart in Cantrell’s pentalogy. In the incom-plete superior type, a bridge of bony tissue exists at thelower ends of the sternal bars, joining the two edges ofthe cleft in a U shape (proximal to the fourth cartilage) orV shape (reaching the xiphoid process). This is frequentlyan isolated entity [9].
There is no explanation for the marked female predi-lection in our series (2 boys and 6 girls) (see Table 1).However, it is similar to that of Gorlin and colleagues [10]and Heron and colleagues [11], who found the number offemale patients was significantly greater when a sternaldefect was accompanied by a supraumbilical raphe butnot by a facial hemangioma. The unexplained associationbetween cleft sternum and cervicofacial hemangiomas orvascular dysplasias, which has been reported by someauthors in the literature [9, 12], was not confirmed in anyof our patients. According to Firmin and coworkers [3],major defects of the sternum make the chest wall unsta-ble, allowing the thoracic viscera to move paradoxicallyduring respiration. Therefore, some infants could sufferattacks of cyanosis and develop recurrent chest infec-tions. None of our patients suffered such attacks.
A considerable variety of procedures for sternal cleftrepair have been reported in the literature [1, 2, 7, 13–15],but it is an undisputed concept that sternal clefts shouldbe corrected in the neonatal period within the first monthof life [3, 8, 16]. At this stage, the sternal bars can be easilyapproximated by simple sutures, owing to the chest’sflexibility. This also permits approximation of the sternalbars with less danger of cardiac compression.
Nevertheless, patients who have not undergone repairduring this period may require reconstruction later on.The increasing rigidity of the chest wall and the physio-logic accommodation of the thoracic organs to a certaincircumference of the chest determine that simple approx-imation is impossible without seriously compromisingthe heart and lungs. This distinguishes these patientsfrom newborns. One of the earliest successful proceduresfor correction was devised by Sabiston in 1958 [7]. Byusing multiple bilateral sliding chondrotomies he wasable to bring the sternal halves together while simulta-neously increasing chest wall dimensions and flexibility.After that, miscellaneous techniques were developed, eg,split ribs, costal cartilage grafts, and segments of costalmargin; stainless steel wire mesh [1]; segments of carti-lage divided laterally and swung medially to cover thedefect [17]; autogenous periosteal graft raised from thetibia in the lower limb [13]; and perichondral flap eleva-
tion and pectoralis muscle transposition [14]. In previousreports of repair in older patients, the use of prostheticmaterials such as Marlex mesh, Teflon, silicone elas-tomer, or perforated acrylic plate has also been adaptedby different authors [18, 19].
In addition to being effective, our procedure of build-ing a PSW with periosteal flaps raised from the sternalbars, together with the chondral grafts, prepares a natu-ral bed for new bone formation which, despite thereabsorption of the grafts, will provide a genuine bonesternum to protect the mediastinal structures. Our pro-posal lies between two techniques recently published inThe Annals of Thoracic Surgery. Suri and colleagues [20]reported a case of complete sternal cleft in a 25-year-oldman. Successful repair was accomplished using autoge-nous tissue (iliac bone and a V-Y myoplasty of thepectoralis major muscle) with “good cosmetic results andpreservation of the already existing anatomic and me-chanical sanctity of the thoracic cage, without using anysynthetic material.” Santini and associates [21], in a letterto the Editor regarding this technique, reported a 52-year-old man with a congenital total cleft sternum asso-ciated with an atrial septal defect, a large conoventricularseptal defect, and pulmonary stenosis. This patient wassuccessfully treated by direct approximation of the ster-nal bars. We agree with Santini and associates that repairshould be accomplished by the simplest and least inva-sive procedure. However, direct closure in some casesseems impossible and even dangerous owing to thehemodynamic consequences as already well docu-mented since 1983 [22]. In the same report, Santini andassociates mentioned that surgical management of me-diastinitis complicating cardiac surgical procedures offers“a model of the repair of a complete sternal cleft inadults.” From our point of view, there is no comparison.
Whether dealing with older children or young adults,the rigidity of the chest wall and the lack of new space foraccommodation of the intrathoracic organs must be con-sidered, especially when the defect is too large to beclosed directly. The heart is the least tolerant organ toreduced space inside the thoracic cage. Enlargement ofthe thoracic cage diameter is the main reason for ourdecision to use the PSW, apart from the fact that in oldergroups approximation of the sternal bars is almost phys-ically and anatomically impossible. We also concur withKnox and colleagues [16], who in 1994 stated that“autologous repair with rib grafts can be accomplishedsafely without the use of prosthetic material whichreduces the risk of infectious complications while al-lowing normal growth of the chest wall and providingsufficient strength and rigidity in the neosternum, withexcellent cosmetic results.” In 2 patients, however, smallstrips of Marlex mesh (2 3 3 and 2 3 4 cm) were used,not as a substitute for the chest wall, but as a bridge forthe major pectoralis muscles that could not be sutureddespite wide mobilization.
It was unnecessary in any of our patients to suture thesternohyoid and sternothyroid muscles or to slide theorigins of the sternocleidomastoid medially to “stabilizethe thorax aperture and avoid the tendency toward
1153Ann Thorac Surg de CAMPOS ET AL1998;66:1151–4 STERNAL CLEFT
by on June 8, 2013 ats.ctsnetjournals.orgDownloaded from

herniation of the lungs and pulsation in the neck,” asproposed by Asp and Sulamaa in 1961, modified byDaum and Hecker in 1964 [1], and used by Greenbergand colleagues in 1991 [14]. On the other hand, we agreewith the Greenberg and colleagues and with Salley andStewart [23] regarding the advantages of contact betweenthe cartilaginous tissue of the two sternal bars, as occurswhen the periosteal flaps are raised to facilitate primaryunion. We also concur that mobilization of the pectoralismuscles may further protect the repair site, reducing site,reducing lateral tension of the advanced rib segmentsdue to approximation of the sternal bars.
According to the literature [14, 16, 20] and our opinion,it is always better to avoid the use of prosthetic materials,considering the risks of infection and the inability ofthese inert materials to grow with the patient. Thosetechniques are described to emphasize the feasibility ofthe repair without resorting to the use of a prostheticmaterial, regardless of the patient’s age. Included in thisreport is a computed tomographic scan of patient 6 (seeTable 1) taken 5 years after primary repair of an incom-plete superior cleft sternum. The new sternum is shownprotecting the mediastinal structures (Fig 2).
References
1. Ravitch MM. Congenital deformities of the chest wall andtheir operative correction. Philadelphia: Saunders, 1977:23–5.
2. Burton JF. Method of correction of ectopic cordis: two cases.Arch Surg 1947;54:79–81.
3. Firmin RK, Fragomeni LS, Lenox SC. Complete cleft ster-num. Thorax 1980;35:303–6.
4. Kotzot D, Huk W, Pfeiffer RA. Genetic counseling of cleftsternum. Genet Counsel 1994;5:147–50.
5. Haque KN. Isolated asternia: an independent entity. ClinGenet 1984;25:362–5.
6. Ramirez-Solis AR, Zheng H, Whiting J, Krumlauf R, BradleyA. Hoxb-4 (Hox-2.6) mutant mice show homeototic transfor-mation of a cervical vertebra and defects in the closure of thesternal rudiments. Cell 1993;73:279–94.
7. Sabiston DC. The surgical management of congenital bifidsternum with partial ectopia cordis. J Thorac Surg 1958;35:118–22.
8. Samarrai AR, Charmolockly AM, Attra AA. Complete cleftsternum: classification and surgical repair. Int Surg 1985;70:71–3.
9. Opitz JM. Editorial comment on the paper by Hersh et al.and Kaplan et al. on sternal cleft. Am J Med Genet 1985;21:201–2.
10. Gorlin RJ, Kantaputra P, Aughton DJ, Muluken JB. Markedfemale predilection in some syndromes associated withfacial hemangiomas. Am J Med Genet 1994;52:130–5.
11. Heron D, Lyonnet S, Iserin L, Munnich A, Padovani JP.Sternal cleft: case report and review of a series of ninepatients. Am J Med Genet 1995;59:154–6.
12. Hersh JH, Waterfill LD, Rutledge J, et al. Sternal malforma-tion/vascular dysplasia association. Am J Med Genet 1985;21:177–86.
13. Valla JS, Bechraqui T, Belghith M, Daoud N, Grinda A.Fissure sternale congenitale. Chir Pediatr 1989;30:219–21.
14. Greenberg BM, Becker JM, Pletcher BA. Congenital bifidsternum: repair in early infancy and literature review. PlasticReconstr Surg 1991;88:886–9.
15. Snyder BJ, Robbins RC, Ramos D. Primary repair of com-plete sternal cleft with pectoralis major muscle flaps. AnnThorac Surg 1996;61:984–6.
16. Knox L, Tuggle D, Knott-Craig J. Repair of congenital sternalclefts in adolescence and infancy. J Ped Surg 1994;29:1513–6.
17. Meissner F. Fissura sterni congenita. Zentralbl Chir 1963;48:1832–9.
18. Daoud S, Jacob Y, Lefort G, Mourad H. Corretion de labifidite sternale par une prothese en silastic. Chir Pediatr1980;21:415–7.
19. Krontiris A, Tsironis A. Bifid sternum—successful repair byuse of an acrylic plaque: report of a case. J Int Coll Surg 1964;41:301–7.
20. Suri KR, Sharma KR, Jha NK, Sharma BK. Complete con-genital sternal cleft in an adult: repair by autogenous tissues.Ann Thorac Surg 1996;62:573–5.
21. Santini F, Faggian G, Pessoto R, Mazzucco A. Repair ofcomplete congenital sternal cleft in an adult [Letter]. AnnThorac Surg 1997;63:918–9.
22. Ravitch MM. Disorder of the sternum and the thoracic wall.In: Sabiston DC, Spencer FC, eds. Gibbon’s surgery of thechest, 4th ed. Philadelphia: Saunders, 1983:318–60.
23. Salley RK, Stewart S. Superior sternal cleft: repair in thenewborn. Ann Thorac Surg 1985;39:582–3.
Fig 2. Computed tomographic scan of the chest (patient 6) showingthe “new sternum” protecting the mediastinal structures.
1154 de CAMPOS ET AL ANN THORAC SURGSTERNAL CLEFT 1998;66:1151–4
by on June 8, 2013 ats.ctsnetjournals.orgDownloaded from

1998;66:1151-1154 Ann Thorac SurgHélio Minamoto, Eduardo de Campos Werebe and Fabio B. Jatene
José Ribas M. de Campos, Luiz T.B. Filomeno, Angelo Fernandez, Raul Lopes Ruiz, Repair of congenital sternal cleft in infants and adolescents
& ServicesUpdated Information
http://ats.ctsnetjournals.org/cgi/content/full/66/4/1151including high-resolution figures, can be found at:
References http://ats.ctsnetjournals.org/cgi/content/full/66/4/1151#BIBL
This article cites 21 articles, 5 of which you can access for free at:
Citationshttp://ats.ctsnetjournals.org/cgi/content/full/66/4/1151#otherarticlesThis article has been cited by 7 HighWire-hosted articles:
Permissions & Licensing
[email protected]: orhttp://www.us.elsevierhealth.com/Licensing/permissions.jsp
in its entirety should be submitted to: Requests about reproducing this article in parts (figures, tables) or
Reprints [email protected]
For information about ordering reprints, please email:
by on June 8, 2013 ats.ctsnetjournals.orgDownloaded from







![4* • Pharingeal grooves/cleft : 4 • [Pharyngeal membrane]](https://static.fdokumen.com/doc/165x107/6334ea00b9085e0bf5093ec7/4-pharingeal-groovescleft-4-pharyngeal-membrane.jpg)












