
Congenital Heart Disease and Multimodality Imaging
12
ORIGINAL ARTICLE Original Article Congenital Heart Disease and Multi-modality Imaging Rajesh Puranik, PhD a,b,∗ , Vivek Muthurangu, MD a , David S. Celermajer, PhD b and Andrew M. Taylor, MD a a Cardiovascular Magnetic Resonance Unit, Great Ormond St Hospital, UK b Department of Cardiology, Royal Prince Alfred Hospital, Sydney, Australia The increasing prevalence of adult congenital heart disease (CHD) can be attributed to major improvements in diagno- sis and treatment of children with CHD. Although, echocardiography is the most commonly used imaging modality for diagnosis and follow up of subjects with CHD, the evolution of both cardiovascular magnetic resonance (MR) imaging and computed tomography (CT) does offer new ways to visualise the heart and great vessels. Cardiovascular MR tech- niques such as spin-echo and gradient-echo imaging, velocity-encoded phase-contrast MR and gadolinium-enhanced MR angiography allow comprehensive assessment of cardiac anatomy and function. This provides information about the long-term sequelae of the underlying anatomy, haemodynamic assessment of residual post-operative lesions and complications of surgery. Similarly, the development of spiral and subsequently multi-detector CT enables the acquisi- tion of data during a single breath-hold and during the first pass of a contrast bolus, so that images can be reconstructed in any two-dimensional plane or in three-dimensions. As much of the functional data in CHD patients was traditionally acquired with invasive X-ray angiography, non-invasive alternatives such as cardiovascular MR and CT are desirable. This review evaluates the role of imaging modalities in the management of subjects with CHD, particularly detailing recent developments in imaging techniques as they relate to the various CHD diagnoses commonly encountered in practice. (Heart, Lung and Circulation 2010;19:133–144) © 2010 Published by Elsevier Inc on behalf of Australasian Society of Cardiac and Thoracic Surgeons and the Cardiac Society of Australia and New Zealand. Keywords. Adult congenital heart disease; Cardiovascular magnetic resonance; Computed tomography Epidemiology: The Problem at Hand C ongenital cardiac malformations occur in 6–7 per 1000 live births [1]. Major improvements in the diagno- sis and treatment of congenital heart disease (CHD) have led to increased patient survival, even for the most com- plex of malformations. It is estimated that more than 80% of affected children will survive into adulthood and soon there will be more adults than children with CHD [2]. Recent population-based reports confirm increased prevalence rates for severe CHD (Tetralogy of Fallot, truncus arteriosus, transposition complexes, endocardial cushion defects and univentricular hearts) from between 1985 and 2000, where the numbers of adults and children alive with severe CHD were nearly equal [3]. In this report the prevalence of total CHD and severe CHD in the pop- ulation was 4.09 per 1000 and 0.38 per 1000 respectively. Extrapolation of such data to an Australian sized popu- lation corresponds to approximately 96,000 patients with CHD and 9000 patients with severe CHD [3]. ∗ Corresponding author at: Department of Cardiology, Royal Prince Alfred Hospital, Missenden Rd, Camperdown 2050, Syd- ney, NSW, Australia. Tel.: +61 295156111/+61 411035624; fax: +61 295506262. E-mail address: [email protected] (R. Puranik). Adult physicians are therefore increasingly likely to encounter a range of patients with CHD, who will need ongoing surveillance and often further medical or surgi- cal intervention. The goals in the management of CHD have moved from simply improving survival during child- hood to lifetime management aimed at optimising life expectancy as well as patient quality of life. A key component of the management of these patients is the requirement for serial imaging. There is thus a need to streamline protocols and clinical algorithms in adult CHD in order to better treat the long-term sequelae of congenital heart disease, including late post-operative complications. In this review we discuss the use of echocardiogra- phy, magnetic resonance (MR) and computed tomography (CT) in the diagnosis and management of various CHD conditions, with a particular focus on pathologies more commonly encountered in grown-up CHD (GUCH). Spe- cific techniques which have evolved to optimise image quality and acquisition will be highlighted. Overview of Imaging Techniques Echocardiography remains the most commonly used tool for diagnosis and follow up of patients with CHD. © 2010 Published by Elsevier Inc on behalf of Australasian Society of Cardiac and Thoracic Surgeons and the Cardiac Society of Australia and New Zealand. 1443-9506/04/$36.00 doi:10.1016/j.hlc.2010.01.001
Transcript of Congenital Heart Disease and Multimodality Imaging

OR
IGIN
AL
AR
TIC
LE
Original Article
Congenital Heart Disease and Multi-modalityImaging
Rajesh Puranik, PhD a,b,∗, Vivek Muthurangu, MD a,David S. Celermajer, PhD b and Andrew M. Taylor, MD a
a Cardiovascular Magnetic Resonance Unit, Great Ormond St Hospital, UKb Department of Cardiology, Royal Prince Alfred Hospital, Sydney, Australia
The increasing prevalence of adult congenital heart disease (CHD) can be attributed to major improvements in diagno-sis and treatment of children with CHD. Although, echocardiography is the most commonly used imaging modality fordiagnosis and follow up of subjects with CHD, the evolution of both cardiovascular magnetic resonance (MR) imagingand computed tomography (CT) does offer new ways to visualise the heart and great vessels. Cardiovascular MR tech-niques such as spin-echo and gradient-echo imaging, velocity-encoded phase-contrast MR and gadolinium-enhancedMR angiography allow comprehensive assessment of cardiac anatomy and function. This provides information aboutthe long-term sequelae of the underlying anatomy, haemodynamic assessment of residual post-operative lesions andcomplications of surgery. Similarly, the development of spiral and subsequently multi-detector CT enables the acquisi-tion of data during a single breath-hold and during the first pass of a contrast bolus, so that images can be reconstructediard
K
E
Cslp8s[ptc1atuElC
∗PnfE
©S
n any two-dimensional plane or in three-dimensions. As much of the functional data in CHD patients was traditionallycquired with invasive X-ray angiography, non-invasive alternatives such as cardiovascular MR and CT are desirable. Thiseview evaluates the role of imaging modalities in the management of subjects with CHD, particularly detailing recentevelopments in imaging techniques as they relate to the various CHD diagnoses commonly encountered in practice.
(Heart, Lung and Circulation 2010;19:133–144)© 2010 Published by Elsevier Inc on behalf of Australasian Society of Cardiac and Thoracic Surgeons and the Cardiac
Society of Australia and New Zealand.
eywords. Adult congenital heart disease; Cardiovascular magnetic resonance; Computed tomography
pidemiology: The Problem at Hand
ongenital cardiac malformations occur in 6–7 per 1000live births [1]. Major improvements in the diagno-
is and treatment of congenital heart disease (CHD) haveed to increased patient survival, even for the most com-lex of malformations. It is estimated that more than0% of affected children will survive into adulthood andoon there will be more adults than children with CHD2]. Recent population-based reports confirm increasedrevalence rates for severe CHD (Tetralogy of Fallot,
runcus arteriosus, transposition complexes, endocardialushion defects and univentricular hearts) from between985 and 2000, where the numbers of adults and childrenlive with severe CHD were nearly equal [3]. In this reporthe prevalence of total CHD and severe CHD in the pop-lation was 4.09 per 1000 and 0.38 per 1000 respectively.xtrapolation of such data to an Australian sized popu-
ation corresponds to approximately 96,000 patients withHD and 9000 patients with severe CHD [3].
Corresponding author at: Department of Cardiology, Royalrince Alfred Hospital, Missenden Rd, Camperdown 2050, Syd-ey, NSW, Australia. Tel.: +61 295156111/+61 411035624;
ax: +61 295506262.-mail address: [email protected] (R. Puranik).
Adult physicians are therefore increasingly likely toencounter a range of patients with CHD, who will needongoing surveillance and often further medical or surgi-cal intervention. The goals in the management of CHDhave moved from simply improving survival during child-hood to lifetime management aimed at optimising lifeexpectancy as well as patient quality of life. A keycomponent of the management of these patients is therequirement for serial imaging. There is thus a needto streamline protocols and clinical algorithms in adultCHD in order to better treat the long-term sequelae ofcongenital heart disease, including late post-operativecomplications.
In this review we discuss the use of echocardiogra-phy, magnetic resonance (MR) and computed tomography(CT) in the diagnosis and management of various CHDconditions, with a particular focus on pathologies morecommonly encountered in grown-up CHD (GUCH). Spe-cific techniques which have evolved to optimise imagequality and acquisition will be highlighted.
Overview of Imaging TechniquesEchocardiography remains the most commonly usedtool for diagnosis and follow up of patients with CHD.
2010 Published by Elsevier Inc on behalf of Australasian Society of Cardiac and Thoraciceala
1443-9506/04/$36.00
urgeons and the Cardiac Society of Australia and New Z nd. doi:10.1016/j.hlc.2010.01.001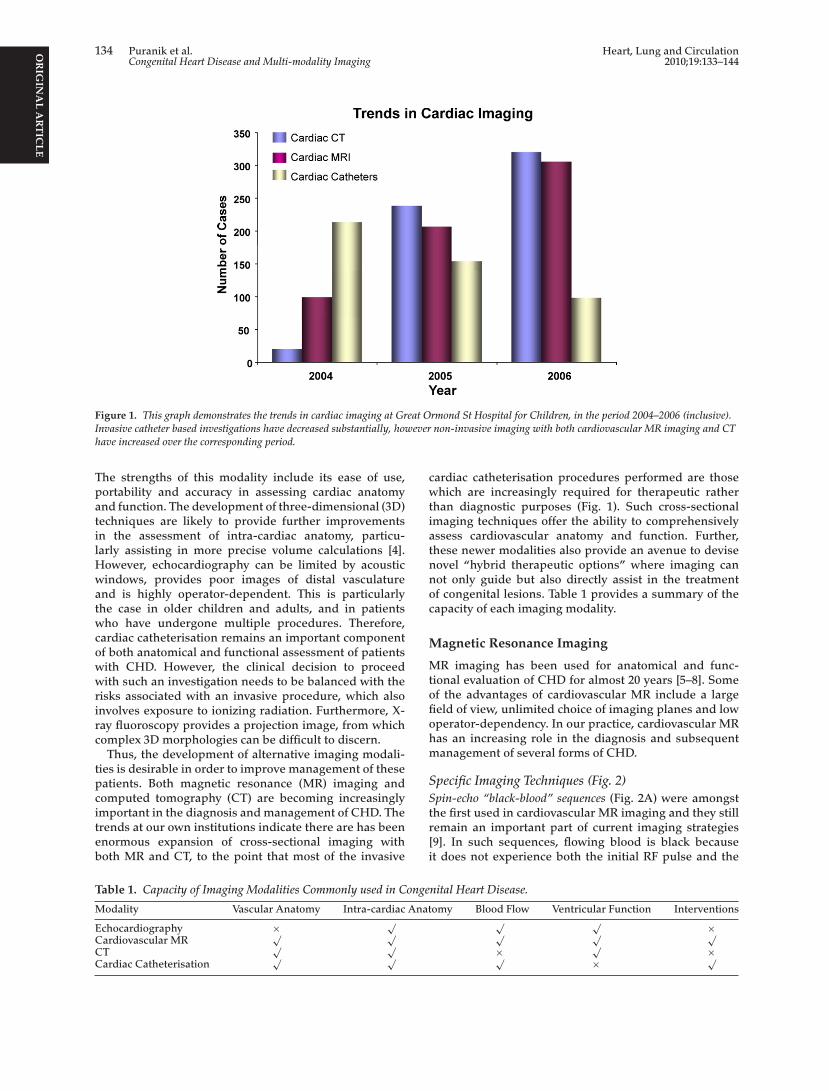
OR
IGIN
AL
AR
TIC
LE
134 Puranik et al. Heart, Lung and CirculationCongenital Heart Disease and Multi-modality Imaging 2010;19:133–144
Figure 1. This graph demonstrates the trends in cardiac imaging at Great Ormond St Hospital for Children, in the period 2004–2006 (inclusive).Invasive catheter based investigations have decreased substantially, however non-invasive imaging with both cardiovascular MR imaging and CThave increased over the corresponding period.
The strengths of this modality include its ease of use,portability and accuracy in assessing cardiac anatomyand function. The development of three-dimensional (3D)techniques are likely to provide further improvementsin the assessment of intra-cardiac anatomy, particu-larly assisting in more precise volume calculations [4].However, echocardiography can be limited by acousticwindows, provides poor images of distal vasculatureand is highly operator-dependent. This is particularlythe case in older children and adults, and in patientswho have undergone multiple procedures. Therefore,cardiac catheterisation remains an important componentof both anatomical and functional assessment of patientswith CHD. However, the clinical decision to proceedwith such an investigation needs to be balanced with therisks associated with an invasive procedure, which alsoinvolves exposure to ionizing radiation. Furthermore, X-ray fluoroscopy provides a projection image, from whichcomplex 3D morphologies can be difficult to discern.
Thus, the development of alternative imaging modali-ties is desirable in order to improve management of thesepatients. Both magnetic resonance (MR) imaging andcomputed tomography (CT) are becoming increasinglyimportant in the diagnosis and management of CHD. Thetrends at our own institutions indicate there are has beenenormous expansion of cross-sectional imaging withboth MR and CT, to the point that most of the invasive
cardiac catheterisation procedures performed are thosewhich are increasingly required for therapeutic ratherthan diagnostic purposes (Fig. 1). Such cross-sectionalimaging techniques offer the ability to comprehensivelyassess cardiovascular anatomy and function. Further,these newer modalities also provide an avenue to devisenovel “hybrid therapeutic options” where imaging cannot only guide but also directly assist in the treatmentof congenital lesions. Table 1 provides a summary of thecapacity of each imaging modality.
Magnetic Resonance Imaging
MR imaging has been used for anatomical and func-tional evaluation of CHD for almost 20 years [5–8]. Someof the advantages of cardiovascular MR include a largefield of view, unlimited choice of imaging planes and lowoperator-dependency. In our practice, cardiovascular MRhas an increasing role in the diagnosis and subsequentmanagement of several forms of CHD.
Specific Imaging Techniques (Fig. 2)Spin-echo “black-blood” sequences (Fig. 2A) were amongstthe first used in cardiovascular MR imaging and they stillremain an important part of current imaging strategies[9]. In such sequences, flowing blood is black becauseit does not experience both the initial RF pulse and the
onge
Anat
Table 1. Capacity of Imaging Modalities Commonly used in C
Modality Vascular Anatomy Intra-cardiac
Echocardiography × √Cardiovascular MR
√ √CT
√ √Cardiac Catheterisation
√ √
nital Heart Disease.
omy Blood Flow Ventricular Function Interventions√ √ ×√ √ √× √ ×√ × √

OR
IGIN
AL
AR
TIC
LEHeart, Lung and Circulation Puranik et al. 135
2010;19:133–144 Congenital Heart Disease and Multi-modality Imaging
Figure 2. (A) Sagittal oblique black-blood image of a patient with severe coarctation of the aorta. Note the excellent delineation of the vessel wallin this black-blood sequence. (B) Transverse oblique 2D steady-state free precession image of a patient with an atrio-ventricular septal defect, atrialisomerism and a total cavo-pulmonary shunt. (C and D) Velocity-encoded phase-contrast image (modulus and phase) of the left ventricular outflowtract in a patient with supravalvular aortic stenosis. Note the high velocity signal (bright white signal) in the phase image at the level of theobstruction. (E) Gadolinium-enhanced MR angiogram of a patient with repaired Tetralogy of Fallot showing severe proximal left pulmonary arterystenosis.
refocusing pulse. This sequence is ideally suited to imag-ing sites of vascular stenosis/obstruction, valvar stenosisand potentially also implanted metallic stents, where therefocusing pulse compensates for increased T2* effects.This is useful as the majority of stents are safe to imagewithin the MRI environment [10]. Despite this potentialto image stents with ‘black-blood’ sequences, our ownpreliminary data suggests that ‘black-blood’ imagesshould be interpreted with caution as they may be falselyreassuring. In our experience, CT imaging is more reliablefor defining intra-stent stenosis and the adjacent anatomy(e.g. aneurysm in close proximity to stents) in this setting.
Gradient-echo imaging (Fig. 2B) has revolutionised car-diovascular MR as it allows dynamic imaging of cardiacanatomy. Gradient sequences have shorter repeat timesand therefore have higher temporal resolution. The fastacquisition enables multiple phases of the cardiac cycle tobe acquired, which can then be reconstructed into a cineMR image representing one full cardiac cycle. Single-slice
two-dimensional (2D) balanced steady-state free preces-sion (b-SSFP) imaging allows qualitative assessment of allcardiac chambers, valvular dysfunction, and dynamic vas-cular anatomy. Multi-slice, 2D b-SSFP imaging is currentlyregarded the best available in vivo method of assessingventricular volumetry [11], as it is not reliant on complexgeometric models.
Velocity-encoded phase-contrast MR (Fig. 2C and D)enables accurate non-invasive blood flow quantificationin major vessels. Cardiac output, pulmonary-to-systemicflow ratio and quantification of gradients across stenosesand valvar regurgitation can all be accurately determinedusing this technique. The quantification of regurgitant vol-ume using this technique has been demonstrated to besuperior to echocardiography [12].
Gadolinium-enhanced MR angiography (Gd-MRA) (Fig. 2E)relies on the T1-shortening effect of dilute gadoliniumto provide high contrast within the vessel lumen and ithas been shown to be useful in delineating thoracic vas-

OR
IGIN
AL
AR
TIC
LE
136 Puranik et al. Heart, Lung and CirculationCongenital Heart Disease and Multi-modality Imaging 2010;19:133–144
Figure 3. Supracardiac total anomalous pulmonary venous drainage. 3D volume-rendered MDCT angiogram viewed from left anterior obliqueshowing a supracardiac total anomalous pulmonary venous drainage. The pulmonary veins (arrow) drain into an ascending vein (triangle) andthen into the brachiocephalic vein (“BCV”) and SVC which drains into the right atrium.
cular anatomy. Gd-MRA is useful in identifying stenoticvessels and correlates well with modalities such as X-ray angiography and surgical findings [13]. It should benoted MRA imaging is not ECG-gated and thus dimen-sions measured from these images represent an average ofdimensions throughout the cardiac cycle. Recently, a syn-drome known as Nephrogenic Systemic Fibrosis has beenidentified following high doses of Gadolinium in patientswith significant renal failure. In those patients withpotential renal problems, an estimated glomerular filtra-tion rate should be calculated and appropriate nationalguidelines followed (www.rcr.ac.uk/docs/radiology/pdf/BFCR0714 Gadolinium NSF guidanceNov07.pdf).
The current guidelines do not recommend that patientswith devices such as pacemakers or defibrillators bescanned with MR imaging.
Computed Tomography
Although MR of the heart and great vessels is often usedin the assessment of CHD, both in grown-up cases andmore recently in neonates, infants and younger children[14], multi-detector computed tomography (MDCT) withits increasing availability and utility is now becomingestablished as a further method of imaging CHD. Thedevelopment of spiral [15,16] and subsequently MDCT[17,18] enables the acquisition of data during a single
acquire a spiral of data of the body (somewhat analogousto an apple core). Increasing the number of detectors used,increases the thickness of data that can be acquired perrevolution of the CT gantry, reducing the total acquisi-tion time without reducing the overall resolution of theimage acquired. For a 16-slice MDCT with 0.75 mm beamcollimation and a table feed of 15 mm/rotation, a data setthrough the thorax of a neonate can be acquired in 3–6 s,and even less for a 64-slice scanner. In order that the vas-cular structures are visualised, iodinated contrast must beadministered – in effect all images are CT angiograms.
Triggering of the MDCT acquisition is crucial, andshould coincide with the peak contrast enhancement inthe vascular region of interest. MDCT can be triggeredeither automatically or by the CT operator. For both meth-ods, an optimal axial slice is defined at the level of theascending aorta for aortic pathology, pulmonary trunkfor pulmonary artery pathology, or left atrium for pul-monary venous pathology. To reduce radiation exposurea tube current of between 15 and 27 mA at 100 kV isused for the majority of neonates and infants; also theanatomical coverage is limited to the thorax (thoracicinlet to the diaphragm), and no pre-contrast images areobtained. For children older than 6 years of age, MDCTcan usually be performed without sedation; feed andwrap techniques can be used for neonates; and sedationcan be used for infants. General anaesthesia is generally
breath-hold and during the first pass of a contrast bolus, sothat images can be reconstructed in any two-dimensionalplane or in 3D (Fig. 3A and B)
MDCT Imaging Techniques“Slip-ring” technology allows the CT gantry to rotatesmoothly with many revolutions per second. When thisis combined with motion of the CT table the effect is to
only required after failure of sedation or in critically ill,intubated patients. In awake children and those imagedunder general anaesthesia, imaging is performed duringa breath-hold at end-expiration.
Images are acquired with an axial spiral volume, andreformatted in sagittal, coronal and oblique planes. 3Dvolume-rendered images can be created for the major-ity of subjects. MDCT scanning will undoubtedly become

OR
IGIN
AL
AR
TIC
LEHeart, Lung and Circulation Puranik et al. 137
2010;19:133–144 Congenital Heart Disease and Multi-modality Imaging
Figure 4. CT image demonstrating tracheal compression from acomplete vascular ring – double aortic arch. The oesophagus(diamond), right aortic arch (white arrow) and left aortic arch (blackarrow) are shown.
more rapid, with installation of 64-slice and 256-slicescanners. This will enable even faster data acquisition,improving spatial and temporal resolution. Also, ECG-gated images of cardiac anatomy will be feasible even athigh heart rates. The assessment of cardiac function willthen be routinely possible. Furthermore, such equipmentwill facilitate accurate non-invasive assessment of coro-nary artery disease
In our own practice, we currently use MDCT for thefollowing indications in patients with CHD.
• Aortic pathology, in particular aortic arch vascular rings(+airways imaging) (Fig. 4).
• Pulmonary artery anatomy (only if no functional infor-mation is required).
• Post-operative systemic to pulmonary shunts – size andpatency.
• Pulmonary venous anatomy – total and partial anoma-lous pulmonary venous drainage [15] (Fig. 3).
• Vascular stent imaging (Fig. 5).• Contraindication to MR imaging – permanent pace-
maker, defibrillators, cerebral aneurysm clips, etc.
MR Versus MDCT
A major advantage of the recent advances in CT technol-ogy over MR is the very rapid acquisition time. Imagingcan now be performed in a comfortable single breath-holdagrliis
tion or vascular flow (e.g. pulmonary incompetence) isrequired, cardiovascular MR scanning is performed undergeneral anaesthesia. For subjects older than 7 years of age,and no contraindications, we will perform MR imagingin the first instance. If there are contraindications to MRimaging (permanent pacemaker, cerebral aneurysm clipsetc.) or when stent imaging is necessary (metal artefact onMR imaging), we will perform cardiovascular MDCT.
There are two main disadvantages of MDCT com-pared with MR imaging. The first is the use of ionizingradiation. This can be kept to a minimum, by usinglow kV, low mA acquisitions, with current modulation,and image acquisition over the minimal area of interest.Using such protocols, our mean dose for non-cardiac-gated cardiovascular MDCT in children is 1.2 ± 0.57 mSv.This equates to approximately 60 chest radiographs (stan-dard PA chest radiograph = 0.02 mSv) or 6 months ofbackground radiation exposure (UK average backgroundradiation = 2.2 mSv per year) [19] [1]. Furthermore, in criti-cally ill patients the ability to perform a rapid examinationwithout the need for general anaesthesia or even sedationmay be more crucial, as the risk of prolonged sedationmay be greater than that of radiation [18]. The seconddisadvantage of current MDCT techniques is that easyquantification of cardiac function (at high heart rates) andarterial flow are not possible especially when comparedwith cardiac-gated MR imaging.
wfci[
SC
AA
mwptpa
batitat
aiorc[
t the peak of the contrast bolus, reducing the need foreneral anaesthesia and sedation in young children. Cur-ently, it is our policy to perform MR imaging in childreness than 7 years of age under general anaesthesia. Thus,n this age group, when anatomical information alones needed, we will perform a MDCT scan (unsedated oredated). However, if quantification of ventricular func-
Importantly, as our GUCH population ages, patientsill become more prone to ischaemic heart disease. In the
uture, MDCT will become increasingly used to assess theoronary arteries, and is arguably the best method to non-nvasively investigate chest pain in this patient population20–22].
pecific CHD Conditions and Imagingonsiderations
cyanotic Heart DefectsTRIAL SEPTAL DEFECT. Atrial septal defects (ASD) are theost common congenital heart defects detected in adults,ith an incidence of 941 per million live births [23]. Theresence of an ASD allows left-to-right shunting, leading
o atrial and ventricular dilatation which can then predis-ose to arrhythmia and volume overload. ASDs are alson independent risk factor for thrombo-embolic stroke.Echocardiography: Complete evaluation is usually possi-
le. Important findings include the presence of right atrialnd right ventricular dilatation. Although the atrial sep-um is best directly visualised from a sub-costal approach,maging is often sub-optimal in adults. Hence, sizing ofhe defect and suitability for device closure (assessingdequacy of margins) is more ideally performed usingrans-oesophageal echo.
Cardiovascular MR: Multi-slice SSFP short-axis imagingccurately quantifies the degree of ventricular overload,nformation which is critical in determining the timingf invasive intervention [11,24]. Quantification of left-to-ight shunts using velocity-encoded phase-contrast MRompares well with invasive catheterisation derived data25]. Pulmonary venous abnormalities which often accom-

OR
IGIN
AL
AR
TIC
LE
138 Puranik et al. Heart, Lung and CirculationCongenital Heart Disease and Multi-modality Imaging 2010;19:133–144
Figure 5. (A) MDCT demonstrating stent fracture at the site of aortic coarctation. (B) Aortic stent fracture shown at high magnification derivedfrom MDCT imaging. (C) Volume-rendered MDCT image demonstrating stent fracture are the site of the previously treated aortic coarctation.
pany sinus venous defects are well defined on Gd-MRA[26] (Fig. 6).
CT evaluation: Role mostly to examine pulmonaryvenous abnormalities if MR not possible.
Cardiac catheterisation: Mostly used if pulmonary hyper-tension is suspected and for percutaneous intervention.
VENTRICULAR SEPTAL DEFECT. Excluding bicuspid aorticvalves, ventricular septal defects (VSD) are the mostcommon CHD defects with an incidence of 3570 permillion live births [23]. The pathophysiology of a VSD isdetermined by the size of the VSD and the pulmonaryvascular resistance. VSDs may be associated with severalother cardiac malformations.
Echocardiography: Accurate and reliable methods ofassessing the ventricular septum are routinely possible.Defect sizing and relationship to cardiac structures canbe determined. Doppler studies aid in the determininghaemodynamic data regarding shunting. Colour flow isable to detect very small defects, often missed clinicallyand on 2D imaging.
Cardiovascular MR: Has the advantage of offering anon-invasive method of quantifying left-to-right shuntsvia velocity-encoded phase-contrast MR, which compareswell with traditional invasive catheterisation methods [25].Multi-slice 2D gradient-echo techniques can be used toassess the dynamic 3D anatomy of the defect. In addi-tion, multi-planar re-formatting of this data can be used
AORTIC PATHOLOGIES. Coarctation accounts for 6–8% of livebirths with CHD and refers to an area of narrowing of thethoracic aorta in the region of insertion of the arterial ductwith or without additional abnormalities of the aortic arch[28]. Detailed serial follow up is mandatory as recoarc-tation occurs in 3–35% of surgically treated patients [14].Added to this is the fact that a third of patients remainor become hypertensive as well as having an increasedlifetime risk of atherosclerosis and end-organ damage.Imaging should also be used to identify other secondarypathologies in these patients, including: assessment forthe presence of dilatation of the ascending or descendingaorta: aortic valve stenosis and regurgitation; and quan-tification of ventricular function and mass.
Aortic dilatation and/or dissection are critical to boththe diagnosis and prognosis of subjects with Marfan syn-drome. MRI provides definitive measurements of aorticdimensions, which are essential for the diagnosis of aorticinvolvement and serial follow up measurements [29].
Echocardiography: Views from the suprasternal notchallow assessment of the severity of aortic arch obstruction(Doppler-derived gradient), size of the transverse aorticarch and branching pattern of the head and neck ves-sels. The distal portion of the ascending aorta is often notwell visualised. Assessment of left ventricular contractil-ity and wall thickness is also an important aspect of theexamination.
to produce image planes that are useful in planning inter-ventional procedures [27]. For example, the relationship ofthe VSD to valvar structures is an important considerationwhen deciding on transcatheter closure (Fig. 2B).
CT evaluation: Limited role.Cardiac catheterisation: Used in evaluation of pulmonary
vascular resistance or transcatheter VSD closure.
Cardiovascular MR: Spin-echo imaging provides excel-lent information of stenotic areas and collateral pathways[30]. 3D Gd-MRA can display the severity and extent ofinvolvement without spin dephasing artifacts and par-tial volume errors [31]. The severity of the stenosis at thelevel of the coarctation can be accurately determined usingMR flow mapping [32,33]. 3D post-processing techniquescan be performed on MRA data allowing abnormalities

OR
IGIN
AL
AR
TIC
LEHeart, Lung and Circulation Puranik et al. 139
2010;19:133–144 Congenital Heart Disease and Multi-modality Imaging
Figure 6. (A) b-SSFP image through a secundum atrial septal defect. Note there is no posterior rim; precluding insertion of an ASD closure device.(B) The dotted line is the plane for through-plane phase-encode velocity flow mapping. (C) Instantaneous flow-against-time curve, through theASD. The total flow through the ASD is 52 ml/beat in a left-to-right direction.
to be viewed from different orientations. Cine imagingof the heart should always accompany these studies, forassessment of left ventricular function/mass and detec-tion of associated intra-cardiac lesions [34]. MR alsoenables the assessment of aortic biophysical properties,such as decreased aortic distensibility and increased flowwave velocity. These parameters have been shown to bepresent prior to overt aortic dilatation in subjects withMarfan syndrome. Finally, black-blood imaging providesthe possibility of imaging aortic stents as the artefactualT2* effects identified on cine gradient-echo imaging arecompensated for by the 180◦ refocusing pulse [35]; how-ever, in our experience, CT is more reliable (see below)(Fig. 7).
CT evaluation: Aortic pathology, in particular aortic archvascular rings are well visualised with CT. The added ben-efit is the possibility of airways imaging on the same study,
especially in cases of suspected compression. There arean increasing number of patients being treated with aor-tic stents for both coarctation [36] and aneurysms [37].Although these metallic implants are safe to image underMR, gradient-echo sequences are prone to field inhomo-geneity effects (T2*) related to the presence of the stent.Hence CT scanning to assess for stent placement andintegrity has an integral role in follow up protocols.
Cardiac catheterisation: Although angiography has beenpreviously regarded as the ‘gold standard’ for the assess-ment of coarctation, both MR and CT are now emergingas commoner, informative methods of assessment.
ANOMALOUS CORONARY ARTERIES. Anomalous coronary arteryorigin and proximal course is a recognised cause ofmyocardial ischaemia and sudden death [38].
Echocardiography: Limited role especially in adult cases.

OR
IGIN
AL
AR
TIC
LE
140 Puranik et al. Heart, Lung and CirculationCongenital Heart Disease and Multi-modality Imaging 2010;19:133–144
Figure 7. MRI of aortic coarctation. Images from various subjects. (A) Black-blood turbo-spin-echo oblique sagittal image through the aortashowing a tight discrete aortic coarctation at the aortic isthmus (arrow). (B) Velocity map images of a more distal moderate coarctation (arrow). (C)Volume-rendered 3D reconstruction of contrast-enhanced MR angiography data in a third subject, showing severe coarctation (arrow) and multiplecollateral vessels.
Cardiovascular MR: Findings from MR angiography cor-relate well and eliminate exposure to X-ray radiation,especially in the assessment of proximal coronary arterycourse [39]. Additionally, cardiovascular MR can also beused to assess myocardial perfusion and infarct size [40],which are powerful predictors of prognosis. However,evaluation of distal coronary course and assessment ofstenoses provide a limitation to the use of MR.
CT evaluation: CT represents the non-invasive methodof choice for the assessment of coronary course and detec-tion of coronary stenoses. This is especially important inthe GUCH population. 3D re-formatting allows apprecia-tion of the relationship of the coronary arteries to adjacentstructures, such as the great vessels.
Cardiac catheterisation: X-ray angiography is regarded asthe ‘gold standard’ for evaluation of anomalous coronaryarteries,
Cyanotic Heart DefectsTETRALOGY OF FALLOT AND PULMONARY ATRESIA. Tetralogy ofFallot (ToF) is the most common cyanotic congenital heartdefect, with an incidence of approximately 420 per mil-lion live births [23]. Mal-alignment of the septum leadsto right ventricular outflow tract (RVOT) obstruction,a sub-aortic VSD with aortic override, and right ven-tricular hypertrophy. Pulmonary atresia, regarded as an
niques, pulmonary regurgitation remains a common latepost-operative complication. The degree of pulmonaryregurgitation determines long-term functional outcomes,risk of arrhythmia and/or sudden cardiac death [43,44].Precise quantifications of RV volumes and function havebecome a key part of treatment protocols [45,46].
Echocardiography: Imaging method of choice prior tosurgical repair, with evaluation of mal-aligned VSD,over-riding aorta, the presence and degree of right ven-tricular outflow tract obstruction (infundibular, valvular,and/or pulmonary arterial stenosis), size and confluence ofbranch pulmonary arteries and detection of associated car-diac malformations. Post-operative complications such asRVOT conduit stenosis are ideally assessed with Doppler-echo, where a Vmax and gradient for the obstruction arepossible. It should be noted that the varied anterior posi-tion of conduits can often make echo views difficult toobtain. The presence of a tricuspid regurgitation jet incombination with the modified Bernoulli equation can beused to estimate the RV and pulmonary artery systolicpressure.
Cardiovascular MR: The main role of MR is in the assess-ment of post-operative complications in ToF. Pulmonaryregurgitation is the most common late post-operativecomplication [47,48]. Current strategies for the manage-ment of severe pulmonary regurgitation include surgicaland transcatheter approaches, which rely on accurate
extreme variant of ToF, is defined as a lack of continuitybetween the RVOT and the central pulmonary arteries,with a variable degree of hypoplasia of these structures.Current management consists of early single-stage recon-structive surgery [41], with staged reconstruction nowreserved for cases with significant hypoplasia of the centralpulmonary arteries [42]. Despite improved surgical tech-
quantification of regurgitation and definition of the RVOTanatomy [49]. 2D spin-echo black-blood and b-SSFPsequences can be used to define RVOT anatomy andquantitatively assess RVOT dilatation or stenosis. Velocity-encoded phase-contrast MR can accurately quantify thedegree of pulmonary regurgitation and can be used tomeasure peak velocities at the level of RVOT obstruc-
OR
IGIN
AL
AR
TIC
LEHeart, Lung and Circulation Puranik et al. 141
2010;19:133–144 Congenital Heart Disease and Multi-modality Imaging
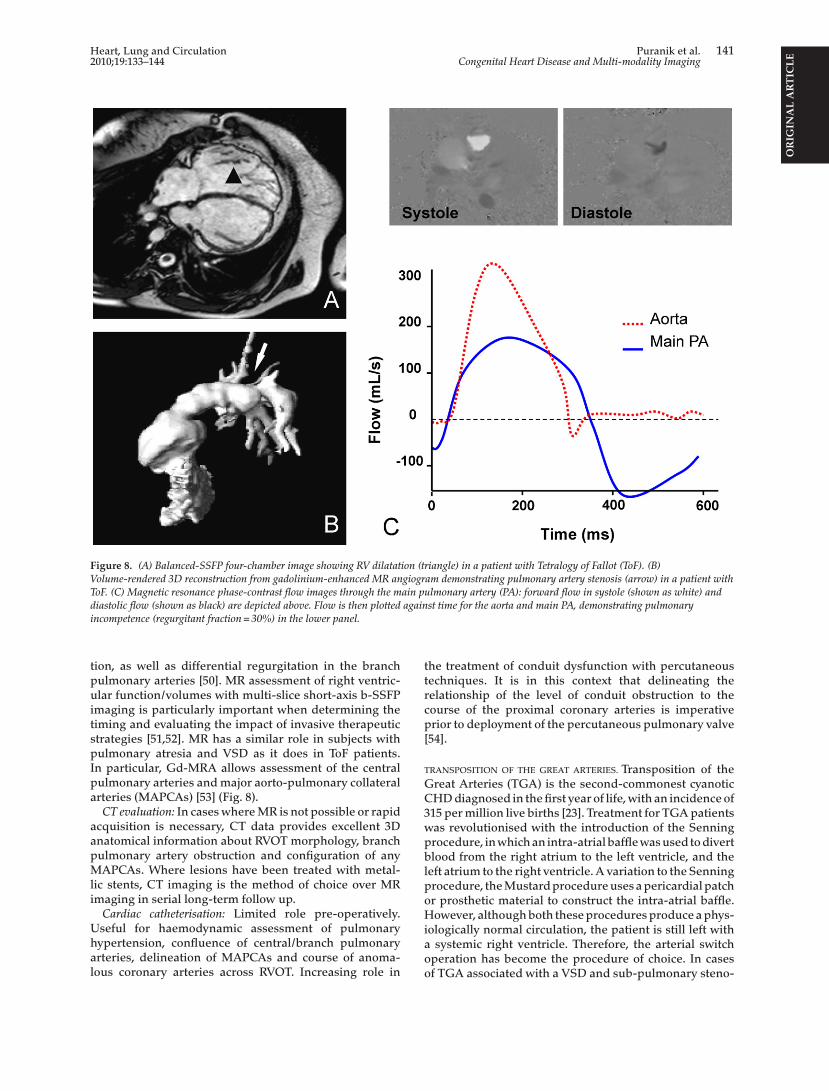
Figure 8. (A) Balanced-SSFP four-chamber image showing RV dilatation (triangle) in a patient with Tetralogy of Fallot (ToF). (B)Volume-rendered 3D reconstruction from gadolinium-enhanced MR angiogram demonstrating pulmonary artery stenosis (arrow) in a patient withToF. (C) Magnetic resonance phase-contrast flow images through the main pulmonary artery (PA): forward flow in systole (shown as white) anddiastolic flow (shown as black) are depicted above. Flow is then plotted against time for the aorta and main PA, demonstrating pulmonaryincompetence (regurgitant fraction = 30%) in the lower panel.
tion, as well as differential regurgitation in the branchpulmonary arteries [50]. MR assessment of right ventric-ular function/volumes with multi-slice short-axis b-SSFPimaging is particularly important when determining thetiming and evaluating the impact of invasive therapeuticstrategies [51,52]. MR has a similar role in subjects withpulmonary atresia and VSD as it does in ToF patients.In particular, Gd-MRA allows assessment of the centralpulmonary arteries and major aorto-pulmonary collateralarteries (MAPCAs) [53] (Fig. 8).
CT evaluation: In cases where MR is not possible or rapidacquisition is necessary, CT data provides excellent 3Danatomical information about RVOT morphology, branchpulmonary artery obstruction and configuration of anyMAPCAs. Where lesions have been treated with metal-lic stents, CT imaging is the method of choice over MRimaging in serial long-term follow up.
Cardiac catheterisation: Limited role pre-operatively.Useful for haemodynamic assessment of pulmonaryhypertension, confluence of central/branch pulmonaryarteries, delineation of MAPCAs and course of anoma-lous coronary arteries across RVOT. Increasing role in
the treatment of conduit dysfunction with percutaneoustechniques. It is in this context that delineating therelationship of the level of conduit obstruction to thecourse of the proximal coronary arteries is imperativeprior to deployment of the percutaneous pulmonary valve[54].
TRANSPOSITION OF THE GREAT ARTERIES. Transposition of theGreat Arteries (TGA) is the second-commonest cyanoticCHD diagnosed in the first year of life, with an incidence of315 per million live births [23]. Treatment for TGA patientswas revolutionised with the introduction of the Senningprocedure, in which an intra-atrial baffle was used to divertblood from the right atrium to the left ventricle, and theleft atrium to the right ventricle. A variation to the Senningprocedure, the Mustard procedure uses a pericardial patchor prosthetic material to construct the intra-atrial baffle.However, although both these procedures produce a phys-iologically normal circulation, the patient is still left witha systemic right ventricle. Therefore, the arterial switchoperation has become the procedure of choice. In casesof TGA associated with a VSD and sub-pulmonary steno-

OR
IGIN
AL
AR
TIC
LE
142 Puranik et al. Heart, Lung and CirculationCongenital Heart Disease and Multi-modality Imaging 2010;19:133–144
Figure 9. Balanced-SSFP images of intra-atrial baffles in a patient who has undergone the atrial switch Senning operation: (A) Baffle takingpulmonary venous blood into the right atrium (arrow), (B) baffles taking systemic venous blood into the left atrium, superior pathway (arrow),inferior pathway (diamond).
sis, the Rastelli procedure (where blood from the LV ischannelled through the VSD to the aorta) is preferred.
Echocardiography: Imaging modality of choice forpre-operative diagnosis and assessment. Importantechocardiographic features include: confirmation ofatrio-ventricular concordance and ventriculo-arterial dis-cordance; adequacy of inter-atrial communication, semi-lunar valve morphology and function; presence of VSDs,exclusion of left ventricular outflow obstruction and aorticcoarctation; patency of arterial duct and pattern of originof coronary arteries.
Cardiovascular MR: As in ToF, the main role of MR isin diagnosis of post-operative complications, particularlythose that develop as the child grows older. MR is notconstrained by the intra-thoracic position of vessels andis ideal for imaging the RVOT and branch pulmonaryarteries, the sites where complications after the arterialswitch procedure are commonly identified [55,56]. Despiteintra-atrial repair being superseded by the arterial switchoperation, there are a significant numbers of patients whohave undergone either a Senning or Mustard operation.As the venous pathways have a complex 3D structurethey may be difficult to accurately assess with echocar-diography. Gd-MRA can completely demonstrate the 3DSenning-Mustard anatomy and detect any luminal nar-rowing [57]. Spin-echo sequences can accurately measurestatic baffle obstruction [58], while 2D and 3D b-SSFP
imaging is of particular importance to patient prognosis(Fig. 9).
CT evaluation: In cases where MR is not possible or rapidacquisition is necessary CT data provides excellent 3Danatomical information about RVOT morphology, branchpulmonary artery obstruction and baffle anatomy. Againwhere metallic stents have been placed, CT provides theideal method of serial assessment.
Cardiac catheterisation: A less common complication ofthe arterial switch procedure is coronary stenoses sec-ondary to the re-implantation procedure. Angiography isthe preferred investigation in this situation.
Conclusion
The recent improvements in non-invasive cross-sectionalcardiovascular imaging modalities (MR and CT) haveresulted in a change in our approach to the assessmentand follow up of patients with CHD. The precise role ofthese imaging modalities will evolve over time. Currently,our own clinical practice is to use echocardiography in allcases of CHD. However, echocardiography can be techni-cally difficult to perform, providing sub-optimal imaging.In these situations we use cardiovascular MR to furtherdefine CHD anatomy and physiology. This is particu-larly important prior to and following corrective surgicaland interventional procedures. Cardiovascular MR is crit-
sequences can delineate dynamic anatomy of intra-atrialbaffles [58]. The combination of Gd-MRA and spin-echosequences has been shown to be superior to echocardio-graphy and compares favourably with conventional X-rayangiography in detecting significant lesions [59]. Velocity-encoded phase-contrast MR can be used to measure peakvelocities at the level of the obstruction and calculate pres-sure gradients. Finally, MR assessment of systemic/rightventricular function with multi-slice short-axis b-SSFP
ical to the non-invasive assessment of ventricular/valvularfunction and blood flow through haemodynamically sig-nificant lesions and shunts. We specifically use MDCT inthe initial diagnostic assessment of great vessel anatomyin young children, especially in circumstances where func-tional information is not required. Finally we use cardiaccatheterisation/angiography if haemodynamic informa-tion is required (pulmonary vascular resistance studies),or if there is a high degree of suspicion of coronary artery

OR
IGIN
AL
AR
TIC
LEHeart, Lung and Circulation Puranik et al. 143
2010;19:133–144 Congenital Heart Disease and Multi-modality Imaging
abnormalities. This approach can improve non-invasivediagnosis and reveal detailed anatomy that is importantfor both clinical decision-making and surgical planning.
Acknowledgements
RP is the Neil Hamilton Fairley NHMRC/NHF of AustraliaOverseas Post-doctoral Fellow and Medical FoundationFellow, University of Sydney. VM is funded by a grantfrom UCL Institute of Child Health. AMT is funded by theHigher Education Funding Council of England (HEFCE).
References
[1] Anderson RH, Baker EJ, Macartney FJ, et al., editors. Paediatriccardiology. 2nd ed. London: Churchill Livingstone; 2002.
[2] Deanfield J, Thaulow E, Warnes C, Webb G, Kolbel F, HoffmanA, Sorenson K, Kaemmer H, Thilen U, Bink-Boelkens M, et al.Management of grown up congenital heart disease. Eur HeartJ 2003;24:1035–84.
[3] Marelli AJ, Mackie AS, Ionescu-Ittu R, Rahme E, Pilote L.Congenital heart disease in the general population: changingprevalence and age distribution. Circulation 2007;115:163–72.
[4] Heusch A, Rubo J, Krogmann ON, Bourgeois M. Vol-umetric analysis of the right ventricle in children withcongenital heart defects: comparison of biplane angiographyand transthoracic 3-dimensional echocardiography. CardiolYoung 1999;9:577–84.
[5] Fellows KE, Hubbard AM. MRI: complacency or ascendancy
[1
[1
[1
[1
[1
[1
[1
dimensional helical computed tomographic angiography inneonates and infants with complex congenital heart disease.Am Heart J 2000;139:654–60.
[17] Lawler LP, Fishman EK. Multi-detector row CT of thoracicdisease with emphasis on 3D volume rendering and CTangiography. Radiographics 2001;21:1257–73.
[18] Siegel MJ. Multiplanar and three-dimensional multi-detectorrow CT of thoracic vessels and airways in the pediatric popu-lation. Radiology 2003;229:641–50.
[19] Allen JK, Hensley WJ, Nicholls AV, Whitfield JB. An enzymicand centrifugal method for estimating high-density lipopro-tein cholesterol. Clin Chem 1979;25:325–7.
[20] Achenbach S, Ropers D, Kuettner A, Flohr T, OhnesorgeB, Bruder H, Theessen H, Karakaya M, Daniel WG, BautzW, et al. Contrast-enhanced coronary artery visualization bydual-source computed tomography—initial experience. Eur JRadiol 2006;57:331–5.
[21] Achenbach S, Ropers D, Pohle FK, Raaz D, von Erffa J, Yil-maz A, Muschiol G, Daniel WG. Detection of coronary arterystenoses using multi-detector CT with 16 × 0.75 collimationand 375 ms rotation. Eur Heart J 2005;26:1978–86.
[22] Mollet NR, Cademartiri F, de Feyter PJ. Non-invasive multi-slice CT coronary imaging. Heart 2005;91:401–7.
[23] Hoffman JI, Kaplan S. The incidence of congenital heart dis-ease. J Am Coll Cardiol 2002;39:1890–900.
[24] Fogel MA, Rychik J. Right ventricular function in congeni-tal heart disease: pressure and volume overload lesions. ProgCardiovasc Dis 1998;40:343–56.
[25] Beerbaum P, Korperich H, Barth P, Esdorn H, Gieseke J,Meyer H. Noninvasive quantification of left-to-right shunt
[2
[2
[2
[2
[3
[3
[3
[3
[3
[3
in the evaluation of congenital heart disease. Pediatr Radiol1999;29:491–5.
[6] Smith HJ. Cardiac MR imaging. Acta Radiol 1999;40:1–22.[7] Didier D, Ratib O, Beghetti M, Oberhaensli I, Friedli B.
Morphologic and functional evaluation of congenital heartdisease by magnetic resonance imaging. J Magn Reson Imag-ing 1999;10:639–55.
[8] de Roos A, Roest AA. Evaluation of congenital heart diseaseby magnetic resonance imaging. Eur Radiol 2000;10:2–6.
[9] Higgins CB, Byrd 3rd BF, Farmer DW, Osaki L, Silverman NH,Cheitlin MD. Magnetic resonance imaging in patients withcongenital heart disease. Circulation 1984;70:851–60.
0] Shellock FG, Shellock VJ. Metallic stents: evaluation of MRimaging safety. AJR Am J Roentgenol 1999;173:543–7.
1] Bellenger NG, Marcus NJ, Rajappan K, Yacoub M, Banner NR,Pennell DJ. Comparison of techniques for the measurementof left ventricular function following cardiac transplantation.J Cardiovasc Magn Reson 2002;4:255–63.
2] Rebergen SA, Chin JG, Ottenkamp J, van der Wall EE, deRoos A. Pulmonary regurgitation in the late postoperativefollow-up of tetralogy of Fallot. Volumetric quantitation bynuclear magnetic resonance velocity mapping. Circulation1993;88:2257–66.
3] Taylor AM, Dymarkowski S, Hamaekers P, Razavi R, Gewil-lig M, Mertens L, Bogaert J. MR coronary angiography andlate-enhancement myocardial MR in children who under-went arterial switch surgery for transposition of great arteries.Radiology 2005;234:542–7.
4] Alam R. Chemokines in allergic inflammation. J Allergy ClinImmunol 1997;99:273–7.
5] Westra SJ, Hill JA, Alejos JC, Galindo A, Boechat MI, LaksH. Three-dimensional helical CT of pulmonary arteries ininfants and children with congenital heart disease. AJR Am JRoentgenol 1999;173:109–15.
6] Kawano T, Ishii M, Takagi J, Maeno Y, Eto G, Sugahara Y,Toshima T, Yasunaga H, Kawara T, Todo K, et al. Three-
in pediatric patients: phase-contrast cine magnetic reso-nance imaging compared with invasive oximetry. Circulation2001;103:2476–82.
6] Puvaneswary M, Leitch J, Chard RB. MRI of partial anoma-lous pulmonary venous return (scimitar syndrome). AustralasRadiol 2003;47:92–3.
7] Miquel ME, Hill DL, Baker EJ, Qureshi SA, Simon RD, KeevilSF, Razavi RS. Three- and four-dimensional reconstructionof intra-cardiac anatomy from two-dimensional magneticresonance images. Int J Cardiovasc Imaging 2003;19:239–54,discussion 255–6.
8] Abu-Soud HM, Hazen SL. Nitric oxide is a physiolog-ical substrate for mammalian peroxidases. J Biol Chem2000;275:37524–32.
9] Kersting-Sommerhoff BA, Sechtem UP, Fisher MR, HigginsCB. MR imaging of congenital anomalies of the aortic arch.AJR Am J Roentgenol 1987;149:9–13.
0] Holmqvist C, Stahlberg F, Hanseus K, Hochbergs P, Sand-strom S, Larsson EM, Laurin S. Collateral flow in coarctationof the aorta with magnetic resonance velocity mapping: corre-lation to morphological imaging of collateral vessels. J MagnReson Imaging 2002;15:39–46.
1] Debatin JF, Hany TF. MR-based assessment of vascular mor-phology and function. Eur Radiol 1998;8:528–39.
2] Mohiaddin RH, Kilner PJ, Rees S, Longmore DB. Magneticresonance volume flow and jet velocity mapping in aorticcoarctation. J Am Coll Cardiol 1993;22:1515–21.
3] Fattori R, Nienaber CA. MRI of acute and chronic aor-tic pathology: pre-operative and postoperative evaluation. JMagn Reson Imaging 1999;10:741–50.
4] Higgins CB, Sakuma H. Heart disease: functional evaluationwith MR imaging. Radiology 1996;199:307–15.
5] Fattori R, Napoli G, Lovato L, Grazia C, Piva T, RocchiG, Angeli E, Di Bartolomeo R, Gavelli G. Descending tho-racic aortic diseases: stent-graft repair. Radiology 2003;229:176–83.

OR
IGIN
AL
AR
TIC
LE
144 Puranik et al. Heart, Lung and CirculationCongenital Heart Disease and Multi-modality Imaging 2010;19:133–144
[36] Hamdan MA, Maheshwari S, Fahey JT, Hellenbrand WE.Endovascular stents for coarctation of the aorta: initialresults and intermediate-term follow-up. J Am Coll Cardiol2001;38:1518–23.
[37] Dake MD, Miller DC, Mitchell RS, Semba CP, Moore KA,Sakai T. The “first generation” of endovascular stent-graftsfor patients with aneurysms of the descending thoracic aorta.J Thorac Cardiovasc Surg 1998;116:689–703, discussion 703–4.
[38] Taylor AJ, Byers JP, Cheitlin MD, Virmani R. Anomalousright or left coronary artery from the contralateral coronarysinus: “high-risk” abnormalities in the initial coronary arterycourse and heterogeneous clinical outcomes. Am Heart J1997;133:428–35.
[39] Taylor AM, Thorne SA, Rubens MB, Jhooti P, Keegan J, Gate-house PD, Wiesmann F, Grothues F, Somerville J, Pennell DJ.Coronary artery imaging in grown up congenital heart dis-ease: complementary role of magnetic resonance and X-raycoronary angiography. Circulation 2000;101:1670–8.
[40] Giorgi B, Dymarkowski S, Rademakers FE, Lebrun F, BogaertJ. Single coronary artery as cause of acute myocardial infarc-tion in a 12-year-old girl: a comprehensive approach with MRimaging. AJR Am J Roentgenol 2002;179:1535–7.
[41] Lillehei CW, Varco RL, Cohen M, Warden HE, Gott VL, DeWallRA, Patton C, Moller JH. The first open heart corrections oftetralogy of Fallot. A 26–31 year follow-up of 106 patients. AnnSurg 1986;204:490–502.
[42] Marshall AC, Love BA, Lang P, Jonas RA, del Nido PJ, MayerJE, Lock JE. Staged repair of tetralogy of Fallot and diminu-tive pulmonary arteries with a fenestrated ventricular septaldefect patch. J Thorac Cardiovasc Surg 2003;126:1427–33.
[
[
[
[
[
[48] Nollert G, Fischlein T, Bouterwek S, Bohmer C, Klinner W,Reichart B. Long-term survival in patients with repair of tetral-ogy of Fallot: 36-year follow-up of 490 survivors of the first yearafter surgical repair. J Am Coll Cardiol 1997;30:1374–83.
[49] Bonhoeffer P, Boudjemline Y, Qureshi SA, Le Bidois J, IserinL, Acar P, Merckx J, Kachaner J, Sidi D. Percutaneous insertionof the pulmonary valve. J Am Coll Cardiol 2002;39:1664–9.
[50] Kang IS, Redington AN, Benson LN, Macgowan C, Valsan-giacomo ER, Roman K, Kellenberger CJ, Yoo SJ. Differentialregurgitation in branch pulmonary arteries after repair oftetralogy of Fallot: a phase-contrast cine magnetic resonancestudy. Circulation 2003;107:2938–43.
[51] Vliegen HW, van Straten A, de Roos A, Roest AA, Schoof PH,Zwinderman AH, Ottenkamp J, van der Wall EE, HazekampMG. Magnetic resonance imaging to assess the hemodynamiceffects of pulmonary valve replacement in adults late afterrepair of tetralogy of Fallot. Circulation 2002;106:1703–7.
[52] Razavi R, Miquel M, Baker E. Diagnosis of hemi-truncus arte-riosis by three-dimensional magnetic resonance angiography.Circulation 2004;109:E15–6.
[53] Geva T, Greil GF, Marshall AC, Landzberg M, Powell AJ.Gadolinium-enhanced 3-dimensional magnetic resonanceangiography of pulmonary blood supply in patients with com-plex pulmonary stenosis or atresia: comparison with X-rayangiography. Circulation 2002;106:473–8.
[54] Khambadkone S, Coats L, Taylor A, Boudjemline Y, Der-rick G, Tsang V, Cooper J, Muthurangu V, Hegde SR,Razavi RS, et al. Percutaneous pulmonary valve implanta-tion in humans: results in 59 consecutive patients. Circulation2005;112:1189–97.
[
[
[
[
[
43] Carvalho JS, Shinebourne EA, Busst C, Rigby ML, RedingtonAN. Exercise capacity after complete repair of tetralogy of Fal-lot: deleterious effects of residual pulmonary regurgitation. BrHeart J 1992;67:470–3.
44] Gatzoulis MA, Elliott JT, Guru V, Siu SC, Warsi MA, Webb GD,Williams WG, Liu P, McLaughlin PR. Right and left ventricularsystolic function late after repair of tetralogy of Fallot. Am JCardiol 2000;86:1352–7.
45] Oosterhof T, van Straten A, Vliegen HW, Meijboom FJ,van Dijk AP, Spijkerboer AM, Bouma BJ, Zwinderman AH,Hazekamp MG, de Roos A, et al. Preoperative thresholdsfor pulmonary valve replacement in patients with correctedtetralogy of Fallot using cardiovascular magnetic resonance.Circulation 2007;116:545–51.
46] Therrien J, Provost Y, Merchant N, Williams W, ColmanJ, Webb G. Optimal timing for pulmonary valve replace-ment in adults after tetralogy of Fallot repair. Am J Cardiol2005;95:779–82.
47] Nollert G, Fischlein T, Bouterwek S, Bohmer C, Dewald O,Kreuzer E, Welz A, Netz H, Klinner W, Reichart B. Long-termresults of total repair of tetralogy of Fallot in adulthood: 35years follow-up in 104 patients corrected at the age of 18 orolder. Thorac Cardiovasc Surg 1997;45:178–81.
55] Haas F, Wottke M, Poppert H, Meisner H. Long-term survivaland functional follow-up in patients after the arterial switchoperation. Ann Thorac Surg 1999;68:1692–7.
56] Gutberlet M, Boeckel T, Hosten N, Vogel M, Kuhne T,Oellinger H, Ehrenstein T, Venz S, Hetzer R, Bein G, et al. Arte-rial switch procedure for D-transposition of the great arteries:quantitative midterm evaluation of hemodynamic changeswith cine MR imaging and phase-shift velocity mapping-initial experience. Radiology 2000;214:467–75.
57] Fogel MA, Hubbard A, Weinberg PM. A simplified approachfor assessment of intracardiac baffles and extracardiacconduits in congenital heart surgery with two- and three-dimensional magnetic resonance imaging. Am Heart J2001;142:1028–36.
58] Sampson C, Kilner PJ, Hirsch R, Rees RS, Somerville J, Under-wood SR. Venoatrial pathways after the Mustard operation fortransposition of the great arteries: anatomic and functionalMR imaging. Radiology 1994;193:211–7.
59] weHardy CE, Helton GJ, Kondo C, Higgins SS, Young NJ,Higgins CB. Usefulness of magnetic resonance imaging forevaluating great-vessel anatomy after arterial switch oper-ation for D-transposition of the great arteries. Am Heart J1994;128:326–32.




















