
Alberta Centre for Child, Family & Community Research (ACCFCR) "There is so much more to a child...
95
Alberta Centre for Child, Family & Community Research (ACCFCR) Rempel, G. (PI), Magill-Evans, J., Wiart, L., Mackie, A., Rinaldi, C., Nicholas, D., Ray, L., Ravindran, V., Alton, G., Heffern, W., Krizan, A., & Palmer, J. (2011-2014). Strengthening family resilience by assessing demands and resources for parents whose children have complex cross-sectoral service needs. ACCFCR Investigator-Driven Research Grant. “There is so much more to a child than their heart” Supports and Services for Children with Complex Congenital Heart Disease and Their Parents FINAL REPORT Photo used with permission http://hlhsbabies.blogspot.ca /
-
Upload
athabascau -
Category
Documents
-
view
0 -
download
0
Transcript of Alberta Centre for Child, Family & Community Research (ACCFCR) "There is so much more to a child...
Alberta Centre for Child, Family & Community Research (ACCFCR)
Rempel, G. (PI), Magill-Evans, J., Wiart, L., Mackie, A., Rinaldi, C., Nicholas, D., Ray, L., Ravindran, V., Alton, G., Heffern, W., Krizan, A., & Palmer, J. (2011-2014). Strengthening family resilience by assessing demands and resources for parents whose children have complex cross-sectoral service needs. ACCFCR Investigator-Driven Research Grant.
“There is so much more to a child than their heart”
Supports and Services for Children with Complex
Congenital Heart Disease and Their Parents FINAL REPORT
Photo used with permission
http://hlhsbabies.blogspot.ca
/

1 Acknowledgments
We extend our appreciation and gratitude to the
wonderful parents and professionals who participated in
the research that informed this report. You have been
generous with your time and patient as you wait for
change.
This ACCFCR-funded study was conducted within G.
Rempel’s Safeguarding the Heart Children research unit.
We thank ACCFCR for the grant and also thank the Faculty
of Nursing (FON) -University of Alberta (U of A), Alberta
Innovates Health Solutions, Stollery Children’s Hospital,
Western Canadian Children’s Heart Network, Heart and
Stroke Foundation of Canada, Mazankowski Alberta Heart
Institute and TD Bank Financial Group for supporting G.
Rempel’s research program at the U of A.
Research Staff and Trainees
The dedication of research staff members Lousia Fricker
and Laura Rogers made this research possible as did the
valuable contributions of trainees – Vinitha Ravindran,
Doctoral student; Tamara Dorfman and Anra Lee, MN
students; Nicole Dahl and Ross Ballantyne, BScN-Honors
students and WCHRI summer students; Health Ulmer,
FON Undergraduate summer student.
Report
Prepared By:
Gwen R. Rempel
PhD, RN
Laura G. Rogers
MScRS, OT(C)
Joyce Magill-
Evans
PhD, OT(C)
Lesley Wiart
PhD, PT
Please direct
questions about
this report to Gwen
Rempel at
gwen.rempel@
ualberta.ca
or call her toll free
1-855-833-5699

i | P a g e
FOREWORD – VOICES FOR CHANGE
Voice of Parent & Advocate for Change
As a parent of a child with HLHS it is incredibly hard to find places where the system could do more for us. Not because all of our needs are being met, but we trip and stumble over our already overwhelming gratitude.
Without the early intervention of the world class medical care that our daughter received we wouldn’t be worried about whether or not she was keeping pace with her reading.
Without the money and resources that were poured into her in the first three years of her life we wouldn’t worry about how she handles sports day. Trust me sports day at a school where no one understands her issues is more stressful than you could imagine.
Without the wonderful follow-up that she receives with her clinic team we’d still be worried about her ticking time bomb of a heart. So now instead we have the luxury of worrying about when we will start to see other delays or difficulties that make her path in this world a little more challenging. We live waiting for the next shoe to drop.
Gwen’s group asked very hard questions. They asked parents to look past their gratitude and thankfulness and to frankly describe the reality of our lives, and our needs.
The problem is that if my child has ADHD the school knows what to do. If my child has a peanut allergy the sports teams know what to do. If my child has asthma the school, sports teams, and doctors all likely know what to do.
When you tell a teacher, coach, or another parent that your child has a complex congenital heart defect they don’t know what to do with it. Often people counter with terror or complacency. People don’t know where to put it or what to do with that information. Above all they focus on the physical. But there is so much more to
a child than their heart.
It is as though I’ve been handed a dot to dot puzzle but there are no numbers on the dots, nothing to guide me in making my connections. I have concerns but I don’t know where to put them. Conventional answers don’t work; trust us we have tried.
As a parent, all I would like is a place within the system where I could take my concerns and the people involved would understand and help me connect the dots. They could provide the missing information so we could guide our daughter through this puzzle of life.
Needing more doesn’t negate our gratefulness. I would just like to see my child not only reach adulthood, but become the beautiful successful adult I know she can be.
Thanks,
Roberta Davis
ii | P a g e
Voice of Researcher/Nurse
As I work in my rural kitchen for healthier food that still pleases the palate, I present a new and improved cookie to my husband. And time and time again his response is:
If it isn’t broken, don’t fix it.
As I work in my urban research office for improved care for families of children with complex congenital heart disease (CHD), a contrary message is before me:
It is broken, and it must be fixed.
What is broken? The interconnected multi-sectoral system that is meant to support parents as they provide long-term complex care for their children with CHD is broken. And this fragmentation is in contrast to the well-functioning system of high technology, life-saving acute care services for children born with life-threatening congenital heart malformations. The irony is that parents repeatedly hear that their child’s heart is fixed, and yet we launch them into a broken system that leaves them feeling stressed, overwhelmed, and guilty that they cannot address the complex needs of their child who has survived so much.
My hope is that through this report, you too will see what needs to be fixed and join me by declaring and responding to:
IF IT IS BROKEN, WE MUST FIX IT
It is time to fix what is broken; what is separated into pieces, what is not working properly, what has been disrupted by change, what has been made weak.
http://jacksonhardy.blogspot.ca/

iii | P a g e
MAIN MESSAGES
Issues
Children with complex CHD:
• have regulatory challenges (sleep, feeding, sensory and behaviour) that require intervention • miss valuable linkages with early intervention and community support due to timing of necessary surgeries • are not being adequately monitored and supported at school age for developmental and learning challenges • experience stress reactions, especially during their third surgery, the Fontan at 2-4 years of age, related to trauma from previous life-saving interventions
Parents of children with complex CHD:
• have lived through traumatic experiences with their child • face their child’s uncertain future • experience significant financial burden with little or inconsistent financial compensation within a funding system that does not understand their needs • are on their own to navigate a complex system that is not prepared for their child’s and family’s needs • do not know how to prepare their child for the Fontan, and are traumatized by their child’s stress reactions
The system
• lacks coordinated community support for the child and their family outside of the inpatient hospital setting
The health care professionals
• who recognize the family’s needs are powerless to secure services for them within the current service and funding structure and definitions • are unable to provide outpatient support beyond medical monitoring and follow-up
Solutions
• A lifespan approach to services to address child and family needs beyond the life-saving surgeries and inpatient environment.
• A coordinated approach to outpatient care including new outpatient roles (nurse practitioner and social worker are top priority) based within the pediatric cardiology clinic at Stollery to provide consultation and develop integrated community services.
• Specialized outpatient interdisciplinary teams who understand the needs of this and other complex medical populations to provide
a. Consultation, treatment, and referrals for specialized needs including medical trauma, sleep, feeding and behavioural issues
b. Service coordination, patient navigation and community education to facilitate access to and expansion of community-based rehabilitation and support services.
c. Parent support and advocacy for all families that is independent of child morbidity.
• A comprehensive plan for addressing the financial needs of these families, for which Family Support for Children with Disabilities has not been adequately meeting.
• Increased support for the well-established Complex Pediatric Therapies Follow-Up program that monitors child outcomes, and extends follow-up beyond the 4-year-old assessment to include school age and adolescent children.
vi | P a g e
EXECUTIVE SUMMARY
The GOOD News! On the Map for Saving Babies
It is an exclusive number of specialty pediatric referral centres that successfully perform life-saving heart surgeries in infants born with congenital heart disease (CHD). Stollery Children’s Hospital, Edmonton, Canada has achieved this status and has been on the world stage for the last decade for saving babies who have the most lethal form of CHD, hypoplastic left heart syndrome (HLHS). These babies often spend their first few months of life in the hospital recovering from their first open heart surgery that occurs soon after they are born. They return for another heart surgery by 6 months of age and then a third surgery, the Fontan, is between 2 and 4 years of age. Parents consistently express gratitude for this life-saving care and their children require life-long specialized care and monitoring through pediatric and adult congenital heart disease programmes. In Alberta these hospital-based outpatient programs exist in Calgary and Edmonton.
Fortunately, pediatric developmental specialists in Alberta have taken the lead to develop a world class Complex Pediatric Therapies Follow-Up program. Nearly all of the children who have heart surgery at Stollery Children’s Hospital, a surgical referral centre for western Canada, are followed from infancy until they are 4 years of age for learning and developmental status. Referrals to community programs are facilitated. Additional services available to families of children with complex needs in Alberta are early intervention, community based education and rehabilitation, and for children classified by Family Support for Children with Disabilities (FSCD) as disabled, financial assistance.
The BAD News! Resources to Support Survival Not Keeping Up
Unfortunately, the extent of support and services that children with HLHS, their parents and other family members require following life-saving surgery has not been appropriately anticipated or developed. The negative results of the gap between needs and services are striking for both the child and the parents. Although the research reported here is based on findings from HLHS families, the findings can be applied to children with many health and developmental concerns; they highlight what is not working in the health and education systems. The system is broken and needs fixing with benefits for many.
Three equally concerning issues have emerged in this rigorous investigation of the needs of parents in relation to their key role of ensuring the ongoing survival and optimal development and learning progress of their child with CHD.
First, the system that saves the baby at an enormous financial cost has not yet provided comprehensive, ongoing support and care for the child within the community and family context; care that comes at a fraction of the cost of the existing life-saving treatment. Second, the celebrated survival of children with complex CHD is being overshadowed by developmental, behavioural, and emotional problems that become increasingly evident as the child undergoes the Fontan operation at 2-4 years of age and then again as they enter the school system. Many of these children require access to specialized educational and rehabilitation services in the early years and into their school years. Third, the emotional cost to parents of safeguarding the survival of their children with complex needs within a multi-sectoral health and education system that has not been prepared for them is profound. The broken system is breaking the parents, and this is
vii | P a g e
putting their children at risk for cumulative behavioural and emotional issues, secondary to their regulatory, developmental and learning problems. Parents require ready access to health care professionals who are “in-the-know” about their child, and can provide proactive assessment and intervention to support their coping and mental health.
The Results are In…
Extensive data were generated over a two–year period from parents of 29 children with HLHS and 38 professionals involved in the care of these children in Calgary (Alberta Children’s Hospital) and Edmonton (Stollery Children’s Hospital, and the Complex Pediatric Therapies Follow-up program). While the parent-participants in this study were mostly educated, middle-class, partnered, and resilient, there was still evidence of extreme struggle as they tried to meet their child’s complex needs. Health care professionals described the parents as being traumatized by their inpatient experiences, and, because of system shortages, they felt powerless to address the parents’ mental health needs. They also emphasized the families’ significant financial hardships.
Findings that need attention from those who can fix the broken system are:
1. Children with complex CHD: • have regulatory challenges (sleep, feeding, sensory and behaviour) that require intervention • miss valuable linkages with early intervention and community support due to timing of necessary surgeries • are not being adequately monitored and supported at school age for developmental and learning challenges • experience stress reactions, especially during their third surgery, the Fontan at 2-4 years of age, related to trauma from previous life-saving interventions
2. Parents of children with complex CHD • have lived through traumatic experiences with their child • face an uncertain future with their child • experience significant financial burden with little or inconsistent financial compensation within a funding system that does not understand their needs • are on their own to navigate a complex system that is not prepared for their child and family needs • do not know how to prepare their child for the Fontan, and are traumatized by their child’s stress reactions
3. The Fontan surgery is a litmus test for the broken system as both the child and parent are ill-prepared for how the surgery impacts them emotionally and practically. The parents’ previous experiences work against them because the system assumes that they can manage when in fact, they have cumulated trauma that emerges alongside their child’s stress reactions.
4. The system lacks coordinated community support for the child and their family outside of the inpatient hospital setting.
5. The health care professionals recognize the child, parent and family needs and are: • powerless to support the families who are an anomaly within the current service and funding structure and definitions • unable to provide outpatient support beyond medical monitoring and follow-up

viii | P a g e
Solutions are Within Reach
Parents and service providers have had a voice in formulating the following solutions:
• A comprehensive approach to life-long services to address the child’s and family’s needs beyond the world recognized life changing surgery and inpatient environment. • A coordinated approach to outpatient care including new outpatient roles (nurse practitioners and social workers are top priority) based within the pediatric cardiology clinics at Stollery. • Specialized outpatient interdisciplinary teams who understand the needs of this and other complex medical populations to provide
a. Consultation, treatment, and referrals for specialized needs including medical trauma, sleep, feeding and behavioural issues
b. Case coordination, patient navigation and community education to facilitate access to and expansion of community-based rehabilitation and support services.
c. Parent support and advocacy for families that is independent of child morbidity. • A comprehensive plan for addressing the financial needs of these families, whose needs are not understood or recognized by the current funding system, FSCD.
• Increased funding for the well-established Complex Pediatric Therapies Follow-Up program that monitors child outcomes to age 4 to extend follow-up to include monitoring of school age and adolescent children and referral as needed.
Next Steps
Service providers and decision makers responsible for the life-saving care of children with complex CHD must initiate changes within the system so that parents are supported emotionally, practically, and financially to care for their child with complex physical, emotional, developmental and learning needs from infancy to their transition to adulthood and adult CHD care. Although a repeated message from health care professionals was that parents needed to be advocating for their needs by lobbying hospital executives and government officials, it is important to be aware that these parents are already burdened. Those who have championed the high profile life-saving pediatric care in Alberta and Western Canada must advocate for increased system awareness of the services needed for the child survivors and their families. As one HCP stated, “The Stollery could be a leader of it [if they] accepted that the whole child needs to be managed in any program that it supports”.
Parents consistently describe clinicians “in-the-know” as their lifelines. Increasing direct care through service coordination/ navigation services at the surgical centre, Stollery Children’s Hospital, is an essential first step. Increased services for children and families through an interdisciplinary outpatient team that also initiates program development along with the community to support children and families is the next crucial step.
As services are refined to better meet the needs of families, research is required to evaluate parent and child-focused interventions to address the regulatory and emotional needs of the children, and the emotional needs of the parents, especially related to pediatric medical trauma and traumatic stress responses. Leading a new area of research in pediatric cardiology has the potential to address parent and child traumatic experiences so that further trauma is prevented.

ix | P a g e
TABLE OF CONTENTS
FOREWORD – VOICES FOR CHANGE .............................................................................................................. i
MAIN MESSAGES .................................................................................................................................................. iii
EXECUTIVE SUMMARY ...................................................................................................................................... vi
CONTEXT .................................................................................................................................................................. 1
Purpose of Current Study .............................................................................................................................. 2
IMPLICATIONS ....................................................................................................................................................... 2
APPROACH ............................................................................................................................................................... 3
RESULTS ................................................................................................................................................................... 4
The Children with HLHS – Who are they? ............................................................................................... 4
The Children with HLHS – How are they doing? .................................................................................. 5
The Children with HLHS: What about trauma? ..................................................................................... 8
The Children with HLHS: What is needed? ............................................................................................. 9
The Parents – Who are they? .................................................................................................................... 10
The Parents – How are they doing? ........................................................................................................ 10
Stress and trauma: “Deer in the headlights” -..................................................................................... 10
Living with persistent uncertainty ......................................................................................................... 14
Living with Financial Burden .................................................................................................................... 15
Lost in the system .......................................................................................................................................... 20
Fontan ................................................................................................................................................................ 21
RECOMMENDATIONS....................................................................................................................................... 23
Overarching recommendations ............................................................................................................... 23
Specific recommendations ......................................................................................................................... 24
EPILOGUE .............................................................................................................................................................. 26
REFERENCES ....................................................................................................................................................... 28
APPENDICES ........................................................................................................................................................ 30

1 | P a g e
CONTEXT
The amazing advances since the first open heart surgeries for children with congenital heart disease (CHD) were successfully performed in the late 1950s have been accompanied by challenges for parents and professionals alike.1 Persistent uncertainty about child outcomes have worried service providers2 and parents as they have struggled to advocate for their child and balance other family demands.3 The “treat your child normally” mantra has prevailed4 but there is increasing evidence that children with surgically-treated congenital heart disease are born with brain abnormalities.5 They have undergone extraordinarily invasive surgical treatment to alter the structure of their heart and require lifelong specialized care and monitoring.
Fortunately, a history of overcoming inevitable barriers has contributed to improved care for children and families. G. Rempel, the principal investigator for this study and the research program Safeguarding the Heart Child, has witnessed such progress. As a nursing student at the University of British Columbia in the early 1980s, she worked with a family whose 5-year old child’s opportunity for surgery was jeopardized because of the surgical risk in the presence of Down syndrome. When this mother asked the pediatric cardiologist what her son would be like at 30 years of age if he did not get surgery the answer was “He won’t be able to walk a block”. Parents pushed for the surgery that closed an “atrial septal defect the size of a quarter” along with “5 stitches to improve the mitral valve” [Personal communication, April 29, 2012]. Health professionals took a risk to operate on Russell and his parents supported his survival and ongoing quality of life. His mother reports that her 36-year old son “has been living on his own in a condo … has worked part-time at Thrifty’s Foods for the past 15 years ... enjoys spending time with his friends and participates in 7 sports with Special Olympics. When he needed an aortic valve replacement in 2005, he decided that a mechanical valve would be best and that managing anticoagulation would be better than having to come back for surgery.”
In the late 1980s when the prenatal diagnosis of CHD was taking hold, Rempel conducted one of the first qualitative studies by interviewing parents whose baby with CHD had been diagnosed antenatally. Women’s accounts of receiving the devastating news of life-threatening CHD while still lying, unclothed on the ultrasound table prompted program changes6 and a further study about decision making.7 Practice guidelines have subsequently been published.8,9 This is an example of supports in the system catching up with technological advances; the system was not ready for these parents but made changes in response to systematic inquiry. These changes in health professional communication influenced interactions beyond the prenatal diagnostic encounter.
In the late 1990s, a frontier in pediatric cardiac care was achieved in Alberta with the successful surgical treatment of children born with one of the most life-threatening forms of CHD, hypoplastic left heart syndrome (HLHS). This three-staged surgical approach had the first surgery occurring a short time after the baby’s birth, the second surgery a few months later, and a third surgery a couple of years later.10 Cardiac surgeries are performed at Stollery Children’s Hospital. Pediatric cardiology services there and at Alberta Children’s Hospital (ACH) provide ongoing care and monitoring. Since 1999, these infants have been enrolled in the Complex Pediatric Therapies Follow-up program (CPTP); they are assessed by an inter-disciplinary team at 6 and 18 months, and 4 years of age and referred for
2 | P a g e
community-based rehabilitation and educational services.11 Although the controversy about whether to even offer high-risk surgical treatment for a condition that is otherwise lethal has lessened,12,13 concern for the long-term outcomes for these children persists with developmental14-16 and functional17,18 morbidity.
Since 1999, Rempel has focused her research on the pioneering parents of children with HLHS, alerting service providers to parent needs as they navigate a multi-sectoral system that has not been ready for them. Rempel’s research has provided direction for clinical practice with relevance beyond children with HLHS, to parenting children with other forms of complex CHD. Rempel’s study of parents whose children were among the first to survive their HLHS in western Canada (i.e., classic Norwood cohort where there was a 2-year mortality rate of 52%) showed that parents safeguarded the physical survival of their young child with HLHS while safeguarding their own emotional survival as parents.19 In a subsequent study of parents and grandparents of children whose chances for survival had improved significantly (i.e., Sano-Norwood cohort where there was a 2-year mortality rate of 23%), Parenting under Pressure characterized an iterative social process of family, parent and child interactions. While fear for their children’s physical survival was less in these mothers and fathers, parents were keenly aware of their children’s precarious survival while growing increasingly attached. In addition, they had the heavy responsibility of recognizing potential problems, finding and accessing appropriate care for their child.20 Encountering new challenges over the course of their young children’s illness trajectory contributed to persistent uncertainty that influenced parent wellbeing, parent-child interaction and family functioning. A further outcome of this study was development of a model to inform parent-focused intervention (Facets of Parenting Intervention Model)
[Appendix A).21 The critical need to help parents identify and utilize support to manage child and family needs informed the current study.
Purpose of Current Study
The purpose of this study was to delineate needs from the perspective of parents and service providers of children with HLHS and to identify the services and resources used and needed by parents to support themselves, their children, and their family.
IMPLICATIONS
Successful surgical treatment of HLHS has heralded new challenges. Complex ongoing morbidity for the child and parents is
serving as a litmus test for what is not working in our system of technology driven acute care services and fragmented community services that expects parents to manage their child’s ongoing physical, developmental, social and emotional challenges with minimal support from the service providers who know their children best.
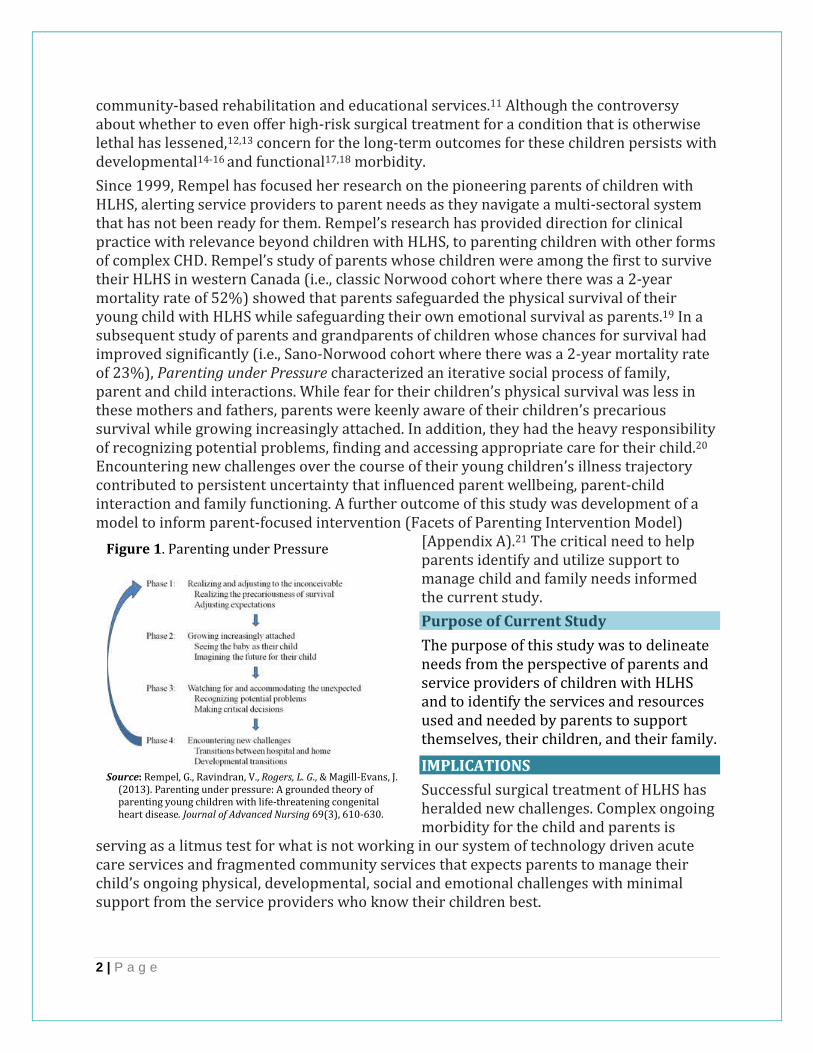
Figure 1. Parenting under Pressure
Source: Rempel, G., Ravindran, V., Rogers, L. G., & Magill-Evans, J.
(2013). Parenting under pressure: A grounded theory of parenting young children with life-threatening congenital heart disease. Journal of Advanced Nursing 69(3), 610-630.
3 | P a g e
Successful HLHS intervention puts tertiary surgical centres “on the map.” Despite the gratitude parents feel towards acute care staff who cared for their child, parents remain overwhelmed. This study determined the service needs of families while also assessing parenting stress, resilience, and family management of CHD through questionnaires and interviews. The initial results were taken back to parents and professionals
through focus groups. Key areas for change were presented to professionals through a Delphi survey to elicit priorities and recommendations for service changes. Although recommendations are based on the HLHS population, the resounding message from parents and professionals was that parents of children with other forms of CHD face similar challenges. Although amazing advancements are saving babies and children, the children have significant challenges that have the potential to affect their quality of life over time. Cognitive and motor disability is well documented,22-24 with growing evidence of emotional challenges over the child’s lifetime.25-27 The struggle for parents and families is also increasingly evident. The world class Complex Pediatric Therapies Follow-up program has systematically assessed child outcomes in first 8 years of life. A systematic approach to assessment and evaluation of interventions targeted at supporting families is also needed.
APPROACH
In this mixed methods study we invited parents and health care professionals (HCPs) to tell us about the service needs of children with complex CHD, specifically regarding education, rehabilitation and mental health. We also gathered data about how the parents’ resilience, parenting stress and family management of their child’s complex health condition. As part of a rigorous research protocol, multiple sources of data included mailed questionnaires for parents; in-person or telephone interviews with parents, focus groups with parents and service providers; and a Delphi survey with service providers. The University of Alberta Health Research Ethics Board and the University of Calgary Health Ethics Research Board approved the study.
Data collection occurred from June 2012 to June 2014. At the outset of the study there were 64 families in Alberta of children who had survived HLHS, the oldest child being 16 years old. The Western Canadian Children’s Heart Network sent out questionnaire packages to 59 families (5 missing addresses). At least one parent from 26 families returned questionnaires for a response rate of 44%. An additional 3 families joined the study through interview and/or focus group participation but did not complete questionnaires. The questionnaires addressed resilience, parenting stress and family management of CHD (Appendix B) to provide quantitative information about parent and family strengths and challenges. Parents also completed a questionnaire about the child’s health, development and schooling (Appendix C) and part way through the study we added the Vineland™-II to assess the child’s adaptive behavior. Parents had the opportunity to opt in for an individual, in-person interview as well.
Telephone or in-person interviews elicited accounts of day-to-day parenting in relation to their child with HLHS using a structured interview guide (Appendix D). Data about what services parents needed and accessed were generated through questions like: “Thinking of
Service changes will benefit
all families of children with
CHD, and apply to other
complex pediatric
populations with medical
and developmental issues.

4 | P a g e
what you have gone through related to child’s HLHS what or who has helped you the most/least?” and “Regarding [child]’s development, what do you worry about the most/least?” Parents were also invited to make recommendations for priority setting by responding to the Facets of Parenting Intervention model (Appendix A).
Questionnaire data were entered in REDCap, a secure web-based data capture system and the transcribed interview data was managed through NVivo. Descriptive statistics of the numeric data and content and thematic analysis of the qualitative data contributed to an in-depth understanding of the service needs of parents in relation to parenting their child with CHD. Findings were presented to stakeholders at local, national and international meetings over the course of the two-year study period (Appendix E). Key findings were presented and discussed through focus groups in Calgary and Edmonton with parents and service providers [Appendix F]. An additional knowledge translation initiative was a Delphi survey (Appendix G) of service providers (May-June 2014) to elicit service providers’ expert opinions regarding priority setting for system changes to enhance services children with HLHS and their parents/families.
RESULTS
Multiple perspectives about needs, services and resources were provided by 46 parents (2 single parents) of 29 children with HLHS who had their surgical treatment at the Stollery and were living in Alberta, along with 38 professionals who provided care for children with complex CHD at the Stollery, ACH, or through the CPTP or community based pediatric services. Thirty-nine parents (25 mothers) completed questionnaires, 29 parents (16 mothers) participated in interviews, and 14 parents (13 mothers) were present in 3 focus groups (Edmonton & Calgary). The 38 professionals attended one of 7 focus groups (Edmonton & Calgary) and 32 participated in the Delphi survey. Professionals were from cardiology, cardiac surgery, inpatient, outpatient, and advance practice nursing, general pediatrics, social work, child life, speech pathology, physical and occupational therapy, audiology, and management.
The Children with HLHS – Who are they?
The 29 children included 18 boys (62%) and ages were from 9 months to 16 years (Figure 2). Many children were functioning well in relation to their cardiac issues, including
participation in sports. Almost all of the children, however, had challenges in one or more areas on the Educational/Rehab Services Questionnaire and/or described by parents during interviews. It is well documented in published research that many children with HLHS have lower than average mental and motor development scores as measured by the Bayley Scales of Infant Development.22 Two-year data of the children born between 1996 and 2005 (the older children in this study) indicated that almost a quarter of children had mental delay and almost a third of the children had psychomotor delay.22 This study provides the results of comprehensive data collection with families of 29
Figure 2. Age breakdown
Age range N (%)
Under 3 years 8 (28%)
3-5 years 8 (28%)
6-12 years 9 (31%)
13-16 years 2 (7%)
unknown 2 (7%)
Total 29
5 | P a g e
children, for which the questionnaire and interview data in combination provided detailed parental accounts about the children’s day-to-day struggles and behaviours.
From a medical perspective, four children were medically fragile. Two older children had recent significant health challenges. For children who had at least one surgery in the Norwood approach, two had a heart transplant and two were on the transplant list. Eight children had a total of 10 surgeries in addition to heart surgery. Several children had a G- or J-tubes currently or in the past. One child had a profound hearing loss, one had a progressive hearing loss and two were being monitored. Four children had at least one stroke. One child had a complex syndrome. One child died during the study period.
From a developmental perspective there was delayed/disordered motor and language skills, anxiety; sleeping, eating/feeding and behaviour issues; sensory sensitivities; and delays in self-help. Four preschool children had received or were receiving provincial educational funding supporting children with severe developmental needs. Two children had hearing loss and developmental delays, two children had experienced strokes in addition to autism(n=1) and developmental delay (n=1). Eight of the ten 6-16-year olds for whom we had child data had challenges in one or more areas of learning and executive functioning.
The Children with HLHS – How are they doing?
The sequelae of survival including developmental, learning, self-care, regulatory, and emotional/ psychological needs were not readily addressed unless the child was severely affected or had an accompanying syndrome with developmental challenges.
Addressing child morbidity in the early years. Children with HLHS experience a spectrum of morbidity. Two of the 29 children in this study had no developmental and learning issues and 4 children had severe developmental needs who received services during their preschool years.
All infants with HLHS are routinely enrolled for follow-up through CPTP and are followed at the Glenrose in Edmonton or ACH in Calgary. Although most parents bring their children for follow-up appointments, parents in this study did not consistently report these services or articulate the role the program had in addressing their child’s developmental and learning needs. Parents were satisfied to very satisfied with rehabilitation at the Glenrose, Stollery, or ACH for children under three who had received treatment. These were primarily children who had severe developmental needs related to stroke(s). While HCPs from inpatient settings expected the Glenrose or ACH to address the children’s ongoing developmental and learning needs, this follow-up now only goes to the age of 4 years, prior to school entry. Additionally, services for the young children whose individual profiles in each domain (i.e., learning, motor, self-care) were classified as mild-to-moderate were not routinely linked to community-based services. In addition to developmental and learning issues, many of these children can have significant regulatory adaptive behaviour and self-care needs.28 This cohort included preschool and school-aged children who had residual and complex sleeping, feeding, anxiety, self-care and motor planning issues as well as sensory sensitivities that required specific intervention, that they did not receive (Figure 3).

6 | P a g e
Cumulative multiple domains of mild to
moderate difficulty resulted in a child with
developmental, learning, self-care, and
regulatory problems for whom parents struggled
to secure services.
Only one parent reported getting help for the child’s sleeping and anxiety issues. “It was a lot of a lack of sleep for us, ‘cause he had been used to being in the hospital and getting poked on an hourly basis. It took probably a good 2 years to get him into a bed routine so he’d sleep through the night.” Children were followed for feeding intervention when they had a tube inserted but none of the children received the intensive intervention required for their food aversions and sensitivities.
For young children with mild to moderate self-care, motor and language challenges it was difficult for parents to access available community-based early intervention
services. There were several contributing factors. First, their child had many medical appointments for health concerns and these concerns influenced parents to keep their child home to avoid infections. Although their babies’ health improved following the second surgery, the third surgery (Fontan) loomed on the horizon. So the children whose parents received recommendations through CPTP to seek early intervention for mild to moderate challenges were unlikely to seek services. Children who were not identified as needing services during CPTP appointments at 6 and 18 months missed the opportunity for ongoing developmental surveillance that would have been provided through attending widely available early intervention programming in Alberta because they did not attend these programs. Second, while there are well-developed links from follow-up clinics to provincial funding programs for severely affected children, parents in this cohort of children with mild to moderate challenges were not connected with Community Rehabilitation Services. Third, the community programs and school systems were not aware of the potential needs of children with complex CHD and so were not proactive in getting services for these children.
The key challenge that parents faced as they navigated a system that was ill-
prepared for their children was the prevailing attitude that their child’s heart had
been fixed and that there were no other problems to address.
A mother of a school age child spoke about meeting with the vice-principal relating to the child’s complex medical needs and frailty (and not even getting into any of the
Figure 3. Data from 26/29 children
Challenge N/26 (%)
Feeding 11/26 (42%)
Anxiety 9/26 (35%)
Sleep 9/26 (35%)
Sensory sensitivities 6/26 (23%)
Significant behaviour issues
5/26 (19%)
Significant need for routines
5/26 (19%)
Delayed toileting 3/26 (12%)
“I couldn’t put him in the
preschool or take him [and
siblings] or anything to
Gymboree. His life was very
secluded those first few
years because we were
waiting for heart surgery.”

7 | P a g e
developmental and learning needs), “So this vice-principal’s like, ‘Oh, well, I can’t believe he’s this sick.’ And I said, ‘But he’s always been this sick,’ and she said, ‘Yeah, but he had surgeries.’’ Fourth, even if language, motor, learning and behaviour problems were identified, access to community rehabilitation and education services was limited. Last, parents had to contend with their child’s troubled sleep, feeding, anxiety and behaviour issues following each surgery before they could attend to less urgent but still important developmental and learning concerns.
Addressing child morbidity in the school years. Early developmental issues inevitably translated to learning/school problems, a repeated message from parents of the school-aged children. Schools seemed unaware of the children’s needs, who presented with disordered developmental and learning profiles, rather than just delays. Typically the school would modify the physical education program but were unprepared for the complex language processing, motor planning, and learning issues. Some children had shared aides, but parents perceived that teachers were not aware of the complexity of the children’s disorders. Access to therapy was limited. Parents who were already stressed financially found and often paid for rehabilitation, psychology and remedial educational services because the wait list was too long and there was the chance that their child would be assessed as ineligible for school-based services.
We paid $175.00 a session [for Speech therapy] twice a month February to June. … So you have to pay for it yourself. These kids, with them being, not scattered, disordered, they need that help.
If the eating and self-care issues were not addressed in the preschool years they persisted, and in many cases children experienced increasing feeding challenges. Appropriate intervention, although available, was not offered.
I’ve talked to the pediatrician and she says what he should eat, and she tells him, but he doesn’t really listen. The cardiologist brought in a dietitian... He’s not interested in eating those things. I mean, I know what he should eat, but just figure out how to get him to just eat.” Several children had a need for control and order. “Sometimes he’s a little over-the-top with it, because if you move something, he gets frustrated if things aren’t the way he wants
them to be. He is a very happy little boy, very particular, very organized, but he’s very fussy. So fussy, meaning it’s got to be clean; if there’s a spot on his shirt, he’s not happy about that.
Children with HLHS typically struggle with independence in self-care, but do not receive therapy to address the sensory and motor planning components. The parents were often blamed for the children’s dependence, without considering emotional and learning factors.
While only 19% of this cohort had behavioural difficulties, these were severe, and parents did not receive assistance. Parents questioned how these difficulties related to the heart problem:
A father summed up the issue related to his school age child: “You have to lay your head on
the pillow at night knowing
that you’ve exhausted every
avenue. … He’s had some pretty
big obstacles to overcome, and
a lot of them have been out of
our control, but education is
one that’s in our control, as
parents, our spot to shine in—
make sure that he’s getting
every possible assistance.”

8 | P a g e
You ask him to stop doing something, and he just doesn’t stop doing it. You ask him to do something, and he forgets, and he goes off and gets carried away with something else. Sometimes I wonder is it his capability. That’s the frustrating part: you don’t know; it’s unanswered; because of his lower oxygen levels and that, does it affect his brain processing?
KEY MESSAGES
Children with complex CHD: • have regulatory challenges (sleep, feeding, sensory and behaviour) that require intervention • miss valuable linkages with widely available early intervention and community support due to timing of necessary surgeries during the early years • are not being adequately monitored and supported at school age for their disordered development and learning challenges
The Children with HLHS: What about trauma?
With increasing awareness of and resources to address pediatric medical traumatic stress29 it behooves HCPs to acknowledge that children with HLHS undergo repeated potentially traumatic medical events, including pediatric intensive care unit (PICU) stays in wakeful states. Although the parents provided accounts of resilience in the face of potentially traumatizing experiences, their vivid stories reflected traumatic stress reactions. Parents described, in detail, their child’s behaviours when thinking about returning to the hospital for other tests or surgeries, or when the child was told that there was a possible return to the hospital. Several of the children had a needle phobia. Nurses in the focus groups spoke about how difficult it was when the children returned to the hospital for the 3rd surgery, the Fontan, and the difficult behaviours displayed in the hospital. A mother of a 3-year old said:
As soon as we show him the striped pyjamas, he’s like ‘No’ and then he starts getting upset. Or if I go onto a unit, he just shuts down and he won’t talk to anyone. He was so mad that I would leave him there. He would just scream at the nurses; he wouldn’t talk to anybody with a white jacket.” The father spoke about the effects of needles. “I was saying to my wife, ‘These needles, he’s going to have post-traumatic stress syndrome,’ ‘cause we’re sleeping and he just wakes up screaming. Then the nightmares stopped. What happened to stop it? I think it was not getting any more needles. ‘Cause … he’d wake up screaming, ‘No pokes! No pokes, Daddy!
His mother described another stress reaction: “I had a cider. And then my son says, ‘Mommy, it smells like poke in here.’ It was the alcohol.” Another parent talked about how long it took their child to get over his hospital experiences.
When we first got him home, even up until I think he was about 3, he just—anybody who looked like a nurse, he wouldn’t go anywhere near them. We had friends who would come and see him, and he would stay away from them. So it took him a long time to get over that.
Some children handled the stress of the hospitalizations and tests better, especially as they got older and were able to talk about their experiences. As parents of a 6-year old said,
9 | P a g e
Because of all he’s been through, like I said, he’s got a control problem. He’s got white-coat syndrome, I think. It’s better now because he can talk and everything, but the worst part was when he couldn’t when he was younger.
Even a teenager had difficulty with thoughts of going back to the hospital. “When [pediatric cardiologist] brought this up the other day, my daughter started to cry, which was interesting, and I can understand why, - the pediatric cardiologist said, ‘This is not open heart surgery.’ Scary, just the thought of going [to the hospital], so that’s what she remembers. So she’s still telling me she’s not doing it. ”
The most severe traumatic stress reactions were reported by a mother of an 11-year old boy. As a toddler after the first two surgeries “he used to just scream with nightmares, … he’d be, ‘No, no, don’t hurt me’ and ‘Don’t let them take me’.” His mom described taking him for his Fontan at age 4: He was in the hospital pyjamas and when they came to get him, he went hysterical. He was frightened. I was
holding him, and he was crawling right up me, over my shoulder to get away … and they were grabbing him—trying to grab him. He was “Please don’t let them take me, don’t let them take me, don’t let them hurt me.”
His mother reported that her son also had to deal with traumatic things he witnessed in the PICU.
He was off the respirator and aware of everything that’s going on, and he had to stay in there. So he saw a lot of awful things. He saw things being done to other kids. So he had nightmares for a long time, too. He fell into a severe depression. I’ve never seen a child so sad in my life. He wouldn’t talk for—he didn’t talk for 2, 3 months—like, not a word to us. Nobody—like, no psychologist came to him; that wasn’t offered.
He went back into the hospital for a catheterization at age 5. He was just angry having to go back to the hospital … We explained to him he was going back to the hospital but he wasn’t going to have anything really bad or anything done, and he’d have to stay one night. When we drove up to the hospital, he was, “No, no, please don’t take me in here! They hurt me, they hurt me here!”
KEY MESSAGE
Children with complex CHD: • experience stress reactions, especially during their third surgery, the Fontan at 2-4 years of age, related to trauma from previous life-saving interventions
The Children with HLHS: What is needed?
There is a need for an interdisciplinary team of professionals to address the needs of the child from a holistic perspective, who can become experts in knowing and understanding their needs and conveying this information to community providers. Systems are in place for addressing the needs of children in the community with many other diagnostic
Witnessing your child’s traumatic experience is difficult. Not getting help for your child is more difficult.
‘No one ever talked to him
about his feelings, about his
emotions. To me, that’s the
biggest thing. And [as he got
older] I asked many times,
‘Could he maybe see a child
psychologist?’ but it just always
fell on deaf ears.”
10 | P a g e
conditions but the children with complex medical needs as well as complex learning needs are a new area. This team needs to not only address the medical, developmental and learning needs of the children, but also their difficulties with sleeping, eating, behaviour, anxieties, rigidities and medical trauma. While the service delivery system tends to focus on young children, this group requires focus on acute medical needs when they are young, but they still require the developmental support later on.
The Parents – Who are they?
Parent participants included 28 mothers and 18 fathers with 17dyads (mother and father of same child). Thirty-nine of the 46 parents (25 mothers and 14 fathers) provided questionnaire data. Three quarters (29/39) of parents were university/college graduates. Only one parent had less than high school education. All the fathers were employed fulltime while 44% (11/25) of mothers were employed fulltime outside of the home, 2 worked part time, 44% were fulltime homemakers, and one was on maternity leave. Of the 25 households represented in the questionnaire data, 11 (44%) had a yearly family income greater than $85,000, 4 had an income of $66,000 -85,000, 6 were between 46,000 and 65,000 and the single mothers had family incomes of $36,000 to $45,000. No family had an income less than $36,000. Two parents did not provide income information including a mother on maternity leave. Parents were partnered except for two single mothers and one
divorced mother. Most parents identified themselves as white/Caucasian; 2 parents were Hispanic; and 2 were South Asian.
The Parents – How are they doing?
Despite the potential for resilience reflected in the demographic profile, these parents were not without significant struggle. Almost 20% of the parents scored in the
post-traumatic stress category of the Connor-Davidson Resilience Measure, and 29% scored in the clinically significant range of the Parenting Stress Index. In addition, 29% of parents (4 dyads and 2 single parents) fell into the problematic or somewhat problematic on the Family Management Measure. Analysis of the qualitative data helped us understand these concerning numbers.
No matter how well or poorly their child was doing, there were common experiences of parental stress and trauma, persistent uncertainty concerning the present and future health of their child with HLHS, financial burden related to long and repeated hospitalizations, care requirements at home, frequent follow-up appointments and a sense of being lost in the system.
Stress and trauma: “Deer in the headlights” -
Data from both the parents and the HCPs raised strong concern for the mental health of these parents of children with complex CHD, children who are not unlike those with other forms of CHD requiring surgical treatment early in life. Both parents and professionals repeatedly referred to “stress”, “stress levels”, “post traumatic stress”, and “post traumatic stresses” without the interviewers ever using those terms. Sources of stress and trauma included having to become “nurses over parents” to safeguard their baby’s survival following initial infant surgery, witnessing the death of other babies with CHD and
Parents experienced
stress, trauma,
exhaustion, financial
burden, survivor
guilt, and felt lost in
the system.

11 | P a g e
experiencing survival guilt, and being excluded from the care team during hospitalizations. These stresses were superimposed on pre-existing, ongoing stresses of family and work life. Stress reactions were self-reported by the parents and described in detail by the HCPs. Physiological and emotional aversions during return hospital visits and exhaustion were two key stress reactions. Pushing through without support also characterized the parents’ experiences that undoubtedly added to their stress.
Becoming nurses over parents. Transitioning home after their baby’s first surgery was particularly stressful. Health care professionals placed high expectations on parents to do the 24/7 care required with minimal support, and then expressed how bad they felt for the parents. One professional remarked, “It’s very sad to hear, because they feel that they need to be nurses over parents. And that’s one thing that I hear a lot, is that they’re going out so fast, so quick, with not much information, not a lot of support.” Another HCP’s perspective was:
So parents are going out like absolute deer in the headlights -no matter what you say to them, no matter how much you try to prepare them … A little bit less when their child’s not tube-feeding, but when their child is tube-fed, if you really sit and speak with a parent—I talk about trauma, and they are traumatized; I see post-traumatic stress immediately.
Round the clock care also included injectable medications. One mother struggled:
I didn’t like the whole feeling that it’s going into his skin; like, that whole initial poke. ‘Cause you pinch it, and then you feel it, and you just feel it, and I didn’t like that. That’s my toughest part. I can handle the driving in, I can handle the doctors’ appointments … I can handle the long days … but the meds has been the most challenging.
No matter how well each child was doing, a social worker emphasized that each family had been through “the same process - post traumatic stress.” The lack of support for parents was emphasized by the HCPs, not the parents. They described the gap between the supports parents had while their child was in the hospital with the lack of supports when at home: “Cause one thing I find is when they’re in the system [the hospital], there’s people that help them navigate it. But I get phone calls all the time from people that are at home and they don’t—they’ve tried to get a hold of their cardiologist and they’ve tried to, they’re hitting, walls, and then they don’t know what to do.” No matter how many times things were explained to parents before their child was discharged home “they get home, and I’ve talked to lots of parents that say that at the beginning, they’re just in complete shock, and when they get home, it all hits them, and then there’s the grief and then they have a million questions, ‘cause now they can kind of understand.´ The repeated message was that the parents needed to have access to “people that are in the know”, HCPs from Stollery, the surgical centre.
Fear and survival guilt. Another significant source of stress was what parents observed in the hospital, and what other parents and children were going through. In addition to the fear they felt for their own child’s life, they had fears for other children. One mother recalled:
I’d push the “call” button for these little babies, ‘cause no one could come and check on them because the machines are beeping, beeping, beeping, beeping, beeping; you know, like, their SATS are dropping, and their heart rates are going through the roof. It just terrified me.

12 | P a g e
Parents recalled how close to death their children had been and one mom described how she had figured out the fear-provoking reality of the “back row” in NICU:
They’re in rows. You know, these rows are going for surgery and [another for] the sick kids and, the back row is almost the death kids; it’s just like that. So when you get moved there, you’re a nervous wreck. So I know they say there’s no rhyme or reason to it, but they forget that when you’re in that situation, you see it. When we were in that back row, we watched two parents say good-bye to their kids. It’s things like that that I think nurses and doctors have to realize that we’re not stupid; we’re there longer than they are a lot of times; we live in that hospital, … and we can tell what’s going on. So yeah, that was very scary.
Adding to their own stress was the experience of someone else’s baby dying. “Like, one of the people we got closest to, their baby passed away while we were there, —that was really difficult to [pause] kind of, yeah, go through. We left and we came back 3 months later, and some of them were still there, and it’s just, like, you almost have survivor guilt, which is weird, because he has significant health issues and challenges, and yet I feel like he’s, like—I’m kind of, like, ‘I’ve got a kid who’s doing so well, and you’re still here and not leaving any time soon.’”
Traumatic stress superimposed on existing stress. Surgeries and hospitalizations never occurred in isolation from the rest of the parents’ lives. As much as they tried to cocoon themselves and focus on their sick baby, they had other life events to deal with, which added to their stress. As one mother said “we do have lives outside of this, and there’s—everything plays into it [stress].” Their “outside lives” included death of a parent’s brother, diagnosis of cancer in a parent’s mother, significant financial issues, house renovations, and the everyday needs of siblings who were being shifted from place to place. As nurses over parents they pushed through: “So between being—finding out we’re pregnant, his heart issues, being laid off three times, my mom getting sick, dying, starting school, shipping the [siblings] off for 2 or 3 months, working out of town for a month. [My wife] kept asking me, “Why are you not snapping?” You have to handle it; you have to; you don’t have a choice. So I did.”
Stress reactions. One mother described going back for the Fontan after being at home as “creepy.” Her physiological reaction was:
A sense on that floor where the PICU is, when you come off the elevator and turn the corner—‘cause the OR is there—there’s some kind of smell there that just turns me inside out, and I don’t know what it is, if it’s a smell in the air or obviously something in the hospital. My husband has a videotape of [son] being in the hospital; he was playing it, actually, the other day, and the beep-beep-beep of the monitors…
A father of a teenager who recently had to be put on oxygen said “so they brought the oxygen in. Oooh, boy, that brought back a lot of strange memories.” Another mom described her extreme negativity when back “in Edmonton” with her child: “There was days where you’d go and you’d get up and you’d leave the Ronald McDonald House and you’d just [go down] that hallway and with every ounce of energy you had to say, ‘Okay, I need to go in there.’” This mother articulated the extreme stress of not being validated for her extensive knowledge of her child when back in the hospital. As much as she valued the HCPs, she felt talked down to in the hospital. Many parents reiterated the message that HCPs did not

13 | P a g e
convey an understanding or appreciation of the responsibility parents had for their child’s care when not in hospital, which for the parents was most of the child’s life despite prolonged hospitalizations. Even though they wanted to be with their child as much as possible they had to muster their courage to enter the hospital doors and for one mom the long walk from the parking lot to her child’s bedside felt “like a walk of shame going in there. It’s such a long walk through the parking lot.”
Most parents described exhaustion and not being able to bounce back. A mother of a 5-year old put it this way.
I cannot do any more, I’m exhausted. Nothing gives me rest; I am very restless. Like, before I was able to deal with the situation or deal with the stress very well, and I don’t see my—I lost that. My patience—not my patience, but my way of handling things is not the same any more. Like, right now, I have less tolerance to be able to handle a lot of things and stuff like that. I know that not only you have to take care of your body, but also you have to take care of your mind. So in this situation, for parents and everything, is very, very—is a hard situation.
An insightful mother of a teenager reflected on the longer term effects of past and cumulative stress, her perceived pressure to not show her stress, and how stress reactions caught her off guard:
I think the tricky thing with parents is that [stress] catches you off-guard. We went through all this health stuff, all this while we [had other things going on in our lives], and I fell apart. Like, couldn’t cope, was a mess, I couldn’t cope with the stress levels that we were in the middle of, and it had nothing to do with the health. And I still, to this day, blame it on all the stress you can’t show, right? ‘Cause you can’t show where you’re at, especially if you’ve got
more than one [child]. It happens in places you just don’t expect, right? I mean, I have to watch at school, ‘cause if the teacher presses a certain button, I’m ready to lose it, and I have to calm down and just say this, but I mean, I have to monitor myself really carefully and be really rational about what am I feeling. And I think maybe if I’d done a little study about post traumatic stresses closer to the time when it all happened … it might have helped.
Lack of support. Parents would have liked more emotional support, both during hospitalizations and afterwards. “It was very surreal and terrifying. I don’t remember them offering me, like, say, a social worker or anything. Maybe someone did talk to us briefly, but I think I was in such a daze back then, I just—and not sleeping. I think somebody did come to the bedside, I remember someone talking to us a little bit, but not, like, getting into my feelings and things like that, about how things were.”
A parent of a 5-year old felt that she had still not processed all that had gone on in the first three years.
But the most difficulty is to keep yourself under control, basically. Like, is very emotional, parents go through a lot, and I think that is very difficult to recover from anything like that. At this moment, I don’t feel like I have recovered from any of that; I don’t feel like I had a chance to actually being able to [pause] to kind of deal with the
“I wish I could have just
talked to somebody
about my feelings and
my fears.”
14 | P a g e
situation. You need to basically be very strong to keep going through everything, and keep going and keep going and doing what is best for your child. But it comes to the point when it gets you—it gets you—and if you don’t have the support and you don’t have who to talk to or anything like that, is very hard. I think it’s [parent support]—it’s just as important or even more than the child, because the child will get the best medical attention, they are getting all these programs, but it’s the parent who is the one who has to be fighting for your child, because they cannot fight for themselves. So you are fighting for two people; you’re staying alive and trying to deal with your emotions, and then you are fighting for your child.
Parents and HCPs felt that one main source of support was other parents. However, HCPs cautioned that there were factors for consideration when matching families. Often parents would find their own support through parent groups or others in the hospital at the same time. Repeatedly the parents said that only another parent could understand what they had gone through.
Living with persistent uncertainty
Parents lived with ever-present uncertainty, but also described how they intentionally placed concerns about their child’s uncertain future in the background and chose to be hopeful. Although ongoing survival fuelled hope, uncertainty increased as the child got older and experienced medical episodes. A father of a 6-year old expressed a sentiment common to many families.
You don’t know if you got that boy in your arms for 2 weeks or 20 years. So that’s—that’s pretty big. … I can’t say that either of us live through rose-coloured glasses. I know that just because of what we’ve gone through. I almost think of it as a marathon and there’s been other runners that have fallen out of the race sooner than we have, kids that have died, kids that have died right in the room next to us. … I know there is a chance something could happen and he might need a transplant someday, he might die at an early age. But that doesn’t mean we live in fear about it.
Parents of children at all ages spoke about uncertainty. The father of a thriving 3-year old wondered “how well his heart is going to hold up in the long term, like when he’s 20 or when he wants to play hockey or baseball.” A mother of a 6-year old believed that things could change at any time: “I’d say you live waiting for the other shoe to drop—well, I do. You could
forget about it, but you’re always aware that this could all be just, just be snatched away, right?” Another mother reflected on coming home after the last surgery:
When the surgeries and everything were finally over and you come home and you start to exhale, and you start thinking about things and going, “Well, that was quite the journey, and it’s not over,… But we live for today, we don’t think about the future. We know he is palliative. We don’t know how long he’s going to live for; we don’t know if he’s going to need a heart transplant. So we just don’t live there, because I think I
Parents knew that their child
with HLHS was paving the way
and that there were not many
answers about their child’s
future but they kept asking: “To
the cardiologist, we always ask
the question, ‘What is the
future going to hold? What are
you seeing?’ and just to pry into
that.”
15 | P a g e
wouldn’t be able to handle it if we did. It’s really hard.”
For parents of school-age children or teens, the uncertainty persisted, and, depending on the complications and crises that they had lived through, the uncertainty could increase.
For the most part, [the heart condition] is not in the forefront, it’s not something that we really talk about and think about every day. … I’m just always concerned about his health. I mean, you’ll wake up in the middle of the night, it’s just, like, it just closes around you and it scares you, you know what I mean? But other than that, you tend to put it behind you and keep looking forward. But [as far as the future, there is ] just everything, from mortality to what’s he going to do as an adult, what kind of job is he going to have, what are his limitations going to be. ‘Cause he has so many issues with school and learning and stuff like that, it’s like these issues, they’re not going to disappear, so how do we deal with it in the future, how can we support him or how can we help him to support himself. That’s probably the biggest concern.”
The parent of a 16-year old was happy that “she has had her education.” Uncertainty, however, persisted about her future:
She’s got big desires. I know that she’s going to kick some butt in this world, but the stuff she wants to do, it just worries me, because [her chosen] career takes lots of hard work and lots of hours, and I really don’t think her health can handle that. I understand her drive, but I’m just worried that if she works lots of hours, does school, is not getting enough sleep, not eating, she will get sick. So in my mind, I’m kind of, like, going, I hear you and I know you’re capable of just conquering whatever, but that worries me. She will just get sick instantly, and then when she gets sick, it just gets really intense, and sometimes it will last way longer than it would a normal person with a healthy heart.
Living with Financial Burden
Financial burden related to having a child with a complex health condition was distressing for many of the parents. The difficulties accessing government support for children with complex CHD was discussed at all focus groups and was of particular concern in the majority (19/26) of parent interviews. This topic was by far the most frequently discussed in response to the question: “What support and services have been most (and least) helpful in your HLHS experience to date?” There was a universal need for financial support. The financial burdens from the child’s first three years of life impacted the family’s financial future.
The common perception reported by parents and HCPs of funding agencies such as Family Supports for Children with Disabilities (FSCD)30 and preschool and school funders, was that after the third surgery the agencies perceived the child’s heart was fixed and there were no further problems. The palliative nature of the treatment was not recognized or acknowledged. One mother of a preschooler living in an urban centre said, “FSCD is very difficult to get and they do not help with the support children and parents need. They [FSCD] will say no, because hypoplastic is so complex and at the same time, is not a familiar thing. They don’t think HLHS is a disability.”
The reality of the financial burden. Financial burden affected a majority of families; some recovered more easily than others did. Their financial situation before the surgeries and whether they received financial help from families and friends were factors. “My boss
16 | P a g e
supported me right through – it was incredible – what do you do when you don’t have that?” and “We had lots of family support. I didn’t lose any income. I got paid. And we had some money put away. It took a while to recover from that. We had some family friends that helped us out with lodging in Edmonton.”
Financial issues occurred when the parents were highly stressed, with little reserves. “When she was in the hospital, I tried to get paternity leave. Or EI, whatever it was, and at the government office they said ‘no you don’t qualify for it because you’re not looking after your child. Your child’s in the hospital, the hospital’s looking after her, you’re not.’ I just didn’t have the energy to fight. And my boss said – just go.” A parent who said they both made good wages said,” Well, you don’t ever recover from the first part; it just doesn’t happen. And it costs a lot of money. And it’s—I’ve often tried to think back of—it’s not—like, the costs build up because you’re missing work, things like that, but there’s other—so many other subsidiary things that come in from the sides that you don’t even think about. I mean, we stayed in my mom and dad’s trailer for a while up there, just ‘cause I thought it was better, and I think it was better. A little more privacy, but like, looking back at all those different costs is [pause] is—I don’t even know what the number would be; be scary.”
Only one parent reported no financial problems, and his child had not completed the three surgeries, and had not had complications. “Financially, no problems, but we live in Edmonton. I mean, aside from taking a little bit of time off work, it wasn’t a problem.” This father was acutely aware of what other families were going through financially.
Families, who did not live within a short drive of the surgical centre, were particularly burdened by accommodation, childcare, and living expenses for weeks and sometimes months while away from home. In numerous situations, the mother had to leave work or work part time for years, or the father lost his job, to attend to the required medical needs of the child. A mother who lost her career said, “It was never my plan to be at home for 5 years till he went to Grade 1, working part-time.” For a family who had to re-locate, the father could not continue the family business, and they had significant financial issues.
We didn’t have a lot of money. We went through [a time] when neither of us was working. It was very scary. When there’s nothing coming in, it ruins your life for years. Our small community had a supper for us and work did a 50/50 draw. So we were lucky to have community support.
There was one couple, they had to go right now back to Edmonton, and they had to fork out for a hotel. Like, dad’s the only one working. So it’s hard. And we went through that, too, the first time, but thank God my mom gave us that money, ‘cause I would have been—like, I think I worked 13 hours in August—in a month—and I’ve got a $2000 mortgage; … I think accommodations [need to be available], especially out of town. I know it’s only Edmonton, it’s 3 hours, but you have to stay there.”
One family, whose child recently had his third surgery, described their dire financial circumstances. “I haven’t been working for 6 months, and 5 weeks with my husband off [during the Fontan], we’re pretty much in financial ruin. 5 weeks is a long time when you still have rent and [pause] everything.” These parents were also paying all of their expenses to travel to and live in Edmonton for surgeries.

17 | P a g e
We met a Social Worker [at the Stollery] during the Glenn, and it was, like, ‘Oh, you could have gotten all this funding and this funding and this funding to help you out,’ ‘cause we were in Edmonton for 7 weeks the first time around. Maybe I should have looked into it more, but I don’t know, like I said, I thought I was going to go to pre-admission clinic and, you know, meet everyone, kind of, and have that support there. I ended up applying for something after the Glenn; I think it was FSCD? And we didn’t qualify. But you know, I asked the social worker on the ward there, [pause] ‘Is there anything we could get, like a parking pass or’—and I was pretty much met with, ‘Well, those are for people who are really in need.’ Okay, so 2 weeks in, we’re not those people yet, but when the 5th week hits, it’s, like, okay, now we’re those people who have nothing; like, we’re drained.”
When asked what she would spend money on now if there was money available, she said, “rent, food”, and for the future… “Make sure the kids from Calgary get the POC [Point of Care] machine, and make sure that nobody else has to go through all of this. I did have a friend who saw [sobs] what we were going through, and she [cries] raised some money for us. Got all her friends, you know. I mean, $20 here and $100 there, I mean, really made a huge difference. I mean, we’re not in a good place now; I mean, I couldn’t even imagine how or where we’d be if she [and a relative] hadn’t of stepped up and helped us out.” This mother blamed herself for not looking into and asking the right questions to get help. “Maybe [pause] [sighs] [I should have] done more research as to what was available to help us.”
It was difficult for parents to find out about and access FSCD. Many families were either never linked up with government support from FSCD, or were not told of the services until discharged after the first surgery. Families typically did not find out about applying for funding until they had been in the hospital, or even discharged after the first surgery.
We didn’t find out about FSCD until he was pretty much done his first stay, his first little stint in the hospital, which turned out to be 75 days. It could have made a huge difference in the stress level. When we got home, that’s when FSCD is brought to our attention by the NICU social worker. What happened, though, through this whole 3 months, 75 days that we were in hospital, my dad is talking to social workers: ‘We need help for this family. Is there anything that we can do? We need somebody to watch the healthy kids at home. The parents are working. Please, we need help. Is there some kind of babysitting, nanny services that we could hire? What can we do to help this family?’ ‘Cause no one was at home to empty the dishwasher; the [siblings] weren’t able to sleep in their own beds, just because there might be—there were so many times we were called to come to the hospital in the middle of the night, and both my husband and I want to go to the hospital, because if they’re calling us, something’s going on, right? When the [Social Worker] gave us the paperwork, she said, ‘You probably won’t be approved, but it’s worth a shot.’”
A Calgary family commented how helpful it was to qualify to get accommodation for their young family. “We didn’t even qualify [for accommodation] that very first time; we ended up staying at a hotel, but we did have the support that, hang on to your receipt for parking and meals and so forth, and they were to reimburse you for some of it. But then the second surgery, we stayed—at [Ronald McDonald House] and that’s a huge, huge, huge, huge help.
18 | P a g e
Being there, it’s just phenomenal. I mean, it is so much help just being there and knowing that you’re close by and you’ve got your kids with you there.”
Many families were told that they did not qualify for FSCD. Other than families who had a child with severe co-morbidities, most families did not receive support and the repeated
message given to families was that “FSCD does not fund heart children, because it is a medical issue and not a developmental issue”. “So it was, like, with heart kids, it’s always you’re kind of right on the line, I remember her [FSCD] interview; it’s like, ‘She’s not physically handicapped.’” Professionals and parents described that even when
the child had a stroke or had other developmental needs such as hearing loss, FSCD was not available to them.
There were inconsistencies for whom and for how long families received services. It was readily apparent in the data that there were system inconsistencies that did not relate to child or family differences. The family of a 3-year old from Calgary said “We get all of our trips to Edmonton, our gas, our food, our hotels,” while another Calgary family of a 3-year old “did not get as much as a parking pass.” Even though the course of the three surgeries for the families was consistent, it was clear that the access to FSCD was not universally available to families, and as one mother put it, “… if you don’t ask for it, you don’t get it, that’s not fair.” Those that were more knowledgeable about the system, had help with access to services, or were strong advocates for their child appeared more likely to get funding from FSCD.
My [relative] is a social worker so I sent out all the echo reports and stuff [before he was born] so that FSCD knew he was coming. They cover parking, meals, like overnights and stuff. They do mileage and meals if you stay. And they help you out. If I needed childcare for her, they’d help with that and stuff. So yeah, no, they’re good.
When you first get there, it’s really overwhelming. The social worker, the first day we were there, came and met us at the Stollery and explained what we could do, keep receipts. [My wife] had experience with this kind of program, so she knew what to ask.
Children who had a severe co-morbidity such as a syndrome or autism received more services. Not all children, however, with co-morbidities received services, even in the presence of physical and learning problems as a result of one or multiple strokes. In some instances, funding policies changed: “We had FSCD for a couple of years, and then they said ‘No more heart kids’.” The process for receiving funded services was difficult and cumbersome. Common themes were having to “fight” to get services and the cumbersome claims processes. The system put the onus on parents to find out what resources were available at a time when they were entering an unknown system with a severely ill child, were stressed themselves, and did not know who to ask and what might be available. Parents described the process.
Social workers and other
professionals described the
differences in FSCD support
dependent on region, with
some rural areas receiving
support, or some families
receiving more support than
others within a region.
Parking was
huge; that was
a lot of dough.”
19 | P a g e
We’ve had to fight for every single thing. We’ve been scrutinized, we’ve had to prove it, it’s a lot of work, it’s a lot of documentation. I realize that we’re spending other people’s money; I get it. But man—it just gets worse and worse and worse.
And the problem is you fight, and you’re tired and you’re sad and you’re stressed out. And a lot of women just are, like, ‘Okay, you said no. I give up.’”
Another family described the process of trying to get therapy services for her developmentally delayed toddler.
I said, “It’s a doctor’s order that my child have this.” [The response was] “Well, just because [pediatric cardiac surgeon] writes it, it doesn’t mean it’s going to happen.” And I was sitting there thinking, “So you’re saying, then, if it’s a doctor’s order, you’re not going to match it or figure out what you guys”—“No, we don’t have to do that.” But guess what? Five days later, it was happening because [pediatric cardiac surgeon] wanted it. So why was there such resistance and scaring of a family?”
Adding to the fight for services was the claims processes: “ We got FSCD, and I had it for a few years and I had to fight like crazy. I am very well organized and I had my documents, all my papers, I had to fight really hard, super hard for FSCD. I made a case, but for me it has been a constant fight.
The process was difficult for busy, stressed families, summed up by a mother who had four preschoolers, “My husband never did turn in any of those receipts!”
Rarely did families receive formal respite care. The care requirements of the child, particularly between the first two surgeries, have been described as 24/7, with often round the clock administrations of feedings (often G-tube feeds), medicines, and ongoing monitoring of the child’s oxygen saturation.18 Even though these care requirements have been well documented in the literature, and the child is not discharged until the parents can do the care, only two families received respite care. One was a family with a set of multiples, and the other was a medically fragile child. In some cases if this was in place, the child could have been discharged sooner, thus saving the medical inpatient system. “It would have been a help to have received respite care for my child so that myself and my husband could have a rest. Our son could have come home much sooner had we had a little help as he was very sick before he had the Glenn.” It was difficult to get funding for rehabilitation
and psychology services. While much of the discussion was around financial support while the child was in hospital, some families of school age children requiring rehabilitation therapy or psychology services found that it was difficult to access and get funding for services. Parents often had to pay out of pocket for services their child needed to function at home and school.
He has an IPP at school. He would have fallen through the cracks, but I had documentation to
A parent who worked in the school system said, “Well, it’d be
interesting to see if there could
be a code attached to some of
these [HLHS kids], right?
Because once there’s a code
attached, then there’s money
attached.”
“It would just be nice — if you
know a child or a family is in
this situation, and you’ve had
numerous doctors tell you this,
you can see how many
hospitalizations, how many
surgeries, why do I still need to
keep proving and fighting and
begging?”
20 | P a g e
take to them and say, “Here’s the psychologist’s report” that we had to pay $1500.00 to get. He needs Occupational Therapy, and the school said “Why don’t you just go get FSCD funding?” I said “That’s not FSCD’s responsibility, it’s yours.”
Lost in the system
Parents and professionals spoke in detail about how there was intensive support from a comprehensive team while in hospital. When families were discharged to the community, however, they did not have a central outpatient contact person and felt lost in navigating the system both in the acute recovery stage after each surgery, and over time as they recognized the developmental, learning, behavioural and emotional needs of their child. Parents were clear about having to contact a health care provider for post-operative concerns about feeding and weight gain, medications and oxygen levels and once connected with a pediatrician they could usually get their concerns addressed in a timely fashion. Often however, parents had concerns that were either not dealt with to their satisfaction by community-based providers or had difficulty accessing someone who could address their concerns although they had “a piece of red paper with black numbers on it, and there was probably about 45 different numbers. I started calling all the numbers, and I couldn't get a hold of anyone.” A possible wound infection was something that parents wanted Stollery “in-the-know” clinicians to address. The clinic nurses were not as available as some parents desired and often the parents did not have the same connection with these nurses as, for example, they had with the inpatient nurse practitioner. Parents expressed difficulties in finding out about rehabilitation and education services for their child, both in the preschool and school years. Only under exceptional circumstances did parents secure assistance for their children:
The only thing that’s really probably pulled us through the educational part is when [mother] was on mat leave [for younger sibling], being able to do all of the, I call it the “private investigative work” herself. For everything - hearing, where to go; OT, where to go; special programs for special needs kids-all of that, she sourced all of that out.
Professionals had consistent messages about why parents were lost in the system. There was no one designated case manager or patient navigator for the families from diagnosis to outpatient follow-up; rather several disciplines fulfill this role at different stages. The surgical coordinator was the initial contact with the inpatient system and around the booking of the surgeries; the cardiologist, nursing staff and social workers were contacts during the inpatient admission; and the cardiologist and nurses were identified for follow-up clinic visits. Some identified the pediatrician as the navigator, but parents indicated that they typically did not become involved with a pediatrician until discharge. In addition, there were responses indicating that existing services were not well coordinated. Responses from professionals included “Does anybody do this?” and “This is not well coordinated”, and “I have no idea”. Given the confusion of the professionals, it is no wonder that the parents struggled.
Parents could get answers from various disciplines when they were an inpatient; however, the difficulty with navigating the system came when they were in the community. Professionals indicated that there is a clear need for assisting parents in navigating the system, whether this was through an established Patient Navigator role, or through comprehensive Care Map planning. “Parents need to be able to connect with a consistent
21 | P a g e
person who guides them to navigate the system from the time of diagnosis to rehabilitation.” “A navigator [is needed] for consistent follow-up for preadmission, in hospital and for post discharge follow-up.” Some felt a case manager role would fulfill this need. “Ideally a case manager should be assigned to all these families.” Some did not think that a new role was needed, but that better coordination within the current system would facilitate this. “I am not sure that there are new services, rather a coordinated approach to care with existing services – possibly a care map with roles and responsibilities clearly laid out. In the care map, identify needs at different stages, equipment, medications required, funding options, - sign off the care map along the way – the parents could keep a copy of the care map so that they know what to expect and who is doing what and when it is done.”
KEY MESSAGES
Parents of children with complex CHD • have lived through traumatic experiences with their child • face an uncertain future with their child • experience significant financial burden with little or inconsistent financial compensation within a funding system that does not understand their needs • are on their own to navigate a complex system that is not prepared for their child and family needs
Fontan
Although parents and HCPs clearly articulated the challenges of accessing appropriate services at the appropriate time for the child, the parents, and other family members, accounts of the Fontan provided alarming data of behavioural and emotional difficulties for the child and emotional difficulties for the parents. Although practice and research literature abounds regarding pre-operative preparation of children for surgery, there were no accounts of preoperative preparation for the Fontan surgery by professionals or parents. Without a patient navigator or case manager to direct parents to pre-operative resources for the child, siblings and parents, pre-operative preparation was minimal. In this context, the negative accounts of the Fontan experience and the professionals’ concerns for the children and families are not surprising. Traumatic stress responses in relation to earlier surgeries followed by the Fontan experience with minimal support or preparation resulted in additional traumatizing experiences. The child’s Fontan experience. Parents spoke ardently about the child feeling betrayed by the parents once they woke up after surgery. Difficulties ranged from the child being clingy to a child being selectively mute for weeks. Nurses described the children as being “out of control” behaviourally. Parents and staff were at a loss as to how to deal with the child’s emotions and behaviour. Parents had not known how to prepare their child for the surgery. They described the child screaming and pleading not to have to go back when they saw the hospital.
It would have been nice to have support to know how to handle this, to tell him, to explain to him what was going to be going on. ‘Cause this poor kid, he had no idea at all; he just thought he was going up for tests, and all of a sudden, people are taking him. Then the next thing he knew, he’s just looking around, he didn’t know where he was, he’s in a diaper all of a sudden when he’s potty-trained for all those years, he’s in a diaper. I mean, he must have felt like a Mack truck hit him.
22 | P a g e
Even children who had previously done well developmentally and medically experienced the Fontan as an exceedingly difficult experience. She took longer to recover, and you know, it’s day-by-day, because something can go wrong, and then can really, really get bad. We kind of forgot after the Glenn, because she did so well, how stressful it is. … She was a really, really happy kid, and then when she came out of the Fontan, she was looking very, very sad, she didn’t want to talk, she wouldn’t have ice cream. She was, like, “Why are you allowing this to happen to me? Aren’t you going to tell them not to?” So it was
very tough at that time. The parents’ Fontan experience. Service providers and parents consistently said that the parents were not prepared for the Fontan. The parents all reported learning about the Fontan surgery at the time of their child’s diagnosis of HLHS, but did not recall learning about how the surgery would impact their child. Professionals and parents spoke about the anticipatory anxiety as the surgery approached. There were no accounts of how parents were counselled for their child’s Fontan; nor were there any accounts of professionals initiating pre-operative preparation activities for the child. Parents did not know how or even that they needed to prepare their child for the Fontan, or how to prepare themselves. “Three years later, I didn’t even know where to start, ‘because he’s fine in every other way. You wouldn’t even know, unless you saw the scars. I think I blocked a lot of it out, I was completely unprepared.” Parents were especially not prepared for how “hands on” they would need to be with their child related to their child’s fears. “… I couldn’t even go to the bathroom, I couldn’t walk across the room to get a cup of water; he wouldn’t let me leave.” For a mother of an 11-year old, the memories had stayed with her:
I don’t think I’ll ever get over that for the rest of my life, that I didn’t explain to him, ‘cause I mean, we owed that to him. Then I had to poke his fingers because I had to learn how to do it, so it was like—the look he gave me, like, “Not you too, Mommy”— it was just sort of the last straw for him. It was horrible.”
Warfarin and monitoring machine. Several parents spoke about the shock of their child having to be on anticoagulants and the ongoing monitoring and child activity limitations. Professionals spoke about the lack of consistency especially with the use of Warfarin, as prescription practices are based on cardiology preferences, without best practice guidelines. This made it difficult to prepare the families. Families from Calgary were especially concerned about their access to the monitoring machines, and the Heartbeats parent group was providing funding for this. Edmonton families typically did not have the same access problem. Several families ended up purchasing the expensive home monitoring machine from personal funds. Strategies for Fontan preparation. Professionals felt that an interdisciplinary team should be in place to assist parents in preparing them and their child, and an appointment was the most preferred method chosen by professionals. The team would include cardiology, surgery, nursing, social work, and child life, as well as other disciplines if needed (i.e., psychology, rehab, thrombosis team). The team would meet with the parents
“Before his first surgery, we
went up to Edmonton and
talked to everyone. We had the
teleconference, we had social
workers, everything. This
surgery, ‘Here’s your date.
Show up.’ To try and remember
everything that you went
through 3 years ago, even
though nothing’s going to be
the same.

23 | P a g e
ahead of time and the child would be prepared for what was to be done. Professionals also thought it would be valuable for the family to meet a family who had gone through the Fontan. Other strategies included a brochure, provision of a monitored webinar for parents, and videos. They also thought it was important to assess the child, parent, and family needs pre-operatively: “what has helped for pain control in the past,” “what pain scale do they use,” “explore the child’s level of preparedness for the surgery”, and “plan for financial needs.” A parent described a successful approach that prepare her child for a different procedure, and wished that it could have been similar for the Fontan. “He had an MRI done, and they were good; we had Child Life then, and she explained; we went to a little thing about a week before. They had a miniature MRI machine and a little puppet, a little doll that you put through it. So he made a little video, a little movie of putting the doll through this to take home. So I think with any procedure they have to go through, if they could have somebody talk to them about it and talk them through it first, it would help.”
KEY MESSAGES
Parent of children with CHD
• do not know how to prepare their child for the Fontan, and are traumatized by their child’s stress reactions
RECOMMENDATIONS
The strength of this study was that we elicited the perspectives of parents and HCPs on the needs of parents as they seek to support the health and development of their child with HLHS. The strength of the results is that the parents and professionals conveyed similar messages regarding a broken system in urgent need of repair and development. Based on these messages we propose the following recommendations.
Overarching recommendations
1. Develop plan for lifespan approach to services for child and parents
A lifespan perspective on specialized services to address the child, parent, and family needs beyond life-saving surgery and inpatient care is required. This plan would extend from diagnosis (often antenatal) through the transition to adulthood and beyond.
2. Provide patient navigation/ case coordination for families
Parents require support in navigating the different cross-sectorial services to meet the needs of their child and family.
3. Address urgent need to address the financial burdens of the families
This is an urgent concern. Funding agencies must be more aware of the needs of this population.
4. Address the complex developmental and health needs of the children from birth
to eighteen years
This includes expansion of the cardiology clinic to an interdisciplinary team knowledgeable about this population, as well as expansion of the world-renowned Complex Therapies program to monitor children with complex CHD at key transition times beyond age 4 and refer as needed.

24 | P a g e
5. Provide family support and advocacy
Families require access to services to deal with their stress and mental health issues. These services need to be independent of child morbidity and available to all members of the family – child with HLHS if needed, parents if needed, and siblings if needed.
6. Address the immediate concerns about the Fontan surgery
Parents require specific direction regarding preparing their child and themselves for the Fontan operation and resources and services to access in the preparation process.
Specific recommendations
1. Develop plan for life-long specialized services for child and parents • This plan would address the inpatient, outpatient and community access needs of this specialized population, and planning could also generalize to other pediatric populations with complex surgical, developmental and mental health needs. • The planning team could include but is not limited to representation from parents, adults with congenital CHD, interdisciplinary service providers (Stollery, ACH and Glenrose), policy makers, the Complex Therapies program, the Stollery Family Centred Care program, the Western Canadian Children’s Heart network, and community agencies (e.g., FSCD) and service providers.
2. Provide patient navigation/ case coordination for families • Immediate expansion of the outpatient cardiology clinic to include new full time positions for case management and program development
o Nurse Practitioner
Begin to address patient navigation issues, including developing a single point of contact for parents
Provide follow-up for post-surgical complications through NP clinic.
o Social Work dedicated to outpatients
Address family support post-discharge Facilitate access to community supports including Glenrose Coordinate a plan to address urgent financial issues Liaise with Family centred care (Heather McCrady) to tap into existing
endeavors, including formal training and support for parents providing parent-to-parent peer support
3. Address urgent need for resolution of financial burdens of the families • A comprehensive plan for addressing the financial needs of these families, whose needs are not understood or recognized by the current funding system, FSCD. • These children and families have needs that span across ministries, plus have unique medical needs, thus do not clearly fit the mandate of a system designed for children with disabilities. These children have developmental, health, regulatory, and psychosocial needs requiring specialized care and therapies. Parents require instrumental supports and access to trained respite care personnel.

25 | P a g e
4. Address the complex developmental and health needs of the children from birth
to eighteen years • Develop specialized outpatient interdisciplinary teams who understand the needs of this (and other complex medical populations). This could be an expansion of the current cardiology clinic adding nurse practitioner, social worker, child life, psychology, medical specialities including psychiatry, rehabilitation therapists (OT, PT, SLP), dietitian and others. This service could:
o Provide case coordination, and patient navigation. o Provide access for families to interdisciplinary team through clinic
appointments o Provide education and consultation to existing community services o Address, through development of services or referrals, regulatory and mental
health issues of the child, family and siblings. This would include sleeping, eating/feeding, emotional well-being, general health and participation (for needs beyond what the pediatrician is addressing, i.e. pediatricians could refer to this service).
Facilitate linkages to specialized community services that currently exist including feeding and sleep clinics, mental health services (CASA), Community Rehabilitation program, and Glenrose programs.
o Develop interdisciplinary services unique to the inpatient surgical population regarding post-traumatic stress of child, sibling and family. These would be integrated with current services.
o Provide support for liaison to adult cardiology and specialty medical services. All services should have a research component, further investigation of medical trauma, and the nature of the developmental, learning, sensory, language, and motor problems experienced by this population. • Secure funding for the Complex Pediatric Therapies Follow-up program to assess
children with complex CHD beyond age 4; at age 8, 12 and 16 years of age
5. Provide parent support and advocacy that is independent of child morbidity. • All services being developed should include a parent support component, independent of child morbidity. This would include services for mothers, fathers, other family members including siblings • Provide a mechanism for access to parent-to-parent support. • Link with Family Centred care (Heather McCrady)
6. Address immediate concerns about the Fontan surgery
Develop an interdisciplinary plan to support children and parents pre/post Fontan by • Pre-surgery preparation of child and family though a combination of appointment, phone call, and or brochure • Interdisciplinary monitoring of mental health issues of child and family immediately post-surgery and after discharge • Linkages with community services for complex traumatized children • Planning for provision of INR machines for Alberta families living outside of Edmonton.
26 | P a g e
EPILOGUE
I have spoken to parents about their families’ lives with their children with HLHS.
I have read every line of every transcript and I have analyzed every line of the Delphi.
I have listened to every focus group recording.
I have reviewed the parents’ questionnaire data honing in on what each parent reported
about their child’s abilities and challenges.
In doing so, I have entered into the most intimate parts of these parents’ and families’ lives.
I see children and parents who have been traumatized.
I see parents who struggle within a system that is not ready for them and their needs.
I see parents who are judged as being too vigilant but who are expected to carry out
intensive medical care for their babies to return home.
I see siblings who have suffered within their families.
I see families torn apart by financial stress.
I see professionals who know the needs of the families and are powerless to help.
I also see professionals who do not get it; who perceive that the developmental and
learning needs of the children are not a cardiac issue.
I see parents who worship their cardiac surgeons and cardiologists, who see them as family
friends and devoted human beings. Parents owe these people their child’s life.
Above all, I see remarkable, resilient parents, who live so intentionally, who understand
what life is all about, who give up everything for their child’s life and quality of life.
We live in an amazing age of technological revolution where we can save babies and be on
the world stage; yet we leave these families to their own devices after they are moved out
of the hospital and are in a community that has not let them down, as the professionals say,
but rather a community that simply does not get these children, is not ready for them, and
is incapable of meeting their complex needs.
We have a financial system that is so stressed that there are mandates that say disabled
children get funding but if you have all of the developmental issues and more, and also have
a complex ongoing palliative medical condition and have survived life-saving surgeries
requiring months of 24/7 parent medical care
You don’t qualify for funding or we drown the families in paperwork.
Professionals assess the children using standardized measures, and those who are the most
severe are referred for education and rehabilitation support. Those who are less severe,
who would benefit greatly by a small amount of therapy to improve the quality of their
lives, are left with nothing, and parents are left on their own.
27 | P a g e
Moreover, in assessing the children, professionals do not always ask the right questions.
We assess whether the children can climb stairs, articulate each sound, and hold a pencil,
but do we ask about eating, sleeping, and managing in a sensory overwhelming world?
In addition, what about their emotions? How are these children organizing their big
emotions?
We say “These children are doing well considering all they have gone through.”
However, it is more than delayed development; it is disordered development and we do not
have enough services to set them on a path to successful learning and independence.
Although not always getting it right, I see dedicated professionals who care intensely for
these children and their parents; and the professionals are struggling too;
I see glimpses of a traumatized group.
I see a different form of the increasingly referred to “pediatric medical trauma.”
Social workers see post-traumatic stress in the families and are powerless in a system that
is not even broken, because it does not exist.
I see professionals jaded by the system, who believe that asking for services, is a lost cause,
and who quip that the way to meet the financial needs is to win a lottery, or ask the parents
to do their own fundraising and advocating.
We have significant, meaningful, and comprehensive data on a small group of families who
have encountered the best and worst we have to offer.
These families also represent other families who have undergone similar intensive life-
saving interventions, who have the same challenges and stresses.
There is so much we can learn from families who have endured so much,
yet are living life to their fullest.
If we are to save the lives of these children, let’s do more than just make their heart work
better and say we have done our best to fix them.
Let’s offer them and their families a better life.
And, let’s fix the system.
Safeguarding the Heart Child ♥
Family Resilience Study
http://jacksonhardy.blogspot.ca/

28 | P a g e
REFERENCES
1. Rempel GR. Technological advances in pediatrics: Challenges for parents and nurses. J Pediatr Nurs. 2004;19(1):13-24.
2. Kern JH, Hinton VJ, Nereo NE, Hayes CJ, Gersony WM. Early developmental outcome after the Norwood procedure for hypoplastic left heart syndrome. Pediatrics. 1998;102(5):1148-1152.
3. Lawoko S, Soares JJF. Distress and hopelessness among parents of children with congenital heart disease, parents of children with other diseases, and parents of healthy children. J Psychosom Res. 2002;52(4):193-208.
4. Rempel GR, Harrison MJ, Williamson DL. Is "treat your child normally" helpful advice for parents of survivors of treatment of hypoplastic left heart syndrome? Cardiol Young. 2009;19(2):135-144. doi: 10.1017/S1047951109003485.
5. Limperopoulos C, Majnemer A, Shevell MI, Rosenblatt B, Rohlicek C, Tchervenkov C. Neurologic status of newborns with congenital heart defects before open heart surgery. Pediatrics. 1999 Feb;103(2):402-408.
6. Rempel, G., & Cender, L. (1998). Knowing but not knowing: Finding out about your baby’s heart problem before your baby is born. Parent Education Booklet. Vancouver, BC.
7. Rempel, G., Cender, L. M., Lynam, M. J., Sandor, G. G., & Farquharson, D. (2004). Parents’ perspectives on decision making after antenatal diagnosis of congenital heart disease. Journal of Obstetric, Gynecologic, and Neonatal Nursing, 33(1), 64-70. doi:10.1177/0884217503261092
8. Allan L, Dangel J, Fesslova V, et al. Recommendations for the practice of fetal cardiology in Europe. Cardiol Young. 2004;14(1):109-114.
9. Donofrio MTC, MoonGrady AJ, Hornberger LK, et al. Diagnosis and treatment of fetal cardiac disease: A scientific statement from the American Heart Association. Circulation. 2014;129(21):2183-2242.
10. Feinstein JA, Benson DW, Dubin AM, Cohen MS, Maxey DM, Mahle WT, Pahl E, Villafane J, Bhatt AB, Peng LF, Johnson BA, Marsden AL, Daniels CJ, Rudd NA, Caldarone CA, Mussatto KA, Morales DL, Ivy DD, Gaynor JW, Tweddell JS, Deal BJ, Furck AK, Rosenthal GL, Ohye RG, Ghanayem NS, Cheatham JP, Tworetzky W, Martin GR. Hypoplastic left heart syndrome: Current considerations and expectations. J Am Coll Cardiol. 2012;59:S1-42.
11. Robertson CM, Joffe AR, Sauve RS, et al. Outcomes from an interprovincial program of newborn open heart surgery. J Pediatr. 2004;144(1):86-92.
12. Osiovich H, Phillipos E, Byrne P, Robertson M. Hypoplastic left heart syndrome: "to treat or not to treat". Journal of Perinatology. 2000;20(6):363-365.
13. Ross, L., & Frader, J. (2009). Hypoplastic left heart syndrome: A paradigm case for examining conscientious objection in pediatric practice. Journal of Pediatrics, 155, 12–15, http://dx.doi.org/10.1016/j.jpeds.2009. 03.008
14. Tabbutt S, Nord AS, Jarvik GP, Bernbaum J, Wernovsky G, Gerdes M, Zackai E, Clancy RR, Nicolson SC, Spray TL, Gaynor JW. Neurodevelopmental outcomes after staged palliation for hypoplastic left heart syndrome. Pediatrics. 2008;121:476-483.

29 | P a g e
15. Creighton DE, Robertson CM, Sauve RS, et al. Neurocognitive, functional, and health outcomes at 5 years of age for children after complex cardiac surgery at 6 weeks of age or younger. Pediatrics. 2007;120(3):e478-86
16. Brosig CL, Mussatto KA, Kuhn EM, Tweddell JS. Neurodevelopmental outcome in preschool survivors of complex congenital heart disease: Implications for clinical practice. J Pediatr Health Care 2007;21(1):3-12.
17. Shillingford AJ, Glanzman MM, Ittenbach RF, Clancy RR, Gaynor JW, Wernovsky G. Inattention, hyperactivity, and school performance in a population of school-age children with complex congenital heart disease. Pediatrics 2008;121(4):E759-E767.
18. Granberg M, Rydberg A, Fisher AG. Activities in daily living and schoolwork task performance in children with complex congenital heart disease. Acta Paediatrica. 2008;97(9):1270-1274.
19. Rempel G, Harrison M. Safeguarding precarious survival: Parenting children who have life-threatening heart disease. Qualitative Health Research. 2007;17(6):824-837.
20. Rempel G, Ravindran V, Rogers L, Magill-Evans J. Parenting under pressure: A grounded theory of parenting young children with life-threatening congenital heart disease. Journal of Advanced Nursing. 2013;69(3):610-630.
21. Rempel G, Rogers LG, Ravindran V, Magill-Evans J. Facets of parenting a child with hypoplastic left heart syndrome. Nursing Research and Practice. 2012;2012:Article ID 714178, 9 pages. doi: 10.1155/2012/714178.
22. Atallah J, Dinu IA, Joffe AR, et al. Two-year survival and mental and psychomotor outcomes after the Norwood procedure: An analysis of the modified Blalock-Taussig shunt and right ventricle-to-pulmonary artery shunt surgical eras. Circulation. 2008;118(14):1410-1418. doi: 10.1161/CIRCULATIONAHA.107.741579.
23. Snookes SH, Gunn JK, Eldridge BJ, et al. A systematic review of motor and cognitive outcomes after early surgery for congenital heart disease. Pediatrics. 2010;125(4):818-827.
24. Bjarnason-Wehrens B, Dordel S, Schickendantz S, et al. Motor development in children with congenital cardiac diseases compared to their healthy peers. Cardiol Young. 2007;17(5):487-498.
25. Connolly D, McClowry S, Hayman L, Mahony L, Artman M. Posttraumatic stress disorder in children after cardiac surgery. J Pediatr 2004;144(4):480-4.
26. Latal B, Helfricht S, Fischer JE, Bauersfeld U, Landolt MA. Psychological adjustment and quality of life in children and adolescents following open-heart surgery for congenital heart disease: A systematic review. BMC Pediatrics 2009;9(6):10.
27. Norozi K, Zoege M, Buchhorn R, Wessel A., Geyer S. The influence of congenital heart disease on psychological conditions in adolescents and adults after corrective surgery. Congenital Heart Disease. 2006;1(6):282-8.
28. Alton G, Rempel G, Robertson C, Newburn-Cook C, Norris C. Functional outcomes after neonatal open heart surgery: Comparison of survivors of the Norwood staged procedure and the arterial switch operation. Cardiology in the Young. 2010;20(6):668-675. doi: 10.1017/S1047951110000971.
29. http://www.nctsn.org/ 30. http://humanservices.alberta.ca/disability-services/15777.html

30 | P a g e
APPENDICES
Appendix A: Facets of Parenting Intervention Model
Appendix B: Parent questionnaires
Appendix C: Education and Rehabilitation Services Questionnaire
Appendix D: Structured interview guide
Appendix E: Knowledge translation activities during the grant
Appendix F: Focus group questions
Appendix G: Delphi survey

Appendix A: Facets of Parenting Intervention Model

Taking charge of
child’s health &
developmental needs in
home & community settings
Expert parenting “She became a nurse”
Educational Intervention:
Teaching caregivers’ skills
Facets
of
Parenting
a child
with HLHS
Facets of Parenting Intervention Model

Appendix B: Parent questionnaires
Parent Questionnaires
To be completed by each parent separately.
Gwen Rempel, Principal Investigator
Safeguarding the Heart Child Research Program
Faculty of Nursing
University of Alberta
Edmonton, Alberta T6G 2T4
Code No: _________________________
Family Management Study 1
~ Thank you ~
for taking the time to complete these questionnaires.
Form completed by
(relationship to child):
[ ] Biological mom [ ] Biological dad [ ] Other (specify)
Form completed on:
Year Month Day
Note: Whenever the form refers to “your child” this means your child or adolescent with HLHS.
Instructions:
• We are collecting data from both mothers and fathers when possible. Please complete the surveys
independently from each other. Feel free to discuss your responses to these surveys with each other
only after you have completed them.
• All questions are optional. We understand that some of the questions are direct, even blunt. We
appreciate all the responses you are willing to provide and be assured, your responses will be kept
strictly confidential.
• Unless the instructions say otherwise, answer the questions for how things are now.
• It will take 30-45 minutes to complete all the questionnaires. Feel free to do them one at a time or all
at once, whatever works best for you.
• Please return the questionnaires in the stamped envelope when complete.
Two key consent questions to start with:
Do you understand that you have been asked to be in a research study?
Yes No
Do you understand that the questionnaire data you provide for this study may be analyzed in
future studies?
Yes No
Family Management Study 2
Demographic Questions
About you
Age
Any health issues
Ethnic background
Education [ ] University or college graduate
[ ] Some university or college
[ ] High school graduate
[ ] Some high school education
[ ] Less than high school education
[ ] Other:
Employment [ ] Working full time
[ ] Working part time
[ ] Full time student
[ ] Full time homemaker
[ ] Laid off
[ ] Unemployed
[ ] Maternity leave
[ ] Other:
Occupation
Yearly family income [ ] Less than $25, 000
[ ] $26,000 to 35,000
[ ] $36,000 to 45,000
[ ] $46,000 to 65,000
[ ] $66,000 to 85,000
[ ] Greater than $85,000
Marital status

Family Management Study 3
About your family
Siblings living in the home:
Age Gender Any health issues
Others living in the home:
Age Gender Relationship to child (for grandparents, indicate maternal or paternal)
Your child’s primary caregiver (who ensures medical regime is adhered to, meds taken on time, diet
restrictions followed, stays home with sick child):

Family Management Study 4
How Our Family Manages
This questionnaire is about how your family manages caring for a child with a chronic condition.
Instructions For each statement in this questionnaire, you are asked to rate your response to the statement on a scale of 1
to 5, with 1 indicating “Strongly disagree” and 5 indicating “Strongly agree.” Please respond to each statement
in this questionnaire based on what you think, not on how you think others might respond. If your child has
more than one chronic condition the word “condition” refers to all of their diagnoses together. Also, many of
these questions use the word “family.” This refers to those people living in your household who you think of as
family.
Section 1: to be completed by everyone Please check the boxes or circle your answers.
Strongly
Disagree
1 2 3 4
Strongly
Agree
5
1. Our child’s everyday life is similar to that of other children his/her
age. 1 2 3 4 5
2. Our child’s condition gets in the way of family relationships. 1 2 3 4 5
3. Our child’s condition requires frequent visits to the clinic. 1 2 3 4 5
4. In the future we expect our child to take care of the condition. 1 2 3 4 5
5. Our child enjoys life less because of the condition. 1 2 3 4 5
6. Taking care of our child’s condition is often overwhelming. 1 2 3 4 5
7. Our child’s condition is like a roller coaster with lots of ups and
downs. 1 2 3 4 5
8. Our child’s condition is the most important thing in our family. 1 2 3 4 5
9. It is very hard for us to take care of our child’s condition. 1 2 3 4 5
10. Our child takes part in activities he/she wishes to despite the
condition. 1 2 3 4 5
11. Because of the condition, we worry about our child’s future. 1 2 3 4 5
12. Our child’s condition doesn’t take a great deal of time to manage. 1 2 3 4 5
13. We have some definite ideas about how to help our child live with the
condition. 1 2 3 4 5
14. Despite the condition, we expect our child to live away from home in
the future. 1 2 3 4 5
15. We have enough money to manage our child’s condition. 1 2 3 4 5
16. Our child is different from other children his/her age because of the
condition. 1 2 3 4 5
Family Management Study 5
Strongly
Disagree
1 2 3 4
Strongly
Agree
5
17. It is difficult to know when our child’s condition must come first in the
family. 1 2 3 4 5
18. We are looking forward to a happy future with our child. 1 2 3 4 5
19. When something unexpected happens with our child’s condition, we
usually know how to handle it. 1 2 3 4 5
20. Our child’s friendships are different because of the condition. 1 2 3 4 5
21. We expect to be devoting less time to our child’s condition in the
future. 1 2 3 4 5
22. A condition like the one our child has makes family life very difficult. 1 2 3 4 5
23. Our child’s condition rarely interferes with other family activities. 1 2 3 4 5
24. Our child’s condition requires frequent hospital stays. 1 2 3 4 5
25. We feel we are doing a good job taking care of our child’s condition. 1 2 3 4 5
26. People with our child’s condition have a normal length of life. 1 2 3 4 5
27. It’s often difficult to know if we need to be more protective of our
child. 1 2 3 4 5
28. We often feel unsure about what to do to take care of our child’s
condition. 1 2 3 4 5
29. Our child’s condition will be harder to take care of in the future. 1 2 3 4 5
30. We think about our child’s condition all the time. 1 2 3 4 5
31. It seems as if our child’s condition controls our family life. 1 2 3 4 5
32. Many conditions are more serious than our child’s. 1 2 3 4 5
33. It is hard to get anyone else to help us with our child’s condition. 1 2 3 4 5
34. We have not been able to develop a routine for taking care of our
child’s condition. 1 2 3 4 5
35. It takes a lot of organization to manage our child’s condition. 1 2 3 4 5
36. We are sometimes undecided about how to balance the condition
and family life. 1 2 3 4 5
37. It is hard to know what to expect of our child’s condition in the
future. 1 2 3 4 5
38. Even though our child has the condition, we have a normal family life. 1 2 3 4 5
39. Our child would do better in school if he/she didn’t have the
condition. 1 2 3 4 5
40. We are confident that we can take care of our child’s condition. 1 2 3 4 5
41. We have goals in mind to help us manage our child’s condition. 1 2 3 4 5
Family Management Study 6
Strongly
Disagree
1 2 3 4
Strongly
Agree
5
42. It is difficult to fit care of our child’s condition into our usual family
routine. 1 2 3 4 5
43. Dealing with our child’s condition makes family life more difficult. 1 2 3 4 5
44. We know when our child needs to be a child. 1 2 3 4 5
45. A condition like the one our child has makes it very difficult to live a
normal life. 1 2 3 4 5
This ends Section 1.
Section 2 covers aspects of family management when there are adult partners in a household. The term
“partner” refers to a spouse or partner living in the same household.
Do you have a spouse or adult partner living in your
home? Yes No
If you answered YES, please proceed to the next page. If you answered NO, please skip ahead to the next
questionnaire.

Family Management Study 7
Section 2 The questions in the next section relate to you and your partner. For each statement in this section, rate your
response to the statement on a scale of 1 to 5, with 1 indicating “Strongly disagree” and 5 indicating “Strongly
agree.” Again, please respond to each statement in this questionnaire based on how YOU feel, not on how you
think your partner or others might respond.
Strongly
Disagree
1 2 3 4
Strongly
Agree
5
46. We are a closer family because of how we deal with our child’s
condition. 1 2 3 4 5
47. My partner and I have different ideas about how serious our child’s
condition is. 1 2 3 4 5
48. I am pleased with how my partner and I work together to manage our
child’s condition. 1 2 3 4 5
49. My partner and I argue about how to manage our child’s condition. 1 2 3 4 5
50. My partner and I consult with each other before we make a decision
about our child’s care. 1 2 3 4 5
51. My partner and I have similar ideas about how we should be raising
our child. 1 2 3 4 5
52. I am unhappy about the way my partner and I share the management
of our child’s condition. 1 2 3 4 5
53. My partner and I support each other in taking care of our child’s
condition. 1 2 3 4 5
Source: Family Management Measure by K. Knafl, J. Deatrick, A. Gallo, J. Dixon, & M. Grey.

Family Management Study 8
How I See Myself
Instructions For each item, please mark an “x” in the box below that best indicates how much you agree with the following
statements as they apply to you over the last month. If a particular situation has not occurred recently,
answer according to how you think you would have felt.
Not at
all true
0
Rarely
true
1
Sometimes
true
2
Often
true
3
True
nearly all
the time
4
1. I am able to adapt when changes occur. 0 1 2 3 4
2. I have at least one close and secure relationship which helps me
when I am stressed. 0 1 2 3 4
3. When there are no clear solutions to my problems, sometimes
fate or God can help. 0 1 2 3 4
4. I can deal with whatever comes my way. 0 1 2 3 4
5. Past successes give me confidence in dealing with new challenges
and difficulties. 0 1 2 3 4
6. I try to see the humorous side of things when I am faced with
problems. 0 1 2 3 4
7. Having to cope with stress can make me stronger. 0 1 2 3 4
8. I tend to bounce back after illness, injury, or other hardships. 0 1 2 3 4
9. Good or bad, I believe that most things happen for a reason. 0 1 2 3 4
10. I give my best effort, no matter what the outcome may be. 0 1 2 3 4
11. I believe I can achieve my goals, even if there are obstacles. 0 1 2 3 4
12. Even when things look hopeless, I don't give up. 0 1 2 3 4
13. During times of stress/crisis, I know where to turn for help. 0 1 2 3 4
14. Under pressure, I stay focused and think clearly. 0 1 2 3 4
15. I prefer to take the lead in solving problems, rather than letting
others make all the decisions. 0 1 2 3 4
16. I am not easily discouraged by failure. 0 1 2 3 4
17. I think of myself as a strong person when dealing with life's
challenges and difficulties. 0 1 2 3 4
18. I can make unpopular or difficult decisions that affect other
people, if it is necessary. 0 1 2 3 4
19. I am able to handle unpleasant or painful feelings like sadness,
fear and anger. 0 1 2 3 4

Family Management Study 9
Not at
all true
0
Rarely
true
1
Sometimes
true
2
Often
true
3
True
nearly all
the time
4
20. In dealing with life's problems, sometimes you have to act on a
hunch, without knowing why. 0 1 2 3 4
21. I have a strong sense of purpose in life. 0 1 2 3 4
22. I feel in control of my life. 0 1 2 3 4
23. I like challenges. 0 1 2 3 4
24. I work to attain my goals, no matter what roadblocks I encounter
along the way. 0 1 2 3 4
25. I take pride in my achievements. 0 1 2 3 4
Source: Connor-Davidson Resiliency Scale. All rights reserved. No part of this document may be reproduced or transmitted in any form, or by any
means, electronic or mechanical, including photocopying, or by any information storage or retrieval system, without permission in writing from Dr.
Davidson: Box 3812, Duke University Medical Center, Durham NC 27710; e-mail: [email protected]. Copyright © 2001, 2003, 2007, 2009 by
Kathryn M. Connor, M.D.and Jonathan R. T. Davidson, M.D.

Family Management Study 10
Parenting Stress
Instructions The Parenting Stress Index (PSI Short Form) is attached. Please do not write your name on the form.
Thank you again for taking the time to complete these questionnaires!
Rempel Family Resilience Study Protocol
A paper copy of the Parenting Stress Index will be included in the Family and Parent Questionnaire Booklet. Sample for review purposes only.

Appendix C: Education and Rehabilitation Services Questionnaire
Child Questionnaires
For Children and Teens (Age 5-18)
To be completed once per family, by either or both parents together.
Gwen Rempel, Principal Investigator
Safeguarding the Heart Child Research Program
Faculty of Nursing
University of Alberta
Edmonton, Alberta T6G 2T4
Code No: _________________________

Family Management Study 1
~ Thank you ~
for taking the time to complete this questionnaire.
Form completed by
(relationship to child):
[ ] Biological mom [ ] Biological dad [ ] Other (specify)
Form completed on:
Year Month Day
Note: Whenever the form refers to your “child” this means your child or adolescent with HLHS.
Instructions:
• This questionnaire need only be completed once per family as most of the questions are factual, not
opinion-based. Feel free to have one parent complete it alone, or for both to complete it together.
• All questions are optional. We understand that some of the questions are direct, even blunt. We
appreciate all the responses you are willing to provide and be assured, your responses will be kept
strictly confidential.
• Unless the instructions say otherwise, answer the questions for how things are now.
• It will take 15-30 minutes to complete the questionnaire.
• Please return the questionnaire in the stamped envelope when complete.
Two key consent questions to start with:
Do you understand that you have been asked to be in a research study?
Yes No
Do you understand that the questionnaire data you provide for this study may be analyzed in
future studies?
Yes No
Family Management Study 2
Demographic Questions
About your child
Gender: [ ] Male
[ ] Female
Age: Grade:
Date of Birth:
Birth Location (city/town, province):
Current Residence (city/town, province):
About your child’s health
Child’s cardiac diagnosis:
[ ] Prenatal diagnosis: Diagnosis made at __________ weeks gestation.
OR
[ ] Postnatal diagnosis: Diagnosis made at child’s age of ____________________.
Cardiac surgeries (complete to your best recollection):
Date Child’s
age
Name of operation Surgical centre (e.g.
name of hospital)
Length of hospitalization
Family Management Study 3
Other procedures and/or hospitalizations (complete to your best recollection):
Date Child’s
age
Purpose Length of hospitalization
Medications your child is on currently:
Other health information (e.g. any conditions other than cardiac):
Any learning issues identified by you or your child’s school:
Family Management Study 4
Education and Rehab Services
Instructions
Please check the boxes that are most appropriate and write additional comments where asked.
I: Schooling
1. What type of school does your child attend?
Public/separate (regular school)
Private (regular school)
Special needs school
Other (e.g., home school)
Specify:
2. What grade is your child in? _____________
3. My child:
Attends a regular school in a regular class
Is in a regular class but receives tutoring after school
Is in a regular class but has educational/resource support (e.g. special education, resource teacher)
Specify:
Is in a special education class in a regular school
Is in a school for children with special needs
4. My child receives classroom aide support
Full time
Part time
Access to classroom aide
5. If your child receives additional educational support or resources, what are these services addressing?
(indicate all that apply)
Communication/language
Class work/education
Class participation/socialization
Handwriting/printing
Reading
Math
Behaviour
Physical activity and mobility (e.g. gym class, stairs)
Other
Specify:
Family Management Study 5
6. If your child is not receiving services at school, do you think they should be?
Yes
No
7. If yes, in what area do you think your child needs services?
Communication/language
Class work/education
Class participation/socialization
Handwriting/printing
Reading
Math
Behaviour
Physical activity and mobility (e.g. gym class, stairs)
Other
Specify:
II: Early Years
8. Which community-based services did you access during the first few years of your child’s life?
A Parent Link Centre in your community
o Drop-In activities
o Positive Parenting Program (Triple P)
The Virtual Parent Link Centre
o The Talk Box
o Ages and Stages information
Health Unit for:
o Immunizations
o Other services
Specify:
Early Intervention Services (0 to 3 years of age)
o Home visits
o Parent child groups
o Developmental screening
o Access to rehabilitation therapies
Specify (e.g., OT, PT, Speech/language):
Other community based activities
o Library programs
o Recreation centres
o Other
Specify:

Family Management Study 6
III: Services We Use (A)
Occupational
Therapy Physical Therapy
Speech Language
Pathology Audiology
9. Is your child
receiving
these services
now?
Yes
Please answer
questions 10-14.
No
Please answer
questions 15-17.
Yes
Please answer
questions 10-14.
No
Please answer
questions 15-17.
Yes
Please answer
questions 10-14.
No
Please answer
questions 15-17.
Yes
Please answer
questions 10-14.
No
Please answer
questions 15-17.
If your child IS currently receiving these services…
10. Who referred
your child to
these
services?
Family physician
Pediatrician
Medical specialist
Specify:
Other health care
professional
Specify:
Complex Pediatric
Therapies Follow-Up
Program
Neonatal/Perinatal
Follow-up Program
Outpatient
rehabilitation facility
School
Self-referred
Other
Specify:
I don’t know
Family physician
Pediatrician
Medical specialist
Specify:
Other health care
professional
Specify:
Complex Pediatric
Therapies Follow-Up
Program
Neonatal/Perinatal
Follow-up Program
Outpatient
rehabilitation facility
School
Self-referred
Other
Specify:
I don’t know
Family physician
Pediatrician
Medical specialist
Specify:
Other health care
professional
Specify:
Complex Pediatric
Therapies Follow-Up
Program
Neonatal/Perinatal
Follow-up Program
Outpatient
rehabilitation facility
School
Self-referred
Other
Specify:
I don’t know
Family physician
Pediatrician
Medical specialist
Specify:
Other health care
professional
Specify:
Complex Pediatric
Therapies Follow-Up
Program
Neonatal/Perinatal
Follow-up Program
Outpatient
rehabilitation facility
School
Self-referred
Other
Specify:
I don’t know
11. Where is your
child receiving
these
services?
(check all that
apply)
Hospital
Outpatient
rehabilitation facility
At school
Home-based
services (e.g. private
practice, agency)
Other
Specify:
Hospital
Outpatient
rehabilitation facility
At school
Home-based
services (e.g. private
practice, agency)
Other
Specify:
Hospital
Outpatient
rehabilitation facility
At school
Home-based
services (e.g. private
practice, agency)
Other
Specify:
Hospital
Outpatient
rehabilitation facility
At school
Home-based
services (e.g. private
practice, agency)
Other
Specify:

Family Management Study 7
Occupational
Therapy Physical Therapy
Speech Language
Pathology Audiology
12. How
frequently is
your child
receiving
these
services?
Once a week or
more
Twice monthly
Once a month
Every 3 months
Every 6 months
Once a year
Other
Specify:
Once a week or
more
Twice monthly
Once a month
Every 3 months
Every 6 months
Once a year
Other
Specify:
Once a week or
more
Twice monthly
Once a month
Every 3 months
Every 6 months
Once a year
Other
Specify:
Once a week or
more
Twice monthly
Once a month
Every 3 months
Every 6 months
Once a year
Other
Specify:
13. How are
these services
covered
financially?
(check all that
apply)
Provincial health
insurance
Private health
insurance
Other provincial
funding (e.g. At
Home Program,
Family Supports for
Children with
Disabilities (FSCD))
Education funding
(e.g. PUF)
Personal finances
Other
Specify:
Provincial health
insurance
Private health
insurance
Other provincial
funding (e.g. At
Home Program,
Family Supports for
Children with
Disabilities (FSCD))
Education funding
(e.g. PUF)
Personal finances
Other
Specify:
Provincial health
insurance
Private health
insurance
Other provincial
funding (e.g. At
Home Program,
Family Supports for
Children with
Disabilities (FSCD))
Education funding
(e.g. PUF)
Personal finances
Other
Specify:
Provincial health
insurance
Private health
insurance
Other provincial
funding (e.g. At
Home Program,
Family Supports for
Children with
Disabilities (FSCD))
Education funding
(e.g. PUF)
Personal finances
Other
Specify:
14. How satisfied
are you with
these
services?
Very dissatisfied
Somewhat
dissatisfied
Neutral
Somewhat satisfied
Very satisfied
Other
Specify:
Very dissatisfied
Somewhat
dissatisfied
Neutral
Somewhat satisfied
Very satisfied
Other
Specify:
Very dissatisfied
Somewhat
dissatisfied
Neutral
Somewhat satisfied
Very satisfied
Other
Specify:
Very dissatisfied
Somewhat
dissatisfied
Neutral
Somewhat satisfied
Very satisfied
Other
Specify:

Family Management Study 8
Occupational
Therapy Physical Therapy
Speech Language
Pathology Audiology
If your child is NOT currently receiving these services…
15. Has your child
ever received
these services
in the past?
Yes
Age:
Reason:
No
Yes
Age:
Reason:
No
Yes
Age:
Reason:
No
Yes
Age:
Reason:
No
16. Do you think
that your
child should
be receiving
these services
now?
Yes
Comment:
No
Yes
Comment:
No
Yes
Comment:
No
Yes
Comment:
No
17. If yes, what
are the
barriers to
receiving
these
services?
(check all that
apply)
No one has referred
my child for services
I am not sure what
type of
rehabilitation
services would
benefit my child
The cost of services
is too high
The location of the
service provider is
inconvenient
We are currently on
a waiting list
My child does not
qualify for services
Reason:
Other
Specify:
No one has referred
my child for services
I am not sure what
type of
rehabilitation
services would
benefit my child
The cost of services
is too high
The location of the
service provider is
inconvenient
We are currently on
a waiting list
My child does not
qualify for services
Reason:
Other
Specify:
No one has referred
my child for services
I am not sure what
type of
rehabilitation
services would
benefit my child
The cost of services
is too high
The location of the
service provider is
inconvenient
We are currently on
a waiting list
My child does not
qualify for services
Reason:
Other
Specify:
No one has referred
my child for services
I am not sure what
type of
rehabilitation
services would
benefit my child
The cost of services
is too high
The location of the
service provider is
inconvenient
We are currently on
a waiting list
My child does not
qualify for services
Reason:
Other
Specify:
Family Management Study 9
IV: Services We Use (B)
For “Other” please specify any other services (e.g. homecare nurse, dietitian, etc.) that your child receives
currently, has received in the past, or should be receiving.
Psychology Social Work Other/Specify:
Other/Specify:
18. Is your child
receiving
these services
now?
Yes
Please answer
questions 19-23.
No
Please answer
questions 24-26.
Yes
Please answer
questions 19-23.
No
Please answer
questions 24-26.
Yes
Please answer
questions 19-23.
No
Please answer
questions 24-26.
Yes
Please answer
questions 19-23.
No
Please answer
questions 24-26.
If your child IS currently receiving these services…
19. Who referred
your child to
these
services?
Family physician
Pediatrician
Medical specialist
Specify:
Other health care
professional
Specify:
Complex Pediatric
Therapies Follow-Up
Program
Neonatal/Perinatal
Follow-up Program
Outpatient
rehabilitation facility
School
Self-referred
Other
Specify:
I don’t know
Family physician
Pediatrician
Medical specialist
Specify:
Other health care
professional
Specify:
Complex Pediatric
Therapies Follow-Up
Program
Neonatal/Perinatal
Follow-up Program
Outpatient
rehabilitation facility
School
Self-referred
Other
Specify:
I don’t know
Family physician
Pediatrician
Medical specialist
Specify:
Other health care
professional
Specify:
Complex Pediatric
Therapies Follow-Up
Program
Neonatal/Perinatal
Follow-up Program
Outpatient
rehabilitation facility
School
Self-referred
Other
Specify:
I don’t know
Family physician
Pediatrician
Medical specialist
Specify:
Other health care
professional
Specify:
Complex Pediatric
Therapies Follow-Up
Program
Neonatal/Perinatal
Follow-up Program
Outpatient
rehabilitation facility
School
Self-referred
Other
Specify:
I don’t know
20. Where is your
child receiving
these
services?
(check all that
apply)
Hospital
Outpatient
rehabilitation facility
School
Home-based
services (e.g. private
practice, agency)
Other
Specify:
Hospital
Outpatient
rehabilitation facility
School
Home-based
services (e.g. private
practice, agency)
Other
Specify:
Hospital
Outpatient
rehabilitation facility
School
Home-based
services (e.g. private
practice, agency)
Other
Specify:
Hospital
Outpatient
rehabilitation facility
School
Home-based
services (e.g. private
practice, agency)
Other
Specify:

Family Management Study 10
Psychology Social Work Other/Specify:
Other/Specify:
21. How
frequently is
your child
receiving
these
services?
Once a week or
more
Twice monthly
Once a month
Every 3 months
Every 6 months
Once a year
Other
Specify:
Once a week or
more
Twice monthly
Once a month
Every 3 months
Every 6 months
Once a year
Other
Specify:
Once a week or
more
Twice monthly
Once a month
Every 3 months
Every 6 months
Once a year
Other
Specify:
Once a week or
more
Twice monthly
Once a month
Every 3 months
Every 6 months
Once a year
Other
Specify:
22. How are
these services
covered
financially?
(check all that
apply)
Provincial health
insurance
Private health
insurance
Other provincial
funding (e.g. At
Home Program,
Family Supports for
Children with
Disabilities (FSCD))
Education funding
(e.g. PUF)
Personal finances
Other
Specify:
Provincial health
insurance
Private health
insurance
Other provincial
funding (e.g. At
Home Program,
Family Supports for
Children with
Disabilities (FSCD))
Education funding
(e.g. PUF)
Personal finances
Other
Specify:
Provincial health
insurance
Private health
insurance
Other provincial
funding (e.g. At
Home Program,
Family Supports for
Children with
Disabilities (FSCD))
Education funding
(e.g. PUF)
Personal finances
Other
Specify:
Provincial health
insurance
Private health
insurance
Other provincial
funding (e.g. At
Home Program,
Family Supports for
Children with
Disabilities (FSCD))
Education funding
(e.g. PUF)
Personal finances
Other
Specify:
23. How satisfied
are you with
these
services?
Very dissatisfied
Somewhat
dissatisfied
Neutral
Somewhat satisfied
Very satisfied
Other
Specify:
Very dissatisfied
Somewhat
dissatisfied
Neutral
Somewhat satisfied
Very satisfied
Other
Specify:
Very dissatisfied
Somewhat
dissatisfied
Neutral
Somewhat satisfied
Very satisfied
Other
Specify:
Very dissatisfied
Somewhat
dissatisfied
Neutral
Somewhat satisfied
Very satisfied
Other
Specify:

Family Management Study 11
Psychology Social Work Other/Specify:
Other/Specify:
If your child is NOT currently receiving these services…
24. Has your child
ever received
these services
in the past?
Yes
Age:
Reason:
No
Yes
Age:
Reason:
No
Yes
Age:
Reason:
No
Yes
Age:
Reason:
No
25. Do you think
that your
child should
be receiving
these services
now?
Yes
Comment:
No
Yes
Comment:
No
Yes
Comment:
No
Yes
Comment:
No
26. If yes, what
are the
barriers to
receiving
these
services?
(check all that
apply)
No one has referred
my child for services
I am not sure what
type of
rehabilitation
services would
benefit my child
The cost of services
is too high
The location of the
service provider is
inconvenient
We are currently on
a waiting list
My child does not
qualify for services
Reason:
Other
Specify:
No one has referred
my child for services
I am not sure what
type of
rehabilitation
services would
benefit my child
The cost of services
is too high
The location of the
service provider is
inconvenient
We are currently on
a waiting list
My child does not
qualify for services
Reason:
Other
Specify:
No one has referred
my child for services
I am not sure what
type of
rehabilitation
services would
benefit my child
The cost of services
is too high
The location of the
service provider is
inconvenient
We are currently on
a waiting list
My child does not
qualify for services
Reason:
Other
Specify:
No one has referred
my child for services
I am not sure what
type of
rehabilitation
services would
benefit my child
The cost of services
is too high
The location of the
service provider is
inconvenient
We are currently on
a waiting list
My child does not
qualify for services
Reason:
Other
Specify:

Family Management Study 12
If you have any further comments to make about services that your child receives currently, has received in
the past, or should be receiving, please use this page.
Source: Adapted from: Majnemer, A., Mazer, B., Lecker, E., Leduc Carter, A., Limperopoulos, C., Shevell, M., et al. (2008). Patterns of use of
educational and rehabilitation services at school age for children with congenitally malformed hearts. Cardiology in the Young, 18(3), 288-296.

Family Management Study 13
Vineland
Instructions
The Vineland booklet and instructions are attached. Please do not write your name on the booklet.
Thank you again for taking the time to complete these questionnaires!

Rempel Family Resilience Study Protocol Vineland Adaptive Behavior Scales A paper copy of the Vineland Adaptive Behavior Scales: Parent/Caregiver Rating Form will be included in the Child Questionnaire Booklet. Partial sample of the Vineland form shown below; for review purposes only.
Vineland overview:
Image source: http://psychcorp.pearsonassessments.com/HAIWEB/Cultures/en-us/Productdetail.htm?Pid=Vineland-II

Appendix D: Structured interview guide

Family Resilience Study - Parent Interview Guiding Questions
1. Tell me about your child with HLHS.
Probes: Any concerns? How was his/her last appointment with the pediatric cardiologist?
How is your child now compared to when he/she was a baby? a toddler? a preschooler? at school
age?
What’s his/her favourite activity?
2. How are you doing as [name of child with HLHS]’s parent?
How is your spouse/partner doing?
Probes: What are you most proud of? Who worries the most?
3. What is life like for your family right now, especially related to your child with HLHS?
Probes: Tell be about the most enjoyable thing you have recently done as a family.
What is the hardest time of day for your family?
4. When you think of [name of child with HLHS]’s future what comes to your mind?
Probes: Do you think differently about [name of child with HLHS]’s when compared to your other
children or other children his/her age?
5. What has been the most rewarding aspect of parenting [name of child with HLHS]?
6. What has been the most challenging aspect of parenting [name of child with HLHS]?
7. Thinking of what you have gone through related to [name of child with HLHS]’s HLHS what or who
has helped you the most? the least?
Supports and Services; Informational, Emotional, and Practical; Formal and Informal
8. What supports and services have you accessed since your child was last in the hospital?
9. Thinking specifically about your child’s needs, what resources have helped you the most? the least?
10. What supports and services have helped you as a parent the most? the least?
11. What supports and services have helped your family the most? the least?
12. Construct and discuss genogram (Family Structure) and ecomap
13. Probes: What was it like to travel to a specialized centre for surgery? Or What was it like to have
specialized surgery available so close to where you lived?
14. What are your current needs in parenting your child?
• Regarding [child]’s development, what do you worry about the most?
• Regarding [child]’s development, what do you worry about the least?
Probe based on results of the Vineland Adaptive Behavior Scales, Educational and
Rehabilitation Services Questionnaire, Family Management Measure]
15. What resources do you currently need? Are they available?
16. Were there supports and services that you needed in the past that were not available?
Probe: tell me about what happened; what did you do? How did things turn out?
17. What stands out in your mind about the supports and services you received at different times along
the way:

Family Resilience Study - Parent Interview Guiding Questions
− At the time of diagnosis
− Hospitalization for first surgery – Norwood or Sano-Norwood
− Going home after first surgery
− Hospitalization for second surgery – Glenn
− Going home after second surgery
− Hospitalization for third surgery – Fontan
− Going home after third surgery
− Linking with preschool and school services
18. Some parents talk about having lingering thoughts about what their child has been through. Is that
something that resonates for you? If so, tell me about that.

Appendix E: Knowledge translation activities during the grant

Life-of-Grant Knowledge Translation Activities
Published abstracts:
Ballantyne, R. T., Dorfman, T., Dahl, N., Rogers, L., Magill-Evans, J., Mackie, A. S. & Rempel, G.
(2013). The relationship of parent well-being, family management, and service
utilization in families of children with hypoplastic left heart syndrome from the
perspective of mothers and fathers. Circulation, 128(22S), A19104.
Rempel, G., Dorfman, T. L., Dahl, N., Rogers, L. G., & Magill-Evans, J. (2013). The relationship
of child and family functioning in families of children with complex congenital heart
disease: A pilot study. SA Heart Journal, 10(1), 378.
Rempel, G., & Fricker, L. (2013, February). What is the timing, setting, and nature of parent
interventions for mothers and fathers of children with congenital heart disease: A
scoping review. SA Heart Journal, 10(1), 378
International conference -Peer reviewed papers:
Rempel, G. R., Dorfman, T. D., Rogers, L. G., Magill-Evans, J. (2013, June). The relationship of
child and family functioning in families of children with complex congenital heart
disease: A pilot study. Paper presented at the 11th International Family Nursing
Conference, Minneapolis, MN.
Rogers, L. G. & Rempel, G. R. (2013, June). Contextualizing narrative data from children with
family-oriented data from parents: Development of a research protocol. Paper
presented at the 11th International Family Nursing Conference, Minneapolis, MN.
Invited Presentations:
Rempel, G. R., Rogers, L. G., & Ravindran, V., (2013 June). Facilitating family caregiving:
Theory-driven intervention development and evaluation. 11th International Family
Nursing Conference, Minneaoplis, MN.
Rempel, G. (2013, May). Family Resilience: Parenting children with complex cross-sectoral
service needs. ACCFCR 10th Anniversary Research Showcase, Edmonton, AB.
Rempel, G. & Rogers, L. (2013 May). Circle of Trust: how to help your child feel safe when
our own world is turned upside down? University Infant Toddler Centre Annual
General Meeting, Edmonton, AB.
Rempel, G. (2013, February). Quality of life and parental concerns after the Norwood. In
Rebeyka, I. (Chair), Hypoplastic left heart syndrome from the prairies to the Rockies:
Edmonton and WCCHN cardiac program experience. Symposium conducted at the
World Congress of Paediatric Cardiology & Cardiac Surgery, Cape Town, South Africa.
Local conferences - Peer reviewed papers and posters
Dahl, N., Fricker, L., Dorfman, T., McConnan, L., Davis, R., & Rempel, G. (2012, October).
Leading the way for children and families: The patient navigator role in pediatric
Life-of-Grant Knowledge Translation Activities
settings in Canada. Paper presented at Margaret Scott Wright (MSW) Research Day,
Calgary, AB.
Dorfman, T., Dahl, N., Rogers, L. G., Magill-Evans, J., & Rempel, G. (2012, October). The
relationship of child and family functioning in families of children with complex
congenital heart disease: A pilot study. Paper presented at Margaret Scott Wright
(MSW) Research Day, Calgary, AB.
Dahl, N., Fricker, L., Dorfman, T., McConnan, L., Davis, R., & Rempel, G. (2012, November).
Leading the way for children and families: The patient navigator role in pediatric
settings in Canada. Poster presented at WCHRI Research Day, Edmonton, AB.
Meakins, L., Ray, L., Hegadoran, K., & Rempel, G. (2012, October). Parental vigilance in
caring for their children with hypoplastic left heart syndrome. Poster presented at the
Canadian Cardiovascular Congress, Toronto, ON.
Dahl, N. D., Dorfman, T., Rogers, L. G., Magill-Evans, J., & Rempel, G. (2012, October). Child
and family functioning when a child has complex congenital heart disease: A pilot
study. Poster presented at Glenrose Spotlight on Research Breakfast & Symposium,
Edmonton, AB.
Rogers, L. G., Rempel, G., Dorfman, T., Dahl, N., Wiart, L., Alton, G., & Magill-Evans, J. (2012,
October). Rehabilitation services utilization for children with hypoplastic left heart
syndrome. Poster presented at Glenrose Spotlight on Research Breakfast &
Symposium, Edmonton, AB.
Dahl, N. D., Dorfman, T., Rogers, L. G., Magill-Evans, J., & Rempel, G. (2012, June). The
relationship of child and family functioning in families of children with complex
congenital heart disease: A pilot study. Poster presented at Mazankowski Cardiac
Sciences Day, Edmonton, AB.

Appendix F: Focus group questions
Study Title: Strengthening Family Resilience Principal Investigator: Gwen Rempel, RN, PhD (780) 435-8167 Associate Adjunct Professor [email protected] Faculty of Nursing, University of Alberta Calgary Investigator: Kim Myers, MD, FRCPC (403) 955-7858 Clinical Assistant Professor, Pediatric Cardiology [email protected] University of Calgary/Alberta Children’s Hospital
Safeguarding the Heart Child [email protected]
Parent Focus Group Guiding Questions 1. Briefly tell us about your current parenting situation with your child with HLHS.
2. What concerns you most about accessing services for your child with HLHS? 3. We are interested in learning about the types of services that would benefit parents of children
with HLHS. In our recent interviews with parents, several components of a parent-focused intervention were identified as important: (See Facets of Parenting diagram)
What do you think are the most important components of a parent-focused intervention for these families? Why do you believe those components are important?
4. We are interested in optimal timing of services for families. When do you think a parent-focussed
intervention would be most effective?
5. We are interested in determining the most appropriate way to provide intervention for parents. For example, clinic based, community-based, peer-support, telephone, web-based are all examples of different ways to provide the intervention. What do you think would be the most effective way to provide the services you described
earlier? Who should provide the service? What is feasible given the current organization of services for parents and families in your community?
6. Summary questions: All things considered, what would be the most helpful thing we could do for you to help you help your child with HLHS? What is the one thing that we could do for you to help you help your family? Why are these things not happening for you and your family?
For the focus groups that include parents from rural areas: What are the unique challenges for you as a parent who lives rurally?
Study Title: Strengthening Family Resilience
Principal Investigator: Gwen Rempel, RN, PhD (780) 435-8167 Associate Adjunct Professor [email protected] Faculty of Nursing, University of Alberta Safeguarding
the Heart Child [email protected]
Focus Group Guiding Questions – SERVICE PROVIDERS 1. Briefly tell us about your current role with families of children with HLHS.
2. What concerns you most about these children and their families? 3. We are interested in learning about the types of services that would benefit parents of children
with HLHS. We have recently conducted interviews with parents and they identified the following components of a parent-focussed intervention as important: (list).
Based on your experience working with families and the responses that we heard from parents, what do you think are the most important components of a parent-focussed intervention for these families? [PROBE- why do you believe those components are important?]
4. We are interested in optimal timing of services for these families. When do you think a parent-
focussed intervention would be most effective? [PROBE- determine timing of different components of intervention]
5. We are interested in determining the most appropriate way to provide intervention with families.
For example, clinic based, community-based, peer-support, telephone, web-based are all examples of different ways to provide the intervention. What do you think would be the most effective way to provide the services you described
earlier? Who should provide the service? What is feasible given the current organization of services for families in your community?
6. Summary questions: All things considered, what is the one that we could do for parents that would help them help their child with HLHS? What is the one thing that we could do for parents that strength the resilience of their family? What is keeping us from providing this service for parents? [What are the barriers to service provision?]
For the focus groups in urban centres: 7. We will conduct focus groups in rural areas – who in those communities or surrounding area
could you recommend based on their involvement with children with HLHS and their families? For the focus groups in rural areas: 8. What are the unique challenges for the parents in your service area who live rurally?

Appendix G: Delphi survey
5/13/2014 HLHS Delphi - Family Resilience Study
https://docs.google.com/a/ualberta.ca/forms/d/1wFiCxgSub45u9u_dxuoEM45yszxsxzzuTkw8jb2L45E/viewform 1/1
Pow ered by
HLHS Delphi - FamilyResilience StudyDATA ARE IN~Alberta parents of children with HLHS have told us they are struggling. ~Health care providers, such as yourself, have also told us about your concerns. ~We have questionnaire, interview, and focus group data from 42 parents and 38 service providers.
TIME FOR ACTION~There are important, even pressing system, parent, and child issues to address. ~Please answer the following questions so we can formulate an action plan.
DELPHI ~A delphi is a quick way of gathering expert opinion ~This one takes 10 minutes to complete; longer if you choose fill in all comment boxes. ~If you do not want to comment, please type in something like "no comment" to keep moving through the questions.~Your responses are received anonymously.
* Requ ir ed
Please confirm informed consent * I have received the INFORMATION LETTER for this study .
I understand that this Delphi Panel is part of the Family Resilience study .
Answering these questions indicates my willingness to participate in this study .
20% completed
This form w as created inside of University of Alberta.
Report Abuse - Terms of Service - Additional Terms
Continue »
Edit this form

5/13/2014 HLHS Delphi - Family Resilience Study
https://docs.google.com/a/ualberta.ca/forms/d/1wFiCxgSub45u9u_dxuoEM45yszxsxzzuTkw8jb2L45E/formResponse 1/4
HLHS Delphi - FamilyResilience Study* Requ ir ed
Your Role
Where do you work? Alberta Children's Hospital
Community Rehabilitation Serv ices
Glenrose Rehabilitation Hospital
Home Care
Stollery Children's Hospital
Other:
What is your discipline? * Cardiac Surgery
Pediatric Cardiology
General Pediatrics
Nursing - inpatient
Nursing- outpatient
Advance Practice Nursing - Nurse Practitioner
Child Life
Dietitian
OT
PT
SLP
Psy chology
Social Work
Other:
Edit this form
5/13/2014 HLHS Delphi - Family Resilience Study
https://docs.google.com/a/ualberta.ca/forms/d/1wFiCxgSub45u9u_dxuoEM45yszxsxzzuTkw8jb2L45E/formResponse 2/4
When you meet with children with congenital heart diseaseand their parents, what issues do you address? *Please check all boxes that apply .
Child’s cardiac function
Child’s exercise tolerance
Child’s play /sports participation
Child’s school issues
Child’s emotional/behavioural difficulties
Child’s motor delay s
Child’s language processing issues
Child’s sensory processing difficulties
Parent’s emotional needs
Parent's financial concerns
Parent's questions regarding access to preschool community serv ices
Parent's questions regarding access to school age community serv ices
Sibling’s social/emotional needs
Other:
If not my role, whose role is it?
If you do not address these CHILD issues, who does it best? *You can only choose one. NOTE: Use slide bar to v iew all options.
Peds cardiology
Nursinpt
Nursoutpt NP Child
life OT PT SLP Socialwork Psy ch Pediatrician
Cardiac function
Exercise tolerance
Play /sportsparticipation
Emotional/Behavioural
Motor delay s
Speech/Language
Sensory processing
Development/Learning

5/13/2014 HLHS Delphi - Family Resilience Study
https://docs.google.com/a/ualberta.ca/forms/d/1wFiCxgSub45u9u_dxuoEM45yszxsxzzuTkw8jb2L45E/formResponse 3/4
Pow ered by
Comments:
If you do not address these PARENT/FAMILY issues, whodoes it best?You can only choose one. Make sure y ou v iew all options.
Peds cardiology
Nursinpt
Nursoutpt NP Child
life OT PT SLP Socialwork Psy ch Pediatrician Not
sure
Parentemotional needsFamily financialneedsReferrals forpreschooldevelopmentalissuesReferrals forschool learningissuesSiblingsocial/emotionalneeds
Comments:
40% completed
This form w as created inside of University of Alberta.
« Back Continue »

5/13/2014 HLHS Delphi - Family Resilience Study
https://docs.google.com/a/ualberta.ca/forms/d/1wFiCxgSub45u9u_dxuoEM45yszxsxzzuTkw8jb2L45E/formResponse 4/4
Report Abuse - Terms of Service - Additional Terms

5/13/2014 HLHS Delphi - Family Resilience Study
https://docs.google.com/a/ualberta.ca/forms/d/1wFiCxgSub45u9u_dxuoEM45yszxsxzzuTkw8jb2L45E/formResponse 1/2
HLHS Delphi - FamilyResilience Study* Requ ir ed
Fontan PreparationParents and children need more preparation for the FONTAN surgery , especially because the child is older compared to surgeries done during infancy .
Please rate some strategies from least helpful (0) to mosthelpful (4)
Brochure? *
0 1 2 3 4
Least helpful Most helpful
A phone call? *
0 1 2 3 4
Least helpful Most helpful
An appointment? *
0 1 2 3 4
Least helpful Most helpful
A webinar that the parents can access? *
0 1 2 3 4
Least helpful Most helpful
Edit this form
5/13/2014 HLHS Delphi - Family Resilience Study
https://docs.google.com/a/ualberta.ca/forms/d/1wFiCxgSub45u9u_dxuoEM45yszxsxzzuTkw8jb2L45E/formResponse 2/2
Pow ered by
Other strategies to help parents and children prepare for theFONTAN?Please note any ideas y ou hav e.
Who should be involved in the design and provision of theseservices for FONTAN preparation? *Please note any ideas y ou hav e.
60% completed
This form w as created inside of University of Alberta.
Report Abuse - Terms of Service - Additional Terms
« Back Continue »

5/13/2014 HLHS Delphi - Family Resilience Study
https://docs.google.com/a/ualberta.ca/forms/d/1wFiCxgSub45u9u_dxuoEM45yszxsxzzuTkw8jb2L45E/formResponse 1/3
HLHS Delphi - FamilyResilience Study* Requ ir ed
Navigating the SystemParents struggle to NAVIGATE THE SY STEM, especially when their child is discharged home.
Currently, who helps parents NAVIGATE the system,including accessing information and services at differentstages of their child’s HLHS trajectory? *
What NEW services or roles do we need to help parentsnavigate the system? *
Who needs to LEAD this initiative? *
Edit this form
5/13/2014 HLHS Delphi - Family Resilience Study
https://docs.google.com/a/ualberta.ca/forms/d/1wFiCxgSub45u9u_dxuoEM45yszxsxzzuTkw8jb2L45E/formResponse 2/3
Financial Burden
What would you suggest to ease the FINANCIAL BURDEN forfamilies of children with HLHS? *
Who is the person or group to work with funding agencies toaddress financial burden for these families? *
Who is in a position to make changes to help the familiesfinancially? *
5/13/2014 HLHS Delphi - Family Resilience Study
https://docs.google.com/a/ualberta.ca/forms/d/1wFiCxgSub45u9u_dxuoEM45yszxsxzzuTkw8jb2L45E/formResponse 3/3
Pow ered by
80% completed
This form w as created inside of University of Alberta.
Report Abuse - Terms of Service - Additional Terms
« Back Continue »
5/13/2014 HLHS Delphi - Family Resilience Study
https://docs.google.com/a/ualberta.ca/forms/d/1wFiCxgSub45u9u_dxuoEM45yszxsxzzuTkw8jb2L45E/formResponse 1/4
HLHS Delphi - FamilyResilience Study* Requ ir ed
Developmental and Behavioural ChallengesMany children with HLHS have DEVELOPMENTAL AND BEHAVIOUR CHALLENGES for which they have not received education, support, or therapies.
How can we facilitate appropriate referrals for children withdevelopmental learning and behavioural difficulties who donot qualify for a Program Unit Fund?
Who is the person or group to work with agencies to addresslack of services for these children? *
Who is in a position to make changes to help these childrendevelopmentally and behaviourally? *
Edit this form
5/13/2014 HLHS Delphi - Family Resilience Study
https://docs.google.com/a/ualberta.ca/forms/d/1wFiCxgSub45u9u_dxuoEM45yszxsxzzuTkw8jb2L45E/formResponse 2/4
Anything else?
What else needs to change to help children with HLHS andtheir families?
Taking Action
We need direction for priority setting. *
High priority Medium priority Low priority
Behaviour Issues
DevelopmentalIssues
Financial Burden
Fontan Preparation
Another Priority?

5/13/2014 HLHS Delphi - Family Resilience Study
https://docs.google.com/a/ualberta.ca/forms/d/1wFiCxgSub45u9u_dxuoEM45yszxsxzzuTkw8jb2L45E/formResponse 3/4
How urgent is this priority? High priority
Medium priority
Low priority
Another Priority?
How urgent is this priority? High priority
Medium priority
Low priority
Final Comments?

5/13/2014 HLHS Delphi - Family Resilience Study
https://docs.google.com/a/ualberta.ca/forms/d/1wFiCxgSub45u9u_dxuoEM45yszxsxzzuTkw8jb2L45E/formResponse 4/4
Pow ered by
Thank you for your contributing your expertise!
100%: Y ou made it.
This form w as created inside of University of Alberta.
Report Abuse - Terms of Service - Additional Terms
« Back SubmitNever submit passwords through Google Forms.

5/13/2014 Thanks!
https://docs.google.com/a/ualberta.ca/forms/d/1wFiCxgSub45u9u_dxuoEM45yszxsxzzuTkw8jb2L45E/formResponse 1/1
HLHS Delphi - Family ResilienceStudyY our response has been recorded.
Edit your response
This form was created using GoogleForms.Create your own




















