Usefulness of Real-Time Three-Dimensional Echocardiography to Identify Right Ventricular Dysfunction...
8
Usefulness of Real-Time Three-Dimensional Echocardiography to Identify Right Ventricular Dysfunction in Patients With Congenital Heart Disease Heleen B. van der Zwaan, MD a, *, Willem A. Helbing, MD, PhD b,c , Eric Boersma, PhD d , Marcel L. Geleijnse, MD, PhD a , Jackie S. McGhie, MSc a , Osama I.I. Soliman, MD, PhD a , Jolien W. Roos-Hesselink, MD, PhD a , and Folkert J. Meijboom, MD, PhD e Because right ventricular (RV) dysfunction predicts a poor outcome in patients with congenital heart disease (CHD), regular monitoring of RV function is indicated. To date, cardiac magnetic resonance (CMR) imaging has been the reference method. A more practical, more accessible, and accurate tool would be preferred. We defined normality regarding RV systolic function using healthy controls and tested the ability of real-time 3-dimensional echocardiographic (RT3DE) findings to identify patients with CHD with RV dysfunction. The cutoff values for the RV volumes and ejection fraction (EF) were derived from the CMR imaging findings from 41 healthy controls (mean age 27 8 years, 56% men). In 100 patients with varying CHDs (mean age 27 11 years, 65% men), both RT3DE data sets (iE33) and short-axis CMR imaging (1.5 T) were obtained within 2 hours. The RT3DE and CMR RV volumes and EF were calculated using commercially available software. Receiver operating characteristic curves were created to obtain the sensitivity and specificity of the RT3DE data to identify RV dysfunction. Applying the cutoff values derived from the healthy controls using the CMR data of patients with CHD, we identified 23 patients with an enlarged indexed end-diastolic volume, 29 patients with an enlarged indexed end-systolic volume, and 21 patients with an impaired RVEF. The best cutoff values predicting RV dysfunction using the RT3DE findings were identified (indexed end-diastolic volume >105 ml/m 2 , indexed end-systolic volume >54 ml/m 2 , and EF <43%). The RT3DE findings revealed 23 patients with impaired RVEF, with 95% sensitivity, 89% specificity, and a negative predictive value of 99%. In conclusion, real-time 3-dimen- sional echocardiography is a very sensitive tool to identify RV dysfunction in patients with CHD and could be applied clinically to rule out RV dysfunction or to indicate additional quantitative analysis of RV function. © 2010 Elsevier Inc. All rights reserved. (Am J Cardiol 2010;106:843– 850) The ideal index to assess right ventricular (RV) contrac- tility—independent of the pre- and afterload, independent of heart size and mass, easy and safe to apply, and proven useful in the clinical setting— does not yet exist. 1 Thus, determination of the ejection fraction (EF) is still the most commonly used method to assess systolic RV performance. Cardiac magnetic resonance (CMR) imaging has become the reference method for the assessment of RVEF but has a number of drawbacks, including limited availability, high costs, and time-consuming acquisition and analysis. 2,3 Ow- ing to the complex RV geometry and the presence of myo- cardial trabeculae, 2-dimensional echocardiography is con- sidered inaccurate and a 3-dimensional imaging technology, such as real-time 3-dimensional echocardiography (RT3DE), is mandatory. 4 Earlier studies have shown that RT3DE can assess RV volumes and EF in various patient groups. 5–7 If proved to be a robust and reliable technique, RT3DE might replace CMR imaging for RV systolic functional assessment in a substantial proportion of patients. To be usable in clinical practice, a prerequisite is the reliability of RT3DE to detect RV dysfunction. This has not been previously studied. The pur- poses of the present study were to define normality regarding systolic RV function using CMR values derived from healthy controls and to test the ability of RT3DE to accurately identify RV dysfunction in patients with congenital heart disease (CHD), according to the reference method CMR imaging. For the purposes of the present study, the cutoff values for the RV volumes and EF were identified and applied to differentiate a Department of Cardiology, Thoraxcenter, Erasmus University Medical Center, Rotterdam, The Netherlands; b Department of Pediatrics, Division of Cardiology, Sophia Children’s Hospital, Erasmus University Medical Center, Rotterdam, The Netherlands; c Department of Radiology, Erasmus University Medical Center, Rotterdam, The Netherlands; d Department of Epidemiology and Statistics, Erasmus University Medical Center, Rotter- dam, The Netherlands; and e Department of Pediatrics, Division of Cardi- ology, Wilhelmina Children’s Hospital, University Medical Center Utre- cht, Utrecht, The Netherlands. Manuscript received March 30, 2010; manuscript received and accepted May 3, 2010. *Corresponding author: Tel: (0031) 10-70-35994; fax: (0031) 10-70- 35498. E-mail address: [email protected] (H.B. van der Zwaan). 0002-9149/10/$ – see front matter © 2010 Elsevier Inc. All rights reserved. www.ajconline.org doi:10.1016/j.amjcard.2010.05.008
Transcript of Usefulness of Real-Time Three-Dimensional Echocardiography to Identify Right Ventricular Dysfunction...

thudcC
CoCUEdocm
3
0d
Usefulness of Real-Time Three-Dimensional Echocardiographyto Identify Right Ventricular Dysfunction in Patients
With Congenital Heart Disease
Heleen B. van der Zwaan, MDa,*, Willem A. Helbing, MD, PhDb,c, Eric Boersma, PhDd,Marcel L. Geleijnse, MD, PhDa, Jackie S. McGhie, MSca, Osama I.I. Soliman, MD, PhDa,
Jolien W. Roos-Hesselink, MD, PhDa, and Folkert J. Meijboom, MD, PhDe
Because right ventricular (RV) dysfunction predicts a poor outcome in patients withcongenital heart disease (CHD), regular monitoring of RV function is indicated. To date,cardiac magnetic resonance (CMR) imaging has been the reference method. A morepractical, more accessible, and accurate tool would be preferred. We defined normalityregarding RV systolic function using healthy controls and tested the ability of real-time3-dimensional echocardiographic (RT3DE) findings to identify patients with CHD withRV dysfunction. The cutoff values for the RV volumes and ejection fraction (EF) werederived from the CMR imaging findings from 41 healthy controls (mean age 27 � 8 years,56% men). In 100 patients with varying CHDs (mean age 27 � 11 years, 65% men), bothRT3DE data sets (iE33) and short-axis CMR imaging (1.5 T) were obtained within 2 hours.The RT3DE and CMR RV volumes and EF were calculated using commercially availablesoftware. Receiver operating characteristic curves were created to obtain the sensitivity andspecificity of the RT3DE data to identify RV dysfunction. Applying the cutoff valuesderived from the healthy controls using the CMR data of patients with CHD, we identified23 patients with an enlarged indexed end-diastolic volume, 29 patients with an enlargedindexed end-systolic volume, and 21 patients with an impaired RVEF. The best cutoffvalues predicting RV dysfunction using the RT3DE findings were identified (indexedend-diastolic volume >105 ml/m2, indexed end-systolic volume >54 ml/m2, and EF <43%). TheRT3DE findings revealed 23 patients with impaired RVEF, with 95% sensitivity, 89%specificity, and a negative predictive value of 99%. In conclusion, real-time 3-dimen-sional echocardiography is a very sensitive tool to identify RV dysfunction in patientswith CHD and could be applied clinically to rule out RV dysfunction or to indicateadditional quantitative analysis of RV function. © 2010 Elsevier Inc. All rights
reserved. (Am J Cardiol 2010;106:843– 850)tncicssiaprapdpscR(t
The ideal index to assess right ventricular (RV) contrac-ility—independent of the pre- and afterload, independent ofeart size and mass, easy and safe to apply, and provenseful in the clinical setting—does not yet exist.1 Thus,etermination of the ejection fraction (EF) is still the mostommonly used method to assess systolic RV performance.ardiac magnetic resonance (CMR) imaging has become
aDepartment of Cardiology, Thoraxcenter, Erasmus University Medicalenter, Rotterdam, The Netherlands; bDepartment of Pediatrics, Divisionf Cardiology, Sophia Children’s Hospital, Erasmus University Medicalenter, Rotterdam, The Netherlands; cDepartment of Radiology, Erasmusniversity Medical Center, Rotterdam, The Netherlands; dDepartment ofpidemiology and Statistics, Erasmus University Medical Center, Rotter-am, The Netherlands; and eDepartment of Pediatrics, Division of Cardi-logy, Wilhelmina Children’s Hospital, University Medical Center Utre-ht, Utrecht, The Netherlands. Manuscript received March 30, 2010;anuscript received and accepted May 3, 2010.
*Corresponding author: Tel: (0031) 10-70-35994; fax: (0031) 10-70-5498.
vE-mail address: [email protected] (H.B. van der Zwaan).
002-9149/10/$ – see front matter © 2010 Elsevier Inc. All rights reserved.oi:10.1016/j.amjcard.2010.05.008
he reference method for the assessment of RVEF but has aumber of drawbacks, including limited availability, highosts, and time-consuming acquisition and analysis.2,3 Ow-ng to the complex RV geometry and the presence of myo-ardial trabeculae, 2-dimensional echocardiography is con-idered inaccurate and a 3-dimensional imaging technology,uch as real-time 3-dimensional echocardiography (RT3DE),s mandatory.4 Earlier studies have shown that RT3DE canssess RV volumes and EF in various patient groups.5–7 Ifroved to be a robust and reliable technique, RT3DE mighteplace CMR imaging for RV systolic functional assessment in
substantial proportion of patients. To be usable in clinicalractice, a prerequisite is the reliability of RT3DE to detect RVysfunction. This has not been previously studied. The pur-oses of the present study were to define normality regardingystolic RV function using CMR values derived from healthyontrols and to test the ability of RT3DE to accurately identifyV dysfunction in patients with congenital heart disease
CHD), according to the reference method CMR imaging. Forhe purposes of the present study, the cutoff values for the RV
olumes and EF were identified and applied to differentiatewww.ajconline.org

bd
M
rauhCigoptf
puc
c
vTaui
aq
sTapqEam
iobs
Fc
844 The American Journal of Cardiology (www.ajconline.org)
etween normal and impaired RV function—to define RVysfunction.
ethods
A total of 41 healthy controls underwent full-volumeeal-time 3-dimensional echocardiography and CMR im-ging to establish the reference RV volume and EF val-es. The controls were employees of the university orospital or their relatives who were willing to undergo aMR scan. They were eligible for inclusion in the study
f they had no medical history or current symptoms sug-estive of cardiovascular disease, including hypertensionr a systemic illness with a potential cardiovascular com-onent such as diabetes or thyroid disease. Participantsaking any cardiovascular medications were excludedrom the present study.
In all included healthy controls the heart rate and bloodressure were measured (with the subject supine), and theynderwent routine 2-dimensional echocardiography to ex-lude cardiac abnormalities.
A total of 100 consecutive patients, in sinus rhythm, with
igure 1. Display from the 4-dimensional RV function Tomtec analysis pontours can be applied in any cross-section or phase of the cardiac cycle
omplex and/or surgically repaired CHD underwent full- v
olume RT3DE and CMR acquisition of the right ventricle.hey were referred for CMR imaging for a quantitativenalysis of their cardiac function for clinical reasons andnderwent a RT3DE examination within 2 hours of CMRmaging to pursue comparable loading conditions.
The medical ethical committee approved the study, andll healthy controls, patients, and/or their parents (if re-uired) provided written informed consent.
CMR images were acquired using a Signa 1.5 Teslacanner (GE Medical Systems, Milwaukee, Wisconsin).he subjects were positioned supine with dedicated phased-rray cardiac surface coils placed over the thorax. The CMRrotocol included cine steady-state, free precision se-uences in the short-axis planes to assess the RV volumes.lectrocardiographic gating and repeated breath holds werepplied to minimize the influence of cardiac and respiratoryotion.The RV volumes were measured from a multisection
mage set of 8 to 12 contiguous slices parallel to the planef the atrioventricular valves and covering the full-length ofoth ventricles. The imaging parameters were as follows:lice thickness 7 to 10 mm, interslice gap 0 mm, field of
showing final stage of contour detection in which manual correction of
rogram.iew 280 to 370 mm, phase field of view 0.75, matrix 160

�fl
dvtSTtows
uNwestghrosadsswatptt
uvomueg
atd
1p((tmfiviteebtirsd
TB
V
PAAAHSDHWBB
TC
P
TAPPTTCEDDVAPC
845Congenital Heart Disease/Three-Dimensional Echocardiography for RV Dysfunction
128 mm, repetition time 3.5 ms, echo time 1.5 ms, andip angle 45°.
One physician (HBZ) analyzed the CMR RV volumetricata set quantitatively on a commercially available Ad-anced Windows workstation (GE Medical Systems) usinghe Advanced Windows, version 5.1, of the MR Analyticaloftware System (Medis Medical Imaging Systems, Leiden,he Netherlands). The RV end-diastolic volume, end-sys-
olic volume and EF were calculated using manual detectionf the endocardial borders in end-systole and end-diastoleith exclusion of trabeculae, as described by Robbers-Vis-
er et al.8
RT3DE harmonic imaging was performed using the iE33ltrasound system (Philips Medical Systems, Best, Theetherlands) equipped with an X3-1 matrix array transducerith the patient in the left lateral decubitus position. To
ncompass the entire right ventricle into the RT3DE dataet, a full-volume scan was acquired from a modified apicalransducer position in harmonic mode from 7 R-wave–ated subvolumes during a single end-expiratory breath-old. The output therefore was not truly real-time but waseconstructed from the 7 subvolumes. The depth and anglef the ultrasound sector were adjusted to a minimal level,till encompassing the entire right ventricle. Before eachcquisition, the images were optimized for endocardial bor-er visualization by modifying the time gain and compres-ion and increasing the overall gain. An average of 3 dataets was acquired per patient to ensure optimal data setsithout motion artifacts that might have occurred during the
cquisition. The mean volume rate was 25 frames (range 14o 38) per cardiac cycle. The data sets were digitally ex-orted to a Tomtec server (Tomtec Imaging Systems, Un-erschleißheim, Germany) connected to a terminal worksta-ion for additional analyses.
The digital RT3DE RV data sets were analyzed off-linesing the Tomtec 4-dimensional RV Function Program,ersion 4.0, by an investigator (HBZ) unaware of the resultsf the CMR measurements. This software performs 3-di-ensional semiautomated border detection of the RV vol-
mes over one cardiac cycle. It uses a physics-based mod-ling algorithm that makes no assumptions regarding RV
able 1aseline characteristics
ariable Healthy Control
All Men
atients (n) 41 23ge (years) 27 � 8 26 � 9ge at initial repair (years) (n � 94) — —ge at reoperation (years) (n � 51) — —eart rate (beats/min) 64 � 13 64 � 14ystolic blood pressure (mm Hg) 121 � 14 128 � 13iastolic blood pressure (mm Hg) 73 � 8 74 � 7eight (cm) 177 � 8 181 � 6eight (kg) 70 � 11 73 � 10
ody mass index (kg/m2) 22 � 3 22 � 3ody surface area (m2) 1.9 � 0.2 1.9 � 0.1
Data are presented as mean � SD.* Difference between healthy controls and patients with CHD.
eometry. The analysis of a RT3DE data set was judged a
ccurate, when the apex and lateral wall were both visible inhe 4-chamber view, allowing adequate tracing of the en-ocardial border.
The functioning of the Tomtec analysis program (Figure) has been previously reported in detail.6 In brief, therogram starts with a screen displaying a short-axis viewtop), an apical 4-chamber view (left), and a coronal viewright). The right ventricle must be outlined in the middle ofhe data set. Next, by movement of a horizontal axis, land-arks can be placed in the tricuspid and mitral valve ori-ces and apex. Subsequently the end-diastolic (largest RVolume) and end-systolic (smallest RV volume) phases aredentified. The endocardial border contours are drawn ontohe apical 4-chamber still frames in both end-diastole andnd-systole. Using these contours, 2 reference markers arextrapolated onto the sagittal view in which the endocardialorder contours are traced with care to include the 2 ex-rapolated reference markers. Next, the contours are drawnn the coronal view, again with attention to include the 3eference markers extrapolated from the 4-chamber andagittal views. After these steps, the software automaticallyelineates the RV endocardial border from the end-diastolic
Patients With CHD p Value*
omen All Men Women
18 100 65 35 0.33� 7 27 � 10 26 � 10 28 � 11 0.89— 5 � 10 6 � 10 6 � 12 —— 11 � 10 11 � 10 10 � 10 —� 14 72 � 12 70 � 13 75 � 11 �0.001� 12 125 � 18 126 � 17 123 � 20 0.29� 9 72 � 10 71 � 10 73 � 11 0.58� 5 172 � 13 176 � 13 165 � 7 0.04� 11 68 � 15 70 � 17 63 � 12 0.36� 3 22 � 4 22 � 5 23 � 4 0.80� 0.1 1.8 � 0.3 1.8 � 0.4 1.7 � 0.2 0.04
able 2ongenital heart diseases (CHDs) studied
athologic Finding Patients(n)
etralogy of Fallot 38ortic valve abnormality 17ulmonary stenosis with or without ventricular septal defect 12ulmonary atresia with or without ventricular septal defect 4ransposition of great arteries, atrial switch 10ransposition of great arteries, arterial switch 9oarctation of aorta 2bstein’s anomaly 2ouble outlet right ventricle 1ouble inlet left ventricle 1entricular septal defect 1nomalous pulmonary venous connection 1erinatal tricuspid insufficiency 1ongenital hypertrophic cardiomyopathy 1
s
W
28
6311471
1716623
1.8
nd end-systolic phases, and by sequential analysis the

smtR
Pcnmwa
baw
s
iUttdm
ieS
dctcRttfiTts
R
(C
TC
V
A
N
TR
V
A
N
846 The American Journal of Cardiology (www.ajconline.org)
oftware creates an RV mathematic dynamic 3-dimensionalodel—referred to as “Beutel”—that represents changes in
he RV cavity over the cardiac cycle. From this Beutel, theV volumes and EF are calculated.
Statistical analysis was done using the Statisticalackage for Social Sciences, version 15.0 (SPSS, Chi-ago, Illinois). The categorical data are summarized asumbers and percentages and the continuous data as theean � SD. Differences between patients and controlsere analyzed using chi-square tests or Student’s t tests,
s appropriate.Both RT3DE and CMR volumes were indexed to the
ody surface area. The body surface area was calculatedccording to the formula by Dubois: body surface area (m2) �eight (kg)0.425 � height (cm)0.725 � 71.84 � 10�4.All statistical tests were 2-sided, and p �0.05 was con-
idered statistically significant.Because no standard on definition of RV dysfunction
s available,9 we defined RV dysfunction as follows.sing the CMR volumetric data from the healthy con-
rols, we identified a range of normal RV function usinghe mean � 2 SDs. Next, we defined the indexes of RVysfunction either as a diminished RVEF (less than the
able 3ardiac magnetic resonance (CMR) imaging: right ventricular (RV) volum
ariable Healthy Contro
All Men
bsolute valuesEnd-diastolic volume (ml) 158 � 32 172 � 29End-systolic volume (ml) 65 � 18 70 � 17Stroke volume (ml) 93 � 19 107 � 18Ejection fraction (%) 60 � 6 60 � 6ormalized to body surface areaIndexed end-diastolic volume (ml/m2) 86 � 21 90 � 15Indexed end-systolic volume (ml/m2) 35 � 11 37 � 9Indexed stroke volume (ml/m2) 51 � 12 53 � 9
Data are presented as mean � SD.* Difference between healthy controls and patients with CHD.
able 4eal-time 3-dimensional echocardiography: right ventricular (RV) volume
ariable Healthy Contro
All Men
bsolute valuesEnd-diastolic volume (ml) 127 � 32 144 � 31End-systolic volume (ml) 58 � 16 66 � 14Stroke volume (ml) 69 � 19 78 � 20Ejection fraction (%) 55 � 5 54 � 5ormalized to body surface areaIndexed end-diastolic volume (ml/m2) 68 � 18 73 � 14Indexed end-systolic volume (ml/m2) 31 � 9 34 � 6Indexed stroke volume (ml/m2) 37 � 11 39 � 9
Data are presented as mean � SD.* Difference between healthy controls and patients with CHD.
ean minus 2 SDs in healthy controls), an enlarged T
ndexed end-diastolic volume or an enlarged indexednd-systolic volume (both greater than the mean plus 2Ds in healthy controls).
Using these cutoff values, we dichotomized the CMRata derived from our CHD group. Receiver operatingharacteristic curves were created to predict RV dysfunc-ion using the RT3DE data. From the receiver operatingharacteristic curves, the sensitivity and specificity of theT3DE findings were derived, as well as the area under
he curves. Next, 2 by 2 tables were created to calculatehe positive and negative predictive values of the RT3DEndings to identify RV dysfunction using the CMR data.he cutoff RT3DE values to obtain the maximum sum of
he sensitivity and specificity, the greatest sensitivity andpecificity, were calculated.
esults
The baseline characteristics of the healthy controlsmean age 27 � 8 years, 56% men) and the patients withHD (mean age 27 � 10 years, 65% men) are listed in
ejection fraction (EF)
Patients With CHD p Value*
omen All Men Women
9 � 27 193 � 72 195 � 72 190 � 75 �0.0018 � 17 94 � 47 96 � 49 91 � 46 �0.0012 � 15 100 � 34 101 � 34 99 � 36 0.159 � 6 53 � 9 52 � 10 53 � 8 �0.001
9 � 13 109 � 37 108 � 36 112 � 39 �0.0013 � 9 54 � 25 53 � 26 54 � 24 �0.0016 � 6 56 � 18 55 � 17 59 � 20 0.04
jection fraction (EF)
Patients With CHD p Value*
omen All Men Women
8 � 22 170 � 61 175 � 60 160 � 61 �0.0018 � 10 96 � 44 98 � 44 79 � 35 �0.0010 � 14 80 � 26 80 � 24 80 � 30 0.0016 � 5 48 � 9 46 � 9 52 � 7 �0.001
6 � 10 96 � 31 97 � 30 94 � 32 �0.0017 � 5 51 � 22 53 � 23 46 � 19 �0.0013 � 6 45 � 14 44 � 12 47 � 16 0.005
es and
ls
W
13585
734
s and e
ls
W
10465
623
able 1. The patients with CHD had a greater heart rate
(c
Ehsosp�
iEddvips
Fv
847Congenital Heart Disease/Three-Dimensional Echocardiography for RV Dysfunction
p �0.001) and shorter stature (p � 0.04) than the healthyontrols. Table 2 lists the types of CHD the patients had.
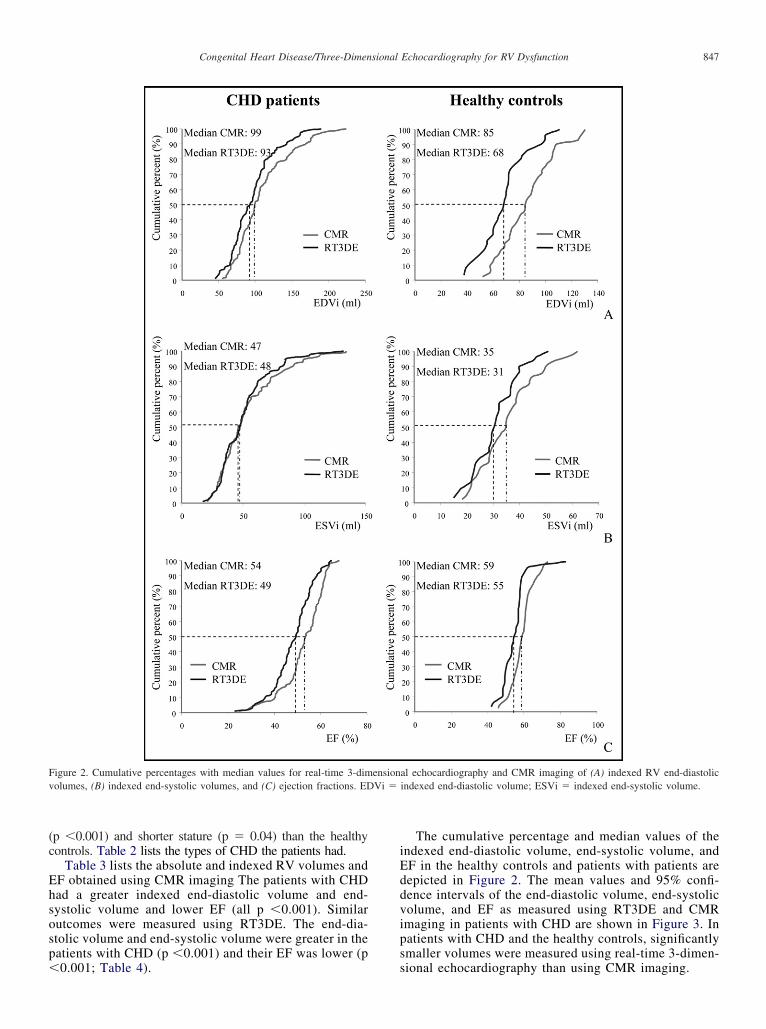
Table 3 lists the absolute and indexed RV volumes andF obtained using CMR imaging The patients with CHDad a greater indexed end-diastolic volume and end-ystolic volume and lower EF (all p �0.001). Similarutcomes were measured using RT3DE. The end-dia-tolic volume and end-systolic volume were greater in theatients with CHD (p �0.001) and their EF was lower (p
igure 2. Cumulative percentages with median values for real-time 3-dimolumes, (B) indexed end-systolic volumes, and (C) ejection fractions. ED
0.001; Table 4). s
The cumulative percentage and median values of thendexed end-diastolic volume, end-systolic volume, andF in the healthy controls and patients with patients areepicted in Figure 2. The mean values and 95% confi-ence intervals of the end-diastolic volume, end-systolicolume, and EF as measured using RT3DE and CMRmaging in patients with CHD are shown in Figure 3. Inatients with CHD and the healthy controls, significantlymaller volumes were measured using real-time 3-dimen-
al echocardiography and CMR imaging of (A) indexed RV end-diastolicindexed end-diastolic volume; ESVi � indexed end-systolic volume.
ensionVi �
ional echocardiography than using CMR imaging.

hevcweiw
RFa
oprFviwpd�npsa
D
vgfewusv�p8sfis
appvwtifamoPngsdpfd
cw
Fdp
848 The American Journal of Cardiology (www.ajconline.org)
We derived cutoff values from the CMR data fromealthy controls as indicators of RV dysfunction (indexednd-diastolic volume �129 ml/m2, indexed end-systolicolume �58 ml/m2, and RVEF �48%). Using theseutoff values for CMR data from the patients with CHD,e identified 23 patients (23%) with an enlarged indexed
nd-diastolic volume, 29 patients (29%) with an enlargedndexed end-systolic volume, and 21 patients (21%)
igure 3. Correlations between (A) RT3DE-derived and (B) CMR imaging-erived volumes and (C) EF. Dotted lines represent best cutoff valuesredicting RV dysfunction.
ith an impaired RVEF. Of the 21 patients with impaired p
V function according to the RVEF, ½ had tetralogy ofallot and ¼ had undergone a Mustard or Senning oper-tion for transposition of the great arteries.
Receiver operating characteristic curves were created tobtain the sensitivity, specificity, and positive and negativeredictive values of real-time 3-dimensional echocardiog-aphy to identify systolic RV dysfunction (Table 5 andigures 3 and 4). Scatter plots of the indexed end-diastolicolume, end-systolic volume, and EF measured using CMRmaging in healthy controls are shown in Figure 3, togetherith the best cutoff values predicting RV dysfunction inatients with CHD using the RT3DE data (indexed end-iastolic volume �105 ml/m2, indexed end-systolic volume54 ml/m2, and EF �43%). In Table 5, 3 alternative sce-
arios are listed. Real-time 3-dimensional echocardiogra-hy could either be a test with a maximum sum of theensitivity and specificity, a test with optimal sensitivity, ortest with optimal specificity.
iscussion
The backbone of the present study was the data on RVolumes and EF we measured using CMR imaging in aroup of 41 healthy controls. These data, consistent thoserom with previous studies,10–14 have provided normal ref-rence data for the definition of RV function. Combinedith the predetermined cutoff values for normality derivedsing the CMR data, the RT3DE data proved to be highlyensitive to identify RV systolic dysfunction in patients witharious CHDs. RV systolic dysfunction, defined as a RVEF43%, could be identified from the RT3DE findings in 23
atients (23%), with a sensitivity of 95%, specificity of9%, and negative predictive value of 99%. The high sen-itivity and negative predictive value imply that the RT3DEndings can be used as a screening tool to exclude RVystolic dysfunction in patients with CHD.
It is important to accurately measure the RV volumesnd EF because impaired RV function is known to be aredictor of adverse outcomes and poor remodeling afterulmonary valve replacement. The relation between the RVolumes and/or EF with the long-term outcome in patientsith CHD has been studied in both the subpulmonary and
he systemic right ventricle.15–17 Knauth et al15 published annteresting study in which they identified the cutoff valuesor the indexed end-diastolic volume, end-systolic volume,nd EF measured using CMR imaging as predictors ofajor adverse cardiac events in patients late after tetralogy
f Fallot repair. In patients with systemic right ventricles,iran et al16 found that a RVEF �35% was a strong prog-ostic risk factor for the development of heart failure. Ineneral, experts have agreed that a systemic RVEF � 50%hould be considered normal.18 When we compared theseata with our own data, we found that only 10% of theatients we studied had a systemic right ventricle. RV dys-unction was present in ½ of them according to their CMRata.
Discussion remains on the relevance of defining absoluteutoff values for impaired systolic RV function in patientsith CHD. Earlier studies based their judgment of RV
erformance on visualization of the 2-dimensional echocar-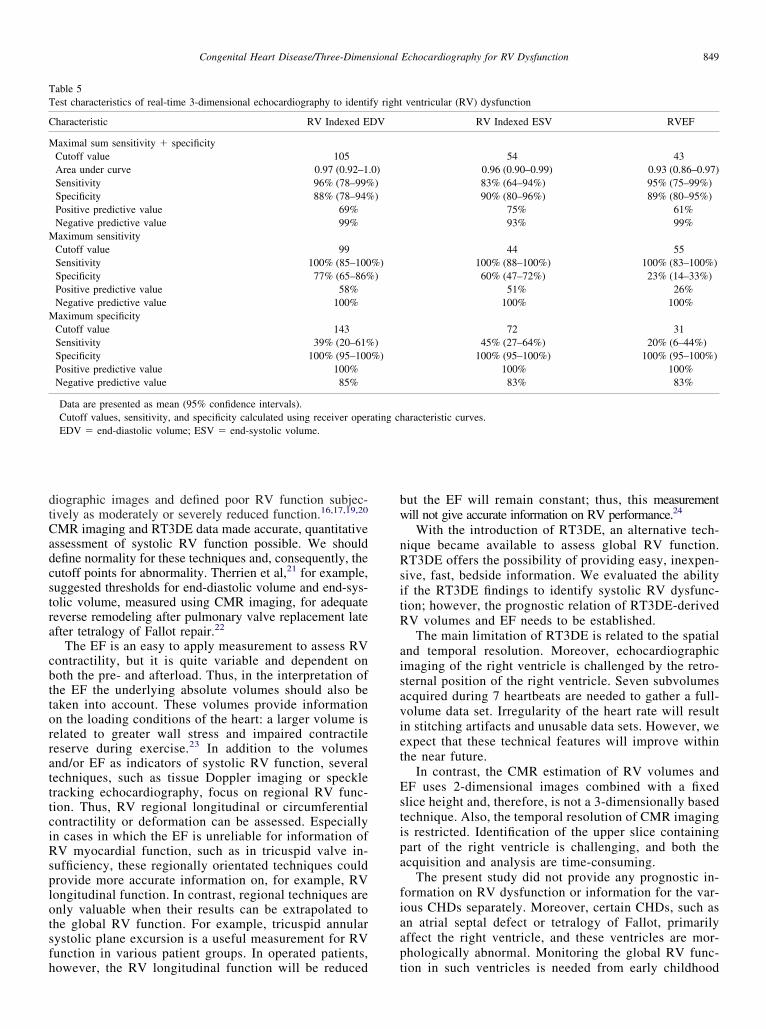
dtCadcstra
cbttorratttciRsplotsfh
bw
nRsitR
aisaviet
Estipa
fiaap
TT
C
M
M
M
849Congenital Heart Disease/Three-Dimensional Echocardiography for RV Dysfunction
iographic images and defined poor RV function subjec-ively as moderately or severely reduced function.16,17,19,20
MR imaging and RT3DE data made accurate, quantitativessessment of systolic RV function possible. We shouldefine normality for these techniques and, consequently, theutoff points for abnormality. Therrien et al,21 for example,uggested thresholds for end-diastolic volume and end-sys-olic volume, measured using CMR imaging, for adequateeverse remodeling after pulmonary valve replacement latefter tetralogy of Fallot repair.22
The EF is an easy to apply measurement to assess RVontractility, but it is quite variable and dependent onoth the pre- and afterload. Thus, in the interpretation ofhe EF the underlying absolute volumes should also beaken into account. These volumes provide informationn the loading conditions of the heart: a larger volume iselated to greater wall stress and impaired contractileeserve during exercise.23 In addition to the volumesnd/or EF as indicators of systolic RV function, severalechniques, such as tissue Doppler imaging or speckleracking echocardiography, focus on regional RV func-ion. Thus, RV regional longitudinal or circumferentialontractility or deformation can be assessed. Especiallyn cases in which the EF is unreliable for information ofV myocardial function, such as in tricuspid valve in-
ufficiency, these regionally orientated techniques couldrovide more accurate information on, for example, RVongitudinal function. In contrast, regional techniques arenly valuable when their results can be extrapolated tohe global RV function. For example, tricuspid annularystolic plane excursion is a useful measurement for RVunction in various patient groups. In operated patients,
able 5est characteristics of real-time 3-dimensional echocardiography to identi
haracteristic RV Indexed E
aximal sum sensitivity � specificityCutoff value 105Area under curve 0.97 (0.92–1Sensitivity 96% (78–99%Specificity 88% (78–94%Positive predictive value 69%Negative predictive value 99%aximum sensitivity
Cutoff value 99Sensitivity 100% (85–100Specificity 77% (65–86%Positive predictive value 58%Negative predictive value 100%aximum specificity
Cutoff value 143Sensitivity 39% (20–61%Specificity 100% (95–100Positive predictive value 100%Negative predictive value 85%
Data are presented as mean (95% confidence intervals).Cutoff values, sensitivity, and specificity calculated using receiver operEDV � end-diastolic volume; ESV � end-systolic volume.
owever, the RV longitudinal function will be reduced t
ut the EF will remain constant; thus, this measurementill not give accurate information on RV performance.24
With the introduction of RT3DE, an alternative tech-ique became available to assess global RV function.T3DE offers the possibility of providing easy, inexpen-
ive, fast, bedside information. We evaluated the abilityf the RT3DE findings to identify systolic RV dysfunc-ion; however, the prognostic relation of RT3DE-derivedV volumes and EF needs to be established.
The main limitation of RT3DE is related to the spatialnd temporal resolution. Moreover, echocardiographicmaging of the right ventricle is challenged by the retro-ternal position of the right ventricle. Seven subvolumescquired during 7 heartbeats are needed to gather a full-olume data set. Irregularity of the heart rate will resultn stitching artifacts and unusable data sets. However, wexpect that these technical features will improve withinhe near future.
In contrast, the CMR estimation of RV volumes andF uses 2-dimensional images combined with a fixedlice height and, therefore, is not a 3-dimensionally basedechnique. Also, the temporal resolution of CMR imagings restricted. Identification of the upper slice containingart of the right ventricle is challenging, and both thecquisition and analysis are time-consuming.
The present study did not provide any prognostic in-ormation on RV dysfunction or information for the var-ous CHDs separately. Moreover, certain CHDs, such asn atrial septal defect or tetralogy of Fallot, primarilyffect the right ventricle, and these ventricles are mor-hologically abnormal. Monitoring the global RV func-
ventricular (RV) dysfunction
RV Indexed ESV RVEF
54 430.96 (0.90–0.99) 0.93 (0.86–0.97)83% (64–94%) 95% (75–99%)90% (80–96%) 89% (80–95%)
75% 61%93% 99%
44 55100% (88–100%) 100% (83–100%)60% (47–72%) 23% (14–33%)
51% 26%100% 100%
72 3145% (27–64%) 20% (6–44%)
100% (95–100%) 100% (95–100%)100% 100%83% 83%
aracteristic curves.
fy right
DV
.0)))
%))
)%)
ating ch
ion in such ventricles is needed from early childhood

oy
1
1
1
1
1
1
1
1
1
1
2
2
2
2
2
Fa
850 The American Journal of Cardiology (www.ajconline.org)
nward. In the present study, we did not investigate suchoung children.
1. Carabello BA. Evolution of the study of left ventricular function:everything Old is new again. Circulation 2002;105:2701–2703.
2. Babu-Narayan SV, Gatzoulis MA, Kilner PJ. Non-invasive imaging inadult congenital heart disease using cardiovascular magnetic reso-nance. J Cardiovasc Med 2007;8:23–29.
3. Bleeker GB, Steendijk P, Holman ER, Yu CM, Breithardt OA, Kaan-dorp TA, Schalij MJ, van der Wall EE, Nihoyannopoulos P, Bax JJ.Assessing right ventricular function: the role of echocardiography andcomplementary technologies. Heart 2006;92(Suppl 1):i19–i26.
4. Lai WW, Gauvreau K, Rivera ES, Saleeb S, Powell AJ, Geva T.Accuracy of guideline recommendations for two-dimensional quanti-fication of the right ventricle by echocardiography. Int J Cardiovasc
igure 4. Plots of sensitivity versus specificity for (A) indexed end-diastolicnd (B) end-systolic volumes and (C) ejection fraction.
Imaging 2008;24:691–698.
5. Sugeng L, Mor-Avi V, Weinert L, Niel J, Ebner C, Steringer-Mas-cherbauer R, Bartolles R, Baumann R, Schummers G, Lang RM,Nesser HJ. Multimodality comparison of quantitative volumetric anal-ysis of the right ventricle. JACC Cardiovasc Imaging. 2010;3:10–18.
6. van der Zwaan HB, Helbing WA, McGhie JS, Geleijnse ML, Luijnen-burg SE, Roos-Hesselink JW, Meijboom FJ. Clinical value of real-time three-dimensional echocardiography for right ventricular quanti-fication in congenital heart disease: validation with cardiac magneticresonance imaging. J Am Soc Echocardiogr 2010;23:134–140.
7. Tamborini G, Marsan NA, Gripari P, Maffessanti F, Brusoni D, Mu-ratori M, Caiani EG, Fiorentini C, Pepi M. Reference values for rightventricular volumes and ejection fraction with real-time three-dimen-sional echocardiography: evaluation in a large series of normal sub-jects. J Am Soc Echocardiogr 2010;23:109–115.
8. Robbers-Visser D, Boersma E, Helbing WA. Normal biventricularfunction, volumes, and mass in children aged 8 to 17 years. J MagnReson Imaging 2009;29:552–559.
9. Puchalski MD, Williams RV, Askovich B, Minich LL, Mart C, TaniLY. Assessment of right ventricular size and function: echo versusmagnetic resonance imaging. Congenit Heart Dis 2007;2:27–31.
0. Alfakih K, Plein S, Thiele H, Jones T, Ridgway JP, Sivananthan MU.Normal human left and right ventricular dimensions for MRI as as-sessed by turbo gradient echo and steady-state free precession imagingsequences. J Magn Reson Imaging 2003;17:323–329.
1. Teo KS, Carbone A, Piantadosi C, Chew DP, Hammett CJ, Brown MA,Worthley SG, Cardiac MRI. Assessment of left and right ventricularparameters in healthy Australian normal volunteers. Heart Lung Circ2008;17:313–317.
2. Maceira AM, Prasad SK, Khan M, Pennell DJ. Reference right ven-tricular systolic and diastolic function normalized to age, gender andbody surface area from steady-state free precession cardiovascularmagnetic resonance. Eur Heart J 2006;27:2879–2888.
3. Hudsmith LE, Petersen SE, Francis JM, Robson MD, Neubauer S.Normal human left and right ventricular and left atrial dimensionsusing steady state free precession magnetic resonance imaging. J Car-diovasc Magn Reson 2005;7:775–782.
4. Lorenz CH, Walker ES, Morgan VL, Klein SS, Graham TP Jr. Normalhuman right and left ventricular mass, systolic function, and genderdifferences by cine magnetic resonance imaging. J Cardiovasc MagnReson 1999;1:7–21.
5. Knauth AL, Gauvreau K, Powell AJ, Landzberg MJ, Walsh EP, LockJE, del Nido PJ, Geva T. Ventricular size and function assessed bycardiac MRI predict major adverse clinical outcomes late after tetral-ogy of Fallot repair. Heart 2008;94:211–216.
6. Piran S, Veldtman G, Siu S, Webb GD, Liu PP. Heart failure andventricular dysfunction in patients with single or systemic right ven-tricles. Circulation 2002;105:1189–1194.
7. Rutledge JM, Nihill MR, Fraser CD, Smith OE, McMahon CJ, BezoldLI. Outcome of 121 patients with congenitally corrected transpositionof the great arteries. Pediatr Cardiol 2002;23:137–145.
8. Davlouros PA, Niwa K, Webb G, Gatzoulis MA. The right ventricle incongenital heart disease. Heart 2006;92(Suppl 1):i27–i38.
9. Meijboom F, Szatmari A, Deckers JW, Utens EM, Roelandt JR, Bos E, HessJ. Long-term follow-up (10 to 17 years) after mustard repair for transpositionof the great arteries. J Thorac Cardiovasc Surg 1996;111:1158–1168.
0. Roos-Hesselink JW, Meijboom FJ, Spitaels SE, van Domburg R, vanRijen EH, Utens EM, McGhie J, Bos E, Bogers AJ, Simoons ML.Decline in ventricular function and clinical condition after mustardrepair for transposition of the great arteries (a prospective study of22–29 years). Eur Heart J 2004;25:1264–1270.
1. Therrien J, Provost Y, Merchant N, Williams W, Colman J, Webb G.Optimal timing for pulmonary valve replacement in adults after tetral-ogy of Fallot repair. Am J Cardiol 2005;95:779–782.
2. Buechel ER, Dave HH, Kellenberger CJ, Dodge-Khatami A, Pretre R, BergerF, Bauersfeld U. Remodelling of the right ventricle after early pulmonaryvalve replacement in children with repaired tetralogy of Fallot: assessment bycardiovascular magnetic resonance. Eur Heart J 2005;26:2721–2727.
3. Apitz C, Sieverding L, Latus H, Uebing A, Schoof S, Hofbeck M. Rightventricular dysfunction and B-type natriuretic peptide in asymptomatic pa-tients after repair for tetralogy of Fallot. Pediatr Cardiol 2009;30:898–904.
4. Tamborini G, Muratori M, Brusoni D, Celeste F, Maffessanti F, CaianiEG, Alamanni F, Pepi M. Is right ventricular systolic function reducedafter cardiac surgery? A two- and three-dimensional echocardio-
graphic study. Eur J Echocardiogr 2009;10:630–634.