
Value of transesophageal echocardiography during repair of congenital heart defects
7
Value of Transesophageal Echocardiography During Repair of Congenital Heart Defects Maurizio Dan, MD, Raffaele Bonato, MD, Alessandro Mazzucco, MD, Uberto Bortolotti, MD, Giuseppe Faggian, MD, Gianpiero Giron, MD, and Vincenzo Gallucci, MD Departments of Anesthesiology and Cardiovascular Surgery, University of Padova Medical School, Padova, Italy Two-dimensional transesophageal color Doppler echo- cardiography was employed intraoperatively in 30 chil- dren undergoing repair of a variety of simple and com- plex cardiac malformations. There were 16 female and 14 male patients, with a mean age of 9 f 3 years (range, 4 to 13 years) and a mean weight of 31 f 9 kg (range, 16 to 50 kg), 16 children weighing less than 30 kg. A standard, commercially available transesophageal echocardiog- raphy probe (5 MHz, 64 elements) was used in all patients without complications. Transesophageal echo- cardiography proved helpful in selecting the surgical approach, in assessing the adequacy of surgical repair, in detecting residual intracardiac shunts, and in allowing uninterrupted monitoring of ventricular performance throughout the procedure. Our initial experience sug- gests that transesophageal echocardiography is a valu- able tool to be used in children with congenital cardiac malformations, particularly in those requiring complex intracardiac procedures. The amount of information ob- tained by the surgeon should favor the routine use of transesophageal echocardiography during open heart procedures and stimulate the development of probes to be safely used even in infants and newborns. (Ann Thorac Surg 1990;50:63743) ransesophageal echocardiography (TEE) is currently T gaining increasing popularity as a means of continu- ous cardiac imaging during open heart operations [l, 21; its ability to monitor left ventricular function and wall motion abnormalities and to assess the adequacy of sur- the technical feasibility of 2-D TEE and its potential advantages for the cardiac surgeon. Material and Methods a , gical repair is well defined in adult patients [3, 41. With the recent introduction of color-flow Doppler technology in transesophageal imaging, TEE has become even more suitable for intraoperative application and its indications are extended to all situations in which detec- tion of abnormal intracardiac blood flow is needed [5]. For this reason patients with congenital heart defects should benefit most from the intraoperative use of TEE. Experi- ence in this field, however, is at present very limited [6, 71, mainly because pediatric-size probes were not com- mercially available until very recently, while epicardial color flow imaging has received increasing acceptance for intraoperative application in children [8]. The latter, how- ever, presents many limitations, such as the need for temporary discontinuation of the operative procedure, impossibility of continuous imaging, poor surface contact, heart compression with potential rhythm disturbances, and, above all, limited time allowed for evaluation [9]. We present here our initial experience with two- dimensional (2-D) color Doppler TEE used intraopera- tively in a series of children undergoing repair of various congenital heart malformations. This report focuses on Accepted for publication June 11, 1990 Address reprint requests to Dr Dan, Istituto di Anestesiologia e Rianimazi- one, Universita di Padova, Via C. Battisti, 267, 35121 Padova, Italy. Patient Population During the interval October 1988 to September 1989, 2-D TEE was used intraoperatively in 30 children undergoing surgical repair of various congenital heart defects. The criteria to be enrolled in the study were a body weight preferably above 20 kg and absence of any documented pathology of the upper gastrointestinal tract. There were 16 female and 14 male patients, with a mean age at operation of 9 & 3 years (range, 4 to 13 years) and a mean weight of 31 ? 9 kg (range, 16 to 50 kg), 16 weighing less than 30 kg. Twenty-seven patients had primary repair of various intracardiac malformations, 1 patient had reoper- ation for residual pulmonary stenosis and ventricular septa1 defect (VSD) due to patch detachment after correc- tion of tetralogy of Fallot, 1 had reoperation because of subaortic stenosis after repair of interrupted aortic arch and VSD, and 1 had an open chest biopsy of a left ventricular hemangioma (Table 1). The preoperative diagnosis was made with standard 2-D echocardiographic and hemodynamic investigations in 13 and by 2-D echocardiography alone in 17. With the exception of the patient undergoing left ventricular biopsy all children were operated on with standard cardiopulmo- nary bypass and moderate systemic hypothermia. Myo- cardial protection was achieved in all cases with the use of cold potassium cardioplegia combined with topical cool- 0 1990 by The Society of Thoracic Surgeons 0003-4975/90/$3.50
Transcript of Value of transesophageal echocardiography during repair of congenital heart defects

Value of Transesophageal Echocardiography During Repair of Congenital Heart Defects Maurizio Dan, MD, Raffaele Bonato, MD, Alessandro Mazzucco, MD, Uberto Bortolotti, MD, Giuseppe Faggian, MD, Gianpiero Giron, MD, and Vincenzo Gallucci, MD Departments of Anesthesiology and Cardiovascular Surgery, University of Padova Medical School, Padova, Italy
Two-dimensional transesophageal color Doppler echo- cardiography was employed intraoperatively in 30 chil- dren undergoing repair of a variety of simple and com- plex cardiac malformations. There were 16 female and 14 male patients, with a mean age of 9 f 3 years (range, 4 to 13 years) and a mean weight of 31 f 9 kg (range, 16 to 50 kg), 16 children weighing less than 30 kg. A standard, commercially available transesophageal echocardiog- raphy probe (5 MHz, 64 elements) was used in all patients without complications. Transesophageal echo- cardiography proved helpful in selecting the surgical approach, in assessing the adequacy of surgical repair, in
detecting residual intracardiac shunts, and in allowing uninterrupted monitoring of ventricular performance throughout the procedure. Our initial experience sug- gests that transesophageal echocardiography is a valu- able tool to be used in children with congenital cardiac malformations, particularly in those requiring complex intracardiac procedures. The amount of information ob- tained by the surgeon should favor the routine use of transesophageal echocardiography during open heart procedures and stimulate the development of probes to be safely used even in infants and newborns.
(Ann Thorac Surg 1990;50:63743)
ransesophageal echocardiography (TEE) is currently T gaining increasing popularity as a means of continu- ous cardiac imaging during open heart operations [l, 21; its ability to monitor left ventricular function and wall motion abnormalities and to assess the adequacy of sur-
the technical feasibility of 2-D TEE and its potential advantages for the cardiac surgeon.
Material and Methods a ,
gical repair is well defined in adult patients [3, 41. With the recent introduction of color-flow Doppler
technology in transesophageal imaging, TEE has become even more suitable for intraoperative application and its indications are extended to all situations in which detec- tion of abnormal intracardiac blood flow is needed [5]. For this reason patients with congenital heart defects should benefit most from the intraoperative use of TEE. Experi- ence in this field, however, is at present very limited [6, 71, mainly because pediatric-size probes were not com- mercially available until very recently, while epicardial color flow imaging has received increasing acceptance for intraoperative application in children [8]. The latter, how- ever, presents many limitations, such as the need for temporary discontinuation of the operative procedure, impossibility of continuous imaging, poor surface contact, heart compression with potential rhythm disturbances, and, above all, limited time allowed for evaluation [9].
We present here our initial experience with two- dimensional (2-D) color Doppler TEE used intraopera- tively in a series of children undergoing repair of various congenital heart malformations. This report focuses on
Accepted for publication June 11, 1990
Address reprint requests to Dr Dan, Istituto di Anestesiologia e Rianimazi- one, Universita di Padova, Via C. Battisti, 267, 35121 Padova, Italy.
Patient Population During the interval October 1988 to September 1989, 2-D TEE was used intraoperatively in 30 children undergoing surgical repair of various congenital heart defects. The criteria to be enrolled in the study were a body weight preferably above 20 kg and absence of any documented pathology of the upper gastrointestinal tract. There were 16 female and 14 male patients, with a mean age at operation of 9 & 3 years (range, 4 to 13 years) and a mean weight of 31 ? 9 kg (range, 16 to 50 kg), 16 weighing less than 30 kg. Twenty-seven patients had primary repair of various intracardiac malformations, 1 patient had reoper- ation for residual pulmonary stenosis and ventricular septa1 defect (VSD) due to patch detachment after correc- tion of tetralogy of Fallot, 1 had reoperation because of subaortic stenosis after repair of interrupted aortic arch and VSD, and 1 had an open chest biopsy of a left ventricular hemangioma (Table 1).
The preoperative diagnosis was made with standard 2-D echocardiographic and hemodynamic investigations in 13 and by 2-D echocardiography alone in 17. With the exception of the patient undergoing left ventricular biopsy all children were operated on with standard cardiopulmo- nary bypass and moderate systemic hypothermia. Myo- cardial protection was achieved in all cases with the use of cold potassium cardioplegia combined with topical cool-
0 1990 by The Society of Thoracic Surgeons 0003-4975/90/$3.50

638 DANETAL INTRAOPERATIVE TRANSESOPHAGEAL ECHOCARDIOGRAPHY
Ann Thorac Surg 1990;50:63743
Table 1 . Preoperative Diagnosis and Surgical Procedures
No. of Disease Patients Operation
Ostium I1 ASD + PAPVC
+PS
Ostium I ASD
Fibrous SAS
VSD + PS
+ A1
Aortic stenosis
TOF
+CAVC
TGA, VSD, PS
Single ventricle, CAVC
Ebstein’s anomaly TV” VSD patch
detachment, PSb Fibrous SAS, AIc LV hemangioma
5 1
1
5
4
1 2
2
1
1
1
1
1
1 1
1 1
ASD patch closure ASD patch closure, intraatrial
tunnel ASD patch closure, pulmonary
valvotomy ASD patch closure, mitral
valvoplasty (3) Blunt resection, septal
myotomy (2) VSD patch closure VSD patch closure, pulmonary
valvotomy (l), right ventricular muscle band resection (1)
VSD patch closure, aortic valvoplasty
Commissurotomy and valvoplasty
TOF repair with transannular patch
TOF repair with transannular patch, CAVC repair with double patch
Rastelli procedure with aortic homograft
Modified Fontan, atrial partitioning
Tricuspid valve replacement VSD closure, transannular
Blunt resection Left ventricular biopsy
patch
a Underwent successful orthotopic heart transplantation because of biven- tricular failure after 20 hours of mechanical support. Reoperation after previous repair of TOF. ‘ Reoperation after previous repair of interrupted aortic arch and VSD closure. A1 = aortic incompetence; CAVC = complete atrioventricular canal; LV = left ventricular; PAPVC = partial anomalous pulmonary venous connection; PS = pulmonary stenosis; SAS = subaortic stenosis; TGA = transposition of great arteries; TOF = tetralogy of Fallot; TV = tricuspid valve; VSD = ventricular septal defect.
ASD = atrial septal defect;
ing. Details of the surgical techniques employed are summarized in Table 1.
Technique of Two- Dimensional Transesophageal Echocard iography A 64-element, 5-MHz, commercially available phased array transducer (HP 21362 A, Hewlett-Packard Co, An- dover, MA) interfaced with a Hewlett-Packard ultrasono- graph (HP 77020 AC) was used in all cases. This system allows color-flow Doppler examination as well as high- resolution 2-D imaging.
Insertion of the probe was performed in the anesthe- tized patient after endotracheal intubation, either blindly
or under direct visualization of the pharynx with the neck moderately flexed. Advancement of the generously lubri- cated probe was accomplished very gently in the flexible mode with the control unlocked. Tilting of the transducer tip in both the anteroposterior and lateral planes was intentionally avoided in patients weighing less than 30 kg.
Transesophageal echocardiographic monitoring was started before skin incision and continued throughout the entire procedure, being temporarily suspended during cardiopulmonary bypass to minimize the risk of esopha- geal damage due to probe heating and temperature gra- dient during this period. At the end of each procedure, just before transfer of the patient from the operating room to the intensive care unit, the probe was removed. When indicated, 2-D TEE studies were also performed in the postoperative period while the patient was still intubated.
Cardiac views were obtained from both the esophagus and stomach as described by Seward and associates (101. Longitudinal four-chamber or four-chamber and left ven- tricular outflow tract views were mainly used; additional views such as basal short-axis, transgastric short-axis, and transgastric four-chamber were also obtained when con- sidered of particular interest for the study. For color-flow mapping long-axis views were almost exclusively used, as blood flow must be parallel to the Doppler source for optimal signal processing.
Results Surgical Results There were two hospital deaths (less than 30 days). One 12-year-old boy died of septic shock 4 days after total repair of tetralogy of Fallot and complete atrioventricular canal, and a 12-year-old girl died of heart failure on postoperative day 1 after a modified Fontan procedure with atrial partitioning for single ventricle and complete atrioventricular canal. Finally, a 12-year-old boy showed severe biventricular failure after tricuspid valve replace- ment for Ebstein’s anomaly; he was supported with extracorporeal circulation for 20 hours before undergoing successful orthotopic heart transplantation. No major postoperative complications were observed in the remain- ing patients.
Technical Aspects of Transesophageal Echocardiography Two-dimensional transesophageal echocardiography monitoring was performed 32 times, once in 28 patients and twice in 2. In the latter it was repeated in the intensive care unit within 24 hours after operation: in the patient with low output state after a modified Fontan procedure, to assess left ventricular performance, and in the patient with tetralogy of Fallot and complete atrioventricular canal repair to verify the effect of vasodilator administra- tion on the degree of residual mitral incompetence.
The probe was successfully inserted without problems in all cases and was left in place for the entire surgical procedure in all but 1. In this patient, the smallest of our series (a 6-year-old, 16-kg boy), the probe was withdrawn during the period of cardiopulmonary bypass. The quality of 2-D TEE was considered satisfactory in all cases,
Ann Thorac Surg 1990;50:637-43
including smaller patients (less than 30 kg in weight) in whom probe manipulation was intentionally avoided.
The addition of color-flow mapping, performed at a mean pulse repetition frequency of 3 to 4 KHz, was considered to represent a substantial improvement to the examination in all cases. Nevertheless, in some instances "ghost" color signals were derived from fast-moving cardiac structures instead of only from the bloodstream. This phenomenon was observed particularly when the heart rate exceeded 140 beats/min, as occurred in some of our children during weaning from cardiopulmonary by- pass; in such cases time was allowed for rhythm stabili- zation while evaluation of color data was in the meantime performed through frame by frame analysis.
DANETAL 639 INTRAOPERATIVE TRANSESOPHAGEAL ECHOCARDIOGRAPHY
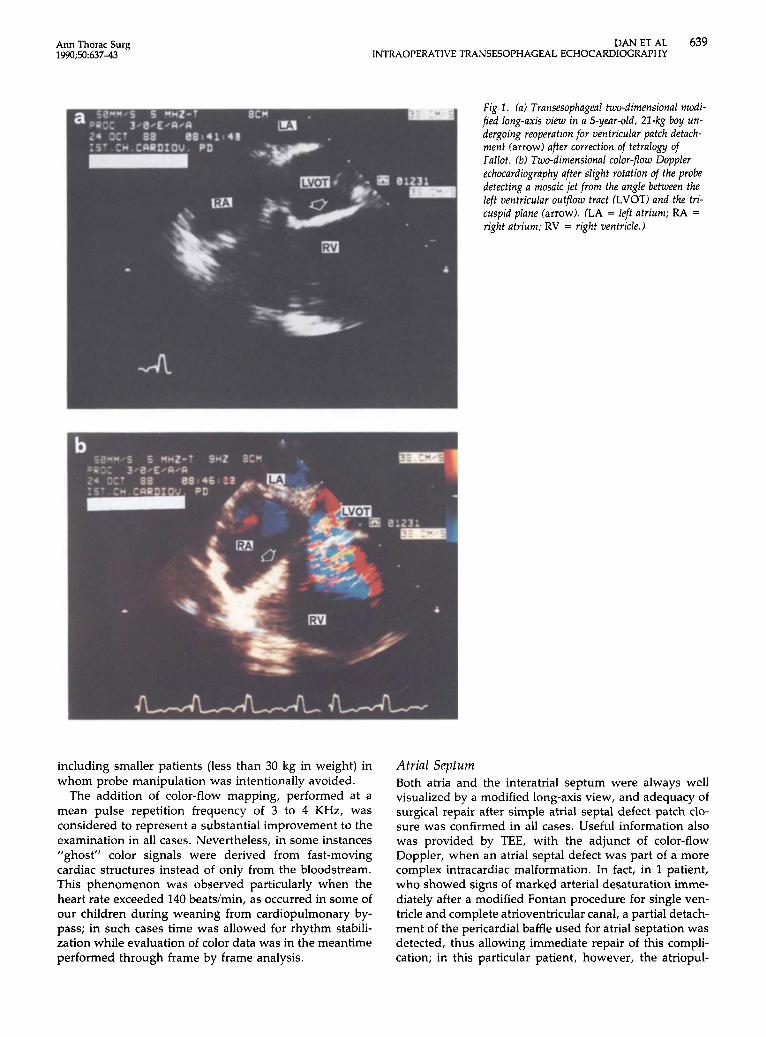
Fig 2 . ( a ) Transesophageal two-dimensional modi- fied long-axis view in a 5-year-old, 22-kg boy un- dergoing reoperation for ventricular patch detach- ment farrow) after correction of tetralogy of Fallot. (b) Two-dimensional color-flow Doppler echocardiography after slight rotation of the probe detecting a mosaic jet from the angle between the left ventricular outflow tract (LVOT) and the tri- cuspid plane (arrow). (LA = left atrium; RA = right atrium; RV = right ventricle.)
Atrial Septum Both atria and the interatrial septum were always well visualized by a modified long-axis view, and adequacy of surgical repair after simple atrial septal defect patch clo- sure was confirmed in all cases. Useful information also was provided by TEE, with the adjunct of color-flow Doppler, when an atrial septal defect was part of a more complex intracardiac malformation. In fact, in 1 patient, who showed signs of marked arterial desaturation imme- diately after a modified Fontan procedure for single ven- tricle and complete atrioventricular canal, a partial detach- ment of the pericardial baffle used for atrial septation was detected, thus allowing immediate repair of this compli- cation; in this particular patient, however, the atriopul-

640 DANETAL INTRAOPERATIVE TRANSESOPHAGEAL ECHOCARDIOGRAPHY
Fig 2 . (a) Preoperative transesoph- ageal two-dimensional long-axis view of the left ventricular outflow tract (LVOT) in a 10-year-old, 37-kg boy showing a subaortic ridge (arrow). (b) Postoperative control in the same view demonstrating complete resec- tion of the ridge. (LA = left atrium; LV = left ventricle.)
monary anastomosis could not be effectively visualized. In another patient, in whom preoperative catheterization had shown a VSD and raised the suspicion of an atrial septa1 defect on the basis of oxymetric data, intraoperative TEE showed an intact interatrial septum; this finding was confirmed at direct inspection and the high oxygen satu- ration was shown to be caused by the combination of ventricular shunting and tricuspid regurgitation second- ary to valve dysplasia.
Ventricular Septum The ventricular septum was best visualized with a stan- dard long-axis view. In all patients with perimembranous and malalignment VSD TEE was helpful to assess the adequacy of operation and to exclude any residual inter- ventricular shunt. Particularly, in 1 child undergoing reoperation after tetralogy of Fallot repair it allowed exact
Ann Thorac Surg 1990;50:637-43
identification of the site of patch detachment, not clearly shown at angiography (Fig 1).
Left Ventricular Outflow Tract and Aortic Valve Both left ventricular outflow tract and aortic valve were always well identified through a long-axis view; in addi- tion a basal short-axis view was also helpful in imaging the aortic valve. In patients with subaortic stenosis TEE allowed us to immediately verify the complete resection of the subaortic membrane and to exclude any iatrogenic complication such as a VSD or aortic regurgitation (Fig 2). Both aortic valve and left ventricular outflow tract were easily examined also in patients with aortic incompetence or stenosis to assess the early result of valve repair.
Pulmonary Artery When needed, the main pulmonary trunk and right pulmonary artery were well visualized through a basal

Ann Thorac Surg 1990;5063743
DANETAL 641 INTRAOPERATIVE TRANSESOPHAGEAL ECHOCARDIOGRAPHY
short-axis view. In 1 patient stenosis of the right pulmo- nary artery could be demonstrated after VSD patch clo- sure even though intraoperative measurements failed to reveal any clinically significant pressure gradient (Fig 3). However, in the child who had a Rastelli procedure for transposition of the great arteries the right ventricular to pulmonary artery conduit could not be visualized, nor could the right ventricular outflow tract and pulmonary valve in many patients.
Atrioventricular Valves Both atrioventricular valves were always well identified in a long-axis, four-chamber view. Transesophageal echocar- diography was of particular value in the evaluation of mitral anatomy and dynamics because of the favorable position of this valve with regard to the esophageal window; consequently, immediate evaluation of the ade- quacy of mitral valvoplasty was always possible. Further- more, in the patient with tetralogy of Fallot and complete atrioventricular canal, TEE helped to assess the degree of residual mitral incompetence after repair of a severely dysplastic mitral component and to monitor the effect of vasodilator therapy in weaning the patient from cardio- pulmonary bypass (Fig 4).
Cardiac Performance Variations of cardiac function due to hypovolemia or hypo- contractility were instantaneously recognized by TEE in all patients, allowing us to select the most proper treatment in each situation. However, quantitative analysis was often impractical mainly because of the hemodynamic instability of most patients with complex intracardiac repair early after cardiopulmonary bypass.
Comment The clinical experience with the intraoperative use of TEE in children so far has been very limited. Recently, Cyran
Fig 3, Transesophageal two-dimensional basal short-axis view after closure of a ventricular septal defect in a 7-year-old, 24-kg boy showing stenosis of the origin of the right pulmonary artery (ar- rowheads). ( A 0 = aorta; PA = main pulmo- nary artery; RVOT = right ventricular outflow tract.)
and co-workers (61 demonstrated the efficacy of this technique in children undergoing operation for congenital heart disease. They employed a 32-element, 3.5-MHz transducer mounted on a gastroscope with an 11-mm external diameter shaft and a 15-mm external diameter tip in all patients except 1, in whom they used a smaller and more technologically advanced second-generation probe. They demonstrated the feasibility of TEE in patients older than 7 years and the great potential of this technique in assessing the adequacy of surgical repair of complex cardiac lesions.
In all patients in our series we used a second-generation TEE imaging system that has a higher number of ele- ments, 64, with an emission frequency of 5 MHz and smaller dimensions (10-mm external diameter shaft and 12 x 14-mm external dimension tip) and incorporates color-flow Doppler echocardiography. These features have further enhanced the utility of intraoperative TEE in pediatric patients undergoing open heart operations by allowing a higher resolution in the near field and, what is more important, a better understanding of normal and abnormal intracardiac blood flow before and after correc- tion.
Transesophageal echocardiography was employed in 30 children between 4 and 13 years of age who had a mean weight of 31 * 9 kg and a variety of simple and complex cardiac malformations. We were able to study children with a body weight as low as 16 kg by employing probes of smaller dimensions when compared with those used by others [6]. Although subsequent endoscopic examination was not performed in any patient in this series, no apparent complications related to probe insertion were observed, most likely because some technical guidelines were routinely followed. These included generous lubri- cation of the probe, moderate nuchal flexion, direct laryn- goscopic visualization in the presence of even minimal resistance to probe advancement into the pharynx, and

642 DANETAL INTRAOPERATIVE TRANSESOPHAGEAL ECHOCARDIOGRAPHY
Fig 4. (a) Postoperative transesophageal two-di- mensional four-chamber view in a 12-year-old, 50-kg boy with tetralogy of Fallot and complete atrioventricular canal. The two patches used to repair the septal defects are evident (arrows). (b) The same image with color Doppler shows a re- gurgitant jet (mosaic systolic pattern) into the left atrium due to residual mitral incompetence. (LA = left atrium; LV = left ventricle; RA = right atrium; RV = right ventricle.)
temporary suspension of monitoring during cardiopulmo- nary bypass. Whether the probe should be withdrawn in children weighing less than 20 kg or during deep hypo- thermic circulatory arrest is still not clear; however, we believe the latter may be a useful precaution despite the safety of prolonged use of TEE as demonstrated experi- mentally by the absence of injury to the esophageal mucosa even in small animals [ll].
The results of this study, although performed in a group of patients with a wide spectrum of cardiac anom- alies, show the potential advantages of the intraoperative use of TEE. Transesophageal echocardiography is proba- bly not needed when dealing with simple congenital heart defects such as an atrial septal defect; nevertheless, appli- cation of this technique in these patients has helped to achieve enough expertise, especially from the technical point of view, enabling us to confidently employ it in
Ann Thorac Surg 1990;50:637-43
more complex cases and in progressively smaller children. The benefits of TEE, greatly enhanced by the addition of color-flow mapping, are particularly evident for patients with complex intracardiac anatomy who require elaborate surgical procedures. Intracardiac flow abnormalities, for example, can be easily detected, thus rendering TEE equivalent to an intraoperative angiography. This appears particularly helpful in detecting the presence and exact site of any residual intracardiac shunt and the amount of any transvalvular reflux, thus allowing the surgeon to make the most appropriate decision for each individual patient before discontinuation of cardiopulmonary by- pass. This occurred in 1 of our patients in whom partial detachment of the atrial partitioning patch was detected after a modified Fontan procedure.
Transesophageal echocardiography permits uninter- rupted monitoring of cardiac performance throughout the

Ann Thorac Surg 1990;5063743
DANETAL 643 INTRAOPERATIVE TRANSESOPHAGEAL ECHOCARDIOGRAPHY
surgical procedure and therefore evaluation of the effec- tiveness of any inotropic or vasoactive drug administered [12]. This clearly represents an advantage over intraoper- ative epicardial 2-D echocardiography as poor surface contact and heart compression with consequent arrhyth- mias are avoided and temporary discontinuation of the operation is not required.
Nevertheless, TEE has some deficiencies that at the present time may be represented mainly by the limited number of scanning planes, which does not allow in most cases a clear visualization of structures such as the right ventricular outflow tract and the pulmonary valve. Fur- thermore, despite the fact that in all our patients TEE monitoring was judged to be satisfactory, in some cases, particularly when the heart rate rose above 140 beats/min, color signals derived from fast-moving cardiac structures temporarily impaired the quality of images. The low signal to noise ratio observed in such situations may probably be solved with more sophisticated probes espe- cially designed for small children, as recently reported by Kyo and colleagues [7].
Our preliminary data suggest that TEE is a valuable tool to be used intraoperatively in children during open heart operations, particularly during correction of complex con- genital heart malformations. From this experience it ap- pears that a standard, commercially available, adult probe can be safely used in children weighing more than 20 kg. However, the amount of information obtained by the surgeon with this technique should favor its routine use and stimulate development of probes to be employed even in small infants and newborns.
References 1. Kremer P, Cahalan M, Beaupre P, et al. Intraoperative
monitoring using transesophageal 2-dimensional echocar- diography. Anaesthesist 1985;34:111-7.
2. Goldman ME, Mindich BP. Intraoperative 2-dimensional echocardiography. New application of an old technique. J Am Coll Cardiol 1986;7:37&82.
3. Kyo S, Takamoto S, Matsumura M, et al. Immediate and early postoperative evaluation of results of cardiac surgery by transesophageal two-dimensional Doppler echocardiog- raphy. Circulation 1987;76(Suppl 5):113-21.
4. Shiller NB. Evaluation of cardiac function during surgery by transesophageal 2-dimensional echocardiography. In: Hanrath P, Bleifeld W, Souquet J, eds. Cardiovascular diag- nosis by ultrasound: transesophageal, computerized, con- trast, Doppler echocardiography. The Hague: Martinus Nij-
5. De Bruijn NP, Clements FM, Kisslo JA. Intraoperative trans- esophageal color flow mapping: initial experience. Anesth Analg 1987;66:386-90.
6. Cyran SE, Kimball TR, Meyer RA, et al. Efficacy of intraop- erative transesophageal echocardiography in children with congenital heart disease. Am J Cardiol 1989;63:594-8.
7. Kyo S, Koike K, Takanawa E, et al. Impact of transesophageal Doppler echocardiography on pediatric cardiac surgery. Int J Card Imag 1989;4:41-2.
8. Ungerleider R. Decision making in pediatric cardiac surgery using intraoperative echo. Int J Card Imag 1989;4:33-5.
9. Sutherland GR, van Daele MERM, Stumper OFW, et al. Epicardial and transesophageal echocardiography during surgery for congenital heart disease. Int J Card Imag 1989;4: 3740.
10. Seward JB, Khandheria BK, Oh JK, et al. Transesophageal echocardiography: technique, anatomic correlations, imple- mentation and clinical applications. Mayo Clin Proc 1988;63:
11. OShea JP, DAmbra MN, Magro C, et al. Transesophageal echocardiography: is it safe to the esophagus? An in vivo study [Abstract]. Circulation 1988;78(Suppl 2):440.
12. Switzer DF, Nanda NC. Doppler color flow mapping. Ultra- sound Med Biol 1985;11:403-16.
hoff, 1982:289-93.
649-80.



















