Congenital Posterior Mediastinal Teratoma with Intraspinal Extension

Ablation of Atrial Flutter inComplex Congenital HeartDisease
Marwan M. Refaat, MD, Edward P. Gerstenfeld, MD*KEYWORDS
� Transposition of the great arteries � Atrial switch � Mustard procedure � Electrophysiology� Radiofrequency ablation
KEY POINTS
� Even in patients with complex congenital heart disease, typical atrial flutter remains the mostcommon supraventricular arrhythmia.
� The flutter circuit in Mustard patients is nearly always in the pulmonary venous atrium.
� Proof of block in the flutter isthmus is critical to achieving long term success.
� Knowledge of the underlying anatomy is critical for guiding mapping and ablation in adult congenitalheart disease patients.
CLINICAL PRESENTATION
A 38-year-old manwho had a history of D-transpo-sition of the great arteries (D-TGA) status postMustard atrial switch procedure and a dual-chamber pacemaker for sinus node dysfunctionpresented with palpitations. His electrocardiogram(ECG) showed a narrow-complex tachycardia at198 beats/min (Fig. 1). After slowing of the ventric-ular rate, the underlying rhythm was consistentwith an atrial flutter. He was treated with diltiazemand flecainide but continued to have episodes ofpalpitations, chest pain, fatigue, and decreasedexercise tolerance. He was thus referred for elec-trophysiology study and possible ablation.
om
ELECTROPHYSIOLOGY STUDY
A contrast injection into the systemic venous atriumvia a 6F pigtail catheter was first performed toexclude baffle obstruction and delineate the atrialanatomy. A 7F deflectable decapolar catheter wasplaced in the high systemic venous atrium (HSVA),a 5F quadripolar catheter was placed in the low
Conflict of interest: None.Cardiology Division, Department of Medicine, UniversityMUE-434, Box 1354, San Francisco, CA 94143-1354, USA* Corresponding author.E-mail address: [email protected]
Card Electrophysiol Clin 4 (2012) 591–596http://dx.doi.org/10.1016/j.ccep.2012.08.0401877-9182/12/$ – see front matter � 2012 Elsevier Inc. All
SVA (LSVA), and a 5F deflectable quadripolar cath-eter was placed in the morphologic left ventricularapex (LVA) via the right femoral vein. A detailed 3-dimensional electroanatomic map (CARTO3; Bio-sense Webster, Diamond Bar, CA) (Fig. 2A) of thesystemic venous atrium during the tachycardiawas acquired using a 3.5-mm open-irrigatedmapping/ablation catheter (Thermocool; BiosenseWebster). Bipolar electrograms (30–500 Hz) weredisplayed and stored using a digital recordingsystem (EP MedSystems, West Berlin, NJ).
Mapping of the systemic venous atriumrevealed a pattern of high to low activation. Theresponse to overdrive ventricular pacing at thesite of earliest activation is shown in Fig. 2B. Isthe origin of the tachycardia in the SVA?
Entrainment of the tachycardia shows a post-pacing interval (PPI) more than 30 millisecondslonger than the tachycardia cycle length (TCL).Therefore, the SVA is not part of the tachycardiacircuit. Femoral arterial access was obtained anda retrograde aortic approach to access the pulmo-nary venous atrium (PVA) was performed. Detailedactivation mapping of the SVA and PVA is shown
of California San Francisco, 500 Parnassus Avenue,
rights reserved. cardiacEP.th
eclinics.c
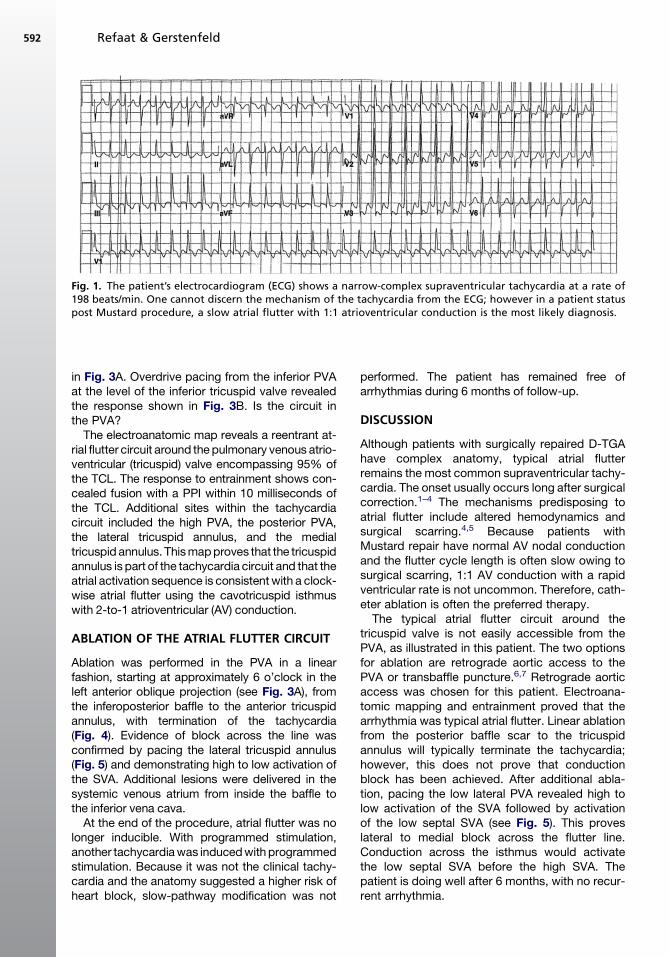
Fig. 1. The patient’s electrocardiogram (ECG) shows a narrow-complex supraventricular tachycardia at a rate of198 beats/min. One cannot discern the mechanism of the tachycardia from the ECG; however in a patient statuspost Mustard procedure, a slow atrial flutter with 1:1 atrioventricular conduction is the most likely diagnosis.
Refaat & Gerstenfeld592
in Fig. 3A. Overdrive pacing from the inferior PVAat the level of the inferior tricuspid valve revealedthe response shown in Fig. 3B. Is the circuit inthe PVA?The electroanatomic map reveals a reentrant at-
rial flutter circuit around the pulmonary venous atrio-ventricular (tricuspid) valve encompassing 95% ofthe TCL. The response to entrainment shows con-cealed fusion with a PPI within 10 milliseconds ofthe TCL. Additional sites within the tachycardiacircuit included the high PVA, the posterior PVA,the lateral tricuspid annulus, and the medialtricuspid annulus. Thismapproves that the tricuspidannulus is part of the tachycardia circuit and that theatrial activation sequence is consistentwith a clock-wise atrial flutter using the cavotricuspid isthmuswith 2-to-1 atrioventricular (AV) conduction.
ABLATION OF THE ATRIAL FLUTTER CIRCUIT
Ablation was performed in the PVA in a linearfashion, starting at approximately 6 o’clock in theleft anterior oblique projection (see Fig. 3A), fromthe inferoposterior baffle to the anterior tricuspidannulus, with termination of the tachycardia(Fig. 4). Evidence of block across the line wasconfirmed by pacing the lateral tricuspid annulus(Fig. 5) and demonstrating high to low activation ofthe SVA. Additional lesions were delivered in thesystemic venous atrium from inside the baffle tothe inferior vena cava.At the end of the procedure, atrial flutter was no
longer inducible. With programmed stimulation,another tachycardiawas inducedwithprogrammedstimulation. Because it was not the clinical tachy-cardia and the anatomy suggested a higher risk ofheart block, slow-pathway modification was not
performed. The patient has remained free ofarrhythmias during 6 months of follow-up.
DISCUSSION
Although patients with surgically repaired D-TGAhave complex anatomy, typical atrial flutterremains the most common supraventricular tachy-cardia. The onset usually occurs long after surgicalcorrection.1–4 The mechanisms predisposing toatrial flutter include altered hemodynamics andsurgical scarring.4,5 Because patients withMustard repair have normal AV nodal conductionand the flutter cycle length is often slow owing tosurgical scarring, 1:1 AV conduction with a rapidventricular rate is not uncommon. Therefore, cath-eter ablation is often the preferred therapy.The typical atrial flutter circuit around the
tricuspid valve is not easily accessible from thePVA, as illustrated in this patient. The two optionsfor ablation are retrograde aortic access to thePVA or transbaffle puncture.6,7 Retrograde aorticaccess was chosen for this patient. Electroana-tomic mapping and entrainment proved that thearrhythmia was typical atrial flutter. Linear ablationfrom the posterior baffle scar to the tricuspidannulus will typically terminate the tachycardia;however, this does not prove that conductionblock has been achieved. After additional abla-tion, pacing the low lateral PVA revealed high tolow activation of the SVA followed by activationof the low septal SVA (see Fig. 5). This proveslateral to medial block across the flutter line.Conduction across the isthmus would activatethe low septal SVA before the high SVA. Thepatient is doing well after 6 months, with no recur-rent arrhythmia.

Fig. 2. (A) Electroanatomic activation map of the systemic venous atrium. The activation pattern appears passive.Entrainment from the area marked with the star is shown in B. (B) Entrainment from the systemic venous atriumsite. S, pacing stimulus.
Mustard Flutter 593

Fig. 3. (A) Electroanatomic activation map of both the systemic venous atrium (SVA) and pulmonary venousatrium (PVA) in a left anterior oblique (LAO) projection. The pink circles denote sites with fractionated signals,the light blue circles are sites with double potentials, the dark blue circles are sites where entrainment of thetachycardia yielded a postpacing interval less than 20 milliseconds longer than the tachycardia cycle length,and the yellow circles represent the His-bundle region. (B) Overdrive pacing from the ablation cathether (arrow)located at the inferior PVA. S, pacing stimulus.
Refaat & Gerstenfeld594

Fig. 4. Termination of the atrial flutter with radiofrequency ablation.
Fig. 5. Pacing the lateral tricuspid annulus (Lat TA) reveals lateral to medial block across the ablation line. Acti-vation proceeds superiorly, activating the high SVA catheter from distal to proximal followed by the low SVAcatheter (blue arrow on electrograms, yellow arrows on fluoroscopy). If there was conduction through the abla-tion line, the low SVA catheter would be activated before the proximal high SVA catheter, however the low SVAis activated last (red star). RFA, radiofrequency ablation.
Mustard Flutter 595

Refaat & Gerstenfeld596
This case illustrates typical mapping and abla-tion of atrial flutter in a patient after Mustard repairof D-TGA.
REFERENCES
1. Dos L, Teruel L, Ferreira IJ, et al. Late outcome of Sen-
ning and Mustard procedures for correction of trans-
position of the great arteries. Heart 2005;91(5):652–6.
2. Zrenner B, Dong J, Schreieck J, et al. Delineation of
intra-atrial reentrant tachycardia circuits after Mustard
operation for transposition of the great arteries using
biatrial electroanatomic mapping and entrainment
mapping. J Cardiovasc Electrophysiol 2003;14(12):
1302–10.
3. Sokoloski MC, Pennington JC 3rd, Winton GJ, et al.
Use of multisite electroanatomic mapping to facilitate
ablation of intra-atrial reentry following the Mustard
procedure. J Cardiovasc Electrophysiol 2000;11(8):
927–30.
4. Li W, Somerville J. Atrial flutter in grown-up congenital
heart (GUCH) patients. Clinical characteristics of
affectedpopulation. Int J Cardiol 2000;75(2–3):129–37.
5. Kanter RJ, Garson A Jr. Atrial arrhythmias during
chronic follow-up of surgery for complex congenital
heart disease. Pacing Clin Electrophysiol 1997;
20(2 Pt 2):502–11.
6. Perry JC, Boramanand NK, Ing FF. “Transseptal”
technique through atrial baffles for 3-dimensional
mapping and ablation of atrial tachycardia in patients
with d-transposition of the great arteries. J Interv Card
Electrophysiol 2003;9(3):365–9.
7. El-Said HG, Ing FF, Grifka RG, et al. 18-year experi-
ence with transseptal procedures through baffles,
conduits, and other intra-atrial patches. Catheter Car-
diovasc Interv 2000;50(4):434–9.
Copyright © 2022 FDOKUMEN