
Palatal Wound Healing: The Effects of Scarring on Growth
13
14.1 Introduction Cleft palate patients often develop growth distur- bances of the midfacial region after primary surgery. Factors such as intrinsic developmental deficiencies and functional distortions are initially involved but palatal repair seems to be a main factor in these growth disturbances [64–70]. A strong indication for the involvement of iatrogenic factors is the largely undisturbed maxillary growth in untreated patients [20, 46, 59]. In treated patients, the healing of surgical wounds originating from palatal repair is probably re- sponsible for the growth disturbances [38]. This chap- ter gives an overview of the wound healing process with emphasis on wound contraction and scar forma- tion since they are considered to be key events. Some specific features of the palatal wound healing process are highlighted. Further, the effects of palatal repair on growth of the maxilla and development of the den- tition are reviewed, as well as possible means to im- prove the clinical outcome. This review is based on clinical evaluations, experimental research in animal models, and on in vitro experiments using cell cultur- ing and tissue engineering techniques. 14.2 Wound Healing 14.2.1 Skin and Oral Mucosa The general function of wound healing is to restore the integrity and function of the tissue. In tissues like skin and oral mucosa, wound healing involves a partly overlapping sequence of inflammation, tissue formation and tissue remodeling (Fig. 14.1). During inflammation, hemostasis is restored and bacteria and debris are removed from the wound. Subsequent- ly, the defect is closed by the formation of new tissues and by wound contraction. Finally, tissue remodeling takes place during maturation of the newly formed tissues, which generally leads to the formation of a scar. Palatal Wound Healing:The Effects of Scarring on Growth Johannes W.Von den Hoff, Jaap C. Maltha,Anne Marie Kuijpers-Jagtman 14 Fig. 14.1. Phases in wound healing. The wound healing process can be divided into three partly overlapping phases. Wound contraction is an early phenomenon while scar formation is a late phenomenon in wound healing (arrows)
-
Upload
khangminh22 -
Category
Documents
-
view
5 -
download
0
Transcript of Palatal Wound Healing: The Effects of Scarring on Growth
14.1 Introduction
Cleft palate patients often develop growth distur-bances of the midfacial region after primary surgery.Factors such as intrinsic developmental deficienciesand functional distortions are initially involved butpalatal repair seems to be a main factor in thesegrowth disturbances [64–70]. A strong indication forthe involvement of iatrogenic factors is the largelyundisturbed maxillary growth in untreated patients[20, 46, 59]. In treated patients, the healing of surgicalwounds originating from palatal repair is probably re-sponsible for the growth disturbances [38]. This chap-ter gives an overview of the wound healing processwith emphasis on wound contraction and scar forma-tion since they are considered to be key events. Somespecific features of the palatal wound healing processare highlighted. Further, the effects of palatal repairon growth of the maxilla and development of the den-tition are reviewed, as well as possible means to im-prove the clinical outcome. This review is based on
clinical evaluations, experimental research in animalmodels, and on in vitro experiments using cell cultur-ing and tissue engineering techniques.
14.2 Wound Healing
14.2.1 Skin and Oral Mucosa
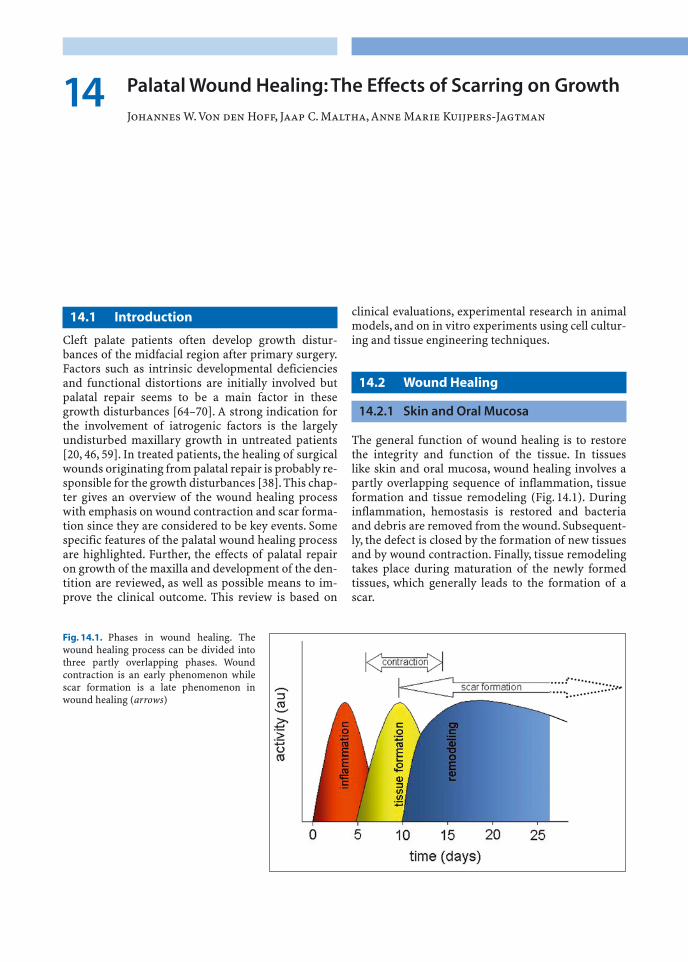
The general function of wound healing is to restorethe integrity and function of the tissue. In tissues like skin and oral mucosa, wound healing involves apartly overlapping sequence of inflammation, tissueformation and tissue remodeling (Fig. 14.1). Duringinflammation, hemostasis is restored and bacteriaand debris are removed from the wound. Subsequent-ly, the defect is closed by the formation of new tissuesand by wound contraction. Finally, tissue remodelingtakes place during maturation of the newly formedtissues, which generally leads to the formation of ascar.
Palatal Wound Healing: The Effects of Scarring on Growth
Johannes W.Von den Hoff, Jaap C. Maltha, Anne Marie Kuijpers-Jagtman14
Fig. 14.1. Phases in wound healing. Thewound healing process can be divided intothree partly overlapping phases. Woundcontraction is an early phenomenon whilescar formation is a late phenomenon inwound healing (arrows)
In intraoral wounds, the wound healing process isgenerally faster than in skin and generates less scartissue. Therefore, intraoral wounds are sometimesconsidered to be more similar to fetal wounds [57].This may be related to the presence of lower levels ofpro-inflammatory and pro-fibrotic cytokines in mu-cosal wounds [84]. The intraoral wound healingprocess is also influenced by the presence of saliva andlarge numbers of bacteria [94]. Saliva contains manygrowth factors such as epidermal growth factor(EGF). In addition, phenotypic differences betweenskin and mucosal fibroblasts may be involved [99].These considerations, however, mainly apply to buccalmucosa, which has a quite different morphology thanthe palatal mucosa (Fig. 14.2).
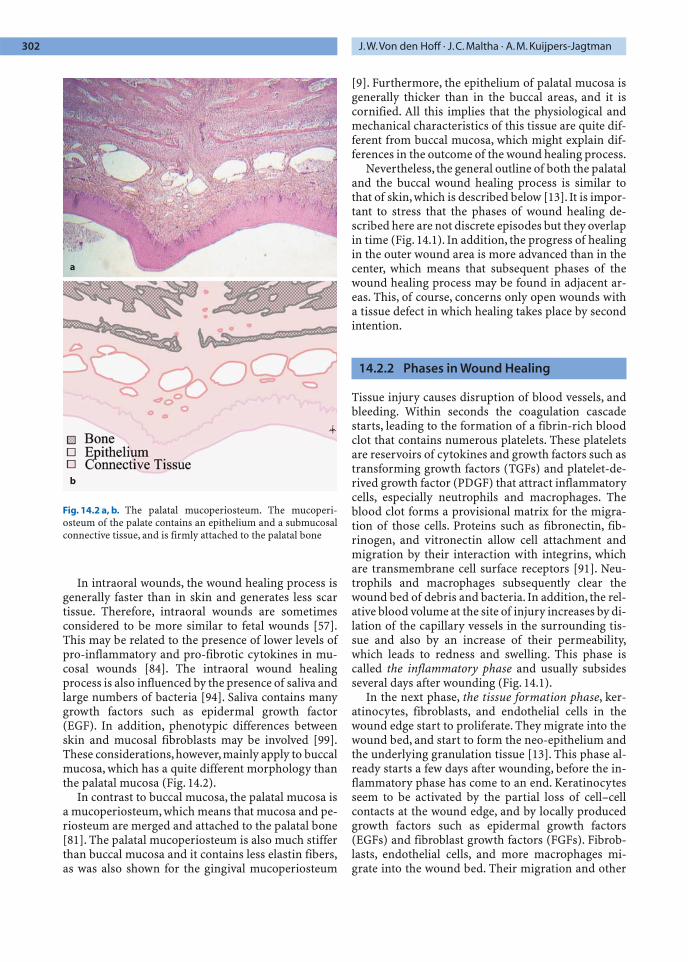
In contrast to buccal mucosa, the palatal mucosa isa mucoperiosteum, which means that mucosa and pe-riosteum are merged and attached to the palatal bone[81]. The palatal mucoperiosteum is also much stifferthan buccal mucosa and it contains less elastin fibers,as was also shown for the gingival mucoperiosteum
[9]. Furthermore, the epithelium of palatal mucosa isgenerally thicker than in the buccal areas, and it iscornified. All this implies that the physiological andmechanical characteristics of this tissue are quite dif-ferent from buccal mucosa, which might explain dif-ferences in the outcome of the wound healing process.
Nevertheless, the general outline of both the palataland the buccal wound healing process is similar tothat of skin, which is described below [13]. It is impor-tant to stress that the phases of wound healing de-scribed here are not discrete episodes but they overlapin time (Fig. 14.1). In addition, the progress of healingin the outer wound area is more advanced than in thecenter, which means that subsequent phases of thewound healing process may be found in adjacent ar-eas. This, of course, concerns only open wounds witha tissue defect in which healing takes place by secondintention.
14.2.2 Phases in Wound Healing
Tissue injury causes disruption of blood vessels, andbleeding. Within seconds the coagulation cascadestarts, leading to the formation of a fibrin-rich bloodclot that contains numerous platelets. These plateletsare reservoirs of cytokines and growth factors such astransforming growth factors (TGFs) and platelet-de-rived growth factor (PDGF) that attract inflammatorycells, especially neutrophils and macrophages. Theblood clot forms a provisional matrix for the migra-tion of those cells. Proteins such as fibronectin, fib-rinogen, and vitronectin allow cell attachment andmigration by their interaction with integrins, whichare transmembrane cell surface receptors [91]. Neu-trophils and macrophages subsequently clear thewound bed of debris and bacteria. In addition, the rel-ative blood volume at the site of injury increases by di-lation of the capillary vessels in the surrounding tis-sue and also by an increase of their permeability,which leads to redness and swelling. This phase iscalled the inflammatory phase and usually subsidesseveral days after wounding (Fig. 14.1).
In the next phase, the tissue formation phase, ker-atinocytes, fibroblasts, and endothelial cells in thewound edge start to proliferate. They migrate into thewound bed, and start to form the neo-epithelium andthe underlying granulation tissue [13]. This phase al-ready starts a few days after wounding, before the in-flammatory phase has come to an end. Keratinocytesseem to be activated by the partial loss of cell–cellcontacts at the wound edge, and by locally producedgrowth factors such as epidermal growth factors(EGFs) and fibroblast growth factors (FGFs). Fibrob-lasts, endothelial cells, and more macrophages mi-grate into the wound bed. Their migration and other
302 J.W.Von den Hoff · J.C. Maltha · A.M. Kuijpers-Jagtman
Fig. 14.2 a, b. The palatal mucoperiosteum. The mucoperi-osteum of the palate contains an epithelium and a submucosalconnective tissue, and is firmly attached to the palatal bone
a
b

activities are regulated by complex interactions withgrowth factors and extracellular matrix componentswithin the provisional matrix [91]. Again, integrinsplay a major role in the interaction between cells andthe extracellular matrix. The binding of matrix pro-teins to integrins is required for attachment and mi-gration, and it also leads to the transmission of addi-tional regulatory signals into the cells [63]. Cellmigration furthermore requires the activity of matrixmetalloproteinases (MMPs), enzymes that pave theway for cells by cleaving extracellular matrix proteins[49].
During migration into the wound, fibroblasts grad-ually switch to a more synthetic phenotype, a switchthat involves the action of TGFb. The fibroblasts startto produce large quantities of collagen, with collagentype III as the main species, but elastin is not synthe-sized in the wound. Within this matrix, endothelialcells form numerous capillaries to nourish the newlyformed tissue. This process is called neo-angiogenesisand FGFs, vascular endothelial growth factor (VEGF),and many other growth factors are implicated in itsregulation as shown by in vitro studies [13]. As soonas the wound is filled with granulation tissue and theneo-epidermis is formed, the collagen production isreduced, which requires interferon-g (IFNg). A nega-tive feedback mechanism based on the accumulatedcollagen may also contribute to the decrease in colla-gen synthesis. This event marks the beginning of thethird and last phase, the remodeling phase.
The remodeling phase starts within 1 week afterwounding and will ultimately lead to the formation ofscar tissue. The remodeling of the extracellular matrixis mainly carried out by fibroblasts. It involves thedegradation of collagen type III by matrix metallo-proteinases [49] and the concurrent deposition oftype I collagen by fibroblasts. In the second week afterinjury, fibroblasts also start to produce proteoglycans.The mechanical properties of the tissue are not onlydetermined by collagens, but to a large extent also by these proteoglycans, since they can bind largeamounts of water. In addition, many proteoglycanshave been shown to regulate cell function, either bydirect modulation of cell adhesion and proliferation,or indirectly through the binding or release of growthfactors [53].
At the start of the remodeling phase, part of the fi-broblasts within the granulation tissue differentiatesinto myofibroblasts that possess contractile proper-ties. These specialized cells are strongly involved inthe process of wound contraction. Their differentia-tion seems to be governed mainly by mechanical ten-sion within the matrix, by TGFb, and by a specificvariant of fibronectin, the ED-A fibronectin [85].Wound contraction causes a rapid reduction of thesurface area of the wound and a concomitant re-
arrangement of the collagen fibers. In the mean timethe neo-epidermis is maturing into a fully differenti-ated stratified epithelium. After 1–2 weeks, no furthercontraction takes place because the myofibroblastshave disappeared, probably by apoptosis [22]. The in-duction of apoptosis is not completely understood,but several genes are known to govern the process.The expression of these genes is regulated by growthfactors as well as by changes in the interaction be-tween the cells and their extracellular matrix. In thenext several months many of the fibroblasts, but alsoendothelial cells, disappear by apoptosis, which grad-ually renders the tissue less vascularized and less cellrich. The slow remodeling of the collagen fibers by re-maining fibroblasts, which is part of the transition toscar tissue, can go on for a long time.
14.2.3 Contraction and Scarring
Wound contraction and scarring seem to be the twomain processes in wound healing responsible for thegrowth disturbances after cleft palate repair, and aretherefore reviewed here in more detail. Wound con-traction is the reduction of the wound surface area byapproximation of the wound edges and it may accountfor up to 80%–90% of wound closure [47]. The evolu-tionary function of this feature obviously is to speedup wound closure and thereby reduce the risk ofinfection and dehydration. Scar formation might be anegative side effect of this primarily beneficialprocess.
The cause of wound contraction is not yet exactlyknown. Two main theories have been described in lit-erature. The first one states that fibroblasts, which mi-grate from the wound margins into the wound bed,cause traction in the extracellular matrix. This ten-sional force would be sufficient to contract the wound[24]. This theory does not require specialized cells toexplain wound contraction. The second theory as-sumes that a specialized subtype of fibroblasts, themyofibroblast, is responsible for wound contraction[21, 27]. During wound contraction, fibroblastscontaining intracellular stress-fibers are found withinthe granulation tissue. These stress-fibers have been shown to contain alpha-smooth muscle actin(ASMA), a cytoskeletal protein also present in smoothmuscle cells. This protein seems to be required for thecontraction of myofibroblasts within the granulationtissue. The coordinated contraction of myofibrob-lasts, attached to the extracellular matrix, causes thereduction of the wound surface.
Nowadays, the two theories have merged into aconsensus theory stating that both fibroblasts andmyofibroblasts are involved in wound contraction[85]. Initially, migrating fibroblasts in the wound area
Chapter 14 Palatal Wound Healing:The Effects of Scarring 303

generate tension within the matrix. The resultingstrain within the matrix triggers the differentiation offibroblasts into myofibroblasts, which also requiresthe presence of TGFb1. The coordinated action of my-ofibroblasts strongly increases tension within thewound tissue, which subsequently contracts. Thus, inthe consensus theory, both fibroblasts and myofibro-blasts contribute to wound contraction.
During contraction of the granulation tissue, ex-tensive collagen remodeling takes place in whichMMPs play a prominent role [49].As a consequence ofthis remodeling, collagen type III is gradually re-placed by collagen type I. The new collagen is deposit-ed in an orientation that is guided by the main lines oftension within the extracellular matrix [71, 31]. Thereorientation of collagen fibers and the substitution of type I collagen for type III collagen mark the startof scar tissue formation. If a uniform direction oftension exists within the contracting granulation tissue, the new collagen fibers will also be deposited in a uniform orientation. Consequently, the resultingtissue will develop the properties of a scar, a processthat may slowly progress for several months to years[71].
During scar tissue formation, the number of en-dothelial cells and fibroblasts within the developingscar tissue slowly decreases, a process in which apop-tosis is involved. The final scar tissue therefore ispoorly vascularized and has a low cell density. In ad-dition, elastin fibers, which provide elasticity to nor-mal mucosa and skin, are not resynthesized duringwound healing and scar tissue formation. Their ab-sence and the presence of highly oriented collagenfibers make the scar a rigid and stiff tissue. A specificfeature of palatal wound healing is the attachment ofthe scar tissue to the palatal bone (see Sect. 4.1). Thismay cause palatal repair to have considerable effectson maxillary growth.
14.3 Effects of Palatal Repair on Growth
Apart from embryonic distortions and intrinsicgrowth deficiencies, facial growth in cleft lip andpalate patients may be affected by surgical repair, or-thodontic treatment, and functional adaptations [38,64–70, 72, 76]. Since the landmark studies of Graber[49] and Dahl [19], numerous descriptive cephalo-metric studies have been published (for an overview,see [76]). It is reasonably well established that cleftsurgery, in particular lip and palate repair, can disturbnormal growth and development of the maxilla incleft patients [7, 38]. However, the possible growth ef-fects of surgery should be evaluated in relation to theintrinsic abnormalities of craniofacial growth in cleftpalate patients. This requires that unoperated cleft lip
and palate patients should be studied as well [11, 20,39, 46].
Of all surgical procedures that are used in cleft lipand palate patients, palatal surgery has attracted thegreatest amount of attention. The reason is that dur-ing this procedure mucoperiosteal flaps are created onthe palate to close the cleft, leaving areas of denudedbone. The scar tissue that is formed during healingmight be a potential inhibitor of subsequent maxillarygrowth and dental arch development. Many studiesover the past 50 years have focused on the effects ofspecific techniques of primary palate repair on midfa-cial growth and development. The effects of palatalclosure seem to be mainly confined to the maxillarybase and arch [77, 38]. The maxilla is shown to be nar-rower, shorter, and displaced posteriorly relative tothe cranial base.The dentoalveolar processes are oftendeflected to the median, resulting in anterior andtransverse cross bites. However, since both lip andpalatal surgery are generally performed, it is difficultto distinguish between the effects of the two types ofsurgery.
A problem with the evaluation of the literature onthis subject is that the majority of the publicationssuffer from major methodological drawbacks, whichminimizes their value [38, 69]. Hardly any studies areavailable that directly compare two types of treatmentin a prospective research design. In contrast, there is avast amount of retrospective studies available that allattempted to relate specific maxillary growth effectsto particular surgical procedures. The most compre-hensive study of this type is the multicenter study byRoss [64–70]. By comparing lateral cephalometric ra-diographs collected from 15 cleft palate centers fromaround the world, they concluded that it was difficultto isolate the effects of individual palate repair tech-niques. However, an inhibition of anterior growth andtranslation of the maxilla was a common finding. An-other problem that is only addressed by few, is that notonly the surgical technique but in particular the skillsof the surgeon are very important for the long-termoutcome in terms of growth and development [38, 78].
In conclusion, strong consensus exists that primarysurgery is a major factor in the impairment of den-tomaxillary growth. The extent of growth impairmentmay be influenced by the specific techniques, the tim-ing and sequence of operations, the use of orthopedicappliances, and possibly the most important of all, theskills of the surgeon. No particular technique hasbeen shown to produce consistently better growth re-sults than any other.Assuming that scar tissue is a pri-mary etiological factor in maxillofacial growth distur-bances, most contemporary repair techniques attemptto minimize scarring. Animal experiments are verywell suited to determine the exact effects of specificsurgical procedures. For a better understanding of the
304 J.W.Von den Hoff · J.C. Maltha · A.M. Kuijpers-Jagtman

biological mechanisms in wound healing, and for thegoal-directed modulation of healing, experimentalstudies are of major importance. Results of such stud-ies are discussed in the next section.
14.4 Experimental Research
Extensive research in animal models has been per-formed to evaluate the effects of cleft surgery ongrowth and development of the maxilla, and to studythe wound healing process. Animal models are alsoused to develop new surgical techniques that may re-duce the unfavorable effects of surgery. Tissue engi-neered constructs are being developed to prevent at-tachment of scar tissue to the bone, or as a substitutefor the lacking mucosal tissue. A lot of in vitro re-search is also aimed at the elucidation of aspects of theoral wound healing process.
14.4.1 Effects of Surgery on Growth
Since suitable animal models for congenital clefts arenot available, the effects of reconstructive surgery areevaluated with surgically created clefts in dogs, rab-bits, and rats. Two different approaches have beenused to evaluate the effects of surgery on midfacialgrowth and development of the dentition. The firstapproach is to create a cleft in the soft tissue and thepalatal bone by surgical means. This cleft is subse-quently closed again as the actual experimental inter-vention. It is obvious, however, that a surgically creat-ed cleft is different from a congenital one. Such a cleftcreates a surgical trauma that might act as a con-founding factor for the interpretation of the results.Only if the bony cleft is considered to be essential forevoking the disturbances in growth and developmentdoes this approach make sense. Bardach and cowork-ers have used this model since 1975. They performedsome of the earliest experiments on the possible neg-ative effect of lip repair [1–6]. Lip repair in rabbits andbeagle dogs with surgically created complete unilater-al clefts, was found to result in a significant increase inlip pressure and a corresponding maxillary growthdeficiency. The authors therefore suggested a causalrelationship between the two.
The second approach is based on the assumptionthat the soft tissue intervention is crucial for thegrowth disturbances after cleft palate surgery.Alreadyin the late 1960s Kremenak and coworkers performedmucoperiosteal excisions without affecting the palatalbone in young beagle dogs as a model for the clinicalsituation after cleft palate repair. This approach led togrowth disturbances that were similar to those aftersurgical cleft closure in children. Kremenak therefore
concluded that “in this model, mucoperiosteal de-nudation of palatal shelf bone adjacent to deciduousmolars is the single surgical variable responsible forthe maxillary growth disturbances seen” [37]. This isin agreement with later dog studies in which a mid-palatal soft tissue cleft was created that was subse-quently closed by von Langenbeck’s technique (e.g.,[88, 89]). Their results not only show the same effectson growth, but also that the extent of this effect is re-lated to the age at which surgery is performed. Growthdisturbances turned out to be most prominent whensurgery is performed before shedding of the decidu-ous dentition. Furthermore, these studies, as well asrecent studies in rats [36], show that the deviations inmaxillary arch dimensions are not only caused by adecreased sutural growth but also by a palatal tippingof the teeth in the lateral areas. In dogs, this tipping isespecially prominent when surgery is performed at ayoung age, and it becomes apparent only after shed-ding of the deciduous dentition.
An explanation for this effect can be found in thehealing of the soft tissue wounds and more specifical-ly in wound contraction and scar tissue formation.Wound contraction in dog mucoperiosteum is mostprominent in the first week after surgery. In palatalwounds in rats it has been shown that the number ofmyofibroblasts increases considerably in that period[17], which also seems to be the case in dogs. There-after, the maturing granulation tissue is characterizedby a gradual decrease in the number of fibroblasts andinflammatory cells, and an increase in number andthickness of collagen type I fibers [74]. Elastic fibersare not present in the granulation tissue, or in the scartissue at later stages.
A specific feature of the healing of open wounds inthe mucoperiosteum is the deposition of callus-likecancellous bone on the palate. The granulation tissueadjacent to the palatal bone acquires an osteogenicpotential, or osteogenic cells migrate into that areafrom adjacent periosteal tissues, and new bone isformed. This phenomenon is also known from othercraniofacial bones and from long bones, where re-moval or mobilization of the periosteum leads to cal-lus formation. Most of the collagen fibers of the scarare oriented in a transverse direction, but many fibersalso show a vertical orientation. These vertical fibersbecome embedded in the cancellous palatal bone asSharpey’s fibers, generating a strong attachment ofthe scar tissue to the underlying palatal bone(Fig. 14.3).
The transverse fibers appear to be continuous withthe cervical periodontal ligament, thus forming a me-chanical connection between the teeth and the mu-coperiosteal scar tissue [89, 36]. At the end of thegrowth period, the teeth alongside the scar tissueshow a palatal tipping which is probably caused by the
Chapter 14 Palatal Wound Healing:The Effects of Scarring 305

traction of the scar tissue on the erupting permanentdentition. These findings have led to the hypothesisthat the iatrogenic effects of palatal surgery are ini-tially caused by wound contraction, but scar tissueformation and the accompanying attachment of thescar tissue to the palatal bone and the teeth are prob-ably the most important features. This leads to a re-striction of maxillary growth and to a palatal tippingof erupting teeth in that region.
14.4.2 Modification of Surgical Techniques
Several researchers have tried to modify cleft palatesurgery in order to avoid the appearance of denudedbone areas and the subsequent growth impairment.Perko [60] was the first to use a mobilized mucosalsplit flap for palatal closure. The disadvantage of histechnique was the high risk of necrosis because theflap was only pedicled at the dorsal side. This tech-nique has been modified by Leenstra et al. to obtain a
flap that is pedicled both at the dorsal and the ventralside [41, 42]. They used a partially split flap, leavingthe lateral bone covered with the osteogenic layer ofthe mucoperiosteum, without impairment of the ma-jor neurovascular bundles [42]. In dogs this techniquewas promising, since it led to less attachment of themucoperiosteum to the underlying bone, and an im-proved transversal growth and development of thedentition [42, 43], and also in a clinical setting the re-sults were promising [41].
The denuded bone can also be covered with a bio-material, which can either be applied as such or sup-plemented with cultured cells. This type of approachbelongs to the field of tissue engineering.
14.4.3 Tissue Engineering
Tissue engineering has been defined in the late 1980sas “the application of principles and methods of engi-neering and life sciences toward fundamental under-
306 J.W.Von den Hoff · J.C. Maltha · A.M. Kuijpers-Jagtman
Fig. 14.3 a–d. Palatal scar tissue. a shows the scar tissue adja-cent to the teeth. The organization of the tissue is shownschematically in b. c and d shows an enlargement of the squared
section. Note the thick perpendicular collagen fibers (Sharpey’sfibers) running in to the bone, which are more clear when seenin polarized light (d)
a b
c d

standing of structure-function relationships in normaland pathological mammalian tissues and the develop-ment of biological substitutes to restore, maintain orimprove tissue functions” [79].
With respect to cleft palate surgery a variety of ap-proaches have been chosen to improve the outcome ofthe wound healing process. Firstly, biocompatiblemembranes have been used to prevent attachment ofthe scar tissue to the palatal bone or to reduce con-traction and scar formation. A second approach is theengineering of mucosal substitutes to replenish thetissue defects. To this end, thin layers of keratinocyteshave been cultured that can be used as epithelialgrafts.Alternatively, keratinocytes have been culturedon top of a dermal substrate to produce a bilayered orcomposite graft, which is a substitute for the entiremucosa. The dermal substrate may consist of a col-lagenous matrix without cells or a matrix with cul-tured fibroblasts.
14.4.3.1 Biocompatible Membranes
Biocompatible synthetic membranes have been usedto inhibit the attachment of scar tissue to the palatalbone by covering the denuded bone areas after sur-gery. Initially, the principles of guided tissue regener-ation were used by inserting membranes in the mu-coperiosteal defects [33]. These membranes weresupposed to cover the palatal bone, inhibit osteogenicprocesses and thereby prevent the formation ofSharpey’s fibers. Bio-resorbable poly-(L-) lactic acidmembranes and nonresorbable polymer membranesyielded unsatisfactory results. This was caused by anuncontrollable degradation of the lactic acid mem-branes, and exfoliation or incomplete coverage of thebone by the nonresorbable membranes [45].
Next to synthetic membranes, collagen-basedmembranes have been used for intraoral surgery. Ate-locollagen membranes have been successfully used toimprove gingival healing in a rat model [50]. Similarmembranes were used later in a model for cleft palaterepair in young rabbits [26]. In a split-mouth design,the membranes were implanted on the denudedpalatal bone at the experimental side, while the con-trol side was left open. The authors report that im-plantation reduced contraction, and allowed more fa-vorable growth of the palatal bone and normaldevelopment of the dentition.
To further improve collagen-based membranes,suitable growth factors might be added to promoteangiogenesis and regeneration of the submucosa andthe overlying epithelium [103].
14.4.3.2 Epithelial Sheets
Oral keratinocytes, obtained from a mucosal biopsy,can be cultured to form an epithelial sheet. The ker-atinocytes are generally expanded using the Rhein-wald and Green method or a modification thereof[62]. Grafts cultured from autologous keratinocytesseem to behave as a permanent epithelial substituteafter transplantation [86, 8]. If allogeneic ker-atinocytes are used, however, the graft behaves as atemporary wound dressing that only accelerates re-epithelialization [83]. Similar results were obtainedafter skin grafting with cultured epidermal ker-atinocytes. Several studies indicate that wound con-traction and scar formation may still occur after theapplication of a cultured epidermal graft [14, 90]. Inaddition, the epithelial sheets are very fragile anddifficult to handle.
14.4.3.3 Composite Substitutes
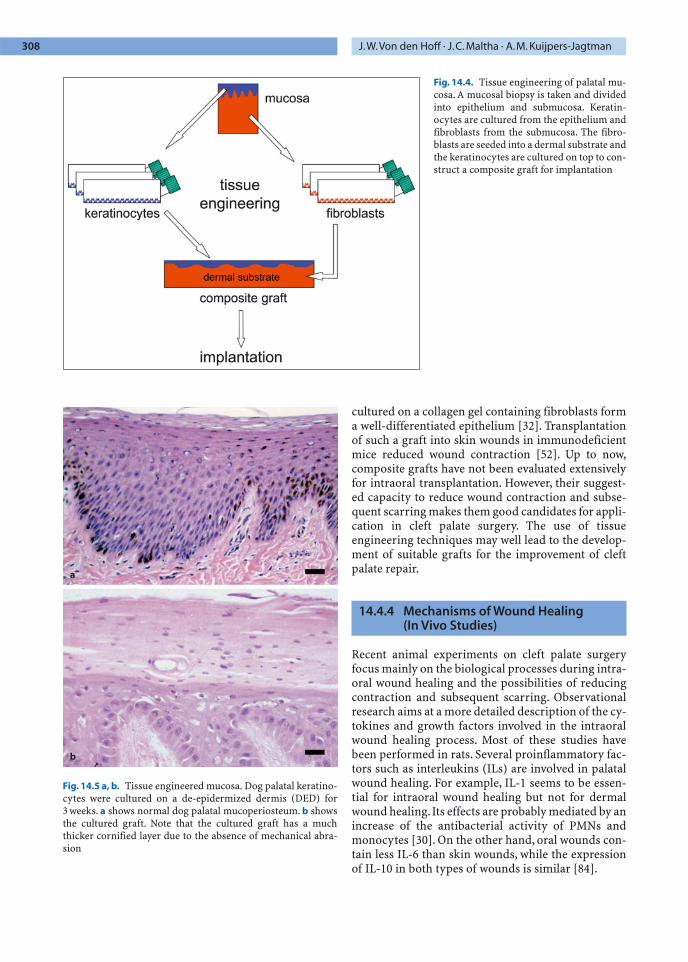
An approach that is more widely used nowadays wasdeveloped for the grafting of full-thickness burnwounds on the skin. In this approach, the epitheliumis cultured on a dermal substrate to produce a com-posite graft [61]. The presence of a dermal substrate issupposed to diminish contraction and subsequentscar formation. It can be derived from human dermisor prepared from purified collagen and additional ex-tracellular matrix components. Also, fibroblasts andgrowth factors may be included within the dermalsubstrate to improve vascularization and epithelialdifferentiation. An overview of the production of acomposite cultured graft is given in Fig. 14.4.
If dog palatal keratinocytes are cultured on skin-derived substrates they form an epithelium similar tothat in vivo [58] (Fig. 14.5). Such a composite graftcontaining human keratinocytes showed a good clin-ical take rate after intraoral grafting. Compared to asubstrate without cells, the composite graft showedenhanced epithelialization, and maturation of thesubmucosa [34]. Grafts composed of a collagen sub-strate and human keratinocytes inside the matrixhave been implanted in full-thickness skin wounds inimmunodeficient mice [10]. They showed a reducedwound contraction and a stimulation of epithelialmaturation.
Composite grafts containing both keratinocytesand fibroblasts have also been constructed. Thefibroblasts within the dermal substrate seem to en-hance the differentiation of the overlying epithelium.Preliminary studies have shown that keratinocytes
Chapter 14 Palatal Wound Healing:The Effects of Scarring 307
cultured on a collagen gel containing fibroblasts forma well-differentiated epithelium [32]. Transplantationof such a graft into skin wounds in immunodeficientmice reduced wound contraction [52]. Up to now,composite grafts have not been evaluated extensivelyfor intraoral transplantation. However, their suggest-ed capacity to reduce wound contraction and subse-quent scarring makes them good candidates for appli-cation in cleft palate surgery. The use of tissueengineering techniques may well lead to the develop-ment of suitable grafts for the improvement of cleftpalate repair.
14.4.4 Mechanisms of Wound Healing (In Vivo Studies)
Recent animal experiments on cleft palate surgeryfocus mainly on the biological processes during intra-oral wound healing and the possibilities of reducingcontraction and subsequent scarring. Observationalresearch aims at a more detailed description of the cy-tokines and growth factors involved in the intraoralwound healing process. Most of these studies havebeen performed in rats. Several proinflammatory fac-tors such as interleukins (ILs) are involved in palatalwound healing. For example, IL-1 seems to be essen-tial for intraoral wound healing but not for dermalwound healing. Its effects are probably mediated by anincrease of the antibacterial activity of PMNs andmonocytes [30]. On the other hand, oral wounds con-tain less IL-6 than skin wounds, while the expressionof IL-10 in both types of wounds is similar [84].
308 J.W.Von den Hoff · J.C. Maltha · A.M. Kuijpers-Jagtman
Fig. 14.4. Tissue engineering of palatal mu-cosa. A mucosal biopsy is taken and dividedinto epithelium and submucosa. Keratin-ocytes are cultured from the epithelium andfibroblasts from the submucosa. The fibro-blasts are seeded into a dermal substrate andthe keratinocytes are cultured on top to con-struct a composite graft for implantation
Fig. 14.5 a, b. Tissue engineered mucosa. Dog palatal keratino-cytes were cultured on a de-epidermized dermis (DED) for3 weeks. a shows normal dog palatal mucoperiosteum. b showsthe cultured graft. Note that the cultured graft has a muchthicker cornified layer due to the absence of mechanical abra-sion
b
a

TGFbs and FGFs are also very important in the ear-ly phases of wound healing, as they are involved in thedifferentiation of myofibroblasts. TGFb1 is supposedto upregulate FGF receptor-1 and FGF receptor-2 onpalatal fibroblasts and thus increasing the susceptibil-ity of these cells to FGFs. The latter factors are mainlyproduced by macrophage-like cells and cause an in-crease in the number of myofibroblasts [25, 35, 93]. Onthe other hand, IFNg inhibits the differentiation ofmyofibroblasts from rat palatal fibroblasts in vitro[93] and in vivo [16]. FGF2 is also involved in the re-epithelialization of palatal mucosa since a singletopical application already speeds up this process[56]. After the completion of wound contraction andre-epithelialization, myofibroblasts disappear, proba-bly through apoptosis that again is influenced byTGFb1 and FGF2 [25]. The same processes have beendescribed for skin wounds, but they seem to proceedat a slower pace [55].
In the later phases of palatal wound healing thenumber of cells and the amount of collagen is higherthan in the normal mucoperiosteum. The collagentype I fibers are densely packed and transverselyaligned, indicating a distinct scar tissue [15] with adecreased vascular density [12]. Since IFNs possessantifibrotic and anticontractive properties, they havebeen used for experimental research on skin woundcontraction and the reduction of keloids. IFNa in-hibits wound contraction [54], IFNb downregulatescollagen synthesis of dermal fibroblasts in vitro [23],and IFNg downregulates collagen synthesis in skinwounds [29].
Strong evidence for the involvement of growth fac-tors in the regulation of wound contraction and scarformation has been obtained from studies on fetalwound healing. Intrauterine wound healing in mam-malian fetuses occurs without contraction and scarformation up to a certain gestational age [101]. In thisearly phase of gestation, myofibroblasts do not occurduring wound healing and the regenerated tissue isindistinguishable from normal tissue. This scarlesshealing seems to depend on a specific growth factorprofile within the wound and on the typical intrauter-ine environment. Several researchers have utilizedthese characteristics of fetal wound healing to per-form prenatal cleft palate surgery in animals [94, 98,105]. These studies are debatable since they involveonly surgically created clefts.
Recently, a model for congenital cleft palate ingoats was described in which clefting was induced bythe teratogen anabasine [106]. In affected fetuses,palatoplasty was performed in utero using a modifiedvon Langenbeck technique at 85 days’ gestation. At6 months of age, the mucoperiosteum of the palatehad healed without scarring, and the function of thesoft palate and the architecture of the velum were sim-
ilar to that of unclefted controls. However, it is highlyunlikely that prenatal surgery for cleft palate repairwill soon be common practice because of diagnosticand ethical problems [102]. The effects of specificgrowth factors that are possibly involved in scarlessfetal healing can be further investigated by in vitrostudies.
14.4.5 Mechanisms of Wound Healing (In Vitro Studies)
Several cell culture models are exploited to investigateaspects of fibroblast and keratinocyte biology that arerelevant to the oral wound healing process. Thesestudies often aim to elucidate the differences betweenoral and dermal wound healing or to find pharmaco-logical means to modify the oral wound healingprocess. Two-dimensional monolayer cultures aresuitable to study the expression of certain proteins orthe proliferation and migration of cells. However, tostudy the interactions of cells with their extracellularmatrix, a three-dimensional culture model is re-quired.An additional advantage of three-dimensionalculture models is that the physiology of the cells ismore similar to that in vivo [51].
In two-dimensional monolayer cultures, humanoral keratinocytes constitutively express higher levelsof hepatocyte growth factor and keratinocyte growthfactor than skin keratinocytes [57]. In addition theyexpress higher levels of IL-6 after stimulation withother cytokines [100]. These differences may con-tribute to the preferential healing of mucosal woundsin comparison with skin wounds. For rat palatalwound fibroblasts, it was shown that interferons canreduce their collagen synthesis, which seems to be fa-vorable in the light of scar reduction [15]. Oral fibro-blasts have also been shown to possess a lower migra-tion capacity in vitro compared with skin fibroblasts[99]. Fibroblasts, taken from subsequent phases in ratpalatal wound healing, show distinct expression pat-terns of integrins and cytoskeletal proteins [87]. Thisindicates that specific subpopulations of fibroblastsmay be responsible for wound contraction and scar-ring.
Fibroblasts cultured in three-dimensional collagenlattices contract this lattice in a time-dependent way[96]. The contraction is caused by attachment of thecells to the collagen and their migration through thelattice. This model therefore represents some aspectsof the wound contraction process in vivo. Several in-vestigators have used this model to compare thecontraction capacity of oral and dermal fibroblasts[40, 97, 104]. In general, these studies show that oralfibroblast have a higher contraction capacity thandermal fibroblasts, similar to that of fetal fibroblasts
Chapter 14 Palatal Wound Healing:The Effects of Scarring 309

[97]. The contraction of all three types of fibroblasts isinhibited by IL-1b. Fibroblast-populated collagen lat-tices were also used to investigate the migration of fi-broblasts into a wound [95]. To this end an experi-mental wound was made in the lattice, and themigration of fibroblasts into the wound was meas-ured. Wound repopulation by mucosal fibroblasts wasgreater than that by age-matched dermal fibroblasts.These in vitro models contribute to the understand-ing of cellular processes during oral wound healingand the identification of factors with potential thera-peutic value. Eventually, this may lead to new strate-gies to reduce intraoral wound contraction and scar-ring, and subsequent growth disturbances.
14.5 Application of Experimental Results
The available data from clinical as well as experimen-tal research clearly indicate that primary palatal sur-gery is an important factor in the maxillary growthdisturbances in cleft palate patients. Experimental re-search in animal models shows that wound contrac-tion and subsequent scarring in the surgical woundsare key events. More specifically, the attachment of thescar tissue to the palatal bone and the periodontalfiber system inhibits sutural growth and normal de-velopment of the dentition. This can only be partiallyprevented by modifications of the surgical techniquesuch as the split flap technique, which avoids the de-nudation of palatal bone. Another development is theuse of tissue engineering techniques to construct asubstitute for oral mucosa, which can be used to cov-er the denuded bone areas. There are some indica-tions that this may reduce contraction and subsequentscarring on the palate. Whether this approach willyield better growth parameters after palatal surgeryremains to be established. A third approach might bethe pharmacological reduction of contraction andscarring after palatal surgery. In vitro studies haveshown that some cytokines have the capacity to inhib-it specific aspects of scar formation such as the differ-entiation of myofibroblasts and excessive collagendeposition. Only few of these factors have also shownfavorable effects in vivo. However, the efficient deliv-ery of the factor into the wound and the targeting tospecific cells are practical problems that have to besolved.
References
1. Bardach J. Lip repair and facial growth in beagles. Plast Re-constr Surg 1989; 83:1079–1080.
2. Bardach J, Eisbach KJ. The influence of primary unilateralcleft lip repair on facial growth. Cleft Palate J 1977; 14:88–97.
3. Bardach J, Kelly KM, Salyer KE. A comparative study offacial growth following lip and palate repair performed insequence and simultaneously: An experimental study inbeagles. Plast Reconstr Surg 1993; 91:1008–1016.
4. Bardach J, Klalusner EC, Eisbach KJ. The relationship be-tween lip pressure and facial growth after cleft lip repair.Cleft Palate J 1979; 16:137–146.
5. Bardach J, Roberts DM, Yale R, Rosewall D, Mooney M. Theinfluence of simultaneous cleft lip and palate repair onfacial growth in rabbits. Cleft Palate J 1980; 17:309–318.
6. Bardach, J. The influence of cleft lip repair on facial growth.Cleft Palate J 1990; 27:76–78.
7. Berkowitz S. Cleft lip and palate research: an updated stateof the art. Section III. Orofacial growth and dentistry. CleftPalate J 1977; 14:288-301.
8. Bodner L, Grossman N. Autologous cultured mucosal graftto cover large intraoral mucosal defects: a clinical study.J Oral Maxillofac Surg 2003; 61:169–173.
9. Bourke KA, Haase H, Li H, Daley T, Bartold PM. Distribu-tion and synthesis of elastin in porcine gingival and alveo-lar mucosa. J Periodont Res 2000; 35:361–368.
10. Butler CE, Navarro FA, Park CS, Orgill DP. Regeneration ofneomucosa using cell-seeded collagen-GAG matrices inathymic mice. Ann Plast Surg 2002; 48:298–304.
11. Capelozza Filho FL, Normando AD, da Silva Filho OG. Iso-lated influences of lip and palate surgery on facial growth:comparison of operated and unoperated males adults withUCLP. Cleft Palate Craniofac J 1996; 33:51–56.
12. Chu S, Ishikawa H, Kim T, Yoshida S. Analysis of scar tissuedistribution on rat palates: a laser Doppler flowmetricstudy. Cleft Palate Craniofac J 2000; 37:488–496.
13. Clark RAF. Wound repair: Overview and general consider-ations. In: Clark RAF (ed.) The molecular and cellular biol-ogy of wound repair. New York: Plenum Press; 1996. p. 3–35.
14. Cooper ML, Andree C, Hansborough JF, Zapata-Sirvent RL,Spielvogel RL. Direct comparison of a cultured compositeskin substitute containing human keratinocytes and fibro-blasts to an epidermal sheet graft containing human kera-tinocytes on athymic mice. J Invest Dermatol 1993; 101:811–819.
15. Cornelissen AMH, Maltha JC, Von den Hoff HW, Kuijpers-Jagtman AM. Palatal mucosal wound healing in the rat. EurJ Oral Sci 1999; 107:344–351
16. Cornelissen AMH, Maltha JC, Von den Hoff JW, Kuijpers-Jagtman AM. Local injection of IFN-gamma reduces thenumber of myofibroblasts and the collagen content inpalatal wounds. J Dent Res 2000b; 79:1782–1788.
17. Cornelissen AMH, Stoop R, Von den Hoff HW, Maltha JC,Kuijpers-Jagtman AM. Myofibroblasts and matrix compo-nents in healing palatal wounds in the rat. J Oral Pathol Med2000a; 29:1–7.
18. Cornelissen AMH, Von den Hoff JW, Maltha JC, Kuijpers-Jagtman AM. Effects of locally injected interferon-beta onpalatal mucoperiosteal wound healing. J Oral Pathol Med2002; 31:518–525.
310 J.W.Von den Hoff · J.C. Maltha · A.M. Kuijpers-Jagtman
19. Dahl E. Craniofacial morphology in congenital clefts of thelip and palate.An X-ray cephalometric study of young adultmales. Acta Odont Scand 1970; 28(Suppl. 57):1–167.
20. Derijcke A, Kuijpers-Jagtman AM, Lekkas C, HardjowasitoW, Latief B. Dental arch dimensions in unoperated adultcleft-palate patients: an analysis of 37 cases. J CraniofacGenet Dev Biol 1994; 14:69–74.
21. Desmouliere A,Gabbiani G.The role of the myofibroblast inwound healing and fibrocontractive diseases. In: Clark RAF(ed) The molecular and cellular biology of wound repair.New York: Plenum Press; 1996. p. 391–414.
22. Desmouliere A, Redard M, Darby I, Gabbiani G. Apoptosismediates the decrease in cellularity during the transitionbetween granulation tissue and scar. Am J Pathol 1995;146:56–66.
23. Duncan MR, Hasan A, Berman B. Pentoxifylline, penti-fylline, and interferons decrease type I and III procollagenmRNA levels in dermal fibroblasts: evidence for mediationby nuclear factor 1 down regulation. J Invest Dermatol1995; 104:282–286.
24. Ehrlich HP, Rajaratnam JB. Cell locomotion forces versuscell contraction forces for collagen lattice contraction: an in vitro model of wound contraction. Tissue Cell 1990; 22:407–417.
25. Funato N, Moriyama K, Baba Y, Kuroda T. Evidence of apop-tosis induction in myofibroblasts during palatal mucope-riosteal repair. J Dent Res 1999; 78:1511–1517.
26. Fujioka M, Fujii T. Maxillary growth following atelocolla-gen implantation on mucoperiosteal denudation of thepalatal process in young rabbits: implications for clinicalcleft palate repair. Cleft Palate Craniofac J 1997; 34:297–308.
27. Gabbiani G. The myofibroblast in wound healing and fibro-contractive diseases. J Pathol 2003; 200:500–503.
28. Graber TM. Craniofacial morphology in cleft palate andcleft lip deformities. Surg Gynec Obs 1949; 88:359–368.
29. Granstein RD, Deak MR, Jacques SL, Margolis RJ, Flotte TJ,Whitaker D, Long FH,Amento EP. The systemic administra-tion of gamma interferon inhibits collagen synthesis andacute inflammation in a murine skin wounding model.J Invest Dermatol 1989; 93:18–27.
30. Graves DT, Nooh N, Gillen T, Davey M, Patel S, Cottrell D,Amar S. IL-1 plays a critical role in oral, but not dermal,wound healing. J Immunol 2001; 167:5316–5320.
31. Huang D, Chang TR,Aggarwal A, Lee RC, Ehrlich HP. Mech-anisms and dynamics of mechanical strengthening in liga-ment-equivalent fibroblast-populated collagen matrices.Ann Biomed Eng 1993; 21:289–305.
32. Igarashi M, Irwin CR, Locke M, Mackenzie IC. Constructionof large area organotypical cultures of oral mucosa andskin. J Oral Pathol Med 2003; 32:422–430.
33. In de Braekt MM, van Alphen FA, Kuijpers-Jagtman AM,Maltha JC. Wound healing and wound contraction afterpalatal surgery and implantation of poly-(L-lactic) acidmembranes in beagle dogs. J Oral Maxillofac Surg 1992;50:359–364.
34. Izumi K, Feinberg SE, Lida A, Yoshizawa M. Intraoral graft-ing of an ex vivo produced oral mucosa equivalent: a pre-liminary report. Int J Oral Maxillofac Surg 2003; 32:188–197.
35. Kanda T, Funato N, Baba Y, Kuroda T. Evidence for fibro-blast growth factor receptors in myofibroblasts duringpalatal mucoperiosteal repair. Arch Oral Biol 2003; 48:213–221.
36. Kim T, Ishikawa H, Chu S, Handa A, Iida J, Yoshida S. Con-striction of the maxillary dental arch by mucoperiostealdenudation of the palate. Cleft Palate Craniofac J 2002; 39:425–431.
37. Kremenak CR Jr, Huffman WC, Olin WH. Maxillary growthinhibition by mucoperiosteal denudation of palatal shelfbone in non-cleft beagles. Cleft Palate J 1970; 7:817–825.
38. Kuijpers-Jagtman AM, Long Jr RE. State of the art: The in-fluence of surgery and orthopedic treatment on maxillofa-cial growth and maxillary arch dimensions in patientstreated for orofacial clefts. Cleft Palate-Craniofac J 2000;37:527/1–527/12.
39. Lambrecht JT, Kreusch T, Schulz L. Position, shape, anddimension of the maxilla in unoperated cleft lip and palatepatients: review of the literature. Clin Anat 2000; 13:121–133.
40. Lee HG, Eun HC. Differences between fibroblasts culturedfrom oral mucosa and skin: implications to wound healing.J Dermatol Sci 1999; 21:176–182.
41. Leenstra TS, Kohama GI, Kuijpers-Jagtman AM, FreihoferHPM. Supraperiosteal flap technique versus mucope-riosteal flap technique in cleft palate surgery. Cleft PalateCraniofac J 1996; 33:501–506.
42. Leenstra TS, Kuijpers-Jagtman AM, Maltha JC, FreihoferHPM. Palatal surgery without denudation of bone favoursdentoalveolar development in dogs. Int J Oral MaxillofacSurg 1995b; 24:440–444.
43. Leenstra TS, Maltha JC, Kuijpers-Jagtman AM, SpauwenPH.Wound healing in beagle dogs after palatal repair with-out denudation of bone. Cleft Palate Craniofac J 1995a;32:363–369.
44. Leenstra TS, Maltha JC, Kuijpers-Jagtman AM. Biodegrada-tion of non-porous films after submucoperiosteal implan-tation on the palate of beagle dogs. J Mater Sci Mater Med1995c; 6:445–450.
45. Leenstra TS, Kuijpers-Jagtman AM, Maltha JC. The healingprocess of palatal tissues after palatal surgery with andwithout implantation of membranes: An experimentalstudy in dogs. J Mater Sci Mater Med 1998; 9:249–255.
46. Mars M, Houston WJ. A preliminary study of facial growthand morphology in unoperated male unilateral cleft lip andpalate subjects. Cleft Palate J 1990; 27:7–10.
47. McGrath MH, Simon RH.Wound geometry and the kineticsof wound contraction. Plast Reconstr Surg 1983; 72:66–73.
48. McPherson JM. Polypeptide growth factors: targeted deliv-ery systems. Biomaterials 1997; 18:1201–1225.
49. Mignatti P, Rifkin DB, Welgus HG, Parks WC. Proteinasesand tissue remodeling. In: Clark RAF (ed) The molecularand cellular biology of wound repair. New York: PlenumPress; 1996. p. 427–461.
50. Minabe M, Kodama T, Hori T, Watanabe Y. Effects of atelo-collagen on the wound healing reaction following palatalgingivectomy in rats. J Periodont Res 1989; 24:178–185.
51. Mio T,Adachi Y, Romberger DJ, Ertl TF, Rennard SI. Regula-tion of fibroblast proliferation in three-dimensional colla-gen gel matrix. In Vitro Cell Dev Biol Anim 1996; 32:427–433.
52. Moriyama T, Asahina I, Ishii M, Oda M, Ishii Y, Enomoto S.Development of composite cultured oral mucosa utilizingcollagen sponge matrix and contracted collagen gel: a pre-liminary study for clinical applications. Tissue Eng 2001;7:415–427.
Chapter 14 Palatal Wound Healing:The Effects of Scarring 311
53. Nakato H, Kimata K. Heparan sulphate fine structure andspecificity of proteoglycan functions. Biochim BiophysActa 2002; 1573:312–318.
54. Nedelec B, Dodd CM, Scott PG, Ghahary A, Tredget EE.Effect of interferon-alpha2b on guinea pig wound closureand the expression of cytoskeletal proteins in vivo. WoundRepair Regen 1998; 6:202–212.
55. Nukumi K, Masuda M, Obata A, Yumoto E. Differences inexpression of basic fibroblast growth factor during woundhealing between oral mucosa and skin. Wound Repair Re-gen 2004; 12:A7.
56. Oda Y, Kagami H, Ueda M. Accelerating effects of basicfibroblast growth factor on wound healing of rat palatalmucosa. J Oral Maxillofac Surg 2004; 62:73–80.
57. Okazaki M, Yoshimura K, Uchida G, Harii K. Elevated ex-pression of hepatocyte and keratinocyte growth factor incultured buccal-mucosa-derived fibroblasts compared withnormal-skin-derived fibroblasts. J Dermatol Sci 2002;30:108–115.
58. Ophof R, van Rheden RE, Von den Hoff JW, Schalkwijk J,Kuijpers-Jagtman AM. Oral keratinocytes cultured on der-mal matrices form a mucosa-like tissue. Biomaterials 2002;23:3741–3748.
59. Ortiz-Monasterio F, Serrano A, Barrera G, Rodriguez-Hoff-man H, Vinageras E. A study of untreated adult cleft palatepatients. Plast Reconstr Surg 1966; 38:36–41.
60. Perko MA.Primary closure of the cleft palate using a palatalmucosal flap: an attempt to prevent growth impairment.J Maxillofac Surg 1974; 2:40–43.
61. Pomahac B, Svensjo T, Yao F, Brown H, Eriksson E. Tissueengineering of skin. Crit Rev Oral Biol Med 1998; 9:333–344.
62. Rheinwald JG, Green H. Serial cultivation of strains of hu-man epidermal keratinocytes: the formation of keratiniz-ing colonies from single cells. 1975; Cell 6:331–344.
63. Rojas AI, Ahmed AR. Adhesion receptors in health and dis-ease. Crit Rev Oral Biol Med 1999; 10:337–358.
64. Ross RB. Treatment variables affecting facial growth incomplete unilateral cleft lip and palate. Part 1: treatmentaffecting growth. Cleft Palate J 1987a; 24:5–23.
65. Ross RB. Treatment variables affecting facial growth incomplete unilateral cleft lip and palate. Part 2: presurgicalorthopedics. Cleft Palate J 1987b; 24:24–30.
66. Ross RB. Treatment variables affecting facial growth incomplete unilateral cleft lip and palate. Part 3: alveolus re-pair and bone grafting. Cleft Palate J 1987c; 24:33–44.
67. Ross RB. Treatment variables affecting facial growth in uni-lateral cleft lip and palate. Part 4: repair of the cleft lip. CleftPalate J 1987d; 24:45–53.
68. Ross RB. Treatment variables affecting facial growth in uni-lateral cleft lip and palate. Part 5: Timing of palate repair.Cleft Palate J 1987e; 24:54–63.
69. Ross RB. Treatment variables affecting facial growth in cleftlip and palate. Part 6: Techniques of palate repair. CleftPalate J 1987f; 24:64–70.
70. Ross RB. Treatment variables affecting facial growth in cleftlip and palate. Part 7: an overview of treatment and facialgrowth. Cleft Palate J 1987g; 24:71–77.
71. Rudolph R, Vande Berg J, Ehrlich HP. Wound contractionand scar contracture. In: Cohen IK, Diegelman RT, LindbladWJ (eds.) Wound healing: biochemical and physical as-pects. Philadelphia: WB Saunders; 1992. p. 96–114.
72. Rygh P, Tindlund RS. Orthopedic expansion and protrac-tion of the maxilla in cleft palate patients – a new treatmentrationale. Cleft Palate J 1982; 19:104–112.
73. Schendel SA, Pearl RM, De Armond SJ. Pathophysiology ofcleft lip muscles following the initial repair. Plast ReconstrSurg 1991; 88:19–200.
74. Searls JC, Kremenak CR, Rittman BR. Quantitative charac-terization of changes in cellularity and collagen fiber size incontracting palatal wounds. Cleft Palate J 1979; 16:373–380.
75. Selliseth NJ, Selvig KA (1995). Revascularization of an exci-sional wound in gingiva and oral mucosa. A scanning elec-tron microscopic study using corrosion casts in rats. Scan-ning Microscop 9:455–467.
76. Semb G, Shaw WC. Facial growth in orofacial clefting disor-ders. In: Turvey TA,Vig KWL, Fonseca RJ (eds.) Facial cleftsand craniosynostosis. Principles and management. Phila-delphia: WB Saunders; 1996. p. 28–56.
77. Semb G, Shaw WC. Facial growth after different methods ofsurgical intervention in patients with cleft lip and palate.Acta Odontol Scand 1998; 56:352–355.
78. Shaw WC, Semb G, Nelson P, Brattström V, Møsted K, Prahl-Andersen B. The Eurocleft Project 1996–2000. Amsterdam:IOS Press; 2000.
79. Skalak R, Fox CF. Preface. In: Skalak R, Fox CF (eds.) Tissueengineering. New York: Alan R Liss; 1988
80. Sloan P. Current concepts of the role of fibroblasts and ex-tracellular matrix in wound healing and their relevance tooral implantology. J Dent 1991; 19:107–109.
81. Squier CA,Hill MW.Oral mucosa. In: Ten Cate AR (ed.) Oralhistology: development, structure and function. 5th ed. St.Louis: Mosby Year Book; 1998. p. 345–385.
82. Stephens P, Davies KJ, Occleston N, Pleass RD, Kon C,Daniels J, Khaw PT, Thomas DW. Skin and oral fibroblastsexhibit phenotypic differences in extracellular matrix reor-ganization and matrix metalloproteinase activity. Br J Der-matol 2001; 144:229–237.
83. Sumi Y, Hata KI, Sawaki Y, Mizuno H, Ueda M. Clinical ap-plication of cultured oral epithelium for palatal wounds af-ter palatoplasty: a preliminary report. Oral Dis 1999;5:307–312.
84. Szpaderska AM, Zuckerman JD, DiPietro LA. Differentialinjury responses in oral and cutaneous wounds. J Dent Res2003; 82:621–626.
85. Tomasek JJ, Gabbiani G, Hinz B, Chaponnier C, Brown RA.Myofibroblasts and mechano-regulation of connective tis-sue remodeling. Nat Rev Mol Cell Biol 2002; 3:349–363.
86. Tsai CY, Ueda M, Hata K, Horie K, Hibino Y, Sugimura Y,Toriyama K, Torii S. Clinical results of cultured epithelialcell grafting in the oral and maxillofacial region. J Cran-iomaxillofac Surg 1997; 25:4–8.
87. Van Beurden HE, Snoek PAM, Von den Hoff JW, TorensmaR, Kuijpers-Jagtman AM. Fibroblast subpopulations in in-traoral wound healing. Wound Rep Regen 2003; 11:55–63.
88. Wijdeveld MGMM, Grupping EM, Kuijpers-Jagtman AM,Maltha JC. Maxillary arch dimensions after palatal surgeryat different ages on beagle dogs. J Dent Res 1989; 68:1105–1109.
89. Wijdeveld MGMM, Maltha JC, Grupping EM, De Jonge J,Kuijpers-Jagtman AM. A histological study of tissue re-sponse to simulated cleft palate surgery at different ages inbeagle dogs. Arch Oral Biol 1991; 36:837–843.
312 J.W.Von den Hoff · J.C. Maltha · A.M. Kuijpers-Jagtman

90. Willimson JS, Snelling CF, Clugston P, Macdonald IB, Ger-mann E. Cultured epithelial autograft: five years of clinicalexperience with twenty-eight patients. J Trauma 1995; 39:309–319.
91. Yamada KM, Clark RAF. Provisional matrix. In: Clark RAF(ed.) The molecular and cellular biology of wound repair.New York: Plenum Press; 1996. p. 51–82.
92. Yokozeki M, Baba Y, Shimokawa H, Moriyama K, Kuroda T.Interferon-g inhibits the myofibroblastic phenotype of ratpalatal fibroblasts induced by transforming growth factorb1 in vitro. FEBS Lett 1999; 442:61–64.
93. Yokozeki M, Moriyama K, Shimokawa H, Kuroda T. Trans-forming growth factor-beta 1 modulates myofibroblasticphenotype of rat palatal fibroblasts in vitro. Exp Cell Res1997; 231:328–336.
94. Zelles T, Purushotham KR, Macaulay SP, Oxford GE,Humphreys-Beher MG. Saliva and growth factors: thefountain of youth resides in us all. J Dent Res 1995; 74:1826–1832.
94. Adzick NS, Longaker MT. Animal models for the study offetal tissue repair. J Surg Res 1991; 51:216–222.
95. al-Khateeb T, Stephens P, Shepherd JP, Thomas DW. An in-vestigation of preferential fibroblast wound repopulationusing a novel in vitro wound model. J Periodontol 1997;68:1063–1069.
96. Grinnell F. Fibroblasts, myofibroblasts and wound contrac-tion. J Cell Biol 1994; 124:401–404.
97. Irwin CR, Myrillas T, Smyth M, Doogan J, Rice C, Schor SL.Regulation of fibroblast-induced collagen gel contractionby interleukin-1 beta. J Oral Pathol Med 1998; 27:255–259.
98. Kaban LB, Dodson TB, Longaker MT, Stern M, Umeda H,Adzick S. Fetal cleft lip repair in rabbits: long-term clinicaland cephalometric results. Cleft Palate Craniofac J 1993;30:13–21.
99. Lepekhin E, Gron B, Berezin V, Bock E, Dabelsteen E. Dif-ferences in motility pattern between human buccal fibro-blasts and periodontal and skin fibroblasts. Eur J Oral Sci2002; 110:13–20.
100. Li J, Farthing PM, Ireland GW, Thornhill MH. IL-1 alphaand IL-6 production by oral and skin keratinocytes: simi-larities and differences in response to cytokine treatmentin vitro. J Oral Pathol Med 1996; 25:157–162.
101. Longaker MT, Adzick NS. The biology of fetal wound heal-ing: a review. Plast Reconstr Surg 1991; 87:788–798.
102. Molsted K. Treatment outcome in cleft lip and palate: issuesand perspectives. Crit Rev Oral Biol Med 1999; 10:225–239.
103. Nimni ME. Polypeptide growth factors: targeted deliverysystems. Biomaterials 1997; 18:1201–1225.
104. Stephens P, Davies KJ, al-Khateeb T, Shepherd JP, ThomasDW. A comparison of the ability of intra-oral and extra-oral fibroblasts to stimulate extracellular matrix reorgani-zation in a model of wound contraction. J Dent Res 1996;75:1358–1364.
105. Sullivan WG. In utero cleft lip repair in the mouse withoutan incision. Plast Reconstr Surg 1989; 84:723–730.
106. Weinzweig J, Panter KE, Spangenberger A, Harper JS,McRae R, Edstrom LE. The fetal cleft palate: III. Ultrastruc-tural and functional analysis of palatal development fol-lowing in utero repair of the congenital model. Plast Re-constr Surg 2002; 109:2355–2362.
Chapter 14 Palatal Wound Healing:The Effects of Scarring 313




















