Trauma Ginjal
39
TRAUMA GINJAL SUB BAGIAN UROLOGI BAGIAN/SMF BEDAH FK UNS/RSUD Dr. MOEWARDI
-
Upload
euffrasia-monica-atikka-sugiarto -
Category
Documents
-
view
241 -
download
4
description
TRAUMA GINJAL
Transcript of Trauma Ginjal

TRAUMA GINJAL
SUB BAGIAN UROLOGIBAGIAN/SMF BEDAHFK UNS/RSUD Dr. MOEWARDI

PENDAHULUAN
10% trauma abdomen trauma traktus urogenitalis
Trauma urogenitalis trauma ginjal >>> 5% trauma abdomen
Dewasa muda sekitar 74%, usia tua 15%, dan anak-anak 9%
Sering bersama trauma organ lain (multiorgan trauma).
AS : trauma ginjal bersama hepar (40%), lien (5-7%), pankreas (13%), kolon (7%) dan usus halus / gaster (3%)

ETIOLOGITrauma tumpul (Blunt Injury) 80-85%Mekanisme trauma tumpul ginjal :1. Trauma langsung pinggang kosta 11 & 12
fraktur melukai ginjal2. Trauma tumpul bagian depan abdomen 3. Jatuh terduduk dari ketinggian

AAST Renal Injury Grading ScaleGrade* Description of Injury
1 Contusion or non-expanding subcapsular haematoma
No laceration
2 Non-expanding peri-renal haematoma
Cortical laceration < 1 cm deep without extravasation
3 Cortical laceration < 1 cm without urinary extravasation
4 Laceration: through corticomedullary junction into collecting system
Or
Vasculary: segmental renal artery or vein injury with contained haematoma, or partial vassel laceration, or vessel thrombosis
5 Laceration: shattered kidney
Or
Vascular: renal pedicle or avulsion

ETIOLOGI
Trauma tembus (penetrating injury) 1. luka tusuk (stab wound)2. luka tembak (gun shot) 80% luka tembus ginjal
trauma visera intraabdomen intervensi operatif

KLASIFIKASI

DIAGNOSIS
1. Riwayat trauma2. Hematuria (95%)3. Hematoma di regio flank4. Fraktur costa bawah 5. Hemodinamik tidak stabil
(hipotensi)

History and Physical ExaminationRecommendations GR
Haemodynamic stability should be decided upon admission B
History should be taken from conscious patient, witnesses and rescue team personnel with regard to the time and setting of the incident
C
Past renal surgery, and known pre-existing renal abnormalities (ureteropelvic junction obstruction, large cysts, lithiasis) should be recorded
B
A though examination should be made of the thorax, abdomen, flanks and back for penetrating wounds B
Findings on physical examination such as haematuria, flank pain, flank absasions and ecchymoses, fractured ribs, abdominal tenderness, distension or mass, could indicate possible renal involvement
B

Laboratory Evaluation
Recommendations GR
Urine from a patient with suspected renal injury should be inspected grossly and then by dipstick analysis B
Serial haematocrit measurement indicates blood loss. However, until evaluation is complete. It not be clean whether it is due to renal trauma and or associated injuries.
B
Creatinine measurement could highlight patient who had impaired renal function prior to injury C

PEMERIKSAAN IMEJING GINJALDahulu: IVP skg: CT Scan kontrasJk fasilitas CT Scan (-) pakai IVPIndikasi:1. Trauma tembus regio flank /
abdomen tdk lihat derajat hematuria
2. Trauma tumpul dewasa dg gross hematuria /mikrohematuria + shock (sistolik < 90 mmHg)
3. Trauma deselerasi4. Trauma mayor berhubungan trauma
intra-abdominal & mikrohematuria5. Trauma abdomen / flank penderita
anak dengan hematuria

ImagingRecommendation GR
Blunt trauma patients with macroscopic or microscopic haematurial (at least 5rbc/hpf) with hypotention (systolic blood preassure <90mmHg) should undergo radiographic evaluation
B
Radiographic evaluation is also recommended for all patients with a history of rapid declaration injury and/or significant associated injuries.
B
All patients with any degree of haematuria after penetrating abdominal or thoracic injury require urgent renal imaging
B
Ultrasonograpy can be informative during the primary evaluation o polytrauma patients and for the follow-up of recuperating patients, although more data is required to suggest this modality university
C
A CT scan with enchancement of intravenous contrast material is the best imaging study for the diagnosis and staging of renal injuries in haemodynamically stable patients
B
Unstable patients who require emergency surgical exploration should undergo a one-shot IVP with bolus intravenous unjection of 2mL/kg contrast
C
Formal IVP/, MRI and radiographic scintigraphy are acceptable second-line alternative for imaging renal trauma when CT is not availabel
C
Angiography can be used for diagnosis and simultaneous selective embolisation of bleeding vessels
B

PENGELOLAAN NONOPERATIF98% trauma tumpul renal Penderita hemodinamik stabil &
staging (+) & CT Scan (+)Trauma tembus luka tembak / tusuk
staging hati-hati dg CT Scan monitor ketat
55% trauma tusuk & 24% trauma luka tembak nonoperatif
Trauma derajat III & IV monitor ketat (serial hematokrit & CT Scan)
perdarahan persisten angiografi embolisasi

Non-operative Management of Renal InjuriesRecommendations GR
Following grade 1-4 blunt renal trauma, stable patients should be manage conservatively with bed-rest, prophylactics antibiotic and continuous of vital signs until haematurial resolves
B
Following grade 1-3 stab and low-velocity gunshot wounds, stable patients, after complete staging, should be selected expectant management
B
Indicated for surgical management includeHaemodynamic instabilityExploration for associated injuriesExpanding or pulsatile peri-renal haematoma identified during laparotomyGrade 5 injury
Incidental finding of pre-existing renal pathology requiring surgical therapy B
Renal reconstructing should be attempted in cases with where the primary goal of controlling haemorrhage is achieved and sufficient amount of renal parenchyma is viable
B

EKSPLORASI GINJALINDIKASI ABSOLUT1. perdarahan ginjal yang
persisten hematoma meluas, denyut, hematom retroperitoneal
2. trauma renal derajat V

EKSPLORASI GINJAL
INDIKASI RELATIF1. Trauma tumpul & tembus ginjal
komplikasi: ekstravasasi urin persisten, abses perinefrik, urinoma terinfeksi, & perdarahan
2. trauma derajat III & IV dg jar non-vital luas & trauma organ intraperitoneal
3. trauma grade IV dg laserasi pelvis renalis, parenkim ginjal & sistem kolektivus & avulsi UPJ
4. trauma tumpul dg hematom retroperitoneal & kelainan pd ’single shot’ IVP

Algoritma Pengelolaan Trauma Ginjal

(a) IVP pada trauma tumpul ginjal dengan trauma pada pelvis renalis yang ditunjukkan ekstravasasi kontras
(b) Tomogram yang menunjukkan trauma ginjal mengenai kaliks pole bawah

TRAUMA VASKULAR Trauma vaskular renal (50%) syok (+) mortalitas
10-50% Trauma arteri renalis sulit utk diselamatkan &
rekonstruksi Pembedahan rekonstruksi < 12 jam >>>
diselamatkan keberhasilan revaskularisasi 10-30%, ↓ fs ginjal
CT Scan ginjal menunjukkan absen komplit kontras pada ginjal kiri oleh karena adanya avulsi komplit pedikel renal

TROMBOSIS ARTERI RENALIS NEFREKTOMI
Pergerakan ginjal ok deselerasi peregangan arteri renalis ruptur intima trombus
CT Scan ginjal kiri dengan trombosis arteri renalis, menunjukkan kurangnya perfusi kontras ke ginjal (kiri); Arteriografi menunjukkan oklusi komplit arteri renalis kiri sekunder akibat trombus

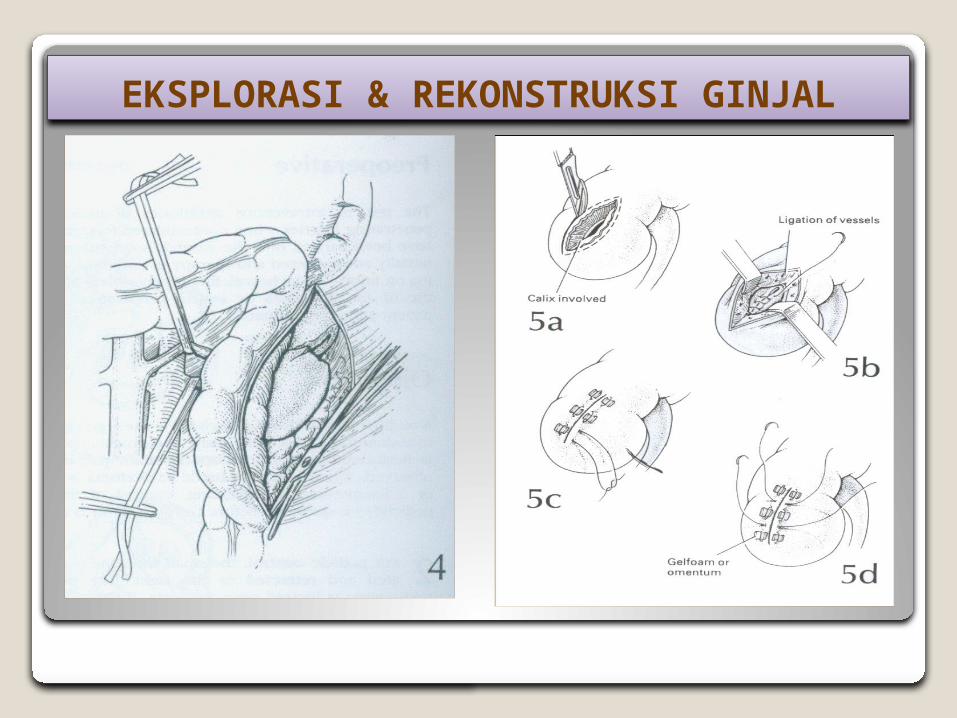
EKSPLORASI & REKONSTRUKSI GINJAL
Insisi midline transabdominal dr proc xiphoideus - simfisis pubis
Kolon transversum rongga dada (bungkus kasa lembab) Identifikasi cab a. mesenterika pd usus halus Angkat usus keatas dan ke kanan retroperitoneum
tampak Insisi vertikal di atas aorta superior dr a. mesenterika
superior smp retroperitoneum perluas keatas dr lig Treitz V. mesenterika inf petunjuk insisi diseksi hingga ant
perm aorta Diseksi smp sup hingga v. renalis sin tanda identifikasi
pd renalis tegel dipasang Kontrol perdrhan dg kompresi manual parenkim ginjal jk
perdarahan (+) klem vena waktu iskemik < 30’

EKSPLORASI & REKONSTRUKSI GINJAL
Kontrol PD (+) evakuasi hematom retroperitoneal Insisi fasia Gerota di lateral ginjal terpapar
evaluasi pelvis renalis, parenkim & pdRekonstruksi debridement adekuat: jar mati dibuang
preservasi kapsula renalis utk penutupan ginjal Ligasi PD parenkim kromik 4/0Laserasi sistem kolektivus dijahit scr kedap air
(watertight fashion) kromik 4/0. Inj metilen blue ke pelvis renalis identifikasi trauma
lain & penutupan sistem kolektivusTutup kapsula renalis reaproksimasi tepi parenkim
jahitan interrupted Vicryl 3/0 Jk defek ginjal luas packing dg agen hemostasis
(Avitene, Tissel, lemak perinefrik)

EKSPLORASI & REKONSTRUKSI GINJAL
Segmen pole ginjal tidak vital (+) parsial nefrektomi (amputasi & penutupan sistem kolektivus) pakai omentum utk tutup defek pole ginjal jk kapsula renalis (-)
Pasang Penrose drain (drainase retroperitoneum) Suction drain tidak boleh

EKSPLORASI & REKONSTRUKSI GINJAL

EKSPLORASI & REKONSTRUKSI GINJAL

EKSPLORASI & REKONSTRUKSI GINJAL
EKSPLORASI & REKONSTRUKSI GINJAL

EKSPLORASI & REKONSTRUKSI GINJAL

DAMAGE CONTROL
Coburn (2002): keuntungan ↑ penyelamatan ginjal
packing dg laparotomy pads kontrol perdrhn & dibuka kembali dalam 24 jam eksplorasi & evaluasi luas trauma
mencegah nefrektomi total

NEFREKTOMI
Indikasi :Trauma ginjal ekstensif, hemodinamik
tidak stabil, suhu tubuh rendah, & koagulasi buruk renal repair tdk mgkn (fs ginjal kontralateral N)
Nash dkk (1995) 77% nefrektomi (+) ok perdrhn parenkim luas, vaskular & kombinasi, 23% ok hemodinamik tdk stabil dg ginjal dpt direkonstruksi.

ComplicationRecommendations GR
Complication following renal trauma require a thorough radiographic evaluation B
Medical management and minimally invasive technique should be the first choice for the management of complications C
Renal salvage should be the surgeon’s aim for patients in whom surgical intervention is necessary C

KOMPLIKASI
Ekstravasasi urin persisten urinoma, infeksi perinefrik & kehilangan ginjal
Obs ketat & AB tepatPerdarahan ginjal tertunda (21 hari) bedrest, hidrasi, angiografi &
embolisasi hipertensi arterial

Post Operative Care and Follow-UpRecommendations GR
Repeat imaging is recommended for all hospitalized patients within 2-4 days of significant renal trauma (although no specific data exists). Repeat imaging is always recommended in cases of fever, flank pain, or falling haematrocrit
B
Nuclear scintigraphy before discharge from the hospital is useful for documenting functional recovery C
Within 3 month of major renal injury, patients follow-up should involve: 1. Physical examination2. Urinalysis3. Individualized radiological investigation4. Serial blood pressure measurement5. Serum determination of renal function
C
Long-term follow-up should be dedicated on a case-by-case basis but should at the very last involve monitoring for renovascular hypertension
C

Paediatric Renal TraumaRecommendations GR
Indications for radiography evaluation of children suspect of renal trauma include:1. Blund and penetrating trauma patients with any level of
haematuria2. Patient with associated abdominal injury regardless of the
findings of urinalysis3. Patient with normal urinaluses who sustained a rapid
deceleration event, direct flank trauma, or all a fall from a height
B
Ultrasonography is the considered a reliable method of screening and monitoring blunt renal injuries by some researchers, but is not universally accepted
B
CT scanning is the imaging study of choice for staging renal injuries B
Haemodynamic instability and a diagnoses grade 5 injury are absolute indications for surgical exploration B

Renal Injury in The Polytrauma Patient
Recommendations GR
Polytrauma patients with associated renal injuries should be evaluated on the basic of the most threatening injury C
In case where surgical intervention is chosen, all associated injuries be evaluated simultaneously C
The decision for conservative management should consider all injuries independently C
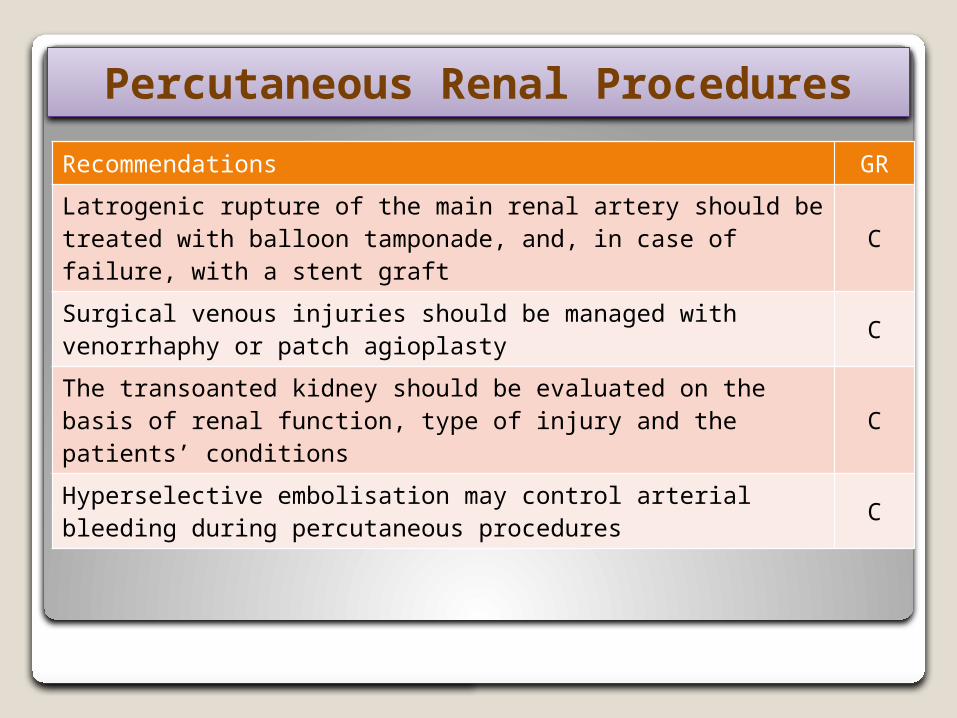
Percutaneous Renal Procedures
Recommendations GR
Latrogenic rupture of the main renal artery should be treated with balloon tamponade, and, in case of failure, with a stent graft
C
Surgical venous injuries should be managed with venorrhaphy or patch agioplasty C
The transoanted kidney should be evaluated on the basis of renal function, type of injury and the patients’ conditions C
Hyperselective embolisation may control arterial bleeding during percutaneous procedures C

Paediatric renal trauma
Blunt Penetrating
>50 rbc/hpf or
deceleration
<50 rbc/hpf or haemodynamicall
y stable
>5 rbc/hpf
CT Scan Abdominal exploration
Observes Renal exploration
IVP
Observes Renal exploration
CT Scan Abdominal exploration
Observes Renal exploration
IVP
Observes Renal exploration
UA UAUA
Stable UnstableStable Unstable
NL ABNL
NL ABNL
Algorithm for The Management of Paediatric Renal Trauma
Suspected adult blunt Renal trauma
Determine haemodynamic stability
Stable Unstable
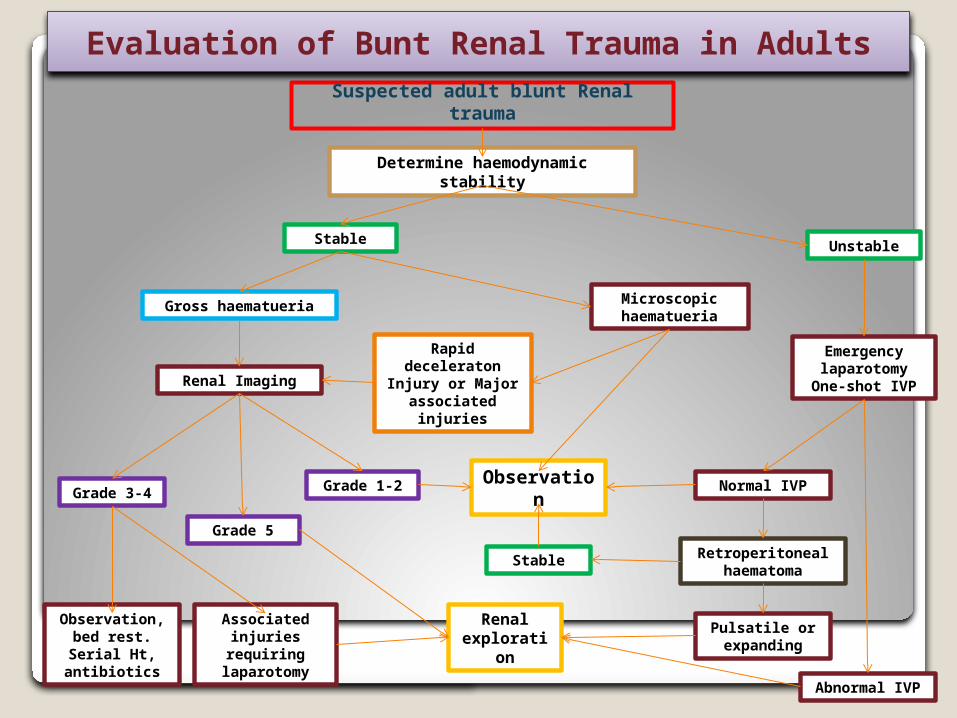
Gross haematueria
Renal ImagingRapid deceleraton
Injury or Major associated injuries
Microscopic haematueria
Grade 1-2Grade 3-4 Observation
Stable
Normal IVP
Retroperitoneal haematoma
Emergency laparotomy One-
shot IVP
Observation, bed rest. Serial Ht, antibiotics
Associated injuries requiring
laparotomy
Renal exploration
Pulsatile or expanding
Abnormal IVP
Grade 5
Evaluation of Bunt Renal Trauma in Adults

Suspected adult blunt Renal trauma
Determine haemodynamic stability
Stable Unstable
Renal Imaging
Grade 1-2Grade 3 Grade 4-5
Observation, bed rest. Serial Ht, antibiotics
Observation
Stable
Normal IVP
Retroperitoneal haematoma
Emergency laparotomy One-
shot IVP
Associated injuries requiring
laparotomy
Renal exploration
Pulsatile or expanding
Abnormal IVP
Evaluation of Penetrating Renal Trauma in Adults

Terima kasih