Osteoporosis
28
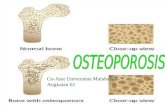
OSTEOPOROSIS Definisi Osteoporosis adalah suatu penyakit kelainan pada tulang yang ditandai dengan berkurangnya massa tulang, kerusakan tubuh atau arsitektur tulang sehingga tulang mudah patah. Osteoporosis adalah penyakit degeneratif yaitu suatu penyakit yang berhubungan dengan usia. Tapi Osteoporosis bisa dihindari atau dicegah agar jangan terjadi akibat yang lebih fatal yaitu patah tulang.
-
Upload
fadilkampus -
Category
Documents
-
view
64 -
download
0
description
kjk
Transcript of Osteoporosis

OSTEOPOROSIS
DefinisiOsteoporosis adalah suatu penyakit kelainan pada tulang yang ditandai dengan berkurangnya massa tulang, kerusakan tubuh atau arsitektur tulang sehingga tulang mudah patah. Osteoporosis adalah penyakit degeneratif yaitu suatu penyakit yang berhubungan dengan usia. Tapi Osteoporosis bisa dihindari atau dicegah agar jangan terjadi akibat yang lebih fatal yaitu patah tulang.

Patogenesis / Terjadinya Osteoporosis
Secara normal di tubuh kita terjadi suatu tahapan yang disebut REMODELLING TULANG, yaitu suatu proses pergantian tulang yang sudah tua untuk diganti dengan tulang yang baru. Hal ini sudah terjadi pada saat pembentukan tulang mulai berlangsung sampai selama kita hidup.
Proses Remodelling tulang tersebut dapat digambarkan seperti gambar dibawah ini :
Setiap saat terjadi remodeling tulang di tulang manusia. Proses remodeling ini dimulai dengan terjadinya resorpsi atau penyerapan atau penarikan tulang oleh sel tulang yaitu OSTEOKLAS, kemudian tulang yang sudah diserap itu tadi akan diisi oleh tulang yang baru dengan bantuan sel tulang yang bernama OSTEOBLAS.
Kejadian ini adalah suatu keadaan yang normal, dimana pada saat proses pembentukan tulang sampai umur 30 – 35 tahun, jumlah tulang yang diserap atau diresorpsi sama dengan jumlah tulang baru yang mengisi atau menggantikan sehingga terbentuk PUNCAK MASSA TULANG, tapi setelah berumur 35 tahun keadaan ini tidak berjalan dengan seimbang lagi dimana jumlah tulang yang diserap lebih besar dari jumlah tulang baru yang menggantikan. Hal inilah yang mengakibatkan terjadinya penurunan massa tulang yang berakibat pada OSTEOPOROSIS.
Perubahan Fisik yang terjadi karena Osteoporosis
Bagian tubuh mana yang sering terkena Osteoporosis?
1. Tulang Punggung 2. Tulang jari tangan 3. Tulang pangkal paha

Faktor Penyebab Osteoporosis
Ada beberapa faktor yang menjadi penyebab atau faktor–faktor yang beresiko terkena osteoporosis, antara lain :
Wanita, wanita lebih beresiko terhadap pria Berusia di atas 50 tahun Post menopause Kekurangan hormon estrogen Mengalami pengangkatan rahim / ovarium Kurang kalsium Kurang sinar matahari dan kurang vit. D Kurang aktifitas fisik Histori keluarga ada yang osteoporosis Perawakan kurus, tulang kecil Orang asia lebih beresiko dibanding orang eropa Perokok Peminum kopi dan cola / minuman bersoda Peminum alcohol Pengguna obat–obatan seperti Kortison, Prednison, Anti konvulsan, hormon tiroid
Menurut Penelitian : 24 % dari Wanita umur 40–59 tahun sudah mengalami osteoporosis dan 62 % dari wanita berumur 60 – 70 tahun mengalami osteoporosis
Mengapa wanita lebih beresiko osteoporosis dibanding pria??
Wanita memiliki hormon estrogen yang dihasilkan setiap mengalami siklus menstruasi, dimana hormon ini merupakan suatu hormon yang berfungsi sebagai PELINDUNG TULANG. Jadi bagi wanita yang mengalami gangguan siklus haid beresiko mengalami osteoporosis. Bila wanita mengalami MENOPAUSE yaitu suatu fase dimana wanita sudah tidak bisa haid lagi, maka hormon estrogen sama sekali tidak bisa dihasilkan. Hal ini akan mengakibatkan tidak adanya hormon yang melindungi tulang, sehingga tulang mudah patah.
Gejala-Gejala Osteoporosis
Osteoporosis adalah suatu penyakit yang biasanya tidak diikuti gejala, makanya sering disebut sebagai THE SILENT THIEF. Tapi ada beberapa gejala yang bisa jadi dasar untuk menentukan seseorang terkena osteoporosis atau tidak :
Adanya nyeri di tulang belakang, pergelangan tangan, pangkal paha Adanya nyeri dan rasa sakit pada tulang leher Adanya kecenderungan penurunan tinggi badan Postur tubuh kelihatan memendek
Akibat Osteoporosis Nyeri pada tulang Tubuh makin lama makin memendek (bungkuk) Tulang menjadi mudah patah
o Biaya perawatan besar o Kecacatan o Ketergantungan pada orang lain o Kualitas hidup menurun o Kematian

Data di Amerika menunjukkan kalau terdapat kasus PATAH TULANG sebanyak 1,5 juta kasus per tahun.
Dan yang bertanggung jawab atas terjadinya patah tulang ini adalah OSTEOPOROSIS
Biasanya orang baru menyadari terkena osteoporosis setelah mengalami PATAH TULANG( FRAKTUR ). Untuk itu bila diantara kita mempunyai factor resiko terkena OSTEOPOROSIS cegahlah dari sekarang biar nanti jangan menjadi fatal.
Deteksi Dini Osteoporosis
Karena osteoporosis merupakan suatu penyakit yang biasanya tidak diawali dengan gejala, maka langkah yang paling penting dalam mencegah dan mengobati osteoporosis adalah : Pemeriksaan secara dini untuk mengetahui apakah kita sudah terkena atau belum OSTEOPOROSIS, sehingga dari pemeriksaan ini, kita akan tahu langkah selanjutnya.
Bagaimana cara Pemeriksaan Dini Osteoporosis? Untuk mengetahui apakah kita terkena OSTEOPOROSIS atau tidak, maka kita perlu mengetahui keadaan MASSA TULANG kita dari sekarang..
Ada tiga cara pemeriksaan dini Osteoporosis :
1. DENSITOMETRY 2. LABORATORIUM 3. RADIOLOGI
Diantara ketiga pemeriksaan diatas, DENSITOMETRY merupakan pemeriksaan yang paling akurat karena yang diukur adalah MASSA TULANG.
Prinsip Pemeriksaan Densitometry :
Pada pengukuran dengan alat DENSITOMETRY, si pasien akan diukur BMDnya. BMD itu adalah ukuran kepadatan tulang.
Angka BMD –1 sampai Positif termasuk NORMAL Angka BMD –1 s.d –2,5 termasuk OSTEOPENIA
Angka BMD dibawah –2,5 termasuk OSTEOPOROSIS
Dari pengukuran BMD ini kita bisa mengantisipasi untuk hal – hal yang lebih parah dengan prinsip:

Bila BMD kita NORMAL, maka usahayang kita lakukan adalah mempertahankan agar tetap NORMAL
Bila BMD kita OSTEOPENIA, kita harus terapi atau obati agar menjadi NORMAL Bila BMD kita OSTEOPOROSIS, kita harus obati agar jangan menjadi parah yang bisa
mengakibatkan tulang patah
Terapi Dan Pengobatan Osteoporosis
Pencegahan Osteoporosis1. Kalsium yang cukup, kira-kira 800–1200 mg per hari 2. Vitamin D3 yang cukup
Kalsium dan Vit. D3 bisa didapatkan dari bahan makanan tapi untuk lebih praktis dan dengan dosis yang tepat, di pasaran sudah beredar EPOCALDI dengan kalsium dan Vit.D3
3. Olah raga yang teratur 4. Hindari merokok, minuman alkohol dan kafein (kopi) 5. Melakukan pemeriksaan tulang untuk mengetahui osteporosis secara dini
MAKANAN TINGGI CALCIUM, VITAMIN C DAN PROTEIN
Susu dan Daging Hewani, pilih yang rendah lemak Sayur-sayuran segar Buah-buahan segar seperti jeruk Ikan termasuk tulang-tulangnya
Kandungan Kalsium dalam Makanan
Jenis makanan Kandungan Kalsium (mg/100)
Susu kambing 98
Susu kerbau 216
Susu bubuk (full cream) 895
Susu bubuk skim 1.300
Keju 777
Kacang kedelai basah 196
Kacang kedelai kering 227
Kacang tanah 730
Tempe kedelai 129
Tahu 124
Daun lamtoro 1.500
Daun kelor 440
Bayam merah 368
Bayam hijau 267
Daun talas 302
Daun melinjo 219

Rebon segar 757
Udang kering 1.209
Udang segar 136
Teri kering 1.200
Teri segar 500
Pengobatan Osteoporosis
Tujuan Pengobatan Osteoporosis
1. Meningkatkan kepadatan tulang 2. Mencegah terjadinya patah tulang Osteoporosis 3. Menjaga keseimbangan metabolisme tulang 4. Mengembalikan kualitas tulang
Ada beberapa standard pengobatan Osteoporosis, yaitu :
1. Kalsium dan Vitamin D3 2. Terapi Hormon Pengganti Pada Wanita Menopause 3. Golongan Bisfosfonate : Alovell®
Alovell spesifik bekerja menghambat sel osteoklast yang menyerap dan meresorpsi tulang (ingat… kalau osteoporosis terjadi karena aktifitas penyerapan tulang lebih besar dari pembentukan, sehingga penyerapan tulang ini harus dihentikan, dan obat yang berfungsi untuk menghentikan dan menghambat penyerapan tulang ini adalah ALOVELL
4. Olah Raga yang cukup
Prinsip Olah raga :
1. Pemanasan : 5 – 10 menit 2. Bertahap 3. Rutin 4. Cooling down : 10 – 15 menit 5. Minum yang cukup

Post menopause and what happens after the change
by Dixie Mills, MD, FACS
Who is the post-menopausal woman? Exactly what is menopause, and what does “post-menopause” mean? Literally, the term means after the menopause or the stopping of periods. To be more precise, most providers consider a woman to be post-menopausal when she hasn’t had a vaginal bleed for one year.
But for many women, it’s difficult to calculate when exactly their last period was because you don’t know it was the last until 12 months later. We often see women who hope that a particular month’s bleeding is the last, only to have another period several months later and have to start counting all over again. So it’s understandable how we could conflate what is actually premenopause with menopause. (For more information, see our article on the beginning of hormonal change.)
Aside from transitioning into menopause naturally as described above, some women have their ovaries removed surgically, and are considered post-menopause after the operation because there is no longer any chance they will have another period. On the other hand, women who stop having periods during chemotherapy might resume them after treatment is over. Even if the treatment causes their periods to stop for a whole year, most doctors do not consider these women to be post-menopausal without checking their FSH levels. Also, women who are taking any type of hormone replacement therapy (HRT), even if they’ve not had a period in 12 months, may not be technically post-menopausal because once they stop therapy they usually have some of the symptoms of menopause again.
So are all post-menopausal women the same? The answer, of course, is a resounding NO.
The range of menopause symptoms, related diseases, and quality of health for post-menopausal women is gigantic. Some women get very few hot flashes; others have night

sweats into their 70’s. We don’t even know what the average age is when women stop having hot flashes because the number is affected by too many variables to be accurate.
Post menopausal and what it means
But then someone should be asking: Are you post-menopause until you die? Theoretically, yes, but the same could be said for post-puberty and post-partum. The difference is that these other life stages seem to have natural endings when a new one begins. But what is the new stage after menopause?
We are considering offering a contest to pick a new heading for the time in a woman’s life that we now call post-menopause. The present terms just are not satisfactory! For the possible 40 or even 50 years of life after menopause to be labeled as simply post-menopausal seems terribly anticlimactic.
The years between 20 and 50 are often referred to as “the childbearing years.” This term is not perfect either, but at least it carries none of the negative connotations of menopause, because we are creating. But what are we doing if we are “post-menopausal?”
With all the baby-boomer women reaching the age of menopause, we are sure to create a new expression. What will it be? The term “midlife” obviously won’t last, and no one wants to be called elderly — even “young elderly” isn’t going to sit well with my friends. I imagine my friends as hip 80-year-olds, driving around in Smart Cars and keeping connected with the latest Blackberry–like devices.
The female midlife crisis, or a new beginning?
Society allows men to have midlife crises and buy red sports cars or find new wives. Women’s midlife crises are bracketed by hot flashes, weight gain, and a vapid sex drive. But what do both sexes discover? Usually that those times of crisis were just a transition, beyond which lies so much more. They may reexamine their values and redefine what they really appreciate — it’s different things for different folks. They realize that the journey is what’s important and that it is far from over!
We contend that menopause brings many benefits along with its changes. But unfortunately we see and hear the negative side effects of menopause emphasized while the joys of post-menopause are neglected.
Our grandmothers and even most of our mothers did not talk about their bodies, let alone their periods. I have read several famous women’s autobiographies to find out if they shared their experiences of menopause or post-menopause. Jane Addams took to her bed in the 40’s with undiagnosed fatigue and headaches. Was it menopause, or just rheumatism as thought at the time? Eleanor Roosevelt never once mentioned a hot flash in her diaries or columns. This did not stem my curiosity about what menopause meant for women of yesteryear. Margaret Mead did write about post-menopausal zest, but then, anthropology is a holistic science, and perhaps this gave her greater license!
Discover the joys of post-menopause
There are many things to love about being post-menopausal. There is a light at the end of the tunnel of heavy bleeding and hot flashes. No more Kotex pads or Tampax! No more worry about pregnancy. Most women find their voice and have no qualms about raising it. This does not happen overnight of course, and for many women it takes time to stop feeling bad about speaking up — but they realize they have nothing to lose and much to gain!

Many women find another avocation of sorts for their second act. With children out of the house, they can spend time on themselves, go back to school and take a class in the area they have always dreamt about. Many pick up a paint brush for the first time or try a musical instrument. I have a patient who was formerly an accountant for a large university, and she decided to resign and open a knitting café that sells organic coffee and green tea! Of course, this wasn’t a snap decision and took months if not years of meditation and consultation with family and friends. But the possibilities are endless. Another patient, once her youngest was in college, enrolled in theology school to satisfy her spiritual quest. Yet another patient for her 60th birthday packed up her husband and her house and began a year-long trek through Europe to explore her ancestral heritage and leave a legacy for her children.
Post-menopausal women are not going to be invisible anymore. There are too many of us to just slip away into anonymity. As a collective we are rediscovering ourselves. Some, maybe including yourself, are going through a lot of angst and discomfort, and we don’t want to trivialize that. But there are answers, and once you begin to feel better you can re-live your passions and really explore with zest! There is no need to grin and bear it — instead, go ahead, scream and dig into it. Let’s make these years truly golden ones. Send your ideas and let us know what you love about being in post-menopause.
Estrogen levels as related to estrogen dominanceby Marcelle Pick, OB/GYN NP
Most conventional doctors still tell women that menopause — and all the menopause symptoms — is the result of a drop in estrogen production. In their view the solution is estrogen supplementation, or HRT, usually with synthetic hormones.
In contrast, many alternative practitioners believe that women have too much estrogen, leading to a condition known as “estrogen dominance.” The late healthcare pioneer, Dr. John Lee broke new ground when he claimed that estrogen dominance was the real cause of menopause and pre-menopause symptoms, especially in younger women. In his view the obvious solution was to rebalance the ratio of estrogen to progesterone through progesterone supplementation.
This idea has led to the marketing of hundreds of brands of progesterone creme and other progesterone products — all promising a quick fix and miraculous results in curing menopausal and pre-menopause symptoms.
Unfortunately, both of these views are simplistic and misleading for women. We’ve written other articles telling you the truth behind the estrogen deficiency theory and our view about synthetic HRT versus bioidentical hormones.
Let’s focus today on the concept of estrogen dominance, the incredible claims being made for the efficacy of progesterone, and what it all means for you and your health.
What is estrogen dominance?
Estrogen and progesterone are two of the primary female sex hormones. During a normal menstrual cycle, they take turns driving the process of maturing and releasing an egg and preparing the uterus for possible pregnancy: estrogen rises in the first half of the cycle, peaks at ovulation, then falls in the second half as progesterone rises. Progesterone is released by

the rupturing of the egg follicle during ovulation. If there is no pregnancy, you have a period and the whole cycle begins again.
When estrogen and progesterone are doing their jobs, they work together. How much or how little of each hormone is made at any one time relies on a complicated feedback system between the brain: specifically the hypothalamus and the pituitary gland, which release LH (luteinizing hormone) and FSH (follicle stimulating hormone), and the ovaries. Stress and diet affect that feedback system and so directly impact your hormonal balance.
© 2006 Women to Women *
What’s critical here is the role of progesterone, which “opposes” the estrogen by helping the body break it down into metabolites that are absorbed and removed in the process. Estrogen stimulates tissue growth, and progesterone signals the body to slough it off.
The original concept of estrogen dominance was very simple. Dr. Lee argued that the first sign of menopause is a drop in progesterone production (not estrogen deficiency!). Without enough “opposing” progesterone, estrogen levels stay unnaturally high in the second half of the menstrual cycle. This causes discomfort in a great many women and can lead over time to some severe health consequences.
(The history of HRT contains a tragic example of the effects of unopposed estrogen. For many years after the creation of synthetic estrogen — Premarin — it was prescribed to women without any accompanying progesterone. The result was an epidemic of uterine cancer that led to the bundling of Premarin with Provera, a synthetic progesterone — i.e., a progestin — which was called Prempro, for decades now the most widely prescribed synthetic HRT in the world.)

Over time, Dr. Lee’s concept of estrogen dominance evolved to promote another, powerful argument: that our overall estrogen levels (in women and men) are too high because of xenoestrogens — chemicals in the environment that mimic estrogen in our bodies and act as endocrine disruptors even at minute concentrations.
Scientific study of wildlife — specifically, frogs and fish — is proving this unfortunate reality to be without doubt.
In an interesting twist, researchers worldwide have observed that fish in our lakes and rivers are actually switching gender due to the high levels of effluent estrogens. Even though mainstream media has only begun to recognize this as “news,” experts have been discussing the problem of pharmaceutical pollution for over 25 years, and have known about “gender-bent” fish for more than 10 years now! Some surmise these changes to be caused in part by excessive levels of steroids — largely excreted by humans using birth control pills and hormonal replacement therapy (HRT). Our water treatment facilities are not designed to remove hormonal pollutants.
Myriad studies indict environmental estrogens as the cause of reproductive abnormalities in small life forms. So it should come as no surprise that these and other widespread contaminants are now suspected of negatively impacting humans as well, contributing to the problems of estrogen dominance and infertility.
As evidence, it’s often noted that women in Western Europe and the US have estrogen levels that are much higher than women in underdeveloped countries. Many experts link these high levels of estrogen with the rise in breast cancer, autoimmune diseases, infertility and other health issues. They question whether or not xenoestrogens are the cause.
The truth about estrogen dominance
While we all owe a huge debt of gratitude to Dr. Lee for his groundbreaking work on the importance of progesterone in relation to estrogen, to my mind the concept of estrogen dominance is too simplistic, as is the concept of progesterone supplementation.
Since Dr. Lee’s death in October 2003, we have witnessed huge leaps in our biochemical understanding. If he were still with us, I’m sure he would feel vindicated to learn that the latest research indicates many women actually have normal levels of circulating progesterone. Just as Dr. Lee himself noted, what throws the balance off is an excess of estrogen, caused by environmental, dietary, and lifestyle factors.
What this all means is that the theory of estrogen dominance is very real, but its significance lies in the overall ratio of estrogen to progesterone — and this ratio is an individualized one. Of all women experiencing symptoms of estrogen dominance, some with low levels of progesterone may do very well with progesterone supplementation, whereas others with normal progesterone levels may be better off focusing on changes that can reduce their estrogen levels. How do you know where you fit in? The only way to really tell is to have your hormone levels checked and take action from there.
It is true that estrogen is often too high relative to progesterone. Most of us who have had PMS are familiar with this temporary, benign form of excess estrogen. You can see by the chart above how progesterone levels gradually fall during the course of a regular menstrual cycle. In some women this drop may be more precipitous and cause symptoms of PMS.
During pre-menopause it’s common for estrogen levels to decrease slowly while progesterone levels plummet — a natural result of fewer ovulations, fewer burst follicles and less progesterone. This can cause many of our worst symptoms. (See our article on irregular periods to learn more.)

Calling this state “estrogen dominance” is catchy but misleading. It implies there is one problem, which isn’t true; and not all women experience the condition anyway. And it implies there is one solution, which also isn’t true. Most of the tens of thousands of women we have treated for pre-menopause symptoms have suffered not from simple estrogen dominance but from a more fundamental disruption of the body’s ability to maintain hormonal balance. There are usually multiple causes, including stress, emotional factors, and the estrogen-like chemicals in our environment called xenoestrogens.
The truth is, healthy hormonal balance is complicated. It isn’t just a matter of not enough progesterone. That’s a little like arguing that menopause is caused by not enough estrogen.
There’s no simple test for estrogen dominance. But if you have severe symptoms of PMS, pre-menopause or menopause that don’t respond to a program of increased support for your body within a month or two, you may have persistently higher than normal levels of estrogen. Let’s talk about why it’s important to pay attention to these symptoms.
What are the health consequences of estrogen dominance?
Another of Dr. Lee’s contributions was to raise women’s awareness of the profound connections between hormonal imbalance and health.
When estrogen levels are high in relation to our progesterone we experience many severe symptoms, among them anxiety, breast tenderness, cyclical headaches or migraines, depression, digestive issues, fuzzy thinking, palpitations, food cravings, irregular bleeding, water retention, weight gain and more.
(Note that a number of these symptoms are also indicative of the exact opposite condition — a deficiency of estrogen — another example of why the concept of estrogen dominance is too simplistic.)
If estrogen levels stay unopposed, women may develop infertility, endometriosis, amenorrhea (skipped periods), hypermenorrhea (heavy bleeding), fibroids, uterine cancer, stroke, and decreased cognitive ability, among other conditions.
And while we share many of the precepts set forth by Dr. Lee, we are less inclined to think of estrogen, even high levels of estrogen, as universally harmful. We believe every woman is unique, and what may cause harm in one may be fine for another. There have been studies and speculation for example about the connection between high levels of estrogen and breast cancer. We think many unanswered questions remain about this link; to learn more, read Dr. Dixie Mills’ article on estrogen and breast cancer.
Estrogen has many wonderful qualities. It creates our fertility, protects our health in myriad ways, and serves as a powerful anti-inflammatory. But we are very concerned about environmental estrogens. They’re another story entirely.
Awash in a sea of xenoestrogens
For the most part, our bodies are amazingly resilient. We are hard-wired to resist threats to our equilibrium. What our bodies are not designed for is exposure to the many endocrine disruptors in our environment, among them the family of chemicals known as xenoestrogens.
Many of these xenoestrogens are proven carcinogens. They are also well known for their ability to damage the immune system and interrupt hormonal balance. Our cells can’t always distinguish fully between our own estrogen and xenoestrogens. Every cell has estrogen receptors that recognize and open to the shape of an estrogen molecular chain, regardless of where it comes from.

Pesticides are perhaps the biggest source of xenoestrogens. Most bioaccumulate, meaning they are stored in fat cells of fish, poultry and other food sources in increasing concentration until they reach the top of the food chain — where you and I consume them! They are highly estrogenic, and some experts estimate that the average American ingests over a pound of pesticides a year.
A second major source of xenoestrogens is the many growth hormones given to livestock and poultry, most of which contain fat-soluble estrogens. When we consume those animals or their milk, we ingest that estrogen. Organochlorides like dioxin (a by-product of chlorine when it is burned or processed), PCB’s, PVC’s, and some plasticizers are just a few of the many chemicals that act like estrogen in our bodies. Many others have the effect of interrupting our normal endocrine function, hence the term “endocrine disruptors.”
Mainstream medicine is finally paying attention because xenoestrogens not only affect the cells of women, but those of men and children. Sperm counts have dropped by 50% in some studies, a significant factor in the epidemic of infertility. The age at which girls develop secondary sex characteristics (breasts and pubic hair) is also dropping. It is not exactly clear what role endocrine disruptors as a whole have in the steady rise of chronic diseases in children (at earlier ages!), but studies are underway to evaluate this.
It is easy to see why Dr. Lee’s advice to support our bodies with extra progesterone makes some sense. Let’s examine the role progesterone plays in our bodies and how it can help in hormonal balance.
The role of progesterone
Progesterone is the building block for many other major hormones. Cortisol, DHEA, testosterone and estrogen are all made from progesterone in a process that begins with cholesterol. Take a look at the chart below of the metabolic pathway.

© 2005 Women to Women
These hormones are present in our bodies to varying degrees at all times, but only progesterone is readily converted into its sister hormones if needed. Importantly, if we are under a lot of stress and our adrenals are pumping out cortisol, our bodies will take any available progesterone and divert it to meet that demand. If too much progesterone gets diverted for cortisol, as happens when you suffer from adrenal fatigue, there is not enough to make the testosterone needed for a woman’s sexual response — let alone to oppose rising levels of estrogen. No wonder we feel sick, lethargic, and uninterested in sex when we’re under stress!
Insufficient progesterone is hard on our health in other ways because, in addition to reproductive function, all women need normal levels of progesterone to spur new bone growth (and ward off osteoporosis), convert fat into energy, metabolize glucose, and perform many other vital cell functions.
But it’s equally obvious that just adding progesterone isn’t the answer. If stress is creating your hormonal imbalance, adding progesterone will just treat the symptom, not the cause. Hormonal balance is never a matter of taking a magic pill. Let’s talk about how to find a solution that works for you.
Your unique path to hormonal balance

In looking at the illustration of the metabolic pathways of progesterone, it’s helpful to think of your endocrine system as a kind of orchestra, and hormonal balance as its music. Each of us has a unique body and biography, so each of us has a unique orchestra and a unique symphony. We all make different demands on our bodies; we all need different kinds of support. Adding any one element to the exclusion of others may make you feel worse, not better. For instance, many women convert progesterone immediately into estrogen; for them, a progesterone supplement will only worsen their imbalance.
There are many women whose bodies, either naturally or due to external factors, produce an abundance of estrogen. I call these patients highly estrogenic, and they are more susceptible to experiencing severe symptoms. They also feel the most dramatic improvement when they add progesterone to their routine.
While genetics have some influence, lifestyle is the single biggest factor in the production and storage of estrogen, progesterone and our other hormones. Our modern diet, filled with refined flour and sugar, simple carbohydrates and artificial ingredients, combined with our lack of exercise, promotes metabolic irregularities that lead to insulin resistance, obesity, digestive problems, and cardiovascular disease, which in turn affect the healthy flow of hormone production shown in the chart above.
Stress plays a major role in estrogen overproduction by triggering an elevated level of cortisol, which interrupts the feedback loop between the brain, pituitary, and the ovaries that regulates hormones. I’m sure most of you have had the experience of skipping a period or two when you are under stress. At the practice we have learned that most women don’t understand that unhappiness is a form of stress. To make the point, I sometimes actually write a patient a prescription that says “Play!”
Limiting our exposure to xenoestrogens is also very important. Thoroughly wash or peel all produce to remove at least some of the pesticides. Eating only lean, organic meat and dairy products is wise. Heat food in metal or porcelain containers, not plastic, and definitely not in the microwave with plastic wrap! Drinking out of glass containers instead of plastic, previously used water bottles, or Styrofoam cups is also a good choice.
A diet rich in phytoestrogens is thought to be protective. Phytoestrogens are plant-based substances found in soybeans, licorice, yams, and alfalfa that naturally mimic estrogen in a healthy way when consumed. This action supposedly protects the cell receptors from accepting the more damaging xenoestrogens.
In addition to making healthy choices in our diet, I recommend taking a high-quality daily nutritional supplement as a very important step towards restoring hormonal balance naturally.
How and when to use natural progesterone supplementation
Additional progesterone can be a shot in the arm for many women with moderate to severe symptoms — especially at the beginning of pre-menopause — and particularly when used as part of a comprehensive plan. We’ve seen women respond extremely well to small amounts of progesterone in over-the-counter formulations for just weeks or months; others need therapeutic doses over longer time periods.
If you are experiencing moderate to severe, persistent symptoms of hormonal imbalance, or weaning yourself off HRT, you probably would benefit from additional progesterone. As long as you’re receiving regular medical check-ups to rule out any serious problem, it’s relatively safe to experiment with non-prescription strength bioidentical progesterone. However, if you don’t respond well to that, I always recommend having your health practitioner do a hormone panel. A simple saliva test, and possibly a blood test, will show whether or not you have a serious progesterone deficiency that warrants a prescription-strength version.

Conventional doctors will often prescribe synthetic progesterone, or progestins, to women who experience major discomfort. In my experience, progestins help with heavy bleeding but only in the short term, and they may make PMS and depression worse. Longer exposure can cause even more problems.
Progestins are large synthetic molecules that do not bind with the progesterone receptors in a cell. In other words, they are not bioidentical — their shape does not quite fit the cell receptor — so the cell has a diminished capacity to accept it. However, your body does register the presence of these synthetic progestin molecules in your bloodstream and consequently downgrades its own progesterone-release mechanism. So by using synthetic progesterone you diminish your body’s own ability to generate the natural form!
The most effective method for delivering progesterone support to our bodies is by way of a bioidentical formulation. We’ve had superior results with a transdermal cream containing micronized progesterone USP. (“USP” means the progesterone meets the standards set by the US Pharmacopeia, which works closely with the FDA.)
Progesterone USP is real progesterone, not a phytoestrogen. The wild Mexican yam contains a phytoestrogen that is closely related to human progesterone, but requires a simple molecular manipulation to become identical. That is why yam creams alone are not effective; their phytoestrogens must be transformed into progesterone USP to be truly therapeutic. If you’ve tried some over-the-counter progesterone products and been disappointed, you may still benefit from the right kind of progesterone support in the right dosage for you. If your symptoms are moderate to severe, like most women’s, you also need to combine progesterone use with other forms of support.
I recommend to my patients that they apply 30–40 mg of high-quality, micronized progesterone USP cream to the inner part of the wrists for two weeks, starting at the mid-point of their monthly cycle. Since everyone is different, some women need more while some need less to restore their equilibrium. We find our progesterone cream is so safe that we can experiment with dosages to see what works best in our patients.
In all but the most severe cases I prefer using progesterone in a skin cream form because transdermal delivery is more natural than oral delivery in pill form. The hormone is absorbed through the skin directly into the bloodstream, which allows us to achieve the desired results with lower dosages than those required to survive the digestive tract. We’ve found the progesterone cream in our Personal Program to be the most efficient, most recognizable, most natural way to give your body what it needs. You don’t have to use ours, but you should look for a progesterone cream with the following attributes:
Contains pharmaceutical-grade progesterone USP Micronized Bioidentical All natural Hypoallergenic
When patients with severe PMS, heavy bleeding or other severe symptoms don’t respond to progesterone cream, I often switch them to a pill form because it’s easier to deliver the necessary higher dosage orally, and because oral dosage delivery is standardized.
Like Dr. Lee, we think progesterone supplementation can be an important step towards rejuvenating hormonal balance, but we don’t recommend using progesterone cream for the rest of your life. And we strongly advise that you have your hormone levels monitored on a regular basis. Our belief is that the smallest intervention that restores hormonal balance is best. In most cases we recommend you use progesterone as a bridge, and curtail its use or drop it entirely when doing so won’t result in a return of your pre-menopause symptoms.

A special note about progesterone use after menopause: although there is no evidence that it’s unsafe, it clearly is not natural to add progesterone to your body indefinitely after menopause, and we feel adequate long-term study is needed before making this assumption. We tell our post-menopausal patients they may safely use additional progesterone for up to a year. These women often benefit immediately from the extra progesterone, but it’s wisest to use it as a bridge to a new, more natural balance in their bodies.
Remember, progesterone can’t do it alone!
I hope it’s helpful for you to read up on how our bodies really seek hormonal balance, and what each of us can do to find a solution that works for us. Viewing our symptoms as simply a sign of estrogen dominance is as misleading as attributing them to estrogen deficiency alone. And a combination approach works better than any kind of magic pill. Improving our nutrition, adding a robust nutritional supplement, reducing stress, and minimizing xenoestrogens are measures that are just as important as adding progesterone. Together they will help support the demands on your body and restore the vitality and good health that come from natural hormonal balance.

OSTEOPOROSIS
Your bone is living tissue like your liver or kidneys. Bone is constantly renewing itself; old bone is taken away and replaced with new bone.
Bone loss can start right after menopause. In fact, women can lose up to 20% of their bone mass in the first 5 to 7 years after menopause. Over time, bone loss can lead to osteoporosis. Based on the 2004 Report of the Surgeon General on Bone Health and Osteoporosis, nearly three times as many women have osteoporosis than report having the disease.
With osteoporosis, cells that break down bone work faster than cells that regenerate bone. While you may not feel it happening, osteoporosis can make bones weak, brittle and vulnerable to fracture.
Risk factors and causes of osteoporosis
A small percentage of women will get true osteoporosis. Osteoporosis occurs earlier and more severely in white women of Northern European descent who are small-boned and thin. And despite the claims made by the calcium supplement makers, the highest rate of osteoporosis is seen in cultures that eat the most dairy.
Other risk factors for osteoporosis include:
post-menopause, either natural or surgical maternal history of osteoporosis delayed puberty, persistent amenorrhea, low hormone levels or other endocrine
disorders poor diet, including vitamin D, calcium, and/or magnesium deficiency gastrointestinal disorders that interfere with natural mineral absorption eating disorders advanced age heavy alcohol consumption smoking under or over-exercising less than 15% body fat elevated blood acid levels use of corticosteroids or other medical drugs thyroid or kidney disorders bone cancers or other malignancies

Drugs for osteopenia and osteoporosis
Research on HRT in the 1970’s showed that estrogen therapy (and later the combined estrogen plus progesterone therapy) helped inhibit bone loss for about seven years after menopause.
This news meant that prescriptions for HRT were written increasingly for the prevention of diseases like osteoporosis — not for relief — and as a result, women were put on hormone therapy whether or not they were experiencing symptoms of menopause. And the truth is that HRT does help bone density — at least in some women.
No wonder HRT was the most frequently prescribed drug in this country by 2001! A year later, when the WHI released its data on the real risks of HRT, this became a dubious practice.
Another fact women weren’t told is that once hormone therapy is discontinued, bone loss accelerates to reach its age-appropriate rate — the nominal gains are “wiped out.” Most HRT studies are rarely carried out for longer than a few years, at which point bone loss may have stabilized itself anyway. And there’s no indication that HRT therapy has any long-term effect on fracture risk in women over 75 — when most fractures occur. And there are no studies of the long-term effects on bone health of HRT therapy.
Fosamax charged into the osteoporosis market as HRT receded. Fosamax works by inhibiting bone resorption. Unfortunately that’s not as good as it may sound. Remember that bone function is a two-way street: if resorption is delayed, then so is formation — so no bone is lost, but no new bone is made.
Evista (raloxifene) is a selective estrogen receptor modulator similar to tamoxifen. It is increasingly prescribed to women with or at risk for osteoporosis. Developers claim it reduces fractures without the risks of HRT. Side effects include increased hot flashes, leg cramps, flu-like symptoms, blood clots and peripheral edema. These symptoms of inflammation are obviously not good for you. Studies are currently underway looking at this drug’s potential to prevent breast cancer.
Osteoporosis prevention and hormones
Before menopause, it’s important to promote your body’s natural hormonal balance so bone growth stays consistent. After menopause, your body has many natural mechanisms to boost estrogen levels and maintain bone health.
One is to store a little extra weight (that’s one of the reasons that recent weight gain is so stubborn). Estrogen is made and stored in fat cells, so keeping a few more around is actually good for your bones. This is one case where thin is not better!
Testosterone, a potent steroid hormone, increases muscle mass, which in turn helps build bone density. After menopause, testosterone can be one of the substances your body converts into estrogen. (Click here for a diagram of how hormones are made in your body.) When you exercise, your body releases testosterone — just one of the reasons physical activity is a natural antidote to bone loss.
But what about women who don’t make enough hormones naturally?

Osteoporosis, irregular periods, and hysterectomy
Much of the information on estrogen and bone loss comes from women who’ve undergone a full hysterectomy and received HRT therapy in their 20’s and early 30’s — the stage at which they are supposed to be maximizing bone density.
Teenagers and young women who’ve experienced hormonal deficiencies characterized by frequent amenhorrhea due to malnutrition, eating disorders, over-exercising, or other factors are at a greater risk for osteoporosis for the same reason.
These women just haven’t had the steady supply of sex hormones to store up a good base of bone to age with. If any of these factors sound familiar, talk to your practitioner about your risk of osteoporosis and the usefulness of a pursuing a course of bioidentical hormone therapy that includes the proper balance of estrogen, progesterone, and testosterone.
And keep in mind that a risk is just that — a risk — not your destiny. Instead of worrying so much about bone loss, most women would benefit by focusing more on natural steps to improving bone health.
Calcium and bone health
Healthy bones store about 99% of the body’s calcium; the rest is used throughout the body for other vital functions. Bones also house about 85% of the body’s phosphorous and 50% of the body’s total sodium and magnesium.
Calcium is one of the most important minerals in the body, not only for bone health but for other physiological functions, including nerve transmission, blood clotting, muscle growth and contraction, heart function, hormone function, and metabolism.
But calcium makes you work for it. It requires a lot of digestive teamwork, including the presence of stomach acid, a whole alphabet of vitamins, magnesium, other essential minerals, and a well-functioning GI tract to deliver calcium’s many benefits. If you have deficiencies anywhere along the line, it won’t matter how much calcium you eat, your body will take it (and whatever other minerals it needs) from your bones. This usually shows up first in non-vital areas like your teeth, hair, and nails.
To test how easily your calcium supplement breaks down in a healthy stomach, put it in a glass of vinegar and stir occasionally. It should dissolve completely in twelve hours.
Bones release calcium by upping the rate of resorption. Whatever doesn’t get used gets excreted through the kidneys — this is why doctors test your urine for calcium as one marker of bone loss. In Chinese medicine the bones are said to be ruled by the kidneys, so interlocked are their functions.
But increasing calcium is not the answer: too much is as problematic as too little, causing other difficulties, like kidney stones, gallstones and hypercalcemia. Our American diets have plenty of available calcium and we still have osteoporosis — what many of us lack is the ability to successfully use the calcium we get.
If you have GI issues, including IBS or celiac disease, you can’t absorb the calcium you need from your food. Older women often lack the digestive acids necessary to break down calcium. Ironically, women are told that antacids like TUMS are good calcium supplements — but antacids oppose the very stomach acid (hydrochloric acid) needed for calcium absorption. Protonics, like Nexium, have the same problem.

Nutrition and calcium absorption
Vitamin D is crucial to moving calcium from the small intestine into the bloodstream, in conjunction with stomach acids and other vitamins. In one study up to 30–40% of older patients with hip fractures had a vitamin D deficiency or insufficiency. Maybe the real health risk for bone fractures is vitamin D deficiency, not low bone density! (For more information on the importance of vitamin D, see our article.)
Magnesium increases calcium absorption from the blood into the bone. Dairy products contain little magnesium and alcohol depletes it. Ironically, too much calcium blocks the absorption of magnesium, leading to a deficiency characterized by hair loss, muscle cramps, irritability, trembling, and disorientation.
A good balance between calcium and phosphorous (about 5:1) is crucial to bone strength, but too much phosphorous depletes calcium. Soda and red meat — two staples of the American diet — are full of this mineral, so much so that now some sodas have extra calcium to counteract the deleterious effect of drinking so much phosphorous.
Trace minerals like boron, selenium, copper, silicon, manganese, and zinc are also important in supporting the healthy balance that makes bone. For an in-depth explanation of all this and more, I encourage you to read Annemarie Colbin’s wonderful book, Food and Our Bone s .
Good calcium digestion is dependent on a lot of other factors too, but I’ll cover only two other substances here because of their prescription use in osteoporosis treatment: calcitonin and parathyroid hormone. The former is secreted by the thyroid gland, the latter by the parathyroid gland.
Calcitonin stabilizes high levels of calcium by inhibiting osteoclast activity (the agents in bone resorption). It’s now available as a prescription nasal spray but is most effective in women who have osteoporosis as a result of corticosteroid use. It causes nasal irritation, headache and joint pain.
Parathyroid hormone (PTH) is normally triggered by high levels of phosphorous in the blood with corresponding low levels of calcium. Daily injections seem to stimulate bone formation and are being used to treat women with severe osteoporosis. High doses of the medication caused bone cancer in rats so treatment is not recommended for more than two years

BEBAS GEJALA MENOPOUSE DGN TERAPI SULIH HORMON
Terapi sulih hormon efektif untuk meringankan gejala menopause dan mencegah osteoporosis, plus menjaga kestabilan berat badan.
Setiap wanita pasti akan mengalami menopause, yaitu masa di mana jumlah estrogen yang dihasilkan ovarium sedikit dan wanita tidak dapat hamil lagi. Masa menopause wanita secara umum terbagi dalam tiga bagian, yaitu pre menopause yang dimulai pada usia 48 tahun ; perimenopause yang dimulai pada usia 50 tahun dan post menopause yang dimulai pada usia 52 tahun.
Masing-masing wanita mengalami gejala menopause yang berbeda-beda. Beberapa keluhan yang dialami wanita menopause antara lain haid tak teratur, sukar tidur, jantung berdebar, pusing, kulit keriput, libido menurun, gangguan berkemih, dan gejolak panas.
Dalam kurun waktu terakhir, topik tentang menopause menjadi salah satu hal penting dalam hal kedokteran. Ini karena meningkatnya tingkat usia harapan hidup wanita di dunia, termasuk di Indonesia. Meski usia wanita meningkat, tetapi usia saat memasuki masa menopause tetap, sehingga wanita akan mengalami tahun-tahun yang panjang tanpa hormon estrogen.
Padahal, berkurangnya hormon estrogen membawa bermacam resiko kesehatan dan secara serius dapat mempengaruhi kualitas hidup wanita.
Sebagaimana diketahui bahwa wanita menopause juga cenderung mengalami osteoporosis (tulang rapuh). Jumlah wanita yang meninggal akibat komplikasi retak pinggul akibat osteoporosis ternyata lebih besar dibandingkan mereka yang meninggal akibat kanker. Selain itu dibutuhkan biaya yang tinggi untuk pengobatan retak pinggul.
Hormon pengganti
Pada saat tubuh kekurangan hormon estrogen, terapi yang paling tepat agar wanita dapat beraktivitas seperti biasa adalah terapi pemberian hormon atau lebih dikenal dengan sebutan terapi sulih hormon/ Hormon Replacement Therapy (HRT). Tujuan dari terapi ini adalah agar estrogen yang semakin berkurang dapat terisi kembali.
"Hormon bukanlah obat untuk mengobati penyakit, pemberian hormon ini untuk mencegah gejala-gejala menopause yang dialami wanita," kata Prof. Marco Gambacciani, ahli obstetrick dan ginekolog dari Universitas Pisa, Italia, saat memberikan presentasi di hadapan wartawan beberapa waktu lalu di Jakarta.
Selama ini beredar mitos yang salah tentang HRT. Dalam penelitian yang dilakukan Prof. Gambacianni, terbukti bahwa persepsi terapi hormon akan meningkatkan berat badan tidak terbukti. Selain itu, wanita-wanita yang menggunakan terapi estrogen dalam jangka waktu lama, resiko terkena kanker payudara lebih kecil.
Ada beberapa macam jenis HRT, yaitu dengan estrogen saja, serta dengan kombinasi estrogen dan progesteron. "HRT kombinasi estrogen dan progesteron merupakan pilihan yang efektif
untuk mengatasi gejala menopause," ujar Prof. Gambacciani lagi.
Pada tahun 1993 National Education Cholesterol Program di AS mengakui pentingnya peranan terapi estrogen di dalam memperbaiki profil lipid (kolesterol) dan memperkecil risiko penyakit
jantung. Mereka merekomendasikan terapi estrogen bagi wanita yang telah mengalami menopause yang level kolesterolnya tidak dapat dinormalkan sepenuhnya dengan diet dan
olahraga.

Kini hadir HRT terbaru dengan estrogen Estradiol Hemyhidrate dan Drospirenone, yaitu Angelic, produksi Schering, sebuah perusahaan farmasi yang juga memproduksi pil KB. Drospirenone merupakan salah satu jenis dari progesteron.
Estradiol Hemyhidrate memiliki beberapa keunggulan, yaitu merupakan estrogen alami yang lebih ditoleransi oleh tubuh, sehingga lebih efektif dan tidak memberatkan kerja liver. Angeliq juga terbukti efektif untuk mengatasi gelaja hot flushes (gejolak panas), menjaga kestabilan berat badan dan membantu mengontrol tekanan darah.
Beberapa suplemen estrogen yang dijual bebas di pasaran ternyata mengandung black cohosh, sehingga berbahaya untuk liver. Di Inggris sudah dikeluarkan larangan untuk penjualan vitoestrogen yang mengandung black cohosh.
Mengingat gejala menopause pada tiap wanita berbeda, maka dosis Angeliq yang diberikan juga disesuaikan dengan usia dan riwayat medis tiap wanita. Karenanya, harus dikonsultasikan dulu dengan dokter sebelum mengkonsumsi Angeliq. Dengan mengeluarkan dana sebesar Rp 230 ribu, Anda bisa mendapatkan Angeliq berisi 28 butir.
Selain melakukan terapi sulih hormon, wanita yang sudah menopause juga disarankan untuk tetap aktif berolahraga, karena selain menyehatkan juga dapat memperbaiki suasana hati
What is Calcium?
Calcium is the most abundant mineral in the body, essential to life itself, with 99 percent of calcium found in bones and teeth. Calcium is vital for bone health, but in addition to building strong bones, calcium is essential for normal heart beat, muscle contraction and relaxation, transmission of nerve impulses, stimulation of hormone secretion, activation of enzyme reactions, and for coagulation of the blood. Uses:
Develop strong bones and teeth Prevent osteoporosis and broken bones Reduce your blood pressure Keep your heart regular Reduce cramps and moodiness from premenstrual syndrome Reduce irritability, insomnia, depression, and headaches during
menopause Reduce risks of pregnancy, such as high blood pressure and
preeclampsia Prevent gum disease Prevent cancer of the colon and rectum Prevent kidney stones May be associated with a decrease in body fat
Blood to clot
Where do we get Calcium?
While many foods contain calcium, dairy products are the most significant source. Milk, yogurt, cheese and buttermilk contain about 300mg of calcium per serving.

Some green, leafy vegetables — including broccoli, collard greens, kale, mustard greens, turnip greens and bok choy or Chinese cabbage — are good sources of calcium. Canned salmon and sardines,shellfish, almonds, Brazil nuts and dried beans are also good dietary sources of calcium. A number of other food products, such as breads, cereals and orange juice, are now enriched with calcium, making them a significant source of calcium for people who are lactose intolerant or whose dietary intake of calcium is otherwise inadequate. There is no apparent difference between eating calcium-fortified foods and eating foods that are naturally rich in calcium. However, calcium-fortified cereals may also contain phytate, which can interfere with calcium absorption. In addition, high-fiber diets – although healthy – contribute to low calcium levels because the presence of a lot of fiber in the intestines reduces the absorption of many nutrients, including calcium. The fiber “rushes” the food through the intestines so fast that maximum absorption of nutrients may not occur.