inadekuat pemeriksaan fisik
6
7/23/2019 inadekuat pemeriksaan fisik http://slidepdf.com/reader/full/inadekuat-pemeriksaan-fisik 1/6 Inadequacies of Physical Examination as a Cause of Medical Errors and Adverse Events: A Collection of Vignettes Abraham Verghese, MD, a Blake Charlton, MD, b Jerome P. Kassirer, MD, c Meghan Ramsey, MD, a John P.A. Ioannidis, MD, DSc d a The Program in Bedside Medicine and d Stanford Prevention Research Center, Stanford University School of Medicine, Stanford, Calif; b Department of Internal Medicine,University of California, San Francisco; c Department of Internal Medicine, Tufts University School of Medicine, Boston, Mass. ABSTRACT BACKGROUND: Oversights in the physical examination are a type of medical error not easily studied by chart review.Theymaybe amajorcontributortomissedordelayed diagnosis,unnecessaryexposuretocontrastand radiation, incorrect treatment, and other adverse consequences. Our purpose was to collect vignettes of physical examination oversights and to capture the diversity of their characteristics and consequences. METHODS: A cross-sectional study using an 11-question qualitative survey for physicians was distributed electron- ically, with data collected from February to June of 2011. The participants were all physicians responding to e-mail or social media invitations to complete the survey. There were no limitations on geography, specialty, or practice setting. RESULTS: Of the 208 reported vignettes that met inclusion criteria, the oversight was caused by a failure to perform the physical examination in 63%; 14% reported that the correct physical examination sign was elicited but misinterpreted, whereas 11% reported that the relevant sign was missed or not sought. Consequence of the physical examination inadequacy included missed or delayed diagnosis in 76% of cases, incorrect diagnosis in 27%, unnecessary treatment in 18%, no or delayed treatment in 42%, unnecessary diagnostic cost in 25%, unnecessary exposure to radiation or contrast in 17%, and compli- cations caused by treatments in 4%. The mode of the number of physicians missing the nding was 2, but many oversights were missed by many physicians. Most oversights took up to 5 days to identify, but 66 took longer. Special attention and skill in examining the skin and its appendages, as well as the abdomen, groin, and genitourinary area could reduce the reported oversights by half. CONCLUSIONS: Physical examination inadequacies are a preventable source of medical error, and adverse events are caused mostly by failure to perform the relevant examination. 2015 Elsevier Inc. All rights reserved. The American Journal of Medicine (2015) 128, 1322-1324 KEYWORDS: Attending rounds; Bedside; Bedside teaching; Diagnostic error; Electronic medical record; EMR; Error; Medical error; Medical mistakes; Mistakes; Oversights; Patient examination; Physical diagnosis; Physical examination; Resident; Teaching SEE RELATED ARTICLE p. 1263 According to theInstitute of Medicine’s reportentitled “ToErr is Human,” 1 medical errors cause nearly 100,000 deaths per year. The causes are systemic problems of inadequate organi- zation, a culture of nondisclosure, and cognitive diagnostic errors. 2-4 A potentially important type of error that has been givenmeagerattentionisde cienciesin physicalexamination. The high-tech transformation of medical care has resulted in diminishing direct patient-physician interaction. Hospi- talists in America might spend only 18% of their on-duty time in direct patient care, 5 and duty-hour restrictions have Funding: None. Conict of Interest: None. Authorship: All authors had access to the data and a role in writing the manuscript. Requests for reprints should be addressed to Abraham Verghese, MD, Stanford University, Department of Medicine, 300 Pasteur Drive, S102, Stanford, CA 94305-5110. E-mail address: [email protected] 0002-9343/$ -see front matter 2015 Elsevier Inc. All rights reserved. http://dx.doi.org/10.1016/j.amjmed.2015.06.004 CLINICAL RESEARCH STUDY
-
Upload
rahmawati-aliwarman -
Category
Documents
-
view
213 -
download
0
Transcript of inadekuat pemeriksaan fisik

7232019 inadekuat pemeriksaan fisik
httpslidepdfcomreaderfullinadekuat-pemeriksaan-fisik 16
Inadequacies of Physical Examination as a Cause
of Medical Errors and Adverse Events A Collectionof VignettesAbraham Verghese MDa Blake Charlton MDb Jerome P Kassirer MDc Meghan Ramsey MDa
John PA Ioannidis MD DScd
aThe Program in Bedside Medicine and d Stanford Prevention Research Center Stanford University School of Medicine Stanford Calif b Department
of Internal Medicine University of California San Francisco c Department of Internal Medicine Tufts University School of Medicine Boston Mass
ABSTRACT
BACKGROUND Oversights in the physical examination are a type of medical error not easily studied by chart review They maybe a major contributor to missed or delayed diagnosis unnecessary exposure to contrast and
radiation incorrect treatment and other adverse consequences Our purpose was to collect vignettes of
physical examination oversights and to capture the diversity of their characteristics and consequences
METHODS A cross-sectional study using an 11-question qualitative survey for physicians was distributed electron-
ically with data collectedfrom February to June of 2011 Theparticipants were allphysicians responding to e-mail or
socialmedia invitations to complete the survey There were no limitations on geography specialty or practice setting
RESULTS Of the 208 reported vignettes that met inclusion criteria the oversight was caused by a failure to
perform the physical examination in 63 14 reported that the correct physical examination sign was
elicited but misinterpreted whereas 11 reported that the relevant sign was missed or not sought
Consequence of the physical examination inadequacy included missed or delayed diagnosis in 76
of cases incorrect diagnosis in 27 unnecessary treatment in 18 no or delayed treatment in 42
unnecessary diagnostic cost in 25 unnecessary exposure to radiation or contrast in 17 and compli-
cations caused by treatments in 4 The mode of the number of physicians missing the 1047297
nding was 2 but many oversights were missed by many physicians Most oversights took up to 5 days to identify but 66
took longer Special attention and skill in examining the skin and its appendages as well as the abdomen
groin and genitourinary area could reduce the reported oversights by half
CONCLUSIONS Physical examination inadequacies are a preventable source of medical error and adverse
events are caused mostly by failure to perform the relevant examination
2015 Elsevier Inc All rights reserved The American Journal of Medicine (2015) 128 1322-1324
KEYWORDS Attending rounds Bedside Bedside teaching Diagnostic error Electronic medical record EMR Error
Medical error Medical mistakes Mistakes Oversights Patient examination Physical diagnosis
Physical examination Resident Teaching
SEE RELATED ARTICLE p 1263
According t o the Institute of Medicinersquos report entitled ldquoTo Err is Humanrdquo1 medical errors cause nearly 100000 deaths per
year The causes are systemic problems of inadequate organi-
zation a culture of nondisclosure and cognitive diagnostic
errors2-4 A potentially important type of error that has been
given meager attention is de1047297ciencies in physical examination
The high-tech transformation of medical care has resulted
in diminishing direct patient-physician interaction Hospi-
talists in America might spend only 18 of their on-duty
time in direct patient care5 and duty-hour restrictions have
Funding None
Con1047298ict of Interest None
Authorship All authors had access to the data and a role in writing the
manuscript
Requests for reprints should be addressed to Abraham Verghese MD
Stanford University Department of Medicine 300 Pasteur Drive S102
Stanford CA 94305-5110
E-mail address abrahamvstanfordedu
0002-9343$ -see front matter 2015 Elsevier Inc All rights reservedhttpdxdoiorg101016jamjmed201506004
CLINICAL RESEARCH STUDY
7232019 inadekuat pemeriksaan fisik
httpslidepdfcomreaderfullinadekuat-pemeriksaan-fisik 26
resulted in Internal Medicine interns spending on average
only 12 of their time wit h patients but 40 of their time
on computer-related tasks6
Diminished focus on the physical examination may result in
important errors We asked physicians to contribute clinical
vignettes of oversights and errors in physical examination and
adverse consequences that resulted
from them This database wascreated to identify the diverse types
and characteristics of errors that can
be made relating to the physical
examination
METHODSWe designed an 11-question qual-
itative survey for physicians who
were asked to send us vignettes of
known instances of oversights in
physical examination and to answer related multiple choice questions
The study was approved by the
Stanford University Institutional
Review Board the detailed instructions to the respondent and
the questionnaire can be found online at wwwsurveymonkey
coms8S6DL7V
A link to the questionnaire was sent to approximately 5000
physicians of diverse specialties using a commercial medical e-
mail marketing service (MMS Inc Woodale Ill) with an esti-
mated 2800 of these having teaching af 1047297liations In addition we
used social media sites to disseminate the link and we
encouraged physicians to share the link There were no limita-tions regarding type of specialty and clinical practice setting
Data were gathered from February to June of 2011 Each
entry was reviewed by 2 physicians We excluded entries that
did not form a vignette (eg ldquoresidents donrsquot do rectal exams
often enoughrdquo) entries missing critical information to form a
vignette (eg a failure to state what precisely was omitted
misinterpreted) entries with 2 or more vignettes combined
when it became impossible to parse out which one was being
addressed in the multiple choice questions We corrected a
response only when the answer to a multiple choice question
clearly contradicted the vignette suggesting the respondent
selected the wrong box (eg the narrative describes a missedhernia in a patient with pain because the abdominal exami-
nation was not done but the respondent ticks ldquo1047297nding elicited
but misinterpretedrdquo in lieu of ldquofailure to do relevant exam rdquo)
RESULTSOf the 263 responses received 55 were excluded of the 208
remaining responses 27 were corrected by the criteria
described in Methods
Sixty-three percent of vignettes reported that the over-
sight was caused by a failure to perform the physical
examination 14 reported that the correct physical exam-ination sign was elicited but misinterpreted Eleven percent
reported that the relevant sign was missed or not sought and
12 reported ldquoother rdquo as the cause of the de1047297ciency
Consequence of the physical examination inadequacy
included missed or delayed diagnosis in 76 of cases
incorrect diagnosis in 27 unnecessary treatment in 18 no
or delayed treatment in 42 unnecessary diagnostic cost in
25 unnecessary exposure to
radiation or contrast in 17 andcomplications caused by treat-
ments in 4
The person thought responsible
for the oversight was most often
an intern or resident (reported
in 95 of 208 cases or 46) a
primary care physician (84 40)
a specialist (79 40) or fellow
(18 9) Though there was no
multiple choice option available to
implicate onersquos self as the person
responsible 9 responders (4)indicated themselves as the
physician responsible
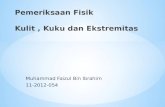
The number of physicians
thought to have missed an important aspect of the examina-
tion is shown in Figure 1 The oversight was typically
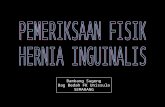
discovered within 5 days (Figure 2) When participants
were asked to estimate what percentage of practicing
physicians have made a similar error to the one described
they estimated it to be gt95 in 43 instances (20)
50-95 in 42 instances (20) and 5-50 in 78 oversights
(375) and less than 5 in 28 instances (28)
The list of 1047297ndings overlooked is long and diverse but those that were missed more than 5 times included abdominal
massorganomegaly (n frac14 21 including 3 pregnancies and
2 distended bladders) diagnostic skin 1047297nding (nfrac1415 such as
cafeacute au lait spots neur 1047297broma erythema migrans syphilitic
lesions and meningococcemia lesions but not including
herpes zoster) neurologic 1047297ndings (n frac14 18) murmursrubs
(n frac14 13 including 4 missed aortic stenosis 3 missed
pericardial rubs) lymphadenopathy (n frac14 10) groin hernia
(n frac14 10) or scrotaltesticular pathology (n frac14 6) signs of
peritonitis (n frac14 10) breast masses (n frac14 9) fracture or
orthopedic 1047297nding (n frac14 9) congestive heart failure (n frac14 8)
Figure 1 Distribution of number of overlookers for 208
oversights in physical exam
CLINICAL SIGNIFICANCE
Most errors in the physical examinationthat lead to consequences are related tonot performing an examination
Failure to undress the patient andexamine the skin is a frequent cause of error
In a patient with abdominal painfailure to examine the groin rectal area
and hernia ori1047297ces can have direconsequences
Verghese et al Oversights in the Physical Examination 1323
7232019 inadekuat pemeriksaan fisik
httpslidepdfcomreaderfullinadekuat-pemeriksaan-fisik 36
absent or abnormal pulses (n frac14 6) wound or ulcer (n frac14 6)
bruising (n frac14 6) and herpes zoster (n frac14 5)
Forty-seven oversights involved the skin and its append-
ages including the breast 37 were related to the abdominal
examination 37 involved the cardiovascular system and 36
involved the groingenitalrectal area Supplementary
Table 1 (available online) lists all items that were missed
DISCUSSIONRecent publications describe the decline of physical exam-
ination skills7-12 Our study highlights the consequences and
suggests that many adverse events are preventable Our
survey suggests that the major cause for error is simply that
the examination is not performed1213 In addition to diag-
nostic consequences approximately half of the vignettes
report treatment consequences Most oversights pertained to
a limited number of overlookers suggesting that some er-rors may be remedied if several people examine the patient
Although the majority of the errors were corrected within 5
days even a delay of 1 hour might affect patient outcomes
Examining a patient presenting with a complaint (as
opposed to the ldquoroutine physicalrdquo) is a low-cost procedure
that when done with skill can avoid the majority of over-
sights listed Many diseases involving the skin or the
nervous system cannot easily be diagnosed except by the
examination and for others the appropriate diagnostic test is
indicated by the examination The drop-down boxes of the
electronic medical record deceptively suggest every patient
has been thoroughly examined (and therefore can be billed)but it will be the responsibility of educators and professional
organizations to make sure the electronic medical record
truthfully re1047298ects what was done
A short checklist is suggested by our study physicians
should seek full exposure of the patient there must be a
mandate to examine hernial ori1047297ces and the genital
and rectal areas in acutely ill patients or with pain Pain
should prompt a search for the lesions of shingles Non-
neurologists need a sound neurologic skill set because im-
aging does not show the functional de1047297cits resulting from a
lesion seen For diseases like Wernickersquos encephalopathy or
Bellrsquos palsy imaging may not be diagnostic Finally there
should be a greater emphasis on actually performing the
examination In short physicians in training must be taught
and evaluated at the bedside to diminish this kind of error
Our survey was not designed to determine prevalence but
to generate an anthology of physical examination oversights
along with their characteristics The vignettes are subject to
recall and response biases We set no time limitation on re-
ports and did not ask responders to specify where they prac-
ticed medicine Finally even though we contacted thousandsof physicians only a small minority contributed vignettes
suggesting a cultural reluctance to admit and share errors
unlike for example in the aviation industry We as physicians
might work in an ldquoignorance traprdquo in which our physical ex-
amination oversights are rarely reported back to us
Diligence in actually teaching and performing the phys-
ical examination and continuing efforts to improve bedside
skills would diminish one kind of medical error and its
consequences for the patient
ACKNOWLEDGMENT The authors thank Ralph Horwitz MD for his encouragement of the First Stanford Symposium on Bedside Medicine in
2009 and for his helpful discussions in planning this study
References1 Kohn KT Corrigan JM Donaldson MS To Err Is Human Building a
Safer Health System Washington DC National Academy Press 1999
2 Kassirer JP Kopelman RI Cognitive errors in diagnosis instantiation
classi1047297cation and consequences Am J Med 198986(4)433-441
3 Graber ML Franklin N Gordon R Diagnostic error in internal
medicine Arch Intern Med 2005165(13)1493-1499
4 Singh H Graber ML Kissam SM et al System-related interventions
to reduce diagnostic errors a narrative review BMJ Qual Saf
201221(2)160-1705 OrsquoLeary KJ Liebovitz DM Baker DW How hospitalists spend their
time insights on ef 1047297ciency and safety J Hosp Med 20061(2)88-93
6 Block L Habicht R Wu AW et al In the wake of the 2003 and 2011
duty hour regulations how do internal medicine interns spend their
time J Gen Intern Med 201328(8)1042-1047
7 Feddock CA The lost art of clinical skills Am J Med 2007120(4)
374-378
8 Rahmani S Ring BN Lowe R et al A pilot study assessing knowledge
of clinical signs and physical examination skills in incoming medicine
residents J Grad Med Educ 20102(2)232-235
9 Willett LL Estrada CA Castiglioni A Does residency training
improve performance of physical examination skills Am J Med Sci
2007333(2)74-77
10 Sharma S A single-blinded direct observational study of PGY-1 in-terns and PGY-2 residents in evaluating their history-taking and
physical-examination skills Perm J 201115(4)23-29
11 Jauhar S The demise of the physical examination N Engl J Med
2006354(6)548-551
12 Ortiz-Neu C Walters CA Tenenbaum J Colliver JA Schmidt HJ
Error patterns of 3rd-year medical students on the cardiovascular
physical examination Teach Learn Med 200113(3)161-166
13 Bordage G Why did I miss the diagnosis Some cognitive explanations
and educational implications Acad Med 199974(10 suppl)S138-S143
SUPPLEMENTARY DATASupplementary table accompanying this article can be found
in the online version at httpdxdoiorg101016jamjmed201506004
Figure 2 Distribution of time to discovery for 208 oversights
in physical exam
1324 The American Journal of Medicine Vol 128 No 12 December 2015
7232019 inadekuat pemeriksaan fisik
httpslidepdfcomreaderfullinadekuat-pemeriksaan-fisik 46
Supplementary Table 1 Complete List of Items Missed as
Reported in Returned Questionnaires
Missed skin 1047297nding of subcutaneous emphysema
Missed pulse absence in ischemic foot
Missed pregnancy with twins before hysterectomy
Missed hip fracture labeled as right lower quadrant pain
Missed Bell rsquo s palsy
Missed liver mass abdominal mass in cholangiocarcinoma
Missed funduscopic 1047297nding of cupping
Missed strangulated groin hernia in small bowel obstruction
Missed incarcerated femoral hernia
Missed crackles in a patient with pulmonary edema
Missed 1047297nger pressure necrosis on microvascular free 1047298 ap
Missed peritoneal signs and free air on plain 1047297lm
Missed peritonitis in patient with gangrenous perforated gall
bladder
Missed adenopathy and therefore chronic lymphocytic leukemia
Missed thyromegaly in patient with tachycardia
Missed strangulated hernia
Missed fungating breast mass
Missed pelvic examination and therefore missed tubo-ovarian
abscess
Missed pregnancy by missed gynecologic examination in patient
with seizures
Missed pyoderma gangrenosum in skin
Missed Fournier rsquo s gangrene in groinmdashno genital examination
Missed clonus and hyperre1047298 exia
Missed abdominal examination 1047297nding of tenderness and Grey
Turner signs
Missed neuro1047297broma and cafeacute au lait spots
Missed large abdominal mass
Missed heart failure signs of cardiomyopathy after 1047298 u in a young
person
Missed pulse extremity examination missed Buerger rsquo sMissed testicular mass in teen
Missed massive splenomegaly
Missed second cervix
Missed abrasion on forehead clue to subdural
Missed bruising signs of abuse in child
Missed prostate mass with elevated prostate-speci1047297c antigen
Missed decreased pulses arterial occlusion in elderly man after hip
fracture
Missed strangulated femoral hernia in 88-year-old with emesis
Missed loud bruit in patient with renal failure and hypertension
Missed ruptured spleen after trauma
Missed ectopic pregnancy because no pelvic examination done
Missed obvious congestive heart failure (CHF) signs labeled asbronchitis
Missed rotatory and vertical nystagmus in patient with basilar
artery aneurysm
Missed abdominal examination old scar mislabeled as hernia scar
and patient operated on for ldquorecurrent rdquo hernia and nothing found
Missed pulses in patient with peripheral vascular disease
Missed tuberculosis signs in chest
Missed vital sign of tachypnea on 1047297rst visit in a patient later found
with bacteremic pneumonia
Missed adenopathy in lymphoma
Missed clavicle fracture labeled ldquorule out myocardial infarctionrdquoMissed the tan of hemochromatosis
Supplementary Table 1 Continued
Missed femoral fracture
Missed acute myocardial infarction by focusing on neck pain ear
pain
Missed hyperre1047298 exia and cord compression in Potts disease
Missed rectal and missed prostatic abscess
Missed supraclavicular mass in lung cancer
Missed splenomegaly and delayed diagnosis of chronic
myelogenous leukemia
Missed psoriasis and its signs
Missed groin cellulitis
Missed dislocated shoulder on examination
Missed adenopathy in germ cell tumor
Missed marked pallor in elderly anemic
Missed pulsatile abdominal aneurysm
Missed adenopathy in patient with Waldenstromrsquo s disease
Missed penetrating foreign body in vaginal 1047297stula
Missed gastric bypass scar in patient with malnutrition and
beriberi
Missed signs of CHF in a young patient
Missed femoral hernia in patient with vomiting
Missed signs of hypothyroidism and neck scar in unresponsive
patient
Missed retinal lesions in a child with poor vision
Missed signs of myocarditis and CHF especially the tachycardia in
a child
Misconstrued bruit from an aortofemoral bypass as a cardiac
murmur
Missed obvious CHF signs
Missed obvious pregnancy and labor
Missed huge spleen in cirrhosis
Missed previous appendectomy scar and made diagnosis of
appendicitis again
Missed ulnar nerve transection after traumaMissed male breast mass
Missed distended bladder
Missed incarcerated hernia
Missed breast mass and metastases
Missed zoster presenting as abdominal pain
Missed femoral hernia
Missed orchitis and diagnosed it as hernia
Missed aortic stenosis murmur preoperatively
Missed breast mass
Missed anus present in patient stated to have abdomino-perineal
resection when they had Hartman procedure
Missed prolapsing rectal cancer rectal examination not done
Missed incarcerated groin herniaMissed bruises of abuse
Missed large melanoma over scapula
Missed hoarseness puf 1047297ness and signs of hypothyroidism
Missed decubitus ulcer causing ldquoback painrdquoMissed leg ulcers and sores as a cause of fever in alcoholic
Missed skin 1047297ndings of secondary syphilis
Missed hip fracture in patient who could not walk
Missed gouty nodules
Missed breast mass
Missed mucor wound on hand in immunocompromised patient
Missed zoster in patient with chest pain
Missed foot ulcer in diabetic with fever
Verghese et al Oversights in the Physical Examination 1324e1
7232019 inadekuat pemeriksaan fisik
httpslidepdfcomreaderfullinadekuat-pemeriksaan-fisik 56
Supplementary Table 1 Continued
Missed signs of Parkinsonrsquo s in elderly being worked up for falls
Missed lymph node in a patient with breast cancer
Missed abdominal mass lymphoma in patient complaining of pain
Missed skin ash leaf macule in child with hypertension
Missed anterior cruciate ligament tear with classic signs
Missed giant ovarian cyst labeled as ascites
Missed giant ovarian cyst again thought to be ascites
Missed loud murmur of ruptured mitral valve chordae tendinae
Missed murmur and signs of subacute bacterial endocarditis
Missed cutaneous abscess in compromised patient with fever
Missed obvious CHF in 33-year-old with cardiomyopathy
Missed appendicitis signs
Missed strangulated hernia
Missed Downrsquo s syndrome on examination in 6 month old
Missed acute central vein occlusion in patient with decreased
visionmdashno fundoscopy done
Missed anal cancer said to be hemorrhoids
Missed peritonitis signs in patient with Crohn rsquo s
Missed dentures in mouth during intubation
Missed signi1047297cant murmur of mitral stenosis called it aortic
stenosis
Missed abdominal mass turned out to be lymphoma
Missed aortic stenosis in preoperative examination
Missed scrotal mass until after surgery for abdominal mass Was
testicular tumor with metastases
Missed supraclavicular nodes in patient with lung cancer
Missed hyperre1047298 exia and clonus from epidural abscess
Missed adenopathy in non-Hodgkinrsquo s lymphoma with fever of
unknown originmdashcalled a hernia
Missed neck nodes
Missed pelvic in1047298 ammatory disease because no pelvic examination
done
Missed gunshot entrance wound in emergency roomMissed large abdominal masses in patient with bloating
Missed pregnancy in patient with large belly
Missed signs of CHF in patient presenting with ldquoscrotal swellingrdquoMissed liver laceration after trauma because focus on head
Missed enlarged tonsil that was cancer
Missed clavicle fracture in patient with syncope
Missed ecchymosis in patient from a fall and the left arm pain
assumed to be cardiac
Missed contact dermatitis
Missed constrictive pericarditis signs
Missed breast mass in patient with shoulder pain
Missed breast mass in patient with deep vein thrombosis
Missed rapid growth in head circumferenceMissed splinters and signs of subacute bacterial endocarditis
Missed systolic murmur cardiac labeled carotid bruits
Missed pericardial rub and pericarditis
Missed zoster rash
Missed hip disease as a cause of joint pain
Missed femoral pathologic fracture in patient with knee pain
Missed large liver in patient with diabetic ketoacidosis
Missed zoster as cause of chest pain
Missed watch battery in umbilicus in child
Missed purulence in tonsils
Missed normal ear examination labeled as perforation by not doing
pneumatic otoscopy
Supplementary Table 1 Continued
Missed breast mass in patient with chest pain and metastasis
Missed pregnancy called it constipation
Missed meningococcemia skin lesion in patient with fever
Missed CHF 1047297ndings in patient with postpartum cardiomyopathy
Missed hoarseness and laryngeal mass in patient labeled asthma
Missed rectal mass by gastrointestinal consultant after primary
care physician feels massmdashsigmoidoscopy negative but tumor
develops
Missed appendicitis by focus on chest
Missed rales and crackles
Missed obvious pleural effusion no examination
Missed signs of myasthenia in patient with weight loss
Missed signs of bowel obstruction
Missed signs of mitral regurgitation from torn lea1047298 et
Missed hepatomegaly and hepatocellular carcinoma in patient with
vague symptoms
Missed metastatic node from breast cancer in patient with weight
loss
Missed stone in urethra causing recurrent urinary tract infection
Missed pelvic examination in adolescent and missed pelvic
in1047298 ammatory disease
Missed radiculopathy causing abdominal pain
Missed signs of peritonitis
Missed fungating breast mass
Missed abdominal mass in patient with back pain
Missed pelvic examination and missed procidentia
Missed skin signs of calcinosis in patient with mixed connective
tissue disease
Missed breast mass in patient being worked up for metastasis
Missed skin erythema migrans in patient with Bell rsquo s palsy
Missed abnormal pulses of combined aortic stenosisaortic
regurgitation and focused on treating high blood pressure and
pulse pressureMissed aortic stenosis murmur
Missed abdominal mass expanding aortic aneurysm in patient with
abdominal pain
Missed pericardial friction rub in chest pain
Missed nasal septal hematoma
Missed scrotal infection in diabetic
Missed Korsakoff rsquo s signs in many neurologic examinations
Missed zoster in patient with chest pain who had coronary
angiogram
Missed pelvic examination and missed ovarian cyst
Missed adenopathy and hepatomegaly in patient with anemia and
weight loss
Missed in1047298 ammatory knee effusion in intensive care unit patient with fever
Missed distended bladder labeled abdominal mass
Missed rectal examination and therefore missed prostatitis
Missed doing pulsus paradoxus in patient with tamponade
Missed abnormal decreased pulse and blood pressure in one arm
Missed purulence around IV catheter as cause of fever
Mistaken diagnosis of peritonitis bias from x-rays showing
pneumatosis intestinalis
Missed lytic lesions as cause of left-sided weakness in limbs
Missed CHF signs
Missed purulence at bone marrow biopsy site in patient with fever
Missed clubbing in patient with shoulder pain who has lung cancer
1324e2 The American Journal of Medicine Vol 128 No 12 December 2015
7232019 inadekuat pemeriksaan fisik
httpslidepdfcomreaderfullinadekuat-pemeriksaan-fisik 66
Supplementary Table 1 Continued
Missed hernia because of missed groin examination
Missed edema from hypoproteinemia labeled CHF
Missed peritonitis and perforation
Missed murmur of critical aortic stenosis
Missed butter 1047298 y bruises of factitious injury
Missed neurogenic bladder
Missed costochondritis in patient labeled as rule out myocardial
infarctions
Missed epididymitis in patient with abdominal pain
Missed scrotal examination
Missed erythema migrans in patient with fever and headache
Missed large abdominal mass on both pelvic and seated abdominal
examination
Missed embolic arterial occlusion
Missed uremic calciphylaxis in patient on dialysis
Verghese et al Oversights in the Physical Examination 1324e3

7232019 inadekuat pemeriksaan fisik
httpslidepdfcomreaderfullinadekuat-pemeriksaan-fisik 26
resulted in Internal Medicine interns spending on average
only 12 of their time wit h patients but 40 of their time
on computer-related tasks6
Diminished focus on the physical examination may result in
important errors We asked physicians to contribute clinical
vignettes of oversights and errors in physical examination and
adverse consequences that resulted
from them This database wascreated to identify the diverse types
and characteristics of errors that can
be made relating to the physical
examination
METHODSWe designed an 11-question qual-
itative survey for physicians who
were asked to send us vignettes of
known instances of oversights in
physical examination and to answer related multiple choice questions
The study was approved by the
Stanford University Institutional
Review Board the detailed instructions to the respondent and
the questionnaire can be found online at wwwsurveymonkey
coms8S6DL7V
A link to the questionnaire was sent to approximately 5000
physicians of diverse specialties using a commercial medical e-
mail marketing service (MMS Inc Woodale Ill) with an esti-
mated 2800 of these having teaching af 1047297liations In addition we
used social media sites to disseminate the link and we
encouraged physicians to share the link There were no limita-tions regarding type of specialty and clinical practice setting
Data were gathered from February to June of 2011 Each
entry was reviewed by 2 physicians We excluded entries that
did not form a vignette (eg ldquoresidents donrsquot do rectal exams
often enoughrdquo) entries missing critical information to form a
vignette (eg a failure to state what precisely was omitted
misinterpreted) entries with 2 or more vignettes combined
when it became impossible to parse out which one was being
addressed in the multiple choice questions We corrected a
response only when the answer to a multiple choice question
clearly contradicted the vignette suggesting the respondent
selected the wrong box (eg the narrative describes a missedhernia in a patient with pain because the abdominal exami-
nation was not done but the respondent ticks ldquo1047297nding elicited
but misinterpretedrdquo in lieu of ldquofailure to do relevant exam rdquo)
RESULTSOf the 263 responses received 55 were excluded of the 208
remaining responses 27 were corrected by the criteria
described in Methods
Sixty-three percent of vignettes reported that the over-
sight was caused by a failure to perform the physical
examination 14 reported that the correct physical exam-ination sign was elicited but misinterpreted Eleven percent
reported that the relevant sign was missed or not sought and
12 reported ldquoother rdquo as the cause of the de1047297ciency
Consequence of the physical examination inadequacy
included missed or delayed diagnosis in 76 of cases
incorrect diagnosis in 27 unnecessary treatment in 18 no
or delayed treatment in 42 unnecessary diagnostic cost in
25 unnecessary exposure to
radiation or contrast in 17 andcomplications caused by treat-
ments in 4
The person thought responsible
for the oversight was most often
an intern or resident (reported
in 95 of 208 cases or 46) a
primary care physician (84 40)
a specialist (79 40) or fellow
(18 9) Though there was no
multiple choice option available to
implicate onersquos self as the person
responsible 9 responders (4)indicated themselves as the
physician responsible
The number of physicians
thought to have missed an important aspect of the examina-
tion is shown in Figure 1 The oversight was typically
discovered within 5 days (Figure 2) When participants
were asked to estimate what percentage of practicing
physicians have made a similar error to the one described
they estimated it to be gt95 in 43 instances (20)
50-95 in 42 instances (20) and 5-50 in 78 oversights
(375) and less than 5 in 28 instances (28)
The list of 1047297ndings overlooked is long and diverse but those that were missed more than 5 times included abdominal
massorganomegaly (n frac14 21 including 3 pregnancies and
2 distended bladders) diagnostic skin 1047297nding (nfrac1415 such as
cafeacute au lait spots neur 1047297broma erythema migrans syphilitic
lesions and meningococcemia lesions but not including
herpes zoster) neurologic 1047297ndings (n frac14 18) murmursrubs
(n frac14 13 including 4 missed aortic stenosis 3 missed
pericardial rubs) lymphadenopathy (n frac14 10) groin hernia
(n frac14 10) or scrotaltesticular pathology (n frac14 6) signs of
peritonitis (n frac14 10) breast masses (n frac14 9) fracture or
orthopedic 1047297nding (n frac14 9) congestive heart failure (n frac14 8)
Figure 1 Distribution of number of overlookers for 208
oversights in physical exam
CLINICAL SIGNIFICANCE
Most errors in the physical examinationthat lead to consequences are related tonot performing an examination
Failure to undress the patient andexamine the skin is a frequent cause of error
In a patient with abdominal painfailure to examine the groin rectal area
and hernia ori1047297ces can have direconsequences
Verghese et al Oversights in the Physical Examination 1323
7232019 inadekuat pemeriksaan fisik
httpslidepdfcomreaderfullinadekuat-pemeriksaan-fisik 36
absent or abnormal pulses (n frac14 6) wound or ulcer (n frac14 6)
bruising (n frac14 6) and herpes zoster (n frac14 5)
Forty-seven oversights involved the skin and its append-
ages including the breast 37 were related to the abdominal
examination 37 involved the cardiovascular system and 36
involved the groingenitalrectal area Supplementary
Table 1 (available online) lists all items that were missed
DISCUSSIONRecent publications describe the decline of physical exam-
ination skills7-12 Our study highlights the consequences and
suggests that many adverse events are preventable Our
survey suggests that the major cause for error is simply that
the examination is not performed1213 In addition to diag-
nostic consequences approximately half of the vignettes
report treatment consequences Most oversights pertained to
a limited number of overlookers suggesting that some er-rors may be remedied if several people examine the patient
Although the majority of the errors were corrected within 5
days even a delay of 1 hour might affect patient outcomes
Examining a patient presenting with a complaint (as
opposed to the ldquoroutine physicalrdquo) is a low-cost procedure
that when done with skill can avoid the majority of over-
sights listed Many diseases involving the skin or the
nervous system cannot easily be diagnosed except by the
examination and for others the appropriate diagnostic test is
indicated by the examination The drop-down boxes of the
electronic medical record deceptively suggest every patient
has been thoroughly examined (and therefore can be billed)but it will be the responsibility of educators and professional
organizations to make sure the electronic medical record
truthfully re1047298ects what was done
A short checklist is suggested by our study physicians
should seek full exposure of the patient there must be a
mandate to examine hernial ori1047297ces and the genital
and rectal areas in acutely ill patients or with pain Pain
should prompt a search for the lesions of shingles Non-
neurologists need a sound neurologic skill set because im-
aging does not show the functional de1047297cits resulting from a
lesion seen For diseases like Wernickersquos encephalopathy or
Bellrsquos palsy imaging may not be diagnostic Finally there
should be a greater emphasis on actually performing the
examination In short physicians in training must be taught
and evaluated at the bedside to diminish this kind of error
Our survey was not designed to determine prevalence but
to generate an anthology of physical examination oversights
along with their characteristics The vignettes are subject to
recall and response biases We set no time limitation on re-
ports and did not ask responders to specify where they prac-
ticed medicine Finally even though we contacted thousandsof physicians only a small minority contributed vignettes
suggesting a cultural reluctance to admit and share errors
unlike for example in the aviation industry We as physicians
might work in an ldquoignorance traprdquo in which our physical ex-
amination oversights are rarely reported back to us
Diligence in actually teaching and performing the phys-
ical examination and continuing efforts to improve bedside
skills would diminish one kind of medical error and its
consequences for the patient
ACKNOWLEDGMENT The authors thank Ralph Horwitz MD for his encouragement of the First Stanford Symposium on Bedside Medicine in
2009 and for his helpful discussions in planning this study
References1 Kohn KT Corrigan JM Donaldson MS To Err Is Human Building a
Safer Health System Washington DC National Academy Press 1999
2 Kassirer JP Kopelman RI Cognitive errors in diagnosis instantiation
classi1047297cation and consequences Am J Med 198986(4)433-441
3 Graber ML Franklin N Gordon R Diagnostic error in internal
medicine Arch Intern Med 2005165(13)1493-1499
4 Singh H Graber ML Kissam SM et al System-related interventions
to reduce diagnostic errors a narrative review BMJ Qual Saf
201221(2)160-1705 OrsquoLeary KJ Liebovitz DM Baker DW How hospitalists spend their
time insights on ef 1047297ciency and safety J Hosp Med 20061(2)88-93
6 Block L Habicht R Wu AW et al In the wake of the 2003 and 2011
duty hour regulations how do internal medicine interns spend their
time J Gen Intern Med 201328(8)1042-1047
7 Feddock CA The lost art of clinical skills Am J Med 2007120(4)
374-378
8 Rahmani S Ring BN Lowe R et al A pilot study assessing knowledge
of clinical signs and physical examination skills in incoming medicine
residents J Grad Med Educ 20102(2)232-235
9 Willett LL Estrada CA Castiglioni A Does residency training
improve performance of physical examination skills Am J Med Sci
2007333(2)74-77
10 Sharma S A single-blinded direct observational study of PGY-1 in-terns and PGY-2 residents in evaluating their history-taking and
physical-examination skills Perm J 201115(4)23-29
11 Jauhar S The demise of the physical examination N Engl J Med
2006354(6)548-551
12 Ortiz-Neu C Walters CA Tenenbaum J Colliver JA Schmidt HJ
Error patterns of 3rd-year medical students on the cardiovascular
physical examination Teach Learn Med 200113(3)161-166
13 Bordage G Why did I miss the diagnosis Some cognitive explanations
and educational implications Acad Med 199974(10 suppl)S138-S143
SUPPLEMENTARY DATASupplementary table accompanying this article can be found
in the online version at httpdxdoiorg101016jamjmed201506004
Figure 2 Distribution of time to discovery for 208 oversights
in physical exam
1324 The American Journal of Medicine Vol 128 No 12 December 2015
7232019 inadekuat pemeriksaan fisik
httpslidepdfcomreaderfullinadekuat-pemeriksaan-fisik 46
Supplementary Table 1 Complete List of Items Missed as
Reported in Returned Questionnaires
Missed skin 1047297nding of subcutaneous emphysema
Missed pulse absence in ischemic foot
Missed pregnancy with twins before hysterectomy
Missed hip fracture labeled as right lower quadrant pain
Missed Bell rsquo s palsy
Missed liver mass abdominal mass in cholangiocarcinoma
Missed funduscopic 1047297nding of cupping
Missed strangulated groin hernia in small bowel obstruction
Missed incarcerated femoral hernia
Missed crackles in a patient with pulmonary edema
Missed 1047297nger pressure necrosis on microvascular free 1047298 ap
Missed peritoneal signs and free air on plain 1047297lm
Missed peritonitis in patient with gangrenous perforated gall
bladder
Missed adenopathy and therefore chronic lymphocytic leukemia
Missed thyromegaly in patient with tachycardia
Missed strangulated hernia
Missed fungating breast mass
Missed pelvic examination and therefore missed tubo-ovarian
abscess
Missed pregnancy by missed gynecologic examination in patient
with seizures
Missed pyoderma gangrenosum in skin
Missed Fournier rsquo s gangrene in groinmdashno genital examination
Missed clonus and hyperre1047298 exia
Missed abdominal examination 1047297nding of tenderness and Grey
Turner signs
Missed neuro1047297broma and cafeacute au lait spots
Missed large abdominal mass
Missed heart failure signs of cardiomyopathy after 1047298 u in a young
person
Missed pulse extremity examination missed Buerger rsquo sMissed testicular mass in teen
Missed massive splenomegaly
Missed second cervix
Missed abrasion on forehead clue to subdural
Missed bruising signs of abuse in child
Missed prostate mass with elevated prostate-speci1047297c antigen
Missed decreased pulses arterial occlusion in elderly man after hip
fracture
Missed strangulated femoral hernia in 88-year-old with emesis
Missed loud bruit in patient with renal failure and hypertension
Missed ruptured spleen after trauma
Missed ectopic pregnancy because no pelvic examination done
Missed obvious congestive heart failure (CHF) signs labeled asbronchitis
Missed rotatory and vertical nystagmus in patient with basilar
artery aneurysm
Missed abdominal examination old scar mislabeled as hernia scar
and patient operated on for ldquorecurrent rdquo hernia and nothing found
Missed pulses in patient with peripheral vascular disease
Missed tuberculosis signs in chest
Missed vital sign of tachypnea on 1047297rst visit in a patient later found
with bacteremic pneumonia
Missed adenopathy in lymphoma
Missed clavicle fracture labeled ldquorule out myocardial infarctionrdquoMissed the tan of hemochromatosis
Supplementary Table 1 Continued
Missed femoral fracture
Missed acute myocardial infarction by focusing on neck pain ear
pain
Missed hyperre1047298 exia and cord compression in Potts disease
Missed rectal and missed prostatic abscess
Missed supraclavicular mass in lung cancer
Missed splenomegaly and delayed diagnosis of chronic
myelogenous leukemia
Missed psoriasis and its signs
Missed groin cellulitis
Missed dislocated shoulder on examination
Missed adenopathy in germ cell tumor
Missed marked pallor in elderly anemic
Missed pulsatile abdominal aneurysm
Missed adenopathy in patient with Waldenstromrsquo s disease
Missed penetrating foreign body in vaginal 1047297stula
Missed gastric bypass scar in patient with malnutrition and
beriberi
Missed signs of CHF in a young patient
Missed femoral hernia in patient with vomiting
Missed signs of hypothyroidism and neck scar in unresponsive
patient
Missed retinal lesions in a child with poor vision
Missed signs of myocarditis and CHF especially the tachycardia in
a child
Misconstrued bruit from an aortofemoral bypass as a cardiac
murmur
Missed obvious CHF signs
Missed obvious pregnancy and labor
Missed huge spleen in cirrhosis
Missed previous appendectomy scar and made diagnosis of
appendicitis again
Missed ulnar nerve transection after traumaMissed male breast mass
Missed distended bladder
Missed incarcerated hernia
Missed breast mass and metastases
Missed zoster presenting as abdominal pain
Missed femoral hernia
Missed orchitis and diagnosed it as hernia
Missed aortic stenosis murmur preoperatively
Missed breast mass
Missed anus present in patient stated to have abdomino-perineal
resection when they had Hartman procedure
Missed prolapsing rectal cancer rectal examination not done
Missed incarcerated groin herniaMissed bruises of abuse
Missed large melanoma over scapula
Missed hoarseness puf 1047297ness and signs of hypothyroidism
Missed decubitus ulcer causing ldquoback painrdquoMissed leg ulcers and sores as a cause of fever in alcoholic
Missed skin 1047297ndings of secondary syphilis
Missed hip fracture in patient who could not walk
Missed gouty nodules
Missed breast mass
Missed mucor wound on hand in immunocompromised patient
Missed zoster in patient with chest pain
Missed foot ulcer in diabetic with fever
Verghese et al Oversights in the Physical Examination 1324e1
7232019 inadekuat pemeriksaan fisik
httpslidepdfcomreaderfullinadekuat-pemeriksaan-fisik 56
Supplementary Table 1 Continued
Missed signs of Parkinsonrsquo s in elderly being worked up for falls
Missed lymph node in a patient with breast cancer
Missed abdominal mass lymphoma in patient complaining of pain
Missed skin ash leaf macule in child with hypertension
Missed anterior cruciate ligament tear with classic signs
Missed giant ovarian cyst labeled as ascites
Missed giant ovarian cyst again thought to be ascites
Missed loud murmur of ruptured mitral valve chordae tendinae
Missed murmur and signs of subacute bacterial endocarditis
Missed cutaneous abscess in compromised patient with fever
Missed obvious CHF in 33-year-old with cardiomyopathy
Missed appendicitis signs
Missed strangulated hernia
Missed Downrsquo s syndrome on examination in 6 month old
Missed acute central vein occlusion in patient with decreased
visionmdashno fundoscopy done
Missed anal cancer said to be hemorrhoids
Missed peritonitis signs in patient with Crohn rsquo s
Missed dentures in mouth during intubation
Missed signi1047297cant murmur of mitral stenosis called it aortic
stenosis
Missed abdominal mass turned out to be lymphoma
Missed aortic stenosis in preoperative examination
Missed scrotal mass until after surgery for abdominal mass Was
testicular tumor with metastases
Missed supraclavicular nodes in patient with lung cancer
Missed hyperre1047298 exia and clonus from epidural abscess
Missed adenopathy in non-Hodgkinrsquo s lymphoma with fever of
unknown originmdashcalled a hernia
Missed neck nodes
Missed pelvic in1047298 ammatory disease because no pelvic examination
done
Missed gunshot entrance wound in emergency roomMissed large abdominal masses in patient with bloating
Missed pregnancy in patient with large belly
Missed signs of CHF in patient presenting with ldquoscrotal swellingrdquoMissed liver laceration after trauma because focus on head
Missed enlarged tonsil that was cancer
Missed clavicle fracture in patient with syncope
Missed ecchymosis in patient from a fall and the left arm pain
assumed to be cardiac
Missed contact dermatitis
Missed constrictive pericarditis signs
Missed breast mass in patient with shoulder pain
Missed breast mass in patient with deep vein thrombosis
Missed rapid growth in head circumferenceMissed splinters and signs of subacute bacterial endocarditis
Missed systolic murmur cardiac labeled carotid bruits
Missed pericardial rub and pericarditis
Missed zoster rash
Missed hip disease as a cause of joint pain
Missed femoral pathologic fracture in patient with knee pain
Missed large liver in patient with diabetic ketoacidosis
Missed zoster as cause of chest pain
Missed watch battery in umbilicus in child
Missed purulence in tonsils
Missed normal ear examination labeled as perforation by not doing
pneumatic otoscopy
Supplementary Table 1 Continued
Missed breast mass in patient with chest pain and metastasis
Missed pregnancy called it constipation
Missed meningococcemia skin lesion in patient with fever
Missed CHF 1047297ndings in patient with postpartum cardiomyopathy
Missed hoarseness and laryngeal mass in patient labeled asthma
Missed rectal mass by gastrointestinal consultant after primary
care physician feels massmdashsigmoidoscopy negative but tumor
develops
Missed appendicitis by focus on chest
Missed rales and crackles
Missed obvious pleural effusion no examination
Missed signs of myasthenia in patient with weight loss
Missed signs of bowel obstruction
Missed signs of mitral regurgitation from torn lea1047298 et
Missed hepatomegaly and hepatocellular carcinoma in patient with
vague symptoms
Missed metastatic node from breast cancer in patient with weight
loss
Missed stone in urethra causing recurrent urinary tract infection
Missed pelvic examination in adolescent and missed pelvic
in1047298 ammatory disease
Missed radiculopathy causing abdominal pain
Missed signs of peritonitis
Missed fungating breast mass
Missed abdominal mass in patient with back pain
Missed pelvic examination and missed procidentia
Missed skin signs of calcinosis in patient with mixed connective
tissue disease
Missed breast mass in patient being worked up for metastasis
Missed skin erythema migrans in patient with Bell rsquo s palsy
Missed abnormal pulses of combined aortic stenosisaortic
regurgitation and focused on treating high blood pressure and
pulse pressureMissed aortic stenosis murmur
Missed abdominal mass expanding aortic aneurysm in patient with
abdominal pain
Missed pericardial friction rub in chest pain
Missed nasal septal hematoma
Missed scrotal infection in diabetic
Missed Korsakoff rsquo s signs in many neurologic examinations
Missed zoster in patient with chest pain who had coronary
angiogram
Missed pelvic examination and missed ovarian cyst
Missed adenopathy and hepatomegaly in patient with anemia and
weight loss
Missed in1047298 ammatory knee effusion in intensive care unit patient with fever
Missed distended bladder labeled abdominal mass
Missed rectal examination and therefore missed prostatitis
Missed doing pulsus paradoxus in patient with tamponade
Missed abnormal decreased pulse and blood pressure in one arm
Missed purulence around IV catheter as cause of fever
Mistaken diagnosis of peritonitis bias from x-rays showing
pneumatosis intestinalis
Missed lytic lesions as cause of left-sided weakness in limbs
Missed CHF signs
Missed purulence at bone marrow biopsy site in patient with fever
Missed clubbing in patient with shoulder pain who has lung cancer
1324e2 The American Journal of Medicine Vol 128 No 12 December 2015
7232019 inadekuat pemeriksaan fisik
httpslidepdfcomreaderfullinadekuat-pemeriksaan-fisik 66
Supplementary Table 1 Continued
Missed hernia because of missed groin examination
Missed edema from hypoproteinemia labeled CHF
Missed peritonitis and perforation
Missed murmur of critical aortic stenosis
Missed butter 1047298 y bruises of factitious injury
Missed neurogenic bladder
Missed costochondritis in patient labeled as rule out myocardial
infarctions
Missed epididymitis in patient with abdominal pain
Missed scrotal examination
Missed erythema migrans in patient with fever and headache
Missed large abdominal mass on both pelvic and seated abdominal
examination
Missed embolic arterial occlusion
Missed uremic calciphylaxis in patient on dialysis
Verghese et al Oversights in the Physical Examination 1324e3

7232019 inadekuat pemeriksaan fisik
httpslidepdfcomreaderfullinadekuat-pemeriksaan-fisik 36
absent or abnormal pulses (n frac14 6) wound or ulcer (n frac14 6)
bruising (n frac14 6) and herpes zoster (n frac14 5)
Forty-seven oversights involved the skin and its append-
ages including the breast 37 were related to the abdominal
examination 37 involved the cardiovascular system and 36
involved the groingenitalrectal area Supplementary
Table 1 (available online) lists all items that were missed
DISCUSSIONRecent publications describe the decline of physical exam-
ination skills7-12 Our study highlights the consequences and
suggests that many adverse events are preventable Our
survey suggests that the major cause for error is simply that
the examination is not performed1213 In addition to diag-
nostic consequences approximately half of the vignettes
report treatment consequences Most oversights pertained to
a limited number of overlookers suggesting that some er-rors may be remedied if several people examine the patient
Although the majority of the errors were corrected within 5
days even a delay of 1 hour might affect patient outcomes
Examining a patient presenting with a complaint (as
opposed to the ldquoroutine physicalrdquo) is a low-cost procedure
that when done with skill can avoid the majority of over-
sights listed Many diseases involving the skin or the
nervous system cannot easily be diagnosed except by the
examination and for others the appropriate diagnostic test is
indicated by the examination The drop-down boxes of the
electronic medical record deceptively suggest every patient
has been thoroughly examined (and therefore can be billed)but it will be the responsibility of educators and professional
organizations to make sure the electronic medical record
truthfully re1047298ects what was done
A short checklist is suggested by our study physicians
should seek full exposure of the patient there must be a
mandate to examine hernial ori1047297ces and the genital
and rectal areas in acutely ill patients or with pain Pain
should prompt a search for the lesions of shingles Non-
neurologists need a sound neurologic skill set because im-
aging does not show the functional de1047297cits resulting from a
lesion seen For diseases like Wernickersquos encephalopathy or
Bellrsquos palsy imaging may not be diagnostic Finally there
should be a greater emphasis on actually performing the
examination In short physicians in training must be taught
and evaluated at the bedside to diminish this kind of error
Our survey was not designed to determine prevalence but
to generate an anthology of physical examination oversights
along with their characteristics The vignettes are subject to
recall and response biases We set no time limitation on re-
ports and did not ask responders to specify where they prac-
ticed medicine Finally even though we contacted thousandsof physicians only a small minority contributed vignettes
suggesting a cultural reluctance to admit and share errors
unlike for example in the aviation industry We as physicians
might work in an ldquoignorance traprdquo in which our physical ex-
amination oversights are rarely reported back to us
Diligence in actually teaching and performing the phys-
ical examination and continuing efforts to improve bedside
skills would diminish one kind of medical error and its
consequences for the patient
ACKNOWLEDGMENT The authors thank Ralph Horwitz MD for his encouragement of the First Stanford Symposium on Bedside Medicine in
2009 and for his helpful discussions in planning this study
References1 Kohn KT Corrigan JM Donaldson MS To Err Is Human Building a
Safer Health System Washington DC National Academy Press 1999
2 Kassirer JP Kopelman RI Cognitive errors in diagnosis instantiation
classi1047297cation and consequences Am J Med 198986(4)433-441
3 Graber ML Franklin N Gordon R Diagnostic error in internal
medicine Arch Intern Med 2005165(13)1493-1499
4 Singh H Graber ML Kissam SM et al System-related interventions
to reduce diagnostic errors a narrative review BMJ Qual Saf
201221(2)160-1705 OrsquoLeary KJ Liebovitz DM Baker DW How hospitalists spend their
time insights on ef 1047297ciency and safety J Hosp Med 20061(2)88-93
6 Block L Habicht R Wu AW et al In the wake of the 2003 and 2011
duty hour regulations how do internal medicine interns spend their
time J Gen Intern Med 201328(8)1042-1047
7 Feddock CA The lost art of clinical skills Am J Med 2007120(4)
374-378
8 Rahmani S Ring BN Lowe R et al A pilot study assessing knowledge
of clinical signs and physical examination skills in incoming medicine
residents J Grad Med Educ 20102(2)232-235
9 Willett LL Estrada CA Castiglioni A Does residency training
improve performance of physical examination skills Am J Med Sci
2007333(2)74-77
10 Sharma S A single-blinded direct observational study of PGY-1 in-terns and PGY-2 residents in evaluating their history-taking and
physical-examination skills Perm J 201115(4)23-29
11 Jauhar S The demise of the physical examination N Engl J Med
2006354(6)548-551
12 Ortiz-Neu C Walters CA Tenenbaum J Colliver JA Schmidt HJ
Error patterns of 3rd-year medical students on the cardiovascular
physical examination Teach Learn Med 200113(3)161-166
13 Bordage G Why did I miss the diagnosis Some cognitive explanations
and educational implications Acad Med 199974(10 suppl)S138-S143
SUPPLEMENTARY DATASupplementary table accompanying this article can be found
in the online version at httpdxdoiorg101016jamjmed201506004
Figure 2 Distribution of time to discovery for 208 oversights
in physical exam
1324 The American Journal of Medicine Vol 128 No 12 December 2015
7232019 inadekuat pemeriksaan fisik
httpslidepdfcomreaderfullinadekuat-pemeriksaan-fisik 46
Supplementary Table 1 Complete List of Items Missed as
Reported in Returned Questionnaires
Missed skin 1047297nding of subcutaneous emphysema
Missed pulse absence in ischemic foot
Missed pregnancy with twins before hysterectomy
Missed hip fracture labeled as right lower quadrant pain
Missed Bell rsquo s palsy
Missed liver mass abdominal mass in cholangiocarcinoma
Missed funduscopic 1047297nding of cupping
Missed strangulated groin hernia in small bowel obstruction
Missed incarcerated femoral hernia
Missed crackles in a patient with pulmonary edema
Missed 1047297nger pressure necrosis on microvascular free 1047298 ap
Missed peritoneal signs and free air on plain 1047297lm
Missed peritonitis in patient with gangrenous perforated gall
bladder
Missed adenopathy and therefore chronic lymphocytic leukemia
Missed thyromegaly in patient with tachycardia
Missed strangulated hernia
Missed fungating breast mass
Missed pelvic examination and therefore missed tubo-ovarian
abscess
Missed pregnancy by missed gynecologic examination in patient
with seizures
Missed pyoderma gangrenosum in skin
Missed Fournier rsquo s gangrene in groinmdashno genital examination
Missed clonus and hyperre1047298 exia
Missed abdominal examination 1047297nding of tenderness and Grey
Turner signs
Missed neuro1047297broma and cafeacute au lait spots
Missed large abdominal mass
Missed heart failure signs of cardiomyopathy after 1047298 u in a young
person
Missed pulse extremity examination missed Buerger rsquo sMissed testicular mass in teen
Missed massive splenomegaly
Missed second cervix
Missed abrasion on forehead clue to subdural
Missed bruising signs of abuse in child
Missed prostate mass with elevated prostate-speci1047297c antigen
Missed decreased pulses arterial occlusion in elderly man after hip
fracture
Missed strangulated femoral hernia in 88-year-old with emesis
Missed loud bruit in patient with renal failure and hypertension
Missed ruptured spleen after trauma
Missed ectopic pregnancy because no pelvic examination done
Missed obvious congestive heart failure (CHF) signs labeled asbronchitis
Missed rotatory and vertical nystagmus in patient with basilar
artery aneurysm
Missed abdominal examination old scar mislabeled as hernia scar
and patient operated on for ldquorecurrent rdquo hernia and nothing found
Missed pulses in patient with peripheral vascular disease
Missed tuberculosis signs in chest
Missed vital sign of tachypnea on 1047297rst visit in a patient later found
with bacteremic pneumonia
Missed adenopathy in lymphoma
Missed clavicle fracture labeled ldquorule out myocardial infarctionrdquoMissed the tan of hemochromatosis
Supplementary Table 1 Continued
Missed femoral fracture
Missed acute myocardial infarction by focusing on neck pain ear
pain
Missed hyperre1047298 exia and cord compression in Potts disease
Missed rectal and missed prostatic abscess
Missed supraclavicular mass in lung cancer
Missed splenomegaly and delayed diagnosis of chronic
myelogenous leukemia
Missed psoriasis and its signs
Missed groin cellulitis
Missed dislocated shoulder on examination
Missed adenopathy in germ cell tumor
Missed marked pallor in elderly anemic
Missed pulsatile abdominal aneurysm
Missed adenopathy in patient with Waldenstromrsquo s disease
Missed penetrating foreign body in vaginal 1047297stula
Missed gastric bypass scar in patient with malnutrition and
beriberi
Missed signs of CHF in a young patient
Missed femoral hernia in patient with vomiting
Missed signs of hypothyroidism and neck scar in unresponsive
patient
Missed retinal lesions in a child with poor vision
Missed signs of myocarditis and CHF especially the tachycardia in
a child
Misconstrued bruit from an aortofemoral bypass as a cardiac
murmur
Missed obvious CHF signs
Missed obvious pregnancy and labor
Missed huge spleen in cirrhosis
Missed previous appendectomy scar and made diagnosis of
appendicitis again
Missed ulnar nerve transection after traumaMissed male breast mass
Missed distended bladder
Missed incarcerated hernia
Missed breast mass and metastases
Missed zoster presenting as abdominal pain
Missed femoral hernia
Missed orchitis and diagnosed it as hernia
Missed aortic stenosis murmur preoperatively
Missed breast mass
Missed anus present in patient stated to have abdomino-perineal
resection when they had Hartman procedure
Missed prolapsing rectal cancer rectal examination not done
Missed incarcerated groin herniaMissed bruises of abuse
Missed large melanoma over scapula
Missed hoarseness puf 1047297ness and signs of hypothyroidism
Missed decubitus ulcer causing ldquoback painrdquoMissed leg ulcers and sores as a cause of fever in alcoholic
Missed skin 1047297ndings of secondary syphilis
Missed hip fracture in patient who could not walk
Missed gouty nodules
Missed breast mass
Missed mucor wound on hand in immunocompromised patient
Missed zoster in patient with chest pain
Missed foot ulcer in diabetic with fever
Verghese et al Oversights in the Physical Examination 1324e1
7232019 inadekuat pemeriksaan fisik
httpslidepdfcomreaderfullinadekuat-pemeriksaan-fisik 56
Supplementary Table 1 Continued
Missed signs of Parkinsonrsquo s in elderly being worked up for falls
Missed lymph node in a patient with breast cancer
Missed abdominal mass lymphoma in patient complaining of pain
Missed skin ash leaf macule in child with hypertension
Missed anterior cruciate ligament tear with classic signs
Missed giant ovarian cyst labeled as ascites
Missed giant ovarian cyst again thought to be ascites
Missed loud murmur of ruptured mitral valve chordae tendinae
Missed murmur and signs of subacute bacterial endocarditis
Missed cutaneous abscess in compromised patient with fever
Missed obvious CHF in 33-year-old with cardiomyopathy
Missed appendicitis signs
Missed strangulated hernia
Missed Downrsquo s syndrome on examination in 6 month old
Missed acute central vein occlusion in patient with decreased
visionmdashno fundoscopy done
Missed anal cancer said to be hemorrhoids
Missed peritonitis signs in patient with Crohn rsquo s
Missed dentures in mouth during intubation
Missed signi1047297cant murmur of mitral stenosis called it aortic
stenosis
Missed abdominal mass turned out to be lymphoma
Missed aortic stenosis in preoperative examination
Missed scrotal mass until after surgery for abdominal mass Was
testicular tumor with metastases
Missed supraclavicular nodes in patient with lung cancer
Missed hyperre1047298 exia and clonus from epidural abscess
Missed adenopathy in non-Hodgkinrsquo s lymphoma with fever of
unknown originmdashcalled a hernia
Missed neck nodes
Missed pelvic in1047298 ammatory disease because no pelvic examination
done
Missed gunshot entrance wound in emergency roomMissed large abdominal masses in patient with bloating
Missed pregnancy in patient with large belly
Missed signs of CHF in patient presenting with ldquoscrotal swellingrdquoMissed liver laceration after trauma because focus on head
Missed enlarged tonsil that was cancer
Missed clavicle fracture in patient with syncope
Missed ecchymosis in patient from a fall and the left arm pain
assumed to be cardiac
Missed contact dermatitis
Missed constrictive pericarditis signs
Missed breast mass in patient with shoulder pain
Missed breast mass in patient with deep vein thrombosis
Missed rapid growth in head circumferenceMissed splinters and signs of subacute bacterial endocarditis
Missed systolic murmur cardiac labeled carotid bruits
Missed pericardial rub and pericarditis
Missed zoster rash
Missed hip disease as a cause of joint pain
Missed femoral pathologic fracture in patient with knee pain
Missed large liver in patient with diabetic ketoacidosis
Missed zoster as cause of chest pain
Missed watch battery in umbilicus in child
Missed purulence in tonsils
Missed normal ear examination labeled as perforation by not doing
pneumatic otoscopy
Supplementary Table 1 Continued
Missed breast mass in patient with chest pain and metastasis
Missed pregnancy called it constipation
Missed meningococcemia skin lesion in patient with fever
Missed CHF 1047297ndings in patient with postpartum cardiomyopathy
Missed hoarseness and laryngeal mass in patient labeled asthma
Missed rectal mass by gastrointestinal consultant after primary
care physician feels massmdashsigmoidoscopy negative but tumor
develops
Missed appendicitis by focus on chest
Missed rales and crackles
Missed obvious pleural effusion no examination
Missed signs of myasthenia in patient with weight loss
Missed signs of bowel obstruction
Missed signs of mitral regurgitation from torn lea1047298 et
Missed hepatomegaly and hepatocellular carcinoma in patient with
vague symptoms
Missed metastatic node from breast cancer in patient with weight
loss
Missed stone in urethra causing recurrent urinary tract infection
Missed pelvic examination in adolescent and missed pelvic
in1047298 ammatory disease
Missed radiculopathy causing abdominal pain
Missed signs of peritonitis
Missed fungating breast mass
Missed abdominal mass in patient with back pain
Missed pelvic examination and missed procidentia
Missed skin signs of calcinosis in patient with mixed connective
tissue disease
Missed breast mass in patient being worked up for metastasis
Missed skin erythema migrans in patient with Bell rsquo s palsy
Missed abnormal pulses of combined aortic stenosisaortic
regurgitation and focused on treating high blood pressure and
pulse pressureMissed aortic stenosis murmur
Missed abdominal mass expanding aortic aneurysm in patient with
abdominal pain
Missed pericardial friction rub in chest pain
Missed nasal septal hematoma
Missed scrotal infection in diabetic
Missed Korsakoff rsquo s signs in many neurologic examinations
Missed zoster in patient with chest pain who had coronary
angiogram
Missed pelvic examination and missed ovarian cyst
Missed adenopathy and hepatomegaly in patient with anemia and
weight loss
Missed in1047298 ammatory knee effusion in intensive care unit patient with fever
Missed distended bladder labeled abdominal mass
Missed rectal examination and therefore missed prostatitis
Missed doing pulsus paradoxus in patient with tamponade
Missed abnormal decreased pulse and blood pressure in one arm
Missed purulence around IV catheter as cause of fever
Mistaken diagnosis of peritonitis bias from x-rays showing
pneumatosis intestinalis
Missed lytic lesions as cause of left-sided weakness in limbs
Missed CHF signs
Missed purulence at bone marrow biopsy site in patient with fever
Missed clubbing in patient with shoulder pain who has lung cancer
1324e2 The American Journal of Medicine Vol 128 No 12 December 2015
7232019 inadekuat pemeriksaan fisik
httpslidepdfcomreaderfullinadekuat-pemeriksaan-fisik 66
Supplementary Table 1 Continued
Missed hernia because of missed groin examination
Missed edema from hypoproteinemia labeled CHF
Missed peritonitis and perforation
Missed murmur of critical aortic stenosis
Missed butter 1047298 y bruises of factitious injury
Missed neurogenic bladder
Missed costochondritis in patient labeled as rule out myocardial
infarctions
Missed epididymitis in patient with abdominal pain
Missed scrotal examination
Missed erythema migrans in patient with fever and headache
Missed large abdominal mass on both pelvic and seated abdominal
examination
Missed embolic arterial occlusion
Missed uremic calciphylaxis in patient on dialysis
Verghese et al Oversights in the Physical Examination 1324e3

7232019 inadekuat pemeriksaan fisik
httpslidepdfcomreaderfullinadekuat-pemeriksaan-fisik 46
Supplementary Table 1 Complete List of Items Missed as
Reported in Returned Questionnaires
Missed skin 1047297nding of subcutaneous emphysema
Missed pulse absence in ischemic foot
Missed pregnancy with twins before hysterectomy
Missed hip fracture labeled as right lower quadrant pain
Missed Bell rsquo s palsy
Missed liver mass abdominal mass in cholangiocarcinoma
Missed funduscopic 1047297nding of cupping
Missed strangulated groin hernia in small bowel obstruction
Missed incarcerated femoral hernia
Missed crackles in a patient with pulmonary edema
Missed 1047297nger pressure necrosis on microvascular free 1047298 ap
Missed peritoneal signs and free air on plain 1047297lm
Missed peritonitis in patient with gangrenous perforated gall
bladder
Missed adenopathy and therefore chronic lymphocytic leukemia
Missed thyromegaly in patient with tachycardia
Missed strangulated hernia
Missed fungating breast mass
Missed pelvic examination and therefore missed tubo-ovarian
abscess
Missed pregnancy by missed gynecologic examination in patient
with seizures
Missed pyoderma gangrenosum in skin
Missed Fournier rsquo s gangrene in groinmdashno genital examination
Missed clonus and hyperre1047298 exia
Missed abdominal examination 1047297nding of tenderness and Grey
Turner signs
Missed neuro1047297broma and cafeacute au lait spots
Missed large abdominal mass
Missed heart failure signs of cardiomyopathy after 1047298 u in a young
person
Missed pulse extremity examination missed Buerger rsquo sMissed testicular mass in teen
Missed massive splenomegaly
Missed second cervix
Missed abrasion on forehead clue to subdural
Missed bruising signs of abuse in child
Missed prostate mass with elevated prostate-speci1047297c antigen
Missed decreased pulses arterial occlusion in elderly man after hip
fracture
Missed strangulated femoral hernia in 88-year-old with emesis
Missed loud bruit in patient with renal failure and hypertension
Missed ruptured spleen after trauma
Missed ectopic pregnancy because no pelvic examination done
Missed obvious congestive heart failure (CHF) signs labeled asbronchitis
Missed rotatory and vertical nystagmus in patient with basilar
artery aneurysm
Missed abdominal examination old scar mislabeled as hernia scar
and patient operated on for ldquorecurrent rdquo hernia and nothing found
Missed pulses in patient with peripheral vascular disease
Missed tuberculosis signs in chest
Missed vital sign of tachypnea on 1047297rst visit in a patient later found
with bacteremic pneumonia
Missed adenopathy in lymphoma
Missed clavicle fracture labeled ldquorule out myocardial infarctionrdquoMissed the tan of hemochromatosis
Supplementary Table 1 Continued
Missed femoral fracture
Missed acute myocardial infarction by focusing on neck pain ear
pain
Missed hyperre1047298 exia and cord compression in Potts disease
Missed rectal and missed prostatic abscess
Missed supraclavicular mass in lung cancer
Missed splenomegaly and delayed diagnosis of chronic
myelogenous leukemia
Missed psoriasis and its signs
Missed groin cellulitis
Missed dislocated shoulder on examination
Missed adenopathy in germ cell tumor
Missed marked pallor in elderly anemic
Missed pulsatile abdominal aneurysm
Missed adenopathy in patient with Waldenstromrsquo s disease
Missed penetrating foreign body in vaginal 1047297stula
Missed gastric bypass scar in patient with malnutrition and
beriberi
Missed signs of CHF in a young patient
Missed femoral hernia in patient with vomiting
Missed signs of hypothyroidism and neck scar in unresponsive
patient
Missed retinal lesions in a child with poor vision
Missed signs of myocarditis and CHF especially the tachycardia in
a child
Misconstrued bruit from an aortofemoral bypass as a cardiac
murmur
Missed obvious CHF signs
Missed obvious pregnancy and labor
Missed huge spleen in cirrhosis
Missed previous appendectomy scar and made diagnosis of
appendicitis again
Missed ulnar nerve transection after traumaMissed male breast mass
Missed distended bladder
Missed incarcerated hernia
Missed breast mass and metastases
Missed zoster presenting as abdominal pain
Missed femoral hernia
Missed orchitis and diagnosed it as hernia
Missed aortic stenosis murmur preoperatively
Missed breast mass
Missed anus present in patient stated to have abdomino-perineal
resection when they had Hartman procedure
Missed prolapsing rectal cancer rectal examination not done
Missed incarcerated groin herniaMissed bruises of abuse
Missed large melanoma over scapula
Missed hoarseness puf 1047297ness and signs of hypothyroidism
Missed decubitus ulcer causing ldquoback painrdquoMissed leg ulcers and sores as a cause of fever in alcoholic
Missed skin 1047297ndings of secondary syphilis
Missed hip fracture in patient who could not walk
Missed gouty nodules
Missed breast mass
Missed mucor wound on hand in immunocompromised patient
Missed zoster in patient with chest pain
Missed foot ulcer in diabetic with fever
Verghese et al Oversights in the Physical Examination 1324e1
7232019 inadekuat pemeriksaan fisik
httpslidepdfcomreaderfullinadekuat-pemeriksaan-fisik 56
Supplementary Table 1 Continued
Missed signs of Parkinsonrsquo s in elderly being worked up for falls
Missed lymph node in a patient with breast cancer
Missed abdominal mass lymphoma in patient complaining of pain
Missed skin ash leaf macule in child with hypertension
Missed anterior cruciate ligament tear with classic signs
Missed giant ovarian cyst labeled as ascites
Missed giant ovarian cyst again thought to be ascites
Missed loud murmur of ruptured mitral valve chordae tendinae
Missed murmur and signs of subacute bacterial endocarditis
Missed cutaneous abscess in compromised patient with fever
Missed obvious CHF in 33-year-old with cardiomyopathy
Missed appendicitis signs
Missed strangulated hernia
Missed Downrsquo s syndrome on examination in 6 month old
Missed acute central vein occlusion in patient with decreased
visionmdashno fundoscopy done
Missed anal cancer said to be hemorrhoids
Missed peritonitis signs in patient with Crohn rsquo s
Missed dentures in mouth during intubation
Missed signi1047297cant murmur of mitral stenosis called it aortic
stenosis
Missed abdominal mass turned out to be lymphoma
Missed aortic stenosis in preoperative examination
Missed scrotal mass until after surgery for abdominal mass Was
testicular tumor with metastases
Missed supraclavicular nodes in patient with lung cancer
Missed hyperre1047298 exia and clonus from epidural abscess
Missed adenopathy in non-Hodgkinrsquo s lymphoma with fever of
unknown originmdashcalled a hernia
Missed neck nodes
Missed pelvic in1047298 ammatory disease because no pelvic examination
done
Missed gunshot entrance wound in emergency roomMissed large abdominal masses in patient with bloating
Missed pregnancy in patient with large belly
Missed signs of CHF in patient presenting with ldquoscrotal swellingrdquoMissed liver laceration after trauma because focus on head
Missed enlarged tonsil that was cancer
Missed clavicle fracture in patient with syncope
Missed ecchymosis in patient from a fall and the left arm pain
assumed to be cardiac
Missed contact dermatitis
Missed constrictive pericarditis signs
Missed breast mass in patient with shoulder pain
Missed breast mass in patient with deep vein thrombosis
Missed rapid growth in head circumferenceMissed splinters and signs of subacute bacterial endocarditis
Missed systolic murmur cardiac labeled carotid bruits
Missed pericardial rub and pericarditis
Missed zoster rash
Missed hip disease as a cause of joint pain
Missed femoral pathologic fracture in patient with knee pain
Missed large liver in patient with diabetic ketoacidosis
Missed zoster as cause of chest pain
Missed watch battery in umbilicus in child
Missed purulence in tonsils
Missed normal ear examination labeled as perforation by not doing
pneumatic otoscopy
Supplementary Table 1 Continued
Missed breast mass in patient with chest pain and metastasis
Missed pregnancy called it constipation
Missed meningococcemia skin lesion in patient with fever
Missed CHF 1047297ndings in patient with postpartum cardiomyopathy
Missed hoarseness and laryngeal mass in patient labeled asthma
Missed rectal mass by gastrointestinal consultant after primary
care physician feels massmdashsigmoidoscopy negative but tumor
develops
Missed appendicitis by focus on chest
Missed rales and crackles
Missed obvious pleural effusion no examination
Missed signs of myasthenia in patient with weight loss
Missed signs of bowel obstruction
Missed signs of mitral regurgitation from torn lea1047298 et
Missed hepatomegaly and hepatocellular carcinoma in patient with
vague symptoms
Missed metastatic node from breast cancer in patient with weight
loss
Missed stone in urethra causing recurrent urinary tract infection
Missed pelvic examination in adolescent and missed pelvic
in1047298 ammatory disease
Missed radiculopathy causing abdominal pain
Missed signs of peritonitis
Missed fungating breast mass
Missed abdominal mass in patient with back pain
Missed pelvic examination and missed procidentia
Missed skin signs of calcinosis in patient with mixed connective
tissue disease
Missed breast mass in patient being worked up for metastasis
Missed skin erythema migrans in patient with Bell rsquo s palsy
Missed abnormal pulses of combined aortic stenosisaortic
regurgitation and focused on treating high blood pressure and
pulse pressureMissed aortic stenosis murmur
Missed abdominal mass expanding aortic aneurysm in patient with
abdominal pain
Missed pericardial friction rub in chest pain
Missed nasal septal hematoma
Missed scrotal infection in diabetic
Missed Korsakoff rsquo s signs in many neurologic examinations
Missed zoster in patient with chest pain who had coronary
angiogram
Missed pelvic examination and missed ovarian cyst
Missed adenopathy and hepatomegaly in patient with anemia and
weight loss
Missed in1047298 ammatory knee effusion in intensive care unit patient with fever
Missed distended bladder labeled abdominal mass
Missed rectal examination and therefore missed prostatitis
Missed doing pulsus paradoxus in patient with tamponade
Missed abnormal decreased pulse and blood pressure in one arm
Missed purulence around IV catheter as cause of fever
Mistaken diagnosis of peritonitis bias from x-rays showing
pneumatosis intestinalis
Missed lytic lesions as cause of left-sided weakness in limbs
Missed CHF signs
Missed purulence at bone marrow biopsy site in patient with fever
Missed clubbing in patient with shoulder pain who has lung cancer
1324e2 The American Journal of Medicine Vol 128 No 12 December 2015
7232019 inadekuat pemeriksaan fisik
httpslidepdfcomreaderfullinadekuat-pemeriksaan-fisik 66
Supplementary Table 1 Continued
Missed hernia because of missed groin examination
Missed edema from hypoproteinemia labeled CHF
Missed peritonitis and perforation
Missed murmur of critical aortic stenosis
Missed butter 1047298 y bruises of factitious injury
Missed neurogenic bladder
Missed costochondritis in patient labeled as rule out myocardial
infarctions
Missed epididymitis in patient with abdominal pain
Missed scrotal examination
Missed erythema migrans in patient with fever and headache
Missed large abdominal mass on both pelvic and seated abdominal
examination
Missed embolic arterial occlusion
Missed uremic calciphylaxis in patient on dialysis
Verghese et al Oversights in the Physical Examination 1324e3

7232019 inadekuat pemeriksaan fisik
httpslidepdfcomreaderfullinadekuat-pemeriksaan-fisik 56
Supplementary Table 1 Continued
Missed signs of Parkinsonrsquo s in elderly being worked up for falls
Missed lymph node in a patient with breast cancer
Missed abdominal mass lymphoma in patient complaining of pain
Missed skin ash leaf macule in child with hypertension
Missed anterior cruciate ligament tear with classic signs
Missed giant ovarian cyst labeled as ascites
Missed giant ovarian cyst again thought to be ascites
Missed loud murmur of ruptured mitral valve chordae tendinae
Missed murmur and signs of subacute bacterial endocarditis
Missed cutaneous abscess in compromised patient with fever
Missed obvious CHF in 33-year-old with cardiomyopathy
Missed appendicitis signs
Missed strangulated hernia
Missed Downrsquo s syndrome on examination in 6 month old
Missed acute central vein occlusion in patient with decreased
visionmdashno fundoscopy done
Missed anal cancer said to be hemorrhoids
Missed peritonitis signs in patient with Crohn rsquo s
Missed dentures in mouth during intubation
Missed signi1047297cant murmur of mitral stenosis called it aortic
stenosis
Missed abdominal mass turned out to be lymphoma
Missed aortic stenosis in preoperative examination
Missed scrotal mass until after surgery for abdominal mass Was
testicular tumor with metastases
Missed supraclavicular nodes in patient with lung cancer
Missed hyperre1047298 exia and clonus from epidural abscess
Missed adenopathy in non-Hodgkinrsquo s lymphoma with fever of
unknown originmdashcalled a hernia
Missed neck nodes
Missed pelvic in1047298 ammatory disease because no pelvic examination
done
Missed gunshot entrance wound in emergency roomMissed large abdominal masses in patient with bloating
Missed pregnancy in patient with large belly
Missed signs of CHF in patient presenting with ldquoscrotal swellingrdquoMissed liver laceration after trauma because focus on head
Missed enlarged tonsil that was cancer
Missed clavicle fracture in patient with syncope
Missed ecchymosis in patient from a fall and the left arm pain
assumed to be cardiac
Missed contact dermatitis
Missed constrictive pericarditis signs
Missed breast mass in patient with shoulder pain
Missed breast mass in patient with deep vein thrombosis
Missed rapid growth in head circumferenceMissed splinters and signs of subacute bacterial endocarditis
Missed systolic murmur cardiac labeled carotid bruits
Missed pericardial rub and pericarditis
Missed zoster rash
Missed hip disease as a cause of joint pain
Missed femoral pathologic fracture in patient with knee pain
Missed large liver in patient with diabetic ketoacidosis
Missed zoster as cause of chest pain
Missed watch battery in umbilicus in child
Missed purulence in tonsils
Missed normal ear examination labeled as perforation by not doing
pneumatic otoscopy
Supplementary Table 1 Continued
Missed breast mass in patient with chest pain and metastasis
Missed pregnancy called it constipation
Missed meningococcemia skin lesion in patient with fever
Missed CHF 1047297ndings in patient with postpartum cardiomyopathy
Missed hoarseness and laryngeal mass in patient labeled asthma
Missed rectal mass by gastrointestinal consultant after primary
care physician feels massmdashsigmoidoscopy negative but tumor
develops
Missed appendicitis by focus on chest
Missed rales and crackles
Missed obvious pleural effusion no examination
Missed signs of myasthenia in patient with weight loss
Missed signs of bowel obstruction
Missed signs of mitral regurgitation from torn lea1047298 et
Missed hepatomegaly and hepatocellular carcinoma in patient with
vague symptoms
Missed metastatic node from breast cancer in patient with weight
loss
Missed stone in urethra causing recurrent urinary tract infection
Missed pelvic examination in adolescent and missed pelvic
in1047298 ammatory disease
Missed radiculopathy causing abdominal pain
Missed signs of peritonitis
Missed fungating breast mass
Missed abdominal mass in patient with back pain
Missed pelvic examination and missed procidentia
Missed skin signs of calcinosis in patient with mixed connective
tissue disease
Missed breast mass in patient being worked up for metastasis
Missed skin erythema migrans in patient with Bell rsquo s palsy
Missed abnormal pulses of combined aortic stenosisaortic
regurgitation and focused on treating high blood pressure and
pulse pressureMissed aortic stenosis murmur
Missed abdominal mass expanding aortic aneurysm in patient with
abdominal pain
Missed pericardial friction rub in chest pain
Missed nasal septal hematoma
Missed scrotal infection in diabetic
Missed Korsakoff rsquo s signs in many neurologic examinations
Missed zoster in patient with chest pain who had coronary
angiogram
Missed pelvic examination and missed ovarian cyst
Missed adenopathy and hepatomegaly in patient with anemia and
weight loss
Missed in1047298 ammatory knee effusion in intensive care unit patient with fever
Missed distended bladder labeled abdominal mass
Missed rectal examination and therefore missed prostatitis
Missed doing pulsus paradoxus in patient with tamponade
Missed abnormal decreased pulse and blood pressure in one arm
Missed purulence around IV catheter as cause of fever
Mistaken diagnosis of peritonitis bias from x-rays showing
pneumatosis intestinalis
Missed lytic lesions as cause of left-sided weakness in limbs
Missed CHF signs
Missed purulence at bone marrow biopsy site in patient with fever
Missed clubbing in patient with shoulder pain who has lung cancer
1324e2 The American Journal of Medicine Vol 128 No 12 December 2015
7232019 inadekuat pemeriksaan fisik
httpslidepdfcomreaderfullinadekuat-pemeriksaan-fisik 66
Supplementary Table 1 Continued
Missed hernia because of missed groin examination
Missed edema from hypoproteinemia labeled CHF
Missed peritonitis and perforation
Missed murmur of critical aortic stenosis
Missed butter 1047298 y bruises of factitious injury
Missed neurogenic bladder
Missed costochondritis in patient labeled as rule out myocardial
infarctions
Missed epididymitis in patient with abdominal pain
Missed scrotal examination
Missed erythema migrans in patient with fever and headache
Missed large abdominal mass on both pelvic and seated abdominal
examination
Missed embolic arterial occlusion
Missed uremic calciphylaxis in patient on dialysis
Verghese et al Oversights in the Physical Examination 1324e3

7232019 inadekuat pemeriksaan fisik
httpslidepdfcomreaderfullinadekuat-pemeriksaan-fisik 66
Supplementary Table 1 Continued
Missed hernia because of missed groin examination
Missed edema from hypoproteinemia labeled CHF
Missed peritonitis and perforation
Missed murmur of critical aortic stenosis
Missed butter 1047298 y bruises of factitious injury
Missed neurogenic bladder
Missed costochondritis in patient labeled as rule out myocardial
infarctions
Missed epididymitis in patient with abdominal pain
Missed scrotal examination
Missed erythema migrans in patient with fever and headache
Missed large abdominal mass on both pelvic and seated abdominal
examination
Missed embolic arterial occlusion
Missed uremic calciphylaxis in patient on dialysis
Verghese et al Oversights in the Physical Examination 1324e3