Endocrinologist - Thyroid - Thyrax - TSH _ Candesartan
66
Endocrinologist – Terapi Pengganti (Thyrax) – TSH Level – Candesartan 1 Terapi Pengganti (Replacement Therapy) Sesudah Pengangkatan Kelenjar Tiroid 1. Sumber: http://mediasehat.com/tanyajawab3482 Thyrax adalah obat yang berisi levothyroxin, yaitu hormon sintetik untuk tiroksin (salah satu hormon tiroid). Levothyroxin diberikan untuk kondisi-kondisi dimana seseorang tidak mampu memproduksi hormon tiroid pada jumlah yang cukup, misalnya pada penderita hipotiroid, atau dalam kasus Bapak, karena mengalami pengangkatan kelenjar tiroid. Levothyroxin juga diberikan untuk mereka yang mengalami penyakit gondok (pembesaran kelenjar tiroid) akibat kekurangan iodium. Dosis obat sebaiknya tidak Anda stop atau dikurangi, atau dilebihkan, di luar anjuran dokter. Hal ini karena bisa menyebabkan Anda menderita hipotiroid (kekurangan hormon tiroid) atau malah hipertiroid (kelebihan hormon tiroid). Kedua kondisi tersebut akan berakibat buruk pada kesehatan Bapak (untuk kondisi tersebut bisa di-search di mediasehat tentang hipotiroid dan hipertiroid). Namun jika Anda mengalami gejala-gejala hipertiroid, sebaiknya diskusikan kembali dengan dokter Anda untuk kemungkinan meninjau kembali dosisnya. Jangan pernah mengambil kesimpulan sendiri untuk menambah ataupun mengurangi karena yang Anda konsumsi adalah hormon, dan dampak lebih/kurang akan berakibat langsung pada fungsi tubuh Anda. Selama Anda berada dalam jalur yang benar, artinya mengkonsumsi obat dalam jumlah yang tepat, justru Anda akan baik-baik saja. Karena Thyrax fungsinya bukan mengobati, tapi melengkapi apa yg kurang. Secara medis disebut sebagai terapi pengganti (replacement therapy). Pengangkatan kelenjar tiroid menyebabkan tubuh Anda kehilangan 'pabrik' hormon tiroid, dan fungsi Thyrax adalah untuk melengkapi apa yang hilang dari tubuh Anda. Jadi fungsinya lebih untuk menjaga agar semua aktivitas yang terjadi pada tubuh Anda berjalan normal, atau setidaknya diusahakan agar tetap berjalan normal. Efek samping akan muncul justru jika Anda tidak mengkonsumsi secara benar. 2. Sumber: http://www.kerjanya.net/faq/8035-thyrax.html Thyrax tersedia dalam bentuk tablet dengan isi sebesar 100 mcg. Dosis dewasa dan anak di atas 12 tahun adalah sebesar 150 – 200 mcg per hari. Sedangkan anak- anak usia 6-12 tahun 100-150 mcg, 1-5 tahun 75-100 mcg, 6-12 bulan 50-75 mcg, <6 bulan 25-50 mcg. Biasanya obat harus diberikan secara terus menerus seumur hidup. Dosis obat tidak boleh dikurangi atau ditambahkan sendiri di luar anjuran dokter. Kekurangan atau kelebihan dosis dapat menyebabkan gangguan pada tubuh
-
Upload
yoppy-soleman-st-mt -
Category
Documents
-
view
51 -
download
4
description
Endocrine - Thyroid - Thyrax - TSH Level - Candesartan
Transcript of Endocrinologist - Thyroid - Thyrax - TSH _ Candesartan

Endocrinologist – Terapi Pengganti (Thyrax) – TSH Level – Candesartan
1
Terapi Pengganti (Replacement Therapy) Sesudah Pengangkatan
Kelenjar Tiroid
1. Sumber: http://mediasehat.com/tanyajawab3482
Thyrax adalah obat yang berisi levothyroxin, yaitu hormon sintetik untuk tiroksin(salah satu hormon tiroid). Levothyroxin diberikan untuk kondisi-kondisi dimanaseseorang tidak mampu memproduksi hormon tiroid pada jumlah yang cukup,misalnya pada penderita hipotiroid, atau dalam kasus Bapak, karena mengalamipengangkatan kelenjar tiroid. Levothyroxin juga diberikan untuk mereka yangmengalami penyakit gondok (pembesaran kelenjar tiroid) akibat kekurangan iodium.
Dosis obat sebaiknya tidak Anda stop atau dikurangi, atau dilebihkan, di luar anjurandokter. Hal ini karena bisa menyebabkan Anda menderita hipotiroid (kekuranganhormon tiroid) atau malah hipertiroid (kelebihan hormon tiroid). Kedua kondisitersebut akan berakibat buruk pada kesehatan Bapak (untuk kondisi tersebut bisadi-search di mediasehat tentang hipotiroid dan hipertiroid). Namun jika Andamengalami gejala-gejala hipertiroid, sebaiknya diskusikan kembali dengan dokterAnda untuk kemungkinan meninjau kembali dosisnya. Jangan pernah mengambilkesimpulan sendiri untuk menambah ataupun mengurangi karena yang Andakonsumsi adalah hormon, dan dampak lebih/kurang akan berakibat langsung padafungsi tubuh Anda.
Selama Anda berada dalam jalur yang benar, artinya mengkonsumsi obat dalamjumlah yang tepat, justru Anda akan baik-baik saja. Karena Thyrax fungsinya bukanmengobati, tapi melengkapi apa yg kurang. Secara medis disebut sebagai terapipengganti (replacement therapy). Pengangkatan kelenjar tiroid menyebabkan tubuhAnda kehilangan 'pabrik' hormon tiroid, dan fungsi Thyrax adalah untuk melengkapiapa yang hilang dari tubuh Anda. Jadi fungsinya lebih untuk menjaga agar semuaaktivitas yang terjadi pada tubuh Anda berjalan normal, atau setidaknya diusahakanagar tetap berjalan normal. Efek samping akan muncul justru jika Anda tidakmengkonsumsi secara benar.
2. Sumber: http://www.kerjanya.net/faq/8035-thyrax.html
Thyrax tersedia dalam bentuk tablet dengan isi sebesar 100 mcg. Dosis dewasa dan
anak di atas 12 tahun adalah sebesar 150 – 200 mcg per hari. Sedangkan anak-
anak usia 6-12 tahun 100-150 mcg, 1-5 tahun 75-100 mcg, 6-12 bulan 50-75 mcg,
<6 bulan 25-50 mcg. Biasanya obat harus diberikan secara terus menerus seumur
hidup.
Dosis obat tidak boleh dikurangi atau ditambahkan sendiri di luar anjuran dokter.
Kekurangan atau kelebihan dosis dapat menyebabkan gangguan pada tubuh

Endocrinologist – Terapi Pengganti (Thyrax) – TSH Level – Candesartan
2
penderita. Selain itu, untuk mencegah terjadinya ketidakcocokan dosis, maka
penderita harus memeriksakan diri ke dokter untuk menyesuaikan dosisnya. Agar
efektif, thyrax harus diberikan dalam keadaan perut kosong atau sekitar setengah
jam sebelum makan. Perlu diketahui juga, beberapa jenis obat juga dapat
mengganggu penyerapan thyrax antara lain kalsium, zat besi, atau obat maag.
3. Sumber: http://www.medicinenet.com/thyroid_replacement-oral/page2.htm
Pharmacy Author: Eni Williams, PharmD, PhDMedical and Pharmacy Editor: Jay W. Marks, MD
What are the side effects of thyroid replacement hormones?
Thyroid replacement hormones usually are well tolerated. Symptoms that occur
during treatment are often due to toxic, elevated levels of thyroid hormones and
resulting symptoms from hyperthyroidism. Symptoms may include chest pain,
increased heart rate or pulse rate, excessive sweating, heat intolerance,
nervousness, headache, insomnia, diarrhea, vomiting, weight loss, and fever. Some
women may experience irregular menstrual cycles.
What are some examples of thyroid replacement hormones?
The following is a list of the thyroid replacement hormones that are available in the
United States:
levothyroxine sodium (Levothroid, Levoxyl, Synthroid, Tirosint, Unithroid)
liothyronine sodium (Cytomel, Triostat)
liotrix (Thyrolar)
For what conditions are thyroid replacement hormones used?
Thyroid replacement hormones are used to treat hypothyroidism (low production of
thyroid hormone) and myxedema, a condition that is caused by prolonged
hypothyroidism. Thyroid replacement hormones prevent thyroid hormone release
from cancerous thyroid nodules and are used therefore to treat thyroid cancers.
They also are used to manage thyrotoxicosis, a condition in which there are high
levels of thyroid hormones resulting from over-active thyroid glands and too much
thyroid hormone. Thyrotoxicosis may progress to hypothyroidism or cause the
growth of goiters necessitating the use of thyroid replacement hormones.
Are there any differences among the different types of thyroid replacement
hormones?

Endocrinologist – Terapi Pengganti (Thyrax) – TSH Level – Candesartan
3
There is conflicting evidence regarding which hormone replacement therapy should
be preferred. The American Association of Clinical Endocrinologists recommends
that clinical hypothyroidism is best treated with synthetic T4 levothyroxine (for
example levothyroxine and sodium [Synthroid, Levoxyl and Levothroid]). There is
variability between the absorption and distribution of generic T4 compared to brand
name preparations. Hence it is recommended that patients remain with specific
brand names during treatment. There is also variability between generic formulations
and brand names of pure T3 (liothyronine [Cytomel, Triostat]), combined T4/T3
formulations (liotrix [Thyrolar]) and thyroid extracts from animal sources (Armour
Thyroid, Nature-Throid etc.). Thyroid extracts from animal sources are no longer
available in the United States. Emerging information shows that combination of
T4/T3 therapy may have some advantages over T4 in cognitive performance and
mood but studies are not conclusive.
With which drugs do thyroid replacement hormones interact?
Thyroid replacement hormones should be used cautiously in people with diabetes
since starting or discontinuing therapy may lead to a loss of control of the blood
sugar requiring adjustments in doses of insulin or oral antidiabetic drugs (for
example, glyburide [Micronase]). The effects of blood thinners such as warfarin
(Coumadin) may be increased by thyroid replacement hormones warranting a
decrease in the dose of warfarin in addition to monitoring of blood clotting.
Intravenous epinephrine administration in patients with coronary artery disease who
are taking thyroid replacement hormones may increase the risk of complications
such as difficulty in breathing and possibly heart attacks. The effectiveness of some
beta blockers [for example, metoprolol (Lopressor) orpropranolol (Inderal)] may be
reduced when a patient is converted from a state of hypothyroidism (under activity)
to a normal state (euthyroid state). It also may be necessary to modify the dose of
digoxin (Lanoxin) and theophylline (Slo-Bid) when a patient is converted from
hypothyroidism (under activity) to a normal state (euthyroid state). There is
increased elimination of theophylline in a euthyroid state compared to a state of
hypothyroidism.
The effectiveness of thyroid replacement hormones may be decreased when given
with drugs such as calcium carbonate, ferrous sulphate, cholestyramine (Questran)
and colestipol (Colestid) that binds thyroid replacement hormones and prevent their
absorption. This interaction may be reduced by separating the administration of
these drugs from thyroid replacement hormones by four hours.
4. Sumber: http://www.thyroid.org/thyroid-hormone-treatment/
THYROID HORMONE REPLACEMENT THERAPY

Endocrinologist – Terapi Pengganti (Thyrax) – TSH Level – Candesartan
4
Many people have a thyroid gland that cannot make enough thyroid hormone for the
body’s needs. This is called Hypothyroidism and may be caused by a non-
functioning thyroid gland (for example Hashimoto’s disease), by destruction of
thyroid gland by surgery or radiation treatment or by a non-functioning pituitary gland
(see Hypothyroidism Brochure). Hypothyroidism, is the most common reason for
needing thyroid hormone replacement.
The goal of thyroid hormone treatment is to closely replicate normal thyroid
functioning. Pure, synthetic thyroxine (T4) works in the same way as a patient’s own
thyroid hormone would. Thyroid hormone is necessary for the health of all the cells
in the body. Therefore, taking thyroid hormone is different from taking other
medications, because its job is to replace a hormone that is missing. The only safety
concerns about taking thyroid hormone are taking too much or too little. Your thyroid
function will be monitored by your physician to make sure this does not happen.
When thyroid hormone is used to treat hypothyroidism, the goal of treatment is to
keep thyroid function within the same range as people without thyroid problems.
Keeping the TSH level in the normal range does this. The best time to take thyroid
hormone is probably first thing in the morning on an empty stomach. This is because
food in the stomach can affect the absorption of thyroid hormone. However, the most
important thing is to be consistent, and take your thyroid hormone at the same time,
and in the same way, every day. If you are taking several other medications, you
should discuss the timing of your thyroid hormone dose with your physician.
Do not stop your thyroid hormone without discussing this with your physician. Most
thyroid problems are permanent, and therefore most patients require thyroid
hormone for life. If you miss a dose of thyroid hormone, it is usually best to take the
missed dose as soon as you remember. It is also safe to take two pills the next day;
one in the morning and one in the evening. It is very important that your thyroid
hormone and TSH levels are checked periodically, even if you are feeling fine, so
that your dose of thyroid hormone can be adjusted if needed.
Warning – Too Much Thyroid HormoneIncreases Bone Fractures In The Elderly
References: Singer PA, Cooper DS, Levy EG, Ladenson PW, Braverman LE, Daniels G,
Greenspan FS, McDougall IR, Nikolai TF 1995 Treatment guidelines for patientswith hyperthyroidism and hypothyroidism. Standards of Care Committee, AmericanThyroid Association. J A M A 273:808-812
Canaris GJ, Manowitz NR, Mayor G, Ridgway EC 2000 The Colorado thyroiddisease prevalence study. Arch Int Med 160:526-534

Endocrinologist – Terapi Pengganti (Thyrax) – TSH Level – Candesartan
5
Sheppard MC, Holder R, Franklyn JA 2002 Levothyroxine treatment and occurrenceof fracture of the hip. Arch Int Med 162:338-343
Bauer DC, Ettinger B, Nevitt MC, Stone KL 2001 Risk for fracture in women withlow serum levels of thyroid-stimulating hormone. Ann Int Med 134:561-568
Murphy E, Williams GR 2004 The thyroid and the skeleton. Clinical Endocrinology61:285-298
Imam A, Iqbal J, Blair HC, Davies TF, Huang CL, Zallone A, Zaidi M, Sun L 2009Role of the pituitary-bone axis in skeletal pathophysiology. Curr Op Endocrinol Diab16:423-429
Flynn RW, Bonellie SR, Jung RT, MacDonald TM, Morris AD, Leese GP 2010Serum thyroid-stimulating hormone concentration and morbidity from cardiovasculardisease and fractures in patients on long-term thyroxine therapy. J Clin EndocrinolMetab 95:186-193
Turner MR, Camacho X, Fischer HD, Austin PC, Anderson GM, Rochon PA,Lipscombe LL 2011 Levothyroxine dose and risk of fractures in older adults: nestedcase-control study. BMJ 342:d2238
Syed FA, Ng AC 2010 The pathophysiology of the aging skeleton. Curr OsteoporosRep
Kabadi UM 1997 Influence of age on optimal daily levothyroxine dosage in patientswith primary hypothyroidism grouped according to etiology. Southern MedicalJournal 90:920-924
Sawin CT, Herman T, Molitch ME, London MH, Kramer SM 1983 Aging and thethyroid. Decreased requirement for thyroid hormone in older hypothyroid patients.Am J Med 75:206-209
Boucai L, Hollowell JG, Surks MI 2011 An approach for development of age-,gender-, and ethnicity-specific thyrotropin reference limits. Thyroid 21:5-11
Cooper DS, Doherty GM, Haugen BR, Kloos RT, Lee SL, Mandel SJ, Mazzaferri EL,McIver B, Pacini F, Schlumberger M, Sherman SI, Steward DL, Tuttle RM 2009Revised American Thyroid Association management guidelines for patients withthyroid nodules and differentiated thyroid cancer. Thyroid 19:1167-1214
For many years the American Thyroid Association has recommended close
monitoring of all patients treated with thyroid hormone (1). The reason for this
recommendation is that many patients are either overtreated or undertreated based
on their blood TSH (thyroid stimulating hormone) levels (2), which may lead to
adverse effects .
This problem has been found to be especially important in post menopausal women
and older men (3) who are at increased risk for fractures from worsening
osteoporosis when overtreated with thyroid hormones (4). Thyroid hormones have a
direct action on bone cells leading to bone loss (5) . TSH, which may play a role in
protecting bone (6), is also low in overtreated patients. On the other hand, patients
with hypothyroidism treated with doses of thyroxine that keep TSH within the normal
range, do not appear to be at increased risk of fracture (4,7). For this reason, regular
monitoring of thyroid replacement therapy every 6-12 months once stabilized, using
serum TSH as a gauge, is the current standard of care (1).
This issue is again emphasized by a new study from Toronto, Canada published in
the British Medical Journal examining the health records of 213,511 patients over
the age of 70 years who were taking thyroxine over a 3.8 year period (8). 10.4% had
a fracture during this time and 88% of the fractures were in women. The risk of
fracture was almost double for those currently taking thyroid hormone as compared
to those who only used it years ago. Those patients taking higher doses of thyroxine

Endocrinologist – Terapi Pengganti (Thyrax) – TSH Level – Candesartan
6
were more likely to have had a fracture than those taking lower doses. Unfortunately
serum TSH data were not available so it is not certain which patients were properly
treated, but it is plausible that many patients were overtreated, especially those who
received higher doses. This supports the importance of avoiding overtreatment with
thyroxine by adjusting the dose carefully through TSH monitoring.
Age itself is a risk factor for osteoporosis and fracture (9). Additionally, older patients
need less thyroxine to maintain a euthyroid state (10,11). Failure to recognize the
relationship of age and thyroxine requirements will lead to over dosage if the dose of
thyroxine is not titrated down as patients age. Unnecessary treatment of elderly
patients adds to this danger. The diagnosis of thyroid failure in the elderly needs to
be carefully evaluated with the knowledge that the upper normal value for TSH in
people over 80 yrs is ~7.5 uU/ml, compared to 4.0 uU/ml in young adults (12).
Therefore careful selection of which elderly patients should be treated with thyroxine
is critical. Thyroid hormone overtreatment of elderly patients is an avoidable
problem.
Individuals vary in their absorption of thyroxine, sometimes because of use of
interfering medications, higher thyroxine doses may be required for some patients to
achieve normal TSH levels. This should not contribute to bone loss as long as
overtreatment is avoided. Further, some patients with thyroid cancer need to have a
lower TSH levels to prevent cancer recurrence (13). In these selected patients the
risk of bone loss is outweighed by beneficial effects on control of the cancer. Hence,
it is important is to adjust the dose of thyroxine to achieve TSH levels that are
appropriate for each individual patient.
5. Sumber: http://www.cancer.org/cancer/thyroidcancer/detailedguide/thyroid-cancer-
treating-thyroid-hormone-therapy
Thyroid hormone therapy
Taking daily pills of thyroid hormone (thyroid hormone therapy) can serve 2
purposes:
It can help maintain the body’s normal metabolism (by replacing missing
thyroid hormone after surgery).
It can help stop any remaining cancer cells from growing (by lowering TSH
levels).
After a thyroidectomy, the body can no longer make the thyroid hormone it needs, so
patients must take thyroid hormone (levothyroxine) pills to replace the loss of the
natural hormone.
Taking thyroid hormone may also help prevent some thyroid cancers from returning.
Normal thyroid function is regulated by the pituitary gland. The pituitary makes a
hormone called TSH that causes the thyroid gland to make thyroid hormone for the

Endocrinologist – Terapi Pengganti (Thyrax) – TSH Level – Candesartan
7
body. TSH also promotes growth of the thyroid gland and probably of thyroid cancer
cells. The level of TSH, in turn, is regulated by how much thyroid hormone is in the
blood. If the level of thyroid hormone is low, the pituitary makes more TSH. If the
level of thyroid hormone is high, not as much TSH is needed, so the pituitary makes
less of it.
Doctors have learned that by giving higher than normal doses of thyroid hormone,
TSH levels can be kept very low. This may slow the growth of any remaining cancer
cells and lower the chance of some thyroid cancers (especially high-risk cancers)
coming back.
Possible side effects
Taking higher than normal levels of thyroid hormone seems to have few short-term
side effects, but some doctors have expressed concerns about taking them for long
periods of time. High levels of thyroid hormone can lead to problems with a rapid or
irregular heartbeat. Over the long run, high doses of thyroid hormone can lead to
weak bones (osteoporosis). Because of this, high doses of thyroid hormone may be
reserved for people with differentiated thyroid cancers who are at high risk of
recurrence.
TSH (thyroid-stimulating hormone) Level
1. Sumber: http://www.everydayhealth.com/hs/healthy-living-with-
hypothyroidism/understanding-test-results/
Understanding Your Hypothyroidism Test Results
By Beth W. Orenstein Reviewed by Farrokh Sohrabi, MD
A simple regular blood test is used to guide treatment for hypothyroidism and
monitor the condition. Here's what the numbers mean.
If there’s a bright side to hypothyroidism, or an underactive thyroid, it’s that treatment
usually just involves taking daily medication, and testing is limited to a simple blood
test. Your hypothyroidism test results are your doctor’s blueprint for prescribing the
right dose of synthetic thyroid hormone medication and tracking how well it’s
working.
Thyroid Hormones: Names and Numbers
The main job of the thyroid gland is to make the hormone thyroxine, also known as
T4 because it has four iodine molecules. The thyroid also makes the hormone
triiodothyronine, known as T3 because it has three iodine molecules, but in smaller
amounts, explains Cathy Doria-Medina, MD, an endocrinologist with HealthCare
Partners Medical Group in Torrance, Calif. “The thyroid gland makes mostly T4,

Endocrinologist – Terapi Pengganti (Thyrax) – TSH Level – Candesartan
8
[and] the T4 has to be converted to T3 because T3 is the part of thyroxine that
actually does the work," she says.
The pituitary gland at the base of the brain controls hormone production in your
body. It makes thyroid-stimulating hormone, or TSH, which tells the thyroid gland
how much T4 and T3 to produce. The TSH level in your blood reveals how much T4
your pituitary gland is asking your thyroid gland to make. If your TSH levels are
abnormally high, it could mean you have an underactive thyroid, or hypothyroidism.
“TSH levels go in the opposite direction of your thyroid hormone,” Dr. Doria-Medina
explains. “If you’re making too little thyroid hormone, your TSH will go up. If you’re
making too much thyroid hormone, your TSH will go down.”
What’s normal can vary, depending on a number of factors, including the laboratory
where your blood test is done, she adds. A normal range for TSH in most
laboratories is 0.4 milliunits per liter (mU/L) to 4.0 mU/L.
If your TSH is higher than 4.0 mU/L on repeat tests, you probably have
hypothyroidism.
Your doctor may also order a T4 test. Most of the T4 in your blood attaches to a
protein, and when it does, it can’t get into your cells. Only T4 that is unattached or
“free” can get into your cells to go to work. A blood test can measure how much free
T4 is available.
Hypothyroidism Tests: A Measure of Treatment Success
Hypothyroidism is treated with daily medication. Taking synthetic thyroid hormone
medication can bring your T4 and TSH levels back to their normal ranges. Once
you’re on the right dose, you should have no symptoms.
When you first start taking medication, your doctor will need to monitor your blood to
fine- tune the dosage. “Initially you will need to be tested more frequently,” Doria-
Medina says. “A person who is newly diagnosed and taking medication for
hypothyroidism should be tested every six weeks until the dosage is just right.”
The dose you start with is your doctor’s educated guess about what’s best for you,
most likely the lowest dose possible to avoid side effects, which can include a rapid
heartbeat and restlessness.
Medication for hypothyroidism is slow-acting, and it can take several weeks for your
body to adjust. If your TSH is still high and your symptoms haven’t subsided after six
to 10 weeks, your doctor will likely increase the dose, and you’ll need your blood
tested again after another six to 10 weeks.
Keeping Hypothyroidism Under Control
Because you’ll need to take thyroid medication every day for the rest of your life,
even after the right dose is found, your hormone levels will be monitored regularly to
be sure that your treatment is working properly. “Eventually, most people with
hypothyroidism can just be seen yearly by their doctor,” Doria-Medina says.
Endocrinologist – Terapi Pengganti (Thyrax) – TSH Level – Candesartan
9
The American Thyroid Association recommends that you keep your TSH within a
narrow range of 0.5 to 2.0 mU/L, but don’t be alarmed if your test results vary a little.
Some variation is normal because your pituitary gland sends out TSH in pulses, not
a steady stream. Also, the time of day you're tested can make a difference. TSH
levels are likely to be higher at night and lower during the day.
If you have new or worsening symptoms or your health-status changes — such as if
you become pregnant, go through menopause, or are given another medicine that
can interfere with your thyroid hormones — you should see your doctor and have
your blood tested again, even if it’s ahead of schedule.
Making the Most of Your Hypothyroidism TreatmentBy Dennis Thompson, Jr. Reviewed by Niya Jones, MD, MPH
Determining the right dose for levothyroxine can be tricky. Find out how to get
your medication right and discover the pitfalls of getting it wrong.
For people with hypothyroidism, the most common medication is levothyroxine, a
synthetic form of thyroid hormone. It's an effective hypothyroidism treatment, but
it's also a very tricky one — it can take weeks or even months to figure out the
daily dosage that works best for you. Even then, if you don't follow your doctor’s
instructions closely and take your medication properly, you could throw your
hormone levels out of whack.
Finding the Right Dose of Thyroid Medication
To determine your levothyroxine dosage, your doctor will draw your blood to test
for thyroid-stimulating hormone (TSH). This test measures how much thyroid
hormone your body is asking your thyroid gland to make. The higher your TSH
level, the more starved your body is for thyroid hormone — a sign that your
doctor needs to increase your dose of the synthetic replacement hormone.
Unless your TSH levels are unusually high, your doctor typically will start you out
at a low dose of about 50 micrograms a day. Then you'll probably have a TSH
test every three to four weeks, and the readings from those tests will be used to
determine your precise hypothyroidism treatment. Based on the test results, your
doctor may increase or decrease the dose until your thyroid hormone levels
stabilize.
"You’ll likely get to a steady level in around a month, and then four to six weeks is
the rule of thumb to re-check your levels again," says Stephanie Lee, MD, PhD
associate chief of endocrinology, nutrition, and diabetes at Boston Medical
Center and an associate professor at the Boston University School of Medicine.
If you find that your levels are not stabilizing, you and your doctor will need to
discuss alternatives. Your doctor might prescribe another type of levothyroxine or
Endocrinologist – Terapi Pengganti (Thyrax) – TSH Level – Candesartan
10
see if you respond better to natural thyroid hormone or a combination of different
thyroid hormones.
Following Thyroid Treatment Instructions
It's very important to follow your doctor's instructions when taking medication as
part of your hypothyroidism treatment. If you don't, your body may not be able to
fully absorb the levothyroxine and your hormone levels could fluctuate.
"This hormone is potent in very small amounts, so any little change in your
routine can change your hormone levels," says Laura Pizzi, PharmD, a professor
at the Jefferson School of Pharmacy at Thomas Jefferson University in
Philadelphia.
Small changes that can influence the effect of thyroid medication on your body
include:
Changing the time of day you take your dose
Taking the medication on an empty stomach, then switching to taking it
with food
Switching brands of levothyroxine
For the best levothyroxine absorption, Hossein Gharib, MD, a professor of
endocrinology at the Mayo Clinic in Rochester, Minn., recommends that it be
taken in a fasting state, just after you wake up. "If you can't take it in a fasting
state, they you should take it in the evening, two to three hours after your
evening meal,” Dr. Gharib says.
Watching for Interactions With Levothyroxine
Other drugs and some dietary supplements can interact with levothyroxine. For
example, iron and calcium supplements can interfere with the absorption of
levothyroxine. The iron or calcium can bind with the synthetic hormone,
preventing your body from using it. "You're basically snatching away some of the
levothyroxine that otherwise would’ve been absorbed into the body," Dr. Pizzi
says.
The hormone estrogen also can interfere with the body's ability to use
levothyroxine. That means women taking birth control pills may need an
increased dose of thyroid medication, Pizzi says.
Other medications that can interfere with the absorption of levothyroxine include:
Aspirin
Amphetamines
Anticoagulants
Some antidepressants
Anti-anxiety drugs
Arthritis medications
Beta blockers
Insulin

Endocrinologist – Terapi Pengganti (Thyrax) – TSH Level – Candesartan
11
Monitoring Potential Side Effects of Thyroid Medication
Not taking levothyroxine the right way or experiencing drug interactions can
make your thyroid hormone levels swing high or low and cause side effects.
Elevated hormone levels can make you feel shaky, jittery, and jumpy, Pizzi says.
You might notice your heart racing or have trouble sleeping at night. You might
even lose some weight.
Hormone levels that are too low can cause fatigue and sluggishness. You might
experience a slow heart rate, lose some of your hair, feel depressed, or gain
weight.
If you experience any of these problems, call your doctor. "Your doctor will likely
ask you to come in and get your blood checked," Pizzi says. Based on the
results, he or she will probably change your thyroid medication dosage to
address the side effect.
Overall, if you establish and maintain a regular routine with your hypothyroidism
treatment, the condition should have little effect on your long-term health and
well-being, Pizzi says.
2. Sumber: http://www.md-health.com/High-Tsh.html
What Does a High TSH Mean?What does a high TSH mean? High levels of TSH in the blood stream typically
signal that the thyroid is underperforming. High TSH levels are a common signal
of hypothyroidism that will require medical treatment to avoid potential health
risks.
TSH or thyroid stimulating hormone is a hormone produced in the anterior
pituitary gland. This is used to help stimulate the thyroid to produce
triiodothyronine (T3) or thyroxine (T4), hormones that help stimulate the
metabolism. If your pituitary gland is producing TSH trying to stimulate the thyroid
but the thyroid does not respond, it can result in an excessive amount of TSH in
the bloodstream. This can be caused by stress, illness, an obstruction or surgery
causing the thyroid to malfunction or be sluggish.
What is a TSH Test?
A TSH test is a lab test that analyzes your blood to determine the body's overall
TSH levels. If you begin to show signs of a malfunctioning thyroid your doctor my
order a test to check for the TSH levels in your system. If these show a high level
of TSH you may have a sluggish thyroid, but low levels of TSH signal that your
thyroid may be overactive.
During a TSH test, your doctor will take a blood sample to check the hormone
levels. A needle will be placed in a sterilized are of your arm, then attached to a

Endocrinologist – Terapi Pengganti (Thyrax) – TSH Level – Candesartan
12
tube to collect the blood. After this is finished the needle removed and you will be
asked to put pressure and a bandage on the site to stop the bleeding. In some
cases an elastic band may be placed around the arm to make it easier to collect
the blood. You should not feel a great deal of pain from the elastic band or the
needle, though you may develop a bruise at the injection site.
Your doctor will be focusing on the two hormones that control the metabolism,
triiodothyronine (T3) and thyroxine (T4). Results of the TSH test are typically
available 2-3 days after the test is given. If your hormones do not fall within a
healthy range your doctor will explain what may be going wrong and what you
can do treat this condition.
What is the Normal Range of TSH?
There are a range of levels that your TSH levels can be. Learning what these
levels mean will help you work with your doctor to address your condition
adequately.
Normal TSH - Adults should have TSH hormone levels that range from
0.4-4.2 mU/L. This indicates that the signals from your pituitary gland
match the activity of your thyroid gland. Your doctor will use this hormone
level alongside the other signals and side affects you may be showing to
determine if there is an underlying health issue at hand.
Low TSH - Low TSH levels can be a sign that you are dealing with an
overactive thyroid gland from conditions such as goiter, noncancerous
tumors or Graves's disease. The thyroid may also become overactive
during the first trimester of pregnancy. If you are already being treated for
thyroid issues, you may develop low TSH levels if you are taking too much
thyroid medication. If you are not showing signs of overactive thyroid you
may have damaged the pituitary gland, causing it to produce less TSH.
High TSH - High levels of TSH are typically caused by an underactive
thyroid or hypothyroidism. This is typically caused by Hashimoto's
thyroiditis. If you are already being treated for a thyroid disorder this can
be a sign that you need to increase your medication. In rare cases, you
may be showing high TSH levels because you have developed a tumor
that is causing the pituitary gland to over-produce TSH.
Conditions that Cause High TSH
Once it is determined that you have excessive levels of TSH in your system, your
doctor will start narrowing down what is causing the trouble.
Hypothyroidism - Hypothyroidism is a condition that is defined by your
body failing to produce enough hormones to adequately manage your
metabolism. Patients suffering from this condition will typically experience
dry skin, increased sensitivity to cold, thinning hear, impaired memory,
muscle aches, puffy face, unexplained weight gain, constipation, fatigue,
hoarseness, elevated cholesterol, irregular menstrual periods or
depression. A number of circumstances such as surgery, taking
psychiatric medications, radiation therapy or an autoimmune disease can

Endocrinologist – Terapi Pengganti (Thyrax) – TSH Level – Candesartan
13
lead to this condition. Hypothyroidism is typically managed with
medication that will artificially replace these hormones.
Pituitary Tumors - In rare cases, excessive TSH levels are a sign that your
pituitary gland is not functioning properly. In some cases this is because a
group of cells has begun to grow on top of the gland. In most cases these
tumors are not cancerous, but they can cause interference in your bodily
functions that can lead to other negative side effects which could be
dangerous to the body. The overproduction of TSH can lead to an
overactive thyroid.
Thyroid Disorder - Thyroid disorders such as enlarged thyroid gland,
cancer or abnormal hormone production can cause the thyroid to function
poorly. Some of these conditions are harmless, but many will require
medical intervention to avoid unpleasant side effects such as a sluggish
metabolism that will lead to damage throughout the body.
3. Sumber: http://www.endocrineweb.com/conditions/thyroid/hypothyroidism-too-
little-thyroid-hormone-
Hypothyroidism: Too Little Thyroid Hormone
Part 1: Introduction, Causes, and Symptoms of Hypothyroidism
Written by James Norman MD, FACS, FACE
Hypothyroidism is a condition in which the body lacks sufficient thyroid hormone.
Since the main purpose of thyroid hormone is to "run the body's metabolism," it is
understandable that people with this condition will have symptoms associated
with a slow metabolism. The estimates vary, but approximately 10 million
Americans have this common medical condition. In fact, as many as 10% of
women may have some degree of thyroid hormone deficiency. Hypothyroidism
is more common than you would believe, and millions of people are currently
hypothyroid and don't know it. For an overview of how thyroid hormone is
produced and how its production is regulated, check out our thyroid hormone
production page.
Hypothyroidism Slideshow: Causes, Symptoms, and Treatments
Causes of Hypothyroidism
There are two fairly common causes of hypothyroidism. The first is a result of
previous (or currently ongoing) inflammation of the thyroid gland, which leaves a
large percentage of the cells of the thyroid damaged (or dead) and incapable of
producing sufficient hormone. The most common cause of thyroid gland failure is
called autoimmune thyroiditis (also called Hashimoto's thyroiditis), a form of
thyroid inflammation caused by the patient's own immune system.
The second major cause is the broad category of "medical treatments." The
treatment of many thyroid conditions warrants surgical removal of a portion or all
of the thyroid gland. If the total mass of thyroid producing cells left within the

Endocrinologist – Terapi Pengganti (Thyrax) – TSH Level – Candesartan
14
body are not enough to meet the needs of the body, the patient will develop
hypothyroidism. Remember, this is often the goal of the surgery for thyroid
cancer.
But at other times, the surgery will be to remove a worrisome nodule, leaving half
of the thyroid in the neck undisturbed. Sometimes, this remaining thyroid lobe
and isthmus will produce enough hormone to meet the demands of the body. For
other patients, however, it may become apparent years later that the remaining
thyroid just can't quite keep up with demand.
Similarly, goiters and some other thyroid conditions can be treated with
radioactive iodine therapy. The aim of the radioactive iodine therapy (for benign
conditions) is to kill a portion of the thyroid to prevent goiters from growing larger
or producing too much hormone (hyperthyroidism).
Occasionally, the result of radioactive iodine treatment will be that too many cells
are damaged so the patient often becomes hypothyroid within a year or two.
However, this is usually greatly preferred over the original problem.
There are several other rare causes of hypothyroidism, one of them being a
completely "normal" thyroid gland that is not making enough hormone because of
a problem in the pituitary gland. If the pituitary does not produce enough thyroid
stimulating hormone (TSH) then the thyroid simply does not have the "signal" to
make hormone. So it doesn't.
Symptoms of Hypothyroidism
Fatigue
Weakness
Weight gain or increased difficulty losing weight
Coarse, dry hair
Dry, rough pale skin
Hair loss
Cold intolerance (you can't tolerate cold temperatures like those around
you)
Muscle cramps and frequent muscle aches
Constipation
Depression
Irritability
Memory loss
Abnormal menstrual cycles
Decreased libido
Each individual patient may have any number of these symptoms, and they will
vary with the severity of the thyroid hormone deficiency and the length of time the
body has been deprived of the proper amount of hormone.
You may have one of these symptoms as your main complaint, while another will
not have that problem at all and will be suffering from an entirely different
symptom. Most people will have a combination of these symptoms. Occasionally,

Endocrinologist – Terapi Pengganti (Thyrax) – TSH Level – Candesartan
15
some patients with hypothyroidism have no symptoms at all, or they are just so
subtle that they go unnoticed.
If you have these symptoms, you need to discuss them with your doctor.
Additionally, you may need to seek the skills of an endocrinologist. If you have
already been diagnosed and treated for hypothyroidism and continue to have any
or all of these symptoms, you need to discuss it with your physician.
Potential Dangers of Hypothyroidism
Because the body is expecting a certain amount of thyroid hormone the pituitary
will make additional thyroid stimulating hormone (TSH) in an attempt to entice the
thyroid to produce more hormone. This constant bombardment with high levels of
TSH may cause the thyroid gland to become enlarged and form a goiter (termed
a "compensatory goiter").
Left untreated, the symptoms of hypothyroidism will usually progress. Rarely,
complications can result in severe life-threatening depression, heart failure, or
coma.
Hypothyroidism can often be diagnosed with a simple blood test. In some
persons, however, it's not so simple and more detailed tests are needed. Most
importantly, a good relationship with a good endocrinologist will almost surely be
needed.
Hypothyroidism is completely treatable in many patients simply by taking a small
pill once a day. However, this is a simplified statement, and it's not always so
easy. There are several types of thyroid hormone preparations and one type of
medicine will not be the best therapy for all patients. Many factors will go into the
treatment of hypothyroidism and it is different for everybody.
Hypothyroidism: Too little thyroid hormone
Part 2: Diagnosis and Treatments of Hypothyroidism.
Too little thyroid hormone produced.Since hypothyroidism is caused by too little
thyroid hormone secreted by the thyroid, the diagnosis of hypothyroidism is
based almost exclusively upon measuring the amount of thyroid hormone in the
blood. There are normal ranges for all thyroid hormones which have been
calculated by computers which measured these hormones in tens of thousands
of people. If your thyroid hormone levels fall below the normal range, that is
consistent with hypothyroidism These tests are very accurate and reliable and
are so routine that they are available to everybody. More about these tests on
another page. However, its not always so simple...keep reading.
REMEMBER
hypo = too little
thyroidism = disease of the thyroid
Thus, hypo-thyroidism = a disease of too little thyroid activity.

Endocrinologist – Terapi Pengganti (Thyrax) – TSH Level – Candesartan
16
The idea is to measure blood levels of T4 and TSH. In the typical person with an
under-active thyroid gland, the blood level of T4 (the main thyroid hormone) will
be low, while the TSH level will be high. This means that the thyroid is not
making enough hormone and the pituitary recognizes it and is responding
appropriately by making more Thyroid Stimulating Hormone (TSH) in an attempt
to force more hormone production out of the thyroid. In the more rare case of
hypothyroidism due to pituitary failure, the thyroid hormone T4 will be low, but the
TSH level will also be low. The thyroid is behaving "appropriately" under these
conditions because it can only make hormone in response to TSH signals from
the pituitary. Since the pituitary is not making enough TSH, then the thyroid will
never make enough T4. The real question in this situation is what is wrong with
the pituitary? But in the typical and most common form of hypothyroidism, the
main thyroid hormone T4 is low, and the TSH level is high.
The next question is: When is low too low, and when is high too high? Blood
levels have "normal" ranges, but other factors need to be taken into account as
well, such as the presence or absence of symptoms. You should discuss your
levels with your doctor so you can interpret how they are helping (or not?) fix
your problems.
Oh, if only it were this simple all the time! Although the majority of individuals
with hypothyroidism will be easy to diagnose with these simple blood tests, many
millions will have this disease in mild to moderate forms which are more difficult
to diagnose. The solution for these people is more complex and this is due to
several factors. First we must realize that not all patients with hypothyroidism are
the same. There are many degrees of this disease from very severe to very mild.
Additionally, and very importantly, we cannot always predict just how bad (or
good) an individual patient will feel just by examining his/her thyroid hormone
levels. In other words, some patients with very "mild" deviations in their thyroid
laboratory test results will feel just fine while others will be quite symptomatic.
The degree of thyroid hormone abnormalities often, but NOT ALWAYS will
correlate with the degree of symptoms. It is important for both you and your
physician to keep this in mind since the goal is not necessarily to make the lab
tests go into the normal range, but to make you feel better as well! We must also
keep in mind that even the "normal" thyroid hormone levels in the blood have a
fairly large range, so even if a patient is in the "normal" range, it may not be the
normal level for them.
For the majority of patients with hypothyroidism, taking some form of thyroid
hormone replacement (synthetic or natural, pill or liquid, etc) will make the
"thyroid function tests" return to the normal range, AND, this is accompanied by a
general improvement in symptoms making the patient feel better. This does not
happen to all individuals, however, and for these patients it is very important to
find an endocrinologist who will listen and be sympathetic. (We aim to help you
find this type of doctor.) Because most patients will be improved (or made
completely better) when sufficient thyroid hormone is provided on a daily basis to
make the hormone levels in the blood come into the normal range, physicians will
often will rely on test results to determine when a patient is on the appropriate
dose and therefore doing well. Remember, these tests have a wide normal
Endocrinologist – Terapi Pengganti (Thyrax) – TSH Level – Candesartan
17
range. Find a doctor who helps make you FEEL better, not just make your labs
better because once given this diagnosis, you are likely to carry it for a long, long
time. There is more than one drug, there is more than one lab test, and there is
a "just right" doctor for everybody.
Treatment of Hypothyroidism
Hypothyroidism is usually quite easy to treat (for most people)! The easiest and
most effective treatment is simply taking a thyroid hormone pill (Levothyroxine)
once a day, preferably in the morning. This medication is a pure synthetic form of
T4 which is made in a laboratory to be an exact replacement for the T4 that the
human thyroid gland normally secretes. It comes in multiple strengths, which
means that an appropriate dosage can almost always be found for each patient.
The dosage should be re-evaluated and possibly adjusted monthly until the
proper level is established. The dose should then be re-evaluated at least
annually. If you are on this medication, make sure your physician knows it so
he/she can check the levels at least yearly. Note: Just like we discussed above,
however, this simple approach does not hold true for everybody. Occasionally
the correct dosage is a bit difficult to pin-point and therefore you may need an
exam and blood tests more frequently. Also, some patients just don't do well on
some thyroid medications and will be quite happy on another. For these reasons
you should not be shy in discussing with your doctor your blood hormone tests,
symptoms, how you feel, and the type of medicine you are taking. The goal is to
make you feel better, make your body last longer, slow the risk of heart disease
and osteoporosis...in addition to making your blood levels normal! Sometimes
that's easy, when its not, you need a physician who is willing to spend the time
with you that you deserve while you explore different dosages other types of
medications (or alternative diagnoses).
Some patients will notice a slight reduction in symptoms within 1 to 2 weeks, but
the full metabolic response to thyroid hormone therapy is often delayed for a
month or two before the patient feels completely normal. It is important that the
correct amount of thyroid hormone is used. Not enough and the patient may have
continued fatigue or some of the other symptoms of hypothyroidism. Too high a
dose could cause symptoms of nervousness, palpitations or insomnia typical of
hyperthyroidism. Some recent studies have suggested that too much thyroid
hormone may cause increased calcium loss from bone increasing the patient's
risk for osteoporosis. For patients with heart conditions or diseases, an optimal
thyroid dose is particularly important. Even a slight excess may increase the
patient's risk for heart attack or worsen angina. Some physicians feel that more
frequent dose checks and blood hormone levels are appropriate in these
patients.
After about one month of treatment, hormone levels are measured in the blood to
establish whether the dose of thyroid hormone which the patient is taking is
appropriate. We don't want too much given or subtle symptoms of
hyperthyroidism could ensue, and too little would not alleviate the symptoms
completely. Often blood samples are also checked to see if there are antibodies
against the thyroid, a sign of autoimmune thyroiditis. Remember, this is the most
common cause of hypothyroidism. Once treatment for hypothyroidism has been

Endocrinologist – Terapi Pengganti (Thyrax) – TSH Level – Candesartan
18
started, it typically will continue for the patient's life. Therefore, it is of great
importance that the diagnosis be firmly established and you have a good
relationship with a physician you like and trust.
Synthetic T4 can be safely taken with most other medications. Patients taking
cholestyramine (a compound used to lower blood cholesterol) or certain
medications for seizures should check with their physician about potential
interactions. Women taking T4 who become pregnant should feel confident that
the medication is exactly what their own thyroid gland would otherwise make.
However, they should check with their physician since the T4 dose may have to
be adjusted during pregnancy (usually more hormone is needed to meet the
increased demands of the mother's new increased metabolism). There are other
potential problems with other drugs including iron-containing vitamins. Once
again, pregnant women (and all women and men for that matter) taking iron
supplements should discuss this with your physician. There are three brand
name Levothyroxine tablets now available. You may want to consult with your
physician or pharmacist on the most cost effective brand since recent studies
suggest that none is better than the other.
4. Sumber: http://www.endocrineweb.com/conditions/thyroid/thyroid-gland-function
Thyroid Gland Function TestsCommon Tests to ExamineWritten by James Norman MD, FACS, FACE
Some information on this page is a little more advanced. If you have troubleunderstanding the process of normal thyroid function, please go to our page describingthis process first.
As we have seen from our overview of normal thyroidphysiology, the thyroid gland produces T4 and T3. But thisproduction is not possible without stimulation from thepituitary gland (TSH) which in turn is also regulated by thehypothalamus's TSH Releasing Hormone. Now, withradioimmunoassay techniques it is possible to measurecirculating hormones in the blood very accurately.Knowledge of this thyroid physiology is important inknowing what thyroid test or tests are needed to diagnosedifferent diseases. No one single laboratory test is 100%accurate in diagnosing all types of thyroid disease; however,a combination of two or more tests can usually detect even the slightest abnormalityof thyroid function.
For example, a low T4 level could mean a diseased thyroid gland ~ OR ~ a non-functioning pituitary gland which is not stimulating the thyroid to produce T4. Since thepituitary gland would normally release TSH if the T4 is low, a high TSH level wouldconfirm that the thyroid gland (not the pituitary gland) is responsible for the

Endocrinologist – Terapi Pengganti (Thyrax) – TSH Level – Candesartan
19
hypothyroidism.
If the T4 level is low and TSH is not elevated, the pituitary gland is more likely to bethe cause for the hypothyroidism. Of course, this would drastically effect the treatmentsince the pituitary gland also regulates the body's other glands (adrenals, ovaries, andtesticles) as well as controlling growth in children and normal kidney function. Pituitarygland failure means that the other glands may also be failing and other treatment than justthyroid may be necessary. The most common cause for the pituitary gland failure is atumor of the pituitary and this might also require surgery to remove.
Modern measurement of thyroid hormones is done by a new technique, radioimmunoassay(RIA), discovered by Dr. Solomon Berson and Dr. Rosalyn Yallow. They were awarded the 1977Nobel Prize in Medicine for this discovery which revolutionized the study of thyroid disease aswell as the entire field of endocrinology.
The following are commonly used thyroid tests
Measurement of Serum Thyroid Hormones: T4 byRIAT4 by RIA (radioimmunoassay) is the most used thyroidtest of all. It is frequently referred to as a T7 whichmeans that a resin T3 uptake (RT3u) has been done to correct for certain medicationssuch as birth control pills, other hormones, seizure medication, cardiac drugs, or evenaspirin that may alter the routine T4 test. The T4 reflects the amount of thyroxine inthe blood. If the patient does not take any type of thyroid medication, this test is usuallya good measure of thyroid function.
Measurement of Serum Thyroid Hormones: T3 by RIAAs stated on our thyroid hormone production page, thyroxine (T4) represents 80% of thethyroid hormone produced by the normal gland and generally represents the overallfunction of the gland. The other 20% is triiodothyronine measured as T3 by RIA.Sometimes the diseased thyroid gland will start producing very high levels of T3 but stillproduce normal levels of T4. Therefore measurement of both hormones provides an evenmore accurate evaluation of thyroid function.
Thyroid Binding GlobulinMost of the thyroid hormones in the blood are attached to a protein called thyroid bindingglobulin (TBG). If there is an excess or deficiency of this protein it alters the T4 or T3measurement but does not affect the action of the hormone. If a patient appears to havenormal thyroid function, but an unexplained high or low T4, or T3, it may be due to anincrease or decrease of TBG. Direct measurement of TBG can be done and will explainthe abnormal value. Excess TBG or low levels of TBG are found in some families as anhereditary trait. It causes no problem except falsely elevating or lowering the T4 level.These people are frequently misdiagnosed as being hyperthyroid or hypothyroid, but theyhave no thyroid problem and need no treatment.
Measurement of Pituitary Production of TSHPituitary production of TSH is measured by a method referred to as IRMA(immunoradiometric assay). Normally, low levels (less than 5 units) of TSH are sufficientto keep the normal thyroid gland functioning properly. When the thyroid gland becomesinefficient such as in early hypothyroidism, the TSH becomes elevated even though theT4 and T3 may still be within the "normal" range. This rise in TSH represents thepituitary gland's response to a drop in circulating thyroid hormone; it is usually thefirst indication of thyroid gland failure. Since TSH is normally low when the thyroidgland is functioning properly, the failure of TSH to rise when circulating thyroid

Endocrinologist – Terapi Pengganti (Thyrax) – TSH Level – Candesartan
20
hormones are low is an indication of impaired pituitary function. The new "sensitive"TSH test will show very low levels of TSH when the thyroid is overactive (as a normalresponse of the pituitary to try to decrease thyroid stimulation). Interpretations of theTSH level depends upon the level of thyroid hormone; therefore, the TSH is usuallyused in combination with other thyroid tests such as the T4 RIA and T3 RIA.
TRH TestIn normal people TSH secretion from the pituitary can be increased by giving a shotcontaining TSH Releasing Hormone (TRH...the hormone released by the hypothalamuswhich tells the pituitary to produce TSH). A baseline TSH of 5 or less usually goes up to10-20 after giving an injection of TRH. Patients with too much thyroid hormone(thyroxine or triiodothyronine) will not show a rise in TSH when given TRH. This "TRHtest" is presently the most sensitive test in detecting early hyperthyroidism. Patients whoshow too much response to TRH (TSH rises greater than 40) may be hypothyroid. Thistest is also used in cancer patients who are taking thyroid replacement to see if they areon sufficient medication. It is sometimes used to measure if the pituitary gland isfunctioning. The new "sensitive" TSH test (above) has eliminated the necessity ofperforming a TRH test in most clinical situations.
Iodine Uptake ScanA means of measuring thyroid function is to measure how much iodine is taken up by thethyroid gland (RAI uptake). Remember, cells of the thyroid normally absorb iodine fromour blood stream (obtained from foods we eat) and use it to make thyroid hormone(described on our thyroid function page). Hypothyroid patients usually take up too littleiodine and hyperthyroid patients take up too much iodine. The test is performed by givinga dose of radioactive iodine on an empty stomach. The iodine is concentrated in thethyroid gland or excreted in the urine over the next few hours. The amount of iodine thatgoes into the thyroid gland can be measured by a "Thyroid Uptake". Of course, patientswho are taking thyroid medication will not take up as much iodine in their thyroid glandbecause their own thyroid gland is turned off and is not functioning. At other times thegland will concentrate iodine normally but will be unable to convert the iodine intothyroid hormone; therefore, interpretation of the iodine uptake is usually done inconjunction with blood tests.
Thyroid ScanTaking a "picture" of how well the thyroid gland isfunctioning requires giving a radioisotope to the patientand letting the thyroid gland concentrate the isotope (justlike the iodine uptake scan above). Therefore, it isusually done at the same time that the iodine uptake test isperformed. Although other isotopes, such as technetium, will be concentrated by thethyroid gland; these isotopes will not measure iodine uptake which is what we really wantto know because the production of thyroid hormone is dependent upon absorbing iodine.It has also been found that thyroid nodules that concentrate iodine are rarely cancerous;this is not true if the scan is done with technetium. Therefore, all scans are now done withradioactive iodine. Both of the scans above show normal sizedthyroid glands, but the one on the left has a "HOT" nodule in thelower aspect of the right lobe, while the scan on the right has a"COLD" nodule in the lower aspect of the left lobe (outlined in redand yellow). Pregnant women should not have thyroid scansperformed because the iodine can cause development troubles withinthe baby's thyroid gland.
Two types of thyroid scans are available. A camera scan is performedmost commonly which uses a gamma camera operating in a fixedposition viewing the entire thyroid gland at once. This type of scan takes only five to tenminutes. In the 1990's, a new scanner called a Computerized Rectilinear Thyroid (CRT)

Endocrinologist – Terapi Pengganti (Thyrax) – TSH Level – Candesartan
21
scanner was introduced. The CRT scanner utilizes computer technology to improve theclarity of thyroid scans and enhance thyroid nodules. It measures both thyroid functionand thyroid size. A life-sized 1:1 color scan of the thyroid is obtained giving the size insquare centimeters and the weight in grams. The precise size and activity of nodules inrelation to the rest of the gland is also measured. CTS of the normal thyroid gland Inaddition to making thyroid diagnosis more accurate, the CRT scanner improves theresults of thyroid biopsy. The accurate sizing of the thyroid gland aids in the follow-up ofnodules to see if they are growing or getting smaller in size. Knowing the weight of thethyroid gland allows more accurate radioactive treatment in patients who have Graves'disease.
Thyroid Scans are used for the following reasons:
Identifying nodules and determining if they are "hot" or "cold". Measuring the size of the goiter prior to treatment. Follow-up of thyroid cancer patients after surgery. Locating thyroid tissue outside the neck, i.e. base of the tongue or in the chest.
Thyroid UltrasoundThyroid ultrasound refers to the use of high frequency sound waves to obtain an image ofthe thyroid gland and identify nodules. It tells if a nodule is "solid" or a fluid-filled cyst,but it will not tell if a nodule is benign or malignant. Ultrasound allows accuratemeasurement of a nodule's size and can determine if a nodule is getting smaller or isgrowing larger during treatment. Ultrasound aids in performing thyroid needle biopsy byimproving accuracy if the nodule cannot be felt easily on examination. Several morepages are dedicated to the use of ultrasound in evaluating thyroid nodules.
Thyroid AntibodiesThe body normally produces antibodies to foreign substances such as bacteria; however,some people are found to have antibodies against their own thyroid tissue. A conditionknown as Hashimoto's Thyroiditis is associated with a high level of these thyroidantibodies in the blood. Whether the antibodies cause the disease or whether the diseasecauses the antibodies is not known; however, the finding of a high level of thyroidantibodies is strong evidence of this disease. Occasionally, low levels of thyroidantibodies are found with other types of thyroid disease. When Hashimoto's thyroiditispresents as a thyroid nodule rather than a diffuse goiter, the thyroid antibodies may not bepresent.
Thyroid Needle BiopsyThis has become the most reliable test to differentiate the "cold" nodule that is cancerfrom the "cold" nodule that is benign ("hot" nodules are rarely cancerous). It providesinformation that no other thyroid test will provide. While not perfect, it will providedefinitive information in 75% of the nodules biopsied. A very extensive discussion ofThyroid Needle Biopsy is found on another page.
Do I need to stop taking my thyroid pills for these tests?
Since Euthyrox or Synthroid (and most other thyroid pills) behave exactly as normalhuman thyroid hormone, they are not rapidly cleared from the body as other medicationsare. Most thyroid pills have a half life of 6.7 days which means they must be stopped forfour to five weeks (five half lives) before accurate thyroid testing is possible. Anexception to the long half life of thyroid medication is Cytomel - a thyroid pill with a halflife of only forty-eight hours. Therefore it is possible to change a person's thyroidreplacement to Cytomel for one month to allow time for his regular pills to clear thebody. Cytomel is then stopped for ten days (five half lives) and the appropriate test can
Endocrinologist – Terapi Pengganti (Thyrax) – TSH Level – Candesartan
22
then be done. Usually patients, even those who have no remaining thyroid function,tolerate being off thyroid replacement only ten days quite well.
Normal Laboratory Values
Test Abbreviation Typical Ranges
Serum thyroxine T4 4.6-12 ug/dl
Free thyroxine fraction FT4F 0.03-0.005%
Free Thyroxine FT4 0.7-1.9 ng/dl
Thyroid hormone binding ratio THBR 0.9-1.1
Free Thyroxine index FT4I 4-11
Serum Triiodothyronine T3 80-180 ng/dl
Free Triiodothyronine l FT3 230-619 pg/d
Free T3 Index FT3I 80-180
Radioactive iodine uptake RAIU 10-30%
Serum thyrotropin TSH 0.5-6 uU/ml
Thyroxine-binding globulin TBG 12-20 ug/dl T4 +1.8 ugm
TRH stimulation test Peak TSH 9-30 uIU/ml at 20-30 min
Serum thyroglobulin l Tg 0-30 ng/m
Thyroid microsomal antibody titer TMAb Varies with method
Thyroglobulin antibody titer TgAb Varies with method
How Your Thyroid Works
Controlling hormones essential to your metabolism
Written by Robert M. Sargis MD, PhD
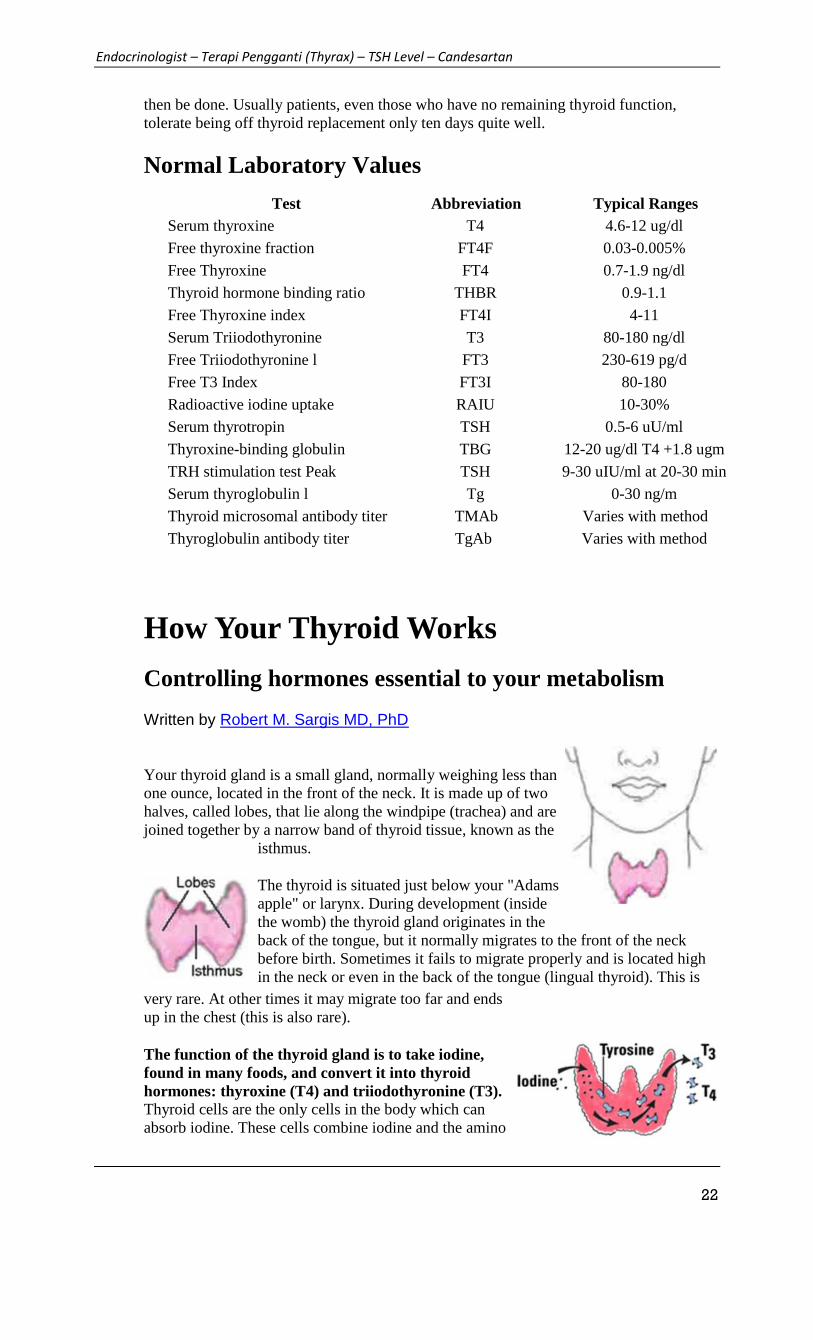
Your thyroid gland is a small gland, normally weighing less thanone ounce, located in the front of the neck. It is made up of twohalves, called lobes, that lie along the windpipe (trachea) and arejoined together by a narrow band of thyroid tissue, known as the
isthmus.
The thyroid is situated just below your "Adamsapple" or larynx. During development (insidethe womb) the thyroid gland originates in theback of the tongue, but it normally migrates to the front of the neckbefore birth. Sometimes it fails to migrate properly and is located highin the neck or even in the back of the tongue (lingual thyroid). This is
very rare. At other times it may migrate too far and endsup in the chest (this is also rare).
The function of the thyroid gland is to take iodine,found in many foods, and convert it into thyroidhormones: thyroxine (T4) and triiodothyronine (T3).Thyroid cells are the only cells in the body which canabsorb iodine. These cells combine iodine and the amino

Endocrinologist – Terapi Pengganti (Thyrax) – TSH Level – Candesartan
23
acid tyrosine to make T3 and T4. T3 and T4 are then released into the blood stream andare transported throughout the body where they control metabolism (conversion ofoxygen and calories to energy).
Every cell in the body depends upon thyroid hormones for regulation of theirmetabolism. The normal thyroid gland produces about 80% T4 and about 20% T3,however, T3 possesses about four times the hormone "strength" as T4.
The thyroid gland is under the control of the pituitarygland, a small gland the size of a peanut at the base of thebrain (shown here in orange). When the level of thyroidhormones (T3 & T4) drops too low, the pituitary glandproduces Thyroid Stimulating Hormone (TSH) whichstimulates the thyroid gland to produce more hormones.Under the influence of TSH, the thyroid will manufactureand secrete T3 and T4 thereby raising their blood levels.
+The pituitary senses this and responds by decreasing itsTSH production. One can imagine the thyroid gland as afurnace and the pituitary gland as the thermostat.
Thyroid hormones are like heat. When the heat gets back to the thermostat, it turns thethermostat off. As the room cools (the thyroid hormone levels drop), the thermostat turnsback on (TSH increases) and the furnace produces more heat (thyroid hormones).
The pituitary gland itself is regulated by another gland, known as the hypothalamus(shown in the picture above in light blue). The hypothalamus is part of the brain andproduces TSH Releasing Hormone (TRH) which tells the pituitary gland to stimulatethe thyroid gland (release TSH). One might imagine the hypothalamus as the person whoregulates the thermostat since it tells the pituitary gland at what level the thyroid shouldbe set.
Thyroid Gland, How it Functions,Symptoms of Hyperthyroidism andHypothyroidism
Written by Bridget Brady MD, FACS

Endocrinologist – Terapi Pengganti (Thyrax) – TSH Level – Candesartan
24
The thyroid gland is a butterfly-shaped organ located inthe base of your neck. It releases hormones that control metabolism—the way your bodyuses energy. The thyroid's hormones regulate vital body functions, including:
Breathing Heart rate Central and peripheral nervous systems Body weight Muscle strength Menstrual cycles Body temperature Cholesterol levels Much more!
The thyroid gland is about 2-inches long and lies in front of your throat below theprominence of thyroid cartilage sometimes called the Adam's apple. The thyroid has twosides called lobes that lie on either side of your windpipe, and is usually connected by astrip of thyroid tissue known as an isthmus. Some people do not have an isthmus, andinstead have two separate thyroid lobes.
How the Thyroid Gland WorksThe thyroid is part of the endocrine system, which is made up of glands that produce,store, and release hormones into the bloodstream so the hormones can reach the body'scells. The thyroid gland uses iodine from the foods you eat to make two main hormones:
Triiodothyronine (T3) Thyroxine (T4)
It is important that T3 and T4 levels are neither too high nor too low. Two glands inthe brain—the hypothalamus and the pituitary communicate to maintain T3 and T4balance.
The hypothalamus produces TSH Releasing Hormone (TRH) that signals the pituitaryto tell the thyroid gland to produce more or less of T3 and T4 by either increasing ordecreasing the release of a hormone called thyroid stimulating hormone (TSH).

Endocrinologist – Terapi Pengganti (Thyrax) – TSH Level – Candesartan
25
When T3 and T4 levels are low in the blood, the pituitary gland releases more TSH totell the thyroid gland to produce more thyroid hormones.
If T3 and T4 levels are high, the pituitary gland releases less TSH to the thyroid glandto slow production of these hormones.
Why You Need a Thyroid GlandT3 and T4 travel in your bloodstream to reach almost every cell in the body. Thehormones regulate the speed with which the cells/metabolism work. For example, T3 andT4 regulate your heart rate and how fast your intestines process food. So if T3 and T4levels are low, your heart rate may be slower than normal, and you may haveconstipation/weight gain. If T3 and T4 levels are high, you may have a rapid heart rateand diarrhea/weight loss.
Listed below are other symptoms of too much T3 and T4 in your body(hyperthyroidism):
Anxiety Irritability or moodiness Nervousness, hyperactivity Sweating or sensitivity to high temperatures Hand trembling (shaking) Hair loss Missed or light menstrual periods
The following is other symptoms of too little T3 and T4 in your body(hypothyroidism):
Trouble sleeping Tiredness and fatigue Difficulty concentrating Dry skin and hair Depression Sensitivity to cold temperature Frequent, heavy periods

Endocrinologist – Terapi Pengganti (Thyrax) – TSH Level – Candesartan
26
Joint and muscle pain
5. Sumber : www.mayoclinic.org
Diseases and Conditions
Hypothyroidism (underactive thyroid)
Tests and diagnosis
By Mayo Clinic Staff
Because hypothyroidism is more prevalent in older women, some doctors
recommend that older women be screened for the disorder during routine annual
physical examinations. Some doctors also recommend that pregnant women or
women thinking about becoming pregnant be tested for hypothyroidism.
In general, your doctor may test for an underactive thyroid if you're feeling
increasingly tired, have dry skin, constipation and weight gain, or have had
previous thyroid problems or goiter.
Blood tests
Diagnosis of hypothyroidism is based on your symptoms and the results of blood
tests that measure the level of TSH and sometimes the level of the thyroid
hormone thyroxine. A low level of thyroxine and high level of TSH indicate an
underactive thyroid. That's because your pituitary produces more TSH in an effort
to stimulate your thyroid gland into producing more thyroid hormone.
In the past, doctors weren't able to detect hypothyroidism until symptoms were
fairly advanced. But by using the sensitive TSH test, doctors are able to diagnose
thyroid disorders much earlier — often before you experience symptoms.
Because the TSH test is the best screening test, your doctor will likely check TSH
first and follow with a thyroid hormone test if needed. TSH tests also play an
important role in managing hypothyroidism. They help your doctor determine the
right dosage of medication, both initially and over time.
In addition, TSH tests are used to help diagnose a condition called subclinical
hypothyroidism, which usually causes no outward signs or symptoms. In this
condition, you have normal blood levels of triiodothyronine and thyroxine, but
higher than normal levels of TSH.
6. Sumber: https: www.synthroid.com
Endocrinologist – Terapi Pengganti (Thyrax) – TSH Level – Candesartan
27
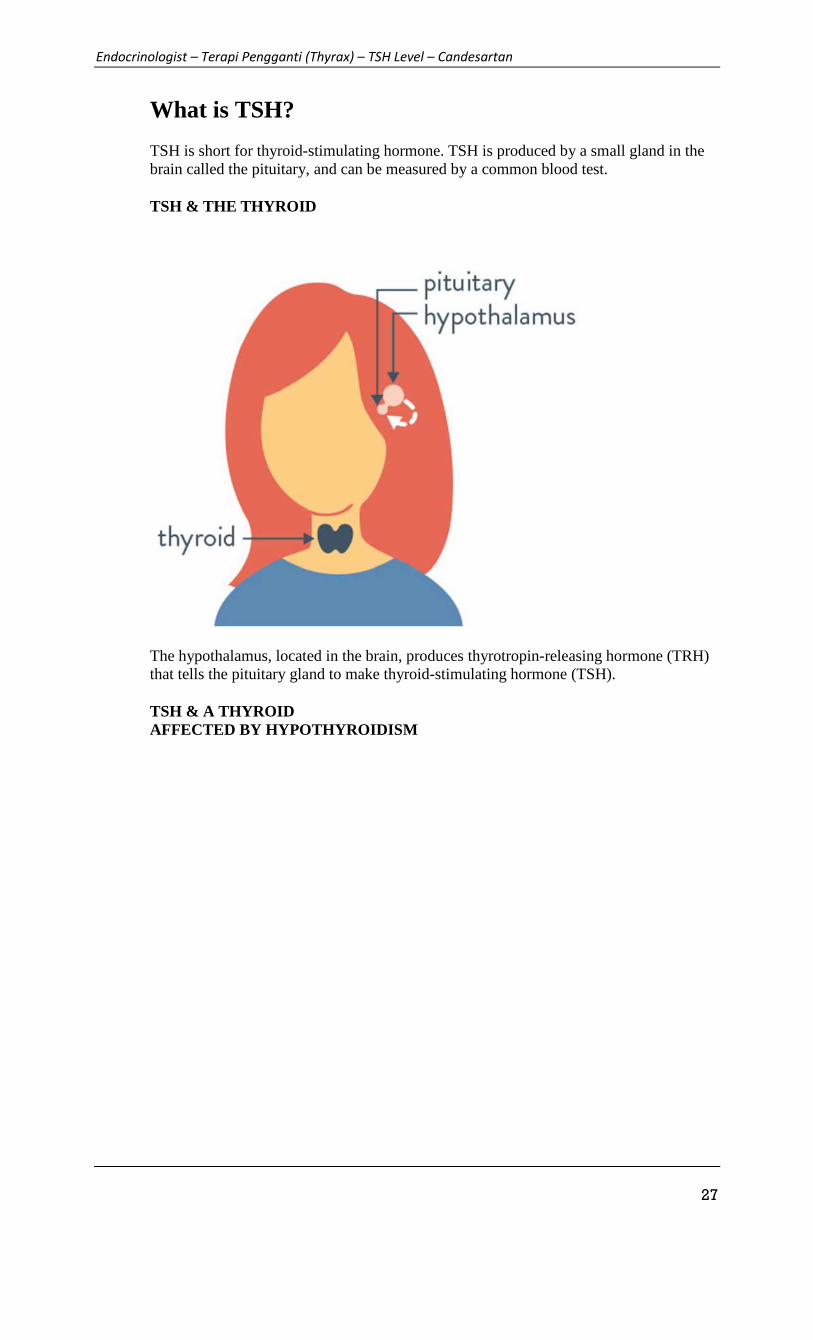
What is TSH?
TSH is short for thyroid-stimulating hormone. TSH is produced by a small gland in thebrain called the pituitary, and can be measured by a common blood test.
TSH & THE THYROID
The hypothalamus, located in the brain, produces thyrotropin-releasing hormone (TRH)that tells the pituitary gland to make thyroid-stimulating hormone (TSH).
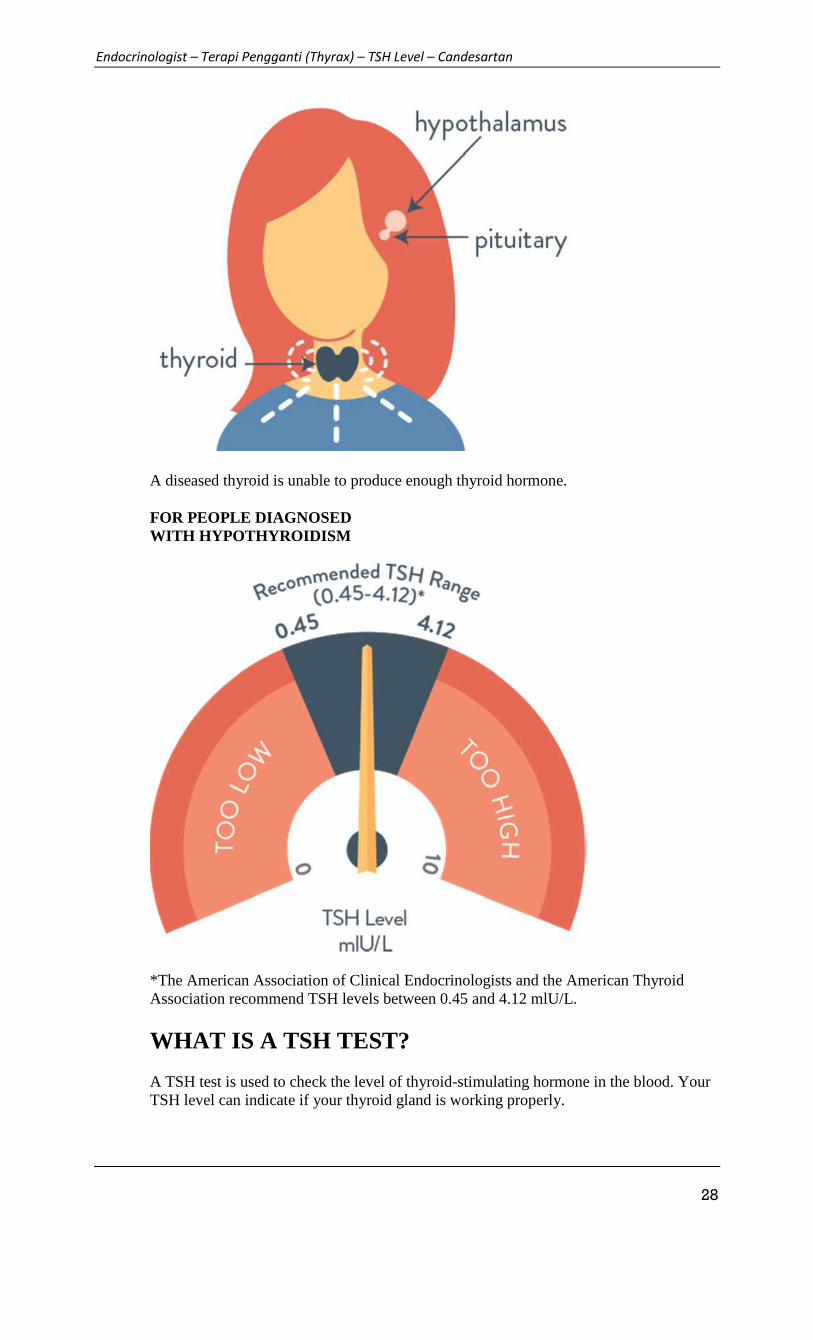
TSH & A THYROIDAFFECTED BY HYPOTHYROIDISM
Endocrinologist – Terapi Pengganti (Thyrax) – TSH Level – Candesartan
28
A diseased thyroid is unable to produce enough thyroid hormone.
FOR PEOPLE DIAGNOSEDWITH HYPOTHYROIDISM
*The American Association of Clinical Endocrinologists and the American ThyroidAssociation recommend TSH levels between 0.45 and 4.12 mlU/L.
WHAT IS A TSH TEST?
A TSH test is used to check the level of thyroid-stimulating hormone in the blood. YourTSH level can indicate if your thyroid gland is working properly.

Endocrinologist – Terapi Pengganti (Thyrax) – TSH Level – Candesartan
29
While a TSH test is usually used as the initial blood test to detect hypothyroidism, thedoctor may need to order additional tests to diagnose hypothyroidism. The doctor alsomay check your level of FT4, or free thyroxine, which is the amount of thyroxine in yourbody.
It’s important to know that blood tests are not the only way the doctor determines yourhypothyroidism diagnosis. Asking how you’re feeling is just as important. Reviewingyour TSH results and discussing all your symptoms helps the doctor see the biggerpicture.
Use
SYNTHROID® (levothyroxine sodium tablets, USP) is a prescription, man-madethyroid hormone that is used to treat a condition called hypothyroidism, except in casesof temporary hypothyroidism, which is usually associated with an inflammation of thethyroid gland (thyroiditis). It is meant to replace a hormone that is usually made by yourthyroid gland. Generally, thyroid replacement treatment is to be taken for life.
Important Safety Information
Thyroid hormones, including SYNTHROID, should not be used either alone orin combination with other drugs for the treatment of obesity or weight loss. Inpatients with normal thyroid levels, doses of SYNTHROID used daily forhormone replacement are not helpful for weight loss. Larger doses may resultin serious or even life-threatening events, especially when used in combinationwith certain other drugs used to reduce appetite.
Do not use SYNTHROID if you have hyperthyroidism or over-active thyroid,uncorrected adrenal problems, are having symptoms of a heart attack, or are allergicto any of its ingredients.
In women, long-term treatment with SYNTHROID has been associated withincreased bone loss, especially in women who are on high doses or those who are onhigh doses after menopause.
Tell your doctor if you are allergic to any foods or drugs, are pregnant or plan tobecome pregnant, are breast-feeding or are taking any other drugs, as well asprescription and over-the-counter products.
Tell your doctor about any other medical conditions you may have, especially heartdisease, diabetes, blood clotting problems, and adrenal or pituitary gland problems.The dose of other drugs you may be taking to control these conditions may have tobe changed while you are taking SYNTHROID. If you have diabetes, check yourblood sugar levels and/or the glucose in your urine, as ordered by your doctor andimmediately tell your doctor if there are any changes. If you are taking bloodthinners, your blood clotting status should be checked often.
Use SYNTHROID only as ordered by your doctor. Do not stop or change theamount you take, or how often you take it, unless told to do so by your doctor.
Products such as iron and calcium supplements and antacids can lower your body’sability to absorb SYNTHROID, so SYNTHROID should be taken 4 hours before orafter taking these products.
Take SYNTHROID as a single dose, preferably on an empty stomach, one-half toone hour before breakfast. Your body’s ability to absorb SYNTHROID is improvedwhen you take it on an empty stomach.
Tell your doctor if you develop any of the following symptoms: rapid or abnormalheartbeat, chest pain, difficulty catching breath, leg cramps, headache, feelingnervous, irritability, sleeplessness, shaking, change in appetite, weight gain or loss,throwing up, diarrhea, increased sweating, unable to tolerate heat, fever, changes inmenstrual periods, swollen red bumps on the skin or skin rash, or any other unusualmedical event.

Endocrinologist – Terapi Pengganti (Thyrax) – TSH Level – Candesartan
30
Tell your doctor or dentist that you are taking SYNTHROID before any surgery. Once your body’s response to SYNTHROID has stabilized, it is important to have
lab tests done, as ordered by your doctor, at least once a year.
This is the most important safety information you should know aboutSYNTHROID. For more information, talk with your doctor.
7. Sumber: http://www.medscape.com/viewarticle/705879
How do You Approach the Problem ofTSH Elevation in a Patient on High-doseThyroid Hormone Replacement?
John C. Morris
Int J Qual Health Care. 2009;70(5):671-673.
Abstract and Introduction
Abstract
Persistent elevation of TSH levels in patients under treatment for hypothyroidism is arelatively common clinical problem in endocrinology practice. The most common causefor this phenomenon is poor patient compliance with their thyroid hormone tablets. In thecompliant patient, however, multiple aetiologies are possible and a methodological andstepwise approach to the patient's problem will uniformly identify a cause, or at least aresolution.
Introduction
Thyroid hormone therapy is generally one of the most gratifying and effective hormonereplacements within the clinician's armamentarium. Most patients are satisfactorilymanaged with a single tablet of synthetically derived levothyroxine daily. To make thatpossible, a wide variety of tablet sizes are available from a number of manufacturers andfeature both brand-name products and several generic preparations. Although the averagedose for effective and optimal replacement varies somewhat from patient to patient, mosthypothyroid patients are managed within a fairly narrow dose window that variesaccording to body weight, the average being near 1·6–1·8 μg/kg.[1] Although total bodyweight is a convenient measurement upon which to base initial dosing, correctreplacement dosing correlates better with lean body mass than total body weight. [2] Inmost patients the circulating concentration of TSH serves as a reflection of thyroidhormone effect upon the pituitary and thereby as an effective marker of the adequacy ofthe replacement dose. However, one of the common clinical problems that I am asked toreview is that of the patient who requires higher doses of levothyroxine for normalizationof their TSH or whose TSH level remains persistently elevated despite these high doses.
For example, a recent patient I was referred was a 40-year-old woman from aneighbouring community who was diagnosed with hypothyroidism 1 year prior to hervisit. In brief, at that time she expressed symptoms compatible with hypothyroidism, such

Endocrinologist – Terapi Pengganti (Thyrax) – TSH Level – Candesartan
31
as severe constipation, fatigue and a modest amount of weight gain, and her thyroid glandwas firm, moderately diffusely enlarged but without nodularity, suggestive ofautoimmune thyroid disease. Laboratory investigation demonstrated marked TSHelevation (145 mIU/l, normal 0·3–5·0 mIU/l) and low free thyroxine (3·9 pmol/l, normal10·3–23·2 pmol/l). Her primary care physician started thyroxine replacement at standarddoses and adjusted the dosage upwards on three occasions because of persistentlyelevated TSH levels. After taking 300 μg of levothyroxine for 6 weeks, she was referred for further evaluation when her TSH remained elevated (77 mIU/l) and free thyroxineremained low at 7·7 pmol/l.
My approach to this patient and those with persistently elevated TSH levels despite dosesof thyroid hormone that should be adequate is outlined below. I recommend followingthese steps, although the order of them and the number that may need further pursuit mayvary from one patient to the next, based upon the individual patient's circumstances.
(1) Confirm the diagnosis and laboratory results. Frank primary hypothyroidism bylaboratory definition requires low levels of thyroid hormones (total and free T4 and T3)and elevated TSH. The finding of a persistently elevated TSH level is not enough toconfirm the diagnosis here, it is also crucial to measure thyroid hormone levels (T4 andT3). Markedly elevated TSH levels without low or at least low-normal thyroid hormonessuggests other diagnoses or reasons for the discrepant dose requirements such asheterophilic antibody interference with TSH measurements, TSH secreting pituitarytumours, or thyroid hormone resistance syndromes. If the thyroid hormone levels are notlow, more investigation and establishing the correct diagnosis are essential. Elevatedthyroid hormone levels that indicate the patient is taking and absorbing the thyroxinetablets appropriately suggest that investigations including more careful quenching of theserum samples for heterophilic antibody interference by the laboratory, serial dilution ofthe TSH sample, screening of the family members or genetic testing for thyroid hormoneresistance, and pituitary imaging for evidence of pituitary tumours may be helpful.Measurement of free T4 and/or free T3 by equilibrium dialysis may at times be helpful asthese more direct methods of assay are less susceptible to the effects of thyroxine bindingproteins.
(2) Ask about compliance. The most common reason for unusually high thyroid hormonedose requirements in my practice is poor compliance with the daily dosing oflevothyroxine. One day's tablet accounts for 14% of the total weekly dose and because ofthe long half-life of levothyroxine, missing a day will have an influence on thyroidhormone and TSH levels that is manifest over several days. Thus, having a discussionwith the patient about compliance should always be the first step in the process. Manypatients will acknowledge forgetting their tablets occasionally if asked in anonaccusatory, nonjudgemental manner. What is sometimes difficult here is determininghow often 'occasionally’ occurs.
(3) Check the patient's medication bottles and tablets. At times the patient's reported dosemay differ from that prescribed and of course errors by the pharmacist also occur,resulting in tablets inside the bottle that differ from those reported on the label. Thecolour coding of thyroxine tablets is helpful for determining the dose the patient is taking,but many patients, and occasionally their physicians, have colour vision deficienciesmaking actual inspection of the tablets an important step in understanding exactly whatthe patient is currently ingesting. Confirming records of prescriptions and refill recordswith the pharmacy may also be helpful in documenting compliance, or lack thereof.
(4) Review the thyroxine ingestion history. The most efficient and reproducible way oftaking levothyroxine is to ingest the tablets on an empty stomach and avoid ingestingother medications or food for 30–60 min afterwards. A fairly large and still growingnumber of medications, supplements and even food items can alter the fraction of aningested dose that is absorbed.[3,4] The ingestion of one or more of these items at or near

Endocrinologist – Terapi Pengganti (Thyrax) – TSH Level – Candesartan
32
the time of dosing with thyroxine can substantially change the dose requirement in anindividual patient, especially when practised as routine. The most common offenders thatI see are calcium and iron supplements. Some multivitamin preparations may alsoinfluence thyroxine absorption but the effect does not seem as clear or commonlyproblematic as that for calcium and iron supplements. A list of medications that mayinterfere is included in Table 1 , but this list is certainly incomplete as new offendingmedications are reported frequently.
(5) Investigate for malabsorption. Unfortunately, levothyroxine is not fully absorbed afteroral ingestion. On average, only about 70–80% of the available tablet dose is absorbed ineuthyroid individuals.[5] Interindividual variability in the efficiency of gastrointestinal(GI) absorption is fairly large and this variability accounts for most of the range ofrequirement seen between compliant patients after adjustment for body size.Malabsorption syndromes increase the requirement for levothyroxine by further reducingthe fraction of the ingested dose that is absorbed. Patients with short bowel from priorsmall bowel bypass or resection commonly require higher than expected T4 doses. If thepatient has frequent, voluminous stools, a malabsorption disorder may be evident andmeasurements of stool fat can confirm this diagnosis. However, thyroxine malabsorptionhas been reported as the initial finding in patients with otherwise asymptomaticmalabsorptive syndromes, especially coeliac disease.[6] I screen patients that get this faralong the diagnostic pathway with measurement of tissue transglutaminase antibodiesand, if positive, send them for GI evaluation, usually including small bowel biopsy andstool fat measurements. Correction of the malabsorption will normalize or at leastimprove thyroxine absorption in these patients. Helicobacter pylori infection, especiallywhen accompanied by atrophic gastritis and achlorhydria, has been reported to impairthyroxine absorption by up to 37% in patients with multinodular goitre. Antibiotictreatment of the H. pylori infection was also demonstrated to improve absorption andreduce thyroxine requirement in those patients.[7]
(6) Consider increased turnover or excretion. A number of drugs or clinical conditionsmay increase the turnover or excretion of thyroid hormone and thereby increaseconsiderably the requirement in individuals that are thyroid hormone dependent. Someexamples are phenytoin, carbamazapine and rifampin. Several of the new kinaseinhibitors, such as imatinib and sunitinib, that are entering the clinic for variousmalignancies appear to influence thyroxine requirements in this manner and this may be aclass effect, although reports to date are few.[8–10] In addition, patients with nephroticsyndrome who excrete large quantities of albumin may have increased thyroxinerequirements due to binding of T4 to the excreted albumin.[11,12] Women experienceincreased thyroxine requirements during normal pregnancy, that may reach as much as50% at its peak.[13]
(7) Perform a thyroxine absorption test. A clinical test to estimate thyroxine absorptionhas been proposed that may have utility in patients who have unexpectedly high T4requirements. This test involves administration of a single large dose of levothyroxine,usually in the range of 1000 μg, then monitoring T4 levels in blood over time.[4]
Although I have occasionally performed this test, I do not find it to be generally helpfulunless it demonstrates completely 'normal’ results, thereby supporting patientnoncompliance. Unfortunately, there is no well-established standard to which individualpatient results can be compared, especially one done in hypothyroid patients with normalabsorption. In the few circumstances when I have asked a patient to perform the test, theresults indicate that the patient does absorb thyroxine when exposed to a large dose, butleaves me wondering if it is a normal amount or not, because of the lack of adequatenormal standards. Furthermore, severe hypothyroidism itself may impair absorption,presumably due to oedema of the small bowel mucosa and this cannot be quantified bythe test. Thus, I have not found that this test helps me very much in the decision-makingprocess in individual patients.

Endocrinologist – Terapi Pengganti (Thyrax) – TSH Level – Candesartan
33
(8) Treat the patient. If an error by the pharmacy or patient, or a compliance-relatedcause, is identified, correction of these underlying factors will help to resolve thesituation. In some circumstances compliance issues are best treated by increasing thetablet size, assuming that compliance will continue at a similar rate. As a 'last resort’ inpatients with continued poor compliance, evidence supports successful use of thyroxineadministered once weekly. This quantity is roughly equivalent to the entire weekly totalas calculated above, but given as a single oral dose,[14] and administration can bemonitored if needed. Removing interfering drugs or changing ingestion patterns whenpresent can also be helpful when possible. In many patients the best course is to increasethe patient's T4 dose and titrate upwards until the TSH and T4 levels normalize. Exceptin patients with surgical small bowel syndromes, I have not yet seen a patient whorequired parenteral administration of thyroid hormone for maintenance. Even relativelylarge doses of levothyroxine administered orally are less expensive and better toleratedthat intravenous or intramuscular injections.
The patient described at the beginning of this article was very convincing in herdescription of faithfully ingesting her thyroxine tablets and had for several months beendoing so in the absence of other, potentially interfering medications or supplements afteradvice from her primary care provider. Although she still described symptoms ofhypothyroidism, I could not elicit symptoms suggestive of malabsorption. Her thyroidfunction tests confirmed inadequately replaced primary hypothyroidism in that her TSHremained elevated at 29·4 mIU/l and her free and total thyroxine levels were at the lowerend of the normal range, this after ingesting 300 μg of thyroxine for approximately 8 weeks. The screens for malabsorption and coeliac disease (transglutaminase antibodiesand stool fat measurement) were negative and urinalysis was normal. I elected to increaseher levothyroxine dose to 400 μg daily and 6 weeks later her TSH was below normal (0·2 mIU/l) and free thyroxine was elevated (25·7 pmol/l). We reduced the thyroxine dose to350 μg daily and after 8 weeks found that her TSH and free thyroxine levels had returned to normal. Her fatigue and constipation also improved and she stated that she felt muchbetter than before.
I have seen a small number of patients (unreported) that appear to have selectivemalabsorption of thyroxine. These patients clearly absorb levothyroxine poorly but do nothave evidence of generalized malabsorption or of coeliac disease and respond well toincreasing the levothyroxine to levels well above those considered usual, in the range of400–600 μg per day. At present I am not aware of a physiological explanation for these findings but I suspect one will be forthcoming with further investigation into thyroxinetransport and absorption. The patient described above may be a representative.
8. Sumber: http://www.medscape.com/viewarticle/722086_5
The Challenges and Complexities ofThyroid Hormone Replacement
Shayri M. Kansagra, BS; Christopher R. McCudden, PhD; Monte S. Willis, MD, PhD

Endocrinologist – Terapi Pengganti (Thyrax) – TSH Level – Candesartan
34
Lab Med. 2010;41(6):229-348.
T4/T3 Combination Compared with T4 Monotherapy
The recent resurgence into hypothyroidism treatment research derives from theexperience of clinicians who found that some patients remain symptomatic while onprescribed T4 replacement therapy. For example, 1 survey conducted in the UnitedKingdom revealed that patients treated with T4 had significantly more psychologicalmorbidity compared with euthyroid controls.[37] This was supported by findings in animalmodels, where hypothyroid rats realized normal thyroid hormone levels on a combinationof T3 and T4 (in the ratio normally secreted by the rat thyroid gland) but not with T4monotherapy.[38] This led to a landmark study by Bunevicius and colleagues whoassessed whether T4/T3 combination therapy had any advantages over T4 monotherapyfor hypothyroidism (Table 1).[19] To compare therapies, they used a crossover studydesign with 33 patients on different regimens of monotherapy and combination therapyover 2 different 5-week periods.[19] Combination therapy was achieved by replacing 50μg of the patient's usual T4 dose (ranging from 100–300 μg/day) with 12.5 μg of T3.[19]
Patients who received combination therapy had lower total and free T4 levels and higherT3 levels than patients who received T4 monotherapy. It was reported that cognitiveperformance and mood were significantly improved or normalized after treatment. [19]
These findings prompted a series of papers aimed at assessing the potential advantages ofcombination therapy over monotherapy for hypothyroidism.[19,39–43]
Following the landmark paper, Bunevicius and colleagues performed a second crossovertrial in women who had undergone a subtotal thyroidectomy as a treatment for Graves'disease (Table 1).[44] In this study, T4 therapy consisted of either the patient's regulardose of T4 or combination therapy, which was achieved by replacing 50 μg of the usual T4 dose with 10 μg of T3. After a period of 5 weeks, the patients were crossed over blindly to the opposite treatment. In patients who received combination therapy, theseverity of symptoms of hypothyroidism and hyperthyroidism had a tendency todecrease, as indicated by patient scores on a standard symptom scale. Mental status alsotended to improve with combination therapy compared with monotherapy, based onapparent improvement in mood (indicated by Visual Analogue Scale [VAS] scores).However, there was no difference in cognitive performance improvement (indicated byimproved scores on the Digit Symbol and Digit Span tests of the Wechsler AdultIntelligence Scale). Although this study was small (n=13), the authors concluded itsfindings were consistent with those of their earlier study in terms of demonstrating arelationship between T4/T3 combination therapy and improved mental function. [44]
Lab Med. 2010;41(6):229-348. © 2010 American Society for Clinical Pathology
Table 1. Summary of Major Studies to Date Which Compared Combined T3/T4 Therapies to Single T4 Monotherapies for
Hypothyroidism
Bunevicius, et
al 1999[7]
Bunevicius
2002[32]
Clyde, et al
2003[28]
Sawka, et al
2003[29]Walsh, et al 2003[31]
Siegmund, et al
2004[30]
Rodriguez, et al
2005[33]
Escobar-
Morreale 2005[34]
Saravanan
2005[35]
Number of
study
participants
(n)/cohort
33 10 46 40 110 23 27 28 697
Patients with
chronic
autoimmune
thyroiditis or
thyroid cancer
treated by near-
total
thyroidectomy
Women with
sub-total
thyroid-
ectomy for
Graves'
disease
Ages 24–65 with
primary
hypothyroidism
Patients with
depressive
symptoms and
primary
hypothyroidism
85% autoimmune or
idiopathic
hypothyroidism.
Remaining had post-
surgical hypo-
thyroidism,Graves'
disease, and
Hashimoto's
Hypothyroidism due
to
surgery/radioiodine
(21) or auto-immune
thyroiditis (2)
Primary
hypothyroidism
Women with
overt primary
hypothyroidism
Family practice
patients 18–75
with T4 dose >
100 mcg/day and
no T4 adjustments
in the past 3
months. Thyroid
CA and
Secondary

Endocrinologist – Terapi Pengganti (Thyrax) – TSH Level – Candesartan
35
disease. Hypothyroidism
excluded.
Study design
Randomized
control,
crossover-
design
Double blind,
cross-over
study
Randomized
control trial
Randomized
control trial
Double blind,
randomized control
trial with cross-over
Design
Double blind,
randomized control
trial with cross-over
design
Double blind,
randomized
control trial with
cross-over
design
Double blind,
randomized
cross-over trial
Double blind,
randomized cross-
over trial
Treatment
Original T4
dosage at
baseline vs
original dosage
minus 50 mcg
T4 replaced by
12.5 mcg of T3
per day.
Original T4
dosage at
baseline vs
original
dosage minus
50 mcg T4
replaced by
10 mcg T3
per day.
Original T4
dosage at
baseline vs
original dosage
minus 50 mcg T4
replaced with 7.5
mcg T3 given
twice a day.
Original T4 dose
at baseline vs
half of original
T4 dosage plus
12.5 mcg of T3
twice a day.
Original T4 dosage
vs original dose
minus 50 mcg T4
plus 10 mcg T3 once
a day.
Original T4 dosage
vs original does
minus 5% T4
replaced by T3 in
that amount once a
day.
Original T4
dosage vs
original dose
minus 50 mcg
T4 replaced by
10 mcg T3 once
a day.
100 mcg T4e vs
75 mcg T4 plus 5
mcg T3. All pts
received 87.5
mcg thyroxine
plus 7.5 mcg T3
per day during
the last 8 weeks.
Original T4
dosage vs original
dose minus 50
mcg T4 plus 10
mcg T3 per day.
Length of
study periods
(in weeks)
5 5 16 15 10 12 6 8 12
All material on this website is protected by copyright, Copyright © 1994-2015 by WebMD LLC. This
website also contains material copyrighted by 3rd parties.
9. Sumber: http://emedicine.medscape.com/article/122393-medication
HypothyroidismAuthor: Philip R Orlander, MD; Chief Editor: George T Griffing, MD
Practice Essentials
Hypothyroidism is a common endocrine disorder resulting from deficiency of thyroidhormone. In the United States and other areas of adequate iodine intake, autoimmunethyroid disease (Hashimoto disease) is the most common cause of hypothyroidism;worldwide, iodine deficiency remains the foremost cause.
The image below depicts the hypothalamic-pituitary-thyroid axis.

Endocrinologist – Terapi Pengganti (Thyrax) – TSH Level – Candesartan
36
The hypothalamic-pituitary-thyroidaxis. Levels of circulating thyroid hormones are regulated by a complex feedback systeminvolving the hypothalamus and pituitary gland.
Signs and symptoms
Hypothyroidism commonly manifests as a slowing in physical and mental activity butmay be asymptomatic. Symptoms and signs are often subtle and neither sensitive norspecific.
The following are symptoms of hypothyroidism:
Fatigue, loss of energy, lethargy Weight gain Decreased appetite Cold intolerance Dry skin Hair loss Sleepiness Muscle pain, joint pain, weakness in the extremities Depression Emotional lability, mental impairment Forgetfulness, impaired memory, inability to concentrate Constipation Menstrual disturbances, impaired fertility Decreased perspiration Paresthesia and nerve entrapment syndromes Blurred vision Decreased hearing Fullness in the throat, hoarseness
The following are symptoms more specific to Hashimoto thyroiditis:
Feeling of fullness in the throat Painless thyroid enlargement Exhaustion Transient neck pain, sore throat, or both
Endocrinologist – Terapi Pengganti (Thyrax) – TSH Level – Candesartan
37
Physical signs of hypothyroidism include the following:
Weight gain Slowed speech and movements Dry skin Jaundice Pallor Coarse, brittle, straw-like hair Loss of scalp hair, axillary hair, pubic hair, or a combination Dull facial expression Coarse facial features Periorbital puffiness Macroglossia Goiter (simple or nodular) Hoarseness Decreased systolic blood pressure and increased diastolic blood pressure Bradycardia Pericardial effusion Abdominal distention, ascites (uncommon) Hypothermia (only in severe hypothyroid states) Nonpitting edema (myxedema) Pitting edema of lower extremities Hyporeflexia with delayed relaxation, ataxia, or both
Myxedema coma is a severe form of hypothyroidism that most commonly occurs inindividuals with undiagnosed or untreated hypothyroidism who are subjected to anexternal stress. Features are as follows:
Altered mental status Hypothermia Bradycardia Hypercarbia Hyponatremia Cardiomegaly, pericardial effusion, cardiogenic shock, and ascites may be present
See Clinical Presentation for more detail.
Diagnosis
Third-generation thyroid-stimulating hormone (TSH) assays are generally the mostsensitive screening tool for primary hypothyroidism.[1] If TSH levels are above thereference range, the next step is to measure free thyroxine (T4) or the free thyroxineindex (FTI), which serves as a surrogate of the free hormone level. Routine measurementof triiodothyronine (T3) is not recommended.
Results in patients with hypothyroidism are as follows:
Elevated TSH with decreased T4 or FTI Elevated TSH (usually 4.5-10.0 mIU/L) with normal free T4 or FTI is considered
mild or subclinical hypothyroidism
Abnormalities in the complete blood count and metabolic profile that may be found inpatients with hypothyroidism include the following[2] :
Anemia Dilutional hyponatremia Hyperlipidemia

Endocrinologist – Terapi Pengganti (Thyrax) – TSH Level – Candesartan
38
Reversible increases in creatinine [2]
Elevations in transaminases and creatinine kinase
No universal screening recommendations exist for thyroid disease for adults. TheAmerican Thyroid Association recommends screening at age 35 years and every 5 yearsthereafter, with closer attention to patients who are at high risk, such as the following[3] :
Pregnant women Women older than 60 years Patients with type 1 diabetes or other autoimmune disease Patients with a history of neck irradiation
See Workup for more detail.
Management
Monotherapy with levothyroxine (LT4) remains the treatment of choice forhypothyroidism. Aspects of LT4 treatment are as follows:
Otherwise young and healthy patients can be started on LT4 at anticipated fullreplacement doses
In elderly patients and those with known ischemic heart disease, begin with onefourth to one half the expected dose and adjust the dose in small increments after noless than 4-6 weeks
For most cases of mild to moderate hypothyroidism, a starting LT4 dose of 50-75 µgdaily will suffice
Clinical benefits begin in 3-5 days and level off after 4-6 weeks Achieving a TSH level within the reference range may take several months LT4 dosing changes should be made every 6-8 weeks until the patient’s TSH is in
target range
After dose stabilization, patients can be monitored with annual clinical evaluations andTSH monitoring. Patients should be monitored for symptoms and signs ofovertreatment, which include the following:
Tachycardia Palpitations Atrial fibrillation Nervousness Tiredness Headache Increased excitability Sleeplessness Tremors Possible angina
In patients who continue to have symptoms (eg, weight gain, fatigue) despitenormalization of their TSH level, consideration should be given to causes other thanhypothyroidism. In some cases, however, the persistence of symptoms results fromimpaired conversion of T4 to T3 in the brain; these patients may benefit fromcombination LT4/liothyronine (LT3) therapy.[4]
The updated guidelines on hypothyroidism issued by the American Thyroid Associationin 2014 maintain the recommendation of levothyroxine as the preparation of choice forhypothyroidism, with the following considerations:[5, 6]

Endocrinologist – Terapi Pengganti (Thyrax) – TSH Level – Candesartan
39
If levothyroxine dose requirements are much higher than expected, considerevaluating for gastrointestinal disorders such as Helicobacter pylori –relatedgastritis, atrophic gastritis, or celiac disease; if such disorders are detected andeffectively treated, re-evaluation of thyroid function and levothyroxine dosage isrecommended.
Initiation or discontinuation of estrogen and androgens should be followed byreassessment of serum TSH at steady state, since such medications may alterlevothyroxine requirement.
Serum TSH should be reassessed upon initiation of agents such as tyrosine kinaseinhibitors that affect thyroxine metabolism and thyroxine or triiodothyroninedeiodination.
Serum TSH monitoring is advisable when medications such as phenobarbital,phenytoin, carbamazepine, rifampin, and sertraline are started.
When deciding on a starting dose of levothyroxine, the patient’s weight, lean bodymass, pregnancy status, etiology of hypothyroidism, degree of TSH elevation, age,and general clinical context, including the presence of cardiac disease, should beconsidered. The serum TSH goal appropriate for the clinical situation should also beconsidered.
Thyroid hormone therapy should be initiated as an initial full replacement or aspartial replacement with gradual increments in the dose titrated upward using serumTSH as the goal.
Dose adjustments should be made upon significant changes in body weight, withaging, and with pregnancy; TSH assessment should be performed 4-6 weeks afterany dosage change.
Reference ranges of serum TSH levels are higher in older populations (eg, >65years), so higher serum TSH targets may be appropriate.
Updated recommendations concerning hypothyroidism treatment in pregnant women areas follows:[5, 6]
Pregnant women with overt hypothyroidism should receive levothyroxinereplacement therapy with the dose titrated to achieve a TSH concentration within thetrimester-specific reference range.
Serial serum TSH levels should be assessed every 4 weeks during the first half ofpregnancy to adjust levothyroxine dosing to maintain TSH within the trimester-specific range.
Serum TSH should be reassessed during the second half of pregnancy. In women already taking levothyroxine, 2 additional doses per week of the current
levothyroxine dose, given as one extra dose twice weekly with several days’separation, may be started as soon as pregnancy is confirmed.
Treatment of myxedema coma is as follows:
Intravenous (IV) LT4 at a dose of 4 µg/kg of lean body weight, or approximately200-250 µg, as a bolus in a single or divided dose, depending on the patient’s risk ofcardiac disease
After 24 hours, 100 µg LT4 IV, then 50 µg/day IV Stress doses of IV glucocorticoids Subsequent adjustment of the LT4 dose can be based on clinical and laboratory
findings

Endocrinologist – Terapi Pengganti (Thyrax) – TSH Level – Candesartan
40
10. Sumber: http://www.ncbi.nlm.nih.gov/books/NBK83492/
Screening and Treatment ofSubclinical Hypothyroidism orHyperthyroidism
Introduction
Background
A mildly elevated thyroid stimulating hormone (TSH – also called thyrotropin)concentration is the most common thyroid function test abnormality encountered ineveryday practice. Most patients who have a mildly elevated TSH have a normal freethyroxine (T4) level. The treatment of such patients is controversial, particularly whenthey have few or no symptoms and no other clinical evidence of thyroid disease. Lessfrequently, clinicians encounter patients who have a low or undetectable serum TSH andnormal triiodothyronine (T3) and free T4 levels. The management of these patients is alsounclear.
The main purpose of this review is to compare the effectiveness of different strategies formanaging individuals who have mildly elevated serum TSH concentrations and thosewho have mildly diminished TSH concentrations with normal free T3 and/or free T4. Wealso address the evidence for whether the primary care clinician should screen for thyroidfunction in patients who have no specific indication for thyroid testing and who come tothe clinician for other reasons. For the purposes of this review, we considered overtthyroid disease to be a well-defined clinical entity that has clear signs and symptoms, andthus, outside the scope of our review.
This topic was also the focus of a 2004 U.S. Preventive Services Task Force review.1
Description of Condition
Disorders of the thyroid gland are among the most common endocrine conditions thatU.S. clinicians evaluate and treat. Hyperthyroidism or hypothyroidism affects about fivepercent of adults in the United States.2
The thyroid gland is involved in metabolic homeostasis in adults. It accomplishes thisthrough secretion of two hormones, thyroxine (T4) and triiodothyronine (T3), and isregulated by thyroid stimulating hormone (TSH), which is secreted by the anteriorpituitary. Hypothyroidism is the under-secretion of thyroid hormones, whilehyperthyroidism is the over-secretion of these hormones.
Symptoms of overt hypothyroidism are subtle and nonspecific and may include fatigue,feeling cold, weight gain, hair loss, poor concentration, dry skin, and constipation (Table1). If overt hypothyroidism is allowed to progress due to lack of treatment or under-treatment, then myxedema coma, a life-threatening condition, can occur. Myxedemacoma is generally seen in the elderly and may be precipitated by factors that impairrespiration; it is marked by hypothermia, hypoventilation, decreased level ofconsciousness, and sometimes seizures and death.3

Endocrinologist – Terapi Pengganti (Thyrax) – TSH Level – Candesartan
41
Table 1. Symptoms and signs of overt thyroid dysfunction
Hypothyroidism Hyperthyroidism
Symptoms Coarse, dry skin and hair Nervousness and irritability
Cold intolerance Heat intolerance
Constipation Increased frequency of stools
Deafness Muscle weakness
Diminished sweating Increased sweating
Physical tiredness Fatigue
Hoarseness Blurred or double vision
Paresthesias Erratic behavior
Periorbital puffiness Restlessness
Heart palpitations
Restless sleep
Decrease in menstrual cycle
Increased appetite
Signs Slow cerebration Distracted attention span
Slow movement Tremors
Slowing of ankle jerk Tachycardia
Weight gain Weight Loss
Goiter Goiter
Symptoms and signs of overt thyroid dysfunction.
Symptoms of overt hyperthyroidism may include palpitations, heat intolerance, andsweating, weight loss, hyperactivity, and fatigue. Thyroid storm is a life-threateningcondition that results from an acute illness superimposed on undiagnosed or under-treatedhyperthyroidism. It is accompanied by fever, delirium, seizures, and coma.3
Subclinical thyroid dysfunction includes subclinical hypo- and hyperthyroidism. Sincethe development of sensitive TSH assays, these conditions have been defined as follows(Table 2):
High or low serum thyroid stimulating hormone (TSH) levels Normal free T4 and T3 levels The absence of signs and symptoms of overt thyroid dysfunction.3
Table 2. Classification of thyroid dysfunction: Biochemical definition
Condition TSH Thyroid
hormones
Comments
Overt hyperthyroidism < 0.1 mIU/L or undetectable Elevated T4
or T3
Overt hypothyroidism > 4.5 mIU/L Low T4
Subclinical hyperthyroidism TSH < 0.1 mIU/LNormal T4
and T3Clearly low serum TSH

Endocrinologist – Terapi Pengganti (Thyrax) – TSH Level – Candesartan
42
Condition TSH Thyroid
hormones
Comments
0.1 mIU/L <= TSH < 0.4 mIU/LNormal T4
and T3Low but detectable
Subclinical hypothyroidism
4.5 mIU/L < TSH < 10 mIU/L Normal T4 Mildly elevated TSH
TSH >= 10 mIU/L Normal T4 Markedly elevated TSH
Abbreviation: TSH=thyroid stimulating hormone.
For the purposes of this report, the term ‘subclinical thyroid dysfunction’ is used todefine the state of having an abnormal TSH in the context of normal free T4 and T3levels. It includes those with ‘sub-clinical thyroid disease,’ i.e. those who have a high riskof disease progression or other adverse consequences, but also those whose prognosis isnot well understood.
Patients with subclinical hypothyroidism are further categorized into those with mildlyelevated TSH (4.5–10 mIU/L), and those with markedly increased serum TSH levels(>10 mIU/L).4Similarly, TSH levels below the lower reference limit can be classified as“low but detectable” (serum TSH 0.1-0.4mIU/L) and “clearly low serum TSH” (less than0.1mIU/L).
Although widely used in the literature, these thresholds are arbitrary. For example,longitudinal studies have demonstrated that the risk of progression to overthypothyroidism increases as the initial serum TSH level increases, but do not support thecommon notion of a threshold at either 4.5 mIU/L or at 10 mIU/L.1 Nevertheless, becausemany guidelines and studies use these thresholds, we use them in this report.
The biochemical definition has several limitations. First, the term “subclinical” usuallyimplies that symptoms and signs are absent, whereas, in actual practice, the morecommon situation is that patients have nonspecific symptoms such as cold intolerance orfeeling tired. As Cooper has noted, “Although subclinical hypothyroidism is the termmost frequently used…, it is not necessarily apt, since on close questioning many patientsdisclose mild nonspecific symptoms. Mild hypothyroidism may be a more appropriateterm for this very common syndrome, which is defined by an isolated elevated serumTSH level in the setting of normal serum thyroid hormone levels, in the presence orabsence of symptoms.”5 Importantly, the presence of such symptoms does not mean theyare related to the finding of an abnormal TSH test. In epidemiologic studies, individualswho had one or two nonspecific symptoms, such as cold intolerance or feeling “a littletired,” were no more likely to have subclinical thyroid dysfunction, or be at increasedhealth risk, than were asymptomatic individuals in the general population.6-10
Second, the biochemical, TSH-based definition of subclinical thyroid dysfunction doesnot take into account clinical factors that affect the natural history. Subclinicalhypothyroidism can be caused by recent hospitalization for severe illness; previouslytreated Graves disease or nodular thyroid disease; thyroiditis and recovery fromthyroiditis; or untreated adrenal insufficiency. The lack of clinical context has causedconfusion about the applicability of evidence from patients with overt thyroid disease toasymptomatic, otherwise healthy individuals who have an abnormal TSH level. Forexample, a frequently cited randomized trial of treatment for subclinical hypothyroidismrecruited patients who had undergone treatment for Graves disease.11 Such patients

Endocrinologist – Terapi Pengganti (Thyrax) – TSH Level – Candesartan
43
predictably and rapidly progress to symptomatic hypothyroidism if not treated. While thestudy demonstrated quite convincingly that early treatment can prevent symptoms inpatients who have undergone thyroid ablation, patients who have no history of thyroiddisease and no clinical findings or symptoms attributable to the thyroid are unlikely toprogress as rapidly, so treatment has much less effect on symptoms in the short term. Thevast majority of patients identified by screening in the clinic or population-based settingsare in the latter group.
Third, there is no consensus on what TSH level should be used as the cut off to diagnosesubclinical hypothyroidism or hyperthyroidism. Differences among assays make itdifficult to establish a universal upper limit.12 Most studies define an abnormal TSH testresult as the upper and lower limits of the assay’s 95 percent reference range,approximately 0.1 to 4.5 mIU/L.
This method, although widely used in laboratory medicine, is not appropriate foridentifying a threshold for diagnosing or treating subclinical hypothyroidism.13 As forother clinical measures, such as blood pressure, bone density, or serum lipid levels, thethreshold should depend on the risk associated with a particular level as well as thebalance of benefits and harms of treatment. Some have argued that the threshold forsubclinical hypothyroidism should be raised above the upper limit of the reference range.The rationale is that otherwise healthy individuals who have a TSH in the range 4.5mIU/L to 8 mIU/L or 9 mIU/L have not been shown to benefit from detection andtreatment. Other experts argue that, because a TSH within the upper end of the usualreference range (2.5 to 4.5 mIU/L) confers some additional risk of progressing to overthypothyroidism over time, the threshold for diagnosing subclinical hypothyroidismshould be lowered to 2.5 mIU/L.14-16 Approximately 9.7 percent of the U.S. adultpopulation, representing 20.6 million Americans, has a TSH in this range and would beidentified as having subclinical hypothyroidism if this change were made.4
The appropriate level for decisionmaking can only be decided by better evidence aboutthe adverse consequences in untreated individuals and the benefits and harms oftreatment at different TSH thresholds.1,4,13,17 Because it depends on the risk ofcomplications in a particular population, the appropriate TSH cutoff for definingsubclinical hypothyroidism might vary with age, gender, and race.18
Fourth, although the definition of subclinical thyroid dysfunction requires a “normal” freeT4 level, the definition is not necessarily applicable to the individual patient. Someexperts argue that if a patient’s TSH level is mildly elevated, then even if their thyroidhormone levels are within the normal range, they “are not truly normal for thatindividual.”19 Put differently, while higher levels of thyroid-stimulating hormone increasethyroid hormone production, the additional production does not fully compensate for theunderlying deficiency. According to this view, subclinical hypothyroidism represents“early thyroid failure,” that is, less than full compensation for the diminished function ofthe thyroid gland.
Prevalence and Course of Mild Thyroid Dysfunction
Using the upper limit of the reference range as a cut off, approximately 5 percent ofwomen and 3 percent of men have subclinical thyroid dysfunction (i.e., TSH > 4mIU/L).1 Approximately one in four of these individuals has a markedly elevated TSHconcentration (>10 mIU/L). Such patients are likely to progress to overt hypothyroidismover 20 years.20
The other 75 percent of individuals with subclinical hypothyroidism have mildly elevatedTSH levels (4 mIU/L < TSH ≤ 10 mIU/L). In this group, age, sex, geographic region, and the presence of thyroid auto-antibodies are strong predictors of the rate of progression to

Endocrinologist – Terapi Pengganti (Thyrax) – TSH Level – Candesartan
44
overt hypothyroidism. From one-third to two-thirds of these individuals have antithyroidantibodies. Depending on age, sex, and TSH level, 50 percent to 70 percent of theseindividuals will progress to overt disease over 20 years. In those who do not haveantithyroid antibodies, the risk of progression is lower.20
In general, prevalence increases with age, is higher among whites compared with blacks,and higher in women compared with men.21 Estimates of the prevalence of subclinicalhypothyroidism vary based on demographic factors and differences in the defined uppernormal limit for TSH. A systematic review and meta-analysis of good-quality cross-sectional studies1 estimated that the prevalence in women ranged from 1.2 percent amongnon-Hispanic, African-American women to 5.8 percent in non-Hispanic, white womenand from 4 percent in women age 18-44 to over 17 percent in women over 75 years. Inthe NHANES sample, estimates ranged from 1.8 percent among non-Hispanic, African-American men to 2.4 percent among Mexican-American men.22 In a population-basedepidemiological study in Whickham, England, the prevalence ranged from 1 percentamong men 18-65 to 6.2 percent among men 65 or older.23
Strategies for Detecting and Managing SubclinicalThyroid Dysfunction
Screening Strategies
Screening can be defined as “the application of a test to detect a potential disease orcondition in a person who has no known signs or symptoms of that condition at the timethe test is done.”24 In case-finding, testing for thyroid dysfunction is performed amongpatients who come to their clinicians for unrelated reasons. When the test is abnormal, thepatient is called back for a detailed thyroid-directed history and confirmatory testing.Subclinical hypothyroidism is diagnosed if the TSH remains elevated and the free T4remains normal for a period of 3-6 months. While hypothyroidism and hyperthyroidismare distinctly different disorders, with different symptoms and potential complications,screening for both subclinical hypo- and hyperthyroidism is accomplished through testingof serum TSH, with testing of serum free T4 if the TSH is high, and of T3 as well as freeT4 if the TSH falls below the normal range.3
Management Strategies
Subclinical Hypothyroidism
For patients with subclinical hypothyroidism, the alternative management strategies aretreatment with thyroid replacement hormone versus watchful waiting. A detailed strategyfor routine treatment is described elsewhere.12 Treatment strategies vary, but all beginwith repeat testing to confirm that the TSH is still elevated. If the TSH is >10 mIU/L onrepeat testing, treatment with levothyroxine is initiated. If the TSH is mildly elevated(above the reference range but below 10 mIU/L), some experts recommend routinetreatment. Others recommend measurement of serum thyroid peroxidase antibodies andtreatment with levothyroxine if antibody levels are high. All guidelines recommendlevothyroxine rather than triiodothyronine or both as the drug of choice. The preferencefor levothyroxine is based on the results of randomized trials of levothyroxine aloneversus combination therapy for patients with overt hypothyroidism that show no clearbenefit of combination therapy over levothyroxine alone.25
“Watchful waiting” encompasses two different strategies—“expectant management” or“active surveillance.” Expectant management means closely watching a patient’scondition and treating if symptoms develop or laboratory results change. Activesurveillance means repeating thyroid function tests and taking a thyroid-directed history

Endocrinologist – Terapi Pengganti (Thyrax) – TSH Level – Candesartan
45
at a particular interval; then, if symptoms or laboratory results change, beginningtreatment. The appropriate time-interval for retesting individuals with subclinical thyroiddysfunction is unknown.
A recent British guideline26 offered the following typical strategy for active surveillance:
If screening is performed, and a high serum TSH concentration and normal free T4 isfound, repeat measurement 3-6 months later after excluding nonthyroidal illness anddrug interference
If the TSH is mildly elevated (above the reference range but below 10 mIU/L), obtainserum thyroid peroxidase antibodies
If antibody levels are high, repeat measurement of TSH annually. If they are low,repeat measurement of TSH every 3 years. Initiate treatment if the TSH level isgreater than 10 mIU/L or the patient develops clinical findings of hypothyroidism.
Practice styles vary widely. A well-conducted chart review study of 500 patients withsubclinical hypothyroidism seen at the Mayo Clinic in 1995-1996 found that clinicianstreated 38.7 percent of patients who had a TSH between 5.1 and 10.0 mIU/L.27
Unfortunately, more recent data and primary care-based practice patterns are notavailable.
Subclinical Hyperthyroidism
For subclinical hyperthyroidism, some experts 21,28 recommend repeating thyroid functiontests after 3 months and, if the TSH remains suppressed, obtaining ultrasonography and a24-hour Radioactive Iodine Uptake (RAIU) thyroid scan. These guidelines recommendantithyroid treatment if the patient has a persistent TSH level less than 0.1 mIU/L and isfound to have Graves or nodular thyroid disease. Treatments include medications, such aspropylthiouracil, or ablation with radioactive iodine or surgery. The guidelinerecommended against routine treatment in those whose TSH was between 0.1 and 0.45mIU/L.
Guidelines on Early Detection and Treatment
A review of the history of guidelines for subclinical thyroid dysfunction provides insightinto the reason for practice variation (see also Appendix E). In 1990 and again in 1998,the American College of Physicians found “it is reasonable to screen women older than50 years of age for unsuspected but symptomatic thyroid disease.” The guidelinespecified that the goal of routine testing was to find overt, but overlooked, thyroiddysfunction, not subclinical hypothyroidism. Because the clinical significance of mildlyelevated TSH test results was uncertain, the guideline recommended obtaining a free T4test only when the TSH level was undetectable or 10 mIU/L or more. The ACP guidelinepanel used a systematic review of the literature to arrive at its recommendations.10Theseguidelines expired in 2003.
In 1999, the American Association of Clinical Endocrinologists recommended screeningasymptomatic women over the age of 60.29In 2000, the American Thyroid Associationrecommended screening all patients over 35 years of age every 5 years (more frequentlyif the patient is at increased risk).30 These organizations used a consensus process todevelop guidelines and did not use systematic reviews in arriving at theirrecommendations.
In 2003, the Institute of Medicine (IOM) published a volume entitled “MedicareCoverage of Routine Screening for Thyroid Disease,” which examined the issue ofscreening for thyroid dysfunction in the Medicare population and concluded that “there isinsufficient evidence to recommend periodic, routine screening for thyroid dysfunctionamong asymptomatic persons using serum TSH levels.”31 In 2004, the USPSTF

Endocrinologist – Terapi Pengganti (Thyrax) – TSH Level – Candesartan
46
determined that the evidence was poor that treatment of screen-detected adults, in eitherthe general population or in specific high-risk groups, improves clinically importantoutcomes and concluded that there was insufficient evidence to recommend for or againstscreening for thyroid disease in adults. These groups used essentially identical systematicreviews to arrive at their recommendations.1,31 The USPSTF issued an “I”recommendation, indicating that the evidence was insufficient to recommend for oragainst routine screening for thyroid disease in adults.32The conclusions about theevidence were:
There is fair evidence that the thyroid stimulating hormone (TSH) test can detectsubclinical thyroid dysfunction in people without symptoms of thyroid dysfunction,but poor evidence that treatment improves clinically important outcomes in adultswith screen-detected thyroid disease
Although the yield of screening is greater in certain high-risk groups (e.g., postpartumwomen, people with Down’s syndrome, and the elderly), there is poor evidence thatscreening these groups leads to clinically important benefits
There is the potential for harm caused by false positive screening tests; however, themagnitude of harm is not known
There is good evidence that overtreatment with levothyroxine occurs in a substantialproportion of patients, but the long-term harmful effects of overtreatment are notknown. As a result, the balance of benefits and harms of screening asymptomaticadults for thyroid disease could not be determined.
In 2004, a panel sponsored by the American Association of Clinical Endocrinologists, theAmerican Thyroid Association, and the Endocrine Society evaluated data regarding themanagement of subclinical thyroid dysfunction.21 Unlike the older AACE and ATAguidelines, the panel used a systematic review of the evidence to arrive at itsrecommendations.33 The panel adopted the strength of evidence rating of the USPSTF inits assessment. The panel found insufficient evidence to support population-basedscreening and recommended against population-based screening for thyroid disease,though it did advocate aggressive case-finding in those considered high-risk, includingpregnant women and women older than 60. They also recommended against routinetreatment of patients with subclinical hypothyroidism with serum TSH levels of 4.5 -10.0 mIU/L. Specifically, the panel found insufficient evidence to support routinetreatment of individuals who have a mildly elevated TSH (Table 3). The findings aboutthe evidence regarding the complications of subclinical hypothyroidism and the effects oftreatment agreed with those of the IOM and USPSTF.
Table 3. Evidence for the association of subclinical hypothyroidism (TSH4.5-10 mIU/L) and adverse health outcomes and quality of evidence forrisks and benefits of treatment: Findings of the American Association ofClinical Endocrinologists, the American Thyroid Association, and theEndocrine Society Panel
Complication
Strength of evidence forassociation with complications
Strength of evidenceregarding benefitsand harms oftreatment
Progression to overthypothyroidism
Gooda Not applicabled
Adverse cardiac end points Insufficientb No evidence
Elevation in serumcholesterol and LDL-Clevels
Insufficientc Insufficient
Cardiac dysfunction Insufficientc Insufficient
Endocrinologist – Terapi Pengganti (Thyrax) – TSH Level – Candesartan
47
Complication
Strength of evidence forassociation with complications
Strength of evidenceregarding benefitsand harms oftreatment
Symptoms ofhypothyroidism
No evidence Insufficient
Psychiatric symptoms No evidence Insufficient
(Adapted from JAMA 200421)
a Good: Evidence includes consistent results from well-designed, well-conductedstudies in representative populations that directly assess effects on healthoutcomes.b Insufficient: Evidence is insufficient to assess the effects on health outcomesbecause of limited number or power of studies, important flaws in their design orconduct, gaps in the chain of evidence, or lack of information on important healthoutcomes.c Data did not distinguish between serum TSH concentrations between 4.5-10mIU/L and > 10 mIU/L.d Thyroid hormone therapy normalizes serum TSH at any TSH concentration.
Evidence for the association of subclinical hypothyroidism (TSH 4.5-10 mIU/L) andadverse health outcomes and quality of evidence for risks and benefits of treatment:Findings of the American Association of Clinical Endocrinologists, the AmericanThyroid (more...)
In 2005, the three professional societies that sponsored the evidence-based panel issued aconsensus statement rejecting its recommendations.34 While acknowledging that theindependent review panel found insufficient evidence to recommend treatment of patientswith subclinical hypothyroidism in the range of 4.5-10.0 mIU/L, the counter argued that“lack of definitive evidence for a benefit does not equate to evidence for lack of benefit”and recommended that most patients with TSH levels between 4.5 and 10.0 mIU/Lshould be considered for treatment. Their rationale for recommending screening despitegaps in the evidence about treatment is discussed in detail in the next section of thisreport (“Rationale for Screening and Treatment”).
In 2006, three British professional associations (Association for Clinical Biochemistry,the British Thyroid Association, and the British Thyroid Foundation) publishedguidelines for using thyroid function tests.26 The guideline panel found that “screeningfor thyroid dysfunction in a healthy adult population is not warranted.” It recommendedagainst routine treatment of patients who have a TSH concentration above the referencerange but below 10 mIU/L but said that “a therapeutic trial of thyroxine [should beconsidered] on an individual patient basis.” The British panel noted that that there wasgrowing evidence against the use of thyroxine in elderly patients, in whom an elevatedTSH concentration “may reflect an adaptive mechanism to prevent excessivecatabolism.” Like the ACP and AACE guidelines, the British panel recommendedaggressive case-finding in women with non-specific symptoms. The panel usedsystematic reviews in their process for developing guidelines.35
In 2007, The American College of Obstetricians and Gynecologists (ACOG)recommended against routine screening in pregnant women. It stated that there is noevidence that identifying and treating pregnant women with subclinical hypothyroidismimproved either maternal or infant outcomes.36
Rationale for Screening and Treatment

Endocrinologist – Terapi Pengganti (Thyrax) – TSH Level – Candesartan
48
Subclinical Hypothyroidism
Although there is wide agreement that the long-term benefits of early treatment ofsubclinical thyroid dysfunction have not been proven, there is disagreement about what todo until better evidence is available. This disagreement reflects differing views of theclinical relevance of research about the complications of subclinical thyroid dysfunction.
Proponents argue that thyroid dysfunction is common and associated with significantmorbidity. Additionally, a serum TSH test is relatively inexpensive, accurate, readilyavailable, and generally a very acceptable test for patients to undergo.30,34Symptoms ofovert thyroid dysfunction also can be vague and at times difficult to diagnose, andtherefore, thyroid screening may allow the diagnosis of overt disease earlier in theclinical course, thus reducing morbidity.30,34,37 For subclinical hypothyroidism, treatmentwith levothyroxine is noninvasive and inexpensive. Finally, proponents argue that thepotential harms of screening are small in relation to the potential benefits: “Because thepotential harm of early detection and treatment appear to be so minor and preventable, itseems prudent to err on the side of early detection and treatment until there is sufficientdata to address these issues definitively.”34
Since 2005, the most important, widely cited argument for early treatment of thyroiddysfunction is the association of untreated subclinical hypothyroidism with other riskfactors for heart disease and with incident coronary disease or heart failure later in life.Subclinical hypothyroidism may be a risk factor for atherosclerosis and myocardialinfarction, but epidemiologic studies of this question have had mixed results.38-42 Fourrecent meta-analyses have evaluated the association of subclinical thyroid disorder oncardiac mortality or all-cause mortality.
One meta-analysis included six cohort studies and found that those with subclinicalhypothyroidism had a relative risk (RR) of 1.53 (1.31-1.79) of having coronary arterydisease (CAD) at baseline.43 Subclinical hypothyroidism was associated with a RR of1.188 (1.024-1.379) of developing CAD in followup (included studies followup rangedfrom 4 to 20 years), but was not found to be associated with all-cause mortality.43 Thesecond review (of 14 cohort and two case-control studies) found no association withsubclinical hyperthyroidism and circulatory or all-cause mortality.44 With regard tosubclinical hypothyroidism, the association with circulatory mortality was not statisticallysignificant, but a hazard ratio of 1.25 (1.3-1.53) was found for all-cause mortality.44 Thethird review, which included 10 population-based prospective studies and two studies ofconvenience samples of cardiac patients or patients with a history of stroke or hipreplacement, found no overall statistically significant association between eithersubclinical hypothyroidism or subclinical hyperthyroidism and total mortality or coronarymorbidity or mortality.45 A statistically significant, but small, increased risk for heartdisease was found for individuals younger than 65.45 The last meta-analysis included 15studies (six population-based cross-sectional studies and nine longitudinal cohort studies)with 2,531 subclinical hypothyroid participants and 26,491 euthyroid individuals.46 Fivestudies provided longitudinal data on the risk of coronary events; in these, overall therewas no difference in incident ischemic heart disease (IHD) in subclinical hypothyroidparticipants and euthyroid participants (OR 1.27 [0.95–1.69]). In a subgroup analysis, instudies of subjects younger than 65 years, the odds ratio was 1.68 (1.27–2.23), but forolder subjects, there was no relationship between subclinical hypothyroidism and incidentIHD (OR 1.02 [0.85–1.22]).46
The epidemiological studies included in these reviews had serious limitations. Manyincluded individuals who had known thyroid disease, ischemic heart disease, or TSHlevels within the reference range. Many included subjects who underwent treatment withlevothyroxine during the followup period. In general, the studies did not adequatelycontrol for potential confounders, such as lipid levels and blood pressure.
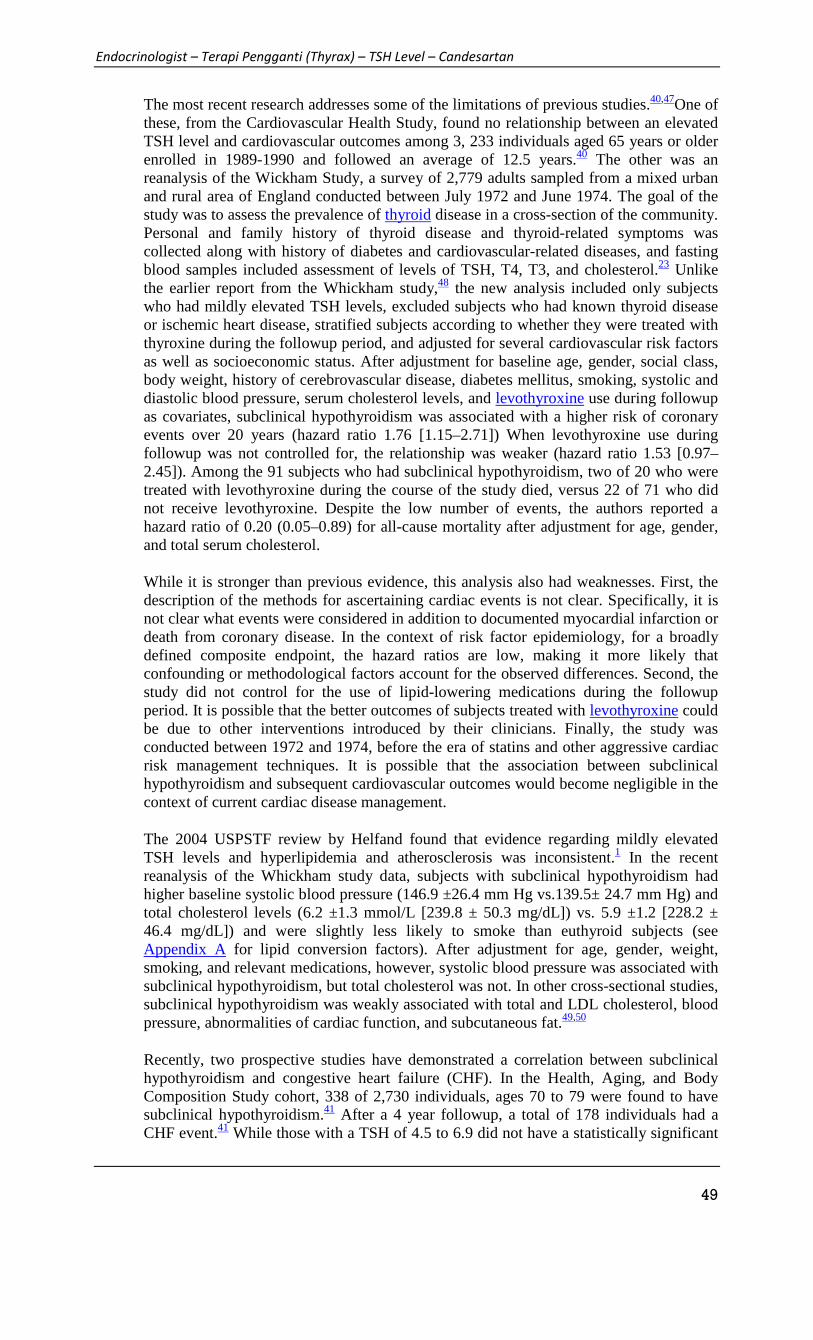
Endocrinologist – Terapi Pengganti (Thyrax) – TSH Level – Candesartan
49
The most recent research addresses some of the limitations of previous studies.40,47One ofthese, from the Cardiovascular Health Study, found no relationship between an elevatedTSH level and cardiovascular outcomes among 3, 233 individuals aged 65 years or olderenrolled in 1989-1990 and followed an average of 12.5 years.40 The other was anreanalysis of the Wickham Study, a survey of 2,779 adults sampled from a mixed urbanand rural area of England conducted between July 1972 and June 1974. The goal of thestudy was to assess the prevalence of thyroid disease in a cross-section of the community.Personal and family history of thyroid disease and thyroid-related symptoms wascollected along with history of diabetes and cardiovascular-related diseases, and fastingblood samples included assessment of levels of TSH, T4, T3, and cholesterol.23 Unlikethe earlier report from the Whickham study,48 the new analysis included only subjectswho had mildly elevated TSH levels, excluded subjects who had known thyroid diseaseor ischemic heart disease, stratified subjects according to whether they were treated withthyroxine during the followup period, and adjusted for several cardiovascular risk factorsas well as socioeconomic status. After adjustment for baseline age, gender, social class,body weight, history of cerebrovascular disease, diabetes mellitus, smoking, systolic anddiastolic blood pressure, serum cholesterol levels, and levothyroxine use during followupas covariates, subclinical hypothyroidism was associated with a higher risk of coronaryevents over 20 years (hazard ratio 1.76 [1.15–2.71]) When levothyroxine use duringfollowup was not controlled for, the relationship was weaker (hazard ratio 1.53 [0.97–2.45]). Among the 91 subjects who had subclinical hypothyroidism, two of 20 who weretreated with levothyroxine during the course of the study died, versus 22 of 71 who didnot receive levothyroxine. Despite the low number of events, the authors reported ahazard ratio of 0.20 (0.05–0.89) for all-cause mortality after adjustment for age, gender,and total serum cholesterol.
While it is stronger than previous evidence, this analysis also had weaknesses. First, thedescription of the methods for ascertaining cardiac events is not clear. Specifically, it isnot clear what events were considered in addition to documented myocardial infarction ordeath from coronary disease. In the context of risk factor epidemiology, for a broadlydefined composite endpoint, the hazard ratios are low, making it more likely thatconfounding or methodological factors account for the observed differences. Second, thestudy did not control for the use of lipid-lowering medications during the followupperiod. It is possible that the better outcomes of subjects treated with levothyroxine couldbe due to other interventions introduced by their clinicians. Finally, the study wasconducted between 1972 and 1974, before the era of statins and other aggressive cardiacrisk management techniques. It is possible that the association between subclinicalhypothyroidism and subsequent cardiovascular outcomes would become negligible in thecontext of current cardiac disease management.
The 2004 USPSTF review by Helfand found that evidence regarding mildly elevatedTSH levels and hyperlipidemia and atherosclerosis was inconsistent.1 In the recentreanalysis of the Whickham study data, subjects with subclinical hypothyroidism hadhigher baseline systolic blood pressure (146.9 ±26.4 mm Hg vs.139.5± 24.7 mm Hg) andtotal cholesterol levels (6.2 ±1.3 mmol/L [239.8 ± 50.3 mg/dL]) vs. 5.9 ±1.2 [228.2 ±46.4 mg/dL]) and were slightly less likely to smoke than euthyroid subjects (seeAppendix A for lipid conversion factors). After adjustment for age, gender, weight,smoking, and relevant medications, however, systolic blood pressure was associated withsubclinical hypothyroidism, but total cholesterol was not. In other cross-sectional studies,subclinical hypothyroidism was weakly associated with total and LDL cholesterol, bloodpressure, abnormalities of cardiac function, and subcutaneous fat.49,50
Recently, two prospective studies have demonstrated a correlation between subclinicalhypothyroidism and congestive heart failure (CHF). In the Health, Aging, and BodyComposition Study cohort, 338 of 2,730 individuals, ages 70 to 79 were found to havesubclinical hypothyroidism.41 After a 4 year followup, a total of 178 individuals had aCHF event.41 While those with a TSH of 4.5 to 6.9 did not have a statistically significant

Endocrinologist – Terapi Pengganti (Thyrax) – TSH Level – Candesartan
50
higher rate of CHF events compared to those without subclinical hypothyroidism, thosewith a TSH of 7 to 9.9 had a hazard ratio of 2.58 (95% CI, 1.19-5.60) and those with aTSH >10 had a hazard ratio of 3.26 (95% CI, 1.37-7.77).41 Additionally, of the 2,555without a history of CHF, those with a TSH of > 7 had a hazard ratio of 2.33 (95% CI,1.1.0-4.96) of developing a incident CHF event.41 In the Cardiovascular Health Studycohort, 474 of 3044 subjects older than 65 years who had no history of CHF hadsubclinical hypothyroidism, 46 of whom had a TSH of > 10.51 After a median of 12 yearsof followup, those with a TSH >10 had a hazard ratio of 1.88 (95% CI,1.05-3.34) ofdeveloping a CHF event, while those with a TSH of 4.5 to 9.9 were not more likely tohave a CHF event.51
These two relatively large prospective cohort studies do indicate that an isolated TSHmight be a risk factor for the development of CHF, particularly for individuals with aTSH of > 10. This association deserves further study. However, it is still unknown ifthyroid replacement therapy would modify this potential risk.
Subclinical Hyperthyroidism
Cross-sectional studies have shown untreated subclinical hyperthyroidism to beassociated with tachycardia, increased left ventricular mass leading to diastolicdysfunction, atrial arrhythmias, and a decline in bone mass density increasing the risk offractures.1,21 Only atrial fibrillation and disease progression have been associated withsubclinical hyperthyroidism in longitudinal studies.1 In a recent longitudinal study of 102women who had a TSH between 0.1 to 0.4 mIU/L, three progressed to overthyperthyroidism and 24 reverted to a normal TSH.52
In summary, progression to overt disease is the best established complication ofsubclinical thyroid dysfunction. Epidemiologic data suggest that subclinicalhypothyroidism is associated with cardiovascular disease in subjects younger than 65years, but the magnitude of risk is low. Evidence about the relationship of a mildlyelevated TSH to symptoms and to other cardiac risk factors, including the metabolicsyndrome, is weak. Subclinical hyperthyroidism is less common and less studied, andthus, its natural history and effects are less clear.
Scope of Review
The main question addressed in this review was whether individuals who have mildlyabnormal TSH values will either benefit from or be harmed by screening and potentialsubsequent treatment. We also addressed the question of whether the primary careclinician should screen for thyroid function in patients seen in general medical practicewho have no specific indication for thyroid testing and who come to the clinician forother reasons. For the purposes of this review, we considered overt thyroid disease to be awell-defined clinical entity that has clear signs and symptoms, and thus, outside the scopeof our review.
In order for a condition to be a good candidate for screening in the general population,several conditions need to be met. First, the condition needs to be relatively prevalent,having a significant impact on the health of the population or an easily identified specialpopulation. Second, there needs to be a test that is readily available to the generalpopulation that is of reasonable cost and accuracy and is acceptable to individuals toundergo. Finally, there needs to be an intervention that is of reasonable cost andtolerability that when administered in a timely fashion will alter the disease state toprevent morbidity and/or morality.
The Helfand (2004) review established that subclinical thyroid disease is quite prevalent;may be responsible for morbidity; and that the serum TSH test is a readily available,
Endocrinologist – Terapi Pengganti (Thyrax) – TSH Level – Candesartan
51
reliable, and acceptable test to detect the condition with a sensitivity above 98 percentand specificity greater than 92 percent.1 However, in 2004, it remained unclear whether,if detected, treating patients with subclinical thyroid disease would reduce morbidity.
As evidence of prevalence, test yield, and test performance have already been adequatelyestablished,1 this current review focuses on whether new evidence demonstrates thattreatment improves clinically important outcomes in adults with screen-detected thyroiddisease.
Key Questions and Analytic Framework
We reviewed published studies to answer the following key questions:
Key Question 1
Does screening for subclinical thyroid dysfunction reduce morbidity or mortality?
Key Question 2
What are the harms of screening? Specifically, how frequently and how severely dopatients screened for subclinical thyroid dysfunction experience adverse psychologicalimpacts or other harms of work-up from screening?
Key Question 3
Does treatment of patients with subclinical hypothyroidism or subclinicalhyperthyroidism detected by screening affect outcomes?
Key Question 4
What are the harms of treatment of subclinical hypothyroidism and subclinicalhyperthyroidism? Specifically, what are the consequences of over-treatment, includingeffects on bone mineral density and incidence of atrial fibrillation, and how frequently dothey occur?
We developed the final analytic framework shown in Figure 1 to guide the literaturereview. The analytic framework shows the populations, classification, intermediateoutcomes, and health outcomes we examined in the review. We defined the targetpopulation as community-living, non-pregnant adults, without a history of thyroid diseaseor symptoms of overt hypothyroidism or hyperthyroidism, who might be representativeof those seen in primary care settings.

Endocrinologist – Terapi Pengganti (Thyrax) – TSH Level – Candesartan
52
Analytic framework. Note: A. fibrillation=atrial fibrillation; CAD=coronary arterydisease; CHF=congestive heart failure; DEXA=dual-energy x-ray absorptiometry;NNS=number needed to screen; NNT=number needed to treat; S=subclinical;TSH=thyroid stimulating (more...)
In the framework, Arrow 1 represents studies directly comparing the effects of screeningversus not screening on important health outcomes (Key Question 1). Arrow 2,corresponding to Key Question 2, represents evidence about the potential harms ofscreening. Arrow 3 represents studies comparing different strategies (treatment vs.monitoring) for managing individuals who are found to have borderline high or low TSHlevels (Key Question 3). Arrow 4 represents studies of the harms of treatment. Outcomesof interest for subclinical hypothyroidism were cardiovascular morbidity and mortality,measures of well-being including but not limited to cognition and memory, weightchange, blood pressure changes, and changes in lipid levels. For subclinicalhyperthyroidism, outcomes of interest were cardiovascular morbidity and mortality,osteoporotic fractures, measures of well-being including but not limited to cognition andmemory, weight changes, blood pressure changes, changes in bone mineral density, andchanges in lipid levels.
Copyright NoticeBookshelf ID: NBK83492

Endocrinologist – Terapi Pengganti (Thyrax) – TSH Level – Candesartan
53
11. Sumber: http://www.todaysgeriatricmedicine.com/archive/110612p6.shtml
Elevated TSH Levels:
To Treat or Not to Treat?
By Juliann Schaeffer
Aging Well
Vol. 5 No. 6 P. 6
Physicians are accustomed to checking thyroid-stimulating hormone (TSH) in
older adults with symptoms of an over- or underactive thyroid, as it’s a fairly
accurate and routine measure of thyroid function. But a new study suggests that
for many patients, treatment for mild TSH elevations may no longer be
warranted.
“As increasing numbers of people live into their 80s and 90s, it is important to
know how to manage their health, including thyroid function,” says Anne
Cappola, MD, ScM, an associate professor of medicine at the Perelman School
of Medicine at the University of Pennsylvania and lead study author. “We sought
to describe what happens to thyroid function in older people over time and to
determine the relationship between thyroid function and mortality in this
population.”
The study, accepted for publication in The Endocrine Society’s Journal of
Clinical Endocrinology & Metabolism, questions the assertion that slightly
elevated TSH levels are linked to an increase in mortality and suggests that
such elevations may actually be a normal part of healthful aging.
Study Particulars
The study first examined 5,888 men and women aged 65 and older between
1989 and 1992. Then in 2005, researchers reexamined 843 surviving
participants’ thyroid function for any changes in physical and cognitive function.
Study participants ranged in age from 77 to 102, with a mean age of 85.
“We found that levels of TSH gradually increase during the aging process, which
means that more older people are outside of standard reference ranges and
could be labeled with the diagnosis of subclinical hypothyroidism,” Cappola
says. “However, older people [mean age of 85] with subclinical hypothyroidism
did not have a higher death rate and, if anything, there was a suggestion that
having subclinical hypothyroidism was protective.
“In addition, higher levels of thyroid hormone itself were associated with a higher
risk of death,” she adds. “Gradual increases in TSH have been shown in
younger populations, and it was gratifying to be able to extend these longitudinal

Endocrinologist – Terapi Pengganti (Thyrax) – TSH Level – Candesartan
54
findings into our older population. Based on our work and those of other groups,
we hypothesized that subclinical hypothyroidism would not be associated with
mortality. Ours is the largest study in older people to show this.”
Cappola says elevated TSH levels are relatively common in older adults, seen
“in approximately 15% of US adults aged 65 and older, and it’s more common in
women than in men,” she says, noting that previous research suggests it
becomes more common in patients in their 70s and tends to run in families.
When to Treat
Cappola notes that older adults with only a mild elevation in TSH are unlikely to
see their levels progress to a dangerous level. “We have shown in previous
studies that the mildly elevated TSH level tends to persist or revert to normal
and rarely progresses to a dangerous level. Others have shown an annual rate
of progression of 2% to 4%,” she says.
What are considered mild vs. extreme in TSH increases? According to Cappola,
her research regarded mildly elevated TSH levels as those in the 4.5 to 7 mU/L
range, while very elevated TSH levels were considered to be those greater than
20 mU/L. “The 7 to 10 and 10 to 20 mU/L ranges are somewhat gray zones,”
she says, “but most would treat persistently elevated TSH levels in this range,
regardless of the patient’s age. The treatment is thyroid hormone replacement
with levothyroxine.”
While Cappola stresses that very elevated TSH levels are a separate matter
altogether and still need to be treated, she notes that milder increases haven’t
yet shown to be a risk to older adults’ health. “There are serious risks to not
treating very elevated TSH levels,” she explains. “Our research group is looking
for risks to leaving mildly elevated TSH levels untreated in older adults, and we
have not found any so far.”
“An important point is that for elderly patients, and increasingly as the patient
ages, doctors need to think carefully about both the indications and ramifications
of any treatment,” notes Rosemary Laird, MD, MHSA, AGSF, medical director of
the Health First Aging Institute and past president of the Florida Geriatrics
Society.
“Certainly, with subclinical disease there is no perceived loss of quality of life, so
treatment of any kind should be carefully considered. For clinicians, these
results support watchful waiting and serial reassessment for most older adults
with only mildly elevated TSH levels. It even suggests some evidence of
potential harm from higher levels of thyroid hormone, so all the more reason to
carefully choose one’s response to mildly elevated TSH,” she posits.
“We can also use this [study’s findings] as a reminder that geriatric care needs
to be care that is individually tailored and reactive to an individual’s overall
quality of life and life expectancy, since both of these foundational pieces of
information make the difference in clinical decision making,” Laird adds.

Endocrinologist – Terapi Pengganti (Thyrax) – TSH Level – Candesartan
55
It is Cappola’s hope that these findings take hold in the clinical community,
prompting geriatricians and primary care physicians to think twice before
treating their much older patients for such mild elevations that, in her opinion
and from recent evidence, prove unlikely to do any harm on their own while
focusing instead on those with more aggressive leaps in TSH.
“Our study shows that a gradual increase in TSH occurs during healthy aging
and that mild increases in TSH are not harmful in the oldest old,” she says.
“Beyond that, we found that higher levels of thyroid hormone are associated with
increased mortality. These findings raise concern for reflexively treating older
people with mild elevations in TSH with thyroid hormone replacement.”
— Juliann Schaeffer is an associate editor at Great Valley Publishing Company.
12. Sumber: https://labtestsonline.org/understanding/analytes/tsh/tab/test/
The Test
1. How is it used?2. When is it ordered?3. What does the test result mean?4. Is there anything else I should know?
How is it used?
The thyroid-stimulating hormone (TSH) test is often the test of choice for evaluatingthyroid function and/or symptoms of a thyroid disorder, including hyperthyroidism orhypothyroidism.
TSH is produced by the pituitary gland, a tiny organ located below the brain and behindthe sinus cavities. It is part of the body's feedback system to maintain stable amounts ofthe thyroid hormones thyroxine (T4) and triiodothyronine (T3) in the blood and to helpcontrol the rate at which the body uses energy.
A TSH test is frequently ordered along with or preceding a free T4 test. Other thyroidtests that may be ordered include a free T3 test and thyroid antibodies (if autoimmune-related thyroid disease is suspected). Sometimes TSH, free T4 and free T3 are orderedtogether as a thyroid panel.
TSH testing is used to:
Diagnose a thyroid disorder in a person with symptoms Screen newborns for an underactive thyroid Monitor thyroid replacement therapy in people with hypothyroidism Monitor anti-thyroid treatment in people with hyperthyroidism Help diagnose and monitor infertility problems in women Help evaluate the function of the pituitary gland (occasionally)

Endocrinologist – Terapi Pengganti (Thyrax) – TSH Level – Candesartan
56
Screen adults for thyroid disorders, although expert opinions vary on who canbenefit from screening and at what age to begin
When is it ordered?
A health practitioner may order a TSH test when someone has symptoms ofhyperthyroidism or hypothyroidism and/or when a person has an enlarged thyroid gland(goiter).
Signs and symptoms of hyperthyroidism may include:
Increased heart rate Anxiety Weight loss Difficulty sleeping Tremors in the hands Weakness Diarrhea (sometimes) Light sensitivity, visual disturbances The eyes may be affected: puffiness around the eyes, dryness, irritation, and, in some
cases, bulging of the eyes.
Signs and symptoms of hypothyroidism may include:
Weight gain Dry skin Constipation Cold intolerance Puffy skin Hair loss Fatigue Menstrual irregularity in women
TSH may be ordered at regular intervals when an individual is being treated for a knownthyroid disorder. When a person's dose of thyroid medication is adjusted, the AmericanThyroid Association recommends waiting 6-8 weeks before testing the level of TSHagain.
TSH screening is routinely performed in the United States on newborns soon after birthas part of each state's newborn screening program.
In 2004, the U.S. Preventive Services Task Force found insufficient evidence torecommend for or against routine screening for thyroid disease in asymptomatic adults.However, the American Thyroid Association and the American Association of ClinicalEndocrinologists released clinical practice guidelines in 2012 that recommend thatscreening for hypothyroidism should be considered in people over the age of 60.Because the signs and symptoms of both hypothyroidism and hyperthyroidism are sosimilar to those seen in many common disorders, health practitioners often need to ruleout thyroid disease even though the patient has another problem.
What does the test result mean?
A high TSH result may mean that:
The person tested has an underactive thyroid gland that is not responding adequatelyto the stimulation of TSH due to some type of acute or chronic thyroid dysfunction

Endocrinologist – Terapi Pengganti (Thyrax) – TSH Level – Candesartan
57
A person with hypothyroidism or who has had their thyroid gland removed isreceiving too little thyroid hormone replacement medication and the dose may needto be adjusted
A person with hyperthyroidism is receiving too much anti-thyroid medication andthe dose needs adjusting
There is a problem with the pituitary gland, such as a tumor producing unregulatedlevels of TSH
A low TSH result may indicate:
An overactive thyroid gland (hyperthyroidism) Excessive amounts of thyroid hormone medication in those who are being treated for
an underactive (or removed) thyroid gland Insufficient anti-thyroid medication in a person being treated for hyperthyroidism;
however, it may take a while for TSH production to resume after successful anti-thyroid treatment. This is why the American Thyroid Association recommendsmonitoring this treatment with tests for thyroid hormones (T4 and T3) as well asTSH levels.
Damage to the pituitary gland that prevents it from producing adequate amounts ofTSH
Whether high or low, an abnormal TSH indicates an excess or deficiency in the amountof thyroid hormone available to the body, but it does not indicate the reason why. Anabnormal TSH test result is usually followed by additional testing to investigate thecause of the increase or decrease.
The following table summarizes some examples of typical test results and their potentialmeaning.
TSH Free T4Free ortotal T3
Probable Interpretation
High Normal Normal Mild (subclinical) hypothyroidism
High LowLow ornormal
Hypothyroidism
Low Normal Normal Mild (subclinical) hyperthyroidism
LowHigh ornormal
High ornormal
Hyperthyroidism
LowLow ornormal
Low ornormal
Non-thyroidal illness; pituitary(secondary) hypothyroidism
Normal High High
Thyroid hormone resistance syndrome(a mutation in the thyroid hormonereceptor decreases thyroid hormonefunction)
Is there anything else I should know?
It is important to note that TSH, free T4, and free T3 tests are a "snapshot" of what isoccurring within a dynamic system. An individual person's thyroid testing results mayvary and may be affected by:
Increases, decreases, and changes (inherited or acquired) in the proteins that bindT4 and T3
Pregnancy Estrogen and other drugs Liver disease

Endocrinologist – Terapi Pengganti (Thyrax) – TSH Level – Candesartan
58
Systemic illness Resistance to thyroid hormones
Many medications — including aspirin and thyroid-hormone replacement therapy —may affect thyroid gland function test results and their use should be discussed with thehealth practitioner prior to testing.
Illnesses not directly related to the thyroid, "nonthyroidal illnesses," can affect thyroidhormones levels. In particular, the level of T3 can be low in nonthyroidal illness (NTI).Typically, the thyroid hormone levels return to normal after a person recovers from thenonthyroidal illness. Historically, this condition was referred to as "euthyroid sicksyndrome" but that term is controversial because there is some question as to whetherthose affected have a thyroid gland that is functioning normally (euthyroid).
When a health practitioner adjusts a person's thyroid hormone replacement dosage, it isimportant to wait at least one to two months before checking the TSH again so that thenew dose can have its full effect.
Extreme stress and acute illness may affect TSH test results. It is generallyrecommended that thyroid testing be avoided in hospitalized patients or deferred untilafter a person has recovered from an acute illness.
Results may be low during the first trimester of pregnancy.
CandesartanCOMMON BRAND NAME(S): AtacandGENERIC NAME(S): CANDESARTAN CILEXETIL
1. Sumber : https://en.wikipedia.org/wiki/Candesartan
Candesartan
Candesartan

Endocrinologist – Terapi Pengganti (Thyrax) – TSH Level – Candesartan
59
Systematic (IUPAC) name2-ethoxy-1-({4-[2-(2H-1,2,3,4-tetrazol-5-yl)phenyl]phenyl}methyl)-1H-
1,3-benzodiazole-7-carboxylic acid
Clinical data
Trade names Atacand
AHFS/Drugs.com monograph
MedlinePlus a601033
Pregnancycategory
AU: D
Legal status ℞ (Prescription only)
Routes ofadministration
oral
Pharmacokinetic data
Bioavailability15% (candesartancilexetil)
Metabolism
Candesartan cilexetil:intestinal wall;candesartan: hepatic(CYP2C9)
Biological half-life 9 hours
Excretion Renal 33%, faecal 67%
Identifiers
CAS RegistryNumber
139481-59-7
ATC code C09CA06
PubChem CID: 2541
IUPHAR/BPS 587
DrugBank DB00796
ChemSpider 2445
UNII S8Q36MD2XX
KEGG D00626
ChEBI CHEBI:3347
ChEMBL CHEMBL1016
Chemical data
Formula C24H20N6O3
Molecular mass 440.45 g/mol
SMILES[show]
InChI[show]

Endocrinologist – Terapi Pengganti (Thyrax) – TSH Level – Candesartan
60
(what is this?) (verify)
Candesartan (rINN) /ˌkændɨˈsɑrtən/ is an angiotensin II receptor antagonist used mainly forthe treatment of hypertension. The prodrug candesartan cilexetil is marketed byAstraZeneca and Takeda Pharmaceuticals, commonly under the trade names Blopress,Atacand, Amias, and Ratacand. It is available in generic form.[1]
Contents
1 Clinical useo 1.1 Prehypertensiono 1.2 Combination with diuretic 2 Chemistry and pharmacology 3 Development history 4 See also 5 References 6 External links
Clinical use
Main article: Angiotensin II receptor antagonist
As with other angiotensin II receptor antagonists, candesartan is indicated for the treatmentof hypertension. Results from the CHARM study (early 2000s) demonstrated the morbidityand mortality reduction benefits of candesartan therapy in congestive heart failure.[2] Thus,while ACE inhibitors are still considered first-line therapy in heart failure, candesartan can beused in combination with an ACE to achieve improved mortality and morbidity vs. an ACEalone and additionally is an alternative in patients intolerant of ACE inhibitor therapy.
Prehypertension
In a four-year randomized controlled trial, candesartan was compared to placebo to seewhether it could prevent or postpone the development of full-blown hypertension in peoplewith so-called prehypertension. During the first two years of the trial, half of participantswere given candesartan, and the others received placebo; candesartan reduced the risk ofdeveloping hypertension by nearly two-thirds during this period. In the last two years of thestudy, all participants were switched to placebo. By the end of the study, candesartan hadsignificantly reduced the risk of hypertension, by more than 15%. Serious side effects wereactually more common among participants receiving placebo than in those givencandesartan.[3]
Combination with diuretic
Candesartan is also available in a combination formulation with a low dose of the thiazidediuretic hydrochlorothiazide, to achieve an additive antihypertensive effect.Candesartan/hydrochlorothiazide combination preparations are marketed under various tradenames including Atacand HCT, Hytacand, Blopress Plus, Advantec and Ratacand Plus.
Endocrinologist – Terapi Pengganti (Thyrax) – TSH Level – Candesartan
61
Candesartan cilexetil
Chemistry and pharmacology
Candesartan is marketed as the cyclohexyl 1-hydroxyethyl carbonate (cilexetil) ester, knownas candesartan cilexetil. Candesartan cilexetil is metabolised completely by esterases in theintestinal wall during absorption to the active candesartan moieity.
The use of a prodrug form increases the bioavailability of candesartan. Despite this, absolutebioavailability is relatively poor at 15% (candesartan cilexetil tablets) to 40% (candesartancilexetil solution). Its IC50 is 15 µg/kg.
Development history
The compound known as TCV-116 (candesartan) was studied by Japanese scientists usingstandard laboratory rats. Animal studies were published showing the effectiveness of thecompound in 1992-1993, with a pilot study on humans published in the summer of 1993. [4][5]
See also
Discovery and development of angiotensin receptor blockers
References
http://www.sandoz.com/cs/www.sandoz.com-v4/assets/media/shared/documents/Candesartan_PR.pdf Pfeffer M, Swedberg K, Granger C, Held P, McMurray J, Michelson E, Olofsson B,Ostergren J, Yusuf S, Pocock S (2003). "Effects of candesartan on mortality and morbidity inpatients with chronic heart failure: the CHARM-Overall programme". Lancet 362 (9386):759–66. doi:10.1016/S0140-6736(03)14282-1. PMID 13678868. Julius S, Nesbitt SD, Egan BM; et al. (July 2006). "Feasibility of treatingprehypertension with an angiotensin-receptor blocker". New England Journal of Medicine354 (16): 1685–97. doi:10.1056/NEJMoa060838. PMID 16537662. Mizuno, K.; et al. (1992). "Hypotensive activity of TCV-116, a newly developedangiotensin II receptor antagonist, in spontaneously hypertensive rats.". Life Sci. 51 (20):PL183–187. PMID 1435062. Ogihara, T.; et al. (Jul–Aug 1993). "Pilot study of a new angiotensin II receptor
antagonist, TCV-116: effects of a single oral dose on blood pressure in patients with
essential hypertension.". Clin Ther. 15 (4): 684–91. PMID 8221818.
2. Sumber: http://www.webmd.com/drugs/2/drug-8183/candesartan-oral/details
candesartan
COMMON BRAND NAME(S): Atacand
GENERIC NAME(S): CANDESARTAN CILEXETIL
I want to save to My MedicineYES

Endocrinologist – Terapi Pengganti (Thyrax) – TSH Level – Candesartan
62
WARNINGS:
This drug can cause serious (possibly fatal) harm to an unborn baby if used during pregna...
Uses
Candesartan is used to treat high blood pressure (hypertension). Lowering high bloodpressure helps prevent strokes, heart attacks, and kidney problems. Candesartan belongs to aclass of drugs called angiotensin receptor blockers (ARBs). It works by relaxing bloodvessels so blood can flow more easily.
This medication is also used to treat heart failure.
This medication is not recommended for use in children younger than 1 year due toincreased risk of side effects.
OTHER USES: This section contains uses of this drug that are not listed in the approvedprofessional labeling for the drug but that may be prescribed by your health careprofessional. Use this drug for a condition that is listed in this section only if it has been soprescribed by your health care professional.
This drug may also be used to help protect the kidneys from damage due to diabetes.
How to use candesartan
Read the Patient Information Leaflet if available from your pharmacist before you starttaking candesartan and each time you get a refill. If you have any questions, ask your doctoror pharmacist.
Take this medication by mouth with or without food as directed by your doctor, usuallyonce or twice daily.
The dosage is based on your medical condition and response to treatment. In children, thedosage is also based on weight.
Use this medication regularly to get the most benefit from it. To help you remember, take itat the same time(s) each day. It is important to continue taking this medication even if youfeel well. Most people with high blood pressure do not feel sick. For the treatment of highblood pressure, it may take up to 6 weeks before you get the full benefit of this drug.
Tell your doctor if your condition does not improve or if it worsens (such as your bloodpressure readings remain high or increase).
What conditions does candesartan treat?
conditions
What conditions does candesartan treat?
candesartan oral is used to treat the following:
High Blood Pressure, Chronic Heart Failure
candesartan oral may also be used to treat:

Endocrinologist – Terapi Pengganti (Thyrax) – TSH Level – Candesartan
63
Kidney Disease from Diabetes, Diastolic Heart Failure, Nondiabetic ProteinuricNephropathy
3. Sumber: http://drugs.webmd.boots.com/drugs/drug-71-Candesartan.aspx
CANDESARTAN
Brand Name(s) : Amias
CANDESARTAN WARNINGS
Candesartan should be used with caution in:
patients with kidney disease or who have had a kidney transplant, patients with liver orheart disease, with renal artery stenosis, those with abnormally low blood pressure,patients who are about to have anaesthetics and surgery (including dental surgery),obstructive hypertrophic cardiomyopathy, primary hyperaldosteronism,hyperkalaemia, severe congestive heart failure.
It should not be used in:
women who are more than 3 months pregnant (it is also better to avoid candesartan inearly pregnancy), patients who are allergic to candesartan or to any of the ingredientsin the medicine; severe liver disease or biliary obstruction (a problem with thedrainage of the bile from the gall bladder).
Also see list of precautions and interactions
STORAGE
Do not store above 30 °C
CANDESARTAN USES
Candesartan is used to lower blood pressure by relaxing your blood vessels, making iteasier for your heart to pump your blood around your body.
It is an angiotensin II receptor antagonist, sometimes known as an angiotensin receptorblocker (ARB).
It is used to lower your blood pressure.

Endocrinologist – Terapi Pengganti (Thyrax) – TSH Level – Candesartan
64
In general this drug is used to treat high blood pressure (hypertension). It is also used totreat heart failure when combined with a specific type of medicines called angiotensin-converting-enzyme inhibitors (ACE inhibitors) or when ACE inhibitors are considered notsuitable
Benefits of being on this drug can include lowering of blood pressure and treating heartfailure
Listed below are the typical uses of Candesartan.
Treatment of high blood pressure in adult patients Treatment of heart failure with reduced heart muscle function in addition to an
angiotensin converting enzyme (ACE) inhibitor or when ACE inhibitors cannot beused, in adult patients.
On occasion your doctor may prescribe this medicine to treat a condition not on the abovelist.
HOW TO USE/TAKE
How often do I take it?
Take this medication orally usually once a day, with or without food. Use this medication regularly in order to get the most benefit from it. Remember to use it at the same time each day - unless specifically told otherwise by
your doctor. It may take up to 4 weeks before the full benefit of this drug takes effect. Certain medical conditions may require different dosage instructions as directed by
your doctor.
What dose?
Dosage is based on your age, gender, medical condition, response to therapy, and use ofcertain interacting medicines.
Do I need to avoid anything?
When driving vehicles or operating machines it should be taken into account thatdizziness or weariness may occur during treatment. Consult your doctor or pharmacistfor more details.
When can I stop?
It is important to continue taking this medication even if you feel well, unless your doctortells you to stop.
CANDESARTAN SIDE EFFECTS
Vertigo, headache, nausea, hepatitis, blood disorders, back pain, joint pain (arthralgia), muscle pain (myalgia), rash,

Endocrinologist – Terapi Pengganti (Thyrax) – TSH Level – Candesartan
65
urticaria, pruritus, dizziness, cold or flu-like symptoms/respiratory infections, hypotension (low blood pressure). changes in kidney function and potassium and sodium levels swelling of the face, lips, tongue and/or throat, jaundice (yellow skin and/or eyes), hepatitis (inflamed liver), changes in red blood cell levels and decreased levels of white blood cells.
If any of these persist or you consider them severe then contact your doctor or pharmacist.
Stop taking candesartan and tell your doctor immediately if you develop any of thefollowing symptoms: swollen face, lips, tongue, eyes and or throat; jaundice.
Remember that your doctor has prescribed this medication because he or she has judgedthat the benefit to you is greater than the risk of side effects. Many people using thismedication do not have serious side effects.
A serious allergic reaction to this drug is unlikely, but seek immediate medical attention ifit occurs. Symptoms of a serious allergic reaction include: rash, itching/swelling (especiallyof the face/tongue/throat), dizziness, trouble breathing.
This is not a complete list of possible side effects. If you notice other effects not listedabove, contact your doctor or pharmacist.
The Yellow Card Scheme allows you to report suspected side effects from any type ofmedicine (which includes vaccines, herbals and over the counter medicines) that you aretaking. It is run by the medicines safety watchdog called the Medicines and Healthcareproducts Regulatory agency (MHRA). Please report any suspected side effect on theYellow Card Scheme website.
CANDESARTAN PRECAUTIONS
This medication should not be used if you have certain medical conditions. Before usingthis medicine, consult your doctor or pharmacist if you have: severe liver disease or biliaryobstruction; are pregnant or are planning to become pregnant; breastfeeding.
Before using this medication, tell your doctor or pharmacist your medical history,especially any of the following: kidney disease or kidney transplant; liver disease; renalartery stenosis; abnormally low blood pressure; obstructive hypertrophic cardiomyopathy;primary hyperaldosteronism; hyperkalaemia (high potassium levels); severe congestiveheart failure; intolerance to any of the ingredients.
Before having surgery, tell your doctor or dentist that you are taking this medication.
Does alcohol intake affect this drug?
If you are being treated for heart failure, your doctor may recommend that you avoidalcohol.
The elderly. Candesartan can be used in the elderly.
Pregnancy and breastfeeding - please ensure you read the detailed information below
PREGNANCY

Endocrinologist – Terapi Pengganti (Thyrax) – TSH Level – Candesartan
66
Candesartan is not safe to take if you are, or are planning to become, pregnant.
It is sensible to limit use of medication during pregnancy whenever possible. However, yourdoctor may decide that the benefits outweigh the risks in individual circumstances and aftera careful assessment of your specific health situation.
If you have any doubts or concerns you are advised to discuss the medicine with your doctoror pharmacist.
BREAST FEEDING
Candesartan is not safe to take if you are breastfeeding.
It is sensible to limit use of medication during breastfeeding whenever possible. However,your doctor may decide that the benefits outweigh the risks in individual circumstances andafter a careful assessment of your specific health situation.
If you have any doubts or concerns you are advised to discuss the medicine with your doctoror pharmacist.
CANDESARTAN INTERACTIONS
Your doctor or pharmacist may already be aware of any possible drug interactions and maybe monitoring you for them. Do not start, stop, or change the dosage of any medicine beforechecking with them first.
This drug should not be used with the following medications because very serious, possiblyfatal interactions may occur: none known.
Before using this medication, tell your doctor or pharmacist of all prescription and non-prescription/herbal products you may use, especially of:
Lithium for mania and depression Potassium sparing diuretics (e.g. amiloride, triamteren, spironolactone) Potassium supplements Salt substitutes containing potassium heparin ACE inhibitors (such as enalapril, captopril, lisinopril or ramipril) Diuretics (water tablets) Non-steroidal anti-inflammatory painkillers (such as ibuprofen, naproxen or
diclofenac) COX-2 inhibitors (such as celecoxib or etoricoxib) More than 3 g of aspirin
This information does not contain all possible interactions. Therefore, before usingCandesartan, tell your doctor or pharmacist of all the products you use.