
WT1 Expression Distinguishes Astrocytic Tumor Cells from Normal and Reactive Astrocytes
31
Author pre-print version, final version Brain Pathol. 2008 Jul;18(3):344-53. doi: 10.1111/j.1750-3639.2008.00127.x. WT1 expression distinguishes astrocytic tumor cells from normal and reactive astrocytes Jens Schittenhelm 1* , Michel Mittelbronn 1* , Thai-Dung Nguyen*, Richard Meyermann * , Rudi Beschorner* * Institute of Brain Research, University Hospital of Tuebingen, Tuebingen, Germany 1 These two authors contributed equally to this study. Running title: WT1 in reactive and neoplastic astrocytes Corresponding author: Jens Schittenhelm, MD Institute of Brain Research University of Tuebingen Calwerstr. 3 D-72076 Tuebingen Tel.: +49-7071-2982293 Fax: +49-7071-294846 Email: [email protected] Key words: WT1, astrocytoma, astrogliosis, neoplastic astrocytes, normal brain This manuscript contains 4 tables and 6 figures.
-
Upload
independent -
Category
Documents
-
view
1 -
download
0
Transcript of WT1 Expression Distinguishes Astrocytic Tumor Cells from Normal and Reactive Astrocytes

Author pre-print version, final version Brain Pathol. 2008 Jul;18(3):344-53.
doi: 10.1111/j.1750-3639.2008.00127.x.
WT1 expression distinguishes astrocytic tumor cells from normal and reactive
astrocytes
Jens Schittenhelm1*, Michel Mittelbronn1*, Thai-Dung Nguyen*, Richard Meyermann*,
Rudi Beschorner*
*Institute of Brain Research, University Hospital of Tuebingen, Tuebingen, Germany
1 These two authors contributed equally to this study.
Running title: WT1 in reactive and neoplastic astrocytes
Corresponding author:
Jens Schittenhelm, MD
Institute of Brain Research
University of Tuebingen
Calwerstr. 3
D-72076 Tuebingen
Tel.: +49-7071-2982293
Fax: +49-7071-294846
Email: [email protected]
Key words: WT1, astrocytoma, astrogliosis, neoplastic astrocytes, normal brain
This manuscript contains 4 tables and 6 figures.

Abstract
Particularly in small brain biopsies it might be difficult to distinguish reactive
astrogliosis from low-grade or infiltration zones of high-grade astrocytomas. So far no
immunohistochemical marker allows a reliable distinction. Recently the over-
expression of Wilms’ tumor gene product WT1 was reported in astrocytic tumor cells.
However, no sufficient data on WT1 expression in normal or reactive astrocytes are
available. Therefore, we investigated WT1 expression in paraffin-embedded brain
sections from 28 controls, 48 cases with astrogliosis of various etiology and 219
astrocytomas (WHO grade I to IV) by immunohistochemistry. In normal brains and in
astrogliosis expression of WT1 was restricted to endothelial cells. In astrocytomas,
WT1 positive tumor cells were found in pilocytic astrocytomas (66.7% of cases),
diffuse astrocytomas WHO grade II (52.7%), anaplastic astrocytomas (83.4%) and
glioblastomas (98.1%). Overall, the majority of all astrocytic neoplasms (84.5%)
expressed WT1. Establishing a cut off value of 0% immunoreactive tumor cells
served to recognize neoplastic astrocytes with 100% specificity and 68% sensitivity
and was associated with positive and negative predictive values of 1 and 0.68
respectively. Therefore, WT1 expression in astrocytes indicates a neoplastic origin
and might represent an important diagnostic tool to differentiate reactive from
neoplastic astrocytes by immunohistochemistry.
Introduction
In the central nervous system, morphological features of astrocytic neoplasms
overlap with reactive astrogliosis occurring within or around brain lesions of various
etiologies. Especially the distinction between astrogliosis and low-grade
astrocytomas or infiltration zones of high-grade astrocytomas may be difficult (9). In
the normal human brain astrocytes are associated with structural support, metabolic
homoeostasis and energy supply (13,45,49). They produce adhesion molecules,
neurotrophic factors and extracellular matrix substances that are essential for
structural integrity and repair (10). As a reaction to pathological changes they
increase in number and size and secrete additional extracellular matrix components
(1,38) through inhibition of membrane-bound Na+/K+-ATPase (5) or activation of
Epidermal Growth Factor Receptor (EGFR), a transmembrane receptor with tyrosine
kinase activity (30). Reactive (non-neoplastic) astrocytes may become very large and
may even display pleomorphic nuclei resembling neoplastic tumor cells (9). These
morphologic features are especially observed in progressive multifocal
leukoencephalopathy (PML) (12). Therefore, in small biopsy specimens this may
result in a diagnostic dilemma leading to inconclusive diagnosis (14) and might be
the main reason for interobserver variability (42). Especially if both atypical astrocytes
and mitotic figures are present in reactive lesions, an erroneous diagnosis of an
astrocytic neoplasm might occur (56). So far, no tool is available to reliably proof
neoplastic nature of astrocytes in pathology routine diagnosis. Expression
upregulation of glial fibrillary acidic protein (GFAP) (10), vimentin (53) and N-cadherin
(44) are the hallmarks of astrocytic activation and may also be observed in distant
areas of the lesion due to gap junction signalling (15). Under physiological conditions
the level of GFAP expression in CNS is low. The increase of GFAP in reactive
astrocytes makes GFAP an excellent immunohistochemical marker in histopathology

for labelling these cells (11). But its diagnostic usefulness in differentiating reactive
and neoplastic astrocytes is very limited since GFAP is also commonly observed in
astrocytomas (4,55). Previous studies have examined EGFR controlling cellular
functions in various gliomas (43). EGFR is not detected in normal astrocytes,
however reappearance occurs in reactive astrocytes under various
pathophysiological conditions (20,41). Other authors suggested that
immunohistochemical presence of p53 protein might detect neoplastic transformation
in glial tissue. However, it became evident that p53 is also expressed in a subset of
reactive astrocytes (26, 54). The cell-surface receptor for hyaluronic acid, CD44 was
considered to be significantly upregulated in astrocytic neoplasms compared to
normal brain (25). Later it became evident that normal brain, as well as neoplastic
tissues share the same splicing variant (35). In addition we were able to demonstrate
in a previous study that CD44 upregulation also occurs in reactive astrocytes at the
border of infiltrative neoplasms of non-glial origin (57). Therefore, a reliable method
to distinguish neoplastic from normal or reactive astrocytes suitable for routine
diagnosis has not yet been established.
The Wilms’ Tumor supressor gene encodes for a zinc-finger transcription factor
(WT1) and is associated with genito-urinary malformations due to reduced protein
levels in human development (8). Allelic losses or mutations of the gene result in
nephroblastoma, a common pediatric solid malignancy of the kidney (19). The WT1
protein is involved in proliferation, differentiation and apoptosis (21). Interaction with
other transcription factors like EGR-1 and p53 shows that WT1 has oncogenic
properties (31). Recent reports indicate that WT1 is expressed in glioblastoma cell
lines (32) and in astrocytic tumor tissue (39) among other types of solid cancer. In
addition it has been shown that WT1 might be useful to differentiate between
proliferating endothelial lesions and vascular malformations (28). In order to

characterize the astrocytic WT1 expression pattern and its diagnostic usefulness, we
investigated normal, reactive and neoplastic human CNS tissue specimens by
immunohistochemistry for differences.
Materials and Methods
Patient data
In total 295 cases from the tissue archives of the Institute of Brain Research
(Neuropathology), University Hospital of Tuebingen were enrolled in this study,
including normal brains (28 cases) and reactive CNS tissues (48 cases). The reactive
CNS tissue samples were derived from different pathological conditions such as
vascular malformations, brain metastasis, infiltrating meningiomas and ischemia
(details on cases are shown in table 1). Furthermore, astrocytic neoplasms (219
samples) consisting of WHO grade I pilocytic astrocytomas (n=24), WHO grade II
astrocytomas (n=36), WHO grade III anaplastic astrocytomas (n=54) as well as WHO
grade IV glioblastomas (n=105) were included in the present study. These patients
underwent surgical treatment between 1995 and 2005 (epidemiologic details are
shown in table 2). Histological diagnosis and grading were performed according to
the WHO classification system by at least two experienced neuropathologists (23).
Immunohistochemistry
After surgical removal all specimens were fixed in 4% formalin (pH 7.4) and
embedded in paraffin. Immunohistochemistry was performed using the established
monoclonal WT1-antibody, clone 6F-H2 (dilution 1:50, Dako, Glostrup, Denmark).
The antibody reacts with all isoforms of the full-length WT1 protein. In addition a
polyclonal GFAP antibody (Z0334, dilution 1:1000, Dako) was used. Sections were
deparaffinized, rehydrated and immunostained using the Benchmark

immunohistochemistry system (Ventana Medical Systems, Strasbourg, France). The
automated standard protocol is based on an indirect biotin-avidin system and
consists of a cell conditioning pretreatment, use of I-View inhibitor (Ventana) for 4
min, application of the WT1 antibody for 20 min or GFAP-antibody for 6 min followed
by an incubation of amplifier Systems A and B (Ventana), avidin-botin blocking for 4
min and one drop of I-View Biotin Ig (Ventana). For visualization the sections were
incubated with one drop of I-View SA-HRP for 8 min and then with DAB/H2O2 for
additional 8 min. The sections were finally incubated with a copper enhancer
(Ventana) for 4 min and counterstained with hematoxylin. Wilms tumor tissue
specimens were used as positive control displaying a distinct nuclear staining pattern
of tumor and endothelial cells. Negative control slides were processed in parallel with
each batch of staining. To exclude unspecific binding of the monoclonal antibody,
IgG isotype controls using the same IgG-concentrations as in the replaced primary
antibody solutions were performed (IgG1, Dako).
Evaluation and Statistics
Only samples showing WT1 expression in endothelial cells serving as internal control
were scored (28). Tumor cells were considered positive, when cytoplasmic staining of
cells matched at least the intensity observed in endothelial cells (47). The scores of
WT1+ tumour cells of the whole neoplastic specimen available was estimated
independently by three raters (JS, MM, RB) using a semiquantitative score including
0 (no staining), 1 (singular positive cells - <1%), 2 (2-19%), 3 (20-50%) and 4 (>50%)
allowing fast and easy scoring of the tissue. Only if two or more scores were identical
for the same case, this score was taken into account. Ordinal logistic regression was
performed for each comparison followed by a Likelihood Ratio Chi-square test. To
test interobserver variability of the three experienced neuropathologists in the WT1

assessment, a weighted kappa statistic was calculated. A summary kappa was
calculated both for each pairwise combination and for all raters as a group. Kappa
values of 0—0.20 have been defined as slight, 0.21—0.40 as fair, 0.41—0.60 as
moderate, 0.61—0.80 as substantial and 0.81—1.0 as almost perfect (27). JMP 7.0
was used for statistical analysis (* p≤0.05, ** ≤0.01, *** p≤0.0001).

Results
The applied WT1 scoring method is an easy and reproducible method.
Interobserver variability for all cases examined was at most one score level. The
agreement about the WT1 scores between the three raters taken as a group was
substantial (κ=0.683). Furthermore, all individual pairwise comparisons showed
substantial agreement ranging for κ=0.613 (SD=0.033) to κ=0.758 (SD=0.029).
Agreement across categories was almost perfect (κ=0.9560) for WT1 score 0 (no
WT1 expression) which is the most relevant factor for the diagnosis of positive and
negative cases.
WT1 expression in normal brain is restricted to endothelial cells
In all 28 normal human brains expression of WT1 was limited to endothelial cells of
small blood vessels, both in gray and in white matter (internal control). No astrocytes,
oligodendroglia, ependymal or neuronal cells showed WT1 immunoreactivity (score
0; figures 1A and 1B). Weak cytoplasmic staining of the epithelial choroid plexus
lining was considered nonspecific as it did not match endothelial staining of
capillaries and small vessels of CNS and leptomeninges (not shown). Regions
examined included samples from all four cerebral lobes, cerebellum, diencephalon
and brainstem. In Wilms’ tumor (positive control) a strong nuclear expression of WT1
was observed in tumor cells and in endothelial cells (figure 1C).
Reactive astrocytes lack WT1 expression
In all 48 brain specimens comprising of reactive astrogliosis due to various
pathological conditions (table 1) an increased number of astrocytes showed
gemistocytic morphology and marked expression of GFAP (figure 2). Reactive CNS
tissue around cavernomas (figure 2A) and arteriovenous malformations displayed
strong GFAP expression in reactive astrocytes close to the pathologic vessels (figure
2B). The same areas remained negative except for endothelial vessels on
consecutive sections stained with WT1 antibody (figure 2C). Gemistocytic astrocytes
around infarct lesions (figure 2D) showed prominent GFAP immunostaining (figure
2E) compared with the surrounding neuropil. These all showed a lack of WT1
expression (figure 2F). Non-primary brain tumors as invasive meningiomas,
melanomas and carcinoma metastases (figure 2G) showed reactive gliotic changes
at the tumor border with strong GFAP expression too (figure 2H) but remained
negative for WT1 (figure 2I). Expression of WT1 was always detectable in endothelial
cells of CNS and tumors (internal control) but was never observed in astrocytes
includig those with gemistocytic morphology (score 0). For the record, all 7
melanomas used in our study exhibited at least focally some cytoplasmic (7/7) or
nuclear (2/7) WT1 staining of tumor cells (not shown). Two cases of progressive
multifocal leucoencephalopathy (PML) with presence of JC-virus DNA confirmed by
molecular genetic methods did not express WT1 including their pleomorphic
astrocytes.
Expression of WT1 in astrocytomas differs significantly from normal brain and
reactive gliosis
Among all 219 glioma samples cytoplasmic WT1 imunoreactivity occurred in
endothelial cells and altogether 185 tumors (84.5%) showed WT1 expression in their
astrocytic cells. The distribution of WT1 positive tumor cells varied between different
WHO grades (table 3). Score variability in astrocytic tumors is exemplarily illustrated
in different glioblastomas (figure 3). Numbers of WT1 positive tumor samples were
higher in pilocytic astrocytomas (16/24) than in WHO grade II astrocytomas (19/36).
There was a significant increase of WT1 positive tumors in anaplastic astrocytomas

(45/54) with almost all glioblastomas showing WT1 positive tumor cells (103/105).
Likelihood Ratio Chi-square test showed that the distribution scores of astrocytic
tumors together and reactive CNS were significantly different (p<0.0001).
Comparison of WT1 expression in astrogliosis and astrocytomas together also
showed significant differences (table 4). Detailed p-values in comparison of normal
brain, gliosis and astrocytomas of different WHO grade are summarized in table 4.
Normal brain and astrocytomas (WHO grade I, II, III and IV, respectively) also
differed significantly (p<0.0001, each). Similarly, comparison of gliosis and
astrocytomas (WHO grade I, II, III and IV, respectively) revealed significant results
(p<=0.0001, each). The frequency distribution of different WT1 scores observed in
normal brain, gliosis and astrocytomas WHO grade I-IV is illustrated in figure 4. Using
score 0 as a cut off value, neoplastic astrocytes are recognized with 100% specificity
and 68% sensitivity and are associated with positive and negative predictive values
of 1 and 0.68 respectively. Using score 1 (<1% immunoreactive cells) instead for cut
off, neoplastic astrocytes are recognized with 100% specificity and 52% sensitivity
and are associated with positive and negative predictive values of 1 and 0.52,
respectively.
Expression patterns of WT1 in neoplastic astrocytes
In the majority of high-grade astrocytomas the tumor cells showed a strong
cytoplasmic staining including delicate cell processes. With few exceptions of
glioblastomas most astrocytomas were devoid of nuclear staining. A considerable
upregulation of WT1 immunoreactivity was observed in areas of pseudopalisading
around necrosis (figure 5A). Except for a thin internally located endothelial layer of
WT1 positive cells, proliferating vessels were immunonegative for WT1 (figure 5B).
Infrequently, astrocytes in close vicinity to microvessel proliferation also showed

increased WT1 staining compared to the more distant tumor areas (figure 5B). Cells
with exceptional anaplastic morphology (large, multinucleated tumor cells) in most
instances also displayed strong immunoreactive for WT1 (figure 5C). In anaplastic
astrocytomas there was usually a diffuse spread of WT1 positive tumor cells
intermingled with WT1 negative tumor cells (figure 5D), but in some cases clustering
of WT1-positive cells was present resulting in WT1-positive areas next to WT1-
negative areas. Similar WT1 immunoreactivity of tumor cells was present in
astrocytomas WHO grade II with exception of gemistocytic astrocytomas which
exhibited moderate to strong WT1 expression in most cases (figure 5E). Further,
most pilocytic astrocytomas frequently displayed WT1+ tumor cells including the
delicate piloid processes (figure 5F).
Discussion
Distinction between reactive astrogliosis and an astrocytic neoplasm is often difficult,
especially in cases when diffuse low-grade astrocytoma or the infiltration zone of a
high-grade astrocytoma is considered (9). So far no single immunohistochemical
marker exists to differentiate clearly in these cases. In recent years, attempts to
discriminate between reactive and neoplastic astrocytes have employed various
methods on molecular genetic level including in-situ hybridisations to detect
chromosomal aberrations absent in non-neoplastic tissue (50). However these
methods are elaborate, expensive and cannot replace the usefulness of
immunostaining practices.
There is a known period of transient WT1 upregulation in ependymal cells of brain
and spinal cord during embryogenesis suggesting involvement in differentiation of
glial cells (3,46). There is no evidence of WT1 reactivation in normal brain or reactive
astrogliosis so far (39). Expression of WT1 has previously been reported in

astrocytomas, although the number of tumors examined was rather low (32,39). In
the present study we were able to confirm that WT1 is indeed expressed in astrocytic
neoplasms. The consistent expression of WT1 in blood vessels of the brain even in
cases lacking WT1 expression in tumor cells serves as a good internal control for
immunohistochemistry and has been noted previously in mesotheliomas (24). WT1
expression in the vessels may come surprising at first glance, however recent studies
were able to demonstrate that WT1 transcriptionally regulates vascular endothelial
growth factor (VEGF) through interaction of its zinc finger DNA binding domain and
thus might be not only present in normal endothelium but also associated with
angiogenesis in neoplasia (16,17).
In our study we examined WT1 immunoreactivity in normal brain, reactive CNS tissue
with astrogliosis resulting from various underlying pathologies (e.g. vascular
malformations, brain metastasis, ischemia, PML) and astrocytic tumors of different
WHO grades. We were able to show that normal and reactive astrocytes do not
display any visible WT1 immunoreactivity. Our observations around ischemic CNS
lesions correlate with previous observations of Wagner and colleagues, describing
WT1 upregulation in kidney and heart but not in brain of rats kept under hypoxic
conditions (48).
In contrast to normal and reactive astrocytes, neoplastic astrocytes frequently
express WT1. In our series of 219 astrocytomas WT1+ tumor cells were found in
pilocytic astrocytomas (66.7% of cases examined), astrocytomas WHO grade II
(52.8%), astrocytoma WHO grade III (83.4%) and glioblastomas WHO grade IV
(98.1%). Overall, the majority of all astrocytic tumors (84.5%) expressed WT1 at least
focally. Thus, WT1 is significantly upregulated in astrocytomas of any WHO grade
when compared to normal brain or astrogliosis. Using score 0 (lack of WT1 positive
tumor cells) as a cut off astrocytic neoplasms can be diagnosed with 100% specificity

and 68% sensitivity. In cases where WT1 expression is present on astrocytic cells,
the diagnosis clearly points to an astrocytic neoplasm as there is an excellent
positive predictive value of 1. In cases lacking WT1 immunostaining differentiation
from reactive gliosis remains still difficult with a negative predictive value of 0.68. We
have employed WT1 in our routine diagnostic panel for glial neoplasms and reactive
gliosis for several months as well during the review process and have not
experienced a single false positive case so far. However we are very well aware that
there will be always an exception that proves the rule and expect someone to report
this. It is important to remember that WT1 is known to be expressed not only in
endothelial cells but also in fibroblasts (37). The presence of WT1 in brain tissue
therefore should not prompt a straightforward diagnosis of an astrocytoma. Rather to
rule out the presence of a glial scar on the one side and mesenchymal or
desmoplastic reaction on the other side, the pathologist should apply appropriate
additional stainings when in doubt. Moreover WT1 should not be regarded as an
astrocytoma-specific marker since its expression in other glial neoplasms
(ependymomas, oligodendrogliomas etc) has been demonstrated recently (18). Our
findings in astrocytic tumors are in accordance to a previous report by Oji et al. who
found expression of WT1 protein in 18/18 high-grade gliomas and in 5/6 low-grade
gliomas examined (39). We have limited the current immunohistochemical study to
astrocytic neoplasms since low-grade astrocytic neoplams are most likely prone to
misdiagnoses than other glial neoplasms. In the past months WT-1 staining helped to
clarify several challenging cases in our institute. Some of these cases are illustrated
in Figure 6. It is also noteworthy that the WT1 antibody can be applied on frozen
tissue as well.
It has previously been suggested by some authors that cytoplasmic staining
represents cross-reactivity with an epitope unrelated to WT1 (24). However recent

studies were able to demonstrate presence of WT1 in the cytoplasm via western blot
(36) and RT-PCR (32). In addition immunohistochemical staining of WT1 in the
cytoplasm of several types of cancer has been demonstrated (36). This suggests that
strong overexpression leads to inactive state of the WT1 transcription activity and
after phosphorylation it shuttles back into the nucleus, where it is able to bind DNA
(37). In addition recent identification of an immunogenic T-cell binding epitope within
WT1 suggests a specific tumor-antigen directed immunological approach in therapy
(6).
Tumor-restricted antigens that are not expressed in normal and/or reactive astrocytes
include the intracellular vimentin-binding 300-kilodalton intermediate filament
associated protein IFAP-300kDa (29). Its expression in radial glia of the embryonic
central nervous system is terminated postnatally and re-expression occurs only
during tumorigenesis as demonstrated in seven high-grade gliomas and cultured
cells (52). To date however no informations on expression in low-grade astrocytomas
or in reactive astrocytes have been provided. Integrin alpha3, a 140-kDa protein is
reported to be present in malignant gliomas but does not show antibody reaction
within the normal brain (22). As a cell membrane adhesion molecule its expression
might be a potential target for immunotherapy, yet its role in reactive astrocytes still
needs to be elucidated. One of the best evaluated proteins is the mutated isoform of
the Epidermal Growth Factor Receptor (EGFRvIII). Considered as a marker for
malignancy it is expressed in approximately half of all gliomas examined (2,51),
however immunohistochemical results on paraffin-embedded specimens remain poor
(7). Another interesting marker is the tumor-specific murine antibody 8H9 directed
against a 58 kDa surface antigen expressed among neuroectodermal, mesenchymal,
and epithelial tumors, which has been reported in 15/17 frozen glioblastoma and 6/8
frozen astrocytoma samples and does not react with normal human brain (33).

Recombinant immunotoxins raised against this epitope are currently tested against
various types of cancer (40). To date no information for 8H9 on paraffin-embedded
specimens exists. The common acute lymphoblastic antigen (cALLA, CD10), also
known as neutral endopeptidase was suggested not only as a marker of malignancy
progession but also considered lacking expression in reactive astrocytes in frozen
tissue sections (34). Although showing promising results, routine use of the
previously mentioned antibodies is limited because the staining of paraffin-embedded
specimens is the method of choice in diagnostic pathology.
In conclusion, WT1 immunohistochemistry is a valid and promising diagnostic tool to
distinguish neoplastic astrocytes from normal or reactive astrocytes in routinely
paraffin-embedded tissue. We have also shown that the used scoring method shows
substantial agreement and therefore is a valid and reproducible tool for quick
assessment of WT1 expression.
Acknowledgments
We wish to thank Gudrun Albrecht for the arrangement of the photomicrographs and
Andrea Bob-Schittenhelm for her help with the English.

References
1.Agapova OA, Ricard CS, Salvador-Silva M, Yang P, Hernandez MR (2001)
Expression of matrix metalloproteinases and tissue inhibitors of
metalloproteinases in human optic nerve head astrocytes. Glia 33:205-216.
2.Aldape KD, Ballman K, Furth A, Buckner JC, Giannini C, Burger PC,
Scheithauer BW, Jenkins RB, James CD (2004) Immunohistochemical detection
of EGFRvIII in high malignancy grade astrocytomas and evaluation of prognostic
significance. J Neuropathol Exp Neurol 63:700-707.
3.Armstrong JF, Pritchard-Jones K, Bickmore WA, Hastie ND, Bard JB (1993).
The expression of the Wilms' tumour gene, WT1, in the developing mammalian
embryo. Mech Dev 40:85-97.
4.Asano K, Kubo O, Tajika Y, Huang MC, Takakura K, Ebina K, Suzuki S (1997)
Expression and role of cadherins in astrocytic tumors. Brain Tumor Pathol 14;27-
33.
5.Aschner M, Sonnewald U, Tan KH (2002) Astrocyte modulation of neurotoxic
injury. Brain Pathol 12:475-481.
6.Asemissen AM, Keilholz U, Tenzer S, Müller M, Walter S, Stevanovic S, Schild
H, Letsch A, Thiel E, Rammensee HG, Scheibenbogen C (2006) Identification of
a highly immunogenic HLA-A*01-binding T cell epitope of WT1. Clin Cancer Res
12:7476-7482.
7.Biernat W, Huang H, Yokoo H, Kleihues P, Ohgaki H (2004) Predominant
expression of mutant EGFR (EGFRvIII) is rare in primary glioblastomas. Brain
Pathol 14:131-136.
8.Buckler AJ, Pelletier J, Haber DA, Glaser T, Housman DE (1991) Isolation,
characterization, and expression of the murine Wilms' tumor gene (WT1) during
kidney development. Mol Cell Biol 11:1707-1712.
9.Burger PC, Scheithauer BW, Vogel FS (2002) The Brain – Tumors. In: Surgical
Pathology of the nervous system and its coverings Burger PC, Vogel FC (eds), pp
160-378, 4th edn. Elsevier: Oxford.
10.Eddleston M, Mucke L (1993) Molecular profile of reactive astrocytes--
implications for their role in neurologic disease. Neuroscience 54:15-36.
11.Eng LF, Ghirnikar RS (1994) GFAP and astrogliosis. Brain Pathol 4:229-237.
12. Ellison D, Love S, Chimelli L, Harding BN, Lowe J, Vinters HV (2004)
Neuropathology – a reference text of CNS pathology, 2nd edn. Mosby: London.
13.Forsyth RJ (1996) Astrocytes and the delivery of glucose from plasma to
neurons. Neurochem Int 28:231-241.
14.Gaudin PB, Sherman ME, Brat DJ, Zahurak M, Erozan YS (1997) Accuracy of
grading gliomas on CT-guided stereotactic biopsies: a survival analysis. Diagn
Cytopathol 17:461-466.
15.Giaume C, Venance L (1998) Intercellular calcium signaling and gap junctional
communication in astrocytes. Glia 24:50-64.
16.Graham K, Li W, Williams BR, Fraizer G. Vascular endothelial growth factor
(VEGF) is suppressed in WT1-transfected LNCaP cells (2006) Gene Expr 13: 1-
14.
17.Hanson J, Gorman J, Reese J, Fraizer G (2007) Regulation of vascular
endothelial growth factor, VEGF, gene promoter by the tumor suppressor, WT1.
Front Biosci 12:2279-2290.
18. Hashiba T, Izumoto S, Kagawa N, Suzuki T, Hashimoto N, Maruno M,
Yoshimine T (2007) Expression of WT1 protein and correlation with cellular
proliferation in glial tumors. Neurol Med Chir 47:165-70.
19.Hastie ND (1994) The genetics of Wilms' tumor--a case of disrupted
development. Annu Rev Genet 28:523-558.

20.Junier MP (2000) What role(s) for TGFalpha in the central nervous system?
Prog Neurobiol 62:443-473.
21.Kerr JF, Winterford CM, Harmon BV (1994) Apoptosis. Its significance in
cancer and cancer therapy. Cancer 73:2013-2026.
22.Kishima H, Shimizu K, Tamura K, Miyao Y, Mabuchi E, Tominaga E,
Matsuzaki J, Hayakawa T (1999) Monoclonal antibody ONS-M21 recognizes
integrin alpha3 in gliomas and medulloblastomas. Br J Cancer 79:333-339.
23.von Deimling A, Burger PC, Nakazato Y, Ohgaki H, Kleihues P (2007) Diffuse
astrocytoma. In: WHO classification of Tumours: Pathology & Genetics: Tumours
of the Nervous System. DN Louis, H Ohgaki, OD Wiestler, WK Cavenee (eds) pp
25-29. International Agency for Research on Cancer: Lyon.
24.Kumar-Singh S, Segers K, Rodeck U, Backhovens H, Bogers J, Weyler J, Van
Broeckhoven C, Van Marck E (1997) WT1 mutation in malignant mesothelioma
and WT1 immunoreactivity in relation to p53 and growth factor receptor
expression, cell-type transition, and prognosis. J Pathol 181:67-74.
25.Kuppner MC, Van Meir E, Gauthier T, Hamou MF, de Tribolet N (1992)
Differential expression of the CD44 molecule in human brain tumours. Int J
Cancer 50:572-577.
26.Kurtkaya-Yapicier O, Scheithauer BW, Hebrink D, James CD (2002) p53 in
nonneoplastic central nervous system lesions: an immunohistochemical and
genetic sequencing study. Neurosurgery 51:1246-1254.
27.Landis JR, Koch GG (1977) The Measurement of Observer Agreement for
Categorical Data. Biometrics 33: 159-174.
28.Lawley LP, Cerimele F, Weiss SW, North P, Cohen C, Kozakewich HP,
Mulliken JB, Arbiser JL (2005) Expression of Wilms tumor 1 gene distinguishes

vascular malformations from proliferative endothelial lesions. Arch Dermatol
141:1297-1300.
29.Lieska N, Yang HY, Goldman RD (1985) Purification of the 300K intermediate
filament-associated protein and its in vitro recombination with intermediate
filaments. J Cell Biol 101:802-813.
30.Liu B, Chen H, Johns TG, Neufeld AH (2006) Epidermal growth factor receptor
activation: an upstream signal for transition of quiescent astrocytes into reactive
astrocytes after neural injury. J Neurosci 26:7532-7540.
31.Maheswaran S, Park S, Bernard A, Morris JF, Rauscher FJ 3rd, Hill DE, Haber
DA (1993) Physical and functional interaction between WT1 and p53 proteins.
Proc Natl Acad Sci U S A 90:5100-5104.
32.Menssen HD, Bertelmann E, Bartelt S, Schmidt RA, Pecher G, Schramm K,
Thiel E (2000) Wilms' tumor gene (WT1) expression in lung cancer, colon cancer
and glioblastoma cell lines compared to freshly isolated tumor specimens. J
Cancer Res Clin Oncol 126:226-232.
33.Modak S, Kramer K, Gultekin SH, Guo HF, Cheung NK (2001) Monoclonal
antibody 8H9 targets a novel cell surface antigen expressed by a wide spectrum
of human solid tumors. Cancer Res 61:4048-4054.
34.Monod L, Hamou MF, Ronco P, Verroust P, de Tribolet N (1992) Expression of
cALLa/NEP on gliomas: a possible marker of malignancy. Acta Neurochir 114:3-7.
35.Nagasaka S, Tanabe KK, Bruner JM, Saya H, Sawaya RE, Morrison RS
(1995) Alternative RNA splicing of the hyaluronic acid receptor CD44 in the
normal human brain and in brain tumors. J Neurosurg 82:858-863.
36.Nakatsuka S, Oji Y, Horiuchi T, Kanda T, Kitagawa M, Takeuchi T, Kawano K,
Kuwae Y, Yamauchi A, Okumura M, Kitamura Y, Oka Y, Kawase I, Sugiyama H,

Aozasa K (2006) Immunohistochemical detection of WT1 protein in a variety of
cancer cells. Mod Pathol 19:804-814.
37. Niksic M, Slight J, Sanford JR, Caceres JF, Hastie ND (2004) The Wilms'
tumour protein (WT1) shuttles between nucleus and cytoplasm and is present in
functional polysomes. Hum Mol Genet 13:463-471.
38.Norenberg MD (1994) Astrocyte responses to CNS injury. J Neuropathol Exp
Neurol 53:213-220.
39.Oji Y, Suzuki T, Nakano Y, Maruno M, Nakatsuka S, Jomgeow T, Abeno S,
Tatsumi N, Yokota A, Aoyagi S, Nakazawa T, Ito K, Kanato K, Shirakata T,
Nishida S, Hosen N, Kawakami M, Tsuboi A, Oka Y, Aozasa K, Yoshimine T,
Sugiyama H (2004) Overexpression of the Wilms' tumor gene WT1 in primary
astrocytic tumors. Cancer Sci 95:822-827.
40.Onda M, Wang QC, Guo HF, Cheung NK, Pastan I (2004) In vitro and in vivo
cytotoxic activities of recombinant immunotoxin 8H9(Fv)-PE38 against breast
cancer, osteosarcoma, and neuroblastoma. Cancer Res 64:1419-1424.
41.Planas AM, Justicia C, Soriano MA, Ferrer I (1998) Epidermal growth factor
receptor in proliferating reactive glia following transient focal ischemia in the rat
brain. Glia 23:120-129.
42.Prayson RA, Agamanolis DP, Cohen ML, Estes ML, Kleinschmidt-DeMasters
BK, Abdul-Karim F, McClure SP, Sebek BA, Vinay R (2000) Interobserver
reproducibility among neuropathologists and surgical pathologists in fibrillary
astrocytoma grading. J Neurol Sci 175:33-39.
43.Rasheed BK, Bigner SH (1991) Genetic alterations in glioma and
medulloblastoma. Cancer Metastasis Rev 10:289-299.
44.Redies C (2000) Cadherins in the central nervous system. Prog Neurobiol
61:611-648.

45.Rust RS (1994) Energy metabolism of developing brain. Curr Opin Neurol
7:160-165.
46.Scharnhorst V, Kranenburg O, van der Eb AJ, Jochemsen AG (1997)
Differential regulation of the Wilms' tumor gene, WT1, during differentiation of
embryonal carcinoma and embryonic stem cells. Cell Growth Differ 8:133-143.
47.Timár J, Mészáros L, Orosz Z, Albini A, Rásó E (2005) WT1 expression in
angiogenic tumours of the skin. Histopathology 47:67-73.
48.Wagner KD, Wagner N, Wellmann S, Schley G, Bondke A, Theres H, Scholz H
(2003) Oxygen-regulated expression of the Wilms' tumor suppressor Wt1 involves
hypoxia-inducible factor-1 (HIF-1). FASEB J 17:1364-1366.
49.Waxman SG, Sontheimer H, Black JA, Minturn JE, Ransom BR (1993)
Dynamic aspects of sodium channel expression in astrocytes. Adv Neurol 59:135-
155.
50.Wessels PH, Hopman AH, Ummelen MI, Krijne-Kubat B, Ramaekers FC,
Twijnstra A (2001) Differentiation between reactive gliosis and diffuse
astrocytoma by in situ hybridization. Neurology 56:1224-1227.
51.Wikstrand CJ, Hale LP, Batra SK, Hill ML, Humphrey PA, Kurpad SN,
McLendon RE, Moscatello D, Pegram CN, Reist CJ, Traweek ST, Wong AJ,
Zalutsky MR, Bigner DB (1995) Monoclonal antibodies against EGFRvIII are
tumor specific and react with breast and lung carcinomas and malignant gliomas.
Cancer Res 55:3140-3148.
52.Yang HY, Lieska N, Glick R, Shao D, Pappas GD (1993) Expression of 300-
kilodalton intermediate filament-associated protein distinguishes human glioma
cells from normal astrocytes. Proc Natl Acad Sci U S A 90:8534-8537.

53.Yamada T, Kawamata T, Walker DG, McGeer PL (1992) Vimentin
immunoreactivity in normal and pathological human brain tissue. Acta
Neuropathol 84:157-162.
54.Yaziji H, Massarani-Wafai R, Gujrati M, Kuhns JG, Martin AW, Parker JC
(1996) Role of p53 immunohistochemistry in differentiating reactive gliosis from
malignant astrocytic lesions. Am J Surg Pathol 20:1086-1090
55.Yung WK, Luna M, Borit A (1985) Vimentin and glial fibrillary acidic protein in
human brain tumors. J Neurooncol 3: 35-38.
56.Zagzag D, Miller DC, Kleinman GM, Abati A, Donnenfeld H, Budzilovich GN
(1993) Demyelinating disease versus tumor in surgical neuropathology. Clues to
a correct pathological diagnosis. Am J Surg Pathol 17:537-545.
57.Zeltner L, Schittenhelm J, Mittelbronn M, Roser F, Tatagiba M, Mawrin C, Kim
YJ, Bornemann A (2007) The astrocytic response towards invasive meningiomas.
Neuropathol Appl Neurobiol 33:163-168.
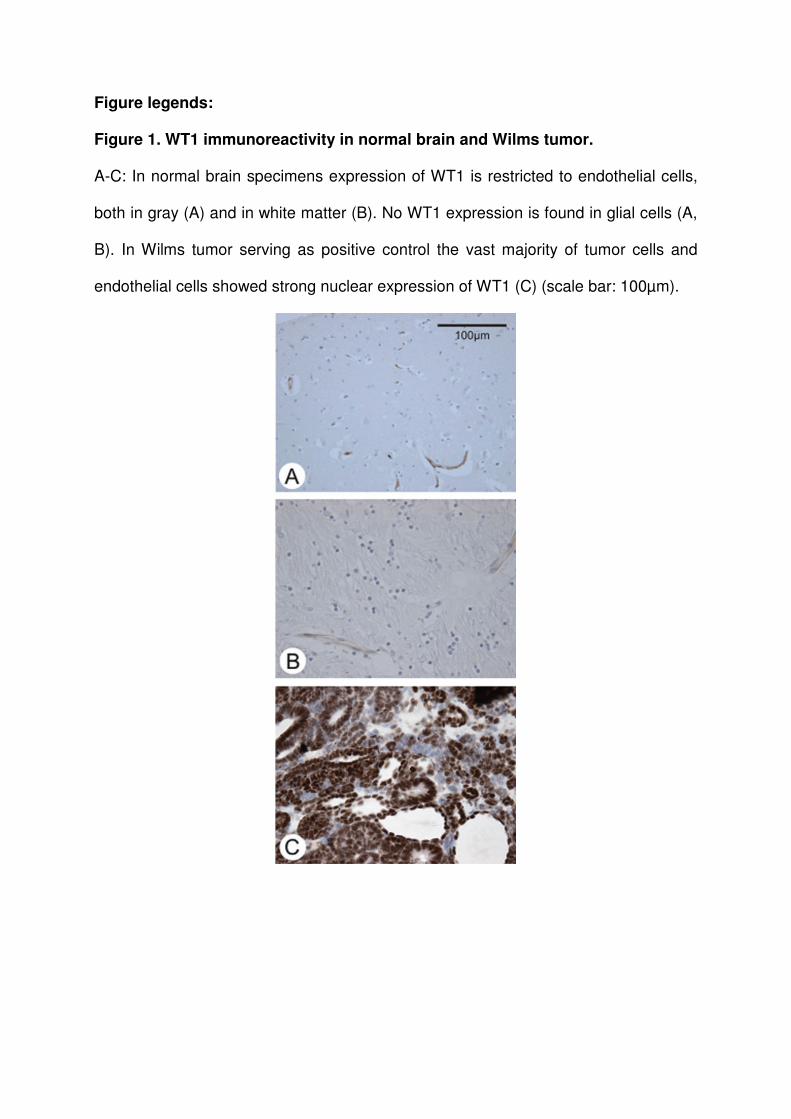
Figure legends:
Figure 1. WT1 immunoreactivity in normal brain and Wilms tumor.
A-C: In normal brain specimens expression of WT1 is restricted to endothelial cells,
both in gray (A) and in white matter (B). No WT1 expression is found in glial cells (A,
B). In Wilms tumor serving as positive control the vast majority of tumor cells and
endothelial cells showed strong nuclear expression of WT1 (C) (scale bar: 100µm).
Figure 2. WT1 immunoreactivity in reactive astrogliosis.
A-C: Thin pathological vessels of a cavernoma (A, H&E) are surrounded by reactive
astrocytes with eosinophilic cytoplasm (inset). Reactive astrocytes are strongly
positive for glial fibrillary acidic protein (GFAP, B), whereas WT1 expression remains
restricted to endothelial cells of capillaries and cavernomatous vessels (C). D-F:
Residual infarction aged 4 months shows glial scar formation with reactive astrocytes
(D, H&E), which express GFAP (E). In the same region WT1 immunoreactivity
remains also restricted to endothelial cells (F). G-I: Astrogliosis due to a brain
metastasis of an adenocarcinoma (G, HE). Reactive astrocytes express GFAP (H)
but not WT1 (I). Note WT1 expression in tumor vessels and in brain capillaries (scale
bars: A-I, 200µm; insets, 50µm).
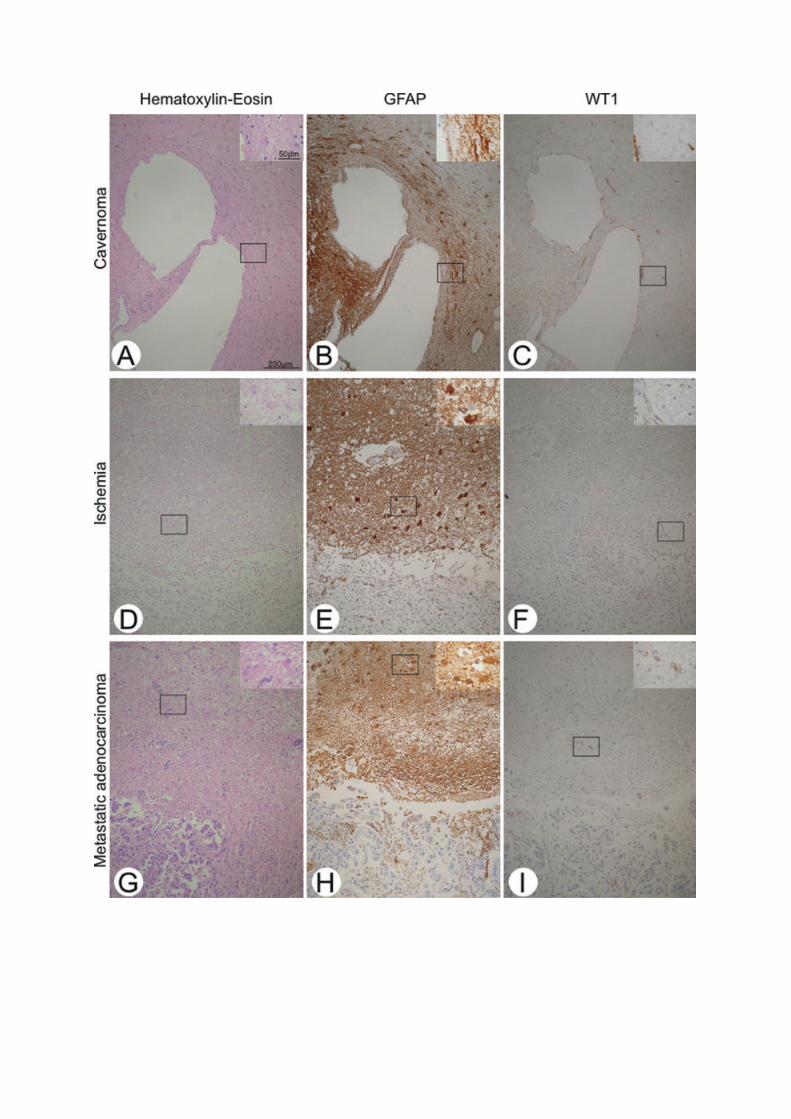

Figure 3. Illustration of WT1 immunoreactivity scores.
Representative photomicrographs illustrating WT1 immunoreactivity scores in
glioblastomas. (A) WT1 expression is limited to endothelial cells of capillaries (score
0). (B) Beside few WT1 positive cell processes also single (<1%) WT1+ tumor cells
(arrows) are present (score 1). Glioblastomas showing WT1 expression in 1-19% (C,
score 2), in 20 to 50% (D, score 3) or in more than 50% of tumor cells (E, score 4).
Isotype control demonstrating specificity of the primary WT1 antibody (F) (scale bar:
A-F, 100µm).

Figure 4. Distribution of different WT1 scores in neoplastic glial cells.
Overall illustration of the frequency of different WT1 scores in astrocytomas grade I-
IV WHO. Note absence of WT1 expression in normal brain and astrogliosis (all cases
score 0, not shown). In astrocytomas of each WHO grade all WT1 scores are present
in variable frequency, respectively.

Figure 5. WT1 immunoreactivity in astrocytomas.
A-F: Immunostaining for WT1 in astrocytic neoplasms. A: Glioblastoma (grade IV
WHO) with areas of pseudopalisading necrosis (score 4), B: Glioblastoma with WT1
enhancement around pathological tumor vessels (score 3), C: Another glioblastoma
with WT1 expression predominating in pleomorphic tumor cells (score 3), D:
Anaplastic astrocytoma, grade III WHO (score 3), E: Gemistocytic astrocytoma grade
II WHO (score 2) and F: Pilocytic astrocytoma grade I WHO (score 3) show
cytoplasmic WT1 in varying number of positive cells (scale bars: A-F, 100µm).

Figure 6. Diagnostic value of WT1 in daily routine.
A-C: 69 year old patient with a left paraventricular mass lesion clinically foremost
considered being a glioblastoma. Stereotactic biopsy specimen showed weak to
moderate increase in cellularity and moderate nuclear pleomorphism but no mitotic
activity, necrosis or microvascular proliferation (A, HE stain). Therefore differential
diagnosis between reactive astrogliosis and infiltration zone of an astrocytoma was
difficult. Assumption of an infiltration zone being more likely was strengthened by
WT1 expression in astrocytic cells (B). The surgery specimen proved neoplastic
nature of the astrocytic lesion and was finally diagnosed as a glioblastoma (C, HE
stain).
D-F: 59-year old patient with a clinically unclear parahippocampal lesion foremost a
glioblastoma or a lymphoma. No steroids were applied prior to biopsy. Due to
complications during the stereotactic procedure only very small tissue specimen
could be achieved for intraoperative diagnosis. The frozen section revealed a
moderate increase in cell density with some gemistocytic astrocytes (D, HE stain).
WT1 expression on frozen-tissue was limited to endothelial cells (E) and there were
no Ki67-positive cells (not shown). Therefore a reactive astrogliosis was considered
to be more likely than an infiltration zone of a glioma. During the following weeks a
rapid spread of the lesion further favoured clinically a glioblastoma. Two months after
stereotaxis an open surgical biopsy was performed yielding the diagnosis of a highly
malignant primary cerebral B-cell lymphoma (F).

Tables
Table 1:
CNS tissue samples with reactive
astrogliosis
No. of cases
(n=76) male/female mean age
Cavernous hemangioma 12 5/7 37
Arteriovenous-Malformation 2 0/2 42
Carcinoma, metastatic 15 10/5 67.6
Meningioma, brain-invasive 6 4/2 60.0
Melanoma 7 3/4 62.1
Ischemia 4 1/3 65.7
Progressive multifocal leukoencephalopathy 2 2/0 55.0
Normal human brain 28 15/13 55.4
Table 2:
Tumor type WHO grade
No. of cases
(n=219) male/female
mean age
Pilocytic astrocytoma I 24 14/10 21.8
Diffuse astrocytoma II 36 24/12 43.9
Anaplastic astrocytoma III 54 36/18 56.1
Glioblastoma IV 105 63/42 58.3
Table 3:
Tissue type Score 0 Score 1 Score 2 Score 3 Score 4
Normal brain 28 0 0 0 0
Gliosis 48 0 0 0 0
Pilocytic astrocytoma 8 6 7 3 0
Diffuse astrocytoma 17 7 8 4 0
Anaplastic astrocytoma 9 13 15 12 5
Glioblastoma 2 8 29 37 29
Table 4:
Level A Level B p-value Gliosis Normal brain (n.s.) all values = 0 Gliosis WHO I <0.0001*** Gliosis WHO II <0.0001*** Gliosis WHO III <0.0001*** Gliosis WHO IV <0.0001*** Normal brain WHO I <0.0001*** Normal brain WHO II <0.0001*** Normal brain WHO III <0.0001*** Normal brain WHO IV <0.0001*** WHO I WHO II 0.3631 (n.s.) WHO I WHO III 0.04 (n.s.) WHO I WHO IV <0.0001*** WHO II WHO III 0.001** WHO II WHO IV <0.0001*** WHO III WHO IV <0.0001*** WHO I-IV Normal brain <0.0001*** WHO I-IV Gliosis <0.0001*** n.s. = not significant, values after Bonferroni-Holm correction







![Astrocytic tracer dynamics estimated from [1-11C]-acetate PET measurements](https://static.fdokumen.com/doc/165x107/6334cca03e69168eaf070c95/astrocytic-tracer-dynamics-estimated-from-1-11c-acetate-pet-measurements.jpg)












