Endovascular treatment of cerebrovascular diseases and intracranial neoplasms
Upload
independentCategory
view
0download
0
IOP PUBLISHING PHYSIOLOGICAL MEASUREMENT
Physiol. Meas. 28 (2007) 465–479 doi:10.1088/0967-3334/28/5/002
Wavelet assessment of cerebrospinal compensatoryreserve and cerebrovascular reactivity
M Latka1, W Kolodziej2, M Turalska1, D Latka2, W Zub3 and B J West4
1 Institute of Physics, Wroclaw University of Technology, Wybrzeze Wyspianskiego 27,50-370 Wroclaw, Poland2 Department of Neurosurgery, Opole Regional Medical Center, Al Witosa 26, 45-401 Opole,Poland3 Department of Neurosurgery, Medical University, 50-420 Wrocław, ul. R. Traugutta 118,Poland4 Mathematical and Information Science Directorate, Army Research Office, PO Box 12211,Research Triangle, NC 27709-2211, USA
E-mail: [email protected]
Received 3 November 2006Published 5 April 2007Online at stacks.iop.org/PM/28/465
AbstractWe introduce a wavelet transfer model to relate spontaneous arterial bloodpressure (ABP) fluctuations to intracranial pressure (ICP) fluctuations. Weemploy a complex continuous wavelet transform to develop a consistentmathematical framework capable of parametrizing both cerebral compensatoryreserve and cerebrovascular reactivity. The frequency-dependent gainand phase of the wavelet transfer function are introduced because ofthe non-stationary character of the ICP and ABP time series. Thegain characterizes the dampening of spontaneous ABP fluctuations and isinterpreted as a novel measure of cerebrospinal compensatory reserve. Fora group of 12 patients who died as a result of cerebral lesions (GlasgowOutcome Scale (GOS) = 1) the average gain in the low-frequency (0.02–0.07 Hz) range was 0.51 ± 0.13 and significantly exceeded that of 17 patientswith GOS = 2 having an average gain of 0.26 ± 0.11 with p = 1×10−4
(Kruskal–Wallis test). A time-averaged synchronization index (which mayvary from 0 to 1) defined in terms of the wavelet transfer function phase yieldsinformation about the stability of the phase difference of the ABP and ICPsignals and is used as a cerebrovascular reactivity index. A low value ofsynchronization index reflects a normally reactive vascular bed, while a highvalue indicates pathological entrainment of ABP and ICP fluctuations. Suchentrainment is strongly pronounced in patients with fatal outcome (for thisgroup the low-frequency synchronization index was 0.69 ± 0.17). The gainand synchronization parameters define a cerebral hemodynamic state space(CHS) in which the patients with GOS = 1 are to large extent partitioned away
0967-3334/07/050465+15$30.00 © 2007 IOP Publishing Ltd Printed in the UK 465

466 M Latka et al
from those with GOS = 2. The concept of CHS elucidates the interplay ofvascular and compensatory mechanisms.
Keywords: brain injury, intracranial hypertension, ICP, compliance, wavelets,synchronization
(Some figures in this article are in colour only in the electronic version)
1. Introduction
In the last decade the list of clinical parameters employed in the management of patients withsevere brain injuries has been steadily growing. Continuous measurement of ECG, arterialand central venous pressure, pulse oximetry (SpO2), and end-tidal carbon dioxide providestandard assessment of systemic cardiovascular and respiratory functions. These physiologicsignals may now be monitored concurrently with intracranial pressure (ICP), jugular venousbulb oxygen saturation (JvO2), flow velocity in major cerebral arteries, regional brain tissueconcentration of O2, CO2, pH, glucose, lactate, and pyruvate (see, for example, Kett-Whiteet al (2002) and references therein). There is a consensus that the technology used to acquiresuch physiologically diverse time series has outpaced algorithms used to analyze them. Forexample, continuous ICP monitoring has been an integral component of the managementof patients with traumatic brain injuries or intracerebral hemorrhages for over two decades.Until recently, the main objective of such monitoring has been confined to the maintenanceof adequate cerebral perfusion pressure. Certainly, severe consequences of even transientcerebral ischemia to some extent provide justification for the status quo. Nevertheless, recentstudies have clearly demonstrated the clinical significance of more sophisticated hemodynamicmetrics derived from ICP waveforms.
For example, Czosnyka et al (1996a) used the moving correlation coefficient betweenthe fundamental harmonic of ICP pulse wave and the mean ICP (RAP index) to assesspressure–volume compensatory reserve. In the same vein, another ICP-derived metric—thepressure-reactivity index (PRx) (Czosnyka et al 1997)—quantifies cerebrovascular pressure-reactivity with the strength of linear correlation between fluctuations of arterial blood pressure(ABP) and ICP. A negative value of PRx reflects a normally reactive vascular bed, as ABPwaves provoke inversely correlated waves in ICP. Positive values of this measure are associatedwith a passive behavior of a non-reactive vascular bed. This index was reported to correlatewith indices of autoregulation based on transcranial Doppler ultrasonography (Czosnyka et al1996b, Lang et al 2002). Furthermore, abnormal values of both PRx and RAP indicate poorautoregulation or reduced cerebrospinal compensatory reserve, respectively. These abnormalvalues have been shown to be predictive of a poor outcome following head injury (Balestreriet al 2004, Czosnyka et al 1996a, 1997, Steiner et al 2002).
However, recent studies (Giller and Mueller 2003, Latka et al 2005, Mitsis and Marmarelis2002, Mitsis et al 2002, Panerai et al 1999, Mitsis et al 2006, Hamner et al 2004) haveemphasized nonlinear, non-stationary and multiscale aspects of cerebral hemodynamics. Thegoal of this paper is to present a novel perspective of the frequency-dependent, non-stationaryaspects of intracranial pressure dynamics. We adopt and extend the mathematical frameworkof complex continuous wavelet transforms to analyze the dynamics of the instantaneous phasedifference between the fluctuations of ABP and ICP (Latka et al 2005). We hypothesize

Wavelet assessment of compensatory reserve and cerebrovascular reactivity 467
that the frequency-dependent strength of synchronization between these two hemodynamictime series reflects reactivity of the cerebrovascular bed. We also test whether the waveletgain which characterizes the dampening of spontaneous arterial blood oscillations within theintracerebral space can quantify cerebrospinal compensatory reserve.
2. Methods
2.1. Patients
The study, approved by the Opole Human Research Committee, comprised 37 patients(29 males and 8 females) treated at the Department of Neurosurgery of the Regional MedicalCenter in Opole, Poland. The median age of subjects was 55 ± 15 years. In the cohort19 patients were diagnosed with subdural hematoma, 7 with spontaneous intracerebralhemorrhage and 6 with subarachnoid hemorrhage from ruptured aneurysm. There were fourcases of cerebral contusions and a single case of traumatic subarachnoid hemorrhage. Thewritten informed consent requirement was waived since only routinely monitored variableswere used in this research.
All of the patients were unconscious at admission. Their initial neurological conditionwas assessed according to the Glasgow Coma Scale (GCS). Five patients had GCS = 3, 14 hadGCS = 4, 8 had GCS = 5, 5 had GCS = 6, 4 had GCS = 7 and 1 had GCS = 8. In all but fourcases the invasive intracranial pressure monitoring followed neurosurgical procedures. Thetip of the ICP strain gauge transducer (Codman) was implanted intraparenchymally into thefrontal lobe, contralaterally to the cerebral lesion. The arterial blood pressure was continuouslymeasured by the radial artery cannulation (Gabarith). The simultaneous monitoring of ICP,ABP and ECG was performed for up to 7 days after ICP gauge implantation.
Postoperative treatment involved mechanical ventilation and optional barbituraneadministration. Cerebral perfusion pressure (CPP) was generally maintained above 70 mmHg.The treatment was scored with Glasgow Outcome Scale (GOS). Twelve out of 37 patientsdied (GOS = 1). For the other patients the scores were distributed as follows: 17 withGOS = 2, 6 with GOS = 3, 1 with GOS = 4 and 1 with GOS = 5. The statistical analysiswas confined to the two largest subgroups, i.e., those with GOS = 1 and those with GOS =2. The physiologic data acquired during monitoring of patients with better clinical condition(GOS > 2) were used for case studies.
2.2. Data analysis
Beat-to-beat average values of blood and intracranial pressures were calculated via waveformintegration of the corresponding signals sampled at 100 Hz and digitized at 16 bits. Innumerical calculations non-uniformly spaced time series were resampled at 2 Hz by cubicspline interpolation.
The wavelet transform is an integral transform which employs basis functions, knownas wavelets, localized in both time and frequency. Such wavelets are constructed from asingle mother wavelet ψ(t) by means of translations and dilations (Mallat 1999). The waveletcoefficient Ws(a, t0) is obtained by filtering the signal:
Ws(a, t0) = 1√a
∫ ∞
−∞ψ∗
(t − t0
a
)s(t) dt (1)
and quantifies the similarity of the signal s(t) to the wavelet dilated by scale a and centered att0 (the asterisk denotes complex conjugation). The instantaneous phase φ(t) associated with

468 M Latka et al
the signal s(t) can be readily extracted by calculating its wavelet transform with a complexmother function to obtain
φ(a, t0) = −i log
[Ws(a, t0)
|Ws(a, t0)|]
. (2)
The dual localization of wavelets makes it possible to associate a pseudofrequency fa with thescale a:
fa = fc
aδt(3)
where fc is the center frequency and δt is the sampling period. Herein, we employ the complexMorlet wavelet:
ψ(t) = 1√πfb
ei2πfct e−t2/fb (4)
and set both the center frequency fc and the bandwidth parameter fb to 1. The detaileddescription of the numerical algorithms used in wavelet analyses may be found in Latka et al(2005, 2003). Herein, we use time-averaged modulus of wavelet coefficients as a frequency-dependent measure of variability of the signal s(t):
Vs(fa) = 〈|Ws(fa, t0)|〉t0 . (5)
We quantify the interdependence of ABP and ICP time series fluctuations with the scale(frequency) dependent synchronization index:
γ ICPABP(a) = 〈sin �φ〉2 + 〈cos �φ〉2 , (6)
where �φ = φABP −φICP is the instantaneous phase difference between the ABP and ICP timeseries. The angular brackets denote averaging over time. The synchronization index lies in theinterval 0 � γ � 1. A vanishing index (γ = 0) corresponds to a uniform distribution of thephase differences (no synchronization) while γ = 1 corresponds to perfect synchronization(phase locking of the two processes).
In the most straightforward approach we define the scale-dependent time-averaged waveletgain η as
ηICPABP(a) ≡ 〈|WICP(a, t0)|〉
〈|WABP(a, t0)|〉 . (7)
The gain quantifies the damping of spontaneous ABP fluctuations. We hypothesize that thesynchronization index γ is determined by reactivity of the vascular bed, while the gain η maybe used as a novel measure of cerebrospinal compensatory reserve.
A transfer function transforms an input signal (ABP time series) into an output signal(ICP time series) and represents the influence of an intervening dynamic process that couplesthe two phenomena together (dynamics of the vascular bed). In frequency space the Fouriertransform of the transfer function is a filter with amplitude and phase, the amplitude beingcalled the gain. The Fourier transform of the signal yields a function that depends only onfrequency, whereas the wavelet transform of that signal depends on both frequency and time.This distinction becomes important when the signal is a non-stationary stochastic process, inwhich case the frequency spectrum of the input changes over time. This time change is illdefined for a Fourier spectrum, but is well defined for a wavelet spectrum. Consequently, thewavelet gain at a given scale is more than a simply filtered input at that scale, but determinesthe influence of the input on the output across scales due to nonlinearities in the underlyingdynamics.

Wavelet assessment of compensatory reserve and cerebrovascular reactivity 469
0.00
0.20
0.40
0.60
0.80
GOS=1 GOS=2
η
0.00
0.25
0.50
0.75
1.00
GOS=1 GOS=2
γ
(a) (b)
Figure 1. Box-and-whiskers plots of wavelet gain ηICPABP (a) and synchronization index ηICP
ABP (b).The plots visualize the data presented in the last two columns of table 1.
2.3. Statistics
Mean values and standard deviations of ABP, ICP, CPP, R–R interval, wavelet gain andsynchronization were calculated first over the 15 min data segments for each patient, and thengroup averaged. For each patient we used up to ten different data segments. Kruskal–Wallisnon-parametric test was used to assess statistical significance of differences in mean values ofphysiological variables in the two outcome groups. The circular variant of the t-test (Batschelet1981) was applied to the group averaged frequency dependent phase difference between theABP and ICP fluctuations. For both tests the significance level was set to p < 0.05.
3. Results
For each patient up to ten different 15 min data segments were used to calculate the low-frequency (0.02–0.07 Hz) ICP-derived indices (ηICP
ABP and γ ICPABP). These physiological variables,
averaged over all available data segments, are reported in table 1 along with the correspondingclinical information and standard hemodynamic parameters. The group-averaged values andstandard deviation of physiological variables in the two outcome groups are presented intable 2. The distribution of values of wavelet gain and synchronization index (the two lastcolumns of table 1) are visualized by the box-and-whiskers plots (figure 1). We can seethat for patients who died the average low-frequency gain ηICP
ABP = 0.51 ± 0.13 significantlyexceeds that of patients with GOS = 2: ηICP
ABP = 0.26 ± 0.11 (p = 1 × 10−4). The averagesynchronization parameter is also different in the two cohorts: γ ICP
ABP = 0.69±0.17 (GOS = 1)and γ ICP
ABP = 0.54 ± 0.23 (GOS = 2).The first row of figure 2 shows the spontaneous fluctuations of arterial (figure 2(a))
and intracranial (figure 2(d)) pressure fluctuations for a patient with normal ICP. Timeevolution of the modulus of the wavelet coefficient for scale a = 10 (this scale corresponds topseudofrequency 0.2 Hz) is presented in figure 2(b) (ABP) and figure 2(e) (ICP). In the thirdrow of figure 2 we display the density plot of the modulus of the wavelet coefficients as afunction of time and frequency. The horizontal color bar at the bottom of the figure reveals theassignments of colors to the values of wavelet coefficients. Figure 3 illustrates the outcomeof the same wavelet analysis used on the data depicted in figure 2 for a patient with severecerebral hypertension.

470 M Latka et al
Table 1. Mean values of physiological variables and ICP-derived indices (ηICPABP and γ ICP
ABP) for thepatients in the two outcome groups.
Age ABP ICP CPP RRPatient (y) G (mmHg) (mmHg) (mmHg) (ms) η γ
GOS = 11 52 M 187 75 112 777 0.38 ± 0.03 0.62 ± 0.322 70 M 85 43 42 972 0.54 ± 0.16 0.80 ± 0.153 43 F 121 67 54 774 0.37 ± 0.07 0.66 ± 0.144 36 M 111 46 64 787 0.57 ± 0.09 0.78 ± 0.155 22 M 87 31 56 735 0.55 ± 0.21 0.61 ± 0.086 64 F 78 21 57 702 0.46 ± 0.01 0.75 ± 0.237 69 M 105 23 82 506 0.41 ± 0.08 0.65 ± 0.128 74 M 98 9 88 643 0.33 ± 0.10 0.28 ± 0.079 50 F 113 59 54 598 0.67 ± 0.11 0.77 ± 0.09
10 50 M 94 101 −7 714 0.46 ± 0.12 0.53 ± 0.2411 15 F 84 71 14 686 0.71 ± 0.23 0.95 ± 0.0212 53 M 90 77 13 899 0.68 ± 0.07 0.86 ± 0.13
GOS = 21 58 M 102 32 70 590 0.36 ± 0.04 0.66 ± 0.062 44 F 111 44 67 670 0.40 ± 0.01 0.99 ± 0.013 59 M 84 12 72 932 0.20 ± 0.05 0.67 ± 0.064 68 F 110 12 97 462 0.12 ± 0.06 0.33 ± 0.195 57 M 102 14 88 680 0.10 ± 0.07 0.32 ± 0.106 55 M 90 20 70 635 0.17 ± 0.06 0.71 ± 0.127 42 M 108 14 93 602 0.14 ± 0.03 0.46 ± 0.198 57 M 107 32 75 933 0.39 ± 0.09 0.82 ± 0.229 55 M 85 17 68 662 0.33 ± 0.12 0.25 ± 0.17
10 65 M 98 7 91 664 0.23 ± 0.14 0.20 ± 0.0311 53 M 101 15 86 754 0.17 ± 0.04 0.46 ± 0.1312 64 M 90 28 62 773 0.30 ± 0.07 0.48 ± 0.1413 70 M 92 30 63 418 0.38 ± 0.15 0.60 ± 0.1514 62 M 86 12 74 1058 0.12 ± 0.03 0.46 ± 0.1015 51 M 70 8 62 654 0.25 ± 0.06 0.38 ± 0.1216 40 M 124 33 91 556 0.31 ± 0.06 0.49 ± 0.1417 42 M 92 51 42 547 0.42 ± 0.06 0.90 ± 0.05
Table 2. Mean values and standard deviation of physiological variables and ICP-derived indices(ηICP
ABP and γ ICPABP) in the two outcome groups.
GOS = 1 GOS = 2 p-value
ABP (mmHg) 104.66 ± 29.03 97.21 ± 12.91 0.8246ICP (mmHg) 51.81 ± 27.73 22.40 ± 12.81 0.0040a
CPP (mmHg) 52.85 ± 34.39 74.81 ± 14.52 0.0189a
RR (ms) 735.71 ± 127.45 682.56 ± 169.30 0.1565η 0.51 ± 0.13 0.26 ± 0.11 0.0001a
γ 0.69 ± 0.17 0.54 ± 0.23 0.0063a
a Statistically significant (p < 0.05).

Wavelet assessment of compensatory reserve and cerebrovascular reactivity 471
(a) (d)
(b) (e)
(c) (f)
Figure 2. Wavelet analysis of arterial (left column) and intracranial (right column) pressurefluctuations for a patient with normal intracranial pressure. First row: the spontaneous fluctuationsaveraged over a cardiac beat. Second row: time evolution of the modulus of the wavelet coefficientfor scale a = 10 (this scale corresponds to pseudofrequency 0.2 Hz). Third row: the density plotof the modulus of the wavelet coefficients. The horizontal color bar at the bottom of the figurereveals the assignments of colors to values of wavelet coefficients. All coefficients with modulusgreater than 6 are marked as dark brown. Strong damping of ABP fluctuations is characteristic ofphysiological cerebral hemodynamics.
In figure 4 the wavelet gain is plotted as a function of frequency for the case studies shownin figures 2 and 3. The next graph shows group averaged ηICP
ABP (figure 5). The thick solidline corresponds to the 12 patients with GOS = 1 and the dashed line to the 17 patients withGOS = 2. The thin lines represent the standard error of the experimental data about the mean.With decreasing frequency, the mean gain for both groups starts to diverge at approximately0.2 Hz.
Variability of ABP and ICP time series is analyzed in figure 6. In particular, thegroup-averaged complex modulus of the wavelet coefficients of ABP (figure 6(a)) and ICP(figure 6(b)) are plotted as a function of frequency. Surprisingly high variability of arterialblood pressure in the higher frequency range (∼0.2 Hz) is a direct consequence of mechanicalventilation.
Figure 7 shows evolution of frequency dependent normalized phase difference �φ/2π
between ABP and ICP fluctuations for a patient with normal ICP (a) and severe hypertension(b). The frequency dependence of synchronization parameter γ ICP
ABP for both case studiesand two cohorts is analyzed in figures 8 and 9, respectively. While the differences insynchronization between the cohorts are not as large as were the differences in wavelet gainthey are again most strongly pronounced in the low-frequency part of the spectrum (figure 9).

472 M Latka et al
(a)
(b)
(c)
(d)
(e)
(f)
Figure 3. Wavelet analysis of arterial (left column) and intracranial (right column) pressurefluctuations for a patient with severe cerebral hypertension. First row: the spontaneous fluctuationsaveraged over a cardiac beat. Second row: time evolution of the modulus of the wavelet coefficientfor scale a = 10 (this scale corresponds to pseudofrequency 0.2 Hz). Third row: the density plotof the modulus of the wavelet coefficients. The horizontal color bar at the bottom of the figurereveals the assignments of colors to values of wavelets coefficients. All coefficients with modulusgreater than 6 are marked as dark brown. Weak damping of ABP fluctuations stems from severecerebral swelling.
1.00
0.80
0.60
0.40
0.20
0.000.0 0.1 0.2 0.3 0.4 0.5
η
f [Hz]
GOS=1GOS=3
0.60
0.40
0.20
0.000.0 0.1 0.2 0.3 0.4 0.5
η
f [Hz]
GOS=1GOS=2
Figure 4. Frequency dependence of wavelet gain for apatient without (dashed line) and with (solid line) cerebralhypertension.
Figure 5. Group averaged wavelet gain as a function offrequency. The thick solid line corresponds to the patientswho died (GOS = 1) and the dashed line to those withGOS = 2. The thin lines represent the correspondingstandard error of the mean.

Wavelet assessment of compensatory reserve and cerebrovascular reactivity 473
(a) (b)
0.25
0.50
0.75
1.00
1.25
0.0 0.1 0.2 0.3 0.4 0.5
V(f
)
f [Hz]
ABP
GOS=1GOS=2
0.00
0.20
0.40
0.60
0.0 0.1 0.2 0.3 0.4 0.5
V(f
)
f [Hz]
ICP
GOS=1GOS=2
Figure 6. Group-averaged complex modulus of the wavelet coefficients of ABP (a) and ICP (b).The thick solid line corresponds to the patients who died (GOS = 1) and the dashed line to thosewith GOS = 2. The thin lines represent the corresponding standard error of the mean.
(a) (b)
Figure 7. Time evolution of frequency dependent normalized phase difference (�φ/2π ) betweenfluctuations of arterial and intracranial pressure fluctuations for a patient with (a) normal ICP(cf figure 1) and (b) severe hypertension (cf figure 2).
1.00
0.80
0.60
0.40
0.20
0.000.0 0.1 0.2 0.3 0.4 0.5
γ
f [Hz]
GOS=1GOS=3
1.00
0.80
0.60
0.40
0.20
0.000.0 0.1 0.2 0.3 0.4 0.5
γ
f [Hz]
GOS=1GOS=2
Figure 8. Frequency dependence of synchronizationparameter for a patient with normal ICP (dashed line)and severe (solid line) cerebral hypertension.
Figure 9. Group-averaged synchronization parameter asa function of frequency. The thick solid line correspondsto the patients who died (GOS = 1) and the dashed lineto those with GOS = 2. The thin lines represent thecorresponding standard error of the mean.

474 M Latka et al
50
25
0
-25
-500.0 0.1 0.2 0.3 0.4 0.5
∆φ
f [Hz]
GOS=1GOS=2
Figure 10. The time averaged angle between ABP and ICP fluctuations for patients withGOS = 1 (thick solid line) and GOS = 2 (thick dashed line). The thin lines delineate 95%confidence intervals.
Figure 11. Rationale of RAP index. The pulse amplitude of ICP (AMP) is associated with pulsatilechanges in cerebral blood volume via the pressure–volume curve (shown in this figure with thethick line). This curve has two zones: a flat zone, expressing good compensatory reserve, and anexponential zone, depicting poor compensatory reserve. The pulse amplitude of ICP is low anddoes not depend on mean ICP in the first zone, resulting in values of RAP close to 0. The pulseamplitude increases linearly with mean ICP in the zone of poor compensatory reserve, resulting inRAP close to 1. Adopted from Czosnyka et al (2004).
The synchronization parameter may be considered as a significance test in the determination ofa time-averaged phase difference between two signals. Strong phase locking for both groupsof patients allows us to characterize cerebral hemodynamics in terms of the time-averagedvalue of the phase difference between the ABP and ICP waveforms. Figure 10 shows such aphase as a function of frequency. As in the case of wavelet gain, with decreasing frequencythe group-averaged values diverge at 0.2 Hz. For example, at f = 0.05 Hz the correspondingdifference for GOS = 1 is equal to 10◦, in sharp contrast to the mean value of 44◦ for patientswith GOS = 2 (p = 1 × 10−4).
4. Discussion
It is apparent that the fundamental Fourier component of intracranial pressure waveform hasa frequency equal to the heart rate. Czosnyka et al (1996a) argue that linear correlationbetween the amplitude of the pulse harmonic (AMP) and mean intracranial pressure providesinformation about accessible intracerebral space. More specifically, the relation between ICPand this volume is given by a nonlinear, sigmoid pressure–volume curve. The rationale ofthis approach is elucidated by figure 11, which was adopted from Czosnyka et al (2004). At

Wavelet assessment of compensatory reserve and cerebrovascular reactivity 475
low ICP this curve is flat, indicating good compensatory reserve. With increasing pressurethe relation becomes exponential. The second flat zone, seen at very high ICP, reflectsderangement of normal cerebrovascular responses. More specifically, they define the RAPindex as the coefficient of correlation between 40 consecutive, time-averaged data points ofAMP and ICP acquired over 6.4 s. The values of RAP close to 0 indicate good pressure–volume compensatory reserve at low ICP. Even though the simplicity and clinical relevanceof the discussed approach is appealing, the fundamental question arises as to whether theresponse to changes in intracranial blood volume is frequency dependent.
In figures 2 and 3 we compare time evolution of the modulus of wavelet coefficientsof ABP and ICP fluctuations for two patients: with normal ICP and cerebral hypertension,respectively. On the basis of these case studies one can hypothesize that strong dampingof spontaneous ABP fluctuations is characteristic of physiologic hemodynamics. Thus, thewavelet gain η which quantifies such attenuation is a plausible metric for pressure–volumecompensatory reserve. In figure 4 we plot the gain as a function of frequency for the casesanalyzed in figures 2 and 3. The elevated value of wavelet gain over the entire frequency rangeis evident for a subject with severe cerebral swelling. It is also worth pointing out that thedamping of ABP fluctuations is significantly weaker (as indicated by higher values of gain) inthe low-frequency part of the spectrum. These conclusions are corroborated by the statisticalanalysis of the wavelet gain for two groups of patients: those with GOS = 1 and those withGOS = 2 (cf figure 5).
Balestreri et al (2004) have shown that the magnitude of slow ICP waves decreasesin severe head-injury patients who died with respect to patients with favorable outcome(GOS = 4.5). In principle, the increased gain for GOS = 1 patients might originate fromthe reduced amplitude of slow ABP fluctuations. To verify such a hypothesis, in figure 6we quantify variability of ABP and ICP time series with the magnitude of complex Morletwavelet coefficients. The average magnitude of low-frequency ABP wavelet coefficients forthe patients with GOS = 1 (0.52 ± 0.20) is not statistically different from the average valueof 0.69 ± 0.29 for the GOS = 2 cohort (p = 0.13). Neither does the average low-frequencymagnitude of ICP wavelet coefficients for the patients with fatal outcome (0.25 ± 0.11) differin a statistically significant way from the mean value of 0.17 ± 0.13 for patients who survived(p = 0.07). Thus, the statistically insignificant changes in the low-frequency ABP variabilityfor two cohorts cannot alone account for the distinct difference in the wavelet gain values infigure 5. Thus, it is not the absolute variability of the wavelet coefficients that is of interestin this study but rather the variability of the ICP coefficients relative to the ABP coefficients.We would like to emphasize that damping of slow ABP fluctuations, while physiologicallyimportant, is just one of the many facets of cerebral hemodynamics. When the vascular bed isactive ABP fluctuations may influence ICP dynamics via nonlinear and multiscale interactions.Such interactions may in principle increase wavelet gain. Consequently, quantification of thecerebrovascular reactivity is indispensable for the correct assessment of clinical condition ofpatients with brain injuries.
In the phenomenological description of cerebral hemodynamics, fluctuations of ABP,due to pressure reactivity of cerebral vessels, lead to fluctuations of ICP. The vascular originof the ICP slow waves through intracranial blood volume variations is commonly accepted(Steinmeier et al 1996). Nevertheless, the quantitative description of this clinically significanteffect is the subject of ongoing research. To shed new light on the interplay of ABP and ICP weemployed complex wavelet transforms to study the time evolution of the instantaneous phasedifference between the two time series. Figure 7 exemplifies such an approach for the twopreviously discussed case studies. Upon inspection of both density plots in this figure one findsthat the presence of the horizontal multicolor strip for a subject with normal ICP (figure 7(a))

476 M Latka et al
is just a manifestation of low-frequency phase variability. Such variability is almost entirelylost during severe hypertension (figure 7(b)). Synchronization strength between fluctuationsof ABP and ICP can be quantified by the synchronization parameter γ , which is plotted as afunction of frequency for both subjects in figure 8. The very high values of γ for the patientwith GOS = 1 reflect pathological entrainment of ABP and ICP time series. Such entrainmentcan also be observed in figure 9, which shows the synchronization parameter averaged overboth groups. For this hemodynamic metric the differences between the groups are not asstrongly pronounced across the displayed frequency range as were the differences in waveletgain (figure 5, table 2). In principle, one might argue that for both groups cerebrovascularreactivity was compromised. However, strong phase locking allows us to characterize cerebralhemodynamics also in terms of the time-averaged value of the phase difference between theABP and ICP waveforms.
We can see in figure 10 that the frequency dependence of the group averaged phasedifference mimics that of wavelet gain. Namely, the differences between the two cohorts arestrongly manifested in the low-frequency part of the spectrum. The low-frequency variabilityof the phase difference between the spontaneous oscillations of ABP and blood flow velocityin major cerebral arteries is the hallmark of intact cerebral autoregulation (Giller 1990, Latkaet al 2005). Therefore, we hypothesize that in patients who died the impairment of cerebralautoregulation is followed by the breakdown of residual pressure reactivity. It is worthemphasizing that such insight is unique to the wavelet analysis. In the PRx approach thegradual loss of cerebrovascular bed pressure reactivity is manifested solely by the index’svalue approaching one.
In the pioneering studies of the cerebrospinal fluid system (Marmarou 1973) postulatedan exponential volume–pressure relation. Such interdependence of variables underlies thePVI index, which quantifies the compliance over the whole physiological range of ICP.Miller et al (1973) advocated the volume–pressure response (VPR) as a measure of elastance(inverse of compliance) which is independent of the functional relation between craniospinalvolume and pressure. In both approaches, now commonly accepted as the gold standards, thecorresponding indices are calculated from the pressure change resulting from volume injectionor withdrawal of fluid from the CSF space. An exhaustive list of relevant references is givenin Reilly and Bullock (2005).
Physiological causes of elevated ICP may be broadly classified into vascular and non-vascular. Vascular mechanisms are associated with either passive or active vasolidation of thecerebrovascular bed. Active vasolidation may be brought about by increased concentrationof CO2 and/or, within the operating range of pressure autoregulation, decreased cerebralperfusion pressure. The list of non-vascular causes is long and includes increases in brainwater content (edema), intracerebral, extradural or subdural mass, as well as CSF outflowresistance (Reilly and Bullock 2005).
Marmarou et al (1987) demonstrated that in patients with severe head-injury elevatedICP can, to a large extent, be attributed to vascular mechanisms. Gray and Rosner (1987a,1987b) determined that PVI and CPP may be linearly anticorrelated or correlated dependingon whether the CPP range is beyond or within the autoregulating range. Detrimental influenceof low CPP on intracranial compliance has been recently corroborated by Portella et al (2005).Interestingly enough, cerebrovascular compensatory reserve is also time-dependent. Anile,Portnoy and Branch found that VPR indices derived from slow, medium and rapid bolusinjection differ (Anile et al 1987). The differences result from the existence of two distinctcomponents of craniospinal compliance. The short-time physical compliance is determinedby such factors as spinal dura matter expansion while the time constant of physiologicalcompliance associated with cerebrovascular alterations (e.g. venous outflow resistance) is

Wavelet assessment of compensatory reserve and cerebrovascular reactivity 477
(a) (b)
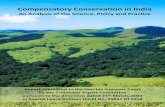
Figure 12. The values of wavelet gain and synchronization index, averaged over the low-frequencypart of the spectrum (0.02–0.07 Hz), were used as the coordinates of points representing thehemodynamic condition of patients with GOS = 1 (left plot) and GOS = 2 (right plot). Thevertical color bar shows the assignment of colors to values of intracranial pressure. Each dotcorresponds to a 15 minute monitoring interval.
significantly longer. Thus, to fully understand the intricate interplay of craniospinal volumeand pressure, the dynamic and the viscoelastic properties of CSF, nervous tissue and vascularfactors must all be considered.
To address this issue in the most straightforward way, the values of wavelet gain andsynchronization index, averaged over the low-frequency part of the spectrum, were used asthe coordinates of points representing the overall hemodynamic condition (figure 12). We dubsuch representation cerebral hemodynamic state space (CHS). We can see that in such spacepatients with GOS = 1 are to a large extent partitioned away from those with GOS = 2. Itcomes as no surprise that the high-synchronization high-gain region of the CHS to a large extentcoincides with high values of intracranial pressure. Nevertheless, one can easily find caseswith relatively high wavelet gain, moderate ICP and largely intact reactivity of the vascularbed. Thus, further studies should explore whether the onset of severe cerebral hypertension ispreceded by high-gain episodes. If such episodes were sufficiently long they could becomethe cornerstone of a ICP hypertension prediction algorithm. It is also worth pointing outthat overnight ICP monitoring may be used in the diagnosis of patients with hydrocephalussymptoms or shunt malfunctions (Czosnyka et al 2004). The frequency-dependent aspectsof cerebrospinal fluid dynamics discussed herein give strong indications that such monitoringcan provide more detailed assessment of patients’ clinical conditions than do limited timeinfusion tests. From the clinical point of view, the studies of time evolution of the waveletgain in patients with normotensive hydrocephalus are particularly important.
Diverse approaches have been used to elucidate interrelations between intracranialpressure and other hemodynamic variables. Most of the research effort has been focused onpropagation of the pulse wave from the arterial bed to the intracranial space (Aboy et al 2003,Daley et al 1995, Pettorossi et al 1978, Portnoy and Chopp 1981, Portnoy et al 1982, Avezaatet al 1979). However, during the last decade, the clinical significance of low-frequencyICP waves has been repeatedly emphasized (Steinmeier et al 1996). Herein we presenteda mathematical framework capable of quantifying intrinsically non-stationary properties ofcerebral hemodynamics across the broad range of physiologically relevant frequencies. Weare convinced that optimal therapy management of patients with cerebral lesions hinges onthorough, qualitative assessment of their clinical condition. Further validation of the proposed

478 M Latka et al
assessment of compensatory reserve and cerebrovascular reactivity will involve the comparisonwith the gold standards (Diehl 2002, Reilly and Bullock 2005) as well as the methods whichfairly recently have gained clinical acceptance (Piper et al 1999, 1990). This issue is thesubject of our ongoing research.
Acknowledgments
We gratefully acknowledge the financial support of the US Army Research Office (GrantDAAD19-03-1-0349) and Polish Ministry of Science and Information Society Technologies(Grant 3 T11E 023 29).
References
Aboy M, McNames J, Cuesta-Frau D, Wakeland W, Thong T, Lai S and Goldstein B 2003 Significance of intracranialpressure pulse morphology in pediatric traumatic brain injury Proc. Ann. Int. Conf. IEEE Engineering inMedicine and Biology (Cancun, Mexico, 17–21 September 2003) pp 2491–4
Anile C, Portnoy H D and Branch C 1987 Intracranial compliance is time-dependent Neurosurgery 20 389–95Avezaat C J, van Eijndhoven J H and Wyper D J 1979 Cerebrospinal fluid pulse pressure and intracranial volume-
pressure relationships J. Neurol. Neurosurg. Psychiatry 42 687–700Balestreri M, Czosnyka M, Steiner L A, Schmidt E, Smielewski P, Matta B and Pickard J D 2004 Intracranial
hypertension: what additional information can be derived from ICP waveform after head injury? Acta Neurochir.(Wien) 146 131–41
Batschelet E 1981 Circular Statistics in Biology (New York: Academic)Czosnyka M, Czosnyka Z, Momjian S and Pickard J D 2004 Cerebrospinal fluid dynamics Physiol. Meas. 25 R51–76Czosnyka M, Guazzo E, Whitehouse M, Smielewski P, Czosnyka Z, Kirkpatrick P, Piechnik S and Pickard J D
1996a Significance of intracranial pressure waveform analysis after head injury Acta Neurochir. (Wien)138 531–41, discussion 41–2
Czosnyka M, Smielewski P, Kirkpatrick P, Laing R J, Menon D and Pickard J D 1997 Continuous assessment of thecerebral vasomotor reactivity in head injury Neurosurgery 41 11–7, discussion 7–9
Czosnyka M, Smielewski P, Kirkpatrick P, Menon D K and Pickard J D 1996b Monitoring of cerebral autoregulationin head-injured patients Stroke 27 1829–34
Daley M L, Pasupathy H, Griffith M, Robertson J T and Leffler C W 1995 Detection of loss of cerebral vascular toneby correlation of arterial and intracranial pressure signals IEEE Trans. Biomed. Eng. 42 420–4
Diehl R R 2002 Cerebral autoregulation studies in clinical practice Eur. J. Ultrasound 16 31–6Giller C A 1990 The frequency-dependent behavior of cerebral autoregulation Neurosurgery 27 362–8Giller C A and Mueller M 2003 Linearity and non-linearity in cerebral hemodynamics Med. Eng. Phys. 25 633–46Gray W J and Rosner M J 1987a Pressure-volume index as a function of cerebral perfusion pressure. Part 1: the
effects of cerebral perfusion pressure changes and anesthesia J. Neurosurg. 67 369–76Gray W J and Rosner M J 1987b Pressure-volume index as a function of cerebral perfusion pressure. Part 2: the
effects of low cerebral perfusion pressure and autoregulation J. Neurosurg. 67 377–80Hamner J W, Cohen M A, Mukai S, Lipsitz L A and Taylor J A 2004 Spectral indices of human cerebral blood flow
control: responses to augmented blood pressure oscillations J. Physiol. 559 965–73Kett-White R, Hutchinson P J, Czosnyka M, Boniface S, Pickard J D and Kirkpatrick P J 2002 Multi-modal monitoring
of acute brain injury Adv. Tech. Stand Neurosurg. 27 87–134Lang E W, Mehdorn H M, Dorsch N W and Czosnyka M 2002 Continuous monitoring of cerebrovascular
autoregulation: a validation study J. Neurol. Neurosurg. Psychiatry 72 583–6Latka M, Turalska M, Glaubic-Latka M, Kolodziej W, Latka D and West B J 2005 Phase dynamics in cerebral
autoregulation Am. J. Physiol. Heart Circ. Physiol. 289 H2272–9Latka M, Was Z, Kozik A and West B J 2003 Wavelet analysis of epileptic spikes Phys. Rev. E Stat. Nonlin. Soft
Matter. Phys. 67 052902Mallat S G 1999 A Wavelet Tour of Signal Processing (Cambridge: Academic)Marmarou A 1973 A theoretical and experimental evaluation of the cerebrospinal fluid system PhD Thesis Drexel
University, Philadelphia, PAMarmarou A, Maset A L, Ward J D, Choi S, Brooks D, Lutz H A, Moulton R J, Muizelaar J P, DeSalles A and
Young H F 1987 Contribution of CSF and vascular factors to elevation of ICP in severely head-injured patientsJ. Neurosurg. 66 883–90

Wavelet assessment of compensatory reserve and cerebrovascular reactivity 479
Miller J D, Garibi J and Pickard J D 1973 Induced changes of cerebrospinal fluid volume. Effects during continuousmonitoring of ventricular fluid pressure Arch. Neurol. 28 265–9
Mitsis G D and Marmarelis V Z 2002 Modeling of nonlinear physiological systems with fast and slow dynamics: I.Methodology Ann. Biomed. Eng. 30 272–81
Mitsis G D, Zhang R, Levine B D and Marmarelis V Z 2002 Modeling of nonlinear physiological systems with fastand slow dynamics: II. Application to cerebral autoregulation Ann. Biomed. Eng. 30 555–65
Mitsis G D, Zhang R, Levine B D and Marmarelis V Z 2006 Cerebral hemodynamics during orthostatic stress assessedby nonlinear modeling J. Appl. Physiol. 101 354–66
Panerai R B, Dawson S L and Potter J F 1999 Linear and nonlinear analysis of human dynamic cerebral autoregulationAm. J. Physiol. 277 H1089–99
Pettorossi V E, Di Rocco C, Caldarelli M, Mancinelli R and Velardi F 1978 Influences of phasic changes in systemicblood pressure on intracranial pressure Eur. Neurol. 17 216–25
Piper I R, Miller J D, Whittle I R and Lawson A 1990 Automated time-averaged analysis of craniospinal compliance(short pulse response) Acta Neurochir. Suppl. (Wien) 51 387–90
Piper I, Spiegelberg A, Whittle I, Signorini D and Mascia L 1999 A comparative study of the Spiegelberg compliancedevice with a manual volume-injection method: a clinical evaluation in patients with hydrocephalus Br. J.Neurosurg. 13 581–6
Portella G, Cormio M, Citerio G, Contant C, Kiening K, Enblad P and Piper I 2005 Continuous cerebral compliancemonitoring in severe head injury: its relationship with intracranial pressure and cerebral perfusion pressure ActaNeurochir. (Wien) 147 707–13
Portnoy H D and Chopp M 1981 Cerebrospinal fluid pulse wave form analysis during hypercapnia and hypoxiaNeurosurgery 9 14–27
Portnoy H D, Chopp M, Branch C and Shannon M B 1982 Cerebrospinal fluid pulse waveform as an indicator ofcerebral autoregulation J. Neurosurg. 56 666–78
Reilly P and Bullock R 2005 Head Injury: Pathophysiology and Management (London, New York: Hodder Arnold)Steiner L A, Czosnyka M, Piechnik S K, Smielewski P, Chatfield D, Menon D K and Pickard J D 2002 Continuous
monitoring of cerebrovascular pressure reactivity allows determination of optimal cerebral perfusion pressurein patients with traumatic brain injury Crit. Care Med. 30 733–8
Steinmeier R, Bauhuf C, Hubner U, Bauer R D, Fahlbusch R, Laumer R and Bondar I 1996 Slow rhythmic oscillationsof blood pressure, intracranial pressure, microcirculation, and cerebral oxygenation. Dynamic interrelation andtime course in humans Stroke 27 2236–43
Copyright © 2022 FDOKUMEN