USO DO TESTE DE LEVANTAR E SENTAR DA CADEIRA ...
45
UNIVERSIDADE DE BRASÍLIA - UnB FACULDADE DE CEILÂNDIA - FCE CURSO DE FISIOTERAPIA FELIPE AUGUSTO RIBEIRO GABRIELA DA SILVA FREIRE USO DO TESTE DE LEVANTAR E SENTAR DA CADEIRA PARA IDENTIFICAR FRAQUEZA MUSCULAR DE MEMBROS INFERIORES EM IDOSOS BRASÍLIA 2020
-
Upload
khangminh22 -
Category
Documents
-
view
0 -
download
0
Transcript of USO DO TESTE DE LEVANTAR E SENTAR DA CADEIRA ...

UNIVERSIDADE DE BRASÍLIA - UnB
FACULDADE DE CEILÂNDIA - FCE
CURSO DE FISIOTERAPIA
FELIPE AUGUSTO RIBEIRO
GABRIELA DA SILVA FREIRE
USO DO TESTE DE LEVANTAR E SENTAR DA
CADEIRA PARA IDENTIFICAR FRAQUEZA
MUSCULAR DE MEMBROS INFERIORES EM
IDOSOS
BRASÍLIA
2020

FELIPE AUGUSTO RIBEIRO
GABRIELA DA SILVA FREIRE
USO DO TESTE DE LEVANTAR E SENTAR
DA CADEIRA PARA IDENTIFICAR
FRAQUEZA MUSCULAR DE MEMBROS
INFERIORES EM IDOSOS
Trabalho de Conclusão de Curso apresentado
à Universidade de Brasília - UNB -
Faculdade de Ceilândia como requisito
parcial para obtenção do título de bacharel
em Fisioterapia.
Orientadora: Profa. Dra. Patrícia Azevedo
Garcia
BRASÍLIA
2020

FELIPE AUGUSTO RIBEIRO
GABRIELA DA SILVA FREIRE
USO DO TESTE DE LEVANTAR E SENTAR DA
CADEIRA PARA IDENTIFICAR FRAQUEZA
MUSCULAR DE MEMBROS INFERIORES EM
IDOSOS
Brasília, 20/04/2020.
COMISSÃO EXAMINADORA
Prof.ª Drª. Patrícia Azevedo Garcia
Faculdade de Ceilândia - Universidade de Brasília-UnB
Orientadora
Prof.ª Drª. Aline Araújo do Carmo
Faculdade de Ceilândia - Universidade de Brasília-UnB
Ft. Ms. Cristiane de Almeida Nagata
Prefeitura Municipal de Goiânia

Dedicatória
Este trabalho é dedicado à Deus e as nossas famílias

AGRADECIMENTOS
Por Felipe Augusto Ribeiro
O desenvolvimento desse trabalho contou com ajuda de várias partes, onde eu devo
agradecer:
Aos meus Pais, que me apoiaram por todos esses anos, me incentivando, me guiando e
tornando possível alcançar meus objetivos;
À minha Irmã, que até mesmo durante os momentos difíceis, arrancou de mim várias risadas
e momentos bons, mesmo quando estive muito estressado;
Aos meus incríveis bichinhos de estimação, que mantem à alegria em minha casa e deixam
todos felizes a qualquer momento;
Aos amigos da faculdade, que dividiram momentos bons e ruins durante essa longa
caminhada;
À Professora Patrícia, que durante todos esses semestres foi como uma mãe para nós,
ajudando muito, não só no trabalho de conclusão, mas com conselhos, histórias, projetos e
todo o apoio super pontual possível;
À minha linda Gabi, a pessoa mais incrível e competente que pude conhecer e ter o prazer
de ter ao lado, que sem ela não teria chegado aonde cheguei e nem vencido diversos desafios
impostos durante esses semestres;
E por fim, à UnB por fornecer um apoio durante anos e transmitir diversos ensinamentos
durante o curso.
Por Gabriela da Silva Freire
Primeiramente, agradecer à Deus, pelo privilégio da vida e por me dar a oportunidade de
estar neste curso, realizando tantos sonhos, me abençoando e protegendo em toda a
caminhada;
Aos meus pais, Nazareno da Mota Freire e Maria Aparecida da Silva Freire, por serem meu
alicerce, agradeço por me tornarem quem sou e por nunca deixarem de acreditar em mim,
que durante minha vida nunca mediram esforços para me apoiar em todos os meus sonhos;
À minha irmã, Ana Carolina da Silva Freire, por ser minha companheira durante toda a
vida, por estar ao meu lado desde quando nasci para me proteger e me ensinar o melhor
caminho, e por todo apoio e ajuda durante a graduação;
Ao meu filho de quatro patas, Flea, por entrar na minha família para nos ensinar sobre amor
incondicional e resiliência, pelo companheirismo durante os estudos e a escrita deste
trabalho;

Ao grande parceiro da minha vida, namorado e melhor amigo, Felipe Augusto Ribeiro, por
todo amor, apoio e compreensão desde o início do curso. Obrigada pelo companheirismo
durante esta jornada, por todas as dificuldades que vencemos juntos. Não seria a mesma
coisa se eu tivesse que passar por tudo isso sem você;
À minha professora e orientadora, Patrícia Azevedo Garcia, um exemplo de fisioterapeuta,
competência e dedicação, por todo apoio e confiança em relação ao Trabalho de Conclusão
de Curso, Programa de Extensão e Programa de Iniciação Científica. Muito obrigada por
todo conhecimento compartilhado e pelas oportunidades que me deu. Serei sempre grata;
Ao CNPq, pelo apoio financeiro durante minhas duas iniciações científicas;
À todos os pacientes, pela confiança que depositaram em mim, sendo instrumentos
fundamentais para meu aprendizado. Vocês contribuíram para meu crescimento, não só
como fisioterapeuta, mas também como ser humano;
Aos amigos que fiz na faculdade, com os quais dividi os meus anseios, alegrias e conquistas
ao longo da graduação, que estiveram ao meu lado durante essa jornada, e participaram
deste processo de amadurecimento e crescimento pessoal que é a graduação;
À Universidade de Brasília, aos funcionários e aos mestres que tive o prazer de aprender e
me inspirar a cada dia. Tenho muito orgulho de ter feito parte desta instituição e ter
convivido com tantas pessoas especiais.

“Nunca deixe que lhe digam que não vale a
pena acreditar no sonho que se tem ou que
os seus planos nunca vão dar certo ou que
você nunca vai ser alguém” (Legião Urbana)

RESUMO
Introdução: A capacidade de levantar a partir da posição sentada é um pré-requisito para a
independência funcional dos idosos. Para a avaliação dessa tarefa, o teste de levantar e sentar da
cadeira é comumente utilizado por pesquisadores e clínicos como indicador da força muscular de
membros inferiores em idosos. O objetivo deste estudo foi investigar a acurácia do teste de levantar
e sentar da cadeira para identificar fraqueza muscular de membros inferiores em idosos. Métodos:
Trata-se de um estudo observacional transversal, com 264 idosos comunitários (69,85±6,50 anos). O
desempenho funcional foi avaliado por meio do teste de Levantar e Sentar (TLS) cinco vezes. O pico
de torque por peso corporal (PT) e potência média (PM) dos músculos flexores plantares e
dorsiflexores de tornozelo, flexores e extensores de joelho e quadril, e abdutores e adutores do quadril
foram avaliados por meio do dinamômetro isocinético. Para cada variável de função muscular
isocinética os participantes foram categorizados em “fracos” ou “fortes” de acordo com o percentil
25. A curva ROC (Receiver Operating Charascteristic) foi construída para verificar a capacidade do
TLS para discriminar deficiência de PT e PM de cada grupo muscular estudado. Resultados: Os
idosos apresentaram TLS médio de 11,60 segundos. O ponto de corte ótimo foi de 10 segundos. Entre
os idosos com deficiência de PT e PM de flexores plantares e de flexores e extensores de joelho, de
PT de dorsiflexores de tornozelo e de PM de flexores de quadril, mais de 80% foi corretamente
identificado pelo TLS maior que 10 segundos. Um TLS negativo (< 10 segundos) identificou
corretamente mais de 88% dos idosos com esses grupos musculares fortes. Conclusão: Em idosos,
um TLS maior que 10 segundos identifica satisfatoriamente fraqueza muscular de flexores plantares
e dorsiflexores de tornozelo, extensores e flexores de joelho e flexores de quadril.
Palavras-chave: Força Muscular; Desempenho Físico Funcional; Programas de Rastreamento;
Idoso.

ABSTRACT
Background and Purpose: The performance of the task of sit to stand from a chair is a prerequisite
for the functional independence of the older adults. For the assessment of this task, the Sit-to-Stand
test (STS) is commonly used by researchers and clinicians as an indicator of lower limb muscle
strength in the older adults. The purpose of this study was to investigate the accuracy of the Sit-to-
Stand test to identify muscle weakness of lower limbs in the older adults. Methods: This is a cross-
sectional observational study, with 264 community-dwelling older adults (69.85 ± 6.50 years).
Functional performance was assessed using the Sit-to-Stand test (STS) five times. The peak torque
by body weight (PT) and average power (AP) of the plantar flexor and ankle dorsiflexor muscles,
knee and hip flexors and extensors, and hip abductors and adductors were assessed using the
isokinetic dynamometer. For each variable of isokinetic muscle function, participants were
categorized as “weak” or “strong” according to the 25th percentile. The ROC (Receiver Operating
Charascteristic) curve was constructed to verify the STS capacity for discriminating PT and AP of
each muscle group studied. Results and Discussion: The older adults have an average STS of 11.60
seconds. The optimum cutoff point was 10 seconds. Among the older adults with PT and AP
deficiency in plantar flexors and knee flexors and extensors, PT in ankle dorsiflexors and AP in hip
flexors, more than 80% were correctly identified by TLS greater than 10 seconds. A negative STS
(<10 seconds) correctly identified more than 88% of the older adults with these muscle groups strong.
Conclusions: In the older adults, a STS greater than 10 seconds satisfactorily identifies muscle
weakness of plantar flexors and ankle dorsiflexors, knee extensors and flexors and hip flexors and
abductors.
Key words: Muscle Strength; Physical Functional Performance; Mass Screening; Aged.

LISTA DE TABELAS E FIGURAS
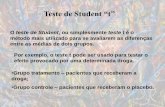
Figura 1. Fluxograma da amostra ....................................................................................... 17
Tabela 1. Características sociodemográficas e clínicas dos participantes .......................... 18
Tabela 2. Dados do Teste de Levantar e Sentar e de pico de torque e potência muscular
isocinética de membros inferiores ....................................................................................... 19
Tabela 3. Capacidade do Teste de Levantar e Sentar para identificar deficiência de pico de
torque e potência muscular de membros inferiores ............................................................. 20
Tabela 4. Acurácia do ponto de corte sugerido de 10 segundos no Teste de Levantar e Sentar
para identificar deficiência de força e potência muscular de membros inferiores .............. 21

LISTA DE ABREVIATURAS
ADM – Amplitude de Movimento
AUC – Area Under the Curve
AVE – Acidente Vascular Encefálico
CAAE – Certificado de Apresentação de Apreciação Ética
DF – Distrito Federal
DP – Desvio Padrão
E – Especificidade
GO – Goiás
IC – Intervalo de Confiança
IMC – Índice de Massa Corporal
Kg – Quilogramas
MEEM – Mini-Exame do Estado Mental
MMII – Membros Inferiores
Nm – Newton.Metros
ROC - Receiver Operating Characteristic curve
S – Sensibilidade
TCLE – Termo de Consentimento Livre e Esclarecido
TLS – Teste de Levantar e Sentar da cadeira
VPN – Valor Preditivo Negativo
VPP – Valor Preditivo Positivo
W – Watt

SUMÁRIO
1 – INTRODUÇÃO ............................................................................................................. 12
2 – MÉTODOS .................................................................................................................... 13
3 – RESULTADOS ............................................................................................................. 17
4 – DISCUSSÃO ................................................................................................................. 21
5 – CONCLUSÃO ............................................................................................................... 23
6 – REFERÊNCIAS ............................................................................................................ 24
ANEXO A – Aprovação do Comitê de Ética da Universidade Federal de Minas Gerais ... 28
ANEXO B - Aprovação do Comitê de Ética da Faculdade de Ceilândia ........................... 29
ANEXO C - Aprovação do Comitê de Ética da Faculdade de Ceilândia ........................... 30
ANEXO D – Normas da Revista Científica ........................................................................ 31

12
1 - INTRODUÇÃO
Após os 75 anos de idade, há uma redução similar em ambos os sexos de aproximadamente 60% da
força muscular e de 30% da capacidade para levantar e sentar de uma cadeira1. A capacidade de
levantar a partir da posição sentada é um pré-requisito para a independência funcional dos idosos2.
Apesar da atividade de levantar e sentar representar um movimento funcional complexo explicado
por fatores sensório-motores, psicológicos e de equilíbrio, pesquisadores observaram que a força dos
membros inferiores também é um importante preditor do desempenho desta atividade, explicando em
até 48% da sua variância2,3.
Para avaliação dessa tarefa diferentes variações do teste de levantar e sentar da cadeira (TLS)
são comumente utilizadas no cenário clínico e de pesquisa, sendo a versão com cinco repetições a
mais popular entre elas4. Em idosos, o TLS é considerado um teste válido e pontos de corte variando
de 10 a 16,4 segundos4–10 têm se mostrado bons preditores para diversos desfechos em saúde, como
disfunção do equilíbrio3,11, distúrbios vestibulares11, risco de quedas4,7,10, risco de incapacidade
funcional7,9,12, sarcopenia13,14 e fraqueza muscular dos membros inferiores3,6,15–17.
Especificamente para fraqueza muscular, diante da indisponibilidade do método padrão-ouro
(dinamômetro isocinético18) para avaliação da maioria dos idosos, pesquisadores e clínicos
frequentemente têm analisado o desempenho no TLS para avaliar a força muscular de membros
inferiores1,4,10,17,19. Para isso, baseiam-se em estudos que mostraram associações entre os resultados
do TLS e a função muscular de membros inferiores6,9,15,18,20. Nesses estudos, a força muscular do
quadríceps femoral, tem se destacado entre os fatores responsáveis pela variabilidade no tempo do
TLS, contribuindo com 12 a 47%3,15,17,20, sendo uma incapacidade funcional para levantar e sentar da
cadeira em 12 segundos observada entre idosos nos percentis inferiores de pico de torque de
extensores de joelho18. Em análise multifatorial, o papel da função muscular dos flexores plantares
do tornozelo explicou de 43% a 53% da variabilidade2,16 e apresentou correlação moderada2 com o
tempo gasto para levantar e sentar da cadeira dez vezes. O pico de torque dos músculos flexores de
quadril, em associação com outros fatores, apresentou correlação moderada e influenciou em 48% a
capacidade de sentar e levantar2. Músculos extensores de quadril e flexores de joelho até o momento

13
foram menos investigados e apresentaram baixa correlação com o desempenho para levantar e sentar
de uma cadeira2,5,20.
Desta forma, parece que a avaliação da capacidade para levantar e sentar de uma cadeira pode
consistir em uma estratégia útil para identificar idosos com maior risco de apresentar deficiência de
força e potência muscular de membros inferiores. Entretanto, o efeito da força dessas musculaturas
no TLS ainda não foi completamente elucidado. A maioria dos estudos têm restringido a investigação
aos músculos extensores de joelho5,15,17,18,21, analisado pequenos tamanhos amostrais2,11,12,14,17,20,
avaliado a capacidade da força muscular predizer o desempenho no TLS3,5,6,15,17,18,20 e pouca
informação está disponível sobre a acurácia de pontos de corte do TLS para identificar fraqueza
muscular considerando as três grandes articulações de membros inferiores2. Nesse sentido, o principal
objetivo deste estudo foi investigar a acurácia do teste de levantar e sentar da cadeira para identificar
fraqueza muscular de membros inferiores em idosos.
2 - MÉTODOS
Delineamento do estudo e aspectos éticos
O presente estudo teve delineamento transversal e foi aprovado pelo Comitê de Ética em Pesquisa da
Universidade Federal de Minas Gerais (CAAE 0370.0.203.013-11) e pelo Comitê de Ética em
Pesquisa da Faculdade de Ceilândia da Universidade de Brasília (sob pareceres nº 2.339.074 e nº
3.067.277). Todos os participantes assinaram o Termo de Consentimento Livre e Esclarecido
(TCLE).
Participantes
A amostra deste estudo foi extraída de um banco de dados de 300 idosos recrutados de
setembro de 2011 a janeiro de 2019 em programas de atenção à saúde do idoso nas cidades de
Ceilândia – DF e Goiânia - GO, compondo uma amostra de conveniência.
A amostra foi constituída por idosos comunitários, com 60 anos ou mais, com marcha
independente, com capacidade para realização dos testes de avaliação do desempenho funcional, ,

14
sem disfunções graves no sistema visual (cegueira), sem histórico de amputação, uso de prótese ou
fraturas recentes nos membros inferiores (MMII) (ocorridas durante os seis meses anteriores à
realização da pesquisa); sem histórico de condições clínicas específicas, como Artrite Reumatoide,
Doença de Parkinson, Acidente Vascular Encefálico (AVE), Doença arterial obstrutiva periférica e
doenças cardiorrespiratórias graves e/ou Vestibulopatias. Foram excluídos das análises os
participantes com ausência de informação sobre o teste de levantar e sentar da cadeira e/ou com dados
ausentes para todas as variáveis de função muscular isocinética dos membros inferiores, e ainda
aqueles que apresentaram alterações cognitivas segundo o Mini-Exame do Estado Mental (MEEM)22.
Procedimentos de estudo
As avaliações foram realizadas nos Laboratórios de Desempenho Funcional Humano da
Faculdade de Ceilândia da Universidade de Brasília (FCE/UnB) e no Laboratório de Pesquisa em
Musculoesquelética (LAPEME) da Universidade Estadual de Goiás - Campus Goiânia (ESEFFEGO).
Para descrição sociodemográfica e clínica dos participantes foram investigados a idade (em
anos), o sexo, a escolaridade (em anos de estudo), o estado nutricional, os medicamentos em uso
contínuo (quantidade) e a prática de exercício físico regular (mínimo de 150 minutos por semana). O
estado nutricional foi determinado por meio do cálculo do Índice de Massa Corporal (IMC) [IMC =
massa corporal (kg)/estatura² (m²)] e os idosos foram classificados em baixo peso (IMC < 22 Kg/m²),
eutrofia (IMC 22-27 Kg/m²) ou sobrepeso (IMC > 27 Kg/m²) 23. Para determinar o nível de atividade
física foram questionados quantos minutos por semana o idoso praticava exercício físico de moderada
a vigorosa intensidade, sendo classificados em ativos (≥ 150 minutos de atividade por semana) ou
sedentários24. No presente estudo a função muscular isocinética de membros inferiores foi
considerada como padrão de referência e o teste de sentar e levantar 5 vezes (TLS) como o teste
index.
A função muscular isocinética do membro inferior dominante foi avaliada utilizando o
dinamômetro Biodex System 4 Pro® (Biodex Medical Systems Inc., Shirley, NY, USA). Foram
investigadas medidas de pico de torque relativo ao peso corporal e de potência média dos músculos

15
flexores, extensores, abdutores e adutores do quadril, flexores e extensores do joelho e flexores
plantares e dorsiflexores do tornozelo. O pico de torque relativo ao peso corporal foi obtido por meio
da divisão do valor máximo de torque pelo peso corporal do indivíduo ([Nm/kg]*100) e avaliado a
60º/s (cinco repetições)2,18,25. A potência muscular foi obtida por meio da divisão do trabalho total
pelo tempo de execução (expressa em Watts, W) e avaliada a 120º/s para tornozelo (6 repetições) e
quadril (15 repetições) e 180º/s para joelho (15 repetições)25. Na articulação do tornozelo o teste foi
realizado na posição sentada, com o joelho posicionado a 30º de flexão tendo como referência o eixo
do dinamômetro alinhado com o maléolo lateral do indivíduo. A amplitude de movimento (ADM)
testada foi de 10º de dorsiflexão a 30º de flexão plantar26. Na articulação do joelho o teste foi realizado
na posição sentada na cadeira com 85º de inclinação do encosto, com o eixo do aparelho alinhado ao
epicôndilo lateral do fêmur. A ADM testada foi de 85º a partir do ângulo de 90º de flexão do joelho26.
Para articulação do quadril o teste de flexão e extensão foi realizado em decúbito dorsal tendo o eixo
rotacional posicionado superior e anteriormente ao trocânter maior do fêmur enquanto o membro
inferior encontrava-se na posição neutra. A ADM de flexão-extensão do quadril foi de 0º a 60º26. Para
articulação do quadril o teste de abdução e adução foi realizado em decúbito lateral, com o membro
a ser testado para cima, com o eixo da articulação coxofemoral (superior e medial ao trocânter maior)
alinhado com o eixo do dinamômetro. A amplitude máxima estabelecida foi de 30° de abdução,
partindo da posição inicial de 10° de adução27. Para coleta calibrou-se o equipamento antes do início
de cada sessão de teste e os participantes foram posicionados a fim de promover estabilização e
garantir o alinhamento articular. Os participantes foram familiarizados com o exercício isocinético
por meio de 3 repetições em esforço submáximo nas mesmas velocidades dos testes e aquecimento
de 5 minutos em cicloergômetro2.
O teste de Levantar e Sentar (TLS) foi avaliado ao cronometrar o tempo gasto pelos
participantes para se levantaram e se sentaram cinco vezes, na maior velocidade possível, em uma
cadeira com medida de altura padronizada de 43 centímetros. O encosto da cadeira foi apoiado contra
a parede, e os idosos foram instruídos a cruzarem os braços sobre o tórax antes de iniciar o teste. O
cronômetro foi disparado a partir da posição sentada inicial e pausado ao final da última repetição,

16
sendo considerado para as análises o tempo total em segundos para desempenhar a atividade do
teste2,10,18.
A coleta iniciou com a investigação dos dados clínicos e sociodemográficos seguida da
avaliação físico-funcional na mesma semana. As avaliações físicas e funcionais iniciaram com as
medidas da massa e estatura corporal para o cálculo do Índice de Massa Corporal (IMC), seguidas da
aplicação do teste Sentar e Levantar da cadeira e da avaliação da função muscular isocinética dos
membros inferiores, intencionalmente mantido como a última avaliação visando prevenir a possível
influência da fadiga muscular decorrente da avaliação isocinética na capacidade de levantar e sentar
da cadeira. Os examinadores que realizaram a avaliação isocinética foram cegados para o resultado
do teste de levantar e sentar da cadeira.
Análises Estatísticas
Os dados foram expressos em média e desvio-padrão para as variáveis contínuas e em
porcentagem e frequência absoluta para as variáveis categóricas. A normalidade da distribuição dos
dados foi confirmada utilizando o teste Kolmogorov-Smirnov. Para cada variável de função muscular
isocinética os participantes foram categorizados em “fracos” ou “fortes” de acordo com o percentil
25. A Receiver Operating Characteristic curve (curva ROC) foi construída para verificar a
capacidade do TLS para discriminar deficiência de pico de torque e potência dos oito grupos
musculares de membros inferiores e a área abaixo da curva ROC (com 95% de intervalo de confiança)
foi calculada para cada curva. Para as curvas que apresentaram AUC estatisticamente significativa os
pontos de corte ‘ótimos’ do TLS foram identificados. Foram calculados a sensibilidade (S),
especificidade (E), valor preditivo positivo (VPP) e valor preditivo negativo (VPN), considerando os
casos falso-positivo, falso-negativo, verdadeiro-negativo e verdadeiro-positivo. O ponto de corte
ótimo foi considerado como o tempo para desempenho o TLS com a melhor combinação de
sensibilidade e especificidade. O ponto de corte do TLS que apresentou melhores valores de
sensibilidade e valor preditivo negativo foi considerado o melhor indicador clínico de deficiência de
função muscular de membros inferiores. Foram considerados valores de sensibilidade e

17
especificidade adequados aqueles maiores que 50%, sendo que valores de 51% a 69% caracterizaram
fraca/limitada acurácia e os valores acima de 70% representaram boa acurácia. Os valores de AUC
entre 0,51 e 0,69 representaram fraca capacidade discriminativa e os valores de AUC iguais ou
maiores a 0,70 determinaram satisfatória capacidade discriminativa. O nível de significância de 5%
foi considerado (α = 0,05). As análises dos dados foram realizadas utilizando-se o programa
Statistical Package for Social Sciences (SPSS), versão 21.0.
3 - RESULTADOS
Foram analisados dados de 264 idosos comunitários (Fluxograma, Figura 1). As características dos
participantes estão presentes na Tabela 1, sendo 82,6% do sexo feminino, 50,4% com excesso de peso
e 51,9% classificados como ativos.
Figura 1. Fluxograma da amostra

18
Tabela 1. Características sociodemográficas e clínicas dos participantes
Variável Dados válidos
(n)
Valores
Idade (anos)‡
60 a 69†
70 a 79†
80 a 89†
264 69,85 (6,50)
52,3 (138)
39,4 (104)
8,3 (22)
Sexo†
Feminino
Masculino
264
82,6 (218)
17,4 (46)
Escolaridade (anos)‡ 264 7,66 (6,39)
IMC‡
Baixo peso†
Eutrofia†
Excesso de peso†
264 27,66 (4,82)
10,2 (27)
39,4 (104)
50,4 (133)
Medicamentos (quantidade)‡ 259 3,87 (2,54)
MEEM (escore)‡ 264 26,22 (3,04)
Prática de exercício regular (sim)† 264 51,9 (137)
IMC = Índice de Massa Corporal. †Valores em percentual (frequência absoluta); ‡Valores de
média (desvio-padrão).
Os idosos apresentaram média de 11,60 (DP = 4,27) segundos, variando de 5,63 a 44,74
segundos para completar o teste de levantar e sentar da cadeira. Os valores de pico de torque e
potência muscular da amostra geral e dos grupos de idosos categorizados como fracos e fortes de
acordo com percentil 25% estão apresentados na Tabela 2.

19
Tabela 2. Dados do teste de levantar e sentar e de pico de torque e potência muscular isocinética de
membros inferiores
Variável Dados válidos
(n)
Amostra geral Fracos Fortes
n Valores n Valores
TLS (s)† 264 11,60 (4,27)
[5,63 – 44,74]
- - - -
Flexores plantares de tornozelo
Pico de torque 115 47,19 (17,83) 29 26,22 (6,82) 86 54,26 (14,51)
Potência 107 19,99 (9,98) 27 8,55 (2,06) 80 23,85 (8,51)
Dorsiflexores de tornozelos
Pico de torque 115 24,24 (6,23) 30 17,47 (2,70) 85 26,64 (5,28)
Potência 107 12,58 (4,82) 27 7,51 (1,45) 80 14,30 (4,33)
Extensores de joelho
Pico de torque 261 124,51 (37,69) 66 77,74 (18,74) 195 140,34 (28,11)
Potência 256 72,43 (28,52) 65 41,01 (9,99) 191 83,12 (24,61)
Flexores de joelho
Pico de torque 261 59,14 (19,92) 66 35,01 (8,70) 195 67,31 (15,53)
Potência 256 36,17 (18,71) 65 14,13 (6,98) 191 43,68 (15,18)
Flexores de quadril
Pico de torque 111 72,93 (26,62) 28 41,15 (9,48) 83 83,66 (21,43)
Potência 106 31,20 (17,59) 27 12,28 (3,37) 79 37,66 (15,71)
Extensores de quadril
Pico de torque 111 94,29 (42,32) 28 49,67 (14,58) 83 109,34 (37,73)
Potência 106 36,63 (25,31) 27 8,08 (4,73) 79 46,14 (22,26)
Abdutores de quadril
Pico de torque 113 84,97 (25,67) 29 53,33 (11,58) 84 95,90 (19,33)
Potência 111 42,09 (17,56) 28 21,66 (4,84) 83 48,99 (14,68)
Adutores de quadril
Pico de torque 113 71,14 (28,11) 29 35,63 (10,98) 84 83,40 (20,81)
Potência 111 21,56 (16,97) 28 2,70 (2,19) 83 27,93 (14,91) †Valores de média (desvio-padrão); [mínimo=-máximo]. Valores de pico de torque em (Nm/Kg)
*100. Valores de potência muscular média expressos em Watts. TLS = Teste de Levantar e Sentar
cinco vezes.
As áreas abaixo das curvas ROC, os pontos de corte ótimos identificados e os respectivos
indicadores de validade estão apresentados na Tabela 3. Os pontos de corte ótimos para o TLS
identificados para rastrear idosos com deficiência de pico de torque e potência muscular dos oito
grupos musculares investigados variaram de 10,14 a 11,23 segundos. Entretanto, o ponto de corte
único, com número inteiro, que apresentou os melhores valores de sensibilidade e valor preditivo
negativo para identificar deficiência de função muscular de membros inferiores foi 10 segundos. Os
indicadores de validade deste ponto de corte para identificar deficiência de pico de torque e potência
muscular estão apresentados na Tabela 4.

20
A investigação da acurácia do teste de levantar e sentar da cadeira para identificar deficiência
de força e potência muscular dos oito grupos musculares avaliados revelou satisfatória capacidade
discriminativa deste teste para reconhecer deficiência de pico de torque e potência de flexores
plantares de tornozelo, extensores e flexores de joelho, flexores e abdutores de quadril e de pico de
torque de dorsiflexores de tornozelo (AUC ≥ 0,70). Entre os idosos com deficiência de pico de torque
e de potência muscular de flexores plantares, de extensores e flexores de joelho, de potência de
flexores de quadril, e de pico de torque de dorsiflexores de tornozelo, mais de 80% foi corretamente
identificado pelo TLS positivo (> 10 segundos). Adicionalmente, um TLS negativo (≤ 10 segundos)
identificou corretamente mais de 88% dos idosos sem deficiência nesses grupos musculares.
Tabela 3. Capacidade do Teste de Levantar e Sentar para identificar deficiência de pico de torque e
potência muscular de membros inferiores
Parâmetro da
função
muscular
Ponto de corte
identificado
(TLS; s)
S
(%)
E
(%)
VPP
(%)
VPN
(%)
AUC
[IC 95%]
p-valor
Flexores plantares de tornozelo
Pico de torque 10,44 72,4 66,3 42,0 87,7 0,790 [0,690 – 0,890] <0,001 Potência 10,84 74,1 68,8 88,7 44,4 0,759 [0,655 – 0,862] <0,001 Dorsiflexores de tornozelo Pico de torque 10,40 80,0 67,1 46,2 90,5 0,776 [0,678 – 0,873] <0,001 Potência 10,40 70,4 61,3 38,0 86,0 0,661 [0,545 – 0,778] 0,013 Extensores de joelho Pico de torque 10,75 71,2 57,4 85,5 36,2 0,721 [0,647 – 0,794] <0,001 Potência 10,91 75,4 62,8 88,2 40,8 0,764 [0,696 – 0,832] <0,001 Flexores de joelho Pico de torque 10,52 72,7 55,4 85,7 35,6 0,704 [0,631 – 0,777] <0,001 Potência 11,23 70,8 71,7 87,8 46,0 0,773 [0,709 – 0,836] <0,001 Flexores de quadril Pico de torque 10,17 67,9 55,4 83,6 33,9 0,704 [0,593 – 0,815] 0,001 Potência 10,70 70,4 67,1 42,2 86,9 0,773 [0,675 – 0,872] <0,001 Extensores de quadril Pico de torque 10,14 71,4 55,4 85,2 35,1 0,662 [0,549 – 0,774] 0,011 Potência 10,40 66,7 60,8 36,7 84,2 0,689 [0,584 – 0,794] 0,003 Abdutores de quadril Pico de torque 10,17 72,4 56,0 85,5 36,2 0,701 [0,588 – 0,814] 0,001 Potência 10,44 71,4 65,1 40,8 87,1 0,739 [0,623 – 0,856] <0,001 Adutores de quadril Pico de torque - - - - - 0,560 [0,436 – 0,683] 0,341 Potência 10,70 65,1 64,3 38,3 84,4 0,679 [0,556 – 0,802] 0,005
S = Sensibilidade. E = Especificidade. VPP = Valor Preditivo Positivo. VPN = Valor Preditivo
Negativo. AUC = Area Under the Curve.

21
Tabela 4. Acurácia do ponto de corte sugerido de 10 segundos no Teste de Levantar e
Sentar para identificar deficiência de força e potência muscular de membros inferiores
Parâmetro da função
muscular
S (%) E (%) VPP
(%)
VPN (%)
Flexores plantares de tornozelo Pico de torque 86,2 50,0 36,8 91,5 Potência 88,9 47,5 36,4 92,7 Dorsiflexores de tornozelo Pico de torque 86,7 50,6 38,2 91,5 Potência 81,5 45,0 33,3 87,8
Extensores de joelho Pico de torque 83,3 45,1 34,0 88,9 Potência 86,2 46,1 35,2 90,7 Flexores de joelho Pico de torque 80,3 44,1 32,7 86,9 Potência 86,2 46,1 35,2 90,7 Flexores de quadril Pico de torque 71,4 48,2 31,7 83,3 Potência 81,5 49,4 35,5 88,6 Extensores de quadril
Pico de torque 75,0 49,4 33,3 85,4
Potência 81,5 49,4 35,5 88,6
Abdutores de quadril Pico de torque 75,9 48,8 33,8 85,4 Potência 75,0 47,0 32,3 84,8 Adutores de quadril
Pico de torque - -- - -
Potência 67,9 44,6 29,2 80,4
S = Sensibilidade. E = Especificidade. VPP = Valor Preditivo Positivo. VPN = Valor
Preditivo Negativo.
4 - DISCUSSÃO
Este estudo foi delineado para avaliar a capacidade do teste de levantar e sentar da cadeira no rastreio
de deficiência de pico de torque e potência muscular de oito grupos musculares de membros inferiores
em idosos. Os valores das estimativas de sensibilidade e de valor preditivo negativo indicaram que o
ponto de corte ótimo de 10 segundos rastreou satisfatoriamente idosos com deficiência de pico de
torque e potência muscular de flexores plantares, flexores e extensores de joelho, pico de torque de
dorsiflexores de tornozelo e potência de flexores de quadril. Esse ponto de corte pode ser utilizado
no ambiente clínico no intuito de rastrear idosos lentos na atividade de levantar e sentar da cadeira
para serem submetidos a avaliações mais específicas do componente de força muscular ou para
encaminhá-los apropriadamente para programas de reabilitação e treinamento resistido.

22
No presente estudo, os participantes apresentaram média de idade de 69,85 anos e a média
dos valores dos tempos do TLS de 11,60 segundos. Esse resultado é compatível com os valores de
referência para o teste de sentar e levantar da cadeira estabelecidos em revisão sistemática com meta-
análise de acordo com a faixa etária, sendo 11,4 segundos para faixa de 60 a 69 anos8. O ponto de
corte ótimo de 10 segundos para o TLS também foi observado em estudo anterior para identificar
risco de incapacidade9. Porém, esse ponto de corte é relativamente rápido comparado com pontos de
corte identificados de 12 segundos para rastrear limitação funcional18, 13,6 segundos para indicação
de maior incapacidade e morbidade28 e de 15 segundos para prever quedas recorrentes e fraqueza
muscular13,29.
A maioria das pesquisas2,3,5,15–18 sobre a associação entre o desempenho muscular e a
atividade de levantar e sentar da cadeira tem investigado a relação contrária à do presente estudo, no
intuito de responder se pontos de corte da força muscular de membros inferiores (mais frequentemente
de extensores de joelho5,15,17) podem predizer o risco de limitação funcional, ou para identificar o
quanto a força muscular determina o desempenho no TLS2,3,17,20. A força de flexão3,20 e extensão2,3,3,17
de joelho, de flexão plantar2,16 e dorsiflexão de tornozelo3 e de flexão de quadril2 tem se mostrado
como importante componente na explicação da variação nos tempos de execução do TLS. Dentre
esses grupos musculares, o mais popularmente investigado como preditor do TLS é o extensor de
joelho5,10, que chega a explicar 16,5%3 do desempenho funcional para essa atividade. Entretanto,
músculos flexores de quadril e flexores plantares de tornozelo, apesar de pouco pesquisados,
destacam-se por explicar, respectivamente, 48% e 43% da variância no TLS2.
No presente estudo, o TLS foi mais acurado para prever o pico de torque de flexores plantares
(AUC = 0,790 [IC 95% 0,690 – 0,890]). A importância da força desse grupamento muscular também
foi identificada por McCarthy et al.2 como a que mais contribuiu para predizer o desempenho do TLS
entre os principais músculos dos membros inferiores, seguida dos músculos flexores de quadril e
extensores de joelho. Essa importante contribuição dos músculos flexores plantares parece não se
restringir apenas à força, mas ao papel desse grupo muscular como estabilizador do corpo na posição
em pé ao final da tarefa de levantar da cadeira ao se completar repetidamente esse movimento2,30,31,32.

23
Entretanto, no presente estudo, o ponto de corte de 10 segundos no TLS também apresentou
indicadores de validade adequados para identificar deficiência de pico de torque e potência média dos
músculos extensores e flexores de joelho, pico de torque de dorsiflexores e potência de flexores de
quadril. Apesar desses grupos musculares não serem mecanicamente independentes, e seus limiares
mecânicos serem resultantes de sinergias e de antagonismos33, a contribuição de cada um desses
músculos parece variar de acordo com a fase da atividade de levantar da cadeira2. Nível suficiente de
força muscular de flexores de quadril parecem essenciais no momento de flexão durante a primeira
fase dessa tarefa2. A força muscular de extensores de joelho é fundamental durante todos os
movimentos na tarefa de sentar e levantar de uma cadeira33, mas ganha destaque na fase de
transferência para o peso do corpo afastar-se da cadeira e deslocar-se para os pés e na fase de extensão
para atingir máxima velocidade de extensão dessa articulação2,34.
O presente estudo tem pontos fortes e limitações. A amostra relativamente grande de idosos
e a avaliação do pico de torque e da potência isocinética de oito grupos musculares de membros
inferiores são pontos fortes. A tentativa de indicar um ponto de corte único do TLS para rastreio de
fraqueza muscular dos oito grupos musculares avaliados também deve ser destacada. Mas nossos
resultados devem ser interpretados com cautela, pois a heterogeneidade dos tamanhos amostrais para
cada grupo muscular pode ter influenciado nas análises e a não estratificação por sexo e faixa etária
impossibilita identificar pontos de corte específicos para cada grupo. Apesar disso, nós reforçamos a
possibilidade do uso do teste de levantar e sentar cinco vezes para identificar idosos com fraqueza
muscular de membros inferiores. Nós trouxemos uma contribuição clínica importante indicando o
ponto de corte de 10 segundos para rastreio simples e de baixo custo com o TLS visando reconhecer
precocemente deficiência dos principais grupos musculares dos membros inferiores e encaminhar
para implementação de medidas preventivas ou de reabilitação.
5 - CONCLUSÃO
Nosso estudo identificou o ponto de corte de 10 segundos no teste de levantar e sentar da cadeira
cinco vezes, trazendo assim uma importante contribuição clínica de rastreio simples, que é capaz de

24
identificar satisfatoriamente fraqueza muscular de flexores plantares e dorsiflexores de tornozelo,
extensores e flexores de joelho e flexores de quadril. Estes resultados são importantes para a prática
clínica, pois representam o valor e a utilidade do teste de levantar e sentar da cadeira como uma
medida de força muscular dos membros inferiores.
Colaboradores
Gabriela da Silva Freire, Felipe Augusto Ribeiro, Cristiane de Almeida Nagata, Tânia Cristina Dias
da Silva Hamu e Patrícia Azevedo Garcia trabalharam na elaboração, redação, delineamento,
interpretação dos dados, correção e edição final.
REFERÊNCIAS
1. Landi F, Calvani R, Tosato M, et al. Age-Related Variations of Muscle Mass ,
Strength , and Physical Performance in Community-Dwellers : Results From the
Milan EXPO Survey. JAMDA J. 2016;18(1):88.e17-88.e24.
2. Mccarthy EK, Horvat MA, Holtsberg PA, Wisenbaker JM. Repeated Chair Stands as
a Measure of Lower Limb Strength in Sexagenarian Women. J Gerentology Ser A
Biol Sci Med Sci. 2004;54(11):1207-1212.
3. Lord SR, Murray SM, Chapman K, Munro B, Tiedemann A. Sit-to-Stand
Performance Depends on Sensation , Speed , Balance , and Psychological Status in
Addition to Strength in Older People. J gerontoly Med Sci. 2002;57(8):m539-m543.
4. Buatois S, Perret-guillaume C, Gueguen R, Miget P, Perrin P, Benetos A. A Simple
Clinical Scale to Stratify Risk of Recurrent Falls in Community- and Older. Phys
Ther. 2010;90(4):550-560.
5. Bohannon RW, Bubela DJ, Magasi SR, Wang Y. Sit-to-stand test : Performance and
determinants across the age-span. Isoknetics Exerc Sci. 2010;18(4):235-240.
doi:10.3233/IES-2010-0389
6. Bergquist R, Weber M, Schwenk M, et al. Performance-based clinical tests of
balance and muscle strength used in young seniors : a systematic literature review.

25
BMC Geriatr. 2019;19(9):1-14.
7. Zhang F, Ferrucci L, Culham E, Metter EJ, Guralnik J, Deshpande N. Performance
on five times sit-to-stand task as a predictor of subsequent falls and disability in
older persons. J Aging Health. 2013;25(3):478-492. doi:10.1177/0898264313475813
8. Bohannon RW. Reference Values for the Five-Repetition Sit-To-Stand Test: a
Descriptive Meta-Analysis of Data From Elders. Percept Mot Skills.
2006;103(5):215. doi:10.2466/pms.103.5.215-222
9. Makizako H, Shimada H, Doi T, et al. Predictive Cutoff Values of the Five-Times
Sit-to-Stand Test and the Timed “Up & Go” Test for Disability Incidence in Older
People Dwelling in the Community. Phys Ther. 2017;97(4):417-424.
10. Tiedemann A, Shimada H, Sherrington C, Murray S, Lord S. The comparative
ability of eight functional mobility tests for predicting falls in community-dwelling
older people. Age Ageing. 2008;37(4):430-435. doi:10.1093/ageing/afn100
11. Whitney SL, Wrisley DM, Marchetti GF, Gee MA, Redfern MS. Clinical
Measurement of Sit-to-Stand Performance in People With Balance Disorders :
Validity of Data for the five-times-sit-to-stand test. Phys Ther. 2005;85(10):1034-
1045.
12. Goldberg A, Chavis M, Watkins J, Wilson T. The five-times-sit-to-stand test:
Validity, reliability and detectable change in older females. Aging - Clin Exp Res.
2012;24(4):339-344. doi:10.1007/BF03325265
13. Cruz-Jentoft AJ, Bahat G, Bauer J, et al. Sarcopenia: Revised European consensus
on definition and diagnosis. Age Ageing. 2019;48(1):16-31.
doi:10.1093/ageing/afy169
14. Cruz-Jentoft AJ, Baeyens JP, Bauer JM, et al. Sarcopenia : European consensus on
definition and diagnosis Report of the European Working Group on Sarcopenia in
Older People. Age Ageing. 2010;39(4):412-423. doi:10.1093/ageing/afq034
15. Barbat-Artigas S, Rolland Y, Cesari M, Abellan Van Kan G, Vellas B, Aubertin-
Leheudre M. Clinical relevance of different muscle strength indexes and functional
impairment in women aged 75 years and older. Journals Gerontol - Ser A Biol Sci

26
Med Sci. 2013;68(7):811-819. doi:10.1093/gerona/gls254
16. Suzuki T, Jonathan F. Bean M, Fielding and RA. Muscle Power of the Ankle
Flexors Predicts Functional Performance in Community-Dwelling Older Women. J
Am Geriatr Soc. 2011;49(9):1161-1167. doi:10.1007/BF00635870
17. Crockett K, Ardell K, Hermanson M, Penner A, Lanovaz J. The Relationship of
Knee-Extensor Strength and Rate of Torque Development to Sit-to-Stand
Performance in Older Adults. Physiother Canada. 2013;65(3):229-235.
doi:10.3138/ptc.2012-04
18. Pereira JC, Gonçalves S, Neri R, et al. Normative Values of Knee Extensor
Isokinetic Strength for Older Women and Implications on Physical Function. Geriatr
Phys Ther. 2018;0(0):1-7. doi:10.1519/JPT.0000000000000198
19. Lindemann U, Claus ÆH, Stuber ÆM. Measuring power during the sit-to-stand
transfer. Eur J Appl Physiol. 2003;89(5):466-470. doi:10.1007/s00421-003-0837-z
20. Jung H, Yamasaki M. Association of lower extremity range of motion and muscle
strength with physical performance of community-dwelling older women. J Physiol
Anthropol. 2016;35(1):1-7. doi:10.1186/s40101-016-0120-8
21. Visser M, Goodpaster BH, Kritchevsky SB, et al. Muscle Mass , Muscle Strength ,
and Muscle Fat Infiltration as Predictors of Incident Mobility Limitations in Well-
Functioning Older Persons. J gerontoly Med Sci. 2005;60(3):324-333.
22. Neri AL, Yassuda MS, Araujo LF, et al. Metodologia e perfil sociodemográfico ,
cognitivo e de fragilidade de idosos comunitários de sete cidades brasileiras : Estudo
FIBRA Methodology and social , demographic , cognitive , and frailty profiles of
community-dwelling elderly from seven Brazilian. Cad Saúde Pública.
2013;29(4):778-792.
23. Lipschitz DA. Screening for nutritional status in the elderly. Prim care.
1994;21(1):55-67.
24. Piercy KL, Troiano RP, Ballard RM, et al. The Physical Activity Guidelines for
Americans. JAMA. 2018;320(19):2020-2028. doi:10.1001/jama.2018.14854
25. Perrin DH. Isokinetic Exercise and Assessment.; 1993.

27
26. Garcia PA, Dias JMD, Dias RC, Santos P, Zampa CC. Estudo da relação entre
função muscular , mobilidade funcional e nível de atividade física em idosos
comunitários. Rev Bras Fisioter. 2011;15(1):15-22.
27. Lourencin FT, Macedo OGDC, Scarpellini S. Evaluation of hip adductor and
abductor muscles using an isokinetic dynamometer Evaluation of hip adductor and
abductor muscles using an isokinetic dynamometer. Acta Fisiátrica. 2017;19(1):16-
20. doi:10.5935/0104-7795.20120004
28. Guralnik JM, Ferrucci L, Pieper CF, et al. Lower extremity function and subsequent
disability: Consistency across studies, predictive models, and value of gait speed
alone compared with the short physical performance battery. Journals Gerontol - Ser
A Biol Sci Med Sci. 2000;55(4):221-231. doi:10.1093/gerona/55.4.M221
29. Buatois S, Miljkovic D, Manckoundia P, Gueguen R, Miget P, Vançon G, Perrin P
BA. Five times sit to stand test is a predictor of recurrent falls in healthy community-
living subjects aged 65 and older. J Am Geriatr Soc. 2008;56(8):1575-1577.
30. Khemlani MM, Carr JH, Crosbie WJ. Muscle synergies and joint linkages in sit-to-
stand under two initial foot positions. Clin Biomech. 1999;14(4):236-246.
doi:10.1016/S0268-0033(98)00072-2
31. Magnan A, McFadyen BJ, St-Vincent G. Modification of the sit-to-stand task with
the addition of gait initiation. Gait Posture. 1996;4(3):232-241. doi:10.1016/0966-
6362(95)01048-3
32. Rodrigues-De-Paula Goulart F, Valls-Solé J. Patterned electromyographic activity in
the sit-to-stand movement. Clin Neurophysiol. 1999;110(9):1634-1640.
doi:10.1016/S1388-2457(99)00109-1
33. Yoshioka S, Nagano A, Hay DC, Fukashiro S. The minimum required muscle force
for a sit-to-stand task. J Biomech. 2012;45(4):699-705.
doi:10.1016/j.jbiomech.2011.11.054
34. Wretenberg P, Arborelius UP. Power and work produced in different leg muscle
groups when rising from a chair. Eur J Appl Physiol Occup Physiol. 1994;68(5):413-
417. doi:10.1007/BF00843738

28
ANEXO A – Aprovação do Comitê de Ética da Universidade Federal de Minas Gerais

29
ANEXO B – Aprovação do Comitê de Ética da Faculdade de Ceilândia

30
ANEXO C – Aprovação do Comitê de Ética da Faculdade de Ceilândia

31
ANEXO D – Normas da Revista Científica
The Journal of Geriatric Physical Therapy (JGPT) is the official publication of
the Academy of Geriatric Physical Therapy of the American Physical Therapy
Association. The JGPT is published four times a year and offers articles that advance the
science and practice of geriatric physical therapy.
JGPT Mission Statement
“The Journal of Geriatric Physical Therapy is the leading source of clinically applicable
evidence for achieving optimal health, wellness, mobility, and physical function across the
continuum of health status for the aging adult.” Evidence published in the JGPT supports the
provision of best practice physical therapy and facilitates advocacy for optimal aging.
Important information for authors regarding the three-stage review process
All manuscripts submitted to the JGPT are first screened by the Editor-in-Chief for
suitability, scientific impact and rigor, clinical relevance, originality, proper format, and
high-quality scientific writing in American English; please see below for further clarification
of these requirements. Acceptable manuscripts are then assigned to an Associate Editor who
performs a second Editor’s review. Submissions judged to have strong scientific merit and
substantial clinical relevance then undergo masked peer review. Authors may wish to read
the JGPT Reviewers Read-Along checklist to obtain a better understanding of reviewer
expectations; download here: http://links.lww.com/ES/A149
• Suitability: Manuscripts may address any scientific or clinical aspect of physical
therapy care for older adults. Manuscripts may focus on, for example, health
promotion/wellness care, risk factor abatement, examination/evaluation methods and
strategies, performance on clinical measures of well and impaired older
adults, efficacy/effectiveness of interventions to reduce risk, decrease impairment,
and/or improve function and participation in aging adults with activity restriction,
movement dysfunction in later life, and theoretical models of examination/evaluation
or care of older adults. Studies not focused on older adults, and those exploring age-
related topics that are not pertinent to the actual clinical practice of geriatric physical
therapy, are not considered a good match.
• Scientific Impact and Rigor: The reported study should do all of the following:
o Address an important problem and add new knowledge to bridge a knowledge
gap
o Include sufficient sample size(s) to achieve adequate statistical power
o Use reliable and valid measures appropriate to the population under study
o For multivariate studies, employ multivariate statistical analyses with
correction to control for inflated Type 1 error, e.g., MANOVA or RM-
MANOVA with planned post-hoc tests. When necessary, control for baseline
between-group differences, e.g., MANCOVA or RM-MANCOVA with
planned post-hoc tests.
o Report both statistical and clinical significance values

32
• Clinical Relevance: The reported study should do all of the following:
o Address a problem that is (1) within the [geriatric] physical therapy scope of
practice, and (2) clinically important to address
o Include a population that represents older adults with a health condition
commonly seen in, or appropriate for referral to, geriatric physical therapy
practice; studies reporting normative data on healthy older adults exempted.
o Explore a practice component that is within the [geriatric] physical therapy
scope of practice, and related to improved client care, management, and
outcomes
▪ Comparative effectiveness studies are highly clinically relevant, e.g.,
a comparison of two or more interventions, two or more screening or
diagnostic tests, etc.
▪ These studies are the most relevant when the comparison
group or test is highly valid, e.g. comparing two exercise
programs (e.g., “usual care” versus studied intervention) is
more valid than comparing exercise to no exercise; adding a
third group with no exercise (control) is even better.
o Use client-centered outcome measures
▪ Measures of physiologic variables (e.g., muscle mass, bone density,
etc.) and impairment-level variables (body structure and function,
such as strength, range of motion, etc.) by themselves (in the absence
of additional measures) are less clinically relevant than activity- and
participation-level measures (functional independence or community
ambulation, return to life roles, etc.) and quality of life measures.
However, studies that examine the relationship between physiologic
or impairment-level variables and activity-level, participation- level,
or quality of life measures are also highly clinically relevant.
o Report measures of clinical significance (in addition to statistical
significance)
▪ Depending on the type of study, these may include:
▪ Effect sizes
▪ Confidence intervals
▪ Minimal Detectable Change (MDC)
▪ Minimally Clinically Important Difference (MCID)
▪ Risk ratios (RR) or Odds ratios (OR)
▪ Number needed to treat (NNT)
o Explicitly discuss current or future clinical impact or clinical application of
the findings
• Originality: Manuscripts should present novel findings that bridge a critical
knowledge gap. The work must be that of the submitting authors, cannot be
substantially identical to the author’s prior work, and must not have been submitted
elsewhere.
• Proper format: Manuscripts must conform to AMA Style guidelines. Manuscripts
of interest to the JGPT that are improperly formatted are immediately rejected and
sent back to the author with invitation to resubmit; this delays the processing of

33
manuscripts significantly as the resubmitted manuscript ‘moves to the back of the
line’.
• High-quality scientific writing in American English: Manuscripts of interest to the
JGPT that reveal sub-standard use of written English are immediately rejected and
sent back to the author with invitation to resubmit; this delays the processing of
manuscripts significantly as the resubmitted manuscript ‘moves to the back of the
line’.
o Responsibility for proof-reading and copy-editing lies with the authors, not
with the JGPT editors and reviewers.
o English-language editing services are available from our publisher; link may
be found on the JGPT home page under the ‘For Authors’ tab
(https://wkauthorservices.editage.com/editing/?center=&PlacementPage:edit
ing-image&PlacementButton/Link:editing). Other English-language editing
services may be used, however, a certificate of completed professional service
must be attached to the submission.
Manuscript Categories and Standardized Reporting Requirements
The Editors will consider systematic reviews of the literature, quantitative research reports
(experimental, quasi-experimental, or descriptive), and qualitative studies. Submissions that
represent a higher level of evidence (systematic reviews, RCTs, etc.) are much more likely
to be accepted than those demonstrating lower levels of evidence (outcomes research, case
series, etc.).
• True pilot intervention studies may be considered, see:
o Vogel S, Draper-Rodi J. The importance of pilot studies, how to write them
and what they
mean. https://www.journalofosteopathicmedicine.com/article/S1746-
0689(17)30013-5/fulltext, and
o Thabane L et al. A tutorial on pilot studies: the what, why and how. (See
especially Section
5.) https://bmcmedresmethodol.biomedcentral.com/articles/10.1186/1471-
2288-10-1
• Under-powered (small sample) intervention studies are not considered true pilot
studies in the absence of an appropriate focus on findings related to the conduct of
the study (versus the participant outcomes).
• Case reports and case series are generally not considered unless they have exceptional
potential to advance clinical practice.
• Authors intending to submit a special interest paper should contact the Editor-in-
Chief prior to submission.
Standardized Reporting Guidelines: Standardized reporting guidelines (with checklists)
specific to manuscript categories are required with submission as follows:
• PRISMA for systematic reviews
• CONSORT for randomized controlled trials

34
• Table 3 checklist from Thabane et. Al, 2010 (BMC Medical Research
Methodology; www.biomedcentral.com/1471-2288/10/1) for preliminary, pilot, or
feasibility studies
• STROBE for observational studies
• STARD for diagnostic accuracy studies
• GRAAS for reliability and agreement studies
• COSMIN for measurement properties studies
• CHERRIES for internet survey studies
• TRIPOD for clinical prediction rule studies
• QUALRES for qualitative studies
• CARE for case reports or case report series
• SCRIBE for single-subject design studies
• TIDieR for intervention studies (in addition to the appropriate checklist specified
above)
Authors are required to include the appropriate checklist complete with manuscript page
numbers to indicate where the required information appears in the manuscript. These
checklists and additional information are available on the Enhancing the Quality and
Transparency of Health Research (EQUATOR) network website (www.equator-
network.org). When indicated by guidelines, the participant flow chart should also be
submitted as a Figure when submitting a manuscript for review.
Human subjects research: All studies reporting the results of investigation with human
subjects must comply with the Declaration of Helsinki and state explicitly that the that the
study was approved by an institutional review board (IRB) or that the requirement for such
approval was formally waived. Studies must also state that participants or their guardians
signed an informed consent, or that the need for consent was waived by the IRB.
Commercial devices: Submissions reporting the results of investigation of or with
commercial devices should at the first mention of the device provide the commercial name,
manufacturer, city and state; thereafter refer to the device using a generic name.
Reporting statistically significant results: The needed sample size to achieve adequate
statistical power (> 0.80) should be determined ‘a priori’; many authors use G*Power
(http://www.psychologie.hhu.de/arbeitsgruppen/allgemeine-psychologie-und-
arbeitspsychologie/gpower.html). Following analyses, the actual statistical power to detect
differences should be reported. Studies that are under-powered (< 0.80) are likely to
be rejected. When significance tests have been used, actual P values (to 3 decimal places)
should be reported. All P values < 0.001 should be reported as “p < 0.001”.
Reporting clinical test results: For each clinical test used in the study, the reliability, validity
and minimal detectable change (MDC) and/or Minimally Clinically Important Difference
(MCID) of the test in the population under study should be included in the Methods section.
In the Results section, in addition to statistical significance, authors should also report
whether or not results were clinically significant, i.e., tables should include confidence
intervals, effect sizes, and whether pre- to post-test changes met or exceeded the MDC or
MCID for each test.
Manuscript Categories:

35
Systematic Reviews and Scoping Reviews: A balanced and unbiased synthesis of evidence
related to a defined clinical question relevant to geriatric physical therapy. This type of article
applies a systematic approach to exploring current evidence in the literature, assessing the
strength of evidence, synthesizing the findings of individual studies, and interpreting the
results. The manuscript should include the following headings: Introduction, Methods,
Results, Discussion and Conclusion.
• For systematic reviews and meta-analyses, authors should use the PRISMA
Statement: Preferred Reporting Items for Systematic Reviews and Meta-Analyses
and include the checklist with page numbers to indicate where the required
information appears in the manuscript (http://www.prisma-statement.org). If the
systematic review has been registered, include the registry hyperlink in the Methods
section.
• For scoping reviews, authors should follow the related guidelines found on the
EQUATOR Network website (http://www.equator-network.org/wp-
content/uploads/2016/06/Gerstein-Library-scoping-reviews_May-12.pdf).
Quantitative Research Reports: Research on a topic of interest to physical therapists caring
for aging adults, including clinical trials, cohort studies, mechanistic experiments, case-
control studies, and single-subject design studies. The manuscript should include the
following headings: Introduction, Methods, Results, Discussion and Conclusion.
• For randomized clinical trials comparing outcomes of intervention, authors should
use the CONSORT-NPT 2017 Statement (Consolidated Standards of Reporting
Trials, non-pharmacological treatment interventions) available
at http://www.consort-statement.org/extensions/interventions/non-pharmacologic-
treatment-interventions/, and include the checklist with page numbers to indicate
where the required information appears in the manuscript.
• NOTE! JGPT requires the registration of clinical intervention trials per the National
Institutes of Health (https://clinicaltrials.gov/ct2/manage-
recs/background#WhyRegister; see also https://clinicaltrials.gov/ct2/manage-
recs/how-register for instructions on how to register). Clinical trials may be
registered retrospectively until December 31, 2019; prospective registration is
required after January 1, 2020. Clinical trials may be registered with
clinicaltrials.gov or another registry (see links above for alternatives), and the registry
hyperlink must be included in the Methods section.
• For observational or prognostic studies using cross-sectional, cohort or case control
designs, authors should use the STROBE Statement (Strengthening the Reporting of
Observational studies in Epidemiology) available at http://www.strobe-
statement.org/index.php?id=available-checklists, and include the checklist with page
numbers to indicate where the required information appears in the manuscript
• For diagnostic studies, authors should use the STARD Statement (Standards for the
Reporting of Diagnostic accuracy studies) available at http://www.stard-
statement.org, and include the checklist with page numbers to indicate where the
required information appears in the manuscript.
http://www.consort-statement.org/extensions/interventions/non-pharmacologic-treatment-interventions/

36
• For preliminary, pilot, or feasibility studies authors should use the Table 3 checklist
from Thabane et al 2010 (BMC Medical Research
Methodology; www.biomedcentral.com/1471-2288/10/1), and include the
checklist with page numbers to indicate where the required information appears in
the manuscript.
• For studies of the measurement properties of measurement instruments, authors
should use the COSMIN checklist (http://www.cosmin.nl), and include the
checklist with page numbers to indicate where the required information appears in
the manuscript.
• For single-subject design studies, authors should use the SCRIBE checklist, and
include the checklist with page numbers to indicate where the required information
appears in the manuscript.
Qualitative Studies: Exploration of phenomena or experiences using semi-structured
methods such as in-depth interviews, focus groups, participant observation, ethnography, and
textual analysis to understand human behavior by exploring beliefs, experiences, behaviors,
attitudes, and interactions that might explain findings. Headings in the manuscript should
include Introduction (Background), Objectives (Purpose), Design, Methods, Results, and
Conclusions.
• Authors should use the QualRes Guidelines (Qualitative Research Guidelines Project
of the Robert Wood Johnson Foundation) available
at http://www.qualres.org/HomeGuid-3935.html, and include the checklist with page
numbers to indicate where the required information appears in the manuscript.
Case Report or Case Series: Reports of the examination and intervention of an individual
or small group of aging adults who are receiving physical therapy for movement dysfunction
are generally of low priority for publication. Infrequent exceptions may be made for reports
with exceptional potential to advance clinical practice. Case reports must systematically
describe patient history, review of systems, use of standardized measures, examination
strategies and findings, evaluation, physical therapy diagnosis, physical therapy prognosis
and goals, and physical therapy intervention and outcomes of those interventions. Each
component must include discussion of clinical decision-making in selection of measures,
interpretation of results and selection of intervention. Case reports do not test hypotheses,
establish causal relationships, or demonstrate effectiveness. For a case series, information
pertinent to the planning of a larger research study (e.g., effect size) is encouraged.
• Authors of case reports or case series should use the CARE guidelines available
at http://care-statement.org and include the completed CARE checklist with
submission, and include the checklist with page numbers to indicate where the
required information appears in the manuscript.
• Authors must also include a statement indicating that their institutional HIPPA
(Health Insurance Portability and Accountability Act) policy requirements have been
met.
Special Interest Papers: Topics of special interest to physical therapy care of aging adults,
including---but not limited to---topical reviews, theoretical perspectives, reviews of
techniques, equipment, or instructional materials. Consult with the Editor prior to
submission.

37
Conflicts of Interest
Authors must state all possible conflicts of interest in the Title Page of the manuscript,
including financial, consultant, institutional and other relationships that might lead to bias or
a conflict of interest. If there is no conflict of interest, this should also be explicitly stated as
“none declared”.
All sources of funding must be acknowledged in the Title Page of the manuscript. Grant
funding, from any source, must be listed clearly on the title page. All relevant conflicts of
interest and sources of funding should be included on the title page of the manuscript with
the heading “Conflicts of Interest and Source of Funding:”.
For example:
Conflicts of Interest and Source of Funding: Author A has received honoraria from Company
Z. Author B is currently receiving a grant (#12345) from Organization Y, and is on the
speaker’s bureau for Organization X – the CME organizers for Company Z. For the
remaining authors none were declared.
Copyright Transfer
In addition, each author must complete and submit the journal's copyright transfer agreement,
which includes a section on the disclosure of potential conflicts of interest based on the
recommendations of the International Committee of Medical Journal Editors, "Uniform
Requirements for Manuscripts Submitted to Biomedical Journals"
(www.icmje.org/update.html).
A copy of the form is made available to the submitting author within the Editorial Manager
submission process. Co-authors will automatically receive an Email with instructions on
completing the form upon submission. Each author should proactively ensure that their
email system will accept automated emails from the Editorial Manager system. Manuscript
processing cannot progress until all forms are signed and returned. Once published, all
material is copyrighted by JGPT.
Manuscript Preparation
• Authorship: The JGPT endorses the Uniform Requirements for Manuscripts
Submitted to Biomedical Journals published by the International Committee of
Medical Journal Editors (ICMJE), and follows their guidelines on requirements for
authorship (http://www.icmje.org/recommendations/browse/roles-and-
responsibilities/defining-the-role-of-authors-and-contributors.html).
• AMA Guidelines: Manuscripts should follow the style outlined in the American
Medical Association (AMA) Manual of Style: A Guide for Authors and Editors, 10th
Ed, Oxford University Press, 2009. Please review Sections 7-15 to ensure that your
manuscript follows these guidelines for: 7/Grammar, 8/Punctuation, 9/Plurals,
10/Capitalization, 11/Correct and Preferred Usage, 12/Non-English Words, Phrases
and Accent Marks, 13/Medical Indexes, 14/Abbreviations, and 15/Nomenclature.
• Headings: Major headings should be in bold with all capital letters, minor headings
should be in bold with only the first letter of each word capitalized, and sub-headings
should be in italics with only the first letter of the first word capitalized. Sub-headings

38
begin the paragraph and run into the first sentence. Headings are left-justified (not
indented).
• Paragraph Indentations: The first paragraph beginning immediately below a major
or minor heading is not indented, while all subsequent paragraphs are indented. Sub-
headings begin the paragraph and run into the first sentence.
• Person-first language must be used throughout the manuscript (i.e., a “individuals
with stroke” rather than “stroke patients”). Text must be free of ageist and sexist
terminology.
o Do not use the term “elderly”, replace with “older adults” or similar terms.
o Do not use the term “subjects”, replace with “participants” or “volunteers” or
similar terms.
• Abbreviations and Acronyms: All abbreviations/acronyms should be spelled out
completely at first usage, with abbreviation in parentheses immediately following.
Subsequently abbreviations are acceptable unless the abbreviation is used
infrequently. Do not begin a sentence with an abbreviation/acronym.
• Numerals should be used in all cases except for the following, when the number
should be spelled out:
o at the beginning of a sentence
o ordinal representation first through ninth, then 10th, 11th, etc.
o common fractions
o when the original source includes the spelled number (eg, quote or title)
o when numbers abut, as in “The sample included fourteen 100-year old
women.”
• Acknowledgements should appear at the end of the text after the article’s conclusion,
prior to the reference section.
• Page numbers are required and must be centered at the bottom of the page.
• Line numbers are required, beginning with the abstract and running consecutively
through the text of the manuscript. Line numbers are not required for references or
for tables and figures.
• Blinding/Masking for peer-review: Online submissions should include
one Reviewer Copy of the manuscript, in which
o the Title page has been stripped of all author information, and
o any Manuscript Text identifying the institution or authors should be redacted
or replaced with substitute or generic text.
▪ It is OK for reviewers to know the country, but not the city, university,
health care institution, or location of data collection.
1. Title page. The title page of the complete manuscript version should include:
• The title of the manuscript (in bold, with the first letter of all major words capitalized),
• Authors’ full names, academic and clinical credentials (e.g., PT, PhD), underneath
the title, with superscripted numbers to indicate institutional affiliation(s)
• The [numbered] institutional affiliation, and phone, fax and email information for
each author.
• Corresponding author information must contain the same as above, as well as a postal
address.
• Disclosure of any conflicts of interest, and any funding sources including grant
funding received for the work from any source, including: National Institutes of
Health (NIH); Wellcome Trust; Howard Hughes Medical Institute (HHMI); and
other(s).

39
• If the manuscript reflects work previously presented at a scientific meeting, a
statement detailing that presentation should be included on the title page.
2. Abstract. An abstract not exceeding 325 words should be submitted on a separate page,
following the Title page and before the Introduction. All abstracts should be typed double-
spaced 11 or 12 font size, and include 3 to 5 key words following the text of the abstract.
• For Research Articles, abstract content should be organized according to the
following headings: Background and Purpose, Methods, Results and Discussion, and
Conclusions. The Conclusion should include a statement of the clinical relevance,
impact, or application of the findings.
• For Case Reports and Case Series, abstract content should be organized according to
the following headings: Background and Purpose, Case Description, Intervention,
Outcomes, Discussion.
3. Video Abstract. After an article has been Accepted for Publication, authors can prepare
a Video Abstract and submit this digital file along with the final draft of the manuscript.
Guidelines for preparation of the Video Abstract, along with links to sample Video Abstracts,
can be found here – http://journals.lww.com/jgpt/Documents/LWW_Toolkit_-
_How_to_Create_a_Video_Abstract.pdf.
4. Manuscript Text. The text of the manuscript (after the Abstract and prior to the Reference
List) should be typed double-spaced and limited to 15 (8.5 x 11 inch) pages with 11 or 12
font size. Tables, Figure Legends, and Figures are not inserted into the text; see below.
• For research reports, the text is divided into sections including: Introduction, Methods
(including study design), Results, Discussion, and Conclusions.
• For case reports and case series, the text is divided into sections including:
Introduction, Case Description, Intervention, Outcomes, Discussion and Summary.
• For other articles, appropriate headings should be chosen to provide organization and
clarity to the paper.
5. Reference citations in the text. References should be indicated by consecutive
superscript numbers after punctuation. Forty or fewer references are preferred, excepting
systematic or scoping reviews.
Example:
Older adults are at high risk of nursing home placement. In developed countries, 1.5% to 8%
of older adults 65 years or older are living in nursing homes.1 Most older adults prefer to stay
in their familiar home environment rather than transfer to a nursing home because the
transition to nursing home can cause loss of autonomy and independence, poor quality of
life, and negative psychological impacts.2,3 In addition, the cost of nursing home placement
is substantial and imposes a huge burden on patients and their family as well as heath care
systems, stretching limited health care resources.4-6
6. Reference List. The reference list should be double-spaced and arranged numerically. The
reference list includes only those references cited in the text, in the order cited in the text.
Forty or fewer references are preferred, excepting systematic or scoping reviews. References
should be formatted according to the style of the AMA (American Medical Association

40
Manual of Style, 10th Ed., Oxford University Press, New York, New York). Reference
format should be checked carefully. Consulting the Reference List of articles previously
published in the Journal may be useful, some examples are provided below.
Examples:
Journal article (1-6 authors):
Trudelle-Jackson E, Jackson, AW. Do older adults who meet 2008 Physical Activity
Guidelines have better physical performance than those who do not meet? Jour Geriatr Phys
Ther. 2018. 41(3):180-185.
• NOTE! In the article title, only the first letter of the first word and proper nouns are
capitalized. The article title is not italicized. The journal name is abbreviated per
PubMed (available here: https://www.ncbi.nlm.nih.gov/nlmcatalog/journals) and is
in italics; the first letter of each word is capitalized. Please be sure to include all of
the following: Year. Issue (Volume): start page-end page. Do not include the DOI
unless the journal is an electronic journal.
Journal article (more than 6 authors):
Lusardi MM, Fritz S, Middleton A, et al. Determining the risk of falls in community-dwelling
older adults: A systematic review and meta-analysis using posttest probability. Jour Geriatr
Phys Ther. 2017. 40(1):1-36.
• Note the use of the first three authors followed by “et al.”
Journal article with no named author or group:
Centers for Disease Control and Prevention (CDC). QuickStats: Rate of nonfatal, medically
consulted fall injury episodes, by age group. MMWR Morb Mortal Wkly Rep. 2012. 61(4):81.
Electronic journal article with DOI (preferred):
Shokrvash B, Saeid A , Saeieh SE, Khasti MY, Salehi L. A psychometric property of the
Attitudes Toward Health Care Teamwork Scale among university students. Shiraz E-Med
J. 2019. 20(2):1-6. doi: 10.5812/semj.69726.
Electronic journal article without DOI:
Shokrvash B, Saeid A , Saeieh SE, Khasti MY, Salehi L. A psychometric property of the
Attitudes Toward Health Care Teamwork Scale among university students. Shiraz E-Med
J. 2019. 20(2):1-6. file:///C:/Users/rover/Downloads/semj-20-2-69726.pdf Accessed
January 10, 2019.
Entire Book:
Bonder BR & Dal Bello-Haas V. Functional Performance in Older Adults. 4th ed.
Philadelphia, PA: F.A. Davis; 2018.

41
• Note that in the book title the first letter of each major word is capitalized, and the
title is in italics. Second and subsequent editions must be specified, and the included
year must be the year that edition was published.
Book Chapter:
Schulte OJ, Stephans J, Ann J. Aging, dementia and disorders of cognition. In: Umphred DA,
ed. Umphred’s Neurological Rehabilitation. 6th ed. St. Louis, MO: Mosby; 2013:835-861.
• Note that in the chapter title only the first letters of the first word and proper nouns
are capitalized. The chapter title is not in italics. In the book title, the first letter of all
major words is capitalized, and the book title is in italics. Second and subsequent
editions must be specified, and the included year must be the year that edition was
published. Start and end pages must be included.
Electronic Book:
Moore GE, Durstine JL, Painter, PL. ACSM’s Exercise Management for Persons with
Chronic Diseases and Disability. Champaign, IL: Human Kinetics;
2016. https://us.humankinetics.com/products/ACSMs-Exercise-Management-for-Persons-
With-Chronic-Diseases-and-Disabilities-4th-Edition-eBook Accessed January 10, 2019.
Internet document:
National Council on Aging. Bingocize® Program Summary. https://www.ncoa.org/wp-
content/uploads/Bingocize-Program-Summary.pdf Accessed January 10, 2019.
7. Tables. Each table should be prepared double-spaced on a separate page at the end of the
manuscript document. Each table should have a brief title and should be numbered
consecutively in the order of their citation in the text. Any references cited within a table
must be numbered in sequence with the preceding text relative to the location at which the
table is to be inserted. The use of lines to demarcate columns and rows is recommended.
Numbers contained within cells should be centered, both left/right and top/bottom. Units of
measure must be specified in row or column headings.
8. Figure legend. Figure captions should be prepared double-spaced on a separate page.
9. Figures. Figures should be numbered consecutively in the order of their citation in the
text. Units of measure must be specified within the visual image (e.g., on the axes, etc.).
Sharp, crisp, camera-ready figures are required for high quality reproduction. Submit figures
in final form; acceptable file formats include: MS Office (DOC, PPT), PDF, jpeg, gif and tiff
files. All graphics and PDFs MUST be at least 300 dpi to assure quality printing. A signed
patient release form must be submitted for figures in which an individual is recognizable.
Color figures: The journal accepts color figures for publication that will enhance an article.
The price for the first color figure is $750. The charge for each additional color figure is
$150. Authors who submit color figures and decide not to pay for color reproduction in print,
can request that the figures be converted to black and white at no charge. Authors should
print a black and white copy of the color figures to ensure that all relevant visual information
is properly conveyed. All color figures can appear in color in the online version of the journal

42
at no charge (Note: this includes the online version on the journal website and Ovid, but not
the iPad edition currently.)
Supplemental Digital Content (SDC) (including Video Abstract for Accepted
manuscripts)
Authors may submit SDC via Editorial Manager to LWW journals that enhance their article’s
text to be considered for online posting. SDC may include standard media such as text
documents, graphs, audio, video, etc. For Systematic or Scoping Reviews, extensive, multi-
page tables should be submitted as a SDC file. On the Attach Files page of the submission
process, please select Supplemental Audio, Video, or Data for your uploaded file as the
Submission Item. If an article with SDC is accepted, our production staff will create a URL
with the SDC file. The URL will be placed in the call-out within the article. SDC files are
not copy-edited by LWW staff, they will be presented digitally exactly as submitted. For a
list of all available file types and detailed instructions, please
visit http://links.lww.com/A142.
SDC Call-outs in the Manuscript Text
Supplemental Digital Content must be cited consecutively in the text of the submitted
manuscript. Citations should include the type of material submitted (Audio, Figure, Table,
etc.), be clearly labeled as “Supplemental Digital Content,” include the sequential list
number, and provide a description of the supplemental content. All descriptive text should
be included in the call-out as it will not appear elsewhere in the article.
Example:
We performed many tests on the degrees of flexibility in the elbow (see Video, Supplemental
Digital Content 1, which demonstrates elbow flexibility) and found our results inconclusive.
List of Supplemental Digital Content
A listing of Supplemental Digital Content must be submitted at the end of the manuscript
file. Include the SDC number and file type of the Supplemental Digital Content. This text
will be removed by our production staff and not be published.
Example:
Supplemental Digital Content 1.wmv
SDC File Requirements
All acceptable file types are permissible up to 10 MBs. For audio or video files greater than
10 MBs, authors should first query the journal office for approval. For a list of all available
file types and detailed instructions, please visit http://links.lww.com/A142.
Submission Guidelines
All manuscripts must be submitted on-line through the Editorial Manager Web site
at http://www.editorialmanager.com/jgpt.
First-time users: Click the "Register" button from the main menu (on the upper banner) and
enter the requested information. On successful registration, you will be sent an e-mail
indicating your user name and password. Save a copy of this information for future reference.
Then log into the system as an author.

43
Return users: If you have received an e-mail from us with an assigned user ID and password
as an author or as a reviewer, do not register again. Just log in as an author. Once you have
an assigned ID and password, you do not have to re-register, even if your status changes (that
is, author, reviewer, or editor).
After you log in as an author, you can submit your manuscript according to the step-by-step
instructions on the Web page. You will receive an automated e-mail confirmation from the
Editorial Manager system after the manuscript is submitted; the e-mail will contain
instructions on how to track the progress of your manuscript through the system. Please
ensure that your email system, and that of each and every co-author, is set up to permit
receipt of automated emails from Editorial Manager. If you experience any problems,
please refer to the detailed "Author Tutorial" guide available on the Editorial Manager web
site. If you still need assistance, contact the Editor, Leslie Allison,
All submissions not initially rejected in the sequential Editor’s Reviews are peer-reviewed,
with recommendations made by an Associate Editor and final decisions made by the Editor-
in-Chief. Outcomes may include acceptance for publication, opportunity to revise and
resubmit, recommendations to submit to a different journal, or rejection of the manuscript.
When resubmission is requested, authors are expected to revise the manuscript as requested,
or to explain why they have chosen to do otherwise in an accompanying cover letter. More
than one resubmission/revision may be required. Requests for resubmission or revision do
not guarantee acceptance.
• Authors should revise and resubmit their manuscript within 12 weeks of receipt of
the Editor’s correspondence requesting revisions.
• Resubmitted revised manuscripts must include a revised cover letter that specifies, in
a point-by-point fashion, how the authors responded to the requests for changes,
including where in the text the change may be found. This cover letter should either
replace or follow the original cover letter.
Submissions should include:
• Cover letter,
o The cover letter should include (1) the manuscript category, (2) a statement
that all authors have substantially contributed to the work, (3) a statement that
the work is not under review elsewhere and has not been previously published,
and (4) the complete contact information for the corresponding author
(address, phone, fax, email).
• Standardized Reporting Guideline Checklist with manuscript page numbers,
• Title page,
• Abstract with key words,
• Complete manuscript (including files for figures and graphics), and
• Signed Copyright Release form each author.
After Acceptance
Page proofs and corrections: Corresponding authors will receive electronic page proofs to
check the copyedited and typeset article before publication. Portable document format (PDF)
files of the typeset pages and support documents (e.g., reprint order form) will be sent to the

44
corresponding author by e-mail. Complete instructions will be provided with the e-mail for
downloading and printing the files and for faxing the corrected page proofs to the publisher. It
is the author’s responsibility to ensure that there are no errors in the proofs. Changes that
have been made to conform to journal style will stand if they do not alter the authors'
meaning. Only the most critical changes to the accuracy of the content will be made. Changes
that are stylistic or are a reworking of previously accepted material will be disallowed. The
publisher reserves the right to deny any changes that do not affect the accuracy of the content.
Compliance with NIH and Other Research Funding Agency Accessibility
Requirements
A number of research funding agencies now require or request authors to submit the post-
print (the article after peer review and acceptance but not the final published article) to a
repository that is accessible online by all without charge. As a service to our authors, LWW
will identify to the National Library of Medicine (NLM) articles that require deposit and will
transmit the post-print of an article based on research funded in whole or in part by the
National Institutes of Health, Wellcome Trust, Howard Hughes Medical Institute, or other
funding agencies to PubMed Central.
Open Access
Authors of accepted peer-reviewed articles have the choice to pay a fee to allow perpetual
unrestricted online access to their published article to readers globally, immediately upon
publication. Authors may take advantage of the open access option at the point of acceptance
to ensure that this choice has no influence on the peer review and acceptance process. These
articles are subject to the journal's standard peer-review process and will be accepted or
rejected based on their own merit.
The article processing charge (APC) is charged on acceptance of the article and should be
paid within 30 days by the author, funding agency or institution. Payment must be processed
for the article to be published open access. For a list of journals and pricing please visit
our Wolters Kluwer Open Health Journals page.
Authors retain copyright
Authors retain their copyright for all articles they opt to publish open access. Authors grant
Wolters Kluwer an exclusive license to publish the article and the article is made available
under the terms of a Creative Commons user license.
Creative Commons license
Open access articles are freely available to read, download and share from the time of
publication under the terms of the Creative Commons License Attribution-NonCommerical
No Derivative (CC BY-NC-ND) license. This license does not permit reuse for any
commercial purposes nor does it cover the reuse or modification of individual elements of
the work (such as figures, tables, etc.) in the creation of derivative works without specific
permission.
Compliance with funder mandated open access policies
An author whose work is funded by an organization that mandates the use of the Creative
Commons Attribution (CC BY) license is able to meet that requirement through the available
open access license for approved funders. Information about the approved funders can be
found here: http://www.wkopenhealth.com/inst-fund.php.