Upper limit of normal serum alanine aminotransferase levels in Japanese subjects
12
Original Article Upper limit of normal serum alanine aminotransferase levels in Japanese subjects Kenichi Tanaka, 1,2 Hideyuki Hyogo, 4 Masafumi Ono, 5 Hirokazu Takahashi, 1,2 Yoichiro Kitajima, 1,3 Naofumi Ono, 1 Takahisa Eguchi, 1 Kazuma Fujimoto, 2 Kazuaki Chayama, 4 Toshiji Saibara, 5 Keizo Anzai, 2 Yuichiro Eguchi 3 and the Japan Study Group of Non-alcoholic Fatty Liver Disease (JSG-NAFLD)* 1 Clinical Gastroenterology, Eguchi Hospital, 2 Department of Internal Medicine, Saga Medical School, 3 Division of Hepatology, Saga Medical School, Saga, 4 Department of Medicine and Molecular Sciences, Graduate School of Biomedical Sciences, Hiroshima University, Hiroshima, and 5 Department of Gastroenterology and Hepatology, Kochi Medical School, Nankoku, Japan Aim: Serum alanine aminotransferase (ALT) is important for screening, diagnosis and management of chronic liver dis- eases. The incidence of non-alcoholic fatty liver disease (NAFLD)/non-alcoholic steatohepatitis (NASH), which is con- sidered a hepatic manifestation of lifestyle-related diseases, is increasing worldwide. However, the upper limit of the normal ALT level has not yet been established because of not excluding many lifestyle-related diseases. The aim of this study was to evaluate the upper limit of normal serum ALT levels in Japanese subjects. Methods: We analyzed the serum ALT levels of 11 404 Japa- nese subjects negative for hepatitis B surface antigen and hepatitis C virus antibody, and who received health check- ups. Lifestyle factors related to ALT levels were determined by multivariate analysis. Subjects with all factors identified by multivariate analysis within the normal range were defined as “healthy” subjects. The 90th percentile of ALT levels in healthy subjects was defined as the upper limit of normal ALT. Results: Whereas alcohol intake was not a significant factor, the following were independently associated with ALT con- centration by multivariate analysis: sex; age; body mass index; waist circumference; concentrations of total choles- terol, high-density lipoprotein cholesterol, triglycerides and fasting blood glucose; and fatty liver on ultrasonography. Healthy subjects consisted of 1462 (21.2%) men and 2046 (45.4%) women, and the 90th percentiles of the ALT levels in the two groups were 29 and 23 IU/L, respectively. Conclusion: The upper limits of normal ALT when consider- ing lifestyle factors in Japanese subjects were 29 IU/L in men and 23 IU/L in women. Key words: fatty liver, health check-up, lifestyle, non-alcoholic fatty liver disease, non-alcoholic steatohepatitis, normal range INTRODUCTION S ERUM ALANINE AMINOTRANSFERASE (ALT) levels reflect damage to liver cells, and assays of serum ALT are used in daily practice to screen, diagnose and follow-up subjects with liver diseases. 1,2 Chronic liver diseases associated with increased serum ALT levels include viral hepatitis, alcoholic hepatitis, non- alcoholic fatty liver disease (NAFLD)/non-alcoholic steatohepatitis (NASH), autoimmune hepatitis, primary biliary cirrhosis and congenital disorders. In Japan, viral hepatitis has been the most frequent cause of chronic hepatitis, liver cirrhosis and liver cancer. 3,4 Recently, the prevalence of hepatitis B surface antigen (HBsAg) and hepatitis C antibody (HCVAb) negative chronic hepati- tis and liver cirrhosis has increased. 5–7 In particular, NAFLD/NASH, a condition closely related to lifestyle, has been increasing in Japan as well as worldwide. 8–10 Because elevated liver enzyme levels may be the only indicator of asymptomatic mild liver diseases, 11,12 a proper diagnosis of NAFLD/NASH requires a Correspondence: Dr Hirokazu Takahashi, Department of Internal Medicine, Saga Medical School, 5-1-1 Nabeshima, Saga 849-8501, Japan. Email: [email protected] *Japan Study Group of Non-alcoholic Fatty Liver Disease (JSG-NAFLD): Yasuaki Suzuki, Norio Aoki, Masato Yoneda, Kento Imajyo, Masafumi Ono, Yoshio Sumida, Hideki Fujii, Hideyuki Hyogo, Takumi Kawaguchi, Yuichiro Eguchi and Takeshi Okanoue. Conflicts of interest: None. Received 12 August 2013; revision 14 November 2013; accepted 16 December 2013. Hepatology Research 2014; 44: 1196–1207 doi: 10.1111/hepr.12293 © 2013 The Japan Society of Hepatology 1196
Transcript of Upper limit of normal serum alanine aminotransferase levels in Japanese subjects

Original Article
Upper limit of normal serum alanine aminotransferaselevels in Japanese subjects
Kenichi Tanaka,1,2 Hideyuki Hyogo,4 Masafumi Ono,5 Hirokazu Takahashi,1,2
Yoichiro Kitajima,1,3 Naofumi Ono,1 Takahisa Eguchi,1 Kazuma Fujimoto,2
Kazuaki Chayama,4 Toshiji Saibara,5 Keizo Anzai,2 Yuichiro Eguchi3 andthe Japan Study Group of Non-alcoholic Fatty Liver Disease (JSG-NAFLD)*1Clinical Gastroenterology, Eguchi Hospital, 2Department of Internal Medicine, Saga Medical School, 3Division ofHepatology, Saga Medical School, Saga, 4Department of Medicine and Molecular Sciences, Graduate School ofBiomedical Sciences, Hiroshima University, Hiroshima, and 5Department of Gastroenterology and Hepatology,Kochi Medical School, Nankoku, Japan
Aim: Serum alanine aminotransferase (ALT) is important forscreening, diagnosis and management of chronic liver dis-eases. The incidence of non-alcoholic fatty liver disease(NAFLD)/non-alcoholic steatohepatitis (NASH), which is con-sidered a hepatic manifestation of lifestyle-related diseases,is increasing worldwide. However, the upper limit of thenormal ALT level has not yet been established because of notexcluding many lifestyle-related diseases. The aim of thisstudy was to evaluate the upper limit of normal serum ALTlevels in Japanese subjects.
Methods: We analyzed the serum ALT levels of 11 404 Japa-nese subjects negative for hepatitis B surface antigen andhepatitis C virus antibody, and who received health check-ups. Lifestyle factors related to ALT levels were determined bymultivariate analysis. Subjects with all factors identified bymultivariate analysis within the normal range were defined as“healthy” subjects. The 90th percentile of ALT levels in healthysubjects was defined as the upper limit of normal ALT.
Results: Whereas alcohol intake was not a significant factor,the following were independently associated with ALT con-centration by multivariate analysis: sex; age; body massindex; waist circumference; concentrations of total choles-terol, high-density lipoprotein cholesterol, triglycerides andfasting blood glucose; and fatty liver on ultrasonography.Healthy subjects consisted of 1462 (21.2%) men and 2046(45.4%) women, and the 90th percentiles of the ALT levels inthe two groups were 29 and 23 IU/L, respectively.
Conclusion: The upper limits of normal ALT when consider-ing lifestyle factors in Japanese subjects were 29 IU/L in menand 23 IU/L in women.
Key words: fatty liver, health check-up, lifestyle,non-alcoholic fatty liver disease, non-alcoholicsteatohepatitis, normal range
INTRODUCTION
SERUM ALANINE AMINOTRANSFERASE (ALT)levels reflect damage to liver cells, and assays of
serum ALT are used in daily practice to screen, diagnose
and follow-up subjects with liver diseases.1,2 Chronicliver diseases associated with increased serum ALTlevels include viral hepatitis, alcoholic hepatitis, non-alcoholic fatty liver disease (NAFLD)/non-alcoholicsteatohepatitis (NASH), autoimmune hepatitis, primarybiliary cirrhosis and congenital disorders. In Japan, viralhepatitis has been the most frequent cause of chronichepatitis, liver cirrhosis and liver cancer.3,4 Recently, theprevalence of hepatitis B surface antigen (HBsAg) andhepatitis C antibody (HCVAb) negative chronic hepati-tis and liver cirrhosis has increased.5–7 In particular,NAFLD/NASH, a condition closely related to lifestyle,has been increasing in Japan as well as worldwide.8–10
Because elevated liver enzyme levels may be theonly indicator of asymptomatic mild liver diseases,11,12
a proper diagnosis of NAFLD/NASH requires a
Correspondence: Dr Hirokazu Takahashi, Department of InternalMedicine, Saga Medical School, 5-1-1 Nabeshima, Saga 849-8501,Japan. Email: [email protected]*Japan Study Group of Non-alcoholic Fatty Liver Disease(JSG-NAFLD): Yasuaki Suzuki, Norio Aoki, Masato Yoneda,Kento Imajyo, Masafumi Ono, Yoshio Sumida, Hideki Fujii,Hideyuki Hyogo, Takumi Kawaguchi, Yuichiro Eguchi andTakeshi Okanoue.Conflicts of interest: None.Received 12 August 2013; revision 14 November 2013; accepted 16December 2013.
bs_bs_banner
Hepatology Research 2014; 44: 1196–1207 doi: 10.1111/hepr.12293
© 2013 The Japan Society of Hepatology1196

determination of the normal range and upper limit ofALT. Although the upper limit of normal (ULN) ALT hasbeen re-evaluated in various populations, it has not yetbeen evaluated in Japan.1,13,14 Therefore, we assessed theULN of serum ALT levels in a large Japanese population.
METHODS
Study population
THE CROSS-SECTIONAL STUDY population con-sisted of 15 785 subjects who received general
health check-ups from 2009 to 2010 at three healthcenters in Japan: Eguchi Hospital Health Center in SagaPrefecture, Kawamura Clinic Heath Center in Hiro-shima Prefecture, and Kochi Medical School Hospitalin Kochi Prefecture. The general medical check-upincluded physical and physiological examinations,abdominal ultrasonography and a blood screening test.We excluded 379 subjects positive for HBsAg or HCVAbor those taking potentially hepatotoxic drugs. We alsoexcluded 1108 subjects being treated for lifestyle-relateddiseases such as hypertension, dyslipidemia and diabe-tes mellitus; and 2984 subjects with missing data. Thefinal subject population consisted of 11 404 individu-als; 6894 men and 4510 women.
All subjects provided written informed consent foranonymous use of their data in this epidemiologicalstudy. The study design was approved by the relevantinstitutional review board (IRB) at each institution(Saga Medical School IRB for Eguchi Hospital [approvalno. 2011-2006-04]; Hiroshima University IRB forKawamura Clinic Health Center [approval no. Eki-241];and Kochi Medical School IRB for Kochi Medical SchoolHospital [approval no. 23–74]). The study was con-ducted in accordance with the Declaration of Helsinki.
Physical examination andserum biochemistryBodyweight and height were measured, and body massindex (BMI) was then calculated. Waist circumference(WC) was measured at the umbilical level. The normalrange of alcohol intake in the non-alcoholic popula-tion was defined as less than 20 g of alcohol per day.Venous blood samples were taken from all subjects fol-lowing a 12-h overnight fast, and aspartate amino-transferase (AST), ALT, !-glutamyltransferase (GGT),total cholesterol (TC), high-density lipoprotein (HDL-C), triglycerides (TG) and fasting plasma glucose(FPG) concentrations were measured using standardtechniques.
Definition of fatty liver and borderlinefatty liverAll subjects underwent abdominal ultrasonography forassessment of fatty liver, which was diagnosed accordingto the criteria of the American Gastroenterology Asso-ciation.15 The presence of steatosis was recognized as amarked increase in hepatic echogenicity, poor penetra-tion of the posterior segment of the right lobe of theliver, and poor or no visualization of the hepatic vesselsand diaphragm. The severity of the hepatic steatosis wasnot graded due to differences in ultrasonography equip-ment and examiners. The liver was considered normal ifthe hepatic parenchyma was homogeneous with noacoustic attenuation, the portal veins were visible, thediaphragm was well-visualized, and the echogenicitywas similar to or slightly higher than that of the renalcortex.
Ultrasonography was performed using a LOGIQ 7with a 4-MHz convex array transducer (GE Healthcare,Chalfont St Giles, UK) at Eguchi Hospital, a ProSoundAlpha 10 with a 3.5-MHz convex array transducer(Hitachi Aloka Medical, Tokyo, Japan) at KawamuraClinic Health Center, and a Xario with a 3.5-MHzconvex array transducer (Toshiba Medical Systems,Tokyo, Japan) at Kochi Medical School. All examina-tions were performed by experienced sonographers,trained by gastroenterologists, and with more than5 years’ experience. The technical parameters wereadjusted for each subject using standard protocols, aspreviously described.5 The certified gastroenterologistsindependently reviewed the images and evaluated thelivers for the presence of steatosis.
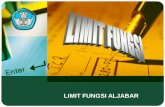
Study designThe flow chart of the study design is shown in Figure 1.Multivariate analysis was performed to identify factorscontributing to increased ALT levels. Factors consideredincluded age; gender; BMI; WC; AST, ALT, GGT, TC,HDL-C, TG and FPG levels; alcohol consumption; andfatty liver. We defined “healthy” subjects as those withfactors identified on multivariate analysis within normalranges. The 90th and 95th percentiles of the serum ALTlevels were calculated separately for men and women.
Statistical analysisMeans and standard deviations were calculated for allcontinuous variables and Student’s t-test was performedfor parametric analysis. The Mann–Whitney U-test,Kruskal–Wallis test and post-hoc test (Bonferroniadjustment) were performed for non-parametric analy-
Hepatology Research 2014; 44: 1196–1207 Normal serum ALT levels in Japan 1197
© 2013 The Japan Society of Hepatology

sis. Multivariate analysis using a generalized linearmodel was performed to identify the factors contribut-ing to ALT levels. In the generalized linear model, ALTlevel was assumed to fit a Poisson distribution and con-verted to a logarithm by the link function. Differenceswere considered significant at P < 0.05. All analyses wereperformed using IBM SPSS Statistics version 21 (SPSS,Chicago, IL, USA).
RESULTS
Baseline characteristics
THE CLINICAL CHARACTERISTICS of the subjects inthis study are summarized in Table 1. The study
population consisted of 6894 men (60.5%) with a meanage of 50.6 years (range, 19–87) and 4510 women(39.5%) with a mean age of 48.8 years (range, 21–82).Mean ALT levels were 27.0 1 19.7 IU/L in men and17.6 1 11.4 IU/L in women. Habitual alcohol intakewas observed in 47.7% of men and 10.5% of women(P < 0.001), and the prevalence of fatty liver was signifi-cantly higher in men than in women (P < 0.001).
Factors associated with elevated serum ALTContinuous variables, (excluding HDL-C and age) werecategorized by the upper limit of their normal rangesusing a generalized linear model. HDL-C was catego-rized according to the lower limit of the normal rangeand age was categorized as less than 50 years or 50 yearsor more because normal ALT levels have been reportedto change between 40 and 50 years of age.16 We alsoanalyzed the data using cut-offs of 40, 45 and 55 years.We found that any cut-offs of age; sex; BMI; WC; levelsof TC, HDL-C, TG and FPG; and fatty liver, were factorssignificantly contributing to ALT levels (P < 0.001),whereas systolic blood pressure (sBP) and alcohol
15785 subjects involved in health check up
11404 subjects enrolled in study
Multivariate Analysis
“Healthy” subjects(N=3508)
90% tile of serum ALT levelsin “healthy” male (N=1462)
90% tile of serum ALT levelsin “healthy” female (N=2046)
“Non-healthy” subjects(N=7896)
Excluding : HCV-Ab or HBs-Ag positive (N=329),treatment for lifestyle related disease (N=1018),taking any hepatotoxic agents (N=50) and datadeficient (N=2984)
Figure 1 Flowchart of the study design. ALT, alanine amino-transferase; HCVAb, hepatitis C virus antibody; HBsAg, hepa-titis B virus antigen.
Table 1 Characteristics of men and women in the overall population
Variables Men (n = 6894) Women (n = 4510)
Age (years) 50.6 1 9.8 (19–87) 48.8 1 9.4 (21–82)BH (cm) 170 1 6.0 (146–195) 157 1 5.4 (136–175)BW (kg) 68.1 1 9.9 (38.0–143.0) 53.5 1 8.3 (32.7–116)BMI (kg/m2) 23.6 1 3.0 (14.8–47.2) 21.8 1 3.3 (14.2–51.3)WC (cm) 84.8 1 3.0 (49.4–137) 79.0 1 9.1 (57.6–142)sBP (mmHg) 119 1 16 (73–187) 109 1 17 (69–183)dBP (mmHg) 73 1 12 (42–117) 67 1 12 (31–115)AST (IU/L) 23.5 1 12.4 (9–185) 20.1 1 7.71 (9–192)ALT (IU/L) 27.0 1 19.7 (4–246) 17.6 1 11.4 (3–215)GGT (IU/L) 57.4 1 66.1 (8–1241) 24.7 1 28.3 (5–719)TC (mg/dL) 201 1 42.0 (93–392) 205 1 43.7 (90–366)HDL-C (mg/dl) 57.5 1 15.3 (9–223) 69.9 1 15.7 (31–156)TG (mg/dL) 138 1 100 (20–1737) 87.2 1 58.2 (22–1197)FPG (mg/dL) 105 1 19.6 (52–378) 95.5 1 14.2 (42–284)Alcohol 320 g/day (%) 47.7% (n = 3289) 10.5% (n = 475)Fatty liver (+) 37.8% (n = 2608) 14.3% (n = 646)
Data are means 1 standard deviation (range).ALT, alanine aminotransferase; AST, aspartate aminotransferase; BMI, body mass index; BH, body height; BW, bodyweight; FPG, fastingplasma glucose; GGT, !-glutamyltransferase; HDL-C, high-density lipoprotein cholesterol; TC, total cholesterol; TG, triglycerides; sBP,systolic blood pressure; dBP, diastolic blood pressure; WC, waist circumference.
1198 K. Tanaka et al. Hepatology Research 2014; 44: 1196–1207
© 2013 The Japan Society of Hepatology

intake were not significant factors. Fatty liver hadthe greatest influence on ALT levels (odds ratio[OR] = 1.340) (Table 2). The model with sBP of130 mmHg or more alternative to 140 mmHg was alsoanalyzed and the result was not significant (P = 0.743).Because diastolic blood pressure (dBP) was a confound-ing factor with sBP, dBP was not used for the modelshown in Table 2. In the model with dBP of 85 mmHgor more alternative to sBP, dBP of 85 mmHg or morewas not a significant factor for ALT levels (P = 0.161).
Characteristics of the healthy populationNormal ranges were less than 25 kg/m2 for BMI; lessthan 85 cm for WC in men and less than 90 cm
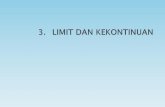
in women; less than 110 mg/dL for FPG; less than220 mg/dL for TC; 40 mg/dL or more for HDL-C; lessthan 150 mg/dL for TG; and the absence of fatty liver.The subjects within the normal range for all of thesefactors, as identified by multivariate analysis, weredefined as healthy subjects and their characteristics areshown in Table 3. We found that 1462 of the 6894 men(21.2%) and 2046 of the 4510 women (45.4%) werehealthy. Figure 2 shows the distribution of the ALTlevels in men and women. The ALT levels in the healthysubjects showed a non-normal distribution in both menand women. The mean and median ALT levels inhealthy men were 19.4 1 10.5 and 17 IU/L, respectively,whereas the mean and median ALT levels in all menwere 27.0 1 19.7 and 22 IU/L, respectively. The meanand median ALT levels were 15.0 1 7.6 and 13 IU/L,respectively, in healthy women and 17.6 1 11.4 and15 IU/L, respectively, in all women.
ULN of serum ALT levelsTable 4 compares ALT levels in healthy subjects andthose having one or more factors in an abnormal range,as shown by multivariate analysis (Table 2). In “non-healthy” men, the mean and median ALT levels were29.1 1 21.0 and 24 IU/L, respectively, significantlyhigher than in healthy men (P < 0.001). In non-healthywomen, the mean and median ALT levels were19.7 1 13.5 and 16 IU/L, respectively, significantlyhigher than in healthy women (P < 0.001). Because ALTlevels showed a non-normal distribution in bothhealthy men and women, the higher percentile valuecould be statistically considered the ULN of ALT. Wedefined the ULN of ALT as the 90th percentile, 29 IU/Lin men and 23 IU/L in women. The 95th percentile ofALT, which can also be used to determine ULN, was36 IU/L in men and 27 IU/L in women. To ensure that
Table 2 Factors associated with ALT level
Variables Oddsratio
95% CI P-value
Age (350 years) 0.942 0.934–0.950 <0.001Sex (male) 1.276 1.263–1.288 <0.001BMI (325 kg/m2) 1.154 1.141–1.166 <0.001WC (385 cm in men
and 95 cm in women)1.113 1.101–1.125 <0.001
sBP (3140 mmHg) 1.005 0.992–1.018 0.446TC (3220 mg/dL) 1.106 1.097–1.115 <0.001HDL-C (<40 mg/dl) 1.116 1.099–1.134 <0.001TG (3150 mg/dL) 1.152 1.141–1.163 <0.001FPG (3110 mg/dL) 1.166 1.149–1.183 <0.001Alcohol (320 g/day) 1.000 0.991–1.009 0.975Fatty Liver (+) 1.340 1.327–1.352 <0.001
ALT, alanine aminotransferase; AST, aspartate aminotransferase;BMI, body mass index; BH, body height; BW, bodyweight; CI,confidence interval; FPG, fasting plasma glucose; GGT,!-glutamyltransferase; HDL-C, high-density lipoproteincholesterol; TC, total cholesterol; TG, triglycerides; sBP, systolicblood pressure; dBP, diastolic blood pressure; WC, waistcircumference.
Table 3 Characteristics of the “healthy” population
Variables “Healthy” men “Healthy” women
n = 1462 (21.2%) n = 2046 (45.4%)Age (years) 47.2 1 10.4 (19–87) 45.3 1 8.71 (21–82)BMI (kg/m2) 21.2 1 1.80 (15.3–24.9) 20.3 1 1.99 (14.3–24.9)WC (cm) 77.4 1 4.91 (49.4–84.8) 75.0 1 6.44 (58.2–89.8)TC (mg/dL) 185 1 21.0 (122–219) 187 1 21.2 (105–219)HDL-C (mg/dL) 62.8 1 13.2 (40–124) 70.1 1 13.0 (40–116)TG (mg/dL) 81.3 1 26.5 (26–149) 65.9 1 24.8 (22–148)FPG (mg/dL) 96.0 1 6.86 (71–109) 91.6 1 7.08 (67–109)
Data are means 1 standard deviation (range).BMI, body mass index; FPG, fasting plasma glucose; HDL-C, high-density lipoprotein cholesterol; TC, total cholesterol; TG, triglycerides;WC, waist circumference.
Hepatology Research 2014; 44: 1196–1207 Normal serum ALT levels in Japan 1199
© 2013 The Japan Society of Hepatology

differences related to the ultrasonography equipmentand institution did not affect the results, we comparedthe median ALT level in healthy subjects and the ULN ofALT among the institutions. The median and 90th per-centile of ALT was not significantly different among theinstitutions: 17 and 30 in men, respectively, and 13 and24 in women, respectively, from Eguchi Hospital HealthCenter; 17 and 28 in men, respectively, and 13 and 23in women, respectively, from Kawamura Clinic HeathCenter; and 18 and 34.6 in men, respectively, and 13and 21 in women, respectively, from Kochi MedicalSchool Hospital (P = 0.074 in men and 0.143 inwomen).
Figures 3 and 4 show the histograms and boxplots ofthe ALT levels in healthy subjects divided into threegroups by age: 40 years and less, 41–60 years, and 61years or more. The distribution of ALT was non-normalin all three groups. The 90th percentile was higher inelderly than in younger men and women (Fig. 3). Inmen of these three age groups, the median ALT levels
were 17, 17 and 17 IU/L, respectively, with no signifi-cant differences. In women of these three age groups, themedian ALT levels were 12, 13 and 17 IU/L, respectively,and were significantly higher in women aged 61 years ormore than in those aged 40 years or less (P < 0.001) and41–60 years (P < 0.001).
Comparison of the characteristics amongthe age-specific groups in the healthypopulationWe compared the characteristics among the age-specificgroups in the healthy population (Table 5). In bothmen and women, several lifestyle-related factors andliver function tests were significantly different amongthe groups. In men, WC, sBP, dBP, AST, ALT, GGT, TC,HDL and FPG were higher in subjects more than 61years of age than in younger groups, and the number ofsubjects with alcohol intake of more than 20 g/day washigher in 41–60-year-old subjects than in 18"40-year-
(n)
400 Male
300
200
100
00 20 40 60
ALT level (IU/L)80 100
(n)400 Female
300
200
100
00 20 40 60
ALT level (IU/L)80 100
Figure 2 Frequency distribution ofserum alanine aminotransferase (ALT)levels. “Healthy” subjects (1462 menand 2046 women) are shown as whitebars and overall subjects as black bars.ALT levels were non-normally distrib-uted in both overall and healthysubjects.
Table 4 Serum ALT levels in “healthy” and “non-healthy” populations
Men (n = 6894) Women (n = 4510)
“Healthy”(n = 1462)
“Non-healthy”(n = 5432)
“Healthy”(n = 2046)
“Non-healthy”(n = 2464)
Mean 1 SD (IU/L) 19.4 1 10.5 * 29.1 1 21.0 15.0 1 7.6 * 19.7 1 13.5Median (IU/L) 17 * 24 13 * 1690th percentile (IU/L) 29 — 23 —95th percentile (IU/L) 36 27
*P < 0.05 vs “healthy” by Student’s t-test or Mann–Whitney U-test.SD, standard deviation.
1200 K. Tanaka et al. Hepatology Research 2014; 44: 1196–1207
© 2013 The Japan Society of Hepatology

old subjects. In women, all parameters were significantlydifferent among the groups.
Relationship between alcohol intake andALT levelAlthough multivariate analysis showed that alcoholintake did not contribute significantly to ALT levels,alcohol intake causes liver injury, fatty liver and livercirrhosis.17–19 Therefore, we compared ALT levels inhealthy subjects with an alcohol intake of 20 g or
less and more than 20 g/day, but found no significantdifferences in either men (P = 0.239) or women(P = 0.186) (Table 6).
Interaction between blood pressure andALT levels in the healthy populationWhile the relationship between blood pressure and ALTlevels was not significant in the multivariate analysis inoverall subjects, we performed a comparison analysis tovalidate the interaction of blood pressure with ALT
100
(a) Male
50
00 20 40
ALT level (IU/L)60
n=499
90% tile: 29 IU/L
18-40 years
(n)
100
50
00 20 40
ALT level (IU/L)60
n=842
90% tile: 29 IU/L
41-60 years
(n)
100
50
00 20 40
ALT level (IU/L)60
n=121
90% tile: 35 IU/L
Over 61 years
(n)
150
100
(b) Female
50
0
0 20 40
ALT level (IU/L)
60
n=776
90% tile: 20 IU/L
18-40 years
(n)
150
100
50
0
0 20 40
ALT level (IU/L)
60
n=1199
90% tile: 24 IU/L
41-60 years
(n)
150
100
50
0
0 20 40
ALT level (IU/L)
60
n=71
90% tile: 33 IU/L
Over 61 years
(n)
Figure 3 Age-specific frequency distribution and 90th percentiles of the serum alanine aminotransferase (ALT) levels in “healthy”(a) men and (b) women. Median ALT levels in subjects aged 19–40, 41–60 and 61 years or more were 17, 17 and 17 IU/L,respectively, in men and 12, 13 and 17 IU/L, respectively, in women.
Hepatology Research 2014; 44: 1196–1207 Normal serum ALT levels in Japan 1201
© 2013 The Japan Society of Hepatology

levels in the healthy population (Table 7). ALT levelswere not significantly different with respect to the sBP/dBP in men. Interestingly, ALT levels were significantlyhigher in female subjects with sBP of more than140 mmHg than in women with sBP of less than140 mmHg, and also significantly higher in womenwith sBP of more than 130 mmHg than in those withsBP of less than 130 mmHg.
Characteristics of the healthy populationwith ALT levels under ULNThe characteristics of the healthy population with ALTlevels under the ULN (29 IU/L in men and 23 IU/L inwomen) were analyzed and compared to subjects withALT levels over the ULN (Table 8). In men, sBP and dBPwere higher in subjects with normal ALT levels thanwith in those with abnormal ALT levels. Also, thenumber of subjects with sBP of more than 130 mmHgor with dBP of more than 85 mmHg was higher insubjects with abnormal ALT levels than in those withnormal ALT levels (sBP, 21.8% vs 12.8%, respectively,P = 0.003; and sBP, 14.8% vs 7.2%, respectively,P = 0.004, data not shown). Female subjects with abnor-mal ALT levels had significantly higher TC and TG levelsthan female subjects with normal ALT levels.
Factors associated with ALT levels inthe healthy populationWe performed multivariate analysis using a generalizedlinear model (Table 9) to clarify the factors related toALT levels in the healthy population. Age was an inde-pendent factor affecting the ALT levels in both men andwomen. Interestingly, dBP in men and sBP and dBP in
women were significant factors. Also, while TG levels inthe healthy population were within the normal range,TG was a significant factor in both men and women.
DISCUSSION
TO OUR KNOWLEDGE, this is the first study in Japa-nese subjects to examine the ULN of ALT relative to
lifestyle factors. The main advantage of this study was itslarge sample size. Also, the definition of healthy subjectswas based not only on the results of the blood testsbut also on the alcohol consumption, as determinedby careful interviews, and fatty liver diagnosed byultrasound. This strict definition of healthy subjectsenhanced the reliability of our determined ULN for ALT.Multiple regression analysis showed that, of thelifestyle-related factors, fatty liver had the greatest effecton ALT levels, followed by TG and BMI. Abnormalvalues of these independent factors may also indicateelevated ALT.
We defined the ULN of ALT as the 90th percentilein healthy subjects, 29 IU/L in men and 23 IU/L inwomen. ALT levels were non-normally distributed inboth the overall population and in healthy subjects.Therefore, the use of the 90th percentile was regarded asmore appropriate for defining the ULN of ALT than theupper limit of the 95% confidence interval.20,21 We alsodetermined the 95th percentiles of ALT levels in healthysubjects: 36 IU/L in men and 27 IU/L in women.Although both the overall and healthy subject popula-tions were strictly selected, both populations includedsubjects with extreme values or outliers. These subjectscould have been eliminated by outlier exclusion, but
Male
17 IU/L 17 IU/L 17 IU/L40
30
20
10
019-40 41-60
Age (years)
seru
m A
LT le
vels
(IU
/L)
Over 61
Female
12 IU/L
* *
*
13 IU/L17 IU/L
40
30
20
10
019-40 41-60
Age (years)
seru
m A
LT le
vels
(IU
/L)
Over 61
Figure 4 Boxplots and comparisons ofserum alanine aminotransferase (ALT)levels among the age groups in the“healthy” population. Serum ALT levelwas not significantly different amongthe three age groups in men, but signifi-cantly increased with age in women.The line and error bars in each boxrepresent the median and quantiledeviation, respectively. *P < 0.001 bypost-hoc test.
1202 K. Tanaka et al. Hepatology Research 2014; 44: 1196–1207
© 2013 The Japan Society of Hepatology

this would have introduced possible arbitrariness intoour analysis. Also, the ULN should be sufficiently sen-sitive for screening examinations; therefore, we adoptedthe 90th percentile of ALT as the ULN.
Recently, several reports have evaluated the ULN ofALT. A study in Italy, involving 6835 HCV negativeblood donors, found that BMI, dyslipidemia and carbo-hydrate metabolism were independent contributors to
Table 5 Characteristics of the “healthy” population in age-specific groups
Male 18–40 years (n = 499) 41–60 years (n = 842) 361 years (n = 121)
Age (years) 35.9 1 3.9 (19–40) 51.0 1 5.6 (41–60)a 66.7 1 4.6 (61–87)b,c
BMI (kg/m2) 21.1 1 1.9 (16.1–24.9) 21.3 1 1.8 (15.3–24.9) 21.2 1 1.6 (17.7–24.4)WC (cm) 76.3 1 5.1 (61.6–84.8) 78.0 1 4.8 (49.4–84.8)a 78.6 1 4.2 (67.1–84.5)b
sBP (mmHg) 109.6 1 10.6 (83–147) 114.8 1 15.8 (73–169)a 124.3 1 18.7 (83–168)b,c
dBP (mmHg) 64.9 1 8.8 (44–99) 70.0 1 11.6 (44–115)a 71.8 1 12.8 (46–108)b
AST (IU/L) 19.6 1 5.8 (11–68) 20.8 1 7.8 (11–166)a 25.2 1 17.8 (10–185)b,c
ALT (IU/L) 19.1 1 8.7 (5–80) 19.0 1 9.3 (5–119) 22.7 1 20.2 (7–179)GGT (IU/L) 31.1 1 24.1 (11–191) 38.6 1 32.9 (10–333)a 45.6 1 51.0 (12–379)b
TC (mg/dL) 181.2 1 21.9 (122–219) 187.9 1 20.1 (123–219) 185.9 1 20.5 (140–219)b
HDL-C (mg/dL) 60.3 1 11.5 (40–106) 63.9 1 13.9 (40–124)a 65.2 1 13.1 (41–99)b
TG (mg/dL) 80.2 1 26.4 (27–149) 82.2 1 26.5 (26–149) 79.6 1 26.7 (29–144)FPG (mg/dL) 95.2 1 6.5 (71–109) 96.3 1 7.0 (73–109)a 97.8 1 7.2 (79–109)b
Alcohol 320 g/day (%) 33.5% (n = 167) 47.6% (n = 401)a 40.5% (n = 49)
Female 18–40 years (n = 776) 41–60 years (n = 1199) 361 years (n = 71)
Age (years) 36.7 1 3.6 (21–40) 49.6 1 5.3 (41–60)a 65.9 1 4.7 (61–82)b,c
BMI (kg/m2) 20.0 1 1.9 (14.8–25.0) 20.6 1 2.0 (14.3–25.0)a 20.6 1 2.0 (16.3–24.8)c
WC (cm) 73.2 1 6.0 (58.5–89.7) 75.8 1 6.4 (58.2–89.8)a 78.4 1 7.3 (61.0–89.6)b,c
sBP (mmHg) 100.8 1 12.3 (75–153) 106.9 1 15.6 (73–161)a 114.4 1 17.2 (76–152)b,c
dBP (mmHg) 62.3 1 9.8 (40–98) 65.1 1 11.2 (31–107)a 66.0 1 12.0 (31–97)c
AST (IU/L) 17.4 1 4.3 (9–50) 19.4 1 6.5 (9–138)a 23.9 1 10.4 (12–87)b,c
ALT (IU/L) 13.6 1 5.7 (4–55) 15.6 1 8.3 (3–196)a 19.7 1 10.5 (9–69)b,c
GGT (IU/L) 17.6 1 13.0 (7–172) 19.9 1 14.6 (5–191)a 25.2 1 17.3 (7–133)b,c
TC (mg/dL) 179.6 1 21.8 (105–219) 191.4 1 19.6 (113–219)a 191.4 1 19.2 (133–219)c
HDL-C (mg/dL) 70.0 1 12.5 (40–114) 70.4 1 13.1 (40–116)a 65.2 1 12.8 (43–103)c
TG (mg/dL) 60.0 1 22.5 (22–147) 68.7 1 25.3 (24–148)a 81.7 1 26.2 (36–141)b,c
FPG (mg/dL) 90.6 1 6.7 (70–109) 92.0 1 7.2 (67–109)a 94.8 1 8.1 (73–109)b,c
Alcohol 320 g/day (%) 12.2% (n = 95) 10.0% (n = 120) 2.8% (n = 2)b,c
Data are means 1 standard deviation (range).aP < 0.05 between 18"40 vs 41"60 years.bP < 0.05 between 41"60 vs >61 years.cP < 0.05 between 48–40 vs >61 yearsALT, alanine aminotransferase; AST, aspartate aminotransferase; BH, body height; BMI, body mass index; BW, bodyweight; CI,confidence interval; dBP, diastolic blood pressure; FPG, fasting plasma glucose; GGT, !-glutamyltransferase; HDL-C, high-densitylipoprotein cholesterol; sBP, systolic blood pressure; TC, total cholesterol; TG, triglycerides; WC, waist circumference.
Table 6 ALT levels in “healthy” men and women with alcohol intake <20 g/day and 320 g/day
Alcohol intake “Healthy” male (n = 1462) “Healthy” female (n = 2046)
<20 g/day (n = 845) 320 g/day (n = 617) <20 g/day (n = 1829) 320 g/day (n = 217)
Mean 1 SD (IU/L) 19.2 1 10.7 19.6 1 10.2 15.1 1 7.80 14.2 1 5.56Median (IU/L) 17 18 13 13
P < 0.05 by Student’s t-test or Mann–Whitney U-test.ALT, alanine aminotransferase; SD, standard deviation.
Hepatology Research 2014; 44: 1196–1207 Normal serum ALT levels in Japan 1203
© 2013 The Japan Society of Hepatology

elevated ALT, with an ULN of 30 IU/L for men and19 IU/L for women.1 In the USA, the ULN of ALT in acohort of 18 518 non-Hispanic whites, non-Hispanicblacks and Mexican Americans was 29 IU/L for menand 22 IU/L for women.13 However, we cannot directlycompare these results with ours because of markedethnic differences in physique and normal BMI range insubjects from Japan and those of Western countries. Inaddition, fatty liver was not evaluated in those studies.Although a study of 34 346 subjects who underwenthealth screening in Taiwan found that the ULN of ALTwas 29 IU/L in men and 22 IU/L in women, the studydid not include an evaluation of alcohol intake,14 pre-venting a direct comparison with our results. Our studyincluded daily alcohol intake in the multiple regressionanalysis analyzing factors associated with ALT levels. Wefound that alcohol intake was not an independent factorassociated with ALT, and that the mean ALT level didnot differ in healthy men and women who consumedmore than 20 g/day and 20 g/day or less alcohol.
Multiple regression analysis in overall subjectsshowed that age was an independent contributor toelevated ALT level. Indeed, in the female healthy popu-lation, the ALT level was higher in subjects aged 61 yearsor older than in younger age groups. Also, age was theindependent factor affecting the ALT level of healthypopulation men and women when the backgroundcharacteristics were matched. Age has been reported tobe significantly associated with ALT levels.22,23 NormalALT has been reported to increase until the age of 40–50years and decreases thereafter;16 however, the study didnot exclude subjects with lifestyle-related chronic liverdiseases, such as NAFLD and NASH, suggesting that
age-related changes in ALT might have been associatedwith the inclusion of these subjects. A study from Koreafound that age-related changes in ALT were significantafter exclusion of subjects with metabolic syndrome andinsulin resistance.22 The mechanisms underlying age-related changes in ALT remain unclear. Because ourstudy included too few healthy subjects aged more than61 years to analyze the age-specific ULN of ALT, furtherstudies will be needed. However, our findings suggestthat the normal range of ALT changes with age and thatthis should be considered when treating patients withvarious liver diseases.
In our study, parameters related to lipid metabolismand blood pressure were significant factors contributingto the ALT level in the healthy subjects. Because thehealthy subjects were selected to be within the normalrange of the parameters identified in the multiple regres-sion analysis in the overall subjects, the TC and TGlevels of all of the healthy subjects were within normalranges. These data suggest that minor elevations of theALT level, with possible liver injury or inflammation,could be caused by relatively higher levels of TC and TGthat remain with normal ranges. The risk of cardiovas-cular diseases reportedly increases according to theserum TG level even when less than 150 mg/dL.24 Toobtain the actual normal ALT level, we may need theliver-specific normal range of lipid metabolism-relatedparameters. According to previous studies, blood pres-sure was higher in subjects with ALT of more than40 IU/L than in those with blood pressure of less than40 IU/L.14 Our results also suggested that ALT level wascorrelated to blood pressure. The mechanism of therelationship between ALT and blood pressure remains
Table 7 Interaction between blood pressure and ALT levels in the “healthy” population
“Healthy” men (n = 1462) “Healthy” women (n = 2046)
sBP <140 mmHg (n = 1379) 3140 mmHg (n = 83) <140 mmHg (n = 1993) 3140 mmHg (n = 53)
Mean 1 SD (IU/L) 19.2 1 10.5 21.3 1 13.7 14.9 1 7.6 17.8 1 8.6*Median (IU/L) 17 17 13 15*
sBP <130 mmHg (n = 1262) 3130 mmHg (n = 200) <130 mmHg (n = 1903) 3130 mmHg (n = 143)
Mean 1 SD (IU/L) 19.2 1 10.2 20.5 1 11.9 14.9 1 7.6 16.4 1 7.1*Median (IU/L) 17 17 13 15
dBP <85 mmHg (n = 1339) 385 mmHg (n = 123) <85 mmHg (n = 1953) 385 mmHg (n = 93)
Mean 1 SD (IU/L) 19.1 1 10.1 21.8 1 13.8 15.0 1 7.6 15.3 1 6.7Median (IU/L) 17 18 13 14
*P < 0.05 by t-test or Mann–Whitney U-test.ALT, alanine aminotransferase; dBP, diastolic blood pressure; sBP, systolic blood pressure; SD, standard deviation.
1204 K. Tanaka et al. Hepatology Research 2014; 44: 1196–1207
© 2013 The Japan Society of Hepatology

unclear; however, it was recently reported that ALT levelsof more than 31 IU/L in men and more than 19 IU/L inwomen produced a significant risk of atherogenesis inasymptomatic subjects.25 Because ALT levels could belinked to atherosclerosis and cardiovascular diseases,strict blood pressure control may contribute to prevent-ing minor ALT elevations as well as cardiovasculardiseases.
A limitation of this study is the unavoidable inclusionof subjects with asymptomatic latent liver dysfunction(e.g. autoimmune hepatitis, primary biliary cirrhosis,congenital hepatitis, hemochromatosis and drug-induced liver damage). Another limitation is thatalcohol consumption was self-reported by the subjects.Heavy drinkers might have underreported their alcoholconsumption, masking the contribution of alcohol to
elevated ALT. Also, patients with NAFLD/NASH mayhave normal ALT levels, with 42% and 16% of patientswith liver biopsy-proven NAFLD/NASH and ALT of lessthan 0.5 times the ULN having steatohepatitis and sig-nificant fibrosis, respectively.26 Therefore, a diagnosis ofNAFLD/NASH should not be based solely on elevatedALT. Evaluation of lifestyle-related factors, other serummarkers, imaging findings and liver biopsy is importantfor the diagnosis of NAFLD/NASH.
The ULN of ALT determined in this cross-sectionalstudy of a large number of subjects may contribute tothe control of lifestyle-related chronic liver diseases.Future studies should include the validation of the ULNof ALT levels determined here and a long-term follow upevaluating the incidence of liver-related disease in thesesubjects, as well as prognosis and mortality.
Table 8 Characteristics of the “healthy” population with ALT levels under the ULN
Male ALT 229 (n = 1320) ALT >29 (n = 142) P-value
Age (years) 47.0 1 10.4 (19.0–87.0) 48.7 1 10.8 (30–74) 0.135BMI (kg/m2) 21.2 1 1.8 (15.3–24.9) 21.3 1 1.8 (16.3–24.9) 0.789WC (cm) 77.4 1 4.9 (49.4–84.8) 78.0 1 4.9 (62.4–84.6) 0.128sBP (mmHg) 113.4 1 14.9 (73–167) 117.6 1 15.7 (83–169) 0.001dBP (mmHg) 68.1 1 11.0 (44–110) 71.3 1 12.1 (47–115) 0.004AST (IU/L) 19.4 1 4.6 (10–50) 33.5 1 19.9 (18–185) <0.001ALT (IU/L) 17.0 1 5.1 (5–29) 41.6 1 18.7 (30–179) <0.001GGT (IU/L) 33.2 1 26.1 (10–316) 68.3 1 58.3 (13–379) <0.001TC (mg/dL) 185.4 1 20.8 (123–219) 185.7 1 22.3 (122–218) 0.676HDL-C (mg/dL) 62.7 1 13.1 (40–124) 63.2 1 13.4 (40–104) 0.685TG (mg/dL) 81.0 1 26.3 (26–149) 84.3 1 27.8 (27–148) 0.147FPG (mg/dL) 96.0 1 6.9 (71–109) 96.2 1 6.9 (76–109) 0.710Alcohol 320 g/day (%) 42.1% (n = 556) 43.0% (n = 61) 0.848
Female ALT 223 (n = 1854) ALT >23 (n = 192) P-value
Age (years) 44.8 1 8.5 (21–82) 49.6 1 9.7 (26–74) <0.001BMI (kg/m2) 20.3 1 2.0 (14.3–24.9) 20.4 1 2.2 (15.4–24.9) 0.809WC (cm) 74.9 1 6.3 (58.2–89.8) 75.5 1 7.6 (60–89.6) 0.224sBP (mmHg) 104.7 1 14.8 (73–161) 105.8 1 16.1 (69–149) 0.253dBP (mmHg) 64.1 1 10.7 (40–107) 63.7 1 11.5 (31–97) 0.616AST (IU/L) 17.7 1 4.0 (9–45) 29.3 1 11.3 (14–138) <0.001ALT (IU/L) 13.4 1 3.8 (3–23) 31.0 1 13.8 (24–196) <0.001GGT (IU/L) 17.4 1 10.1 (5–172) 36.0 1 29.0 (9–191) <0.001TC (mg/dL) 186.6 1 21.3 (105–219) 190.2 1 20.5 (133–219) 0.022HDL-C (mg/dL) 70.0 1 12.7 (40–116) 70.9 1 14.6 (40–109) 0.527TG (mg/dL) 65.2 1 24.7 (22–147) 72.3 1 25.4 (25–148) <0.001FPG (mg/dL) 91.5 1 7.0 (67–109) 92.1 1 7.7 (70–109) 0.267Alcohol 3 20 g/day (%) 11.0% (n = 204) 6.8% (n = 13) 0.070
ALT, alanine aminotransferase; AST, aspartate aminotransferase; BH, body height; BMI, body mass index; BW, bodyweight; CI,confidence interval; dBP, diastolic blood pressure; FPG, fasting plasma glucose; GGT, !-glutamyltransferase; HDL-C, high-densitylipoprotein cholesterol; sBP, systolic blood pressure; TC, total cholesterol; TG, triglycerides; WC, waist circumference.
Hepatology Research 2014; 44: 1196–1207 Normal serum ALT levels in Japan 1205
© 2013 The Japan Society of Hepatology

In conclusion, the ULN of ALT for Japanese subjects,considering lifestyle factors, was 29 IU/L for men and23 IU/L for women.
ACKNOWLEDGMENTS
THE AUTHORS THANK Professor Kyuichi Tanikawa(International Institute for Liver Research) for excel-
lent advice; the entire medical staff at Eguchi Hospital,Kochi Medical School and Kawamura Clinic for assis-tance; and members of the Japan Study Group of Non-alcoholic Fatty Liver Disease (JSG-NAFLD) for excellentadvice. This work was supported by a Grant-in-Aid fromthe Ministry of Education, Culture, Sports, Science andTechnology of Japan (2010) (nos. 22590741 to Y. E.and 20590785 to M. O.).
REFERENCES1 Pratt DS, Kaplan MM. Evaluation of abnormal liver-
enzyme results in asymptomatic patients. N Engl J Med2000; 342: 1266–71.
2 Kim WR, Flamm SL, Di Bisceglie AM, Bodenheimer HC;Public Policy Committee of the American Association forthe Study of Liver Disease. Serum activity of alanine ami-notransferase (ALT) as an indicator of health and disease.Hepatology 2008; 47: 1363–70.
3 Ikai I, Kudo M, Arii S et al. Report of the 18th follow-upsurvey of primary liver cancer in Japan. Hepatol Res 2010;40: 1043–59.
4 Ikai I, Arii S, Ichida T et al. Report of the 16th follow-upsurvey of primary liver cancer. Hepatol Res 2005; 32: 163–72.
5 Eguchi Y, Hyogo H, Ono M et al. Prevalence and associatedmetabolic factors of nonalcoholic fatty liver disease in thegeneral population from 2009 to 2010 in Japan: a multi-center large retrospective study. J Gastroenterol 2012; 47:586–95.
6 Argo CK, Caldwell SH. Epidemiology and natural historyof nonalcoholic steatohepatitis. Clin Liver Dis 2009; 13:511–31.
7 Everhart JE, Bambha KM. Fatty liver: think globally.Hepatology 2010; 51: 1491–3.
8 Angulo P. Nonalcoholic fatty liver disease. N Engl J Med2002; 346: 1221–31.
9 Neuschwander-Tetri BA, Caldwell SH. Nonalcoholicsteatohepatitis: summary of an AASLD single topic confer-ence. Hepatology 2003; 37: 1202–19.
10 Kojima S, Watanabe N, Numata M, Ogawa T, MatsuzakiS. Increase in the prevalence of fatty liver in japanover the past 12 years: analysis of clinical background.J Gastroenterol 2003; 38: 954–61.
11 Hultcrantz R, Glaumann H, Lindberg G, Nilsson LH. Liverinvestigation in 149 asymptomatic patients with moder-ately elevated activities of serum aminotransferases. ScandJ Gastroenterol 1986; 21: 106–13.
12 Kundrotas LW, Clement DJ. Serum alanine amino-transferase (ALT) elevation in asymptomatic US AirForce basic trainee blood donors. Dig Dis Sci 1993; 38:2145–50.
13 Ruhl CE, Everhart JE. Upper limits of normal for alanineaminotransferase activity in the United States population.Hepatology 2012; 55: 447–54.
14 Wu WC, Wu CY, Wang YJ et al. Updated thresholdsfor serum alanine aminotransferase level in a large-scalepopulation study composed of 34 346 subjects. AlimentPharmacol Ther 2012; 36: 560–8.
15 Sanyal AJ. AGA technical review on nonalcoholic fatty liverdisease. Gastroenterology 2002; 123: 1705–25.
16 Siest G, Henry J, Schiele F, Young DS. Interpretation ofClinical Laboratory Tests: Reference Values and Their BiologicalVariation. Foster City, CA: Biomedical Publications, 1985;459.
Table 9 Factors associated with ALT levels in the “healthy”population
Male Oddsratio
95% CI P-value
Age 1.002 1.001–1.003 0.004BMI 1.021 1.011–1.032 <0.001WC 1.005 1.001–1.009 0.012sBP 1.000 0.999–1.002 0.750dBP 1.002 1.001–1.004 0.006TC 1.000 0.999–1.000 0.314HDL-C 1.001 1.000–1.002 0.103TG 1.002 0.996–1.000 <0.001FPG 0.998 0.996–1.000 0.032Alcohol 320 g/day (%) 0.989 0.964–1.014 0.379
Female Oddsratio
95% CI P-value
Age 1.012 1.011–1.014 <0.001BMI 1.003 0.995–1.011 0.477WC 0.999 0.996–1.001 0.276sBP 1.003 1.001–1.004 <0.001dBP 0.996 0.994–0.998 <0.001TC 1.000 0.999–1.001 0.850HDL-C 1.001 1.001–1.002 0.151TG 1.003 1.001–1.004 <0.001FPG 1.000 0.998–1.001 0.884Alcohol 320 g/day (%) 0.956 0.920–0.993 0.020
ALT, alanine aminotransferase; AST, aspartate aminotransferase;BH, body height; BMI, body mass index; BW, bodyweight; CI,confidence interval; dBP, diastolic blood pressure; FPG, fastingplasma glucose; GGT, !-glutamyltransferase; HDL-C, high-densitylipoprotein cholesterol; sBP, systolic blood pressure; TC, totalcholesterol; TG, triglycerides; WC, waist circumference.
1206 K. Tanaka et al. Hepatology Research 2014; 44: 1196–1207
© 2013 The Japan Society of Hepatology

17 Bedogni G, Miglioli L, Masutti F et al. Incidence andnatural course of fatty liver in the general population: theDionysos study. Hepatology 2007; 46: 1387–91.
18 Pendino GM, Mariano A, Surace P et al. Prevalence andetiology of altered liver tests: a population-based survey ina Mediterranean town. Hepatology 2005; 41: 1151–9.
19 Ruhl CE, Everhart JE. Joint effects of body weight andalcohol on elevated serum alanine aminotransferase in theUnited States population. Clin Gastroenterol Hepatol 2005;3: 1260–8.
20 CLSI. Defining, Establishing, and Verifying Reference Intervalsin the Clinical Laboratory: Approved Guideline, 3rd edn.Wayne, PA: Clinical and Laboratory Standards Institute,2008.
21 Hyndman RH, Fan Y. Sample quantiles in statistical pack-ages. Am Stat 1996; 50: 361–5.
22 Kang HS, Um SH, Seo YS et al. Healthy range for serum ALTand the clinical significance of “unhealthy” normal ALT
levels in the Korean population. J Gastroenterol Hepatol2011; 26: 292–9.
23 Dufour DR, Lott JA, Nolte FS, Gretch DR, Koff RS, Seeff LB.Diagnosis and monitoring of hepatic injury. I. Perfor-mance characteristics of laboratory tests. Clin Chem 2000;46: 2027–49.
24 Iso H, Naito Y, Sato S et al. Serum triglycerides and risk ofcoronary heart disease among Japanese men and women.Am J Epidemiol 2001; 153: 490–9.
25 Siddiqui MS, Sterling RK, Luketic VA et al. Associationbetween high-normal levels of alanine aminotransferaseand risk factors for atherogenesis. Gastroenterology 2013;145: 1271–9.
26 Wong VW, Wong GL, Tsang SW et al. Metabolic and histo-logical features of non-alcoholic fatty liver disease patientswith different serum alanine aminotransferase levels.Aliment Pharmacol Ther 2009; 29: 387–96.
Hepatology Research 2014; 44: 1196–1207 Normal serum ALT levels in Japan 1207
© 2013 The Japan Society of Hepatology