
University of Groningen Fetal growth restriction Tanis, Jozijntje ...
146
University of Groningen Fetal growth restriction Tanis, Jozijntje Christina IMPORTANT NOTE: You are advised to consult the publisher's version (publisher's PDF) if you wish to cite from it. Please check the document version below. Document Version Publisher's PDF, also known as Version of record Publication date: 2015 Link to publication in University of Groningen/UMCG research database Citation for published version (APA): Tanis, J. C. (2015). Fetal growth restriction: Prenatal predictors of neonatal and late functional outcome. University of Groningen. Copyright Other than for strictly personal use, it is not permitted to download or to forward/distribute the text or part of it without the consent of the author(s) and/or copyright holder(s), unless the work is under an open content license (like Creative Commons). The publication may also be distributed here under the terms of Article 25fa of the Dutch Copyright Act, indicated by the “Taverne” license. More information can be found on the University of Groningen website: https://www.rug.nl/library/open-access/self-archiving-pure/taverne- amendment. Take-down policy If you believe that this document breaches copyright please contact us providing details, and we will remove access to the work immediately and investigate your claim. Downloaded from the University of Groningen/UMCG research database (Pure): http://www.rug.nl/research/portal. For technical reasons the number of authors shown on this cover page is limited to 10 maximum. Download date: 10-01-2022
-
Upload
khangminh22 -
Category
Documents
-
view
1 -
download
0
Transcript of University of Groningen Fetal growth restriction Tanis, Jozijntje ...
University of Groningen
Fetal growth restrictionTanis, Jozijntje Christina
IMPORTANT NOTE: You are advised to consult the publisher's version (publisher's PDF) if you wish to cite fromit. Please check the document version below.
Document VersionPublisher's PDF, also known as Version of record
Publication date:2015
Link to publication in University of Groningen/UMCG research database
Citation for published version (APA):Tanis, J. C. (2015). Fetal growth restriction: Prenatal predictors of neonatal and late functional outcome.University of Groningen.
CopyrightOther than for strictly personal use, it is not permitted to download or to forward/distribute the text or part of it without the consent of theauthor(s) and/or copyright holder(s), unless the work is under an open content license (like Creative Commons).
The publication may also be distributed here under the terms of Article 25fa of the Dutch Copyright Act, indicated by the “Taverne” license.More information can be found on the University of Groningen website: https://www.rug.nl/library/open-access/self-archiving-pure/taverne-amendment.
Take-down policyIf you believe that this document breaches copyright please contact us providing details, and we will remove access to the work immediatelyand investigate your claim.
Downloaded from the University of Groningen/UMCG research database (Pure): http://www.rug.nl/research/portal. For technical reasons thenumber of authors shown on this cover page is limited to 10 maximum.
Download date: 10-01-2022
Fetal Growth Restriction
Prenatal predictors of neonatal
and late functional outcome
Jozien C. Tanis
Fetal growth restriction.
Prenatal predictors of neonatal and late functional outcome.
© 2015, J.C. Tanis, the Netherlands
ISBN 978-94-6299-208-5
ISBN 978-94-6299-209-2
The printing of this thesis was financially supported by:
BMA BV (Mosos), Chiesi Pharmaceuticals BV, ChipSoft BV, Covidien, Nutricia Early Life Nutrition, Rijksuniveriteit Groningen, Universitair Medisch Centrum Groningen, and postgraduate school for Behavioral and Cognitive Neurosciences.
Cover design: Amanda Gautier, Gautier Scientific Illustration
Layout : Jos Hendrix
Printed by: Ridderprint BV, Ridderkerk, the Netherlands
Fetal Growth Restriction
Prenatal predictors of neonataland late functional outcome
Proefschrift
ter verkrijging van de graad van doctor aan deRijksuniversiteit Groningen
op gezag van derector magnificus prof. dr. E. Sterken
en volgens besluit van het College voor Promoties.
De openbare verdediging zal plaatsvinden op
woensdag 9 december 2015 om 14.30 uur
door
Jozijntje Christina Tanis
geboren op 16 augustus 1988te Harlingen

PromotoresProf. dr. A.F. BosProf. dr. C.M. Bilardo
Beoordelingscommissie Prof. dr. H. LafeberProf. dr. S.A. ScherjonProf. dr. G.H.A. Visser
ParanimfenEline L. VegterLaura V. de Vries
Contents
Chapter 1 Introduction
Part I Cardiac function in FGR
Chapter 2 Online versus offline spatiotemporal image correlation (STIC) M-mode for the evaluation of cardiac longitudinal annular displacement in fetal growth restriction
Submitted
Part II Prenatal predictors of neonatal outcome in FGR
Chapter 3 Prenatal Doppler flow patterns and neonatal circulation in fetal growth restriction
Ultrasound in Obstetrics & Gynecology 2015 Sept 11. doi 10.1002/uog.14744
Chapter 4 General movements after fetal growth restriction in relation to prenatal Doppler flow patterns
Provisionally accepted Ultrasound in Obstetrics & Gynecology
Part III Follow-up at school age after FGR
Chapter 5 Functional outcome of very preterm-born and small-for-gestational-age children at school age
Pediatric Research 2012 Dec;72(6):641-8
Chapter 6 Functional outcomes at age 7 years of moderate preterm and full term children born small for gestational age
Journal of Pediatrics 2015 Mar;166(3):552-558
Chapter 7 General discussion
Chapter 8 English summary Nederlandse samenvatting Abbreviations Dankwoord Curriculum vitae List of publications
9
21
23
37
39
55
71
73
93
109
125

Chapter 1
Introduction

10
Chapter 1
Introduction
11
1
Dating pregnancy accurately begins with establishing the estimated date of con�inement on the basis of information about the last menstrual period. The most commonly used clinical tool for assessing growth of the pregnancy is serial measurement of uterine fundal height in centimeters, from the symphysis pubis across the uterus to the top of the fundus.(1)
Fetal growth
Normalfetalgrowthtakesninemonths,or40weeks,or280daysfromthelastmenstrualperiod. During pregnancy, a fetus develops from a single cell into an unborn infantwithavarietyofcomplexstructuresandfunctions.Growthdoesnotoccurlinearly,butproceedsatadifferentpaceindifferentphases.
growth / /: 1) The process of increasing in size. 2) The process of developing physically, mentally, or spiritually. 3) The process of increasing in amount, value, or importance. (Oxford English Dictionary)
Fetal growth restriction (FGR) refers to a condition of inadequate quantitativedevelopmentofthefetus.Often,growthdoesoccur,butitislessthanexpected.Inotherde�initionsofFGR,fetalweightorfetalsizeiscomparedtopopulationreferencecurves.Commonlyusedcut-offsareaweightbelowthe10th,5th,or3rdpercentile,orminus2standarddeviations.FGRcanalsobede�inedasde�lectingfetalgrowth,regardlessofthepercentile.Itisstillunderdebatewhichcut-offshouldbeusedandwhichisbestsuitedforclinicaluse. Being too small in utero can have several causes: congenital and/or syndromicabnormalities, fetal infection, placental disease, or being constitutionally small.Congenital and/or syndromic abnormalities and fetal infection are easily detectedandtheyhavetheirownpathophysiologicalmechanisms.Thereforetheyareexcludedfromthede�initionofFGR, leavingplacentaldiseaseandbeingconstitutionallysmallas the causesof anestimated fetalweight (EFW)below the10thpercentile.Dopplerabnormalitiesofthefetalandmaternalvesselsoftendetectplacentaldisease,butnotinallcases.Itisofgreatclinicalimportance,however,todistinguishbetweenplacentaldiseaseandbeingconstitutionallysmall.FGRduetoalackofnutrientsandoxygen,i.e.placentaldisease, results inan increasedriskofperinatalmortalityandwidespreadmorbidity.(2)However,newevidencesuggeststhatseeminglyhealthy,constitutionallysmallfetusesalsohaveanincreasedriskofabnormaloutcome.(3,4) Long-termmorbidityduetolowbirthweightwas�irststudiedin1989byBarkeretal.(5)Theyfoundthatmaleswithabirthweightof5.5pounds,approximately2.5kg,orless,hadthehigheststandardmortalityratiosforischemicheartdiseaseinlaterlife.
12
Chapter 1
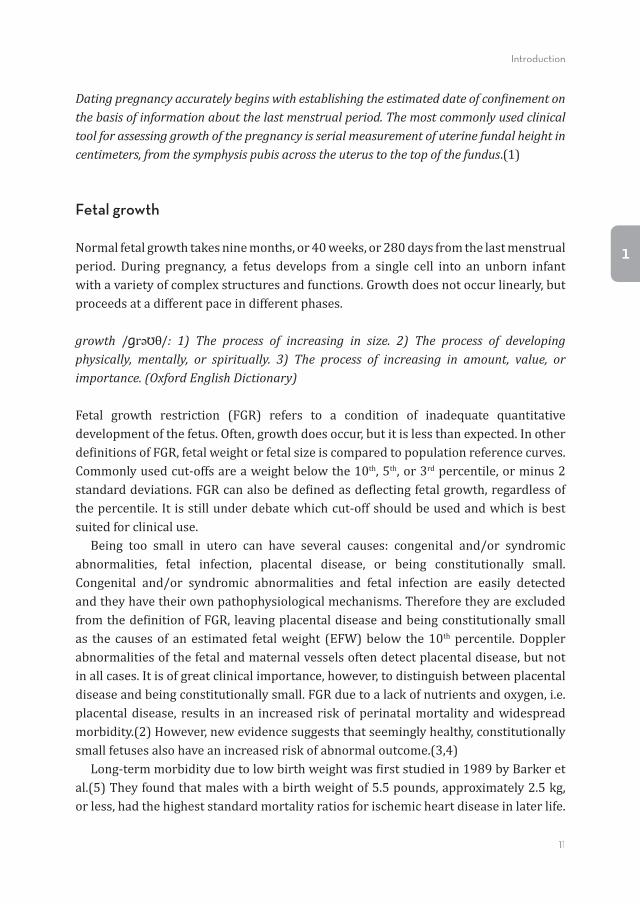
Apparently,cardiovascularremodelingoccursinsmallfetusesandhasitseffectatleastuntiladulthood.FGRisalsoknownforitsshort-termconsequences.FGRcanresultinperinataldeathandgivesanincreasedriskofneonatalmorbidity,suchasnecrotizingenterocolitis (NEC), respiratory distress syndrome (RDS), intracranial hemorrhage,sepsis,andasphyxia,seealsoFigure1.(2,6,7)Inordertoreducethesemortalityandmorbidityrates,itiscrucialtodetectFGR,anditsunderlyingcause,early.Subsequently,suitablemonitoringandinterventioncanbeimplemented.
Figure 1. Morbidity and mortality in 1560 small-for-gestational-age fetuses. From Manning FA, ed. Fetal Medicine: Principles and practice. Norwalk, CT: Appleton and Lange; 1195.
Monitoring of fetal growth
Duringthepastdecades,ultrasoundhasbeenincorporatedintoantenatalsurveillance.In 1967, ultrasound was �irst applied in obstetrics to estimate fetal maturity, fetalposition,andintrauterinefetaldeath.(8)Soonitbecameanessentialtoolformonitoringfetalgrowth,sincefundalheightmeasurementisunreliableuptoonethirdofthetime.Nowadays,ultrasoundisusedtodeterminegestationalagebymeasuringthecrown-rumplength,anditprovestobemoreaccuratethanusingthelastmenstrualperiod.Therefore, itreducesthe incidenceofposttermpregnanciesaswellas false-positivediagnosesofFGR.(1)
Introduction
13
1
Laterinpregnancy,ultrasoundisusedtoestablishtheEFWbyapplyingaformula;themostcommonlyusedonebeingHadlock’sformula.(9)Thisformulausesmeasurementsoftheheadcircumference,abdominalcircumference,andfemurlengthtocalculateEFW.Growthassessmentthroughoutpregnancyisbetterachievedbyrepeatedbiometricalmeasurements, i.e. at leastonceevery tendays, inorder tominimizemeasurementserrors. Once FGR has been established, additional ultrasound measurements should beperformed. An important non-invasive technique is Doppler ultrasound. It uses theprincipleoftheDopplereffecttomeasureblood�low.Movingredbloodcellsre�lecttheultrasoundbeam,andcauseafrequencyshiftinthere�lectedsignal,whichisdetectedbytheultrasoundreceiverandproducesasonogramcontinuouswithtime.(10)Next,thepulsatilityindex(PI)canbecalculatedas(peaksystolicheight–minimumdiastolicheight)/meanwaveformheight.(11)Itrepresentsthelevelofvascularresistanceandis,therefore,usedinFGRasanindicatorofplacentalfunction.Wladimiroffetalwerethe�irsttoapplyDopplerultrasoundoftheumbilicalartery(UA)inFGR.(12)Thereafter,Doppler ultrasoundwas used tomeasure themiddle cerebral artery (MCA), ductusvenosus(DV),andmaternaluterinearteries(UtA).(13-15) Anothermethod tomonitor the growth restricted fetus is the biophysical pro�ilescoredescribedforthe�irsttimebyManningetal.(16)Itincorporatesfetalmovement,fetaltone,fetalbreathing,amniotic�luidindex,andfetalheartrateintoascorere�lectingfetalwellbeing.Fetalheartrateismonitoredelectronicallywithcardiotocography.Thebiophysicalpro�ilenevergainedpopularityinEurope.
Circulation and FGR
Thefetalheartstartsfunctioningaroundthefourthweekofgestationanditsformationiscompletedwithinthenexttwoweeks.Theheartpumpsoxygen-depletedbloodtotheplacentathroughtheUA,whereitbecomeshighlyoxygenatedandpassesthroughtheumbilicalveinandDVbacktothefetalheart.(17)IncaseofFGR,hemodynamicadaptationmayoccurwherebythefetuspreferentiallydivertsitscardiacoutputtoitsvitalorgans.(17)Sincetheheartisthemostimportantorganinfetalcirculation,itismostaffectedbyhemodynamicchanges,asprovenbytheincreasedriskofcardiovasculardiseaseinadulthoodafter lowbirthweight.(5)Therefore, it isofgreat importance toestablishfetal cardiac functioning and changes thereindue toFGR.Themost commonlyusedmethodtodoso isbymeansofcardiac longitudinalannulardisplacement(LAD),aneasyandreproduciblemethodthatmeasuresmyocardialmotion.(18)Insevere,early-onsetFGR,LADwasfoundtobedecreasedincomparisontocontrols.(19)However,itsapplicationtolesssevereFGRhasnotyetbeeninvestigated.

14
Chapter 1
Hemodynamic adaptations in FGR can be monitored non-invasively by Dopplerultrasound.Redistributionoffetalblood�lowoccursinmoreadvancedstagesofFGR,and isexpressedasa raisedPIof theUAandDV.Since thebrain isoneof themostimportantorgans requiringoxygenandnutrients, cerebral vesselsdilate inorder topreservecerebralblood�low.ThisisdemonstratedbyadecreasedPI(lowerresistance)oftheMCAordecreasedcerebroplacentalratio(CPR),anadaptivemechanismknownasbrainsparing.(3,20) IncaseofFGR,itisunknownwhetherfetalcirculatoryredistributioncontinuesafterbirthornot.PreviousstudiesreportedalackofincreaseinleftventricularoutputinFGRinfantsduringthe�irstdaysafterbirth,asmeasuredwithechocardiography.(21)Therefore,FGRinfantsseemtofallshortinadaptingtheircirculationtothepostnatalsituation.However, these �indingshaveneverbeencomparedwithprenatalDopplermeasurements. Anon-invasivemethodtostudyneonatalhemodynamicsismultisitenear-infraredspectroscopy(NIRS),a light-based technologyused tomeasure tissueoxygenstatus.(22,23)NIRS isgenerallybelieved tobeavaluable tool formonitoring trends in theindividual patient. Moreover, it is a useful tool for comparing different groups ofinfants exposed to a variety of risk factors.(24) By means of NIRS, regional tissueoxygensaturation(rSO2),whichre�lectsthevenous-weightedoxygensaturationoftheunderlyingtissue,canbemeasured.Fractionaltissueoxygenextraction(FTOE)re�lectsthebalancebetweentissueoxygensupplyandconsumption,andcanbecalculatedas(arterialoxygensaturation–rSO2)/arterialoxygensaturation.AsFTOEisin�luencedby tissueoxygenationandtissueoxygendemand, itcouldbeusedasan indicatoroftissueperfusion.WhenNIRSmeasurementsareappliedtomultiplesites,aratiocanbecalculatedofcerebraltoabdominaltissueoxygenstatus.Herewith,neonatalcirculatorydistributioncanbedeterminedandthisenablesustoestimatewhetherornotbrainsparingpersistsafterbirth.
Neurodevelopment and FGR
FGRnotonlyaffectsgeneralgrowthandcirculation,italsoin�luencesbraindevelopment.Brainvolumesofbothsevereandnon-severeFGRfetuseswerefoundtobereduced,asmeasuredwiththree-dimensionalultrasoundandfetalMRI.(25-27)Previously,brainsparingwasthoughttobeaprotectivemechanism,butgrowingevidencesuggests itmightbeanexpressionofcirculatoryfailure.(4)Figuerasetalcon�irmthissuggestion.TheyfoundthatbrainsparingisassociatedwithneurobehavioralimpairmentaroundtheduedateinpretermFGRnewborns.(3)Furthermore,neonatalMRIsinFGRinfantswhoexperiencedbrainsparingrevealreducedmyelination.(28)Apparently,therefore,
Introduction
15
1
notonlyispostnatalgrowthaffectedbyFGR,butneurodevelopmentaswell.Whattheunderlyingpathophysiologicalmechanismsareregardingneurologicaldevelopmentintheseinfantsisstillunderdebate,asisthequestionhowneurodevelopmentcorrespondswithprenatalDopplermeasurements. Qualitativeassessmentofgeneralmovements(GMs)isasuitablemethodtofollowtheneurologicaloutcomeofinfantsfromnewlybornuntilseveralmonthsofage.(29-31) GMs are part of an infant’s spontaneousmovement repertoire and are presentfrom the early fetal periodonwardsuntil the endof the �irst half a year afterbirth.(32)GMsaregrossmovements involving thewholebody.Theymay last froma fewsecondstoseveralminutes.ThecharacteristicaspectofGMsinhealthyinfantsistheir�luentandelegantcharacterandthecomplexandvariablesequenceofarm,leg,neck,andtrunkmovements.Theintensity,force,andspeedofthemovementsarevariable.(33)IfthenervoussystemisimpairedthequalityoftheGMschanges.Thequalityoftheso-called�idgetygeneralmovements(FMs),presentbetween9and20weeksposttermandde�inedascontinuoussmallmovementsofmoderatespeedinalldirections,isaparticularlyaccuratemarker forneurologicaloutcome.Most infants (96%)withnormal FMs have normal neurological outcome,whilemost infants (95%) inwhomFMsareabsentduringthisparticularagespandevelopcerebralpalsy.(29)Recently,itwasreportedthatdetailedaspectsoftheGMs,asre�lectedinamotoroptimalityscore(MOS),alsohavepredictivevalueformildmotorabnormalitieslaterinlife.(34) TheneurologicaldevelopmentalcourseofFGRchildrencanalsobefollowedupuntillaterinchildhood,i.e.schoolage.Inapreviousstudy,childrenbornafterlate-onsetFGRwereshowntohavealowerintelligentquotientandexperiencedneuropsychologicaldif�icultiesmorefrequentlyattheageofnineyears.(35)This�inding,however,appliestochildrenbornatameangestationalageof37weeks.Thequestionarosehowthese�indingsapplytoseparategroupsofgestationalage,suchasverypreterm-bornversusmoderatelypreterm-bornand full termchildren.Furthermore,assessing intelligencequotientsisnottheonlyre�lectionofchildren’sperformance.Otherfunctionsmakeamajorcontributiontodeterminetheabilitytoperformeverydaytasks,suchasattention,memory, executive functioning, behavior, and motor skills.(36) We felt the need,therefore,foranextensivefollow-upatschoolagetoestablishlong-termconsequencesofFGR.
16
Chapter 1
Aim of this thesis
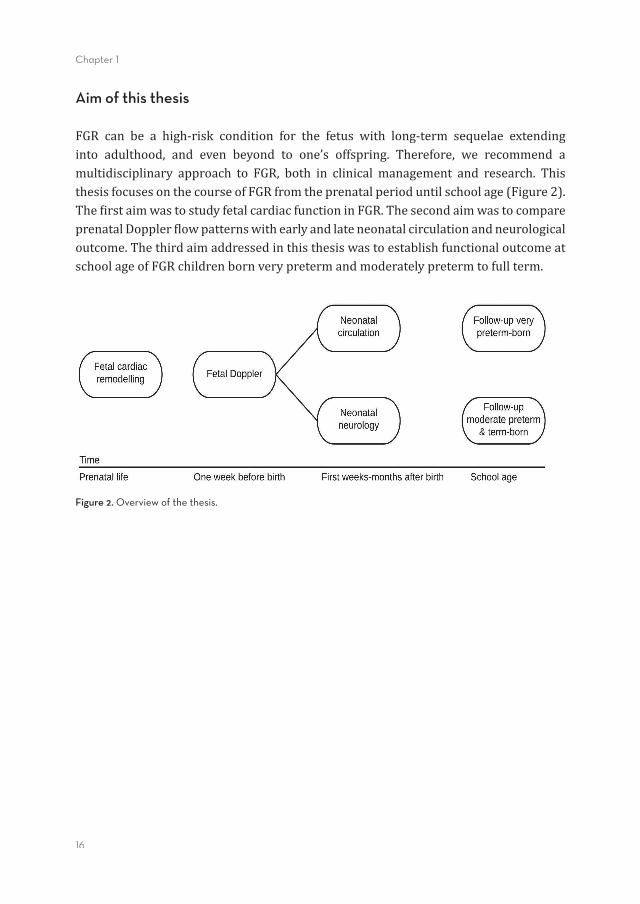
FGR can be a high-risk condition for the fetus with long-term sequelae extendinginto adulthood, and even beyond to one’s offspring. Therefore, we recommend amultidisciplinary approach to FGR, both in clinical management and research. ThisthesisfocusesonthecourseofFGRfromtheprenatalperioduntilschoolage(Figure2).The�irstaimwastostudyfetalcardiacfunctioninFGR.ThesecondaimwastocompareprenatalDoppler�lowpatternswithearlyandlateneonatalcirculationandneurologicaloutcome.ThethirdaimaddressedinthisthesiswastoestablishfunctionaloutcomeatschoolageofFGRchildrenbornverypretermandmoderatelypretermtofullterm.
Figure 2. Overview of the thesis.

Introduction
17
1
Outline
Part I. Cardiac function in FGRIn Chapter 2, we present a comparison of online M-mode ultrasound with of�linespatiotemporal image correlation (STIC) M-mode for the assessment of cardiaclongitudinalannulardisplacement(LAD)inFGRandcontrols.
Part II. Prenatal predictors of neonatal outcome in FGRInChapter3,wedescribe the associationbetween fetalDopplermeasurements andneonatalcirculation,measuredwithnear-infraredspectroscopy(NIRS).InChapter4,wereportonthesamestudygroupasinChapter3,focusingontheassociationbetweenfetal Doppler measurements and infants’ neurological development assessed withgeneralmovements(GMs).
Part III. Follow-up at school age after FGRPart III focuses on the long-term functional consequences of FGR. Chapter 5 is anoutline of neuropsychological outcome at the age of eight years of children bornverypretermand small for gestational age. InChapter6,we elaborate on the sameoutcomemeasures,nowstudiedinchildrenbornmoderatepretermorfullterm,andsmall for gestational age. In both studies, follow-up consisted of a series of tests inordertodetermineintelligence,attention,memory,visuomotorintegration,executivefunctioning,behavior,andmotorskills.
The thesis is concludedwith a general discussion that integrates the results of thestudiesincludedintheseparateparts.Wediscusstheimplicationsofour�indingsbyprovidingfutureperspectivesforclinicalpracticeandresearch.
18
Chapter 1
References(1) Gibbs R, Karlan B, Haney A, Nygaard I. Danforth’s Obstetrics and Gynecology. 10th edition ed.
Philadelphia,USA:WoltersKluwer;2008.(2) ResnikR.Intrauterinegrowthrestriction.ObstetGynecol2002Mar;99(3):490-496.(3) FiguerasF,Cruz-MartinezR,Sanz-CortesM,ArranzA,IllaM,BotetF,etal.Neurobehavioraloutcomes
in preterm, growth-restricted infants with and without prenatal advanced signs of brain-sparing.UltrasoundObstetGynecol2011Sep;38(3):288-294.
(4) EixarchE,MelerE,IraolaA,IllaM,CrispiF,Hernandez-AndradeE,etal.Neurodevelopmentaloutcomein 2-year-old infants who were small-for-gestational age term fetuses with cerebral blood �lowredistribution.UltrasoundObstetGynecol2008Dec;32(7):894-899.
(5) BarkerDJ,WinterPD,OsmondC,MargettsB,SimmondsSJ.Weightininfancyanddeathfromischaemicheartdisease.Lancet1989Sep9;2(8663):577-580.
(6) Bernstein IM, Horbar JD, Badger GJ, Ohlsson A, Golan A.Morbidity andmortality among very-low-birth-weightneonateswithintrauterinegrowthrestriction.TheVermontOxfordNetwork.AmJObstetGynecol2000Jan;182(1Pt1):198-206.
(7) DamodaramM,StoryL,KulinskayaE,RutherfordM,KumarS.Earlyadverseperinatalcomplicationsinpretermgrowth-restrictedfetuses.AustNZJObstetGynaecol2011Jun;51(3):204-209.
(8) Taylor ES, Thompson HE, Gottesfeld KR, Holmes JH. Clinical use of ultrasound in obstetrics andgynecology.AmJObstetGynecol1967Nov1;99(5):671-682.
(9) HadlockFP,HarristRB,SharmanRS,DeterRL,ParkSK.Estimationoffetalweightwiththeuseofhead,body,andfemurmeasurements--aprospectivestudy.AmJObstetGynecol1985Feb1;151(3):333-337.
(10) HarringtonK,CampbellS.AcolouratlasofDopplerultrasonographyinobstetrics.Anintroductiontoitsuseinmaternalfetalmedicine.London,GreatBritain:EdwardArnold;1995.
(11) GoslingRG,KingDH.ArterialassessmentbyDoppler-shiftultrasound.ProcRSocMed1974Jun;67(6Pt1):447-449.
(12)WladimiroffJW,TongeHM,StewartPA,ReussA.Severeintrauterinegrowthretardation;assessmentofitsoriginfromfetalarterial�lowvelocitywaveforms.EurJObstetGynecolReprodBiol1986Jun;22(1-2):23-28.
(13) vandenWijngaardJA,GroenenbergIA,WladimiroffJW,HopWC.CerebralDopplerultrasoundofthehumanfetus.BrJObstetGynaecol1989Jul;96(7):845-849.
(14) RudolphAM.Distributionandregulationofblood�lowinthefetalandneonatallamb.CircRes1985Dec;57(6):811-821.
(15) CampbellS,Diaz-RecasensJ,Grif�inDR,Cohen-OverbeekTE,PearceJM,WillsonK,etal.Newdopplertechniqueforassessinguteroplacentalblood�low.Lancet1983Mar26;1(8326Pt1):675-677.
(16) ManningFA,BaskettTF,MorrisonI,LangeI.Fetalbiophysicalpro�ilescoring:aprospectivestudyin1,184high-riskpatients.AmJObstetGynecol1981Jun1;140(3):289-294.
(17) BahtiyarMO, Copel JA. Cardiac changes in the intrauterine growth-restricted fetus. SeminPerinatol2008Jun;32(3):190-193.
(18) CarvalhoJS,O’SullivanC,ShinebourneEA,HeneinMY.Rightandleftventricularlong-axisfunctioninthefetususingangularM-mode.UltrasoundObstetGynecol2001Dec;18(6):619-622.
(19) Cruz-LeminiM,CrispiF,Valenzuela-AlcarazB,FiguerasF,SitgesM,GomezO,etal.ValueofannularM-modedisplacementvs tissueDopplervelocities toassess cardiac function in intrauterinegrowthrestriction.UltrasoundObstetGynecol2013Aug;42(2):175-181.
(20) Baschat AA, Gembruch U. The cerebroplacental Doppler ratio revisited. Ultrasound Obstet Gynecol2003Feb;21(2):124-127.
(21) Fouzas S, Karatza AA, Davlouros PA, Chrysis D, Alexopoulos D, Mantagos S, et al. Neonatal cardiacdysfunctioninintrauterinegrowthrestriction.PediatrRes2014May;75(5):651-657.
(22)Wyatt JS, Cope M, Delpy DT, Wray S, Reynolds EO. Quanti�ication of cerebral oxygenation andhaemodynamics in sick newborn infants by near infrared spectrophotometry. Lancet 1986 Nov8;2(8515):1063-1066.
(23) Pellicer A, Bravo Mdel C. Near-infrared spectroscopy: a methodology-focused review. Semin FetalNeonatalMed2011Feb;16(1):42-49.
Introduction
19
1
(24) vanBelF,LemmersP,NaulaersG.Monitoringneonatalregionalcerebraloxygensaturationinclinicalpractice:valueandpitfalls.Neonatology2008;94(4):237-244.
(25) BusinelliC,deWitC,VisserGH,PistoriusLR.Ultrasoundevaluationofcorticalbraindevelopmentinfetuseswithintrauterinegrowthrestriction.JMaternFetalNeonatalMed2014Sep10:1-6.
(26) Egana-Ugrinovic G, Sanz-CortesM, Figueras F, Couve-Perez C, Gratacos E. FetalMRI insular corticalmorphometryand itsassociationwithneurobehavior in late-onsetsmall-for-gestational-age fetuses.UltrasoundObstetGynecol2014Sep;44(3):322-329.
(27) Egana-Ugrinovic G, Sanz-Cortes M, Figueras F, Bargallo N, Gratacos E. Differences in corticaldevelopmentassessedbyfetalMRIinlate-onsetintrauterinegrowthrestriction.AmJObstetGynecol2013Aug;209(2):126.e1-126.e8.
(28)RamenghiLA,MartinelliA,DeCarliA,BrusatiV,MandiaL,FumagalliM,etal.CerebralmaturationinIUGRandappropriateforgestationalagepretermbabies.ReprodSci2011May;18(5):469-475.
(29) PrechtlHF, Einspieler C, Cioni G, BosAF, Ferrari F, SontheimerD. An earlymarker for neurologicalde�icitsafterperinatalbrainlesions.Lancet1997May10;349(9062):1361-1363.
(30) EinspielerC,PrechtlHF.Prechtl’sassessmentofgeneralmovements:adiagnostictoolforthefunctionalassessmentoftheyoungnervoussystem.MentRetardDevDisabilResRev2005;11(1):61-67.
(31) Bruggink JL,EinspielerC,ButcherPR,VanBraeckelKN,PrechtlHF,BosAF.Thequalityof theearlymotorrepertoireinpreterminfantspredictsminorneurologicdysfunctionatschoolage.JPediatr2008Jul;153(1):32-39.
(32) EinspielerC,PrechtlHF,FerrariF,CioniG,BosAF.Thequalitativeassessmentofgeneralmovementsinpreterm,termandyounginfants--reviewofthemethodology.EarlyHumDev1997Nov24;50(1):47-60.
(33) PrechtlHF.Qualitativechangesofspontaneousmovementsinfetusandpreterminfantareamarkerofneurologicaldysfunction.EarlyHumDev1990Sep;23(3):151-158.
(34) BrugginkJL,EinspielerC,ButcherPR,StremmelaarEF,PrechtlHF,BosAF.Quantitativeaspectsoftheearlymotorrepertoireinpreterminfants:dotheypredictminorneurologicaldysfunctionatschoolage?EarlyHumDev2009Jan;85(1):25-36.
(35) GevaR,EshelR,LeitnerY,ValevskiAF,HarelS.Neuropsychologicaloutcomeofchildrenwithintrauterinegrowthrestriction:a9-yearprospectivestudy.Pediatrics2006Jul;118(1):91-100.
(36) RozeE,TaBD,vanderReeMH,TanisJC,vanBraeckelKN,HulscherJB,etal.Functionalimpairmentsatschoolageofchildrenwithnecrotizingenterocolitisorspontaneousintestinalperforation.PediatrRes2011Dec;70(6):619-625.

Part I
Cardiac function in FGR
Chapter 2
Online versus offline spatiotemporal image correlation (STIC) M-mode
for the evaluation of cardiac longitudinal annular displacement
in fetal growth restriction
Jozien C. Tanis, Nuruddin Mohammed, Mar Bennasar, Josep Maria Martinez, Bart Bijnens, Fatima Crispi, and Eduard Gratacos
Submitted
24
Chapter 2
Abstract
ObjectivesOur �irst aim was to compare online M-mode with of�line spatiotemporal imagecorrelation(STIC)M-mode forassessing longitudinalannulardisplacement(LAD) ingrowthrestrictedfetuses(FGR).OursecondaimwastocompareLADmeasuresofFGRcaseswithcontrols.
MethodsProspective study including 40 FGR cases (de�ined estimated fetalweight and birthweight<10thcentile)and72normallygrownfetusespairedwithcasesbygestationalageatscan.LADwasmeasuredwithonlineM-modeandof�lineSTICM-modeattheleftandrightventricularfreewallsandseptuminallfetuses.
ResultsFGRcaseshadasigni�icantdecreaseinLADbySTICinallsites(e.g.rightLADinFGRmean6.7mm (SD1.2) vs controls 7.2mm (1.2), P=0.033) as compared to controls.Therewasanon-signi�icanttrendforlowervaluesinFGRwhenusingonlineM-mode(e.g.rightLADinFGR6.9mm(1.5)vscontrols7.4mm(1.5),P=0.084).
ConclusionSTICM-modeseemsabettermethodthanonlineM-modefordetectingsubtlechangesinmyocardialmotion.STICpresentsmorepreciseresultsandallowsanidealplacementof the M-mode arrow. These results con�irm previous data suggesting decreasedlongitudinalmotioninFGR.
Cardiac function in FGR
25
6
2
Introduction
Evaluation of cardiac function is increasingly used for the characterization andunderstanding of fetal diseases. Fetal cardiac function assessment is technicallychallenging, and the development of reproducible methods is critical to allowcomparability among studies. Longitudinal annular displacement (LAD) is themostcommonlyusedparameter,becauseitisaneasyandreproduciblemethodtomeasuremyocardialmotion.(1-10)LADisnormallyevaluatedbyonlinemotionmode(M-mode)atthefreeventricularwallsandtheinterventricularseptum.However,onlineM-modehasa fewdisadvantages.Amain limitationofM-modeis thedif�icultyofobtainingaperfectaligmentoftheM-modelinewiththeventricularwallsatananglecloseto0°,particularlyintheleftfreewall.Thismightintroducesomebiasinthedetectionofmildchangesinventricularmotion,bothinprenatalandpostnatalevaluations.Inaddition,obtainingaperfect4-chamberview, i.e,withsimilarlysized left/rightchambersandatrioventricularvalves,formeasuringLADintheoptimalpositionisoftenchallenging. Spatiotemporal image correlation (STIC) provides an of�line method for four-dimensional(4D)analysisofthefetalheart.(11-13)STICwouldallowtomeasureLADattheangleofchoiceandalsotorotatethevolumeforobtaininganoptimal4-chamberview. In thisstudy,wehypothesized thatLADmeasuredwithSTICcouldbeabettermethodtodetectdifferencesinfetaldiseasesascomparedtoonlineM-mode.Totestthishypothesis,weusedfetalgrowthrestriction(FGR)asdiseasemodel.InFGR,theheartisacentralorganintheadaptivemechanismstoplacentalinsuf�iciency(14,15)displayingprofoundstructuralandfunctionalchangesprenatally,(16)whichpersistintochildhood.(17,18)Brie�ly,FGRisassociatedwithcardiacremodelingtomoreglobularhearts, with impaired relaxation and decreased longitudinal myocardial motion asmeasuredbyonlineM-mode.(19,20) Our�irstaimwastoperformaprospectivestudytocompareLADmeasuresusingonline conventional M-mode versus of�line STIC M-mode in 40 FGR cases and 72normallygrownfetuses.OursecondaimwastocompareLADmeasuresofFGRcaseswithcontrols.
Methods
Study design and populationThestudydesignwasaprospectivecohortstudyincluding40casesubjectswithFGRand72controlsubjects.ThesourcepopulationconsistedofwomenwithasingletonpregnancyattendingtheDepartmentofMaternal-FetalMedicineatHospitalClinic inBarcelonafromJanuary2013toOctober2014.FGRwasde�inedbybothestimatedfetal
26
Chapter 2
weight(EFW)belowthe10thcentileandbirthweightbelowthe10thcentile,accordingtolocalstandards.(21)Clinicalfollow-upofFGRcasesfollowedthestage-basedprotocolformanagingFGR.(22)Controlswereselectedamonglow-riskpregnancieswithEFWandbirthweightabovethe10thcentileandpairedwithcasesbygestationalageatscan(±1week). Gestational age at scanwas calculated based on the crown-rump lengthobtainedat�irsttrimesterscan.Structural/chromosomalabnormalitiesorcaseswithevidenceoffetalinfectionwereexcluded.Thestudyprotocolwasapprovedbythelocalethicscommitteeandallpatientsprovidedinformedconsent. All women underwent ultrasound examination using a Voluson E8 (GE MedicalSystems,Milwaukee,WI,USA) that includedestimationof fetalweightand standardfeto-placentalDoppler evaluation in cases. At delivery, gestational age, birthweight,birth weight centile, mode of delivery, Apgar scores, presence of preeclampsia andadmissiontotheneonatalintensivecareunitwererecorded.
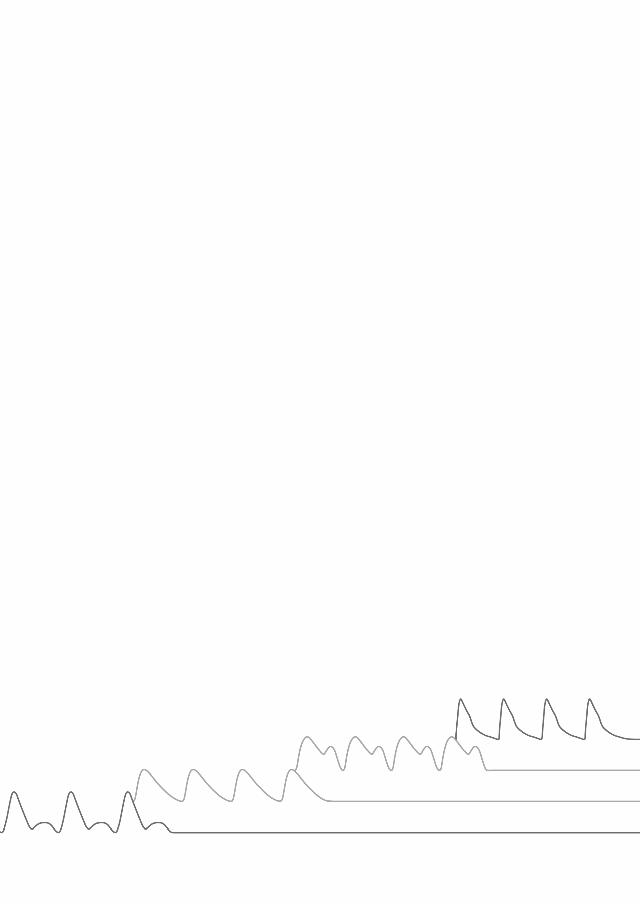
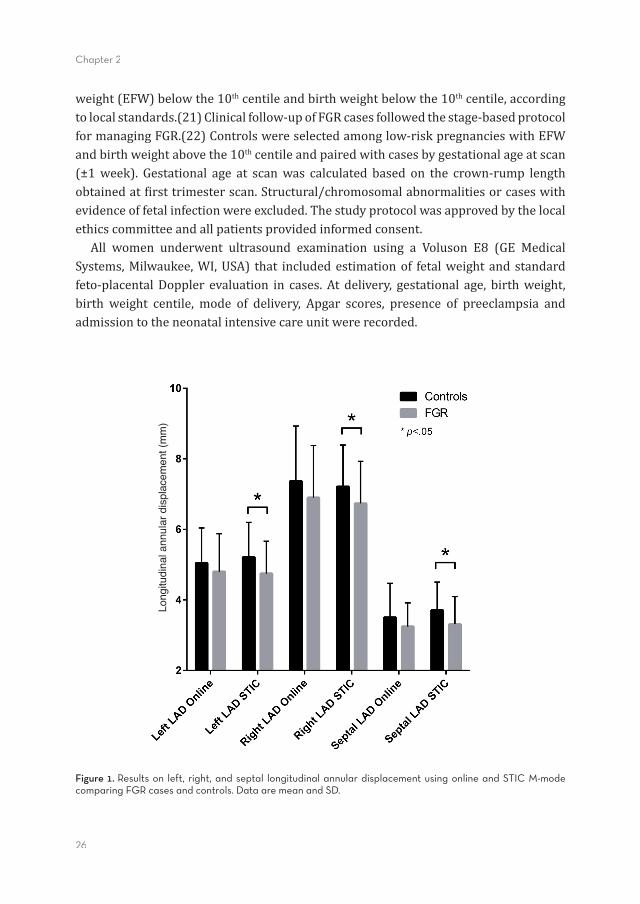
Figure 1. Results on left, right, and septal longitudinal annular displacement using online and STIC M-mode comparing FGR cases and controls. Data are mean and SD.
Long
itudi
nal a
nnul
ar d
ispl
acem
ent (
mm
)
Cardiac function in FGR
27
6
2
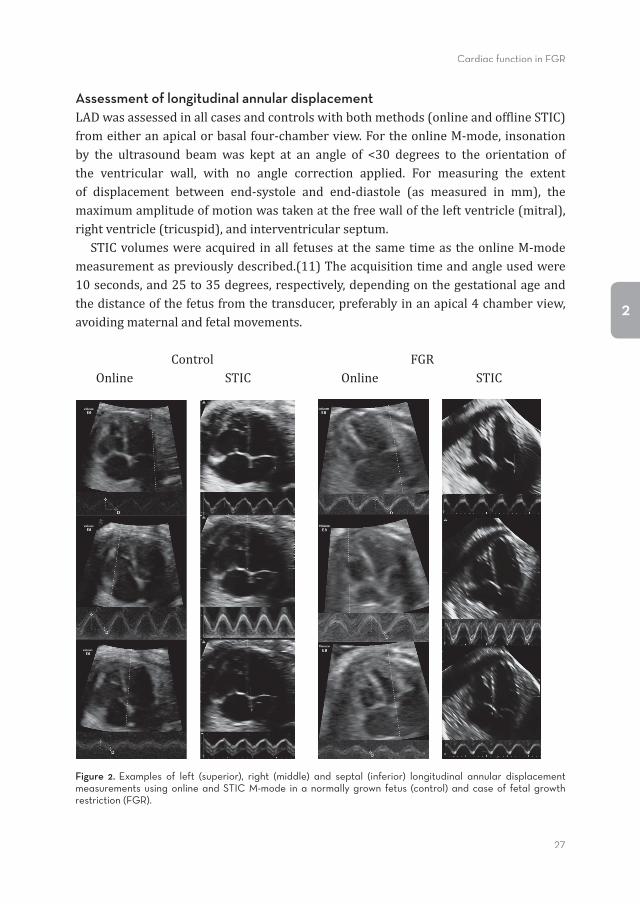
Assessment of longitudinal annular displacementLADwasassessedinallcasesandcontrolswithbothmethods(onlineandof�lineSTIC)fromeitheranapicalorbasalfour-chamberview.FortheonlineM-mode,insonationby the ultrasound beamwas kept at an angle of <30 degrees to the orientation ofthe ventricular wall, with no angle correction applied. For measuring the extentof displacement between end-systole and end-diastole (as measured in mm), themaximumamplitudeofmotionwastakenatthefreewalloftheleftventricle(mitral),rightventricle(tricuspid),andinterventricularseptum. STICvolumeswereacquired inall fetusesat thesametimeas theonlineM-modemeasurementaspreviouslydescribed.(11)Theacquisitiontimeandangleusedwere10seconds,and25to35degrees,respectively,dependingonthegestationalageandthedistanceofthefetusfromthetransducer,preferablyinanapical4chamberview,avoidingmaternalandfetalmovements.
Control FGROnline STIC Online STIC
Figure 2. Examples of left (superior), right (middle) and septal (inferior) longitudinal annular displacement measurements using online and STIC M-mode in a normally grown fetus (control) and case of fetal growth restriction (FGR).

28
Chapter 2
STICM-modeanalysiswasblindlyperformedbyoneexperiencedinvestigator.Of�line,theoperatoradjustedtheSTICvolumebyscrollingthroughthevolumeslicesandadjustingX,Y,Zaxis,andcontrast.LADwasmeasuredinthesamewayasonline,exceptfortheangleofinsonation.DuetothepossibilityofplacingtheM-modearrowaspreferred,theinsonationanglewasalwaysparalleltotheinterventricularseptumorthelateralwalls.6Inordertooptimizethemeasuringconditions,thespeedwasadjustedtoseethreeto�ivecardiaccyclesandtheY-axiswasmaximized.OnthethusobtainedM-modeimages,themaximumdistanceoftheresultingwaveformwasmeasured(Figure2).Inthe4chamberview,wealsomeasuredcardiacsizeascardiaclongaxisfromapextobase.
Statistical analysisData were analyzed using IBM SPSS Statistics 19 (IBM Corporation, Armonk, NY).ComparisonbetweenstudygroupswasperformedbyStudentTtestforindependentsamplesandthechi-squaretestwhereappropriate.P<0.05wasconsideredstatisticallysigni�icant.Inordertoadjustforcardiacsize,asubanalysisincluding40FGRcasesand40controlspairedbycardiaclongaxisdimensionwasalsoperformed(Supplementaldata).
Results
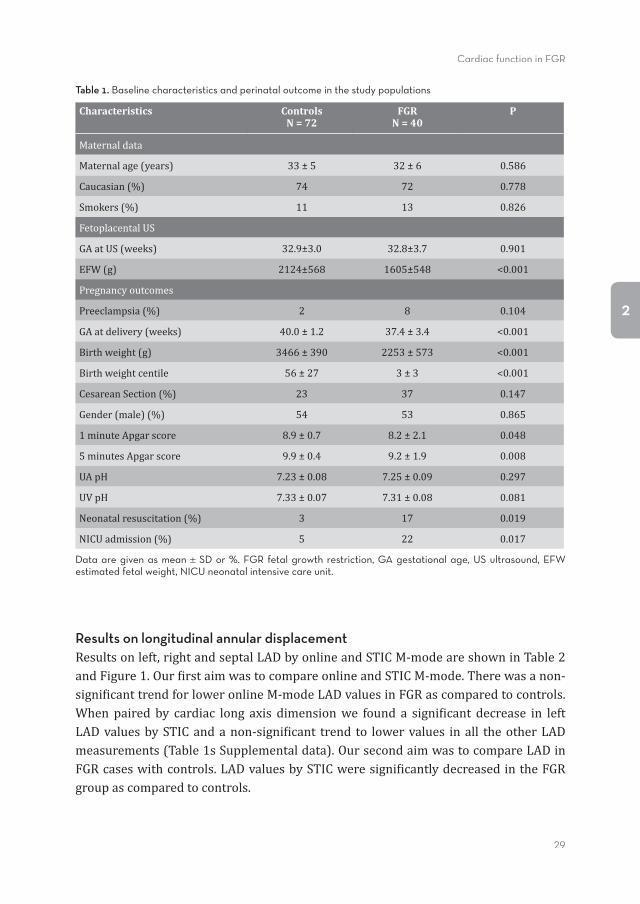
Study populationsCharacteristicsofthestudypopulationsareshowninTable1.Baselinecharacteristicsweresimilarincasesandcontrolsregardingmaternaldata,gestationalageatultrasound,gender,umbilicalarteryandveinpH,andpreeclampsiaandcesareansectionrate. Asexpected,FGRcasesshoweda lowerestimatedfetalweight,birthweight,birthweightcentile,gestationalageatbirthandApgarscore.InFGRcases,27%hadabnormalDopplerPIvalues(above95thcentile)ofthemeanuterineartery,7%abnormalumbilicalartery,2%abnormal(below5thcentile)middlecerebralartery,2%abnormalductusvenosus,2%abnormalaortic isthmus.Gestationalagerangeatultrasoundwas25.0-40.2withameanof32.9weeks.
Cardiac function in FGR
29
6
2
Table 1. Baseline characteristics and perinatal outcome in the study populations
Characteristics ControlsN = 72
FGRN = 40
P
Maternaldata
Maternalage(years) 33±5 32±6 0.586
Caucasian(%) 74 72 0.778
Smokers(%) 11 13 0.826
FetoplacentalUS
GAatUS(weeks) 32.9±3.0 32.8±3.7 0.901
EFW(g) 2124±568 1605±548 <0.001
Pregnancyoutcomes
Preeclampsia(%) 2 8 0.104
GAatdelivery(weeks) 40.0±1.2 37.4±3.4 <0.001
Birthweight(g) 3466±390 2253±573 <0.001
Birthweightcentile 56±27 3±3 <0.001
CesareanSection(%) 23 37 0.147
Gender(male)(%) 54 53 0.865
1minuteApgarscore 8.9±0.7 8.2±2.1 0.048
5minutesApgarscore 9.9±0.4 9.2±1.9 0.008
UApH 7.23±0.08 7.25±0.09 0.297
UVpH 7.33±0.07 7.31±0.08 0.081
Neonatalresuscitation(%) 3 17 0.019
NICUadmission(%) 5 22 0.017
Data are given as mean SD or %. FGR fetal growth restriction, GA gestational age, US ultrasound, EFW estimated fetal weight, NICU neonatal intensive care unit.
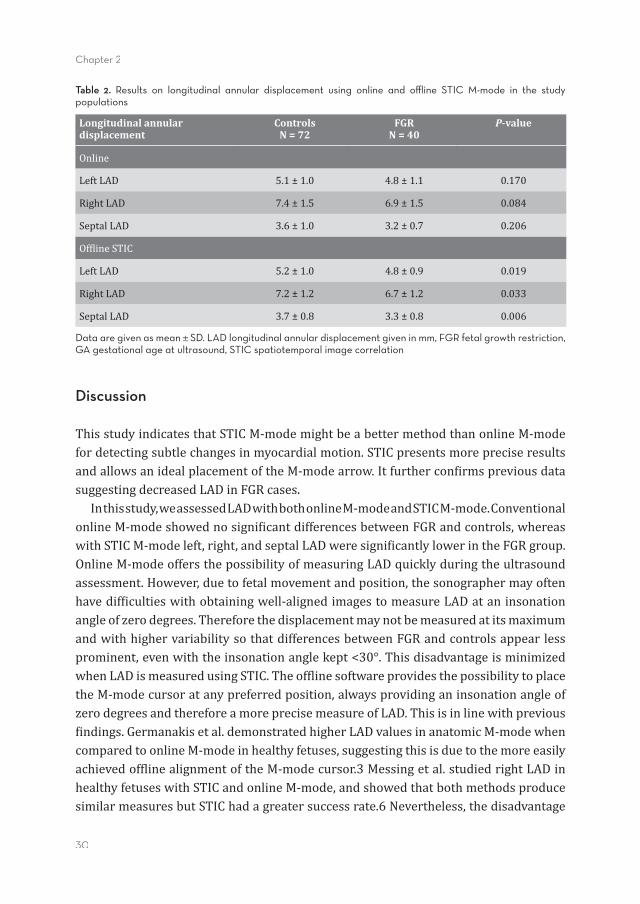
Results on longitudinal annular displacementResultsonleft,rightandseptalLADbyonlineandSTICM-modeareshowninTable2andFigure1.Our�irstaimwastocompareonlineandSTICM-mode.Therewasanon-signi�icanttrendforloweronlineM-modeLADvaluesinFGRascomparedtocontrols.When paired by cardiac long axis dimensionwe found a signi�icant decrease in leftLADvaluesbySTICandanon-signi�icant trend to lowervalues inall theotherLADmeasurements(Table1sSupplementaldata).OursecondaimwastocompareLADinFGRcaseswithcontrols.LADvaluesbySTICweresigni�icantlydecreasedintheFGRgroupascomparedtocontrols.
30
Chapter 2
Table 2. Results on longitudinal annular displacement using online and offl ine STIC M-mode in the study populations
Longitudinal annular displacement
ControlsN = 72
FGRN = 40
P-value
Online
LeftLAD 5.1±1.0 4.8±1.1 0.170
RightLAD 7.4±1.5 6.9±1.5 0.084
SeptalLAD 3.6±1.0 3.2±0.7 0.206
Of�lineSTIC
LeftLAD 5.2±1.0 4.8±0.9 0.019
RightLAD 7.2±1.2 6.7±1.2 0.033
SeptalLAD 3.7±0.8 3.3±0.8 0.006
Data are given as mean SD. LAD longitudinal annular displacement given in mm, FGR fetal growth restriction, GA gestational age at ultrasound, STIC spatiotemporal image correlation
Discussion
ThisstudyindicatesthatSTICM-modemightbeabettermethodthanonlineM-modefordetectingsubtlechangesinmyocardialmotion.STICpresentsmorepreciseresultsandallowsanidealplacementoftheM-modearrow.Itfurthercon�irmspreviousdatasuggestingdecreasedLADinFGRcases. Inthisstudy,weassessedLADwithbothonlineM-modeandSTICM-mode.ConventionalonlineM-modeshowednosigni�icantdifferencesbetweenFGRandcontrols,whereaswithSTICM-modeleft,right,andseptalLADweresigni�icantlylowerintheFGRgroup.OnlineM-modeoffersthepossibilityofmeasuringLADquicklyduringtheultrasoundassessment.However,duetofetalmovementandposition,thesonographermayoftenhavedif�icultieswithobtainingwell-alignedimagestomeasureLADataninsonationangleofzerodegrees.ThereforethedisplacementmaynotbemeasuredatitsmaximumandwithhighervariabilitysothatdifferencesbetweenFGRandcontrolsappearlessprominent,evenwiththeinsonationanglekept<30°.ThisdisadvantageisminimizedwhenLADismeasuredusingSTIC.Theof�linesoftwareprovidesthepossibilitytoplacetheM-modecursoratanypreferredposition,alwaysprovidinganinsonationangleofzerodegreesandthereforeamoreprecisemeasureofLAD.Thisisinlinewithprevious�indings.Germanakisetal.demonstratedhigherLADvaluesinanatomicM-modewhencomparedtoonlineM-modeinhealthyfetuses,suggestingthisisduetothemoreeasilyachievedof�linealignmentoftheM-modecursor.3Messingetal.studiedrightLADinhealthyfetuseswithSTICandonlineM-mode,andshowedthatbothmethodsproducesimilarmeasuresbutSTIChadagreatersuccessrate.6Nevertheless,thedisadvantage
Cardiac function in FGR
31
6
2
ofSTICM-modeliesinthetimeittakestodotheof�lineanalysisaswellasapotentiallylowertemporalresolution. Inconclusion,whileonlineM-mode isa fasterandeasiermethodandmaybeusedtomeasureLADinmoreseverecases,STICseemstobemoresuitabletodetectsubtledifferencesinmildFGR. We coulddemonstrate a signi�icant reductionof LAD in the left, right, and septalwall in FGR cases, which is consistent with previous data suggesting decreasedlongitudinalmotioninsevereearlygrowthrestrictedfetuses.(19)Wehavepreviouslydemonstrated signi�icant lower LADmeasuredwith onlineM-mode in severe IUGRcasesbornbeforeagestationalageof34weeks, thusbeingearly-onsetandwithanabnormal umbilical artery Doppler pulsatility index.(19) Therefore, that populationcontainedmoresevereFGRcasesascomparedtothepresentstudy(includingmainlylate-onset cases with normal feto-placental Doppler). These group differences mayexplainthenon-signi�icanttrendinonlineM-modeinthepresentstudy.Thepresentstudyisthe�irstreportdemonstratingsigni�icantchangesinLADinnon-severeFGRbyusingSTICM-mode.Sincebothdisplacementandvelocityrelatetolongitudinalmotion,our�indingsarecomplementarywithpreviousstudiesdemonstratinglowerE’andA’annularpeakvelocitiesbytissueDopplerinlate-onsetsmall-for-gestationalagefetusesascomparedtocontrols.(19,23,24) Weacknowledgethatthisstudyhasseveralstrengthsandlimitations.Wetookgreatcare in data acquisition; onlineM-mode and 4D STIC loop acquisition took place indirectconsecutiveorder.OneexperiencedinvestigatorperformedSTICM-modeof�lineanalysis,blinded forcasesorcontrols.Therefore,unfortunately,wecouldnotassessinter-observer variability. In addition,we did not perform intra-observer variability.AnotherlimitationisthatoursamplesizepreventsustosubdivideFGRcasesaccordingtoDoppler �indings. Furthermore, our limited sample sizemay partially explain thenon-signi�icanttrendintheonlineM-moderesults.Ourstudypopulationwaspairedbygestationalageatscaninordertoadjustformaturationalchangesthroughoutgestationincardiacfunctionparameters.However,weacknowledgethatlongitudinalaxismotionisalsostronglyrelatedtocardiacsize.Inordertoadjustforthat,asubanalysisincludingcases and controls paired by cardiac sizewas also performed (Supplemental data),whichleadtosimilarconclusions;asigni�icantdecreaseinleftLADvaluesbySTICandalsoanon-signi�icanttrendtolowervaluesinalltheotherLADmeasurements.Futurestudies arewarranted to con�irmour results and furthervalidate theuseof STICMmodeinthedetectionofearlychangesincardiacfunction.
32
Chapter 2
Conclusion
These data support the hypothesis that STIC is feasible for the assessment of LADinuteroand itcould improveconventionalonlineM-mode in thedetectionofsubtledifferences in cardiac dysfunction. Since reduced right LADhas been proposed as apredictivemarker for postnatal hypertension and arterial remodeling in FGR,(25) itmightbeofusefortheprenataldetectionofthoseFGRcasesathighercardiovascularriskandthatmightbene�itfrompostnatalinterventionsinordertopotentiallyimprovetheirfuturecardiovascularhealth.
AcknowledgementsThisstudywassupportedbygrantsfromtheGraduateSchoolofMedicalSciencesoftheUniversityofGroningen,theresearchinstituteBCN-BRAIN,theMinisteriodeEconomiayCompetitividad(ref.SAF2012-37196),theInstitutodeSaludCarlosIII(ref.PI11/00051,PI11/01709,PI12/02230)integradoenelPlanNacionaldeI+D+Iyco�inanciadoporelISCIII-SubdirecciónGeneraldeEvaluaciónyelFondoEuropeodeDesarrolloRegional(FEDER)“OtramaneradehacerEuropa”,theCerebraFoundationfortheBrainInjuredChild(Carmarthen,Wales,UK),ObraSocial“laCaixa”,theFundaciónMutuaMadrileña,andAGAUR2014SGRgrantnº928.
Cardiac function in FGR
33
6
2
References1 CarvalhoJS,O’SullivanC,ShinebourneEA,HeneinMY.Rightandleftventricularlong-axisfunctioninthe
fetususingangularM-mode.UltrasoundObstetGynecol2001Dec;18(6):619-622.2 GardinerHM,PasquiniL,WolfendenJetal.MyocardialtissueDopplerandlongaxisfunctioninthefetal
heart.IntJCardiol2006Oct26;113(1):39-47.3 Germanakis I, Pepes S, Sifakis S, Gardiner H. Fetal longitudinal myocardial function assessment by
anatomicM-mode.FetalDiagnTher2012;32(1-2):65-71.4 GodfreyME,MessingB,ValskyDVetal.Fetalcardiacfunction:M-modeand4Dspatiotemporalimage
correlation.FetalDiagnTher2012;32(1-2):17-21.5 Jurgens J, Chaoui R. Three-dimensionalmultiplanar time-motion ultrasound or anatomicalM-mode
of the fetal heart: a new technique in fetal echocardiography. Ultrasound Obstet Gynecol 2003Feb;21(2):119-123.
6 Messing B, Gilboa Y, LipschuetzM et al. Fetal tricuspid annular plane systolic excursion (f-TAPSE):evaluationoffetalrightheartsystolicfunctionwithconventionalM-modeultrasoundandspatiotemporalimagecorrelation(STIC)M-mode.UltrasoundObstetGynecol2013Aug;42(2):182-188.
7 Bazaz R, Edelman K, Gulyasy B, Lopez-Candales A. Evidence of robust coupling of atrioventricularmechanicalfunctionoftherightsideoftheheart: insightsfromM-modeanalysisofannularmotion.Echocardiography2008Jul;25(6):557-561.
8 GhioS,RecusaniF,KlersyCetal.Prognosticusefulnessofthetricuspidannularplanesystolicexcursioninpatientswithcongestiveheartfailuresecondarytoidiopathicorischemicdilatedcardiomyopathy.AmJCardiol2000Apr1;85(7):837-842.
9 KoestenbergerM,NagelB,RavekesWet al. Systolic right ventricular function inpretermand termneonates:referencevaluesofthetricuspidannularplanesystolicexcursion(TAPSE)in258patientsandcalculationofZ-scorevalues.Neonatology2011;100(1):85-92.
10 HuK,LiuD,HerrmannSetal.Clinicalimplicationofmitralannularplanesystolicexcursionforpatientswithcardiovasculardisease.EurHeartJCardiovascImaging2013Mar;14(3):205-212.
11 DeVoreGR, Falkensammer P, SklanskyMS, Platt LD. Spatio-temporal image correlation (STIC): newtechnologyforevaluationofthefetalheart.UltrasoundObstetGynecol2003Oct;22(4):380-387.
12 Goncalves LF, Lee W, Espinoza J, Romero R. Examination of the fetal heart by four-dimensional(4D) ultrasound with spatio-temporal image correlation (STIC). Ultrasound Obstet Gynecol 2006Mar;27(3):336-348.
13 YagelS,CohenSM,ShapiroI,ValskyDV.3Dand4Dultrasoundinfetalcardiacscanning:anewlookatthefetalheart.UltrasoundObstetGynecol2007Jan;29(1):81-95.
14 HecherK,CampbellS,DoylePetal.AssessmentoffetalcompromisebyDopplerultrasoundinvestigationofthefetalcirculation.Arterial,intracardiac,andvenousblood�lowvelocitystudies.Circulation1995Jan1;91(1):129-138.
15 MakikallioK,VuolteenahoO,JouppilaP,RasanenJ.Ultrasonographicandbiochemicalmarkersofhumanfetalcardiacdysfunctioninplacentalinsuf�iciency.Circulation2002Apr30;105(17):2058-2063.
16 Leipala JA,BoldtT,TurpeinenUet al. Cardiachypertrophyandalteredhemodynamicadaptation ingrowth-restrictedpreterminfants.PediatrRes2003Jun;53(6):989-993.
17 CrispiF,BijnensB,FiguerasFetal.Fetalgrowthrestrictionresultsinremodeledandlessef�icientheartsinchildren.Circulation2010Jun8;121(22):2427-2436.
18 DemichevaE,CrispiF.Long-termfollow-upofintrauterinegrowthrestriction:cardiovasculardisorders.FetalDiagnTher2014;36(2):143-153.
19 Cruz-LeminiM,CrispiF,Valenzuela-AlcarazBetal.ValueofannularM-modedisplacementvstissueDoppler velocities to assess cardiac function in intrauterine growth restriction. Ultrasound ObstetGynecol2013Aug;42(2):175-181.
20 Crispi F, Bijnens B, Sepulveda-Swatson E et al. Postsystolic shortening by myocardial deformationimagingasasignofcardiacadaptationtopressureoverloadinfetalgrowthrestriction.CircCardiovascImaging2014Sep;7(5):781-787.
21 FiguerasF,MelerE, IraolaAetal.CustomizedbirthweightstandardsforaSpanishpopulation.EurJObstetGynecolReprodBiol2008Jan;136(1):20-24.
34
Chapter 2
22 FiguerasF,GratacosE.Updateonthediagnosisandclassi�icationoffetalgrowthrestrictionandproposalofastage-basedmanagementprotocol.FetalDiagnTher2014;36(2):86-98.
23 LarsenLU,PetersenOB,SlothE,UldbjergN.ColorDopplermyocardialimagingdemonstratesreduceddiastolic tissue velocity in growth retarded fetuses with �low redistribution. Eur J Obstet GynecolReprodBiol2011Apr;155(2):140-145.
24 Comas M, Crispi F, Cruz-Martinez R et al. Tissue Doppler echocardiographic markers of cardiacdysfunctioninsmall-for-gestationalagefetuses.AmJObstetGynecol2011Jul;205(1):57.e1-57.e6.
25 Cruz-Lemini M, Crispi F, Valenzuela-Alcaraz B et al. A fetal cardiovascular score to predict infanthypertension and arterial remodeling in intrauterine growth restriction. Am JObstet Gynecol 2014Jun;210(6):552.e1-552.e22.
Cardiac function in FGR
35
6
2
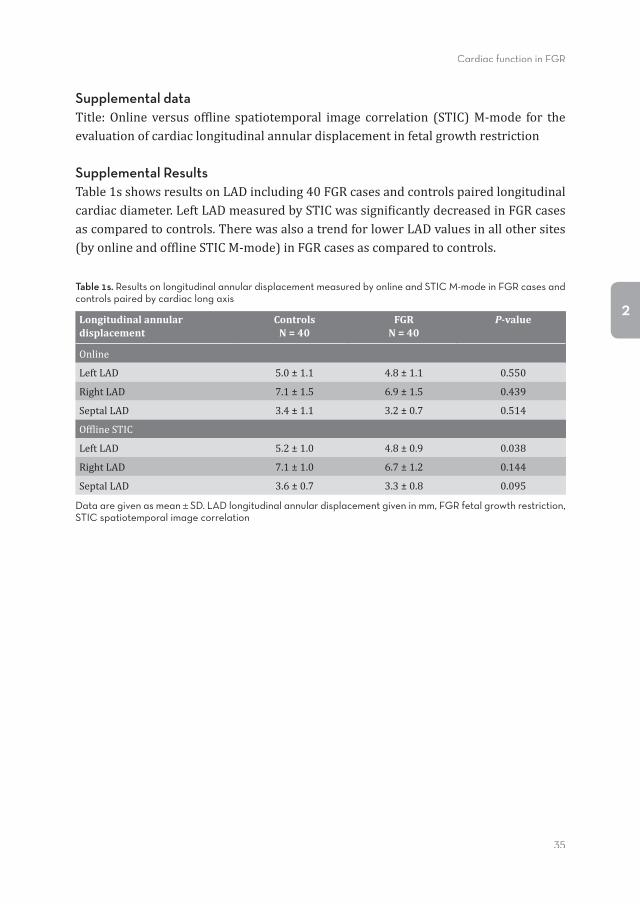
Supplemental dataTitle:Online versus of�line spatiotemporal image correlation (STIC)M-mode for theevaluationofcardiaclongitudinalannulardisplacementinfetalgrowthrestriction
Supplemental ResultsTable1sshowsresultsonLADincluding40FGRcasesandcontrolspairedlongitudinalcardiacdiameter.LeftLADmeasuredbySTICwassigni�icantlydecreasedinFGRcasesascomparedtocontrols.TherewasalsoatrendforlowerLADvaluesinallothersites(byonlineandof�lineSTICM-mode)inFGRcasesascomparedtocontrols.
Table 1s. Results on longitudinal annular displacement measured by online and STIC M-mode in FGR cases and controls paired by cardiac long axis
Longitudinal annular displacement
ControlsN = 40
FGRN = 40
P-value
Online
LeftLAD 5.0±1.1 4.8±1.1 0.550
RightLAD 7.1±1.5 6.9±1.5 0.439
SeptalLAD 3.4±1.1 3.2±0.7 0.514
Of�lineSTIC
LeftLAD 5.2±1.0 4.8±0.9 0.038
RightLAD 7.1±1.0 6.7±1.2 0.144
SeptalLAD 3.6±0.7 3.3±0.8 0.095
Data are given as mean SD. LAD longitudinal annular displacement given in mm, FGR fetal growth restriction, STIC spatiotemporal image correlation

Part II
Prenatal predictors of neonatal outcome in FGR
Chapter 3
Prenatal Doppler flow patterns and neonatal circulation in
fetal growth restriction
Jozien C. Tanis, Maaike R. Boelen, Danique M. Schmitz, Lucia Casarella, Michelle E. van der Laan, Arend F. Bos, and Caterina M. Bilardo
Ultrasound in Obstetrics & Gynecology 2015 Sept 11. doi 10.1002/uog.14744

40
Chapter 3
Abstract
ObjectivesToinvestigate,ingrowth-restrictedfetuses,whetherprenatalDopplerparametersarecorrelatedwithneonatalcirculatorychanges.
MethodsIn43casesofsuspectedFGR,serialDopplermeasurementsoftheumbilicalartery(UA)andthemiddlecerebralartery(MCA)wereperformed(lastmeasurement,closesttodelivery:<1weekbeforebirth).Neonatalcirculationwasassessedfor2hours/dayonDays1-5,8, and15bynear-infrared spectroscopy (NIRS)of the cerebral, renal, andsplanchnic regions.The followingratioswerecalculated: cerebroplacental (CPR), i.e.MCA/UA, cerebrorenal (CRR), i.e. cerebral/renalNIRS, and cerebrosplanchnic (CSR),i.e.cerebral/splanchnicNIRS.Correlationcoef�icientswerecalculatedbetweenDopplerparametersandneonatalNIRS.Theseanalyseswerecarriedoutfortheentiregroup,andseparatelyforearlyFGR(casesdeliveredbefore34weeks’GA)andlateFGR(≥34weeks’GA).
ResultsOnDays1-3postnatally, fetalDopplerparameters correlated stronglywithneonatalNIRS:UAcorrelatedwithrenalNIRS(Day1:rho=.454,P <.01)andCRR(Day1:rho=-.517,P<.001).MCAcorrelatedwithcerebralNIRSonDays2and3,butnotonDay1(Day2:rho=.469,P<.01).CPRcorrelatedwithCRR(Day1:rho=.474,P<.01).InearlyandlateFGRseparately,mostassociationslosttheirstatisticalsigni�icance.
ConclusionLowMCApulsatilityindex(PI)andlowCPR,indicatingbrainsparingbeforebirth,areassociatedwithlowCRRafterbirth,indicatingrelativelygreaterbloodvolumestothecerebrum than to the renal region.Basedon the results from this study, it couldbespeculatedthatifbrainsparingispresentinfetalcirculation,itpersistsduringthe�irstthreedaysafterbirth.
Prenatal predictors of neonatal outcome in FGR
41
3
Introduction
Thecirculationofgrowth-restrictedfetusesadaptstodiminishedavailabilityofoxygenandnutrientsinsuchawayastosparethebrain-amechanismknownasbrainsparing.(1,2)Infetalgrowthrestriction(FGR),itisunderdebatewhetherbrainsparingfunctionsasaprotectivemechanism,orwhetheritisasanexpressionofcirculatoryfailure.(3,4)Inaddition,consequencesofbrainsparingmightbedifferentbetweenearlyFGRandlateFGR. Dopplervelocimetryoftheumbilicalartery(UA)andofthemiddlecerebralartery(MCA) is a well-established, non-invasive, and reproducible method to measurefetoplacentalcirculation.(2)Abnormal �lowpatternsof theUAandMCAcanbeusedasanindicatoroftheseverityofFGRandthedegreeoffetalhypoxemia.(5-8)Theratiobetweenthecerebralandfetoplacentalcirculation,alsoknownasthecerebroplacentalratio(CPR),i.e.MCA/UA,hasbeensuggestedasastrongpredictoroffetaloutcome.(9-13) AlthoughDoppleradaptationsduringfetallifeinFGRhavebeenwidelystudied,littleisknownaboutthepersistenceofhemodynamicadjustmentswhen,afterbirth,chronichypoxiaceases.Insightintocirculatorychangesofthegrowthrestrictedinfantmayaidneonatalcare. Near-infrared spectroscopy (NIRS), a light-based technology used tomeasure thestatus of tissue oxygen, is a non-invasivemethod to study neonatal hemodynamics.(14-16)NIRSsensorsareeasilyapplicableanddonotdisturbthevulnerableneonate.Therefore, particularly in a neonatal intensive care setting, it is preferred over, forexample, Doppler ultrasound. Previously, NIRSwas used solely tomeasure cerebralperfusion.(17)Lately,multisiteNIRShasbeenintroduced.Itprovidestheopportunitytomeasurenotonlythecerebral,butrenalandsplanchniccirculationaswell–hencethede�initionmultisite.(18-20)SinceNIRSmeasuresperfusion,aratioofcerebraltorenalandcerebraltosplanchnicperfusioncanbecalculated.(21)Theseratiosmayrepresentneonatalcirculatorydistributionandare,therefore,apossiblepostnatalequivalentofthefetalDopplerCPR. The aim of this studywas to investigatewhether in early and late FGR, Dopplervelocimetry of the fetal circulation are associated with measurements of neonatalcirculation.
Methods
A prospective observational cohort study was performed between June 2012 andSeptember 2014 at the Department of Obstetrics and the Fetal Medicine Unit of
42
Chapter 3
UniversityMedical Center Groningen (UMCG), in theNetherlands. Exclusion criteriaweremultiplepregnancy,structuraland/orchromosomalabnormalities,orevidenceoffetalinfection.AllpregnanciesweredeliveredatUMCG.Ifindicated,neonateswereadmittedtotheNeonatologywardofthesamehospital.Dataonobstetric,birth,andneonatalcharacteristicswerecollected fromthe twodepartments.Written informedparentalconsentwasobtainedinallcases.Thestudywasapprovedbythehospital’sMedicalBoardandMedicalResearchEthicsCommittee. We de�ined FGR as fetal abdominal circumference or estimated fetalweight (22)below the 10th percentile, or de�lecting fetal growth of at least 30 percentiles withrespect topreviousmeasurements (reducedgrowthaccording to the fetus’expectedgrowthpotential).Onaverage,priortomaternaladmission,fetalDopplerparametersweremeasuredseriallyonceaweek,andtwiceaweekforthedurationofadmission.We used themeasurement thatwas closest to delivery,with amaximumof 1weekbeforebirth.MeasurementsincludedPIoftheUAandMCA.Carewastakentoperformthelastmeasurementasclosetothedayofdeliveryaspossibleandneveratanintervalofmorethanoneweektodelivery.LeftandrightmaternaluterinearteryDopplersweremeasuredduringthe�irstvisit.TwoexperiencedoperatorsperformedalltheDopplermeasurements.Allthemeasurementsweretransformedtozscores(standarddeviationfromthegestationalagemean)forfurtheranalysis.(23,24)Incaseofabsentenddiastolic�lowintheUA,thePIwascalculatedbymanuallytracingtheenddiastolicvelocityalongthetimeaxis.Thecerebroplacentalratio(CPR)wascalculatedasMCAdividedbyUA.(9,11) ForpostnatalhemodynamicmeasurementsweusedtheINVOS5100Cnear-infraredspectrometer (Covidien, Mans�ield, MA, USA). NIRS is a non-invasive method toassess tissueoxygendeliveryandconsumption.TomeasureNIRS,weusedneonatalSomaSensors (Covidien). The optical sensor measures the quantity of re�lectedlight photons as a function of two wavelengths (730 and 805 nm) and determinesthe spectral absorption of the underlying tissue. As oxygenated and deoxygenatedhaemoglobin have distinct absorption spectra, NIRS can differentiate between thetwo.Theratioofoxygenatedhaemoglobin to totalhaemoglobinre�lects theregionaltissueoxygensaturation(rSO2)oftheunderlyingtissue.(25-27)Whentranscutaneousarterialoxygensaturation(spO2)ismeasuredsimultaneously,fractionaltissueoxygenextraction (FTOE) can be calculated as FTOE = (spO2- rSO2)/ spO2. If tissue oxygenmetabolismisconstant,FTOEmayserveasanindicatoroftissueperfusion.Moreblood�low toa tissueresults ina lowerFTOE,whereas lessblood �lowresults inahigherFTOE.WeusedFTOEasameasureofpostnataltissueperfusion.Wethencalculatedthecerebrorenalratio(CRR)andcerebrosplanchnicratio(CSR)ascerebralFTOEdividedby renal and splanchnicFTOE, respectively.NIRS sensorswereplacedon the left orright frontoparietal sideof the infant’sheaddependingon thepositionof the infant(cerebral),ontheleftlateralposterior�lank(renal),andinfraumbilicalonthecentral
Prenatal predictors of neonatal outcome in FGR
43
3
abdomen(splanchnic).WemeasuredrSO2usingNIRSduringa2-hourperiodonDays1(within18hoursafterbirth),2,3,4,5,8,and15afterbirth.
Statistical analysesMeanandmedianvaluesforrSO2andFTOEwerecalculatedforthe2-hourrecordingperiod.FortheanalysesweusedonlyFTOE.SpearmanrankordercorrelationtestswereusedtodeterminecorrelationsbetweenDopplerandNIRSparameters.TheanalyseswererepeatedfortheearlyFGRgroup(<34weeks’GA)andthelateFGRgroup(≥34weeks’GA).DatawereanalysedwithIBMSPSSStatistics22(IBMCorp.,Armonk,NY,USA).APvalue<.05wasconsideredstatisticallysigni�icant.
Results
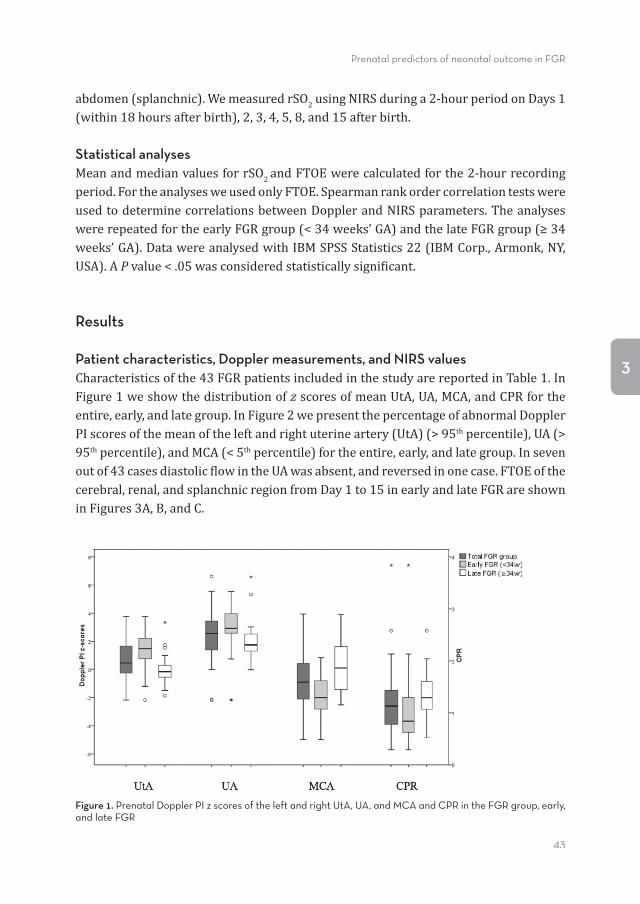
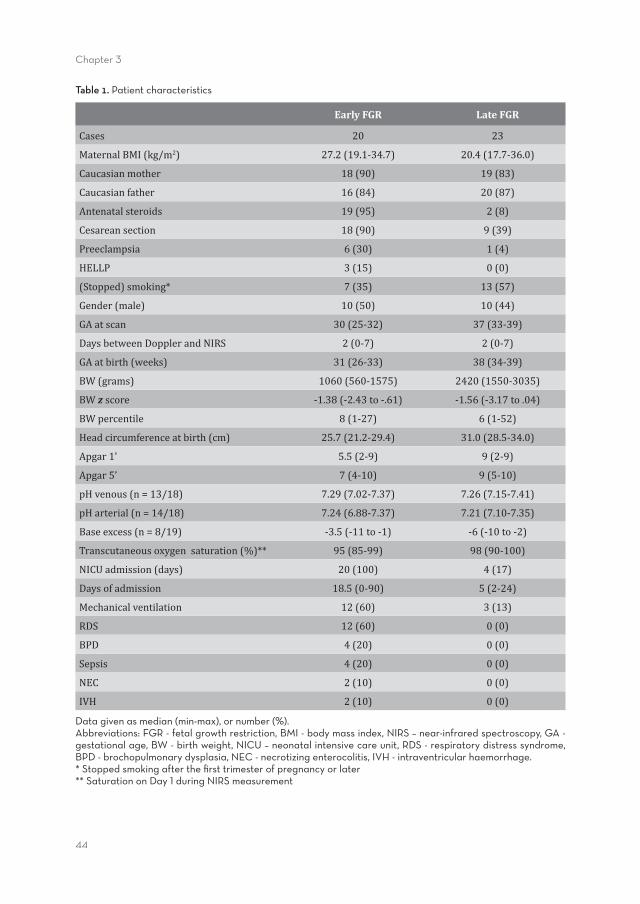
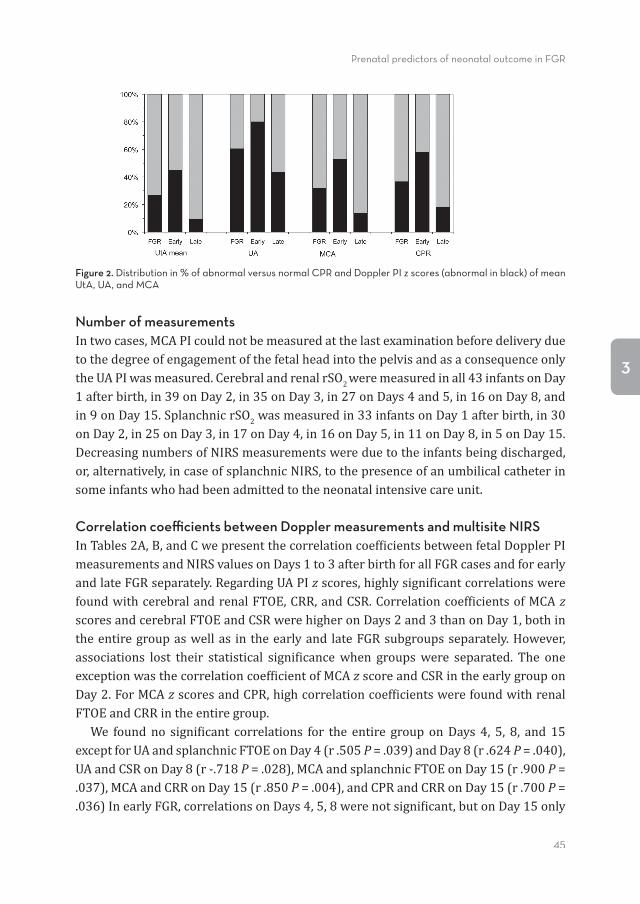
Patient characteristics, Doppler measurements, and NIRS valuesCharacteristicsofthe43FGRpatientsincludedinthestudyarereportedinTable1.InFigure1weshowthedistributionofz scoresofmeanUtA,UA,MCA,andCPRfortheentire,early,andlategroup.InFigure2wepresentthepercentageofabnormalDopplerPIscoresofthemeanoftheleftandrightuterineartery(UtA)(>95thpercentile),UA(>95thpercentile),andMCA(<5thpercentile)fortheentire,early,andlategroup.Insevenoutof43casesdiastolic�lowintheUAwasabsent,andreversedinonecase.FTOEofthecerebral,renal,andsplanchnicregionfromDay1to15inearlyandlateFGRareshowninFigures3A,B,andC.
Figure 1. Prenatal Doppler PI z scores of the left and right UtA, UA, and MCA and CPR in the FGR group, early, and late FGR
44
Chapter 3
Table 1. Patient characteristics
Early FGR Late FGR
Cases 20 23
MaternalBMI(kg/m2) 27.2(19.1-34.7) 20.4(17.7-36.0)
Caucasianmother 18(90) 19(83)
Caucasianfather 16(84) 20(87)
Antenatalsteroids 19(95) 2(8)
Cesareansection 18(90) 9(39)
Preeclampsia 6(30) 1(4)
HELLP 3(15) 0(0)
(Stopped)smoking* 7(35) 13(57)
Gender(male) 10(50) 10(44)
GAatscan 30(25-32) 37(33-39)
DaysbetweenDopplerandNIRS 2(0-7) 2(0-7)
GAatbirth(weeks) 31(26-33) 38(34-39)
BW(grams) 1060(560-1575) 2420(1550-3035)
BWz score -1.38(-2.43to-.61) -1.56(-3.17to.04)
BWpercentile 8(1-27) 6(1-52)
Headcircumferenceatbirth(cm) 25.7(21.2-29.4) 31.0(28.5-34.0)
Apgar1’ 5.5(2-9) 9(2-9)
Apgar5’ 7(4-10) 9(5-10)
pHvenous(n=13/18) 7.29(7.02-7.37) 7.26(7.15-7.41)
pHarterial(n=14/18) 7.24(6.88-7.37) 7.21(7.10-7.35)
Baseexcess(n=8/19) -3.5(-11to-1) -6(-10to-2)
Transcutaneousoxygensaturation(%)** 95(85-99) 98(90-100)
NICUadmission(days) 20(100) 4(17)
Daysofadmission 18.5(0-90) 5(2-24)
Mechanicalventilation 12(60) 3(13)
RDS 12(60) 0(0)
BPD 4(20) 0(0)
Sepsis 4(20) 0(0)
NEC 2(10) 0(0)
IVH 2(10) 0(0)
Data given as median (min-max), or number (%). Abbreviations: FGR - fetal growth restriction, BMI - body mass index, NIRS – near-infrared spectroscopy, GA - gestational age, BW - birth weight, NICU – neonatal intensive care unit, RDS - respiratory distress syndrome, BPD - brochopulmonary dysplasia, NEC - necrotizing enterocolitis, IVH - intraventricular haemorrhage.* Stopped smoking after the fi rst trimester of pregnancy or later** Saturation on Day 1 during NIRS measurement
Prenatal predictors of neonatal outcome in FGR
45
3
Figure 2. Distribution in % of abnormal versus normal CPR and Doppler PI z scores (abnormal in black) of mean UtA, UA, and MCA
Number of measurementsIntwocases,MCAPIcouldnotbemeasuredatthelastexaminationbeforedeliveryduetothedegreeofengagementofthefetalheadintothepelvisandasaconsequenceonlytheUAPIwasmeasured.CerebralandrenalrSO2weremeasuredinall43infantsonDay1afterbirth,in39onDay2,in35onDay3,in27onDays4and5,in16onDay8,andin9onDay15.SplanchnicrSO2wasmeasuredin33infantsonDay1afterbirth,in30onDay2,in25onDay3,in17onDay4,in16onDay5,in11onDay8,in5onDay15.DecreasingnumbersofNIRSmeasurementswereduetotheinfantsbeingdischarged,or,alternatively,incaseofsplanchnicNIRS,tothepresenceofanumbilicalcatheterinsomeinfantswhohadbeenadmittedtotheneonatalintensivecareunit.
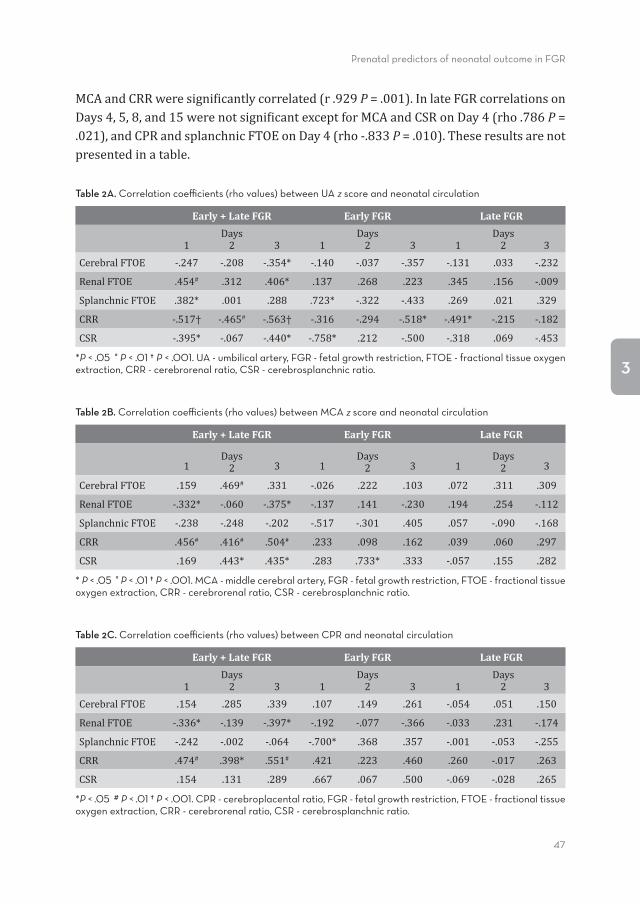
Correlation coeffi cients between Doppler measurements and multisite NIRSInTables2A,B,andCwepresentthecorrelationcoef�icientsbetweenfetalDopplerPImeasurementsandNIRSvaluesonDays1to3afterbirthforallFGRcasesandforearlyandlateFGRseparately.RegardingUAPIz scores,highlysigni�icantcorrelationswerefoundwithcerebralandrenalFTOE,CRR,andCSR.Correlationcoef�icientsofMCAz scoresandcerebralFTOEandCSRwerehigheronDays2and3thanonDay1,bothintheentiregroupaswellas in theearlyand lateFGRsubgroupsseparately.However,associations lost their statistical signi�icancewhen groupswere separated. The oneexceptionwasthecorrelationcoef�icientofMCAz scoreandCSRintheearlygrouponDay2.ForMCAz scoresandCPR,highcorrelationcoef�icientswerefoundwithrenalFTOEandCRRintheentiregroup. We foundno signi�icant correlations for the entire group onDays 4, 5, 8, and15exceptforUAandsplanchnicFTOEonDay4(r.505P =.039)andDay8(r.624P =.040),UAandCSRonDay8(r-.718P =.028),MCAandsplanchnicFTOEonDay15(r.900P =.037),MCAandCRRonDay15(r.850P =.004),andCPRandCRRonDay15(r.700P =.036)InearlyFGR,correlationsonDays4,5,8werenotsigni�icant,butonDay15only
46
Chapter 3
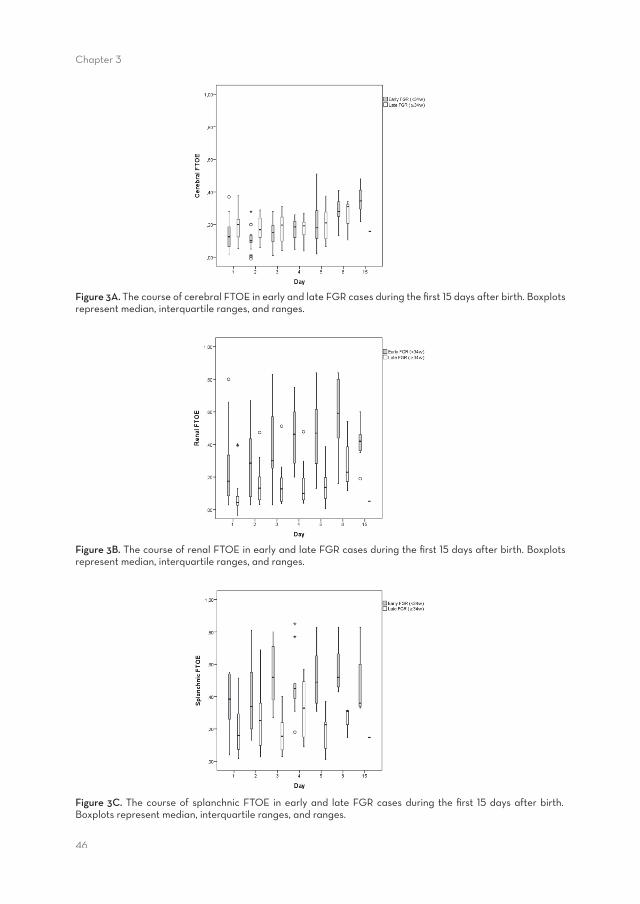
Figure 3A. The course of cerebral FTOE in early and late FGR cases during the fi rst 15 days after birth. Boxplots represent median, interquartile ranges, and ranges.
Figure 3B. The course of renal FTOE in early and late FGR cases during the fi rst 15 days after birth. Boxplots represent median, interquartile ranges, and ranges.
Figure 3C. The course of splanchnic FTOE in early and late FGR cases during the fi rst 15 days after birth. Boxplots represent median, interquartile ranges, and ranges.
Prenatal predictors of neonatal outcome in FGR
47
3
MCAandCRRweresigni�icantlycorrelated(r.929P =.001).InlateFGRcorrelationsonDays4,5,8,and15werenotsigni�icantexceptforMCAandCSRonDay4(rho.786P =.021),andCPRandsplanchnicFTOEonDay4(rho-.833P =.010).Theseresultsarenotpresentedinatable.
Table 2A. Correlation coeffi cients (rho values) between UA z score and neonatal circulation
Early + Late FGR Early FGR Late FGR
1Days2 3 1
Days2 3 1
Days2 3
CerebralFTOE -.247 -.208 -.354* -.140 -.037 -.357 -.131 .033 -.232
RenalFTOE .454# .312 .406* .137 .268 .223 .345 .156 -.009
SplanchnicFTOE .382* .001 .288 .723* -.322 -.433 .269 .021 .329
CRR -.517† -.465# -.563† -.316 -.294 -.518* -.491* -.215 -.182
CSR -.395* -.067 -.440* -.758* .212 -.500 -.318 .069 -.453
*P < .05 # P < .01 † P < .001. UA - umbilical artery, FGR - fetal growth restriction, FTOE - fractional tissue oxygen extraction, CRR - cerebrorenal ratio, CSR - cerebrosplanchnic ratio.
Table 2B. Correlation coeffi cients (rho values) between MCA z score and neonatal circulation
Early + Late FGR Early FGR Late FGR
1Days2 3 1
Days2 3 1
Days2 3
CerebralFTOE .159 .469# .331 -.026 .222 .103 .072 .311 .309
RenalFTOE -.332* -.060 -.375* -.137 .141 -.230 .194 .254 -.112
SplanchnicFTOE -.238 -.248 -.202 -.517 -.301 .405 .057 -.090 -.168
CRR .456# .416# .504# .233 .098 .162 .039 .060 .297
CSR .169 .443* .435* .283 .733* .333 -.057 .155 .282
* P < .05 # P < .01 † P < .001. MCA - middle cerebral artery, FGR - fetal growth restriction, FTOE - fractional tissue oxygen extraction, CRR - cerebrorenal ratio, CSR - cerebrosplanchnic ratio.
Table 2C. Correlation coeffi cients (rho values) between CPR and neonatal circulation
Early + Late FGR Early FGR Late FGR
1Days2 3 1
Days2 3 1
Days2 3
CerebralFTOE .154 .285 .339 .107 .149 .261 -.054 .051 .150
RenalFTOE -.336* -.139 -.397* -.192 -.077 -.366 -.033 .231 -.174
SplanchnicFTOE -.242 -.002 -.064 -.700* .368 .357 -.001 -.053 -.255
CRR .474# .398* .551# .421 .223 .460 .260 -.017 .263
CSR .154 .131 .289 .667 .067 .500 -.069 -.028 .265
*P < .05 # P < .01 † P < .001. CPR - cerebroplacental ratio, FGR - fetal growth restriction, FTOE - fractional tissue oxygen extraction, CRR - cerebrorenal ratio, CSR - cerebrosplanchnic ratio.
48
Chapter 3
Discussion
This study demonstrated the continuity between hemodynamic adjustments beforeandafterbirthincaseofFGR.WefoundthatprenatalDopplerparameters,indicativeofpreferentialredistributionofblood�lowtothebrain,wereassociatedwithcirculatoryparametersassessedbyNIRSafterbirth.Strongassociationswerefoundforthe�irstthreedaysafterbirthbetweenUAandrenalFTOE/CRR,betweenCPRandCRR,betweenCPRandCSRand, starting fromDay2afterbirth,betweenMCAandcerebralFTOE.To our knowledge this is the �irst study on associations between prenatal DopplermeasurementsandpostnatalmultisiteNIRSinFGRwhichshowedthathemodynamicadaptationspresentbeforebirthcontinueinthepostnatalperiod. Brainsparingcontinueduntilthe�irstthreedaysafterbirthasseenbyarelativelyhighcerebralperfusion(lowFTOE)comparedtorenalperfusion.PrenatalbrainsparingcanbeexpressedashighUAandlowMCAPIorlowCPR.Theseparameterswerepositivelyassociated with low cerebral FTOE and high renal FTOE, and negatively associatedwith lowCRR.Since theseNIRSvaluescanbe interpretedaspostnatalhighcerebralperfusioninrelationtorenalperfusion,ourdatasuggestthathemodynamicchangespresentbeforebirthpersistatleastforthe�irstdaysafterbirth.Theseassociationslostsigni�icancestartingfromDay4.Thismightbeduetothedisappearanceofthebrainsparingeffect,oralternatively,tothedecreasingnumberofmeasurementsstartingfromDay4.SincenootherstudieshavepreviouslyreportedassociationsbetweenprenatalDopplermeasurementsandpostnatalNIRSmeasurements,weareunabletocompareour results. Reports on solely cerebral FTOE in FGR do exist, but show con�lictingresults.The�irstthreedaysafterbirth,cerebralFTOEwasfoundtobeconsistentlylowinSGAinfants,(17)toincreaseinsevereFGRinfants,(28)andisrelativelyhighinverypretermextremelylowbirthweightinfants.(29)Thesedifferencesmaybeexplainedbytimingofthemeasurementsandgroupcharacteristics. Inthisstudy,anexceptiontothecontinuationofbrainsparingafterbirth,isthe�irstpostnatal daywhereMCA and cerebral FTOEwere not associated. Previous studiesreportedalackofincreaseinleftventricularoutputinSGAinfantsthe�irstdaysafterbirth, measured with echocardiography.(30-32) Therefore, SGA infants seem to fallshortinadaptingtheircirculationtothepostnatalsituation.Apparently,onthe�irstdayafterbirthanacuteadaptationoccursafterFGR.Infetalcirculationthereispreferentialblood�lowtothefetalbrainandheart.(1)Wespeculatethatthesuddenchangeinbloodgasesdirectlyafterbirthtriggersanabruptreductionofpreferentialblood�lowtothebrain. Brain sparing is not as protective as previously thought, butmight contribute toneurologicalde�icits.(33)MorerecentstudiesreportthatFGRfetuseswithanabnormalMCAPIareatriskofabnormalneurologicalmaturationorsubtleneurodevelopmental
Prenatal predictors of neonatal outcome in FGR
49
3
de�icits.(3,4)Inaddition,inverypreterminfantsfetalbrainsparingwasassociatedwithpoorcognitiveoutcome.(34)Wespeculatethatbrainsparinginduceshyperoxygenationofcerebraltissueafterbirth.Higherregionalcerebraltissueoxygencontentisknownto be associatedwith poor cognition at three years.(35) Therefore, the presence offetalandpostnatalbrainsparingisimportanttobothobstetriciansandpaediatricians.TheyshouldbeawarethatcirculatorychangesinFGRcouldbeprolongeduntilafterbirth.Duetobrainsparing,abdominalorgansarevulnerableandarethereforemoresusceptible for e.g. sepsis. Paediatricians should be aware of the vulnerability ofabdominalorgansofFGRinfantsbornafterprenatalbrainsparing.Inaddition,brainsparingcouldrepresentariskfactorforlaterneurodevelopmentalabnormalities. AssociationsbetweenprenatalDopplervelocimetryandpostnatalNIRSmeasurementsseem to bemainly determined by the early FGR group. Correlations (R values)werenot statistically signi�icant for separate groups, nevertheless they were high in earlyFGR.WeoffertwopossibleexplanationsforthepredominanceintheearlyFGRgroup.Firstly,mostoftheearlyFGRcaseswerebornpretermduetotheseverityoftheirgrowthrestrictionandmay,therefore,havehadmorepronouncedblood�lowredistribution.Thenon-signi�icantassociationsinthegrowthrestrictedgroupswhentheywereconsideredseparatelymightthenhavebeenduetothesmallersamplesizes.ThesecondexplanationmightbethedifferenceinrenalandsplanchnicFTOEduetoprematurity.PreviousstudiesreportedlowermeanrenalandsplanchnicrSO2valuesinpreterminfantsthaninterminfants.(36,37)LowerrSO2valuescorrespondwithhigherFTOEvalues.WealsofoundhigherFTOEvaluesintherenalandsplanchnicregionsinpreterminfants,comparedwithterminfants.Itsuggeststhat,apartfromFGR,preterm-borninfantshavearelativelylowperfusionoftheabdominalareainthe�irstdaysafterbirth,comparedwithterminfants.Wespeculatethatthismightbeduetoimmaturityoftheabdominalorgansinpreterminfants.Asaconsequence,CRRandCSRhavemoreextremevaluesintheearlyFGRgroup,whichmightexplainthefactthatcorrelationsbetweenDopplermeasurementsandNIRSratioswereespeciallypresentinthepretermgroup. This study has several strengths and limitations.We performedNIRS atmultiplesitesandduringthe�irsttwoweeksafterbirth,whichimpliesaveryextensiveneonatalfollow-up.We also recognize some limitations. Associationswere found in the totalgroup,but they lost signi�icancewhen theearly and lateFGRgroupswereanalyzedseparately.Thismaybedue to thesmall samplesizesof thesubgroups.Wealsodidnot include a control group, asDopplermeasurements andNIRS arenotperformedroutinelyaspartofthestandardcareofhealthyfetusesandinfants.Anotherlimitationistheunknowndurationofbrainsparingbeforebirth.WeonlyincludedthelastDopplermeasurement before birth. Therefore, we could not investigate whether the FGRfetuseswithprolongedbrainsparingweretheonesshowingcerebralvasodilatationasneonates.Moreover,wedidnotperformfollow-upatlaterage.

50
Chapter 3
Inconclusion,prenatalhemodynamicchangesduetoFGRseemtopersistafterbirth.LowMCAPIandlowCPRbeforebirth,indicatingbrainsparing,arestronglyassociatedwith a low CRR, indicating a higher neonatal blood supply and, therefore, oxygendeliverytothebraincomparedtotherenalregion.Wespeculatethatifbrainsparingispresentprenatally,itpersistsforthe�irstthreedaysafterbirth.
AcknowledgementsThisstudywaspartoftheresearchprogramoftheSchoolforBehaviouralandCognitiveNeurosciences, University Medical Center Groningen, University of Groningen. WewouldliketothankSaraKuik,MirtheMebius,AnnevanZoonen,andAnneliesOlthuisfortheirhelpwithdatacollectionandacknowledgethehelpofDr.T.vanWulfftenPaltheforeditorialassistance.
Prenatal predictors of neonatal outcome in FGR
51
3
References (1) RudolphAM.Distributionandregulationofblood�lowinthefetalandneonatallamb.CircRes1985
Dec;57(6):811-821.(2) WladimiroffJW,TongeHM,StewartPA,ReussA.Severeintrauterinegrowthretardation;assessmentof
itsoriginfromfetalarterial�lowvelocitywaveforms.EurJObstetGynecolReprodBiol1986Jun;22(1-2):23-28.
(3) FiguerasF,Cruz-MartinezR, Sanz-CortesM,ArranzA, IllaM,BotetF,Costas-MoragasC,GratacosE.Neurobehavioraloutcomesinpreterm,growth-restrictedinfantswithandwithoutprenataladvancedsignsofbrain-sparing.UltrasoundObstetGynecol2011Sep;38(3):288-294.
(4) Eixarch E, Meler E, Iraola A, Illa M, Crispi F, Hernandez-Andrade E, Gratacos E, Figueras F.Neurodevelopmentaloutcome in2-year-old infantswhoweresmall-for-gestationalage termfetuseswithcerebralblood�lowredistribution.UltrasoundObstetGynecol2008Dec;32(7):894-899.
(5) KingdomJC,BurrellSJ,KaufmannP.PathologyandclinicalimplicationsofabnormalumbilicalarteryDopplerwaveforms.UltrasoundObstetGynecol1997Apr;9(4):271-286.
(6) BilardoCM,WolfH,StigterRH,VilleY,BaezE,VisserGH,Hecher,K.Relationshipbetweenmonitoringparametersandperinataloutcomeinsevere,earlyintrauterinegrowthrestriction.UltrasoundObstetGynecol2004Feb;23(2):119-125.
(7) Hernandez-Andrade E, Stampalija T, Figueras F. Cerebral blood �low studies in the diagnosis andmanagementofintrauterinegrowthrestriction.CurrOpinObstetGynecol2013Apr;25(2):138-144.
(8) Morsing E, Asard M, Ley D, Stjernqvist K, Marsal K. Cognitive function after intrauterine growthrestrictionandverypretermbirth.Pediatrics2011Apr;127(4):e874-82.
(9) ArbeilleP,RoncinA,BersonM,PatatF,PourcelotL.Explorationofthefetalcerebralblood�lowbyduplexDoppler--linear array system in normal and pathological pregnancies. Ultrasound Med Biol 1987Jun;13(6):329-337.
(10) GramelliniD,FolliMC,RaboniS,VadoraE,MerialdiA.Cerebral-umbilicalDopplerratioasapredictorofadverseperinataloutcome.ObstetGynecol1992Mar;79(3):416-420.
(11) Baschat AA, Gembruch U. The cerebroplacental Doppler ratio revisited. Ultrasound Obstet Gynecol2003Feb;21(2):124-127.
(12) Flood K, Unterscheider J, Daly S, Geary MP, Kennelly MM, McAuliffe FM, O’Donoghue K, Hunter A,MorrisonJJ,BurkeG,DickerP,TullyEC,MaloneFD.Theroleofbrainsparinginthepredictionofadverseoutcomes in intrauterine growth restriction: results of the multicenter PORTO Study. Am J ObstetGynecol2014Sep;211(3):288.e1-288.e5.
(13) FiguerasF,SavchevS,TriunfoS,CrovettoF,GratacosE.Anintegratedmodelwithclassi�icationcriteriato predict small-for-gestational-age fetuses at risk of adverse perinatal outcome.UltrasoundObstetGynecol2014Oct31.
(14) EdwardsAD,WyattJS,RichardsonC,DelpyDT,CopeM,ReynoldsEO.Cotsidemeasurementofcerebralblood�lowinillnewborninfantsbynearinfraredspectroscopy.Lancet1988Oct1;2(8614):770-771.
(15)Wyatt JS, Cope M, Delpy DT, Wray S, Reynolds EO. Quanti�ication of cerebral oxygenation andhaemodynamics in sick newborn infants by near infrared spectrophotometry. Lancet 1986 Nov8;2(8515):1063-1066.
(16) Pellicer A, Del Carmen BravoM. Near-infrared spectroscopy: amethodology-focused review. SeminFetalNeonatalMed2011Feb;16(1):42-49.
(17) IshiiH,TakamiT,FujiokaT,MizukakiN,KondoA,SunoharaD,HoshikaA,AkutagawaO,IsakaKeiichi.Comparison of changes in cerebral and systemic perfusion between appropriate- and small-for-gestational-ageinfantsduringthe�irstthreedaysafterbirth.BrainDev2014May;36(5):380-387.
(18) DaniC,PratesiS,BarpJ,BertiniG,GozziniE,MeleL,ParriniL.Near-infraredspectroscopymeasurementsof splanchnic tissue oxygenation during continuous versus intermittent feedingmethod in preterminfants.JPediatrGastroenterolNutr2013Jun;56(6):652-656.
(19) SchatTE,vanderLaanME,SchurinkM,HulscherJB,HulzebosCV,BosAF,KooiEMW.Abdominalnear-infraredspectroscopyinpreterminfants:acomparisonofsplanchnicoxygensaturationmeasurementsattwoabdominallocations.EarlyHumDev2014Jul;90(7):371-375.
(20) Mintzer JP, Parvez B, ChelalaM, Alpan G, LaGammaEF. Quiescent variability of cerebral, renal, andsplanchnic regional tissueoxygenation invery lowbirthweightneonates. JNeonatalPerinatalMed2014Jan1;7(3):199-206.

52
Chapter 3
(21) FortunePM,WagstaffM,PetrosAJ.Cerebro-splanchnicoxygenationratio(CSOR)usingnearinfraredspectroscopy may be able to predict splanchnic ischaemia in neonates. Intensive Care Med 2001Aug;27(8):1401-1407.
(22) HadlockFP,HarristRB,SharmanRS,DeterRL,ParkSK.Estimationoffetalweightwiththeuseofhead,body,andfemurmeasurements--aprospectivestudy.AmJObstetGynecol1985Feb1;151(3):333-337.
(23) Parra-Cordero M, Lees C, Missfelder-Lobos H, Seed P, Harris C. Fetal arterial and venous Dopplerpulsatilityindexandtimeaveragedvelocityranges.PrenatDiagn2007Dec;27(13):1251-1257.
(24) GomezO,FiguerasF,FernandezS,BennasarM,Martinez JM,PuertoB,GratacosE.Referencerangesforuterinearterymeanpulsatilityindexat11-41weeksofgestation.UltrasoundObstetGynecol2008Aug;32(2):128-132.
(25) BrazyJE,LewisDV,MitnickMH,JobsisvanderVlietFF.Noninvasivemonitoringofcerebraloxygenationinpreterminfants:preliminaryobservations.Pediatrics1985Feb;75(2):217-225.
(26) LemmersPM,ToetM,vanSchelvenLJ,vanBelF.Cerebraloxygenationandcerebraloxygenextractioninthepreterminfant:theimpactofrespiratorydistresssyndrome.ExpBrainRes2006Aug;173(3):458-467.
(27) Verhagen EA, TerHorst HJ, Keating P,Martijn A, Van Braeckel KN, Bos AF. Cerebral oxygenation inpreterm infantswith germinalmatrix-intraventricular hemorrhages. Stroke 2010Dec;41(12):2901-2907.
(28) BozzettiV,PaterliniG,BelFV,VisserGH,TosettiL,GazzoloD,TagliabuePE.CerebralandsomaticNIRS-determinedoxygenationinIUGRpreterminfantsduringtransition.JMaternFetalNeonatalMed2015Jan21:1-4.
(29) Takami T, Sunohara D, Kondo A, Mizukaki N, Suganami Y, Takei Y, Miyajima T, Hoshika A. Changesin cerebral perfusion in extremely LBW infants during the �irst 72 h after birth. Pediatr Res 2010Nov;68(5):435-439.
(30) Leipala JA, Boldt T, Turpeinen U, Vuolteenaho O, Fellman V. Cardiac hypertrophy and alteredhemodynamicadaptationingrowth-restrictedpreterminfants.PediatrRes2003Jun;53(6):989-993.
(31) Sehgal A, Doctor T, Menahem S. Cardiac function and arterial biophysical properties in small forgestationalageinfants:postnatalmanifestationsoffetalprogramming.JPediatr2013Nov;163(5):1296-1300.
(32) FouzasS,KaratzaAA,DavlourosPA,ChrysisD,AlexopoulosD,MantagosS,DimitriouG.Neonatalcardiacdysfunctioninintrauterinegrowthrestriction.PediatrRes2014May;75(5):651-657.
(33) ScherjonSA,OostingH,Smolders-DeHaasH,ZondervanHA,KokJH.Neurodevelopmentaloutcomeatthreeyearsofageafterfetal‘brain-sparing’.EarlyHumDev1998Aug28;52(1):67-79.
(34) ScherjonS,BrietJ,OostingH,KokJ.Thediscrepancybetweenmaturationofvisual-evokedpotentialsandcognitiveoutcomeat�iveyearsinverypreterminfantswithandwithouthemodynamicsignsoffetalbrain-sparing.Pediatrics2000Feb;105(2):385-391.
(35) Verhagen EA, VanBraeckel KN, van der Veere CN, GroenH, Dijk PH,Hulzebos CV, Bos AF. Cerebraloxygenationisassociatedwithneurodevelopmentaloutcomeofpretermchildrenatage2to3years.DevMedChildNeurol2014Nov8.
(36) McNeillS,GatenbyJC,McElroyS,EngelhardtB.Normalcerebral,renalandabdominalregionaloxygensaturationsusingnear-infraredspectroscopyinpreterminfants.JPerinatol2011Jan;31(1):51-57.
(37) BaileySM,Hendricks-MunozKD,MallyP.Cerebral,renal,andsplanchnictissueoxygensaturationvaluesinhealthytermnewborns.AmJPerinatol2014Apr;31(4):339-344.
Prenatal predictors of neonatal outcome in FGR
53
3
Chapter 4
General movements after fetal growth restriction in relation to prenatal Doppler flow patterns
Jozien C. Tanis, Danique M. Schmitz, Maaike R. Boelen, Lucia Casarella, Paul P. van den Berg, Caterina M. Bilardo, and Arend F. Bos
Provisionally accepted Ultrasound in Obstetrics & Gynecology
56
Chapter 4
Abstract
AimToinvestigatewhetherinfetalgrowthrestriction(FGR)DopplerPImeasurementsofthefetalcirculationareassociatedwithneonatalgeneralmovements(GMs).
MethodFGRdiagnosiswasbasedonabdominalcircumferenceorestimatedfetalweight<P10orde�lectingfetalgrowth.FetalDopplerparametersoftheumbilicalartery(UA),middlecerebralartery(MCA),andductusvenosus(DV)weremeasuredmaximally1weekpriortodelivery.Cerebroplacentalratio(CPR)wascalculatedasMCAdividedbyUAPI.WeassessedthequalityofGMsonday7afterbirth,aroundtheduedateifcaseswerebornpreterm,andatthreemonthspostterm.Additionally,weperformedadetailedanalysisofthemotorrepertoirebycalculatingamotoroptimalityscore(MOS).
Results Forty-eightFGRcaseswereincludedwithamedianGAof35(range26-40)weeks.UAPI,MCAPI,andCPRcorrelatedstrongly(rho.374-.472,p<.01)withMOSonday7afterbirth,DVdidnot.DopplerPImeasurementsdidnotcorrelatewithMOSatthreemonthspostterm.
Conclusion FetalarterialDopplermeasurementsareassociatedwiththequalityofneonatalGMsoneweekafterbirth,butthisassociationisnolongerevidentatthreemonthsposttermage.BrainsparinginparticularassociatedstronglywithabnormalqualityofGMs.
Prenatal predictors of neonatal outcome in FGR
57
4
Introductory section
Fetalgrowthrestriction(FGR)isoneoftheleadingcausesofperinatalandlong-termadverseoutcomes.(1)FGRoccursinbothearlyandlatestagesofpregnancy,eachwithitsownpathofysiologicalmechanism.During fetal life,Dopplerpulsatility index (PI)measurementsofarterialandvenousvesselsareused for fetalmonitoring.PreviousstudiessuggestthatabnormalPIvaluesoftheumbilicalartery(UA),middlecerebralartery(MCA),andductusvenosus(DV)arepredictiveofperinataloutcomeincludinglong-termneurodevelopment.(2-4)Speci�ically,absentorreversedend-diastolic �low(AREDF) of the UA is associated with long-term neurodevelopmental delay.(3) It isunknown,however,whethertheentirerangeofDopplermeasurementsareassociatedwithneurodevelopmentaldelay,andhowabnormalPIof theUA,MCA,andDVaffectneurologicdevelopmentshortlyafterbirth.Previousstudiesreportahigherincidenceofabnormalgeneralmovements(representativeofneurologicalfunctioning)ingrowthrestrictedinfantswhencomparedtocontrols.(5,6)However,theydidnotcomparetheseresultswithfetalDopplermeasurements.Therefore,itremainsunknownwhetherfetalDopplermeasurementsareassociatedwithshort-termneurologicalfunctioningofthenewborninFGR,andifso,whichDopplermeasurements. A reliable method to determine neurological functioning, is Prechtl’s method ofassessingqualityofgeneralmovements(GMs).(7,8)Chronologically,twotypesofGMscanbedistinguished.Up to termage,GMsarenormally characterizedbyvariability,complexity,and�luency.Atthreemonthspostterm,�idgetyGMs(FMs)emerge,de�inedascontinuoussmall,circularmovementsofmoderatespeedinalldirections.ThequalityofGMsandFMsarepredictiveofabnormalneurologicaldevelopment.(8)Therefore,abnormalGMsinFGRinfantsmaybeare�lectionofpossiblebraindamage. TogaininsightintotherelationshipbetweenprenatalDopplerPImeasurementsandshorttermpostnatalneurologyinFGR,weaimedtodetermineassociationsbetweenDopplerPIoftheUA,MCA,andDVandthequalitativeandquantitativeassessmentofGMsandFMs.Sincepretermandterm-bornFGRinfantsmighthavedifferentunderlyingpathofysiologicalmechanisms,wealsoaimedtostudyassociationsforbothgroupsseparately.
58
Chapter 4
Methods
ParticipantsAprospectiveobservationalcohortstudywasperformedfromJune2012toSeptember2014attheDepartmentsofObstetricsandFetalMedicineofUniversityMedicalCenterGroningen (UMCG) in The Netherlands. Exclusion criteria weremultiple pregnancy,structural and/or chromosomal abnormalities or evidence of fetal infection. Allpregnancies were delivered at UMCG and, if indicated, neonates were admitted tothe Neonatology ward of the same hospital. Data on obstetric, birth, and neonatalcharacteristicswere collected from the twodepartments.Written informedparentalconsentwas obtained in all cases. The studywas approved by the hospitalMedicalBoardandMedicalResearchEthicsCommittee. Wede�inedFGRasafetalabdominalcircumferenceorestimatedfetalweight(9)belowthe10thcentile,orde�lectingfetalgrowthofatleast30centileswithrespecttopreviousmeasurements (reduced growth according to the fetus’ expected growth potential).On average, prior to maternal admission, fetal Doppler parameters were measuredseriallyonceaweek,andtwiceaweekforthedurationofadmission.Carewastakentoperformthelastmeasurementasclosetothedayofdeliveryaspossibleandneveratanintervalofmorethanoneweektodelivery.Onlythelastmeasurementwasusedforanalysis.MeasurementsincludedPIofUA,MCA,andDV.LeftandrightmaternaluterinearteryDopplersweremeasuredduringthe�irstvisit,thenmeanuterineartery(UtA)PI was calculated. Two experienced operators performed all measurements. All themeasurementsweretransformedtoz scores(standarddeviationfromthegestationalagemean)forfurtheranalysis.(10,11)Incaseofabsentenddiastolic�lowintheUA,thePIwascalculatedbymanuallytracingtheenddiastolicvelocityalongthetimeaxis.Thecerebroplacentalratio(CPR)wascalculatedasMCAPIdividedbyUAPI.(12)
Recording of general movementsWevideorecordedeachinfant’sgeneralmovementsfor30to60minutesonday7afterbirth.Preterm-borninfantswereagainrecordedaroundduedate(40weeksGA)withthesamerecordingtime.Atthreemonthspostterm,allinfantswererecordedfor10minutes.TiminganddurationofrecordingwereasadvisedbyEinspieleretal.(8)Theinfantswere�ilmednakedorwearingonlyadiaper,lyinginsupineposition,andbeingabletomovetheirlimbsandtrunkfreely.Weplacedthevideocamerahighabovetheinfantatthefootofthechangingmatorplaypen,orincaseofpretermbornorillinfants,theincubator.GMsduringcrying,hiccupping,orsuckingonadummywereexcludedfromanalysis.

Prenatal predictors of neonatal outcome in FGR
59
4
Analysis of general movementsTwooftheauthors(JCTandAFB)assessedthequalityofGMsaccordingtoPrechtl’smethod, on the basis of visual Gestalt perception.(7) They did so blinded for theprenatal data. Both are certi�ied by the GM Trust. Interobserver reliability was notdeterminedinthisstudy,buthaspreviouslybeenstudiedextensivelyandreportedasgoodtoexcellent.(8)NormalGMsinvolvetheinfant’sentirebody,canlastafewsecondstoseveralminutes,andarecharacterizedbyacomplexandvariablesequenceofarms,legs,neck,andtrunk.GMsarescoredasabnormaliftheylackcomplexity,variability,and�luency.TherearethreetypesofabnormalGMsthatapplytothepretermandtermperiod: poor repertoire, chaotic, and cramped-synchronized GMs.(5,13) If GMs areabsentorveryshort(<3s),theinfantwasassessedasbeinghypokinetic.(14)Nextweperformedadetailedanalysisbycalculatingamotoroptimalityscore(MOS)usingtheGMOptimalityList.(14)Eightdifferentaspects,includingGMquality,aredistinguished.MOSrangesfrom8to18(lowtohighoptimality). Atapproximately theendof thesecondmonthpost term,during theso-calledmajorneural transformation, GMs acquire a �idgety character.(15)Normal �idgetymovements(FMs)arecircularmovementsofsmallamplitude,moderatespeed,andvariableaccelerationofneck, trunk,and limbs inalldirections.(16)FMsarescoredasbeingabnormalwhencircularmovementsresemblingFMsarepresent,butwithexaggeratedspeed,amplitudeorjerkiness.Theyarescoredasabsent(severelyabnormal)iftheyareneverobservedduringvideorecordingsbetween9and16weekspostterm.Next,weusedtheMotorOptimalityList forFidgetyMovements toassessaMOS.(17)Fiveaspects, includingFMquality,aredistinguished.Duringthisperiod,MOSrangesfrom5to28(lowtohighoptimality).
Statistical analysisWe performed a sample size calculation. We expected Doppler PI of the UA to beabnormalintwothirdofthecases(ratio2:1).OurmainendpointwasMOSat3monthspost term age, range 8-18, standard deviation 3.1.We considered a difference of 4MOSpointsrelevant.Therefore,atapowerof0.8andPvalue0.05,38infantsshouldbe included in this study.However,due toanotnormaldistributionof theMOS,weadd10%tothisnumber,andtheminimumnumberofinclusionshouldbe42.Duetopracticalitieswefollowed43infantsupuntil3monthspostterm. WeusedtheSpearmanrankordercorrelationtesttodeterminecorrelationsbetweenDopplerparametersandMOS,andBWcentilesandMOS.TheanalyseswererepeatedinthepretermFGRgroup(below37weeksGA)andinthetermFGRgroup(≥37weeksGA),andinamildFGRgroup(BW>P5)andsevereFGRgroup(BW≤P5).ChisquaretestwasusedtoevaluatecategorisedDopplerandGMvariables,andwhensigni�icantunivariateandmultiplelogisticregressionanalyseswereperformed.AP valueof<.05wasconsideredstatisticallysigni�icant.
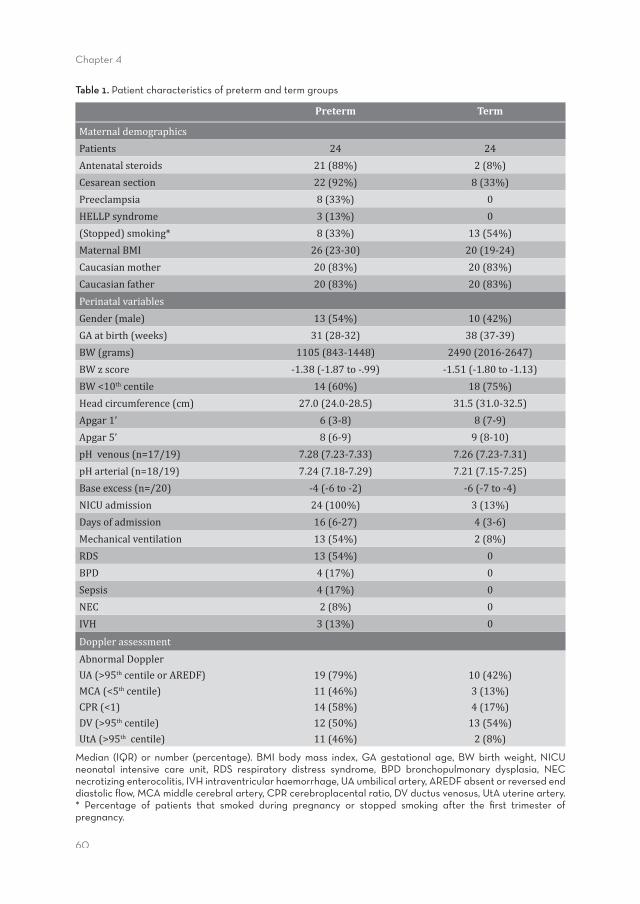
60
Chapter 4
Table 1. Patient characteristics of preterm and term groups
Preterm Term
MaternaldemographicsPatients 24 24Antenatalsteroids 21(88%) 2(8%)Cesareansection 22(92%) 8(33%)Preeclampsia 8(33%) 0HELLPsyndrome 3(13%) 0(Stopped)smoking* 8(33%) 13(54%)MaternalBMI 26(23-30) 20(19-24)Caucasianmother 20(83%) 20(83%)Caucasianfather 20(83%) 20(83%)PerinatalvariablesGender(male) 13(54%) 10(42%)GAatbirth(weeks) 31(28-32) 38(37-39)BW(grams) 1105(843-1448) 2490(2016-2647)BWzscore -1.38(-1.87to-.99) -1.51(-1.80to-1.13)BW<10thcentile 14(60%) 18(75%)Headcircumference(cm) 27.0(24.0-28.5) 31.5(31.0-32.5)Apgar1’ 6(3-8) 8(7-9)Apgar5’ 8(6-9) 9(8-10)pHvenous(n=17/19) 7.28(7.23-7.33) 7.26(7.23-7.31)pHarterial(n=18/19) 7.24(7.18-7.29) 7.21(7.15-7.25)Baseexcess(n=/20) -4(-6to-2) -6(-7to-4)NICUadmission 24(100%) 3(13%)Daysofadmission 16(6-27) 4(3-6)Mechanicalventilation 13(54%) 2(8%)RDS 13(54%) 0BPD 4(17%) 0Sepsis 4(17%) 0NEC 2(8%) 0IVH 3(13%) 0
DopplerassessmentAbnormalDopplerUA(>95thcentileorAREDF)MCA(<5thcentile)CPR(<1)DV(>95thcentile)UtA(>95thcentile)
19(79%)11(46%)14(58%)12(50%)11(46%)
10(42%)3(13%)4(17%)13(54%)2(8%)
Median (IQR) or number (percentage). BMI body mass index, GA gestational age, BW birth weight, NICU neonatal intensive care unit, RDS respiratory distress syndrome, BPD bronchopulmonary dysplasia, NEC necrotizing enterocolitis, IVH intraventricular haemorrhage, UA umbilical artery, AREDF absent or reversed end diastolic fl ow, MCA middle cerebral artery, CPR cerebroplacental ratio, DV ductus venosus, UtA uterine artery.* Percentage of patients that smoked during pregnancy or stopped smoking after the fi rst trimester of pregnancy.
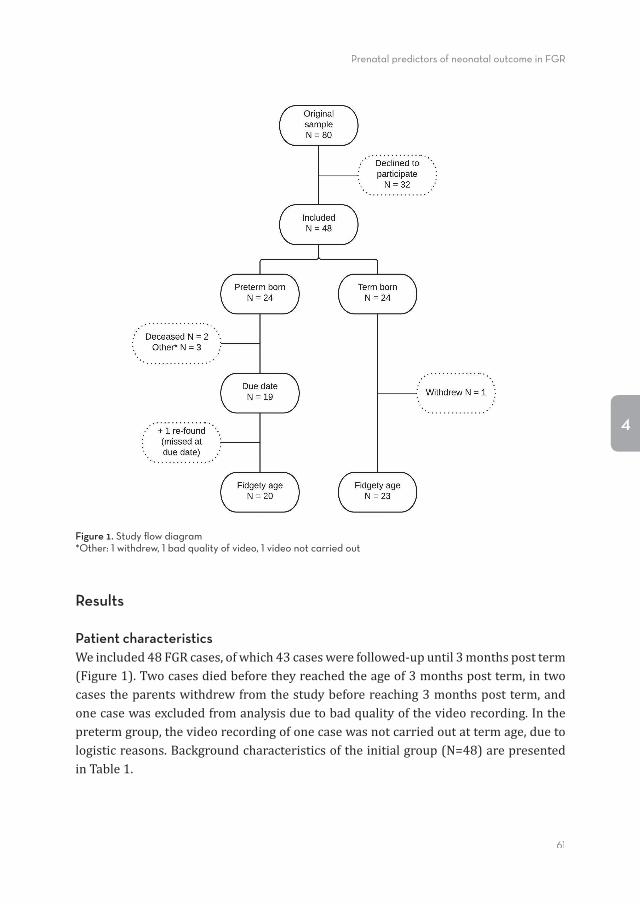
Prenatal predictors of neonatal outcome in FGR
61
4
Figure 1. Study fl ow diagram*Other: 1 withdrew, 1 bad quality of video, 1 video not carried out
Results
Patient characteristicsWeincluded48FGRcases,ofwhich43caseswerefollowed-upuntil3monthspostterm(Figure1).Twocasesdiedbeforetheyreachedtheageof3monthspostterm,intwocasestheparentswithdrewfromthestudybeforereaching3monthspostterm,andonecasewasexcludedfromanalysisduetobadqualityofthevideorecording.Inthepretermgroup,thevideorecordingofonecasewasnotcarriedoutattermage,duetologisticreasons.Backgroundcharacteristicsoftheinitialgroup(N=48)arepresentedinTable1.
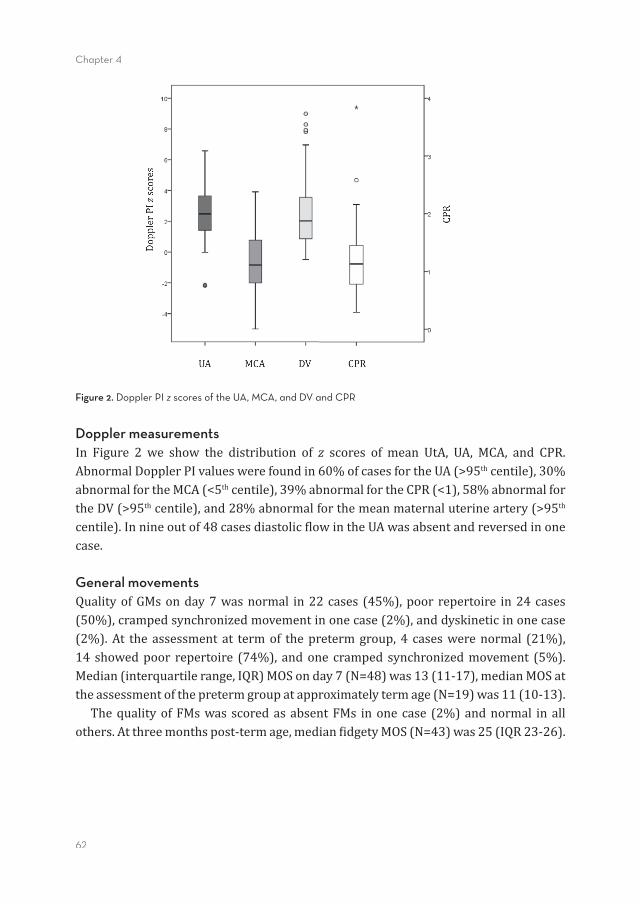
62
Chapter 4
Doppler measurements In Figure 2 we show the distribution of z scores of mean UtA, UA, MCA, and CPR.AbnormalDopplerPIvalueswerefoundin60%ofcasesfortheUA(>95thcentile),30%abnormalfortheMCA(<5thcentile),39%abnormalfortheCPR(<1),58%abnormalfortheDV(>95thcentile),and28%abnormalforthemeanmaternaluterineartery(>95thcentile).Innineoutof48casesdiastolic�lowintheUAwasabsentandreversedinonecase.
General movementsQualityofGMsonday7wasnormal in22cases (45%),poorrepertoire in24cases(50%),crampedsynchronizedmovementinonecase(2%),anddyskineticinonecase(2%).At the assessment at termof thepretermgroup,4 caseswerenormal (21%),14 showedpoor repertoire (74%), andone cramped synchronizedmovement (5%).Median(interquartilerange,IQR)MOSonday7(N=48)was13(11-17),medianMOSattheassessmentofthepretermgroupatapproximatelytermage(N=19)was11(10-13). ThequalityofFMswasscoredasabsentFMs inonecase (2%)andnormal inallothers.Atthreemonthspost-termage,median�idgetyMOS(N=43)was25(IQR23-26).
Figure 2. Doppler PI z scores of the UA, MCA, and DV and CPR
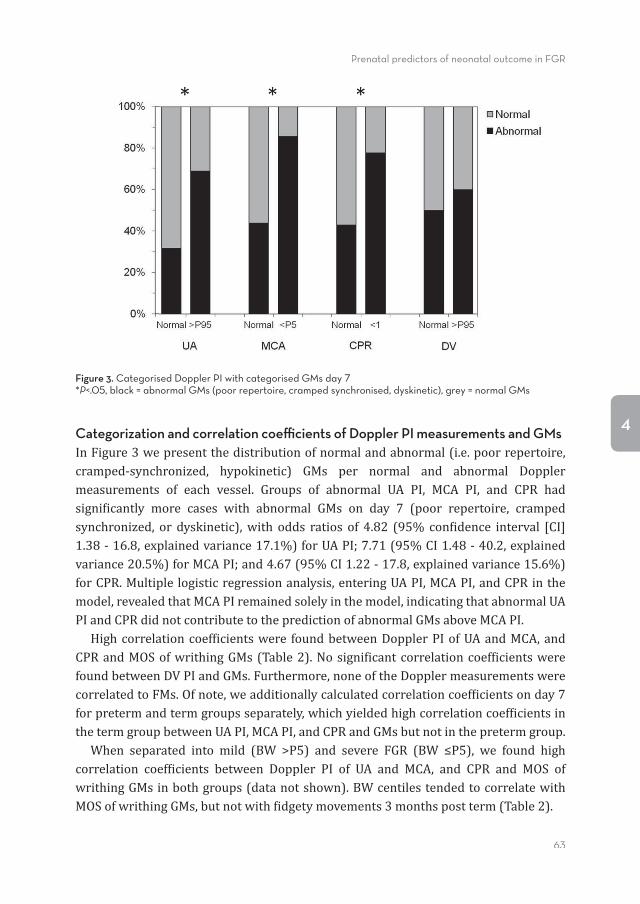
Prenatal predictors of neonatal outcome in FGR
63
4Categorization and correlation coeffi cients of Doppler PI measurements and GMsInFigure3wepresentthedistributionofnormalandabnormal(i.e.poorrepertoire,cramped-synchronized, hypokinetic) GMs per normal and abnormal Dopplermeasurements of each vessel. Groups of abnormal UA PI, MCA PI, and CPR hadsigni�icantly more cases with abnormal GMs on day 7 (poor repertoire, crampedsynchronized, or dyskinetic),with odds ratios of 4.82 (95% con�idence interval [CI]1.38-16.8,explainedvariance17.1%)forUAPI;7.71(95%CI1.48-40.2,explainedvariance20.5%)forMCAPI;and4.67(95%CI1.22-17.8,explainedvariance15.6%)forCPR.Multiplelogisticregressionanalysis,enteringUAPI,MCAPI,andCPRinthemodel,revealedthatMCAPIremainedsolelyinthemodel,indicatingthatabnormalUAPIandCPRdidnotcontributetothepredictionofabnormalGMsaboveMCAPI. Highcorrelationcoef�icientswere foundbetweenDopplerPIofUAandMCA,andCPRandMOSofwrithingGMs(Table2).Nosigni�icantcorrelationcoef�icientswerefoundbetweenDVPIandGMs.Furthermore,noneoftheDopplermeasurementswerecorrelatedtoFMs.Ofnote,weadditionallycalculatedcorrelationcoef�icientsonday7forpretermandtermgroupsseparately,whichyieldedhighcorrelationcoef�icientsinthetermgroupbetweenUAPI,MCAPI,andCPRandGMsbutnotinthepretermgroup. When separated into mild (BW >P5) and severe FGR (BW ≤P5), we found highcorrelation coef�icients between Doppler PI of UA and MCA, and CPR and MOS ofwrithingGMsinbothgroups(datanotshown).BWcentilestendedtocorrelatewithMOSofwrithingGMs,butnotwith�idgetymovements3monthspostterm(Table2).
Figure 3. Categorised Doppler PI with categorised GMs day 7*P<.05, black = abnormal GMs (poor repertoire, cramped synchronised, dyskinetic), grey = normal GMs
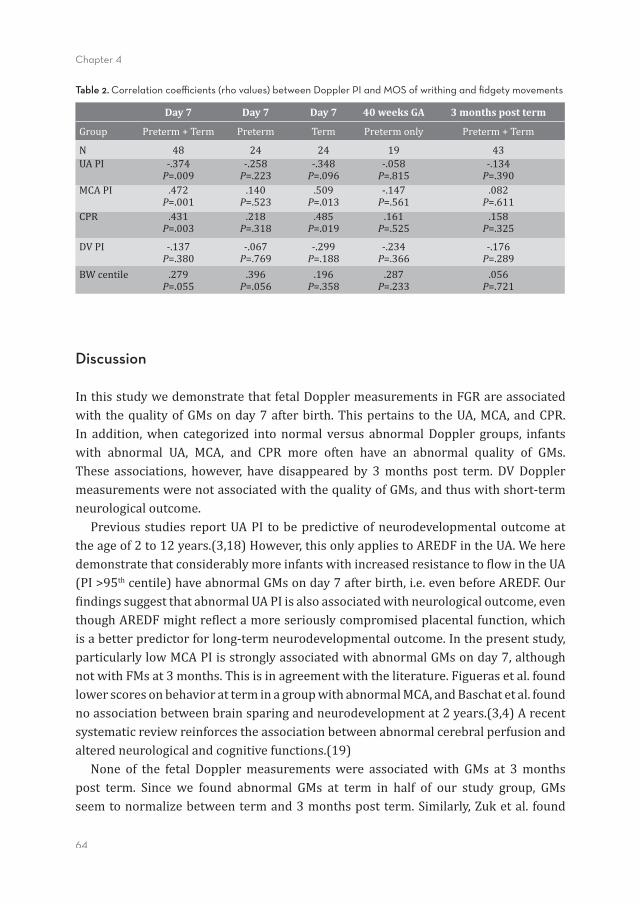
64
Chapter 4
Table 2. Correlation coeffi cients (rho values) between Doppler PI and MOS of writhing and fi dgety movements
Day 7 Day 7 Day 7 40 weeks GA 3 months post term
Group Preterm+Term Preterm Term Pretermonly Preterm+Term
N 48 24 24 19 43UAPI -.374
P=.009-.258
P=.223-.348
P=.096-.058
P=.815-.134
P=.390MCAPI .472
P=.001.140
P=.523.509
P=.013-.147
P=.561.082
P=.611CPR .431
P=.003.218
P=.318.485
P=.019.161
P=.525.158
P=.325
DVPI -.137P=.380
-.067P=.769
-.299P=.188
-.234P=.366
-.176P=.289
BWcentile .279P=.055
.396P=.056
.196P=.358
.287P=.233
.056P=.721
Discussion
InthisstudywedemonstratethatfetalDopplermeasurementsinFGRareassociatedwith thequalityofGMsonday7afterbirth.Thispertains to theUA,MCA,andCPR.In addition,when categorized into normal versus abnormalDoppler groups, infantswith abnormal UA, MCA, and CPR more often have an abnormal quality of GMs.These associations, however, have disappeared by 3months post term. DVDopplermeasurementswerenotassociatedwiththequalityofGMs,andthuswithshort-termneurologicaloutcome. PreviousstudiesreportUAPI tobepredictiveofneurodevelopmentaloutcomeattheageof2to12years.(3,18)However,thisonlyappliestoAREDFintheUA.Weheredemonstratethatconsiderablymoreinfantswithincreasedresistanceto�lowintheUA(PI>95thcentile)haveabnormalGMsonday7afterbirth,i.e.evenbeforeAREDF.Our�indingssuggestthatabnormalUAPIisalsoassociatedwithneurologicaloutcome,eventhoughAREDFmightre�lectamoreseriouslycompromisedplacentalfunction,whichisabetterpredictorforlong-termneurodevelopmentaloutcome.Inthepresentstudy,particularlylowMCAPIisstronglyassociatedwithabnormalGMsonday7,althoughnotwithFMsat3months.Thisisinagreementwiththeliterature.Figuerasetal.foundlowerscoresonbehavioratterminagroupwithabnormalMCA,andBaschatetal.foundnoassociationbetweenbrainsparingandneurodevelopmentat2years.(3,4)Arecentsystematicreviewreinforcestheassociationbetweenabnormalcerebralperfusionandalteredneurologicalandcognitivefunctions.(19) None of the fetal Dopplermeasurementswere associatedwith GMs at 3monthspost term. Since we found abnormal GMs at term in half of our study group, GMsseemtonormalizebetweentermand3monthspostterm.Similarly,Zuketal. found
Prenatal predictors of neonatal outcome in FGR
65
4
thatoutof32growthrestrictedinfants,16hadabnormalGMsattermand7ofthemnormalizedat9-11weekspostterm(oneinfantdroppedout).(6)Bosetal.alsofoundthatthemajorityofgrowthrestrictedinfantswithabnormalGMsatpretermandtermperiod had normalized at approximately 3months post term.(5) In Zuk’s study, allof the7 infantswithnormalizedGMshadanormalneurodevelopmentaloutcomeat2 years.However, abnormalGMs inpreterm infants recordedprior to 8weekspostterm,despitenormalizationlateron,areassociatedwithalowerIQatschoolage.(20)Apparently, inspiteofnormalization,abnormalGMsatterminFGRinfantsmaybeare�lectionofpossiblebraindamage.Morespeci�ically,abnormalGMsaroundtermareassociatedwith cerebralwhitematter pathology.(21)We speculate that FGR infantswithnormalizationofGMs fromtermto3monthspost termarestillat riskof latercognitivedelayandsubtlebraindysfunction. AssociationsbetweenUA,MCA,andCPRandGMsatday7seemtobemainlyduetothetermFGRgroup.WeperformedextraanalysesforpretermandtermFGRgroupsseparately, and found that in the term group, associationswere even stronger thanintheentiregroup,whereasinthepretermgroupassociationswereweakerandlostsigni�icance. One possible explanation is a higher incidence of comorbidity in thepreterm group.(22) Serious complications in the �irst days after birth may induceabnormalGMs,andobscuretheoriginalassociationbetweenDopplermeasurementsandGMs.Conversely,infantsbornattermafterFGRarelesslikelytohavecomorbidity,sincetheirFGRwasmildenoughtoallowa full-termpregnancy. Inthesecases,GMspurelyre�lecttheneonatalneurologicalstatus. In previous studies DVwas predictive of poor neonatal outcome,(2,23) postnatalbrainfunctionseemstobepositivelyin�luencedbyaclinicalmanagementofFGRbasedonDVchanges.(24)GMsonday7to3monthsposttermwerenotassociatedwithDVinourstudy.Therefore,webelievethatabnormalityinDV�low,alateeventonlypresentinearlyandsevereFGR,mayhaveamorecomplexrelationshipwithneurologicaloutcome,than,forinstance,alonglastingabnormalcerebralperfusion.(19)Anunexpectedandinexplicable�indingwasthattheproportionofcaseswithabnormalDVPIinthetermgroupwashigherthantheproportionofabnormalUAPI. Werecognizeseveralstrengthsand limitations inthisstudy.Astrength is thatweperformed an extensive postnatal neurological follow-up, until 3 months post termage.Alimitationmaybetheheterogeneityofthegroup(earlyandlateFGR,variableseverityof thecondition),preventingstatisticallysigni�icantassociations.Becauseofthe inclusion criteria (abdominal circumference below the 10th centile, or de�lectinggrowthpattern),thestudygroupconsistsmainlyofmildFGR,assuggestedbythefactthatonlyonecasehadabsentFMsat3monthsposttermage. Our �indingsmighthave clinical implications.Despite the lossof associationwithDoppler measurements in the �idgety period, normalization of GMs from term to
66
Chapter 4
3monthspost termmight stillbea risk factor for subtlebraindysfunction.Medicalcaregivers,suchasneonatologists,generalpaediatricians,andnursesshouldbeawareoftheconsequencesoffetalbrainsparingininfantsbornafterFGR.
Conclusion
Thisisthe�irstreportontheassociationbetweenfetalDopplerparametersandGMsinFGR.UA,MCA,andCPRarestronglyassociatedwithGMsonday7,buttheassociationisnolongerevidentat3monthsposttermage.BrainsparinginparticularassociatedstronglywithabnormalqualityofGMs.
AcknowledgementsThisstudywaspartoftheresearchprogramofthePostgraduateSchoolforBehaviouralandCognitiveNeurosciences(BCN),UniversityofGroningen.J.C.Taniswas�inanciallysupportedbyaUniversityofGroningenJuniorScienti�icMasterClassgrant.WewouldliketothankD.H.Baptist,J.C.Holwerda,M.E.vanderLaan,andT.E.Schatfortheirhelpindatacollection.Theauthorsgreatlyacknowledgethehelpofprof.dr.A.E.J.Duboisforeditorialassistance.
Prenatal predictors of neonatal outcome in FGR
67
4
References(1) BarkerDJ,OsmondC,GoldingJ,KuhD,WadsworthME.Growthinutero,bloodpressureinchildhood
andadultlife,andmortalityfromcardiovasculardisease.BMJ1989Mar4;298(6673):564-567.(2) Bilardo CM,Wolf H, Stigter RH, Ville Y, Baez E, Visser GH, et al. Relationship between monitoring
parametersandperinataloutcomeinsevere,earlyintrauterinegrowthrestriction.UltrasoundObstetGynecol2004Feb;23(2):119-125.
(3) BaschatAA,ViscardiRM,Hussey-GardnerB,HashmiN,HarmanC.Infantneurodevelopmentfollowingfetal growth restriction: relationship with antepartum surveillance parameters. Ultrasound ObstetGynecol2009Jan;33(1):44-50.
(4) FiguerasF,Cruz-MartinezR,Sanz-CortesM,ArranzA,IllaM,BotetF,etal.Neurobehavioraloutcomesin preterm, growth-restricted infants with and without prenatal advanced signs of brain-sparing.UltrasoundObstetGynecol2011Sep;38(3):288-294.
(5) BosAF,vanLoonAJ,Hadders-AlgraM,MartijnA,OkkenA,PrechtlHF.Spontaneousmotilityinpreterm,small-for-gestationalageinfants.II.Qualitativeaspects.EarlyHumDev1997Nov24;50(1):131-147.
(6) Zuk L, Harel S, Leitner Y, Fattal-Valevski A. Neonatal general movements: an early predictor forneurodevelopmental outcome in infants with intrauterine growth retardation. J Child Neurol 2004Jan;19(1):14-18.
(7) PrechtlHF.Qualitativechangesofspontaneousmovementsinfetusandpreterminfantareamarkerofneurologicaldysfunction.EarlyHumDev1990Sep;23(3):151-158.
(8) EinspielerC,PrechtlHF.Prechtl’sassessmentofgeneralmovements:adiagnostictoolforthefunctionalassessmentoftheyoungnervoussystem.MentRetardDevDisabilResRev2005;11(1):61-67.
(9) HadlockFP,HarristRB,SharmanRS,DeterRL,ParkSK.Estimationoffetalweightwiththeuseofhead,body,andfemurmeasurements--aprospectivestudy.AmJObstetGynecol1985Feb1;151(3):333-337.
(10) Parra-Cordero M, Lees C, Missfelder-Lobos H, Seed P, Harris C. Fetal arterial and venous Dopplerpulsatilityindexandtimeaveragedvelocityranges.PrenatDiagn2007Dec;27(13):1251-1257.
(11) Gomez O, Figueras F, Fernandez S, Bennasar M, Martinez JM, Puerto B, et al. Reference ranges foruterine arterymeanpulsatility index at 11-41weeks of gestation.UltrasoundObstetGynecol 2008Aug;32(2):128-132.
(12) Baschat AA, Gembruch U. The cerebroplacental Doppler ratio revisited. Ultrasound Obstet Gynecol2003Feb;21(2):124-127.
(13) FerrariF,CioniG,PrechtlHF.Qualitativechangesofgeneralmovementsinpreterminfantswithbrainlesions.EarlyHumDev1990Sep;23(3):193-231.
(14) deVriesNK,ErwichJJ,BosAF.Generalmovementsinthe�irstfourteendaysoflifeinextremelylowbirthweight(ELBW)infants.EarlyHumDev2008Nov;84(11):763-768.
(15) Bos AF, Einspieler C, Prechtl HF. Intrauterine growth retardation, general movements, andneurodevelopmentaloutcome:areview.DevMedChildNeurol2001Jan;43(1):61-68.
(16) PrechtlHF, Einspieler C, Cioni G, BosAF, Ferrari F, SontheimerD. An earlymarker for neurologicalde�icitsafterperinatalbrainlesions.Lancet1997May10;349(9062):1361-1363.
(17) BrugginkJL,EinspielerC,ButcherPR,StremmelaarEF,PrechtlHF,BosAF.Quantitativeaspectsoftheearlymotorrepertoireinpreterminfants:dotheypredictminorneurologicaldysfunctionatschoolage?EarlyHumDev2009Jan;85(1):25-36.
(18) SchreuderAM,McDonnellM,GaffneyG,JohnsonA,HopePL.Outcomeatschoolagefollowingantenataldetectionofabsentorreversedenddiastolic�lowvelocityintheumbilicalartery.ArchDisChildFetalNeonatalEd2002Mar;86(2):F108-14.
(19) Meher S, Hernandez-Andrade E, Basheer SN, Lees C. Impact of cerebral redistribution onneurodevelopmental outcome in small for gestational age or growth restrictedbabies: a systematicreview.UltrasoundObstetGynecol2015Feb14.
(20) BrugginkJL,VanBraeckelKN,BosAF.Theearlymotorrepertoireofchildrenbornpretermisassociatedwithintelligenceatschoolage.Pediatrics2010Jun;125(6):e1356-63.
(21) SpittleAJ,BrownNC,DoyleLW,BoydRN,HuntRW,BearM,etal.Qualityofgeneralmovementsisrelatedtowhitematterpathologyinverypreterminfants.Pediatrics2008May;121(5):e1184-9.
(22) GouyonJB,IacobelliS,FerdynusC,BonsanteF.Neonatalproblemsoflateandmoderatepreterminfants.SeminFetalNeonatalMed2012Jun;17(3):146-152.

68
Chapter 4
(23) BaschatAA,CosmiE,BilardoCM,WolfH,BergC,RiganoS,etal.Predictorsofneonataloutcomeinearly-onsetplacentaldysfunction.ObstetGynecol2007Feb;109(2Pt1):253-261.
(24) Lees CC, Marlow N, van Wassenaer-Leemhuis A, Arabin B, Bilardo CM, Brezinka C, et al. 2 yearneurodevelopmentaland intermediateperinataloutcomes in infantswithverypretermfetalgrowthrestriction(TRUFFLE):arandomisedtrial.Lancet2015Mar4.
Prenatal predictors of neonatal outcome in FGR
69
4

Part III
Follow-up at school age after FGR

Chapter 5
Functional outcome of very preterm-born and
small-for-gestational-age children at school age
Jozien C. Tanis, Meike H. van der Ree, Elise Roze, Anna E. Huis in ’t Veld, Paul P. van den Berg, Koenraad N.J.A. Van Braeckel, and Arend F. Bos
Pediatric Research 2012 Dec;72(6):641-8

74
Chapter 5
Abstract
BackgroundOur aimwas to determine functional outcome of very preterm-born and small-for-gestational-age(SGA)childrenascomparedwithmatchedcontrolsatschoolage.
MethodsWe included 28 very preterm SGA children (GA <32wk, birth weight (BW) <10thpercentile), born in2000–2001.Wealso included28verypretermbut appropriate-for-gestational-age(AGA)children,matchedforGA,gender,andbirthyear,ascontrols.Weassessedmotorskills, intelligencequotient(IQ),attention,verbalmemory,visualperception,visuomotorintegration,executivefunctioning,andbehaviorofbothsetsofchildrenatschoolage.
ResultsTheSGAchildrenhadamedianGAof29.7wkandBWof888g,whereasthecontrolshadamedianGAof29.4wkandBWof1,163g.at8.6y,themediantotalIQoftheSGAchildrenwas94ascomparedwith95inthecontrols(notsigni�icant).PerformanceIQwassigni�icantlylowerinSGAchildren(89vs.95,P =0.043),whereasverbalIQwasnot(95vs.95).Totalmotorskills(P =0.048)and�inemotorskills(P =0.021)wereworseinSGAchildren.Furthermore,SGAchildrenscoredloweronselectiveattention(P =0.026)andvisualperception(P =0.025).Otherscoresdidnotdiffersigni�icantlybetweengroups.
ConclusionThe differences we found between the groups were small. This suggests that theimpairedfunctioningofverypreterm–bornSGAchildrenisattributabletotheirhavingbeenbornverypretermratherthantobeingSGA.

Follow-up at school age after FGR
75
5
Introduction
Ithasbeenshownthatchildrenwhoarebornverypreterm(<32wkofgestation)areat increased risk of impaired neurodevelopmental outcome.(1–4) In addition, it hasbeenshownthatchildrenbornsmallforgestationalage(SGA)arealsoatriskforpoorneurodevelopmental outcome.(5,6) This holds good for SGA children born at termand also for thosebornpreterm (<37wk).(5) Lower intelligencequotients (IQs) arereportedinfulltermandmoderatelypretermSGAchildreninparticular.(7,8)ItwouldbeinterestingtoascertainwhethersimilardomainsareaffectedinverypretermSGAchildren, given that thepathophysiologicmechanisms relating tobraindevelopmentmay be different in these infants. Studies on very preterm SGA children are scarce,andthe �indingsarecontradictory.Somestudiesreport lowerIQscores(6,9,10)andmorebehavioralproblemsorattentionde�icitsinthesechildren(9)ascomparedwithcontrols,(6)whereasothershavefoundnodifferencesasregardsbehavioralproblemsandattentionde�icits(6,10).CognitiveimpairmentwasrestrictedtoverbalIQonly.(10)Severalspeci�icneuropsychologicfunctionssuchasmotorskills,executivefunctioning,memory,visuomotorintegration,andvisualperceptionwerenotstudied.Furthermore,these follow-upstudies inverypretermSGAchildrenwereperformedatarelativelyyoung age, i.e., up to the age of 5 y. For determining functional outcome, however,neuropsychologicaltestsperformedatschoolagearemorereliable.(1)Atschoolage,functional demands are higher than at preschool age. In addition, from~6 y of ageonward,alargervarietyoftestsareavailableforassessingvariousmotor,cognitive,andbehavioraldomains.Finally,becauseschoolchildrenareusedtotestsatschool,theyaremorecompliantintestsituations.Therefore,testingfunctionaloutcomeislikelytobebothreliableandvalidatschoolage. Asyet,knowledgeon the functionaloutcomes inSGAchildrenbornverypretermis limited.We expect that their functional outcomeswould be poorer than those ofverypretermbut appropriateforgestationalage (AGA) children.(6,9,10)Thequestioniswhether this poor functional outcome at school age can be attributed to pretermbirthalone,orwhetherbeingbornSGAposesadditionalrisks.Ouraimwasthereforetoassess theperformanceofverypreterm–bornandSGAchildren invariousmotor,cognitive,andbehavioraldomainsand tocompare theirperformanceswith thoseofverypreterm–bornAGAcontrolsatschoolage.

76
Chapter 5
Methods
Patients This was a case–control study. As cases, we included children born very preterm(<32wkGA)whowerealsoSGA,de�inedashavingaBWlowerthanthe10thpercentile(z score−1.28)oftheDutchKloostermangrowthcharts.(11)Atbirth,thesechildrenhadbeenadmittedtotheNICUoftheUniversityMedicalCenterGroningenduringtheyears2000and2001.Wefoundthesecasechildrenbysearchingthepatientdatabaseonthebasisofthediagnoses“SGA”and“IUGR.”Thosewithchromosomalandcongenitalabnormalities were excluded. As controls, we included very preterm–born children(matchedforageandgenderwiththecasechildren)whohadalsobeenadmittedtothesameNICUduringthesameperiod,withbirthtimesclosest(eitherbeforeorafter)toeachSGAcasebutwithBWsthatwereAGA.ClinicalcharacteristicssuchasApgarscoresandheadcircumference(HC)atbirthwerecollectedfromthemedical�iles.ThestudywasapprovedbytheMedicalEthicsCommitteeoftheUniversityMedicalCenterGroningen.
Testing procedure This was a hypothesisgenerating study. Therefore, tests on multiple domains wereperformed.All theparentsgave theirwritten informedconsent toparticipate in thefollow-upprogram. Follow-up consisted of a battery of tests that took~2.5 h to complete, includingbreaks.ThetesterwasblindedastothediagnosisofSGAinthechildren.Duringthesevisitswealsomeasuredthechildren’sHC,whichwetransformedintoz scores.Duringtesting,thechildwasinaseparateroomwiththetester,whileoneorbothoftheparentswere�illingoutquestionnairesinanotherroom.Testscoresgeneratedwhenachildwastootiredand/oruncooperative(asassessedbythetrainedtester)wereexcluded,aswerethoseaccompaniedbyincompletequestionnaires.
Cognitive measures Beforetestingthechildren,we�irstdeterminedwhetherthechildrenattendedregularschool or received special education, andwhether they had repeated classes at anytime.Cognitiveoutcomewasassessedusingseveralstandardizedtests. A short form of the Wechsler Intelligence Scale for Children, 3rd edition, Dutchversion,wasusedtodetermineintelligence.(12,13)WecalculatedtotalIQonthebasisoftheverbalIQandperformanceIQsubtests.Selectiveattentionandattentionalcontrolweremeasuredusingtwosubtests,“MapMission”and“OppositeWorlds,”oftheTestof Everyday Attention for Children.(14)We assessed verbal memory using the ReyAuditoryVerbalLearningTest.(15)Thistestconsistsofa15wordlistthatisrepeated
Follow-up at school age after FGR
77
5
tothechild�ivetimes.Aftereachtrialwetestedimmediaterecall.Delayedrecallwasassessedafteranintervalof20min.Forassessingvisualperceptionandvisuomotorintegration,weused two subtests, “GeometricPuzzles” and “DesignCopying,” of theNeuropsychologicalAssessment,2ndedition.(16)ExecutivefunctioningindailylifewasassessedusingtheBehaviorRatingInventoryofExecutiveFunctionquestionnaire,(17)whichwas�illedoutbytheparents.
Motor measures MotoroutcomewasassessedusingtheMovementABC.(18)Thisisastandardizedtestthatmeasurestotalmotorperformancebasedonsubscoresformanualdexterity(�inemotor skills), ball skills, and static–dynamic balance (coordination). The higher thescore,thepoorertheoutcome.
Behavioral measures Weusedtwoquestionnairestoassessthechildren’sbehavior.EmotionalandbehavioralproblemswereassessedusingtheCBCL.(19)SymptomsofADHDwereassessedusingtheDutchADHDquestionnaire.(20)
Potential confounders Toestimatethedegreeofillnessexperiencedbythechildrenduringtheneonatalperiod,weusedtwoscoringsystems.TheseweretheNurseryNeurobiologicRiskScore(21)andtheSNAPII.(22)TheNeurobiologicRiskScoreestimatesthedegreeofillnessduringtheentireperiodofadmissionandisbasedonpHvalue,theneedformechanicalventilation,andthepresenceofbrainwhitematterabnormalities,infections,convulsions,cerebralhemorrhages,andhypoglycemia.TheSNAPIIassessesseverityofillnessonthe�irstdayoflife.Itisbasedonbloodpressure,lowesttemperature,PO2/FiO2(fractionofinspiredoxygen) ratio, lowest serumpH, thepresenceofmultiple seizures, andurineoutputduringthe�irst24h. We also considered SES as a possible confounder. SES was determined using aclassi�ication of occupations developed in TheNetherlands.(23)We categorized SESintothreeclassesbasedontheparents’occupations,takingthehigheroftheoccupationlevels of the two parents of each child. Class 1 corresponds with the lowerleveloccupations,class3withhigherleveloccupations.
Statistical analysis SPSS 16.0 software for Windows was used for all data analyses. IQ scores werecalculatedonthebasisofthemeanscoresontheverbalandperformancesubtestsoftheWechslerIntelligenceScaleforChildren.Weusednormscoresfromthemanualsfor cognitive outcome (Test of Everyday Attention for Children, Auditory Verbal

78
Chapter 5
Learning Test, Neuropsychological Assessment), motor outcome (Movement ABC),and the questionnaires (ADHD questionnaire, CBCL, Behavior Rating Inventory ofExecutiveFunction).PercentilesonthestandardizationsamplesoftheMovementABCand each cognitive testwere used to classify scores into normal (>15th percentile),borderline(5thto15thpercentile),andabnormal(<5thpercentile).Weusedasimilarclassi�icationfortheCBCL,BehaviorRatingInventoryofExecutiveFunction,andADHDquestionnaires,onthebasisofthecriteriasetoutinthemanuals.Wetransformedtherawtotalmotorscoresof theMovementABC intopercentilesandsubsequently intoz scores,inaccordancewiththeinstructionsinthemanual.Wedidsotodojusticetothevariabilityinthemotorskillsofthegroupofchildrenbelowthe1stpercentilewho,whileshowingawiderangeofrawtotalmotorscores,couldnotbedifferentiatedonthebasisofthepercentiles.Whereappropriate,weusedtheMannWhitneyUtest,Fisher’sexact test, andχ2 test for trend to test fordifferencesbetween thecaseandcontrolgroups,bothforoutcomemeasuresandforpotentialconfounders.WeusedSpearman’srank correlation to test the correlation between clinical characteristics (e.g., HC z scoresatbirth)andconfoundersontheonehand,andcognitive,motor,andbehavioraloutcomescoresontheother.WealsotestedwhetherSGAchildrenwithbrainsparing(de�inedasHCz scores−BWz scores>0.75SD)haddifferentoutcomesascomparedtoSGAchildrenwithoutbrainsparing.Throughouttheanalyses,P <0.05(twotailed)wasconsideredtobestatisticallysigni�icant. We used univariate logistic regression analyses to calculate ORs for abnormaloutcomesaccordingtogroup.Wedidsotwice:�irstwetookborderlineandabnormaloutcomestogethervs.normaloutcome,andnextwetookabnormaloutcomevs.normalandborderlineoutcomes.Wethenperformedmultivariatelogisticregressionanalyses.Inthemultivariatemodel,weincludedthepotentialconfoundersthatwereassociatedwithgroupallocationoroutcomemeasuresatP ≤0.1. SESwasalso included in themultivariatemodel.WedecidedtoreportallORswithP ≤0.1,bothintheunivariateandinthemultivariatemodels.
Results
In2000and2001,atotalof275verypretermchildrenwereadmittedtotheneonatalintensiveareunit(NICU)atourhospital.Amongthisgroup,56childrenwereSGA,18(32%)ofwhomdiedintheneonatalperiod.Ofthesurvivors,�ivechildrenwereexcludedbecause of major chromosomal and con genital abnormalities (one child with XXYsyndrome,onechildwithcongenitalupperairwayobstructionrequiringtracheotomy,andthreechildrenwithcardiacdefects,i.e.,tetralogyofFallot,truncusarteriosus,andatriumseptaldefectwithalargelefttorightshunt).Theother33childrenwereeligible
Follow-up at school age after FGR
79
5
forfollow-up.Ofthese,wewereunabletotracethreechildren,andtheparentsoftwootherchildrendeclinedtoparticipate.Wethereforehad28(85%)childreninthefollow-upprogram. As controls we included 28 very preterm–born AGA children free of congenitalabnormalitiesadmittedin2000and2001toourhospital’sNICU.
Patient characteristics InTable1,wepresentanoverviewofthepatientdemographicsoftheSGAcasechildrenandtheAGAcontrolchildren.(11,24)The�iveSGAchildrenwhodidnotparticipateinthestudyhadsimilarGAandbirthweight(BW)values(median30.1wk,930g,respectively)tothoseofthe28SGAchildrenweincluded.Atfollow-upat2yofagetheneurologic�indingswerenormal inall these �ivechildren.Theparentsof twochildrenreportedbehavioralproblems,andonechildshowedalanguagedelay.TheSGAchildrenwhodiedintheneonatalperiodhadamedianGAof29.1wk,BW730g,andHCof24.5cm. Thedemographicsofthechildreninthestudydidnotdifferbetweengroups,apartfrom the fact that 100%of the SGA childrenwere delivered by cesarean section ascomparedwith61% in theAGAgroup.TheHCatbirthwas lower in theSGAgroupthan in theAGAgroup. In11of theSGAchildren (39%),z scoresofHCwerebelow−1.28, i.e., below the10thpercentile,whereas17 (61%)hadnormalHCvalues.TheScore for Neonatal Acute Physiology, second version (SNAPII) scores of the SGAchildrenalsoappearedtobeslightlyhigher,indicatinggreaterseverityofillness;however,thisdifferencefelljustshortofsigni�icance(Table1).Retinopathyofprematurity(maximumstageIIwithoutplusdisease)occurredinfourchildrenintheSGAgroupandinonechildintheAGAcontrolgroup.Noneofthesechildrenbecameblind. Themedianageatfollow-upforthisstudywas8.6y(interquartilerange8.3–9.1).Bythistime,themedianz scoresoftheHCaccordingtoagewere−0.91(interquartilerange−1.55to−0.24)intheSGAchildren,and−1.05(interquartilerange−1.60to0.29)intheAGAchildren(notsigni�icant). Noneofthechildrendevelopedcerebralpalsy.
Cognitive outcome Ofthe28childrenincludedintheSGAcasegroup,24(86%)attendedregularschoolsand 4 (14%) received special education, 3 of them because of learning dif�icultiesand1becauseofdevelopmentalcoordinationdisorder.Inaddition,9(32%)ofthe28childrenhadhadtorepeataclassorclassesinelementaryschool(startingattheageof4y)atleastonce.OnechildintheAGAcontrolgroupreceivedspecialeducationandalltheotherswenttoregularschools.Ofthe28controlchildren,9(32%)hadhadtorepeataclassorclasses.Neitherthelevelofeducationnortherepeatingofclasseswassigni�icantlydifferentbetweenthetwogroups.
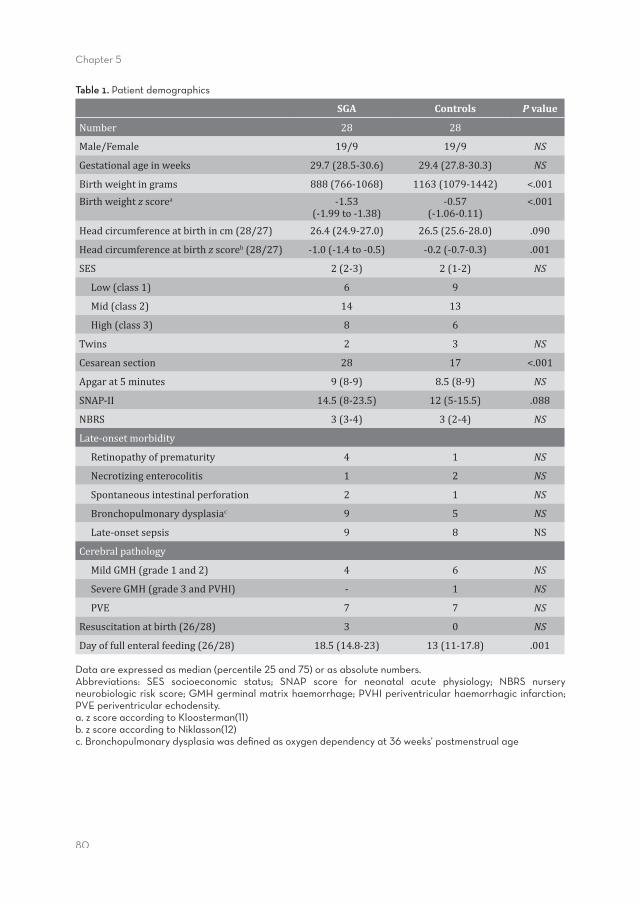
80
Chapter 5
Table 1. Patient demographics
SGA Controls P value
Number 28 28
Male/Female 19/9 19/9 NS
Gestationalageinweeks 29.7(28.5-30.6) 29.4(27.8-30.3) NS
Birthweightingrams 888(766-1068) 1163(1079-1442) <.001Birthweightzscorea -1.53
(-1.99to-1.38)-0.57
(-1.06-0.11)<.001
Headcircumferenceatbirthincm(28/27) 26.4(24.9-27.0) 26.5(25.6-28.0) .090
Headcircumferenceatbirthzscoreb(28/27) -1.0(-1.4to-0.5) -0.2(-0.7-0.3) .001
SES 2(2-3) 2(1-2) NS
Low(class1) 6 9
Mid(class2) 14 13
High(class3) 8 6
Twins 2 3 NS
Cesareansection 28 17 <.001
Apgarat5minutes 9(8-9) 8.5(8-9) NS
SNAP-II 14.5(8-23.5) 12(5-15.5) .088
NBRS 3(3-4) 3(2-4) NS
Late-onsetmorbidity
Retinopathyofprematurity 4 1 NS
Necrotizingenterocolitis 1 2 NS
Spontaneousintestinalperforation 2 1 NS
Bronchopulmonarydysplasiac 9 5 NS
Late-onsetsepsis 9 8 NS
Cerebralpathology
MildGMH(grade1and2) 4 6 NS
SevereGMH(grade3andPVHI) - 1 NS
PVE 7 7 NS
Resuscitationatbirth(26/28) 3 0 NS
Dayoffullenteralfeeding(26/28) 18.5(14.8-23) 13(11-17.8) .001
Data are expressed as median (percentile 25 and 75) or as absolute numbers. Abbreviations: SES socioeconomic status; SNAP score for neonatal acute physiology; NBRS nursery neurobiologic risk score; GMH germinal matrix haemorrhage; PVHI periventricular haemorrhagic infarction; PVE periventricular echodensity.a. z score according to Kloosterman(11) b. z score according to Niklasson(12)c. Bronchopulmonary dysplasia was defi ned as oxygen dependency at 36 weeks’ postmenstrual age
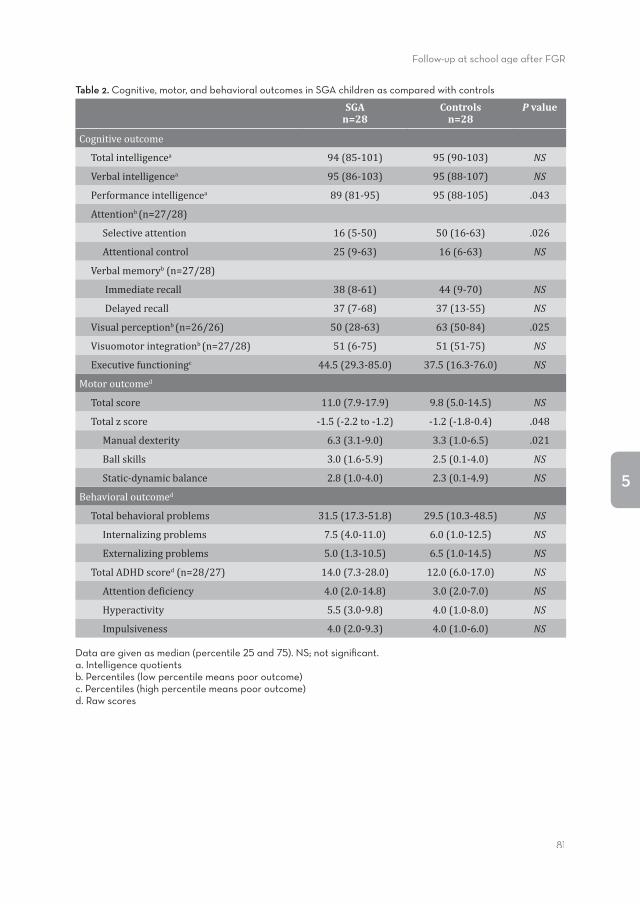
Follow-up at school age after FGR
81
5
Table 2. Cognitive, motor, and behavioral outcomes in SGA children as compared with controls
SGAn=28
Controlsn=28
P value
Cognitiveoutcome
Totalintelligencea 94(85-101) 95(90-103) NS
Verbalintelligencea 95(86-103) 95(88-107) NS
Performanceintelligencea 89(81-95) 95(88-105) .043
Attentionb(n=27/28)
Selectiveattention 16(5-50) 50(16-63) .026
Attentionalcontrol 25(9-63) 16(6-63) NS
Verbalmemoryb(n=27/28)
Immediaterecall 38(8-61) 44(9-70) NS
Delayedrecall 37(7-68) 37(13-55) NS
Visualperceptionb(n=26/26) 50(28-63) 63(50-84) .025
Visuomotorintegrationb(n=27/28) 51(6-75) 51(51-75) NS
Executivefunctioningc 44.5(29.3-85.0) 37.5(16.3-76.0) NS
Motoroutcomed
Totalscore 11.0(7.9-17.9) 9.8(5.0-14.5) NS
Totalzscore -1.5(-2.2to-1.2) -1.2(-1.8-0.4) .048
Manualdexterity 6.3(3.1-9.0) 3.3(1.0-6.5) .021
Ballskills 3.0(1.6-5.9) 2.5(0.1-4.0) NS
Static-dynamicbalance 2.8(1.0-4.0) 2.3(0.1-4.9) NS
Behavioraloutcomed
Totalbehavioralproblems 31.5(17.3-51.8) 29.5(10.3-48.5) NS
Internalizingproblems 7.5(4.0-11.0) 6.0(1.0-12.5) NS
Externalizingproblems 5.0(1.3-10.5) 6.5(1.0-14.5) NS
TotalADHDscored(n=28/27) 14.0(7.3-28.0) 12.0(6.0-17.0) NS
Attentionde�iciency 4.0(2.0-14.8) 3.0(2.0-7.0) NS
Hyperactivity 5.5(3.0-9.8) 4.0(1.0-8.0) NS
Impulsiveness 4.0(2.0-9.3) 4.0(1.0-6.0) NS
Data are given as median (percentile 25 and 75). NS; not signifi cant.a. Intelligence quotientsb. Percentiles (low percentile means poor outcome)c. Percentiles (high percentile means poor outcome)d. Raw scores
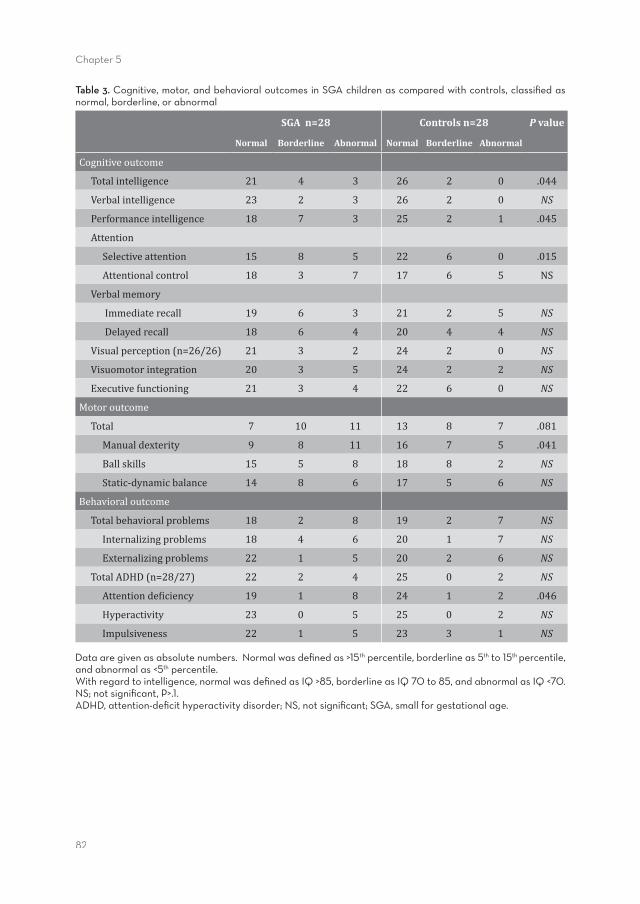
82
Chapter 5
Table 3. Cognitive, motor, and behavioral outcomes in SGA children as compared with controls, classifi ed as normal, borderline, or abnormal
SGA n=28 Controls n=28 P value
Normal Borderline Abnormal Normal Borderline Abnormal
Cognitiveoutcome
Totalintelligence 21 4 3 26 2 0 .044
Verbalintelligence 23 2 3 26 2 0 NS
Performanceintelligence 18 7 3 25 2 1 .045
Attention
Selectiveattention 15 8 5 22 6 0 .015
Attentionalcontrol 18 3 7 17 6 5 NS
Verbalmemory
Immediaterecall 19 6 3 21 2 5 NS
Delayedrecall 18 6 4 20 4 4 NS
Visualperception(n=26/26) 21 3 2 24 2 0 NS
Visuomotorintegration 20 3 5 24 2 2 NS
Executivefunctioning 21 3 4 22 6 0 NS
Motoroutcome
Total 7 10 11 13 8 7 .081
Manualdexterity 9 8 11 16 7 5 .041
Ballskills 15 5 8 18 8 2 NS
Static-dynamicbalance 14 8 6 17 5 6 NS
Behavioraloutcome
Totalbehavioralproblems 18 2 8 19 2 7 NS
Internalizingproblems 18 4 6 20 1 7 NS
Externalizingproblems 22 1 5 20 2 6 NS
TotalADHD(n=28/27) 22 2 4 25 0 2 NS
Attentionde�iciency 19 1 8 24 1 2 .046
Hyperactivity 23 0 5 25 0 2 NS
Impulsiveness 22 1 5 23 3 1 NS
Data are given as absolute numbers. Normal was defi ned as >15th percentile, borderline as 5th to 15th percentile, and abnormal as <5th percentile. With regard to intelligence, normal was defi ned as IQ >85, borderline as IQ 70 to 85, and abnormal as IQ <70. NS; not signifi cant, P>.1.ADHD, attention-defi cit hyperactivity disorder; NS, not signifi cant; SGA, small for gestational age.
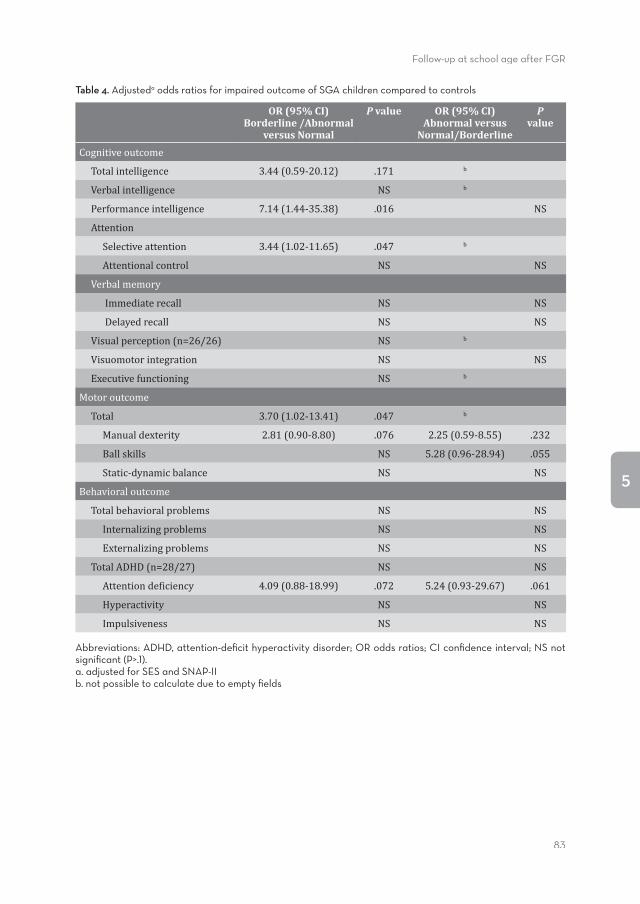
Follow-up at school age after FGR
83
5
Table 4. Adjusteda odds ratios for impaired outcome of SGA children compared to controls
OR (95% CI)Borderline /Abnormal
versus Normal
P value OR (95% CI)Abnormal versus
Normal/Borderline
Pvalue
Cognitiveoutcome
Totalintelligence 3.44(0.59-20.12) .171 b
Verbalintelligence NS b
Performanceintelligence 7.14(1.44-35.38) .016 NS
Attention
Selectiveattention 3.44(1.02-11.65) .047 b
Attentionalcontrol NS NS
Verbalmemory
Immediaterecall NS NS
Delayedrecall NS NS
Visualperception(n=26/26) NS b
Visuomotorintegration NS NS
Executivefunctioning NS b
Motoroutcome
Total 3.70(1.02-13.41) .047 b
Manualdexterity 2.81(0.90-8.80) .076 2.25(0.59-8.55) .232
Ballskills NS 5.28(0.96-28.94) .055
Static-dynamicbalance NS NS
Behavioraloutcome
Totalbehavioralproblems NS NS
Internalizingproblems NS NS
Externalizingproblems NS NS
TotalADHD(n=28/27) NS NS
Attentionde�iciency 4.09(0.88-18.99) .072 5.24(0.93-29.67) .061
Hyperactivity NS NS
Impulsiveness NS NS
Abbreviations: ADHD, attention-defi cit hyperactivity disorder; OR odds ratios; CI confi dence interval; NS not signifi cant (P>.1).a. adjusted for SES and SNAP-II b. not possible to calculate due to empty fi elds
84
Chapter 5
InTable2,wepresent themedianscoresoncognitive tests.Onechild in theSGAgrouphaddif�icultieswithallcognitivetestsbecauseofverylowintelligence,asseenbyIQscores(totalIQ<55).IntwoSGAchildrenandtwoAGAcontrols,thevisualperceptiontestwasnotadministeredreliably.IncomparisontoAGAcontrols,SGAchildrenscoredsigni�icantlyloweronperformanceIQ,selectiveattention,andvisualperception.ScoresontotalandverbalIQ,attentionalcontrol,verbalmemory,visuomotorintegration,andexecutivefunctioningdidnotdiffersigni�icantlybetweenthegroups. InTable3,weclassi�iedthechildren’sscoresintothecategoriesnormal(>15thpercentile),borderline (5th to 15th percentiles), and abnormal (<5th percentile). The child whoseneuropsychologicalfunctionscouldnotbeassessedbecauseofverylowintelligencewasclassi�iedas“abnormal.”Beforeadjustment,theoddsratios(ORs)forimpairedoutcomeintheSGAgroupforborderline/abnormalvs.normal,were4.33(95%con�idenceinterval(CI),0.81–23.10,P =0.086)fortotalIQ,4.63(95%CI,1.11–19.26,P =0.035)forperformanceIQ,and3.18(95%CI,0.99–10.23,P =0.053)forselectiveattention.TheORsforabnormalvs.borderline/normalwerenotsigni�icant.InTable4,wepresenttheORsafteradjustmentforSNAPIIandsocioeconomicstatus(SES).Aftertheseadjustments,theORswerelowerfortotalIQandhigherforperformanceIQandselectiveattention. ThedatashowninTables3and4con�irmtheanalysesofthemedianscoresasshowninTable2,exceptwithrespecttovisualperception.Totalintelligencewassigni�icantlylowerintheSGAgroupbutonlyafterwecategorizedoutcomesinthisdomain.
Motor outcome We were able to assess the motor skills of all the children, using the MovementAssessmentBatteryforChildren(MovementABC).Manualdexteritywassigni�icantlymoreimpairedinSGAchildren(Table2).ThetotalscorespertheMovementABCwerealsohigher (i.e.,poorer)andreachedsigni�icancewhenwe transformedthem intoz scores.Moreover,agreaterproportionofthechildrenintheSGAgroupwereclassi�iedas borderline or abnormal for total scores inMovement ABC aswell as formanualdexterity (Table3).Before adjustment, theORs for impairedoutcome in children inthe SGA group for borderline/abnormal vs. normal were 2.60 (95% CI, 0.84–8.07,P =0.098)fortotalmotorscoresand2.82(95%CI,0.95–8.38,P =0.063)formanualdexterity.Forabnormalvs.normal/borderline,theORswere2.98(95%CI,0.87–10.17,P = 0.082) for manual dexterity and 5.20 (95% CI, 0.99–27.23, P = 0.051) for ballskills.AfteradjustmentforSNAPIIandSES,theORswerelowerformanualdexterity(abnormalvs.normal/borderline),higherfortotalmotoroutcome,andunchangedformanualdexterity(borderline/abnormalvs.normal)aswellasforballskills(abnormalvs.normal/borderline)(Table4).
Follow-up at school age after FGR
85
5
Behavioral outcome Theparentsofallthechildren�illedoutdetailsintheChildBehaviorCheckList(CBCL).ForonechildintheAGAcontrolgroup,theresultsoftheattentionde�icithyperactivitydisorder (ADHD) questionnaire were lacking because it had not been �illed outcompletely.Medianscoreswerenotsigni�icantlydifferentbetweenthegroups(Table2).When the childrenwere classi�ied asnormal, borderline, or abnormal,we foundthatmoreSGAchildrenhadattentionde�icits(Table3).Beforeadjustment,theORsforattentionde�icitsintheSGAchildrenwere3.79(95%CI,0.90–15.97,P =0.070)whenclassi�iedasborderline/abnormalvs.normal,and5.00(95%CI,0.95–26.23,P =0.057)when classi�ied as abnormal vs. normal/borderline. The adjusted ORswere slightlyhigher,therebycon�irmingthese�indings(Table4).
Relation between functional outcome, head size at birth, and at follow-upWithinthegroupofSGAchildren,thez scoresforHCatbirthdidnotcorrelatewithanyoftheoutcomemeasures,apartfromthesubscale“Impulsiveness”intheDutchADHDquestionnaire. Lowerz scoresofHCcorrelatedwithhigher scoreson impulsiveness(Spearman’sr =−0.501,P =0.007).NodifferencesexistedbetweenSGAchildrenwithbrainsparingandthosewithout. The z scores of theHC in children in the SGA group at follow-up correlatedwithmotor skills and behavior per the CBCL but not with scores on the cognitive tests.Lowerz scoresforHCcorrelatedwithpoorerscoresontotalmotorskills,inparticularstaticanddynamicbalance(Spearman’sr =−0.415,P =0.039andr =−0.517,P =0.008,respectively).Manualdexterityandballskillsdidnotcorrelatewithheadsizeatfollow-up.Asregardsbehavior,thelowerz scoresforHCcorrelatedwithpoorerscoresontotalbehavioralproblems(r =−0.520,P =0.008),externalizingproblems(r =−0.410,P =0.042),andinternalizingproblems(r =−0.501,P =0.011).
Discussion
Theaimofourstudywas toassess,at schoolage, theperformance levels invariousmotor,cognitive,andbehavioraldomainsinchildrenwhohadbeenbornverypretermandSGA,andtocomparetheseperformancelevelswiththoseofchildrenwhohadalsobeenbornverypretermbutwithbodyweightsAGA.WefoundthattheSGAchildrenperformedlesswellonperformanceintelligence,selectiveattention,visualperception,andmotorskills(particularly�inemotorskills)ascomparedwiththeverypretermAGAgroup.Wefoundnosigni�icantdifferencesasregardstotalandverbalintelligence,grossmotorskills(balanceandballskills),verbalmemory,visuomotorintegration,executivefunctioning,orbehavior.
86
Chapter 5
WithregardtoIQ,thedifferencesbetweentheSGAchildrenandthecontrolsweresmall.TotalIQandverbalIQdidnotdifferbetweenthegroups,andonlyperformanceIQwas~0.5SDlowerintheSGAgroup.ContrarytosomeotherstudiesthathadreportedlowertotalIQinSGAchildren,(6,9)our�indingssuggestthatbeingbornpretermaffectsIQmorethandoesgrowthrestriction.ThisismoresoinverbalIQthaninperformanceIQ(10).Alargepopulationbasedcohortstudyreportedfollow-updataoftheEPIPAGEcohortat5yofage.(6)Theirinclusionrateforthecognitivetestswasonly~65%.Thismayhavecausedbias in theresults.Ofnote, in theEPIPAGEcohort, lower IQswerefoundinSGAchildrenwithGA29–32wk,whereastherewasnosuch�indinginSGAchildrenwithGA24–28wk.TwootherstudiesthatfoundapoorertotalandverbalIQinSGAchildrenincludedapproximatelythesamenumberofchildrenasourstudydid.(9,10)Oneofthesestudieswasperformedinchildren3yofage(9)andtheotherinchildren5yofage.(10)Inourstudy,thechildrenweretestedbetweentheagesof7and10y.Byimplication,thismaymeanthat,astheygrowolder,verypretermSGAchildrencatchuponintelligencelagbutnotonperformanceIQ. Ascomparedwiththecontrols, theSGAchildreninourstudyalsoobtainedlowerscoresonselectiveattentionandvisualperception.These�indingscon�irmthedatafromotherfollow-upstudiesofverypretermSGAchildren.(5–7,9)Apparently,attentionisavulnerableneuropsychologicaldomaininverypretermSGAchildren.AttentionisalsoveryoftenaffectedinSGAchildrenbornmoderatelypretermoratfullterm.(5,7)Earlier,lowerscoresonvisualperceptionwerefoundinfulltermandmoderatelypretermSGAchildren.(7) Inourstudy,wefoundthat�inemotorskillsinparticularwereslightlymoreaffectedintheverypretermSGAchildren.Inastudythatusedastandardneurologicexamination,Guellecet al. couldnotdemonstratedifferencesinmotoroutcomebetweenverypretermSGAcasesandAGAcontrolsassessedattheageof5y.(6)Con�lictingresultsonoutcomeasregardsmotorskillshavebeenreportedinpretermSGAchildrenwhenthede�initionofprematurityisextendedto37wkGA.(5)Padillaet al. foundnodifferencesbetweenSGAcasesandAGAcontrolswithrespect toeithergrossor �inemotorskills.(25)Bycontrast,Matilainenet al. reported that both gross and �inemotor skillsweremoreimpaired inSGAchildren.(26)Otherstudieshavealsoreported increased incidencesofspasticmotoroutcomesandgrossmotorimpairment.(27,28)Ofnote,inourstudymotorskillswereobservedtobeaffectedinasmanyas~50%ofthechildreninboththeSGAandAGAgroups.ThissuggeststhatGAratherthangrowthrestrictionisthemajordeterminantoftheriskofdevelopingimpairmentin�inemotorskills.(6) With regard to behavioral problems, we did not �ind any signi�icant differencesbetweenthetwogroupsofverypretermchildren.Anearlierstudyhadreportedmorebehavioralproblems inverypretermSGAchildren,(29)whereasotherstudies failedtocon�irmthese�indings.(6,30)AsregardsADHD,wefoundnosigni�icantdifference
Follow-up at school age after FGR
87
5
betweentheSGAchildrenandthecontrols.Thisisinlinewiththeresultsofpreviousstudies.(6,10) A higher incidence of behavioral problems and ADHD is consistentlyfound inpretermchildrenas comparedwith childrenbornat term,(1,3,31)and thiswascon�irmedinourstudy. Wedidnot �ind theoutcomes tobeworse in the SGA childrenas comparedwiththeAGAcontrolsinsuchcognitivedomainsasverbalmemory,verbalIQ,andexecutivefunctioning.Furthermore, thepercentageof childrenwhorepeatedclasses inschoolwassimilarinthetwogroups.CognitiveskillshaveveryrarelybeenassessedinchildrenbornverypretermandSGA;moststudiesreportinginthedomainsofcognitiveskillsstudiedSGAchildrenbornupto37wkGAorthosebornfullterm.Thestudiesreportedpoorer performances by these children with respect to these neuropsychologicaldomains.(7,8,26,32)Inourstudy,theratesofabnormalandborderlinescoresinnearlyalldomainsexceededthoseonewouldexpectinanormalpopulation. Although children born very preterm and SGA have poorer cognitive and �inemotoroutcomes,thedifferencesinoutcomesascomparedwiththematchedcontrols(childrenbornverypretermbutAGA)were small, andbehaviordidnot seem tobedifferentbetweenthetwogroups.VerypretermbirthinitselfisassociatedwithpoorIQ, poor motor skills,(1,2,4) and behavioral problems.(31) Apparently, intrauterinegrowthrestriction (IUGR)doesnot contributemuch tomakingoutcomesworse.Weoffertwoexplanationsforthis�inding.First,ourstudygroupconsistedofchildrenbornverypretermandSGA.GiventheirlowerBW,SGAinfantshaveahighermortalityratethanAGAinfantsdo.(6,33)ThereforeverypretermSGAchildrenwhodosurvivemayhavebeen lessgrowthrestricted thanSGAchildrenbornat full term.Second, inourgroup,IUGRoccurredratherearlyinpregnancy,aswasre�lectedbythehighpercentage of childrenwithHC values lower than the 10thpercentile. If growth restrictionhad occurred later in pregnancy, it could have led to other patterns of brain injury.WespeculatethatthesetwofactorspartlyexplainsomeofthesmallerdifferencesinoutcomemeasuresbetweenSGAcasesandAGAcontrols. SeveralcausesmayleadtoaninfantbeingbornSGA.Someofthesearecongenitalorchromosomalabnormalities,pathologyoftheplacenta(withIUGRasaconsequence),andbeingconstitutionallysmallbecauseoftheshortstatureoftheparents.Inourstudy,weexcludedthe�irstofthesepossiblecauses,andthereforethestudygroupconsistedofthosewhohadexperiencedIUGRandthosewhowereconstitutionallysmall.Boththese factorsmight slightlydelayoralterbraindevelopment inutero, and thereforesmalldifferencesinfunctionaloutcomemaybeseenbetweenverypreterm–bornSGAchildrenandverypreterm–bornAGAchildren. Nevertheless,inseveralneuropsychologicaldomainstheoutcomeswefoundintheSGAchildrenwerede�initelypoorerthanintheAGAcontrols.Themoststriking�indingswere lower levels of performance IQ, selective attention, and �ine motor skills. We
88
Chapter 5
consideredseveralpotentialexplanationsforour�indings.Theclinicalcharacteristicsdidnotdifferbetweenthegroups,apartfromhigherSNAPIIscoresintheSGAgroup;indeed,theresultsremainedsimilarafteradjustmentforSNAPIIscores.Therewasalsoasigni�icantdifferenceincesareansectionratesbetweenthetwogroups,beinghigherintheSGAgroup.ThissuggeststhattheSGAchildrenexperiencedsigni�icantlygreaterdistressinutero thanthecontrolsdid,possiblycontributingtotheobserveddifferencesinoutcomes.However,Apgarandneurobiologicriskscoresdidnotdifferbetweenthegroups.WithintheSGAcasegroup,wecouldnotdemonstrateanassociationbetweenIQandsmallHC,eitheratbirthorat follow-up.Thiswas in contrast to the �indingsreportedbyGevaet al.,whostudiedneuropsychologicaloutcomesofmainlyfulltermgrowthrestricted children.(7) However, small head size at follow-up appeared tohavesomeassociationwithbehavioralproblemsand impairedmotorskills.PossiblydecreaseinneuralconnectivityandinthecomplexityoftheneuralnetworksplayedaroleinthedifferenceswefoundbetweenverypretermSGAandAGAchildren,butthisishighlyspeculative. Tothebestofourknowledge,thisisoneofthefewstudiesthatreportsfunctionaloutcomeatschoolageofvariousdevelopmentaldomains inverypreterm–bornSGAchildren.Thestrengthofourstudyisthatalargearrayofneuropsychologicaldomains,relevant for everyday functioning, was tested. We took great care in selecting anappropriatecontrolgroup.ControlswerematchedforGA,gender,andbirthyear. Wealsorecognizesomelimitationsofourstudy.Thiswasasinglecenterstudy,andthismay limit thegeneralizabilityofourresults.Wereportedononlya smallgroupofverypretermSGAchildren.Executivefunctioningwasassessedonlybymeansofaquestionnaire.Weusedtheparent’soccupationasanindicatorofSESinsteadof(forexample)education.Nevertheless,webelievethatthe�indingsinourcohortrepresentthefunctionalskillsanddisabilitiesinverypretermSGAchildreningeneral. Our �indings suggest that care should be taken to closely monitor preterm SGAchildrenduringfollow-up,particularlyinthedomainsofattention,performanceIQ,and�inemotor skills. Future research should focus on thepathophysiological process ofbraindevelopmentinIUGR,andonthepreventionofthesefunctionalde�icits.
Conclusion
Very preterm–born SGA children performed worse on performance intelligence,selectiveattention,visualperception,andmotorskills(inparticular,�inemotorskills)ascomparedwithmatchedAGAcontrols.Thedifferences,however,weresmall.Thissuggeststhat theobservedimpairment inthe functioningofverypreterm–bornSGAchildren isattributable to theirverypre termbirthper se rather than tobeingSGA.
Follow-up at school age after FGR
89
5
Ourdataalsosuggestthatverypreterm–bornSGAchildrenshouldbefollowed-upandscreenedfor�inemotorandattentionde�icitsatschoolage.
Statement of fi nancial supportNo�inancialassistancehasbeenreceivedinsupportofthisstudy.
AcknowledgementsThis studywas part of the research program of the Research school for Behavioraland Cognitive Neurosciences, university of Groningen, the Netherlands. We greatlyappreciate the help of Titia Brantsma–vanWulfften Palthe in correcting the Englishmanuscript.

90
Chapter 5
References(1) JohnsonS.Cognitiveandbehaviouraloutcomesfollowingverypretermbirth.SeminFetalNeonatalMed
2007;12:363–73.(2) FawkeJ.Neurologicaloutcomesfollowingpretermbirth.SeminFetalNeonatalMed2007;12:374–82.(3) BhuttaAT,ClevesMA,CaseyPH,CradockMM,AnandKJ.Cognitiveandbehavioraloutcomesofschool-
agedchildrenwhowerebornpreterm:ametaanalysis.JAMA2002;288:728–37.(4) AarnoudseMoens CS, WeisglasKuperus N, van Goudoever JB, Oosterlaan J. Metaanalysis of
neurobehavioral outcomes in very preterm and/or very low birth weight children. Pediatrics2009;124:717–28.
(5) Bos AF, Einspieler C, Prechtl HF. Intrauterine growth retardation, general movements, andneurodevelopmentaloutcome:areview.DevMedChildNeurol2001;43:61–8.
(6) GuellecI,LapillonneA,RenolleauS,etal.;Neurologicoutcomesatschoolageinverypreterminfantsbornwithsevereormildgrowthrestriction.Pediatrics2011;127:e883–91.
(7) GevaR,EshelR,LeitnerY,ValevskiAF,HarelS.Neuropsychologicaloutcomeofchildrenwithintrauterinegrowthrestriction:a9yearprospectivestudy.Pediatrics2006;118:91–100.
(8) LeitnerY,FattalValevskiA,GevaR,etal.Neurodevelopmentaloutcomeofchildrenwith intrauterinegrowthretardation:alongitudinal,10yearprospectivestudy.JChildNeurol2007;22:580–7.
(9) Sung IK, Vohr B, OhW. Growth and neurodevelopmental outcome of very low birthweight infantswithintrauterinegrowthretardation:comparisonwithcontrolsubjectsmatchedbybirthweightandgestationalage.JPediatr1993;123:618–24.
(10) Morsing E, Asard M, Ley D, Stjernqvist K, Marsál K. Cognitive function after intrauterine growthrestrictionandverypretermbirth.Pediatrics2011;127:e874–82.
(11) Kloosterman GJ. On intrauterine growth: the signi�icance of prenatal care. Int J Gynaecol Obstet1970;8:895–912.
(12) KortW,CompaanEL,BleichrodtN,etal.WISC-IIINL: Wechsler Intelligence Scales for Children,3rdedn,Dutchversion.Amsterdam,TheNetherlands:NIPDienstencentrum,2002.
(13) GregoireJ.ComparisonofthreeshortformsoftheWechslerintelligencescaleforchildrenthirdedition(WISCIII).EurRevApplPsychol2000;50:437–41.
(14) ManlyT,AndersonV,NimmoSmithI,TurnerA,WatsonP,RobertsonIH.Thedifferentialassessmentofchildren’sattention:theTestofEverydayAttentionforChildren(TEACh),normativesampleandADHDperformance.JChildPsycholPsychiatry2001;42:1065–81.
(15) vandenBurgW,KingmaA.Performanceof225DutchschoolchildrenonRey’sAuditoryVerbalLearningTest(AVLT):paralleltestretestreliabilitieswithanintervalof3monthsandnormativedata.ArchClinNeuropsychol1999;14:545–59.
(16) KorkmanM,KirkU,KempSL.NEPSY II: Clinical and Interpretative Manual.SanAntonio,TX:PsychCorp,2007.
(17) Gioia GA, Isquith PK, Guy SC, Kenworthy L. Behavior rating inventory of executive function. ChildNeuropsychol2000;6:235–8.
(18) SmitsEngelsman BCM.Movement Assessment Battery for Children. Lisse, The Netherlands: Swets &Zeitlinger,1998.
(19) AchenbachTM,EdelbrockC.Manual for the Child Behavior Checklist: 4-8 and 1991 Pro�ile.Burlington,Vermont:UniversityofVermont,DepartmentofPsychiatry,1991.
(20) ScholteEM,vanderPloegJD.[ADHD-questionnaire (AVL) manual]. Houten, The Netherlands: BohnSta�leuVanLoghum,2004.
(21) Brazy JE, Eckerman CO, Oehler JM, Goldstein RF, O’Rand AM. Nursery Neurobiologic Risk Score:importantfactorinpredictingoutcomeinverylowbirthweightinfants.JPediatr1991;118:783–92.
(22) RichardsonDK, Corcoran JD, Escobar GJ, Lee SK. SNAPII and SNAPPEII: Simpli�ied newborn illnessseverityandmortalityriskscores.JPediatr2001;138:92–100.
(23) DivisieSocialeenRuimtelijkestatistieken.Standard Classi�ication Of Occupations 1992, edition 2001.Voorburg/Heerlen,TheNetherlands:CentraalBureauvoordeStatistiek,2001.
(24) NiklassonA,AlbertssonWiklandK.Continuousgrowth reference from24thweekof gestation to24monthsbygender.BMCPediatr2008;8:8.
Follow-up at school age after FGR
91
5
(25) PadillaN,PerapochJ,CarrascosaA,AcostaRojasR,BotetF,GratacósE.Twelvemonthneurodevelopmentaloutcome in preterm infants with and without intrauterine growth restriction. Acta Paediatr2010;99:1498–503.
(26) MatilainenR,HeinonenK,SirenTiusanenH,JokelaV,LaunialaK.Neurodevelopmentalscreeningofinuterogrowthretardedprematurelybornchildrenbeforeschoolage.EurJPediatr1987;146:453–7.
(27) HaddersAlgraM,HuisjesHJ,TouwenBC.Pretermorsmallforgestationalageinfants.Neurologicalandbehaviouraldevelopmentattheageof6years.EurJPediatr1988;147:460–7.
(28) ClaasMJ,BruinseHW,KoopmanC,vanHaastertIC,PeelenLM,deVriesLS.Twoyearneurodevelopmentaloutcomeofpretermbornchildren≤750gatbirth.ArchDisChildFetalNeonatalEd2011;96:F169–77.
(29) Zubrick SR, Kurinczuk JJ, McDermott BM, McKelvey RS, Silburn SR, Davies LC. Fetal growth andsubsequentmentalhealthproblemsinchildrenaged4to13years.DevMedChildNeurol2000;42:14–20.
(30) vandenBroekAJ,KokJH,HoutzagerBA,ScherjonSA.Behaviouralproblemsattheageofelevenyearsinpretermbornchildrenwithorwithoutfetalbrainsparing:aprospectivecohortstudy.EarlyHumDev2010;86:379–84.
(31) ReijneveldSA,deKleineMJ,vanBaarAL,etal.Behaviouralandemotionalproblemsinverypretermandverylowbirthweightinfantsatage5years.ArchDisChildFetalNeonatalEd2006;91:F423–8.
(32) GutbrodT,WolkeD,SoehneB,OhrtB,RiegelK.Effectsofgestationandbirthweightonthegrowthanddevelopmentofverylowbirthweightsmallforgestationalageinfants:amatchedgroupcomparison.ArchDisChildFetalNeonatalEd2000;82:F208–14.
(33) RegevRH,LuskyA,Dol�inT,LitmanovitzI,ArnonS,ReichmanB.Excessmortalityandmorbidityamongsmallforgestationalageprematureinfants:apopulationbasedstudy.JPediatr2003;143:186–91.
Chapter 6
Functional outcomes at age 7 years of moderate
preterm and full term children born small for gestational age
Jozien C. Tanis, Koenraad N.J.A. Van Braeckel, Jorien M. Kerstjens, Inger F.A. Bocca-Tjeertes, Sijmen A. Reijneveld, and Arend F. Bos
Journal of Pediatrics 2015 Mar;166(3):552-558
94
Chapter 6
Abstract
Objective To compare functional outcomes of 7-year-old (school age) children born small forgestationalage(SGA;ie,abirthweightz score≤-1SD),withappropriateforgestationalage(AGA)peers,bornmoderatelypretermorfullterm.
Study design Data were collected as part of the Longitudinal Preterm Outcome Project study, acommunity- based, prospective cohort study of 336 AGA and 42 SGA born children(mediangestationalage35weeks,range31-41).OftheSGAchildren,32weremoderatelypreterm,10werefullterm;oftheAGA,thesenumberswere216and120,respectively.At6.9years,weassessedintelligence,verbalmemory,attention,visuomotorintegration,and motor skills and we collected the parent-reported executive functioning. WecomparedtheoutcomesoftheSGAchildrenwiththoseoftheirAGApeers.
Results The performance of SGA childrenwas similar to that of their AGApeers, except forattentioncontrolwhichwasabnormalmoreoften inSGAchildren (OR3.99,95%CI1.32-12.12).The IQof SGA childrenwas3points lower, but thisdifference failed toreachsigni�icance.
Conclusions Atschoolage,childrenbornSGAhaveagreaterriskofabnormaltestscoresonattentioncontrolthanchildrenbornAGA,independentofgestationalage.Theirmotorandmanyother cognitive functions are similar. The impact of these outcomes seems limited.Nevertheless,theconsequencesforschoolperformancedeserveattention.
Follow-up at school age after FGR
95
6
Introduction
Aninfantbornsmallforgestationalage(SGA)isconsideredtobeatriskofimpaireddevelopmentinchildhood.(1)ReportsontheoutcomesofSGA-bornchildrenvaryfromminortomajorde�icitsincomparisonwiththeirappropriateforgestationalage(AGA)peers.(2-7)Thesede�icitsmayleadtoimpairedneurocognitiveoutcomeatschoolage.(8) Another risk factor associated with impaired neurodevelopmental outcomesis preterm birth.(9,10) Very preterm birth (<32 weeks’ gestational age [GA]) cancause serious perinatal complications and neurodevelopmental sequelae.(11) ThecombinationofverypretermbirthandbornSGA,posesanadditionalrisk,(12)buttowhatextentisstillunderdebate.Previously,withanothercohort,wefoundthatchildrenbornverypretermandSGAhavepoorertotaland�inemotorskills,selectiveattention,andvisualperceptioncomparedwiththeirverypreterm,AGApeers.(13)AnotherstudyshowedlowerintelligenceintheverypretermSGAchildren.(14)
ThemajorityofSGAchildren,however,arebornmoderatelypreterm(MPT)orfulltermratherthanverypreterm.AswithbeingbornSGA,MPTbirthalsoappearstobeariskfactorassociatedwithimpairedoutcome.(15-18)Theadditionaleffects,however,ofSGAbirthinMPTsandfulltermsonneurodevelopmentarenotyetunderstood.PreviousstudiesonfunctionaloutcomesofMPTandfulltermSGAchildrenreportedcon�lictingresults.(19-21)Differencesinoutcomesmaybetheresultofthevarietyofsubgroups,thede�initionofSGA, the inclusionofpreterm-bornor full term-bornchildren,or tothefactthatmostweresingle-centerstudies.Becauseourstudygroupisacommunity-basedcohort,our�indingsmightaddtotheknowledgeonneurodevelopmentofMPTand full term-born SGA children. Our aimwas, therefore, to compare the functionaloutcomesof7-year-old(schoolage)MPTandfulltermchildrenbornSGAwiththatoftheirAGApeersinacommunity-basedcohort,whiletakingintoaccountsexandGA.
Methods
ThisstudywaspartoftheLongitudinalPretermOutcomeProject,astudyongrowth,development,andgeneralhealthofpreterm-bornchildren.(22)Childrenwererecruitedfrom13DutchPreventiveChildHealthCareCentersat theageof4years.Fromthiscommunity-based cohort of 45446 children born during 2002 and 2003, all 1843preterms(<36weeks’GA)andamatchedrandomsampleof674fullterms(38-41+6
weeks’GA)wereincluded.Thematchedfulltermgroupcomprisedthe�irstsubsequentchildfromthesamebirthyearasapretermbornchildwithaGAbetween38+0and41+6weeksthatwas�iledaftereachsecondpretermchild.TheGAswerecalculated

96
Chapter 6
from the date of lastmenstruation, and in themajority of cases con�irmedby earlyultrasoundmeasurements.Weexcludedchildrenwithmajorcongenitalmalformations,congenitalinfections,orsyndromes. At 7 years of age,we invited all children from the cohort to participatewho hadparticipatedattheageof4yearsandwhowerelivinginthe3northernprovincesofTheNetherlands(Groningen,Friesland,andDrenthe):341MPTs(32-35+6weeks’GA)and195fullterms(38-41+6weeks’GA).Theparentsof93MPTchildrenand65fulltermchildrencouldnotbe tracedor theydeclinedtoparticipate in the follow-up, leadingtoaparticipationpercentageof71%.Wefoundnosigni�icantdifferencesbetweentheoutcomesofchildrenwhoparticipatedinthepresentstudyandthosewhodroppedout.Altogether,248bornMPT(138boys,110girls,medianGA34weeks)and130fulltermchildren(58boys,72girls,medianGA40weeks)participatedinourstudy. Forthepresentstudy,weusedthesamecohorttocomparethefunctionaloutcomesofMPTandfulltermchildrenbornSGAwiththoseoftheirAGApeers.WecategorizedtheMPTandfulltermchildreninto1of2groups:birthweight<-1SDandbirthweight>-1SDaccordingtoGAusingtheDutchKloostermancurve.(23)Wetookasomewhatlowercut-offforSGA(-1SD,belowthe16thpercentile)accordingtothe�indingsoftheEtudeEpidemiologiquesurlesPetitsAgesGestationnelsstudy,(24)andalsotoincreasethepowerofpotentialdifferencesbetween thegroups.Wedenoted thestudygroup(birthweight<-1SD)asSGA.Of42SGAchildren32(76%)wereMPT,and10(24%)werefullterm.Eighteenofthe32MPTand5ofthe10fulltermchildrenwerebelowthe10thpercentile. Medicaldatawereextracted fromhospitalcharts.ThestudywasapprovedbytheEthics Review Board of University Medical Center Groningen. Examinations wereperformed in accordance with the institutional and international ethical standards,withwritteninformedconsentfromallparents. ChildrenandtheirparentswereinvitedtovisitUniversityMedicalCenterGroningenor a well-baby clinic in their neighborhood for a 3-hour assessment comprising anumberof standardizedneuropsychologic tests andaquestionnaire.Each childwastested individuallybya trainedpsychologist,whowasblindas togroupassignment,whereastheparentscompletedthequestionnaireinthewaitingroom.
Cognitive outcomes Weassessedcognitiveoutcomesbyusingseveralstandardizedtests.Ashort formoftheWechslerIntelligenceScaleforChildren,ThirdEdition,Dutchversionwasusedtodetermine intelligence.(25,26)We calculated total IQ on the basis of the verbal andperformanceIQsubtests.Wemeasuredselectiveattentionandattentioncontrolwith“MapMission”and“OppositeWorlds,”2subtestsoftheTestofEverydayAttentionforChildren.(27)Selectiveattentionreferstoachild’sabilitytoselecttargetinformation
Follow-up at school age after FGR
97
6
froman arrayof distractors.Attention control refers to the ability to shift attention�lexibly and adaptively. To assess verbal memory, we used Rey’s Auditory VerbalLearningTest.(28)Itconsistsofa15-wordlistthatisrepeatedtothechild5times.Aftereach trial,we tested immediate recall. Delayed recallwas assessed after an intervalof 20 minutes. To assess visuomotor integration, we used “Design Copying” of theNeuropsychologicalAssessment,SecondEdition.(29)Visuomotorintegrationinvolvestheintegrationofvisualinformationwith�inger-handmovements. We used the Behavior Rating Inventory of Executive Function questionnaire,(30)
whichwas �illedout by theparents, to assess executive functioning indaily life.Wetransformed the percentile rank scores (high percentile means poor outcome) ofthe global executive composition score into percentiles (low percentilemeans pooroutcome).Wedidthistopresentalloutcomemeasuresinthesameway.
Motor outcome WeusedtheMovementAssessmentBatteryforChildren(MovementABC)(31)toassessmotoroutcomes.This is a standardized test thatmeasures totalmotorperformancebasedon subscoresusingDutchnorms formanualdexterity (�inemotor skills), ballskills,andstatic-dynamicbalance(coordination).Thegreaterthescore,thepoorertheoutcome.
Statistical analyses MPTand full termgroupswere combined for analyses.We tested thedifferences inpatientdemographicsbetweenSGAandAGAgroupswiththeMann-WhitneyUtestortheχ2 testwhereappropriate.Regarding functionaloutcomes,we testeddifferencesin continuous outcome scores between the SGA and AGA groups bymultiple linearregressionanalyses.Next,weadjustedforGA(MPT/full term),sex,andassessedtheinteractionofSGA/AGAbyGAcategory.GAwasdichotomizedastoavoidtheassumptionof exponential associations between determinant and outcome, a peculiarity of thelogistic model. Second, we classi�ied functional outcomes into 3 categories; normal(>15th percentile, IQ ≥85), borderline (5-15th percentile, IQ 70-84), and abnormal(<5thpercentile, IQ<70).Themotoroutcomeclassi�icationwasbasedon theDutchnormsinthemanual.Third,wecalculatedORviamultiplelogisticregressionanalysesandinvestigatedORforborderline/abnormalvsnormalandforabnormalvsnormal/borderline outcomes. Next, we adjusted for GA and sex, and again assessed theinteractionof SGA/AGAwithGA category.Weadjusted forGAand sex as thesemayactasconfounderseveniftheydonotdifferwithstatisticalsigni�icancebetweenthe2groups.
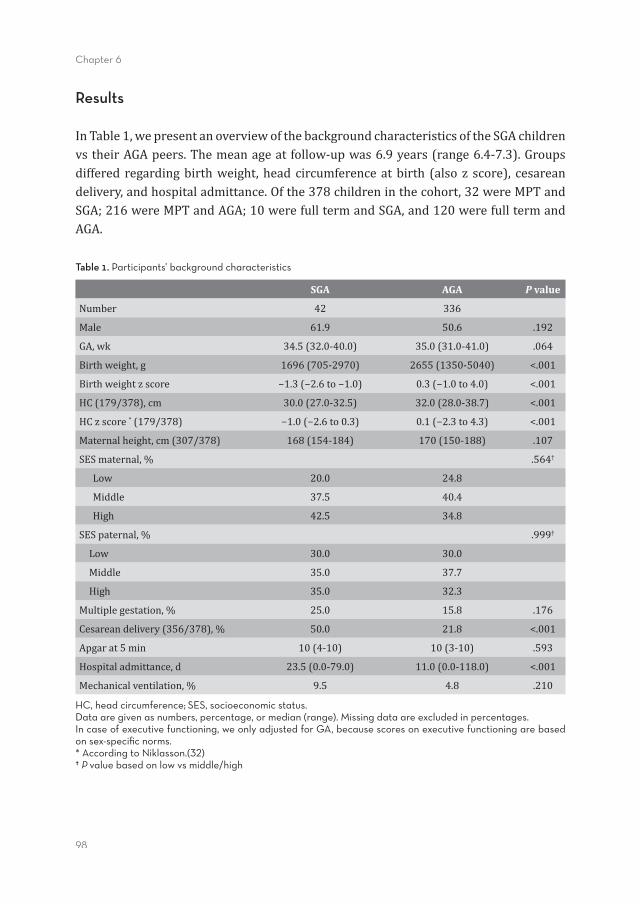
98
Chapter 6
Results
InTable1,wepresentanoverviewofthebackgroundcharacteristicsoftheSGAchildrenvstheirAGApeers.Themeanageat follow-upwas6.9years(range6.4-7.3).Groupsdiffered regardingbirthweight,headcircumferenceatbirth (also z score), cesareandelivery,andhospitaladmittance.Ofthe378childreninthecohort,32wereMPTandSGA;216wereMPTandAGA;10werefulltermandSGA,and120werefulltermandAGA.
Table 1. Participants’ background characteristics
SGA AGA P value
Number 42 336
Male 61.9 50.6 .192
GA,wk 34.5(32.0-40.0) 35.0(31.0-41.0) .064
Birthweight,g 1696(705-2970) 2655(1350-5040) <.001
Birthweightzscore −1.3(−2.6to−1.0) 0.3(−1.0to4.0) <.001
HC(179/378),cm 30.0(27.0-32.5) 32.0(28.0-38.7) <.001
HCzscore*(179/378) −1.0(−2.6to0.3) 0.1(−2.3to4.3) <.001
Maternalheight,cm(307/378) 168(154-184) 170(150-188) .107
SESmaternal,% .564†
Low 20.0 24.8
Middle 37.5 40.4
High 42.5 34.8
SESpaternal,% .999†
Low 30.0 30.0
Middle 35.0 37.7
High 35.0 32.3
Multiplegestation,% 25.0 15.8 .176
Cesareandelivery(356/378),% 50.0 21.8 <.001
Apgarat5min 10(4-10) 10(3-10) .593
Hospitaladmittance,d 23.5(0.0-79.0) 11.0(0.0-118.0) <.001
Mechanicalventilation,% 9.5 4.8 .210
HC, head circumference; SES, socioeconomic status.Data are given as numbers, percentage, or median (range). Missing data are excluded in percentages.In case of executive functioning, we only adjusted for GA, because scores on executive functioning are based on sex-specifi c norms.* According to Niklasson.(32) † P value based on low vs middle/high
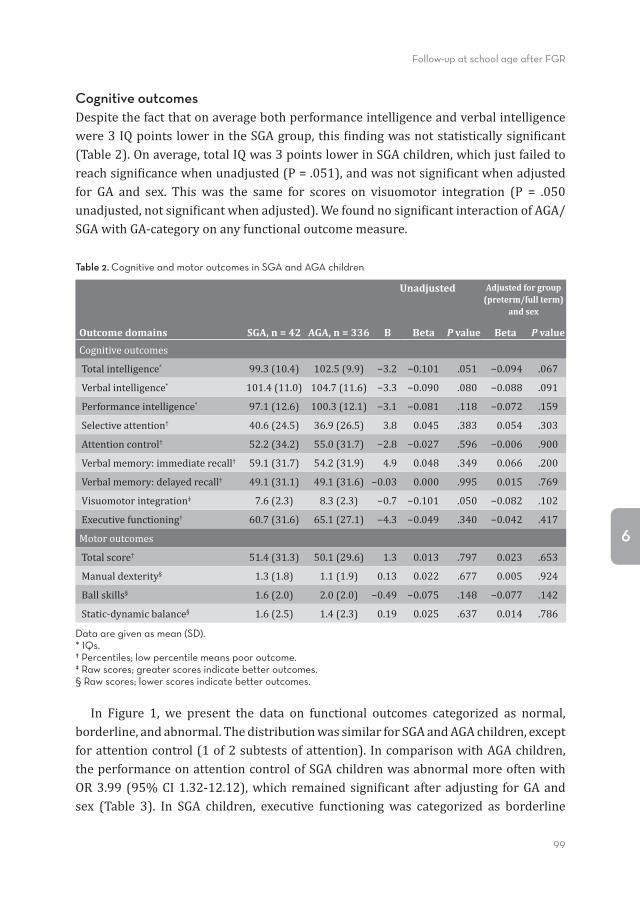
Follow-up at school age after FGR
99
6
Cognitive outcomes Despitethefactthatonaveragebothperformanceintelligenceandverbalintelligencewere3IQpointslowerintheSGAgroup,this�indingwasnotstatisticallysigni�icant(Table2).Onaverage,totalIQwas3pointslowerinSGAchildren,whichjustfailedtoreachsigni�icancewhenunadjusted(P=.051),andwasnotsigni�icantwhenadjustedfor GA and sex. This was the same for scores on visuomotor integration (P = .050unadjusted,notsigni�icantwhenadjusted).Wefoundnosigni�icantinteractionofAGA/SGAwithGA-categoryonanyfunctionaloutcomemeasure.
Table 2. Cognitive and motor outcomes in SGA and AGA children
Outcome domains SGA, n = 42 AGA, n = 336
Unadjusted Adjusted for group (preterm/full term)
and sex
B Beta P value Beta P value
Cognitiveoutcomes
Totalintelligence* 99.3(10.4) 102.5(9.9) −3.2 −0.101 .051 −0.094 .067
Verbalintelligence* 101.4(11.0) 104.7(11.6) −3.3 −0.090 .080 −0.088 .091
Performanceintelligence* 97.1(12.6) 100.3(12.1) −3.1 −0.081 .118 −0.072 .159
Selectiveattention† 40.6(24.5) 36.9(26.5) 3.8 0.045 .383 0.054 .303
Attentioncontrol† 52.2(34.2) 55.0(31.7) −2.8 −0.027 .596 −0.006 .900
Verbalmemory:immediaterecall† 59.1(31.7) 54.2(31.9) 4.9 0.048 .349 0.066 .200
Verbalmemory:delayedrecall† 49.1(31.1) 49.1(31.6) −0.03 0.000 .995 0.015 .769
Visuomotorintegration‡ 7.6(2.3) 8.3(2.3) −0.7 −0.101 .050 −0.082 .102
Executivefunctioning† 60.7(31.6) 65.1(27.1) −4.3 −0.049 .340 −0.042 .417
Motoroutcomes
Totalscore† 51.4(31.3) 50.1(29.6) 1.3 0.013 .797 0.023 .653
Manualdexterity§ 1.3(1.8) 1.1(1.9) 0.13 0.022 .677 0.005 .924
Ballskills§ 1.6(2.0) 2.0(2.0) −0.49 −0.075 .148 −0.077 .142
Static-dynamicbalance§ 1.6(2.5) 1.4(2.3) 0.19 0.025 .637 0.014 .786
Data are given as mean (SD).* IQs.† Percentiles; low percentile means poor outcome.‡ Raw scores; greater scores indicate better outcomes.§ Raw scores; lower scores indicate better outcomes.
In Figure 1, we present the data on functional outcomes categorized as normal,borderline,andabnormal.ThedistributionwassimilarforSGAandAGAchildren,exceptforattentioncontrol(1of2subtestsofattention).IncomparisonwithAGAchildren,theperformanceonattentioncontrolofSGAchildrenwasabnormalmoreoftenwithOR3.99 (95%CI1.32-12.12),which remainedsigni�icantafteradjusting forGAandsex (Table 3). In SGA children, executive functioning was categorized as borderline
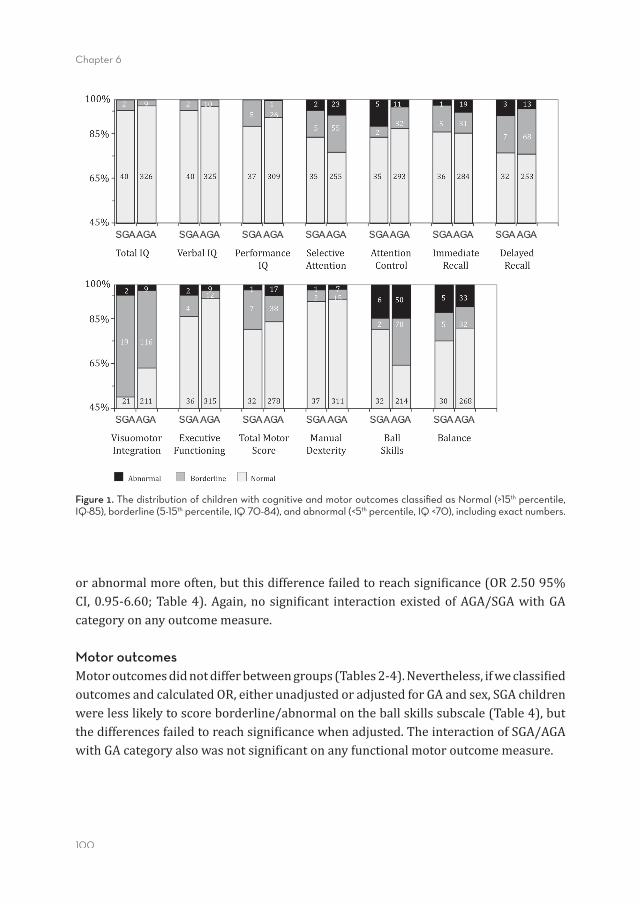
100
Chapter 6
orabnormalmoreoften,butthisdifferencefailedtoreachsigni�icance(OR2.5095%CI,0.95-6.60;Table4).Again,nosigni�icant interactionexistedofAGA/SGAwithGAcategoryonanyoutcomemeasure.
Motor outcomes Motoroutcomesdidnotdifferbetweengroups(Tables2-4).Nevertheless,ifweclassi�iedoutcomesandcalculatedOR,eitherunadjustedoradjustedforGAandsex,SGAchildrenwerelesslikelytoscoreborderline/abnormalontheballskillssubscale(Table4),butthedifferencesfailedtoreachsigni�icancewhenadjusted.TheinteractionofSGA/AGAwithGAcategoryalsowasnotsigni�icantonanyfunctionalmotoroutcomemeasure.
Figure 1. The distribution of children with cognitive and motor outcomes classifi ed as Normal (>15th percentile, IQ≥85), borderline (5-15th percentile, IQ 70-84), and abnormal (<5th percentile, IQ <70), including exact numbers.
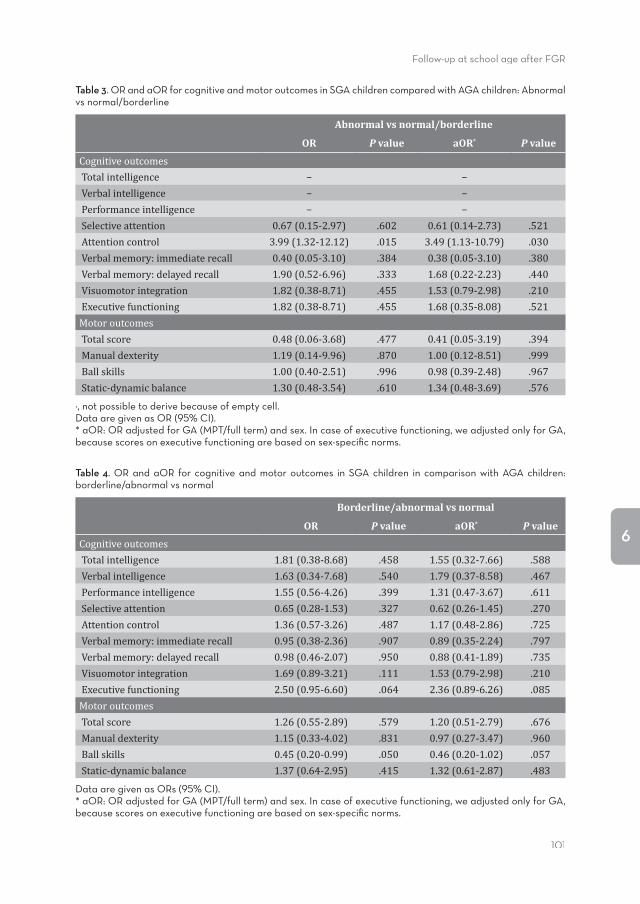
Follow-up at school age after FGR
101
6
Figure 1. The distribution of children with cognitive and motor outcomes classifi ed as Normal (>15th percentile, IQ≥85), borderline (5-15th percentile, IQ 70-84), and abnormal (<5th percentile, IQ <70), including exact numbers.
Table 3. OR and aOR for cognitive and motor outcomes in SGA children compared with AGA children: Abnormal vs normal/borderline
Abnormal vs normal/borderline
OR P value aOR* P value
CognitiveoutcomesTotalintelligence − −Verbalintelligence − −Performanceintelligence − −Selectiveattention 0.67(0.15-2.97) .602 0.61(0.14-2.73) .521Attentioncontrol 3.99(1.32-12.12) .015 3.49(1.13-10.79) .030Verbalmemory:immediaterecall 0.40(0.05-3.10) .384 0.38(0.05-3.10) .380Verbalmemory:delayedrecall 1.90(0.52-6.96) .333 1.68(0.22-2.23) .440Visuomotorintegration 1.82(0.38-8.71) .455 1.53(0.79-2.98) .210Executivefunctioning 1.82(0.38-8.71) .455 1.68(0.35-8.08) .521MotoroutcomesTotalscore 0.48(0.06-3.68) .477 0.41(0.05-3.19) .394Manualdexterity 1.19(0.14-9.96) .870 1.00(0.12-8.51) .999Ballskills 1.00(0.40-2.51) .996 0.98(0.39-2.48) .967Static-dynamicbalance 1.30(0.48-3.54) .610 1.34(0.48-3.69) .576
−, not possible to derive because of empty cell.Data are given as OR (95% CI).* aOR: OR adjusted for GA (MPT/full term) and sex. In case of executive functioning, we adjusted only for GA, because scores on executive functioning are based on sex-specifi c norms.
Table 4. OR and aOR for cognitive and motor outcomes in SGA children in comparison with AGA children: borderline/abnormal vs normal
Borderline/abnormal vs normal
OR P value aOR* P value
CognitiveoutcomesTotalintelligence 1.81(0.38-8.68) .458 1.55(0.32-7.66) .588Verbalintelligence 1.63(0.34-7.68) .540 1.79(0.37-8.58) .467Performanceintelligence 1.55(0.56-4.26) .399 1.31(0.47-3.67) .611Selectiveattention 0.65(0.28-1.53) .327 0.62(0.26-1.45) .270Attentioncontrol 1.36(0.57-3.26) .487 1.17(0.48-2.86) .725Verbalmemory:immediaterecall 0.95(0.38-2.36) .907 0.89(0.35-2.24) .797Verbalmemory:delayedrecall 0.98(0.46-2.07) .950 0.88(0.41-1.89) .735Visuomotorintegration 1.69(0.89-3.21) .111 1.53(0.79-2.98) .210Executivefunctioning 2.50(0.95-6.60) .064 2.36(0.89-6.26) .085MotoroutcomesTotalscore 1.26(0.55-2.89) .579 1.20(0.51-2.79) .676Manualdexterity 1.15(0.33-4.02) .831 0.97(0.27-3.47) .960Ballskills 0.45(0.20-0.99) .050 0.46(0.20-1.02) .057Static-dynamicbalance 1.37(0.64-2.95) .415 1.32(0.61-2.87) .483
Data are given as ORs (95% CI).* aOR: OR adjusted for GA (MPT/full term) and sex. In case of executive functioning, we adjusted only for GA, because scores on executive functioning are based on sex-specifi c norms.

102
Chapter 6
Discussion
Ouraimwas tocompare functionaloutcomesof7-year-old (schoolage)MPTand fulltermchildrenbornSGAwiththeirAGApeersinacommunity-basedcohortandtakingintoaccountGAandsex.Theoutcomesofthe2groupsweresimilar,exceptforattentioncontrol.TheoddsofSGAchildrentohaveabnormalscoresonattentioncontrolwere4timesgreaterthanthatoftheirAGApeers.ThisresultheldafteradjustingforGAandsex.Oneshouldbeaware,however,thatattentioncontrolonlydiffersbetweenSGAandAGAwhencategorized.Becausenodifferencesinattentioncontrolwerefoundinthelinearanalysis,thismightbeachance�inding.Furthermore,theriskofproblemsonselectiveattention,theotheraspectofattentionweassessed,didnotdifferbetweenthe2groups. Previously,3studiesreportedonattentionwithcon�lictingresults.(20,21,33)Leitneret al (21) investigated attention span and found poorer outcomes in SGA childrenconsistentwithour�indings.Emondetal,(20)whoalsoinvestigatedattentioncontrol,foundnodifferences.TheycomparedfulltermSGAchildren(birthweight1500-2500g) with full term controls (birth weight 3000-3500 g) at the age of 8, whereas westudiedmainlyMPT-bornSGAchildren.Thispossiblyexplainsthediscrepancybetweenthe�indingsofEmondetal(20)andours.Viggedaletal(33)foundnodifferencesinattentionbetweenSGAsandtheirAGApeers.TheyusedadifferenttestfromtheoneweusedandtheystudiedtheSGAchildrenat24yearsofage.Ifthedifferencesbetweentheir�indingsandourswerenotbasedontestspeci�ics,thenitmightimplythatour�inding—moreSGA childrenwith abnormal attention control—will diminishas theygrowolder. Regardingintelligence,themeanscoresoftotal,verbal,andperformanceIQwereonaverage3IQpointslowerintheSGAgroup,yetthedifferencesfailedtoreachstatisticalsigni�icance.These �indingsare in linewith thoseofEmondetal,(20)whoreporteda total IQ4points lower in theSGAgroup,basedonverbal IQ (3points lower)andperformance IQ (5points lower).Yet, their �indingsalso failed to reach signi�icance.Theodoreetal(34)foundnosigni�icantdifferencesinIQat7yearsbetweenfulltermSGA children (birth weight <10th percentile) and controls. In a study on full termintrauterinegrowthrestriction(IUGR;birthweight<5thpercentile)childrenat6years,performanceIQshowedthegreatestoutcomedifferenceswithAGApeers.(35)Otherstudiesdid�indsigni�icantdifferencesinIQ.(19,21,33,36)Gevaetal(19)andLeitneretal(21)reportedthatmainIQoutcomeswere10pointslowerinchildrenbornwithIUGR;birthweight<P10andprovenplacentainsuf�iciency.(19,21)AnexplanationmaybethattheimpactoflowbirthweightongeneralcognitivedevelopmentissmallerthantheimpactofIUGR. AsindicatedbythelowerscoresofSGAchildren,theirvisuomotorintegrationwasmoreaffectedthanthatofAGAchildren.Yet,thisdifferencefailedtoreachstatistical
Follow-up at school age after FGR
103
6
signi�icance.WedrawattentiontothefactthatthescoresoftheAGAchildrenwerelowincomparisonwiththestandardscoresinthepopulation,yetintheSGAgrouptheywereeven lower.Theseresultsweresimilar to the �indingsofpreviousstudies.(19,21,35)Becausevisuomotorintegrationwasassessedwith“DesignCopying,”thequestionriseswhethertheaveragepoorerscoresintheSGAgroupwererelatedtopoorercognitivetransformation of the visual information intomotor action (manipulating a pencil),ortoa�inemotorproblem.LikeEmondetal,(20)wefoundnodifferencesinmanualdexterity(motoroutcome)betweenSGAandAGAchildren;thus,weassumethatbeingbornSGAaffectstheintegrationofvisualinformationand�inemotorfunctioning. MeantotalscoresonmotorfunctioningweresimilarfortheSGAandAGAgroups.Surprisingly, SGA children performed slightly better on the ball skill subtest. Morespeci�ically,moreAGAchildrenperformedintheborderlinerange(thuspoorer)onballskillsthantheSGAgroup,butthis�indingwasnotsigni�icantlydifferent.Apparently,theabilitytocontrolaballisnotaffectedbybeingbornSGA.Thisunexpected�indingwasalsoreportedbyEvensenetal,wherenoneofthefulltermSGA(<P10)childrenhadabnormalballskillsvs3of71fulltermcontrols(MovementABC).(37) Other long-term follow-up studies con�lict with our results: Emond et al (20)
foundnodifferences inmanualdexterity,whereastheydid inballskillsandbalance(MovementABC).Conversely,Sommerfeltetal(38)foundpoorermanualdexterityintheirstudygroupandnodifferencesinballskillsandbalance(PeabodyDevelopmentalMotorScales).Differencesinmotoroutcomesbetweenthesestudiesandoursmaybeexplainedbytheagedifferenceofthegroups(14vs7years)andbythetypeoftestsused. Overall,we found fewdifferencesbetweenSGAchildrenand theirAGApeers.Weoffer2explanations.Oneconcernsthede�initionofourstudygroup.Wede�inedSGAasbirthweight<-1SD.WedidsoaccordingtotheEtudeEpidemiologiquesurlesPetitsAgesGestationnelsstudy(24);Guellecetal(24)foundanincreasedriskofcognitiveandbehavioral impairmentat theageof5years inpretermbornmildSGAchildrende�inedas10th-19thpercentile.Therefore,wetookthecutoffbelow-1SD,representingthechildrenwithbirthweightsbelowthe16thpercentile.Thiscoversalargerandthusapossiblylessimpairedgroupthan,forexample,astudygroupwithbirthweight<P2.3(-2SD).Nevertheless,withSGAde�inedasbirthweight<-1SD,westillfoundoneaspectofattention,ie,attentioncontrol,tobepoorerinSGAchildrenthanintheirAGApeers.The second explanation is that we may have included constitutionally small non-IUGR children unintentionally, whereas others studied IUGR children speci�ically.Unfortunately,wedidnothaveaccesstoprenatalultrasoundinformationthuswewereunabletodistinguishIUGRfromSGA.Maternalheightwas2cmlessintheSGAthanintheAGAgroup,butthisdifferencewasnotstatisticallysigni�icant.However,thisdoesnotexcludethepossibilitythatsomechildrenoftheSGAgroupwerenotgrowthretarded
104
Chapter 6
but,instead,constitutionallysmall.Otherresearchers,suchasGevaetal,(19)studiedchildrenwithIUGRandfoundlargerdifferencesinfunctionaloutcomesatschoolagein comparison to controls. This resultmight indicate that IUGR in particular affectsoutcomemorethanSGAitself.Evenso,itisofgreatimportancetoknowtheoutcomesoftheseSGAchildren,becauseitisnotalwayspossibletodistinguishbetweenIUGRandSGAafterbirth.Furthermore,ourstudywasperformedinacommunity-basedcohort,whichispossiblythebestrepresentationoftheentirepopulation. FunctionaloutcomedifferencesbetweenSGAandAGAchildrenshowednointeractionwithGA,whichindicatesthatfunctionaloutcomesofMPTSGAchildrenarenotdifferenttothoseoffulltermSGAchildren.OvertheGArangefrom32weeksbeyondtermage,wefoundthatSGAchildrenperformpooreronlyonattentioncontrol.ThismaybedifferentfortheGArangeyoungerthan32weeks.PreviouslywereportedthatverypretermSGAchildrenhadpoorerfunctionaloutcomesatschoolagethantheirAGApeers,onseveralmore domains, including performance IQ, selective attention, and visual perception.(13)This�indingindicatesthatbeingbornSGAmayhavemoreimpactonfunctionaloutcomesinchildrenbornbefore32weeks’GAthaninthosebornafter32weeks.Ofnote,somemeasureofattentionwasaffectedinSGAchildrenoverthefullGArange,beitselectiveattentionorattentioncontrol. We recognize some limitations. The measurements at age 7 of the LongitudinalPretermOutcomeProjectcohortoriginallyweredesignedtoinvestigateMPTchildren,comparing themwith full term controls. In this study we used the same cohort tocompareSGAandAGAchildren,amongbothMPTandfulltermchildren.ThisresultedinarathersmallnumberofchildrenbornSGA,particularlyfortheGAsubgroups,whichhaslimitedthepowertodetectsmalldifferences.Evenso,tothebestofourknowledgethis is oneof the few studies comparingSGAwithAGApeers in apopulation-basedregionalcohort.Anotherlimitationisthefactthatour�indingsmayseeminconsistent.Forexample,nodifferenceswerefoundinattentioncontrolmeasuredasacontinuousvariable, but differenceswere foundwhen this variablewas categorized in normal,subclinical,andabnormal.Our�indingsshouldthusbeinterpretedwithcaution,theycouldbebasedonchance�indings.Itmight,however,alsobethatthedistributionofthescores,particularlyofthoseabovethe5thpercentile,leadstononsigni�icantdifferences,whereasthenumbersofindividualinfantswithscoresbelowthe5thpercentileindeedaredifferent.Ifso,thisisrelevantfordailypractice. Because attention plays an important role in adequate school performance,(27)
impairedattentioncontrolinSGAchildrenmayaffectthedevelopmentoftheiracademicskills.Cliniciansandteachersshouldbeawareofthispossiblede�icitinthecognitivepro�ileofMPTandfulltermchildrenbornSGA.
Follow-up at school age after FGR
105
6
AcknowledgementsWe thank the participating Preventive ChildHealth Care Centers and physicians fortheircontributiontothe�ieldworkofthestudy.WegreatlyappreciatethehelpofTitiavanWulfftenPaltheforcorrectingtheEnglishmanuscript.
106
Chapter 6
References(1) ArcangeliT,ThilaganathanB,HooperR,KhanKS,BhideA.Neurodevelopmentaldelayinsmallbabiesat
term:asystematicreview.UltrasoundObstetGynecol2012;40:267-75.(2) BassanH,StolarO,GevaR,EshelR,Fattal-ValevskiA,LeitnerY,etal. Intrauterinegrowth-restricted
neonatesbornattermorpreterm:howdifferent?PediatrNeurol2011;44:122-30.(3) CamposD,SantosDC,GoncalvesVM,GotoMM,Campos-ZanelliTM.Motorperformanceofinfantsborn
smallorappropriateforgestationalage:acomparativestudy.PediatrPhysTher2008;20:340-6.(4) Jelliffe-PawlowskiLL,HansenRL.Neurodevelopmentaloutcomeat8monthsand4yearsamonginfants
bornfull-termsmall-for-gestational-age.JPerinatol2004;24:505-14.(5) O’Keeffe MJ, O’Callaghan M, Williams GM, Najman JM, Bor W. Learning, cognitive, and attentional
problemsinadolescentsbornsmallforgestationalage.Pediatrics2003;112:301-7.(6) SimicKlaricA,KolundzicZ,GalicS,MejaskiBosnjakV.Languagedevelopment inpreschoolchildren
bornafterasymmetricalintrauterinegrowthretardation.EurJPaediatrNeurol2012;16:132-7.(7) StreimishIG,EhrenkranzRA,AllredEN,O’SheaTM,KubanKC,PanethN,etal.Birthweight-andfetal
weight-growthrestriction:impactonneurodevelopment.EarlyHumDev2012;88:765-71.(8) WalkerDM,MarlowN.Neurocognitiveoutcomefollowingfetalgrowthrestriction.ArchDisChildFetal
NeonatalEd2008;93:F322-5.(9) JohnsonS.Cognitiveandbehaviouraloutcomesfollowingverypretermbirth.SeminFetalNeonatalMed
2007;12:363-73.(10) LipkindHS,SlopenME,PfeifferMR,McVeighKH.School-ageoutcomesoflatepreterminfantsinNew
YorkCity.AmJObstetGynecol2012;206:222.e1-6.(11) FawkeJ.Neurologicaloutcomesfollowingpretermbirth.SeminFetalNeonatalMed2007;12:374-82.(12) Grisaru-GranovskyS,ReichmanB,Lerner-GevaL,BoykoV,HammermanC,SamueloffA,etal.Mortality
and morbidity in preterm small-for-gestational-age infants: a population-based study. Am J ObstetGynecol2012;206:150.e1-7.
(13) TanisJC,vanderReeMH,RozeE,Huisin’tVeldAE,vandenBergPP,VanBraeckelKN,etal.Functionaloutcome of very preterm-born and small-for-gestational-age children at school age. Pediatr Res2012;72:641-8.
(14) Morsing E, Asard M, Ley D, Stjernqvist K, Marsal K. Cognitive function after intrauterine growthrestrictionandverypretermbirth.Pediatrics2011;127:e874-82.
(15) CserjesiR,VanBraeckelKN,ButcherPR,Kerstjens JM,ReijneveldSA,BoumaA,etal.Functioningof7-year-oldchildrenbornat32to35weeks’gestationalage.Pediatrics2012;130:e838-46.
(16) McGowanJE,AlderdiceFA,HolmesVA,JohnstonL.Earlychildhooddevelopmentoflate-preterminfants:asystematicreview.Pediatrics2011;127:1111-24.
(17) Morse SB, Zheng H, Tang Y, Roth J. Early school-age outcomes of late preterm infants. Pediatrics2009;123:e622-9.
(18) Taylor HG. Outcomes of late preterm birth: who is at risk and for what? Am J Obstet Gynecol2012;206:181-2.
(19) GevaR,EshelR,LeitnerY,ValevskiAF,HarelS.Neuropsychologicaloutcomeofchildrenwithintrauterinegrowthrestriction:a9-yearprospectivestudy.Pediatrics2006;118:91-100.
(20) EmondAM,LiraPI,LimaMC,Grantham-McGregorSM,AshworthA.Developmentandbehaviouroflow-birthweightterminfantsat8yearsinnortheastBrazil:alongitudinalstudy.ActaPaediatr2006;95:1249-57.
(21) LeitnerY,Fattal-ValevskiA,GevaR,EshelR,Toledano-AlhadefH,RotsteinM,etal.Neurodevelopmentaloutcomeofchildrenwithintrauterinegrowthretardation:alongitudinal,10-yearprospectivestudy.JChildNeurol2007;22:580-7.
(22) Kerstjens JM,BosAF, tenVergertEM, deMeerG,ButcherPR,Reijneveld SA. Support for the globalfeasibilityoftheAgesandStagesQuestionnaireasdevelopmentalscreener.EarlyHumDev2009;85:443-7.
(23) Kloosterman GJ. On intrauterine growth: the signi�icance of prenatal care. Int J Gynaecol Obstet1970;8:895-912.
Follow-up at school age after FGR
107
6
(24) GuellecI,LapillonneA,RenolleauS,CharlalukML,RozeJC,MarretS,etal.Neurologicoutcomesatschoolageinverypreterminfantsbornwithsevereormildgrowthrestriction.Pediatrics2011;127:e883-91.
(25) KortW,CompaanE,BleichrodtN.WISC-IIINL:WechslerIntelligenceScalesforChildren.Dutchversion.3rded.Amsterdam,TheNetherlands:NIPDienstencentrum;2002.
(26) GregoireJ.ComparisonofthreeshortformsoftheWechslerintelligencescaleforchildren-thirdedition(WISC-III).EurRevApplPsychol2000;50:437-41.
(27) ManlyT,AndersonV,Nimmo-SmithI,TurnerA,WatsonP,RobertsonIH.Thedifferentialassessmentofchildren’sattention:theTestofEverydayAttentionforChildren(TEA-Ch),normativesampleandADHDperformance.JChildPsycholPsychiatry2001;42:1065-81.
(28) vandenBurgW,KingmaA.Performanceof225DutchschoolchildrenonRey’sAuditoryVerbalLearningTest(AVLT):paralleltest-retestreliabilitieswithanintervalof3monthsandnormativedata.ArchClinNeuropsychol1999;14:545-59.
(29) Korkman M, Kirk U, Kemp SL. NEPSY II. Clinical and interpretative manual. San Antonio (TX):PsychologicalCorporation;2007.
(30) Gioia GA, Isquith PK, Guy SC, Kenworthy L. Behavior rating inventory of executive function. ChildNeuropsychol2000;6:235-8.
(31) Smits-EngelsmanBCM.MovementAssessmentBatteryforChildren.Lisse,TheNetherlands:Swets&Zeitlinger;1998.
(32) NiklassonA,Albertsson-WiklandK.Continuousgrowthreferencefrom24thweekofgestationto24monthsbygender.BMCPediatr2008;8:8.
(33) ViggedalG,LundalvE,CarlssonG,Kjellmer I.Neuropsychological follow-up intoyoungadulthoodofterminfantsbornsmallforgestationalage.MedSciMonit2004;10:CR8-16.
(34) TheodoreRF,ThompsonJM,WaldieKE,BecroftDM,RobinsonE,WildCJ,etal.Determinantsofcognitiveabilityat7years:alongitudinalcase-controlstudyofchildrenbornsmall-for-gestationalageatterm.EurJPediatr2009;168:1217-24.
(35) LeitnerY,Fattal-ValevskiA,GevaR,BassanH,PosnerE,KutaiM,etal.Six-yearfollow-upofchildrenwithintrauterinegrowthretardation:long-term,prospectivestudy.JChildNeurol2000;15:781-6.
(36) Sommerfelt K, Andersson HW, Sonnander K, Ahlsten G, Ellertsen B, Markestad T, et al. Cognitivedevelopmentoftermsmallforgestationalagechildrenat�iveyearsofage.ArchDisChild2000;83:25-30.
(37) EvensenKA,SkranesJ,BrubakkAM,VikT.Predictivevalueofearlymotorevaluationinpretermverylowbirthweightandtermsmallforgestationalagechildren.EarlyHumDev2009;85:511-8.
(38) SommerfeltK,SonnanderK,SkranesJ,AnderssonHW,AhlstenG,EllertsenB,etal.Neuropsychologicandmotorfunctioninsmall-for-gestationpreschoolers.PediatrNeurol2002;26:186-91.
Chapter 7
General discussion
110
Chapter 7
Thisthesiscomprisesstudiesonfetalgrowthrestriction(FGR)fromtheprenatalperiodtoschoolagewiththeemphasisonprenatalandneonatalcirculatoryadaptationsandneurologicaloutcome.Our�irstaimwastoassessprenatalcardiacfunctioninFGR.InChapter2,therefore,wemeasuredlongitudinalannulardisplacement(LAD)ingrowth-restricted fetuses. Our second aim was to determine whether prenatal ultrasoundmeasurementsofgrowth-restricted fetusareassociatedwithearlyand lateneonataldistribution of circulation and neurological functioning. Doppler pulsatility indices(PIs)ofthefetalvesselswereassessedandwecomparedthemwithneonatalmultisitenear-infraredspectroscopy(NIRS)(Chapter3)andgeneralmovements(GMs)(Chapter4). Our third aimwas to investigate functional outcome at school age of small-for-gestational-age (SGA) children born very preterm on the one hand, andmoderatelypreterm-born to full-term infants on the other hand. To this end,we performed anextensive follow-up study at the age of seven and eight years of children born SGA(Chapters5and6).
Cardiac function in FGRInPartIwepresentastudyoncardiacfunctioninFGRwithprenatalultrasound.Wefoundthatleft,right,andseptalLADmeasuredwithspatiotemporalimagecorrelation(STIC) was reduced in FGR in comparison to age-matched controls (Chapter 2).CardiacLAD,commonlyusedinadultechocardiography,isaparameterthatmeasuresmyocardialmotion.(1,2)In2001,CarvalhoetalappliedLADtofetalechocardiographyandfoundittobeausefultooltoassesssystolicanddiastolicfunctionofthefetalheartforclinicalpurposes.(3)InFGR,theheartisacentralorganintheadaptivemechanismsfollowing placental insuf�iciency and it can already display profound structural andfunctionalchangesprenatally.(4-6)InapreviousreportLADwasdecreasedinagroupwithsevereFGR.(7)InFGR,however,LADwasonlymeasuredonlinewithmotionmode(M-mode).Thishasseveraldisadvantages,onebeingthatLADmeasurementsarelessprecise due to fetalmovements. Anothermethod, spatiotemporal image correlation(STIC),allowsLADtobemeasuredof�linebyusingfour-dimensional(4D)ultrasoundanalysis.WehypothesizedthatSTICisthebettermethodtomeasurecardiacfunction.Totestthishypothesis,wecomparedtheonlineM-modeofmeasuringLADinFGRwiththeof�line STICmethod (Chapter2).TheSTICmethodproved tobebetter than theonlineM-modeindetectingreducedcardiacmotion.ThedisadvantageofusingSTIC,however,isthattheclinicianhastoinvesttimeinlearningtousethetechniqueandhowtoanalyzeit.Thelattermethodmight,therefore,bebettersuitedforuseinaresearchsetting.IftheclinicianisabletoinvestinlearninghowtousetheSTICtechnique,theadvantageisthatitisausefulaidinclinicaldecision-making.Theof�linetechniqueisnotonlyofvalueinFGRmanagement,butaddsintheclinicalapproachofvariousfetalcardiacanomalies.(8)STICallowsclinicianstostorea4Dimageofthefetalhearttobe
General discussion
111
7
viewedwhenevertheneedarises.Thisenablesclinicianstoquietlyreexamineafetalcardiacdefectafterclinichoursand,ifneedbe,consultacolleagueabouttheanomalywiththe4Dimageofthefetalheartathand.WerecommendimplementingSTICaspartofclinicalpracticeofobstetricians involved inFGRand fetalassessmentofpotentialcongenitalcardiacdefects.
Prenatal predictors of neonatal distribution of circulationInPartIIwepresentastudyonprenatalDopplermeasurementsanditsassociationswithneonatalcirculatoryconsequencesofFGR(Chapter3).Lowmiddlecerebralartery(MCA)PIsandlowcerebroplacentalratio(CPR),indicatingbrainsparingbeforebirth,were strongly associatedwith a low cerebrorenal ratio afterbirth, indicatinghigherpostnatalbloodsupplyto thecerebrumthantotherenalregion.Wespeculatedthatifbrainsparingispresentinfetalcirculation,redistributionofthecirculationpersistsduring the �irst threedays afterbirth.Thenoveltyof this study is thatwewere the�irsttostudyhemodynamicchangesduetoFGRfromtheprenatalperiodtotwoweeksafter birth. Previous studies report on the relationship between prenatal Dopplermeasurements and, inter alia, neonatal cranial ultrasound and echocardiography inFGR,butnotNIRS.ScherjonetalperformedcranialultrasoundinFGRneonateswithan interval of several hours after birthuntil oneweekpostpartum.They found thatfetalbrainsparing isrelatedtoahigherneonatalcerebralblood �lowvelocity in theMCA.(9)Thus,prenatalbrainsparing isassociatedwithpostnatalpreferentialblood�low to the brain,which is in linewith our �indings (Chapter 3).However, Scherjonetalonlystudiedneonatalcerebralblood�low,whereasweinvestigatedtherelationbetweencerebralandsystemicblood�lowandoveralldistribution.Recently,TuranetalstudiedtherelationbetweenprenatalDopplermeasurementsinFGRandneonatalechocardiography.(10)Intheirstudy,umbilicalartery(UA)PIswerenotpredictiveofneonatal echocardiographic �indings, but neonates with mild placental dysfunctiondidshowvisualevidenceofimpairedcardiaccontractility.Thismaybeduetothefactthatnoassociationexists.Alternatively,thechangesshownbytheneonatalheartarevery subtle andmight, therefore, not prove an association. By contrast,we did �indassociations between prenatal Doppler measurements and neonatal circulation, inparticularredistributionofthecirculation.WespeculatethatNIRSisasensitivemethodtoestablishdistributionofcirculationinFGRinthetransitionalperiod.
Pathophysiological process of FGRIncaseofFGR,thecirculationofthefetusadaptstodiminishedavailabilityofoxygenand nutrients. Baschat hypothesized about this pathophysiological process in termsofthreephases;preclinical,clinical,anddecompensation-thelattercorrespondingtofetaldemise.(11)Weadaptedthe�irsttwophasesofthishypothesisandvisualizedit
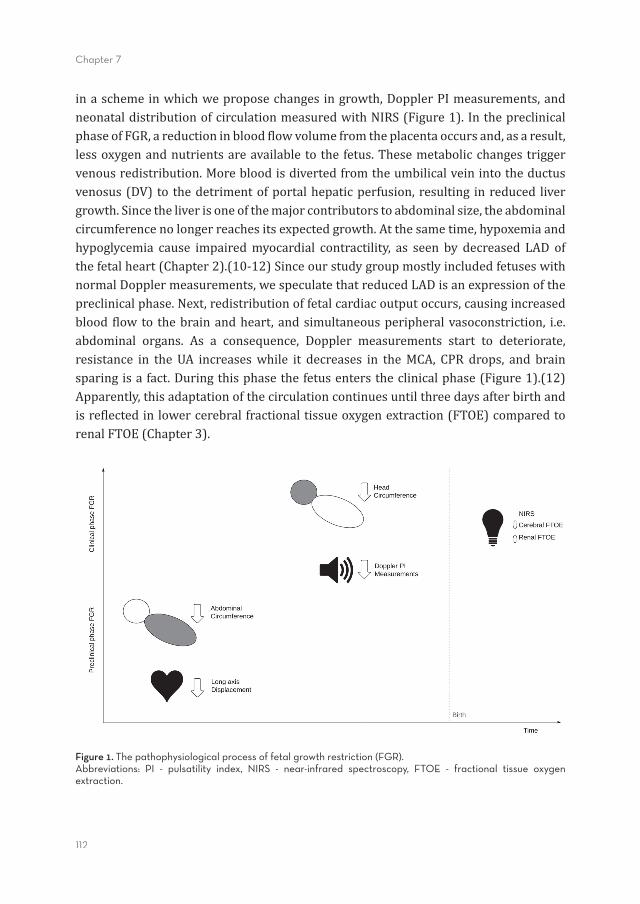
112
Chapter 7
inaschemeinwhichweproposechangesingrowth,DopplerPImeasurements,andneonataldistributionofcirculationmeasuredwithNIRS(Figure1).InthepreclinicalphaseofFGR,areductioninblood�lowvolumefromtheplacentaoccursand,asaresult,lessoxygenandnutrientsareavailabletothe fetus.Thesemetabolicchangestriggervenousredistribution.Morebloodisdivertedfromtheumbilicalveinintotheductusvenosus(DV) to thedetrimentofportalhepaticperfusion,resulting inreduced livergrowth.Sincetheliverisoneofthemajorcontributorstoabdominalsize,theabdominalcircumferencenolongerreachesitsexpectedgrowth.Atthesametime,hypoxemiaandhypoglycemia cause impairedmyocardial contractility, as seen by decreased LAD ofthefetalheart(Chapter2).(10-12)SinceourstudygroupmostlyincludedfetuseswithnormalDopplermeasurements,wespeculatethatreducedLADisanexpressionofthepreclinicalphase.Next,redistributionoffetalcardiacoutputoccurs,causingincreasedblood �low to thebrainandheart,andsimultaneousperipheralvasoconstriction, i.e.abdominal organs. As a consequence, Doppler measurements start to deteriorate,resistance in the UA increaseswhile it decreases in theMCA, CPR drops, and brainsparingisafact.Duringthisphasethefetusenterstheclinicalphase(Figure1).(12)Apparently,thisadaptationofthecirculationcontinuesuntilthreedaysafterbirthandisre�lectedinlowercerebralfractionaltissueoxygenextraction(FTOE)comparedtorenalFTOE(Chapter3).
Figure 1. The pathophysiological process of fetal growth restriction (FGR). Abbreviations: PI - pulsatility index, NIRS - near-infrared spectroscopy, FTOE - fractional tissue oxygen extraction.
General discussion
113
7
Brain sparingThe association betweenDopplermeasurements andNIRS in FGR is new.Wewereintriguedto�indthatbrainsparingcontinueduntilthreedaysafterbirth.Previously,BozettietalstudiedtheuseofNIRSinFGR,butwithoutconsideringprenatalDopplermeasurements,andcon�irmedthepostnatalpresenceofbrainsparinguptothreedaysafterbirth(13)Atmean12hoursaswellasmean63hoursafterbirth,cerebralFTOEwaslowerthansplanchnicFTOEinFGRinfants.Unfortunately,theydidnotmeasureNIRSafter72hours.Therefore,our�indingthatbrainsparinghaddisappearedonDay4afterbirthcouldnotbecon�irmed.Scherjonetaldid�indasigni�icantlyhighermeanvelocityoftheMCAduringthe�irstweekofpostnatallifeininfantswithanabnormalfetal CPR compared to a normal CPR.(9) They studied infantswith abnormal CPRs,butonlyhalfofthemhadabirthweightbelowthe10thpercentile.Wespeculatethatiffetusesexperiencebrainsparing,itisassociatedwithabnormalblood�lowoftheMCAforatleastoneweekafterbirth.InFGRinfantswhoexperiencebrainsparing,however,redistributionof theentireneonatalcirculationseemstoadjust fromfourdaysafterbirth.Apparently,brainsparingitselfaffectsneonatalcerebralblood�lowlongerthanFGRdoes,whereasFGRhasmorein�luenceonthedistributionofcirculationthroughoutthebody. Brainsparingnotonlyin�luencespostnatalcirculationafterFGR,italsoaffectsthequality of generalmovements (GMs)oneweekafterbirth (Chapter4). Inour study,abnormalDopplerPIsoftheUAandMCA,andtheCPR(thusbrainsparing)correlatedstronglywithabnormalqualityofGMsonDay7afterbirth,whereasDVPIsdidnot.Anothermethodtoestablishtheinfant’swellbeingshortlyafterbirthistheneonatalbehavioralassessmentscale(NBAS).Usingthismethod,pretermandterm-bornFGRinfantswithbrainsparingwerestudiedandtheywerefoundtohaveabnormalscoresinthemotorarea.(14,15)Unfortunately,thesestudiesdidnotincludefollow-upatlaterages.WereassessedGMsatthreemonthsposttermandfoundthat�idgetyGMs(FMs)wereno longerassociatedwithprenatalDopplermeasurements.This is in linewiththe�indingsofZuketalwhofoundthatneurodevelopmentaloutcomeattwoyearswasnormalininfantswithnormalizedGMs.(16)Nevertheless,aswespeculateinChapter4,normalizationofGMsfromtermtothreemonthsposttermmightstillbeariskfactorforsubtlebraindysfunction.Namely,attheageofone-and-a-halfandtwoyears,FGRinfantswithbrainsparingwerefoundtohavebehavioralproblemsmoreoften,(17,18)andat�iveyearstheymoreoftenhavelowerIQs.(19)OnepossibleexplanationforimpairedneurodevelopmentaloutcomeafterbrainsparingisofferedbyHernandez-Andradeetal.TheystudiedregionalcerebralbloodperfusionatdifferenthemodynamicstagesinsevereFGRandfoundthatdeteriorationofthefetalcondition,startingwithabnormalUAandMCAPIs,wasassociatedwithadecreaseinfrontalbrainperfusion.(20)Therefore,theysuggestedthatanabnormalMCAPI(increasedperfusion)becomesvisibleonly

114
Chapter 7
after thedeclineofhemodynamicprotectionof the frontal area.Thus,brain sparingmightnotbeaprotectivemechanism,butthe�irstsignofdeterioration.Conversely,inadifferentstudy,noassociationswerefoundbetweenbrainsparingandbehaviorattheageofeleven.(21)Wespeculatethatoncegrowth-restrictedinfantsreachschoolage,theymight,inthemeantime,havecompensatedthepoorbrainperfusionexperiencedduringtheprenatalperiod.
Neurodevelopmental course after FGRIn Part III we present an extensive follow-up study at school age of children bornsmallforgestationalage(SGA).WereferredtothemasSGAandnotFGR,sincewehadno prenatal background information such as Doppler measurements. The childrenparticipatinginthestudyinPartIIIwerefromdifferentcohortsthantheinfantsinthestudypresented inPart II. In comparison tomatched controls, in verypretermSGAchildrenwe found lower scores on performance IQ, selective attention, total motorskills,andmanualdexterity(Chapter5).ModeratepretermandfulltermSGAchildrenmoreoftenhadabnormalscoresonattentioncontrol,andtheyshowedanon-signi�icanttrendtowardslowerIQsthancontrols(Chapter6).Strikingly,manyneuropsychologicaltestscoresinSGAchildrenatschoolagewerecomparablewiththeirpeerswhowereborn appropriate for gestational age. Exceptions were attention and, only in verypretermchildren,performanceIQ.Atschoolage,attentionwastheonlyareaaffectedinbothpretermandterm-bornchildrenbornSGA.Previousstudiesonthistopicreportedcon�lictingresults.At�ivetoeightyears,attentionde�icitdisorderscoresdidnotdifferbetweenpreterm-bornSGAchildrenandcontrols, although thismightbedue to theuseofaquestionnaireratherthanastandardizedfollow-uptest.(22)Atsixyears,beingbornSGAisariskfactorforattentionproblems,butthisriskhasdisappearedattheageofeight.(23)Thus,attentionproblemsseemtobepresentatschoolageinchildrenborn SGA, but apparently they disappear as children grow older.(24)We speculatethat inSGAchildren,attentionproblemsarepresentuntilacertainstage inachild’scognitivedevelopment,andthattheseproblemsmaydisappearovertime.Tothebestof our knowledge, it is unknownwhich factors contribute to this so-called catch-upphenomenon (25) of attention skills, but perhaps the severity of growth restriction,underlyingplacentalpathology,andgenderdifferencesmayexertin�luence.(26,27) The percentage of children with neurodevelopmental abnormalities after FGRseemstodecreaseovertime(Figure2).IntheFGRgroupswestudied,thequalityofGMsonDay7afterbirthwasabnormalinmorethanhalfoftheinfants.Subsequently,althoughthequalityofFMsatthreemonthsposttermwasonlyabnormalinoneinfant,half of the infantshadaquantitatively abnormal score, i.e. amotoroptimality score(MOS)oflessthan25.(28)Atschoolage,wemostlyfoundabnormalscoresincognitivefunctionsofSGAchildren(follow-upinFigure2),whichisinlinewiththeliterature.
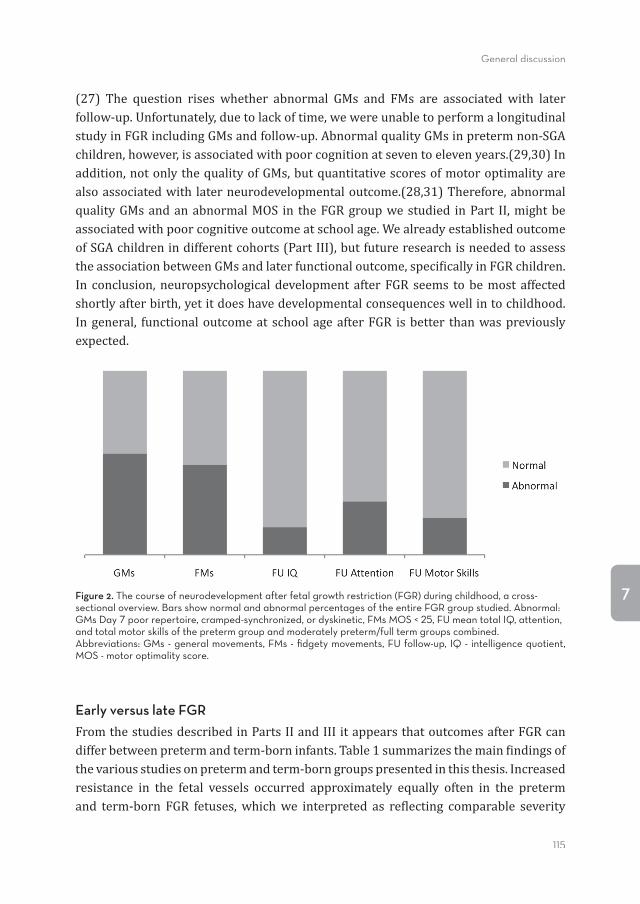
General discussion
115
7
(27) The question rises whether abnormal GMs and FMs are associated with laterfollow-up.Unfortunately,duetolackoftime,wewereunabletoperformalongitudinalstudyinFGRincludingGMsandfollow-up.AbnormalqualityGMsinpretermnon-SGAchildren,however,isassociatedwithpoorcognitionatseventoelevenyears.(29,30)Inaddition,notonlythequalityofGMs,butquantitativescoresofmotoroptimalityarealsoassociatedwith laterneurodevelopmentaloutcome.(28,31)Therefore,abnormalqualityGMsandanabnormalMOS in theFGRgroupwestudied inPart II,mightbeassociatedwithpoorcognitiveoutcomeatschoolage.WealreadyestablishedoutcomeofSGAchildrenindifferentcohorts(PartIII),butfutureresearchisneededtoassesstheassociationbetweenGMsandlaterfunctionaloutcome,speci�icallyinFGRchildren.In conclusion,neuropsychologicaldevelopment afterFGR seems tobemost affectedshortlyafterbirth,yetitdoeshavedevelopmentalconsequenceswellintochildhood.Ingeneral, functionaloutcomeat schoolageafterFGR isbetter thanwaspreviouslyexpected.
Figure 2. The course of neurodevelopment after fetal growth restriction (FGR) during childhood, a cross-sectional overview. Bars show normal and abnormal percentages of the entire FGR group studied. Abnormal: GMs Day 7 poor repertoire, cramped-synchronized, or dyskinetic, FMs MOS < 25, FU mean total IQ, attention, and total motor skills of the preterm group and moderately preterm/full term groups combined. Abbreviations: GMs - general movements, FMs - fi dgety movements, FU follow-up, IQ - intelligence quotient, MOS - motor optimality score.
Early versus late FGRFromthestudiesdescribedinPartsIIandIIIitappearsthatoutcomesafterFGRcandifferbetweenpretermandterm-borninfants.Table1summarizesthemain�indingsofthevariousstudiesonpretermandterm-borngroupspresentedinthisthesis.Increasedresistance in the fetal vessels occurred approximately equally often in the pretermand term-born FGR fetuses,whichwe interpreted as re�lecting comparable severity
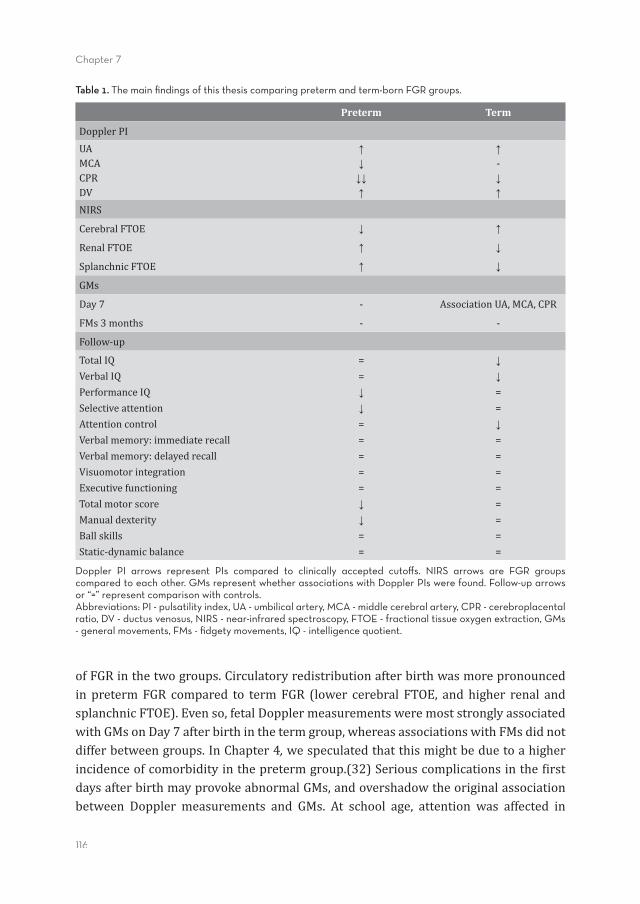
116
Chapter 7
ofFGRinthetwogroups.Circulatoryredistributionafterbirthwasmorepronouncedin pretermFGR compared to termFGR (lower cerebral FTOE, and higher renal andsplanchnicFTOE).Evenso,fetalDopplermeasurementsweremoststronglyassociatedwithGMsonDay7afterbirthinthetermgroup,whereasassociationswithFMsdidnotdifferbetweengroups.InChapter4, wespeculatedthatthismightbeduetoahigherincidenceofcomorbidityinthepretermgroup.(32)Seriouscomplicationsinthe�irstdaysafterbirthmayprovokeabnormalGMs,andovershadowtheoriginalassociationbetween Doppler measurements and GMs. At school age, attention was affected in
Table 1. The main fi ndings of this thesis comparing preterm and term-born FGR groups.
Preterm Term
DopplerPIUAMCACPRDV
↑↓↓↓↑
↑-↓↑
NIRS
CerebralFTOE ↓ ↑
RenalFTOE ↑ ↓
SplanchnicFTOE ↑ ↓
GMs
Day7 - AssociationUA,MCA,CPR
FMs3months - -
Follow-up
TotalIQVerbalIQPerformanceIQSelectiveattentionAttentioncontrolVerbalmemory:immediaterecallVerbalmemory:delayedrecallVisuomotorintegrationExecutivefunctioningTotalmotorscoreManualdexterityBallskillsStatic-dynamicbalance
==↓↓=====↓↓==
↓↓==↓========
Doppler PI arrows represent PIs compared to clinically accepted cutoff s. NIRS arrows are FGR groups compared to each other. GMs represent whether associations with Doppler PIs were found. Follow-up arrows or “=” represent comparison with controls.Abbreviations: PI - pulsatility index, UA - umbilical artery, MCA - middle cerebral artery, CPR - cerebroplacental ratio, DV - ductus venosus, NIRS - near-infrared spectroscopy, FTOE - fractional tissue oxygen extraction, GMs - general movements, FMs - fi dgety movements, IQ - intelligence quotient.
General discussion
117
7
bothpretermandtermgroups,albeitindifferentsubtests.Intheverypretermgroup,motorfunctionwasalsoaffected,whereasinthemoderatelypretermandtermgroupthiswasnotthecase. IQscoresdidnotdiffersigni�icantlywiththoseofthecontrolsinbothgroups,butwedidseeatrendtowardslowerscoresonperformanceIQinthepretermgroupincontrasttothetermgroupthathadlowerscores,(butnotstatisticallysigni�icant)thannon-SGAcontrolsonbothtotalandverbalIQ. Preterm-born FGR infants are at higher risk of perinatalmorbidity andmortalitythantermFGRinfants,especiallywhenbornbefore32weeksofgestation.(33)Inalargeprospective cohort study, Bassan et al reported lowerneonatal neurodevelopmentalscores in preterm-born FGR infants together with increased perinatal morbidityin comparison toFGR infantsborn at term.(34) In this light, our �indingsofmore apronounced neonatal redistribution of circulation in preterm FGR infants might bein linewiththesepreviousstudies.Surprisingly,Bassanetal foundnodifferences inneurodevelopmentaloutcomebetweenpretermandtermFGRinfantsat twoandsixyears’follow-upofthesamecohort.Thisisinlinewithour�indingsatsevenandeightyears(PartIIIandTable1),sinceinbothgroupsoutcomesdidnotdiffermuchfromthoseofcontrols–attentionbeingtheexception.Weconcludethatpreterm-bornFGRinfants initiallyhaveahigherriskofcomplications.Oncetheyoutgrowtheperinatalperiod,brain functionno longer seems tobeaffectedandcatch-upmightevenhavetakenplace.Theimplicationmightbethat,incaseofFGR,earlydeliveryisconsideredaviableoptionwhenfetal-placentalabnormalitiesareevident,(34)whereasafter36weeksofgestationnon-interventionissafe.(35)
Limitations of this thesis Thestudiesdescribed inthis thesisweresubject topotential limitations.Allstudies,except the study presented in Chapter 6, were single-center studies. Therefore, thegeneralizabilityof theresultsneedstobeestablished inpopulationstudies.Anotherconsequencewasthatthestudygroupsweresmall.Furthermore,westudiedacrosssectionoftheFGRgroups:alongitudinalstudyofgrowth-restrictedcaseswasnotpartof the studydesignspresented in this thesis.Wedid, however, provide an extensiveoverviewoftheconsequencesofFGRatdifferentpointsintime,encompassingthefetalperiodtoschoolage. Inthisthesisweuseddifferentde�initionsofFGR.InPartI,wede�inedFGRasanEFWbelowthe10thpercentile.SevenpercentoftheFGRgrouphadabnormalPIsoftheUA.InPartII,wede�inedFGRasanEFWorabdominalcircumferencebelowthe10thpercentile,orde�lectingfetalgrowth,andUAPIwasabnormalin60%ofthecases.InPartIII,wereferredtothechildrenasSGA,sincenoprenatalDopplermeasurementswereavailable.Wede�inedSGAasabirthweightbelowthe10thpercentile (Chapter5)andbelow-1standarddeviationinordertoincreasestatisticalpower(Chapter6).
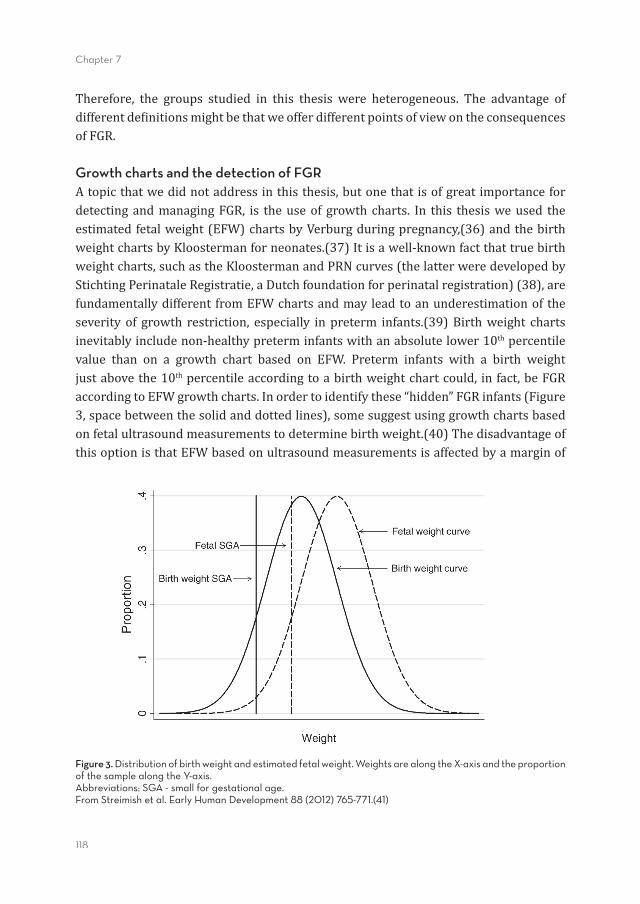
118
Chapter 7
Therefore, the groups studied in this thesis were heterogeneous. The advantage ofdifferentde�initionsmightbethatweofferdifferentpointsofviewontheconsequencesofFGR.
Growth charts and the detection of FGRAtopicthatwedidnotaddressinthisthesis,butonethatisofgreatimportancefordetectingandmanagingFGR, is theuseof growth charts. In this thesisweused theestimatedfetalweight(EFW)chartsbyVerburgduringpregnancy,(36)andthebirthweightchartsbyKloostermanforneonates.(37)Itisawell-knownfactthattruebirthweightcharts,suchastheKloostermanandPRNcurves(thelatterweredevelopedbyStichtingPerinataleRegistratie,aDutchfoundationforperinatalregistration)(38),arefundamentallydifferent fromEFWchartsandmayleadtoanunderestimationoftheseverity of growth restriction, especially inpreterm infants.(39)Birthweight chartsinevitablyincludenon-healthypreterminfantswithanabsolutelower10thpercentilevalue than on a growth chart based on EFW. Preterm infants with a birth weightjustabovethe10thpercentileaccordingtoabirthweightchartcould, infact,beFGRaccordingtoEFWgrowthcharts.Inordertoidentifythese“hidden”FGRinfants(Figure3,spacebetweenthesolidanddottedlines),somesuggestusinggrowthchartsbasedonfetalultrasoundmeasurementstodeterminebirthweight.(40)ThedisadvantageofthisoptionisthatEFWbasedonultrasoundmeasurementsisaffectedbyamarginof
Figure 3. Distribution of birth weight and estimated fetal weight. Weights are along the X-axis and the proportion of the sample along the Y-axis. Abbreviations: SGA - small for gestational age.From Streimish et al. Early Human Development 88 (2012) 765-771.(41)
General discussion
119
7
±10%ofthetrueweight,duetomeasurementvariation.(40)WhenitcomestothestudypresentedinPartIII,inwhichweusedbirthweightcurvestode�ineSGA,wehavetokeepinmindthatwemighthavemissedthe“hidden”SGAcases.InChapter6,however,wede�inedSGAasabirthweightof-1standarddeviationormore,thusbelowthe16thpercentile.Therefore,inthischapter,wemightalreadyhaveincludedthe“hidden”SGAchildren.Itisimportanttorealizethataccurateknowledgeofthedurationofpregnancyisessentialtoassesstheadequacyoffetalgrowthandtodeterminewhetherafetusisgrowth-restricted.
Conclusions and implicationsThisthesisprovidesinsightintothedevelopmentalcourseofinfantswhoexperiencedgrowth restriction in utero.We found that in FGR, of�line assessment of LAD usingSTICcouldimproveconventionalonlineM-mode,soastodetectsubtledifferencesinfetal cardiacdysfunction.Therefore, thismethodmaybeuseful todetect,prenatally,thoseFGRinfantsatriskofcardiovascularproblems,whomightbene�itfrompostnatalinterventionstoimprovetheirfuturecardiovascularhealth.Next,inthedevelopmentfrom fetus to newborn infant, fetal brain sparing was associated with neonatalredistributionof circulation andwithneurological functioning oneweek after birth.Sincecardiovascularinstabilitymaybecausedbymyocardialdysfunction,theeffectsof persistent fetal circulation might become important in modifying early neonatalmanagement.(10) Medical caregivers, such as neonatologists, general pediatricians,andnursesshouldbeawareoftheconsequencesoffetalbrainsparingininfantsbornafterFGR. Atschoolage,differencesinfunctionaloutcomeweresmallbetweenchildrenwhoexperiencedgrowthrestriction inuteroandcontrols.Attentionwastheexception. Itwasimpairedinbothpretermandterm-bornchildren.Inaddition,totaland�inemotorskillswerepoorerinpretermSGAchildrenthaninmatchedpretermnon-SGAcontrols.Even though abnormal neuropsychological outcomes after FGR seem to decrease aschildrengrowolder, attentionproblems shouldnotbedismissed.Especiallyparentsandteachers,whoexperiencethesechildrenineverydaylife,shouldbeawareofthesepotentialde�icitsduetoFGR. In thestudiespresentedhere, long-termneuropsychologicalconsequencesofFGRseemmoderate.Thisdoes,however,notimplythatconsequencesofFGRinotherareasshouldbeneglected.Weemphasizetheeffectthatsmallbirthsizemighthaveonthecardiovascularsystem.FGRinduces,forexample,primarycardiacandvascularchangesat�iveyears,(42)whichmightberelatedtoanincreasedriskofischemicheartdiseaseinlaterlife.(43)

120
Chapter 7
Future perspectivesFor future studies we suggest examining whether associations between prenatalDopplermeasurements andneonatal circulation andneurology canbe con�irmed inlarger samples. Furthermore, associations between prenatal Dopplermeasurementsand neonatal circulation and neurologymight become clearer if study groupswerede�ined by Doppler abnormalities. Not only studies on perinatal consequences ofgrowth restriction, but also long-term neuropsychological research would bene�itfromultrasounddata being included. SinceDopplermeasurements have, nowadays,enteredthestandardmanagementprotocolofFGR,soontheseparametersshouldbemade accessible for long-term follow-up.We also urgently recommend that the 48infantsstudiedinPartIIarefollowedupuntilschoolageinordertoassesswhetherGMsareassociatedwithlatefunctionaloutcomeingrowth-restrictedchildren.Finally,werecommendamultidisciplinaryapproachtoFGR,bothinclinicalmanagementandresearch.
General discussion
121
7
References(1) Bazaz R, Edelman K, Gulyasy B, Lopez-Candales A. Evidence of robust coupling of atrioventricular
mechanicalfunctionoftherightsideoftheheart: insightsfromM-modeanalysisofannularmotion.Echocardiography2008Jul;25(6):557-561.
(2) Ghio S, Recusani F, Klersy C, Sebastiani R, Laudisa ML, Campana C, et al. Prognostic usefulness ofthe tricuspidannularplanesystolicexcursion inpatientswithcongestiveheart failuresecondary toidiopathicorischemicdilatedcardiomyopathy.AmJCardiol2000Apr1;85(7):837-842.
(3) CarvalhoJS,O’SullivanC,ShinebourneEA,HeneinMY.Rightandleftventricularlong-axisfunctioninthefetususingangularM-mode.UltrasoundObstetGynecol2001Dec;18(6):619-622.
(4) HecherK,CampbellS,DoyleP,HarringtonK,NicolaidesK.AssessmentoffetalcompromisebyDopplerultrasoundinvestigationofthefetalcirculation.Arterial,intracardiac,andvenousblood�lowvelocitystudies.Circulation1995Jan1;91(1):129-138.
(5) MakikallioK,VuolteenahoO,JouppilaP,RasanenJ.Ultrasonographicandbiochemicalmarkersofhumanfetalcardiacdysfunctioninplacentalinsuf�iciency.Circulation2002Apr30;105(17):2058-2063.
(6) Leipala JA, Boldt T, Turpeinen U, Vuolteenaho O, Fellman V. Cardiac hypertrophy and alteredhemodynamicadaptationingrowth-restrictedpreterminfants.PediatrRes2003Jun;53(6):989-993.
(7) Cruz-LeminiM,CrispiF,Valenzuela-AlcarazB,FiguerasF,SitgesM,GomezO,etal.ValueofannularM-modedisplacementvs tissueDopplervelocities toassess cardiac function in intrauterinegrowthrestriction.UltrasoundObstetGynecol2013Aug;42(2):175-181.
(8) YagelS,CohenSM,ShapiroI,ValskyDV.3Dand4Dultrasoundinfetalcardiacscanning:anewlookatthefetalheart.UltrasoundObstetGynecol2007Jan;29(1):81-95.
(9) ScherjonSA,OostingH,KokJH,ZondervanHA.Effectoffetalbrainsparingontheearlyneonatalcerebralcirculation.ArchDisChildFetalNeonatalEd1994Jul;71(1):F11-5.
(10) Turan S, Turan OM, Salim M, Berg C, Gembruch U, Harman CR, et al. Cardiovascular transition toextrauterinelifeingrowth-restrictedneonates:relationshipwithprenatalDoppler�indings.FetalDiagnTher2013;33(2):103-109.
(11) BaschatAA.Neurodevelopmentfollowingfetalgrowthrestrictionanditsrelationshipwithantepartumparametersofplacentaldysfunction.UltrasoundObstetGynecol2011May;37(5):501-514.
(12) SeveriFM,RizzoG,BocchiC,D’AntonaD,VerzuriMS,ArduiniD.Intrauterinegrowthretardationandfetalcardiacfunction.FetalDiagnTher2000Jan-Feb;15(1):8-19.
(13) BozzettiV,PaterliniG,BelFV,VisserGH,TosettiL,GazzoloD,etal.CerebralandsomaticNIRS-determinedoxygenationinIUGRpreterminfantsduringtransition.JMaternFetalNeonatalMed2015Jan21:1-4.
(14) FiguerasF,Cruz-MartinezR,Sanz-CortesM,ArranzA,IllaM,BotetF,etal.Neurobehavioraloutcomesin preterm, growth-restricted infants with and without prenatal advanced signs of brain-sparing.UltrasoundObstetGynecol2011Sep;38(3):288-294.
(15) Cruz-MartinezR,FiguerasF,OrosD,PadillaN,MelerE,Hernandez-AndradeE, et al. Cerebralbloodperfusionandneurobehavioralperformanceinfull-termsmall-for-gestational-agefetuses.AmJObstetGynecol2009Nov;201(5):474.e1-474.e7.
(16) Zuk L, Harel S, Leitner Y, Fattal-Valevski A. Neonatal general movements: an early predictor forneurodevelopmental outcome in infants with intrauterine growth retardation. J Child Neurol 2004Jan;19(1):14-18.
(17) RozaSJ,SteegersEA,VerburgBO,JaddoeVW,MollHA,HofmanA,etal.Whatissparedbyfetalbrain-sparing? Fetal circulatory redistribution and behavioral problems in the general population. Am JEpidemiol2008Nov15;168(10):1145-1152.
(18) EixarchE,MelerE,IraolaA,IllaM,CrispiF,Hernandez-AndradeE,etal.Neurodevelopmentaloutcomein 2-year-old infants who were small-for-gestational age term fetuses with cerebral blood �lowredistribution.UltrasoundObstetGynecol2008Dec;32(7):894-899.
(19) ScherjonS,BrietJ,OostingH,KokJ.Thediscrepancybetweenmaturationofvisual-evokedpotentialsandcognitiveoutcomeat�iveyearsinverypreterminfantswithandwithouthemodynamicsignsoffetalbrain-sparing.Pediatrics2000Feb;105(2):385-391.
(20) Hernandez-AndradeE,Figueroa-DieselH, JanssonT,Rangel-NavaH,GratacosE.Changes inregionalfetal cerebral blood �low perfusion in relation to hemodynamic deterioration in severely growth-restrictedfetuses.UltrasoundObstetGynecol2008Jul;32(1):71-76.
122
Chapter 7
(21) vandenBroekAJ,KokJH,HoutzagerBA,ScherjonSA.Behaviouralproblemsattheageofelevenyearsinpreterm-bornchildrenwithorwithoutfetalbrainsparing:aprospectivecohortstudy.EarlyHumDev2010Jun;86(6):379-384.
(22) Morsing E, Asard M, Ley D, Stjernqvist K, Marsal K. Cognitive function after intrauterine growthrestrictionandverypretermbirth.Pediatrics2011Apr;127(4):e874-82.
(23) Eryigit-MadzwamuseS,WolkeD.Attentionproblemsinrelationtogestationalageatbirthandsmallnessforgestationalage.EarlyHumDev2015Feb;91(2):131-138.
(24) ViggedalG,LundalvE,CarlssonG,Kjellmer I.Neuropsychological follow-up intoyoungadulthoodofterminfantsbornsmallforgestationalage.MedSciMonit2004Jan;10(1):CR8-16.
(25) Paulson JF, Chauhan SP, Hill JB, Abuhamad AZ. Severe small size for gestational age and cognitivefunction:catch-upphenomenonpossible.AmJObstetGynecol2012Aug;207(2):119.e1-119.e5.
(26) O’Keeffe MJ, O’Callaghan M, Williams GM, Najman JM, Bor W. Learning, cognitive, and attentionalproblemsinadolescentsbornsmallforgestationalage.Pediatrics2003Aug;112(2):301-307.
(27) GevaR,EshelR,LeitnerY,ValevskiAF,HarelS.Neuropsychologicaloutcomeofchildrenwithintrauterinegrowthrestriction:a9-yearprospectivestudy.Pediatrics2006Jul;118(1):91-100.
(28) BrugginkJL,EinspielerC,ButcherPR,StremmelaarEF,PrechtlHF,BosAF.Quantitativeaspectsoftheearlymotorrepertoireinpreterminfants:dotheypredictminorneurologicaldysfunctionatschoolage?EarlyHumDev2009Jan;85(1):25-36.
(29) BrugginkJL,VanBraeckelKN,BosAF.Theearlymotorrepertoireofchildrenbornpretermisassociatedwithintelligenceatschoolage.Pediatrics2010Jun;125(6):e1356-63.
(30) ButcherPR,vanBraeckelK,BoumaA,EinspielerC,StremmelaarEF,BosAF.Thequalityofpreterminfants’spontaneousmovements:anearlyindicatorofintelligenceandbehaviouratschoolage.JChildPsycholPsychiatry2009Aug;50(8):920-930.
(31) HitzertMM,RozeE,VanBraeckelKN,BosAF.Motordevelopmentin3-month-oldhealthyterm-borninfantsisassociatedwithcognitiveandbehaviouraloutcomesatearlyschoolage.DevMedChildNeurol2014Sep;56(9):869-876.
(32) GouyonJB,IacobelliS,FerdynusC,BonsanteF.Neonatalproblemsoflateandmoderatepreterminfants.SeminFetalNeonatalMed2012Jun;17(3):146-152.
(33) SavchevS,FiguerasF,Sanz-CortesM,Cruz-LeminiM,TriunfoS,BotetF,etal.Evaluationofanoptimalgestationalagecut-off forthede�initionofearly-and late-onset fetalgrowthrestriction.FetalDiagnTher2014;36(2):99-105.
(34) BassanH,StolarO,GevaR,EshelR,Fattal-ValevskiA,LeitnerY,etal. Intrauterinegrowth-restrictedneonatesbornattermorpreterm:howdifferent?PediatrNeurol2011Feb;44(2):122-130.
(35) BoersKE,VijgenSM,BijlengaD,vanderPostJA,BekedamDJ,KweeA,etal.Inductionversusexpectantmonitoringforintrauterinegrowthrestrictionatterm:randomisedequivalencetrial(DIGITAT).BMJ2010Dec21;341:c7087.
(36) VerburgBO,SteegersEA,DeRidderM,SnijdersRJ,SmithE,HofmanA,etal.Newchartsforultrasounddatingofpregnancyandassessmentoffetalgrowth:longitudinaldatafromapopulation-basedcohortstudy.UltrasoundObstetGynecol2008Apr;31(4):388-396.
(37) KloostermanGJ.Onintrauterinegrowth:thesigni�icanceofprenatalcare.1970(8):895-912.(38) Visser GH, Eilers PH, Elferink-Stinkens PM, Merkus HM, Wit JM. New Dutch reference curves for
birthweightbygestationalage.EarlyHumDev2009Dec;85(12):737-744.(39) WolfH,SchaapAH.Whatisthenormalfetalweight?NedTijdschrGeneeskd2009May2;153(18):844-
847.(40) EhrenkranzRA.Estimatedfetalweightsversusbirthweights:shouldthereferenceintrauterinegrowth
curvesbasedonbirthweightsberetired?ArchDisChildFetalNeonatalEd2007May;92(3):F161-2.(41) StreimishIG,EhrenkranzRA,AllredEN,O’SheaTM,KubanKC,PanethN,etal.Birthweight-andfetal
weight-growthrestriction:impactonneurodevelopment.EarlyHumDev2012Sep;88(9):765-771.(42) CrispiF,BijnensB,FiguerasF,BartronsJ,EixarchE,LeNobleF,etal.Fetalgrowthrestrictionresultsin
remodeledandlessef�icientheartsinchildren.Circulation2010Jun8;121(22):2427-2436.(43) BarkerDJ,WinterPD,OsmondC,MargettsB,SimmondsSJ.Weightininfancyanddeathfromischaemic
heartdisease.Lancet1989Sep9;2(8663):577-580.
General discussion
123
7
Chapter 8
English summaryNederlandse samenvatting
AbbreviationsDankwoord
Curriculum vitaeList of publications

126
Chapter 8
English summary
127
8
English summary
Fetal growth restriction (FGR) is an inadequatedevelopmentof the fetus.Growth ispresent,butnotasmuchasexpected.FGRisoftende�inedasanestimatedfetalweight(EFW)belowthe10thpercentileaccordingtopopulationreferencecurves.OneofthemostimportantcausesofFGRisplacentalpathology,whichisassociatedwithperinatalmortalityandshort-termandlong-termmorbidity.Pleasenote,growthrestrictedisnotthesameasbeingbornpreterm;FGRisde�inedasbeingsmallaccordingtogestationalage,whereaspretermmeansbeingborntooearly.
ThisthesisreportsonstudiesinvestigatingthecourseofFGRfromtheprenatalperioduntil school age. Our �irst aim was to study the reliability of prenatal ultrasoundmeasuresofthefetalcardiacfunctioningrowthrestrictedfetuses.OursecondaimwastocompareprenatalDopplermeasurementswithearlyand lateneonatal circulationand neurological development after FGR. Our third aim was to establish functionaloutcomeatschoolageofFGRchildrenbornverypretermandmoderatepretermtofullterm.
InPartIwereportonourstudyofcardiacfunctioningrowthrestrictedfetusesusingprenatalultrasound.Chapter2describesthelongaxisdisplacementofthefetalheart(LAD)inFGR,comparingonlinemotionmode(M-mode)withof�linefour-dimensionalspatiotemporal image correlation (STIC). We found that left, right, and septal LADmeasuredwithSTICwasreducedinFGRwhencomparedtoage-matchedcontrols.Anon-signi�icanttrendforlowervaluesinFGRwasfoundwhenusingonlineM-mode.STICprovedbetterabletodetectreducedcardiacmotionthanonlineM-mode.Eventhoughseveral advantages and disadvantages exist for STIC, we recommend implementingSTICinclinicalpracticeforobstetriciansmanagingFGR.Itmayalsobeusedincaseofcongenitalcardiacdefects. InPart II of this thesiswe reportonour studyofprenatalpredictorsofneonataloutcome in FGR. In Chapter 3, we describe the association between fetal Dopplerparameters and neonatal circulation, measured with near-infrared spectroscopy(NIRS).FetalDopplerparameterscorrelatedstronglywithneonatalNIRSonDays1to3afterbirth.Pulsatilityindex(PI)oftheumbilicalartery(UA)correlatedwithrenalNIRSandthecerebrorenalNIRSratio(CRR).Middlecerebralartery(MCA)PIcorrelatedwithcerebralNIRSonDays2and3butnotonDay1.Cerebroplacentalratio(CPR)correlatedwithCRR.WhenanalyzingearlyandlateFGRseparately,associationswerestrongestintheearlyFGRgroup.Thus,lowMCAandlowCPR,indicatingbrainsparingbeforebirth,are strongly associatedwith low CRR after birth, indicating relatively greater blood
128
Chapter 8
volumestothecerebrumthantotherenalregion.Wespeculatedthatifbrainsparingispresentinthefetalcirculation,thiscirculatoryadaptationpersistsduringthe�irstthreedaysafterbirth. InChapter4,wepresentourresultsonthesamegroupaswasreportedoninChapter3,butinthischapterwedescribedtheassociationbetweenfetalDopplerparametersand the infant’s neurological development assessedwith generalmovements (GMs).UA,MCA,andCPRcorrelatedstronglywiththemotoroptimalityscore(MOS)ofGMsonDay7afterbirth,whereasductusvenosus(DV)didnot.DopplermeasurementsdidnotcorrelatewithMOSatthreemonthspostterm.Again,brainsparinginparticularwasstronglyassociatedwithGMsofabnormalquality,butonlyduringthe�irstweekafterbirth.Theassociationshaddisappearedthreemonthspostterm.Wespeculatedthat,despitenormalizationofGMs,FGRinfantsmaystillbeatriskoflatercognitivedelayandsubtlebraindysfunction. TheresultspresentedinPartIIdemonstratethatprenatalbrainsparingpersistsuntilthreedaysafterbirth,andthatitisassociatedwithGMsofabnormalqualityoneweekafterbirth.Therefore,brainsparingmaynotbeasprotectiveaspreviouslythought,butthatshortlyafterbirthitcontributestoanalteredneonatalcirculationandneurologicalmanifestation. InPartIII,wedescribedlong-termfunctionalconsequencesatschoolageofchildrenbornsmallforgestationalage(SGA).WerefertothemasSGAandnotFGR,sincewehadnoprenatalbackgroundinformationsuchasDopplermeasurements.ThechildrenwestudiedinPartIIIwerefromdifferentcohortsthantheinfantsstudiedinPartII.Follow-upconsistedofaseriesofneuropsychologicaltestsinordertodetermineintelligencequotient (IQ), attention, memory, visuomotor integration, executive functioning,behavior,andmotorskills. InChapter5,wepresentour�indingthateight-year-oldchildrenbornverypretermandSGAhad lower scoresonperformance IQ, selective attention, visual perception,totalmotorskillsand�inemotorskills,comparedwithcontrols.Otherscores,suchastotalandverbal IQ,memory,visuomotor integration,executive functioning,behavior,ballskills,andbalancedidnotdifferbetweengroups.Alltogether,thedifferenceswefoundweresmall.Thissuggeststhat impairedfunctioningofverypreterm-bornSGAchildren isattributable to theirhavingbeenbornverypretermrather than tobeingSGA. InChapter6,wepresentourcomparisonofmoderatepretermandfull termbornSGAchildrenwithcontrols,whotookpartintheLongitudinalPretermOutcomeProject,acommunity-based,prospectivecohortstudy.TheoutcomeofSGAchildrenwassimilartothatoftheirpeers,exceptforattentioncontrol.AlthoughtheIQofSGAchildrenwasthreepointslower,thisdifferencefailedtoreachsigni�icance.Therefore,atschoolage,childrenbornSGAhaveagreaterriskofobtainingabnormaltestscoresonattention
English summary
129
8
control than controls, independent of gestational age. Even though the impact oftheseoutcomesseemslimited,theconsequencesforschoolperformancedeserveourattention. Strikingly,manyneuropsychologicaltestscoresinSGAchildrenatschoolagewerecomparable with their appropriate for gestational age born peers. Exceptions wereattention and, only in very preterm children, performance IQ. We speculated thatfunctionalproblemsdue tobeingbornSGAareonly temporarilypresent inachild’scognitivedevelopment,andseemtodisappearlaterinlife.
ThestudiesreportedoninthisthesisprovideinsightintothecourseofFGRfromtheprenatal perioduntil school age. InFGR fetuses and infants,we found reduced fetalcardiacmotion,neonatalcontinuationofbrain sparinganditsassociationwithabnormalneurologicalperformanceoneweekafterbirth.Atschoolage,however,differencesinfunctional outcome between children who experienced growth restriction in uteroandcontrolsbecamesmall.Basedonthe�indingspresentedinthisthesis,weadvocatethatmedicalcaregiversshouldbeawareoftheconsequencesoffetalbrainsparing,inbothfetusesandinfantssubjectedtoFGR.AdequatepostnatalcarefromparentsandattentionbyeducatorsmaycontributetowardsfurtherreducingthesmalldifferencesweobservedinfunctionaloutcomebetweenSGAchildrenandcontrolsatschoolage.

130
Chapter 8
131
8
Nederlandse samenvatting
Nederlandse samenvatting
Bij foetale groeirestrictie (FGR) is er sprake van onvoldoende ontwikkeling van defoetus.Groeiisvaakwelaanwezig,maarblijftachter.FGRwordtmeestalgede�inieerdalshetgeschattefoetalegewicht(estimated fetal weight,EFW)onderhet10depercentielvolgens de referentiecurve van de populatie. De belangrijkste oorzaak van FGR isplacentapathologie,datgeassocieerdismetperinatalesterfteenziekteopkorteenlangetermijn.Er isoverigenseenverschil tussenFGRenvroeggeboorte:FGRbetekentdatdefoetustekleinisvoordezwangerschapsduur.Daarbijkanvroeggeboorteoptredenmaarhetisookmogelijkdatdezwangerschapvoldragenwordt.
DitproefschriftrichtzichopFGRengevolgendaarvanvanafdeprenataleperiodetotschoolleeftijd.Heteerstedoelwasomdebetrouwbaarheidvanprenataleechometingenvandehartfunctieindegroeivertraagdefoetusvasttestellen.Hettweededoelwasomechometingenvandebloedsomloopvoordegeboortetevergelijkenmetvroegeenlateneonataleuitkomsten:circulatieenneurologie.HetderdedoelvanditproefschriftwasomdefunctioneleontwikkelingtebepalenvanFGRkinderendietevroegendieoptijdgeborenzijn.
In deel 1 hebben we cardiale veranderingen door FGR onderzocht met prenataleechoscopie.Hoofdstuk2beschrijftdecardialelongitudinal annular displacement(LAD)inFGR,waarbijweonline motion mode (M-mode)vergelekenmetof�linevierdimensionalespatiotemporal image correlation (STIC).Linker,rechterenseptaalLADwarenlagerinFGRvergelekenmetcontrolesmetgelijkezwangerschapsduurwanneergemetenmetSTIC.MetonlineM-modevondenweeenniet-signi�icantetrendvoorlagereLADinFGR.DaarmeeconcluderenwedatSTICeenbeterdetectievermogenheeftdanM-modeinhetmetenvanverminderdeLAD inFGR.Ondankshet feitdatSTICalsmethodeeenaantalnadelenheeft,adviserenwehetgebruikvanSTICindedagelijksepraktijkvandeperinatoloog.STICkanzowelvoorFGRalsmogelijkecongenitalehartafwijkingenwordeningezet. Het tweede deel van dit proefschrift richt zich op prenatale voorspellers voorneonataleuitkomstinFGR(deelII).Inhoofdstuk3beschrijvenwedeassociatietussenfoetaleDopplerparametersenneonatalecirculatieinFGR,gemetenmetnear-infrared spectroscopy (NIRS). Foetale Doppler parameterswaren de eerste drie dagen na degeboortesterkgecorreleerdmetNIRS.Depulsatility index (PI)vandearteriaumbilicalis(UA) correleerde sterk met renale NIRS en de cerebrorenale NIRS ratio (CRR). DetweedeenderdedagnageboortecorreleerdedePIvandearteriacerebrimedia(MCA)met cerebrale NIRS, maar niet de eerste dag postpartum. Cerebroplacentaire ratio
132
Chapter 8
(CPR) correleerdemet CRR. Bij het apart analyseren van vroege en late FGR bleekdatdeassociatieshetsterkstwarenvoorvroegeFGR.OpbasisvandezebevindingenconcluderenwedateenlageMCAenlageCPR,beidewijzendopbrain sparing,sterkgeassocieerd zijnmet lage CRR na de geboorte. Dit betekent dat een relatief groterbloedvolumenaardehersenengaatdannaarderenaleregio.HetlijkterdusopdatbijkinderenmetFGRdecirculatoireveranderingenvanbrain sparingvoordegeboortetotdriedagennadegeboortevoortduren. In hoofdstuk 4 presenterenwe dezelfde studiegroep als in hoofdstuk 3,maar nubeschrijvenwedeassociatie tussen foetaleDopplerparametersendeneurologischeontwikkelingvanFGRkinderennadegeboorte.Neurologischeontwikkelinghebbenweonderzochtdoorgeneral movements(GMs)tebeoordelen.UA,MCAenCPRcorreleerdensterkmetdemotor optimality score (MOS)vandeGMsopdag7nadegeboorte,maardit gold niet voor de ductus venosus (DV). MOS drie maanden na de uitgerekendedatum correleerde nietmeermet deDoppler parameters. Opnieuw isbrain sparinggeassocieerdmet neonatale uitkomst, numet abnormale kwaliteit van de GMs eenweeknadegeboorte.DitzoukunnenbetekenendatkinderenmetFGRenbrain sparingmeerrisicolopenopeencognitieveachterstandenmildeontwikkelingsproblemen.HetisnamelijkbekenddatbijkinderenmetafwijkendeneonataleGMsdiedriemaandennadeuitgerekendedatumzijn genormaliseerd,mildeontwikkelingsproblemenvaakvoorkomen. Inhetderdedeelvanditproefschriftbeschrijvenwedegevolgenoplangetermijnvoorkinderendiegeborenzijnals small for gestational age (SGA).WenoemendezegroephierSGAennietFGR,omdatwegeenprenataleinformatiehaddenzoalsDopplerparameters. De kinderen diewe onderzocht hebben voor deel III komenuit anderecohortendan indeel II.Ookde tweehoofdstukkenonderlingbevattenverschillendestudiegroepen.Middelsneuropsychologischetestenhebbenwedevolgendefunctioneleuitkomstmatenbepaald: intelligentiequotient(IQ),aandacht,geheugen,visuomotoreintegratie,executievefuncties,gedragenmotoriek. Inhoofdstuk5vondenwedattevroeggeborenSGAkinderenop8-jarigeleeftijdtenopzichtevantevroeggeboren,maarniet-SGAkinderenlagerscoordenopperformaleIQ,selectieveaandacht,visueleperceptie,totaleen�ijnemotoriek.Andereuitkomstmaten,zoals totaal en verbaal IQ, geheugen, visuomotore integratie, executieve functies,gedrag, balvaardigheid en balans verschilden niet tussen SGA en controle kinderen.Deverschillendiewevonden,warenklein.Ditsuggereertdatvroeggeboortevoorde32eweekmeerbijdraagt aanverminderd functionerenop schoolleeftijddanSGAopzichzelf. Hoofdstuk6gaat inopfunctioneleuitkomstvankinderendieSGAenmatigvroeggeboren of op tijd geboren zijn. Dit onderzoekwas onderdeel van het Longitudinal Preterm Outcome Project, een prospectief cohort onderzoek naar vroeggeboorte.
133
8
Nederlandse samenvatting
De uitkomst van SGA kinderen was vergelijkbaar met de controle kinderen. Eenuitzonderingwasaandacht.HoewelhettotaalIQdriepuntenlagerwasinSGAkinderendanindecontrolekinderen,wasditverschilnietsigni�icant.Weconcluderendaaromdat kinderen die matig vroeg of op tijd geboren zijn en SGA zijn, een groter risicohebben om afwijkende test scores te hebben voor aandacht, ona�hankelijk van dezwangerschapsduur.Deimpactvandezeuitkomstlijktbeperkt,maarisdesalnietteminvanbelangvoordeschoolprestatiesenverdientdeaandachtvanoudersendocentenvanSGAkinderen. Opvallend is dat SGA kinderen op schoolleeftijd bijna vergelijkbare testscoreshaddenalsdecontrolekinderen.Eenuitzonderingwasaandacht,enalleeninmatigtevroeggeborenSGAkinderenooknoghetperformaleIQ.HetlijkteropdatSGAalleentoteenbepaaldeleeftijdinvloedheeftopdefunctioneleuitkomstvankinderenendatcognitieveproblementoegeschrevenaanSGAopdenduurweerkunnenverdwijnen.
Dit proefschrift geeft inzicht in het beloop van FGR, geobserveerd van de prenataleperiodetotschoolleeftijd.Wevondenlagerelong axis displacementbijFGRfoetussen.Indienbrain sparingprenataalaanwezigisbijFGRlijktditzichdeeerstedriedagennadegeboortevoorttezetten.Tevensisprenatalebrain sparinginFGRgeassocieerdmetafwijkendeneurologieeenweeknadegeboorte.Later,opschoolleeftijd,zijnverschillentussenSGAkinderenencontrolesechterklein,maarnietverwaarloosbaar.Opbasisvanditproefschriftattenderenweobstetrici,kinderartsenenanderemediciopdegevolgenvan foetalebrain sparing inFGR,zowel tijdensdezwangerschapalsnadegeboorte.OndankskleineverschilleninfunctioneleuitkomstopschoolleeftijdbijSGAkinderen,moetenoudersendocentenzichbewustzijnvandemogelijkegevolgenvanSGA.

134
Chapter 8
135
8
Abbreviations
AbbreviationsAGA appropriateforgestationalageAREDF absentorreversedend-diastolic�lowBMI bodymassindexBPD bronchopulmonarydysplasiaBW birthweightCI con�idenceintervalCPR cerebroplacentalratioCRR cerebrorenalratioCSR cerebrosplanchnicratioDV ductusvenosusEFW estimatedfetalweightFGR fetalgrowthrestrictionFMs �idgetygeneralmovementsFTOE fractionaltissueoxygenextractionGA gestationalageGMs generalmovementsHC headcircumferenceIUGR intrauterinegrowthrestrictionIQ intelligencequotientIVH intraventricularhemorrhageLAD longitudinalannulardisplacementM-mode motionmodeMCA middlecerebralarteryMOS motoroptimalityscoreMPT moderatepretermNEC necrotizingenterocolitisNIRS near-infraredspectroscopyOR oddsratioPI pulsatilityindexRDS respiratorydistresssyndromerSO2 regionaltissueoxygensaturationSD standarddeviationSES socioeconomicstatusSGA smallforgestationalageSTIC spatiotemporalimagecorrelationUA umbilicalarteryUtA uterinearteryUS ultrasound

136
Chapter 8
137
8
Dankwoord
Dankwoord
Beste lezer, promoveren doe je niet alleen. Daarom wil ik iedereen bedanken diemij de afgelopen jaren opwat voormanier dan ook geholpen heeft dit proefschriftwerkelijkheidtelatenworden.
BesteArie,in2008mochtikalsderdejaarsstudentbijjoualsprofessorlangskomen.Webesprakendemogelijkhedenomnaastmijnstudieeenkleinonderzoeksprojecttestarten.Nietalleenwasjeenthousiasmerendoverdeinhoud,jenamdetijdommedeNICUtelatenzienensteldejetoegankelijkop.Alsnelmerkteikdatikhetonderzoekleuk vond enwerd door jou steeds gestimuleerd om verder te gaan. Zo volgde eenwetenschappelijke stage en later het MD PhD traject. Je hebt me altijd het volstevertrouwen gegeven en je nodigdemij en de andere studenten uit om op de grotewereldcongressenvoorkindergeneeskundeonsonderzoektepresenteren.Arie,jouwvertrouwen,optimismeeninzetheeftmijnpromotietrajectglansgegeven.Ikhebnietalleeninhoudelijkveelvanjegeleerd,maarookvanjoualspersoon.Dankjewel.
BesteKatia,voormijnMDPhDtrajectwildeikgraagvakgroepoverstijgendonderzoekdoen:bijdeobstetrieenneonatologie.WatwasikblijdatjijonlangsnaarGroningenwasgekomenenmijwildebegeleideninhetonderzoeknaarfoetalegroeirestrictie.Bijdestartvanmijnpromotieonderzoekmaaktejijvandenoodeendeugdengafjemijderuimteommijdeechoscopieeigentemaken.Ineenaantalmaandenhebikveelgeleerdvanjouenjecollega’sbijdeprenatalediagnostiek.Maarnietalleeninhoudelijkhebikveelvan jegeleerd. Jehebtzelfeen internationaleroutebewandeld in jecarrièreenwenstemijdatooktoe.Nogvoordatikerzelfdevoordelenvanzag,hadjijmijnstageinBarcelonaalgeregeld.Ikbenjedaarontzettenddankbaarvoor,omdathetmezowelalswetenschapperenalspersoonrijkerheeftgemaakt.
Graagwil ikde ledenvande leescommissiebedankenvoorhun tijd en inzetbij hetbeoordelenvanditproefschrift:prof.dr.H.Lafeber,prof.dr.S.A.Scherjonenprof.dr.G.H.A.Visser.
Dear doctora Crispi, dear Fatima, thank you for welcoming me with open arms inBarcelona.ProfessorGratacos,thankyouforgivingmetheopportunitytoworkinyourwell-knownresearchcenter.DoctoraBennasar,Mar, evenaftermy in�initequestionsabout4Dultrasound,youkepthelpingmewithasmile,atanytime.Ofcourse,allmydirectcolleguesoftheDepartmentofMaternal-FetalMedicine,thankyouformakingmytimeworthwhileinBarcelona.Istilllongforthelunchesandyogaclasseswehadin

138
Chapter 8
theHeliosgardens.ElenaandAudrey,thanksforlearningmehowtotakegoodcoffeebreaks.Inparticular,IwouldliketothankGülçin,forbeingmydearfriend.
ToallICFOnians:youhavemademytimeinBarcelonaworthremembering.
Lievecollega’s,lievemedebewonersvandekrochtenderTriadegebouw.Lamellendicht,verdieping -1 onderde grond, vreemdegeluiden vandeboven- enoverburen,maartoch.Ikhadhetnietwillenmissen.Wathebbenweeenlolgehad,daarzoafgezonderdvandebedrijvigheidvanwat iknoemdehethoofdgebouw.Een lekkerekof�iehalen?Daarmoestenwetienminutenwandeltijdvooroverhebben.Maarvervolgenskondenweurenzittengenietenvandat(tedure?)kopjekof�ie.Datvervolgenshelaasweleensdoordebazenopgemerktwerd. Michelle,mijnmaatje op links,wat heb ik veelmet je gelachen,maar ook tranengedeeld. Je hebt altijd voorme klaar gestaan, meegedacht bij problemen,metingengedaan enmijn statistische vragen beantwoord.Wat heerlijk dat onze bureaus zo’nwereld van verschil zijn (bij jou status na ontplof�ing, bij mij neurotische netheid),misschienjuistdaaromkunjemezogoeddespiegelvoorhouden.Janyte,materfamilias,east-sider,oprjochteFries.Watkondenwelekkerdebatterenovermuziek,wantlatenwewelwezen:oversmaakvaltniettetwisten.JijNewKidsontheBlock,ikKinderenVoorKinderen. Tussen die hitjes door kon ook een goed gesprek nietmissen. ChrisPeter,toendeinwonersvanTenBoeroptelevisieverscheneninjanuari2012wegensde overstroming, zaten wij dagenlang gekluisterd aan het journaal. Het begin vaneengezellig jaar,metuitermategoedevrijdagmiddaghitjes!Anne,nogeeneast-sider,watsuperdatjealsnogdelaatstemaandenmetonsindekelderdoorhebtgebracht.Annemiek,waarmoetikbeginnen.Vrolijkenoot,rasoptimist,sarcast.Maarookbenjeeenheledierbarevriendinvanmegeworden,metveleritjesopderace�iets,biertjesvoor-tijdens-en-naetenstijdenveleanderewijntjesenAperolspritz.Numaarhopendatwedatallemaalnogtotindentreurekunnenblijvendoenenzonderkleerscheurener vanaf komen. Marrit, mijn evenbeeld. Altijd lollig als we weer eens door elkaargehaaldwerden.NadatjejepromotieafgerondhadenvertrokuithetTriadegebouw,misteikonzeklop-signalenviademuur!EliseRoze,bijjoustartteikmijnonderzoekalsderdejaarsgeneeskundestudent.Ikkonjealtijddemeestbasalevragenstellen,diejemevervolgensmetplezieruitlegde.Jehebtmedestijdsnogeenstukjeenthousiastergemaakt voor het onderzoek. Andere vrienden en collega’s uit het Triadegebouw:Danique,Djoeke,EliseRoze,EliseVerhagen,Esther,Floris-Jan,Karen,Karin,Mark-Jan,Martijn,Menno,Mirthe,Nicole,Nynke,Sara,Sietske,TjitskeenWillemijnwatwarenhetlekkeretaartjes!
139
8
Dankwoord
Roos enDanique,wat �ijn dat jullie het stokje overnamen toen ik co-schappen liep.In het bijzonderwil ik jullie bedanken voor alle ritjes de provincie in om te �ilmenenweekenddagenenavondendiejullieacuutnaarhetziekenhuiszijngegaanomdemetingentestarten.Super!OokwilikAnnelies,Dyvonne,Janyte,Michelle,Mirthe,Nynke,SaraenSietskebedankenvoorhetverzamelenvandedatavoormijnproefschrift.Lucia,thankyouforyourcommitmentandhoursofperformingultrasoundformythesis.
Alleneonatologenennatuurlijkkinderneuropsychologen(KoenenAnne):bedanktvoorjulliescherpeaanwijzingenbijderesearchbesprekingenennatuurlijkdeontzettendleukeavondentijdensdecongressen!
Ookwilikgraagallegynaecologen,arts-assistenten,verloskundigenenechoscopistenvan het UMCG bedanken voor de hulp bij het includeren van patiënten. Door julliesamenwerking hebben we deel II van dit proefschrift werkelijkheid kunnen latenworden.
Ina,Ineke,JoséenLida,besteresearchnursesvandegynaecologie,watontzettend�ijndatjulliemetmemeedachtenbijhetincluderenentracerenvanpatiënten.
VerpleegkundigenvandeNICUenK3inhetUMCG,zonderjulliegeenmetingen!Julliehebbenmegeleerddeallerkleinstenmetzorgtebenaderenenlietenaltijdhetbelangvandekinderenvooropstaan.
Joke, Janette en Heidi, wat moest ik zonder jullie. Altijd wisten jullie een gaatje tevindenindeagendavanArie.Maarnogveelbelangrijker,julliehebbenmegeholpenomklussendieweleensveelwerkophaddenkunnenleveren,ineenhandomdraaiklaartespelen.Verderwil ikJannieTjassingenAadvanMourikhartelijkbedanktvoordeorganisatorischeen�inanciëlehulpdeafgelopenjaren.
BesteTitiavanWulfftenPalthe,onzettendbedanktvoorallehulpbijdecorrectiesvandeEngelseteksten.Uheeftdemanuscriptennaareenhogerniveaugebracht.
GraagwilikallemedewerkersvandeJuniorScienti�icMasterclassbedankenvoorhetmogelijkmakenvanmijnMDPhDtraject.
BesteAmanda(GautierScienti�icIllustration),jehebteenprachtigenpassendontwerpgemaaktvoordeomslagvanditproefschrift.Dankjewelvoorjeinzetengeduld.
140
Chapter 8
Oudersvanallekinderendiemeehebbengedaanaandeinditproefschriftvermeldeonderzoeken, dankjulliewel voor jullie vertrouwen.Maar ookwil ik de kinderendieik als foetus, pasgeborene, of jonge scholier heb leren kennen bedanken, voor julliebijdrageaandewetenschap.
Laura, lieve Lau, najaar 2008 enwe vertrokken naar Berlijn. Studenten bij ISCOMSwarenweenwehaddenhetonderzoekalsgemenedeler.Datbleekalgauwhetbeginvan een bijzondere vriendschap. Wat kende je me al goed die koninginnenacht in2009,waarbij jijweldoorhaddat ikbestuurvan ISCOMSwildedoen.HetwerdeenonvergetelijkbestuursjaarendaarnavooronsbeidedestartvaneenMDPhDtraject.Weproosttensamenoponzetoelating,toenwistenwenognietwatpromoverenéchtinzouhouden.Maaraltijdstakjemeeenhartonderderiemalshetonderzoekwééreenstegenzat.Op9decemberstajenaastme,ikkanmegeendierbaarderparanimfwensen.
Eline,lieveElie,ookonzevrienschapbegonbijISCOMS.AlsnelgingenwesamenopreisnaarMaleisië,waarwepromotiemaaktenvooronscongresmaarvooralookgenotenvanhetmooieweer. Jij, geen rijbewijs, zoumij (wel een rijbewijs)wel eens scooterlerenrijden.Dathebbenwegeweten,toenwedelokalepolitietegenkwamen.Naonsbestuursjaarwerdenweof�iciëlemaatjestijdensdejuniorco-schappen.Hoehaddenzehetzobedacht.Metblauwenagellakverschenenwijoppractica,waarbijdedocentonsweesoponzeiatrogeneperiferecyanose.Inmiddelsbenjeookaanhetpromoveren,watmaaktdatikopallevlakkenmetjekansparren.Ikvindhetontzettend�ijndatjijmijnparanimfbent,maarnog�ijnerdatjemijnvriendinbent.
LieveDurvina,oudstezus.Alskindalverwonderdeikmeoverjouwprecisie,hoemooiennetjesjekonkleuren.Jehaddeliefdeenhetgeduldommij,metdemotoriekvaniemanddievierjaarjongeris,bijnanetzomooitelatenkleuren.Nogsteedshebjeallesinhet levenzogoedvoorelkaarenweet jeookvandaagdedagmijte latengroeien.Huib, jebent inmiddelsalseenbroervoorme,endevadervanmijn lievenichtjeennee�je-KatelijneenJilles.Julliebiedenmealtijdeenwarmthuis,dankjulliewel.
Lieve Rinske,wat kondenwe het oneens zijn als tieners. Hetwas dan ook een gokomsamen inGroningengeneeskunde te studeren.Maarwatben ikblijdatweonzestudententijdsamenhebbendoorgebracht.Jebentinmiddelsnietalleenmijnzus,maarookmijnmaatje.Alsgeenanderweetjijmedespiegelvoortehoudenenmeopz’ntijdtewijzenopallebureaucratischezakendienoggeregeldmoetenworden.Ikwaardeerjeenormenheberallevertrouwenindatjeeengoedehuisartswordt.

141
8
Dankwoord
Lievepapaenmama.Ditproefschrifthadernietgelegenzonderjullie.Alvanjongsafaanhebbenjulliemijgemotiveerdomopzoektegaannaarwatikleukvindengestimuleerdombegonnenzakenaf temaken.Toen ik julliehetMDPhD trajectvoorlegdewarenjullie gelijk enthousiast en zijn dat tot vandaag gebleven. Ook al hebben jullie eenmedischeachtergrond,dewetenschappelijkewereld is jullienietaltijdevenbekend.Desondankshebbenjullieallekleineengrotestappenindeafgelopenjarenmetveelpleziergevolgdenmedaaringesteund.Nietvoornietshebikjulliedanookgeciteerd:eenweloverwogenkeuzeiseenjuistekeuze.Dankjulliewel.
LieveJanny,ikherinnerje.
142
Chapter 8
143
8
Curriculum vitae
Curriculum vitae
JozienwasbornasJozijntjeChristinaTanisonAugust16,1988inHarlingen,Friesland,TheNetherlands.ShegrewupinFranekerwithherparentsKlaasenMintsjeandtwoeldersistersDurvinaandRinske.Whenshewas12yearsold,JozienstartedVoorgezet Wetenschappelijk Onderwijs at theRegionale Scholen Gemeenschap Simon Vestdijk inHarlingen,fromwhichshegraduatedin2006.InSeptemberofthesameyearshestartedstudyingmedicineattheUniversityofGroningen.In2008,JozieninitiatedherresearchattheDepartmentofNeonatologyoftheUniversityMedicalCenterGroningen(UMCG),which subsequently led to admission to the MD PhD programme in 2012. Becauseofherinterest inthe�ieldofObstetrics,shecombinedherresearchinthis�ieldwithNeonatologyresearch.In2013,shedidhermedicalinternshipsattheIsalahospitalinZwolle.InadditiontoherPhD,JozienwenttoBarcelona,Spainforaresearchproject,in 2014. Next to her studies, she did several extracurricular activities. For instance,she was president of the International Student Congress of (bio)Medical Sciences(ISCOMS)andtreasureroftheGroningerStudentenorkestMira.InDecember2015shehassuccessfullycompletedbothhermedicalstudiesandtheMDPhDprogramme.Herwhishesaretobecomeagynecologist.

144
Chapter 8
145
8
List of publications
List of publications
Tanis JC,NuriddinM,BennasarM,MartinezJM,BijnensB,CrispiF,GratacosE.Cardiaclongaxisdisplacementinfetalgrowthrestriction:onlineversusof�linespatiotemporalimagecorrelation(STIC)M-mode.Submitted.
vanderLaanME,RoofthooftMTR,FriesMWA,BergerRMF,SchatTE,vanZoonenAGJF,Tanis JC,BosAF,KooiEMW.Regionaltissueoxygenationinrelationtoechocardiographicparameters of a hemodynamically signi�icant patent ductus arteriosus in preterminfants.Provisionally accepted Neonatology
Tanis JC, SchmitzDM,BoelenMR,CasarellaL, vandenBergPP,BilardoCM,BosAF.GeneralmovementsafterfetalgrowthrestrictioninrelationtoprenatalDoppler�lowpatterns.Provisionally accepted Ultrasound in Obstetrics & Gynecology
Tanis JC,BoelenMR,SchmitzDM,CasarellaL,vanderLaanME,BosAF,BilardoCM.PrenatalDoppler�lowpatternsandneonatalcirculationinearlyandlatefetalgrowthrestriction.Ultrasound Obstetrics Gynecol 2015 Sept 11. doi 10.1002/uog.14744
Tanis JC, Van Braeckel KNJA, Kerstjens JM, Bocca-Tjeertes IF, Reijneveld SA, Bos AF.Functionaloutcomesatage7yearsofmoderatepretermandfulltermchildrenbornsmallforgestationalage.JPediatr.2015Mar;166(3):552-558.
BosAF,VanBraeckelKNJA,HitzertMM,Tanis JC,RozeE.Developmentof�inemotorskillsinpreterminfants.DevMedChildNeurol.2013Nov;55Suppl4:1-4.
Tanis JC, vanderReeMH,RozeE,Huis in ‘tVeldAE,vandenBergPP,VanBraeckelKNJA,BosAF.Functionaloutcomeofverypreterm-bornandsmall-for-gestational-agechildrenatschoolage.PediatrRes.2012Dec;72(6):641-8.
van der ReeM,Tanis JC, Van Braeckel KN, Bos AF, Roze E. Functional impairmentsat school age of pretermborn childrenwith late-onset sepsis. EarlyHumDev. 2011Dec;87(12):821-6.
Roze E, Ta BD, van der ReeMH,Tanis JC, van Braeckel KNJA, Hulscher JB, Bos AF.Functional impairments at school age of children with necrotizing enterocolitis orspontaneousintestinalperforation.PediatrRes.2011Dec;70(6):619-25.




















