Treatment of HCV, Infectious disease, infections by immigrants ...
11
American Journal of Computational and Applied Mathematics 2012, 2(1): 10-20 DOI: 10.5923/j.ajcam.20120201.02 Modelling the Effect of Treatment and Infected Immigrants on the Spread of Hepatitis C Virus Disease with Acute and Chronic Stages Neterindwa Ainea 1 , Estomih S. Massawe 1,* , Oluwole Daniel Makinde 2 1 Mathematics Department, University of Dar es Salaam, P. O. Box 35062, Dar es Salaam, Tanzania 2 Institute for Advance Research in Mathematical Modelling and Computations, Cape-Peninsula University of technology, P. O. Box 1906, Bellville 7535, South Africa Abstract This paper examines the effect of Treatment and Infected Immigrants on the spread of Hepatitis C Virus (HCV) disease with Acute and Chronic stages. A nonlinear mathematical model for the problem is proposed and analysed qualitatively using the stability theory of the differential equations. The results show that the disease free equilibrium is locally stable at threshold parameter less than unity and unstable at threshold parameter greater than unity. Globally, the disease free equilibrium is not stable due existence of forward bifurcation at threshold parameter equal to unity. However the disease becomes more endemic due to the presence of infected immigrants in the community. It is also shown that in the presence of treatment, the rate of infected immigrants (acute and chronic) decreases and consequently the treated in- fected individuals decreases continuously. Numerical simulation of the model is implemented to investigate the sensitivity of certain key parameters on the treatment and infected immigrants on the spread of the disease with acute and chronic stages. Keywords Treatment Of HCV, Infectious Disease, Infections By Immigrants, Spread Of Infectious Disease 1. Introduction Hepatitis (plural hepatitides) is an inflammation of the liver characterized by the presence of inflammatory cells in the tissue of the organ[1]. The inflammation of liver causes soreness and swelling. Hepatitis is most commonly caused by one of the 5 hepatitis viruses; hepatitis A, hepatitis B, hepatitis C, hepatitis D and hepatitis E. Hepatitis C is usually spread through contact with blood products[2]. Blood products have been the main agents through which HCV is transmitted, but ever since 1992, when it became possible to detect the virus in blood, transmissions through transfusions, and organ transmissions have been minimal. Most common avenues through which HCV is spread are unprotected sex, sharing of contaminated needles among drug addicts and those with other STDs[3]. Some people also get this virus from tattoo and piercing salons. It is also possible to contract HCV at birth, as it can be transmitted from mother to baby. A HCV infection can be categorized into two stages, firstly an acute infection (following initial infection) and secondly a chronic infection. Acute means ‘new ‘or illness of * Corresponding author: [email protected] (Estomih S. Massawe) Published online at http://journal.sapub.org/ajcam Copyright © 2012 Scientific & Academic Publishing. All Rights Reserved a short period. A chronic hepatitis C infection is when the infection lasts for longer than six months. The goal of treatment is to reduce the amount of the HCV in the blood to levels that can't be detected after 24 weeks of therapy. HCV is treated with drugs that slow or stop the virus from damaging the liver. The treatment of HCV has ad- vanced in recent years which have greatly improved the outlook for people with HCV. The usual treatment of HCV is a combination of two different medicines called pegylated interferon and ribavirin[2]. [4] made an analysis on the immigration status, race and language barriers on chronic hepatitis virus infection man- agement and treatment outcomes. The researchers found that HCV endemic regions of the word are diagnosed with HCV infection after immigration and subsequently referred to viral hepatitis chronics for disease management. They suggested that optimal care to all patients, indentifying and under- standing barriers to care related to immigrant status, race and language in HCV management must be provided. [5] found that chronic HCV is a progressive condition that accounts for at least one quarter of all cases of chronic liver disease[6] predicted that the prevalence of chronic HCV (CH-C) remains high and the complications of infection are common[7] discovered that chronic HCV complications are increasing, especially among people older than 60 years[8] conducted a study on disease progression of Acute HCV[9] analyzed the screening of HCV in a Health maintenance
-
Upload
khangminh22 -
Category
Documents
-
view
0 -
download
0
Transcript of Treatment of HCV, Infectious disease, infections by immigrants ...
American Journal of Computational and Applied Mathematics 2012, 2(1): 10-20 DOI: 10.5923/j.ajcam.20120201.02
Modelling the Effect of Treatment and Infected Immigrants on the Spread of Hepatitis C Virus Disease
with Acute and Chronic Stages
Neterindwa Ainea1, Estomih S. Massawe1,*, Oluwole Daniel Makinde2
1Mathematics Department, University of Dar es Salaam, P. O. Box 35062, Dar es Salaam, Tanzania 2Institute for Advance Research in Mathematical Modelling and Computations, Cape-Peninsula University of technology, P. O. Box 1906,
Bellville 7535, South Africa
Abstract This paper examines the effect of Treatment and Infected Immigrants on the spread of Hepatitis C Virus (HCV) disease with Acute and Chronic stages. A nonlinear mathematical model for the problem is proposed and analysed qualitatively using the stability theory of the differential equations. The results show that the disease free equilibrium is locally stable at threshold parameter less than unity and unstable at threshold parameter greater than unity. Globally, the disease free equilibrium is not stable due existence of forward bifurcation at threshold parameter equal to unity. However the disease becomes more endemic due to the presence of infected immigrants in the community. It is also shown that in the presence of treatment, the rate of infected immigrants (acute and chronic) decreases and consequently the treated in-fected individuals decreases continuously. Numerical simulation of the model is implemented to investigate the sensitivity of certain key parameters on the treatment and infected immigrants on the spread of the disease with acute and chronic stages.
Keywords Treatment Of HCV, Infectious Disease, Infections By Immigrants, Spread Of Infectious Disease
1. Introduction Hepatitis (plural hepatitides) is an inflammation of the
liver characterized by the presence of inflammatory cells in the tissue of the organ[1]. The inflammation of liver causes soreness and swelling. Hepatitis is most commonly caused by one of the 5 hepatitis viruses; hepatitis A, hepatitis B, hepatitis C, hepatitis D and hepatitis E. Hepatitis C is usually spread through contact with blood products[2]. Blood products have been the main agents through which HCV is transmitted, but ever since 1992, when it became possible to detect the virus in blood, transmissions through transfusions, and organ transmissions have been minimal.
Most common avenues through which HCV is spread are unprotected sex, sharing of contaminated needles among drug addicts and those with other STDs[3]. Some people also get this virus from tattoo and piercing salons. It is also possible to contract HCV at birth, as it can be transmitted from mother to baby.
A HCV infection can be categorized into two stages, firstly an acute infection (following initial infection) and secondly a chronic infection. Acute means ‘new ‘or illness of
* Corresponding author: [email protected] (Estomih S. Massawe) Published online at http://journal.sapub.org/ajcam Copyright © 2012 Scientific & Academic Publishing. All Rights Reserved
a short period. A chronic hepatitis C infection is when the infection lasts for longer than six months.
The goal of treatment is to reduce the amount of the HCV in the blood to levels that can't be detected after 24 weeks of therapy. HCV is treated with drugs that slow or stop the virus from damaging the liver. The treatment of HCV has ad-vanced in recent years which have greatly improved the outlook for people with HCV. The usual treatment of HCV is a combination of two different medicines called pegylated interferon and ribavirin[2].
[4] made an analysis on the immigration status, race and language barriers on chronic hepatitis virus infection man-agement and treatment outcomes. The researchers found that HCV endemic regions of the word are diagnosed with HCV infection after immigration and subsequently referred to viral hepatitis chronics for disease management. They suggested that optimal care to all patients, indentifying and under-standing barriers to care related to immigrant status, race and language in HCV management must be provided.
[5] found that chronic HCV is a progressive condition that accounts for at least one quarter of all cases of chronic liver disease[6] predicted that the prevalence of chronic HCV (CH-C) remains high and the complications of infection are common[7] discovered that chronic HCV complications are increasing, especially among people older than 60 years[8] conducted a study on disease progression of Acute HCV[9] analyzed the screening of HCV in a Health maintenance

American Journal of Computational and Applied Mathematics 2012, 2(1): 10-20 11
Organization[10], investigated the effects of a HCV educa-tional intervention or a motivational intervention on alcohol use and sexual risk behaviours among injection drug users
[11] investigated the dynamic behaviour of an SEI (Sus-ceptible- Exposed- Infective) model with acute and chronic stages. However the integration of treatment and infective immigrants to the population was not incorporated. In this paper, it is intended to study and analyze a model which incorporates the impact of treatment and infective immi-grants on the spread of HCV transmission dynamics. Thus we study and analyse a deterministic model of the effect of treatment and infected immigrants on the spread of HCV disease with acute and chronic stages.
2. Model Formulation A non linear mathematical model is proposed and ana-
lyzed to study the effect of treatment and infected immi-grants on the spread of HCV disease with acute and chronic stages.
In modelling the dynamics, the population is divided into five groups: Susceptible individuals ′S′; Exposed individuals ′E′’ who are not yet infectious; Acute infected class ′𝐼𝐼′ who are individuals initially infected; Chronic infected class ''V , who are infectious individuals; Treated group ′𝑇𝑇′ but not yet cured.
The interaction between the classes will be assumed as follows: Exposed ( )E acute infected ( )I and chronic
infected ( )V immigrants enter into the population with the
rates 1 2 3 δ , δ , δ , respectively. Susceptible individuals (𝑆𝑆)
are shifted to exposed class (𝐸𝐸) by the rate 1δ . Also sus-
ceptible individuals ( )S may become acute infectious ( )I and chronic infectious ( )V shifted to Treatment class ( )T at the rates 1 2, π π respectively. The number of new infec-tious individuals produced is therefore
1 2 3( )I V T S
N
β β β+ + where 1 2 3, , β β β are the effective
contact rate of individuals with acute hepatitis C chronic hepatitis C, and the individual still undergoing Treatment but not yet cured respectively.
In formulating the model, the following assumptions are taken into consideration:
i. Both treatment ( )T and chronic infectious individuals
( )V recover with the constant rates >0 ρ and >0 α re-
spectively,
ii. The recovered individuals go back to susceptible ( )S
group,
iii. The rate of transmission is directly proportional to the susceptible population and also to the ratio between the infected population and the total population. Total popula-tion at time 𝑡𝑡 is given by
( ) ( ) ( ) ( ) ( ) ( )N t = S t + E t + I t + T t +V t , (1)
iv. Following the interactions of susceptible, exposed class, acute individuals, chronic infective and treated group in everyday activities, susceptible acquire HCV infection with the force of infection υ , v. The population is homogeneously mixed and each
susceptible individual has equal chance of acquiring HCV infection when he/she comes into contact with infectious individual, vi. The population under study comprise of persons with at least fifteen (15) years old. In this case, it is assumed that there is no vertical transmission and all recruitments are immigrants.
vii. All parameters in population are positive and all com-partments suffer natural mortality at a rate µ .
Taking into account the above considerations, we then have the following schematic flow diagram (Figure1):
Figure 1. Model flowchart.
From the above flow chart, and with
SN
TVI )( 321 βββυ ++= ,
the model will be governed by the following system of equations:
1 2 31 2 3
( )(1 )
I V T SdSN
dt N
β β βδ δ δ λ
+ += − − − −
V T Sα ρ µ+ + −
1 2 31
( )( )
I V T SdEN E
dt N
β β βδ λ ε µ
+ += + − +
2 ( )dI
N E k Idt
δ λ ε µ= + − +
1 2 ( )dT
kI V Tdt
π π ρ µ= + − +
Nλδ1
υ
Nλ
Sµ
Tρ
TµV2π
kI1πkI
Iµ Vµ
Eµ
Eε Nλδ 2 Nλδ3
T
Vα

12 Neterindwa Ainea et al.: Modelling the Effect of Treatment and Infected Immigrants on the Spread of Hepatitis C Virus Disease with Acute and Chronic Stages
3 1 2(1 ) ( )dV
N kI Vdt
δ λ π π α µ= + − − + + (2)
with nonnegative initial conditions and 0)0( >N . where
(i=1,2,3)iβ are the effective contact rates of individuals with acute hepatitis C, chronic hepatitis C, and the individual still undergoing treatment but not yet cured,
(i=1,2,3)iδ are the rates at which exposed ( )E , acute
infected ( )I and chronic infected ( )V immigrants enter into the population respectively,
λ is the recruitment rate, µ is the death rate, k is the rate of progression from acute infected class to
both treatment and chronic infected class, ε is the rate of progression from the exposed to acute
infected class,
1π , 2π are the rates of progression from acute infected and chronic infected groups to treatment respectively,
ρ , α are the rates of progression for treatment from acute infected and chronic infected group respectively
Since the model is homogeneous of degree one, the vari-ables can be normalized by setting /s S N= , /e E N= ,
/i I N= , /h T N= , /v V N= . This leads to the normal-ized system
1 2 31ds ( δ δ δ s)λdt
= − − − −
1 2 3(β i β v β h)s αv ρh− + + + +
1 1 2 3( ) ( )de e i v h s edt
δ λ β β β ε= − + + + −
2( )di i e kidt
δ λ ε= − + −
1 2 ( )dh ki v hdt
π π ρ λ= + − +
3 1 2( ) (1 )dv v ki v vdt
δ λ π π α= − + − − − (3)
3. Model Analysis The nonlinear system in Equation (1) will be qualitatively
analyzed so as to find the conditions for existence and sta-bility a disease free equilibrium points[12]. Analysis of the model allows us to determine the effect of treatment with infected immigrants on the spread of HCV disease with acute and chronic stages. Also on finding the reproductive number
0R , one can determine if the disease become endemic in a population or not.
3.1. Disease Free Equilibrium (DFE) The disease free equilibrium of the normalised model
system of equations (3) is obtained by setting
0ds de di dh dvdt dt dt dt dt
= = = = = .
At disease free equilibrium we have 1, 0s e i h v= = = = = Thus the system (3) becomes
0sλ λ− = . Therefore the disease free equilibrium (DFE) denoted by
0€ of the normalised model system (3) is given by
( ) ( )0 0 0 0 0 1 0 0 0 0€ s, , , , , , , ,= = .
3.2. Local Stability of Disease Free Equilibrium The disease free equilibrium of the normalised model
system (3) was given by
( ) ( )0€ , 0, 0, 0, 0 1, 0, 0, 0, 0s= = . The local stability of 0€ is established by using the next
generation operator method on the normalised model system (3). The basic reproduction number 0R is defined as the effective number of secondary infections caused by typical infected individual during his/her entire period of infec-tiousness[13]. This definition is given for the models that represent spread of infection in a population. It is obtained by taking the largest (dominant) Eigen value, (spectral radius) of
1
0 0(€ ) (€ ).i i
j
F V
X Xj
−∂ ∂
∂ ∂
(4)
where
iF is the rate of appearance of new infection in com-
partment i , iV is the transfer of individuals out of the compartment i
by all other means,
0€ is the disease free equilibrium. Therefore
1 1 2 3
2
3
4
( )000
i
F i v h sF
FFF
β β β+ +
= =
(5)
By linearization approach, the associated matrix at disease free equilibrium is obtained as
1 0 1 0 1 0 1 0
2 0 2 0 2 0 2 0
3 0 3 0 3 0 3 0
4 0 4 0 4 0 4 0
(€ ) (€ ) (€ ) (€ )
(€ ) (€ ) (€ ) (€ )
(€ ) (€ ) (€ ) (€ )
(€ ) (€ ) (€ ) (€ )
F F F F
e i h vF F F F
e i h vF F F F
e i h vF F F F
e i h v
∂ ∂ ∂ ∂
∂ ∂ ∂ ∂∂ ∂ ∂ ∂
∂ ∂ ∂ ∂=∂ ∂ ∂ ∂
∂ ∂ ∂ ∂∂ ∂ ∂ ∂
∂ ∂ ∂ ∂
F (6)
American Journal of Computational and Applied Mathematics 2012, 2(1): 10-20 13
This gives
1 3 200 0 0 00 0 0 00 0 0 0
β β β
=
F (7)
The transfer of individuals from the compartment i is given by
1 1
2 2
3 1 2
2 3 14
( )( )
( )( ) (1 )
i
V eV k i e
VV h ki v
v kiV
ε λ λδλ δ λ ε
ρ λ π ππ α λ δ λ π
+ −+ − −
= =+ − −
+ + − − −
(8)
Again, by linearization approach, the associated matrix at disease free equilibrium is given by
1 0 1 0 1 0 1 0
2 0 2 0 2 0 2 0
3 0 3 0 3 0 3 0
4 0 4 0 4 0 4 0
(€ ) (€ ) (€ ) (€ )
(€ ) (€ ) (€ ) (€ )
(€ ) (€ ) (€ ) (€ )
(€ ) (€ ) (€ ) (€ )
V V V Ve i h v
V V V Ve i h v
V V V Ve i h v
V V V Ve i h v
∂ ∂ ∂ ∂∂ ∂ ∂ ∂
∂ ∂ ∂ ∂∂ ∂ ∂ ∂=
∂ ∂ ∂ ∂∂ ∂ ∂ ∂
∂ ∂ ∂ ∂∂ ∂ ∂ ∂
V
This gives
1 2
1 2
0 0 00 0
00 (1 ) 0
kk
k
ε λε λ
π λ ρ ππ α π λ
+− +
=− + −
− − + +
V (9)
With
11
1 1 2 1 2
1 1
1 1 2 1 2
10 0
10
( )( ) ( )1
( )( )( ) ( )( )
θ δ λθ
θ δ λ γ δ λ γ δ λθγ γ
θ δ λ γ δ λ σ λ γ δ λ σ λ σ λ
−
+ +
=+ + + + + +
+ + + + + + + + +
V (10)
Therefore
0 0 0 010 0 0 00 0 0 0
M N R Q
− =
FV (11)
Where ( )3 1 1 21
( )( ) ( )( )( )( )2
kM
k kβ ε π α π λ πβ ε
ε λ λ ε λ λ λ ρ α π λ+ +
= ++ + + + + + +
2 1
2
( 1 )( )( )( )
kk
β π εε λ λ α π λ
− +−
+ + + +
3 1 1 21
2
( )( ) ( )( )( )
kN
k kβ π α π λ πβ
λ λ λ ρ α π λ+ +
= ++ + + + +
2 1
2
( 1 )( )( )
kkβ πλ α π λ− +
−+ + +
3
( )R
βλ ρ
=+
and
λπαβ
λπαρλπβ
+++
+++=
2
2
2
23
))((Q
The Eigen values of 1−FV are ( )0, 0, 0, Z where
3 1 1 21
2
( )( )( ) ( )( )( )( )
kZ
k kβ ε π α π λ πβ ε
ε λ λ ε λ λ λ ρ α π λ+ +
= ++ + + + + + +
2 1
2
( 1 )( )( )( )
kk
β π εε λ λ α π λ
− +−
+ + + +
It follows that the basic reproduction number for the normalised model system (3) with infective immigrant and treatment denoted by 0R is given by
10 ( )( )
Rk
β ε
ε λ λ=
+ +
3 1 1 2
2
( )
( )( )( )( )
k
k
β ε π α π λ π
ε λ λ λ ρ α π λ
+ ++
+ + + + +
2 1
2
( 1 )
( )( )( )
k
k
β π ε
ε λ λ α π λ
− +−
+ + + + (12)
The disease free equilibrium of the treatment model sys-tem (3) with infective immigrants is locally asymptotically stable if 0 1R < and unstable if 0 1R > . In order to assess the contribution of , i ν and h in terms of 1 2, β β and
3β respectively from equation (12) above, we let
10 ( )( )iR
k
β ε
ε λ λ=
+ +,
2 10
2
( 1 )
( )( )( )
kR v
k
β π ε
ε λ λ α π λ
− += −
+ + + +,
3 1 1 20
2
( )
( )( )( )( )hk
Rk
β ε π α π λ π
ε λ λ λ ρ α π λ
+ +=
+ + + + + (13)
Then
0 0 0 0i v hR R R R= + + .
Lemma 1 The disease free equilibrium of the treatment model sys-
tem (3) with infective immigrants is locally asymptotically stable if 0 1R < and unstable If 0 1R > .
Remark:From the equations (14) above, it is clear that
0 00i vhR R R> > which implies that acute infective ' 'i have a significant contribution on the transmission of the HCV infection followed by individuals who are still under-going treatment but not yet cured ′ℎ′ which keep the disease endemic (i.e. 0 1R > ) in the population through 1 1'' , ''β δ
and 3 3'' , ''β δ respectively compared to chronic infective ‘ v ’ under 2 2'' , ''β δ .
In the absence of infection, the population size approaches the steady state for a normalized model system (3). The results by[11] on 0R 𝑅𝑅0 are recovered only when 𝛽𝛽3 = 0 and 𝜋𝜋1 = 𝜋𝜋2 = 0 from equation (12) above.

14 Neterindwa Ainea et al.: Modelling the Effect of Treatment and Infected Immigrants on the Spread of Hepatitis C Virus Disease with Acute and Chronic Stages
3.3. Endemic Equilibrium and Local Stability
To obtain an endemic equilibrium Ε∗ , we set each equa-tion in the model (3) equal to zero. Solving the system while expressing each equilibrium point in terms of *i at steady state, we get ( )*s t , ( )*e t , ( )* i t , ( )*h t , and ( )*v t as an endemic equilibrium point. Thus
( )( ) ( )( ) ( )( ) ( )( ) ( )( )( )* * * * *, , , , Ε s t e t i t h t v t∗ = is an endemic equilibrium where
( )3 4
0 1 2
r r is
R r i rλ
∗∗
∗
+=
+ +
( ) ( )( )( )( )
1 0 1 2 0 1 2 3 4
0 1 2
R r i r R r i r r r ie
R r i r
δ λ λ
λ λ ε
∗ ∗ ∗∗
∗
+ + + + +=
+ + +
( )( )
1 1 2 2 3
2( )ki
hλπ απ π π δ λ
ρ λ λ π α
∗∗ + + +=
+ + +
2 1
2
(1 )kiv
δ λ πλ π α
∗∗ + −=
+ +
and ( )
1( )k
rε λ λ
ε+ +
= , ( )( )( )
2 3 3 2 32
2r
β δ λ ρ λ β π δ λρ λ λ π α
+ +=
+ + +
( ) ( ) ( )( )( )
2 1 2 3 3 2 33
2
( ) 1r
λ ρ λ λ π α δ δ δ ρ λ αδ λ ρπ δ λ
ρ λ λ π α
+ + + − − − + + +=
+ + + ( ) ( )
( )1 1 1 2
42
1 ( )
( )
k kr
ρ λ α π ρ λπ απ π
ρ λ λ π α
+ − + + +=
+ + +
We note that * * * *, v , s , h e are always positive and this will happen if and only if 0 0R > .
3.4. Global Stability of DFE
Theorem 1: If 0 1R > , the endemic equilibrium Ε∗ of the model (3) is globally asymptotically stable.
Proof: To establish the global stability of the endemic equilibrium Ε∗ , we construct the following Lyapunov func-tion:
* * * * *( , , , , ) log sV s e i h v s s ss
∗∗ ∗
= − −
log loge ie e e i i ie i
∗ ∗∗ ∗ ∗ ∗
+ − − + − −
log logh vh h h v v vh v
∗ ∗∗ ∗ ∗ ∗
+ − − + − −
By directly calculating the derivation of V along the so-lution of (3) we get
dV s s ds e e dedt s dt e dt
∗ ∗ − −= +
i i di h h dh v v dvi dt h dt v dt
∗ ∗ ∗ − − −+ + +
(14)
which gives dV a bdt
= −
Where
( ) ( )2
1 2 3s s
a i v hs
β β β∗
∗ ∗ ∗ −= + +
( )1 2 3s
v h i s v s h ss
α ρ β β β∗
∗ ∗ ∗+ + + + +
1 2 3( )δ δ δ λ+ + +
( )1 2 3 1 2 3e
i s v s h s is vs hse
β β β β β β∗
∗ ∗ ∗ ∗ ∗ ∗+ + + + + +
( ) ( )1 2 1 h vki v ki kih v
π π π∗ ∗
∗ ∗ ∗+ + + +
2 1 2 3( )v h v kiα ρ π λ λ δ δ δ+ + + + + + + +
2 3 1e vs hs isε β β β+ + + + and
( ) ( )2
1 2 3s s
b i v hs
λ β β β∗−
= + + +
( ) ( ) ( ) ( )2 2e e i i
ke i
λ ε λ∗ ∗− −
+ + + +
( ) ( ) ( ) ( )2 2
2h h v v
h vρ λ λ π α
∗ ∗− −+ + + + +
( )2 3 1s
v h vs hs iss
λ α ρ β β β∗
+ + + + + +
( )1 1 2 3 1 2 3e
is vs hs i s v s h s ee
δ λ β β β β β β ε∗
∗ ∗ ∗ ∗ ∗ ∗+ + + + + + + +
( )2 1+ i
e ki sii
δ λ ε β∗
+ + +
( )1 2 3h
ki v h shh
π π ρ β∗
+ + + +
( )1 3 2 2v ki ki v v svv
π δ λ α π β∗
∗+ + + + + + +
1 2 3( )δ δ δ λ+ + +
Thus from (14), if a b< then dVdt
will be negative
definite, implying that 0dVdt
< . Also 0dVdt
= if and only
if ., , , , s s e e i i h h v v∗ ∗ ∗ ∗ ∗= = = = = Therefore, the largest compact invariant set in
American Journal of Computational and Applied Mathematics 2012, 2(1): 10-20 15
{ }* * * * *( , , , , ) : 0dV
s e i h vdt
∈Γ = is the singleton { }∗Ε ,
where ∗Ε is endemic equilibrium of the normalised system (3). By LaSalle’s invariant principle, it then implies that ∗Ε is globally asymptotically stable in Γ if a b< .
3.5. Determination of Forward or Backward Bifurcation
The existence and stability of endemic equilibrium is de-termined through the investigation of the possibility of ex-istence of the backward or forward bifurcation due to exis-tence of endemic equilibrium using the the centre manifold theory [14]. As a disease invades the population, it reduces the number of susceptible individuals in the population, which tends to reduce its reproductive rates.
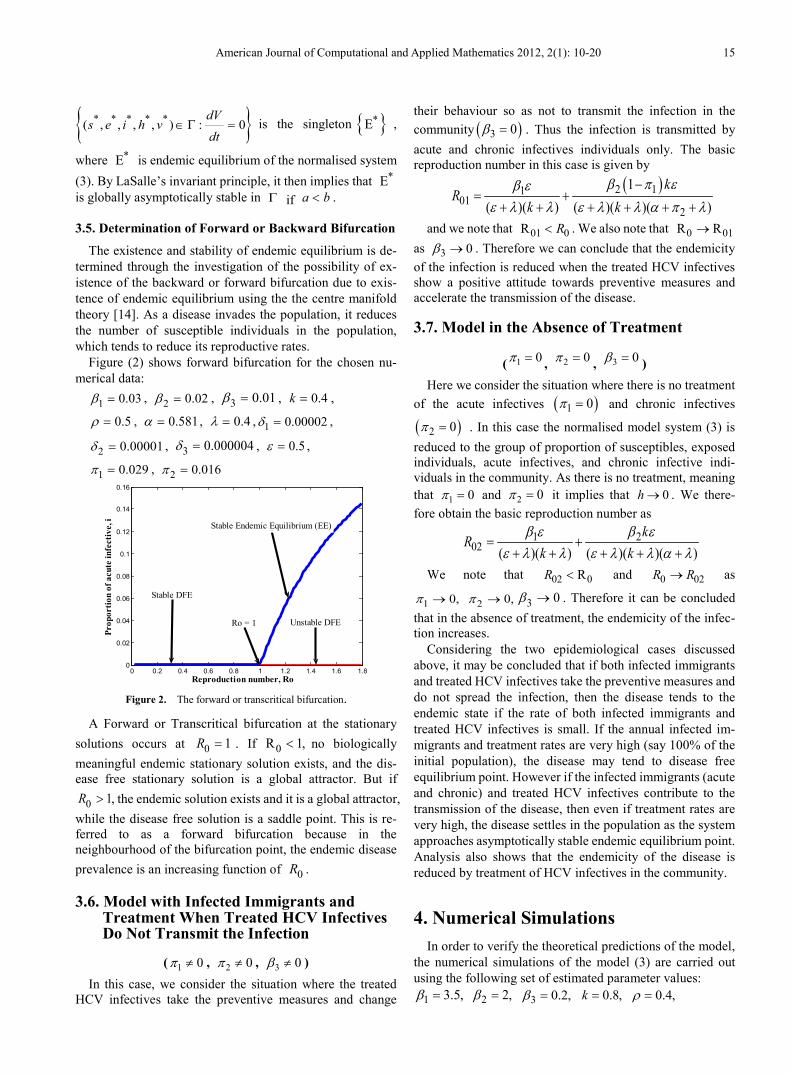
Figure (2) shows forward bifurcation for the chosen nu-merical data:
1 0.03β = , 2 0.02β = , 3 0.01β = , 0.4k = ,
0.5ρ = , 0.581α = , 0.4λ = , 1 0.00002δ = ,
2 0.00001δ = , 3 0.000004δ = , 0.5ε = ,
1 0.029π = , 2 0.016π =
Figure 2. The forward or transcritical bifurcation.
A Forward or Transcritical bifurcation at the stationary solutions occurs at 0 1R = . If 0 R 1,< no biologically meaningful endemic stationary solution exists, and the dis-ease free stationary solution is a global attractor. But if
0 1,R > the endemic solution exists and it is a global attractor, while the disease free solution is a saddle point. This is re-ferred to as a forward bifurcation because in the neighbourhood of the bifurcation point, the endemic disease prevalence is an increasing function of 0R .
3.6. Model with Infected Immigrants and Treatment When Treated HCV Infectives Do Not Transmit the Infection
( 1 0π ≠ , 2 0π ≠ , 3 0β ≠ ) In this case, we consider the situation where the treated
HCV infectives take the preventive measures and change
their behaviour so as not to transmit the infection in the community ( )3 0β = . Thus the infection is transmitted by acute and chronic infectives individuals only. The basic reproduction number in this case is given by
( )2 1101
2
1( )( ) ( )( )( )
kR
k kβ π εβ ε
ε λ λ ε λ λ α π λ−
= ++ + + + + +
and we note that 01 0R R< . We also note that 0 01R R→ as 3 0β → . Therefore we can conclude that the endemicity of the infection is reduced when the treated HCV infectives show a positive attitude towards preventive measures and accelerate the transmission of the disease.
3.7. Model in the Absence of Treatment
( 1 0π = , 2 0π = , 3 0β = ) Here we consider the situation where there is no treatment
of the acute infectives ( )1 0π = and chronic infectives
( )2 0 π = . In this case the normalised model system (3) is reduced to the group of proportion of susceptibles, exposed individuals, acute infectives, and chronic infective indi-viduals in the community. As there is no treatment, meaning that 1 0π = and 2 0π = it implies that 0h → . We there-fore obtain the basic reproduction number as
1 202 ( )( ) ( )( )( )
kR
k kβ ε β ε
ε λ λ ε λ λ α λ= +
+ + + + +
We note that 02 0RR < and 0 02R R→ as
1 20, 0,π π→ → 3 0β → . Therefore it can be concluded that in the absence of treatment, the endemicity of the infec-tion increases.
Considering the two epidemiological cases discussed above, it may be concluded that if both infected immigrants and treated HCV infectives take the preventive measures and do not spread the infection, then the disease tends to the endemic state if the rate of both infected immigrants and treated HCV infectives is small. If the annual infected im-migrants and treatment rates are very high (say 100% of the initial population), the disease may tend to disease free equilibrium point. However if the infected immigrants (acute and chronic) and treated HCV infectives contribute to the transmission of the disease, then even if treatment rates are very high, the disease settles in the population as the system approaches asymptotically stable endemic equilibrium point. Analysis also shows that the endemicity of the disease is reduced by treatment of HCV infectives in the community.
4. Numerical Simulations In order to verify the theoretical predictions of the model,
the numerical simulations of the model (3) are carried out using the following set of estimated parameter values:
1 3.5,β = 2 2,β = 3 0.2,β = 0.8,k = 0.4,ρ =
0 0.2 0.4 0.6 0.8 1 1.2 1.4 1.6 1.80
0.02
0.04
0.06
0.08
0.1
0.12
0.14
0.16
Prop
ortio
n of
acu
te in
fect
ive,
i
Reproduction number, Ro
Stable Endemic Equilibrium (EE)
Ro = 1 Unstable DFE
Stable DFE
16 Neterindwa Ainea et al.: Modelling the Effect of Treatment and Infected Immigrants on the Spread of Hepatitis C Virus Disease with Acute and Chronic Stages
0.581,α = ,8.0=λ ,5.0=ε 1 0.6,π = 2 0.3,π =,
1 0.00002,δ = 2 0.00001,δ = 3 0.000004.δ =
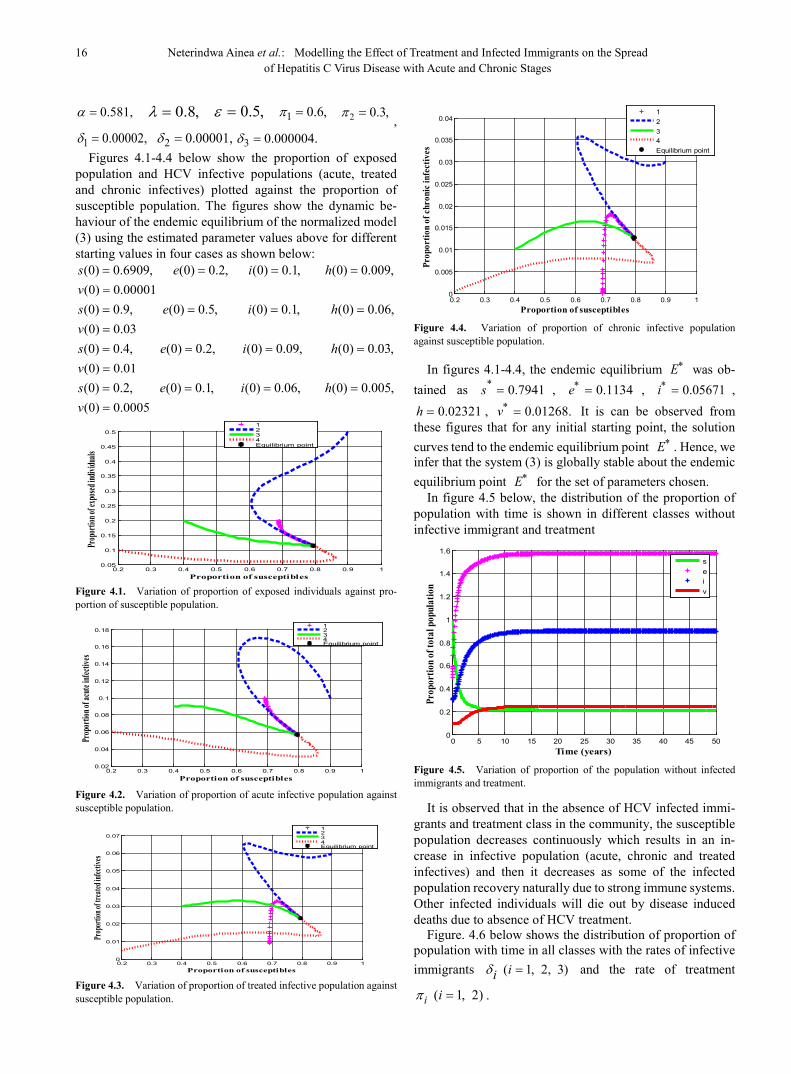
Figures 4.1-4.4 below show the proportion of exposed population and HCV infective populations (acute, treated and chronic infectives) plotted against the proportion of susceptible population. The figures show the dynamic be-haviour of the endemic equilibrium of the normalized model (3) using the estimated parameter values above for different starting values in four cases as shown below:
(0) 0.6909,s = (0) 0.2,e = (0) 0.1,i = (0) 0.009,h =(0) 0.00001v = (0) 0.9,s = (0) 0.5,e = (0) 0.1,i = (0) 0.06,h = (0) 0.03v = (0) 0.4,s = (0) 0.2,e = (0) 0.09,i = (0) 0.03,h = (0) 0.01v = (0) 0.2,s = (0) 0.1,e = (0) 0.06,i = (0) 0.005,h = (0) 0.0005v =
Figure 4.1. Variation of proportion of exposed individuals against pro-portion of susceptible population.
Figure 4.2. Variation of proportion of acute infective population against susceptible population.
Figure 4.3. Variation of proportion of treated infective population against susceptible population.
Figure 4.4. Variation of proportion of chronic infective population against susceptible population.
In figures 4.1-4.4, the endemic equilibrium Ε∗ was ob-tained as * 0.7941s = , 0.1134e∗ = , 0.05671i∗ = ,
0.02321h = , 0.01268.v∗ = It is can be observed from these figures that for any initial starting point, the solution curves tend to the endemic equilibrium point Ε∗ . Hence, we infer that the system (3) is globally stable about the endemic equilibrium point Ε∗ for the set of parameters chosen.
In figure 4.5 below, the distribution of the proportion of population with time is shown in different classes without infective immigrant and treatment
Figure 4.5. Variation of proportion of the population without infected immigrants and treatment.
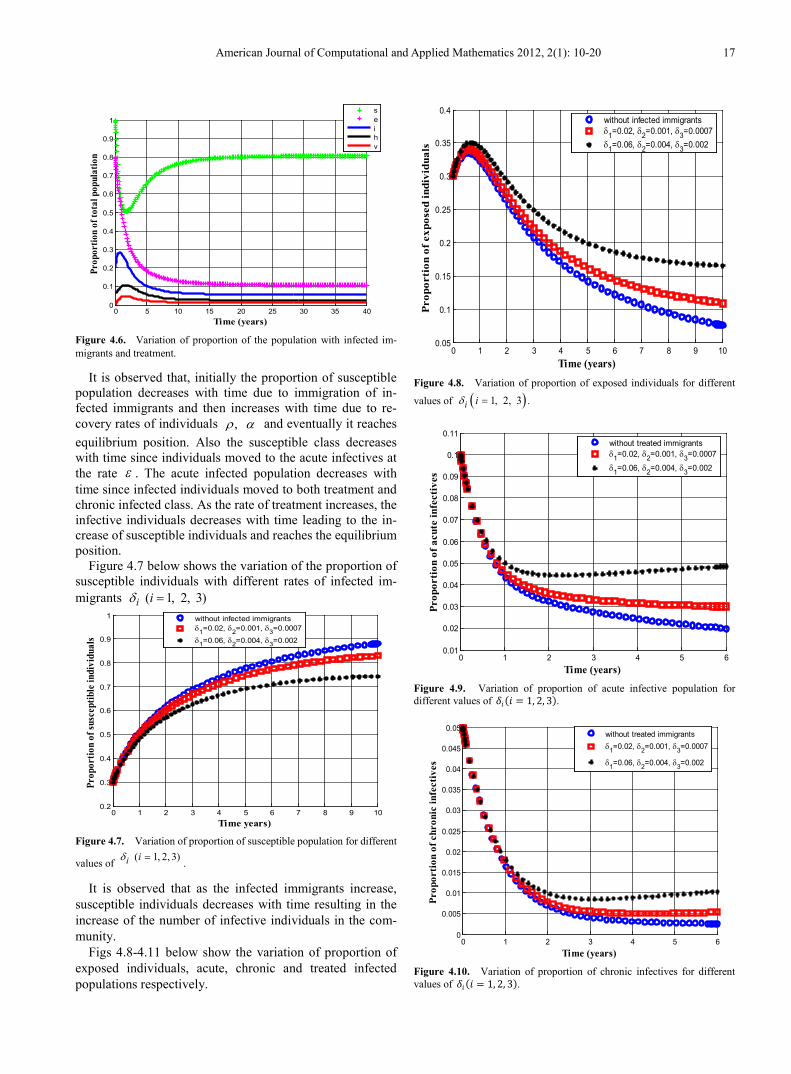
It is observed that in the absence of HCV infected immi-grants and treatment class in the community, the susceptible population decreases continuously which results in an in-crease in infective population (acute, chronic and treated infectives) and then it decreases as some of the infected population recovery naturally due to strong immune systems. Other infected individuals will die out by disease induced deaths due to absence of HCV treatment.
Figure. 4.6 below shows the distribution of proportion of population with time in all classes with the rates of infective immigrants ( 1, 2, 3)iiδ = and the rate of treatment
( 1, 2)i iπ = .
0.2 0.3 0.4 0.5 0.6 0.7 0.8 0.9 10.05
0.1
0.15
0.2
0.25
0.3
0.35
0.4
0.45
0.5
Proportion of susceptibles
Prop
ortion
of ex
posed
indiv
iduals
1234Equilibrium point
0.2 0.3 0.4 0.5 0.6 0.7 0.8 0.9 10.02
0.04
0.06
0.08
0.1
0.12
0.14
0.16
0.18
Proportion of susceptibles
Prop
ortio
n of a
cute
infect
ives
1234Equilibrium point
0.2 0.3 0.4 0.5 0.6 0.7 0.8 0.9 10
0.01
0.02
0.03
0.04
0.05
0.06
0.07
Proportion of susceptibles
Prop
ortion
of tr
eated
infect
ives
1234Equilibrium point
0.2 0.3 0.4 0.5 0.6 0.7 0.8 0.9 10
0.005
0.01
0.015
0.02
0.025
0.03
0.035
0.04
Proportion of susceptibles
Prop
ortio
n of
chro
nic i
nfec
tives
1234Equilibrium point
0 5 10 15 20 25 30 35 40 45 500
0.2
0.4
0.6
0.8
1
1.2
1.4
1.6
Time (years)
Prop
ortio
n of
tota
l pop
ulat
ion
seiv
American Journal of Computational and Applied Mathematics 2012, 2(1): 10-20 17
Figure 4.6. Variation of proportion of the population with infected im-migrants and treatment.
It is observed that, initially the proportion of susceptible population decreases with time due to immigration of in-fected immigrants and then increases with time due to re-covery rates of individuals , ρ α and eventually it reaches equilibrium position. Also the susceptible class decreases with time since individuals moved to the acute infectives at the rate ε . The acute infected population decreases with time since infected individuals moved to both treatment and chronic infected class. As the rate of treatment increases, the infective individuals decreases with time leading to the in-crease of susceptible individuals and reaches the equilibrium position.
Figure 4.7 below shows the variation of the proportion of susceptible individuals with different rates of infected im-migrants ( 1, 2, 3)i iδ =
Figure 4.7. Variation of proportion of susceptible population for different
values of ( 1, 2, 3)i iδ = .
It is observed that as the infected immigrants increase, susceptible individuals decreases with time resulting in the increase of the number of infective individuals in the com-munity.
Figs 4.8-4.11 below show the variation of proportion of exposed individuals, acute, chronic and treated infected populations respectively.
Figure 4.8. Variation of proportion of exposed individuals for different
values of ( ) .1, 2, 3i iδ =
Figure 4.9. Variation of proportion of acute infective population for different values of 𝛿𝛿𝑖𝑖(𝑖𝑖 = 1, 2, 3).
Figure 4.10. Variation of proportion of chronic infectives for different values of 𝛿𝛿𝑖𝑖(𝑖𝑖 = 1, 2, 3).
0 5 10 15 20 25 30 35 400
0.1
0.2
0.3
0.4
0.5
0.6
0.7
0.8
0.9
1
Time (years)
Prop
ortio
n of
tota
l pop
ulat
ion
seihv
0 1 2 3 4 5 6 7 8 9 100.2
0.3
0.4
0.5
0.6
0.7
0.8
0.9
1
Time years)
Prop
ortio
n of
susc
eptib
le in
divi
dual
s
without infected immigrantsδ1=0.02, δ2=0.001, δ3=0.0007
δ1=0.06, δ2=0.004, δ3=0.002
0 1 2 3 4 5 6 7 8 9 100.05
0.1
0.15
0.2
0.25
0.3
0.35
0.4
Time (years)
Prop
orti
on o
f exp
osed
indi
vidu
als
without infected immigrantsδ1=0.02, δ2=0.001, δ3=0.0007δ1=0.06, δ2=0.004, δ3=0.002
0 1 2 3 4 5 60.01
0.02
0.03
0.04
0.05
0.06
0.07
0.08
0.09
0.1
0.11
Time (years)
Prop
orti
on o
f acu
te in
fect
ives
without treated immigrantsδ1=0.02, δ2=0.001, δ3=0.0007
δ1=0.06, δ2=0.004, δ3=0.002
0 1 2 3 4 5 60
0.005
0.01
0.015
0.02
0.025
0.03
0.035
0.04
0.045
0.05
Time (years)
Prop
orti
on o
f chr
onic
infe
ctiv
es
without treated immigrantsδ1=0.02, δ2=0.001, δ3=0.0007
δ1=0.06, δ2=0.004, δ3=0.002
18 Neterindwa Ainea et al.: Modelling the Effect of Treatment and Infected Immigrants on the Spread of Hepatitis C Virus Disease with Acute and Chronic Stages
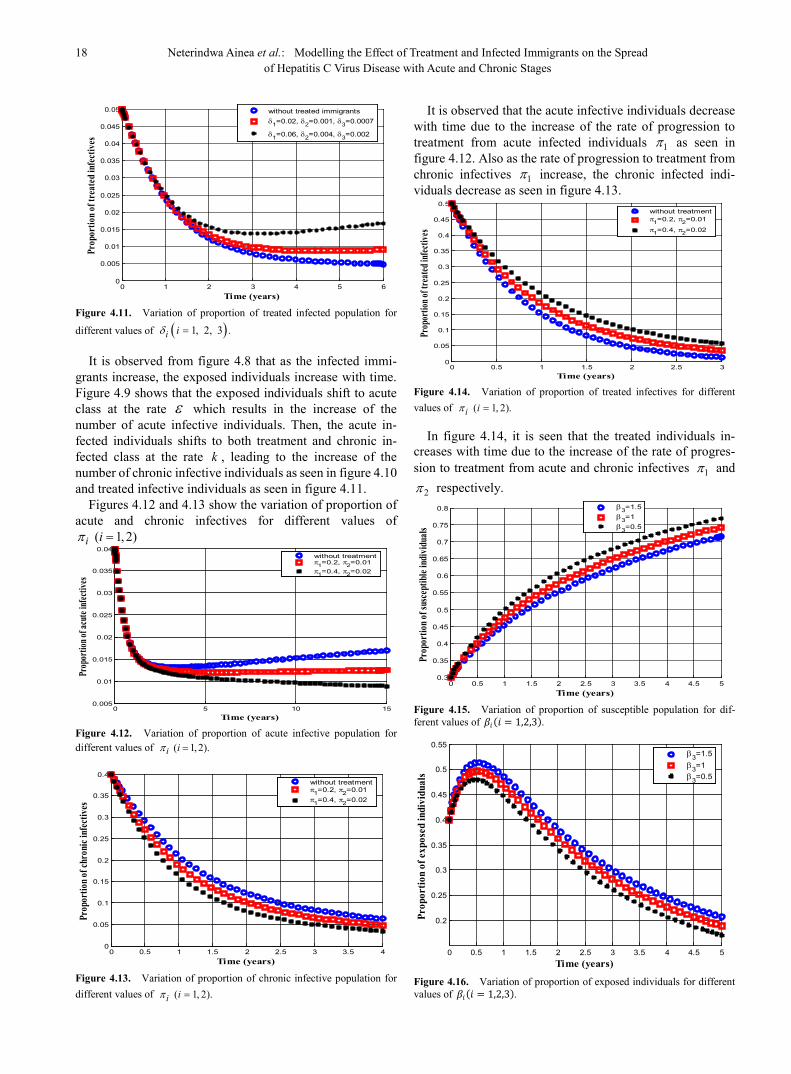
Figure 4.11. Variation of proportion of treated infected population for
different values of ( ) .1, 2, 3i iδ =
It is observed from figure 4.8 that as the infected immi-grants increase, the exposed individuals increase with time. Figure 4.9 shows that the exposed individuals shift to acute class at the rate ε which results in the increase of the number of acute infective individuals. Then, the acute in-fected individuals shifts to both treatment and chronic in-fected class at the rate k , leading to the increase of the number of chronic infective individuals as seen in figure 4.10 and treated infective individuals as seen in figure 4.11.
Figures 4.12 and 4.13 show the variation of proportion of acute and chronic infectives for different values of
( 1, 2)i iπ =
Figure 4.12. Variation of proportion of acute infective population for different values of ( 1, 2).i iπ =
Figure 4.13. Variation of proportion of chronic infective population for different values of ( 1, 2).i iπ =
It is observed that the acute infective individuals decrease with time due to the increase of the rate of progression to treatment from acute infected individuals 1 π as seen in figure 4.12. Also as the rate of progression to treatment from chronic infectives 1 π increase, the chronic infected indi-viduals decrease as seen in figure 4.13.
Figure 4.14. Variation of proportion of treated infectives for different values of ( 1, 2).i iπ =
In figure 4.14, it is seen that the treated individuals in-creases with time due to the increase of the rate of progres-sion to treatment from acute and chronic infectives 1π and
2π respectively.
Figure 4.15. Variation of proportion of susceptible population for dif-ferent values of 𝛽𝛽𝑖𝑖(𝑖𝑖 = 1,2,3).
Figure 4.16. Variation of proportion of exposed individuals for different values of 𝛽𝛽𝑖𝑖(𝑖𝑖 = 1,2,3).
0 1 2 3 4 5 60
0.005
0.01
0.015
0.02
0.025
0.03
0.035
0.04
0.045
0.05
Time (years)
Prop
ortio
n of t
reat
ed in
fect
ives
without treated immigrantsδ1=0.02, δ2=0.001, δ3=0.0007
δ1=0.06, δ2=0.004, δ3=0.002
0 5 10 150.005
0.01
0.015
0.02
0.025
0.03
0.035
0.04
Time (years)
Prop
ortio
n of a
cute
infec
tives
without treatmentπ1=0.2, π2=0.01π1=0.4, π2=0.02
0 0.5 1 1.5 2 2.5 3 3.5 40
0.05
0.1
0.15
0.2
0.25
0.3
0.35
0.4
Time (years)
Prop
ortio
n of c
hron
ic inf
ectiv
es
without treatmentπ1=0.2, π2=0.01π1=0.4, π2=0.02
0 0.5 1 1.5 2 2.5 30
0.05
0.1
0.15
0.2
0.25
0.3
0.35
0.4
0.45
0.5
Time (years)
Prop
ortio
n of t
reate
d infe
ctive
s
without treatmentπ1=0.2, π2=0.01
π1=0.4, π2=0.02
0 0.5 1 1.5 2 2.5 3 3.5 4 4.5 50.3
0.35
0.4
0.45
0.5
0.55
0.6
0.65
0.7
0.75
0.8
Time (years)
Prop
ortio
n of s
usce
ptibl
e ind
ividu
als
β3=1.5β3=1β3=0.5
0 0.5 1 1.5 2 2.5 3 3.5 4 4.5 5
0.2
0.25
0.3
0.35
0.4
0.45
0.5
0.55
Time (years)
Prop
ortio
n of
expo
sed
indi
vidu
als
β3=1.5β3=1β3=0.5
American Journal of Computational and Applied Mathematics 2012, 2(1): 10-20 19
It is observed from figures. 4.15 and 4.16 that when the effective contact rate of individuals still undergoing treat-ment 3β become very small, the susceptible population increase with time.(see figure 4.15) and if the susceptible population increase, the number of exposed individuals decrease (see figure 4.16).
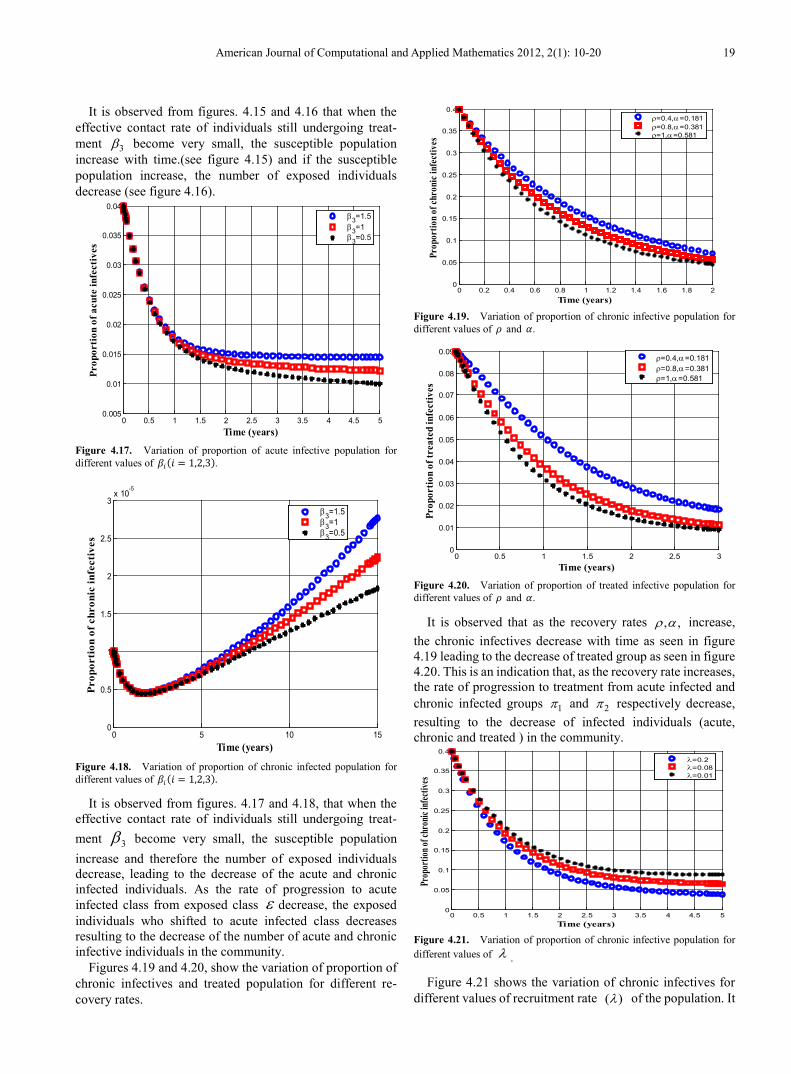
Figure 4.17. Variation of proportion of acute infective population for different values of 𝛽𝛽𝑖𝑖(𝑖𝑖 = 1,2,3).
Figure 4.18. Variation of proportion of chronic infected population for different values of 𝛽𝛽𝑖𝑖(𝑖𝑖 = 1,2,3).
It is observed from figures. 4.17 and 4.18, that when the effective contact rate of individuals still undergoing treat-ment 3β become very small, the susceptible population increase and therefore the number of exposed individuals decrease, leading to the decrease of the acute and chronic infected individuals. As the rate of progression to acute infected class from exposed class ε decrease, the exposed individuals who shifted to acute infected class decreases resulting to the decrease of the number of acute and chronic infective individuals in the community.
Figures 4.19 and 4.20, show the variation of proportion of chronic infectives and treated population for different re-covery rates.
Figure 4.19. Variation of proportion of chronic infective population for different values of 𝜌𝜌 and 𝛼𝛼.
Figure 4.20. Variation of proportion of treated infective population for different values of 𝜌𝜌 and 𝛼𝛼.
It is observed that as the recovery rates , ,ρ α increase, the chronic infectives decrease with time as seen in figure 4.19 leading to the decrease of treated group as seen in figure 4.20. This is an indication that, as the recovery rate increases, the rate of progression to treatment from acute infected and chronic infected groups 1π and 2π respectively decrease, resulting to the decrease of infected individuals (acute, chronic and treated ) in the community.
Figure 4.21. Variation of proportion of chronic infective population for different values of λ .
Figure 4.21 shows the variation of chronic infectives for different values of recruitment rate ( )λ of the population. It
0 0.5 1 1.5 2 2.5 3 3.5 4 4.5 50.005
0.01
0.015
0.02
0.025
0.03
0.035
0.04
Time (years)
Prop
orti
on o
f acu
te in
fect
ives
β3=1.5β3=1β3=0.5
0 5 10 150
0.5
1
1.5
2
2.5
3x 10
-5
Time (years)
Prop
orti
on o
f chr
onic
infe
ctiv
es
β3=1.5β3=1β3=0.5
0 0.2 0.4 0.6 0.8 1 1.2 1.4 1.6 1.8 20
0.05
0.1
0.15
0.2
0.25
0.3
0.35
0.4
Time (years)
Prop
ortio
n of
chro
nic i
nfec
tives
ρ=0.4,α=0.181ρ=0.8,α=0.381ρ=1,α=0.581
0 0.5 1 1.5 2 2.5 30
0.01
0.02
0.03
0.04
0.05
0.06
0.07
0.08
0.09
Time (years)
Prop
ortio
n of
trea
ted
infe
ctiv
es
ρ=0.4,α=0.181ρ=0.8,α=0.381ρ=1,α=0.581
0 0.5 1 1.5 2 2.5 3 3.5 4 4.5 50
0.05
0.1
0.15
0.2
0.25
0.3
0.35
0.4
Time (years)
Prop
ortio
n of c
hron
ic inf
ectiv
es
λ=0.2λ=0.08λ=0.01

20 Neterindwa Ainea et al.: Modelling the Effect of Treatment and Infected Immigrants on the Spread of Hepatitis C Virus Disease with Acute and Chronic Stages
is clear from the figure that as the recruitment rate increases, the chronic infected population decrease. This might be due to the effect of treatment in the community which leads to the decline of infected individuals (acute, chronic and treated infectives) in the community.
5. Discussions and Conclusions In this paper, a mathematical model of HCV showing the
effects of treatment and infected immigrants on the spread of HCV disease with acute and chronic stages has been estab-lished. Both qualitative and numerical analysis of the model was done. The model incorporates the assumption that in-fected immigrants enter the homogenous population. It was shown that there exists a feasible region where the model is well posed in which a unique disease free equilibrium point exists.
The disease free and endemic equilibrium points were obtained and their stabilities investigated. A numerical study of the model has been conducted to see the effect of certain key parameters on the spread of the disease. It was observed that the disease become more endemic due to the presence of infected immigrants in the community. As the infected im-migrants increase, the acute and chronic infective individuals also increase in the population. It was also shown that in the presence of treatment, the rate of infected individuals (acute and chronic) decrease and consequently the treated infected individuals decrease continuously. It was therefore shown that the disease can be eliminated at some point due to treatment and natural immunity of chronic infected indi-viduals in the community.
Finally from the analysis, it may be hypothesized that preventive measures, through reducing rates of transmission of HCV are therefore necessary to the community. Reduced transmission leads to lower prevalence of the disease in the long-term. The national health cares to HCV should there-fore seek to ensure that all people at risk or that have been at risk in the past, have access to and are supported in the use of HCV education and prevention services, regardless of their social and economic status.
REFERENCES [1] J. Wales, L. Sanger, 2001. Acute hep C virus infection:
Transmission, Diagnosis, Prevention and Treatment. Wi-kimedia Foundation, Inc
[2] L. A. Moyer, E. E. Mast, M. J. Alter, 1999, Hepatitis C: Prevention counseling and medical evaluation. American Academy of Family Physicians
[3] J. Wong, 2000,. “Silent killer”. American Journal of Public Health", Vol 90
[4] C. Giordano, E. F. Drugts, G. Garber, C. Cooper, Evaluation of immigration status, race and language barriers on chronic hepatitis C virus infection management and treatment out-comes, Wolters Kluwer Health: Lippincott Williams and Wilkins, 2008
[5] A. Mehta, R. Pawson, S. Rajan, G. Hazlehurst, G. Dusheiko, R. Miller, P. Hewitt (1999) “Hepatitis C lookback programme: a single hospital experience”, Transfusion Medicine , 9 (3) 189 - 193
[6] G. L. Davis, K. Yalamanchili, S. Saadeh, R. Lepe, 2009, The prevalence of hepatitis C virus infection in Taxes: Implica-tions for future health care. Baylcr University Medical centre
[7] L. Highleyman, 2010, “Chronic Hepatitis C Complications are Increasing, Especially among People Older than 60 Years”. Gastroenterology
[8] C. D. Mazoff (2008), Disease Progression: Acute Hepatitis C. Alan Franciscus
[9] L. R. Fischer, D. H. Tope, S. Kathleen, R. N. Conboy, B. D. Hedblom, E. Ronberg, D. K. Shewmake, J. C. Butter, 2000. Screening for hepatitis C virus in a health maintenance orga-nisatio, American Medical Association
[10] W. A. Zule, E. C. Costenbader, C. M. Coomes, W. M. Wechsberg, 2009. Effects of a hepatitis C virus educational intervention or a motivational intervention on alcohol use, injection drug use, and sexual risk behaviours among injec-tion drug users. National centre for Biotechnology Informa-tion, U. S. National Library of Medicine, Bethesda MD, USA
[11] L. Cai, X. Li, A note on global stability of an SEI epidemic model with acute and chronic stages. Beijing Institute of In-formation Control, PR China, 2007
[12] G. M. Gomes, L. J. White, G. F. Medley, 2004, Infection, reinfection, and vaccination under suboptimal immune pro-tection: epidemiological perspectives, J. Theor. Biol. 228, p. 539-549
[13] O. Diekmann, J. A. P. Heesterbeek and J. A. P. Metz, 1990, On the definition and computation of the basic reproduction ratio 0R in the model of infectious disease in heterogeneous populations. Journal. Math. Biol. 2(1), 265-382
[14] A. Gumel, C. Castillo-Chavez, R. E. Mickens and D. P. Clemence, 2009, Simulation of the pertusis epidemiology in the united states: Effects of Adult booster doses, maths equa-tions and application of Biology and industry, www.publc.asu.edu/…/pubs.htm retrieved on 9 April, 2011