IB 6.3 Defence against infectious disease
47
6.3 Defence against infectious disease Plan 1 Skin and mucous membranes as barriers to infection 2 Cuts, platelets and blood clotting 3 Coronary thrombosis 4 Phagocytes and Lymphocytes 5 HIV/AIDS 6 Antibiotics 2 3 4 1 Xavier DANIEL, Ph.D. IB 5
-
Upload
independent -
Category
Documents
-
view
4 -
download
0
Transcript of IB 6.3 Defence against infectious disease
6.3 Defence against infectious disease
Plan
1 Skin and mucous membranes as barriers to infection
2 Cuts, platelets and blood clotting
3 Coronary thrombosis
4 Phagocytes and Lymphocytes
5 HIV/AIDS
6 Antibiotics
2
3
4
1
Xavier DANIEL, Ph.D. IB
5
Xavier DANIEL, Ph.D. IB
Introduction
Disease: A pathological condition of a part, organ, or system of an organism
resulting from infection, genetic defect, or environmental stress, and
characterized by an identifiable group of signs or symptoms.
Ex.: Cholera, Malaria, Tuberculosis, HIV/AIDS, Smallpox, Measles
Pathogen: An agent that causes disease by infection, e.g. a living
microorganism such as a bacterium, a fungus or a virus.
Ex.: Vibrio cholerae, Plasmodium, Mycobacterium tuberculosis, HIV virus,
Variola viruses, Measles virus
Xavier DANIEL, Ph.D. IB
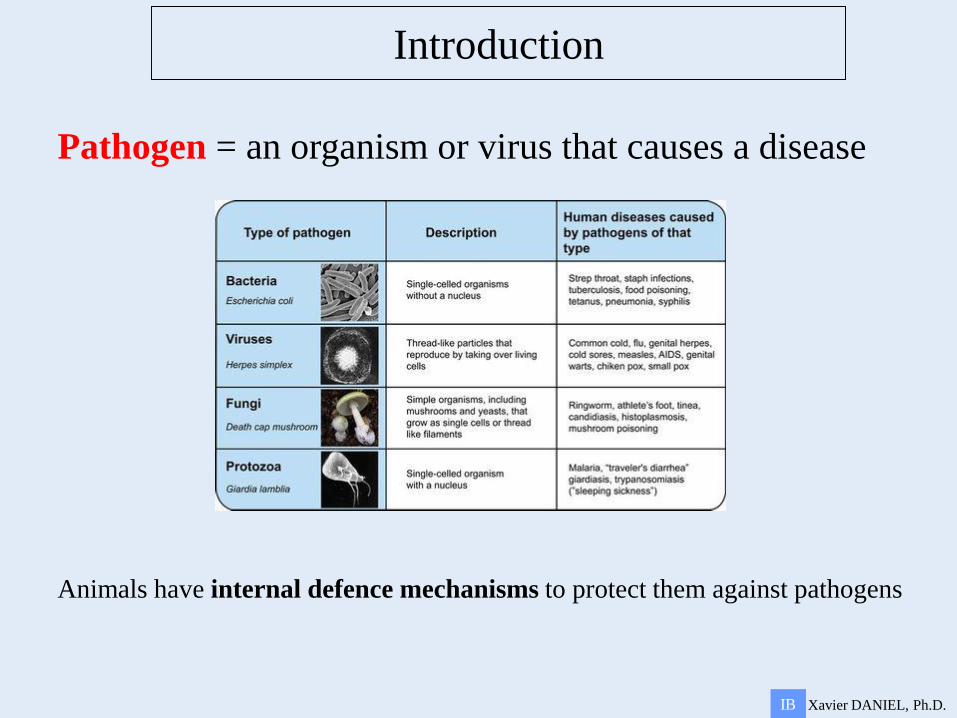
Introduction
Pathogen = an organism or virus that causes a disease
Animals have internal defence mechanisms to protect them against pathogens
Xavier DANIEL, Ph.D. IB
Introduction
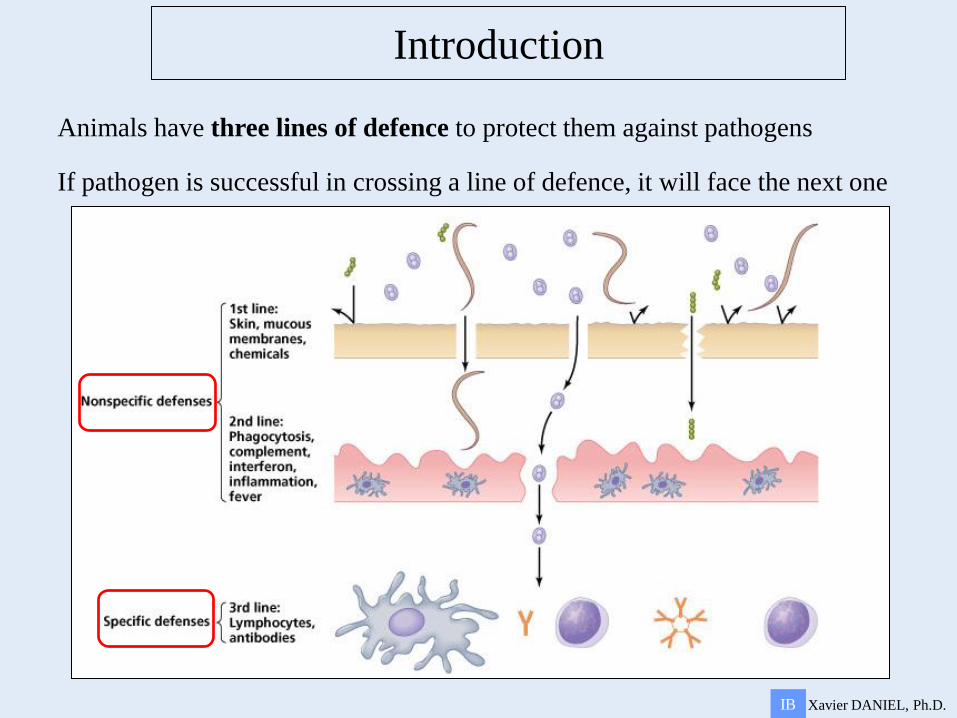
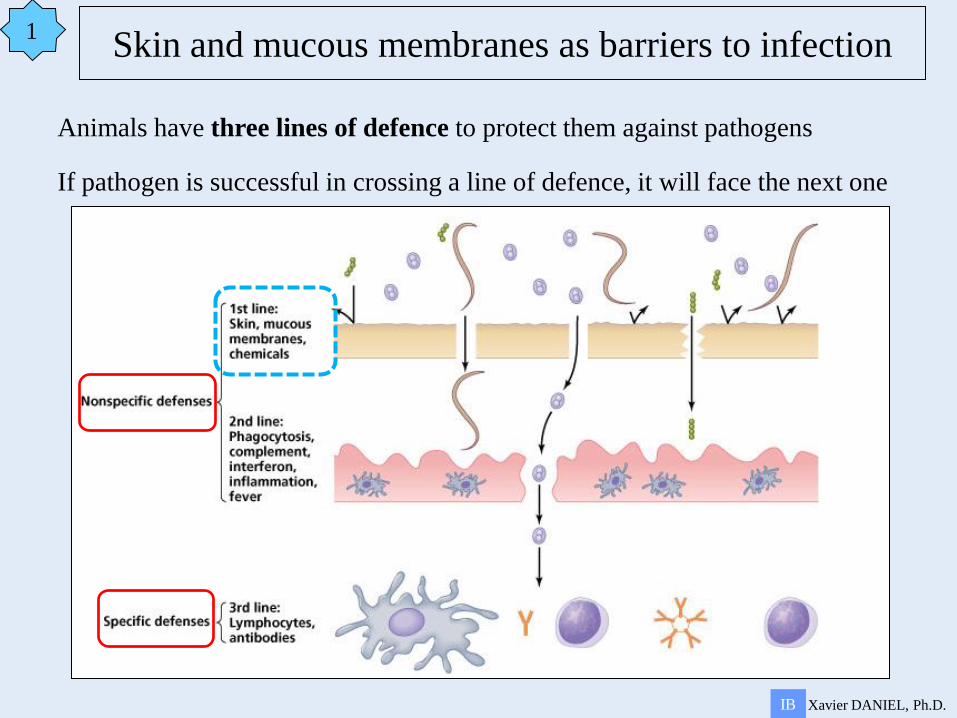
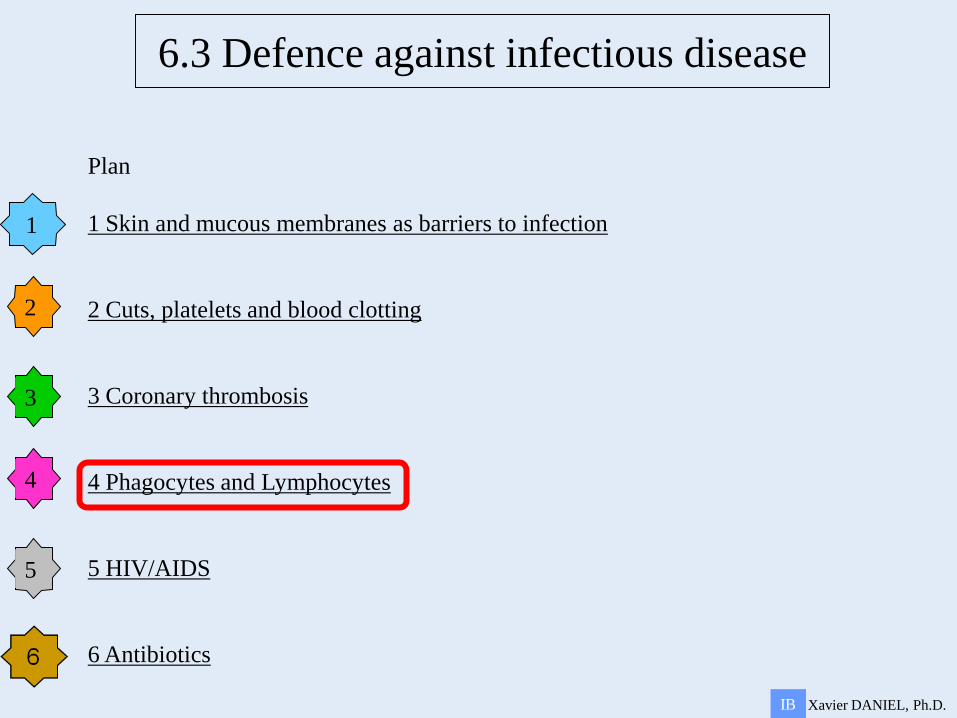
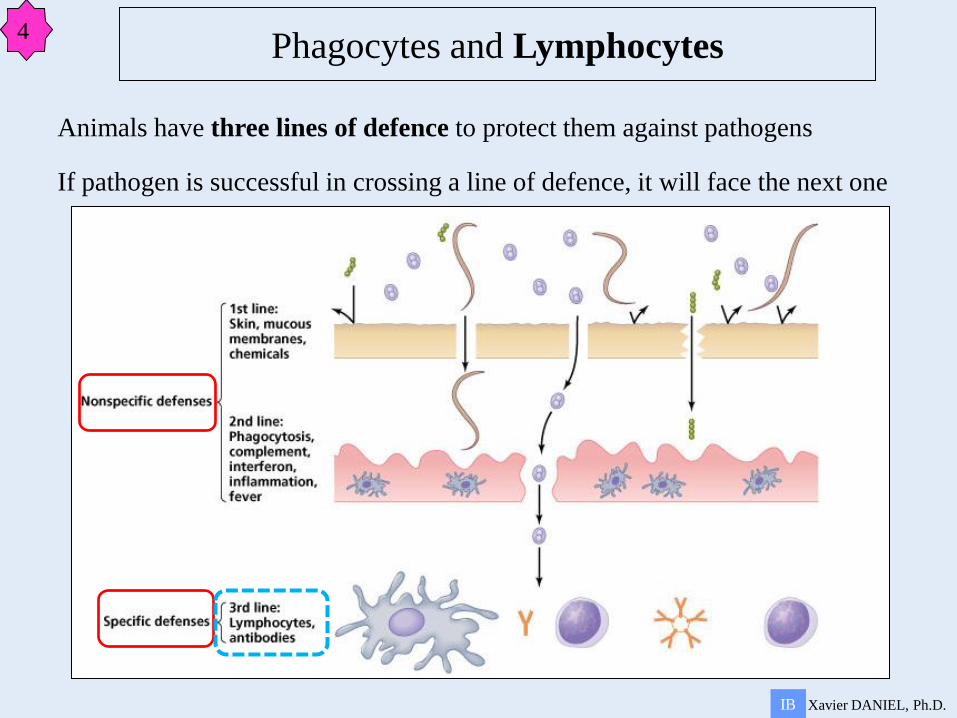
Animals have three lines of defence to protect them against pathogens
If pathogen is successful in crossing a line of defence, it will face the next one
6.3 Defence against infectious disease
Plan
1 Skin and mucous membranes as barriers to infection
2 Cuts, platelets and blood clotting
3 Coronary thrombosis
4 Phagocytes and Lymphocytes
5 HIV/AIDS
6 Antibiotics
2
3
4
1
Xavier DANIEL, Ph.D. IB
5
Xavier DANIEL, Ph.D. IB
Animals have three lines of defence to protect them against pathogens
If pathogen is successful in crossing a line of defence, it will face the next one
Skin and mucous membranes as barriers to infection 1
1
Xavier DANIEL, Ph.D. IB
Skin and mucous membranes as barriers to infection
sweat
1
Xavier DANIEL, Ph.D. IB
Skin and mucous membranes as barriers to infection
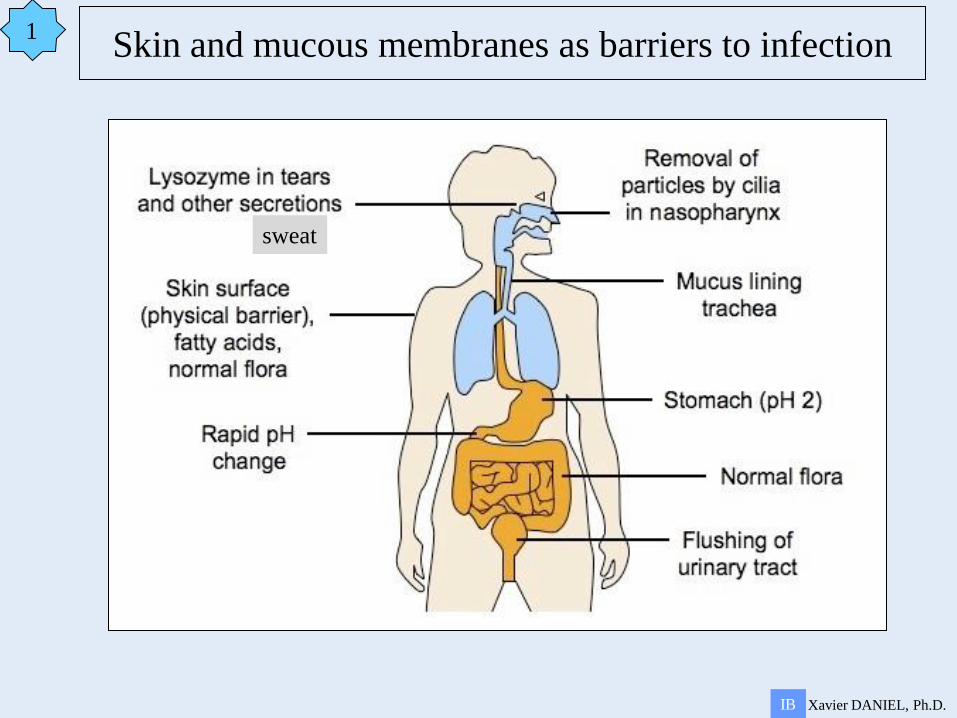
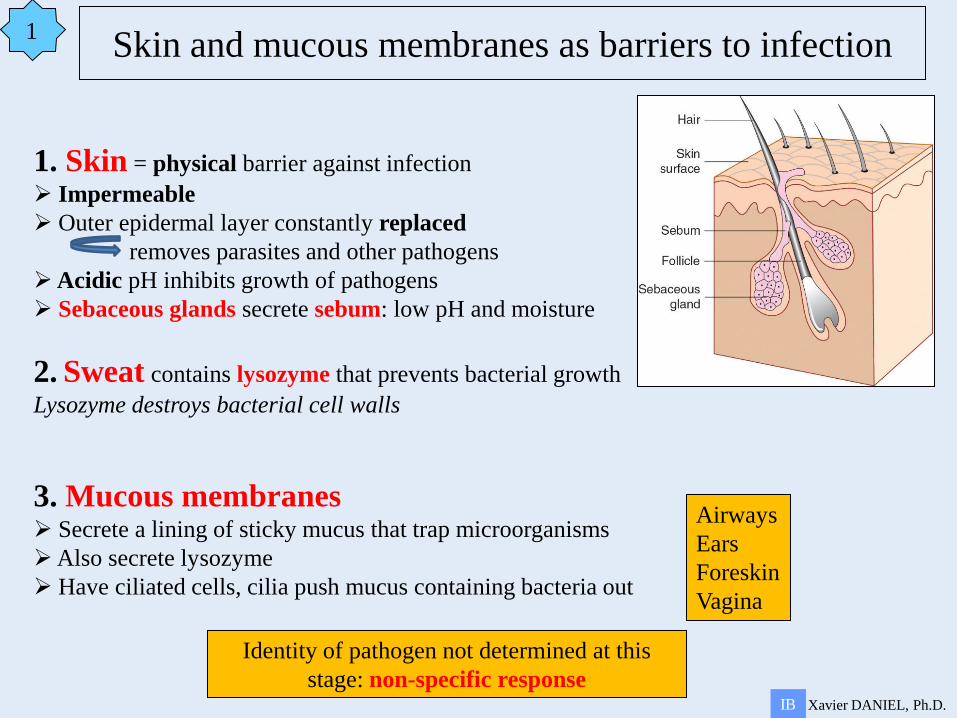
1. Skin = physical barrier against infection
Impermeable
Outer epidermal layer constantly replaced
removes parasites and other pathogens
Acidic pH inhibits growth of pathogens
Sebaceous glands secrete sebum: low pH and moisture
2. Sweat contains lysozyme that prevents bacterial growth
Lysozyme destroys bacterial cell walls
3. Mucous membranes Secrete a lining of sticky mucus that trap microorganisms
Also secrete lysozyme
Have ciliated cells, cilia push mucus containing bacteria out
Airways
Ears
Foreskin
Vagina
Identity of pathogen not determined at this
stage: non-specific response
6.3 Defence against infectious disease
Plan
1 Skin and mucous membranes as barriers to infection
2 Cuts, platelets and blood clotting
3 Coronary thrombosis
4 Phagocytes and Lymphocytes
5 HIV/AIDS
6 Antibiotics
2
3
4
1
Xavier DANIEL, Ph.D. IB
5
Xavier DANIEL, Ph.D. IB
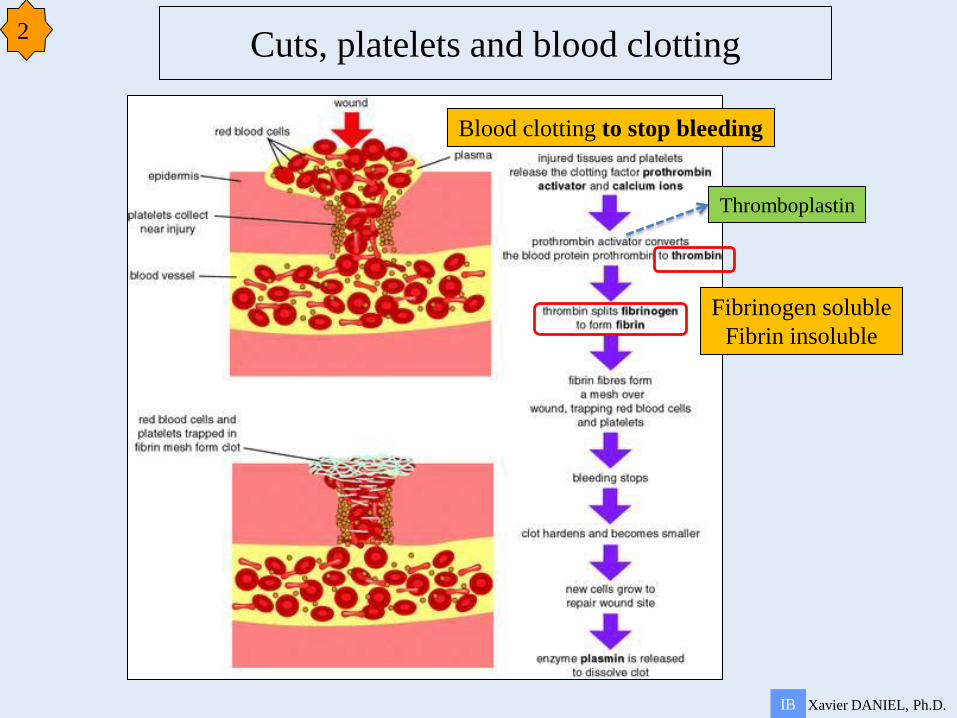
Cuts, platelets and blood clotting 2
Thromboplastin
Blood clotting to stop bleeding
Fibrinogen soluble
Fibrin insoluble
6.3 Defence against infectious disease
Plan
1 Skin and mucous membranes as barriers to infection
2 Cuts, platelets and blood clotting
3 Coronary thrombosis
4 Phagocytes and Lymphocytes
5 HIV/AIDS
6 Antibiotics
2
3
4
1
Xavier DANIEL, Ph.D. IB
5
Xavier DANIEL, Ph.D. IB
Coronary thrombosis 3
Atherosclerosis = progressive degeneration of artery walls
1.Endothelial damage
2.Plaque formation
3.Raised blood pressure
4.Rupture of lining
5.Inflammatory response in lumen
6.Thrombus
7.Embolus
8.Death of cells downstream blood clot
Xavier DANIEL, Ph.D. IB
Coronary thrombosis 3
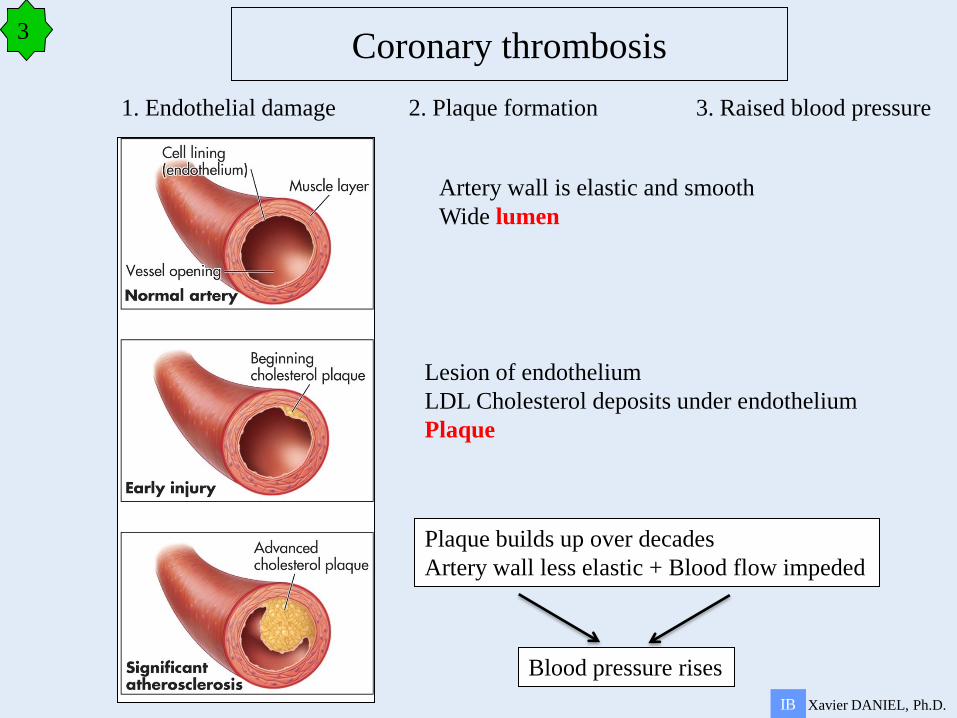
1. Endothelial damage 2. Plaque formation 3. Raised blood pressure
Artery wall is elastic and smooth
Wide lumen
Lesion of endothelium
LDL Cholesterol deposits under endothelium
Plaque
Plaque builds up over decades
Artery wall less elastic + Blood flow impeded
Blood pressure rises
Xavier DANIEL, Ph.D. IB
Coronary thrombosis 3
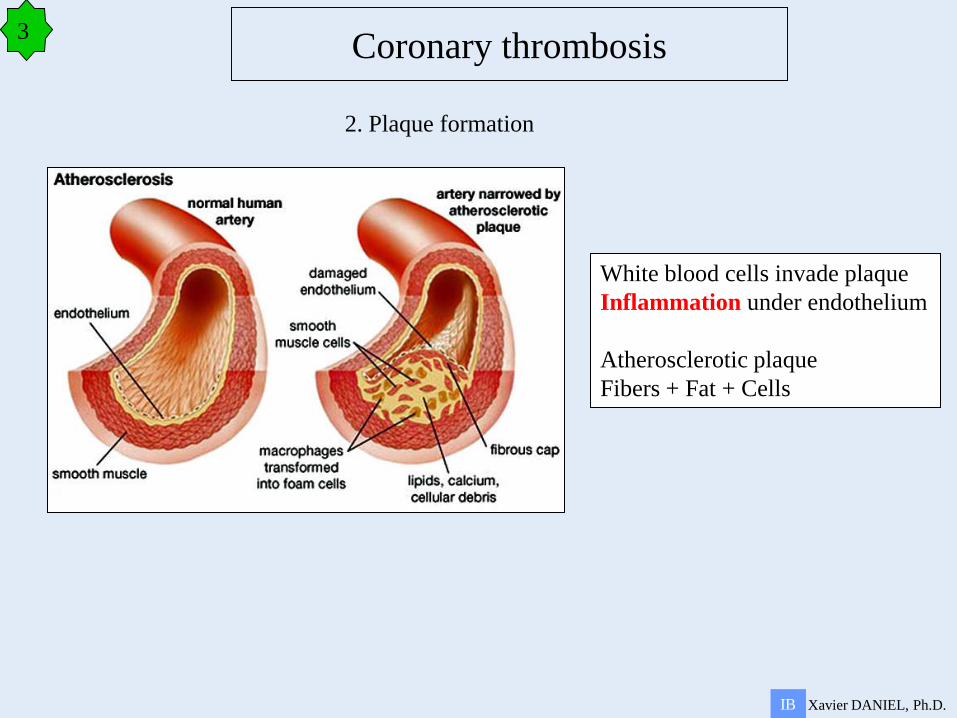
2. Plaque formation
White blood cells invade plaque
Inflammation under endothelium
Atherosclerotic plaque
Fibers + Fat + Cells
Xavier DANIEL, Ph.D. IB
Coronary thrombosis 3
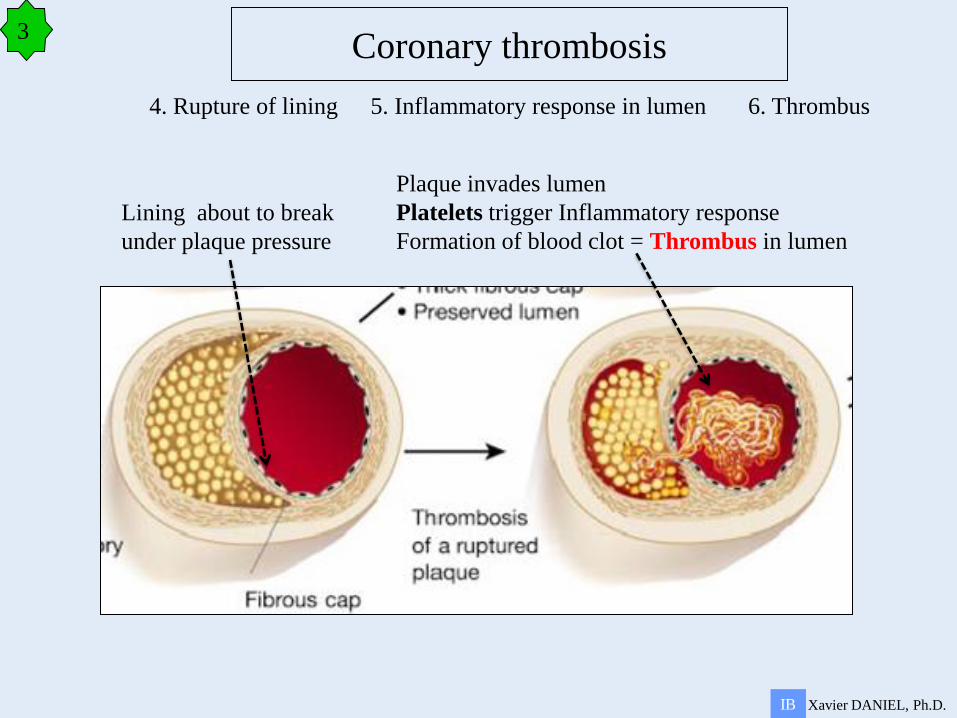
4. Rupture of lining 5. Inflammatory response in lumen 6. Thrombus
Lining about to break
under plaque pressure
Plaque invades lumen
Platelets trigger Inflammatory response
Formation of blood clot = Thrombus in lumen
Xavier DANIEL, Ph.D. IB
Coronary thrombosis 3
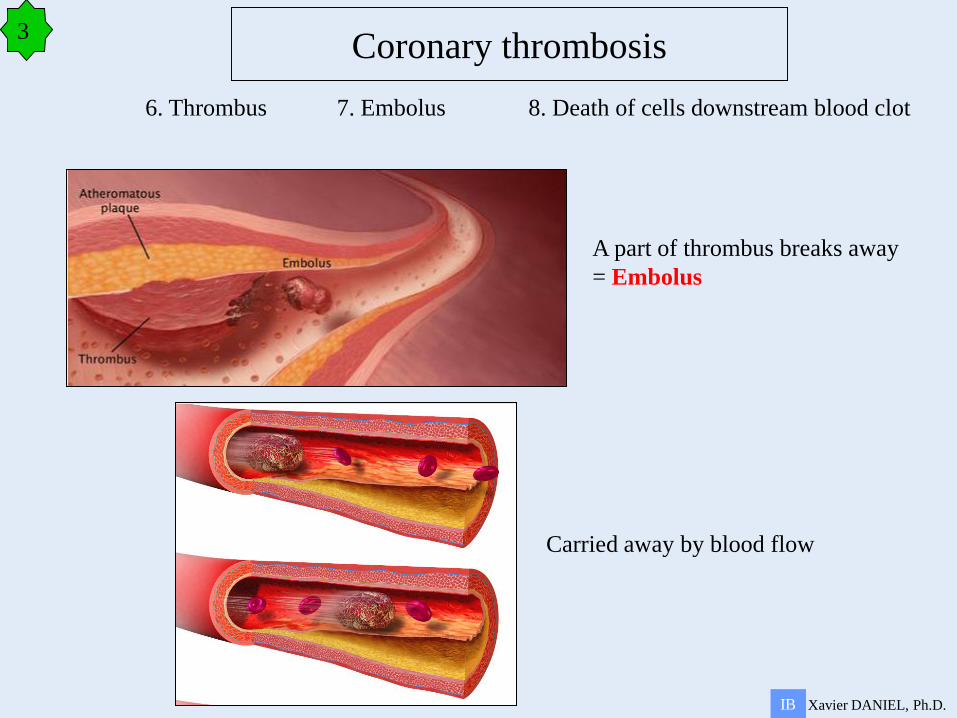
6. Thrombus 7. Embolus 8. Death of cells downstream blood clot
A part of thrombus breaks away
= Embolus
Carried away by blood flow
Xavier DANIEL, Ph.D. IB
Coronary thrombosis 3
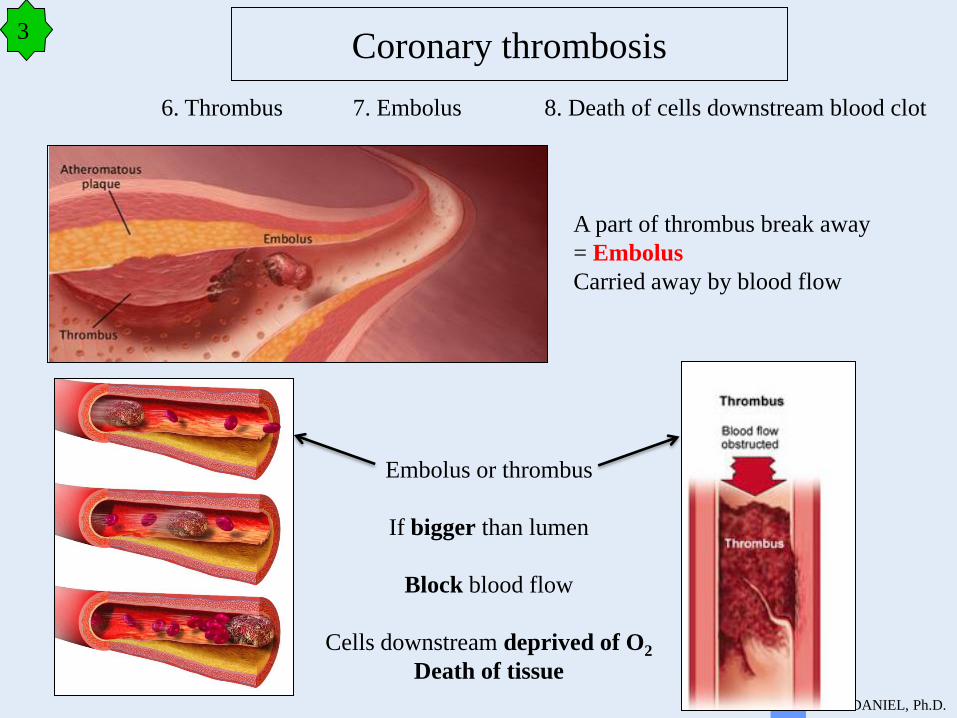
6. Thrombus 7. Embolus 8. Death of cells downstream blood clot
A part of thrombus break away
= Embolus
Carried away by blood flow
Embolus or thrombus
If bigger than lumen
Block blood flow
Cells downstream deprived of O2
Death of tissue
Xavier DANIEL, Ph.D. IB
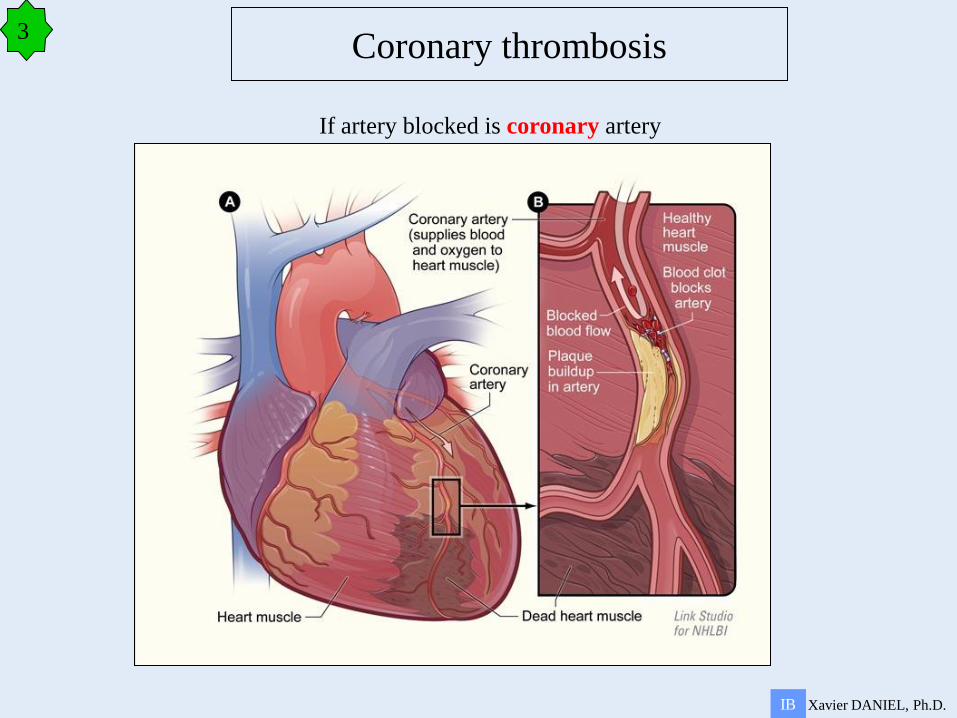
Coronary thrombosis 3
If artery blocked is coronary artery
Xavier DANIEL, Ph.D. IB
Coronary thrombosis 3
Main factors increasing risks of coronary thrombosis
Smoking
High blood cholesterol concentration
High blood pressure
Diabetes I and II
Obesity
Lack of exercise
Xavier DANIEL, Ph.D. IB
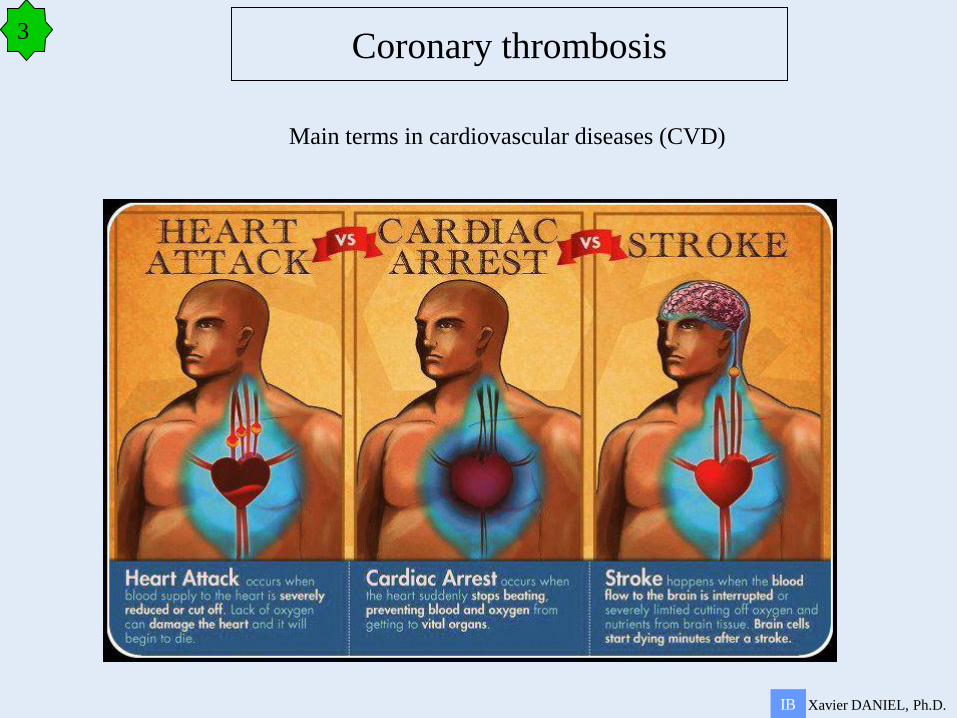
Coronary thrombosis 3
Main terms in cardiovascular diseases (CVD)
6.3 Defence against infectious disease
Plan
1 Skin and mucous membranes as barriers to infection
2 Cuts, platelets and blood clotting
3 Coronary thrombosis
4 Phagocytes and Lymphocytes
5 HIV/AIDS
6 Antibiotics
2
3
4
1
Xavier DANIEL, Ph.D. IB
5
Xavier DANIEL, Ph.D. IB
Animals have three lines of defence to protect them against pathogens
If pathogen is successful in crossing a line of defence, it will face the next one
Phagocytes and Lymphocytes 4
Xavier DANIEL, Ph.D. IB
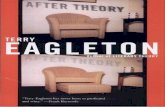
Phagocytes and Lymphocytes 4
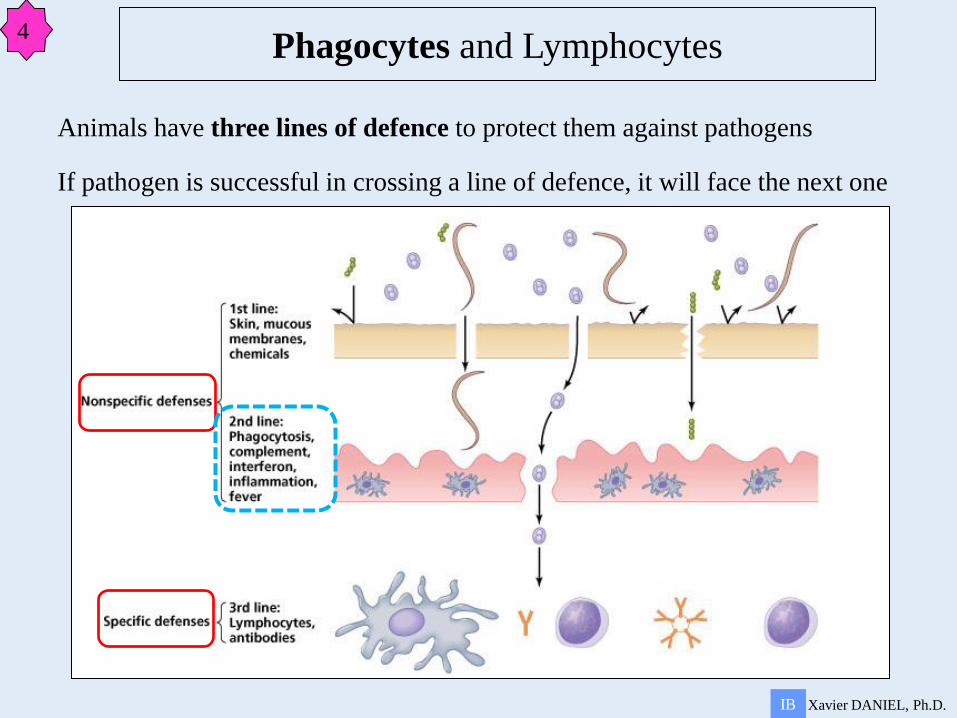
Pathogen crosses the first line of defence
Pathogen enters the body
Second line of defence = white blood cells
Many kinds of WBC, i.e. Macrophages (= Phagocytes) and Lymphocytes
All cells have specific proteins on their surface
Cells of the body have self proteins on their surface
Pathogens have non-self proteins on their surface
Phagocytes recognize non-self
Change shape to engulf pathogen: phagocytosis
Identity of pathogen not determined at this
stage: non-specific response
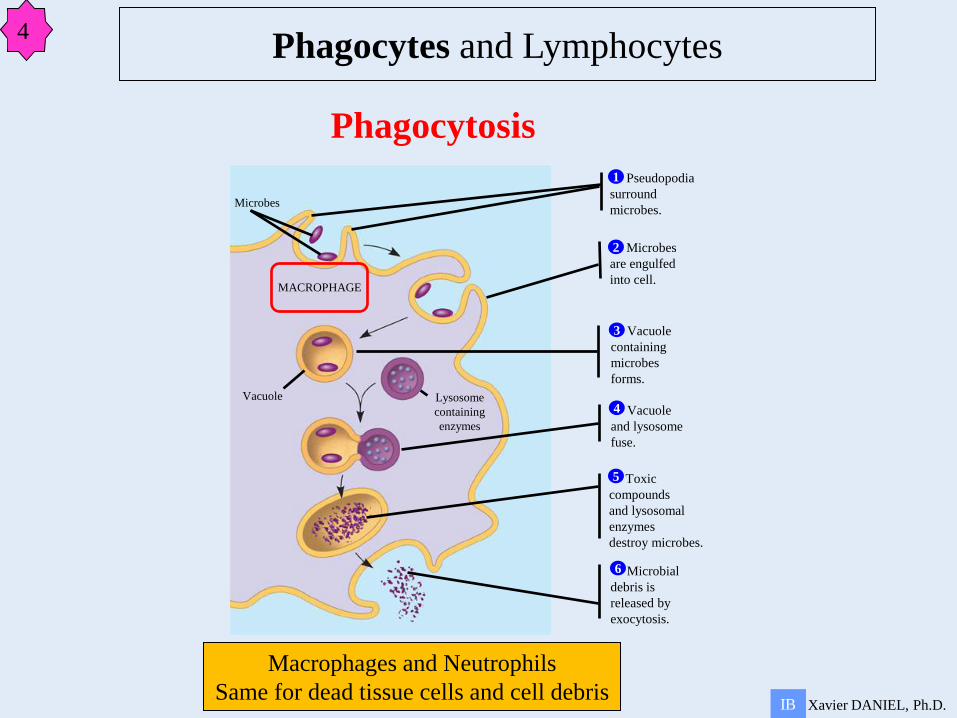
Macrophages and Neutrophils
Same for dead tissue cells and cell debris Xavier DANIEL, Ph.D. IB
Pseudopodia
surround
microbes.
1
Microbes
are engulfed
into cell.
2
Vacuole
containing
microbes
forms.
3
Vacuole
and lysosome
fuse.
4
Toxic
compounds
and lysosomal
enzymes
destroy microbes.
5
Microbial
debris is
released by
exocytosis.
6
Microbes
MACROPHAGE
Vacuole Lysosome
containing
enzymes
Phagocytosis
Phagocytes and Lymphocytes 4
Xavier DANIEL, Ph.D. IB
Animals have three lines of defence to protect them against pathogens
If pathogen is successful in crossing a line of defence, it will face the next one
Phagocytes and Lymphocytes 4
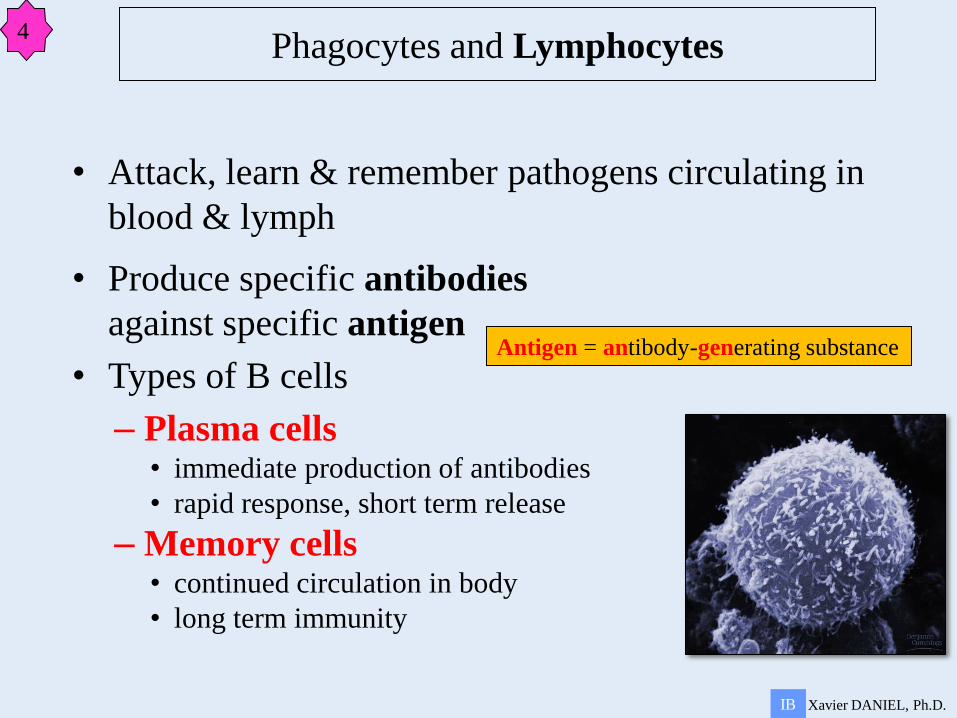
• Attack, learn & remember pathogens circulating in
blood & lymph
• Produce specific antibodies
against specific antigen
• Types of B cells
– Plasma cells • immediate production of antibodies
• rapid response, short term release
– Memory cells • continued circulation in body
• long term immunity
Xavier DANIEL, Ph.D. IB
Phagocytes and Lymphocytes 4
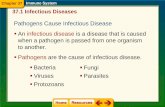
Antigen = antibody-generating substance
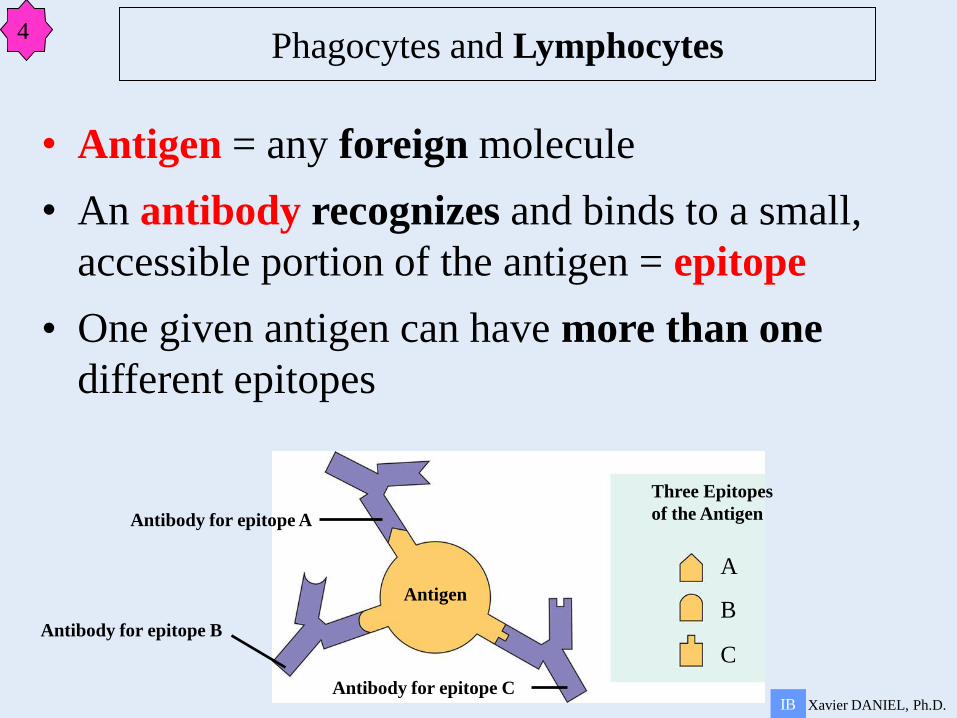
Antibody for epitope A
Antigen
Antibody for epitope B
Antibody for epitope C
Three Epitopes
of the Antigen
• Antigen = any foreign molecule
• An antibody recognizes and binds to a small,
accessible portion of the antigen = epitope
• One given antigen can have more than one
different epitopes
A
B
C
Xavier DANIEL, Ph.D. IB
Phagocytes and Lymphocytes 4
s s
s s
s s
s s
s s
s s
s s
s s
s s
s s
s
s s
s s
s
s s
s s
s s
s s
s s
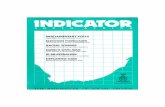
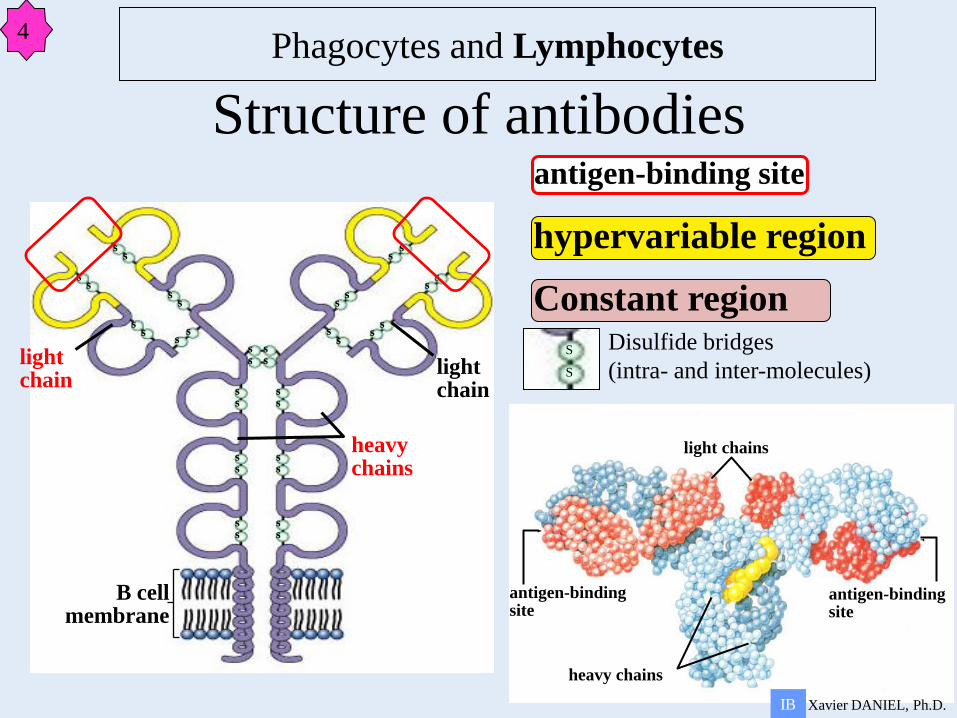
Structure of antibodies
light chains
antigen-binding site
heavy chains
antigen-binding site
light chain
B cell membrane
heavy chains
light chain
hypervariable region
antigen-binding site
Constant region
S
S
Disulfide bridges
(intra- and inter-molecules)
Xavier DANIEL, Ph.D. IB
Phagocytes and Lymphocytes 4
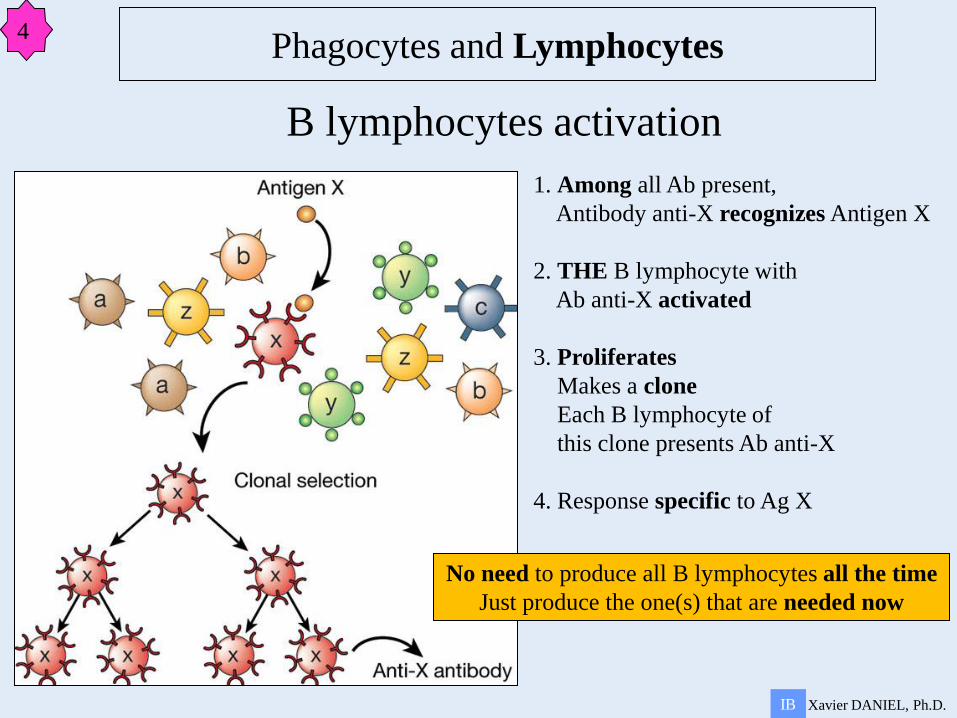
1. Among all Ab present,
Antibody anti-X recognizes Antigen X
2. THE B lymphocyte with
Ab anti-X activated
3. Proliferates
Makes a clone
Each B lymphocyte of
this clone presents Ab anti-X
4. Response specific to Ag X
B lymphocytes activation
No need to produce all B lymphocytes all the time
Just produce the one(s) that are needed now
Xavier DANIEL, Ph.D. IB
Phagocytes and Lymphocytes 4
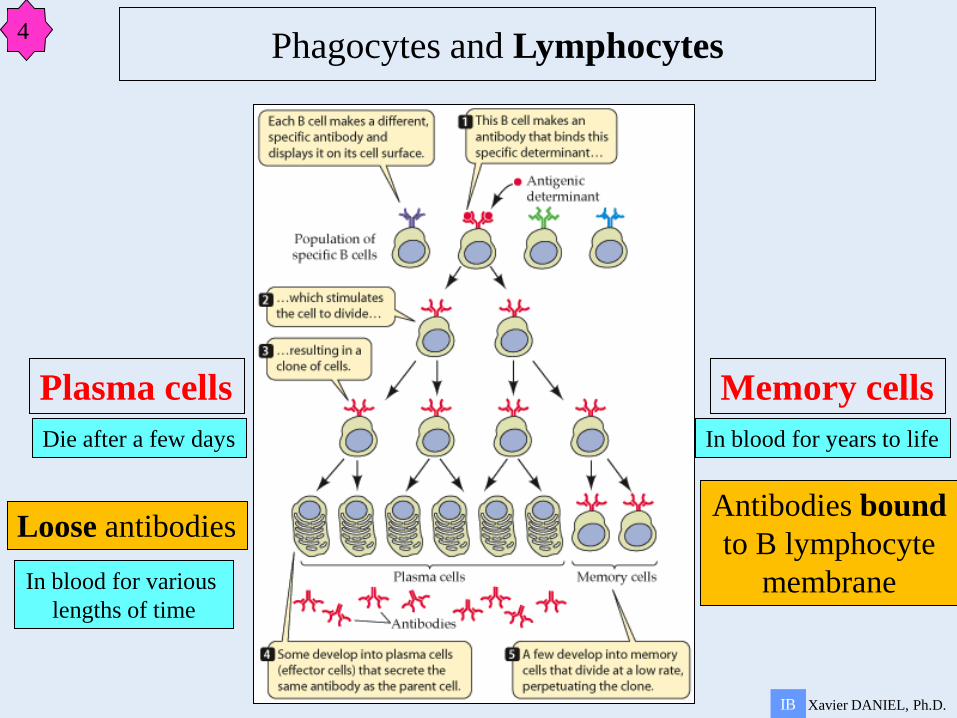
Loose antibodies Antibodies bound
to B lymphocyte
membrane
Plasma cells Memory cells
Die after a few days
In blood for various
lengths of time
In blood for years to life
Xavier DANIEL, Ph.D. IB
Phagocytes and Lymphocytes 4
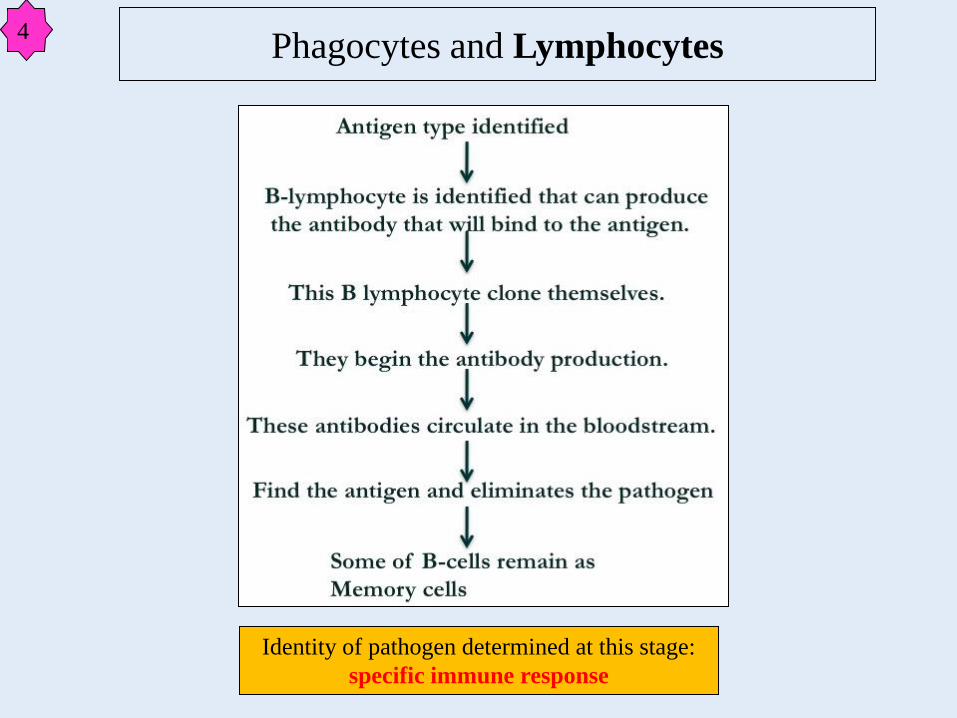
Phagocytes and Lymphocytes 4
Identity of pathogen determined at this stage:
specific immune response
• “Anti-self” B lymphocytes are destroyed
before Clonal Selection
– This has to occur since the antigen receptors are
formed from RANDOM gene rearrangements
– Could accidentally produce a receptor that
recognizes a body cell/molecule
– Autoimmune diseases result when clonal
selection fails
B lymphocytes activation
Xavier DANIEL, Ph.D. IB
Phagocytes and Lymphocytes 4
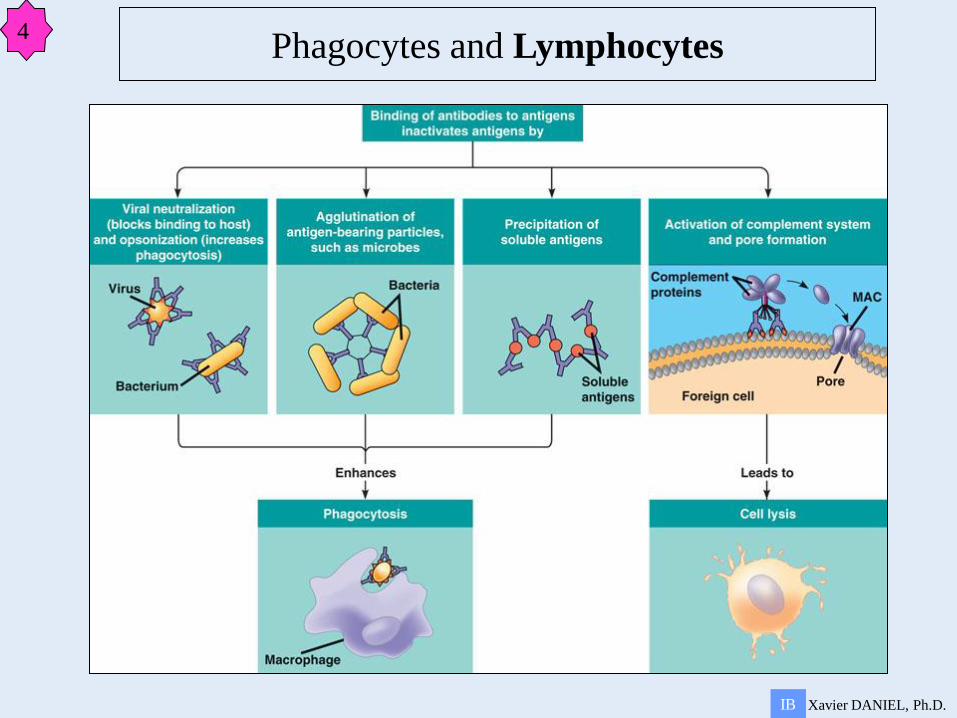
Neutralization
Loose antibodies
Plasma cells
production
Agglutination Precipitation Cell lysis
Xavier DANIEL, Ph.D. IB
Phagocytes and Lymphocytes 4
Xavier DANIEL, Ph.D. IB
Phagocytes and Lymphocytes 4
6.3 Defence against infectious disease
Plan
1 Skin and mucous membranes as barriers to infection
2 Cuts, platelets and blood clotting
3 Coronary thrombosis
4 Phagocytes and Lymphocytes
5 HIV/AIDS
6 Antibiotics
2
3
4
1
Xavier DANIEL, Ph.D. IB
5
Xavier DANIEL, Ph.D. IB
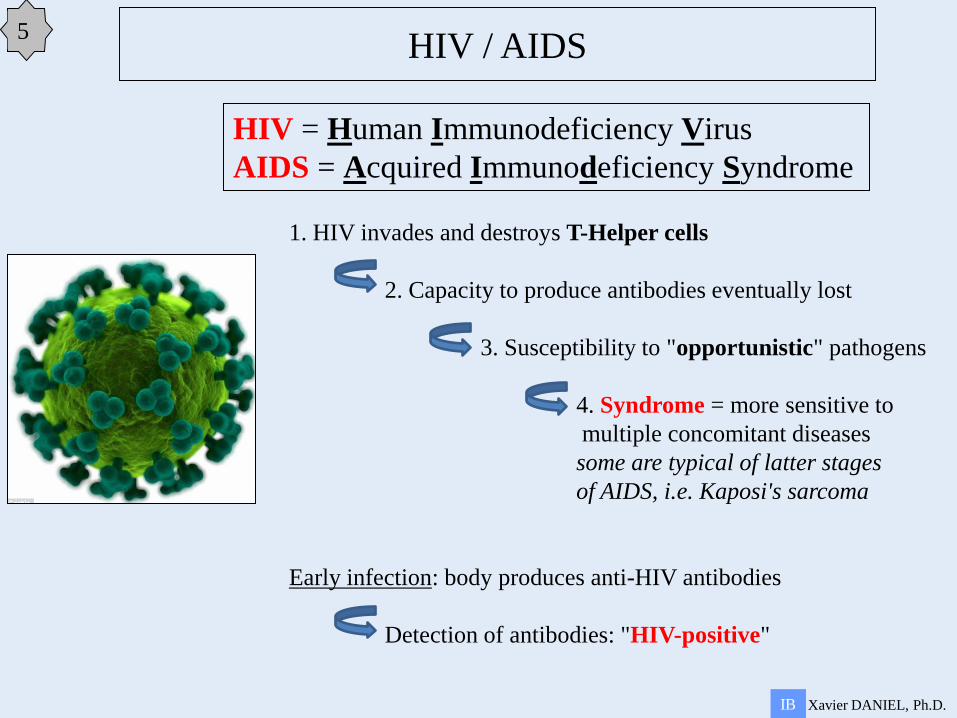
HIV / AIDS 5
HIV = Human Immunodeficiency Virus
AIDS = Acquired Immunodeficiency Syndrome
1. HIV invades and destroys T-Helper cells
2. Capacity to produce antibodies eventually lost
3. Susceptibility to "opportunistic" pathogens
4. Syndrome = more sensitive to
multiple concomitant diseases
some are typical of latter stages
of AIDS, i.e. Kaposi's sarcoma
Early infection: body produces anti-HIV antibodies
Detection of antibodies: "HIV-positive"
Xavier DANIEL, Ph.D. IB
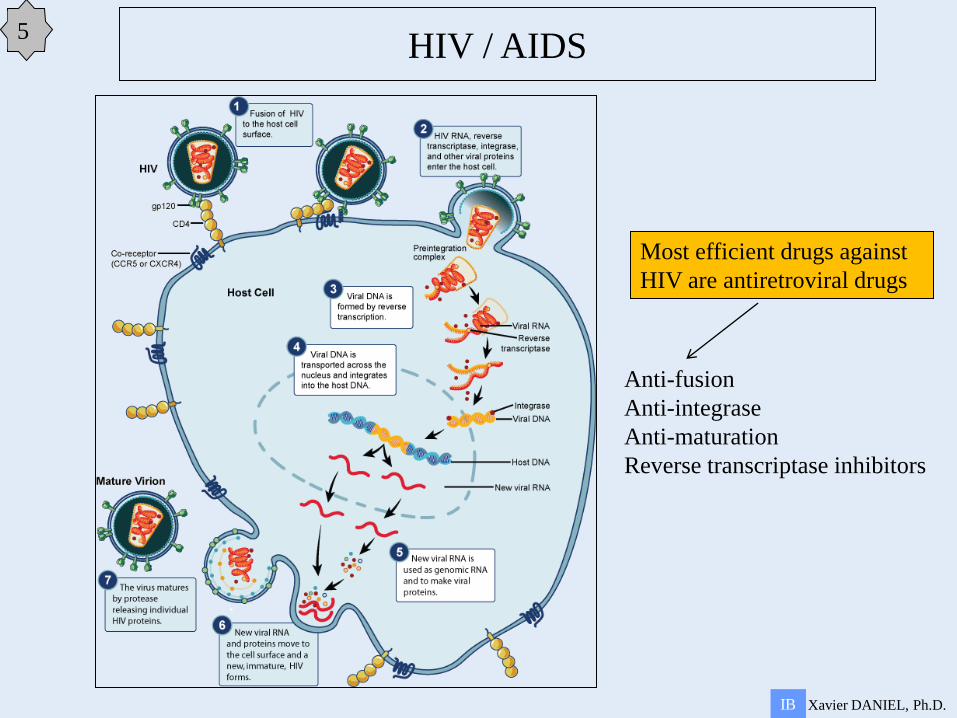
HIV / AIDS 5
Most efficient drugs against
HIV are antiretroviral drugs
Anti-fusion
Anti-integrase
Anti-maturation
Reverse transcriptase inhibitors
Xavier DANIEL, Ph.D. IB
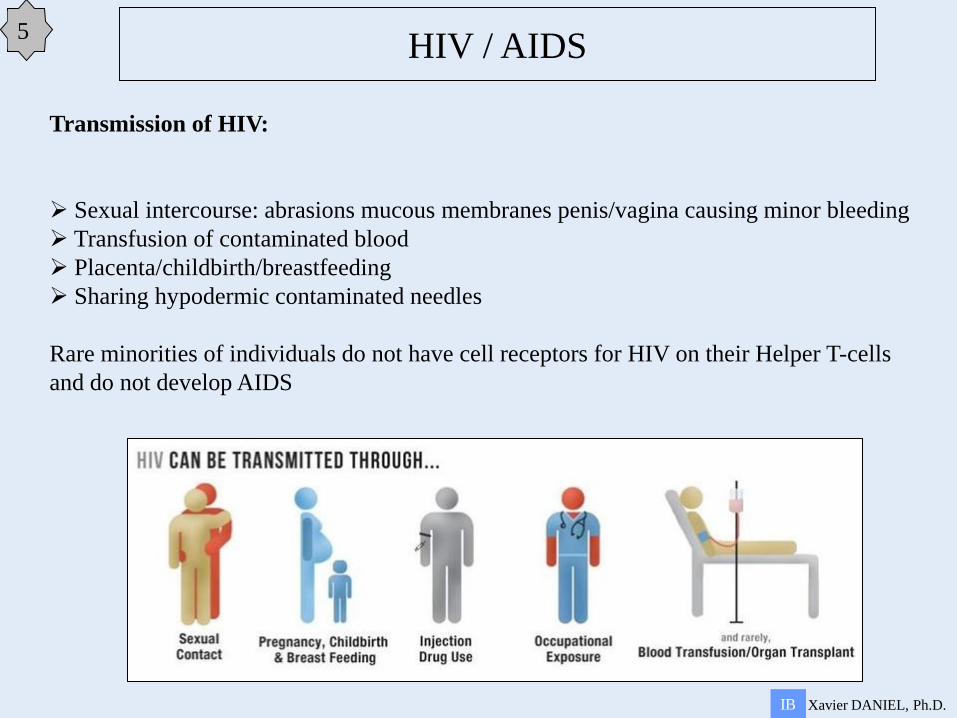
HIV / AIDS 5
Transmission of HIV:
Sexual intercourse: abrasions mucous membranes penis/vagina causing minor bleeding
Transfusion of contaminated blood
Placenta/childbirth/breastfeeding
Sharing hypodermic contaminated needles
Rare minorities of individuals do not have cell receptors for HIV on their Helper T-cells
and do not develop AIDS
6.3 Defence against infectious disease
Plan
1 Skin and mucous membranes as barriers to infection
2 Cuts, platelets and blood clotting
3 Coronary thrombosis
4 Phagocytes and Lymphocytes
5 HIV/AIDS
6 Antibiotics
2
3
4
1
Xavier DANIEL, Ph.D. IB
5
Xavier DANIEL, Ph.D. IB
Antibiotics
Antibiotics can be
Antibiotic : anti life
Only living organisms are affected by ATB
Viruses are NOT targets of ATB
Most ATB target bacterial pathogens
Prokaryotes (bacteria) and eukaryotes show differences in metabolism
ATB take advantages of these differences
ATB are specific for prokaryotic metabolic processes
Antibiotics = chemicals that can kill or damage prokaryotic cells but not eukaryotic cells
bactericidal (kill bacteria)
bacteriostatic (making bacteria inactive)
Xavier DANIEL, Ph.D. IB
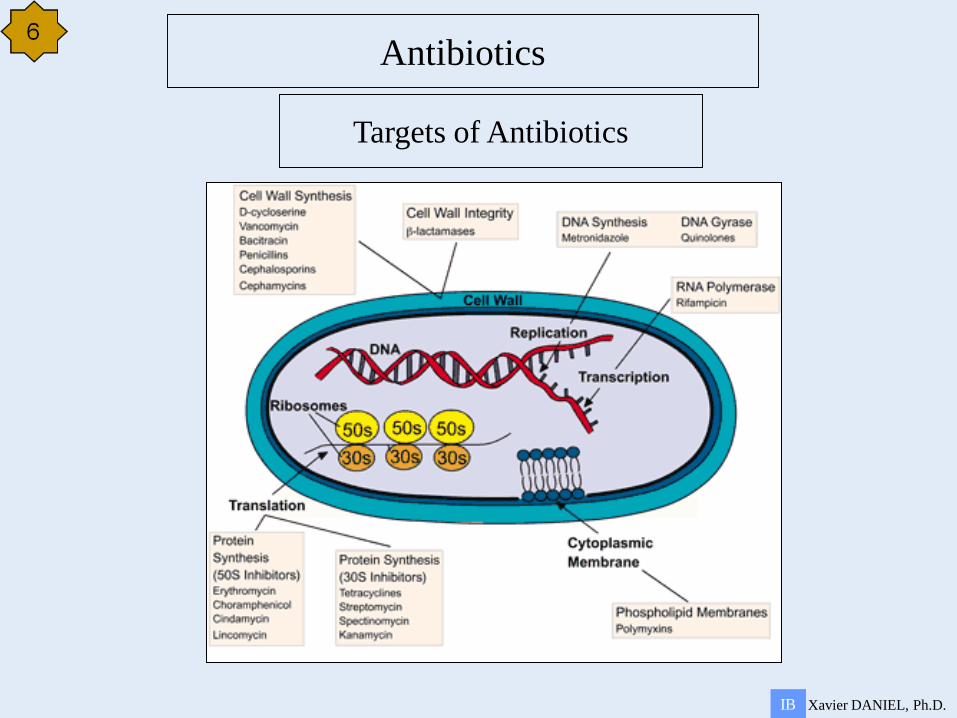
Antibiotics
Targets of Antibiotics
Xavier DANIEL, Ph.D. IB
Antibiotics
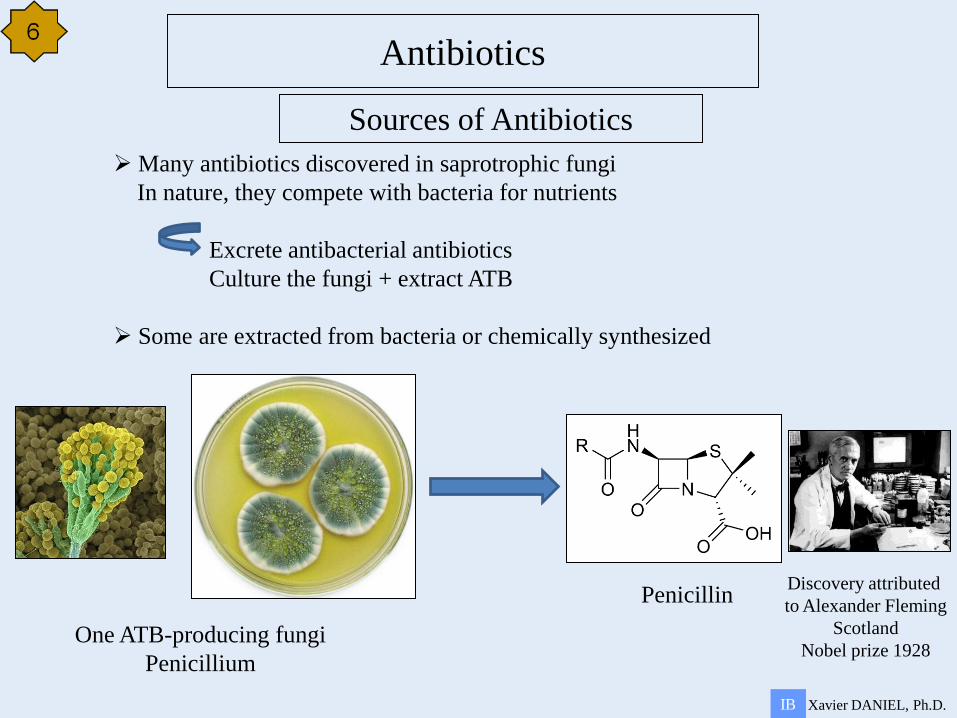
Many antibiotics discovered in saprotrophic fungi
In nature, they compete with bacteria for nutrients
Excrete antibacterial antibiotics
Culture the fungi + extract ATB
Some are extracted from bacteria or chemically synthesized
One ATB-producing fungi
Penicillium
Penicillin Discovery attributed
to Alexander Fleming
Scotland
Nobel prize 1928
Sources of Antibiotics
Xavier DANIEL, Ph.D. IB
Antibiotics
Testing Penicillin
Stage 1:Growing the penicillin
This was a combination of the latest freeze-drying technology and some much more traditional equipment: thousands of milk bottles (in which to grow the bacteria), milk churns, a dog bath and a
hand pump! From this, the team were able to gather a few grams of pure penicillin.
Stage 2: Testing penicillin on animals
There was enough penicillin to test it on eight mice. They were injected with a deadly bacteria (streptococci). Four of the mice were then given penicillin. 24 hours later the mice which had not
been injected with penicillin were dead. Those who had been injected were healthy.
Stage 3: The first human trial of penicillin
By 1941 the team had enough penicillin to test it on a human. The patient had terrible abscesses which had spread from his mouth to his scalp, eyes, arm and even his lung. He was going to die –
there was nothing to lose by trying penicillin. After four days of treatment he was much improved and was sitting up in bed – penicillin worked. However, they did not have enough, and after five days the
supply ran out – the patient relapsed and died.
Xavier DANIEL, Ph.D. IB
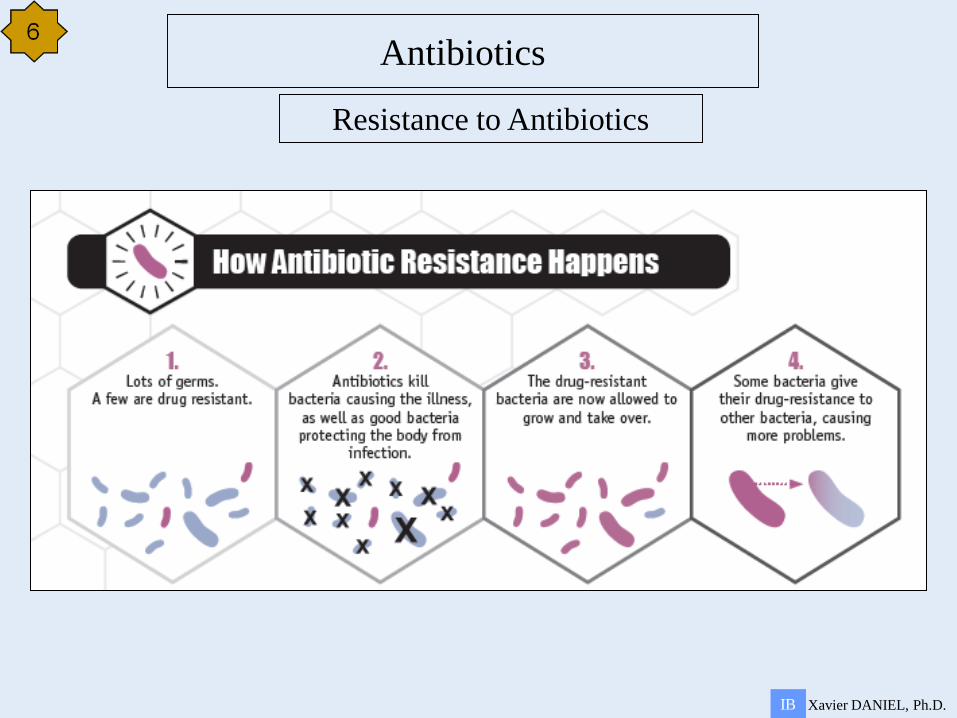
Antibiotics
Resistance to Antibiotics
Xavier DANIEL, Ph.D. IB
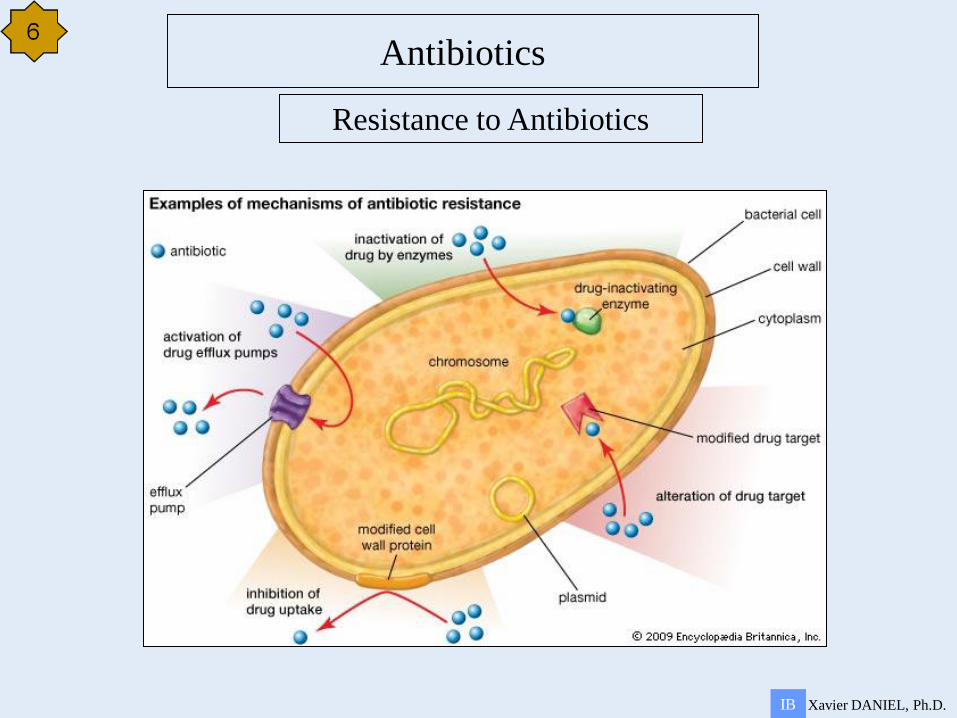
Antibiotics
Resistance to Antibiotics
Xavier DANIEL, Ph.D. IB
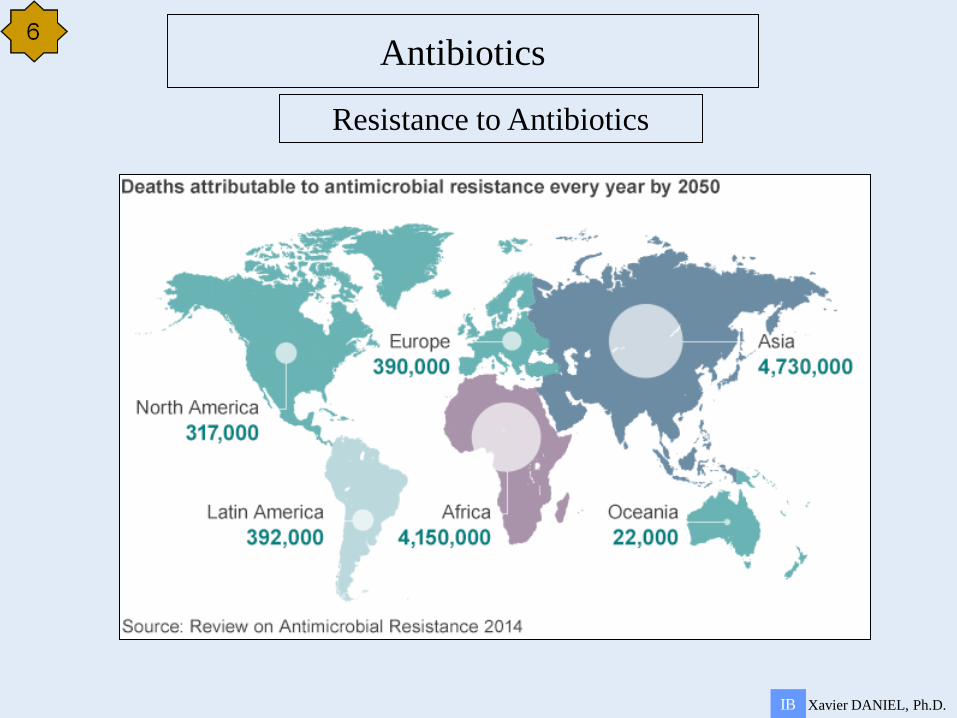
Antibiotics
Resistance to Antibiotics
Xavier DANIEL, Ph.D. IB
Antibiotics
Resistance to Antibiotics
Required measures
Doctors prescribe ATB only for serious bacterial infections
Patients complete full courses of ATB to eliminate the infections completely
High hygiene standards maintained in hospitals to prevent cross-infections
Farmers not using ATB in animals feeding
Develop new ATB