Treatment of chronic myeloid leukaemia in first chronic phase with idarubicin and cytarabine:...
8
Treatment of chronic myeloid leukaemia in first chronic phase with idarubicin and cytarabine: mobilization of Philadelphia-negative peripheral blood stem cells E. A. C HALMERS , 1 I. M. F RANKLIN, 1 S. M. K ELSEY, 2 A. C. NEWLAND, 2 R. E. C LARK , 3 A. M. S PROUL , 1 G. C ROTTY, 4 S. R. MC C ANN, 4 A. F IELDING , 5 A. H. G OLDSTONE , 5 A. H EPPLESTONE , 6 W. WATSON, 7 R. A. S HARP 8 AND P. TANSEY 8 1 Glasgow Royal Infirmary, 2 Royal London Hospital, 3 Royal Liverpool Hospital, 4 St James’ Hospital Dublin, 5 University College London Hospital, 6 Ninewells Hospital Dundee, 7 Monklands Hospital, Airdrie, 8 Victoria Infirmary, Glasgow Received 28 June 1996; accepted for publication 7 November 1996 Summary. Peripheral blood stem cell (PBSC) mobilization using idarubicin and cytarabine was investigated in 40 patients with chronic myeloid leukaemia in first chronic phase (CML CP1). Disease contamination was evaluated in harvests from 41/44 (93%) mobilization episodes. Using cytogenetics, 22/37 (59%) showed a complete or major response; Southern blot analysis demonstrated a complete or major response in 9/17 (53%). No harvests were RT-PCR negative. In the 41 evaluable episodes, more complete or major responses were seen when PBSC mobilization occurred within 24 months [17/23 (74%) versus 6/18 (33%); P ¼ 0 : 02] and within 12 months of diagnosis [10/11 (91%) versus 13/30 (43%); P ¼ 0 : 018]. 20 patients under- went PBSC transplantation and 18/20 successfully engrafted. Post-transplant cytogenetic analysis was available on 15 cases, of whom five achieved a major cytogenetic response at 1–3 months, with five partial cytogenetic remissions. Two of 40 patients died during mobilization therapy (5%) and three of 20 after the transplant (15%). Overall mortality was high at five of 40 patients, and the procedural mortality was 20%. This study demonstrates that Ph-negative PBSCs can be mobilized in a significant proportion of patients with CML CP1, with the best results observed within a year of diagnosis. These cells can subsequently be used for autologous transplantation, how- ever, the impact on long-term survival requires longer follow-up, and potential benefits may be compromised by the high mortality. Keywords: chronic myeloid leukaemia, peripheral blood stem cells, autologous transplantation, idarubicin, cytarabine. For the majority of patients with chronic myeloid leukaemia (CML), current treatment strategies remain unsatisfactory, Allogeneic bone marrow transplantation (BMT) is potentially curative and can result in prolonged disease-free survival, but its use is restricted to younger patients for whom a suitably matched donor can be found (Kantarjian et al, 1993). Alpha interferon (IFN-a) has recently been shown to prolong survival when compared with conventional chemotherapy, but only a relative small percentage of patients actually achieve a complete cytogenetic response with this agent (Italian Cooperative Study Group on Chronic Myeloid Leukaemia, 1994; Allan et al, 1995). Autologous transplantation carried out in advanced stage disease, using bone marrow or peripheral blood cells collected at diagnosis, can temporarily restore chronic phase (CP) in a proportion of cases and if performed during first chronic phase (CP1), may prolong survival (Butturini et al, 1990; Hoyle et al, 1994; McGlave et al, 1994). It has also been noted that in some cases transient restoration of Ph-negative haemopoiesis occurs following autologous transplantation and convincing evidence now exists to support the presence of residual Ph negative cells in many patients with CML, at least in the early stages of their disease (Butturini et al, 1990; Leemhuis et al, 1993). These observations have generated considerable interest in attempts to select out putatively normal Ph-negative progenitor cells for subsequent reinfusion following high- dose therapy. Various approaches are currently under British Journal of Haematology , 1997, 96, 627–634 627 q 1997 Blackwell Science Ltd Correspondence: Professor Ian M. Franklin, Department of Medicine, Glasgow Royal Infirmary, Alexandra Parade, Glasgow G31 2ER.
-
Upload
xn--jhhjhkl-rbb -
Category
Documents
-
view
0 -
download
0
Transcript of Treatment of chronic myeloid leukaemia in first chronic phase with idarubicin and cytarabine:...

Treatment of chronic myeloid leukaemia in first chronic phasewith idarubicin and cytarabine: mobilization ofPhiladelphia-negative peripheral blood stem cells
E. A. CHALMERS,1 I. M. FRANKLIN,1 S. M. KELSEY,2 A. C. NEWL AND,2 R. E. CLARK,3 A. M. SPRO UL,1 G. CROTTY,4
S. R. MCCANN,4 A. FIELDING,5 A. H. GOLDSTONE,5 A. HEPPLES TONE,6 W. WATSON,7 R. A. SHARP8
AND P. TANSEY8
1Glasgow Royal Infirmary, 2Royal London Hospital, 3Royal Liverpool Hospital, 4St James’ Hospital Dublin,5University College London Hospital, 6Ninewells Hospital Dundee, 7Monklands Hospital, Airdrie,8Victoria Infirmary, Glasgow
Received 28 June 1996; accepted for publication 7 November 1996
Summary. Peripheral blood stem cell (PBSC) mobilizationusing idarubicin and cytarabine was investigated in 40patients with chronic myeloid leukaemia in first chronicphase (CML CP1). Disease contamination was evaluated inharvests from 41/44 (93%) mobilization episodes. Usingcytogenetics, 22/37 (59%) showed a complete or majorresponse; Southern blot analysis demonstrated a complete ormajor response in 9/17 (53%). No harvests were RT-PCRnegative. In the 41 evaluable episodes, more complete ormajor responses were seen when PBSC mobilizationoccurred within 24 months [17/23 (74%) versus 6/18(33%); P ¼ 0:02] and within 12 months of diagnosis [10/11(91%) versus 13/30 (43%); P ¼ 0:018]. 20 patients under-went PBSC transplantation and 18/20 successfullyengrafted. Post-transplant cytogenetic analysis was availableon 15 cases, of whom five achieved a major cytogenetic
response at 1–3 months, with five partial cytogeneticremissions. Two of 40 patients died during mobilizationtherapy (5%) and three of 20 after the transplant (15%).Overall mortality was high at five of 40 patients, and theprocedural mortality was 20%. This study demonstrates thatPh-negative PBSCs can be mobilized in a significantproportion of patients with CML CP1, with the best resultsobserved within a year of diagnosis. These cells cansubsequently be used for autologous transplantation, how-ever, the impact on long-term survival requires longerfollow-up, and potential benefits may be compromised by thehigh mortality.
Keywords: chronic myeloid leukaemia, peripheral blood stemcells, autologous transplantation, idarubicin, cytarabine.
For the majority of patients with chronic myeloidleukaemia (CML), current treatment strategies remainunsatisfactory, Allogeneic bone marrow transplantation(BMT) is potentially curative and can result in prolongeddisease-free survival, but its use is restricted to youngerpatients for whom a suitably matched donor can befound (Kantarjian et al, 1993). Alpha interferon (IFN-a)has recently been shown to prolong survival whencompared with conventional chemotherapy, but only arelative small percentage of patients actually achieve acomplete cytogenetic response with this agent (ItalianCooperative Study Group on Chronic Myeloid Leukaemia,1994; Allan et al, 1995).
Autologous transplantation carried out in advanced stagedisease, using bone marrow or peripheral blood cellscollected at diagnosis, can temporarily restore chronicphase (CP) in a proportion of cases and if performed duringfirst chronic phase (CP1), may prolong survival (Butturiniet al, 1990; Hoyle et al, 1994; McGlave et al, 1994). It hasalso been noted that in some cases transient restoration ofPh-negative haemopoiesis occurs following autologoustransplantation and convincing evidence now exists tosupport the presence of residual Ph negative cells in manypatients with CML, at least in the early stages of their disease(Butturini et al, 1990; Leemhuis et al, 1993).
These observations have generated considerable interestin attempts to select out putatively normal Ph-negativeprogenitor cells for subsequent reinfusion following high-dose therapy. Various approaches are currently under
British Journal of Haematology, 1997, 96, 627–634
627q 1997 Blackwell Science Ltd
Correspondence: Professor Ian M. Franklin, Department of Medicine,Glasgow Royal Infirmary, Alexandra Parade, Glasgow G31 2ER.

investigation for the selection of Ph-negative progenitor cellsincluding in vitro purging techniques using chemotherapy,antisense oligonucleotides and long-term liquid cultures(Carlo-Stella et al, 1991; Kirkland et al, 1993; Barnett et al,1994). An alternative approach involves the collection ofperipheral blood stem cells (PBSCs) during the earlyregenerative phase following myelosuppressive chemo-therapy when, at least in some cases, Ph-negative progenitorcells appear to have a short-term growth advantage. Thisapproach was originally investigated by Carella et al (1993a, b),who reported the successful mobilization of PBSCs whichwere not only Ph-negative by cytogenetic analysis, but werealso negative by polymerase chain reaction (PCR) in somecases when the bcr-abl transcript was sought by reversetranscriptase (RT)-PCR. We have recently investigated thisapproach in a cohort of patients with chronic-phase diseaseusing a mobilizing regimen modified from the original ‘ICE’protocol used by Carella et al (1993a, b).
PATIENTS AND METHODS
Patients. Between January 1993 and January 1995, 40patients with Ph-positive CML were entered into this pilotstudy. These patients were recruited from five centres in theU.K. and Ireland. The median age in this cohort was 45 years(range 25–58 years); 19 patients were female and 21 male.Apart from one patient who had previously had a localizedblast crisis in a single rib lesion, all patients were in CP1. Theduration of CP1 varied widely, with a median duration of 18months (range 2–90 months) (Table I). All cases wereconsidered ineligible for allogeneic BMT either due to theirage or the lack of a suitable donor. Prior to receivingmobilizing chemotherapy, 34/40 (83%) were either un-responsive (previous failure to achieve a major cytogeneticresponse) or intolerant to IFN-a; two patients (UPN 20, 31)were in cytogenetic relapse having previously achieved acomplete cytogenetic response to IFN-a; the remaining sixpatients had not been exposed to IFN-a.
Following mobilization and collection of PBSC in thisstudy, some patients progressed directly to autologoustransplantation (n ¼ 20), whereas others were given atrial of further IFN-a. This division was a centre-basedeffect, and in the main the earlier patients enrolled had thetrial of IFN-a. Data on the transplant outcomes arepresented in order to demonstrate the potential of thePBSC to engraft post-autograft, although the mainanalysis relates to the PBSC quality in terms of Phcontamination.
Mobilization therapy and harvesting. All patients received‘IDAC 2 þ 5’ as mobilizing chemotherapy. This regimenconsists of idarubicin administered intravenously in a doseof either 8, 10 or 20 mg/m2/d for 2 d with cytarabine 1 g/m2
as a continuous intravenous infusion over 5 d. They alsoreceived growth factor stimulation with granulocyte colonystimulating factor (G-CSF) 263–300 mg/d from day þ9 (dosedepended upon whether filgrastim (300 mg) or lenograstim(263 mg) was used).
PBSC harvesting was performed using either a COBESpectra or Baxter CS3000þ continuous flow centrifuge. The
timing of the first collection was planned to coincide with theearly phase of white cell regeneration and in general it wasaimed to commence harvesting once the white count hadrisen >0:5 × 109/l. Additional harvests were performed onsubsequent days. PBSC harvests were then processed with-out the use of additional purging or selection techniques,cryopreserved in DMSO and stored in liquid nitrogen.Samples were taken from each individual harvest prior tocryopreservation for the analysis of progenitor cell contentand estimation of Ph-positive cell contamination. In themajority of patients, back-up bone marrow harvests wereperformed following white cell regeneration and cryopre-served in the same way.
Analysis of PBSC harvests. Cytogenetic analysis was carriedout on metaphases prepared from fresh PBSC samplesfollowing short-term culture (24–48 h) without the use ofmitogens or additional growth factors. The chromosomeswere then G-banded prior to analysis. Where possible, atleast 20 metaphases were analysed from each harvestsample.
Genomic DNA was purified from fresh material using‘Nucleon II’ (Scotlab, U.K.) and resuspended in 10 : 1 T.E.buffer (10 mM TRIS, 1 mM EDTA, pH 8.0) at approximately1 mg/ml. The BCR gene breakpoint was localized for eachpatient using DNA stored at presentation. Restrictionenzyme digestion of 10 mg aliquots of DNA was carried outusing BamH1, BGl II, Hind III and EcoR1 (Life Technologies,Paisley, Scotland). Digested DNA was separated on 0.8%agarose gels and transferred to PALL Biodyne B (PALL,Portsmouth) and hybridized with probes specific for the 59and 39 regions of the M-BCR as previously described (Millset al, 1989). Once the BCR breakpoint had been establishedfor each patient, the most appropriate combination restric-tion enzyme and probe was then used for the analysis ofPBSC harvest samples.
Total cellular RNA was prepared using ‘RNAzol’ (Bio-genesis) as recommended by the manufacturer. After thefinal ethanol precipitation the resulting RNA pellet waswashed with 70% followed by 100% ethanol, air dried andresuspended in diethylpyrocarbonate treated water at aconcentration of approximately 1 mg/ml. cDNA synthesisand RT PCR was carried out using the ‘Geneamp’ kit(Applied Biosystems, U.K.) using 1 mg of RNA. PCR primersfor the BCR gene were as described by Martiat et al (1990)and for all the ABL exon a3 as described by Cross et al(1993). Primers were purchased from Oswell (Edinburgh,Scotland) and thermal cycling was carried out on a PerkinElmer 9600 thermal cycler. 35 cycles of amplification wereperformed for the first round of amplification and wherenecessary a further 30 cycles were performed using nestedprimers. Amplification products were analysed on 2%agarose gels.
In order to determine the CFU-GM content of eachcollection, fresh PBSC samples were routinely set up inculture at a concentration of 1 × 105/ml. The culturemedium comprised 0.9% methyl cellulose (Methocell,Fluka, Gillingham) rehydrated in Iscove’s modifiedDulbecco’s medium (IMDM) (Life Technologies, Paisley,Scotland), supplemented with 25% fetal bovine serum
q 1997 Blackwell Science Ltd, British Journal of Haematology 96: 627–634
628 E. A. Chalmers et al
629Peripheral Blood Stem Cell Mobilization in Chronic Myeloid Leukaemia
q 1997 Blackwell Science Ltd, British Journal of Haematology 96: 627–634
(FBS) (Globepharm, Esher, Surrey), 1% bovine serumalbumin (BSA) (Sigma, Poole, Dorset), 5 × 10¹5
M 2-mercaptoethanol (BDH, Poole, Dorset), 10 ng/ml humanstem cell factor (SCF) (Advanced Protein Products Ltd,Brierley Hill, West Midlands) and 10 ng/ml human granulo-cyte macrophage colony stimulating factor (GM-CSF) (Life
Technologies). Duplicate aliquots of 1 ml were plated out in35 mm suspension culture dishes (Nunclon, Life Tech-nologies) and cultured for 14 d at 378C with 5% CO2 in afully humidified atmosphere. Using an inverted microscope(Labovert, Leica, Milton Keynes) cultures were scored forCFU-GM colonies containing >50 cells per colony.
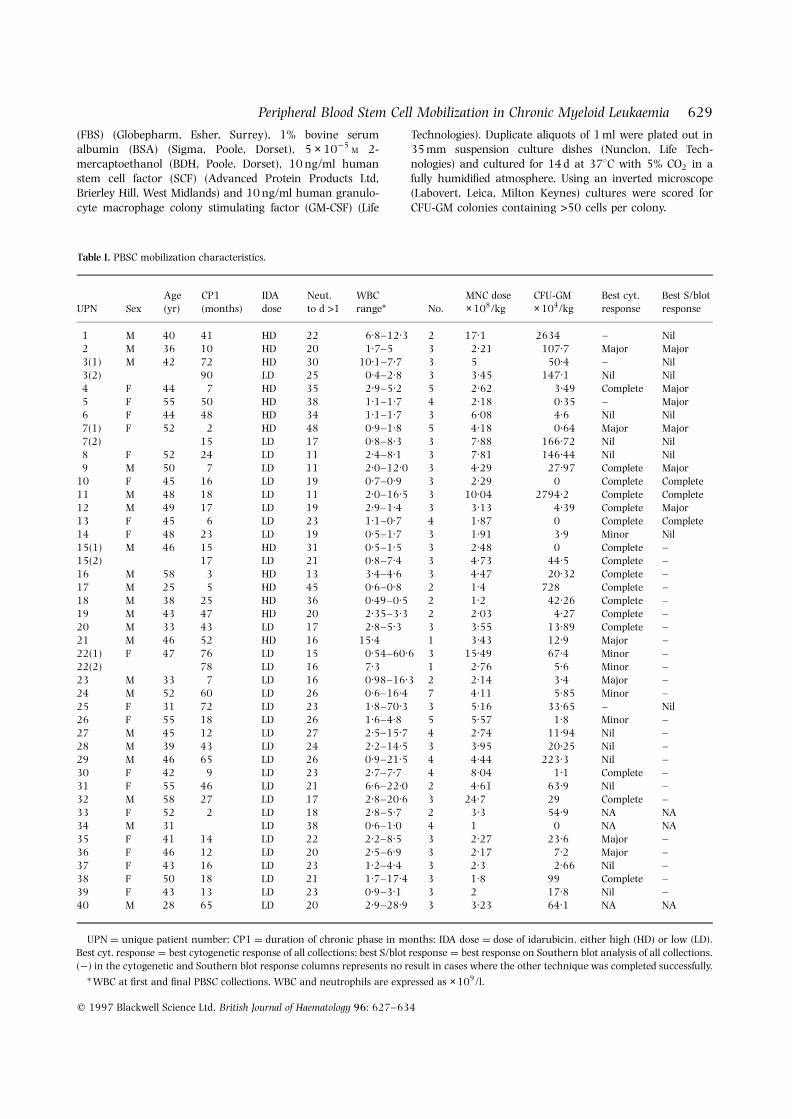
Table I. PBSC mobilization characteristics.
Age CP1 IDA Neut. WBC MNC dose CFU-GM Best cyt. Best S/blotUPN Sex (yr) (months) dose to d >1 range* No. × 108/kg × 104/kg response response
1 M 40 41 HD 22 6.8–12.3 2 17.1 2634 – Nil2 M 36 10 HD 20 1.7–5 3 2.21 107.7 Major Major3(1) M 42 72 HD 30 10.1–7.7 3 5 50.4 – Nil3(2) 90 LD 25 0.4–2.8 3 3.45 147.1 Nil Nil4 F 44 7 HD 35 2.9–5.2 5 2.62 3.49 Complete Major5 F 55 50 HD 38 1.1–1.7 4 2.18 0.35 – Major6 F 44 48 HD 34 1.1–1.7 3 6.08 4.6 Nil Nil7(1) F 52 2 HD 48 0.9–1.8 5 4.18 0.64 Major Major7(2) 15 LD 17 0.8–8.3 3 7.88 166.72 Nil Nil8 F 52 24 LD 11 2.4–8.1 3 7.81 146.44 Nil Nil9 M 50 7 LD 11 2.0–12.0 3 4.29 27.97 Complete Major
10 F 45 16 LD 19 0.7–0.9 3 2.29 0 Complete Complete11 M 48 18 LD 11 2.0–16.5 3 10.04 2794.2 Complete Complete12 M 49 17 LD 19 2.9–1.4 3 3.13 4.39 Complete Major13 F 45 6 LD 23 1.1–0.7 4 1.87 0 Complete Complete14 F 48 23 LD 19 0.5–1.7 3 1.91 3.9 Minor Nil15(1) M 46 15 HD 31 0.5–1.5 3 2.48 0 Complete –15(2) 17 LD 21 0.8–7.4 3 4.73 44.5 Complete –16 M 58 3 HD 13 3.4–4.6 3 4.47 20.32 Complete –17 M 25 5 HD 45 0.6–0.8 2 1.4 728 Complete –18 M 38 25 HD 36 0.49–0.5 2 1.2 42.26 Complete –19 M 43 47 HD 20 2.35–3.3 2 2.03 4.27 Complete –20 M 33 43 LD 17 2.8–5.3 3 3.55 13.89 Complete –21 M 46 52 HD 16 15.4 1 3.43 12.9 Major –22(1) F 47 76 LD 15 0.54–60.6 3 15.49 67.4 Minor –22(2) 78 LD 16 7.3 1 2.76 5.6 Minor –23 M 33 7 LD 16 0.98–16.3 2 2.14 3.4 Major –24 M 52 60 LD 26 0.6–16.4 7 4.11 5.85 Minor –25 F 31 72 LD 23 1.8–70.3 3 5.16 33.65 – Nil26 F 55 18 LD 26 1.6–4.8 5 5.57 1.8 Minor –27 M 45 12 LD 27 2.5–15.7 4 2.74 11.94 Nil –28 M 39 43 LD 24 2.2–14.5 3 3.95 20.25 Nil –29 M 46 65 LD 26 0.9–21.5 4 4.44 223.3 Nil –30 F 42 9 LD 23 2.7–7.7 4 8.04 1.1 Complete –31 F 55 46 LD 21 6.6–22.0 2 4.61 63.9 Nil –32 M 58 27 LD 17 2.8–20.6 3 24.7 29 Complete –33 F 52 2 LD 18 2.8–5.7 2 3.3 54.9 NA NA34 M 31 LD 38 0.6–1.0 4 1 0 NA NA35 F 41 14 LD 22 2.2–8.5 3 2.27 23.6 Major –36 F 46 12 LD 20 2.5–6.9 3 2.17 7.2 Major –37 F 43 16 LD 23 1.2–4.4 3 2.3 2.66 Nil –38 F 50 18 LD 21 1.7–17.4 3 1.8 99 Complete –39 F 43 13 LD 23 0.9–3.1 3 2 17.8 Nil –40 M 28 65 LD 20 2.9–28.9 3 3.23 64.1 NA NA
UPN ¼ unique patient number; CP1 ¼ duration of chronic phase in months: IDA dose ¼ dose of idarubicin, either high (HD) or low (LD).Best cyt. response ¼ best cytogenetic response of all collections: best S/blot response ¼ best response on Southern blot analysis of all collections.(¹) in the cytogenetic and Southern blot response columns represents no result in cases where the other technique was completed successfully.
* WBC at first and final PBSC collections. WBC and neutrophils are expressed as × 109/l.
CD34-positive cell analysis of the harvests. This was notperformed because at the time the study opened this procedurewas not widely available, and no consistent method wasagreed. Further, in pilot studies at one institution, CD34 cellnumbers proved difficult to enumerate in the CML samples, incontrast to collections from patients with, for example, non-Hodgkin lymphoma (data not shown).
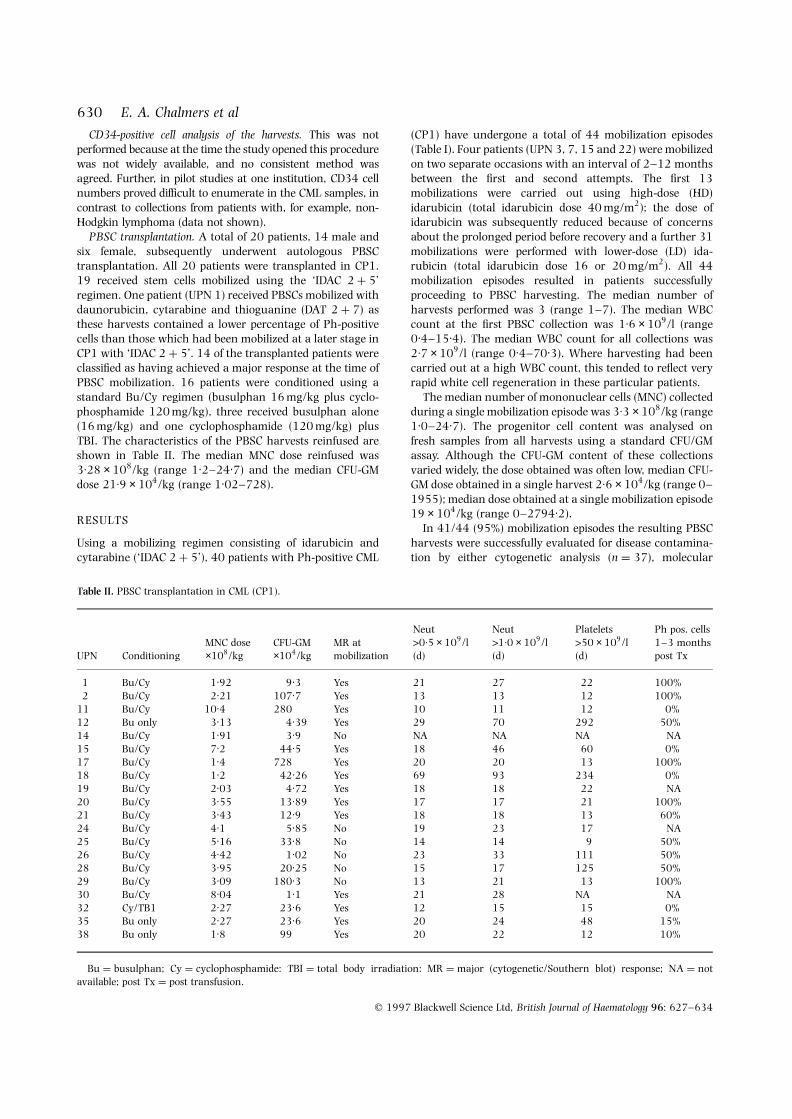
PBSC transplantation. A total of 20 patients, 14 male andsix female, subsequently underwent autologous PBSCtransplantation. All 20 patients were transplanted in CP1.19 received stem cells mobilized using the ‘IDAC 2 þ 5’regimen. One patient (UPN 1) received PBSCs mobilized withdaunorubicin, cytarabine and thioguanine (DAT 2 þ 7) asthese harvests contained a lower percentage of Ph-positivecells than those which had been mobilized at a later stage inCP1 with ‘IDAC 2 þ 5’. 14 of the transplanted patients wereclassified as having achieved a major response at the time ofPBSC mobilization. 16 patients were conditioned using astandard Bu/Cy regimen (busulphan 16 mg/kg plus cyclo-phosphamide 120 mg/kg), three received busulphan alone(16 mg/kg) and one cyclophosphamide (120 mg/kg) plusTBI. The characteristics of the PBSC harvests reinfused areshown in Table II. The median MNC dose reinfused was3:28 × 108/kg (range 1.2–24.7) and the median CFU-GMdose 21:9 × 104/kg (range 1.02–728).
RESULTS
Using a mobilizing regimen consisting of idarubicin andcytarabine (‘IDAC 2 þ 5’), 40 patients with Ph-positive CML
(CP1) have undergone a total of 44 mobilization episodes(Table I). Four patients (UPN 3, 7, 15 and 22) were mobilizedon two separate occasions with an interval of 2–12 monthsbetween the first and second attempts. The first 13mobilizations were carried out using high-dose (HD)idarubicin (total idarubicin dose 40 mg/m2); the dose ofidarubicin was subsequently reduced because of concernsabout the prolonged period before recovery and a further 31mobilizations were performed with lower-dose (LD) ida-rubicin (total idarubicin dose 16 or 20 mg/m2). All 44mobilization episodes resulted in patients successfullyproceeding to PBSC harvesting. The median number ofharvests performed was 3 (range 1–7). The median WBCcount at the first PBSC collection was 1:6 × 109/l (range0.4–15.4). The median WBC count for all collections was2:7 × 109/l (range 0.4–70.3). Where harvesting had beencarried out at a high WBC count, this tended to reflect veryrapid white cell regeneration in these particular patients.
The median number of mononuclear cells (MNC) collectedduring a single mobilization episode was 3:3 × 108/kg (range1.0–24.7). The progenitor cell content was analysed onfresh samples from all harvests using a standard CFU/GMassay. Although the CFU-GM content of these collectionsvaried widely, the dose obtained was often low, median CFU-GM dose obtained in a single harvest 2:6 × 104/kg (range 0–1955); median dose obtained at a single mobilization episode19 × 104/kg (range 0–2794.2).
In 41/44 (95%) mobilization episodes the resulting PBSCharvests were successfully evaluated for disease contamina-tion by either cytogenetic analysis (n ¼ 37), molecular
q 1997 Blackwell Science Ltd, British Journal of Haematology 96: 627–634
630 E. A. Chalmers et al
Table II. PBSC transplantation in CML (CP1).
Neut Neut Platelets Ph pos. cellsMNC dose CFU-GM MR at >0:5 × 109/l >1:0 × 109/l >50 × 109/l 1–3 months
UPN Conditioning ×108/kg ×104/kg mobilization (d) (d) (d) post Tx
1 Bu/Cy 1.92 9.3 Yes 21 27 22 100%2 Bu/Cy 2.21 107.7 Yes 13 13 12 100%
11 Bu/Cy 10.4 280 Yes 10 11 12 0%12 Bu only 3.13 4.39 Yes 29 70 292 50%14 Bu/Cy 1.91 3.9 No NA NA NA NA15 Bu/Cy 7.2 44.5 Yes 18 46 60 0%17 Bu/Cy 1.4 728 Yes 20 20 13 100%18 Bu/Cy 1.2 42.26 Yes 69 93 234 0%19 Bu/Cy 2.03 4.72 Yes 18 18 22 NA20 Bu/Cy 3.55 13.89 Yes 17 17 21 100%21 Bu/Cy 3.43 12.9 Yes 18 18 13 60%24 Bu/Cy 4.1 5.85 No 19 23 17 NA25 Bu/Cy 5.16 33.8 No 14 14 9 50%26 Bu/Cy 4.42 1.02 No 23 33 111 50%28 Bu/Cy 3.95 20.25 No 15 17 125 50%29 Bu/Cy 3.09 180.3 No 13 21 13 100%30 Bu/Cy 8.04 1.1 Yes 21 28 NA NA32 Cy/TB1 2.27 23.6 Yes 12 15 15 0%35 Bu only 2.27 23.6 Yes 20 24 48 15%38 Bu only 1.8 99 Yes 20 22 12 10%
Bu ¼ busulphan; Cy ¼ cyclophosphamide: TBI ¼ total body irradiation: MR ¼ major (cytogenetic/Southern blot) response; NA ¼ notavailable; post Tx ¼ post transfusion.

631Peripheral Blood Stem Cell Mobilization in Chronic Myeloid Leukaemia
q 1997 Blackwell Science Ltd, British Journal of Haematology 96: 627–634
analysis (n ¼ 17) or a combination of both techniques(n ¼ 13). Of the 37 episodes evaluated by cytogeneticanalysis, a complete cytogenetic response (no Ph-positivecells detected in one or more harvests) was documented in16/37 (43%), with a further 6/37 (16%) showing a majorcytogenetic response (<20% Ph-positive cells in one or moreharvests). Together this gives an overall complete/majorcytogenetic response rate of 59%. Five (14%) mobilizationsresulted in a minor cytogenetic response (<85% Ph positivecells in one or more harvests) and in 10 mobilizations (27%)no significant cytogenetic response was observed (>85% Ph-positive cells detected in all harvests) (Table III).
PBSC harvests from 17 mobilization episodes were analysedby Southern blot analysis of the BCR gene rearrangement. In6/17 (35%) there was a major response (defined arbitrarily asa BCR gene rearrangement quantified by scanning densito-metry at <20% of the total DNA) and in three cases (18%) therearranged band was undetectable following prolongedexposure (defined as a complete response). In the remaining8/17 (47%) Southern blot analysis was strongly positive (nosignificant response) (Table III). PBSC harvests from these 17mobilization episodes were also analysed by RT-PCR. In 16cases all harvests were RT-PCR positive following one round ofamplification; in the final case nested RT-PCR was required forthe detection of the abnormal transcript. No harvests weretherefore recorded as being completely RT-PCR negative.
In 10/13 cases analysed by both cytogenetic and South-ern blot techniques there was complete agreement in termsof the level of disease contamination detected by the two
methodologies. In the other three cases Southern blotanalysis remained weakly positive in the presence of anegative cytogenetic result, suggesting that this techniquemay be marginally more sensitive in this situation.
In an attempt to predict which patients are likely toachieve a major response using this mobilization strategy wehave analysed a number of patient and disease character-istics. In this group of patients the duration of CP1 was foundto be an important predictor of outcome. We have observed acomplete or major response (as defined by cytogenetic orSouthern blot analysis) in 74% of those treated within 24months of diagnosis compared with 33% in patients treatedlater in CP (P ¼ 0:02) (Table IV). Although the total patientnumbers are smaller the results are even more striking inpatients treated within 12 months of diagnosis with acomplete or major response rate of 91% versus 43% for thosetreated later (P ¼ 0:018). The dose of idarubicin alsoappears to have had an effect on outcome with a higherresponse rate seen in patients treated with the HD idarubicinregimen (77% versus 46%).
Haemopoietic recovery following mobilizing chemother-apy was also related to the dose of idarubicin used. Recoveryto >1:0 × 109
=l neutrophils occurred at a median of 31 d(range 13–48) using the HD idarubicin schedule and 21 d(range 11–38) using the LD regimen. With the high-doseregimen, therefore, some patients experienced markedlyprolonged periods of neutropenia. Two patients died follow-ing mobilization chemotherapy (UPN 10 and 27) giving amortality of 4.5% for each mobilization episode (2/44mobilizations), and an overall mortality of 5% (2/40patients). Both deaths occurred following white cell regen-eration but were related to sepsis. In one case this wasthought clinically to be fungal in origin, the other was due toPseudomonas septicaemia. Additional cytogenetic abnormal-ities were observed in three patients following haemopoieticregeneration and in two cases (UPN 6 and 8) specifictranslocations were documented (t(1;17), t(3;12)) whichwere clonal and persistent. In one case (UPN 8) this appearedto be associated with progression to a more acceleratedphase of the disease.
PBSC transplantationOf the 20 patients who proceeded to PBSC transplantation18/20 (90%) successfully engrafted. Of the two who failed toengraft, one (UPN 18) was salvaged using buffy coat cellswhich had been cryopreserved at presentation; the otherpatient (UPN 14) died of sepsis related to graft failure despite
Table III. Results of PBSC mobilization.
No.
Cytogenetic resultsComplete cytogenetic response 16 (43%)Major cytogenetic response 6 (16%)Minor cytogenetic response 5 (14%)No cytogenic response 10 (27%)
Total 37 (100%)
Southern blot resultsComplete response 3 (18%)Major response 6 (35%)No response 8 (47%)
Total 17 (100%)
Table IV. Effect of duration of first chronic phase on outcome of PBSC mobilization.
CP1 CP1 CP1 CP1Response <24 months >24 months <12 months >12 months
Complete/major 17 (74%) 6 (33%) 10 (91%) 13 (43%)Minor/nil 6 (26%) 12 (67%) 1 (9%) 17 (57%)
Total 23 18 11 30ðP ¼ 0:02Þ ðP ¼ 0:018Þ

reinfusion of bone marrow cells stored prior to transplanta-tion. Excluding the latter patient who failed to engraft, themedian time to achieve a neutrophil count of >0:5 × 109/lwas 18 d (range 10–69) and to regenerate platelets to>50 × 109/l was 19 d (range 11–93) (Table II). Threepatients in this cohort died following transplantation ofnon-disease-related problems, one (UPN 14) as alreadymentioned due to early graft failure, and two (UPN 12 and14) of interstitial pneumonitis/pneumonia at day 100 andday 189 respectively. At this time there is only limited dataon the cytogenetic status of these patients post transplant.Results are currently available on bone marrow samplesfrom 15 cases analysed at 1–3 months post transplant. Infive cases there was a major cytogenetic response (<20% Ph-positive cells detected), four of whom appeared to be incytogenetic remission. Another five cases had a partialresponse with 50–60% Ph-positive cells detected, and theremaining five regenerated with 100% Ph-positive cells(Table II).
The outcome of these transplanted patients has beenupdated at a median follow-up for surviving patients of 24months. Two further patients have died, both havingprogressed to accelerated or blast phase. One died of CMLcomplications, the other following an unrelated donor BMT.Three other patients are in accelerated phase, one definedonly by the presence of an additional Ph chromosome. 12remain in chronic phase, all except one of these patients areon some form of therapy. Four remain chimaeric for the Phchromosome at a median of 18 months post-autograft. Onlyone is haematologically normal and on no therapy, but has25% Ph metaphases in the marrow.
DISCUSSION
Haemopoietic stem cells capable of long-term haemopoieticreconstitution following high-dose therapy can be mobilizedinto the peripheral blood following myelosuppressive chemo-therapy with or without the use of additional growth factorstimulation (Richman et al, 1977; Siena et al, 1989). In CMLthere is increasing evidence to suggest that Ph-negativeprogenitor cells may, at least in some patients, predominatein the peripheral blood during the early phase of post-chemotherapy regeneration. Harvesting of cells mobilized inthis way can therefore potentially provide an enriched sourceof Ph-negative progenitor cells for subsequent autologoustransplantation.
Optimal methods for Ph-negative PBSC mobilization inCML and the timing of such procedures remain to beadequately defined. In this study we have investigated PBSCmobilization following idarubicin and cytarabine (‘IDAC2 þ 5’) in a cohort of patients with CML CP1 of variableduration. We have demonstrated a significant cytogeneticresponse in almost 60% of mobilization episodes evaluatedby this technique (complete in 43% and major in 16%), withsimilar responses documented by Southern blot analysis. Noharvests were bcr-abl negative by RT-PCR analysis, reflectingthe greater sensitivity of this technique. Overall ourcytogenetic results are very similar to those published byCarella using the ‘ICE’ regimen (idarubicin, cytarabine and
etoposide) for mobilization in patients in CP1 (Catella et al,1993a, b). Unlike the Italian data, however, where 5/17cytogenetically negative harvests were also RT-PCR negative,we did not document any bcr-abl negative harvests by RT-PCR analysis which suggests a higher level of Ph-positive cellcontamination in our patients.
Although there was a tendency for the first collection of aseries to be the least contaminated with Ph metaphases,these also tended to have the fewest CFU-GM numbers.Therefore, a minimum of three harvests would appearprudent. Some patients had Ph-negative collections evenwhen the total WBC was high, again supporting collectingregardless and awaiting detailed analysis of the qualitybefore deciding which to use for autologous transplantation.
In terms of trying to predict the optimal timing forsuccessful PBSC mobilization in CML, it is already clear thatpatients mobilized during chronic phase achieve betterresults than those who are in an accelerated phase or blastcrisis (Carella et al, 1993a; Kantarjian et al, 1995). In thisstudy we have clearly documented significantly better resultsin patients treated during the early stages of chronic phase,particularly those mobilized within the first year of diagnosis.The mechanism of progenitor release into the peripheralcirculation following chemotherapy is not understood, butmay involve alterations in adhesion molecules or activeprogenitor cell proliferation. Similarly, in CML, the reasonfor the short-term proliferative advantage of Ph-negativecells in this situation is not well defined; however, ourresults suggest that this advantage may be lost as thedisease progresses, perhaps due to an overall reduction inthe number of residual Ph-negative cells present in themarrow.
Whether patients with CML who are potential candidatesfor autologous transplantation should undergo PBSC mobi-lization at diagnosis or following a trial of IFN-a remainscontroversial. Carella et al (1994) have recently presenteddata suggesting that the best PBSC mobilization results areobtained in patients mobilized at diagnosis, who havereceived either no treatment or hydroxyurea only. Theseresults have to be balanced against the potential risks(procedural mortality ¼ 4.5% for the mobilization therapy inour study) associated with early mobilization therapy for the20% or so of patients who might achieve a completecytogenetic response and prolongation of survival with IFN-aalone. In addition, prior failure to respond to IFN-a in ourstudy did not seem to preclude a good cytogenetic response toPBSC mobilization therapy.
As well as the timing of the mobilization procedure, theintensity of the chemotherapy used may have an effect onoutcome. In this study we have looked at the effect ofdifferent dose intensities of idarubicin and have observed abetter response using a more intensive schedule. Again,however, these results have to be weighed against thetendency to prolonged neutropenia seen with HD idarubicintherapy despite the administration of G-CSF.
The optimal method for quantification of residual Ph-positive cells in PBSC harvest material also requires furtherinvestigation. Conventional cytogenetic analysis of unstimu-lated cells provides information on mitotic cells but may fail
q 1997 Blackwell Science Ltd, British Journal of Haematology 96: 627–634
632 E. A. Chalmers et al

633Peripheral Blood Stem Cell Mobilization in Chronic Myeloid Leukaemia
q 1997 Blackwell Science Ltd, British Journal of Haematology 96: 627–634
to reflect the true Ph status of primitive progenitor cells ifthey have, as might be predicted, low mitotic activity. Someof these problems may be overcome by the use of interphasefluorescence in situ hybridization (FISH) analysis, which canalso be combined with simultaneous phenotypic analysis ofindividual cells (Arnoldus et al, 1990). However, this is not aroutinely available technique in all centres at the presenttime. With regard to molecular analysis, immunopheno-typing of PBSC collections reveals that >90% of the cellsharvested are T lymphocytes. Although T cells are notthought to be involved in CML and do not therefore containthe bcr-abl gene rearrangement (Garicochea et al, 1994),these cells may act to dilute out residual Ph-positive cells,potentially to below the level of detection. This is most likelyto be a problem with Southern blot analysis, a techniquewith a relatively low sensitivity in terms of its ability to detectminimal residual disease. Problems of sensitivity may beovercome by PCR analysis, but this requires a quantitativeanalysis in order to provide meaningful data.
Only relatively small numbers of patients with chronic-phase CML have so far undergone autologous transplanta-tion using PBSCs mobilized in this way. We have clearlydemonstrated the ability of chemotherapy mobilized PBSCsto facilitate engraftment in the majority of patients despitethe relatively low CFU-GM content of some harvests,although one patient died from engraftment failure andtwo others from pneumonitis after engraftment. There isonly limited follow-up to date on the disease status of thesepatients post transplant, but it is clear that some patientsmay regenerate with Ph-negative haemopoiesis. UnlikeTalpaz et al (1995), who recently reported the results ofPBSC transplantation in a group of CML patients withadvanced disease, we have not, however, seen an absolutecorrelation between the Ph status of the harvests reinfusedand the percentage of Ph-positive cells present in the marrowpost transplant. Longer follow-up will be required todocument the impact of this procedure on survival in CMLand to examine the effect of IFN-a therapy in patients whohave undergone a high-dose procedure, a question whichwill be addressed in the forthcoming MRC CML IV trial(Spencer et al, 1995). Furthermore, the mortality in ourseries was high, five of 40 patients dying at some point oftreatment, and this will need to be lower if any benefit overmore conventional therapy is to be seen.
ACKNOWLEDGMENT
S.M.K. and A.C.N. wish to thank Chugai Pharma UK Ltd fortheir financial support.
REFERENCES
Allan, N.C., Shepherd, P.C.A. & Richards, S.M. (1995) UK MedicalResearch Council randomised multicentre trial of interferon-an1for chronic myeloid leukaemia: improved survival irrespective ofcytogenetic response. Lancet, 345, 1392–1397.
Arnoldus, E.P.J., Wiegant, J., Noordermeer, I.A., Wessels, J.W.,Beverstock, G.C., Grosveld, G.C., van der Ploeg, M. & Raap, A.K.(1990) Detection of the Philadelphia chromosome in interphasenuclei. Cytogenetics and Cell Genetics, 54, 108–112.
Barnett, M.J., Eaves, C.J., Phillips, G.L., Gascoyne, R.D., Hogge, D.E.,Horseman, D.E., Humphries, R.K., Klingemann, H.G., Lansdorp,P.M., Nantel, S.H., Reece, D.E., Shepherd, J.D., Spinelli, J.J.,Sutherland, H.J. & Eaves, A.C. (1994) Autografting with culturedmarrow in chronic myeloid leukemia: results of a pilot study.Blood, 84, 724–732.
Butturini, A., Keating, A., Goldman, J.M. & Gale, R.P. (1990) Autotrans-plants in chronic myeloid leukaemia. Lancet, 335, 1255–1258.
Carella, A.M., Frassoni, F., Pollicardo, N., Pungolino, E., Podesta, M.,Giordano, D., Ferrero, R., Soracco, M., Benvenuto, F. & Figgari, O.(1994) Ph-negative blood progenitor cells (BPCs) can be recruitedafter chemotherapy and G-CSF during early haemopoietic recoveryin patients at diagnosis of CML or pretreated only with hydroxyurea.Bone Marrow Transplantation, 14, (Suppl. 3), S34–S35.
Carella, A.M., Podesta, M., Frassoni, F., Pungolino, E., Pollicardo, N.,Raffo, M.R., Ferrero, R., Benvenuto, F., Figari, O., Giordano, D.,Lercari, G., Carlier, P., Valbonesi, V., Parodi, M., Gallamini, A.,Saglio, G. & Marmont, A.M. (1993a) Selective overshoot of Ph-negative blood haemopoietic cels after intensive idarubicincontaining regimen and their repopulating capacity afterreinfusion. Stem Cells, 11, (Suppl. 3), 67–72.
Carella, A.M., Pollicardo, N., Pungolino, E., Raffo, M.R., Podesta, M.,Ferrero, R., Pierluigi, D., Nati, S., Naibo, K., Congui, A.,Spriano, M., Vimercati, R., Figari, O., Rosso, C., Saglio, G.,Sessarego, M., Lercari, G., Valbonesi, M., Carlier, P., Vitale, V.,Corvo, P. & Parodi, M. (1993b) Mobilization of cytogenetically‘normal’ blood progenitor cells by intensive conventional chemo-therapy for chronic myeloid and acute lymphoblastic leukemia.Leukemia and Lymphoma, 9, 477–483.
Carlo-Stella, C., Mangoni, L., Piovani, G., Almici, C., Garau, D.,Caramatti, C. & Rizzoli, V. (1991) In vitro marrow purging inchronic myelogenous leukemia: effect of mafosfamide andrecombinant granulocyte-macrophage colony stimulating factor.Bone Marrow Transplantation, 8, 265–273.
Cross, N.C., Hughes, T.P., Feng, L., O’Shea, P., Bungey, J., Marks, D.I.,Ferrant, A., Martiat, P. & Goldman, J.M. (1993) Minimal residualdisease after allogeneic bone marrow transplantation for chronicmyeloid leukaemia in first chronic phase: correlations with acutegraft-versus-host disease and relapse. British Journal ofHaematology, 84, 67–74.
Garicochea, B., Chase, A., Lazaridou, A. & Goldman, J.M. (1994) Tlymphocytes in chronic myeloid leukemia (CML): no evidence ofthe BCR/ABL fusion gene detected by fluorescence in situhybridization in 14 patients. Leukemia, 8, 1197–1201.
Hoyle, C., Gray, R. & Goldman, J.M. (1994) Autografting for patientswith CML in chronic phase: an update. British Journal ofHaematology, 86, 76–81.
Italian Cooperative Study Group on Chronic Myeloid Leukaemia(1994) Interferon alpha-2a as compared with conventionalchemotherapy for the treatment of chronic myeloid leukemia.New England Journal of Medicine, 330, 820–825.
Kantarjian, H.M., Deisseroth, A., Kurzrock, R., Estrov, Z. & Talpaz, M.(1993) Chronic myeloid leukemia: a concise update. Blood, 82,691–703.
Kantarjian, H.M., Talpaz, M., Hester, J., Feldman, E., Korbling, M.,Liang, J., Rios, M.B., Smith, T.L., Calvert, L. & Deisseroth, A.B.(1995) Collection of peripheral blood diploid cells from chronicmyelogenous leukemia patients early in the recovery phase frommyelosuppression induced by intensive dose chemotherapy.Journal of Clinical Oncology, 13, 553–559.
Kirkland, M.A., O’Brien, S.G., McDonald, C., Davidson, R.J., Cross,N.C.P. & Goldman, J.M. (1993) BCR-ABL antisense purging inchronic myeloid leukaemia. (Letter). Lancet, 342, 614.
Leemhuis, T., Leibowitz, D., Cox, G., Silver, R., Srour, E.F., Tricot, G. &Hoffman, R. (1993) Identification of BCR/ABL negative primitive

hemopoietic progenitor cells within chronic myeloid leukemiamarrow. Blood, 81, 801–807.
Martiat, P., Maisin, D., Philippe, M., Ferrant, A., Michaux, J.L.,Cassiman, J.J., Van den Berghe, H. & Sokal, G. (1990) Detection ofresidual BCR/ABL transcripts in chronic myeloid leukaemiapatients in complete remission using the polymerase chain reactionand nested primers. British Journal of Haematology, 75, 355–358.
McGlave, P.B., De Fabritiis, P., Deisseroth, A., Goldman, J.M., Barnett,M., Reiffers, J., Simonsson, B., Carella, A. & Aeppli, D. (1994)Autologous transplant therapy for chronic myeloid leukaemiaprolongs survival: results from eight transplant groups. Lancet,343, 1486–1491.
Mills, K.I., Hynds, S.A., Burnett, A.K., MacKenzie, E.D. & Birnie, G.D.(1989) Further evidence that the site of the breakpoint in themajor breakpoint cluster region (M-ber) may be a prognosticindicator. Leukemia, 3, 837–841.
Richman, C.M., Weiner, R.S. & Yankee, R.A. (1977) Increase incirculating stem cells following chemotherapy in man. Blood, 47,1031–1039.
Siena, S., Bregni, M., Brando, B., Ravagnani, F., Bonadonna, G. &Gianni, A.M. (1989) Circulation of CD34þ hemopoietic stem cellsin the peripheral blood of high-dose cyclophosphamide treatedpatients: enhancement by intravenous granulocyte-macrophage-colony-stimulating factor. Blood, 74, 1905–1914.
Spencer, A., O’Brien, S.G. & Goldman, J.M. (1995) Options fortherapy in chronic myeloid leukaemia. British Journal ofHaematology, 91, 2–7.
Talpaz, M., Kantarjian, H., Liang, J., Calvert, L., Hamer, J., Tibbits, P.,Durett, A., Claxton, D., Giralt, S., Khouri, I., Przepiorka, D.,Besien, K.V., Anderson, B., Mehra, R., Gajewski, J., Seong, D.,Hester, J., Estey, E., Korbling, M., Pollicardo, N., Berenson, R.,Heinfield, S., Champlin, R. & Deisseroth, A.B. (1995) Percentageof Philadelphia chromosome (Ph)-negative and Ph-positive cellsfound after autologous transplantation for chronic myeloidleukemia depends on the percentage of diploid cells induced byconventional-dose chemotherapy before collection of autologouscells. Blood, 85, 3257–3263.
q 1997 Blackwell Science Ltd, British Journal of Haematology 96: 627–634
634 E. A. Chalmers et al




















