Surfactant alteration and replacement in acute respiratory distress syndrome
Upload
polysaccharidesCategory
view
6download
0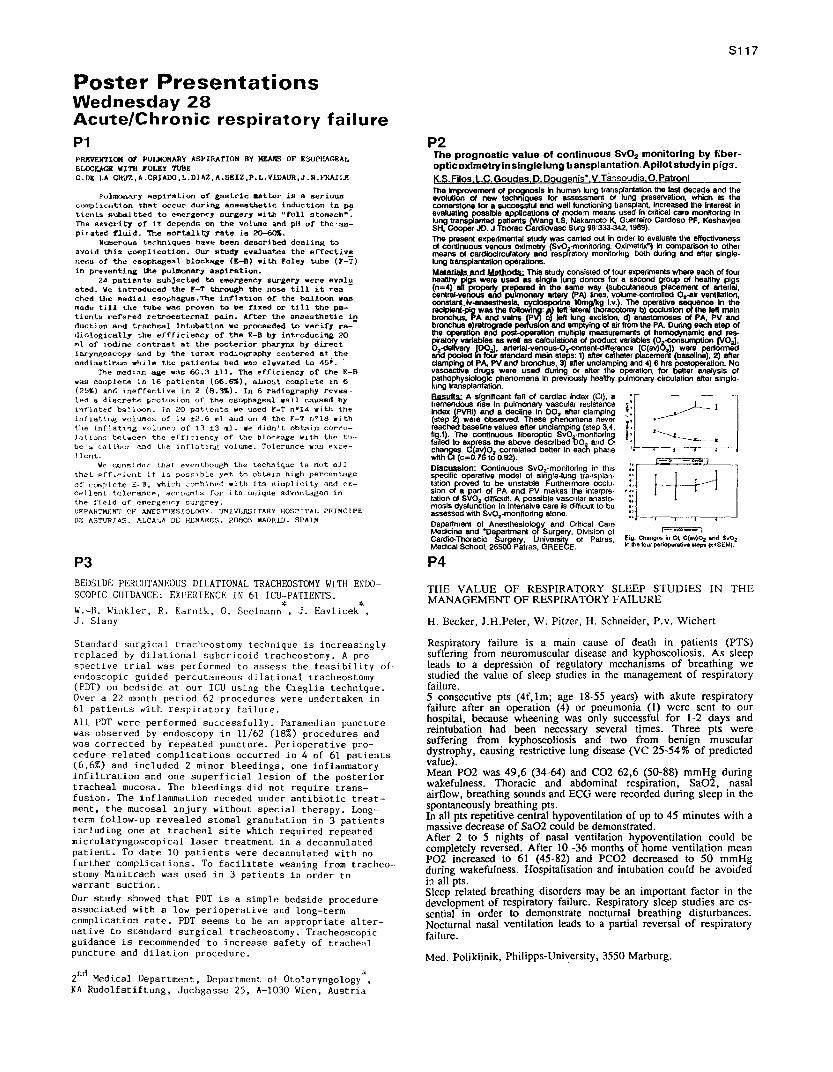
Poster PresentationsWednesday 28Acute/Chronic respiratory failureP1PRKVEN'l'ION OF PUJ.lOIOIfARY ASPIRATION BY MEANS OF K50PHAC".E...L
BLOCY.AGIl "'1r11 FOLEY TUllEC.DK LA CRUZ.A.CRJADO.L.or...z ..... sEIZ.P.L.VlDAUR.J.R.}~JLE
?ulmo~~1 ~ap1ration of gastric aetter is a seriouscomplicn~ion that occur during anaesthetic induction in patients subl2li tted 'to entergency surger,.. with lIf'ull stomach":The severity of it depends 00 the yollJnle and pH of t.he vaa-,pirated ~luid. The mortalit1 rate is ~.
N~erous techniques haY~ been described dealing toavoid this. comp j t ca t Lon , OUr" "stud7 evaluates the e r'recuj ver.e~s of the esopt~eal block~e (£-B) with Foley tube (r-T)in preventing the pulmonary aspiration.
24 patients subjected to emergency surgery were eValua t.ed , We introduced 'the Y-T through the nose till it rca--ched the ~edial esophagus.The in~lation or the balloon wasmade till the tube was proven to be fixed or till the pa-ticnta rcf'er-ed r-e ta-oee t.er-na.I pain. After 1:hc anaesthetic induction and tracheal intubation we proceeded to verify ra--<Jiologically the eHficiency of the E-B by introducing 20ml of iodi ne con t.r-ae t at the po~tcrior phar-ynx by directlaryngoscopy and by the torax radiography centered at th~
raedd as t Lrnaa whi le the patients bed was elevated to 45; ..The median age "3~ 60.3 ±11. The efficiency of the E-B
was conplete in 16 patients (66.~). almo~t complete in 6(2~%) anG ineffective in 2 (6.3%)_ In 6 radiography revea-led a discrete protusion or the csophage~l wall caused byinrlated balloon. In 20 pottent3 we used F-T n~14 with theLnf'Le t i ng volumes of 1'::1 ~2_6 ml and on 4 the F-T n!'18 withthe inflating vc Lumc n of 13 13 11.1. We didn't cbt.a i n cor ce-:La t i onn be t.veen the efficiency of the b Lookage With th~ t-u-.Le':;; c a Li bcr and t.he t nr l a t.t ng volume. To Ler-ance W3.H e'X.ce-] lent.
We c,onsi dc r- t ha t evc n t.hough the technique \6 not l'lJ.lthat eff ~t:ient it is POSf;) b Le yet to ob t-a Ln high per-ccn t.agcof complete E--B. whi,~h corab.i ned with its a i rapLi c i t.y and (>x-eel lent t.o j er-ance , acc ourrt.s for its. unique advaut.agen inthe field of emergency sIJrgrey.UgPAH'!"Mf.PIT OF ANESTIfF.SJOLOGY. IJNIVr;m51TARY I-IOSPITAL PRTNCIPEDr.: AST'lJRJAS. I'.LCAI..A DE HLNARES. 2B80~ MAJ)RID. SPAIN
P3BEDSIDE PERCIITANEOUS DILATIONAL TRACHEOSTOMY WITH ENDO-SCOPIC GUIDANCE: EXPERIENCE IN 61 ICU-PATIENTS.
W.-B. Winkler, R. Karnik. O. Seelmann*, J. Havlicek*,J. Slany
Standard surgical tracheostomy technique is increasinglyreplaced by dilational subcricoid tracheostomy. A pro-spective trial was performed to assess the feasibility of·endoscopic gUided percutaneous dilational tracheostomy(PDT) on bedSide at our ICU using the Ciaglia technique.Over a 22 month period 62 procedures were undertaken in61 patients with respiratory failure.
All PDT were performed successfully. Paramedian puncturewas observed by endoscopy in 11/62 (18%) procedures andwas corrected by repeated puncture. Perioperative pro-cedure related complications occurred in 4 of 61 patients(6.6%) and included 2 minor bleedings, one inflammatoryinfiltration and one superficial lesion of the posteriortracheal mucosa. The bleedings did not require trans-fusion. The inflammation receded under antibiotic treat-ment, the mucosal injury without special therapy. Long-term follow-up revealed stomal granulation in 3 patientsincluding one at tracheal site which required repeatedmicrolaryngoscopical laser treatment in a decannulatedpatient. To date 10 patients were decannulated with nofurther complications. To facilitate weaning from tracheo-stomy Minitrach was used in 3 patients in order towarrant suction.
Our study showed that PDT is a simple bedside procedureassociated with a low perioperative and long-termcomplication rate. PDT seems to be an appropriate alter-native to standard surgical tracheostomy. TracheoscopicgUidance is recommended to increase safety of trachealpuncture and dilation procedure.
2nd
Medical Department, Department of Otolaryngology".KA Rudolfstiftung, Juchgasse 25. A-1030 Wien. Austria
8117
P2The prognostic value of continuous Sv02 monitoring by fiber-opticoximetryinsingle lung transplantation. Apllot studyin pigs.K.S. Filos. i.c. Goudas, O.Dougenis·.V, Tassoudis O.PatronlThe Improvsment of prOQnosls In human lung transplantation the last decade and theevolutiOn of new technIques lor assessment 01 lung preservation. which Is thecornsNllone for a successful and wellfunctioning transplant, Increased the Intsrest Inevaluating possible applications of modam means used In crllical care monllorlng Inlungtransplantad patIents (Wang LS. Nakamoto K, Guerrelro Cardoso PF. KeshavjeeSH. CoopSrJD. J Thorac Cardlovasc Surg 98:333-342, 1989).Ths present experimental atudy was earned out Inorderto evaluatelhe effectivansss01 continuous venous oxlmstry (SvO~·monllorinQ. Oximetrlx") Incompanson to othsrmsans of cardioclrculatory and resplfatory monlloring, both during and alter single·lungtransplantation operations.Malerlals and MetbodS- This study consisted of four experiments where each ot fourhealthy pigs were used as single lung donors for a second group of heallhy pigs(n=4) all propel1y prepared In the same way (subcutaneous placement of artsrlalcentral-vsnous and pulmOlllllY art8f}' (PA) Nnes. volume-eontrolled O.-air ventilation:~.Iv-anasstheslB, cyclosporlne 10mgJkg I.v.). The operative sequence In thersclptent..ptg was ths fofIOW~:IJ) Ialt Iaterafthoracotomy b) occlusion of the IellmalnbronchUS; PA and veins llj Iell lung excision, d) anastomoses of PA, PV andbronchus a)ratrograde pe and emptying of airfromthe PA. During each step 01the operatiOn and post-operatlon muftipte measurements 01 hemodynamiC and res-piratory variables as well as calculations01product vanables(0 -consumption (V0alO.-dellvsry ID0al. arterlal-venous-O.-content-dilference [C(av)6.n were pelformadarid pooled il loUr standard main steps: 1) aftercalhaterplacement(baseline) 2) altsrclampl~ 01PA,PVand bronchus, 3) alterunclamplng and 4)6 hrs postope"illon. NovasoactIVe. d~s were used during or aner the operation, for better analysis of~~~ra';r.~?~~..:icfn~anomena In previously heallhy pulmonary circulation anar single·
I!lls.uI1ll.: A significant fall of cardiac Index (CI), atremendous rise In pUlmonary vascular rssistanceIndex (PVRI) and a decline In 00. alter clamping(step 2) were.observed. These phenomena naverreached baselinevalues aller unclamping (step 3,4;
r~i~ci tJ:':x cr~~nt~:~~r~~~~rl~1\i~~"Ji~changes. Wcav)o.correlated better In each phasewllh CI(c=0.16to 0.92).Discussloo- Continuous Sv02·monl1oring In thisspecific operative model of single-lung transptan-lotion proved to be unstabls F'urthermoreocclu·sion of a part 01 PA and PV makes the Interpre·tatlonof SVO. dilficutl. A possible vascular anasto-mosis dysfunction In Intensivs care Is difficull to boassessad wllh SvO.-mon~orlng 810ne.Department 01 Anesthesiology and Crnical CamMedicine and "Department of Surgery, Division of 1-- •.02__ ICar~io.Thoraclc Surgery, University of Patras, f.ig. Changes In ct C(all)~ and Sv02Medical School, 26500 Patras, GREECE, In the four perioperative 118ps (xtSEM).
P4
THE VALUE OF RESPIRATORY SLEEP STUDIES IN THEMANAGEMENT OF RESPIRATORY FAILURE
H. Becker. J.H.Peter, W. Pitzer, H. Schneider, P.v. Wichert
Respiratory failure is a main cause of death in patients (PTS)suffering from neuromuscular disease and kyphoscoliosis. As sleepleads to a depression of regulatory mechanisms of breathing westudied the value of sleep studies in the management of respiratoryfailure.5 consecutive pts (4f,lm; age 18-55 years) with akute respiratoryfailure after an operation (4) or pneumonia (1) were sent to OUf
hospital. because wheening was only successful for 1-2 days andreintubation had been necessary several times. Three pts weresuffering from kyphoscoliosis and two from benign musculardystrophy, causing restrictive lung disease (VC 25-54 % of predictedvalue).Mean P02 was 49,6 (34-64) and CO2 62,6 (50-88) mmHg during~akefulness. !horacic and abdominal respiration, Sa02, nasalairflow, breathing sounds and ECG were recorded during sleep in thespontaneously breathing pts,In all pts repetitive central hypoventilation of up to 45 minutes with amassive decrease of Sa02 could be demonstrated.After 2 to 5 nights of nasal ventilation hypoventilation could becompletely reversed. After 10 -36 months of home ventilation meanP02 increased to 61 (45-82) and PC02 decreased to 50 mmHgduring wakefulness. Hospitalisation and intubation could be avoidedin all pts.Sleep related breathing disorders may be an important factor in thedevelopment of respiratory failure. Respiratory sleep studies are es-sential in order to demonstrate nocturnal breathing disturbances.Nocturnal nasal ventilation leads to a partial reversal of respiratoryfailure.
Med. Poliklinik, Philipps-University, 3550 Marburg.
S118
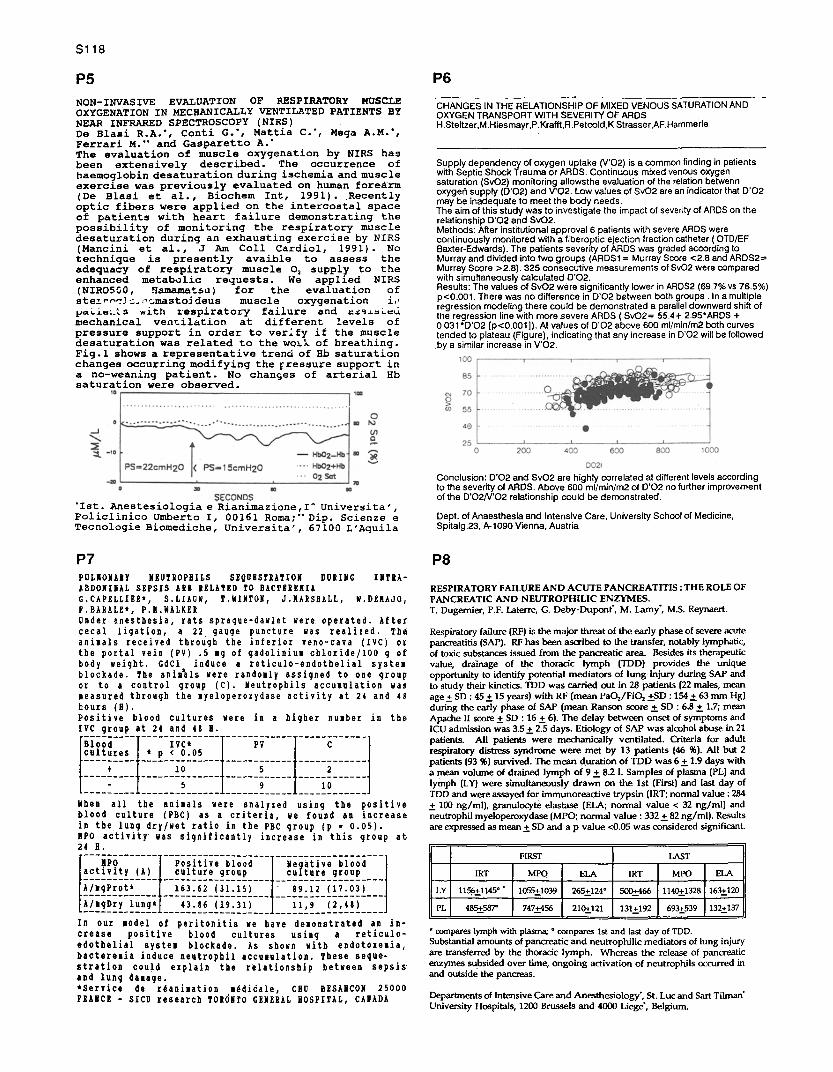
P5NON-INVASIVE EVALUATION OF RESPIRATORY MUSCLEOXYGENATION IN MECHANICALLY VENTILATED PATIENTS BYNEAR INFRARED SPECTROSCOPY (NIRS)De Blasi R.A.', Conti G.*, Mattia C.*, Mega A.M.',Ferrari M. and Gasparetto A.The evaluation of muscle oxygenation by NIRS hasbeen extensively described. The occurrence ofhaemoglobin desaturation during ischemia and muscleexercise was previously evaluated on human foreärm(De Blasi et al., Biochem Int, 1991). Recentlyoptic fibers were applied on the intercostal spaceof patients with heart failure demonstrating thepossibility of monitoring the respiratory muscledesaturation during an exhausting exercise by NIRS(Mancini et al., J Am Coll Cardiol, 1991). Notechnique is presently avaible to assess theadequacy of respiratory muscle 0 2 supply to theenhanced metabolic requests. We applied NIRS(NIRO500, Hamamatsu) for the evaluation ofatemm^-!_.;••:;mastoidens muscle oxygenation i,'
s with respiratory failure and as^a.eümechanical ventilation, at different levels ofpressure support in order to verify if the muscledesaturation was related to the woLk of breathing.Fig.1 shows a representative trend of Hb saturationchanges occurring modifying the pressure support ina no-weaning patient. No changes of arterial Hbsaturation were observed.
P6
CHANGES IN THE RELATIONSHIP OF MIXED VENOUS SATURATION ANDOXYGEN TRANSPORT WITH SEVERITY OF ARDSH. Steltzer,M. Hiesmayr,P.Krafft,R.Petcold,K.Strasser,AF.Hammerle
Supply dependency of oxygen uptake (V'02) is a common finding in patientswith Septic Shock Trauma or ARDS. Continuous mixed venous oxygensaturation (SvO2) monitoring allowsthe evaluation of the relation betwennoxygen supply (D'O2) and V'02. Low values of Sv02 are an indicator that D'02may be inadequate to meet the body needs.The aim of this study was to investigate the impact of severity of ARDS on therelationship D'02 and SvO2.Methods: After institutional approval 6 patients with severe ARDS werecontinuously monitored with a fiberoptic ejection fraction catheter (OTD/EFBaxter-Edwards). The patients severity of ARDS was graded according toMurray and divided into two groups (ARDS1 = Murray Score <2.8 and ARDS2=Murray Score >2.8). 325 consecutive measurements of Sv02 were comparedwith simultaneously calculated 002.Results: The values of SvO2 were significantly lower in ARDS2 (69.7% vs 76.5%)p<0.001. There was no difference in D'02 between both groups . In a multipleregression modeling there could be demonstrated a parallel downward shift ofthe regression line with more severe ARDS (SvO2= 55.4+ 2.95*ARDS +0.031•D02 [p<0.001]). At values of D'02 above 600 ml/min/m2 both curvestended to plateau (Figure), indicating that any increase in D'02 will be followedby a similar increase in V'O2.
'Ist. Anestesiologia e Rxanimazione,I Universita',Policlinico Umberto I, 00161 Roma;" Dip. Scienze eTecnologie Biomediche, Universita', 67100 L'Aquila
P7PULNONAYY NEUTROPHILS SEQUESTRATION DURING INTYA-ABDOMINAL SEPSIS ARE RELATED TO BACTEREMIAG.CAPELLIER*, S.LIAUW, T.WINTON, J.NARSHALL, W.DENAJO,F.BARALE*, P.M.WALKERUnder anesthesia, rats sprague-dawlet were operated. Aftercecal ligation, a 22 gauge puncture was realized. Theanimals received through the inferior veno-cava (IVC) orthe portal vein (PV) .5 n g of gadoliniun chloride/100 g ofbody weight. GdCl induce a reticulo-endothelial systemblockade. The animals were randomly assigned to one groupor to a control group (C). Neutrophils accumulation wasmeasured through the myeloperoxydase activity at 24 and 48hours (H).Positive blood cultures were in a higher number in theIVC group at 24 and 48 H.--------- ----------- -- -- --------- ------------Blood IVC* PV Ccultures * p < 0.05--------- -------------- ------5---- - ------------
2----_--- ---- 0---- - ----- 5- - -
10- --- -- ------9----- ----10--- ---
When all the animals were analyzed using the positiveblood culture (PBC) as a criteria, we found an increasein the lung dry/wet ratio in the PBC group (p = 0.05).MPO activity was significantly increase in this group at24 H.------------- -------------------
NPO Positive blood Ne g ative bloodactivity (A) culture group culture group------------- ------------------- ---------------- --A/igProt* 163.62 (31.15) 89.12 (17.03)------------ ------- -- -- ---- -------------------
A/mgDry lung* 43.86 (19.31) 11,9 (2,48)
In our model of peritonitis we have demonstrated an in-crease positive blood cultures using a reticulo-edotbelial system blockade. As shown with endotoxeiia,bactere.ia induce neutrophil accumulation. These seque-stration could explain the relationship between sepsis'and lung damage.*Service de rdaniaation n Edidale, CHU BESANCON 25000FRANCE - SICU research T0EÖNTO GENERAL HOSPITAL, CANADA
Conclusion: D'O2 and SvO2 are highly correlated at different levels accordingto the severity of ARDS. Above 600 ml/min/m2 of D'02 no further improvementof the D'02N'02 relationship could be demonstrated.
Dept. of Anaesthesia and Intensive Care, University School of Medicine,Spitalg.23, A-1090 Vienna, Austria
P8
RESPIRATORY FAILURE AND ACUTE PANCREATITIS : THE ROLE OFPANCREATIC AND NEUTROPHILIC ENZYMES.T. Dugernier, P.F. Laterre, G. Deby-Dupont, M. Lamy, M.S. Reynaert.
Respiratory failure (RF) is the major threat of the early phase of severe acutepancreatitis (SAP). RF has been ascribed to the transfer, notably lymphatic,of toxic substances issued from the pancreatic area. Besides its therapeuticvalue, drainage of the thoracic lymph (TDD) provides the uniqueopportunity to identify potential mediators of lung injury during SAP andto study their kinetics. TDD was carried out in 28 patients (22 males, meanage ± SD : 45 ± 15 years) with RF (mean PaO2/FiO2 ±SD : 154 ± 63 mm Hg)during the early phase of SAP (mean Ranson score ± SD : 6.8 ± 1.7; meanApache II score ± SD : 16±6). The delay between onset of symptoms andICU admission was 3.5 + 2.5 days. Etiology of SAP was alcohol abuse in 21patients. All patients were mechanically ventilated. Criteria for adultrespiratory distress syndrome were met by 13 patients (46 %). All but 2patients (93 %) survived. The mean duration of TDD was 6 ± 1.9 days witha mean volume of drained lymph of 9±8.2 1. Samples of plasma (PL) andlymph (LY) were simultaneously drawn on the 1st (First) and last day ofTDD and were assayed for immunoreactive trypsin (IRT; normal value: 284± 100 ng/ml), granulocyte elastase (ELA; normal value < 32 ng/ml) andneutrophil myeloperoxydase (MPO; normal value : 332 + 82 ng/ml). Resultsare expressed as mean + SD and a p value <0.05 was considered significant.
FIRST LAST
IRT MPO ELA IRT MPO ELk
LY, 1156+1145°' 1055+1039 265+124° 500+466 1140+1328 163.s-1 Jj
PL 485+587° 747+456 210+121 131+192 693+539 132+137
* compares lymph with plasma; ° compares ist and last day of TDD.Substantial amounts of pancreatic and neutrophilic mediators of lung injuryare transferred by the thoracic lymph. Whereas the release of pancreaticenzymes subsided over time, ongoing activation of neutrophils occurred inand outside the pancreas.
Departments of Intensive Care and Anesthesiology', St. Luc and Sart TilmanUniversity Hospitals, 1200 Brussels and 4000 Liege, Belgium.
P9CLIIICIL 31D ROIOIAGICGL CEM ti1AMIIATIa c011PARED MIS C01P0'TBRISEDTOIMIGRIF9Y 11 !NR IlW AJICALLI V91HLÄM PATIf311T.P.Navarrete, G.VScyuea, R.Rivera, E.Fernandei, A. Hdrida and J.N. Boch'.
Conventional clinical examination using chest auscultation and inspection(A/I), along with bedside radiology (X-ray), are the normally accepted methodsfor the morphological evaluation of the pleura and lung In the patient onaechanical ventilatiolr(MV). Both methods provide limited information in thissituation. on the other hand coeputerised. tomography of the chest (CrC)provides very reliable images.This study's objective is the evaluation of the efficacy of clinical (A/I) andradiological (X-ray) exploration at the bedside comparing it with CIC as anideal reference method.
Ne studied 23 patients, age 36±9.5 and APACH II score of 19.315 who were onIN for acute respiratory failure. A/I exaination of the anterior andposterior tones in each ben!-thorax evaluated the Increase and decrease inrespiratory sounds transmission (Vt 10 al/kg),and/or the presence of cracklesand/or thoracic assynetry, and these were compared with simultaneous chest I-ray and CTC findings for pulmonary condenation,collapse,pleural effusion andpneuaotborax.Tbe three tests were carried out separately by differentspecialists.In pleural pathology: of 8 cases of anterior pneuuothorax identified by CXC,none were detected by X-ray (0/8.0t),and b/I was positive in 3 cases(3/8.37.5%). Of the 21 cases of pleural effusion (by CPC) 12 were positive byX-ray (12/21. 57.1%) and 15 by A/I (15/21.71.4%).In pulmonary pathology:of 29 cases of segmental condensation (CXC), X-ray only identified 16(16/29. 55.1%) while of 7 lobar cases, X-ray identified 6 (6/7. 85.7%) and A/I7 (7/7.100%).In conclusion, chest X-ray and clinical methods are neither very sensitive norspecific with a high incidence of false negatives in the evaluation of pleuraland pulmonary pathologies in the ventilated patient, with CTC being thereference technique.
Services of Intensive Medicine and Radiology tVirgen de las lieves Nospital.Granada. Spain.
S119
P10FOLLOW UP OF ARDS - SURVIVORS BY CLINICAL INVESTIGA-TION AND HIGH-RESOLUTION COMPUTED TOMOGRAPHYK Strasser, R Petcold, K Eibenberger*, C Herold*, W Schlick **,H Slettzer
While patients during ARDS are meticulously monitored with respectto their respiratory function and thoracic imaging, the respiratorystatus of this patient population after surviving ARDS has received lessattention. In order to point out any correlation between severity ofARDS and health-status of survivors, 12 patients (age mean 21, rangefrom 7 to 69 years) were Investigated 12 t 4 months after dismissal fromICU. We discriminated moderate from severe ARDS by following para-meters: chest-x-ray, PaO2IFiO2, PEEP, and compliance (JF Murray:Am Rev Resp Dis 136:720, 1988). 7 patients with an index < 2.5 enteredgroup I for moderate and 5 patients with -e 2.5 group II for severeARDS.Our clinical Index consisted of following parameters: age, duration ofstay at ICU, number of additional organ failures, sepsis, degree of dia-gnostic and therapeutic efforts as pulmonary artery catheter, hemo-filtration, prostaglandine-therapy and inversed ratio ventilation.In the follow up study pulmonary findings were documented and sco-red (Pistolesi et al.: Intens Crit Care Dig 7:2-4, 1988) by high-resolutioncomputed tomography (HRCT). Furthermore cardiac state (ECG,NYHA, LOWN), degree of dyspnea and state of social reintegrationwere investigated, spirometry, blood gas analysis and a check-up ofneuromuscular function were performed.No correlation was seen between Murray-index representing severity ofARDS and our follow up index (hyp.-test for HO 0,86) includingHRCT-index (hyp.-test for HO 0,065).In conclusion, neither the severity of ARDS nor the pulmonary struc-ture as assessed by HRC'I' determine the health status of ARDS-survivors
Department of Anesthesia and General Intensive Care, Department ofRadiology*, Department II of Surge ry **,University of Vienna, Spitalgasse 23, A - 1090 Vienna, Austria.
P11
PULMONARY VASOCONSTRICTION IN RESPIRATORY DISTRESSIN PIGSR.M.J.L van der Heijde, H.P. Grotjohan, A. Versprille, C.A. Wagenvoort.
Vasoconstriction was studied in experimentally induced respirato-ry distress (RD). Eighteen pigs were anesthetized with pentobarbi-tal, paralyzed with d-tubocurarine and mechanically ventilated at arate of 10 per minute and an F,a, of 0.6. In six animals RD wasinduced by a pair of lung lavages followed after one hour byanother pair (group L). In a second group (n=6) a series of 0.1 mloleic acid injections was given (group OA). A third control group(group C. n=6) was ventilated for about 8 h. A similar Pw2 whichwas stable for 4-6 hours was induced in groups L (53 t 13mmHg) and OA (57 f 8 mmHg). Pulmonary arterial pressure (PP,)was significantly higher in group OA compared with group L: 36± 2 mmHg vs 31 ± 6 mmHg respectively (p<0.01). The animalswere killed with pentobarbital. As a measure of muscular vaso-constriction medial thickness (MT) as percentage of externaldiameter of muscular pulmonary arteries was determined invarious parts of the lungs. In group L MT was 7.7 t 2.9 % andin group OA it was 8.1 ± 3.2 % INS). In group C Pao, was 284t 21 mmHg, P,. was 14 ± 4 mmHg and MT was 3.8 ± 1.7 %.All these variables were different at p<0.01 from group L andOA. MT in corresponding lung regions was not statistical differentbetween group L and OA, implying a severe but similar degree ofmuscular vasoconstriction. As P„ was higher in group OA weconclude that besides muscular vasoconstriction other factorssuch as vasculitis and compression by lung edema were involvedin the development of pulmonary hypertension after oleic acid.
Pathophysiological Lab., Dept. of Pulmonary Diseases, ErasmusUniversity EE 2251, P.O.Box 1738, 3000 DR Rotterdam, TheNetherlands.
P12CENTRAL VASCULAR SURGERY AND PULMONARY VASCULAR INJURY.P. G. H. M. Raijmakere', A.B.J. Groeneveld', A.J.Schneider', J.A. Rauwerda 2, G.J.J. Teule', L.G. Thije'.
Ischaemia and reperfusion of the lower body duringcentral vascular surgery may release proinflammatorymediators that lead to a pulmonary vascular injury. Wetherefore studied tranevascular protein transport inthe lung. in 25 consecutive patients undergoing electivecentral vascular surgery (with aortic cross-clamping,Group 1, n=19) or reconstruction of the femoral artery(Group 2, n=6). Tranavascular protein transport wasmeasured one day before (preop) and after surgery(postop)1 y recording kinetics of intravenously in-jected ";Gallium-transferrin and 'Technetium-erythro-cytes in blood (sampling) and in the lung (externaldetection with a probe). A protein leak index (PLI,xlO''.min'') was calculated.
In Group 1, the mean (±SD) PLI rose from 96±28preop to 342±174, 3 hours postop (p<0.005, n=12). In asecond series of Group 1 patients (n=7) the PLI was97±42 preop and 115±40 (p>0.05) 24 hours postop. ForGroup 2, the PLI was 111*30 preop and 130±22 postop(p>0.05).
Hence, tranevascular protein transport in thelung increases about three-fold following surgery withaortic cross-clamping. However, the phenomenon istransient. No increase is observed following peripheralvascular surgery. Hence, ischaemia and reperfusion ofthe lower body may result in release of proinflammatorymediators, that transiently increase permeability ofthe pulmonary vasculature.
Medical intensive care unit', Dep. of Nuclear Medicine 3 ,Dep. of Surgery', Free University Hospital, Boelelaan1117, 1081 HV Amsterdam, The Netherlands.
This research was supported by a grant from the Dutch'stichting Maatschappij tot Redding van Drenkelingen'.
8120
P13HAEMODYNAMIC EFFECTS OFHYPERINFLATIONM Singer, J Vermaat, G Hall, G Latter, M Patel
Chest hyperinflation (HI) isa commonly usedICUprocedure during whichallerations in heartrateandblood pressure arefrequently seen. However,the relationship between tidalvolumes andinspiratory pressuresgenerated by HIandchanges in cardiac output (CO)havenotbeenelucidated. Cardiovascular derangements during 6 HIusinga 2 litrerebreathing baganda flowrateof 151itres O;>/min were thusstudied usingcontinuous beat-by-beat oesophageal Doppler monitoring of CO(ODM,Dellex, UK).A pressure transducer placed at the endof thecathetermount recorded ontoa chartrecorder thepeakinspiratory pressure (PIP)during (i) mechanical ventilation and(ii)HI.Thetidalvolumes (TV)generated by HI weremeasured with a spirometer. Thenurses performingthe HIwerekeptblinded to these additional measurements. Fifteenmechanically ventilated patients (age range 19-87y.)werestudied on 17occasions before, during, andat 1,5, 10and15minsafterHI.
I preHI I dunnQ HI 1 min 15min 10mln 15mlnIGO 7.0±0.6 6.2±0.Stt 64±O.6tt 6.S±0.St 6.6±O.S' 6.8±06
IHR 90±6 88±S 89±6 90±6 90±6 92±6
meanBP 77±3 7S±4 7S±3 7S+3 77+3 77+3
mean± SE p<O.OS' p<0.01f p<O.OOS" p<0.OO1tt
Significant (>10%) fallsor increases in BP(n=6) were bothassociatedwith falls inCO.A goodcorrelation (r=-o.64) wasseen between the%change in CO (range +5to -26%) andthe %rise in tidalvolume (range-33to +127%). There wasnocorrelation (r = 0.04)between the%fall inCOandthe %increase in PIP(range -30 to +167%). Neither thepresenceof Inotropic/pressor support (n=4) northeneedfor increased ventilatorysupport (n=9) wasrelated to a fall inCOduring HI.Falls inCO,which maytakeupto 15minutes to recover, are related to thedegree of HIbutnot to thepeak inspiratory pressure generated. AsHI ispoorly assessed bythe operator, a volume limiting device in thecircuitmayprove beneficial.
Bloomsbury Institute of Intensive Care Medicine, University College &Middlesex Hospitals, London, WC1 E 6JJ, UK
P14EFFECTS OF PEEP IN EARLY RESPIRATORY DISTRESS IN PIGSINDUCED BY LAVAGES AND OLEIC ACID ADMINISTRATIONH.P. Grotjohan, R.M.J.L van der Heijde, A. Versprille, J.R.C. Jansen.
This study was aimed at the evaluation of variables duringapplication of PEEP, which predict maximal oxygen delivery inearly respiratory distress, and therefore indicate the "best" level ofPEEP. Twentyfour pigs (9.4 ± 0.8 kg body weight) wereanesthetized with pentobarbital sodium, paralyzed withtubocurarine, and mechanically ventilated at 10 per min with anFI0 2 of 0.6. Respiratory distress was induced in 12 animals by astandardized protocol of two pairs of lung lavages at one hourinterval (group L), and in the other 12 by multiple small oleic acidinjections of 0.1 ml (group OA). In both groups a stable p. 0 2below 60 mmHg was established. Six animals of each groupserved as controls and revealed a stable hypoxaemia for 4-6hours. In. the remaining 6 animals of each group PEEP wasincreased in steps of 2 cmH20 from PEEP2 (PEEP of 2 cmH 20) upto PEEP12 and reset to PEEP 2 . Each level was maintained for 30min. p.0 2 increased in group L from 55 ± 14 mmHg to 218 ± 94mmHg at PEEP 12 and in group OA from 56 ± 7 mmHg at PEEP2to 226 ± 45 mmHg. End-expiratory lung volume (VEE) increasedin groups L from 12 ± 2 ml.kg-1 to 46 ± 9 ml.kg-1 and group OAfrom 16 ± 3 ml.kg-1 to 50 ± 3 rnl.kq". Central venous pressureincreased and cardiac output decreased linearly in both g'·oups."Best PEEP" was on average at PEEPe. At "best PEEP" VEE wassimilar to control values before induction of respiratory distress.Mixed venous P0 2 (Pii0 2 ) correlated significantly with oxygendelivery (00 2 ) in five animals of group L and in four of group OA.Physiological dead space, arterial to end tidal Pe 0 2 gradient, totalrespiratory compliance and venous admixture did not correlatewith 0 0 2 , We concluded that Pii 0 2 and VEE are useful indicators of"best PEEP" in early respiratory distress.
Pathophysiological. Lab., Dept. of Pulmonary Diseases, ErasmusUniversity EE2250, P.O. Box 1738, 3000 DR Rotterdam, TheNetherlands.
P15 P16
Hospital for the diseases of the Chest. Athens-Greece152 Messogeion Avenue.
14( 100%)14(100%)14(100%)
7(50%)9(64.2%)
11(78.5%)11(78.5%)
13 days14( 100%)10(70.1%)45 days2(14.2%)
1436.78-7080.5%
Table IIPreceeding infect.WeaknessSensory symptomsSymmetric facial
weaknessPharyngeal paresisAbnonnal CXRABG-s abnonnal.
level of CSFprotein andabsence of cells 14(100%)Plasmapheresis 6(42.8%)
Our results suggest that the meticulous attention to smalldetails of daily care is of greater importance in the careof GBS than any available treatment directed specificallyat the disease. Plasmapheresis seems to have a beneficialeffect on rate of improvement of Guillain-Barre syndrome.
GUILLAIN-BARRE SYNDROME IN THE leuL.Gregorakos. Ch.Katsanos. A.Michalopoulos. V.Malessios.D.Mavropanou. J.Nicolopoulos. K.Karageorgiou.
During the period 1984-1991. 14 patients (pts) with thediagnosis of Guillain-Barre syndrome (GBS) were admittedto our ICU because of respiratory failure. The presenta-tion and the main symptoms of pts are summarized in thetable below:
Table INumber of casesAverage ageAge rangePrior illnessOnset to maximaldeficit and plateauRespiratory failureMechanical ventil.Average hospital.Mortality
F.Bordct, A.Mercatello, B.Coronel, M'Brct, J.D.Tlgaud,E.Archimbaud,J.F.Moskovtchcnko
ACUTE RESPIRATORY FAILURE I:-.IDUeED BY ALVEOLARHEMORRHAGE IN HEMATOLOGICAL PATIENTS.
Service de Reanimation, Pavilion P cr Service d'Hcmatologic, PavilIon E;h6pital Ed. Herriot, 69437 Lyon Cedcx 03, France.
Several different life-threatening pulmonary complications are common inhematologicalpatients which could be transferredin ICU. These are dependentupon multiple factors, including the type of diseases, the nature and the timecourse of treatment, and the presence or absenceof neutropenia. At the onsetofthe disease, acute respiratory failure (ARF) is infrequent. In these cases, aninfection or a hyperieukocytic reaction are generally found. In the formersituation,chemotherapy are postponed. In the later, cytapheresisare performed.The aim of this study is to describe an other etiology of ARF at the auack ofdisease:diffuse pulmonary alveolar hemorrhage(DPAH).Five patients (I female) aged 47±1Owere admitted in ICU for ARF. Underlyingdiseases were: acute leukemia (3) and non-Hodgkin lymphoma (2). Initialphysical examination revealed a systolic blood pressure at 137±10 mmHg, aheart rate at 74±16 beat/min, a respiratory rate at 35±4 breath/min and acutaneous temperature at 37.2±0.4 °C. Two patients had episodes ofhemoptysie.Arterial blood gas determination with oxygen supplementrevealeda pH of7.4±O.I, PC02 of 4.6±O.5 kPa, P02 of 5.5±1.6kPa. Plateletcountswereunder range in 4 cases and intravascularcoagulationwas foundin 3 cases. In allcases, chest radiograph showed bilateral infiltrates. In 4 cases, bronchoalveolarlavage (BAL) fluids were bloody and negative for bacteria, virus, fungus andparasites.Clinical status and radiographicabnormalitiesrapidlyworsened. In allcases, treatments were specific chemotherapies associated with respiratorysupport (mechanical ventilation by oro-trachealintubation in 4 patient' and via afacial mask in one). In 4 cases, dyspnea, Pa02 and chest radiograph improvedprogressively and in these cases mechanical ventilationcould be stopped.Twopatients are discharged from ICU. The other 3 patients died because of theevolutionof the underlying diseases.In conclusion. DPAH is a life-threatening complication at the attack ofhematological disease. The Occurrence of DPAH is a sign of serious andprogressivediseases. DPAH diagnosis was made on the context, the hemoptysieand the bloody BAL fluid. A rapid specific treatmentbefore results of BALareessential for the improvement of ARF. The prognosisof this patients seem to besimilar to those which have other complications leading to intensive careadmissions.

P17RESPIRATORY DISTRESS TREATED BY POSITVE PRESSUREVENTILATION THROUGH A FACIAL MASK IN HEMATOLOGICALPATIENTS E.Tognet, A.Mercatello, B.Coronel, P.Polo, Y.Devaux, M.Bret,E.Archimbaud, D.Fitre,J.F.Moskovtchcnko.
Patients with hematological disease need sometimes respiratory support (RS)for acute respiratory failure (ARF). Unfortunately the mortality rate of patientsrequiring endotracheal intubation and mechanical ventilation is from 50 to 80% inrelation to the nosocomial complications and to the degree of aplasia. In thosepatients, both endotracheal intubation and mechanical ventilation inducenumerous complications. Therefore, there is a need for methods of ventilatoryassistance that could obviate the necessity for intubation in hematologicalpatients. Ventilation has been assisted non invasively by means of positivepressure ventilation administered through a facial mask (FM). Inspiratory-pressure support (IPS) is a new method of partial ventilatory assistance in whichconstant positive pressure is applied during the patient's spontaneous inspirationThis mode of RS reduces respiratory-muscle work. But this technique is difficultto use routinely because it requires numerous conditions including: cooperationfrom patient and ability to tolerate FM. The aim of this study is to test IPSthrough a FM in hematological patients.
15 patients (7 females) aged 36 years and treated for acute leukemia (14) ormyeloma (1) were prospectively ventilated through FM. The onset of ARFoccurred in 4 cases just before the induction of chemotherapy, 7 during aplasiaand 4 at the end of aplasia. The causes of ARF were alveolar hemorrhages (2cases), infections (9), hemodynamic edema (2) and unknown (2). At the time ofadmission in ICU, respiratory rate (RR) was 35 breaths/min and Pa02 lesser than6kPa while the patients were breathing air room. Intermittent treatment with IPSwas instituted at a level of pressure from 16 to 20 cm of water (Servo ventilatortype C, Siemens). The Fi02 was adapted to the result of Pa02 (40<FiO2<70%).
Out of 15 patients, 4 had immediate failure which resulted in endotrachealintubation within 3 hours. The causes of failure were : impossibility to adapt IPSto the patient (3) and cardiac arrest (1). 5 patients were incubated during IPS(seizure [1J, gastric dilatation [1], hemoptysie [1] and impossibility to adapt IPSto the patient [3]). These 9 patients . died. IPS was achieved with success in 6patients who were discharged from ICU. In the 11 patients treated by IPS, theduration of the treatment period was from 3 to 24 It per day (mean 13 h) and thenumber of days during which treatment was administered ranged from I to 16(mean 5.4 days). RR decreased from 33 to 23, Pa02 increased (17,7kPa); PaCO2remained stable (4,2kPa). Any hemodynamic change was noticed. Localtolerance of FM was excellent.
In conclusion, our results show that inspiratory pressure support delivered by afacial mask can obviate the need for conventional mechanical ventilation inhematological patients with acute respiratory distress.Services d'Anesthesie et d'Hematologie: Pavillons P et E, Hbpital Ed.
_ Herrint,_69437 I y, n edexAM France.---
P19PRESSURE CONTROL VENTILATION : WHAT THE BENEFITS?E. De Blasio,E. Iannuzzi,A. De Sio,F. Ferraro,F.Schiraldi,GF.Mostarda.Pressure Control Ventilation seems to be able to improvegas exchange reducing the risks of barotrauma and hemodynamit deternoration.10 patients with mild to severe respirat o
ry failure(Pa02/FiO2 ratio=168+87; Static Compliance=33+ 13),previously sedated and paralyzed,were ventilated employinga randomized sequence of Volume Control Mode with squareflow wave(VCMsq),Volume Control Mode with decelerating flow
wave(VCMdec) and Pressure Control Ventilation(PCV),keepingconstant respiratory rates,tidal volumes,inspiratory time(33%),Fi02 and peep.After 1 hour of each mode of vuntilat i
on a full set of ventilatory, hemodynamic and blood gas m e
asurements was obtained.The results are shown in the table.It has been suggested that the decelerating inspiratoryflow curve could account for the better results during PCV.Our experience confirms the benefits of PCV and suggests nore .complex mechanisms,even not fully understood,as thecomparision with VCMdec demonstrates.Parameters VCMsq PCV VCMdecPIP cmH20 41 +20 33+ 15w 37+17*P5wcmH2O 14+ 5// 14+ 6 15+ 6CI 1/m/m 4+ 1 4+ 1 4 + 1D02 ml/m/m 703+256 735+247k 706+248Pa02 mmHg 68+21 73+20 69+18Sa02 % 88+ 7 90+ 5 89+ 7Compl.eff. 19+ 6 22+10 t 15+ 90pp<0.01 vs VCMsq // p<0.01 vs VCMdec
p<0.05 vs VCMsq t p<0.001 vs VCMsq$p(0. 05 vs VCMdec 0 p<0.05 vs PCV
Servizio di Serapia Intensiva—I° Policlinico UniversitarioVia Pansini, 5 Pad. 17 80131 Napoli— Italia
S121
P18INVERSE RATIO VENTILATION: EFFECT ONEND-EXPIRATORY LUNG VOLU)E AND AUTO-PEEPP.Valta, J. Takala
We compared the effects of inverse ratio venti-lation (IRV) and PEEP on dynamic hyperinflationand auto-PEEP in 9 patients with ARDS and 10postoperative patients after coronary artery by-pass (CABG). During volume controlled mechanicalventilation with constant tidal volume (V 12ml/kg) and respiratory rate (12/min) two experi-ments were carried out; (1) with constant I:Eratio PEEP was increased in steps of 2 cmH 20 from0 to 12 cmHZO, and (2) with no PEEP I:E ratio waschanged stepwise from 1:4 to 4:1. PEEPtot wasmeasured while occluding the airway in end-expiration. Changes in end-expiratory lung volume(EELV) were measured with respiratory inductiveplethysmograph. We found that, (1) changing PEEPfrom 0 to 12 and IRV from 1:4 to 4:1 causedsimilar increase in EELV in ARDS (379±69 ml and390±83 ml), but in CABG the increase in EELV wasgreater with PEEP (1001±98m1 and 655±58m1), (2)when compared at the same levels of PEEPtot theincrease in EELV was similar with PEEP and IRV inboth groups, (3) EELV increased significantly inARDS with Te < 2.5 s and in CABG with Te < 2.0 s,and 4) peak inspiratory pressures were onlymarginally lower with the IRV (at EELV 150 mlwith IRV 2:1 and PEEP 8, Ppeak 37±3 and 4313 inARDS). We conclude that the effect of reducedexpiratory time on end-expiratory lung volume andpressure during volume controlled IRV is similarto the use of PEEP.
From the Critical Care Research Program, Depart-ment of Intensive Care, Kuopio University Hospi-tal, P.O.B. 1777, 70211 Kuopio, Finland
P20INVERSED RATIO VENTILATION WITH REDUCED PEEP INPATIENTS WITH ACUTE RESPIRATORY FAILUREN. Spannbrucker, U. Kiesow, R. Kleinschmidt
In patients with acute respiratory failure reduction of PEEP is recom-mended to avoid barotrauma of the lungs. Thirteen critically ill patientsfree of any factor known to alter chest wall mechanics were studiedprospectively. Continuous positiv pressure ventilation (CPPV) with aninspiratory : exspiratory (I:E) ratio of 1:2 and a PEEP of 10 mm Hgand CPPV with an I:E ratio of 2:1 and reduction of PEEP to 5 mmHg were administered to each patients in a random order for a 1 hperiod. Gas flow, tidal volume, tracheal pressure, blood gas concen-trations and hemodynamic parameters were measured.JIemodynamic parameters remained unchanged in both ventilatoryregimens. Inversed ratio ventilation with reduced PEEP tended toincrease Pa02 and decreased PaCO2 significantly from 44.3 mm Hgto 35.1 mm Hg (p <0.05). Without significant changes in minuteventilation and tidal volume inversed I:E ratio ventilation decreasedmean inspiratory pressure from 34.5 mm Hg to 29.6 mm Hg andincreased static respiratory compliance from 39 ml/mm Hg to 53ml/mm Hg significantly.
We conclude that in patients with severe respiratory failure inversedI:E ratio ventilation is superior to ventilation with I:E ratio of 1:2providing reduction in airway pressure and improvement in pulmonarygas exchange.
Medizinische Universitätsklinik Bonn - Allgemeine Innere Medizin -Sigmund Freud Str. 25, 5300 Bonn 1, FRG
S122
P21INTEREST OF COMBINED HIGH FREQUENCY PERCI'SSIV'E %*ENTI-L.ATION DURING ACUTE RESPIRATORY FAILURE AFTER SMOKELNIL.%LATIONP REPER'. E MARION '. E VAN HILLE '.H DE NEFF, W. HEYMANS',D YSEBAERT'. R VAN HOOF'. A VANDERKELEN -.
Smoke inhalation injury and bacterial pneumonia represent sonic of the mostimportant causes of mortality in burn patients.We described eleven severely burned patients (mean Burn Surface Area 49.7±24.2 %)with acute respiratory failure under conventional respiratory support (CRS)(Dräger UV l - LT 1:2 - Tidal Volume 10 to 20 mlikg) 8 to 32 hours after inhalationinjury.High frequency percussive ventilation (HFPV) is a recent ventilatory mode, whichcombines advantages of conventional ventilation with some of high frequencyventilation (1); HFPV was initially instituted as salvage therapy achieving in eachcase a dramatic improvement (within 14 to 32 hours)of blood oxygenation, PaCO 2
and ventilatory pressures(VDR4 - Percussionnaire Corp. - USA) (High frequencypercussions 300 to 900/min; conventional frequency 8 to 14 ,min).
CRS HFPV p (Wilcoxon test)m PaO,/FiO, 85.7±21.6 303.4±55.3 <0.003m PaCO, mmHg 54.4±6.2 34.3±4.6 <0.003m PEEP cmHO 10.5±1.2 10.5±2.1 ' NSm PIP cmHO 50.1±6.8 30.6±5.2 <0.003PIP=Peak Inspiratory Pres sure, PEEP=Positive End Expiratoy Pressure
Seven patients (63°/o) developed pulmonary infection during the acute phase; onepatient died of multiple organ failure on day 25.All the other patients survived; two developed bronchiolitis obliterans symptomsbefore discharge. No side effects were noted and hemodynamic tolerance of HFP Vwas excellent.This observation suggests that HFPV could improve pulmonary function and bloodoxygenation in these catastrophic pulmonary failures after smoke inhalation.Further studies are necessary to confirm this initial experience.(1) Cioffi and coil. J. of Trauma, 1989; 29-3: 350-54.
I Bums Center Brussels - 2 Centre €pidemiologiqueRoyal Military Hospital - Belgium
P22EFFECTS OF HIGH FREQUENCY PERCUSSIVE VENTILATION ONHEMODYNAMICS AND BLOOD OXYGENATION IN CRITICALLY ILLPATIENTSP. REPER', E. MARION', F. VAN 1-BLLE', D. YSEBAERT', M. ELSEN 2 ,
W. HEYMANS', R. VAN HOOF', A. VANDERKELEN'.
High frequency percussive ventilation (HFPV) is a recent ventilatory mode whichcombines advantages of conventional respiratory support with some of highfrequency ventilation: high frequency oscillations (300 to 900 cycles/min) areassociated with conventional cycles.Nine severely burned patients (mean Burn Surface Area 37±12%) were studiedunder conventional ventilation (Dräger Evita) and under HFPV (at two differentfrequency rates: 600 and 900/min) (VDR4 - Percussionaire Corp. - USA) underconstant FiO, and for periods of one hour (measurements every 30 minutes) insteady state.Under I-WPV, hemodynamic data are not significantly modified (heart rate (HR),cardiac index (CI), pulmonary wedge pressure (PWP), central venous pressure(CVP) and mean arterial pressure (MAP)). Peak inspiratory pressure (PIP) andconventional ventilatory frequency (CVF) were significantly lower under HFPV;blood oxygenation (Pa02 ) and CO, elimination were significantly improved afterone hour under HFPV. The oscillatory frequency rates don't influence theseconstations.
CV HFPV 600 HFPV 900 CV pHR 102.8±6.8 106.2±4.3 105.6±4.6 104.3±3.1CI 4.88±0.6 5.11±0.6 5.21±0.62 4.9±0.53PEEP 7±1 2 6.4±1 2 6.3±1 6.9±1.05PIP 36.9±3.2 26.3±2.1 24.6±1.6 36±2.9CVF 15.6±2.2 9.8±1.2 7.4±0. 15.3±3.1Pa0, 88.8±4.6 101.2±2.4 138.1±3.6 90.8±2.8PaCO5 36.9±2.2 30.2±1.9 27.8±2.8 36.4±2.8
• Wilcoxon p < 0.003
This observation suggests that HFPV represents a usefull ventilatory mode whichallows to ventilate at lower FiO, and under lower ventilatory pressures with anexcellent hemodynamic tolerance.
I Bum Center Brussels - 2 Centre EpidemiologiqueRoyal Military Hospital - Belgium
P23USEFULNESS OF NON INVASIVE PRESSURE SUPPORTVENTILATION (NIPSV) BY MASK IN THE CARE OF TRAUMAPATIENTS WITH RESPIRATORY FAILURE (RF).C. Gregoretti, F. Beltrame, G. Conti, L. Burbi, V. Antonaglia, U. Lucangelo,P. Biolino, P.M. Giugiaro, F. Sasso.
This five-year study evaluates physiological benefits in trauma patients withRF undergoing NIPSV. Patients were selected in three different centersfrom July 87 to July 91. The mean age was 39±19 years. Including criteriawere PaO2/FiO2 less than 200 mmHg, clinical signs of respiratory fatigue,respiratory rate (RR) higher than 30 breaths /min, tidal volume (TV) less than5 ml/Kg or CO2 retention during spontaneous or non invasive continuousflow CPAP. We performed 158 trials with 68 patients on NIPSV, InvasivePSV (IPSV) and spontaneous breathing (SB) recording gas exchange andrespiratory pattern. Respiratory support was delivered by Siemens ServoVentilator C in the PSV mode through endotracheat tube or face and nasalmasks modified to allow nasogastric tube insertion and to improve long termtolerance. Representative results (mean ±SD) are shown below.-------------------------------------------------------------------
SB IPSV NIPSVPa02/FiO2 146±42 238±77 * 275±107 §PaCO2 mmHg 41.7±10.2 38.8±6.1 38.3±5.1 §Ve 1/min 17.4±17.9 14.2±2.5 14.7±16.3TV ml 375.9±117.1 774±128' 710.8±193.1 §RR c/min 32±5 18.6±3.2 * 18.6±4.3 §PSV cmH20 - 12.4±9.3 13.5±5.8one-way ANOVA 'P< 0.05, SB vs. IPSV; § SB vs. NIPSV.-------------------------------------------------------------------------------Pa02/FiO2 increased significantly with both IPSV and NIPSV. The TVincreased with a concomitant reduction in RR so that Ve and PaCO2remained constant. No difference between IPSV and NIPSV was found.Although not statistically significant the better oxygenation observed withNIPSV is likely due to a better stimulus for coughing, which might haveincreased sputum production. Mask ventilation was performed for anaverage 67±65 hours long period. Only eight patients treated with NIPSVrequired intubation.Three for mask intolerance, five for occurred septicsyndrome. We conclude that NIPSV can safely substitute endotrachealintubation as a mean of delivering ventilatory support in most of consciousand collaborating trauma patients.
Department of Anesthesiology and Intensive Care, CTO Torino, via Zuretti,29 Torino, Italy.
P24NASAL POSITIVE PRESSURE VENTILATION FOR
TREATMENT OF NOCTURNAL HYPO VENTILATIONIN PATIENTS WITH SEVERE COPD
Schneider H, Becker H, Cassel W, Peter JH, von Wiehert P
Med. Poliklinik, ZIM, Philipps-Universität Marburg, Germany
Patients with COPD and sleep related breathing disorders(SRBD) have often exacerbation of hypoxemia, to life-threateninglevels that might be related to the higher mortality of these patients.The hypothesis of this study was that specific treatment of sleeprelated alveolar hypoventilation in patients with severe COPDimproves respiratory function, daytime sleepiness (EDS) andreduces the individual risk.
6 patients, mean age 57 yrs. mean BMI 30,8 kg/m 2, withsevere airway obstruction (FEV1 < 1,51), excessive daytimesleepiness (EDS) and alveolar hypoventilation (mean daytime P0257 mmHG pCO2 49 mmHG) were hospitalizized and treated byconventional regime (CR) of aggressive secretion clearencetechniques, antibiotics, corticosteroids, bronchodilatators, cardio-vascular support and supplemental oxygen. Respiration, SaO2 andEEG was recorded by standard polysomnography (PSG). Sleepinesswas documented by means of a standardized questionaire. Positivepressure ventilation (PPV) was established via nasal mask nasalusing BiPAP-ST (Respironics) or Bear 33 home ventilator.
During treatment with CR there was no significantinprovement of both the # of apneas, hypopneas, oxygendesaturation, EEG-arousal and daytime sleepiness (EDS). Duringtreatment with nasal PPV there was a significant decrease of # ofapneas (181-^17) hypopneas (281-27), oxygen desaturation (43432) and EEG arousal (243-.31). The reported EDS was diminishedwith this regime..
In order to prevent life threatening events in patients withsevere COPD it is important to record respiration during sleep. Theapplication of nasal positive pressure ventilation reduces the risk ofnocturnal hypoventilation. We conclude that the interaction of sleeprelated breathing disorders with COPD is a main factor in thedevelopment of severe respiratory failure and may be responsiblefor the higher mortality in COPD patients with nocturnalhypoventilation.
P25PRESSURE CONTROLLED INVERSE RATIO VENTILATION IN OLEICACID INDUCED LUNG INJURYUlf Ludwigs, Christer Klingstedt, Svante Bachrendtz and Göran Hedenstierna
Pressure controlled inverse ratio ventilation (PCIRV) has been proposed asan alternative ventilatory tedmique in severe lung injury. In order to clarifythe effects of PCIRV and the relative importance of the componentsconstituting this complex concept, a study has been carried out in an animalmodel of lung injury.Ten pigs (25 *_ dkg) were anaesthetized and mechanically ventilated. Lunginjury was induced by iv injection of oleic acid (0.15 ml/kg) and becamemanifest within two It Four ventilatory modes (volume controle zero PEEPI:E ratio 1:2 (VCZ 1:2), volume controle 10 cm H 0 PEEP (VCP 1:2),volume controle zero PEEP I:E ratio 4:1 (VCZ 4:1) and pressure controlezero PEEP I:E ratio 4:1 (PCZ 4:1)) were employed in random order. Centralhemodynamics, respiratory mechanics and gas exchange were measured aftera 30 minute stabilization neriod.
VCZ 1:2 VCP 1:2 VCZ 4:1 PCZ 4:1
Paw cm H O 41±8" 44±7" 41±7" 36±5a
Paw (cm 1-IZO) 11±3n 17±2c 22±3n 30±5"
FRC ml 207±90r 4221149" 373F173" 432±164"
Pao, (kPa) 10.5±6.0a 14.8±9.5"a 15.1±9.1"I 21.6±13.3"
Os Ot % 39±24" 23*_12v 23±16v 17±158
DO ml min 300±120" 344$71" 295±75" 263+52"
N=10. Mean values±SD. Letters in superscript refers to analysis of variancebetween ventilatory modes after lung injury. Values in overlapping 95 % Tukeyir.(ervais hui'e identical superscripts.
In this model, PCIRV did Icad to substantial improvements in gas exchangeand respiratory mechanics compared to conventional volume controlled PEEPventilation. The effects seem to be mediated principally by decelerating flowin combination with increased inspiratory time. PCIRV allows not only forreduction in Paw and minute ventilation but also for a decrease in inspiredoxygen fraction. Eviderrtly, in the light of new knowledge concerning lunginjury caused by high Paw, large tidal volumes and/or high inspired oxygenconcentrations, the beneficial effects of PCIRV are important and need to beinvestigated further in clinical studies on ARF.
Dept of Cardiology, Södersjukhuset, S-118 83 Stockholm, Sweden
S123
P26EFFECTS OF HIGH FREQUENCY PERCUSSIVE VENTILATION ONHEMODYNAMICS AND BLOOD OXYGENATION IN CRITICALLY ILLPATIENTSP. REPER', E. MARION', F. VAN HILLE', D. YSE13AERT 1 , M. ELSEN z,
W. HEYMANS', R. VAN HOOF', A. VANDERKELEN'.
High frequency percussive ventilation (JFPV) is a recent ventilatory mode whichcombines advantages of conventional respiratory support with some of highfrequency ventilation: high frequency oscillations (300 to 900 cycles/min) areassociated with conventional cycles.Nine severely burned patients (mean Burn Surface Area 37±12%) were studiedunder conventional ventilation (Dräger Evita) and under HFPV (at two differentfrequency rates: 600 and 900/min) (VDR4 - Percussionaire Corp. - USA) underconstant FiO. and for periods of one hour (measurements every 30 minutes) insteady state.Under HFPV, hemodynamic data are not significantly modified (heart rate (HR),cardiac index (CI), pulmonary wedge pressure (PWP), central venous pressure(CVP) and mean arterial pressure (MAP)). Peak inspiratory pressure (PIP) andconventional ventilatory frequency (CVF) were signficantly lower under HFPV;blood oxygenation (PaO,) and CO. elimination were significantly improved afterone hour under HFPV. The oscillatory frequency rates don't influence theseconstations.
CV
I-IFPV 600 HFPV 900 CVFIR 102.8f6.8
106.2±4.3
105.6±4.6 104.3±3.1
C 1 4.88±0.6
5.1110.6
5.21±0.62 4.910.53PEEP 7±1.2
6.4 +. 1.2
6.3±1 6.9±1.05PIP 36.9±3.2
26.312.1
24.6±1.6 36±2.9CVF 15.6±2.2
9.8+1.2
7.4±0. 15.3±3.1PaO, 88.8±4.6
101.2±2.4
138.1±3.6 90.8±2.8PaCO2 . 36.9±2.2
30.2±1.9
27.8±2.8 36.4±2.8• Wilcoxon p < 0.003
This observation suggests that HFPV represents a usefull ventilatory mode whichallows to ventilate at lower FiO, and under lower ventilatory pressures with anexcellent bemodynamic tolerance.
I Bum Center Brussels - 2 Centre EpidemiologiqueRoyal Military Hospital - Belgium
P27INTEREST OF COMBINED HIGH FREQUENCY" PERCUSSIVE VENTI-LATION DURING ACUTE RESPIRATORY FAILURE AFTER SMOKEINHALATIONP. REPER', E. MARION', F. VAN HILLE', H. DE NEEF', W. HEYMANS',D. YSEBAERT', R. VAN HOOF', A. VANDERKELEN'.
Smoke inhalation injury and bacterial pneumonia represent some of the mostimportant causes of mortality in burn patients.We describedeleven severely burnedpatients (mean Burn Surface Area49.7±24.2%)with acute respiratory failure under conventional respiratory support (CRS)(Dräger UV I - UE 1:2 -Tidal Volume l0 to 20 ml/kg) 8 to 32 hours after inhalationinjury.High frequency percussive ventilation (HFPV) is a recent ventilatory mode, whichcombines advantages of conventional ventilation with some of high frequencyventilation (1); HFPV was initially instituted as salvage therapy achieving in eachcase a dramatic improvement (within 14 to 32 hours)of blood oxygenation, PaCO,and ventilatory pressures(VDR4 - Percussionnaire Corp. - USA) (High frequencypercussions 300 to 900/min; conventional frequency 8 to 14/min).
CRS HFPV p (Wilcoxon test)in PaO/FiO. 85.7±21.6 303.4±55.3 <0.003in PaCO, mmHg 54.4±6.2 34.3±4.6 <0.003in PEEP cmH2O 10.5±1.2 10.5±2.1 NSin PIP cmli50 50.136.8 30.6±5.2 <0.003PIP=Peak Inspiratory Pressure; PEEP=Positive End Expiratoy Pressure
Seven patients (63%) developed pulmonary infection during the acute phase; onepatient died of multiple organ failure on day 25.All the other patients survived; two developed bronchiolitis obliterans symptomsbefore discharge. No side effects were noted and hemodynamic tolerance of HFPVwas excellent.This observation suggests that HFPV could improve pulmonary function and bloodoxygenation in these catastrophic pulmonary failures after smoke inhalation.Further studies are necessary to confirm this initial experience.(1) Cioffi and coil. J. of Trauma, 1989; 29-3: 350-54.
I Burns Center Brussels - 2 Centre epid6miologiqueRoyal Military Hospital - Belgium
P28
CICLIC VARIATIONS OF CO2-END TIDAL DURING VENTILATIONWITH TWO LEVELS OF CPAP (BIPAP).
Gomez V, De is Casa R, Anon JM, Pascual C, Jimenez M.and Yus S.
General Intensive Care Unit. Hospital "La Paz". MADRID
In last year we have started to use the mechanicalventilation mode called BIPAP (Ventilation with twoCPAP levels) as a method to ventilate and "weaning"patients. In this report we show the results ofmonitoring tidal volumes, espired CO2 and CO2-ET withthis technique.Twelve patients were included, 9 men and 3 women, whosemean age was 45+-8.4 years. The mean period undermechanical mentilation was 7+-3.2 days. The previousstatic compliance was 44+-18.39 ml/cm H20.The setting of the volumetric ventilator -EVITA,Dragger Corporation- was stablished as follows: P1 12,P2 6 cm H2O T1 6 seconds, T2 6 seconds. Espired CO2 wasmeasured with two capnographs: DATEX MODEL cd-101 andOHMEDA model OXICAP. Data are expressed as mean andstandart desviation.
Results:1.- The employment of BIPAP produced the followingvalues of CO2-ET: With PI 27.65+-10.74 mm Hg wasobtained and with P2 38.11+-12.54 mm Hg 2- The tidalvolumes ranged with both pressions from 205+-91.3 ml to559+-193.9 ml 3.- The difference between paCO2 and CO2-ET was 9.6+-7.6
Conclussions:During mechanical ventilation with BIPAP mode, periodicchanges are produced in Co2-ET in coincidence with theoscilations of psessions. Since the difference betweenpaCO2 and CO2-ET are minimal, we think this parametercould become into a guide of the ventilatory situationof patients in weaning phase by BIPAP method.

S124
P29MOIITHIIG REA1 £11101 P11090001 00EIIG HYBRID IBITILATIO1 (Combined
BFJI-CHT):Hot informing is it?P. Angoaridakis, E. Sofianoc, M. Anastasaki, 0. Prantiesios, E.Askitopoalot
Daring clinical application of hybrid ventilation,(cosbioed High FrequencyJet Yeetilation=HFJ1 and Conventional fecbaoical fettitatioa=C111), themain concerns are those of monitoring the attained intrapaltonary volumes(l j r bad intraalveolar pressures (Pall). The BFJ Teatilator's safetycontrol system is based on monitoring the mean airway pressure (Paean),which has been suggested as a reliable index of both Il l and Pali.Methods: It order to test the hypothesis that the Paean is tot an accaretemonitor of Pali and Ti., ender variable conditions of lang coapliaace(Ct)and airway resistance (law), to studied it a long model the effects ofchanges in CL and law, on lat,Paly and l i p toiler constant reetilatorysettings. He teed the Penlon Bronsgrove Jet ventilator, the Brager 01-1conventional ventilator and the Drager ling sitelator with an endotrachialtobe Bi -lo Jet Mallincrodt B.So ID, which icorporates a linen with adistal opening fr •eassaring the airway pressares. Palo aid l i p wererecorded. The BPJI was set at a driving pressure of 40 psi 25% ieepiratorytime and 10th/an respiratory rate (I1). These settings were chosen asthey reunited in a •atitaf jet f r _700t1 for a mean airway pressure(Pueao)=I0cuI10. The CRY ras net at a flow of lit/sec, RRrtb/tin, tidalrolsue (0r)=I00e1, and 0 PEEP.Oar results showed that for Ct=IO0al/csH i Oand Fat=2ca/el.sec the marital for Paean=l0 iotrapilaonary volume tag
2500el and Palv:l4ca. Then Pat increased ep to 64c.ful.sec the lit reduceddown to 1400 and Palo descreased to Hera/rt. On the contrary by decreasingthe C L from 100 to 15al/c.B0O the l tr reduced down to 400x1 and Paloincreased from 14 to 40c.B10. This study has shorn that Paean is not asate monitor of the iotrapaltonary volumes and alveolar pressures daringhybrid ventilation under conditions of variable C l, and Rae.
Anesthetic Dep/vent, ICU of University Hospital of Iraklion, GREECE
P30INFLUENCE OF PRESSURE LIMITED AND VOLUME LIMITATEDVENTILATION ON INTRACRANIAL PRESSURE IN HEAD INJUREDPATIENTSR.Priem, R.Schuttheiss, C.Cedzich
Introduction:Head injured patients with intracranial hypertension must be treated byintubation, respiratory support and sedation. Dramatic results in preventionand treatment of respiratory complications and ARDS were obtained bypressure limited ventilation. This study compares the influence of pressureand volume limitated ventilation on intracranial pressure (ICP) and cerebralperfusion pressure.Patients and Methods:18 patients admitted to ICU after a severe head injury (GCS<_5), SAH (H&HIV-V) or ICH (Fisher 3-4) had a continuous and simultaneous monitoring ofRCP and CPP. All patients were treated with intubation, sedation andmechanical ventilation. They were divided into two groups; (A) the initialrespiratory support was a pressure limitated ventilation (PLV) and (B) avolume limitated ventilation (VLV). Every 24 hours the ventilation design waschanged from PLV to VLV and vice versa, unless pulmonary complicationsmade a PLV necessary. All patients were sedated.Results:In the long term follow-up there was no significant increase or decrease ofICP after the change from VLV to PLV (p<0.01) and vice versa, with amaintained PEEP. Only immediately 1-3 hours after the change or after ansignificant increase of the maximum pressure border in PLV there was anincrease of about 20% in RCP which always became stabilized to the previousvalues within half an hour.Conclusion:A pressure limitated ventilation does not induce a significant and persistentincrease of RCP. Thus, all advantages of PLV may be gained even inneurotraumatized patients without influencing the most importantmonitoring parameter (RCP and CPP) in these patients.
Clinic of Neurosurgery, University of Bonn, Sigmund-Freud-Str.25,5300 Bonn, FRG
P31
PRESSURE SUPPORT VENTILATION BY FACIAL MASK INIMMUNOCOMPROMISED PATIENTS WITH RESPIRATORY FAILUREA Rabbat. M f Garrouste G Nahmias J R Le Gall 8 Schlemmer
Irnmunocompromrsed ( IC ) patients weih acute respiratory failure ( ARF )recgrunng enclotracheal intubation and mechanical ventilation ( MV ) have a verypoor prognostic. The aim of this prospective study was to evaluate the efficacy ora non invasive ventilatory assistance pressure support by means of a face mask( PSFM) in IC patients with ART METHODS ARF was defined by a respiratory
rate ( RR 1» 25/mn and Pa02 < 55 mmHg at room air or Pa02 / F102 < 250 mmHgand bilateral infiltrates on the chest X- ray The pressure support at a levelbetween 8 to 25 cm of water was delivered through a tight titling facial mask by aCesar ( CFPO I ventilator A PEP 01 5 cm of water was addedRESULTS 19 IC patients ( 13 AIDS 6 neutropenics with hematologicalmalignencies I. SAPS = 11 8 x 4 1. aged 38 z 9 years 17 males were initiallytreated with PSFM The ARF was due to infection in 15 cases In 12 patients PSI`Mwas a succes avoiding tracheal intubation 7 patients were incubated ( 5 deaths )
Entry Hat H+24 Dischargen= 19 n^ 19 n= 1 r n- 12
RR(/ mn) 38--7 29-5 2,-7 2t r3'HR(/mn) 109xl7 105_2) 9t,-2'i 84_r,AllAP (nlml fig) 850177 85019 89.11ß 75.1PaCO2 (rrrrJigi 34.7 36-6 3o.3 3b.4Pa02 / F102 143-55 259.91- 246.124' 318.171'(mfg) ' p.- 0 (J01 vs entryAll patients lulerahnoj well the PSI M ventilation Mean da ly administration ofPSFM was 6 x 2 hours (2-12) during 1 to 21 days Timte of incubation ( failure ofPSFM I was early (< 48 h (tor 5 patients 2 septic shocks (2 deaths) 1 massivepulmonary hervorrage (dead) 2 after BAI- (2 alive?) or late for 2 patients will,severe ARD; ors day 13 arid day 21 (7 deaths(CONCLUSIONS Pressure support ventilation delivered by face mask inunrnunorompromised patients with respiratory failure result in early physiologicrmproverrr nt and may redur-e the need for intubation arid hrechanrcal ventilation
Departrnc;nt of ir.tynslvn; cart IJnrversrty Hospital Saint I ours75010 Pans FHANr,f
P32A MORPHOLOGICAL STUDY OF PRESSURE CONTROLLED INVERSERiTIO VENTILATION IN OLEIC ACID INDUCED LUNG INJURY.t' If Ludwi>s, Christer Ktingstedt, Svante Baehrendtz, Güran Wegenius andDoran Hedcnsticrna
Pre'.sure controlled inverse ratio ventilation (PCIRV) has been proposed asan alternative ventilatory technique in severe lung injury. In order to clarifythe morphological effects of this ventilatory mode, it has been investi gated inin animal model of acute respiratory failure (ARF). A mow phological analysisI b computerized tomography has been performed and PCIRV has beencompared with conventional PEEP ventilation.Six pigs (25 ± 4 kg) were anaesthetized and mechanically ventilated. Lungi njury was induced by iv injection of oleic acid (0.15 ml/kg) and becamemanifest within two h Four ventilatory modes volume controle zero PEEPLE ratio 1:2 (VCZ 1:2), volume controle 10 cm HO PEEP (VCP 1:2),vutume controle zero PEEP I:E ratio 4:1 (VCZ 4:1 ) and pressure controlezero PEEP I:E ratio 4:1 (PCZ 4:1)) were employed in random order.Respiratory mechanics, gas exchange and central hemodynamics weremeasured and structure and density of the lungs studied by CT scanning(Somatomc HiQ, Siemens Elema). A transverse scan just above the level ofthe dia phragm was obtained during four seconds in end-expiratory a pnea.Mean density expressed as Hounsfield units (HU) and proportion ofatelectatic and poorly aerated lung was then calculated.Vereins admixture was strongly correlated to the ma gn itude of atelectatic lungrc giuns (r-0.86).Mean density during VCZ 1:2 (-216 HU) xiU) was a promatelyhalf of that registered during ventilation with VCP 12 ( 389 HU , VCZ 41 (-31,0 fIU) and PCZ 4:1 (-411 HU). No statistically significant differencesbctwecn the latter three modes were observed. The pro portion of of poorlyaerated regions (-200 to -100 HU) was about 14% with VCZ 1:2 and 10% inthe other ventilatory modes. The quantity of atelectatic area (-100 to 100Iltl was 44% with VCZ 1:2 and considerably smaller with VCP 1.2 (24%
4:1 (29%) and PCZ 4:1 (32%). Thus, during VCZ 1:2, almost 60% othe lung area was poorly aerated or atelecatic. The three other modesresulted in su perior aeration with corresponding percentages of 34% (VCP1.2). 35 (VCZ 4:1) and 32% (PCZ 4:1),I (:1R V (cads to a reduction in atelectatic and poorly aerated lun g regions.'I hest effects correlate to the magnitude of venous admixture and are of thesiehe magnitude as seen with conventional PEEP ventilation and seem to be0: l,Icd lu the presence of positive end-expiratory pressure.
Dept of C ardiulogy, Södersjukhuset, S-118 83 Stockholm, Sweden
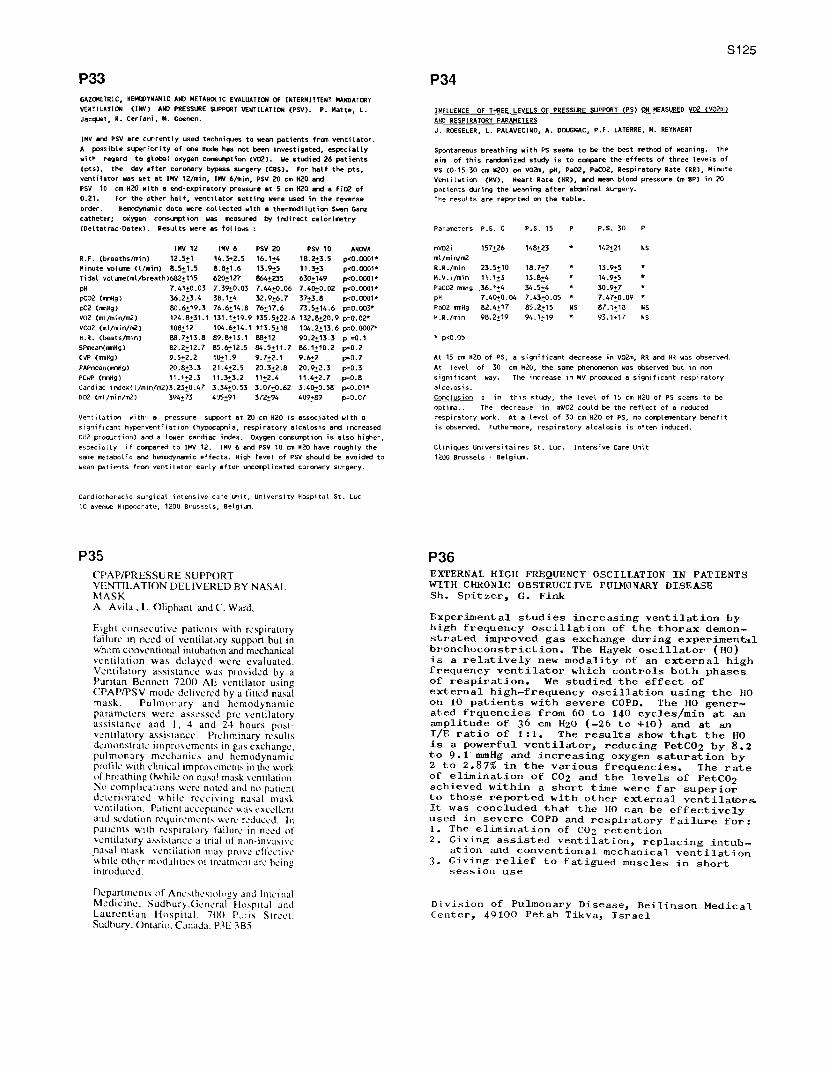
P33GAZOMETRIC, HEMC YNAMIC AND METABOLIC EVALUATION OF INTERMITTENT MANDATORY
VENTILATION (IMV) AND PRESSURE SUPPORT VENTILATION (PSV). P. Matte, L.
Jacquet, R. Cerieni, M. Goenen.
IMV and PSV are currently used techniques to wean patients from ventilator.
A possible superiority of one mode has not been investigated, especially
with regard to global oxygen consumption (V02). Ne studied 26 patients
(pts), the day after coronary bypass surgery (CBS). For half the pts,
ventilator was set at INV 12/min, INV 6/min, PSV 20 cm H2O and
PSV 10 cm H2O with a end- expiratory pressure at 5 cm H2O and a Fi02 of
0.21. For the other half, ventilator setting were used in the reverse
order. Hemndynarnic data were collected with a thermodilution Swan Ganz
catheter; oxygen consumption was measured by indirect calorimetry
(Deltatrac-Datex). Results were as follows
INV 12 IMV 6 PSV 20 PSV 10 ANOVA
R.F. (breaths/min) 12.5+1 14.3+_2.5 16.1±4 18.2+3.5 p<0.0001*
Minute volume (1/ein) 8.5 + 1.5 8.8+ 1.6 13.9+5 11.3+3 peO.0001*
Tidal vol umetmt/breath)682 + 115 620+127 864+235 630+149 p<0.0001•
pH 7.41 +0.03 7.39+0.03 7.44+0.06 7.40!0.02 pc0.0001*
pCO2 (moig) 36.2+3.4 38.1+4 32.9+6.7 37+3.8 p<0.00010
p02 (mmHg) 80.6+19.3 76.6«14.8 76+ 17.6 73.5+ 14.6 p=0.003*
V02 (m1/min/m2) 124.8+31.1 131.1 + 19.9 135.5+ 22.6 132.8+20.9 p=0.02*
VCO2 (ml/mirVm2) 108+ 12 104.6+ 14.1 113.5+ 18 104.2+ 13.6 p=0.0007"
H.R. (beats/min) 88.7+13.8 89.8+13.1 88+ 12 90.2+ 13-3 p =0.1
BPmean(mmHg) 82.2 +12.7 85.6!12.5 84.5+11.7 86.1 + 10.2 p=0.2
COP (mmHg) 9.5 + 2.2 10!1.9 9.7+ 2.1 9.6+2 p=0.7
PAPmean(mr5ig) 20.8+3.3 21.4+ 2,5 20.3+2.8 20.9+2.3 p=0.3
PCwP (mmHg) 11.1 +2.3 11.3+ 3.2 11+2.4 11.4+2.7 p=0.8
Cardiac ireJex(t/min/m2 )3.23+0.47 3.34+ 0,53 3.07+0.62 3.40!0.58 p=0.01*
D02 (ml/min/m2) 394+73 495+91 372+94 409+89 p4.07
ventilation with a pressure support at 20 cm H2O is associated with a
significant hyperventilation (hypocapnia, respiratory atcglos is and increased
CU2 prod,ction) and a lower cardiac index. Oxygen consumption is also higher,
especially if compared to IMV 12. INV 6 and PSV 10 on H2O have roughly the
same metabolic and hemodynamic effects. High level of PSV should be avoided to
wean patients from ventilator early after uncomplicated coronary surgery.
S125
P34
INFLUENCE OF THREE LEVELS OF PRESSURE SUPPORT (PS) ON MEASURED V02 (V02n.0
AND RESPIRATORY PARAMETERS
J. ROESELER, L. PALAVECINO, A. DOUGNAC, P.F. LATERRE, M. REYNAERT
Spontaneous breathing with PS seems to be the best method of weaning. The
aim of this randomized study is to compare the effects of three levels of
PS (0-15-30 cm 820) on V02m, pH, Pa02, PaCO2, Respiratory Rate (RR), Minute
Ventilation (MV), Heart Rate (HR), and mean blood pressure (m BP) in 20
patients during the weaning after abdminat surgery.
The results are reported on the table.
Parameters P.S. 0 P.S. 15 P P.S. 30 P
mV02i 157+26 148+ 23 * 142+ 21 NS
ml/mirVm2
R.R./min 23.5+10 18.7+7 * 13.9+5 *
M.V.I/min 11.1_3 13.8+4 * 14.9+5
PaCO2 0mH9 36.1 +4 34.5 +4 * 30.9+7 *
pH 7.40+ 0.04 7.43 +0.05 * 7.47+0.09
Pa02 mmHg 82.4+ 17 85.2+15 NS 87.1 + 18 NS
N.R./min 98.2+19 94.1,19 * 93.1+17 NS
* p<0.05
At 15 cm H2O of PS, a significant decrease in V02m, RR and HR was observed.
At level of 30 cm 820. the same phenomenon was observed but in non
significant way. The increase in MV produced a significant respiratory
alcolosis.
Conclusion : in this study, the level of 15 cm H2O of PS seems to be
optimal. The decrease in mVO2 could be the reflect of a reduced
respiratory work. At a level of 30 cm H2O of PS, no complementary benefit
is observed. Futhermore, respiratory alcalosis is often induced.
Cliniques Universitaires St. Luc. Intensive Care Unit
1200 Brussels - Belgium.
Cardiothoracic surgical intensive care unit, University Hospital St. Luc
10 avenue Hippocrate, 1200 Brussels, Belgium.
P35
CPAP/PRESSURE SUPPORT
VENTILATION DELIVERED BY NASAL
MASK
A. Avila , L. Oliphant and C. Ward,
Eight consecutive patients with respiratory
failure in need of ventilatory support but in
whom conventional intuhation and mechanical
ventilation was delayed were evaluated.
Ventilatory assistance was provided by aPuritan Bennett 7200 AE ventilator usingCPAP/PSV mode delivered by a fitted nasal
mask. Pulmonary and hemodynamic
parameters were assessed pre-ventilatory
assistance and 1, 4 and 24 hours post-
ventilatory assistance. Preliminary results
demonstrate improvements in gas exchange,
pulmonary mechanics and hemodynamic
profile with clinical improsemcntti in the work
of breathing Owhile on nasal mask ventilation.No complications were noted and no patientdeteriorated while receiving nasal mask
ventilation. Patient acceptanc • was excellent
and sedation requirements were reduced. In
patients with respiratory failure in need ofs entilatory assistance a trial of non-inn asinCnasal mask ventilation may prove effective
while other modalities of treatment are beingintroduced.
Department~ of Ancsth •si l y and Internal
Medicine. Sudhury.General Hospital and
Laurentian Hospital. 70(1 P,:ris Street.
Sudbury, Ontaio, Canada, PIE 3B5
P36EXTERNAL HIGH FREQUENCY OSCILLATION IN PATIENTSWITH CHRONIC OBSTRUCTIVE FULMONARY DISEASESh. Spitzer, G. Fink
Experimental studies increasing ventilation byhigh frequency oscillation of the thorax demon-strated improved gas exchange during experimentalbronchoconstriction. The Hayek oscillator (HO)is a relatively new modality of an external highfrequency ventilator which controls both phasesof respiration. We studied the effect ofexternal high-frequency oscillation using the HOon 10 patients with severe COPD. The HO gener-ated frquencies from 60 to 140 cycles/min at anamplitude of 36 cm H2O (-26 to +10) and at anI/E ratio of 1:1. The results show that the HOis a powerful ventilator, reducing PetCO2 by 8.2to 9.1 mmHg and increasing oxygen saturation by2 to 2.87% in the various frequencies. The rateof elimination of CO2 and the levels of PetCO2achieved within a short time were far superiorto those reported with other external ventilators.It was concluded that the HO can be effectivelyused in severe COPD and respiratory failure for:1. The elimination of CO2 retention2. Giving assisted ventilation, replacing intub-
ation and conventional mechanical ventilation3. Giving relief to fatigued muscles in short
session use
Division of Pulmonary Disease, Beilinson MedicalCenter, 49100 Petah Tikva, Israel

S126
P37'ABNORMAL' FLOW, AIRWAY PRESSURE, AND CAPNOGRAPHY WAVEFORMS
DURING NORMAL AIRWAY PRESSURE RELEASE VENTILATIONC: Putensen, M. Leon, G. Putensen-Himmer
-Airway pressure release ventilation (APRV) is based on intermittent time-cycledrelease of continuous positive airway pressure (CPAP) to a lower pressure level.APRV augments ventilation by passive lung deflation from a baseline lung volumeestablished by CPAP and is designed to allow unrestricted spontaneous breathingthroughout the ventilator cycle. As a result extraordinary gas flow (V), airway pressure(Paw), CO2 concentration(CO2) waveforms are observed during routine monitoring.This waveforms may not be interpreted correctly by monitors or by physicans notfamilar with APRV. This study describes such "abnormal" V. Paw, and CO2waveforms observed during uncomplicated APRV.
Ten pigs weighing 25-30 kg, were anesthetized with pentobarbital (7 mg/kg/h),and then tracheotomized. The pigs remained in the supine position andspontaneous breathing was augmented by APRV using a commercial availableventilator (PPG, IRSA). Gas flow was measured with a pneumotachograph betweenthe endotracheal tube and the ventilator's Y-piece. Paw and CO2 fractions weremeasured at the endotracheal tube. All signals were sampled by an A/D boardinstalled in a computer (IBM P/S2 70) operating under custom designed software.Digitized signals were stored in real-time for computeraided off-line analysis. Tostudy V. Paw, and CO2 pattern during different APRV settings, CPAP varied from 5 to15 , release pressure was 0 cm H2O. Release time varied from 1 to 2 s, CPAP timefrom 2to45.
The figures show examples of "abnormal looking" V, Paw, and CO2 waveformsrecorded during APRV. Fig. 1 shows spontaneous breathing during the CPAPrelease period that is merged with CPAP restoration. Fig 2. shows CPAP restorationimmediately followed by a spontaneous breath. In both cases the presence of twomajor expiratory flow waves (e, e') for each inspiration (i) is noticeable. First expiratoryflow wave (e) is due to CPAP release, the second (e') results exclusively fromexpiration of a tidal volume due to spontaneous breathing. The inspiratory flow wave(i) combines spontaneous inspiration and CPAP restoration components.Fio.1 Fig .2602 \^ f — — ^f _ l
Paw ~^
V e r e ' y- Ve
"Abnormal" V, Paw, and CO2 waveforms are frequent observed during normalAPRV. These waveforms provide important clinical information, but differentiation ofmechanical and spontaneous components may not be easy for unexperiencedclinicians and respiratory monitors. Knowledge of what is, and is not normal, isnecessary for appropriate application arid monitoring of APRV.
Department of Anesthesiology, University of South Florida, Tampa 33612, USA
Shock IP38
A STUDY OF THE DETERMINANTS OF CENTRAL VENOUS CO2 TEN-SION (PVCO2) IN SEPSIS. I. Glovanninl, C. Chiarla', G.Boldrini' 8 , M. Castagneto`.
Data from 260 measurements in 72 critically ill septicpts were used to assess determinants and correlates ofPVCO2. Arterial and central venous blood gas analyseswere associated with determinations of pulmonary shunt(Qs/Qr), ventilation/perfusion ratio (VA/Qr), 02 consum-ption (VOz), respiratory quotient (RQ), cardiac index(CI), 02 extraction (O2Ex) and other indices. Venous-arterial CO2 concentration difference (v-aDCOz,ml/100ml) was calculated by an original model (Perspec-tives in Critical Care 2:139, 1989) with the specificquantification of its Haldane component (HALD = Oz -
linked COs exchange, % of total v-aDCOz).Regression analysis showed that arterial CO2 tension(PaCO2) was the main determinant of PVCO2 and explained90% of its variability (rz= 0.9, p < 0.0001).At any given PaCOz, PVCO2 was principally set by HALO,v-aDCO2 and central venous pH, which explained together89% of the variability of the PvCOz-PaCOz gradient(mmHg): (PvCO2-PaCO2) = 38.1/HALD+1.5(v-aDCO2) -8.6(pHv)(rz= 0.89, p < 0.0001). HALD was inversely related toVA/Qr and RQ, directly related to VOz, OzEx and CI, andshowed a complex relationship to Qs/QT. Changes inVA/Qr, RQ and VOz explained together 80% of the variabi-lity of HALD (rz= 0.8, p < 0.0001).The level of PVCO2 depends on PaCOz and on the balancebetween C0z exchange and transport, which may be affec-ted by metabolic acidosis, changes in CO2-binding pro-perties of blood, and specific cardiorespiratory inte-ractions. This is relevant for defining the correct Im-plications of altered PVCO2 levels in clinical settings.
'Centro Studio Fisiopatologia Shock CNR, 'Divlsione diChirurgia Geriatrics Istltuto'di Patologia Chirurgica,Catholic University, Largo Gemelli 8, I-00168 Roma,Italy
P39
COMPPRISON OF HAE1()DYNBMIC AND OXYGEN TRANSPORT
RESPONSE TO HATASTARCH AND MODIFIED FLUIDGELATIN IN CRITICALLY ILL PATIENTSBeards SC, Watt T, Edwards JD and Nightingale P.The Intensiv. Care Unit. University HospitalSouth Manchester, Uk.
The effects of rapid (< 10 minutes) infusion of500mls of modified fluid gelatin (group A) or
hydroxyetylated starch (group B) were compared in a
prospective non-randomized, non-crossover study of
patients suffering from acute hypovolemia whilst beingmechanically ventilated for acute respiratory failure
on an intensive care unit. Haemodynamic and oxygentransport variables were determined at baseline, 15minutes and 30 minutes, in summary, in both groupsthere were significant increases in pulmonary artery
wedge pressure, stroke volume and cardiac index. Inneither group did heart rate decrease. In group Aoxygen delivery increased but in did not in group B.This was due to greater'haemodilution in group B.
Copyright © 2022 FDOKUMEN