
Prospective validation of predictive value of abdominal computed tomography scan on time to first...
10
ORIGINAL ARTICLE Prospective validation of predictive value of abdominal computed tomography scan on time to first treatment in Rai 0 chronic lymphocytic leukemia patients: results of the multicenter O-CLL1-GISL study Massimo Gentile 1 , Giovanna Cutrona 2 , Stefano Molica 3 , Fiorella Ilariucci 4 , Francesca R. Mauro 5 , Nicola Di Renzo 6 , Francesco Di Raimondo 7 , Iolanda Vincelli 8 , Katia Todoerti 9 , Serena Matis 10 , Caterina Musolino 11 , Sonia Fabris 12 , Marta Lionetti 12 , Luciano Levato 3 , Simona Zupo 2 , Francesco Angrilli 13 , Ugo Consoli 14 , Gianluca Festini 15 , Giuseppe Longo 16 , Agostino Cortelezzi 9 , Pellegrino Musto 17 , Massimo Federico 18 , Antonino Neri 12 , Manlio Ferrarini 10 , Fortunato Morabito 1 1 Hematology Unit, Department of Onco-Hematology, A.O. of Cosenza, Cosenza; 2 SS Molecular Diagnostics IRCCS S. Martino-IST, Genova; 3 Department of Oncology and Haematology, Pugliese-Ciaccio Hospital, Catanzaro; 4 Division of Haematology, A.O. S. Maria Nuova, Reggio Emilia; 5 Divisione di Ematologia, Universit a La Sapienza, Rome; 6 Hematology Unit, Ospedale Vito Fazzi, Lecce; 7 Division of Haematology, Department of Biomedical Sciences, University of Catania and Ferrarotto Hospital, Catania; 8 Hematology Unit, A.O. of Reggio Calabria, Reggio; 9 Laboratory of Preclinical and Translational Research, IRCCS, Referral Cancer Center of Basilicata, Rionero in Vulture (Pz); 10 Direzione Scientifica IRCCS, San Martino IST, Genova; 11 Division of Haematology, University of Messina, Messina; 12 Department of Clinical Sciences and Community Health, University of Milano and Hematology CTMO, Foundation IRCCS Ca’ Granda Ospedale Maggiore Policlinico, Milan; 13 Department of Hematology, Ospedale Santo Spirito, Pescara; 14 U.O.S. di Emato-Oncologia, Ospedale Garibaldi-Nesima, Catania; 15 Centro di Riferimento Ematologico-Seconda Medicina, Azienda Ospedaliero-Universitaria, Ospedali Riuniti, Trieste; 16 Unit a di Ematologia, Ospedale San Vincenzo, Taormina; 17 Scientific Direction, IRCCS, Referral Cancer Center of Basilicata, Rionero in Vulture (Pz); 18 Department of Onco-hematology, Universit a di Modena Centro Oncologico Modenese, Policlinico Modena, Italy Abstract Objective: We performed an external and multicentric validation of the predictive value of abdominal computed tomography (aCT) on time to first treatment (TTFT) in early stage chronic lymphocytic leukemia (CLL) patients. Methods: aCT was performed at diagnosis in 181 Rai 0 patients enrolled in the O-CLL1- GISL trial (clinicaltrial.gov ID:NCT00917549). Results: Fifty-five patients showed an abnormal aCT. Patients with an abnormal aCT showed a significantly shorter TTFT than those with normal aCT (P < 0.0001). At multivariate analysis, aCT (P = 0.011), b-2 microglobulin (P = 0.019), and CD38 expression (P = 0.047) correlated with TTFT. Following IWCLL 2008 criteria, 112 (61.9%) cases remained at Rai 0, while 69 (38.1%) satisfied the criteria of clinical monoclonal B-cell lymphocytosis (cMBL). Reclassified Rai 0 patients with an abnormal aCT showed a significantly shorter TTFT than those with a normal aCT (P < 0.0001). At multivariate analysis, only aCT (P = 0.011) correlated with TTFT. Eleven cMBL cases (15.9%) showed an abnormal aCT and were reclassified as small lymphocytic lymphomas (SLL); nonetheless, TTFT was similar for cMBLs and SLLs. Conclusion: Our results confirm the ability of the abnormal aCT to predict progression in early stage cases. Key words chronic lymphocytic leukemia; abdominal CT scan; prognosis; early stage; clinical monoclonal B-cell lymphocytosis Correspondence Massimo Gentile, MD and Fortunato Morabito, MD, UOC Ematologia, Azienda Ospedaliera di Cosenza, viale della Repubblica snc, 87100 Cosenza, Italy. Tel: +39 0984 681329; Fax: +39-0984-681329; e-mails: [email protected]; fortunato_ [email protected] Accepted for publication 9 March 2015 doi:10.1111/ejh.12545 © 2015 John Wiley & Sons A/S. Published by John Wiley & Sons Ltd 1 European Journal of Haematology
-
Upload
independent -
Category
Documents
-
view
0 -
download
0
Transcript of Prospective validation of predictive value of abdominal computed tomography scan on time to first...

ORIGINAL ARTICLE
Prospective validation of predictive value of abdominalcomputed tomography scan on time to first treatment in Rai0 chronic lymphocytic leukemia patients: results of themulticenter O-CLL1-GISL studyMassimo Gentile1, Giovanna Cutrona2, Stefano Molica3, Fiorella Ilariucci4, Francesca R. Mauro5,Nicola Di Renzo6, Francesco Di Raimondo7, Iolanda Vincelli8, Katia Todoerti9, Serena Matis10, CaterinaMusolino11, Sonia Fabris12, Marta Lionetti12, Luciano Levato3, Simona Zupo2, Francesco Angrilli13,Ugo Consoli14, Gianluca Festini15, Giuseppe Longo16, Agostino Cortelezzi9, Pellegrino Musto17,Massimo Federico18, Antonino Neri12, Manlio Ferrarini10, Fortunato Morabito1
1Hematology Unit, Department of Onco-Hematology, A.O. of Cosenza, Cosenza; 2SS Molecular Diagnostics IRCCS S. Martino-IST, Genova;3Department of Oncology and Haematology, Pugliese-Ciaccio Hospital, Catanzaro; 4Division of Haematology, A.O. S. Maria Nuova, Reggio Emilia;5Divisione di Ematologia, Universit�a La Sapienza, Rome; 6Hematology Unit, Ospedale Vito Fazzi, Lecce; 7Division of Haematology, Department of
Biomedical Sciences, University of Catania and Ferrarotto Hospital, Catania; 8Hematology Unit, A.O. of Reggio Calabria, Reggio; 9Laboratory of
Preclinical and Translational Research, IRCCS, Referral Cancer Center of Basilicata, Rionero in Vulture (Pz); 10Direzione Scientifica IRCCS, San
Martino IST, Genova; 11Division of Haematology, University of Messina, Messina; 12Department of Clinical Sciences and Community Health,
University of Milano and Hematology CTMO, Foundation IRCCS Ca’ Granda Ospedale Maggiore Policlinico, Milan; 13Department of Hematology,
Ospedale Santo Spirito, Pescara; 14U.O.S. di Emato-Oncologia, Ospedale Garibaldi-Nesima, Catania; 15Centro di Riferimento Ematologico-Seconda
Medicina, Azienda Ospedaliero-Universitaria, Ospedali Riuniti, Trieste; 16Unit�a di Ematologia, Ospedale San Vincenzo, Taormina; 17Scientific
Direction, IRCCS, Referral Cancer Center of Basilicata, Rionero in Vulture (Pz); 18Department of Onco-hematology, Universit�a di Modena Centro
Oncologico Modenese, Policlinico Modena, Italy
Abstract
Objective: We performed an external and multicentric validation of the predictive value of abdominal
computed tomography (aCT) on time to first treatment (TTFT) in early stage chronic lymphocytic leukemia
(CLL) patients. Methods: aCT was performed at diagnosis in 181 Rai 0 patients enrolled in the O-CLL1-
GISL trial (clinicaltrial.gov ID:NCT00917549). Results: Fifty-five patients showed an abnormal aCT. Patients
with an abnormal aCT showed a significantly shorter TTFT than those with normal aCT (P < 0.0001). At
multivariate analysis, aCT (P = 0.011), b-2 microglobulin (P = 0.019), and CD38 expression (P = 0.047)
correlated with TTFT. Following IWCLL 2008 criteria, 112 (61.9%) cases remained at Rai 0, while 69
(38.1%) satisfied the criteria of clinical monoclonal B-cell lymphocytosis (cMBL). Reclassified Rai 0 patients
with an abnormal aCT showed a significantly shorter TTFT than those with a normal aCT (P < 0.0001). At
multivariate analysis, only aCT (P = 0.011) correlated with TTFT. Eleven cMBL cases (15.9%) showed an
abnormal aCT and were reclassified as small lymphocytic lymphomas (SLL); nonetheless, TTFT was similar
for cMBLs and SLLs. Conclusion: Our results confirm the ability of the abnormal aCT to predict
progression in early stage cases.
Key words chronic lymphocytic leukemia; abdominal CT scan; prognosis; early stage; clinical monoclonal B-cell lymphocytosis
Correspondence Massimo Gentile, MD and Fortunato Morabito, MD, UOC Ematologia, Azienda Ospedaliera di Cosenza, viale della
Repubblica snc, 87100 Cosenza, Italy. Tel: +39 0984 681329; Fax: +39-0984-681329; e-mails: [email protected]; fortunato_
Accepted for publication 9 March 2015 doi:10.1111/ejh.12545
© 2015 John Wiley & Sons A/S. Published by John Wiley & Sons Ltd 1
European Journal of Haematology

Chronic lymphocytic leukemia (CLL) patients show a vari-able clinical course with some cases having an almost nor-mal therapy-free life span, while others require therapyshortly after diagnosis (1). Rai and Binet staging systems,which consider the extent of lymphadenopathy, organomeg-aly, and cytopenias, are useful for assessing prognosis (2, 3).However, for patients with early-stage disease it is virtuallyimpossible to predict the clinical course in general, and morespecifically, the time to progression; this represents a majorproblem as most patients are now diagnosed at early stagesand generally belong to the low-risk category (Rai stage 0or Binet stage A) (4–6). The inability of these staging sys-tems to stratify patients with different progression potentialhas led to substantial efforts to identify new prognostic tools,including determination of chromosomal alterations by fluo-rescent in situ hybridization (FISH) (7), of immunoglobulinheavy chain variable (IGHV) mutational status (8, 9), and ofCD38, ZAP-70 (10), and CD49d cellular expression (11), aswell as of serum indicators, that is, b2-microglobulin (12)and free-light chains levels (13). Moreover, with the aim torealize a simplified tool to assess prognosis, both MDAnderson Cancer Center (MDACC) CLL group and GermanCLL Study Group (GCLLSG), through the combination ofparameters independently associated with prognosis, devel-oped two different prognostic indexes to predict survival ofCLL patients (14, 15).Although CT scan is a mandatory staging procedure of
nearly all other lymphoid malignancies (16), the currentstaging systems for CLL patients are based only on clinicalexamination and blood counts, and a CT scan remains adiagnostic procedure not recommended at diagnosis (17, 18).For this reason, abdominal lymphadenopathies are not incor-porated in the staging procedures. Moreover, in somepatients spleen enlargement may go undetected at clinicalexamination and hence not be computed into the stagingdetermination. In this regard, Munta~nola et al. (19) haveshown that among Rai 0 patients, abdominal lymphadenopa-thy or splenomegaly detected by computed tomography (CT)scan predicts disease progression. No further studies address-ing the issue systematically have been published. However,for a widespread application, the predictive power of abdom-inal CT (aCT) scan requires external validation in an inde-pendent series of newly diagnosed Rai 0 CLL patientsevaluated and monitored at multiple institutions at the timeof diagnosis.In this study, we investigated the prognostic value in
terms of time to first treatment (TTFT) of aCT scans in acohort of Rai 0 patients participating in a prospective multi-center observational study. Hence, through this analysis, wewill better understand whether abdominal lymphadenopathyshould be considered an additional lymph node area in thisgroup of CLL patients.As this observational trial started in the 2007 and CLL
diagnosis and staging were based on the NCI-WG 1996
guidelines (17), we have subsequently reclassified Rai 0patients according to IWCLL 2008 guidelines (18) excludingclinical monoclonal B-cell lymphocytosis (cMBL) cases.Thus, we have also performed subanalyses in the setting ofRai 0 (staged according to NCI-WG 2008 guidelines) andcMBL cases, included in this cohort.
Patients
Newly diagnosed CLL patients from several Italian Institu-tions were prospectively enrolled in the O-CLL1-GISL pro-tocol (clinicaltrial.gov identifier: NCT00917540). Theinclusion criteria for CLL diagnosis, employed at the time ofstudy start, followed the NCI-WG guidelines established in1996 requiring >5.000 lymphocytes/lL in the peripheralblood (15). CLL cell phenotype, CD38 and ZAP-70 expres-sion, and IGHV mutational status were centralized at the lab-oratory in Genoa and cytogenetic analyses in Milan. Thisstudy was approved by the ethics committees of the partici-pating centers. All patients provided written informedconsent.To date, of 491 Binet stage A patients enrolled, 384 cases
were at Rai 0 according the NCI-WG guidelines establishedin 1996 (17). As 181 of 384 Rai 0 patients underwent totalbody CT scan at baseline, aCT scan data were available forthese cases and were included in this analysis. Although CTscans are not recommended at diagnosis in CLL (18), thisprocedure was strongly recommended for all patientsenrolled in the O-CLL1-GISL protocol at baseline. Data oftotal body CT scans of 179 of 181 cases have been analyzedto perform a previous study regarding the integration of totalbody scan in the Binet and Rai staging systems (20).Our series was representative of all 384 cases Rai 0
enrolled in the 0-CLL1-GISL protocol, as both subgroupshad a similar distribution of clinical and biological parame-ters (Table S1). Sixty-nine of the 181 cases satisfied theIWCLL 2008 criteria for the definition of cMBL (<5.0 9
109 B lymphocytes/L in the peripheral blood and no appar-ent lymph node, spleen, or liver enlargement) (18).
Indication for therapy
All patients underwent follow-up visits every 6 months. Allphysicians had used the NCI-WG guidelines as reference cri-terion of starting therapy (17, 18). All 181 cases had a mini-mum follow-up of 6 months and were evaluated for TTFT.
Abdominal CT evaluation
CT scans of the abdomen were performed in cranio-caudaldirection, with a 5- to 8-mm collimation. The scans wereroutinely acquired 70 s after the injection of 100 mL ofiodinated contrast material, at a rate of 3 mL/s by poweredinjection.
2 © 2015 John Wiley & Sons A/S. Published by John Wiley & Sons Ltd
Abdominal CT scan for CLL patients Gentile et al.

Radiologists evaluated CT scans according to the follow-ing shared criteria. The assessment of nodal groups statuswas based on size (21), the maximum short-axis diameterof lymph nodes was taken as the most reliable parameter todetermine lymph node size according to standard criteria(22). Lymph nodes >10 mm in diameter were consideredabnormal according to the Binet staging system (3). Fur-thermore, lymph nodes were also considered abnormal ifmultiple nodes measuring <10 mm in the short-axis diame-ter were seen in a single region (23). The abdominal lym-phoid areas were diaphragmatic, celiac, mesenteric, iliac,and retroperitoneal (the latter including periaortic, inter-aortocaval, and pericaval chains). Splenomegaly wasdefined based upon the changes that an enlarged spleencaused in relation to the other abdominal viscera; moreover,spleen volume was calculated according to standard diag-nostic criteria (24). The normal volume for the spleen was<375 cm3 for males and <309.55 cm3 for females (24). CTwas defined as abnormal when one or more anomalouslymph node regions, including spleen enlargement, wereobserved, in accordance with the Spanish criteria (19). Inany hematologic center, participating to this trial, two radi-ologists independently evaluated all CT scans; in case ofdisagreement in their evaluation, a consensus diagnosis wasachieved (19).
Assessment of biological markers
Cytogenetic abnormalities involving deletions at chromo-somes 11q23, 13q14, and 17p13 and trisomy 12 wereevaluated by FISH in purified CD19+ population as previ-ously described (13). Cytogenetic abnormalities were clus-tered in three risk groups [i.e., low risk (del(13q14) andnormal), intermediate risk (trisomy 12), and high risk (del(11q22) and del(17p13)]. CD38-positive leukemic cellswere measured by triple staining with CD19-FITC (BDBiosciences), CD38-PE (BD Biosciences, San Diego, Cali-fornia, USA), and CD5-PC5 (Beckman Coulter). The cellswere analyzed using a FACSCalibur flow-cytometer (BDBiosciences, Franklin Lakes, New Jersey, USA). CD38-positive cases were indicated as those having >30% posi-tive cells. ZAP-70 was determined by flow cytometry witha ZAP-70-FITC (clone 2F3.2; Millipore, Billerica, Massa-chusetts, USA) or an isotype control mAb (mouse IgG2a-FITC; BD Biosciences) as previously described (25, 26).We previously demonstrated that 40% of ZAP-70-positivecells represents the best cutoff value for predicting TTFT(27); therefore, 40% was used as threshold to identifyZAP-70-positive cases. IGHV mutational status wasassessed on cDNA specimens (26). Sequences werealigned to the IMGT directory and analyzed using IMGT/VQUEST software. Sequences differing more than 2%from the corresponding germ-line gene were consideredIGHV-mutated (IGHV-M) (27). NOTCH-1 mutation hotspot
was assessed by next generation deep sequencing as previ-ously described (28).
Statistical analysis
SPSS for Windows, v13.0, 2004 software (SPSS, Portsmouth,Hampshire, UK) was used for all analyses. For categoricalvariables, statistical comparisons were performed using two-way tables for the Fisher’s exact test and multiway tables forthe Pearson’s chi-square test. TTFT analyses were performedusing the Kaplan–Meier method in patients with a minimum6 months follow-up. Statistical significance of associationsbetween individual variables and survival was calculatedusing the log-rank test. Prognostic impact for the outcome var-iable was investigated by univariate and multiple Cox regres-sion analysis. Data are expressed as hazard ratio (HR) and95% confidence interval (CI). A value of P < 0.05 was con-sidered significant.
Results
Patient characteristics
The cohort analyzed included 181 Rai 0 patients diagnosedaccording to the NCI/WG 1996 criteria (17). When thesepatients were reclassified according to the IWCLL 2008 cri-teria (18) 69 (38.1%) met the diagnostic criteria of cMBL,while 112 (61.1%) remained at Rai 0 stage. Baseline patientfeatures are listed in Table 1. Eighty-seven cases (48.1%)were aged <60 yr, and 98 (54.1%) were male; roughly one-third of cases showed an elevated b2-microglobulin level.Fifty-five patients (30.4%) had an IGHV unmutated status(IGHV-UM), 44.8% had positive ZAP-70 expression, and17.1% positive CD38 expression. FISH data, available in171 of 181 cases, identified del(13q14) as the most frequentabnormality (43.9%) followed by trisomy 12 (12.3%), whilethere was a low incidence of del(11q22.3) cases (4.7%) andan even lower percentage of del(17p13) cases (1.8%).The median time from CLL diagnosis to aCT scan was
2 months (range 0–9 months). aCT was defined as pathologicalin 55 patients (30.4%). Detailed distribution of abdominalnodal involvement was as follows: spleen enlargement, 22(40%); iliac, 20 (36.4%); retroperitoneal, 17 (30.9%); mesen-teric, 13 (23.6%); celiac, 6 (10.9%); and diaphragmatic, 1(1.8%). Seven patients showed only splenomegaly, and 18patients showed involvement of at least one lymph node region,including the spleen. Thirty-eight patients showed abdominallymph nodes of 1–1.5 cm in diameter, while in ten patientslymph nodes were of 1.5–3 cm. The median spleen longitudi-nal diameter of patients with radiologic splenomegaly was14.8 cm (range 14–15.6 cm; coefficient of variance 2.81%).After a median follow-up of 40 months (range, 6–82
months), 43 of 181 (23.7%) cases required treatment and 11(6%) patients died. The probability of remaining free from
© 2015 John Wiley & Sons A/S. Published by John Wiley & Sons Ltd 3
Gentile et al. Abdominal CT scan for CLL patients
therapy need was 84% at 3 yr. When the analysis wasrestricted to patients who required treatment, the medianTTFT was 31 months (range 6–82). The overall survival ofthe series was 93% at 3 yr.
Abnormal aCT and clinical variables in Rai 0 casesclassified according to the NCI/WG 1996 criteria
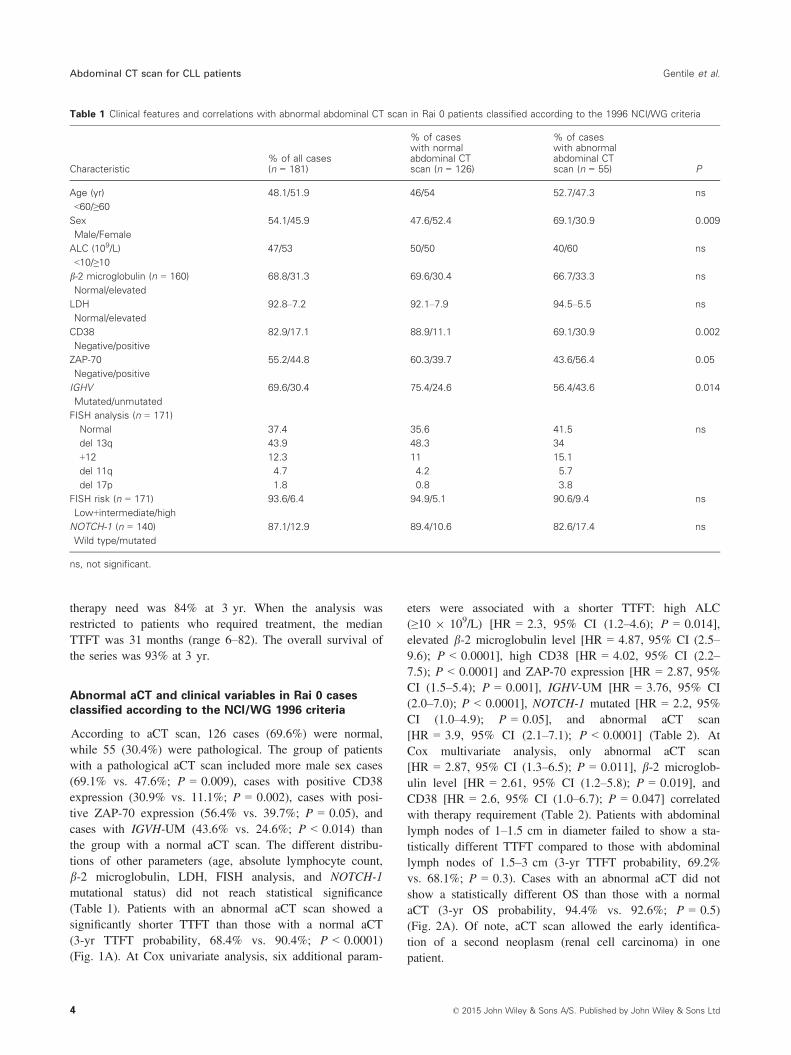
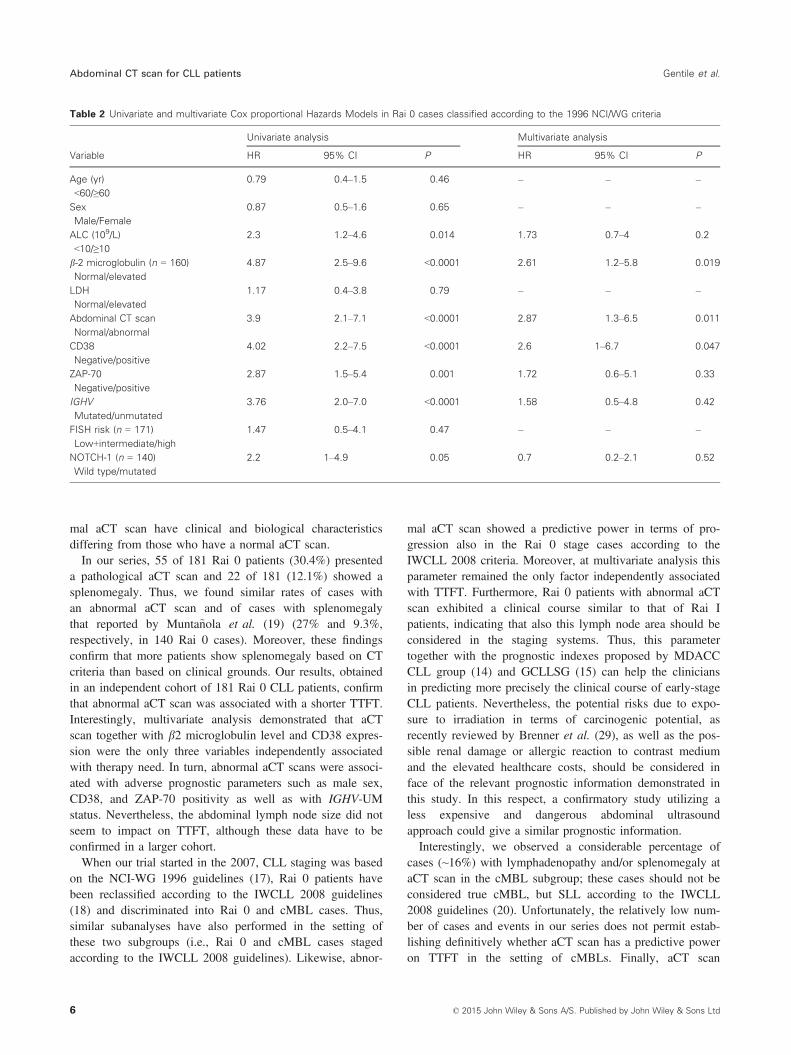
According to aCT scan, 126 cases (69.6%) were normal,while 55 (30.4%) were pathological. The group of patientswith a pathological aCT scan included more male sex cases(69.1% vs. 47.6%; P = 0.009), cases with positive CD38expression (30.9% vs. 11.1%; P = 0.002), cases with posi-tive ZAP-70 expression (56.4% vs. 39.7%; P = 0.05), andcases with IGVH-UM (43.6% vs. 24.6%; P < 0.014) thanthe group with a normal aCT scan. The different distribu-tions of other parameters (age, absolute lymphocyte count,b-2 microglobulin, LDH, FISH analysis, and NOTCH-1mutational status) did not reach statistical significance(Table 1). Patients with an abnormal aCT scan showed asignificantly shorter TTFT than those with a normal aCT(3-yr TTFT probability, 68.4% vs. 90.4%; P < 0.0001)(Fig. 1A). At Cox univariate analysis, six additional param-
eters were associated with a shorter TTFT: high ALC(≥10 9 109/L) [HR = 2.3, 95% CI (1.2–4.6); P = 0.014],elevated b-2 microglobulin level [HR = 4.87, 95% CI (2.5–9.6); P < 0.0001], high CD38 [HR = 4.02, 95% CI (2.2–7.5); P < 0.0001] and ZAP-70 expression [HR = 2.87, 95%CI (1.5–5.4); P = 0.001], IGHV-UM [HR = 3.76, 95% CI(2.0–7.0); P < 0.0001], NOTCH-1 mutated [HR = 2.2, 95%CI (1.0–4.9); P = 0.05], and abnormal aCT scan[HR = 3.9, 95% CI (2.1–7.1); P < 0.0001] (Table 2). AtCox multivariate analysis, only abnormal aCT scan[HR = 2.87, 95% CI (1.3–6.5); P = 0.011], b-2 microglob-ulin level [HR = 2.61, 95% CI (1.2–5.8); P = 0.019], andCD38 [HR = 2.6, 95% CI (1.0–6.7); P = 0.047] correlatedwith therapy requirement (Table 2). Patients with abdominallymph nodes of 1–1.5 cm in diameter failed to show a sta-tistically different TTFT compared to those with abdominallymph nodes of 1.5–3 cm (3-yr TTFT probability, 69.2%vs. 68.1%; P = 0.3). Cases with an abnormal aCT did notshow a statistically different OS than those with a normalaCT (3-yr OS probability, 94.4% vs. 92.6%; P = 0.5)(Fig. 2A). Of note, aCT scan allowed the early identifica-tion of a second neoplasm (renal cell carcinoma) in onepatient.
Table 1 Clinical features and correlations with abnormal abdominal CT scan in Rai 0 patients classified according to the 1996 NCI/WG criteria
Characteristic% of all cases(n = 181)
% of caseswith normalabdominal CTscan (n = 126)
% of caseswith abnormalabdominal CTscan (n = 55) P
Age (yr)
<60/≥60
48.1/51.9 46/54 52.7/47.3 ns
Sex
Male/Female
54.1/45.9 47.6/52.4 69.1/30.9 0.009
ALC (109/L)
<10/≥10
47/53 50/50 40/60 ns
b-2 microglobulin (n = 160)
Normal/elevated
68.8/31.3 69.6/30.4 66.7/33.3 ns
LDH
Normal/elevated
92.8–7.2 92.1–7.9 94.5–5.5 ns
CD38
Negative/positive
82.9/17.1 88.9/11.1 69.1/30.9 0.002
ZAP-70
Negative/positive
55.2/44.8 60.3/39.7 43.6/56.4 0.05
IGHV
Mutated/unmutated
69.6/30.4 75.4/24.6 56.4/43.6 0.014
FISH analysis (n = 171)
Normal 37.4 35.6 41.5 ns
del 13q 43.9 48.3 34
+12 12.3 11 15.1
del 11q 4.7 4.2 5.7
del 17p 1.8 0.8 3.8
FISH risk (n = 171)
Low+intermediate/high
93.6/6.4 94.9/5.1 90.6/9.4 ns
NOTCH-1 (n = 140)
Wild type/mutated
87.1/12.9 89.4/10.6 82.6/17.4 ns
ns, not significant.
4 © 2015 John Wiley & Sons A/S. Published by John Wiley & Sons Ltd
Abdominal CT scan for CLL patients Gentile et al.

Abnormal CT and clinical variables in Rai 0 and cMBLcases classified according to the IWCLL 2008 criteria
When patients were reclassified according to the IWCLL2008 guidelines (18), 69 of 181 cases (38.1%) satisfied thecriteria of cMBL cases, while 112 of 181 (61.9%) remainedat Rai 0 stage. In the setting of patients at Rai 0 stage, 46 of112 cases (41.1%) showed an abnormal aCT scan. The sub-group of patients with abnormal aCT scan was more numer-ous for male sex (70.5% vs. 48.5%; P = 0.031), CD38
positive (29.5% vs. 10.3%; P = 0.012), and ZAP-70 positivecases (56.8% vs. 26.8%; P = 0.05) than the group with anormal aCT scan (Table 3). After a median follow-up of41 months (range, 6–82 months), 36 of 112 cases (32.1%)showed disease progression. Patients with an abnormal aCTscan showed a significantly shorter TTFT than those with anormal aCT (3-yr TTFT probability, 62% vs. 87.1%;P < 0.0001) (Fig. 1B). At Cox univariate analysis, fiveparameters were associated with a shorter TTFT: elevatedb-2 microglobulin level [HR = 4.87, 95% CI (2.5–9.6);P < 0.0001], high CD38 [HR = 4.02, 95% CI (2.2–7.5);P < 0.0001] and ZAP-70 expression [HR = 2.87, 95% CI(1.5–5.4); P = 0.001], IGHV-UM [HR = 3.76, 95% CI (2.0–7.0); P < 0.0001], and abnormal aCT scan [HR = 2.2, 95%CI (1.0–4.9); P = 0.05] (Table 2). At Cox multivariateanalysis, only abnormal aCT scan [HR = 2.87, 95% CI(1.3–6.5); P = 0.011] correlated with progression (Table 4).The OS were not statistically different between cases withan abnormal aCT and those with a normal aCT (3-yr OSprobability, 91.9% vs. 90.4%; P = 0.9) (Fig. 2B).With the aim of evaluating whether Rai stage 0 with
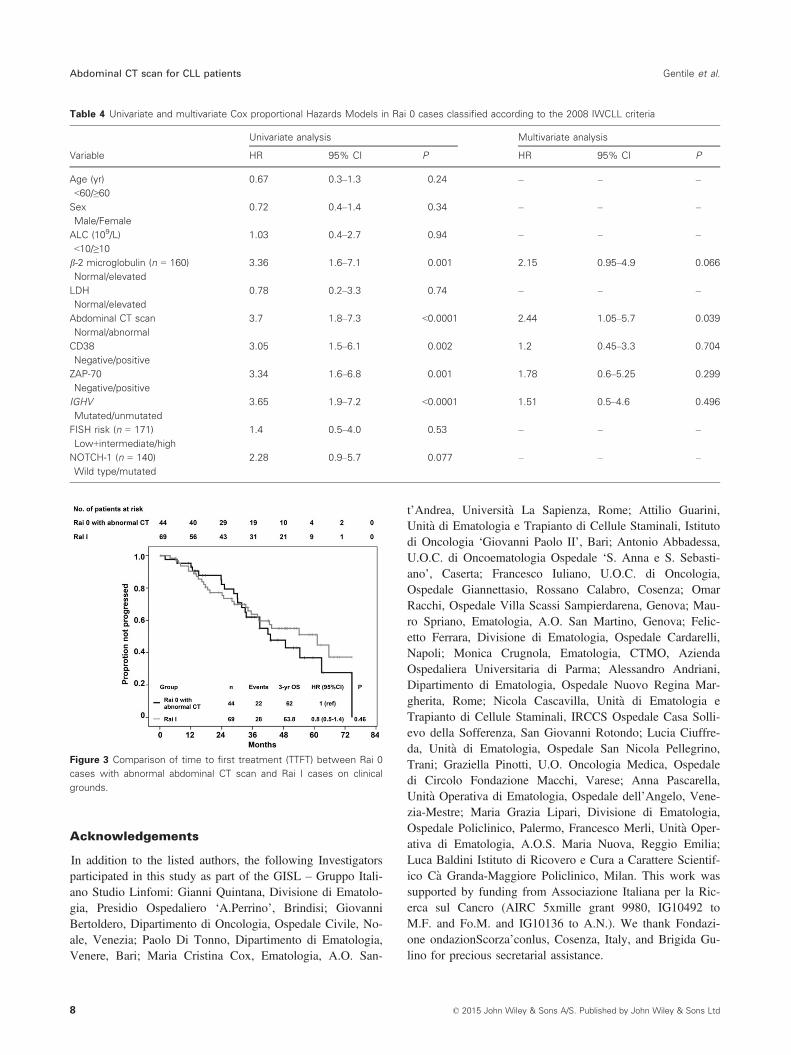
abnormal aCT scan had a clinical course similar to Rai stageI, we compared clinical features and the TTFT of Rai 0cases with abnormal CT with those observed in the 69 Raistage I patients diagnosed on clinical grounds and enrolledin the O-CLL1 study. The distribution of clinical and biolog-ical parameters was not statistically different between thetwo subgroups (Table S2). Moreover, also the TTFT wasnot significantly different between these two groups ofpatients (3-yr TTFT probability, 62% vs. 63.8%; P = 0.46;Fig. 3).Among the 69 cMBL patients, 11 cases (15.9%) showed
an abnormal aCT scan and were reclassified as small lym-phocytic lymphomas (SLL). The different distribution ofclinical features did not reach statistical significance (TableS3). No statistical difference in TTFT was observed betweenSLL and cMBL patients (3-yr PFS probability, 90.9% vs.92.1%; P = 0.44).
Discussion
This study was performed with the aim to validate, in anindependent cohort of newly diagnosed and non-referred Rai0 CLL patients evaluated and monitored at multiple Italianinstitutions, the prognostic significance of the abnormal aCTscan, according to the Spanish criteria (19), in terms ofTTFT. This endpoint, which allowed for a shorter follow-upperiod, is adequate because the standardized criteria for start-ing therapy based upon the NCI Working Group guidelineswere employed by all participating centers. Moreover, thisendpoint is more suitable than overall survival, as it is notinfluenced by subsequent relapses and differing therapeuticapproaches, histologic transformation and non-CLL relateddeaths. Moreover, we evaluated whether patients with abnor-
A
B
Figure 1 Time to first treatment (TTFT) according to abdominal CT
scan in Rai 0 patients classified according to the 1996 NCI/WG criteria
(A); TTFT according to abdominal CT scan in Rai 0 patients classified
according to the 2008 IWCLL criteria (B).
© 2015 John Wiley & Sons A/S. Published by John Wiley & Sons Ltd 5
Gentile et al. Abdominal CT scan for CLL patients
mal aCT scan have clinical and biological characteristicsdiffering from those who have a normal aCT scan.In our series, 55 of 181 Rai 0 patients (30.4%) presented
a pathological aCT scan and 22 of 181 (12.1%) showed asplenomegaly. Thus, we found similar rates of cases withan abnormal aCT scan and of cases with splenomegalythat reported by Munta~nola et al. (19) (27% and 9.3%,respectively, in 140 Rai 0 cases). Moreover, these findingsconfirm that more patients show splenomegaly based on CTcriteria than based on clinical grounds. Our results, obtainedin an independent cohort of 181 Rai 0 CLL patients, confirmthat abnormal aCT scan was associated with a shorter TTFT.Interestingly, multivariate analysis demonstrated that aCTscan together with b2 microglobulin level and CD38 expres-sion were the only three variables independently associatedwith therapy need. In turn, abnormal aCT scans were associ-ated with adverse prognostic parameters such as male sex,CD38, and ZAP-70 positivity as well as with IGHV-UMstatus. Nevertheless, the abdominal lymph node size did notseem to impact on TTFT, although these data have to beconfirmed in a larger cohort.When our trial started in the 2007, CLL staging was based
on the NCI-WG 1996 guidelines (17), Rai 0 patients havebeen reclassified according to the IWCLL 2008 guidelines(18) and discriminated into Rai 0 and cMBL cases. Thus,similar subanalyses have also performed in the setting ofthese two subgroups (i.e., Rai 0 and cMBL cases stagedaccording to the IWCLL 2008 guidelines). Likewise, abnor-
mal aCT scan showed a predictive power in terms of pro-gression also in the Rai 0 stage cases according to theIWCLL 2008 criteria. Moreover, at multivariate analysis thisparameter remained the only factor independently associatedwith TTFT. Furthermore, Rai 0 patients with abnormal aCTscan exhibited a clinical course similar to that of Rai Ipatients, indicating that also this lymph node area should beconsidered in the staging systems. Thus, this parametertogether with the prognostic indexes proposed by MDACCCLL group (14) and GCLLSG (15) can help the cliniciansin predicting more precisely the clinical course of early-stageCLL patients. Nevertheless, the potential risks due to expo-sure to irradiation in terms of carcinogenic potential, asrecently reviewed by Brenner et al. (29), as well as the pos-sible renal damage or allergic reaction to contrast mediumand the elevated healthcare costs, should be considered inface of the relevant prognostic information demonstrated inthis study. In this respect, a confirmatory study utilizing aless expensive and dangerous abdominal ultrasoundapproach could give a similar prognostic information.Interestingly, we observed a considerable percentage of
cases (~16%) with lymphadenopathy and/or splenomegaly ataCT scan in the cMBL subgroup; these cases should not beconsidered true cMBL, but SLL according to the IWCLL2008 guidelines (20). Unfortunately, the relatively low num-ber of cases and events in our series does not permit estab-lishing definitively whether aCT scan has a predictive poweron TTFT in the setting of cMBLs. Finally, aCT scan
Table 2 Univariate and multivariate Cox proportional Hazards Models in Rai 0 cases classified according to the 1996 NCI/WG criteria
Variable
Univariate analysis Multivariate analysis
HR 95% CI P HR 95% CI P
Age (yr)
<60/≥60
0.79 0.4–1.5 0.46 – – –
Sex
Male/Female
0.87 0.5–1.6 0.65 – – –
ALC (109/L)
<10/≥10
2.3 1.2–4.6 0.014 1.73 0.7–4 0.2
b-2 microglobulin (n = 160)
Normal/elevated
4.87 2.5–9.6 <0.0001 2.61 1.2–5.8 0.019
LDH
Normal/elevated
1.17 0.4–3.8 0.79 – – –
Abdominal CT scan
Normal/abnormal
3.9 2.1–7.1 <0.0001 2.87 1.3–6.5 0.011
CD38
Negative/positive
4.02 2.2–7.5 <0.0001 2.6 1–6.7 0.047
ZAP-70
Negative/positive
2.87 1.5–5.4 0.001 1.72 0.6–5.1 0.33
IGHV
Mutated/unmutated
3.76 2.0–7.0 <0.0001 1.58 0.5–4.8 0.42
FISH risk (n = 171)
Low+intermediate/high
1.47 0.5–4.1 0.47 – – –
NOTCH-1 (n = 140)
Wild type/mutated
2.2 1–4.9 0.05 0.7 0.2–2.1 0.52
6 © 2015 John Wiley & Sons A/S. Published by John Wiley & Sons Ltd
Abdominal CT scan for CLL patients Gentile et al.

allowed the early diagnosis of a concomitant neoplasm inone patient. Although CLL patients have a high risk ofdeveloping a second cancer and an increased frequency ofcertain cancer types (30), there are no studies investigatingthe use of CT scans in routine screening or follow-up to pre-cociously detect cancer in CLL. However, a meta-analysisperformed by Eichorst et al. (31) showed that CT scans didnot provide any additional prognostic information for CLLpatients when performed during the follow-up.Overall, these results confirm those reported by Spanish
CLL group (19) that aCT scan allows the identification of asubset of cases with a more aggressive disease in patients
with early-stage disease. These data are also in line with ourprevious report, in which we demonstrated how the integra-tion of total body CT scan in the staging systems, through amore comprehensive evaluation of tumor burden, allowed todistinguish cases with more aggressive clinical coursebetween Binet stage A patients (20). Moreover, we firstlyextended the utility of this prognostic tool in terms ofprogression to the setting of Rai stage 0 staged according toIWCLL 2008 criteria (18). Finally, in patients with<5.0 9 109 B lymphocytes/L, however, aCT scan candifferentiate between true cMBL and SLL cases, it does notallow to individuate cases at high risk of progression.Although CT scan is not routinely recommended for CLLpatient workup as for other low-grade lymphoproliferativedisorders (32), these data together with those reported byMunta~nola et al. (19) provide a basis for performing a radio-logical evaluation of abdominal lymph nodes and spleno-megaly in CLL patients in early stage at diagnosis alongwith other new prognostic parameters in CLL patients.
A
B
Figure 2 OS according to abdominal CT scan in Rai 0 patients classi-
fied according to the 1996 NCI/WG criteria (A); OS according to
abdominal CT scan in Rai 0 patients classified according to the 2008
IWCLL criteria (B).
Table 3 Clinical features and correlations with abnormal abdominal
CT scan in Rai 0 patients classified according to the 2008 IWCLL cri-
teria
Characteristic
% of Rai 0caseswith normalabdominalCT scan (n = 68)
% of Rai 0caseswith abnormalabdominalCT scan(n = 44) P
Age (yr)
<60/≥60
47.1/52.9 59.1/40.9 ns
Sex
Male/Female
48.5/51.5 70.5/29.5 ns
ALC (109/L)
<10/≥10
13.2/86.8 25/75 ns
b-2 microglobulin
(n = 160)
Normal/elevated
65.6/34.4 61.5/38.5 ns
LDH
Normal/elevated
94.4–5.6 93.2–7.8 ns
CD38
Negative/positive
89.7/10.3 70.5/29.5 0.066
ZAP-70
Negative/positive
63.2/26.8 43.2/56.8 ns
IGHV
Mutated/unmutated
73.5/26.5 56.8/43.2 ns
FISH analysis (n = 171)
Normal 33.8 37.2 ns
del 13q 50.8 39.5
+12 9.2 14
del 11q 4.6 7
del 17p 1.5 2.3
FISH risk (n = 171)
Low+intermediate/high
93.8/6.2 90.7/9.3 ns
NOTCH-1 (n = 140)
Wild type/mutated
87.7/12.3 86.8/13.2 0.059
ns, not significant.
© 2015 John Wiley & Sons A/S. Published by John Wiley & Sons Ltd 7
Gentile et al. Abdominal CT scan for CLL patients
Acknowledgements
In addition to the listed authors, the following Investigatorsparticipated in this study as part of the GISL – Gruppo Itali-ano Studio Linfomi: Gianni Quintana, Divisione di Ematolo-gia, Presidio Ospedaliero ‘A.Perrino’, Brindisi; GiovanniBertoldero, Dipartimento di Oncologia, Ospedale Civile, No-ale, Venezia; Paolo Di Tonno, Dipartimento di Ematologia,Venere, Bari; Maria Cristina Cox, Ematologia, A.O. San-
t’Andrea, Universit�a La Sapienza, Rome; Attilio Guarini,Unit�a di Ematologia e Trapianto di Cellule Staminali, Istitutodi Oncologia ‘Giovanni Paolo II’, Bari; Antonio Abbadessa,U.O.C. di Oncoematologia Ospedale ‘S. Anna e S. Sebasti-ano’, Caserta; Francesco Iuliano, U.O.C. di Oncologia,Ospedale Giannettasio, Rossano Calabro, Cosenza; OmarRacchi, Ospedale Villa Scassi Sampierdarena, Genova; Mau-ro Spriano, Ematologia, A.O. San Martino, Genova; Felic-etto Ferrara, Divisione di Ematologia, Ospedale Cardarelli,Napoli; Monica Crugnola, Ematologia, CTMO, AziendaOspedaliera Universitaria di Parma; Alessandro Andriani,Dipartimento di Ematologia, Ospedale Nuovo Regina Mar-gherita, Rome; Nicola Cascavilla, Unit�a di Ematologia eTrapianto di Cellule Staminali, IRCCS Ospedale Casa Solli-evo della Sofferenza, San Giovanni Rotondo; Lucia Ciuffre-da, Unit�a di Ematologia, Ospedale San Nicola Pellegrino,Trani; Graziella Pinotti, U.O. Oncologia Medica, Ospedaledi Circolo Fondazione Macchi, Varese; Anna Pascarella,Unit�a Operativa di Ematologia, Ospedale dell’Angelo, Vene-zia-Mestre; Maria Grazia Lipari, Divisione di Ematologia,Ospedale Policlinico, Palermo, Francesco Merli, Unit�a Oper-ativa di Ematologia, A.O.S. Maria Nuova, Reggio Emilia;Luca Baldini Istituto di Ricovero e Cura a Carattere Scientif-ico C�a Granda-Maggiore Policlinico, Milan. This work wassupported by funding from Associazione Italiana per la Ric-erca sul Cancro (AIRC 5xmille grant 9980, IG10492 toM.F. and Fo.M. and IG10136 to A.N.). We thank Fondazi-one ondazionScorza’conlus, Cosenza, Italy, and Brigida Gu-lino for precious secretarial assistance.
Table 4 Univariate and multivariate Cox proportional Hazards Models in Rai 0 cases classified according to the 2008 IWCLL criteria
Variable
Univariate analysis Multivariate analysis
HR 95% CI P HR 95% CI P
Age (yr)
<60/≥60
0.67 0.3–1.3 0.24 – – –
Sex
Male/Female
0.72 0.4–1.4 0.34 – – –
ALC (109/L)
<10/≥10
1.03 0.4–2.7 0.94 – – –
b-2 microglobulin (n = 160)
Normal/elevated
3.36 1.6–7.1 0.001 2.15 0.95–4.9 0.066
LDH
Normal/elevated
0.78 0.2–3.3 0.74 – – –
Abdominal CT scan
Normal/abnormal
3.7 1.8–7.3 <0.0001 2.44 1.05–5.7 0.039
CD38
Negative/positive
3.05 1.5–6.1 0.002 1.2 0.45–3.3 0.704
ZAP-70
Negative/positive
3.34 1.6–6.8 0.001 1.78 0.6–5.25 0.299
IGHV
Mutated/unmutated
3.65 1.9–7.2 <0.0001 1.51 0.5–4.6 0.496
FISH risk (n = 171)
Low+intermediate/high
1.4 0.5–4.0 0.53 – – –
NOTCH-1 (n = 140)
Wild type/mutated
2.28 0.9–5.7 0.077 – – –
Figure 3 Comparison of time to first treatment (TTFT) between Rai 0
cases with abnormal abdominal CT scan and Rai I cases on clinical
grounds.
8 © 2015 John Wiley & Sons A/S. Published by John Wiley & Sons Ltd
Abdominal CT scan for CLL patients Gentile et al.

Author’s disclosures of potential conflicts of
interest
The authors indicated no potential conflict of interests.
References
1. Chiorazzi N, Rai KR, Ferrarini M. Chronic lymphocytic leu-kemia. N Engl J Med 2005;352:804–15.
2. Rai KR, Sawitsky A, Cronkite EP, et al. Clinical staging ofchronic lymphocytic leukemia. Blood 1975;46:219–34.
3. Binet JL, Auquier A, Dighiero G, et al. A new prognosticclassification of chronic lymphocytic leukemia derived from amultivariate survival analysis. Cancer 1981;48:198–206.
4. Call T, Phyilky R, Noel P, et al. Incidence of chronic lym-phocytic leukemia in Olmsted County, Minnesota, 1935through 1989, with emphasis on changes in initial stage atdiagnosis. Mayo Clin Proc 1994;69:323–8.
5. Molica S, Levato D, Dattilo A. Natural history of earlychronic lymphocytic leukemia. A single institution study withemphasis on the impact of disease-progression on overall sur-vival. Haematologica 1999;84:1094–9.
6. Rozman C, Bosch F, Montserrat E. Chronic lymphocyticleukemia: a changing natural history? Leukemia1997;11:775–8.
7. Dohner H, Stilgenbauer S, Benner A, et al. Genomic aberra-tions and survival in chronic lymphocytic leukemia. N Engl JMed 2000;343:1910–6.
8. Hamblin TJ, Davis Z, Gardiner A, et al. Unmutated Ig V(H)genes are associated with a more aggressive form of chroniclymphocytic leukemia. Blood 1999;94:1848–54.
9. Damle RN, Wasil T, Fais F, et al. Ig V gene mutation statusand CD38 expression as novel prognostic indicators in chroniclymphocytic leukemia. Blood 1999;94:1840–7.
10. Gentile M, Cutrona G, Mosca L, et al. Prospective validationof a risk score based on biological markers for predicting pro-gression free survival in Binet stage A chronic lymphocyticleukemia patients: results of the multicenter O-CLL1-GISLstudy. Am J Hematol 2014;89:743–50.
11. Shanafelt TD, Geyer SM, Bone ND, et al. CD49d expressionis an independent predictor of overall survival in patients withchronic lymphocytic leukaemia: a prognostic parameter withtherapeutic potential. Br J Haematol 2008;140:537–46.
12. Gentile M, Cutrona G, Neri A, et al. Predictive value ofbeta2-microglobulin (beta2-m) levels in chronic lymphocyticleukemia since Binet A stages. Haematologica 2009;94:887–8.
13. Morabito F, De Filippi R, Laurenti L, et al. The cumulativeamount of serum-free light chain is a strong prognosticator inchronic lymphocytic leukemia. Blood 2011;118:6353–61.
14. Wierda WG, O’Brien S, Wang X, et al. Prognostic nomogramand index for overall survival in previously untreated patientswith chronic lymphocytic leukemia. Blood 2007;109:4679–85.
15. Pflug N, Bahlo J, Shanafelt TD, et al. Development of a com-prehensive prognostic index for patients with chronic lympho-cytic leukemia. Blood 2014;124:49–62.
16. Mavromatis BH, Cheson BD. Pre- and post-treatment evalua-tion of non-Hodgkin’s lymphoma. Best Pract Res Clin Hae-matol 2002;15:429–47.
17. Cheson BD, Bennett JM, Grever M, et al. National CancerInstitute-sponsored Working Group guidelines for chroniclymphocytic leukemia: revised guidelines for diagnosis andtreatment. Blood 1996;87:4990–7.
18. Hallek M, Cheson BD, Catovsky D, et al. Guidelines for thediagnosis and treatment of chronic lymphocytic leukemia: areport from the International Workshop on Chronic Lympho-cytic Leukemia updating the National Cancer Institute-Work-ing Group 1996 guidelines. Blood 2008;111:5446–56.
19. Muntanola A, Bosch F, Arguis P, et al. Abdominal computedtomography predicts progression in patients with Rai stage 0chronic lymphocytic leukaemia. J Clin Oncol 2007;25:1576–80.
20. Gentile M, Cutrona G, Fabris S, et al. Total body computedtomography scan in the initial work-up of Binet stage Achronic lymphocytic leukemia patients: results of the prospec-tive, multicenter O-CLL1-GISL study. Am J Hematol2013;88:539–44.
21. Dorfman RE, Alpern MB, Gross BH, et al. Upper abdominallymph nodes: criteria for normal size determined with CT.Radiology 1991;180:319–22.
22. Vinnicombe SJ, Reznek RH. Computerised tomography in thestaging of Hodgkin’s disease and non-Hodgkin’s lymphoma.Eur J Nucl Med Mol Imaging 2003;30(Suppl 1):S42–55.
23. Sutinen E, Jyrkkio S, Varpula M, et al. Nodal staging of lym-phoma with whole-body PET: comparison of. J Nucl Med2000;41:1980–8.
24. Geraghty EM, Boone JM, McGahan JP, Jain K. Normal organvolume assessment from abdominal CT. Abdom Imaging2004;29:482–90.
25. Morabito F, Cutrona G, Gentile M, et al. Definition of pro-gression risk based on combinations of cellular and molecularmarkers in patients with Binet stage A chronic lymphocyticleukaemia. Br J Haematol 2009;146:44–53.
26. Morabito F, Cutrona G, Gentile M, et al. Is ZAP70 still a keyprognostic factor in early stage chronic lymphocytic leukae-mia? Results of the analysis from a prospective multicentreobservational study. Br J Haematol 2015;168:455–9.
27. Cutrona G, Colombo M, Matis S, et al. Clonal heterogeneityin chronic lymphocytic leukemia cells: superior response tosurface IgM cross-linking in CD38, ZAP-70-positive cells.Haematologica 2008;93:413–22.
28. Lionetti M, Fabris S, Cutrona G, et al. High-throughputsequencing for the identification of NOTCH1 mutations inearly stage chronic lymphocytic leukemia: biological and clin-ical implications. Br J Haematol 2014;165:629–39.
29. Brenner DJ, Hall EJ. Computed tomography–an increasingsource of radiation exposure. N Engl J Med 2007;357:2277–84.
30. Tsimberidou AM, Wen S, McLaughlin P, et al. Other malig-nancies in chronic lymphocytic leukemia/small lymphocyticlymphoma. J Clin Oncol 2009;27:904–10.
31. Eichhorst BF, Fischer K, Fink AM, et al. Limited clinical rel-evance of imaging techniques in the follow-up of patients
© 2015 John Wiley & Sons A/S. Published by John Wiley & Sons Ltd 9
Gentile et al. Abdominal CT scan for CLL patients

with advanced chronic lymphocytic leukemia: results of ameta-analysis. Blood 2011;117:1817–21.
32. Armitage JO. Staging non-Hodgkin lymphoma. CA Cancer JClin 2005;55:368–76.
Supporting Information
Additional Supporting Information may be found in theonline version of this article:
Table S1. Comparison of main clinical and biologicalpatient features according to the availability of abdominalCT scan at baseline.Table S2. Comparison of clinical features between Rai 0
cases with abnormal abdominal CT scan and Rai I cases onclinical grounds.Table S3. Clinical features and correlations with abnormal
abdominal CT scan in cMBL patients.
10 © 2015 John Wiley & Sons A/S. Published by John Wiley & Sons Ltd
Abdominal CT scan for CLL patients Gentile et al.




















