
Blast Crisis of Chronic Myeloid Leukaemia (CML): II. CELL SURFACE MARKER ANALYSIS OF...
12
BritishJournal of Haematology, 1976, 34, 167. Blast Crisis of Chronic Myeloid Leukaemia (CML) I. PRESENTATION SIMULATING ACUTE LYMPHOID LEUKAEMIA (ALL) M. E. J. BEARD,’ JILL DURRANT,’ D. CATOVSKY,~ E. WILTSHAW,4 J. L. AMESS,~ R. L. BREARLEY,’ BARBARA KIRK,^ P. F. M. wRIGLEY,3 G. JANOSSY,~ M. F. GREAVES~ AND D. A. G. GAL TON^ ‘Department of Haematology, St Bartholomew’s Hospital, London, 21mperial Cancer Research Fund Tumour lmmunology Unit, Department of Zoology, University College London, 31mperial Cancer Research Fund Department of Medical Oncology, St Bartholomew’s Hospital, London, 4Department of Chemotherapy, Royal Marsden Hospital, Fulham Road, London, ’Horton General Hospital, Banbury, Oxon, and The Radclire Infirmary, Oxford, and 6Medical Research Council Leukaemia Unit, Royal Postgraduate Medical School, London (Received 2 February 1976; acceptedfor publication 16 March 1976) SUMMARY. Seven patients presenting as an acute leukaemia caused difficulty in diagnosis. The lymphoid appearance of the blast cells either initially or during treat- ment suggested acute lymphoid leukaemia (ALL). In each case the Philadelphia chromosome was shown to be present thus suggesting that these cases were exam- ples of chronic myeloid leukaemia (CML) presenting in blast crisis without a detect- able chronic phase. The implications of these findings are discussed and the difficulty in achieving a precise diagnosis in the acute leukaemias is emphasized. Cytogenetic analysis should be carried out whenever the type of acute leukaemia present is of critical importance. The identification of the types of acute leukaemia has been discussed recently by Hayhoe & Cawley (1972), Beard & Hamilton Fairley (1974) and Flandrin & Bernard (1975). Acute myelogenous leukaemia (AML) may be recognized with the aid of simple cytochemistry but the other acute leukaemias, often of lymphoid appearance, constitute a heterogeneous group. The diagnosis of acute lymphoid leukaemia (ALL) has hitherto been subjective, depending on the lymphoid appearance of the Romanowsky-stained blast cells. Greater diagnostic precision has now been achieved by the use of cell surface marker analysis (Seligmann, 197s; Greaves et al, 1975) and most non-myelogenous leukaemias may be divided into ‘T’, ‘B’ or ‘anti ALL’ positive (ALL+)sub-varieties. The presence of T and B markers indicates a lymphoid origin whereas the non-B, non-T, ALL’ type is undifferentiated. In rare ‘null’ non-myelogenous cases, none of these surface markers is found. We now draw attention to a small minority of cases presenting as acute leukaemia, which we believe to be instances of chronic myeloid leukaemias (CML) presenting in blast crisis without a detectable chronic phase. They may have features of AML, ALL, or both, but those Correspondence: Professor D. A. G. Galton, Medical Research Council Leukaemia Unit, Royal Postgraduate Medical School, Du Cane Road, London WIZ oHS. 167
Transcript of Blast Crisis of Chronic Myeloid Leukaemia (CML): II. CELL SURFACE MARKER ANALYSIS OF...

BritishJournal of Haematology, 1976, 34, 167.
Blast Crisis of Chronic Myeloid Leukaemia (CML)
I. PRESENTATION SIMULATING ACUTE LYMPHOID LEUKAEMIA (ALL)
M. E. J. BEARD,’ JILL DURRANT,’ D. CATOVSKY,~ E. WILTSHAW,4 J. L. AMESS,~ R. L. BREARLEY,’ BARBARA KIRK,^ P. F. M. wRIGLEY,3 G. JANOSSY,~ M. F. GREAVES~
AND D. A. G. GAL TON^ ‘Department of Haematology, St Bartholomew’s Hospital, London, 21mperial Cancer Research Fund Tumour lmmunology Unit, Department o f Zoology, University College London, 31mperial Cancer Research Fund Department o f Medical Oncology, St Bartholomew’s Hospital, London, 4Department o f Chemotherapy, Royal Marsden Hospital, Fulham Road, London, ’Horton General Hospital, Banbury, Oxon, and The Radclire Infirmary, Oxford, and 6Medical Research Council
Leukaemia Unit, Royal Postgraduate Medical School, London
(Received 2 February 1976; acceptedfor publication 16 March 1976)
SUMMARY. Seven patients presenting as an acute leukaemia caused difficulty in diagnosis. The lymphoid appearance of the blast cells either initially or during treat- ment suggested acute lymphoid leukaemia (ALL). In each case the Philadelphia chromosome was shown to be present thus suggesting that these cases were exam- ples of chronic myeloid leukaemia (CML) presenting in blast crisis without a detect- able chronic phase.
The implications of these findings are discussed and the difficulty in achieving a precise diagnosis in the acute leukaemias is emphasized. Cytogenetic analysis should be carried out whenever the type of acute leukaemia present is of critical importance.
The identification of the types of acute leukaemia has been discussed recently by Hayhoe & Cawley (1972), Beard & Hamilton Fairley (1974) and Flandrin & Bernard (1975). Acute myelogenous leukaemia (AML) may be recognized with the aid of simple cytochemistry but the other acute leukaemias, often of lymphoid appearance, constitute a heterogeneous group. The diagnosis of acute lymphoid leukaemia (ALL) has hitherto been subjective, depending on the lymphoid appearance of the Romanowsky-stained blast cells. Greater diagnostic precision has now been achieved by the use of cell surface marker analysis (Seligmann, 197s; Greaves et al, 1975) and most non-myelogenous leukaemias may be divided into ‘T’, ‘B’ or ‘anti ALL’ positive (ALL+) sub-varieties. The presence of T and B markers indicates a lymphoid origin whereas the non-B, non-T, ALL’ type is undifferentiated. In rare ‘null’ non-myelogenous cases, none of these surface markers is found.
We now draw attention to a small minority of cases presenting as acute leukaemia, which we believe to be instances of chronic myeloid leukaemias (CML) presenting in blast crisis without a detectable chronic phase. They may have features of AML, ALL, or both, but those
Correspondence: Professor D. A. G. Galton, Medical Research Council Leukaemia Unit, Royal Postgraduate Medical School, Du Cane Road, London WIZ oHS.
167

168
of CML may be overlooked and such cases regarded as uncomplicated ALL or even AML. Accurate diagnosis requires the recognition of their unique appearances and the establishment of the presence of the Philadelphia chromosome. Surface marker analysis of the leukaemia cells helps to define the type of leukaemia present (Janossy et a!, 1976).
M. E. J. Beard et a1
MATERIALS AND METHODS
Seven patients with a diagnosis of chronic myeloid leukaemia presenting in blast crisis were studied. Romanowsky, May-Griinwald-Giemsa (MGG) , Sudan Black (SB), periodic acid- Schiff (PAS) and neutrophil alkaline phosphatase (NAP) stains were performed by standard methods (Dacie & Lewis, 1968). Acid phosphatase activity was demonstrated by the method of Goldberg & Barka (1962). Cytogenetic analysis of both bone-marrow cells and PHA- stimulated peripheral blood lymphocytes were performed by the methods of Tjio & Whang (1962) and Moorhead et al(1960) respectively. Cytogenetic analysis of cells in the cerebro- spinal fluid was carried out after incubation for 72 h without PHA. Methods of surface marker analysis were described by Brown et al(1974) and Greaves et a1 (1975). Cerebrospinal fluid was examined by the cytocentrifuge (Shandon). Serum vitamin BIZ levels were measured by Etrglena gracilis microbiological assay (Anderson, 1964) and unsaturated B1 binding capacity (UBBC) by a modification of the method of Gottlieb et a1 (1965).
TABU I. Clinical features at presentation
Duration of Liver (cm Spleen (cm Case Sex Age symptoms below costal below costal Enlarged Other
(yr) (months) margin) margin) nodes findings ~~
I (B.B) F 38 I 7 I4
2 (T.C.) M 3 1 2 2
3 (J.H.1 F 33 0.3 4
5 (P.H.) M 68 2 2
7 (E.R.1 M 18 0.5 3
4 (J.R.1 F 23 8 Not felt
6 (W.D.) M 68 2 Not felt
Just palpable
6
6 Not felt
9
2
Occipital Bruising, fundal
Axillary Fundal
None None Cervical Bruising None None None None Axillary Papilloedema
haemorrhages
haemorrhage
CASE REPORTS (Tables I-VII) Case I
Miss B.B., aged 38 years, had a I-month history of increasing dyspnoea and pain in the left hypochondrium (see Tables I and 11). The blast cells in the peripheral blood film had a high nuclear cytoplasmic ratio and one to two nucleoli, and a few had scanty azurophilic granules. Cells of lymphoid appearance showed various stages of differentiation. The neutrophils were of normal morphology except for rare hypogranular forms. The bone marrow aspirate showed almost total replacement by abnormal cells, mostly of lymphoid appearance at all

HWNWUW -3.3.I ow Y o(I
~roniyelocytes
Myelocytes
I I*lUl I u 2 ii’ 3
s- - 3
8- t: Prolymphocytes
Nerrtrophils a Si
x v
Metumyelocytes 1 E
Eosinophils
Basophils
Monocytes
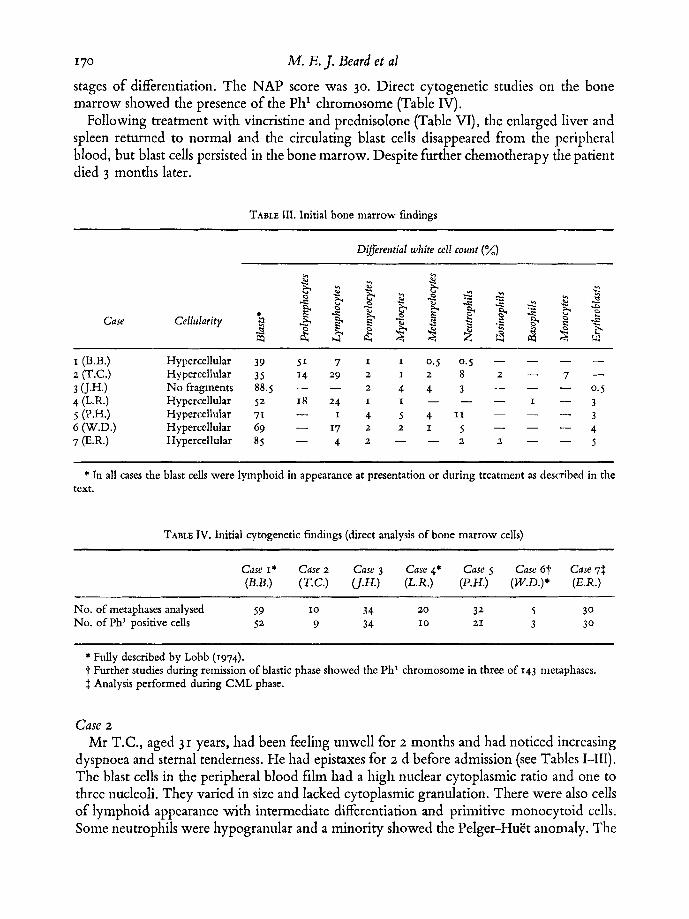
170 M. E.J. Beard et a1
stages of differentiation. The NAP score was 30. Direct cytogenetic studies on the bone marrow showed the presence of the Ph' chromosome (Table IV).
Following treatment with vincristine and prednisolone (Table VI), the enlarged liver and spleen returned to normal and the circulating blast cells disappeared from the peripheral blood, but blast cells persisted in the bone marrow. Despite further chemotherapy the patient died 3 months later.
TABLE 111. Initial bone marrow fmdings
Di&erential white cell count (%)
I (B.B.) Hypercellular 39 5 1 7 I I 0.5 0.5 - - - - 2 (T.C.) Hypercellular 3 5 1 4 2 9 2 1 2 8 2 - 7 -
No fragments 88.5 - - 2 4 4 3 - - - 0.5
4 (L.R.) Hypercellular 52 18 24 I I - 3 3 (J.H.1
5 (P.H.) Hypercellular 71 - 6 (W.D.) Hypercellular 69 - 1 7 2 2 1 5 - - - 4 7 (E.R.1 Hypercellular 85 - 4 2 - - 2 2 - - 5
I - - -
3 - _ - 1 4 5 4 1 1
* In all cases the blast cells were lymphoid in appearance at presentation or during treatment as described in the text.
TABLK IV. Initial cytogenetic findings (direct analysis of bone marrow cells)
Case I* Case 2 Case 3 Case 4* Case 5 Care 67 Case 7$ (B.B.) (T.C.) (J.H.) (L.R.) (P.H.) (W.D.)* (E.R.)
No. of metaphases analysed 59 I0 34 20 32 5 3 0 No. of Ph' positive cells 52 9 34 I 0 21 3 3 0
* Fully described by Lobb (1974). t Further studies during remission of blastic phase showed the Ph' chromosome in three of I43 metaphases. 3 Analysis performed during CML phase.
Case 2
Mr T.C., aged 3 I years, had been feeling unwell for 2 months and had noticed increasing dyspnoea and sternal tenderness. He had epistaxes for z d before admission (see Tables 1-111). The blast cells in the peripheral blood film had a high nuclear cytoplasmic ratio and one to three nucleoli. They varied in size and lacked cytoplasmic granulation. There were also cells of lymphoid appearance with intermediate differentiation and primitive monocytoid cells. Some neutrophils were hypogranular and a minority showed the Pelger-Hutt anomaly. The

TABLE
V. C
ytoc
hem
ical
resu
lts
Case
I
Case
2
Case
3 Ca
se 4
Ca
se 5
Ca
se 6
ca
se 7
E (B
.B.)
(T.C
.)
(JJW
(L
.R)
(P.H
.) (W
.D.)
(E
.R.)
Suda
n B
last
cel
ls N
egat
ive
5%
posi
tive
Neg
ativ
e N
egat
ive
Neg
ativ
e N
egat
ive
Neg
ativ
e b
B
lack
2
2 M
atur
e -3
neut
roph
ils
Posi
tive
Som
e So
me
Posi
tive
Posi
tive
Posi
tive
Posi
tive
$. ne
gativ
e ne
gativ
e G % -.
3
Neg
ativ
e PA
S B
last
cel
ls N
egat
ive
Neg
ativ
e N
egat
ive
Neg
ativ
e W
eak
Initi
ally
ta
0
ther
apy
3
E-
Aci
d B
last
cel
ls N
ot
Fine
Fi
ne
Not
N
ot
Not
N
ot
E-
phos
phat
ase
test
ed
gran
ular
gr
anul
ar
test
ed
test
ed
test
ed
test
ed
- gr
anul
ar
gran
ular
. w
ith ra
re
Blo
cks
bloc
k af
ter
posi
tivity
po
sitiv
ity

172 M. E.]. Beard et a1
bone marrow was almost totally replaced by abnormal ‘lymphoid’ cells at all stages of differ- entiation. The blast cells were PAS negative, an occasional cell was Sudan Black positive and there was fine granular positivity of blasts with the acid phosphatase stain (see Table V). The NAP score was 65, serum vitamin BIZ level was markedly raised at 4760 ng/l. and the UBBC was 245 ng/l. Direct cytogenetic studies of bone-marrow cells showed the presence of the Phi chromosome (Table IV). 85% of the blast cells were positive with ALL antisera.
After four courses of daunorubicin and cytosine arabinoside the blasts disappeared from the peripheral blood, but there was no bone-marrow improvement (Table VI). On multiple-drug therapy (Table VI) he regained normal health but there was no bone-marrow remission. He remained reasonably well, apart from an episode of pneumonia, for 11 months and died I month later. At one stage he responded well to vincristine and prednisolone alone, and the percentage of bone-marrow blasts fell from 70% to 19% of the nucleated cell population.
TABLE VI. Therapy and response
Case Therapy Response Survival (months)
I (B.B.) 2 (T.C.)
~~~ ~
V, P then C and 6MP DNR, Ara-C, 6TG, Ve HU, V, P, C, 6MP V, Ara-C, Asp, Pred 6TG, HU, 6MP, MTX, Ve
6TG, Ara-C, Trampcol*
v, p V, P, DNR, Ara-C, 6MP V, P, Asp
Partial remission Partial remission
4 I2
Complete remission subsequent CNS > I2
leukaemia and marrow relapse. Now in second remission Partial remission 2
Complete remission > Z
Complete remission > 9 Complete remission but CNS leukaemia > 23 11 months later. CNS relapse 21 months later
~~ ~
V = Vincristine; C = Cydophosphamide; P = Prednisone; 6MP = 6 Mercaptopurine; DNR = Daunorubicin; Ara-C = Cytosine arabinoside; 6TG = 6-thioguanine; H U = Hydroxyurea; MTX = Methotrexate; Asp = L-asparaginase; Ve = Vercyte. * See text.
Case 3 Mrs J.H., aged 3 3 years, had a 10 d history of headaches, fever, palpitations and leg weak-
ness. The blast cells in the peripheral blood film had a high nuclear cytoplasmic ratio, a dark blue vacuolated cytoplasm and one to two nucleoli. The majority were small and only occa- sional cells had cytoplasmic granulation. Most granulocytes appeared normal; occasional primitive monocytoid cells were present. The bone marrow was almost completely replaced by blast cells. The blast cells and occasional neutrophils were negative with the Sudan Black stain. The blast cells showed fine, granular positivity with acid phosphatase (Table V). The NAP score was 80. The serum vitamin BIZ level was 880 ng/l. with a UBBC of 2977 ng/l. Direct cytogenetic studies on the bone marrow showed the presence of the Phi chromosome,

CML Presenting in Blast Crisis I73 and of additional chromosome abnormalities in a minority of the metaphases (Table VII). Surface marker analysis of the blast cells gave negative results.
Vincristine, cytosine arabinoside, L-asparaginase, prednisone and 6-thioguanine in combina- tion induced a complete bone-marrow and peripheral blood remission (Table VI), which was maintained for 3 months with hydroxyurea and pipobroman. A second complete remis- sion was induced with the same combination of drugs as used initially, and maintained by daily 6-mercaptopurine and intermittent methotrexate and cyclophosphamide. Cytogenetic studies of the marrow during remission showed one Phl chromosome in each cell and no other abnormality. For subsequent analyses see Table VII.
Nine months after presentation she developed CNS leukaemia. The cells in the cerebro- spinal fluid (3 x 109/l.) were mainly blast cells which were PAS and SB negative but showed a much stronger diffuse granular acid phosphatase positivity than at presentation. They carried the Phi chromosome (Table VII) and were positive with ALL antiserum. The CNS leukaemia was controlled by dexamethazone, and intrathecal chemotherapy. She is now in good health 12 months after the initial diagnosis. The blood and marrow findings are a t present those of CML and there are no abnormal cells in the CSF.
TABLE VII. Sequential cytogenetic studies in J.H. ~
Date
Ph' positive
One Phl with Source of Blasts (%) No. of One Phi additional Ph'
cells metaphases only rearrangements negative
5.11.74 At presentation 5.12.74 First remission 7.3,75 Relapse 4.5.75 Second remission 15.8.75 CNS relapse
while in second remission
remission 22.10.75 Still in second
Bone marrow Bone marrow Bone marrow Bone marrow Bone marrow CSF
Bone marrow Blood after 72 h incubation with PHA
91 3
98 3
95 2
3
3 4 40 20 20
30 I 3
3 0
2 5
24 40
18 30
None
I0
30
None
I0 None
8 None None
I 2
None
None
None None
2 2
None I
None
Case 4 Miss L.R., aged 23 years, had an 8 month history of tiredness, backache and dizziness, and
for I week had noticed swelling of her legs and bruising. The blasts in the peripheral blood included large forms with abundant cytoplasm, some with a high nuclear cytoplasmic ratio and a lymphoid appearance, and lymphoid cells showing intermediate differentiation. Some neutrophils were hypogranular and some were Pelger-HuSt cells. There were occasional nucleated red cells. The bone marrow was largely replaced by lymphoid blast cells which

I74 M. E. I. Beard et a1
were both PAS and SB negative (Table V). The Ph’ chromosome was present (see Table IV). After eight courses of 6-thioguanine and cytosine arabinoside (Table VI) the spleen de-
creased in size, she felt well, and blast cells disappeared from the peripheral blood; bone marrow infiltration persisted. One week after a course of ‘Trampcol’ (6-thioguanine, dauno- rubicin, cytosine arabinoside, methotrexate, prednisone, cyclophosphamide, vincristine and L-asparaginase) she developed a Klebsiella septicaemia and died 4 months after the diagnosis had been made.
Case 5 Mr P.H., aged 68, had complained of increasing weakness and generalized muscular pains
for 2 months, He received blood transfusions, and chemotherapy with vincristine and predni- solone induced a complete clinical and haematological remission. The blast cells at diagnosis gave positive results with anti-ALL serum. Cytogenetic analysis showed the presence of the Ph’ chromosome (Table IV).
Case 6 Mr W.D., aged 68, had felt unwell and complained of left-sided chest pain for 2 months.
Blood and marrow examination suggested a diagnosis of acute undifferentiated leukaemia. After two 5 d courses of cytosine arabinoside (Ara C) and daunorubicin (DNR), and before the third, he was pancytopenic and the marrow was hypoplastic. Nearly all thc cells in the marrow were lymphoid blast cells, the majority showing block PAS positivity. They were positive with anti-ALL serum. Seven days after the third course the pancytopenia had im- proved, and 11% of the cells present in the marrow were blasts. The results of the cytogenetic analysis made on the initial aspirate showed the Ph’ chromosome in three of five metaphases analysed (Table IV). Treatment with vincristine and prednisolone induced complete remis- sion and he remains well 9 months after the initial diagnosis.
Case 7 Mr E.R., aged 18, had complained of headaches, dizziness and malaise for 2 weeks. Early
papilloedema was present but abnormal cells were not found in the CSF. A diagnosis of acute lymphoblastic leukaemia (ALL) was made. Vincristine, prednisolone and L-asparaginase therapy induced complete remission which was maintained with intermittent chemotherapy. Cranial irradiation (2400 r) and intrathecal methotrexate for prophylaxis of meningeal leukaemia were given immediately after the induction of complete remission. Following a period of 5 weeks without any treatment the leucocyte count rose to 80 x 10~11. of which 62% were neutrophils and neutrophil precursors. No blasts were present. This picture resem- bled that of CML, and analysis of the bone-marrow cells revealed the Ph’ chromosome (Table IV). The original diagnosis was therefore revised to CML presenting in blast crisis. Later, headaches and papilloedema returned and the CSF contained 600 blast cells/pl. The leucocyte count was 18 x 1 0 ~ 1 1 . and the bone marrow, though hypercellular, showed no evidence of relapse of acute leukaemia. Intrathecal chemotherapy via an Ommaya reservoir was given, but a further CNS relapse occurred 10 months later, when CSF blasts were found to be positive with anti-ALL serum(Janossy et al, 1976). Two years after presentation the leucocyte count rose to 190 x 1 0 ~ 1 1 . ~ the differential cell count being that of CML in the chronic phase.
CML Presenting in Blast Crisis I75
RESULTS
Haemutological (Tables I-VI) In case I the correct diagnosis was established only when the cytogenetic analysis revealed
the Ph’ chromosome. CML had not been considered as a possible diagnosis from the clinical and haematological findings. In cases 2-5 the correct diagnosis was suspected by noting abnormalities in the granulocyte series which were thought to be incompatible with the provisional diagnosis of ALL. Initial examination of blood and marrow showed large numbers of blast cells morphologically resembling lymphoblasts. These cells had a high nuclear cyto- plasmic ratio, a rather coarser nuclear chromatin than is usually seen in myeloblasts, and no cytoplasmic granulation. Lymphocytes and lymphoid cells intermediate in differentiation were also present. In case J.H. a minority of blast cells had more plentiful dark blue, often vacuolated cytoplasm similar to that of Burkitt’s lymphoma. The abnormalities in the granu- locyte series included hypogranularity of mature neutrophils on both MGG and SB stains, the Pelger-HuEt anomaly in a proportion of mature granulocytes and the presence of primitive monocytoid cells. The blast cells were SB-negative in cases 3, 4 and 5 , and only 5% were positive in T.C. at presentation. This stain confirmed abnormal hypogranulation in mature neutrophils. Just before death, he had over 200 x 10~11. blast cells in the peripheral blood and all cells were SB negative. The blast cells, though cytochemically undifferentiated, now frequently had a low nuclear cytoplasmic ratio and an abundant dark blue non-vacuolated cytoplasm. In W.D. the correct diagnosis was made because of the persistence of large numbers of ‘lymphoid’ PAS positive blast cells following therapy. In case 7 (E.R.) the peri- pheral blood appearances suggested CML 6 months after the initial diagnosis of ALL.
Cytogenetic Analysis (Table IV) In each case the Ph’ chromosome was present in bone-marrow cells. In J.H. and E.R. all
the metaphases analysed contained the Ph’ chromosome. In J.H. additional cytogenetic changes were associated with the CSF blast-cell line as well as in the bone marrow at presen- tation and in relapse. Both these patients have developed the typical picture of CML while in remission from blast-cell leukaemia. In the remaining five cases, variable proportions of Ph’ negative metaphases were present either initially or following treatment. In T.C. during a prolonged partial remission of blast-cell leukaemia 170 of 200 metaphases analysed were Ph‘ negative. None of these patients has developed a CMLlike picture when in remission of blast-cell leukaemia.
Surface Marker Analysis No tests were carried out on B.B. and C.R. Four patients were negative for ‘T’ and ‘B’
markers and patient E.R. was not tested. When tested with ALL antisera, in T.C. and P.H. the bone marrow blast cells were strongly positive. In J.H. and W.D. blast cells were negative at presentation. Subsequent analysis of bone marrow in W.D. showed 5.5% of cells to be strongly positive with ALL antisera. In J.H. and E.R. when CNS infiltration occurred, the blast cells were positive with ALL antisera (Janossy et al, 1976).
B

176 M. E.J. Beard et a1
DISCUSSION CML usually passes through two phases, a chronic phase which is often prolonged, and a tcrminal phase which is often rapidly fatal and resistant to currently available therapy. Killman (1968, 1972) and Pedersen (1975) regarded CML in the chronic phase as a preleuk- aemic state with a high probability of becoming malignant (the blast crisis). The blast phase may develop at any time during the course of CML, and patients may present for the first time in blast crisis, the presumed previous chronic phase being clinically silent (Hammouda, 1963 ; Kiossoglou et al, 1965; Neerhout, 1968; Bornstein et al, 1972). Usually an initial diag- nosis of AML was revised when the Ph’ chromosome was found.
We believe that in the patients reported here, who presented clinically and haematologic- ally as acute leukaemias, the chronic phase of CML was either short, unusually benign, or had failed to become expressed, and that the acute leukaemic picture at presentation represented the blastic crisis. The misleading clinical and haematological features of our cases initially suggested a diagnosis of undifferentiated leukaemia in case 6 and ALL in the other patients. This initial impression suggested that our cases were similar to those reported as Ph’-positive ALL (Propp & Lizzi, 1970; Schmidt et al, 1975; Van Biervliet et al, 1975). The presence of minor but definite changes, Pelger-HuEt anomaly, hypogranular mature neutrophils, and primitive monocytoid cells in some of the cases, indicated an involvement of the granulocytic series not seen in ordinary ALL.
The acute leukaemias may be divided into AML and non-AML groups. The A M L group can readily be identified by Romanowsky staining supplemented by either the peroxidase or Sudan Black techniques and non-specific esterase reactions. The sub-division of the non-AML group has been highly subjective until recently and agreement between different centres poor or non-existent. A very small percentage of cases in this group could include poorly differenti- ated AML (Bessis, 1973) or CML presenting in blast crisis. On any objective assessment, the non-AML group was essentially undifferentiated even though many cases had a lymphoid appearance. The development of methods to detect cell surface marker systems (Seligmann, 197s; Brown et al, 1974) and leukaemia-specific antigens (Greaves et al, 1975) has enabled this non-AML group to be sub-divided by more objective criteria and has placed the lymphoid nature of some cases in this group on a firmer basis (Janossy et al, 1976). In the non-AML group I-2% are of ‘B’ cell type, 20-25% are of ‘T’ cell type and both these may be regarded as lymphoid in origin. The majority of cases lack B and T markers and most of these are anti- ALL positive (Seligmann, 1975; Greaves et al, 1975).
CML presenting in blast crisis most often resembles AML in that the proliferating cells are clearly myeloid in origin. Such cases will be diagnosed as AML unless there are features to suggest an underlying CML or cytogenetic analyses are carried out routinely in all cases of acute leukaemia. Conventional pointers to CML are an unusually large spleen, high neutro- phi1 and platelet counts, and the presence of large numbers of eosinophils or basophils. In a minority of cases the blast crisis of CML may have a lymphoid appearance (Matht & Seman, 1963 ; Matht et al, 1967; Canellos et al, 1971 ; Marmont & Damasio, 1973 ; Atkinson et al, 1975) as in the cases reported here. The responsiveness of these ‘lymphoid’ cases to vincristine and prednisolone has also been cited as indirect evidence of their lymphoid origin (Marmont & Damasio, 1973). This, however, emphasizes their similarity to common childhood ALL rather than indicating their cellular origin. Several of our cases responded well to these drugs and most have survived for longer than is usually seen in ‘myeloid’ blast crisis. Cases like ours

CML Presenting in Blast Crisis I77 are likely to be placed into the non-AML group, and can only be accurately diagnosed by the demonstration of the Ph’ chromosome.
The Ph’ chromosome originally described by Nowell & Hungerford (1960) is found in approximately 90% of patients diagnosed as CML on haematological grounds. Most Phl- negative cases are atypical. The Ph’ chromosome can thus be regarded as a marker for CML since relatively few Ph’ positive patients have been described in other blood conditions. These include myelofibrosis (Forrester & Louro, 1966), polycythaemia rubra Vera (Kemp et al, 1964) essential thrombocythaemia (Tough et al, 1963), AML (the cases referred to above as CML presenting in blast crisis), ALL (see above), and chronic lymphocytic leukaemia (RoloviC & &riC, 1974). Some of these conditions are chronic myeloproliferative disorders closely related to CML, and might represent CML occurring in atypical form rather than the Phi phenomenon occurring in a different disease. Some cases, including ours, may represent the malignant transformation of the myeloid and premyeloid stem cell line occurring in atypical forms, or alternatively they may represent the Ph’ phenomenon occurring in distinctly different (i.e. lymphoid or prelymphoid) precursors as suggested by Propp & Lizzi (1970). This question is analysed in the subsequent paper where the surface marker analysis of lym- phoid and myeloid CML blast crisis is described. In practice the Ph’ chromosome acts as a marker not only in diagnosis, but also in the assessment of the extent of the disease within the body. It is generally agreed that myeloid cells, granulocytes, erythroblasts, megakaryocytes and monocytes all carry the Ph’ defect but that skin fibroblasts do not. Although the Ph’ chromosome has been reported in lymphocytes (Secker Walker & Hardy, 1975) detailed studies in the late stages of CML have not been published.
The frequency of CML blast crisis presenting as ALL is likely to be very low but should be identified wherever possible because the prognosis is likely to be worse than in common ALL, but appears to be considerably better than in ‘myeloid’ blast crisis. Whenever acute leukaemias are being intensively investigated and in particular when new techniques are applied, the precise diagnosis should be established. In these situations cytogenetic analysis of the blast cells under study is now essential.
We are grateful to the nursing staff and the staff of the Haematology Departments of the hospitals where these patients were cared for. The cytogenetic analyses on L.R. and B.B. were performed under the direction of Dr S. D. Lawler. Dr Lawler also reviewed the findings in J.H. and T.C. and gave much helpful advice. Dr E. Pearce performed the cytogenetic analysis on E.R. and Mr G. Breckon on cases P.H. and W.D. Miss N. Sourial measured the B12 binding capacities on T.C. and J.H.
We also wish to acknowledge the skilful technical help given by Mrs L. Brown and the secretarial assistance of Miss C. Prior.
ACKNOWLEDGMENTS
REFERENCES
ANDERSON, B.B. (1964) Investigations into the Euglena for the assay of the vitamin Biz in serum.]oumal of Clinical Pathology, 17, 14.
ATKINSON, K., KAY, H.E.M., LAWLER, S.D., WBLLS, D.G. & MCELWAIN, T.J. (197s) Meningeal leu- kemia after blastic transformation of chronic myeloid leukemia. Cancer, 35, 529.
BEARD, M.E.J. & HAMILTON FAIRLEY, G. (1974) Acute
Ieukemia in adults. Seminars in ffaematology, 11, 5. BBSSIS, M. (1973) Cytologic diagnosis of leukaemias
by electron microscopy. Recent Advances in Cancer Research, 43, 63.
Chronic myelogenous leukemia presenting in blastic crisis. Cancer, 30.939.
BORNSTEIN, R.S., NBSBIT, M. & KBNNBDY, B.J. (1972)
BROWN, G., GRBAVES, M.F., LISTFiR, T.A., RAPSON, N.

M. E. J. Beard et af & PAPAMICHAEL, M. (1974) Expression of human T and B lymphocyte cell-surface markers on leu- kaemic cells. Lancet, ii, 753.
CANELLOS, G.P., DEVITA, V.T., WHANG-PENG, J. & CARBONE, P.P. (1971) Hematologic and cytogenetic remission of blastic transformation in chronic granulocytic leukemia. Blood, 38, 671.
DACIE, J.V. & LEWIS, S.M. (1968) Practical Haema- tology, 4th edn. Churchill. London.
FLANDRIN, G. & BERNARD, J. (1975) Cytological classification of acute leukemias. A survey of 1400 cases. Blood Cells, I, 7.
FORRESTER, R.H. & LOURO, J.M. (1966) Philadelphia chromosome abnormality in agnogenic myeloid metaplasia. Annals of Internal Medicine, 64, 622.
GOLDBERG, A.F. & BARKA, T. (1962) Acid phosphatase activity in human blood cells. Nature, 195, 297.
GOTTLIEB, C., LAU, K.-S., WASSERMAN, L.R. & HERBERT, V. (1965) Rapid charcoal assay for intrinsic factor (IF), gastric juice unsaturated BIZ binding capacity, antibody to IF, and serum un- saturated Blz binding capacity. Blood, 25, 875.
GREAVES, M.F., BROWN, G., RAPSON, N.T. & LISTER, T.A. (1975) Antisera to acute lymphoblastic leukaemia cells. Clinical Immunology and Immuno-
HAMMOUDA, F. (1963) Chromosome abnormality in acute leukaemia. Lancet, ii. 410.
HAMMOUDA, F., QUAGLINO. D. & HAYHOE, F.G.J. (1964) Blast aisis in chronic granulocytic leukaemia. Cytochemical, cytogenetic, and autoradiographical studies in four cases. Britich Medical]ournal, i. 1275.
HAYHOE, F.G.J. & CAWLEY, J.C. (1972) Acute leu- kaemia: cellular morphology, cytochemisny and fine structure. Clinics in Haematology, I, 49.
JANOSSY, G., GREAVES, M.F., REVESZ, T., LISTER, T.A., ROBERTS, M., DURRANT, J., KIRK, B., CATOVSKY, D. & BEARD, M.E.J. (1976) Blast crisis of chronic myeloid leukaeniia (CML). 11. Cell surface marker analysis of ‘lymphoid’ and myeloid cases. British
Journal of Haematology, 34, 179. KBMP, N.H., STAFFORD, J.L. & TANNER, R. (1964)
Chromosome studies during early and terminal chronic niyeloid leukaemia. British Medical ]ournal, i, 1010.
KHAN, M.H. & MARTIN, H. (1967) Myeloblasten- leukaemie mit Philadelphia-Chromosom. Klinisch Wochenschrifr, 45. 821.
KILLMAN, S.-A. (1968) Acute leukemia: develop- ment, remission/relapse pattern, relationship be- tween normal and leukemic hemopoiesis and the ‘sleeper-to-feeder’ stem cell hypothesis. Series Haematologica, I. (3). 103.
KILLMAN, S.-A. (1972) Chronic myelogenous leukaemia: Preleukaemia or leukaemia? Haemato- logica (Pavia), 57, 641.
KIOSSOGLOU, K.A., MITUS, W.J. & DAMESHBK, W. (1965) Two Phi chromosomes in acute grando- cytic leukaemia. A study oftwo cases. Lancet, ii. 665.
pathology, 4, 67.
LOBB, D.S. (1974) A cytogenetic study of Philadelphia positive chromosome positive cases of chronic myeloid leukaemia. Thesis for M.Phil., University of London.
MARMONT, A.M. & DAMASIO, E.E. (1973) The treat- ment of terminal metamorphosis of chronic granulocytic leukaemia with corticosteroids and vincristine. Acta Haematologica, 50, I.
MA&, G. & SEMAN, G. (1963) Aspects Histologiques et Cytologiques de Leucemies et Ha~matosorcomer. Lib- raire Maloine S.A., Paris.
MATH$, G., TUBIANA, M., CALMAN, F., SCHLUM- BERGER, J.R., BERUMEN, L., CHOQUET, c . , CATTAN, A. & SCHNEIDER, M. (1967) Les syndromes de leucCmie aigne (SLA) appraisant au cours de l’evolution des haematosarcomes et des 1eucCmies chroniques (analyse clinique). Nouvelle Revue Franpise d’Himatologie, 7, 543.
MOORHEAD, P.S., NOWELL, P.C., MELLMAN, W.J., BATTIPS, D.M. & HUNGERPORD, D.A. (1960) Chromosome preparations of leukocytes cultured from human peripheral blood. Experimental Cell Research, ao, 613.
NBBRHOUT, R.C. (1968) Chronic granulocytic leu- kemia. Early blast crisis simulating acute leukemia. American Journal of Diseases of Children, 115, 66.
NOWELL, P.C. & HUNGERPORD, D.A. (1960) A minute chromosome in human granulocytic leukaemia. (Abstract). Science, 132, 1497.
PBDERSEN, B. (1975) Clonal evolution and progression in chronic myeloid leukaemia. Blood Cells, I, 227.
PROPP, S. & LIZZI, F.A. (1970) Philadelphia chromo- some in acute lymphocytic leukemia. Blood, 36, 3 53.
ROLOVIC, Z. & C h C , M. (1974) Phl-positive cells in chronic lymphocytic leukemia bone marrow. Blood, 4, 623.
SCHMIDT, T.A., DAR, H., SANTORXNEOU, M. & SEKINE, I. (1975) Philadelphia chromosome and loss and reappearance of the Y chromosome in acute lym- phocytic leukaemia. Lancet, i, 1145.
SBCKER WALKER, L.H. & HARDY, J.D. (1975) Phila- delphia chromosome in PHA-stimulated lympho- cytes in acute leukaemia. Lancet, ii, 1301.
SELIGMANN, M. (1975) Membrane cell markers in human leukaemias and lymphomas. British Journal ojlfuematology, 31 (Suppl.), I.
TJIO, J.H. & WHANG, J. (1962) Chromosome prepara- tions of bone marrow cells without prior in vitro or in uiuo colchicine administration. Stain Technology, 37. 17.
TOUGH, I.M., JACOBS, P.A., COURT-BROWN, W.M., BAKIE, A.G. & WILLIAMSON, E.R.D. (1963) Cyto- genetic studies on bone marrow in chronic myeloid leukaemia. Luncet, i, 844.
VAN BIBRVLIET, J.P., VAN HEMEL, J., GEURTS, K., PUNT, K. & DB BOER-VAN WERINC (1975) Phila- delphia chromosome in acute lymphocytic leu- kaemia. Lancet, ii, 617.




















