
Value of transfusion independence in severe aplastic anemia ...
Upload
independentCategory
view
3download
0
Transfusion related acute lung injury in the critically ill: prospective nested case-control
study
Ognjen Gajic1
Rimki Rana1
Jeffrey L. Winters2
Murat Yilmaz1
Jose L. Mendez1
Otis B. Rickman1
Megan M O’Byrne3
Laura K. Evenson1
Michael Malinchoc 3
Steven R DeGoey2
Bekele Afessa1
Rolf D. Hubmayr1
S. Breanndan Moore2
1Division of Pulmonary and Critical Care Medicine 2Division of Transfusion Medicine
3Division of Biostatistics
Mayo Clinic College of Medicine
Rochester, Minnesota
Address correspondence to: Ognjen Gajic, M.D. Mayo Clinic 200 First Street SW Rochester, MN 55905 Telephone: 507-255-6051 Fax: 507-255-4267 E-mail: [email protected]
This study was supported by NHLBI 1 K23 HL087843-01A1 and the grant from National Blood Foundation, NBF 2004-05 Running Title: TRALI in the Critically Ill Descriptor Number: 2 Word Count: 2,328
This article has an online data supplement, which is accessible from this issue's table of content
online at www.atsjournals.org
AJRCCM Articles in Press. Published on July 12, 2007 as doi:10.1164/rccm.200702-271OC
Copyright (C) 2007 by the American Thoracic Society.

1
ABSTRACT
Rationale: Acute lung injury (ALI) that develops six hours after transfusion (TRALI) is the
leading cause of transfusion-related mortality. Several transfusion characteristics have been
postulated as risk factors for TRALI, but the evidence is limited to retrospective studies.
Objective: To compare patient and transfusion risk factors between the patients who do and do
not develop ALI
Methods: In this prospective cohort study, consecutive transfused critically ill patients were
closely observed for development of ALI. Donor samples were collected from the transfusion
bags. Risk factors were compared between patients who did develop ALI following transfusion
and transfused controls, matched by age, gender and admission diagnosis.
Measurements and main results: Seventy-four out of 901 transfused patients developed ALI
within 6 hours after transfusion (8%). Compared to transfused controls, ALI patients were more
likely to have sepsis (37% vs 22%, p=0.016), and a history of chronic alcohol abuse (37% vs
18%, p=0.006). When adjusted for patient characteristics, transfusion of plasma from female
(odds ratio-OR 5.09, 95%CI 1.37-18.85), rather than male donors (OR 1.60, 95%CI 0.76 to
3.37), number of pregnancies among the donors (OR 1.19, 95%CI 1.05 to 1.34), number of
donor units positive for antigranulocyte (OR 4.85, 95%CI, 1.32-17.86) and HLA class II
antibodies (OR 3.08, 95%CI 1.15-8.25), and the concentration of lysophosphatidylcholine in the
donor product (OR 1.69, 95%CI 1.10 to 2.59) were associated with development of ALI.
Conclusions: Both patient and transfusion risk factors determine the probability of ALI after
transfusion. Transfusion factors represent attractive targets for prevention of ALI
Abstract Word Count 250

2
Keywords: Fresh-frozen plasma; Platelet transfusion, Transfusion; Outcome study; Pulmonary edema; Respiratory Distress Syndrome, Acute; Female; Blood Donors

3
INTRODUCTION
Since the original description twenty years ago (1), Transfusion-Related Acute Lung Injury
(TRALI) has emerged as the most important cause of morbidity and mortality resulting from
blood transfusion (2-4), in part due to the decrease in morbidity and mortality from other
adverse effects of transfusion. While the exact etiology is not known, uncontrolled clinical
studies and animal models have suggested an important role of donor derived anti-leukocyte
antibodies as well as biologic response modifiers accumulated during blood storage (5-9). Anti-
leukocyte antibodies (anti HLA class I, class II and antigranulocyte) are known to be commonly
present in the plasma of donors exposed to the foreign tissue during previous pregnancy or
transfusion and have been implicated in multiple case series and case reports (1, 3-5). Indeed,
anti-HLA antibodies have been detected in up to 25% of multiparous women donors (10).
TRALI is thought to be under-diagnosed and under-reported (4, 5, 11), particularly in critically
ill patients who often have multiple risk factors for acute lung injury (ALI). It is possible that
current TRALI cases reported to the blood bank represent the "tip of the iceberg" and that
transfusion factors play a mechanistic role in many more patients with ALI, as one of "multiple
hits" required for the full expression of this syndrome (12-14). Indeed, transfusion (massive) has
long been recognized as one of the most important ALI risk factors (15). Submassive transfusion
of all blood products, and particularly high plasma volume products have been recently identified
as independent risk factors for development of ALI in the critically ill(16, 17). In animal studies
the presence of additional ALI risk factors has been found to modulate both the development and
severity of TRALI (multiple-hit hypothesis) (8, 9). The lack of standardized definition, however,
posed a significant limitation on previous clinical studies(3, 4).
Two recent expert consensus panels have proposed a standardized TRALI definition (3, 4).
Using the proposed definition, we reported retrospective data showing a much higher incidence

4
of TRALI in critically ill patients than previously suggested (18, 19). In this prospective study
we aimed to determine the incidence, risk factors and outcome of ALI which develops 0-6 hours
after the transfusion of blood products in a cohort of patients admitted to the medical intensive
care unit (ICU). Using a matched case-control design, we compared types of blood
products transfused by donor and storage characteristics, the prevalence of anti-leukocyte
antibodies (anti-granulocyte, anti-HLA class I and class II)(1, 5) and the amount of biologic
response modifiers (interleukin 8, IL8 and lysophosphatidil choline, Lyso-PC)(20) in the samples
of donor blood units given to patients who did or did not develop ALI after transfusion.
Some of the results of this study have been previously reported in the form of an abstract.(21)
MATERIALS AND METHODS
In this two year prospective cohort study, all patients transfused in a medical ICU of a tertiary
care medical center were closely observed for 24 h after transfusion. Detailed methods are
provided in online data supplement. The Institutional Review Board approved the study protocol.
Patients who refused research authorization were excluded. Monitoring logs reflecting
cardiopulmonary function, chest radiographs and arterial blood gases were reviewed and
followed until 24 hours after each transfusion allowing for identification of patients who had any
worsening of respiratory status 0-24 hours after the transfusion (see online data supplement).
Expert intensivists blinded to specific transfusion factors, subsequently reviewed all clinical data
and assigned the diagnosis of ALI within 6 hours of transfusion (suspected or possible TRALI)
based on the standard clinical definition (4, 22, 23). Inter-observer agreement was measured
using Kappa statistics. Two of the reviewers (JLM and OBR) re-reviewed the discordant cases
together and resolved any disagreements.
In the nested case control part of the study the patients’ and transfusion factors were compared
between patients who developed ALI after transfusion and transfused controls matched by age

5
±10 years, gender and admission diagnostic group (19). Predictor variables were grouped as
follows:
1. ALI risk factors prior to transfusion: Severity of illness was determined by calculating
Acute Physiology and Chronic Health Evaluation (APACHE III) scores(24) prior to
transfusion. Sepsis and pneumonia were defined according to standard clinical criteria
(25, 26). Aspiration was defined as witnessed or suspected aspiration of gastric contents
into the airways. Chronic alcohol abuse was defined as a known diagnosis of chronic
alcoholism or a previous admission for alcohol detoxification or alcohol withdrawal(27)
2. Transfusion factors: Units given 0-6 hours prior to the development of ALI (in cases) or
0-6 hours after the beginning of the first transfusion (controls) were considered associated
units. The exposure time for each control was matched to the exposure time of the
corresponding case (see online data supplement). The data on type of blood product,
storage age and donor gender were collected from the institutional transfusion database.
Female donors were contacted to obtain pregnancy history unless available from the
medical record of the donor. Transfused plasma volume was calculated based on the
average plasma content in specific blood products (19). Fresh frozen plasma (FFP) and
platelet transfusions were considered high plasma volume components(28).
3. Donor plasma samples: Throughout the study period transfusion bags and tubing were
collected at the end of each transfusion and stored for subsequent testing. Anti HLA class
I and class II antibodies were measured by multiplexed, microsphere-based flow
cytometric assay, ABScreenTM PRA (One Lambda, Inc, Canoga Park, CA) (29).
Antigranulocyte antibodies were detected by standard indirect immunofluorescence
method (30). LysoPC was measured by high performance lipid chromatography (31).
Interleukin (IL)-8 was measured using standard ELISA Quantikine HS Immunoassay

6
(R&D Systems Inc. Minneapolis, MN). If insufficient amount of plasma was obtained
from the transfusion bag, antibody (but not LysoPC and IL8) testing was performed on
available donor product or donor sample from subsequent donation.
Statistical Analysis: Paired parametric and non parametric testing was used in univariate
analyses as appropriate. We anticipated that approximately 80% of cases, and 40% of controls,
will have received at least one unit of donor blood that tests positive for anti-leukocyte
antibodies (6, 20). It was determined that a 1:1 matched case/control study with 50 cases and 50
controls would provide >80% power to detect a significant difference in the number of positive
antibody tests between groups using a two-sided, alpha=0.05 level test. Conditional logistic
regression was used to compare specific transfusion factors after the adjustment for pre-
transfusion ALI risk factors. SAS statistical software was used for all the analysis (SAS Version
9, SAS Institute Inc., Cary, North Carolina).
RESULTS
We prospectively observed 901 critically ill patients who were transfused in the medical ICU
over the two year study period (see outline of the study in Figure 1). Among 6588 blood product
units transfused during the ICU stay 3383 (51%) were packed RBCs, 2728 (41%) FFP, 306 (5%)
platelets and 171 (3%) cryoprecipitate. Waste plasma samples were stored from 3813 (57%)
transfusions for subsequent laboratory studies. Seventy-four (8%) patients developed ALI within
6 h of transfusion (Figure 1). Inter-observer agreement was moderately good (kappa 0.6).
Tables 1 describes clinical and transfusion characteristics of patients who developed ALI after
transfusion and matched controls. Gastrointestinal bleeding was the most common reason for
ICU admission (Table 1). Compared to patients who had no respiratory worsening after
transfusion, patients who developed ALI were more likely to have sepsis, liver disease and a
history of chronic alcohol abuse (Table 1).

7
ALI cases were more likely to have received plasma-rich blood products (FFP or platelets). They
were also more likely to have received blood products from female donors and larger volumes of
plasma from female donors (Table 1). Five cases (7%) and 4 controls (5%) received massive
(≥10 units) transfusion during the exposure period. Donors of patients who developed ALI had a
higher number of pregnancies and tested positive for anti-leukocyte antibodies (Table 1 and 2)
more often. There was no difference in IL8 or storage age of red cell products between patients
who developed ALI and matched controls. The concentration of LysoPC was significantly higher
in blood products given to ALI cases than controls (Table 2). At least one of the associated units
was tested for anti-leukocyte antibodies on 82% of cases and 80% of controls. LysoPC and IL8
were tested on at least one associated unit in 73% of cases and 78% of controls (Table 2).
Table 3 provides the unadjusted and adjusted ALI odds ratios for specific transfusion risk
factors. When adjusted for baseline APACHE III scores, sepsis and alcohol abuse in the
conditional logistic regression analysis, several transfusion factors remained associated with the
development of ALI (Table 3). The results were similar after additional adjustment for baseline
liver disease (Table E2, online data supplement). The distribution of transfusion factors were
similar in subgroups of patients who had significant additional ALI risk factors (“possible
TRALI”) and those who did not (“suspected” TRALI), Table E1, online data supplement..
Of 74 patients who developed ALI, 58 were treated with mechanical ventilation (48 invasive, 10
noninvasive) and 16 were treated with oxygen supplementation via face mask. Median duration
of mechanical ventilation was 3.6 (1.6 to 7.1) days. Twenty seven cases and 27 controls were
mechanically ventilated at the time of transfusion. Additional 31 cases were started on
mechanical ventilation (26 invasive, 5 noninvasive) because of development of ALI. Hospital
mortality was higher in patients who developed ALI (41%) than in matched controls (23%),
p<0.01), see also online data supplement.

8
DISCUSSION
The principal findings of our study are the following: 1) In a cohort of critically ill medical
patients, the development of ALI shortly after transfusion was more common than usually
appreciated and an order of magnitude more common than what is reported to blood banks 2)
Both underlying patient characteristics (“first hit”) and specific transfusion factors (“second hit”)
were associated with the development of ALI after blood transfusion. 3) Our results support both
of the proposed TRALI mechanisms as well as general multiple hit model of TRALI and ALI.
To our knowledge, this is the first time the recommended standardized clinical definition (3, 4,
22) was implemented in a prospective study of TRALI. In critically ill medical patients admitted
to a tertiary care medical center, clinically defined TRALI appears to be more common than
previously thought, supporting the general notion that TRALI is grossly under-recognized and
under-reported (3-5). Rather than concentrating on clinically suspected TRALI reactions
reported to the blood bank, we prospectively examined consecutive transfused critically ill
medical patients. Patients who developed ALI after transfusion often had other important ALI
risk factors not related to transfusion itself, sepsis and a history of chronic alcohol abuse. The
fact that potentially modifiable transfusion risk factors (such as donor gender, parity and
alloimmunization) are commonly associated with development of ALI may have important
implications on prevention and treatment of ALI in critically ill medical patients. Observational
data already suggest a decrease in incidence of ALI in patients treated with less liberal
transfusion policy (32, 33). Moreover, preliminary data from UK suggest a significant decrease
in postoperative ALI associated with a decreased use of FFP from female donor plasma(34).
Our results to some extent support both of the main proposed mechanisms for TRALI (6, 7, 35,
36) as well as the overall multiple-hit paradigm in ALI development (13, 14). Both the presence
of anti-leukocyte antibodies and the concentration of bioactive lipid factors in the donor product

9
were higher in patients who developed ALI than in matched controls both with and without
adjustment for baseline characteristics (“first hit”). Although the small sample size precludes
wider inferences, the closer look at the distribution of antibodies and LysoPC across different
blood products (Tables E3 and E4, online data supplement) reveals a trend towards more
antibody positive units given to ALI patients vs controls across each of the blood products (RBC,
FFP, platelets). On the other hand, a higher concentration of LysoPC seems to merely reflect the
larger number of high plasma volume products (platelets and FFP) given to ALI patients vs
controls. Our study design did not allow us to determine the sensitivity and specificity of
laboratory diagnosis of TRALI, nor to assess the specific etiologic (as opposed to a biomarker)
role of anti-leukocyte antibodies and LysoPC.
The association between infusion of plasma from female donors and the subsequent development
of lung injury is an intriguing finding of our study and has important implications with regards to
the etiology and prevention of TRALI. Our findings support the results of the small randomized
trial by Palfi et al, in which the plasma transfusion from multiparous female donors lead to
worsening in oxygenation and increased inflammatory response(35). The United Kingdom blood
system recently nearly eliminated female donors from the production of high plasma volume
products (FFP) and the first reports suggest a significant decrease in TRALI reactions reported to
the national transfusion surveillance system (SHOT-serious hazards of transfusion) (37). AABB
TRALI working group recently recommended similar guidelines for North American Blood
Centers, with a plan to eliminate transfusion of high plasma volume products from donors at high
risk of leukocyte alloimunization (including previously pregnant female donors) by November of
2008 (28). Since this intervention may be associated with costs and/or shortage of blood products
in some blood centers, further studies will have to assess if benefit of this intervention outweighs
the costs.

10
Relatively high mortality of our suspected or possible TRALI cases is comparable to a report
from Wallis et al (38) and our recent retrospective study in the critically ill (19), but higher than
in some other epidemiological studies (6). It is important to emphasize the characteristics of the
population studied: medical ICU patients in a tertiary care medical center, a group with
inherently high mortality rate. The observed mortality may or may not be attributable to TRALI
as these critically ill patients had multiple additional risk factors for both ALI and poor outcome.
We need to point out limitations of our study design. The study was conducted in a single
medical ICU in tertiary care center and, while internal validity may be high, external validity is
limited. In addition, the observational nature of the study does not allow independent estimation
of the cause and effect relationship between the predictors and outcome. Residual confounding
is always an issue in observational studies but is unlikely to fully explain our observed
differences in donor product characteristics (anti-leukocyte antibodies from previously pregnant
female donors and the concentration of LysoPC). Since there is no way that clinicians could have
specifically ordered “male” or “low LysoPC product in our institution, indication bias should be
less of an issue. While the trend towards higher amount of total plasma could explain some of the
observed differences it is again unlikely to explain the association between the donor gender and
pregnancy and the development of ALI.
Important limitation of our study is that we did not test for corresponding leukocyte antigens and
were not able to determine the specificities of donor antibodies. We did not perform additional
testing or treatment of the sera (e.g. adsorption of HLA Class I antibodies with platelets) to
confirm if our GIF+ samples were indeed directed against granulocyte specific antigens.
Because the fresh granulocyte panels used for the assay could not be selected to include all
possible granulocyte antigens, the potential exists that antibodies directed toward uncommon
granulocyte antigens would not be detected. Therefore, we could not distinguish between the

11
etiologic, rather than a biomarker role of specific antibodies. In a number of units given to both
cases and controls we were unable to extract an adequate sample for laboratory analysis. While
the proportion of units tested for anti-leukocyte antibodies was similar in cases and controls,
somewhat higher proportion of control units were tested for IL 8 and LysoPC. This difference, if
anything, would make it less likely to detect a significant difference by chance alone.
While the differences in pre-transfusion risk factors to some may point to the limitation of our
matching procedure, we were able to distinguish important, but not as well appreciated patient
risk factors, i.e. chronic alcohol abuse. Moss et al previously reported a strong independent
association between alcohol use and development of ALI (27). Laboratory experiments suggest
the depletion of antioxidant glutathione stores associated with chronic alcohol abuse as the most
plausible mechanistic explanation (39). Since a neutrophil mediated oxidative injury is the
hallmark of TRALI (7, 8, 36, 40), it seems plausible that antioxidant depletion may be associated
with greatly increased risk of this type of ALI.
In conclusion, by prospectively applying the standardized clinical definition, we have found a
high incidence of suspected and possible TRALI among transfused critically ill medical patients.
The association between specific donor and transfusion characteristics and subsequent
development of ALI has important implications relative to both the etiology and prevention of
this syndrome. Ongoing multicenter studies in transfused patients with and without underlying
critical illness will allow us to further elucidate the incidence and mechanisms of TRALI and the
effect of potential preventive strategies.

12
REFERENCES
1. Popovsky, M. A., M. D. Abel, and S. B. Moore. 1983. Transfusion-related acute lung
injury associated with passive transfer of antileukocyte antibodies. Am Rev Respir Dis
128(1):185-9.
2. Holness, L., M. A. Knippen, L. Simmons, and P. A. Lachenbruch. 2004. Fatalities caused
by TRALI. Transfus Med Rev 18(3):184-8.
3. Toy, P., M. A. Popovsky, E. Abraham, D. R. Ambruso, L. G. Holness, P. M. Kopko, J.
G. McFarland, A. B. Nathens, C. C. Silliman, and D. Stroncek. 2005. Transfusion-related acute
lung injury: definition and review. Crit Care Med 33(4):721-6.
4. Kleinman, S., T. Caulfield, P. Chan, R. Davenport, J. McFarland, S. McPhedran, M.
Meade, D. Morrison, T. Pinsent, P. Robillard, and P. Slinger. 2004. Toward an understanding of
transfusion-related acute lung injury: statement of a consensus panel. Transfusion 44(12):1774-
89.
5. Kopko, P. M., C. S. Marshall, M. R. MacKenzie, P. V. Holland, and M. A. Popovsky.
2002. Transfusion-Related Acute Lung Injury: Report of a Clinical Look-Back Investigation.
JAMA 287(15):1968-1971.
6. Popovsky, M. A., and S. B. Moore. 1985. Diagnostic and pathogenetic considerations in
transfusion-related acute lung injury. Transfusion 25(6):573-7.
7. Silliman, C. C., A. J. Paterson, W. O. Dickey, D. F. Stroneck, M. A. Popovsky, S. A.
Caldwell, and D. R. Ambruso. 1997. The association of biologically active lipids with the
development of transfusion-related acute lung injury: a retrospective study. Transfusion
37(7):719-26.

13
8. Sachs, U. J., K. Hattar, N. Weissmann, R. M. Bohle, T. Weiss, U. Sibelius, and J. Bux.
2005. Antibody-induced neutrophil activation as a trigger for transfusion-related acute lung
injury in an ex vivo rat lung model. Blood:2005-04-1744.
9. Silliman, C. C., N. F. Voelkel, J. D. Allard, D. J. Elzi, R. M. Tuder, J. L. Johnson, and D.
R. Ambruso. 1998. Plasma and lipids from stored packed red blood cells cause acute lung injury
in an animal model. J Clin Invest 101(7):1458-67.
10. Densmore, T., L. Goodnough, S. Ali, M. Dynis, and H. Chaplin. 1999. Prevalence of
HLA sensitization in female apheresis donors. Transfusion 39(1):103-106.
11. Looney, M. R., M. A. Gropper, and M. A. Matthay. 2004. Transfusion-Related Acute
Lung Injury: A Review. Chest 126(1):249-258.
12. Boshkov, L. 2005. Transfusion-related acute lung injury and the ICU. Crit Care Clin
21(3):479-95.
13. Silliman, C. C., D. R. Ambruso, and L. K. Boshkov. 2004. Transfusion-related acute lung
Injury (TRALI). Blood:2004-07-2929.
14. Matthay, M. A., G. A. Zimmerman, C. Esmon, J. Bhattacharya, B. Coller, C. M.
Doerschuk, J. Floros, M. A. Gimbrone, Jr., E. Hoffman, R. D. Hubmayr, M. Leppert, S. Matalon,
R. Munford, P. Parsons, A. S. Slutsky, K. J. Tracey, P. Ward, D. B. Gail, and A. L. Harabin.
2003. Future research directions in acute lung injury: summary of a National Heart, Lung, and
Blood Institute working group. Am J Respir Crit Care Med 167(7):1027-35.
15. Hudson, L. D., J. A. Milberg, D. Anardi, and R. J. Maunder. 1995. Clinical risks for
development of the acute respiratory distress syndrome. Am J Respir Crit Care Med 151(2 Pt
1):293-301.

14
16. Khan, H., J. Belsher, M. Yilmaz, B. Afessa, S. B. Moore, R. D. Hubmayr, and O. Gajic.
2007. Fresh frozen plasma and platelet transfusions are associated with development of acute
lung injury in critically ill medical patients. Chest.
17. Gong, M. N., B. T. Thompson, P. Williams, L. Pothier, P. D. Boyce, and D. C. Christiani.
2005. Clinical predictors of and mortality in acute respiratory distress syndrome: potential role of
red cell transfusion. Crit Care Med 33(6):1191-8.
18. Gajic, O., R. Rana, J. L. Mendez, O. B. Rickman, J. F. Lymp, R. D. Hubmayr, and S. B.
Moore. 2004. Acute lung injury after blood transfusion in mechanically ventilated patients.
Transfusion 44(10):1468-74.
19. Rana, R., E. R. Fernandez-Perez, S. A. Khan, S. Rana, J. L. Winters, T. G. Lesnick, S. B.
Moore, and O. Gajic. 2006. Transfusion-related acute lung injury and pulmonary edema in
critically ill patients: a retrospective study. Transfusion 46(9):1478-83.
20. Silliman, C. C., L. K. Boshkov, Z. Mehdizadehkashi, D. J. Elzi, W. O. Dickey, L.
Podlosky, G. Clarke, and D. R. Ambruso. 2003. Transfusion-related acute lung injury:
epidemiology and a prospective analysis of etiologic factors. Blood 101(2):454-462.
21. Gajic, O., R. Rana, J. L. Winters, J. L. Mendez, O. B. Rickman, L. K. Evenson, M.
Malinchoc, M. Yilmaz, S. R. DeGoey, D. L. Rasmussen, R. D. Hubmayr, and S. B. Moore. 2007.
Transfusion related acute lung injury in the medical critically ill patients: nested case-control
study. Am J Respir Crit Care Med 175:A965.
22. Bernard, G. R., A. Artigas, K. L. Brigham, J. Carlet, K. Falke, L. Hudson, M. Lamy, J. R.
Legall, A. Morris, and R. Spragg. 1994. The American-European Consensus Conference on
ARDS. Definitions, mechanisms, relevant outcomes, and clinical trial coordination. Am J Respir
Crit Care Med 149(3 Pt 1):818-24.

15
23. Gajic, O., M. A. Gropper, and R. D. Hubmayr. 2006. Pulmonary edema after transfusion:
how to differentiate transfusion-associated circulatory overload from transfusion-related acute
lung injury. Crit Care Med 34(5 Suppl):S109-13.
24. Knaus, W. A., D. P. Wagner, E. A. Draper, J. E. Zimmerman, M. Bergner, P. G. Bastos,
C. A. Sirio, D. J. Murphy, T. Lotring, A. Damiano, and et al. 1991. The APACHE III prognostic
system. Risk prediction of hospital mortality for critically ill hospitalized adults. Chest
100(6):1619-36.
25. Bone, R. C., R. A. Balk, F. B. Cerra, R. P. Dellinger, A. M. Fein, W. A. Knaus, R. M.
Schein, and W. J. Sibbald. 1992. Definitions for sepsis and organ failure and guidelines for the
use of innovative therapies in sepsis. The ACCP/SCCM Consensus Conference Committee.
American College of Chest Physicians/Society of Critical Care Medicine. Chest 101(6):1644-55.
26. Bartlett, J. G., S. F. Dowell, L. A. Mandell, T. M. File Jr, D. M. Musher, and M. J. Fine.
2000. Practice guidelines for the management of community-acquired pneumonia in adults.
Infectious Diseases Society of America. Clin Infect Dis 31(2):347-82.
27. Moss, M., B. Bucher, F. A. Moore, E. E. Moore, and P. E. Parsons. 1996. The role of
chronic alcohol abuse in the development of acute respiratory distress syndrome in adults. Jama
275(1):50-4.
28. 2006. Transfusion-Related Acute Lung Injury. AABB, Association Bulletin #06-07
(November 3, 2006) Bethesda, MD.
29. Pei, R., J. Lee, T. Chen, S. Rojo, and P. I. Terasaki. 1999. Flow cytometric detection of
HLA antibodies using a spectrum of microbeads. Hum Immunol 60(12):1293-302.
30. Verheugt, F. W., A. E. von dem Borne, F. Decary, and C. P. Engelfriet. 1977. The
detection of granulocyte alloantibodies with an indirect immunofluorescence test. Br J Haematol
36(4):533-44.

16
31. Silliman, C. C., K. L. Clay, G. W. Thurman, C. A. Johnson, and D. R. Ambruso. 1994.
Partial characterization of lipids that develop during the routine storage of blood and prime the
neutrophil NADPH oxidase. J Lab Clin Med 124(5):684-94.
32. Ciesla, D., E. Moore, J. Johnson, C. Cothren, A. Banerjee, J. Burch, and A. Sauaia. 2006.
Decreased progression of postinjury lung dysfunction to the acute respiratory distress syndrome
and multiple organ failure. Surgery 140(4):640-8.
33. Yilmaz M, Afessa B, Keegan MT, Hubmayr RD, and G. O. The effect of ventilation and
transfusion protocols on prevention of acute lung injury in mechanically ventilated patients. Crit
Care Med 2006 Dec; 43(12 Suppl):A85.
34. Wright, S., S. Athey, A. Leaver, C. Snowden, D. Roberts, J. Clarkson, C. Chapman, and
J. Wallis. 2007. The effect of male-donor-only fresh frozen plasma on the incidence of acute
lung injury following ruptured abdominal aortic aneurysm repair. Critical Care 11(Suppl
2):P374.
35. Palfi, M., S. Berg, J. Ernerudh, and G. Berlin. 2001. A randomized controlled trial
oftransfusion-related acute lung injury: is plasma from multiparous blood donors dangerous?
Transfusion 41(3):317-322.
36. Seeger, W., U. Schneider, B. Kreusler, E. von Witzleben, D. Walmrath, F. Grimminger,
and J. Neppert. 1990. Reproduction of transfusion-related acute lung injury in an ex vivo lung
model. Blood 76(7):1438-44.
37. Chapman, C. E., L. M. Williamson, and H. e. a. Cohen. 2006. The impact of using male
only plasma on hemovigilance reports of transfusion-related acute lung injury (TRALI) in the
UK (abstract). Vox Sang 91(Suppl 3):227.
38. Wallis, J. P., A. Lubenko, A. W. Wells, and C. E. Chapman. 2003. Single hospital
experience of TRALI. Transfusion 43(8):1053-1059.

17
39. Moss, M., D. M. Guidot, M. Wong-Lambertina, T. Ten Hoor, R. L. Perez, and L. A.
Brown. 2000. The effects of chronic alcohol abuse on pulmonary glutathione homeostasis. Am J
Respir Crit Care Med 161(2 Pt 1):414-9.
40. Looney, M. R., X. Su, J. A. Van Ziffle, C. A. Lowell, and M. A. Matthay. 2006.
Neutrophils and their Fc gamma receptors are essential in a mouse model of transfusion-related
acute lung injury. J Clin Invest 116(6):1615-23.

FIGURE LEGENDS
Figure 1. Outline of the study. ALI = Acute Lung Injury, TACO = Transfusion Associated
Circulatory Overload

Table 1 Demographics, admission diagnostic groups pre-transfusion ALI risk factors and transfusion characteristics of patients who developed ALI after transfusion and matched controls
ALI n=74
Matched Controls n=74
P value
Age (years), median (IQR) 64 (52 to 78) 61 (53 to 73) - Female gender, n (%) 37(50%) 37(50%) - ICU admission diagnoses -
Gastrointestinal, n (%) 28 (38%) 28 (38%) Respiratory, n (%) 18 (24%) 18 (24%)
Cardiovascular, n (%) 17 (23%) 17 (23%) Genitourinary, n (%) 6(8%) 5 (7%)
Hematology, n (%) 4 (6%) 5 (7%) Metabolic, n (%) 1 (1%) 1 (1%)
Baseline APACHE III score 61 (44 to 75) 57 (45 to 81) 0.586 Sepsis, n (%) 27 (37%) 16 (22%) 0.016 Pneumonia, n (%) 5 (7%) 7 (9%) 0.683 Aspiration, n (%) 8 (11.4%) 13 (18.6%) 0.225 History of heavy alcohol use, n (%) 27 (36.5%) 13 (17.6%) 0.006 Liver disease, n (%) 20 (27.4%) 11(15.1%) 0.039 Pancreatitis, n (%) 5 (6.8%) 1 (1.4%) 0.102 DIC, n (%) 10 (13.9%) 5 (6.9%) 0.132 Patients receiving RBC transfusion, n (%)
46 (62.2%) 54 (73%) 0.144
Patients receiving high plasma volume components (FFP or platelet), n (%)
44 (59.5%) 27 (36.5%) 0.006
Average RBC storage age (days) (N=35 matched pairs), median (IQR)
22.9 (17 to 31) 22.9 (15 to 30) 0.801
Number of associated units, median (IQR)*
3 (1 to 5) 2 (1 to 3) 0.063
RBC 1 (0 to 2) 2 (0 to 2) 0.77 FFP 1 (0 to 4) 0 (0 to 1) 0.08 Platelet** 0 (0 to 0) 0 (0 to 0) 0.06
Number of units from female donors, median (IQR)
1 (1 to 2) 1 (0 to 2) 0.016
Number of pregnancies among donors (n=68 matched pairs), median (IQR)
2 (0 to 5) 0 (0 to 3) 0.030
Amount of plasma (L), median (IQR) 0.27 (0.07 to 1.03) 0.07 (0.07 to 0.32) 0.047 Amount of plasma from female donors (L), median (IQR)
0.16 (0.04 to 0.5) 0.04 (0 to 0.1) 0.013
Amount of plasma (L) from female donors with at least one pregnancy (n=68 matched pairs), median (IQR)
0.04 (0 to 0.25) 0 (0 to 0.07) 0.038

RBC; red blood cells, FFP fresh frozen plasma, ALI acute lung injury, IQR interquartile range, DIC disseminated intravascular coagulation, APACHE Acute physiology and chronic health evaluation * Units transfused within 0-6 hours of the development of ALI in cases and 0-6h after the first transfusion in controls **Of 16 platelet units given to cases, 10 were aphaeresis platelets and 6 were pooled platelets; of 6 platelet units given to controls, 3 were aphaeresis platelets and 3 were pooled platelets

Table 2.Specific laboratory testing of donor samples that were given to patients who developed ALI after transfusion and matched controls*
ALI
Matched Controls
P value
IL8 (pg/dL), median (IQR), (n=47 matched pairs)
2.5 (2.5 to 6.4) 2.5 (2.5 to 7.7) 0.448
LysoPC 16 umol/L, median (IQR), (n=47 matched pairs)
46 (21 to 109) 25 (18 to 72) 0.004
LysoPC 18 umol/L, median (IQR), (n=47 matched pairs)
15 (4.9 to 33) 7.25 (2.5 to 19) 0.005
Number of antibody + tests, median (IQR)**, (n=52 matched pairs)
1 (0 to 2) 0 (0 to 1) 0.014
Received any HLA class I + units, n (%), (n=52 matched pairs)
21 (40.4%) 12 (23.1%) 0.072
Received any HLA class II + units, n (%), (n=52 matched pairs)
17 (32.7%) 10 (19.2%) 0.108
Received any GIF + units, n (%), (n=52 matched pairs)
13 (25%) 4 (7.7%) 0.020
Percentage of associated units tested for anti-leukocyte antibodies, median (IQR)
67% (24 to 100%) 90% (33 to 100%) 0.341
Percentage of associated units tested for IL8 and LysoPC, median (IQR),
50% (0 to 100%) 67% (33 to 100%) 0.036
*HLA class I, II and GIF antibodies were analyzed in 52 matched pairs, IL8 and LysoPC were analyzed in 47 matched pairs **If the associated unit tested positive for more than one antibody (for example both HLA1 and HLA2) each of these was counted as a positive test. GIF granulocyte immunofluorescence, HLA human leukocyte antigen, LysoPC lysophosphatidyl choline, ALI acute lung injury, IQR interquartile range

Table 3 Transfusion-related risk factors for acute lung injury: *unadjusted and **adjusted for baseline APACHE III score, sepsis and chronic alcohol abuse
Variable OR (95% CI)* P-Value OR (95% CI)** P-ValueAny high plasma volume components (FFP or platelets)
2.55 (1.27,5.11) 0.009 2.78 (1.21,6.38) 0.016
Number of units 1.09 (0.99,1.20) 0.081 1.11 (0.99,1.25) 0.086 Number of units from female donors 1.30 (1.03,1.66) 0.029 1.51 (1.08, 2.12) 0.016 Amount of male plasma (L) 1.55 (0.79,3.06) 0.202 1.60 (0.76,3.37) 0.215 Amount of female plasma (L) 3.23 (1.17,8.91) 0.024 5.09 (1.37,18.85) 0.015 Amount of plasma from female donors with at least one pregnancy (L)
4.41 (1.00,19.55) 0.050 9.48 (1.38,65.35) 0.022
Number of pregnancies among donors 1.11 (1.00,1.22) 0.047 1.19 (1.05,1.34) 0.007 Number of HLA class I + units 1.81 (0.97,3.38) 0.061 1.70 (0.94,3.09) 0.098 Number of HLA class II + units 1.93 (0.88,4.28) 0.103 3.08 (1.15,8.25) 0.025 Number of GIF + units 4.19 (1.22,14.32) 0.023 4.85 (1.32,17.86) 0.018 Mean LysoPC 16 (per 10 umol/L) 1.16 (1.04,1.30) 0.011 1.16 (1.02,1.32) 0.022 Mean LysoPC 18 (per 10 umol/L) 1.58 (1.10,2.26) 0.013 1.61 (1.08,2.38) 0.018
OR odds ratio, CI confidence interval, RBC red blood cell, FFP fresh frozen plasma, GIF granulocyte immunofluorescence, HLA human leukocyte antigen, LysoPC lysophosphatidyl choline, APACHE Acute Physiology and Chronic Health Evaluation, ALI acute lung injury For continuous variables odds ratios were calculated per each unit of measurement: for each additional unit transfused, for each additional liter of plasma (1L of plasma corresponds to a usual dose of ~ four units of FFP), for each 10 umol/L increase in LysoPC)

Figure 1.

Transfusion related acute lung injury in critically ill medical patients: prospective
nested case-control study
Online Data Supplement
Ognjen Gajic Rimki Rana
Jeffrey L. Winters
Murat Yilmaz
Jose L. Mendez Otis B. Rickman
Megan M O’Byrne
Laura K. Evenson
Michael Malinchoc
Stever R DeGoey
Bekele Afessa
Rolf D. Hubmayr
S. Breanndan Moore

Materials and Methods:
Prospective screening and case identification: Figure E1 outlines the prospective review
of monitoring logs used to identify respiratory worsening after transfusion. Respiratory
worsening was defined as the sustained (more than two hours) change in two out of three
respiratory monitoring parameters: 1) continuous arterial oxygen saturation measured by
pulse oximetry (decrease of 5% or below 90%), 2) oxygen supplementation (increase in
FiO2 by 10% or more) and 3) respiratory rate (increase by 10 or above 30 per minute).
ALI was defined as acute onset (within 6 h of transfusion) of hypoxemia: arterial oxygen
tension to fraction of inspired oxygen ratio (PaO2/FIO2) <300 mm Hg and bilateral
infiltrates on chest radiography, in the absence of left atrial hypertension as the principal
cause of pulmonary edema (1).
Experts used standardized algorithm to assign the probability of acute lung injury (ALI)
and TRALI as opposed to hydrostatic pulmonary edema including transfusion associated
circulatory overload (TACO) (2). The patient’s history, physical exam, echocardiogram,
electrocardiogram, biomarkers of myocardial injury, digital portable chest radiographs,
fluid balance, and data from invasive monitoring were integrated with the clinical course
and response to therapy in order to determine whether the onset of acute pulmonary
edema in these patients was mainly due to hydrostatic (TACO) or permeability (ALI)
mechanism. The experts further classified ALI patients into “possible” and “suspected”
TRALI based on the presence or absence of clear temporal relationship to another non-
transfusion related ALI risk factor (sepsis, overdose, aspiration) (3, 4).
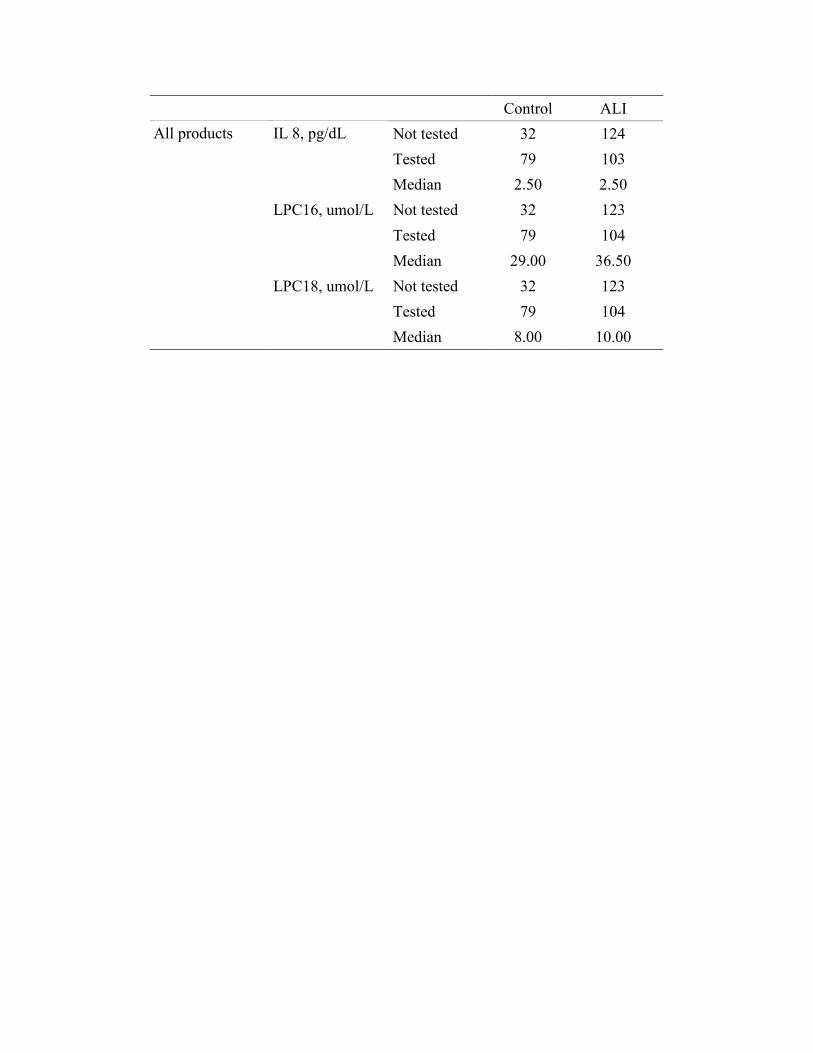
Sample collection and testing:

Throughout the study period, transfusion bags and tubing were collected at the end of the
transfusion by the bedside nurse and sent to the transfusion laboratory by the hospital
pneumatic tube system (Figure E2). The remaining blood product was extracted,
centrifuged at 3000 rpm for 10 minutes and the supernatant stored at -70C for subsequent
analysis. Units given 0-6 hours prior to ALI (in cases) and 0-6h after the onset of first
transfusion were considered associated units and were subsequently tested for anti-
leukocyte antibodies, IL-8 and LysoPC. The exposure time for each control was matched
to the exposure time of the corresponding case.
Anti HLA Class I and Class II antibodies were identified using flow cytometry analysis
of antibody binding to antigen coated microbead plates (5). ABScreenTM PRA (One
Lambda, Inc, Canoga Park, CA) allows combination of up to 100 different beads in one
suspension for a single test. Corresponding antibodies present in the test sample bind to
the antigens and then are labeled with R-Phycoerythrin (PE)-conjugated goat anti-human
IgG. The LABScan 100TM flow analyzer detects the fluorescent emission of PE from
each bead and the accompanying software assists in detection of the proteins of interest.
Testing for antigranulocyte antibodies was performed at the Mayo Clinic Tissue Typing
Laboratory using standard indirect immunofluorescence method (6). After incubation of
the sample with paraformaldehyde the presence of specific antibody is detected by the
addition of a fluorescein labeled antihuman globulin and examination with a fluorescent
microscopy. Serum was not absorbed against platelets and therefore a positive result
could represent antibodies directed toward granulocyte specific antigens or antibodies to
HLA Class I. The panel of fresh granulocytes used for the GIF studies were not selected
to include a full complement of granulocyte antigens.

IL-8 was measured using standard ELISA Quantikine HS Immunoassay (R&D Systems
Inc. Minneapolis, MN). In a quantitative sandwich enzyme immunoassay, the specimen
is added onto a microplate pre-coated with monoclonal antibody. After washing away
unbound substances and addition of enzyme-linked specific polyclonal antibody and the
substrate, the enzyme activity is measured which is proportional to the amount of the
cytokine bound in the first step
Lysophosphatidylcholines (LysoPC) have been described as important biologic response
modifiers which stimulate neutrophils by increasing concentration of intracellular
calcium(7). LysoPC 18 (18 acyl carbon) and lyso PC 16 (16 acyl carbon) were
determined using standard high performance lipid chromatography (HPLC)(8)
Remaining plasma was extracted with 3 mL butanol after the addition of 1 µmol/L 17:0
LysoPC as internal standard. After vortexing and centrifugation, the upper phase was
collected, evaporated under nitrogen at 50°C, and reconstituted in 200-µL of methanol.
HPLC was performed by autosampler injection of 5 µL of the reconstituted specimen
onto a Phenomenex C8 50x2 mm column. The mobile phase (methanol: 100 mM
ammonium acetate: formic acid, 90: 10: 0.05 was pumped over the HPLC analytical
column at the rate of 300 µL/min. LysoPC elute apart from the bulk of the specimen
matrix at a retention time of approximately 1.5 minutes. 16:0 and 18:0 LysoPC were
quantitated using 17:0 LysoPC as internal standard from calibration over a concentration
range 0.1-5.0 µmol/L.
Transfused plasma volume was calculated based on the average plasma content in
specific blood products: 250 mL for fresh frozen plasma (FFP) and platelets, 150 mL for
cryoprecipitate and 37 mL for packed red blood cells (RBCs) (4).
To assure similar exposure time to possible risk factors between cases and control the
exposure time for each control was matched to the exposure time of the corresponding
case. That means if the earliest unit given to the TRALI case was x hours prior to the
onset of TRALI then the control recipient had his/her transfusion data tabulated for the
same number of hours subsequent to the first transfusion
Results
Table E 1 demonstrates a comparison of ALI patients who did (“possible TRALI”) or did
not (“suspected TRALI”) have a temporal relationship to another risk factor for acute
lung injury (2).
Table E2 presents the association between the transfusion risk factors and ALI after
adjustment for baseline liver disease in addition to chronic alcohol abuse, sepsis,
APACHE III scores in a conditional regression analysis
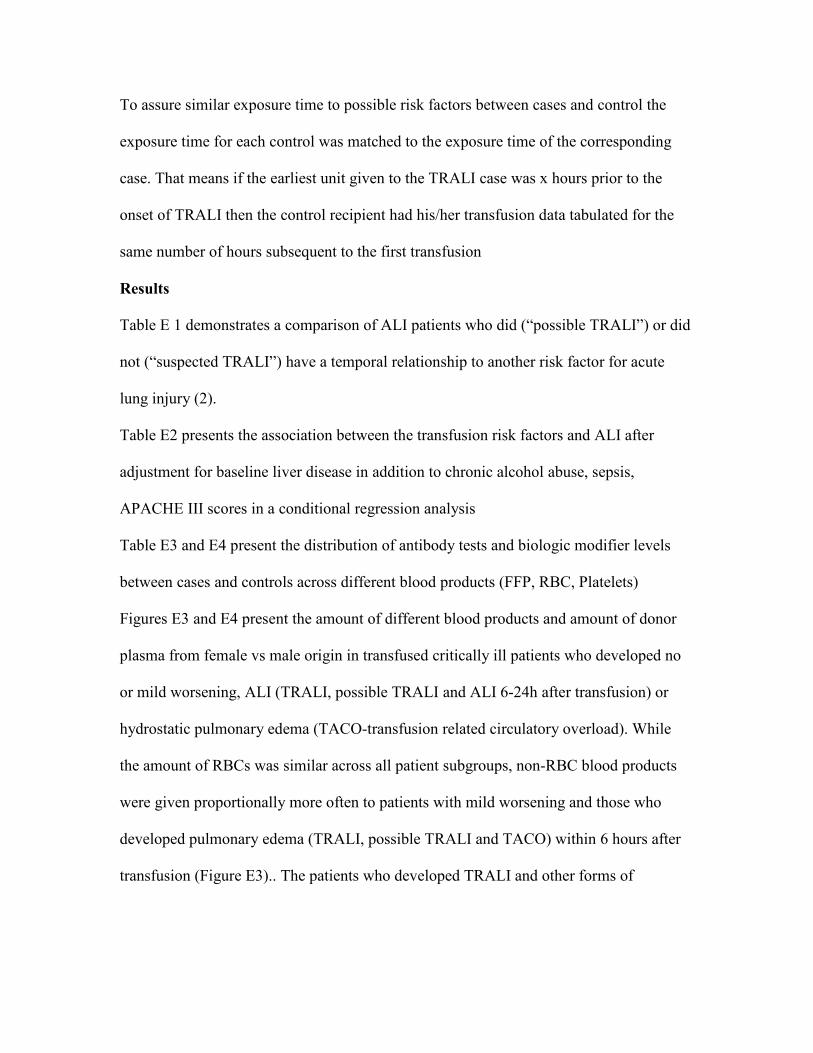
Table E3 and E4 present the distribution of antibody tests and biologic modifier levels
between cases and controls across different blood products (FFP, RBC, Platelets)
Figures E3 and E4 present the amount of different blood products and amount of donor
plasma from female vs male origin in transfused critically ill patients who developed no
or mild worsening, ALI (TRALI, possible TRALI and ALI 6-24h after transfusion) or
hydrostatic pulmonary edema (TACO-transfusion related circulatory overload). While
the amount of RBCs was similar across all patient subgroups, non-RBC blood products
were given proportionally more often to patients with mild worsening and those who
developed pulmonary edema (TRALI, possible TRALI and TACO) within 6 hours after
transfusion (Figure E3).. The patients who developed TRALI and other forms of

pulmonary edema associated with transfusion received a larger amount of plasma.
(Figure E4)
Table E5 presents a post-hoc multivariate logistic regression analysis for mortality. When
adjusted for age, APACHE III, sepsis and liver disease, ALI was not independently
associated with hospital mortality (table E5).

References
E1. Bernard, G. R., A. Artigas, K. L. Brigham, J. Carlet, K. Falke, L. Hudson, M.
Lamy, J. R. Legall, A. Morris, and R. Spragg. 1994. The American-European Consensus
Conference on ARDS. Definitions, mechanisms, relevant outcomes, and clinical trial
coordination. Am J Respir Crit Care Med 149(3 Pt 1):818-24.
E2. Gajic, O., M. A. Gropper, and R. D. Hubmayr. 2006. Pulmonary edema after
transfusion: how to differentiate transfusion-associated circulatory overload from
transfusion-related acute lung injury. Crit Care Med 34(5 Suppl):S109-13.
E3. Kleinman, S., T. Caulfield, P. Chan, R. Davenport, J. McFarland, S. McPhedran,
M. Meade, D. Morrison, T. Pinsent, P. Robillard, and P. Slinger. 2004. Toward an
understanding of transfusion-related acute lung injury: statement of a consensus panel.
Transfusion 44(12):1774-89.
E4. Rana, R., E. R. Fernandez-Perez, S. A. Khan, S. Rana, J. L. Winters, T. G.
Lesnick, S. B. Moore, and O. Gajic. 2006. Transfusion-related acute lung injury and
pulmonary edema in critically ill patients: a retrospective study. Transfusion 46(9):1478-
83.
E5. Pei, R., J. Lee, T. Chen, S. Rojo, and P. I. Terasaki. 1999. Flow cytometric
detection of HLA antibodies using a spectrum of microbeads. Hum Immunol
60(12):1293-302.
E6. Jiang, A. F., and P. Lalezari. 1975. A micro-technique for detection of leukocyte
agglutinins. J Immunol Methods 7(1):103-8.
E7. Silliman, C. C., D. J. Elzi, D. R. Ambruso, R. J. Musters, C. Hamiel, R. J.
Harbeck, A. J. Paterson, A. J. Bjornsen, T. H. Wyman, M. Kelher, K. M. England, N.

McLaughlin-Malaxecheberria, C. C. Barnett, J. Aiboshi, and A. Bannerjee. 2003.
Lysophosphatidylcholines prime the NADPH oxidase and stimulate multiple neutrophil
functions through changes in cytosolic calcium
10.1189/jlb.0402179. J Leukoc Biol 73(4):511-524.
E8. Silliman, C. C., K. L. Clay, G. W. Thurman, C. A. Johnson, and D. R. Ambruso.
1994. Partial characterization of lipids that develop during the routine storage of blood
and prime the neutrophil NADPH oxidase. J Lab Clin Med 124(5):684-94.

Table E1. Characteristics of patients who developed ALI after transfusion: “suspected”
versus “possible” TRALI as determined by post-hoc expert assessment
Suspected TRALI
n=28
Possible TRALI
n=46
P value
Age (years) 62 (52 to 79) 60 (54 to 71) 0.42
Female gender 18 (64) 19 (41) 0.06
APACHE III score before the
transfusion
50 (33 to 63) 67 (54 to 80) <0.01
Sepsis 5 (18) 22 (48) <0.01
Aspiration 5 (18) 3 (7) 0.15
Pancreatitis 2 (7) 3 (7) 0.94
Alcohol abuse 14 (50) 13 (28) 0.06
Liver disease 9 (32) 11 (24) 0.48
DIC 3 (11) 7 (16) 0.55
WBC count before 9.6 (8 to 15) 11.4 (6 to 18) 0.91
WBC count after 9.9 (6 to 15) 11.5 (11 to 18) 0.92
Any RBC 15 (54) 31 (67) 0.24
Any FFP 16 (57) 23 (50) 0.55
Any Platelet 8 (29) 5 (11) 0.07
Average RBC storage (days) 24 (15 to 29) 21 (17 to 30) 0.78
# of Units 4(2 to 6) 3 (1 to 5) 0.28
Any Units from female
donors
18 (64) 23 (55) 0.52

# Units from female donors 1 (1 to 2) 1 (1 to 2) 0.85
# Units from female donors
with at least one pregnancy
1 (0 to 2) 1 (0 to 2) 0.56
Number of donor pregnancies 2 (0 to 8) 1 (0 to 5) 0.28
Median amount of plasma (L) 0.66 (0.1 to 1.1) 0.25 (0.1 to 1.0) 0.12
Median amount
of female plasma (L)
0.25 (0.1 to 0.5) 0.04 (0.04 to 0.5) 0.10
Median amount of plasma
from female donors with at
least one pregnancy
0.06 (0 to 0.5) 0.04 (0 to 0.3) 0.23
Received any HLA I + units 12 (44) 13 (38) 0.64
Received any HLA II + units 9 (33) 11 (32) 0.94
Received any GIF + units 7 (26) 6 (18) 0.43
Received any Ab+ units 15 (56) 16 (47) 0.51
# of Antibody + tests (N=52)* 1 (0 to 2) 0 (0 to 2) 0.56
Mean IL8 (pg/dL) (N=47) 2.5 (3 to 12) 2.5 (3 to 6) 0.54
Mean LPC16 umol/L(N=47) 79 (29 to 111) 43 (21 to 95) 0.16
Mean LPC18 umol/L (N=47) 21 (8 to 38) 13 (4 to 30) 0.17
Mechanically ventilated
Invasive
Noninvasive
15 (54)
5 (18)
33 (73)
5 (11)
0.224

Hospital mortality 10 (36) 20 (44) 0.46
*If the associated unit tested positive for more than one antibody (for example both
HLA1 and HLA2) each of these was counted as a positive test.

Table E2 Transfusion-related risk factors for acute lung injury adjusted for baseline liver disease, APACHE III score, sepsis and chronic alcohol abuse
Variable OR (95% CI)** P-ValueAny high plasma volume components (FFP or platelets)
2.55 (1.1,5.9) 0.029
Number of units 1.13 (0.99,1.29 0.064 Number of units from female donors 1.53 (1.06, 2.20) 0.021 Amount of male plasma (L) 1.87 (0.83, 4.21) 0.131 Amount of female plasma (L) 5.52 (1.34,22.79) 0.018 Amount of plasma from female donors with at least one pregnancy (L)
17.9 (1.72 ,186) 0.016
Number of pregnancies among donors 1.20 (1.06,1.37) 0.005 Number of HLA class I + units 1.69 (0.93,3.08) 0.088 Number of HLA class II + units 3.19 (1.18,8.62) 0.022 Number of GIF + units 5.04 (1.35,18.85) 0.018 Mean LysoPC 16 (per 10 umol/L) 1.19 (1.02,1.38) 0.023 Mean LysoPC 18 (per 10 umol/L) 1.76 (1.11,2.80) 0.017
OR odds ratio, CI confidence interval, RBC red blood cell, FFP fresh frozen plasma, GIF granulocyte immunofluorescence, HLA human leukocyte antigen, LysoPC
lysophosphatidyl choline, APACHE Acute Physiology and Chronic Health Evaluation, ALI acute lung
injury

Table E3 Distribution of antibody tests between cases and controls across different associated blood products (RBC. Platelet, FFP)
Control ALI product
Not tested 19 20 Tested 60 65 # positive 8 17
HLA I
% positive 13.3 26.2 Not tested 19 20 Tested 60 65 # positive 4 9
HLA II
% positive 6.7 13.8 Not tested 19 20 Tested 60 65 # positive 4 8
RBC
GIF
% positive 6.7 12.3 Not tested 2 5Tested 1 9# positive 0 1
HLA I
% positive 0.0 11.1 Not tested 2 5Tested 1 9# positive 1 1
HLA II
% positive 100.0 11.1 Not tested 2 5Tested 1 9# positive 0 3
Platelets
GIF
% positive 0.0 33.3

Control ALI Not tested 11 71 Tested 30 56 # positive 5 13
HLA I
% positive 16.7 23.2 Not tested 11 71 Tested 30 56 # positive 6 11
HLA II
% positive 20.0 19.6 Not tested 11 71 Tested 30 56 # positive 0 4
FFP
GIF
% positive 0.0 7.1 Not tested 32 96 Tested 91 130 # positive 13 31
HLA I
% positive 14 24 Not tested 32 96 Tested 91 130 # positive 11 21
HLA II
% positive 12 16 Not tested 32 96 Tested 91 130 # positive 4 15
All products
GIF
% positive 4 12

Table E4 Distribution of IL8 and LysoPC between cases and controls across different associated blood products (RBC. Platelet, FFP)
Control ALI product
Not tested 22 30 Tested 52 52
IL 8, pg/dL
Median 2.50 2.50 Not tested 22 29 Tested 52 53
LPC16, umol/L
Median 19.00 21.00 Not tested 22 29 Tested 52 53
RBC
LPC18, umol/L
Median 5.00 6.00 Not tested 2 5Tested 0 8
IL 8, pg/dL
Median 8.00 Not tested 2 5Tested 0 8
LPC16, umol/L
Median 213.50 Not tested 2 5Tested 0 8
Platelets
LPC18, umol/L
Median 78.00 Not tested 7 77 Tested 25 41
IL 8, pg/dL
Median 2.50 2.50 Not tested 7 77 Tested 25 41
LPC16, umol/L
Median 103.00 104.00 Not tested 7 77 Tested 25 41
FFP
LPC18, umol/L
Median 33.00 31.00
Control ALI Not tested 32 124 Tested 79 103
IL 8, pg/dL
Median 2.50 2.50 Not tested 32 123 Tested 79 104
LPC16, umol/L
Median 29.00 36.50 Not tested 32 123 Tested 79 104
All products
LPC18, umol/L
Median 8.00 10.00

Table E5 Risk factors for hospital mortality in a multivariate logistic regression analysis
OR 95% CI p-value
ALI 2.16 0.98 4.88 0.059
Age 1.03 1.00 1.06 0.049
APACHE III 1.02 1.00 1.04 0.019
Sepsis 2.07 0.89 4.85 0.091
Liver disease 2.79 1.07 7.47 0.037
OR odds ratio, ALI acute lung injury, CI – confidence interval, APACHE – Acute Physiology and Chronic Health Evaluation

Figure E1 Snapshot of a monitoring log identifying worsening in respiratory status after
transfusion
FIO2
RR
MABP
O2 sat
FFP
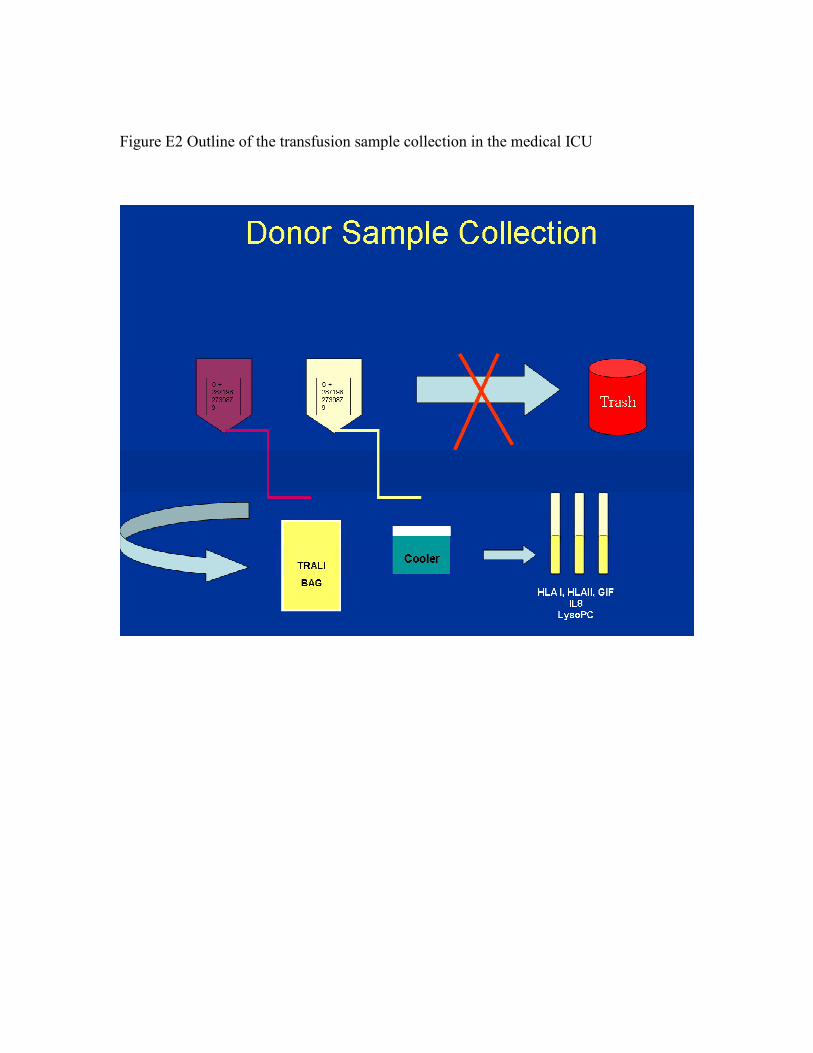
Figure E2 Outline of the transfusion sample collection in the medical ICU

Figure E3 Type of blood products given to the patients who developed ALI (TRALI and
possible TRALI), TACO, mild worsening, ALI 24h after the transfusion, matched
controls and other controls

Figure E4 The amount of male vs female donor plasma given to the patients who
developed ALI (TRALI and possible TRALI), TACO, mild worsening, ALI 24h
after the transfusion, matched controls and other ontrols
Copyright © 2022 FDOKUMEN




















