Haematological effects of zidovudine prophylaxis in newborn ...
Upload
independentCategory
view
1download
0
F E T A L A N D N E O N A T A L
M E D I C I N E Richard E. Behrman, Editor
Prevention of transfusion-acquired cytomegalovirus infections in newborn infants
Transfusion-acquired cytomegalovirus infections occurred in 13.5% of 74 infants of seronegative mothers
who were exposed to one or more blood donors who had a CM V indirect hemagglutination titer of 1:8
or higher None of 90 infants of seronegative mothers exposed only to donors with CMV 1HA titers of
less than 1:8 became infected Ten of 41 (24%) infants of seronegative mothers who received more than
50 ml of packed red blood cells and who were exposed to at least one seropositive donor became infected.
None of 23 infants of seronegative mothers who received this amount of blood but who were exposed
only to seronegative donors became infected. Fatal or serious symptoms developed in 50% of the infected
infants of seronegative mothers and in none of the 32 infected infants of seropositive mothers. Acquired
CMV infections occurred in 15% of infants of seropositive mothers who were exposed to the red blood
cells of seropositive donors and in 17.6% of infants of seropositive mothers exposed only to seronegative
donors. Use of seronegative donors reduced the prevalence of excretion of CM V among hospitalized
infants who were 4 weeks of age or older from 12.5 to 1.8% and eliminated acquired CMV infections in
infants of seronegative mothers.
Anne S. Yeager, M.D.,* F. Carl Grumet, M.D.,
Elizabeth B. Hafleigh, M.T. (ASCP)SBB, Ann M. Arvin, M.D.,
John S. Bradley, M,D., and Charles G. Prober, M.D., S tan ford , Cali f .
IN UTERO INFECTION with cytomegalovirus is a well- known cause of damage to the fetus. '-'~ The frequency and
severity of infections acquired by premature infants from blood transfusions are less well appreciated. 7 .... CMV causes pneumonia, hepatitis, thrombocytopenia, and hemolytic anemia, which add to the morbidity of infants who already have pulmonary, hepatic, and marrow dys- function resulting from prematurity per se5 The rate of excretion of CMV by young infants who have not been transfused is 11 to 14%. 1 . . . . The majority of these infec- tions result from transmission of virus from mother to
From the Departments of Pediatrics and Pathology, Stanford University School of Medicine.
Supported by Grant (HD 09872)from the National Institutes of Health, a grant from the National Foundation-March of Dimes, and a grant (RR-81)
from the General Clinical Research Center's program of the Division of Research Resources, National Institutes of Health.
*Reprint address: Department of Pediatrics, Room $322, Stanford University Medical Center, Stanford, CA 94305.
infant at the time of birth. Among transfused infants,
however, the rate of excretion is twice as high, suggesting that transfusion of blood products frequently results in infectionS " Fourteen to 31% of sick newborn infants who have been transfused and who remain hospitalized for longer than four weeks excrete CMV?" lo
Abbreviations used C M V : cytomegalovirus IHA: indirect hemagglutination assay CMV Ab-: CMV seronegative CMV Ab+: CMV seropositive CPD: citrate-phosphate-dextrose RBC: red blood cells FI%: fraction of inspired oxygen
The purpose of this study was to determine if transfu- sion-associated CMV infections could be avoided by using blood donors who had no serologic evidence of having had a CMV infection, and whose blood products, therefore, had a low probability of being able to transmit CMV to the infant. The indirect hemagglutination assay
281 The Journal of P E D I A T R I C S 0022-3476/81/020281 +07500.70/0 �9 1981 The C. V. Mosby Co. Vol. 98, No. 2, pp. 281-287

2 8 2 Yeager et al. The Journal of Pediatrics February 1981
Table 1. Infected infants according to antibody status of their mothers and blood donors
Seronegative mother
CMV Ab+ red blood cells
CMV Ab-- red blood cells
Seropositive mother
CMV Ab+ red CMV A b - red blood cells blood cells
Total number 74 Number with birth weight < 1,200 gm 22 Mean birth weight (gin) 1,980 Number infected (%) 10
03.5%)
90 60 131 16 15 25
2,089 1,905 1,947 0 9 23
(0%) (15%) (17.6%)
was chosen as the means of testing the donor's blood because of its sensitivity and its adaptability to rapid,
large scale testing. The data demonstrate that the use of blood donors with CMV IHA titers of less than 1:8 significantly reduced transfusion-acquired CMV infec- tions in newborn infants. Other factors affecting infection rates and morbidity in this high-risk population were also identified.
M E T H O D S
Measurement of antibody to CMV. Glutaraldehyde-
fixed, tanned sheep, or human 0 red blood cells were sensitized with antigen derived from the stock strain of CMV, Ad169, and used in the IHA test as previously described.' ..... Liquid nitrogen storage of sensitized cells
made it possible to test, in 1.5 to 2 hours, the 20 to 30 freshly drawn donor samples necessary to select donors to
supply the nursery for each three- to four-day period.
Donors with IHA titers of less than 1:8 were considered seronegative and those with IHA titers of 1:8 or higher were considered seropositive.
Cultures. Each infant's urine was cultured at the time of admission and twice a week until discharge. Infants who were congenitally infected were eliminated from the study. Saliva and freshly voided urine were cultured from infants six to 12 weeks following the last transfusion.
All cultures were performed in human foreskin fibro- blasts maintained in Earle minimum essential medium
containing 2% fetal calf serum, penicillin, gentamicin, and amphotericin. Specimens were inoculated immediately and observed for four weeks for the typical cytopathic effect caused by CMV.
Preparation of red blood cells. Blood to be used for red cell transfusions in the intensive care nurseries was drawn
into the primary bag of a quadruple citrate-phosphate- dextrose pack (Fenwal Laboratories) two times a week. Red blood cells from freshly drawn CPD whole blood units were divided into three or four bags in a closed system. One bag, which was less than 72 hours old, was dispensed to the nursery refrigerator (1 to 6~ for each of
three or four consecutive 24-hour periods. In the nursery, aliquots were withdrawn from each bag through a multi- ple injection site as needed. Fresh-frozen CPD plasma was transfused within six hours of thawing.
Assignment of blood to infants. From January, 1976, to February, 1978, infants received transfusions from either random donors or preselected CMV A b - donors accord- ing to the last digit of the infant's hospital number. Because all of the morbidity associated with CMV infec- tions occurred in recipients of CMV A b + RBC, only CMV A b - donors were used after February, 1978. The study was continued until September, 1979, so that more recipients of CMV A b - RBC who had high transfusion requirements could be studied. The written consent of a parent was obtained. Infants receiving blood from non- protocol units were not included in the data analysis.
Infants receiving RBC from one or more CMV A b+ donors were classified as recipients of CMV Ab+ RBC regardless of whether or not CMV Ab-- RBC were also given. Infants receiving blood exclusively from CMV Ab-- donors were classified as recipients of CMV A b - RBC. The same system was used for designating the use of fresh-frozen plasma from CMV A b + or CMV A b - donors.
Infants were also separated according to whether or not their mothers had serologic evidence of having had a CMV infection in the past. Maternal blood was available for 278 (79%) of the infants. Cord blood was used to
determine the serologic status of the mothers in 75 (21%) of the cases. Despite the prematurity of the infants, the concordance between maternal and cord sera as regards the presence or absence of antibody was 95.2% in 187 pairs tested.
Human milk. None of the infants received fresh milk from a donor other than his or her own mother.
R E S U L T S
Incidence of infections. The 353 transfused infants
studied received RBC from 1,354 donors and had an average of 3.8 donors per infant. In evaluating the risk of

Volume 98 Prevention of transfusion-acquired CM V 2 8 3 Number 2
>_12
11
10
9
8
7
6
5
4 0 3
tz: 3 O z 2 O
1 r
kl,.
O r,- >__12 U.I
'~ 11
D 10 Z
9
8
7
6
5
4
3
2
I I I
A b - M O T H E R 8 ~ Ab + RBC
QO O0
#o o
oo o~o O0
0 O0
0 o
0880 ~o o�9 NN ~ o
I I I 0 - 4 9 e c 50--99ee >_100ee
I I
Ab + MOTHER A b + R B C
O O
O O
O O O O
o
OO O
~ o
I I 0 - 4 9 e c 50-99c'c
I
8~88
0
I I
O0
0
I > 100cc
CC
Fig. 1. Infected (e) and uninfected (o) infants of CMV Ab-- CMV Ab + or A b - donors according to volume of red blood
I I I
A b - M O T H E R oo
_ A b - RBC oo
O
~ o
"- O O<3
~
o o
~ 8 8 8 8 8 8 8 O O
. ~ o
I I 0--49ee
= Ab+MOTHER A b - RBC
O0 o
o
0 o
c~o o
I
5 0 - 9 9 c c >100cc
I I
~ 8
o e
( 3 0 0 o
o o
gl o
O O
o% oe
o
O
I ,,
5 0 - 9 9 c c > - 1 0 0 c c
o ' i ~ 8#o
o8~o
1--40cc
RBC RECEIVED
and Ab + mothers who received red blood cells from ceils received and number of donors.
acquiring a CMV infection, the immune status of the
mother as well as the donor was considered. Blood donors
were the only expected source of infection for infants of
seronegative mothers. Infants of seropositive mothers had
two potential sources of in fec t ion-donors and maternal
secretions.
As shown in Table I, 74 infants of seronegative mothers
were exposed to a CMV A b + donor. Ninety infants of
seronegative mothers were exposed only to CMV A b -
donors. Transfusion-acquired infections occurred in
13.5% of the 74 infants who were exposed to a CMV A b +
donor and in none of 90 infants who received blood from
CMV A b - donors. Nine of the ten infected infants had
been exposed to five or more donors. As shown in Fig. 1,
none of the 33 infants of seronegative mothers who
received less than 50 ml of RBC became infected despite
exposure to a CMV A b + donor. However, of 41 infants
of seronegative mothers who were exposed to one or more
CMV A b + donors and to 50 ml or more RBC, 10 (24%)
became infected. In contrast, none of the 23 infants of
seronegative mothers who received 50 ml or more RBC
but who were exposed only to CMV A b - donors became
infected (P = 0.01; Fisher exact test).
Infants of seropositive mothers acquired CMV infec-
tions at a similar rate regardless of whether or not they
were exposed to the RBC o f C M V Ab + donors. As shown
in Table I and Fig. 1, 15% of 60 infants exposed to a
seropositive mother as well as to a CMV A b + donor
became infected. Of 131 infants of seropositive mothers
exposed only to CMV A b - donors, 17.6% became

2 8 4 Yeager et aL The Journal of Pediatrics February 1981
Fig. 2. This premature infant was born 8/18 and weighed 910 gm. By 9/11 the FIo~ had been decreased from 52% to 23%, although the infant still required assisted ventilation. The last negative culture for CMV was obtained on 9/13. The first positive culture for CMV was obtained 9/20.
infected. Infections were not restricted to infants receiving 50 ml or more of RBC. Thirteen of 88 (15%) infants who received less than 50 ml and nine of 43 (20%) who received more than 50 ml of RBC became infected. Fifty-two percent of the infected infants of seropositive mothers had only one or two donors and only 35% had five or more donors.
The donors of plasma were also screened for antibody to CMV. Twenty-two of the 90 infants of seronegative mothers who received RBC exclusively from CMV Ab-- donors received fresh-frozen plasma from one or more CMV Ab+ donors. Although none of these infants became infected, 73% were exposed to only one CMV Ab + donor and none had five or more donors. Although no infections attributable to plasma were identified, it was not possible to evaluate whether or not transmission of CMV by fresh-frozen plasma could occur in circum-
stances in which large volumes and multiple donors were used.
Morbidity and mortality of acquired CMV infections.
The infected infants of seronegative mothers experienced significant morbidity. Two of the ten (20%) had fatal
infections. CMV pneumonia developed in a 30-day-old premature infant who had weighed 910 gm at birth. Her pulmonary function had been steadily improving and her FI% had been decreased from 52% to 23%. The infant began shedding CMV between 26 and 33 days of age. The development of pneumonia (Fig. 2) was associated with the onset of excretion of CMV, hepatomegaly, a rise in SGOT from 25 IU to 41 IU and a fall in platelets from 330,000/mm' to 27,000/mm'. CMV was isolated in a titer of 10:' from lung tissue obtained at autopsy. The second infant died after a long illness complicated by hepatitis, thrombocytopenia, chorioretinitis, cerebral edema (as
Volume 98 Prevention o f transfusion-acquired C M V 2 8 5 Number 2
assessed by computerized tomography), and pleocytosis; the head circumference increased from twenty-fifth to
ninetieth percentile. Three other infected infants of sero- negative mothers had serious symptoms. These included
combinations of pneumonia, hepatitis, hemolytic anemia, and/or a decline in platelet count of > 100,000/mm:'. Two of these three infants died of chronic lung disease one day and four months, respectively, following dis-
charge. These deaths increased the fatality rate among infected infants of Seronegative mothers to 40%. The expected mortality rate for 1,735 consecutive admissions
to the neonatal intensive care unit during this study period was 6.6% during hospitalization and 1.3% following dis-
charge. All of the fatal or serious infections in infants of
seronegative mothers occurred among the seven infected infants who weighed less than 1,200 gm and who, there- fore, had gestational ages of less than 28 weeks.':' Howev- er, six infected infants of seropositive mothers also weighed less than 1,200 gm but did not develop symp- toms.
None of the 32 infected infants of seropositive mothers had fatal or serious symptoms attributable to CMV.
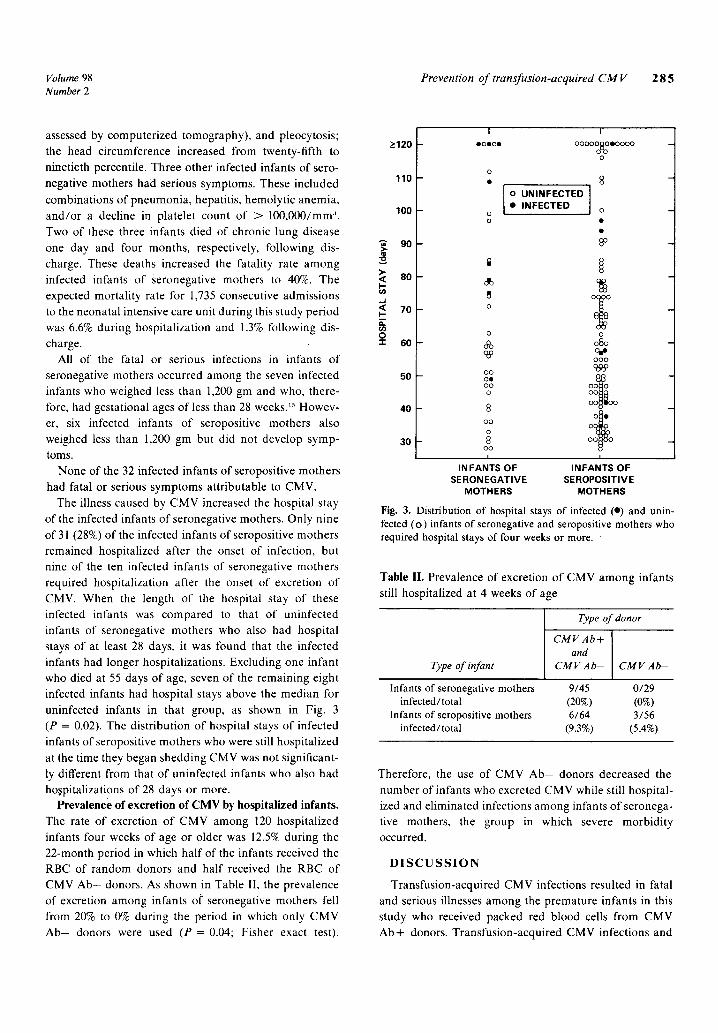
The illness caused by CMV increased the hospital stay of the infected infants of seronegative mothers. Only nine of 31 (28%) of the infected infants of seropositive mothers remained hospitalized after the onset of infection, but nine of the ten infected infants of seronegative mothers required hospitalization after the onset of excretion of CMV. When the length of the hospital stay of these infected infants was compared to that of uninfected infants of seronegative mothers who also had hospital stays of at least 28 days, it was found that the infected infants had longer hospitalizations. Excluding one infant who died at 55 days of age, seven of the remaining eight infected infants had hospital stays above the median for uninfected infants in that group, as shown in Fig. 3 (P = 0.02). The distribution of hospital stays of infected infants of seropositive mothers who were still hospitalized
at the time they began shedding CMV was not significant- ly different from that of uninfected infants who also had hospitalizations of 28 days or more.
Prevalence of excret ion of C M V by hospitalized infants.
The rate of excretion of CMV among 120 hospitalized infants four weeks of age or older was 12.5% during the 22-month period in which half of the infants received the RBC of random donors and half received the RBC of CMV Ab-- donors. As shown in Table II, the prevalence of excretion among infants o1" seronegative mothers fell from 20% to 0% during the period in which only CMV A b - donors were used (P = 0.04; Fisher exact test).
I I > 120 ooeoe oooOOScOeOOOO -
o o
110 �9 8 - o U N I N F E C T E D I
INFECTED o 100 o o �9
m
8 o _
o o
0% 080 -
o o o od~ o o
50 oe o~8~L - O0 O0 0 O0
40 8 o
O0 0 0 0 ~ 0
30 ; o oo
i I INFANTS OF INFANTS OF
SERONEGATIVE SEROPOSlTIVE MOTHERS MOTHERS
Fig. 3. Distribution of hospital stays of infected (�9 and unin- fected (o) infants of seronegative and seropositive mothers who required hospital stays of four weeks or more.
.~ 80 I -
..J < 70 I - E r,~ o �9 I- 6o
Table II. Prevalence of excretion of CMV among infants still hospitalized at 4 weeks of age
Type of in fan t
Type of donor
CMV Ab+ and
CMV A b - CMV A b -
Infants of seronegative mothers 9/45 0/29 infected / total (20%) (0%)
Infants of seropositive mothers 6/64 3/56 infected/total (9.3%) (5.4%)
Therefore, the use of CMV A b - donors decreased the
number of infants who excreted CMV while still hospital- ized and eliminated infections among infants of seronega- tive mothers, the group in which severe morbidity occurred.
D I S C U S S I O N
Transfusion-acquired CMV infections resulted in fatal and serious illnesses among the premature infants in this study who received packed red blood cells from CMV Ab+ donors. Transfusion-acquired CMV infections and

2 8 6 Yeager et al. The Journal of Pediatrics February 1981
the associated morbidity were not seen among infants
who received cells from CMV Ab-- donors. All of the infections in infants of seronegative mothers
occurred among infants who had transfusion require-
ments of 50 ml or more of RBC and who had been exposed to a CMV Ab + donor. Twenty-four percent of these infants became infected. The CMV infection was the
immediate cause of death or a contributing cause of death in four of ten infected infants. Pneumonia, hemolytic anemia, and thrombocytopenia developed in association with the onset of excretion of CMV, as had been described previously7 . . . . . . . In addition, one infant developed a disseminated infection with involvement of the central nervous system and chorioretinitis. The severity of this transfusion-acquired infection was identical to that of the most severe form of intrauterine infection.
The use of CMV A b - donors successfully eliminated transfusion-acquired CMV infections among 90 infants of seronegative mothers, including the 23 infants who had received more than 50 ml of RBC. No maternally derived infections occurred in the infants whose mothers had CMV IHA titers of less than 1:8, whereas 16.7% of the infants of seropositive mothers became infected despite the fact that they were exposed only to CMV A b - donors. The CMV IHA titer, therefore, was accurate in predicting the immune status and the potential for transmission of CMV from the blood donors and the mothers.
In contrast to the severe morbidity experienced by infected infants of CMV A b - mothers, none of the infected infants of CMV Ab+ mothers had fatal or serious symptoms attributable to CMV. All five of the serious infections among infants of seronegative mothers occurred among the seven infants who weighed less than 1,200 gm at birth; however, six infected infants of seropos- itive mothers also weighed less than 1,200 gm at birth and none developed serious symptoms. Maternally derived antibody may have modified the infection in these infants. Reynolds et aW have shown that maternally transmitted
infections occur despite the presence of passively trans- ferred maternal antibody in the baby. Most of these infections are asymptomatic, although pneumonia can occur in otherwise healthy babies. TM Similarly, immunity
derived from past infections ameliorates symptoms, but does not prevent shedding of CMV in renal transplant patients. 1~-~1 Infants acquire antibody but not cellular immunity transplacentally from mothers who have been infected with CMV in the past. Since the severity of symptoms was less in infected infants who derived anti- body from their mothers than in infected infants who did not, this study suggests that antibody alone may be capable of modifying the severity of CMV infections.
Infants exposed to CMV Ab + donors as well as to their
own seropositive mothers had the same incidence of infections as infants exposed only to seropositive mothers. Antibody alone does not prevent transmission of virus from mother to infant, but it is likely that the inoculation site is mucosal rather than intravascular and that secretory
antibody is lackings Circulating antibody may be capa- ble of neutralizing a small inoculum ~ introduced intravas- cularly by donor blood.
Fifty percent of the infections in infants who began to excrete CMV while still hospitalized proved to be transfu- sion acquired. The elimination of these infections is important for epidemiologic reasons, as well as for the sake of the infant. The prevention of transfusion-acquired infections in the nursery reduced the risk of exposing pregnant hospital personnel to CMV, and eliminated the possibility that seronegative mothers of infants with transfusion-acquired infections would acquire the infec- tion from their infant during a subsequent pregnancy.
The use of donors with CMV IHA titers of less than 1:8 was successful in reducing the prevalence rate of excretion of CMV among hospitalized infants from 12.5 to 1.8% and eliminated all of the symptomatic infections among infants of CMV A b - mothers. Other techniques for measuring CMV antibody are rapid and comparable in sensitivity to the IHA assay used in this study, including the fluorescent antibody test and its modification, the anticomplement fluorescent antibody test. ~:~-~ In addition, the concordance between the Cytomegelisa test (M.A. Bioproducts) and the IHA test was 96% in distinguishing seronegative from seropositive donors in 100 sera tested
(unpublished observation). Of the 353 infants in this study, 137 (39%) had transfu-
sion requirements of 50 ml or more for RBC, which was the volume associated with symptomatic infections among infants of seronegative mothers. Other ways of avoiding
transfusion-acquired infections have been suggested, and include the use of leukocyte-poor blood or frozen bloods ~7 Neither of these methods appears to be as practical as the use ofCMV Ab-- donors. The use of CMV Ab-- units or a CMV A b - donor pool can be expected to decrease CMV infections in the nursery and, more impor- tantly, to decrease the morbidity of prematurity. Other immunocompromised patients may also benefit from the use of blood products derived from CMV A b - do- nors. zs
Infections acquired from human milk have the same potential for causing symptoms in infants of seronegative mothers as infections acquired from blood products. Therefore, donors of fresh milk should also be restricted to CMV Ab-- donors or to the baby's own mother. "~

Volume 98 Prevention of transfusion-acquired CM V 2 8 7 Number 2
The authors thank Laurie May, Lenore Urbani, Laura Dollar, Linda Lew, and Barbara Peppin for technical assistance, Drs. Paula Duke, Philip Sunshine, John Johnson, and Ronald Ariag- no, and Natalie Malachowski, Division of Neonatology, and the Stanford University Blood Bank and Transfusion Service for their cooperation. The sustained support of Aida Huggins, Laine Gigler, Sandy Fuller, Donna Arellano, and Sonia Hofferd, and of the nursing staff of the intensive care nurseries is especially appreciated. Bradley Effron offered helpful advice regarding the nature of the statistical problems.
R E F E R E N C E S
1. Starr JG, Bart RD, and Gold E: Inapparent congenital cytomegalovirus infection, N Engl J Med 282:1075, 1970.
2. Monif GRG, Egan EA, Held B, and Eitzman DV: The correlation of maternal cytomegalovirus infection during varying stages in gestation with neonatal involvement. J PEDIATR 80:17, 1972.
3. Stern H, and Tucker SM: Prospective study of cytomegalo- virus infection in pregnancy, Br J Med 2:268, 1973.
4. Hanshaw JB, Scheiner AP, Moxley AW, Gaev L, Abal V, and Scheiner B: School failure and deafness after "silent" congenital cytomegalovirus infection, N Engl J Med 295:468, 1976.
5. Stagno S, Reynolds DW, Amos CS, et al: Auditory and visual defects resulting from symptomatic and subclinical congenital cytomegaloviral and toxoplasma infections, Pediatrics 59:669, 1977.
6. Davis GL, Spector GJ, Strauss M, and Middlekamp JN: Cytomegalovirus endolabyrinthitis, Arch Pathol Lab Med 101:118, 1977.
7. Yeager AS: Transfusion-acquired cytomegalovirus infec- tion in newborn infants, Am J Dis Child 128:478, 1974.
8. Pass MA, Johnson JD, Schulman IA, et al: Evaluation of a walking-donor blood transfusion program in an intensive care nursery, J PEDIATR 89:646, 1976.
9. Spector SA, Schmidt K, Ticknor W, and Grossman M: Cytomegaloviruria in older infants in intensive care nur- series, J PEDIATR 95:444, 1979.
10. Ballard RA, Drew WL, Hufnagle KG, and Reidel PA: Acquired cytomegalovirus infection in preterm infants, Am J Dis Child 133:482, 1979.
11. Levinsohn EM, Foy HM, Kenny GE, Wentworth BB, and Grayston JT: Isolation of cytomegalovirus from a cohort of 100 infants throughout the first year of life (34345), Proc Soc Exp Biol Med 132:957, 1969.
12. Stagno S, Reynolds DW, Tsiantos A, Fucillo DA, Long W, and Alford CA: Comparative serial virologic and serologic studies of symptomatic and subclinical congenital and natally acquired cytomegalovirus, J Infect Dis 132:568, 1975.
13. Bernstein MT, and Stewart JA: Indirect hemagglutination test for detection of antibodies to cytomegalovirus, Appl Microbiol 21:84, 1971.
14. Yeager AS: Improved indirect hemagglutination test for
cytomegalovirus using human O erythrocytes in lysine, J Clin Microbiol 10:64, 1979.
15. Cunningham GC, Hawes WE, Madore C, Norris FD, and Williams RC: Intrauterine growth and neonatal risk in California, Sacramento, California, 1966-70, Infant Health Section, Maternal and Child Health, State of California Department of Health.
16. King-Lewis PA, and Gardner SD: Congenital cytomegalic inclusion disease following intrauterine transfusion, Br Med J 2:603, 1969.
17. Reynolds DW, Stagno S, Reynolds R, and Alford CA: Perinatal cytomegalovirus infection: influence of placental- ly transferred maternal antibody, J Infect Dis 137:564, 1978.
18. Whitley RJ, Brasfield D, Reynolds DW, Stagno S, Tiller RE, and Alford CA: Protracted pneumonitis in young infants associated with perinatally acquired cytomegaloviral infection, J PEDIATR 89:16, 1976.
19. HO M, Suwansirikul S, Dowling JN, Youngblood LA, and Armstrong JA: The transplanted kidney as a source of cytomegaloyirus infection, N Engl J Med 293:1109, 1975.
20. Betts RF, Freeman RB, Douglas RG, and Talley TE: Clinical manifestations of renal allograft derived primary cytomegalovirus infection, Am J Dis Child 131:759, 1977.
21. Pass RF, Long WK, Whitley RJ, et al: Productive infection with cytomegalovirus and herpes simplex virus in renal transplant recipients: role of source of kidney, J Infect Dis 137:556, 1978.
22. Reynolds DW, Stagno S, Hosty TS, Tiller M, and Alford CA: Maternal cytomegalovirus excretion and perinatal infection, N Engl J Med 289:1, 1973.
23. Betts RF, George SD, Rundell BB, Freeman RB, and Douglas RG: Comparative activity of immunofluorescent antibody and complement-fixing antibody in cytomegalovi- rus infection, J Clin Microbiol 4:151, 1976.
24. Kettering JD, Schmidt NJ, Gallo D, and Lennette EH: Anti-complement immunofluorescence test for antibodies to human cytomegalovirus, J Clin Microbiol 6:627, 1977
25. Rao N, Waruszewki DT, Atchison RW, and Ho M: Evalu- ation of anti-complement immunofluorescence test in cytomegalovirus infection, J Clin Microbiol 6:633, 1977.
26. Lang DJ, Ebert PA, Rodgers BM, Boggess HP, and Rixse RS: Reduction of postperfusion cytomegalovirus-infections following the use of leukocyte depleted blood, Transfusion 17:391, 1977.
27. Betts RF, Cestero RUM, Freeman RB, and Douglas RG: Epidemiology of cytomegalovirus infection in end stage renal disease, J Med Virol 4:89, 1979.
28. Neiman PE, Reeves W, Ray G, et al: A prospective analysis of interstitial pneumonia and opportunistic viral infection among recipients of allogenic bone marrow grafts, J Infect Dis 136:754, 1977.
29. Stagno S, Reynolds DW, Pass RF, and Altbrd CA: Breast milk and the risk of cytomegalovirus infection, N Engl J Med 19:1973, 1980.
Copyright © 2022 FDOKUMEN