Melatonin and Mental Capacities in Newborn Infants
6
Melatonin and Mental Capacities in Newborn Infants Sari Goldstein Ferber, PhD, Heidelise Als, PhD, Gloria McAnulty, PhD, Hava Peretz, PhD, and Nava Zisapel, PhD Objectives To investigate the role of melatonin in the emergence of mental capacities in the newborn infant. Study design Assessment of Preterm Infant Behavior examination was performed at 2 weeks post-term age for 39 (21 preterm and 18 term) infants. 6-Suphatoxymelatonin from nocturnal urine samples was analyzed by enzyme- linked immunosorbent assays, and the Mental Developmental Index, assessed by Bayley scales, was correlated at 4, 6, and 9 months’ corrected age. Results Multivariate analysis of variance with repeated measures showed that improved autonomic function at 2 weeks of age was associated with higher Mental Developmental Index scores at 9 months when related to the amount of melatonin at 4, 6, and 9 months of age. Conclusions Early compromised autonomic system function in preterm infants is associated with lower mental capacities and is related to lower melatonin levels at later ages. (J Pediatr 2011;159:99-103). W hen compared with term infants of comparable postmenstrual ages, medically low-risk preterm infants score on average 5 to 10 points lower on the Mental Developmental Index (MDI) of the Bayley Scales of Infant Development. 1,2 Medically high-risk preterm infants demonstrate even greater deficits. 3-6 The lower MDI scores and the compromised attention control may be attributed to environmentally stressful conditions in the Neonatal Intensive Care Unit (NICU) 7 and differences in preterm infant brain development. 8 Suprachiasmatic nucleus (SCN) cells, the primary controllers of circadian rhythms, and SCN afferent and efferent pathways, emerge in fetal life and continue to develop after birth. The SCN can be identified in humans around mid-gestation and completes its development at 18 months post-term age, on average. 9 Fetal rhythms during pregnancy correspond to the external circadian rhythm due to the effect of the mother’s hormonal activity and the environmental cycles to which she is exposed. 10 The newborn infant loses the coordinating signal, apparently produced by the mother. Blood and urine melatonin levels are not detected before 8 weeks after term. 11 Melatonin rhythmicity is established at about 8 to 12 weeks after a term delivery. 12 Higher vagal tone is associated with better mental function, 13 and higher oxygenation levels are associated with improved sleep patterns in preterm infants. 14 This suggests a link between the melatonin metabolism and the development of the autonomic system in preterm as compared with term infants. Reduced secretion of melatonin potentially causes suboptimal oxygenation of the frontal lobe, thus compromising the development of cognitive capacities of the newborn infant. Delayed mel- atonin production in preterm infants has been well documented. 11,15 Melatonin is considered a powerful and readily available an- tioxidant and a scavenger of free radicals. 16,17 In light of the sympathetic control of melatonin production, the antioxidant effect of melatonin and its recent clinical use for treatment of respiratory distress syndrome, 18,19 we asked if the development of melatonin production is a mediator of the autonomic system’s impact on mental development. Methods The study was approved by the institutional review board. Because seasonal effects on melatonin production in early life have been reported, 20 the infants participating in the study were all winter-born (October to March) and the recruitment process was completed within 6 months. Study inclusion criteria were (1) healthy mothers with singleton and twin infants born at 38 to 42 weeks of gestation for term subjects or born at 28 to 34 weeks of gestation for the preterm sample; (2) Apgar scores equal or better than 7 at 1 and 5 minutes after birth; and (3) 10 th to 90 th percentile in weight, and head circumference according to Israeli growth curves. Study exclusion criteria included diagnosis of genetic anomalies, congenital heart malformations, gastrointestinal dis- turbances, and central nervous system abnormalities. Infants and their mothers who met study criteria were randomly selected from a successive list of preterm and term births at a large urban medical center in Israel and were recruited with informed consent between 2 to 9 days after delivery. The singletons and twins and boys and girls were matched between preterm and term groups. In the 6-month recruitment period, 46 infants qualified for From the Department of Neurobiology (S.G.F., N.Z.), Tel Aviv University, Tel Aviv, Israel; the Department of Psychiatry (H.A., G.M.), Harvard Medical School and Children’s Hospital, Boston, MA; and the Clinical Biochemistry Laboratory (H.P.), Tel-Aviv Sorasky Medical Center, Sackler School of Medicine, Tel-Aviv University, Tel-Aviv, Israel Supported by the BiNational American Israeli Science Foundation and the Fulbright New Century Scholars Award (to S.G.F.). The authors declare no conflicts of interest. 0022-3476/$ - see front matter. Copyright ª 2011 Mosby Inc. All rights reserved. 10.1016/j.jpeds.2010.12.032 APIB Assessment of Preterm Infant Behavior MANCOVA Multivariate analysis of covariance MDI Mental Developmental Index NICU Neonatal Intensive Care Unit SCN Suprachiasmatic nucleus 99
-
Upload
independent -
Category
Documents
-
view
0 -
download
0
Transcript of Melatonin and Mental Capacities in Newborn Infants

Melatonin and Mental Capacities in Newborn Infants
Sari Goldstein Ferber, PhD, Heidelise Als, PhD, Gloria McAnulty, PhD, Hava Peretz, PhD, and Nava Zisapel, PhD
Objectives To investigate the role of melatonin in the emergence of mental capacities in the newborn infant.Study design Assessment of Preterm Infant Behavior examination was performed at 2 weeks post-term age for39 (21 preterm and 18 term) infants. 6-Suphatoxymelatonin from nocturnal urine samples was analyzed by enzyme-linked immunosorbent assays, and the Mental Developmental Index, assessed by Bayley scales, was correlated at4, 6, and 9 months’ corrected age.Results Multivariate analysis of variance with repeated measures showed that improved autonomic function at2 weeks of age was associated with higher Mental Developmental Index scores at 9 months when related to theamount of melatonin at 4, 6, and 9 months of age.Conclusions Early compromised autonomic system function in preterm infants is associated with lower mentalcapacities and is related to lower melatonin levels at later ages. (J Pediatr 2011;159:99-103).
When compared with term infants of comparable postmenstrual ages, medically low-risk preterm infants score on average5 to 10 points lower on theMentalDevelopmental Index (MDI) of the Bayley Scales of InfantDevelopment.1,2Medicallyhigh-risk preterm infants demonstrate even greater deficits.3-6 The lower MDI scores and the compromised attention
control may be attributed to environmentally stressful conditions in the Neonatal Intensive Care Unit (NICU)7 and differencesin preterm infant brain development.8 Suprachiasmatic nucleus (SCN) cells, the primary controllers of circadian rhythms, andSCN afferent and efferent pathways, emerge in fetal life and continue to develop after birth. The SCN can be identified in humansaround mid-gestation and completes its development at 18 months post-term age, on average.9 Fetal rhythms during pregnancycorrespond to the external circadian rhythm due to the effect of the mother’s hormonal activity and the environmental cycles towhich she is exposed.10 The newborn infant loses the coordinating signal, apparently produced by the mother. Blood and urinemelatonin levels are not detected before 8 weeks after term.11 Melatonin rhythmicity is established at about 8 to 12 weeks aftera term delivery.12 Higher vagal tone is associated with better mental function,13 and higher oxygenation levels are associatedwith improved sleep patterns in preterm infants.14 This suggests a link between the melatonin metabolism and the developmentof the autonomic system in preterm as compared with term infants. Reduced secretion of melatonin potentially causes suboptimaloxygenation of the frontal lobe, thus compromising the development of cognitive capacities of the newborn infant. Delayed mel-atonin production in preterm infants has been well documented.11,15 Melatonin is considered a powerful and readily available an-tioxidant and a scavenger of free radicals.16,17 In light of the sympathetic control ofmelatonin production, the antioxidant effect ofmelatonin and its recent clinical use for treatment of respiratory distress syndrome,18,19 we asked if the development of melatoninproduction is a mediator of the autonomic system’s impact on mental development.
APIB Assessment of Preterm In
MANCOVA Multivariate analysis of co
MDI Mental Developmental Ind
NICU Neonatal Intensive Care U
SCN Suprachiasmatic nucleus
Methods
The study was approved by the institutional review board. Because seasonal effects on melatonin production in early life havebeen reported,20 the infants participating in the study were all winter-born (October toMarch) and the recruitment process wascompleted within 6 months. Study inclusion criteria were (1) healthy mothers with singleton and twin infants born at 38 to 42weeks of gestation for term subjects or born at 28 to 34weeks of gestation for the preterm sample; (2) Apgar scores equal or betterthan 7 at 1 and 5minutes after birth; and (3) 10th to 90th percentile in weight, and head circumference according to Israeli growthcurves. Study exclusion criteria included diagnosis of genetic anomalies, congenital heart malformations, gastrointestinal dis-turbances, and central nervous system abnormalities. Infants and their mothers who met study criteria were randomly selected
From the Department of Neurobiology (S.G.F., N.Z.), TelAviv University, Tel Aviv, Israel; the Department ofPsychiatry (H.A., G.M.), Harvard Medical School andChildren’s Hospital, Boston, MA; and the Clinical
from a successive list of preterm and term births at a large urbanmedical center inIsrael andwere recruitedwith informed consent between 2 to 9 days after delivery.
The singletons and twins and boys and girls were matched between pretermand term groups. In the 6-month recruitment period, 46 infants qualified for
Biochemistry Laboratory (H.P.), Tel-Aviv SoraskyMedical Center, Sackler School of Medicine, Tel-AvivUniversity, Tel-Aviv, Israel
Supported by the BiNational American Israeli ScienceFoundation and the Fulbright New Century ScholarsAward (to S.G.F.). The authors declare no conflicts ofinterest.
0022-3476/$ - see front matter. Copyright ª 2011 Mosby Inc.
All rights reserved. 10.1016/j.jpeds.2010.12.032
fant Behavior
variance
ex
nit
99

THE JOURNAL OF PEDIATRICS � www.jpeds.com Vol. 159, No. 1
the study. Of these, two refused to participate. Thus, 44 in-fants (22 term and 22 preterm) infants and their mothersconstituted the study sample. Five infants (two pairs ofterm twins and a singleton preterm infant) were later ex-cluded because of spoiled urine samples. Additional samplecharacteristics are shown in Table I.
Power analysis indicated that a sample size of 30 mother-infant dyads would be sufficient to show a significant effectfor melatonin levels with a power of 90% and 5% risk oftype a error. This calculation was based on the effect sizefound in term and preterm infants’ melatonin secretionlevels.15,21
The examiners of the neurobehavioral assessment, melato-nin assays, and Bayley scales were all blind to infant groupstatus and other developmental data. Mothers were blindto the research question associating melatonin to the emerg-ing mental capacities and were only aware of the research title‘‘melatonin in the first year of life.’’
ProceduresThe preterm-born infants were exposed to bright intensivecare lighting for 24 hours (day and night) until dischargefrom the hospital and then to natural cyclical day-night light-ing at home for the rest of the study period. The term-borninfants were exposed to 24 hours of bright lighting for 2days after birth until discharged from the hospital and then
Table I. Demographic and medical background
Variable Group
Gestational age at birth PretermTerm
Apgar 1 min PretermTerm
Apgar 5 min PretermTerm
Birth weight PretermTerm
Birth weight percentile PretermTerm
Head circumference at birth PretermTerm
Head circumference percentile at birth PretermTerm
Maternal age PretermTerm
Paternal age PretermTerm
Paternal education PretermTerm
Maternal education PretermTerm
Mode of delivery (number of vaginal deliveries,number of cesarean section deliveries)
PretermTerm
Mode of feeding (number of breast-fed infants,number of formula- and breast-fed infants,number of formula-only–fed infants
PretermTerm
Surfactants (n) PretermTerm
Bronchodilators (n) PretermTerm
Respirator assistance (days range, 1-9) (n) PretermTerm
Intravenous feeding (n) PretermTerm
100
to natural cyclical day-night lighting at home for the rest ofthe study period. The participating NICU implemented dim-ming of light of all infants upon completion of this study.
Melatonin MeasurementThe mothers were instructed to collect their infants’ night-time diapers containing urine from 7 p.m. to 7 a.m. (1900to 0700) at the ages of 4, 6, and 9 months’ correctedage.20,21 The procedures of urine extraction from the diapersand the enzyme-linked immunosorbent assay for determin-ing the amounts of the melatonin metabolite 6-sulfatoxyme-latonin in the urine of young infants were as describedpreviously.20,21
Neurobehavioral AssessmentThe Assessment of Preterm Infant Behavior (APIB)22 isawidely used, comprehensive newborn behavioral assessmentwith sensitivity to differentiate among subgroups of infants ofvarying gestational ages and degrees of risk status assessed at 2weeks’ corrected age.23 The APIB appears to be sensitive to theincrease in cortical gray and white matter as well as onset ofmyelination in the last trimester.24,25 The assessment presentsincreasingly demanding environmental inputs in a graded se-quence of distal and proximal stimulus presentations, whichare based on the Neonatal Behavioral Assessment Scale.26
The APIB six summary system variables were used in this
Mean/n SD T/c2 P
3138
11
16.1 <.0001
88
11
0.9 NS
910
0.60.3
1.8 NS
16423073
353424
11.4 <.001
5951
2020
1.1 NS
2833
21
8.9 <.001
4551
2219
0.8 NS
3331
75
1.2 NS
3634
56
0.9 NS
1312
22
1.4 NS
1314
1 1.2 NS
9, 1213, 7
16.6 <.001
0,9,1213,2,3
28.4 <.03
70
16.0 <.001
80
13.5 <.001
80
13.5 <.001
190
35. 1 <.001
Goldstein Ferber et al

Table II. Means and SDs as shown in MANCOVA onneurobehavioral measures of the Assessment of PretermInfant Behavior Six Systems Scores
Group Mean SD F P
July 2011 ORIGINAL ARTICLES
study in accordance with previous studies with this outcomemeasure.7 These variables range in score from 1 to 9, with lowscores denoting well-modulated and well-organized behav-ioral regulation. The approximately 45-minute examinationwas performed in the course of a home visit and 1 hour beforethe infant’s next expected feeding, typically with the infant insleep state at the beginning of the examination. All infantswere assessed with the APIB at 2 weeks post-term age. The as-sessment was conducted by an NFI-certified (National NID-CAP Federation International) APIB examiner, purposefullyblinded to the group status of the infants.
Mental Developmental IndexTheMDImeasure of the Bayley Scales of Infant Development– Second Edition (Bayley-II)2 was used at 4, 6, and 9 months’corrected age. The test was conducted at a home visit by oneof two psychologists trained in administration of the Bayley-II and blinded to the group status of the infants.
Statistical AnalysisOne-way multivariate analysis of variance (MANCOVA) wasused to evaluate differences between groups (preterm versusterm) in the APIB systems scores at 42 weeks after the lastmenstrual period. Repeated-measures ANOVAs were usedto test the differences between groups in melatonin produc-tion over time and separately in the behavioral indices of theMDI scores at 4, 6, and 9 months. MANCOVA was used toassess group differences with melatonin production servingas the dependent repeated-measure variable at 4, 6, and 9months, and the APIB system scores were entered as a covari-ate constant across time to assess the role of each of the APIBsystem scores on melatonin secretion. To examine the differ-ences between groups and the differences between subjectswith high versus low autonomic APIB system scores, a 2 �2 � 3 MANCOVA (group � autonomic system score �time) with repeated-measures on time (MDI scores at thethree time points of measurement) and the three melatoninmeasures as covariates was used.
Pearson correlations were used to assess the relationshipbetween melatonin and the APIB system scores as well asbetween the APIB system scores and the MDI scores at thedifferent age points.
Autonomic Term 2.0 1.1 204.6 <.0001Preterm 6.2 0.6
Motor Term 2.1 1.3 138.3 <.0001Preterm 6.4 0.8
State Term 3.7 1.4 20.0 <.0001Preterm 5.5 0.9
Attention Term 3.7 2.3 38.5 <.0001Preterm 7.2 0.9
Self-regulation Term 2.5 1.5 142.9 <.0001Preterm 6.3 0.5
Examinerfacilitation
Term 2.7 1.5 161.3 <.0001
Preterm 6.8 0.7
Results
Although there were no significant differences betweengroups for demographic background variables, expected dif-ferences in gestational age, weight, and head circumference atbirth were found between the preterm and term-born infants(Table I). Additionally, no significant differences betweenterm singleton and twin infants nor between females andmales were found in the APIB system scores, or the MDI orthe amounts of melatonin at 4, 6, and 9 months’ correctedage.
Multivariate analysis of variance revealed a significant dif-ference between the preterm and term infants on the six
Melatonin and Mental Capacities in Newborn Infants
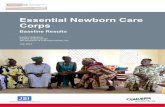
APIB system scores (Table II). Repeated-measures analysisof variance for melatonin at 4, 6, and 9 months revealeda significant time effect (F (1, 36) = 25.2, P < .0001) anda significant group � time interaction effect (F (2, 36) = 3.5,P < .04) (Figure 1). Analyses of simple effects to reveal thesource of the interaction showed a significant effect of theincrease in melatonin secretion in both the preterm [F (1,19) = 21.5] and the term [F (16) = 11.8] groups. Furtheranalyses of contrasts between the time points in each groupshowed significant differences of melatonin secretionbetween 4 and 6 months [F (1, 20) = 43.3 P < .0001] andbetween 6 and 9 months [F (1, 20) = 10.2, P < .005] for thepreterm group. For the term group, a significant differencewas found between 4 and 6 months [F (1, 17) = 17.8, P >.001] but not between 6 and 9 months. A 2 � 3 ANOVA(group � time) with repeated measures (the MDI scores at4, 6, and 9 months) revealed a significant difference favoringthe term group in terms of MDI scores across all time points(F (1, 29) = 29.8, P < .0001) and at each time pointseparately (Figure 2).A group � time MANCOVA, with melatonin production
at 4, 6, and 9 months as repeated measures, with each of theAPIB system scores entered each time separately as a covariate,revealed a significant effect of the autonomic system covariate(F (2, 35) = 3.5, P< .028) that goes beyond the effects of groupstatus. Higher levels of melatonin were associated with moreoptimal scores of the APIB autonomic system score.To analyze the role of the autonomic system and the
groups as independent variables, the autonomic APIB systemscores were divided into high (above the group mean of 6.25for preterm infants and above the group mean of 2.02 forterm infants) and low scores (below the means as statedabove for the preterm infants and term infants, respectively).A 2 � 2 � 3 MANCOVA (group � high/low scores in auto-nomic system score � time) with repeated measures on thethree time points of the MDI measurement and with the
101

Figure 1. Distribution of the significantly different rhythms ofmelatonin levels in the preterm group compared with the termgroup.
THE JOURNAL OF PEDIATRICS � www.jpeds.com Vol. 159, No. 1
melatonin measures at 4, 6, and 9 months as covariatesrevealed a significant interaction effect of melatonin at4 months with MDI at 4, 6, and 9 months (F (2,31) = 5.4,P < .01). This analysis revealed a significant interaction be-tween the MDI at 4, 6, and 9 months and the autonomicAPIB system score (F (2, 31) = 6.1, P < .006) as well, beyondgroup effect. Higher levels of melatonin at 4, 6, and 9 monthswere associated with more optimal scores of the APIB auto-nomic system scores.
Significant correlations were found between melatoninproduction at 6 and 9 months and the following APIB systemscores: the autonomic system, the self-regulation system, andexaminer facilitation. In addition, significant correlationswere found between the APIB state organization and atten-tion systems scores and melatonin production at 9 months(Table III; available at www.jpeds.com). Higher scores ofmelatonin at 6 and 9 months were significantly correlatedwith more mature neurobehavioral performance on theAPIB at 42 weeks. These results show that theneurobehavioral differences precede the melatonindifferences and the melatonin maturation.
Figure 2. Significant differences between Mental Develop-mental Index scores at 4, 6, and 9months in the preterm groupcompared with the term group.
102
Significant correlations were found between all the APIBsystems scores and the MDI at 4, 6, and 9 months; the lowerAPIB system scores that represent more optimal functioningreached highly significant correlations, that is, higher MDIscores on the Bayley-II.
Discussion
We demonstrate that preterm infants have different profilesof development than term infants. Preterm profiles arecharacterized by compromised autonomic and motorfunctioning, state organization, self-regulation, and attentioncapacities at 2 weeks corrected age, as well as by delayed mel-atonin production and slower mental development up to 9months of age when compared with term infants. Accordingto our results, melatonin level at 4 months was responsiblefor the variance of the MDI at all ages, and the source ofthe statistic interactions was the rapid catch-up of the termgroup in melatonin secretion between 4 and 6 months ascompared with the pattern of the melatonin maturation inthe preterm group. The maturation of early brain globalfunctioning precedes the melatonin maturation, as the auto-nomic system measured at 42 weeks significantly explainedchanges in melatonin over time at older ages. These resultsalso show high validity of this study as two well-acceptedand widely used neurobehavioral tests, the MDI and theAPIB, were highly correlated. This is in keeping with previousmelatonin and cognitive studies.1,3-6,11,15
The autonomic systemwas a variable that interacts with themediating function ofmelatonin in supporting the emergenceof mental capacities of the newborn infant. This may suggesta role for melatonin in the emergence of mental capacities,beyond its photic reactivity and multimetabolite characteris-tics.16 The maturation of the thalamocortical network mayhave a positive impact on mental development through theprotective impact of melatonin by its reduction of oxidativestress.17 Because melatonin synthesis is affected by noradren-ergic stimulation,18,19 the irregularity in sympathetic activityin preterm infants may affect the maturation of melatoninproduction. This is buttressed by the results of the currentstudy, which shows long-term correlations between the integ-rity of the autonomic system at 2 weeks corrected age and themelatonin levels up to 9 months. The compromised norad-renergic effect on melatonin production on one hand, andthe resulting lack ofmelatonin facilitation for reduction of ox-idative stress on the other, may be a bidirectional processaffecting sympathetic stability in preterm infants. Such a bidi-rectional coregulatory paradigm for explaining processes inthe developing brain was suggested.27-29 This bidirectionalprocess may have an impact on the maturation of the thala-mocortical network and thus on the development of mentalcapacities through negative coregulatory feedback amongthe various components.
The emergence of mental capacities is among the mostchallenging and complex processes of the human brain.The rhythm of neurobehavioral development depends on
Goldstein Ferber et al

July 2011 ORIGINAL ARTICLES
many genetic and postnatal components, as identified in theextensive literature on nature-nurture effects.30 We suggestthat melatonin may be an important specific componentthat contributes to the development of mental capacities, in-dependent of the clock and dependent on the autonomicfunctioning. This study adds another significant aspect tothe body of literature that shows the importance of dimmingof lights in NICUs. n
The investigators are most thankful to Sandra Kosta, BA, Departmentof Psychiatry, Harvard Medical School and Children’s Hospital Bos-ton, as well as to Irit Tavori, MD, Israel.
Submitted for publication Jul 15, 2010; last revision received Nov 15, 2010;
accepted Dec 22, 2010.
Reprint requests: Dr Sari Goldstein Ferber, PhD, c/o Prof Nava Zisapel,
Department of Neurobiology, Faculty of Life Sciences, Tel Aviv University,
69978, Tel Aviv, Israel. E-mail: [email protected]
References
1. Bhutta AT, Cleves MA, Casey PH, Cradock MM, Anand KJS. Cognitive
and behavioral outcomes of school-aged children who were born pre-
term: a meta-analysis. JAMA 2002;288:728-37.
2. Bayley N. Bayley Scales of Infant Development. 2nd edition. San Anto-
nio, TX: The Psychological Corporation; 1993.
3. Maitre NL, Marshall DD, Price WA, Slaughter JC, O’Shea TM,
Maxfield C, et al. Neurodevelopmental outcome of infants with unilat-
eral or bilateral periventricular hemorrhagic infarction. Pediatrics
2009;124:1153-60.
4. Saldir M, Sarici SU, Bakar EE, Ozcan O. Neurodevelopmental status of
preterm newborns at infancy, born at a tertiary care center in Turkey.
Am J Perinatol 2010;27:121-8.
5. Sun J, Mohay H, O’Callaghan MA. Comparison of executive function in
very preterm and term infants at 8months corrected age. Early HumDev
2009;85:225-30.
6. Aylward GP. Cognitive and neuropsychological outcomes: more than IQ
scores. Ment Retard Dev Disabil Res Rev 2002;8:234-40.
7. Als H, Duffy FH, McAnulty GB, Rivkin MJ, Vajapeyam S, Mulkern RV,
et al. Early experience alters brain function and structure. Pediatrics
2004;113:846-57.
8. Swaab DF, Hofman MA, Honnebier MB. Development of vasopressin
neurons in the human suprachiasmatic nucleus in relation to birth.
Brain Res Dev Brain Res 1990;52:289-93.
9. Houghton DC, Young IR,McMillen IC. Evidence for hypothalamic con-
trol over the diurnal rhythms in PRL andmelatonin in fetal sheep during
late gestation. Endocrinology 1995;136:218-23.
10. McMillen IC, Nowak R. The pre- and postnatal development of hormonal
circadian rhythms. Baillieres Clin Endocrinol Metab 1989;3:707-21.
11. Kennaway DJ, Stamp GE, Goble FC. Development of melatonin produc-
tion in infants and the impact of prematurity. J Clin Endocrinol Metab
1992;75:367-9.
12. Ser�on-Ferr�e M, Torres-Farf�an C, Forcelledo ML, Valenzuela GJ. The de-
velopment of circadian rhythms in the fetus and neonate. Semin Perina-
tol 2001;25:363-70.
Melatonin and Mental Capacities in Newborn Infants
13. Doussard-Rossevelt J, Porges SW, McClenny BD. Behavioral sleep states
in very low birth weight preterm neonates: relation to neonatal health
and vagal maturation. J Pediatr Psychol 1996;21:785-802.
14. Simakajornboon N, Beckerman RC, Mack C, Sharon D, Gozal D. Effect
of supplemental oxygen on sleep architecture and cardiorespiratory
events in preterm infants. Pediatrics 2002;110:884-8.
15. Ferber SG, Makhoul IR. Prematurely-born infants produce less melato-
nin than term-born infants at 9 and 12months of age: a randomized con-
trolled trial. J Pediatr Neurol 2010;8:381-4.
16. Tan DX, Manchester LC, TerronMP, Flores LJ, Reiter RJ. One molecule,
many derivatives: a never-ending interaction of melatonin with reactive
oxygen and nitrogen species? J Pineal Res 2007;42:28-42.
17. Gitto E, Pellegrino S, Gitto P, Barberi I, Reiter RJ. Oxidative stress of the
newborn in the pre- and postnatal period and the clinical utility of mel-
atonin. J Pineal Res 2009;46:128-39.
18. Gitto E, Reiter RJ, Amodio A, Romeo C, Cuzzocrea E, Sabatino G, et al.
Early indicators of chronic lung disease in preterm infants with respira-
tory distress syndrome and their inhibition by melatonin. J Pineal Res
2004;36:250-5.
19. Mu~noz-Hoyos A, Bonillo-Perales A, Avila-Villegas R, Gonz�alez-
Ripoll M, Uberos J, Florido-Nav�ıo J, et al. Melatonin levels during the
first week of life and their relation with the antioxidant response in
the perinatal period. Neonatology 2007;92:209-16.
20. Sivan Y, Laudon M, Tauman R, Zisapel N. Melatonin production in
healthy infants: evidence for seasonal variations. Pediatr Res 2001;49:
63-8.
21. Ferber SG, Laudon M, Kuint J, Weller A, Zisapel N. Massage therapy by
mothers enhanced the adjustment of circadian rhythms to the nocturnal
period in full term infants. J Dev Behav Pediatr 2002;23:410-5.
22. Als H, Lester BM, Tronick EZ, Brazelton TB. Manual for the assessment
of preterm infants’ behavior (APIB). In: Fitzgerald HE, Lester BM,
Yogman MW, eds. Theory and Research in Behavioral Pediatrics. New
York: Plenum Press; 1982. p. 65-132.
23. Duffy FH, Als H, McAnulty GB. Behavioral and electrophysiological
evidence for gestational age effects in healthy preterm and fullterm in-
fants studied two weeks after expected due date. Child Dev 1990;61:
271-86.
24. Duffy FH, Als H,McAnulty GB. Infant EEG spectral coherence data dur-
ing quiet sleep: Unrestricted Principal Components Analysis: relation of
factors to gestational age, medical risk, and neurobehavioral status. Clin
Electroencephalogr 2003;34:54-69.
25. H€uppi PS, Schuknecht B, Boesch C, Bossi E, Felblinger J, Fusch C, et al.
Structural and neurobehavioral delay in postnatal brain development of
preterm infants. Pediatr Res 1996;39:895-901.
26. Brazelton TB. Neonatal Behavioral Assessment Scale. Philadelphia, PA:
Lippincott; 1973.
27. Jan JE, Reiter RJ, Wasdell MB, Bax M. The role of the thalamus in sleep,
pineal melatonin production, and circadian rhythm sleep disorders. J Pi-
neal Res 2009;46:1-7.
28. Simonneaux V, Ribelayga C. Generation of the melatonin endocrine
message in mammals: a review of the complex regulation of melatonin
synthesis by norepinephrine, peptides, and other pineal transmitters.
Pharmacol Rev 2003;55:325-95.
29. Ferber SG. Co-regulation of stress in uterus and during early infancyme-
diates gender differences in attachment styles: evolutionary, genetic and
endocrinal perspectives. Behav Brain Sci 2009;32:29-30.
30. Sameroff AJ. Environmental risk factors in infancy. Pediatrics 1998;102:
1287-92.
103

Table III. Pearson correlations between the Assessment of Preterm Infants’ Behavior System scores at 2 weeks of age andmelatonin amounts (in micrograms) at 4, 6, and 9 months
Variable Motor State AttentionSelf-
regulationExaminerfacilitation
Melatonin,4months
Melatonin,6 months
Melatonin,9 months
APIB autonomic system .97† .75† .79† .96† .96† .10 �.34* �.35*APIB motor system .76† .79† .97† .97† .097 �.32* �.30APIB state system .80† .80† .77† �.002 �.19 �.30*APIB attention system .82† .80† .037 �.23 �.37*APIB self-regulation system .98† .018 �.35* �.33*APIB examiner facilitation system .069 �.32* �.31*Melatonin, 4 months .20 .33*Melatonin, 6 months .32*
*Significance adjusted at .05 level.†significance adjusted at .01 level.
THE JOURNAL OF PEDIATRICS � www.jpeds.com Vol. 159, No. 1
103.e1 Goldstein Ferber et al