
University of Groningen Groningen Growth and Development ...
Upload
khangminh22Category
view
4download
0
University of Groningen
Influenza vaccination in primary and secondary immunodeficienciesvan Assen, Sander
IMPORTANT NOTE: You are advised to consult the publisher's version (publisher's PDF) if you wish to cite fromit. Please check the document version below.
Document VersionPublisher's PDF, also known as Version of record
Publication date:2011
Link to publication in University of Groningen/UMCG research database
Citation for published version (APA):van Assen, S. (2011). Influenza vaccination in primary and secondary immunodeficiencies. [s.n.].
CopyrightOther than for strictly personal use, it is not permitted to download or to forward/distribute the text or part of it without the consent of theauthor(s) and/or copyright holder(s), unless the work is under an open content license (like Creative Commons).
The publication may also be distributed here under the terms of Article 25fa of the Dutch Copyright Act, indicated by the “Taverne” license.More information can be found on the University of Groningen website: https://www.rug.nl/library/open-access/self-archiving-pure/taverne-amendment.
Take-down policyIf you believe that this document breaches copyright please contact us providing details, and we will remove access to the work immediatelyand investigate your claim.
Downloaded from the University of Groningen/UMCG research database (Pure): http://www.rug.nl/research/portal. For technical reasons thenumber of authors shown on this cover page is limited to 10 maximum.
Download date: 04-07-2022
Influenza vaccinationin primary and secondary
immunodeficiencies
Layout: Luite van AssenPrint: Ipskamp Drukkers, Enschede, The Netherlands
ISBN (printed): 978-90-367-5035-6ISBN (digital): 978-90-367-5034-9©2011 Sander van Assen
Financial support for studies in this thesis (in alphabetical order):Abbott B.V., EULAR, Jan Kornelis de Cock Stichting, Roche Nederland B.V.
Financial support for publication of this thesis (in alphabetical order):Abbott B.V., Baxter, BD Biosciences, Boehringer-Ingelheim B.V., Gilead Sciences Netherlands B.V., GlaxoSmithKline, GUIDE, MSD, Roche Nederland B.V., Sanofi-Pasteur MSD N.V., Sanquin, ViiV Healthcare
RIJKSUNIVERSITEIT GRONINGEN
Influenza vaccination in primary and
secondary immunodeficiencies
Proefschrift
ter verkrijging van het doctoraat in de
Medische Wetenschappen
aan de Rijksuniversiteit Groningen
op gezag van de
Rector Magnificus, dr. E. Sterken,
in het openbaar te verdedigen op
woensdag 21 september 2011
om 16:15 uur
door
Sander van Assen
geboren op 24 september 1970
te Leeuwarden

Promotor: Prof. dr. C.G.M. Kallenberg
Copromotores: Dr. M. Bijl Dr. A. de Haan
Beoordelingscommissie: Prof. dr. J.W.J. Bijlsma Prof. dr. J.T. van Dissel Prof. dr. H.G.M. Niesters

Paranimfen: Sander van der Beek Arto Boeken Kruger
6
Con
tent
s
9
25
41
61
81
99
113
Contents
Chapter 1 Introduction
Part 1 Influenza vaccination in patients with humoral primary immunodeficiency
Chapter 2 Patients with humoral primary immunodeficiency do not develop protective anti-influenza antibody titers after vaccination with trivalent subunit influenza vaccine Clinical Immunology 2010 Aug;136(2):228-235
Chapter 3 Cell-mediated immune responses to inactivated trivalent influenza-vaccination are decreased in patients with common variable immunodeficiency Clinical Immunology. In press
Part 2 Influenza vaccination in patients with auto-immune inflammatory rheumatic diseases
Chapter 4 Studies of cell-mediated immune responses to influenza vaccination in systemic lupus erythematosus Arthritis & Rheumatism 2009 Aug;60(8):2438-2447
Chapter 5 Effect of a second, booster, influenza vaccination on antibody responses in quiescent systemic lupus erythematosus: an open, prospective, controlled study Rheumatology (Oxford) 2009 Oct;48(10):1294-1299
Chapter 6 Humoral responses after influenza vaccination are severely reduced in patients with rheumatoid arthritis treated with rituximab Arthritis & Rheumatism 2010 Jan;62(1):75-81
Chapter 7 Polyclonal and influenza-specific cell-mediated immune responses are hampered in rheumatoid arthritis patients treated with rituximab Submitted
7
Con
tent
s
Part 3 eULAR recommendations for vaccination in patients with auto-immune inflammatory rheumatic diseases
Chapter 8 Vaccination in adult patients with auto-immune inflammatory rheumatic diseases: a systematic literature review for the European League Against Rheumatism evidence-based recommendations for vaccination in adult patients with auto-immune inflammatory rheumatic diseases Autoimmunity Reviews 2011 Apr;10(6):341-352
Chapter 9 European League Against Rheumatism recommendations for vaccination in adult patients with autoimmune inflammatory rheumatic diseases Annals of Rheumatic Diseases 2011 Mar;70(3):414-422
Chapter 10 Summary, general discussion and future perspectives
Chapter 11 Nederlandse samenvatting Dankwoord List of selected publications
135
171
197
213 223 227

CHAPT
ER 1INTRODUCTION


11
Cha
pter
1
INTRODUCTIONVaccination has been one of the most effective measures to reduce mortality [1, 2]. It has led to the eradication of naturally occurring smallpox and the control of diphtheria, tetanus, pertussis, yellow fever, Haemophilus influenzae b, poliomye-litis, measles, mumps, rubella, typhoid and rabies [2]. The aim of vaccination is to prevent or mitigate diseases by artificially inducing immunity. Active vaccination triggers the immune system to provide (protective) humoral and cell-mediated immune responses against the vaccine-preventable disease, while passive vac-cination refers to the administration of exogenously produced antibodies for pro-tection.
History of vaccination
In 430 BC the Greek already knew that survivors of the plague were resistant to the plague when a new epidemic occurred [3, 4]. In the 10th century the Chinese transferred dried material from smallpox pustules to susceptible individuals in order to prevent them from contracting smallpox. This was done by putting a cotton with the dried material from a pustule in the nostrils. In India non-immune children were wrapped in pox-laden blankets from children suffering from small-pox during a mild smallpox epidemic, in order to transmit a less virulent smallpox virus to the non-immune children. Also subcutaneous instillation of fresh matter from a ripe smallpox pustule in an incision made in a non-immune person’s fo-rearm, referred to as inoculation or variolation, was performed. The latter term was derived from the Latin word varius (meaning “stained”) or varus (meaning “mark on the skin”) [2, 4, 5].
After being practiced in China, India and Africa, in the 17th century variolation was introduced in the Turkish Ottoman Empire, possibly by Circassian traders or Circassian women, who were in great demand in the Sultan’s harem for their extreme beauty [5].
In the beginning of the 18th century variolation was introduced in Europe. Lady Mary Worthley Montagu, the wife of the British ambassador of “The Sublime Por-te” (the Ottoman government in Constantinople) Lord Worthley Montagu, noti-ced during her stay in Turkey in 1717 that the smallpox was much less of a threat than in the UK and attributed this to variolation, or “engrafting”. She had great respect for the disease as her brother had died of it at the age of 20, while she herself survived the illness, but at the cost of permanent scars on her face. To her friend she wrote: ‘the smallpox, so fatal, and so general amongst us, is here enti-rely harmless, by the intervention of engrafting, which is the term they give it…’. Although several years earlier two Ottoman inoculators of Greek origin, Emma-

12
Cha
pter
1
nouel Timonius and Jacobus Pylorinos, send papers on variolation to the Royal Society in 1713 and 1716, respectively, it was Lady Montagu who popularized vari-olation in Europe. After variolation of her daughter by Charles Maitland, who also variolated her sons some years earlier in Turkey, and of several others, many members of the upper class had themselves variolated. Although skepticism remained among British doctors, variolation received official approval from the Royal College of Physicians. In 1757, at the age of 8 years, a boy called Edward Jen-ner was inoculated in Gloucester [5].
The same Edward Jenner, a country doctor, was elected a Fellow of the Royal Society in 1789 for his work on cuckoos: he demonstrated that the newly-hatched cuckoo ejected the eggs and nestlings of its foster-parents. In 1796 Jenner started his experiments on inoculating persons with cowpox in order to prevent them from smallpox. Cowpox was removed from the hand of the dairymaid Sarah Nelmes and Jenner inserted this in two superficial incisions in the arm of a boy named James Phipps. Six weeks later the boy was variolated with freshly remo-ved smallpox: no disease ensued, even when the challenge was repeated after several months [3]. Jenner published his findings at his own costs, since the Presi-dent of the Royal Society rejected his manuscript with the addition that he should be concerned for his reputation and his colleague’s esteem [6]. Hereafter his me-thods of vaccination were adopted in most European countries and subsequently in the USA. Although Jenner deserves credits for carrying out the experiments to test the hypothesis that vaccination with cowpox protects for smallpox, he was neither the first who noticed the protective effect of cowpox infection, nor the first to vaccinate with cowpox. The protective effect of cowpox was already known to farmers from North Dorset, England, who observed that dairymaids did not contract smallpox after contracting cowpox from handling cows’ udders. Knowing this, the cattle breeder Benjamin Jesty deliberately infected his wife and two children with cowpox using his wife’s knitting needle in order to protect them for smallpox, and he proved his right when even after several exposures to smallpox his boys did not acquire the disease. This was 22 years before Jenner performed his experiments. These were the first recorded vaccinations. In 1829 John Fosbroke, surgeon, wrote that if Jenner did not have had fortune, fame and high alliance, his merit would have been crushed or faintly supported [7, 8]. Jen-ner was awarded grants by the House of Commons in 1802 of 10.000 pounds and of 20.000 pounds in 1807 for his discovery of vaccination for smallpox. However, during the committee’s deliberations, it was pointed out that inoculation had been practiced previous to Edward Jenner’s experiments. Therefore, the Original Vac-cine Pock Institution invited Benjamin Jesty in 1805. He was cross-examined and presented with a long testimonial and pair of gold mounted lancets. The verbal

13
Cha
pter
1
evidence of their examination was published in the Edinburgh Medical and Surgi-cal Journal [2, 4, 7].
After vaccination for smallpox, several other vaccines were developed. It took until the forties of the 20th century until an influenza vaccine was available. An influenza vaccine was most welcome, since the influenza pandemic occurring in 1918, the so-called “Spanish Flu”, led to an estimated 40 million deaths worldwide. Also, many soldiers fighting in World War I became victim of the influenza pande-mic and therefore the US army supported the development of a vaccine.
However, to be able to develop an influenza vaccine, researchers had to deter-mine the causative micro-organism of influenza, which was initially thought to be bacterial. In 1892 Pfeiffer discovered a new organism from the secretions of flu patients, named by Pfeiffer Bacillus influenzae (later Haemophilus influenzae), by others Pfeiffer’s bacillus. Since this organism could only be isolated from a mi-nority of flu patients during the 1918 pandemic, the causal relation with influenza was rejected. The same held true for many other bacteria, among which Dialister pneumosintes that was isolated in 1918 from nasal secretions of influenza patients, but which turned out to be related with periodontal disease, and played no role in influenza [9].
It was Richard Shope who in 1931 was the first to isolate influenza virus from swine during epizootic periods of hog flu [10]. Shortly thereafter, Thomas Francis, an American virologist, isolated influenza type A in 1934 from humans for the first time, and he was also the first to grow influenza type B, in 1940 [11, 12]. Thomas Francis and Jonas Salk, a protégé of Francis and best remembered for his con-tributions to the development of polio vaccine, worked on an influenza vaccine in Ann Arbor for the US army. They developed a vaccine from an influenza type A strain that had led to an outbreak of atypical pneumonia in 1943 and tested the vaccine in the winter of 1943-1944 on male residents of a mental institution. The vaccine turned out to induce resistance to challenge with active virus. Later on, a large randomized, double-blind, placebo-controlled trial, including 6.236 vaccina-ted men and 6.211 controls who received placebo, was performed in the fall of 1943 and demonstrated an attack rate of influenza of 2.22% in the vaccinated group, while this was 7.11% in the unvaccinated group [13]. Since then, nothing much chan-ged with regard to influenza vaccines currently used, except for purification of the vaccine, which resulted in split and subunit influenza vaccines. These are as immunogenic as the whole inactivated virus (WIV) vaccines that Salk and Francis developed, but are less reactogenic and therefore cause less adverse events. Un-til very recently these vaccines were also still grown on the chorio-allantoic mem-branes of developing chick-embryos [14]. The in 1941 developed hemagglutination

14
Cha
pter
1
inhibition assay, which uses the capacity of influenza-specific antibodies in the human serum to inhibit agglutination of chicken, turkey and guinea pig erythrocy-tes by hemagglutinin, is still the gold standard for determination of the humoral response following influenza vaccination, in particular to determine seroprotec-tion [15].
Vaccination immunology with a focus on influenza vaccination
Virus-neutralizing immune effector responses are antibody or immune cell me-diated. Most vaccines confer protection by eliciting B-cell responses leading to the production of antibodies directed against infectious or toxic agents. This also holds true for influenza vaccines, which induce the production of influenza neu-tralizing antibodies in order to prevent binding of the virus to epithelium of the respiratory tract. These are mainly IgG antibodies directed against influenza surf-ace antigens. Mucosal influenza-specific IgA antibodies play an important role in the protection against infection with influenza. However, subunit influenza vac-cine induces only production of IgG and/or IgM antibodies. Only the mucosal ap-plied live-attenuated influenza vaccine leads to the synthesis of anti-influenza IgA antibodies.
Besides neutralizing antibodies, cytotoxic CD8+ T-lymphocytes (CTL) can serve as immune effectors following vaccination by recognizing and killing infected cells or by secreting antiviral cytokines. Influenza-specific CTL responses have been shown to mitigate the course of influenza infection [16] and influenza-spe-cific CTL responses following influenza vaccination (as measured by granzyme B production, an effector mechanism of CTL) correlate with protection for labora-tory confirmed influenza in elderly [17]. CTL responses are not induced by surface antigens, and therefore also not by subunit vaccines. In contrast, WIV influenza vaccine and live-attenuated influenza vaccine do elicit CTL responses, since they contain many other influenza antigens besides surface antigens.
To support the generation and maintenance of these B-cell and CTL responses CD4+ T-lymphocytes (T-helper cells) secrete growth factors and give signals. Moreover, T-cell help results in the induction of long term memory leading to a faster, larger and more specific immune response on a second encounter of the antigen [2].
The influenza vaccines used in the studies presented are trivalent subunit influ-enza vaccines, containing mainly hemagglutinin, one of the two surface protein-antigens of influenza, of the two influenza A-strains and the one B-strain for the particular season. To a smaller extent the vaccines contain neuraminidase (the other surface protein-antigen), and only very little internal antigens such as ma-

15
Cha
pter
1
trixprotein and nucleoprotein. Influenza is capable of changing composition and therefore also epitopes, as a form of immune evasion, referred to as “antigenic drift”. Therefore, every year the composition of influenza vaccine is evaluated and adjusted to the changes in hemagglutinin and neuraminidase, based on the most recent circulating influenza strains. Since the mutations that lead to the an-tigenic drift can not be predicted, the efficacy of the vaccine may differ from year to year based on the similarity of the vaccine strains and the natural oc-curring influenza strains. Nonetheless, antibody production following influenza vaccination generally correlates well with protection for influenza infection. An anti-influenza antibody titer of ≥40 as determined by hemagglutination inhibition assay is considered protective [15], although it should be noted that this has only been demonstrated in young healthy volunteers, and that for elderly and immuno-compromised persons, for example, it remains unclear whether the same titer can be presumed to be protective.
Following intramuscular administration of influenza subunit vaccine the vaccine antigens will reach the draining lymph node as free proteins or associated with dendritic cells. The vaccine antigens can be recognized by naïve B-cells and bound to their IgM-receptor, leading to activation of the B-cells and migration of the B-cells to the outer T-cell zone of the lymph node. Here the B-cell is exposed to and T-helper cells by activated dendritic cells , which provide help to differentiate into immunoglobulin secreting plasma cells. T-helper cells also drive immunoglobulin class switch from IgM towards IgG, but there is no hypermutation, so affinity of the immunoglobulins is low [2].
To produce more antibodies and antibodies with a better fit (higher affinity), and, thus, a higher capacity to neutralize the influenza virus, a so-called germinal cen-ter reaction needs to be elicited. Antigen-specific B-cells and follicular T-cells are attracted by follicular denditric cells towards B-cell follicles in the germinal cen-ter. Here follicular T-helper cells provide help to B-cells through costimulatory molecules. An optimal interplay between these cells results in clonal expansion of specific B-cells and antibody production, class switch from IgM to IgG and IgA, and affinity maturation of the antibodies by somatic hypermutation. Also diffe-rentiation of germinal center B-cells towards specific antibody secreting plasma cells or memory B-cells takes place. It takes 10-14 days before the highly specific IgG antibodies enter the circulation and these will peak 4 to 6 weeks after vacci-nation. However, after a re-exposure to the vaccine antigen, in case of infection with natural influenza for example, a faster, larger and more specific immune response will result (also referred to as a memory response) [2].
In contrast to B-cell and CD4+ T-cell responses, no or only limited CTL responses

16
Cha
pter
1
are induced by influenza subunit vaccine, since the influenza surface protein from the vaccine is presented by antigen presenting cells in the context of a MHC class II molecule. This is recognized by CD4+ T-cells only, not by CD8+ T-cells. Some pre-sentation of antigen in the context of MHC class I might occur through cross-pre-sentation, leading to CTL responses, but this occurs only to a limited extent [18].
Influenza vaccination in immunocompromised persons
As can be expected based on the former section, an adequately functioning immu-ne system is required to respond with protective immunity following vaccination. Paradoxically, this also means that patients with a compromised immune system, who theoretically profit most from vaccination because they are at increased risk of contracting vaccine-preventable infections and to have a complicated course of these infections, may not be able to elicit protective immune responses.
An immunocompromised state can result from a primary (or hereditary) immu-nodeficiency or from a secondary (or acquired) immunodeficiency. With a preva-lence of up till almost 1 in 200 in Caucasians selective IgA-deficiency is the most common primary immunodeficiency [19]. Most individuals with IgA-deficiency are asymptomatic. The primary immunodeficiency most frequently encountered in the clinic is common variable immunodeficiency (CVID). It is defined by reduced levels of total IgG, in combination with reduced levels of IgM and/or IgA and a poor or absent response on vaccination, despite the presence of normal levels of B-cells in the peripheral blood [20]. The onset of disease is usually in the second or third decade, and it is characterized by recurrent infections of the respiratory and gastrointestinal tracts, auto-immune manifestations, sarcoid-like granuloma for-mation and an increased risk of developing malignancy [21, 22]. The pathogenesis is poorly understood, although many defects in humoral and cell-mediated immu-nity have been described. Ten to 15% of the patients with CVID have a known gene defect causing the disease [23]. Other humoral primary immunodeficiencies are X-linked agammaglobulinemia, autosomal recessive agammaglobulinemia, IgG subclass deficiency and specific antibody response deficiency. In order to prevent infections in patients with humoral primary immunodeficiencies intravenous im-munoglobulins (IVIg) every 2 to 4 weeks or subcutaneous immunoglobulins every 1 to 2 weeks, and prophylactic antibiotics can be administered. Influenza vaccina-tion is recommended for patients with CVID, however, efficacy is unknown. Only a limited proportion of patients with CVID developed an adequate immune res-ponse after vaccination with anti-peptide and anti-polysaccharide vaccines [24].
Secondary immunodeficiencies are acquired during life. Most often the cause is iatrogenic, i.e. treatment with immunosuppressive agents, e.g. corticosteroids,

17
Cha
pter
1
methotrexate or biologics that target specific parts of the immune system, usu-ally in order to prevent the immune system from attacking self antigens or trans-planted organs. In this thesis (combinations of) immunosuppressive agents are addressed that are used in the treatment of auto-immune inflammatory rheuma-tic diseases such as systemic lupus erythematosus (SLE) and rheumatoid arthritis (RA).
SLE is a multisystem, auto-immune, connective-tissue disorder with a broad range of clinical presentations, predominantly occurring in young women, usually in their third or fourth decade. It mainly affects the skin, joints, kidneys, lungs, nervous system, serous membranes and hematopoietic system (but every organ can be affected), and is characterized by a relapsing and remitting disease course [25]. The prevalence in Europe ranges from 25 to 91 per 100.000 persons, but is higher in specific ethnic groups [26]. Treatment depends strongly on the speci-fic organ involvement and might include non-steroidal anti-inflammatory drugs (NSAIDs), and immunosuppressive medication such as systemic corticosteroids, antimalarials, methotrexate, azathioprine, mycophenolate mophetil, cyclophos- phamide, and rituximab.
RA is a chronic inflammatory arthropathy associated with articular damage, at-tendant comorbidities, particularly in the cardiovascular system, and with incre-asing disability and socioeconomic decline [27]. It is an auto-immune disease of unknown cause, and has a prevalence of 1 per 100 persons in Caucasians. The disease usually occurs between 30 and 55 years of age and women are affected 2 to 3 times more often than men. The treatment aims to reduce disease activity to a minimum level as determined by the disease activity score, and start of therapy early in the disease course can prevent irreversible joint damage. Disease modi-fying anti-rheumatic drugs (DMARDs) such as methotrexate, leflunomide, sulp-hasalazine and hydroxychloroquine are the first line treatment, followed by anti-TNFα agents. When anti-TNFα agents fail to induce remission, newer biologics are available: anakinra (IL1 receptor antagonist), abatacept (CTLA4-Ig construct), rituximab (anti-CD20 antibodies) and tocilizumab (anti-IL6 receptor antibodies).
Rituximab is different from other biologics in that it does not block cytokines or costimulatory molecules, but leads to a depletion of CD20+ B-cells in the peripheral blood that persists for 6 to 9 months [28]. It is highly effective in sup-pressing the activity of RA, however, it does not seem to result in a large increase in infection risk, although theoretically one expects humoral immune responses to neo-antigens to be impaired during B-cell depletion [29, 30].
Apart from the immunosuppressive treatments, patients with auto-immune in-flammatory rheumatic diseases might be immunocompromised by the disease
18
Cha
pter
1
itself. SLE often is accompanied by lymphocytopenia. In RA patients, even if not treated with immunosuppressive medication, morbidity and mortality due to in-fections are increased [31].
Immunocompromised patients are at increased risk of contracting potentially life-threatening vaccine-preventable infections, and therefore vaccination seems indicated as an elegant and effective measure to reduce this infection risk. Un-fortunately, many controversies and uncertainties regarding vaccination in this population remain. First, the incidence of vaccine-preventable infections, among which influenza, in immunocompromised patients is largely unknown, since good studies addressing this are lacking. Second, investigations aiming to determine the efficacy of vaccination are based on surrogate parameters, mainly antibody responses, and not on clinical outcome. Also, for only a minority of the availa-ble vaccines correlates of protection have been determined, and if so, in healthy volunteers, but not for immunocompromised populations. Finally, harms of vac-cination are of utmost importance. Concerns regarding new onset or flares of auto-immune diseases triggered by vaccination have arisen after the publication of many case reports. In this context, the studies in this thesis have been designed and performed.
Aims and outline of the thesis
In the studies presented in this thesis we aimed to address the following aspects of influenza vaccination in patients with primary or secondary immunodeficien-cies:
• Efficacy, assessed by the investigation of humoral and cell-mediated immune responses following influenza vaccination
• Impact of immunosuppressive agents on efficacy• Impact of the timing of influenza vaccination following the treatment with
immunosuppressive agents on efficacy• Impact of booster influenza vaccination on efficacy• Safety In part 1 of the thesis the investigations regarding humoral (chapter 2) and cell-mediated (chapter 3) immune responses following influenza vaccination in pa-tients with humoral primary immunodeficiencies, in particular CVID, are analyzed.
In part 2 we focus on secondary immunodeficiencies. We performed studies on efficacy and safety of influenza vaccination in patients with auto-immune inflam-matory rheumatic diseases, especially SLE and RA. In chapter 4 cell-mediated influenza-specific immune responses in SLE patients were investigated, while in

19
Cha
pter
1
chapter 5 the value of a second, booster, influenza vaccination in patients with SLE was evaluated.
Next, studies addressing the influence of rituximab therapy on the efficacy of influenza vaccination in RA patients are described in chapter 6 and chapter 7: in the former with a focus on humoral responses and in the latter on cell-mediated immune responses.
European League Against Rheumatic Diseases (EULAR) recommendations on vaccination in patients with auto-immune inflammatory rheumatic diseases com-plete this thesis (part 3; chapter 9), preceded by the systematic literature review (chapter 8) that summarizes the current evidence on vaccination in patients with auto-immune inflammatory rheumatic diseases, among which articles presented in this thesis, and that served as the basis for the EULAR recommendations.
20
Cha
pter
1
Reference List
(1) Mandell GL, Bennett JE, Dolin R. Principles and practice of infectious diseases. Seventh ed.
Philadelphia: Churchill Livingstone Elsevier, 2010.
(2) Plotkin SA, Orenstein WA, Offit PA. Vaccines. Fifth ed. Philadelphia: Saunders Elsevier, 2008.
(3) Morgan AJ, Parker S. Translational mini-review series on vaccines: The Edward Jenner Museum
and the history of vaccination. Clin Exp Immunol 2007 Mar; 147(3):389-94.
(4) Gross CP, Sepkowitz KA. The myth of the medical breakthrough: smallpox, vaccination, and Jen-
ner reconsidered. Int J Infect Dis 1998 Jul; 3(1):54-60.
(5) Dinc G, Ulman YI. The introduction of variolation ‘A La Turca’ to the West by Lady Mary Montagu
and Turkey’s contribution to this. Vaccine 2007 May 22; 25(21):4261-5.
(6) Jenner E. An inquiry into the causes and effects of the Variolae Vaccinae, a disease discovered
in some of the western countries of England, particularly Gloucestershire, and known by the
name of Cow Pox. 1798.
(7) Hammarsten JF, Tattersall W, Hammarsten JE. Who discovered smallpox vaccination? Edward
Jenner or Benjamin Jesty? Trans Am Clin Climatol Assoc 1979; 90:44-55.
(8) Horton R. Myths in medicine. Jenner did not discover vaccination. BMJ 1995 Jan 7; 310(6971):62.
(9) Scheindlin S. The flu in retrospect: etiology and immunization. Mol Interv 2009 Dec; 9(6):284-90.
(10) Shope RE. Swine influenza: I. Experimental transmission and pathology. J Exp Med 1931 Jul 31;
54(3):349-59.
(11) Francis T, Jr. Transmission of influenza by a filterable virus. Science 1934 Nov 16; 80(2081):457-9.
(12) Francis T, Jr. A new type of virus from epidemic influenza. Science 1940 Nov 1; 92(2392):405-8.
(13) Members of the Commission on Influenza, Board for the Investigation and Control of Influenza
and Other Epidemic Diseases in the Army, Preventive Medicine Service, Office of the Surgeon
General, United States Army. A clinical evaluation of vaccination against influenza: preliminary
report. J Am Med Assoc 1944; 124(14):982-5.
(14) Lambert LC, Fauci AS. Influenza vaccines for the future. N Engl J Med 2010 Nov 18; 363(21):2036-
44.
(15) de Jong JC, Palache AM, Beyer WE, Rimmelzwaan GF, Boon AC, Osterhaus AD. Haemagglutina-
tion-inhibiting antibody to influenza virus. Dev Biol (Basel) 2003; 115:63-73.
(16) Brown LE, Kelso A. Prospects for an influenza vaccine that induces cross-protective cytotoxic T
lymphocytes. Immunol Cell Biol 2009 May; 87(4):300-8.
(17) McElhaney JE, Xie D, Hager WD, et al. T cell responses are better correlates of vaccine protec-
tion in the elderly. J Immunol 2006 May 15; 176(10):6333-9.
(18) Keynan Y, Card CM, Ball BT, Li Y, Plummer FA, Fowke KR. Cellular immune responses to recur-
ring influenza strains have limited boosting ability and limited cross-reactivity to other strains.
Clin Microbiol Infect 2010 Aug; 16(8):1179-86.
(19) Pereira LF, Sapina AM, Arroyo J, Vinuelas J, Bardaji RM, Prieto L. Prevalence of selective IgA
deficiency in Spain: more than we thought. Blood 1997 Jul 15; 90(2):893.
(20) European Society for Immunodeficiencies (ESID). Diagnostic criteria for PID. http://www esid
org/workingparty php?party=3&sub=2&id=73 2010
(21) Cunningham-Rundles C, Bodian C. Common variable immunodeficiency: clinical and immunolo-
gical features of 248 patients. Clin Immunol 1999 Jul; 92(1):34-48.
(22) Oksenhendler E, Gerard L, Fieschi C, et al. Infections in 252 patients with common variable im-

21
Cha
pter
1
munodeficiency. Clin Infect Dis 2008 May 15; 46(10):1547-54.
(23) Park MA, Li JT, Hagan JB, Maddox DE, Abraham RS. Common variable immunodeficiency: a new
look at an old disease. Lancet 2008 Aug 9; 372(9637):489-502.
(24) Goldacker S, Draeger R, Warnatz K, et al. Active vaccination in patients with common variable
immunodeficiency (CVID). Clin Immunol 2007 Sep; 124(3):294-303.
(25) D’Cruz DP, Khamashta MA, Hughes GR. Systemic lupus erythematosus. Lancet 2007 Feb 17;
369(9561):587-96.
(26) Danchenko N, Satia JA, Anthony MS. Epidemiology of systemic lupus erythematosus: a compa-
rison of worldwide disease burden. Lupus 2006; 15(5):308-18.
(27) McInnes IB, O’Dell JR. State-of-the-art: rheumatoid arthritis. Ann Rheum Dis 2010 Nov; 69(11):1898-
906.
(28) Onrust SV, Lamb HM, Balfour JA. Rituximab. Drugs 1999 Jul; 58(1):79-88.
(29) Furst DE. The risk of infections with biologic therapies for rheumatoid arthritis. Semin Arthritis
Rheum 2010 Apr; 39(5):327-46.
(30) Salliot C, Finckh A, Katchamart W, et al. Indirect comparisons of the efficacy of biological antir-
heumatic agents in rheumatoid arthritis in patients with an inadequate response to conventional
disease-modifying antirheumatic drugs or to an anti-tumour necrosis factor agent: a meta-ana-
lysis. Ann Rheum Dis 2010 Nov 19.
(31) Doran MF, Crowson CS, Pond GR, O’Fallon WM, Gabriel SE. Frequency of infection in patients
with rheumatoid arthritis compared with controls: a population-based study. Arthritis Rheum
2002 Sep; 46(9):2287-93.

PART 1I n f l u e n z a vaccination in patients w i t h h u m o r a l p r i m a r y i m m u n o -deficiency

CHAPT
ER2Patients with h u m o r a lp r i m a r yi m m u n o -d e f i c i e n c yd o n o t d e v e l o pp r o t e c t i v eanti-influenzaa n t i b o d ytiters after vaccinat ionwith trivalents u b u n i ti n f l u e n z av a c c i n e
S. van Assen
A. Holvast
D.S.C. Telgt
C.A. Benne
A. de Haan
J. Westra
C.G.M. Kallenberg
M. Bijl
Clinical Immunology 2010 Aug; 136 (2): 228-235
26
Cha
pter
2
AbsTrAcTIntroduction Yearly influenza vaccination is recommended for patients with humoral primary immunodeficiency (hPID). However, humoral respon-ses following vaccination can be expected to be reduced in these patients.
Methods The efficacy of influenza vaccination in patients with hPID was as-sessed in 26 patients with hPID and 26 matched healthy controls (HC) using hemagglutination inhibition assay.
results Following vaccination, geometric mean titers (GMTs) significantly increased for all influenza strains in the HC group, but only for A/H1N1 in the patient group. Fold-increase in anti-influenza titer and seroprotection rates were lower for patients than for HC for A/H3N2 and A/H1N1, leading to postvaccination titer ≥40 in only 29% and 83% vs. 77% and 100%, respectively. Previous vaccination in patients and treatment with IVIg did not result in a higher rate of postvaccination titer ≥40.
conclusion Patients with hPID show hardly any humoral response following influenza vaccination.

27
Cha
pter
2
InTroducTIonInfluenza occurs in seasonal outbreaks of varying extent nearly every winter, and is associated with increased morbidity and mortality. Particularly young children, elderly, patients with chronic illnesses (e.g. cardiac, pulmonary or renal disease, diabetes mellitus) and immunodeficient patients are at increased risk for deve-loping complicated influenza [1]. Influenza-related death is mainly due to cardiac events or influenza pneumonia, with or without secondary bacterial infection [2]. Patients with humoral primary immunodeficiencies (hPID; i.e. IgA deficiency (IgAD), common variable immunodeficiency (CVID), X-linked agammaglobuline-mia (XLA), autosomal recessive agammaglobulinemia, IgG-subclass deficiency (IgGSD), and specific antibody response deficiency), frequently experience recur-rent bacterial infections of the upper and lower respiratory tract. Although these patients seem to be at risk for complicated influenza, the prevalence, morbidity and mortality of influenza in patients with hPID are unknown.
Because of the immunocompromised state and the risk of potentially life threa-tening secondary bacterial respiratory tract infections, influenza vaccination is recommended to patients with hPID [3]. On the other hand, humoral responses to vaccination can be expected to be reduced in these patients; absence of humoral responses to vaccination is even part of the diagnostic criteria for several hPID (http://www.esid.org). Nevertheless, peripheral blood mononuclear cells from a subset of CVID patients have been shown to be capable of producing antibodies in response to influenza antigen in vitro, this in contrast to mononuclear cells from X-linked agammaglobulinemia patients [4]. In vivo, antibody responses to polysaccharide and polypeptide vaccines have been demonstrated in respectively 18% and 23% of CVID patients [5]. Data on in vivo responses following influenza vac-cination in patients with hPID are lacking.
To determine if influenza vaccination results in protective antibody titers against influenza in patients with hPID, we investigated the humoral immune response following vaccination with trivalent subunit influenza vaccine.
MeThods
Patients and healthy controls
All patients had to fulfil the European Society for Immunodeficiencies (ESID) clas-sification criteria for an hPID (http://www.esid.org). Patients and healthy controls (HC) were excluded in case of: (i) no informed consent, (ii) age under 18, (iii) cur-rent infection that needed to be treated with antibiotics, (iv) malignancy, (v) preg-nancy, (vi) known allergy to or former severe reaction following vaccination with trivalent influenza subunit vaccine.

28
Cha
pter
2
Vaccine
Trivalent influenza subunit vaccine for the season 2006-2007 (Influvac®; Solvay Pharmaceuticals, Weesp, The Netherlands) was used, containing isolated hemag-glutinin and neuramidase proteins derived from egg-cultured virus. The following strains were included in the vaccine: A/Wisconsin/67/2005 (H3N2)-like strain (A/Hiroshima/52/2005 IVR-142 reass.); A/New Caledonia/20/99 (H1N1)-like strain (A/New Caledonia/20/99 IVR-116 reass.); and B/Malaysia/2506/2004-like strain (B/Malaysia/2506/2004).
Procedures
Patients and HC received the influenza vaccine intramuscularly between Octo-ber 2006 and January 2007, which was before the onset of the seasonal influ-enza outbreak in The Netherlands [6]. Immediately before and 21 or 28 days ± 3 days after vaccination blood samples were taken. The latter variation depended on the interval between the intravenous immunoglobulins (IVIg) administration that patients received; 21 days was chosen when the interval between consecu-tive IVIg (Nanogam®, Sanquin, Amsterdam, The Netherlands or Kiovig®, Baxter B.V., Utrecht, The Netherlands) administration was 2 weeks, and 28 days when the interval between consecutive IVIg administrations was 3 or 4 weeks or when patients did not receive IVIg, and in HC. Patients treated with IVIg were vaccina-ted 7 days before the administration of IVIg to distinguish possible side effects of vaccination from those of IVIg administration, and to diminish the influence of immunoglobulin substitution during the distribution phase on the outcome of the anti-influenza antibody titers. Measurements of complete blood count, lymp-hocyte subsets (CD19+ B-cells, CD4+ T-cells, CD8+ T-cells, and CD16/56+ NK-cells) and immunoglobulins (IgG, IgA, IgM) were performed according to standard pro-cedures. Information on previous influenza vaccination was obtained from all par-ticipants, and adverse effects occurring in the first 7 days postvaccination were recorded. Adverse effects were classified into local (itching, pain, erythema, and induration at the site of vaccination), systemic (fever, tiredness, sweating, myal-gia, chills, headache, arthralgia, diarrhoea, flu-like symptoms), and the need to use antipyretic drugs.
The study was approved by the ethics committees of both participating centers.
hemagglutination Inhibition Assay and eLIsA
For the detection of influenza antibodies the hemagglutination inhibition assay (HIA) was used. HIAs were performed with guinea pig erythrocytes and using cell grown influenza viruses as antigens, following standard procedures [7] with

29
Cha
pter
2
slight modifications as described elsewhere [8]. Sera were tested for antibodies against all three vaccine strains. The following parameters for efficacy of vac-cination were evaluated: geometric mean titer (GMT); seroconversion, defined as a ≥4-fold titer rise to a postvaccination titer of ≥40; seroprotection, defined as a rise in titer to ≥40 [9]. Hemagglutination inhibition (HI)-titers ≥40 are generally considered to be protective, while a median titer of 28 is estimated to protect 50% of healthy adult vaccinees [10].
To estimate the contribution of anti-influenza antibodies in the IVIg preparations to the levels of anti-influenza antibodies in the patient treated with IVIg, in sam-ples of three batches of IVIg (Nanogam®, Sanquin, Amsterdam, The Netherlands) the levels of anti-influenza antibodies to A/H3N2, A/H1N1 and the B-strain were determined using HIA (procedure described above) and in-house ELISA. For the latter, in short, microtiter plates were coated with 1 μg/ml subunit of A/H3N2 or A/H1N1 and subsequently incubated with IVIg samples. Detection of influenza-specific antibodies was done with mouse-anti-human IgG-HRP and mouse-anti-human IgM-HRP (Southern Biotech, Birmingham, USA) respectively, followed by color reaction with 3’3’5’5’tetramythylbenzidin (TMB) and H2 O2. Absorbance was read at 450-575 nm in an Emax microplate reader and concentration of antibodies was calculated by SOFTmax PRO software (Molecular Devices, Sunnyvale, USA) according to IgG- or IgM-standard curves included on each ELISA plate. The HIA and ELISA were performed on a 1:10 dilution of the IVIg preparations (in PBS) re-sulting in a concentration of 10 g/l, which was comparable with the mean of the total IgG-concentration in patients at the moment of vaccination (11 g/l).
statistical analysis
Data were analysed using SPSS 16.0 for Windows (SPSS Inc.). Wilcoxon signed rank test, Mann-Whitney U test, Chi square test, Fisher’s exact test, and Spear-man’s rank correlation coefficient were used where appropriate. To obtain a po-wer of 90% with an significance level α of 0.05, and considering a drop-out rate of 10%, 26 patients and HC needed to be included, when the expected proportion reaching a postvaccination HI-titer ≥40 was 30% for hPID patients, and 75% for HC.
resuLTs
Patient characteristics
Twenty-six patients from the university medical centers in Groningen (UMCG, n=21) and Nijmegen, The Netherlands (UMC St.Radboud, n=5), and 42 HC, recrui-ted from UMCG-health care workers and their family members, gave informed consent. Twenty-six HC were successfully matched on group level to the partici-
30
Cha
pter
2
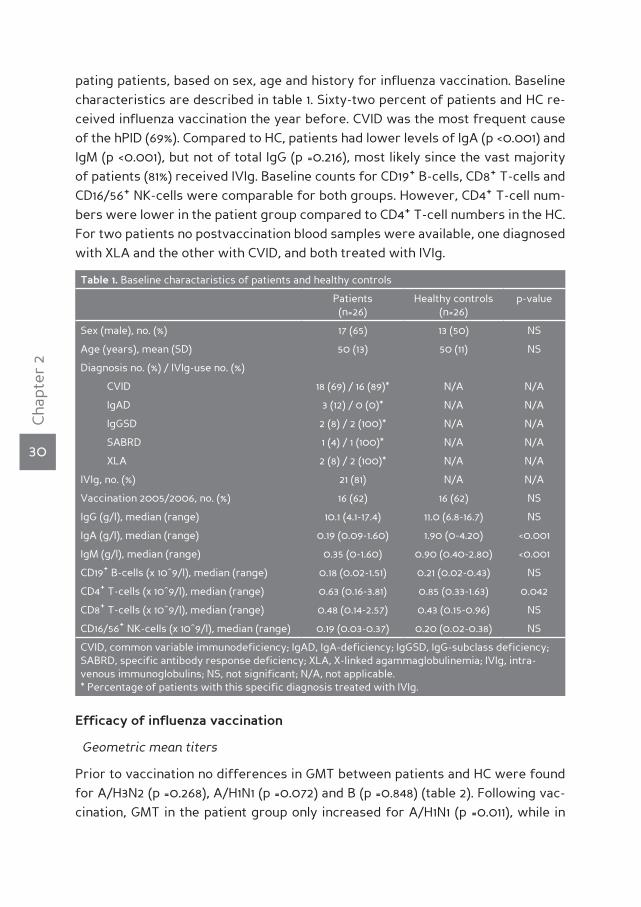
pating patients, based on sex, age and history for influenza vaccination. Baseline characteristics are described in table 1. Sixty-two percent of patients and HC re-ceived influenza vaccination the year before. CVID was the most frequent cause of the hPID (69%). Compared to HC, patients had lower levels of IgA (p <0.001) and IgM (p <0.001), but not of total IgG (p =0.216), most likely since the vast majority of patients (81%) received IVIg. Baseline counts for CD19+ B-cells, CD8+ T-cells and CD16/56+ NK-cells were comparable for both groups. However, CD4+ T-cell num-bers were lower in the patient group compared to CD4+ T-cell numbers in the HC. For two patients no postvaccination blood samples were available, one diagnosed with XLA and the other with CVID, and both treated with IVIg.
Table 1. Baseline charactaristics of patients and healthy controls
Patients (n=26)
Healthy controls (n=26)
p-value
Sex (male), no. (%) 17 (65) 13 (50) NS
Age (years), mean (SD) 50 (13) 50 (11) NS
Diagnosis no. (%) / IVIg-use no. (%)
CVID 18 (69) / 16 (89)* N/A N/A
IgAD 3 (12) / 0 (0)* N/A N/A
IgGSD 2 (8) / 2 (100)* N/A N/A
SABRD 1 (4) / 1 (100)* N/A N/A
XLA 2 (8) / 2 (100)* N/A N/A
IVIg, no. (%) 21 (81) N/A N/A
Vaccination 2005/2006, no. (%) 16 (62) 16 (62) NS
IgG (g/l), median (range) 10.1 (4.1-17.4) 11.0 (6.8-16.7) NS
IgA (g/l), median (range) 0.19 (0.09-1.60) 1.90 (0-4.20) <0.001
IgM (g/l), median (range) 0.35 (0-1.60) 0.90 (0.40-2.80) <0.001
CD19+ B-cells (x 10^9/l), median (range) 0.18 (0.02-1.51) 0.21 (0.02-0.43) NS
CD4+ T-cells (x 10^9/l), median (range) 0.63 (0.16-3.81) 0.85 (0.33-1.63) 0.042
CD8+ T-cells (x 10^9/l), median (range) 0.48 (0.14-2.57) 0.43 (0.15-0.96) NS
CD16/56+ NK-cells (x 10^9/l), median (range) 0.19 (0.03-0.37) 0.20 (0.02-0.38) NS
CVID, common variable immunodeficiency; IgAD, IgA-deficiency; IgGSD, IgG-subclass deficiency; SABRD, specific antibody response deficiency; XLA, X-linked agammaglobulinemia; IVIg, intra-venous immunoglobulins; NS, not significant; N/A, not applicable. * Percentage of patients with this specific diagnosis treated with IVIg.
efficacy of influenza vaccination
Geometric mean titers
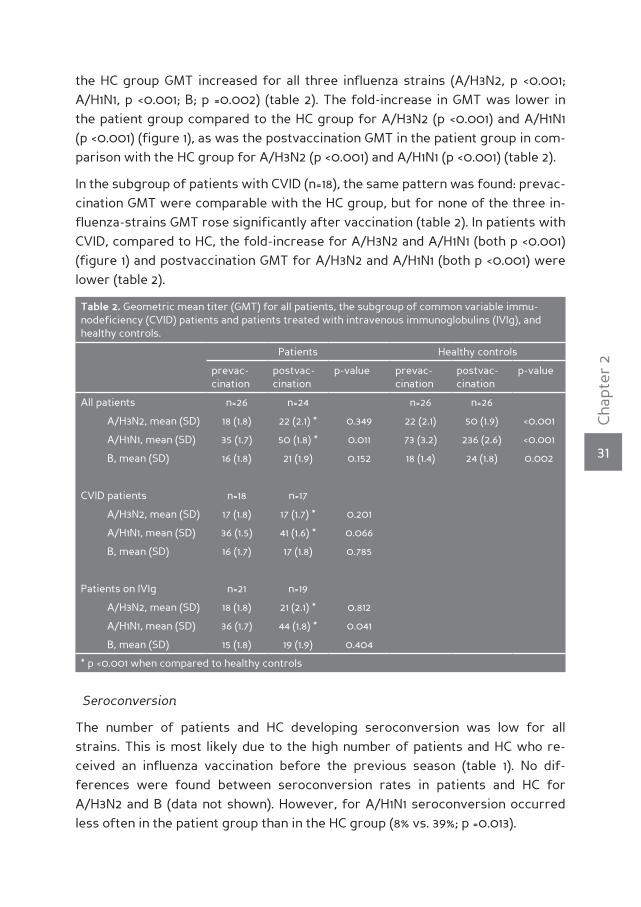
Prior to vaccination no differences in GMT between patients and HC were found for A/H3N2 (p =0.268), A/H1N1 (p =0.072) and B (p =0.848) (table 2). Following vac-cination, GMT in the patient group only increased for A/H1N1 (p =0.011), while in
31
Cha
pter
2
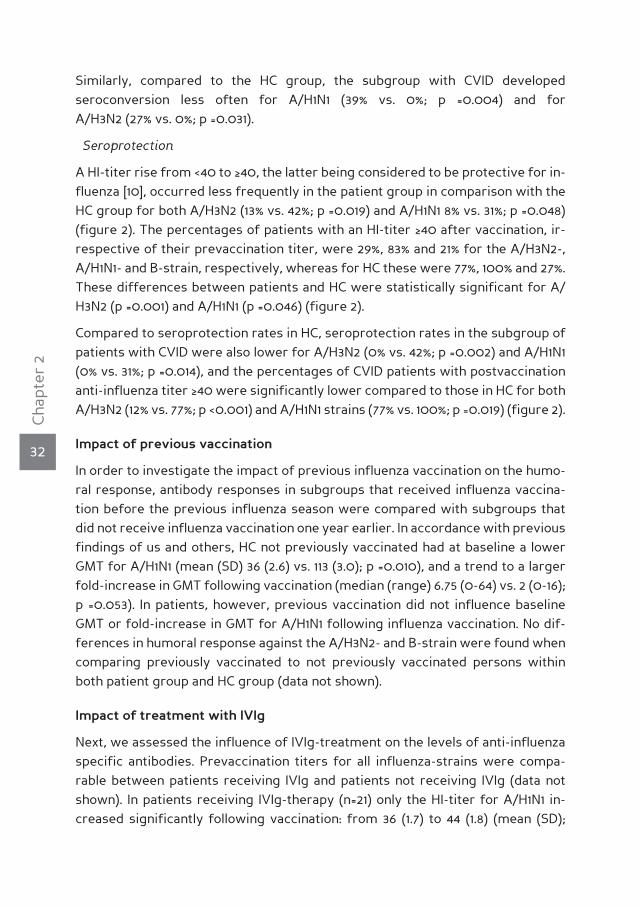
the HC group GMT increased for all three influenza strains (A/H3N2, p <0.001; A/H1N1, p <0.001; B; p =0.002) (table 2). The fold-increase in GMT was lower in the patient group compared to the HC group for A/H3N2 (p <0.001) and A/H1N1 (p <0.001) (figure 1), as was the postvaccination GMT in the patient group in com-parison with the HC group for A/H3N2 (p <0.001) and A/H1N1 (p <0.001) (table 2).
In the subgroup of patients with CVID (n=18), the same pattern was found: prevac-cination GMT were comparable with the HC group, but for none of the three in-fluenza-strains GMT rose significantly after vaccination (table 2). In patients with CVID, compared to HC, the fold-increase for A/H3N2 and A/H1N1 (both p <0.001) (figure 1) and postvaccination GMT for A/H3N2 and A/H1N1 (both p <0.001) were lower (table 2).
Table 2. Geometric mean titer (GMT) for all patients, the subgroup of common variable immu-nodeficiency (CVID) patients and patients treated with intravenous immunoglobulins (IVIg), and healthy controls.
Patients Healthy controls
prevac-cination
postvac-cination
p-value prevac-cination
postvac-cination
p-value
All patients n=26 n=24 n=26 n=26
A/H3N2, mean (SD) 18 (1.8) 22 (2.1) * 0.349 22 (2.1) 50 (1.9) <0.001
A/H1N1, mean (SD) 35 (1.7) 50 (1.8) * 0.011 73 (3.2) 236 (2.6) <0.001
B, mean (SD) 16 (1.8) 21 (1.9) 0.152 18 (1.4) 24 (1.8) 0.002
CVID patients n=18 n=17
A/H3N2, mean (SD) 17 (1.8) 17 (1.7) * 0.201
A/H1N1, mean (SD) 36 (1.5) 41 (1.6) * 0.066
B, mean (SD) 16 (1.7) 17 (1.8) 0.785
Patients on IVIg n=21 n=19
A/H3N2, mean (SD) 18 (1.8) 21 (2.1) * 0.812
A/H1N1, mean (SD) 36 (1.7) 44 (1.8) * 0.041
B, mean (SD) 15 (1.8) 19 (1.9) 0.404
* p <0.001 when compared to healthy controls
Seroconversion
The number of patients and HC developing seroconversion was low for all strains. This is most likely due to the high number of patients and HC who re-ceived an influenza vaccination before the previous season (table 1). No dif-ferences were found between seroconversion rates in patients and HC for A/H3N2 and B (data not shown). However, for A/H1N1 seroconversion occurred less often in the patient group than in the HC group (8% vs. 39%; p =0.013).
32
Cha
pter
2
Similarly, compared to the HC group, the subgroup with CVID developed seroconversion less often for A/H1N1 (39% vs. 0%; p =0.004) and for A/H3N2 (27% vs. 0%; p =0.031).
Seroprotection
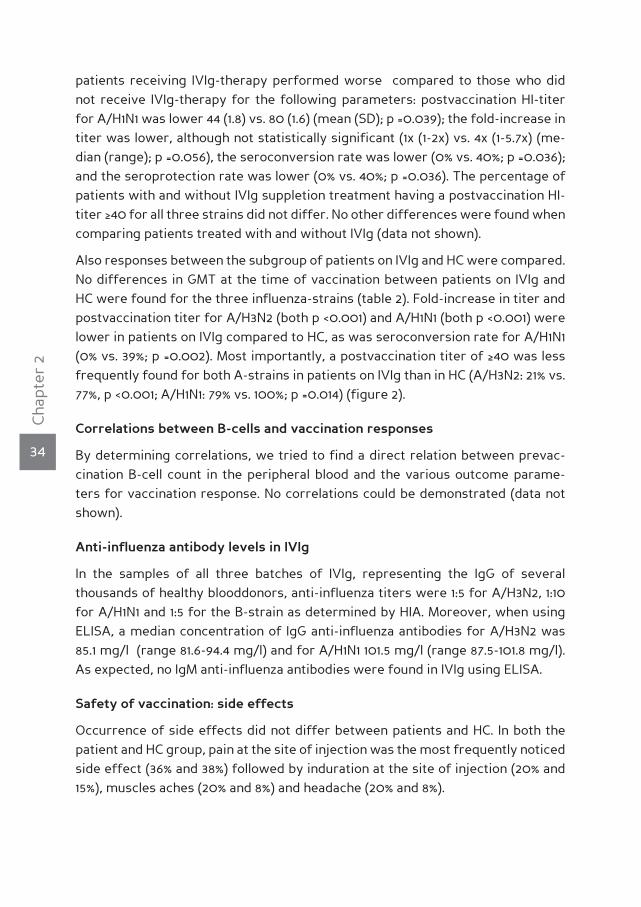
A HI-titer rise from <40 to ≥40, the latter being considered to be protective for in-fluenza [10], occurred less frequently in the patient group in comparison with the HC group for both A/H3N2 (13% vs. 42%; p =0.019) and A/H1N1 8% vs. 31%; p =0.048) (figure 2). The percentages of patients with an HI-titer ≥40 after vaccination, ir-respective of their prevaccination titer, were 29%, 83% and 21% for the A/H3N2-, A/H1N1- and B-strain, respectively, whereas for HC these were 77%, 100% and 27%. These differences between patients and HC were statistically significant for A/H3N2 (p =0.001) and A/H1N1 (p =0.046) (figure 2).
Compared to seroprotection rates in HC, seroprotection rates in the subgroup of patients with CVID were also lower for A/H3N2 (0% vs. 42%; p =0.002) and A/H1N1 (0% vs. 31%; p =0.014), and the percentages of CVID patients with postvaccination anti-influenza titer ≥40 were significantly lower compared to those in HC for both A/H3N2 (12% vs. 77%; p <0.001) and A/H1N1 strains (77% vs. 100%; p =0.019) (figure 2).
Impact of previous vaccination
In order to investigate the impact of previous influenza vaccination on the humo-ral response, antibody responses in subgroups that received influenza vaccina-tion before the previous influenza season were compared with subgroups that did not receive influenza vaccination one year earlier. In accordance with previous findings of us and others, HC not previously vaccinated had at baseline a lower GMT for A/H1N1 (mean (SD) 36 (2.6) vs. 113 (3.0); p =0.010), and a trend to a larger fold-increase in GMT following vaccination (median (range) 6.75 (0-64) vs. 2 (0-16); p =0.053). In patients, however, previous vaccination did not influence baseline GMT or fold-increase in GMT for A/H1N1 following influenza vaccination. No dif-ferences in humoral response against the A/H3N2- and B-strain were found when comparing previously vaccinated to not previously vaccinated persons within both patient group and HC group (data not shown).
Impact of treatment with IVIg
Next, we assessed the influence of IVIg-treatment on the levels of anti-influenza specific antibodies. Prevaccination titers for all influenza-strains were compa-rable between patients receiving IVIg and patients not receiving IVIg (data not shown). In patients receiving IVIg-therapy (n=21) only the HI-titer for A/H1N1 in-creased significantly following vaccination: from 36 (1.7) to 44 (1.8) (mean (SD);

33
Cha
pter
2
Figure 1. Fold-increase in anti-influenza hemagglutination inhibition titer following influenza vaccina-tion for A/H3N2 (A), A/H1N1 (B) and B (C) in all hPID patients (All, n=24), common variable immunode-ficiency patients (CVID, n=17) and patients treated with intravenous immunoglobulins (IVIg, n=19), and healthy controls (HC, n=26). * p ≤0,001 when compared to HC
p =0.041). In patients not receiving IVIg, no significant increase was found follo-wing vaccination: 35 (1.9) to 80 (1.6) (mean (SD); p =0.102). It should be noted, howe-ver, that the number of patients without IVIg-therapy was low (n=5). In contrast,
34
Cha
pter
2
patients receiving IVIg-therapy performed worse compared to those who did not receive IVIg-therapy for the following parameters: postvaccination HI-titer for A/H1N1 was lower 44 (1.8) vs. 80 (1.6) (mean (SD); p =0.039); the fold-increase in titer was lower, although not statistically significant (1x (1-2x) vs. 4x (1-5.7x) (me-dian (range); p =0.056), the seroconversion rate was lower (0% vs. 40%; p =0.036); and the seroprotection rate was lower (0% vs. 40%; p =0.036). The percentage of patients with and without IVIg suppletion treatment having a postvaccination HI-titer ≥40 for all three strains did not differ. No other differences were found when comparing patients treated with and without IVIg (data not shown).
Also responses between the subgroup of patients on IVIg and HC were compared. No differences in GMT at the time of vaccination between patients on IVIg and HC were found for the three influenza-strains (table 2). Fold-increase in titer and postvaccination titer for A/H3N2 (both p <0.001) and A/H1N1 (both p <0.001) were lower in patients on IVIg compared to HC, as was seroconversion rate for A/H1N1 (0% vs. 39%; p =0.002). Most importantly, a postvaccination titer of ≥40 was less frequently found for both A-strains in patients on IVIg than in HC (A/H3N2: 21% vs. 77%, p <0.001; A/H1N1: 79% vs. 100%; p =0.014) (figure 2).
correlations between b-cells and vaccination responses
By determining correlations, we tried to find a direct relation between prevac-cination B-cell count in the peripheral blood and the various outcome parame-ters for vaccination response. No correlations could be demonstrated (data not shown).
Anti-influenza antibody levels in IVIg
In the samples of all three batches of IVIg, representing the IgG of several thousands of healthy blooddonors, anti-influenza titers were 1:5 for A/H3N2, 1:10 for A/H1N1 and 1:5 for the B-strain as determined by HIA. Moreover, when using ELISA, a median concentration of IgG anti-influenza antibodies for A/H3N2 was 85.1 mg/l (range 81.6-94.4 mg/l) and for A/H1N1 101.5 mg/l (range 87.5-101.8 mg/l). As expected, no IgM anti-influenza antibodies were found in IVIg using ELISA.
safety of vaccination: side effects
Occurrence of side effects did not differ between patients and HC. In both the patient and HC group, pain at the site of injection was the most frequently noticed side effect (36% and 38%) followed by induration at the site of injection (20% and 15%), muscles aches (20% and 8%) and headache (20% and 8%).

35
Cha
pter
2
Figure 2. Percentage of patients and healthy controls with a titer ≥40 before vaccination (black bars) and postvaccination (white bars) for A/H3N2 (A), A/H1N1 (B) and B (C) in all hPID patients (All, n=24), common variable immunodeficiency patients (CVID, n=17) and patients treated with intravenous im-munoglobulins (IVIg, n=19), and healthy controls (HC, n=26). * p <0,05 for seroprotection (HI-titer rise from <40 before vaccination to ≥40 after vaccination), compared to HC

36
Cha
pter
2
dIscussIonThe current study is, to our knowledge, the first study evaluating humoral re-sponses following influenza vaccination in patients with hPID. We show that in these patients the humoral response to all three influenza-strains in the vaccine is severely hampered for almost all of the outcome measures. This holds true in particular for influenza A/H3N2 and A/H1N1, the widest circulating and most vi-rulent of the influenza-strains. Most alarming is that patients often did not reach protective anti-influenza HI-titers; 71% and 17% of the studied patients did not have a titer ≥40 of for influenza A/H3N2 and A/H1N1 after vaccination, respectively. For the subgroup of patients with CVID (n=18) the numbers are even worse: 88% and 23%. In comparison, HC responded adequately with 23% and 0% not reaching pro-tective postvaccination titers for A/H3N2 and A/H1N1, respectively.
Previous vaccination in healthy individuals generally results in higher prevacci-nation titers. Following subsequent influenza vaccination postvaccination titers might be higher, similar or even somewhat lower, compared to postvaccination titers in previously unvaccinated HC [11, 12]. Our results show that in previously vaccinated patients with hPID neither a significant higher prevaccination titer, nor higher postvaccination titer, compared to not previously vaccinated patients, are present. Therefore, most likely yearly influenza vaccination in patients with hPID does not result in higher levels of protective anti-influenza titers. This might be expected, since in patients with hPID the decreased number and/or function of memory B-cells is caused by an intrinsic defect instead of a reversible cause underlying the hampered response. While patients with X-linked agammaglobu-linemia have absent or severely reduced numbers of circulating B-cells, a consi-derable number of CVID patients have normal numbers of B-cells , but reduced counts of class-switched memory B-cells [13].
Many patients with hPID (81% in the current study) receive treatment with IVIg to reduce frequency and severity of respiratory infections [14]. IVIg is reserved for those patients with recurrent infections, for whom protection against influenza might be considered to be of great importance. When comparing patients treated with IVIg to patients without IVIg-therapy, patients with IVIg-therapy showed a reduced response to influenza vaccination. This probably reflects the more se-vere immunodeficiency in these patients. Moreover, pre- and postvaccination ti-ters were not protective in a large part of the patients treated with IVIg, despite treatment with IVIg every 2 to 4 weeks. Although anti-influenza antibodies have been detected in IVIg preparations [15, 16], as would be expected since 10-20% of the general population contracts influenza every year, our finding demonstrates that passive immunization with IVIg is not protective for influenza.

37
Cha
pter
2
We found large differences between HI-titers for the different influenza-strains. The relatively high titers for A/H1N1 might be caused by the fact that the A/H1N1-component in the vaccine did not change since 2001, while the A/H3N2 and B-strains were new in the influenza vaccine for the season 2006-2007 [17]. There-fore, more anti-influenza A/H1N1 antibodies might be present in the general population, as is reflected by the high level of anti-influenza A/H1N1 antibodies in the prevaccination samples of the HC, and therefore probably also in IVIg. Testing of the levels of anti-influenza antibodies in the IVIg preparations using HIA did in-deed show higher titers of anti-A/H1N1 antibodies compared to anti-A/H3N2 anti-bodies. When using ELISA, the higher concentrations of anti-A/H1N1 compared to anti-A/H3N2 antibodies could be confirmed. However, it should be noted that the HI assay has not been validated for testing influenza-specific antibodies in IVIg preparations. Responses to the influenza B-strain were low in both patients and HC, but this is a common phenomenon when HIA is used to measure anti-influenza antibodies directed against influenza B-strains [18].
As active immunization with influenza subunit vaccine and “passive immuniza-tion” with IVIg does not result in protective levels of anti-influenza antibodies in patients with hPID, other strategies against influenza are warranted. Reducing exposure to influenza by vaccination for influenza of household contacts and of health care workers of patients at high risk for severe complications from in-fluenza is recommended by ACIP [19], as there is evidence that this strategy can reduce transmission of influenza [20, 21]. Therefore household contacts of pa-tients with hPID should be vaccinated for influenza if no contra-indications exist. Passive immunization with serum from donors with high levels of anti-influenza antibodies shortly before the start of and during the influenza season might be another option to protect these patients, but this needs to be further explored. Finally, prophylactic antiviral treatment with adamantanes and neuraminidase inhibitors reduces the chances of contracting influenza [22], but should be used cautiously, since virtually all A/H3N2 are resistant to adamantanes, while resis-tance to the neuraminidase inhibitor oseltamivir is highly prevalent in A/H1N1. To prevent further resistance, the use of these medications should preferentially be reserved for treatment or post-exposure prophylaxis only and not for prop-hylaxis in patients with hPID [23]. Finally, the cellular immune responses following influenza vaccination should be evaluated in patients with a hPID, since cellular immunity has been shown to play a role in the prevention of clinically manifest influenza in elderly [24].
In conclusion, patients with hPID show severely impaired humoral response fol-lowing vaccination with inactivated trivalent subunit influenza vaccine. Moreover, passive immunization with IVIg is insufficient for the prevention of influenza.
38
Cha
pter
2
reference List
(1) Smith NM, Bresee JS, Shay DK, Uyeki TM, Cox NJ, Strikas RA. Prevention and Control of Influ-
enza: recommendations of the Advisory Committee on Immunization Practices (ACIP). MMWR
Recomm Rep 2006 Jul 28; 55(RR-10):1-42.
(2) Treanor JJ. Mandell, Douglas and Bennett’s principles and practice of infectious diseases. 6th
ed. Philadelphia: Elsevier; 2005
(3) Smith NM, Bresee JS, Shay DK, Uyeki TM, Cox NJ, Strikas RA. Prevention and Control of Influ-
enza: recommendations of the Advisory Committee on Immunization Practices (ACIP). MMWR
Recomm Rep 2006 Jul 28; 55(RR-10):1-42.
(4) Yarchoan R, Schneider HS, Wray BB, Nelson DL. Specific anti-influenza virus antibody produc-
tion in vitro by lymphocytes from a subset of patients with hypogammaglobulinemia. J Clin
Invest 1983 Jun; 71(6):1720-7.
(5) Goldacker S, Draeger R, Warnatz K, et al. Active vaccination in patients with common variable
immunodeficiency (CVID). Clin Immunol 2007 Sep; 124(3):294-303.
(6) de Jong JC, Rimmelzwaan GF, Donker GA, Meijer A, Fouchier RA, Osterhaus AD. [The 2006/’07
influenza season in the Netherlands and the vaccine composition for the 2007/’08 season]. Ned
Tijdschr Geneeskd 2007 Sep 29; 151(39):2158-65.
(7) Harmon MW. Influenza viruses. In: Lennette, ed. Laboratory diagnosis of viral infections, 2nd ed.
New York: Marcel Dekker, Inc, 2004:515-34.
(8) de Jong JC, Ronde-Verloop FM, Veenendaal-van Herk TM, Weijers TF, Bijlsma K, Osterhaus AD.
Antigenic heterogeneity within influenza A (H3N2) virus strains. Bull World Health Organ 1988;
66(1):47-55.
(9) European agency for the evaluation of medicinal products (EMEA). Note for guidance on harmo-
nisation of requirements for influenza vaccines. London, UK; 1997
(10) de Jong JC, Palache AM, Beyer WE, Rimmelzwaan GF, Boon AC, Osterhaus AD. Haemagglutina-
tion-inhibiting antibody to influenza virus. Dev Biol (Basel) 2003; 115:63-73.
(11) Beyer WE, Palache AM, Sprenger MJ, et al. Effects of repeated annual influenza vaccination on
vaccine sero-response in young and elderly adults. Vaccine 1996 Oct; 14(14):1331-9.
(12) Nabeshima S, Kashiwagi K, Murata M, Kanamoto Y, Furusyo N, Hayashi J. Antibody response to
influenza vaccine in adults vaccinated with identical vaccine strains in consecutive years. J Med
Virol 2007 Mar; 79(3):320-5.
(13) Park MA, Li JT, Hagan JB, Maddox DE, Abraham RS. Common variable immunodeficiency: a new
look at an old disease. Lancet 2008 Aug 9; 372(9637):489-502.
(14) Park MA, Li JT, Hagan JB, Maddox DE, Abraham RS. Common variable immunodeficiency: a new
look at an old disease. Lancet 2008 Aug 9; 372(9637):489-502.
(15) Scheiermann N, Kuwert EK. [Studies on human immunoglobulin preparations: I. Viral antibody
profiles (author’s transl)]. Med Klin 1979 May 25; 74(21):820-4.
(16) Weeke-Luttmann M, Schmidt I, Fenyves A, von Wangenheim G, Fischer L. [Neutralizing virus
antibodies in human immunoglobulins for intravenous use]. Immun Infekt 1984 Aug; 12(4):201-7.
(17) Rimmelzwaan GF, de Jong JC, Donker GA, Meijer A, Fouchier RA, Osterhaus AD. [The 2005-
2006 influenza season in the Netherlands and the vaccine composition for the 2006-2007 sea-
son]. Ned Tijdschr Geneeskd 2006 Oct 7; 150(40):2209-14.
(18) Kendal AP, Cate TR. Increased sensitivity and reduced specificity of hemagglutination inhibition

39
Cha
pter
2
tests with ether-treated influenza B/Singapore/222/79. J Clin Microbiol 1983 Oct; 18(4):930-4.
(19) Smith NM, Bresee JS, Shay DK, Uyeki TM, Cox NJ, Strikas RA. Prevention and Control of Influ-
enza: recommendations of the Advisory Committee on Immunization Practices (ACIP). MMWR
Recomm Rep 2006 Jul 28; 55(RR-10):1-42.
(20) Esposito S, Marchisio P, Cavagna R, et al. Effectiveness of influenza vaccination of children
with recurrent respiratory tract infections in reducing respiratory-related morbidity within the
households. Vaccine 2003 Jul 4; 21(23):3162-8.
(21) Ghendon YZ, Kaira AN, Elshina GA. The effect of mass influenza immunization in children on the
morbidity of the unvaccinated elderly. Epidemiol Infect 2006 Feb; 134(1):71-8.
(22) Jefferson T, Demicheli V, Rivetti D, Jones M, Di Pietrantonj C, Rivetti A. Antivirals for influenza
in healthy adults: systematic review. Lancet 2006 Jan 28; 367(9507):303-13.
(23) Poland GA, Jacobson RM, Ovsyannikova IG. Influenza Virus Resistance to Antiviral Agents: A
Plea for Rational Use. Clin Infect Dis 2009 Mar 26.
(24) McElhaney JE, Xie D, Hager WD, et al. T cell responses are better correlates of vaccine protec-
tion in the elderly. J Immunol 2006 May 15; 176(10):6333-9.


CHAPT
ER3Cell-mediatedi m m u n eresponses to inact ivatedt r i v a l e n ti n f l u e n z avaccinat ionare decreasedin patients w i t hc o m m o n v a r i a b l ei m m u n o -d e f i c i e n c y
S. van Assen
A. de Haan
A. Holvast
G. Horst
L. Gorter
J. Westra
C.G.M. Kallenberg
D.S.C. Telgt
A.M. Palache
K.M. Giezeman
M. Bijl
Clinical Immunology In press
42
Cha
pter
3
AbsTrAcTIntroduction Influenza-specific cell-mediated immune (CMI) responses can protect for influenza, but may be decreased in common variable immuno-deficiency (CVID) patients since defects in CMI responses have been de-monstrated in CVID patients.
Methods CMI responses were evaluated in 15 CVID patients and 15 mat-ched healthy controls (HC) by determining frequencies of interferon (IFN)γ-producing PBMC, and frequencies of IFNγ-, interleukin (IL)-2- and tumor necrosis factor (TNF)α-producing CD4+ and CD8+ T-cells before and after influenza vaccination using IFNγ enzyme-linked immunospot (IFNγ-ELISpot) and flow cytometry. Humoral responses were determined using hemagglu-tination inhibition assay.
results In CVID patients the number of spotforming PBMC in the IFNγ-ELISpot did not increase following influenza vaccination, in contrast to HC. In flow cytometry, the frequencies of IFNγ-producing T-cells decreased in CVID patients after influenza vaccination, while in HC the frequencies of IFNγ-production increased.
conclusion CMI responses following influenza vaccination are hampered in CVID patients compared to HC. Additional protective strategies against influenza other than vaccination are warranted.

43
Cha
pter
3
InTroducTIonCommon variable immunodeficiency (CVID) is the primary immunodeficiency most frequently encountered in clinical practice. CVID is primarily characterised by a defective humoral immune response. Recurrent sinopulmonary, and less fre-quently, gastrointestinal infections are the most common clinical manifestations, but CVID patients are also at increased risk for the development of auto-immune diseases, granulomatous disease and hematological and solid malignancies [1].
Because of the immunocompromised state of CVID patients, influenza vaccina-tion is recommended [2]. However, compared to healthy individuals vaccination with polysaccharide and protein vaccines is less efficacious [3, 4]. We demonstra-ted hampered humoral responses following influenza vaccination in patients with CVID, resulting in lower seroprotection rates, defined as an anti-influenza titer as determined by haemagglutinin inhibition assay (HIA) ≥40) in these patients com-pared to healthy controls (HC) [5]
Not only humoral [6], but also cell-mediated immune (CMI) responses following influenza vaccination have been shown to correlate with protection for clinical in-fluenza infection [7]. Although CVID is classified as a humoral immunodeficiency, decreased cellular immune function has been demonstrated in a considerable proportion of CVID patients, consisting of numerical and/or functional defects involving T-cells, natural killer (NK)-cells, dendritic cells (DC), macrophages and monocytes [8-10]. Data regarding the CMI response following influenza vaccinati-on in patients with CVID are lacking. However, in view of their hampered humoral responses, cellular responses should be considered as well when discussing the usefulness of influenza vaccination in these patients.
In this study we investigated the influenza-specific CMI response in patients with CVID before, and 7 and 21-28 days after vaccination with trivalent subunit influen-za vaccine in comparison with that in healthy controls. CMI response on vaccinati-on was determined using interferon (IFN)γ enzyme-linked immunospot (ELISpot) and flow cytometry with intracellular cytokine staining (ICS) for IFNγ, interleukin (IL)-2 and tumor necrosis factor (TNF)α. Finally, a relationship between CMI re-sponses and humoral immune responses was studied.
MATerIAls And MeThods
Patients and healthy controls
Patients were included at the University Medical Center Groningen (UMCG) and the University Medical Center St. Radboud Nijmegen, both in The Netherlands, and had to fulfil the European Society for Immunodeficiencies classification crite-ria for CVID (http://www.esid.org). HC were recruited from the UMCG personnel.

44
Cha
pter
3
Patients and HC were excluded in case of: (i) no informed consent, (ii) age under 18, (iii) current infection that needed treatment with antibiotics, (iv) malignancy, (v) pregnancy, (vi) known allergy to or former severe reaction following vaccina-tion with trivalent influenza subunit vaccine.
Vaccine
Trivalent influenza subunit vaccine for the season 2006-2007 (Influvac®; Solvay Pharmaceuticals, Weesp, The Netherlands) was used, containing isolated hemag-glutinin and neuramidase proteins derived from egg-cultured virus. The vac-cine contained the following strains: A/Wisconsin/67/2005 (A/H3N2)-like strain (A/Hiroshima/52/2005 IVR-142 reass.); A/New Caledonia/20/99 (A/H1N1)-like strain (A/New Caledonia/20/99 IVR-116 reass.); and B/Malaysia/2506/2004-like strain (B/Malaysia/2506/2004).
Procedures
Patients and HC received the influenza vaccine intramuscularly between October 2006 and January 2007, which was before the onset of the seasonal influenza outbreak in The Netherlands. Immediately before, and 7 and 21 or 28 days after vaccination blood samples were taken. The latter variation depended on the inter-val between the intravenous immunoglobulins (IVIg) administration that patients received, to prevent interference of the administration of IVIg with the results of the humoral and cellular immune responses. Twenty-one days was chosen when the interval between consecutive IVIg administrations was 2 weeks, and 28 days when the interval between consecutive IVIg administrations was 3 or 4 weeks or when patients did not receive IVIg, and in HC. Moreover, patients treated with IVIg were vaccinated 7 days before the administration of IVIg to distinguish possible side effects of vaccination from those of IVIg administration, and also to dimi-nish the influence of IVIg on the outcome of the cellular immune responses on day 7. Measurements of complete blood count, lymphocyte subsets (CD4+ T-cells, CD8+ T-cells, CD16/56+ NK-cells and CD19+ B-cells) were performed according to standard procedures. Information on previous influenza vaccination was obtained from all participants.
The study was approved by the ethics committees of both participating centers.
cell-mediated immunity assays
Processing of PBMC and the procedures for the IFNγ-ELISpot assay and flow cy-tometry were as described earlier [11]. Therefore, these procedures will only be described in short.

45
Cha
pter
3
Isolation, storage and thawing of PBMC
PBMC were isolated from BD Vacutainer® CPT™ Cell Preparation Tubes containing 0.1 M sodium citrate anticoagulant and blood separation media composed of a thixotropic polyester gel and a FICOLL™ HYPAQUE™ solution (BD, Franklin Lakes, NJ, USA), according to the instructions of the producer. PBMC were stored in li-quid nitrogen until use in RPMI 1640 (Cambrex BioScience, Verviers, Belgium) sup-plemented with 10% human pool serum, 50 µg/ml of gentamicin (Gibco, Paisley, UK) and 10% dimethylsulfoxide. Prevaccination and postvaccination samples from a patient with CVID and a matched control subject were simultaneously thawed and batch-processed.
Influenza antigens used in assays of cell-mediated responses
PBMC were stimulated with β-propiolactone inactivated whole virus (WIV) of A/New Caledonia/20/99 (IVR-116 reass.; A/H1N1) and A/Hiroshima/52/2005 (IVR-142 reass.; A/H3N2).
IFNγ-ELISpot assay
Immobilon-P membrane plates (Millipore,Billerica,MA,USA) were coated with an-ti-human IFNγ (Mabtech, Nacka Strand, Sweden). 2 x 105 PBMC were added per well and incubated for 8 hours in culture medium (CM), RPMI 1640 (Cambrex Bi-oScience, Verviers, Belgium) supplemented with 10% fetal calf serum, 50 µg/ml of gentamicin (Gibco, Paisley, UK) with WIV A/H1N1 (1 µg/ml) and WIV A/H3N2 (1 µg/ml). Concanavalin A stimulation served as a positive control, a negative con-trol consisted of PBMC in CM alone. Stimulation tests were performed in dupli-cate. Biotinylated anti-human IFNγ, streptavidin-alkaline phosphatase and BCIP/NBT-plus substrate (all Mabtech) were used in order to visualise IFNγ-producing PBMC. Spots were counted using an automated reader (automated ELISpot video-analysis system, Sanquin, Amsterdam, The Netherlands).
Flow cytometry
For stimulations, 1.0–1.5 x 106 PBMC were cultured in CM for 18 hours. Staphylo-coccal enterotoxin B (SEB; Sigma-Aldrich, St. Louis, MO) at 5 µg/ml was used as a positive control. WIV A/H1N1 and WIV A/H3N2 were used at final concentrations of 1 µg of total viral protein/ml. Negative controls were not stimulated (CM only). Pa-cific Blue and Pacific Orange dyes (Invitrogen, Carlsbad, CA), in a different com-bination for each stimulus, were used to enable fluorescent T-cell bar coding. The following monoclonal antibodies were used: allophycocyanin (APC)-Cy7-conjuga-ted anti-CD3, peridinin chlorophyll A protein–conjugated anti-CD8 (Becton Dickin-son Pharmingen, San Diego, CA, USA), phycoerythrin–Cy7 (PE-Cy7)–conjugated anti-CD69 (Biolegend, San Diego,CA, USA), PE–conjugated anti-IFNγ, APC-conju-

46
Cha
pter
3
gated anti-TNFα, and Fluorescein isothiocyanate-conjugated anti–IL-2 (eBiosci-ence, Hatfield, UK) Analysis was performed on a LSR II flow cytometer (Becton Dickinson).
The WinList software package (Verity Software House, Topsham, ME) was used. Percentages of antigen-specific cells were expressed as the percentage of CD69+ cytokine-producing CD4+ or CD8+ T-cells within the total CD4+ or CD8+ T-cell po-pulation. Samples were excluded if the proportion of viable cells after thawing was <85%, and if the proportion of IFNγ- or TNFα-producing CD4+ or CD8+ T-cells was <2.00% upon stimulation with SEB (positive control). For IL-2 no cut-off could be determined since the proportion of cytokine-producing CD4+ and CD8+ T-cells upon stimulation with SEB was generally low.
Antibody response to influenza
For the detection of influenza antibodies the HIA was used. HIA were perfor-med with guinea pig erythrocytes and using cell grown influenza viruses as an-tigens, following standard procedures [12] with slight modifications as described elsewhere [13]. Sera were tested for antibodies against A/New Caledonia/20/99 (A/H1N1) and A/Wisconsin/67/2005 (A/H3N2).
statistical analysis
Since none of the variables were normally distributed, data are presented as me-dian (range). Data were analysed using PASW Statistics 18 (SPSS Inc., Chicago, IL, USA). To determine differences in baseline characteristics between the matched CVID patients and HC, the levels of spotforming cells with IFNγ-ELISpot and the frequencies of cytokine-producing cells with flow cytometry, the Mann-Whitney U test was used. Friedman’s two-way analysis of variance by ranks was used to analyse the presence of differences in CMI responses at the three time points. All cytokine frequencies reported are after background subtraction of the frequen-cy of the identically gated population of cells from the same sample stimulated without antigen. For correlations, Spearman’s rank correlation coefficients were used. A two sided p-value <0.05 was considered statistically significant. A power calculation could not be performed since no data were available with regard to what difference in CMI responses could be expected and would be clinically rele-vant.
resulTs
Patient characteristics
Fifteen eligible CVID patients were included and successfully matched for sex, age
47
Cha
pter
3
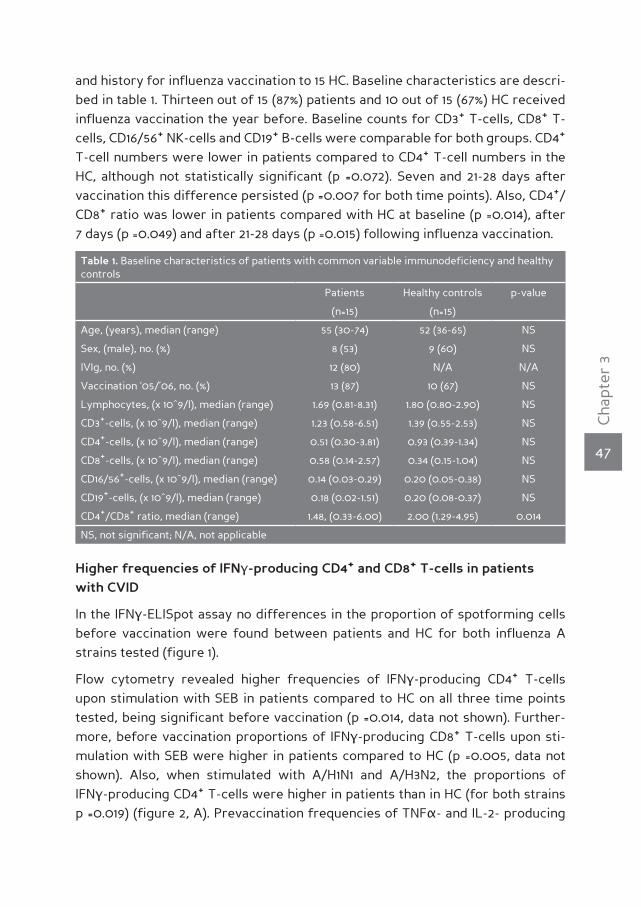
and history for influenza vaccination to 15 HC. Baseline characteristics are descri-bed in table 1. Thirteen out of 15 (87%) patients and 10 out of 15 (67%) HC received influenza vaccination the year before. Baseline counts for CD3+ T-cells, CD8+ T-cells, CD16/56+ NK-cells and CD19+ B-cells were comparable for both groups. CD4+ T-cell numbers were lower in patients compared to CD4+ T-cell numbers in the HC, although not statistically significant (p =0.072). Seven and 21-28 days after vaccination this difference persisted (p =0.007 for both time points). Also, CD4+/CD8+ ratio was lower in patients compared with HC at baseline (p =0.014), after 7 days (p =0.049) and after 21-28 days (p =0.015) following influenza vaccination.
Table 1. Baseline characteristics of patients with common variable immunodeficiency and healthy controls
Patients Healthy controls p-value
(n=15) (n=15)
Age, (years), median (range) 55 (30-74) 52 (36-65) NS
Sex, (male), no. (%) 8 (53) 9 (60) NS
IVIg, no. (%) 12 (80) N/A N/A
Vaccination ‘05/’06, no. (%) 13 (87) 10 (67) NS
Lymphocytes, (x 10^9/l), median (range) 1.69 (0.81-8.31) 1.80 (0.80-2.90) NS
CD3+-cells, (x 10^9/l), median (range) 1.23 (0.58-6.51) 1.39 (0.55-2.53) NS
CD4+-cells, (x 10^9/l), median (range) 0.51 (0.30-3.81) 0.93 (0.39-1.34) NS
CD8+-cells, (x 10^9/l), median (range) 0.58 (0.14-2.57) 0.34 (0.15-1.04) NS
CD16/56+-cells, (x 10^9/l), median (range) 0.14 (0.03-0.29) 0.20 (0.05-0.38) NS
CD19+-cells, (x 10^9/l), median (range) 0.18 (0.02-1.51) 0.20 (0.08-0.37) NS
CD4+/CD8+ ratio, median (range) 1.48, (0.33-6.00) 2.00 (1.29-4.95) 0.014
NS, not significant; N/A, not applicable
higher frequencies of IFnγ-producing cd4+ and cd8+ T-cells in patients with cVId
In the IFNγ-ELISpot assay no differences in the proportion of spotforming cells before vaccination were found between patients and HC for both influenza A strains tested (figure 1).
Flow cytometry revealed higher frequencies of IFNγ-producing CD4+ T-cells upon stimulation with SEB in patients compared to HC on all three time points tested, being significant before vaccination (p =0.014, data not shown). Further-more, before vaccination proportions of IFNγ-producing CD8+ T-cells upon sti-mulation with SEB were higher in patients compared to HC (p =0.005, data not shown). Also, when stimulated with A/H1N1 and A/H3N2, the proportions of IFNγ-producing CD4+ T-cells were higher in patients than in HC (for both strains p =0.019) (figure 2, A). Prevaccination frequencies of TNFα- and IL-2- producing

48
Cha
pter
3
CD4+ and CD8+ T-cells did not differ except for a lower frequency of TNFα-producing CD8+ T-cells upon stimulation with SEB (p =0.022, data not shown) and a higher frequency of IL-2-producing CD8+ T-cells upon stimulation with A/H1N1 (p =0.015, data not shown) in patients compared to HC.
lower cell-mediated responses to A/h1n1 and A/h3n2 following influenza vaccination in patients with cVId
In patients with CVID the IFNγ-ELISpot assay revealed no differences in the pro-portion of spotforming cells between time points 0, 7 and 21-28 days upon stimu-lation with A/H1N1 (p =0.202) or A/H3N2 (p =0.905), whereas for HC significant changes in spotforming cells between the three time points were present upon stimulation with A/H1N1 (p =0.020) and A/H3N2 (p <0.001), representing a CMI res-ponse in HC following influenza vaccination (figure 1).
When using flow cytometry, in CVID patients a decrease was found in the fre-quencies of IFNγ-producing CD4+ T-cells upon stimulation with SEB when com-paring time points 0, 7 and 21-28 days (p =0.035, data not shown). Upon stimu-lation with A/H1N1 and A/H3N2 this was also shown, although the decrease was not statistically significant for the latter (p =0.026 and p =0.060, respectively) (fi-gure 2, A). On the contrary and as expected, in HC the frequencies of A/H1N1- and A/H3N2-specific IFNγ+CD4+ T-cells increased after influenza vaccination (p =0.028 and p =0.016, respectively) (figure 2, A).
Regarding CD8+ T-cells, in CVID patients the frequencies of A/H1N1- and A/H3N2- specific IFNγ+CD8+ T-cells did not differ between the three time points (p =0.909
Figure 1. Influenza-specific IFNγ-production by PBMC before, and 7 and 21-28 days following influ-enza vaccination in healthy controls and patients with CVID, as determined by IFNγ-ELISpot assay. Bars represent medians, whiskers represent interquartile range. P-value as calculated using Friedman’s Two-Way analysis of variance by ranks.
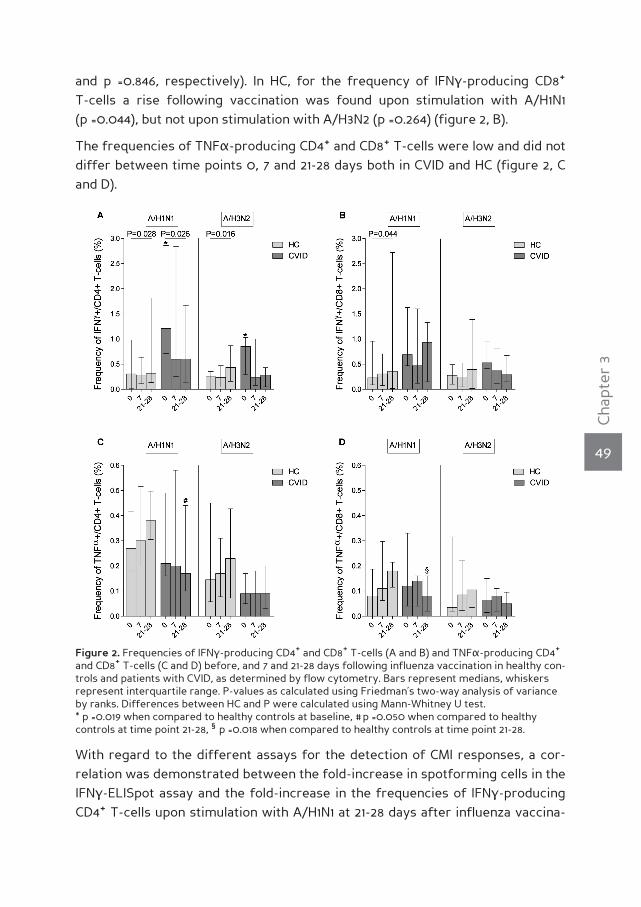
49
Cha
pter
3
and p =0.846, respectively). In HC, for the frequency of IFNγ-producing CD8+ T-cells a rise following vaccination was found upon stimulation with A/H1N1 (p =0.044), but not upon stimulation with A/H3N2 (p =0.264) (figure 2, B).
The frequencies of TNFα-producing CD4+ and CD8+ T-cells were low and did not differ between time points 0, 7 and 21-28 days both in CVID and HC (figure 2, C and D).
With regard to the different assays for the detection of CMI responses, a cor-relation was demonstrated between the fold-increase in spotforming cells in the IFNγ-ELISpot assay and the fold-increase in the frequencies of IFNγ-producing CD4+ T-cells upon stimulation with A/H1N1 at 21-28 days after influenza vaccina-
Figure 2. Frequencies of IFNγ-producing CD4+ and CD8+ T-cells (A and B) and TNFα-producing CD4+ and CD8+ T-cells (C and D) before, and 7 and 21-28 days following influenza vaccination in healthy con-trols and patients with CVID, as determined by flow cytometry. Bars represent medians, whiskers represent interquartile range. P-values as calculated using Friedman’s two-way analysis of variance by ranks. Differences between HC and P were calculated using Mann-Whitney U test. * p =0.019 when compared to healthy controls at baseline, # p =0.050 when compared to healthy controls at time point 21-28, § p =0.018 when compared to healthy controls at time point 21-28.

50
Cha
pter
3
tion for HC (r =0.829, p =0.042) and for patients at 7 days (r =0.750, p =0.052) and at 21-28 days (r =0.667, p =0.071). For A/H3N2 only in patients a correlation was found between the fold-increase in spotforming cells in the IFNγ-ELISpot assay and the fold-increase in the frequencies of IFNγ-producing CD4+ T-cells at 7 days following influenza vaccination (r =0.714; p =0.071).
lower anti-influenza antibody titers as determined by hIA in patients with cVId
The humoral response following influenza vaccination in 18 patients with CVID from the original cohort of 26 patients with a humoral primary immunodeficiency has been described elsewhere [5]. Summarizing, prevaccination geometric mean titers (GMTs) in patients with CVID and HC were comparable. However, for none of the influenza strains GMTs rose significantly after vaccination in patients with CVID. Patients with CVID had, for both A/H1N1 and A/H3N2, lower fold-increase in GMT (both p <0.001), postvaccination GMT (both p <0.001), seroconversion rates (p =0.004 and p =0.031), seroprotection rates (p =0.014 and p =0.002) and propor-tion of patients with protective postvaccination anti-influenza hemagglutination inhibition-titer of ≥40 (p =0.019 and p <0.001), compared to HC.
Inverse correlation between baseline cMI responses to A/h1n1 and A/h3n2 and fold-increase in influenza-specific cMI responses following influenza vaccination
As earlier described by others [14], we found an inverse correlation between influenza-specific CMI responses at baseline and the fold-increase in influenza-specific CMI responses following influenza vaccination. For patients as well as for HC the fold-increase in spotforming cells in the IFNγ-ELISpot assay was in-versely correlated with the prevaccination proportion of spotforming cells upon stimulation with A/H1N1 at 7 days (for CVID r =-0.5152; p =0.130: for HC r =-0.4615; p =0.110) and 21-28 days (for CVID r =-0.8364; p =0.022: for HC r =-0.7636; p =0.009), and upon stimulation with A/H3N2 at 7 (for CVID r =-0.4667; p =0.180: for HC r =-0.8077; p <0.001) and 21-28 days (for CVID r =-0.8364 (p =0.022); for HC r =-0.6545 (p =0.034) following influenza vaccination. Although these correlations were not always statistically significant, these results all point in the same direction.
no correlation between influenza-specific cell-mediated and humoral im-mune response
Next, in order to assess a possible relationship between the influenza-specific CMI responses and influenza-specific antibody responses following influenza vac-cination, we computed correlations between the fold-increase in anti-influenza

51
Cha
pter
3
GMT and the fold-increase in spotforming cells in the IFNγ-ELISpot assay as well as the fold-increase in IFNγ-producing CD4+ and CD8+ T-cells by flow cytometry upon stimulation with A/H1N1 and A/H3N2 at 7 and 21-28 days following influenza vaccination. No correlations were found (data not shown).
dIscussIonTo our knowledge, this study is the first to investigate the CMI response follo-wing influenza vaccination in patients with CVID using two different assays: IFNγ-ELISpot assay and flow cytometry with ICS. Earlier we showed that humoral re-sponses following influenza vaccination are severely hampered in patients with CVID [5].
Following influenza vaccination the patterns of the influenza-specific CMI respon-ses were different in patients with CVID and HC. In HC the proportion of IFNγ-producing cells increased, as determined by ELISpot assay as well as by flow cy-tometry analysis. This held in particular true for CD4+ T-cells, as expected, since subunit material is presented by antigen presenting cells to CD4+ T-cells in the context of MHC-class II molecules. Only a small part is presented to CD8+ T-cells, in the context of MHC-class I molecules by cross-presentation. This might explain the increase in the frequency of IFNγ-producing CD8+ T-cells in HC following in-fluenza vaccination. In contrast, in CVID patients IFNγ-producing cells did not in-crease in frequency following influenza vaccination in the ELISpot assay and even a decrease in the proportion of A/H1N1 and A/H3N2-specific IFNγ-producing CD4+ T-cells could be demonstrated using flow cytometry. These findings suggest that influenza-specific CMI responses are impaired in patients with CVID and fits with studies demonstrating a decreased CMI response after vaccination with recall and neo-antigens in these patients [15, 16].
Several causes may underlie the difference in influenza-specific CMI response in CVID and HC. First, defects in antigen-presenting cells have been described in CVID: DC are decreased in number [17-19], have reduced expression of surface molecules associated with maturity [20], express markedly reduced levels of the costimulatory molecules that are critical for T-cell stimulation [21], have defective TLR9 activation [22] and are impaired in differentiation (in part due to the defici-ency of circulating natural IgG antibodies) [23]. Monocytes of patients with CVID produce less IL-6 and TNFα in response to vaccination with 23-valent polysaccha-ride pneumococcal vaccine [24].
Second, T-cell abnormalities may explain the absence of an increase in CMI res-ponse following influenza vaccination in CVID: reduced numbers of (naïve) CD4+ T-cells and CD8+ T-cells, decrease in regulatory T-cells, reduced thymic output,

52
Cha
pter
3
increased T-cell activation, altered cytokine production (among which elevated levels of IFNγ-producing CD4+ and CD8+ T-cells, as we also found at baseline using FASC/ICS), disruption of CD4+ and CD8+ T-cell receptor repertoires, increased CD4+ and CD8+ T-cell turnover and increased levels of spontaneous apoptosis have all been found [8, 25-29]. Finally, 80% of the included CVID patients were treated with IVIg, which can inhibit T-cell proliferation and cytokine-production, although the exact mechanism remains to be elucidated [30]. IVIg-treatment in patients with CVID does not seem to play a role in their restriction of T-cell re-pertoires [8].
Our findings of a decrease in CD4+ T-cell count following vaccination and a reduc-tion in the proportion of IFNγ-producing CD4+ and CD8+ T-cells upon stimulation with SEB, A/H1N1 and A/H3N2 might be caused by activation-induced apoptosis of CD4+ and CD8+ T-cells, triggered by influenza vaccination or upon their reactiva-tion ex vivo by influenza virus. Influenza virus, but also its major surface protein hemagglutinin, the major constituent of the trivalent subunit influenza vaccine used in this study, can induce activation-induced apoptosis [31, 32]. Also increased pre-activation of T-cells in vivo , as has been demonstrated in CVID patients, make these cells more prone to apoptosis upon their ex vivo culture, thus reducing fre-quencies of influenza-specific T-cells. Furthermore, brefeldin A, used in the flow cytometry assay to inhibit secretion of cytokines and allowing their intracellular detection by monoclonal antibodies, has been shown to provoke apoptosis in hu-man tumor cells. A similar effect may have been induced in the (apoptosis-prone) T-cells, possibly leading to their accelerated apoptosis. This could also explain decreases in IFNγ-production in the flow cytometry assay, but not in the ELISpot assay. Moreover, this may not only be due to the use of brefeldin A but also due to the more extensive handling of the PBMC samples in the flow cytometry assay, as compared to the ELISpot assay.
We could demonstrate correlations between the fold-increase in spotforming PBMC by ELISpot and the fold-increase in the frequencies of INFγ-producing CD4+ T-cells by flow cytometry following influenza vaccination, but not for the individu-al parameters of CMI responses at the same time points. This latter finding most likely depends on the fact that both tests address different aspects of cell-me-diated immunity and therefore also differ in sensitivity [33]. Also an inverse cor-relation between CMI response at baseline and the fold-increase as determined by IFNγ-ELISpot was found. This has previously been demonstrated by others and is suggested to result from the interactions of memory CD4+ T-cells, CD56dim NK-cells and DC, where low memory CD4+ T-cells lead to better DC-function [14].
Although CD4+ T-cell help to B-cells is necessary for adequate antibody responses,

53
Cha
pter
3
B-cells of CVID patients have been shown to have low B-cell activation in res-ponse to stimuli from T-cells [34]. This might be an explanation for the absence of a relationship between humoral immune responses and CMI responses in the CVID patients in the current study. However, this can not explain the absence of a correlation in HC.
A limitation of this study is the low number of patients and HC included. This pre-vented us from analysing the influence of the clinical classification of the CVID patients, of IVIG-treatment and of previous vaccination on the CMI response.
Although influenza vaccination does not lead to the development of protective levels of anti-influenza antibodies [5] and no increase in CMI response using IFNγ- ELISpot and flow cytometry in CVID patients in this study, other parameters of cell-mediated immunity that we did not address (e.g. granzyme B-production by CD8+ T-cells) might lead to protection from influenza in these patients. Of note, correlates of protection from influenza with regard to CMI responses are lac-king. Therefore, influenza vaccination should be offered to patients with CVID, but additional measures for CVID patients to prevent influenza infection are also warranted, such as vaccination for influenza of household contacts and of health care workers of CVID patients [2, 35, 36]. Although prophylactic antiviral treatment with adamantanes and neuraminidase inhibitors reduces the chances of contrac-ting influenza [37], these should preferentially be reserved for treatment or post-exposure prophylaxis only since virtually all A/H3N2 are resistant to adamantanes, while resistance to the neuraminidase inhibitor oseltamivir is highly prevalent in A/H1N1. Passive immunization of CVID patients with serum from donors with high levels of anti-influenza antibodies shortly before the start of and during the influ-enza season might be another option to protect these patients, but this needs to be further explored.
conclusIonIn patients with CVID humoral immune responses as well as CMI responses fol-lowing influenza vaccination are hampered. Additional measures to influenza vac-cination are warranted to prevent patients with CVID from contracting (compli-cated) influenza.

54
Cha
pter
3
reference list
(1) Park MA, Li JT, Hagan JB, Maddox DE, Abraham RS. Common variable immunodeficiency: a new
look at an old disease. Lancet 2008 Aug 9; 372(9637):489-502.
(2) Smith NM, Bresee JS, Shay DK, Uyeki TM, Cox NJ, Strikas RA. Prevention and Control of Influ-
enza: recommendations of the Advisory Committee on Immunization Practices (ACIP). MMWR
Recomm Rep 2006 Jul 28; 55(RR-10):1-42.
(3) Goldacker S, Draeger R, Warnatz K, et al. Active vaccination in patients with common variable
immunodeficiency (CVID). Clin Immunol 2007 Sep; 124(3):294-303.
(4) Rezaei N, Aghamohammadi A, Siadat SD, et al. Serum bactericidal antibody responses to me-
ningococcal polysaccharide vaccination as a basis for clinical classification of common variable
immunodeficiency. Clin Vaccine Immunol 2008 Apr; 15(4):607-11.
(5) van Assen S, Holvast A, Telgt DS, et al. Patients with humoral primary immunodeficiency do not
develop protective anti-influenza antibody titers after vaccination with trivalent subunit influ-
enza vaccine. Clin Immunol 2010 Aug; 136(2):228-35.
(6) de Jong JC, Palache AM, Beyer WE, Rimmelzwaan GF, Boon AC, Osterhaus AD. Haemagglutina-
tion-inhibiting antibody to influenza virus. Dev Biol (Basel) 2003; 115:63-73.
(7) McElhaney JE, Xie D, Hager WD, et al. T cell responses are better correlates of vaccine protec-
tion in the elderly. J Immunol 2006 May 15; 176(10):6333-9.
(8) Giovannetti A, Pierdominici M, Mazzetta F, et al. Unravelling the complexity of T cell abnormali-
ties in common variable immunodeficiency. J Immunol 2007 Mar 15; 178(6):3932-43.
(9) Bayry J, Hermine O, Webster DA, Levy Y, Kaveri SV. Common variable immunodeficiency: the
immune system in chaos. Trends Mol Med 2005 Aug; 11(8):370-6.
(10) Cunningham-Rundles C, Bodian C. Common variable immunodeficiency: clinical and immunolo-
gical features of 248 patients. Clin Immunol 1999 Jul; 92(1):34-48.
(11) Holvast A, van Assen S, de Haan A, et al. Studies of cell-mediated immune responses to influenza
vaccination in systemic lupus erythematosus. Arthritis Rheum 2009 Aug; 60(8):2438-47.
(12) Harmon MW. Influenza viruses. In: Lennette, ed. Laboratory diagnosis of viral infections, 2nd ed.
New York: Marcel Dekker, Inc. 2004:515-34.
(13) de Jong JC, Ronde-Verloop FM, Veenendaal-van Herk TM, Weijers TF, Bijlsma K, Osterhaus AD.
Antigenic heterogeneity within influenza A (H3N2) virus strains. Bull World Health Organ 1988;
66(1):47-55.
(14) He XS, Holmes TH, Sasaki S, et al. Baseline levels of influenza-specific CD4 memory T-cells af-
fect T-cell responses to influenza vaccines. PLoS One 2008; 3(7):e2574.
(15) Kondratenko I, Amlot PL, Webster AD, Farrant J. Lack of specific antibody response in common
variable immunodeficiency (CVID) associated with failure in production of antigen-specific me-
mory T cells. MRC Immunodeficiency Group. Clin Exp Immunol 1997 Apr; 108(1):9-13.
(16) Stagg AJ, Funauchi M, Knight SC, Webster AD, Farrant J. Failure in antigen responses by T
cells from patients with common variable immunodeficiency (CVID). Clin Exp Immunol 1994 Apr;
96(1):48-53.
(17) Martinez-Pomar N, Raga S, Ferrer J, et al. Elevated serum interleukin (IL)-12p40 levels in com-
mon variable immunodeficiency disease and decreased peripheral blood dendritic cells: analy-
sis of IL-12p40 and interferon-gamma gene. Clin Exp Immunol 2006 May; 144(2):233-8.
(18) Viallard JF, Camou F, Andre M, et al. Altered dendritic cell distribution in patients with common

55
Cha
pter
3
variable immunodeficiency. Arthritis Res Ther 2005; 7(5):R1052-R1055.
(19) Yong PF, Workman S, Wahid F, Exley A, Webster AD, Ibrahim MA. Selective deficits in blood den-
dritic cell subsets in common variable immunodeficiency and X-linked agammaglobulinaemia
but not specific polysaccharide antibody deficiency. Clin Immunol 2008 Apr; 127(1):34-42.
(20) Scott-Taylor TH, Green MR, Raeiszadeh M, Workman S, Webster AD. Defective maturation of
dendritic cells in common variable immunodeficiency. Clin Exp Immunol 2006 Sep; 145(3):420-7.
(21) Bayry J, Lacroix-Desmazes S, Kazatchkine MD, et al. Common variable immunodeficiency is as-
sociated with defective functions of dendritic cells. Blood 2004 Oct 15; 104(8):2441-3.
(22) Cunningham-Rundles C, Radigan L, Knight AK, Zhang L, Bauer L, Nakazawa A. TLR9 activation is
defective in common variable immune deficiency. J Immunol 2006 Feb 1; 176(3):1978-87.
(23) Elluru SR, Vani J, Delignat S, et al. Modulation of human dendritic cell maturation and function by
natural IgG antibodies. Autoimmun Rev 2008 Jun; 7(6):487-90.
(24) Hong R, Agrawal S, Gollapudi S, Gupta S. Impaired pneumovax-23-induced monocyte-derived
cytokine production in patients with common variable immunodeficiency. J Clin Immunol 2010
May; 30(3):435-41.
(25) Di Renzo M, Zhou Z, George I, Becker K, Cunningham-Rundles C. Enhanced apoptosis of T cells
in common variable immunodeficiency (CVID): role of defective CD28 co-stimulation. Clin Exp
Immunol 2000 Jun; 120(3):503-11.
(26) Horn J, Manguiat A, Berglund LJ, et al. Decrease in phenotypic regulatory T cells in subsets of
patients with common variable immunodeficiency. Clin Exp Immunol 2009 Jun; 156(3):446-54.
(27) Melo KM, Carvalho KI, Bruno FR, et al. A decreased frequency of regulatory T cells in patients
with common variable immunodeficiency. PLoS One 2009; 4(7):e6269.
(28) Mouillot G, Carmagnat M, Gerard L, et al. B-cell and T-cell phenotypes in CVID patients correlate
with the clinical phenotype of the disease. J Clin Immunol 2010 Sep; 30(5):746-55.
(29) North ME, Webster AD, Farrant J. Primary defect in CD8+ lymphocytes in the antibody defici-
ency disease (common variable immunodeficiency): abnormalities in intracellular production of
interferon-gamma (IFN-gamma) in CD28+ (‘cytotoxic’) and. Clin Exp Immunol 1998 Jan; 111(1):70-5.
(30) Tha-In T, Bayry J, Metselaar HJ, Kaveri SV, Kwekkeboom J. Modulation of the cellular immune
system by intravenous immunoglobulin. Trends Immunol 2008 Dec; 29(12):608-15.
(31) Xie D, Bai H, Liu L, et al. Apoptosis of lymphocytes and monocytes infected with influenza virus
might be the mechanism of combating virus and causing secondary infection by influenza. Int
Immunol 2009 Nov; 21(11):1251-62.
(32) Ohyama K, Nishina M, Yuan B, Bessho T, Yamakawa T. Apoptosis induced by influenza virus-he-
magglutinin stimulation may be related to fluctuation of cellular oxidative condition. Biol Pharm
Bull 2003 Feb; 26(2):141-7.
(33) Karlsson AC, Martin JN, Younger SR, et al. Comparison of the ELISPOT and cytokine flow cyto-
metry assays for the enumeration of antigen-specific T cells. J Immunol Methods 2003 Dec;
283(1-2):141-53.
(34) Rezaei N, Wing JB, Aghamohammadi A, et al. B-cell-T-cell activation and interaction in common
variable immunodeficiency. Hum Immunol 2010 Apr; 71(4):355-62.
(35) Esposito S, Marchisio P, Cavagna R, et al. Effectiveness of influenza vaccination of children
with recurrent respiratory tract infections in reducing respiratory-related morbidity within the
households. Vaccine 2003 Jul 4; 21(23):3162-8.
(36) Ghendon YZ, Kaira AN, Elshina GA. The effect of mass influenza immunization in children on the

56
Cha
pter
3
morbidity of the unvaccinated elderly. Epidemiol Infect 2006 Feb; 134(1):71-8.
(37) Jefferson T, Demicheli V, Rivetti D, Jones M, Di Pietrantonj C, Rivetti A. Antivirals for influenza
in healthy adults: systematic review. Lancet 2006 Jan 28; 367(9507):303-13.


PART 2I n f l u e n z a vaccination in patients w i t h a u t o - i m m u n e i n f l a m -m a t o r y rheumatic d i s e a s e s

CHAPT
ER4S t u d i e s o f c e l l -m e d i a t e di m m u n eresponses to i n f l u e n z a vaccinat ion in systemic l u p u se r y t h e -m a t o s u s
A. Holvast
S. van Assen
A. de Haan
A.L.W. Huckriede
C.A. Benne
J. Westra
A.M. Palache
J.C. Wilschut
C.G.M. Kallenberg
M. Bijl
Arthritis & Rheumatism 2009 Aug;60(8):2438-2447

62
Cha
pter
4
ABSTRACTIntroduction Both antibody and cell-mediated responses are involved in the defense against influenza. In systemic lupus erythematosus (SLE) pa-tients a decreased antibody response to subunit influenza vaccine has been demonstrated. However, cell-mediated responses have not yet been as-sessed.
Methods Fifty-four SLE patients and healthy HC (HC) received subunit influenza vaccine. Peripheral blood mononuclear cells and sera were ob-tained before and one month after vaccination. Cell-mediated responses to A/H1N1 and A/H3N2 were evaluated using interferon (IFN)γ ELISpot and flow cytometry. Antibody responses were measured using the hemagglu-tination inhibition test.
Results Prior to vaccination, SLE patients had fewer IFNγ spotforming cells against A/H1N1 compared to HC and a lower frequency of IFNγ+CD8+ T-cells. After vaccination, the numbers of IFNγ spotforming cells increased in both patients and HC, though it remained lower in patients. Also frequen-cies of CD4+ T-cells producing tumor necrosis factor α and interleukin-2 were lower in patients after vaccination, compared to HC. As expected for a subunit vaccine, vaccination did not induce a CD8+ T-cell response. For A/H3N2-specific responses, results were comparable. Diminished cell-mediated responses to influenza vaccination were associated with the use of prednisone and/or azathioprine. Patients showed a lower increase in A/H1N1-specific and A/H3N2-specific antibody titers after vaccination, as compared to HC.
Conclusion In addition to a decreased antibody response, cell-mediated re-sponses to influenza vaccination are diminished in SLE patients, which may reflect effects of the concomitant use of immunosuppressive drugs. This may render these patients more susceptible for (complicated) influenza infections.
63
Cha
pter
4
InTRoduCTIonSystemic lupus erythematosus (SLE) is a systemic autoimmune disease charac-terized by a remitting and relapsing course. SLE patients have an increased risk of infection, due to both intrinsic disturbances of immune responses and use of immunosuppressive drugs which are often needed to control disease activity. Indeed, infection-related morbidity and mortality occur more frequently in SLE patients [1].
For influenza, infection-related morbidity and mortality are increased in immuno-compromised patients [2]. As influenza infection has a high incidence, with an estimated 5-20% of the general population infected annually [3], influenza vac-cination is a clinically relevant issue in SLE patients. Influenza vaccination of SLE patients is safe, as it has been shown that influenza vaccination does not induce disease activity [4]. Annual vaccination in SLE is therefore recommended [5].
In the immune response to influenza, both antibody and cell-mediated respon-ses, comprised of CD4+ and CD8+ T-cells, are involved. In SLE, antibody responses to influenza vaccination are diminished [6], but T-cell-mediated responses have not been assessed. The latter are relevant, as it has been shown that in certain groups, such as the elderly, cell-mediated responses to influenza vaccination can be a marker of clinical protection, independent from antibody responses [7]. The most frequently used vaccine formulations are split virus or subunit vaccines. With these vaccines, antigens are primarily presented via MHC II, which induces CD4+ T-cell stimulation [8]. However, they are incapable of inducing MHC class I restricted CD8+ T-cell responses [9]. In addition, subunit vaccines, in contrast to split virus and whole virus vaccines, do not contain any of the internal proteins that may more readily (re)activate influenza-specific CD8+ T-cells.
In SLE, decreased T-helper (Th) recall responses to influenza A and tetanus toxoid antigens have been reported in a subset of patients, as measured by interleukin (IL)-2 production upon stimulation. This decreased function could not be accoun-ted for by the use of immunosuppressives alone, and was shown to be associated with disease activity [10]. In addition, lower levels of cell-mediated cytotoxicity against target T-cells infected with influenza A and B have been found in SLE patients [11].
Based on these data, we hypothesized that SLE patients have lower CD4+ T-cell responses to subunit influenza vaccine and lower CD8+ T-cell recall responses to influenza antigens than HC. Cell-mediated responses against influenza in SLE, prior to and following vaccination, were evaluated. In addition, antibody respon-ses were evaluated, and vaccine safety was recorded.
64
Cha
pter
4
MeThodS
Study population
Patients were eligible for the study when they fulfilled at least four of the Ame-rican College of Rheumatology criteria for SLE [12]. Exclusion criteria were preg-nancy and the presence of an indication for yearly influenza vaccination based on concomitant disease according to international guidelines [13]. A control group of healthy individuals was included that was age and sex matched to the vaccinated SLE patients. Pregnancy was an exclusion criterion for participation as HC.
Study design
SLE patients and healthy controls (HC) were included from October to December 2005. Before entry, patients were randomized in a ratio of 2:1 to receive an influ-enza vaccination or to serve as non-vaccinated patient control. At entry (visit 1), patients randomized for vaccination and all HC were vaccinated. Patients and HC were followed up at 28 days (visit 2) and three to four months after inclusion (visit 3). PBMC were isolated from vaccinated participants at visits 1 and 2 (see below). At each visit blood was drawn, and serum was stored at –20° C until use. Also, SLE disease activity index (SLEDAI) [14] was recorded and patients were asked to mark a visual analogue score (VAS) for disease activity on a scale of 0-10, 0 indicating no activity and 10 indicating the highest activity. Information on influenza vac-cination in the previous year was obtained. Adverse effects to vaccination were recorded using a standardized questionnaire which included: itching, pain, ery-thema, induration at the site of vaccination, shivers, myalgia, fever, headache, nausea, arthralgia, diarrhea, use of an analgesic/ antiphlogistic drug. The study was approved by the institutional medical ethics committee, and informed con-sent was obtained from all participants.
Influenza vaccine
A single dose of a trivalent subunit influenza vaccine (Influvac®, 2005-2006, Sol-vay Pharmaceuticals, Weesp, the Netherlands), containing A/New Caledonia/ 20/99 [H1N1], A/NewYork/55/2004 [H3N2] and B/Hong Kong/330/2001, was admi-nistered intramuscularly.
Isolation, storage and thawing of PBMC
PBMC were isolated from heparinized venous blood by density-gradient centrifu-gation on Lymphoprep (Axis-Shield, Oslo, Norway) immediately after blood was drawn. PBMC were frozen in RPMI 1640 (Cambrex BioScience, Verviers, Belgium) supplemented with 10% fetal calf serum (FCS), 50 µg/ml of gentamicin (Gibco,

65
Cha
pter
4
Paisley, UK) and 10% dimethylsulfoxide. PBMC were stored in liquid nitrogen until use. Pre- and postvaccination samples, from a SLE patient and a matched control, were simultaneously thawed and batch-processed. A minimum cell viability of 90%, evaluated by trypan blue staining, was required. Preceding ELISpot assays, PBMC were rested, by overnight incubation at 37° C. Cells were counted before plating, using an automated cell counter (Beckman Coulter, Fullerton, CA, USA).
Influenza antigens used in assays of cell-mediated responses
β-propiolactone whole inactivated virus (WIV) of A/New Caledonia/20/99 (H1N1) and A/Hiroshima/52/2005 (H3N2) were used to stimulate PBMC. A/Hiroshi-ma/52/2005 is a very closely related antigenic variant of the vaccine strain A/NewYork/55/2004.
Interferon (IFn)γ eLISpot assay
Nitrocellulose plates (Nunc, Rochester, NY, USA) were coated overnight at 4° C with 50 µl anti-human IFNγ, 15 µg/ml per well (Mabtech, Nacka Strand, Sweden). Plates were washed and blocked with culture medium (CM; RPMI supplemented with 50 µg/ml gentamicin and 10% FCS) for one hour at room temperature (RT). Subsequently, 2 x 105 PBMC were added per well, in 200 µl, and incubated in CM at 37° C with WIV of A/H1N1 and A/H3N2, at a final concentration of 5 µg total viral protein/ml. Concanavalin A stimulation, 5 µg/ml, was used as a positive control and a negative control consisted of PBMC in CM alone. Stimulation tests were performed in duplo. After 48 hours plates were washed with phosphate buffered saline (PBS), and 50 µl of 1 µg/ml biotinylated anti-human IFNγ (Mabtech) was ad-ded per well for 3 hours at RT. Next, plates were washed again, and 50 µl 1:1000 streptavidin-alkaline phosphatase (Mabtech) per well was added for 1.5 hours at RT. Plates were washed and 100 µl BCIP/NBT plus substrate (Mabtech) was added per well for 10 minutes. Finally, plates were washed with tap water. After drying, spots were counted using an automated reader (automated ELISpot video-ana-lysis system, Sanquin, Amsterdam, The Netherlands). Results are referred to as IFNγ spotforming cells, as IFNγ-producing CD4+ and CD8+ T-cells as well as natu-ral killer (NK) cells, following WIV stimulation, have been described [15].
Flow cytometry
For stimulations, 1.0-1.5 x 106 PBMC were cultured in 200 µl CM, in 5 ml polypropy-lene round-bottom FalconTM tubes (Becton Dickinson and Company (BD), Franklin Lakes, NJ, USA). Staphylococcal enterotoxin B, at 5 µg/ml, (SEB, Sigma-Aldrich, Saint Louis, MO, USA) was used as a positive control. WIV A/New Caledonia (H1N1) and WIV A/Hiroshima (H3N2) were used at final concentrations of 1 µg of total

66
Cha
pter
4
viral protein/ml. WIV and negative control (CM only) cultures were incubated in the presence of 10 µg/ml anti CD28/CD49 (BD). Cells were incubated for 18h at 37° C, the final 16 hours in the presence of 10 µg/ml brefeldin A (Sigma-Aldrich). Following incubation, 10 µl 40mM EDTA in PBS was added, tubes were vortexed and incubated for 10 minutes, to facilitate resuspending. Next, 2 ml FACS lysing solution (BD) was added for 10 minutes. Cells were spun down and washed in PBS-1% bovine serum albumin. Subsequently cells were permeabilized in 500 µl PERM-2 (BD) for 10 minutes in the dark in the presence of pacific blue and orange (Invitrogen, Carlsbad, CA, USA), in a different combination for each stimulus, to enable fluorescent T-cell barcoding [16]. PBS-20% FCS was added for 5 minutes. Cells were washed and pooled per PBMC sample. Next, anti-CD3-FITC, anti-CD4-PE-Cy7, anti-CD8-PercP, anti-CD69-APC-Cy7, anti-IFNγ-Alexa 700, anti-tumor ne-crosis factor (TNF)α-APC and anti-interleukin (IL)-2-PE (all from BD) were added, following the manufacturer’s instruction. After incubation for 30 minutes at RT, cells were washed and immediately analyzed on a LSR II flow cytometer (BD). Data for at least 1 x 106 CD3+ cells were collected. Using the Win-List software package (Verity Software House, Topsham ME, USA), positively and negatively stained populations were gated and Boolean gating was applied. First, lymphocy-tes were gated by CD3 expression and sideward scatter patterns. Next, CD4+ and CD8+ T-cell populations were gated as CD4+CD8- or CD4-CD8+, respectively. Then, cells from different stimulation tubes were separated in a pacific blue/orange plot. Finally CD69+/- cytokine+/- quadrants were set for the different stimuli si-multaneously, according to the negative and positive controls. Percentages of antigen-specific cells were expressed as the percentage of CD69+ cytokine+ CD4+ or CD8+ T-cells within the total CD4+ or CD8+ T-cell population.
Antibody response to influenza
For quantitative detection of anti-influenza antibodies the hemagglutination in-hibition assay (HIA) was employed, following standard procedures [17]. Influenza A/New Caledonia/20/99 [H1N1] and A/NewYork/55/2004 [H3N2] were provided by Solvay Pharmaceuticals (Weesp, the Netherlands). Seroconversions were defined as a fourfold rise in titer one month after vaccination, and seroprotection was defined as a titer ≥40. Titers <10 (below detection level) were assigned a value of 5 for calculation purposes [18].
Statistical analysis
Data were analyzed using SPSS 14 (SPSS Inc., Chicago, IL, USA). Titers were log transformed prior to testing of geometric mean titers. For comparisons of T-cell cytokine responses, Mann-Whitney U test and Wilcoxon signed rank test were

67
Cha
pter
4
used. All T-cell frequencies reported are after background subtraction of the fre-quency of the identically gated population of cells from the same sample stimu-lated without antigen. For correlations, Spearman’s rho was used. Age was nor-mally distributed and tested with Student’s t-test. For all other variables Fisher’s exact test and Mann-Whitney U test were used where appropriate. A two sided P value <0.05 was considered statistically significant. No adjustments for multiple testing were made given the explorative design of the study.
ReSuLTS
Patient characteristics
Eighty SLE patients gave informed consent to participate and were randomized: 54 for the vaccination group and 26 for the non-vaccination group. Two patients initially randomized for the non-vaccination group were excluded (due to preg-nancy and withdrawal, respectively). Patient groups did not differ in sex, age, and medication use. More patients in the vaccination group had received an influenza vaccination the year before as compared to patients not receiving vaccination and HC (table 1).
Cell-mediated responses against A/H1N1 and A/H3N2 were measured in a subset
Table 1. Baseline characteristics and disease parameters
SLE patients HC
Non-vaccinated Vaccinated Vaccinated
(n=24) (n=54) (n=54)
Sex, males 2 (8.3%) 10 (18.5%) 11 (20.4%)
Age, mean (SD) 45.5 (11.5) 44.8 (13.6) 43.1 (10.9)
Influenza vaccination in previous year 9 (37.5%) 34 (63.0%) * 3 (5.6%) **
Without immunosuppressives 5 (20.8%) 5 (9.3%) N/A
Prednisone 10 (41.7%) 28 (51.9%) N/A
median (range), in users (mg/day) 6.25 (2.5-15) 5 (1.25-15) N/A
Hydroxychloroquine 10 (41.7%) 30 (55.6%) N/A
median (range), in users (mg/day) 400 (200-800) 400 (200–1000) N/A
Azathioprine 6 (25%) 17 (31.5%)
median (range), in users (mg/day) 87.8 (50-125) 125 (75–200) N/A
Other immunosuppressive drugs 0 (0%) 6 (11.1%) # N/A
SLEDAI, median (range) t=0 2 (0-8) 2 (0-12) N/A
VAS, median (range) t=0 2.2 (0-5.6) 1.6 (0-6.6) N/A
SLE, systemic lupus erythematosus; HC, healthy controls; SLEDAI, systemic lupus erythematosus disease activity index; VAS, visual analogue score; N/A, not applicable # Methotrexate, 5 patients used 15 mg per week, 1 used 25 mg per week; * p <0.05 (vaccinated SLE patients versus non-vaccinated SLE patients); ** p <0.001 (HC versus vaccinated SLE patients)

68
Cha
pter
4
of vaccinated SLE patients (n=38) and HC (n=38), matched for age and sex. This subset was based on availability of a matched control and proper acquisition of PBMC prior to and one month following vaccination. Mean age (SD) in this sub-group was 43.4 years (10.2); 24% were male.
Lower prevaccination cell-mediated responses to A/h1n1 and A/h3n2 in SLe patients
In ELISpot, prior to vaccination, SLE patients had fewer IFNγ spotforming cells against A/H1N1 and A/H3N2 as compared to HC (figure 1). In flow cytometry, the fre-quency of CD4+TNFα+ T-cells upon A/H1N1 stimulation was lower in SLE patients than in HC (figure 2, A). SLE patients also had a lower frequency of IFNγ+CD8+ T-cells upon A/H1N1 stimulation as well as lower frequencies of IFNγ- and TNFα-producing CD8+ T-cells upon A/H3N2 stimulation (figure 3, A and B).
Lower cell-mediated responses to A/h1n1 and A/h3n2 in SLe patients fol-lowing influenza vaccination
Following vaccination, 68.4% of SLE patients and 71.1% of HC showed a rise in IFNγ spotforming cells against A/H1N1; for A/H3N2 60.5% of patients and 73.7% of HC showed a rise. Rises were similar in SLE patients and HC. After vaccination, the number of IFNγ spotforming cells remained lower in SLE patients, compared to HC (figure 1).
Figure 1. Enzyme-linked immunospot assay of interferon (IFN)γ spot-forming cells per 2 x 10^5 peripheral blood mononuclear cells in patients with systemic lupus erythematosus (SLE) and healthy controls (HC) in response to A/H1N1 and A/H3N2 stimulation before vaccination (t=0 days) and 4 weeks after vaccination (t=28 days). Results are corrected for responses in unstimulated cultures from the same sample. Bars show the median and interquartile range.
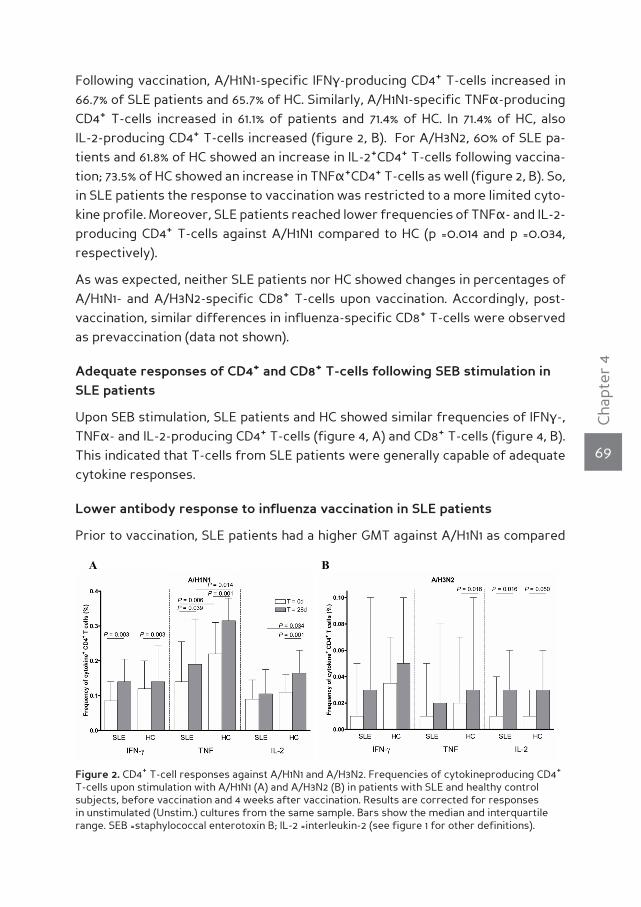
69
Cha
pter
4
Following vaccination, A/H1N1-specific IFNγ-producing CD4+ T-cells increased in 66.7% of SLE patients and 65.7% of HC. Similarly, A/H1N1-specific TNFα-producing CD4+ T-cells increased in 61.1% of patients and 71.4% of HC. In 71.4% of HC, also IL-2-producing CD4+ T-cells increased (figure 2, B). For A/H3N2, 60% of SLE pa-tients and 61.8% of HC showed an increase in IL-2+CD4+ T-cells following vaccina-tion; 73.5% of HC showed an increase in TNFα+CD4+ T-cells as well (figure 2, B). So, in SLE patients the response to vaccination was restricted to a more limited cyto-kine profile. Moreover, SLE patients reached lower frequencies of TNFα- and IL-2- producing CD4+ T-cells against A/H1N1 compared to HC (p =0.014 and p =0.034, respectively).
As was expected, neither SLE patients nor HC showed changes in percentages of A/H1N1- and A/H3N2-specific CD8+ T-cells upon vaccination. Accordingly, post-vaccination, similar differences in influenza-specific CD8+ T-cells were observed as prevaccination (data not shown).
Adequate responses of Cd4+ and Cd8+ T-cells following SeB stimulation in SLe patients
Upon SEB stimulation, SLE patients and HC showed similar frequencies of IFNγ-, TNFα- and IL-2-producing CD4+ T-cells (figure 4, A) and CD8+ T-cells (figure 4, B). This indicated that T-cells from SLE patients were generally capable of adequate cytokine responses.
Lower antibody response to influenza vaccination in SLe patients
Prior to vaccination, SLE patients had a higher GMT against A/H1N1 as compared
Figure 2. CD4+ T-cell responses against A/H1N1 and A/H3N2. Frequencies of cytokineproducing CD4+ T-cells upon stimulation with A/H1N1 (A) and A/H3N2 (B) in patients with SLE and healthy control subjects, before vaccination and 4 weeks after vaccination. Results are corrected for responses in unstimulated (Unstim.) cultures from the same sample. Bars show the median and interquartile range. SEB =staphylococcal enterotoxin B; IL-2 =interleukin-2 (see figure 1 for other definitions).
A B
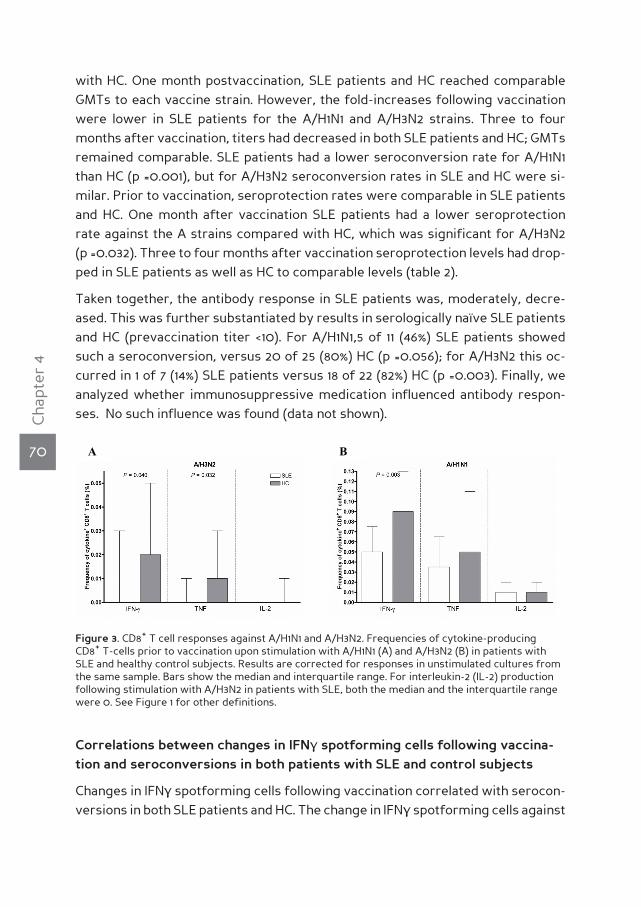
70
Cha
pter
4
with HC. One month postvaccination, SLE patients and HC reached comparable GMTs to each vaccine strain. However, the fold-increases following vaccination were lower in SLE patients for the A/H1N1 and A/H3N2 strains. Three to four months after vaccination, titers had decreased in both SLE patients and HC; GMTs remained comparable. SLE patients had a lower seroconversion rate for A/H1N1 than HC (p =0.001), but for A/H3N2 seroconversion rates in SLE and HC were si-milar. Prior to vaccination, seroprotection rates were comparable in SLE patients and HC. One month after vaccination SLE patients had a lower seroprotection rate against the A strains compared with HC, which was significant for A/H3N2 (p =0.032). Three to four months after vaccination seroprotection levels had drop-ped in SLE patients as well as HC to comparable levels (table 2).
Taken together, the antibody response in SLE patients was, moderately, decre-ased. This was further substantiated by results in serologically naïve SLE patients and HC (prevaccination titer <10). For A/H1N1,5 of 11 (46%) SLE patients showed such a seroconversion, versus 20 of 25 (80%) HC (p =0.056); for A/H3N2 this oc-curred in 1 of 7 (14%) SLE patients versus 18 of 22 (82%) HC (p =0.003). Finally, we analyzed whether immunosuppressive medication influenced antibody respon-ses. No such influence was found (data not shown).
Correlations between changes in IFnγ spotforming cells following vaccina-tion and seroconversions in both patients with SLe and control subjects
Changes in IFNγ spotforming cells following vaccination correlated with serocon-versions in both SLE patients and HC. The change in IFNγ spotforming cells against
Figure 3. CD8+ T cell responses against A/H1N1 and A/H3N2. Frequencies of cytokine-producing CD8+ T-cells prior to vaccination upon stimulation with A/H1N1 (A) and A/H3N2 (B) in patients with SLE and healthy control subjects. Results are corrected for responses in unstimulated cultures from the same sample. Bars show the median and interquartile range. For interleukin-2 (IL-2) production following stimulation with A/H3N2 in patients with SLE, both the median and the interquartile range were 0. See Figure 1 for other definitions.
A B
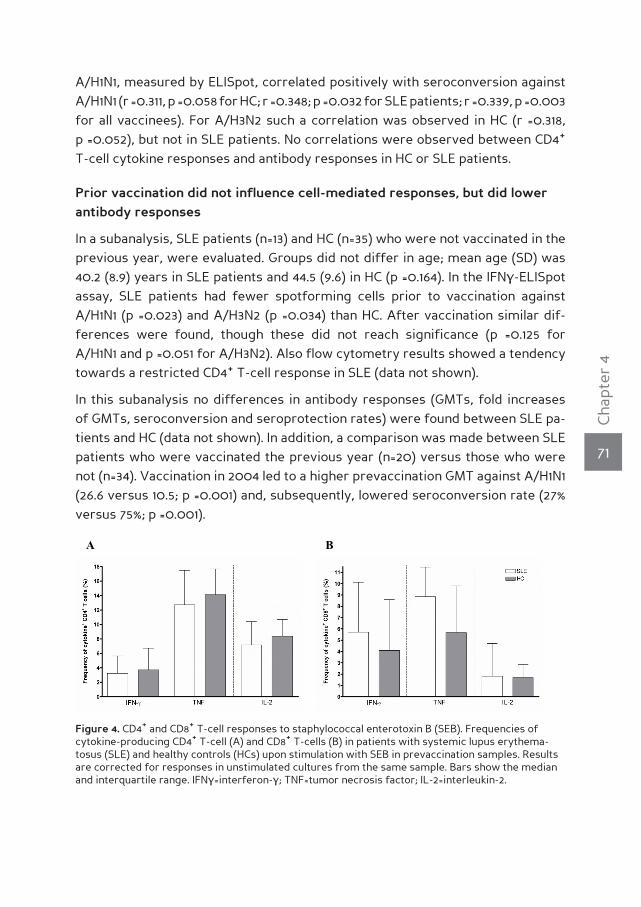
71
Cha
pter
4
A/H1N1, measured by ELISpot, correlated positively with seroconversion against A/H1N1 (r =0.311, p =0.058 for HC; r =0.348; p =0.032 for SLE patients; r =0.339, p =0.003 for all vaccinees). For A/H3N2 such a correlation was observed in HC (r =0.318, p =0.052), but not in SLE patients. No correlations were observed between CD4+ T-cell cytokine responses and antibody responses in HC or SLE patients.
Prior vaccination did not influence cell-mediated responses, but did lower antibody responses
In a subanalysis, SLE patients (n=13) and HC (n=35) who were not vaccinated in the previous year, were evaluated. Groups did not differ in age; mean age (SD) was 40.2 (8.9) years in SLE patients and 44.5 (9.6) in HC (p =0.164). In the IFNγ-ELISpot assay, SLE patients had fewer spotforming cells prior to vaccination against A/H1N1 (p =0.023) and A/H3N2 (p =0.034) than HC. After vaccination similar dif-ferences were found, though these did not reach significance (p =0.125 for A/H1N1 and p =0.051 for A/H3N2). Also flow cytometry results showed a tendency towards a restricted CD4+ T-cell response in SLE (data not shown).
In this subanalysis no differences in antibody responses (GMTs, fold increases of GMTs, seroconversion and seroprotection rates) were found between SLE pa-tients and HC (data not shown). In addition, a comparison was made between SLE patients who were vaccinated the previous year (n=20) versus those who were not (n=34). Vaccination in 2004 led to a higher prevaccination GMT against A/H1N1 (26.6 versus 10.5; p =0.001) and, subsequently, lowered seroconversion rate (27% versus 75%; p =0.001).
Figure 4. CD4+ and CD8+ T-cell responses to staphylococcal enterotoxin B (SEB). Frequencies of cytokine-producing CD4+ T-cell (A) and CD8+ T-cells (B) in patients with systemic lupus erythema-tosus (SLE) and healthy controls (HCs) upon stimulation with SEB in prevaccination samples. Results are corrected for responses in unstimulated cultures from the same sample. Bars show the median and interquartile range. IFNγ =interferon-γ ; TNF=tumor necrosis factor; IL-2=interleukin-2.
B A

72
Cha
pter
4
The use of prednisone and/or azathioprine was associated with lower cell-mediated responses to influenza vaccination
Patients using prednisone and/or azathioprine (PRED/AZA; n=22) were compa-red to patients who did not use these drugs (n=16). In this subanalysis, no diffe-rences were noted prior to vaccination. Following vaccination, patients on PRED/AZA had fewer IFNγ spotforming cells against A/H1N1 and A/H3N2 (p =0.004 and p =0.007, respectively) and lower frequencies of A/H1N1-specific IFNγ-, TNFα- and IL-2-producing CD4+ T-cells (p =0.004, p =0.033 and p =0.036, respectively) as well as A/H3N2-specific IFNγ-producing CD4+ T-cells (p =0.023). No differences in CD8+ T-cell responses to A/H1N1 and A/H3N2 were observed (data not shown). In patients not using prednisone and/or azathioprine, cell mediated responses to influenza vaccination were not significantly lower than in HC (data not shown).
no increase in disease activity following influenza vaccination, but more adverse effects in SLe than in hC
Prior to inclusion (Table 1), and during follow-up, vaccinated and non-vaccinated patient groups did not differ in SLEDAI and VAS scores. At visit 2, median (range) SLEDAI scores were 2 (0–13) in vaccinated SLE patients versus 2 (0–8) in non-vaccinated patients and at visit 3 these were 2 (0–10) versus 2 (0–4), respectively. For VAS scores, median (range) scores at visit 2 were 1.4 (0–8.1) in vaccinated SLE patients versus 2.1 (0–7.4) in non-vaccinated patients, at visit 3 these were 1.8 (0–9.4) versus 2.2 (0–8.9) respectively. Following vaccination, SLE patients more often reported itching (18% vs. 2% in HC; p =0.006), erythema (24% vs. 4%; p =0.003) and induration (30% vs. 11% p =0.026) at the site of vaccination, and arthralgia (16% vs. 4%; p =0.046). All adverse effects were mild and short-lasting.
dISCuSSIonTo our knowledge, this is the first study to evaluate cell-mediated immune re-sponses to subunit influenza vaccine in patients with a systemic autoimmune disease. To do so, we used ELISpot and flow cytometry. ELISpot is the more sensi-tive assay, whereas flow cytometry allows phenotyping and detection of multiple cytokines, which offers additional information on the gamma of the response [19].
Cell-mediated recall responses to influenza were lower in SLE patients. Prior to vaccination, SLE patients had considerably fewer IFNγ spotforming cells than HC against both A/H1N1 and A/H3N2. CD4+ T-cell responses to A/H1N1 were lower in SLE patients, which reached significance for TNFα-producing CD4+ T-cells. Also CD8+ T-cell responses were lower in SLE patients than in HC, for both A/H1N1 (IFNγ-production) and A/H3N2 (IFNγ and TNFα-production).

73
Cha
pter
4
Following influenza vaccination, cell-mediated responses to influenza remained lower in SLE patients. Although both SLE patients and HC showed an increase in IFNγ spotforming cells upon vaccination, for A/H1N1 as well as A/H3N2, numbers remained lower in SLE patients. SLE patients showed an increase in cytokine-pro-ducing A/H1N1-specific and A/H3N2-specific CD4+ T-cells following vaccination, however, this increase was restricted with respect to cytokine profile compa-red to HC. Moreover, SLE patients reached lower frequencies of A/H1N1-specific TNFα-producing and IL-2-producing CD4+ T-cells after vaccination. As expected, we did not observe a change in cytokine-producing CD8+ T-cells following vac-cination in either SLE patients or HC.
As CD4+ and CD8+ T-cell responses to SEB were normal in SLE patients, the de-creased cell-mediated response to influenza vaccination could not be attributed to a decreased responsiveness of T-lymphocytes in general. Furthermore, the observed differences in cell-mediated responses were, at least largely, indepen-dent of previous influenza vaccination status as well. The degree of influenza vac-cination in the previous year was higher in SLE patients, but in a subanalysis com-paring previously unvaccinated SLE patients with HC, SLE patients still showed considerably lower responses. Importantly, the use of medications played a major role, as the use of prednisone and/or azathioprine was associated with lower cell-mediated responses against both A/H1N1 and A/H3N2 following vaccination.
A diminished T-helper cell response in SLE patients to influenza has been repor-ted previously [20], as measured by IL-2 secretion in the supernatant of influen-za-stimulated PBMC of unvaccinated patients. We found a decreased CD8+ T-cell recall response in SLE patients to influenza antigens, which is in accordance with a previous study [11]. WIV, as used in this study, is able to induce CD8+ T-cell re-sponses in vivo and to reactivate memory CD8+ T-cells in vitro [21]. However, WIV might be a weaker stimulus of CD8+ T-cells as compared to live virus, due to lower antigen presentation on MHC I.
Importantly, fewer influenza-specific PBMC in SLE may be of clinical relevance. Recently, it was shown that numbers of spotforming cells correlate with clini-cal protection from, culture-confirmed, influenza in young children [22]. These numbers may vary depending on antigen type and influenza strain, as median numbers in our assays were higher than in assays in which hemagglutinin (HA) or vaccine components were used [23-26], and as in the present study A/H3N2-specific cell-mediated responses were lower than A/H1N1-specific responses. WIV contains core antigens in addition to surface antigens. Also, the uptake and presentation of WIV is more efficient [27]. Both factors might contribute to higher responses to WIV compared to HA or vaccine components.
74
Cha
pter
4
SLE patients showed normal T-cell cytokine responses to SEB. Previous reports reported a normal capacity of PBMC from SLE patients to respond to different stimuli, though diminished cell-mediated responses may be present during ac-tive disease [28-31]. As our cohort of SLE patients predominantly had quiescent disease, this may explain their normal responses to SEB. In addition, previous studies reported decreased proliferation of PBMC [32-34], whereas others found normal proliferative capacity [35], or heterogeneous results [36].
Diminished cell-mediated responses to influenza vaccination in SLE patients ap-pear to reflect, in particular, effects of immunosuppressive drugs. Effects of previous influenza vaccinations, or natural infections, could not be completely excluded. Whether intrinsic defects are involved, such as a defective antigen-presenting cell function [37, 38], is uncertain.
In SLE, antibody production upon influenza vaccination is lower than in the general population [39]. In the present study, we too found lower antibody responses in SLE patients, as reflected by lower fold-increases in titers, a trend towards lo-wer postvaccination GMTs and fewer seroconversions in serologically naïve SLE patients. Notably, antibody titers are the gold standard for protection and with regard to seroprotection rates, little differences were observed between SLE pa-tients and HC. Influenza vaccination in the previous year was associated with a lower seroconversion rate to A/H1N1; both vaccines contained the same A/H1N1 strain. Effects of previous influenza vaccination on antibody responses remain subject to discussion, as some studies reported decreased antibody responses [40-42], whereas others found similar [43-45] or improved responses [46].
We evaluated relationships between antibody and cell-mediated responses, as CD4+ T-cell help is necessary for antibody responses [47]. However, we did not find a correlation between CD4+ T-cell responses and antibody responses using flow cytometry. We did observe a, modest, correlation in SLE patients between changes in IFNγ spotforming cells against A/H1N1, measured by ELISpot, upon vaccination and seroconversion to A/H1N1. This suggests that in a subset of poor-er responding patients both cell-mediated and antibody responses are affected. Possibly, no correlation between CD4+ T-cell responses and antibody responses was observed due to the lower sensitivity of flow cytometry as compared to ELISpot [48].
Finally, we showed that influenza vaccination did not induce disease activity over a period of three to four months. This confirms previous studies, reviewed in [49].
Our study has some limitations. First, the sample size was relatively small and multiple comparisons were made. However, a proper power analysis was not

75
Cha
pter
4
possible as this is the first study to explore cell-mediated responses to influenza vaccination in SLE patients. Second, medication use in vaccinated SLE patients was heterogeneous. Third, more vaccinated SLE patients than HC had received an influenza vaccination in the previous year, which was of influence upon antibody responses. Fourth, there are no well-defined correlates between cell-mediated responses to influenza and the risk of influenza infection, which limits transla-tion of our results to clinical implications. Fifth, phenotypes of cells responding in ELISpot assays are unknown. It can be speculated that NK cells are among the cells which have responded in our ELISpot assay [50].
Despite these limitations, we conclude that the combined data point towards di-minished cell-mediated immune responses to influenza vaccination in a cohort of SLE patients representative for daily practice. Diminished cell-mediated respon-ses may reflect effects of the concomitant use of immunosuppressive drugs. The antibody response to influenza vaccination is also reduced in SLE patients. Clinici-ans should be aware that this combined defect might increase the morbidity and mortality due to influenza virus infection, in particular in patients on prednisone and/or azathioprine. Therefore evaluation of clinical protection from influenza in SLE patients, following influenza vaccination, seems indicated in order to assess if more effective influenza vaccines, or vaccination strategies, are warranted.
76
Cha
pter
4
Reference List
(1) Fessler BJ. Infectious diseases in systemic lupus erythematosus: risk factors, management and
prophylaxis. Best Pract Res Clin Rheumatol 2002 Apr; 16(2):281-91.
(2) Hayden FG. Prevention and treatment of influenza in immunocompromised patients. Am J Med
1997 Mar 17; 102(3A):55-60.
(3) Prevention and control of influenza: recommendations of the Advisory Committee on Immuni-
zation Practices (ACIP). MMWR Recomm Rep 1999 Apr 30; 48(RR-4):1-28.
(4) Abu-Shakra M, Press J, Buskila D, Sukenik S. Influenza vaccination of patients with systemic
lupus erythematosus: Safety and immunogenecity issues. Autoimmun Rev 2007 Sep; 6(8):543-6.
(5) Gluck T, Muller-Ladner U. Vaccination in patients with chronic rheumatic or autoimmune disea-
ses. Clin Infect Dis 2008 May 1; 46(9):1459-65.
(6) Holvast A, Huckriede A, Wilschut J, et al. Safety and efficacy of influenza vaccination in systemic
lupus erythematosus patients with quiescent disease. Ann Rheum Dis 2006 Jul; 65(7):913-8.
(7) McElhaney JE, Xie D, Hager WD, et al. T cell responses are better correlates of vaccine protec-
tion in the elderly. J Immunol 2006 May 15; 176(10):6333-9.
(8) Huckriede A, Bungener L, Stegmann T, et al. The virosome concept for influenza vaccines. Vac-
cine 2005 Jul 8; 23 Suppl 1:S26-S38.
(9) Vogt A, Mahe B, Costagliola D, et al. Transcutaneous anti-influenza vaccination promotes both
CD4 and CD8 T cell immune responses in humans. J Immunol 2008 Feb 1; 180(3):1482-9.
(10) Bermas BL, Petri M, Goldman D, et al. T helper cell dysfunction in systemic lupus erythematosus
(SLE): relation to disease activity. J Clin Immunol 1994 May; 14(3):169-77.
(11) Pons VG, Reinertsen JL, Steinberg AD, Dolin R. Decreased cell-mediated cytotoxicity against
virus-infected cells in systemic lupus erythematosus. J Med Virol 1979; 4(1):15-23.
(12) Tan EM, Cohen AS, Fries JF, et al. The 1982 revised criteria for the classification of systemic
lupus erythematosus. Arthritis Rheum 1982 Nov; 25(11):1271-7.
(13) Influenza vaccines. Wkly Epidemiol Rec 2005 Aug 19; 80(33):279-87.
(14) Bombardier C, Gladman DD, Urowitz MB, Caron D, Chang CH. Derivation of the SLEDAI. A disease
activity index for lupus patients. The Committee on Prognosis Studies in SLE. Arthritis Rheum
1992 Jun; 35(6):630-40.
(15) Long BR, Michaelsson J, Loo CP, et al. Elevated frequency of gamma interferon-producing
NK cells in healthy adults vaccinated against influenza virus. Clin Vaccine Immunol 2008 Jan;
15(1):120-30.
(16) Krutzik PO, Nolan GP. FluorescenT cell barcoding in flow cytometry allows high-throughput
drug screening and signaling profiling. Nat Methods 2006 May; 3(5):361-8.
(17) Harmon MW. Influenza viruses. In: Lennette, ed. Laboratory diagnosis of viral infections, 2nd ed.
New York: Marcel Dekker, Inc, 2004:515-34.
(18) European Medicines Agency (EMEA). Note for guidance on harmonisation of requirements for
influenza vaccines. 1997 Mar 12. Report No.: CPMP/BWP/214/96.
(19) Karlsson AC, Martin JN, Younger SR, et al. Comparison of the ELISPOT and cytokine flow cyto-
metry assays for the enumeration of antigen-specific T cells. J Immunol Methods 2003 Dec;
283(1-2):141-53.
(20) Bermas BL, Petri M, Goldman D, et al. T helper cell dysfunction in systemic lupus erythematosus
(SLE): relation to disease activity. J Clin Immunol 1994 May; 14(3):169-77.
77
Cha
pter
4
(21) Sawai T, Itoh Y, Ozaki H, et al. Induction of cytotoxic T-lymphocyte and antibody responses
against highly pathogenic avian influenza virus infection in mice by inoculation of apathogenic
H5N1 influenza virus particles inactivated with formalin. Immunology 2008 Jun; 124(2):155-65.
(22) Forrest BD, Pride MW, Dunning AJ, et al. Correlation of cellular immune responses with protec-
tion against culture-confirmed influenza virus in young children. Clin Vaccine Immunol 2008 Jul;
15(7):1042-53.
(23) Cheong HJ, Song JY, Park JW, et al. Humoral and cellular immune responses to influenza vac-
cine in patients with advanced cirrhosis. Vaccine 2006 Mar 20; 24(13):2417-22.
(24) Deng Y, Jing Y, Campbell AE, Gravenstein S. Age-related impaired type 1 T cell responses to
influenza: reduced activation ex vivo, decreased expansion in CTL culture in vitro, and blunted
response to influenza vaccination in vivo in the elderly. J Immunol 2004 Mar 15; 172(6):3437-46.
(25) Vogt A, Mahe B, Costagliola D, et al. Transcutaneous anti-influenza vaccination promotes both
CD4 and CD8 T cell immune responses in humans. J Immunol 2008 Feb 1; 180(3):1482-9.
(26) Forrest BD, Pride MW, Dunning AJ, et al. Correlation of cellular immune responses with protec-
tion against culture-confirmed influenza virus in young children. Clin Vaccine Immunol 2008 Jul;
15(7):1042-53.
(27) Huckriede A, Bungener L, Stegmann T, et al. The virosome concept for influenza vaccines. Vac-
cine 2005 Jul 8; 23 Suppl 1:S26-S38.
(28) Alcocer-Varela J, Alarcon-Segovia D. Decreased production of and response to interleukin-2 by
cultured lymphocytes from patients with systemic lupus erythematosus. J Clin Invest 1982 Jun;
69(6):1388-92.
(29) Bermas BL, Petri M, Goldman D, et al. T helper cell dysfunction in systemic lupus erythematosus
(SLE): relation to disease activity. J Clin Immunol 1994 May; 14(3):169-77.
(30) Draeger AM, Swaak AJ, van den Brink HG, Aarden LA. T cell function in systemic lupus erythe-
matosus: normal production of and responsiveness to interleukin 2. Clin Exp Immunol 1986 Apr;
64(1):80-7.
(31) Nies K, Boyer R, Stevens R, Louie J. Anti-tetanus toxoid antibody synthesis after booster im-
munization in systemic lupus erythematosus. Comparison of the in vitro and in vivo responses.
Arthritis Rheum 1980 Dec; 23(12):1343-50.
(32) Gottlieb AB, Lahita RG, Chiorazzi N, Kunkel HG. Immune function in systemic lupus erythema-
tosus. Impairment of in vitro T cell proliferation and in vivo antibody response to exogenous
antigen. J Clin Invest 1979 May; 63(5):885-92.
(33) Hernandez-Fuentes MP, Reyes E, Prieto A, et al. Defective proliferative response of T lymphocy-
tes from patients with inactive systemic lupus erythematosus. J Rheumatol 1999 Jul; 26(7):1518-
26.
(34) Lockshin MD, Eisenhauer AC, Kohn R, Weksler M, Block S, Mushlin SB. Cell-mediated immunity in
rheumatic diseases. II. Mitogen responses in RA, SLE, and other illnesses: correlation with T- and
B-lymphocyte populations. Arthritis Rheum 1975 May; 18(3):245-50.
(35) Defreitas ME, Kondracki E, Perez-Rojas G, Bianco NE. Further aspects of T cell function in syste-
mic lupus erythematosus. Immunol Commun 1982; 11(2):113-20.
(36) Stekman IL, Blasini AM, Leon-Ponte M, Baroja ML, Abadi I, Rodriguez MA. Enhanced CD3-media-
ted T lymphocyte proliferation in patients with systemic lupus erythematosus. Arthritis Rheum
1991 Apr; 34(4):459-67.
(37) Via CS, Tsokos GC, Bermas B, Clerici M, Shearer GM. T cell-antigen-presenting cell interactions

78
Cha
pter
4
in human systemic lupus erythematosus. Evidence for heterogeneous expression of multiple
defects. J Immunol 1993 Oct 1; 151(7):3914-22.
(38) Scheinecker C, Zwolfer B, Koller M, Manner G, Smolen JS. Alterations of dendritic cells in sys-
temic lupus erythematosus: phenotypic and functional deficiencies. Arthritis Rheum 2001 Apr;
44(4):856-65.
(39) Abu-Shakra M, Press J, Buskila D, Sukenik S. Influenza vaccination of patients with systemic
lupus erythematosus: Safety and immunogenecity issues. Autoimmun Rev 2007 Sep; 6(8):543-6.
(40) Govaert TM, Sprenger MJ, Dinant GJ, Aretz K, Masurel N, Knottnerus JA. Immune response to
influenza vaccination of elderly people. A randomized double-blind placebo-controlled trial. Vac-
cine 1994 Oct; 12(13):1185-9.
(41) Gross PA, Sperber SJ, Donabedian A, et al. Paradoxical response to a novel influenza virus vac-
cine strain: the effect of prior immunization. Vaccine 1999 May 4; 17(18):2284-9.
(42) Pyhala R, Kumpulainen V, Alanko S, Forsten T. HI antibody kinetics in adult volunteers immunized
repeatedly with inactivated trivalent influenza vaccine in 1990-1992. Vaccine 1994 Aug; 12(10):947-
52.
(43) de Bruijn I, Remarque EJ, Jol-van der Zijde CM, van Tol MJ, Westendorp RG, Knook DL. Quality
and quantity of the humoral immune response in healthy elderly and young subjects after an-
nually repeated influenza vaccination. J Infect Dis 1999 Jan; 179(1):31-6.
(44) Keitel WA, Cate TR, Couch RB. Efficacy of sequential annual vaccination with inactivated influ-
enza virus vaccine. Am J Epidemiol 1988 Feb; 127(2):353-64.
(45) Keitel WA, Cate TR, Couch RB, Huggins LL, Hess KR. Efficacy of repeated annual immunization
with inactivated influenza virus vaccines over a five year period. Vaccine 1997 Jul; 15(10):1114-22.
(46) de Bruijn I, Remarque EJ, Beyer WE, le CS, Masurel N, Ligthart GJ. Annually repeated influenza
vaccination improves humoral responses to several influenza virus strains in healthy elderly.
Vaccine 1997 Aug; 15(12-13):1323-9.
(47) LeBien TW, Tedder TF. B lymphocytes: how they develop and function. Blood 2008 Sep 1;
112(5):1570-80.
(48) Karlsson AC, Martin JN, Younger SR, et al. Comparison of the ELISPOT and cytokine flow cyto-
metry assays for the enumeration of antigen-specific T cells. J Immunol Methods 2003 Dec;
283(1-2):141-53.
(49) Gluck T, Muller-Ladner U. Vaccination in patients with chronic rheumatic or autoimmune disea-
ses. Clin Infect Dis 2008 May 1; 46(9):1459-65.
(50) Long BR, Michaelsson J, Loo CP, et al. Elevated frequency of gamma interferon-producing
NK cells in healthy adults vaccinated against influenza virus. Clin Vaccine Immunol 2008 Jan;
15(1):120-30.


CHAPT
ER5A s e c o n d , b o o s t e r , i n f l u e n z a vaccinat ion has l imiteda d d i t i o n a le f f e c t o na n t i b o d y r e s p o n s e s in quiescents y s t e m i c l u p u se r y t h e -m a t o s u s
A. Holvast
S. van Assen
A. de Haan
A.Huckriede
C.A. Benne
J. Westra
A.M. Palache
J. Wilschut
C.G.M. Kallenberg
M. Bijl
Rheumatology (Oxford) 2009 Oct;48(10):1294-1299

82
Cha
pter
5
AbsTrAcTIntroduction In systemic lupus erythematosus (SLE), a decreased antibody response upon influenza vaccination has been reported. In this study, we assessed whether a booster vaccination could improve antibody respon-ses, as determined by seroprotection rates, in SLE patients.
Methods SLE patients (n=52) with quiescent disease (SLE disease activi-ty index; SLEDAI ≤4) and healthy controls (HC; n=28) received subunit in-fluenza vaccine in October - December 2007. After four weeks, only SLE patients received a second vaccination. Sera were obtained prior to both vaccinations, and four weeks after the second vaccination. At each visit, SLE disease activity was recorded. The hemagglutination inhibition as-say was used to measure antibody titers. Seroprotection was defined as a titer ≥40.
results Following the first vaccination seroprotection rates and geometric mean titers (GMTs) to each vaccine strain increased in both SLE patients and HC, to comparable levels. Seroprotection rates in SLE patients after the first vaccination were 86.5% to A/H1N1, 80.8% to A/H3N2 and 61.5% to the B strain; GMTs were 92.6, 56.2 and 39.2, respectively. Overall, the booster vaccination did not lead to a further rise of seroprotection rates and GMTs in SLE patients. However, in patients not vaccinated in the previous year, GMTs and seroconversion rate to A/H1N1 did rise following the booster vac-cination. Both influenza vaccinations did not increase SLEDAI scores.
conclusion Additional value of a booster influenza vaccination in SLE is li-mited to patients who were not vaccinated in the previous year.

83
Cha
pter
5
InTroducTIonInfections are a frequent cause of death in systemic lupus erythematosus (SLE) patients, accounting for up to 20–55% of all deaths [1]. An increased risk of infec-tion in SLE is related to both intrinsic disturbances of immune responses and use of immunosuppressive drugs which are often needed to control disease activity.
One of the most frequent infections is influenza, with an estimated 5% of the adult population infected annually [2]. In immunocompromised patients, influenza has a higher morbidity and mortality [3]. Vaccination is considered the cornerstone for prevention of influenza related morbidity and mortality, and is recommen-ded in immunocompromised patients [4]. As influenza vaccination does not induce disease activity in SLE, there is an increasing support for annual influenza vacci-nation of SLE patients [5, 6].
However, several studies have reported a decreased antibody response in SLE patients. Seroprotection (titer ≥40) rates were lower in SLE patients than in heal-thy adults, which may limit clinical protection from influenza in (part of) vaccina-ted SLE patients [7]. Several strategies have been developed to increase antibody responses to influenza vaccination, the most important being addition of an ad-juvans, administration of booster vaccinations, increase of antigen dosage in the vaccine and intradermal instead of intramuscular vaccine administration. All have been reported to have additional value in certain patient groups, as compared to conventional vaccination [8-11]. We chose to evaluate a booster vaccination in our SLE cohort, as this strategy has two advantages over the others. First, in contrast to other strategies, the safety profile of conventional subunit vaccine in SLE has been established. This is important as triggering of autoimmunity is a concern in systemic autoimmune disease. Second, this strategy would be easiest to imple-ment within current vaccination practice.
In liver transplantation patients, an increase of the antibody response following trivalent booster vaccination has been shown [11]. Moreover, in SLE, a booster of A/H1N1 solely, one month after a first vaccination, increased geometric mean titer (GMT) [12]. However, there are also patient groups in which a booster vaccination had no additional value, such as dialysis patients, bone marrow transplant reci-pients and severely immunocompromised HIV patients [10, 13-17].
Based on previous data from our group, we hypothesized that influenza vacci-nation would result in a lower seroprotection rate in SLE patients [18], and that administration of a booster vaccination would increase seroprotection rate up to the level of seroprotection reached in healthy adults after a single vaccination. To test this hypothesis, we administered a booster dose of influenza subunit vac-cine to SLE patients with quiescent disease, four weeks after a first vaccination.

84
Cha
pter
5
Antibody responses were determined prior to the first and second vaccination, and four weeks after the booster vaccination.
MeThods
Patients and controls
SLE patients were eligible for the study when they fulfilled at least four of the American College of Rheumatology criteria for SLE [19] and had quiescent disease, defined as a SLE disease activity index (SLEDAI 20) ≤4. Exclusion criteria were pregnancy, malignancy and the use of prednisone >30 mg/day. A control group of healthy individuals was included that was age and sex matched to the patients on group level. Pregnancy was an exclusion criterion for participation as healthy control (HC).
study design
We conducted an open, prospective, controlled study. SLE patients and HC were included from October - December 2007. At entry (t=0), patients and HC re-ceived intramuscularly a single dose of trivalent subunit influenza vaccine (In-fluvac® 2007-2008, Solvay Pharmaceuticals, Weesp, the Netherlands), containing A/Solomon Islands/3/2006 [H1N1], A/Wisconsin/67/2005 [H3N2] and B/Malay-sia/2506/2004. After four weeks (t=1), patients received a second, booster, vac-cination. HC were not given a booster vaccination, because this does not increase antibody responses [11, 15, 17, 21]. Serum was obtained at t=0 and t=1 in patients and HC, and four weeks thereafter (t=2) in patients alone. At each visit, the SLEDAI was recorded. Routine measures were used to determine anti-double-stranded DNA (by Farr assay) and complement C3 and C4. From all participants, informa-tion on influenza vaccination in the previous year was obtained. Adverse effects to vaccination were recorded using a standardized questionnaire which included: itching, pain, erythema, induration at the site of vaccination, shivers, myalgia, fever, headache, nausea, arthralgia, diarrhea, use of an analgesic/ antiphlogistic drug. The study was approved by the institutional medical ethics committee, and informed consent was obtained from all participants.
Antibody response to influenza
For quantitative detection of influenza antibodies the hemagglutination inhibition assay (HIA) was used. HIA were performed in duplo with guinea pig erythrocytes following standard procedures [22] with slight modifications as described else-where [23]. Seroprotection was defined as a titer ≥40, seroconversion was de-fined as ≥ fourfold rise in titer; titers <10 (below detection level) were assigned a
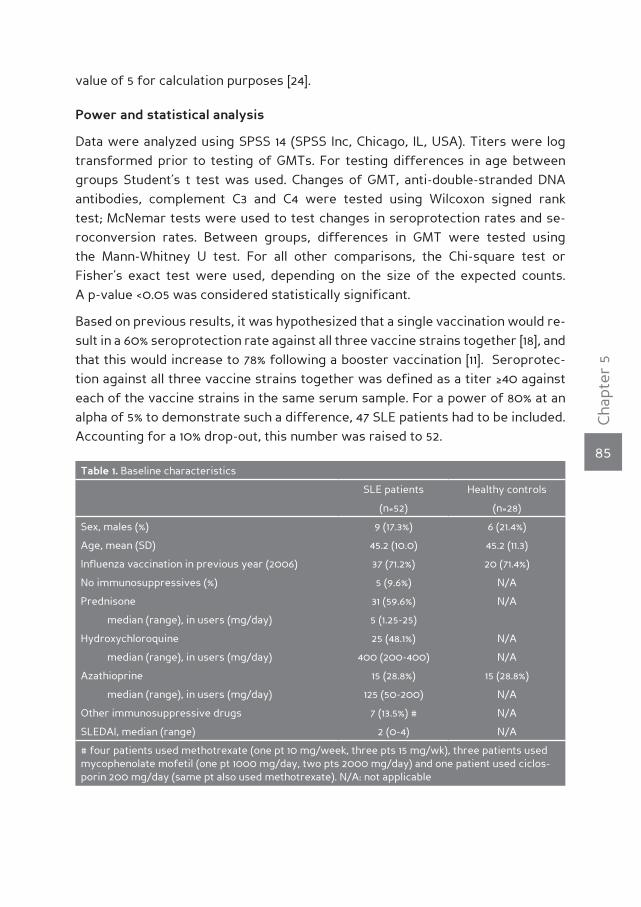
85
Cha
pter
5
value of 5 for calculation purposes [24].
Power and statistical analysis
Data were analyzed using SPSS 14 (SPSS Inc, Chicago, IL, USA). Titers were log transformed prior to testing of GMTs. For testing differences in age between groups Student’s t test was used. Changes of GMT, anti-double-stranded DNA antibodies, complement C3 and C4 were tested using Wilcoxon signed rank test; McNemar tests were used to test changes in seroprotection rates and se-roconversion rates. Between groups, differences in GMT were tested using the Mann-Whitney U test. For all other comparisons, the Chi-square test or Fisher’s exact test were used, depending on the size of the expected counts. A p-value <0.05 was considered statistically significant.
Based on previous results, it was hypothesized that a single vaccination would re-sult in a 60% seroprotection rate against all three vaccine strains together [18], and that this would increase to 78% following a booster vaccination [11]. Seroprotec-tion against all three vaccine strains together was defined as a titer ≥40 against each of the vaccine strains in the same serum sample. For a power of 80% at an alpha of 5% to demonstrate such a difference, 47 SLE patients had to be included. Accounting for a 10% drop-out, this number was raised to 52.
Table 1. Baseline characteristics
SLE patients Healthy controls
(n=52) (n=28)
Sex, males (%) 9 (17.3%) 6 (21.4%)
Age, mean (SD) 45.2 (10.0) 45.2 (11.3)
Influenza vaccination in previous year (2006) 37 (71.2%) 20 (71.4%)
No immunosuppressives (%) 5 (9.6%) N/A
Prednisone 31 (59.6%) N/A
median (range), in users (mg/day) 5 (1.25-25)
Hydroxychloroquine 25 (48.1%) N/A
median (range), in users (mg/day) 400 (200-400) N/A
Azathioprine 15 (28.8%) 15 (28.8%)
median (range), in users (mg/day) 125 (50-200) N/A
Other immunosuppressive drugs 7 (13.5%) # N/A
SLEDAI, median (range) 2 (0-4) N/A
# four patients used methotrexate (one pt 10 mg/week, three pts 15 mg/wk), three patients used mycophenolate mofetil (one pt 1000 mg/day, two pts 2000 mg/day) and one patient used ciclos-porin 200 mg/day (same pt also used methotrexate). N/A: not applicable
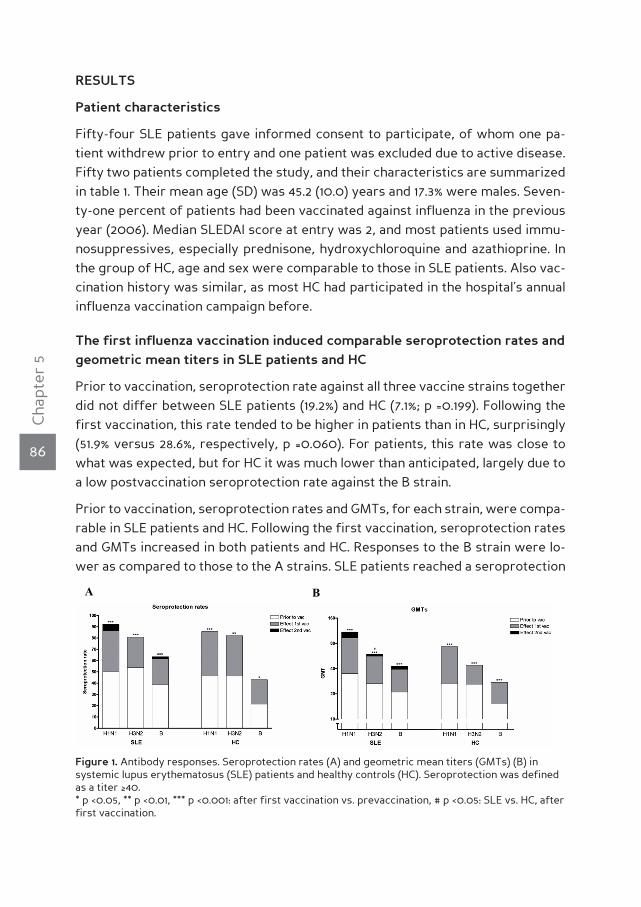
86
Cha
pter
5
resulTs
Patient characteristics
Fifty-four SLE patients gave informed consent to participate, of whom one pa-tient withdrew prior to entry and one patient was excluded due to active disease. Fifty two patients completed the study, and their characteristics are summarized in table 1. Their mean age (SD) was 45.2 (10.0) years and 17.3% were males. Seven-ty-one percent of patients had been vaccinated against influenza in the previous year (2006). Median SLEDAI score at entry was 2, and most patients used immu-nosuppressives, especially prednisone, hydroxychloroquine and azathioprine. In the group of HC, age and sex were comparable to those in SLE patients. Also vac-cination history was similar, as most HC had participated in the hospital’s annual influenza vaccination campaign before.
The first influenza vaccination induced comparable seroprotection rates and geometric mean titers in sle patients and hc
Prior to vaccination, seroprotection rate against all three vaccine strains together did not differ between SLE patients (19.2%) and HC (7.1%; p =0.199). Following the first vaccination, this rate tended to be higher in patients than in HC, surprisingly (51.9% versus 28.6%, respectively, p =0.060). For patients, this rate was close to what was expected, but for HC it was much lower than anticipated, largely due to a low postvaccination seroprotection rate against the B strain.
Prior to vaccination, seroprotection rates and GMTs, for each strain, were compa-rable in SLE patients and HC. Following the first vaccination, seroprotection rates and GMTs increased in both patients and HC. Responses to the B strain were lo-wer as compared to those to the A strains. SLE patients reached a seroprotection
Figure 1. Antibody responses. Seroprotection rates (A) and geometric mean titers (GMTs) (B) in systemic lupus erythematosus (SLE) patients and healthy controls (HC). Seroprotection was defined as a titer ≥40. * p <0.05, ** p <0.01, *** p <0.001: after first vaccination vs. prevaccination, # p <0.05: SLE vs. HC, after first vaccination.
A B

87
Cha
pter
5
rate of 86.5% for A/H1N1, 80.8% for A/H3N2 and 61.5% for the B strain. Their post-vaccination GMT was 92.6 for A/H1N1, 56.2 for A/H3N2 and 39.2 for the B strain. HC reached comparable seroprotection rates and GMTs (figure 1). Also fold increases in GMT were comparable in SLE patients and HC. SLE patients showed fold incre-ases of 2.7, 2.1 and 1.9 for strains A/H1N1, A/H3N2 and B, respectively. HC showed fold increases in GMT of 2.7, 1.7 and 1.8 for strains A/H1N1, A/H3N2 and B, respec-tively.
A booster influenza vaccination did not increase seroprotection rates and GMTs in sle patients
Primary focus was the effect of booster vaccination upon seroprotection rates in SLE patients. The second vaccination did not further increase these seroprotec-tion rates (figure 1, A). Accordingly, at t=2, the proportion of patients with serop-rotection to all vaccine strains was 55.8%, demonstrating that there was no signi-ficant increase following the second vaccination. Similarly, the second vaccination did not induce a significant rise in GMTs (figure 1, B).
low seroconversion rates in both patients and hc
Seroconversion rates were low in both SLE patients and HC. After the first vac-cination, seroconversion rates to A/H1N1 were 34.6% in SLE patients and 28.6% in HC, for A/H3N2 rates were 25.0% and 10.7% and for B rates were 19.2% and 10.7%, respectively. Following the booster vaccination (t=2 vs. t=1), five (9.6%) SLE pa-tients showed a seroconversion to A/H1N1 whereas none of the patients showed a seroconversion to either A/H3N2 or the B strain. In SLE patients, when using baseline titers (t=0) as reference, for A/H1N1, the seroconversion rate tended to be higher after the second vaccination (t=2 vs. t=0) than after the first vaccination (46.2% versus 34.6%; p =0.070). However, the booster vaccination did not lead to a further increase of seroconversion rates for A/H3N2 and the B strain.
Influence of previous influenza vaccinations
A large part of SLE patients (71.2%) and HC (71.4%) had received an influenza vaccination in the previous year. Vaccination in the previous year led to higher prevaccination seroprotection rates, which reached significance for strains A/H3N2 (p =0.016) and B (p =0.027) in patients, and for A/H1N1 in HC (p =0.038) (figure 2, A). Accordingly, prevaccination GMTs were higher in previously vac-cinated participants; in patients this difference was significant again for strains A/H3N2 (p =0.001) and B (p =0.026), and in HC for A/H1N1 (p =0.004) (figure 2, B). Influenza vaccination in the previous year did not influence titers and se-roprotection rates after the first vaccination, except for the B strain in HC. The
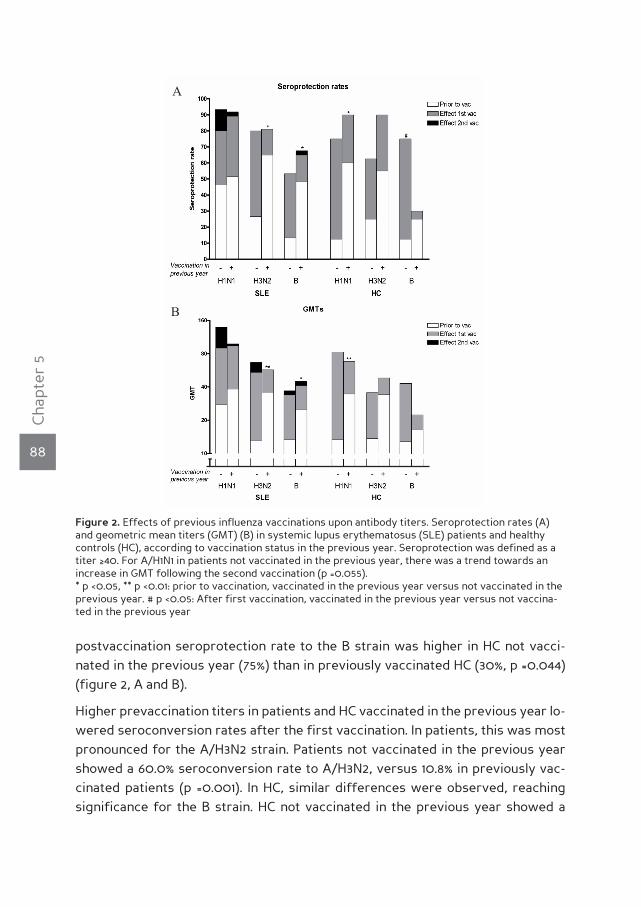
88
Cha
pter
5
postvaccination seroprotection rate to the B strain was higher in HC not vacci-nated in the previous year (75%) than in previously vaccinated HC (30%, p =0.044) (figure 2, A and B).
Higher prevaccination titers in patients and HC vaccinated in the previous year lo-wered seroconversion rates after the first vaccination. In patients, this was most pronounced for the A/H3N2 strain. Patients not vaccinated in the previous year showed a 60.0% seroconversion rate to A/H3N2, versus 10.8% in previously vac-cinated patients (p =0.001). In HC, similar differences were observed, reaching significance for the B strain. HC not vaccinated in the previous year showed a
Figure 2. Effects of previous influenza vaccinations upon antibody titers. Seroprotection rates (A) and geometric mean titers (GMT) (B) in systemic lupus erythematosus (SLE) patients and healthy controls (HC), according to vaccination status in the previous year. Seroprotection was defined as a titer ≥40. For A/H1N1 in patients not vaccinated in the previous year, there was a trend towards an increase in GMT following the second vaccination (p =0.055). * p <0.05, ** p <0.01: prior to vaccination, vaccinated in the previous year versus not vaccinated in the previous year. # p <0.05: After first vaccination, vaccinated in the previous year versus not vaccina-ted in the previous year
A
B

89
Cha
pter
5
37.5% seroconversion rate to the B strain, versus 0% of the previously vaccinated HC (p =0.017).
Notably, for A/H1N1, vaccinations in the previous year influenced the response to the booster vaccination. In SLE patients not vaccinated in the previous year, the booster tended to increase the GMT to A/H1N1, but not to A/H3N2 and the B strain. Following the booster vaccination, the GMT to A/H1N1 increased from 89.8 to 139.3 (p =0.055). In previously vaccinated patients, the GMT was not influenced (figure 2, B). For seroconversion rate, a similar effect was found; in SLE patients not vaccinated in previous year, the seroconversion rate increased from 46.7% to 80% (p =0.062) but in previously vaccinated patients the seroconversion rate did not change (29.7% vs. 32.4%).
The use of prednisone and/or azathioprine was associated with lower anti-body responses to influenza vaccination
The use of immunosuppressives was heterogeneous, but stable during the du-ration of the study. Previous studies have reported lower antibody responses to influenza vaccination in SLE patients treated with steroids and azathioprine, but not in patients treated with hydroxychloroquine [18, 25-27]. We performed a suba-nalysis in which patients using prednisone and/or azathioprine (PRED/AZA; n=28) were compared with patients using no immunosuppressives or hydroxychloro-quine only (NO-imm/HCQ; n=17); patients using other immunosuppressive drugs then prednisone, azathioprine and hydroxychloroquine were excluded because of low numbers (n=7). PRED/AZA patients were somewhat younger than NO-imm/HCQ patients, but the groups did not differ with regard to influenza vaccination in the preceding year. PRED/AZA patients had a lower antibody response to influ-enza vaccination as compared to NO imm/HCQ patients, reflected by a lower GMT against A/H1N1 and A/H3N2 following the first vaccination, and a lower serocon-version rate for A/H1N1. The second vaccination had a slight additional effect for A/H1N1 within PRED/AZA patients (table 2).
Disease parameters did not increase following the influenza vaccinations and ad-verse effects of both vaccinations were mild in SLE patients
SLEDAI scores and levels of anti-double stranded DNA antibodies did not increase following the vaccinations. Levels of C3 and C4 remained almost stable during this period; slight increases of C3 and C4 levels were observed (Table 3). More SLE patients (19.6%) experienced erythema after both the first and second vaccination, compared to HC (0%; p =0.013). In SLE patients, adverse effects to the first and second vaccination were comparable (data not shown).

90
Cha
pter
5
Tab
le 2
. Eff
ects
of
imm
unos
uppr
essi
ve d
rugs
on
anti
body
res
pons
es
SLE
pati
ents
Pre
dnis
one/
AZ
AP
atie
nts
not
usin
g im
mun
osup
pres
sive
s/H
CQ
(n=2
8)(n
=17)
t=0
t=1
t=2
t=0
t=1
t=2
Age
, mea
n ±
SD, y
ears
42.1
± 9.
248
.4 ±
10*
Infl
uenz
a va
ccin
atio
n in
pre
viou
s ye
ar (2
00
6), n
(%)
21 (7
5)12
(70
.6)
SP r
ate,
n (%
)
H1N
114
(50
)23
(82.
1)25
(89.
3)8
(47.
1)16
(94.
1)16
(94.
1)
H3N
210
(35.
7)19
(67.
9)19
(67.
9)13
(76.
5)*
16 (9
4.1)
***
16 (9
4.1)
***
B11
(39.
3)17
(60
.7)
17 (6
0.7
)7
(41.2
)11
(64.
7)10
(58.
8)
GM
T
H1N
139
.572
.592
.8#
3213
0.5
*13
0.5
H3N
220
3941
39.2
*78
.4*
83.3
*
B22
.936
.740
18.4
40.8
43.4
SC r
ate,
n (%
)
H1N
1N
/A4
(14.
3)3
(10
.7)
N/A
11 (6
4.7)
**1 (
5.9)
H3N
2N
/A5
(17.
9)0
N/A
5 (2
9.4)
0
BN
/A3
(10
.7)
0N
/A5
(29.
4)0
t=0
: pri
or t
o va
ccin
atio
n; t
=1: 4
wee
ks a
fter
the
fir
st v
acci
nati
on; t
=2: 8
wee
ks a
fter
the
fir
st v
acci
nati
on, 4
wee
ks a
fter
the
sec
ond
vacc
inat
ion.
A
ZA
, aza
thio
prin
e; H
CQ
, hyd
roxy
chlo
roqu
ine;
SP
rat
e, s
erop
rote
ctio
n ra
te; S
C r
ate,
ser
ocon
vers
ion
rate
; N/A
, not
app
licab
le*
p <0
.05;
**p
<0
.01;
***
p =0
.064
(SLE
pat
ient
s us
ing
pred
niso
ne a
nd/o
r A
ZA
vs
pati
ents
usi
ng n
o im
mun
osup
pres
sive
dru
gs o
r H
CQ
onl
y); #
p <
0.0
5 (t
=2 v
s t=
1).

91
Cha
pter
5
dIscussIonIn SLE, a hampered antibody response to influenza vaccination has been reported in several studies [7]. As seroprotection rates are related to clinical protection from influenza, strategies to improve antibody responses are relevant in SLE. In the present study, we evaluated whether a second, booster, influenza vaccination could increase antibody titers. We did not find such an enhancing effect. Follo-wing the first vaccination, seroprotection rates and GMTs rose for each strain, but these did not rise further following the second vaccination. As an exception, there was a clear trend in the response to A/H1N1 in SLE patients who were not vaccinated in the previous year. This response did increase following the booster vaccination, in terms of GMT and seroconversion rate. The booster vaccination had mild adverse effects and did not increase SLEDAI scores.
Our findings regarding A/H1N1 in patients not vaccinated in the previous year ap-pear to be in accordance with a previous study in SLE patients, in which boosting was performed for A/H1N1 solely and was found to increase GMTs [12]. In this stu-dy, no information is presented regarding previous influenza vaccinations but it is likely that most patients had not received an influenza vaccination before, since there was much uncertainty regarding safety of vaccination in SLE [5].
In liver transplantation patients, a trivalent booster vaccination (28 days after the first vaccination) led to higher GMTs to all vaccine strains. Furthermore, the seroprotection rate against all three strains increased from >68% after the first vaccination to >80% after the booster vaccination [11]. Also in frail elderly, a boos-ter vaccination after 84 days increased GMTs, as detected by ELISA assay [28]. In healthy elderly, increases in seroconversion rate and GMT following a booster vaccination have been reported [21], however, the majority of studies did not find an additional effect [29, 30]. Similarly, in other patient groups such as bone mar-row transplant recipients [16], severely immunocompromised HIV patients [17] and dialysis patients [10, 13-15], booster vaccination did not have additional value. Also in healthy adults, booster vaccination did not increase antibody responses [11, 15,
Table 3. Disease parameters
t=0 t=1 t=2
SLEDAI, median (range) 2 (0-4) 2.5 (0-8) 2 (0-8)
Anti-dsDNA, median (range) (units/ml) 16 (<3-397) 18.5 (<3-275) 18.5 (<3-261)
C3, median (range) (g/l) 0.91 (0.42-1.42) 0.91 (0.35-1.45) 0.93 (0.31-1.45)*
C4, median (range) (g/l) 0.14 (<0.02-0.52) 0.15 (<0.02-0.52) 0.16 (0.02-0.50)**
t=0: prior to vaccination; t=1: four weeks after the first vaccination; t=2: eight weeks after the first vaccination, four weeks after the second vaccination; Anti-dsDNA: anti-double-stranded DNA; C3, C4: complement C3 and C4. * p < 0.05, ** p<0.01: at t=8 weeks vs. t=0 (prior to vaccination)
92
Cha
pter
5
17, 21].
Why booster vaccination did not improve the antibody response to influenza in SLE patients remains speculative. First, previous vaccinations appear to limit the effect of a booster vaccination, as reported in this study. Second, it may be ar-gued that booster vaccination can only have effect in patients with a low titer (<40) after a first vaccination. In this study, over 80% of patients had achieved protective titers to the A strains after the first vaccination and for these strains this may have hindered a further increase. This does not apply for the B strain as the seroprotection rate was 61.5% after the first vaccination. Nevertheless, the seroprotection rate to the B strain did not increase either following the booster vaccination.
Responses and titers to the B strain were low in both patients and HC. Generally, antibody titers to B strains are lower than titers to A strains [16, 31, 32]. This may be due to lower immunogenicity of the B strain as compared to the A strains, or a lower sensitivity of the HIA. The HIA for influenza B with whole virus particles, which is standard and was applied here, was previously found to be less sensitive than testing with influenza B virus disrupted with ether [33].
In accordance with previous reports, the use of prednisone and/or azathioprine was associated with lower antibody responses to influenza vaccination in SLE pa-tients [18, 25-27].
As a secondary study question, we evaluated whether a booster vaccination, sup-posed it were effective, would increase antibody responses in SLE patients up to levels reached in HC after a single vaccination. However, we did not observe differences in antibody responses between SLE patients and HC. Patients showed similar responses as in a previous study, but the responses of HC were lower than expected [18]. Although also some previous studies did not find differences between patients and HC [26, 34-36], most have shown antibody responses in SLE patients to be lower than in HC [12, 18, 25, 27, 37]. Furthermore, we found that cell-mediated responses to influenza vaccination, which correlate to clinical protec-tion from influenza infection, are hampered in SLE as well [38].
It is not clear why in the present study, SLE patients and HC did not differ in anti-body responses, but several factors could be involved. First, lack of power, as the study was not powered to study this question. Second, lower immunogenicity of current vaccine strains could have restrained differences between patients and HC. Third, HC had a higher degree of previous influenza vaccinations as compared to a previous study, while they did not differ with regard to age and sex [18]. Pos-sibly, influenza vaccinations in the preceding year hindered antibody responses
93
Cha
pter
5
[39-41], in which case previous findings of impaired responses were (partly) due to differences in vaccination history between SLE patients and HC. This implicates that actual differences between SLE patients and HC may be less than expected. In an extensive overview, Beyer et al. reported that especially for the B strain there is a general tendency to a lower postvaccination GMT and seroprotection rate in previously vaccinated groups [31], as we observed in our HC. It has been suggested that vaccines which are antigenically close to a prior vaccine may be partially eliminated by pre-existent cross-reactive antibodies, thus reducing the immune response [42].
Finally, the influenza vaccinations did not affect disease activity, which is in ac-cordance with previous studies [5]. However, it has been reported previously that although SLEDAI scores remain stable after influenza vaccination, levels of auto-antibodies may transiently increase [43].
In this study, a control group of SLE patients vaccinated once was not included, which might be a limitation. Here, SLE patients functioned as their own controls with regard to the effects of the first and the booster vaccination. This increased the statistical power to detect the expected additional effect of a booster vacci-nation, as it enabled a matched samples analysis. This has been done previously [11, 12, 14-17, 21, 32], though indeed some studies included a patient group vaccina-ted once and a patient group vaccinated twice [10, 13, 28-30].
In summary, booster vaccination with subunit influenza vaccine had no additional value in annually vaccinated SLE patients. In this study we did not find differences between SLE patients and HC in the antibody response to subunit influenza vacci-ne. However, the study was not designed and powered to detect such a difference. Therefore, we do not challenge previous studies showing decreased responses in SLE patients after influenza vaccination. As such, other strategies to improve antibody responses, mentioned earlier, should be considered. For example, the use of an MF59-adjuvanted influenza vaccine, which has a higher immunogenicity than conventional trivalent inactivated vaccine in adults with chronic diseases [8]. Another option would be to use an increased vaccine dose. In hemodialysis pa-tients, not using immunosuppressive drugs, a booster influenza vaccination did not have an additional effect upon titers, but a single double-dose vaccine did have additional value [10]. Finally, intradermal application of conventional influ-enza vaccine was reported to have higher immunogenicity in elderly as compared to intramuscular vaccination [9]. Whether these strategies enhance the immune response to influenza vaccination in SLE should be studied in controlled studies.
We conclude that the positive effect of a booster influenza vaccination on antibo-dy responses was limited to SLE patients who were not vaccinated in the previous

94
Cha
pter
5
year. These findings are restricted to patients with quiescent disease. Our results implicate that there is no additional value in offering a booster to annually vacci-nated SLE patients. This is of clinical importance, as annual influenza vaccination is recommended in SLE patients. Finally, it should be noted that in SLE patients who were not vaccinated in the previous year, administration of a booster vac-cination may be considered.
95
Cha
pter
5
reference list
(1) Fessler BJ. Infectious diseases in systemic lupus erythematosus: risk factors, management and
prophylaxis. Best Pract Res Clin Rheumatol. 16, 281-291 (2002).
(2) Nicholson KG, Wood JM & Zambon M. Influenza. Lancet 362, 1733-1745 (2003).
(3) Hayden FG. Prevention and treatment of influenza in immunocompromised patients. Am J Med.
102, 55-60 (1997).
(4) Influenza vaccines. Wkly Epidemiol Rec. 80, 279-287 (2005).
(5) Conti F, Rezai S & Valesini G. Vaccination and autoimmune rheumatic diseases. Autoimmun Rev.
8, 124-128 (2008).
(6) Gluck T. Vaccinate your immunocompromised patients! Rheumatology. (Oxford) 45, 9-10 (2006).
(7) Holvast B, Huckriede A, Kallenberg CG & Bijl M. Influenza vaccination in systemic lupus erythe-
matosus: safe and protective? Autoimmun Rev. 6, 300-305 (2007).
(8) Baldo V, Baldovin T, Floreani A, Carraro AM & Trivello R. MF59-adjuvanted influenza vaccine
confers superior immunogenicity in adult subjects (18-60 years of age) with chronic diseases
who are at risk of post-influenza complications. Vaccine 25, 3955-3961 (2007).
(9) Holland D et al. Intradermal influenza vaccine administered using a new microinjection system
produces superior immunogenicity in elderly adults: a randomized controlled trial. J Infect Dis.
198, 650-658 (2008).
(10) Rautenberg P, Proppe D, Schutte A & Ullmann U. Influenza subtype-specific immunoglobulin A
and G responses after booster versus one double-dose vaccination in hemodialysis patients. Eur
J Clin Microbiol Infect Dis. 8, 897-900 (1989).
(11) Soesman NM et al. Efficacy of influenza vaccination in adult liver transplant recipients. J Med
Virol. 61, 85-93 (2000).
(12) Brodman R, Gilfillan R, Glass D & Schur PH. Influenzal vaccine response in systemic lupus erythe-
matosus. Ann Intern Med. 88, 735-740 (1978).
(13) Song JY et al. Active influenza immunization in hemodialysis patients: comparison between
single-dose and booster vaccination. Am J Nephrol. 26, 206-211 (2006).
(14) Tanzi E et al. Lack of effect of a booster dose of influenza vaccine in hemodialysis patients. J
Med Virol. 79, 1176-1179 (2007).
(15) Versluis DJ et al. Value of booster immunisation with influenza vaccine in patients undergoing
haemodialysis. Br Med J (Clin Res Ed). 294, 348 (1987).
(16) Engelhard D et al. Antibody response to a two-dose regimen of influenza vaccine in allogeneic T
cell-depleted and autologous BMT recipients. Bone Marrow Transplant. 11, 1-5 (1993).
(17) Kroon FP, van Dissel JT, de Jong JC & van Furth R. Antibody response to influenza, tetanus and
pneumococcal vaccines in HIV-seropositive individuals in relation to the number of CD4+ lymp-
hocytes. AIDS 8, 469-476 (1994).
(18) Holvast A et al. Safety and efficacy of influenza vaccination in systemic lupus erythematosus
patients with quiescent disease. Ann Rheum Dis. 65, 913-918 (2006).
(19) Mackenzie JS. Influenza subunit vaccine: antibody responses to one and two doses of vaccine
and length of response, with particular reference to the elderly. Br Med J. 1, 200-202 (1977).
(20) Tan EM et al. The 1982 revised criteria for the classification of systemic lupus erythematosus.
Arthritis Rheum. 25, 1271-1277 (1982).
(21) Bombardier C, Gladman DD, Urowitz MB, Caron D, & Chang CH. Derivation of the SLEDAI. A
96
Cha
pter
5
disease activity index for lupus patients. The Committee on Prognosis Studies in SLE. Arthritis
Rheum. 35, 630-640 (1992).
(22) Harmon MW. Influenza viruses. In: Lennette, editor. Laboratory diagnosis of viral infections, 2nd
ed. New York, Marcel Dekker, Inc, 2004:515-34.
(23) de Jong JC et al. Antigenic heterogeneity within influenza A (H3N2) virus strains. Bull World
Health Organ. 66, 47-55 (1988).
(24) European Medicines Agency (EMEA). Note for guidance on harmonisation of requirements for
influenza vaccines. Report No.: CPMP/BWP/214/96 (1997).
(25) Abu-Shakra M et al. Specific antibody response after influenza immunization in systemic lupus
erythematosus. J Rheumatol. 29, 2555-2557 (2002).
(26) Herron A et al. Influenza vaccination in patients with rheumatic diseases. Safety and efficacy.
JAMA 242, 53-56 (1979).
(27) Williams GW et al. Influenza immunization in systemic lupus eruthematosus. A double-blind trial.
Ann Intern Med. 88, 729-734 (1978).
(28) Roos-Van Eijndhoven DG et al. Randomized controlled trial of seroresponses to double dose and
booster influenza vaccination in frail elderly subjects. J Med Virol. 63, 293-298 (2001).
(29) Gross PA et al. Immunization of elderly people with two doses of influenza vaccine. J Clin Micro-
biol. 25, 1763-1765 (1987).
(30) McElhaney JE, Hooton JW, Hooton N & Bleackley RC. Comparison of single versus booster dose
of influenza vaccination on humoral and cellular immune responses in older adults. Vaccine 23,
3294-3300 (2005).
(31) Beyer WE et al. Effects of repeated annual influenza vaccination on vaccine sero-response in
young and elderly adults. Vaccine 14, 1331-1339 (1996).
(32) Neuzil KM et al. Immunogenicity and reactogenicity of 1 versus 2 doses of trivalent inactivated
influenza vaccine in vaccine-naive 5-8-year-old children. J Infect Dis. 194, 1032-1039 (2006).
(33) Berlin BS, McQueen JL, Minuse E & Davenport FM. A method for increasing the sensitivity of the
hemagglutination-inhibition test with equine influenza virus. Virology 21, 665-666 (1963).
(34) Del Porto F et al. Influenza vaccine administration in patients with systemic lupus erythemato-
sus and rheumatoid arthritis. Safety and immunogenicity. Vaccine 24, 3217-3223 (2006).
(35) Kanakoudi-Tsakalidou F, Trachana M, Pratsidou-Gertsi P, Tsitsami E & Kyriazopoulou-Dalaina V.
Influenza vaccination in children with chronic rheumatic diseases and long-term immunosup-
pressive therapy. Clin Exp Rheumatol. 19, 589-594 (2001).
(36) Louie JS et al. Clinical and antibody responses after influenza immunization in systemic lupus
erythematosus. Ann Intern Med. 88, 790-792 (1978).
(37) Ristow SC, Douglas RG, Jr. & Condemi JJ. Influenza vaccination of patients with systemic lupus
erythematosus. Ann Intern Med. 88, 786-789 (1978).
(38) McElhaney JE et al. T cell responses are better correlates of vaccine protection in the elderly. J
Immunol. 176, 6333-6339 (2006).
(39) Govaert TM et al. Immune response to influenza vaccination of elderly people. A randomized
double-blind placebo-controlled trial. Vaccine 12, 1185-1189 (1994).
(40) Gross PA et al. Paradoxical response to a novel influenza virus vaccine strain: the effect of prior
immunization. Vaccine.17, 2284-2289 (1999).
(41) Pyhala R, Kumpulainen V, Alanko S & Forsten T. HI antibody kinetics in adult volunteers immu-
nized repeatedly with inactivated trivalent influenza vaccine in 1990-1992. Vaccine 12, 947-952

97
Cha
pter
5
(1994).
(42) Smith DJ, Forrest S, Ackley DH & Perelson AS. Variable efficacy of repeated annual influenza
vaccination. Proc Natl Acad Sci. 96, 14001-14006 (1999).
(43) Abu-Shakra M, Press J, Sukenik S & Buskila D. Influenza virus vaccination of patients with SLE:
effects on generation of autoantibodies. Clin Rheumatol. 21, 369-372 (2002).

CHAPT
ER6H u m o r a l r e s p o n s e s a f t e r i n f l u e n z a vaccinat ion are severely reduced in p a t i e n t s w i t h rheumatoid a r t h r i t i s t r e a t e d w i t h r i t u x i m a b
S. van Assen
A. Holvast
C.A. Benne
M.D. Posthumus
M.A. van Leeuwen
A.E. Voskuyl
M. Blom
A.P. Risselada
A. de Haan
J. Westra
C.G.M. Kallenberg
M. Bijl
Arthritis & Rheumatism 2010 Jan;62(1):75-81

100
Cha
pter
6
AbsTrAcTIntroduction For patients with rheumatoid arthritis (RA), yearly influenza vaccination is recommended. However, its efficacy in patients treated with rituximab is unknown. The objectives of this study were to investigate the efficacy of influenza vaccination in RA patients treated with rituximab and to investigate the duration of the possible suppression of the humoral im-mune response following rituximab treatment. We also undertook to as-sess the safety of influenza vaccination and the effects of previous influ-enza vaccination.
Methods Trivalent influenza subunit vaccine was administered to 23 RA patients who had received rituximab (4–8 weeks after rituximab for 11 pa-tients [the early rituximab subgroup] and 6–10 months after rituximab for 12 patients [the late rituximab subgroup]), 20 RA patients receiving metho-trexate (MTX), and 29 healthy controls (HC). Levels of antibodies against the three vaccine strains were measured before and 28 days after vaccination using hemagglutination inhibition assay. The Disease Activity Score in 28 joints (DAS28) was used to assess RA activity.
results Following vaccination, geometric mean titers (GMTs) of anti-in-fluenza antibodies significantly increased for all influenza strains in the MTX-treated group and in HC, but for no strains in the rituximab-treated group. However, in the late rituximab subgroup, a rise in GMT for the A/H3N2 and A/H1N1 strains was demonstrated, in the absence of a repopu-lation of CD19+ cells at the time of vaccination. Seroconversion and serop-rotection occurred less often in the rituximab-treated group than in the MTX-treated group for the A/H3N2 and A/H1N1 strains, while seroprotecti-on occurred less often in the rituximab-treated group than in the HC for the A/H1N1 strain. Compared with unvaccinated patients in the rituximab-tre-ated group, previously vaccinated patients in the rituximab-treated group had a higher pre- and postvaccination GMT for the A/H1N1 strain. The DAS28 did not change after vaccination.
conclusion Rituximab reduces humoral responses following influenza vaccination in RA patients, with a modestly restored response 6–10 months after rituximab administration. Previous influenza vaccination in rituximab- treated patients increases pre- and postvaccination titers. RA activity was not influenced.

101
Cha
pter
6
InTroducTIonPatients with rheumatoid arthritis (RA) are considered immunocompromised and at increased risk of infection [1]. Therefore, although the exact prevalence, morbi-dity, and mortality of influenza in patients with RA are unknown, yearly influenza vaccination is recommended [2]. Influenza vaccination is safe and results in pro-tective levels of anti-influenza antibodies in most RA patients, even when they are treated with prednisone, disease-modifying antirheumatic drugs (DMARDs), or tumor necrosis factor α–blocking agents [3, 4]. A growing number of RA patients are being treated with rituximab, depleting B-cells for 6–9 months. Theoretically, humoral responses to neoantigens cannot be elicited during B-cell depletion. Anti- influenza antibody response after influenza vaccination has been shown to be blunted in RA patients treated with rituximab [5, 6]. However, the exact level and duration of suppression of the humoral immune response and the influence of previous influenza vaccination on antibody response after treatment with rituxi-mab remain unclear.
In order to make recommendations for the usefulness and timing of influenza vaccination in RA patients treated with rituximab, we investigated humoral re-sponses in RA patients following vaccination with trivalent subunit influenza vac-cine 4–8 weeks or 6–10 months after treatment with rituximab. The responses were compared with responses in RA patients treated with methotrexate (MTX) and with responses in healthy controls (HC). In addition, the influence of previous influenza vaccination on antibody response and the safety of influenza vaccina-tion were assessed.
PATIenTs And MeThods
Patients and healthy controls
Patients had to fulfill the American College of Rheumatology (formerly, the Ame-rican Rheumatism Association) 1987 revised criteria for the classification of RA. Two groups of RA patients were defined. The first group of RA patients (the ri-tuximab group) received influenza vaccination either 4–8 weeks after treatment with rituximab (the early rituximab subgroup) or 6–10 months after treatment with rituximab (the late rituximab subgroup). Rituximab was administered intra-venously (IV) in 2 cycles of 1,000 mg with 100 mg IV methylprednisolone, except for one patient who instead received 4 cycles of 375 mg/m2 based on a proto-col for concomitant mixed cryoglobulinemia. The second group (the MTX group) consisted of RA patients who were treated with MTX at a minimum dosage of 10 mg/week, eventually with additional DMARDs. Health care workers served as HC. Patients in the rituximab group were recruited in all 4 participating Dutch univer-
102
Cha
pter
6
sity medical centers. RA patients receiving MTX and HC were recruited from the University Medical Center Groningen.
Exclusion criteria were no informed consent, age <18 years, malignancy, preg-nancy, or known allergy to or former severe reaction following vaccination with trivalent influenza subunit vaccine.
Vaccine
We used trivalent influenza subunit vaccine (Influvac® 2007–2008; Solvay Phar-maceuticals, Weesp, The Netherlands) containing purified hemagglutinin and neuramidase of the following strains: A/Wisconsin/67/2005 (H3N2)–like strain (A/H3N2 strain), A/Solomon Islands/3/2006 (H1N1)–like strain (A/H1N1 strain), and B/Malaysia/2506/2004-like strain (B strain).
Procedures
Patients and HC received the influenza vaccine intramuscularly from October 2007 until January 2008. Immediately before and 28 ± 3 days (mean ± SD) after vaccination, blood was drawn for measurement of CD19+ cell count, C-reactive protein level, erythrocyte sedimentation rate, and anti-influenza antibodies. The Disease Activity Score in 28 joints (DAS28) was recorded before and 7 and 28 days after vaccination. Information on previous influenza vaccination was obtained from all participants, and adverse effects occurring in the first 7 days postvac-cination were recorded. The study was approved by the ethics committees of all participating centers.
hemagglutination inhibition assay
The hemagglutination inhibition assay (HIA) was used for the detection of anti-influenza antibodies. HIAs were performed with guinea pig erythrocytes in ac-cordance with standard procedures [7]. The following parameters for efficacy of vaccination based on anti-influenza antibody response were evaluated: geometric mean titer (GMT), fold increase in titer, ≥4-fold titer rise resulting in a postvac-cination level of ≥40 (seroconversion), and titer rise to ≥40 (seroprotection). HIA titers ≥40 are generally considered to be protective in healthy adults [8].
statistical analysis
All other data are presented as the median and range, except for GMTs, which are shown as the mean ± SD. Data were analyzed using SPSS 16.0 for Windows (SPSS, Chicago, IL). Analysis of variance, Student’s t-test with Bonferroni correction, the Kruskal-Wallis test, Friedman’s test, Wilcoxon’s signed rank test, the Mann-
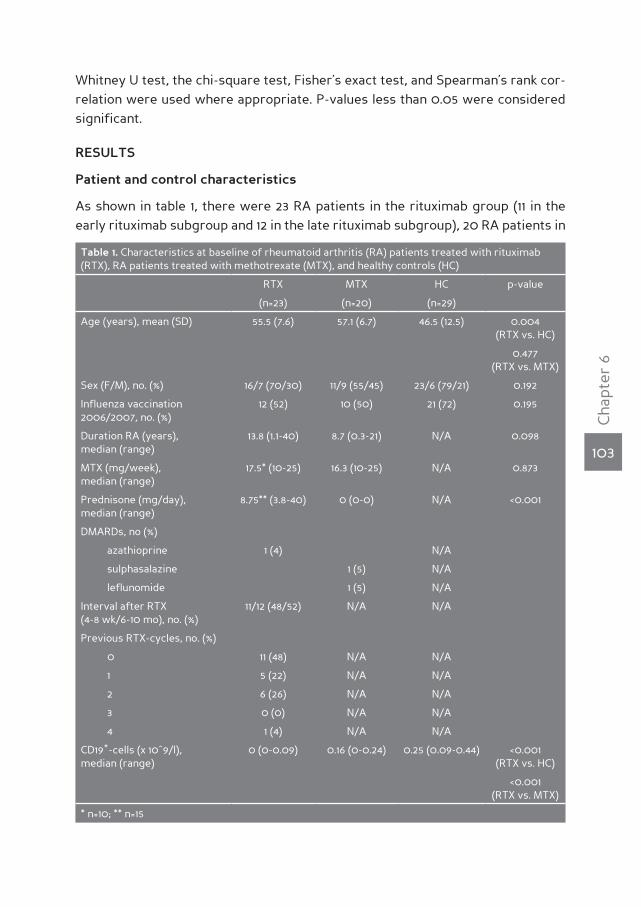
103
Cha
pter
6
Whitney U test, the chi-square test, Fisher’s exact test, and Spearman’s rank cor-relation were used where appropriate. P-values less than 0.05 were considered significant.
resulTs
Patient and control characteristics
As shown in table 1, there were 23 RA patients in the rituximab group (11 in the early rituximab subgroup and 12 in the late rituximab subgroup), 20 RA patients in
Table 1. Characteristics at baseline of rheumatoid arthritis (RA) patients treated with rituximab (RTX), RA patients treated with methotrexate (MTX), and healthy controls (HC)
RTX MTX HC p-value
(n=23) (n=20) (n=29)
Age (years), mean (SD) 55.5 (7.6) 57.1 (6.7) 46.5 (12.5) 0.004 (RTX vs. HC)
0.477 (RTX vs. MTX)
Sex (F/M), no. (%) 16/7 (70/30) 11/9 (55/45) 23/6 (79/21) 0.192
Influenza vaccination 2006/2007, no. (%)
12 (52) 10 (50) 21 (72) 0.195
Duration RA (years), median (range)
13.8 (1.1-40) 8.7 (0.3-21) N/A 0.098
MTX (mg/week), median (range)
17.5* (10-25) 16.3 (10-25) N/A 0.873
Prednisone (mg/day), median (range)
8.75** (3.8-40) 0 (0-0) N/A <0.001
DMARDs, no (%)
azathioprine 1 (4) N/A
sulphasalazine 1 (5) N/A
leflunomide 1 (5) N/A
Interval after RTX (4-8 wk/6-10 mo), no. (%)
11/12 (48/52) N/A N/A
Previous RTX-cycles, no. (%)
0 11 (48) N/A N/A
1 5 (22) N/A N/A
2 6 (26) N/A N/A
3 0 (0) N/A N/A
4 1 (4) N/A N/A
CD19+-cells (x 10^9/l), median (range)
0 (0-0.09) 0.16 (0-0.24) 0.25 (0.09-0.44) <0.001 (RTX vs. HC)
<0.001 (RTX vs. MTX)
* n=10; ** n=15
104
Cha
pter
6
the MTX group, and 29 HC. The mean age of patients in the rituximab group did not differ significantly from that in the MTX group (p =0.477) but was higher than that in the healthy control group (p =0.004). Patients in the rituximab group had higher baseline DAS28 scores than patients in the MTX group (p =0.001) and lower B-cell counts than patients in the MTX group and HC (both p <0.001).
efficacy of influenza vaccination
Geometric mean titers (table 2)
As expected, the GMTs of antibodies against the A/H3N2 and B strains prior to vaccination were higher in HC (p =0.002 and p =0.008, respectively, versus the rituximab and MTX groups combined), since more HC had received an influenza vaccination in the 2006–2007 season. Compared with GMTs before vaccination, GMTs following vaccination increased for all 3 influenza strains both in the HC (p =0.001 for the A/H3N2 strain, p <0.001 for the A/H1N1 strain, p <0.001 for the B strain) and in the MTX group (p <0.001 for the A/H3N2 strain, p <0.001 for the A/H1N1 strain, p =0.022 for the B strain). In contrast, no significant increase in GMT after vaccination was found in the rituximab group as a whole. Postvaccina-tion titers were higher for all 3 strains in the HC and for the A/H3N2 and A/H1N1 strains in the MTX group than in the rituximab group. Compared with the rituxi-mab group, the fold increase in titer was larger in the HC for the A/H1N1 strain (p =0.001) and the B strain (p =0.030) and larger in the MTX group for the A/H3N2 and A/H1N1 strains (both p <0.001).
GMT rose after vaccination in the late rituximab subgroup for the A/H3N2 strain (p =0.040) and the A/H1N1 strain (p =0.042), but not in the early rituximab sub-group, resulting in higher postvaccination GMT (p =0.040 for the A/H3N2 strain, p =0.003 for the A/H1N1 strain, p =0.007 for the B strain) and larger fold increase (p =0.041 for the A/H3N2 strain, p =0.043 for the A/H1N1 strain) in the late rituximab subgroup, thereby indicating some recovery of the humoral immune response 6–10 months after treatment with rituximab. At baseline, the peripheral blood CD19+ cell count was comparable for the early and late rituximab subgroups (me-dian [range] 0 x 109/liter [0 to 0.01] versus 0 x 109/liter [0 to 0.08], respectively; p =0.072). However, 28 days after vaccination, significantly more B-cells were present in the late rituximab subgroup than in the early rituximab subgroup (me-dian [range] 0.01 x 109/liter [0 to 0.10] versus 0 x 109/liter [0 to 0]; p =0.004).
Seroconversion
Seroconversion occurred more often in the MTX group than in the rituximab group for the A/H3N2 strain (p =0.011) and the A/H1N1 strain (p =0.020). Seroconversion for any of the 3 influenza strains occurred in only 3 patients in the rituximab group
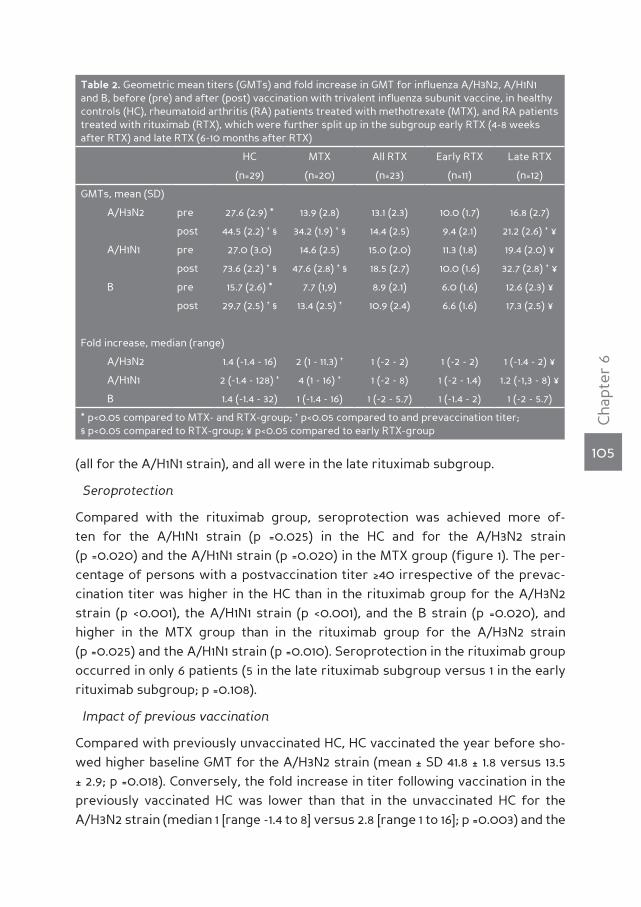
105
Cha
pter
6
(all for the A/H1N1 strain), and all were in the late rituximab subgroup.
Seroprotection
Compared with the rituximab group, seroprotection was achieved more of-ten for the A/H1N1 strain (p =0.025) in the HC and for the A/H3N2 strain (p =0.020) and the A/H1N1 strain (p =0.020) in the MTX group (figure 1). The per-centage of persons with a postvaccination titer ≥40 irrespective of the prevac-cination titer was higher in the HC than in the rituximab group for the A/H3N2 strain (p <0.001), the A/H1N1 strain (p <0.001), and the B strain (p =0.020), and higher in the MTX group than in the rituximab group for the A/H3N2 strain (p =0.025) and the A/H1N1 strain (p =0.010). Seroprotection in the rituximab group occurred in only 6 patients (5 in the late rituximab subgroup versus 1 in the early rituximab subgroup; p =0.108).
Impact of previous vaccination
Compared with previously unvaccinated HC, HC vaccinated the year before sho-wed higher baseline GMT for the A/H3N2 strain (mean ± SD 41.8 ± 1.8 versus 13.5 ± 2.9; p =0.018). Conversely, the fold increase in titer following vaccination in the previously vaccinated HC was lower than that in the unvaccinated HC for the A/H3N2 strain (median 1 [range -1.4 to 8] versus 2.8 [range 1 to 16]; p =0.003) and the
Table 2. Geometric mean titers (GMTs) and fold increase in GMT for influenza A/H3N2, A/H1N1 and B, before (pre) and after (post) vaccination with trivalent influenza subunit vaccine, in healthy controls (HC), rheumatoid arthritis (RA) patients treated with methotrexate (MTX), and RA patients treated with rituximab (RTX), which were further split up in the subgroup early RTX (4-8 weeks after RTX) and late RTX (6-10 months after RTX)
HC MTX All RTX Early RTX Late RTX
(n=29) (n=20) (n=23) (n=11) (n=12)
GMTs, mean (SD)
A/H3N2 pre 27.6 (2.9) * 13.9 (2.8) 13.1 (2.3) 10.0 (1.7) 16.8 (2.7)
post 44.5 (2.2) † § 34.2 (1.9) † § 14.4 (2.5) 9.4 (2.1) 21.2 (2.6) † ¥
A/H1N1 pre 27.0 (3.0) 14.6 (2.5) 15.0 (2.0) 11.3 (1.8) 19.4 (2.0) ¥
post 73.6 (2.2) † § 47.6 (2.8) † § 18.5 (2.7) 10.0 (1.6) 32.7 (2.8) † ¥
B pre 15.7 (2.6) * 7.7 (1,9) 8.9 (2.1) 6.0 (1.6) 12.6 (2.3) ¥
post 29.7 (2.5) † § 13.4 (2.5) † 10.9 (2.4) 6.6 (1.6) 17.3 (2.5) ¥
Fold increase, median (range)
A/H3N2 1.4 (-1.4 - 16) 2 (1 - 11.3) † 1 (-2 - 2) 1 (-2 - 2) 1 (-1.4 - 2) ¥
A/H1N1 2 (-1.4 - 128) † 4 (1 - 16) † 1 (-2 - 8) 1 (-2 - 1.4) 1.2 (-1,3 - 8) ¥
B 1.4 (-1.4 - 32) 1 (-1.4 - 16) 1 (-2 - 5.7) 1 (-1.4 - 2) 1 (-2 - 5.7)
* p<0.05 compared to MTX- and RTX-group; † p<0.05 compared to and prevaccination titer; § p<0.05 compared to RTX-group; ¥ p<0.05 compared to early RTX-group
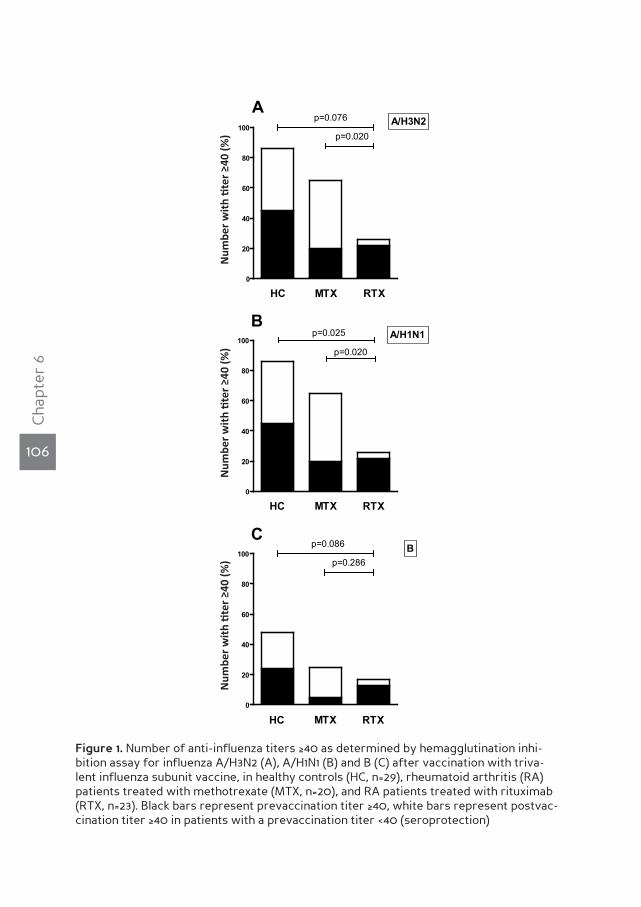
106
Cha
pter
6
Figure 1. Number of anti-influenza titers ≥40 as determined by hemagglutination inhi-bition assay for influenza A/H3N2 (A), A/H1N1 (B) and B (C) after vaccination with triva-lent influenza subunit vaccine, in healthy controls (HC, n=29), rheumatoid arthritis (RA) patients treated with methotrexate (MTX, n=20), and RA patients treated with rituximab (RTX, n=23). Black bars represent prevaccination titer ≥40, white bars represent postvac-cination titer ≥40 in patients with a prevaccination titer <40 (seroprotection)
0
20
40
60
80
100
HC MTX RTX
p=0.020
p=0.076
Num
ber w
ith ti
tre³ 4
0 (%
)
0
20
40
60
80
100p=0.020
RTX
p=0.025
MTXHC
Num
ber w
ith ti
tre³ 4
0 (%
)
0
20
40
60
80
100p=0.286
p=0.086
RTXMTXHC
Num
ber w
ith ti
tre³ 4
0 (%
)
Figure 1A
B
C
A/H3N2
A/H1N1
B
Num
ber
wit
h ti
ter
≥40
(%)
Num
ber
wit
h ti
ter
≥40
(%)
Num
ber
wit
h ti
ter
≥40
(%)

107
Cha
pter
6
B strain (median 1.4 [range -1.4 to 8] versus 2.8 [range 1 to 32]; p =0.023). In the MTX group, higher baseline GMT in vaccinated patients than in unvaccinated patients were shown for the A/H1N1 strain (mean ± SD 31.8 ± 2.1 versus 9.7 ± 2.7; p =0.019) and the B strain (mean ± SD 10.4 ± 2.0 versus 5.7 ± 1.6; p =0.015). In the MTX group, there was a lower fold increase in the previously vaccinated patients than in the unvac-cinated patients for the A/H3N2 strain (median 1.4 [range 1 to 4] versus 4 [range 2 to 11.3]; p =0.003), the A/H1N1 strain (median 2 [range 1 to 5.7] versus 6.7 [range 1 to 16]; p =0.018), and the B strain (median 1 [range -1.4 to 1] versus 3.4 [range 1 to 16]; p =0.001). In the rituximab group, compared with patients who were not pre-viously vaccinated, patients who were previously vaccinated had higher baseline antibody titers against the A/H1N1 strain (mean ± SD 19.4 ± 1.8 versus 11.3 ± 2.0; p =0.036) as well as higher postvaccination antibody titers against the A/H1N1 strain (mean ± SD 30.8 ± 2.6 versus 10.7 ± 2.0; p =0.007).
Seroconversion occurred more often for the A/H3N2 strain in the unvaccinated MTX group than in the vaccinated MTX group (50% versus 0%; p =0.016), but not for the HC or the rituximab group for any of the influenza strains (data not shown).
Previously unvaccinated HC more often developed seroprotection for the influ-enza B strain than did previously vaccinated HC (75% versus 9.5%; p =0.001). Previ-ously unvaccinated patients in the MTX group developed seroprotection for strain A/H3N2 (70% versus 20%; p =0.035) and strain B (40% versus 0%; p =0.043) more frequently than patients vaccinated the year before. However, the number of pa-tients with a postvaccination titer ≥40, irrespective of prevaccination titer, did not differ between previously vaccinated and unvaccinated patients in the rituximab group (data not shown).
Correlations between B-cell numbers and vaccination responses
In the rituximab group, CD19+ B-cells tended to increase 4 weeks after vaccina-tion (from median 0 x 109/liter [range 0 to 0.08] to 0 x 109/liter [range 0 to 0.10]; p =0.058) due to regeneration of B-cells in the late rituximab subgroup; B-cells in the late rituximab subgroup increased following vaccination (from median 0 x 109/liter [range 0 to 0.08] to 0.01 x 109/liter [range 0 to 0.10]; p =0.031) in contrast to B-cells in the early rituximab subgroup (from median 0 x 109/liter [range 0 to 0.01] to 0 x 109/liter [range 0 to 0]; p =0.317). However, in both the early and late rituximab subgroups, there were no correlations between B-cell count and pre-vaccination GMT, postvaccination GMT, fold increase in GMT, rates of serocon-version, and rates of seroprotection (data not shown).
Safety of vaccination - side effects and RA activity
There were no differences between the 3 groups in the occurrence of side ef-

108
Cha
pter
6
fects. RA activity, assessed with the DAS28 prior to and 7 and 28 days after vac-cination, was not influenced by influenza vaccination in either the MTX group (me-dian 3.04 [range 0.77 to 5.17] versus 2.93 [range 0.49 to 3.71] versus 2.59 [range 1.00 to 4.22], respectively; p =0.287) or the rituximab group (median 3.95 [range 2.15 to 5.71] versus 3.97 [range 2.15 to 6.26] versus 4.02 [range 2.04 to 6.77], respectively; p =0.834).
dIscussIonThe present study clearly shows that humoral responses to influenza subunit vac-cine in RA patients receiving rituximab are severely hampered compared with those in RA patients receiving MTX and compared with those in HC. This holds true for almost all outcomes. Our results are in line with those from a study in 4 RA patients, which evaluated humoral responses following influenza vaccination 84 days after treatment with rituximab [6]. A larger study by Oren et al that included 14 RA patients receiving rituximab showed only a lower GMT for influenza B strain and reduced rates of achieving a combined end point of seroconversion and se-roprotection for influenza A/H3N2 strain in patients receiving rituximab, compa-red with 29 RA patients receiving various DMARDs and 21 HC [5]. The discrepancy between our results and those of Oren et al might be explained by the larger time span between treatment with rituximab and influenza vaccination in the study by Oren et al (18 months, versus 10 months in our late rituximab subgroup); further, only 7 patients received influenza vaccination in the first 6 months after rituximab in the study by Oren et al.
The hampered response seems temporary since a significant rise in GMT after influenza vaccination in the late rituximab subgroup was found, while there was no increase in GMT in the early rituximab subgroup. Moreover, the only 3 cases of seroconversion in the rituximab group occurred in the late rituximab subgroup, and of the 6 cases of seroprotection in the rituximab group, 5 occurred in the late rituximab subgroup.
Although B-cells are required for the development of humoral immune responses to neoantigens, and depletion of B-cells following rituximab would be expected to reduce humoral immune responses to neoantigens, no correlation could be de-monstrated between B-cell count and the humoral responses following influenza vaccination in the 3 groups studied. This might be attributed to insufficient sensi-tivity of the standard quantitative assessment of B-cells (the lowest measurable B-cell count being 0.01 x 109/liter) [9]. Responders to influenza vaccination in the late rituximab subgroup probably already achieved some level of B-cell repopula-tion that was undetectable using standard methods. Another explanation could be that the number of B-cells in lymphoid tissues (i.e., sites where vaccine-mediated

109
Cha
pter
6
immune responses are initiated) is not correctly reflected by the peripheral blood B-cell numbers; CD19+CD20- B-cells have been shown to remain in the bone mar-row after 2 cycles of rituximab in RA patients [10].
Yearly repeated influenza vaccination leads to higher prevaccination anti- influenza antibody titers during the following year [11] and to a reduction in mortality [12]. In the current study we indeed found higher prevaccination GMT and lower fold increase in titer in previously vaccinated HC and patients in the MTX group compared with previously unvaccinated HC and patients in the MTX group. However, in addition to a higher prevaccination titer for the A/H1N1 strain, previously vaccinated patients in the rituximab group had a higher postvaccination titer. Notably, peripheral blood B-cells after recovery from rituxi-mab-induced B-cell depletion mainly consist of immature and naive B-cells, and low numbers of B-cells remain for up to 2 years [13, 14]. Our findings may there-fore point to the persistence of memory B-cells in compartments other than the peripheral blood that are capable of responding to the vaccine, and indicate that repeated yearly vaccination could be of additional value in achieving adequate levels of anti-influenza antibodies following influenza vaccination of RA patients treated with rituximab. Influenza vaccination was safe. Side effects in the study groups were comparable, and influenza vaccination did not increase RA activity. Finally, one should keep in mind that the correlates of protection for influenza following influenza vaccination in immunocompromised patients are not well de-fined. Anti-influenza titers ≥40 determined by HIA are considered protective, and 50% of persons with a titer of 28 are estimated to be protected; however, this has only been validated in young healthy adults [8]. Moreover, cellular immune responses have been shown to be of major importance in vaccination-mediated protection against influenza [15], and these are affected by rituximab as well. Since even titers <28 might provide some level of protection, even small increases in anti-influenza titer can be of clinical relevance. Therefore, the modest rise in titer in the late rituximab subgroup might be valuable.
Our study has some limitations. First, although this is the largest study to evalu-ate the response to influenza vaccination in RA patients treated with rituximab, the number of patients is still relatively small. However, the results were uni-form, and statistical significance was reached for many parameters. Second, the HC were younger than the RA patients, and age is an important factor in influenza vaccination response [2]. Since the age of patients in the MTX and ri-tuximab groups was comparable, and HIA titers were significantly higher in the MTX group than in the rituximab group, the difference in HIA titers between HC and patients in the rituximab group was unlikely to be caused by differen-ces in age. Third, although the use of additional DMARDs was not standardized,

110
Cha
pter
6
most of the patients in the rituximab group who had been taking DMARDs were receiving MTX, and only 1 patient was receiving high-dose corticosteroids. In the MTX group, only 2 patients had taken DMARDs other than MTX. Therefore, we do not believe that the unrestricted use of DMARDs influenced the study out-come. Moreover, the allowance of additional DMARDs offers the possibility to extrapolate our data to daily practice, where use of additional DMARDs is com-mon. The difference in corticosteroid use between the MTX and rituximab groups probably did not change the outcome, since even prednisone at a dosage of >7.5 mg/day has been shown not to affect the humoral response following influenza vaccination in RA patients [3;4].
In conclusion, this study shows a severely hampered humoral immune response to trivalent subunit influenza vaccine in RA patients treated with rituximab com-pared with RA patients receiving MTX and compared with HC. This response was slightly restored but still reduced 6–10 months after rituximab treatment. Previ-ously vaccinated patients in the rituximab group achieved higher anti-influenza titers following influenza vaccination for the A/H1N1 strain than did patients in the rituximab group who were not previously vaccinated. We recommend yearly influenza vaccination for RA patients. For those patients who start rituximab tre-atment, preemptive influenza vaccination should be considered.

111
Cha
pter
6
reference list
(1) Wolfe F, Mitchell DM, Sibley JT, et al. The mortality of rheumatoid arthritis. Arthritis Rheum 1994
Apr; 37(4):481-94.
(2) MMWR Recomm Rep. 2006;55(RR-10):1-48
(3) Fomin I, Caspi D, Levy V, et al. Vaccination against influenza in rheumatoid arthritis: the effect
of disease modifying drugs, including TNF alpha blockers. Ann Rheum Dis 2006 Feb; 65(2):191-4.
(4) Chalmers A, Scheifele D, Patterson C, et al. Immunization of patients with rheumatoid arthritis
against influenza: a study of vaccine safety and immunogenicity. J Rheumatol 1994 Jul; 21(7):1203-6.
(5) Oren S, Mandelboim M, Braun-Moscovici Y, et al. Vaccination against influenza in patients with
rheumatoid arthritis: the effect of rituximab on the humoral response. Ann Rheum Dis 2008 Jul;
67(7):937-41.
(6) Gelinck LB, Teng YK, Rimmelzwaan GF, van den Bemt BJ, Kroon FP, van Laar JM. Poor serolo-
gical responses upon influenza vaccination in patients with rheumatoid arthritis treated with
rituximab. Ann Rheum Dis 2007 Oct; 66(10):1402-3.
(7) Holvast A, Huckriede A, Wilschut J, et al. Safety and efficacy of influenza vaccination in systemic
lupus erythematosus patients with quiescent disease. Ann Rheum Dis 2006 Jul; 65(7):913-8.
(8) de Jong JC, Palache AM, Beyer WE, Rimmelzwaan GF, Boon AC, Osterhaus AD. Haemagglutina-
tion-inhibiting antibody to influenza virus. Dev Biol (Basel) 2003; 115:63-73.
(9) Dass S, Rawstron AC, Vital EM, Henshaw K, McGonagle D, Emery P. Highly sensitive B cell ana-
lysis predicts response to rituximab therapy in rheumatoid arthritis. Arthritis Rheum 2008 Oct;
58(10):2993-9.
(10) Teng YK, Levarht EW, Hashemi M, et al. Immunohistochemical analysis as a means to predict
responsiveness to rituximab treatment. Arthritis Rheum 2007 Dec; 56(12):3909-18.
(11) Beyer WE, Palache AM, Sprenger MJ, et al. Effects of repeated annual influenza vaccination on
vaccine sero-response in young and elderly adults. Vaccine 1996 Oct; 14(14):1331-9.
(12) Voordouw AC, Sturkenboom MC, Dieleman JP, et al. Annual revaccination against influenza and
mortality risk in community-dwelling elderly persons. JAMA 2004 Nov 3; 292(17):2089-95.
(13) Roll P, Dorner T, Tony HP. Anti-CD20 therapy in patients with rheumatoid arthritis: predictors of
response and B cell subset regeneration after repeated treatment. Arthritis Rheum 2008 Jun;
58(6):1566-75.
(14) Roll P, Palanichamy A, Kneitz C, Dorner T, Tony HP. Regeneration of B cell subsets after transient
B cell depletion using anti-CD20 antibodies in rheumatoid arthritis. Arthritis Rheum 2006 Aug;
54(8):2377-86.
(15) McElhaney JE, Xie D, Hager WD, et al. T cell responses are better correlates of vaccine protec-
tion in the elderly. J Immunol 2006 May 15; 176(10):6333-9.

CHAPT
ER7Polyclonal andi n f l u e n z as p e c i f i cc e l l - m e d i a t e di m m u n eresponses are hampered in rheumatoida r t h r i t i sp a t i e n t st r e a t e d w i t h r i t u x i m a b
S. van Assen
A. de Haan
A.E. Voskuyl
A. Holvast
G. Horst
J. Westra
M.D. Posthumus
M.A. van Leeuwen
M. Blom
A.P. Risselada
C.G.M. Kallenberg
M. Bijl
Submitted
114
Cha
pter
7
AbsTrAcTIntroduction Yearly influenza vaccination is recommended for rheumatoid arthritis (RA) patients. However, humoral immune responses following influenza vaccination are severely hampered in RA patients treated with rituximab. Influenza-specific cell-mediated immune (CMI) responses follo-wing vaccination also contribute to protection against influenza. Therefore, we investigated CMI responses before and after influenza vaccination in RA patients treated with rituximab.
Methods 40 RA patients and 22 matched healthy controls (HC) were vacci-nated with trivalent influenza subunit vaccine. 21 RA patients had received rituximab and 19 RA patients were on methotrexate (MTX). Polyclonal and influenza-specific CMI responses were measured before, 7, and 28 days af-ter vaccination using flow cytometry, CFSE dye dilution proliferation assay and IFNγ-ELISpot.
results Before influenza vaccination, lower frequencies of polyclonally activated IL-2-producing CD4+ and CD8+ T-cells were observed in the rituximab-group compared to the MTX-group. Also, proliferation of polyclonally activated T-cells was lower in the rituximab-group compared with HC. Numbers of Influenza A/H1N1- specific IL-2+CD8+ and TNFα+CD8+ T-cells were lower in the rituximab-group compared to the MTX-group and HC. No differences were seen for A/H3N2-specific cells. After influenza vaccination, increased numbers of influenza A/H1N1-specific IL-2+CD8+ T-cells and an increased proliferative capacity of A/H1N1-specific T-cells were observed in HC. In contrast, in the MTX- and rituximab-group such incre-ased influenza-specific CMI responses were not seen, although responses tended to be higher in MTX-treated patients than in rituximab-treated RA patients.
conclusion Rituximab therapy reduces polyclonal T-cell responses in RA patients. Also influenza-specific CMI responses before and following influ-enza vaccination are hampered.

115
Cha
pter
7
InTroducTIonPatients with rheumatoid arthritis (RA) are at increased risk of infection, due to immune dysregulation inherent to the underlying autoimmune disease and the immunosuppressive treatment that these patients generally need to reduce RA disease activity. In a large prospective cohort study with a long follow-up on 3.501 RA patients, pulmonary infections were observed as the cause of death 5.3 times more often than expected [1]. Although the causative microorganisms of pulmo-nary infections in RA patients have not been well documented, mainly common bacteria and viruses causing respiratory infections, including influenza, are con-sidered to be involved.
Influenza is associated with increased morbidity and mortality, in particular in certain risk groups, such as young children, elderly and patients with chronic ill-nesses such as cardiac, pulmonary or renal disease, diabetes mellitus, and pa-tients with an immunocompromised state, among which RA patients treated with immunomodulating agents [2]. Although the exact prevalence, morbidity and mortality of influenza in RA patients are unknown, yearly influenza vaccination is recommended for RA patients [3].
Influenza vaccination is efficacious in most RA patients, even when treated with prednisone, disease modifying antirheumatic drugs (DMARDs) or TNF-α blocking agents [4]. However, as we and others demonstrated, following treatment with rituximab, RA patients are unable to mount adequate anti-influenza antibody re-sponses after seasonal influenza vaccination [5-9].
Besides humoral immune responses, cell-mediated immune (CMI) responses have been shown to be important for the prevention of influenza [10]. However, little is known about CMI responses in patients treated with rituximab. In order to evaluate CMI responses in RA patients treated with rituximab we analysed the polyclonal and influenza-specific CMI responses in these patients before and fol-lowing influenza vaccination.
PATIenTs And MeThods
Patients and healthy controls
Patients had to fulfil the American College of Rheumatology (ACR) clinical clas-sification criteria for RA. Two groups of RA patients were defined. One group consisted of RA patients who were treated with rituximab (rituximab-group), either at 4-8 weeks (early rituximab-subgroup) or 6-10 months (late rituximab-subgroup) after treatment. Rituximab was administered in 2 cycles of 1000 mg IV with 100 mg methylprednisolone IV, except for one patient who instead received 4 cycles of 375 mg/m2 based on a protocol for concomitant mixed cryoglobuline-
116
Cha
pter
7
mia. The other group consisted of RA patients treated with MTX, at a minimum dose of 10 mg/week orally or subcutaneously, with or without additional DMARDs. This group served as a disease control group (MTX-group). Health care workers and their family members served as healthy controls (HC-group). Patients in the rituximab-group were recruited from the four participating Dutch university me-dical centers in Groningen, Amsterdam, Nijmegen and Utrecht. MTX patients and HC were recruited from the University Medical Center Groningen. Exclusion crite-ria were: (i) no informed consent, (ii) age under 18, (iii) malignancy, (iv) pregnancy, (v) known allergy to or former severe reaction following vaccination with trivalent influenza subunit vaccine.
Vaccine
Trivalent influenza subunit vaccine (season 2007-2008; Influvac®; Abbott BV, Weesp, The Netherlands) was used. The vaccine contained purified hemaggluti-nin and neuramidase proteins from the following strains: A/Wisconsin/67/2005 (H3N2)-like strain (reassortant virus IVR-142, derived from A/Hiroshima/52/2005), A/Solomon Islands/3/2006 (H1N1)-like strain (reassortant virus IVR-145, derived from A/Solomon Islands/3/2006), and B/Malaysia/2506/2004-like strain (derived from B/Malaysia/2506/2004).
Procedures
Before the onset of influenza activity in The Netherlands, patients and HC received the influenza vaccine intramuscularly from October 2007 up till January 2008. Immediately before, and 7 and 28 ± 3 days after vaccination blood was drawn for measurement of lymphocyte subsets (CD4+ T-cells, CD8+ T-cells, CD16/56+ NK-cells and CD19+ B-cells), C-reactive protein and erythrocyte sedimentation rate, and for isolation of PBMC in order to determine CMI responses using interferon (IFN)-γ ELISpot, intracellular cytokine staining (ICS) using flow cytometry, and CFSE dye dilution proliferation assay. DAS28 was recorded before vaccination, and after 7 and 28 days as a validated measure for RA activity. From all partici-pants information on previous influenza vaccination was obtained. The study was approved by the ethics committees of all four participating centers.
cell-mediated immunity assays
Processing of PBMC and the procedures for the IFNγ ELISpot assay and flow cy-tometry were as described earlier [11]. Therefore, these procedures will only be described briefly.

117
Cha
pter
7
Isolation, storage and thawing of PBMC
PBMC were isolated from BD Vacutainer® CPT™ Cell Preparation Tubes containing 0.1 M sodium citrate anticoagulant and blood separation media composed of a thixotropic polyester gel and a FICOLL™ HYPAQUE™ solution (BD, Franklin Lakes, NJ, USA), according to the instructions of the producer. PBMC were stored in li-quid nitrogen until use in RPMI 1640 (Cambrex BioScience, Verviers, Belgium) sup-plemented with 10% human pool serum, 50 µg/ml of gentamicin (Gibco, Paisley, UK) and 10% dimethylsulfoxide. Prevaccination and postvaccination samples from a RA patient treated with rituximab, a RA patient treated with MTX, and a matched HC were simultaneously thawed and batch-processed.
Influenza antigens used in assays of cell-mediated responses
PBMC were stimulated with whole β-propiolactone-inactivated virus (WIV) or subunit of A/Solomon Islands/3/2006 (IVR-145 reass.; A/H1N1) and A/Hiroshi-ma/52/2005 (IVR-142 reass.; A/H3N2).
IFNγ-ELISpot assay
Before testing thawed PBMC were rested for 24 hours in culture medium (CM; RPMI 1640 [Cambrex BioScience, Verviers, Belgium] supplemented with 10% fetal calf serum, 50µg/ml of gentamicin [Gibco,Paisley, UK]), overnight at 37°C. Immobi-lon-P membrane plates (Millipore,Billerica,MA,USA) were coated with anti-human IFNγ (Mabtech, Nacka Strand, Sweden). 2 x 105 PBMC were added per well and incubated for 48 hours with A/H1N1 subunit (1 µg/ml) and A/H3N2 subunit (1 µg/ml) in CM. Concanavalin A stimulation served as a positive control, a negative control consisted of PBMC in CM alone. Stimulation tests were performed in duplicate. After incubation, biotinylated anti-human IFNγ was added, streptavidin-alkaline phosphatase and BCIP/NBT-plus substrate (all Mabtech) were used in order to visualise IFNγ-producing PBMC. Spots were counted using an automated reader (automated Aelvis ELISpot scanning system, Sanquin, Amsterdam, The Nether-lands).
Flow cytometry
For stimulations, 1.0–1.5 × 106 PBMC were cultured in CM. Staphylococcal ente-rotoxin B (SEB; Sigma-Aldrich, St. Louis, MO) was used as a polyclonal T-cell sti-mulus. WIV A/H1N1 and WIV A/H3N2 were used at final concentrations of 1 µg of total viral protein/ml. Negative controls were incubated in CM only. Pacific Blue and Pacific Orange dyes (Invitrogen, Carlsbad, CA), in a different combination for each stimulus, were used to enable fluorescent T-cell bar coding [12]. The fol-lowing monoclonal antibodies were used: allophycocyanin (APC)-Cy7-conjugated anti-CD3, peridinin chlorophyll A protein–conjugated anti-CD8 (Becton Dickinson
118
Cha
pter
7
Pharmingen, San Diego, CA, USA), phycoerythrin–Cy7 (PE-Cy7)–conjugated anti-CD69 (Biolegend, San Diego,CA, USA), PE–conjugated anti-IFNγ, APC-conjugated anti-TNFα, and Fluorescein isothiocyanate-conjugated anti–IL-2 (eBioscience, Hatfield, UK). Analysis was performed on a LSR II flow cytometer (Becton Dickin-son). At least 300.000 events were recorded.
The WinList software package (Verity Software House, Topsham, ME, USA) was used. Percentages of antigen-specific cells were expressed as the percentage of CD69+ cytokine-producing CD4+ or CD8+ T-cells within the total CD4+ or CD8+
T-cell population. Samples were excluded if the percentage of viable cells after thawing was <80%, and if the frequencies of IFNγ- or TNFα-producing CD4+ or CD8+ T-cells were <2.0% upon stimulation with SEB.
CFSE dye dilution proliferation assay
PBMC were washed with and resuspended in PBS at a concentration of 1x107/100 µl. Carboxyfluorescein succinimidyl ester (CFSE; Invitrogen, Carlsbad, CA, USA) was added to the PBMC at a final concentration of 5 µg/ml. After PBMC were incubated for 10 minutes at 37˚C while protected for light, 10 ml RPMI + 10% FCS was added followed by two washing steps with RPMI + 10% FCS. The cell pellet was resuspended in CM (RPMI + 10% HPS), making a dilution containing 1x106 PBMC/ml.
Subsequently, 1x105 labeled cells per well were stimulated for 7 days in a 96-wells plate (Greiner bio-one Cellstar 650 180) with CM alone or CM with anti-CD3/CD28 as a polyclonal activation (anti-CD3 hybridoma supernatant clone WT32; anti-CD28 hybridoma supernatant clone 20-4996), A/H1N1 (5 µg/ml) subunit, or A/H3N2 sub-unit (1 µg/ml).
At day 7 cell pellets were washed with PBS and treated with FACS lysing solution (1:10; Becton Dickinson Pharmingen, San Diego, CA, USA). After washing with PBS supplemented with 0.3% heparin, cells were stained with anti-CD3-APC and anti-CD8-PercP, and subsequently analysed on a BD FACSCalibur. The degree of T-cell proliferation was analysed with Modfit LT 3.2 (Verity House Software) software and expressed as proliferation-index, defined as the average number of divisions of proliferating cells.
statistical analysis
Data were analysed using SPSS 16 (SPSS Inc., Chicago, IL, USA) and are presented as median (range), except for age, which is presented as mean (SD). Analysis of variance, Kruskal-Wallis test, Friedman’s two-way analysis of variance by ranks, Mann-Whitney U test, and Pearson’s chi square test were used where appropri-ate. Differences between two of the three groups were only addressed with the
119
Cha
pter
7
Mann-Whitney U test if the Kruskal-Wallis test revealed a statistically significant difference between the three groups. A p-value <0.05 was considered statisti-cally significant.
resulTs
Patient characteristics
Twenty-one RA patients were included in the rituximab-group; 10 received influ-enza vaccination 4-8 weeks after their last rituximab infusion and 11 received influ-enza vaccination 6-10 months after rituximab therapy (table 1). Nine patients (43%) received their first cycle of rituximab, 5 (24%) their second, 6 (28%) their third and 1 (5%) her fifth. As controls, 19 RA patients on MTX and 22 HC were included. Medication use is depicted in table 1. Before vaccination the rituximab-group had higher baseline DAS28 scores than the MTX-group (p =0.003). Lower B-cells were found in the rituximab-group than in the MTX- and HC-group (p <0.001) and CD3+ and CD4+ T-cells were also lower in the rituximab-group (p =0.001 and p =0.002). No significant differences between groups were present for age, sex, influenza vaccination in the previous season (2006/2007), CD8+ T-cells, CD16/56+ cells, and the duration of RA.
Prevaccination polyclonal cMI responses
PBMC taken before vaccination were stimulated with Staphylococcal Enterotoxin B (SEB) to induce a strong polyclonal activation of T-cells that express SEB-bin-ding TCR Vβ families. A statistically significant difference between the HC, the MTX-group and the rituximab-group was found regarding the frequencies of IL-2-producing CD4+ and CD8+ T-cells upon SEB stimulation (p =0.009 and p =0.041, respectively, as determined by Kruskal-Wallis test). The differences in the fre-quencies of IL-2+CD4+ and CD8+ T-cells could be attributed to lower frequencies of the RTX-group in comparison to the MTX-group (p =0.020 and p =0.016, respec-tively) (figure 1, A). No differences between groups were found for frequencies of IFNγ- and TNFα-producing CD4+ or CD8+ T-cells upon SEB stimulation.
In the proliferation assay, polyclonal stimulation of T-cells was done using anti-CD3/28 antibodies. The proliferation-index of CD4+ T-cells in response to CD3/28 stimulation was different between the three groups (p =0.050 as determined by Krusal-Wallis test) (figure 1, B), which was due to a decreased response in the rituximab-group: the proliferation-index in HC was not statistically significantly different from the MTX-group, but was lower in the rituximab-group compared to HC (p =0.033) (figure 1, B). The proliferation-index for CD8+ T-cells was compa-rable between the three groups (figure 1, B).
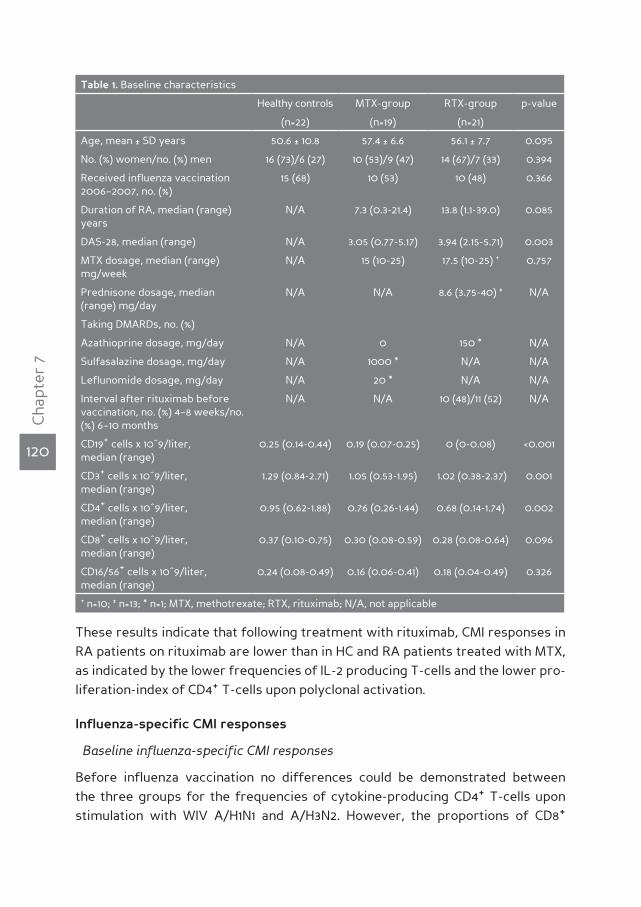
120
Cha
pter
7
These results indicate that following treatment with rituximab, CMI responses in RA patients on rituximab are lower than in HC and RA patients treated with MTX, as indicated by the lower frequencies of IL-2 producing T-cells and the lower pro-liferation-index of CD4+ T-cells upon polyclonal activation.
Influenza-specific cMI responses
Baseline influenza-specific CMI responses
Before influenza vaccination no differences could be demonstrated between the three groups for the frequencies of cytokine-producing CD4+ T-cells upon stimulation with WIV A/H1N1 and A/H3N2. However, the proportions of CD8+
Table 1. Baseline characteristics
Healthy controls MTX-group RTX-group p-value
(n=22) (n=19) (n=21)
Age, mean ± SD years 50.6 ± 10.8 57.4 ± 6.6 56.1 ± 7.7 0.095
No. (%) women/no. (%) men 16 (73)/6 (27) 10 (53)/9 (47) 14 (67)/7 (33) 0.394
Received influenza vaccination 2006–2007, no. (%)
15 (68) 10 (53) 10 (48) 0.366
Duration of RA, median (range) years
N/A 7.3 (0.3-21.4) 13.8 (1.1-39.0) 0.085
DAS-28, median (range) N/A 3.05 (0.77-5.17) 3.94 (2.15-5.71) 0.003
MTX dosage, median (range) mg/week
N/A 15 (10-25) 17.5 (10-25) † 0.757
Prednisone dosage, median (range) mg/day
N/A N/A 8.6 (3.75-40) ‡ N/A
Taking DMARDs, no. (%)
Azathioprine dosage, mg/day N/A 0 150 * N/A
Sulfasalazine dosage, mg/day N/A 1000 * N/A N/A
Leflunomide dosage, mg/day N/A 20 * N/A N/A
Interval after rituximab before vaccination, no. (%) 4–8 weeks/no. (%) 6–10 months
N/A N/A 10 (48)/11 (52) N/A
CD19+ cells x 10^9/liter, median (range)
0.25 (0.14-0.44) 0.19 (0.07-0.25) 0 (0-0.08) <0.001
CD3+ cells x 10^9/liter, median (range)
1.29 (0.84-2.71) 1.05 (0.53-1.95) 1.02 (0.38-2.37) 0.001
CD4+ cells x 10^9/liter, median (range)
0.95 (0.62-1.88) 0.76 (0.26-1.44) 0.68 (0.14-1.74) 0.002
CD8+ cells x 10^9/liter, median (range)
0.37 (0.10-0.75) 0.30 (0.08-0.59) 0.28 (0.08-0.64) 0.096
CD16/56+ cells x 10^9/liter, median (range)
0.24 (0.08-0.49) 0.16 (0.06-0.41) 0.18 (0.04-0.49) 0.326
† n=10; ‡ n=13; * n=1; MTX, methotrexate; RTX, rituximab; N/A, not applicable
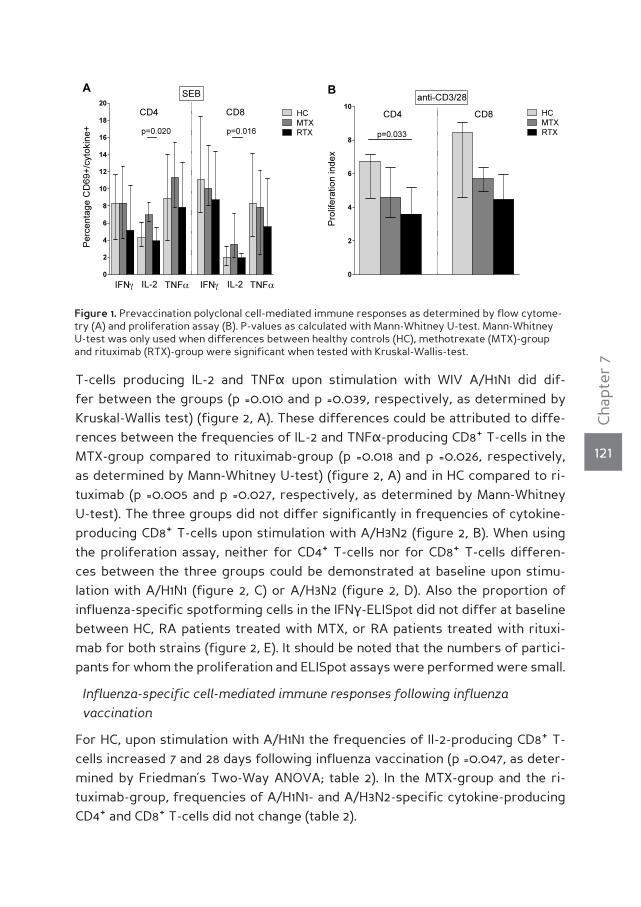
121
Cha
pter
7
T-cells producing IL-2 and TNFα upon stimulation with WIV A/H1N1 did dif-fer between the groups (p =0.010 and p =0.039, respectively, as determined by Kruskal-Wallis test) (figure 2, A). These differences could be attributed to diffe-rences between the frequencies of IL-2 and TNFα-producing CD8+ T-cells in the MTX-group compared to rituximab-group (p =0.018 and p =0.026, respectively, as determined by Mann-Whitney U-test) (figure 2, A) and in HC compared to ri-tuximab (p =0.005 and p =0.027, respectively, as determined by Mann-Whitney U-test). The three groups did not differ significantly in frequencies of cytokine-producing CD8+ T-cells upon stimulation with A/H3N2 (figure 2, B). When using the proliferation assay, neither for CD4+ T-cells nor for CD8+ T-cells differen-ces between the three groups could be demonstrated at baseline upon stimu-lation with A/H1N1 (figure 2, C) or A/H3N2 (figure 2, D). Also the proportion of influenza-specific spotforming cells in the IFNγ-ELISpot did not differ at baseline between HC, RA patients treated with MTX, or RA patients treated with rituxi-mab for both strains (figure 2, E). It should be noted that the numbers of partici-pants for whom the proliferation and ELISpot assays were performed were small.
Influenza-specific cell-mediated immune responses following influenza vaccination
For HC, upon stimulation with A/H1N1 the frequencies of Il-2-producing CD8+ T-cells increased 7 and 28 days following influenza vaccination (p =0.047, as deter-mined by Friedman’s Two-Way ANOVA; table 2). In the MTX-group and the ri-tuximab-group, frequencies of A/H1N1- and A/H3N2-specific cytokine-producing CD4+ and CD8+ T-cells did not change (table 2).
Figure 1. Prevaccination polyclonal cell-mediated immune responses as determined by flow cytome-try (A) and proliferation assay (B). P-values as calculated with Mann-Whitney U-test. Mann-Whitney U-test was only used when differences between healthy controls (HC), methotrexate (MTX)-group and rituximab (RTX)-group were significant when tested with Kruskal-Wallis-test.
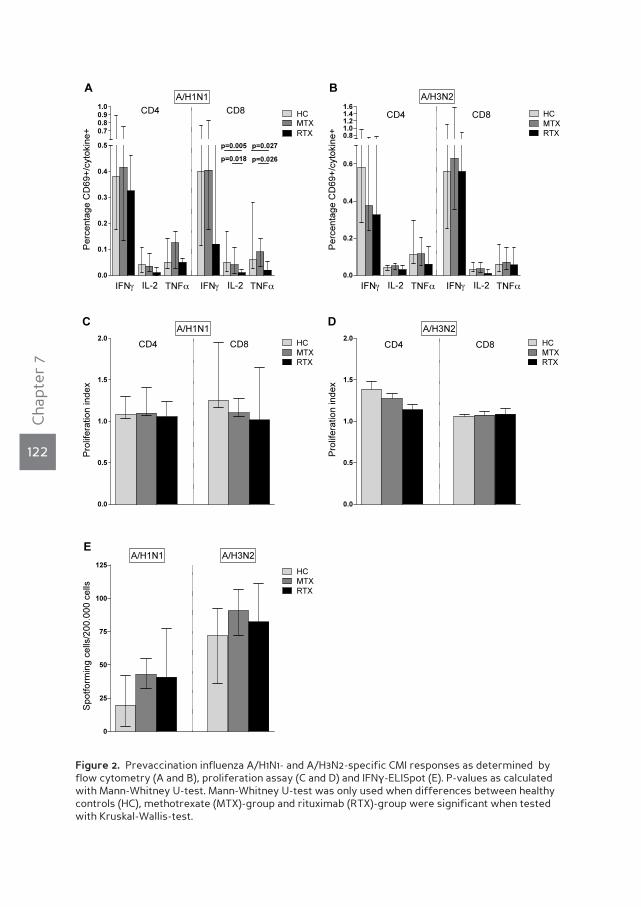
122
Cha
pter
7
Figure 2. Prevaccination influenza A/H1N1- and A/H3N2-specific CMI responses as determined by flow cytometry (A and B), proliferation assay (C and D) and IFNγ-ELISpot (E). P-values as calculated with Mann-Whitney U-test. Mann-Whitney U-test was only used when differences between healthy controls (HC), methotrexate (MTX)-group and rituximab (RTX)-group were significant when tested with Kruskal-Wallis-test.

123
Cha
pter
7
Tab
le 2
. CM
I res
pons
es b
efor
e, 7
and
28
follo
win
g in
flue
nza
vacc
inat
ion
as d
eter
min
ed b
y fl
ow c
ytom
etry
, in
heal
thy
cont
rols
, RA
pat
ient
s tr
eate
d w
ith
met
ho-
trex
ate
(MT
X) a
nd R
A p
atie
nts
trea
ted
wit
h ri
tuxi
mab
(RT
X).
Num
bers
rep
rese
nt m
edia
n (r
ange
) fre
quen
cies
of
cyto
kine
+ CD
4+ or
CD
8+ T-c
ells
..
Hea
lthy
con
trol
s (n
=17)
MT
X (n
=14)
RT
X (
n=13
)
Bef
ore
728
P-v
alue
Bef
ore
728
P-v
alue
Bef
ore
728
P-v
alue
CD
4+ T-c
ells
, A/H
1N1
IFNγ
0.3
9 (0
.04-
1.31)
0.2
5 (0
.05-
1.97)
0.2
7 (0
.04-
1.86)
0.8
980
.42
(0.0
4-1.8
4)0
.26
(0-2
.28)
0.3
5
0.0
9-2.
35)
0.13
30
.33
(0.0
3-1.8
4)0
.18
(0.0
7-2.
46)
0.2
6 (0
.02-
3.37
)0
.794
IL-2
0.0
4 (0
-0.3
1)0
.05
(0-0
.20
)0
.04
(0-0
.73)
0.0
710
.04
(0-1
.01)
0.0
3 (0
-0.13
)0
.04
(0-0
.20
)0
.694
0.0
1 (0
-0.0
9)0
.02
(0-0
.82)
0.0
3 (0
-0.3
8)0
.90
9
TN
Fα0
.05
(0-0
.67)
0.10
(0
-0.3
2)0
.10
(0-0
.43)
0.0
690
.13
(0.0
1-1.1
3)0
.11
(0-0
.32)
0.14
(0
.02-
0.4
1)0
.256
0.0
5 (0
-0.16
)0
.10
(0-1
.25)
0.0
5 (0
-0.2
8)0
.923
CD
4+ T-c
ells
, A/H
3N2
IFNγ
0.5
0
(0.10
-1.7
8)0
.50
(0
.05-
1.78)
0.5
9 (0
.07-
1.92)
0.5
540
.38
(0.0
6-1.5
1)0
.25
(0.0
7-2.
21)
0.3
8 (0
.09-
2.36
)0
.880
0.3
3 (0
.06-
2.60
)0
.39
(0.14
-3.9
3)0
.79
(0.0
8-4.
88)
0.5
84
IL-2
0.0
4 (0
.01-
0.14
)0
.0
(0-0
.09)
0.0
3 (0
-0.3
1)0
.884
0.0
5 (0
-0.13
)0
.02
(0-0
.12)
0.0
4 (0
-0.10
)0
.40
40
.05
(0-0
.13)
0.0
2 (0
.0.12
)0
.04
(0-0
.10)
0.7
26
TN
Fα0
.12
(0.0
3-0
.50
)0
.10
(0.0
1-0
.92)
0.15
(0
-1.5
4)0
.580
0.12
(0
-0.5
5)0
.14
(0-0
.61)
0.13
(0
04-
0.8
1)0
.797
0.0
6 (0
.02-
0.4
2)0
.08
(0.0
2-1.6
9)0
.14
(0-0
.58)
0.9
23
CD
8+ T-c
ells
, A/H
1N1
IFNγ
0.4
0
(0.0
2-3.
15)
0.2
5 (0
.07-
4.0
0)
0.2
4 (0
-2.3
9)0
.627
0.4
1 (0
.07-
3.22
)0
.27
(0.0
1-2.
16)
0.2
7 (0
.08-
3.29
)0
.171
0.12
(0
.04-
3.61
)0
.23
(0.0
3-4.
79)
0.2
0
(0-6
.87)
0.5
00
IL-2
0.0
5 (0
-0.6
5)0
.04
(0-0
.15)
0.0
7 (0
-0.7
3)0
.047
0.0
4 (0
-0.2
2)0
.04
(0-0
.30
)0
.07
(0-0
.69)
0.2
450
.01
(0-0
.07)
0.0
3 (0
.0.4
7)0
.0
(0-0
.23)
0.2
25
TN
Fα0
.06
(0-1
.58)
0.0
7 (0
-0.5
2)0
.08
(0-0
.62)
0.8
190
.09
(0-0
.33)
0.10
(0
-0.2
8)0
.10
(0.0
2-0
.61)
0.3
05
0.0
2 (0
-0.18
)0
.03
(0-0
.51)
0.0
8 (0
-1.3
50
.922
CD
8+ T-c
ells
, A/H
3N2
IFNγ
0.5
6 (0
-1.7
0)
0.5
5 (0
.06-
3.0
1)0
.52
(0-2
.56)
0.2
360
.63
(0.0
9-3.
01)
0.5
8 (0
.03-
3.27
)0
.60
(0
.09-
2.73
)0
.880
0.5
6 (0
.04-
4.28
)0
.39
(0.12
-2.4
6)0
.48
(0.0
6-2.
61)
0.6
62
IL-2
0.0
3 (0
-0.2
4)0
.03
(0-0
.12)
0.0
5 (0
-0.2
9)0
.650
0.0
4 (0
-0.3
7)0
.02
(0-0
.25)
0.0
4 (0
-0.3
7)0
.119
0.0
1 (0
-0.15
)0
.02
(0-0
.44)
0.2
0
(0-0
.38)
0.2
97
TN
Fα0
.06
(0-0
.60
)0
.07
(0-0
.49)
0.0
8 (0
-0.4
7)0
.938
0.0
7 (0
-1.2
0)
0.0
8 (0
-0.2
7)0
.06
(0.0
1-0
.43)
0.3
900
.06
(0-0
.18)
0.0
7 (0
.01-
0.9
6)0
.11
(0.0
1-1.3
0)
0.6
62

124
Cha
pter
7
Also, the proliferation-index for CD4+ T-cells rose in HC following influenza vac-cination upon stimulation with A/H1N1 (p =0.042, as determined by Mann-Whitney U-test), but not upon stimulation with A/H3N2 and not for CD8+ T-cells. Further-more, no change in proliferation-index for CD4+ and CD8+ T-cells could be demon-strated 7 and 28 days following influenza vaccination upon stimulation with A/H1N1 or A/H3N2 in the MTX- and rituximab-group (data not shown).
Since it is unknown what increase in influenza-specific CMI response is of clinical relevance, we categorised the proliferation assay results qualitatively as “rise” or “no rise” in proliferation-index. Five out of 5 (100%) HC, 3 out of 6 MTX patients (50%) and 1 out of 4 rituximab patients (25%) demonstrated a rise following vac-cination for CD4+ T-cells for A/H1N1 (figure 3, A), and 4 out of 5 (80%) HC, 4 out of 6 MTX patients (67%) and 3 out of 4 rituximab patients (75%) for A/H3N2 (figure 3, A). For CD8+ T-cells 3 out of 3 (100%) HC, 4 out of 5 MTX patients (80%) and 2 out of 4 rituximab patients (50%) demonstrated a rise following vaccination for A/H1N1 (figure 3, A), and 3 out of 4 (75%) HC, 3 out of 5 MTX patients (60%) and 3 out of 4 rituximab patients (75%) for A/H3N2 (figure 3, A).
In the subgroup of study participants for whom an IFNγ-ELISpot assay could be performed, comparisons of the proportions of spotforming cells did not reveal any significant changes following influenza vaccination in all three groups upon stimulation with WIV A/H1N1 (table 2). From the 7 HC, 6 (86%) had a rise in spotfor-ming cells upon stimulation with A/H1N1 at day 7 following influenza vaccination, compared to 4 out of 6 (67%) MTX patients and 1 out of 5 (20%) rituximab patients (figure 3, B). No difference was found upon stimulation with A/H3N2 (figure 3, B).
Figure 3. Percentage of healthy controls (HC), methotrexate (MTX) and rituximab (RTX) patients with a rise in proliferation index as determined by proliferation assay (A) and in spotforming cells as determined by IFNγ-ELISpot (B) 7 days after influenza vaccination.
125
Cha
pter
7
dIscussIonInfluenza-specific CMI responses following influenza vaccination are important for the protection from clinical influenza [10]. This is of particular importance in patients who are unable to mount sufficient influenza-specific humoral immune responses. RA patients treated with rituximab have been shown to have severely hampered humoral responses following influenza vaccination and seroprotection rates for influenza hardly increase in response to influenza vaccination [5-8]. Therefore, we investigated influenza-specific CMI responses before and follo-wing influenza vaccination, using three different techniques. Flow cytometry was used to determine frequencies of IFNγ-, IL-2- and TNFα-producing CD4+ T-cells and CD8+ T-cells upon stimulation with WIV of the two influenza A-strains as pre-sent in the used vaccine. Moreover, IFNγ-ELISpot was performed since this test has been shown to be more sensitive than flow cytometry with intracellular cyto-kine staining [11, 13]. Finally, proliferation of CD4+ and CD8+ T-cells upon stimulation with influenza-subunit was investigated. This is the first study to address pre- and postvaccination polyclonal and influenza-specific CMI responses in rituximab-treated RA patients this extensively.
Before vaccination we demonstrated lower frequencies of IL-2-producing CD4+
and CD8+ T-cells upon stimulation with SEB in the rituximab-group than in the MTX-group, while the MTX-group and HC performed similarly. Proliferation upon stimulation with anti-CD3/28 was also reduced in the rituximab-group compared to HC. Furthermore, rituximab patients had lower influenza-specific CMI respon-ses at baseline. Following influenza vaccination, flow cytometry showed an incre-ase in frequencies of IL-2- and TNFα-producing CD4+ T-cells and IL-2-producing CD8+ T-cells in HC only, although not all increases were statistically significant. IFNγ-ELISpot and proliferation assay further supported the reduced vaccination responses in rituximab-treated RA patients, taking into account that numbers of patients included in these assays were low.
The lower CMI responses that we found at baseline in the rituximab-group upon stimulation with SEB and anti-CD3/28 indicate that RA patients treated with ri-tuximab have a lower ability to mount CMI responses. This likely explains the de-creased influenza-specific CMI responses in these patients. Little is known on CMI responses in RA patients following treatment with rituximab. Delayed type hy-persensitivity T-cell responses to Candida as measured by skin testing 24 weeks after treatment with rituximab have been shown to be comparable between RA patients treated with rituximab and RA patients treated with MTX [14]. Arad et al. investigated influenza-specific CMI responses following influenza vaccination in RA patients treated with rituximab. Only the frequency of IFNγ-producing CD4+ T-cells was addressed using flow cytometry with intracellular cytokine staining [8].
126
Cha
pter
7
At baseline, a lower frequency of IFNγ-producing CD4+ T-cells upon stimulation with a mixture containing WIV of the A/H1N1, A/H3N2- and B-strain was found in ri-tuximab patients than in HC. The current study, however, did not find differences in IFNγ-producing CD4+ T-cells at baseline, but demonstrated lower frequencies of IL-2- and TNFα-producing CD4+ and CD8+ T-cells in rituximab patients, as mea-sured by flow cytometry. This discrepancy might have been caused by the fact that methods differed: we measured responses to A/H1N1 and A/H3N2 separately.
Our findings are in line with experimental animal studies, which revealed that in mice B-cell depletion leads to reduced CD4+ T-cell recall responses to keyhole limpet hemocyanin, and CD4+ T-cell expansion was significantly reduced upon im-munization with ovalbumin in these mice. In response to infection with Listeria monocytogenes B-cell depleted mice had a reduced frequency of dividing CD4+ T-cells and CD8+ T-cell proliferation was reduced. Furthermore, in B-cell depleted mice IL-2- and IFNγ-production by CD4+ T-cells was limited. Finally, it was shown that B-cells were necessary in addition to dendritic cells for optimally inducing CD4+ T-cell responses, pointing at the important role of B-cells with regard to antigen presentation. CD8+ T-cells demonstrated the same responses in B-cell depleted mice as in their littermates that were not B-cell depleted [15]. The re-duced responses in CD8+ T-cells that were found in this study, may therefore be caused by other factors. CD8+ T-cells, as well as CD4+ T-cells, can be driven towards apoptosis by glucocorticoids in vitro [16], and 13 of 21 (62%) of the included RA patients that received rituximab used prednisone. Moreover, five of 21 (24%) rituximab patients used a combination of low dose prednisone and MTX. Schuer-wegh et al. investigated the influence of the use of the combination of low dose MTX (7.5-10 mg/day) and low dose prednisone (5-10 mg/day), comparable to the doses used by our patients, on the production of IFNγ, IL-2 and IL-4 by CD4+ and CD8+ T-cells of 20 RA patients. After 12 months of treatment a significant reduc-tion of the absolute numbers of IL-2 and IFNγ-producing CD4+ and CD8+ T-cells compared to pre-treatment values was found [17]. Therefore, the use of the com-bination of MTX and prednisone might have contributed to the reduction in the frequencies of IL-2 producing CD8+ T-cells in our rituximab-treated RA patients.
Only limited influenza-specific CMI responses following influenza vaccination as determined by flow cytometry were found in all participants, including HC. This might have had several causes. Flow cytometry has been shown to be less sen-sitive than IFNγ-ELISpot [11, 13], and, therefore, a rise in IFNγ-producing CD4+ or CD8+ T-cells might have been missed. However, using the more sensitive method of IFNγ-ELISpot, we found a trend towards a rise in spotforming cells in HC, des-pite the small number of included HC (n=6). Second, a large proportion of the stu-dy participants were vaccinated during the previous year. This was in particular

127
Cha
pter
7
true for HC, of whom 68% received influenza vaccine during the previous year. It has been shown that persons who received influenza vaccination the year before can have blunted influenza-specific CMI responses [18]. This may have contributed to the limited CMI responses in both patient groups and HC, following influenza vaccination. In contrast to our results, Arad et al. found a rise in the frequency of influenza-specific IFNγ-producing CD4+ T-cells after influenza vaccination in pa-tients treated with rituximab. However, it was not stated whether or not the rise reached statistical significance [8]. Surprisingly, they demonstrated a drop in the frequency of influenza-specific IFNγ-producing CD4+ T-cells after influenza vac-cination in HC, which could not be confirmed by our results.
It has been assumed that blunted CMI responses in patients treated with rituximab account for the occurrence of opportunistic infections that have been documented in these patients. Opportunistic infections are typically found in patients with cel-lular immunodeficiencies. In particular progressive multifocal leucencephalopathy due to JC-polyoma virus has been described, however, the majority of cases oc-curred in patients with lymphoproliferative disorders treated with rituximab [19]. A meta-analysis performed on the overall incidence of severe infections in lymphoma patients treated with CHOP with or without rituximab did not find an increase in risk in the group treated with rituximab [20]. Another meta-analysis including three randomized controlled trials on treatment of RA patients with rituximab also did not reveal a statistically significant increased risk of serious infection due to the use of rituximab. In the included studies most patients treated with rituxi-mab were also treated with MTX 10-25 mg/week [21]. Therefore, despite the loss of humoral responses following rituximab and the blunted CMI responses that we demonstrated, the immune system seems to be sufficiently redundant to com-pensate for these defects. It is well known that many immune defects by itself do not lead to clinical consequences. For example, a large drop in CD4+ T-cells is mandatory in HIV patients before opportunistic infections occur [22], and hypo-gammaglobulinemia not necessarily is accompanied by infections, which depends largely on the level and the class of immunoglobulins that are decreased [23].
We recognize that our study has some limitations. The number of participating patients and HC was relatively small, although no larger studies have been per-formed so far. At the start of the study no data were available regarding CMI responses following influenza vaccination in RA patients treated with rituximab and RA patients treated with MTX. Therefore, a power calculation could not be performed. Also, treatment in patients with rituximab was not standardized with regard to immunosuppressive co-medication. Therefore, the differences found between the rituximab-group and the two control groups might have been influ-enced by this co-medication. Furthermore, a correlate of protection regarding

128
Cha
pter
7
influenza-specific CMI responses has not been determined. Therefore, it remains unknown if the differences found in our study have any clinical relevance with regard to the protection for influenza. Finally, more HC received influenza vac-cination the year before, which could have influenced the CMI response following influenza vaccination as well.
In conclusion, we demonstrated that prior to influenza vaccination RA patients treated with rituximab, compared to RA patients treated with MTX and HC, have reduced influenza-specific CMI responses, but also lower CMI responses upon strong polyclonal stimuli. Moreover, in response to influenza vaccination, no in-crease in CMI responses was found in rituximab-treated patients. Although a cor-relate of protection for influenza with regard to influenza-specific CMI responses has to be determined yet, our findings support the recommendation to offer in-fluenza vaccination to RA patients before treatment with rituximab [3].
129
Cha
pter
7
reference list
(1) Wolfe F, Mitchell DM, Sibley JT, et al. The mortality of rheumatoid arthritis. Arthritis Rheum 1994
Apr; 37(4):481-94.
(2) Treanor JJ. Principles and pracice of infectious diseases. Influenza virus. 6th ed. Elsevier, 2008.
(3) van Assen S, Agmon-Levin N, Elkayam O, et al. EULAR recommendations for vaccination in adult
patients with autoimmune inflammatory rheumatic diseases. Ann Rheum Dis 2011 Mar; 70(3):414-
22.
(4) van Assen S, Elkayam O, Agmon-Levin N, et al. Vaccination in adult patients with auto-immune
inflammatory rheumatic diseases: A systematic literature review for the European League
Against Rheumatism evidence-based recommendations for vaccination in adult patients with
auto-immune inflammatory rheumatic diseases. Autoimmun Rev 2011 Apr; 10(6):341-52.
(5) Gelinck LB, Teng YK, Rimmelzwaan GF, van den Bemt BJ, Kroon FP, van Laar JM. Poor serolo-
gical responses upon influenza vaccination in patients with rheumatoid arthritis treated with
rituximab. Ann Rheum Dis 2007 Oct; 66(10):1402-3.
(6) Oren S, Mandelboim M, Braun-Moscovici Y, et al. Vaccination against influenza in patients with
rheumatoid arthritis: the effect of rituximab on the humoral response. Ann Rheum Dis 2008 Jul;
67(7):937-41.
(7) van Assen S, Holvast A, Benne CA, et al. Humoral responses after influenza vaccination are seve-
rely reduced in patients with rheumatoid arthritis treated with rituximab. Arthritis Rheum 2009
Dec 28; 62(1):75-81.
(8) Arad U, Tzadok S, Amir S, et al. The cellular immune response to influenza vaccination is pre-
served in rheumatoid arthritis patients treated with rituximab. Vaccine 2011 Feb 11; 29(8):1643-8.
(9) Rehnberg M, Brisslert M, Amu S, Zendjanchi K, Hawi G, Bokarewa MI. Vaccination response to
protein and carbohydrate antigens in patients with rheumatoid arthritis after rituximab treat-
ment. Arthritis Res Ther 2010; 12(3):R111.
(10) McElhaney JE, Xie D, Hager WD, et al. T-cell responses are better correlates of vaccine protec-
tion in the elderly. J Immunol 2006 May 15; 176(10):6333-9.
(11) Holvast A, van Assen S, de Haan A, et al. Studies of cell-mediated immune responses to influenza
vaccination in systemic lupus erythematosus. Arthritis Rheum 2009 Aug; 60(8):2438-47.
(12) Krutzik PO, Nolan GP. Fluorescent cell barcoding in flow cytometry allows high-throughput drug
screening and signaling profiling. Nat Methods 2006 May; 3(5):361-8.
(13) Karlsson AC, Martin JN, Younger SR, et al. Comparison of the ELISPOT and cytokine flow cyto-
metry assays for the enumeration of antigen-specific T cells. J Immunol Methods 2003 Dec;
283(1-2):141-53.
(14) Bingham CO, III, Looney RJ, Deodhar A, et al. Immunization responses in rheumatoid arthritis
patients treated with rituximab: Results from a controlled clinical trial. Arthritis Rheum 2009
Dec 28; 62(1):64-74.
(15) Bouaziz JD, Yanaba K, Venturi GM, et al. Therapeutic B cell depletion impairs adaptive and auto-
reactive CD4+ T cell activation in mice. Proc Natl Acad Sci U S A 2007 Dec 26; 104(52):20878-83.
(16) Lanza L, Scudeletti M, Puppo F, et al. Prednisone increases apoptosis in in vitro activated human
peripheral blood T lymphocytes. Clin Exp Immunol 1996 Mar; 103(3):482-90.
(17) Schuerwegh AJ, Van Offel JF, Bridts CH, Stevens WJ, De Clerck LS. Influence of longterm the-
rapy with methotrexate and low dose corticosteroids on type 1 and type 2 cytokine production
130
Cha
pter
7
in CD4+ and CD8+ T lymphocytes of patients with rheumatoid arthritis. J Rheumatol 2001 Aug;
28(8):1793-9.
(18) Keynan Y, Card CM, Ball BT, Li Y, Plummer FA, Fowke KR. Cellular immune responses to recur-
ring influenza strains have limited boosting ability and limited cross-reactivity to other strains.
Clin Microbiol Infect 2010 Aug; 16(8):1179-86.
(19) Cooper N, Arnold DM. The effect of rituximab on humoral and cell mediated immunity and infec-
tion in the treatment of autoimmune diseases. Br J Hematol 2010 Apr; 149(1):3-13.
(20) Lanini S, Molloy AC, Fine PE, Prentice AG, Ippolito G, Kibbler CC. Risk of infection in patients
with lymphoma receiving rituximab: systematic review and meta-analysis. BMC Med 2011 Apr 12;
9(1):36.
(21) Salliot C, Dougados M, Gossec L. Risk of serious infections during rituximab, abatacept and ana-
kinra treatments for rheumatoid arthritis: meta-analyses of randomised placebo-controlled tri-
als. Ann Rheum Dis 2009 Jan; 68(1):25-32.
(22) Kaplan JE, Benson C, Holmes KH, Brooks JT, Pau A, Masur H. Guidelines for prevention and
treatment of opportunistic infections in HIV-infected adults and adolescents: recommendations
from CDC, the National Institutes of Health, and the HIV Medicine Association of the Infectious
Diseases Society of America. MMWR Recomm Rep 2009 Apr 10; 58(RR-4):1-207.
(23) Furst DE. Serum immunoglobulins and risk of infection: how low can you go? Semin Arthritis
Rheum 2009 Aug; 39(1):18-29.


PART 3E U L A R recomen- d a t i o n s for vacci- n a t i o n in patients w i t h a u t o - i m m u n e i n f l a m -m a t o r y rheumatic d i s e a s e s

CHAPT
ER8V a c c i n a t i o n i n a d u l t patients with auto-immune inflammatory r h e u m a t i c d i s e a s e s : a systematic l i t e r a t u r e review for the E U L A R e v i d e n c e -b a s e d r e c o m m e n -d a t i o n s for vaccination i n a d u l t patients with auto-immune inflammatory r h e u m a t i c d i s e a s e s
S. van Assen
O. Elkayam
N. Agmon-Levin
R. Cervera
M.F. Doran
M. Dougados
P. Emery
P. Geborek
J.P.A. Ioannidis
D.R.W. Jayne
C.G.M. Kallenberg
U. Müller-Ladner
Y. Shoenfeld
L. Stojanovich
G. Valesini
N.M. Wulffraat
M. Bijl
Autoimmunity Reviews 2011 Apr;10(6):341-352

136
Cha
pter
8
ABSTRACTObjectives To present the systematic literature review (SLR), which for-med the basis for the European League Against Rheumatism (EULAR) evi-dence-based recommendations for vaccination in adult patients with auto-immune inflammatory rheumatic diseases (AIIRD).
Methods AIIRD, vaccines and immunomodulating drugs, as well as eight key questions were defined by the multidisciplinary expert committee commissioned by EULAR for developing the recommendations. A SLR was performed using MedLine through to October 2009 and including data from meta-analyses, systematic reviews, randomized trials, and observa-tional studies, excluding case series with ≤5 participants. Articles in English and regarding patients ≥16 years of age, were eligible.
Results Several vaccine-preventable infections (VPI) occur more often in AIIRD patients and most vaccines are efficacious in AIIRD patients, even when treated with immunomodulating agents, except rituximab. There does not appear to be an increase in vaccination-related harms in vacci-nated patients with AIIRD in comparison with unvaccinated patients with AIIRD. However, these studies are underpowered and therefore not conclu-sive.
Conclusion Based on the current evidence from the literature, recom-mendations for vaccination in patients with AIIRD were made. However, more research is needed in particular regarding incidence of VPI, harms of vaccination and the influence of (new and established) immunomodulating agents on vaccinationefficacy.

137
Cha
pter
8
InTROduCTIOnPatients with auto-immune inflammatory rheumatic diseases (AIIRD) are at incre-ased risk of contracting infections, associated with considerable morbidity and mortality [1-11]. Certain infections might be prevented by vaccination. The effi-cacy of vaccinations may, however, be reduced in patients with AIIRD. Moreover, safety of vaccination in patients with AIIRD is an important issue, because of the potential risk of AIIRD-flares following vaccination.
In order to prepare recommendations for vaccination in patients with AIIRD the European League Against Rheumatism (EULAR) commissioned a task force [12]. The exercise performed by the task force involved both evidence-based and ex-pert opinion-based approaches. The current review reports the results of the systematic literature review (SLR) that formed the basis for these recommen-dations.
METHOdSThe expert committee formulated eight key questions to be addressed for the SLR, performed by SvA, MB, NAL and OE. Twenty-seven predefined AIIRD con-ditions, 29 vaccines and 17 immunosuppressive medications (table 1) were used as search terms, using Medline (via PubMed; from 1966 to October 2009) and the abstracts from the meetings of EULAR 2008 and 2009 and the American College of Rheumatology (ACR) 2007 and 2008. Only articles in English and concerning patients older than 16 years of age were included. Additional papers considered relevant in the opinion of the experts could be added (figure 1). Meta-analyses, systematic reviews, randomized trials, and observational studies (both analytic and descriptive) were eligible and scored according to table 2. Case reports and case series (≤5 patients) were not included.
RESuLTS
Question 1. Is the risk of infections for which vaccines are available incre-ased in patients with AIIRd in general, and specifically in those with active disease, and in those using immunomodulating agents?
Influenza
Two retrospective studies showed an increased risk of influenza in elderly pa-tients (≥65 years) with rheumatic diseases, vasculitis, chronic renal failure, de-mentia or stroke (all considered at intermediate risk of complicated influenza). Compared to low-risk elderly, the odds ratio was 1.56 (95% confidence interval [CI] 1.23-2.02) for hospital admission for either pneumonia or influenza and 2.67 (CI 2.26-3.16) for death, measured over 6 seasons [13]. In another study 4.5-7% of
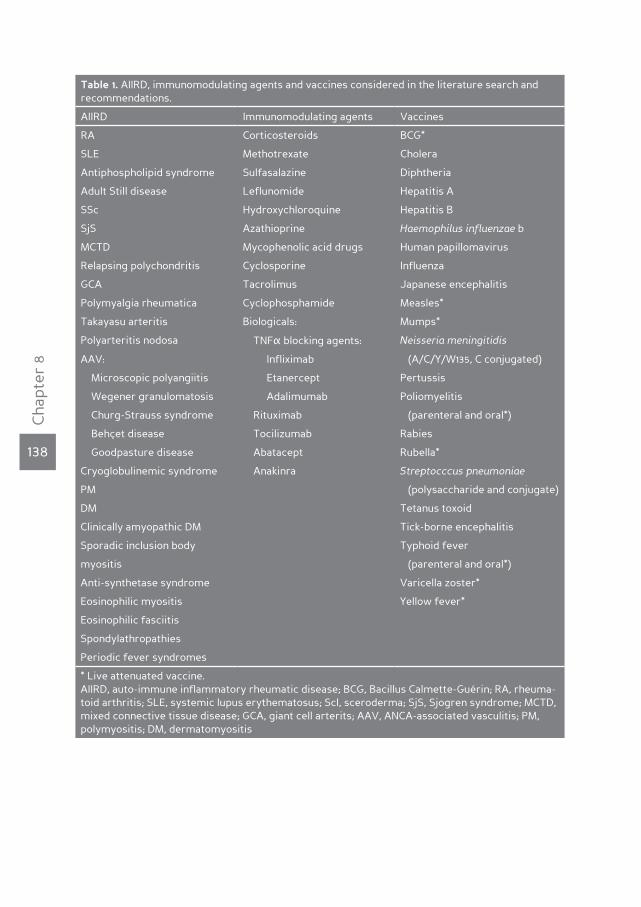
138
Cha
pter
8
Table 1. AIIRD, immunomodulating agents and vaccines considered in the literature search and recommendations.
AIIRD Immunomodulating agents Vaccines
RA Corticosteroids BCG*
SLE Methotrexate Cholera
Antiphospholipid syndrome Sulfasalazine Diphtheria
Adult Still disease Leflunomide Hepatitis A
SSc Hydroxychloroquine Hepatitis B
SjS Azathioprine Haemophilus influenzae b
MCTD Mycophenolic acid drugs Human papillomavirus
Relapsing polychondritis Cyclosporine Influenza
GCA Tacrolimus Japanese encephalitis
Polymyalgia rheumatica Cyclophosphamide Measles*
Takayasu arteritis Biologicals: Mumps*
Polyarteritis nodosa TNFα blocking agents: Neisseria meningitidis
AAV: Infliximab (A/C/Y/W135, C conjugated)
Microscopic polyangiitis Etanercept Pertussis
Wegener granulomatosis Adalimumab Poliomyelitis
Churg-Strauss syndrome Rituximab (parenteral and oral*)
Behçet disease Tocilizumab Rabies
Goodpasture disease Abatacept Rubella*
Cryoglobulinemic syndrome Anakinra Streptocccus pneumoniae
PM (polysaccharide and conjugate)
DM Tetanus toxoid
Clinically amyopathic DM Tick-borne encephalitis
Sporadic inclusion body Typhoid fever
myositis (parenteral and oral*)
Anti-synthetase syndrome Varicella zoster*
Eosinophilic myositis Yellow fever*
Eosinophilic fasciitis
Spondylathropathies
Periodic fever syndromes
* Live attenuated vaccine. AIIRD, auto-immune inflammatory rheumatic disease; BCG, Bacillus Calmette-Guérin; RA, rheuma-toid arthritis; SLE, systemic lupus erythematosus; Scl, sceroderma; SjS, Sjogren syndrome; MCTD, mixed connective tissue disease; GCA, giant cell arterits; AAV, ANCA-associated vasculitis; PM, polymyositis; DM, dermatomyositis
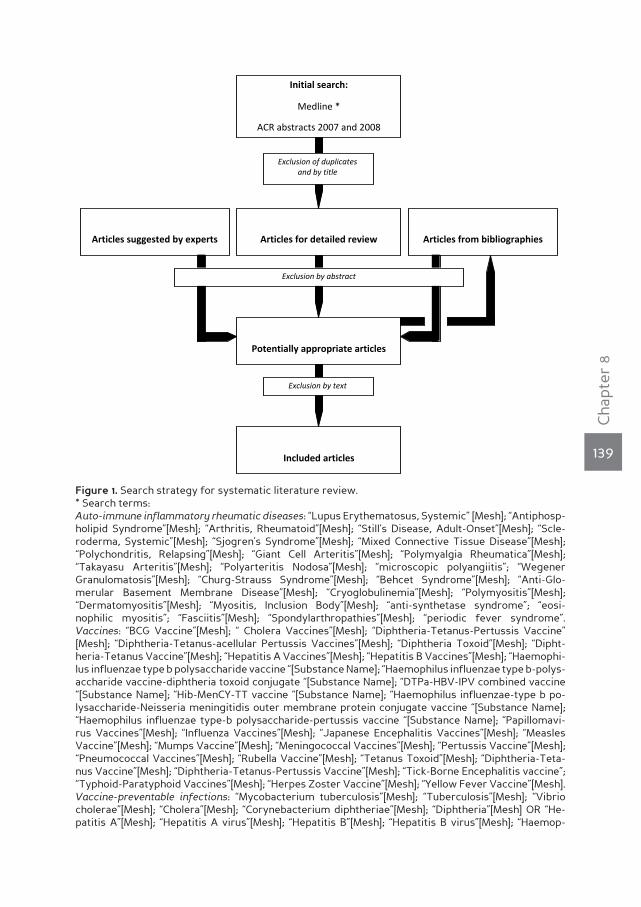
139
Cha
pter
8
Initial search:
Medline *
ACR abstracts 2007 and 2008
EULAR abstracts 2008 and 2009
Articles for detailed review
Potentially appropriate articles
Included articles
Articles from bibliographies
Exclusion of duplicates and by title
Articles suggested by experts
Exclusion by abstract
Exclusion by text
Figure 1. Search strategy for systematic literature review. * Search terms: Auto-immune inflammatory rheumatic diseases: “Lupus Erythematosus, Systemic” [Mesh]; “Antiphosp-holipid Syndrome”[Mesh]; “Arthritis, Rheumatoid”[Mesh]; “Still’s Disease, Adult-Onset”[Mesh]; “Scle-roderma, Systemic”[Mesh]; “Sjogren’s Syndrome”[Mesh]; “Mixed Connective Tissue Disease”[Mesh]; “Polychondritis, Relapsing”[Mesh]; “Giant Cell Arteritis”[Mesh]; “Polymyalgia Rheumatica”[Mesh]; “Takayasu Arteritis”[Mesh]; “Polyarteritis Nodosa”[Mesh]; “microscopic polyangiitis”; “Wegener Granulomatosis”[Mesh]; “Churg-Strauss Syndrome”[Mesh]; “Behcet Syndrome”[Mesh]; “Anti-Glo-merular Basement Membrane Disease”[Mesh]; “Cryoglobulinemia”[Mesh]; “Polymyositis”[Mesh]; “Dermatomyositis”[Mesh]; “Myositis, Inclusion Body”[Mesh]; “anti-synthetase syndrome”; “eosi-nophilic myositis”; “Fasciitis”[Mesh]; “Spondylarthropathies”[Mesh]; “periodic fever syndrome”. Vaccines: “BCG Vaccine”[Mesh]; “ Cholera Vaccines”[Mesh]; “Diphtheria-Tetanus-Pertussis Vaccine” [Mesh]; “Diphtheria-Tetanus-acellular Pertussis Vaccines”[Mesh]; “Diphtheria Toxoid”[Mesh]; “Dipht-heria-Tetanus Vaccine”[Mesh]; “Hepatitis A Vaccines”[Mesh]; “Hepatitis B Vaccines”[Mesh]; “Haemophi-lus influenzae type b polysaccharide vaccine “[Substance Name]; “Haemophilus influenzae type b-polys-accharide vaccine-diphtheria toxoid conjugate “[Substance Name]; “DTPa-HBV-IPV combined vaccine “[Substance Name]; “Hib-MenCY-TT vaccine “[Substance Name]; “Haemophilus influenzae-type b po-lysaccharide-Neisseria meningitidis outer membrane protein conjugate vaccine “[Substance Name]; “Haemophilus influenzae type-b polysaccharide-pertussis vaccine “[Substance Name]; “Papillomavi-rus Vaccines”[Mesh]; “Influenza Vaccines”[Mesh]; “Japanese Encephalitis Vaccines”[Mesh]; “Measles Vaccine”[Mesh]; “Mumps Vaccine”[Mesh]; “Meningococcal Vaccines”[Mesh]; “Pertussis Vaccine”[Mesh]; “Pneumococcal Vaccines”[Mesh]; “Rubella Vaccine”[Mesh]; “Tetanus Toxoid”[Mesh]; “Diphtheria-Teta-nus Vaccine”[Mesh]; “Diphtheria-Tetanus-Pertussis Vaccine”[Mesh]; “Tick-Borne Encephalitis vaccine”; “Typhoid-Paratyphoid Vaccines”[Mesh]; “Herpes Zoster Vaccine”[Mesh]; “Yellow Fever Vaccine”[Mesh]. Vaccine-preventable infections: “Mycobacterium tuberculosis”[Mesh]; “Tuberculosis”[Mesh]; “Vibrio cholerae”[Mesh]; “Cholera”[Mesh]; “Corynebacterium diphtheriae”[Mesh]; “Diphtheria”[Mesh] OR “He-patitis A”[Mesh]; “Hepatitis A virus”[Mesh]; “Hepatitis B”[Mesh]; “Hepatitis B virus”[Mesh]; “Haemop-

140
Cha
pter
8
hilus influenzae type b”[Mesh]; “Human papillomavirus 6”[Mesh]’; “Human papillomavirus 18”[Mesh]; “Human papillomavirus 11”[Mesh]; “Human papillomavirus 16”[Mesh]; “Influenza, Human”[Mesh]; “Influenza A Virus, H1N1 Subtype”[Mesh]; “Influenza B virus”[Mesh]; “Influenza A virus”[Mesh]; “In-fluenza A Virus, H3N2 Subtype”[Mesh]; “Encephalitis, Japanese”[Mesh]; “Encephalitis Virus, Japanese”[Mesh]; “Measles”[Mesh]; “Measles virus”[Mesh]; “Mumps”[Mesh]; “Mumps virus”[Mesh]; “Neisseria meningitidis”[Mesh]; “Whooping Cough”[Mesh]; “Bordetella pertussis”[Mesh]; “Poliomyelitis”[Mesh]; “Poliovirus”[Mesh]; “Rabies”[Mesh]; “Rabies virus”[Mesh]; “Rubella”[Mesh]; “Rubella virus”[Mesh]; “Streptococcus pneumoniae”[Mesh]; “Pneumococcal Infections”[Mesh]; “Tetanus”[Mesh]; “Clostridium tetani”[Mesh]; “Encephalitis Viruses, Tick-Borne”[Mesh]; “Encep-halitis, Tick-Borne”[Mesh]; “Typhoid Fever”[Mesh]; “Salmonella typhi”[Mesh]; “Encephalitis, Va-ricella Zoster”[Mesh]; “Herpes Zoster”[Mesh]; “Yellow Fever”[Mesh]; “Yellow fever virus”[Mesh] Limits: Humans, English, Adolescent: 13-18 years, Adult: 19-44 years, Middle Aged: 45-64 years, Middle Aged + Aged: 45+ years, Aged: 65+ years, 80 and over: 80+ years
patients with rheumatic diseases, vasculitis, dementia or stroke who were unvac-cinated for influenza were admitted for pneumonia/influenza or death, compared to 0.8% in unvaccinated healthy controls (HC) [14].
Streptococcus pneumoniae
In a prospective cohort of 45 systemic lupus erythematosus (SLE) patients tre-ated with rituximab, cyclophosphamide and methylprednisolone, one patient developed pneumococcal pneumonia and septicaemia [15]. Retrospective cohort studies in SLE showed invasive pneumococcal infection in 1.34% of patients over an unknown period of time, in 1.9% over 25 years and in 2.40% over 9 years, res-pectively [16-18]. However, comparisons with the general population are lacking. No data are available regarding the incidence of pneumococcal infection for AIIRD other than SLE.
Herpes zoster (HZ)
In rheumatoid arthritis (RA), prospective cohort studies found an incidence of HZ ranging from 0.55 up to 11.1/1000 patient-years (PY) [19-22] and in retrospective cohort studies from 5.6 up to 14.5/1000 PY [23-28]. RA per se is a risk factor for HZ (adjusted hazard ratio 1.65 and 1.91 compared to HC respectively in two large databases [25]). Additional risk factors are the use of steroids (relative risk [RR] point estimates 1.41-2.52) [20, 24, 25, 27], use of anti-TNFα (in particular infliximab/adalimumab [RR point estimates 1.38-2.44]) [20, 24, 25, 28] and the combination of TNFα-blocking agents and steroids (RR estimate 2.44) [25]. Non-biologic DMARDs also increase the risk [24, 25], especially cyclophosphamide (4.2-fold), azathioprine (2.1-fold) and leflunomide (1.4-fold) [27]. Furthermore, combination therapy of non-biologic DMARDs and steroids increases the risk 2.39-fold [25]. Etanercept and methotrexate (MTX) do not seem to increase the risk for HZ [21, 29].
In SLE, one prospective cohort study shows an incidence of HZ of 18.3/1000 PY [30]. In retrospective studies the incidence ranges between 16-91.5/1.000 PY [31-
141
Cha
pter
8
36]. The percentage of SLE patients developing HZ is 3.2-46.6%, unfortunately the duration of follow-up in most of these studies has not been well documented [31, 33-43]. Compared to the general population the risk is increased by a factor ran-ging from 5 to 16-fold [31-33], and 3-fold compared to patients with musculo-ske-letal diseases [44]. HZ correlates with the use of cyclophosphamide, azathioprine and steroids in combination with other immunosuppressive drugs [30, 31, 33, 42]. The risk may be lower for mycophenolic acid compared with cyclophosphamide (RR 0.36) [45]. Fifty-two-week follow-up safety data from a randomized controlled trial (RCT) showed that 15.4% of SLE patients treated with rituximab, along with background immunosuppressives including steroids, developed HZ, compared with 8% in the placebo-groups [46]. One study showed that there was no increase in incidence of HZ during flares of SLE [30].
In a RCT in which Wegener granulomatosis (WG)-patients were randomized to receive etanercept or placebo along with standard immunosuppressives, the inci-dence of HZ (both groups together) was 45/1000 PY, compared with 1.2-4.8/1000 PY in the general population. A serum creatinine ≥1.5 mg/dl increased the risk of developing HZ by 6.3 [47].
In patients with polymyositis/dermatomyositis (PM/DM) the incidence of HZ was 27.2/1.000 PY in a retrospective cohort study [34]. There was no comparator-group in this study.
Tuberculosis (TB)
The incidence of TB differs strongly according to geographic area, ranging in RA patients from 0 (England, when using DMARDs) to 36.3/1000 PY (Morocco, when using DMARDs) [19, 48-74]. The highest incidence in an European country was 18.93/1000 PY in Spain among RA patients treated with infliximab, before screening for latent TB infection (LTBI) was recommended [51]. Compared to the general population, RA patients have an increased risk for contracting TB (RR point estimates ranging from 2.0 to 10.9 when treated with non-biologic DMARDs [48, 50-52, 55, 58, 62] and from 4 to 90.1 when treated with TNFα blocking agents
Table 2. Evidence-categories
Category Evidence
1A Meta-analysis of randomized controlled trials
1B Randomized controlled trial
2 Prospective controlled intervention study without randomization
3 Descriptive/analytic study (including case-control, cross-sectional, case series)
4 Expert committee reports or opinion or clinical experience of respected authori-ties or both
142
Cha
pter
8
[51, 52, 58, 62]. Within the group of RA patients non-biologic DMARDs increase the risk of TB by 1.2 and 3.0-fold [49, 50], in particular MTX (1.7 and 3.4-fold) and leflu-nomide (10.2 and 11.7-fold) [50, 75]. Steroids are also a risk factor (HR estimates 1.4-2.4) [49, 50, 75]. TNFα-blocking agents increase the risk for TB 1.5-8.7-fold, es-pecially infliximab (1.6-19.9-fold) [48, 49, 51, 58, 62-64, 68, 70]. As a result of these findings, in subsequent studies on biologics, all patients were screened for LTBI before inclusion. For RA patients treated with etanercept TB-risk was compara-ble to placebo-treated patients or the general population [21, 72]. Rituximab [60, 71, 76], anakinra [76] and the recently registered anti-IL6 agent tocilizumab [61, 66] do not seem to increase the risk for TB. For tozilizumab this was confirmed in a meta-analysis, where none of 1870 patients treated with tocilizumab (with or wit-hout additional non-biologic DMARD) developed TB [69]. Of 378 patients treated with abatacept three developed TB in a time span of five years, but there was no comparator group [77].
Only retrospective studies are performed regarding the incidence of TB in SLE patients showing incidences ranging from 2.61/1000 PY in Spain to 20/1000 PY in Korea [56, 68, 78-80]. The percentage of patients in the cohorts developing TB ranges from 0.66%/10 years up to 11.6%/5 years [39, 81-88]. Most studies come from South-East Asian countries, where TB is more prevalent than in most European countries. TB occurs more often in SLE patients than in the general population: 7.9 vs. 2.3/1000 PY [56]; 17 vs. 1.1/1000 PY [80]; 20 vs. 3.93/1000 PY [78] and 11.6%/5 years vs. 1.4-2.6%/5 years [81]. Patients who developed TB were on higher daily prednisone doses [78, 86] steroid pulse therapy [78], had a higher cumulative dose of steroids [80, 86], or lupus-nephritis [78]. Two cohort-studies addressing TB-incidence in ankylosing spondylitis (AS) found an incidence of 0 and 0.34/1000 PY respectively [68, 73]. Percentages of AS patients developing TB vary from 0% up to 12%/4 years [51, 53, 68, 72, 89, 90]. One RCT studying the treatment of AS with infliximab found one TB-case in 20 AS patients [91]. Prospective and retrospective cohorts of AS patients treated with infliximab, etanercept and adalimumab, with follow-up up to 5, 7 and 3 years respectively, did not show any cases of active TB [72, 92-98].
In one prospective cohort-study evaluating the treatment of psoriatic arthritis (PsA) with adalimumab the incidence of TB was 3/1000 PY [73].
TB occurred in 1.5%/13 years of patients with giant cell arteritis (GCA) in a retro-spective cohort study [99]. Three prospective cohort studies found that TB was the cause of death in 0.9-1.13% of patients with GCA/polymyalgia rheumatica [100-102].
Among patients with Sjögren’s syndrome (SjS) TB was not found in a retrospec-

143
Cha
pter
8
tive cohort of Spanish AIIRD patients, duration of follow-up was not stated [68].
Human Papillomavirus (HPV)
HPV-infection occurs more often in SLE patients compared with HC (24.6 vs. 10.4%) [103, 104], also with the high-risk subtype HPV-16 (4.7-53% vs. 1.2-6.7%) [103, 105] and the cumulative prevalence rises from 13.1% at baseline (11.7% high-risk sub-type) to 25.5% (21.4% high-risk subtype) after 3 years. Incidence for HPV infection was 17/1000 patient-months. The most common newly acquired HPV-subtype was HPV-16 (1.7/1000 patient-months), followed by HPV-18, -56 and -58 (1.2/1000 patient-months). Only 31.8% of all incident infections was cleared [106]. Risk fac-tors for HPV-infection in SLE patients are the same as those for the general po-pulation, but also ANA>320 [103, 106, 107].
Question 2. do vaccines decrease the risk of infections in patients with AIIRd in general, and specifically in those with unstable disease, and in those using immunomodulating agents?
Influenza vaccine (table 3)
Just one study addressed a clinical endpoint after vaccination as the primary end point, and found a reduction in pneumonitis, acute bronchitis or viral infection in RA patients and SLE patients who received influenza vaccine compared to those who did not [108]. Other studies evaluated the development of a protective level of antibodies (≥40, as measured by the hemagglutination inhibition assay). The majority of these studies have shown similar efficacy of influenza vaccination in RA patients, compared to HC. Neither DMARDs, nor TNFα-blocking treatment diminished the humoral response [109-120]. Only two studies reported a modestly impaired response in anti-TNFα users, not resulting in a lower percentage of se-roprotection [114, 121]. In contrast, rituximab severely hampers the immune res-ponse [120, 122, 123]: influenza vaccination in the first eight weeks after treatment with rituximab did not induce an antibody response. The antibody response was partially restored six to ten months after rituximab [120].
In one RCT [124] and three controlled studies [125-127] a modestly reduced res-ponse to influenza vaccination in SLE patients was found. In two other studies SLE patients showed a similar [110] or a slightly reduced in vitro response to immuni-sation [119], compared to disease controls (RA patients). In SLE several controlled studies on the efficacy of subunit influenza vaccine have shown a similar humoral response in SLE patients compared to HC [115, 128-131]. In most studies the use of immunosuppressive drugs did not affect the vaccination response [124, 126, 128, 131], however, a lower response to vaccination in SLE patients on azathioprine [125, 132], steroids [115], and hydroxychloroquine [127] has also been observed.

144
Cha
pter
8
Patients with WG develop similar humoral responses following influenza vacci-nation compared to HC. Use of immunosuppressive drugs did not to affect the humoral response [133, 134].
Also in 46 patients with systemic sclerosis (SSc) (virosomal) influenza vaccination was effective in terms of humoral and cellular immune response [135].
Pneumococcal vaccine (table 4)
The efficacy of pneumococcal vaccination is difficult to determine as no generally accepted response criteria are available. Moreover, different vaccines (polysac-charide and conjugate vaccine) are available containing antigens with different numbers of pneumococcal serotypes.
In RA, both similar [116, 136-138] and lower [138-141] responses to pneumococcal vac-cination have been reported. TNFα-blocking agents were not demonstrated to reduce efficacy of pneumococcal vaccination [116, 136-138], except for two studies, where a reduced response was demonstrated [137, 141]. Two other papers repor-ted an impaired response to pneumococcal vaccination in RA patients on the com-bination of MTX and anti-TNFα, [136, 138]. These papers also reported an impaired response in those treated with MTX alone [136, 138]. Finally, rituximab reduced the response to pneumococcal polysaccharide vaccine in a study of 69 RA patients vaccinated 28 weeks after rituximab-administration [139].
Similar [17, 142, 143] as well as a reduced/low responses [140, 144-147] were ob-served in several controlled and uncontrolled studies in SLE patients, without in-fluence of the combined use of steroids and azathioprine or cyclophosphamide [140, 143, 144, 146].
In patients with PsA (n=184) or AS (n=5) responses after pneumococcal vaccination were equal in patients with or without use of TNFα-blocking agents [148, 149].
Pneumococcal vaccination resulted in a protective antibody level to at least three out of four tested serotypes in 83% of 18 SSc-patients in an uncontrolled study [150].
Hepatitis B vaccine (table 5)
The efficacy of hepatitis B (HBV) vaccination has been addressed in patients with RA [151], SLE [152], AS [148] and Behçet disease (BD) [153]. In the majority of patients, irrespective of the underlying AIIRD and the use of steroids or DMARDs, a vacci-nation response could be demonstrated. Only use of TNFα-blocking agents seve-rely hampered the response to HBV vaccine in AS patients [148], However, a clear conclusion can not be drawn due to low numbers (n=20 for RA; n=28 for SLE; n=30 for AS; n=13 for BD) and the lack of appropriately controlled studies.
145
Cha
pter
8
Tetanus toxoid vaccine (table 6)
Tetanus toxoid vaccination seems to be efficacious in RA patients in two pros-pective controlled studies [111, 154]. The use of steroids or DMARDs did not reduce efficacy. Also treatment with rituximab did not diminish response to tetanus vac-cine in 69 RA patients when administered 24 weeks after rituximab [139].
In SLE, controlled studies revealed similar responses to tetanus toxoid vaccina-tion compared to HC [154-156]. A larger, uncontrolled study confirmed these fin-dings: >90% of the 73 SLE patients achieved an adequate response [147]. Only one small study showed a diminished response to tetanus vaccination in SLE patients. The use of steroids or DMARDs did not reduce response rates [157].
Haemophilus influenza B (HIB) vaccine (table 7)
In an uncontrolled study HIB vaccination resulted in protection in 88% of the 73 in-cluded SLE patients. A trend towards a lower response was observed in patients on immunosuppressive drugs [147].
Question 3. do vaccines cause any significant harm in patients with AIIRd in general, and specifically in those with unstable disease, and in those using immunomodulating agents?
Influenza vaccine (table 3)
In one RCT including 126 RA patients and one controlled study including 20 RA patients, RA patients who received influenza vaccine did not have an increased disease activity compared to those who were not vaccinated [109, 110]. Also in other pre-post studies RA patients did not experience increased disease activity following influenza vaccination [112-114, 116, 120, 123].
SLE patients who are vaccinated for influenza do not develop more disease fla-res than unvaccinated SLE patients, as demonstrated in one RCT [124] and three non-randomized comparative studies [108, 110, 132]. Other studies in SLE patients found either no flares [125, 126], mild flares (up to 35%) [115, 128] or renal flares with glomerulonephritis (one of 29 SLE patients) [129, 131]. Since these studies did not include disease-controls, the interpretation is difficult: the flares may have represented the natural course of SLE. In a single study systemic side effects of influenza vaccination occurred more often in SLE patients (in 19 of 56 patients) than in HC [125].
No difference in the occurrence of disease flares was found in WG patients recei-ving influenza vaccination compared to WG patients that did not receive influenza vaccination in two prospective studies [133, 134] and one large retrospective study [158].
146
Cha
pter
8
In 46 SSc patients who received (virosomal) influenza vaccine no flares of SSc were registered [135].
Of note, in all aforementioned studies inactivated influenza vaccine was used.
Pneumococcal vaccine (table 4)
No studies have been performed that compared disease activity following pneu-mococcal vaccination in RA patients with those who did not receive pneumococ-cal vaccine. Uncontrolled pre-post studies showed no increase in disease activity following vaccination [116, 136, 139-141].
In all three studies comparing SLE patients who did (n=20, 18 and 38) and did not (n=20, 8 and 23) receive pneumococcal vaccination, disease activity after vacci-nation did not differ significantly [17, 142, 144]. Other studies, comparing SLE pa-tients receiving pneumococcal vaccine with RA patients and/or HC [140, 143-146], or case series of SLE patients receiving pneumococcal vaccine [143, 147, 159] could not demonstrate an increase in SLE activity following pneumococcal vaccination. Case series in patients with PsA [149] and SjS [160] did not show increased disease activity following pneumococcal vaccination.
Hepatitis B vaccine (table 5)
HBV vaccination did not lead to increased disease activity in 22 vaccinated RA patients compared to 22 unvaccinated RA patients [151].
One uncontrolled prospective study regarding HBV vaccination in 28 SLE patients revealed no significant change in SLEDAI-score after each vaccine dose. The number of flares following vaccination was similar to that observed in the year before vaccination (21%) [152].
In a study of 13 Behçet patients three developed oral aphtae following HBV vac-cination but otherwise no increase in disease activity was observed [153].
Question 4. does the timing of vaccination in relation to disease activity and in relation to the receipt of immunomodulating agents affect the effective-ness of vaccination in patients with AIIRd?
There are no studies comparing the efficacy of vaccination in AIIRD patients with stable and unstable disease: generally, studies performed in patients with AIIRD included typically patients with stable, quiescent disease.
Influenza vaccine
Three studies addressing the influence of disease activity on the humoral response in RA patients found that the degree of disease activity did not affect

147
Cha
pter
8
Tab
le 3
. Eff
icac
y an
d sa
fety
of
infl
uenz
a va
ccin
atio
n in
AIIR
D p
atie
nts
Aut
hor/
Year
Des
ign
No.
cas
esEf
fica
cyIn
flue
nce
of IS
on
effi
cacy
Safe
tyLo
E
Cha
lmer
s [10
9]R
CT
64 R
A-P
VN
o di
ffer
ence
No
No
diff
eren
ce1B
1994
22 R
A n
ot-P
V
40
RA
-IS
64
HC
Kai
ne [1
16]
RC
T99
RA
-AD
AN
o di
ffer
ence
No
No
flar
es1B
20
07
109
RA
Den
man
[111
]C
ontr
olle
d20
RA
No
diff
eren
ceN
oN
/A2
1970
39 R
A-D
C
20
HC
Kap
etan
ovic
[121
]C
ontr
olle
d50
RA
-ant
i-T
NF+
MT
XR
educ
ed in
RA
-ant
i-R
educ
ed o
n T
NF+
MT
XN
/A2
200
762
RA
-ant
i-T
NF+
MT
Xan
d R
A-a
nti-
TN
F co
mpa
red
TN
F+D
MA
RD
to R
A-M
TX
37 R
A-M
TX
18 H
C
Kub
ota
[117]
Con
trol
led
27 R
A-a
nti-
TN
FN
o di
ffer
ence
Incr
ease
d on
ant
i-T
NF
N/A
2
20
07
36 R
A-D
C
52
HC
Ore
n [12
3]C
ontr
olle
d29
RA
Red
uced
in R
A-R
TX
Red
uced
on
RT
XN
o fl
ares
2
20
08
14 R
A-R
TX
21
HC
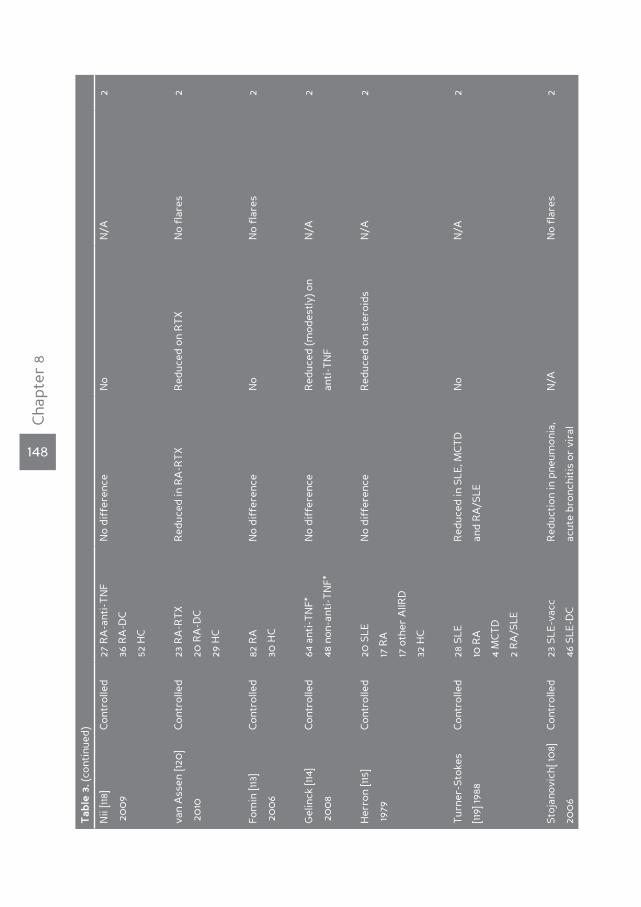
148
Cha
pter
8
Tab
le 3
. (co
ntin
ued)
Nii
[118]
Con
trol
led
27 R
A-a
nti-
TN
FN
o di
ffer
ence
No
N/A
2
20
09
36 R
A-D
C
52
HC
van
Ass
en [1
20]
Con
trol
led
23 R
A-R
TX
Red
uced
in R
A-R
TX
Red
uced
on
RT
XN
o fl
ares
2
20
1020
RA
-DC
29
HC
Fom
in [1
13]
Con
trol
led
82 R
AN
o di
ffer
ence
No
No
flar
es2
20
06
30 H
C
Gel
inck
[114
]C
ontr
olle
d64
ant
i-T
NF*
No
diff
eren
ceR
educ
ed (m
odes
tly)
on
N/A
2
20
08
48 n
on-a
nti-
TN
F*an
ti-T
NF
Her
ron
[115]
Con
trol
led
20 S
LEN
o di
ffer
ence
Red
uced
on
ster
oids
N/A
2
1979
17 R
A
17
oth
er A
IIRD
32
HC
Tur
ner-
Stok
esC
ontr
olle
d28
SLE
Red
uced
in S
LE, M
CT
DN
oN
/A2
[119]
1988
10 R
Aan
d R
A/S
LE
4
MC
TD
2
RA
/SLE
Stoj
anov
ich[
108]
Con
trol
led
23 S
LE-v
acc
Red
ucti
on in
pne
umon
ia,
N/A
No
flar
es2
200
646
SLE
-DC
acut
e br
onch
itis
or
vira
l
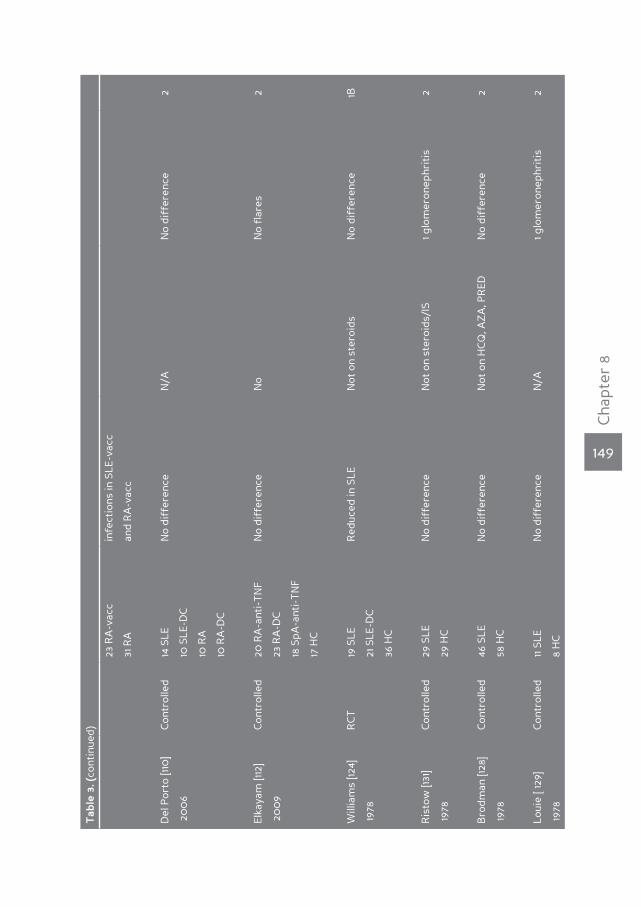
149
Cha
pter
8
Tab
le 3
. (co
ntin
ued)
23 R
A-v
acc
infe
ctio
ns in
SLE
-vac
c
31 R
Aan
d R
A-v
acc
Del
Por
to [1
10]
Con
trol
led
14 S
LEN
o di
ffer
ence
N/A
No
diff
eren
ce2
20
06
10 S
LE-D
C
10
RA
10
RA
-DC
Elka
yam
[112
]C
ontr
olle
d20
RA
-ant
i-T
NF
No
diff
eren
ceN
oN
o fl
ares
2
20
09
23 R
A-D
C
18
SpA
-ant
i-T
NF
17
HC
Will
iam
s [12
4]R
CT
19 S
LER
educ
ed in
SLE
Not
on
ster
oids
No
diff
eren
ce1B
1978
21 S
LE-D
C
36
HC
Ris
tow
[131
]C
ontr
olle
d29
SLE
No
diff
eren
ceN
ot o
n st
eroi
ds/I
S1 g
lom
eron
ephr
itis
2
1978
29 H
C
Bro
dman
[128
]C
ontr
olle
d46
SLE
No
diff
eren
ceN
ot o
n H
CQ
, AZ
A, P
RED
No
diff
eren
ce2
1978
58 H
C
Loui
e [ 1
29]
Con
trol
led
11 S
LEN
o di
ffer
ence
N/A
1 glo
mer
onep
hrit
is2
1978
8 H
C
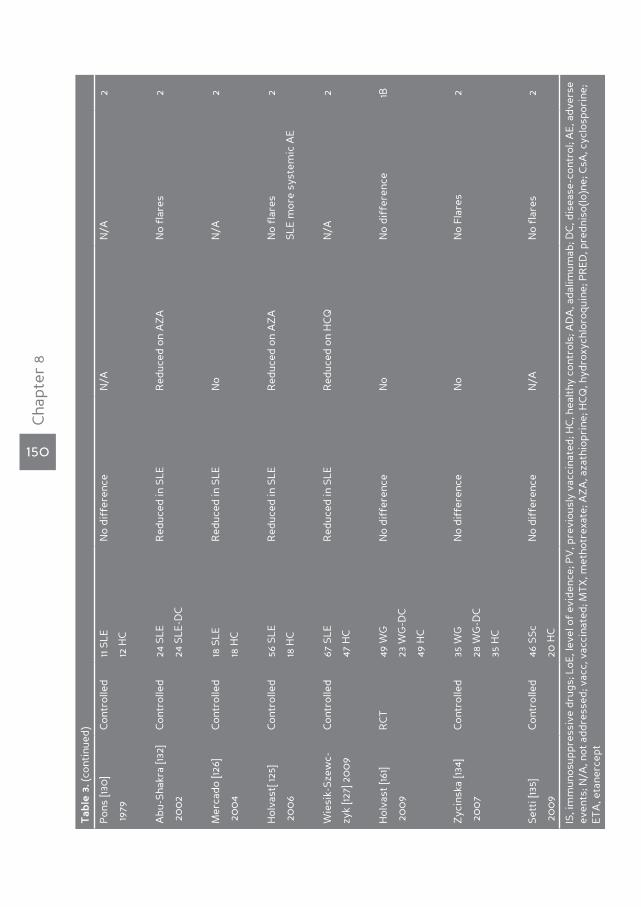
150
Cha
pter
8
Tab
le 3
. (co
ntin
ued)
Pon
s [13
0]
Con
trol
led
11 S
LEN
o di
ffer
ence
N/A
N/A
2
1979
12 H
C
Abu
-Sha
kra
[132]
Con
trol
led
24 S
LER
educ
ed in
SLE
Red
uced
on
AZ
AN
o fl
ares
2
20
02
24 S
LE-D
C
Mer
cado
[126
]C
ontr
olle
d18
SLE
Red
uced
in S
LEN
oN
/A2
20
04
18 H
C
Hol
vast
[ 125
]C
ontr
olle
d56
SLE
Red
uced
in S
LER
educ
ed o
n A
ZA
No
flar
es2
20
06
18 H
CSL
E m
ore
syst
emic
AE
Wie
sik-
Szew
c-C
ontr
olle
d67
SLE
Red
uced
in S
LER
educ
ed o
n H
CQ
N/A
2
zyk
[127]
20
09
47 H
C
Hol
vast
[161
]R
CT
49 W
GN
o di
ffer
ence
No
No
diff
eren
ce1B
20
09
23 W
G-D
C
49
HC
Zyc
insk
a [13
4]C
ontr
olle
d35
WG
No
diff
eren
ceN
oN
o Fl
ares
2
20
07
28 W
G-D
C
35
HC
Sett
i [13
5]C
ontr
olle
d46
SSc
No
diff
eren
ceN
/AN
o fl
ares
2
20
09
20 H
C
IS, i
mm
unos
uppr
essi
ve d
rugs
; LoE
, lev
el o
f ev
iden
ce; P
V, p
revi
ousl
y va
ccin
ated
; HC
, hea
lthy
con
trol
s; A
DA
, ada
limum
ab; D
C, d
isea
se-c
ontr
ol; A
E, a
dver
se
even
ts; N
/A, n
ot a
ddre
ssed
; vac
c, v
acci
nate
d; M
TX
, met
hotr
exat
e; A
ZA
, aza
thio
prin
e; H
CQ
, hyd
roxy
chlo
roqu
ine;
PR
ED, p
redn
iso(
lo)n
e; C
sA, c
yclo
spor
ine;
ET
A, e
tane
rcep
t
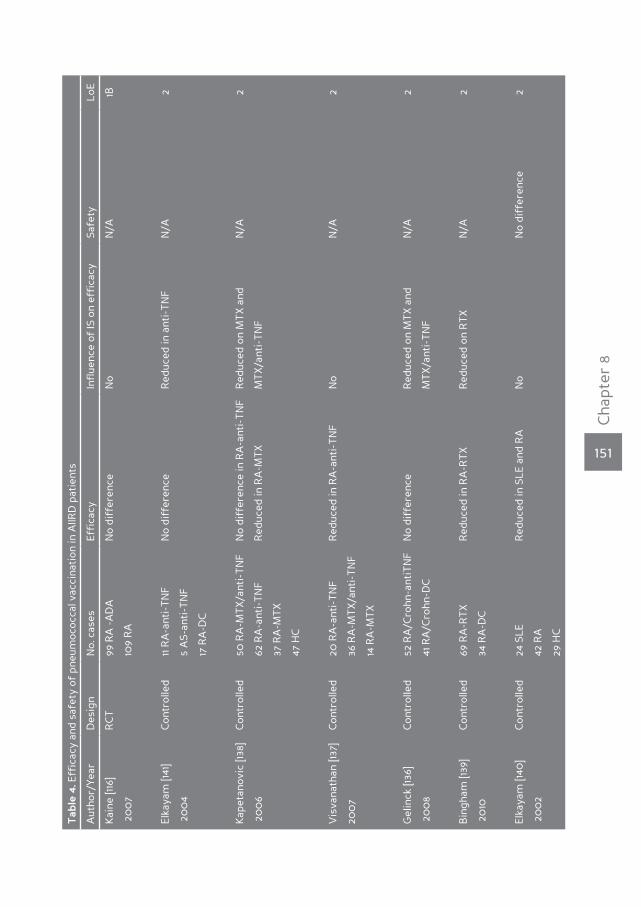
151
Cha
pter
8
Tab
le 4
. Eff
icac
y an
d sa
fety
of
pneu
moc
occa
l vac
cina
tion
in A
IIRD
pat
ient
s
Aut
hor/
Year
Des
ign
No.
cas
esEf
fica
cyIn
flue
nce
of IS
on
effi
cacy
Safe
tyLo
E
Kai
ne [1
16]
RC
T99
RA
-A
DA
No
diff
eren
ceN
oN
/A1B
20
07
109
RA
Elka
yam
[141
]C
ontr
olle
d11
RA
-ant
i-T
NF
No
diff
eren
ceR
educ
ed in
ant
i-T
NF
N/A
2
20
04
5 A
S-an
ti-T
NF
17
RA
-DC
Kap
etan
ovic
[138
]C
ontr
olle
d50
RA
-MT
X/a
nti-
TN
FN
o di
ffer
ence
in R
A-a
nti-
TN
FR
educ
ed o
n M
TX
and
N/A
2
20
06
62 R
A-a
nti-
TN
FR
educ
ed in
RA
-MT
XM
TX
/ant
i-T
NF
37
RA
-MT
X
47
HC
Vis
vana
than
[137
]C
ontr
olle
d20
RA
-ant
i-T
NF
Red
uced
in R
A-a
nti-
TN
FN
oN
/A2
200
736
RA
-MT
X/a
nti-
TN
F
14
RA
-MT
X
Gel
inck
[136
]C
ontr
olle
d52
RA
/Cro
hn-a
ntiT
NF
No
diff
eren
ceR
educ
ed o
n M
TX
and
N
/A2
20
08
41 R
A/C
rohn
-DC
MT
X/a
nti-
TN
F
Bin
gham
[139
]C
ontr
olle
d69
RA
-RT
XR
educ
ed in
RA
-RT
XR
educ
ed o
n R
TX
N/A
2
20
1034
RA
-DC
Elka
yam
[140
]C
ontr
olle
d24
SLE
Red
uced
in S
LE a
nd R
AN
oN
o di
ffer
ence
2
20
02
42 R
A
29
HC
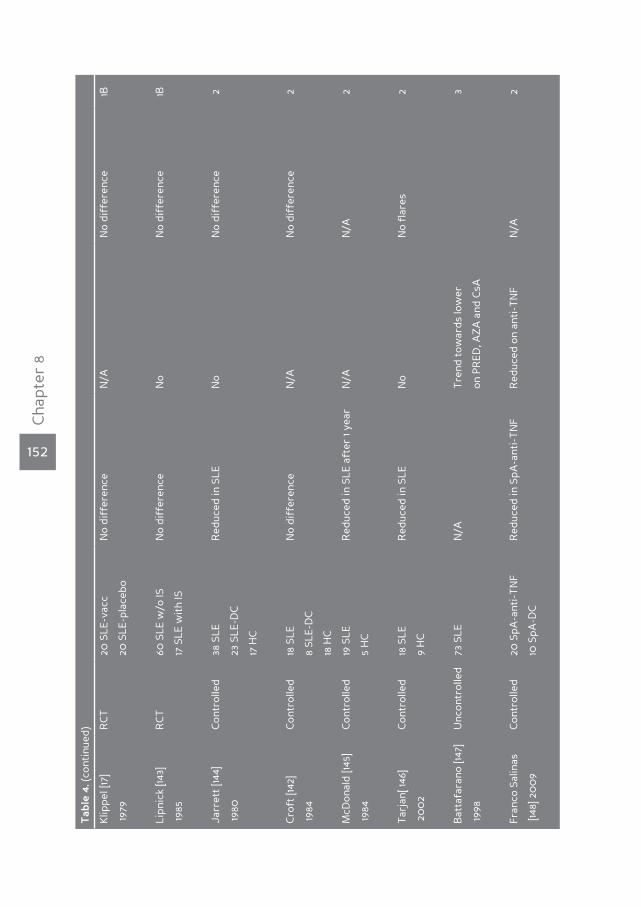
152
Cha
pter
8
Tab
le 4
. (co
ntin
ued)
Klip
pel [
17]
RC
T20
SLE
-vac
cN
o di
ffer
ence
N/A
No
diff
eren
ce1B
1979
20 S
LE-p
lace
bo
Lipn
ick
[143]
RC
T60
SLE
w/o
ISN
o di
ffer
ence
No
No
diff
eren
ce1B
1985
17 S
LE w
ith
IS
Jarr
ett
[144]
Con
trol
led
38 S
LER
educ
ed in
SLE
No
No
diff
eren
ce2
1980
23 S
LE-D
C
17
HC
Cro
ft [1
42]
Con
trol
led
18 S
LEN
o di
ffer
ence
N/A
No
diff
eren
ce2
1984
8 SL
E-D
C
18
HC
McD
onal
d [14
5]C
ontr
olle
d19
SLE
Red
uced
in S
LE a
fter
1 ye
arN
/AN
/A2
1984
5 H
C
Tar
jan[
146]
Con
trol
led
18 S
LER
educ
ed in
SLE
No
No
flar
es2
20
02
9 H
C
Bat
tafa
rano
[147
]U
ncon
trol
led
73 S
LEN
/AT
rend
tow
ards
low
er
3
1998
on P
RED
, AZ
A a
nd C
sA
Fran
co S
alin
asC
ontr
olle
d20
SpA
-ant
i-T
NF
Red
uced
in S
pA-a
nti-
TN
FR
educ
ed o
n an
ti-T
NF
N/A
2
[148
] 20
09
10 S
pA-D
C
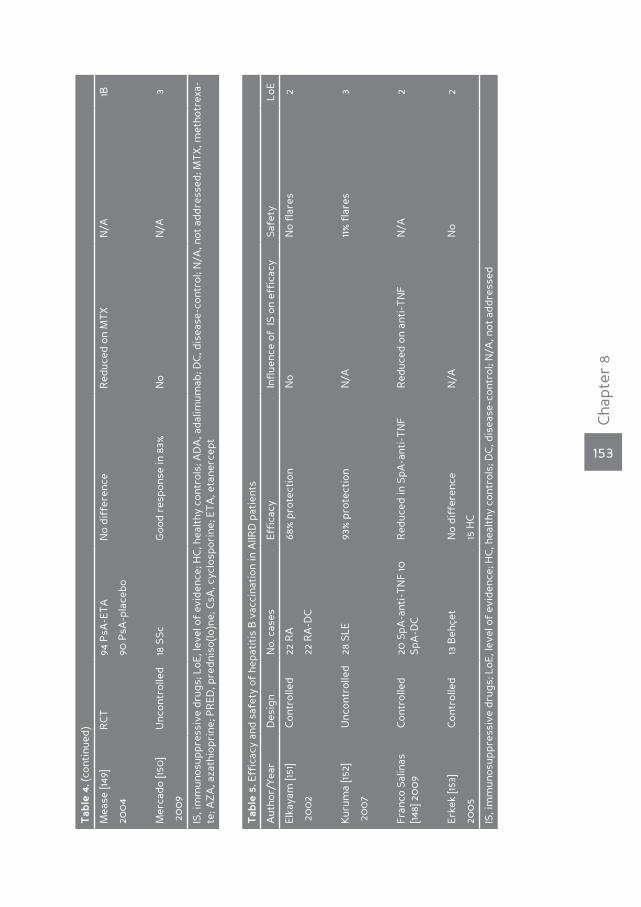
153
Cha
pter
8
Tab
le 4
. (co
ntin
ued)
Mea
se [1
49]
RC
T94
PsA
-ET
AN
o di
ffer
ence
Red
uced
on
MT
XN
/A1B
200
490
PsA
-pla
cebo
Mer
cado
[150
]U
ncon
trol
led
18 S
ScG
ood
resp
onse
in 8
3%N
oN
/A3
20
09
IS, i
mm
unos
uppr
essi
ve d
rugs
; LoE
, lev
el o
f ev
iden
ce; H
C, h
ealt
hy c
ontr
ols;
AD
A, a
dalim
umab
; DC
, dis
ease
-con
trol
; N/A
, not
add
ress
ed; M
TX
, met
hotr
exa-
te; A
ZA
, aza
thio
prin
e; P
RED
, pre
dnis
o(lo
)ne;
CsA
, cyc
losp
orin
e; E
TA
, eta
nerc
ept
Tab
le 5
. Eff
icac
y an
d sa
fety
of
hepa
titi
s B
vac
cina
tion
in A
IIRD
pat
ient
s
Aut
hor/
Year
Des
ign
No.
cas
esEf
fica
cyIn
flue
nce
of I
S on
eff
icac
ySa
fety
LoE
Elka
yam
[151
]C
ontr
olle
d22
RA
68%
pro
tect
ion
No
No
flar
es2
20
02
22 R
A-D
C
Kur
uma
[152]
Unc
ontr
olle
d28
SLE
93%
pro
tect
ion
N/A
11%
fla
res
3
20
07
Fran
co S
alin
as
[148]
20
09
Con
trol
led
20 S
pA-a
nti-
TN
F 10
Sp
A-D
CR
educ
ed in
SpA
-ant
i-T
NF
Red
uced
on
anti
-TN
FN
/A2
Erke
k [15
3]C
ontr
olle
d13
Beh
çet
No
diff
eren
ceN
/AN
o2
200
515
HC
IS, i
mm
unos
uppr
essi
ve d
rugs
; LoE
, lev
el o
f ev
iden
ce; H
C, h
ealt
hy c
ontr
ols;
DC
, dis
ease
-con
trol
; N/A
, not
add
ress
ed
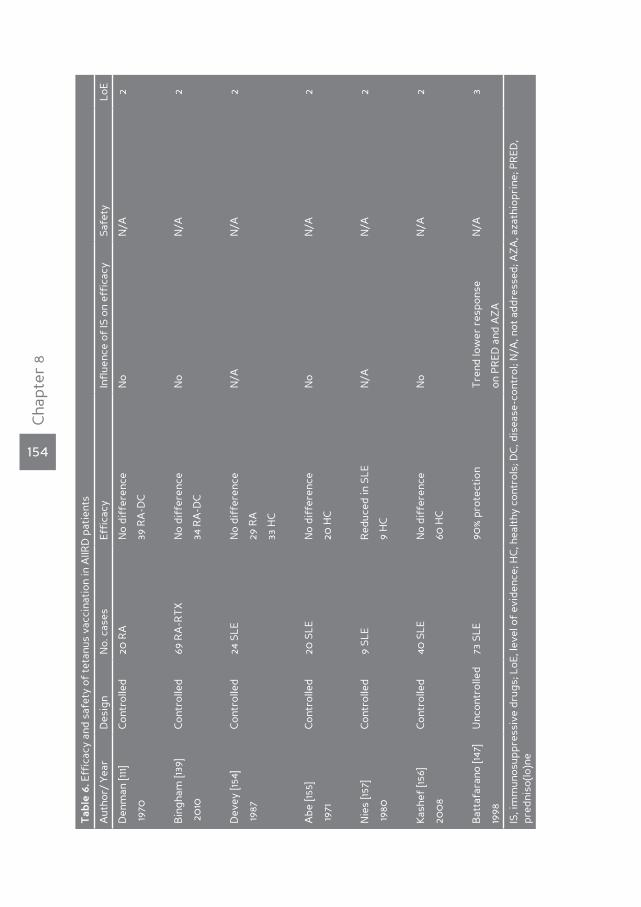
154
Cha
pter
8
Tab
le 6
. Eff
icac
y an
d sa
fety
of
teta
nus
vacc
inat
ion
in A
IIRD
pat
ient
s
Aut
hor/
Yea
rD
esig
nN
o. c
ases
Effi
cacy
Infl
uenc
e of
IS o
n ef
fica
cySa
fety
LoE
Den
man
[111
]C
ontr
olle
d20
RA
No
diff
eren
ceN
oN
/A2
1970
39 R
A-D
C
Bin
gham
[139
]C
ontr
olle
d69
RA
-RT
XN
o di
ffer
ence
No
N/A
2
20
1034
RA
-DC
Dev
ey [1
54]
Con
trol
led
24 S
LEN
o di
ffer
ence
N/A
N/A
2
1987
29 R
A
33
HC
Abe
[155
]C
ontr
olle
d20
SLE
No
diff
eren
ceN
oN
/A2
1971
20 H
C
Nie
s [15
7]C
ontr
olle
d9
SLE
Red
uced
in S
LEN
/AN
/A2
1980
9 H
C
Kas
hef
[156]
Con
trol
led
40 S
LEN
o di
ffer
ence
No
N/A
2
200
8 60
HC
Bat
tafa
rano
[147
]U
ncon
trol
led
73 S
LE90
% p
rote
ctio
nT
rend
low
er r
espo
nse
N/A
3
1998
on P
RED
and
AZ
A
IS, i
mm
unos
uppr
essi
ve d
rugs
; LoE
, lev
el o
f ev
iden
ce; H
C, h
ealt
hy c
ontr
ols;
DC
, dis
ease
-con
trol
; N/A
, not
add
ress
ed; A
ZA
, aza
thio
prin
e; P
RED
, pr
edni
so(lo
)ne

155
Cha
pter
8
Tab
le 7
. Eff
icac
y an
d sa
fety
of
H. i
nflu
enza
e b
vacc
inat
ion
in A
IIRD
pat
ient
s
Aut
hor/
Year
Des
ign
No.
cas
esEf
fica
cyIn
flue
nce
of IS
on
effi
cacy
Safe
tyLo
E
Bat
tafe
rano
[147
]U
ncon
trol
led
73 S
LE88
% p
rote
ctio
nT
rend
low
er o
n P
RED
,N
/A3
1998
AZ
A a
nd C
sA
IS, i
mm
unos
uppr
essi
ve d
rugs
; LoE
, lev
el o
f ev
iden
ce; N
/A, n
ot a
ddre
ssed
; AZ
A, a
zath
iopr
ine;
PR
ED, p
redn
iso(
lo)n
e; C
sA, c
yclo
spor
ine
156
Cha
pter
8
this response [112, 113, 123]. One study investigated the influence of timing of the in-fluenza vaccination in relation to the receipt of infliximab in RA and AS patients. A trend towards a lower immune response was observed in RA patients vaccinated three weeks after the administration of infliximab as compared with those vacci-nated on the day of infliximab administration [112]. In another study in RA patients treated with rituximab the humoral response after influenza vaccination was se-verely hampered in the group that received their influenza vaccination four to eight weeks after rituximab, while six to ten months after rituximab a slight reco-very of the humoral response was observed [120].
In SLE, most studies assessing the effect of disease activity on the humoral res-ponse following influenza vaccination did not show a reduced response in patients with active disease [119, 126, 128, 132, 133], although some reported a diminished response [127, 131]. With regard to the influence of immunomodulating agents on the timing of vaccination, no data are available in SLE patients.
Pneumococcal vaccine
In four studies no effect of disease activity on the efficacy of pneumococcal vac-cination in RA patients was shown [137, 138, 140, 141].
Also in SLE, disease activity did not influence the efficacy of vaccination [17, 140, 144], although one open trial demonstrated a trend towards a reduced response in patients with active lupus [147].
Hepatitis vaccine
A single study in RA patients did not show an effect of disease activity on anti-body response to HBV vaccination [151].
Tetanus toxoid vaccine
The efficacy of tetanus booster in RA patients has not been shown to be affec-ted by the degree of disease activity [154]. Also rituximab, when administered 24 weeks before tetanus vaccination, did not reduce the humoral response to teta-nus vaccination [139].
In SLE, the efficacy of tetanus vaccination may be reduced in SLE patients with active disease [147, 155], although data are conflicting [154, 156].
Question 5. does the timing of vaccination in relation to disease activity and in relation to receipt of immunomodulating agents affect important harms of vaccination in patients with AIIRd?
Only two studies addressed the timing of vaccination in patients with AIIRD with regard to harms. In patients with RA or AS, influenza vaccination on the day of

157
Cha
pter
8
infliximab infusion or three weeks afterwards did not result in a significant dif-ference in adverse events and no increase in disease activity was observed [112]. Disease activity did not change following influenza vaccination regardless of whether administered 4-8 weeks or 6-10 months after treatment with rituximab [120].
Question 6. does revaccination with any vaccines increase the effectiveness in patients with AIIRd?
The usefulness of a second vaccination in AIIRD patients was addressed by one study. In SLE patients a booster influenza vaccination four weeks after the first vaccination did not lead to a further rise of seroprotection rates and geometric mean titres (GMTs). However, in the subgroup of SLE patients who have not been vaccinated in the previous year, GMT and seroconversion rate to A/H1N1 did rise following the booster vaccination [161].
Question 7. does revaccination with any vaccine increase significant harms in patients with AIIRd?
There are no data available on the harms of revaccination in AIIRD patients.
Question 8. Is vaccination in patients with AIIRd cost-effective?
There are no data available on the cost-effectiveness of vaccination specifically in AIIRD patients.
dISCuSSIOnThis SLR summarizes the available evidence regarding vaccination is patients with AIIRD. By defining eight key questions we were able to address the most im-portant issues, mainly the indication, the efficacy and the possible harms of vacci-
Table 8. Research agenda
1. Set-up of a vaccination registry for patients with AIIRD with a focus on safety and efficacy
2. Prospective studies evaluating the prevalence and identification of causative micro-organisms of infection in patients with AIIRD, and the outcome of vaccine preventable infections in these patients
3. Evaluation of the impact of therapies on safety and efficacy of vaccination
4. Evaluation of the impact of new therapies on prevalence of (vaccine preventable) infections
5. Research for efficacy and safety of new vaccines (such as herpes zoster, pandemic H1N1 Influ-enza A, HPV)
6. Evaluation of the implementation of vaccination recommendations
7. Research for the safety and efficacy regarding adjuvants and specific risk groups (e.g. preg-nancy)

158
Cha
pter
8
nation in these patients. Unfortunately, studies investigating the incidence of VPI in AIIRD patients are scarce and no RCT with clinical primary endpoints regarding efficacy were available. Moreover, although vaccination did not lead to signifi-cant harms in the available comparative studies, these studies were too small and had too short follow-up to draw firm conclusions. Safety of vaccination is considered to be of major importance in particular in patients with auto-immune diseases, because of the potential risk for flares of their underlying disease. Although many case series and case reports regarding side effects of vaccination in patients with AIIRD have been published, these were not included since these can not distinguish natural course of the underlying AIIRD from possible adverse effects caused by vaccination. On the other hand, use of live attenuated vaccines in immunocompromised patients is generally considered unsafe, but only case reports are available to support this concern. Finally, cost-effectiveness was con-sidered, but no studies were found to address this issue specifically in AIIRD pa-tients, and results from cost-effectiveness analyses in the general population for these same vaccines may not be applicable for AIIRD.
In conclusion, the currently available evidence was systematically reviewed to make evidence-based recommendations for vaccination in patients with AIIRD [12]. However, because of the lack of adequately large, well-designed studies, there is a need for further research (table 8) regarding the incidence of VPI, the efficacy of vaccination in patients with AIIRD (in particular in relation to treat-ment with traditional and/or new immunosuppressive agents and the timing of vaccination with regard to these immunosuppressive medications), and potential harms of vaccination in patients with AIIRD.
159
Cha
pter
8
Reference List
(1) Falagas ME, Manta KG, Betsi GI, Pappas G. Infection-related morbidity and mortality in patients
with connective tissue diseases: a systematic review. Clin Rheumatol 2007 May; 26(5):663-70.
(2) Bosch X, Guilabert A, Pallares L, et al. Infections in systemic lupus erythematosus: a prospective
and controlled study of 110 patients. Lupus 2006; 15(9):584-9.
(3) Doran MF, Crowson CS, Pond GR, O’Fallon WM, Gabriel SE. Frequency of infection in patients
with rheumatoid arthritis compared with controls: a population-based study. Arthritis Rheum
2002 Sep; 46(9):2287-93.
(4) Wolfe F, Mitchell DM, Sibley JT, et al. The mortality of rheumatoid arthritis. Arthritis Rheum 1994
Apr; 37(4):481-94.
(5) Cervera R, Khamashta MA, Font J, et al. Morbidity and mortality in systemic lupus erythemato-
sus during a 10-year period: a comparison of early and late manifestations in a cohort of 1,000
patients. Medicine (Baltimore) 2003 Sep; 82(5):299-308.
(6) Steen VD, Medsger TA. Changes in causes of death in systemic sclerosis, 1972-2002. Ann Rheum
Dis 2007 Jul; 66(7):940-4.
(7) Ruangjutipopan S, Kasitanon N, Louthrenoo W, Sukitawut W, Wichainun R. Causes of death and
poor survival prognostic factors in thai patients with systemic sclerosis. J Med Assoc Thai 2002
Nov; 85(11):1204-9.
(8) Hoffman GS, Kerr GS, Leavitt RY, et al. Wegener granulomatosis: an analysis of 158 patients. Ann
Intern Med 1992 Mar 15; 116(6):488-98.
(9) Reinhold-Keller E, Beuge N, Latza U, et al. An interdisciplinary approach to the care of patients
with Wegener’s granulomatosis: long-term outcome in 155 patients. Arthritis Rheum 2000 May;
43(5):1021-32.
(10) Little MA, Nightingale P, Verburgh CA, et al. Early mortality in systemic vasculitis: relative con-
tribution of adverse events and active vasculitis. Ann Rheum Dis 2009 Jul 1.
(11) Marie I, Hachulla E, Cherin P, et al. Opportunistic infections in polymyositis and dermatomyosi-
tis. Arthritis Rheum 2005 Apr 15; 53(2):155-65.
(12) van Assen S, Agmon-Levin N, Elkayam O, et al. EULAR recommendations for vaccination in adult
patients with autoimmune inflammatory rheumatic diseases. Ann Rheum Dis 2010 Dec 3.
(13) Nichol KL, Wuorenma J, von Sternberg T. Benefits of influenza vaccination for low-, intermedi-
ate-, and high-risk senior citizens. Arch Intern Med 1998 Sep 14; 158(16):1769-76.
(14) Hak E, Nordin J, Wei F, et al. Influence of high-risk medical conditions on the effectiveness of in-
fluenza vaccination among elderly members of 3 large managed-care organizations. Clin Infect
Dis 2002 Aug 15; 35(4):370-7.
(15) Isenberg DA, Lu TY, Ng KP, Cambridge G, Leandro MJ, Ehrenstein M et al. A Retrospective Se-
ven-year Analysis Of The Use Of B-cell Depletion Therapy In Systemic Lupus Erythematosus At
University College London Hospital: The First Fifty Patients. ACR 2008; abstract 1075
(16) Yee AM, Ng SC, Sobel RE, Salmon JE. Fc gammaRIIA polymorphism as a risk factor for invasive
pneumococcal infections in systemic lupus erythematosus. Arthritis Rheum 1997 Jun; 40(6):1180-
2.
(17) Klippel JH, Karsh J, Stahl NI, Decker JL, Steinberg AD, Schiffman G. A controlled study of pneu-
mococcal polysaccharide vaccine in systemic lupus erythematosus. Arthritis Rheum 1979 Dec;
22(12):1321-5.

160
Cha
pter
8
(18) Naveau C, Houssiau FA. Pneumococcal sepsis in patients with systemic lupus erythematosus.
Lupus 2005; 14(11):903-6.
(19) Favalli EG, Desiati F, Atzeni F, et al. Serious infections during anti-TNFalpha treatment in rheu-
matoid arthritis patients. Autoimmun Rev 2009 Jan; 8(3):266-73.
(20) Strangfeld A, Listing J, Herzer P, et al. Risk of herpes zoster in patients with rheumatoid arthritis
treated with anti-TNF-alpha agents. JAMA 2009 Feb 18; 301(7):737-44.
(21) Gordon KB, Gottlieb AB, Gianinni EH, Mease PJ, Chon Y, Weng HH et al. Clinical Trial Safety Data
of Events of Interest in Patients Receiving Etanercept (ENBREL®) across Approved Indications.
ACR 2007: abstract 960
(22) Weinblatt M, Genovese M, Bathon J, Kremer J, Fleischmann R, Schiff M et al. Safety and Efficacy
of Etanercept (Enbrel®) Treatment in North American Patients With Early and Long-Standing
Rheumatoid Arthritis: 10 Years of Clinical Experience. ACR 2008: abstract 1007
(23) Antonelli MA, Moreland LW, Brick JE. Herpes zoster in patients with rheumatoid arthritis trea-
ted with weekly, low-dose methotrexate. Am J Med 1991 Mar; 90(3):295-8.
(24) McDonald JR, Zeringue AL, Caplan L, et al. Herpes zoster risk factors in a national cohort of
veterans with rheumatoid arthritis. Clin Infect Dis 2009 May 15; 48(10):1364-71.
(25) Smitten AL, Choi HK, Hochberg MC, et al. The risk of herpes zoster in patients with rheumatoid
arthritis in the United States and the United Kingdom. Arthritis Rheum 2007 Dec 15; 57(8):1431-8.
(26) Speerstra F, Boerbooms AM, van de Putte LB, van Beusekom HJ, Kruijsen MW, Vandenbroucke
JP. Side-effects of azathioprine treatment in rheumatoid arthritis: analysis of 10 years of expe-
rience. Ann Rheum Dis 1982; 41 Suppl 1:37-9.
(27) Wolfe F, Michaud K, Chakravarty EF. Rates and predictors of herpes zoster in patients with rheu-
matoid arthritis and non-inflammatory musculoskeletal disorders. Rheumatology (Oxford) 2006
Nov; 45(11):1370-5.
(28) Perez-Zafrilla B, Garcia Doval I, Carmona L. Rates of herpes zoster in patients with rheumatoid
arthritis and treatment with TNF antagonists. Incidence rate in Biobadaser cohort in comparison
with Emecar cohort. Ann Rheum Dis 2008;67 (suppl2):327
(29) Salliot C, Bombardier C, van der Heide D. Long term safety of methotrexate in rheumatoid
arthritis; a systematic literature review. Ann Rheum Dis 2008;67 (suppl II):204
(30) Ginzler E, Diamond H, Kaplan D, Weiner M, Schlesinger M, Seleznick M. Computer analysis of
factors influencing frequency of infection in systemic lupus erythematosus. Arthritis Rheum
1978 Jan; 21(1):37-44.
(31) Kahl LE. Herpes zoster infections in systemic lupus erythematosus: risk factors and outcome. J
Rheumatol 1994 Jan; 21(1):84-6.
(32) Kang TY, Lee HS, Kim TH, Jun JB, Yoo DH. Clinical and genetic risk factors of herpes zoster in
patients with systemic lupus erythematosus. Rheumatol Int 2005 Mar; 25(2):97-102.
(33) Manzi S, Kuller LH, Kutzer J, et al. Herpes zoster in systemic lupus erythematosus. J Rheumatol
1995 Jul; 22(7):1254-8.
(34) Nagaoka S, Tani K, Ishigatsubo Y, et al. Herpes zoster in patients with polymyositis and derma-
tomyositis. Kansenshogaku Zasshi 1990 Nov; 64(11):1394-9.
(35) Nagasawa K, Yamauchi Y, Tada Y, Kusaba T, Niho Y, Yoshikawa H. High incidence of herpes zoster
in patients with systemic lupus erythematosus: an immunological analysis. Ann Rheum Dis 1990
Aug; 49(8):630-3.
(36) Wang F, Chua CT, Bosco J. Herpes zoster in patients with systemic lupus erythematosus. Singa-
161
Cha
pter
8
pore Med J 1983 Aug; 24(4):218-20.
(37) Dubois EL, Tuffanelli DL. Clinical manifestations of systemic lupus erythematosus. Computer
analysis of 520 cases. JAMA 1964 Oct 12; 190:104-11.
(38) Ishikawa O, Abe M, Miyachi Y. Herpes zoster in Japanese patients with systemic lupus erythe-
matosus. Clin Exp Dermatol 1999 Jul; 24(4):327-8.
(39) Janwityanuchit S, Totemchokchyakarn K, Krachangwongchai K, Vatanasuk M. Infection in syste-
mic lupus erythematosus. J Med Assoc Thai 1993 Oct; 76(10):542-8.
(40) Moutsopoulos HM, Gallagher JD, Decker JL, Steinberg AD. Herpes zoster in patients with syste-
mic lupus erythematosus. Arthritis Rheum 1978 Sep; 21(7):798-802.
(41) Della-Torre E, Bozzolo E, Baldini M, Ferrante L, Bonavida G, Baldissera E et al. Individualized the-
rapy provides better outcome in patients with proliferative lupus nephritis: follow up of a cohort
of Italian patients. Ann Rheum Dis 2009;68 (suppl3):247
(42) Medeiros AC, Martin P, Ribeiro AR, Gonçalves R, Borba EF. Associated Factors and Outcome of
Herpes Zoster in Systemic Lupus Erythematosus (SLE) Patients . ACR 2007: abstract 1950
(43) Tanaka Y, Tokunaga M, Nawata M, Suzuki K, Iwata S, Yamaoka K et al. Long-Term Follow Up of
Rituximab (Anti-CD20) Therapy for Refractory Systemic Lupus Erythematosus. ACR 2007: ab-
stract 1939
(44) Pope JE, Krizova A, Ouimet JM, Goodwin JL, Lankin M. Close association of herpes zoster reac-
tivation and systemic lupus erythematosus (SLE) diagnosis: case-control study of patients with
SLE or noninflammatory nusculoskeletal disorders. J Rheumatol 2004 Feb; 31(2):274-9.
(45) Mak A, Tan JY, Su HC, Ho RC. Mycophenolate Mofetil Confers Survival Benefit And Is Safer Than
Cyclophosphamide In The Treatment Of Proliferative Lupus Nephritis: A Comprehensive Meta-
analysis of 445 Patients In 8 Controlled Trials. ACR 2008: abstract 1066
(46) Merrill JT, Neuwelt CM, Wallace DJ, Shanahan JC, Latinis KM, Oates JC et al. Rituximab in extra-
renal SLE patients showed no significant difference compared to placebo at 52 weeks in the
randomized, double-blind phase II/III study EXPORER. Ann Rheum Dis 2009;68 (suppl3):249
(47) Wung PK, Holbrook JT, Hoffman GS, et al. Herpes zoster in immunocompromised patients: inci-
dence, timing, and risk factors. Am J Med 2005 Dec; 118(12):1416.
(48) Askling J, Fored CM, Brandt L, et al. Risk and case characteristics of tuberculosis in rheumatoid
arthritis associated with tumor necrosis factor antagonists in Sweden. Arthritis Rheum 2005
Jul; 52(7):1986-92.
(49) Brassard P, Kezouh A, Suissa S. Antirheumatic drugs and the risk of tuberculosis. Clin Infect Dis
2006 Sep 15; 43(6):717-22.
(50) Brassard P, Lowe AM, Bernatsky S, Kezouh A, Suissa S. Rheumatoid arthritis, its treatments, and
the risk of tuberculosis in Quebec, Canada. Arthritis Rheum 2009 Mar 15; 61(3):300-4.
(51) Gomez-Reino JJ, Carmona L, Valverde VR, Mola EM, Montero MD. Treatment of rheumatoid
arthritis with tumor necrosis factor inhibitors may predispose to significant increase in tuber-
culosis risk: a multicenter active-surveillance report. Arthritis Rheum 2003 Aug; 48(8):2122-7.
(52) Seong SS, Choi CB, Woo JH, et al. Incidence of tuberculosis in Korean patients with rheumatoid
arthritis (RA): effects of RA itself and of tumor necrosis factor blockers. J Rheumatol 2007 Apr;
34(4):706-11.
(53) Sichletidis L, Settas L, Spyratos D, Chloros D, Patakas D. Tuberculosis in patients receiving anti-
TNF agents despite chemoprophylaxis. Int J Tuberc Lung Dis 2006 Oct; 10(10):1127-32.
(54) Wolfe F, Michaud K, Anderson J, Urbansky K. Tuberculosis infection in patients with rheumatoid

162
Cha
pter
8
arthritis and the effect of infliximab therapy. Arthritis Rheum 2004 Feb; 50(2):372-9.
(55) Yamada T, Nakajima A, Inoue E, et al. Increased risk of tuberculosis in patients with rheumatoid
arthritis in Japan. Ann Rheum Dis 2006 Dec; 65(12):1661-3.
(56) Yun JE, Lee SW, Kim TH, et al. The incidence and clinical characteristics of Mycobacterium tu-
berculosis infection among systemic lupus erythematosus and rheumatoid arthritis patients in
Korea. Clin Exp Rheumatol 2002 Mar; 20(2):127-32.
(57) Allali F, Rkain H, Faik A, El Hassani S, Hajjaj-Hassouni N. Prevalence and clinical characteristics of
tuberculosis in rheumatoid arthritis patients. Clin Rheumatol 2005 Nov; 24(6):656-7.
(58) Askling J. Risk for tuberculosis following treatment of rheumatoid arthritis with anti-TNF the-
rapy - the Swedish experience 1998-2008. Ann Rheum Dis 2009;68 (suppl3):422
(59) Doran JPW, Ng CT, Veale DJ, Fitzgerald O, Bresnihan B. Late-onset tuberculosis infection in
patients receiving anti-TNF therapy. Ann Rheum Dis 2009;68 (suppl3):423
(60) van Vollenhoven RF, Emery P, Bingham III CO, Keystone E, Fleischmann RM, Furst DE et al. Long-
term safety of rituximab: follow-up of the RA clinical trials and re-treatment population. Ann
Rheum Dis 2009;68 (suppl3):76
(61) van Vollenhoven RF, Nishimoto N, Yamanaka H, Woodworth T, Schiff MH, Taylor A et al. Expe-
rience with mycobacterium tuberculosis infection reported in the tocilizumab worldwide RA
safety database. Ann Rheum Dis 2009;68 (suppl3):567
(62) Baronnet L, Kahn V, Lacoin C, Barnetche T, Schaeverbeke T. Tuberculosis incidence in rheuma-
toid arthritis affected patients. Ann Rheum Dis 2008;67 (suppl2):544
(63) Tubach F, Salmon D, Ravaud P, Lequerré T, Goupille P, Schaeverbeke T et al. The risk of tubercu-
losis with anti-TNF is higher with monoclonal antibodies than with the soluble receptor. Results
of the French 3-year prospective RATIO observatory. Ann Rheum Dis 2008;67 (suppl2):52
(64) Dixon WG, Hyrich KL, Watson KD, Lunt M, BSRBR consortium, Symmons DPM. Specific risk of
tuberculosis in patients with rheumatoid arthritis treated with anti-TNF therapy: results from
the BSR Biologic Register (BSRBR). Ann Rheum Dis 2008;67 (suppl2):178
(65) Mines D, Gu Y, Liu Q, Horne LN, Harrison MJ. Risk of active tuberculosis (TB) among biologic-
naive patients: retrospective cohort study in a US claims database. Ann Rheum Dis 2008;67(sup-
pl2):91
(66) Nishimoto N, Miyasaka N, Yamamoto K, Kawai S, Takeuchi T, Ito K et al. Safety profile of toci-
lizumab in Japanese patients with rheumatoid arthritis -incidences of infections in Japanese
long-term clinical studies-. Ann Rheum Dis 2008;67 (suppl2):335
(67) Burmester GR, Matuci Cerinic M, Mariette X, Navarro Blasco F, Oezer U, Unnebrink K et al. Safety
and effectiveness of adalimumab (Humira®) is maintained in patients with rheumatoid arthritis
- three-year reults of REALISE, a post-marketing observational study. Ann Rheum Dis 2008;67
(suppl2):176
(68) Vadillo C, Abásolo L, Hernández C, Iajas C, Martines Prada C, Pato E et al. Incidence Of Tuberculo-
sis In Patients With Autoimmune Disorders In A Tertiary Hopsital Of Spain. The Role Of Biologic
Drugs. ACR 2008: abstract 1448
(69) Smolen JS, Beaulieu AD, Dikranian A, Fenton I, Fisheleva E Alecock E et al. Safety of Tocilizumab
in Patients with Rheumatoid Arthritis: Pooled Analysis of Five Phase 3 Clinical Trials. ACR 2008:
abstract 1669
(70) Dixon WG, Hyrich KL, Watson KD, Lunt M, Symmons DP. Drug-Specific Risk of Tuberculosis in
Patients with Rheumatoid Arthritis Treated with Anti-TNF Therapy: Results from the BSRBR.
163
Cha
pter
8
ACR 2008: abstract 1263
(71) Keystone EC, Fleischmann RM, Emery P, Chubick A, Dougados MR, Baldassare AR et al. Efficacy
and Safety of Repeat Treatment Courses of Rituximab (RTX) in RA Patients (pts) with Inade-
quate Response (IR) to Tumor Necrosis Factor (TNF) Inhibitors: Long-term Experience from the
REFLEX study. ACR 2008: abstract 367
(72) Wajdula J, MacPeek D, Lin S, Hamza S, Fatenejad S. Tuberculosis Incidence Low in Double-Blind
and Open-Label Etanercept Studies in Patients With Rheumatoid Arthritis. ACR 2007: abstract
1022
(73) Burmester GR, Mease PJ, Dijkmans BA, Gordon KB, Lovell DJ, Panaccione R et al. Adalimumab
Safety Profile in Global Clinical Trials and Reduction in Standardized Mortality Ratios (SMR)
Across Multiple Indications. ACR 2007: abstract 959
(74) Weinblatt ME, Keystone EC, Furst DE, Kavanaugh AF, Perez JL, Segurado OG. Change Over Time
in the Safety, Efficacy, and Remission Profiles of Patients With Rheumatoid Arthritis Receiving
Adalimumab for Up to 7 Years. ACR 2007: abstract 294
(75) Bernatsky S, Bombardier C, Bhamani A, Cividino A, Hux JE, Paterson M et al. Tuberculosis in a
population-based cohort of seniors with rheumatoid arthritis. Ann Rheum Dis 2009;68 (sup-
pl3):568
(76) Salliot C, Dougados M, Gossec L. Risk of serious infections during rituximab, abatacept and ana-
kinra treatments for rheumatoid arthritis: meta-analyses of randomised placebo-controlled tri-
als. Ann Rheum Dis 2009 Jan; 68(1):25-32.
(77) Kremer JM, Russell AS, Emery P, Abud-Mendoza C, Szechinski J, Becker JC et al. Abatacept
demonstrates consistent safey and sustained improvements in efficacy through 5 years of tre-
atment in biologic-naive patients with RA. Ann Rheum Dis 2009;68 (suppl3):444
(78) Kim HA, Yoo CD, Baek HJ, et al. Mycobacterium tuberculosis infection in a corticosteroid-treated
rheumatic disease patient population. Clin Exp Rheumatol 1998 Jan; 16(1):9-13.
(79) Mok MY, Lo Y, Chan TM, Wong WS, Lau CS. Tuberculosis in systemic lupus erythematosus in an
endemic area and the role of isoniazid prophylaxis during corticosteroid therapy. J Rheumatol
2005 Apr; 32(4):609-15.
(80) Tam LS, Li EK, Wong SM, Szeto CC. Risk factors and clinical features for tuberculosis among pa-
tients with systemic lupus erythematosus in Hong Kong. Scand J Rheumatol 2002; 31(5):296-300.
(81) Balakrishnan C, Mangat G, Mittal G, Joshi VR. Tuberculosis in patients with systemic lupus ery-
thematosus. J Assoc Physicians India 1998 Aug; 46(8):682-3.
(82) Feng PH, Tan TH. Tuberculosis in patients with systemic lupus erythematosus. Ann Rheum Dis
1982 Feb; 41(1):11-4.
(83) Hou CL, Tsai YC, Chen LC, Huang JL. Tuberculosis infection in patients with systemic lupus
erythematosus: pulmonary and extra-pulmonary infection compared. Clin Rheumatol 2008 May;
27(5):557-63.
(84) Purice S, Mitu S, Popescu T, Guran M, Vintila M, Suta G. The relationship between systemic lupus
erythematosus and tuberculosis. Med Interne 1982 Jul; 20(3):191-6.
(85) Rovensky J, Kovalancik M, Kristufek P, et al. Contribution to the problem of occurrence of tuber-
culosis in patients with systemic lupus erythematosus. Z Rheumatol 1996 May; 55(3):180-7.
(86) Sayarlioglu M, Inanc M, Kamali S, et al. Tuberculosis in Turkish patients with systemic lupus ery-
thematosus: increased frequency of extrapulmonary localization. Lupus 2004; 13(4):274-8.
(87) Shyam C, Malaviya AN. Infection-related morbidity in systemic lupus erythematosus: a clinico-

164
Cha
pter
8
epidemiological study from northern India. Rheumatol Int 1996; 16(1):1-3.
(88) Wang J, Pan HF, Su H, Li XP, Xu JH, Ye DQ. Tuberculosis in systemic lupus erythematosus in
Chinese patients. Trop Doct 2009 Jul; 39(3):165-7.
(89) Crompton GK, Cameron SJ, Langlands AO. Pulmonary fibrosis, pulmonary tuberculosis and an-
kylosing spondylitis. Br J Dis Chest 1974 Jan; 68(1):51-6.
(90) Ho HH, Lin MC, Yu KH, Wang CM, Wu YJ, Chen JY. Pulmonary tuberculosis and disease-related
pulmonary apical fibrosis in ankylosing spondylitis. J Rheumatol 2009 Feb; 36(2):355-60.
(91) Van den Bosch F, Kruithof E, Baeten D, et al. Randomized double-blind comparison of chimeric
monoclonal antibody to tumor necrosis factor alpha (infliximab) versus placebo in active spon-
dylarthropathy. Arthritis Rheum 2002 Mar; 46(3):755-65.
(92) Heldmann F, Brandt J, van der Horst-Bruinsma I, Landewe R, Sieper J, Burmester G et al. Eu-
ropean ankylosing spondylitis infliximab cohort (EASIC): safety of longterm therapy with in-
fliximab in patients with ankylosing spondylitis (AS). Ann Rheum Dis 2009;68 (suppl3):626
(93) Hoehle M, Finkenstaedt M, Maas R. Efficacy and safety of etanercept monotherapy in patients
with ankylosing spondylitis - treatment period of >7 years. Ann Rheum Dis 2009;68 (suppl68):631
(94) Sieper J, Meng T, Neeck G, Klopsch T, Loeschmann P. A Drug Utilisation Observation (DUO)
Study To Evaluate The Safety And Effectiveness Of Enbrel (etanercept) In Patients With Ankylo-
sing Spondylitis (AS). ACR 2008: abstract 1110
(95) Martin Mola E, van der Linden S, Wishneski, Robertson D, Freundlich BF, Koenig AS. Five-Year
Efficacy and Safety, Including Patient-Reported Outcomes, With Etanercept in Ankylosing Spon-
dylitis. ACR 2008: abstract 1119
(96) Dijkmans BA, Sieper J, van der Linden S, Martin-Mola E, Leirisalo-Repo M, Freundlich B et al.
Long Term Efficacy and Safety, Including Reports of Ocular Inflammation, in Ankylosing Spon-
dylitis Patients Treated with Etanercept for 4 Years. ACR 2007: abstract 1161
(97) van der Heijde D, Schiff MH, Sieper J, Dijkmans BA, Mease PJ, Kupper H et al. 2-Year Safety
and Efficacy Results From the Adalimumab Trial Evaluating Long-Term Efficacy and Safety in
Ankylosing Spondylitis (ATLAS). ACR 2007: abstract 581
(98) van der Heijde D, Sieper J, Dijkmans BAC, Schiff MH, Kivitz A, Westhovens R et al. Three-year
safety and efficacy results from the adalimumab (Humira®) trial evaluting long-term efficacy
and safety in ankylosing spondylitis. Ann Rheum Dis 2008;67 (suppl2):519
(99) Jonasson F, Cullen JF, Elton RA. Temporal arteritis. A 14-year epidemiological, clinical and prog-
nostic study. Scott Med J 1979 Apr; 24(2):111-7.
(100) Schmidt J, Duhaut P, Smail A, Salle V, Chatelain D Bosshard S et al. Severe infections during Gi-
ant Cell Arteritis and Polymyalgia Rheumatica course: incidence and mortality. The prospective,
multicenter cohort GRACG study. ACR 2008: abstract 2015
(101) Schmidt J, Duhaut P, Smail A, Salle V, Chatelain D, Bosshard S et al. Severe infections during
giant cell arteritis (GCA) course: incidence and mortalitiy. The prospective, multicenter double
cohort CRACG study. Ann Rheum Dis 2009;68 (suppl3):80
(102) Schmidt J, Duhaut P, Smail A, Salle V, Chatelain D, Bosshard S et al. Survival and causes of death
in giant cell arteritis (GCA) and polymyalgia rheumatica (PMR): the prospective, multicenter
double cohort CRACG study. Ann Rheum Dis 2009;68 (suppl3):600
(103) Tam LS, Chan AY, Chan PK, Chang AR, Li EK. Increased prevalence of squamous intraepithe-
lial lesions in systemic lupus erythematosus: association with human papillomavirus infection.
Arthritis Rheum 2004 Nov; 50(11):3619-25.

165
Cha
pter
8
(104) Lee Y, Choe J, Kim J, Park Y, Lee S, Kang Y et al. Prevalence and Risk Factors for Human Papil-
lomavirus Infection and Cervical Cytological Abnormalities in Korean Patients with Systemic
Lupus Erythematosus. ACR 2007: abstract 1105
(105) Nath R, Mant C, Luxton J, et al. High risk of human papillomavirus type 16 infections and of deve-
lopment of cervical squamous intraepithelial lesions in systemic lupus erythematosus patients.
Arthritis Rheum 2007 May 15; 57(4):619-25.
(106) Tam L, Chan PS, Ho S, Cheung T, Yim S, Wong MC et al. Natural history of cervical human papil-
lomavirus infection among women with systemic lupus erythematosus. Ann Rheum Dis 2009;68
(suppl3):128
(107) Lee Y, Choe J, Kim J, Park Y, Lee S Kang Y et al. Prevalence and Risk Factors for Human Papil-
lomavirus Infection and Cervical Cytological Abnormalities in Korean Patients with Systemic
Lupus Erythematosus. ACR 2007: abstract 1105
(108) Stojanovich L. Influenza vaccination of patients with systemic lupus erythematosus (SLE) and
rheumatoid arthritis (RA). Clin Dev Immunol 2006 Jun; 13(2-4):373-5.
(109) Chalmers A, Scheifele D, Patterson C, et al. Immunization of patients with rheumatoid arthritis
against influenza: a study of vaccine safety and immunogenicity. J Rheumatol 1994 Jul; 21(7):1203-
6.
(110) Del Porto F, Lagana B, Biselli R, et al. Influenza vaccine administration in patients with systemic
lupus erythematosus and rheumatoid arthritis. Safety and immunogenicity. Vaccine 2006 Apr
12; 24(16):3217-23.
(111) Denman EJ, Denman AM, Greenwood BM, Gall D, Heath RB. Failure of cytotoxic drugs to sup-
press immune responses of patients with rheumatoid arthritis. Ann Rheum Dis 1970 May;
29(3):220-31.
(112) Elkayam O, Bashkin A, Mandelboim M, et al. The Effect of Infliximab and Timing of Vaccination
on the Humoral Response to Influenza Vaccination in Patients with Rheumatoid Arthritis and
Ankylosing Spondylitis. Semin Arthritis Rheum 2009 Feb 24.
(113) Fomin I, Caspi D, Levy V, et al. Vaccination against influenza in rheumatoid arthritis: the effect
of disease modifying drugs, including TNF alpha blockers. Ann Rheum Dis 2006 Feb; 65(2):191-4.
(114) Gelinck LB, van der Bijl AE, Beyer WE, et al. The effect of anti-tumour necrosis factor alpha tre-
atment on the antibody response to influenza vaccination. Ann Rheum Dis 2008 May; 67(5):713-6.
(115) Herron A, Dettleff G, Hixon B, et al. Influenza vaccination in patients with rheumatic diseases.
Safety and efficacy. JAMA 1979 Jul 6; 242(1):53-6.
(116) Kaine JL, Kivitz AJ, Birbara C, Luo AY. Immune responses following administration of influ-
enza and pneumococcal vaccines to patients with rheumatoid arthritis receiving adalimumab. J
Rheumatol 2007 Feb; 34(2):272-9.
(117) Kubota T, Nii T, Nanki T, et al. Anti-tumor necrosis factor therapy does not diminish the immune
response to influenza vaccine in Japanese patients with rheumatoid arthritis. Mod Rheumatol
2007; 17(6):531-3.
(118) Nii T, Kubota T, Nanki T, et al. Reevaluation of antibody titers 1 year after influenza vaccination in
patients with rheumatoid arthritis receiving TNF blockers. Mod Rheumatol 2009; 19(2):216-8.
(119) Turner-Stokes L, Cambridge G, Corcoran T, Oxford JS, Snaith ML. In vitro response to influenza
immunisation by peripheral blood mononuclear cells from patients with systemic lupus erythe-
matosus and other autoimmune diseases. Ann Rheum Dis 1988 Jul; 47(7):532-5.
(120) van Assen S, Holvast A, Benne CA, et al. Humoral responses after influenza vaccination are seve-

166
Cha
pter
8
rely reduced in patients with rheumatoid arthritis treated with rituximab. Arthritis Rheum 2009
Dec 28; 62(1):75-81.
(121) Kapetanovic MC, Saxne T, Nilsson JA, Geborek P. Influenza vaccination as model for testing
immune modulation induced by anti-TNF and methotrexate therapy in rheumatoid arthritis pa-
tients. Rheumatology (Oxford) 2007 Apr; 46(4):608-11.
(122) Gelinck LB, Teng YK, Rimmelzwaan GF, van den Bemt BJ, Kroon FP, van Laar JM. Poor serolo-
gical responses upon influenza vaccination in patients with rheumatoid arthritis treated with
rituximab. Ann Rheum Dis 2007 Oct; 66(10):1402-3.
(123) Oren S, Mandelboim M, Braun-Moscovici Y, et al. Vaccination against influenza in patients with
rheumatoid arthritis: the effect of rituximab on the humoral response. Ann Rheum Dis 2008 Jul;
67(7):937-41.
(124) Williams GW, Steinberg AD, Reinertsen JL, Klassen LW, Decker JL, Dolin R. Influenza immuniza-
tion in systemic lupus eruthematosus. A double-blind trial. Ann Intern Med 1978 Jun; 88(6):729-34.
(125) Holvast A, Huckriede A, Wilschut J, et al. Safety and efficacy of influenza vaccination in systemic
lupus erythematosus patients with quiescent disease. Ann Rheum Dis 2006 Jul; 65(7):913-8.
(126) Mercado U, Acosta H, Avendano L. Influenza vaccination of patients with systemic lupus erythe-
matosus. Rev Invest Clin 2004 Jan; 56(1):16-20.
(127) Wiesik-Szewczyk E, Romanowska M, Mielnik P, et al. Anti-influenza vaccination in systemic lupus
erythematosus patients: an analysis of specific humoral response and vaccination safety. Clin
Rheumatol 2010 Jun; 29(6):605-13.
(128) Brodman R, Gilfillan R, Glass D, Schur PH. Influenzal vaccine response in systemic lupus erythe-
matosus. Ann Intern Med 1978 Jun; 88(6):735-40.
(129) Louie JS, Nies KM, Shoji KT, et al. Clinical and antibody responses after influenza immunization
in systemic lupus erythematosus. Ann Intern Med 1978 Jun; 88(6):790-2.
(130) Pons VG, Reinertsen JL, Steinberg AD, Dolin R. Decreased cell-mediated cytotoxicity against
virus-infected cells in systemic lupus erythematosus. J Med Virol 1979; 4(1):15-23.
(131) Ristow SC, Douglas RG, Jr., Condemi JJ. Influenza vaccination of patients with systemic lupus
erythematosus. Ann Intern Med 1978 Jun; 88(6):786-9.
(132) Abu-Shakra M, Press J, Varsano N, et al. Specific antibody response after influenza immuniza-
tion in systemic lupus erythematosus. J Rheumatol 2002 Dec; 29(12):2555-7.
(133) Holvast A, Stegeman CA, Benne CA, et al. Wegener’s granulomatosis patients show an adequate
antibody response to influenza vaccination. Ann Rheum Dis 2009 Jun; 68(6):873-8.
(134) Zycinska K, Romanowska M, Nowak I, Rybicka K, Wardyn KA, Brydak LB. Antibody response to in-
activated subunit influenza vaccine in patients with Wegener’s granulomatosis. J Physiol Phar-
macol 2007 Nov; 58 Suppl 5(Pt 2):819-28.
(135) Setti M, Fenoglio D, Ansaldi F, et al. Flu vaccination with a virosomal vaccine does not affect clini-
cal course and immunological parameters in scleroderma patients. Vaccine 2009 May 26;27(25-
26):3367-72.
(136) Gelinck LB, van der Bijl AE, Visser LG, et al. Synergistic immunosuppressive effect of anti-TNF
combined with methotrexate on antibody responses to the 23 valent pneumococcal polysaccha-
ride vaccine. Vaccine 2008 Jun 25; 26(27-28):3528-33.
(137) Visvanathan S, Keenan GF, Baker DG, Levinson AI, Wagner CL. Response to pneumococcal vac-
cine in patients with early rheumatoid arthritis receiving infliximab plus methotrexate or me-
thotrexate alone. J Rheumatol 2007 May; 34(5):952-7.

167
Cha
pter
8
(138) Kapetanovic MC, Saxne T, Sjoholm A, Truedsson L, Jonsson G, Geborek P. Influence of metho-
trexate, TNF blockers and prednisolone on antibody responses to pneumococcal polysaccharide
vaccine in patients with rheumatoid arthritis. Rheumatology (Oxford) 2006 Jan; 45(1):106-11.
(139) Bingham CO, III, Looney RJ, Deodhar A, et al. Immunization responses in rheumatoid arthritis
patients treated with rituximab: Results from a controlled clinical trial. Arthritis Rheum 2009
Dec 28; 62(1):64-74.
(140) Elkayam O, Paran D, Caspi D, et al. Immunogenicity and safety of pneumococcal vaccination in
patients with rheumatoid arthritis or systemic lupus erythematosus. Clin Infect Dis 2002 Jan 15;
34(2):147-53.
(141) Elkayam O, Caspi D, Reitblatt T, Charboneau D, Rubins JB. The effect of tumor necrosis factor
blockade on the response to pneumococcal vaccination in patients with rheumatoid arthritis and
ankylosing spondylitis. Semin Arthritis Rheum 2004 Feb; 33(4):283-8.
(142) Croft SM, Schiffman G, Snyder E, Herrmann K, James K, Jarrett MP. Specific antibody response
after in vivo antigenic stimulation in systemic lupus erythematosus. J Rheumatol 1984 Apr;
11(2):141-6.
(143) Lipnick RN, Karsh J, Stahl NI, Blackwelder WC, Schiffman G, Klippel JH. Pneumococcal immu-
nization in patients with systemic lupus erythematosus treated with immunosuppressives. J
Rheumatol 1985 Dec; 12(6):1118-21.
(144) Jarrett MP, Schiffman G, Barland P, Grayzel AI. Impaired response to pneumococcal vaccine in
systemic lupus erythematosus. Arthritis Rheum 1980 Nov; 23(11):1287-93.
(145) McDonald E, Jarrett MP, Schiffman G, Grayzel AI. Persistence of pneumococcal antibodies after
immunization in patients with systemic lupus erythematosus. J Rheumatol 1984 Jun; 11(3):306-8.
(146) Tarjan P, Sipka S, Marodi L, et al. No short-term immunological effects of Pneumococcus vac-
cination in patients with systemic lupus erythematosus. Scand J Rheumatol 2002; 31(4):211-5.
(147) Battafarano DF, Battafarano NJ, Larsen L, et al. Antigen-specific antibody responses in lupus
patients following immunization. Arthritis Rheum 1998 Oct; 41(10):1828-34.
(148) Franco Salinas G, de Rycke L, Cantaert T, Remans P, van der Burg M, Barendregt B et al. TNF
blockade impairs T cell dependent antibody responses. Ann Rheum Dis 2009;68 (suppl3):238
(149) Mease PJ, Ritchlin CT, Martin RW, et al. Pneumococcal vaccine response in psoriatic arthritis
patients during treatment with etanercept. J Rheumatol 2004 Jul; 31(7):1356-61.
(150) Mercado U, Acosta H, Diaz-Molina R. Antibody response to pneumococcal polysaccharide vac-
cine in systemic sclerosis. J Rheumatol 2009 Jul; 36(7):1549-50.
(151) Elkayam O, Yaron M, Caspi D. Safety and efficacy of vaccination against hepatitis B in patients
with rheumatoid arthritis. Ann Rheum Dis 2002 Jul; 61(7):623-5.
(152) Kuruma KA, Borba EF, Lopes MH, de Carvalho JF, Bonfa E. Safety and efficacy of hepatitis B vac-
cine in systemic lupus erythematosus. Lupus 2007; 16(5):350-4.
(153) Erkek E, Ayaslioglu E, Erkek AB, Kurtipek GS, Bagci Y. Response to vaccination against hepatitis
B in patients with Behcet’s disease. J Gastroenterol Hepatol 2005 Oct; 20(10):1508-11.
(154) Devey ME, Bleasdale K, Isenberg DA. Antibody affinity and IgG subclass of responses to tetanus
toxoid in patients with rheumatoid arthritis and systemic lupus erythematosus. Clin Exp Im-
munol 1987 Jun; 68(3):562-9.
(155) Abe T, Homma M. Immunological reactivity in patients with systemic lupus erythematosus. Hu-
moral antibody and cellular immune responses. Acta Rheumatol Scand 1971; 17(1):35-46.
(156) Kashef S, Ghazizadeh F, Derakhshan A, Farjadian S, Alyasin S. Antigen-specific antibody res-
168
Cha
pter
8
ponse in juvenile-onset SLE patients following routine immunization with tetanus toxoid. Iran J
Immunol 2008 Sep; 5(3):181-4.
(157) Nies K, Boyer R, Stevens R, Louie J. Anti-tetanus toxoid antibody synthesis after booster im-
munization in systemic lupus erythematosus. Comparison of the in vitro and in vivo responses.
Arthritis Rheum 1980 Dec; 23(12):1343-50.
(158) Stassen PM, Sanders JS, Kallenberg CG, Stegeman CA. Influenza vaccination does not result
in an increase in relapses in patients with ANCA-associated vasculitis. Nephrol Dial Transplant
2008 Feb; 23(2):654-8.
(159) Elkayam O, Paran D, Burke M, et al. Pneumococcal vaccination of patients with systemic lupus
erythematosus: effects on generation of autoantibodies. Autoimmunity 2005 Nov; 38(7):493-6.
(160) Karsh J, Pavlidis N, Schiffman G, Moutsopoulos HM. Immunization of patients with Sjogren’s
syndrome with pneumococcal polysaccharide vaccine: a randomized trial. Arthritis Rheum 1980
Nov; 23(11):1294-8.
(161) Holvast A, van Assen S, de Haan A, et al. Effect of a second, booster, influenza vaccination on
antibody responses in quiescent systemic lupus erythematosus: an open, prospective, control-
led study. Rheumatology (Oxford) 2009 Oct; 48(10):1294-9.


CHAPT
ER9E U L A R recommen-d a t i o n s f o r v a c c i - n a t i o n i n a d u l t p a t i e n t s w i t ha u t o - i m m u n e inflammatory r h e u m a t i c d i s e a s e s
S. van Assen
N. Agmon-Levin
O. Elkayam
R. Cervera
M.F. Doran
M. Dougados
P. Emery
P. Geborek
J.P.A. Ioannidis
D.R.W. Jayne
C.G.M. Kallenberg
U. Müller-Ladner
Y. Shoenfeld
L. Stojanovich
G. Valesini
N.M. Wulffraat
M. Bijl
Annals of Rheumatic Diseases 2011 Mar;70(3):414-422

172
Cha
pter
9
AbsTrAcTObjectives To develop evidence-based European League Against Rheu-matism (EULAR) recommendations for vaccination in patients with auto-immune inflammatory rheumatic diseases (AIIRD).
Methods A EULAR task force was composed of experts representing 11 European countries, consisting of eight rheumatologists, four clinical im-munologists, one rheumatologist/clinical immunologist, one infectious disease physician, one nephrologist, one paediatrician/rheumatologist and one clinical epidemiologist. Key questions were formulated and the eligible spectrum of AIIRD, immunosuppressive drugs and vaccines were defined, in order to perform a systematic literature review. We searched Medline from 1966 to October 2009, as well as abstracts from the EULAR meetings of 2008 and 2009 and the American College of Rheumatology meetings of 2007 and 2008. Evidence was graded in categories 1-4, the strength of recommendations was graded in categories A-D, and Delphi voting was ap-plied to determine the level of agreement between the experts of the task force.
results Eight key questions and 13 recommendations addressing vacci-nation in patients with AIIRD were formulated. The strength of each re-commendation was determined. Delphi voting revealed a very high level of agreement with the recommendations among the experts of the task force. Finally, a research agenda was proposed.
conclusion Recommendations for vaccination in patients with AIIRD based on the currently available evidence and expert opinion were formulated. More research is needed in particular regarding incidence of vaccine-preventable infectious diseases and the safety of vaccination in patients with AIIRD.
173
Cha
pter
9
InTrOducTIOnPatients with auto-immune inflammatory rheumatic diseases (AIIRD) are at incre-ased risk of contracting infections [1-10]. The increased susceptibility to infection can be attributed to by any of the following: the immunosuppressive effect of the underlying AIIRD, the occurrence of a “locus minoris resistentiae” as a sequel of the AIIRD and the use of immunomodulatory medication to treat the AIIRD. The possible contribution of biologic agents to infection risk is of particular interest, especially since increasingly more indications are being recognized for their use, they are increasingly being used earlier in the course of AIIRD, and newer agents are becoming available [11-23].
Vaccination is an attractive method to prevent certain infections. The efficacy of vaccinations in patients with AIIRD, however, may be reduced, and there is a po-tential risk of flares of the underlying AIIRD following vaccination.
Our aim was to develop recommendations for vaccination in Patients with AIIRD, in line with the European League Against Rheumatism (EULAR)’s standard ope-rating procedures, combining evidence from clinical studies with expert opinion when sufficient evidence was lacking. Our recommendations target all physicians and nurses who are involved in the care for patients with AIIRD.
MeThOds
The expert committee
The committee consisted of eight rheumatologists (OE, MFD, MD, PE, PG, UML, LS, GV), four clinical immunologists (NAL, RC, CGMK, YS), one rheumatologist/cli-nical immunologist (MB), one infectious disease physician (SvA), one nephrologist (DRWJ), one paediatrician/rheumatologist (NW) and one clinical epidemiologist (JPAI), representing 11 European countries.
definitions
In these recommendations the term efficacy represents the capability of a vac-cine to mount a protective immune response, because vaccination studies in pa-tients with AIIRD addressing clinical endpoints are scarce. Moreover, it should be acknowledged that in vitro immune responses may not always correlate well with clinical effectiveness. This should be taken into account when interpreting the available evidence for these recommendations.
development of recommendations
The experts were invited to define the AIIRD, the vaccines and the immunosup-pressive medications, which were to be used as search terms for the systematic
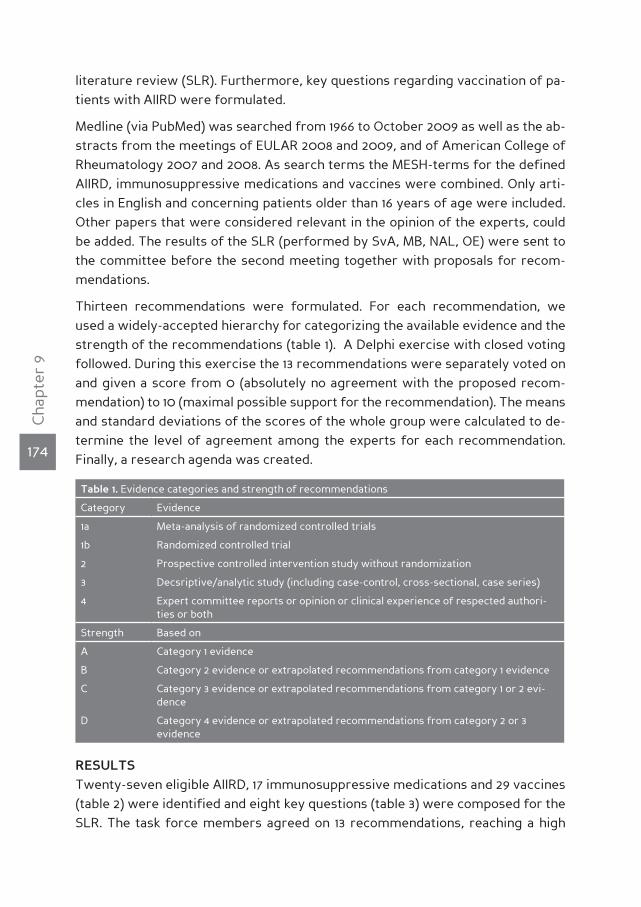
174
Cha
pter
9
literature review (SLR). Furthermore, key questions regarding vaccination of pa-tients with AIIRD were formulated.
Medline (via PubMed) was searched from 1966 to October 2009 as well as the ab-stracts from the meetings of EULAR 2008 and 2009, and of American College of Rheumatology 2007 and 2008. As search terms the MESH-terms for the defined AIIRD, immunosuppressive medications and vaccines were combined. Only arti-cles in English and concerning patients older than 16 years of age were included. Other papers that were considered relevant in the opinion of the experts, could be added. The results of the SLR (performed by SvA, MB, NAL, OE) were sent to the committee before the second meeting together with proposals for recom-mendations.
Thirteen recommendations were formulated. For each recommendation, we used a widely-accepted hierarchy for categorizing the available evidence and the strength of the recommendations (table 1). A Delphi exercise with closed voting followed. During this exercise the 13 recommendations were separately voted on and given a score from 0 (absolutely no agreement with the proposed recom-mendation) to 10 (maximal possible support for the recommendation). The means and standard deviations of the scores of the whole group were calculated to de-termine the level of agreement among the experts for each recommendation. Finally, a research agenda was created.
Table 1. Evidence categories and strength of recommendations
Category Evidence
1a Meta-analysis of randomized controlled trials
1b Randomized controlled trial
2 Prospective controlled intervention study without randomization
3 Decsriptive/analytic study (including case-control, cross-sectional, case series)
4 Expert committee reports or opinion or clinical experience of respected authori-ties or both
Strength Based on
A Category 1 evidence
B Category 2 evidence or extrapolated recommendations from category 1 evidence
C Category 3 evidence or extrapolated recommendations from category 1 or 2 evi-dence
D Category 4 evidence or extrapolated recommendations from category 2 or 3 evidence
resulTsTwenty-seven eligible AIIRD, 17 immunosuppressive medications and 29 vaccines (table 2) were identified and eight key questions (table 3) were composed for the SLR. The task force members agreed on 13 recommendations, reaching a high

175
Cha
pter
9
level of agreement according to the Delphi scores (table 4).
recommendations
Each recommendation is followed in parenthesis with the grade of the evidence, the strength of the recommendation and the Delphi voting score.
1. The vaccination status should be assessed in the initial work-up of patients with AIIRD. (no grade of evidence possible; strength of recommendation D; Delphi vote 9,50)
In order to make recommendations for the individual patient with AIIRD, it is ne-cessary to know which vaccines the patient received in the past according to ta-ble 5. Catch-up vaccination might be considered for missed vaccinations that are recommended for the general population. Also adverse events and flares of the underlying AIIRD following former vaccinations should be queried, since these might be (relative) contraindications for certain future vaccinations.
2. Vaccination in patients with AIIRD should ideally be administered during sta-ble disease. (no grade of evidence possible; strength of recommendation D; Delphi vote 8,88)
No studies have been performed comparing efficacy and harms between patients with AIIRD with stable and unstable disease. Moreover, almost all vaccination stu-dies in patients with AIIRD addressed patients with quiescent disease. Studies that also included patients with moderate or severe disease activity did not show more frequent side effects or disease flares, or decreased efficacy in patients with AIIRD, compared with healthy controls [24-26]. However, the numbers of pa-tients in these studies were too small to conclude that vaccination during active disease is safe and efficacious. Therefore, based on theoretical risks of disease flare following vaccination in unstable patients with AIIRD, vaccination is prefe-rentially administered during stable disease, according to expert opinion.
3. Live attenuated vaccines should be avoided whenever possible in immunosup-pressed patients with AIIRD. (grade of evidence 4; strength of recommendation D; Delphi vote 9,25)
Live attenuated vaccines (table 2) might lead to (severe) infections in immuno-suppressed patients. It is unknown what level of immunosuppression renders pa-tients to be at risk for infections caused by these vaccines and this risk should be balanced to the risk of (severe) infection the vaccine aims to prevent. Measles-, mumps- and rubella (MMR) vaccine has been administered without subsequent infection to paediatric patients two years after bone marrow transplantation [27] and varicella vaccine has been administered without subsequent infection in HIV-
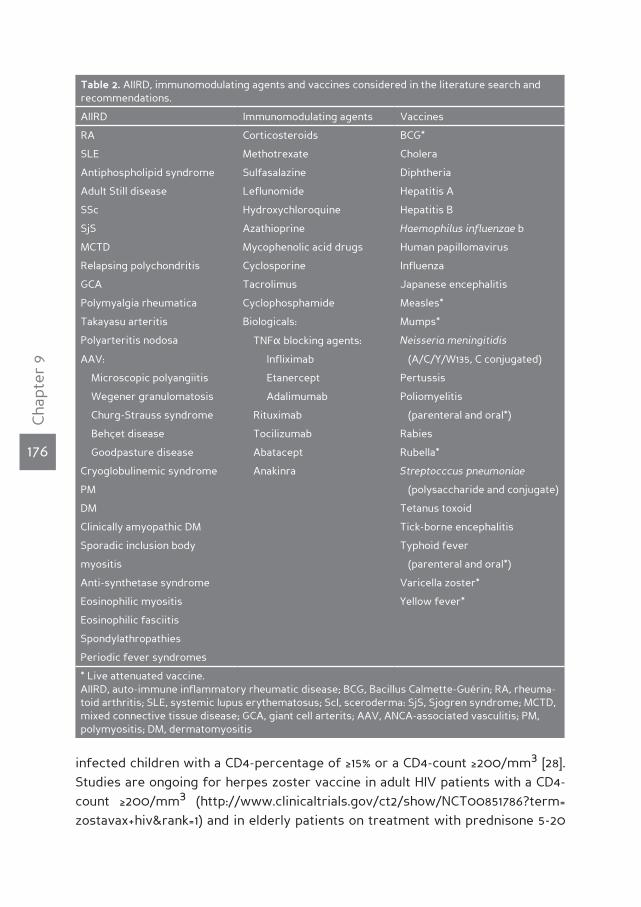
176
Cha
pter
9
Table 2. AIIRD, immunomodulating agents and vaccines considered in the literature search and recommendations.
AIIRD Immunomodulating agents Vaccines
RA Corticosteroids BCG*
SLE Methotrexate Cholera
Antiphospholipid syndrome Sulfasalazine Diphtheria
Adult Still disease Leflunomide Hepatitis A
SSc Hydroxychloroquine Hepatitis B
SjS Azathioprine Haemophilus influenzae b
MCTD Mycophenolic acid drugs Human papillomavirus
Relapsing polychondritis Cyclosporine Influenza
GCA Tacrolimus Japanese encephalitis
Polymyalgia rheumatica Cyclophosphamide Measles*
Takayasu arteritis Biologicals: Mumps*
Polyarteritis nodosa TNFα blocking agents: Neisseria meningitidis
AAV: Infliximab (A/C/Y/W135, C conjugated)
Microscopic polyangiitis Etanercept Pertussis
Wegener granulomatosis Adalimumab Poliomyelitis
Churg-Strauss syndrome Rituximab (parenteral and oral*)
Behçet disease Tocilizumab Rabies
Goodpasture disease Abatacept Rubella*
Cryoglobulinemic syndrome Anakinra Streptocccus pneumoniae
PM (polysaccharide and conjugate)
DM Tetanus toxoid
Clinically amyopathic DM Tick-borne encephalitis
Sporadic inclusion body Typhoid fever
myositis (parenteral and oral*)
Anti-synthetase syndrome Varicella zoster*
Eosinophilic myositis Yellow fever*
Eosinophilic fasciitis
Spondylathropathies
Periodic fever syndromes
* Live attenuated vaccine. AIIRD, auto-immune inflammatory rheumatic disease; BCG, Bacillus Calmette-Guérin; RA, rheuma-toid arthritis; SLE, systemic lupus erythematosus; Scl, sceroderma: SjS, Sjogren syndrome; MCTD, mixed connective tissue disease; GCA, giant cell arterits; AAV, ANCA-associated vasculitis; PM, polymyositis; DM, dermatomyositis
infected children with a CD4-percentage of ≥15% or a CD4-count ≥200/mm3 [28]. Studies are ongoing for herpes zoster vaccine in adult HIV patients with a CD4-count ≥200/mm3 (http://www.clinicaltrials.gov/ct2/show/NCT00851786?term= zostavax+hiv&rank=1) and in elderly patients on treatment with prednisone 5-20
177
Cha
pter
9
mg/day (http://www.clinicaltrials.gov/ct2/show/NCT00546819?term=zostavax+corticosteroid&rank=1). The Advisory Committee on Immunization Practices (ACIP) stated, that herpes zoster vaccine may be administered to patients when treated with short-term corticosteroid therapy (<14 days); low-to-moderate dose corti-costeroids (<20 mg/day of prednisone or equivalent); intra-articular, bursal, or tendon corticosteroids injections; long-term alternate-day treatment with low to moderate doses of short-acting systemic corticosteroids; therapy with metho-trexate (MTX; <0.4 mg/kg/week), azathioprine (<3.0 mg/kg/day), or 6-mercapto-purine (<1.5 mg/kg/day) [29]. It must be emphasized that these recommendations are based on expert opinion only and require further investigation.
The EULAR task force on vaccination recommends avoiding the use of live at-tenuated vaccines in immunosuppressed patients with AIIRD whenever possible. MMR, varicella and herpes zoster vaccine might be exceptions to this rule, and may be considered in mildly immunosuppressed patients with AIIRD on a case-by-case basis. Temporary discontinuation of immunosuppressive medication be-fore vaccination with live attenuated vaccines might also be considered, but there are no studies to support this strategy.
4. Vaccination in patients with AIIRD can be administered during the use of disease modifying anti-rheumatic drugs (DMARDs) and tumor necrosis factor (TNF) α-blocking agents, but should ideally be administered before starting B-cell depleting biological therapy. (grade of evidence 2a; strength of recommendation B; Delphi vote 9,13)
The efficacy of vaccination during the use of DMARDs, glucocorticoids and/or TNFα-blocking agents has been studied in patients with rheumatoid arthritis (RA), systemic lupus erythematosus (SLE), ANCA-associated vasculitis (AAV) and sys-
Table 3. Key questions
1. Is the risk of infections for which vaccines are available increased in patients with AIIRD in general, and specifically in those with active disease, and in those using immunomodulating agents?
2. Do vaccines decrease the risk of infections in patients with AIIRD in general, and specifically in those with unstable disease, and in those using immunomodulating agents?
3. Do vaccines cause any significant harm in patients with AIIRD in general, and specifically in those with unstable disease, and in those using immunomodulating agents?
4. Does the timing of vaccination in relation to disease activity and receipt of immunomodulating agents affect the effectiveness of vaccination in patients with AIIRD
5. Does the timing of vaccination in relation to disease activity and receipt of immunomodulating agents affect important harms of vaccination in patients with AIIRD?
6. Does revaccination with any vaccines increase the effectiveness in patients with AIRD?
7. Does revaccination with any vaccine increase significant harms in patients with AIRD?
8. Is vaccination in patients with AIIRD cost-effective?

178
Cha
pter
9
temic sclerosis (SSc). Influenza, pneumococcal, hepatitis B, tetanus toxoid and Haemophilus influenzae b vaccination were addressed. Most controlled studies showed responses in patients with AIIRD following vaccination comparable to tho-se in healthy controls [24, 25, 30-36, 36-62], while some showed slightly reduced efficacy [38, 43, 45, 47, 49, 61, 63-67]. Of note, azathioprine hampered the response following influenza vaccination in SLE patients, but the majority of patients still develop protective levels of antibodies [63, 68]. The combination of TNFα- bloc-king agents and MTX reduced the response to pneumococcal vaccination in RA patients [45, 67, 69]. Finally, humoral responses following influenza vaccination 2-3 months after treatment with rituximab [38, 41, 69, 70] as well as humoral respon-ses following pneumococcal vaccination 28 weeks after treatment with rituximab [71] are severely hampered. Tetanus toxoid vaccination led to adequate immune responses 24 weeks following rituximab administration [71]. Vaccines should ide-ally be administered before B-cell depleting biological therapy is started, or, when patients are on such a treatment already, at least six months after start, but four weeks before the next course.
5. Inactivated influenza vaccination should be strongly considered for patients with AIIRD. (grade of evidence 1b-3; strength of recommendation B-C; Delphi vote 9,00)
Although the exact incidence of influenza is unknown in patients with AIIRD, their risk of dying from pulmonary infections is increased [4, 5, 72]. Influenza vacci-nation has been shown to reduce admissions for and mortality from influenza/pneumonia in elderly RA patients [73, 74] and is efficacious in RA, SLE, AAV and SSc patients, even when treated with DMARDs, infliximab, etanercept or adali-mumab [24-26, 30-40, 47-50, 63, 67, 68, 75-77], but with rituximab as an exception [41, 70, 78]. Adverse events of influenza vaccination in patients with AIIRD seem comparable with those in healthy controls, although there are no studies that are sufficiently powered with regard to safety. This recommendation regards seaso-nal influenza vaccination as well as pandemic swine flu vaccination, although no studies have been performed on efficacy and safety of swine flu vaccination in patients with AIIRD. Because some of the swine flu vaccines contain the adjuvant MF-59, an oil-in-water emulsion that potentiates the humoral response, it is reas-suring that a large meta-analysis showed no difference in the occurrence of ad-verse events that were of auto-immune origin between persons vaccinated with influenza vaccine with and without MF-59 [79].

179
Cha
pter
9
6. 23-valent polysaccharide pneumococcal vaccination (23-PPV) should be strongly considered for patients with AIIRD. (grade of evidence 1b-3; strength of recommendation B-C; Delphi vote 8,19)
As stated above, patients with AIIRD are at increased risk of dying from pulmo-nary infections compared to the general population [2, 4, 5, 72], with pneumococci being considered to be one of the main causative pathogens. Pneumococcal vac-cination induces an adequate to slightly reduced humoral response in patients with RA, SLE, psoriatic arthritis, ankylosing spondylitis and SSc, even when tre-ated with immunosuppressive drugs [36, 42-45, 47, 51-54, 62, 70, 80]. MTX, with or without TNFα-blocking agents [45, 69], and in particular rituximab [71] reduce the humoral response following pneumococcal vaccination. It is unknown if and when revaccination should take place and if the new conjugated pneumococcal vaccines, whether or not in combination with 23-PPV (so-called prime-and-boost strategy), induce more and/or more durable immunity to pneumococci in patients with AIIRD. Pneumococcal vaccination seems safe in patients with AIIRD, but again the available studies were not adequately powered for analyzing safety.
7. Patients with AIIRD should receive tetanus toxoid vaccination in accordance to recommendations for the general population. In case of major and/or con-taminated wounds in patients who received rituximab within the last 24 weeks, passive immunization with tetanus immunoglobulins should be administered. (grade of evidence 2a; strength of recommendation B-D; Delphi vote 9,19)
In RA and SLE patients efficacy for tetanus toxoid vaccination has been demon-strated to be comparable with healthy controls [30, 46, 58, 59]. This also holds true for RA patients on immunosuppressive drugs, including those who have been treated with rituximab 24 weeks earlier [71]. However, since no data are available regarding the efficacy of tetanus toxoid vaccine within 24 weeks after treatment with rituximab [71], we recommend to immunize patients with AIIRD who are tre-ated with rituximab less then 24 weeks earlier passively with tetanus immuno-globulins in case of a serious risk to contract tetanus i.e. in case of major and/or contaminated wounds.
8. Herpes zoster vaccination may be considered in patients with AIIRD. (grade of evidence 3-4; strength of recommendation C-D; Delphi vote 8,00)
Compared to the general population patients with RA, SLE, AAV and polymyositis/dermatomyositis have an increased risk of developing herpes zoster [81-99]. RA is in itself a risk factor and the risk of developing herpes zoster is further incre-ased in patients with AIIRD treated with corticosteroids, TNFα-blocking agents and non-biologic DMARDs, in particular cyclophosphamide , azathioprine and
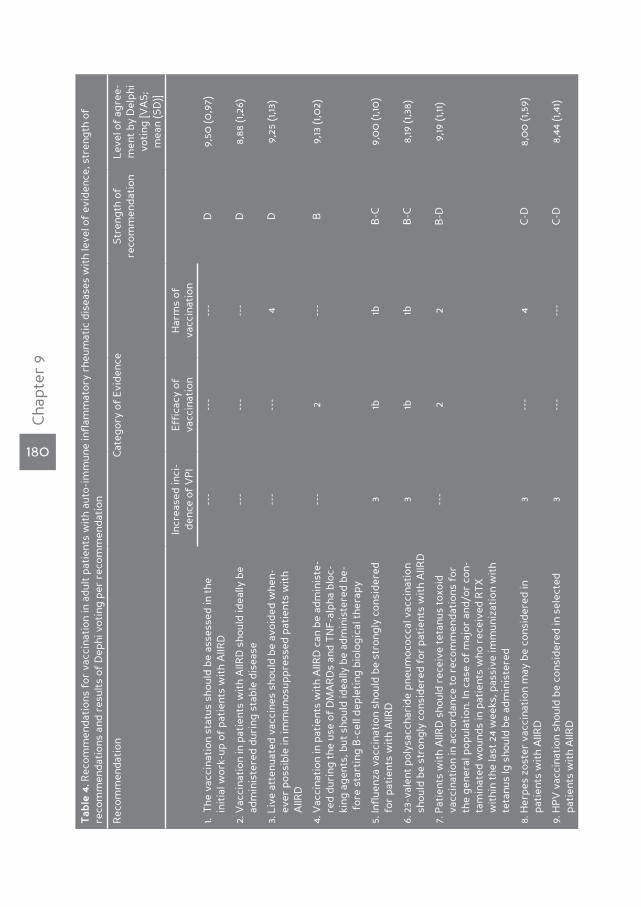
180
Cha
pter
9
Tab
le 4
. Rec
omm
enda
tion
s fo
r va
ccin
atio
n in
adu
lt p
atie
nts
wit
h au
to-i
mm
une
infl
amm
ator
y rh
eum
atic
dis
ease
s w
ith
leve
l of
evid
ence
, str
engt
h of
re
com
men
dati
ons
and
resu
lts
of D
ephi
vot
ing
per
reco
mm
enda
tion
Rec
omm
enda
tion
Cat
egor
y of
Evi
denc
eSt
reng
th o
f re
com
men
dati
onLe
vel o
f ag
ree-
men
t by
Del
phi
voti
ng [V
AS;
m
ean
(SD
)]
Incr
ease
d in
ci-
denc
e of
VP
IEf
fica
cy o
f va
ccin
atio
nH
arm
s of
va
ccin
atio
n
1. T
he v
acci
nati
on s
tatu
s sh
ould
be
asse
ssed
in t
he
in
itia
l wor
k-up
of
pati
ents
wit
h A
IIRD
---
---
---
D9,
50 (0
,97)
2. V
acci
nati
on in
pat
ient
s w
ith
AIIR
D s
houl
d id
eally
be
adm
inis
tere
d du
ring
sta
ble
dise
ase
---
---
---
D8,
88 (1
,26)
3. L
ive
atte
nuat
ed v
acci
nes
shou
ld b
e av
oide
d w
hen-
eve
r po
ssib
le in
imm
unos
uppr
esse
d pa
tien
ts w
ith
A
IIRD
---
---
4D
9,25
(1,13
)
4. V
acci
nati
on in
pat
ient
s w
ith
AIIR
D c
an b
e ad
min
iste
-
red
dur
ing
the
use
of D
MA
RD
s an
d T
NF-
alph
a bl
oc-
k
ing
agen
ts, b
ut s
houl
d id
eally
be
adm
inis
tere
d be
-
for
e st
arti
ng B
-cel
l dep
leti
ng b
iolo
gica
l the
rapy
---
2--
-B
9,13
(1,0
2)
5. In
flue
nza
vacc
inat
ion
shou
ld b
e st
rong
ly c
onsi
dere
d
for
pat
ient
s w
ith
AIIR
D3
1b1b
B-C
9,0
0 (1
,10)
6. 2
3-va
lent
pol
ysac
char
ide
pneu
moc
occa
l vac
cina
tion
sho
uld
be s
tron
gly
cons
ider
ed f
or p
atie
nts
wit
h A
IIRD
31b
1bB
-C8,
19 (1
,38)
7. P
atie
nts
wit
h A
IIRD
sho
uld
rece
ive
teta
nus
toxo
id
v
acci
nati
on in
acc
orda
nce
to r
ecom
men
dati
ons
for
the
gen
eral
pop
ulat
ion.
In c
ase
of m
ajor
and
/or
con-
tam
inat
ed w
ound
s in
pat
ient
s w
ho r
ecei
ved
RT
X
w
ithi
n th
e la
st 2
4 w
eeks
, pas
sive
imm
uniz
atio
n w
ith
t
etan
us Ig
sho
uld
be a
dmin
iste
red
---
22
B-D
9,19
(1,11
)
8. H
erpe
s zo
ster
vac
cina
tion
may
be
cons
ider
ed in
pat
ient
s w
ith
AIIR
D3
---
4C
-D8,
00
(1,5
9)
9. H
PV
vac
cina
tion
sho
uld
be c
onsi
dere
d in
sel
ecte
d
p
atie
nts
wit
h A
IIRD
3--
---
-C
-D8,
44 (1
,41)

181
Cha
pter
9
Tab
le 4
. (co
ntin
ued)
10. I
n hy
posp
leni
c/as
plen
ic p
atie
nts
wit
h A
IIRD
infl
uenz
a
pn
eum
ococ
cal,
Hae
mop
hilu
s in
flue
nzae
b a
nd m
e-
ning
ococ
cal C
vac
cina
tion
s ar
e re
com
men
ded
4--
---
-D
9,50
(0,8
2)
11.
Hep
atit
is A
and
/or
B v
acci
nati
on is
onl
y re
com
men
-
ded
in p
atie
nts
wit
h A
IIRD
at
risk
---
2*3*
D9,
13 (0
,89)
12. A
IIRD
pat
ient
s w
ho p
lan
to t
rave
l are
rec
omm
ende
d
t
o re
ceiv
e th
eir
vacc
inat
ions
acc
ordi
ng t
o ge
nera
l
rul
es, e
xcep
t fo
r liv
e-at
tenu
ated
vac
cine
s, w
hich
sho
uld
be a
void
ed w
hene
ver
poss
ible
in im
mun
osup
-
pre
ssed
pat
ient
s w
ith
AIIR
D
---
---
---
D9,
25 (1
,24)
13. B
CG
vac
cina
tion
is n
ot r
ecom
men
ded
in p
atie
nts
wit
h A
IIRD
3--
---
-D
9,38
(1,0
9)
* fo
r he
pati
tis
B o
nly
VP
, vac
cine
-pre
vent
able
; AIIR
D, a
uto-
imm
une
infl
amm
ator
y di
seas
e; Ig
, im
mun
oglo
bulin
s; H
PV
, hum
an p
apill
omav
irus

182
Cha
pter
9
leflunomide [82-85, 90, 91, 98] but not MTX [100]. One study found an increased risk for herpes zoster in SLE patients when treated with rituximab [101]. Lupus disease activity is not a risk factor for herpes zoster [88]. Herpes zoster vaccine has been shown to reduce herpes zoster and post-herpetic neuralgia in patients over 60 years [102], but no studies have been performed in patients with AIIRD. Because of the high burden of herpes zoster in patients with AIIRD, herpes zoster vacci-nation may be considered in these patients, but only when less severely immu-nosuppressed. The ACIP suggested criteria for immunosuppressed patients who can receive herpes zoster vaccine, however, it must be emphasized that these recommendations are not validated but are based on expert opinion, and require further investigation [29]. It seems prudent to administer herpes zoster vaccine only to patients with AIIRD who are seropositive for varicella zoster antibodies, in order to prevent primary varicella infection with the vaccine-strain.
9. Human Papillomavirus (HPV) vaccination should be considered in selected patients with AIIRD. (grade of evidence 3; strength of recommendation C-D; Delphi vote 8,44)
It has been shown that HPV infection occurs more often in SLE patients, also with the high-risk (oncogenic) subtypes of the virus [103-105]. A lower percentage of these infections (31,8%) is spontaneously cleared by SLE patients [106], leading to an increased risk of developing cervical cancer. The risk factors for contracting HPV infection are the same in SLE patients as in the general population [103;105]. The efficacy of HPV vaccination has not been investigated in patients with AIIRD. HPV vaccination is recommended for young females in many countries, and HPV vaccination should be considered for women with SLE until the age of 25 years. The quadrivalent (q) HPV vaccine has been associated with venous thromboem-bolic events (VTE). However, of the 31 cases (0,2/100.000 doses of qHPV vaccine) that had objectified VTE, 90% had a known risk factor for VTE, being antiphospho-lipid syndrome in two cases [107].
10. In hyposplenic/asplenic patients with AIIRD influenza, pneumococcal, Hae-mophilus influenzae b and meningococcal C vaccinations are recommended. (grade of evidence 4; strength of recommendation D; Delphi vote 9,50)
Hyposplenic/asplenic patients are at risk of contracting a so-called “overwhel-ming post-splenectomy infection (OPSI)”. OPSI is caused by encapsulated bac-teria (e.g. S. pneumoniae, H. influenzae b, N. meningitidis) and the mortality of OPSI is up to 70% [108-112]. OPSI can occur as a secondary infection after infection with influenza. No studies have addressed the efficacy of vaccination to prevent OPSI in patients who are hyposplenic/asplenic, but the general consensus is to vaccinate these patients against influenza, S. pneumoniae, H. influenzae b and N.

183
Cha
pter
9
meningitides C [113]. When hyposplenic/asplenic patients with AIIRD plan to travel to or live in areas where other meningococcal strains are endemic (A, Y, W135), vaccination for these meningococcal subtypes is also indicated [114]. Prophylactic or on-demand antibiotics and preventive measures for malaria and babesiosis are beyond the scope of these recommendations.
11. Hepatitis A and/or B vaccination is only recommended in patients with AIIRD at risk. (grade of evidence 2a-3; strength of recommendation B-D; Delphi vote 9,13)
Data on incidence of hepatitis A and B infection in patients with AIIRD are lacking. Reactivation of hepatitis B infection in patients with AIIRD has been described following treatment with immunosuppressive medication or immediately after discontinuing immunosuppressive medication (among which anti-TNFα agents). However, no comparative studies have been published. Therefore it is impossible to distinguish whether the immunosuppressive treatment, the disease activity of the AIIRD or the natural course of chronic hepatitis B infection was the cause of the hepatitis flare. Hepatitis B vaccination is efficacious in most patients with AIIRD [55-57]. Vaccination for hepatitis A and/or B is only recommended when the risk of contracting these infections is increased (travel to or residence in endemic countries for hepatitis A and/or B; increased risk of exposure or proven exposure to hepatitis A and/or B (e.g. because of medical profession, infected family mem-ber or contacts) and when protective antibodies against hepatitis A and/or B are absent.
12. AIIRD patients who plan to travel are recommended to receive their vaccinati-ons according to general rules, except for live-attenuated vaccines, which should be avoided whenever possible in immunosuppressed patients with AIIRD. (no grade of evidence; strength of recommendation D; Delphi vote 9,25)
It is unknown whether patients with AIIRD have an increased risk of contracting travel-related vaccine-preventable infections (VPI). In RA patients and SLE pa-
Table 5. Vaccinations to be checked during initial workup (by history taking)
Haemophilus influenzae b
Hepatitis A
Hepatitis B
Human papillomavirus
Influenza
Neisseria meningitides
Rubella (for women of child-baring age)
Streptococcus pneumoniae
Tetanus toxoid

184
Cha
pter
9
tients the risk of tuberculosis (TB) is increased (also see recommendation 13) [115-129]. However, the majority of these TB cases represent reactivations from earlier contracted latent TB infection, and BCG vaccination has not been clearly demon-strated to prevent tuberculosis in adults. Influenza is endemic in subtropical and tropical climates during the entire year and is the most frequent VPI among tra-vellers to subtropical and tropical countries [130, 131]. The incidence of influenza in patients with AIIRD is not known. Also the incidence of cholera, diphtheria, hepati-tis A, meningococcal infection, poliomyelitis, rabies, tetanus, tick-borne encepha-litis, typhoid fever and yellow fever is unknown. Studies addressing the efficacy of influenza vaccination (in RA, SLE, SSc and AAV patients) [24-26, 30-41, 47-50, 63, 68, 75, 76] and tetanus toxoid vaccination (in RA and SLE patients) [30, 46, 58, 59] generally showed responses comparable to those in healthy controls .
To protect patients with AIIRD from contracting travel-related VPI, they should receive the vaccinations that are recommended to the general population. Excep-tions are vaccinations with BCG vaccine, oral poliomyelitis vaccine, oral typhoid fever vaccine and yellow fever vaccine, which contain live attenuated micro-or-ganisms and therefore might lead to life threatening infection in immunosup-pressed patients with AIIRD.
13. BCG vaccination is not recommended in patients with AIIRD. (grade of evidence 3; strength of recommendation C-D; Delphi vote 9,38)
The incidence of tuberculosis is increased in patients with AIIRD, in particular when treated with immunosuppressive drugs (DMARDs, corticosteroids [115-119, 121-124, 127-129], and especially TNFα-blocking agents [116-119, 122, 127-129]. The large majority of these cases of active tuberculosis are reactivations of earlier con-tracted latent tuberculosis infections, which cannot be prevented by vaccination. Moreover, BCG vaccination has not been clearly demonstrated to be efficacious
Table 6. Research agenda
1. Set-up of a vaccination registry for patients with AIIRD with a focus on safety and efficacy
2. Prospective studies evaluating the prevalence and identification of causative micro-organisms of infection in patients with AIIRD, and the outcome of vaccine preventable infections in these patients
3. Evaluation of the impact of therapies on safety and efficacy of vaccination
4. Evaluation of the impact of new therapies on prevalence of (vaccine preventable) infections
5. Research for efficacy and safety of new vaccines (such as herpes zoster, pandemic H1N1 Influ-enza A, HPV)
6. Evaluation of the implementation of vaccination recommendations
7. Research for the safety and efficacy regarding adjuvants and specific risk groups (e.g. preg-nancy)

185
Cha
pter
9
in preventing tuberculosis in adults. Finally, BCG vaccine contains attenuated my-cobacteria, and vaccination with BCG vaccine has been shown to induce BCG-itis in immunosuppressed patients [132-134].
research agenda
The EULAR Task Force for vaccination in patients with AIIRD agreed on the re-search agenda as represented in table 6.
dIscussIOnThe recommendations for vaccination in patients with AIIRD, as presented abo-ve, are based on the current evidence resulting from the SLR and the opinion of selected experts in the fields of rheumatology, clinical immunology, nephrology, paediatric rheumatology/immunology and infectious diseases from 11 European countries. Unfortunately no randomized controlled studies were available that addressed efficacy of vaccination in patients with AIIRD on clinical endpoints. Therefore the highest strength of these recommendations can be strength B (ta-ble 1). We did not systematically review the literature on vaccines in the general population without AIIRD, but the experts did take into account their knowledge of this wider literature in formulating the recommendations. In general, it should be noted that even for the general population, conceptions about the efficiency and efficacy of vaccination have varied over time. Especially for influenza and pneumococcal vaccines there is strong evidence that adequate immune respon-ses are achieved with vaccines, but this may not always translate to equally high efficiency at the clinical protection level [135-137].
Other infection-preventive measures than vaccination are not addressed in these recommendations, and we suggest a new EULAR task force should be set up to recommend on important issues like general hygienic measures and antibiotic prophylaxis for patients with AIIRD to further reduce infection-related morbidity and mortality in patients with AIIRD.
Our literature search focused essentially on three important aspects of vaccina-tion in patients with AIIRD: the incidence of infectious diseases for which vaccines are available; the efficacy of vaccinations that are indicated; and the harms of vac-cination. We should acknowledge that the grading of the available evidence can differ between the three aforementioned aspects: often little evidence is availa-ble for the incidence of VPI, and most studies are underpowered with regard to adverse events, while efficacy is best studied for most vaccines. The results of the Delphi voting to the traditional level of evidence are therefore of particular importance, since these represent the overall interpretation of the evidence on all aforementioned aspects of vaccination in patients with AIIRD by the panel of

186
Cha
pter
9
experts.
The morbidity and mortality for most VPI increase for patients who are more se-verely immunosuppressed, e.g. when treated with a more intensive immunosup-pressive regimen. Therefore we like to stress that the recommendations regar-ding vaccination in patients with AIIRD should be followed more stringently for more immunosuppressed patients. However, because efficacy can be reduced by immunosuppressive treatment, offering vaccination prior to (intensive) immuno-suppressive treatment, in particular rituximab, is started is advisable.
A note of caution is warranted with regard to the safety of vaccination in pa-tients with AIIRD. Although many case reports have been published demonstra-ting flares of AIIRD or new onset auto-immune diseases following vaccination, these adverse events remain rare and a causal relationship has not been proved. Moreover, several controlled studies show no difference in the occurrence of fla-res of AIIRD after vaccination, although these studies have not been powered to address specific adverse events, but efficacy. Because of the lack of sufficiently powered studies focusing on harms, these issues remain an important item on the research agenda.
Finally, there are different vaccination schemes that have been developed and proposed in different European countries. The exact implementation of the cur-rent recommendations may need to take into account local differences in specific countries and settings. Moreover, the recommendations need to be updated on a regular basis (every 3 years, since new evidence will become available with re-gard to current and new vaccines, and current and new immunomodulating tre-atments.
187
Cha
pter
9
reference list
(1) Falagas ME, Manta KG, Betsi GI, Pappas G. Infection-related morbidity and mortality in patients
with connective tissue diseases: a systematic review. Clin Rheumatol 2007 May; 26(5):663-70.
(2) Bosch X, Guilabert A, Pallares L, et al. Infections in systemic lupus erythematosus: a prospective
and controlled study of 110 patients. Lupus 2006; 15(9):584-9.
(3) Doran MF, Crowson CS, Pond GR, O’Fallon WM, Gabriel SE. Frequency of infection in patients
with rheumatoid arthritis compared with controls: a population-based study. Arthritis Rheum
2002 Sep; 46(9):2287-93.
(4) Wolfe F, Mitchell DM, Sibley JT, et al. The mortality of rheumatoid arthritis. Arthritis Rheum 1994
Apr; 37(4):481-94.
(5) Cervera R, Khamashta MA, Font J, et al. Morbidity and mortality in systemic lupus erythemato-
sus during a 10-year period: a comparison of early and late manifestations in a cohort of 1,000
patients. Medicine (Baltimore) 2003 Sep; 82(5):299-308.
(6) Steen VD, Medsger TA. Changes in causes of death in systemic sclerosis, 1972-2002. Ann Rheum
Dis 2007 Jul; 66(7):940-4.
(7) Ruangjutipopan S, Kasitanon N, Louthrenoo W, Sukitawut W, Wichainun R. Causes of death and
poor survival prognostic factors in thai patients with systemic sclerosis. J Med Assoc Thai 2002
Nov; 85(11):1204-9.
(8) Hoffman GS, Kerr GS, Leavitt RY, et al. Wegener granulomatosis: an analysis of 158 patients. Ann
Intern Med 1992 Mar 15; 116(6):488-98.
(9) Reinhold-Keller E, Beuge N, Latza U, et al. An interdisciplinary approach to the care of patients
with Wegener’s granulomatosis: long-term outcome in 155 patients. Arthritis Rheum 2000 May;
43(5):1021-32.
(10) Marie I, Hachulla E, Cherin P, et al. Opportunistic infections in polymyositis and dermatomyosi-
tis. Arthritis Rheum 2005 Apr 15; 53(2):155-65.
(11) Furst DE, Breedveld FC, Kalden JR, et al. Updated consensus statement on biological agents for
the treatment of rheumatic diseases, 2007. Ann Rheum Dis 2007 Nov; 66 Suppl 3:iii2-22.
(12) Chen YF, Jobanputra P, Barton P, et al. A systematic review of the effectiveness of adalimumab,
etanercept and infliximab for the treatment of rheumatoid arthritis in adults and an economic
evaluation of their cost-effectiveness. Health Technol Assess 2006 Nov; 10(42):iii-xiii, 1.
(13) Kremer JM, Genant HK, Moreland LW, et al. Effects of abatacept in patients with methotrexa-
te-resistant active rheumatoid arthritis: a randomized trial. Ann Intern Med 2006 Jun 20;
144(12):865-76.
(14) Genovese MC, Becker JC, Schiff M, et al. Abatacept for rheumatoid arthritis refractory to tumor
necrosis factor alpha inhibition. N Engl J Med 2005 Sep 15; 353(11):1114-23.
(15) Cohen SB, Moreland LW, Cush JJ, et al. A multicentre, double blind, randomised, placebo con-
trolled trial of anakinra (Kineret), a recombinant interleukin 1 receptor antagonist, in patients
with rheumatoid arthritis treated with background methotrexate. Ann Rheum Dis 2004 Sep;
63(9):1062-8.
(16) Nuki G, Bresnihan B, Bear MB, McCabe D. Long-term safety and maintenance of clinical improve-
ment following treatment with anakinra (recombinant human interleukin-1 receptor antagonist)
in patients with rheumatoid arthritis: extension phase of a randomized, double-blind, placebo-
controlled trial. Arthritis Rheum 2002 Nov; 46(11):2838-46.
188
Cha
pter
9
(17) Keystone E, Fleischmann R, Emery P, et al. Safety and efficacy of additional courses of rituximab
in patients with active rheumatoid arthritis: an open-label extension analysis. Arthritis Rheum
2007 Dec; 56(12):3896-908.
(18) Edwards JC, Szczepanski L, Szechinski J, et al. Efficacy of B-cell-targeted therapy with rituxi-
mab in patients with rheumatoid arthritis. N Engl J Med 2004 Jun 17; 350(25):2572-81.
(19) Emery P, Fleischmann R, Filipowicz-Sosnowska A, et al. The efficacy and safety of rituximab in
patients with active rheumatoid arthritis despite methotrexate treatment: results of a phase IIB
randomized, double-blind, placebo-controlled, dose-ranging trial. Arthritis Rheum 2006 May;
54(5):1390-400.
(20) McLeod C, Bagust A, Boland A, et al. Adalimumab, etanercept and infliximab for the treatment
of ankylosing spondylitis: a systematic review and economic evaluation. Health Technol Assess
2007 Aug; 11(28):1-iv.
(21) Lequerre T, Quartier P, Rosellini D, et al. Interleukin-1 receptor antagonist (anakinra) treatment
in patients with systemic-onset juvenile idiopathic arthritis or adult onset Still disease: prelimi-
nary experience in France. Ann Rheum Dis 2008 Mar; 67(3):302-8.
(22) Pijpe J, van Imhoff GW, Spijkervet FK, et al. Rituximab treatment in patients with primary Sjog-
ren’s syndrome: an open-label phase II study. Arthritis Rheum 2005 Sep; 52(9):2740-50.
(23) Smolen JS, Beaulieu A, Rubbert-Roth A, et al. Effect of interleukin-6 receptor inhibition with
tocilizumab in patients with rheumatoid arthritis (OPTION study): a double-blind, placebo-con-
trolled, randomised trial. Lancet 2008 Mar 22; 371(9617):987-97.
(24) Louie JS, Nies KM, Shoji KT, et al. Clinical and antibody responses after influenza immunization
in systemic lupus erythematosus. Ann Intern Med 1978 Jun; 88(6):790-2.
(25) Ristow SC, Douglas RG, Jr., Condemi JJ. Influenza vaccination of patients with systemic lupus
erythematosus. Ann Intern Med 1978 Jun; 88(6):786-9.
(26) Zycinska K, Romanowska M, Nowak I, Rybicka K, Wardyn KA, Brydak LB. Antibody response to in-
activated subunit influenza vaccine in patients with Wegener’s granulomatosis. J Physiol Phar-
macol 2007 Nov; 58 Suppl 5(Pt 2):819-28.
(27) King SM, Saunders EF, Petric M, Gold R. Response to measles, mumps and rubella vaccine in
paediatric bone marrow transplant recipients. Bone Marrow Transplant 1996 Apr; 17(4):633-6.
(28) Levin MJ, Gershon AA, Weinberg A, Song LY, Fentin T, Nowak B. Administration of live varicella
vaccine to HIV-infected children with current or past significant depression of CD4(+) T cells. J
Infect Dis 2006 Jul 15; 194(2):247-55.
(29) Harpaz R, Ortega-Sanchez IR, Seward JF. Prevention of herpes zoster: recommendations of the
Advisory Committee on Immunization Practices (ACIP). MMWR Recomm Rep 2008 Jun 6; 57(RR-
5):1-30.
(30) Denman EJ, Denman AM, Greenwood BM, Gall D, Heath RB. Failure of cytotoxic drugs to sup-
press immune responses of patients with rheumatoid arthritis. Ann Rheum Dis 1970 May;
29(3):220-31.
(31) Herron A, Dettleff G, Hixon B, et al. Influenza vaccination in patients with rheumatic diseases.
Safety and efficacy. JAMA 1979 Jul 6; 242(1):53-6.
(32) Turner-Stokes L, Cambridge G, Corcoran T, Oxford JS, Snaith ML. In vitro response to influenza
immunisation by peripheral blood mononuclear cells from patients with systemic lupus erythe-
matosus and other autoimmune diseases. Ann Rheum Dis 1988 Jul; 47(7):532-5.
(33) Chalmers A, Scheifele D, Patterson C, et al. Immunization of patients with rheumatoid arthritis
189
Cha
pter
9
against influenza: a study of vaccine safety and immunogenicity. J Rheumatol 1994 Jul; 21(7):1203-
6.
(34) Del Porto F, Lagana B, Biselli R, et al. Influenza vaccine administration in patients with systemic
lupus erythematosus and rheumatoid arthritis. Safety and immunogenicity. Vaccine 2006 Apr
12; 24(16):3217-23.
(35) Fomin I, Caspi D, Levy V, et al. Vaccination against influenza in rheumatoid arthritis: the effect
of disease modifying drugs, including TNF alpha blockers. Ann Rheum Dis 2006 Feb; 65(2):191-4.
(36) Kaine JL, Kivitz AJ, Birbara C, Luo AY. Immune responses following administration of influ-
enza and pneumococcal vaccines to patients with rheumatoid arthritis receiving adalimumab. J
Rheumatol 2007 Feb; 34(2):272-9.
(37) Kubota T, Nii T, Nanki T, et al. Anti-tumor necrosis factor therapy does not diminish the immune
response to influenza vaccine in Japanese patients with rheumatoid arthritis. Mod Rheumatol
2007; 17(6):531-3.
(38) Gelinck LB, van der Bijl AE, Beyer WE, et al. The effect of anti-tumour necrosis factor alpha tre-
atment on the antibody response to influenza vaccination. Ann Rheum Dis 2008 May; 67(5):713-6.
(39) Nii T, Kubota T, Nanki T, et al. Reevaluation of antibody titers 1 year after influenza vaccination in
patients with rheumatoid arthritis receiving TNF blockers. Mod Rheumatol 2009; 19(2):216-8.
(40) Elkayam O, Bashkin A, Mandelboim M, et al. The Effect of Infliximab and Timing of Vaccination
on the Humoral Response to Influenza Vaccination in Patients with Rheumatoid Arthritis and
Ankylosing Spondylitis. Semin Arthritis Rheum 2009 Feb 24.
(41) van Assen S, Holvast A, Benne CA, et al. Humoral responses after influenza vaccination are seve-
rely reduced in patients with rheumatoid arthritis treated with rituximab. Arthritis Rheum 2009
Dec 28; 62(1):75-81.
(42) Elkayam O, Paran D, Caspi D, et al. Immunogenicity and safety of pneumococcal vaccination in
patients with rheumatoid arthritis or systemic lupus erythematosus. Clin Infect Dis 2002 Jan 15;
34(2):147-53.
(43) Elkayam O, Caspi D, Reitblatt T, Charboneau D, Rubins JB. The effect of tumor necrosis factor
blockade on the response to pneumococcal vaccination in patients with rheumatoid arthritis and
ankylosing spondylitis. Semin Arthritis Rheum 2004 Feb; 33(4):283-8.
(44) Visvanathan S, Keenan GF, Baker DG, Levinson AI, Wagner CL. Response to pneumococcal vac-
cine in patients with early rheumatoid arthritis receiving infliximab plus methotrexate or me-
thotrexate alone. J Rheumatol 2007 May; 34(5):952-7.
(45) Kapetanovic MC, Saxne T, Sjoholm A, Truedsson L, Jonsson G, Geborek P. Influence of metho-
trexate, TNF blockers and prednisolone on antibody responses to pneumococcal polysaccharide
vaccine in patients with rheumatoid arthritis. Rheumatology (Oxford) 2006 Jan; 45(1):106-11.
(46) Devey ME, Bleasdale K, Isenberg DA. Antibody affinity and IgG subclass of responses to tetanus
toxoid in patients with rheumatoid arthritis and systemic lupus erythematosus. Clin Exp Im-
munol 1987 Jun; 68(3):562-9.
(47) Mercado U, Acosta H, Avendano L. Influenza vaccination of patients with systemic lupus erythe-
matosus. Rev Invest Clin 2004 Jan; 56(1):16-20.
(48) Pons VG, Reinertsen JL, Steinberg AD, Dolin R. Decreased cell-mediated cytotoxicity against
virus-infected cells in systemic lupus erythematosus. J Med Virol 1979; 4(1):15-23.
(49) Williams GW, Steinberg AD, Reinertsen JL, Klassen LW, Decker JL, Dolin R. Influenza immuniza-
tion in systemic lupus eruthematosus. A double-blind trial. Ann Intern Med 1978 Jun; 88(6):729-34.

190
Cha
pter
9
(50) Brodman R, Gilfillan R, Glass D, Schur PH. Influenzal vaccine response in systemic lupus erythe-
matosus. Ann Intern Med 1978 Jun; 88(6):735-40.
(51) Lipnick RN, Karsh J, Stahl NI, Blackwelder WC, Schiffman G, Klippel JH. Pneumococcal immu-
nization in patients with systemic lupus erythematosus treated with immunosuppressives. J
Rheumatol 1985 Dec; 12(6):1118-21.
(52) Croft SM, Schiffman G, Snyder E, Herrmann K, James K, Jarrett MP. Specific antibody response
after in vivo antigenic stimulation in systemic lupus erythematosus. J Rheumatol 1984 Apr;
11(2):141-6.
(53) Tarjan P, Sipka S, Marodi L, et al. No short-term immunological effects of Pneumococcus vac-
cination in patients with systemic lupus erythematosus. Scand J Rheumatol 2002; 31(4):211-5.
(54) Jarrett MP, Schiffman G, Barland P, Grayzel AI. Impaired response to pneumococcal vaccine in
systemic lupus erythematosus. Arthritis Rheum 1980 Nov; 23(11):1287-93.
(55) Kuruma KA, Borba EF, Lopes MH, de Carvalho JF, Bonfa E. Safety and efficacy of hepatitis B vac-
cine in systemic lupus erythematosus. Lupus 2007; 16(5):350-4.
(56) Elkayam O, Yaron M, Caspi D. Safety and efficacy of vaccination against hepatitis B in patients
with rheumatoid arthritis. Ann Rheum Dis 2002 Jul; 61(7):623-5.
(57) Erkek E, Ayaslioglu E, Erkek AB, Kurtipek GS, Bagci Y. Response to vaccination against hepatitis
B in patients with Behcet’s disease. J Gastroenterol Hepatol 2005 Oct; 20(10):1508-11.
(58) Kashef S, Ghazizadeh F, Derakhshan A, Farjadian S, Alyasin S. Antigen-specific antibody res-
ponse in juvenile-onset SLE patients following routine immunization with tetanus toxoid. Iran J
Immunol 2008 Sep; 5(3):181-4.
(59) Abe T, Homma M. Immunological reactivity in patients with systemic lupus erythematosus. Hu-
moral antibody and cellular immune responses. Acta Rheumatol Scand 1971; 17(1):35-46.
(60) Battafarano DF, Battafarano NJ, Larsen L, et al. Antigen-specific antibody responses in lupus
patients following immunization. Arthritis Rheum 1998 Oct; 41(10):1828-34.
(61) Nies K, Boyer R, Stevens R, Louie J. Anti-tetanus toxoid antibody synthesis after booster im-
munization in systemic lupus erythematosus. Comparison of the in vitro and in vivo responses.
Arthritis Rheum 1980 Dec; 23(12):1343-50.
(62) Mease PJ, Ritchlin CT, Martin RW, et al. Pneumococcal vaccine response in psoriatic arthritis
patients during treatment with etanercept. J Rheumatol 2004 Jul; 31(7):1356-61.
(63) Holvast A, Huckriede A, Wilschut J, et al. Safety and efficacy of influenza vaccination in systemic
lupus erythematosus patients with quiescent disease. Ann Rheum Dis 2006 Jul; 65(7):913-8.
(64) Franco Salinas G, de Rycke L, Cantaert T et al. TNF blockade impairs T-cell dependant antibody
respons. Ann Rheum Dis 2009;68(Suppl3):238
(65) Wiesik-Szewczyk E, Romanowska M, Mielnik P, et al. Anti-influenza vaccination in systemic lupus
erythematosus patients: an analysis of specific humoral response and vaccination safety. Clin
Rheumatol 2010 Jun; 29(6):605-13.
(66) Wiesik-Szewczyk E et al. Predictors of antigen-specific response for influenza vaccination on
lupus patients. Ann Rheum Dis 2009;68(Suppl3):263
(67) Kapetanovic MC, Saxne T, Nilsson JA, Geborek P. Influenza vaccination as model for testing
immune modulation induced by anti-TNF and methotrexate therapy in rheumatoid arthritis pa-
tients. Rheumatology (Oxford) 2007 Apr; 46(4):608-11.
(68) Abu-Shakra M, Press J, Varsano N, et al. Specific antibody response after influenza immuniza-
tion in systemic lupus erythematosus. J Rheumatol 2002 Dec; 29(12):2555-7.

191
Cha
pter
9
(69) Gelinck LB, van der Bijl AE, Visser LG, et al. Synergistic immunosuppressive effect of anti-TNF
combined with methotrexate on antibody responses to the 23 valent pneumococcal polysaccha-
ride vaccine. Vaccine 2008 Jun 25; 26(27-28):3528-33.
(70) Oren S, Mandelboim M, Braun-Moscovici Y, et al. Vaccination against influenza in patients with
rheumatoid arthritis: the effect of rituximab on the humoral response. Ann Rheum Dis 2008 Jul;
67(7):937-41.
(71) Bingham CO, III, Looney RJ, Deodhar A, et al. Immunization responses in rheumatoid arthritis
patients treated with rituximab: Results from a controlled clinical trial. Arthritis Rheum 2009
Dec 28; 62(1):64-74.
(72) Little MA, Nightingale P, Verburgh CA, et al. Early mortality in systemic vasculitis: relative con-
tribution of adverse events and active vasculitis. Ann Rheum Dis 2009 Jul 1.
(73) Nichol KL, Goodman M. The health and economic benefits of influenza vaccination for healthy
and at-risk persons aged 65 to 74 years. Pharmacoeconomics 1999; 16 Suppl 1:63-71.
(74) Hak E, Nordin J, Wei F, et al. Influence of high-risk medical conditions on the effectiveness of in-
fluenza vaccination among elderly members of 3 large managed-care organizations. Clin Infect
Dis 2002 Aug 15; 35(4):370-7.
(75) Holvast A, Stegeman CA, Benne CA, et al. Wegener’s granulomatosis patients show an adequate
antibody response to influenza vaccination. Ann Rheum Dis 2009 Jun; 68(6):873-8.
(76) Setti M, Fenoglio D, Ansaldi F, et al. Flu vaccination with a virosomal vaccine does not affect
clinical course and immunological parameters in scleroderma patients. Vaccine 2009 May 26;
27(25-26):3367-72.
(77) Stojanovich L. Influenza vaccination of patients with systemic lupus erythematosus (SLE) and
rheumatoid arthritis (RA). Clin Dev Immunol 2006 Jun; 13(2-4):373-5.
(78) Gelinck LB, Teng YK, Rimmelzwaan GF, van den Bemt BJ, Kroon FP, van Laar JM. Poor serolo-
gical responses upon influenza vaccination in patients with rheumatoid arthritis treated with
rituximab. Ann Rheum Dis 2007 Oct; 66(10):1402-3.
(79) Pellegrini M, Nicolay U, Lindert K, Groth N, Della Cioppa G. MF59-adjuvanted versus non-adju-
vanted influenza vaccines: integrated analysis from a large safety database. Vaccine 2009 Nov
16; 27(49):6959-65.
(80) McDonald E, Jarrett MP, Schiffman G, Grayzel AI. Persistence of pneumococcal antibodies after
immunization in patients with systemic lupus erythematosus. J Rheumatol 1984 Jun; 11(3):306-8.
(81) Favalli EG, Desiati F, Atzeni F, et al. Serious infections during anti-TNFalpha treatment in rheu-
matoid arthritis patients. Autoimmun Rev 2009 Jan; 8(3):266-73.
(82) Strangfeld A, Listing J, Herzer P, et al. Risk of herpes zoster in patients with rheumatoid arthritis
treated with anti-TNF-alpha agents. JAMA 2009 Feb 18; 301(7):737-44.
(83) McDonald JR, Zeringue AL, Caplan L, et al. Herpes zoster risk factors in a national cohort of
veterans with rheumatoid arthritis. Clin Infect Dis 2009 May 15; 48(10):1364-71.
(84) Smitten AL, Choi HK, Hochberg MC, et al. The risk of herpes zoster in patients with rheumatoid
arthritis in the United States and the United Kingdom. Arthritis Rheum 2007 Dec 15; 57(8):1431-8.
(85) Wolfe F, Michaud K, Chakravarty EF. Rates and predictors of herpes zoster in patients with rheu-
matoid arthritis and non-inflammatory musculoskeletal disorders. Rheumatology (Oxford) 2006
Nov; 45(11):1370-5.
(86) Antonelli MA, Moreland LW, Brick JE. Herpes zoster in patients with rheumatoid arthritis trea-
ted with weekly, low-dose methotrexate. Am J Med 1991 Mar; 90(3):295-8.

192
Cha
pter
9
(87) Speerstra F, Boerbooms AM, van de Putte LB, van Beusekom HJ, Kruijsen MW, Vandenbroucke
JP. Side-effects of azathioprine treatment in rheumatoid arthritis: analysis of 10 years of expe-
rience. Ann Rheum Dis 1982; 41 Suppl 1:37-9.
(88) Ginzler E, Diamond H, Kaplan D, Weiner M, Schlesinger M, Seleznick M. Computer analysis of
factors influencing frequency of infection in systemic lupus erythematosus. Arthritis Rheum
1978 Jan; 21(1):37-44.
(89) Kang TY, Lee HS, Kim TH, Jun JB, Yoo DH. Clinical and genetic risk factors of herpes zoster in
patients with systemic lupus erythematosus. Rheumatol Int 2005 Mar; 25(2):97-102.
(90) Manzi S, Kuller LH, Kutzer J, et al. Herpes zoster in systemic lupus erythematosus. J Rheumatol
1995 Jul; 22(7):1254-8.
(91) Kahl LE. Herpes zoster infections in systemic lupus erythematosus: risk factors and outcome. J
Rheumatol 1994 Jan; 21(1):84-6.
(92) Nagasawa K, Yamauchi Y, Tada Y, Kusaba T, Niho Y, Yoshikawa H. High incidence of herpes zoster
in patients with systemic lupus erythematosus: an immunological analysis. Ann Rheum Dis 1990
Aug; 49(8):630-3.
(93) Wang F, Chua CT, Bosco J. Herpes zoster in patients with systemic lupus erythematosus. Singa-
pore Med J 1983 Aug; 24(4):218-20.
(94) Pope JE, Krizova A, Ouimet JM, Goodwin JL, Lankin M. Close association of herpes zoster reac-
tivation and systemic lupus erythematosus (SLE) diagnosis: case-control study of patients with
SLE or noninflammatory nusculoskeletal disorders. J Rheumatol 2004 Feb; 31(2):274-9.
(95) Nagaoka S, Tani K, Ishigatsubo Y, et al. Herpes zoster in patients with polymyositis and derma-
tomyositis. Kansenshogaku Zasshi 1990 Nov; 64(11):1394-9.
(96) Wung PK, Holbrook JT, Hoffman GS, et al. Herpes zoster in immunocompromised patients: inci-
dence, timing, and risk factors. Am J Med 2005 Dec; 118(12):1416.
(97) Gordon KB, Gottlieb AB, Gianinni EH et al. Clinical Trial Safety Data of Events of Interest in Pa-
tients Receiving Etanercept (ENBREL®) across Approved Indications. ACR 2007: abstract 960
(98) Weinblatt ME, Genovese MC, Moreland LW et al. Efficacy and Safety of up to 10 Years of Etaner-
cept (Enbrel®) Therapy in North American Patients With Early and Long-Standing Rheumatoid
Arthritis ACR Annual Meeting 2007; abstract 957.
(99) Perez-Zafrilla B, Garcia Doval I, Carmona L. Rates of herpes zoster in patients with rheumatoid
arthritis and treatment with TNF antagonists. Incidence rate in Biobadaser cohort in comparison
with Emecar cohort. Ann Rheum Dis 2008;67 (suppl2):327
(100) Salliot C, Bombardier C, van der Heide D. Long term safety of methotrexate in rheumatoid
arthritis; a systematic literature review. Ann Rheum Dis 2008;67 (suppl II):204
(101) Merrill JT, Neuwelt CM, Wallace DJ et al. Rituximab in extra-renal SLE patients showed no signi-
ficant difference compared to placebo at 52 weeks in the randomized, double-blind phase II/III
study EXPORER. Ann Rheum Dis 2009;68 (suppl3):249
(102) Oxman MN, Levin MJ, Johnson GR, et al. A vaccine to prevent herpes zoster and postherpetic
neuralgia in older adults. N Engl J Med 2005 Jun 2; 352(22):2271-84.
(103) Tam LS, Chan AY, Chan PK, Chang AR, Li EK. Increased prevalence of squamous intraepithe-
lial lesions in systemic lupus erythematosus: association with human papillomavirus infection.
Arthritis Rheum 2004 Nov; 50(11):3619-25.
(104) Nath R, Mant C, Luxton J, et al. High risk of human papillomavirus type 16 infections and of deve-
lopment of cervical squamous intraepithelial lesions in systemic lupus erythematosus patients.
193
Cha
pter
9
Arthritis Rheum 2007 May 15; 57(4):619-25.
(105) Lee Y, Choe J, Kim J et al. Prevalence and Risk Factors for Human Papillomavirus Infection and
Cervical Cytological Abnormalities in Korean Patients with Systemic Lupus Erythematosus. ACR
2007: abstract 1105
(106) Tam L, Chan PS, Ho S et al. Natural history of cervical human papillomavirus infection among
women with systemic lupus erythematosus. Ann Rheum Dis 2009;68 (suppl3):128
(107) Slade BA, Leidel L, Vellozzi C, et al. Postlicensure safety surveillance for quadrivalent human
papillomavirus recombinant vaccine. JAMA 2009 Aug 19; 302(7):750-7.
(108) Kyaw MH, Holmes EM, Toolis F, et al. Evaluation of severe infection and survival after splenec-
tomy. Am J Med 2006 Mar; 119(3):276-7.
(109) Brigden ML, Pattullo AL. Prevention and management of overwhelming postsplenectomy infec-
tion--an update. Crit Care Med 1999 Apr; 27(4):836-42.
(110) Lynch AM, Kapila R. Overwhelming postsplenectomy infection. Infect Dis Clin North Am 1996
Dec; 10(4):693-707.
(111) Styrt B. Infection associated with asplenia: risks, mechanisms, and prevention. Am J Med 1990
May; 88(5N):33N-42N.
(112) Green JB, Shackford SR, Sise MJ, Fridlund P. Late septic complications in adults following sple-
nectomy for trauma: a prospective analysis in 144 patients. J Trauma 1986 Nov; 26(11):999-1004.
(113) Davies JM, Barnes R, Milligan D. Update of guidelines for the prevention and treatment of infec-
tion in patients with an absent or dysfunctional spleen. Clin Med 2002 Sep; 2(5):440-3.
(114) Watson DA. Pretravel health advice for asplenic individuals. J Travel Med 2003 Mar; 10(2):117-21.
(115) Brassard P, Lowe AM, Bernatsky S, Kezouh A, Suissa S. Rheumatoid arthritis, its treatments, and
the risk of tuberculosis in Quebec, Canada. Arthritis Rheum 2009 Mar 15; 61(3):300-4.
(116) Askling J, Fored CM, Brandt L, et al. Risk and case characteristics of tuberculosis in rheumatoid
arthritis associated with tumor necrosis factor antagonists in Sweden. Arthritis Rheum 2005
Jul; 52(7):1986-92.
(117) Brassard P, Kezouh A, Suissa S. Antirheumatic drugs and the risk of tuberculosis. Clin Infect Dis
2006 Sep 15; 43(6):717-22.
(118) Gomez-Reino JJ, Carmona L, Valverde VR, Mola EM, Montero MD. Treatment of rheumatoid
arthritis with tumor necrosis factor inhibitors may predispose to significant increase in tuber-
culosis risk: a multicenter active-surveillance report. Arthritis Rheum 2003 Aug; 48(8):2122-7.
(119) Seong SS, Choi CB, Woo JH, et al. Incidence of tuberculosis in Korean patients with rheumatoid
arthritis (RA): effects of RA itself and of tumor necrosis factor blockers. J Rheumatol 2007 Apr;
34(4):706-11.
(120) Bernatsky S, Bombardier C, Bhamani A et al. Tuberculosis in a population-based cohort of seni-
ors with rheumatoid arthritis. Ann Rheum Dis 2009;68 (suppl3):568
(121) Askling J. Risk for tuberculosis following treatment of rheumatoid arthritis with anti-TNF the-
rapy - the Swedish experience 1998-2008. Ann Rheum Dis 2009;68(Suppl3):422
(122) Baronnet L, Kahn V, Lacoin C, et al. Tuberculosis incidence in rheumatoid arthritis affected pa-
tients. Ann Rheum Dis 2008;67 (suppl2):544
(123) Mines D, Gu Y, Liu Q et al. Risk of active tuberculosis (TB) among biologic-naive patients: retro-
spective cohort study in a US claims database. Ann Rheum Dis 2008;67(suppl2):91
(124) Tubach F, Salmon D, Ravaud P et al. The risk of tuberculosis with anti-TNF is higher with mono-
clonal antibodies than with the soluble receptor. Results of the French 3-year prospective RATIO

194
Cha
pter
9
observatory. Ann Rheum Dis 2008;67 (suppl2):52
(125) Dixon WG, Hyrich KL, Watson KD et al. Specific risk of tuberculosis in patients with rheumatoid
arthritis treated with anti-TNF therapy: results from the BSR Biologic Register (BSRBR). Ann
Rheum Dis 2008;67 (suppl2):178
(126) Dixon WG, Hyrich KL, Watson KD et al. Drug-Specific Risk of Tuberculosis in Patients with Rheu-
matoid Arthritis Treated with Anti-TNF Therapy: Results from the BSRBR. ACR 2008: abstract
1263
(127) Kim HA, Yoo CD, Baek HJ, et al. Mycobacterium tuberculosis infection in a corticosteroid-treated
rheumatic disease patient population. Clin Exp Rheumatol 1998 Jan; 16(1):9-13.
(128) Sayarlioglu M, Inanc M, Kamali S, et al. Tuberculosis in Turkish patients with systemic lupus ery-
thematosus: increased frequency of extrapulmonary localization. Lupus 2004; 13(4):274-8.
(129) Tam LS, Li EK, Wong SM, Szeto CC. Risk factors and clinical features for tuberculosis among pa-
tients with systemic lupus erythematosus in Hong Kong. Scand J Rheumatol 2002; 31(5):296-300.
(130) Marti F, Steffen R, Mutsch M. Influenza vaccine: a travelers’ vaccine? Expert Rev Vaccines 2008
Jul; 7(5):679-87.
(131) Mutsch M, Tavernini M, Marx A, et al. Influenza virus infection in travelers to tropical and subtro-
pical countries. Clin Infect Dis 2005 May 1; 40(9):1282-7.
(132) Karpelowsky JS, Alexander AG, Peek SD, Millar AJ, Rode H. Surgical complications of bacille
Calmette-Guerin (BCG) infection in HIV-infected children: time for a change in policy. S Afr Med
J 2008 Oct; 98(10):801-4.
(133) Hesseling AC, Johnson LF, Jaspan H, et al. Disseminated bacille Calmette-Guerin disease in HIV-
infected South African infants. Bull World Health Organ 2009 Jul; 87(7):505-11.
(134) Kawashima H, Hasegawa D, Nakamura M, et al. Hazards of early BCG vaccination: BCGitis in a
patient with chronic granulomatous disease. Pediatr Int 2007 Jun; 49(3):418-9.
(135) Jefferson T, Di Pietrantonj C, Rivetti A, Bawazeer GA, Al Ansary LA, Ferroni E. Vaccines for
preventing influenza in healthy adults. Cochrane Database Syst Rev 2010; 7:CD001269.
(136) Jefferson T, Di Pietrantonj C, Al Ansary LA, Ferroni E, Thorning S, Thomas RE. Vaccines for
preventing influenza in the elderly. Cochrane Database Syst Rev 2010; 2:CD004876.
(137) Huss A, Scott P, Stuck AE, Trotter C, Egger M. Efficacy of pneumococcal vaccination in adults: a
meta-analysis. CMAJ 2009 Jan 6; 180(1):48-58.



CHAPT
ER10Summary,g e n e r a l discussion and future perspectives


199
Cha
pter
10
SummAryPatients with primary and secondary immunodeficiencies are at increased risk of contracting common and/or opportunistic infections [1, 2]. Moreover, these in-fections more often follow a complicated course, with increased morbidity and mortality [1, 2]. One of the interventions to prevent or mitigate the course of in-fections in these patients is vaccination. However, paradoxically, for an optimal response following vaccination an adequately functioning immune systems is re-quired (also see introduction to this thesis).
In order to make recommendations on the usefulness of influenza vaccination in patients with primary and secondary immunodeficiencies, we investigated the humoral and cell-mediated immune (CMI) responses following influenza vaccina-tion in these patients. Moreover, the timing of vaccination in relation to immuno-suppressive treatment was studied as well as a strategy to optimize the immune response to influenza vaccination: administration of a second, booster, influenza vaccination.
Following chapter 1, where we summarized the history of the discovery of vac-cination, the immune response to influenza vaccination, and the primary and se-condary immunodeficiencies that are addressed in the thesis, part 1 describes the vaccination studies that we performed in patients with humoral primary immuno-deficiencies (hPID). Chapter 2 addresses the humoral immune response following inactivated trivalent subunit influenza vaccination in patients with hPID. Following vaccination, as expected, hPID-patients developed humoral responses that were clearly inferior to those found in healthy controls (HC), as measured by geometric mean titers (GMTs), fold-increase in GMT, and seroprotection rates. In contrast to HC, who responded to all three influenza strains, patients were able to respond with a significant rise in GMT only for the A/H1N1-strain. Moreover, previous vac-cination and treatment with intravenous immunoglobulin (IVIg) did not result in higher postvaccination GMTs or higher rate of seroprotection (defined as titer ≥40).
Since CMI responses are also of importance for the clearance of influenza from infected individuals, in the study presented in chapter 3 we investigated the cell-mediated recall responses following influenza vaccination in patients with com-mon variable immunodeficiency (CVID), a subgroup of the hPID-patients that were included in the study described in chapter 2. Although cellular immune responses are affected in patients with CVID at many different levels, the cellular response following influenza vaccination had never been addressed before by others. We found impaired recall responses following influenza vaccination in the CVID-pa-tients when using interferon (IFN)γ-ELISpot. Flow cytometry with intracellular cy-

200
Cha
pter
10
tokine staining revealed a decrease in influenza-specific IFNγ and tumor necrosis factor (TNF)α producing CD4+ and CD8+ T-cells in patients following vaccination compared to baseline, while HC demonstrated an increase in influenza-specific cytokine producing T-cells. In vitro activation-induced cell death of CD4+ and CD8+ T-cells might be the explanation for this fall in T-cell numbers after influenza vac-cination as increased pre-activation of T-cells in vivo has been demonstrated in CVID patients.
Part 2, addressing immune responses to influenza vaccination in patients with se-condary immunodeficiencies, in particular those suffering from auto-inflamma-tory rheumatic diseases (AIIRD), starts with two studies on influenza vaccination in patients with systemic lupus erythematosus (SLE). The first focused on the humoral and CMI responses before and after influenza vaccination (chapter 4). SLE patients showed a decreased antibody response to A/H1N1 and A/H3N2, com-pared to HC. Cell-mediated influenza-specific responses were also found to be lower in SLE-patients in comparison with HC. Using FACS analysis, SLE-patients showed increases in frequencies of influenza-specific CD4+ T-cells for fewer cy-tokines following influenza vaccination as compared to HC. Impaired cell-medi-ated influenza-specific responses were associated with the use of prednisone and/or azathioprine. The second study (chapter 5) investigated a strategy to im-prove the outcome of vaccination in SLE-patients, since an earlier study (chap-ter 4) demonstrated sub-optimal humoral responses in these patients. In this re-vaccination study, the efficacy of administration of a second, booster, influenza vaccination four weeks after the first one was studied. In contrast to previous data, with in part other influenza strains, this study did not find differences in the influenza-specific antibody responses between SLE patients and HC after the first vaccination. The booster vaccination did not result in a further rise in GMT, seroconversion rates or seroprotection rates, except for SLE patients who were not vaccinated in the previous year, who tended to have an additional increase in GMT and seroconversion rate for the A/H1N1 influenza-strain.
Chapter 6 describes a study that was initiated to investigate the influence of tre-atment with rituximab, a B-cell depleting anti-CD20 monoclonal antibody, on the antibody response following influenza vaccination in patients with rheumatoid arthritis (RA). In B-cell depleted individuals no influenza-specific antibodies were produced following influenza vaccination. This was expected, as influenza vac-cine antigens are considered (in part) to be neo-antigens. The antigens are yearly adjusted to the changes in the influenza virus caused by antigenic drift. Vacci-nation within 4 to 8 weeks after administration of rituximab showed no humoral response at all. However, 6 to 10 months following rituximab therapy, when recur-rence of B-cells in the peripheral blood occurred, a significant, but still hampered,

201
Cha
pter
10
antibody response to both A-strains in the vaccine could be demonstrated.
Within the same study population that was studied in chapter 6, the CMI respon-ses before and after influenza vaccination (using IFNγ-ELISpot, proliferation as-says and flowcytometry with intracellular cytokine staining) were determined, as described in chapter 7. Before vaccination, flow cytometry demonstrated that polyclonal and influenza-specific CMI responses were reduced in RA-patients tre-ated with rituximab. Moreover, influenza-specific CMI responses following influ-enza vaccination were hampered.
Finally, part 3 presents the systematic literature review (SLR) (chapter 8) that was performed to form the basis of evidence-based recommendations on vaccination in patients with auto-immune inflammatory rheumatic diseases (AIIRD).
After the multidisciplinary expert committee commissioned by EULAR defined the AIIRD, vaccines and immunomodulating drugs to be included in the search, eight key questions were answered. The EULAR recommendations for vaccina-tion in adult patients with AIIRD based on this SLR and expert opinion, using Delphi voting, can be found in chapter 9. Although more research is needed, in particu-lar regarding incidence of vaccine preventable infections (VPI), harms of vacci-nation and the influence of (new and established) immunomodulating agents on vaccination efficacy, 13 recommendations were formulated. Moreover, a research agenda was proposed.
GenerAl diScuSSionIn the studies described in this thesis, we evaluated humoral and CMI responses following influenza vaccination in patients with primary and secondary immuno-deficiencies in order to determine the usefulness of influenza vaccination in these categories of patients. Moreover, (influenza) vaccination can be used as a tool to measure the residual immune response as the resultant of the immunosuppres-sion in immunocompromised patients. When administrating identical antigenic stimuli such as influenza vaccine, the immune response is mainly dependent on host factors.
occurrence of influenza in primary and secondary immunodeficiencies
Influenza infection is clinically asymptomatic in 30-50% of infected cases. It gene-rally presents with an acute illness characterized by fever, chills, sore throat, my-algias, headache and fatigue. Symptoms last an average of 7 days [1, 2]. However, gastro-intestinal symptoms may be most prominent in children, but during the novel influenza A/H1N1 pandemic in 2009 with the influenza virus strain A/H1N1/California/2009 also in adults abdominal complaints frequently occurred as one

202
Cha
pter
10
of the presenting symptoms (3).
Influenza is usually a self-limiting disease, but complications may occur in particu-lar in young children, elderly and immunocompromised hosts. Common complica-tions are exacerbations of underlying respiratory or heart disease. Viral pneumo-nia may occur as well as secondary bacterial pneumonia [1-3]. The last pandemic confirmed the vulnerability of young children, patients with underlying cardiopul-monary diseases and immunocompromised patients [3, 4].
For the specific patient groups addressed in this thesis, however, little is known on the occurrence, morbidity and mortalitiy of influenza infection. Patients with hypogammaglobulinemia (chapter 2 and 3) frequently experience bacterial upper and lower respiratory tract infections [5-7], and it seems logical to assume that the risk of contracting influenza and its morbidity and mortality are increased in patients with hypogammaglobulinemia, because humoral immunity following influenza vaccination correlates with protection from or mitigation of influen-za infection [8]. Moreover, an increasing amount of data supports the role CMI responses in the clearance of influenza [9, 10]. CMI responses are hampered in patients with CVID [5, 11-20]. However, no data are available regarding viral pa-thogens causing respiratory infection is these patients. Therefore, not only the mortality and morbidity resulting from influenza infection remains unknown, it is also impossible to estimate the efficacy of influenza vaccination on clinical end-points in these patients.
In patients with secondary immunodeficiencies (SLE and RA, treated with immu-nosuppressive medication) that we studied in chapter 4, 5, 6, and 7 it has been shown that morbidity and mortality from pulmonary infections is increased, but no studies assessed the causative micro-organisms that led to these pulmonary infections. Two studies that included elderly patients with an increased risk of contracting influenza, among whom patients with rheumatic diseases and vas-culitis, found an increased risk for hospital admission for either pneumonia or influenza and for death, compared to low-risk elderly [21, 22]. A subgroup analysis of patients with rheumatic diseases or vasculitis, however, was not performed. Still, patients with rheumatic diseases should be considered at increased risk of influenza and a complicated course of influenza.
efficacy of influenza vaccination
The aim of vaccination is to reduce the morbidity and mortality, directly or in-directly provoked by the vaccine-preventable disease. Therefore, studies eva-luating the efficacy of vaccination should ideally use clinical endpoints. In case of influenza vaccination, the reduction of microbiologically confirmed influenza

203
Cha
pter
10
infection, the occurrence of influenza-like illness (ILI), influenza-related hospital admission, pneumonia and death have been used as clinical endpoints of studies evaluating the efficacy of influenza vaccination.
On the other hand, ILI can also be caused by many infections other than influenza and for a long time it has been hard to confirm influenza microbiologically, becau-se no sensitive tests for influenza were available (only viral culture and serology). Moreover, vaccine efficacy also depends on the homology between the influenza-strains in the vaccine and the actually circulating influenza-strains. Since influ-enza strains yearly undergo an antigenic change, efficacy of influenza vaccination varies per year and per strain [1, 2]. Therefore, studies investigating efficacy of influenza vaccination on clinical endpoints should investigate their study partici-pants for influenza on a regular basis with a sensitive microbiological test, include large numbers of participants and cover multiple influenza seasons. Such a study is difficult to accomplish, and therefore many studies assessed the efficacy of influenza vaccination by determining surrogate outcome measures.
The most important surrogate parameter is the humoral immune response as determined by hemagglutination inhibition assay (HIA), because this parameter has been shown to correlate with protection from influenza. Hemagglutination inhibition (HI)-titer ≥40 is protective in young healthy adults, and in 90% of healthy young adults HI-titers rise to ≥40 after vaccination [8]. In elderly and most im-munocompromised persons the humoral response following influenza vaccinati-on is suboptimal [23-26]. Moreover, it has never been demonstrated which HI-titer should be strived for in elderly or immunocompromised patients. For example, elderly with very high HI-titers might not be protected from influenza [27-29].
The fact that despite so-called protective antibody levels individuals might not be protected from influenza might be due to an impaired cellular response. The influenza-specific cell mediated immune (CMI) responses following influenza vac-cination are important for the clearance of influenza after infection [10, 27, 29] and can be induced by influenza vaccination, in particular when using whole in-activated virus (WIV)-vaccine or live attenuated influenza-vaccine. In children the production of IFNγ-production has been shown to correlate with protection from influenza [30]. In elderly granzyme-B (as a measure of the effector mechanism of cytotoxic T-lymphocytes), and the ratio between IFNγ and interleukin(IL)-4 (as a measure of the balance between the Th1- and Th2-response) was demonstrated to correlate better with protection from clinical influenza than the HI-titer [27, 29].
In the studies reported in this thesis we evaluated both humoral and CMI respon-ses to determine the efficacy of influenza vaccination in our patient groups with hypogammaglobulinemia, SLE and RA. The humoral immune response was deter-
204
Cha
pter
10
mined with the generally accepted HIA, the CMI response by using IFNγ-ELISpot, flow cytometry with intracellular cytokine staining for IFNγ, IL-2 and tumor ne-crosis factor (TNF)α and CFSE-dye dilution proliferation assay. IFNγ-ELISpot has been demonstrated to be sensitive, but only determines the production of one cytokine by PBMC, a mixture of different white blood cells. The advantage of flow cytometry with intracellular cytokine staining is its capability to determine the production of several cytokines in well defined subsets of PBMC, but it is a la-bour-intensive technique and less sensitive than ELISpot [31]. Finally, the CFSE-dye dilution proliferation assay is the most functional assay, assessing an important aspect of the CMI response: the capability of predefined cell types to proliferate in a clonal fashion in response to a specific antigen. However, none of these para-meters of cellular immunity have been shown to correlate with protection from influenza in the investigated study populations.
In patients with hypogammaglobulinemia, especially in patients with CVID, ham-pered humoral and CMI responses were recorded (chapter 2 and 3). Influenza vaccination did not lead to an increase in seroprotection rates. Pre-existent anti-influenza HI-titers might have resulted from earlier infections or treatment with IVIg. SLE patients seem to have humoral responses following influenza vaccina-tion comparable to HC, but might benefit from a second, booster vaccination if not previously vaccinated. CMI responses following influenza vaccination in SLE-patients did increase, but were lower compared to HC, before as well as following vaccination (chapter 4 and 5). Finally, RA patients treated with rituximab, will not respond to influenza vaccination with a rise in HI-titer or increase in seropro-tection rates, unless the interval after the last administration of rituximab is at least 6-10 months. Also these RA patients demonstrated reduced CMI responses at baseline and following influenza vaccination, indicating an important role for B-cells also in CMI responses.
clinical implications of the findings in this thesis
It is hard to determine the clinical implications of influenza vaccination in the pa-tients categories assessed in this thesis realising that the burden of influenza in these patients is unknown. However, as it is generally accepted that immunocom-promised patients “not-otherwise-defined” are at increased risk of contracting influenza and of a complicated course of influenza, our studies do have implica-tions.
The reduced humoral as well as to CMI responses to influenza vaccination in hy-pogammaglobulinemia patients, especially CVID patients, requests for additional measures to prevent influenza in these patients. Influenza vaccination should be

205
Cha
pter
10
offered to persons caring for or residing with patients with hypogammaglobuli-nemia and post-exposure prophylactic antiviral treatment should be considered in these patients. When influenza is suspected, these patients should be treated empirically.
Recommendations for vaccination in patients with AIIRD (chapter 9), based on a systematic literature research (chapter 8), have recently been developed for the European League against Rheumatism (EULAR). The articles regarding influ-enza vaccination in patients with SLE, and RA patients treated with rituximab, performed by our research group (chapter 5 and 7), contributed to these recom-mendations. Because of the increased risk of pulmonary infections in AIIRD pa-tients, they should be offered influenza vaccination. A booster can be considered in previously unvaccinated patients, as also supported by the reduced response in AIIRD patients vaccinated with the novel non-adjuvanted A/H1N1-vaccine [32]. Furthermore, vaccination of patients treated with rituximab should be administe-red before the start of rituximab, since rituximab severely hampers the immune response to influenza vaccine.
Besides recommendations on influenza vaccination in patients with AIIRD, also all other in Europe available vaccines were addressed in the EULAR recommenda-tions on vaccination in patients with AIIRD (chapter 9). The next, last, step in the assessment of the clinical implications of vaccination is of course the implemen-tation of these recommendations. Several studies show that, despite recommen-dations and guidelines supporting influenza vaccination in patients with AIIRD, only a small proportion of these patients do receive influenza vaccination [33-36]. Therefore, care givers should be informed about the recent EULAR recommen-dations for vaccination in patients with AIIRD during symposia and conferences. For practical implementation general practitioners, and doctors and nurses spe-cialised in the care for patients with AIIRD, need to offer and actually administer the vaccines. One Dutch study revealed that, despite an indication for influenza vaccination according to the guidelines, 262 of 595 patients were not vaccinated. Half of them was not advised about the vaccination, or was even advised to res-train from vaccination. In contrast, 86% of patients with an indication for influenza vaccination according to the guidelines was vaccinated when advised to [37].
FuTure PerSPecTiveSAlthough some questions have been answered in the studies in this thesis, and practical recommendations based in the currently available evidence have been formulated regarding vaccination in patients with AIIRD, still many questions remain unanswered and some additional questions came up. Therefore, there are many opportunities for further research.

206
Cha
pter
10
epidemiology of influenza and its complications in patients with primary im-munodeficiencies and Aiird
As discussed in the general discussion, it is unknown what the extent is of influen-za-related morbidity and mortality in patients with primary immunodeficiencies and AIIRD. Without these data, the efficacy of and also the indication for influenza vaccination remain largely unknown in these patient groups. Also cost-efficacy can not be addressed without this knowledge. Studies investigating the frequen-cy of influenza infection and the morbidity and mortality associated herewith should be performed. Serological studies before and following the influenza sea-son 2009-2010, when the novel influenza A/H1N1 occurred, might provide insight in the epidemiology, although the occurrence of a pandemic is exceptional and because of the large proportion of patients vulnerable for a new influenza virus strain reduces the possibility to extrapolate these data to seasonal flu. Another option would be to determine reference centres treating patients with primary immunodeficiencies and AIIRD that investigate the incidence of particular vacci-ne-preventable infections, among which influenza, during a predefined period. Those reference centers can also evaluate the safety of vaccinations in patients with AIIRD, as limited (however reassuring) data are available, in particular about safety of vaccination in patients treated with newer biologic therapies and/or ac-tive disease.
correlates of protection for influenza
Since large studies assessing clinical endpoint will remain hard to perform in sub-groups of immunocompromised patients, there is a need for good correlates of protection from influenza. Not only should those parameters be determined in healthy adults, also correlates of protection should be defined for immunocom-promised patients, since currently it is uncertain if a HI-titer ≥40 also correlates with protection in these patients. It should also be investigated which parameters for CMI responses following influenza are protective. A good candidate could be granzyme-B [27, 29, 38]. Standardised assays for granzyme-B have recently be-come available. Also the IFNγ/IL-4 ratio should be further explored [27, 29, 38].
more effective immunization of patients with primary immunodeficiency or Aiird
Since influenza-specific immune responses are hampered in the patient groups we investigated in this thesis, more effective immunizations are needed to pro-vide protection from influenza. For example, adjuvants can be added. Alum is well known for its role as an adjuvant. Since it shifts the immune response towards a Th2-response, it leads to better antibody production [39]. Also oil-in-water emul-

207
Cha
pter
10
sion adjuvants, i.e. MF59 and AS03, which enhance the recruitment and activation of antigen presenting cells and therefore induces stronger immune responses following influenza vaccination [40], might be used. Moreover, addition of MF59 leads to cross-protection against influenza-strains that were not included in the vaccine [41]. MF59-adjuvanted influenza A/H1N1v vaccination did not result in an increase in disease activity scores in patients with RA, SLE, or ankylosing spondy-litis [42]. A stronger Th1 response can be induced by using whole virus vaccines, unfortunately these are also more reactogenic [38, 43]. Furthermore, antigens can be offered within a constructed virus envelope, so called virosomes or virus-like particles, leading to both humoral and CTL-responses [43-48]. Besides hemagglu-tinin (HA) and neuraminidase (NA), internal proteins of influenza virus, that are more conserved than HA and NA, can the offered in the virosomes for a better CMI response [48]. Stimulation of Toll-like receptors along with the administration of influenza antigens might lead to better Th1 responses and potentially better protection from influenza [49;50]. Finally, intradermal administration of influenza vaccine could be an option to ameliorate the immune response following influen-za vaccination, since resident dendritic cells in the dermis are able to stimulate in-nate immunity thereby increasing the adaptive immune response to vaccination. This has been shown to be safe and feasible in immunocompromised patients in one study, but CMI responses were not assessed [51].
For all these strategies it remains important to realise that the immune system is stimulated more profoundly and therefore the chance of side effects is incre-ased. In particular for patients with (an increased risk of) auto-immune diseases, the benefit of better influenza-specific immune responses may not outweigh the risks of developing auto-immune phenomena in patients with primary immuno-deficiencies or of disease flares in patients with pre-existent AIIRD.
implementation of the recently developed recommendation for vaccination of patients with Aiird
Finally, the evidence-based recommendations that we developed need to be implemented, so that all patients with AIIRD can take advantage of the available vaccines. Little has been published on implementation of influenza vaccination in these specific patient groups. The available evidence shows increasing coverage when a positive vaccination advise is given by the treating physicians and nurses [37].

208
Cha
pter
10
reference list
(1) Plotkin SA, Orenstein WA, Offit PA. Vaccines. Fifth ed. Philadelphia: Saunders Elsevier, 2008.
(2) Treanor JJ. Mandell, Douglas, and Bennett’s principles and practice of infectious diseases. Influ-
enza virus. 7th ed. Elsevier, 2008.
(3) Bautista E, Chotpitayasunondh T, Gao Z, et al. Clinical aspects of pandemic 2009 influenza A
(H1N1) virus infection. N Engl J Med 2010 May 6; 362(18):1708-19.
(4) Kim YJ, Boeckh M, Englund JA. Community respiratory virus infections in immunocompromised
patients: hematopoietic stem cell and solid organ transplant recipients, and individuals with
human immunodeficiency virus infection. Semin Respir Crit Care Med 2007 Apr; 28(2):222-42.
(5) Cunningham-Rundles C, Bodian C. Common variable immunodeficiency: clinical and immunolo-
gical features of 248 patients. Clin Immunol 1999 Jul; 92(1):34-48.
(6) Oksenhendler E, Gerard L, Fieschi C, et al. Infections in 252 patients with common variable im-
munodeficiency. Clin Infect Dis 2008 May 15; 46(10):1547-54.
(7) Park MA, Li JT, Hagan JB, Maddox DE, Abraham RS. Common variable immunodeficiency: a new
look at an old disease. Lancet 2008 Aug 9; 372(9637):489-502.
(8) Stambas J, Guillonneau C, Kedzierska K, Mintern JD, Doherty PC, La Gruta NL. Killer T cells in
influenza. Pharmacol Ther 2008 Nov; 120(2):186-96.
(9) Thomas PG, Keating R, Hulse-Post DJ, Doherty PC. Cell-mediated protection in influenza infec-
tion. Emerg Infect Dis 2006 Jan; 12(1):48-54.
(10) Giovannetti A, Pierdominici M, Mazzetta F, et al. Unravelling the complexity of T cell abnormali-
ties in common variable immunodeficiency. J Immunol 2007 Mar 15; 178(6):3932-43.
(11) Bayry J, Lacroix-Desmazes S, Kazatchkine MD, et al. Common variable immunodeficiency is as-
sociated with defective functions of dendritic cells. Blood 2004 Oct 15; 104(8):2441-3.
(12) Cunningham-Rundles C, Radigan L, Knight AK, Zhang L, Bauer L, Nakazawa A. TLR9 activation is
defective in common variable immune deficiency. J Immunol 2006 Feb 1; 176(3):1978-87.
(13) Elluru SR, Vani J, Delignat S, et al. Modulation of human dendritic cell maturation and function by
natural IgG antibodies. Autoimmun Rev 2008 Jun; 7(6):487-90.
(14) Kondratenko I, Amlot PL, Webster AD, Farrant J. Lack of specific antibody response in common
variable immunodeficiency (CVID) associated with failure in production of antigen-specific me-
mory T cells. MRC Immunodeficiency Group. Clin Exp Immunol 1997 Apr; 108(1):9-13.
(15) Martinez-Pomar N, Raga S, Ferrer J, et al. Elevated serum interleukin (IL)-12p40 levels in com-
mon variable immunodeficiency disease and decreased peripheral blood dendritic cells: analy-
sis of IL-12p40 and interferon-gamma gene. Clin Exp Immunol 2006 May; 144(2):233-8.
(16) Scott-Taylor TH, Green MR, Raeiszadeh M, Workman S, Webster AD. Defective maturation of
dendritic cells in common variable immunodeficiency. Clin Exp Immunol 2006 Sep; 145(3):420-7.
(17) Stagg AJ, Funauchi M, Knight SC, Webster AD, Farrant J. Failure in antigen responses by T
cells from patients with common variable immunodeficiency (CVID). Clin Exp Immunol 1994 Apr;
96(1):48-53.
(18) Viallard JF, Camou F, Andre M, et al. Altered dendritic cell distribution in patients with common
variable immunodeficiency. Arthritis Res Ther 2005; 7(5):R1052-R1055.
(19) Yong PF, Workman S, Wahid F, Exley A, Webster AD, Ibrahim MA. Selective deficits in blood den-
dritic cell subsets in common variable immunodeficiency and X-linked agammaglobulinaemia
but not specific polysaccharide antibody deficiency. Clin Immunol 2008 Apr; 127(1):34-42.

209
Cha
pter
10
(20) Hak E, Nordin J, Wei F, et al. Influence of high-risk medical conditions on the effectiveness of in-
fluenza vaccination among elderly members of 3 large managed-care organizations. Clin Infect
Dis 2002 Aug 15; 35(4):370-7.
(21) Nichol KL, Wuorenma J, von Sternberg T. Benefits of influenza vaccination for low-, intermedi-
ate-, and high-risk senior citizens. Arch Intern Med 1998 Sep 14; 158(16):1769-76.
(22) de Jong JC, Palache AM, Beyer WE, Rimmelzwaan GF, Boon AC, Osterhaus AD. Haemagglutina-
tion-inhibiting antibody to influenza virus. Dev Biol (Basel) 2003; 115:63-73.
(23) Kroon FP, van Dissel JT, de Jong JC, Zwinderman K, van Furth R. Antibody response after in-
fluenza vaccination in HIV-infected individuals: a consecutive 3-year study. Vaccine 2000 Jul 1;
18(26):3040-9.
(24) Kroon FP, van Dissel JT, de Jong JC, van Furth R. Antibody response to influenza, tetanus and
pneumococcal vaccines in HIV-seropositive individuals in relation to the number of CD4+ lymp-
hocytes. AIDS 1994 Apr; 8(4):469-76.
(25) Thompson WW, Shay DK, Weintraub E, et al. Mortality associated with influenza and respiratory
syncytial virus in the United States. JAMA 2003 Jan 8; 289(2):179-86.
(26) Kunisaki KM, Janoff EN. Influenza in immunosuppressed populations: a review of infection fre-
quency, morbidity, mortality, and vaccine responses. Lancet Infect Dis 2009 Aug; 9(8):493-504.
(27) McElhaney JE, Xie D, Hager WD, et al. T cell responses are better correlates of vaccine protec-
tion in the elderly. J Immunol 2006 May 15; 176(10):6333-9.
(28) Gravenstein S, Drinka P, Duthie EH, et al. Efficacy of an influenza hemagglutinin-diphtheria
toxoid conjugate vaccine in elderly nursing home subjects during an influenza outbreak. J Am
Geriatr Soc 1994 Mar; 42(3):245-51.
(29) McElhaney JE, Ewen C, Zhou X, et al. Granzyme B: Correlates with protection and enhanced CTL
response to influenza vaccination in older adults. Vaccine 2009 Apr 21; 27(18):2418-25.
(30) Forrest BD, Pride MW, Dunning AJ, et al. Correlation of cellular immune responses with protec-
tion against culture-confirmed influenza virus in young children. Clin Vaccine Immunol 2008 Jul;
15(7):1042-53.
(31) Karlsson AC, Martin JN, Younger SR, et al. Comparison of the ELISPOT and cytokine flow cyto-
metry assays for the enumeration of antigen-specific T cells. J Immunol Methods 2003 Dec;
283(1-2):141-53.
(32) Saad CG, Borba EF, Aikawa NE, et al. Immunogenicity and safety of the 2009 non-adjuvanted
influenza A/H1N1 vaccine in a large cohort of autoimmune rheumatic diseases. Ann Rheum Dis
2011 Jun; 70(6):1068-73.
(33) Bridges MJ, Coady D, Kelly CA, Hamilton J, Heycock C. Factors influencing uptake of influenza
vaccination in patients with rheumatoid arthritis. Ann Rheum Dis 2003 Jul; 62(7):685.
(34) Pradeep J, Watts R, Clunie G. Audit on the uptake of influenza and pneumococcal vaccination in
patients with rheumatoid arthritis. Ann Rheum Dis 2007 Jun; 66(6):837-8.
(35) Doe S, Pathare S, Kelly CA, Heycock CR, Binding J, Hamilton J. Uptake of influenza vaccination in
patients on immunosuppressant agents for rheumatological diseases: a follow-up audit of the
influence of secondary care. Rheumatology (Oxford) 2007 Apr; 46(4):715-6.
(36) Feuchtenberger M, Kleinert S, Schwab S, et al. Vaccination survey in patients with rheumatoid
arthritis: a cross-sectional study. Rheumatol Int 2011 Feb 15.
(37) Meynaar IA, ‘t Wout JW, Vandenbroucke JP, van Furth R. [Implementation of influenza vaccina-
tion in 3 hospitals]. Ned Tijdschr Geneeskd 1992 Jan 25; 136(4):180-3.

210
Cha
pter
10
(38) Jordan MB, Mills DM, Kappler J, Marrack P, Cambier JC. Promotion of B cell immune responses
via an alum-induced myeloid cell population. Science 2004 Jun 18; 304(5678):1808-10.
(39) Durando P, Icardi G, Ansaldi F. MF59-adjuvanted vaccine: a safe and useful tool to enhance and
broaden protection against seasonal influenza viruses in subjects at risk. Expert Opin Biol Ther
2010 Apr; 10(4):639-51.
(40) Ansaldi F, Canepa P, Parodi V, et al. Adjuvanted seasonal influenza vaccines and perpetual viral
metamorphosis: the importance of cross-protection. Vaccine 2009 May 26; 27(25-26):3345-8.
(41) Ori E, Sharon A, Ella M, et al. The efficacy and safety of vaccination against pandemic 2009 influ-
enza a (H1N1) virus among patients with rheumatic diseases. Arthritis Care Res (Hoboken ) 2011
Mar 18.
(42) McElhaney JE. Influenza vaccination in the elderly: seeking new correlates of protection and
improved vaccines. Aging health 2008 Dec 1; 4(6):603-13.
(43) Saurwein-Teissl M, Zisterer K, Schmitt TL, Gluck R, Cryz S, Grubeck-Loebenstein B. Whole virus
influenza vaccine activates dendritic cells (DC) and stimulates cytokine production by peripheral
blood mononuclear cells (PBMC) while subunit vaccines support T cell proliferation. Clin Exp Im-
munol 1998 Nov; 114(2):271-6.
(44) Bungener L, Huckriede A, de Mare A, Vries-Idema J, Wilschut J, Daemen T. Virosome-mediated
delivery of protein antigens in vivo: efficient induction of class I MHC-restricted cytotoxic T
lymphocyte activity. Vaccine 2005 Jan 26; 23(10):1232-41.
(45) Herzog C, Hartmann K, Kunzi V, et al. Eleven years of Inflexal V-a virosomal adjuvanted influenza
vaccine. Vaccine 2009 Jul 16; 27(33):4381-7.
(46) Huckriede A, Bungener L, Ter Veer W, et al. Influenza virosomes: combining optimal presenta-
tion of hemagglutinin with immunopotentiating activity. Vaccine 2003 Feb 14; 21(9-10):925-31.
(47) Huckriede A, Bungener L, Stegmann T, et al. The virosome concept for influenza vaccines. Vac-
cine 2005 Jul 8; 23 Suppl 1:S26-S38.
(48) Song JM, Van Rooijen N, Bozja J, Compans RW, Kang SM. Vaccination inducing broad and impro-
ved cross protection against multiple subtypes of influenza A virus. Proc Natl Acad Sci U S A 2011
Jan 11; 108(2):757-61.
(49) Geeraedts F, Goutagny N, Hornung V, et al. Superior immunogenicity of inactivated whole virus
H5N1 influenza vaccine is primarily controlled by Toll-like receptor signalling. PLoS Pathog 2008;
4(8):e1000138.
(50) Taylor DN, Treanor JJ, Strout C, et al. Induction of a potent immune response in the elderly
using the TLR-5 agonist, flagellin, with a recombinant hemagglutinin influenza-flagellin fusion
vaccine (VAX125, STF2.HA1 SI). Vaccine 2011 May 16.
(51) Gelinck LB, van den Bemt BJ, Marijt WA, et al. Intradermal influenza vaccination in immunocom-
promized patients is immunogenic and feasible. Vaccine 2009 Apr 21; 27(18):2469-74.


CHAPT
ER11Nederlandse s a m e n -v a t t i n g
D a n k w o o r d
L i s t o f s e l e c t e d publications


215
Cha
pter
11
NederlANdse sAmeNvATTiNg
introductie
Eind 18de eeuw verscheen de eerste wetenschappelijke publicatie over vaccina-tie, toen nog “variolatie” genoemd. Al ruim voordien, ca. 400 jaar voor Christus, was het de Grieken opgevallen dat iemand die eenmaal de pokken had gehad, dit vervolgens de rest van zijn leven niet meer zou krijgen. Deze waarneming is in feite de basis voor vaccinatie, waarbij van dit principe gebruik wordt gemaakt. Rond het jaar 1000 na Christus probeerde men in China en India door het toedie-nen van een gedroogde vorm van pus van personen met pokken een besmetting op te wekken die niet fataal was, maar wel bescherming voor pokken bood na-dien. Via de Kaukasus bereikte deze strategie Turkije, waar het gunstige effect van variolatie in het begin van de 18de eeuw werd opgemerkt door de echtge-note van de Britse ambassadeur in Constantinopel, Lady Mary Worthley Montagu. Zij liet haar kinderen varioleren en gaf bekendheid aan variolatie onder de Britse upperclass. Edward Jenner, Brits plattelandsdokter en zelf gevarioleerd in 1750 als 8-jarige jongen, was in 1798 de eerste die publiceerde over zijn experimenten waarin hij koepokken i.p.v. de echte pokken toediende aan o.a. een 8-jarige jongen genaamd James Phipps. Dit bleek effectief om pokken te voorkomen, en tevens veel veiliger dan toediening van echte pokken. Jenner was echter niet de eerste die koepokken gebruikte om pokken te voorkomen. Benjamin Jesty, een veehou-der in North Dorset, had al eerder opgemerkt dat melkmeisjes na het oplopen van koepokken geen pokken meer kregen, ondanks blootstelling aan pokken. Jesty bracht, 22 jaar vóór de experimenten van Jenner, met een breinaald koepokken in in de huid van zijn vrouw en zoons en zij bleken daarna beschermd voor pokken tijdens vele daaropvolgende blootstellingen. Nadat Jenner al uitgebreid was ge-lauwerd als ontdekker van vaccinatie, werd in 1805 Benjamin Jesty alsnog geëerd voor zijn bijdrage aan de ontdekking van het beschermende effect van koepokken tegen pokken. De echtgenote van Jesty liet op zijn grafsteen ingraveren dat hij de eerste was die koepokken toediende ter preventie van pokken. Inmiddels is door vaccinatie pokken uitgeroeid en heeft vaccinatie geleid tot een enorme daling in sterfte aan en ziekte door diverse infectieziekten. Hiertoe behoort ook influenza, waartegen in de jaren ’40 van de vorige eeuw een vaccin werd uitgevonden dat nog steeds de basis vormt voor de huidige influenzavaccins.
de werking van vaccinatie
Om te voorkomen dat een micro-organisme het lichaam binnendringt en ziek maakt, beschikt het lichaam over een afweersysteem. Dit afweersysteem is op-gebouwd uit verschillende componenten, die kunnen worden onderscheiden in

216
Cha
pter
11
niet-specifieke en specifieke componenten van de afweer. De niet-specifieke af-weer geeft een algemene bescherming tegen een micro-organismen. Voorbeel-den hiervan zijn de huid die geen bacteriën naar binnen laat of de urinestroom naar buiten toe waardoor bacteriën moeilijk via de plasbuis de blaas kunnen be-reiken. Als deze barrières zijn doorbroken zijn er niet-specifieke afweereiwitten (zoals complement) en niet-specifieke afweercellen (zoals macrofagen en neu-trofiele granulocyten) die bescherming bieden, ongeacht de precieze structuur van het micro-organisme dat probeert binnen te dringen. Hiertoe behoren ook zgn. antigeenpresenterende cellen (APCs), die als stofzuigers de indringende micro-organismen opnemen en vervolgens deze in onderdelen aanbieden aan afweercellen van het specifieke afweersysteem. Het specifieke afweersysteem bestaat uit cellen die antistoffen maken specifiek gericht tegen een bepaald mi-cro-organisme (B-lymfocyten, plasmacellen), afweercellen die geïnfecteerde li-chaamscellen aanvallen (cytotoxische T-cellen, ofwel CD8+ T-cellen) en zgn. CD4+ T-cellen, die hulp bieden aan de B-lymfocyten en cytotoxische T-cellen om hun functie optimaal uit te voeren.
Als het specifieke afweersysteem tegen een bepaald micro-organisme al eens eerder een afweerreactie heeft gemaakt, ontstaan er tevens geheugencellen. Hierdoor kan bij een nieuwe blootstelling aan dit micro-organisme het afweer-systeem sneller optreden door binnen een korte termijn de geheugencellen van het specifieke afweersysteem in actie te laten komen. Verder zullen bij een her-haalde blootstelling kwalitatief betere afweercellen en antistoffen geproduceerd worden dan bij een eerste blootstelling. Op dit geheugen is het principe van vac-cinatie gebaseerd. Door het afweersysteem reeds voordat een bepaald micro-organisme is binnengedrongen kennis te laten maken met (onderdelen van) dit micro-organisme door ermee te vaccineren, kan men het afweersysteem alvast laten oefenen om een specifieke reactie hiertegen te maken. Bij werkelijke bloot-stelling aan het micro-organisme heeft het afweersysteem vervolgens sneller en effectiever de verdediging paraat.
Om infectie met influenzavirus te voorkómen zijn vooral de vorming van antistof-fen door het specifieke afweersysteem tegen eiwitten op het oppervlak van het influenzavirus (hemagglutinine en in mindere mate neuraminidase) van belang. Omdat de oppervlakte-eiwitten van influenza (vrijwel) jaarlijks enigszins veran-deren en met grotere tussenpozen geheel veranderen, dient het influenzavaccin elk jaar aangepast te worden aan deze veranderingen. Naast antistoffen blijken ook cytotoxische T-cellen en CD4+ T-cellen een rol te spelen bij het voorkómen van influenza. De cytotoxische T-cellen en CD4+ T-cellen zijn niet alleen tegen oppervlakte eiwitten van influenza gericht, maar ook tegen interne eiwitten en structuren van influenza. Een vaccin dat goed deze cellen stimuleert, maakt dat

217
Cha
pter
11
jaarlijkse aanpassing van het vaccin misschien niet meer nodig is, omdat deze interne eiwitten niet een jaarlijkse verandering ondergaan. Bovendien zou een dergelijk vaccin bescherming kunnen bieden aan personen die niet in staat zijn om antistoffen te produceren, bijvoorbeeld omdat de antistofproducerende cel-len onvoldoende aanwezig zijn door een aangeboren afweerstoornis of door me-dicatie zijn verdwenen.
Uit bovenstaande blijkt dat voor het verkrijgen van het beoogde effect van vac-cinatie, nl. een gerichte afweerreactie oproepen, er een adequaat functionerend afweersysteem moet zijn. Dit brengt met zich mee dat bij personen met een min-der goed functionerend afweersysteem vaccinatie ter preventie van een infectie in veel gevallen minder effectief zal zijn dan bij gezonde personen. Anderzijds zijn het juist personen met een verminderd functionerend afweersysteem die veel baat zouden kunnen hebben bij vaccinatie, omdat zij een verhoogd risico lopen infecties te krijgen en deze infecties vaak ernstiger verlopen dan bij mensen met een normale afweer.
doelstellingen van het onderzoek beschreven in dit proefschrift
De onderzoeken beschreven in dit proefschrift zijn uitgevoerd bij personen met een verminderde afweer, waarbij wij verschillende aspecten van de afweerre-actie voor en na toediening van influenzavaccinatie hebben onderzocht. Het be-treft hierbij verschillende categorieën van afweerstoornis. Ten eerste hebben we onderzoek gedaan naar influenzavaccinatie bij patiënten met een aangebo-ren (primaire) afweerstoornis. In dit proefschrift zijn dat patiënten bij wie het afweersysteem onvoldoende antistoffen produceert, een zgn. hypogammaglo-bulinemie. Door dit tekort aan antistoffen is bij deze patiënten de kans verhoogd op het oplopen van bijholteontstekingen, longontstekingen, maag/darm infecties, maar ook op auto-immuunziekten en sommige vormen van kanker. Bovendien blijkt bij een groot deel van de patiënten met een hypogammaglobulinemie ver-oorzaakt door de aandoening “common variable immunodeficiency” er niet alleen een tekort te zijn aan antistoffen, maar ook van niet goed functionerende afweer-cellen. Deze patiënten wordt geadviseerd zich jaarlijks te laten vaccineren tegen influenza, echter de vraag is hoe effectief dat is bij hun ondermaats functione-rende afweersysteem. Daarom werd dit door ons onderzocht. Ten tweede onder-zochten we de effectiviteit en veiligheid van influenzavaccinatie bij patiënten met een verworven (niet-aangeboren, secundaire) afweerstoornis. In dit proefschrift zijn twee patiëntengroepen bestudeerd met verschillende auto-immuunziekten: systemische lupus erythematodes en reumatoïde artritis. Beide ziektes worden veroorzaakt door een ontregeling van het afweersysteem, waardoor de afweer lichaamseigen cellen aanvalt. De ziekten zelf kunnen leiden tot verminderd func-
218
Cha
pter
11
tioneren van de afweer, bijvoorbeeld door een tekort aan (bepaalde soorten van) witte bloedcellen of van complementeiwitten. Ook wordt de afweer verminderd bij deze ziekten door het gebruik van afweeronderdrukkende medicijnen, met als doel om de afweer die zich tegen de eigen organen heeft gekeerd tot rust te brengen. Voorbeelden van deze medicijnen zijn prednison, methotrexaat, TNFα-blokkers en rituximab. Rituximab is een medicament dat leidt tot totale verwij-dering uit het bloed van B-lymfocyten, die essentieel zijn voor de productie van antistoffen. Door het gebruik van afweeronderdrukkende medicatie worden deze patiënten echter ook vatbaarder voor infecties. Daarom wordt ook aan patiënten met een secundaire afweerstoornis geadviseerd om zich jaarlijks te laten vac-cineren tegen influenza, maar ook voor hen geldt dat onzeker is hoe effectief dit is. Bovendien is de veiligheid van vaccinatie van speciaal belang bij patiënten met een auto-immuunziekte, omdat verondersteld wordt dat door stimulatie van het afweersysteem door vaccinaties ook de aanwezige auto-immuunziekte kan verergeren.
De doelstelling van het onderzoek beschreven in dit proefschrift was het ver-krijgen van meer inzicht in de effectiviteit en veiligheid van influenzavaccinatie bij patiënten met een primaire (aangeboren) en secundaire (verworven) afweer-stoornis, en tot het komen van goed onderbouwde aanbevelingen voor vaccinatie van deze patiëntengroepen.
Uitkomsten van de in dit proefschrift beschreven onderzoeken
Deel 1 van dit proefschrift beschrijft het onderzoek dat we uitvoerden bij patiën-ten met een primaire afweerstoornis waarbij er sprake is van een aangeboren tekort aan antistoffen, een zgn. hypogammaglobulinemie. Patiënten met een hy-pogammaglobulinemie blijken onvoldoende in staat te zijn om na een influenza-vaccinatie beschermende antistoffen tegen influenza te vormen (hoofdstuk 2). Ook toonden we aan dat de patiënten die lijden aan een “common variable im-munodefeciency”, een vorm van hypogammaglobulinemie, ook in mindere mate in staat zijn een tegen influenza gerichte afweerreactie door afweercellen als cy-totoxische T-cellen en CD4+ T-cellen op gang te brengen na influenzavaccinatie (hoofdstuk 3). Daarom lijkt het verstandig bij deze patiënten niet te vertrouwen op alleen een influenzavaccinatie ter bescherming van influenza, maar aanvullende maatregelen te nemen: vaccineren van de huisgenoten en verzorgenden van deze patiënten en vroegtijdig behandelen met medicijnen tegen influenza bij een ver-denking op een infectie met influenza.
In deel 2 wordt het onderzoek beschreven naar influenzavaccinatie bij patiënten met een secundaire afweerstoornis t.g.v. auto-immuunziekten en de behande-
219
Cha
pter
11
ling met afweeronderdrukkende medicatie. Hoofdstukken 4 en 5 betreffen beide studies naar effect van influenzavaccinatie bij patiënten met systemische lupus erythematodes, waarbij in hoofdstuk 4 zowel antistofproductie tegen influenza en afweer door afweercellen werd onderzocht. De antistofproductie na influen-zavaccinatie bleek lager te zijn in vergelijking met gezonde controlepersonen. Ook de afweerreactie tegen influenza door specifieke afweercellen van het im-muunsysteem bleek zich na vaccinatie minder goed te hebben ontwikkeld, in het bijzonder als de patiënten prednison of azathioprine gebruikten, twee afweeron-derdrukkende medicamenten. Met als doel de antistofproductie tegen influenza na vaccinatie te verbeteren, werd in hoofdstuk 5 in plaats van één maal nu twee maal tegen influenza gevaccineerd. De tweede, zgn. boostervaccinatie, vond vier weken na de eerste vaccinatie plaats. Helaas had dit geen toegevoegde waarde bij de onderzochte patiënten, met uitzondering van de patiënten die het jaar ervoor niet voor influenza waren gevaccineerd. Zij hadden wel extra baat bij een tweede influenzavaccinatie.
Een ander groep patiënten met een secundaire afweerstoornis die we onderzoch-ten waren reumapatiënten die waren behandeld met rituximab (hoofdstukken 6 en 7). Rituximab leidt tot het verdwijnen uit het bloed van B-cellen, die een sleutel-rol spelen bij antistofproductie, maar ook een rol vervullen bij het aanbieden van (onderdelen van) micro-organismen en andere lichaamsvreemde substanties aan CD4+ T-cellen. Daarom werden zowel de antistofproductie als de afweer door af-weercellen bestudeerd bij met rituximab behandelde reumapatiënten (hoofdstuk 6). Er werden twee groepen gevormd: een groep van patiënten die 4-8 weken te-voren met rituximab waren behandeld en geen aantoonbare hoeveelheden B-cel-len meer in hun bloed hadden, en een groep patiënten die 6-10 maanden tevoren met rituximab waren behandeld, het tijdstip waarop doorgaans de B-cellen weer in het bloed terugkeren. Patiënten die met rituximab waren behandeld waren niet in staat een beschermende hoeveelheid antistoffen tegen influenza te maken. Bij het deel van de patiënten die 6-10 maanden tevoren rituximab hadden ontvangen was wel enige stijging van de hoeveelheid antistoffen tegen influenza door de vaccinatie, maar nog altijd onvoldoende om bescherming te bieden tegen influ-enza. Ook de afweercellen bleken bij patiënten met rituximab-behandeling niet zo goed te functioneren tegen influenza als bij gezonde personen (hoofdstuk 7). Bo-vendien bleek dat bij de patiënten die rituximab gebruikt hadden de stimulatie van de afweercellen met een algemene stimulus, waarop de afweercellen doorgaans signaalstoffen gaan produceren, te leiden tot een verminderde afweerreactie ten opzichte van gezonde personen. Hieruit kan afgeleid worden dat het verstandig is reumapatiënten te vaccineren met influenzavaccin een aantal weken voordat de behandeling met rituximab wordt gestart.

220
Cha
pter
11
Een vertaling van de onderzoeksresultaten van de bovengenoemde studies (en vele andere) naar de praktijk werd gemaakt in deel 3 van dit proefschrift. Namens de European League Against Rheumatism (EULAR) werden door een team van internationale experts op het gebied van reumatologie, klinische immunologie, nierziekten, infectieziekten, kinder-reumatologie/immunologie en klinische epi-demiologie aanbevelingen opgesteld, gebaseerd op de beschikbare wetenschap-pelijke medische literatuur (hoofdstuk 9). Gezocht werd naar literatuur over alle auto-immuun reumatsche aandoeningen in combinatie met alle in Europa beschik-bare vaccins. Bovendien werd de invloed van afweeronderdrukkende medicatie op de effectiviteit en veiligheid van deze vaccins bij deze patiënten nagegaan. Om te komen tot de 13 aanbevelingen werden acht belangrijke vragen opgesteld t.a.v. vaccinatie bij patiënten met een auto-immuun reumatische aandoening. De antwoorden op deze vragen, voor zover mogelijk gebaseerd op de wetenschap-pelijke bewijzen in de medische literatuur, zijn terug te vinden in hoofdstuk 8.
Conclusies en een blik op de toekomst
De respons op influenzavaccinatie is gestoord bij patiënten met een humorale primaire afweerstoornis, patiënten met systemische lupus erythematodes en pa-tiënten met reumatoïde artritis. Dit geldt zowel voor de productie van antistoffen als voor de afweer door specifieke afweercellen. Daarom zouden bij patiënten met een primaire humorale afweerstoornis huisgenoten en verzorgenden ge-vaccineerd moet worden, zodat de kans verkleind wordt dat influenza door deze personen overgebracht wordt op de patiënt. Ook dienen deze patiënten bij een verdenking op infectie met influenza hiervoor behandeld te worden.
Patiënten met systemische lupus erythematodes dienen influenzavaccinatie te ontvangen, waarbij overwogen kan worden om een boostervaccinatie toe te die-nen bij patiënten die in het jaar ervoor geen influenzavaccinatie hebben ontvan-gen.
Vaccinatie voor influenza lijkt de eerste vier tot acht weken na behandeling met rituximab niet zinvol. Daarom zou een influenzavaccinatie toegediend moeten worden vóór het starten van de behandeling met rituximab. Aangezien voor alle patiënten met reumatoïde artritis jaarlijkse influenzavaccinatie wordt aanbevo-len, en rituximab pas wordt toegediend in de fase dat andere reumabehandelin-gen onvoldoende effect hebben gehad, zou dit gemeengoed moeten zijn.
Onderzoek is nooit klaar, over het algemeen werpt het meer vragen op. In de toekomst zou onderzoek zich moeten richten op het verkrijgen van een beter inzicht in de werkelijke hoeveelheid influenza infecties bij patiënten met een afweerstoornis en ook hoe ernstig die gevallen verlopen. Aangezien influenza-
221
Cha
pter
11
vaccinatie minder effectief blijkt te zijn bij de patiëntengroepen beschreven in dit proefschrift, zijn nieuwe vaccinatie strategieën nodig om de effectiviteit van influenzavaccinatie bij deze patiënten te vergroten. De ontwikkeling van nieuwe influenzavaccins die op andere wijze het afweersysteem stimuleren of van an-dere toedieningswijzen, om zo een krachtigere respons op te wekken, is in volle gang. Zeker bij patiënten met auto-immuunziekten is nog meer inzicht nodig in de veiligheid van vaccinatie. De huidige beschikbare onderzoeken betreffen te kleine aantallen patiënten om met voldoende zekerheid te kunnen stellen dat vaccinatie bij patiënten met een auto-immuunziekte veilig is, alhoewel deze onderzoeken wel alle in dezelfde richting wijzen, nl. dat de bijwerkingen niet toegenomen zijn. Tot slot verschijnen er met grote regelmaat nieuwe afweerdrukkende medica-menten op de markt, die gebaseerd zijn op nieuwe werkingsmechanismen. Ken-nis van de effectiviteit en veiligheid van vaccinatie tijdens gebruik van deze nieu-were middelen is uiteraard ook noodzakelijk.
Kortom, wordt vervolgd…


223
Cha
pter
11
dANkwoord U hebt het dankwoord gevonden, maar nu is de vraag: staat u erin? De kans is klein, omdat ik vind dat hier alleen diegenen bedankt moeten worden die wer-kelijk een substantiële bijdrage hebben geleverd aan het tot stand komen van dit proefschrift. Hiermee volg ik voorschriften van de Leidse faculteit Sociale Wetenschappen, die stellen dat het dankwoord niet bedoeld is om je dank uit te spreken naar “God, hond en jaarclub”. Overigens hebben deze alle drie geen plaats in mijn leven.Om te beginnen wil ik alle patiënten en gezonde vrijwilligers die mee hebben ge-daan aan de in dit proefschrift beschreven studies ontzettend bedanken voor de tijd en moeite die ze hiervoor hebben genomen. Zeker voor een aantal patiënten was dit geen sinecure, maar hun motivatie was bewonderenswaardig.
Dan de personen die mij begeleid hebben bij het onderzoek: van hen wil ik als eer-ste mijn promotor Cees Kallenberg bedanken. Je goede naam en grote kwaliteiten waren bij mijn vertrek uit Nijmegen al door Jos van der Meer genoemd en er was geen woord onwaar. En naast je enorme deskundigheid als onderzoeker (zie de vele andere dankwoorden in door Cees begeleide proefschriften), waarvan ik heb mogen profiteren, wil ik graag benadrukken dat je ook nog eens (ik zou bijna zeg-gen desondanks) een bijzonder aimabele en bindende persoon bent. We zullen je missen na jouw emeritaat, al hoop ik ook daarna nog eens een djogo met jou en Dieneke te mogen delen.
Marc Bijl, jou ben ik zeker de meeste dank verschuldigd. Een betere copromotor had ik mij niet kunnen wensen. Ondanks goede redenen om eens een keer niet thuis te geven, stond je altijd klaar met altijd weer even terechte en consistente commentaren. Ooit hoop ik net zo goed in onderzoek te worden als jij, een toga zou je niet misstaan! Het Martini ziekenhuis zij gefeliciteerd met jouw keuze voor hen.
Aalzen de Haan, mijn tweede copromotor, hopelijk blijf jij voorlopig wel in het UMCG. Veel dank ben ik je verschuldigd voor je optreden als “routeplanner” bij mijn tocht door de voor mij ondoorgrondelijke jungle genaamd immunologie. “Quick and dirty” kregen door jouw invulling een nieuwe, zelfs positieve betekenis.
Verder wil ik Bert Holvast bedanken. Zeker in mijn positie, als parttime promo-vendus, heb ik enorm kunnen en mogen profiteren van al jouw verkennende werk en je hulp bij mijn studies. Hopelijk kruisen onze wegen elkaar weer in onder-zoeksland na het afronden van jouw opleiding tot kinderarts.
Zonder input en output vanuit het immunologie laboratorium was dit onderzoek niet mogelijk geweest. Hannie Westra en Gerda Horst, jullie hebben zowel een be-

224
Cha
pter
11
langrijke inhoudelijke bijdrage geleverd als een enorme hoop werk uit mijn klun-zige handen genomen (het meten van de cel-gemedieerde immuunresponsen). Heel erg bedankt! Van het Laboratorium voor Infectieziekten wil ik René Benne, Gioia Smid en Eline Bloemink bedanken voor hun denk- en handwerk bij de he-magglutinatie remmingstest. Ook alle andere analisten die mij hebben geholpen bedank ik: Johan Bijzet, Berber Doornbos-v/d Meer, Minke Huitema, Marcel v/d Leij en Bessel Schaap, en daarnaast studenten Linda Gorter en Kim van Lieshout.
Veel hulp heb ik gehad bij ditjes en DAS’jes van de stafleden, nurse practitioners, AIOS en administratieve medewerkers van de afdeling reumatologie/klinische immunologie, in het bijzonder van Miek van Leeuwen, Marcel Posthumus, Judith Vierdag, Ina Holwerda, Eefke Eppinga en Diana Nijborg, waarvoor mijn dank.
Mijn mede-auteurs dank ik voor hun inbreng in de studies en manuscripten.
Promotie onderzoek doen tijdens een fulltime baan viel niet (altijd) mee. Gelukkig hebben mijn collega’s van de werkgroep infectieziekten mij regelmatig kunnen ontzien waardoor ik net even een paar extra uurtjes had om tot een afronding te komen. Herman, Piet, Tjip, Jan, Rita, Wouter, Cari, Dorien, Ymkje en Kasper (in volgorde van anciënniteit), bedankt! Ik zal jullie steun ook nog hard nodig hebben voor het binnenhalen van de begeerde opleiding in het aandachtsgebied infectie-ziekten.
Rijk Gans, als afdelingshoofd van de interne geneeskunde wil ik je bedanken voor je vertrouwen dat ik de eindstreep zou halen.
Zelf vind ik dit proefschrift esthetisch ook zeer verantwoord. Alle lof daarvoor komt mijn broer Luite toe. Luite, je bent niet alleen altijd heel creatief en perfec-tionistisch, maar ook uitermate gezellig om langdurig mee achter de MacBook te zitten. We moeten op zoek naar een andere reden om elkaar zo regelmatig te blijven zien, spreken en SMS-en.
Sander en Arto, jullie bereidheid om je op te laten tuigen tot mijn paranimfen leidt tot een heugelijk feit: de hereniging van “Medrieco”, de drie aan de Rusthoflaan in het Rotterdamse Crooswijk wonende medico’s. We zien elkaar te weinig, maar wat telt is de kwaliteit!
Ik sluit mijn dankwoord af met Hilma, Sam en Sophie. Ik zal niet beweren dat het proefschrift zonder jullie er nooit was gekomen, maar dan wel zonder jullie liefde, warmte, steun en kritiek. Ik ga hier ook niet zeggen hoe veel ik van jullie houd. Er zijn vele andere manieren om dat te laten merken en daar ga ik nu maar eens werk van maken!



227
Cha
pter
11
lisT of seleCTed PUbliCATioNs(1) van Assen S, de Haan A, Voskuyl AE, Holvast A,Horst G, Westra J, Posthumus MD, van Leeuwen
MA, Blom M, Risselada AP, Kallenberg CGM, Bijl M. Polyclonal and influenza-specific cell-medi-
ated immune responses are hampered in rheumatoid arthritis patients treated with rituximab.
Submitted
(2) van Assen S, de Haan A, Holvast A, Horst G, Gorter L, Westra J, Kallenberg CGM, Telgt DCS,
Palache AM, Giezeman KM, Bijl M. Cell-mediated immune responses to inactivated trivalent
influenza-vaccination are decreased in patients with common variable immunodeficiency. Clin
Immunol. In press
(3) Arends JE, van Assen S, Stek CJ, Wensing AMJ, Fransen JH, Schellens IM, Spijkers SNM,
Mudrikova T, van Baarle D, Sprenger HG, Hoepelman AIM. Peginterferon-alfa mono-therapy
leads to low response rates in HIV-infected patients with acute hepatitis C. Antiviral Ther. In
press
(4) Rachinger A, Groeneveld PH, van Assen S, Lemey P, Schuitemaker H. Time-measured phyloge-
nies of gag, pol and env sequence data reveal the direction and time interval of HIV-1 transmis-
sion. AIDS 2011 May;25(8):1035-9
(5) van Assen S, Elkayam O, Agmon-Levin N, Cervera R, Doran MF, Dougados M, Emery P, Geborek
P, Ioannidis JP, Jayne DR, Kallenberg CG, Müller-Ladner U, Shoenfeld Y, Stojanovich L, Valesini
G, Wulffraat NM, Bijl M. Vaccination in adult patients with auto-immune inflammatory rheu-
matic diseases: a systematic literature review for the European League Against Rheumatism
evidence-based recommendations for vaccination in adult patients with auto-immune inflam-
matory rheumatic diseases. Autoimmun Rev 2011 Apr;10(6):341-52
(6) van Assen S, Agmon-Levin N, Elkayam O, Cervera R, Doran MF, Dougados M, Emery P, Geborek
P, Ioannidis JP, Jayne DR, Kallenberg CG, Müller-Ladner U, Shoenfeld Y, Stojanovich L, Valesini
G, Wulffraat NM, Bijl M. EULAR recommendations for vaccination in adult patients with autoim-
mune inflammatory rheumatic diseases. Ann Rheum Dis. 2011 Mar;70(3):414-22
(7) Stek CJ, van Eijk JJ, Jacobs BC, Enting RH, Sprenger HG, van Alfen N, van Assen S. Neuralgic
amyotrophy associated with Bartonella henselae infection. J Neurol Neurosurg Psychiatry 2011
Jun;82(6):707-8
(8) van Assen S, Holvast A, Telgt DS, Benne CA, de Haan A, Westra J, Kallenberg CG, Bijl M. Patients
with humoral primary immunodeficiency do not develop protective anti-influenza antibody ti-
ters after vaccination with trivalent subunit influenza vaccine. Clin Immunol 2010 Aug;136(2):228-
35
(9) Alffenaar JW, van Assen S, de Monchy JG, Uges DR, Kosterink JG, van der Werf TS. Intravenous
voriconazole after toxic oral administration. Antimicrob Agents Chemother 2010 Jun;54(6):2741-
2
(10) van Assen S, Holvast A, Benne CA, Posthumus MD, van Leeuwen MA, Voskuyl AE, Blom M, Risse-
lada AP, de Haan A, Westra J, Kallenberg CG, Bijl M. Humoral responses after influenza vaccina-
tion are severely reduced in patients with rheumatoid arthritis treated with rituximab. Arthritis
Rheum 2010 Jan;62(1):75-81
(11) Hagen F, van Assen S, Luijckx GJ, Boekhout T, Kampinga GA. Activated dormant Cryptococcus
gattii infection in a Dutch tourist who visited Vancouver Island (Canada): a molecular epidemio-
logical approach. Med Mycol 2010 May;48(3):528-31

228
Cha
pter
11
(12) Holvast A, van Assen S, de Haan A, Huckriede A, Benne CA, Westra J, Palache A, Wilschut J, Kal-
lenberg CG, Bijl M. Effect of a second, booster, influenza vaccination on antibody responses in
quiescent systemic lupus erythematosus: an open, prospective, controlled study. Rheumatology
(Oxford) 2009 Oct;48(10):1294-9
(13) Holvast A, van Assen S, de Haan A, Huckriede A, Benne CA, Westra J, Palache A, Wilschut J,
Kallenberg CG, Bijl M. Studies of cell-mediated immune responses to influenza vaccination in
systemic lupus erythematosus. Arthritis Rheum 2009 Aug;60(8):2438-47
(14) Holvast A, de Haan A, van Assen S, Stegeman CA, Huitema MG, Huckriede A, Benne CA, Westra
J, Palache A, Wilschut J, Kallenberg CG, Bijl M. Cell-mediated immune responses to influenza
vaccination in Wegener’s granulomatosis. Ann Rheum Dis 2010 May;69(5):924-7
(15) Alffenaar JW, van Assen S, van der Werf TS, Kosterink JG, Uges DR. Omeprazole significantly
reduces posaconazole serum trough level. Clin Infect Dis 2009 Mar 15;48(6):839
(16) Rachinger A, Navis M, van Assen S, Groeneveld PH, Schuitemaker H. Recovery of viremic con-
trol after superinfection with pathogenic HIV type 1 in a long-term elite controller of HIV type 1
infection. Clin Infect Dis 2008 Dec 1;47(11):e86-9
(17) Huits RM, Bremmer R, Enting RH, Sprenger HG, van Assen S. Return of meningeal symptoms in
a patient treated for cryptococcal meningitis. J Neurol 2007 Oct;254(10):1443-4
(18) Meeuse JJ, Sprenger HG, van Assen S, Leduc D, Daenen SM, Arends JP, van der Werf TS. Rho-
dococcus equi infection after alemtuzumab therapy for T-cell prolymphocytic leukemia. Emerg
Infect Dis 2007 Dec;13(12):1942-3
(19) van Assen S, Houwerzijl EJ, van den Dungen JJ, Koopmans KP. Vascular graft infection due to
chronic Q fever diagnosed with fusion positron emission tomography/computed tomography.
J Vasc Surg 2007 Aug;46(2):372
(20) de Vries JJ, van Assen S, Mulder AB, Kampinga GA. Positive blood culture with Plasmodium
falciparum: case report. Am J Trop Med Hyg 2007 Jun;76(6):1098-9
(21) Huits RM, van Assen S, Wildeboer-Veloo AC, Verschuuren EA, Koeter GH. Prevotella bivia necro-
bacillosis following infectious mononucleosis. J Infect 2006 Aug;53(2):e59-63
(22) van Assen S, Bakker SJ. Did syphilis truly strike the kidneys this time? Nephrol Dial Transplant
2005 Jun;20(6):1029-31
(23) van Assen S, Bosma F, Staals LM, Kullberg BJ, Melchers WJ, Lammens M, Kornips FH, Vos PE,
Fikkers BG. Acute disseminated encephalomyelitis associated with Borrelia burgdorferi. J Neu-
rol 2004 May;251(5):626-9
(24) Van Damme PA, Keuter M, Van Assen S, DeWilde PC, Beckers PJ. A rare case of oral leishmani-
asis. Lancet Infect Dis 2004 Jan;4(1):53
(25) van Assen S, Bootsma GP, Verweij PE, Donnelly JP, Raemakers JM. Aspergillus tracheobronchi-
tis after allogeneic bone marrow transplantation. Bone Marrow Transplant 2000 Nov;26(10):1131-
2
(26) van Roijen JH, van Assen S, van der Kwast TH, de Rooij DG, Boersma WJ, Vreeburg JT, Weber
RF. Androgen receptor immunoexpression in the testes of subfertile men. J Androl 1995 Nov-
Dec;16(6):510-6

Copyright © 2022 FDOKUMEN




















