
Incidence, Etiology, Histologic Findings, and Course of Thoracic Inflammatory Aortopathies
Upload
meduniwienCategory
view
2download
0
GYNECOLOGIC ONCOLOGY 67, 20–26 (1997)ARTICLE NO. GO974815
The Relevance of Angiogenesis in Benign and Malignant EpithelialTumors of the Ovary: A Quantitative Histologic Study
Hermann Brustmann, M.D., Ph.D.,* Paul Riss, M.D.,† and Susanna Naude, M.D.*
*Department of Pathology and †Department of Obstetrics and Gynecology, Landeskrankenhaus, A-2340 Moedling/Vienna, Austria
Received February 3, 1997
neoplasms at an early stage. The use of ultrasound imagingThe ability of a tumor to grow and eventually to infiltrate adja- with color Doppler technology allows the visualization of
cent tissues requires a sufficient blood supply. Many malignant blood flow in ovarian tumors, which may permit early diag-neoplasms have been shown to induce neovascularization. We nosis and treatment [5–7]. However, the relationship be-asked whether it is possible to characterize ovarian epithelial tu- tween the pattern of blood flow in ovarian tumors and themors on the basis of vascularization and whether vascularization histologic characteristics has yet to be established. We there-can be used to differentiate between benign and malignant neo-
fore asked whether it is possible to characterize ovarian epi-plasms. We examined 14 cases of benign cystadenomas and 18thelial tumors on the basis of microvascularization andcarcinomas. The microvessels were identified by immunohisto-whether microvascularization can be used to differentiatechemical staining of endothelial cells for factor VIII. They werebetween benign and malignant neoplasms.counted within the most vascular area of a tumor (neovascular
‘‘hot spot’’) on a 1100 and a 1400 field. Mean vessel countswere 51.64 [standard error of the mean (SEM), 5.7] in the benign MATERIALS AND METHODScystadenomas and 131.05 (SEM, 6.7) in the group of carcinomasat a 1100 magnification. The mean microvessel counts per 1400 We examined specimens from 32 patients whose ovarianfield were 14.4 (SEM, 1.9) in the benign and 33.7 (SEM, 3.45) in tumors were classified at our institute. They consisted of 14the malignant tumors investigated. These differences were signifi- benign cystadenomas (10 serous and 4 mucinous type) andcant (t test for independent samples, P õ 0.001). Since our study 18 carcinomas (14 serous, 2 clear cell, 1 endometroid, andshows significantly fewer small blood vessels in the benign cystade- 1 undifferentiated). All cases were surgical specimens, ex-nomas than in the malignant tumors, the histologically determin-
cept 1 which was retrieved from an autopsy case. The origi-able vascular density may be the basis for imaging blood flow bynal pathological reports as well as all tumor sections whichmeans of color ultrasound. q 1997 Academic Presswere stained with hematoxylin and eosin were reviewed.From each case a representative tissue block was chosen.Patient age, tumor size, type, and staging are shown in TablesINTRODUCTION1 and 2.
The blood vessels in the paraffin-embedded tissues wereThe ability of a malignant tumor to grow and eventuallyto infiltrate adjacent tissue requires a sufficient blood supply. highlighted by immunohistochemical staining of endothelial
cells for factor VIII. Briefly, we performed a standard immu-Folkman [1] has shown experimentally that tumor growthin culture in the absence of vascularization is limited to a nohistochemical technique using a prediluted ready-to-use
polyclonal antiserum for factor VIII-related antigen (DAKOdiameter of 1 or 2 mm. Implantation of such tumor cellaggregates in host tissue leads to angiogenesis from the sur- Corporation). This antibody was applied to the 3-mm-thick
sections for 30 min at room temperature. No previous diges-rounding stroma and further growth occurs. Experiences indifferent tumor types suggest that their vascularization is an tion was performed. The antibody was used with a DAKO
LSAB kit, alkaline phosphatase.important factor in their clinical behavior [2, 3]. Thus, newcapillary blood vessels have to be formed, increasing in turn We counted microvessels within the tumors as described
previously [2]. Any red-stained endothelial cell or endothe-the opportunity for tumor cells to enter the circulation andto metastasize. It is not surprising, therefore, that the study lial cell cluster with or without lumen that was clearly sepa-
rate from adjacent microvessels, tumor cells, and other con-of angiogenesis in tumors has attracted increased attentionin recent years [4]. nective tissue elements was considered an individually
countable blood vessel. Vessel lumen, although usually pres-In clinical practice, it is often difficult to diagnose ovarian
200090-8258/97 $25.00Copyright q 1997 by Academic PressAll rights of reproduction in any form reserved.
AID Gyn 4815 / 6d23$$$$81 09-16-97 05:26:38 goas AP: GYN
21ANGIOGENESIS IN EPITHELIAL TUMORS OF THE OVARY
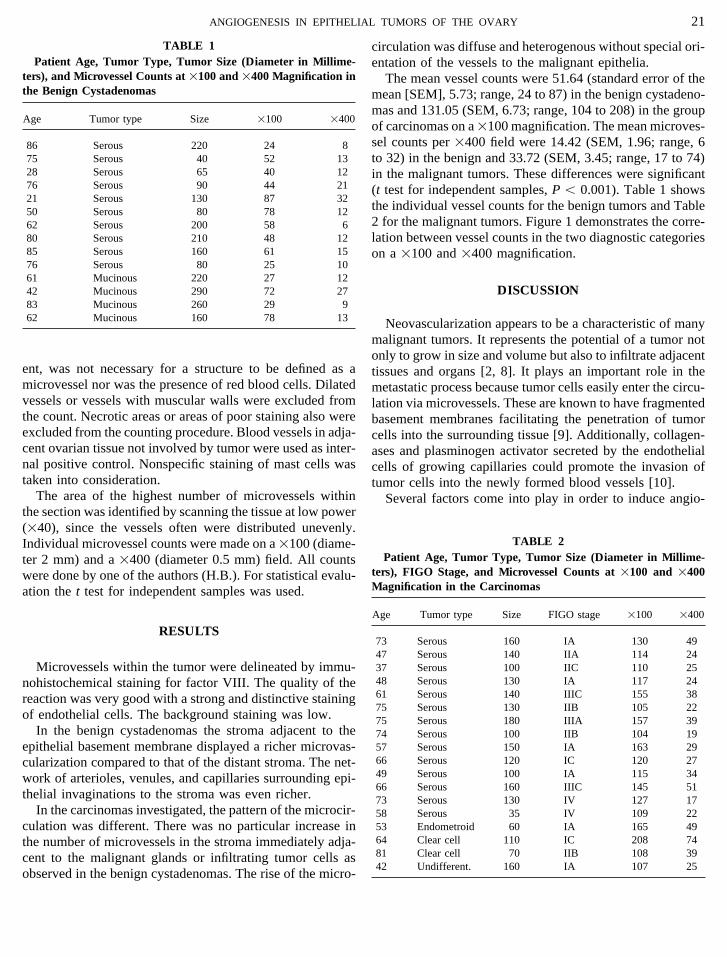
TABLE 1 circulation was diffuse and heterogenous without special ori-Patient Age, Tumor Type, Tumor Size (Diameter in Millime- entation of the vessels to the malignant epithelia.
ters), and Microvessel Counts at 1100 and 1400 Magnification in The mean vessel counts were 51.64 (standard error of thethe Benign Cystadenomas mean [SEM], 5.73; range, 24 to 87) in the benign cystadeno-
mas and 131.05 (SEM, 6.73; range, 104 to 208) in the groupAge Tumor type Size 1100 1400
of carcinomas on a1100 magnification. The mean microves-sel counts per 1400 field were 14.42 (SEM, 1.96; range, 686 Serous 220 24 8
75 Serous 40 52 13 to 32) in the benign and 33.72 (SEM, 3.45; range, 17 to 74)28 Serous 65 40 12 in the malignant tumors. These differences were significant76 Serous 90 44 21 (t test for independent samples, P õ 0.001). Table 1 shows21 Serous 130 87 32
the individual vessel counts for the benign tumors and Table50 Serous 80 78 122 for the malignant tumors. Figure 1 demonstrates the corre-62 Serous 200 58 6
80 Serous 210 48 12 lation between vessel counts in the two diagnostic categories85 Serous 160 61 15 on a 1100 and 1400 magnification.76 Serous 80 25 1061 Mucinous 220 27 12
DISCUSSION42 Mucinous 290 72 2783 Mucinous 260 29 962 Mucinous 160 78 13 Neovascularization appears to be a characteristic of many
malignant tumors. It represents the potential of a tumor notonly to grow in size and volume but also to infiltrate adjacent
ent, was not necessary for a structure to be defined as a tissues and organs [2, 8]. It plays an important role in themicrovessel nor was the presence of red blood cells. Dilated metastatic process because tumor cells easily enter the circu-vessels or vessels with muscular walls were excluded from lation via microvessels. These are known to have fragmentedthe count. Necrotic areas or areas of poor staining also were basement membranes facilitating the penetration of tumorexcluded from the counting procedure. Blood vessels in adja- cells into the surrounding tissue [9]. Additionally, collagen-cent ovarian tissue not involved by tumor were used as inter- ases and plasminogen activator secreted by the endothelialnal positive control. Nonspecific staining of mast cells was cells of growing capillaries could promote the invasion oftaken into consideration. tumor cells into the newly formed blood vessels [10].
The area of the highest number of microvessels within Several factors come into play in order to induce angio-the section was identified by scanning the tissue at low power(140), since the vessels often were distributed unevenly.
TABLE 2Individual microvessel counts were made on a 1100 (diame-Patient Age, Tumor Type, Tumor Size (Diameter in Millime-ter 2 mm) and a 1400 (diameter 0.5 mm) field. All counts
ters), FIGO Stage, and Microvessel Counts at 1100 and 1400were done by one of the authors (H.B.). For statistical evalu-Magnification in the Carcinomasation the t test for independent samples was used.
Age Tumor type Size FIGO stage 1100 1400
RESULTS73 Serous 160 IA 130 4947 Serous 140 IIA 114 2437 Serous 100 IIC 110 25Microvessels within the tumor were delineated by immu-48 Serous 130 IA 117 24nohistochemical staining for factor VIII. The quality of the61 Serous 140 IIIC 155 38reaction was very good with a strong and distinctive staining75 Serous 130 IIB 105 22
of endothelial cells. The background staining was low. 75 Serous 180 IIIA 157 39In the benign cystadenomas the stroma adjacent to the 74 Serous 100 IIB 104 19
57 Serous 150 IA 163 29epithelial basement membrane displayed a richer microvas-66 Serous 120 IC 120 27cularization compared to that of the distant stroma. The net-49 Serous 100 IA 115 34work of arterioles, venules, and capillaries surrounding epi-66 Serous 160 IIIC 145 51
thelial invaginations to the stroma was even richer. 73 Serous 130 IV 127 17In the carcinomas investigated, the pattern of the microcir- 58 Serous 35 IV 109 22
53 Endometroid 60 IA 165 49culation was different. There was no particular increase in64 Clear cell 110 IC 208 74the number of microvessels in the stroma immediately adja-81 Clear cell 70 IIB 108 39cent to the malignant glands or infiltrating tumor cells as42 Undifferent. 160 IA 107 25
observed in the benign cystadenomas. The rise of the micro-
AID Gyn 4815 / 6d23$$$$82 09-16-97 05:26:38 goas AP: GYN

22 BRUSTMANN, RISS, AND NAUDE
FIG. 1. Correlation between microvessel counts in benign (correlation coefficient r Å 0.58) and malignant (r Å 0.84) epithelial tumors of the ovary.The abscissa is the 1100, the ordinate the 1400 magnification.
genesis. First, tumor cells may release angiogenic molecules situ of the breast (CIS angiogenesis [2]), suggesting that theproduction of angiogenic factors is a property of the neoplas-into the tumor stroma [11]. For example, in cervical intraepi-
thelial neoplasia (CIN) there are significantly more mi- tic epithelial cells themselves [4]. Second, host immune cellssuch as macrophages are known to be able to secrete trans-crovessels beneath dysplastic epithelia compared to the adja-
cent normal epithelia. This CIN angiogenesis is not related forming growth factor a, angiotropin, tumor necrosis factora, and basic fibroblast growth factor [11, 13–20]. Mast cellsto the number of macrophages within the CIN lesion [12].
Similar observations were reported for ductal carcinoma in are often found near or within tumors. They contain heparin,
FIG. 2. Serous cystadenoma of the ovary stained with antibody to factor VIII. There are few microvessels in the stroma adjacent to the epithelium.
AID Gyn 4815 / 6d23$$$$82 09-16-97 05:26:38 goas AP: GYN

23ANGIOGENESIS IN EPITHELIAL TUMORS OF THE OVARY
FIG. 3. Serous cystadenocarcinoma of the ovary stained with antibody to factor VIII showing many capillaries and single-stained endothelial cells.
which in turn is known to mobilize the angiogenic substance be concentrated in the stroma close to the epithelium (Fig.2). An analogous observation was described in the prostatebasic fibroblast growth factor from the extracellular matrix,
protect it from degradation, and potentiate its angiogenic [28]. In malignant epithelial tumors of the ovary we foundan increase in the number of microvessels which were dis-effects [21]. However, in a study of angiolipomas and hem-
angiomas of the human skin, Shea et al. found mast cells tributed in a heterogenous pattern in the tumor stroma. Themicrovessel density varied from tumor to tumor and alsorelated to the maturation of blood vessels rather than to the
early steps of angiogenesis [22]. Also, in the nonneoplastic within one and the same tumor (Figs. 3 and 4). Wu et al.assessed angiogenesis in ovarian neoplasms by color Dopp-ovary vascular permeability factor/vascular endothelial
growth factor, which is thought to induce angiogenesis, is ler ultrasound and reported similar experiences suggestingthat neovascularization may depend on individual tumorexpressed by human granulosa and theca lutein cells during
follicle development [23]. characteristics, although angiogenesis was a common phe-nomenon in the malignant ovarian neoplasms they investi-On the basis of vascularization there are two different
stages to be observed in the development of tumors, the gated [5]. Hollingworth et al. suggest that analysis of neovas-cularization in advanced stage ovarian cancer may be a use-prevascular and the vascular phase [8]. For example, in cuta-
neous melanomas it has been shown that the vascular phase ful prognostic factor [29]. Schoenfeld et al. reportobservations based upon three-dimensional imaging of nor-is associated with rapid tumor growth, bleeding, and the
potential to metastasize [24]. Accordingly, Weidner et al. mal and tumor-induced ovarian angiogenesis. Their findingsshow that tumor-induced angiogenesis creates a bizzare vas-reported for invasive breast carcinoma that the number of
microvessels per 1200 field in the area of most intense cular architecture [30].There was a clear-cut difference in the total number ofneovascularization was found to be an independent predictor
for metastatic disease [2]. This observation has recently been blood vessels per 1100 and 1400 field in our two series.In contrast to other organs such as prostate or skin, the ovaryextended to a number of other tumors like non-small-cell
lung carcinoma [25] and prostate carcinoma [26, 27]. undergoes significant cyclic changes at regular intervals. Infact, in a preliminary series of tumor-like lesions of the ovaryOur studies show an increased microvessel density in ma-
lignant epithelial tumors of the ovary compared to that of (functional ovarian cysts) we found blood vessel countsranging from low to very high, overlapping especially withbenign tumors. In the benign group the capillaries tended to
AID Gyn 4815 / 6d23$$$$82 09-16-97 05:26:38 goas AP: GYN

24 BRUSTMANN, RISS, AND NAUDE
FIG. 4. Clear-cell carcinoma of the ovary immunostained with anti-factor VIII antibody. There is a dense capillary network between sheets andnests of tumor cells.
AID Gyn 4815 / 6d23$$4815 09-16-97 05:26:38 goas AP: GYN

25ANGIOGENESIS IN EPITHELIAL TUMORS OF THE OVARY
5. Wu CC, Lee CN, Chen TM, Shyu MK, Hsieh CY, Chen HY, Hsiehblood vessel counts in carcinomas (unpublished observa-FJ: Incremental angiogenesis assessed by color Doppler ultrasoundtion).in the tumorigenesis of ovarian neoplasms. Cancer 73(4):1251–1256,
The demonstration of tumor vascularity may have im- 1994portant clinical implications [29]. In gynecology, it is now 6. Kurjak A, Shalan H, Kupesic S, Predanic M, Zald I, Breyer B, Jukicpossible to examine blood flow in adnexal tumors by means S: Transvaginal color Doppler sonography in the assessment of pelvicof transvaginal Doppler sonography [5–7]. To our knowl- tumor vascularity. Ultrasound Obstet Gynecol 3:137–154, 1993
edge, a direct correlation between histologically defined vas- 7. Maly Z, Riss P, Deutinger J: Localisation of blood vessels and qualita-tive assessment of blood flow in ovarian tumors. Obstet Gynecol 85:33–cularity of adnexal tumors and blood flow patterns on Dopp-36, 1995ler sonography has not yet been established. It is tempting
8. Folkman J, Watson K, Ingber D, Hanahan D: Induction of angiogenesisto speculate, however, that the increased number of bloodduring transition from hyperplasia to neoplasia. Nature 339:58–61,vessels in malignant epithelial tumors of the ovary is respon-1989
sible for typical changes seen in sonographic blood flow9. Nagy JA, Brown LF, Senger DR: Pathogenesis of tumor stroma genera-
studies [5–7]. In a previous study one of the authors (P.R.) tion: A critical role for leaky blood vessels and fibrin deposition. Bio-and his group described the distribution of blood vessels chim Biophys Acta 948:305–326, 1989within benign and malignant ovarian tumors and the charac- 10. Moscatelli D, Gross JL, Rifkin DB: Angiogenic factors stimulate plas-teristics of the flow curve using color Doppler imaging [7]. minogen activator and collagenase production by capillary endothelial
cells. J Cell Biol 91:201a, 1981They found blood vessels in almost all malignant but only11. Blood CH, Zetter BR: Tumor interactions with the vasculature: Angio-in about two-thirds of the benign tumors. This finding corre-
genesis and tumor metastasis. Biochim Biophys Acta 1032:89–118,lates with our observation that the number of blood vessels is1990significantly higher in malignant compared to benign ovarian
12. Smith-McCune KK, Weidner N, Bishop JM: Cervical intraepithelialtumors. Likewise, they demonstrated blood vessels tendingneoplasia (CIN) is angiogenic. Proc Am Assoc Cancer Res 34:74, 1993
to be located centrally or septally rather than in the periphery13. Folkman J, Klagsbrun M: Angiogenic factors. Science 235:442–447,
of the malignancies. This seems to correspond to the pattern 1987of microvascularization we found. Malignant epithelial tu-
14. Polverini PJ, Leibovich SJ: Induction of neovascularisation in vivo andmors of the ovary display a much more complex growth endothelial proliferation in vivo by tumor associated macrophages. Labpattern, especially toward the central tumor regions and a Invest 51:635–642, 1984diffuse and heterogenous stromal neovascularization. In con- 15. Baird A, Mormede P, Bohlen P: Immunoreactive fibroblast growth
factor in cells of peritoneal exsudate suggests its identity with macro-trast, cystadenomas show central regions that are rather cys-phage-derived growth factor. Biochem Biophys Res Commun 126:358–tic and accentuated microvascularization in the stroma adja-364, 1985cent to the epithelial basement membrane.
16. Frater-Schroder M, Risau W, Hallmann R: Tumor necrosis factor typeIn conclusion, we were able to show that common epithe-a, a potent inhibitor of endothelial cell growth in vitro is angiogenic
lial tumors of the ovary are characterized by the total number in vivo. Proc Natl Acad Sci USA 84:5277–5281, 1987of blood vessels in the section of the tumor with the highest 17. Leibovich SJ, Polverini PJ, Shepard HM: Macrophage-induced angio-vascular density (neovascular hot spot). Benign cystadeno- genesis is mediated by tumor necrosis factor alpha. Nature 329:630–mas had significantly fewer blood vessels than malignant 632, 1987
tumors. Vascular density may be the basis for imaging blood 18. Schreiber AB, Winkler ME, Derynck R: Transforming growth factoralpha: A more potent angiogenic mediator than epidermal growth fac-flow by means of transvaginal color Doppler ultrasound.tor. Science 232:1250–1253, 1986
19. Hockel M, Jung W, Vaupel P: Purified monocyte-derived angiogenicACKNOWLEDGMENTsubstance (angiotropin) induces controlled angiogenesis associated withregulated tissue proliferation in rabbit skin. J Clin Invest 82:1075–
The authors thank Gabi Sagmeister, H.T., for her technical assistance. 1090, 1988
20. Folkman J, Klagsbrun M, Sasse J: Heparin-binding angiogenic pro-REFERENCES tein—basic fibroblast growth factor—is stored within basement mem-
brane. Am J Pathol 133:419–423, 19881. Folkman J: Tumor Angiogenesis, in Holland JF, Frei E, Bast RC (eds): 21. Thornton S, Mueller S, Levine E: Human endothelial cells: Use of
Cancer Medicine, 3rd ed. Philadelphia, Lea & Febiger, 1992, p 153 heparin in cloning and long term serial cultivation. Science 222:623–625, 19832. Weidner N, Semple JP, Welch WR, Folkman J: Tumor angiogenesis
and metastases—Correlation in invasive breast carcinoma. N Engl J 22. Shea CR, Prieto VG: Mast cells in angiolipomas and hemangiomas ofMed 324:1–8, 1991 human skin: Are they important for angiogenesis? J Cutaneous Pathol
21:247–251, 19943. Sillman F, Boyce J, Fruchter R: The significance of atypical vesselsand neovascularisation in cervical neoplasia. Am J Obstet Gynecol 23. Kamat BR, Brown LF, Manseau SJ, Senger DR, Dvorak HF: Expres-139:154–159, 1981 sion of vascular permeability factor/vascular endothelial growth factor
by human granulosa and theca lutein cells. Role in corpus luteum4. Weidner N: Tumor angiogenesis: Review of current applications intumor prognostication. Semin Diagn Pathol 10:302–313, 1993 development. Am J Pathol 146(1):157–165, 1995
AID Gyn 4815 / 6d23$$$$82 09-16-97 05:26:38 goas AP: GYN

26 BRUSTMANN, RISS, AND NAUDE
24. Srivastava A, Laidler P, Davies RP, Horgan K, Hughes LE: The prog- 27. Weidner N, Carroll PR, Flax J, Blumenfeld W, Folkman J: Tumorangiogenesis correlates with metastases in invasive prostate carcinoma.nostic significance of tumor vascularity in intermediate thickness (0,76–Am J Pathol 143:401–409, 19934,0 mm thick) skin melanoma: A quantitative histologic study. Am J
Pathol 133:419–423, 1988 28. Bigler SA, Deering RE, Brawer MK: Comparison of microscopic vas-cularity in benign and malignant prostate tissue. Hum Pathol 24:220–
25. Macchiarini P, Fontaini G, Hardin MJ, Sqartini F, Angeletti CA: Rela-226, 1993
tion of neovasculature to metastases of non-small-cell lung cancer.29. Hollingworth HC, Kohn E, Steinberg S, Rothenberg M, Merino M:
Lancet 340:145–146, 1992Tumor angiogenesis in advanced stage ovarian carcinoma. Am J Pathol147:33–41, 199526. Wakui S, Furusato M, Itoh T, Sasaki H, Akiyama A, Kinoshita I, Asano
K, Tokuda T, Aizawa S: Tumor angiogenesis in prostatic carcinoma 30. Schoenfeld A, Levavi H, Breslavski D, Amir R, Ovadia J: Three-with and without bone marrow metastases: A morphometric study. J dimensional modelling of tumor-induced ovarian angiogenesis. Cancer
Lett 87(1):79–84, 1994Pathol 168:257–262, 1992
AID Gyn 4815 / 6d23$$$$82 09-16-97 05:26:38 goas AP: GYN
Copyright © 2022 FDOKUMEN




















