Sequencing and de novo analysis of a coral larval transcriptome using 454 GSFlx

www.elsevier.com/locate/humpath
Human Pathology (2013) xx, xxx–xxx
Original contribution
The prognostic role of ERG immunopositivity in prostaticacinar adenocarcinoma: a study including 454 cases andreview of the literature☆,☆☆
Bin Xu MD, PhDa,1, Myriam Chevarie-Davis MD, MSc a,1, Simone Chevalier PhDb,Eleanora Scarlata PhDb, Nebras Zeizafoun MDc, Alice Dragomir PhDb,Simon Tanguay MDb, Wassim Kassouf MDb, Armen Aprikian MDb, Fadi Brimo MDa,⁎
aDepartment of Pathology, McGill University Health Center, Montreal, CanadabDepartment of Urology, McGill University Health Center, Montreal, CanadacDepartment of Pathology, St Luke's Roosevelt Hospital Center, New York, NY, USA
Received 3 September 2013; revised 4 October 2013; accepted 10 October 2013
aa
H
0h
Keywords:ERG;TMPRSS2/ERG fusion;Immunohistochemistry;Prostate adenocarcinoma;Biochemical recurrence
Summary TMPRSS2/ERG fusion is among the most frequent genetic anomalies in prostateadenocarcinomas. Although positive immunostaining for ERG has been shown to tightly correlatewith ERG fusion status, the clinical and prognostic significance of a positive ERG stain remainsundetermined. The significance of ERG immunostaining in 454 consecutive prostate adenocarcinomasfrom radical prostatectomies (RPs) using tissue microarrays, herein, is evaluated. A separate set of 59cases of incidental prostate adenocarcinoma detected on transurethral resection of prostate with aGleason score of 6 was also included. ERG translocation was significantly more common inperipheral zone cancer in comparison with cancer of the transitional zone (33% in RP versus 5% intransurethral resection of prostate specimens). In the RP cohort, although ERG positivity wassignificantly associated with younger age at presentation and lower prostate-specific antigen values, itshowed no association with Gleason score or with pathologic stage. In multivariate analysis,biochemical recurrence was only associated with the final RP Gleason score and elevated prostate-specific antigen levels and was unrelated to neither ERG positivity or to its staining intensity. In ourhands, ERG positivity was unrelated to either aggressive local tumor characteristics or a worseoutcome. Our results, as well as an extensive review of the related literature showing conflictingfindings, seem to indicate that ERG immunopositivity cannot be considered as an importantprognostic factor in prostate cancer.© 2013 Elsevier Inc. All rights reserved.
☆ Disclosure and conflict of interests: All contributing authors herebycknowledge the responsibility for the work presented in this manuscriptnd declare no potential conflicts of interests.
☆☆ Funding sources: None.⁎ Corresponding author. Department of Pathology, Montreal General
ospital, Montreal, Quebec, Canada H3G 1A4.E-mail address: [email protected] (F. Brimo).1 Both authors contributed equally to the study.
046-8177/$ – see front matter © 2013 Elsevier Inc. All rights reserved.ttp://dx.doi.org/10.1016/j.humpath.2013.10.012
1. Introduction
Prostate cancer is the most prevalent cancer and thesecond leading cause of cancer death in men world-wide, with an incidence of 206 640 and a mortality of

2 B. Xu et al.
28 088 in the United States [1]. In 2005, Tomlins et al[2] discovered a recurrent chromosome fusion inprostate cancer, involving the androgen-regulated trans-membrane protease serine 2 (TMPRSS2) on chromosome21q22.3 and erythroblast transformation–specific (ETS)regulated gene-1 (ERG) on chromosome 21q22.2,making it the first discovered translocation in thiscancer. Since then, numerous studies have confirmedthat TMPRSS2/ERG fusion is the most common geneticevent in prostate cancer, with a reported prevalence of~50% in radical prostatectomy (RP) and biopsyspecimens [3-24] and ~20% in incidental tumors fromtransurethral resection of prostate (TURP) specimens[4,5,13,25-30]. It has also been reported to be presentin a minority of cases of high-grade prostate intrae-pithelial neoplasia [3,31-33].
ERG is an oncogene that belongs to the ETS familyof transcription factors, which play an important role inregulating cell proliferation, differentiation, apoptosis,and angiogenesis [34,35]. The TMPRSS2/ERG fusionresults in an aberrant expression of a truncated ERGproduct, which can be detected reliably using ERGimmunohistochemistry (IHC). The use of IHC as asurrogate method to detect TMPRSS2/ERG fusion hasbeen previously validated in several large-scale studieswith a reported sensitivity of 95.7% to 100% and aspecificity of 85% to 99% compared with the criterionstandard methods, namely, fluorescent in situ hybridiza-tion (FISH) or reverse transcription polymerase chainreaction (RT-PCR) [6,9,22,29,36,37]. Using FISH, PCR,RT-PCR, and/or IHC techniques, more than 14 000prostate cancer cases have been investigated in multiplestudies in an effort to establish the diagnostic andprognostic values of TMPRSS2/ERG fusion in prostatecancer. However, the results were conflicting, reportinga positive [4,5,11,17,18,26,30,31,38-49], null [4,7,8,10-12,15-18,20,22,26,27,30,38,40,42-47,49-75], or negative[12,15,20,28,42,45,47,50,54,55,59,62,76] association be-tween TMPRSS2/ERG fusion and aggressive clinicopath-ologic parameters including preoperative prostate-specificantigen (PSA) levels, Gleason score, pathologic stage,biochemical recurrence (BCR), and disease-specificmortality.
In an effort to clarify the prognostic value of a positiveERG immunostain in prostate adenocarcinoma, the immu-nopositivity of ERG in a large cohort of 454 cases obtainedfrom RP specimens was evaluated herein, and the ERGimmunoreactivity was correlated with a variety of clinico-pathologic parameters. In addition, we included a separateset of 59 cases of incidental transitional zone adenocarcino-ma detected on TURP specimens to compare the prevalenceof ERG immunoreactivity between peripheral zone andtransitional zone cancers. A comprehensive review of therelated literature was also undertaken, the results of whichare compared with the current study and are presented in thecurrent report.
2. Materials and methods
2.1. Characteristics of the patients and tissuemicroarray construction
Eight tissue microarrays (TMAs) were constructed usingtissues obtained from the surgical pathology archives of theMcGill University Health Centre (Montreal, Quebec,Canada). The TMAs included 454 consecutive RPs contain-ing prostate acinar adenocarcinoma performed between 1993and 2008. Most prostatectomies were sampled, in theirentirety, for histologic examination. The hematoxylin andeosin slides were retrieved and reviewed by a genitourinaryexpert pathologist (F.B.) at the time of TMA construction toconfirm the Gleason score using the current/modifiedgrading system, surgical margin status, and the AmericanJoint Committee on Cancer (AJCC) pathologic stage [77].Each tumor was represented by 2 separate 1-mm cores toaccount for potential intratumoral heterogeneity. The coreswere taken from the representative area of the dominantnodule. In cases in which the dominant nodule had a lowerGleason score than the secondary nodule, the secondarynodule with the highest Gleason score was also sampled toensure that the core Gleason score reflected the final score ofa given case. To provide adequate negative immunohisto-chemical control, 62 cores of randomly selected areas ofbenign prostatic and renal parenchyma were included in theTMA blocks. An additional set of 59 cases of incidentaltransitional zone adenocarcinoma, detected in TURP spec-imens with a Gleason score of 6 and an overall tumor volumeof less than 1% (pT1a), was also included.
Among the 454 patients who underwent RP, 297 patientshad detailed clinical follow-up with a follow-up duration of5.6 ± 0.2 years (mean ± SEM). The Gleason score,pathologic stage, surgical margins status, and ERG positivitywere compatible between patients with and without clinicalfollow-up (data not shown). The primary clinical outcomestudied was BCR, which is defined as a PSA level of 0.4 ng/mL or higher post-RP.
2.2. Immunohistochemistry
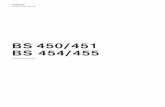
IHC was performed using a Ventana automated systemand Ventana Iview DAB detection kit (Ventana MedicalSystems Inc, Tucson, AZ). A monoclonal mouse antihumanERG antibody (Clone 9FY; Biocare Medical LLC, Concord,CA), with a dilution of 1:100, was used. The evaluation ofimmunostaining was performed by the participating pathol-ogist blinded to the outcome. A case was considered positivefor ERG whenever nuclear staining of tumor cells wasidentified in at least 1 core regardless of its intensity. Inaddition, the intensity of nuclear staining was evaluatedsemiquantitatively using a 4-tiered system as follows: 0,negative; 1, weak staining; 2, moderate staining; and 3,intense staining (Fig. 1).

3ERG immunopositivity in prostate adenocarcinoma
2.3. Statistical analysis
All analyses were performed using the Statistical AnalysisSystem Software (version 9.3; SAS Institute, Cary, NC), andall tests were 2 sided, with a significance threshold of 5%. AStudent t test was used to examine the correlation of ERGstatus and clinical characteristics, for example, age atpresentation and preoperative PSA level. A Pearson χ2 testor a Fisher exact test was performed to correlate the ERGimmunopositivity with BCR, or local tumor characteristics,including AJCC staging (pT or pN) and Gleason score. Theoutcome start point was the date of surgery, whereas theoutcome end point was the date of the last follow-up orBCR.Amultivariate analysis was performed using the Cox propor-tional hazards model to evaluate the association between BCRand prognostic factors including the following: Gleason score,status of surgical margin, and ERG immunopositivity.Separate statistical analyses were performed to study theassociation of ERG staining intensity with clinicopathologiccharacteristics and BCR, which yielded very similar statisticalresults (data not shown). Therefore, only results based on ERGpositivity and negativity are reported in the current article.
3. Results
3.1. Clinicopathologic characteristics and ERGimmunopositivity in RP and TURP
The clinical and pathologic characteristics of the RP cohortare summarized in Table 1. In brief, a total of 454 patients wereincluded in the current study, with an age of 60.7 ± 0.3 years(mean ± SEM) at the time of surgery and a mean preoperativePSA of 8.0 ± 0.4 ng/mL. The most common total Gleasonscore reported in this cohort was 7 (3 + 4 or 4 + 3), accountingfor 62.3% of cases (n = 283). The rest of cases had a Gleasonscore of 6 (n = 133 [29.3%]), 8 (4 + 4, n = 28 [6.2%]), or 9 (n =10 [2.2%]). Most patients (n = 266 [58.6%]) had organ-confined disease (AJCC pT2), whereas 127 patients (28.0%)
Fig. 1 Representative images of ERG IHC in prostate adenocarcinoma1 (B, weak), 2 (C, moderate), and 3 (D, strong).
had extraprostatic extension (AJCC pT3). Sixty-one patients(13.4%) had positive surgical margins in areas of intraprostaticincision (pT2+). Among the 188 patients with lymph nodesampling at the time of radical prostectomy, 3 patients (1.6%)had metastasis to regional lymph nodes (pN1). Of the 297patients with available clinical follow-up of 5.6 ± 0.2 years(mean ± SEM), 80 patients (26.9%) recurred after a meanduration of 2.8 years.
Among the 454 RP specimens, 151 adenocarcinomas(33.3%) demonstrated ERG immunoreactivity including thefollowing: 75 cases (16.5%) with weak, 50 cases (11.0%)with moderate, and 26 cases (5.7%) with strong stainingintensity. The ERG IHC yielded a homogenous stainingpattern in all cores examined, with a compatible stainingintensity among cores taken from the same case. Cauteryartifact that was sometimes encountered in TURP specimensdid not alter the ERG immunostaining in neoplastic orendothelial cells. In comparison, the prevalence of ERGimmunopositivity in incidental adenocarcinoma detected inTURP specimens was significantly lower, with only 3 (5.1%)of 59 cases showing ERG immunopositivity (χ2 test, P b.0001). The 62 cores of benign prostate and renalparenchyma were all negative for the marker.
3.2. ERG immunopositivity in relation toclinicopathologic characteristics
The clinical and pathologic features of ERG-negative andERG-positive prostatic adenocarcinomas are shown inTable 1. Compared with ERG-negative cases, ERG-positivecases were associated with a significantly younger age atdiagnosis (2-tailed Student t test, P = .002) and a lowerpreoperative PSA level (2-tailed Student t test, P = .03). Incontrast, ERG immunoreactivity appeared to have noinfluence on BCR (Pearson χ2 test, P = .66) or local tumoralcharacteristics. The Gleason score and pathologic stage werecomparable between the 2 groups (Pearson χ2 test, P = .69for Gleason score, and P = .45 for AJCC pT stage; Fisherexact test, P = .55).
(×400). The intensity of nuclear staining is scored as 0 (A negative),

Table 1 The association of ERG immunoreactivity and clinicopathologic characteristics of prostatic adenocarcinoma in RP
All ERG negative ERG positive P
n (%) 454 303 (66.7) 151 (33.3)Age at diagnosis (y), mean ± SEM 60.7 ± 0.3 a 61.4 ± 0.3 59.5 ± 0.5 .002 a
Preoperative PSA (ng/mL), mean ± SEM 8.0 ± 0.4 a 8.5 ± 0.6 7.0 ± 0.6 .03 a
Duration of follow-up (y), mean ± SEM 5.6 ± 0.2 a 5.4 ± 0.2 5.8 ± 0.4 .36 a
Gleason score, n (%)3 + 3 133 (29.3) 89 (29.4) 44 (29.1) .69 b
3 + 4/4 + 3 283 (62.3) 185 (61.1) 98 (64.9)4 + 4 28 (6.2) 22 (7.3) 6 (4.0)4 + 5/5 + 4 10 (2.2) 7 (2.3) 3 (2.0)AJCC pT stage, n (%)pT2 266 (58.6) 179 (59.1) 87 (57.6) .45 b
pT2+ 61 (13.4) 43 (14.2) 18 (11.9)pT3a 106 (23.4) 65 (21.5) 41 (27.2)pT3b 21 (4.6) 16 (5.3) 5 (3.3)Lymph node sampling (n = 188), n (%)pN0 185 (98.4) 67 (100) 118 (97.5) .55 c
pN1 3 (1.6) 0 (0) 3 (2.5)BCR (n = 297), n (%)No 217 (73) 71 (74.7) 146 (72.3) .66 b
Yes 80 (27) 24 (25.3) 56 (27.7)a Two-tailed Student t test.b Pearson χ2 test.c Fisher exact test.
4 B. Xu et al.
3.3. ERG expression in relation to BCR
To determinate the potential prognostic role of ERG, amultivariate analysis using the Cox proportional hazardsmodel was performed. BCR was only associated with higherGleason score (hazards ratio, 4.30; 95% confidence interval[CI], 1.78-10.40; P = .001) and elevated preoperative PSAlevels (hazards ratio, 1.03; 95% CI, 1.00-1.05; P = .04). Nosignificant correlation was detected between BCR and age atthe time of diagnosis (hazards ratio, 0.99; 95% CI, 0.95-1.03;P = .47), surgical margin status (hazards ratio, 1.39; 95% CI,0.86-2.24;P = .18), or ERG immunopositivity (hazards ratio =1.04; 95% CI = 0.63-1.71; P = .88). A Kaplan-Meier curverevealed no difference in terms of BCR-free survival betweenERG-positive and ERG-negative groups (Fig. 2).
ig. 2 Kaplan-Meier curve of disease-free survival: the expres-ion of ERG is unrelated to BCR.
4. Discussion
TMPRSS2 and ERG genes are located 3 Mb apart onchromosome 21q. Under the influence of androgens,intrachromosomal interstitial deletion or translocation oc-curs, leading to juxtaposition of the androgen-responsiveTMPRSS2 gene to the transcription unit of ERG [78,79].TMPRSS2/ERG fusion produces a truncated ERG protein,which, in turn, mediates transcription, apoptosis, cellproliferation, differentiation, and invasiveness via multiplemolecular pathways [78-80]. The molecular targets, whichhave been shown to interact with ERG, include the
following: poly(ADP-ribosome) polymerase 1 [81], DNAprotein kinase [81], HDAC1 target genes and WNT/β-catenin signaling pathway [82], matrix metaloproteinases,PIM-1 oncogene, c-MYC oncogene, PI3K-PTEN axis, andEZH2 polycomb group protein [78-80]. Recently, it has beenshown that poly(ADP-ribosome) polymerase 1 inhibitorselectively represses the growth of ERG-positive, but notERG-negative, prostate cancer xenografts, renderingTMPRSS2/ERG fusion a potential molecular therapeutictarget for prostate cancer [81].
The reported incidence of TMPRSS2/ERG fusion inprostate adenocarcinoma ranges from 20% to 68% in RPand biopsy specimens [3-24] and from 0 to 29% in incidentaltumors detected in TURP specimens [4,5,13,25-30]. This
Fs

Table 2 Association of TMPRSS2/ERG fusion or ERGoverexpression with clinicopathologic characteristics:a summary of English literature
Association of ERG fusion with No. of studies No. of men
Preoperative PSALow level 6 6159High level 2 510No association 20 2740Gleason scoreLow score 8 5424High score 9 1734No association 37 6455Pathologic stageLow stage 0 0High stage 10 5540No association 35 6474Recurrence and/or mortalityLow risk 1 150High risk 8 1078No association 30 11 092Total 54 14 376
5ERG immunopositivity in prostate adenocarcinoma
wide range of incidence is influenced by multiple factorsincluding study design, detection methods (PCR, FISH, orIHC), patients' ethnic background, intratumoral immunohe-terogeneity of ERG, interobserver and interstudy variability ofstain interpretation, the clone of the ERG antibody used, andthe molecular difference between transitional and peripheralzone tumors [11,13,24,50-52,76,83-85]. Our study included59 cases of prostatic adenocarcinoma detected in TURPspecimen. Only cancers with a total Gleason score of 6 and anoverall tumor volume of less than 1% of TURP volume wereincluded in an effort to ensure that the adenocarcinoma wereof transitional zone origin rather than an extension of prostaticcancer from the peripheral zone. Consistent with what hasbeen previously reported, we have found that the incidence ofERG immunopositivity in RP (151/454 patients; 33%) wassignificantly higher compared with that of incidental transi-tional zone cancers detected in TURP specimens (3/59patients; 5.1%). The exact significance of such a zonaldifference in terms of ERG expression is unclear, but mostlikely reflects the biological difference between transitionaland peripheral zone cancers [24,84,85].
The main objective of the current study was to investigatewhether ERG immunopositivity was associated with clinicaland pathologic phenotypes of prostate adenocarcinoma, andwhether it could serve as a prognostic biomarker to predictrecurrence and mortality. Numerous studies have beenpublished, in the past decade, which generated conflictingresults. We have reviewed all available English literature,from 2005 to 2013, that focused on the association betweenTMPRSS2/ERG fusion/ERG overexpression in RPs and thefollowing 4 clinicopathologic parameters: (1) preoperativePSA level, (2) Gleason score, (3) AJCC pathologic stage,and (4) recurrence and mortality. Tumor stage, Gleasongrade, and PSA level were selected because they are the 3criteria currently used by clinicians following the D'Amicocriteria to define prognostic risk groups and to guidetreatment [86]. A total of 56 studies [4,5,7,8,10-12,15-18,20,22,26-28,30,31,38,38-76] including 14 571 men withprostate cancer were identified, and the results are summa-rized in Table 2. Details of each study, in terms of the numberof patients, detection methods for ERG, and specimen type(RP, TURP, or biopsy), are provided in Table 3.
The result of this literature review shows that ERG-positive prostate cancer cases tend to have a lowerpreoperative PSA level compared with ERG-negativecases. A total of 6 studies, with 6159 men, including the 4largest-scale studies to date with 481, 1039, 1180, and 2805men [15,54,56,58] and the present study with 454 men, haveshown a significant correlation of ERG positivity with lowPSA levels. In contrast, 20 studies [7,10,11,17,18,20,40,42-45,49-51,56-61], with a samples size of 19 to 254, havereported no correlation between ERG status and PSA level,which might be explained by a lack of statistical power dueto small sample size.
Based on the existing evidence, we cannot conclude, withconfidence, the relationship between ERG status and
Gleason score. Eight studies of 5424 prostate cancers[12,28,42,47,50,55,59,62,76] have reported a significantnegative association; 9 studies of 1734 men [4,5,11,26,39-41,43,44] reported a positive association, and 37 studies of6455 men, including our own, reported a null associationbetween ERG status and high Gleason score [7,8,10,15-17,20,22,27,30,38,38,44,45,45,46,49,51-54,56-61,63-71].
Overall, TMPRSS2/ERG fusion tends to be associated withadvanced AJCC pathologic stage. Ten studies, including 5540men [4,11,30,31,39,42,45,45-47], have found a higherpercentage of advanced disease in ERG-positive cancercompared with ERG-negative cancer, whereas the reversehas not been reported in the literature. The link between ERGpositivity and advanced tumor stage has been further supportedby a meta-analysis across 34 studies and 8003 RPs, in whichTMPRSS2/ERG fusion was associated with more advancedpathologic stage at diagnosis [45]. However, such associationis not always clear-cut. Thirty-five studies of 6474 men[7,8,10,12,15,17,18,20,22,26,27,38,38,40,44,49-51,54,56-58,60-62,64-70,72], including the current study, have shownthat ERG status was independent from pathologic stage.Possible explanations could be that the adverse correlationbetween ERG and tumor stage is biologically trivial, or onlypresent in a small subset of patients. Therefore, suchassociation cannot be readily detected in small-scale studies.
Despite the high prevalence of TMPRSS2/ERG fusion inprostate adenocarcinoma, the fusion carries very little, if any,prognostic value in predicting BCR and cancer-specific death.Overwhelming evidence from 30 studies and 11 092 men[4,7,8,12,15,38,43,44,44-47,50,53-56,58,60-65,67,70,73-75],including the present study, has demonstrated that ERGpositivity was unrelated to recurrence or mortality. Thisconclusion was further supported by the meta-analysis

Table 3 Association of TMPRSS2/ERG fusion or ERGoverexpression with clinicopathologic characteristics:a detailed review of literature
Reference N Assay Type
Low PSA level (6 studies, 6159 men)[54] a 200 FISH Bx
454 IHC RP[15] 481 IHC RP[55] 1039 IHC RP[45] 1180 IHC RP[47] 2805 IHC RPHigh PSA level (2 studies, 510 men)[38] 65 FISH RP[39] 445 FISH RPNo association with PSA level (20 studies, 2740 men)[40] 19 IHC RP[18] 26 RT-PCR RP[44] 45 RT-PCR RP[56] 45 RT-PCR RP[57] 50 FISH RP, TURP[10] 59 FISH RP[45] 90 IHC TURP[49] 122 FISH RP[20] 150 FISH RP[51] 150 FISH RP[7] 163 FISH RP[17] 165 RT-PCR RP[58] 178 FISH Bx[42] 184 TLDA RP[59] 194 RT-PCR RP[43] 197 FISH, RT-PCR RP[11] 209 IHC RP, Bx[60] 214 FISH RP, TURP[61] 226 RT-PCR RP[50] 254 FISH RPLow Gleason score (8 studies, 5424 men)[76] 174 FISH RP[42] 184 TLDA RP[59] 194 RT-PCR RP[62] 253 IHC RP[50] 254 FISH RP[12,28] 521 FISH RP[55] 1039 IHC RP[47] 2805 IHC RPHigh Gleason score (9 studies, 1734 men)[40] 19 IHC RP[41] 75 FISH RP[5] 105 FISH TURP[26] 111 FISH, PCR TURP[43] 197 FISH, RT-PCR RP[11] 209 IHC RP, Bx[44] 261 IHC RP[4] 312 IHC TURP[39] 445 FISH RPNo association with Gleason score (37 studies, 6455 men)[22] 41 IHC, PCR RP[38] 42 FISH RP[44] 45 RT-PCR RP[56] 45 RT-PCR RP
Table 3 (continued)
Reference N Assay Type
[57] 50 FISH RP, TURP[63] 50 RT-PCR RP[30] 54 FISH TURP[64] 54 RT-PCR, FISH RP[10] 59 FISH RP[65] 59 RT-PCR RP[38] 65 FISH RP[66] 82 FISH, RT-PCR RP[67] 84 RT-PCR RP[53] 85 RT-PCR Mets[68] 88 FISH, RT-PCR RP[45] 90 IHC TURP[27] 94 FISH RP[16] 100 FISH Bx[46] 118 FISH RP[49] 122 FISH RP[69] 147 IHC RP[20] 150 FISH RP[51] 150 FISH RP[70] 158 RT-PCR Bx[7] 163 FISH RP[17] 165 RT-PCR RP[58] 178 FISH Bx[71] 180 IHC, FISH RP[59] 194 RT-PCR RP[54] 200 FISH Bx[60] 214 FISH RP, TURP[61] 226 RT-PCR RP[52] 248 FISH RPa 454 IHC RP[15] 481 IHC RP[8] 540 FISH RP[45] 1180 IHC RPLow AJCC stage (0 study)High AJCC stage (10 studies, 5540 men)[30] 54 FISH TURP[45] 90 IHC TURP[46] 118 FISH RP[31] 143 IHC, FISH RP[42] 184 TLDA RP[11] 209 IHC RP, Bx[4] 312 IHC TURP[39] 445 FISH RP[45] 1180 IHC RP[47] 2805 IHC RPNo association with stage (35 studies, 6474 men)[40] 19 IHC RP[18] 26 RT-PCR RP[22] 41 IHC, PCR RP[38] 42 FISH RP[44] 45 RT-PCR RP[56] 45 RT-PCR RP[57] 50 FISH RP, TURP[64] 54 RT-PCR, FISH RP[10] 59 FISH RP[65] 59 RT-PCR RP[38] 65 FISH RP
6 B. Xu et al.

Table 3 (continued)
Reference N Assay Type
[66] 82 FISH, RT-PCR RP[67] 84 RT-PCR RP[68] 88 FISH, RT-PCR RP[27] 94 FISH RP[72] 95 FISH RP[26] 111 FISH, PCR TURP[49] 122 FISH RP[69] 147 IHC RP[20] 150 FISH RP[51] 150 FISH RP[70] 158 RT-PCR Bx[7] 163 FISH RP[17] 165 RT-PCR RP[58] 178 FISH Bx[54] 200 FISH Bx[60] 214 FISH RP, TURP[61] 226 RT-PCR RP[62] 253 IHC RP[50] 254 FISH RPa 454 IHC RP[15] 481 IHC RP[12] 521 FISH RP[8] 540 FISH RP[55] 1039 IHC RPLow risk of recurrence or mortality (1 study, 150 men)[20] 150 FISH RPHigh risk of recurrence or mortality (8 studies, 1078 men)[40] 19 IHC RP[18] 26 RT-PCR RP[45] 90 IHC TURP[48] 100 IHC RP[26] 111 FISH, PCR TURP[49] 122 FISH RP[17] 165 RT-PCR RP[39] 445 FISH RPNo association with clinical outcome (30 studies, 11 092 men)[44] 45 RT-PCR RP[56] 45 RT-PCR RP[63] 50 RT-PCR RP[64] 54 RT-PCR, FISH RP[65] 59 RT-PCR RP[38] 65 FISH RP[73] 67 RT-PCR RP, TURP[67] 84 RT-PCR RP[53] 85 RT-PCR Mets[46] 118 FISH RP[70] 158 RT-PCR Bx[7] 163 FISH RP[58] 178 FISH Bx[43] 197 FISH, RT-PCR RP[54] 200 FISH Bx[60] 214 FISH RP, TURP[61] 226 RT-PCR RP[62] 253 IHC RP[50] 254 FISH RP[44] 261 IHC RP[4] 312 IHC TURP
Table 3 (continued)
Reference N Assay Type
[74] 344 FISH RPa 454 IHC RP[15] 481 IHC RP[12] 521 FISH RP[8] 540 FISH RP[75] 640 FISH RP[55] 1039 IHC RP[45] 1180 IHC RP[47] 2805 IHC RP
Abbreviations: Bx, biopsy; Mets, metastasis; RP, radical prostatectomy;TURP, transurethral resection of prostate; Type, type of the specimen; FISH,fluorescence in situ hybridization; IHC, immunohistochemistry; RT-PCR,real-time polymerase chain reaction; TLDA, TaqMan low-density arrays.
a Current study.
7ERG immunopositivity in prostate adenocarcinoma
performed by Pettersson et al [45] across 19 studies and 5074prostate cancers. Once again, conflicting evidence has beenreported, with 8 studies (1078 men) [17,18,26,39,40,45,48,49]showing a positive association and 1 study (150 men) [20]showing a negative association between ERG fusion and anadverse clinical outcome.
Other than reporting ERG staining in prostate cancer aspositive or negative, only 2 studies, to date, have evaluated theprognostic value of the intensity of ERG staining, which yieldconflicting results [4,48]. Bismar et al [4] have shown anegative correlation between staining intensity and cancer-specific mortality, whereas Spencer et al [48] reported anincreased risk of BCR, metastasis, and cancer-specific death inprostatic cancer with high ERG intensity. In our hands, therewas no association between staining intensity or H-score on onehand and any clinicopathologic or outcome parameters onanother hand.
In summary, the biological relationship betweenTMPRSS2/ERG fusion and clinicopathologic parameters,such as PSA level, Gleason score, pathologic stage, andprognosis, is not well established, and the results of differentstudies lack consistency. That being said, the possibility thatERG status may only influence a small subset of prostatecancer cases bearing a unique histologic or molecularsignature exists, and such a relationship would be dilutedwhen all prostate cancers are pooled into different studies.Further studies incorporating thorough morphologic andimmunophenotypic features, or using advanced moleculartechniques (eg, array-comparative genomic hybridizationand next-generation sequencing) to allow the comparison ofgene profiles, will be required to identify the subgroup ofprostate cancers in which TMPRSS2/ERG fusion may beprognostically important.
5. Conclusions
In this TMA study of 454 prostate adenocarcinomas fromRP and 59 incidental cancers from TURP, we have found

8 B. Xu et al.
that ERG overexpression was much more common inperipheral zone prostate cancers in comparison with thoseof the transitional zone. In our hands, ERG immunopositivitywas unrelated either to aggressive local tumor characteristicsor to a worse outcome.
References
[1] U.S. Cancer Statitics Working Group. United state cancer statistics:1999-2009 incidence and mortality Web-based report. 2012. Atlanta,GA: Department of Health and Human Services, Centers for DiseaseControl and Prevention, and National Cancer Institute.
[2] Tomlins SA, Rhodes DR, Perner S, et al. Recurrent fusion ofTMPRSS2 and ETS transcription factor genes in prostate cancer.Science 2005;310:644-8.
[3] Bismar TA, YoshimotoM, Vollmer RT, et al. PTEN genomic deletion isan early event associated with ERG gene rearrangements in prostatecancer. BJU Int 2011;107:477-85.
[4] Bismar TA, Dolph M, Teng LH, Liu S, Donnelly B. ERG proteinexpression reflects hormonal treatment response and is associated withGleason score and prostate cancer specific mortality. Eur J Cancer2012;48:538-46.
[5] Braun M, Scheble VJ, Menon R, et al. Relevance of cohort design forstudying the frequency of the ERG rearrangement in prostate cancer.Histopathology 2011;58:1028-36.
[6] Chaux A, Albadine R, Toubaji A, et al. Immunohistochemistry forERG expression as a surrogate for TMPRSS2-ERG fusion detection inprostatic adenocarcinomas. Am J Surg Pathol 2011;35:1014-20.
[7] Darnel AD, Lafargue CJ, Vollmer RT, Corcos J, Bismar TA.TMPRSS2-ERG fusion is frequently observed in Gleason pattern 3prostate cancer in a Canadian cohort. Cancer Biol Ther 2009;8:125-30.
[8] Esgueva R, Perner S, LaFargue J, et al. Prevalence of TMPRSS2-ERGand SLC45A3-ERG gene fusions in a large prostatectomy cohort. ModPathol 2010;23:539-46.
[9] Falzarano SM, Zhou M, Carver P, Tsuzuki T, Simmerman K, He H,Magi-Galluzzi C. ERG gene rearrangement status in prostate cancerdetected by immunohistochemistry. Virchows Arch 2011;459:441-7.
[10] Falzarano SM, Zhou M, Hernandez AV, Klein EA, Rubin MA, Magi-Galluzzi C. Single focus prostate cancer: pathological features andERG fusion status. J Urol 2011;185:489-94.
[11] Furusato B, van Leenders GJ, Trapman J, et al. ImmunohistochemicalETS-related gene detection in a Japanese prostate cancer cohort:diagnostic use in Japanese prostate cancer patients. Pathol Int 2011;61:409-14.
[12] Gopalan A, Leversha MA, Satagopan JM, et al. TMPRSS2-ERG genefusion is not associated with outcome in patients treated byprostatectomy. Cancer Res 2009;69:1400-6.
[13] Guo CC, Zuo G, Cao D, Troncoso P, Czerniak BA. Prostate cancer oftransition zone origin lacks TMPRSS2-ERG gene fusion. Mod Pathol2009;22:866-71.
[14] Guo CC, Wang Y, Xiao L, Troncoso P, Czerniak BA. The relationshipof TMPRSS2-ERG gene fusion between primary and metastaticprostate cancers. HUM PATHOL 2012;43:644-9.
[15] Hoogland AM, Jenster G, van Weerden WM, et al. ERG immuno-histochemistry is not predictive for PSA recurrence, local recurrence oroverall survival after radical prostatectomy for prostate cancer. ModPathol 2012;25:471-9.
[16] Mosquera JM, Mehra R, Regan MM, et al. Prevalence of TMPRSS2-ERG fusion prostate cancer among men undergoing prostate biopsy inthe United States. Clin Cancer Res 2009;15:4706-11.
[17] Nam RK, Sugar L, Yang W, et al. Expression of the TMPRSS2:ERGfusion gene predicts cancer recurrence after surgery for localisedprostate cancer. Br J Cancer 2007;97:1690-5.
[18] Nam RK, Sugar L, Wang Z, et al. Expression of TMPRSS2:ERG genefusion in prostate cancer cells is an important prognostic factor forcancer progression. Cancer Biol Ther 2007;6:40-5.
[19] Perner S, Mosquera JM, Demichelis F, et al. TMPRSS2-ERG fusionprostate cancer: an early molecular event associated with invasion. AmJ Surg Pathol 2007;31:882-8.
[20] Saramaki OR, Harjula AE, Martikainen PM, Vessella RL, TammelaTL, Visakorpi T. TMPRSS2:ERG fusion identifies a subgroup ofprostate cancers with a favorable prognosis. Clin Cancer Res 2008;14:3395-400.
[21] Scheble VJ, Braun M, Beroukhim R, et al. ERG rearrangement isspecific to prostate cancer and does not occur in any other commontumor. Mod Pathol 2010;23:1061-7.
[22] van Leenders GJ, Boormans JL, Vissers CJ, et al. Antibody EPR3864is specific for ERG genomic fusions in prostate cancer: implicationsfor pathological practice. Mod Pathol 2011;24:1128-38.
[23] Yaskiv O, Zhang X, Simmerman K, et al. The utility of ERG/P63double immunohistochemical staining in the diagnosis of limitedcancer in prostate needle biopsies. Am J Surg Pathol 2011;35:1062-8.
[24] Zhang S, Pavlovitz B, Tull J, Wang Y, Deng FM, Fuller C. Detectionof TMPRSS2 gene deletions and translocations in carcinoma,intraepithelial neoplasia, and normal epithelium of the prostate bydirect fluorescence in situ hybridization. Diagn Mol Pathol 2010;19:151-6.
[25] Bismar TA, Yoshimoto M, Duan Q, Liu S, Sircar K, Squire JA.Interactions and relationships of PTEN, ERG, SPINK1 and AR incastration-resistant prostate cancer. Histopathology 2012;60:645-52.
[26] Demichelis F, Fall K, Perner S, et al. TMPRSS2:ERG gene fusionassociated with lethal prostate cancer in a watchful waiting cohort.Oncogene 2007;26:4596-9.
[27] Falzarano SM, Navas M, Simmerman K, Klein EA, Rubin MA, ZhouM, Magi-Galluzzi C. ERG rearrangement is present in a subset oftransition zone prostatic tumors. Mod Pathol 2010;23:1499-506.
[28] Fine SW, Gopalan A, Leversha MA, et al. TMPRSS2-ERG genefusion is associated with low Gleason scores and not with high-grademorphological features. Mod Pathol 2010;23:1325-33.
[29] Gopalan A, Leversha MA, Dudas ME, et al. TMPRSS2-ERGrearrangement in dominant anterior prostatic tumours: incidence andcorrelation with ERG immunohistochemistry. Histopathology2013;63:279-86.
[30] Liu S, Yoshimoto M, Trpkov K, et al. Detection of ERG generearrangements and PTEN deletions in unsuspected prostate cancer ofthe transition zone. Cancer Biol Ther 2011;11:562-6.
[31] Gao X, Li LY, Zhou FJ, et al. ERG rearrangement for predictingsubsequent cancer diagnosis in high-grade prostatic intraepithelialneoplasia and lymph node metastasis. Clin Cancer Res 2012;18:4163-72.
[32] Mosquera JM, Perner S, Genega EM, et al. Characterization ofTMPRSS2-ERG fusion high-grade prostatic intraepithelial neoplasiaand potential clinical implications. Clin Cancer Res 2008;14:3380-5.
[33] Shah RB, Tadros Y, Brummell B, Zhou M. The diagnostic use of ERGin resolving an “atypical glands suspicious for cancer” diagnosis inprostate biopsies beyond that provided by basal cell and alpha-methylacyl-CoA-racemase markers. HUM PATHOL 2013;44:786-94.
[34] Clark J, Merson S, Jhavar S, et al. Diversity of TMPRSS2-ERG fusiontranscripts in the human prostate. Oncogene 2007;26:2667-73.
[35] Clark JP, Cooper CS. ETS gene fusions in prostate cancer. Nat RevUrol 2009;6:429-39.
[36] Braun M, Goltz D, Shaikhibrahim Z, et al. ERG protein expression andgenomic rearrangement status in primary and metastatic prostatecancer—a comparative study of two monoclonal antibodies. ProstateCancer Prostatic Dis 2012;15:165-9.
[37] Park K, Tomlins SA, Mudaliar KM, et al. Antibody-based detection ofERG rearrangement-positive prostate cancer. Neoplasia 2010;12:590-8.

9ERG immunopositivity in prostate adenocarcinoma
[38] Mehra R, Tomlins SA, Shen R, et al. Comprehensive assessment ofTMPRSS2 and ETS family gene aberrations in clinically localizedprostate cancer. Mod Pathol 2007;20:538-44.
[39] Attard G, Clark J, Ambroisine L, et al. Duplication of the fusion ofTMPRSS2 to ERG sequences identifies fatal human prostate cancer.Oncogene 2008;27:253-63.
[40] Szasz AM, Majoros A, Rosen P, et al. Prognostic potential of ERG(ETS-related gene) expression in prostatic adenocarcinoma. Int UrolNephrol 2013;45:727-33.
[41] Hofer MD, Kuefer R, Maier C, et al. Genome-wide linkage analysis ofTMPRSS2-ERG fusion in familial prostate cancer. Cancer Res2009;69:640-6.
[42] Paulo P, Barros-Silva JD, Ribeiro FR, et al. FLI1 is a novel ETStranscription factor involved in gene fusions in prostate cancer. GenesChromosomes Cancer 2012;51:240-9.
[43] Rajput AB, Miller MA, De Luca A, et al. Frequency of the TMPRSS2:ERG gene fusion is increased in moderate to poorly differentiatedprostate cancers. J Clin Pathol 2007;60:1238-43.
[44] Furusato B, Tan SH, Young D, et al. ERG oncoprotein expression inprostate cancer: clonal progression of ERG-positive tumor cells andpotential for ERG-based stratification. Prostate Cancer Prostatic Dis2010;13:228-37.
[45] Pettersson A, Graff RE, Bauer SR, et al. The TMPRSS2:ERGrearrangement, ERG expression, and prostate cancer outcomes: acohort study and meta-analysis. Cancer Epidemiol Biomarkers Prev2012;21:1497-509.
[46] Perner S, Demichelis F, Beroukhim R, et al. TMPRSS2:ERG fusion-associated deletions provide insight into the heterogeneity of prostatecancer. Cancer Res 2006;66:8337-41.
[47] Minner S, Enodien M, Sirma H, et al. ERG status is unrelated to PSArecurrence in radically operated prostate cancer in the absence ofantihormonal therapy. Clin Cancer Res 2011;17:5878-88.
[48] Spencer ES, Johnston RB, Gordon RR, et al. Prognostic value of ERGoncoprotein in prostate cancer recurrence and cause-specific mortality.Prostate 2013;73:905-12.
[49] Yoshimoto M, Joshua AM, Cunha IW, et al. Absence of TMPRSS2:ERG fusions and PTEN losses in prostate cancer is associated with afavorable outcome. Mod Pathol 2008;21:1451-60.
[50] Lee K, Chae JY, Kwak C, Ku JH, Moon KC. TMPRSS2-ERG genefusion and clinicopathologic characteristics of Korean prostate cancerpatients. Urology 2010;76:1268-313.
[51] Magi-Galluzzi C, Tsusuki T, Elson P, et al. TMPRSS2-ERG genefusion prevalence and class are significantly different in prostatecancer of Caucasian African-American and Japanese patients. Prostate2011;71:489-97.
[52] Mao X, Yu Y, Boyd LK, et al. Distinct genomic alterations inprostate cancers in Chinese and Western populations suggestalternative pathways of prostate carcinogenesis. Cancer Res 2010;70:5207-12.
[53] Boormans JL, Hermans KG, Made AC, et al. Expression of theandrogen-regulated fusion gene TMPRSS2-ERG does not predictresponse to endocrine treatment in hormone-naive, node-positiveprostate cancer. Eur Urol 2010;57:830-5.
[54] Barros-Silva JD, Ribeiro FR, Rodrigues A, et al. Relative 8q gainpredicts disease-specific survival irrespective of the TMPRSS2-ERGfusion status in diagnostic biopsies of prostate cancer. GenesChromosomes Cancer 2011;50:662-71.
[55] Schaefer G, Mosquera JM, Ramoner R, et al. Distinct ERGrearrangement prevalence in prostate cancer: higher frequency inyoung age and in low PSA prostate cancer. Prostate Cancer ProstaticDis 2013;16:132-8.
[56] Rouzier C, Haudebourg J, Carpentier X, et al. Detection of theTMPRSS2-ETS fusion gene in prostate carcinomas: retrospectiveanalysis of 55 formalin-fixed and paraffin-embedded samples withclinical data. Cancer Genet Cytogenet 2008;183:21-7.
[57] Sun QP, Li LY, Chen Z, et al. Detection of TMPRSS2-ETS fusions bya multiprobe fluorescence in situ hybridization assay for the early
diagnosis of prostate cancer: a pilot study. J Mol Diagn 2010;12:718-24.
[58] Leinonen KA, Tolonen TT, Bracken H, et al. Association of SPINK1expression and TMPRSS2:ERG fusion with prognosis in endocrine-treated prostate cancer. Clin Cancer Res 2010;16:2845-51.
[59] Miyagi Y, Sasaki T, Fujinami K, et al. ETS family-associated genefusions in Japanese prostate cancer: analysis of 194 radicalprostatectomy samples. Mod Pathol 2010;23:1492-8.
[60] FitzGerald LM, Agalliu I, Johnson K, et al. Association of TMPRSS2-ERG gene fusion with clinical characteristics and outcomes: results froma population-based study of prostate cancer. BMC Cancer 2008;8:230.
[61] Rubio-Briones J, Fernandez-Serra A, Calatrava A, et al. Clinicalimplications of TMPRSS2-ERG gene fusion expression in patientswith prostate cancer treated with radical prostatectomy. J Urol2010;183:2054-61.
[62] Kron K, Liu L, Trudel D, et al. Correlation of ERG expression andDNA methylation biomarkers with adverse clinicopathologic featuresof prostate cancer. Clin Cancer Res 2012;18:2896-904.
[63] Winnes M, Lissbrant E, Damber JE, Stenman G. Molecular geneticanalyses of the TMPRSS2-ERG and TMPRSS2-ETV1 gene fusions in50 cases of prostate cancer. Oncol Rep 2007;17:1033-6.
[64] Lapointe J, Kim YH, Miller MA, et al. A variant TMPRSS2 isoformand ERG fusion product in prostate cancer with implications formolecular diagnosis. Mod Pathol 2007;20:467-73.
[65] Wang J, Cai Y, Ren C, Ittmann M. Expression of variantTMPRSS2/ERG fusion messenger RNAs is associated with aggres-sive prostate cancer. Cancer Res 2006;66:8347-51.
[66] Tu JJ, Rohan S, Kao J, Kitabayashi N, Mathew S, Chen YT. Genefusions between TMPRSS2 and ETS family genes in prostate cancer:frequency and transcript variant analysis by RT-PCR and FISH onparaffin-embedded tissues. Mod Pathol 2007;20:921-8.
[67] Bonaccorsi L, Nesi G, Nuti F, et al. Persistence of expression of theTMPRSS2:ERG fusion gene after pre-surgery androgen ablation maybe associated with early prostate specific antigen relapse of prostatecancer: preliminary results. J Endocrinol Invest 2009;32:590-6.
[68] Svensson MA, Lafargue CJ, MacDonald TY, et al. Testing mutualexclusivity of ETS rearranged prostate cancer. Lab Invest 2011;91:404-12.
[69] Verdu M, Trias I, Roman R, et al. ERG expression and prostaticadenocarcinoma. Virchows Arch 2013;462:639-44.
[70] Sabaliauskaite R, Jarmalaite S, Petroska D, et al. Combined analysis ofTMPRSS2-ERG and TERT for improved prognosis of biochemicalrecurrence in prostate cancer. Genes Chromosomes Cancer 2012;51:781-91.
[71] Nagle RB, Algotar AM, Cortez CC, et al. ERG overexpression andPTEN status predict capsular penetration in prostate carcinoma.Prostate 2013;73:1233-40.
[72] Albadine R, Latour M, Toubaji A, et al. TMPRSS2-ERG gene fusionstatus in minute (minimal) prostatic adenocarcinoma. Mod Pathol2009;22:1415-22.
[73] Hermans KG, Boormans JL, Gasi D, et al. Overexpression of prostate-specific TMPRSS2(exon 0)-ERG fusion transcripts corresponds withfavorable prognosis of prostate cancer. Clin Cancer Res 2009;15:6398-403.
[74] Toubaji A, Albadine R, Meeker AK, et al. Increased gene copy numberof ERG on chromosome 21 but not TMPRSS2-ERG fusion predictsoutcome in prostatic adenocarcinomas. Mod Pathol 2011;24:1511-20.
[75] Perner S, Rupp NJ, Braun M, et al. Loss of SLC45A3 protein(prostein) expression in prostate cancer is associated with SLC45A3-ERG gene rearrangement and an unfavorable clinical course. Int JCancer 2013;132:807-12.
[76] Rosen P, Pfister D, Young D, et al. Differences in frequency of ERGoncoprotein expression between index tumors of Caucasian andAfrican American patients with prostate cancer. Urology 2012;80:749-53.
[77] Edge SB, Byrd DR, Compton CC, Fritz AG, Greene FL, Trotti A,editors. AJCC cancer staging manual. Springer; 2009.

10 B. Xu et al.
[78] Hessels D, Schalken JA. Recurrent gene fusions in prostate cancer:their clinical implications and uses. Curr Urol Rep 2013;14:214-22.
[79] Rahim S, Uren A. Emergence of ETS transcription factors asdiagnostic tools and therapeutic targets in prostate cancer. Am JTransl Res 2013;5:254-68.
[80] Rosen P, Sesterhenn IA, Brassell SA, McLeod DG, Srivastava S, DobiA. Clinical potential of the ERG oncoprotein in prostate cancer. NatRev Urol 2012;9:131-7.
[81] Brenner JC, Ateeq B, Li Y, et al. Mechanistic rationale for inhibition ofpoly(ADP-ribose) polymerase in ETS gene fusion-positive prostatecancer. Cancer Cell 2011;19:664-78.
[82] Iljin K, Wolf M, Edgren H, et al. TMPRSS2 fusions with oncogenicETS factors in prostate cancer involve unbalanced genomic rearrange-
ments and are associated with HDAC1 and epigenetic reprogramming.Cancer Res 2006;66:10242-6.
[83] Shaikhibrahim Z, Lindstrot A, Ellinger J, et al. The peripheral zone ofthe prostate is more prone to tumor development than the transitionalzone: is the ETS family the key? Mol Med Rep 2012;5:313-6.
[84] Mehra R, Han B, Tomlins SA, et al. Heterogeneity of TMPRSS2 generearrangements in multifocal prostate adenocarcinoma: molecular evi-dence for an independent group of diseases. Cancer Res 2007;67:7991-5.
[85] Minner S, Gartner M, Freudenthaler F, et al. Marked heterogeneity ofERG expression in large primary prostate cancers. Mod Pathol2013;26:106-16.
[86] Ingels A, de la Taille A, Ploussard G. Radical prostatectomy as primarytreatment of high-risk prostate cancer. Curr Urol Rep 2012;13:179-86.
Copyright © 2022 FDOKUMEN