analysis and evaluation of segmental concrete tunnel linings
Upload
independentCategory
view
2download
0
CLINICAL ARTICLES J Oral Maxillofac Surg
42.771-781. 1984
The Posterior Segmental Maxillary Osteo tomy:
Recent Applications
FRANK MOLONEY, DDS, MD,* PAUL J. W. STOELINGA, DDS, MD,t AND HENK TIDEMAN, DDS, MD*
The application of the posterior segmental maxillary osteotomy to the problem of edentulous space closure was studied in 30 patients so treated. The degree of success was based on several criteria, which included sta- bility, periodontal health, occlusion, and response to treatment. A simpli- fied surgical technique is described and useful surgical aids are demon- strated. The existing literature is reviewed in the light of present findings.
The posterior segmental maxillary osteotomy (PSMO) has most commonly been used for the sur- gical correction of anterior open-bite deformity. Very few reports in the literature refer to its use in the treatment of dentoalveolar problems other than those involving vertical dimension. It is the aim of this paper to review the application of this operation in three groups of patients for whom treatment was planned 1) to close existing edentulous spaces, 2) to “balance” occlusions resulting from other planned osteotomies performed at the same time, or 3) to close the space associated with the palatally impacted canine tooth.
The last group provides the first report of use of the PSMO in the treatment of the palatally impacted canine by the simultaneous advancement of the posterior segment and extraction of the unerupted tooth, either used singly or in combination with or- thodontics or with subsequent restorative dentistry.
Historical Aspects
The PSMO was introduced by Schuchardtr in 1954 as a two-staged procedure used in the surgical correction of open-bite deformity. In 1955? and
* Formerly resident, Department of Oral and Maxillofacial Surgery, Municipal Hospital. Arnhem, The Netherlands; cur- rently Consultant Maxillofacial Surgeon, Royal Brisbane Hos- pital, Herston Road Q 4029, Australia.
+ Consulting Oral Surgeon, Department of Oral and Maxillo- facial Surgery. Municipal Hospital, Arnehm. The Netherlands.
i: Professor of Oral and Maxillofacial Surgery, University of ,4delaide, SA 5001, Australia.
Address correspondence and reprint requests to Dr. Stoelinga: Department of Oral and Maxillofacial Surgery, Municipal Hos- pital. 6800 EE Arnhem. The Netherlands.
19593 Schuchardt reported a technique that in- volved a delay of four to six weeks between the initial palatal osteotomy and the subsequent oste- otomy of the lateral maxillary wall. Although Schu- chardt was the first surgeon to report segmental maxillary surgery for functional correction, the demonstration that part of the upper jaw could be segmentally downfractured and returned to its orig- inal position and that it would then heal without complication was provided as long ago as 1867 by Cheever.4,5 In 1960 Kufner6 described a one-stage modification of the Schuchardt procedure and, in 1968,7 reported his follow-up results. Schuchardt is later reported to have used the one-stage operation als0.s
Several modifications of the PSMO have been de- scribed using either horizontal or vertical buccal in- cisions, a direct or transantral approach to the pal- atal osteotomy, and varying degrees of exposure of the palatal bone before osteotomy.s-‘” A pictorial review of several of these modifications can be found in the textbook of Bell, Proffit. and White. Is The palatal osteotomy is generally carried into the maxillary sinus, although Perko” performs this cut parasagittally into the nasal cavity. Potential prob- lems within the nasal cavity using this variation have been discussed by West and Epker.*
Mohnacr’ utilized the PSMO for both anterior open-bite and posterior cross-bites, and, later,‘s he extended its use in combination with mandibular osteotomies. In 1971 Converse and Wood-SmithI reported their experiences with the PSMO not only for intrusion but also for extrusion of the segment to close a posterior open-bite, filling the resultant defect with bone grafts.
771
772 POSTERIOR SEGMENTAL MAXILLARY OSTEOTOMY
, I , \
i -I I J
I’ I \
‘__-’ : .
s__’
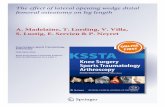
FIGURE 1. Lej?. Interdental and tuberosity buccal incisions; right, transverse palatal incision.
West and Epker* provided the first extensive re- view of the PSMO, listing as the four basic indica- tions for its use:
1. Correction of posterior maxillary alveolar hy- perplasia.
2. Correction of total maxillary alveolar hyper- plasia when combined with a simultaneous anterior osteotomy.
3. Correction of bilateral or unilateral cross-bite. 4. Distal repositioning of the posterior maxillary
alveolar fragment to provide space for an impacted canine or premolar tooth.
Bell and Turvey2’ successfully corrected poste- rior cross-bites with this operation, while its use for edentulous space closure was first reported in 1976 by Bell and McBride.” Use of the PSMO in pre- prosthetic cases to intrude over-erupted posterior maxillary segments and allow restoration of eden- tulous mandibular segments was first described by West and Burk22 and later by Alexander and Sickels.23
Tideman et al.24 demonstrated the versatility of the PSMO, using it for the collapsed minor segment when dealing with simultaneous palatal cleft clo- sure, arch movement in several planes, and oro- nasal fistula closure. One significant advantage of- fered by this technique was the partial or complete elimination of the edentulous space in the region of the alveolar cleft, whether or not the area was grafted. The concept of utilizing the PSMO in cases involving a palatally impacted canine tooth was de- veloped by one of the authors (P.S.) from its suc- cessful application in these more complex palatal and alveolar cleft patients.
Preoperative Evaluation
Model surgery demonstrates the feasibility of segmental arch alteration, attention being directed
to the stability of the planned occlusion and the angulation and rotation of the individual teeth ad- jacent to the proposed interdental osteotomy site. Periapical radiographs are essential for this study. Consultation with the prosthodontist or restorative dentist is often necessary to decide how much space to leave between anterior segments, the degree of esthetic success of the final restoration often de- pending on this decision.
An acrylic wafer is made to key the teeth into the desired position at the time of surgery, along with a full palatal acrylic splint. This palatal splint acts as a protective “dressing” over the palatal wounds, which are not sutured. The use of this simple device reduces operating time and eliminates the tedium of difficult palatal suturing, which experience has shown to be unnecessary. A custom-made arch bar may be constructed if bilateral PSMOs are planned but is not usually necessary in unilateral cases, the teeth being simply ligated to the acrylic wafer. Max- illomandibular fixation is usually not necessary.
Surgical Technique
The case of the impacted canine is used as the basis for this description, the anterior osteotomy cut being placed vertically in the interdental space between the lateral incisor and the first premolar. The anesthetist should be instructed to intubate the patient on the side opposite the planned osteotomy. A vertical incision is made in the buccal mucoperi- osteum of the interdental area (Fig. 1). Inferiorly the incision is carrier over to the palatal side. With the lateral alveolus exposed by reflection of adja- cent tissues, the vertical osteotomy line is com- pleted with a fine tapering fissue bur (Fig. 2). During this maneuver the impacted canine tooth will be sectioned.
Buccally, submucoperiosteal tunneling is carried

MOLONEY ET AL
FIGURE 2. Ti~p /&. Vertical interdental cut completed. Long Lindemann bur begins lateral osteotomy.
FIGURE 3. Top ri,qht. A IO-mm osteotome is used to complete the osteotomy directly through the palatal mucoperiosteum. without direct exposure of the bone.
FIGURE 4. Bottorrr I&. Straight osteotome aimed at 45 degree% to sagittal plane and directed through the tuberosity. Note the posterior extent of palatal osteotomy.
FIGURE 5. B~>ttom rigkf. Third molar removed and alternative use of curved instrument to complete tuherosity osteotomy.
posteriorly toward the tuberosity. A flat, malleable retractor is placed under the buccal pedicle in this tunnel, its distal end in the vicinity of the pterygo- maxillary junction. The lateral horizontal oste- otomy can be performed with relative ease despite the apparent confinement of this approach if a long Lindemann bur is used in an “inside-to-outside” fashion. It is first placed fully into the antrum at the uppermost point of the vertical osteotomy and grad- ually brought to bear against the bone of the lateral wall (Fig. 2). In this manner the posterior extent of the cut can be completed almost to the tuberosity, the last several millimeters finished by careful use of a 4-mm osteotome.
Next, the transverse palatal incision is made as depicted in Figure 1. The transverse palatal oste- otomy can be performed along this line with a bur or osteotome. This is followed by the palatal oste- otomy. Previous authors have resorted to varying degrees of exposure of the palatal bone to visualize the performance of this cut. However, reflection of
the soft tissues is unnecessary, and the palatal bone can be approached in a “blind” manner if certain precautions are taken. The aim is to place the sag- ittal bone cut at the junction of the vertical alveolus with the horizontal palatal process of the maxilla, above the root apices and lateral to the greater pal- atine artery. This can be safely accomplished by first placing a series of punctures into the antrum by angling a 4-mm osteotome at 45 degress to the vertical plane. The osteotomy is completed along this line using a thin-bladed, lo-mm, wood-handled osteotome (Fig. 3). The bone cut posteriorly should just begin to involve the horizontal process of the palatine bone (Fig. 4).
The final step is to approach the tuberosity region where the posterior osteotomy will be performed (Figs. 4, 5). Use of the tuberosity as an alternative osteotomy site to the standard pterygomaxillary junction was described by DuPont et al.?’ in 1974. and again by Bell and Turvey’O later that same year. Trimble et al.16 discussed in detail this simplified

POSTERIOR SEGMENTAL MAXILLARY OSTEOTOM\
FIGURE 6. Top. Preoper ative and (botrnm) postoperative r adio- graphs. Right third molar dis- placed and remaining in situ (arrow).
approach to the posterior osteotomy and reviewed all aspects of this modification. A straight or curved osteotomy is directed at 45 degrees to the sagittal plane (Figs. 4, 5). Excessively anterior angulation of the osteotome may damage the greater palatine vessels at their exit from the foramen or injure the distobuccal root of the second molar. Care is nec- essary to avoid accidental displacement of the third molar into an inaccessible region. Such a case is illustrated in Figure 6. An extremely high third molar may be ignored or avoided during the tuber- osity osteotomy, or extracted from the antrum after the downfracture of the segment.
The posterior segment is now downfractured. This sequence of events is recommended so that the major cuts are completed prior to the potentially more hazardous posterior osteotomy, immediate downfracture being possible in the event of unusual hemorrhage from the pterygotuberosity region.
Following the removal of the sectioned pieces of the canine, bone is removed in the interdental area until the segment can be seated in the splint in the predetermined position. A curved osteotome placed in the tuberosity may aid mobilization and anterior traction (Fig. 7). The acrylic wafer is then ligated to the maxillary arch. Finally, the palatal splint is ligated to adjacent teeth, four wire anchor points
pre-fixed to the splint aiding this final step. Only the anterior vertical buccal incision is sutured. A small amount of periodontal pack may be lightly applied to the interdental area after any grossly re- dundant gingival tissue is trimmed away. This dressing is removed in three to five days. Maxillo- mandibular fixation is not routinely used. If the wires crossing the occlusal wafer are molded by pressure into the mandibular teeth impressions, the
I.___
- ‘.--. FIGURE 7. Curved osteotome in tuberosity region aids for- ward mobilization. Interdental osteotomy has been completed and sectioned canine extracted.
MOLONEY ET AL
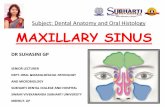
FlGtJRE 8. TcJ~, Preoperative frontal intraoral view showing retained deciduous canines (arrows) and otherwise satisfactory occlu- sion. Middle I#, Panoramic radiograph shows position of palatally impacted canine. Middle right, Right lateral postoperative intraoral view. Bottom icfr, Postoperative radiograph. Botfom right, Left lateral postoperative intraoral view. Note edge-to-edge occlusion of second premolar.
approximate occlusal position can be checked by closure of the mandible as a final step. The palatal splint may be removed after two weeks. The oc-
clusal wafer is removed at the six-week follow up. The stability of the segment is tested at the latter
appointment and generally found to be solidly healed. However, additional splinting is sometimes necessary. Impressions are then taken for the man- ufacture of a retainer device (Hawley-type) worn full-time initially and later at nighttime, as neces- sary. Return to the orthodontist, prosthodontist, or restorative dentist is usually achieved within two to four months after surgery.
Report of Cases
Cuse 1
A 19-year-old young woman presented with bilateral palatally impacted canine teeth. Her occlusion was oth-
erwise satisfactory. She was not interested in long-term orthodontic treatment, and was reluctant to seek expen- sive bridge restorations of the edentulous spaces subse- quent to the loss of her deciduous canines (Fig. 8). Bi- lateral PSMOs were performed without orthodontics. the retention plate being worn for six months postoperatively. Both sides healed solidly without complication. The I- mm gaps present on both sides between the lateral inci- sors and first premolars did not represent an ideal result. Overall, however. the result was considered successful and the patient was extremely pleased with her apprar- ante.
Case 2
A 36-year-old woman had prematurely lost her poste- rior mandibular teeth. She had not sought prosthetic res- toration until such time as the situation was virtually im- possible to treat by conservative means. Figure 9 clearly demonstrates the inferiorly collapsed posterior maxillary segments with almost complete elimination of the pos- terior mandibular dental spaces on jaw closure. Bilateral PSMO’s allowed superior repositioning of both posterior

776 POSTERIOR SEGMENTAL MAXILLARY OSTEOTOMY
FIGURE 9. Vertical collapse of (top Ieff) right and (top right) left posterior maxillary segments. Middle, Pre- and postoperative radiographs demonstrating im- proved freeway space for denture construction. B&torn lqft und
right, Postoperative occlusion with removable prosthesis in po-
segments together with medial movement of the left seg- ment to bring the molars more directly over the mandib- ular alveolus. Prosthetic consultation during model sur- gery helped coordinate the planned segmental movement. A mandibular fixed-removable prosthesis completed the treatment plan (Fig. 9).
Case 3
A 17-year-old young woman presented with a left max- illary alveolar cleft, a missing upper left first premolar and a malaligned upper left canine. The canine was
moved posteriorly by orthodontics to achieve contact with the second premolar, after which the maxillary seg- ment itself was surgically advanced to close the edentu- lous space. At the same time, the alveolar cleft was grafted with cancellous bone. Restorative dentistry is planned pending completion of the retention phase (Fig. 10).
Follow-up Study
Thirty patients were recalled for detailed assess- ment (Table I), all of whom underwent a PSMO for

MOLONEY ET AL 777
one or more of the three reasons previously out- lined. There were 23 females and seven males. The average age at operation was 20 years (range, 13-38 years) and the average follow-up time was 18 months (range, 3-52 months). The results in each case were evaluated by questionnaire, clinical ex- amination, serial study models, extraoral and in- traoral photographs, and panoramic and periapical radiographs.
Clinical evaluation included a critical assessment of the overall esthetic result. Close inspection was made of the occlusion, the contact between teeth adjacent to the interdental osteotomy, and the health of the individual teeth. Electrical pulp testing was performed. Periodontal probing depth was mea- sured in all teeth in and adjacent to the individual segment, and an assessment was made of gingival form and health in the area of the interdental bone cut. Crestal bone height in this area was scored ac- cording to a simple system, shown in Figure 11, through use of the radiographs. Individual teeth were also inspected for color, percussion sensi- tivity, and mobility within the alveolar segment. Other features studied included the presence of periapical pathology; the need for postoperative endodontics; the occlusal stability, with special note of any shift between centric relation (CR) and cen- tric occlusion (CO); the fate of the third molar in the involved tuberosity; the state of the palatal scar; the presence of oronasal or oroantral fistulae; and the presence of other complications, such as sinus infection and dental pain.
Results
Pulpal and Periapical Health
Of 165 teeth tested electrically, 35 (21%) were unresponsive. On only two occasions was there ob- vious pulpal or periapical pathology. Both teeth were adjacent to the interdental bone cut and both required subsequent root canal therapy. No direct damage to these teeth could be discovered when all available periapical tilms were examined. Evidence of damage to the root apices was not found in any other cases. All teeth showed normal color, no per- cussion sensitivity, and were stable, whether they responded positively or negatively to pulp testing.
FIGURE IO. Top. Preoperative condition. Left canine moved
posteriorly to contact second premolar and to open up alveolar cleft. Top center. Postoperative condition, in retention. Bottom center, Preoperative and (bottom) postoperative occlusal radio- graphs. Note consolidation of cancellous bone graft in alveolar cleft (arrow).

778 POSTERIOR SEGMENTAL MAXILLARY OSTEOTOMY
Table 1. Case Types of 30 Cases treated by Posterior Segmental Maxillary Osteotomy*
Type of Case Total No.
Bilateral Orthodontic Cases Cases
Impacted canine (I bilateral case) 13 1 I
Closure of edentulous space 7 4 4
Alveolar cleft case 7 2
Combined with mandibular osteotomies 3 3 3
* Thirty-eight segments were treated.
Periodontal Health
In the majority of cases the results were excel- lent. In 3 1 instances probing depth was 2 mm or less. In four sites the depth was 3 mm; in two, 4 mm; and in one, 5 mm. Of the seven cases where probing depth of the interdental osteotomy area was greater than 2 mm, five showed lack of contact between adjacent teeth. Notably, contact in the other two cases had been achieved by orthodontics in one and full crown coverage of the first premolar in the other. On no occasion was there any obvious ab- normal gingival condition present, the interdental tissues showing normal shape and form.
interdental Areas
Crestal bone height and form were studied from periapical films and classified. Normal anatomy was achieved in the great majority (27) of cases. Three cases showed loss of crest and eight showed vertical bone loss. Of the eight cases in the last category, six were also associated with lack of con- tact between adjacent teeth and, significantly, all of these areas had probing depths of 3 mm or more.
Eight cases showed interdental “healing defects” as described by Shepherd.27 As in his case, bony
union was complete despite the presence of the ra- diolucent line, which almost certainly represents an area of fibrous scar tissue (Fig. 12). Such an area was subjected to surgical exploration in one patient who repeatedly complained of localized pain de- spite the complete absence of clinical signs. Al- though a traumatic neuroma was suspected, the bi- opsy report described only unremarkable scar tissue, which, when removed, cured the patient’s symptoms.
Contact Point Assessment
The interdental areas were examined clinically and by follow-up dental casts to assess where ideal contact had been achieved between teeth adjacent to the osteotomy site. In the 33 instances in which full closure was attempted, 13 had ideal contact (seven orthodontic cases, five restorative dentistry cases, and one surgical case). Fifteen had a l-mm gap and five had a 2-mm gap. In five segments com- plete closure of the edentulous space was not the treatment aim, as this was to be accomplished by postoperative restorative dentistry. Achieving ideal contact purely by surgical means is generally not only impossible but also endangers the adjacent teeth, excessive bone removal being required to achieve this relationship. Only one case had ideal contact achieved purely by surgery.
Occlusion
In 24 instances good occlusal results were achieved. In four cases there was a significant CR/ CO shift with premature contact involving the sur- gical segment. One was related to mandibular re- lapse after advancement surgery, two had partially relapsed into a cusp-to-cusp cross-bite, and one simply had poor interdigitation of the opposing teeth. An additional two cases had less than ideal occlusion; one was a complete cross-bite and the
type A type C
FIGURE Il. Interdental crestal bone healing pat- terns: type A, normal anatomy with complete lamina dura: type B. hori- zontal bone loss; type C. vertical bone loss.

MOLON EY ET AL
other an open-bite between opposing premolars, al- though neither had any CR/CO discrepancy. In the seven cases where orthodontics was coordinated with surgery, the occlusal results were ideal in six cases, the one failure being the mandibular relapse case mentioned.
Stabilit!
In all cases the operated segments were clinically stable in the long-term. On only four occasions was bone-grafting employed, these being alveolar cleft cases. A Hawley-type retainer was routinely in- serted a few days after removal of the acrylic wafer and was worn full-time for a period of two to three months, followed by nighttime and weekend wear for 12 months in some cases, the average time being six months.
Palatal Tisslrrs
All unsutured palatal wounds healed without com- plication, with no cases of oronasal or oroantral fis- tula formation. The palatal splint is thought to have been partially responsible for the good palatal healing.
Fate oj’the Third Molur
Nineteen teeth were removed at the time of sur- gery, and 13 had been extracted previously. In four instances the tooth was not disturbed. On two oc- casions the third molar was displaced during the tuberosity osteotomy and was not found despite careful and prolonged search after downfracture of the segment. Postoperative radiographs showed both of these teeth rotated and displaced superiorly (Fig. 6). In neither case has the position of the tooth altered in the long term, nor have the patients de- veloped any symptoms.
Esthetic Resrdts
All but one patient was pleased with their final appearance. However, six were scored as not ideal but adequate by the examiner, although the patients remained happy. The one “poor” case was a re- lapse into complete cross-bite with a 2-mm sepa- ration between the teeth adjacent to the osteotomy.
Postoperative Pain
Discomfort after the PSMO was minimal. Four patients experienced significant pain, in one of whom it persisted and required reoperation of the interdental osteotomy, as described earlier. An ad- ditional three suffered transient nasal stuffiness and discharge, but significant maxihary sinusitis was
FIGURE 12. Healing defect in interdental osteotomy site (arrow) three months after operation.
not a problem. This low incidence of antral com- plication is similar to the findings of Perko?s after the Le Fort I maxillary operation. Inability to chew hard foods was the persistent complaint of one pa- tient 12 months after surgery, while three experi- enced annoying “prickling” sensations in the teeth of the operated segment three, 16 and 17 months, respectively, after operation.
Patient Satisfaction
General patient response was positive. Only two were unhappy with the overall result, both of whom had to spend an unexpectedly long time in retention (nine and 12 months, respectively). Both of these cases experienced early partial relapse treated by a removable palatal expansion device. Despite this, all 30 patients would recommend the operation for others with similar problems,
Discussion
The PSMO has been viewed with mixed feelings by many operators, particularly for the stable and complete correction of anterior open-bite. Kufner’ had difficulties in achieving a long-term, stable re- sult in six of his 18 patients. He blamed insufficient ostectomy and over-reliance on postoperative aids, such as chin straps. for his partial failures. How- ever, several long-term follow up studiess,‘3.zy-3’ at- test to the usefulness of this operation. West and Epker8 experienced no relapse with the single-stage procedure in 12 patients. They described the use of the retention splint and indicated its usefulness in cases that required lateral movement of the poste- rior segment. Stoker and Epker” commented on
780 POSTERIOR SEGMENTAL MAXILLARY OSTEOTOMY
the same tendency to lingual relapse after lateral movement, especially when intermolar width was expanded beyond 5 mm. They treated these cases “as a rapid orthodontic palatal expansion” and re- tained the maxillary arch for between three and five months. They could find no significant relapse in 11 cases followed for six months to two years. Bell and Turvey20 had success with the PSMO in ten patients, again emphasizing adequate retention during the healing phase. They did, however, utilize maxillomandibular fixation, which is not routine in our clinic, even in bilateral cases.
In an attempt to overcome potential relapse prob- lems, Martis14 advocated long-term immobilization in reporting the results of 67 anterior open-bite cases. Despite up to 12 weeks of maxillomandibular fixation he noted partial re-opening of the bite in 40 cases (60%). Such results do not support the use of extended immobilization.
The physiologic changes associated with the PSMO and other segmental osteotomies have been researched both in animal experiments33l34 and in human follow up studies.27,28*3”-38 Bell and Levy’s33 revascularization and bone healing studies in the Rhesus monkey clearly demonstrated the biologic principles underlying survival of the teeth, bone, and supporting tissues. The greater palatine artery was not crucial to the revascularization of the sec- tioned and mobilized posterior segment. When the area of the interdental osteotomy was studied his- tologically, alveolar crestal bone healing was well- advanced by six weeks, with good gingival cov- erage. However, there was some evidence of wid- ening of the periodontal ligament space due to bone resorption on the tooth side of the cortical plate somewhat akin to the “type C” pattern (Fig. 1 lc). A higher incidence of pulp damage was noted in the teeth adjacent to the interdental osteotomy site. Poswillo36 also studied pulp changes after anterior segmental surgery, and the findings help to explain the lack of return of sensation in teeth whose pulps demonstrated progressive fibrosis, with loss of nerve fibers and odontoblasts, but which remained viable.
Healing of the alveolar crestal bone and the peri- odontal pocket formations after interdental oste- otomy were also looked at by Hutchinson and MacGregor,35 with no significant complications noted. Normal reaction to electrical pulp testing re- turned to 177 of 181 teeth tested in patients followed serially for almost three years. The interpretation of pulp testing by whatever means after segmental osteotomy remains difficult. Mumford originally cautioned about the lack of correlation between test response and the viability of the pulp, which is more dependent on the integrity of pulpal and periodontal
vasculature than on the preservation of nerve con- nections.
Periodontal health after segmental osteotomy has received scant attention in the literature. Shep- herd” found no abnormal pocketing in 58 teeth adjacent to the interdental osteotomy. Bell and Turvey 2o had no periodontal problems, describing instead “minimal loss of interseptal bone” in the inter-radicular bone cut area. Our findings generally agree with previous reports in this regard, only three such areas having probing depths of 4 mm or more. Despite this, caution must be entertained, as the “type C” pattern of bone loss previously de- scribed was present in eight of 38 interdental areas, six of which had probing depths of 3 mm or more, and all of which had lack of contact between adja- cent teeth in the affected area.
Lack of contact between teeth adjacent to the osteotomy site was perhaps the least ideal aspect of our treatment results. This was achieved in only 13 of 33 segments where complete closure was the aim of treatment. Five segments showed a gap of 2 mm between the teeth adjacent to the osteotomy site. The importance of coordinated orthodontics and planned restorative dentistry needs little addi- tional emphasis. However, it is not always possible for the patient to share the benefits of the former and not always an aim of treatment to combine sur- gery with the latter. A critical inspection of the oc- clusion along the lines suggested by Hoh140 revealed a less than satisfactory result in six of our 30 pa- tients, all of whom remain asymptomatic at this point.
The modified technique and simple surgical aids described in this paper have allowed this operation to be performed with relative ease, safety, and speed. The continued use of cast metal cap splints for segmental osteotomies as described by Honore4’ and Glick et al.42 would seem to represent an ex- pensive and unnecessarily complex procedure.
The use of this versatile operation in simulta- neous extraction of a palatally impacted canine tooth and immediate space closure by advancement of the posterior maxillary segment offers an inter- esting solution to a difficult problem. While not ad- vocating its use in every case, and while not offering it as an alternative to orthodontics or conservative measures, its application should be considered when expensive restorative dentistry and prolonged orthodontic therapy are the other alternatives. As demonstrated by this study, close cooperation be- tween several dental specialties may be necessary if ideal results are to be achieved routinely.
The PSMO continues to occupy an important place in the operating armamentarium of the or- thognathic surgeon. Its successful application in the

MOLONEY ET AL 781
correction of dentoalveolar problems in all planes of space has stood the test of time. This report dem- onstrates its additional usefulness in circumstances demanding the closure of edentulous spaces and suggests an interesting solution to the problem of the palatally impacted canine tooth.
Dr. Moloney wishes to thank Dr. Guido de Troyer for his as- sistance with the translation of the German literature.
I Schuchardt K: Chirurgie fur offenen Bisses. in Bier, Braun. Kummel teds): Chirurgische Operationslehre, 7. Aufl. bd. 2. Leipzig. 19.54
2. Schuchardt K: Foramen des offenen Bisses und ihre oper- ativen Behandlungsmogligkeiten. in Schuchardt K, Wass- mund M (eds): Fortschritte der Kiefer-und Gesichtschi- rurgie. I. Stuttgart. George Thieme Verlag, 1955, p 222
3. Schuchardt K: Experiences with the surgical treatment of deformities of the jaws: prognathia, micrognathia and open bite. in Wallace AB (ed): Second Congress of Inter- national Society of Plastic Surgeons (London) 1959. Edin- burgh. ES Livingstone. 1961. p 73
4. Cheever DW: Displacement of the upper jaw. Medical and Surgical reports of the Boston City Hospital, 1870. p 154
5. Moloney F. Worthington P: The origin of the Le Fort I max- illary osteotomy: Cheever’s operation. J Oral Surg 39:73 I, 1981
6. Kufner J: Nove metody chirurgiekeho leceni ostevreneho skusu. Cslka Stomat 60:387. 1960
7. Kufner J: Experience with a modified procedure for correc- tion of open bite, in Walker RV (ed): Transactions of the third Intertmtional Converence on Oral Surgery (London) 1968. Edinburgh, ES Livingstone. 1970. p 18
8. West RA, Epker BN: Posterior maxillary surgery: its place in the treatment of dentofacial deformities. J Oral Surg 30:Sh?. 1972
9. Kapovits M, Pfeifer G: Die chirgurgische Behandlung des offenen Bisses nach Schuchardt (Technik und Erfah- rut-men). Dtsch Zahn- Mund- und Kiefer Heilk 36:268. l96T.
IO. Obwegeser H: Der offenen Biss in chirurgischer Sicht. Schweiz Mschr Zahnheilk 74:668. 1964
1 I. Perko M: Die chirurgische Spatkorrektur von Zahn-und Kiefer-stellunsanomalien bei Staetpatienten. Schweiz Mschr Zahnheilk 79:19, 179. 1969
12. Bell WH: Correction of skeletal type of anterior open bite, J Oral Surg 29:706. 1971
13. Schriver W, Swintak E: Surgical correction of unilateral pos- terior bimaxillary malocclusion. J Maxillofac Surg .5:214. 1977
14. Martis CS: Postoperative results of posterior maxillary os- teotomy after long-term immobilization. J Oral Surg 38:103. 19x0
15. Bell WH. Proffit WR. White RP: Surgical Correction of Den- tofacial Deformities. Philadelphia, WB Saunders. 1980, pp 327-367
16. Reichenbach E: Die chirurgische Benhandlung des offenen Bisses. Fortschr Kieferorthop 21:393. 1960
17. Mohnac AM: Surgical correction of maxillomandibular de- formities. J Oral Surg 23:393. 1965
18. Mohnac AM: Maxillary osteotomy in the management of occlusal deformities. J Oral Surg 24:305, 1966
19. Converse JM, Wood-Smith D: An atlas and classification of
midfacial and craniofacial osteotomies. in Hueston JT (ed): Transactions of the Fifth International Congress on Plastic and Reconstructive Surgery. Melbourne, Butter- worths, 1971. pp 931-962
20. Bell WH. Turvey TA: Surgical correction of posterior cross- bite. J Oral Surg 32:81 I. 1974
21. Bell WH, McBride K: Immediate surgical repositioning of anterior and posterior maxillary dento-osseous segments. J Oral Surg 34:943, 1976
22. West RA, Burk JL: Maxillary osteotomies for preprosthetic surgery. J Oral Surg 32:13. 1974
23. Alexander JM. Van Sickels JE: Posterior maxillary osteot- omies: an aid for a difficult prosthodontic problem. J Prosthet Dent 41:614. 1979
24. Tideman H, Stoelinga PJW, Gallia L: Le Fort 1 advancement with segmental palatal osteotomies in patients with cleft palates. J Oral Surg 38:196. 1980
25. Dupon C. Ciaburro H, Prevost Y: Simplifying the Le Fort I maxillary osteotomy. Plast Reconstr Surg 54:142. I974
26. Thimble LD. Tideman H, Stoelinga PJW: A modification of the pterygoid plate separation in low-level maxillary os- teotomies. J Oral Maxillofac Surg 41:544. 1983
27. Shepherd JP: Long-term effects of segmental alveolar oste- otomy. Int J Oral Surg 8:327. 1979
28. Perko. M: Maxillary sinus and surgical movement of the maxilla. Int J Oral Surg 1:177. 1972
29. Stoker NG, Epker BN: The posterior maxillary osteotomy: a retrospective study of treatment results. In1 J Oral Surg 3:153, 1974
30. Nwoku AL: Eraebnisse der chirurgische Korrektur des of- fenen Bisses-nach Schuchardt.~in Schuchardt K. Steil- math R teds): Fortschritte der Kiefer and Gesichts- Chirurgie. XVIII. Stuttgart. Georg Thieme Verlag. 1974. pp 209-21 I
31.
32.
33.
34.
35.
36.
37.
38.
39.
40.
41.
42.
Holte WJ, Lentrodt J: Indikation, Technik und klinische Er- gebnisse der chirurgischen Behandlung des offenen Bisses durch Osteotomies im seitlichen Oberkiefer nach Schu- chardt, in Schuchardt K. Stellmach R teds): Fortschritte der Kiefer und Gesichts-Chirurgie. XVIII, Stuttgart. Georg Thieme Verlag. 1974. pp ?O?-X6
Schweinzer N: Hat sich die Korrektur des offenen Bisses nach Schuchardt bewahrt? in Schuchardt K. Schwenzer N teds): Fort-schritte der Kiefer und Gesichts-Chirurgie. XXVI, Stuttgart. Georg Thieme Verlag. 1981. pp 117- 121
Bell WH, Levy BM: Revascularization and bone healing after posterior maxillary osteotomy. J Oral Surg ?9:313, 1971
Rontal E, Hohmann A: Lateral alveolo-maxillary osteoto- mies: revascularization studies. Arch Otolarng 95: IX. 1972
Hutchinson D. MacGregor AJ: Tooth survival following var- ious methods of sub-apical osteotomy. Int J Oral Surg l:Sl, 1972
Poswillo DE: Early pulp changes following reduction of open bite by segmental surgery. Int J Oral Surg 187. 1972
Pepersack WJ: Tooth vitality after segmental osteotomy. J Maxillofac Surg 1:85. 1973
Kohn MW, White RP: Evaluation of sensation after seg- mental alveolar osteotomy in 22 patients. J Am Dent Assoc 89:154. 1974
Mumford JM: Pain perception threshold on stimulating human teeth and the histological condition of the pulp. Br Dent J 123:427, 1967
Hohl TH: Occlusal concepts for the orthognathic surgeon. Int J Oral Surg 7:197, 1978
Honore P: Splinting for alveolar osteotomies. Br J Oral Surg 14:213, 1977
Glick D, Gutman 0. Ariely E, et al: A semi-precision cast splint for fixation following segmental osteotomies. Br J Oral Surg 14:214, 1977
Copyright © 2022 FDOKUMEN